A comparative clinical study to evaluate the efficacy of ...
Upload
khangminh22Category
view
0download
0
RADIOLOGIC TECHNIQUES USED TO EVALUATE THETEMPOROMANDIBULAR JOINT; I. Conventional Methods
David Roberts, Ph.D.,* James Pettigrew, D.M.D.,**Carol Ram, B.S.N., Peter M. Joseph, Ph.D.***
*Department of Oral Medicine,** School of Dental Medicine, University of Pennsylvania,Philadelphia, Pa.,*** Department of Radiology, School of Medicine, University of Pennsylvania,Philadelphia, Pa.
SUMMARYSymptoms of temporomandibular joint pathology are present in a relatively high proportion of
the population. Conventional radiographic techniques used to evaluate the morphology of thejoint provide data which may be difficult to interpret. These techniques are reviewed briefly andtheir interpretational shortcomings are noted. Computed tomography is currently being used bysome clinicians to evaluate the joint. This technique may also yield data which are difficult tointerpret. Extended processing of CT data to provide three-dimensional images of the jointenhances the technique as a means of diagnosing hard tissue pathology, but despite reports inthe literature detailing its use in diagnosing soft tissue pathology, CT is not optimal for this pur-pose. The introduction of nuclear magnetic resonance imaging provides a means of examiningthe soft tissues of the joint in either two- or three-dimensional images and has the advantageover all previous techniques in that the patient is not subjected to ionizing radiation during thescan process.
KEY WORDSTemporomandibular joint, radiographic evaluation, conventional radiography, computed tomography, threedimensional imaging, nuclear magnetic resonance
INTRODUCTIONThe incidence of clinical symptomatology
thought to be associated with the temporoman-dibular joint (TMJ) is estimated to be as high as28% in some modern adult populations.1 Thesymptomatology may vary from apparently in-nocuous crepitation of the joint, to a series of broadsyndromes which appear to be progressive interms of both the number of symptoms and the in-tensity of their manifestation. In the later stages ofthe development of such syndromes some or all ofthe following symptoms may be included: intenseintracapsular pain, crepitation and clicking of thejoint, limited ability to open the jaw, deviation ofthe jaw to one side on opening, painful jaw andcervical musculature prone to spasticity, deep,extracapsular facial pain, general neuralgia, and
Accepted for publication July 10, 1984.Address reprint requests to Dr. Roberts, 4001 Spruce Street,
Philadelphia, PA 19104.
various symptoms apparently related to the func-tion of the vestibulo-acoustic systems. The patientmay become completely disabled.2.3.4The evidence for causal relationships between
symptoms and observable intracapsular path-ology is contradictory. In some cases jointcrepitation and clicking, intracapsular pain andlimited jaw function is associated with ratherspecific pathologic conditions, including softtissue derangement (displacement of the car-tilagenous disk)5, and various forms of arthriticchanges.6 In other cases, despite the evidenceof symptoms, no overt pathology is detectable,but the joint relationships may be suspect;localised regions of the joint space may be con-sidered too narrow or too wide; or, the articulareminence may be considered too steep. In stillother cases, the joint may appear to be entirelynormal.1,2,7,8Where intracapsular pathology can be
detected, it is possible to intervene directly viasurgery. The surgical procedures include diskrepositioning or removal, various forms of con-
SEPTEMBER/OCTOBER 1984 197
dylectomy, surgical reshaping of the eminence,and the introduction of prostheses.9
In the current state of the art it is therefore in-cumbent upon the dental clinician or dental diag-nostic radiologist to determine the presence or ab-sence of joint pathology in subjects displaying theappropriate symptoms. Various radiographic tech-niques have been developed and are now con-sidered part of the conventional diagnostic arma-mentarium. Although widely used, these tech-niques have some shortcomings, the chief of whichis that the data they yield often are difficult tointerpret.10The underlying interpretational problem is that,
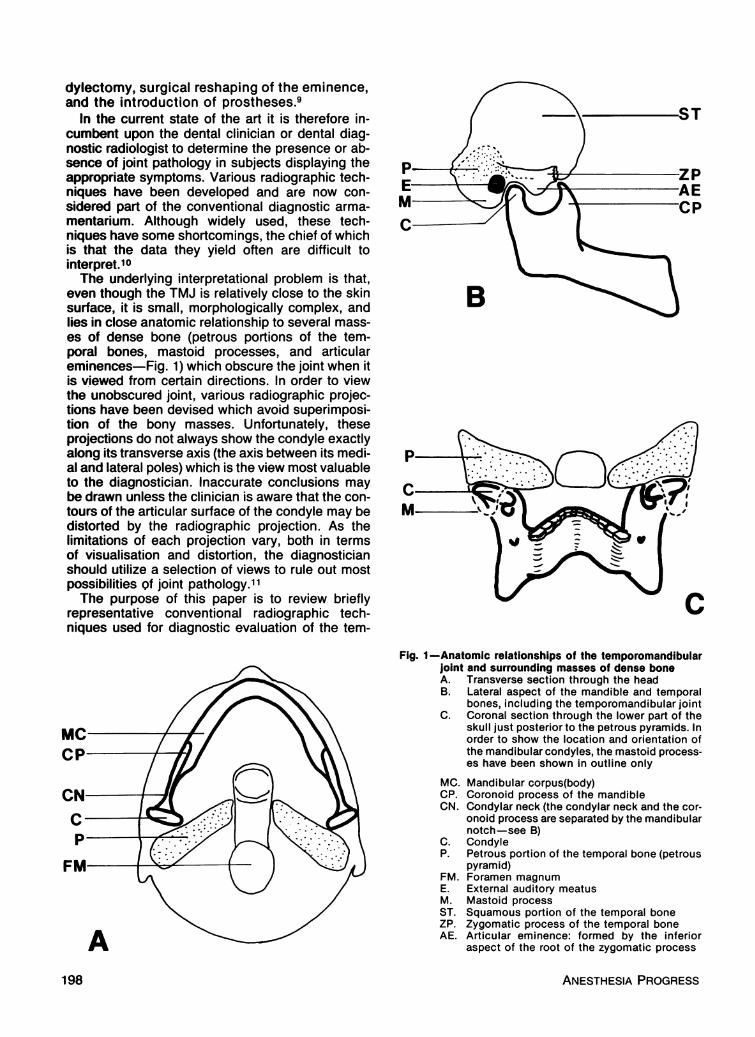
even though the TMJ is relatively close to the skinsurface, it is small, morphologically complex, andlies in close anatomic relationship to several mass-es of dense bone (petrous portions of the tem-poral bones, mastoid processes, and articulareminences-Fig. 1) which obscure the joint when itis viewed from certain directions. In order to viewthe unobscured joint, various radiographic projec-tions have been devised which avoid superimposi-..- .. . . . . . . .ltion ot tne bony masses. unTortunately, tneseprojections do not always show the condyle exactlyalong its transverse axis (the axis between its medi-al and lateral poles) which is the view most valuableto the diagnostician. Inaccurate conclusions maybe drawn unless the clinician is aware that the con-tours of the articular surface of the condyle may bedistorted by the radiographic projection. As thelimitations of each projection vary, both in termsof visualisation and distortion, the diagnosticianshould utilize a selection of views to rule out mostpossibilities of joint pathology.11The ouroose of this Daner is to review briefiv-"_ * - %... r wr .11 torepresentative conventional radiographic tech-
niques used for diagnostic evaluation of the tem-
Fig. 1-Anatomic relationships of the temporomandibularjoint and surrounding masses of dense boneA. Transverse section through the headB. Lateral aspect of the mandible and temporal
bones, including the temporomandibular jointC. Coronal section through the lower part of the
skull just posterior to the petrous pyramids. Inorder to show the location and orientation ofthe mandibular condyles, the mastoid process-es have been shown in outline only
MC. Mandibular corpus(body)CP. Coronoid process of the mandibleCN. Condylar neck (the condylar neck and the cor-
onoid process are separated by the mandibularnotch-see B)
C. CondyleP. Petrous portion of the temporal bone (petrous
pyramid)FM. Foramen magnumE. External auditory meatusM. Mastoid processST. Squamous portion of the temporal boneZP. Zygomatic process of the temporal boneAE. Articular eminence: formed by the inferior
. r . . r . . ..... ~-am% aspect ofthe root ot the zygomatic process
ANESTHESIA PROGRESS198
poromandibular joint, and to describe and discussthe potential of new, alternative techniques such ascomputed tomography (CT) and nuclear magneticresonance (NMR) imaging which yield more readilyinterpretable data.
CURRENT TECHNIQUES INDIAGNOSTIC RADIOLOGY
Conventional radiographic techniques includeplain film radiography (transcranial, transpharyn-geal and anterior-posterior projections) and vari-ous forms of tomography-including panoramic.Contrast arthrography with or without fluoroscopyand tomography are specialized techniques usedmainly to diagnose meniscal derangements.
Generally, conventional diagnostic radiologyof the TMJ seeks to detect and evaluate devia-tions in joint relationships and in the mor-phology, structure and function of the jointcomponents-principally the mandibular con-dyle. Many studies have been published whichcompare conventional techniques and formulaterecommendations regarding which view shouldbe used in specific clinical situations.1213,14,15The criteria for selection of radiographic pro-cedures are based in part on the available clinicalfindings, and the nature of the suspectedpathology. Further limitations may be imposedby the availability of special radiographic equip-ment and expertise. Although the radiation dosefor each of the techniques is relatively low,cumulative risk/benefit factors need to be con-sidered, especially in the younger patient. Final-ly, selection of techniques may be influenced bythe clinician's preference for a specific view onthe basis of the ease with which they feel thedata may be interpreted. Some diagnosticiansprefer transcranial techniques because the com-plete joint is shown in a single view, whereasothers feel that the absence of image superim-position in tomograms compensates for thesegmented data they offer.
Madsen,16 attemped to outline the goals ofthe ideal TMJ radiographic technique. It shouldinclude: 1. demonstration of all parts of the jointwith minimal distortion; 2. simultaneous depic-tion of both joints; 3. patient comfort and naturalposture; and 4. accuracy sufficient to permitreproducible images over time. It has become in-creasihgly obvious that no single technique cansatisfy all of these goals.
In conventional radiography, the x-ray beampasses through all the structures interposed be-tween its source and the x-ray film. This inevitablyresults in superimposition of structures. However,various subtechniques have been devised tominimize the effect of superimposition, allowing im-
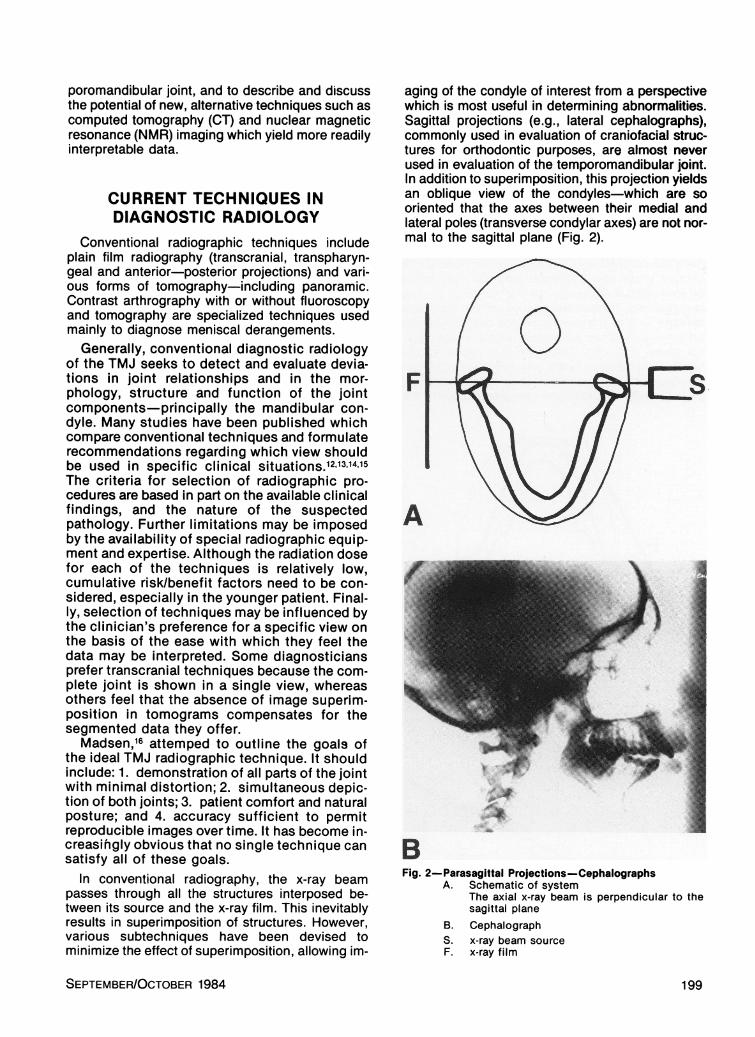
aging of the condyle of interest from a perspectivewhich is most useful in determining abnormalities.Sagittal projections (e.g., lateral cephalographs),commonly used in evaluation of craniofacial struc-tures for orthodontic purposes, are almost neverused in evaluation of the temporomandibular joint.In addition to superimposition, this projection yieldsan oblique view of the condyles-which are sooriented that the axes between their medial andlateral poles (transverse condylar axes) are not nor-mal to the sagittal plane (Fig. 2).
F
A
BFig. 2-Parasagittal Projections-Cephalographs
A. Schematic of systemThe axial x-ray beam is perpendicular to thesagittal plane
B. CephalographS. x-ray beam sourceF. x-ray film
SEPTEMBER/OCTOBER 1984
1.
199
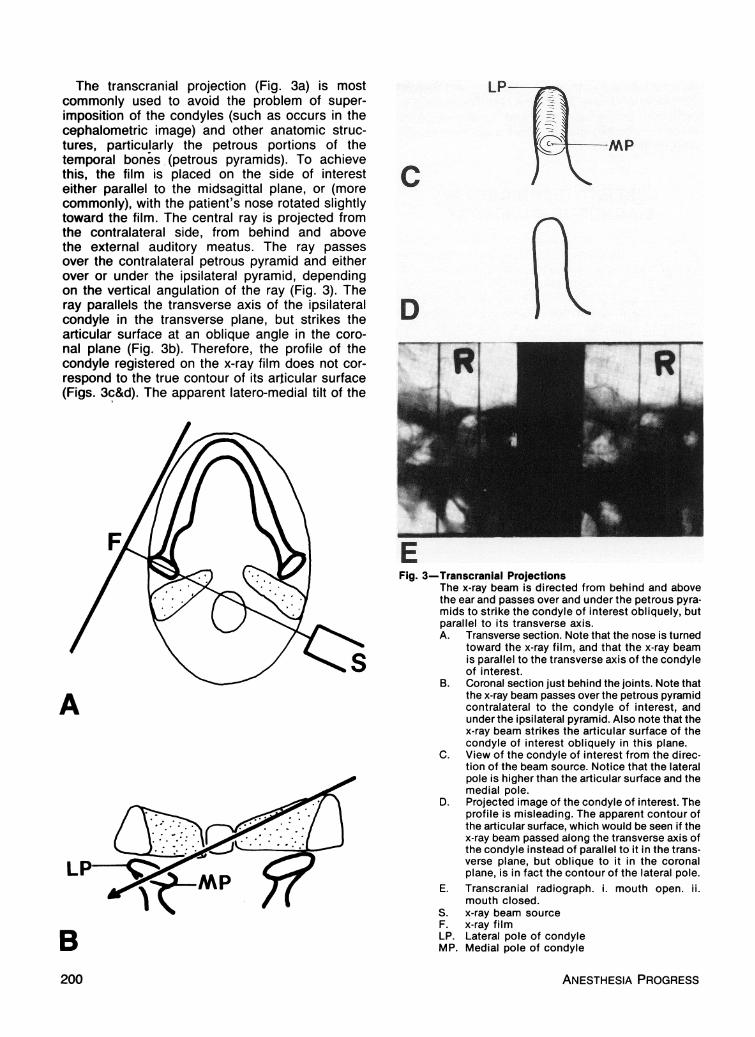
The transcranial projection (Fig. 3a) is mostcommonly used to avoid the problem of super-imposition of the condyles (such as occurs in thecephalometric image) and other anatomic struc-tures, particu!arly the petrous portions of thetemporal bones (petrous pyramids). To achievethis, the film is placed on the side of interest
-: L- -L L --I _ C _ _elther parallel to the mlasagittal plane, or (more -
commonly), with the patient's nose rotated slightlytoward the film. The central ray is projected fromthe contralateral side, from behind and abovethe external auditory meatus. The ray passesover the contralateral petrous pyramid and eitherover or under the ipsilateral pyramid, dependingon the vertical angulation of the ray (Fig. 3). Theray parallels the transverse axis of the ipsilateralcondyle in the transverse plane, but strikes theartiullnr slirface at an ohlin,Iannnle in the onrn-
-MP
LAN &11¥L11ILAN ¥¥A I%¥ V.__.__ A.L ..I ¥II.I 11. , ..11 I.Li _1¥nal plane (Fig. 3b). Therefore, the profile of thecondyle registered on the x-ray film does not cor-respond to the true contour of its articular surface(Figs. 3c&d). The apparent latero-medial tilt of the
EFig. 3-Transcranial Projections
The x-ray beam is directed from behind and abovethe ear and passes over and under the petrous pyra-mids to strike the condyle of interest obliquely, butparallel to its transverse axis.A. Transverse section. Note that the nose is turned
toward the x-ray film, and that the x-ray beamis parallel to the transverse axis of the condyleof interest.
B. Coronal section iust behind the ioints. Note thatthe x-ray beam passes over the petrous pyramidA contralateral to the condyle of interest, andunder the ipsilateral pyramid. Also note that thex-ray beam strikes the articular surface of thecondyle of interest obliquely in this plane.
C. View of the condyle of interest from the direc-tion of the beam source. Notice that the lateral
-I ! L Al i1.I ..o .Z Ii_JLLpole is nigner tnan mte articular surface ana tnemedial pole.
D. Projected image of the condyle of interest. Theprofile is misleading. The apparent contour ofthe articular surface, which would be seen if thex-ray beam passed along the transverse axis ofthe condyle instead of parallel to it in the trans-verse plane, but oblique to it in the coronalplane, is in fact the contour of the lateral pole.
E. Transcranial radiograph. i. mouth open. ii.mouth closed.
S. x-ray beam sourceF. x-ray filmLP. Lateral pole of condyleMP. Medial pole of condyle
ANESTHESIA PROGRESS200
condyle axis means that the clinician sees thesurface of the lateral pole, rather than that of thecentral-potentially load-bearing portion of thearticular surface where morphological anomaliesare most likely to occur.Another approach is to use a transpharyngeal
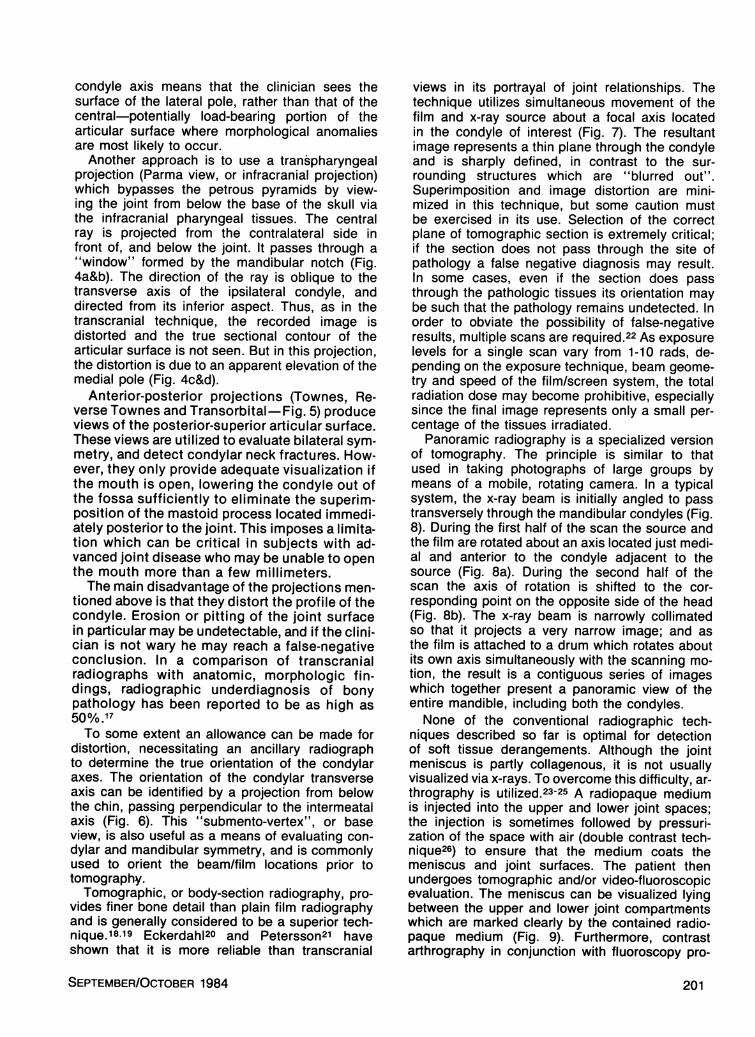
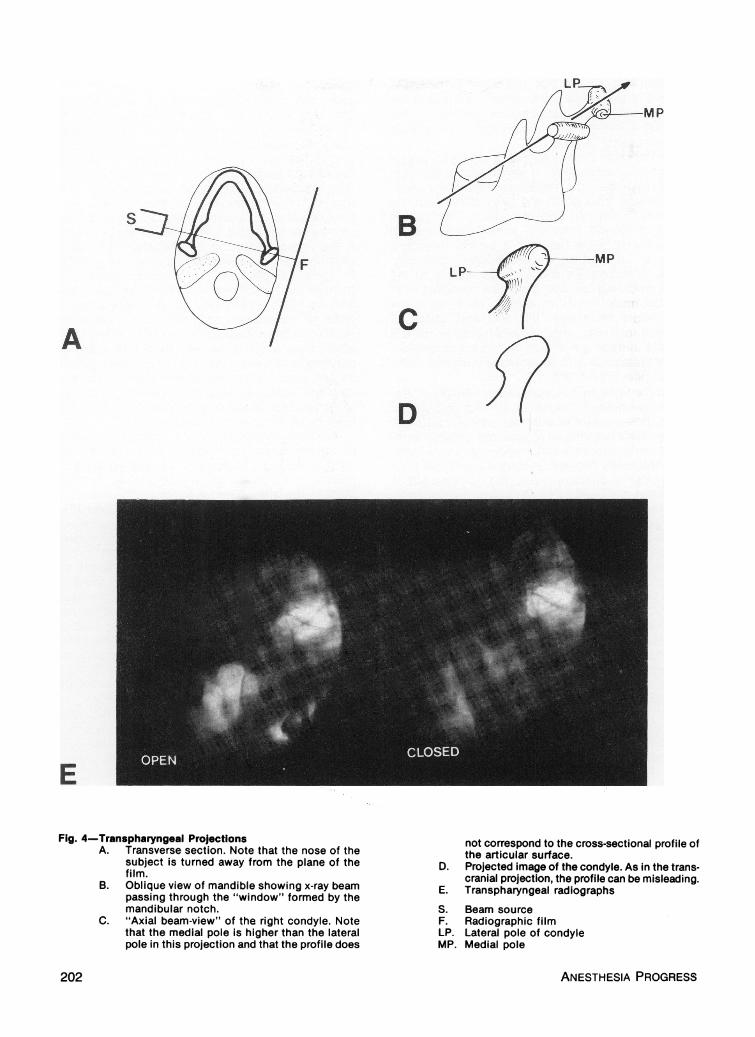
projection (Parma view, or infracranial projection)which bypasses the petrous pyramids by view-ing the joint from below the base of the skull viathe infracranial pharyngeal tissues. The centralray is projected from the contralateral side infront of, and below the joint. It passes through a"window" formed by the mandibular notch (Fig.4a&b). The direction of the ray is oblique to thetransverse axis of the ipsilateral condyle, anddirected from its inferior aspect. Thus, as in thetranscranial technique, the recorded image isdistorted and the true sectional contour of thearticular surface is not seen. But in this projection,the distortion is due to an apparent elevation of themedial pole (Fig. 4c&d).
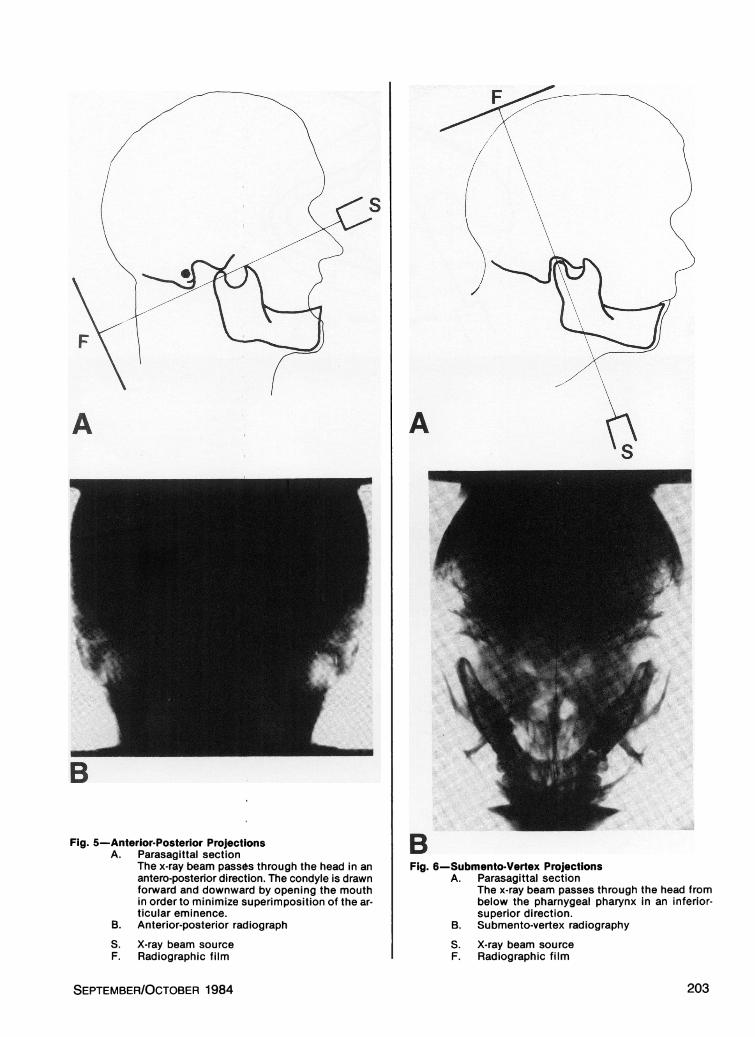
Anterior-posterior projections (Townes, Re-verse Townes and Transorbital-Fig. 5) produceviews of the posterior-superior articular surface.These views are utilized to evaluate bilateral sym-metry, and detect condylar neck fractures. How-ever, they only provide adequate visualization ifthe mouth is open, lowering the condyle out ofthe fossa sufficiently to eliminate the superim-position of the mastoid process located immedi-ately posterior to the joint. This imposes a limita-tion which can be critical in subjects with ad-vanced joint disease who may be unable to openthe mouth more than a few millimeters.The main disadvantage of the projections men-
tioned above is that they distort the profile of thecondyle. Erosion or pitting of the joint surfacein particular may be undetectable, and if the clini-cian is not wary he may reach a false-negativeconclusion. In a comparison of transcranialradiographs with anatomic, morphologic fin-dings, radiographic underdiagnosis of bonypathology has been reported to be as high as50%/0 .17To some extent an allowance can be made for
distortion, necessitating an ancillary radiographto determine the true orientation of the condylaraxes. The orientation of the condylar transverseaxis can be identified by a projection from belowthe chin, passing perpendicular to the intermeatalaxis (Fig. 6). This "submento-vertex", or baseview, is also useful as a means of evaluating con-dylar and mandibular symmetry, and is commonlyused to orient the beam/film locations prior totomography.Tomographic, or body-section radiography, pro-
vides finer bone detail than plain film radiographyand is generally considered to be a superior tech-nique.18.19 Eckerdah120 and Petersson21 haveshown that it is more reliable than transcranial
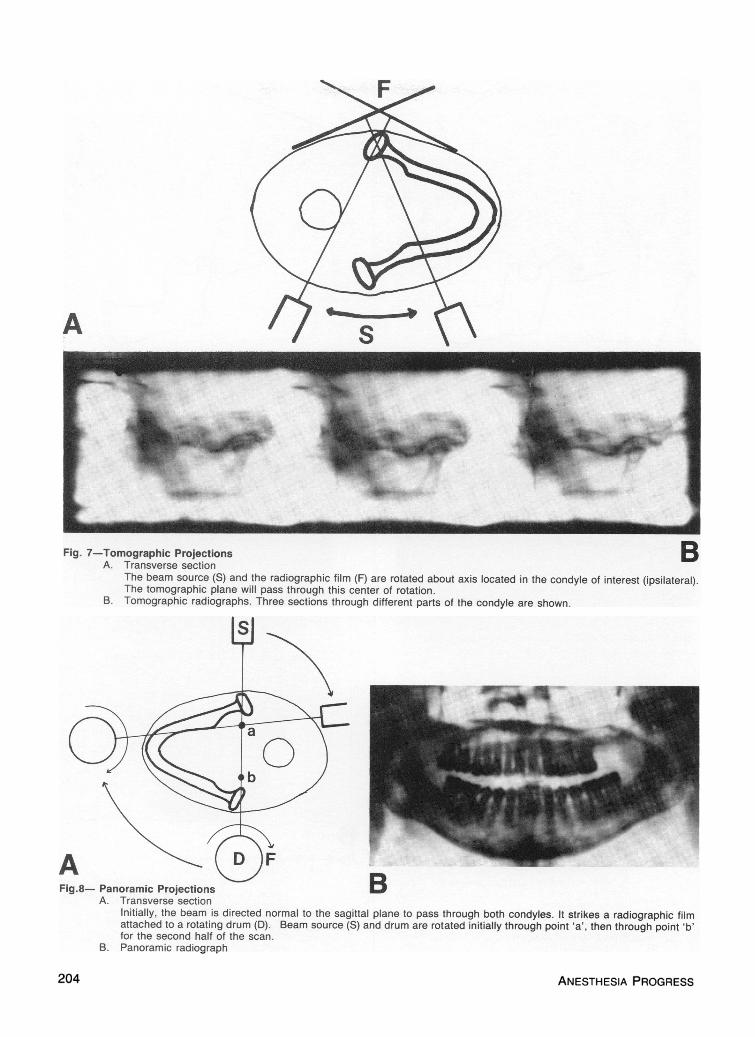
views in its portrayal of joint relationships. Thetechnique utilizes simultaneous movement of thefilm and x-ray source about a focal axis locatedin the condyle of interest (Fig. 7). The resultantimage represents a thin plane through the condyleand is sharply defined, in contrast to the sur-rounding structures which are "blurred out".Superimposition and image distortion are mini-mized in this technique, but some caution mustbe exercised in its use. Selection of the correctplane of tomographic section is extremely critical;if the section does not pass through the site ofpathology a false negative diagnosis may result.In some cases, even if the section does passthrough the pathologic tissues its orientation maybe such that the pathology remains undetected. Inorder to obviate the possibility of false-negativeresults, multiple scans are required.22 As exposurelevels for a single scan vary from 1-10 rads, de-pending on the exposure technique, beam geome-try and speed of the film/screen system, the totalradiation dose may become prohibitive, especiallysince the final image represents only a small per-centage of the tissues irradiated.Panoramic radiography is a specialized version
of tomography. The principle is similar to thatused in taking photographs of large groups bymeans of a mobile, rotating camera. In a typicalsystem, the x-ray beam is initially angled to passtransversely through the mandibular condyles (Fig.8). During the first half of the scan the source andthe film are rotated about an axis located just medi-al and anterior to the condyle adjacent to thesource (Fig. 8a). During the second half of thescan the axis of rotation is shifted to the cor-responding point on the opposite side of the head(Fig. 8b). The x-ray beam is narrowly collimatedso that it projects a very narrow image; and asthe film is attached to a drum which rotates aboutits own axis simultaneously with the scanning mo-tion, the result is a contiguous series of imageswhich together present a panoramic view of theentire mandible, including both the condyles.None of the conventional radiographic tech-
niques described so far is optimal for detectionof soft tissue derangements. Although the jointmeniscus is partly collagenous, it is not usuallyvisualized via x-rays. To overcome this difficulty, ar-thrography is utilized.23-25 A radiopaque mediumis injected into the upper and lower joint spaces;the injection is sometimes followed by pressuri-zation of the space with air (double contrast tech-nique26) to ensure that the medium coats themeniscus and joint surfaces. The patient thenundergoes tomographic and/or video-fluoroscopicevaluation. The meniscus can be visualized lyingbetween the upper and lower joint compartmentswhich are marked clearly by the contained radio-paque medium (Fig. 9). Furthermore, contrastarthrography in conjunction with fluoroscopy pro-
SEPTEMBER/OCTOBER 1984 201
IP
B
CA
LP-
D
E
Fig. 4-Transpharyngeal ProjectionsA. Transverse section. Note that the nose of the
subject is turned away from the plane of thefilm.
B. Oblique view of mandible showing x-ray beampassing through the "window" formed by themandibular notch.
C. "Axial beam-view" of the right condyle. Notethat the medial pole is higher than the lateralpole in this projection and that the profile does
not correspond to the cross-sectional profile ofthe articular surface.
D. Projected image of the condyle. As in the trans-cranial projection, the profile can be misleading.
E. Transpharyngeal radiographs
S. Beam sourceF. Radiographic filmLP. Lateral pole of condyleMP. Medial pole
ANESTHESIA PROGRESS
S
202
A
B
Fig. 5-Anterior-Posterior ProjectionsA. Parasagittal section
The x-ray beam passes through the head in anantero-posterior direction. The condyle is drawnforward and downward by opening the mouthin order to minimize superimposition of the ar-ticular eminence.
B. Anterior-posterior radiographS. X-ray beam sourceF. Radiographic film
Aa
BFig. 6-Submento-Vertex Projections
A. Parasagittal sectionThe x-ray beam passes through the head frombelow the pharnygeal pharynx in an inferior-superior direction.
B. Submento-vertex radiography
S. X-ray beam sourceF. Radiographic film
SEPTEMBER/OCTOBER 1984
m203
A Ss
Fig. 7-Tomographic Projections BA. Transverse section
The beam source (S) and the radiographic film (F) are rotated about axis located in the condyle of interest (ipsilateral).The tomographic plane will pass through this center of rotation.B. Tomographic radiographs. Three sections through different parts of the condyle are shown.
44 DFig.8- Panoramic Projections D
A. Transverse sectionInitially, the beam is directed normal to the sagittal plane to pass through both condyles. It strikes a radiographic filmattached to a rotating drum (D). Beam source (S) and drum are rotated initially through point 'a', then through point 'b'for the second half of the scan.
B. Panoramic radiograph
ANESTHESIA PROGRESS204
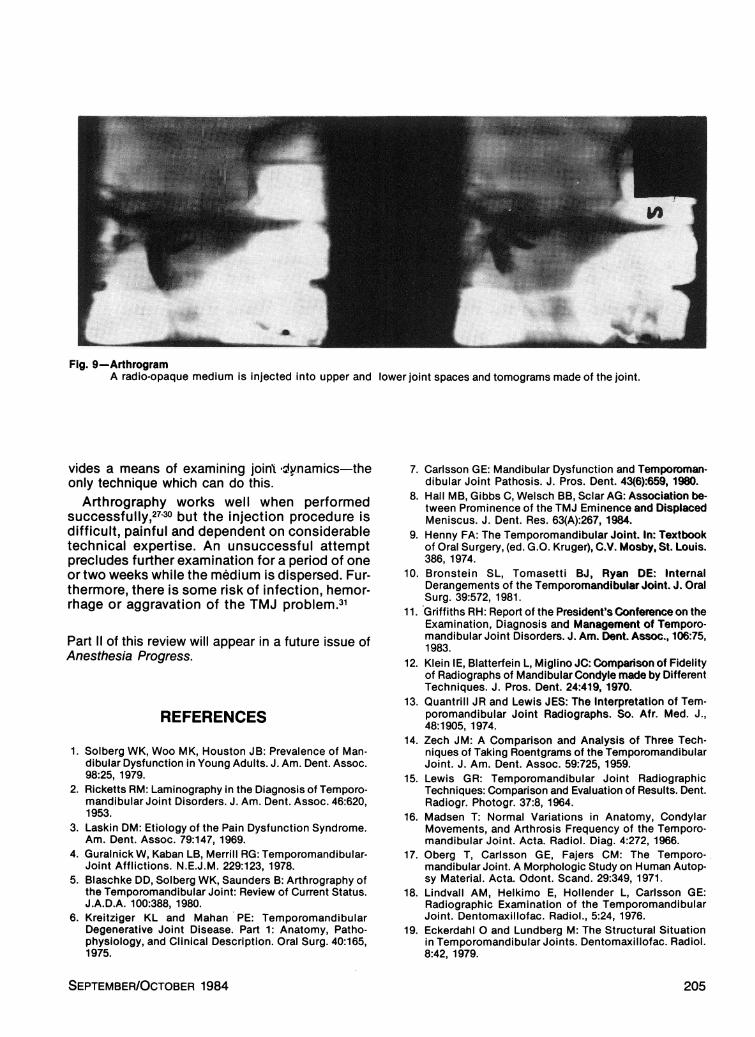
Fig. 9 ArthrogramA radio-opaque medium is injected into upper and lower joint spaces and tomograms made of the joint.
vides a means of examining joint dynamics-theonly technique which can do this.
Arthrography works well when performedsuccessfully,27-30 but the injection procedure isdifficult, painful and dependent on considerabletechnical expertise. An unsuccessful attemptprecludes further examination for a period of oneor two weeks while the medium is dispersed. Fur-thermore, there is some risk of infection, hemor-rhage or aggravation of the TMJ problem.31
Part 11 of this review will appear in a future issue ofAnesthesia Progress.
REFERENCES
1. Solberg WK, Woo MK, Houston JB: Prevalence of Man-dibular Dysfunction in Young Adults. J. Am. Dent. Assoc.98:25, 1979.
2. Ricketts RM: Laminography in the Diagnosis of Temporo-mandibular Joint Disorders. J. Am. Dent. Assoc. 46:620,1953.
3. Laskin DM: Etiology of the Pain Dysfunction Syndrome.Am. Dent. Assoc. 79:147, 1969.
4. Guralnick W, Kaban LB, Merrill RG: Temporomandibular-Joint Afflictions. N.E.J.M. 229:123, 1978.
5. Blaschke DD, Solberg WK, Saunders B: Arthrography ofthe Temporomandibular Joint: Review of Current Status.J.A.D.A. 100:388, 1980.
6. Kreitziger KL and Mahan PE: TemporomandibularDegenerative Joint Disease. Part 1: Anatomy, Patho-physiology, and Clinical Description. Oral Surg. 40:165,1975.
7. Carlsson GE: Mandibular Dysfunction and Temporoman-dibular Joint Pathosis. J. Pros. Dent. 43(6):659, 1980.
8. Hall MB, Gibbs C, Welsch BB, Sclar AG: Association be-tween Prominence of the TMJ Eminence and DisplacedMeniscus. J. Dent. Res. 63(A):267, 1984.
9. Henny FA: The Temporomandibular Joint. In: Textbookof Oral Surgery, (ed. G.O. Kruger), C.V. Mosby, St. Louis.386, 1974.
10. Bronstein SL, Tomasetti BJ, Ryan DE: InternalDerangements of the Temporomandibular Joint. J. OralSurg. 39:572, 1981.
11. Griffiths RH: Report of the President's Conference on theExamination, Diagnosis and Management of Temporo-mandibular Joint Disorders. J. Am. Dent. Assoc., 106:75,1983.
12. Klein IE, Blatterfein L, Miglino JC: Comparison of Fidelityof Radiographs of Mandibular Condyle made by DifferentTechniques. J. Pros. Dent. 24:419, 1970.
13. Quantrill JR and Lewis JES: The Interpretation of Tem-poromandibular Joint Radiographs. So. Afr. Med. J.,48:1905, 1974.
14. Zech JM: A Comparison and Analysis of Three Tech-niques of Taking Roentgrams of the TemporomandibularJoint. J. Am. Dent. Assoc. 59:725, 1959.
15. Lewis GR: Temporomandibular Joint RadiographicTechniques: Comparison and Evaluation of Results. Dent.Radiogr. Photogr. 37:8, 1964.
16. Madsen T: Normal Variations in Anatomy, CondylarMovements, and Arthrosis Frequency of the Temporo-mandibular Joint. Acta. Radiol. Diag. 4:272, 1966.
17. Oberg T, Carlsson GE, Fajers CM: The Temporo-mandibular Joint. A Morphologic Study on Human Autop-sy Material. Acta. Odont. Scand. 29:349, 1971.
18. Lindvall AM, Helkimo E, Hollender L, Carlsson GE:Radiographic Examination of the TemporomandibularJoint. Dentomaxillofac. Radiol., 5:24, 1976.
19. Eckerdahl 0 and Lundberg M: The Structural Situationin Temporomandibular Joints. Dentomaxillofac. Radiol.8:42, 1979.
SEPTEMBER/OCTOBER 1984 205

20. Eckerdahl 0: Tomography of the TemporomandibularJoint. Correlation between Tomographic Image andHistologic Sections in a Three-Dimensional System.Acta. Radiol., Suppl. 329, 1973
21. Petersson A: Radiography of the TemporomandibularJoint. A Comparison of Information Obtained from Dif-ferent Radiographic Techniques. Thesis, Malmo, 1976.
22. Rozencweig D and Martin G: Selective Tomography ofthe TMJ and the Myofacial Pain Dysfunction Syndrome.J. Pros. Dent. 40(1):67-74, 1978.
23. Agerberg G and Lundberg M: Changes in the Temporo-mandibular Joint After Surgical Treatment: A RadiologicFollow-up Study. Oral Surg. 32:865, 1971.
24. Wilkes CH: Arthrography of the Temporomandibular Jointin patients with the TMJ Pain-Dysfunction Syndrome.Minn. Med. 61:645, 1978.
25. FarrarW and McCarty WL, Jr.: Inferior Joint Space Ar-thrography and Characteristics of Condylar Paths in In-ternal Drangements of the TMJ. J. Pros. Dent. 41548,1979.
26. Westesson P: Double Contrast Arthrotomography of theTemporomandibular Joint: Introduction of an Arthro-graphic Technique for Visualization of the Disk andArticular Surfaces. J. Oral and Maxillofac. Surg. 41:163,1983.
27. Katzberg RW, Dolwick MF, Bales DJ, Helms CA: Arthro-tomography of the Temporomandibular Joint: NewTechnique and Preliminary Observations. Am. J. Rad.132:949, 1979.
28. Dolwick MF, Katzberg RW, Helms CA, Bales DJ: Arthro-tomographic Evaluation of the Temporomandibular Joint.J. Oral Surg. 37:793, 1979.
29. Katzberg RW, Dolwick MF, Helms CA, Hopens T, BalesDJ, Coggs GC: Arthrotomography of the Temporoman-dibular Joint. Am. J. Rad. 134:995-1003, 1980.
30. Blaschke DD, Solberg WK, Saunders B: Arthtography ofthe Temporomandibular Joint: Review of Current Status.J. Am. Dent. Assoc. 100:388, 1980.
31. Blaschke DD: Arthrography of the TemporomandibularJoint. In: TMJ Problems: Biologic Diagnosis and Treat-ment. (Solberg, WR and Clark GT, eds.), QuintessencePubI. Co., Chicago, Ill., 69, 1980.
206 ANESTHESIA PROGRESS
Copyright © 2022 FDOKUMEN