Quantitative Magnetic Resonance Perfusion Imaging Detects Anatomic and Physiologic Coronary Artery...
9
Cardiac Imaging Quantitative Magnetic Resonance Perfusion Imaging Detects Anatomic and Physiologic Coronary Artery Disease as Measured by Coronary Angiography and Fractional Flow Reserve Marco A. Costa, MD, PHD, FACC,* Steven Shoemaker, MD,* Hideki Futamatsu, MD, PHD,* Chris Klassen, MD,† Dominick J. Angiolillo, MD, PHD, FACC,* Minh Nguyen, MD,† Alan Siuciak, MS,† Paul Gilmore, MD, FACC,* Martin M. Zenni, MD, FACC,* Luis Guzman, MD, FACC,* Theodore A. Bass, MD, FACC,* Norbert Wilke, MD, FACC*† Jacksonville, Florida Objectives To evaluate the ability of quantitative perfusion cardiac magnetic resonance (CMR) to assess the hemodynamic significance of coronary artery disease (CAD) compared with well-established anatomic and physiologic techniques. Background Fractional flow reserve (FFR) is considered by many investigators to be a reliable stenosis-specific method to determine hemodynamically significant CAD. Quantitative perfusion CMR is a promising noninvasive approach to detect CAD but has yet to be validated against FFR. Methods This is a prospective study in patients with suspected CAD who underwent coronary angiography, FFR, and CMR assessments. The quantitative myocardial perfusion reserve (MPR) was calculated in 720 myocardial sectors (8 sectors/slice). The MPR was calculated from the ratio between stress and rest myocardial flow based on signal intensity time curves using deconvolution analysis. Stress was simulated with adenosine for both FFR and MPR. The MPR assessments were compared to FFR (n 44 coronary segments) and quantitative coronary angiogra- phy (n 108 segments) in the corresponding coronary territories. Results The MPR was 1.54 0.36 in segments with FFR 0.75 (n 14) and 2.11 0.68 in those with FFR 0.75 (n 30; p 0.0054). An MPR cutoff of 2.04 was 92.9% (95% CI 77.9 to 100.0) sensitive and 56.7% (95% CI 32.8 to 80.6) specific in predicting a coronary segment with FFR 0.75. The MPR was 1.54 0.49 in coronary segments with 50% diameter stenosis (DS) (n 47) and 2.13 0.80 in segments with 50% DS (n 61; p 0.001). An MPR cutoff of 2.04 was 85.1% (95% CI 71.1 to 99.2) sensitive and 49.2% (95% CI 33.6 to 64.8) specific in predicting CAD with 50% DS. Conclusions Quantitative perfusion CMR is a safe noninvasive test that represents a stenosis-specific alternative to de- termine the hemodynamic significance of CAD. (J Am Coll Cardiol 2007;50:514–22) © 2007 by the American College of Cardiology Foundation In patients with coronary artery disease (CAD), revascular- ization is deemed appropriate based on combined physio- logic and anatomic data. Quantitative coronary angiography (QCA) remains a well-established technique in the ana- tomic assessment of CAD (1,2), whereas fractional flow reserve (FFR) is an accurate stenosis-specific method to evaluate the hemodynamic significance of CAD (3,4). Both methods are well validated and routinely applied to deter- mine severity of CAD (1,5,6). However, the invasive nature of these diagnostic modalities limits their broad application for screening purposes. Cardiac magnetic resonance (CMR) is a promising non- invasive and ionizing-free radiation imaging modality to evaluate CAD. The first pass of gadolinium through the myocardium can be plotted as signal intensity (SI) versus time. Both relative and absolute blood flows can be quan- tified with reproducibility by first-pass magnetic resonance perfusion (7,8). The high spatial resolution of CMR allows regional quantification of transmural flow gradients (9). From the *Division of Cardiology and the †Division of Radiology, University of Florida Shands Jacksonville, Jacksonville, Florida. Manuscript received August 1, 2006; revised manuscript received February 7, 2007, accepted April 3, 2007. Journal of the American College of Cardiology Vol. 50, No. 6, 2007 © 2007 by the American College of Cardiology Foundation ISSN 0735-1097/07/$32.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2007.04.053
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Quantitative Magnetic Resonance Perfusion Imaging Detects Anatomic and Physiologic Coronary Artery...

Iil(tre
FF
a
Journal of the American College of Cardiology Vol. 50, No. 6, 2007© 2007 by the American College of Cardiology Foundation ISSN 0735-1097/07/$32.00P
Cardiac Imaging
Quantitative Magnetic ResonancePerfusion Imaging Detects Anatomic andPhysiologic Coronary Artery Disease as Measuredby Coronary Angiography and Fractional Flow Reserve
Marco A. Costa, MD, PHD, FACC,* Steven Shoemaker, MD,* Hideki Futamatsu, MD, PHD,*Chris Klassen, MD,† Dominick J. Angiolillo, MD, PHD, FACC,* Minh Nguyen, MD,†Alan Siuciak, MS,† Paul Gilmore, MD, FACC,* Martin M. Zenni, MD, FACC,*Luis Guzman, MD, FACC,* Theodore A. Bass, MD, FACC,* Norbert Wilke, MD, FACC*†
Jacksonville, Florida
Objectives To evaluate the ability of quantitative perfusion cardiac magnetic resonance (CMR) to assess the hemodynamicsignificance of coronary artery disease (CAD) compared with well-established anatomic and physiologictechniques.
Background Fractional flow reserve (FFR) is considered by many investigators to be a reliable stenosis-specific method todetermine hemodynamically significant CAD. Quantitative perfusion CMR is a promising noninvasive approach todetect CAD but has yet to be validated against FFR.
Methods This is a prospective study in patients with suspected CAD who underwent coronary angiography, FFR, and CMRassessments. The quantitative myocardial perfusion reserve (MPR) was calculated in 720 myocardial sectors (8sectors/slice). The MPR was calculated from the ratio between stress and rest myocardial flow based on signalintensity time curves using deconvolution analysis. Stress was simulated with adenosine for both FFR and MPR.The MPR assessments were compared to FFR (n � 44 coronary segments) and quantitative coronary angiogra-phy (n � 108 segments) in the corresponding coronary territories.
Results The MPR was 1.54 � 0.36 in segments with FFR �0.75 (n � 14) and 2.11 � 0.68 in those with FFR �0.75(n � 30; p � 0.0054). An MPR cutoff of 2.04 was 92.9% (95% CI 77.9 to 100.0) sensitive and 56.7% (95% CI32.8 to 80.6) specific in predicting a coronary segment with FFR �0.75. The MPR was 1.54 � 0.49 in coronarysegments with �50% diameter stenosis (DS) (n � 47) and 2.13 � 0.80 in segments with �50% DS (n � 61;p � 0.001). An MPR cutoff of 2.04 was 85.1% (95% CI 71.1 to 99.2) sensitive and 49.2% (95% CI 33.6 to 64.8)specific in predicting CAD with �50% DS.
Conclusions Quantitative perfusion CMR is a safe noninvasive test that represents a stenosis-specific alternative to de-termine the hemodynamic significance of CAD. (J Am Coll Cardiol 2007;50:514–22) © 2007 by theAmerican College of Cardiology Foundation
ublished by Elsevier Inc. doi:10.1016/j.jacc.2007.04.053
mmof
iemttp
n patients with coronary artery disease (CAD), revascular-zation is deemed appropriate based on combined physio-ogic and anatomic data. Quantitative coronary angiographyQCA) remains a well-established technique in the ana-omic assessment of CAD (1,2), whereas fractional floweserve (FFR) is an accurate stenosis-specific method tovaluate the hemodynamic significance of CAD (3,4). Both
rom the *Division of Cardiology and the †Division of Radiology, University oflorida Shands Jacksonville, Jacksonville, Florida.
rManuscript received August 1, 2006; revised manuscript received February 7, 2007,
ccepted April 3, 2007.
ethods are well validated and routinely applied to deter-ine severity of CAD (1,5,6). However, the invasive nature
f these diagnostic modalities limits their broad applicationor screening purposes.
Cardiac magnetic resonance (CMR) is a promising non-nvasive and ionizing-free radiation imaging modality tovaluate CAD. The first pass of gadolinium through theyocardium can be plotted as signal intensity (SI) versus
ime. Both relative and absolute blood flows can be quan-ified with reproducibility by first-pass magnetic resonanceerfusion (7,8). The high spatial resolution of CMR allows
egional quantification of transmural flow gradients (9).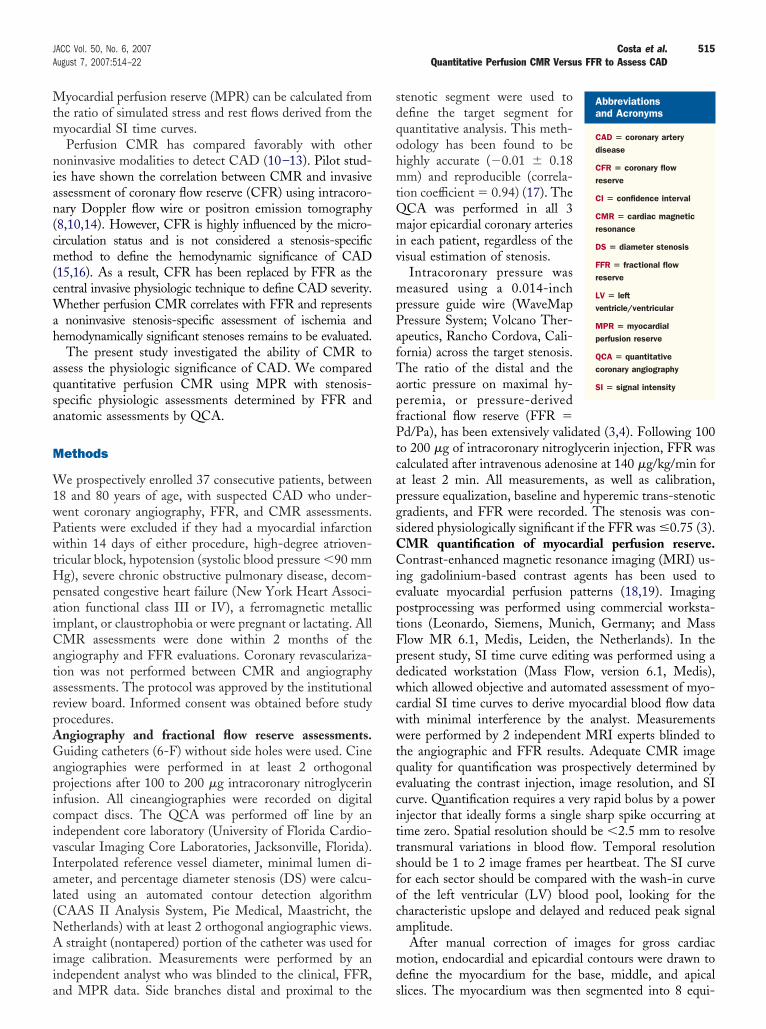
Mtm
nian(cm(cWah
aqsa
M
W1wPwtHpaiCatarpAGapicivIal(NAiia
sdqohmtQmiv
mpPafTapfPtcapgsCCieptFpdwcwwtqecittsfoca
md
515JACC Vol. 50, No. 6, 2007 Costa et al.August 7, 2007:514–22 Quantitative Perfusion CMR Versus FFR to Assess CAD
yocardial perfusion reserve (MPR) can be calculated fromhe ratio of simulated stress and rest flows derived from theyocardial SI time curves.Perfusion CMR has compared favorably with other
oninvasive modalities to detect CAD (10–13). Pilot stud-es have shown the correlation between CMR and invasivessessment of coronary flow reserve (CFR) using intracoro-ary Doppler flow wire or positron emission tomography8,10,14). However, CFR is highly influenced by the micro-irculation status and is not considered a stenosis-specificethod to define the hemodynamic significance of CAD
15,16). As a result, CFR has been replaced by FFR as theentral invasive physiologic technique to define CAD severity.
hether perfusion CMR correlates with FFR and representsnoninvasive stenosis-specific assessment of ischemia and
emodynamically significant stenoses remains to be evaluated.The present study investigated the ability of CMR to
ssess the physiologic significance of CAD. We compareduantitative perfusion CMR using MPR with stenosis-pecific physiologic assessments determined by FFR andnatomic assessments by QCA.
ethods
e prospectively enrolled 37 consecutive patients, between8 and 80 years of age, with suspected CAD who under-ent coronary angiography, FFR, and CMR assessments.atients were excluded if they had a myocardial infarctionithin 14 days of either procedure, high-degree atrioven-
ricular block, hypotension (systolic blood pressure �90 mmg), severe chronic obstructive pulmonary disease, decom-
ensated congestive heart failure (New York Heart Associ-tion functional class III or IV), a ferromagnetic metallicmplant, or claustrophobia or were pregnant or lactating. AllMR assessments were done within 2 months of the
ngiography and FFR evaluations. Coronary revasculariza-ion was not performed between CMR and angiographyssessments. The protocol was approved by the institutionaleview board. Informed consent was obtained before studyrocedures.ngiography and fractional flow reserve assessments.uiding catheters (6-F) without side holes were used. Cine
ngiographies were performed in at least 2 orthogonalrojections after 100 to 200 �g intracoronary nitroglycerinnfusion. All cineangiographies were recorded on digitalompact discs. The QCA was performed off line by anndependent core laboratory (University of Florida Cardio-ascular Imaging Core Laboratories, Jacksonville, Florida).nterpolated reference vessel diameter, minimal lumen di-meter, and percentage diameter stenosis (DS) were calcu-ated using an automated contour detection algorithmCAAS II Analysis System, Pie Medical, Maastricht, theetherlands) with at least 2 orthogonal angiographic views.straight (nontapered) portion of the catheter was used for
mage calibration. Measurements were performed by anndependent analyst who was blinded to the clinical, FFR,
nd MPR data. Side branches distal and proximal to the stenotic segment were used toefine the target segment foruantitative analysis. This meth-dology has been found to beighly accurate (�0.01 � 0.18m) and reproducible (correla-
ion coefficient � 0.94) (17). TheCA was performed in all 3ajor epicardial coronary arteries
n each patient, regardless of theisual estimation of stenosis.
Intracoronary pressure waseasured using a 0.014-inch
ressure guide wire (WaveMapressure System; Volcano Ther-peutics, Rancho Cordova, Cali-ornia) across the target stenosis.he ratio of the distal and the
ortic pressure on maximal hy-eremia, or pressure-derivedractional flow reserve (FFR �d/Pa), has been extensively validated (3,4). Following 100
o 200 �g of intracoronary nitroglycerin injection, FFR wasalculated after intravenous adenosine at 140 �g/kg/min fort least 2 min. All measurements, as well as calibration,ressure equalization, baseline and hyperemic trans-stenoticradients, and FFR were recorded. The stenosis was con-idered physiologically significant if the FFR was �0.75 (3).MR quantification of myocardial perfusion reserve.ontrast-enhanced magnetic resonance imaging (MRI) us-
ng gadolinium-based contrast agents has been used tovaluate myocardial perfusion patterns (18,19). Imagingostprocessing was performed using commercial worksta-ions (Leonardo, Siemens, Munich, Germany; and Masslow MR 6.1, Medis, Leiden, the Netherlands). In theresent study, SI time curve editing was performed using aedicated workstation (Mass Flow, version 6.1, Medis),hich allowed objective and automated assessment of myo-
ardial SI time curves to derive myocardial blood flow dataith minimal interference by the analyst. Measurementsere performed by 2 independent MRI experts blinded to
he angiographic and FFR results. Adequate CMR imageuality for quantification was prospectively determined byvaluating the contrast injection, image resolution, and SIurve. Quantification requires a very rapid bolus by a powernjector that ideally forms a single sharp spike occurring atime zero. Spatial resolution should be �2.5 mm to resolveransmural variations in blood flow. Temporal resolutionhould be 1 to 2 image frames per heartbeat. The SI curveor each sector should be compared with the wash-in curvef the left ventricular (LV) blood pool, looking for theharacteristic upslope and delayed and reduced peak signalmplitude.
After manual correction of images for gross cardiacotion, endocardial and epicardial contours were drawn to
efine the myocardium for the base, middle, and apical
Abbreviationsand Acronyms
CAD � coronary arterydisease
CFR � coronary flowreserve
CI � confidence interval
CMR � cardiac magneticresonance
DS � diameter stenosis
FFR � fractional flowreserve
LV � leftventricle/ventricular
MPR � myocardialperfusion reserve
QCA � quantitativecoronary angiography
SI � signal intensity
lices. The myocardium was then
segmented into 8 equi-
dobaat(waaTscstpstpaw
tauopaSdasTabMflflpms
516 Costa et al. JACC Vol. 50, No. 6, 2007Quantitative Perfusion CMR Versus FFR to Assess CAD August 7, 2007:514–22
istant radial sectors per slice (Fig. 1). The sectors wererdered in a clockwise orientation, with sector number 1eginning at the insertion of the right ventricle to thenterior septal wall of the LV. The distribution of therterial territories within the 24 segments was based onhe 17-segment model for tomographic imaging of the heart20). The left anterior descending artery perfusion territoryas assigned to sectors 8, 1, and 2 for the base, middle, and
pical slices. The diagonal branches perfusion territory wasssigned to sectors 1 and 2 for the middle and apical slices.he circumflex artery and obtuse marginal branches perfu-
ion territories were assigned to sectors 3 and 4. Theircumflex territory included the base, middle, and apicallices, and the obtuse marginal branches territory involvedhe middle and apical slices. The right coronary artery andosterior descending artery perfusion territories were as-igned to sectors 5, 6, and 7. The right coronary arteryerritory included the base, middle, and apical slices, and theosterior descending artery territory was assigned to thepical slice. The posterior lateral artery perfusion territory
Figure 1 Base, Middle, And Apical Short-Axis CMR Slices Divid
(Lower right panel) Schematic representation of the 3 concentric left ventricle shodiac magnetic resonance (CMR) images represents the anterior insertion of the rigdescending (base 1, 2, 8; middle 9, 10, 16; apical 17, 18, 24), diagonal brancheobtuse marginal branches (middle 11, 12; apical 19, 20), right coronary (base 5,and posterior lateral (apical 20,21) arteries.
as assigned to sectors 4 and 5 of the apical slice (Fig. 1). C
Constrained deconvolution analysis using a Fermi func-ion was applied to the first-pass SI curves and provided andjusted or absolute myocardial blood flow measurementsing a custom C�� software program previously devel-ped by our group (7–9). The Fermi function models therobability that a contrast molecule has left the myocardiums a function of time. Deconvolution of the LV blood poolI curve with the Fermi function yields a theoretic myocar-ial SI curve. The theoretic curve is compared against thectual measured myocardial SI data points using leastquares and a repetitive Marquardt-Levenberg algorithm.he initial amplitude of the Fermi function corresponds to
bsolute myocardial blood flow (21–24). This technique haseen validated using radioactive microspheres (25). ThePR was then calculated as the ratio of myocardial blood
ow at maximal hyperemia divided by the myocardial bloodow at rest. The MPR was then normalized by rate pressureroduct, which was calculated for rest and hyperemia at theaximum rate of adenosine infusion, as previously de-
cribed and validated (7,21,24,25). The reproducibility of
to 8 Equidistant Radial Sectors
slices segmented radially on a polar map. The plus (�) sign in blue in the car-tricle. The segments were assigned based on anatomic location of left anteriordle 9, 10; apical 17, 18), circumflex (base 3, 4; middle 11, 12; apical 19, 20),iddle 13, 14, 15; apical 21, 22, 23), posterior descending (apical 21, 22, 23),
ed In
rt-axisht vens (mid6, 7; m
MR first-pass imaging has also been reported and showed

gaaCctSsigfiBpogzTaSrpowadiitaosrstb
gRotwCMpdgmiu
bflsav
laafdovtnfutSdRutMivd9wCVaD
R
D1t�wSictwbpMpBMcmFR8(9
cM
517JACC Vol. 50, No. 6, 2007 Costa et al.August 7, 2007:514–22 Quantitative Perfusion CMR Versus FFR to Assess CAD
ood intraobserver (correlation coefficient � 0.8 to 0.85)nd interobserver (correlation coefficient � 0.81 to 0.97)greements (26).MR imaging protocol. All patients underwent first-pass
ontrast-enhanced CMR perfusion analysis imaging ob-ained at rest and stress on a Sonata 1.5 Tesla (Siemens-onata) magnet (maximum slew rate 150 T/m/s: gradienttrength 40 mT/m) using a 6-channel body coil. Scoutmages were obtained initially to determine the cardiaceometry and to plan subsequent scans. Imaging was per-ormed at rest and simulated stress during intravenousnjection of 0.1-mmol/kg gadolinium-DPTA (Magnevist;erlex Laboratories Inc., St. Louis, Missouri) contrast byower injector (MedRad, Indianola, Pennsylvania) at a ratef 10 ml/s. The pulse sequence used was a single-shotradient echo sequence with saturation-recovery magneti-ation preparation for T1 weighting and linear k-spacing.he parameters were set to repetition time/echo time flip
ngle of 2.4 ms/1.2 ms/18° and a slice thickness of 10 mm.ixty images per slice location were acquired with a spatialesolution of 2 to 3 mm. Simulated stress imaging waserformed using an infusion of adenosine at a concentrationf 140 �g/kg/min for 4 min. First-pass perfusion imagingas obtained at the end of injection, and after 3 min 45 s of
denosine infusion. Subsequently, the scan was repeateduring resting conditions, at least 5 min after the adenosine
nfusion had been stopped. Perfusion was then determinedn 3 LV short-axis slices. The first slice was located closer tohe base of the heart, the second in the middle of the LV,nd the third slice closer to the apex just distal to the basef the papillary muscles. Patients were asked to performhallow breathing for the duration of the scan to minimizeespiratory motion. Blood pressure, heart rate, and anyerious adverse reactions caused by the simulated stresshroughout the CMR imaging examination were monitoredy a physician and nursing personnel.For cinemagnetic resonance imaging, an electrocardiogram-
ated breath hold, segmented truefisp sequence was used withT/TE/flip angle 33 ms/6 ms/25°. In-plane spatial resolutionf the cine sequence was 2 mm � 1.4 mm with a slicehickness and increment of 10 mm. The temporal resolutionas 30 to 50 ms with 14 to 16 cardiac phases per plane.omparisons between MPR, FFR, and QCA. First,PR values for all coronary segments, as described in the
receding, were plotted and compared with QCA and FFRata without any guidance (blind analysis) from the angio-raphic data regarding specific target segments. The mini-um MPR values for the corresponding coronary segment
n each slice (base, middle, and apex) were averaged andsed for comparison.In a second analysis, the location of the stenosis defined
y QCA was used to guide the selection of MPR valuesrom specific myocardial slices corresponding to the stenosisocation (proximal, middle, or distal). This allowed a moretenosis-specific comparison among MPR, QCA, and FFRssessments. Thus, in an ostial stenosis we considered MPR
alues from all 3 slices, whereas for proximal and middle 0ocated stenosis, only MPR values from the middle andpical slices were averaged for comparison. As in the blindnalysis, the lowest MPR from an artery’s territory was usedrom each pertinent slice. At least 2 MPR values fromifferent slices were averaged for comparison. The exceptionccurred with apical stenosis, of which the 2 lowest MPRalues from the artery’s territory were averaged. It is impor-ant to note that, although the selection of MPR values wasot blinded to QCA measurements, the calculation of MPRor each sector (8 per slice) was automatically calculatedsing a computerized workstation by analysts unaware ofhe angiographic data.tatistical analysis. Data are presented as mean � stan-ard deviation. Frequencies are presented as percentage.eceiver-operating curve (ROC) analysis was performedsing MedCalc (MedCalc Software, Mariakerke, Belgium)o define sensitivity, specificity, and optimal cutoff values of
PR to determine anatomic (�50% DS) and hemodynam-cally (FFR �0.75) significant CAD. Positive predictivealue (PPV) and negative predictive value (NPV) were alsoerived using the MPR cutoff from the ROC analysis. The5% confidence intervals (CIs) for sensitivity and specificityere analyzed using SAS 9.1 (SAS Institute Inc., Cary, Northarolina) with PROC SURVEYFREQ and PROC SUR-EYMEANS. Analysis of variance single factor analysis was
lso performed on the MPR data using an FFR of �0.75 andS of �50% as cutoff for those patients with CAD.
esults
emographics of the study population are reported in Table. There were no significant demographic differences be-ween patients with single-vessel CAD who had an FFR of
0.75 or �0.75. One patient was excluded because ofire-induced coronary spasm during FFR measurements.ix patients were excluded because of inadequate MRI
mage quality for quantitative assessment. There were noomplications related to CMR procedures, and all patientsolerated the procedure well. The MPR and FFR valuesere compared in 44 coronary segments, and comparisonetween QCA and MPR involved 108 segments from 30atients. Figure 2 illustrates a typical correlation betweenPR, angiography, and FFR. A typical appearance of a
erfusion defect during stress MRI is illustrated in Figure 3.lind MPR comparisons with FFR and QCA. ThePR and FFR values were compared in 44 corresponding
oronary segments (Table 2). The average MPR in seg-ents with FFR �0.75 (n � 14) was 1.50 � 0.45 and withFR �0.75 (n � 30) was 2.07 � 0.66 (p � 0.0059). TheOC curve demonstrated an MPR cutoff of 1.97 that was5.7% sensitive (95% CI 57.2 to 97.8) and 60.0% specific95% CI 40.6 to 77.3) with a PPV of 50% and an NPV of0% in predicting an FFR of �0.75.The MPR and QCA data were compared in 108
orresponding coronary segments (Table 2). The averagePR in segments with �50% DS (n � 47) was 1.54 �
.51 and with �50% DS (n � 61) was 2.02 � 0.77 (p �

023
aa10c9PC
CMh(SQcM0025a(
bsw
S
C
518 Costa et al. JACC Vol. 50, No. 6, 2007Quantitative Perfusion CMR Versus FFR to Assess CAD August 7, 2007:514–22
.001). The ROC curve demonstrated an MPR cutoff of
.12 that was 85.1% sensitive (95% CI 71.7 to 93.8) and9.3% specific (95% CI 27.1 to 52.7) with a PPV of 63%
Figure 2 Correlation Between MPR and Quantitative Coronary
The myocardial perfusion reserve (MPR) data (left panel) are reported in graphicssponding to left ventricle blood pool). Purple and green lines represent the fittingslice at the bottom of each graphic. Rest and stress flow are also reported in theaverage MPR of 1.79, which corresponds to the left circumflex artery territory. Cormarginal branch of the left circumflex artery, which had a fractional flow reserve oftours. Perfusion magnetic resonance imaging images at both stress and rest are svisualized in the stress image, and was only detected by the quantitative method.
Please see the Appendix for accompanying video.
tudy Population
Table 1 Study Population
Demographics
Age, yrs 65 � 11
Male, n (%) 16 (53%)
Hypertension, n (%) 24 (80%)
Diabetes mellitus, n (%) 7 (23%)
Smoking history, n (%) 6 (20%)
Hyperlipidemia, n (%) 17 (57%)
Peripheral vascular disease, n (%) 3 (10%)
Ejection fraction, per CMR (%) 57 � 13
Creatinine, mg/dl 0.98 � 0.36
Coronary anatomy, n (%)
No significant disease 1 (3%)
1-vessel disease 8 (27%)
2-vessel disease 9 (30%)
3-vessel disease 10 (33%)
Left main disease 2 (7%)
Medications, n (%)
Beta-blockers 21 (70%)
Angiotensin blockers 18 (60%)
Statins 19 (63%)
Calcium-channel blockers 6 (20%)
Nitrates 12 (40%)
MR � cardiac magnetic resonance.
nd an NPV of 84% in predicting �50% DS CAD. Theverage MPR in segments with �70% DS (n � 14) was.46 � 0.53 and with �70% DS (n � 94) was 1.86 �.72 (p � 0.047). The ROC curve demonstrated an MPRutoff of 1.84 that was 85.7% sensitive (95% CI 57.2 to7.8) and 46.8% specific (95% CI 36.4 to 57.4) with aPV of 19% and NPV of 96% in predicting a �70% DSAD.In segments that were most likely to have significant
AD, i.e., FFR �0.75 and �50% DS (n � 12), the averagePR was 1.56 � 0.46. In segments that were least likely to
ave significant CAD, i.e., FFR �0.75 and �50% DSn � 20), the average MPR was 2.2 � 0.72.tenosis-specific correlation of MPR with FFR andCA. A total of 44 segments were analyzed for the
omparison between MPR and FFR (Table 2). The averagePR in segments with FFR �0.75 (n � 14) was 1.54 �
.36 and with FFR �0.75 (n � 30) was 2.11 � 0.68 (p �
.0054). The ROC analysis demonstrated an MPR cutoff of
.04, which was 92.9% sensitive (95% CI 77.9 to 100.0) and6.7% specific (95% CI 32.8 to 80.6) with a PPV of 50%nd an NPV of 94% in predicting a significant FFR (�0.75)Fig. 4).
A total of 108 segments were analyzed for the comparisonetween MPR and QCA (Table 2). The average MPR inegments with �50% DS (n � 47) was 1.54 � 0.49 andith �50% DS (n � 61) was 2.13 � 0.80 (p � 0.001). The
graphy
ividual slices of cardiac magnetic resonance (CMR) (S1 to S8; first graphic corre-for rest and stress, respectively. The MPR values (Pr) are depicted for each
aph, with each bar corresponding to 1 CMR slice. Note that slice S4 shows anngiography (middle bottom panel) revealed a 65% stenosis in the first obtuseMiddle upper panel shows the middle CMR slides with the quantitative con-in the right panels. It is important to note that the perfusion defect was notdiameter stenosis; FFR � fractional flow reserve.
Angio
for indcurvesbar gronary a0.65.hownDS �

R8(8a1(o5a
sF1st
D
TscCCfisCaiscmtcth
tasMadesssmYF
SS
*
519JACC Vol. 50, No. 6, 2007 Costa et al.August 7, 2007:514–22 Quantitative Perfusion CMR Versus FFR to Assess CAD
OC analysis demonstrated an MPR cutoff of 2.04 that was5.1% sensitive (95% CI 71.1 to 99.2) and 49.2% specific95% CI 33.6 to 64.8) with a PPV of 59% and an NPV of3% in predicting significant (50% DS) CAD (Fig. 5). Theverage MPR in segments with �70% DS (n � 14) was.40 � 0.38 and with �70% DS (n � 94) was 1.94 � 0.76p � 0.01). The ROC analysis demonstrated an MPR cutofff 1.85 that was 92.9% sensitive (95% CI 66.1 to 98.8) and0% specific (95% CI 39.5 to 60.5) with a PPV of 22% andn NPV of 98% in predicting significant (�70% DS) CAD.
In segments that were most likely to be hemodynamicallyignificant, according to the invasively derived data, i.e.,FR �0.75 and �50% DS (n � 12), the average MPR was.60 � 0.34. In segments that were least likely to haveignificant CAD, i.e., FFR �0.75 and �50% DS (n � 20),he average MPR was 2.25 � 0.73.
Figure 3 MRI Rest and Stress Perfusion Images (Middle Slices
The stress image shows the perfusion defect in the inferior cardiac wall (lower sigartery. There is no perfusion defect observed in the magnetic resonance imaging (mid perfusion MRI images at rest and stress.
Please see the Appendix for accompanying video.
ummary of Blinded andtenosis-Specific MPR Data
Table 2 Summary of Blinded andStenosis-Specific MPR Data
Blinded MPRStenosis-Specific
MPR
FFR �0.75 1.50 � 0.45* 1.54 � 0.36*
FFR �0.75 2.07 � 0.66 2.11 � 0.68
�50% DS 1.54 � 0.51* 1.54 � 0.49*
�50% DS 2.02 � 0.77 2.13 � 0.80
�70% DS 1.46 � 0.53* 1.40 � 0.38*
�70% DS 1.86 � 0.72 1.94 � 0.76
FFR �0.75 � �50% DS 1.56 � 0.46* 1.60 � 0.34*
FFR �0.75 � �50% DS 2.2 � 0.72 2.25 � 0.73
FFR �0.75 � �70% DS 1.49 � 0.46* 1.56 � 0.29*
FFR �0.75 � �70% DS 2.09 � 0.66 2.14 � 0.68
sp � 0.05 indicates comparison between each category.DS � diameter stenosis; FFR � fractional flow reserve; MPR � myocardial perfusion reserve.
iscussion
he present results suggest that quantitative CMR can beafely used to determine the hemodynamic significance oforonary stenosis and to exclude the presence of significantAD with a high degree of accuracy. Beyond the ability ofMR to detect the presence of ischemia (10,11), thesendings support the hypothesis that MPR represents atenosis-specific measure of the functional significance ofAD. Cardiac magnetic resonance could therefore be used
s a highly sensitive screening tool to exclude hemodynam-cally significant CAD. Likewise, CMR, with its higherpatial resolution compared with single-photon emissionomputerized tomography (SPECT) and its ability to si-ultaneously evaluate myocardial viability, mechanics using
agging or phase-based techniques, and hemodynamics,ould be used synergistically with multislice computerizedomographic angiography to further stratify patients whoave been identified with ambiguous coronary stenosis (27).Myocardial perfusion reserve, similar to other approaches
hat use adenosine as the pharmacologic stimuli, may beffected by endothelial dysfunction and the microcirculationtatus (28–32). Thus, the relatively lower specificity of
PR compared with both FFR and QCA is likely associ-ted with the high prevalence of hypertension, diabetes, andyslipidemia, which are all known risk factors for impairedndothelium and myocardial flow-mediated dependent va-odilation (33). In addition, there were �2 vessels withignificant CAD in 73% of the patients. In the presenttudy, side branches were also included and coronary seg-ents supplying small myocardium territories compared.et, MPR showed high degrees of agreement with bothFR and QCA. Although the FFR has been shown to be
rker image; arrows) corresponding to significant disease in the right coronaryage at rest. The perfusion defect can be appreciated in the video files of the
)
nal, daMRI) im
tenosis specific and an accurate determinant of the need for

cedbk(anC
pchbpfl
cv
(etda(lr(sc
wsSsd
aF
520 Costa et al. JACC Vol. 50, No. 6, 2007Quantitative Perfusion CMR Versus FFR to Assess CAD August 7, 2007:514–22
oronary revascularization (3–6,34), it might still be influ-nced by microvascular disease resulting in elevated valuesespite significant epicardial CAD (34,35). Discrepancyetween QCA data and physiologic measurements has beennown since the early studies comparing CFR and QCA36,37). The possibility of using other pharmacologicgents, such as dobutamine, makes CMR an attractiveoninvasive test for patients who are not candidates forFR, FFR, or other adenosine-based ischemia tests (38).According to the present study, which includes a stable
opulation, a patient with a normal MPR (�2.04) in alloronary segments has a very low probability of havingemodynamically significant CAD. Whether CMR cane used as a guide for therapeutic decision-making inatients with known CAD remains to be evaluated inuture studies with a larger patient population andong-term follow-up (39).
The MPR cutoff values observed in the present studyorrelated well with previously reported significant CFRalues observed in patients with CAD (1,40). Serruys et al.
Figure 4 Sensitivity and Specificity of MPR to Detect CAD Wit
Graphics showing sensitivity (Sens), specificity (Spec), and predictive values of myating curve analysis to detect coronary artery disease (CAD) with fractional flow resevaluated by Welch approximation for unequal variances from the independent-sam
Figure 5 Sensitivity and Specificity of MPR to Detect CAD Wit
Graphics showing sensitivity, specificity, and predictive values of MPR using a cuto�50% DS. Heterogeneity of variance in MPR levels correlated with percentage diafrom the independent-sample t test (p � �0.0001). Abbreviations as in Figure 4.
1) reported that a CFR �2.5 with a �35% DS hadxcellent short- and long-term outcomes after percutaneousransluminal coronary angioplasty. Di Mario et al. (40)emonstrated that a CFR �2.0 with �35% DS wasssociated with similar clinical outcomes. We and others8,10,41,42) have shown the equivalence and direct corre-ation between CFR and MPR values. Bedaux et al. (41)eported an average MPR of 2.7 � 1 and CFR of 3.1 � 0.6p � 0.01) for nonstenosed vessels. Similar to the presenttudy findings, CFR has also been shown to stronglyorrelate with SPECT imaging and QCA (1,40,43,44).
The sensitivity and specificity of MPR in detecting CADhen FFR was used as the gold standard in the present
tudy compared favorably with earlier reports comparingPECT with FFR (45–47). Hacker et al. (46) reported aensitivity of 80% and a specificity of 76% for SPECT inetecting a target vessel with an FFR �0.75.The MPR and QCA data, although correlated, were not
s strong as the correlation observed between MPR andFR in the present study. Similar correlation coefficients
<0.75
al perfusion reserve (MPR) using a cutoff of 2.04 as determined by receiver-oper-FFR) �0.75. Heterogeneity of variance in MPR levels correlated with FFR wastest (p � 0.008).
0% DS
.04 as determined by receiver-operating curve analysis to detect CAD withstenosis (DS) was evaluated by the Welch approximation for unequal variances
h FFR
ocardierve (ple t
h >5
ff of 2meter

b(miaaCbdQ
prasTg
tCnauscSrharistset
rqsacoH3aftFvs
dt(ow
FhiiCFMdproa
ATtW
RAdSdm
R
1
1
1
521JACC Vol. 50, No. 6, 2007 Costa et al.August 7, 2007:514–22 Quantitative Perfusion CMR Versus FFR to Assess CAD
etween SPECT and QCA data have been reported47,48). The present data correlate favorably with a recenteta-analysis demonstrating a sensitivity of 89% and spec-
ficity of 65% when SPECT was compared with coronaryngiography in detecting CAD (48). The limitation ofngiography to determine the hemodynamic significance ofAD and its inability to define microvascular disease haseen previously reported (49) and likely explains some of theiscordance between the noninvasive physiologic data andCA.The MPR cutoff values to exclude significant CAD in the
resent study are relatively higher than those previouslyeported (11,50). The differences in patient demographicsnd degrees of epicardial and microvascular CAD betweentudies may explain these variations in MPR cutoff values.he MPR values have recently been shown to be affected byender, age, and CAD risk factors (32).
The benefit of a noninvasive highly sensitive diagnosticest to evaluate for and exclude physiologically significantAD is unquestionable. Although further studies areeeded to further establish the value of this imagingpproach, the present data suggest that CMR through these of quantitative MPR can be used as an alternativecreening tool to both exclude and localize hemodynami-ally significant CAD.tudy limitations. The relatively small study populationepresents a potential limitation of this study. Our analysis,owever, was based on coronary segments that included 44nd 108 comparisons between MPR, FFR, and QCA,espectively. Indeed, a larger study population would havencreased the statistical power and potentially improved thepecificity of MPR compared with FFR and QCA. Al-hough not pre-specified in the present study, a largerample size would allow subgroup analyses such as specificvaluation of patients with FFR between 0.75 and 0.8 andhose with poor LV function.
The CMR images in 6 patients did not meet the minimalequirements for quantitative analysis, which required ade-uate images at rest and stress, as described in the Methodsection. Suboptimal images in the present study were mainlyssociated with motion artifact or inadequate timing of theontrast bolus. Therefore, the present study findings applynly to patients with optimal CMR image acquisition.opefully, recent CMR technologic advancements such as
-T scanning, 32-channel scanners, and 32-element cardiacrray coils will improve the CMR image quality and lead toewer patients with suboptimal image quality. Nevertheless,he seminal data reported in this study comparing MPR andFR for the first time suffice to demonstrate the potentialalue of MPR as an alternative noninvasive test to demon-trate the physiologic significance of CAD.
Coronary flow reserve data would have been beneficial toetermine the relative contribution of microvascular diseaseo MPR values, and such data have been previously reported8,10). However, CFR data alone do not provide anbjective evaluation of epicardial CAD. The present study
as aimed at investigating the ability of MPR to reproduceFR data, the current gold standard method to assess theemodynamic status of epicardial CAD with minimal
nfluence of microcirculation. The FFR is not absolutelyndependent of the microcirculatory status, but, unlikeFR, microvascular dysfunction has an opposite effect onFR measurements, i.e., it may increase FFR values. ThePR and FFR data correlated well in the present study
espite this peculiar aspect of FFR assessment of coronaryhysiology, which may further strengthen our conclusionsegarding the ability of perfusion MRI to evaluate CAD. Tour knowledge, such a comparative study between MPRnd FFR had not been done previously.
cknowledgmentshe authors thank Otgonbayar Batmunh, MS, for his
echnical support with the MRI imaging analysis and Peterludyka, PhD, for his statistical assistance.
eprint requests and correspondence: Dr. Marco A. Costa,ssistant Professor of Medicine, Director of Research and Car-iovascular Imaging Core Laboratories, University of Floridahands Jacksonville, 655 West 8th Street, ACC Building, Car-iovascular Center, Jacksonville, Florida 32209. E-mail:[email protected].
EFERENCES
1. Serruys PW, Di Mario C, Piek J, et al. Prognostic value of intracoro-nary flow velocity and diameter stenosis in assessing the short- andlong-term outcomes of coronary balloon angioplasty: the DEBATE(Doppler Endpoints Balloon Angioplasty Trial Europe) study. Circu-lation 1997;96:3369–77.
2. Bartunek J, Sys SU, Heyndrickx GR, Pijls NH, De Bruyne B.Quantitative coronary angiography in predicting functional signifi-cance of stenosis in an unselected patient cohort. J Am Coll Cardiol1995;26:328–34.
3. Pijls NHJ, de Bruyne B, Peels K, et al. Measurement of fractional flowreserve to assess the functional severity of coronary-artery stenoses.N Engl J Med 1996;334:1703–8.
4. Pijls NHJ, Van Gelder B, Van der Voot P, et al. Fractional flow reserve.A useful index to evaluate the influence of an epicardial coronary stenosison myocardial blood flow. Circulation 1995;92:3183–93.
5. Bech, GJW, De Bruyne B, Pijls NHJ, et al. Fractional flow reserve todetermine the appropriateness of angioplasty in moderate coronarystenosis: a randomized trial. Circulation 2001;103:2928–34.
6. Bech GJ, Pijls NH, De Bruyne B, et al. Usefulness of fractional flowreserve to predict clinical outcome after balloon angioplasty. Circula-tion 1999;99:883–8.
7. Wilke N, Kroll K, Merkle H, et al. Regional myocardial blood volumeand flow: first-pass MR imaging with polylysine-Gd-DTPA. J MagnReson Imaging 1995;5:227–37.
8. Wilke N, Jerosch-Herold M, Wang Y, et al. Myocardial perfusionreserve: assessment with multisection, quantitative, first-pass MRimaging. Radiology 1997;204:373–84.
9. Wilke N, Simm C, Zhang J, et al. Contrast-enhanced first pass myocar-dial perfusion imaging: correlation between myocardial blood flow in dogsat rest and during hyperemia. Magn Reson Med 1993;29:485–97.
0. Schwitter J, Nanz D, Kneifield S, et al. Assessment of myocardialperfusion in coronary artery disease by magnetic resonance: a compar-ison with positron emission tomography and coronary angiography.Circulation 2001;103:2230–5.
1. Al-Saadi N, Nagel E, Gross M, et al. Noninvasive detection ofmyocardial ischemia from perfusion reserve based on cardiovascularmagnetic resonance. Circulation 2000;101:1379–83.
2. Panting JR, Gatehouse PD, Yang GZ, et al. Echo-planar magneticresonance myocardial perfusion imaging: parametric map analysis and
comparison with thallium SPECT. J Magn Reson Imaging 2001;13:192–200.
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
522 Costa et al. JACC Vol. 50, No. 6, 2007Quantitative Perfusion CMR Versus FFR to Assess CAD August 7, 2007:514–22
3. Sakuma H, Suzawa N, Ichikawa Y, et al. Diagnostic accuracy of stressfirst-pass contrast-enhanced myocardial perfusion MRI comparedwith stress myocardial perfusion scintigraphy. AJR Am J Roentgenol2005;185:95–102.
4. Ibrahim T, Nekolla SG, Schreiber K, et al. Assessment of coronaryflow reserve: comparison between contrast-enhanced magnetic reso-nance imaging and positron emission tomography. J Am Coll Cardiol2002;39:864–70.
5. de Bruyne B, Bartunek J, Sys SU, Pijls NH, Heyndrickx GR, WijnsW. Simultaneous coronary pressure and flow velocity measurements inhumans. Feasibility, reproducibility, and hemodynamic dependence ofcoronary flow velocity reserve, hyperemic flow versus pressure slopeindex, and fractional flow reserve. Circulation 1996;94:1842–19.
6. Vassalli G, Hess OM. Measurement of coronary flow reserve and itsrole in patient care. Basic Res Cardiol 1998; 93:339–53.
7. Haase J, Escaned J, van Swijndregt EM, et al. Experimental validationof geometric and densitometric coronary measurements on the newgeneration Cardiovascular Angiography Analysis System (CAAS II).Cathet Cardiovasc Diagn 1993;30:104–14.
8. Wesbey GE, Englestad BL, Brasch RC. Paramagnetic pharmaceuti-cals for magnetic resonance imaging. Physiol Chem Phys Med NMR1984;16:145–55.
9. Jerosch-Herold M, Wilke N, Wang Y, et al., Cardiac MRI Group. Directcomparison of an intravascular and an extracellular contrast agent forquantification of myocardial perfusion. Int J Card Imaging 1999;15:453–64.
0. Cerqueria MD, Weissman NJ, Dilsizian V, et al. Standardizedmyocardial segmentation and nomenclature for tomographic imagingof the heart: a statement for healthcare professionals from the CardiacImaging Committee of the Council on Clinical Cardiology of theAmerican Heart Association. Circulation 2002;105:539–542.
1. Jerosch-Herold, M, Wilke N, Stillman AE. Magnetic resonance quanti-fication of the myocardial perfusion reserve with a Fermi function modelfor constrained deconvolution. Med Phys 1998;25:73–84.
2. Axel L. Tissue mean transit time from dynamic computed tomographyby a simple deconvolution technique. Invest Radiol 1983;18:94–9.
3. Bassingthwaighte B, Goresky CA. Modeling in the analysis of soluteand water exchange in the microvasculature. In: Renkin EM, MichelCC, editors. Handbook of Physiology: The Cardiovascular System.Bethesda, MD: American Physiology Society, 1984:549–626.
4. Kroll K, Wilke N, Jerosch-Herold M, et al. Modeling regionalmyocardial flows from residue functions of an intravascular indicator.Am J Physiol 1996;271:H1643–55.
5. Kraitchman DL, Wilke N, Hexeberg E, et al. Myocardial perfusionand function in dogs with moderate coronary stenosis. Magn ResonMed 1996;35:771–80.
6. Mühling OM, Dickson ME, Zenovich A, et al. Quantitative magneticresonance first-pass perfusion analysis: inter- and intraobserver agree-ment. J Cardiovasc Magn Reson 2001;3:247–56.
7. Leber AW, Becker A, Knez A, et al. Accuracy of 64-slice computedtomography to classify and quantify plaque volumes in the proximalcoronary system: a comparative study using intravascular ultrasound.J Am Coll Cardiol 2006;47:672–7.
8. Zeiher AM, Drexler H, Wollschlager H, Just H. Endothelial dysfunc-tion of the coronary microvasculature is associated with coronary bloodflow regulation in patients with early atherosclerosis. Circulation1991;84:1984–92.
9. Uren NG, Camici PG, Melin JA, et al. Effect of aging on myocardialperfusion reserve. J Nucl Med 1995;36:2032–6.
0. Nahser PJ Jr., Brown RE, Oskarsson H, Winniford MD, Rossen JD.Maximal coronary flow reserve and metabolic coronary vasodilation inpatients with diabetes mellitus. Circulation 1995;91:635–60.
1. Takiuchi S, Rakugi H, Masuyama T, et al. Hypertension attenuates theefficacy of hypoglycemic therapy for preserving coronary flow reserve inpatients with type 2 diabetes. Hypertens Res 2002;25:893–900.
2. Wang L, Jerosch-Herold M, Jacobs DR Jr., et al. Coronary riskfactors and myocardial perfusion in asymptomatic adults: theMulti-Ethnic Study of Atherosclerosis (MESA). J Am Coll Car-
diol 2006;47:565–72. F3. Thorne S, Mullen MJ, Clarkson P, Donald AE, Deanfield JE. Earlyendothelial dysfunction in adults at risk from atherosclerosis: differentresponses to L-arginine. J Am Coll Cardiol 1998;32:110–6.
4. Yanagisawa H, Chikamori T, Tanaka N, Usui Y, Takazawa K,Yamashina A. Application of pressure-derived myocardial fractionalflow reserve in assessing the functional severity of coronary arterystenosis in patients with diabetes mellitus. Circ J 2004;68:993–8.
5. Tamita K, Akasaka T, Takagi T, et al. Effects of microvasculardysfunction on myocardial fractional flow reserve after percutaneouscoronary intervention in patients with acute myocardial infarction.Catheter Cardiovasc Interv 2002;57:452–9.
6. Gould KL, Kirkeeide RL, Buchi M. Coronary flow reserve as aphysiologic measure of stenosis severity. J Am Coll Cardiol 1990;15:459–74.
7. Uren NG, Melin JA, De Bruyne B, Wijns W, Baudhuin T, CamiciPG. Relation between myocardial blood flow and the severity ofcoronary-artery stenosis. N Engl J Med 1994;330:1782–8.
8. Paetsch I, Jahnke C, Wahl A, et al. Comparison of dobutamine stressmagnetic resonance, adenosine stress magnetic resonance, and adenosinestress magnetic resonance perfusion. Circulation 2004;110:835–42.
9. Selvanayagam JB, Jerosch-Herold M, Porto I, et al. Resting myocar-dial blood flow is impaired in hibernating myocardium: a magneticresonance study of quantitative perfusion assessment. Circulation2005;112:3289–96.
0. Di Mario C, Moses JW, Anderson TJ, et al., DESTINI (DopplerEndpoint Stenting International Investigation) Study Group. Ran-domized comparison of elective stent implantation and coronaryballoon angioplasty guided by online quantitative angiography andintracoronary Doppler. Circulation 2000;102:2938–44.
1. Bedaux WL, Hofman MB, de Cock CC, Stoel MG, Visser CA, vanRossum AC. Magnetic resonance imaging versus Doppler guide wirein the assessment of coronary flow reserve in patients with coronaryartery disease. Coron Artery Dis 2002;13:365–72.
2. Panting JR, Gatehouse PD, Yang GZ, et al. Abnormal subendocardialperfusion in cardiac syndrome X detected by cardiovascular magneticresonance imaging. N Engl J Med 2002;346:1948–53.
3. Miller DD, Donohue TJ, Younis LT, et al. Correlation ofpharmacological99mTc-sestamibi myocardial perfusion imaging withpoststenotic coronary flow reserve in patients with angiographicallyintermediate coronary artery stenoses. Circulation 1994;89:2150–60.
4. Heller LI, Cates C, Popma J, et al., FACTS Study Group. Intracoro-nary Doppler assessment of moderate coronary artery disease: com-parison with201Tl imaging and coronary angiography. Circulation1997;96:484–90.
5. Chamuleau SA, Meuwissen M, van Eck-Smit BLF, et al. Fractionalflow reserve, absolute and relative coronary blood flow velocity reservein relation to the results of technetium-99m sestamibi single-photonemission computed tomography in patients with two-vessel coronaryartery disease. J Am Coll Cardiol 2001;37:1316–22.
6. Hacker M, Rieber J, Schmid R, et al. Comparison of Tc-99msestamibi SPECT with fractional flow reserve in patients with inter-mediate coronary artery stenoses. J Nucl Cardiol 2005;12:645–54.
7. Erhard I, Rieber J, Jung P, et al. The validation of fractional flowreserve in patients with coronary multivessel disease: a comparisonwith SPECT and contrast-enhanced dobutamine stress echocardio-graphy. Z Kardiol 2005;94:321–7.
8. Kim C, Kwok YS, Heagerty P, Redberg R. Pharmacologic stresstesting for coronary disease diagnosis: a meta-analysis. Am Heart J2001;142:934–44.
9. White CW, Wright CB, Doty DB, et al. Does visual interpretation ofthe coronary arteriogram predict the physiologic importance of acoronary stenosis? N Engl J Med 1984;310:819–24.
0. Nagel E, Klein C, Paetsch I, et al. Magnetic resonance perfusionmeasurements for the noninvasive detection of coronary artery disease.Circulation 2003;108:432–7.
APPENDIX
or accompanying videos, please see the online version of this article.