A comparative clinical study to evaluate the efficacy of ...
246
A comparative clinical study to evaluate the efficacy of Triphala choorna with Krishnadi anjana and Triphala choorna in the management of Timira w.s.r. to Senile immature cataract by Santosh Kumar Shaw Dissertation Submitted to the Rajiv Gandhi University of Health Sciences, Karnataka, Bengaluru In partial fulfillment of the requirements for the degree of Ayurveda Dhanwantari Master of Surgery (Ayu) in Shalakya Tantra Under the guidance of Dr. Sujathamma K Department of Post Graduate Studies in Shalakya Tantra Sri Kalabyraveshwaraswamy Ayurvedic Medical College, Hospital & Research centre, Vijayanagar, Bengaluru- 560 104 2015 – 2018
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of A comparative clinical study to evaluate the efficacy of ...

A comparative clinical study to evaluate the efficacy of Triphala choorna with Krishnadi anjana and Triphala choorna in the management of Timira w.s.r. to Senile
immature cataract
by
Santosh Kumar Shaw
Dissertation Submitted to the
Rajiv Gandhi University of Health Sciences, Karnataka, Bengaluru
In partial fulfillment
of the requirements for the degree of
Ayurveda Dhanwantari Master of Surgery (Ayu)
in
Shalakya Tantra
Under the guidance of
Dr. Sujathamma K
Department of Post Graduate Studies in Shalakya Tantra
Sri Kalabyraveshwaraswamy Ayurvedic Medical College, Hospital & Research centre,
Vijayanagar, Bengaluru- 560 104
2015 – 2018
Scanned by CamScanner
Page I
ABBREVIATIONS
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page VI
LIST OF ABBREVIATIONS USED
A. H. Ni. Ashtanga Hridaya Nidanasthana
A. H. Su. Ashtanga Hridaya Sutrasthana
A. H. Ut. Ashtanga Hridaya Uttarasthana
A. S. Sha. Ashtanga Sangraha Sharirasthana
A. S. Su. Ashtanga Sangraha Sutrasthana
A. S. Ut. Ashtanga Sangraha Uttarasthana
B. P. Bhavaprakasha
B. P. Ma. Bhavaprakasha Madhyamakhanda
B. P. N. Bhavaprakasha Nighantu
Bh. Sha. Bhela Sharirasthana
Bh. Su. Bhela Sutrasthana
BID Twice a day
Ch.S.Chi. Charaka Samhita Chikitsasthana
Ch.S.Ni. Charaka Samhita Nidanasthana
Ch.S.Sha. Charaka Samhita Sharirasthana
Ch.S.Su. Charaka Samhita Sutrastana
Ch.S.Si. Charaka Samhita Siddhisthana
C.D. Chakradatta
D Dioptre
Dal. Dalhana tika
G.N. Gada Nigraha
H.S. Harita Samhita
ABBREVIATIONS
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page VII
HS Highly significant
Ka.S. Kashyapa Samhita
M.N. Madhava Nidana
NS Nonsignificant
Pg Page
Pp Printed pages
Rig. Rigveda
S Significant
Sha.S.Pu. Sharangadhara Samhita Purvakhanda
Sha.S.Ut. Sharangadhara Samhita Uttarakhanda
Su.S.Sha. Sushruta Samhita Sharirasthana
Su.S.Su. Sushruta Samhita Sutrastana
Su.S.Ut. Sushruta Samhita Uttaratantra
Y.R. Yoga Ratnakara Uttarardha
V.S. Vangasen Samhita
< Less than
> Greater than
% Percentage
LIST OF TABLES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page VIII
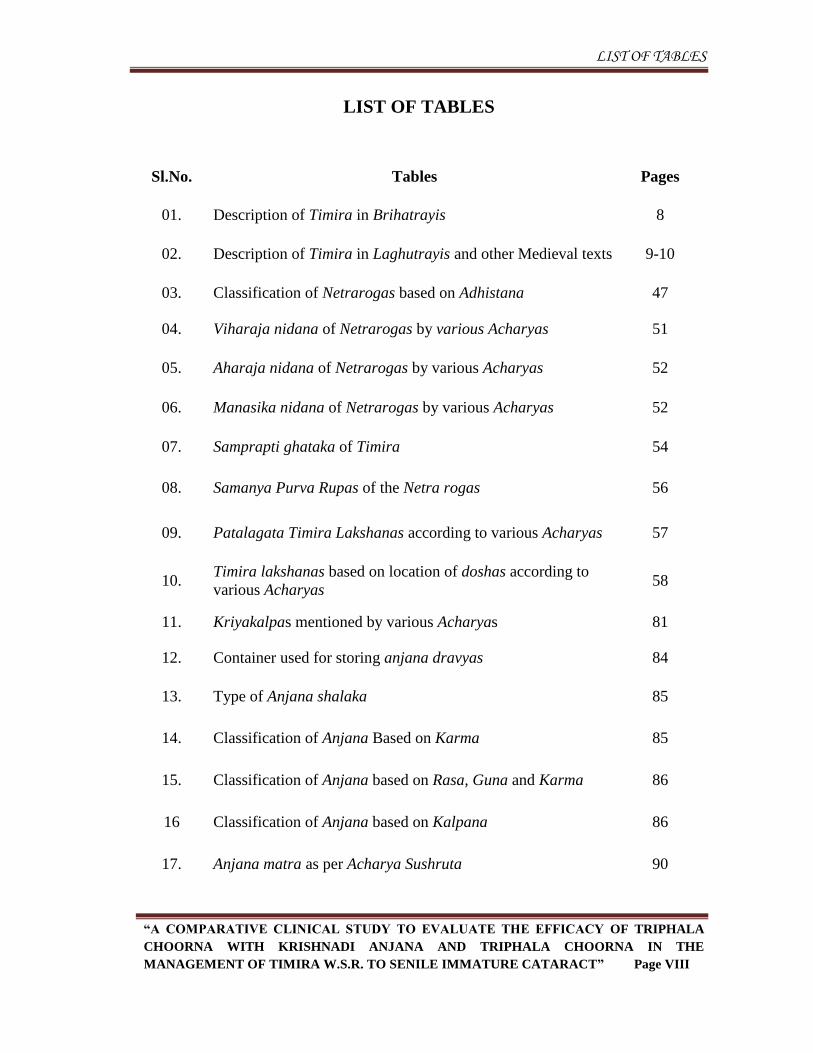
LIST OF TABLES
Sl.No. Tables Pages
01. Description of Timira in Brihatrayis 8
02. Description of Timira in Laghutrayis and other Medieval texts 9-10
03. Classification of Netrarogas based on Adhistana 47
04. Viharaja nidana of Netrarogas by various Acharyas 51
05. Aharaja nidana of Netrarogas by various Acharyas 52
06. Manasika nidana of Netrarogas by various Acharyas 52
07. Samprapti ghataka of Timira 54
08. Samanya Purva Rupas of the Netra rogas 56
09. Patalagata Timira Lakshanas according to various Acharyas 57
10. Timira lakshanas based on location of doshas according to
various Acharyas 58
11. Kriyakalpas mentioned by various Acharyas 81
12. Container used for storing anjana dravyas 84
13. Type of Anjana shalaka 85
14. Classification of Anjana Based on Karma 85
15. Classification of Anjana based on Rasa, Guna and Karma 86
16 Classification of Anjana based on Kalpana 86
17. Anjana matra as per Acharya Sushruta 90
LIST OF TABLES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page IX
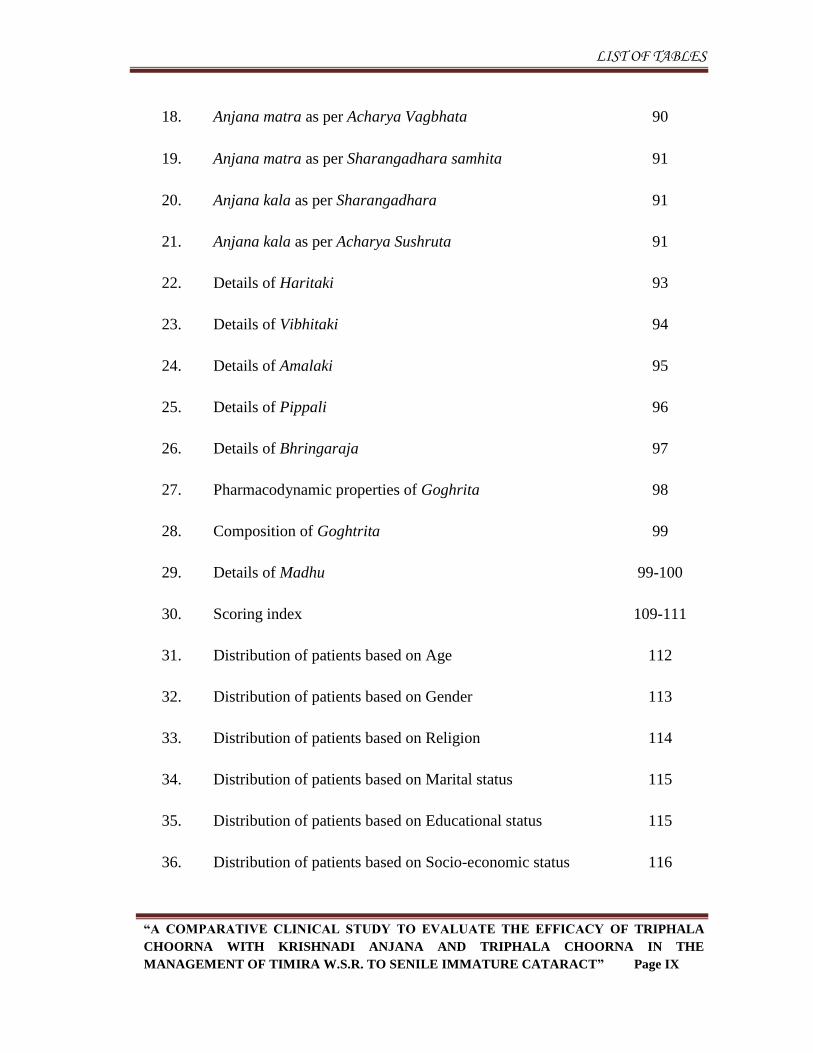
18. Anjana matra as per Acharya Vagbhata 90
19. Anjana matra as per Sharangadhara samhita 91
20. Anjana kala as per Sharangadhara 91
21. Anjana kala as per Acharya Sushruta 91
22. Details of Haritaki 93
23. Details of Vibhitaki 94
24. Details of Amalaki 95
25. Details of Pippali 96
26. Details of Bhringaraja 97
27. Pharmacodynamic properties of Goghrita 98
28. Composition of Goghtrita 99
29. Details of Madhu 99-100
30. Scoring index 109-111
31. Distribution of patients based on Age 112
32. Distribution of patients based on Gender 113
33. Distribution of patients based on Religion 114
34. Distribution of patients based on Marital status 115
35. Distribution of patients based on Educational status 115
36. Distribution of patients based on Socio-economic status 116
LIST OF TABLES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page X
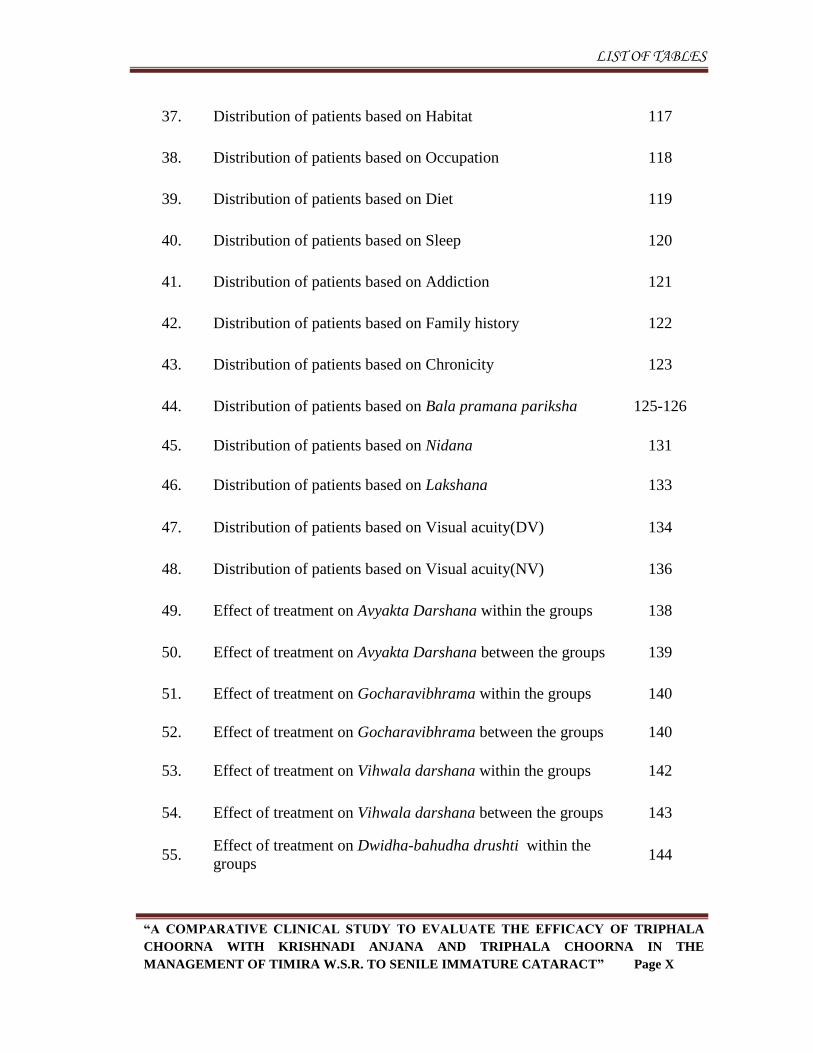
37. Distribution of patients based on Habitat 117
38. Distribution of patients based on Occupation 118
39. Distribution of patients based on Diet 119
40. Distribution of patients based on Sleep 120
41. Distribution of patients based on Addiction 121
42. Distribution of patients based on Family history 122
43. Distribution of patients based on Chronicity 123
44. Distribution of patients based on Bala pramana pariksha 125-126
45. Distribution of patients based on Nidana 131
46. Distribution of patients based on Lakshana 133
47. Distribution of patients based on Visual acuity(DV) 134
48. Distribution of patients based on Visual acuity(NV) 136
49. Effect of treatment on Avyakta Darshana within the groups 138
50. Effect of treatment on Avyakta Darshana between the groups 139
51. Effect of treatment on Gocharavibhrama within the groups 140
52. Effect of treatment on Gocharavibhrama between the groups 140
53. Effect of treatment on Vihwala darshana within the groups 142
54. Effect of treatment on Vihwala darshana between the groups 143
55. Effect of treatment on Dwidha-bahudha drushti within the
groups 144
LIST OF TABLES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page XI
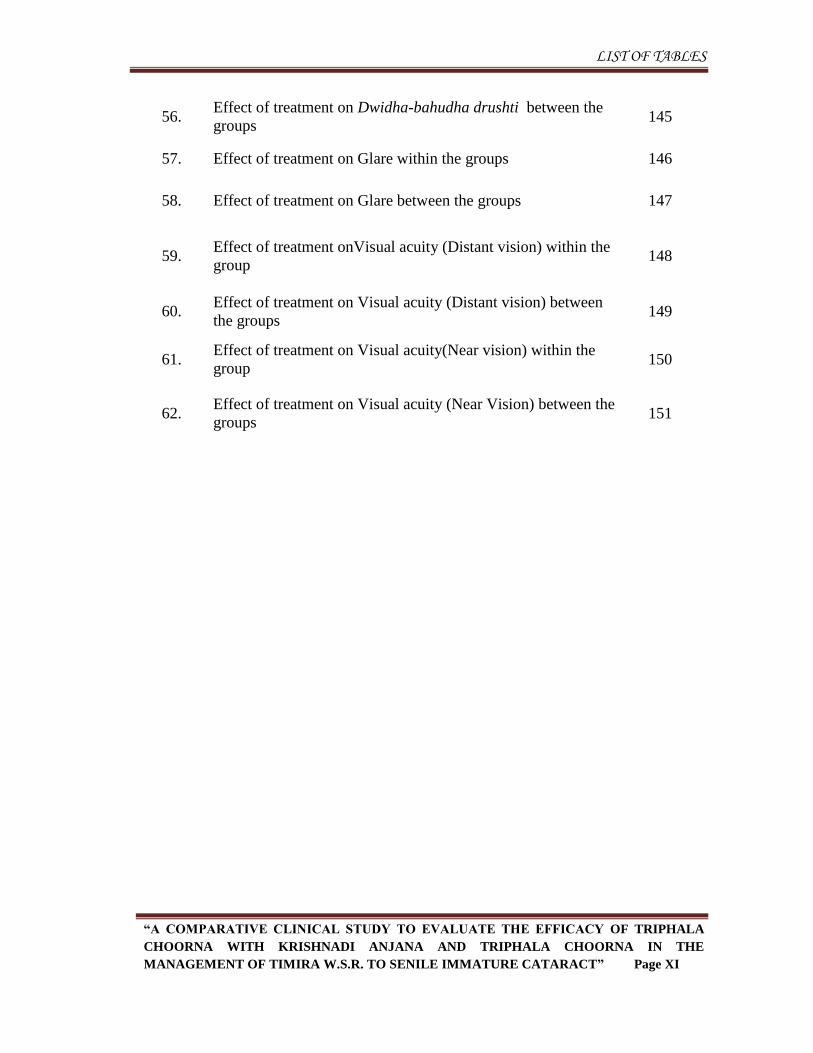
56. Effect of treatment on Dwidha-bahudha drushti between the
groups 145
57. Effect of treatment on Glare within the groups 146
58. Effect of treatment on Glare between the groups 147
59. Effect of treatment onVisual acuity (Distant vision) within the
group 148
60. Effect of treatment on Visual acuity (Distant vision) between
the groups 149
61. Effect of treatment on Visual acuity(Near vision) within the
group 150
62. Effect of treatment on Visual acuity (Near Vision) between the
groups 151
LIST OF FIGURES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page XII
LIST OF FIGURES
Sl. No. Figures Pages
01. Distribution of patients based on Age 112
02. Distribution of patients based on Gender 113
03. Distribution of patients based on Religion 114
04. Distribution of patients based on Marital status 115
05. Distribution of patients based on Educational status 116
06. Distribution of patients based on Socio-economic status 117
07. Distribution of patients based on Habitat 118
08. Distribution of patients based on Occupation 119
09. Distribution of patients based on Diet 120
10. Distribution of patients based on Sleep 121
11. Distribution of patients based on Addiction 122
12. Distribution of patients based on Family history 123
13. Distribution of patients based on Chronicity 124
14. Distribution of patients based on Bala pramana pariksha 126
15. Distribution of patients based on Nidana 131
16. Distribution of patients based on Lakshana 133
17. Distribution of patients based on Visual acuity(DV) 135
LIST OF FIGURES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page XIII
18. Distribution of patients based on Visual acuity(NV) 136
19. Effect of treatment on Avyakta Darshana within the group 139
20. Effect of treatment on Gocharavibhrama within the group 141
21. Effect of treatment on Vihwala darshana within the group 143
22. Effect of treatment on Dwidhabahudha drushti within the group 145
23. Effect of treatment on Glare within the groups 147
24. Effect of treatment on Visual acuity (Distant vision) within the
group 149
25. Effect of treatment on Visual acuity (Near vision) within the
group 151
ABSTRACT
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page XV
ABSTRACT
Title:
A comparative clinical study to evaluate the efficacy of Triphala choorna with
Krishnadi anjana and Triphala choorna in the management of Timira w.s.r. to Senile
immature cataract.
Background & Objectives:
Timira is one among the drishtigata nerta roga explained by our ancient
Acharyas. If proper care is not taken, Timira leads to kaca which in turn to linganasha.1
Based on the clinical manifestations it can be correlated to cataract. Any opacity in the
lens or its capsule, whether developmental or acquired is called as cataract.2 There are no
non-surgical measures which delay, prevent or reverse the development of cataract in
conventional system of medicine, the only definite management is lens extraction once it
reaches matured stage.
Objectives are to evaluate the efficacy of Triphala choorna with Krishnadi
anjana and Triphala choorna in the management of Timira and to compare the clinical
efficacies of both the groups.
Methods:
A randomized clinical study was taken up. 40 patients of Timira were selected
from OPD/IPD of the Shalakya tantra department of SKAMCH&RC, Bengaluru and
made into two groups. Patients of Group A were treated with Krishnadi varti anjana
along with Triphala choorna internally for 48 days. Patients of Group B were treated
ABSTRACT
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page XVI
with Triphala choorna internally for 48 days. The effect of treatment was statistically
analyzed using Unpaired and Paired student’s ‘t’–test.
Results:
The group with both Krishnadi varti anjana and Triphala choorna responded
better when compared to the group with only Triphala choorna based on statistical
analysis indicating the added effect of Krishnadi varti anjana in Group A.
Interpretation & Conclusion:
Krishnadi varti anjana and Triphala choorna are the two effective modalities of
treatment which can be adopted in Timira w.s.r. to Senile immature cataract.
Key words: Timira; Cataract; Triphala choorna; Krishnadi varti anjana.
INTRODUCTION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 1
Title:
A comparative clinical study to evaluate the efficacy of Triphala choorna with
Krishnadi anjana and Triphala choorna in the management of Timira w.s.r. to Senile
immature cataract.
Introduction:
Ayurveda is the most ancient science of life and Shalakya tantra is one of the
branches of Ashtanga Ayurveda which deals with the prevention and treatment of
Urdhwajatrugata rogas including netra.
Eyes are the most precious gift of the God to the living beings. Good vision is
crucial for social and intellectual development of a person. According to Ayurveda,
“sarvendriyanaam nayanam pradhanam” i.e., among all the sense organs, eyes are the
most important. “Everyone should be dedicated enough to protect their vision, throughout
the period of life because for an individual who is blind, day and night are the same and
the beautiful world is useless to him even if he possess lot of wealth.3
Acharya Sushruta explains seventy six netrarogas.4 Among them Timira is an
important disease, explained under Drushtigata rogas. Clinical features of dwiteeya
patalagatha timira and some features of triteeya patalagata timira such as avyakta
darshana, gochara vibhrama and dwidhabahudha drushti is simulated to that of signs
and symptoms of immature cataract. The early symptoms of cataract include blurrness of
vision, glare, polyopia and colour halos.5
According to WHO “In spite of the progress made in surgical techniques in many
countries during the last ten years, cataract (47.9%) remains the leading cause of visual
INTRODUCTION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 2
impairment in all areas of the world, except for developed countries.”6 As per National
Programme for Control of Blindness of Govt. of India about 62.60% blindness is due to
cataract.7
If proper care is not taken at time, Timira leads to kaca which in turn to
linganasha.8
There are no non-surgical measures which delay, prevent or reverse the
development of senile cataract in conventional system of medicine, the only definite
management is lens extraction once it reaches matured stage or complete opacification.
The success rate of cataract surgery is more than 90%9, but complications such as
sensitivity to anaesthesia, injury to the cornea and iris, vitreous loss, expulsive choroidal
haemorrhage, uveitis, retinal detachment, secondary cataract etc may occur which cause
loss of vision.10
The treasure of ancient wisdom depicted in our classical texts has to be
considered at this critical juncture which provides potentiality in probing of disease
and its management through vast scientific advancements.
Ocular therapeutic like Anjana karma11
and internal administration of Triphala
choorna12
are mentioned in Ayurvedic classics for the management of Timira roga. Thus
the present study is being undertaken to scientifically study and validate the effect of
Triphala choorna and Krishnadi varti anjana in the management of Timira.
OBJECTIVES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 3
Objectives
To evaluate the efficacy of Triphala choorna with Krishnadi Anjana in the
management of Timira w.s.r. to Senile Immature Cataract.
To evaluate the efficacy of Triphala choorna in the management of Timira
w.s.r. to Senile Immature Cataract.
To compare and evaluate the clinical efficacies of both the groups.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 4
Review of literature
Historical review
Ayurvedic review:
Development of Ayurveda- “the science of life” has taken place from the
beginning of the creation as it was the necessity of human beings to preserve their health.
Vedas - the oldest records of mankind has vast scattered references about medical
knowledge. History is a root of knowledge in scientific researches. In the initial stage of
planning in any scientific work, it is very important to know the evolution of the present
knowledge, origin of the present knowledge and the basic idea given by ancient
scientists. Hence, at the outset an attempt is made to throw light over the history of the
eye disease, Timira w.s.r. to immature cataract.
Shalakya tantra is one of the renowned branch of Ashtanga Ayurveda is a unique
contribution to the present modern world. A Greek physician Megasthanes (BC 300) who
visited northern part of India in 300BC wrote in his book „Indica‟ that Indians had their
own remedies for curing Urdhwa jatrugata rogas.14
The king of Videha, Rajarshi Nimi was the original expounder of the Shalakya
Tantra; hence it is also called as „Nimi Tantra‟. Nimi got knowledge from Sun God
(Brahma kanda 16). Today Sushruta Samhita is the main source of Shalakya Tantra.
Acharya Sushruta has accepted that the description regarding Shalakya given in
Uttartantra has been taken from Videha Tantra. Gargya Tantra, Galava Tantra, Satyaki
Tantra, Karala Tantra and Shounaka Tantra are other legends of Shalakya Tantra.15
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 5
The references pertaining to netra rogas in general and Timira in specific have been
compiled from the following periods:
Vedic period: (5000BC to 1500BC)
In Vedic periods we find many references in the „Rigveda‟, curing the disease by
medicine as well as surgery by Ashwini kumaras. The word Timira means Andhakara or
sequel of it i.e. Linganasha (loss of vision) is taken into consideration, there are many
references in the Vedic literature to support the same. Here are few examples found in
these literatures which are related to Shalakya Tantra, probably it is the first evidence of
flourished medical knowledge and the treatment of eye diseases have been recorded in
the history.
In „Rigveda‟, we have reference of replacement of injured eye with artificial eye
(1.116.16). There are references available in texts where Ashwini kumaras have
cured the blindness and the persons Kanwa, Rijaswa, Paravrija, Kaksivit, Kavi puru
regained their eyesight. (Rigveda 1.112, 116, 117)
In Yajurveda, various anjanas were mentioned to cure the eye diseases like sisa
anjana and also for Timira roga chikitsa with medicated ghee prepared from
sahadeva, satavari, rasna, guduchi, saireyaka and triphala are described. (Yajurveda
21/36)
Atharva Veda is a vital source of origin of Ayurveda. In Atharva veda there is
description of several indications of Anjana for improvement of vision (7.30.36) and
other local medicaments (19.45.4) has mentioned. (Akshiroga bheshaja 6/16)
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 6
Upanishad period (4000 BC to 1000 BC)
During Upanishad period, various authors wrote several books on the subject of
Shalakya like Nimi Tantra, Videha Tantra, Karala Tantra, Gargya Tantra, Kankayana
Tantra, Galava Tantra, Krishnatreya Tantra, Satyaki Tantra,Chakshushya Tantra,
Shaunaka Tantra but unfortunately none of those books are available today; but
commentators of various Samhitas and other books quote names of these books and some
shlokas.
Brhadaranyaka Upanishad (11.2.3) has narrated that two eyes are Vishwamitra and
Jamadagni; they are located in two of the seven cavities of the skull.
Brhadaranyaka Upanishad (11.2.3) has also mentioned that Urdhwa vartma, Adhara
vartma and three distinct layers of the eye ball as Suklam, Lohinum and Krishnam.
Chandogya Upanishad (1.6.5 and 1.6.6) has described internal features of eye with
its reflections as Shukla-bha, Neela-bha and Krishna-bha. It has identified golden
glow inside the eyes.
Chakshushopanishat is a short summary of prayers to sun, chanting of which
promote eye sight and better health.
Samhita period (2000 BC to 800 AD)
In Samhita period “Netra Rogas” have been elaborately illustrated by all the authors
of the Ayurvedic literatures.
Acharya Charaka (200BC) mentioned the eye diseases as four in Sutra sthana16
and
ninty-six in chikitsa sthana explained some of the names of eye diseases like
Vartmastambha, Vartamasankocha, Timira, Pilla Roga etc., in chikitsa stana.17
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 7
Acharya Charaka has included Timira under the Vata Nanatmaja Vyadhi.18
Statement of Charaka indicates that Shalakya was well established in that period.
Acharya Sushruta (200 AD), the first and the foremost scientist of the
Dhanvantarian School, has given vivid description of Urdhvajatrugata Rogas in
Uttaratantra where he described ailments of netra, karna, nasa and shiro-rogas.
Acharya Sushruta was a pioneer of the Indian Surgery, and hardly left any
specialized branch. His contribution to the surgical field is a most valuable and
priceless gift. He had described ophthalmology in a systematic way. Acharya
Sushruta has devoted first twenty six chapters in Uttara Tantra, last chapter of
Nidana Sthana, 16th chapter of Sutra sthana and 22nd chapter of Chikitsa Sthana for
Shalakya Tantra. He has described Timira roga in detail19
along with its treatment20
in uttaratantra.
In Ashtanga Sangraha21
(600 AD), and Ashtanga Hridaya22
(800 AD), there is
description of ninety-four eye diseases. They have described Timira under 27 types
of Drishtigata rogas. Vagbhata considers Timira, kacha and linganasha as separate
clinical entities and each of them are of six types.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 8
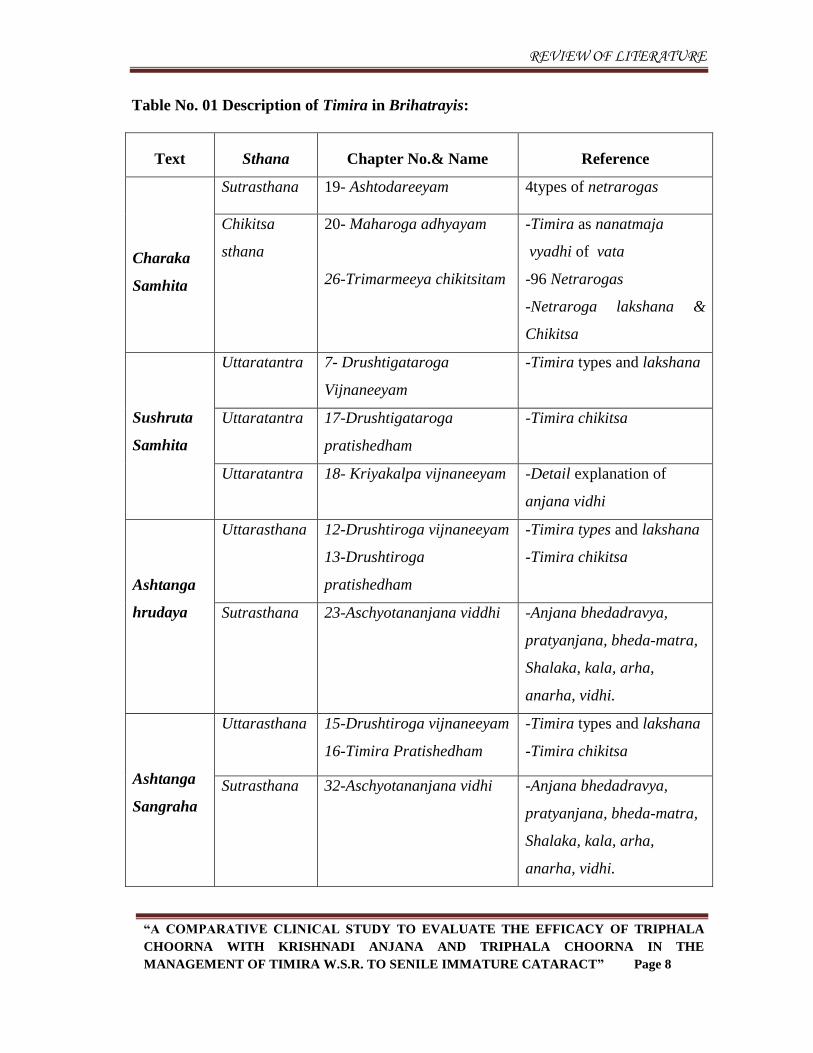
Table No. 01 Description of Timira in Brihatrayis:
Text Sthana Chapter No.& Name Reference
Charaka
Samhita
Sutrasthana 19- Ashtodareeyam 4types of netrarogas
Chikitsa
sthana
20- Maharoga adhyayam
26-Trimarmeeya chikitsitam
-Timira as nanatmaja
vyadhi of vata
-96 Netrarogas
-Netraroga lakshana &
Chikitsa
Sushruta
Samhita
Uttaratantra 7- Drushtigataroga
Vijnaneeyam
-Timira types and lakshana
Uttaratantra 17-Drushtigataroga
pratishedham
-Timira chikitsa
Uttaratantra 18- Kriyakalpa vijnaneeyam -Detail explanation of
anjana vidhi
Ashtanga
hrudaya
Uttarasthana 12-Drushtiroga vijnaneeyam
13-Drushtiroga
pratishedham
-Timira types and lakshana
-Timira chikitsa
Sutrasthana 23-Aschyotananjana viddhi -Anjana bhedadravya,
pratyanjana, bheda-matra,
Shalaka, kala, arha,
anarha, vidhi.
Ashtanga
Sangraha
Uttarasthana 15-Drushtiroga vijnaneeyam
16-Timira Pratishedham
-Timira types and lakshana
-Timira chikitsa
Sutrasthana 32-Aschyotananjana vidhi -Anjana bhedadravya,
pratyanjana, bheda-matra,
Shalaka, kala, arha,
anarha, vidhi.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 9
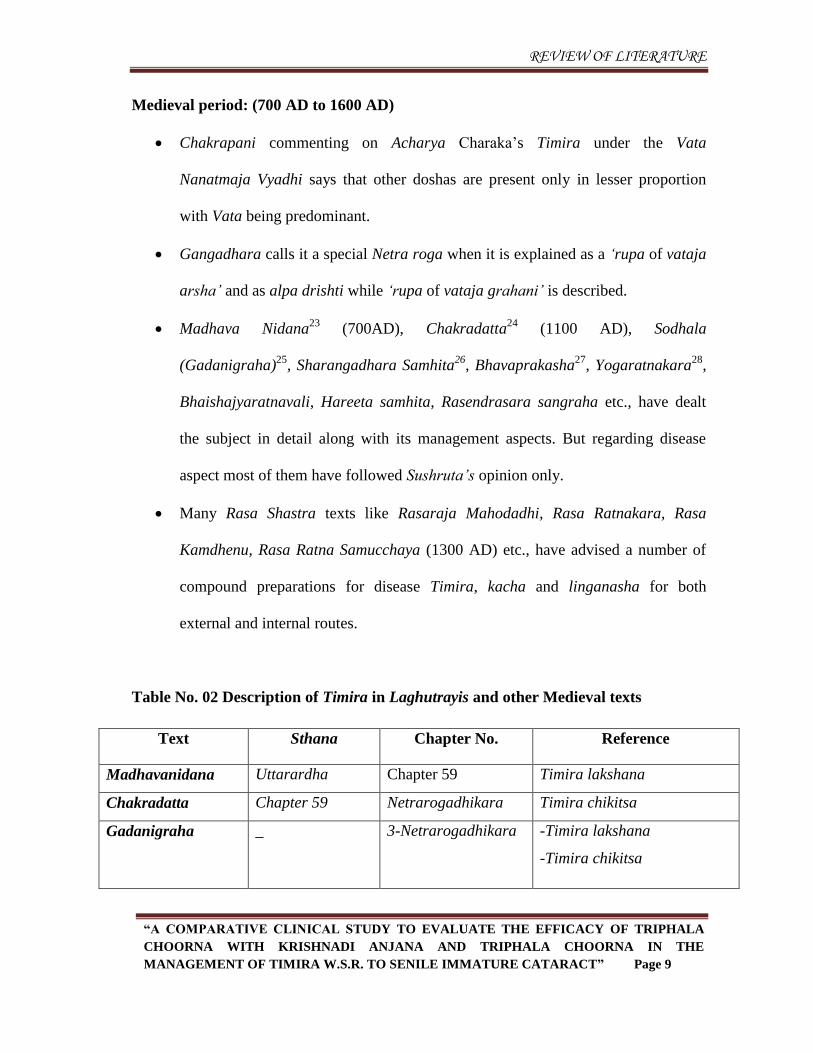
Medieval period: (700 AD to 1600 AD)
Chakrapani commenting on Acharya Charaka‟s Timira under the Vata
Nanatmaja Vyadhi says that other doshas are present only in lesser proportion
with Vata being predominant.
Gangadhara calls it a special Netra roga when it is explained as a „rupa of vataja
arsha‟ and as alpa drishti while „rupa of vataja grahani‟ is described.
Madhava Nidana23
(700AD), Chakradatta24
(1100 AD), Sodhala
(Gadanigraha)25
, Sharangadhara Samhita26
, Bhavaprakasha27
, Yogaratnakara28
,
Bhaishajyaratnavali, Hareeta samhita, Rasendrasara sangraha etc., have dealt
the subject in detail along with its management aspects. But regarding disease
aspect most of them have followed Sushruta‟s opinion only.
Many Rasa Shastra texts like Rasaraja Mahodadhi, Rasa Ratnakara, Rasa
Kamdhenu, Rasa Ratna Samucchaya (1300 AD) etc., have advised a number of
compound preparations for disease Timira, kacha and linganasha for both
external and internal routes.
Table No. 02 Description of Timira in Laghutrayis and other Medieval texts
Text Sthana Chapter No. Reference
Madhavanidana Uttarardha Chapter 59 Timira lakshana
Chakradatta Chapter 59 Netrarogadhikara Timira chikitsa
Gadanigraha _ 3-Netrarogadhikara -Timira lakshana
-Timira chikitsa
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 10
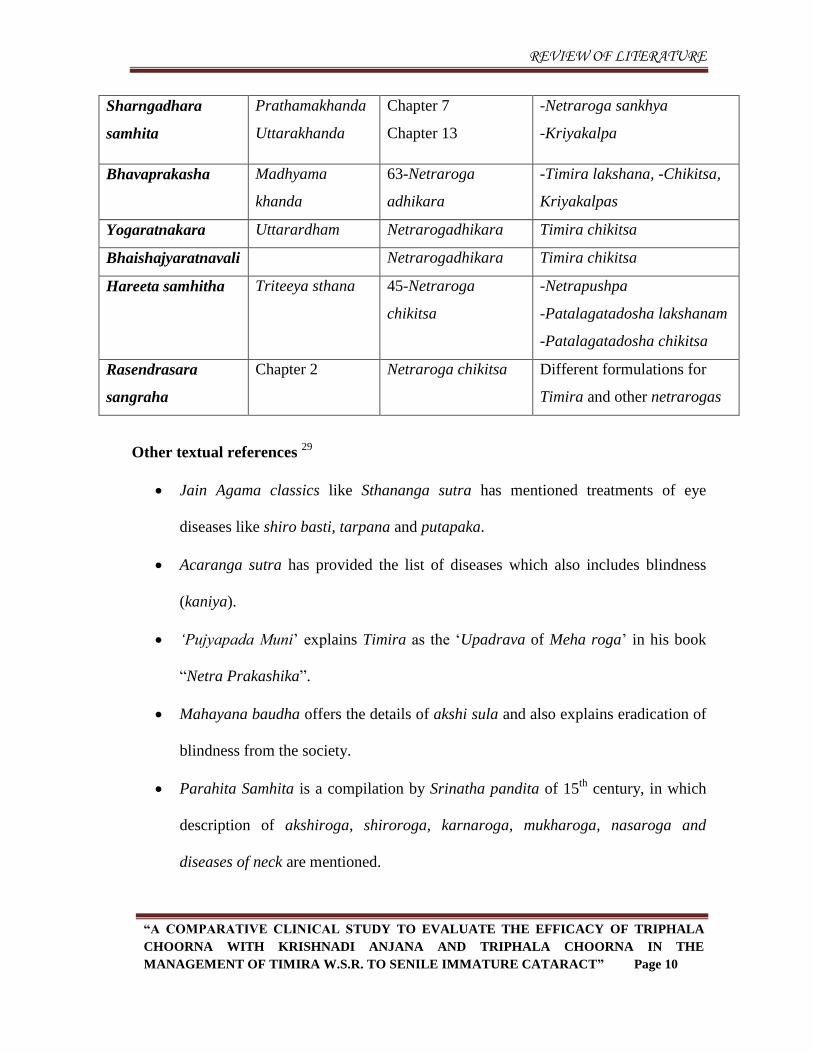
Sharngadhara
samhita
Prathamakhanda
Uttarakhanda
Chapter 7
Chapter 13
-Netraroga sankhya
-Kriyakalpa
Bhavaprakasha Madhyama
khanda
63-Netraroga
adhikara
-Timira lakshana, -Chikitsa,
Kriyakalpas
Yogaratnakara Uttarardham Netrarogadhikara Timira chikitsa
Bhaishajyaratnavali Netrarogadhikara Timira chikitsa
Hareeta samhitha Triteeya sthana 45-Netraroga
chikitsa
-Netrapushpa
-Patalagatadosha lakshanam
-Patalagatadosha chikitsa
Rasendrasara
sangraha
Chapter 2 Netraroga chikitsa Different formulations for
Timira and other netrarogas
Other textual references 29
Jain Agama classics like Sthananga sutra has mentioned treatments of eye
diseases like shiro basti, tarpana and putapaka.
Acaranga sutra has provided the list of diseases which also includes blindness
(kaniya).
„Pujyapada Muni‟ explains Timira as the „Upadrava of Meha roga‟ in his book
“Netra Prakashika”.
Mahayana baudha offers the details of akshi sula and also explains eradication of
blindness from the society.
Parahita Samhita is a compilation by Srinatha pandita of 15th
century, in which
description of akshiroga, shiroroga, karnaroga, mukharoga, nasaroga and
diseases of neck are mentioned.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 11
Modern Review: 30
History of cataract
The oldest documented case of cataract throughout history was reported in a
famous and small statue from the 5th dynasty (about 2457-2467 B.C.) contained
in the Egyptian Museum in Cairo, Egypt.
This fact confirms that old Egyptians knew the disease. By analysis of ancient
surgical instruments it is possible to define the history of medical specialties, and
acquaint the evolution of specific surgical techniques and operations through the
centuries (Aruta et al., 2009). Scientists have often discussed whether cataract was
firstly operated in Ancient Egypt (Bernscherer, 2001). This hypothesis seems
plausible (Ascaso et al., 2009). Thus, a wall painting in the tomb of the master
builder Ipwy at Thebes (about 1200 B.C.) reveals an oculist treating the eye of a
craftsman. Because of the length of the instrument, the scene might also be
interpreted as a cataract surgery by couching of the lens into the vitreous cavity.
Cataract surgery by “couching” (lens depression) was, without a doubt, one of the
oldest surgical procedures. This technique involved using a sharp instrument to
push the cloudy lens to the bottom of the eye. Perhaps this procedure is that which
is mentioned in the articles of the Code of Hammurabi (Cotallo & Esteban, 2008;
Ascaso et al., 2011).
However, there are some doubts about the real meaning of the term “na-kap-tu”,
which someone translated as “cloud”and other directly as “waterfall”. It is even
possible that these articles of the Code of Hammurabi made some reference to
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 12
treatment of corneal pathology instead of cataract (Gorin, 1982). So, couching for
cataract is one of the most ancient surgical procedures.
This method may have been brought to the West by Greek travelers from India
and the Middle East (Wales, 2010). The removal of cataract by surgery was also
introduced into China from India (Lade & Svovboda, 2000).
New revolution: Cataract extraction surgery
Later, “couching” technique would be replaced by cataract extraction surgery.
The lens could be removed by suction through a hollow instrument. Bronze oral
suction instruments that have been unearthed seem to have been used for this
method of cataract extraction during the 2nd century A.C. Such a procedure was
described by the 10th-century Persian physician Muhammad ibn Zakariya al-Razi,
who attributed it to Antyllus, a 2nd-century Greek physician.
The procedure “required a large incision in the eye, a hollow needle, and an
assistant with an extraordinary lung capacity” (Savage-Smith, 2000).
The French ophthalmologist Jacques Daviel (1696–1762) was the first modern
European physician to successfully extract cataracts from the eye. He performed
the first extracapsular cataract extraction on April 8, 1747. It was the first
significant advance in cataract surgery since couching was invented.
John Taylor (1703-1772) was a coucher, or cataract surgeon, who performed
removal of cataracts by breaking them up into pieces.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 13
The era of Intraocular Lenses (IOLs)
Sir Nicholas Harold Lloyd Ridley (1906, Kibworth Harcourt, Leicestershire –
2001, Salisbury, Wiltshire) was an English ophthalmologist who pioneered
artificial intraocular lens transplant surgery for cataract patients.
29 November 1949, Harold Ridley successfully implanted the first IOL at St.
Thomas‟ Hospital in London. The implant was made of an inflexible material
called PMMA. It was not until 1950 that he left an artificial lens permanently in
place in an eye.
The first lens was manufactured by the Rayner Company of Brighton & Hove,
East Sussex (Spalton, 2009).
The modern phacoemulsification technique
In 1967, Charles D. Kelman (1930, Brooklyn, New York–2004, Boca Raton,
Florida), an ophthalmologist pioneer in cataract surgery, introduced
phacoemulsification after being inspired by his dentist's ultrasonic probe. This
technique uses ultrasonic waves to emulsify the nucleus of the crystalline lens in
order to remove the cataracts without a large incision.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 14
Rachana shareera of Netra
In Ayurvedic literature, the references regarding the anatomical description of
netra is scattered in different contexts and it is mentioned as an important sense organ
among the panchagnanendriyas.
Nirukti :
चष्टे रुऩं रुऩवन्तं च प्रकशमतत इतत चऺष् । (Ch.S.Su.8/8)
According to Acharya Charaka „chakshu‟ is one among pancha jnanendriyas
which is responsible for roopa grahana.
तत्र ऩूववाणि ऩंच फषध्दीन्द्न्िमवणि । (Su.S. Sha. 1/4)
Acharya Sushruta mentioned buddhindriya originating from „Roopatanmatra‟
which performed visual perception with the dominance of tejomahabhoota.
Synonyms and its meaning:
Chakshu, Akshi,Drishti, Lochanam, Netram, Nayanam
Chakshu :
1. Cakşa – Darşane + “Sinca Karaņe” Pratyaya31
(Vachaspatyam).
Which is responsible for sight.
2. Cakşa + “us” Pratyaya32
(Shabdakalpadruma)
Which means Darshanendriya.
3. According to Sir Monier Williams - It means eye, vision, faculty to see, Lord
Shiva, name of Maruta, Sage, Sun, responsible for sight.33
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 15
Akshi :
Ashu– to reach + “Ktin Karane” Pratyaya (Shabdakalpadruma)
अश्नषते अनेन 34
(Shabdakalpadruma)
This means source of reaching or seeing.
Drishti :
Driś – to see + “Ktin Karaņe” Pratyaya35
(Shabdakalpadrum)
Means source or tool with which one sees. The word „Drishti‟ has different
meanings in Ayurvedic texts including Netra, „Drishti‟ Mandala, Netrakriya
(vision), Darshana etc.
Lochanam :
Loch– to see + “ Karane lyut ” Pratyaya (Shabdakalpadrum)
Means the tool with which one sees.
रोचते अनेन इतत। 36 (Shabdakalpadruma)
Which has the capacity to see.
Netram :
Ni – to drive + “Ktin Karaņe” Pratyaya37
(Shabdakalpadruma)
Means which leads or drives one towards knowledge.
Nayanam :
Ni – to drive, to lead + “Karaņe Lyut” Pratyaya 38
(Shabdakalpadruma).
Means the source, which drives towards the subject.
Thus it is clear from the above discussion of the synonyms related to the organ of sight
that Akshi, Netra, Nayana and Lochana are the words used in anatomical sense and
Chakshu in functional.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 16
Netra utpatti :
1. As per Acharya Sushruta Ekadasha indriyas are produced from vaikarika
ahankara with the aid of tejasa ahankara. Out of this first five are called
buddhindriyas, Next five are karmendriyas and manas is ubhayatmaka, having
both functions. 39
2. As per Acharya Charaka indriyas are made up of pancamahabhoota; in which
tejomahabhoota in chakshu, akasha in shrotra, prithvi in ghrana, jala in rasana
and vayu in twak are the specially dominated ones. 40
Embryological development of Netra :
The evolution of all sense organs occurs in the 3rd
month of intrauterine life (Ch.S.
Sha. 4/11) and completes at about 7th
month (A.S. Sha. 2/13). There were differences in
opinions among ancient Acharyas regarding the evolution of Netra.
1. According to Kashyapa and Bhela, eye is the first organ to develop in the foetus.
(Ka. S. and Bh.Sha. 4/30).
2. Videha Janaka (Ch.S. Sha. 6/21) opines that all Indriyas are the foremost organ to
develop in the foetus as they are the Adhisthana of Buddhi.
3. According to the opinion of Shaunaka, Shirah is the first organ to develop, as it is
the seat of Indriyas. (Su.S. Sha. 3/32).
4. Atreya and Dhanvantari conclude that all organs in the human body develop
simultaneously (Ch.S. Sha. 6/21 & Su.S. Sha. 3/32).
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 17
Panchabhoutikatwam of Netra :
ऩरं बूवो अन्द्ननतो यक्तं ववतवत ्क्रष ष्िं ससतं जरवत ् आकवशवदश्रषभवगवांश्च च जवमन्ते
नेत्र फषद्फषदे। (Su.S. Ut. 1/11)
Netra is composed of all the five Mahabhutas i.e,
The muscular portion of eye is derived from prithvi, rakta from agni,
krishnabhaga from vayu, shwetabhaga from jala and ashrumarga from
akashamahabhutas.
Tridosha in Netra rachana :
All 3 doshas have active part in normal functioning of eye.
Vata - Pranavayu, Udanavayu, Vyanavayu, Apanavayu
Pitta - Aalochakapitta, Saadhakapitta.
Kapha - Tarpaka kapha, Avalambaka kapha.
तथव कपयक्तववहहनवं स्रोतसवं भहवबूतवनवं च प्रसवदवहदन्द्न्िमवणि तेष्वपऩ च नेत्र ेश्रेष्भि्
प्रसवदवत ्शषक्रभण्डरं च तत ्पऩत्रषजभ ्भध्मे द्र्षन्द्ष्टभण्डरं च तत ्उबमवत्भकभ ्।
(A.S. Sha. 5/48-49)
Mamsa Prithvi
Rakta Agni
Krishna mandala Vayu
Shweta mandala Jala
Ashrumarga Akasha
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 18
Tridoshas play important role in determining the colour of the eye. like Teja in
association with Rakta dhatu results in Raktaksha (reddish eye) the same Teja in
association with Pitta forms Pingaksha (dark brown eyes) and with Kapha causes
Shuklaksha (pale eye), If Tejo Mahabhoota does not reach to Drishti part then child is
born congenitally blind and Vata in association with Tejo mahabhoota causes vikrutakshi.
Dhatus in Netra rachana:
All dhatus have active part in formation and normal functioning of netra.
Rasa, Rakta, Mamsa, Meda, Asthi, Majja, Shukra ( Sarvadehavyaapi)
Pramana and akruti of Netra:
Akshikoota:
It is the orbital cavity which is two in number. It is placed just below the bhru.
The eyeball is placed in akshikoota.
Netrakriti:
सषवतृ ंगोस्तनवकवयं सवाबूतगषिॊद्धवभ ्। (Su.S.Ut.1/10)
Eye ball is round and resembles the tout of a cow in appearance and originates
from all the five elements with their attributes.
Netra pramana:
पवध्मवत ्व्दमंगषरं फवहष ल्मं स्ववंगषष्टॊदय संसभतभ ्।
व्दमंगषर ंसवात: सवधां सबषक् नमन फषद्फषदं ॥ (Su.S.Ut.1/10)
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 19
Taking central part of the patient‟s own thumb as one finger unit, the eyeball
should be known by the clinicians to measure two finger units from before backwards
and a half from side to side. The distance between two eyes is two angulas.
नेत्रवमवभ त्रत्रबवगं तष कृष्िभण्डरभषच्मते ।
कृष्िवत ्सप्तसभच्छन्द्न्त दृन्द्ष्ट दृन्द्ष्टपवशवयदव् ॥ (Su.S.Ut.1/13)
The black circle of the eye is said to be 1/3rd
of the transverse extent of the eye
ball and the eye specialists consider drishti to measure 1/7th
of this black portion.
Parts of Netra :
भण्डरवतन च सन्धधंश्च ऩटरवतन च रोचने मथवक्रभं पवजवनधमवत ्ऩंच षट् च षडवे च।
(Su.S. Ut 1/14)
Parts of eye were described by Acharya Sushruta as five mandalas, six sandhis
and six patalas.
Acharya Vagbhatta, Bhavamishra and Madhavakara have also mentioned same
as Acharya Sushruta.
1) Netra mandala :
ऩंचनेत्र ेचक्रवदवन्तयत् भण्डरवतन । (A.S. Sha. 5/50 Indu teeka)
The consecutive circular layers of the eyes are termed as mandalas.
ऩक्ष्भ वत्भा श्वेत क्रष ष्ििषष्टीनवं भण्डरवतन तष
अनषऩूवां तष ते भध्मवश्च्त्ववयो अन्त्मव मथोत्तयभ।् (Su.S. Ut. 1/15)
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 20
The mandalas are 5 in number. They are pakshma, vartma, shweta, krishna and
drishti. Beginning from the first, the outer four lie successively towards the periphery if
considered from the last (drishti).
a) Pakshma Mandala-
This is the first and outermost mandala of the eye formed by the pakshma.
b) Vartma Mandala-
Upper and lower eyelids jointly form a circle in front of the eyeball, which is
termed as vartma mandala.
c) Shukla Mandala-
This portion appears as whitish and therefore known as shukla mandala.
d) Krishna Mandala-
This portion appears as blackish and therefore known as Krishna mandala.
e) Drishti Mandala:
It is the innermost circular structure of the netra.
भसूयदरभवत्रवं तष ऩंचबूतप्रसवदजवं। खद्मोत पवस्पष सरन्गवबवसभद्धवं तेजोसबयव्मम ्॥
आव्रषतवं ऩटरेनवक्ष्िौ फवह्मेन पववयवक्रष ततभ। शधतसवत्ममवं न्रषिवं िषन्द्ष्टभवहषनामन
चचन्तकव्। (Su.S. Ut.7/3)
The Acharya Sushruta describe size of drishti is like masura dala and it is
originated from the essence of panchabhutas, resembling glow worm and spark,
shining with constant light covered with the outer most layers of eyes, appearing
like a hole and suited for cold.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 21
2) Netra sandhi:
ऩक्ष्भ वत्भागत् सन्द्न्धवात्भाशषक्रगतॊ अऩय् ।
शषक्रकृष्िगतस्त्वन्म: कृष्िदृन्द्ष्टगतॊ अऩय् ।।
तत् कनधतनकगत् षष्ट्श्चवऩवन्ग् स्भृत्। । (Su.S.Ut.1/16)
Netra Sandhis are junctional areas between two mandalas. There are 6 sandhis in netra:
a) Pakshma vartma gata sandhi-
The union line of Pakshma Mandala and Vartma Mandala is called as the
Pakshma Vartmagata Sandhi and it is considered as the lid margin.15
b) Vartma shukla gata sandhi-
The union line of Vartma and Shukla Mandala is called as Vartma Shuklagata
Sandhi. Fornix of the eyeball where the palpebral conjunctiva is reflected on to
the bulbar conjunctiva seems to be Vartma Shuklagata Sandhi.
c) Shukla krishna gata sandhi-
The circular line joining between Shukla Mandala and Krishna Mandala is called
as Shukla Krishnagata Sandhi. This junctional area can be considered as the
sclero - corneal junction i.e., Limbus.
d) Krishna drishti gata sandhi-
The union line of Krishna and Drishti Mandala is called as Krishna – Drishtigata
Sandhi. By considering iris part in Krishna Mandala, this Sandhi can be explained
and the central free margin of the iris, which rests on the anterior capsule of the
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 22
lens, can be considered as the Krishna Drishtigata Sandhi. Otherwise there is no
apparent union line between the cornea and pupil.
e) Kaneenika sandhi-
Acharya Dalhana describes kaneenika sandhi and it can be considered as the
inner or nasal canthus of the eye.
f) Apanga sandhi-
Acharya Dalhana describes apanga sandhi and it can be considered as the outer
canthus of the eye.
3. Netra patalas:
ऩटर दृष्टेयववयकभ ्। चऺषषव ऩयदव इतत बवषव ॥
Patalas means an enclosing membrane of the eye. V.S. Apte, in his Sanskrit –
English dictionary describes the meaning of Patala as a film or coating over the eyes.
According to Monier Williams, it can be considered as a layer of the eyeball.
The term patala denotes a thin membrane with a thickness of 1/5th
of width of drishti.
व्दे वत्भाऩटरे पवध्मवत ्चत्ववरय अन्मवतन चवक्षऺणि ।
जवमते ततसभयं मेषष व्मवचध् ऩयभ दवरुि् ॥ (Su.S.Ut.1/17)
Two patalas should be known to be the eye lids and other in the eye proper itself,
in which Timira, a most formidable disease occurs. The first two patalas are vartma
patala namely urdhwa vartma i.e., the upper eye lid and the adho vartma patala or lower
eyelid.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 23
तेजॊजरवचश्रतं फवह्मं तेषष अन्मत ्पऩसशतवचश्रतभ ्।
भेदस्ततृधम ंऩटरवचश्रतं त्वन्द्स्थ चवऩयभ ्॥
ऩन्चभवंशसभं दृष्टेस्तेषवं फवहष ल्मसभष्मत े॥ (Su.S.Ut.1/18)
Out of them the outer most subsists in the tejas and jala, the next one is the mamsa,
the third patala in the meda and the last one is asthi. Their thickness is said to be 1/5th
of
the drishti. Acharya Dalhana has described the first or outermost patala as
“tejojalashrita” and the word Teja means alochaka pitta and so siragata rakta can be
taken as Teja. Jala, according to him implies rasa dhatu. So it can be considered that the
first patala is supported by rasa and rakta dhatus.
a) Tejojalashrita patala-
It is the outer most among four patalas.
अत्र तेजॊ शब्देनवरॊचक तेज् सभवश्रमं ससयवगत ंयक्त ंफॊध्दव्म ं। जर ंत्वक् गतॊ यस धवतष:
॥ (Dal. Su. S.Ut.1/18)
Acharya Dalhana interprets the word teja as alochaka teja present in the blood of
blood vessels and jala as rasa dhatu in twak. Bahya patala is supported by agni
and ambasi. This patala is nourished by rasa and rakta dhatus.
b) Pishitashrita/ mamsashrita patala-
It is supported by mamsa dhatu.
c) Medoshrita patala-
It is supported by medo dhatu.
d) Asthyashrita patala-
It is supported by asthi and particularly by kalakasthi.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 24
Kriya shareera of Netra
Chakshu is the visual sensual faculty i.e., one of the panchendriyas.
आत्भेन्ि भनो अथवानवं सन्द्न्नकषवात प्रवतात े।
व्मक्तव तदत्वे मव फषन्द्ध्द् प्रत्मऺं स तनरुच्मत े॥ (Ch. S. Su.11/20)
A mental faculty is instantaneously manifested in a particular form as a result of
proximity of the soul, sense faculties, mind and the objects are known as pratyaksha
(percepition or direct observation).
भन् ऩषयस्सयवणि इन्द्न्िमवणि अथाग्रहि सभथवातन बवन्द्न्त । (Ch. S. Su.8/7)
The sense faculties are capable of perceiving their respective objective, only when
they are motivated by mind.
There are five kinds of perception viz., visual, tactile, auditory, gustatory and
olfactory. These are again the products of combination of sense faculties, their objects,
the mind and the soul; they are momentary and determinative.
These perceptions are momentary in the sense that they fade away soon. Even
though they fade away soon, they are determinative in relation to the size, shape etc., of
the objects just as a momentary light of a lamp illuminates its surroundings.
There are things which though existent, cannot directly be perceived due to over
proximity, over distance, weakness of senses, diversion of mind, confusion with other
similar objects, over shadowing and over minuteness.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 25
इन्द्न्िमेि इन्द्न्िमवथां तष स्वं गॄह्िवतत भवनव् ।
न्द्स्थतं तषल्ममोतनत्ववत ्न अन्मेन अन्मसभतत न्द्स्थतत् ॥ (Su.S.Sh.1/15)
Human beings have the perception of the objects of indriyas by that indriyaartha
only because the origin of both is similar. One indriya cannot perceive the object of
another indriya.
Eye which receives the light and light which illuminates the object both are
derivatives of tejo mahabhuta. Hence eye perceives only rupa of the object and not other
characters like sound etc. Rupa is the adhibhuta, surya is the adidaiva of chakshu which
is adhyatma (pertains to soul)
Among 6 indriyas including manas, 3 perform functions with remoteness and 3
with proximation. Amongst these manas, eyes and ears function with remoteness while
nose, tongue and skin with proximation.
Role of alochaka pitta in visual perception:
अन्द्ननयेव शरयये पऩतवन्तगात् …… दशानभदशानभ ्…… । (Ch. S. Su.12/11)
It is agni alone represented by pitta which is responsible for vision or loss of
vision depending on its normal or abnormal state.
दशानवदशाने नेत्रगतस्मवरोचकस्म । (Chak. Ch. S. Su.12/11)
Alochaka pitta present in netra is responsible for vision or loss of vision.
Its function is to form the image of an external object presented to the eye.
रुऩवरॊचनत् स्भृतं दृकस्थभवरोचकं । (A.H.Su.12/14)
Alochaka pitta is situated in the eye and its function is rupa grahana or forming
images presented to it.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 26
स न्द्व्दपवध् चऺषवैशपेषको फषन्द्ध्दवैशपेषकश्चतेत । (Bh. Sha.4/15)
Bhela has envisaged two aspects of alochaka pitta viz, chakshur vaisheshika and
buddhir vaisheshika.
The chakshurvaisheshika alochaka pitta begins its function after the sannikarsha
(union) of atma and manas, when the object has made contact with it, leading to the
production in chitta, the knowledge of the characteristics, form, colour etc., of such
things as flowers, fruits, leaves.
Buddhirvaisheshika is that which is located in shringataka, between the two eye
brows. It seizes subtle objects, retains and recalls them. This is the factor which enables
concentration, responses and cognition.
Role of other doshas in visual perception:
Vayu is the stimulator of all sensory organs and makes them to perceive their
respective objects. Pranavayu attends the function of chakshuradi sense organs.
Vyanavayu is responsible for closing and opening of eyes. The compactness of eye, its
Bandhana are all brought about by kapha.
सशय् संस्थॊ अऺतऩािवत ्तऩाक् । (A.H.Su.12/17)
Akshi Tarpana is the function of tarpaka kapha which is present in Shiras.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 27
Anatomy and Physiology 41, 42
Anatomy of the eye:
The eye is situated in a quadrilateral pyramid-shaped bony cavity called orbit. Eye
ball is a cystic structure, not a sphere but an ablate spheroid. Each eye is protected
anteriorly by two shutters called the eyelids. The anterior part of the sclera and posterior
surface of lids are lined by a thin membrane called conjunctiva. For smooth functioning,
the cornea and conjunctiva are to be kept moist by tears which are produced by lacrimal
gland and drained by the lacrimal passages. These structures (eyelids, eyebrows,
conjunctiva and lacrimal apparatus) are collectively called „the appendages of the eye‟.
Dimensions of an adult eyeball
Anteroposterior diameter - 24 mm
Horizontal diameter - 23.5 mm
Vertical diameter - 23 mm
Circumference - 75 mm
Volume - 6.5 ml
Weight - 7 gm
Coats of the eyeball
The eyeball comprises three coats:
1) Outer - fibrous coat
2) Middle - vascular coat
3) Inner - nervous coat
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 28
1) Fibrous coat:
It is a dense strong wall which protects the intraocular contents.
Anterior 1/6th of this fibrous coat is transparent and is called cornea.
Posterior 5/6th opaque part are called sclera.
Junction of the cornea and sclera is called limbus.
Conjunctiva is firmly attached at the limbus.
2) Vascular coat:
Vascular coat includes three parts from anterior to posterior. These are
iris, ciliary body and choroid.
3) Nervous coat: It includes retina.
Segments and chambers of the eyeball:
1) Anterior segments
2) Posterior segments
1) Anterior segment:
Anterior segment includes:
Crystalline lens (which is suspended from the ciliary body by zonules)
Iris
Cornea
Aanterior and posterior chamber.
Anterior chamber: It is bounded anteriorly by the back of cornea, and posteriorly by the
iris and part of ciliary body. It contains about 0.25 ml of the aqueous humour.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 29
Posterior chamber: It is a triangular space containing 0.06 ml of aqueous humour. It is
bounded anteriorly by the posterior surface of iris and part of ciliary body, posteriorly by
the crystalline lens and its zonules, and laterally by the ciliary body.
3) Posterior segment.
Posterior segment includes- Vitreous humour, Retina, Choroid and Optic disc.
Lens:
Lens is a transparent, biconvex, crystalline structure placed between iris and the
vitreous in a saucer shaped depression, the patellar fossa. The posterior surface of the lens
is in intimate contact with the vitreous in this fossa and is attached to it in a circular area
with ligamentum hyaloideo capsulare (Wiegert‟s ligament). With in this area, is a small
potential space called as retrolental or Berger‟s space. The lens is encircled by the ciliary
process, to which it is attached by the zonular fibres, collectively forming the zonule
holding the lens in place and transmitting the forces stretching the lens except in visual
accommodation. The zonular fibres are inserted into the lens capsule, a basement
membrane completely enclosing the eye.
Dimensions of the lens:
Equatorial diameter: 6.5 mm at birth, increases to 9-10 mm in second decade
then remains constant.
Thickness (Axial/Anteroposterior diameter): 3.5 mm (at birth) to 5 mm (at
extreme of age)
Weight: (0-9 years) - 135 mg, (40-80 years) - 255 mg
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 30
Surfaces: Anterior surface – Less convex (radius of 8 to 14mm.)
Post surface - More curved (radius of 4.5 to 7.5 mm.)
Both surfaces meet at the equator
Poles (and post):
Anterior pole - Centre of the anterior surface
Posterior pole- Centre of the posterior surface
Refractive Index: 1.39
Nucleus - 1.42, Cortex- 1.38
Refractive Power: 16 – 20 D
14-16 D at Birth, 7-8 D at 25 years and 1-2 D at 50 years of age.
Colour: Changes with age
Infants – Transparent, Young Adults - Colourless
By 30 years - Definite yellow finge, Old Eye - Amber colour
Structure of the Lens:
1. Lens capsule:
Capsule is the outer covering of lens. It is thin, transparent, hyaline collagenous
membrane surrounding the lens completely. Though the capsule has no elastic
tissue, it is highly elastic. The elastic nature of lens is of much importance in the
mechanism of accommodation. The lens capsule is secreted by the basal cell area
of the lens epithelium anteriorly and by the basal area of the elongating fibres
posteriorly. The lens capsule is thickest at pre equator regions (14micron) and
thinnest at the posterior pole (3 μ). Light microscopy shows capsule to be as a
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 31
transparent structure. Ultra microscopy reveals the lamellar appearance of the lens
capsule. Each lamella contains fine filaments. During exfoliation of capsule, it is
these superficial lamellae getting separated (splitting off) from deeper layers.
Principally it is composed of type IV collagen and 10% glycosamino glycans and
also contains enzymes, ATP and glycolytic intermediates.
2. Anterior lens epithelium:
Anterior lens epithelium is a single layer of cuboidal nucleated epithelial cells
which lies deep to the anterior capsule. These cells contain all the organelles
found in typical epithelial cells. The entire lens metabolic activities, synthetic and
transport processes of the lens occurs in this layer. It is the cells of this layer,
which are actively involved in dividing and elongating to form new lens fibres
throughout life, but limited to equatorial region. There is no posterior lens
epithelium, as these cells are used up in filling the central cavity of lens vericle
during development of the lens. Anterior lens epithelium has highest metabolic
rate. Have prominent, well characterized cytoskeletal network consisting of actin,
vimentin, spectrin, microtubules, alpha actinin and myosin. Anterior epithelium
can be divided into 3 zones- Central Zone, Intermediate Zone and Germinative
zone.
Central Zone- This zone is of some importance as the age progresses. The
cuboidal epithelium of this region reduces with age and under normal
circumstances do not undergo mitosis. If tissue insult occurs, repair occurs by
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 32
elongating the epithelial cells resembling fibroblasts and as much as up to 10
layers thick cell piling up occurs leading to anterior subcapsular cataract.
Intermediate Zone- Consists of much smaller and more cylindrical cells located
peripheral to central zone.
Germinative zone- Situated most peripheral and cells are actively dividing to
form new cells which migrate posteriorly to become lens fibres. Dysplasia of
these cells results in posterior subcapsular cataract.
3. Lens fibres:
The epithelial cells elongate to form lens fibres which have a complicated
structural form. Mature lens fibres are cells which have lost their nuclei. As the
lens fibres are formed throughout the life, these are arranged compactly as
nucleus and cortex of the lens.
Nucleus-
Nucleus is the central part containing the oldest fibres. It consists of different
zones, which are laid down successively as the development proceeds. In the
beam of slit-lamp these are seen as zones of discontinuity. Depending upon the
period of development, the different zones of the lens nucleus include:
Embryonic nucleus is the innermost part of nucleus which corresponds to the
lens up to the first 3 months of gestation. It consists of the primary lens fibres
which are formed by elongation of the cells of posterior wall of lens vesicle.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 33
Fetal nucleus lies around the embryonic nucleus and corresponds to the lens
from 3 months of gestation till birth. Its fibres meet around sutures which are
anteriorly Y-shaped and posteriorly inverted Y-shaped.
Infantile nucleus corresponds to the lens from birth to puberty, and
Adult nucleus corresponds to the lens fibres formed after puberty to rest of the
life.
Cortex-
It is the peripheral part which comprises the youngest lens fibres.
4. Suspensory ligaments of lens (ciliary zonules):
It consists of a series of fibres which run from the ciliary body and fuse into the
outer layer of the lens capsule around the equatorial zone. Thus, they hold the lens
in position and enable the ciliary muscle to act on it. Structurally, the ciliary
zonules are transparent, stiff and not elastic. Each zonules are composed of
microfibrils and fibres are made up of glycol protein and muco polysaccharides.
They are susceptible for hydrolysis by α-chymotrypsin has been used to
advantage in intracapsular cataract surgery. These zonular fibres are divided into
4 zones- Pars orbicularis, Zonularplexus, Zonular Fork and Zonular limbs.
Apart from these main zonular fibres, there are other supporting fibres/ auxillary
fibres that help lens to maintain its position they are hyaloid zonule, hyalocapsular
zonule and circumferential zonular girdle.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 34
Biochemical composition of lens
Main constituents of the lens are water and proteins. Water constitutes about 65 %
of the lens wet weight of the solids; the highest is protein which constitutes about 34 % of
the total weight of an adult lens. The other constituents present in the lens are lipids,
inorganic ions, carbohydrates particularly glucose and its derivatives, ascorbic acid,
glutathione and amino acids.
Lens water:
Lens is a relatively dehydrated organ, cortex being more hydrated than nucleus.
Lens dehydration is maintained by an active sodium pump that resides with in the
membrane of the cell, in the lens epithelium and in each lens fibre. 80% of water is in
free form while remaining is bound water low amount of water is necessary to
differentiate it from the surrounding acqueous structures in refractive indices.
Proteins:
Lens has richest content of proteins than any other structures/organs of the body.
The structure of these proteins is very important in maintenance of transparency of lens.
The proteins of crystalline lens can be divided into an insoluble fraction at physiological
PH called Albuminoids and the soluble fraction called crystallins.
Various protein fractions in the lens as follows:
Insoluble albuminoid - 12.5%
Alpha- crystalline - 31.7%
Beta- crystalline - 53.4%
Gamma-crystalline or albumin - 1.5%
Mucoproteins - 0.8%
Nucleoproteins - 0.07%
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 35
Beside these few minor proteins like glycoproteins, phosphoprotein, lipoprotein
and fluorescent proteins are reported in the lens.
Crystallins:
As much as 40 % of net weight of lens fibre cells can be accounted for crystalline.
It can be classified as classical and taxon specific. Classical crystallins include members
of the alpha crystallins family and the beta/gamma crystallins super family. All vertebrate
lenses accumulate large amounts of classical crystalline in their lens. There are many
transcription factors which are responsible for high lens specific crystalline gene
expression. Protein structure of alpha crystallins showed that they are members of the
family of small heat shock proteins.
An important function of small heat shock proteins is to stabilize proteins that are
partially unfolded and prevent them from aggravating (chaperone activity). Thus
increases in alpha crystallins prevent protein aggregation. Excessive protein aggregation
could lead to light scattering and cataract formation.
Insoluble proteins:
The chief insoluble protein of lens is albuminoid. It is a mixture since it is only
partly digested by the urea. Amino acid composition of albuminoid is similar to alpha
crystallin. The urea soluble and insoluble albuminoid varies with species.
Amino acids:
Two groups of amino acids are present in the lens: Proteogenic and Non-
proteogenic.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 36
Carbohydrates:
Metabolism of carbohydrates in lens is of highly active and complex. Free
carbohydrate of normal crystalline lens is glucose, fructose and glycogen. Derivates of
sugar found in lens are sorbitol, inositol, ascorbic acid, gluconic acid and glucosamine.
Lenticular glucose has its source in acqueous humor. Fructose is produced from glucose
in the crystalline lens. The concentration of glycogen varies with age and the region of
lens, lenticular glycogen is localized in nucleus where it appears to replace alpha
crystallins normally present there. Sorbitol and inositol is said to have the role in
metabolism of phospholipids.
Lipids:
The main lipids concerned are cholesterol, various phospholipids such as
cephalin, isolecithin, sphingomyelin and glycerides in addition to lipoproteins. Lipids are
present in two forms – free form and bound form (lipoproteins). The lipids are
extensively present in epithelium in young and in cortex in the adults/older. The
membranes of mature fibre cells have an unusual Lipid Composition.
Human lens fibres have the highest proportion of cholesterol of any plasma membrane in
the body and the amount of cholesterol increases as the fibre cells mature. The
cholesterol / phospholipids ratio is nearly 3 fold greater in nuclear than in cortical fiber
cells. Cholesterol content, increases with age especially in nucleus while glycerides
decrease. Similar changes occur in cataract where lecithin is abundant and cholesterol is
frequently evident macroscopically as crystals. The concentration of free lipids increases,
however, lipoprotein decreases.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 37
Electrolytes:
As in any other tissue, Sodium, Potassium, Calcium and Magnesium are present
in lens in relatively large quantities, some being present principally in the extra cellular
fluid of the lens while others predominate within the cell.
Organic phosphates:
Include nucleotides of both adenosine and pyridine. ATP is responsible for
phosphorylation of glucose. Adenosine mono and di-phosphates has also been reported.
Pyridine nucleotides act as co-enzymes to the dehydrogenaces, assisting with the transfer
of hydrogen in oxidation reduction processes. Other co-enzymes assisting in oxidation
reduction during CHO metabolism are co-enzyme 1 (Diphosphopyridine nucleotide) and
co-enzyme 2 (Triphospho pyridine nucleotide). Most of these substances in lens decline
with age and with the development of cataract.
Glutathione:
The level of glutathione in normal individuals varies from 3.5 – 5.5 mm/g net
weight of the lens. The level is altered with age. Its concentration falls with advancing
age. Glutathione is basically an amino acid. It is a tripeptide consisting of 3 amino acids –
glycine, cysteine and glutamic acid. Also known as γ – glutamyl cysteinyl glycine. The
cysteine fraction of glutathione by virtue of the presence of sulph-hydryl group (-SH) is
the most reactive constituent, making glutathione exist in 2 forms – oxidized glutathione
(GSSG) and reduced glutathione (GSH). Lens is constantly exposed to oxidative agents;
indeed there is a high level of hydrogen peroxide in normal aqueous and peroxidase
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 38
activity is also present in the lens 1-1 self. Apart from these, several enzyme systems are
available to minimize the oxidative damage. They include – catalase, superoxide
dismutase, glutathione peroxidase and glutathione-S-transferase. Glutathione is produced
from the interaction between glutamate and cysteine in lens cells. Thiol groups in
proteins are also protected by Glutathione especially in cation-transporting membrane
proteins. (Thus prevents excess hydration).
Ascorbic acid:
5-48 mg/100gm net weight concentration of ascorbic acid is present in lens. The
precise role of ascorbic acid is the conversion between ascorbic acid and the oxidized
form -dehydroascorbic acid, might be coupled with other oxidation reduction systems in
lens.
Physiology of vision
Physiology of vision is a complex phenomenon which is still poorly understood. The
main mechanisms involved in physiology of vision are:
Initiation of vision (Phototransduction), a function of photoreceptors (rods and
cones).
Processing and transmission of visual sensation, a function of image processing
cells of retina an individual pathway, and
Visual perception, a function of visual cortex and related areas of cerebral cortex.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 39
Phototransduction
The rods and cones serve as sensory nerve endings for visual sensation. Light
falling upon the retina causes photochemical changes which in turn trigger a cascade of
biochemical reactions that result in generation of electrical changes. Photochemical
changes occurring in the rods and cones are essentially similar but the changes in rod
pigment (rhodopsin) have been studied in more detail. This whole phenomenon of
conversion of light energy into nerve impulse is known as phototransduction.
Photochemical Changes:
The photochemical changes include:
Rhodopsin bleaching: Rhodopsin refers to the visual pigment present in the rods – the
receptors for night (scotopic) vision. Its maximum absorption spectrum is around 500 nm.
Rhodopsin consists of a colourless protein called opsin coupled with a carotenoid called
retinine (Vitamin A aldehyde or II-cis-retinal). Light falling on the rods converts 11-cis-
retinal component of rhodopsin into all-trans-retinal through various stages. The all trans-
retinal so formed is soon separated from the opsin. This process of separation is called
photodecomposition and the rhodopsin is said to be bleached by the action of light.
Rhodopsin regeneration: The 11-cis-retinal is regenerated from the all-trans-retinal
separated from the opsin (as described above) and vitamin-A (retinal) supplied from the
blood. The 11-cis-retinal then reunites with opsin in the rod outer segment to form the
rhodopsin. This whole process is called rhodopsin regeneration. Thus, the bleaching of
the rhodopsin occurs under the influence of light, whereas the regeneration process is
independent of light, proceeding equally well in light and darkness.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 40
Visual cycle: In the retina of living animals, under constant light stimulation, a steady
state must exist under which the rate at which the photochemicals are bleached is equal to
the rate at which they are regenerated. This equilibrium between the photodecomposition
and regeneration of visual pigments is referred to as visual cycle.
Electrical change: The activated rhodopsin, following exposure to light, triggers a
cascade of complex biochemical reactions which ultimately result in the generation of
receptor potential in the photoreceptors. In this way, the light energy is converted into
electrical energy which is further processed and transmitted via visual pathway.
Processing and transmission of visual impulse
The receptor potential generated in the photoreceptors is transmitted by
electrotonic conduction (i.e., direct flow of electric current, and not as action potential) to
other cells of the retina viz. horizontal cells, amacrine cells, and ganglion cells. However,
the ganglion cells transmit the visual signals by means of action potential to the neurons
of lateral geniculate body and the later to the primary visual cortex. The phenomenon of
processing of visual impulse is very complicated. It is now clear that visual image is
deciphered and analyzed in both serial and parallel fashion.
Serial processing: The successive cells in the visual pathway starting from the
photoreceptors to the cells of lateral geniculate body are involved in increasingly
complex analysis of image. This is called sequential or serial processing of visual
information.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 41
Parallel processing: Two kinds of cells can be distinguished in the visual pathway
starting from the ganglion cells of retina including neurons of the lateral geniculate body,
striate cortex, and extrastriate cortex. These are large cells (magno or M cells) and small
cells (parvo or P cells). There are striking differences between the sensitivity of M and P
cells to stimulus features.
The visual pathway is now being considered to be made of two lanes: one made
of the large cells is called magnocellular pathway and the other of small cells is called
parvocellular pathway. These can be compared to two-lanes of a road. The M pathway
and P pathway are involved in the parallel processing of the image i.e., analysis of
different features of the image.
Visual perception
It is a complex integration of light sense, form sense, sense of contrast and colour
sense. The receptive field organization of the retina and cortex are used to encode this
information about a visual image.
1. The light sense:
It is awareness of the light. The minimum brightness required to evoke a sensation of
light is called the light minimum. It should be measured when the eye is dark adapted for
at least 20-30 minutes. The human eye in its ordinary use throughout the day is capable
of functioning normally over an exceedingly wide range of illumination by a highly
complex phenomenon termed as the visual adaptation. The process of visual adaptation
primarily involves:
Dark adaptation (adjustment in dim illumination),
Light adaptation (adjustment to bright illumination).
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 42
Dark adaptation: It is the ability of the eye to adapt itself to decreasing illumination.
When one goes from bright sunshine into a dimly-lit room, one cannot perceive the
objects in the room until some time has elapsed. During this period, eye is adapting to
low illumination. The time taken to see in dim illumination is called „dark adaptation
time‟. The rods are much more sensitive to low illumination than the cones. Therefore,
rods are used more in dim light (scotopic vision) and cones in bright light (photopic
vision).
When fully dark adapted: The retina is about one lakh times more sensitive to light than
when bleached.
Delayed dark adaptation: Occurs in diseases of rods e.g., retinitis pigmentosa and
vitamin A deficiency.
Light adaptation: When one passes suddenly from a dim to a bright lighted
environment, the light seems intensely and even uncomfortably bright until the eyes
adapt to the increased illumination and the visual threshold rises. The process by means
of which retina adapts itself to bright light is called light adaptation. Unlike dark
adaptation, the process of light adaptation is very quick and occurs over a period of 5
minutes. Strictly speaking, light adaptation is merely the disappearance of dark
adaptation.
2. The form sense:
It is the ability to discriminate between the shapes of the objects. Cones play a
major role in this faculty. Therefore, form sense is most acute at the fovea, where there
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 43
are maximum number of cones and decreases very rapidly towards the peripheral Visual
acuity recorded by Snellen's test chart is a measure of the form sense.
3. Sense of contrast:
It is the ability of the eye to perceive slight changes in the luminance between
regions which are not separated by definite borders. Loss of contrast sensitivity results in
mild fogginess of the vision. Contrast sensitivity is affected by various factors like age,
refractive errors, glaucoma, amblyopia, diabetes, optic nerve diseases and lenticular
changes. Further, contrast sensitivity may be impaired even in the presence of normal
visual acuity.
4. Colour sense:
It is the ability of the eye to discriminate between different colours excited by
light of different wavelengths. Colour vision is a function of the cones and thus better
appreciated in photopic vision. In dim light (scotopic vision), all colours are seen grey
and this phenomenon is called Purkinje shift.
Lens transparency
Factors that play significant role in maintaining outstanding clarity and
transparency of lens are:
Avascularity,
Tightly-packed nature of lens cells,
The arrangement of lens proteins,
Semipermeable character of lens capsule,
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 44
Pump mechanism of lens fibre membranes that regulate the electrolyte and
water balance in the lens, maintaining relative dehydration
Auto-oxidation and high concentration of reduced glutathione in the lens
maintains the lens proteins in a reduced state and ensures the integrity of the
cell membrane pump.
Changes in aging lens
There are three stages of age related changes in the crystalline lens development,
growth and ageing. Changes in ageing lens can be grouped as follows:
Physical changes:
Lens weight and thickness increases steadily with age. This results due to
continued growth of the crystalline lens throughout life building up layers of new
cells from the equator.
Light transmission by the lens especially at lower wavelengths decreases with the
increasing age indicating that light absorbance increases with the age.
Light Scattering is increased with the age. It has been reported to be caused by
aggregation and formation of a gel- like state. Some workers have pursued the
idea that the increased light scattering with age could be attributed to synergism, a
process in which conformational changes to the protein release bound water,
enhancing the difference in refractive index between the drier„ protein region and
its surroundings.
Fluorescence property of lens has been confirmed to increase with the age.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 45
Refractive index in the nucleus of bovine lens is reported to increases with age.
However no such change was found in human lens.
Metabolic changes:
Most of the metabolic activities of the lens decreases with age. A few important ones are
as follows:
The proliferative capacity of human lens epithelial cells declines during adult life.
Many enzyme activities decline in the whole lens with age.
There occurs an increase in the urea- soluble protein at the expense of soluble
proteins, on going from cortex to nucleus.
Three enzymes of glutathione metabolism viz. Glutathione peroxidase,
Glutathione reductase and Glutathione transferase do not significantly decline
with age. However both glutathione and ascorbate level decrease in lens by age.
Both superoxide dismutase and glucose-6-phosphate dehydrogenase activity is
lost with age. But the denatured enzyme protein remains.
Changes in crystallins:
There occurs an age- related loss of gamma- crystallines
The gamma- crystallines fraction in particular shows an increase in disulphide
bondage.
There occurs a limited unfolding of bovine gamma- crystallines with age.

REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 46
Changes of plasma membrane and cytoskeleton:
There occur age-related losses of membrane proteins and lipids and of
cytoskeletal proteins.
A loss of membrane potential and an increase in lens sodium and calcium occurs
with age.
All the large membrane polypeptides are reported to decrease in parallel with age.
Main functional polypeptide is converted into smaller variants with age.
Changes in membrane rigidity- also occur with aging.
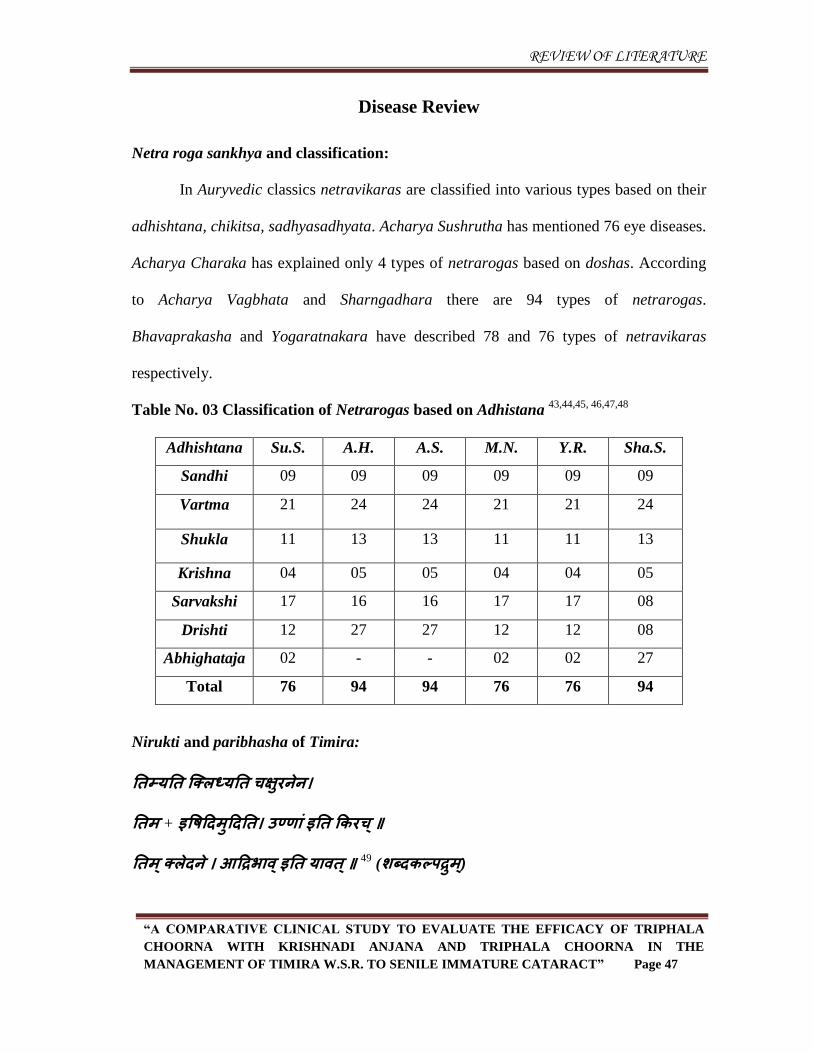
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 47
Disease Review
Netra roga sankhya and classification:
In Auryvedic classics netravikaras are classified into various types based on their
adhishtana, chikitsa, sadhyasadhyata. Acharya Sushrutha has mentioned 76 eye diseases.
Acharya Charaka has explained only 4 types of netrarogas based on doshas. According
to Acharya Vagbhata and Sharngadhara there are 94 types of netrarogas.
Bhavaprakasha and Yogaratnakara have described 78 and 76 types of netravikaras
respectively.
Table No. 03 Classification of Netrarogas based on Adhistana 43,44,45, 46,47,48
Adhishtana Su.S. A.H. A.S. M.N. Y.R. Sha.S.
Sandhi 09 09 09 09 09 09
Vartma 21 24 24 21 21 24
Shukla 11 13 13 11 11 13
Krishna 04 05 05 04 04 05
Sarvakshi 17 16 16 17 17 08
Drishti 12 27 27 12 12 08
Abhighataja 02 - - 02 02 27
Total 76 94 94 76 76 94
Nirukti and paribhasha of Timira:
ततममतत न्द्क्रध्मतत चऺषयनेन।
ततभ + इपषहदभषहदतत। उण्िवं इतत ककयच ्॥
ततभ ्क्रेदने । आहिबवव ्इतत मववत ्॥ 49
(शब्दकल्ऩिषभ)्
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 48
(1) √„Tim‟ + Unadi suffix „Kirach‟ which means:
- The increase of watery substance in the eye,
- Loss of light perception
(2) In Amarakosha, the meaning of Timira is given as darkness.
(3) In Halayudham, Timira means darkness whose enemy is sun.
From this etymological derivation it is clear that Timira means loss of light
perception of darkness or blindness, but this stage is last in Timira Roga. Thus the
nomenclature of this disease was made on the basis of its grave sequeal, which follows
improper treatment of the diseases. So, Timira is a pathological condition in which vision
gets reduced and ultimately leads to blindness- linganasha.
Synonymns of Timira: 50
Andhakara - Darkness
Tamishra - The dark half of the month
Dhwanta - Darkness
Tama - Darkness
Timira - Darkness
Nidana of Timira:
The specific nidana of Timira is not mentioned in the classics. Samanya nidana of
netrarogas is described in classics. In few Ayurvedic classics Timira has been mentioned
as a symptom or sequel of some rogas. Thus Timira roga varies from a symptom to a
full-established disease. Even other urdhvajatrugata rogas can also be the cause of this
roga as many nidanas for other diseases are same as of netra rogas.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 49
The different references regarding etiology of Timira are as follows:
योगव सवे अपऩ भन्दे अननौ, सषतयवभषदयवणि च। (M.N. Udararanidana/1)
Mandagni is the root cause of all diseases. Same way even netra rogas are due to the
hampered agnibala of an individual.
असवत्ममेन्द्न्िमवथा संमोग् प्रज्नवऩयवध् ऩरयिवभश्चतेत त्रमन्द्स्त्रपवधपवकल्ऩव् कवयिं
पवकवयविवभ ्। (Ch.S. Su. 11/43)
As per Acharya Charaka‟s version asatmyendriyartha samyoga, prajna paratha and
parinama are causative factors of diseases.
कवरवथाकभािवं मोगो हीनसभथ्मवहदभवत्रक : सममनमोगश्च पवज्नेमो योगवयोनम क
कवयिभ ्। (A.H. Su. 1/19 )
Acharya Vagbhata has mentioned the samyak yoga of kala, artha and karma is the base
of arogya; If those are not in balance, there will be origin of disease.
योगव् सवेपऩ जवमन्ते वेगोदीयिधवयि ्
तनहदाष्टं सवधनं तत्र बूतमष्ठं मे तष तवन ्प्रतत ।
ततश्चवनेकधव प्रवम् ऩवनो मत्प्रकष प्मतत
अन्नऩवनौषध ंतस्म मषन्जधतवतो अनषरोभनभ ्।। (A.H. Su. 4/22-23)
All diseases are due to the forceful evacuation or withholding of adharaneeyavegas.
In this context, vata is the main prakupita dosha. So anulomana with suitable food,
drinks and medicine plays an important role.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 50
उष्िवसबतप्तस्म जरप्रवेशवत ्दयेूक्ष्िवत ्स्व्प्नपवऩमामवच्च ।।
प्रसक्तसंयोदन कोऩशोक क्रेशवसबघवतवदततभ थषनवच्च ।।
शषक्तवयनवरवमरकष रत्थभवषतनषेविवत ्वेगपवतनग्रहवच्च ।।
स्वेदविजोधूभतनषेविवच्च छदेपवाघवतवत ्वभनवततमोगवत ् ।।
फवष्ऩग्रहवत ्सूक्ष्भतनयीऺिवच्च नेत्र ेपवकवयवन ्जनमन्द्न्त दोषव: ।। (Su. S. Ut. 1/26-27)
Sudden plunging into water after exposure to heat, looking at very distant objects,
improper sleeping habits, prolonged weeping, excess of anger, grief, trauma of head,
excessive intercourse, intake of highly sour foods, horse-gram, black-gram, withholding
natural urges, atiyoga of vamana karma, withholding tears, looking at very minute
objects, atiyoga of sweda karma and exposure to dust and smoke are the causative factors
leading to netraroga.
Acharya Sushruta also highlighted that Abhishyanda is the root cause of all eye
diseases. 51
Atiyoga, heenayoga and mithyayoga of vak-mana-shareera pravrutti are the other
causes mentioned by Acharya Charaka. These have bad effect on all senses including
chakshuindriya. 52
Acharya Harita mentioned intake of ushna, atikshara and katu ahara, injury and
looking at fine object do have harmful effect on netras. 53
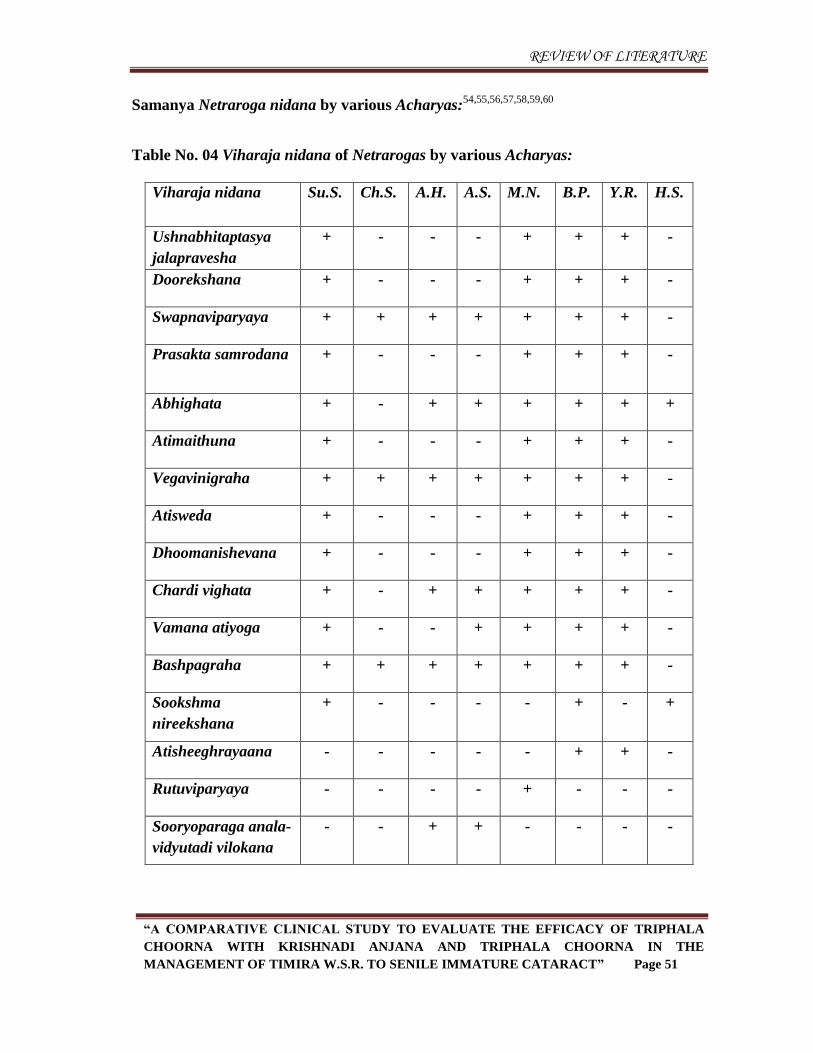
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 51
Samanya Netraroga nidana by various Acharyas:54,55,56,57,58,59,60
Table No. 04 Viharaja nidana of Netrarogas by various Acharyas:
Viharaja nidana Su.S. Ch.S. A.H. A.S. M.N. B.P. Y.R. H.S.
Ushnabhitaptasya
jalapravesha
+ - - - + + + -
Doorekshana + - - - + + + -
Swapnaviparyaya + + + + + + + -
Prasakta samrodana + - - - + + + -
Abhighata + - + + + + + +
Atimaithuna + - - - + + + -
Vegavinigraha + + + + + + + -
Atisweda + - - - + + + -
Dhoomanishevana + - - - + + + -
Chardi vighata + - + + + + + -
Vamana atiyoga + - - + + + + -
Bashpagraha + + + + + + + -
Sookshma
nireekshana
+ - - - - + - +
Atisheeghrayaana - - - - - + + -
Rutuviparyaya - - - - + - - -
Sooryoparaga anala-
vidyutadi vilokana
- - + + - - - -
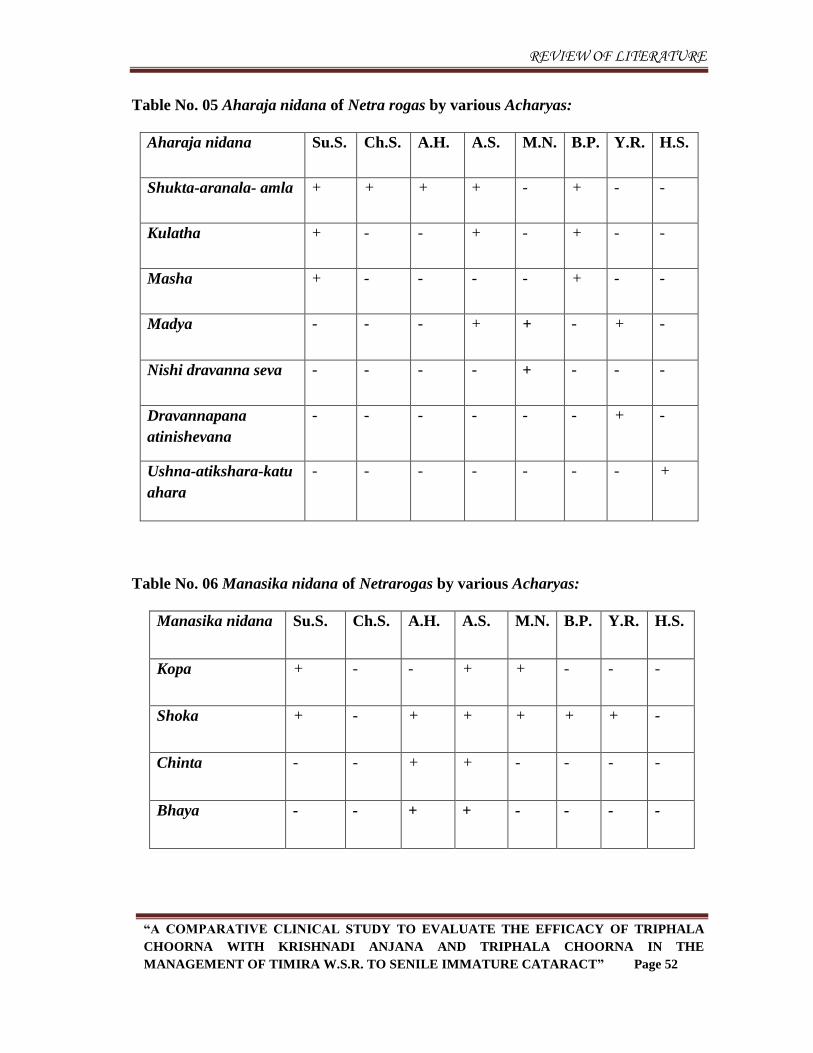
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 52
Table No. 05 Aharaja nidana of Netra rogas by various Acharyas:
Aharaja nidana Su.S. Ch.S. A.H. A.S. M.N. B.P. Y.R. H.S.
Shukta-aranala- amla + + + + - + - -
Kulatha + - - + - + - -
Masha + - - - - + - -
Madya - - - + + - + -
Nishi dravanna seva - - - - + - - -
Dravannapana
atinishevana
- - - - - - + -
Ushna-atikshara-katu
ahara
- - - - - - - +
Table No. 06 Manasika nidana of Netrarogas by various Acharyas:
Manasika nidana Su.S. Ch.S. A.H. A.S. M.N. B.P. Y.R. H.S.
Kopa + - - + + - - -
Shoka + - + + + + + -
Chinta - - + + - - - -
Bhaya - - + + - - - -
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 53
Secondary causes of Timira:
Grahani Roga: Acharya Charaka specifies that if grahani is not treated well results in
Timira.61
Navana Nasya Karma: Acharya Charaka described that a person suffering from fever,
grief or has consumed alcohol, if we give navana nasya karma then he will suffer from
Timira roga. 62
Arsha: According to Acharya Charaka, Timira is a common lakshana of sahaja arsha
and Acharya Vagbhata also describes it as a common symptom of arhsa. 63
Pinasa: Andhatva (blindness) and severe eye ailments are mentioned as complications of
pratishyaya by Acharya Sushruta. 64
Raktasrava: Excessive raktasrava leads to Timira. 65
Bhaspa nigraha leads to Timira as mentioned by Acharya Bhela. 66
Samprapti:
The entire process which represents a sequence from vitiation of doshas to vivid
manifestation of the disease is known as samprapti.67
ससयवनषसवरयसबदोष ् पवगषि रूध्वाभवगत ्
जवमन्ते नेत्रबवगेषष योगव: ऩयभदवरुिव्। (Su.S. Ut 1/20)
Acharya Sushruta has described common samprapti for all the netra rogas. He
explained that vitiated doshas through siras reaches the supra clavicular region and
settles in eyes and cause different eye diseases.
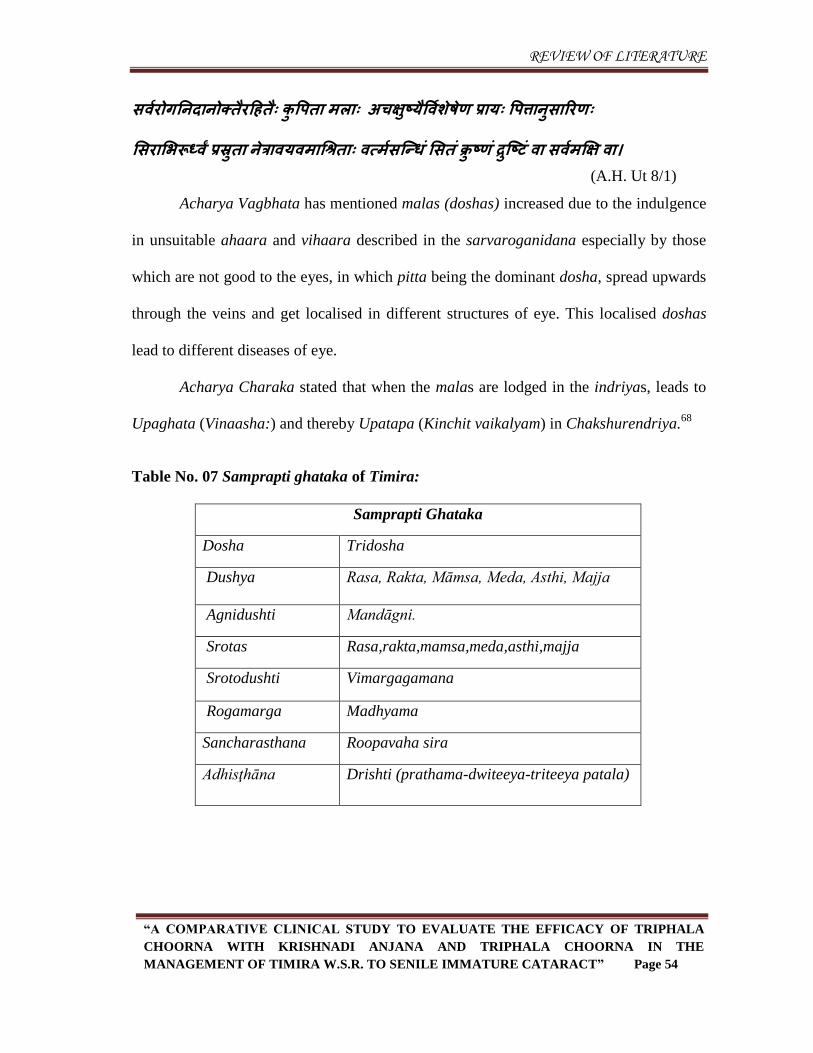
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 54
सवायोगतनदवनोक्त यहहत ् कष पऩतव भरव् अचऺषष्म पवाशषेेि प्रवम् पऩत्तवनषसवरयि्
ससयवसबरूध्वां प्रस्रषतव नेत्रववमवभवचश्रतव् वत्भासन्द्न्ध ंससतं क्रष ष्िं िषन्द्ष्टं वव सवाभक्षऺ वव। (A.H. Ut 8/1)
Acharya Vagbhata has mentioned malas (doshas) increased due to the indulgence
in unsuitable ahaara and vihaara described in the sarvaroganidana especially by those
which are not good to the eyes, in which pitta being the dominant dosha, spread upwards
through the veins and get localised in different structures of eye. This localised doshas
lead to different diseases of eye.
Acharya Charaka stated that when the malas are lodged in the indriyas, leads to
Upaghata (Vinaasha:) and thereby Upatapa (Kinchit vaikalyam) in Chakshurendriya.68
Table No. 07 Samprapti ghataka of Timira:
Samprapti Ghataka
Dosha Tridosha
Dushya Rasa, Rakta, Māmsa, Meda, Asthi, Majja
Agnidushti Mandāgni.
Srotas Rasa,rakta,mamsa,meda,asthi,majja
Srotodushti Vimargagamana
Rogamarga Madhyama
Sancharasthana Roopavaha sira
Adhisţhāna Drishti (prathama-dwiteeya-triteeya patala)
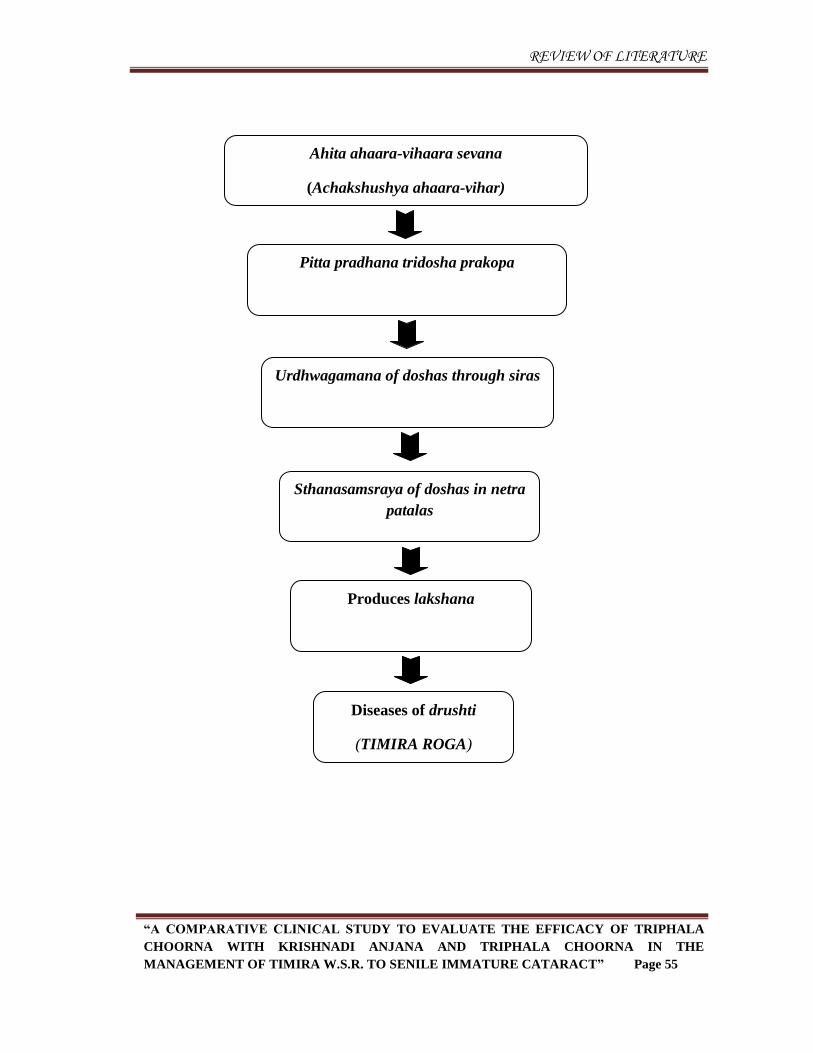
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 55
Ahita ahaara-vihaara sevana
(Achakshushya ahaara-vihar)
Pitta pradhana tridosha prakopa
Urdhwagamana of doshas through siras
Sthanasamsraya of doshas in netra
patalas
Produces lakshana
Diseases of drushti
(TIMIRA ROGA)
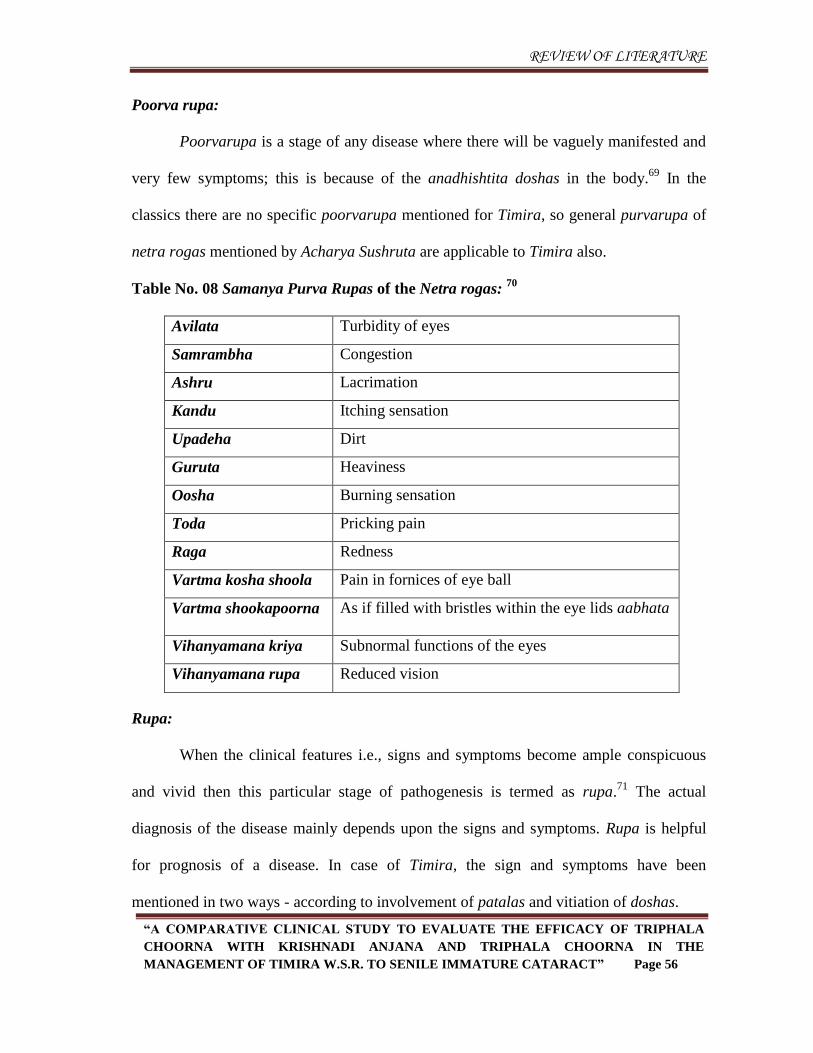
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 56
Poorva rupa:
Poorvarupa is a stage of any disease where there will be vaguely manifested and
very few symptoms; this is because of the anadhishtita doshas in the body.69
In the
classics there are no specific poorvarupa mentioned for Timira, so general purvarupa of
netra rogas mentioned by Acharya Sushruta are applicable to Timira also.
Table No. 08 Samanya Purva Rupas of the Netra rogas: 70
Avilata Turbidity of eyes
Samrambha Congestion
Ashru Lacrimation
Kandu Itching sensation
Upadeha Dirt
Guruta Heaviness
Oosha Burning sensation
Toda Pricking pain
Raga Redness
Vartma kosha shoola Pain in fornices of eye ball
Vartma shookapoorna As if filled with bristles within the eye lids aabhata
Vihanyamana kriya Subnormal functions of the eyes
Vihanyamana rupa Reduced vision
Rupa:
When the clinical features i.e., signs and symptoms become ample conspicuous
and vivid then this particular stage of pathogenesis is termed as rupa.71
The actual
diagnosis of the disease mainly depends upon the signs and symptoms. Rupa is helpful
for prognosis of a disease. In case of Timira, the sign and symptoms have been
mentioned in two ways - according to involvement of patalas and vitiation of doshas.
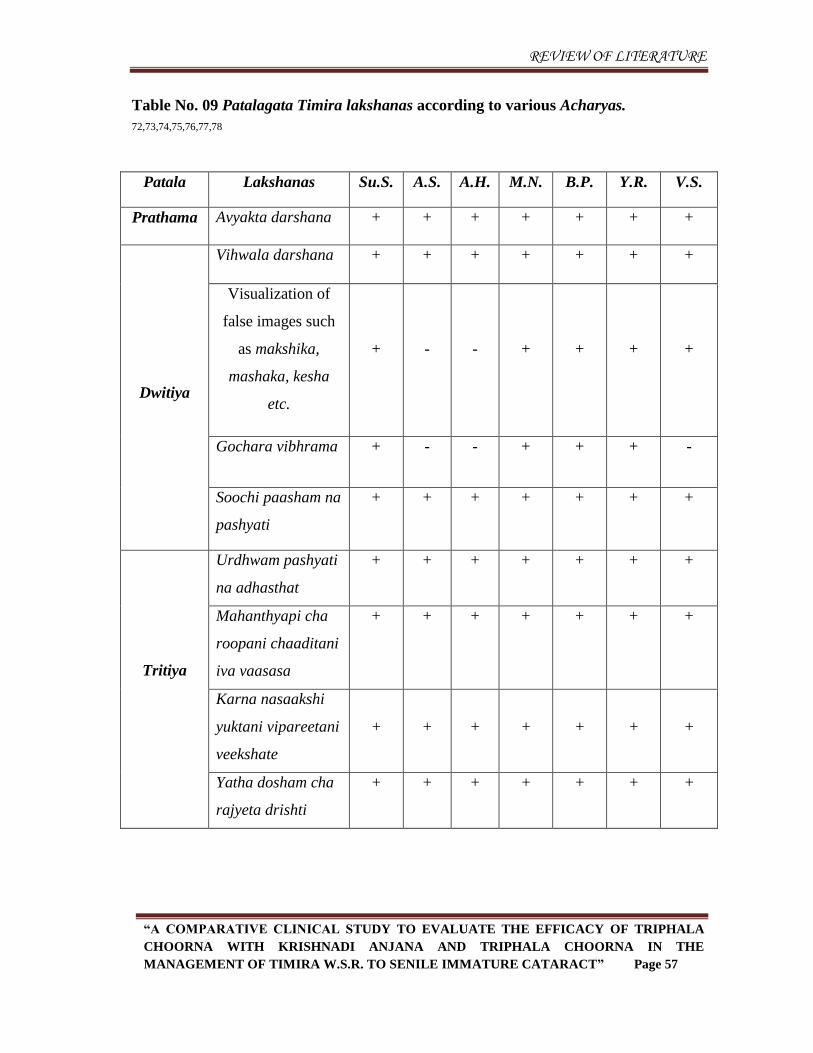
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 57
Table No. 09 Patalagata Timira lakshanas according to various Acharyas.
72,73,74,75,76,77,78
Patala Lakshanas Su.S. A.S. A.H. M.N. B.P. Y.R. V.S.
Prathama Avyakta darshana + + + + + + +
Dwitiya
Vihwala darshana + + + + + + +
Visualization of
false images such
as makshika,
mashaka, kesha
etc.
+
-
-
+
+
+
+
Gochara vibhrama + - - + + + -
Soochi paasham na
pashyati
+ + + + + + +
Tritiya
Urdhwam pashyati
na adhasthat
+ + + + + + +
Mahanthyapi cha
roopani chaaditani
iva vaasasa
+ + + + + + +
Karna nasaakshi
yuktani vipareetani
veekshate
+
+
+
+
+
+
+
Yatha dosham cha
rajyeta drishti
+ + + + + + +
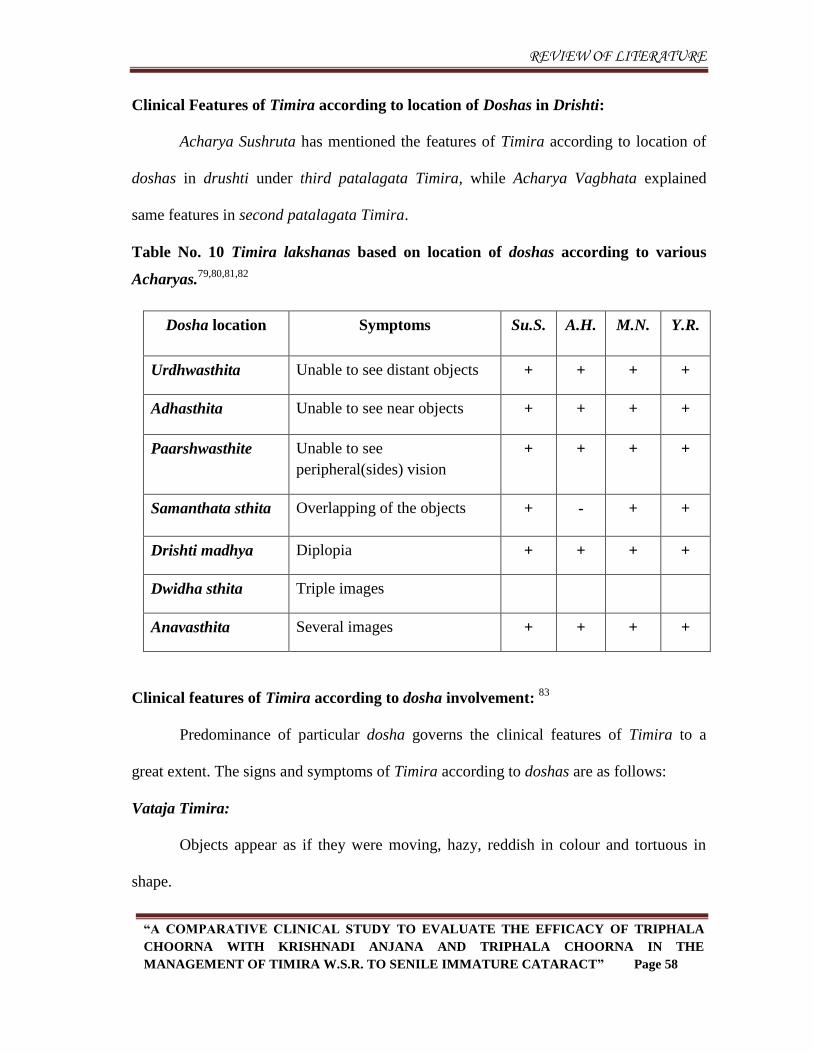
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 58
Clinical Features of Timira according to location of Doshas in Drishti:
Acharya Sushruta has mentioned the features of Timira according to location of
doshas in drushti under third patalagata Timira, while Acharya Vagbhata explained
same features in second patalagata Timira.
Table No. 10 Timira lakshanas based on location of doshas according to various
Acharyas.79,80,81,82
Dosha location Symptoms Su.S. A.H. M.N. Y.R.
Urdhwasthita Unable to see distant objects + + + +
Adhasthita Unable to see near objects + + + +
Paarshwasthite Unable to see
peripheral(sides) vision
+ + + +
Samanthata sthita Overlapping of the objects + - + +
Drishti madhya Diplopia + + + +
Dwidha sthita Triple images
Anavasthita Several images + + + +
Clinical features of Timira according to dosha involvement: 83
Predominance of particular dosha governs the clinical features of Timira to a
great extent. The signs and symptoms of Timira according to doshas are as follows:
Vataja Timira:
Objects appear as if they were moving, hazy, reddish in colour and tortuous in
shape.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 59
Pittaja Timira:
Visualization of false flashes of the light, glow worm, rainbow and the lightening.
Bluish and blackish shades appear as variegated like the feathers of a peacock.
Kaphaja Timira:
Patient sees all the objects as glossy white like the colours of clouds. The patients
can see objects which are not excessively small and visualize moving clouds in the
cloudless sky. All the objects appear as if inundated in water.
Vagbhata described that objects are seen dim or dark.
Raktaja Timira:
Objects appear to be in various colours such as dark greenish, greyish, or blackish
and smoky all around.
Sannipataja Timira:
Due to vitiation of all doshas together, objects appear to be in various colours,
scattered and as having double or manifold images all around. Images appear to be
luminous and are seen to possess more or less than normal parts. Non existing things are
visualised and existing things are improperly visualised.
Parimlayi Timira:
Pitta when associated with tejas of shonita produces the Timira called parimlayi,
the patient sees all sides as yellow and visualizes as if the sun is rising. All trees appear to
be full of glow worms and flashes of the light. Patient‟s vision may improve due to
depletion of doshas.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 60
Chikitsa
Timira is one among the diseases of drishti mandala, which commonly starts from
simple visual disturbances which may turn into complete vision loss so proper care
should be taken to restore vision.
Acharya Vagbhata has mentioned that, if Timira is ignored by the physician or
patient, it leads to Kacha and then into Linganasha i.e., blindness. Thus to
manage Timira, the most dreadful one among the diseases of eye, urgent
measures to be taken. 84
According to Acharya Yogaratnakara, Timira is the main cause of blindness so it
must be treated with all efforts. 85
As per Gada Nigraha Netrarogadhikara, Timira is a condition which can destroy
the drishti shakti. Thus it has to be treated by the physician without any delay. 86
तत्र समबवभवसवद्म मथवदोषं सबषन्द्नजतभ ्पवद्मवन्नेत्रजवयोगव् फरवन्त् स्मषयन्मथव संऺेऩत् कक्रमवमोगो तनदवनऩरयवजानभ ्ववतवदीनवं प्रतधघवतो प्रोक्तो पवस्तयत् ऩषन्।
(Su.S.Ut. 1/25)
Upon recognizing the possibility of development of disease, a proper treatment should be
given according to the affection of doshas, failing which grave eye diseases may develop.
In brief, the management essentially consists of avoidance of the etiological factors; and
specifically in detail, it implies counteracting the increased vata and other doshas.
सेक आश्च्मोतन ंपऩण्डध त्रफडवरस्तऩािं तथव ऩषटऩवको अन्जनं च सब् कल्क ् नेत्रभषऩवचयेत।् (B.P. Ma. 63/136)
According to Bhavaprakasha, the eye has to be treated with procedures like Seka,
Aschyotana, Pindi, Bidalaka, Tarpana, Putapaka and Anjana.

REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 61
Chikitsa sutra:
दोषवनषयोधेन च न कशस्तं स्नेहवस्रपवस्रववियेकनस्म ् उऩवचयेदन्जनभूधाफन्द्स्त
फन्द्स्तकक्रमवतऩािरेऩसेक ् सवभवन्मं सवधनसभदभ।् (A. H. Ut. 13/47)
According to Acharya Vagbhata Snehana, Raktamokshana, Virechana, Nasya,
Anjana, Shirobasti, Basti, Tarpana, Lepa and Seka- these therapies administered several
times suitable to the doshas is the mode of treatment of Timira.
Chikitsa of timira can be classified into two:
1. Shodhana chikitsa
2. Shamana chikitsa
1. Shodhana chikitsa:
Virechana:
The following formulations are mentioned by acharyas for virechana karma in
timira:
Vataja Timira
Dashamoola ghrita pana followed by Virechana with Triphala-Panchamoola
kwatha with ksheera and eranda taila. 87
Pittaja Timira
Virechana with Trivrit choorna mixed with Sharkara, Ela and Madhu. 88
Kaphaja Timira
Virechana with Poogadi kwatha. 89
Raktaja and Pittaja Timira
Ghrita processed with Triphala is good for Virechana. 90
Sannipataja Timira
Virechana by taila processed with Trivrit is desirable. 91
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 62
Nasya:
Depending upon doshadhikya in Timira, the formulation for nasya is selected.
Formulations such as Jeevantyadi taila,92
Jeevaneeya-Sita-Utpala siddha ghrita,93
Hreeberadi taila,94
Bhringarajadya taila, Marichadi taila, Vibheetakadyataila,
Triphalataila, Gomaya taila, Ajita taila and Neelotpaladya taila are useful in Timira.95
Basti:
In vataja timira, nirooha and anuvasana bastis are useful.
Raktamokshana:
In Kaphaja timira, Pittajatimira and Raktaja Timira, Siravyadha is indicated.
Siravyadha is contra-indicated in Ragaprapta timira.96
2. Shamana chikitsa:
Shamana Chikitsa can be devided into:
a) Sthanika Chikitsa
b) Sarvadaihika Chikitsa
a) Sthanika Chikitsa
Tarpana with Patoladi ghrita, Jeevantyadi ghrita, Drakshadi ghrita, and
Shatahwadi ghrita and Triphala ghrita are beneficial for treating timira. 97
Seka with prapoundareekadi kwatha is helful to treating timira. 98
Anjana with Krishnadi varti,99
Triphaladi varti,100
Kumarika varti, Drushtiprada
varti, Hareetakyadivarti, Sukhavativarti, Muktadimahanjana, Bhaskara varti and
Chandrodayadi varti are mentioned by acharyas.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 63
Bidalaka with Pathyadi lepa101
and Rasanjanadi lepa102
are useful in treating
timira.
Pindi with Haridradi pindika is indicated in timira.
103
b) Saarvadaihika Chikitsa
Ghrita Kalpanas - Phalatrikadi Ghrita, Patoladi ghrita, Triphla Ghrita,
Mahatriphaladya ghrita, Dwitiya Triphaladya Ghrita, Laghu Triphala Ghrita,
Rasnadi ghrita, Dashamoola ghritam, Drakshadi ghrita, , Jeevantyadi ghritam,
Shatahwadi ghrita.104, 105
Triphala prayoga- In Pittaja timira regular intake of triphala mixed with ghrita,
in vataja timira triphala mixed with taila and in kaphaja triphala mixed with
madhu is indicated. 106
Pathyapathya for Timira:
Pathya Ahaara
Shigru, bhringaraja, yava, raktashaali, mudga, purana ghrita, kulatha, surana,
patola, varthaka, karkataka, karavellaka, navina mocha, nava moolaka, punarnava,
kakamachi, kumarika, draksha, kustumburu, saindhava lavana, lodra, triphala, madhu,
stanya, candana, karpura, matsyakshi, All tikta and laghu ahara.
Pathya Vihaara
Prasanna manasa, guru pooja, pada raksha dharana, umbrella and shirovestana
to protect uttamanga, shirah snana with cold water, regular practice of shiro abhyanga.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 64
Apathya Ahara
Masha, aranala, sura, dadhi, kalinga, pinyaka, adhika jala paana, matsya, patra
shakha, jangala mamsam, tambulam, veshavara, phanita, kanji, amla- lavana-vidahi-
tikshna-katu-ushna-guru anna and paana.
Apathya Vihara
Diva swapna, suppression of natural urges like ashru, vayu, vinmutra, nidra,
vamana, sukshmekshanam, danta vigharshanam, ratri bhojanam, aatapa sevana,
prajalpanam, vamana karma, exposure to smoke, dust, heat and cold, krodha, klesha,
shoka, bhaya, atimaithuna.
Sadhyasaadhyata:
अयवगध ततसभयं सवध्मभवद्मं ऩटरभवचश्रतभ।् क्रष च्रं द्पवतधमे यवचग स्मवत्त्रषतधमे मवप्मभषच्मते॥
(Su.S. Ut. 17/53)
Prathama patalagata timira which has not attained ragatwa is sadhya, dwitiya
patalagata timira which has not attained ragatwa is krichhrasadhya and tritiya
patalagata timira which has attained ragatwa is yapya.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 65
Modern Aspect
Disease Review107,108,109,110
The term cataract is used loosely to mean the occurrence of an optical
discontinuity in the lens of such magnitude as to cause a noticeable dispersion of light.
Cataracts are considered clinically significant when opacification interferes with visual
function.
Etymology:
The word cataract means a waterfall or floodgate. It is derived from Latin word
cataracta. In Greek, the root word is “katarhaktes” which means broken water; Its
alternative sense in Latin of "portcullis" probably was passed through French to form the
English meaning “eye disease” (early 15century.), on the notion of “obstruction” (to
eyesight).111
Definition:
Opacity in the lens or its capsule, whether developmental or acquired, is called a
cataract.
As per WHO, Cataract is clouding of the lens of the eye which prevents clear
vision.
WHO says, though most of cases of cataract are related to the ageing process,
occasionally children can be born with the condition, or a cataract may be
developed after eye injuries, inflammation, and some other eye diseases.
Etiological factors of cataract:
Age, systemic diseases, dermatological diseases, physical factors and toxic agents
are the basic causes of the cataract.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 66
Age:
Usually Above 50 years
Heredity
UV radiation- Early onset and maturation
Dietary factors -Diet deficient in proteins , amino acids, vitamins &
essential elements
Severe dehydration -Diarrhoea, Cholera, Smoking
Systemic diseases:
Diabetes mellitus, galactosaemia, alport syndrome, lowe‟s syndrome and down
syndrome are the common systemic disorders which can cause loss of transparency of
lens.
Dermatological diseases:
Atopic dermatitis
Icthyosis
Physical factors:
Trauma
Electric Shock
Radiation-Infrared, X-ray, UV-Radiation
Toxic agents:
Gold, Iron, Copper
Pathogenesis:
Following mechanisms lead to opacification or loss of transparency of lens-
Oxidative damage to membranes & proteins, hydration, denaturation of lens
proteins, opacification of lens fibres with fibrous metaplasia, epithelial opacification,
accumulation of pigmented molecules, disturbance of osmotic balance, formation of
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 67
deposits of extracellular materials and failure of ion pumps can leads to the opacification
of lens.
Cataract is caused by the degeneration and opacification of the lens fibres already
formed, the formation of aberrant lens fibres or deposition of other material in their place.
The loss of transparency occurs because of abnormalities of lens proteins and consequent
disorganisation of the lens fibres. Any factor, physical or chemical, which disturbs the
critical intra and extra cellular equilibrium of water and electrolytes or deranges the
colloid system within the fibres tend to bring about opacification. Aberrant lens fibres are
produced when the germinal epithelium of the lens loses its ability to form normal fibres.
Biologically, three factors are evident in the process of cataract formation. In the early
stages of cataract, particularly the rapidly developing forms, hydration is a prominent
feature so that frequently actual droplets of fluid gather under the capsule forming
lacunae between the fibres, and the entire tissue swells (intumescence) and becomes
opaque. To some extent, this process may be reversible and thus opacities formed may
clear up. The second factor is denaturation of lens proteins. If the proteins are denatured
with an increase in insoluble proteins, a dense opacity is produced, a process which is
irreversible; opacities thus constituted do not clear up. Such an alteration occurs typically
in the young lens or the cortex of adult lens where metabolism is relatively active. It is
rarely seen in the older and inactive fibres of the nucleus. Here the usual degenerative
change is rather of third type, one of slow sclerosis. Clinically, when the first process is
predominant the condition is called a soft cataract and third is described as a hard
cataract.112
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 68
Classification:
A. Etiological classification
I. Congenital and developmental cataract
II. Acquired cataract
1. Senile cataract
2. Traumatic cataract
3. Complicated cataract
4. Metabolic cataract
5. Electric cataract
6. Radiational cataract
7. Toxic cataract- i. Corticosteroid-induced cataract
ii. Miotics-induced cataract
iii. Copper (in chalcosis) and iron (in siderosis) induced cataract.
8. Cataract associated with skin diseases (Dermatogenic cataract).
9. Cataract associated with osseous diseases.
10. Cataract with miscellaneous syndromes- i. Dystrophica myotonica
ii. Down's syndrome.
iii. Lowe's syndrome
iv. Treacher - Collin's syndrome
B. Morphological classification
1. Capsular cataract: i. Anterior capsular cataract
ii. Posterior capsular cataract
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 69
2. Subcapsular cataract: It involves the superficial part of the cortex (just below the
capsule): i. Anterior subcapsular cataract
ii. Posterior subcapsular cataract
3. Cortical cataract: It involves the major part of the cortex.
4. Supranuclear cataract: It involves only the deeper parts of cortex (just outside the
nucleus).
5. Nuclear cataract: It involves the nucleus of the crystalline lens.
Senile cataract
Factors affecting age of onset, type and maturation of senile cataract:
It is also called age related cataract and is the commonest type of acquired
cataract. It affected equally persons of either sex usually above the age of 50 years. This
condition is usually bilateral but almost always one eye is affected earlier than the other.
Classically the senile cataract occurs in two forms, the cortical (soft) cataract and nuclear
(hard) cataract. The cortical senile cataracts start as cuneiform or cupuliform. In general
the predominant form can be given as cuneiform (75%), nuclear (25%) and cupuliform
(5%).
Etiology:
Senile cataract is essentially an ageing process. Though its precise
etiopathogenesis is not clear, the following etiopathogenic factors are to be considered.
Heredity
It plays a considerable role in incidence, age of onset and maturation of
cataract in different races and families.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 70
Exposure to Ultraviolet irradiation
More exposure to UV radiation from sunlight has implicated for early onset
and maturation of senile cataract. Recently from animal experiments it has
been confirmed that UV radiation between 290 and 320mm could induce lens
opacification.
It has been proposed that prolonged exposure to UV-rays may initiate
photooxidative damage in the lens. The mechanisms are:
Near UV-light is absorbed by tryptophan.
Tryptophan in sunlight is converted in to N-formyl-kynurenine.
Both these compounds can act as photosensitizers and lead to production of
the free radical single oxygen.
This free radical single oxygen regulates the function of critical lens
enzymes such as Na+/K
+ ATP-ase and lead to lens swelling and
opacification.
Other free radicals generated by near UV-light such as hydrogenperoxide
have been implicated in the dysfunction of hexokinase, an enzyme central to
glucose utilization in lens.
Lipid peroxidation may also play a role in cataractogenesis. Fattyacids can
ultimately produce the compound malondialdehyde, a well known cross
linking agent, which can attach enzymes and membrane components.
Oxygen increasees the rate of photo-oxidation and vitamin E, ascorbic acid
and glutathione reduces the effects of light damage.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 71
Dietary factors
Diet deficient in certain proteins, amino acids, vitamins (riboflavin, vitamin E,
vitamin C), and essential elements have also been blamed for early onset and
maturation of senile cataract.
Dehydrational crisis:
An association with priorepisode of severe dehydrational crisis (due to
diarrhoea, cholera etc.) and age of onset and maturation of cataract is also
suggested.
Smoking: has also been reported to have some effect on the age of onset of
senile cataract. Smoking causes accumulation of pigmented molecules-3
hydroxykynurinine and chromophores, which lead to yellowing. Cyanates in
smoke cause carbamylation and protein denaturation.
Causes of presenile cataract:
The term presenile cataract is used when the cataractous changes similar to senile cataract
occur before 50 years of age. Its common causes are:
Heredity
As mentioned above because of influence of heredity, the cataractous changes
may occur at an earlier age in successive generations.
Diabetes mellitus
Age related cataract occurs earlier in diabetics. Nuclear cataract is more
common and tends to progress rapidly.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 72
Myotonic dystrophy
Associated with posterior subcapsular type of presenile cataract.
Atopic dermatitis
It may be associated with presenile cataract (atopic cataract) in 10% of the
cases.
Mechanism of loss of transparency
It is basically different in nuclear and cortical senile cataracts.
Cortical senile cataract
Its main biochemical features are decreased levels of total proteins, amino
acids and potassium associated with increased concentration of sodium and
marked hydration of the lens, followed by coagulation of proteins.
Nuclear senile cataract
In nuclear senile cataract usual degenerative changes are intensification of the
age related nuclear sclerosis associated with dehydration and compaction of
the nucleus resulting in a hard cataract.
It is accompanied by a significant increase in water insoluble proteins.
However, the total protein content and distribution of cations remain normal.
There may or may not be associated deposition of pigment urochrome and/or
melanin derived from the amino acids in the lens.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 73
Stages of maturation
1. Maturation of the cortical type of senile cataract
a) Stage of lamellar separation:
The earliest senile change is demarcation of cortical fibres owing to their
separation by fluid.
This phenomenon of lamellar separation can be demonstrated by slit-lamp
examination only. These changes are reversible.
b) Stage of incipient cataract:
In this stage early detectable opacities with clear areas between them are seen.
Two distinct types of senile cortical cataracts can be recognized at this stage:
i. Cuneiform senile cortical cataract
It is characterised by wedge-shaped opacities with clear areas in between.
These extend from equator towards centre and in early stages can only be
demonstrated after dilatation of the pupil. They are first seen in the lower
nasal quadrant. These opacities are present both in anterior and posterior
cortex and their apices slowly progress towards the pupil.
On oblique illumination these present a typical radial spoke-like pattern of
greyish white opacities.
On distant direct ophthalmoscopy, these opacities appear as dark lines
against the red fundal glow. Since the cuneiform cataract starts at periphery
and extends centrally, the visual disturbances are noted at a comparatively
late stage.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 74
ii. Cupuliform senile cortical cataract
Here a saucer shaped opacity develops just below the capsule. Usually in the
central part of posterior cortex (posterior subcapsular cataract), which
gradually extends outwards. There is usually a definite demarcation between
the cataract and the surrounding clear cortex.
Cupuliform cataract lies right in the pathway of the axial rays and thus
causes an early loss of visual acuity.
c) Immature senile cataract (ISC):
In this stage, opacification progresses further. The cuneiform or cupuliform
patterns can be recognised till the advanced stage of ISC when opacification
becomes more diffuse and irregular. The lens appears greyish white but clear
cortex is still present and so iris shadow is visible. In some patients, at this stage,
lens may become swollen due to continued hydration. This condition is called
„intumescent cataract'. Intumescence may persist even in the next stage of
maturation. Due to swollen lens anterior chamber becomes shallow.
d) Mature senile cataract (MSC):
In this stage, opacification becomes complete, i.e., whole of the cortex is
involved. Lens becomes pearly white in colour. Such a cataract is also labelled as
„ripe cataract‟
e) Hypermature senile cataract (HMSC):
When the mature cataract is left in situ, the stage of hypermaturity sets in. The
hypermature cataract may occur in any of the two forms-
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 75
i. Morgagnian hypermature cataract
In some patients, after maturity the whole cortex liquefies and the lens is
converted into a bag of milky fluid. The small brownish nucleus settles at the
bottom, altering its position with change in the position of the head. Such a
cataract is called Morgagnian cataract. Sometimes in this stage, calcium deposits
may also be seen on the lens capsule.
ii. Sclerotic type hypermature cataract:
Sometimes after the stage of maturity, the cortex becomes disintegrated and the
lens becomes shrunken due to leakage of water. The anterior capsule is wrinkled
and thickened due to proliferation of anterior cells and a dense white capsular
cataract may be formed in the papillary area. Due to shrinkage of lens, anterior
chamber becomes deep and iris becomes tremulous (iridodonesis).
2. Maturation of nuclear senile cataract
In it, the sclerotic process renders the lens inelastic and hard, decreases its ability to
accommodate and obstructs the light rays. These changes begin centrally and slowly
spread peripherally almost up to the capsule when it becomes mature; however, a very
thin layer of clear cortex may remain unaffected. The nucleus may become diffusely
cloudy (greyish) or tinted (yellow to black) due to depositionof pigments. In practice,
the commonly observed pigmented nuclear cataracts are either amber, brown
(cataracta brunescens) or black (cataracta nigra) and rarely reddish (cataracta rubra) in
colour.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 76
Management of cataract:
Cataract treatment essentially consists of its surgical removal. As discussed in
need for study, until surgery is taken up, in peculiar circumstances, certain non-surgical
measures may be of help. These include-
Non-surgical measure:
1. Treatment of cause of cataract
In acquired cataracts, thorough search should be made to find out the cause of
cataract, treatment of the causative disease, many a time it may stop progression and
sometimes in early stages may cause even regression of cataractous changes and thus
defer the surgical treatment. Some common examples include:
Adequate control of DM, when discovered
Removal of cataractogenic drugs such as cortico-steroids, phenothiazenes and
strong miotics, may delay or prevent cataractogenis
Removal of irradiation (IR or x-rays) may also delay or prevent cataract
formation.
Early and adequate treatment of ocular diseases like uveitis may prevent
occurrence of complicated cataract.
2. Measures to delay progression
Many commercially available preparations containing iodide salts of calcium and
potassium are being prescribed in abundance in early stages of cataract (especially
in senile cataract) in a bid to delay its progression. However, till date no
conclusive results about their role are available. Role of Vitamin E and aspirin in
delaying the process of cataractogenesis is also mentioned.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 77
3. Measures to improve vision in the presence of incipient and immature
cataract
This may be of great solace to the patient. They include-
Refraction, which often changes with considerable rapidity, should be corrected at
frequent intervals.
Arrangement of illumination- Patients with peripheral opacities (pupillary area
still free), may be instructed to use brilliant illumination. Conversely,in the
presence of central opacities, a dull light placed beside and slightly behind the
patient„s head will give the best result.
Use of dark goggles in patients with central opacities is of great value and comfort
when worn outdoors.
Mydriatics: The patients with small axial cataracts frequently may benefit from
pupillary dilatation. This allows the clear paraxial lens to to participate in light
transmission, image formation and focusing. Mydriatics such as 5%
phenylephrine or 1% tropicamide; 1 drop BID in the affected eye may clarify
vision.
Role of diet and nutrition:
Diet and nutrition has an important role in the treatment of cataract. They not only
prevent progression but also reverse the process, thereby helping in early stages of
cataract. Their probable function can be studied on following basis:
Protection from free radical damage: maintaining glutathione levels, Vitamin C,
Vitamin B2, Vitamin E, selenium, α- lipoic acid, N- acetyl cysteine, garlic and
melatonin.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 78
Protein protection: VitB6, acetyl-N- carnosine, amino guanidine
Lens metabolism support: Bioflavonoids, inositol, carnosine
Ocular environment support: Carotenoids, COQ 10, potassium and magnesium.
Levels at which these phyto-chemicals take an important role in protecting the
damage process are:
a) During the process of glycation: they bind to the sugar molecules
exhibiting chaperone activity, inhibits the activity of AR enzymes,
inhibits the formation of AGE‟s there by reduction in free radical
formation, protecting the normal proteins from the toxic effects of
existing AGE‟s
b) In lipid peroxidation: acts on membrane function (fatty acid break down)
and cellular structure (changes in proteins), restores mitochondrial
dysfunction, chaperone activity, lipid solubility nature of these
phytochemicals helping in drug penetration.
c) In UV irradiation: acts on inhibiting DNA strand breakage and repair,
preventing photooxidative stress, inhibition of nonenzymatic glycation,
maintaing the tryptophan levels, maintaining the levels of photochemicals
in 3HKG.
d) In aging: maintaining the levels of glutathione. Here they act preventive
rather than curative.
e) In oxidative damage: preventing the reduction of oxidative damage
resistant cells, scavenging activity of byproducts of lipid peroxidation,
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 79
glycation, UV radiation,regeneration and stimulation of glutathione,
membrane protection from damaging effects of byproducts of oxidative
damage etc, stimulation of NADPH.
f) In protein metabolism: in preventing mutation of protein phakinins,
maintaining normalcy of protein metabolism.
g) In maintenance of low pH: as H2O2 inhibitors, maintaining higher levels
of connexin α- 8 proteins, which abolishes sensitivity to low pH
h) Maintaining patency of aquaporin / removing blockage: maintaining
microcirculation, free radical generation inhibition from changes in
membrane and fibers.
Surgical management
Indications of cataract surgery
1. Visual improvement
It is the most common indication for cataract surgery and it is indicated when the
cataract develops to a degree sufficient to cause difficulty in performing daily
essential activities. Legal prescription of visual acuity in certain jobs also necessitates
the need for surgery.
2. Medical indication:
Sometimes patients may be comfortable from the visual point (due to useful vision
from the other eye or otherwise) but may be advised cataract surgery due to medical
grounds such as:
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 80
Lens induced glaucoma,
Phacoanaphylactic endophthalmitis
Retinal diseases like diabetic retinopathy or retinal detachment, treatment of
which is being hampered by the presence of lens opacities.
3. Cosmetic indication:
Sometimes patient with mature cataract may insist for cataract extraction (even with no
hope of getting improvement in vision), in order to obtain a black pupil.
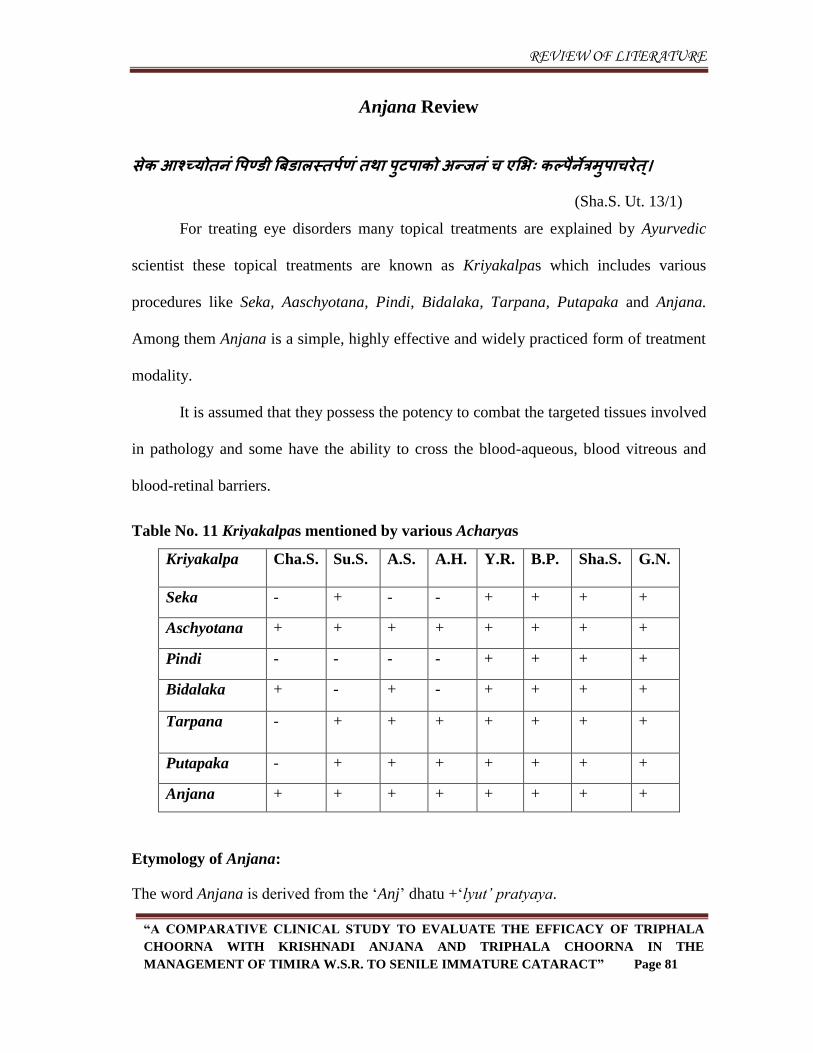
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 81
Anjana Review
सेक आश्च्मोतन ंपऩण्डध त्रफडवरस्तऩािं तथव ऩषटऩवको अन्जनं च एसब् कल्ऩ नेत्रभषऩवचयेत।्
(Sha.S. Ut. 13/1)
For treating eye disorders many topical treatments are explained by Ayurvedic
scientist these topical treatments are known as Kriyakalpas which includes various
procedures like Seka, Aaschyotana, Pindi, Bidalaka, Tarpana, Putapaka and Anjana.
Among them Anjana is a simple, highly effective and widely practiced form of treatment
modality.
It is assumed that they possess the potency to combat the targeted tissues involved
in pathology and some have the ability to cross the blood-aqueous, blood vitreous and
blood-retinal barriers.
Table No. 11 Kriyakalpas mentioned by various Acharyas
Kriyakalpa Cha.S. Su.S.
A.S. A.H. Y.R. B.P. Sha.S. G.N.
Seka - + - - + + + +
Aschyotana + + + + + + + +
Pindi - - - - + + + +
Bidalaka + - + - + + + +
Tarpana - + + + + + + +
Putapaka - + + + + + + +
Anjana + + + + + + + +
Etymology of Anjana:
The word Anjana is derived from the „Anj‟ dhatu +„lyut‟ pratyaya.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 82
Definition of Anjana:
अनन्द्क्त अनेन इतत अन्जनभ।् 113 (Vachaspatyam)
That which spreads in the eye is called Anjana.
An act of applying ointment or pigment.
Black pigment or Collyrium applied to the eyelashes or the inner coat of the
eyelid.
That which cause Vyaktekarana (manifestation) of Dosha.
That which creates movement of Dosha.
The word anjana means both, a substance which is used for application into eyes and
procedure of applying anjana into eyes. For easy understanding the material used for
doing the procedure of anjana is termed as anjana dravya and the procedure of
applying anjana dravya is termed as anjana karma.
Anjana karma is a procedure of application of medicinal pastes or powders to the
inner side of lower lid, either with the help of an applicator ie. Anjana shalaka or by
the finger tip from kaneenaka sandhi to apanga sandhi. 114
Indications of Anjana:
व्मक्तरूऩेषष दोषेषष शषद्धकवमस्म केवरे नेत्र ेएव न्द्स्थते दोष ेप्रवप्त्भन्जनभवचयेत।्
(Su.S. Ut. 18/51)
Acharyas have mentioned anjana in following condictions:
Based on dosha
Anjana can be applied in pitta, kapha, rakta and vata dosha predominant eye
diseases.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 83
Based on avastha of dosha
Anjana should be applied only when dosha show their lakshanas clearly
(vyaktarupeshu dosheshu). It should be applied when the dosha show pakva
linga, i.e. when they manifest their lakshanas clearly. Sushruta had used the term
vyakta roopa of dosha to indicate this condition. It can also be done when the
doshas, i.e pitta, kapha, rakta gets ghanatva (Solidification).
Based on Treatment order
It should be done only after purification therapies of the body (kaya shodhana),
i.e. after performing, vamana, virechana, nasya, vasti and rakta mokshana, which
should be according to the condition of the dosha and vyadhi. This implies that
anjana karma has to be done when the doshas which have been vitiated in the
whole body is initially removed by kaya shodhana procedures and the vitiated
doshas are left only in the eyes.
Based on the Asraya of Dosha
Anjana should be applied only when doshas are present only in the eyes or the
features of dosha dushti are limited only to the eye.
Based on Lakshana
It should be performed when symptoms like edema (shopha), Sliminess or
Stickiness (paichilya), itching (kandu), fatigue (mlanata), Redness (raga), foreign
body sensation (gharshana) and watering (asru) has decreased.
Based on Ritu
In hemanta and shishira ritu, it should be performed at noon (madhyahna), in
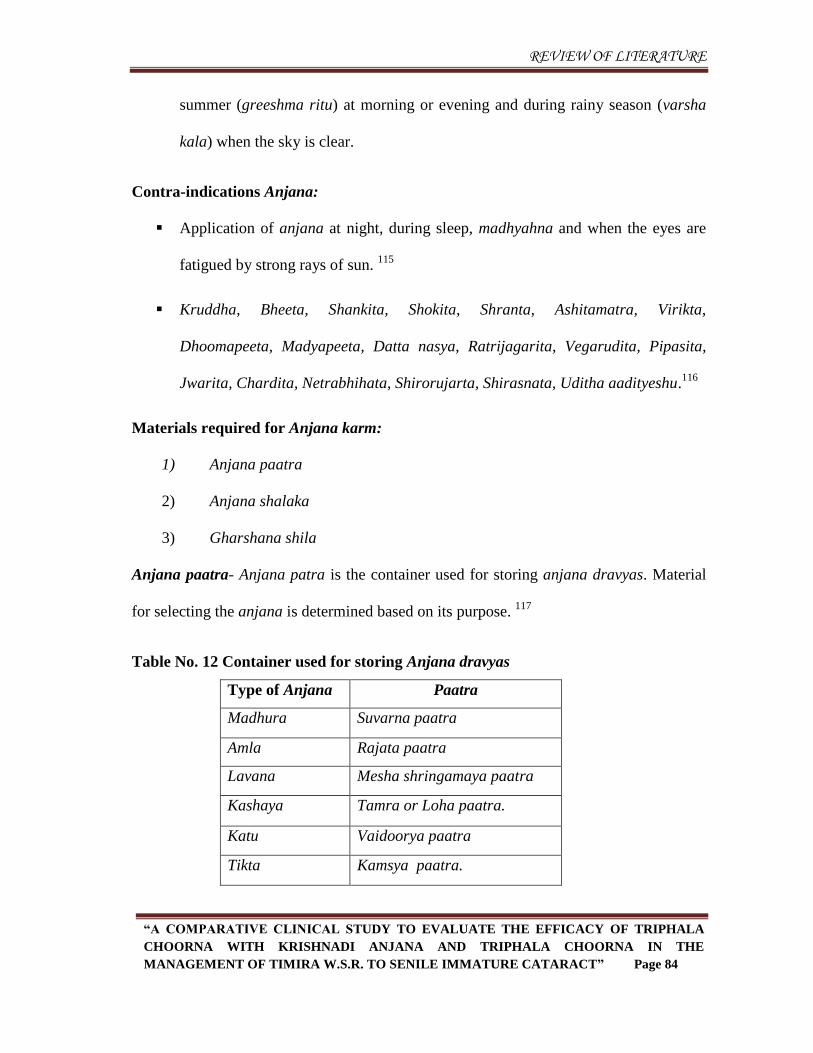
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 84
summer (greeshma ritu) at morning or evening and during rainy season (varsha
kala) when the sky is clear.
Contra-indications Anjana:
Application of anjana at night, during sleep, madhyahna and when the eyes are
fatigued by strong rays of sun. 115
Kruddha, Bheeta, Shankita, Shokita, Shranta, Ashitamatra, Virikta,
Dhoomapeeta, Madyapeeta, Datta nasya, Ratrijagarita, Vegarudita, Pipasita,
Jwarita, Chardita, Netrabhihata, Shirorujarta, Shirasnata, Uditha aadityeshu.116
Materials required for Anjana karm:
1) Anjana paatra
2) Anjana shalaka
3) Gharshana shila
Anjana paatra- Anjana patra is the container used for storing anjana dravyas. Material
for selecting the anjana is determined based on its purpose. 117
Table No. 12 Container used for storing Anjana dravyas
Type of Anjana Paatra
Madhura Suvarna paatra
Amla Rajata paatra
Lavana Mesha shringamaya paatra
Kashaya Tamra or Loha paatra.
Katu Vaidoorya paatra
Tikta Kamsya paatra.
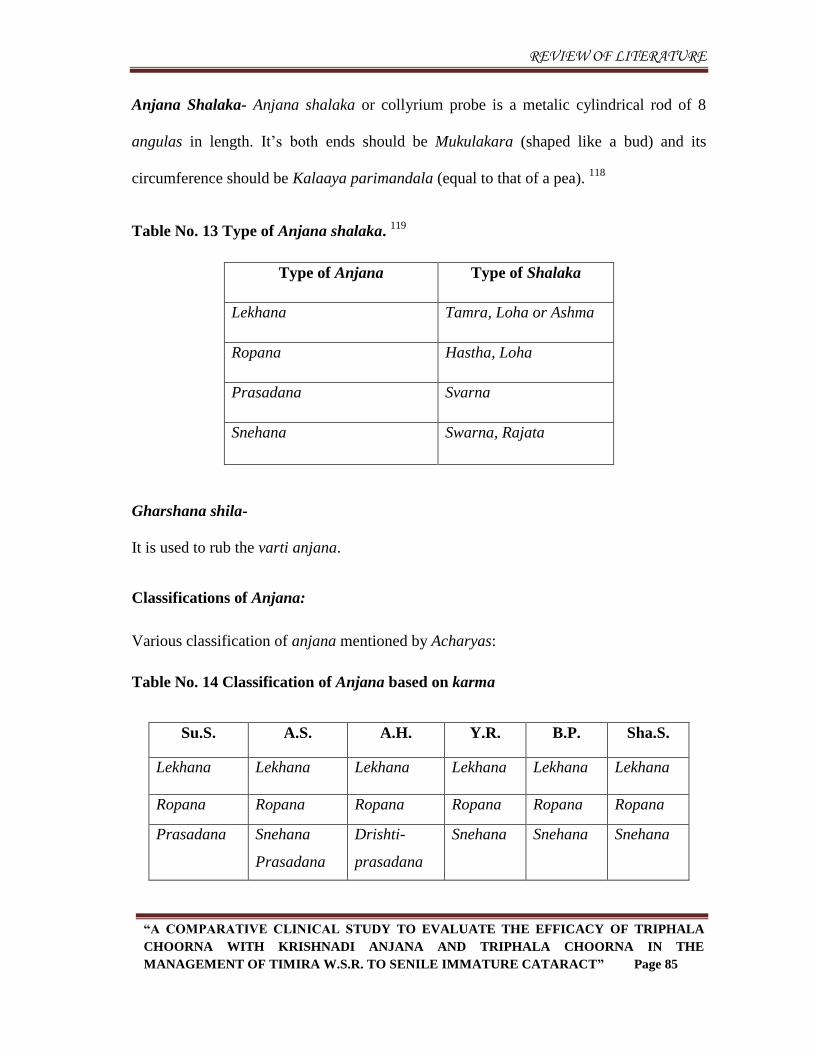
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 85
Anjana Shalaka- Anjana shalaka or collyrium probe is a metalic cylindrical rod of 8
angulas in length. It‟s both ends should be Mukulakara (shaped like a bud) and its
circumference should be Kalaaya parimandala (equal to that of a pea). 118
Table No. 13 Type of Anjana shalaka. 119
Type of Anjana Type of Shalaka
Lekhana Tamra, Loha or Ashma
Ropana Hastha, Loha
Prasadana Svarna
Snehana Swarna, Rajata
Gharshana shila-
It is used to rub the varti anjana.
Classifications of Anjana:
Various classification of anjana mentioned by Acharyas:
Table No. 14 Classification of Anjana based on karma
Su.S. A.S. A.H. Y.R. B.P. Sha.S.
Lekhana Lekhana Lekhana Lekhana Lekhana Lekhana
Ropana Ropana Ropana Ropana Ropana Ropana
Prasadana
Snehana
Prasadana
Drishti-
prasadana
Snehana
Snehana
Snehana
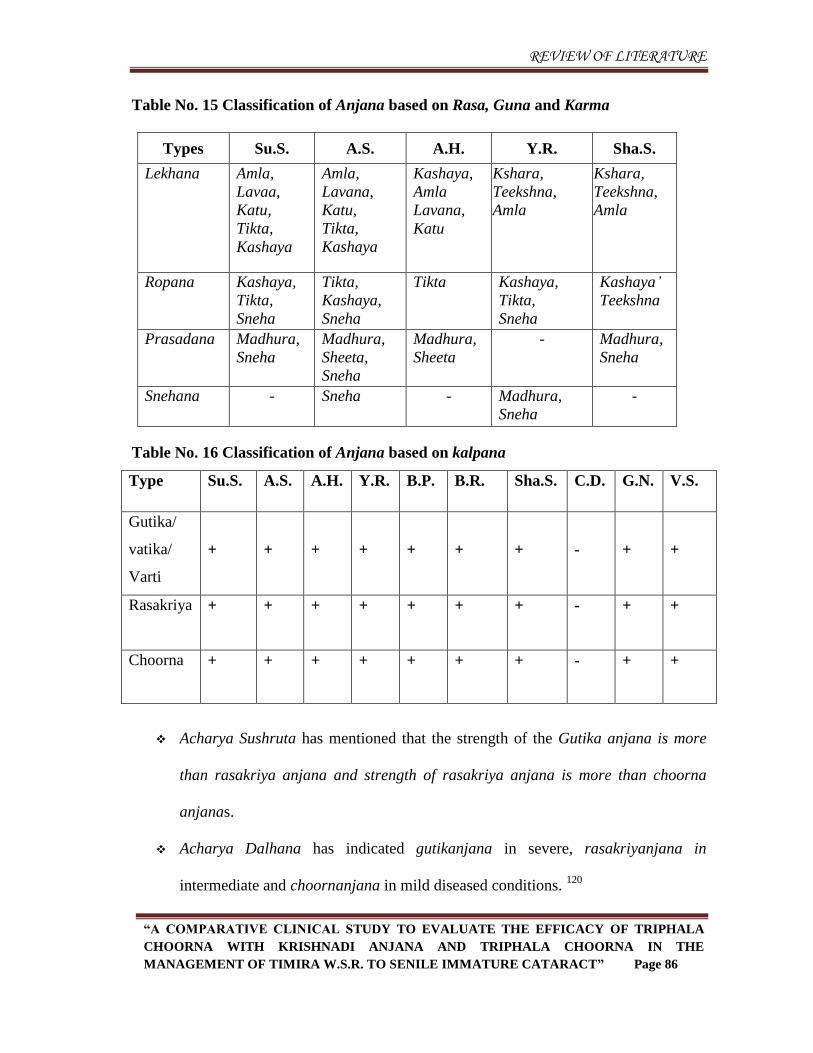
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 86
Table No. 15 Classification of Anjana based on Rasa, Guna and Karma
Types Su.S. A.S. A.H. Y.R. Sha.S.
Lekhana Amla,
Lavaa,
Katu,
Tikta,
Kashaya
Amla,
Lavana,
Katu,
Tikta,
Kashaya
Kashaya,
Amla
Lavana,
Katu
Kshara,
Teekshna,
Amla
Kshara,
Teekshna,
Amla
Ropana Kashaya,
Tikta,
Sneha
Tikta,
Kashaya,
Sneha
Tikta Kashaya,
Tikta,
Sneha
Kashaya‟
Teekshna
Prasadana Madhura,
Sneha
Madhura,
Sheeta,
Sneha
Madhura,
Sheeta
- Madhura,
Sneha
Snehana - Sneha - Madhura,
Sneha
-
Table No. 16 Classification of Anjana based on kalpana
Type Su.S. A.S. A.H. Y.R. B.P. B.R. Sha.S. C.D. G.N. V.S.
Gutika/
vatika/
Varti
+
+
+
+
+
+
+
-
+
+
Rasakriya + + + + + + + - + +
Choorna + + + + + + + - + +
Acharya Sushruta has mentioned that the strength of the Gutika anjana is more
than rasakriya anjana and strength of rasakriya anjana is more than choorna
anjanas.
Acharya Dalhana has indicated gutikanjana in severe, rasakriyanjana in
intermediate and choornanjana in mild diseased conditions. 120
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 87
Types of Anjana
1. Lekhananjana: 121
Selection: It is done according to the dosha vitiation of the disease and it is of
pancharasas ie. “madhura rasa varjita.”
Dosha Selection of rasa
Vata -Amla and Lavana rasa dravyas
Pitta -Tikta and Kashaya rasa dravyas
Kapha -Katu, Tikta and Kashaya rasa dravyas
Raktaja -Tikta and Kashaya rasa dravyas
If vitiated doshas are more in number then 2 or more types of rasa dravyas in
combination can be selected accordingly.
Action: The mode of action of lekhananjana described in Sushruta Samhita is as
follows. Properly applied lekhanajana enters into the eye lids, blood vessels of the
eye, ducts of ashru and “shringataka marma”. Then it causes sravana (flow out)
of vitiated doshas through the mouth, nose and the eyes itself.
Indication: Shukla-Armaadi
Time of application: Morning
Samyak lakshnas of Lekhananjana: 122
There will be Clarity of vision (vaishadyata), Lightness of eyes (laghutva),
stoppage of tear secretion (anasravi), easy movement of eyes (kriyapatu), eyes
become comfortable as before (sunirmalam) and pacification of adverse effects of
anjana (sa shanta upadrava).
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 88
Athiyoga of Lekhananjana:
Squinting of eyes (jihma netra), daruna netra, discoloration of eyes (dur varna),
srastam, severe dryness (ati rooksha), syandana.
Managemant of athiyoga:
Santarpana karma should be adopted in management of atiyoga to pacify vata
dosha.
Heenayoga of Lekhananjana:
If lekhananjana application is insufficient then the doshas get vitiated more
(Ugrataradosha).
Managemant of heenayoga:
The vitiated doshas can be eliminated by dhooma, nasya and again application of
anjana.
2. Ropananjana
Ropana anjana should be prepared with drugs having kashaya, tikta rasa along with
sneha dravyas such as ghee. Due to sneha and sheeta it does varnapradana, dristi bala
vardhana. 123
Action: By the virtue of sneha and sheethalata it does varnya karma and
dristibala vardhana.
Indications: Pitta and rakta vyadhis
Time of administration: Night
Atiyoga and heeneyoga and their management are similar to that of Prasadana
anjana. 124
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 89
3. Drishtiprasadananjana / prasadana anjana:
It should be prepared with madhura rasa and with lot of sneha dravyas. It imparts
tone and vigour to the eye sight and should be used with advantage for all soothing
purposes connected with eyes. 125
Indications: Vataja Rogas, Srotoshodhana, Rookshata of eyes, Vataja timira and
after Lekhananjana.
Time of application: Evening
Samyak lakshnas of drishtiprasadananjana: 126
Samyak lakshnas of prasadananjana are snehavarnabalopetam, prasannam and
doshavarjitam.
Athiyoga of drishtiprasadananjana:
Guruta, avilata, atisnigdhata, ashru, kandu and doshasamutklishta are mentioned
as athiyoga of drishtiprasadananjana.
Managemant of Athiyoga:
It can be treated by using doshahara (ie.kaphahara), rooksha and mrudu (ie.
sheeta veerya) medications and can be achieved by virechana nasya, dhoomapana,
kavala and lekhananjana also.
Heenayoga of drishtiprasadananjana:
In heenayoga disease will not subside, dryness, roughness will persist.
Managemant of Heenayoga:
In such conditions anjana should be continued. Bramhana nasya, Netra trapana is
employed if necessary.
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 90
Pratyanjana:
Application of prasadananjana to the eyes which have become fatigue by the
application of choorna and teekshna anjanas will derive the name „Pratyanjana‟. 127
Complications of anjana:
Applying anjana when there is loss of sleep produces inability for work; when
applied during or after exposure to heavy breeze, produces loss of strength of eye and
vision; when troubled by dust and smoke, it gives rise to red colour, exudation and severe
pain to eye (adhimantha); when applied at the end of Nasya it produces swelling and
pain; when applied during diseases related to head, it produces headache. 128
Anjana matra:
Matra of anjana has mentioned by acharyas as follow:
Table No. 17 Anjana matra as per Acharya Sushruta 129
Table No. 18 Anjana matra as per Acharya Vagbhata 130
Teekshna Pinda Harenumatra
Mrudu Pinda Two Harenumatra
Teekshna Rasakriya Vella matra (vidanga matra)
Mrudu Rasakriya Two vella matra.
Teekshna Choorna Two Shalaka
Mrudu Choorna Three Shalaka
Lekahananjana Harenu matra
Prasadananjana one and half harenu matra
Ropananjana Two harenu matra
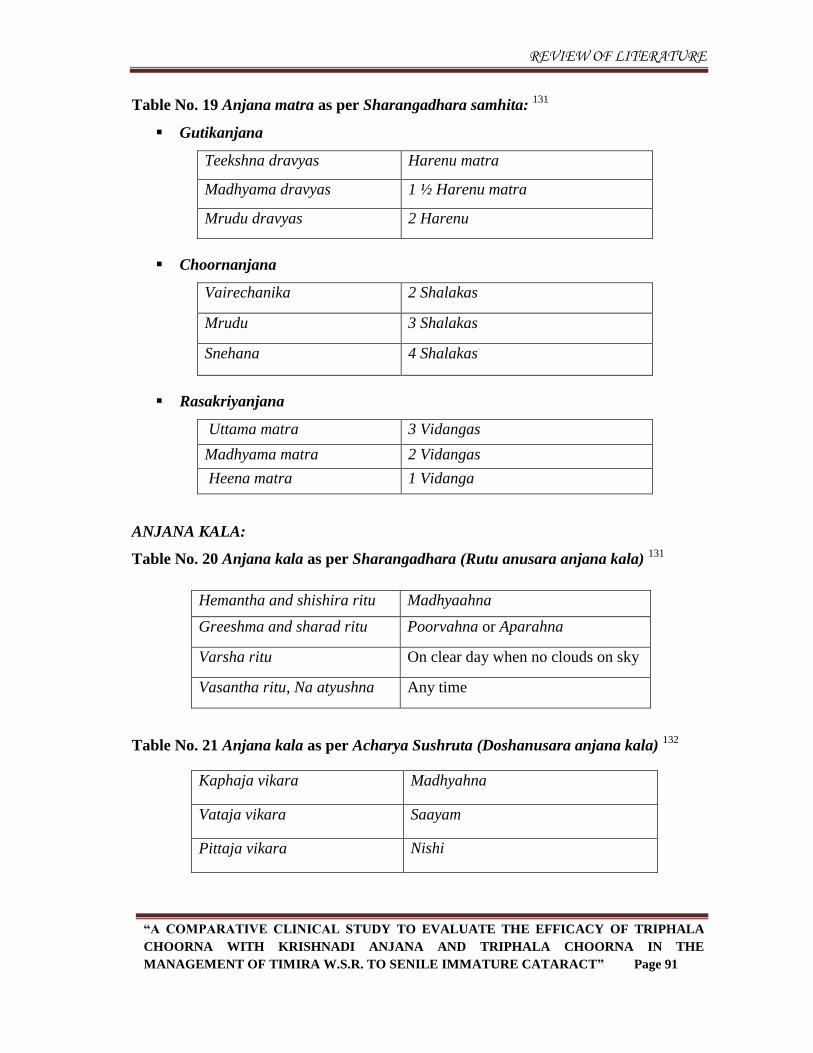
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 91
Table No. 19 Anjana matra as per Sharangadhara samhita: 131
Gutikanjana
Teekshna dravyas Harenu matra
Madhyama dravyas 1 ½ Harenu matra
Mrudu dravyas 2 Harenu
Choornanjana
Vairechanika 2 Shalakas
Mrudu 3 Shalakas
Snehana 4 Shalakas
Rasakriyanjana
Uttama matra 3 Vidangas
Madhyama matra 2 Vidangas
Heena matra 1 Vidanga
ANJANA KALA:
Table No. 20 Anjana kala as per Sharangadhara (Rutu anusara anjana kala) 131
Hemantha and shishira ritu Madhyaahna
Greeshma and sharad ritu Poorvahna or Aparahna
Varsha ritu On clear day when no clouds on sky
Vasantha ritu, Na atyushna Any time
Table No. 21 Anjana kala as per Acharya Sushruta (Doshanusara anjana kala) 132
Kaphaja vikara Madhyahna
Vataja vikara Saayam
Pittaja vikara Nishi
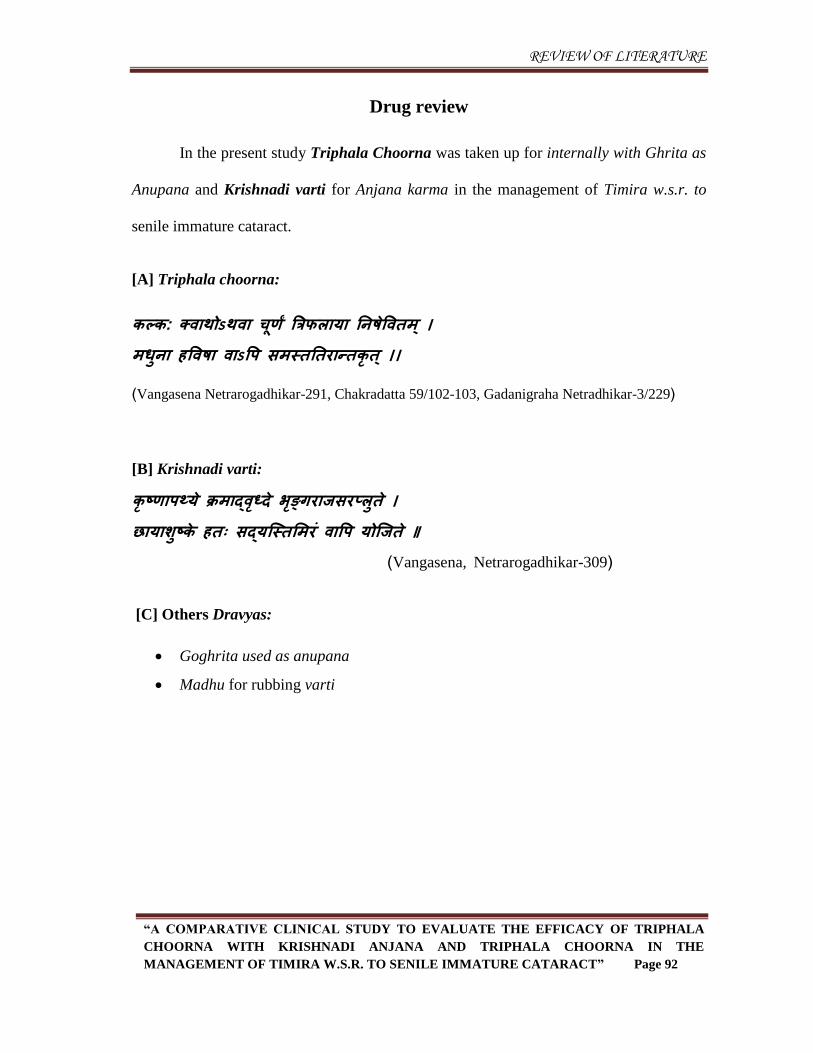
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 92
Drug review
In the present study Triphala Choorna was taken up for internally with Ghrita as
Anupana and Krishnadi varti for Anjana karma in the management of Timira w.s.r. to
senile immature cataract.
[A] Triphala choorna:
कल्क: क्ववथोऽथवव चूिां त्रत्रपरवमव तनषेपवतभ ्। भधषनव हपवषव ववऽपऩ सभस्तततयवन्तकृत ्।।
(Vangasena Netrarogadhikar-291, Chakradatta 59/102-103, Gadanigraha Netradhikar-3/229)
[B] Krishnadi varti:
कृष्िवऩथ्मे क्रभवद्वधृ्दे बङृ्गयवजसयप्रषते । छवमवशषष्के हत् सद्मन्द्स्तसभयं ववपऩ मोन्द्जते ॥ (Vangasena, Netrarogadhikar-309)
[C] Others Dravyas:
Goghrita used as anupana
Madhu for rubbing varti
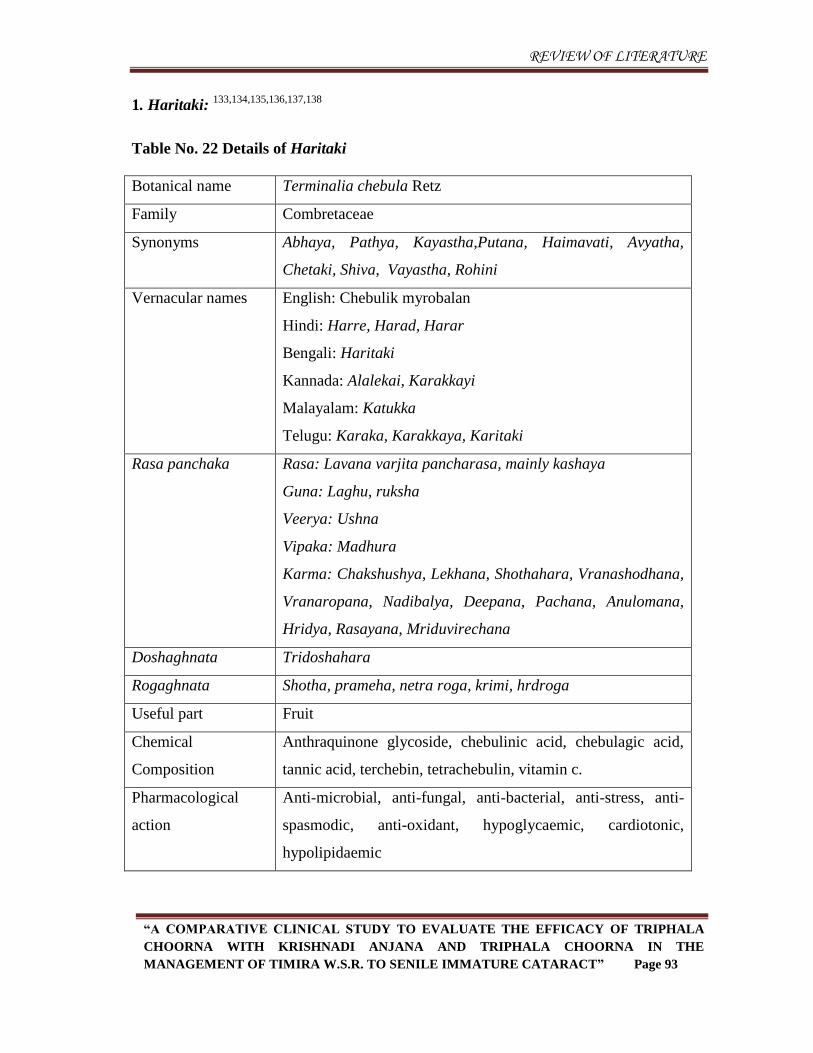
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 93
1. Haritaki: 133,134,135,136,137,138
Table No. 22 Details of Haritaki
Botanical name Terminalia chebula Retz
Family Combretaceae
Synonyms Abhaya, Pathya, Kayastha,Putana, Haimavati, Avyatha,
Chetaki, Shiva, Vayastha, Rohini
Vernacular names English: Chebulik myrobalan
Hindi: Harre, Harad, Harar
Bengali: Haritaki
Kannada: Alalekai, Karakkayi
Malayalam: Katukka
Telugu: Karaka, Karakkaya, Karitaki
Rasa panchaka Rasa: Lavana varjita pancharasa, mainly kashaya
Guna: Laghu, ruksha
Veerya: Ushna
Vipaka: Madhura
Karma: Chakshushya, Lekhana, Shothahara, Vranashodhana,
Vranaropana, Nadibalya, Deepana, Pachana, Anulomana,
Hridya, Rasayana, Mriduvirechana
Doshaghnata Tridoshahara
Rogaghnata Shotha, prameha, netra roga, krimi, hrdroga
Useful part Fruit
Chemical
Composition
Anthraquinone glycoside, chebulinic acid, chebulagic acid,
tannic acid, terchebin, tetrachebulin, vitamin c.
Pharmacological
action
Anti-microbial, anti-fungal, anti-bacterial, anti-stress, anti-
spasmodic, anti-oxidant, hypoglycaemic, cardiotonic,
hypolipidaemic
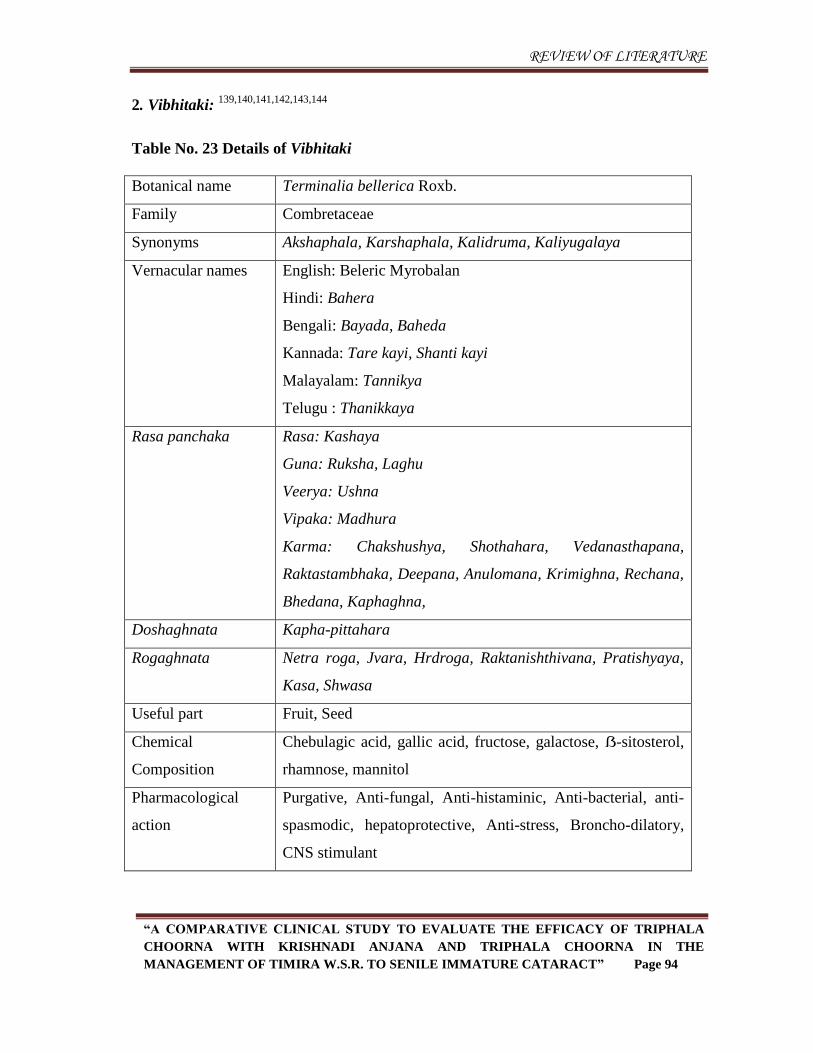
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 94
2. Vibhitaki: 139,140,141,142,143,144
Table No. 23 Details of Vibhitaki
Botanical name Terminalia bellerica Roxb.
Family Combretaceae
Synonyms Akshaphala, Karshaphala, Kalidruma, Kaliyugalaya
Vernacular names English: Beleric Myrobalan
Hindi: Bahera
Bengali: Bayada, Baheda
Kannada: Tare kayi, Shanti kayi
Malayalam: Tannikya
Telugu : Thanikkaya
Rasa panchaka Rasa: Kashaya
Guna: Ruksha, Laghu
Veerya: Ushna
Vipaka: Madhura
Karma: Chakshushya, Shothahara, Vedanasthapana,
Raktastambhaka, Deepana, Anulomana, Krimighna, Rechana,
Bhedana, Kaphaghna,
Doshaghnata Kapha-pittahara
Rogaghnata Netra roga, Jvara, Hrdroga, Raktanishthivana, Pratishyaya,
Kasa, Shwasa
Useful part Fruit, Seed
Chemical
Composition
Chebulagic acid, gallic acid, fructose, galactose, ẞ-sitosterol,
rhamnose, mannitol
Pharmacological
action
Purgative, Anti-fungal, Anti-histaminic, Anti-bacterial, anti-
spasmodic, hepatoprotective, Anti-stress, Broncho-dilatory,
CNS stimulant
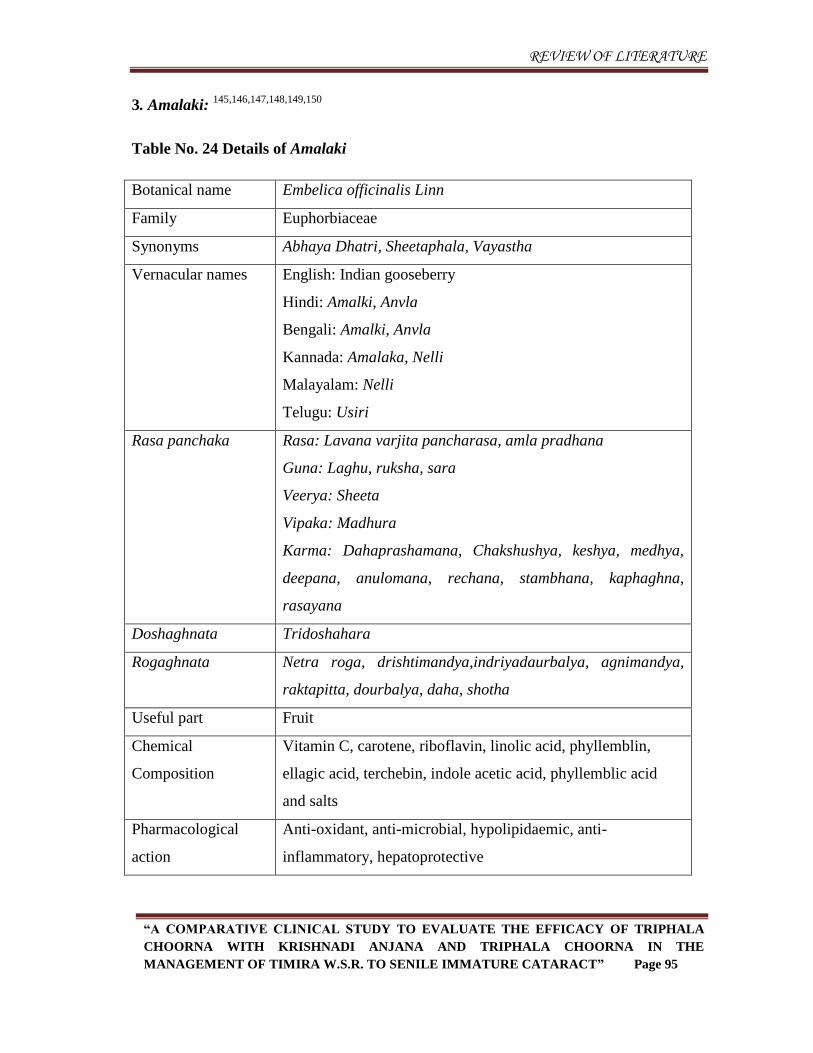
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 95
3. Amalaki: 145,146,147,148,149,150
Table No. 24 Details of Amalaki
Botanical name Embelica officinalis Linn
Family Euphorbiaceae
Synonyms Abhaya Dhatri, Sheetaphala, Vayastha
Vernacular names English: Indian gooseberry
Hindi: Amalki, Anvla
Bengali: Amalki, Anvla
Kannada: Amalaka, Nelli
Malayalam: Nelli
Telugu: Usiri
Rasa panchaka Rasa: Lavana varjita pancharasa, amla pradhana
Guna: Laghu, ruksha, sara
Veerya: Sheeta
Vipaka: Madhura
Karma: Dahaprashamana, Chakshushya, keshya, medhya,
deepana, anulomana, rechana, stambhana, kaphaghna,
rasayana
Doshaghnata Tridoshahara
Rogaghnata Netra roga, drishtimandya,indriyadaurbalya, agnimandya,
raktapitta, dourbalya, daha, shotha
Useful part Fruit
Chemical
Composition
Vitamin C, carotene, riboflavin, linolic acid, phyllemblin,
ellagic acid, terchebin, indole acetic acid, phyllemblic acid
and salts
Pharmacological
action
Anti-oxidant, anti-microbial, hypolipidaemic, anti-
inflammatory, hepatoprotective
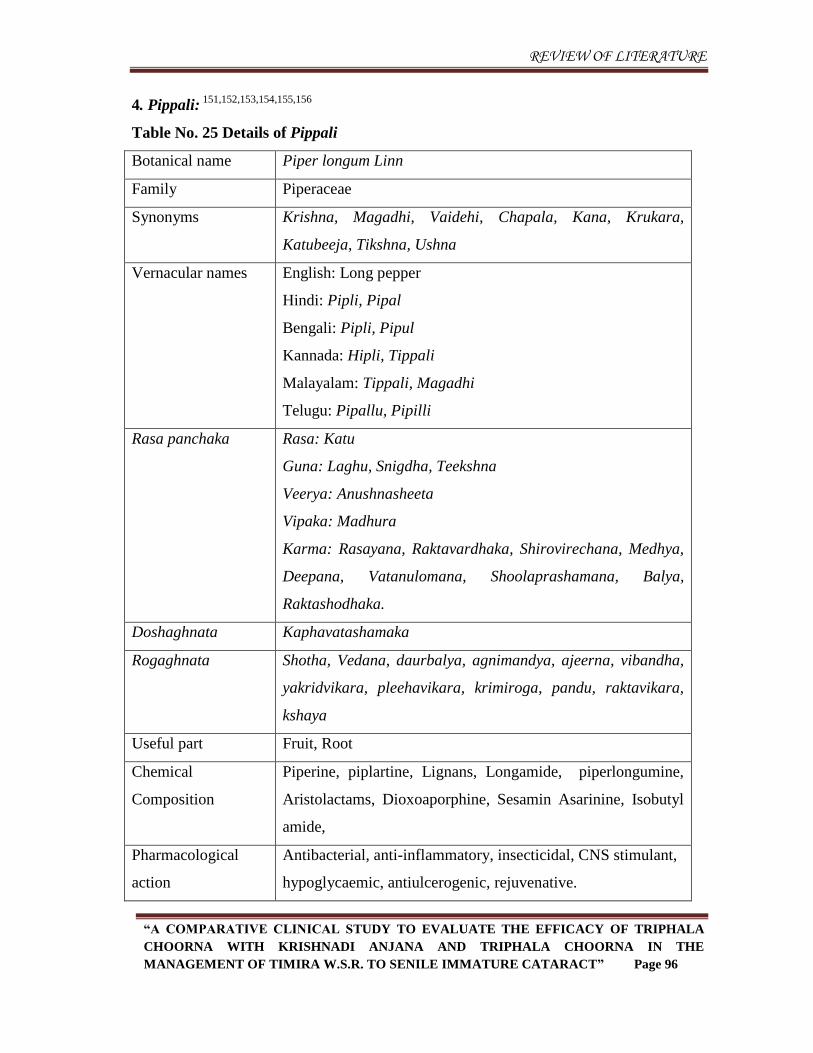
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 96
4. Pippali: 151,152,153,154,155,156
Table No. 25 Details of Pippali
Botanical name Piper longum Linn
Family Piperaceae
Synonyms Krishna, Magadhi, Vaidehi, Chapala, Kana, Krukara,
Katubeeja, Tikshna, Ushna
Vernacular names English: Long pepper
Hindi: Pipli, Pipal
Bengali: Pipli, Pipul
Kannada: Hipli, Tippali
Malayalam: Tippali, Magadhi
Telugu: Pipallu, Pipilli
Rasa panchaka Rasa: Katu
Guna: Laghu, Snigdha, Teekshna
Veerya: Anushnasheeta
Vipaka: Madhura
Karma: Rasayana, Raktavardhaka, Shirovirechana, Medhya,
Deepana, Vatanulomana, Shoolaprashamana, Balya,
Raktashodhaka.
Doshaghnata Kaphavatashamaka
Rogaghnata Shotha, Vedana, daurbalya, agnimandya, ajeerna, vibandha,
yakridvikara, pleehavikara, krimiroga, pandu, raktavikara,
kshaya
Useful part Fruit, Root
Chemical
Composition
Piperine, piplartine, Lignans, Longamide, piperlongumine,
Aristolactams, Dioxoaporphine, Sesamin Asarinine, Isobutyl
amide,
Pharmacological
action
Antibacterial, anti-inflammatory, insecticidal, CNS stimulant,
hypoglycaemic, antiulcerogenic, rejuvenative.
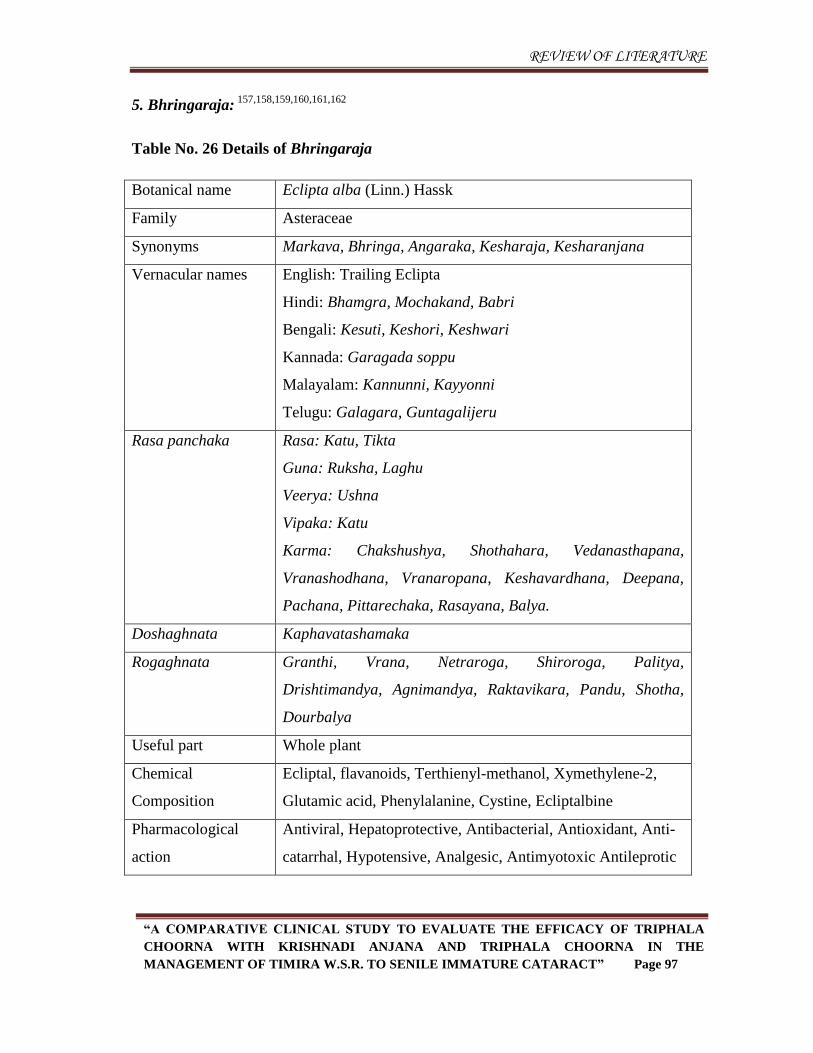
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 97
5. Bhringaraja: 157,158,159,160,161,162
Table No. 26 Details of Bhringaraja
Botanical name Eclipta alba (Linn.) Hassk
Family Asteraceae
Synonyms Markava, Bhringa, Angaraka, Kesharaja, Kesharanjana
Vernacular names English: Trailing Eclipta
Hindi: Bhamgra, Mochakand, Babri
Bengali: Kesuti, Keshori, Keshwari
Kannada: Garagada soppu
Malayalam: Kannunni, Kayyonni
Telugu: Galagara, Guntagalijeru
Rasa panchaka Rasa: Katu, Tikta
Guna: Ruksha, Laghu
Veerya: Ushna
Vipaka: Katu
Karma: Chakshushya, Shothahara, Vedanasthapana,
Vranashodhana, Vranaropana, Keshavardhana, Deepana,
Pachana, Pittarechaka, Rasayana, Balya.
Doshaghnata Kaphavatashamaka
Rogaghnata Granthi, Vrana, Netraroga, Shiroroga, Palitya,
Drishtimandya, Agnimandya, Raktavikara, Pandu, Shotha,
Dourbalya
Useful part Whole plant
Chemical
Composition
Ecliptal, flavanoids, Terthienyl-methanol, Xymethylene-2,
Glutamic acid, Phenylalanine, Cystine, Ecliptalbine
Pharmacological
action
Antiviral, Hepatoprotective, Antibacterial, Antioxidant, Anti-
catarrhal, Hypotensive, Analgesic, Antimyotoxic Antileprotic
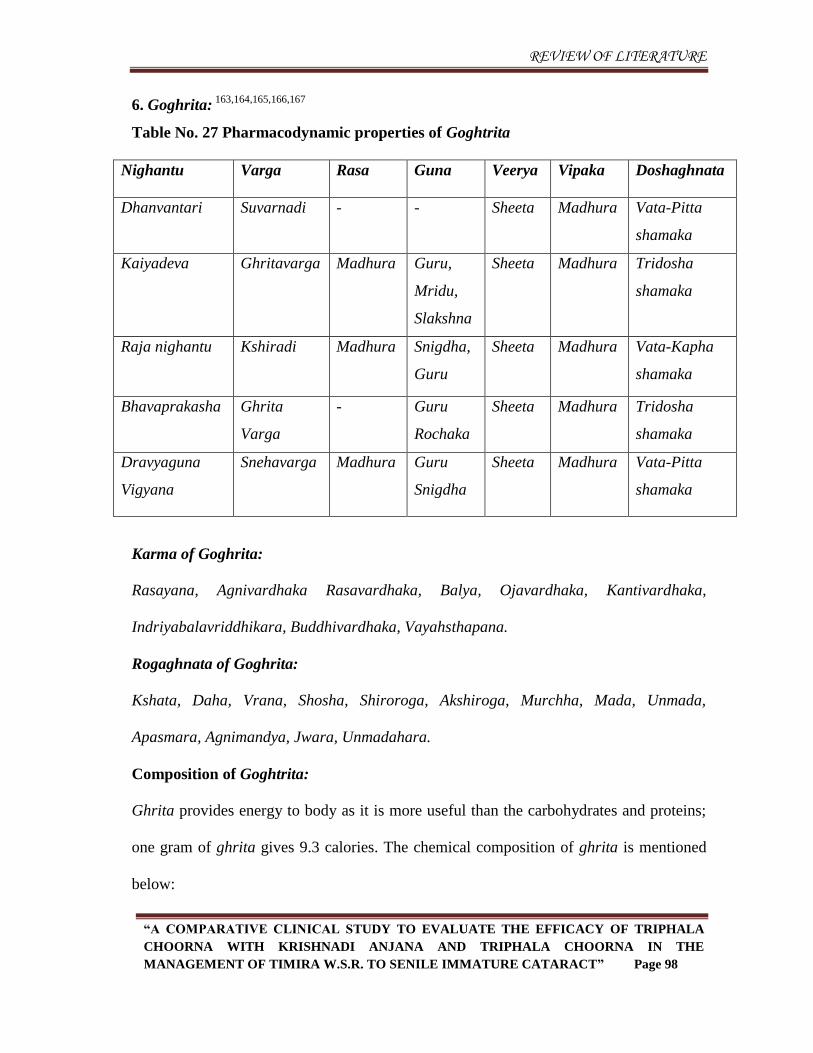
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 98
6. Goghrita: 163,164,165,166,167
Table No. 27 Pharmacodynamic properties of Goghtrita
Nighantu Varga Rasa Guna Veerya Vipaka Doshaghnata
Dhanvantari Suvarnadi - - Sheeta Madhura Vata-Pitta
shamaka
Kaiyadeva Ghritavarga Madhura
Guru,
Mridu,
Slakshna
Sheeta Madhura Tridosha
shamaka
Raja nighantu Kshiradi Madhura Snigdha,
Guru
Sheeta Madhura Vata-Kapha
shamaka
Bhavaprakasha Ghrita
Varga
- Guru
Rochaka
Sheeta Madhura Tridosha
shamaka
Dravyaguna
Vigyana
Snehavarga Madhura Guru
Snigdha
Sheeta Madhura Vata-Pitta
shamaka
Karma of Goghrita:
Rasayana, Agnivardhaka Rasavardhaka, Balya, Ojavardhaka, Kantivardhaka,
Indriyabalavriddhikara, Buddhivardhaka, Vayahsthapana.
Rogaghnata of Goghrita:
Kshata, Daha, Vrana, Shosha, Shiroroga, Akshiroga, Murchha, Mada, Unmada,
Apasmara, Agnimandya, Jwara, Unmadahara.
Composition of Goghtrita:
Ghrita provides energy to body as it is more useful than the carbohydrates and proteins;
one gram of ghrita gives 9.3 calories. The chemical composition of ghrita is mentioned
below:
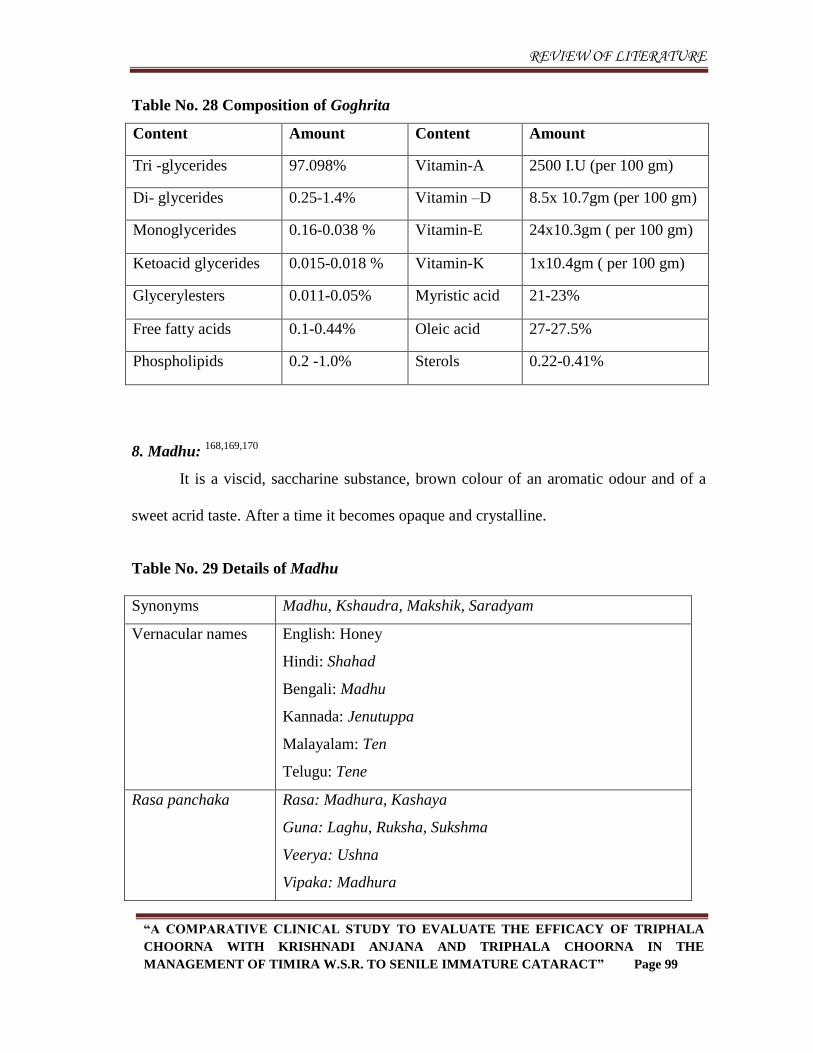
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 99
Table No. 28 Composition of Goghrita
Content Amount Content Amount
Tri -glycerides 97.098% Vitamin-A 2500 I.U (per 100 gm)
Di- glycerides 0.25-1.4% Vitamin –D 8.5x 10.7gm (per 100 gm)
Monoglycerides 0.16-0.038 % Vitamin-E 24x10.3gm ( per 100 gm)
Ketoacid glycerides 0.015-0.018 % Vitamin-K 1x10.4gm ( per 100 gm)
Glycerylesters 0.011-0.05% Myristic acid 21-23%
Free fatty acids 0.1-0.44% Oleic acid 27-27.5%
Phospholipids 0.2 -1.0% Sterols 0.22-0.41%
8. Madhu: 168,169,170
It is a viscid, saccharine substance, brown colour of an aromatic odour and of a
sweet acrid taste. After a time it becomes opaque and crystalline.
Table No. 29 Details of Madhu
Synonyms Madhu, Kshaudra, Makshik, Saradyam
Vernacular names English: Honey
Hindi: Shahad
Bengali: Madhu
Kannada: Jenutuppa
Malayalam: Ten
Telugu: Tene
Rasa panchaka Rasa: Madhura, Kashaya
Guna: Laghu, Ruksha, Sukshma
Veerya: Ushna
Vipaka: Madhura
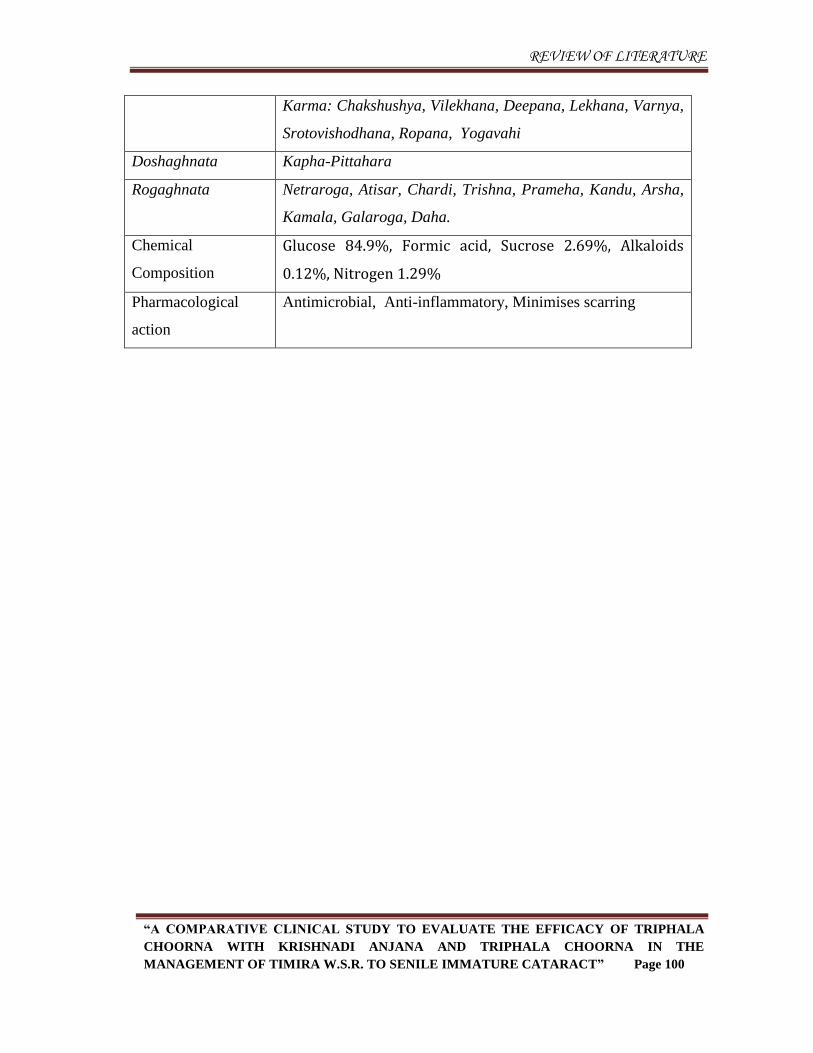
REVIEW OF LITERATURE
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 100
Karma: Chakshushya, Vilekhana, Deepana, Lekhana, Varnya,
Srotovishodhana, Ropana, Yogavahi
Doshaghnata Kapha-Pittahara
Rogaghnata Netraroga, Atisar, Chardi, Trishna, Prameha, Kandu, Arsha,
Kamala, Galaroga, Daha.
Chemical
Composition
Glucose 84.9%, Formic acid, Sucrose 2.69%, Alkaloids
0.12%, Nitrogen 1.29%
Pharmacological
action
Antimicrobial, Anti-inflammatory, Minimises scarring
METHODOLOGY
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 101
Methodology
Null hypothesis
There is no added effect of Krishnadi anjana in the management of Timira w.s.r. to
Senile Immature Cataract.
Alternate hypothesis
There is an effect of Krishnadi anjana in the management of Timira w.s.r. to Senile
Immature Cataract.
Materials and methods
A. Source of data
1. Literary source
Classical Ayurveda texts, Modern literatures and Contemporary text books including
the Websites and Journals were reviewed to gather information about the disease,
therapy and the drugs.
2. Sample source
Patients with clinical features of Timira (Immature cataract) coming under the
inclusion criteria approaching the OPD and IPD of Shalakya Tantra, SKAMCH &
RC, Bengaluru were selected for the study.
The sample collection was initiated with post approval from the Institutional
Ethical Committee.
METHODOLOGY
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 102
3. Drug source
The identified raw drugs required for the preparation of Krishnadi varti anjana and
Triphala choorna were purchased from approved vendors. Post purchase, the raw drugs
were authenticated by the faculty of Dravya Guna, SKAMCH & RC, BENGALURU.
B. Method of collection of data
Study design
Randomized clinical study.
Sampling technique
The subjects who fulfilled the inclusion and exclusion criteria and complying with
the informed consent (IC) were selected using random sampling technique.
Sample size
A comparative clinical study where in 40 Patients diagnosed as Timira of either
sex were randomly assigned into two groups i.e., Group A and Group B
comprising of 20 patients each.
A case proforma containing all the necessary details pertaining to the study was
prepared.
The parameters considered for the study were scored as mentioned in the
proforma.
METHODOLOGY
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 103
Diagnostic criteria
Patients with lakshanas of Timira.
Clinical feature of senile immature cataract.
Diminished visual acuity up to 6/12 and N12.
Immature cataract confirmed by Ophthalmoscopy and Slit lamp biomicroscopy.
Inclusion criteria
Patients with lakshanas of Timira.
Patients with signs and symptoms of Senile immature cataract.
Patients in between the age group of 40 to 70 years.
Exclusion criteria
Post surgical cataract
Mature cataract
Sluggish pupillary reaction
Patients with systemic disorders that may interfere with the course of the study.
Associated with any inflammatory and infective ocular conditions.
METHODOLOGY
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 104
C. Intervention
The study was intervened in one treatment phase
Group Treatments Dose Duration
A 1. Krishnadi
anjana
-1 Harenu matra -Once daily at Morning for
48 days
2. Triphala
choorna Internally
-05 Grams with sufficient
amount of Go ghrita.
-Once daily at night after
food for 48 days
B 1. Triphala
choorna Internally
-05 Grams with sufficient
amount of Go ghrita
-Once daily at night after
food for 48 days
Assessment was done on 49th
day.
Duration of the study:
The total duration of the study in both the groups was 49days.
Method of preparation of medicaments required for the study:-
1. Krishnadi varti
Ingredients and Quantity:
Pippali tandula - 350 grams
Haritaki - 700 grams
Bhringaraja Swarasa - 4 litres (was extracted from fresh Bhringaraja panchanga-
fresh plant)
METHODOLOGY
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 105
Method:
A. Pre-preparatory procedure:
1) The raw drugs required for varti i.e. Pippali tandula and Haritaki were
washed thoroughly and allowed to dry up.
2) The procured Bhringaraja fresh plant was washed thoroughly and kept in the
clean vessel.
B. Preparatory procedure
1. Each of the drugs (Pippali tandula and Haritaki) were crushed and finely
powdered separately in a mixer grinder. Then a homogenous mixture was
prepared by adding these powders.
2. Bhringaraja plant was subjected to grinding using wet grinder until
Bhringaraja was completely grinded. The above paste of Bhringaraja was
placed in a clean cloth and allowed for squeezing by which Bhringaraja
swarasa was extracted and collected in a clean container.
3. The above mixture was subjected for bhavana using Bhringaraja swarasa.
4. The bhavana procedure was continued till it attained the form of kalka fulfil
the Subhavita lakshanas as per classics and then it rolled into varti aakar.
5. Each prepared varti was 2 inches long and about 5 grams weight.
C. Post-preparatory procedure:
1) The prepared vartis were dried in shade.
2) After complete drying, vartis were stored in a clean air tight container.
METHODOLOGY
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 106
2. Triphala choorna:
Ingredients and Quantity:
Amalaki - 5 Kgs
Haritaki - 5 Kgs
Vibhitaki - 5 Kgs
Method:
A. Pre-preparatory procedure:
1. The dry drugs required for Triphala choorna viz., as Amalaki, Haritaki and
Vibhitaki were thoroughly washed to remove the impurities and was dried
completely.
B. Preparatory procedure:
1. Each of the drugs were crushed separately using khalwa yantra and made
fine powder using mixture grinder.
2. The powders were sieved and a homogenous mixture was prepared by mixing
these powders.
C. Post-preparatory procedure:
The prepared choorna was stored in a clean air tight container.
METHODOLOGY
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 107
Procedure
Anjana karma:
The patients of Group A were subjected to Anjana karma with Krishnadi varti.
Materials required
1. Water
2. Madhu
3. Sterilized Steel bowl-2
4. Gharshana shila (sterile)
5. Anjana shalaka (sterile)
6. Sterile gauze-2
7. Sterile Cotton
Procedure
Poorva karma:
In a clean and well light room patient was seated comfortably with head rest.
The eye lids and area around the eyes were wiped with wet sterile gauze dipped
in water.
Pradhana karma:
Under aseptic precautions, the tapered end of the krishnadi varti was rubbed
against a gharshana shila with sufficient quantity of Madhu to get a soft paste.
The patient was asked to open the eyes widely and eye lids were pulled down
with thumb or index finger and the anjana paste was taken on a shalaka in the
dose of one Harenu and applied from Kaninika sandhi to Apanga sandhi in a jerk
free manner and the same is repeated for other eye.
METHODOLOGY
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 108
The patient was then advised to close his eyes and rotate the eye ball in clock wise
and anti clockwise direction once for the uniform spreading of medicine.
Paschat karma:
Wet cotton gauze was kept over each eye after closing, in order to soothe the
burning sensation due to the medicament applied.
When the burning sensation and lacrimation stopped, eyes were washed with
clean water.
Eyes were checked for any remnants of medicament or accumulated akshimala
and if present it was removed with sterile gauze in order to avoid any irritation to
the eyes.
Patient was advised to avoid exposure to dust and excessive eye strain.
Assessment Criteria:
Assessment criteria was designed based on subjective and objective parameters as
per the proforma by adapting a scoring pattern.
The clinical findings were noted in specially prepared case proforma and
assessment was done
Day 1-Before treatment (BT)
Day 49- After treatment (AT)
The parameters considered for the study were graded based on the scoring pattern
0-3 for subjective parameters and 0-6 for distant vision and near vision visual acuity for
the purpose of statistical analysis.

METHODOLOGY
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 109
Scoring index
Table No. 30 Scoring index
1. Avyaktadarshana (Blurriness of vision)
Score Criteria
0 Absent
1 Blurred vision present but can make out the features of an object
clearly
2 Blurred vision present but can make out the features of an object with
straining of the eyes
3 Blurred vision present and cannot make out the features of an object
2. Gocharavibhrama
Score Criteria
0 Can assess the distance
1 Can assess the distance for near objects easily and far objects on
straining the eyes
2 Can assess the distance for both near objects and far objects on
straining the eyes
3 Cannot assess the distance for either far or near objects on straining
the eyes
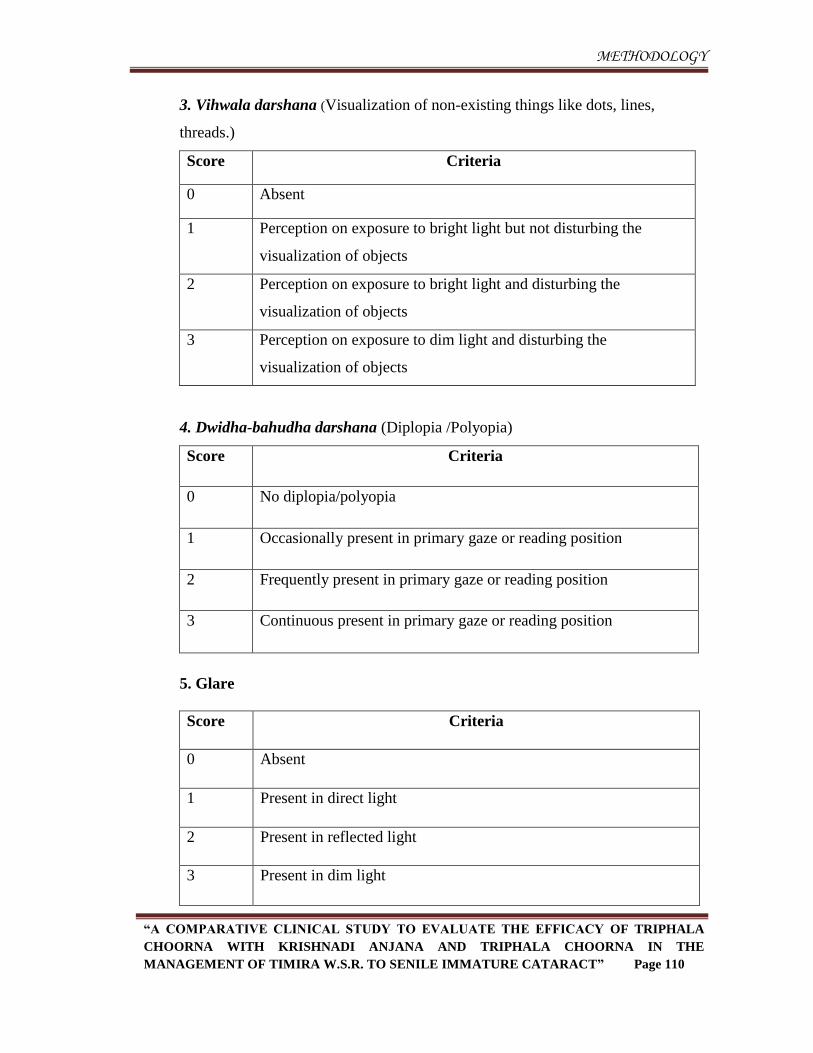
METHODOLOGY
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 110
3. Vihwala darshana (Visualization of non-existing things like dots, lines,
threads.)
Score Criteria
0 Absent
1 Perception on exposure to bright light but not disturbing the
visualization of objects
2 Perception on exposure to bright light and disturbing the
visualization of objects
3 Perception on exposure to dim light and disturbing the
visualization of objects
4. Dwidha-bahudha darshana (Diplopia /Polyopia)
Score Criteria
0 No diplopia/polyopia
1 Occasionally present in primary gaze or reading position
2 Frequently present in primary gaze or reading position
3 Continuous present in primary gaze or reading position
5. Glare
Score Criteria
0 Absent
1 Present in direct light
2 Present in reflected light
3 Present in dim light
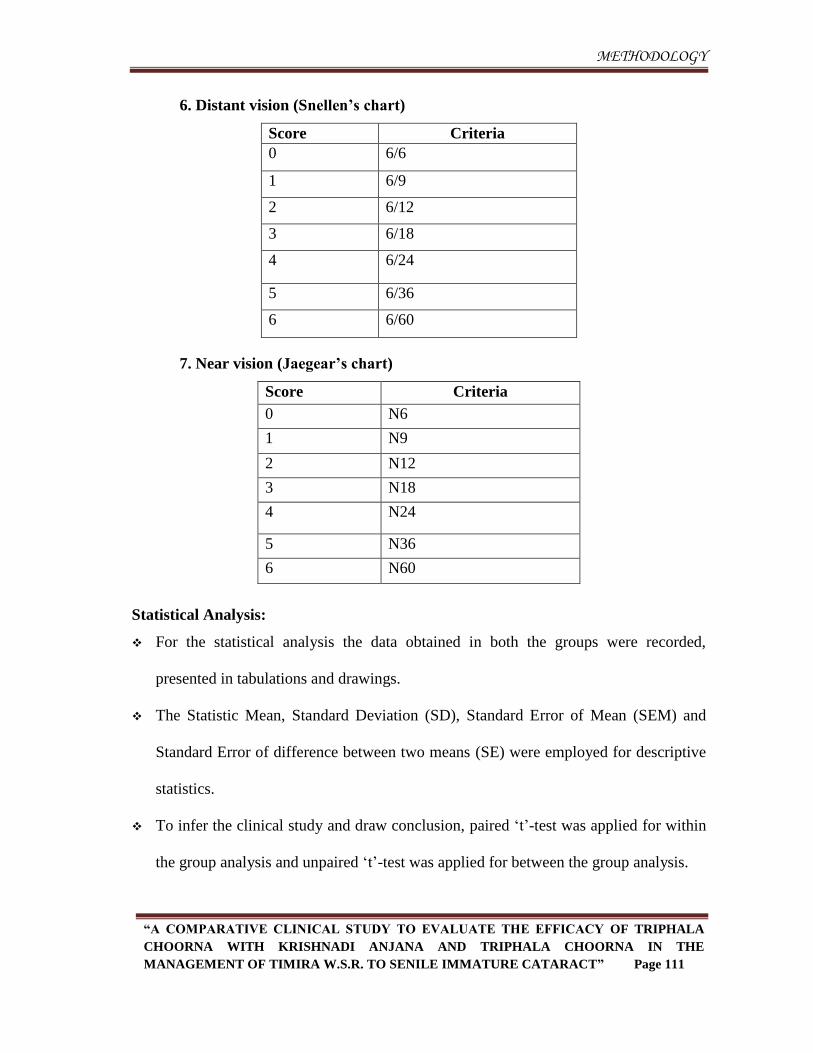
METHODOLOGY
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 111
6. Distant vision (Snellen’s chart)
Score Criteria
0 6/6
1 6/9
2 6/12
3 6/18
4 6/24
5 6/36
6 6/60
7. Near vision (Jaegear’s chart)
Score Criteria
0 N6
1 N9
2 N12
3 N18
4 N24
5 N36
6 N60
Statistical Analysis:
For the statistical analysis the data obtained in both the groups were recorded,
presented in tabulations and drawings.
The Statistic Mean, Standard Deviation (SD), Standard Error of Mean (SEM) and
Standard Error of difference between two means (SE) were employed for descriptive
statistics.
To infer the clinical study and draw conclusion, paired ‘t’-test was applied for within
the group analysis and unpaired ‘t’-test was applied for between the group analysis.
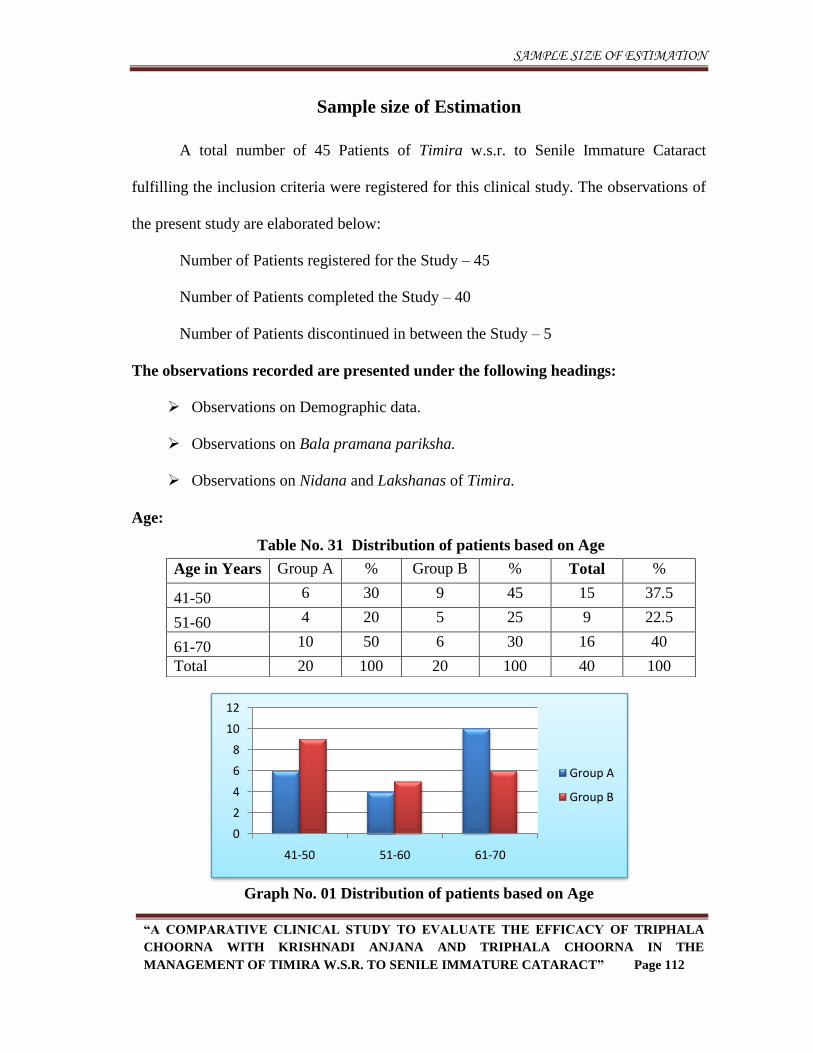
SAMPLE SIZE OF ESTIMATION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 112
Sample size of Estimation
A total number of 45 Patients of Timira w.s.r. to Senile Immature Cataract
fulfilling the inclusion criteria were registered for this clinical study. The observations of
the present study are elaborated below:
Number of Patients registered for the Study – 45
Number of Patients completed the Study – 40
Number of Patients discontinued in between the Study – 5
The observations recorded are presented under the following headings:
Observations on Demographic data.
Observations on Bala pramana pariksha.
Observations on Nidana and Lakshanas of Timira.
Age:
Graph No. 01 Distribution of patients based on Age
0
2
4
6
8
10
12
41-50 51-60 61-70
Group A
Group B
Table No. 31 Distribution of patients based on Age
Age in Years Group A % Group B % Total %
41-50 6 30 9 45 15 37.5
51-60 4 20 5 25 9 22.5
61-70 10 50 6 30 16 40
Total 20 100 20 100 40 100
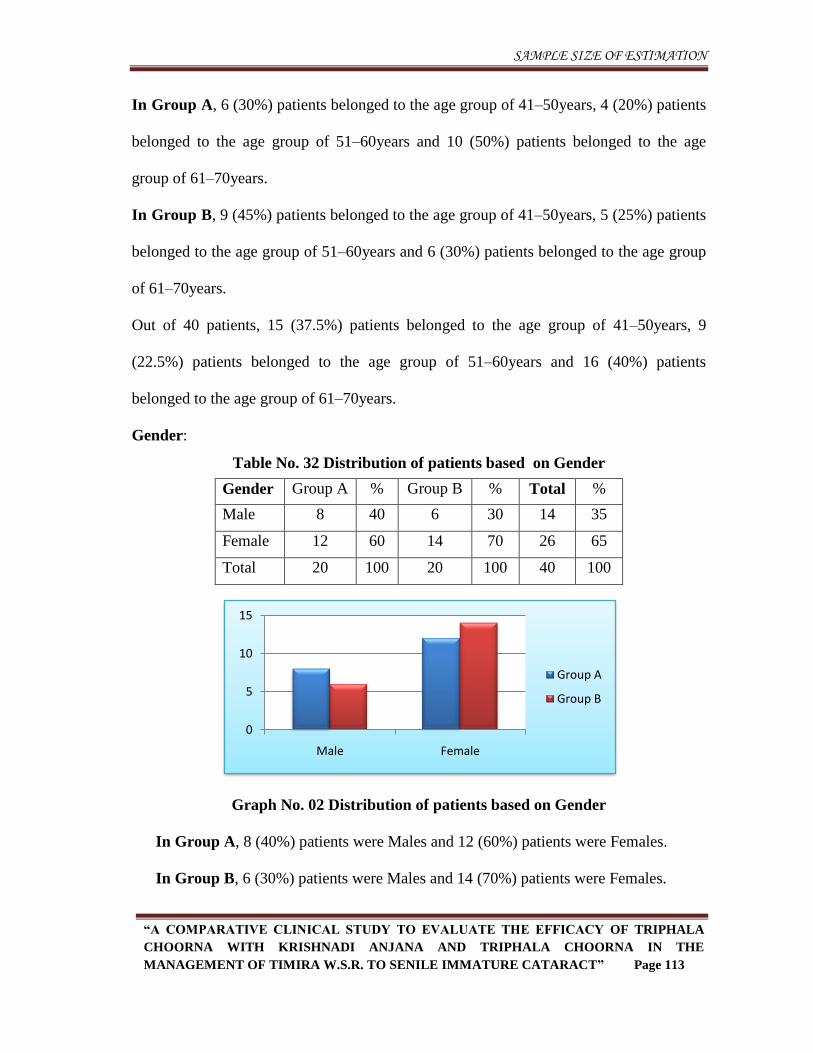
SAMPLE SIZE OF ESTIMATION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 113
In Group A, 6 (30%) patients belonged to the age group of 41–50years, 4 (20%) patients
belonged to the age group of 51–60years and 10 (50%) patients belonged to the age
group of 61–70years.
In Group B, 9 (45%) patients belonged to the age group of 41–50years, 5 (25%) patients
belonged to the age group of 51–60years and 6 (30%) patients belonged to the age group
of 61–70years.
Out of 40 patients, 15 (37.5%) patients belonged to the age group of 41–50years, 9
(22.5%) patients belonged to the age group of 51–60years and 16 (40%) patients
belonged to the age group of 61–70years.
Gender:
Table No. 32 Distribution of patients based on Gender
Gender Group A % Group B % Total %
Male 8 40 6 30 14 35
Female 12 60 14 70 26 65
Total 20 100 20 100 40 100
Graph No. 02 Distribution of patients based on Gender
In Group A, 8 (40%) patients were Males and 12 (60%) patients were Females.
In Group B, 6 (30%) patients were Males and 14 (70%) patients were Females.
0
5
10
15
Male Female
Group A
Group B
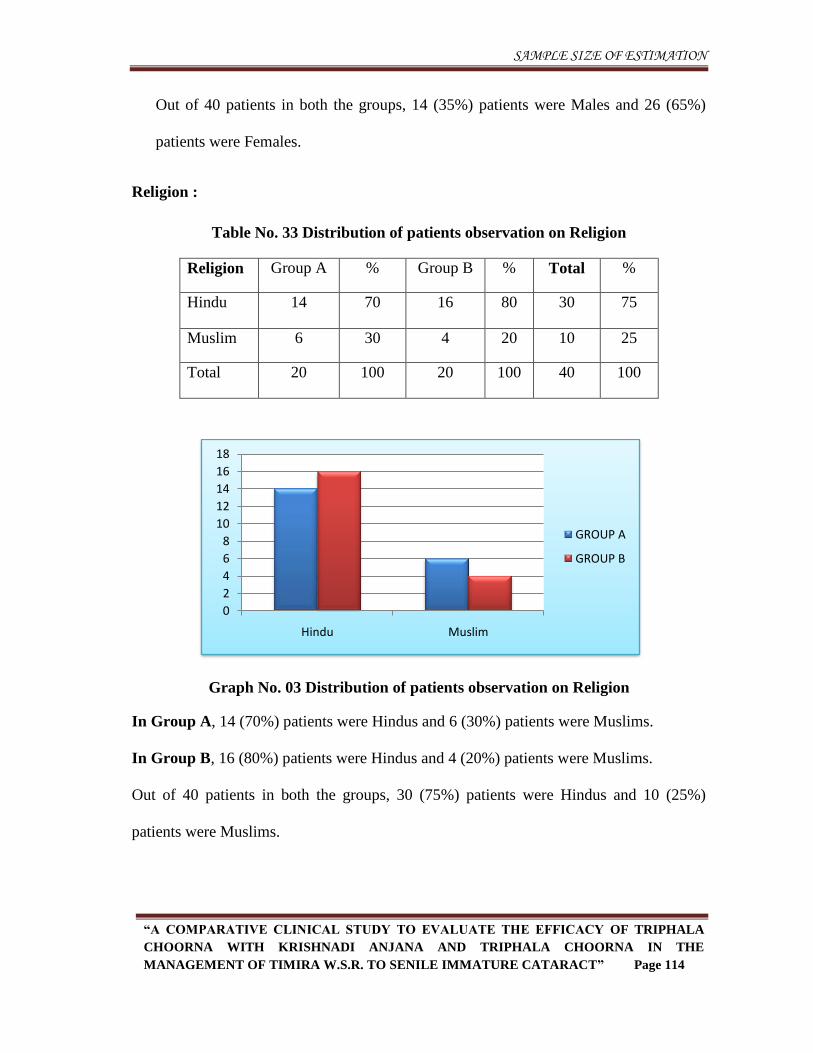
SAMPLE SIZE OF ESTIMATION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 114
Out of 40 patients in both the groups, 14 (35%) patients were Males and 26 (65%)
patients were Females.
Religion :
Table No. 33 Distribution of patients observation on Religion
Religion Group A % Group B % Total %
Hindu 14 70 16 80 30 75
Muslim 6 30 4 20 10 25
Total 20 100 20 100 40 100
Graph No. 03 Distribution of patients observation on Religion
In Group A, 14 (70%) patients were Hindus and 6 (30%) patients were Muslims.
In Group B, 16 (80%) patients were Hindus and 4 (20%) patients were Muslims.
Out of 40 patients in both the groups, 30 (75%) patients were Hindus and 10 (25%)
patients were Muslims.
0
2
4
6
8
10
12
14
16
18
Hindu Muslim
GROUP A
GROUP B
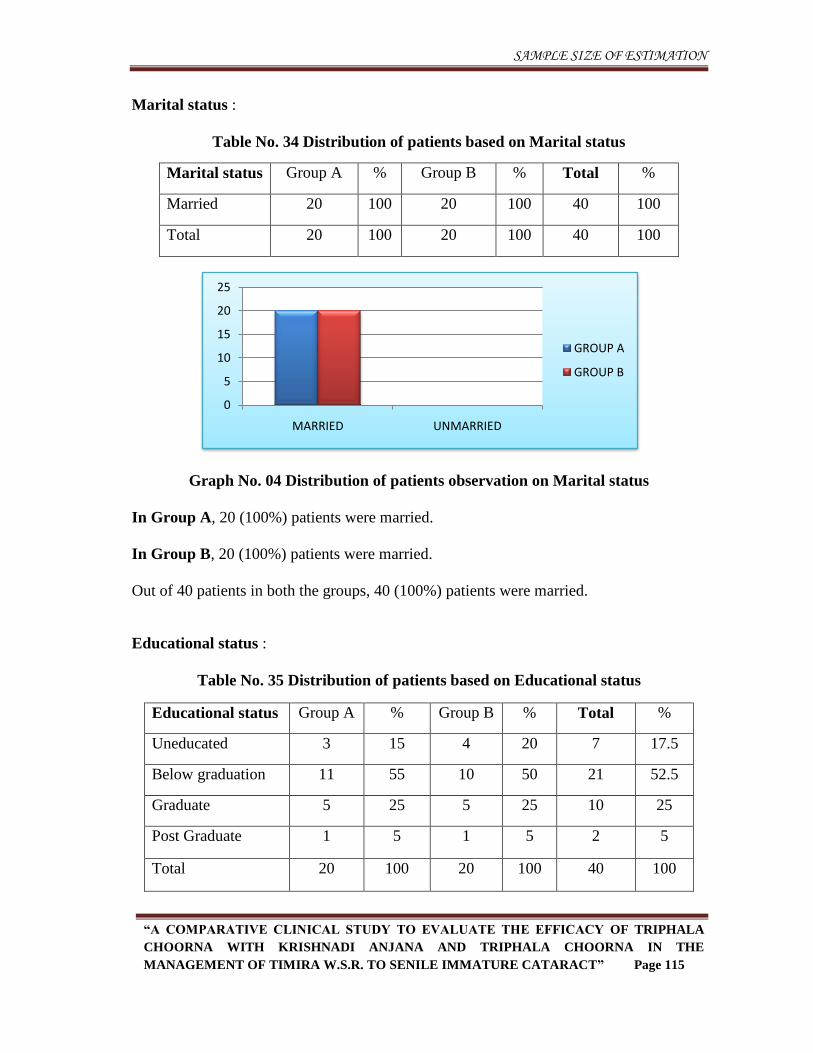
SAMPLE SIZE OF ESTIMATION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 115
Marital status :
Table No. 34 Distribution of patients based on Marital status
Marital status Group A % Group B % Total %
Married 20 100 20 100 40 100
Total 20 100 20 100 40 100
Graph No. 04 Distribution of patients observation on Marital status
In Group A, 20 (100%) patients were married.
In Group B, 20 (100%) patients were married.
Out of 40 patients in both the groups, 40 (100%) patients were married.
Educational status :
Table No. 35 Distribution of patients based on Educational status
Educational status Group A % Group B % Total %
Uneducated 3 15 4 20 7 17.5
Below graduation 11 55 10 50 21 52.5
Graduate 5 25 5 25 10 25
Post Graduate 1 5 1 5 2 5
Total 20 100 20 100 40 100
0
5
10
15
20
25
MARRIED UNMARRIED
GROUP A
GROUP B
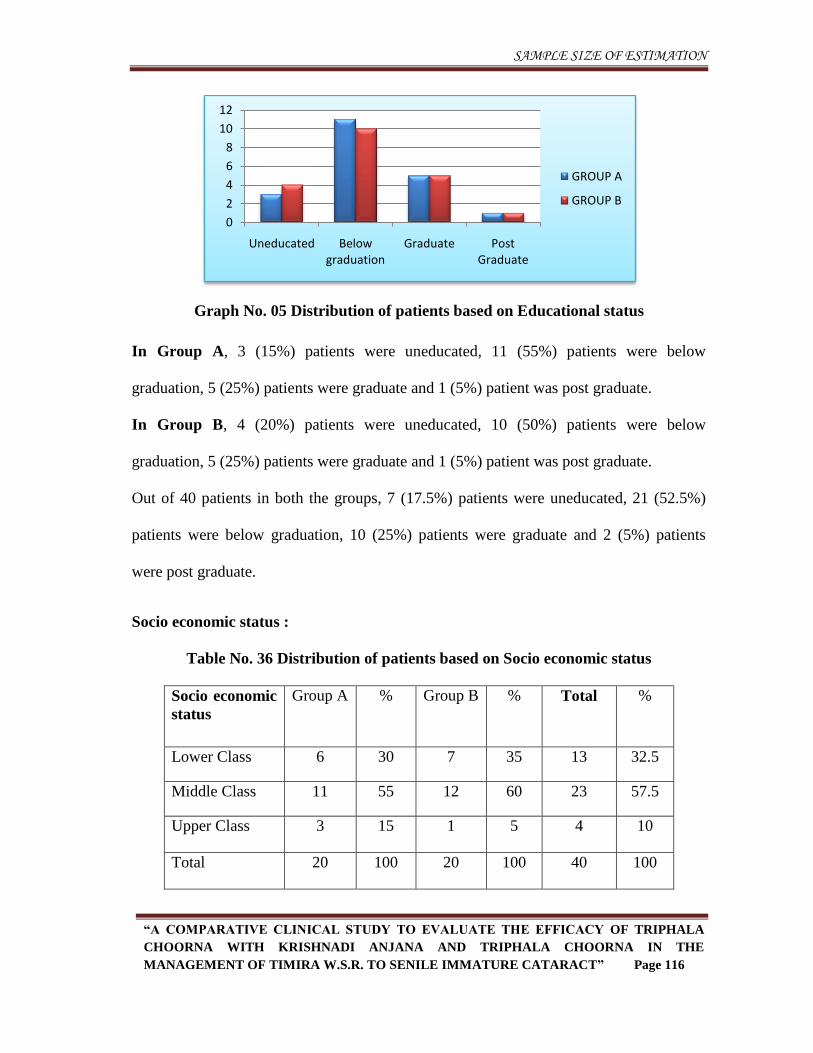
SAMPLE SIZE OF ESTIMATION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 116
Graph No. 05 Distribution of patients based on Educational status
In Group A, 3 (15%) patients were uneducated, 11 (55%) patients were below
graduation, 5 (25%) patients were graduate and 1 (5%) patient was post graduate.
In Group B, 4 (20%) patients were uneducated, 10 (50%) patients were below
graduation, 5 (25%) patients were graduate and 1 (5%) patient was post graduate.
Out of 40 patients in both the groups, 7 (17.5%) patients were uneducated, 21 (52.5%)
patients were below graduation, 10 (25%) patients were graduate and 2 (5%) patients
were post graduate.
Socio economic status :
Table No. 36 Distribution of patients based on Socio economic status
Socio economic
status
Group A % Group B % Total %
Lower Class 6 30 7 35 13 32.5
Middle Class 11 55 12 60 23 57.5
Upper Class 3 15 1 5 4 10
Total 20 100 20 100 40 100
0
2
4
6
8
10
12
Uneducated Below graduation
Graduate Post Graduate
GROUP A
GROUP B
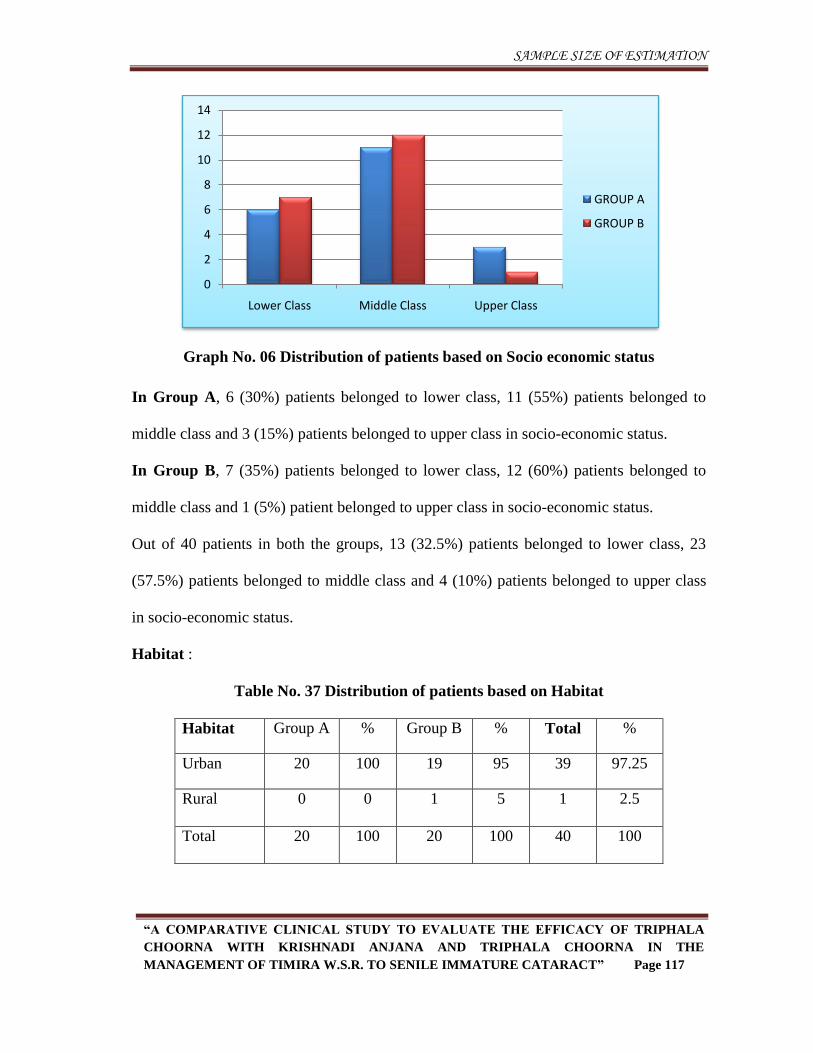
SAMPLE SIZE OF ESTIMATION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 117
Graph No. 06 Distribution of patients based on Socio economic status
In Group A, 6 (30%) patients belonged to lower class, 11 (55%) patients belonged to
middle class and 3 (15%) patients belonged to upper class in socio-economic status.
In Group B, 7 (35%) patients belonged to lower class, 12 (60%) patients belonged to
middle class and 1 (5%) patient belonged to upper class in socio-economic status.
Out of 40 patients in both the groups, 13 (32.5%) patients belonged to lower class, 23
(57.5%) patients belonged to middle class and 4 (10%) patients belonged to upper class
in socio-economic status.
Habitat :
Table No. 37 Distribution of patients based on Habitat
Habitat Group A % Group B % Total %
Urban 20 100 19 95 39 97.25
Rural 0 0 1 5 1 2.5
Total 20 100 20 100 40 100
0
2
4
6
8
10
12
14
Lower Class Middle Class Upper Class
GROUP A
GROUP B
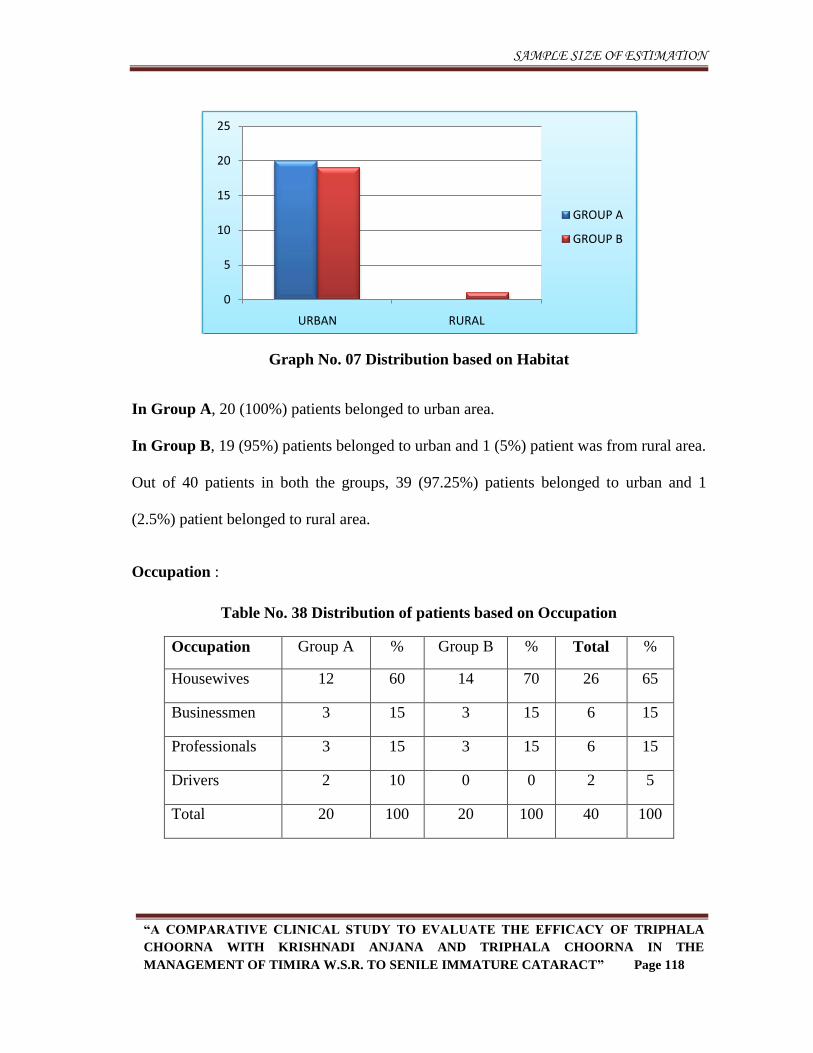
SAMPLE SIZE OF ESTIMATION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 118
Graph No. 07 Distribution based on Habitat
In Group A, 20 (100%) patients belonged to urban area.
In Group B, 19 (95%) patients belonged to urban and 1 (5%) patient was from rural area.
Out of 40 patients in both the groups, 39 (97.25%) patients belonged to urban and 1
(2.5%) patient belonged to rural area.
Occupation :
Table No. 38 Distribution of patients based on Occupation
Occupation Group A % Group B % Total %
Housewives 12 60 14 70 26 65
Businessmen 3 15 3 15 6 15
Professionals 3 15 3 15 6 15
Drivers 2 10 0 0 2 5
Total 20 100 20 100 40 100
0
5
10
15
20
25
URBAN RURAL
GROUP A
GROUP B
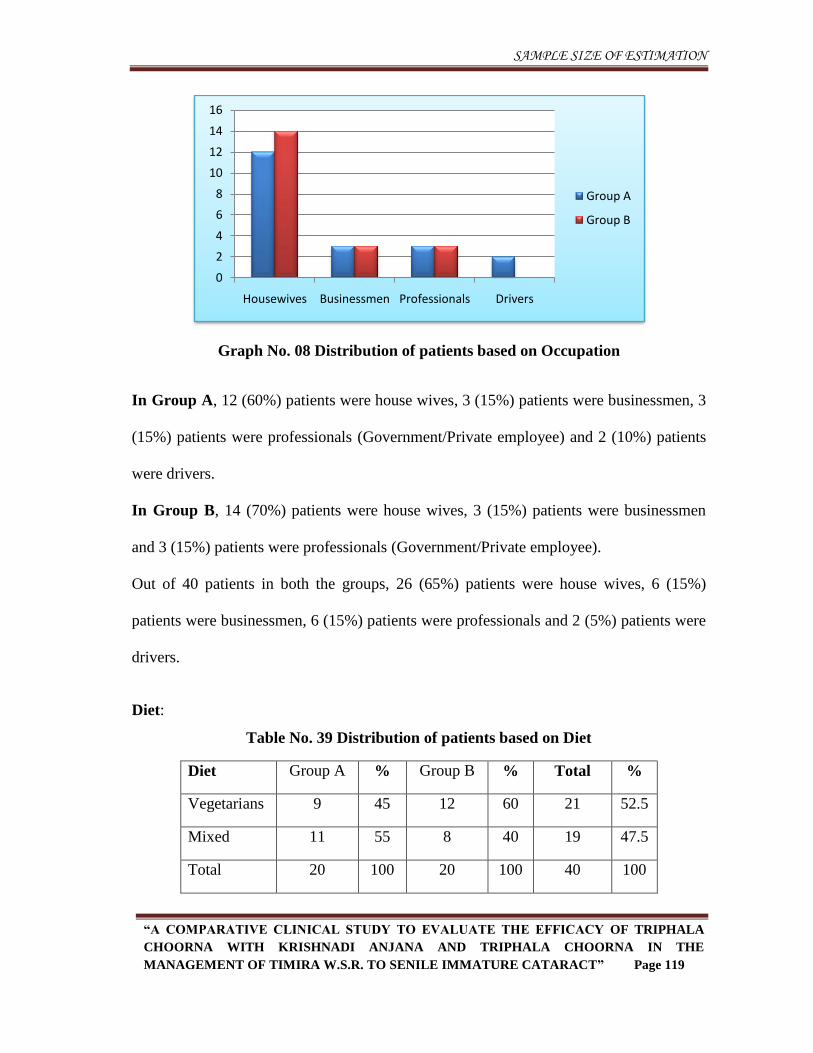
SAMPLE SIZE OF ESTIMATION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 119
Graph No. 08 Distribution of patients based on Occupation
In Group A, 12 (60%) patients were house wives, 3 (15%) patients were businessmen, 3
(15%) patients were professionals (Government/Private employee) and 2 (10%) patients
were drivers.
In Group B, 14 (70%) patients were house wives, 3 (15%) patients were businessmen
and 3 (15%) patients were professionals (Government/Private employee).
Out of 40 patients in both the groups, 26 (65%) patients were house wives, 6 (15%)
patients were businessmen, 6 (15%) patients were professionals and 2 (5%) patients were
drivers.
Diet:
Table No. 39 Distribution of patients based on Diet
Diet Group A % Group B % Total %
Vegetarians 9 45 12 60 21 52.5
Mixed 11 55 8 40 19 47.5
Total 20 100 20 100 40 100
0
2
4
6
8
10
12
14
16
Housewives Businessmen Professionals Drivers
Group A
Group B
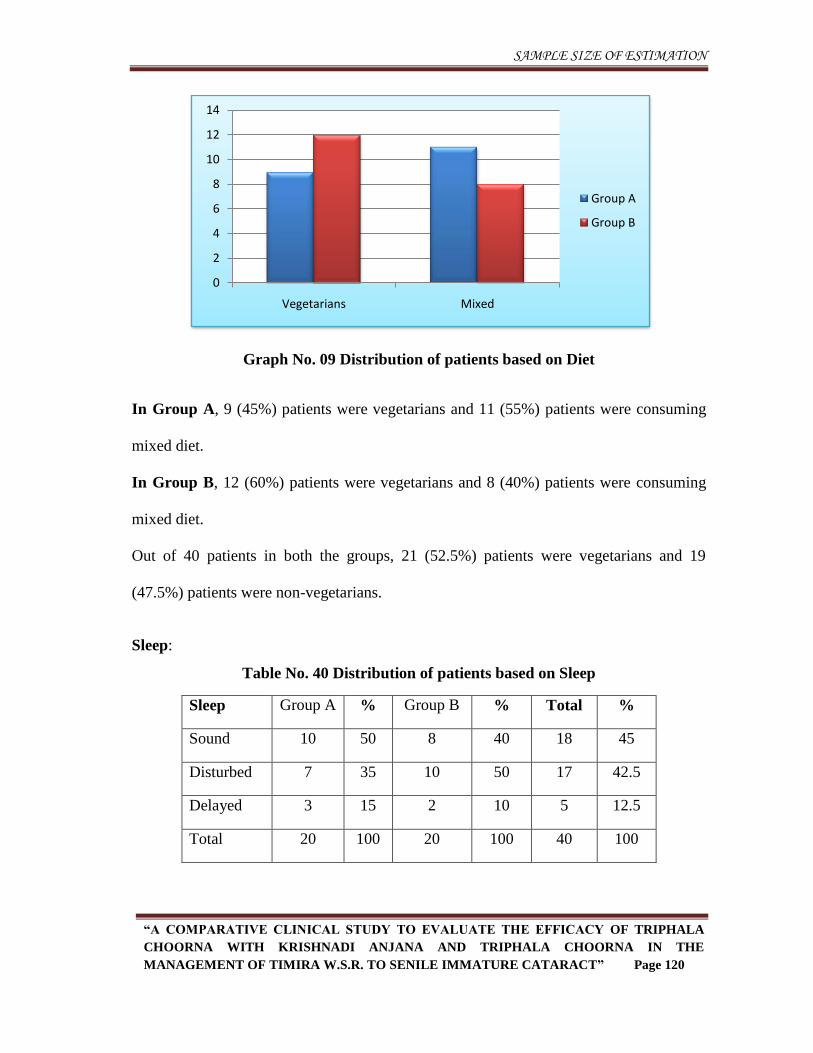
SAMPLE SIZE OF ESTIMATION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 120
Graph No. 09 Distribution of patients based on Diet
In Group A, 9 (45%) patients were vegetarians and 11 (55%) patients were consuming
mixed diet.
In Group B, 12 (60%) patients were vegetarians and 8 (40%) patients were consuming
mixed diet.
Out of 40 patients in both the groups, 21 (52.5%) patients were vegetarians and 19
(47.5%) patients were non-vegetarians.
Sleep:
Table No. 40 Distribution of patients based on Sleep
Sleep Group A % Group B % Total %
Sound 10 50 8 40 18 45
Disturbed 7 35 10 50 17 42.5
Delayed 3 15 2 10 5 12.5
Total 20 100 20 100 40 100
0
2
4
6
8
10
12
14
Vegetarians Mixed
Group A
Group B
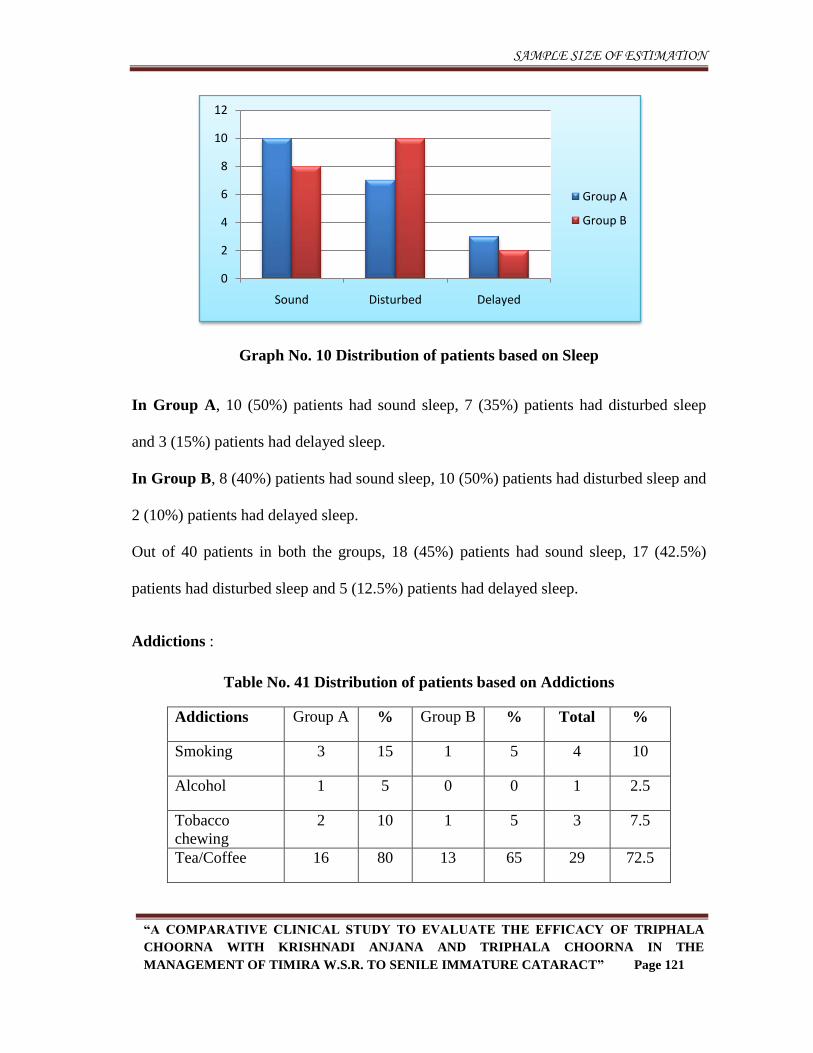
SAMPLE SIZE OF ESTIMATION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 121
Graph No. 10 Distribution of patients based on Sleep
In Group A, 10 (50%) patients had sound sleep, 7 (35%) patients had disturbed sleep
and 3 (15%) patients had delayed sleep.
In Group B, 8 (40%) patients had sound sleep, 10 (50%) patients had disturbed sleep and
2 (10%) patients had delayed sleep.
Out of 40 patients in both the groups, 18 (45%) patients had sound sleep, 17 (42.5%)
patients had disturbed sleep and 5 (12.5%) patients had delayed sleep.
Addictions :
Table No. 41 Distribution of patients based on Addictions
Addictions Group A % Group B % Total %
Smoking 3 15 1 5 4 10
Alcohol 1 5 0 0 1 2.5
Tobacco
chewing
2 10 1 5 3 7.5
Tea/Coffee 16 80 13 65 29 72.5
0
2
4
6
8
10
12
Sound Disturbed Delayed
Group A
Group B
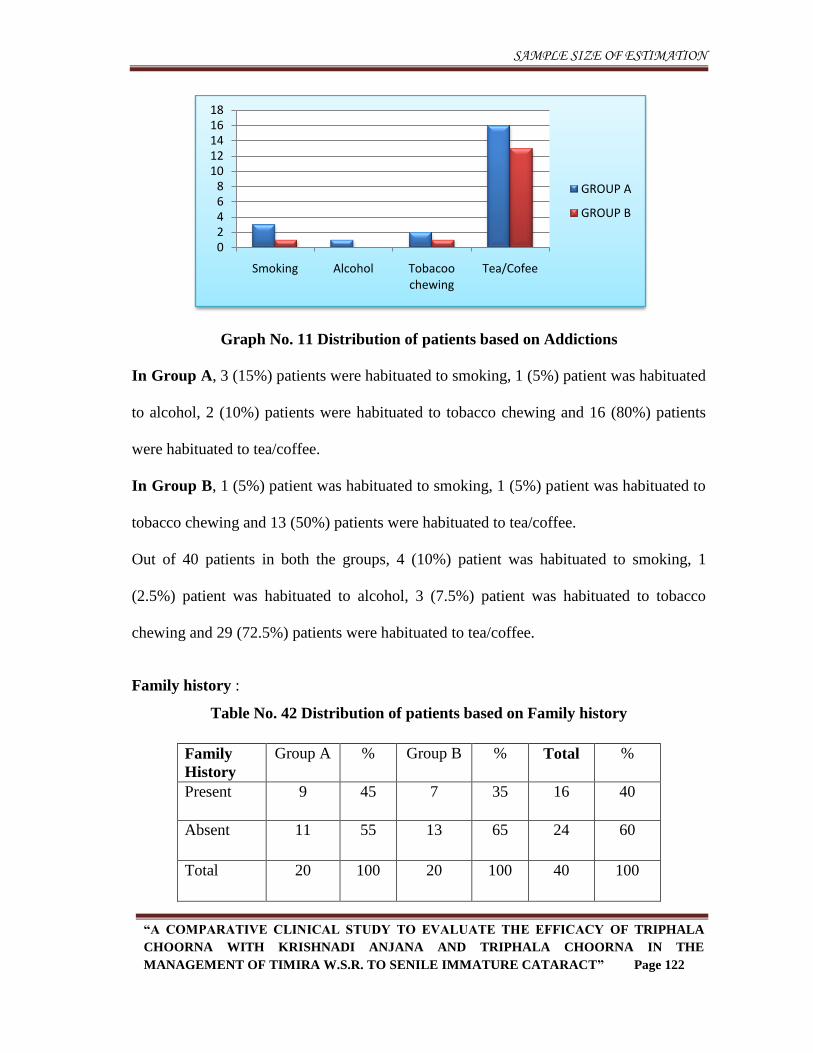
SAMPLE SIZE OF ESTIMATION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 122
Graph No. 11 Distribution of patients based on Addictions
In Group A, 3 (15%) patients were habituated to smoking, 1 (5%) patient was habituated
to alcohol, 2 (10%) patients were habituated to tobacco chewing and 16 (80%) patients
were habituated to tea/coffee.
In Group B, 1 (5%) patient was habituated to smoking, 1 (5%) patient was habituated to
tobacco chewing and 13 (50%) patients were habituated to tea/coffee.
Out of 40 patients in both the groups, 4 (10%) patient was habituated to smoking, 1
(2.5%) patient was habituated to alcohol, 3 (7.5%) patient was habituated to tobacco
chewing and 29 (72.5%) patients were habituated to tea/coffee.
Family history :
Table No. 42 Distribution of patients based on Family history
Family
History
Group A % Group B % Total %
Present 9 45 7 35 16 40
Absent 11 55 13 65 24 60
Total 20 100 20 100 40 100
02468
1012141618
Smoking Alcohol Tobacoo chewing
Tea/Cofee
GROUP A
GROUP B
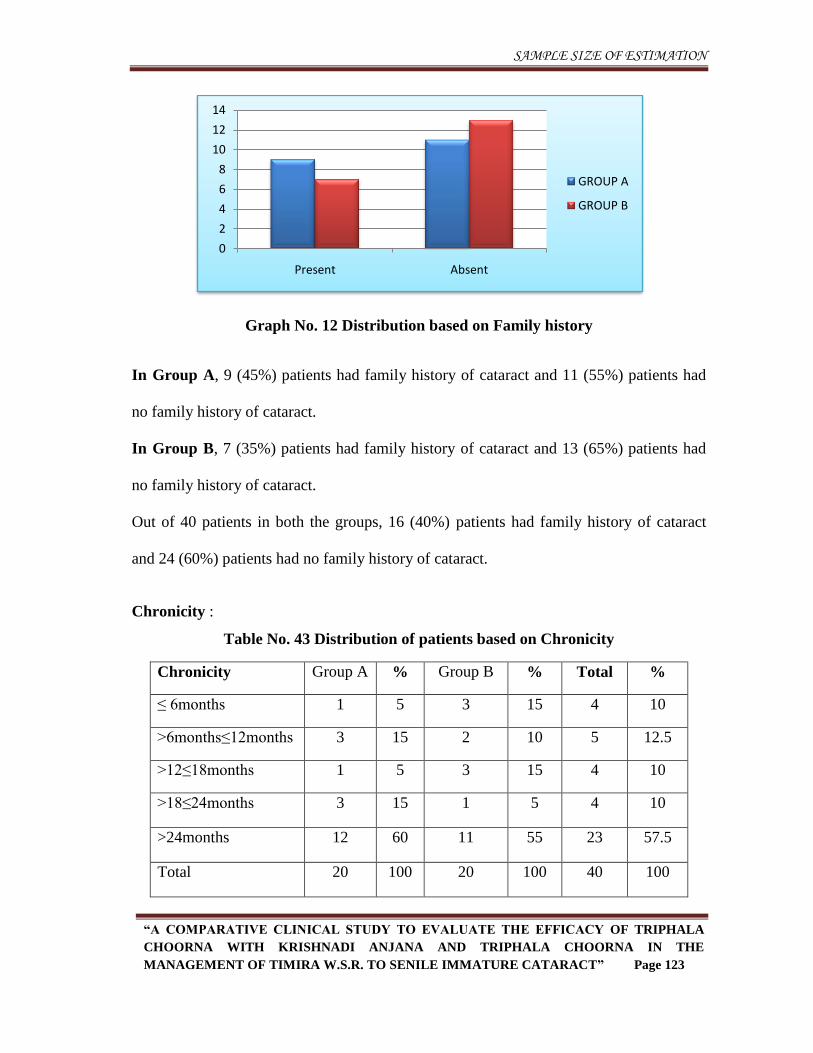
SAMPLE SIZE OF ESTIMATION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 123
Graph No. 12 Distribution based on Family history
In Group A, 9 (45%) patients had family history of cataract and 11 (55%) patients had
no family history of cataract.
In Group B, 7 (35%) patients had family history of cataract and 13 (65%) patients had
no family history of cataract.
Out of 40 patients in both the groups, 16 (40%) patients had family history of cataract
and 24 (60%) patients had no family history of cataract.
Chronicity :
Table No. 43 Distribution of patients based on Chronicity
Chronicity Group A % Group B % Total %
≤ 6months 1 5 3 15 4 10
>6months≤12months 3 15 2 10 5 12.5
>12≤18months 1 5 3 15 4 10
>18≤24months 3 15 1 5 4 10
>24months 12 60 11 55 23 57.5
Total 20 100 20 100 40 100
0
2
4
6
8
10
12
14
Present Absent
GROUP A
GROUP B
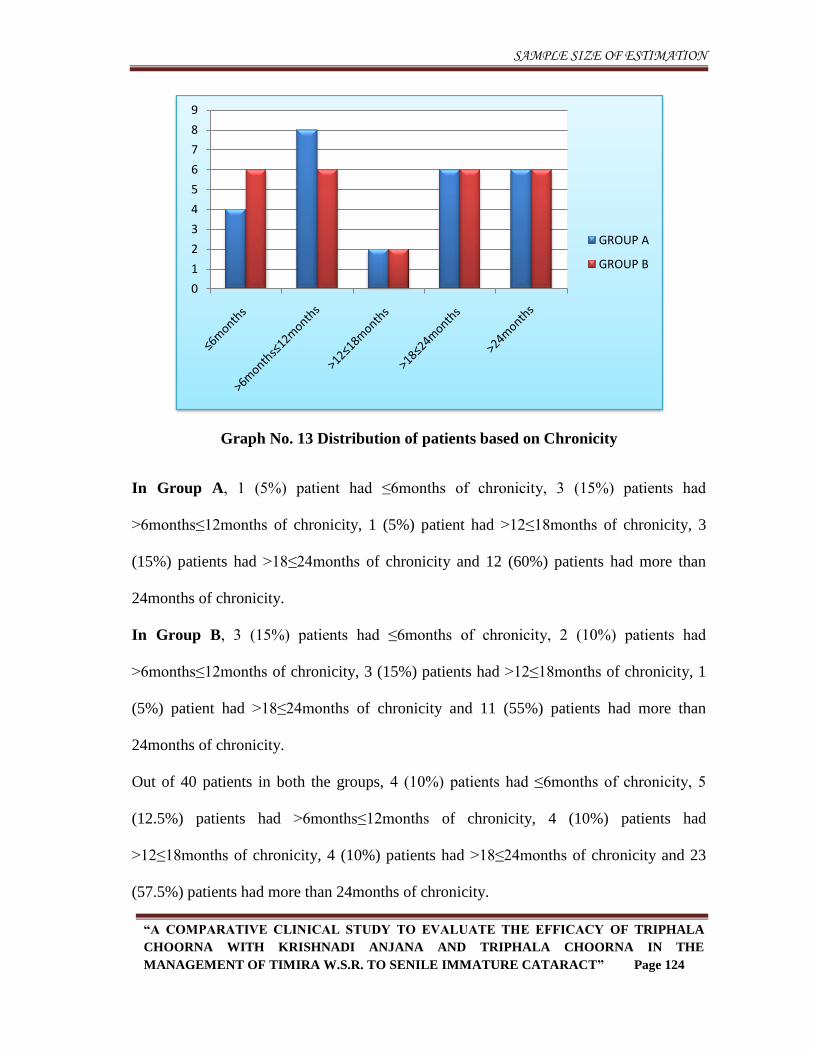
SAMPLE SIZE OF ESTIMATION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 124
Graph No. 13 Distribution of patients based on Chronicity
In Group A, 1 (5%) patient had ≤6months of chronicity, 3 (15%) patients had
>6months≤12months of chronicity, 1 (5%) patient had >12≤18months of chronicity, 3
(15%) patients had >18≤24months of chronicity and 12 (60%) patients had more than
24months of chronicity.
In Group B, 3 (15%) patients had ≤6months of chronicity, 2 (10%) patients had
>6months≤12months of chronicity, 3 (15%) patients had >12≤18months of chronicity, 1
(5%) patient had >18≤24months of chronicity and 11 (55%) patients had more than
24months of chronicity.
Out of 40 patients in both the groups, 4 (10%) patients had ≤6months of chronicity, 5
(12.5%) patients had >6months≤12months of chronicity, 4 (10%) patients had
>12≤18months of chronicity, 4 (10%) patients had >18≤24months of chronicity and 23
(57.5%) patients had more than 24months of chronicity.
0
1
2
3
4
5
6
7
8
9
GROUP A
GROUP B
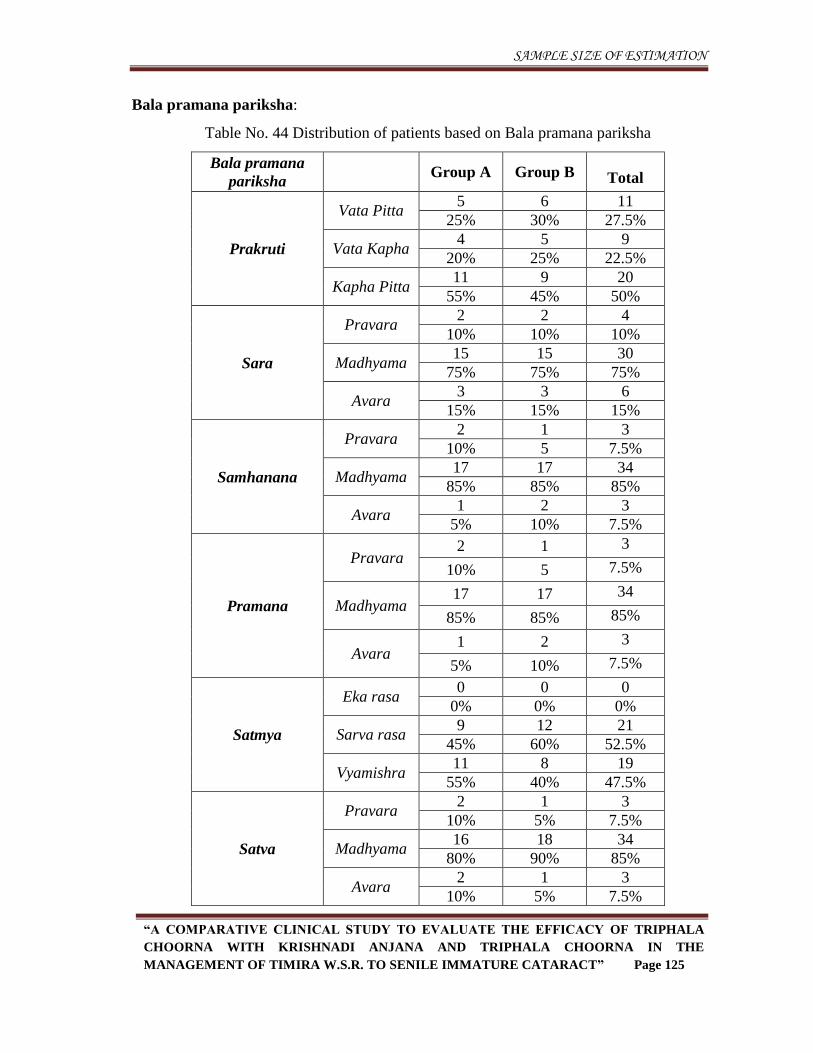
SAMPLE SIZE OF ESTIMATION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 125
Bala pramana pariksha:
Table No. 44 Distribution of patients based on Bala pramana pariksha
Bala pramana
pariksha Group A Group B Total
Prakruti
Vata Pitta 5 6 11
25% 30% 27.5%
Vata Kapha 4 5 9
20% 25% 22.5%
Kapha Pitta 11 9 20
55% 45% 50%
Sara
Pravara 2 2 4
10% 10% 10%
Madhyama 15 15 30
75% 75% 75%
Avara 3 3 6
15% 15% 15%
Samhanana
Pravara 2 1 3
10% 5 7.5%
Madhyama 17 17 34
85% 85% 85%
Avara 1 2 3
5% 10% 7.5%
Pramana
Pravara 2 1 3
10% 5 7.5%
Madhyama 17 17 34
85% 85% 85%
Avara 1 2 3
5% 10% 7.5%
Satmya
Eka rasa 0 0 0
0% 0% 0%
Sarva rasa 9 12 21
45% 60% 52.5%
Vyamishra 11 8 19
55% 40% 47.5%
Satva
Pravara 2 1 3
10% 5% 7.5%
Madhyama 16 18 34
80% 90% 85%
Avara 2 1 3
10% 5% 7.5%
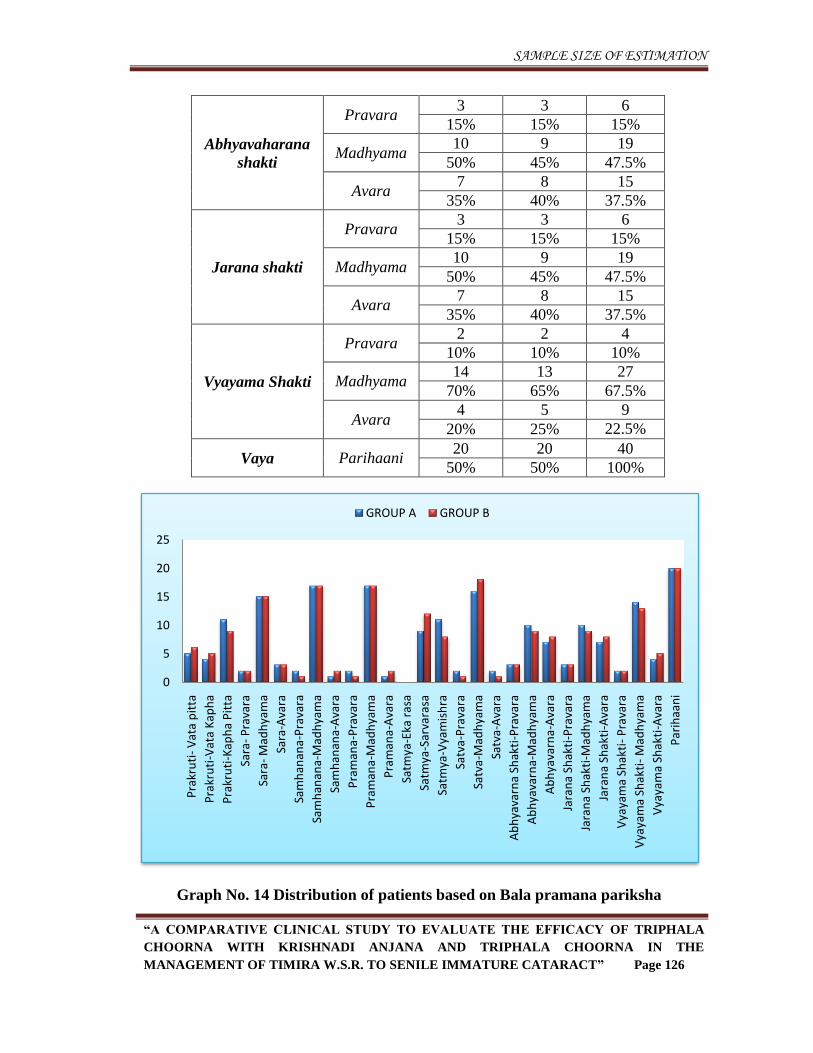
SAMPLE SIZE OF ESTIMATION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 126
Abhyavaharana
shakti
Pravara 3 3 6
15% 15% 15%
Madhyama 10 9 19
50% 45% 47.5%
Avara 7 8 15
35% 40% 37.5%
Jarana shakti
Pravara 3 3 6
15% 15% 15%
Madhyama 10 9 19
50% 45% 47.5%
Avara 7 8 15
35% 40% 37.5%
Vyayama Shakti
Pravara 2 2 4
10% 10% 10%
Madhyama 14 13 27
70% 65% 67.5%
Avara 4 5 9
20% 25% 22.5%
Vaya Parihaani 20 20 40
50% 50% 100%
Graph No. 14 Distribution of patients based on Bala pramana pariksha
0
5
10
15
20
25
Pra
kru
ti-
Vat
a p
itta
Pra
kru
ti-V
ata
Kap
ha
Pra
kru
ti-K
aph
a P
itta
Sara
-P
rava
ra
Sara
-M
adh
yam
a
Sara
-Ava
ra
Sam
han
ana-
Pra
vara
Sam
han
ana-
Mad
hya
ma
Sam
han
ana-
Ava
ra
Pra
man
a-P
rava
ra
Pra
man
a-M
adh
yam
a
Pra
man
a-A
vara
Satm
ya-E
ka r
asa
Satm
ya-S
arva
rasa
Satm
ya-V
yam
ish
ra
Satv
a-P
rava
ra
Satv
a-M
adh
yam
a
Satv
a-A
vara
Ab
hya
varn
a Sh
akti
-Pra
vara
Ab
hya
varn
a-M
adh
yam
a
Ab
hya
varn
a-A
vara
Jara
na
Shak
ti-P
rava
ra
Jara
na
Shak
ti-M
adh
yam
a
Jara
na
Shak
ti-A
vara
Vya
yam
a Sh
akti
-P
rava
ra
Vya
yam
a Sh
akti
-M
adh
yam
a
Vya
yam
a Sh
akti
-Ava
ra
Par
ihaa
ni
GROUP A GROUP B
SAMPLE SIZE OF ESTIMATION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 127
1. Prakruti:
In Group A, 5 (25%) patients belonged to Vata pitta prakruti, 4 (20%) patients belonged
to Vata kapha prakruti and 11 (55%) patients belonged to Kapha pitta prakruti.
In Group B, 6 (30%) patients belonged to Vata pitta prakruti, 5 (25%) patients belonged
to Vata kapha prakruti and 9 (45%) patients belonged to Kapha pitta prakruti.
Out of 40 patients in both the groups, 11 (27.5%) patients belonged to Vata pitta prakruti,
9 (22.5%) patients belonged to Vata kapha prakruti and 20 (50%) patients belonged to
Kapha pitta prakruti.
2. Sara:
In Group A, 2 (10%) patients were of Pravara sara, 15 (75%) patients were of
Madhyama sara and 3 (15%) patients were of Avara sara.
In Group B, 2 (10%) patients were of Pravara sara, 15 (75%) patients were of
Madhyama sara and 3 (15%) patients were of Avara sara.
Out of 40 patients in both the groups, 4 (10%) patients were of Pravara sara, 30 (75%)
patients were of Madhyama sara and 6 (15%) patients were of Avara sara.
3. Samhanana:
In Group A, 2 (10%) patients were of Pravara samhanana, 17 (85%) patients were of
Madhyama samhanana and 1 (5%) patient was of Avara samhanana.
In Group B, 1 (5%) patient was of pravara samhanana, 17 (85%) patients were of
Madhyama samhanana and 2 (10%) patients were of Avara samhanana.
SAMPLE SIZE OF ESTIMATION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 128
Out of 40 patients in both the groups, 3 (7.5%) patients were of Pravara samhanana, 34
(85%) patients were of Madhyama samhanana and 3 (7.5%) patients were of Avara
samhanana.
4. Pramana:
In Group A, 2 (10%) patients were of Pravara pramana, 17 (85%) patients were of
Madhyama pramana and 1 (5%) patient was of Avara pramana.
In Group B, 1 (5%) patient was of Pravara pramana, 17 (85%) patients were of
Madhyama pramana and 2 (10%) patients were of Avara pramana.
Out of 40 patients in both the groups, 3 (7.5%) patients were of Pravara pramana, 34
(85%) patients were of Madhyama pramana and 3 (7.5%) patients were of Avara
pramana.
5. Satmya:
In Group A, 9 (45%) patients belonged to Sarva rasa satmya and 11 (55%) patients
belonged to Vyamishra satmya.
In Group B, 12 (60%) patients belonged to Sarva rasa satmya and 8 (40%) patients
belonged to Vyamishra satmya.
Out of 40 patients in both the groups, 21 (52.5%) patients belonged to Sarva rasa satmya
and 19 (47.5%) patients belonged to Vyamishra satmya.
6. Satva:
In Group A, 2 (10%) patients belonged to Pravara satva, 16 (80%) patients belonged to
Madhyama satva and 2 (10%) patients belonged to Avara satva
SAMPLE SIZE OF ESTIMATION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 129
In Group B, 1 (5%) patient belonged to Pravara satva, 18 (90%) patients belonged to
Madhyama satva and 1 (5%) patient belonged to Avara satva.
Out of 40 patients in both the groups, 3 (7.5%) patients belonged to Pravara Satva, 34
(85%) patients belonged to Madhyama satva and 3 (7.5%) patients belonged to Avara
satva.
7. Abhyavaharanashakti:
In Group A, 3 (15%) patients had Pravara abhyavaharana shakti, 10 (50%) patients had
Madhyama abhyavaharana shakti and 7 (35%) patients had Avara abhyavaharana
shakti.
In Group B, 3 (15%) patients had Pravara abhyavaharana shakti, 9 (45%) patients had
Madhyama abhyavaharana shakti and 8 (40%) patients had Avara abhyavaharana
shakti.
Out of 40 patients in both the groups, 6 (15%) patients had Pravara abhyavaharana
shakti, 19 (47.5%) patients had Madhyama abhyavaharana shakti and 15 (37.5%)
patients had Avara abhyavaharana shakti.
8. Jarana shakti:
In Group A, 3 (15%) patients had Pravara jarana shakti, 10 (50%) patients had
Madhyama jarana shakti and 7 (35%) patients had Avara jarana shakti.
In Group B, 3 (15%) patients had Pravara jarana shakti, 9 (45%) patients had
Madhyama jarana shakti and 8 (40%) patients had Avara jarana shakti.
SAMPLE SIZE OF ESTIMATION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 130
Out of 40 patients in both the groups, 6 (15%) patients had Pravara jarana shakti, 19
(47.5%) patients had Madhyama jarana shakti and 15 (37.5%) patients had Avara jarana
shakti.
9. Vyayama Shakti:
In Group A, 2 (10%) patients belonged to Pravara vyayama shakti, 14 (70%) patients
belonged to Madhyama vyayama shakti and 4 (20%) patients belonged to Avara vyayama
shakti.
In Group B, 2 (10%) patients belonged to Pravara vyayama shakti, 13 (65%) patients
belonged to Madhyama vyayama shakti and 5 (25%) patients belonged to Avara vyayama
shakti.
Out of 40 patients in both the groups, 4 (10%) patients belonged to Pravara vyayama
shakti, 27 (67.5%) patients belonged to Madhyama vyayama shakti and 9 (22.5%)
patients belonged to Avara vyayama shakti.
10. Vaya:
In Group A, all 20 (100%) patients belonged to Parihani avastha.
In Group B, all 20 (100%) patients belonged to Parihani avastha.
Out of 40 patients in both the groups, all 40 (100%) patients belonged to Parihani
avastha.
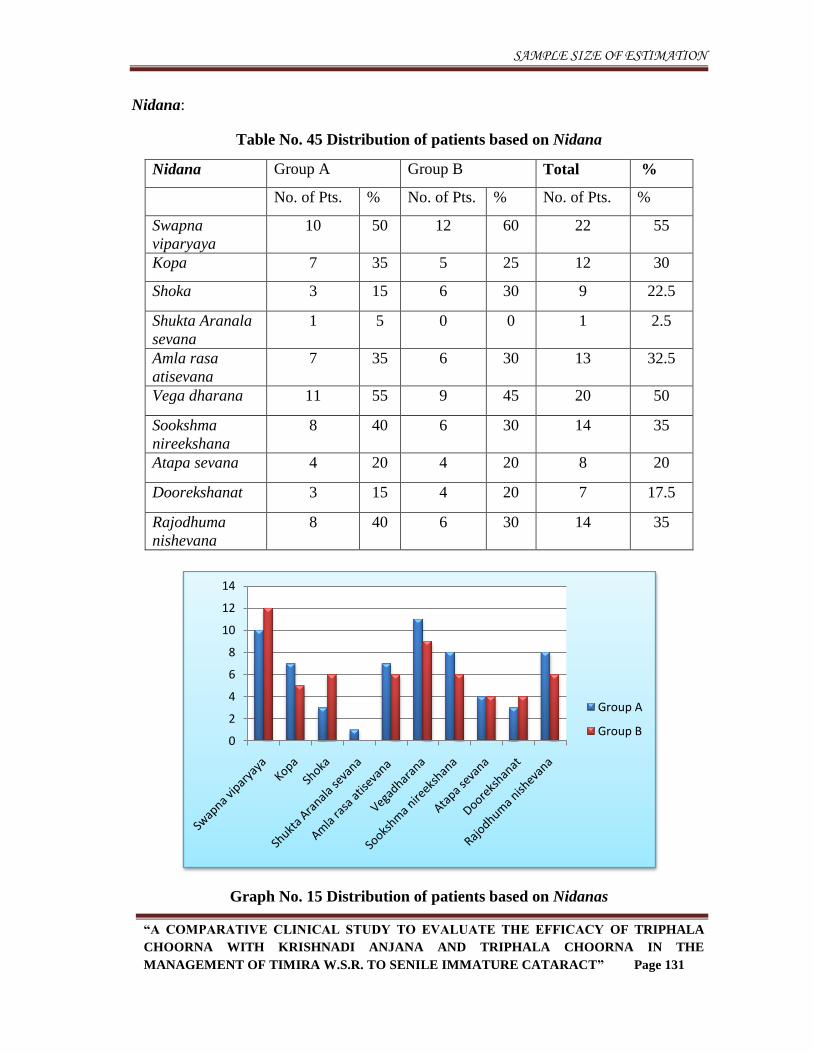
SAMPLE SIZE OF ESTIMATION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 131
Nidana:
Table No. 45 Distribution of patients based on Nidana
Nidana Group A Group B Total %
No. of Pts. % No. of Pts. % No. of Pts. %
Swapna
viparyaya
10 50 12 60 22 55
Kopa 7 35 5 25 12 30
Shoka 3 15 6 30 9 22.5
Shukta Aranala
sevana
1 5 0 0 1 2.5
Amla rasa
atisevana
7 35 6 30 13 32.5
Vega dharana 11 55 9 45 20 50
Sookshma
nireekshana
8 40 6 30 14 35
Atapa sevana 4 20 4 20 8 20
Doorekshanat 3 15 4 20 7 17.5
Rajodhuma
nishevana
8 40 6 30 14 35
Graph No. 15 Distribution of patients based on Nidanas
0
2
4
6
8
10
12
14
Group A
Group B
SAMPLE SIZE OF ESTIMATION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 132
In Group A, 10 (50%) patients had Swapna viparyaya, 7 (35%) patients had Kopa, 3
(15%) patients had Shoka, 1 (5%) patient had a habit of Shukta aranala sevana, 7 (35%)
patients had a habit of Amlarasa atisevana, 11 (55%) patients had Vegadharana
(majority had Mutra, Purisha & Nidra vegadharana), 8 (40%) patients had Sookshma
nireekshana, 4 (20%) patients had Atapa sevana, 3 (15%) patients had Doorekshanat and
8 (40%) had Rajadhuma nishevana as nidanas.
In Group B, 12 (60%) patients had Swapna viparyaya, 5 (25%) patients had Kopa, 6
(30%) patients had Shoka, 6 (30%) patients had a habit of Amlarasa atisevana, 9 (45%)
patients had Vegadharana (majority had Mutra, Purisha & Nidra vegadharana), 6 (30%)
patients had Sookshma nireekshana, 4 (20%) patients had Atapa sevana, 4 (20%)
patients had Doorekshanat and 6 (30%) had Rajadhuma nishevana as Nidanas.
Out of 40 patients in both the groups, 22 (55%) patients had Swapna viparyaya, 12 (30%)
patients had Kopa, 9 (22.5%) patients had Shoka, 1 (2.5%) patient had a habit of Shukta
aranala sevana, 13 (32.5%) patients had a habit of Amlarasa atisevana, 20 (50%)
patients had Vegadharana (majority had Mutra, Purisha & Nidra vegadharana), 14
(35%) patients had Sookshma nireekshana, 8 (20%) patients had Atapa sevana, 7
(17.5%) patients had Doorekshanat and 14 (35%) had Rajadhuma nishevana as nidanas.
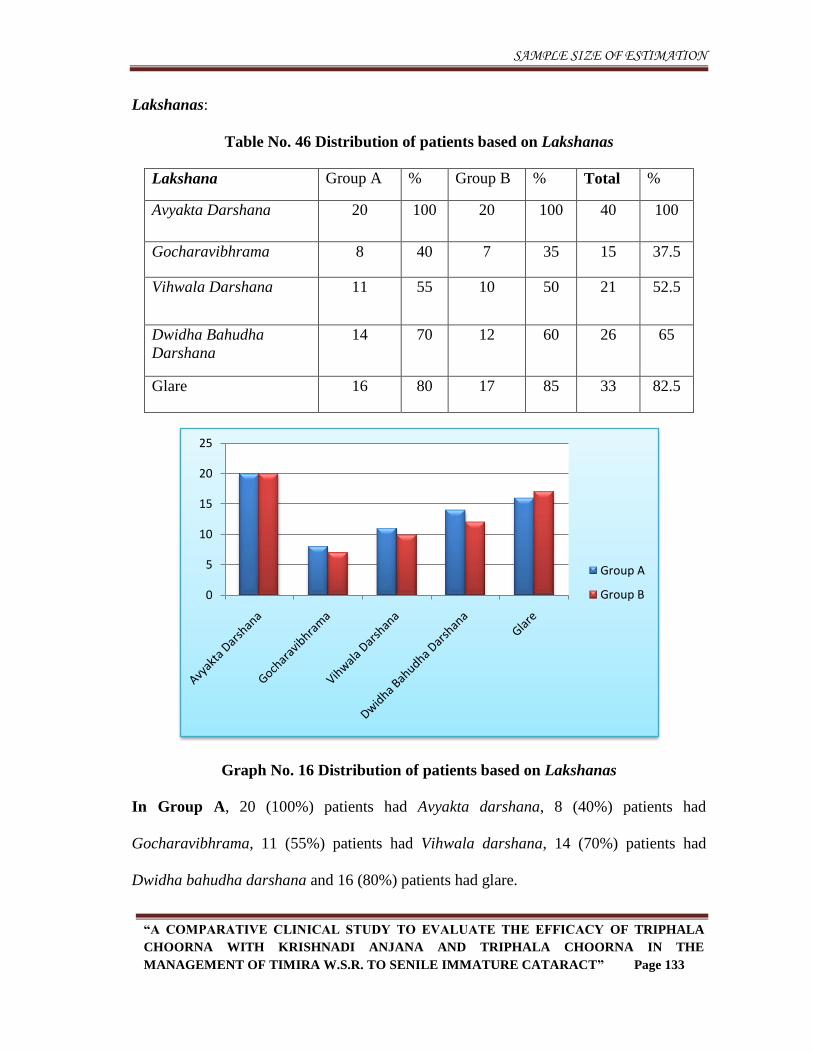
SAMPLE SIZE OF ESTIMATION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 133
Lakshanas:
Table No. 46 Distribution of patients based on Lakshanas
Lakshana Group A % Group B % Total %
Avyakta Darshana 20 100 20 100 40 100
Gocharavibhrama 8 40 7 35 15 37.5
Vihwala Darshana 11 55 10 50 21 52.5
Dwidha Bahudha
Darshana
14 70 12 60 26 65
Glare 16 80 17 85 33 82.5
Graph No. 16 Distribution of patients based on Lakshanas
In Group A, 20 (100%) patients had Avyakta darshana, 8 (40%) patients had
Gocharavibhrama, 11 (55%) patients had Vihwala darshana, 14 (70%) patients had
Dwidha bahudha darshana and 16 (80%) patients had glare.
0
5
10
15
20
25
Group A
Group B
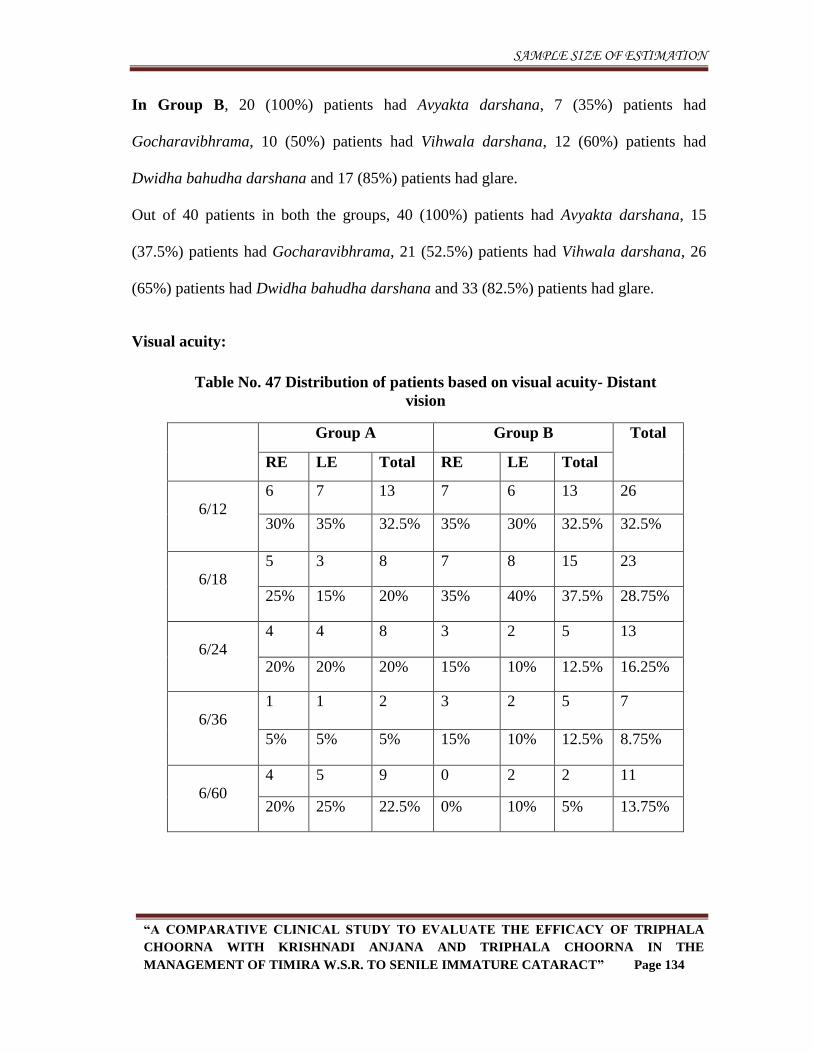
SAMPLE SIZE OF ESTIMATION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 134
In Group B, 20 (100%) patients had Avyakta darshana, 7 (35%) patients had
Gocharavibhrama, 10 (50%) patients had Vihwala darshana, 12 (60%) patients had
Dwidha bahudha darshana and 17 (85%) patients had glare.
Out of 40 patients in both the groups, 40 (100%) patients had Avyakta darshana, 15
(37.5%) patients had Gocharavibhrama, 21 (52.5%) patients had Vihwala darshana, 26
(65%) patients had Dwidha bahudha darshana and 33 (82.5%) patients had glare.
Visual acuity:
Table No. 47 Distribution of patients based on visual acuity- Distant
vision
Group A Group B Total
RE LE Total RE LE Total
6/12
6 7 13 7 6 13 26
30% 35% 32.5% 35% 30% 32.5% 32.5%
6/18
5 3 8 7 8 15 23
25% 15% 20% 35% 40% 37.5% 28.75%
6/24
4 4 8 3 2 5 13
20% 20% 20% 15% 10% 12.5% 16.25%
6/36
1 1 2 3 2 5 7
5% 5% 5% 15% 10% 12.5% 8.75%
6/60
4 5 9 0 2 2 11
20% 25% 22.5% 0% 10% 5% 13.75%
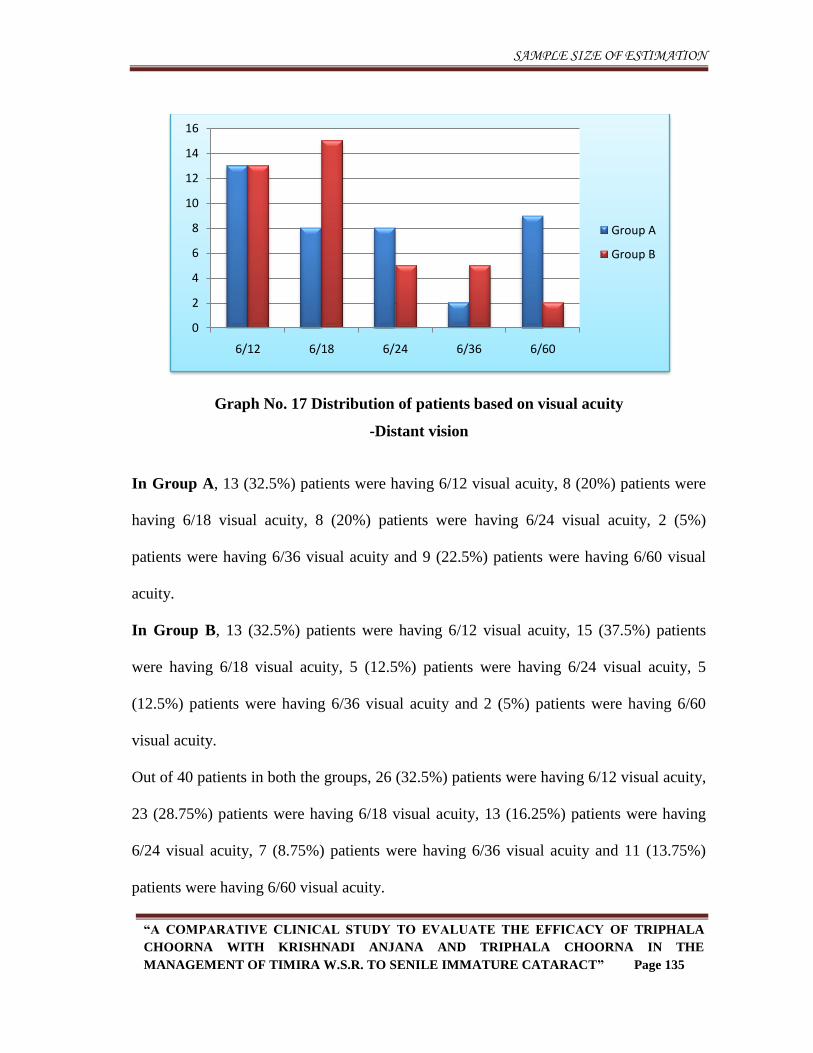
SAMPLE SIZE OF ESTIMATION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 135
Graph No. 17 Distribution of patients based on visual acuity
-Distant vision
In Group A, 13 (32.5%) patients were having 6/12 visual acuity, 8 (20%) patients were
having 6/18 visual acuity, 8 (20%) patients were having 6/24 visual acuity, 2 (5%)
patients were having 6/36 visual acuity and 9 (22.5%) patients were having 6/60 visual
acuity.
In Group B, 13 (32.5%) patients were having 6/12 visual acuity, 15 (37.5%) patients
were having 6/18 visual acuity, 5 (12.5%) patients were having 6/24 visual acuity, 5
(12.5%) patients were having 6/36 visual acuity and 2 (5%) patients were having 6/60
visual acuity.
Out of 40 patients in both the groups, 26 (32.5%) patients were having 6/12 visual acuity,
23 (28.75%) patients were having 6/18 visual acuity, 13 (16.25%) patients were having
6/24 visual acuity, 7 (8.75%) patients were having 6/36 visual acuity and 11 (13.75%)
patients were having 6/60 visual acuity.
0
2
4
6
8
10
12
14
16
6/12 6/18 6/24 6/36 6/60
Group A
Group B
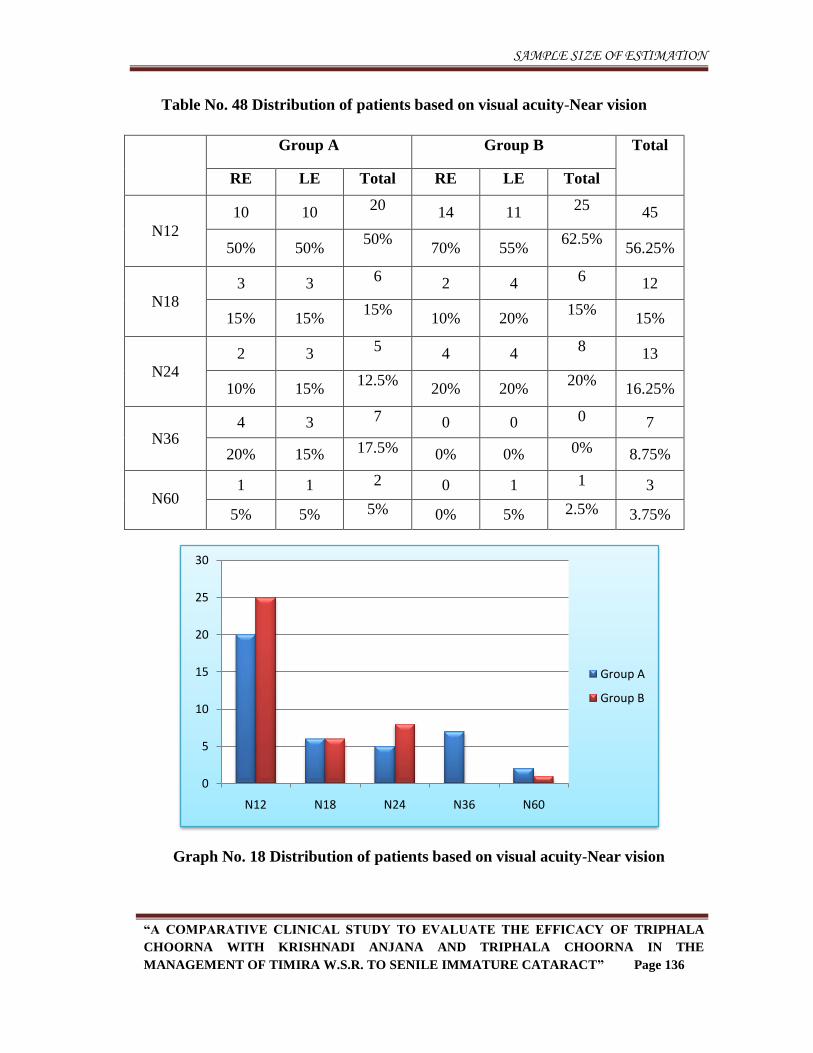
SAMPLE SIZE OF ESTIMATION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 136
Table No. 48 Distribution of patients based on visual acuity-Near vision
Group A Group B Total
RE LE Total RE LE Total
N12
10 10 20
14 11 25
45
50% 50% 50%
70% 55% 62.5%
56.25%
N18
3 3 6 2 4 6 12
15% 15% 15%
10% 20% 15%
15%
N24 2 3
5 4 4
8 13
10% 15% 12.5%
20% 20% 20%
16.25%
N36 4 3 7 0 0 0 7
20% 15% 17.5% 0% 0% 0% 8.75%
N60 1 1 2 0 1 1 3
5% 5% 5% 0% 5% 2.5% 3.75%
Graph No. 18 Distribution of patients based on visual acuity-Near vision
0
5
10
15
20
25
30
N12 N18 N24 N36 N60
Group A
Group B
SAMPLE SIZE OF ESTIMATION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 137
In Group A, 20 (50%) patients were having N12 visual acuity, 6 (15%) patients were
having N18 visual acuity, 5 (12.5%) patients were having N24 visual acuity, 7 (17.5%)
patients were having N36 visual acuity and 2 (5%) patients were having N60 visual
acuity.
In Group B, 25 (62.5%) patients were having N12 visual acuity, 6 (15%) patients were
having N18 visual acuity, 8 (20%) patients were having N24 visual acuity and 1 (2.5%)
patient was having N60 visual acuity.
Out of 40 patients in both the groups, 45 (56.25%) patients were having N12 visual
acuity, 12 (15%) patients were having N18 visual acuity, 13 (16.25%) patients were
having N24 visual acuity, 7 (8.75%) patients were having N36 and 3 (3.75%) patients
were having N60 visual acuity.
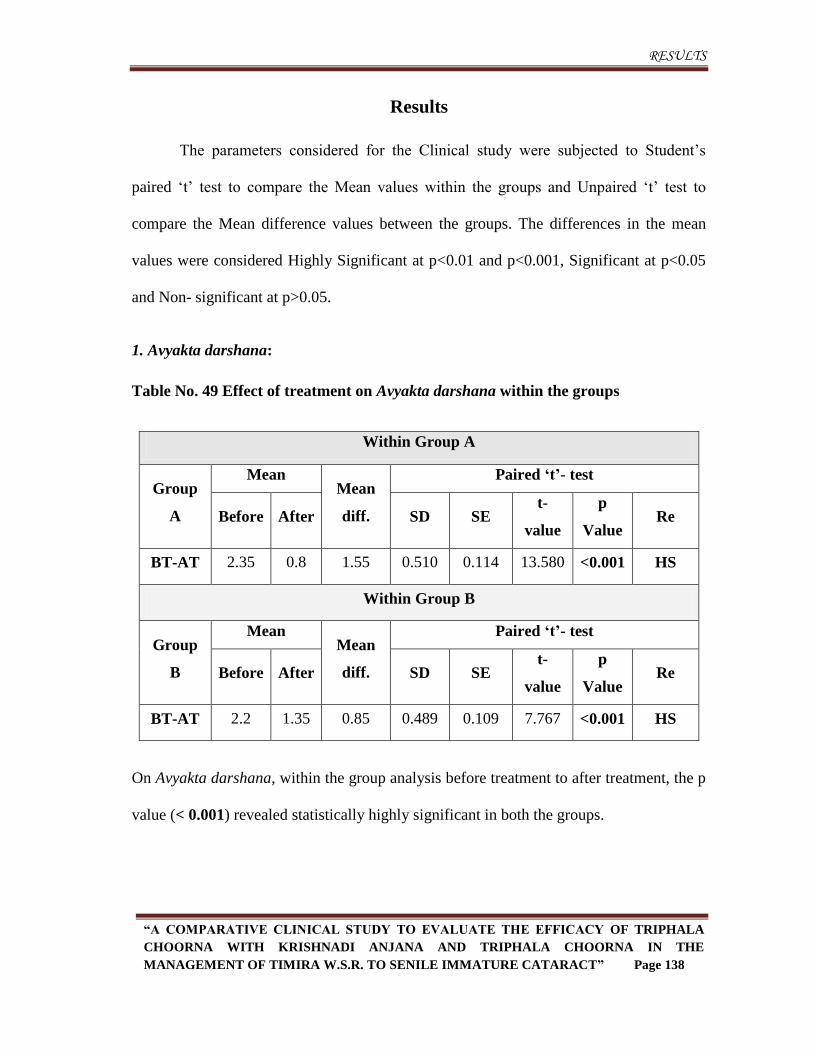
RESULTS
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 138
Results
The parameters considered for the Clinical study were subjected to Student’s
paired ‘t’ test to compare the Mean values within the groups and Unpaired ‘t’ test to
compare the Mean difference values between the groups. The differences in the mean
values were considered Highly Significant at p<0.01 and p<0.001, Significant at p<0.05
and Non- significant at p>0.05.
1. Avyakta darshana:
Table No. 49 Effect of treatment on Avyakta darshana within the groups
Within Group A
Group
A
Mean Mean
diff.
Paired „t‟- test
Before After SD SE t-
value
p
Value Re
BT-AT 2.35 0.8 1.55 0.510 0.114 13.580 <0.001 HS
Within Group B
Group
B
Mean Mean
diff.
Paired „t‟- test
Before After SD SE t-
value
p
Value Re
BT-AT 2.2 1.35 0.85 0.489 0.109 7.767 <0.001 HS
On Avyakta darshana, within the group analysis before treatment to after treatment, the p
value (< 0.001) revealed statistically highly significant in both the groups.
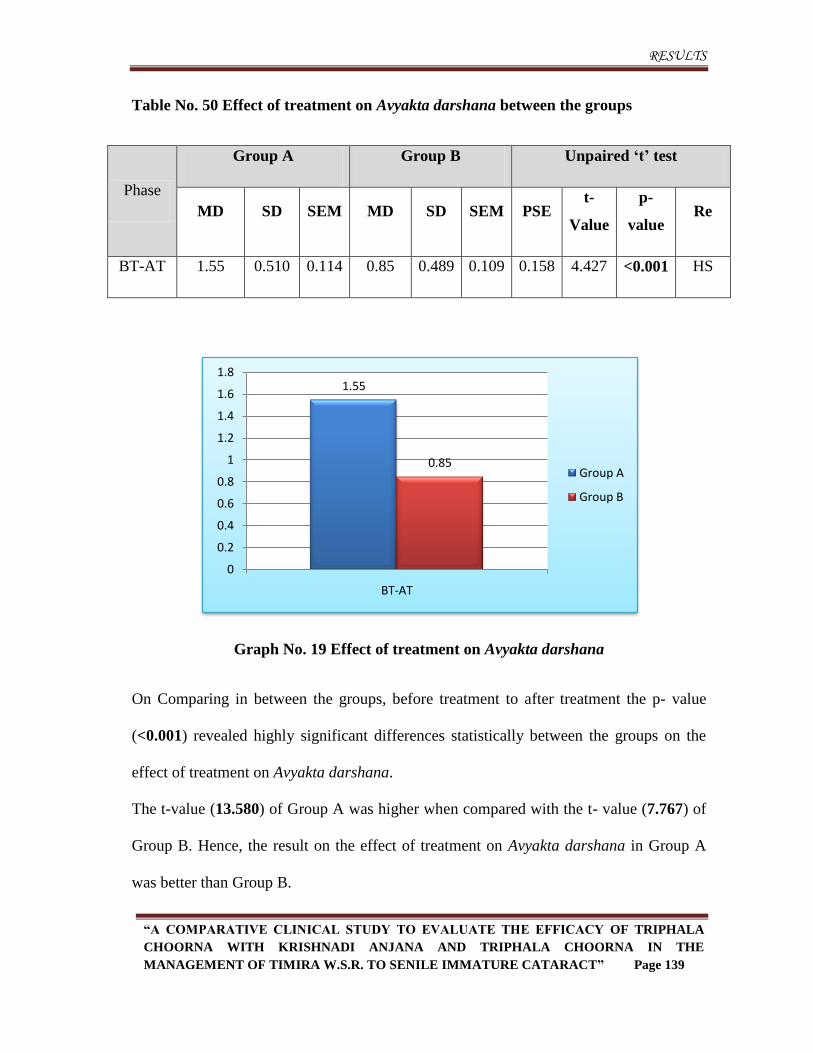
RESULTS
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 139
Table No. 50 Effect of treatment on Avyakta darshana between the groups
Phase
Group A Group B Unpaired „t‟ test
MD SD SEM MD SD SEM PSE t-
Value
p-
value Re
BT-AT 1.55 0.510 0.114 0.85 0.489 0.109 0.158 4.427 <0.001 HS
Graph No. 19 Effect of treatment on Avyakta darshana
On Comparing in between the groups, before treatment to after treatment the p- value
(<0.001) revealed highly significant differences statistically between the groups on the
effect of treatment on Avyakta darshana.
The t-value (13.580) of Group A was higher when compared with the t- value (7.767) of
Group B. Hence, the result on the effect of treatment on Avyakta darshana in Group A
was better than Group B.
1.55
0.85
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
BT-AT
Group A
Group B
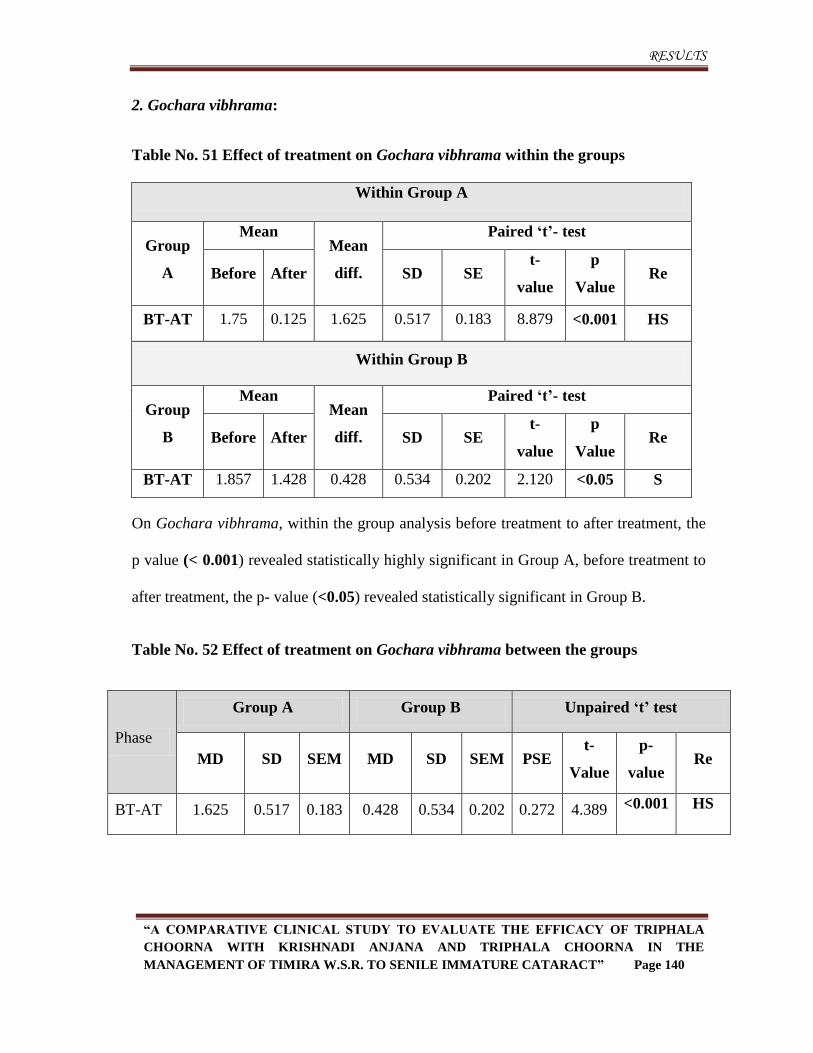
RESULTS
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 140
2. Gochara vibhrama:
Table No. 51 Effect of treatment on Gochara vibhrama within the groups
Within Group A
Group
A
Mean Mean
diff.
Paired „t‟- test
Before After SD SE t-
value
p
Value Re
BT-AT 1.75 0.125 1.625 0.517 0.183 8.879 <0.001 HS
Within Group B
Group
B
Mean Mean
diff.
Paired „t‟- test
Before After SD SE t-
value
p
Value Re
BT-AT 1.857 1.428 0.428 0.534 0.202 2.120 <0.05 S
On Gochara vibhrama, within the group analysis before treatment to after treatment, the
p value (< 0.001) revealed statistically highly significant in Group A, before treatment to
after treatment, the p- value (<0.05) revealed statistically significant in Group B.
Table No. 52 Effect of treatment on Gochara vibhrama between the groups
Phase
Group A Group B Unpaired „t‟ test
MD SD SEM MD SD SEM PSE t-
Value
p-
value Re
BT-AT 1.625 0.517 0.183 0.428 0.534 0.202 0.272 4.389 <0.001 HS
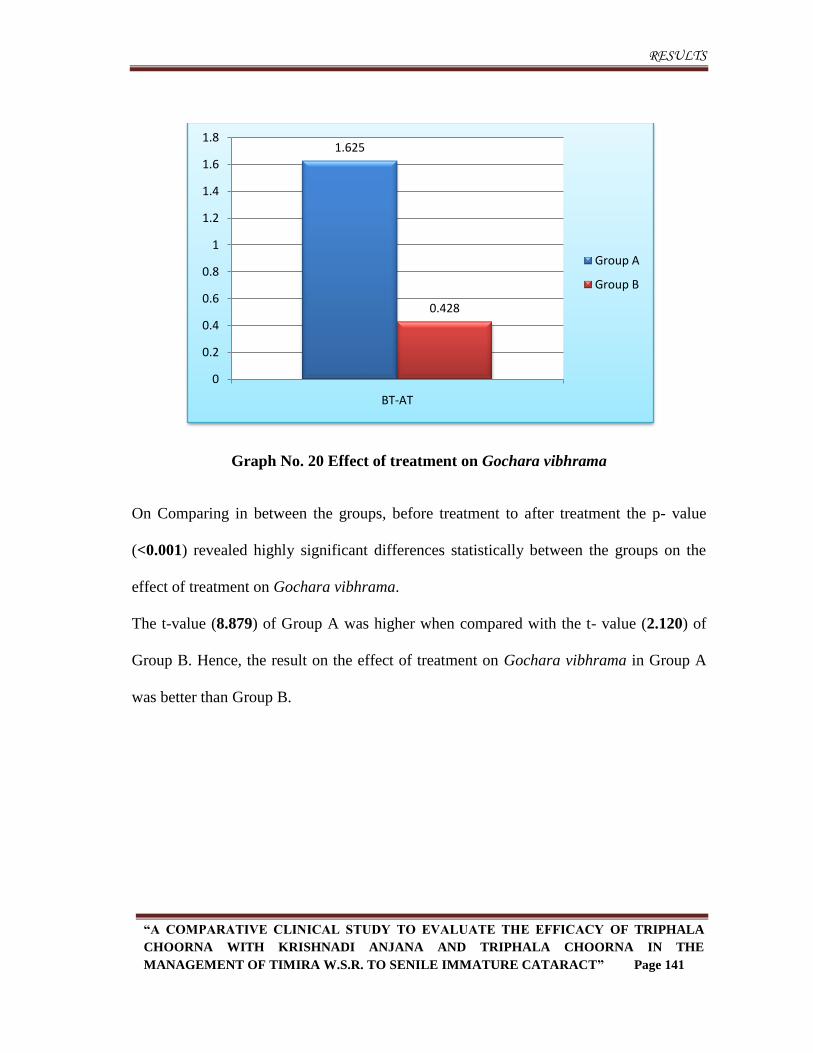
RESULTS
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 141
Graph No. 20 Effect of treatment on Gochara vibhrama
On Comparing in between the groups, before treatment to after treatment the p- value
(<0.001) revealed highly significant differences statistically between the groups on the
effect of treatment on Gochara vibhrama.
The t-value (8.879) of Group A was higher when compared with the t- value (2.120) of
Group B. Hence, the result on the effect of treatment on Gochara vibhrama in Group A
was better than Group B.
1.625
0.428
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
BT-AT
Group A
Group B
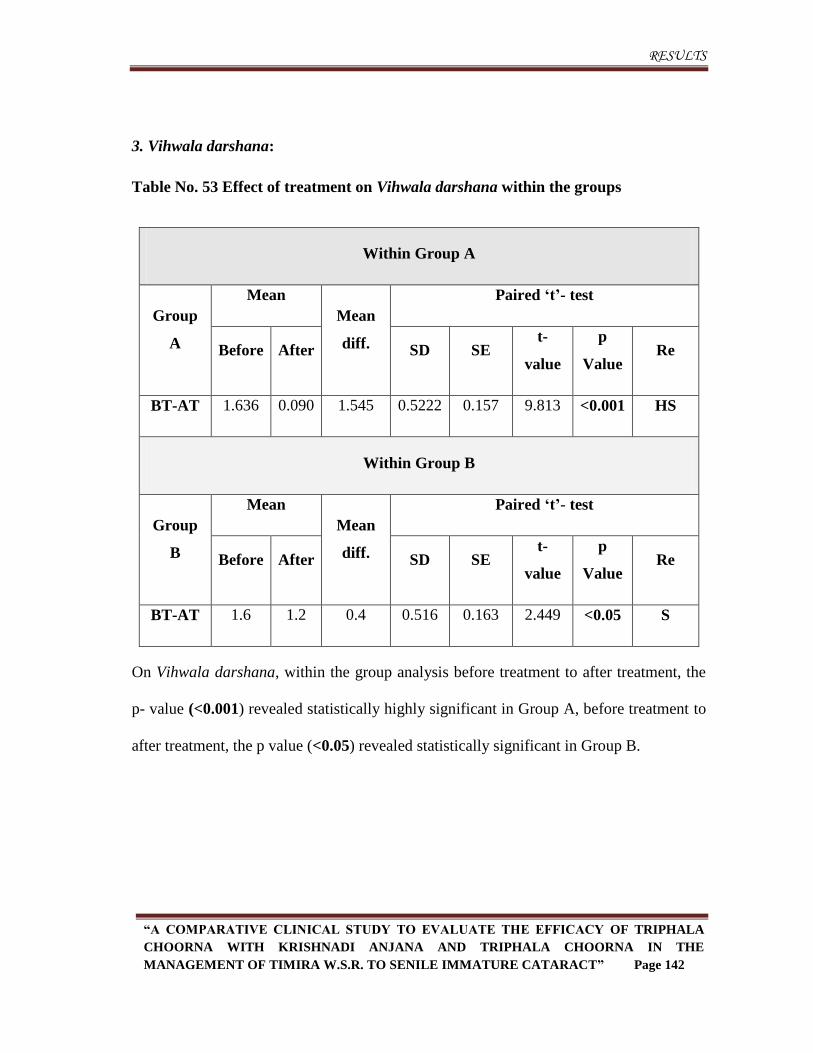
RESULTS
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 142
3. Vihwala darshana:
Table No. 53 Effect of treatment on Vihwala darshana within the groups
Within Group A
Group
A
Mean
Mean
diff.
Paired „t‟- test
Before After SD SE t-
value
p
Value Re
BT-AT 1.636 0.090 1.545 0.5222 0.157 9.813 <0.001 HS
Within Group B
Group
B
Mean
Mean
diff.
Paired „t‟- test
Before After SD SE t-
value
p
Value Re
BT-AT 1.6 1.2 0.4 0.516 0.163 2.449 <0.05 S
On Vihwala darshana, within the group analysis before treatment to after treatment, the
p- value (<0.001) revealed statistically highly significant in Group A, before treatment to
after treatment, the p value (<0.05) revealed statistically significant in Group B.
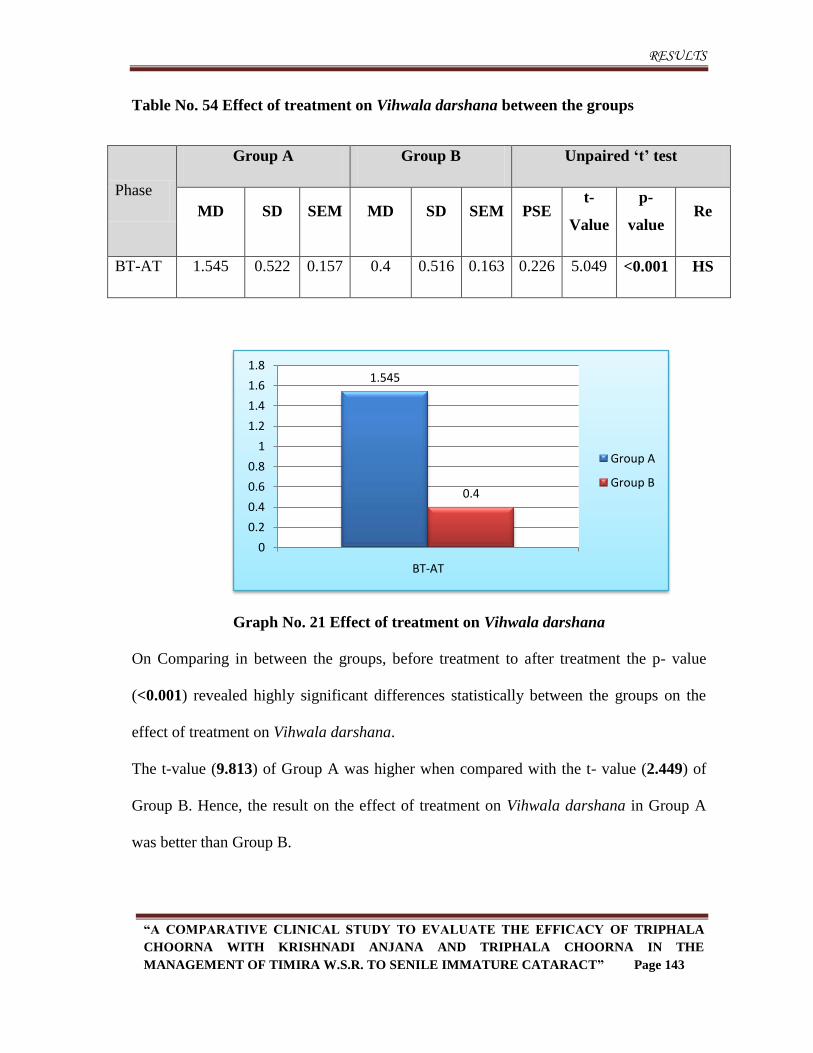
RESULTS
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 143
Table No. 54 Effect of treatment on Vihwala darshana between the groups
Phase
Group A Group B Unpaired „t‟ test
MD SD SEM MD SD SEM PSE t-
Value
p-
value Re
BT-AT 1.545 0.522 0.157 0.4 0.516 0.163 0.226 5.049 <0.001 HS
Graph No. 21 Effect of treatment on Vihwala darshana
On Comparing in between the groups, before treatment to after treatment the p- value
(<0.001) revealed highly significant differences statistically between the groups on the
effect of treatment on Vihwala darshana.
The t-value (9.813) of Group A was higher when compared with the t- value (2.449) of
Group B. Hence, the result on the effect of treatment on Vihwala darshana in Group A
was better than Group B.
1.545
0.4
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
BT-AT
Group A
Group B
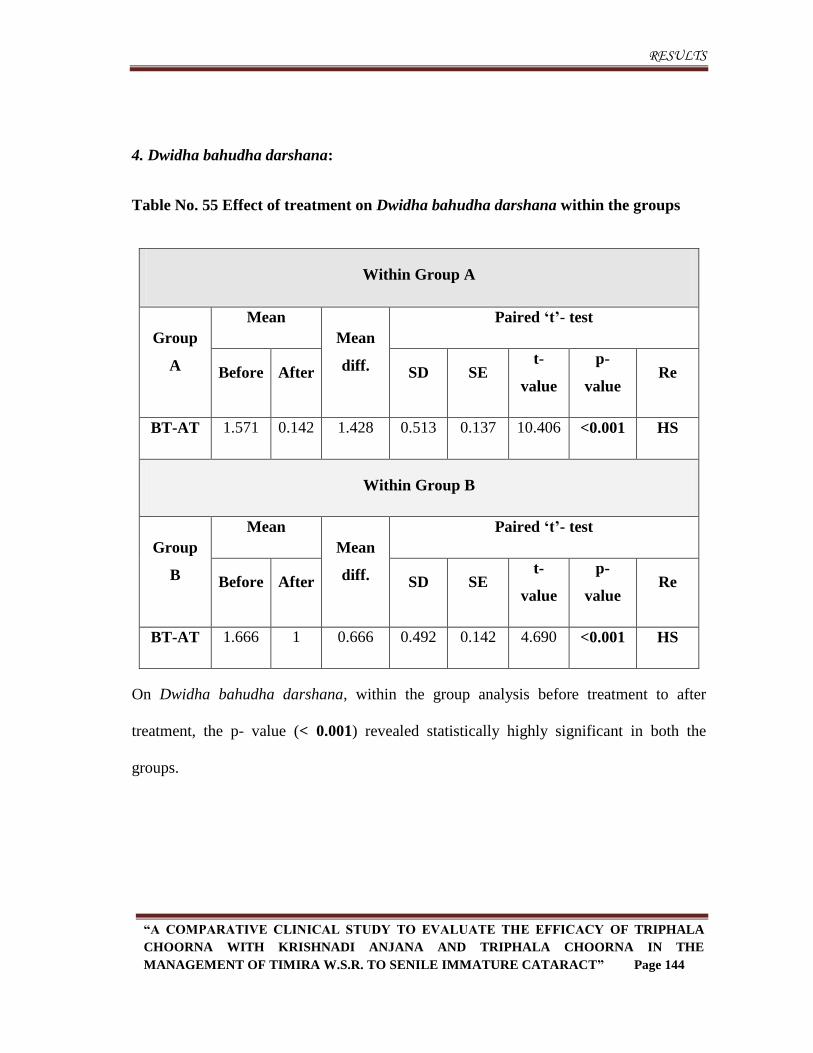
RESULTS
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 144
4. Dwidha bahudha darshana:
Table No. 55 Effect of treatment on Dwidha bahudha darshana within the groups
Within Group A
Group
A
Mean
Mean
diff.
Paired „t‟- test
Before After SD SE t-
value
p-
value Re
BT-AT 1.571 0.142 1.428 0.513 0.137 10.406 <0.001 HS
Within Group B
Group
B
Mean
Mean
diff.
Paired „t‟- test
Before After SD SE t-
value
p-
value Re
BT-AT 1.666 1 0.666 0.492 0.142 4.690 <0.001 HS
On Dwidha bahudha darshana, within the group analysis before treatment to after
treatment, the p- value (< 0.001) revealed statistically highly significant in both the
groups.
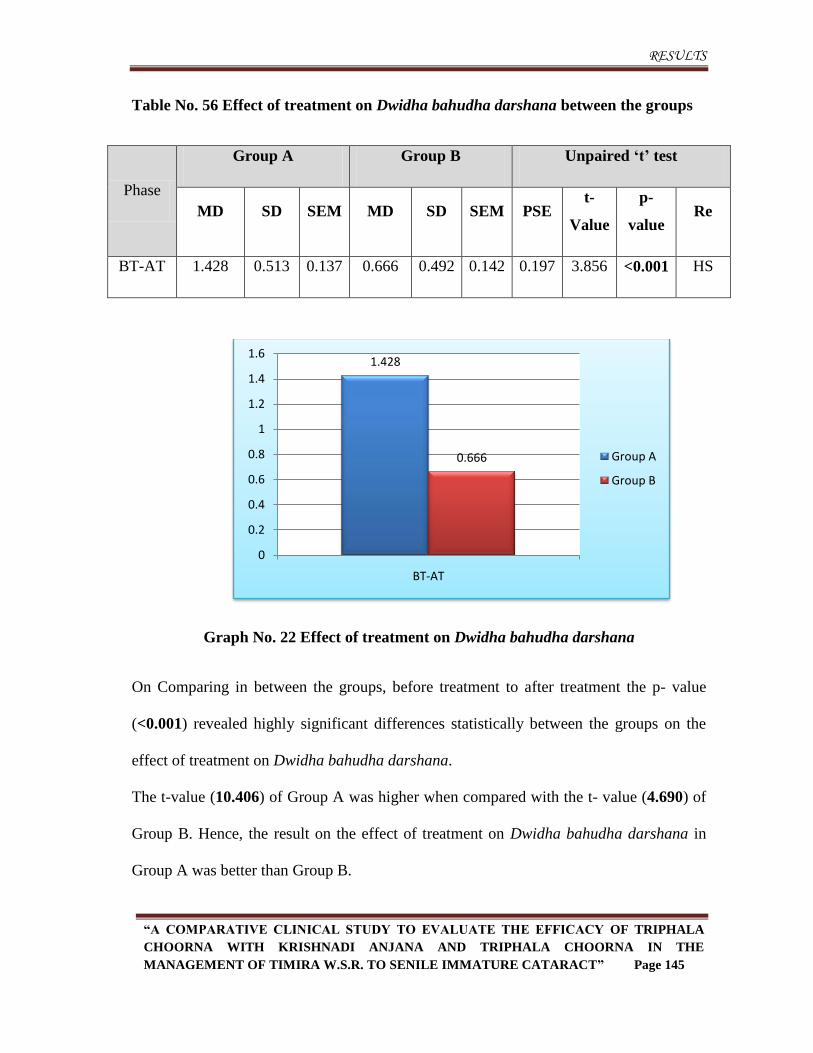
RESULTS
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 145
Table No. 56 Effect of treatment on Dwidha bahudha darshana between the groups
Phase
Group A Group B Unpaired „t‟ test
MD SD SEM MD SD SEM PSE t-
Value
p-
value Re
BT-AT 1.428 0.513 0.137 0.666 0.492 0.142 0.197 3.856 <0.001 HS
Graph No. 22 Effect of treatment on Dwidha bahudha darshana
On Comparing in between the groups, before treatment to after treatment the p- value
(<0.001) revealed highly significant differences statistically between the groups on the
effect of treatment on Dwidha bahudha darshana.
The t-value (10.406) of Group A was higher when compared with the t- value (4.690) of
Group B. Hence, the result on the effect of treatment on Dwidha bahudha darshana in
Group A was better than Group B.
1.428
0.666
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
BT-AT
Group A
Group B
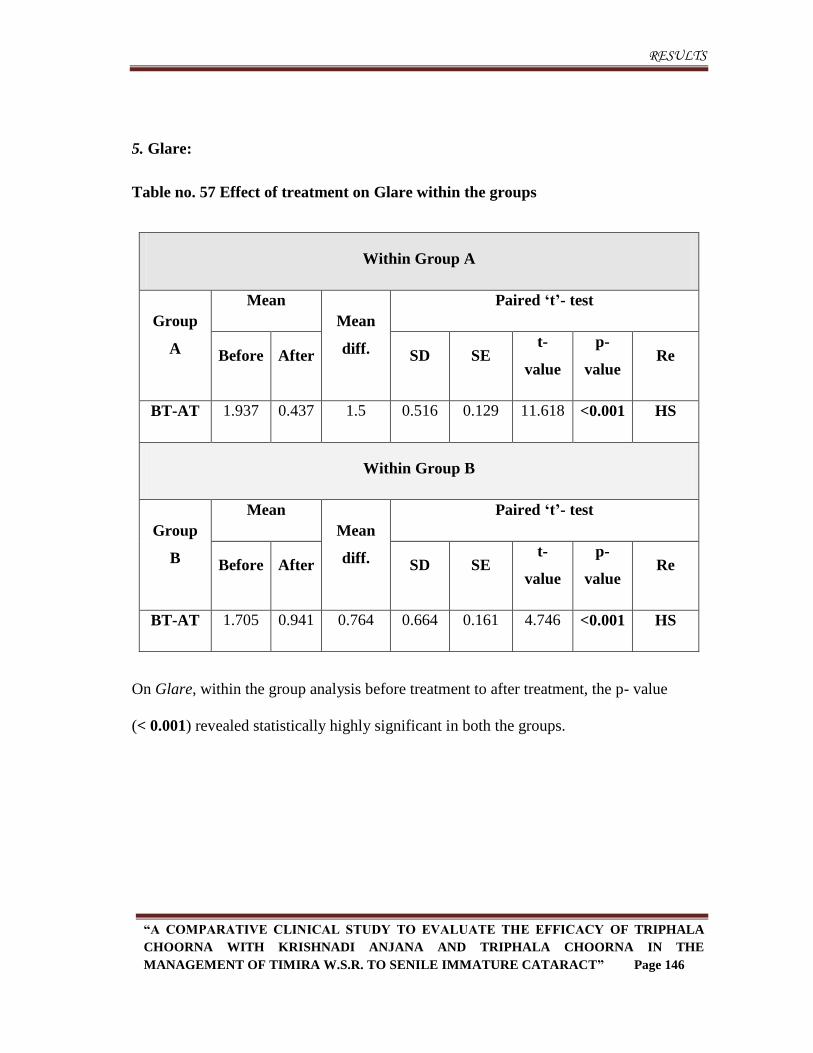
RESULTS
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 146
5. Glare:
Table no. 57 Effect of treatment on Glare within the groups
Within Group A
Group
A
Mean
Mean
diff.
Paired „t‟- test
Before After SD SE t-
value
p-
value Re
BT-AT 1.937 0.437 1.5 0.516 0.129 11.618 <0.001 HS
Within Group B
Group
B
Mean
Mean
diff.
Paired „t‟- test
Before After SD SE t-
value
p-
value Re
BT-AT 1.705 0.941 0.764 0.664 0.161 4.746 <0.001 HS
On Glare, within the group analysis before treatment to after treatment, the p- value
(< 0.001) revealed statistically highly significant in both the groups.
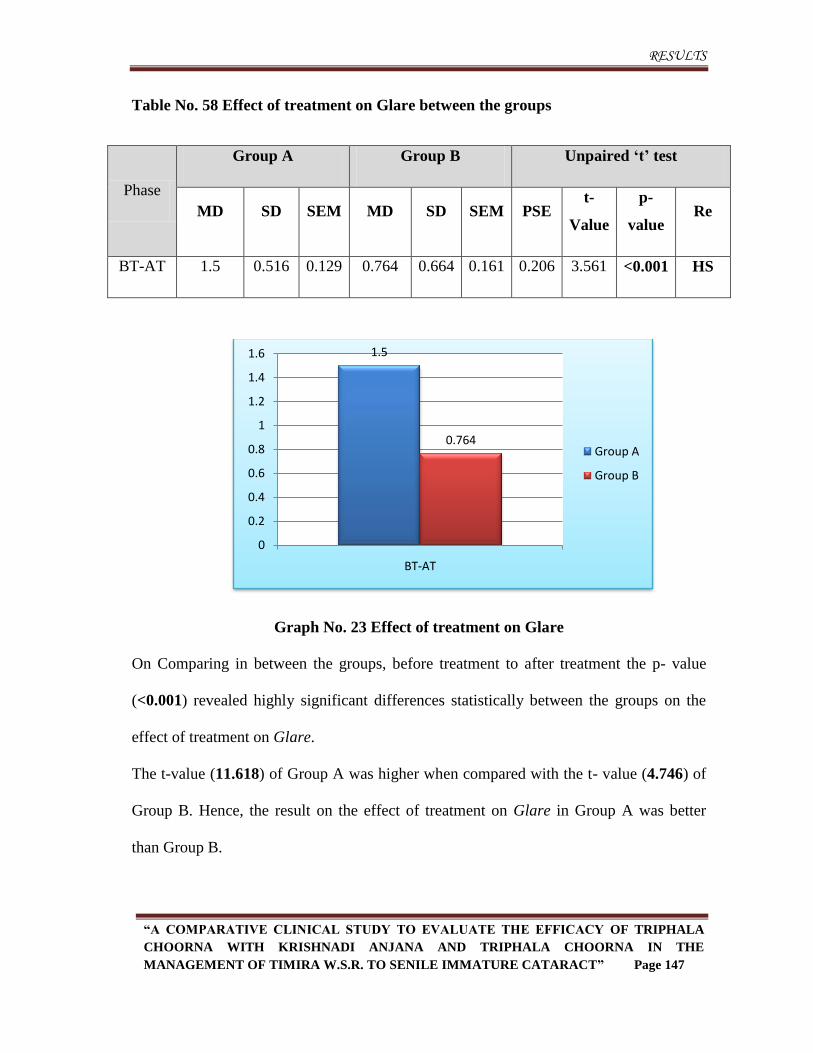
RESULTS
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 147
Table No. 58 Effect of treatment on Glare between the groups
Phase
Group A Group B Unpaired „t‟ test
MD SD SEM MD SD SEM PSE t-
Value
p-
value Re
BT-AT 1.5 0.516 0.129 0.764 0.664 0.161 0.206 3.561 <0.001 HS
Graph No. 23 Effect of treatment on Glare
On Comparing in between the groups, before treatment to after treatment the p- value
(<0.001) revealed highly significant differences statistically between the groups on the
effect of treatment on Glare.
The t-value (11.618) of Group A was higher when compared with the t- value (4.746) of
Group B. Hence, the result on the effect of treatment on Glare in Group A was better
than Group B.
1.5
0.764
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
BT-AT
Group A
Group B
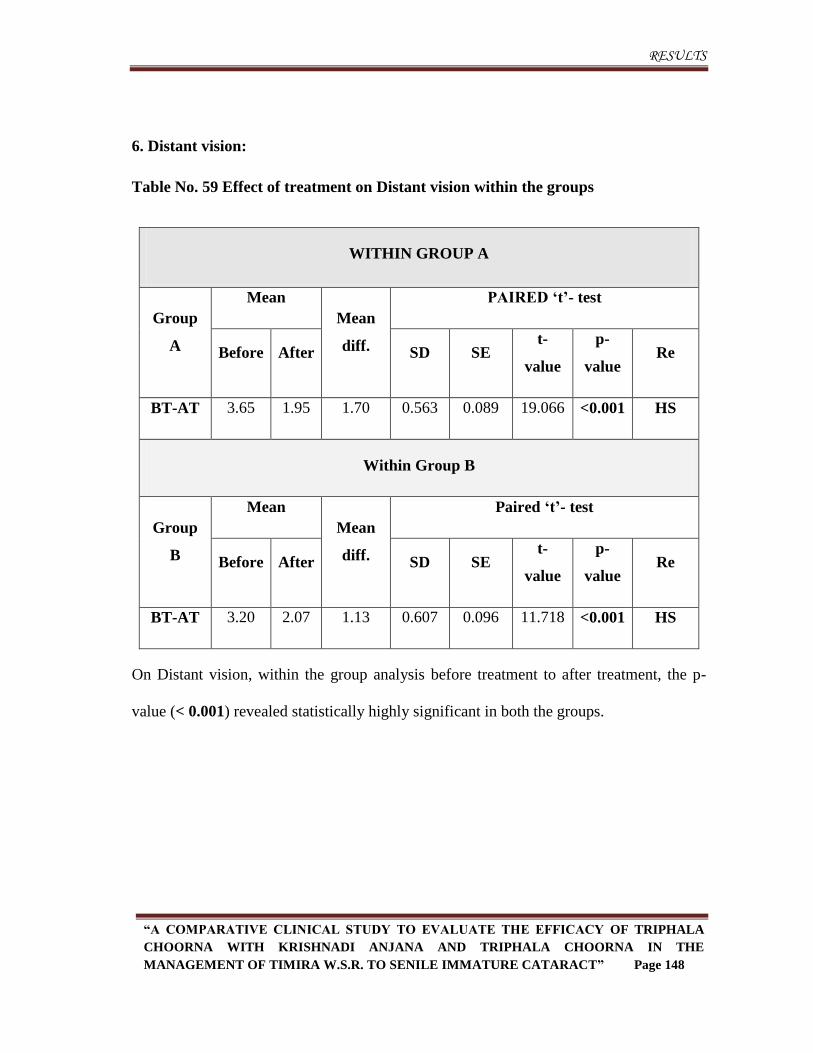
RESULTS
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 148
6. Distant vision:
Table No. 59 Effect of treatment on Distant vision within the groups
WITHIN GROUP A
Group
A
Mean
Mean
diff.
PAIRED „t‟- test
Before After SD SE t-
value
p-
value Re
BT-AT 3.65 1.95 1.70 0.563 0.089 19.066 <0.001 HS
Within Group B
Group
B
Mean
Mean
diff.
Paired „t‟- test
Before After SD SE t-
value
p-
value Re
BT-AT 3.20 2.07 1.13 0.607 0.096 11.718 <0.001 HS
On Distant vision, within the group analysis before treatment to after treatment, the p-
value (< 0.001) revealed statistically highly significant in both the groups.
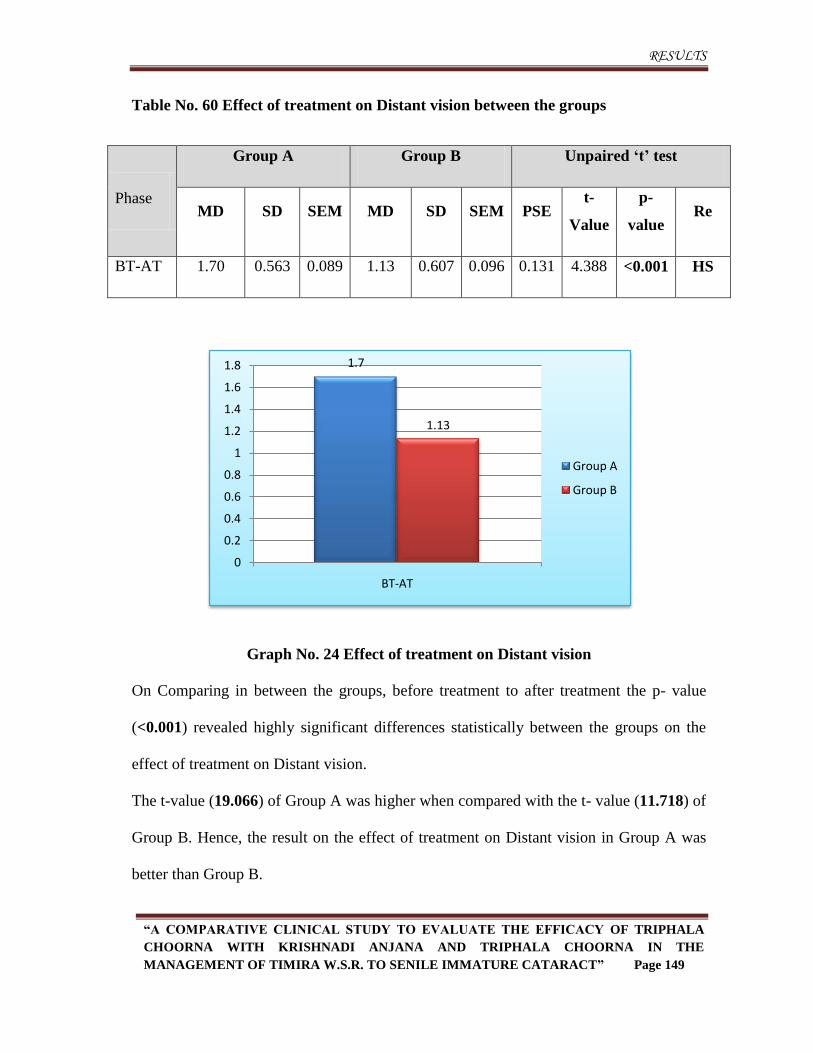
RESULTS
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 149
Table No. 60 Effect of treatment on Distant vision between the groups
Phase
Group A Group B Unpaired „t‟ test
MD SD SEM MD SD SEM PSE t-
Value
p-
value Re
BT-AT 1.70 0.563 0.089 1.13 0.607 0.096 0.131 4.388 <0.001 HS
Graph No. 24 Effect of treatment on Distant vision
On Comparing in between the groups, before treatment to after treatment the p- value
(<0.001) revealed highly significant differences statistically between the groups on the
effect of treatment on Distant vision.
The t-value (19.066) of Group A was higher when compared with the t- value (11.718) of
Group B. Hence, the result on the effect of treatment on Distant vision in Group A was
better than Group B.
1.7
1.13
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
BT-AT
Group A
Group B
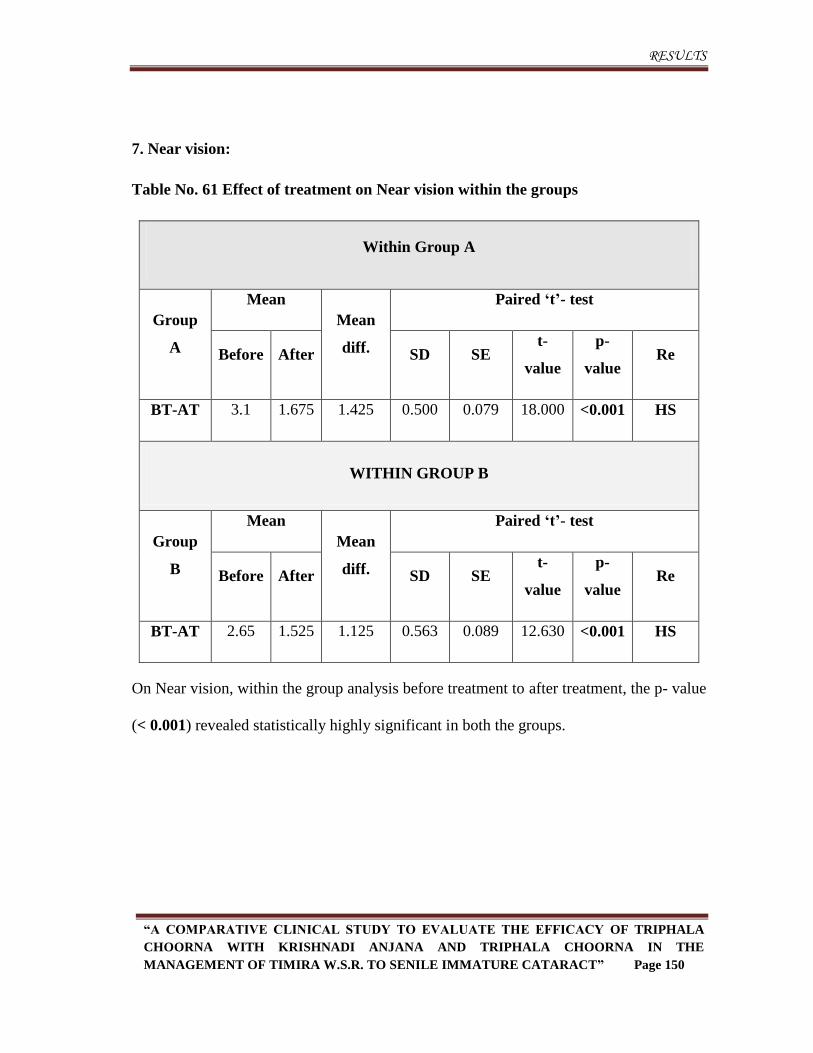
RESULTS
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 150
7. Near vision:
Table No. 61 Effect of treatment on Near vision within the groups
Within Group A
Group
A
Mean
Mean
diff.
Paired „t‟- test
Before After SD SE t-
value
p-
value Re
BT-AT 3.1 1.675 1.425 0.500 0.079 18.000 <0.001 HS
WITHIN GROUP B
Group
B
Mean
Mean
diff.
Paired „t‟- test
Before After SD SE t-
value
p-
value Re
BT-AT 2.65 1.525 1.125 0.563 0.089 12.630 <0.001 HS
On Near vision, within the group analysis before treatment to after treatment, the p- value
(< 0.001) revealed statistically highly significant in both the groups.
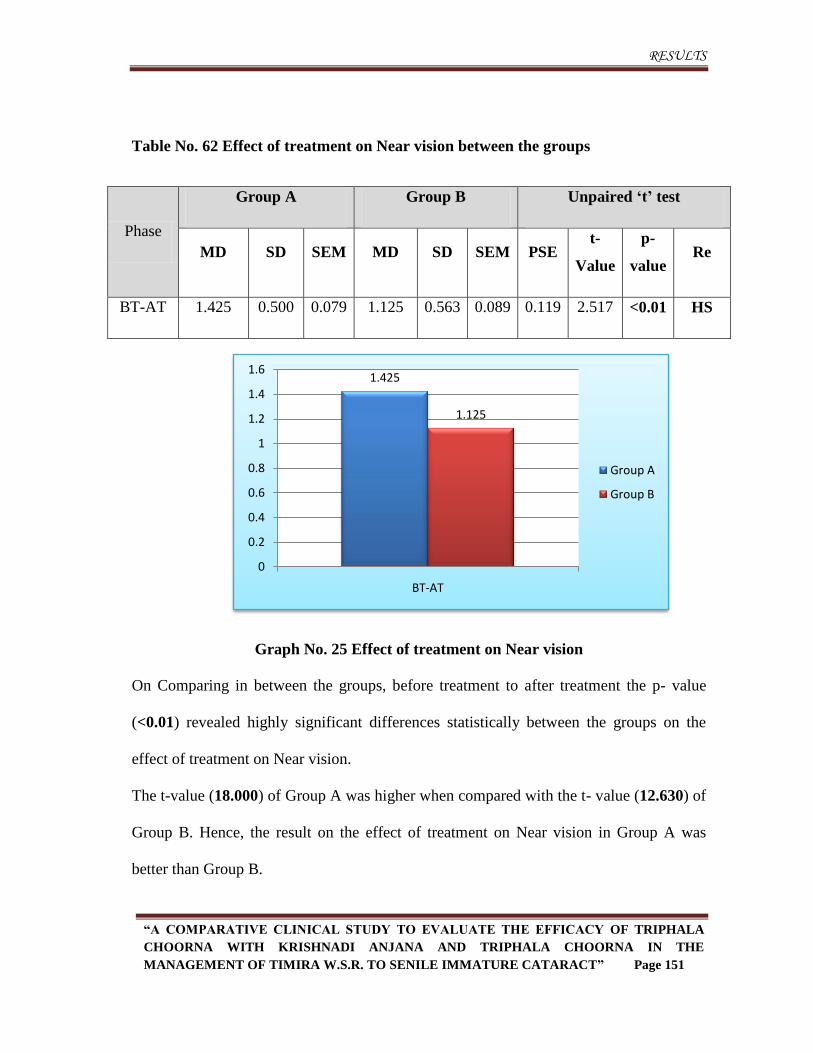
RESULTS
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 151
Table No. 62 Effect of treatment on Near vision between the groups
Phase
Group A Group B Unpaired „t‟ test
MD SD SEM MD SD SEM PSE t-
Value
p-
value Re
BT-AT 1.425 0.500 0.079 1.125 0.563 0.089 0.119 2.517 <0.01 HS
Graph No. 25 Effect of treatment on Near vision
On Comparing in between the groups, before treatment to after treatment the p- value
(<0.01) revealed highly significant differences statistically between the groups on the
effect of treatment on Near vision.
The t-value (18.000) of Group A was higher when compared with the t- value (12.630) of
Group B. Hence, the result on the effect of treatment on Near vision in Group A was
better than Group B.
1.425
1.125
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
BT-AT
Group A
Group B
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 152
Discussion
In any research work discussion plays an important role which sheds light on
logical analysis, reasoning and rational interpretations to ignite new ideas. Discussion
(Upanaya) on Shastra improves the knowledge and becomes the base of establishing the
concept or Conclusion (Nigamana). The theory is accepted only after the proper
reasoning (Tarka) of observations. Hence, here is an attempt to discuss on this topic.
The present study entitled “A comparative clinical study to evaluate the efficacy
of Triphala choorna with Krishnadi anjana and Triphala choorna in the management
of Timira w.s.r. to Senile immature cataract” was carried out on 40 patients with the
following objectives.
To evaluate the efficacy of Triphala choorna with Krishnadi Anjana in the
management of Timira w.s.r. to Senile Immature Cataract.
To evaluate the efficacy of Triphala choorna in the management of Timira
w.s.r. to Senile Immature Cataract.
To compare and evaluate the clinical efficacies of both the groups.
The discussion on the present study is done under the following headings:
DISCUSSION
Discussion on Selection of
Problem
Discussion on Review of Literature
Discussion on Disease
Discussion on Procedure
Discussion on Drugs
Discussion on Clinical study
Discussion on Observations
Discussion on Results
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 153
Discussion on selection of the problem:
Cataract is opacification of the lens of the eye which disturbs the clarity of the
vision. Although most cases of cataract are related to the ageing process, occasionally
children can be born with the condition, or a cataract may develop after eye injuries,
inflammation, drug induced and due to some other local, focal or systemic diseases.
Incidence and prevalence:
According to WHO “In spite of the progress made in surgical techniques in many
countries during the last ten years, cataract (47.9%) remains the leading cause of visual
impairment in all areas of the world, except for developed countries.”6 As per National
Programme for Control of Blindness of Govt. of India about 62.60% blindness is due to
cataract in India.7
Prevention and treatment
Development of Cataract can be prevented or delayed by avoiding exposure to
ultraviolet light and smoking. The additional risk factors considered are Diabetes mellitus
and high body mass index.
In modern system of medicine, the only definite management is lens extraction
once it reaches matured stage or complete opacification. Over 90% cataract surgeries are
successful9 but complications though rare are more serious which includes sensitivity to
anaesthesia, injury to the cornea & iris, vitreous loss, expulsive choroidal haemorrhage,
ocular infections, uveitis, retinal detachment, subluxation of lens, development of
posterior capsule opacification and loss of vision.
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 154
Ayurvedic management of cataract will be of great triumph in low economic
people who cannot afford surgery, in those patients when surgery becomes a
contraindication due to other factors, and in patients who are unwilling for surgery.
Therefore aiming these objectives Cataract in immature stage was selected for the present
study.
Discussion on review of literature
Discussion on disease review:
Timira is a disease included under Drishtigata vikaras by Ayurvedic scientists.
According to Acharya Sushruta the number of Drishtigata rogas is 12 and 27 as per
Acharya Vagbhata. Acharyas have rightly given the name „Timira‟ ie. „andhakara‟ as it
causes the visual impairment in the individual. The degree of blurredness may vary from
a lesser extent to a greater level depending upon the stage of the disease. As per Acharya
Sushruta, the involvement of first three netra patalas can be considered as Prathama,
Dwiteeya and Triteeya patalagata Timira respectively. Once the doshas reach the fourth
patala, there will be complete absence of vision, which is termed as Linganasha.
According to Acharya Vagbhata, the disease Timira is produced when the vitiated doshas
are situated in the first and second patala. When the vitiated doshas affects the third
patala, it is termed as Kacha and when it involves the fourth patala, it is termed as
Linganasha.
As per Acharya Sushsruta, under drishtigata rogas Timira is considered as one
among 76 netra rogas. Prathama-dwithiya-triteeya patalagata timiras and Linganasha
are different stages of the disease Timira itself. Though Acharya Vagbhata has counted
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 155
six types of Timira among 92 types of netra rogas he has described the signs and
symptoms along with Linganasha in three stages- Timira, Kacha and Linganasha. This
fact again proves Timira as different stages of the same and its progressive pathology.
Clinical features of Timira:
Avyakta darshana
Avyakta darshana (Blurring of vision) produced due to affliction of first patala,
which is the cardinal feature of timira and immature cataract. Blurring of vision, which
can be corrected by glasses in early stages, but the power would change rapidly based on
type of cataract, so one of the initial symptom could be frequent change of glasses.
Gochara vibhrama
Patient will have difficulty to perceive distant and near vision due to the
accumulation of water droplets in the lens which attains opacification and patient
develops different refractive index which can be understood as gochara vibhrama.
Vihwala darshana
Visualization of nonexisting things like dots, lines, threads in front of eyes, are
one of the symptom of timira and immature cataract which occurs due to irregular opaque
areas in the lens.
Dwidha bahudha darshana
Uniocular polyopia, another early symptom, is the perception of double or
multiple folds of the objects seen. It is due to the irregular refraction by different parts of
lens as in intumescent stage that several images are formed of each object.
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 156
Causative factors
In Ayurvedic texts, general causative factors of eye diseases are explained
elaborately. Following nidanas play a contributory role in pathogenesis of Timira -
Aharaja nidanas:
Among the ahaaraja factors excessive consumption of Katu, Amla and Lavana
are the most harmful rasas for eyes. The chances of consumption of vidahi aharas of
these rasas in excess are more in this epoch as people are more fond of spicy foods, like
pickles, different spice powders, fried items, over cooked, half cooked, baked foods,
excess of meat, fish and alcohol, consumption of fermented food stuffs like breads, flat
bread, white bread, pan cakes and other foods mainly containing urad dal, refined flour
etc lead to vatadi kopa. As per Acharya Charaka, Timira is a nanatmaja vyadhi of vata
and pitta being a dominant dosha in netra can disturb the functioning of vision. They
both in turn lead to kaphadushti, as netra being an organ situated in kapha sthana. All
these food factors impair the metabolism of the body and also eye in particular.
Transparency of lens is maintained by the normal nutrition and if this normal nutritional
status is altered due to life style modification then there occurs a certain pathological
changes in the lens leading to opacity.
Viharaja nidanas:
Ushnaabhitaptasya jalapraveshaat
Immersion in cold water immediately after getting exposed to heat or sun is the
one of the causative factor for eye diseases. When body is too warm, the vessels
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 157
supplying the eye are dilated and the volume of fluids will be increased. Then if body
temperature is suddenly dropped, the vessels constrict and the vasculature is damaged.
These cause circulatory disturbances, which in turn affects the mechanism of nutrition
leading to eye diseases.
Doorekshanat
Looking at very distant object for a longer time cause strain to cilliary muscle that
alter accommodative power of the lens which disturbs the clarity of the vision.
Swapna viparyaya
Sleeping in day time and keeping awake at night results in aggravation of kapha
and vata respectively. This will lead to impairment of Jatharagni, which in turn disturbs
the lens metabolism leading to improper nutrition to lens. Eyes are modified to work in
the presence of light and to rest in the absence of light. There are two types of
photosensitive pigments to adjust, according to the presence and absence of light rays.
Among these two, cones functions mainly in the presence of light rays where as rods in
dim light. In the presence of light, the cones will be in active form and in the absence of
light cones will be in inactive form. Similarly rods become active when there is a dim
light. Working at night and sleeping during day time leads to derangement of this
mechanism, which in turn cause strain on the ocular system and result into various
diseases including Timira.
Kopa-Shoka-Klesha
The manasika nidanas like kopa-shoka-klesha will lead to pitta and vata vriddhi
respectively, that in turn may accelerate the oxidation process in the cellular level
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 158
including lens tissues, resulting in denaturation of proteins followed by opacification of
lens. These emotional factors also activate autonomic nervous system which in turn
leads to profound vasodialatation which may hamper the circulation and in turn the
metabolism of the lens.
Abhighata
Abhighata is a direct cause for Timira roga. Abhighata gives rise to the disease
first rather than any of the prodromal signs and symptoms either of systemic organ or
organ specific in nature. These damages directly results into the disease of the eye as
cataract.
Traumatic cataract is partly due to mechanical effects of the injury on the lens
fibres and largely due to the entrance of aqueous due to the damage to the capsule, either
secondary to the impairment of its semi permeability or often the result of actual tears.
Sometimes if they are covered by the iris, such tears are rapidly sealed at first with fibrin
and later by the proliferation of the subcapsular epithelium which secretes a new capsule.
In these cases the entrance of aqueous is stopped and the opacity of the lens may remain
stationary or even regress. Alternatively the tear may remain open and opacification may
progress to involve the entire lens.
Ati maithuna
Excessive indulgence in sexual activity results in shukra dhatu kshaya leading to
poorva dhatu kshaya which will hamper the nourishment of ocular tissues that accelerates
the degenerative process in lens may cause opacification of the lens.
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 159
Vegavinigraha
Suppression of urges like adhovaayu, kshudha, baashpa, chardi, mutra purisha
and nidra vitiates vata, which in turn develops various types of eye diseases as per the
classics. Among these fourteen urges nidra and ashru are directly connected with the eye.
Rajodhuma nishevana
Exposure to dust and smoke, including cigarette smoking is considered as harmful
for eyes by both i.e. Ayurveda and modern medicines. As per Ayurveda, smoking will
vitiate pitta because of its teekshana, ushna and laghu gunas, and ultimately lead to vata
prokopa and causes maximum rookshata of the body. Hence it can be considered as one
of the important factors in the causation of Timira. In the context of dhoomapaana,
Acharya explains that inhaling smoke through mouth and discharging through nostrils
will lead to impairment of vision.
Cigarettes contain thousands of chemical substances like formaldehyde, ammonia,
and hydrogen sulphide that act as irritants, carcinogens and inflammatory agents, all of
which can interfere with blood flow and damage eyes. Research has established smoking
as a definitive cause of serious, progressive disorders of the eye that can lead to partial or
total vision loss. Heavy smokers and those who smoke for an extended number of years
are particularly at risk of eye damage. Smoking is responsible for a prolonged attack on
the eyes that can lead to the development of cataracts in two ways. First of all, tobacco
smoke contains harmful free radicals that directly assault the eye, potentially damaging
lens proteins and the fibrous cell membrane in the lens. Secondly, smoking reduces the
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 160
body's levels of antioxidants and certain enzymes which may help to remove damaged
proteins from the lens.
Aatapasevana:
As per Ayurvedic classics Aatapasevana is a direct cause for Timira roga.
Acharya has insisted the use of umbrella as one of the pathya for netra in order to protect
them from sun light. Also, as per modern science, exposure to almost all types of heat
generating activities is known to produce cataract by causing damage to the lens
epithelium. The different radiations which induce cataract are infrared, X-ray, gamma
rays and UV-rays. People who have more exposure to sun light, those who work in glass
factories, inadequately protected technicians, patients those who treated for malignant
tumours and workers of atomic energy plants are more prone to develop radiation
cataract.
Sookshma nireekshana
Watching minute objects for longer duration cause strain to cilliary muscles
which will interfere with normal accommodation of the lens that will disturb the clarity of
the vision.
Samprapti
Vatadi doshas get vitiated due to indulgence in achakshushya nidanas and
become vimargagami, through the siras reach the upper part of the body pathologically
lodged in netra patalas, giving rise to Timira. The mandagni, further leads to the vitiation
of sthanika doshas. The dushyas (rasa, rakta, mamsa, meda and asthi) i.e. substrate
elements of patalas, also become weak and at the same time khavaiguņya of rupavaha
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 161
sira (favourable site for localization of vitiated doshas) and drishti patalas occurs.
Depending upon the involved patalas the various symptoms are produced.
Pathogenesis of cataract
Cataract mainly caused due to degenerative process. The most common factor is
age, and it may be of significance that as age progresses the semi permeability of the
capsule is impaired, the inactive insoluble proteins increase and the antioxidaive
mechanisms become less effective. The normal lens contains sulphydryl-containing
reduced glutathione and ascorbic acid (Vitamin C), both of which decrease with age.
Cataract is produced by the administration of toxic substances like naphthalene, lactose,
galactose, selenite, thallium etc. Cyanate from cigarette smoke causes protein
denaturation. Cataractous changes may follow the use of the anti cholinesterase group of
miotics and after prolonged use of corticosteroids. Physical factors like mechanical
trauma or radiant energy may also induce the formation of cataract.
Oxidative stress is a common problem that the lens deals with daily through
exposure to ultraviolet and other types of irradiation. Molecular oxygen is the cause of
most oxidative damage. Fortunately the lens‟s oxygen tension is very low. This protects
the lens proteins and lipids from oxidative damage. However the lens normally derives a
substantial proportion of its ATP from oxidative phosphorylation which generates free
radicals.
Lens has many anti-oxidant mechanisms to maintain its transparency. These
mechanisms include glutathione, thiol-transferase, catalase and super oxide dismutase.
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 162
With age, the efficacy of endogenous anti-oxidant defences decline and opacification of
the lens increases resulting in cataract.
Prognosis
Prathama and dweetiya patalagata timira are easily curable. Treetiya patalagata
timira is yapya and when the doshas reach to chaturtha patala all the Timira attain the
stage of asadhyata except that of kaphaja variety, which may be curable with the help of
surgical intervention. 158
According to conventional system of medicine, the only remedy is surgical management
which has success rate but posterior capsule opacification remains the most prevalent
long-term complication along with other post-operative complications like subluxation of
the lens, posterior sub-capsular cataract, cystoid macular oedema, retinal detachment and
others which will not benefit the surgery.
Discussion on procedure
Anjana:
Anjana is the one of ocular therapeutics of Ayuveda which is very helpful in the
treating various eye disorders timira is one among them. Application of anjana is
advisable both in healthy and diseased person. In healthy person as a part of dinacharya
and in case of diseased person there is a broad range of indications such as timira,
abhishyanda, adhimantha, arma, shuklagata rogas and krishnagata netrarogas. There
are different types of anjana depending on their mode of action. The basic aim of anjana
prayoga is, eye being an organ which is “tejomayam” ie., one which is predominant with
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 163
tejomahabhuta can easily get afflicted by kapha dosha and by anjana prayoga as a daily
regimen the accumulated kapha can be normalised. In a disease based on the condition
and the pathogenesis involved different types of anjanas has been explained and which
can be employed accordingly. The anjana used in Timira will be of lekhana among its
varieties ie. snehana, ropana, lekhana or prasadana. In case of cataract, the lekhana
anjana is helpful because the lens is hydrated and hard due to denaturated lens fibres.
Discussion on drug
Triphala choorna: 186, 187, 188
Triphala choorna contains haritaki, vibhitaki and amalaki. It has tridoshahara
property that helps to normalise the vitiated doshas which are pathologicaly lodged in the
netra patala and obstructs the vision. Chakshushya and rasayana properties of triphala
helped in delaying the aging process along with nourishing the ocular tissues. Deepana
property enhanced the agni which helps in maintaining normal metabolic reactions of the
lens. Triphala has anti-cataract property which helps in maintaining transparency of the
lens. It acts as a free radical scavenger and removes free radical which is helpful in the
arrangement of the lens fibres. Antioxidant property of triphala helps in delaying
degenerative process in the lens. Vitamin C helps in the maintaining the normal level of
glutathione which is very necessary for normal metabolism of the lens. All these are
beneficial in preventing the progression of cataract.
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 164
Krishnadi varti: 189
Krishnadi varti contains Pippali, Haritaki and Bhringaraja. It has been mentioned
to be useful in Timira in Ayurvedic classics, as the drug possess teekshna guna, ushna
veerya which are beneficial in samprapti vighatana of Timira.
The lekhana (scraping) property of the formulation helped to clear the hydrated lens.
Antioxidant property of ingredients helped in delaying the degenerative process.
Ingredients having Chakshushya, Rasayana, Balya properties helped in revitalizing and
restoring normal ocular functions. Cysteine present in Bhringaraja essential for
maintaining glutathian of the lens which is a vital factor for lens transparency. Deepana
property of ingredients enhanced the agni which helps in maintaining normal metabolic
reactions of the lens. Katu rasa of Bhringaraja is netra virechaka, removes Doshas from
ciliary muscles, also it has the property of Vedana sthapana, inturn remove strain of
ciliary muscles, thereby gives strength and helps in physiological accommodation.
The availability of drugs listed in the preparation was ease and economical. Hence it was
selected for the present study for assessing its efficacy in the management of Timira.
Goghrita: 220,221,222,223,224
In this clinical study goghrita was taken as anupana for triphala choorna which
has tridoshahara property that helped in normalising the pathologically lodged vatadi
dosha in ntra patala.
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 165
Rasayana, chakshusya, rasavardhaka, balya, indriyabalavriddhikara and
vayahsthapana properties of goghrita have delayed the degeneration process and
nourished the ocular tissues.
Madhu: 225,226,227
In this clinical study madhu was taken for rubbing the ajnana varti. Lekhana and
kaphahara property of madhu helped in removing of water droplets from the lens.
Sukshma, laghu and yogavahi gunas promoted deeper penetration of drugs and cross the
barriers. It has srotovishodhana property that cleared the minute channels and helped in
the exchange of nutrients from the aqueous humor. Chakshushya property helped in
nourishing the oclular tissues. It enhanced the agni that helped in maintaining the lens
metabolism which is important for lens transparency. It has property of minimising scar
so helped in the removing the opaque area on the lens which hampered the clarity of
vision.
Probable mode of action of anjana
As described in paribhasha, “anakti anena ithi anjanam” meant for the spreading
and propagation of anjana.
After application of anjana in inner surface of lower palpebral conjunctiva, it
comes in contact with tear and due to blinking of eyelids the drugs get mixed with tear.
The tear mixed drugs now come in contact with conjunctiva and cornea. Due to
hydrophilic nature of conjunctiva the drugs get directly absorbed through conjunctival
sac by the trans cellular pathway. The absorbed drugs through scleral route entered into
the aqueous humor and through aqueous humor reached lens. Due to liphophilic and
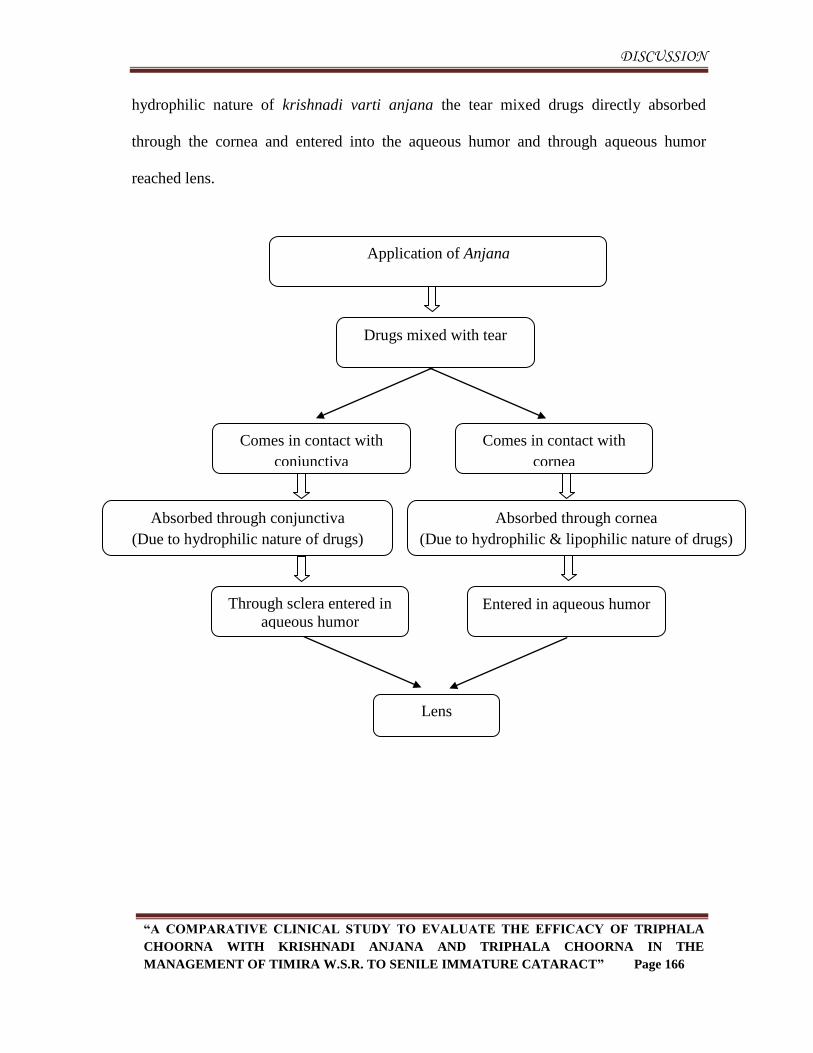
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 166
hydrophilic nature of krishnadi varti anjana the tear mixed drugs directly absorbed
through the cornea and entered into the aqueous humor and through aqueous humor
reached lens.
Application of Anjana
(Inner surface of lower palpebral conjunctiva)
Drugs mixed with tear
Absorbed through conjunctiva
(Due to hydrophilic nature of drugs)
Comes in contact with
cornea
Comes in contact with
conjunctiva
Absorbed through cornea
(Due to hydrophilic & lipophilic nature of drugs)
Through sclera entered in
aqueous humor Entered in aqueous humor
Lens
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 167
Discussion on clinical study
Discussion on observations
Age:
In this clinical study, more number of patients i.e., 40% patients belonged to the age
group of 61–70 years followed by 37.5% patients belonged to the age group of 41–50
years and 22.5% patients belonged to the age group of 51–60 years.
The concentration of glutathione falls with advancing age which maintains the lens
transparency and also metabolic activities of lens decrease with age. It may be a cause to
initiate cataract during the fourth decade of life. According to Ayurveda the Ishat-
parihani avastha starts after the age of 40 years. By the influence of Kala swabhava in
this period, Dhatukshaya and Indriya vishaya grahana asamarthya occurs which can
have an impact on aging lens.
Gender:
In this clinical study, more number of patients i.e., 65% were females and 35% were
males.
The present study supports the higher incidence of Timira- Cataract in females. Lens
capsule is made up of collagen. Recent researches have discovered that collagen
disorders are more often seen in females after the age of 40 years, this is due to the
imbalance in the oestrogen level affecting the collagen and hence resulting in higher risk
of Cataract in females. The higher incidence in females as seen in this study is thus
justifiable.
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 168
Religion:
In the present clinical study 75% of the patients were Hindus and 25% were Muslims.
There is no reference available that establishes the relation between religion and its
associated cultural practices with the incidence of Timira- Cataract. Thus no conclusion
can be drawn from this observation apart from geographical representation.
Marital status:
Here in this clinical study, all patients were married.
None of the studies on cataract reveal any relationship of marital status with the
incidence of Cataract. Hence no inference can be made based on this observation.
Educational status:
More number of the patients i.e., 52.5% were below graduation, 25% of patients were
graduates, 17.5% of patients were uneducated and 5% of patients were post graduates.
As there is no direct relationship between educational status and the incidence of
Cataract, no definite conclusion can be drawn in relation to education and Cataract.
Socio-economic status:
In present study more number of patients i.e., 57.5% belonged to the middle class
followed by 32.5% belonged to lower class and 10% were from upper class.
There is no evidence available regarding the relationship between socio-economic status
and the incidence of cataract.
The percentage of patients in the middle class and lower class were more, it is
possible that they might be taking low nutritious diet, which progresses the degeneration
of the lens leading to Cataract.
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 169
Habitat:
Here in this clinical study, 97.25% patients were from urban area and 2.5% were from
rural area.
The changing life style, dietary habits, working conditions and the environment in
urban population are the contributory factors to impair the lens metabolism which
increases the incidence of Cataract in urban area. Further as the study was conducted in
urban area no definite conclusion can be drawn.
Occupation:
In the occupational category 65% were housewives, 15% were businessmen, 15%
were professionals (Government/Private employee) and 5% were drivers.
Relation between the cataract and the occupation can be ascertained here. In house
wives exposure to heat while cooking acts as predisposing factor for netra rogas
especially Timira- Cataract. In professionals (Government/Private employee) and
business men kopa, kleshla, swapna viparyaya along with improper food habits like
intake of food at irregular timings and excess of junk foods were found to be the nidanas
which increases risk of cataract by disturbing the normal metabolism of lens. In drivers
more exposure to sunlight acts as a risk factor for Cataract.
These above mentioned Nidanas are causative factors for the eye diseases which are
mentioned by Ancient Ayurvedic Scientists and hence the data of present study supports
the same.
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 170
Diet:
More number of patients in this study i.e., 52.5% were consuming vegetarian diet and
47.5% were consuming mixed diet.
Intake of low protentious and minerals deficits diet causes earlier development of
Cataract and recent researches have proved that nutrition can prevent cataract, due to the
small sample size, no conclusion can be made based on this observation. The reasons
could be that many of the patients had faulty food habits like intake of food without
proper nutrients (proteins, vitamins and minerals) along with Adhyashana and
Vishamashana. The above said reasons hasten formation of Cataract.
Sleep:
More number of patients i.e., 45% were having sound sleep, 42.5% were having
disturbed sleep and 12.5% were having delayed sleep in this study.
Sound sleep and disturbed sleep depends on the Prakruti, Circumstances, Life style
and Stress. The disturbed sleep as discussed in the Nidana of Timira will impair the
metabolic reactions of the lens which accelerates the degenerative process and leads to
opacification of the lens.
Addiction:
In the present clinical study, majority of the patients (72.5%) had the habit of having
tea/coffee, 10% of the patients had the habit of smoking, 7.5% of the patients had the
habit of chewing tobacco and 2.5% of patients had the habit of consuming alcohol.
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 171
Acharya Vagbhata in the context of Dhumapana adhyaya quotes that, inhalation of
smoke through the mouth and leaving through the nose is highly harmful for the eyes and
could be a reason for timira.
Though the modern medical science has considered smoking and alcohol as the risk
factors for the manifestation of Cataract, this fact cannot be concluded in the study as
only 10% patients were addicted to smoking and 2.5% were addicted to alcohol,
registered for the study.
There are no such evidences available regarding impact of excess intake of tea/coffee
on changes in lens, it‟s just a part of observation.
Family history
In the present clinical study, 60% patients had no family history of cataract and 40%
had family history of cataract.
Heredity has a considerable role in the incidence, age of onset and maturation of
Cataract in different races and families. As 40% patients had family history of Cataract
the observation of the present study supports the same.
Chronicity:
In this clinical study, 57.5% of patients were having chronicity more than 24months.
Among others 12.5% were having the chronicity of >6months≤12months and 10% of the
patients were having chronicity of ≤ 6months, >12≤18months and >18≤24months.
This emphasizes the chronicity of cataract. Most of the patients neglect to visit the doctor
at early stages as it starts with mild blurrness of vision which does not hamper their
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 172
routine activities. With spectacles correction from optician, patients get improvement in
vision in early stages so they don‟t consult physician but when they experience more
blurrness of vision even with the spectacles then they consult physician.
Bala pramana pareeksha:
Prakruti:
In the present study 50% of the patients were of Kapha-pitta prakruti, 27.5%
were Vata-pitta prakruti and 22.5% were Vata-kapha prakruti.
Due to the small sample size, no definite correlation between Shareera prakruti and
occurrence of Cataract can be established.
Saara, Samhanana and Pramana:
In the present study observation on Sara, Samhanana, Pramana and Satmya shows:
75% of patients were of Madhyama sara, 15% of patients were of Avara sara
and 10% of patients were of Pravara sara.
85% of patients were of Madhyama samhanana, 7.5% of patients were of
Avara and Pravara samhanana.
85% of patients were of Madhyama pramana, 7.5% of patients were of Avara
and Pravara pramana.
Maximum number of patients belonged to Madhyama saara, Madhyama
samhanana and Madhyama pramana. The incidence of Cataract is more in individuals
who are poorly built with low height and low weight. Though this is an established fact,
such observations were not found in this clinical study.
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 173
Saatmya:
In the present study 52.5% of patients were of Sarva rasa satmya and 47.5% of
patients were of Vyamishra satmya.
No conclusive inference can be drawn from this observation to indicate the relation
between Satmya and incidence of Timira.
Satva:
More number of patients, i.e., 85% were having Madhyama satva followed by
7.5% were Avara satva and Pravara satva.
Since more number of patients had Madhyama satva, they were convinced to undergo
treatment for long duration of 48 days and were asked to follow the instructions.
Abhyavaharana shakti and Jarana shakthi:
In the present study 47.5% were having Madhyama abhyavaharana shakti, 37.5%
had Avara abhyavaharana shakti and 15% had Pravara abhyavaharana shakti.
In present study more number of patients i.e., 47.5% were having Madhyama
jarana shakti, 37.5% were having Avara jarana shakti and 15% were having
Pravara jarana shakti.
Maximum patients belonging to Madhyama and Avara Abhyavaranashakthi and
Jaranashakti indicates the relation between age, appetite and food intake which decreases
on increasing age. Agnimandya can impair the metabolic process which inturn disturbs
metabolism of the lens and accelerates the degenerative process causing loss of
transparency of the lens.
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 174
Vyayamashakti:
More number of patients i.e., 67.5.5% were having Madhyama vyayama shakti
followed by 22.5% of patients were having Avara vyayama shakti and 10% of patients
were having Pravara vyayama shakti.
There is no direct relationship between Vyayama shakti and Timira, hence no
conclusion can be drawn from this observation of the present study and has been just
considered as a part of the study‟s observations.
Vaya:
In this clinical study, all patients i.e., 100% belonged to Parihani avastha.
The abilities of human body will gradually reduce in every decade of life. The
visual efficiency, according to Sharangadhara samhita will start diminishing from the
age of sixty years. As per the contemporary science, the degenerative changes in lens
start as age advances, so the incidence of Cataract is more in the old age and loss of
transparency of lens occurs due to ageing and degenerating process. This justifies the
higher incidence of Cataract in old age patients.
Nidana:
In the present clinical study, the probable Nidanas recorded for the manifestation
of Timira possess the following percentages:
Swapna viparyaya (55%), Vegadharana (majority had Mutra, Purisha & Nidra
vegadharana) (50%), Sookshma nireekshana (35%), Rajodhuma nishevana (35%), Amla
rasa atisevana (32.5%), Kopa (30%), Shoka (22.5%), Atapa sevana (20%),
Doorekshanat (17.5%) and Shukta aranala sevana (2.5%).
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 175
As per the literatures, these are the causative factors of Netra rogas and the present
observation supports the same. Due to intake of above mentioned Nidanas, Vatadi doshas
becomes vitiated and pathologically lodge in Netra patalas causing Timira. These
causative factors may be responsible for altering the lens metabolism and increase the
oxidative stress of the lens. Hence the denaturation of lens proteins occurs and ultimately
manifests cataract.
Lakshanas
In the clinical study, all the patients i.e. 100% had Avyakta darshana, 82.5% of
patients had glare, 65% of patients had Dwidha bahudha darshana, 52.5% of patients
had Vihwala darshana, 37.5% of patients had Gocharavibhrama.
Avyakta darshana is the cardinal feature of Timira- Cataract. In Cataract opacification
of lens takes place. These opaque areas obstruct the rays of light coming from the objects
to reach the retina and hence blurriness of vision is seen as early symptom. The velocity
of light varies for different colours and due to increased scattering of light patients
develop glare. In opaque lens accumulation of water droplets causes irregular refraction
and hence double or multiple images are visualised by the patient. As per the literatures,
these are the common changes that occur in the lens as a result of ageing, and the present
observation supports the same.
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 176
Visual acuity- distant vision
In the clinical study, all the patients i.e. 100% had diminished visual acuity for distant
objects.
It is due to de-arrangement of lens fibres and opacity of lens which obstruct the rays
of light to reach retina hence visual acuity for distant objects becomes decreased.
Visual acuity- near vision
In the clinical study, all the patients i.e. 100% had diminished visual acuity for near
objects.
With advancing age, strength of ciliary muscles and accommodative power of opaque
lens decrease, so patients experienced difficulty in near vision.
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 177
Discussion on Results
1. Effect of treatment on Avyakta darshana
The effect of treatment on Avyakta darshana within the group, before treatment
and after treatment, the p value (<0.001) was statistically highly significant in both the
groups.
On comparing between the groups, before treatment to after treatment p value
(<0.001) was statistically highly significant.
Though both the groups showed good results, the t-value (13.580) of Group A
was higher when compared to the t-value (7.767) of Group B, concluding that the effect
of treatment on Avyakta darshana in Group A was better than Group B.
Cataract is caused by the degeneration and opacification of the lens fibres. There
is an accumulation of water droplets in between the fibres, which disturbs its arrangement
and leads to opacification of the lens. As age progresses glutathione content of the lens
decreases, which is an important factor to maintain the transparency of the lens by
controlling anti-oxidative process.
Anti-cataract property of Triphala delays the degeneration of the lens and
Vibhitaki in Triphala choorna helps to remove the accumulated water droplets due to its
Kaphahara property and maintain transparency of the lens.
Due to tikta, kashaya rasa and laghu, ruksha guna of Haritaki in Krishnadi varti, it acts
as lekhya and srotoshodhaka. By its lekhana (scraping) property it minimises the
opacification and by virtue of its srotoshodhaka property it helps to clear the hydrated
lens that would be the reason to form a better image on the retina.
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 178
However the effect of treatment in Group A was better than Group B probably
due to the added effect of Krishnadi anjana.
2. Effect of treatment on Gochara vibhrama
The effect of treatment on Gochara vibhrama within the group, before treatment
and after treatment, the p value (< 0.001) revealed statistically highly significant in Group
A, before treatment to after treatment, the p value (<0.05) revealed statistically significant
in Group B.
On comparing between the groups, before treatment to after treatment p value
(<0.001) was statistically highly significant. The t-value (8.879) of Group A was higher
when compared to the t-values (2.120) of Group B thereby concluding, the effect of
treatment on Gochara vibhrama in Group A was better than Group B.
Patients had difficulty to assess the distance of an object which occurred due to
alteration in the accommodation caused by weak ciliary muscles and reduced
accommodative power of lens due to opacity.
Rasayana property of of Triphala choorna provides strength to ciliary muscles and Anti-
oxidant activity of Go ghrita minimises the degeneration of the lens which improves
accommodative power.
Ciliary muscles are made up of proteins. Cysteine of Bhringaraja in krishnadi
anjana being a building block of proteins helps to strengthen the ciliary muscles so that
there is an improvement in physiological accommodation. Lekhana (scraping) property of
Krishnadi anjana maintains transparency of the lens and improves physical
accommodation.
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 179
In both the groups Triphala choorna rejuvenates the ciliary muscles and provides
strength hence improvement is seen in both the groups. Due to added effect of Krishnadi
anjana Group A showed better results in comparison of Group B on Gochara vibhrama.
3. Effect of treatment on Vihwala darshana
The effect of treatment on Vihwala darshana within the group, before treatment
and after treatment, the p value (<0.001) revealed statistically highly significant in Group
A, before treatment to after treatment, the p value (<0.05) revealed statistically significant
in Group B.
On comparing between the groups, before treatment to after treatment p value
(<0.001) was statistically highly significant. The t-value (9.813) of Group A was higher
when compared to the t-values (2.449) of Group B thereby concluding, the effect of
treatment on Vihwala darshana in Group A was better than Group B.
The vitiated doshas pathologically lodged in Netra patala cause the visualisation
of non-existing things in front of eyes like mosquitoes, flies, hair and net. Irregular
opaque areas on the lens obstructs the rays of light coming from an object which falls
abruptly on retina so patients visualise false moving objects in front of the eye.
Amalaki and Haritaki in Triphala choorna are Tridoshahara dravyas, they help to
remove the pathologically lodged Doshas from the Netra patalas.
Pippali in Krishnadi anjana due to its laghu and snigdha guna crosses the
lipophilic layer of the cornea and through aqueous humour reaches the lens and helps in
maintaining its transparency. Therefore patients got relief in Vihwala darshana in both
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 180
the groups. The effect of treatment on Vihwala darshana in Group A was better than
Group B probably due to the added effect of Krishnadi anjana.
4. Effect of treatment on Dwidha bahudha darshana
The effect of treatment on Dwidha bahudha darshana within the group, before
treatment and after treatment, the p value (<0.001) was statistically highly significant in
both the groups.
On comparing between the groups, before treatment to after treatment p value
(<0.001) was statistically highly significant.
Though both the groups showed good results, the t-value (10.406) of Group A was higher
when compared to the t-value (4.690) of Group B, concluding that the effect of treatment
on Dwidha bahudha darshana in Group A was better than Group B.
In Cataract, cortical spoke opacities in conjunction with water clefts form radial
wedges containing a fluid of lower refractive index than surrounding lens, this is the
cause for diplopia and polyopia.
The Kaphahara property of Vibhitaki in Triphala choorna helps to remove the
accumulated water droplets from the lens fibres and provides uniform refractive index
which corrects the diplopia and polyopia.
Srotoshodhana property of Madhu which is used to rub the Krishnadi anjana
varti, clears the channels, provides uniform refractive index thus minimizes diplopia and
polyopia.
The effect of treatment on Dwidha bahudha darshana in Group A was better
than Group B probably due to the added effect of Krishnadi anjana.
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 181
5. Effect of treatment on Glare
The effect of treatment on Glare within the group, before treatment and after
treatment, the p value (< 0.001) was statistically highly significant in both the groups.
On comparing between the groups, before treatment to after treatment p value (<0.001)
was statistically highly significant.
Though both the groups showed similar effect, the t-value (11.618) of Group A
was higher when compared to the t-value (4.746) of Group B, concluding that the effect
of treatment on Glare in Group A was better than Group B.
Glare is seen as a result of increased scattering of light rays through the opaque
lens.
The anti-cataract and scavenging property of Triphala choorna arrests the
degeneration process in the lens and removes free radicals thereby helps in maintaining
its transparency.
Lekhana property of Haritaki and antioxidant property of Bhringaraja in
Krishnadi anjana, minimizes the opacification of the lens hence scattering of light by
lens is reduced and improvement is seen in both the groups.
Group A was showed better result than Group B on Glare probably due to the
added effect of Krishnadi anjana.
6. Effect of treatment on Distant vision
The effect of treatment on Distant vision within the group, before treatment and
after treatment, the p value (<0.001) revealed statistically highly significant in both the
groups.
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 182
On comparing between the groups, before treatment to after treatment p value
(<0.001) was statistically highly significant.
Though both the groups showed good results, the t-value (19.006) of Group A was higher
when compared to the t-value (11.718) of Group B, concluding that the effect of
treatment on Distant vision in Group A was better than Group B.
The concentration of glutathione falls with advancing age which is a vital for
maintaing the lens transparency by controlling its metabolic activities. Opacification of
lens occurs as a result of decreased metabolic reactions and increased degeneration.
These opaque areas of the lens obstruct the rays of light coming from an object so
patients develop blurrness of vision for distant objects.
Chakshushya and Rasayana properties of Triphala choorna nourishes the lens and
stops further degeneration. Glutathione and ascorbic acid of Amalaki in Triphala choorna
keeps the normal level of glutathione in the lens thereby maintain its transparency.
Lekhana (scraping) and srotoshodhaka properties of Haritaki in Krishnadi varti
anjana helps to clear the hydrated lens and minimizes the obstruction of the light rays.
Therefore improvement is seen in both the groups and the effect of treatment in Group A
was better than Group B probably due to the added effect of Krishnadi anjana.
7. Effect of treatment on Near vision
The effect of treatment on Near vision within the group, before treatment and
after treatment, the p value (<0.001) revealed statistically highly significant in both the
groups.
DISCUSSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 183
On comparing between the groups, before treatment to after treatment p value
(<0.001) was statistically highly significant.
Though both the groups showed similar effect, the t-value (18.000) of Group A
was higher when compared to the t-value (12.630) of Group B, concluding that the effect
of treatment on Near vision in Group A was better than Group B.
Altered physical and physiological accommodation makes deficient near vision.
With the advancing age, strength of the ciliary muscles and accommodative power of the
opaque lens decreases so patients experienced difficulty in near vision.
Ruksha, laghu guna of vibhitaki in Triphala choorna acts as Kaphaghna and
Shoshana helps in dehydration of lens, which is a prime factor in maintaining its
transparency. Ushna virya of Vibhitaki does Deepana and Pachana, enhances the
metabolic activities of the lens and increases the contractility thereby improves physical
accommodation.
Katu rasa of Bhringaraja in Krishnadi anjana is Netra virechaka, removes
Doshas from ciliary muscles, also it has the property of Vedana sthapana, inturn removes
strain of ciliary muscles, thereby gives strength and helps in physiological
accommodation.
In both the groups accommodative power is improving as the result of treatment
and Group A showed better result than Group B probably due to the added effect of
Krishnadi anjana.
CONCLUSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 184
Conclusion
Timira is one among Drushtigata netra rogas, which is commonly encountered in
the present clinical practice.
Kacha and Linganasha are the progressive stages of the disease Timira.
The lakshanas of Timira simulate to that of the clinical entity of Cataract.
Senile Cataract is a geriatric condition which initially can be reversed. With the
gradual development of opacifications, surgery becomes inevitable.
The study was conducted on 40 patients of Timira w.s.r. to Senile Immature
Cataract assigned into two groups- Group A and Group B, comprising of 20
patients.
The patients of Group A were subjected to internal administration of 5 grams
Triphala choorna once daily at night after food with sufficient amount of Go
ghrita as anupana along with Anjana karma with Krishnadi varti once daily at
morning. The patients of Group B were subjected to internal administration of 5
grams Triphala choorna once daily at night after food with sufficient amount of
Go ghrita as anupana.
In the course of study majority of the patients were females.
Predisposing factors described in modern texts and the Nidanas mentioned by our
ancient Acharyas are very much similar.
Nidanas like Swapana viparyaya and Vegadharana were observed more as
Nidana in the present study.
CONCLUSION
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 185
The effect of treatment was statistically assessed by Student’s paired t test to
analyse within the group and unpaired t-test to analyse between the groups. In
both the groups, within the group analysis, the effect of treatment was statistically
highly significant in Avyakta darshana, Dwidha bahudha darshana, Glare, visual
acuity for Distant vision and Near vision, and statistically significant in Gochara
vibhrama and Vihwala darshana.
Though both groups showed highly significant differences, within the group
analysis however on comparing the t- values in between the groups, the t-values
Group A was higher when compared to that of Group B which could be due to
added effects of Krishnadi varti anjana which proved beneficial.
Anjana karma is important procedure for treating diseases of eye. In the present
study, the bio availability of the drugs helps in Samparapti vighatana as they act
on the target tissues effectively. Thus procedure Anjana can be practised for
clinical success.
Triphala choorna has anti-cataract and anti-oxidant properties that help in
delaying the degenerative process of the lens.
Scope for further study:
Considering the doshaja variety of Timira in particular, same clinical study can
further be established.
Owing to the progressive nature of the disease it is recommended to have prolonged
duration of treatment and follow up.
As the sample size was small and the disease is chronic nature. It is recommended to
carry the study on larger sample size.
SUMMARY
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 186
Summary
Chapter-01:
In this chapter, a brief introduction of the present study which gives compact idea
regarding the disease, pathogenesis, treatment aspect and the utility of Triphala choorna
and Anjana karma in Timira is described.
Chapter- 02:
Objectives of the study:
In this chapter, objectives of the study have been mentioned.
Chapter -03:
Review of Literature:
This chapter contains review of literature pertaining to the disease, drug and procedure.
Review of Disease:
In this section, Ayurvedic description of Timira, historical review of Timira, etymology,
definition, Nidana, Samprapti, Samprapti ghataka, Poorvaroopa, Roopa, Sadhya
Asadhyata, Upashaya and Anupashaya, Samanya Chikitsa of Timira, Vishesha Chikitsa
of Timira, Pathya and Apathya are described in detail. It also contains detailed
description of Cataract- definition, synonyms, epidemiology, types, risk factors,
pathology, clinical features, diagnostic tests and treatment.
SUMMARY
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 187
Review of the procedure:
This section deals with the conceptual study of Anjana, in detail comprising of historical
review, etymology, definition, utility and importance, classification according to different
acharyas, procedure, matra, indications of Anjana, mode of action of Anjana, Samyak,
atiyoga and ayoga lakshanas.
Review of Drug:
This Section contains the detailed description of the ingredients of Triphala choorna,
Anjana karma and anupana.
Chapter- 04:
Methodology:
This chapter contains the description regarding the source of data, Method of collection
of data, study design, diagnostic criteria, inclusion criteria, exclusion criteria, intervention
and procedural details of Anjana.
Chapter-05:
Sample Size of Estimation:
The observation of the study in relation to age, sex, religion, marital status, educational
status, socio- economic status, occupation, diet, addictions, sleep, family history,
chronicity, balapramana pareeksha, nidanas and lakshanas are presented in both tabular
and diagrammatic form.
SUMMARY
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page 188
Chapter-06:
Results:
The result of the study in relation to its effect on assessment parameters like Avyakta
darshana, Gochara vibhrama, Vihwala darshana, Dvidhabahudha darshana, Glare,
Distant vision and Near vision were assessed using scoring and grading pattern and were
statistically analyzed within the group and between the groups to draw a valid conclusion
and is represented both in tabular and graphical form.
Chapter -07:
Discussion:
This chapter contains details about the discussion on Anjana and its probable mode of
action, methodology, observations and results along with the logical reasoning.
Chapter-08:
Conclusion:
In this chapter, whole study is concluded by giving a brief description of the disease,
procedure, study design, observation and results.
Chapter- 09:
Summary:
This chapter contains brief explanation of the whole dissertation.
Chapter- 10:
References:
This chapter contains the references in Vancouver's style.
REFERENCES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page i
References
1) Vagbhata, Astangahrdaya, Sarvangasundara of Arunadatta and
Ayurvedarasayana of Hemadri, Chowkhamba Sanskrit Series Office Varanasi,
Edition – 2009, Uthara sthana, Chapter 13, Verse- 1, pp- 956, pg- 818.
2) Parson, Parson’s diseases of the eye, revised by Ramanjit Sihota and Radhika
Tandon, Elsevier India Private Limited New Delhi, 22th
Edition- 2015, chapter
18, pp- 628, pg- 262.
3) Vagbhata, Astangahrdaya, Sarvangasundara of Arunadatta and
Ayurvedarasayana of Hemadri, Chowkhamba Sanskrit Series Office Varanasi,
Edition – 2009, Uthara sthana, Chapter 13, Verse- 98, pp- 956, pg- 825.
4) Sushruta, Sushruta Samhita, Nibandha Samgraha Commentary of Sri
Dalhanacharya and NyayaChandrika Panjika on Nidanasthana Commentary of
Sri Gayadasacharya, by; Vaidya Yadavji Trikramji Acharya, Choukambha
Surabharati Prakashan, Varanasi, edition- 2014, Uttar tantra, Chapter 18,
Verse- 28, pp- 824, pg- 597.
5) A K Khurana, Comprehensive Ophthalmology, The Health Sciences Publisher,
6th
Edition-2015, chapter- 9, pp-623, pg- 190-191.
6) WHO Survey, http://www.who.int/blindness/causes/en/
7) National Programme for Control of Blindness of Govt. of India,
http://npcb.nic.in/
8) Vagbhata, Astangahrdaya, Sarvangasundara of Arunadatta and
Ayurvedarasayana of Hemadri, Chowkhamba Sanskrit Series Office Varanasi,
Edition – 2009, Uthara sthana, Chapter 13, Verse- 1, pp- 956, pg- 818.
9) National eye institute (NEI), US,
https://nei.nih.gov/health/cataract/cataract_facts
10) A K Khurana, Comprehensive Ophthalmology, The Health Sciences Publisher,
6th
Edition-2015, chapter- 9, pp- 623, pg- 211-215.
REFERENCES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page ii
11) Vagbhata, Astangahrdaya, Sarvangasundara of Arunadatta and
Ayurvedarasayana of Hemadri, Chowkhamba Sanskrit Series Office Varanasi,
Edition – 2009, Uthara sthana, Chapter 13, Verse- 47, pp -956, pg- 822
12) Shaligramaji Vaishya, Vangasena Hindi teeka sahita, Khemraj Srikrishnadas
Prakashan, Mumbai, Edition-1996, Chapter- Netrarogadhikara, Verse- 291, pp-
1096, pg- 777.
13) Rajiv Gandhi University of Health Sciences website: www.rguhs.com, and
Ayurvedic research database 6th
edition, IPGTRA, Gujarat Ayurveda
University, Jamnagar; 2014.
14) Dr.K.P. Sreekumari Amma, Ayurveda ithihasam, Publication section,
Government Ayurveda college Thiruvananthapuram, Thiruvananthapuram,
1985, pp- 256, pg- 10
15) Dr.K.P. Sreekumari Amma, Ayurveda ithihasam, Publication section,
Government Ayurveda college Thiruvananthapuram, Thiruvananthapuram,
1985, pp- 256, Pg- 86,88.
16) Agnivesha, Charaka Samhita, Revised by Charaka and Drdhabala, Ayurveda
Dipika Commentry of Chakrapani Datta, Edited by Vaidya Jadavji Trikamji
Acharya, Chowkhamba Krishnadas Academy Varanasi, Reprint-2010, Sutra
sthana, Chapter 19, Verse 5, pp- 738, pg- 110.
17) Agnivesha, Charaka Samhita, Revised by Charaka and Drdhabala, Ayurveda
Dipika Commentry of Chakrapani Datta, Edited by Vaidya Jadavji Trikamji
Acharya, Chowkhamba Krishnadas Academy Varanasi, Reprint-2010, Chikitsa
sthana, Chapter 26, Verse 130, pp- 738, pg- 606.
18) Agnivesha, Charaka Samhita, Revised by Charaka and Drdhabala, Ayurveda
Dipika Commentry of Chakrapani Datta, Edited by Vaidya Jadavji Trikamji
Acharya, Chowkhamba Krishnadas Academy Varanasi, Reprint-2010, Sutra
sthana, Chapter 20, Verse 11, pp- 738, pg- 113.
19) Sushruta, Sushruta Samhita, Nibandha Samgraha Commentary of Sri
Dalhanacharya and NyayaChandrika Panjika on Nidanasthana Commentary of
Sri Gayadasacharya, by; Vaidya Yadavji Trikramji Acharya, Choukambha
REFERENCES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page iii
Surabharati Prakashan, Varanasi, edition-2014, Uttar tantra, Chapter 7, Verse-
6-24, pp- 824, pg- 606-607.
20) Sushruta, Sushruta Samhita, Nibandha Samgraha Commentary of Sri
Dalhanacharya and NyayaChandrika Panjika on Nidanasthana Commentary of
Sri Gayadasacharya, by; Vaidya Yadavji Trikramji Acharya, Choukambha
Surabharati Prakashan, Varanasi, edition-2014, Uttar tantra, Chapter 17, Verse-
29-54, pp- 824, pg- 627-630.
21) Vruddha Vagbhata, Ashtanga Sangraha, with Shasilekha commentary by Indu,
Prologue in Sanskrit and English by Prof. Jyotir Mitra, Chaukamba Sanskrit
Series Varanasi, Reprint 2006, Uttara tantra, Chapter 15, Verse-17, pp- 965,
pg- 705.
22) Vagbhata, Astangahrdaya, Sarvangasundara of Arunadatta and
Ayurvedarasayana of Hemadri, Chowkhamba Sanskrit Series Office Varanasi,
Edition – 2009, Uthara sthana, Chapter 12, Verse- 8-22, pp -956, pg- 816-817.
23) Shri Madhavakara, Madhava Nidana
- by Vijayarakshita & Srikanthadatta,
Chawkhamba Orientalia, Varanasi, Reprint- 2010, Chapter 59, Verse-29, pp-
408, pg- 349.
24) Chakrapanidatta’s, Chakradatta (Chikistasangraha) – Sanskrit text with English
translation by Dr. G. Prabhakara Rao, Chaukamba Orientalia Varanasi, edition-
2014, Chapter 59, pp- 723, pg- 561.
25) Vaidya Sodhala, Gadanigraha, Commentry by Indradeva Tripathi,
Chaukhambha Sanskrit Sansthan, Varanasi, Edition 1994, Chapter 3, pp- 807,
pg-74.
26) Sharangadhara, Sharangadhara Samhita by- Prof. K. R. Srikanthamurthy,
Chaukamba Orientallia, Varanasi, Reprint-2010, Purva Khanda, Chapter 7,
Verse-164, Pg-44, Uttarkhanda, Chapter 13, Verse- 82-84, pg- 336, pp- 267.
27) Sri Bhavamishra, Bhavaprakasha, Vidyotini Hindi Commentary by Pandit Sri
Brahma Shankar Misra, Chaukambha Sanskrit Bhavana Varanasi, Edition-
2010, Madhyama Khanda, Part-II, Chapter 63, pp- 836, pg- 616.
REFERENCES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page iv
28) Yogaratnakara, Vidyotini Hindi Commentary by Acharya Shri Lakshmipati
Shastri, Chawkhamba Prakashan Varanasi, Edition- 2012, Uttarardha,
Netrarogadhikara, pp- 504, pg- 341.
29) A text book of Shalakya tantra by – Prof. Udaya Shankar, Ayurvedic
Ophthalmology, Vol. I, Netra roga, pp-742, pg- 15.
30) The history of cataract surgery – F. J. Ascaso- University of Zaragoza and V.
Huerva- University of Lleida, Spain.
(http://cdn.intechopen.com/pdfs/42710/InTech-The_history_of_cataract_surgery.pdf)
31) Taranatha tarka vachaspati bhattacharya, Vachaspathyam, Chaukhambha
Sanskrit Series office, Varanasi, Edition.3, Vol. 4, pp- 3442, pg- 2842.
32) Rajaradhakanthdeva, Shabdakalpadruma, Chaukhamba Sanskrit Office,
Varanasi, Edition III, 1967. Vol. 2, pg 517.
33) Monier Williams, A sanskrit-english-dictionary, Motilal banarsidass publishers
private limited dehli, 11007. Edition-1, pp-1333, pg- 382.
34) Rajaradhakanthdeva, Shabdakalpadruma, Chaukhamba Sanskrit Office,
Varanasi, Edition III, 1967. Vol.1, pp- 315, pg- 6.
35) Rajaradhakanthdeva, Shabdakalpadruma, Chaukhamba Sanskrit Office,
Varanasi, Edition III, 1967. Vol. 4, pp- 565, pg- 232.
36) Rajaradhakanthdeva, Shabdakalpadruma, Chaukhamba Sanskrit Office,
Varanasi, Edition III, 1967. Vol. 5, pp- 480, pg- 71.
37) Rajaradhakanthdeva, Shabdakalpadruma, Chaukhamba Sanskrit Office,
Varanasi, Edition III, 1967. Vol.4, pp- 565, pg- 327.
38) Rajaradhakanthdeva, Shabdakalpadruma, Chaukhamba Sanskrit Office,
Varanasi, Edition III, 1967. Vol.4, pp- 565, pg- 320.
39) Sushruta, Sushruta Samhita, Nibandha Samgraha Commentary of Sri
Dalhanacharya and NyayaChandrika Panjika on Nidanasthana Commentary of
Sri Gayadasacharya, by; Vaidya Yadavji Trikramji Acharya, Choukambha
Surabharati Prakashan, Varanasi, edition-2014, Sharira sthana, Chapter 1,
Verse- 4, pp- 824, pg- 338.
REFERENCES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page v
40) Agnivesha, Charaka Samhita, Revised by Charaka and Drdhabala, Ayurveda
Dipika Commentry of Chakrapani Datta, Edited by Vaidya Jadavji Trikamji
Acharya, Chowkhamba Krishnadas Academy Varanasi, Reprint-2010, Sutra
sthana, Chapter 8, Verse 14, pp- 738, pg- 57.
41) A K Khurana, Comprehensive Ophthalmology, The Health Sciences Publisher,
6th
Edition-2015, chapter- 9, pp- 623, pg- 179-218.
42) A.K.Khurana and Indu Khurana, Anatomy and Physiology of eye CBS
Publishers & Distributors Pvt. Ld., New Delhi, 2nd edition.
43) Sushruta, Sushruta Samhita, Nibandha Samgraha Commentary of Sri
Dalhanacharya and NyayaChandrika Panjika on Nidanasthana Commentary of
Sri Gayadasacharya, by; Vaidya Yadavji Trikramji Acharya, Choukambha
Surabharati Prakashan, Varanasi, edition- 2014, Uttar tantra, Chapter 2, 3, 4, 5,
6, 7th
, Verse- 3,5-8,3-4,3,3-4,7-45, pp- 824, pg- 598,599,601,602,603,606-609.
44) Vagbhata, Astangahrdaya, Sarvangasundara of Arunadatta and
Ayurvedarasayana of Hemadri, Chowkhamba Sanskrit Series Office Varanasi,
Edition – 2009, Uttara sthana, Chapter 8,10,12,15, pp- 956, pg- 804-830.
45) Vruddha Vagbhata, Ashtanga Sangraha, with Shasilekha commentary by Indu,
Prologue in Sanskrit and English by Prof. Jyotir Mitra, Chaukamba Sanskrit
Series Varanasi, Reprint- 2006, Uttara stana, Chapter- 11,13,15 pp- 965, pg-
686,693,702.
46) Shri Madhavakara, Madhava Nidana
- by Vijayarakshita & Srikanthadatta,
Chawkhamba Orientalia, Varanasi, Reprint- 2010, Chapter 59, Verse-29, pp-
408, pg- 349.
47) Yogaratnakara, Vidyotini Hindi Commentary by Acharya Shri Lakshmipati
Shastri, Chawkhamba Prakashan Varanasi, Edition- 2012, Uttarardha,
Netrarogadhikara, Verse-3, pp- 504, pg- 341.
48) Sharangadhara, Sharangadhara Samhita by- Prof. K. R. Srikanthamurthy,
Chaukamba Orientallia, Varanasi, Reprint-2010, Purva Khanda, Chapter 7,
Verse-164, pp- 336, pg- 44.
REFERENCES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page vi
49) Rajaradhakanthdeva, Shabdakalpadruma, Chaukhamba Sanskrit Office,
Varanasi, Edition III, 1967. Vol 3, pg- 618.
50) Amarakosa, Amarakosa of Amarasimha with the commentary Vyakhyasudha
by Ramasrami of Bhanuji Diksita, Chaukhambha Sanskrit Pratishtan Dehli,
edition-2002, pp-463, pg-87.
51) Sushruta, Sushruta Samhita, Nibandha Samgraha Commentary of Sri
Dalhanacharya and NyayaChandrika Panjika on Nidanasthana Commentary of
Sri Gayadasacharya, by; Vaidya Yadavji Trikramji Acharya, Choukambha
Surabharati Prakashan, Varanasi, edition-2014, Uttar tantra, Chapter 6, Verse-
5, pp- 824, pg- 603.
52) Agnivesha, Charaka Samhita, Revised by Charaka and Drdhabala, Ayurveda
Dipika Commentry of Chakrapani Datta, Edited by Vaidya Jadavji Trikamji
Acharya, Chowkhamba Krishnadas Academy Varanasi, Reprint-2010, Sutra
sthana, Chapter 11, Verse 39-41, pp- 738, pg- 76.
53) Hareeta Samhita, Vaidya Jayamani Pandey, Chaukhambha Visvabharati,
Varanasi, Edition-2010, Chapter 45, Verse-1, pp- 544, pg- 451.
54) Sushruta, Sushruta Samhita, Nibandha Samgraha Commentary of Sri
Dalhanacharya and NyayaChandrika Panjika on Nidanasthana Commentary of
Sri Gayadasacharya, by; Vaidya Yadavji Trikramji Acharya, Choukambha
Surabharati Prakashan, Varanasi, edition-2014, Uttar tantra, Chapter 1, Verse-
26-27, pp- 824, pg- 597.
55) Agnivesha, Charaka Samhita, Revised by Charaka and Drdhabala, Ayurveda
Dipika Commentry of Chakrapani Datta, Edited by Vaidya Jadavji Trikamji
Acharya, Chowkhamba Krishnadas Academy Varanasi, Reprint-2010, Sutra
sthana, Chapter 21, Verse 50, pp-738, pg-119.
56) Agnivesha, Charaka Samhita, Revised by Charaka and Drdhabala, Ayurveda
Dipika Commentry of Chakrapani Datta, Edited by Vaidya Jadavji Trikamji
Acharya, Chowkhamba Krishnadas Academy Varanasi, Reprint-2010, Sutra
sthana, Chapter 7, Verse 23, pp-738, pg- 50.
REFERENCES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page vii
57) Shri Madhavakara, Madhava Nidana
- by Vijayarakshita & Srikanthadatta,
Chawkhamba Orientalia, Varanasi, Reprint- 2010, Chapter 59, Verse- 1-3, pp-
408, pg- 342.
58) Sri Bhavamishra, Bhavaprakasha, Vidyotini Hindi Commentary by Pandit Sri
Brahma Shankar Misra, Chaukambha Sanskrit Bhavana Varanasi, Edition-
2010, Madhyama Khanda, Part-II, Chapter 63, Verse- 7-9, pp- 836, pg- 615.
59) Yogaratnakara, Vidyotini Hindi Commentary by Acharya Shri Lakshmipati
Shastri, Chawkhamba Prakashan Varanasi, Edition- 2012, Uttarardha,
Netrarogadhikara, Verse-7, pp- 504, pg- 341.
60) Hareeta Samhita, Vaidya Jayamani Pandey, Chaukhambha Visvabharati,
Varanasi, Edition-2010, Chapter 45, Verse- 1-2, pp- 544, pg- 451.
61) Agnivesha, Charaka Samhita, Revised by Charaka and Drdhabala, Ayurveda
Dipika Commentry of Chakrapani Datta, Edited by Vaidya Jadavji Trikamji
Acharya, Chowkhamba Krishnadas Academy Varanasi, Reprint-2010, Chikitsa
sthana, Chapter 15, Verse 60, pp-738, pg- 518.
62) Agnivesha, Charaka Samhita, Revised by Charaka and Drdhabala, Ayurveda
Dipika Commentry of Chakrapani Datta, Edited by Vaidya Jadavji Trikamji
Acharya, Chowkhamba Krishnadas Academy Varanasi, Reprint-2010, Siddhi
sthana, Chapter 9, Verse 115, pp- 738, pg- 723.
63) Vagbhata, Astangahrdaya, Sarvangasundara of Arunadatta and
Ayurvedarasayana of Hemadri, Chowkhamba Sanskrit Series Office Varanasi,
Edition – 2009, Nidana sthana, Chapter 7, Verse- 50, pp- 956, pg- 494.
64) Sushruta, Sushruta Samhita, Nibandha Samgraha Commentary of Sri
Dalhanacharya and NyayaChandrika Panjika on Nidanasthana Commentary of
Sri Gayadasacharya, by; Vaidya Yadavji Trikramji Acharya, Choukambha
Surabharati Prakashan, Varanasi, edition-2014, Uttar tantra, Chapter 24, Verse-
17, pp- 824, pg- 652.
65) Sushruta, Sushruta Samhita, Nibandha Samgraha Commentary of Sri
Dalhanacharya and NyayaChandrika Panjika on Nidanasthana Commentary of
Sri Gayadasacharya, by; Vaidya Yadavji Trikramji Acharya, Choukambha
REFERENCES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page viii
Surabharati Prakashan, Varanasi, edition-2014, Sutra sthan, Chapter 14, Verse-
30, pp- 824, pg- 65.
66) Bhela Samhita, by Dr. K. H. Krishnamurthy, Chawkhamba Visvabharati,
Varanasi, Reprint- 2003, Sutra stana, Chapter- 6, Verse- 6, pp-660, pg- 17.
67) Vagbhata, Astangahrdaya, Sarvangasundara of Arunadatta and
Ayurvedarasayana of Hemadri, Chowkhamba Sanskrit Series Office Varanasi,
Edition – 2009, Nidana sthana, Chapter 1, Verse- 8, pp- 956, pg- 443.
68) Agnivesha, Charaka Samhita, Revised by Charaka and Drdhabala, Ayurveda
Dipika Commentry of Chakrapani Datta, Edited by Vaidya Jadavji Trikamji
Acharya, Chowkhamba Krishnadas Academy Varanasi, Reprint-2010, Sutra
sthana, Chapter 28, Verse 20, pp- 738, pg- 179.
69) Vagbhata, Astangahrdaya, Sarvangasundara of Arunadatta and
Ayurvedarasayana of Hemadri, Chowkhamba Sanskrit Series Office Varanasi,
Edition – 2009, Nidana sthana, Chapter 1, Verse- 4, pp- 956, pg- 441.
70) Sushruta, Sushruta Samhita, Nibandha Samgraha Commentary of Sri
Dalhanacharya and NyayaChandrika Panjika on Nidanasthana Commentary of
Sri Gayadasacharya, by; Vaidya Yadavji Trikramji Acharya, Choukambha
Surabharati Prakashan, Varanasi, edition-2014, Uttar tantra, Chapter 1, Verse-
21-23, pp- 824, pg- 597.
71) Vagbhata, Astangahrdaya, Sarvangasundara of Arunadatta and
Ayurvedarasayana of Hemadri, Chowkhamba Sanskrit Series Office Varanasi,
Edition – 2009, Nidana sthana, Chapter 1, Verse- 5, pp- 956, pg- 441.
72) Sushruta, Sushruta Samhita, Nibandha Samgraha Commentary of Sri
Dalhanacharya and NyayaChandrika Panjika on Nidanasthana Commentary of
Sri Gayadasacharya, by; Vaidya Yadavji Trikramji Acharya, Choukambha
Surabharati Prakashan, Varanasi, edition-2014, Uttar tantra, Chapter 7, Verse-
6-17, pp- 824, pg- 606.
73) Vruddha Vagbhata, Ashtanga Sangraha, with Shasilekha commentary by Indu,
Prologue in Sanskrit and English by Prof. Jyotir Mitra, Chaukamba Sanskrit
REFERENCES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page ix
Series Varanasi, Reprint- 2006, Uttara stana, Chapter 15, Verse- 2-5, pp - 965,
pg- 702-703.
74) Vagbhata, Astangahrdaya, Sarvangasundara of Arunadatta and
Ayurvedarasayana of Hemadri, Chowkhamba Sanskrit Series Office Varanasi,
Edition – 2009, Uttar sthana, Chapter 12, Verse 1-7, pp- 956, pg- 816.
75) Shri Madhavakara, Madhava Nidana
- by Vijayarakshita & Srikanthadatta,
Chawkhamba Orientalia, Varanasi, Reprint- 2010, Chapter 59, Verse- 29-40,
pp- 408, pg- 349-352.
76) Sri Bhavamishra, Bhavaprakasha, Vidyotini Hindi Commentary by Pandit Sri
Brahma Shankar Misra, Chaukambha Sanskrit Bhavana Varanasi, Edition-
2010, Madhyama Khanda, Part-II, Chapter 63, Verse- 14-26, pp- 836, pg- 317-
320.
77) Yogaratnakara, Vidyotini Hindi Commentary by Acharya Shri Lakshmipati
Shastri, Chawkhamba Prakashan Varanasi, Edition- 2012, Uttarardha,
Netrarogadhikara, Verse-14-26, pp-504, pg- 342-344.
78) Shaligramaji Vaishya, Vangasena Hindi teeka sahita, Khemraj Srikrishnadas
Prakashan, Mumbai, Edition-1996, Chapter- Netrarogadhikara, Verse- 226-
238, pp- 1096, pg- 771.
79) Sushruta, Sushruta Samhita, Nibandha Samgraha Commentary of Sri
Dalhanacharya and NyayaChandrika Panjika on Nidanasthana Commentary of
Sri Gayadasacharya, by; Vaidya Yadavji Trikramji Acharya, Choukambha
Surabharati Prakashan, Varanasi, edition-2014, Uttar tantra, Chapter 7, Verse-
6-17, pp- 824, pg- 606.
80) Vagbhata, Astangahrdaya, Sarvangasundara of Arunadatta and
Ayurvedarasayana of Hemadri, Chowkhamba Sanskrit Series Office Varanasi,
Edition – 2009, Uttar sthana, Chapter 12, Verse 1-7, pp- 956, pg- 816.
81) Shri Madhavakara, Madhava Nidana
- by Vijayarakshita & Srikanthadatta,
Chawkhamba Orientalia, Varanasi, Reprint- 2010, Chapter 59, Verse- 29-40,
pp- 408, pg- 349-352.
REFERENCES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page x
82) Yogaratnakara, Vidyotini Hindi Commentary by Acharya Shri Lakshmipati
Shastri, Chawkhamba Prakashan Varanasi, Edition- 2012, Uttarardha,
Netrarogadhikara, Verse- 14-26, pp-504, pg- 342-344.
83) Sushruta, Sushruta Samhita, Nibandha Samgraha Commentary of Sri
Dalhanacharya and NyayaChandrika Panjika on Nidanasthana Commentary of
Sri Gayadasacharya, by; Vaidya Yadavji Trikramji Acharya, Choukambha
Surabharati Prakashan, Varanasi, edition-2014, Uttar tantra, Chapter 7, Verse-
18-25, pp- 824, pg- 607.
84) Vagbhata, Astangahrdaya, Sarvangasundara of Arunadatta and
Ayurvedarasayana of Hemadri, Chowkhamba Sanskrit Series Office Varanasi,
Edition – 2009, Uttar sthana, Chapter 13, Verse 1, pp- 956, pg- 818.
85) Yogaratnakara, Vidyotini Hindi Commentary by Acharya Shri Lakshmipati
Shastri, Chawkhamba Prakashan Varanasi, Edition- 2012, Uttarardha,
Netrarogadhikara, Verse- 1-2, pp- 504, pg- 362.
86) Vaidya Sodhala, Gadanigraha, Commentry by Indradeva Tripathi,
Chaukhambha Sanskrit Sansthan, Varanasi, Edition 1994, Chapter 3, Verse
221, pp- 807, pg- 123.
87) Vagbhata, Astangahrdaya, Sarvangasundara of Arunadatta and
Ayurvedarasayana of Hemadri, Chowkhamba Sanskrit Series Office Varanasi,
Edition – 2009, Uttar sthana, Chapter 13, Verse 50, pp- 956, pg- 822.
88) Vagbhata, Astangahrdaya, Sarvangasundara of Arunadatta and
Ayurvedarasayana of Hemadri, Chowkhamba Sanskrit Series Office Varanasi,
Edition – 2009, Uttar sthana, Chapter 13, Verse 63, pp- 956, pg- 823.
89) Vagbhata, Astangahrdaya, Sarvangasundara of Arunadatta and
Ayurvedarasayana of Hemadri, Chowkhamba Sanskrit Series Office Varanasi,
Edition – 2009, Uttar sthana, Chapter 13, Verse 68, pp -956, pg- 823.
90) Sushruta, Sushruta Samhita, Nibandha Samgraha Commentary of Sri
Dalhanacharya and NyayaChandrika Panjika on Nidanasthana Commentary of
Sri Gayadasacharya, by; Vaidya Yadavji Trikramji Acharya, Choukambha
REFERENCES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page xi
Surabharati Prakashan, Varanasi, edition-2014, Uttar tantra, Chapter 17, Verse-
29, pp- 824, pg- 627.
91) Sushruta, Sushruta Samhita, Nibandha Samgraha Commentary of Sri
Dalhanacharya and NyayaChandrika Panjika on Nidanasthana Commentary of
Sri Gayadasacharya, by; Vaidya Yadavji Trikramji Acharya, Choukambha
Surabharati Prakashan, Varanasi, edition-2014, Uttar tantra, Chapter 17, Verse-
30, pp- 824, pg- 627.
92) Vagbhata, Astangahrdaya, Sarvangasundara of Arunadatta and
Ayurvedarasayana of Hemadri, Chowkhamba Sanskrit Series Office Varanasi,
Edition – 2009, Uttar sthana, Chapter 13, Verse 51-52, pp- 956, pg- 822.
93) Vagbhata, Astangahrdaya, Sarvangasundara of Arunadatta and
Ayurvedarasayana of Hemadri, Chowkhamba Sanskrit Series Office Varanasi,
Edition – 2009, Uttar sthana, Chapter 13, Verse 67, pp- 956, pg- 823.
94) Vagbhata, Astangahrdaya, Sarvangasundara of Arunadatta and
Ayurvedarasayana of Hemadri, Chowkhamba Sanskrit Series Office Varanasi,
Edition – 2009, Uttar sthana, Chapter 13, Verse 69, pp- 956, pg- 823.
95) Shaligramaji Vaishya, Vangasena Hindi teeka sahita, Khemraj Srikrishnadas
Prakashan, Mumbai, Edition-1996, Chapter- Netrarogadhikara, Verse- 285,
424-434, pp-1096, pg- 777-791.
96) Sushruta, Sushruta Samhita, Nibandha Samgraha Commentary of Sri
Dalhanacharya and NyayaChandrika Panjika on Nidanasthana Commentary of
Sri Gayadasacharya, by; Vaidya Yadavji Trikramji Acharya, Choukambha
Surabharati Prakashan, Varanasi, edition-2014, Uttar tantra, Chapter 17, Verse-
52, pp- 824, pg- 630.
97) Vagbhata, Astangahrdaya, Sarvangasundara of Arunadatta and
Ayurvedarasayana of Hemadri, Chowkhamba Sanskrit Series Office Varanasi,
Edition – 2009, Uttar sthana, Chapter 13, Verse 2-11 & 58, pp- 956, pg- 819.
98) Yogaratnakara, Vidyotini Hindi Commentary by Acharya Shri Lakshmipati
Shastri, Chawkhamba Prakashan Varanasi, Edition- 2012, Uttarardha,
Netrarogadhikara, Verse- 6, pp- 504, pg- 391.
REFERENCES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page xii
99) Shaligramaji Vaishya, Vangasena Hindi teeka sahita, Khemraj Srikrishnadas
Prakashan, Mumbai, Edition-1996, Chapter- Netrarogadhikara, Verse- 309, pp-
1096, pg- 779.
100) Chakrapanidatta’s, Chakradatta (Chikistasangraha) – Sanskrit text with English
translation by Dr. G. Prabhakara Rao, Chaukamba Orientalia Varanasi,
Edition-2014, Chapter 59, Verse- 115-116, pp- 723, pg- 575.
101) Vaidya Sodhala, Gadanigraha, Commentry by Indradeva Tripathi,
Chaukhambha Sanskrit sansthan, Varanasi, Edition3, 1994, Chapter 3, Verse-
144, pp- 807, pg- 106.
102) Vaidya Sodhala, Gadanigraha, Commentry by Indradeva Tripathi,
Chaukhambha Sanskrit sansthan, Varanasi, Edition3,1994, Chapter 3, Verse-
464, pp- 807, pg- 169.
103) Vaidya Sodhala, Gadanigraha, Commentry by Indradeva Tripathi,
Chaukhambha Sanskrit sansthan, Varanasi, Edition 3, 1994, Chapter 3, Verse-
456, pp- 807, pg- 168.
104) Govindadas Sen, Bhaishajyaratnavali, Mottilal Banarasidas, Mumbai, Edition 8,
1970, Reprint- 2007, Chapter-Netrarogadhikara, pp- 832, pg- 672.
105) Shaligramaji Vaishya, Vangasena Hindi teeka sahita, Khemraj Srikrishnadas
Prakashan, Mumbai, Edition-1996, Chapter- Netrarogadhikara, Verse- 274,
275, 278, pp-1096, pg- 776-791.
106) Sushruta, Sushruta Samhita, Nibandha Samgraha Commentary of Sri
Dalhanacharya and NyayaChandrika Panjika on Nidanasthana Commentary of
Sri Gayadasacharya, by; Vaidya Yadavji Trikramji Acharya, Choukambha
Surabharati Prakashan, Varanasi, edition-2014, Uttar tantra, Chapter 17, Verse-
31-32, pp- 824, pg- 627.
107) A K Khurana, Comprehensive Ophthalmology, The Health Sciences Publisher,
6th
Edition-2015, Chapter 9, pp- 623, pg- 179-218.
108) A.K.Khurana and Indu Khurana, Anatomy and Physiology of eye CBS
Publishers & Distributors Pvt. Ld., New Delhi, 2nd edition.
REFERENCES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page xiii
109) Parson, Parson’s diseases of the eye, revised by Ramanjit Sihota and Radhika
Tandon, Elsevier India Private Limited New Delhi, 22th
Edition-2015, Chapter-
18, pp- 628, pg- 261-286.
110) Jack J Kanshi, Clinical Ophthalmology, A systemic approach, British Libraray
catalouging, 6th Edition, pp-922, pg- 208-209.
111) http://www.etymonline.com/index.php?term=cataract
112) Parson, Parson’s diseases of the eye, revised by Ramanjit Sihota and Radhika
Tandon, Elsevier India Private Limited New Delhi, 22th
Edition-2015, Chapter-
18, pp- 628, pg- 262-263.
113) Taranatha tarka vachaspati bhattacharya, Vachaspathyam, Chaukhambha
Sanskrit Series office, Varanasi, Edition.3, Vol.1, pp.3442, pg- 64.
114) Vruddha Vagbhata, Astanga Samgraha, Shashilekha Sanskrit commentary of
Indu, by; Dr Shivaprasad Sharma, Choukambha Sanskrit Series Office,
Varanasi, Reprint- 2006, Sutrasthana, Chapter 32, Verse 17, pp- 965, pg- 228.
115) Vagbhata, Astangahrdaya, Sarvangasundara of Arunadatta and
Ayurvedarasayana of Hemadri, Chowkhamba Sanskrit Series Office Varanasi,
Edition – 2009, Sutra sthana, Chapter 23, Verse 16-17, pp- 956, pg- 305.
116) Vruddha Vagbhata, Astanga Samgraha, Shashilekha Sanskrit commentary of
Indu, by; Dr Shivaprasad Sharma, Choukambha Sanskrit Series Office,
Varanasi, reprint-2006, Sutrasthana, Chapter 32, Verse- 16, pp- 965, pg- 235.
117) Sushruta, Sushruta Samhita, Nibandha Samgraha Commentary of Sri
Dalhanacharya and NyayaChandrika Panjika on Nidanasthana Commentary of
Sri Gayadasacharya, by; Vaidya Yadavji Trikramji Acharya, Choukambha
Surabharati Prakashan, Varanasi, edition-2014, Uttar tantra, Chapter 18, Verse-
57, pp- 824, pg- 637.
118) Sushruta, Sushruta Samhita, Nibandha Samgraha Commentary of Sri
Dalhanacharya and NyayaChandrika Panjika on Nidanasthana Commentary of
Sri Gayadasacharya, by; Vaidya Yadavji Trikramji Acharya, Choukambha
Surabharati Prakashan, Varanasi, edition-2014, Uttar tantra, Chapter 18, Verse-
61-62, pp- 824, pg- 637.
REFERENCES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page xiv
119) Sharangadhara, Sharangadhara Samhita by- Prof. K. R. Srikanthamurthy,
Chaukamba Orientallia, Varanasi, Reprint-2010, Purva Khanda, Chapter 7,
Verse-164, Pg-44, Uttarkhanda, Chapter 13, Verse- 71-72, pp- 336, pg- 266.
120) Sushruta, Sushruta Samhita, Nibandha Samgraha Commentary of Sri
Dalhanacharya and NyayaChandrika Panjika on Nidanasthana Commentary of
Sri Gayadasacharya, by; Vaidya Yadavji Trikramji Acharya, Choukambha
Surabharati Prakashan, Varanasi, edition-2014, Uttar tantra, Chapter 18, Verse-
57, pp- 824, pg- 637.
121) Sushruta, Sushruta Samhita, Nibandha Samgraha Commentary of Sri
Dalhanacharya and NyayaChandrika Panjika on Nidanasthana Commentary of
Sri Gayadasacharya, by; Vaidya Yadavji Trikramji Acharya, Choukambha
Surabharati Prakashan, Varanasi, edition-2014, Uttar tantra, Chapter 18, Verse-
53-54, pp- 824, pg- 636.
122) Sushruta, Sushruta Samhita, Nibandha Samgraha Commentary of Sri
Dalhanacharya and NyayaChandrika Panjika on Nidanasthana Commentary of
Sri Gayadasacharya, by; Vaidya Yadavji Trikramji Acharya, Choukambha
Surabharati Prakashan, Varanasi, edition-2014, Uttar tantra, Chapter 18, Verse-
75-77, pp- 824, pg- 638.
123) Sushruta, Sushruta Samhita, Nibandha Samgraha Commentary of Sri
Dalhanacharya and NyayaChandrika Panjika on Nidanasthana Commentary of
Sri Gayadasacharya, by; Vaidya Yadavji Trikramji Acharya, Choukambha
Surabharati Prakashan, Varanasi, edition-2014, Uttar tantra, Chapter 18, Verse-
55, pp- 824, pg- 637.
124) Sushruta, Sushruta Samhita, Nibandha Samgraha Commentary of Sri
Dalhanacharya and NyayaChandrika Panjika on Nidanasthana Commentary of
Sri Gayadasacharya, by; Vaidya Yadavji Trikramji Acharya, Choukambha
Surabharati Prakashan, Varanasi, edition-2014, Uttar tantra, Chapter 18, Verse-
81, pp- 824, pg- 639.
125) Sushruta, Sushruta Samhita, Nibandha Samgraha Commentary of Sri
Dalhanacharya and NyayaChandrika Panjika on Nidanasthana Commentary of
REFERENCES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page xv
Sri Gayadasacharya, by; Vaidya Yadavji Trikramji Acharya, Choukambha
Surabharati Prakashan, Varanasi, edition-2014, Uttar tantra, Chapter 18, Verse-
53, pp- 824, pg- 637.
126) Sushruta, Sushruta Samhita, Nibandha Samgraha Commentary of Sri
Dalhanacharya and NyayaChandrika Panjika on Nidanasthana Commentary of
Sri Gayadasacharya, by; Vaidya Yadavji Trikramji Acharya, Choukambha
Surabharati Prakashan, Varanasi, edition-2014, Uttar tantra, Chapter 18, Verse-
79-81, pp- 824, pg- 638.
127) Vruddha Vagbhata, Astanga Samgraha, Shashilekha Sanskrit commentary of
Indu, by; Dr Shivaprasad Sharma, Choukambha Sanskrit Series Office,
Varanasi, reprint-2006, Sutrasthana chapter 32, verse 9, pp- 965, pg- 234.
128) Sushruta, Sushruta Samhita, Nibandha Samgraha Commentary of Sri
Dalhanacharya and NyayaChandrika Panjika on Nidanasthana Commentary of
Sri Gayadasacharya, by; Vaidya Yadavji Trikramji Acharya, Choukambha
Surabharati Prakashan, Varanasi, edition-2014, Uttar tantra, Chapter 18, Verse-
70-73, pp- 824, pg- 638.
129) Sushruta, Sushruta Samhita, Nibandha Samgraha Commentary of Sri
Dalhanacharya and NyayaChandrika Panjika on Nidanasthana Commentary of
Sri Gayadasacharya, by; Vaidya Yadavji Trikramji Acharya, Choukambha
Surabharati Prakashan, Varanasi, edition-2014, Uttar tantra, Chapter 18, Verse-
59, pp- 824, pg- 638.
130) Vagbhata, Astangahrdaya, Sarvangasundara of Arunadatta and
Ayurvedarasayana of Hemadri, Chowkhamba Sanskrit Series Office Varanasi,
Edition – 2009, Sutra sthana, Chapter 23, Verse 14, pp -956, pg- 305.
131) Sharangadhara, Sharangadhara Samhita by- Prof. K. R. Srikanthamurthy,
Chaukamba Orientallia, Varanasi, Reprint-2010, Purva Khanda, Chapter 7,
Verse-164, Pg-44, Uttarkhanda, Chapter 13, Verse- 68-70, pp- 336, pg- 265.
132) Sushruta, Sushruta Samhita, Nibandha Samgraha Commentary of Sri
Dalhanacharya and NyayaChandrika Panjika on Nidanasthana Commentary of
Sri Gayadasacharya, by; Vaidya Yadavji Trikramji Acharya, Choukambha
REFERENCES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page xvi
Surabharati Prakashan, Varanasi, edition-2014, Uttar tantra, Chapter 18, Verse-
53, pp- 824, pg- 638.
133) Dr.J.L.N Sastri, Dravyaguna Vijnana, Chaukhambha Orientalia, Varanasi,
Reprint Edition 2014, Volume 2, pp- 1134, pg- 209.
134) Bapalal G. Vaidya, Nighantu Adarsa, Chaukhambha Bharathi Academy,
Varanasi, Reprint Edition 2013, Volume 1, pg- 550.
135) Sri Bhavamishra, Bhavaprakasha, Vidyotini Hindi Commentary by Pandit Sri
Brahma Shankar Misra, Chaukambha Sanskrit Bhavana Varanasi, Edition-
2007, Purva Khanda, Part-I, Haritakyadi varga, pp- 659, pg- 7.
136) Sri Narhari Pandit, Raj Nighantu, By Dr. Satish Chandra Sankhyadhar and Dr.
Deepika Sankhyadhar, Chaukhambha Orientalia, Varanasi, Edition 2012, pp-
1306, pg- 621.
137) P.C. Sharma, M.B. Yelne; Data base on medicinal plants used in Ayurveda,
Central council for research in Ayurveda & Siddha, New Delhi, Print 2001,
Volume 3, pg- 282.
138) The Ayurvedic Pharmacopoeia of India, Government of India Ministry of
Health and Family Welfare Department of AYUSH, New Delhi, Part 1,
Volume 1, pp- 171, pg- 60.
139) Dr.J.L.N Sastri, Dravyaguna Vijnana, Chaukhambha Orientalia, Varanasi,
Reprint Edition 2014, Volume 2, pp- 1134, pg- 216.
140) Bapalal G. Vaidya, Nighantu Adarsa, Chaukhambha Bharathi Academy,
Varanasi, Reprint Edition 2013, Volume 1, pg- 576.
141) Sri Bhavamishra, Bhavaprakasha, Vidyotini Hindi Commentary by Pandit Sri
Brahma Shankar Misra, Chaukambha Sanskrit Bhavana Varanasi, Edition-
2007, Purva Khanda, Part-I, Haritakyadi varga, pp- 659, pg- 9.
142) Sri Narhari Pandit, Raj Nighantu, By Dr. Satish Chandra Sankhyadhar and Dr.
Deepika Sankhyadhar, Chaukhambha Orientalia, Varanasi, Edition 2012, pp-
1306, pg- 626.
REFERENCES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page xvii
143) P.C. Sharma, M.B. Yelne; Data base on medicinal plants used in Ayurveda,
Central council for research in Ayurveda & Siddha, New Delhi, Print 2001,
Volume 3, pg- 158.
144) The Ayurvedic Pharmacopoeia of India, Government of India Ministry of
Health and Family Welfare Department of AYUSH, New Delhi, Part 1,
Volume 1, pp- 171, pg- 33.
145) Dr.J.L.N Sastri, Dravyaguna Vijnana, Chaukhambha Orientalia, Varanasi,
Reprint Edition 2014, Volume 2, pp-1134, pg- 221.
146) Bapalal G. Vaidya, Nighantu Adarsa, Chaukhambha Bharathi Academy,
Varanasi, Reprint Edition 2013, Volume 2, pg- 403.
147) Sri Bhavamishra, Bhavaprakasha, Vidyotini Hindi Commentary by Pandit Sri
Brahma Shankar Misra, Chaukambha Sanskrit Bhavana Varanasi, Edition-
2007, Purva Khanda, Part-I, Haritakyadi varga, pp- 659, pg- 10.
148) Sri Narhari Pandit, Raj Nighantu, By Dr. Satish Chandra Sankhyadhar and Dr.
Deepika Sankhyadhar, Chaukhambha Orientalia, Varanasi, Edition 2012, pp-
1306, pg- 598.
149) P.C. Sharma, M.B. Yelne; Data base on medicinal plants used in Ayurveda,
Central council for research in Ayurveda & Siddha, New Delhi, Print 2001,
Volume 3, pg- 12.
150) The Ayurvedic Pharmacopoeia of India, Government of India Ministry of
Health and Family Welfare Department of AYUSH, New Delhi, Part 1,
Volume 1, pp- 171, pg- 7.
151) Dr.J.L.N Sastri, Dravyaguna Vijnana, Chaukhambha Orientalia, Varanasi,
Reprint Edition 2014, Volume 2, pp-1134, pg- 452.
152) Bapalal G. Vaidya, Nighantu Adarsa, Chaukhambha Bharathi Academy,
Varanasi, Reprint Edition 2013, Volume 2, pg- 345.
153) Sri Bhavamishra, Bhavaprakasha, Vidyotini Hindi Commentary by Pandit Sri
Brahma Shankar Misra, Chaukambha Sanskrit Bhavana Varanasi, Edition-
2007, Purva Khanda, Part-I, Haritakyadi varga, pp- 659, pg- 15.
REFERENCES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page xviii
154) Sri Narhari Pandit, Raj Nighantu, By Dr. Satish Chandra Sankhyadhar and Dr.
Deepika Sankhyadhar, Chaukhambha Orientalia, Varanasi, Edition 2012, pp-
1306, pg-197.
155) P.C. Sharma, M.B. Yelne; Data base on medicinal plants used in Ayurveda,
Central council for research in Ayurveda & Siddha, New Delhi, Print 2001,
Volume 3, pg- 71.
156) The Ayurvedic Pharmacopoeia of India, Government of India Ministry of
Health and Family Welfare Department of AYUSH, New Delhi, Part 1,
Volume 4, pp- 167, pg- 105.
157) Dr.J.L.N Sastri, Dravyaguna Vijnana, Chaukhambha Orientalia, Varanasi,
Reprint Edition 2014, Volume 2, pp-1134, pg- 296.
158) Bapalal G. Vaidya, Nighantu Adarsa, Chaukhambha Bharathi Academy,
Varanasi, Reprint Edition 2013, Volume 1, pg- 764.
159) Sri Bhavamishra, Bhavaprakasha, Vidyotini Hindi Commentary by Pandit Sri
Brahma Shankar Misra, Chaukambha Sanskrit Bhavana Varanasi, Edition-
2007, Purva Khanda, Part-I, pp- 659, pg- 429.
160) Sri Narhari Pandit, Raj Nighantu, By Dr. Satish Chandra Sankhyadhar and Dr.
Deepika Sankhyadhar, Chaukhambha Orientalia, Varanasi, Edition 2012, pp-
1306, pg- 121.
161) P.C. Sharma, M.B. Yelne; Data base on medicinal plants used in Ayurveda,
Central council for research in Ayurveda & Siddha, New Delhi, Print 2001,
Volume 2, pg- 112.
162) The Ayurvedic Pharmacopoeia of India, Government of India Ministry of
Health and Family Welfare Department of AYUSH, New Delhi, Part 1,
Volume 2, pp- 190, pg- 21.
163) Dr.J.L.N Sastri, Dravyaguna Vijnana, Chaukhambha Orientalia, Varanasi,
Reprint Edition 2014, Volume 3, pg- 46.
164) Sri Bhavamishra, Bhavaprakasha, Vidyotini Hindi Commentary by Pandit Sri
Brahma Shankar Misra, Chaukambha Sanskrit Bhavana Varanasi, Edition-
2007, Purva Khanda, Part-I, Dugdha varga, pp- 659, pg- 775.
REFERENCES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page xix
165) Sri Narhari Pandit, Raj Nighantu, By Dr. Satish Chandra Sankhyadhar and Dr.
Deepika Sankhyadhar, Chaukhambha Orientalia, Varanasi, Edition 2012, pp-
1306, pg- 841.
166) Vaidya. V.M. Gogte, Ayurvedic Pharmacology & Therapeutic uses of
medicinal plants, Dravyaguna vignyan, Chaukhambha publication, edition,
Reprint 2012, pg-841, pp- 765.
167) Inventory of Animal products used in Ayurveda Siddha and Unani, National
Bio-Resources Development Board, Department of Bio-Technology, Ministry
of Science and Technology Government of India, CCRAS, New Delhi, Print
2008, Part 1, pg- 54.
168) Dr.J.L.N Sastri, Dravyaguna Vijnana, Chaukhambha Orientalia, Varanasi,
Reprint Edition 2014, Volume 3, pg- 51.
169) Vaidya. V.M. Gogte, Ayurvedic Pharmacology & Therapeutic uses of
medicinal plants, Dravyaguna vignyan, Chaukhambha publication, edition,
Reprint 2012, pg- 841, pp- 765.
170) Inventory of Animal products used in Ayurveda Siddha and Unani, National
Bio-Resources Development Board, Department of Bio-Technology, Ministry
of Science and Technology Government of India, CCRAS, New Delhi, Print
2008, Part 2, pg-507.
CONSENT FORM
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page xx
WRITTEN INFORMED CONSENT FORM
Certificate by Investigator
I certify that I have disclosed all the details about the study in the terms easily understood
by the patient.
Date: Signature of the investigator
PATIENT’S CONSENT FORM
I the undersigned,
Resident of ……………
Age: yrs. Education:
I am taking the treatment with the Ayurvedic drugs under the supervision of Dr. Santosh
Kumar Shaw, She has explained me the purpose of treatment and I have understood it. I
have come to the hospital on my own and the treatment is for my betterment.
Voluntarily and without any pressure I am willing to undergo this treatment as long as
Physician in-charge asked me to undergo. She has not offered me any rewards. She has
also not made assurance regarding the benefits of cure from this trail. I am aware of my
rights to opt out of the study at any point of time during the study period.
The meaning of the contents of this letter has been explained to me in my own language.
Name of the subject: Name & sign of the investigator
Signature/ thumb impression
Place:
Date:
Page xxi
CASE PROFORMA
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page xxii
CASE PROFORMA
SRI KALABYRAVESHWARASWAMY AYURVEDIC MEDICAL COLLEGE,
HOSPITAL AND RESEARCH CENTRE.
VIJAYANAGAR, BANGALORE-560040.
DEPARTMENT OF POST GRADUATE STUDIES IN SHALAKYA TANTRA
A COMPARATIVE CLINICAL STUDY TO EVALUATE THE
EFFICACY OF TRIPHALA CHOORNA WITH KRISHNADI
ANJANA AND TRIPHALA CHOORNA IN THE MANAGEMENT
OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT
GUIDE : Dr. Sujathamma K. M.D., (Ayu)
RESEARCH SCHOLAR : Dr. Santosh Kumar Shaw, B.A.M.S.
ATURA VIVARANA Sl.No:
Name : O.P.D No:
Age : I.P.D No:
Sex : M / F Ward :
Religion : H / M / C / O Bed No:
Educational status : UE / UG / GR / PG D.O.A:
Marital status : UM / M D.O.D:
Economic status : LC / MC / UC Occupation:
Postal address :
Place/ area : R / U Ph No:
Desha : Anupa / Jangala / Sadharana E-mail ID:
CASE PROFORMA
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page xxiii
Date of commencement of treatment:
Date of completion of treatment: Study Group – A/B:
PRADHANA VEDANA: Duration:
ANUBANDHA VEDANA: Duration:
VEDANAVRUTTANTHA
POORVA VYADHI VRUTTANTA:
CHIKITSA VRUTTANTA:
KAUTUMBIKA VRUTTANTA:
VAIYAKTIKA VRUTTANTA:
1] Ahara: Vegetarian / Non veg/ Lacto ova veg
2] Vyasana:
Beedi / Cigarette - Yes / No , If Yes no........../ day /week Duration
Alcohol - Yes / No , If Yes qnt....................../ day /week/month Duration
CASE PROFORMA
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page xxiv
Tobacco Chewing - Yes / No , If Yes qnt....../ day /week/month Duration
Coffee/Tea -Yes / No , If Yes qnt in ml/cups......../day Duration
Other-
3] Nidra: ......... Hours /day - Sound / Disturbed /delayed
Divaswapna- Yes / No ......... Hours/day, Daily/Occasional
Ratrijagarana- Yes / No ........ Hours /day, Daily /Occasional
Other-
4] Koshta: Mridu/Madhyama/Kroora
5] Mala Visarjana: Regular / Irregular / Constipation / Loose stool
Frequency ........./Day
Colour-
Consistency-
Other-
6] Mutravisarjana – Frequency: Day........times, Night.........../times
Colour -
Other -
7] Vegadharana – Yes/No, Suppression of............................ urge/s regularly/
occasional
VYAVASAYIKA VRUTTANTA:
Work- Sedentary / Labour / Travelling/ House makers
Working hrs / day
Day / Night
CASE PROFORMA
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page xxv
RAJOSAMBANDHI VRUTTANTA:
Menstrual cycle: …… Regular / Irregular
ROGI PAREEKSHA
DASHA VIDHA PAREEKSHA (Atura Balapramanapareeksha ) :
Prakriti :V / P/ K/ VP/ PK/ VK/ VPK
Sara :Pravara / Madhyama / Avara
Samhanana :Pravara / Madhyama / Avara
Pramana :Heena / Madhyama / Uttama
(Dairghya___ cms, Bhara___kgs)
Satmya :Eka rasa / Sarva rasa / Vyamishra
Satva : Shareerika- Pravara / Madhyama / Avara
Manasika- Pravara / Madhyama / Avara
AharaShakti :
Abhyavaharana Shakti- Pravara / Madhyama / Avara
Jarana Shakti- Pravara / Madhyama / Avara
Vyayama Shakti: Pravara / Madhyama / Avara
Vaya : Bala/ Madhyama/Vriddha
Vikruti :P/ M/ A
Hetu - Desha -
Kala - Dosha -
Bala - Dushya -
CASE PROFORMA
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page xxvi
SROTO PAREEKSHA:
General Physical examination:
1. Built and nourishment:
2. Pulse : / min, regular/irregular
3. B.P : / mm of Hg
4. Temperature : F
5. Respiratory rate : / min
6. Tongue :
7. Height : meter
8. Weight : kg
9. Pallor : P / A
10. Icterus : P / A
11. Clubbing : P / A
12. Cynosis : P / A
SYSTEMIC EXAMINATION :
Respiratory System :
Cardiovasular System :
Gastrointestinal System :
Nervous System :
CASE PROFORMA
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page xxvii
OCULAR EXAMINATION
1. VISUAL ACUITY TEST:
Without spectacles With spectacles
DV NV DV NV
Both eye
Right eye
Left eye
2. PIN HOLE OCCLUDER TEST:
Right eye
Left eye
3. REFRACTION CORRECTION:
Right Eye Left Eye
Sph Cyl axis V/A sph cyl axis V/A
DV
NV
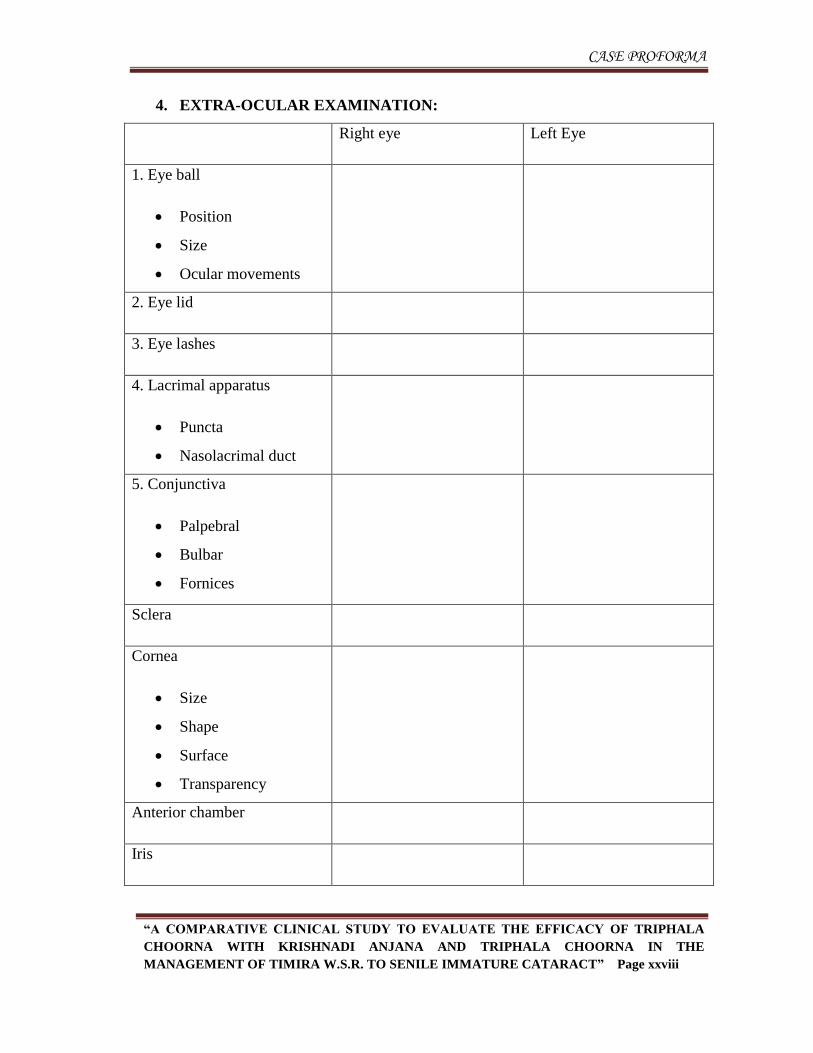
CASE PROFORMA
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page xxviii
4. EXTRA-OCULAR EXAMINATION:
Right eye Left Eye
1. Eye ball
Position
Size
Ocular movements
2. Eye lid
3. Eye lashes
4. Lacrimal apparatus
Puncta
Nasolacrimal duct
5. Conjunctiva
Palpebral
Bulbar
Fornices
Sclera
Cornea
Size
Shape
Surface
Transparency
Anterior chamber
Iris
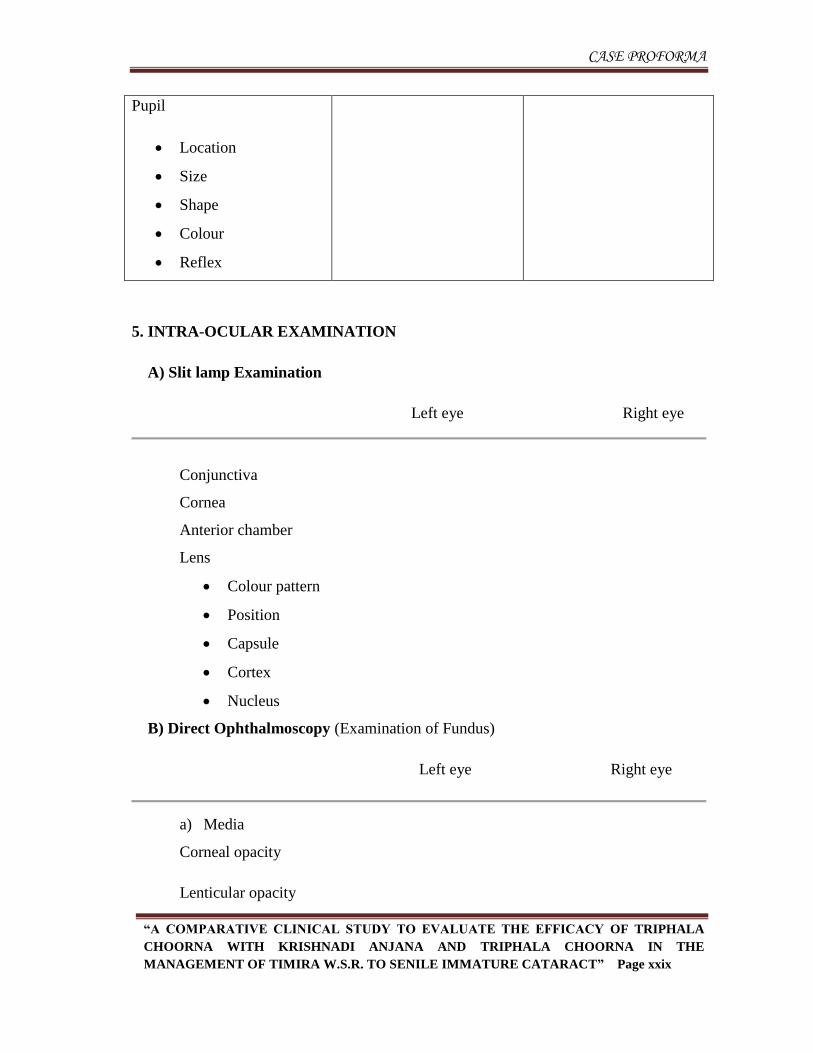
CASE PROFORMA
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page xxix
Pupil
Location
Size
Shape
Colour
Reflex
5. INTRA-OCULAR EXAMINATION
A) Slit lamp Examination
Left eye Right eye
Conjunctiva
Cornea
Anterior chamber
Lens
Colour pattern
Position
Capsule
Cortex
Nucleus
B) Direct Ophthalmoscopy (Examination of Fundus)
Left eye Right eye
a) Media
Corneal opacity
Lenticular opacity
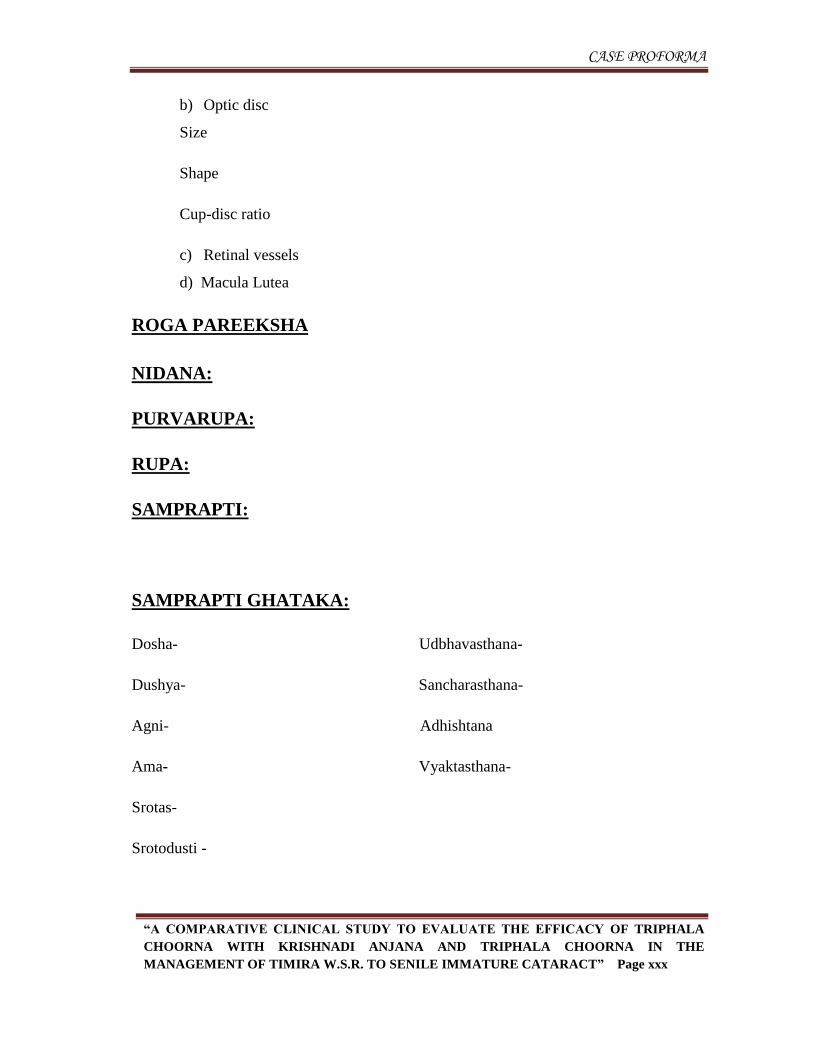
CASE PROFORMA
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page xxx
b) Optic disc
Size
Shape
Cup-disc ratio
c) Retinal vessels
d) Macula Lutea
ROGA PAREEKSHA
NIDANA:
PURVARUPA:
RUPA:
SAMPRAPTI:
SAMPRAPTI GHATAKA:
Dosha- Udbhavasthana-
Dushya- Sancharasthana-
Agni- Adhishtana
Ama- Vyaktasthana-
Srotas-
Srotodusti -
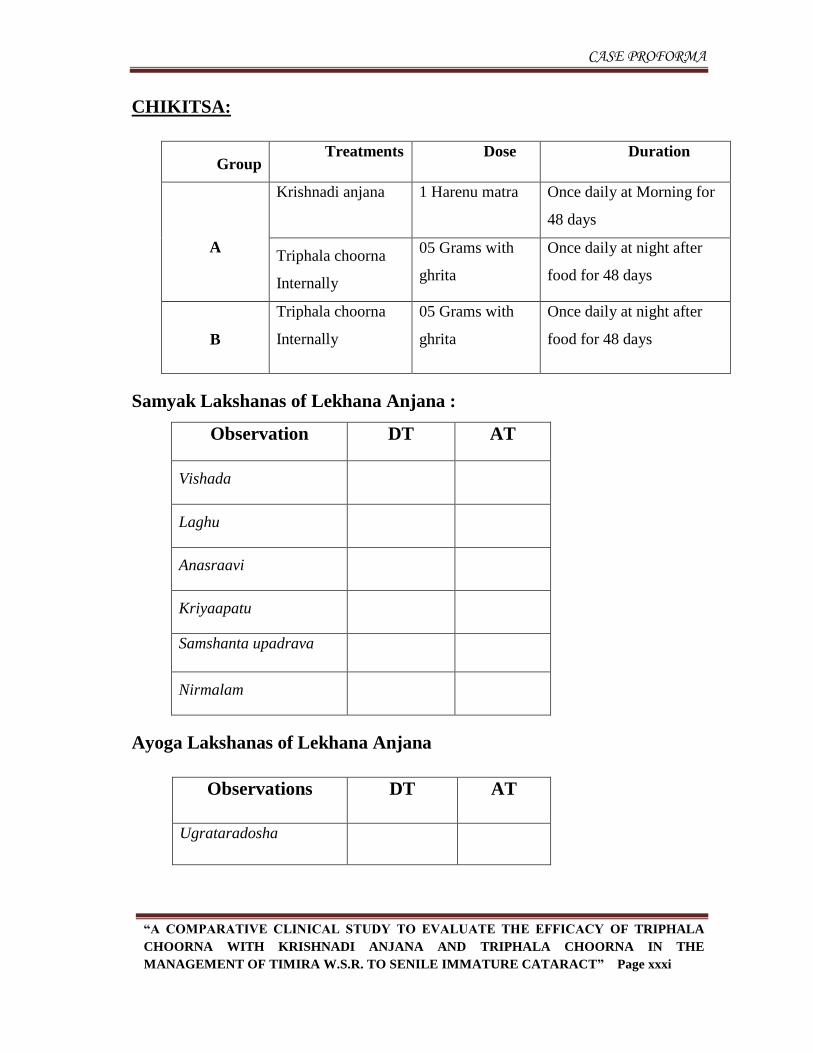
CASE PROFORMA
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page xxxi
CHIKITSA:
Group Treatments Dose Duration
A
Krishnadi anjana 1 Harenu matra Once daily at Morning for
48 days
Triphala choorna
Internally
05 Grams with
ghrita
Once daily at night after
food for 48 days
B
Triphala choorna
Internally
05 Grams with
ghrita
Once daily at night after
food for 48 days
Samyak Lakshanas of Lekhana Anjana :
Observation DT AT
Vishada
Laghu
Anasraavi
Kriyaapatu
Samshanta upadrava
Nirmalam
Ayoga Lakshanas of Lekhana Anjana
Observations DT AT
Ugrataradosha
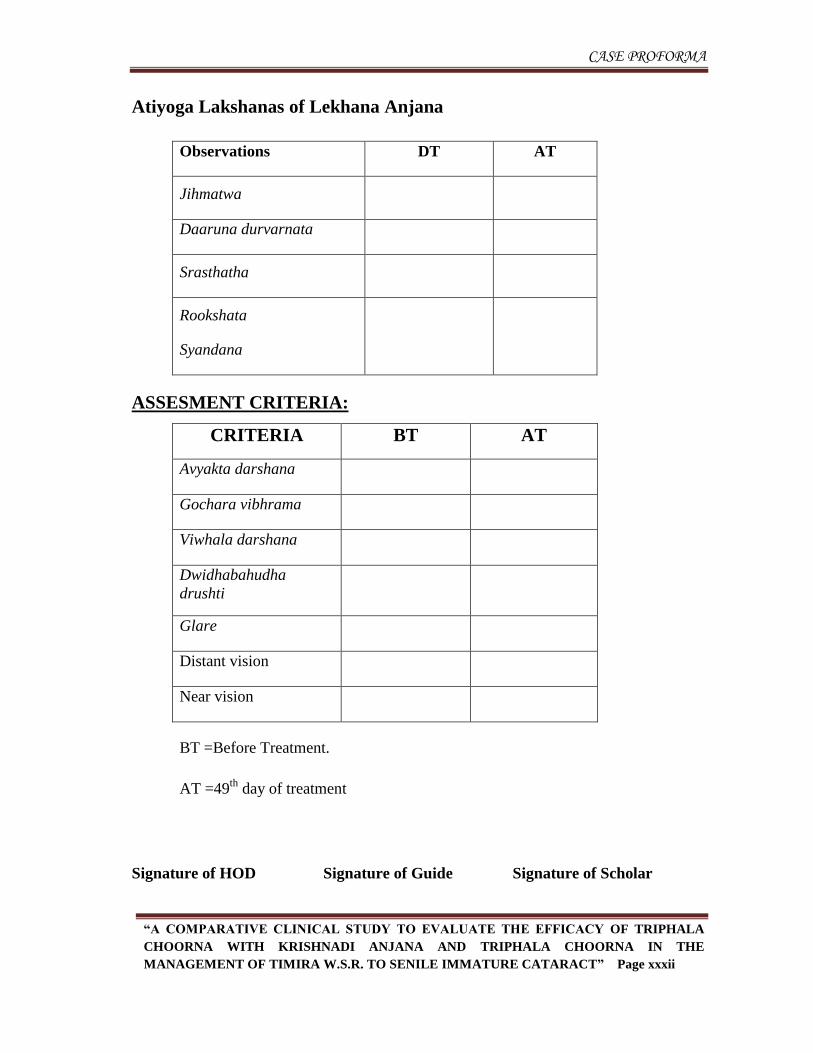
CASE PROFORMA
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page xxxii
Atiyoga Lakshanas of Lekhana Anjana
Observations DT AT
Jihmatwa
Daaruna durvarnata
Srasthatha
Rookshata
Syandana
ASSESMENT CRITERIA:
CRITERIA BT AT
Avyakta darshana
Gochara vibhrama
Viwhala darshana
Dwidhabahudha
drushti
Glare
Distant vision
Near vision
BT =Before Treatment.
AT =49th
day of treatment
Signature of HOD Signature of Guide Signature of Scholar
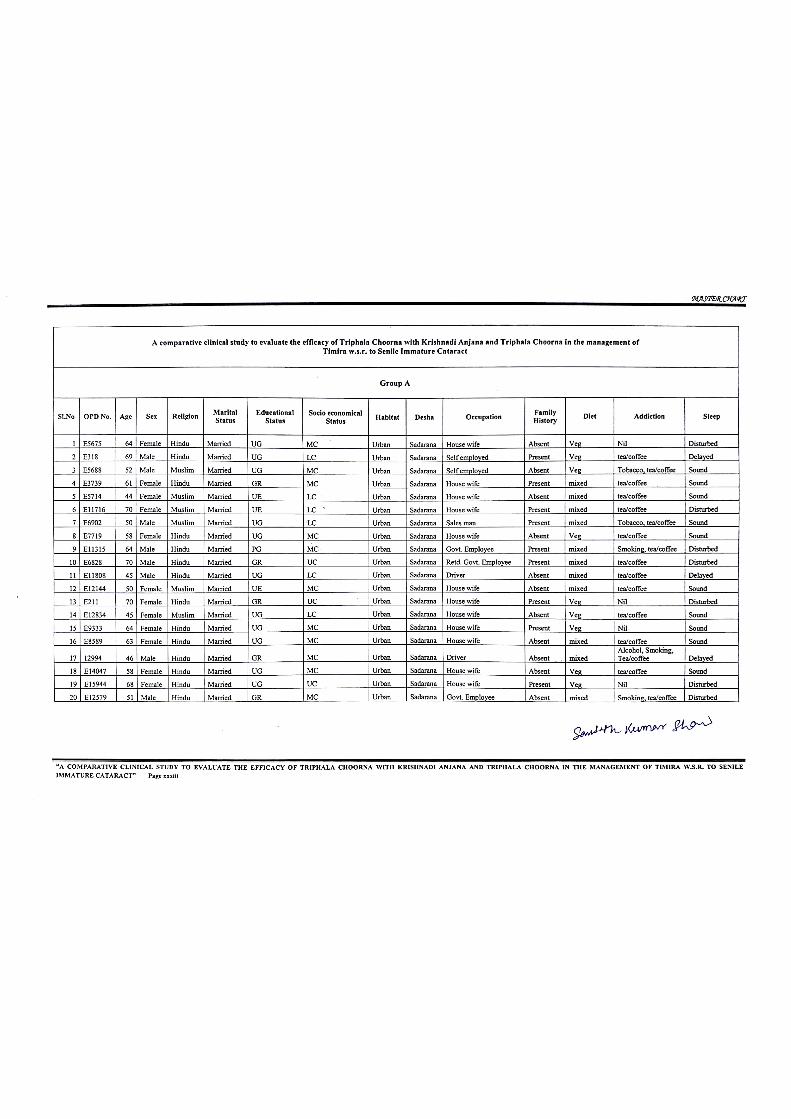
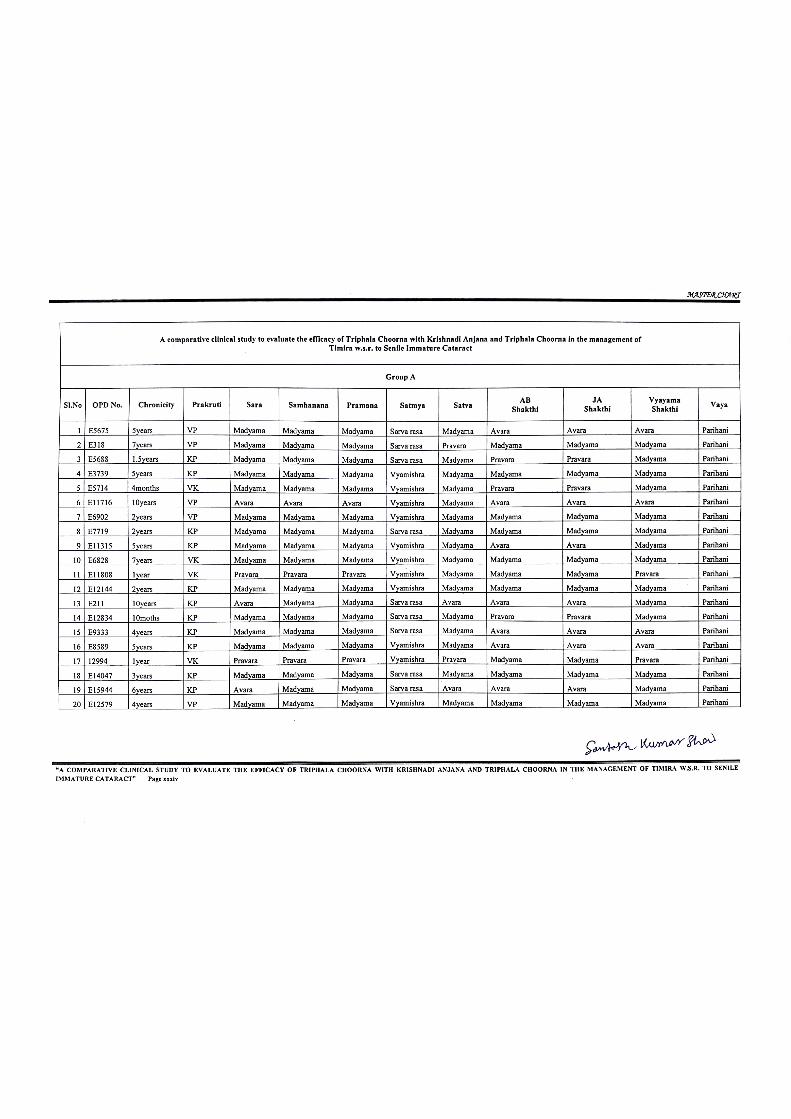
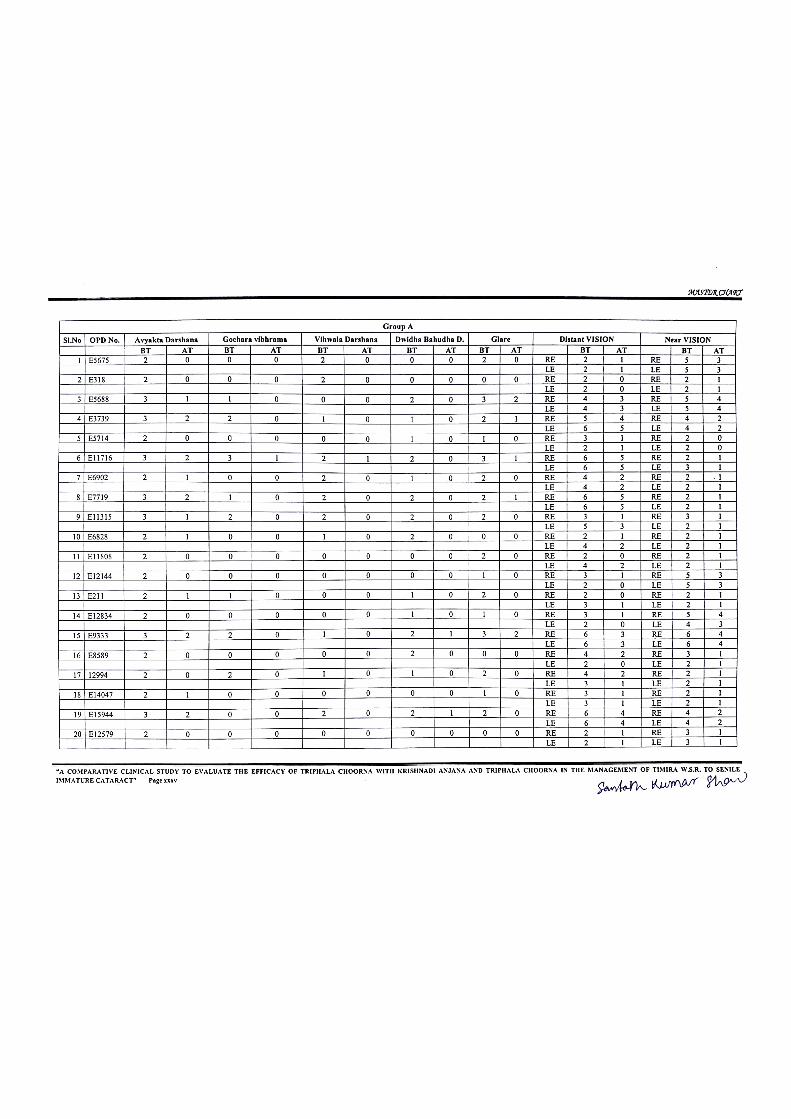
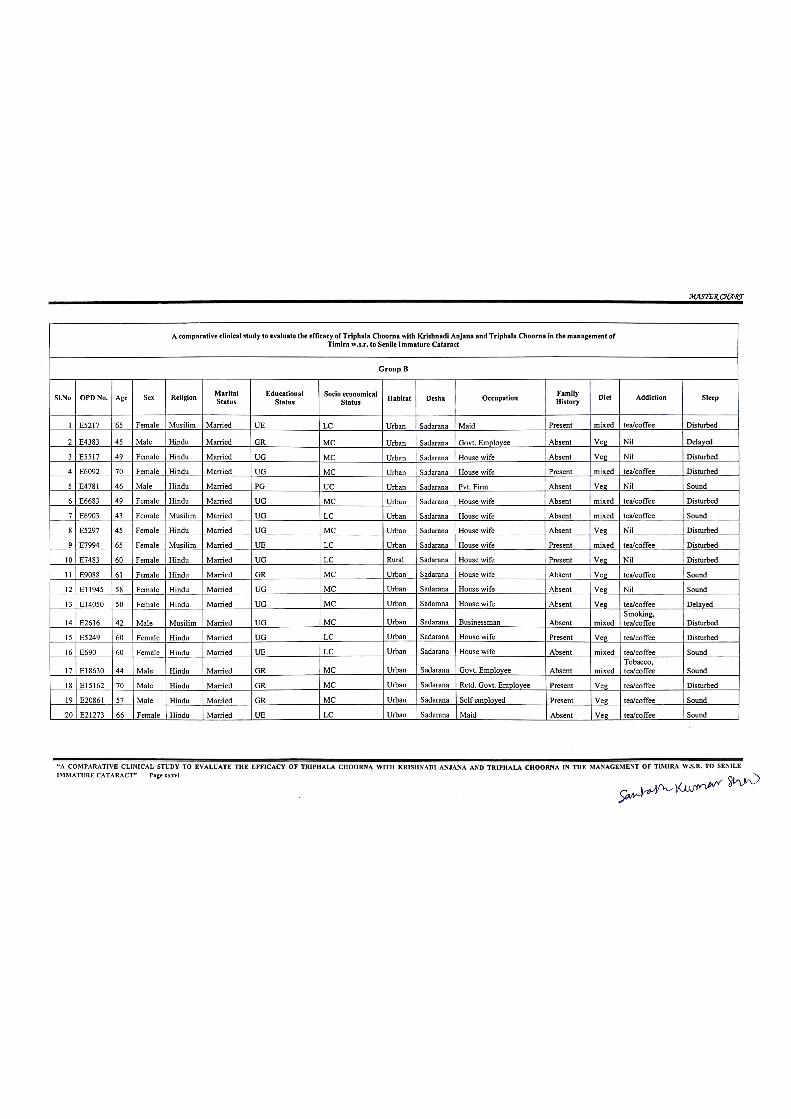
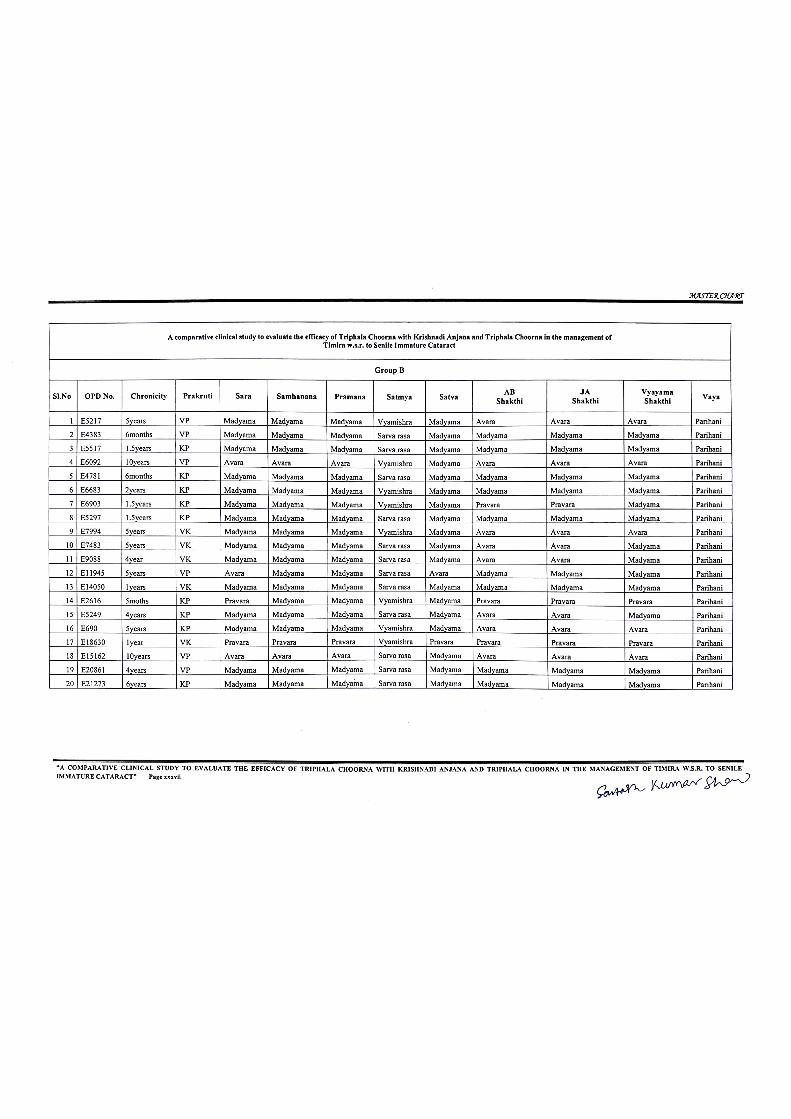
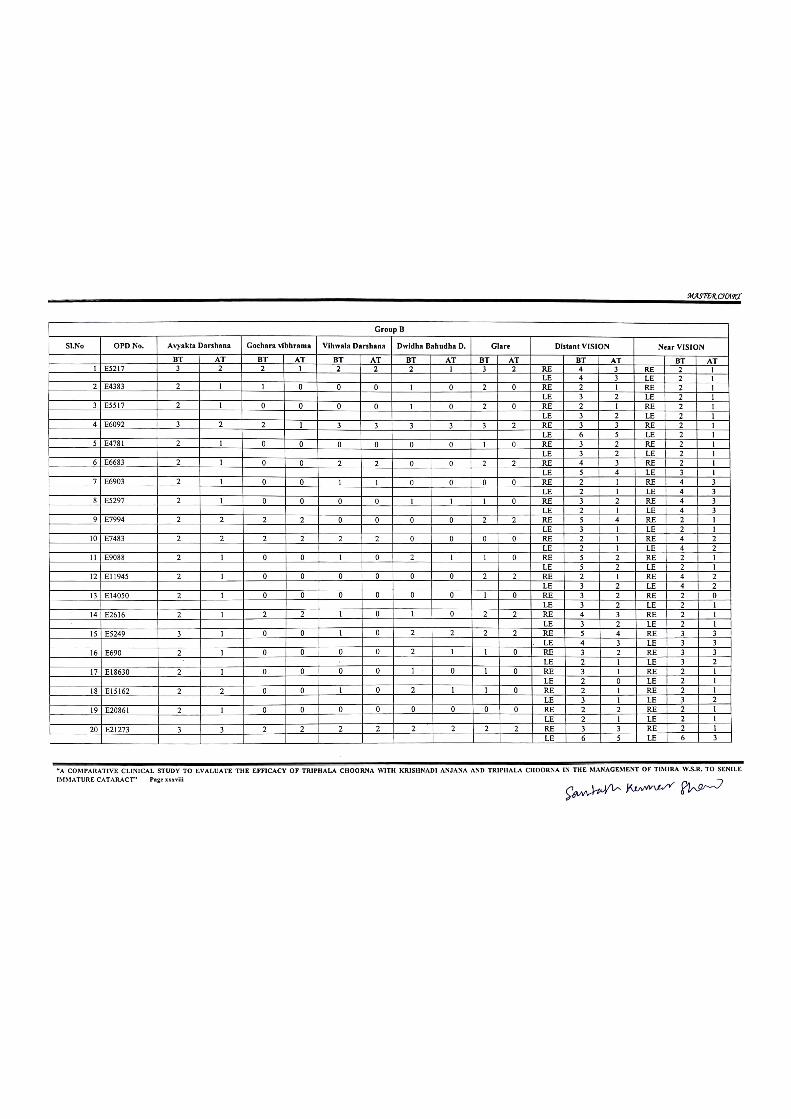
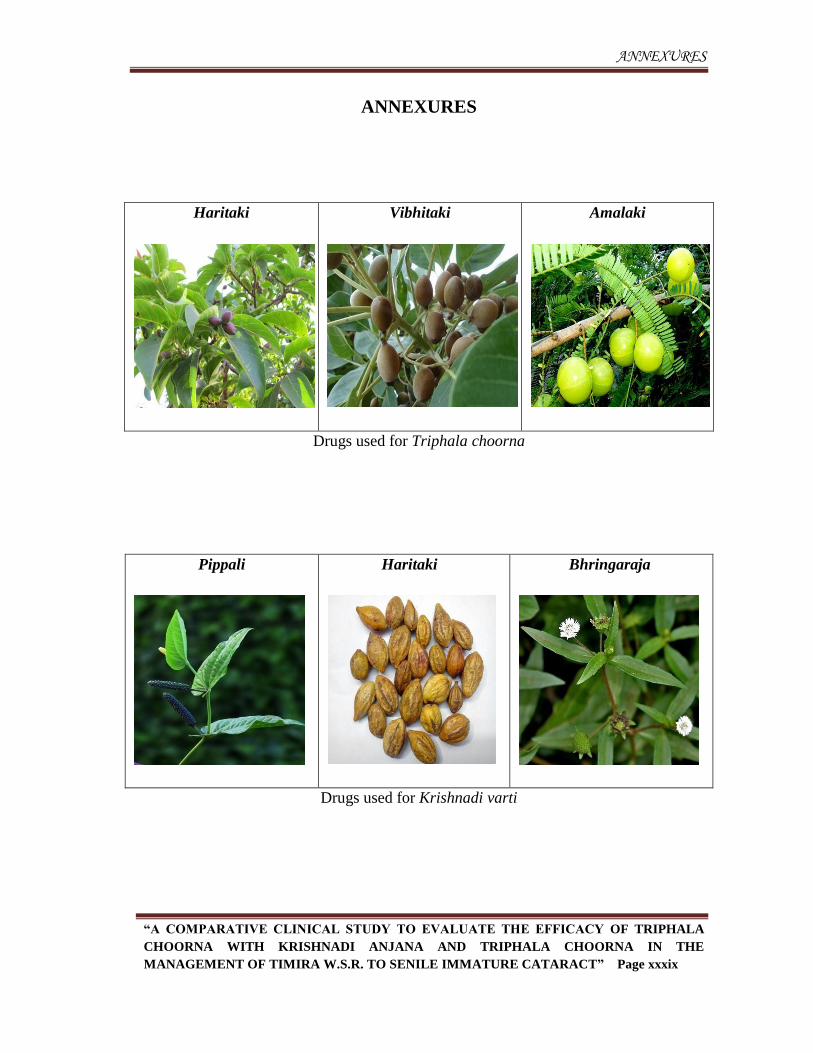
ANNEXURES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page xxxix
ANNEXURES
Haritaki
Vibhitaki
Amalaki
Drugs used for Triphala choorna
Pippali
Haritaki
Bhringaraja
Drugs used for Krishnadi varti

ANNEXURES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page xl
Goghrita used as anupana
Madhu for rubbing Anjana varti
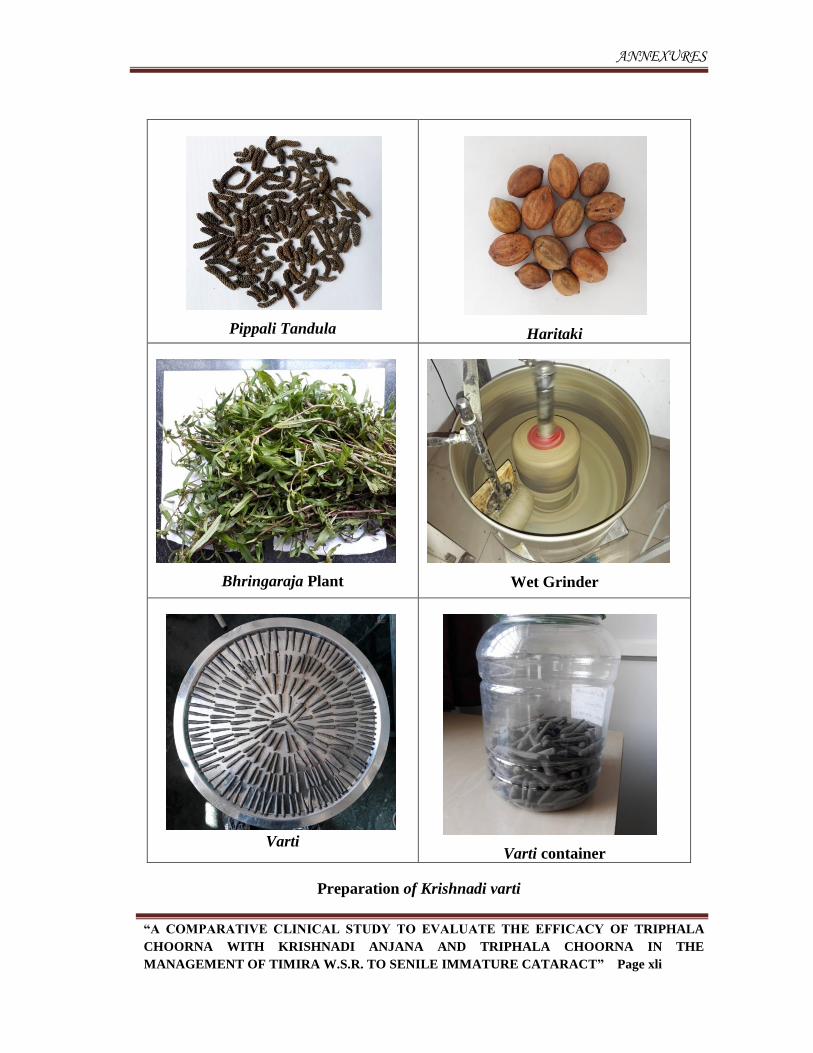
ANNEXURES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page xli
Preparation of Krishnadi varti
Pippali Tandula
Haritaki
Bhringaraja Plant
Wet Grinder
Varti
Varti container
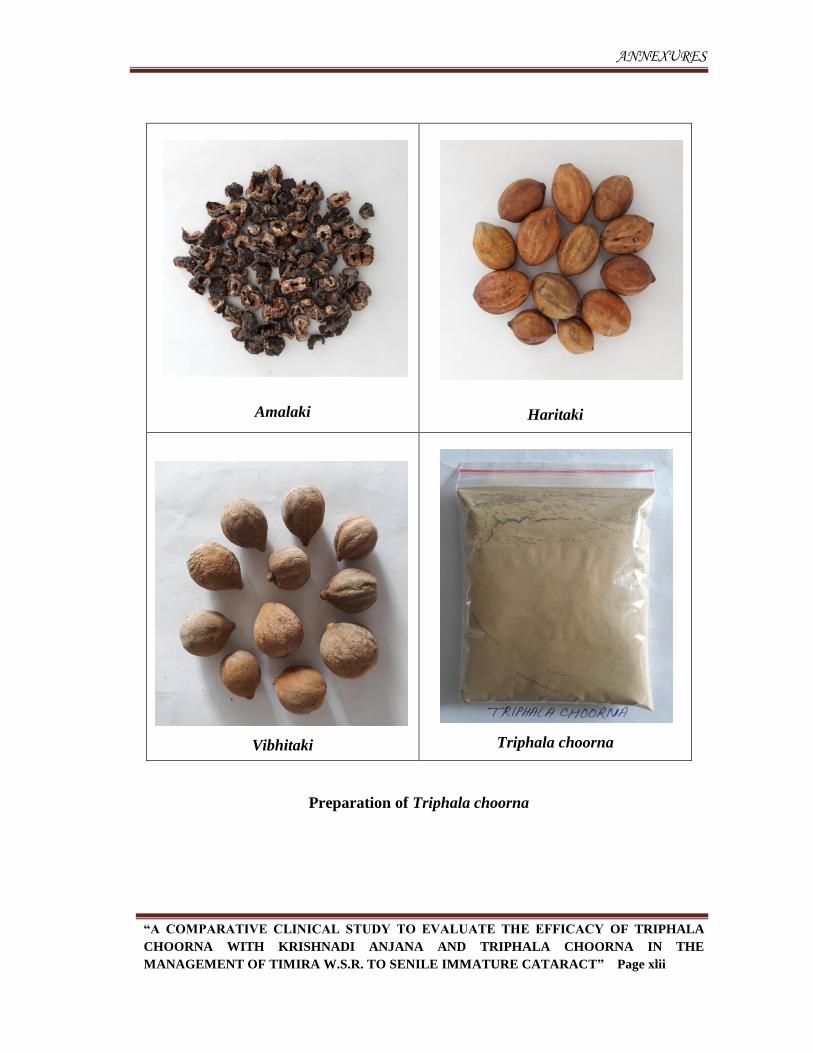
ANNEXURES
“A COMPARATIVE CLINICAL STUDY TO EVALUATE THE EFFICACY OF TRIPHALA
CHOORNA WITH KRISHNADI ANJANA AND TRIPHALA CHOORNA IN THE
MANAGEMENT OF TIMIRA W.S.R. TO SENILE IMMATURE CATARACT” Page xlii
Amalaki
Haritaki
Vibhitaki
Triphala choorna
Preparation of Triphala choorna