Rationale, design, and methods of the systematic treatment enhancement program for bipolar disorder...
15
Rationale, Design, and Methods of the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) Gary S. Sachs, Michael E. Thase, Michael W. Otto, Mark Bauer, David Miklowitz, Stephen R. Wisniewski, Philip Lavori, Barry Lebowitz, Mathew Rudorfer, Ellen Frank, Andrew A. Nierenberg, Maurizio Fava, Charles Bowden, Terence Ketter, Lauren Marangell, Joseph Calabrese, David Kupfer, and Jerrold F. Rosenbaum The Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) was conceived in response to a National Institute of Mental Health initiative seeking a public health intervention model that could generate externally valid answers to treatment effectiveness ques- tions related to bipolar disorder. STEP-BD, like all effectiveness research, faces many design challenges, including how to do the following: recruit a representative sample of patients for studies of readily available treat- ments; implement a common intervention strategy across diverse settings; determine outcomes for patients in mul- tiple phases of illness; make provisions for testing as yet undetermined new treatments; integrate adjunctive psy- chosocial interventions; and avoid biases due to subject drop-out and last-observation-carried-forward data anal- yses. To meet these challenges, STEP-BD uses a hybrid design to collect longitudinal data as patients make transitions between naturalistic studies and randomized clinical trials. Bipolar patients of every subtype with age 15 years are accessioned into a study registry. All patients receive a systematic assessment battery at entry and are treated by a psychiatrist (trained to deliver care and measure outcomes in patients with bipolar disorder) using a series of model practice procedures consistent with expert recommendations. At every follow-up visit, the treating psychiatrist completes a standardized assessment and assigns an operationalized clinical status based on DSM-IV criteria. Patients have independent evaluations at regular intervals throughout the study and remain under the care of the same treating psychiatrist while making transitions between randomized care studies and the standard care treatment pathways. This article reviews the methodology used for the selection and certification of the clinical treatment centers, training study personnel, the general approach to clinical management, and the sequential treatment strategies offered in the STEP-BD standard and randomized care pathways for bipolar de- pression and relapse prevention. Biol Psychiatry 2003; 53:1028 –1042 © 2003 Society of Biological Psychiatry Key Words: Bipolar disorder, effectiveness research, bipolar depression, relapse prevention Introduction T he Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) is a national, longitudi- nal public health initiative designed to examine the effec- tiveness of treatments and their impact on the course of bipolar disorder. The initial proposal was made in re- sponse to a National Institute of Mental Health (NIMH) request (RFP 98-DS-0001) seeking a common interven- tion model for studies of treatment effectiveness. The request for proposal asked for a public health model (Norquist and Hyman 1999; Norquist et al 1999) that enrolled patients with bipolar disorder of all subtypes, severity, and demographic groups. The NIMH funded STEP-BD as a contract to the Massachusetts General Hospital on October 1, 1998. The design and protocol were refined over the following year by committees convened by the STEP-BD Executive Committee and From the Partners Bipolar Treatment Center (GSS, MWO, AAN, MF, JFR), Department of Psychiatry, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts; Western Psychiatric Institute and Clinic (MET, EF, DK); and the Department of Epidemiology, School of Public Health (SRW), University of Pittsburgh, Pittsburgh, Pennsylvania; Department of Psychiatry (MB), Brown University, Providence, Rhode Island; Department of Psychiatry (DM), University of Colorado, Boulder, Colorado; Departments of Psychiatry (TK) and Health Research and Policy (PL), Stanford University School of Medicine, Stanford, California; National Institutes of Mental Health (BL, MR), Bethesda, Maryland; Department of Psychiatry (CB), University of Texas Health Science Center of San Antonio, San Antonio; Department of Psychiatry (LM), Baylor College of Medicine, Houston, Texas; Department of Psychiatry (JC), Case Western Reserve University, Cleveland, Ohio. Address reprint requests to Gary S. Sachs, M.D., Massachusetts General Hospital, Partners Bipolar Treatment Center, 50 Stanford Street, 5th Floor, Boston, MA 02114. Received September 27, 2002; revised January 22, 2003; accepted January 30, 2003. © 2003 Society of Biological Psychiatry 0006-3223/03/$30.00 doi:10.1016/S0006-3223(03)00165-3
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Rationale, design, and methods of the systematic treatment enhancement program for bipolar disorder...

Rationale, Design, and Methods of the SystematicTreatment Enhancement Program for Bipolar Disorder(STEP-BD)
Gary S. Sachs, Michael E. Thase, Michael W. Otto, Mark Bauer, David Miklowitz,Stephen R. Wisniewski, Philip Lavori, Barry Lebowitz, Mathew Rudorfer,Ellen Frank, Andrew A. Nierenberg, Maurizio Fava, Charles Bowden,Terence Ketter, Lauren Marangell, Joseph Calabrese, David Kupfer, andJerrold F. Rosenbaum
The Systematic Treatment Enhancement Program forBipolar Disorder (STEP-BD) was conceived in responseto a National Institute of Mental Health initiative seekinga public health intervention model that could generateexternally valid answers to treatment effectiveness ques-tions related to bipolar disorder. STEP-BD, like alleffectiveness research, faces many design challenges,including how to do the following: recruit a representativesample of patients for studies of readily available treat-ments; implement a common intervention strategy acrossdiverse settings; determine outcomes for patients in mul-tiple phases of illness; make provisions for testing as yetundetermined new treatments; integrate adjunctive psy-chosocial interventions; and avoid biases due to subjectdrop-out and last-observation-carried-forward data anal-yses. To meet these challenges, STEP-BD uses a hybriddesign to collect longitudinal data as patients maketransitions between naturalistic studies and randomizedclinical trials. Bipolar patients of every subtype with age� 15 years are accessioned into a study registry. Allpatients receive a systematic assessment battery at entryand are treated by a psychiatrist (trained to deliver careand measure outcomes in patients with bipolar disorder)using a series of model practice procedures consistentwith expert recommendations. At every follow-up visit, the
treating psychiatrist completes a standardized assessmentand assigns an operationalized clinical status based onDSM-IV criteria. Patients have independent evaluations atregular intervals throughout the study and remain underthe care of the same treating psychiatrist while makingtransitions between randomized care studies and thestandard care treatment pathways. This article reviews themethodology used for the selection and certification ofthe clinical treatment centers, training study personnel,the general approach to clinical management, and thesequential treatment strategies offered in the STEP-BDstandard and randomized care pathways for bipolar de-pression and relapse prevention. Biol Psychiatry 2003;53:1028–1042 © 2003 Society of Biological Psychiatry
Key Words: Bipolar disorder, effectiveness research,bipolar depression, relapse prevention
Introduction
The Systematic Treatment Enhancement Program forBipolar Disorder (STEP-BD) is a national, longitudi-
nal public health initiative designed to examine the effec-tiveness of treatments and their impact on the course ofbipolar disorder. The initial proposal was made in re-sponse to a National Institute of Mental Health (NIMH)request (RFP 98-DS-0001) seeking a common interven-tion model for studies of treatment effectiveness. Therequest for proposal asked for a public health model(Norquist and Hyman 1999; Norquist et al 1999) thatenrolled patients with bipolar disorder of all subtypes,severity, and demographic groups. The NIMH fundedSTEP-BD as a contract to the Massachusetts GeneralHospital on October 1, 1998. The design and protocolwere refined over the following year by committeesconvened by the STEP-BD Executive Committee and
From the Partners Bipolar Treatment Center (GSS, MWO, AAN, MF, JFR),Department of Psychiatry, Massachusetts General Hospital, Harvard MedicalSchool, Boston, Massachusetts; Western Psychiatric Institute and Clinic (MET,EF, DK); and the Department of Epidemiology, School of Public Health(SRW), University of Pittsburgh, Pittsburgh, Pennsylvania; Department ofPsychiatry (MB), Brown University, Providence, Rhode Island; Department ofPsychiatry (DM), University of Colorado, Boulder, Colorado; Departments ofPsychiatry (TK) and Health Research and Policy (PL), Stanford UniversitySchool of Medicine, Stanford, California; National Institutes of Mental Health(BL, MR), Bethesda, Maryland; Department of Psychiatry (CB), University ofTexas Health Science Center of San Antonio, San Antonio; Department ofPsychiatry (LM), Baylor College of Medicine, Houston, Texas; Department ofPsychiatry (JC), Case Western Reserve University, Cleveland, Ohio.
Address reprint requests to Gary S. Sachs, M.D., Massachusetts General Hospital,Partners Bipolar Treatment Center, 50 Stanford Street, 5th Floor, Boston, MA02114.
Received September 27, 2002; revised January 22, 2003; accepted January 30, 2003.
© 2003 Society of Biological Psychiatry 0006-3223/03/$30.00doi:10.1016/S0006-3223(03)00165-3

reviewed by an external advisory committee convened bythe NIMH. STEP-BD commenced clinical operations inNovember 1999 and projects to enroll 5000 bipolar pa-tients in treatment centers across the United States. Theproject is currently funded through 2005.
The purpose of this article is to provide an overview ofthe central purposes and methods of STEP-BD. Amonglarge treatment studies, STEP-BD is notable for ensuringwide representation of the heterogeneity of presentingmood states and comorbidities that represent bipolar dis-order. Moreover, STEP was designed with attention to thegap that can develop between well-controlled treatmenttrials and the ongoing treatment of patients in clinicalsettings. That is, do results in one generalize to the other?By combining a large naturalistic study with seamlessentry of some participants into randomized trials,STEP-BD will be able to compare the results frommethods that enhance internal validity with those thatenhance external validity. In addition, the detailed study ofa specific phase of the disorder will be complemented bydetailed information on what came before and what cameafter the window on outcome offered by the typicalrandomized treatment trial.
Before discussing some of the strategies and innova-tions used in STEP-BD, it is helpful first to place bipolardisorder and its treatment in context.
Rationale: Why a Nationwide Study ofBipolar Disorder?
Bipolar disorder is a major public health concern, recentlyranked as the world’s eighth greatest cause of medicaldisability (Murray and Lopez 1996). Prevalence estimatesrange from 1.0% to 3% of the population of the UnitedStates (Kessler et al 1994; Regier et al 1990; Weissman etal 1988). Moreover, a substantial minority of peoplediagnosed with recurrent depressive episodes is found tohave conditions within the broader spectrum of bipolardisorder (Angst and Sellaro 2000; Goldberg 2001). Bipo-lar patients and their caregivers must contend with thehigh rates of chronicity and recurrent illness associatedwith the disorder (Dunner and Fieve 1974; Fawcett et al1987; Keller et al 1986; Regier et al 1990). These multiplerecurrent episodes are disruptive to family, social, andvocational functioning (Coryell et al 1995; Dunner andFieve 1974; Maj et al 1989). Furthermore, bipolar disorderis associated with a significant risk of substance abuse(Thase and Salloun 2000) and suicide; approximately 25%of those with the disorder attempt suicide at least once(Koukopulos et al 1980), with rates as high as 2% per year(Baldessarini et al 2001). It is estimated that bipolardisorder reduces life expectancy by 10 years and costs the
afflicted individual an average of 9 years of productiveadult life (Lish et al 1994).
These factors make bipolar disorder an extremely costlyproblem for the nation’s health care systems. Over all,affective disorders account for approximately 21% of thedirect costs of all mental illnesses (Wyatt and Henter1995), with the total economic burden of bipolar disorderalone estimated at $45 billion per year as of 1991 (Wyattand Henter 1995). This figure takes into account bothdirect costs (i.e., bipolar patients’ use of psychiatric andother services) and indirect costs (i.e., the loss of economicproductivity of those directly affected by the disorder).Lost occupational earnings alone account for nearly $18billion per year (Wyatt and Henter 1995).
The direct costs shouldered by patients treated forbipolar disorder exceed that of patients treated for depres-sion, diabetes, and general medical conditions (Simon andUnutzer 1999). Additionally, a small subset of bipolarpatients, approximately 5%, account for 95% of the totalcosts for in-patient treatment (Simon and Unutzer 1999).These hazards and costs provide a compelling rationale fordevelopment of effective and well-tolerated treatmentstrategies for bipolar disorder, with attention to the acutetreatment of mood episodes as well as to the prevention ofepisodes over the long term.
This goal, however, has long languished without suffi-cient research attention. Recognition of the antimaniceffects of lithium in 1949 ultimately led to broad use oflithium salts for both acute and preventive treatment by thelate 1960s; subsequent progress has been slow. For exam-ple, in the United States, 24 years elapsed between the U.SFood and Drug Administration (FDA) approvals of lith-ium and divalproex for the treatment of acute mania. Tothis day, only three treatments have FDA approval specif-ically for treatment of any aspect of bipolar disorder:lithium, divalproex, and olanzapine.
At least five characteristics of bipolar disorder and itsinitial treatment may have contributed to a slower devel-opment of outcome research. First, promising results inearly studies may have contributed to overestimates of theeffectiveness of lithium and a false sense that the needs ofbipolar patients had been met. More recent data fromnaturalistic as well as controlled studies find more modestresults (Boerlin et al 1998), such that current estimates ofsustained response to lithium are now less than 50%instead of the 60%–80% previously cited (Goldberg et al1996).
Second, the low cost of lithium medications establisheda challenging cost-effectiveness standard for new treat-ments. Third, research on bipolar depression may haveslowed owing to the erroneous assumption that the effec-tiveness of antidepressants for people with bipolar disor-der can be inferred from studies of non-bipolar depression.
STEP-BD Clinical Effectiveness Methodology 1029BIOL PSYCHIATRY2003;53:1028–1042

This assumption decreased the pressure on the pharma-ceutical industry from the FDA to evaluate the utility ofnovel antidepressants. As a result, no antidepressant haspassed the conventional FDA muster for efficacy inbipolar depression (two positive, placebo controlled clin-ical trials; Thase and Sachs 2000).
Fourth, the complexity of bipolar disorder presentsgreater challenges to treatment researchers. For example,bipolar disorder encompasses four defined abnormal moodstates (mania, depression, mixed disorder, and hypomania)that may emerge at different points in the course of thedisorder and may each dictate specific therapeutic inter-ventions. Indeed, the goal of understanding the uniquefeatures as well as transitions between these states neces-sitates a dauntingly large sample by which to considerclinical subtypes over time.
Finally, to match the many phases characterizing thedisorder, outcome assessment must be multidimensional.No single measure can accurately capture the range oftreatment outcomes. For example, when a bipolar de-pressed patient experiences treatment-emergent maniaduring a course of treatment with a standard antidepressantmedication, this undeniably adverse outcome usually isaccompanied by a decrease in depression symptom ratingscales. Similarly, when interventions intended as treatmentfor mania are followed by a switch to a depressive episode,reporting change scores for rating scales that only indicatethe reduction of manic symptoms falsely conveys theimpression that a clinically well state was achieved.
The Design of STEP-BD
STEP-BD is not a single study but rather a platform orinfrastructure designed to carry out a variety of clinicaltrials and other studies that require a cohort of well-characterized bipolar subjects. From the outset, STEP-BDwas designed to be inclusive of the full spectrum ofbipolar patients presenting for clinical care. Effort in theplanning stage was devoted to capturing the heterogeneityof presentations (e.g., mood states and diagnostic specifi-ers) of the disorder itself, the rich diagnostic comorbiditycharacteristic of the disorder (Kessler 1994), differences intreatment sites and patient populations, and differences inthe strategies employed by the many specialists who treatbipolar disorder. To bring coherence to this heterogeneity,STEP-BD adopted a common set of clinical and assess-ment procedures to the multiple descriptive, naturalistic/quasi-experimental, and randomized studies that run underit. Regardless of whether patients are participating only inthe naturalistic study or are in randomized trials, theyreceive the same ongoing assessments of treatment andoutcome information. Assessment itself makes rich use ofongoing clinical monitoring, as well as the independent
evaluations more characteristic of controlled trials. Toachieve these ends, the role of the treating clinician inproviding ongoing outcome assessments and treatmentinformation is maximized while minimizing intrusion andrespondent burden, because clinical treatment itself isinformed by a set of time-efficient model practiceprocedures.
The combination of this systematic gathering of clinicaldata with serial independent assessment interviews andquestionnaire batteries provides the basis for profiling theclinical state and transitions between states for all partic-ipants during the course of their participation in STEP-BD.Participation itself reflected broad inclusion criteria (seebelow) and virtually no exclusion criteria. These criteriawere adopted to facilitate enrollment of a sample repre-sentative of those bipolar patients seeking treatment.Therefore, entry into the registry sample is limited mainlyby the participant’s willingness to be seen by a STEP-BDphysician and to accept the additional burden of self-ratingbatteries and independent study interviews. These inde-pendent study assessments are scheduled at baseline andquarterly for the first year and semiannually thereafter.
Site Selection
STEP-BD sites were selected from a larger number offormal site applications. Eligible sites described theirclinical services and staff available to deliver care tobipolar patients, the capacity to increase clinical servicesto bipolar patients, and adequate computer and telecom-munication infrastructure to meet the needs of the secureweb data-entry system. As a rough initial screening tool,only sites that had bipolar disorder specialty programscaring for at least 100 active patients were evaluated indetail. From applicants meeting these criteria, sites wereselected to assure geographic balance and demographicdiversity. For example, sites limited to only a Veteran’sHospital clinic or a fee-for-service format were typicallyexcluded. We also limited review to sites within theUnited States. Preference was given to qualified sitesexperienced in the conduct of clinical research withbipolar patients. Sites selected to participate contractedwith the coordinating center to implement the studyprocedures in their clinic.
Before a site could initiate the study, key personnel hadto meet stringent certification criteria for outcome assess-ment, data-entry procedures, and medical education per-taining to bipolar illness. New clinicians and site personnelmust be credentialed before treating patients and gatheringdata within STEP-BD.
Currently, the active sites for the program are the BaylorCollege of Medicine, Case Western Reserve University,Cornell University/New York Presbyterian Hospital,
1030 G.S. Sachs et alBIOL PSYCHIATRY2003;53:1028–1042

Howard University, Massachusetts General Hospital, NewYork University/Bellevue Hospital Center, Portland Vet-eran’s Administration Medical Center, Stanford Univer-sity School of Medicine, University of Colorado HealthSciences Center, University of Louisville Medical School,University of Massachusetts Medical School, Universityof Missouri at Kansas City, University of OklahomaHealth Sciences Center, University of Pennsylvania Med-ical Center, University of Pittsburgh Medical Center/Western Psychiatric Institute, and University of Texas atSan Antonio. Sites that participated in STEP-BD for alimited period of time include Medical University of SouthCarolina, University of Arizona, University of California-San Diego, University of Maryland, State University ofNew York at Buffalo, and Rush–Presbyterian St. Luke’sMedical Center.
Model Practice Procedures for TreatingPsychiatrists
The model practice procedures in STEP-BD include pro-cedures for delivery of treatments and procedures forrecord keeping. Both procedure sets are intended toprovide the common ground necessary to deliver andevaluate the outcome of treatment strategies.
The model practice procedures for pharmacotherapy arebased on the expert consensus guidelines (Sachs et al2000) and other published treatment guidelines (AmericanPsychiatric Association 2002; Bauer et al 1999). Atvarious operationally defined decision points, cliniciansare encouraged to offer treatments from a series of “Menusof Reasonable Choices.” These menus correspond to a listof treatments considered first line in one or more of thepublished guidelines. The sequence of decision points formanagement of the differing phases of the illness isreferred to as a pathway. STEP-BD offers cliniciansinstruction on nine major clinical pathways, each referredto as a Standard Care Pathway (SCP): Acute Depression,Refractory Depression, Acute Mania, Refractory Mania,Rapid Cycling, Relapse Prevention, Pregnancy, SubstanceAbuse, and other Comorbidity.
Training of Treating Psychiatrists
Training in model practice procedures requires treatingpsychiatrists to participate in an accredited continuingmedical education program that offers instruction in theuse of each of the treatments recommended in the study.The goal of the training is to ensure that every clinicianhas been exposed to at least 20 credit hours of basicteaching related to the management of bipolar disorder andto ensure access to additional training necessary to useeach of the treatments recommended in the pathways. Thisis accomplished through a combination of live training, a
continuing medical education–accredited virtual confer-ence series (available 24 hours a day via the Internet), andthe STEP-BD Clinician’s Handbook.
This approach differs from the use of a more formaltreatment algorithm. The study’s leadership recognizedthat limiting clinician choice would be neither practicalnor desirable. Therefore, STEP-BD adopted an encourage-ment design, in which clinicians are provided informationenabling them to use each of the SCP treatment optionsrecommended within the pathways. STEP-BD offers noextra compensation to practitioners but does offer trainingand the materials necessary to accomplish clinical priori-ties in a time-efficient manner. Care in SCPs is thereforeguidance based, in contrast with Randomized Care Path-way care (see below), which is largely protocol-driven oralgorithmic.
Recommended pharmacologic options for differentphases of the disorder consist of several first-line treat-ment recommendations offered by the “Expert ConsensusGuideline for Bipolar Disorder” (Sachs et al 2000) oranother published treatment guideline (American Psychi-atric Association 2002; Bauer et al 1999) and are referredto in training materials as the “Menu of ReasonableChoices” for that pathway.
The model practice procedures for record keepinginvolve specific training in the assessment of clinicalstates using the Clinical Monitoring Form (CMF), whichalso serves as the progress note in the patients’ medicalrecord. The CMF is a one-page assessment tool (seeAppendix 1) developed by the principal investigator(Sachs et al 2002). The CMF consists of nine parts,including modified versions of the Structured ClinicalInterview for DSM-IV Diagnosis (SCID) current moodmodules; associated symptoms, stressors, medical prob-lems, and comorbid conditions; selected mental statusitems; current medications compliance and adverse ef-fects; laboratory data; summary scores (i.e., clinical status,Depression, Mood Elevation, Clinical Global Impression–Severity Scale, and Global Assessment of FunctioningScale) narrative; and treatment plan.
The CMF’s operational conventions for concise clinicalrecord keeping allow it to serve as the source document forkey outcome measures in STEP-BD. Central to the track-ing of outcome is designation of the current clinical state.The clinical states tracked in the study are outlined inTable 1.
Before the initiation of STEP-BD, the CMF subscalesfor depression and mood elevation were found to be highlycorrelated with scores on commonly used rating scales.The CMF Depression subscale score was well correlatedwith the Hamilton Depression Rating Scale (r � .79) andthe Montgomery-Asberg Depression Rating Scale (r �.88). The CMF Mood Elevation subscale correlations with
STEP-BD Clinical Effectiveness Methodology 1031BIOL PSYCHIATRY2003;53:1028–1042

the Young Mania Rating Scale and the Schedule forAffective Disorders and Schizophrenia–Change ManiaRating Scale were r � .84, and r � .86, respectively(Sachs et al 2002).
These assessments of clinical state, checked for accu-racy relative to the independent assessments and otherclinical information (i.e., the occurrence of serious adverseevents), serve as the basis for the primary outcomes in themajority of proposed analyses across the diverse studieswithin STEP-BD. Full instructions for use of the CMF areavailable at www.manicdepressive.org (click on “Toolsfor Patients and Clinicians” button).
To be certified for use of the CMF, treating psychiatristsmust complete standardized training and meet certificationrequirements for establishing interrater agreement withgold standard ratings. Following initial training using aCD-ROM or live instruction, raters had to reach perfectagreement on the clinical status assignment and rate allindividual items within one-half point on a five-pointscale. Once certified, treating psychiatrists are periodicallymonitored to ensure that they are maintaining the stan-dards and avoiding the rater drift often associated withclinical interviews.
Independent Evaluations
Assessment of mood state and treatment information withthe CMF occurs against a backdrop of independent assess-ments that provide a wealth of information on the severityof mood symptoms, the presence and severity of comorbidpsychiatric disorders, social and role functioning, qualityof life, relevant attitudes and personality characteristics,and care utilization. Independent assessment begins atstudy initiation and continues with quarterly evaluationsduring the first year and semiannual evaluations thereafter.A summary of the interview (Table 2) and questionnaire
(Table 3) data collected during the independent evaluationassessments are presented below.
The Young Mania Rating Scale and the Montgomery-Asberg Depression Rating Scale are primary assessmentsof mood symptoms and are also used as a check onclinician ratings. Reliability of raters is checked continu-ally throughout the course of the study by comparing thedistribution of actual formal scale scores from independentraters and those derived from the subscales of the CMFcompleted by the treating psychiatrist. The data are exam-ined on a regular basis for inconsistencies. Rater pairsidentified as outliers are retrained on study ratingprocedures.
Eligibility Criteria for the Study Registry
Participating treatment centers offer STEP-BD enrollmentto all diagnostically eligible patients, both existing andnew, who seek outpatient treatment. Patients are notexcluded by virtue of hospital admission, but the ethicaland practical considerations inherent to tracking longitu-dinal outcomes limit enrollment to those patients willingand able to consent and enroll into the care of a localSTEP-BD certified treating psychiatrist for ongoing clin-ical management.
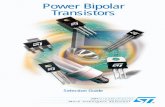
Patients treated in a STEP-BD clinic are informed aboutthe STEP-BD program by their psychiatrists. A flowdiagram is illustrated in Figure 1. Eligibility criteria wereselected based on the aim of effectiveness research: tomaximize the generalizability of study results. TheSTEP-BD registry includes consenting bipolar patientsolder than 15 years. Patients are of all subtypes (bipolar I,bipolar II, bipolar not otherwise specified, or cyclothymia)and in any phase of illness (See Table 4). The diagnosis ofa bipolar spectrum disorder is determined during the
Table 1. Assignment of Clinical Status
Associated Symptoms ofMania or Depression
Assigned Status
DSM-IV STEP-BD
If DSM Criteria for Current Episode: PositiveMajor depression �5 moderate Depression DepressionMania �3 moderate Mania ManiaHypomania �3 moderate Hypomania HypomaniaMajor depression and mania �3 moderate for mania and
�5 moderate for depressionMixed Mixed
If DSM Criteria for Current Episode: NegativeNot recovered from last acute episode �3 moderate Partial recovery Continued symptomaticNot recovered from last acute episode �2 moderate Partial recovery RecoveringRecovered from last acute episode,
if recovered �8 consecutive weeks�2 moderate Recovered Recovered
Recovered from last acute episode �3 moderate — Roughening
STEP-BD, Systematic Treatment Enhancement Program for Bipolar Disorder; DSM-IV, Diagnostic and Statistical Manual of Mental Disorders-Fourth Edition.
1032 G.S. Sachs et alBIOL PSYCHIATRY2003;53:1028–1042

screening and baseline assessments (see below) by usingthe Mini International Neuropsychiatric Interview (MINI;Sheehan et al 1998) and a standardized affective disorderevaluation (ADE; Sachs 1990) as administered by aclinical specialist (a psychologist or social worker) and thetreating psychiatrist, respectively. Eligibility requires thatsubjects receive a consensus bipolar diagnosis on both theMINI and ADE.
The ADE includes a modified version of the mood andpsychosis modules from the SCID intended for routine useby practicing clinicians. The ADE also collects specificdata on age of onset, estimate of number of prior episodes,past treatment response, trauma, childhood psychopathol-ogy, medical conditions, psychoactive substance use, fam-ily history, menstrual history, and mental status. Patientsdiagnosed with the bipolar subtype of schizoaffectivedisorder are also eligible, if the medical record is availableand provides clear documentation of both a manic episodeand a period of recovery without psychosis lasting 6months or longer in the 12 months before study entry.Enrollment is deferred for patients who require inpatientdetoxification; however, enrolled patients in need of inpa-tient detoxification are included in the study.
Standard and Randomized Care Treatment
At any point in the patient’s participation in the registry, sheor he may become eligible for one of the STEP-BD Ran-domized Care Pathways (RCPs). Patients may enter thesepathways if they meet inclusion/exclusion criteria and if anadditional consent is obtained by their psychiatrist. Subjectsnot eligible or unwilling to consent continue to receive SCPtreatment. Subjects may enter each randomized pathway onlyonce. Unlike drug trials, which have predetermined lengthsof treatment within the study and no further assessment forsubjects once off protocol, randomized patients in STEP-BDsimply move back into the SCP once they have completedtreatment or elect to drop out of an RCP. After exiting arandomized pathway, patients may not re-enroll in thatpathway but remain eligible for other randomized pathwayswithin STEP-BD. Therefore, STEP-BD offers greater conti-nuity of care and greater continuity of data than do typicalrandomized clinical trials.
Three RCPs initially offered by STEP-BD includepathways for acute depression, refractory depression, andrelapse prevention. The RCPs are designed to comparefirst-line treatment options under more rigorous condi-
Table 2. STEP-BD Clinician/Observer Data Collection
Clinician Rated Assessment Tools
Standard Care PathwaysRandomized Care
Pathways
OtherStudyEntry
Month3/9
Month6/18
Month12/24
Entry/Exit
AllEvaluations
Treating Psychiatrist–Rated MeasuresAffective Disorders Evaluation (Sachs 1990)a XClinical Monitoring Form (Sachs 1990)
(Sachs et al 2002)All patient visits scheduled with
the treating psychiatrist.Measures Completed by Clinical Specialist or Other Certified Rater
Care Utilization Form X X X X XDemographic Form X XFamily Contacts X XMontgomery-Asberg Depression
Rating Scale (Montgomery 1979)X X X X X
Hospitalization Form X X XRange of Impaired Functioning Tool X X X X XMini International Neuropsychiatric
Interview (Sheehan et al 1998)X
UCLA Social Attainment Scale(Goldstein 1978)
X
Work Impact Form X X X X XYoung Mania Rating Scale
(Young et al 1978)X X X X X
Liebowitz Social Phobia Scale(Liebowitz 1987)
X X Comorbidity pathway only
Panic Disorder Severity Scale X X Comorbidity pathway onlyYale-Brown Obsessive Compulsive Scale X X Comorbidity pathway only
STEP-BD, Systematic Treatment Enhancement Program for Bipolar Disorder; UCLA, University of California at Los Angeles.aThe Affective Disorders Evaluation (ADE) is administered by a treating psychiatrist if a patient was not seen at the clinic before. The clinical specialist may administer the ADE
for patients previously evaluated at the clinic. Administration of the ADE requires certification from the Clinical Coordinating Center for treating psychiatrist and/or clinical specialist.
STEP-BD Clinical Effectiveness Methodology 1033BIOL PSYCHIATRY2003;53:1028–1042

tions. Each of the RCPs has somewhat narrower inclusioncriteria than the SCPs (See Table 4) and randomizesconsenting participants to one of several psychotropicmedication regimens considered to be a first-line treatmentoption (See Table 5).
The Acute Depression and Refractory Depression RCPsalso offer the option of allowing the treating psychiatrist toselect a randomization stratum (Peduzzi et al 2002). Theuse of randomization strata maximizes entry of subjectsinto randomized pathways by allowing doctors the optionof excluding what they or their patient regards as aninappropriate or unacceptable arm of the randomizationschema in the trial. For example, the treating psychiatristcan decide to exclude one of the options in the randomized
acute depression pathway based on the treatment historyor tolerance of an individual patient. For example, path-way-eligible patients for whom paroxetine is unacceptableremain eligible for randomization to adjunctive treatmentwith bupropion or placebo but not paroxetine.
Enhancing Psychosocial Treatment in StandardPharmacologic Care
Recent reports suggest the addition of psychotherapy canimprove the effectiveness of somatic treatment and reducetreatment costs (Craighead and Miklowitz 2000; Huxley etal 2000; Swartz and Frank 2001). But psychotherapy ishardly a monolithic entity, and it is not at all clear that
Table 3. STEP-BD Self-Report Data Collection
Patient Self-Report Assessment Tools
Standard Care PathwaysRandomized Care
Pathways
OtherStudyEntry
Month3/9
Month6/18
Month12/24
Entry/Exit
AllEvaluations
Beck Depression Inventory Version II(Beck et al 1961)
X
Edinbergh Handedness Inventory(Oldfield 1971)
X
Family History (Sachs 1990) XMedication History (Sachs 1990) XMenstrual History (Sachs 1990) X Females onlyNEO Five Factor Inventory
(Costa and McCrae 1985)X X
ADHD Symptom Check List X X Comorbidity pathwayDavidson Trauma Scale
(Davidson et al 1997)X X Comorbidity pathway
Eating Disorders Inventory X X Comorbidity pathwayFear Questionnaire X X Comorbidity pathwayKennerley Blues Questionnaire Administered within 2 weeks
after live birthAttributional Style Scale
(Peterson et al 1982)X
Beck Anxiety Inventory X X X X XBeck Hopelessness Scale
(Beck et al 1974)X X X X
Care Satisfaction Questionnaire X X X XDysfunctional Attitudes Scale
(Hooley 1989)X
Helping Alliance Questionnaire X XInterpersonal Support Evaluation List XLife Experience Survey X X XPerceived Criticism Scale X XPersonality Diagnostic
Questionnaire–Version 4X X
Quality of Life Enjoyment andSatisfaction (Short Form)
X X X X X
Religiosity XSF-36 Health Survey X XSocial Rhythm Metric “Short Form”
(Goldstein 1978)X
STEP-BD, Systematic Treatment Enhancement Program for Bipolar Disorder; ADHD, attention-deficit/hyperactivity disorder; SF-36, Short-Form 36 Item HealthSurvey.
1034 G.S. Sachs et alBIOL PSYCHIATRY2003;53:1028–1042

traditional, psychodynamically oriented interventionshave a prominent role when compared with more focusedpsychoeducational, interpersonal, cognitive–behavioral,and family-oriented interventions. Understanding whichpsychotherapies for which patients might be of clinical
benefit is an obvious need. It is also essential to understandhow psychosocial treatments might reduce the risks asso-ciated with the many nonbiological social and environ-mental factors that can mediate the course of illness,care utilization, work performance, and overall treat-
Figure 1. Evaluation and flow into STEP-BDStandard Care Pathways and RandomizedCare Pathways. On contact with a STEP-BDtreatment center, patients with mood disor-ders are informed about the study and offeredstandardized diagnostic evaluation with aSTEP-BD certified clinician. Those meetingcriteria for any bipolar disorder are offeredentry into the study registry. Consenting pa-tients receive clinical care from a STEP-BDclinician, and all visits are recorded using theClinical Monitoring Form (CMF; see Appen-dix 1). At these follow-up visits, if the pa-tient’s status meets eligibility criteria for arandomized study, consent is requested forentry into that Randomized Care Pathway(RCP). Those ineligible or unwilling to con-sent remain in the Standard Care Pathway.The same clinician treats the patient as theymake transitions from randomized to standardcare. An independent evaluator (not shown)administers formal assessments and self-ratedscales quarterly in year 1 and semiannuallythereafter. STEP-BD, Systemic TreatmentEnhancement Program for Bipolar Disorder.
Table 4. STEP-BD Eligibility Criteria
Pathway Inclusion Criteria Exclusion Criteria
Standard Care Pathways Treatment is open to all participants with a bipolardiagnosis
Unwilling or unable to comply with study requirements
Acute Depression Pathway Meets criteria for current major depression Unresponsive to both paroxetine and bupropion in the pastPatient must currently be taking a mood stabilizer or Unable to tolerate both paroxetine and bupropion
agree to begin treatment with a mood stabilizer Meets criteria for mixed episode or hypomaniaPatient agrees to have all non-study antidepressants Contraindication to lithium, valproate, or carbamazapine
tapered after initiation of study drug Unstable medical condition or other medicalcontraindication
Current alcohol or substance abuse requiring treatmentRefractory Depression
PathwayFailure to respond to treatment in first 12 weeks, or
well-documented failure to respond to at least twotrials of antidepressant, during current depressiveepisode
Meets criteria for depression for 8 weeks prior topathway entry
Currently taking a mood stabilizer or agree to begintreatment with a mood stabilizer
Patient has refused electroconvulsive therapy
Failure to respond to at least two of the following:inositol, lamotrigine, or risperidone
History of intolerance or medical contraindicationto any of the medications listed above
Meets criteria for mixed episode or hypomaniaCurrent substance abuse or dependence
Relapse PreventionPathwya
Index episode (mania, mixed, or hypomania)occurred while receiving treatment with eitherlithium or valproate
Thyroid-stimulating hormone and creatinine levelswithin normal limits
Treatment at time of episode includes both lithium andvalproate
Patient cannot be taking additional moodstabilizers, antidepressant or antipsychotic
Current substance abuse or dependenceAcute episode responded to electroconvulsive therapy
STEP-BD, Systematic Treatment Enhancement Program for Bipolar Disorder.
STEP-BD Clinical Effectiveness Methodology 1035BIOL PSYCHIATRY2003;53:1028–1042

ment response (Craighead and Miklowitz 2000; Frank etal 2000).
A unique feature of STEP-BD is its aim to transformclinical care in the context of the study. The modelpractice procedures and the education programs linked tothem provide one way of achieving this goal. In addition,attention to psychosocial aspects of treatment were en-hanced with the use of a “Collaborative Care” approachand a workbook for patients and families.
The Collaborative Care approach is grounded on theclinical assumption that patients are more likely to besatisfied with their treatment if they are involved in thedecision-making process. Collaborative Care encouragespatients, their clinicians, and clinicians from multipledisciplines and specialties to combine their efforts to decideon the best treatment options for the patient (Sachs 1996).
At the heart of Collaborative Care are attempts toenhance the therapeutic alliance between patients, theirclinicians, and their family members, allowing patientsand their families to be more committed to the treatmentsand to treatment goals. Clinicians are responsible forrecommending reasonable, safe, and effective treatmentoptions, thus passing on to patients the “Menu of Reason-
able Choices” (Sachs 1996). Patients entering STEP-BDare given a workbook and videotape describing theCollaborative Care model.
The Collaborative Care Workbook (available at:www.manicdepressive.org/tools.html) contains informa-tion about bipolar disorder and its treatment, and alsoincludes information on managing stress, poor communi-cation, sleep, dysfunctional cognitions, and other psycho-social factors associated with increased risk of relapse(Otto et al 2003). This workbook culminates in a treatmentcontract that helps patients and their support networkidentify symptoms and early action strategies for helpingmanage bipolar disorder; this contract is to be signed incollaboration with the treating clinician (Otto et al 2003).
Randomized Psychosocial Treatment
The role of psychosocial treatment is evaluated moreformally in the context of a randomized clinical trialexamining the efficacy of a full treatment trial (30 sessionsover 9 months) with one of three psychotherapies—cognitive–behavior therapy (Otto et al 2003), family-focused therapy (Miklowitz et al 2000), or interpersonalpsychotherapy with a social rhythm component (Frank
Table 5. Randomized Pathway Primary Aims and Design Overview
Pathway and Primary Question(s) Design and Duration Randomization Main Outcomes
Randomized Acute DepressionIf a bipolar patient becomes depressed,
is it better to start treatment withoptimized mood stabilizer or treat withcombination of mood stabilizer and astandard antidepressant
Double-blindUp to 24 weeks
MS � PBO vs. MS �paroxetine or MS � PBOvs. MS � bupropion
% recovered% affective switch% drop outCare utilization
Is an intensive psychosocialintervention superior to CollaborativeCare Plus for acute depression?
Collaborative Care Plus vsCognitive–behavioraltherapy/family-focustherapy/interpersonal socialrhythm therapy
Randomized Refractory DepressionIf a bipolar patient remains depressed
despite two trials with standardantidepressants, is greater responseachieved with adjunctive treatmentwith risperidone, inositol, orlamotrigine?
OpenUp to 24 weeks
Inositol vs. risperidone orRisperidone vs. lamotrigineor lamotrigine vs. inositol
% recovered% affective switch% drop outCare utilization
Randomized Relapse PreventionIf a bipolar patient becomes manic
while on lithium or divalproex, is itbetter to increase the current moodstabilizer or treat with combination oflithium and divalproex?
Double-blindUp to 2 years
MS 1 � PBO vs. divalproex� lithium
% clinical status � recoveredTime to event% drop outCare UtilizationTime in remission
Is an intensive psychosocialintervention superior to CC�for relapse prevention?
Collaborative Care Plus vs.Cognitive–behavioraltherapy/family-focustherapy/interpersonal socialrhythm therapy
Functional impairment
MS, mood stabilizer; PBO, placebo; CC�, Collaborative Care Plus.
1036 G.S. Sachs et alBIOL PSYCHIATRY2003;53:1028–1042

et al 2000)—relative to a three-session psychosocial inter-vention using the Collaborative Care model and workbook(Collaborative Care Plus). Each of these full treatmentshave evidence of clinical efficacy (for review see Miklow-itz and Otto, in press), a clinicians’ treatment manual, andeasily assimilated training materials.
Training in psychosocial therapies is accomplished inseveral steps. First, new psychosocial clinicians read thetreatment manuals for each respective treatment. Then, train-ees watch an 8-hour videotaped workshop directed by theauthors of the manuals for each modality. Next, clinicianstake on two treatment cases and receive at least 3 hours oftelephone supervision (and review at least 6 session audio-tapes) from a clinician who champions the modality. Thesupervisor makes regular treatment integrity ratings based oneach clinicians’ ability to administer the modality with skilland adherence to the manual. Successful completion of twocases marks the end of the training phase for that modality.
The design of the psychosocial interventions within theRCPs also represents an innovative feature of STEP-BD.Clinical specialists at each STEP-BD site are responsible foradministering three of the four psychosocial interventions,thus giving this branch of STEP-BD a partly crossed, orinterpolated, design. Specifically, all sites offer the standardclinical management approach, Collaborative Care Plus(which serves as the control group), plus two of the threeestablished interventions described above. This design fea-ture simplifies the process of training clinical specialistsacross the sites: clinical specialists typically learn one mo-dality in their area of expertise and then one other modality.This design feature simplifies the process of training clinicalspecialists across the study, and permits secondary analyseslooking at such issues as allegiance and therapist comfortwith newly learned therapies. Careful supervision of eachmodality decreases the likelihood of overlap or “bleedthrough” from one manualized intervention to another.
Primary Scientific Objectives
The primary objectives are summarized in Table 5.Among the many unmet needs for research on bipolardisorder, the executive committee consensus determinedthe highest priorities for the field were studies of: 1)treatment effectiveness for bipolar depression; and 2)treatment effectiveness for relapse prevention. In the caseof each of these objectives, the urgency of desire foreffectiveness data included determination of the role ofpsychosocial interventions.
The structure of STEP-BD allows examination of ques-tions in the context of well-controlled clinical trials andexamination of the long-term outcome of these patients asthey continue their care after the randomized trial iscomplete. This structure leads to two immediate advan-tages: 1) patients dropping out of the randomized trial are
not lost to follow-up as long as they continue in theregistry and open clinical care with their treating psychi-atrist (providing longer-term intent-to-treat data on therandomization strategy); and 2) follow-up data for therandomized study of treatment of acute and refractorydepression also allow commentary on the efficacy of thesestrategies for preventing relapse (assuming recovery fromdepression). In addition, outcome can be compared be-tween patients receiving a specific treatment in a random-ized trial with those who received that treatment in thesame phase of disorder as part of standard clinical care.Accordingly, STEP-BD should be able to comment onoutcome from designs that separately stress internal andexternal validity for a particularly diverse and broadlydefined sample of bipolar patients across the UnitedStates.
The systematic assessment of outcome in the registrypermits the conduct of quasi-experimental analyses, whichcan address important clinical questions for which nowell-controlled trial is currently feasible. For instance,such quasi-experimental data allows potentially valuablecommentary on the probability of improvement with novelpharmacologic strategies and the use of case–controldesigns to understand how patients with a similar trajec-tory of symptoms faired with alternative agents (e.g., if alithium-treated bipolar depressed patient has not re-sponded to fluoxetine, is lamotrigine treatment moreeffective than treatment with another standardantidepressant?).
Another objective of STEP-BD is to estimate the costsand quality-of-life outcomes of acute treatment and long-term management strategies for bipolar disorder. Theextensive longitudinal data collection of STEP-BD in-cludes a number of functional outcome measures, whichassess the economic and social effects of each patient’sdisorder and treatments, as well as measures addressingthe impact on overall quality of life and satisfaction.
Secondary aims of the study include assessing theprognostic impact of comorbid conditions in the treatmentof bipolar patients. STEP-BD attempts to determine thebenefit of interventions specifically for comorbid psycho-active substance abuse or dependence, anxiety disorders,and eating disorders, all of which frequently co-occur withbipolar disorder and cause obvious difficulties in patients’functionality and treatment. As patients with these com-mon comorbidities are invariably excluded from standardclinical trials, we will have a unique capacity to mountlarge-scale studies, both descriptive and prospective, ofthe more complex forms of bipolar disorder.
Data from STEP-BD will also shed light on the diag-nostic and therapeutic complexities within the bipolardiagnosis itself. Specific interventions for rapid-cycling
STEP-BD Clinical Effectiveness Methodology 1037BIOL PSYCHIATRY2003;53:1028–1042

bipolar disorder, as well as acute and refractory mania,will be assessed, and the benefit of those treatmentstrategies will be determined. Furthermore, the abundanceof high-quality data gathered will allow analysis of thevalidity of specific bipolar diagnoses, such as bipolar I,bipolar II, and cyclothymia, as well as other proposedsubtypes.
Ancillary Studies
The large scale of the STEP-BD program offers an excellentopportunity for independent investigators to examine a widevariety of research hypotheses across the spectrum of bipolardisorders. The first ancillary studies in STEP-BD are threepilot studies focused on women’s health issues related totreatment for bipolar disorder. The largest of these STEP-BDwomen’s studies will compare rates of polycystic ovarysyndrome in women treated with valproate versus othermood stabilizers. Other pilot studies explore rates of treat-ment-emergent affective switching in depressed women witha history of rapid cycling, and the safety and efficacy ofomega 3 fatty acids for bipolar women who are or want tobecome pregnant. These relatively small studies are examplesof projects designed to provide estimates of sample-sizerequirements or explore the feasibility of larger, indepen-dently funded projects.
Human Subjects Study
Despite numerous advantages, there are several significantbarriers to participation in STEP-BD. Unlike most efficacystudies, STEP-BD sites cannot offer free care. STEP-BDrequires that the study group be representative of thosepresenting for treatment, and therefore enrollment requiresthat subjects continue to pay for care at each facility asthey would in the absence of the study. The multiple studyobjectives also produce a greater respondent burden thanrequired in routine care. These factors raise the question ofwhy subjects would enter a study offering treatments thatare generally available.
The coordinating center plans to examine representative-ness at enrollment milestones of 500, 1000, and 2000subjects. As warranted by disparities in the representativenessof the sample, the coordinating center will encourage appro-priate outreach and establish treatment centers at sites servingsubpopulations underrepresented in the enrolled sample.
Statistical Analysis Plan
Data are collected on paper forms, either by self-reportor interview, and data are keyed into a web-based datamanagement system. The web-based data managementsystem is secure to only study personnel, using bothinternet provider restriction and username/password
verification to secure the site. Upon logging on to theweb site, study personnel open a screen to enter thevarious instruments. Upon completion of entry of theinstrument, the data are submitted and immediatelytransferred to the Data Coordinating Center. Minimumon-line edits are employed, such as range and data-typechecks. Double-entry verification is required for se-lected data. Once the data arrive at the Data Coordinat-ing Center, all data pass through an extensive editingprocess to check for logical inconsistencies within thedata.
Reports are available to study personnel via the studyweb site for monitoring recruitment and data quality.These reports are routinely updated to assure that the mostrecent data are being assessed.
All data collection forms and data reports include onlythe subject’s study identification number. No names orpersonal identification information are sent to the DataCoordinating Center or stored in the STEP-BD database.
The analyses of data from the RCPs are complicated bythe fact that participants may indicate preferences tospecific treatments. Preference strata have been created toaccount for these differences. Patients are stratified ac-cording to the preference of the treatments provided in theRCP. For the analyses to compare the treatments, thesample will be restricted to those patients assigned to thosetreatments that were considered acceptable. The data willbe stratified by preference strata, and a Mantel-Haenszel�2 test will be used to make pairwise comparisons of theresponse rates among the treatments.
There are many statistical analyses that will be con-ducted of the data collected from the SCP. Two primaryapproaches outlined below will take advantage of thelongitudinal aspects of the data, as well as the changes inthe clinical states of the patients.
Much of the data collected in the SCP will permit theinvestigators to examine the changes in the character-istics of the patients over time. These characteristicsinclude measures of quality of life, care utilization, andfunction. To do so, mixed-effects regression modelswill be used to model the changes of these characteris-tics over time. Included in the model will be indicatorsof treatment, both pharmacologic and psychosocial,adherence to treatment, and measures of the clinicalstate of the patient.
Additional analyses will be conducted to examine var-ious treatment effects in a variety of subpopulations (e.g.,history of rapid cycling, mixed episode). A cohort will beassembled and followed longitudinally (e.g., those in amixed episode), with information recorded as the patienttransitions from state to state. The amount of time in each“well” state will be estimated and compared over time todetermine whether the length of the “well” period changes
1038 G.S. Sachs et alBIOL PSYCHIATRY2003;53:1028–1042

over time. Because each subject will contribute multiple“well” periods to the analyses, traditional survival analysistechniques will not be appropriate. One possible analytictechnique would be the use of a frailty model, whichpermits multiple transitions over time.
Frailty models will be developed to determine whetherthere is a change in the length of the well period as thenumber of episodes increase. Because patients presentwith different characteristics, it will be important tocontrol for any potential confounding variables. Thesewould include, among others, type of bipolar disorder (I orII), length of illness, and pole before the onset of each wellepisode.
Conclusions
Bipolar mood disorder is a common, chronic, and oftensevere mental illness for which treatment effectivenessresearch is a high public health priority. The complexity ofthe condition, lack of a common intervention model, andthe need for a large sample present daunting obstacles toresearchers and provide compelling rationale for NIMHsponsorship of multisite collaborative research.
STEP-BD consists of a clinical coordinating center, datamanagement center, and a network of collaborating sitesusing common practice procedures to carry out multiplestudies. Overall, the study design corresponds with thoseBauer has proposed as defining effectiveness research(Bauer 2002). STEP-BD uses broad entry criteria aimed ataccrual of a sample that reflects the population of bipolarpatients who present for clinical care. The interventionsare limited to those which can be delivered by a typicalclinic staff without special training or unusual resources.The substantial burden of research data collection isminimized for clinicians by using a standardized formatthat doubles as the clinical progress note and routineincorporation of patient self-report into clinical assess-ments. Similarly, the respondent burden for subjects ismitigated by the close linkage of assessments with clinicalcare. By minimizing the assessments that are pertinent toresearch only and having the bulk of assessments be thosethat are also used for clinical care, respondent burden iskept within acceptable limits. The data analytic plans canmake use of the hybrid design and provide continuedassessment of subjects beyond their participation in a shortterm-intervention. STEP-BD results will have substantialexternal validity and share some of the internal validityadvantages of standard efficacy trials.
STEP-BD is one of several large NIMH-sponsoredinitiatives that provide the funding necessary for effective-ness trials. It is clear that large mental health initiativeslike STEP-BD are necessary and that feasibility dependson establishing a network of collaborators and the opera-
tional support necessary to collect and analyze large datasets. Over the next decade, the stream of data generated bythese studies will greatly improve quantity and quality ofdata available to guide clinicians and policy makers asthey attempt to meet the needs of citizens with severemental illness.
This project has been funded in whole or in part with Federal funds fromthe National Institute of Mental Health (NIMH), National Institutes ofHealth, under Contract N01MH80001. Any opinions, findings, andconclusions or recommendations expressed in this publication are thoseof the authors and do not necessarily reflect the views of the NIMH. Thisarticle was approved by the publication committee of the SystematicTreatment Enhancement Program for Bipolar Disorder (STEP-BD). Coreinvestigators and collaborators for STEP-BD are:
STEP-BD Contract: Gary S. Sachs, M.D. (PI), Michael E. Thase, M.D.(Co-PI)
STEP-BD Clinical Coordinating Center: Gary S. Sachs, M.D.; LeslieLeahy, Ph.D.*; Jane N. Kogan, Ph.D.; Ellen B. Dennehy, Ph.D.; JenniferA. Conley, M.A.; Jamie L. Gradus, B.A.; Stephen M. Gray, B.A.;Jacqueline Flowers, B.A.; Mandy Graves, B.A.
STEP-BD Data Coordinating Center: Stephen Wisniewski, Ph.D.STEP-BD Site Principal Investigators and Co-Principal Investigators:
Lauren B. Marangell, M.D. and James M. Martinez, M.D. at BaylorCollege of Medicine; Joseph R. Calabrese, M.D. and Melvin D. Shelton,M.D. at Case Western Reserve University; Michael W. Otto, Ph.D.*/Andrew A. Nierenberg, M.D. and Gary S. Sachs, M.D. at MassachusettsGeneral Hospital and Harvard Medical School; R. Bruce Lydiard, M.D.at the Medical University of South Carolina*; Joseph F. Goldberg, M.D.at New York Presbyterian Hospital and Weill Medical College of CornellUniversity; James C.-Y. Chou, M.D. and Joshua Cohen, DO at New YorkUniversity School of Medicine; John Zajecka, M.D. at Rush-PresbyterianSt. Luke’s Medical Center*; Terence A. Ketter, M.D. and Po W. Wang,M.D. at Stanford University School of Medicine; Uriel Halbreich, M.D.at State University of New York at Buffalo*; Alan Gelenberg, M.D. atUniversity of Arizona*; Mark Rapaport, M.D. at University of Califor-nia, San Diego*; Marshall Thomas, M.D., Michael H. Allen, M.D., andDavid J. Miklowitz, Ph.D at University of Colorado Health SciencesCenter; Rif S. El-Mallakh, M.D. at University of Louisville School ofMedicine; Peter Hauser, M.D. at University of Maryland*; JayendraPatel, M.D. at University of Massachusetts Medical Center; KemalSagduyu, M.D. at University of Missouri-Kansas City, School ofMedicine. Western Missouri Mental Health Center; Mark D. Fossey,M.D. and William R. Yates, M.D. at University of Oklahoma College ofMedicine; Laszlo Gyulai, M.D. and Claudia Baldassano, M.D. atUniversity of Pennsylvania Medical Center; Michael E. Thase, M.D. andEdward S. Friedman, M.D. at University of Pittsburgh Western Psychi-atric Institute and Clinic; and Charles L. Bowden, M.D. and Cherly LGonzales, M.D. at University of Texas Health Science Center at SanAntonio.
STEP-BD Executive Committee: Mark S. Bauer, M.D., Charles L.Bowden, M.D., Joseph R. Calabrese, M.D., Jennifer Conley, M.A., EllenB. Dennehy, Ph.D., Maurizio Fava, M.D., Gary Gottleib, M.D., EllenFrank, Ph.D., Terence A. Ketter, M.D., Jane N. Kogan, Ph.D., DavidKupfer, M.D., Leslie Leahy, Ph.D.*, Lauren B. Marangell, M.D., DavidJ. Miklowitz, Ph.D., Michael W. Otto, Ph.D., Jerrold F. Rosenbaum,M.D., Matthew V. Rudorfer, M.D., Gary S. Sachs, M.D., Linda Street,Ph.D., Michael E. Thase, M.D., Sean Ward and Stephen Wisniewski,Ph.D.
NIMH Liaisons to STEP-BD: Matthew V. Rudorfer, M.D., JoanneSevere, MS, Linda Street, Ph.D.
STEP-BD Clinical Effectiveness Methodology 1039BIOL PSYCHIATRY2003;53:1028–1042

Aspects of this work were presented at the conference, “PediatricBipolar Disorder,” held March 9, 2002 in Boston, Massachusetts. Theconference was sponsored by the Massachusetts General Hospitalthrough an unrestricted educational grant provided by JanssenPharmaceutica.
* No longer participating in this role in STEP-BD.
ReferencesAmerican Psychiatric Association (2002): Practice guideline for
the treatment of patients with bipolar disorder (revision).Am J Psychiatry 159:1–50.
Angst J, Sellaro R (2000): Historical perspectives and naturalhistory of bipolar disorder. Biol Psychiatry 48:445–457.
Baldessarini R, Tondo L, Hennen J (2001): Treating the suicidalpatient with bipolar disorder: Reducing suicide risk withlithium. Ann N Y Acad Sci 932:24–38.
Bauer MS, Callahan AM, Jampala C, Petty F, Sajatovic M,Schaefer V, et al (1999): Clinical practice guidelines forbipolar disorder from the Department of Veterans Affairs.J Clin Psychiatry 60:9–21.
Beck A, Lester D, Trexler L (1974): The measurement ofpessimism: The hopelessness scale. J Consult Clin Psychol42:861–865.
Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J (1961):An inventory for measuring depression. Arch Gen Psychiatry4:561–571.
Boerlin H, Gitlin M, Zoeller L, Hammen C (1998): Bipolardepression and antidepressant-induced mania: A naturalisticstudy. J Clin Psychiatry 59:374–379.
Bauer MS, Williford WO, Dawson EE, Akiskal HS, Altshuler L,Fye C, et al (2001): Principles of effectiveness trials and theirimplementation in VA Cooperative Study #430: “Reducingthe efficacy-effectiveness gap in bipolar disorder.” J AffectDisord 67:61–78.
Coryell W, Endicott J, Maser JD, Keller MB, Leon AC, AkiskalHS (1995): Long-term stability of polarity distinctions in theaffective disorders. Am J Psychiatry 152:385–390.
Costa PT Jr, McCrae RR (1988): Personality in adulthood: asix-year longitudinal study of self-reports and spouse ratings onthe NEO Personality Inventory. J Pers Soc Psychol 54:853–863.
Craighead W, Miklowitz D (2000): Psychosocial interventionsfor bipolar disorder. J Clin Psychiatry 61(suppl):58–64.
Davidson JR, Book SW, Colket JT, Tupler LA, Roth S, David D,et al (1997): Assessment of a new self-rating scale forpost-traumatic stress disorder. Psychol Med 27:153–160.
Dunner D, Fieve R (1974): Clinical factors in lithium carbonateprophylaxis failure. Arch Gen Psychiatry 30:229–233.
Fawcett J, Scheftner W, Clark D, Hedeker D, Gibbons R, CoryellW (1987): Clinical predictors of suicide in patients withmajor affective disorders: A contolled prospective study.Am J Psychiatry 144:35–40.
Frank E, Swartz H, Kupfer D (2000): Interpersonal and socialrhythms therapy: Managing the chaos of bipolar disorder.Biol Psychiatry 48:593–604.
Goldberg J (2001): Spontaneous depression versus biphasiccycling. Am J Psychiatry 158:325–326.
Goldberg JF, Harrow M, Leon A (1996): Lithium treatment ofbipolar affective disorders under naturalistic followup condi-tions. Psychopharmacol Bull 32:47–54.
Goldstein M (1978): Further data concerning the relation be-tween pre-morbid adjustment and paranoid symptomatology.Schizophr Bull 4:236–243.
Hooley J (1989): Predictors of relapse in unipolar depressives:Expressed emotion, marital distress, and perceived criticism.J Abnorm Psychol 98:229–235.
Huxley NA, Parikh SV, Baldessarini RJ (2000): Effectiveness ofpsychosocial treatment in bipolar disorder: State of theevidence. Harv Rev Psychiatry 8:126–140.
Keller MB, Lavori PW, Coryell W, Andreasen NC, Endicott J,Clayton PJ, et al (1986): Differential outcome of pure manic,mixed/cycling, and pure depressive episodes in patients withbipolar illness. JAMA 255:3138–3142.
Kessler RC (1994): The National Comorbidity Survey of theUnited States. Int Rev Psychiatry 6:365–376.
Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M,Eshleman S, et al (1994): Lifetime and 12-month prevalenceof DSM-III-R psychiatric disorders in the United States.Results from the National Comorbidity Survey. Arch GenPsychiatry 51:8–19.
Koukopulos A, Reginaldi D, Laddomada P, Floris G, Serra G,Tondo L (1980): Course of the manic-depressive cycle andchanges caused by treatments. Pharmacopsychiatry 13:156–167.
Liebowitz (1987). Social phobia. Mod Probl Pharmacopsychia-try 22:141–173.
Lish JD, Dime-Meenan S, Whybrow PC, Price RA, HirschfeldRMA (1994): The National Depressive and Manic-depressiveAssociation (DMDA) survey of bipolar members. J AffectDisord 31:281–294.
Maj M, Pirozzi R, Starace F (1989): Previous pattern of course ofthe illness as a predictor of response to lithium prophylaxis inbipolar patients. J Affect Disord 17:237–41.
Miklowitz DJ, Otto MW (in press): New psychosocial interven-tions for bipolar disorder: A review of literature and intro-duction of the systematic treatment enhancement program.Trends in Evidence-Based Neuropsychiatry.
Miklowitz DJ, Simoneau TL, George EL, Richards JA, KalbagA, Sachs-Ericsson N, et al (2002): Family-focused treatmentof bipolar disorder: 1-year effects of a psychoeducationalprogram in conjunction with pharmacotherapy. Biol Psychi-atry 48:582–592.
Montgomery A (1979): A new depression scale designed to besensitive to change. Br J Psychiatry 134:382–389.
Murray C, Lopez A (1996): Evidence-based health policy—lessons from the Global Burden of Disease Study. Science274:740–743.
Norquist G, Hyman S (1999): Advances in understanding andtreating mental illness: Implications for policy. Health Aff(Millwood) 18:32–47.
Norquist G, Lebowitz B, Hyman S (1999): Expanding thefrontier of treatment research. Prev Treatment. Availableonline at http://journals.apa.org/prevention/volume2/pre0020001a.html.
1040 G.S. Sachs et alBIOL PSYCHIATRY2003;53:1028–1042

Oldfield R (1971): The assessment and analysis of handedness:The Edinburgh inventory. Neuropsychologia 9:97–113.
Otto MW, Reilly-Harrington N, Sachs GS (2003): Psychoeduca-tional and cognitive-behavioral strategies in the managementof bipolar disorder. J Affect Disord 73:171–181.
Peduzzi P, Henderson W, Hartigan P, Lavori P (2002): Analysisof randomized controlled trials. Epidemiol Rev 24:26–38.
Peterson C, Von Baeyer C, Abramson L, Metalsky G, SeligmanM (1982): The attributional style questionnaire. Cognit TherRes 6:287–299.
Regier DA, Farmer ME, Rae DS, Locke BZ, Keith SJ, Judd LL,Goodwin FK (1990): Comorbidity of mental disorders withalcohol and other drug abuse. Results from the EpidemilogicCatchment Area (ECA) Study. JAMA 264:2511–2518.
Sachs G (1990): Use of clonazepam for bipolar affective disor-der. J Clin Psychiatry 51:31–34.
Sachs G (1996): Bipolar mood disorder: Practical strategies foracute and maintenance phase treatment. J Clin Psycho-pharmacol 16:32S–47S.
Sachs G, Printz D, Kahn D, Carpenter D (2000): The expertconsensus guideline series. Medication treatment of bipolardisorder. Postgrad Med Apr;Spec No:1–104.
Sachs GS, Guille C, McMurrich S (2002): A clinical monitoringform for mood disorders. Bipolar Disord 4:323–327.
Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J,Weiller E, et al (1998): The Mini-International Neuropsychi-atric Interview (M.I.N.I.): The development and validation ofa structured diagnostic psychiatric interview for DSM-IV andICD-10. J Clin Psychiatry 59:22–33.
Simon G, Unutzer J (1999): Health care utilization and costsamong patients treated for bipolar disorder in an insuredpopulation. Psychiatr Serv 50:1303–1308.
Swartz H, Frank E (2001): Psychotherapy for bipolar depression:A phase-specific treatment strategy? Bipolar Disord 3:11–22.
Thase M, Sachs G (2000): Bipolar depression: Pharmacotherapyand related therapeutic strategies. Biol Psychiatry 48:558–572.
Thase M, Salloun I (2000): Impact of substance abuse on thecourse and treatment of bipolar disorder. Bipolar Disord2:269–280.
Weissman M, Warner V, Wickamaratne P, Prusoff B (1988):Early-onset major depression in parents and their children. JAffect Disord 15:269–277.
Wyatt RJ, Henter I (1995): An economic evaluation of manic-depressive illness—1991. Soc Psychiatry Psychiatr Epide-miol 30:213–219.
Young RC, Biggs JT, Ziegler VE, Meyer DA (1978): A ratingscale for mania: Reliability, validity, and sensitivity. Br JPsychiatry 133:429–435.
STEP-BD Clinical Effectiveness Methodology 1041BIOL PSYCHIATRY2003;53:1028–1042

Appendix 1. The Clinical Monitoring Form
1042 G.S. Sachs et alBIOL PSYCHIATRY2003;53:1028–1042