Régis Peffault de Latour - MaRIH
40
1 E-MaRIH - Grenoble Régis Peffault de Latour French reference center for aplastic anemia & PNH French network for rare immunological & hematological disorders (MaRIH) Hôpital Saint-Louis, Paris, France Monday April 23 rd , 2018
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Régis Peffault de Latour - MaRIH
1
E-MaRIH - Grenoble
Régis Peffault de Latour French reference center for aplastic anemia & PNH
French network for rare immunological & hematological disorders (MaRIH) Hôpital Saint-Louis, Paris, France
Monday April 23rd, 2018

• Pathophysiology
– Idiopathic aplastic anemia (and PNH)
• Diagnosis
• Management in 2018
2
Idiopathic aplastic anemia Agenda
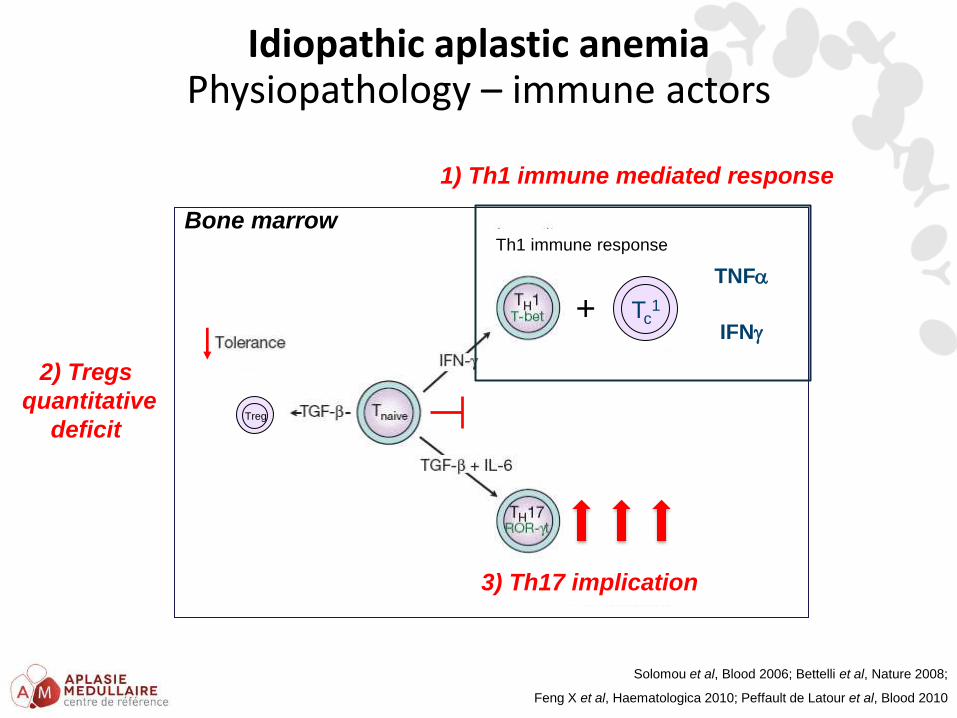
Idiopathic aplastic anemia Physiopathology – immune actors
+ Tc1
TNF
Treg
Th1 immune response
IFN
Bone marrow
Solomou et al, Blood 2006; Bettelli et al, Nature 2008;
Feng X et al, Haematologica 2010; Peffault de Latour et al, Blood 2010
1) Th1 immune mediated response
3) Th17 implication
2) Tregs
quantitative
deficit
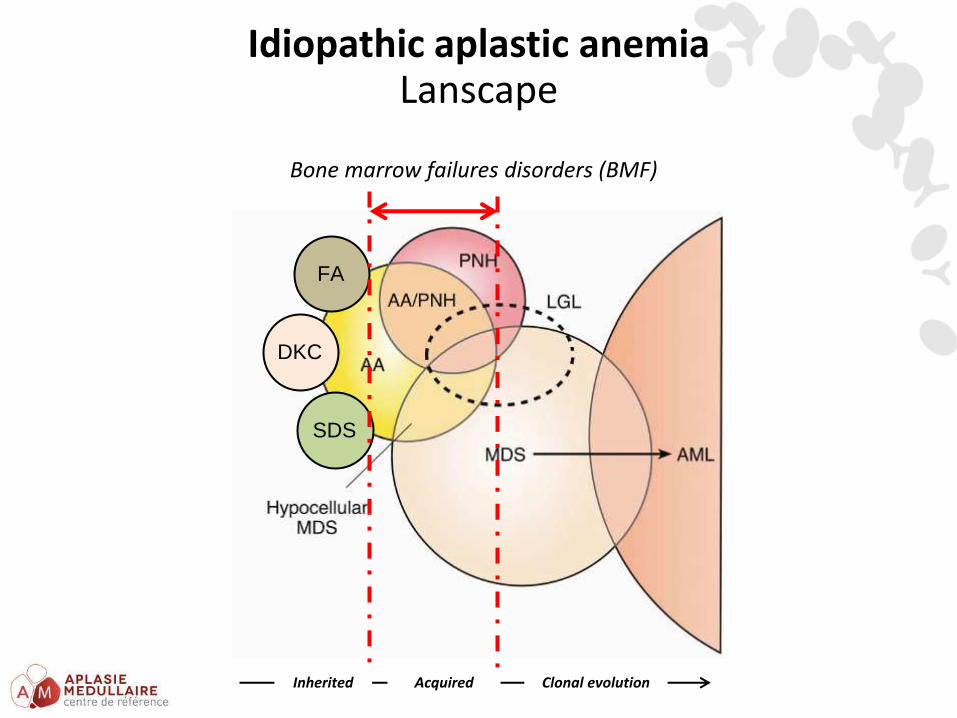
Idiopathic aplastic anemia Lanscape
DKC
SDS
FA
Inherited Acquired Clonal evolution
Bone marrow failures disorders (BMF)
Permission for all content within is covered by our supplier’s RightsDirect Multinational Annual Copyright License, which covers presentation only in educational settings G-REV-1139109
For presentation in response to an unsolicited request for medical information subject to local NP4 approval. Not for distribution.
Idiopathic aplastic anemia Diagnosis
- Pancytopenia (+/- PNH)
• Macrocytosis is common
• Lymphocytes count is usually preserved
• Isolated cytopenia at early stage (thrombocytopenia)
Permission for all content within is covered by our supplier’s RightsDirect Multinational Annual Copyright License, which covers presentation only in educational settings G-REV-1139109
For presentation in response to an unsolicited request for medical information subject to local NP4 approval. Not for distribution.
Idiopathic aplastic anemia Diagnosis
- Pancytopenia (+/- PNH)
• Macrocytosis is common
• Lymphocytes count is usually preserved
• Isolated cytopenia at early stage (thrombocytopenia)
- Bone marrow aspiration
• No abnormal cells
Permission for all content within is covered by our supplier’s RightsDirect Multinational Annual Copyright License, which covers presentation only in educational settings G-REV-1139109
For presentation in response to an unsolicited request for medical information subject to local NP4 approval. Not for distribution.
Idiopathic aplastic anemia Diagnosis
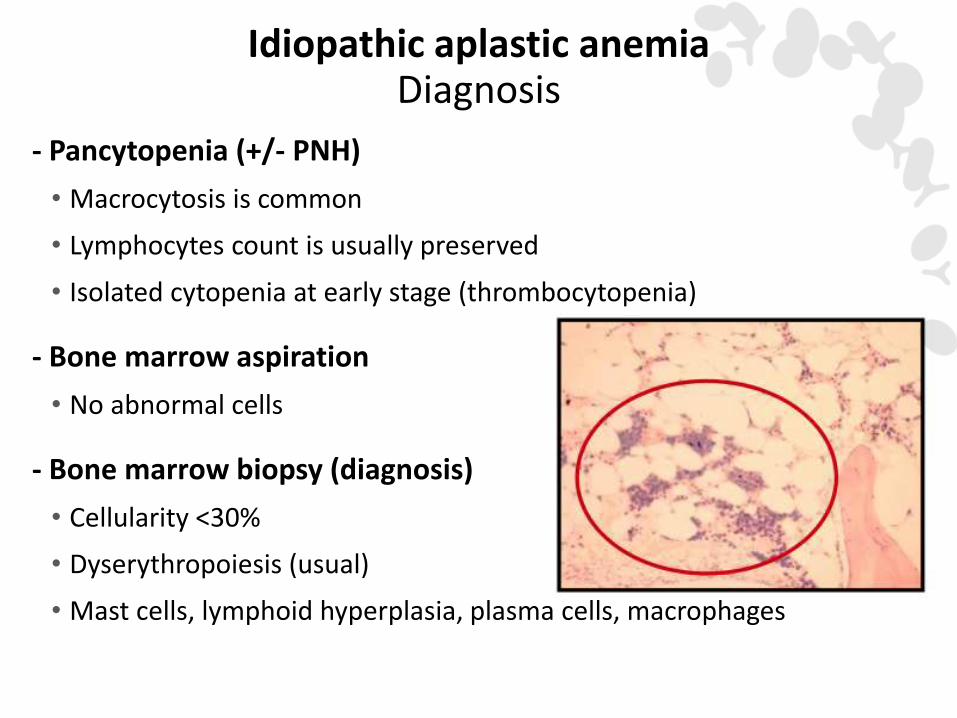
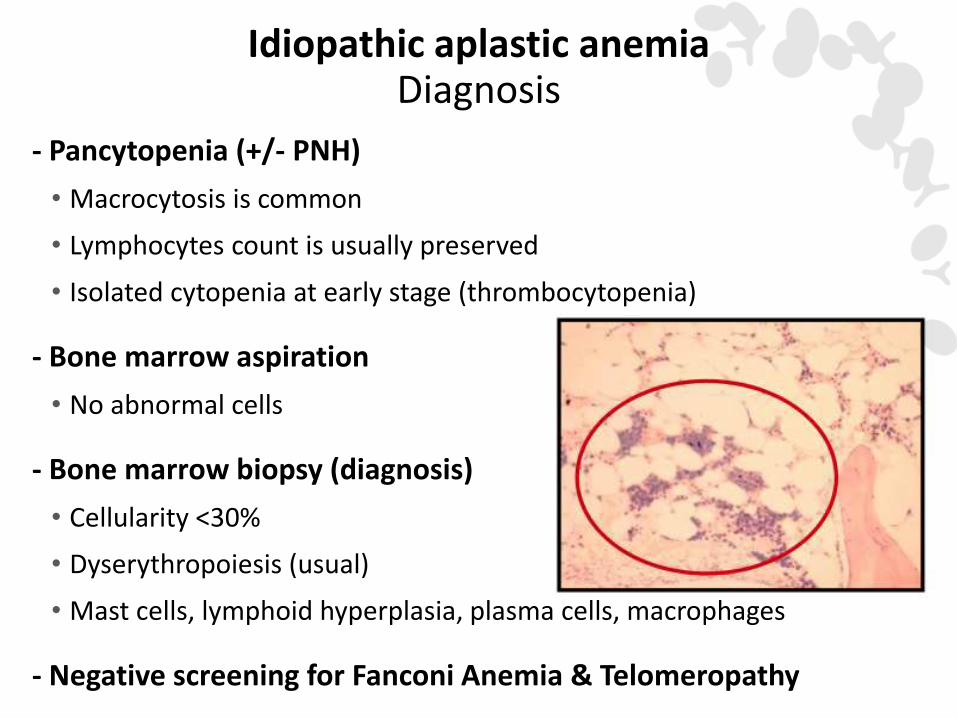
- Pancytopenia (+/- PNH)
• Macrocytosis is common
• Lymphocytes count is usually preserved
• Isolated cytopenia at early stage (thrombocytopenia)
- Bone marrow aspiration
• No abnormal cells
- Bone marrow biopsy (diagnosis)
• Cellularity <30%
• Dyserythropoiesis (usual)
• Mast cells, lymphoid hyperplasia, plasma cells, macrophages
Permission for all content within is covered by our supplier’s RightsDirect Multinational Annual Copyright License, which covers presentation only in educational settings G-REV-1139109
For presentation in response to an unsolicited request for medical information subject to local NP4 approval. Not for distribution.
Idiopathic aplastic anemia Diagnosis
- Pancytopenia (+/- PNH)
• Macrocytosis is common
• Lymphocytes count is usually preserved
• Isolated cytopenia at early stage (thrombocytopenia)
- Bone marrow aspiration
• No abnormal cells
- Bone marrow biopsy (diagnosis)
• Cellularity <30%
• Dyserythropoiesis (usual)
• Mast cells, lymphoid hyperplasia, plasma cells, macrophages
- Negative screening for Fanconi Anemia & Telomeropathy
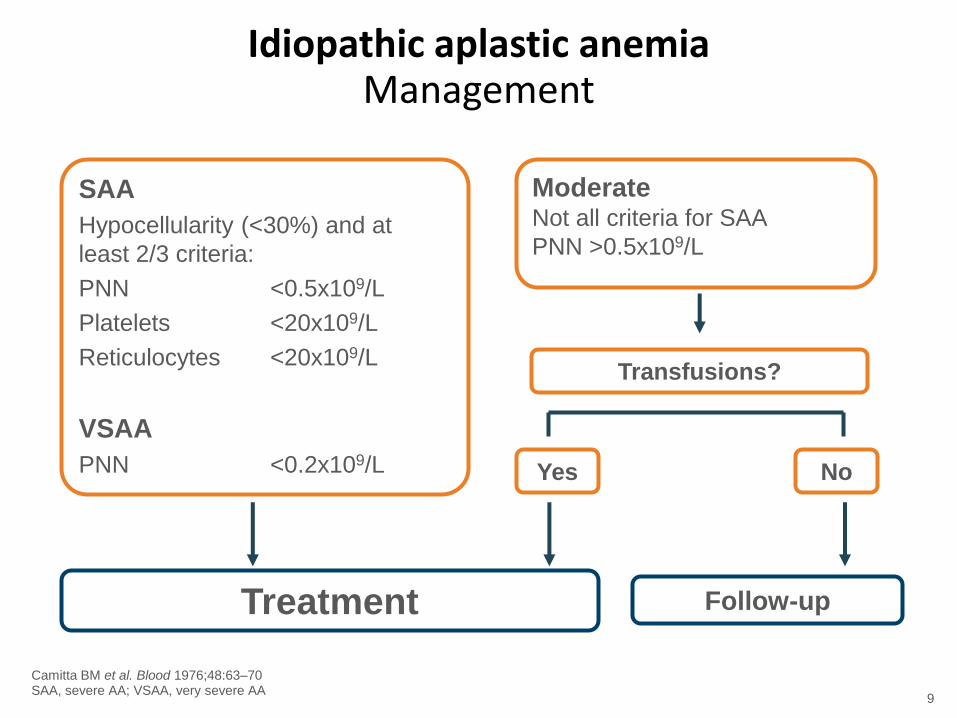
Camitta BM et al. Blood 1976;48:63–70 SAA, severe AA; VSAA, very severe AA
9
SAA
Hypocellularity (<30%) and at
least 2/3 criteria:
PNN <0.5x109/L
Platelets <20x109/L
Reticulocytes <20x109/L
VSAA
PNN <0.2x109/L
Moderate Not all criteria for SAA
PNN >0.5x109/L
Transfusions?
Yes No
Treatment Follow-up
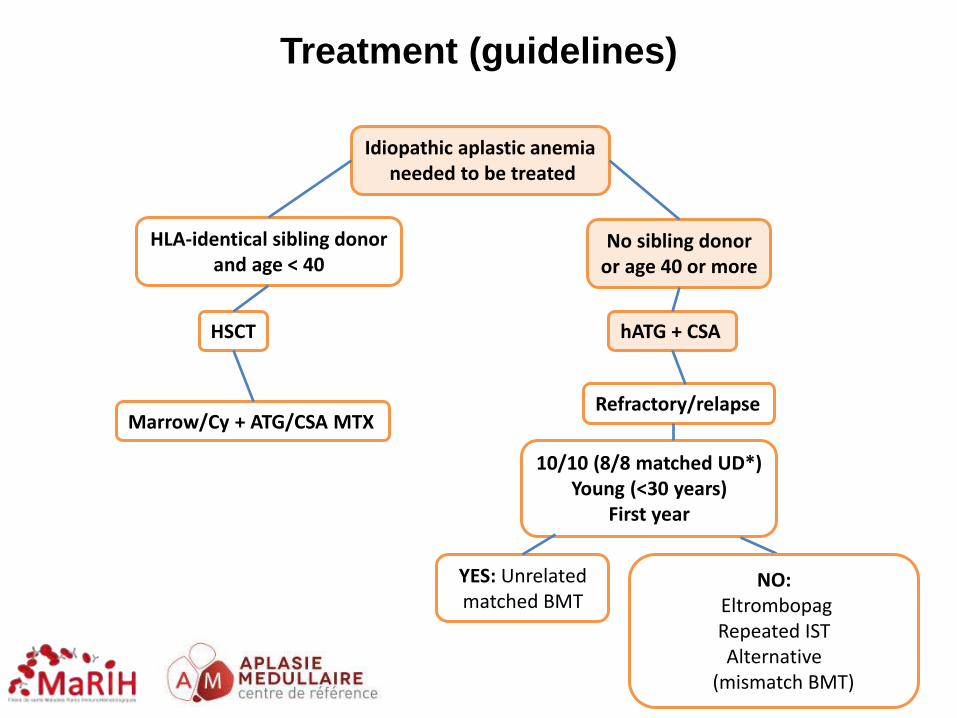
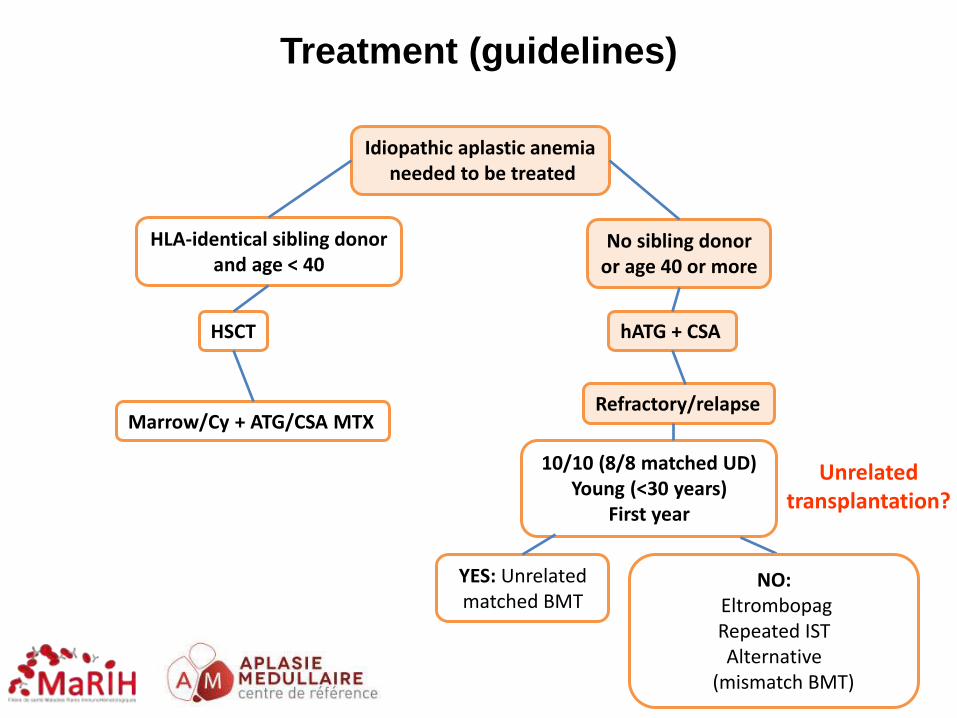
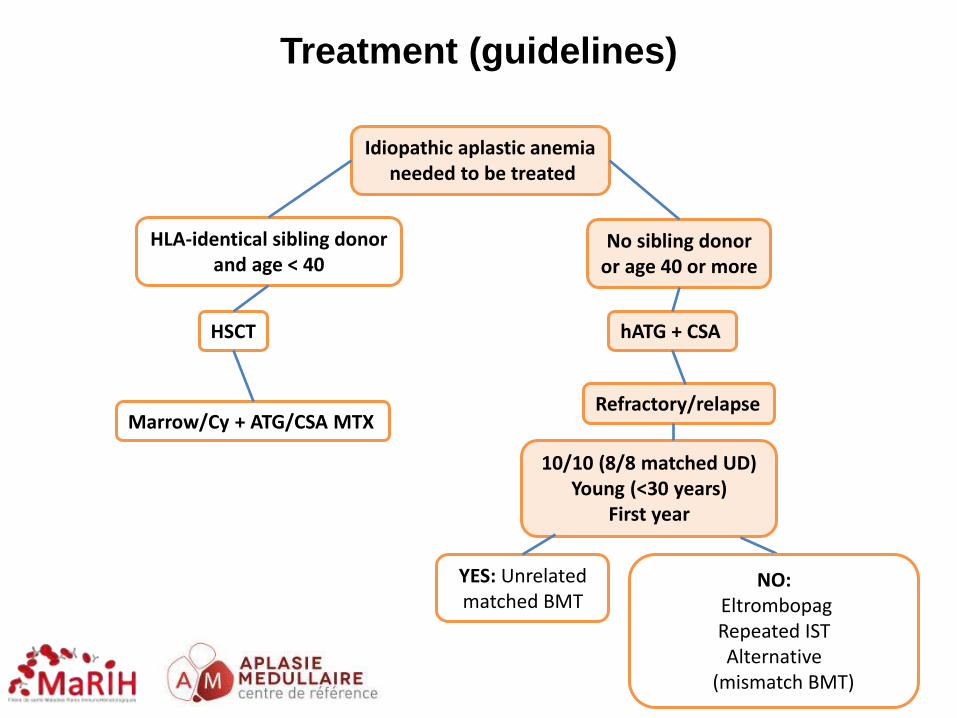
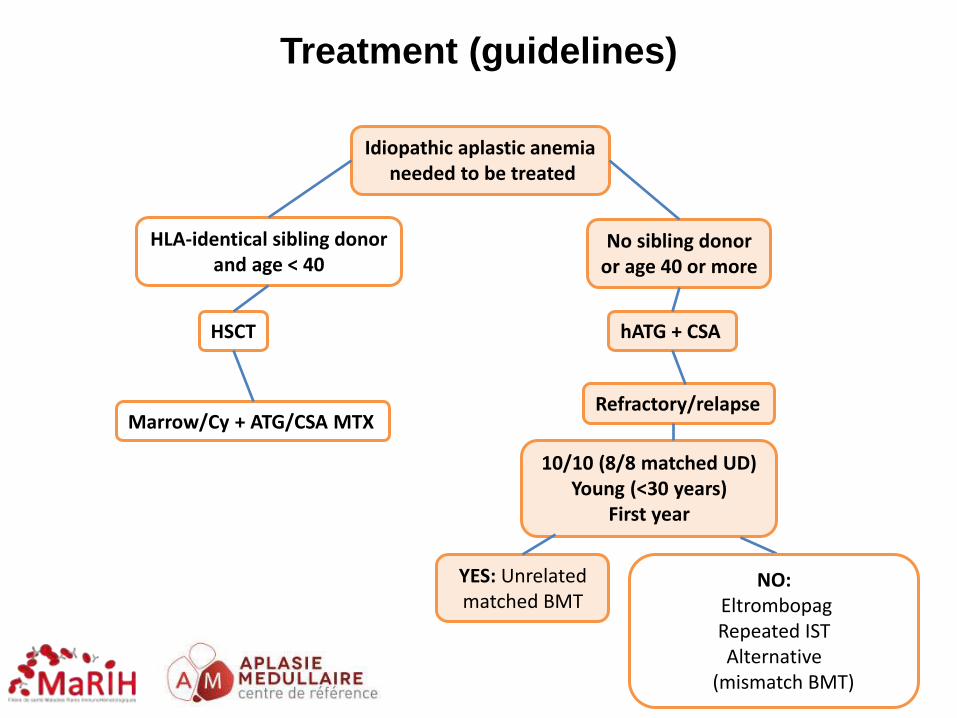
Idiopathic aplastic anemia Management
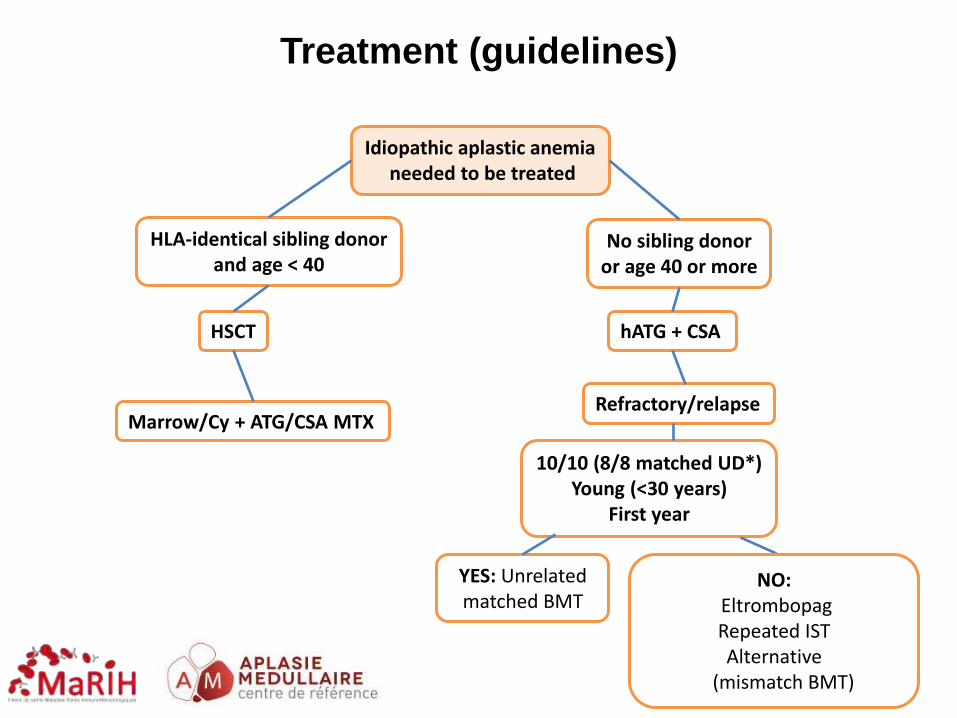
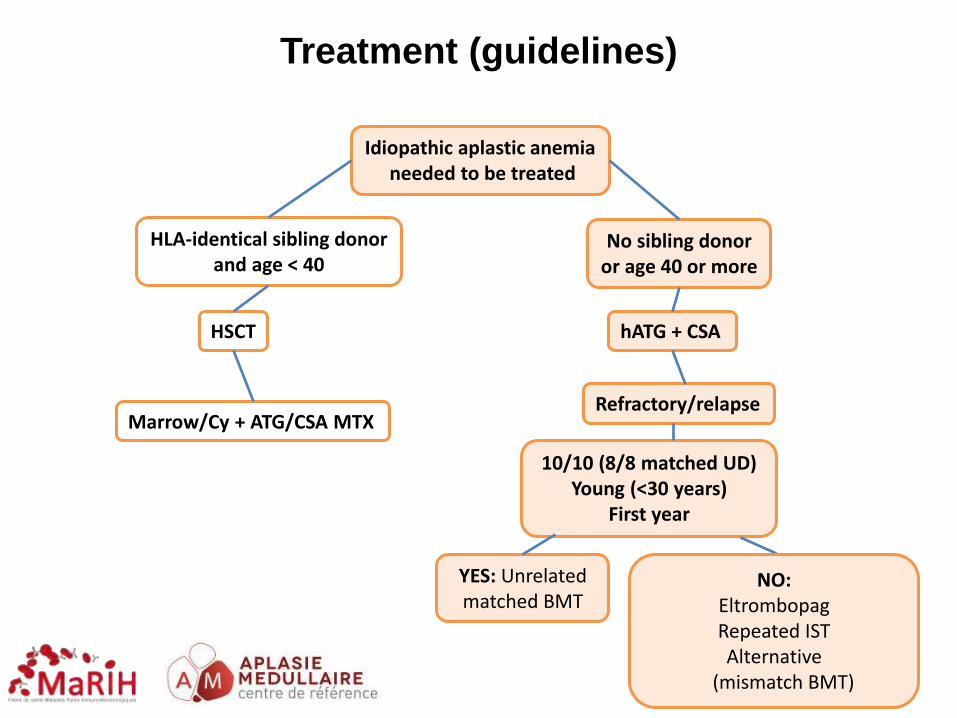
Idiopathic aplastic anemia needed to be treated
HLA-identical sibling donor and age < 40
HSCT
Marrow/Cy + ATG/CSA MTX
No sibling donor or age 40 or more
hATG + CSA
Refractory/relapse
10/10 (8/8 matched UD*) Young (<30 years)
First year
YES: Unrelated matched BMT
Treatment (guidelines)
NO: Eltrombopag Repeated IST Alternative
(mismatch BMT)
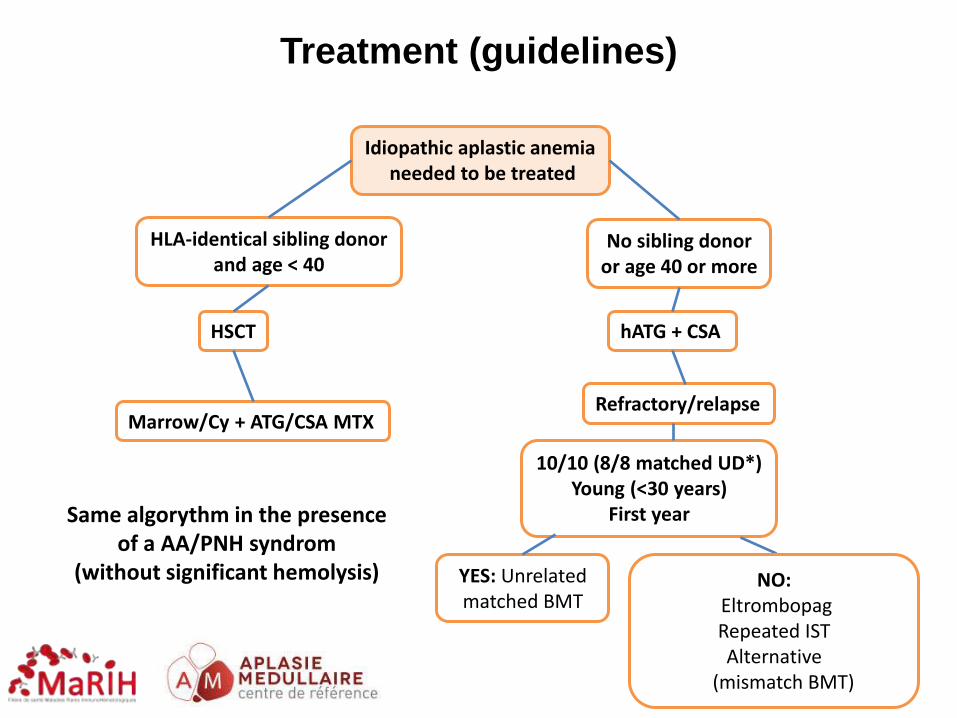
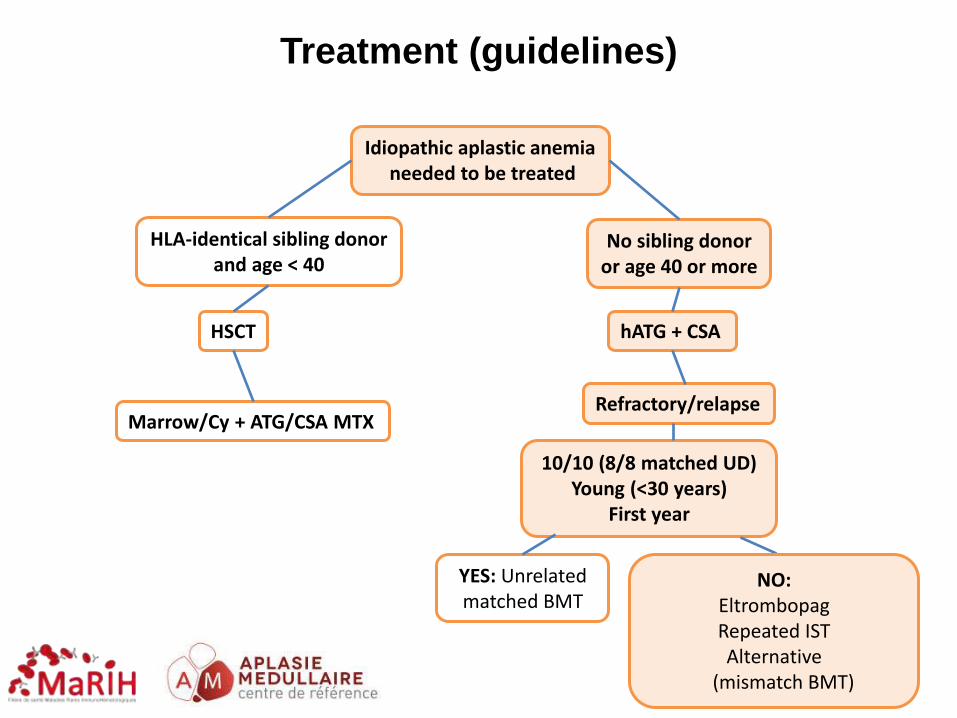
Idiopathic aplastic anemia needed to be treated
HLA-identical sibling donor and age < 40
HSCT
Marrow/Cy + ATG/CSA MTX
No sibling donor or age 40 or more
hATG + CSA
Refractory/relapse
10/10 (8/8 matched UD*) Young (<30 years)
First year
YES: Unrelated matched BMT
Treatment (guidelines)
Same algorythm in the presence of a AA/PNH syndrom
(without significant hemolysis) NO: Eltrombopag Repeated IST Alternative
(mismatch BMT)
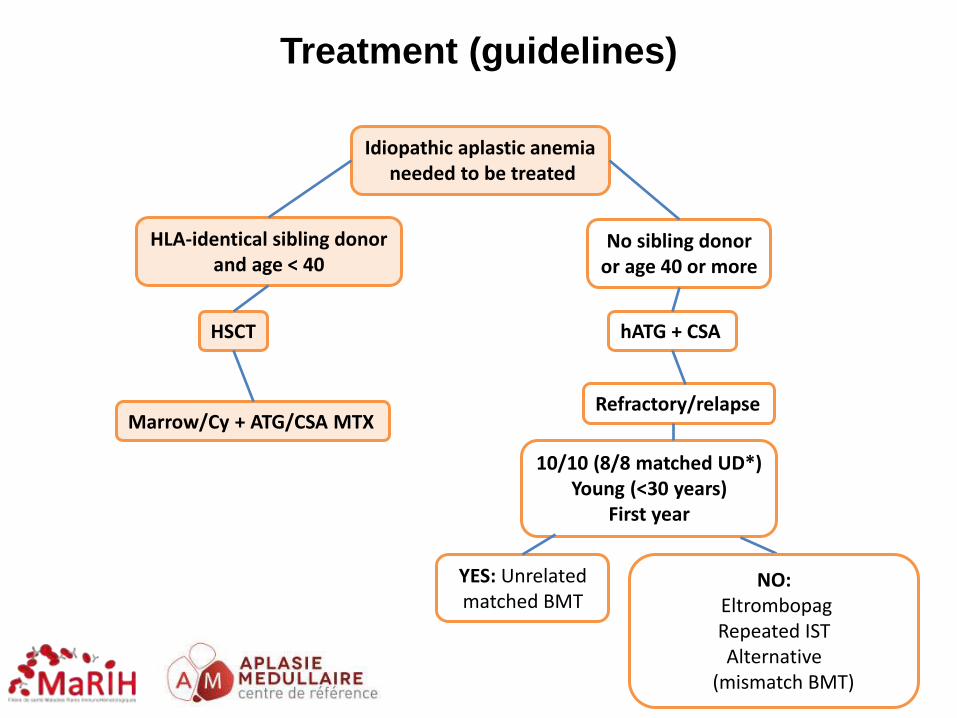
HLA-identical sibling donor and age < 40
HSCT
Marrow/Cy + ATG/CSA MTX
No sibling donor or age 40 or more
hATG + CSA
Refractory/relapse
10/10 (8/8 matched UD*) Young (<30 years)
First year
YES: Unrelated matched BMT
Treatment (guidelines)
Idiopathic aplastic anemia needed to be treated
NO: Eltrombopag Repeated IST Alternative
(mismatch BMT)

Sibling transplantation
Long-term
Event
No of
Events 6yr-CI (%)
Secondary Cancer 1 2 (0-9)
Osteonecrosis 10 21 (10-36)
Cardiovascular
complications
1 2 (0-9)
Endocrine
dysfunctions
7 19 (9-31)
Saint Louis experience. Haematologica. 2012.
61 53 38 35 33 30 28
N. At risk
87,5 % (CI 95%, 78-97)
Surv
ival
Pro
bab
ility
Time (months)
0 12 24 36 48 60 72
0.0
0.2
0.4
0.6
0.8
1.0
Marrow / Cy-ATG / CSA + MTX (standard) As soon as possible (<100 days)
61 patients Median follow-up 77 months
HLA-identical sibling donor and age < 40
HSCT
Marrow/Cy + ATG/CSA MTX
No sibling donor or age 40 or more
hATG + CSA
Refractory/relapse
10/10 (8/8 matched UD*) Young (<30 years)
First year
YES: Unrelated matched BMT
Treatment (guidelines)
Idiopathic aplastic anemia needed to be treated
NO: Eltrombopag Repeated IST Alternative
(mismatch BMT)
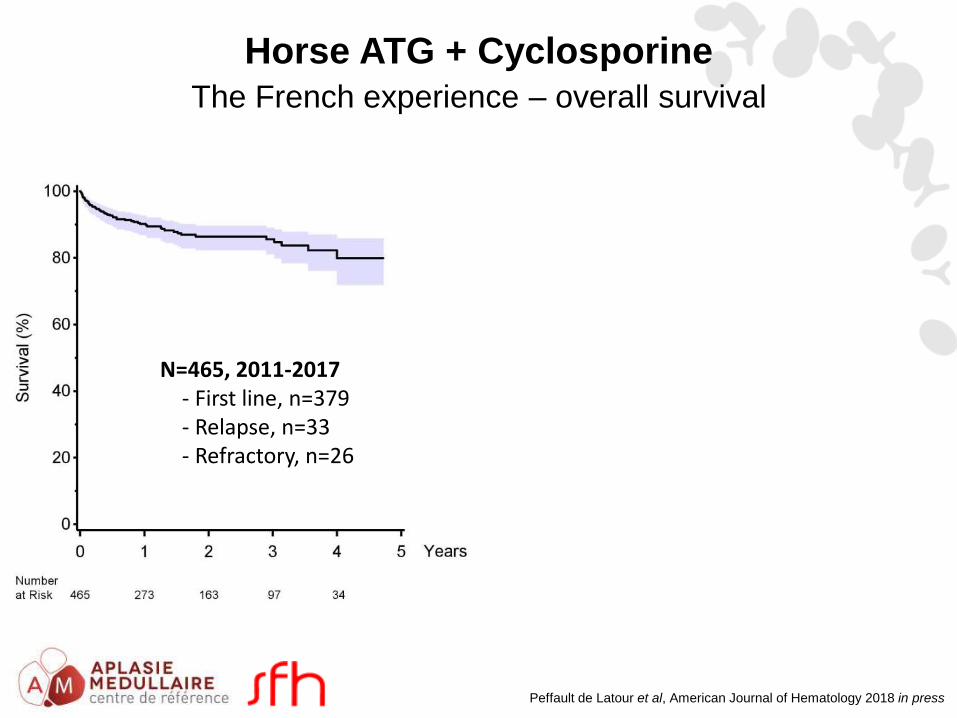
Horse ATG + Cyclosporine
The French experience – overall survival
Peffault de Latour et al, American Journal of Hematology 2018 in press
N=465, 2011-2017 - First line, n=379 - Relapse, n=33 - Refractory, n=26
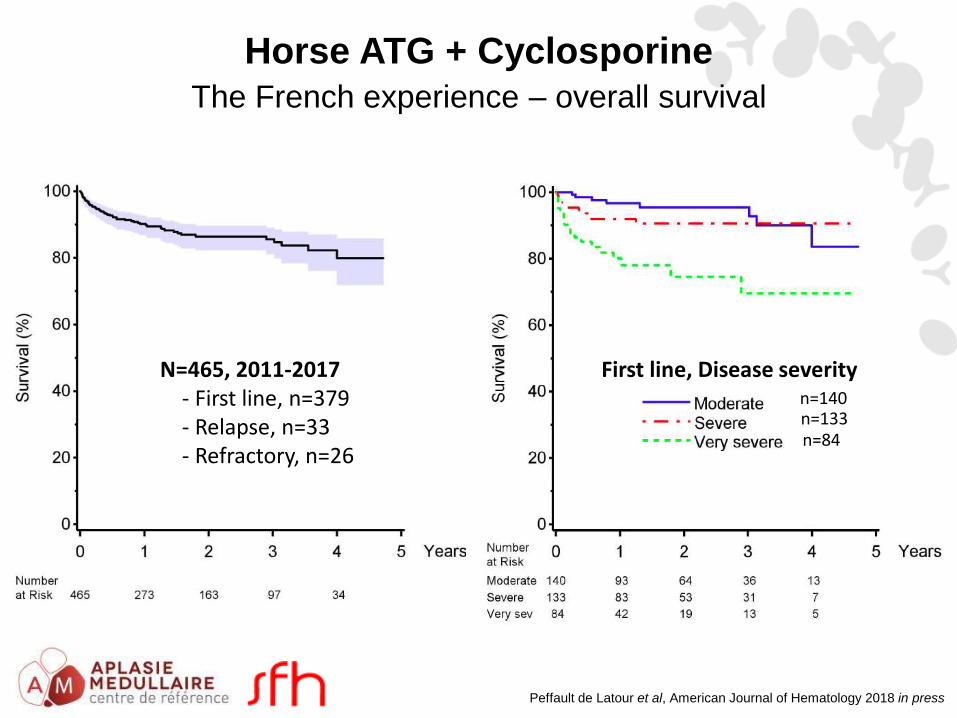
Horse ATG + Cyclosporine
The French experience – overall survival
Peffault de Latour et al, American Journal of Hematology 2018 in press
N=465, 2011-2017 - First line, n=379 - Relapse, n=33 - Refractory, n=26
n=140 n=133 n=84
First line, Disease severity
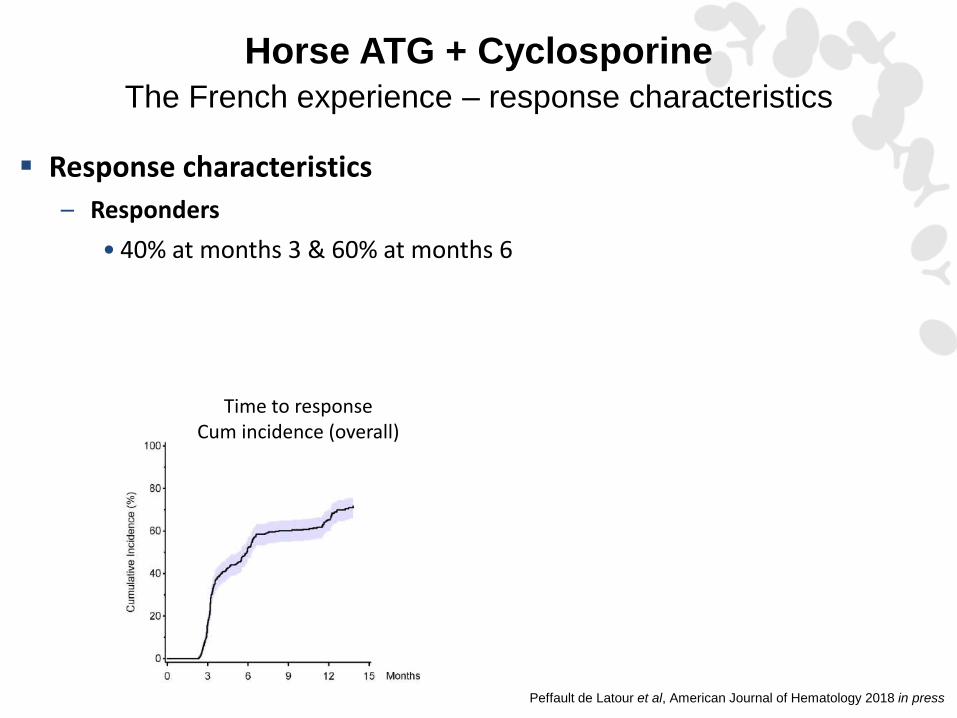
Horse ATG + Cyclosporine
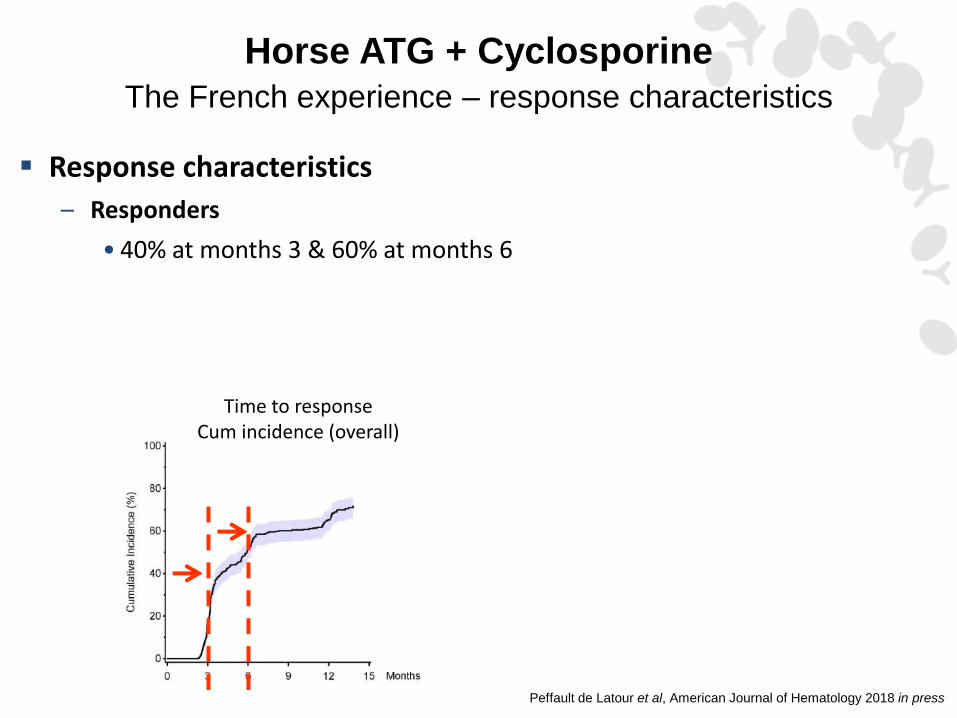
The French experience – response characteristics
Response characteristics
– Responders
• 40% at months 3 & 60% at months 6
Peffault de Latour et al, American Journal of Hematology 2018 in press
Time to response Cum incidence (overall)
Horse ATG + Cyclosporine
The French experience – response characteristics
Response characteristics
– Responders
• 40% at months 3 & 60% at months 6
Peffault de Latour et al, American Journal of Hematology 2018 in press
Time to response Cum incidence (overall)
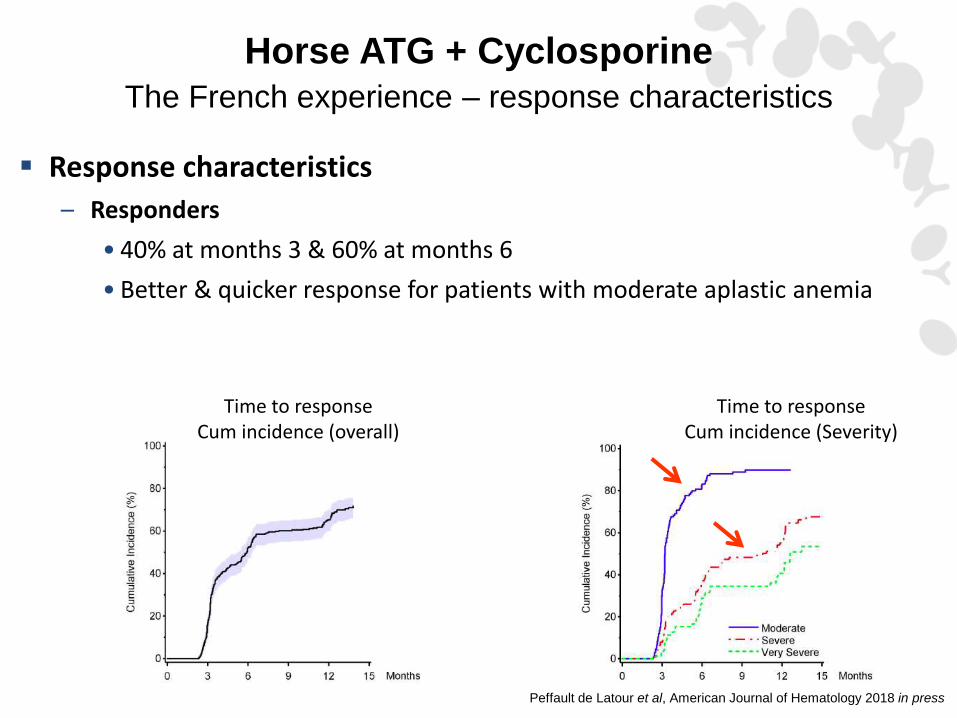
Horse ATG + Cyclosporine
The French experience – response characteristics
Response characteristics
– Responders
• 40% at months 3 & 60% at months 6
• Better & quicker response for patients with moderate aplastic anemia
Peffault de Latour et al, American Journal of Hematology 2018 in press
Time to response Cum incidence (overall)
Time to response Cum incidence (Severity)
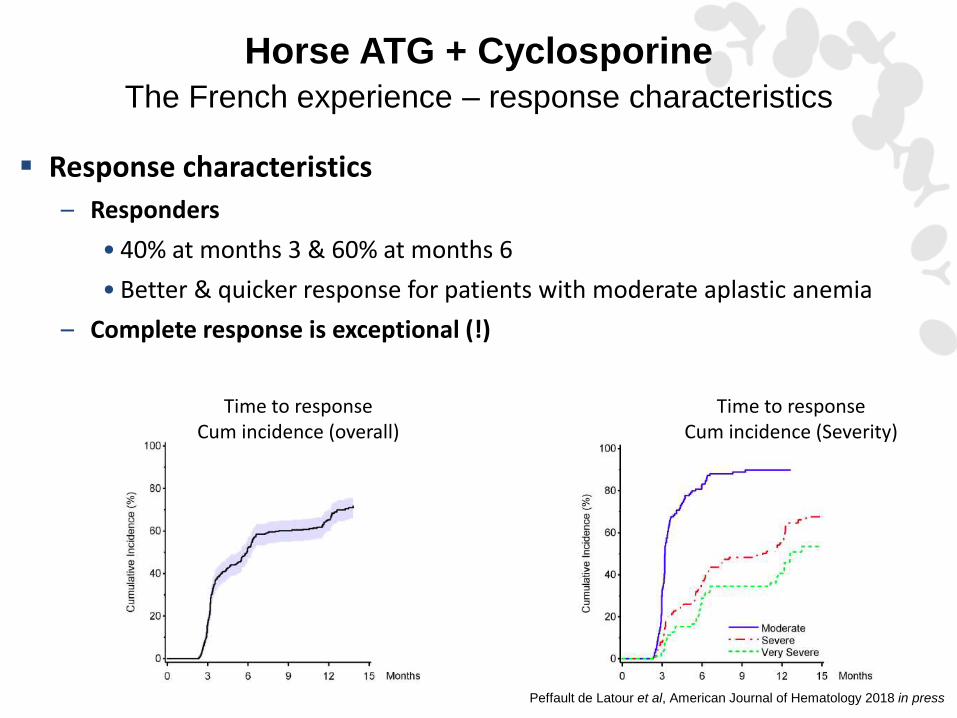
Horse ATG + Cyclosporine
The French experience – response characteristics
Response characteristics
– Responders
• 40% at months 3 & 60% at months 6
• Better & quicker response for patients with moderate aplastic anemia
– Complete response is exceptional (!)
Peffault de Latour et al, American Journal of Hematology 2018 in press
Time to response Cum incidence (overall)
Time to response Cum incidence (Severity)
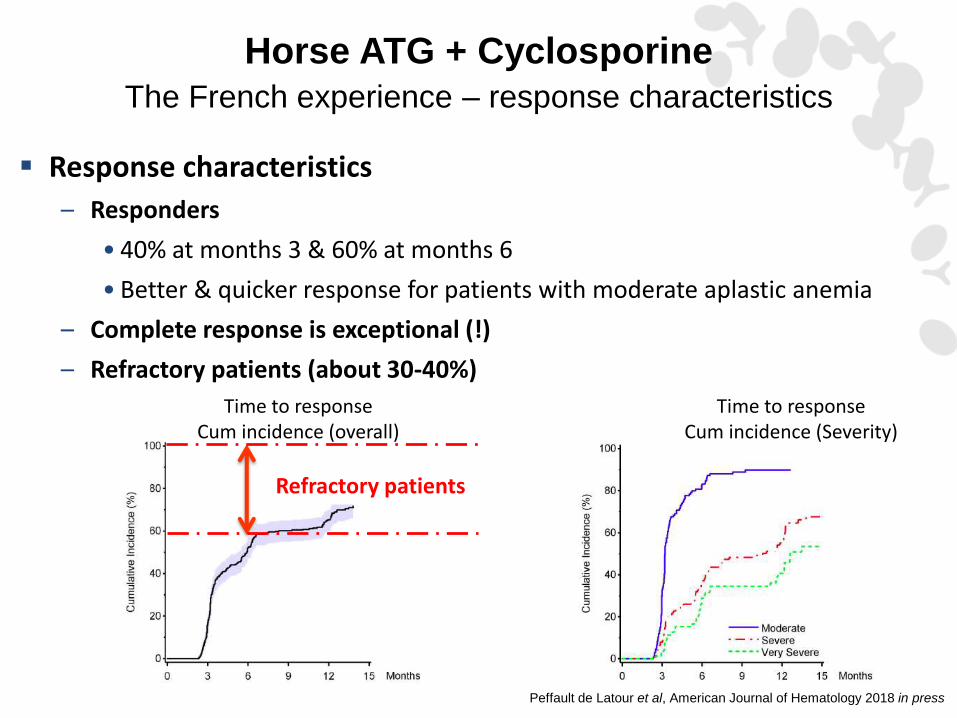
Horse ATG + Cyclosporine
The French experience – response characteristics
Response characteristics
– Responders
• 40% at months 3 & 60% at months 6
• Better & quicker response for patients with moderate aplastic anemia
– Complete response is exceptional (!)
– Refractory patients (about 30-40%)
Peffault de Latour et al, American Journal of Hematology 2018 in press
Time to response Cum incidence (overall)
Time to response Cum incidence (Severity)
Refractory patients
HLA-identical sibling donor and age < 40
HSCT
Marrow/Cy + ATG/CSA MTX
No sibling donor or age 40 or more
hATG + CSA
Refractory/relapse
10/10 (8/8 matched UD) Young (<30 years)
First year
YES: Unrelated matched BMT
Treatment (guidelines)
Idiopathic aplastic anemia needed to be treated
Unrelated transplantation?
NO: Eltrombopag Repeated IST Alternative
(mismatch BMT)
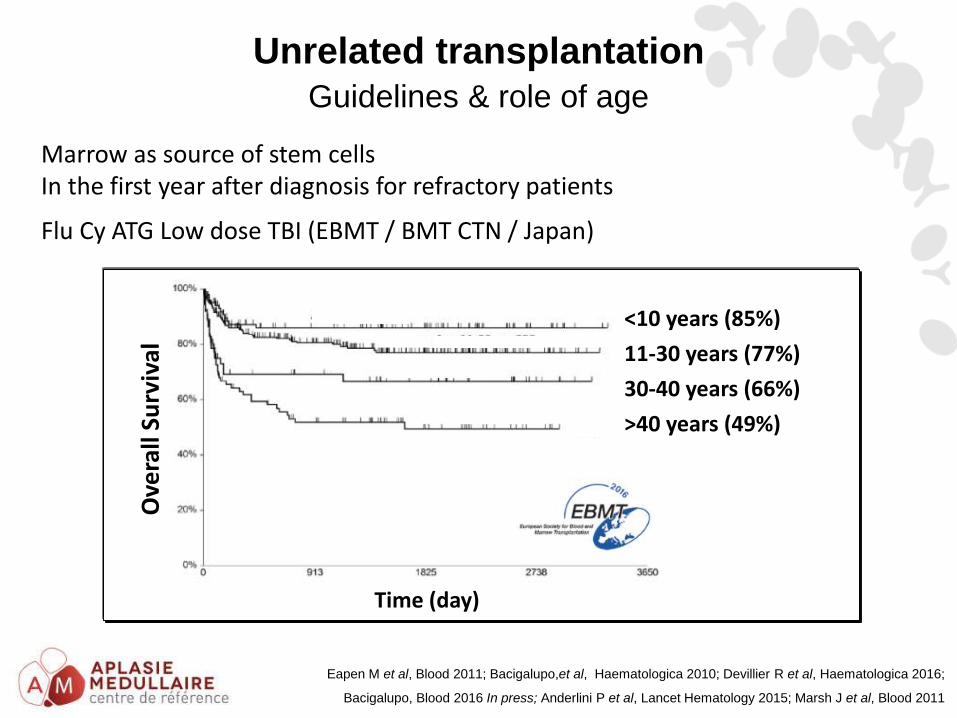
Marrow as source of stem cells In the first year after diagnosis for refractory patients
Flu Cy ATG Low dose TBI (EBMT / BMT CTN / Japan)
Ove
rall
Surv
ival
Eapen M et al, Blood 2011; Bacigalupo,et al, Haematologica 2010; Devillier R et al, Haematologica 2016;
Bacigalupo, Blood 2016 In press; Anderlini P et al, Lancet Hematology 2015; Marsh J et al, Blood 2011
Time (day)
<10 years (85%)
11-30 years (77%)
30-40 years (66%)
>40 years (49%)
Unrelated transplantation
Guidelines & role of age
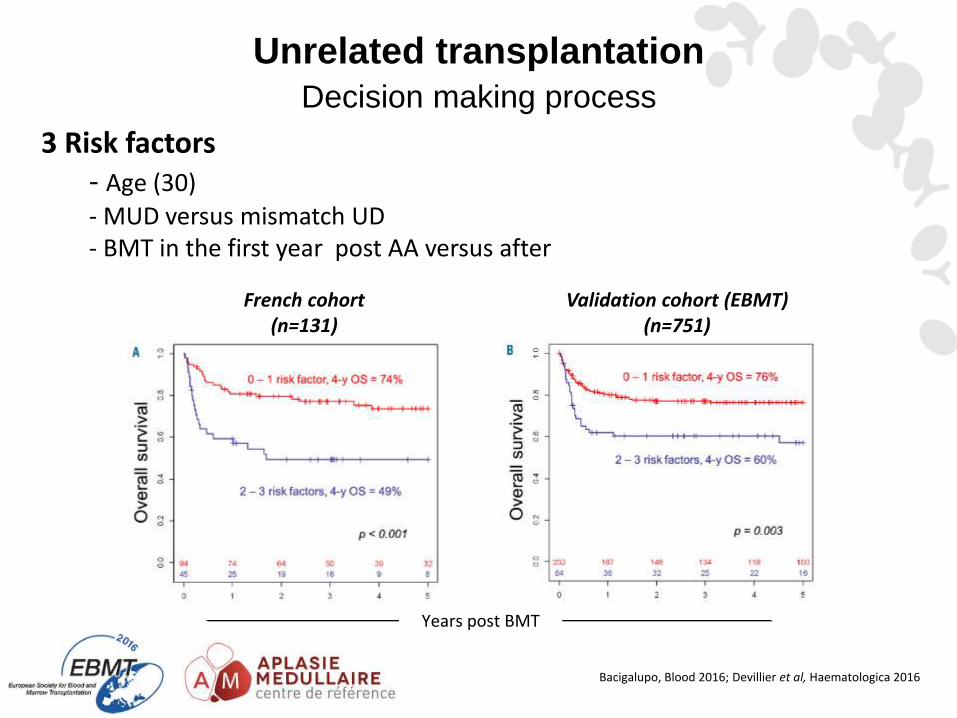
3 Risk factors - Age (30)
- MUD versus mismatch UD - BMT in the first year post AA versus after
Bacigalupo, Blood 2016; Devillier et al, Haematologica 2016
French cohort (n=131)
Validation cohort (EBMT) (n=751)
Years post BMT
Unrelated transplantation
Decision making process
HLA-identical sibling donor and age < 40
HSCT
Marrow/Cy + ATG/CSA MTX
No sibling donor or age 40 or more
hATG + CSA
Refractory/relapse
10/10 (8/8 matched UD) Young (<30 years)
First year
YES: Unrelated matched BMT
Treatment (guidelines)
Idiopathic aplastic anemia needed to be treated
NO: Eltrombopag Repeated IST Alternative
(mismatch BMT)
HLA-identical sibling donor and age < 40
HSCT
Marrow/Cy + ATG/CSA MTX
No sibling donor or age 40 or more
hATG + CSA
Refractory/relapse
10/10 (8/8 matched UD) Young (<30 years)
First year
YES: Unrelated matched BMT
Treatment (guidelines)
Idiopathic aplastic anemia needed to be treated
NO: Eltrombopag Repeated IST Alternative
(mismatch BMT)
27
HLA-identical sibling donor and age < 40
HSCT
Marrow/Cy + ATG/CSA MTX
No sibling donor or age 40 or more
hATG + CSA
Refractory/relapse
10/10 (8/8 matched UD) Young (<30 years)
First year
YES: Unrelated matched BMT
NO: Eltrombopag Repeated IST Alternative
(mismatch BMT)
Treatment (guidelines)
Idiopathic aplastic anemia needed to be treated
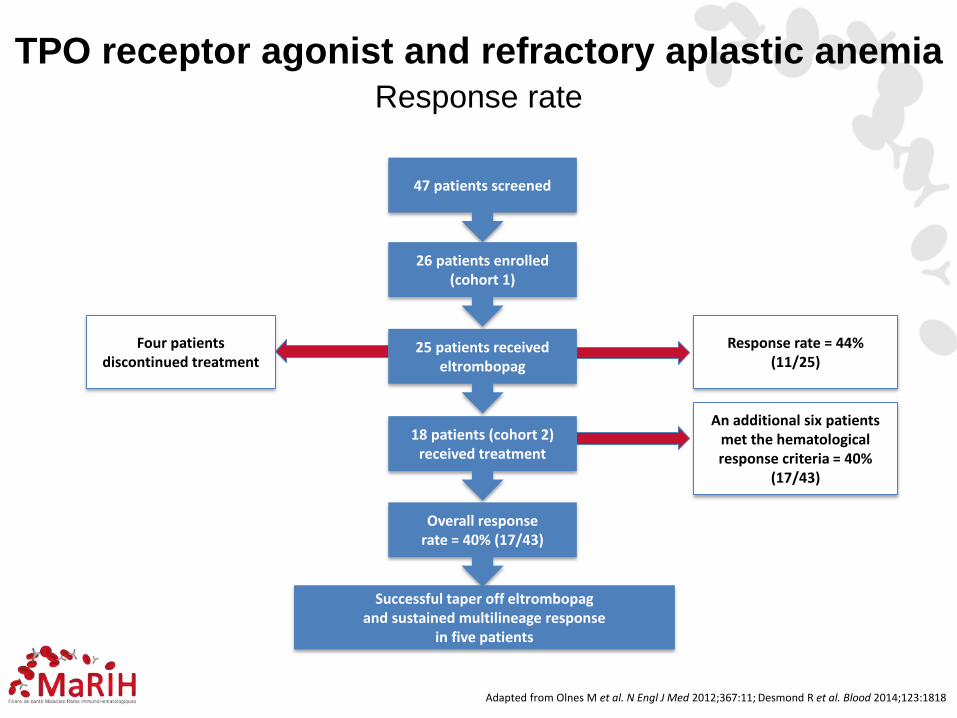
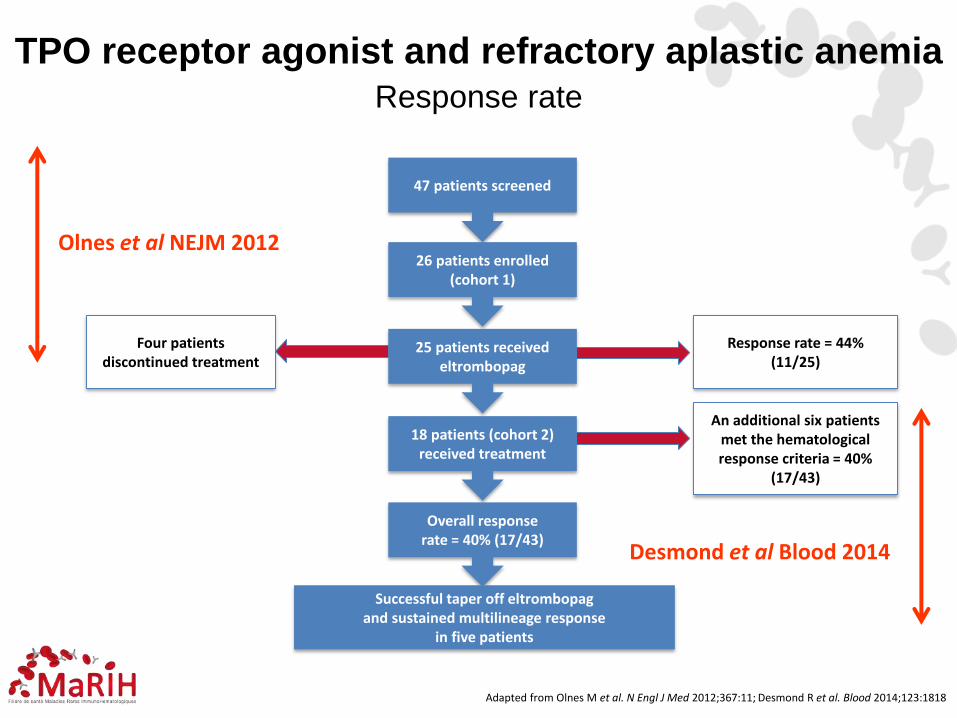
Adapted from Olnes M et al. N Engl J Med 2012;367:11; Desmond R et al. Blood 2014;123:1818
47 patients screened
26 patients enrolled (cohort 1)
25 patients received eltrombopag
Four patients discontinued treatment
Response rate = 44% (11/25)
18 patients (cohort 2) received treatment
An additional six patients met the hematological response criteria = 40%
(17/43)
Overall response rate = 40% (17/43)
Successful taper off eltrombopag and sustained multilineage response
in five patients
TPO receptor agonist and refractory aplastic anemia
Response rate
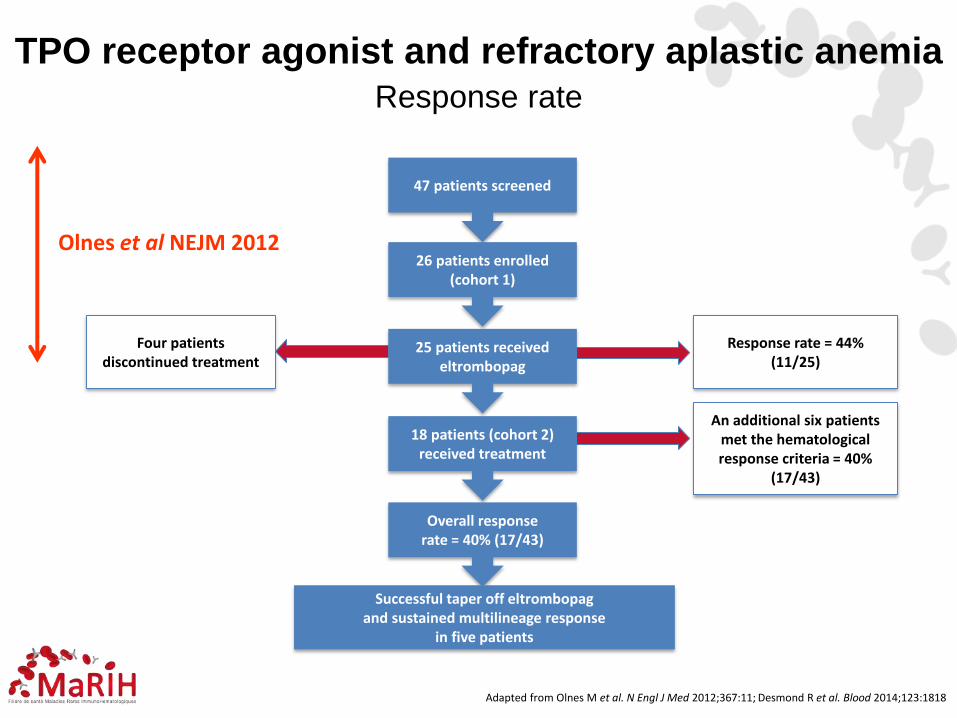
47 patients screened
26 patients enrolled (cohort 1)
25 patients received eltrombopag
Four patients discontinued treatment
Response rate = 44% (11/25)
18 patients (cohort 2) received treatment
An additional six patients met the hematological response criteria = 40%
(17/43)
Overall response rate = 40% (17/43)
Successful taper off eltrombopag and sustained multilineage response
in five patients
TPO receptor agonist and refractory aplastic anemia
Response rate
Olnes et al NEJM 2012
Adapted from Olnes M et al. N Engl J Med 2012;367:11; Desmond R et al. Blood 2014;123:1818
47 patients screened
26 patients enrolled (cohort 1)
25 patients received eltrombopag
Four patients discontinued treatment
Response rate = 44% (11/25)
18 patients (cohort 2) received treatment
An additional six patients met the hematological response criteria = 40%
(17/43)
Overall response rate = 40% (17/43)
Successful taper off eltrombopag and sustained multilineage response
in five patients
TPO receptor agonist and refractory aplastic anemia
Response rate
Olnes et al NEJM 2012
Desmond et al Blood 2014
Adapted from Olnes M et al. N Engl J Med 2012;367:11; Desmond R et al. Blood 2014;123:1818

Subject (age)
Response Baseline Abnormality Time on
Eltrombopag (Months)
Dysplasia Outcome
7 (60) NR 46XY[20] Monosomy 7 3 N Died of progressive
cytopenias
8 (18) NR 46XX[6] Trisomy 8 3 N HSCT
19 (20) NR 46XY[20] Monosomy 7 3 N HSCT
26 (67) R 46XY[20] del(13q) 13 Yes (mild) HSCT
31 (41) NR 46XY[20] Trisomy 21
Monosomy 7
3
6 Yes (mild) Awaiting HSCT
32 (66) R 46XY[20] del(13q) 9 N Under observation
36 (23) NR 46XY[20] Monosomy 7 3 N HSCT
42 (17) NR No
metaphases Chromosome 7 3 N HSCT
HSCT, hematopoietic stem cell transplant; NR, nonresponder; R, responder; TPO-R, TPO, thrombopoietin receptor Desmond R et al. Blood 2014;123:1818–1825; Olnes MJ et al. N Engl J Med 2012;367:11–19
Eight patients (19%) developed cytogenetic abnormalities during eltrombopag treatment
Advise serial bone marrow biopsies
Clonal evolution
TPO receptor agonist and refractory aplastic anemia
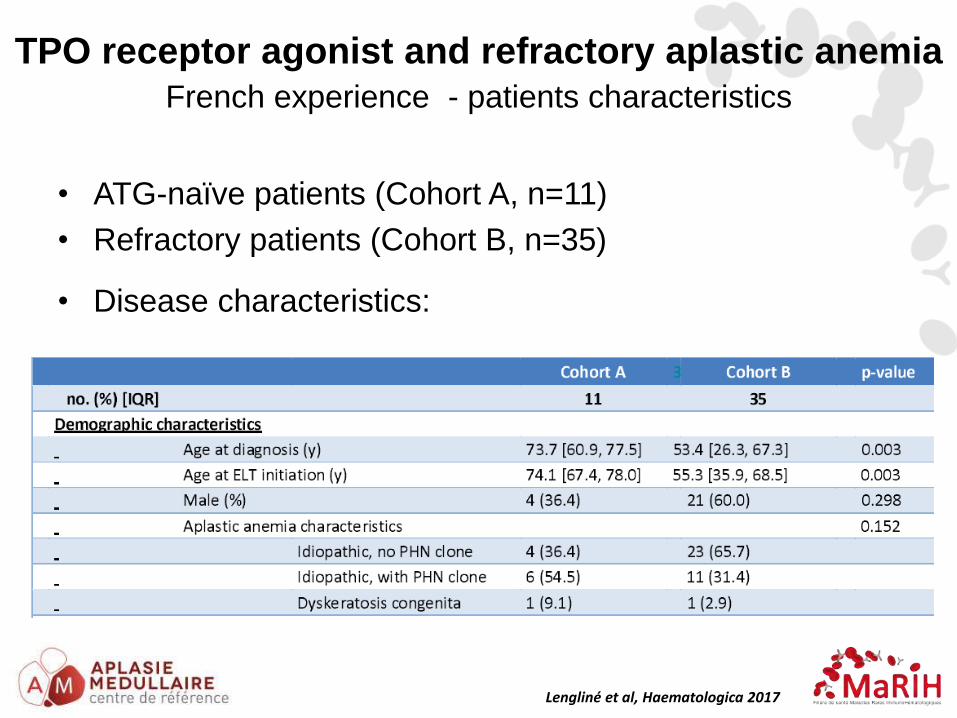
• ATG-naïve patients (Cohort A, n=11)
• Refractory patients (Cohort B, n=35)
• Disease characteristics:
French experience - patients characteristics
Lengliné et al, Haematologica 2017
TPO receptor agonist and refractory aplastic anemia
• Safety
– 1 SAE (liver toxicity)
– Clonal evolution (lack of follow-up …)
French experience - main messages
TPO receptor agonist and refractory aplastic anemia
Lengliné et al, Haematologica 2017
• Safety
– 1 SAE (liver toxicity)
– Clonal evolution (lack of follow-up …)
• Response rate = 40%
• 3 months for refractory patients
• 6 months for 1st line
• Multi-lineage response = 30% among responders
TPO receptor agonist and refractory aplastic anemia
French experience - main messages
Lengliné et al, Haematologica 2017
• Safety
– 1 SAE (liver toxicity)
– Clonal evolution (lack of follow-up …)
• Response rate = 40%
• 3 months for refractory patients
• 6 months for 1st line
• Multi-lineage response = 30% among responders
• Of note
– 20% of non responders responded at a higher dose (225 mg)
– Second IST including ATG (Revolade-ATG-CSA) lead to
excellent results in refractory patients (response rate = 100%
but n=8)
TPO receptor agonist and refractory aplastic anemia
Lengliné et al, Haematologica 2017
French experience - main messages
36
HLA-identical sibling donor and age < 40
HSCT
Marrow/Cy + ATG/CSA MTX
No sibling donor or age 40 or more
hATG + CSA
Refractory/relapse
10/10 (8/8 matched UD) Young (<30 years)
First year
YES: Unrelated matched BMT
NO: Eltrombopag Repeated IST Alternative
(mismatch BMT)
Treatment (guidelines)
Idiopathic aplastic anemia needed to be treated
Conclusions
• Diagnosis
– Inherited versus idiopathic aplastic anemia
• First line treatment in 2018
– Sibling transplantation: patients < 40 years
– Horse ATG + Cyclosporine for the others
• Refractory patients (6 months)
– Matched unrelated transplantation: patients < 30 years
– Experimental transplantation: patients < 20 years (?)
– Eltrombopag (+/- second course of ATG) for the others
Perspectives – Eltrombopag first line
• Phase II study
– Horse ATG + Cyclosporine + Revolade
– Responders 86%; Complete response 37% (6 months)
Patients naïfs clinicaltrials.gov NCT01623167
April 2017
Patients naïfs clinicaltrials.gov NCT02099747
Perspectives – Eltrombopag first line
Accrual 120/200
Thank you!
The French Reference Center for aplastic anemia and PNH in Paris
Saint-Louis Hospital Robert Debré Hospital Institute of Hematology, IUH St-Louis
F Sicre, T Leblanc, A Baruchel, G Socié (clinic)
N Vasquez, W. Cuccuini, J Soulier (Fanconi Team),
C Kannengiesser, E Lainey, L Da Costa (Telomeres team)