
Radiographs in periodonties - CiteSeerX
14
Journal of Clinical Periodontology: 1977: 4: 16-28 Key words: Periodontium - periotloiiial disease - radiographs. .Accepted tor publiculion: Oaober 2^, 1976, Review Article Radiographs in periodontics NiKLAUS P. LANGI AND ROGER W. 'School of Dental Medicine, University of Berne, Switzerland ^Department of Periodontics, School of Dentistry, University of Michigan, Ann Arbor, Michigan, U.S.A. Abstract. Intraoral radiographs are widely used in periodontal diagnosis and research. However, accurate radiographic interpretation is only possible with high quality images. Some of the technical and geometric variables to consider have been presented. Early periodontal lesions are not detected in radiographs. The amount of periodontal destruction in more advanced disease is generally underestimated. The accurate topography of periodontal pockets and the buccai and lingual aspects of the teeth cannot be visualized. Clinical probing is therefore a prerequisite for a complete periodontal diagnosis. How- ever, radiographs are a valuable adjunct for the periodontal diagnosis and the diagnosis of trauma from occlusion. With standardized systems, radiographs may furnish additional quantitative data in clinical research. Radiographs have been used in tnedicine since 1895 when Wilhelm Conrad Rontgen discovered the roentgen rays. One year later, the radiographic technique was used hy Morton in the diagnosis of periodontal disease. With the Introduction of the con- cept of focal infection, radiographs became commonly accepted in dentistry. In periodontics, radiographs have mainly heen used to assess the loss and destruction of alveolar hone and to confirm a clinical diagnosis of trauma from occlusion. Intra- oral radiographs are generally preferred due to tbeir sharpness and ability to demonstrate structural details (Barr 1966). When using radiographs in clinical diagnosis, it has to he kept in mind that a three-dimensional object is projected onto a two-dimensional plane resulting in a complex picture of different anatomical structures super- imposed on each other (Regan & Mitchell 1963). The purpose of this review is to present some of the technical and clinical aspects of dental radiography in order to facilitate correct interpretation of radiographs in the diagnosis and treatment of periodontal dis- ease. Technical Considerations Correct interpretation of radiographs is pos- sihle only if the image of the ohject is well defined and if there is not too much con- trast. Contrast is defined as the difference between various degrees of density making details visible (Fitzgerald 1950). It may he altered by varying the kilovoltage or the processing time (Fitzgerald 1950, Guldener & Beissner 1970) (Fig. la, c). The increase of the kilovoltage from 65 KV to 90 KV produces shorter, more penetrating rays, re- sulting in a film with a dull and almost flat character (Updergrave 1951). This is due to the fact that rays of shorter wave length are more evenly absorbed into all tissues (Fitz- gerald 1950).
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Radiographs in periodonties - CiteSeerX
Journal of Clinical Periodontology: 1977: 4: 16-28
Key words: Periodontium - periotloiiial disease - radiographs.
.Accepted tor publiculion: Oaober 2^, 1976,
Review Article
Radiographs in periodonticsNiKLAUS P. LANGI AND ROGER W .
'School of Dental Medicine, University of Berne, Switzerland^Department of Periodontics, School of Dentistry, University of Michigan,
Ann Arbor, Michigan, U.S.A.
Abstract. Intraoral radiographs are widely used in periodontal diagnosis and research.However, accurate radiographic interpretation is only possible with high quality images.Some of the technical and geometric variables to consider have been presented.
Early periodontal lesions are not detected in radiographs. The amount of periodontaldestruction in more advanced disease is generally underestimated. The accurate topographyof periodontal pockets and the buccai and lingual aspects of the teeth cannot be visualized.Clinical probing is therefore a prerequisite for a complete periodontal diagnosis. How-ever, radiographs are a valuable adjunct for the periodontal diagnosis and the diagnosisof trauma from occlusion. With standardized systems, radiographs may furnish additionalquantitative data in clinical research.
Radiographs have been used in tnedicinesince 1895 when Wilhelm Conrad Rontgendiscovered the roentgen rays. One yearlater, the radiographic technique was usedhy Morton in the diagnosis of periodontaldisease. With the Introduction of the con-cept of focal infection, radiographs becamecommonly accepted in dentistry.
In periodontics, radiographs have mainlyheen used to assess the loss and destructionof alveolar hone and to confirm a clinicaldiagnosis of trauma from occlusion. Intra-oral radiographs are generally preferred dueto tbeir sharpness and ability to demonstratestructural details (Barr 1966). When usingradiographs in clinical diagnosis, it has tohe kept in mind that a three-dimensionalobject is projected onto a two-dimensionalplane resulting in a complex picture ofdifferent anatomical structures super-imposed on each other (Regan & Mitchell1963).
The purpose of this review is to present
some of the technical and clinical aspectsof dental radiography in order to facilitatecorrect interpretation of radiographs in thediagnosis and treatment of periodontal dis-ease.
Technical Considerations
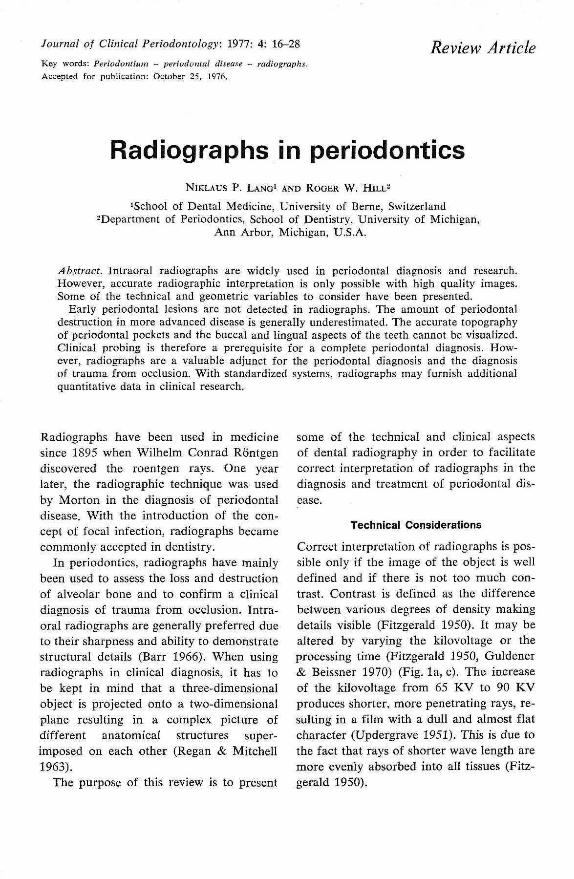
Correct interpretation of radiographs is pos-sihle only if the image of the ohject is welldefined and if there is not too much con-trast. Contrast is defined as the differencebetween various degrees of density makingdetails visible (Fitzgerald 1950). It may healtered by varying the kilovoltage or theprocessing time (Fitzgerald 1950, Guldener& Beissner 1970) (Fig. la, c). The increaseof the kilovoltage from 65 KV to 90 KVproduces shorter, more penetrating rays, re-sulting in a film with a dull and almost flatcharacter (Updergrave 1951). This is due tothe fact that rays of shorter wave length aremore evenly absorbed into all tissues (Fitz-gerald 1950).
RADIOGRAPHS IN PERIODONTICS 17
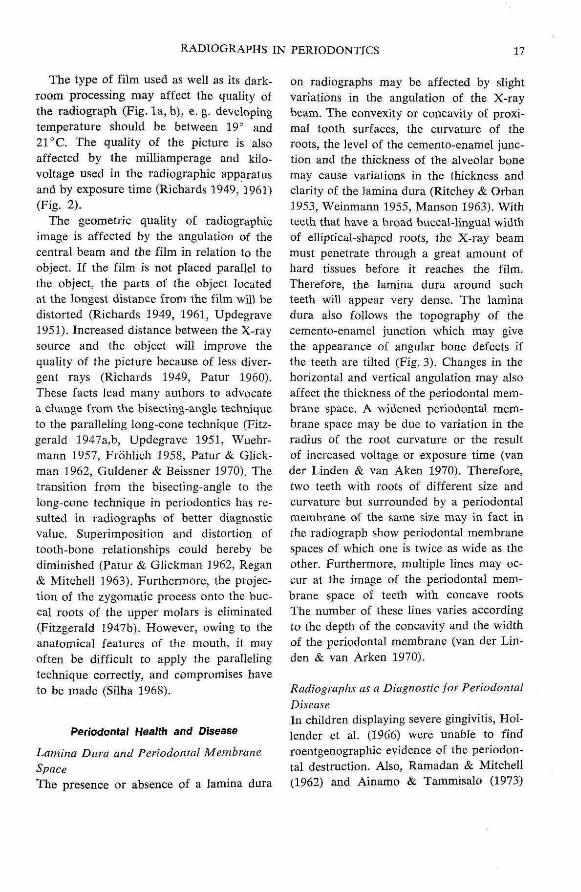
The type of film used as well as its dark-room processing may affect the quality ofthe radiograph (Fig. la, b), e. g. developingtemperature should be between 19" and21 °C. The quality of the picture is alsoaffected by the milhamperage and kilo-voltage nsed in the radiographic apparatusand by exposure time (Richards T949, 1961)(Fig. 2).
The geometric quality of radiographicimage is affected by the angulation of Ihecentral beam and the film in relation to theobject. If the film is not placed parallel tothe object, the parts of the object locatedat the longest distance from the film will bedistorted (Richards 1949, 1961, Updegrave1951). Increased distance between the X-raysource and tbe object will improve thequality of the picture because of less diver-gent rays (Richards 1949, Patur 1960).These facts lead many authors to advocatea change from the bisecting-angle techniqueto the parallehng long-cone technique (Fitz-gerald 1947a,b, Updegrave 1951, Wuehr-mann 1957, Frohlich 195S, Patur & Glick-man 1962, Guldener & Beissner J970). Thetransition from the bisecting-angle to thelong-cone technique in periodontics has re-sulted in radiographs of better diagnosticvalue. Superimposition and distortion oftooth-bone relationships could hereby bediminished (Patur & Glickman J962, Regan& Mitchell 1963). Furthermore, the projec-tion of the zygomatic process onto the buc-cal roots of the upper molars is eliminated(Fitzgerald 1947b). However, owing to theanatomical features of the mouth, it mayoften be difficult to apply the parallelingtechnique correctly, and compromises haveto be made (Siiha 1968).
Periodontal Health and Disease
Lamina Dura and Periodonlal MembraneSpaceThe presence or absence of a lamina dura
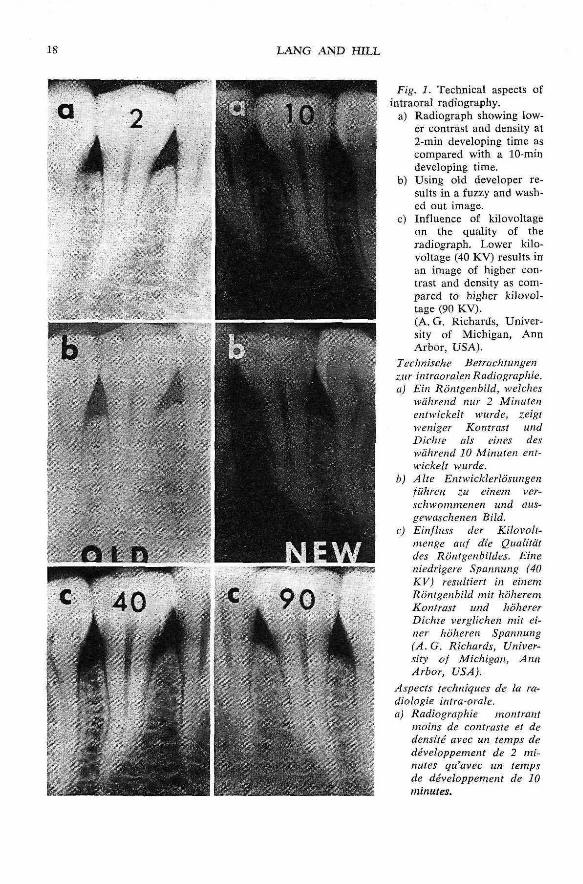
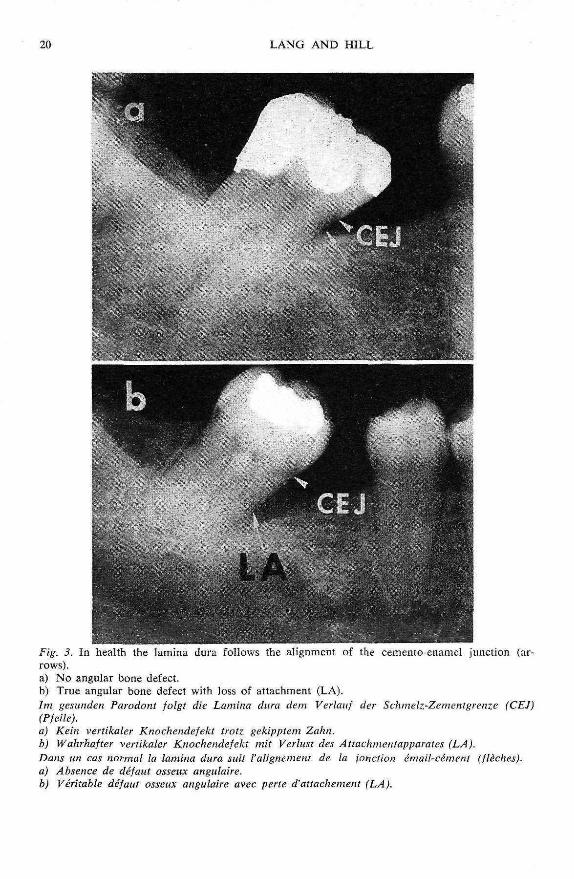
on radiographs may be affected by slightvariations in the angulation of the X-raybeam. The convexity or concavity of proxi-mal tooth surfaces, the curvature of theroots, the level of the cemento-enamel junc-tion and the thickness of the alveolar bonemay cause variations in the thickness andclarity of the lamina dura (Ritchey & Orban1953, Weinmann 1955, Manson 1963). Withteeth that have a broad buccal-lingual widthof elliptical-shaped roots, the X-ray beammust penetrate through a great amount ofhard tissues before it reaches the film.Therefore, the lamina dura around suchteeth will appear very dense. The laminadura also follows the topography of thecemento-enamel junction which may givethe appearance of angular bone defects ifthe teeth are lilted (Fig. 3). Changes in thehorizontal and vertical angulation may alsoaffect the thickness of the periodontal mem-brane space. A widened periodontal mem-brane space may be due to variation in theradius of the root curvature or the resultof increased voltage or exposure time (vander Linden & van Aken 1970). Therefore,two teeth with roots of different size andcurvature but surrounded by a periodontalmembrane of the same size may in fact inthe radiograph show periodontal membranespaces of which one is twice as wide as theother. Furthermore, multiple lines may oc-cur at the image of the periodontal mem-brane space of teeth with concave rootsThe number of these hnes varies accordingto the depth of the concavity and the widthof the periodontal membrane (van der Lin-den & van Arken 1970).
Radiographs as a Diagnostic for PeriodontalDiseaseIn children displaying severe gingivitis, Hol-lender et al. (1966) were unable to findroentgenographic evidence of tbe periodon-tal destruction. Also, Ramadan & Mitchell(1962) and Ainamo & Tammisalo (1973)
IS LANG AND HILL
aFig. J. Technical aspects of
intraoral radiography.a) Radiograph showing low-
er contrast and density at2-min developing time ascompared with a lO-mindeveloping time.
b) Using old developer re-sults in a fuzzy and wash-ed out image.
c) Influence of kilovoltageon the quahty of theradiograph. Lower kilo-voltage (40 KV) resuUs inan image of higher con-trast and density as com-pared to higher kilovol-tage (90 KV).(A. G. Richards, Univer-sity of Michigan, AnnArbor, USA).
Technische Betruchtungenzur intraoralen Radiograph'ie.a) Ein Ronlgenbild, welches
wahrend nur 2 Miiiutenentwickelt wurde, zeigtweniger Kontrast undDichse als eines deswahrend 10 Minuten ent-wickelt wurde.
b) A he Entwicklerlosungenfilhreti zu einem ver-schwommenen und aus-gewaschenen Bild.
c) Einfluss der Kilovolt-meitge auf die QualUiitdes Rontgenhiides. Eineniedrigere Spannung (40KV) resultiert in einemRontgenbild mit IioheremKontrast und hohererDichte verglichen mit ei-ner huheren Spannung(A.G. Richards, Univer-sity of Michigan, AnnArbor, USA).
Aspects techniques de la ra-diologie intra-orale.a) Radiographie montrant
inoins de contraste et dedensite avec un temps dedeveloppeinent de 2 mi-nutes gu'avec un tempsde developpement de 10minutes.
RADIOGRAPHS IN PERIODONTICS 19
Fig. 2. Influence of exposure time as radiographic image. Too high exposure time results in atoo dense image with high contrast resulting in "burn out" of the interproximal alveolar crest.(A. G. Richards, University of Michigan, Ann Arbor, USA).Einfhiss der Belichtung auf das Rontgenbild. Eine zii lange Belichtungszeit kann zu einemzu dichteu Bild mit sehr hohem Kontrast fuhren, was in sogenanntem "Ausbrennen" des Al-veolarkainmes resiiltiert (A. G. Richards, University of Michigan, Ann Arbor, USA).L'infhience dit temps d'exposition sur Vimage radiologique: une exposition trop longue donneitn image trop dense a haut contraste qui resulte en I'elimination de la Crete alveolaire inter-proximale (A. G. Richard, University of Michigan, Ann Arbor, USA).
were unabie to reveal early crestal boneloss in radiographs. From these studies itcan be concluded that radiographs are use-less in the assessment of early destructivechanges in the periodontium.
Several investigations have been carriedout in order to detertnine the amotmt ofbone resorption which can be visualized inradiographs. Lesions produced with burs indried specimens of canceiious hone werenot visible in radiographs unless the corti-
cal bone plates had been eroded extensivelyor penetrated (Goldman et al. 1957, Bender& Seltzer 1961a,b, Wengraf 1964). Like-wise, Ramadan & Mitchell (1962) foundthat interproximal defects produced in driedhuman skulls could not be seen in radio-graphs when the huccal and lingual corticalplates were intact. Defects on the buccaland lingual root surfaces could only be seenif the cortical plate was thick, and a highdegree of contrast existed between the de-
b) L'usage d'un vieux revelateiir donne une image floue et pale.cj L'lnfluence du kilovoltage sur la qualite de la radiographie: un kilovoltage bas (40 KV) re-
sulte en une image d'un contraste et d'une densite plus elevcs qu'avec un kilovoltage eleve(90 KV).(A. G. Richards, University of Michigan, Ann Arbor, USA).
LANG AND HILL
Fig. 3. In health the lamina dura follows the alignment of the cemento-enamel junction (ar-rows).a) No angular bone defect,b) True angular bone defect with loss of attachment (LA).Im gesunden Farodont folgt die Lamina dura dem Verlauf der Schmelz.-Zemenlgrenze (CEJ)(Ffeile).a) Kein vertikaler Knochendefekt trotz. gekipplem Zahn.h) Wahrhafter vertikaler Knochendefekt mit Verlusl des Attachmentapparates (LA).Dans un cas normal la lamina dura suit I'alignement de la jonclion email-cement (fleches).a) Absence de defaut osseux angulaire.b) Veritable defaut osseux angulaire avec perte d'attachement (LA).
RADIOGRAPHS IN PERIODONTICS 21
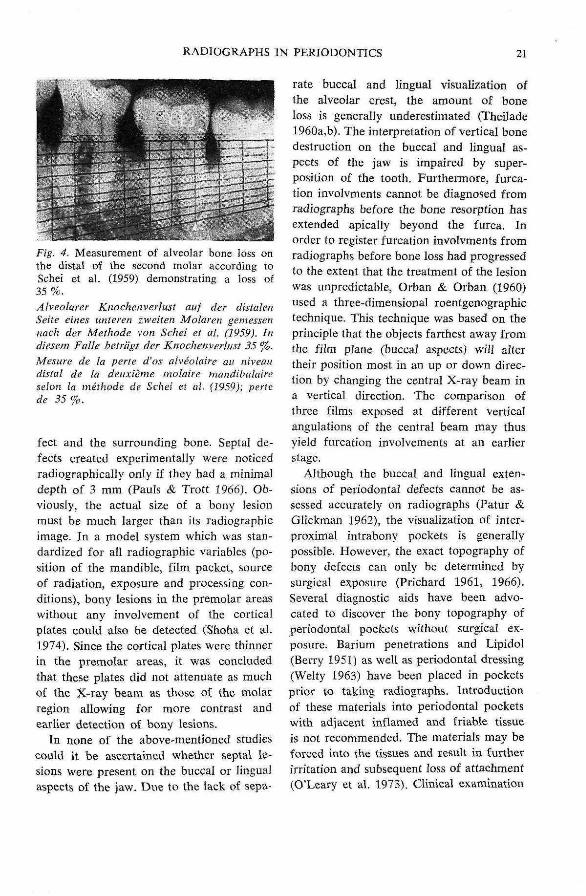
Fig. 4. Measurement of alveolar bone loss onthe distal of the second molar according toSchei et al. (1959) demonstrating a !oss of35%.Alveolarer Knochenverlust auf der dista!enSeite eines unieren iweiten Molareu gemesserinach der Melhode von Schei et al. (1959). Indiesem Falle hetrligt der Knochenverlust 35 %.
Mesure de la perte d'os alveola'ire an niveaiidistal de (a deiixieme molaire mandlbidaireselon la methode de Schei el al. (1959): pertcde 35%.
feet and the surrounding bone. Septa! de-fects created experimentally were noticedradiograph!cally only if lhey had a minimaldepth of 3 mm (Pauls & Trott 1966). Ob-viously, Ihe actual size of a bony lesionmust be much Jarger than its radiographicimage. In a model system which was stan-dardized for all radiographic variables (po-sition of the mandible, film packet, sourceof radiation, exposure and processing con-ditions), bony lesions in the premolar areaswithout any involvement of the corticalplates could also be detected (Shoha et al.1974). Since the cortical plates were thinnerin the premolar areas, it was coacludedthat these plates did not attenuate as muchof the X-ray beam as those of the n:iolarregion allowing for more contrast andearlier detection of bony lesions.
In none of the above-mentioned studiescould it be ascertained whether septal le-sions were present on the buccal or lingua!aspects of the jaw. Due to the lack of sepa-
rate buccal and lingual visualization ofthe alveolar crest, the amount of boneloss is generally underestimated (Theilade1960a,b). The interpretation of vertical bonedestruction on the buccal and lingual as-pects of the jaw is impaired by super-position of the tooth. Furthermore, furca-tion involvments cannot he diagnosed fromradiographs before the bone resorption hasextended apically beyond the furca. Inorder to register furcation involvments fromradiographs before bone loss had progressedto the extent that the treatment of the lesionwas unpredictable, Orban & Orban (1960)used a three-dimensional roentgenographictechnique. This technique was based on theprinciple that the objects farthest away fromthe film plane (buccai aspects) will altertheir position most in an up or down direc-tion by changing the centra! X-ray beam ina vertical direction. The comparison ofthree films exposed at different verticalangulations of the central beam may thusyield furcation involvements at an earlierstage.
Although the bucca! and lingua! exten-sions of periodonta! defects cannot be as-sessed accurately on radiographs (Patur ScGlickman 1962), the visualization of jnter-proximal intrabony pockets is generallypossible. However, the exact topography ofbony defects can only be determined bysurgical exposure (Prichard 1961, 1966).Several diagnostic aids have been advo-cated to diseover the bony topography ofperiodontal pockets without surgical ex-posure. Barium penetrations and Lipidol(Berry 1951) as well as periodontal dressing(Welty 1963) have been placed in pocketsprior to taking radiographs. Introductionof these materials into periodontal pocketswith adiacent inflamed and friable tissueis not recommended. The materials may beforced into the tissues and result in furtherirritation and subsequent loss of attachment(O'Leary et al. 1973). Clinical examination
LANG AND HILL
with a periodontal probe is a safer andmore effective means of determining thedepth and topography of periodontal pock-ets.
Another method used io determinepocket depth is the insertion of calibratedsilver points into the pocket prior to ex-posing the X-ray film. This technique maybe useful to evaluate intrabony pockets andto locate fistulous tracts and periodontalabscesses in relation to the teeth (Hirsch-feld 1953).
In order to visualize three-dimensionalchanges in alveolar crest height, a stereo-scopic technique was introduced (Berg-hagen & Hjelmstrom 1956a,b, Berghagen &Blom ]961). Two films of the same objectwere exposed with different horizontalangulations. The radiographs were then ob-served with stereoscopic viewers. Super-imposed detail may be distinguished anddefinitions improved with this technique.
The diagnosis of absence or presence ofcalculus deposits should not be based onradiographlc interpretation, since smalldeposits are not visible in radiographs (All-
dritt 1954). Radiographs are useful in de-tecting defective margins of restorations(Prichard 1961). However, if there is ex-cessive vertical or horizontal angulation ofthe central X-ray beam, there is a risk ofunderestimating, but not overestimating thesize of the defective margin (Bjorn et al.1973, Haakonson et al. 1973). This empha-sizes the importance of precise parallelingradiographic technique for periodontal dia-gnosis.
Radiographs in Evaluation of PeriodontalTherapy and in Epidemiological Research
Standardization of RadiographsResults of periodontal therapy may incor-rectly be evaluated as successful if the pre-operative radiograph is under-angulated orover-exposed compared to that of the post-operative film (Wuehrmann 1957) (Fig. 2).Several devices have been suggested in or-der to standardize pre- and postoperativeradiographs. Obviousjy, the technical speci-fications of the film and its exposure andprocessing have to be the same. One of
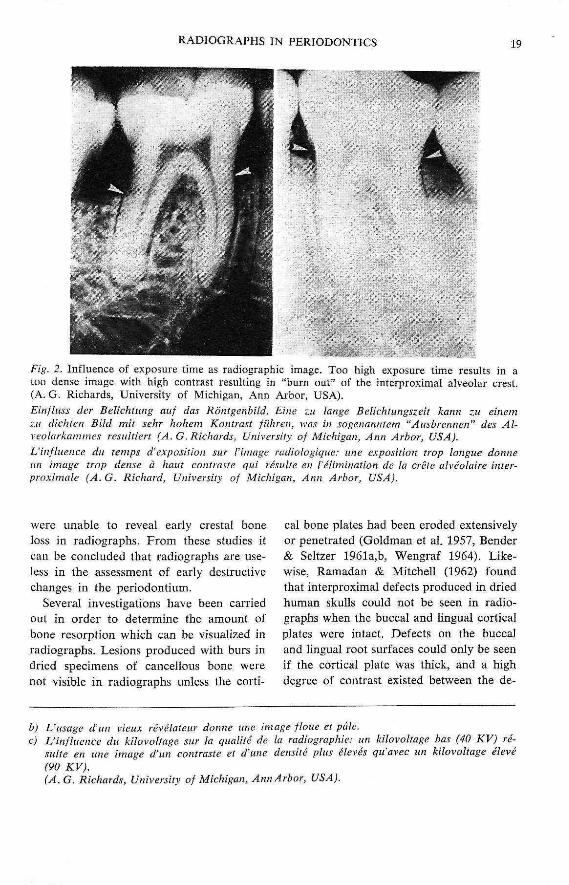
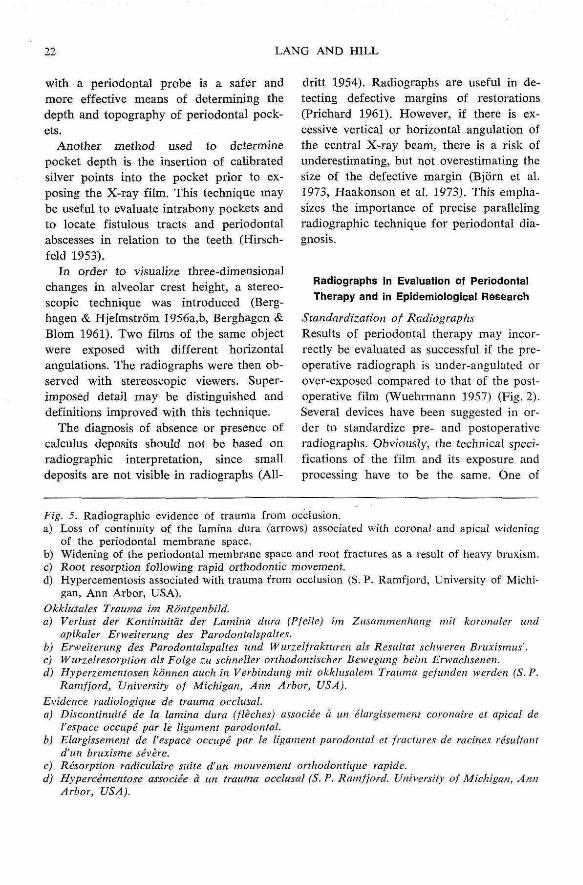
Fig. 5. Radiographic evidence of trauma from occlusion.a) Loss of continuity of the lamina dura (arrows) associated with coronal and apical widening
of the periodontal membrane space.b) Widening of the periodontal memhrane space and root fractures as a result of heavy bruxism.c) Root resorption fdWow'mg rapid orthodontic movement.d) Hypercementosis associated with trauma from occlusion (S. P. Ramfjord, University of Michi-
gan, Ann Arbor, USA).Okklusales Trauma im RdntgenhiJd.a) Verlusl der Kontinuitdt der Lamina dura (Pfeile) im Zusaminenhang init koronaler iind
apikajer Erweiterung des Parodontalspaltes.b) Erweiterung des Parodontalspaltes und Wurzelfrakture/i ah Resultat schweren Bruxismus'.c) Wurzelresorption ah Folge zu schneller orthodonthcher Bewegung beini Erwachsenen.d) Hyperz.ementosen konnen auch in Verbindung mit okkliisalein Trauma gefunden werden (S. P.
Ramfjord, University of Michigan, Ann Arbor, USA).Evidence radiologique de trauma occlusal.a) Discontinuite de la lamina dura (fleches) associee u iin elarghsenicnt. coronaire et apical de
I'espace occupe par le ligament parodontal.b) Elargissement de I'espace occupe par le ligament parodontat et fractures de racines resullani
d'un bruxisme severe.c) Resorption radiculaire suite d'un mouvement orthodontique rapide.d) Hypercementose associee a uii trauma occlusal (S. P. Ramfjord. Universily of Michigan, Ann
Arbor, USA).
RADIOGRAPHS IN PERIODONTICS 23
d
. 5 •

.24 LANG AND HILL
the first devices for identical exposures wasdesigned by Benkow in 1956. This systemconsisted of a tray containing a thermo-plastic compound impression of the occlusaisurfaces in the area to be radiographed. Thefilm was placed in the tray perpendicularto a steel bar which was parallel to theX-ray beam. The bar also assured an iden-tical distance between the film plane andthe cone of the X-ray machine. Using thesame compound impression for the pre- andpostoperative exposures, it was possible toobtain identical pictures. Similar deviceshave been constructed by Benkow (1960),Medwedeff et ai. (1962), Dalitz (1964),Gilbers & Hanan (1968) and Puckett (1968).Recently Rosling et al. (1975) presented adevice based on a similar principle for peri-odic reproducible radiographs. It consistedof an acrylic splint with five quadrangularmetal tubes. A metal rod connecting thesplint with the X-ray cone can be inserted.The splint has five paired tracks on the oralsurface serving as film holders to alloworthoradial projection of either the pre-molar, canine or the incisor regions.
Quantitation of Bone Loss
Several attempts have been made to objec-tively determine the amount of bone lossin advanced cases of periodontal disease.One of the first methods was developed bySchei et al. (1959) who determined thepercentage of alveolar bone on either amesial or distal surface of a tooth. Usinga plastic ruler, they assessed the boneheight relative to the distance betweeti theapex of the root and the "normal" levelof the alveolar crest defined as 1 mm apicalto the cemento-enamel junction (Fig. 4).This method has been modified by Engel-berger et al. (1963) who used the totaltooth length minus 1 mm as the reference.The "normal" bone level was thus between60-70 % of the total length.
Bjdrn and co-workers (1969) modifiedtheir original determination system whichalso based on total tooth length. They intro-duced a scale of 20 units for the total lengthof the tooth as opposed to only 4 scaleunits in their original scoring system (Bjorn& Holmberg 1966, Bjorn et al. 1967).
In an attempt to quantify changes in themineral content of interalveolar bone septa,Omnell (1957) developed a photometricsystem. He compared the density of thebone with a reference object consisting ofan aluminum step wedge. The amount ofradiation transmitted through the radio-graph was compared with the transmissionof radiation through the aluminum stepwedge. With this method is was possible tostudy the healing of interalveolar septalbone following injury.
Several studies have been performed toevaluate the long-term effect of periodontaltherapy (Ramfjord et al. 1973). Radio-graphic assessment of bone loss was posi-tively correlated with tooth mobility, pocketdepth and the level of attachment (Kellyet al. 1975). Stiomi et al. (1968) determinedthe bone height on the basis of radiographicmeasurements, probing prior to and aftersurgical exposure of the bone. They dem-onstrated that there was no significantdifference between radiographic and clinicalmeasurements. These results indicate thatradiographs are useful for an accurateevaluation of the level of alveolar bone, butthat clinical measurements of the attach-ment level yield an equally accurate assess-ment of the periodontal destruction. Sincemeasurements on radiographs require moretime, equipment and money, it is reasonableto assess periodontal destruction in clinicaltrials on the basis of clinical attachmentlevel measurements (Ramfjord 1959, Gla-vind & Loe 1967).
Radiographs have also been used to eval-uate the results of reattachment procedures.The regeneration of the lamina dura asso-
RADIOGRAPHS IN PERIODONTICS 25
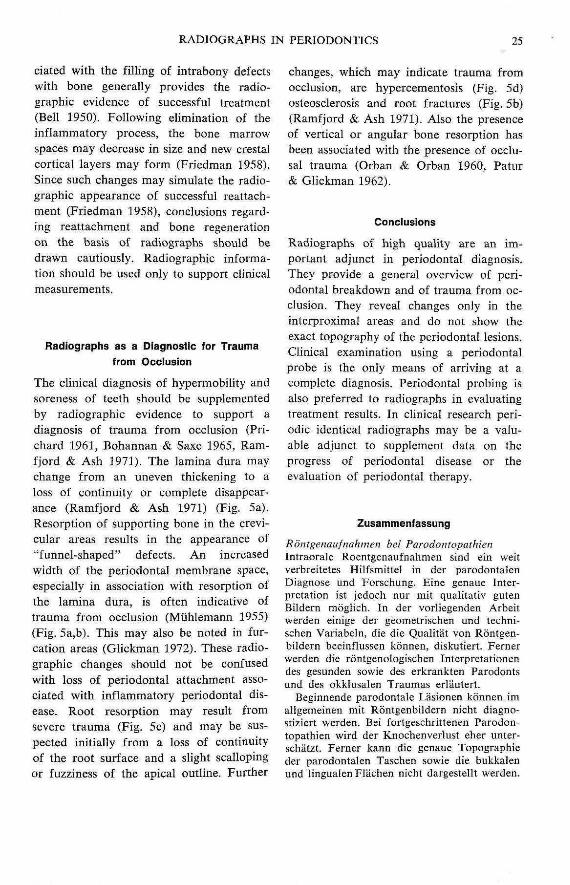
ciated with the filling of intrabony defectswith bone generally provides the radio-graphic evidence of successful treatment(Bell 3950). Following elimination of theinflammatory process, the bone marrowspaces may decrease in size and new crestalcortical layers may form (Friedman 1958).Since such changes may simulate the radio-graphic appearance of successful reattach-ment (Friedman 1958), conclusions regard-ing reattachment and bone regenerationon the basis of radiographs should bedrawn cautiously. Radiograpbic informa-tion should be used only to support clinicalmeasurements.
Radiographs as a Diagnostic for Traumafrom Occiusion
The clinical diagnosis of hypermobility andsoreness of teeth should be supplementedby radiographic evidence to support adiagnosis of trauma from occlusion (Pri-chard 1963, Bohannan & Saxe 3965, Ram-fjord & Ash 3971). The lamina dura maychange from an uneven thickening to aloss of continuity or complete disappear-ance (Ramfjord & Ash 1971) (Fig. 5a).Resorption of supporting bone in the crevi-cular areas results in the appearance of"funnel-shaped" defects. An increasedwidth of the periodontal membrane space,especially in association with resorption ofthe lamina dura, is often indicative oftrauma from occlusion (Muhlemann 1955)(Fig. 5a,b). This may also be noted in fur-cation areas (Giickman 1972). These radio-graphic changes should not be confusedwith loss of periodontal attachment asso-ciated with inflammatory periodontal dis-ease. Root resorption may result fromsevere trauma (Fig. 5c) and may be sus-pected initially from a loss of continuityof the root surface and a slight scallopingor fuzziness of the apical outline. Further
changes, which may indicate trauma fromocclusion, are hypercementosis (Fig. 5d)osteosclerosis and root fractures (Fig. 5b)(Ramfjord & Ash 1971). Also the presenceof vertical or angular bone resorption hasbeen associated with the presence of occlu-sal trauma (Orban & Orban 1960, Patur& Glickman 1962).
Conciusions
Radiographs of high quality are an im-portant adjunct in periodontal diagnosis.They provide a general overview of peri-odontal breakdown and of trauma from oc-clusion. They reveal changes only in theinterproxima! areas and do not show theexact topography of the periodontal lesions.Clinical examination using a periodontalprobe is the only means of arriving at acomplete diagnosis. Periodontal probing isalso preferred to radiographs in evaluatingtreatment results. In clinical research peri-odic identical radiographs may be a valu-able adjunct to supplement data on theprogress of periodontal disease or theevaluation of periodontal therapy.
Zusammenfassung
Rontgenaufnahinen bei FarodontopathienIntraorale Roentgenaufnahmen sind ein weitverbreitetes HilfsmiEtel in der parodontaienDiagnose und Forschting. Eine genaue Inter-pretation ist jedoch nur mit qualitativ gutenBsldern tnoglich. In der vorliegenden Arbeitwerden einige der geometrischen und techni-schen Variabeln, die die Qualitat von Rontgen-bildern beeinflussen kdnnen, diskutiert. Fernerwerden die rontgenologischen Interpretationetides gesunden sowie des erkrankten Parodontsund des okkiusalen Traumas erlautert.
Beginnende parodontale Lasionen konnen imaiigemeinen mit Rontgenbiidern nicht diagno-stiziert werden. Bei fortgeschrittenen Parodon-topathien wird der Knochenverlust eher unter-schatzt. Eerner kann die genaue Topographieder parodontaien Taschen sowie die bukkalenund lingualenFliichen nicht dargestellt werden.
26 LANG AND HILL
Die klinischeUntersuchung mit der Parodontal-sonde ist deshalb absolute Bedingung fiir einegenaue Diagnose der Parodontopathien. DieRontgenbilder Hefem aber einen recht gutentlbersichtshefund und bilden eine gute Ergan-zung zur klinischen Diagnose der Parodontal-erkrankungen und des okklusalen Traumas.Rontgenbilder, die In standardisierten Systemenaufgenommen worden sind, konnen auch zu-satzliche quantitative Resultate in der klini-schen Forschung vermitteln.
Les radiographies en parodontologieLes radiographies intra-orales sont courammentutilisees pour le diagnostic et la rechercheparodontologique. Une interpretation exacten'est possible qu'avec des images de hautequalite. Quelques variables geometdques ettechniques qui infiuencent la qualite des radio-graphies sont discutees. L'interpretation radio-logique du ligament parodontal sain et maladeest evaluee.
Au debut, les lesions parodontales ne peu-vent pas etre diagnostiquees par des radio-graphies. Avec des parodontites plus avanceesla perte de I'os est generalement sous-estimee.En outre, la topographie exacte des pochesparodontates et les surfaces buccales et oralesne sont pas visibles pour le diagnostic. C'estpoiirquoi l'examen clinique avec une sondeparodontale est indispensable pour le diagnos-tic exact des parodontopathies. Les radio-graphies peuvent, par contre, completer etverifier le diagnostic clinique d'une parodon-tite et d'un trauma occlusal. Si les radio-graphies sont executees d'une maniere stan-dardisee, elles peuvent fournir des resultatsquantitatifs dans la recherche ciinique.
References
Ainamo, J. & Tammisalo, E. H. (1973) Com-parison of radiographie and clinical signsof early periodontal disease. ScandinavianJournal of Dental Research 81, 548-552.
AUdritt, W. A. S. (1954) Radiology in peri-odontal practice. Dental Practitioner 5, 123-133.
Barr, J. H. (1961) The scope and iimitationsof roentgenography as a diagnostic proce-dure. Dental Clinics of North America,pp. 379-389, July. Philadelphia: W. B. Saun-ders.
Barr, J. H. (1966) The information yield from
radiographs. Oral Surgeiy, Oral Medicine,Oral Pathology 11, 174-182.
Bell, D. G. (1950) The periodontal lesion ILA roentgenographic evaluation of treatedperiodontal cases. A biological approach.Journal of Periodontology 21, 70-78.
Bender, I. B. & Seltzer, S. (1961a) Roentgeno-graphic and direct observation of experimen-tal lesions in bone: 1. Journal of the Ameri-can Dental Association 62, 152-160.
Bender, L B. & Seltzer, S. (1961h) Roentgeno-graphic and direct observations of experi-mental lesions in bone: 2. Journal of theAmerican Denial Association 62, 708-716.
Benkow, H. H. (1956) Periodisk-identiske ogstereoskopiske intraoraie r0ntgenopptak. DenNorske Tannlaegetidende 66, 239-255.
Benkow, H. H. (1960) New principle for clini-cal roentgenographic tooth measurement.Odontologisk Tidskrift 68, 423-449.
Berghagen, N. & Hjeimstrom. P. (1956a) Three-dimensional intraoral radiography. ActaOdontologica Scandinavica 14, 189-220.
Berghagen, N. & Hjeimstrom, P. (1956b) Radio-graphic measurement of hone changes in thealveolar Hmbus in a case of marginal peri-odontal disease. Acta Odontologica Scan-dinavica 14, 221-229.
Berghagen, N. & Biom, K. (1961) Periodontaipocket studied hy three-dimensional radiog-raphy. Dental Practitioner 12, 10-20.
Berry, H. M. (1951) Radiopaque materials inthe roentgenographic interpretation of peri-odontal lesions: a preliminary report. Jour-nal of the American Dental Association 43,278-284.
Bjorn, H. & Holmberg, K. (1966) Radiographiedetermination of periodontal bone destruc-tion in epidemiological research. Odonto-logisk Revy 17, 232-250.
Bjorn, H., Hoimberg, K. &, Nylander, G.(1967) Maxillary sinus in periodontal dis-ease. A clinical and radiographie investiga-tion. Odontologisk Revy 18, 83-114.
Bjorn, H., Hailing, A. & Thyberg, H. (1969)Radiographie assessment of marginal boneloss. Odontologisk Revy 20, 165-179.
Bjorn, H., Haakansson, H. & Johansson, O.(1973) Roentgenographic assessment of over-hanging margins of dental restorations. I.Significance of variations in longitudinalprojection. Odontologisk Revy 24, 127-140.
Bohannan, H. M. & Saxe, S. R. (1965) Peri-odontal roentgenographie interpretation.Journal of the Tennessee Dental Association45, 406-416.
RADIOGRAPHS IN PERIODONTICS 27
Dalitz, G. D. (3964) Variation of apparatus forobtaining serial roentgenograms. AustralianDental Journal 9, 29-31.
Engelberger, A., Rateitschak, K. H, & Mar-thaler, T. M. (1963) Zur Messung des paro-dontaien Knochenschwundes (Fehierbestim-mung einer Messmethode). Helvetica Odon-lologlca Acta 7, 34-38.
Fitzgerald, G. M. {1947a) Dental roentgeno-graphy. I. An investigation of adumbrationor the factors that control geometric un-sharpness. Journal of the Amerlcafi DentalAssociation 34, 1-20.
Fitzgerald, G. M. (1947b) Dental roentgeno-graphy. 11. Vertical angulation film place-ment and increased object-film distance.Journal of the American Dental Association34, 160-170.
Fitzgerald, G. (1950) Dental roentgenography.IV. The voltage factor (KVP). Journal ofthe American Dental Association 41, 19-28.
Friedman, N. (1958) Reattachment and roent-genograms. Journal of Periodontology 29,98-110.
Frohlich, E. (1958) A comparison between ana-tomical and radiographic interpretation ofmarginal periodontal disease. Paradontologic32, 89-100.
Gilbers, R. R. & Hanan, L. (1968) Duplicationand quality control for intraoral roentgeno-graphic use in clinical periodontics. OralSurgery, Oral Medicine, Oral Pathology 26,31-38.
Glavind, L. & Loe, H. (]967) Errors in theciinical assessment of periodontal destruction.Journal of Periodoutal Research 2, 180-184.
Glickman, I. (1972) Clinical Periodontology,4th ed., pp. 336-339. Philadelphia: W. B.Saunders.
Goldman, H. M., Miilsap, J. S. & Brenman,H. S. (1957) Origin of registration of thearchitectural pattern, the lamina dura, andthe alveolar crest in the dental radiograph.Oral Surgery, Oral Medicine, Oral Pathologyid, 749-758'
Guldener, P. H. A. & Beissner, H. (1970)5 Jahre Erfahrung mit der Langtubus-Roent-gentechnik. Schweizerischc. Monatsschrift fUrZahnhcilkunde 80, 139-162.
Haakansson, H., Johansson, O. & Bjorn, H.(1973) Roentgenographic assessment of over-hanging margins of dental restorations. II.Significance of variations in vertical angula-tion of the roentgen beam. OdontologiskRevy 24, 245-256.
Hirschfeld, L. (1953) A calibrated silver point
for periodontal diagnosis and recording.Journal of Periodontology 24, 94-98.
Hollender, L., Lindhe, J. & Koch, G. (1966)A roentgenographic study of clinical healthyand inflamed periodontal tissues in children.Journal of Periodontai Research I, 146-151.
Keiiy, G. P., Cain, R. J., Knowles, J. W.,Nissle, R. R., Burgett, F. G., Shick, R. A. &Ramfjord, S. P. (1975) Radiographs in clini-cal periodontal trials. Journal of Periodon-tology 46, 381-386.
Manson, J. D. (1963) The lamina dura. OralSurgeiy, Oral Medicine, Oral Pathology 16,432^38.
Medwedeff, F. M., Knox, W. H. & Latiner, P.(1962) New device to reduce patient irradia-tion and improve denial film quality. OralSurgery, Oral Medicine, Oral Pathology 15,1079-1088.
Mtihlemann, H. R. (J955) Parodontale Ront-gendiagnostik. Schweizerischc Monatsschriftfiir Zahnheilkunde 65, 1005-1013.
O'Leary, T. J., Standish, S. M. & Bloomer, R.S. (1973) Severe periodontal destruction fol-lowing impression procedures. Journal ofPeriodontology 44, 43^8.
Omnell, K.-A. (1957) Quantitative roentgeno-logic studies on changes in mineral contentof bone in vivo. Acta Radiologica, Stock-holm, Suppl. 148, 71-79.
Orban, T. R. & Orban, B. I. (1960) Tbrce-dimensional roentgenographic interpretationin periodontal diagnosis. Journal of Peri-odontology 31, 275-282.
Patur, B. (1960) Roentgenographic evaluationof alveolar bone changes in periodontal dis-ease. In Dental Clinics of North America,pp. 47-54. Philadelphia: W. B. Saunders.
Patur, B. & Glickman, I. (1962) Clinical androentgenographic evaluation of the post-treatment healing of infrabony pockets.Journal of Periodontology 33, 164-171.
Pauls, V. & Trott, 3. R. (1966) A radiologicalstudy of experimentally produced lesions inbone. Dental Practitioner 16, 254-258.
Pricbard, J. (1961) Role of the roentgenogramin the diagnosis and prognosis of periodontaldisease. Oral Surgery, Oral Medicine, OralPatholog}' 14, 182-196.
Prichard, J. F. (1966) Criteria for verifyingtopographical changes in alveolar processafter surgical intervention. Periodontics 4,71-76.
Puckett, J. B. (1968) A device for comparingroentgenograms of the same mouth. Journalof Periodontology 39, 160-161.
28 LANG AND HILL
Ramadan, A. E. & Mitchell, D. F. (1962)A roentgenographic study of experimentalbone destruction. Oral Surgery, Oral Medi-cine, Oral Pathology' 15, 934-943.
Kamfjord, S. P. (1959) Indices for prevalenceand incidence of periodonlal disease. Journalof Periodonloiogy 30, 51-59.
Ramfjord, S. P. & Ash, M. M. (1971) Occlu-sion. 2nd ed., pp. 384-397. Philadelphia:W. B. Saunders.
Ramfiord, S. P., Knowles, J, W., Nissle, R. R.,Shick, R. A. & Burgett, F. G. (]973) Longi-tudinal study of periodontal therapy. Journalof Periodontology 44, 6b~ll.
Regan, 3. E. & Mitchell, D. F. (1963) Roent-genographic and dissection measurements ofalveolar crest height. Journal of theAmerican Denial Association 66, 356-359.
Richards, A. G, (1949) Roentgenographic tech-niques made to order. Journal of the Ameri-can Dental Association 39, 396-404.
Richards, A. G. (1961) Technical factors thaicontrol radiographic density. In DentalClinics of North America, pp. 371-377.Philadelphia: W. B. Saunders.
Ritchey, B. & Orban, B. J. (1953) The crestsof the interdental alveolar septa. Journal ofPeriodonloiogy 24, 75-87.
RosHng, B., Hollender, L., Nyman, S. & OIs*son, G. (1975) A radiographic method forassessing changes in alveolar hone heightfollowing periodontal therapy. Journal ofClinical Periodontology 2, 211-217.
Schei, O., Waerhaug, J., L0vdai, A. & Arno, A.(1959) Alveolar bone loss as related to oralhygiene and age. Journal of Periodontology30, 7-16.
Shoha, R. R., Dowson, J. & Richards, A. G.(1974) Radiographic interpretation of experi-mentally produced bony lesions. Oral Sur-gery, Oral Medicine, Oral Pathology 38, 294-303.
Siiha, R. E. (1968) Technical errors with theparalleling technique. Dental Radiography &Photography 41, 51-55, 65-68.
Suomi, J. D., Plumbo, J. & Barbano, J. P.(3968) A comparative study of radiographsand pocket measurements in periodontal dis-ease evaluation. Journal of Periodontology39, 311-315.
Theilade, ] . {1960a) Usikkerheden ved r0nt-genologisk bed0mmelse af marginalt knogle-svind. Tandlaegebladet 64, 351-371.
Theilade, J. (1960b) An evaluation of thereliability of radiographs in the measurementof bone loss in periodontal disease. Journalof Periodotitology 31, 143-153.
Updegrave, W. J. (1951) The paralleling exten-sion-cone technique in intraoral dental radiog-raphy. Oral Surgery, Oral Medicine, OralPathology 4, 1250-1261.
Van der Linden, L. W. J. & van Aken, 1. (1970)The periodontal ligament in the roentgeno-gram. Journal of Periodontology 41, 243-248.
Weimann, J. P. (1955) Variation in the struc-ture of bone and bones and their significancein radiology. Oral Surgery, Oral Medicine,Oral Pathology 8, 988-992.
Weity, A. S. (1963) An evaluation of threeradiographic methods for delineating peri-odontal disease. V -f 37 p. Master Thesis.Ann Arhor: University of Michigan Schoolof Dentistry.
Wengraf, A. (1964) Radiologicaliy occult bonecavities. An experimental study and review.British Dental Journal 117, 532-536.
NVuehrmann, A. H. (1957) The long conetechnique. Practical Dental Monographs,July. .
Address:
University of BerneSchool of Dental MedicineFreiburgstr. 7CH'3O1O BerneSwitzerland





















