Rapid assessment of aortic regurgitation and left ventricular function using cine nuclear magnetic...
8
VAl.VUlAR HEAR7 DlSEASE Rapid Assessment of Aortic Regurgitation and Left Ventricular Function Using Cine Nuclear Magnetic Resonance Imaging and the Proximal Convergence Zone Gregory B. Cranney, MBBS, FRACP, Halima Benjelloun, MD, Gilbert J. Perry, MD, Chaim S. Lotan, MD, Jerry G. Blackwell, MD, Cecil H. Coghlan, MD, and GeraldM. Pohost, MD In patients with aortic regu@tation (AR), knowC edgeoftheseverityofAR,andthedegreeofleft ventticular (W) dysfunction are important for op timal mwagement. Previous nuclear metic msonanw (NMR) studii to - -- ters used multiple tomo@aphic planes that are ti-ming to obtain and analyze, and thus not coddhtive. In addiion, these studii 89 sessedtheseverityofARbylookingsimplyatthe sizeoftheregurgitWjet,aparametefthat* late8 only poorly to regur@tant volume. The PreQ ent study evaluates a rapid, singleglamt, tine NMR approach (scan time 40 minutes), and a new#adingsystemforARthatisbasedonthe presence,sizeandpersistenceofnotontythere gu#tant jet, but also the zone of proximal signal losaComparedwithcolorDopplermi phy (n q 42), the NMR approach detected AR with aspecificityoflOO%andasensitivityof95%. NMR regu@tant jet area correlated well with Cot orDoppler~rgitantjetarea(n=20;r=O.&p cO.Ol), but did not discriminate well between all ~ofARascompareulwithxrayconbastao+ to@aphy (n = 14). Using the new NMR grading c+ teria, AR @ade by NMR was in acco&nce with -ic #ade in 12 patients, differing by only 1 @ade in the remaining 2 patients. NMR @adewasinmncewithinl@adeofDopp ler in all patients compared (n q 20). LV volumes and ejection fraction using this singleplane ap preach correlated well with a previously validated, NMR biplane approach (r ~0.87; n q 18). The NMR appmach enables simuttaneous assessment of LV function and AR, using practical acquisition and analysis timea (Am J Cardiol1993371:10744OSl) From the Division of Cardiovascular Disease, Department of Medicine, University of Alabama at Birmingham, Birmingham, Alabama. Manu- script received March 23, 1992;revised manuscripted received and ac- cepted November 23,1992. Address for reprints: Gregory B. Cranney, MBBS, FRACP, De- partment of Cardiovascular Medicine, Prince Hemy Hospital, Univer- sity of New South Wales, Little Bay, New South Wales 2036, Austra- lia. I n patients with chronic aortic regurgitation (AR), se- rial evaluation of the severity of AR, but more im- portantly the degree of left ventricular (LV) dys- function, is used to guide medical management and de- termine the optimal time for valve replacement.14 Color Doppler echocardiographyvisualizes regurgi- tant jets and provides a semiquantitative noninvasive es- timate of the severity of AR.5 However, for LV volume determinations, echocardiography may not detect ade- quately the endocardial border.6p7 Radionuclide tech- niques, although providing a reliable measurement of LV ejection fraction,s are subjectto variable attenuationfac- tors that limit the accuracy and reproducibility of serial estimations of absolute LV volumes.9 Ultrafast tine computed tomography provides good spatial resolution, but uses ionizing radiation and radiopaque contrast,‘O and is unable to image regurgitant jets. In comparison, nuclear magnetic resonance(NMR), owing to its flow sensitivity11v12 and dimensional accura- Cy,13 can be used to both visualize regurgitant jets1”17 and determine accurately LV volumes1s-20 without us- ing contrast agentsor ionizing radiation. Most previous NMR studies to assess these parameters used multiple tomographic planes that are time-consuming to obtain and cumbersome to analyze,1419 and therefore not cost- effective. For assessing the severity of AR, NMR stud- ies have focused on the more obvious ventricular por- tion of the regurgitant jet. Recent phantom studies21,22 and 1 in vivo study23 suggestthat phenomenaassociat- ed with the proximal flow convergence region may de- scribe regurgitant flow more reliably. The present study evaluates a rapidly acquired, single-plane NMR strategy for: (1) obtaining LV volumes, (2) detecting the pres- ence of AR and (3) grading the severity of AR by using the proximal signal loss zone. METHODS Patients: Cardiovascular NMR studies using a sin- gle, angulated, LV outflow tract plane have been per- formed in our NMR facility since January 1988. Patients were included in the present study if they had a tine acquisition performed using this plane during their NMR imaging study and also had either color Doppler echocardiographicor contrast x-ray aortographic study within 16days (median 2) of the NMR examination. Pa- tients with atrial fibrillation, mechanicalprosthetic valves or recent myocardial infarction were excluded from the 1074 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 71 MAY 1,1993
-
Upload
hadassah-med -
Category
Documents
-
view
4 -
download
0
Transcript of Rapid assessment of aortic regurgitation and left ventricular function using cine nuclear magnetic...

VAl.VUlAR HEAR7 DlSEASE
Rapid Assessment of Aortic Regurgitation and Left Ventricular Function Using Cine Nuclear
Magnetic Resonance Imaging and the Proximal Convergence Zone
Gregory B. Cranney, MBBS, FRACP, Halima Benjelloun, MD, Gilbert J. Perry, MD, Chaim S. Lotan, MD, Jerry G. Blackwell, MD, Cecil H. Coghlan, MD, and Gerald M. Pohost, MD
In patients with aortic regu@tation (AR), knowC edgeoftheseverityofAR,andthedegreeofleft ventticular (W) dysfunction are important for op timal mwagement. Previous nuclear metic msonanw (NMR) studii to - -- ters used multiple tomo@aphic planes that are ti-ming to obtain and analyze, and thus not coddhtive. In addiion, these studii 89 sessedtheseverityofARbylookingsimplyatthe sizeoftheregurgitWjet,aparametefthat* late8 only poorly to regur@tant volume. The PreQ ent study evaluates a rapid, singleglamt, tine NMR approach (scan time 40 minutes), and a new#adingsystemforARthatisbasedonthe presence,sizeandpersistenceofnotontythere gu#tant jet, but also the zone of proximal signal losaComparedwithcolorDopplermi phy (n q 42), the NMR approach detected AR with aspecificityoflOO%andasensitivityof95%. NMR regu@tant jet area correlated well with Cot orDoppler~rgitantjetarea(n=20;r=O.&p cO.Ol), but did not discriminate well between all ~ofARascompareulwithxrayconbastao+ to@aphy (n = 14). Using the new NMR grading c+ teria, AR @ade by NMR was in acco&nce with -ic #ade in 12 patients, differing by only 1 @ade in the remaining 2 patients. NMR @adewasinmncewithinl@adeofDopp ler in all patients compared (n q 20). LV volumes and ejection fraction using this singleplane ap preach correlated well with a previously validated, NMR biplane approach (r ~0.87; n q 18). The NMR appmach enables simuttaneous assessment of LV function and AR, using practical acquisition and analysis timea
(Am J Cardiol1993371:10744OSl)
From the Division of Cardiovascular Disease, Department of Medicine, University of Alabama at Birmingham, Birmingham, Alabama. Manu- script received March 23, 1992; revised manuscripted received and ac- cepted November 23,1992.
Address for reprints: Gregory B. Cranney, MBBS, FRACP, De- partment of Cardiovascular Medicine, Prince Hemy Hospital, Univer- sity of New South Wales, Little Bay, New South Wales 2036, Austra- lia.
I n patients with chronic aortic regurgitation (AR), se- rial evaluation of the severity of AR, but more im- portantly the degree of left ventricular (LV) dys-
function, is used to guide medical management and de- termine the optimal time for valve replacement.14
Color Doppler echocardiography visualizes regurgi- tant jets and provides a semiquantitative noninvasive es- timate of the severity of AR.5 However, for LV volume determinations, echocardiography may not detect ade- quately the endocardial border.6p7 Radionuclide tech- niques, although providing a reliable measurement of LV ejection fraction,s are subject to variable attenuation fac- tors that limit the accuracy and reproducibility of serial estimations of absolute LV volumes.9 Ultrafast tine computed tomography provides good spatial resolution, but uses ionizing radiation and radiopaque contrast,‘O and is unable to image regurgitant jets.
In comparison, nuclear magnetic resonance (NMR), owing to its flow sensitivity11v12 and dimensional accura- Cy,13 can be used to both visualize regurgitant jets1”17 and determine accurately LV volumes1s-20 without us- ing contrast agents or ionizing radiation. Most previous NMR studies to assess these parameters used multiple tomographic planes that are time-consuming to obtain and cumbersome to analyze,1419 and therefore not cost- effective. For assessing the severity of AR, NMR stud- ies have focused on the more obvious ventricular por- tion of the regurgitant jet. Recent phantom studies21,22 and 1 in vivo study23 suggest that phenomena associat- ed with the proximal flow convergence region may de- scribe regurgitant flow more reliably. The present study evaluates a rapidly acquired, single-plane NMR strategy for: (1) obtaining LV volumes, (2) detecting the pres- ence of AR and (3) grading the severity of AR by using the proximal signal loss zone.
METHODS Patients: Cardiovascular NMR studies using a sin-
gle, angulated, LV outflow tract plane have been per- formed in our NMR facility since January 1988. Patients were included in the present study if they had a tine acquisition performed using this plane during their NMR imaging study and also had either color Doppler echocardiographic or contrast x-ray aortographic study within 16 days (median 2) of the NMR examination. Pa- tients with atrial fibrillation, mechanical prosthetic valves or recent myocardial infarction were excluded from the
1074 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 71 MAY 1,1993

study; 2 patients were also excluded because of poor image quality on tine NMR scans. Thus, this study co- hort comprised 46 patients (aged 19 to 79 years; 20 women and 26 men); 42 patients had color Doppler echocardiographic studies, and 14 had aortic root con- trast x-ray angiographic studies (10 had both). In addi- tion, studies from 18 patients, where both the previous- ly validated, biplane NMR scans and the single-plane NMR scan had been obtained, were used to compare LV volumes determined by these 2 approaches.
AOftiCltIOtX~~ Cineangiography was performed in 2 planes (45” right and 60” left anterior oblique with 15” cranial angulation) using 40 to 60 ml of meglumine diatrizoate (Renogralin 76%, Squibb) injected through an 8Fr pigtail catheter positioned 2 to 3 cm above the aortic valve. The severity of AR was graded on a scale of 1 to 5 using the method of Hunt et alz4
Doppler- . Color Doppler examina- tions were performed using commercially available sys- tems (Aloka 870, Hewlett-Packard 500 and Toshiba 16OA). Standard parastemal and apical long-axis views were obtained. The severity of AR by Doppler was graded using the previously validated ratio of jet height to LV outtIow tract diameter.5 Maximal regurgitant jet area was measured from the window that best showed the entire jet (usually apical view).
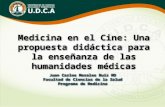
mGuREl.Aligmndofsinglesngulatedleffvsntrlwlar(Lv) 0utbwtractplane(botbm).Planeisdiiuaingcoronal Spitbscho image (top) as scout. Resulht image (battom) is PWpedculatoawanalscoutinYgeandinWsectsaorkic vdve (AV), and IeIt v-lsr outlIow tmct snd apex. LA=leftalxium;MV=mitralvalve;RV=~~.
formed consent was-obtained from all patients before NMR imaging. Studies were performed using a 1.5 Tesla imaging system (Philips Gyroscan, Best, the Nether- lands). Spin-echo scout images were used to determine the orientation of tine NMR planes. The LV outflow tract, long-axis plane was defined as the single angulat- ed plane that is perpendicular to the coronal plane, and intersects the aortic valve, and LV outtlow tract and apex (Figure 1). This plane is carefully positioned to pass through the apposition of the aortic valve leatlets so that the origin of a regurgitant jet is optimally visualized.
For validation of LV volumes obtained using this sin- gle plane, a recently validated biplane NMR approach was used.20 Accordingly, 2 additional long-axis planes (2-chamber and orthogonal 4-chamber) were obtained in 18 patients using methods previously described?0
Cine NMR acquisition parameters were as follows: pulse tlip angle 40 to 45”, echo time 12 to 15 ms, repeti- tion time 30 to 40 ms, 14 to 16 phases and slice thick- ness 8 to 10 mm. Images were obtained with 128 ma- trix resolution interpolated to 256 during reconstruction. The acquisition and reconstruction time for each tine NMR scan was approximately 9 minutes, depending on heart rate. For acquisition of only the coronal scout and single LV outflow tract plane, the time would be ~12 minutes.
-ofaolticregu~bycinenucle ~ma@K+tklWCtWKX Image analysis was performed in a blinded manner. NMR images were displayed in a cineloop for analysis. AR was diagnosed when an area of diastolic signal loss was visualized extending from the aortic valve into the left ventricle (Figure 2).
It is important to standardize window settings for vi- sualization and planimetry of both the jet25 and region of proximal signal loss. Initially images are displayed with the default reconstruction setting (i.e., they are scaled between 0.1 and 99.9% of all pixel intensities). To increase contrast between the jet and the blood pool
FlGURfi2.Leftvu&icularoutflowtmctimageinwhichaor- ticregu~Jetisshownwaread-~lless e-n%fmrn- ofiiiceintokftventWe(krge arow~.2onsofppximalsi&m!kmsisckmly~ onawticsideofaarticvslve(smsllerarrow~.
ASSESSMENT OF AORTIC REGURGITATION USING NMR 1075

TABLE I Grading Criteria for Aortic Regurgitation
Jet Proximal Zone
Max Size Persistence to ED Max Size Persistence to ED
I Small (< 5 cm2)* Never Not seen or small Never II Moderate (5-10 cm2) Not seen or small III Always Moderate (0.4-1.0 cm2) IV Large (> 1 cm2) Always (moderate to large
size) distinct neck
*Regurgitant jet must be visible in > 1 phase of diastole. ED = end-diastolic image; Jet = regurgitant jet seen in left ventricle; Max Size = maximal area of let or proximal zone at any
time during diastole (using standard window levels); areas (cm21 are given es guidelines only; observers did not planimeter areas to perform grading; Proximal Zone = proximal signal loss zone (must be typicallycircularor parbcular).
without increasing unduly the apparent size of the jets, an approach was used based on the following: For gra- dient echo images, the maximal signal intensity should always be in the flowing blood, whereas the minimal signal intensity should always be in the air (i.e., noise in the comers of the image). With our tine NMR acquisitions, the signal intensities in the blood are in the upper 50% of pixel intensities (except in regions of tur- bulence; e.g., jets). Therefore, we developed a standard- ized windowing method, such that the window level is
I
II
III
IV
MAX ED
FlQURE3.Leftvenbicularoutflowtractimagesobtained during-whsnJetisatmaxilnal(MAx)sizeandat ealddidole (ED) for muyin& grads8 of wrtic mom (AR) (I to lV). ha@ window 8ettingr m standardized (see text) to enhance ccntmst betwesn proxinlal signal loss ~and~,and~~ndinlJblood.IeMI(IIIrelpl~ntJet inkftventricuhrouMowbact,notseenatED;II=mode~ atesizemaxinlalJet,slnellatED;verysmallzolleoflJro~ malsi@dlossumbe~scen~&lll=modemteto~eJet thatis~ill~~#8nIlfED;~~,cireular,moderste Si*poxilll8lZOlWdUMlgClhStO@da+tde;XlmdzOneW~llOt
cledyseenbyED;lV=largeJettiriegBde,whichis stillmodemtetokgeatED;pnoximalzoneisl~,has distinctneckendisstillclearlyseenatED.
below the minimal blood pixel intensity, and the win- dow width is decreased to more easily define the bound- ary of the turbulence created by the jet. The window set- tings do not depend on the observer, and can be easily and rapidly obtained on the NMR viewing console: win- dow level = 0.5 X {maximum (blood intensity) - mini- mum (noise intensity)}; (window width = window level). The cardiac phases with the maximal areas of sig- nal loss for the jet and proximal zone were identified, and the corresponding areas underwent planimetry using software available on the system. The maximal length of the jet was also measured. The image representing end-diastole (cardiac phase 1, obtained approximately 20 ms after the R wave) was examined, and the presence and size of a regurgitant jet or zone of proximal signal loss were recorded. These findings were compared with AR grades obtained by x-ray aortography and color Doppler. A new grading system was developed, based on the presence, size and persistence of both the jet and the zone of proximal signal loss (Table 1 and Figure 3).
ventricular vdume dekmnination: LV volumes were determined from the 2- and 4-chamber planes us- ing the biplane area-length algorithm,20~26 and from the LV outflow tract plane using the single-plane algorithm (Figure 4)?6 Calculation of LV volumes from the single tine NMR plane could be performed in ~5 minutes.
Data analysk Collection and analysis of data from the various modalities were performed by independent, blinded investigators. NMR detection of AR was com- pared with color Doppler echocardiography. NMR max- imal jet area was correlated with color Doppler maxi-
ED FlGURE4.LeRventricularcutflowtractimagesatenddi~ tde (ED) and enhystole (ES), showing m and k@hs meiasumd. Left ventricular volumes ere calculated using sirr gieqlme, areah@h algcdthm.
1076 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 71 MAY 1, 1993

ma1 jet area. The NMR grade of AR was determined by was considered “trivial.” Thus, compared with Doppler, the consensus score of the 3 independent observers. the specificity of the single NMR plane approach for de- NMR grading (1 to 4) of AR was then compared with tection of AR was 100% and the sensitivity 95%. both color Doppler echocardiographic (1 to 4) and con- Camparisen of nuclear magnetii ramname jet trast aortographic (1 to 5) grading. Grades 4 and 5 by with &h~ Dopprer jet: In patients with AR (Table II contrast angiography were combined to facilitate com- and Figure 5) the maximal area of diastolic signal loss parison with NMR. LV volumes and ejection fraction by tine NMR correlated with (r = 0.81; p ~0.01) but was calculated from the single NMR plane were compared with the previously validated, biplane, tine NMR method.20
r--
TABLE II Patients with Aortic Regurgitation by Nuclear
Magnetic Resonance
Aortic Regurgitation Grade
Statistical methods: Data are expressed as mean + SD. The paired Student’s t test was used to test for sys- tematic differences between equivalent data. Least- squares regression was used where appropriate to corre- late corresponding data. Observer errors were expressed as the mean coefficient of variation or, in the case of ejection fraction, as the mean absolute difference be- tween observations.
RESULTS Data for patients who had AR detected by NMR are
listed in Table II. Heart rate did not differ signikantly for patients who had both studies (Doppler 76 + 12 vs NMR 76 _+ 13 beats/min; n = 20). However, heart rate during x-ray aortography was significantly greater than during the corresponding NMR studies (83 + 14 vs 74 f 12 beats/mm, p CO.01; n = 14).
-~aolticregu~by-~ netic resonmm NMR confimd the presence of AR in all patients (n = 14) who had contrast aortographic stud- ies performed. Because aortography is usually per- formed only when patients are known to have AR, it could not be used to assess the sensitivity of the NMR technique.
Of 42 patients with both NMR and Doppler studies, 20 had AR detected by both techniques, 21 had no AR by either technique, and 1 had AR by Doppler only. In the latter patient, AR was graded as <l/4 by Doppler and
Heart Rate NMR Pt. Age (yr) No. & Sex NMR CDE CATH A B C CDE CATH
1 56M 95 90 111 1 2 52 M 60 74 333 3 3 49F 80 84 333 2 4 71 F 8% 80 222 2 5 24M 93 90 343 3 6 61M 60 58 232 3 7 79M 55 62 222 2 8 54 M 80 82 222 2 9 2JF 73 74 334 4
10 56 F 80 70 222 1 11 75 F 75 63 84 1 1 1 1 12 66 F 90 92 87 444 3 13 69 F 70 76 80 444 3 14 62 M 57 60 70 222 1 15 25 M 72 79 86 444 4 16 61 M 76 72 84 222 1 17 84 F 103 98 114 111 1 18 37 M 80 82 96 232 3 19 38 F 55 50 58 332 2 20 64M 82 84 86 333 2 21 64 M 60 69 2 2 2 22 24M 70 98 3 3 3 23 67 F 75 86 2 2 2 24 62 M 65 70 3 3 3
CATH = contrast autography; CDE = color Doppler echocardiography; NMR = uclear magnetic resonance (3 independent observers: A, B and CL I
FlGlJRE5.colTcMhoflluclearmagne4- ic wwance (NMR) maximal jet wea with Dcppkr (CDE) maximal jet area (n=20; p <0.01; y=2.4 + 0.52 x).
2 5 4 3 5 2 1 2 3 3 2 3 2 3
201
r n 0.81 see - 2.4 cm2
z-
a
1 10
0 5
CDE JET ARE: (cm2) 20 25
1
ASSESSMENT OF AORTIC REGURGITATION USING NMR 1077

significantly less than the maximal jet area by color Doppler (8.0 + 3.9 vs 10.7 + 6.0 cm*; n = 20; p ~0.01, paired t test).
Comparisonbehveennuclear~B parametersand -I- Doppler lm@: Comparisons between Nh4R parameters and aortographic grade for both maximal and end-diastolic values are shown in Figure 6. NMR jet size (maximal and end-di- astolic) separates grade 1 from 2 and also grade 3 from 4, but does not separate grade 2 from 3. In contrast, the presence and size of the proximal signal loss zone does not separate grades 1 and 2 (as it may not be visible in either), but does separate adjacent grades 2, 3 and 4 both for maximal and end-diastolic values. Jet length does not appear useful for separating any adjacent grades.
Figure 7 shows the relation between NMR jet and proximal signal loss areas for varying grades of AR (de- termined by Doppler if aortography not available). This demonstrates a similar finding in that jet area does not separate grades 2 and 3, whereas proximal signal loss area does not separate grades 1 ‘and 2.
Devdopmentofanewgradingsystem*assee merit of ~OIGC m@t@atiom Based on these observa- tions, a new grading system was developed (Table I and Figure 3). The size of the jet by NMR was used to dis- criminate grade 1 from 2, 3 and 4, whereas the proxi- mal signal loss zone was used to discriminate between grades 2, 3 and 4. The persistence of these phenomena to end-diastole was most helpful in arbitrating border- line cases. After initial training, it is easy to appreciate the size of the jet and proximal signal loss zone. The numeric areas are shown as guidelines only because pla- nimetry of these areas was not necessary for semiquan- titative grading. This system was found to be easy to learn, and fast to use.
VaWation of new grading system: Three observers independently graded the severity of AR using the crite- ria listed in Table I. All images had been windowed as described. The observers focused on the image at end- diastole, and that showing the maximal jet and proximal signal loss zone size. The comparison between NMR grades for the 3 observers is shown in Table II. All ob-
MAX SIZE END-DIASTOLE
NUR JET AREA km’)
0’ 0 1 t s If@
CATH QRADE
NMR JET AREA bm’)
NMR JET LENGTH (mm)
FIGURE 0. Compaison of nuclear - resonance (NMR) re$ur& tantparameterewithaorticregur @tationgmdedetemIinedbycorr trast aottocpaphy (CAllI). Roth maximal (MAX) size at any time dwing diastole and at enddiastok are shown. PSL q proxind signal lo!ss zone.
1078 THEAMERICANJOURNALOFCARDIOLOGY VOLUME 71 MAY1,1993

servers agreed on the grade of AR in 19 of 24 patients; in the other 5 patients, the difference between the vary- ing observer and the other 2 was only 1 grade.
When compared with aortography in 14 patients, NMR grading agreed exactly in 12 patients and differed by only 1 grade in 2 patients (Table III). For the 20 pa- tients who had Doppler examinations and AR detected by NMR, the severity of AR by NMR agreed with
Doppler within 1 grade. In 9 patients the grades were identical, whereas in 11 the difference was 1 grade (Table IV).
Left ventricular volumes ad ejectii liacthm In 18 patients without regional wall motion abnormali- ties, LV volumes and ejection fraction, obtained using the single NMR plane, correlated well with the previ- ously validated biplane approach (Figure 8).
TABLE III Severity of Aortic Regurgitation (nuclear magnetic TABLE IV Severity of Aortic Regurgitation (nuclear magnetic resonance [NMRI vs aortographic grade) resonance [NMRl vs Doppler grade)
Aortography Doppler
n = 14 I II III IV/V
I 1 1 0 0
II 0 4 1 0 NMR
III 0 0 4 0
n = 42 0 I II Ill IV
0 21 1’ 0 0 0 I 0 3 0 0 0
NMR II 0 3 3 2 0 III 0 0 3 2 1 IV 0 0 0 2 1
* <l/IV by Doppler. IV 0 0 0 3
Aortography = contrast x-ray aortography.
FIGURE 7. ccnlparison of nuclear mag- netic maoname (NMR) jet area with proximal signal loss (Pa) mea for vary- ing #des of aortic regu@tatiOn (AR). GWk!3WW9-ll8dby~glWphy
(CATH;n=l4),orDoppler(CDE;n=lO) when aato@aphy was not available. Nu- Cl8iWlW@l6tiC~ncOj6t~does
notsepmategradeas2antl3,whemas lxEmnceandaixeofproximaleignallogs zonedoesnotseparategradesland2.
1
15 m
* 0
ox-.-- !..._.__ -i ..-- .-.-. % .-....
x
I
--
AR GRADE
by CATHICDE
I 0 I x II
L 0 Ill
* IV/V
0 2
EDV (ml) ESV (ml) EF 1%)
300 r - 0.94
see . 19 ml 250
60 w 100 150 ml *w
BIPLANE BIPLANE BIPLANE
1
FIGURE 8. Comlations of left venbicular volumes ad ejection fmction between si- (LVOT) and biplme nuckuw ms(pletic B method (n q 18; p 40.01). EDV P e&diastolic volume (y = -26 + 1.16 x); EF = eJecWn fraction (y = 7.7 + 0.87 x); Esv q enasystoric volume (y q -5.5 + 1.07 x).
ASSESSMENT OF AORTIC REGURGITATION USING NMR 1079

ob#wver Emmy Interobserver errors were as fol- lows: NMR jet area 13% and proximal signal loss area 16%; and single-plane end-diastolic volume lo%, end- systolic volume 11% and ejection fraction 6%. Intraob- server errors were as follows: NMR jet area 6% and proximal signal loss area 11%; and single-plane enddias- tolic volume 3%, end-systolic volume 8% and ejection fraction 4%.
DISCUSSION This study demonstrates the use of a readily applied,
single plane, tine NMR imaging approach for simulta- neous evaluation of LV volumes, and detection of the pres- ence and grading of severity of AR. This plane is compa- rable to the echocardiographic “parastemal long-axis” plane, and visualizes flow in the LV outflow tract and above the aortic valve, while at the same time displaying the left ventricle in a nonforeshortened perspective.
drcaprmant of aottk re@&Wk~ Because regur- gitant volume is difficult to quantitate, the severity of AR has been assessed indirectly by either contrast aor- tography24 or Doppler? Methods that rely on the regur- gitant jet are flawed, because jet area depends not only on the volume of regurgitant flow, but also the size and shape of the regurgitant orifice, and diastolic pressure gradient.27 This study supports this observation. Al- though the NMR regurgitant jet area correlated with the Doppler regurgitant jet area, it did not discriminate well between AR grades as compared with aortography. In comparison, the size of the proximal signal loss zone was a much better predictor of AR grade; this may be because this zone relates to the proximal flow conver- gence region that has been observed by both Doppler and NMR phantom studies.21,22
Physical basis for nuclear magnetic resonance si@al loas in proximal zone: As fluid approaches an orifice, the flow accelerates. It has been suggested that the isovelocity contours (surfaces) proximal to the ori- fice can be described by a series of hemispheres cen- tered around the orifice. *l The greater is the flow rate, the larger the hemisphere for a given isovelocity con- tour. Furthermore, if the isovelocity surfaces are hemi- spheres, then the flow rate through the oriice can be cal- culated if the radius of the hemisphere is known and if a single radial velocity is measured at a point on the hemisphere. Thus, it is clear that the greater the flow, the closer together the isovelocity contours are for a given distance from the orifice (i.e., the greater the spatial ac- celeration for a given distance from the orifice). It is likely that the main mechanism of reduction in NMR signal in this zone is due to spatial acceleration. Increas- ing spatial acceleration will cause a progressive spatial reduction in signal intensity. ** Thus, the greater the flow rate, the further from the orifice that a spatial acceleration threshold is reached and signal loss begins to occur. This mechanism would account for a direct relation between the flow rate through the orifice and the size of this prox- imal signal loss zone at any given window setting.
Difficulty visualizing small proximal signal loss zones relates to their size with respect to slice thickness and plane alignment. A small proximal signal loss zone will have a smaller diameter than the slice thickness and
thus may be obscured or missed if the plane is not per- fectly aligned during diastole. In contrast, the large prox- imal signal loss zones will always be easily visualized, even if the plane is not perfectly aligned.
persistence of proximal m void: Initial consider- ations may suggest that in patients with more severe AR, the persistence of a visible, moderate sized, signal void at end-diastole is contradictory to data obtained by con- tinuous-wave Doppler. In patients with mild AR, there is a high pressure gradient at end-diastole, and thus the velocity through the regurgitant orifice may be greater at end-diastole than in patients with more severe AR. This is manifest by the flatter deceleration slope of the velocity versus time Doppler spectra in mild AR. How- ever, this does not mean that flow is necessarily high at end-diastole in these patients. Conversely, these patients have small regurgitant orifices, and therefore the flow is probably very low at end-diastole.
In contrast, the proximal convergence zone and hence the size of the proximal NMR signal void are re- lated to the flow rate and not the velocity at the orifice. Thus, the presence of a moderate sized, NMR signal void at end-diastole indicates that the flow rate is still significant at that time. Because the regurgitant volume depends not only on the size of the regurgitant orifice but also the duration of AR, this NMR phenomena can logically be associated with more severe grades of AR. This is also consistent with the clinical observation that the duration of the diastolic murmur correlates with the severity of AR.
DifFerence in jet area by nudear magnetic rem nance and color Doppler: Although the NMR regurgi- tant jet area correlates with the Doppler jet area, the NMR jet area tended to be smaller, and in 1 patient with trivial AR, was not visualized at all by NMR. Two hy- potheses may be postulated to explain this observation. First, this difference in measured jet size may be because in Doppler studies, the imaging plane is angled interac- tively to optimize visualization of the maximal jet area, whereas the NMR plane is lixed in advance. Thus, whereas the aortic regurgitant jet is consistently detect- ed by NMR, the full extent of the jet may not be visu- alized if the jet is eccentric.
Alternatively, it is possible that the NMR jets were smaller owing to different properties of the flow distur- bance being examined by the 2 techniques. The signal loss that results in NMR visualization of the regurgitant jet most likely occurs owing to spatial acceleration and deceleration, with subsequent dephasing of spin~.*~-~~ Contrary to previous beliefs, high, constant velocity flow in smooth straight tubes by itself does not cause NMR signal loss, even at high Reynold’s numbers (19,000),28-30 and thus only the most disturbed region of the regurgi- tant jet may be visualized by NMR. In contrast, color Doppler detects the regurgitant jet by its high velocity and abnormal direction. The color Doppler jet encom- passes both a high velocity inner core (which is dis- played as a mosaic of red and blue due to aliasing) and a lower velocity outer layer. The lower velocity outer layer may also consist of flow that has been entrained into the jet from the surrounding blood. Thus, the NMR jets may have been smaller than the color Doppler jets,
1080 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 71 MAY 1,1993

because only the inner portion of the jet has sufficient acceleration and deceleration to cause NMR signal loss, whereas the whole of the regurgitant jet is detected by Doppler.
PotdidlimitaWnsofthism4cleam8@mticrese m method: Patients with ahial fibrillation present problems with current NMR gating strategies and produce inconsistent image quality. Mechanical valves cause re- gional signal loss and often have periprosthetic jets when regurgitant. Severe regional wall motion abnormalities im- pair the accuracy of single-plane LV volumes, and in these circumstances it would be preferable to use either a biplane long-axis2o or stacked-slicelg NMR approach.
It is well known by echocardiographers that a single plane may not visualize optimally an eccentrically directed regurgitant jet. This occurs particularly with mitral regur- gitation where the receiving chamber (left atrium) is large. It is less problematic with AR, where the LV outflow tract, which must contain the proximal portion of the jet, is rel- atively narrow with respect to the thickness of the imaging slice. In 1 of our patients with severe AR, the regurgitant jet was very eccentric and only moderate in size; howev- er, the proximal zone and neck were clearly seen and large, so that it was clear that this patient had grade 4 AR. It ap pears that the proximal signal loss zone is less affected by eccentrically directed jets, unless the regurgitant orilice is located near the edges of the valve (i.e., a lateral perfora- tion or tear).
The area of signal loss in jets is dependent on the echo time used during acquisition.30 We have found that for echo times in the range used in this study (12 to 15 ms), the differences in signal loss area are only on the order of 5%.30
Conclusion: This study demonstrates the use of a single-plane tine NMR approach for the simultaneous assessment of LV function and AR. This approach may be useful when performed in conjunction with NMR studies for evaluation of the thoracic aorta or when seri- al noninvasive evaluation of patients with AR is need- ed. Further studies examining standard windowing meth- ods in different NMR imaging systems are desirable for general application
.Adu~~wled@nent: We wish to gratefully acknowl- edge Navin C. Nanda, MD, for assistance with super- vising and performing Doppler studies, Kristin Adams, BS, for assistance with analysis, Patty Bischoff, RT, CNMT, for technical assistance in obtaining NMR data, Shirley Nolen for secretarial support, Mary Lou Camp, BS, for organizational support, Bruce Carter, ASEE, for maintenance of the NMR system, and Mohammed Benomar, MD, FACC, for support of Dr. Benjelloun during her fellowship at the University of Alabama at Birmingham.
1. Henry WL, Bonow RO, Borer JS, Ware JH, Kent KM, Redwood DR, Mcln- tosh Cl, Morrow AG, Epstein SE. Observations on the optimum time for operative intervention for aortic regurgitation. I. Evaluation of the results of aomic valve re- placement in symptomatic patients. Circulrrrion 1980;61:471483. 2. Borow KM, Green LH, Mann T, Sloss LJ, Braunwald E, Collins JJ, Cohn L, Grossman W. End-systolic volume as a predictor of postoperative left ventricular perfotmance in volume overload from valvular regurgitation. Am J Med 1980;68: 655Jj63. 3. Bonow RO, Rosing DR, Kent KM, Epstein SE. Timing of operation for chron- ic aortic regurgitarion. Am J CardioL 1982;50:325-336.
4. Carabello BA, Usher BW, Hendrix GH, Assey ME, Crawford FA, Leman RB. Predictors of outcome for aottic valve replacement in patients with aattic regurgi- tation and left ventricular dysfunction: a change in the measuring stick. J Am Coil Cardiol 1987;10:991-997. 5. Perry GJ, Helmcke F, Nanda NC, Byard C, Soto B. Evaluation of aottic insuf- ficiency by Doppler color flow mapping. J Am Coil Cardiol 19879~952-959. 6. Schiller NB, Acquatella H, Potts TA, Gocrke J, Ringettz H, Silverman NH, Bmndage B, Botvinick EH, Bowel1 R, Carlsson E, Parmley WW. Left venhicu- lar volume from paired biplane two-dimensional echocardiography. Circulorion 1979;60:547-555. 7. FoIland ED, Parisi AF, Moynihan PF. Jones RD, Feldman CL, Tow DE. As- sessment of left ventricular ejection fraction and volumes by real time hvo-dimen- sional echocardiography. Circulation 1979;60:76C-766. 8. Wackers FJT, Berger H, Johnstone DE, Goldman L, Reduto LA, Langou RA, Gottschalk A, Zaret BL. Multiple gated cardiac blood pool imaging for left ven- tricular ejection fraction: validation of the technique and assessment of variability. Am J Cardiol 1979;43: 1159-l 166. 9. Massie BM, Kramer BL, Gettz EW, Henderson SG. Radionuclide measurement of left ventricular volume: comparison of geometric and count-based methods. Cir- cdafion 1982;65:725-730. 10. Reiter SJ, Rumberger JA, Feiring AJ, Stanford W, Marcus ML. Precision of measurements of right and left ventricular volume by tine computed tomography. Circularion 1986;74:89&903. 11. Lotan CS, Cranney GB, Pohost GM. Cine NMR: an emerging technology. Echocardiography 1988;5:373-382. 12. Cranney GB, Lotan CS, Pohost GM. Nuclear magnetic resonance imaging for assessment and follow-up of patients with valve disease. Circulation 1991;84(suppl 1):216227. 13. Longmore DB, Underwood SR, Bland C, Hounsfield GN, Poole-Wilson PA, D&son D, Klipstein RH, Fi DN, Watanabe M, Fox K, Rees RSO, McNeilly AM. Dimensional accuracy of magnetic resonance in stadies of the heart. Lancer 1985;1:1360-1362. 14. Schiebler M, Axe1 L, Reichek N, Amigemma G, Yeager B, Douglas P, Bogin K, Kressel H. Correlation of tine MR imaging with two-dimensional pulsed Doppler echocardiography in valvular insuftXency. J Compur Assist Tomogr 198x11: 627-632. 15. Utz JA, H&kens RJ, Heinsimer JA, Shimakawa A, Glover G, Pelt N. Valvu- lar regurgitation: dynamic MR imaging. Radiology 1988; 168:91-94. 18. Pflugfelder PW, Landzberg IS, Cassidy MM, Cheitlin MD, Auffennan W, Hig- gins. Comparison of tine MR imaging with Doppler echocardiography for the eval- uation of aottic regurgitation. AJR Am J Roenrgenol 1989;152:729-735. 17. Aurigemma G, Reichek N, Axel L. Evaluation of mitral regurgitation by tine magnetic resonance imaging. Am J Cardial 1990;66:621-625, 18. Baser FT. Aufferman W, Holt WW, Wagner S, Kircher B, Wolfe C, Higgins CB. Noninvasive evaluation of global left ventricular function with use of tine nu- clear magnetic resonance. J Am Coil Cardiol 1989;13: 1294-1300. 19. Sechtem U, pflugfelder PW, Gould RG, Cassidy MM, Higgins CB. Mea- surement of tight and left ventricular volumes in healthy individuals with tine MR imaging. Radiology 1987; 163:697-702. 20. Cranney GB, Lotan CS, Dean L, Baxley W, Bouchard A, Pohost GM. Left venhicular volume measurement using cardiac axis NMR imaging-validation by calibrated ventricular angiography. Circularion 1990;82: 154-163. 21. Recusani F, Bargiggia GS, Yoganathan AP, Raisam A, Valdes-Cmz LM, Sung HW, Bettucci C, Gallati M, Moises VA, Simpson IA, Tromconi L, Sahn DJ. A new method for quantification of regurgitant flow rate using color Doppler flow imaging of the flow convergence region proximal to a discrete orifice. An in vitro study. Circularion 1991:83:594-604. 22. Cranney GB, Walker FG, Cape EG, Pohost GM, Yoganathan AP. Mapping of flow fields proximal to regurgitant orifices using NMR phase velocity encodiig. In: SMRM Annual Meeting Book of Abstracts. Berkeley, California: Society of Magnetic Resonance in Medicine, 1990: 1176. 23. Yoshida K, Yoshikawa J, Hozumi T, Akasaka T, Minagoe A, Nakajima H, Miyamoto T. Assessment of aortic regurgitation by the acceleration flow void prox- imal to the leaking orifice in tine magnetic resonance imaging. Cimrlarion 1991:83:1951-1955. 24. Hunt D, Baxley WA, Kennedy JW, Judge TP, Williams JE, Dodge JT. Quan- tttative evaluation of cineaortography in the assessment of aottic regurgitation. Am J Cardiol 1973;31:696-700. 21. Suzuki J, Caputo GR, Kondo C, Higgins CB. Cine NMR imaging of valvular heart disease: display and imaging parameters affect the size of the signal void caused by valvular regurgitation. AJR Am J Roenrgenol 1990;155:723-727. 26. Grossman W, ed. Cardiac Catheterization and Angiography. 3rd ed. Phila- delphia: Lea & Febiger, 1986:282-289. 27. Simpson IA, Valdes-Cmz LM, Sahn DJ, Muillo Azucena, Tamura T, Chug KJ. Doppler color flow mapping of simulated in vitro regurgitant jew evaluation of the effects of orifice sire and hemodynamic variables. J Am Coil Cardio/ 1989; 13:1195-1207. 28. Poiseau E, Yoganathan AP, Cranney GB. Flow imaging with phase velocity encoding: in vitro study (absu). Radiology 1989; 173(suppl):47. 29. Evans AJ, Blinder RA, He&ens RJ, Spritzer CE, Kuethe DO, Fram EK, Hed- lurid LW. Effects of turbulence on signal intensity in gradient echo images. Invest Radio/ 198X:23:512-518. 30. Cranney GB, Gunter BC, Pohost GM. Mechanism of gradient echo NMR sig- nal loss in a stenotic phantom. In: SMRM Annual Meeting Book of Abstracts, Berkeley, California: Society of Magnetic Resonance in Medicine, 1989; 1:203.
ASSESSMENT OF AORTIC REGURGITATION USING NMR 1081