
Androgen Receptors and Sexual Dimorphisms in the Larynx of the Bullfrog
Upload
kedarunipuneCategory
view
1download
0
Oral Oncology xxx (2009) xxx–xxx
ARTICLE IN PRESS
Contents lists available at ScienceDirect
Oral Oncology
journal homepage: www.elsevier .com/locate /ora loncology
Relationship between molecular markers and treatment responsein a retrospective cohort of Indian patients with primary carcinoma of the larynx
R. Sahoo a, V. Chittibabu a, G. Patil a, S. Rao a, S. Thakur a, G. Dhondalay a, A.J. Kulkarni a, A. Banerjee a,B.S. Ajaikumar b, A. Korlimarla a, A. Nargund a, R.N. Niti b, K.S. Gopinath b, Shilpa Prabhudesai a,R.M. Raghavendra a,b,*
a Triesta Sciences (India) Pv Ltd., No. 8, Kalinga Rao Rd., Sampangiramanagar, Bangalore 560027, Indiab HCG Foundation, No. 8, P. Kalinga Rao Rd., Sampangiramanagar, Bangalore 560027, India
a r t i c l e i n f o
Article history:Received 12 June 2009Received in revised form 16 July 2009Accepted 16 July 2009Available online xxxx
Keywords:p53 MutationCarcinoma of the larynxTreatment responsePrognostic markersCisplatin resistanceLarynx preservation
1368-8375/$ - see front matter � 2009 Elsevier Ltd. Adoi:10.1016/j.oraloncology.2009.07.013
* Corresponding author. Address: Research Head,Triesta Sciences Pvt. Ltd., HCG Towers, No. 8, P. Kalmanagar, Bangalore 560027, India. Tel.: +91 80 40206122485962.
E-mail address: [email protected] (R.M. Rag
Please cite this article in press as: Sahoo R et altients with primary carcinoma of the larynx. Or
s u m m a r y
p53 Mutations and over expression have been shown to predict treatment response in head and neckcancer patients. Failure of organ sparing therapy has been attributed to cisplatin and radiotherapy resis-tance in carcinoma of the larynx patients. In this study, we evaluate the relationships between p53 overexpression/mutations, bcl2 expression and ploidy status in a retrospective cohort of responder andnon-responder carcinoma of the larynx patients.
Tissue samples from 22 patients with histopathologically confirmed carcinoma of the larynx andmatched for age, stage, node status and treatment regimen, were analysed from our tissue biorepository.Differences in the above molecular markers were analysed between the responders and non-respondersto conventional treatment. p53 and bcl2 over expression was checked by IHC and p53 mutation by PCRand direct sequencing. DNA ploidy and S-phase fractions were also analysed. Chi square analysis wasused to identify changes in proportions of these markers in responders and non-responders andlikelihood ratio test was done to determine the best predictor biological marker for treatment response.Bivariate relationships were determined between these variables using Spearman’s rank correlation.
Node negativity at time of diagnosis (p = 0.05), p53 mutation (p = 0.02) and bcl2 negativity (p = 0.05) aresome of the factors that are known to influence treatment response in our study. p53 over expression, S-phase fractions and ploidy status did not seem to influence treatment response. There was a significantinverse correlation between stage of cancer (p = 0.03) and node positivity (p = 0.06) with bcl2 positivity.There was an inverse correlation between mutation category to treatment response (p = 0.01).
The results suggest p53 mutations to be a promising marker in predicting treatment response incarcinoma of the larynx patients.
� 2009 Elsevier Ltd. All rights reserved.
Background
Head and neck cancers constitute a large proportion of cancersin India accounting for 23% of all cancers in males and 6% of all can-cers in females.1 Majority of these cancers are preventable and arerelated to consumption of tobacco, alcohol, poor hygiene, diet andviral infections.2 carcinoma of the larynx and preferably, squamouscell carcinoma constitutes 78% of all head and neck malignancies.The average 5-year survival for head and neck cancer rangesbetween 20% and 90% depending on the site and extent of thedisease.3
ll rights reserved.
Investigator Initiated Trials,inga Rao Road, Sampangira-22/9916488864; fax: +91 80
havendra).
. Relationship between moleculal Oncol (2009), doi:10.1016/j.o
The preferred surgical treatment for advanced laryngeal tumorsremains total laryngectomy (TL), a surgical technique in which lar-yngeal speech is sacrificed. However, of late radiation and chemo-therapy, along with subtotal laryngectomies that form a part of theso-called organ sparing protocols have also resulted in effectiveoutcomes in western populations.4 In India most of these cancerspresent at an advanced stage (stage III and above) thus pittingthe principles of oncologically sound resection against organ pres-ervation. Currently used organ sparing protocols such as cisplatinanalogues and radiotherapy that are used in the treatment of headand neck cancers are not always effective in tumor killing due todevelopment of resistance.5
Cisplatin forms adduct in DNA and is a mutagen in mammaliancells.6–9 Current evidence suggests that cisplatin resistance arisesthrough a combination of mutagenesis that generates highlycisplatin-resistant clones in the surviving population with
ar markers and treatment response in a retrospective cohort of Indian pa-raloncology.2009.07.013

e2 R. Sahoo et al. / Oral Oncology xxx (2009) xxx–xxx
ARTICLE IN PRESS
enrichment of these variants by subsequent cycles of cisplatintreatment. Clearly, identifying the molecular mechanisms of che-motherapy resistance and using this knowledge to develop moreeffective treatment strategies is an important goal.
Among the most common genetic events that occur in the gen-esis of tumors, including Head and Neck Squamous Cell Carcinoma(HNSCC) are mutations in the p53 tumor suppressor gene. Wild-type p53 helps maintain genomic integrity through the inductionof cell growth arrest and/or apoptosis (programmed cell death) fol-lowing DNA damage. p53-induced cell cycle arrest allows the cellto repair damaged DNA. If DNA damage is extensive and repairfails, p53 can induce apoptosis.10–13 Missense mutations of p53that lead to changes in the binding properties or conformation ofthe protein is common. Such changes inactivate its function andenhance the half life and stability of the p53 protein leading to overexpression. Studies show that high expression of p53 is signifi-cantly associated with organ preservation in patients with ad-vanced laryngeal cancer treated with induction chemotherapyand radiation.14 Additionally, in vitro studies with HNSCC cell lineswith mutant p53, as a group, has shown mixed results.15,16 Consis-tent with these in vitro studies; p53 status has been linked to che-motherapy resistance in several tumor types such as breastcancer,17 lymphomas,18 and leukemia’s.19 In general, p53 muta-tions in these tumor types are associated with disease progressionand poor prognosis. Studies also report worse prognosis in caseswith mutant p53 thereby negating the findings from other studiesthat have shown good prognosis.20 The findings are therefore con-troversial with respect to the role of p53 mutants and wild typep53. These findings are also paradoxical in that wild-type p53 nor-mally functions to induce apoptosis in response to DNA-damagingagents, and thus these tumors should be more responsive to cis-platin-based chemotherapy. For example, in bladder cancer, p53mutations were shown to correlate with increased chemosensitiv-ity.21 Similarly, other in vitro studies are consistent with thisobservation and have shown that inactivation or disruption ofp53 function sensitizes tumor cells to DNA-damaging agents, spe-cifically cisplatin.22,23 Thus, the predictive value of p53 status andits clinical impact seem to depend largely on the predominant ef-fect of p53 mutations in a specific tumor type.24
In HNSCC, the prognostic role of p53 mutations is still uncleardue to contradictory reports. The same group could not confirminitial findings that p53 mutations were associated with loco regio-nal treatment failure later.25,26 Others could not confirm the re-ported association of mutations with survival.27,28 In most of theprevious studies, the biochemical consequences of different muta-tions were not considered.29 Furthermore, most studies so far haveexamined mixed tumor cohorts from all head and neck sites. Sincethe tumor site is an established clinical factor of its own, the ana-tomical site might have confounded the role of p53 mutations. Inlaryngeal cancer, some studies have reported an inverse relation-ship between p53 alterations and outcome, i.e., p53 mutationswas associated with decreased survival,30 whereas p53 overexpression was associated with improved larynx preservation butnot better survival.31
In fact, exogenous co expression of wild type p53 and bcl-xLprotects cells from p53-mediated apoptosis. Recent studies showthat bcl-xL is over expressed in 74% and bcl2 in 15% of laryngealtumors. There has been a better response to chemotherapy and lar-ynx preservation in those tumors with low bcl-xL expression.32
Both bcl-xL and bcl2 proteins are frequently over expressed inHNSCC cell lines. In addition, the absence of p53 has been shownto be associated with genomic instability and increasing anneup-loidy and worse prognosis.33 Low p53 and low bcl-xl expressionhas been found to be a strong predictor of larynx preservation.34
Therefore understanding molecular events in these pathways thatoffer resistance to cisplatin or radiotherapy in head and neck can-
Please cite this article in press as: Sahoo R et al. Relationship between molecultients with primary carcinoma of the larynx. Oral Oncol (2009), doi:10.1016/j.o
cers will offer more impetus to develop good organ sparing proto-cols. In this study, we evaluate the relationships between p53 overexpression, p53 mutations, bcl2 expression and ploidy status ontreatment response in a retrospective cohort of carcinoma of thelarynx patients.
Material and methods
Study cohort
Tissue samples from 22 patients with histopathologically pro-ven Carcinoma of Larynx were analysed from the hospital tissuebiorepository. The study was approved by the Institutional ethicscommittee. Clinical, sociodemographic information and responseto treatment were abstracted from case records of all patientswho had been diagnosed with carcinoma of the larynx from years2001 to 2005. Those patients whose records had all follow up infor-mation until recent and whose tissue was stored in the hospitalbiorepository were chosen as study cohorts after consent. Patientswere classified as non-responders if they had any recurrence/relapse/metastases of tumor and responders if they were survivingwithout disease. Patients in both these groups were matched forage, stage of disease, node status, histopathogy type, and cisplatintherapy and treatment regimen. Eleven subjects in each groupmatched for all these variables were chosen as a study cohort.Their tissue samples were analysed for p53overexpression andmutation, bcl2 overexpression,, ploidy status and S-phase fractions.
Molecular markers
p53 and bcl2 overexpression were checked by IHC and p53mutation by PCR and direct sequencing. DNA ploidy and S-phasefractions were analysed on Cyan (DAKO) flow cytometer.
Immunohistochemistry
Briefly, 5-lm serial sections were cut from FFPE blocks andmounted on glass slides coated with 10% poly L-lysin. Sectionswere dewaxed in xylene and rehydrated in graded ethanol. Endog-enous peroxidase activity was blocked by immersion in 3% hydro-gen peroxide in methanol for 20 min. Immunoreactivity of thetarget antigens was enhanced using heat induced antigen retrieval.The sections were placed in a microwave, 0.1 M EDTA buffer,heated to 800 W for 10 min, followed by 200 W at 15 min and thencooled. p53 protein expression was determined by incubating thetissue sections with a ready to use monoclonal antibody DO7(DAKO). This antibody recognizes both wild type and mutant formsof the p53 protein. For analysis of bcl2 protein expression, tissuesections were incubated with bcl2 monoclonal antibody (BioGe-nex, CA, USA). The sections were then incubated with a polymerHRP secondary antibody (DAKO) for 30 min. The bound complexeswere visualized by the application of a 2% solution of 3,30-diam-inobenzidine (DAKO) containing hydrogen peroxide as a substrate,for 3 min. Following incubation, the sections were washed andthen counterstained with hematoxylin, dehydrated, cleared andcover slipped.
Quantification
Scoring of p53 and bcl2 immunostaining was performed bycounting the number of cells showing nuclear staining as a propor-tion of the total tumor cell population, expressed categorically asfollows: 0, 0% tumor cells stained; 1+, 1–25% tumor cells stained;2+, 26–50% tumor cells stained; 3+, 51–75% and 4+, 76–100% tu-mor cells stained. For p53, tumors showing >10% positive cells
ar markers and treatment response in a retrospective cohort of Indian pa-raloncology.2009.07.013

R. Sahoo et al. / Oral Oncology xxx (2009) xxx–xxx e3
ARTICLE IN PRESS
were considered to show abnormal protein staining. bcl2 proteinexpression was considered as positive if neoplastic cells showedcytoplasmic staining.
Mutation analysis
2 � 20 lm section of each sample was taken in 200 ll of 0.5%Tween 20, and heated at 90 �C for 10 min followed by 55 �C for10 min. Twice 2 ll of proteinase K was added within 1-h intervaland incubated overnight at 55 �C. Four hundred microliter of 5%chelex was added and heated to 99 �C for 10 min. Lysate was cen-trifuged for 15 min at 3000 rpm at 4 �C. Two hundred microliterof chloroform was added and lysate incubated at 45 �C for1 min. The lysate was centrifuged again for 15 min at13,000 rpm at 4 �C. DNA from the lysate was precipitated with1/10 vol 3 M sodium acetate and 2 volumes of 100% ethanol.DNA was recovered after incubation at �80 �C for 20 min, centri-fuged for 15 min at 4 �C, and then washed twice with 70% alcohol.Pellet was air dried and dissolved in 50 ll of deionised water andtaken further for PCR.
PCR amplification and gene sequencing
Exons 5, 6, 7 and 8 of the p53 gene were amplified separatelyusing p53 exon specific primers 35 with minor modification inPCR cycling. Briefly, 100 ng of genomic DNA was added to a 25-ll PCR mixture (Eppendorff Cat #130175479). For exon 6, 7, 8,PCR was carried out through 35 cycles at temperatures of 94 �C(30 s), 58 �C (40 s), and 72 �C (1 min). Touch down PCR for exon 5was done at 94 �C (20 s), 61 �C (30 s) with a drop of 0.5 �C/cycle fol-lowed by 72 �C (1 min) for 1st 13 cycles, 94 �C (20 s) for 30 cyclesand 57 �C (30 s) and 72 �C (1 min). PCR products were separated byelectrophoresis in 1% agarose gel. Bands were cut and DNA wasrecovered from gel using gel-purification kit (Eppendorf, Cat No#955152000). Purified products were sequenced and aligned withwild type sequence to detect mutation.
DNA ploidy
50 lM sections were taken for single cell preparation. Sectionswere dewaxed using 2 changes of xylene, (3 ml for 10 min) at roomtemperature and then rehydrated in a sequence of 3 ml of 100%,95%, 70% and 50% alcohol. Sections were washed twice in distilledwater and re-suspended in 1 ml of 0.5% pepsin in 0.9% NaCl, ad-justed to pH of 1.5 with 2 N HCl. Tubes were incubated in a waterbath at 37 �C for 30 min with intermediate vortex mixing. The cellswere filtered using 45l filters. The filtrate was centrifuged, pel-leted and washed with PBS. The pellet was dissolved in stainingsolution of T-X100 (0.1%); RNAses (0.05 ng) and PI, 20 ng/ll. Cellu-lar DNA content was measured using a DAKO flow cytometer at488 nm.
Figure 1 IHC to detect over expression of p53 protein. A representative tumorsample of p53 over expression (1a) and no expression (1b).
Data analysis
Data was analysed using SPSS 10.0 version for windows. Datawere transformed into category variables with various levels to as-sess distribution of proportions in responders and non-responders.Chi square analysis was used to analyze the distribution of propor-tions in treatment responders and non-responders. Likelihood ratiotest was used to assess which molecular or clinical variable pre-dicted treatment response. Spearman’s correlation analysis wasused to identify the bivariate relationships between independentand outcome variables.
Please cite this article in press as: Sahoo R et al. Relationship between molecultients with primary carcinoma of the larynx. Oral Oncol (2009), doi:10.1016/j.o
Results
Eighty two percentage of the study subjects in the study cohortwere male and remaining was female. The percentage of those whosmoked tobacco and chewed tobacco was 50% and 18.2%, respec-tively. All subjects were matched for their age, stage of disease,and treatment regimen. The age range of subjects was between41 and 71 years (54 ± 10.1 years). All of them were diagnosed withcarcinoma of the larynx and had squamous cell carcinoma of vari-ous grades. Analysis of the paraffin blocks was done for p53expression (Fig. 1a and b) and mutation and for bcl2 expression(Fig. 2). 45.5% of the cohort had stage II disease, 54.5% stage III,77.3% were node positive at time of diagnosis, 36.4% received sur-gery followed by radiotherapy and chemotherapy (S+RT+CT) andanother 36.4% received radiotherapy followed by chemotherapyand surgery (RT+CT+S).
p53 expression was categorized as negative (<10%), mild posi-tive (10–20%), moderately positive (20–50%) and strongly positive(>50%). 95.2% of subjects had expression of p53. Mutations wereseen in exon 8 and exon 5 in 31.8% of the patients. bcl2 was positivein 27.3% of patients. 50% were smokers and rest was non-smokers(Table 1).
ar markers and treatment response in a retrospective cohort of Indian pa-raloncology.2009.07.013
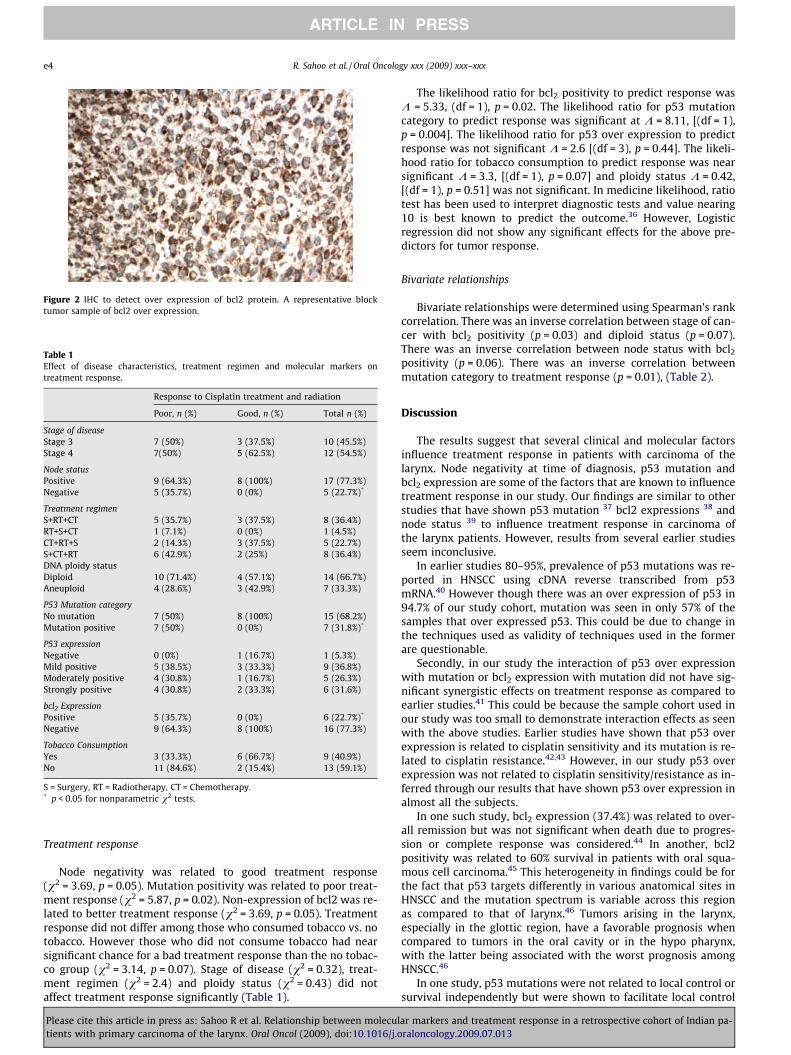
Figure 2 IHC to detect over expression of bcl2 protein. A representative blocktumor sample of bcl2 over expression.
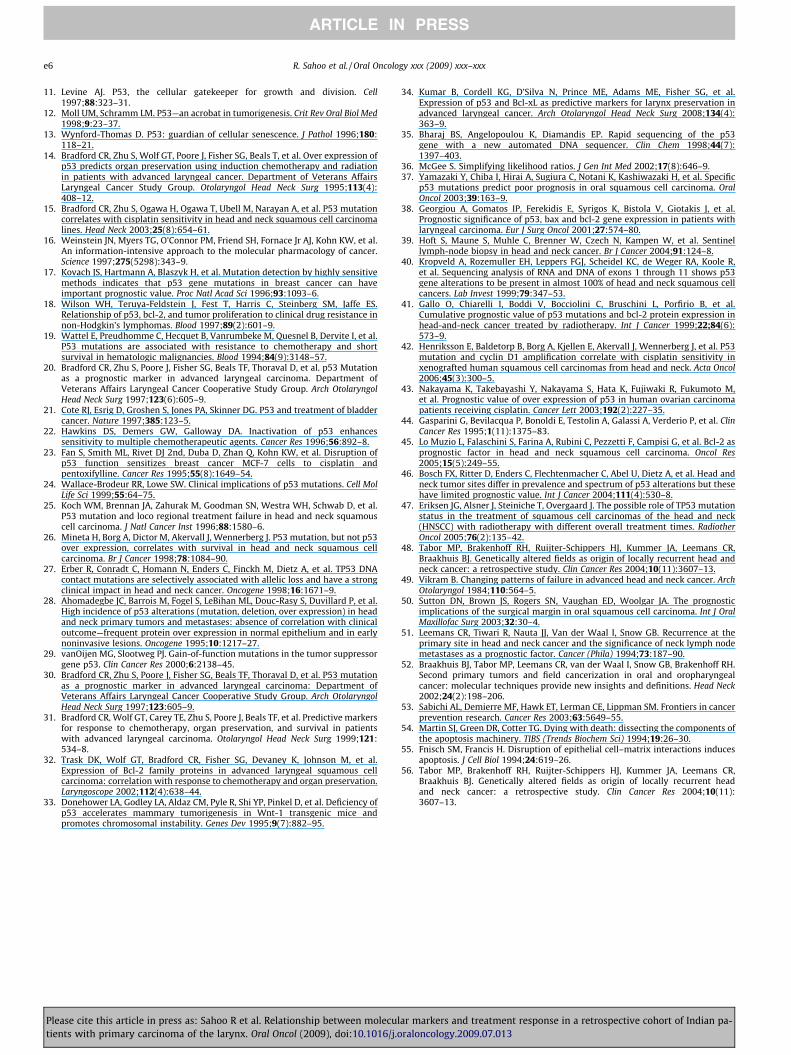
Table 1Effect of disease characteristics, treatment regimen and molecular markers ontreatment response.
Response to Cisplatin treatment and radiation
Poor, n (%) Good, n (%) Total n (%)
Stage of diseaseStage 3 7 (50%) 3 (37.5%) 10 (45.5%)Stage 4 7(50%) 5 (62.5%) 12 (54.5%)
Node statusPositive 9 (64.3%) 8 (100%) 17 (77.3%)Negative 5 (35.7%) 0 (0%) 5 (22.7%)*
Treatment regimenS+RT+CT 5 (35.7%) 3 (37.5%) 8 (36.4%)RT+S+CT 1 (7.1%) 0 (0%) 1 (4.5%)CT+RT+S 2 (14.3%) 3 (37.5%) 5 (22.7%)S+CT+RT 6 (42.9%) 2 (25%) 8 (36.4%)DNA ploidy statusDiploid 10 (71.4%) 4 (57.1%) 14 (66.7%)Aneuploid 4 (28.6%) 3 (42.9%) 7 (33.3%)
P53 Mutation categoryNo mutation 7 (50%) 8 (100%) 15 (68.2%)Mutation positive 7 (50%) 0 (0%) 7 (31.8%)*
P53 expressionNegative 0 (0%) 1 (16.7%) 1 (5.3%)Mild positive 5 (38.5%) 3 (33.3%) 9 (36.8%)Moderately positive 4 (30.8%) 1 (16.7%) 5 (26.3%)Strongly positive 4 (30.8%) 2 (33.3%) 6 (31.6%)
bcl2 ExpressionPositive 5 (35.7%) 0 (0%) 6 (22.7%)*
Negative 9 (64.3%) 8 (100%) 16 (77.3%)
Tobacco ConsumptionYes 3 (33.3%) 6 (66.7%) 9 (40.9%)No 11 (84.6%) 2 (15.4%) 13 (59.1%)
S = Surgery, RT = Radiotherapy, CT = Chemotherapy.* p < 0.05 for nonparametric v2 tests.
e4 R. Sahoo et al. / Oral Oncology xxx (2009) xxx–xxx
ARTICLE IN PRESS
Treatment response
Node negativity was related to good treatment response(v2 = 3.69, p = 0.05). Mutation positivity was related to poor treat-ment response (v2 = 5.87, p = 0.02). Non-expression of bcl2 was re-lated to better treatment response (v2 = 3.69, p = 0.05). Treatmentresponse did not differ among those who consumed tobacco vs. notobacco. However those who did not consume tobacco had nearsignificant chance for a bad treatment response than the no tobac-co group (v2 = 3.14, p = 0.07). Stage of disease (v2 = 0.32), treat-ment regimen (v2 = 2.4) and ploidy status (v2 = 0.43) did notaffect treatment response significantly (Table 1).
Please cite this article in press as: Sahoo R et al. Relationship between molecultients with primary carcinoma of the larynx. Oral Oncol (2009), doi:10.1016/j.o
The likelihood ratio for bcl2 positivity to predict response wasK = 5.33, (df = 1), p = 0.02. The likelihood ratio for p53 mutationcategory to predict response was significant at K = 8.11, [(df = 1),p = 0.004]. The likelihood ratio for p53 over expression to predictresponse was not significant K = 2.6 [(df = 3), p = 0.44]. The likeli-hood ratio for tobacco consumption to predict response was nearsignificant K = 3.3, [(df = 1), p = 0.07] and ploidy status K = 0.42,[(df = 1), p = 0.51] was not significant. In medicine likelihood, ratiotest has been used to interpret diagnostic tests and value nearing10 is best known to predict the outcome.36 However, Logisticregression did not show any significant effects for the above pre-dictors for tumor response.
Bivariate relationships
Bivariate relationships were determined using Spearman’s rankcorrelation. There was an inverse correlation between stage of can-cer with bcl2 positivity (p = 0.03) and diploid status (p = 0.07).There was an inverse correlation between node status with bcl2
positivity (p = 0.06). There was an inverse correlation betweenmutation category to treatment response (p = 0.01), (Table 2).
Discussion
The results suggest that several clinical and molecular factorsinfluence treatment response in patients with carcinoma of thelarynx. Node negativity at time of diagnosis, p53 mutation andbcl2 expression are some of the factors that are known to influencetreatment response in our study. Our findings are similar to otherstudies that have shown p53 mutation 37 bcl2 expressions 38 andnode status 39 to influence treatment response in carcinoma ofthe larynx patients. However, results from several earlier studiesseem inconclusive.
In earlier studies 80–95%, prevalence of p53 mutations was re-ported in HNSCC using cDNA reverse transcribed from p53mRNA.40 However though there was an over expression of p53 in94.7% of our study cohort, mutation was seen in only 57% of thesamples that over expressed p53. This could be due to change inthe techniques used as validity of techniques used in the formerare questionable.
Secondly, in our study the interaction of p53 over expressionwith mutation or bcl2 expression with mutation did not have sig-nificant synergistic effects on treatment response as compared toearlier studies.41 This could be because the sample cohort used inour study was too small to demonstrate interaction effects as seenwith the above studies. Earlier studies have shown that p53 overexpression is related to cisplatin sensitivity and its mutation is re-lated to cisplatin resistance.42,43 However, in our study p53 overexpression was not related to cisplatin sensitivity/resistance as in-ferred through our results that have shown p53 over expression inalmost all the subjects.
In one such study, bcl2 expression (37.4%) was related to over-all remission but was not significant when death due to progres-sion or complete response was considered.44 In another, bcl2positivity was related to 60% survival in patients with oral squa-mous cell carcinoma.45 This heterogeneity in findings could be forthe fact that p53 targets differently in various anatomical sites inHNSCC and the mutation spectrum is variable across this regionas compared to that of larynx.46 Tumors arising in the larynx,especially in the glottic region, have a favorable prognosis whencompared to tumors in the oral cavity or in the hypo pharynx,with the latter being associated with the worst prognosis amongHNSCC.46
In one study, p53 mutations were not related to local control orsurvival independently but were shown to facilitate local control
ar markers and treatment response in a retrospective cohort of Indian pa-raloncology.2009.07.013

Table 2Bivariate relationships (r) between disease characteristics, treatment response and molecular prognostic markers using spearman correlation.
p53 Expression in % (r value) p53 Positivity (r value) bcl2 Positivity (r value) Mutation category (r value) Ploidy status (r value)
Stage of cancer 0.27 0.03 �0.47* �0.36 0.07Node status �0.36 �0.28 �0.39 �0.10 0.16Treatment response �0.11 �0.14 �0.25 �0.52** 0.14Treatment regimen 0.45* 0.06 0.10 �0.26 0.06
* p < 0.05 on Spearman’s rank correlation.** p < 0.01.
R. Sahoo et al. / Oral Oncology xxx (2009) xxx–xxx e5
ARTICLE IN PRESS
with 6 fractions/week of radiotherapy treatment than non mutatedtumors.47 p53 mutations are also known to confer resistance tochemotherapy. This shows that p53 mutation is an importantevent in predicting response to radiotherapy and chemotherapy.This should be accounted for as a biologic marker to determine ifpatients with carcinoma of the larynx can have their larynx pre-served with only radiotherapy and chemotherapy as against sur-gery. Apart from identifying p53 mutations in tumor tissues,identifying them in tumor free margins could possibly indicate aresidual precursor disease that could manifest as local recurrencein future.48 Though significant advances in surgery and radiother-apy have been made over the last decades, the 5-year survival ratesof HNSCC patients have improved only moderately, partly due tothe relatively high rate of locally recurrent cancer. Even whenthe surgical margins are diagnosed as tumor free by histopathol-ogy, the local recurrence rate is still 10–30%.49–51 These new carci-nomas are clonally related to the primary tumor because theydevelop from a common genetically altered field and have there-fore been designated ‘‘second field tumors” [SFTs].52 In addition,current treatment modalities (surgery and/or chemotherapy/radio-therapy) are very effective to eradicate tumor cells, but these maynot be indicated for the treatment of relatively large fields of pre-neoplastic cells. There is a need therefore for the development oftargeted treatment strategies for patients at risk for SFTs.53
There are multiple pathways for induction of apoptosis, onlysome of which are modulated by bcl2 expression. Several geneshave been shown to be involved in activation and inhibition ofapoptosis, including wild-type p53, bcl-x, bax, and c-myc. A diverseco expression of these genes 54 and their interaction with differentextra cellular matrixes 55 may explain the different role played byp53 and bcl2 under different circumstances.
We were not able to demonstrate if these markers were impor-tant predictors for treatment response using regression and multi-variate analysis due to the relatively small sample size in ourstudy. More over we did not characterize the type of mutation inp53 and we looked at mutation in only the hot spots of axons 5–8. Therefore, it is difficult to discern if events outside these regionscould have confounded our observations. However, it should benoted that in earlier study mutations in exon 5 have been foundto be a unique feature of carcinoma of the larynx.56
One of the major strengths of our study was that we studied ahomogenous group of patients with carcinoma of the larynx andmatched them for clinical characteristics such as stage, node sta-tus, age, grade and treatment regimen. This could have nullifiedthe confounding effects of these clinical variables in our analysisstrengthening our hypothesis that p53 mutations are a significantbiomarker in predicting treatment response. The likely hood ratiofor detecting response with p53 mutation was high compared tobcl2, S-phase fractions, ploidy status and p53 over expression. Thisinfact is a novel contribution of this study, as earlier studies havenot validated the efficacy of these biomarkers as predictors oftreatment response.
Even if these data are to be interpreted with caution due to thesmall number of cases studied, and the relatively short period ofobservation, they give novel and potentially useful information to
Please cite this article in press as: Sahoo R et al. Relationship between molecultients with primary carcinoma of the larynx. Oral Oncol (2009), doi:10.1016/j.o
the clinician on the prediction of clinical outcome of patients withcarcinoma of the larynx treated with surgery and concurrent che-mo radiation therapy.
Worthy of note is the observation that the markers tested in thisstudy played a differential role in predicting response to therapyand prognosis. Our results add to the original data on the role ofthe biological markers in carcinoma of the larynx and give poten-tially useful indications to the clinician to predict more accuratelythe response to concurrent chemo radiation therapy and prognosis.However, a prospective randomized cohort study is underway totest the utility of these markers on treatment response in a clinicalsetting thereby moving from bench to bedside. Future studiesshould also unravel the distinct array of p53 alterations, mutationsand putative downstream signaling events that contribute to cis-platin and radiotherapy resistance in laryngeal tumors. Deeperunderstanding of this mechanism will help design strategies toovercome such resistance with new targeted therapies and pre-serve the larynx.
Conflicts of Interest Statement
None declared.
Acknowledgements
The current research work was carried out with full supportfrom Health care Global Foundation. We acknowledge contribu-tions from Ramachandra in providing information on study co-horts. We acknowledge all those patients who consented to givetheir tissue samples for the study.
References
1. National Cancer Registry Programme-Biennial Report (1988-89) of the NationalCancer Registry Programme. New Delhi: Indian Council of Medical Research1992; 3-42.
2. Mehrotra R, Singh M, Kumar D, Pandey AN, Gupta RK, Sinha US. Age specificincidence rate and pathological spectrum of oral cancer in Allahabad. Indian JMed Sci 2003;57:400–4.
3. Mehrotra R, Singh M, Gupta RK, Singh M, Kapoor AK. Trends of prevalence andpathological spectrum of head and neck cancers in North India. Indian J Cancer2005;42(2):89–93.
4. Pfister DG, Laurie SA, Weinstein GS, Mendenhall WM, Adelstein DJ, Ang KK,et al. American Society of Clinical Oncology clinical practice guideline for theuse of larynx-preservation strategies in the treatment of laryngeal cancer. J ClinOncol 2006;24(22):3693–704.
5. Juvekar AS, Amonkar AJ, D’cruz AK, Saikaia T, Pradhan S. Chemosensitivity ofadvanced Larynx Carcinoma cells in vitro and significance of multidrugresistance markers in these tumors. Cancer Biother Radiopharm1998;13(2):81–7.
6. Zamble DB, Lippard SJ. Cisplatin and DNA repair in cancer chemotherapy.Trends Biochem Sci 1995;20:435–9.
7. Wong E, Giandomenico CM. Current status of platinum-based antitumor drugs.Chem Rev 1999;99:2451–66.
8. Vokes EE, Weichselbaum RR, Lippman SM, Hong WK. Head and neck cancer. NEngl J Med 1993;328:184–94.
9. Induction chemotherapy plus radiation compared with surgery plus radiationin patients with advanced laryngeal cancer. The Department of Veterans AffairsLaryngeal Cancer Study Group. N Engl J Med 1991;324:1685–90.
10. el-Deiry WS. P21/p53, cellular growth control and genomic integrity. Curr TopMicrobiol Immunol 1998;227:121–37.
ar markers and treatment response in a retrospective cohort of Indian pa-raloncology.2009.07.013
e6 R. Sahoo et al. / Oral Oncology xxx (2009) xxx–xxx
ARTICLE IN PRESS
11. Levine AJ. P53, the cellular gatekeeper for growth and division. Cell1997;88:323–31.
12. Moll UM, Schramm LM. P53—an acrobat in tumorigenesis. Crit Rev Oral Biol Med1998;9:23–37.
13. Wynford-Thomas D. P53: guardian of cellular senescence. J Pathol 1996;180:118–21.
14. Bradford CR, Zhu S, Wolf GT, Poore J, Fisher SG, Beals T, et al. Over expression ofp53 predicts organ preservation using induction chemotherapy and radiationin patients with advanced laryngeal cancer. Department of Veterans AffairsLaryngeal Cancer Study Group. Otolaryngol Head Neck Surg 1995;113(4):408–12.
15. Bradford CR, Zhu S, Ogawa H, Ogawa T, Ubell M, Narayan A, et al. P53 mutationcorrelates with cisplatin sensitivity in head and neck squamous cell carcinomalines. Head Neck 2003;25(8):654–61.
16. Weinstein JN, Myers TG, O’Connor PM, Friend SH, Fornace Jr AJ, Kohn KW, et al.An information-intensive approach to the molecular pharmacology of cancer.Science 1997;275(5298):343–9.
17. Kovach JS, Hartmann A, Blaszyk H, et al. Mutation detection by highly sensitivemethods indicates that p53 gene mutations in breast cancer can haveimportant prognostic value. Proc Natl Acad Sci 1996;93:1093–6.
18. Wilson WH, Teruya-Feldstein J, Fest T, Harris C, Steinberg SM, Jaffe ES.Relationship of p53, bcl-2, and tumor proliferation to clinical drug resistance innon-Hodgkin’s lymphomas. Blood 1997;89(2):601–9.
19. Wattel E, Preudhomme C, Hecquet B, Vanrumbeke M, Quesnel B, Dervite I, et al.P53 mutations are associated with resistance to chemotherapy and shortsurvival in hematologic malignancies. Blood 1994;84(9):3148–57.
20. Bradford CR, Zhu S, Poore J, Fisher SG, Beals TF, Thoraval D, et al. p53 Mutationas a prognostic marker in advanced laryngeal carcinoma. Department ofVeterans Affairs Laryngeal Cancer Cooperative Study Group. Arch OtolaryngolHead Neck Surg 1997;123(6):605–9.
21. Cote RJ, Esrig D, Groshen S, Jones PA, Skinner DG. P53 and treatment of bladdercancer. Nature 1997;385:123–5.
22. Hawkins DS, Demers GW, Galloway DA. Inactivation of p53 enhancessensitivity to multiple chemotherapeutic agents. Cancer Res 1996;56:892–8.
23. Fan S, Smith ML, Rivet DJ 2nd, Duba D, Zhan Q, Kohn KW, et al. Disruption ofp53 function sensitizes breast cancer MCF-7 cells to cisplatin andpentoxifylline. Cancer Res 1995;55(8):1649–54.
24. Wallace-Brodeur RR, Lowe SW. Clinical implications of p53 mutations. Cell MolLife Sci 1999;55:64–75.
25. Koch WM, Brennan JA, Zahurak M, Goodman SN, Westra WH, Schwab D, et al.P53 mutation and loco regional treatment failure in head and neck squamouscell carcinoma. J Natl Cancer Inst 1996;88:1580–6.
26. Mineta H, Borg A, Dictor M, Akervall J, Wennerberg J. P53 mutation, but not p53over expression, correlates with survival in head and neck squamous cellcarcinoma. Br J Cancer 1998;78:1084–90.
27. Erber R, Conradt C, Homann N, Enders C, Finckh M, Dietz A, et al. TP53 DNAcontact mutations are selectively associated with allelic loss and have a strongclinical impact in head and neck cancer. Oncogene 1998;16:1671–9.
28. Ahomadegbe JC, Barrois M, Fogel S, LeBihan ML, Douc-Rasy S, Duvillard P, et al.High incidence of p53 alterations (mutation, deletion, over expression) in headand neck primary tumors and metastases: absence of correlation with clinicaloutcome—frequent protein over expression in normal epithelium and in earlynoninvasive lesions. Oncogene 1995;10:1217–27.
29. vanOijen MG, Slootweg PJ. Gain-of-function mutations in the tumor suppressorgene p53. Clin Cancer Res 2000;6:2138–45.
30. Bradford CR, Zhu S, Poore J, Fisher SG, Beals TF, Thoraval D, et al. P53 mutationas a prognostic marker in advanced laryngeal carcinoma: Department ofVeterans Affairs Laryngeal Cancer Cooperative Study Group. Arch OtolaryngolHead Neck Surg 1997;123:605–9.
31. Bradford CR, Wolf GT, Carey TE, Zhu S, Poore J, Beals TF, et al. Predictive markersfor response to chemotherapy, organ preservation, and survival in patientswith advanced laryngeal carcinoma. Otolaryngol Head Neck Surg 1999;121:534–8.
32. Trask DK, Wolf GT, Bradford CR, Fisher SG, Devaney K, Johnson M, et al.Expression of Bcl-2 family proteins in advanced laryngeal squamous cellcarcinoma: correlation with response to chemotherapy and organ preservation.Laryngoscope 2002;112(4):638–44.
33. Donehower LA, Godley LA, Aldaz CM, Pyle R, Shi YP, Pinkel D, et al. Deficiency ofp53 accelerates mammary tumorigenesis in Wnt-1 transgenic mice andpromotes chromosomal instability. Genes Dev 1995;9(7):882–95.
Please cite this article in press as: Sahoo R et al. Relationship between molecultients with primary carcinoma of the larynx. Oral Oncol (2009), doi:10.1016/j.o
34. Kumar B, Cordell KG, D’Silva N, Prince ME, Adams ME, Fisher SG, et al.Expression of p53 and Bcl-xL as predictive markers for larynx preservation inadvanced laryngeal cancer. Arch Otolaryngol Head Neck Surg 2008;134(4):363–9.
35. Bharaj BS, Angelopoulou K, Diamandis EP. Rapid sequencing of the p53gene with a new automated DNA sequencer. Clin Chem 1998;44(7):1397–403.
36. McGee S. Simplifying likelihood ratios. J Gen Int Med 2002;17(8):646–9.37. Yamazaki Y, Chiba I, Hirai A, Sugiura C, Notani K, Kashiwazaki H, et al. Specific
p53 mutations predict poor prognosis in oral squamous cell carcinoma. OralOncol 2003;39:163–9.
38. Georgiou A, Gomatos IP, Ferekidis E, Syrigos K, Bistola V, Giotakis J, et al.Prognostic significance of p53, bax and bcl-2 gene expression in patients withlaryngeal carcinoma. Eur J Surg Oncol 2001;27:574–80.
39. Hoft S, Maune S, Muhle C, Brenner W, Czech N, Kampen W, et al. Sentinellymph-node biopsy in head and neck cancer. Br J Cancer 2004;91:124–8.
40. Kropveld A, Rozemuller EH, Leppers FGJ, Scheidel KC, de Weger RA, Koole R,et al. Sequencing analysis of RNA and DNA of exons 1 through 11 shows p53gene alterations to be present in almost 100% of head and neck squamous cellcancers. Lab Invest 1999;79:347–53.
41. Gallo O, Chiarelli I, Boddi V, Bocciolini C, Bruschini L, Porfirio B, et al.Cumulative prognostic value of p53 mutations and bcl-2 protein expression inhead-and-neck cancer treated by radiotherapy. Int J Cancer 1999;22;84(6):573–9.
42. Henriksson E, Baldetorp B, Borg A, Kjellen E, Akervall J, Wennerberg J, et al. P53mutation and cyclin D1 amplification correlate with cisplatin sensitivity inxenografted human squamous cell carcinomas from head and neck. Acta Oncol2006;45(3):300–5.
43. Nakayama K, Takebayashi Y, Nakayama S, Hata K, Fujiwaki R, Fukumoto M,et al. Prognostic value of over expression of p53 in human ovarian carcinomapatients receiving cisplatin. Cancer Lett 2003;192(2):227–35.
44. Gasparini G, Bevilacqua P, Bonoldi E, Testolin A, Galassi A, Verderio P, et al. ClinCancer Res 1995;1(11):1375–83.
45. Lo Muzio L, Falaschini S, Farina A, Rubini C, Pezzetti F, Campisi G, et al. Bcl-2 asprognostic factor in head and neck squamous cell carcinoma. Oncol Res2005;15(5):249–55.
46. Bosch FX, Ritter D, Enders C, Flechtenmacher C, Abel U, Dietz A, et al. Head andneck tumor sites differ in prevalence and spectrum of p53 alterations but thesehave limited prognostic value. Int J Cancer 2004;111(4):530–8.
47. Eriksen JG, Alsner J, Steiniche T, Overgaard J. The possible role of TP53 mutationstatus in the treatment of squamous cell carcinomas of the head and neck(HNSCC) with radiotherapy with different overall treatment times. RadiotherOncol 2005;76(2):135–42.
48. Tabor MP, Brakenhoff RH, Ruijter-Schippers HJ, Kummer JA, Leemans CR,Braakhuis BJ. Genetically altered fields as origin of locally recurrent head andneck cancer: a retrospective study. Clin Cancer Res 2004;10(11):3607–13.
49. Vikram B. Changing patterns of failure in advanced head and neck cancer. ArchOtolaryngol 1984;110:564–5.
50. Sutton DN, Brown JS, Rogers SN, Vaughan ED, Woolgar JA. The prognosticimplications of the surgical margin in oral squamous cell carcinoma. Int J OralMaxillofac Surg 2003;32:30–4.
51. Leemans CR, Tiwari R, Nauta JJ, Van der Waal I, Snow GB. Recurrence at theprimary site in head and neck cancer and the significance of neck lymph nodemetastases as a prognostic factor. Cancer (Phila) 1994;73:187–90.
52. Braakhuis BJ, Tabor MP, Leemans CR, van der Waal I, Snow GB, Brakenhoff RH.Second primary tumors and field cancerization in oral and oropharyngealcancer: molecular techniques provide new insights and definitions. Head Neck2002;24(2):198–206.
53. Sabichi AL, Demierre MF, Hawk ET, Lerman CE, Lippman SM. Frontiers in cancerprevention research. Cancer Res 2003;63:5649–55.
54. Martin SJ, Green DR, Cotter TG. Dying with death: dissecting the components ofthe apoptosis machinery. TIBS (Trends Biochem Sci) 1994;19:26–30.
55. Fnisch SM, Francis H. Disruption of epithelial cell–matrix interactions inducesapoptosis. J Cell Biol 1994;24:619–26.
56. Tabor MP, Brakenhoff RH, Ruijter-Schippers HJ, Kummer JA, Leemans CR,Braakhuis BJ. Genetically altered fields as origin of locally recurrent headand neck cancer: a retrospective study. Clin Cancer Res 2004;10(11):3607–13.
ar markers and treatment response in a retrospective cohort of Indian pa-raloncology.2009.07.013
Copyright © 2022 FDOKUMEN




















