The Co-emergence Model of Reinforcement: A Rationale for Mindfulness Integration
Upload
khangminh22Category
view
0download
0
IMMEDIATE FUNCTIONAL LOAD OFMANDIBULAR IMPLANT OVERDENTURES:A SURGICAL AND PROSTHODONTICRATIONALE OF 2 IMPLANT MODALITIES
Jaime L. Lozada, DDSAladdin J. Al-Ardah, DDSKitichai Rungcharassaeng,DDS,MSJoseph Y. K. Kan, DDS, MSAlejandro Kleinman, DDS
KEY WORDS
Endosseous implantsOsseointegrationOverdenturesImmediate functional loadingSubperiostal implant
Jaime L. Lozada, DDS, is a professor anddirect or, Aladdin J. Al-A rdah , D DS, is anassistant professor, Joseph Y. K. Kan,DDS, MS, and Alejandro KleinmanDDS, are associate professors, andKitichai Rungcharassaeng, DDS, MS,is an assistant professor of the GraduateProgram in Implant Dentistry,Loma LindaUniversity, School of DentistryCenter for Implant Dentistry,Loma Linda, Calif.
Address correspondence to Dr Lozada at11092 Anderson St, Suite 4411,Loma Linda, CA. 92350(e-mail: [email protected]).
Classic guidelines in osseointegration for root-form dental implants
include a long healing period, during which functional load should
be avoided. However, the long healing period might impose an
intolerable situation on some patients, especially in the completely
edentulous situation. Subperiosteal dental implant guidelines dem-
onstrate that the implant upon insertion can be put into immediate
function and be restored with the final prosthesis soon after surgery.
Studies on immediately functional loaded implant-supported pros-
theses in patients who are completely edentulous have been reported,
exhibiting high success rates comparable with conventionally loaded
implants. This article describes the surgical and prosthodontic
procedure for the immediately functional loaded mandibular implant
overdentures in 2 different dental implant modalities, as well as its
clinical rationale.
INTRODUCTION
The viability andpredictability ofosseointegrated en-dosseous implantsin treating patientswho are completely
and partially edentulous havebeen supported with the highsuccess rates reported in numer-ous studies.1–4 Classic guidelinesfor osseointegration includea long healing period, duringwhich functional load should beavoided. Periods of 3 to 4 monthsand 4 to 6 months have been
recommended as healing timesfor osseointegrated implantsplaced in the mandible and max-illa, respectively.5,6 The long heal-ing periods might impose anintolerable situation esthetically,functionally, psychologically, andsocially on some patients, espe-cially in a completely edentuloussituation.
In 1986, Babbush et al7
described a technique of immedi-ately loading 4 titanium plasma-sprayed implants placed in themandibular symphysis with anoverdenture. The implants were
Journal of Oral Implantology 297
SPECIAL REPORTD
ownloaded from
http://meridian.allenpress.com
/joi/article-pdf/30/5/297/2033444/0686_1.pdf by guest on 13 February 2022

rigidly splinted with a metal bar,and the denture was relined withsoft liner within 2 to 3 days afterthe surgery. The final prosthesiswith the clips was placed 2 weekslater. The authors reported a cu-mulative failure rate of 12% after8 years of follow-up. Since then,several studies have focused onboth fixed and removable imme-diately loaded implant-supportedprostheses in patients who arecompletely edentulous, and highsuccess rates comparable withconventionally loaded implantshave been reported.
The success rates of subperios-teal dental implants have beendisputed.8,9Minimal documentedevidence of the predictability ofthese devices has lessened thebenefits that the implant offersfor patientswith severely atrophicmandibles.10,11 One of the guide-lines of these particular implantmodality dictates that the implantupon insertion be loaded withaprovisional overdenture. Inmostcases, the patient’s existing den-ture is modified so it can be usedas a provisional denture for 3months before the final prosthesisis inserted.
The purpose of this article is todescribe the surgical and pros-thodontic procedure for the im-mediately loaded mandibularimplant overdenture of 2 differ-ent implant modalities: root-formimplant overdenture and sub-periosteal implant overdenture.The clinical rationale and out-comes of each modality are alsodiscussed.
MATERIALS AND METHODS
Patient selection for theroot-form implant modality
The patients selected for immedi-ately loaded mandibular implantbar overdentures fulfilled thefollowing criteria: (1) had com-
pletely edentulous maxilla andmandible (Figure 1), (2) hadenough bone between the mentalforamina to allow for placementof 4 endosseous root-form im-plants with a minimum lengthof 12 mm, (3) had bone qualitybetter than type IV according toLekholm and Zarb,12 and (4) hada medical history that did notcontraindicate implant treatment.
Patient selection for thesubperiosteal implant modality
The patients selected for imme-diately loaded mandibular sub-periosteal implant bar overdenturesfulfilled the following criteria:(1) had completely edentulousmaxilla and mandible (Figure 1),(2) had enough bone to allow forplacement of a subperiosteal im-plant framework without havingto augment the mandible withsimultaneous bone graft (divisionC according to Misch13), and (3)had a medical history that did notcontraindicate implant treatment.
Presurgical prosthodonticprocedures
After thepatienthadbeen selectedas a candidate for immediatelyloaded mandibular implant over-denture, new maxillary and man-dibular complete dentures withproper extensions as well as prop-er occlusal schemes were fabricat-ed. Adjustments were made sothat the patient was as comfort-able as possible with the newdentures. A radiographic tem-plate was then fabricated withclear acrylic resin (Splint ResinPolymer, Great Lakes Orthodon-tics, Towanda,NY) by duplicatingthemandibular complete denture.Radiopaquemarkers, such as gut-ta percha (Dental stopping, Col-tene-Whaledent, Cuyahoga Falls,OH) or barium sulfate (E-Z-HD,E-Z-EM), were used during com-puterized tomography (CT) scan-
ning to determine the implantposition and data to produce forthe subperiostal implant protocola 3-dimensional life-size cast ormodel of the mandible by stereo-lithography methods.14–16 (Figure2). The radiographic templatewaslater modified into a surgical tem-plate.
Surgical procedure for theroot-form implant modality
Implant placement surgery wasperformed under local anesthesiaby infiltration in the mandible. Amidcrestal incision was made,a full-thickness flap was reflected,and the mental foramina wereidentified bilaterally. The surgicaltemplate was then placed in posi-tion for evaluation of the clearancefor the attachment system. In thepatient shown in Figure 3, alveo-loplasty was necessary because ofthe space inadequacy.
The maxillary complete den-ture was used to locate the mid-line, and a slight mark was madeon the mandible. The 2 posteriorimplants were located approxi-mately 5 mm anterior to themental foramina. The 2 anteriorimplants were about 7 to 10 mmanterior to the posterior implants;the anterior implants should beequidistant from the midline. Allimplant positions should bewithin the confines of the sur-gical template (Figure 4).
A complete series of osteoto-mies were performed accordingto the manufacturer’s protocol,and the implants were placed intothe osteotomy sites. The surgicaltemplate and maxillary completedenture were used to verify buc-colingual andmesiodistal angula-tion of the implants, respectively.
Transmucosal abutments ofappropriate heights to create aproper plane for the frameworkfabrication were placed with theappropriate abutment wrench.
IMPLANT MODALITIES FOR MANDIBULAR IMPLANT OVERDENTURES
298 Vol. XXX/No. Five/2004
Dow
nloaded from http://m
eridian.allenpress.com/joi/article-pdf/30/5/297/2033444/0686_1.pdf by guest on 13 February 2022
The tops of the transmucosalabutments should follow the an-terior occlusal plane of the maxil-lary complete denture. Therecommended torque for the abut-ments should not be attempted,because this might cause the im-plant to thread into a deeper level.
Plastic bridge copings wereroughened to create a retentivesurface and were placed on top ofthe transmucosal abutments. The
flapwas then preliminarily closedwith Gore-Tex sutures (3i/WLGore, Newark, Del). English-Don-nelle-Staubi (EDS) plastic bars(Attachments International, SanMateo, Calif) were prepared tothe proper lengths and placedbetween the plastic bridge cop-ings. The bar and the bridgecopings were joined with auto-polymerizing acrylic resin (GCPattern Resin, Alsip, Ill). The
anterior bar should be parallel tothe occlusal plane of themaxillarycomplete denture and perpendic-ular to the line bisecting themandible (Figure 5).
The resin pattern was left toset intraorally for approximately20 minutes. It was then removedand transferred to the laboratory,where the metal framework wasfabricated in type IV gold alloy(Monogram IV, Leach & Dillon,
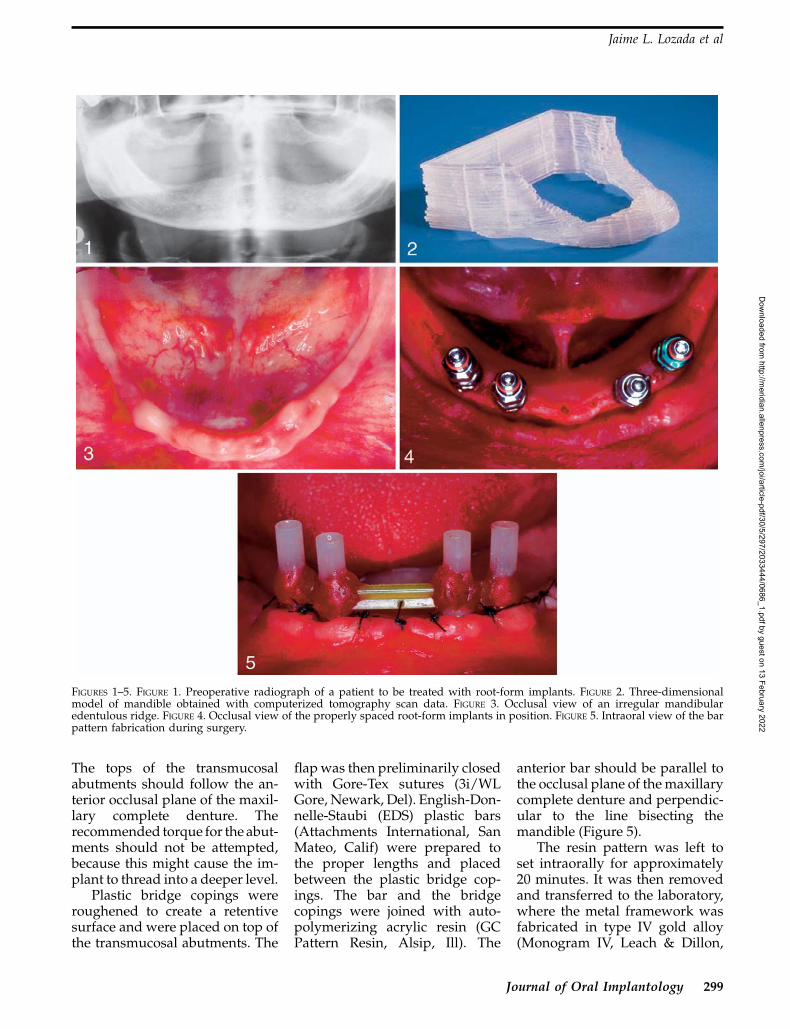
FIGURES 1–5. FIGURE 1. Preoperative radiograph of a patient to be treated with root-form implants. FIGURE 2. Three-dimensionalmodel of mandible obtained with computerized tomography scan data. FIGURE 3. Occlusal view of an irregular mandibularedentulous ridge. FIGURE 4. Occlusal view of the properly spaced root-form implants in position. FIGURE 5. Intraoral view of the barpattern fabrication during surgery.
Jaime L. Lozada et al
Journal of Oral Implantology 299
Dow
nloaded from http://m
eridian.allenpress.com/joi/article-pdf/30/5/297/2033444/0686_1.pdf by guest on 13 February 2022
Cranston, RI). Meanwhile, theprotective titanium healing capswere placed on the transmucosalabutments and the final flapclosure was performed, leavingthe healing caps exposed.
Amoxicillin 500 mg andibuprofen (Motrin, Upjohn, Kala-mazoo, Mich) 800 mg were pre-scribed for antibiotic coverageand pain control. The patientwas instructed to use 0.12% chlo-rhexidine gluconate (Peridex,Procter & Gamble, Cincinatti,Ohio) twice a day for 2 weeksand to start brushing the barregularly with an end-tuftedbrush (John O. Butler, Chicago,Ill) 1 week after the surgery. Thepatient was placed on a liquiddiet for the next 2 weeks.
Postsurgical prosthodonticprocedure for the root-form
implant modality
The try-in of the metal frameworkwas completed within 24 hours
after the surgery. After satisfac-tory fit and stability of the frame-work were verified both clinicallyand radiographically, the bar wasplaced in the patient’s mouth(Figures 6 and 7). The patient didnot wear the mandibular dentureduring the soft-tissue healing.
The sutures were removed 2weeks after the surgery (Figure 8).The mandibular denture was re-lieved so that it was not touchingthe bar when placed in position.The pickup impression of the barwas made with the mandibulardenture with polyvinyl siloxaneimpression material (Reprosil,Dentsply, York, Pa). The metalhousing for the EDS clip (Attach-ments International) was incor-porated during the relining of themandibular overdenture. Aftertissue surface adjustment, theEDS clip was placed in the metalhousing. Clinical remount wasperformed, and occlusion wasadjusted for bilaterally balanced
occlusion. Afterward, the finalprostheses were placed in thepatient’s mouth (Figure 9). Oralhygiene instructions were rein-forced. Although no food restric-tion was imposed, the patient wasrecommended to follow a soft dietfor the first 2 to 3 weeks afterprosthesis placement.
The patient was asked toreturn the next day for a post-insertion check and any necessaryadjustments. Follow-ups werescheduled at 1, 3, and 6 monthsafter prosthesis placement andevery 6 months thereafter.
Surgical procedure for thesubperiosteal implant modality
After the protocol outlined byTruitt et al17 for the morpho-logical replication of mandibles byusing 3-dimensional (3-D) model-ing and sterelithoradiography,subperiosteal implants weredesigned and fabricated fromsurgical-grade Vitallium (How-
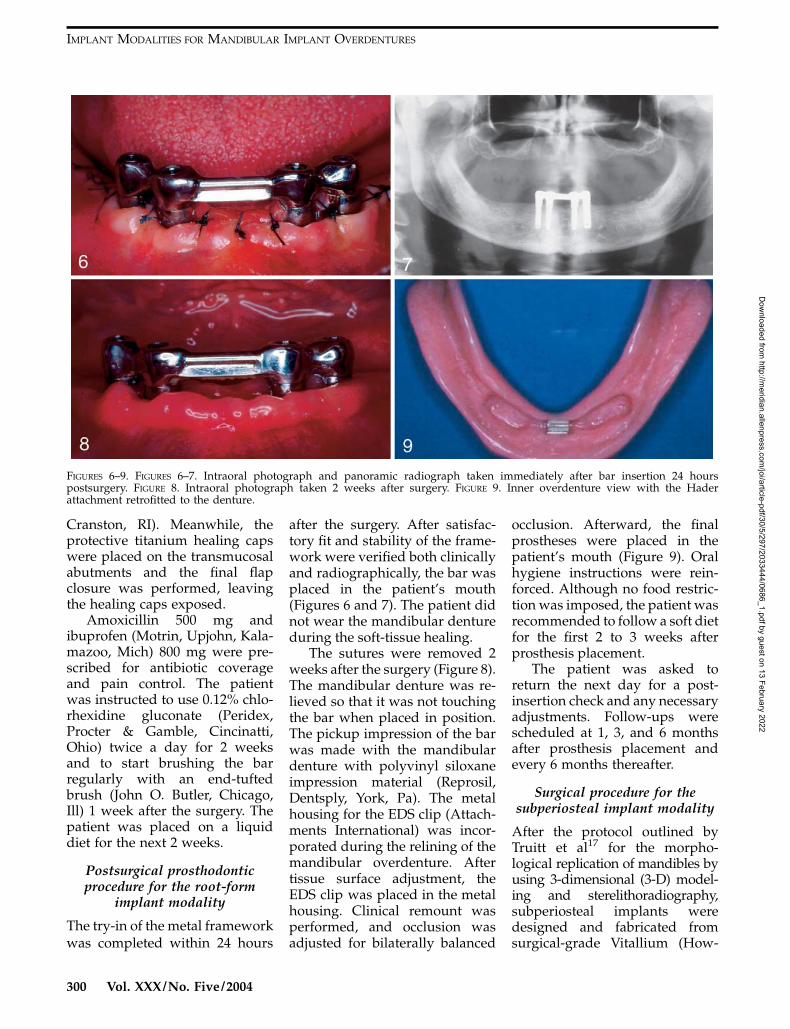
FIGURES 6–9. FIGURES 6–7. Intraoral photograph and panoramic radiograph taken immediately after bar insertion 24 hourspostsurgery. FIGURE 8. Intraoral photograph taken 2 weeks after surgery. FIGURE 9. Inner overdenture view with the Haderattachment retrofitted to the denture.
IMPLANT MODALITIES FOR MANDIBULAR IMPLANT OVERDENTURES
300 Vol. XXX/No. Five/2004
Dow
nloaded from http://m
eridian.allenpress.com/joi/article-pdf/30/5/297/2033444/0686_1.pdf by guest on 13 February 2022

medica, Kalamazoo, Mich)(27% chrome, 66% cobalt, 7%molybdenum) and coated withhydroxyapatite (HA). They werealso fabricated in 1 piece with thecontinuous intraoral bar in placeas part of the implant at the timeof insertion (Figure 10). The in-traoral incisions were made fromthe right retromolar pad and
extended along the crest of theridge to the contralateral retro-molar pad. By using periostealelevators, the mucoperiosteumwas reflected from the bone, bothbuccally and lingually; the mentalforamina were identified; and thedissection was completed withminimal trauma to the neuro-vascular bundles. During implan-
tation, the tissues were carefullyretracted with nylon-covered in-struments to prevent transfer ofmetal to the passivated orHA-coated implant. When theimplants were fully seated, theapproximation of bone to metalwas noted and recorded, andany discrepancies were thenfilled with an appropriate graft
FIGURES 10–14. FIGURE 10. Subperiosteal implant seated on 3-dimensional cast. Note design features. FIGURE 11. Intraoperativephotograph of implant placement before suturing. FIGURE 12. Postoperative view. Notice satisfactory tissue healing. FIGURE 13.Preexisting denture showing the flanges removed and relined for immediate insertion after surgery. FIGURE 14. Modified immediatecompletely implant-supported overdenture inserted minutes after surgery.
Jaime L. Lozada et al
Journal of Oral Implantology 301
Dow
nloaded from http://m
eridian.allenpress.com/joi/article-pdf/30/5/297/2033444/0686_1.pdf by guest on 13 February 2022

material. The tissues were closedwith 4-0 vicryl sutures (Figures 11and 12).
Postsurgical prosthodonticprocedure for the subperiosteal
implant modality
Immediately after implant place-ment and complete closure, thepatient’s existing denture wasmodified and adapted for use asa transitional denture. The den-ture modification consisted of re-moval of a portion of the buccaland lingual flanges of the dentureand the relining of the same den-ture at the correct vertical di-mension of occlusion (Figures 13and 14).
The modified denture wassubsequently adapted and re-lined, thereby increasing its re-tention and function for 2 monthsbefore the final prosthesis wasfabricated.
For the final mandibular over-denture, record bases were madeat the time of implant fabrication,which accurately fit on the in-traoral bar. These record basesfacilitated the intraoral bar andborder molding impressions andwere also used to obtain theinterocclusal records. The recordbases had Dolder clips (Attach-ments International) added tothem for retention purposes.Once the interocclusal recordswere obtained, the subsequentsteps involved conventional den-ture fabrication procedures.
DISCUSSION
Surgical and prosthodonticrationale of the root-form andsubperiosteal implant modality
Recently, clinical studies havereported comparably high im-plant success rates (85%–100%)in immediate loading in patients
who were completely edentu-lous.7,18–24 Peri-implant bone re-sponse of the immediately loadedimplants is also favorable andcomparable with that of conven-tional delayed-loading im-plants.24 It is difficult to comparesubperiosteal implant overden-tures with root-form implantoverdentures; however, some ele-ments are common and can be thebases for evaluation of thesemodalities.
Bone Quality
Root-form implants. Dense tra-becular bone provides betterintimacy of initial fit and im-plant-bone contact area, whichtranslates to better primarystability.25–27 It has also beendocumented that implant failurerates in type IV bone are signifi-cantly higher than in type I toIII bone.28–30 In addition, Schnit-man et al21 reported that 3 of 4failed immediately loaded im-plants were placed distal to themental foramen, where the bonequality is inferior to the symphy-sis area.
Subperiosteal implants. Nocom-parative studies have reportedthe success rate of subperiostealimplants among the differentbone types; however, some anec-dotal reports describe significantlyhigher failure rates in the maxillathan in the mandible.
Bone Quantity
Root-form implants. Bone quan-tity dictates the implant diameterand length. Wider-diameter orlonger implants provide greatersurface area for initial bone-im-plant contact as well as forosseointegration. Positive correla-tion has been established betweenimplant diameter or length andthe removal torque or push-outforce values.31–33 Higher implant
failures for short implants (�10mm) were also reported in bothimmediate21,22 (??) and delayedloadings.30,34–36 Although imme-diate loading of wide-diameterimplants has not been reported, itshould be considered when avail-able bone permits the placementof such implants.
Subperiosteal implants. The au-thors of this article have limitedthe application of the subperios-teal implant to the severely atro-phic mandible. Considering thearguments against the use of shortendosseous implants, class D ac-cording Misch,13 mandibles cansuccessfully be treated with sub-periosteal implants without bonegrafting. The authors haveachieved positive results in thetreatment of severely atrophicmandibles.
Implant Geometry
Root-form implants. Threadedimplants should be used in im-mediate loading situations be-cause they provide the strongestimmediate mechanical retentionafter placement.37
Subperiosteal implants. The de-sign according to James has theonly documented evidence aboutthe benefits of the lateral supportvs the designs with support fromonly the crest of the ridge. Since1983, the authors of the currentpaper have exclusively used theavowed design. The implant, ingeneral, uses maximum supportfor the body of the mandible andis HA coated.
Implant Surface Characteristics
Root-form implants. Althoughno significant differences havebeen in the implant success ratesbetween smooth and rough im-plant surfaces, recent literatureseems to favor a rough surface inachieving a greater magnitudeand faster rate of osseointegra-
IMPLANT MODALITIES FOR MANDIBULAR IMPLANT OVERDENTURES
302 Vol. XXX/No. Five/2004
Dow
nloaded from http://m
eridian.allenpress.com/joi/article-pdf/30/5/297/2033444/0686_1.pdf by guest on 13 February 2022

tion.38–41 Therefore, in immediateloading situations where maxi-mum magnitude and rate ofosseointegration are desired, im-plants with surface treatmentsshould be considered.
Subperiosteal implants. Humanhistology has demonstrated thebenefits of HA-coated subperios-teal implants. Positive correlationhas been found in the quality ofsurvival between the coated andthe noncoated subperiostealimplants.42
Bicortication
Root-form implants. Engagingboth the superior and the inferiorcortical bone significantly in-creases the implant stability andthe removal torque.43 In addition,Chiapasco et al23 found nocorrelation between the implantlength and the success rates aslong as there was bicortical stabi-lization. Bicortical initial stabili-zation could also be enhanced byminimal countersinking.20
It has been frequently statedthat implant surgery is prosthet-ically driven; this is especiallytrue in an immediate loadingsituation. The final prosthesesdictate implant position, angula-tion, number, and distribution aswell as bar length and orienta-tion. The interarch distance andthe attachment systems dictatethe depth at which the implantsare placed. Therefore, fabricationof the final prostheses beforeimplant surgery is very impor-tant. The use of the maxillarycomplete denture and surgicaltemplate is very essential duringimplant surgery. The maxillarycomplete denture is used to locatethe midline, as a guide for mesio-distal implant angulation andimplant level, and as a guide forhorizontal bar orientation. Thesurgical template is used to eval-uate the clearance for the attach-ment system, confine the implant
positions, guide buccolingual im-plant orientation, and guidesagittaly bar orientation.
Attachment Systems
The attachment system used inimmediate loading situationsshould involve prompt, rigidsplinting of the implants. Lumet al42 showed that direct bone-implant interface was achievedwhen immediately loading HA-coated blade-form implants withrigid fixation to a firm naturaltooth. Babbush et al7 also showed,in the immediate loading study,that apart from infection, failurewas related to delayed applica-tion of a rigid splinting bar. Theauthors of the current paper havealso previously reported on therecommended guidelines for im-mediate functional load, whichinclude the immediate rigidsplinting bar placed in the pa-tient’s mouth within 24 hoursafter surgery.44 In this report,and in the case of the root-formimplant modality, the EDS bar-and-clip system was used and therigid splinting bar was placed inthe patient’s mouth within thesame period after the implantsurgery. The Dolder bar-and-clipsystem has been used since 1984for the subperiosteal implant mo-dality. During the fabrication ofthe subperiosteal implant, theintraoral bar is incorporated tothe wax pattern and correspondsto the same bar dimensions of theDolder system.
Bar Length and Orientation
Root-form implants. The barorientation should be parallel tothe arbitrary transverse horizon-tal axis horizontally and sagit-taly.45,46 Because the plastic barpattern is fabricated at the time ofsurgery, the bar cannot be alignedparallel to the condylar compo-nents in the articulator. However,
the anterior occlusal plane of themaxillary complete denture andthe surgical template can be usedas the guides for horizontal andsagittal bar orientations, respec-tively. The bar should be parallelto the anterior occlusal plane ofthe maxillary complete dentureand perpendicular to the lineconnecting the lingual frenumand the midline of the surgicaltemplate.
Improper bar length can causeunfavorable force distribution,which may lead to peri-implantbone resorption.47 The optimalbar length has been postulatedas 18 to 23 mm, which corre-sponds to a distance of 22 to 27mm between the centers of theimplants.47 Nevertheless, this barlength may not be routinelyachieved because of anatomiclimitations such as the arch formand the location of the mentalforamen.
Subperiosteal implants. The lo-cation of the intraoral bar forsubperiosteal implants is basedon the evaluation of the CT scandata in relation to the radiogra-phic templates. The intraoral baris traced on the 3-D generatedmodel of the mandible followingspecific guidelines. The radi-opaque material present in theradiographic template aids in thelocation of the transmucosal poststhat interconnect the intraoral bar.The main advantage of this mo-dality is that the bar is an integralpart of the implant; it is attachedto it from the time of insertionand, in essence, is ready to receivea transitional overdenture imme-diately after surgery.
Implant Number and Distribution
Root-form implants. Althoughthe implant success rates of man-dibular overdentures supportedby 2 and 4 conventionally loadedimplants were not different,4,48–50
Jaime L. Lozada et al
Journal of Oral Implantology 303
Dow
nloaded from http://m
eridian.allenpress.com/joi/article-pdf/30/5/297/2033444/0686_1.pdf by guest on 13 February 2022

Rangert et al51suggested that loadtransferred to individual im-plants could vary because of thenumber of the implants and theirpositions. They have shown thatwhen implants are in line (usuallyin situations with 2 implants), thebending moment encountered ishigher than when the implantsare in configurations (eg, tripodor quadrilateral) that create off-sets. In immediate loading situa-tions, excessive load in anydirection can be detrimental. Toprovide the offset configurationas well as to allow anterior barorientation to be parallel to thetransverse horizontal axis, 4 im-plants may be the ideal minimumnumber.
Implant Position and Angulation
Root-form implants. The im-plants should be placed withinthe confines of the surgical tem-plate. To avoid any neurovascularinjury, the posterior implants areplaced approximately 5 mm an-terior to the mental foramina. Theanterior implants are positionedso that the optimal bar length isachieved without encroachinginto the tongue space, and thedistance between the centers ofthe anterior and posterior im-plants is at least 7 mm for hygienepurposes. During implant place-ment, the implant angulationshould be perpendicular to theocclusal plane to avoid any un-due overloading.52 The maxillarycomplete denture and surgicaltemplate can be used as guidesfor mesodistal and buccolingualimplant angulation, respectively.
Subperiosteal implants. The lo-cation of the implant posts as wellas the height of the bar in relationof to the crest of the ridge is‘‘prosthetically driven,’’ and, spe-cifically, the implant designs usedin this report were done accord-ing to the concepts outlined byJames et al.10
Clinical Outcomes
Root-form implants. Followingthe described protocol, whichwas approved by the InstitutionalReview Board of Loma LindaUniversity, a prospective studywas conducted on 5 patients.24
Twenty implants were placed,and all remained successfullyosseointegrated after 1 year ofloading. The mean marginal boneloss was 1.16 mm at 12 months.24
Although no major complica-tions or loss of osseointegrationwere encountered, a precaution-ary measure should be taken. Inthe case of early failures (less than3 months after the implant place-ment surgery) of 1 or more im-plants, it is recommended that theunaffected implants be left un-loaded until they are fully inte-grated for subsequent restorationin the conventional manner. Ifthe remaining implants are notadequate for supporting a man-dibular overdenture, more im-plants should be implementedaccordingly. The patient must beinformed of such a possibilitybefore the treatment.
The advantages of immedi-ately functional loaded implantprostheses include the shortertreatment time and the elimina-tion of the provisional stage aswell as the second-stage surgery.This article describes the surgicaland prosthodontic procedure ofthe immediately loaded mandib-ular implant bar overdenturealong with its clinical rationale.Although the high implant suc-cess rates reported with thistreatment modality might sug-gest that it is a viable and pre-dictable treatment option, carefulpatient selection and treatmentplanning are still as important asor even more important than thetreatment itself.
Achieving primary stabilityand maximizing the magnitude
and the rate of osseointegrationseem to be the key elements inachieving and maintaining os-seointegration in such situations.
Subperiosteal implants. Follow-ing the described protocol, whichwas approved by the InstitutionalReview Board of Loma LindaUniversity, a retrospective study(unpublished thesis) was con-ducted on the last 5 patientstreated with superiosteal im-plants from June 1995 to June2000 who had immediate oveden-tures in function for at least 3years. After 1 year of loading, all 5implants that were placed havesuccessfully provided immediatefunctional load since the day ofthe surgery. Bone loss aroundsubperiosteal dental implants isoften difficult to measure becauseof the metal superimpositionfrom the implant struts. Radio-graphs were taken of each im-plant post at implant placementand at 3-, 6-, 9-, and 12-monthintervals. The detectable meanmarginal bone loss was 1.2 mmat 1 year.
No major complications orloss of implants occurred; how-ever, some observations are inorder. It must be emphasized asreported previously that many ofthese implants required ‘‘minorcorrective’’ soft-tissue surgery. Inthis particular report, 3 of the 5implants placed required correc-tive surgery.
CONCLUSIONS
The surgical and prosthodonticprocedures for the immediatelyfunctional loadedmandibular im-plant overdentures described inthis article demonstrate the differ-ences between the 2 modalities.The subperiosteal implant modal-ity provides an overdenture thatis supported by the implant in itsentirety. The technique appears tobe highly sensitive and, apart
IMPLANT MODALITIES FOR MANDIBULAR IMPLANT OVERDENTURES
304 Vol. XXX/No. Five/2004
Dow
nloaded from http://m
eridian.allenpress.com/joi/article-pdf/30/5/297/2033444/0686_1.pdf by guest on 13 February 2022

from the information presentedhere, lacks documented repro-ducible data. The root-form im-plant overdenture modality usesthe retention given by the implantbar-and-clip system and partialsupport given by the edentulousridge. The technique is simplerand has been reproduced andreported by other clinicians.Within the limitations of thisarticle, both techniques achievethe goal of providing predictableimmediate function after surgery.
REFERENCES
1. Adell R, Eriksson B, Lekholm U,Branemark P-I, Jemt T. A long-termfollow-up study of osseointegrated im-plants in the treatmet of totally edentu-lous jaws. Int J Oral Maxillofac Implants.1990;5:347–359.
2. Naert I, Quirynen M, van Steen-berghe D. A six-year prosthodontic studyof 509 consecutively inserted implants forthe treatment of partial edentulism.J Prosthet Dent. 1992;67:236–245.
3. Andersson B, Odman P, LindvallAM. Single tooth restorations supportedby osseointegrated implants: results andexperiences from a prospective studyafter 2 to 3 years. Int J Oral MaxillofacImplants. 1995;10:702–711.
4. Jemt T, Chai J, Harnett J, et al. A 5-year prospective multicenter follow-upreport on overdentures supported byosseointegrated implants. Int J Oral Max-illofac Implants. 1996;11:291–298.
5. Albrektsson T, Branemark P-I,Hansson HA, Lindstrom J. Osseointe-grated titanium implants. Requirementsfor ensuring a long-lasting, direct bone-to-implant anchorage in man. Acta OrthopScand. 1982;52:155–170.
6. Branemark P-I. Osseointegrationand its experimental background. J Pros-thet Dent. 1983;50:399–410.
7. Babbush CA, Kent JN, Misiek DJ.Titanium plasma sprayed (TPS) screwimplants for the reconstruction of theedentulous mandible. J Oral MaxillofacSurg. 1986;44:274–282.
8. Schnitman PA, Shulman LB.Dental Implants: Benefit and Risk. NIHHarvard Consensus Development Con-ference, US Dept of Health and HumanSciences; 1980. Publication 81:1531.
9. James RA. Subperiostal implantdesign based on peri-implant tissuebehavior. NYJD. 1983;53:407–413.
10. James RA, Lozada JL, Truit PH,Foust BE, Jovanovic SA. Subperiostalimplants. J Calif Dent Assoc. January1988:10–14.
11. Minichetti JC. Analysis of HA-coated subperiosteal implants. J OralImplantol. 2003;3:111–116.
12. Lekholm U, Zarb GA. Patientselection and preparation. In: BranemarkP-I, Zarb GA, Albrektsson T, eds. Tissue-Integrated Prostheses. Osseointegration inClinical Dentistry. Chicago, Ill: Quintes-sence; 1985:199–210.
13. Misch CE. Contemporary ImplantDentistry. 2nd ed. St Louis, Mo: Mosby;1999:94–106.
14. James RA, Lozada JL, Truitt HP.Computer tomography (CT) applicationsin implant dentistry. J Oral Implantol.1991;17:10–15.
15. Tardieu PB, Vrielinck L, EscolanoE. Computer-assisted implant placement.A case report: treatment of the mandible.J Oral Maxillofac Implants. 2003;18:599–604.
16. Sarment DP, Al-Shammari K,Kazor CE. Stereolithographic surgicaltemplates for placement of dental im-plants in complex cases. Int J PeriodontRestor Dent. 2003;23:287–295.
17. Truit HP, James RA, Altman A,Boyne P. Use of computer tomography insubperiostal implant therapy. J ProsthetDent. 1988;59;474–477.
18. Buser DA, Shroeder A, Sutter F,Lang NP. The new concept of ITI hollow-cylinder and hollow-screw implants. Part2. Clinical aspects, indications, and earlyclinical results. Int J Oral Maxillofac Im-plants. 1988;3:173–181.
19. Schnitman PA, Wohrle PS, Ru-benstein JE. Immediate fixed interimprostheses supported by two-stagethreaded implants. Methodology andresults. J Oral Implantol. 1990;16:96–105.
20. Salama H, Rose LF, Salama M,Betts NJ. Immediate loading of bilateral-ly splinted titanium root-form implants infixed prosthodontics—a technique reex-amined: two case reports. Int J PeriodontRestor Dent. 1995;15:345–361.
21. Schnitman PA, Wohrle PS, Ru-benstein JE, DaSilva JD, Wang NH. Ten-year results for Branemark implantsimmediately loaded with fixed prosthe-ses at implant placement. Int J OralMaxillofac Implants. 1997;12:495–503.
22. Tarnow DP, Emtiaz S. Classi A.Immediate loading of threaded implantsat stage 1 surgery in surgery in edentu-lous arches: ten consecutive case reportswith 1- to 5-year data. Int J Oral MaxillofacImplants. 1997;12:319–324.
23. Chiapasco M, Gatti C, Rossi E,Haefliger W, Markwalder TH. MImplant
retained mandibular overdentures withimmediate loading. Clin Oral ImplantsRes. 1997;8:48–57.
24. Rungcharassaeng K, Lozada JL,Kan JYK, Campagni WV, Munoz CA.Marginal bone change around immedi-ately loaded threaded HA-coated im-plants: one-year results. Paper presentedat: 14th Annual Meeting of the Academyof Osseointegration; March 4–6, 1999;Palm Springs, Calif.
25. Truhlar RS, Lauciello F, MorrisHF, Ochi S. The influence of bone qualityon periotest values of endosseous dentalimplants at stage II surgery. J OralMaxillofac Surg. 1997;55:55–61.
26. Tricio J, van Steenberghe D,Rosenberg D, Duchateau L. Implantstability related to insertion torque forceand bone density; an in vitro study. JProsthet Dent. 1995;74:608–612.
27. Misch CE. Density of bone: effecton treatment plans, surgical approach,healing, and progressive bone loading.Int J Oral Implantol. 1990;6:23–31.
28. Jaffin RA, Berman CL. The exces-sive loss of Branemark fixtures in type IVbone: a five year analysis. J Periodontol.1991;62:2–4.
29. Engquist B, Bergendal T, KallusT, Linden U. A retrospective multicenterevaluation of osseointegrated implantssupporting overdentures. Int J Oral Max-illofac Implants. 1988;3:129–134.
30. Goodacre CJ, Kan JYK, Run-gcharassaeng K. Clinical complicationsof osseointegrated implants. J ProsthetDent. 1999;81:537–552.
31. Ivanoff CJ, Sennerby L, Johans-son C, Rangert B, Lekholm U. Influenceof implant diameters on the integrationof screw implants. An experimentalstudy in rabbits. Int J Oral MaxillofacSurg. 1997;26:141–148.
32. Ochi S, Morris HF, Winkler S. Theinfluence of implant type, material, coat-ing, diameter, and length on periotestvalues at second-stage surgery: DICRGinterim report no. 4. Dental ImplantClinical Research Group. Implant Dent.1994;3:159–162.
33. Block MS, Delgado A, FontenotMG. The effect of diameter and length ofhydroxylapatite-coated dental implantson ultimate pullout force in dog alveolarbone. J Oral Maxillofac Surg. 1990;48:174–178.
34. Gunne J, Jemt T, Linden B.Implant treatment in partially edentulouspatients: a report on prostheses after 3years. Int J Prosthodont. 1994;7:143–148.
35. Friberg B, Jemt T, Lekholm U.Early failures in 4,641 consecutivelyplaced Branemark dental implants:
Jaime L. Lozada et al
Journal of Oral Implantology 305
Dow
nloaded from http://m
eridian.allenpress.com/joi/article-pdf/30/5/297/2033444/0686_1.pdf by guest on 13 February 2022

a study from stage 1 surgery to theconnection of completed prostheses. IntJ Oral Maxillofac Implants. 1991;6:142–146.
36. Jemt T, Lekholm U. Implanttreatment in edentulous maxillae: a 5-year follow-up report on patients withdifferent degrees of jaw resorption. Int JOral Maxillofac Implants. 1995;10:303–310.
37. Brunski JB. Biomechanical fac-tors affecting the bone-dental implantinterface [review paper]. Clin Mater.1992;10:153–201.
38. Buser D, Nydegger T, Hirt HP,Cochran DL, Nolte LP. Removal torquevalue of titanium implants in the maxillaof miniature pigs. Int J Oral MaxillofacImplants. 1998;13:611–619.
39. Klokkevold PR, Nishimura RD,Adachi M, Caputo A. Osseointegrationenhanced by chemical etching of thetitanium surface. A torque removal studyin the rabbit. Clin Oral Implants Res.1997;8:442–447.
40. Wennerberg A, Ektessabi A,Alberktson T, Johansson C, AnderssonB. A 1-year follow-up of implants ofdiffering surface roughness placed inrabbit bone. Int J Oral Maxillofac Im-plants. 1997;12:486–494.
41. Wong M, Eulenberger J, SchenkR, Hunziker E. Effect of surface topologyon the osseointegration of implant mate-rials in trabecular bone. J Biomed MaterRes. 1995;29:1567–1575.
42. Lum LB, Beirne OR, Curtis DA.Histologic evaluation of hydroxyapatite-coated versus uncoated titanium bladeimplants in delayed and immediatelyloaded applications. Int J Oral MaxillofacImplants. 1991;6:456–462.
43. Ivanoff CJ, Sennerby L, LekholmU. Influence of mono-and bicorticalanchorage on the integration of titaniumimplants. A study in the rabbit tibia. Int JOral Maxillofac Surg. 1996;2:229–235.
44. Babbush CA. Titanium plasmaspray screw implant system for recon-struction of the edentulous mandible.Dent Clin North Am. 1986;30:117–131.
45. Zarb GA, Bolender CL, CarlssonGE. Boucher’s Prosthodontic Treatment forEdentulous Patients. 11th ed. St Louis, Mo:Mosby; 1997:522–523.
46. Spiekermann H, Donath K, Has-sel T, Jovanovic S, Richter J. Implantology.New York, NY: Thieme Medical;1995:152–159.
47. Hertel RC, Kalk W. Influence ofthe dimensions of implant superstructure
on peri-implant bone loss. Int J Prostho-dont. 1993;6:18–24.
48. Cune MS, de Putter C, Hoogstrat-en J. Treatment outcome with implant-retained overdenture: part I—clinicalfindings and predictability of clinicaltreatment outcome. J Prosthet Dent.1994;72:144–151.
49. Leimola-Virtanen R, Peltola J,Oksana E, Helenius H, Happonen RP.ITI titanium plasma- sprayed screw im-plants in the treatment of edentulousmandibles: a follow-up study of 39patients. Int J Oral Maxillofac Implants.1995;10:595–603.
50. Wismeyer D, van Waas MAJ,Vermeeren JIJF. Overdentures supportedby ITI implants: a 6.5-year evaluation ofpatient satisfaction and prosthetic after-care. Int J Oral Maxillofac Implants.1995;10:744–749.
51. Rangert BR, Sullivan RM, JemtTM. Load factor control for implants in theposterior partially edentulous segment.Int J Oral Maxillofac Implants. 1997;12:360–370.
52. Weinberg LA, Kruger B. A com-parision of implant/prosthesis loadingwith four clinical variables. Int J Prostho-dont. 1995;8:421–433.
IMPLANT MODALITIES FOR MANDIBULAR IMPLANT OVERDENTURES
306 Vol. XXX/No. Five/2004
Dow
nloaded from http://m
eridian.allenpress.com/joi/article-pdf/30/5/297/2033444/0686_1.pdf by guest on 13 February 2022
Copyright © 2022 FDOKUMEN