
Psychosocial predictors of smoking among secondary school students in Al-Hassa, Saudi Arabia
15
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/49803524 Psychosocial predictors of smoking among secondary school students in Al-Hassa, Saudi Arabia Article in Journal of Behavioral Medicine · February 2011 DOI: 10.1007/s10865-011-9319-7 · Source: PubMed CITATIONS 13 READS 116 3 authors, including: Some of the authors of this publication are also working on these related projects: Diabetic foot ulcer: pattern of risk among Egyptians View project Tarek Tawfik Amin Cairo University 72 PUBLICATIONS 551 CITATIONS SEE PROFILE Mostafa Amr Mansoura University 89 PUBLICATIONS 528 CITATIONS SEE PROFILE All content following this page was uploaded by Mostafa Amr on 03 February 2014. The user has requested enhancement of the downloaded file. All in-text references underlined in blue are linked to publications on ResearchGate, letting you access and read them immediately.
Transcript of Psychosocial predictors of smoking among secondary school students in Al-Hassa, Saudi Arabia

Seediscussions,stats,andauthorprofilesforthispublicationat:https://www.researchgate.net/publication/49803524
PsychosocialpredictorsofsmokingamongsecondaryschoolstudentsinAl-Hassa,SaudiArabia
ArticleinJournalofBehavioralMedicine·February2011
DOI:10.1007/s10865-011-9319-7·Source:PubMed
CITATIONS
13
READS
116
3authors,including:
Someoftheauthorsofthispublicationarealsoworkingontheserelatedprojects:
Diabeticfootulcer:patternofriskamongEgyptiansViewproject
TarekTawfikAmin
CairoUniversity
72PUBLICATIONS551CITATIONS
SEEPROFILE
MostafaAmr
MansouraUniversity
89PUBLICATIONS528CITATIONS
SEEPROFILE
AllcontentfollowingthispagewasuploadedbyMostafaAmron03February2014.
Theuserhasrequestedenhancementofthedownloadedfile.Allin-textreferencesunderlinedinbluearelinkedtopublicationsonResearchGate,lettingyouaccessandreadthemimmediately.

1 23
Journal of Behavioral Medicine ISSN 0160-7715Volume 34Number 5 J Behav Med (2011) 34:339-350DOI 10.1007/s10865-011-9319-7
Psychosocial predictors of smokingamong secondary school students in Al-Hassa, Saudi Arabia
Tarek Tawfik Amin, Mostafa AbdelMonhem Amr & Burhan Omar Zaza

1 23
Your article is protected by copyright and
all rights are held exclusively by Springer
Science+Business Media, LLC. This e-offprint
is for personal use only and shall not be self-
archived in electronic repositories. If you
wish to self-archive your work, please use the
accepted author’s version for posting to your
own website or your institution’s repository.
You may further deposit the accepted author’s
version on a funder’s repository at a funder’s
request, provided it is not made publicly
available until 12 months after publication.

Psychosocial predictors of smoking among secondary schoolstudents in Al-Hassa, Saudi Arabia
Tarek Tawfik Amin • Mostafa Abdel Monhem Amr •
Burhan Omar Zaza
Received: March 27, 2010 / Accepted: January 19, 2011 / Published online: February 1, 2011
� Springer Science+Business Media, LLC 2011
Abstract The objective of this study was to determine
the prevalence and determinants of the current smoking
status among secondary school students in Al-Hassa, Saudi
Arabia. A total of 1,652 secondary school adolescents were
selected by multistage proportionate sampling method.
Data collection was carried out through self-administered
anonymous questionnaire including: Arabic version of the
Global Youth Tobacco Survey, modified Fagerstrom Test
for Nicotine Dependence and Patient Health Questionnaire
to asses for anxiety and depressive disorders. This study
revealed that the prevalence of current smokers was 21.7.
Seventy-one percent of current cigarette smokers were
minimally nicotine dependent. Major depressive and anx-
iety disorders were significantly higher among current
smokers. Hierarchical regression analysis shows that, male,
older age, smoking of close relatives and friends, anxiety
disorders and socializing motives were statistically signif-
icant determinants of current smoking status among the
included adolescents. Family members should be made
aware of the detrimental influence their smoking behavior
has on their youth. Counseling and preventive psychiatric
services should be an integral part of the clinical facilities
caring for secondary school students.
Keywords Smoking � Smoking predictors �Secondary schools � Adolescents � Saudi Arabia
Introduction
The World Health Organization (WHO) attributes 4.9
million deaths a year to tobacco use, a figure expected to
rise to[10 millions by 2030 if the current trend continues
(Peto and Lopez 2001). Almost 70% of these premature
deaths will be in the developing countries, one-third (*2.3
millions) of which will be among children (WHO 1999).
Morbidity and mortality associated with tobacco use is
shifting from the developed to developing countries,
especially low and middle-income Arab countries (Jha and
Chaloupka 2000). According to the WHO reports, smoking
prevalence among young people in Arab countries differs
greatly: 7% in Oman, 14% in Iran, 18% in Kuwait, 23% in
Iraq, 25% in Jordan, 31% in Syria, 43% in Yemen and 53%
in Lebanon (WHO 2001). Smoking is a major public health
problem in Saudi Arabia and it is increasing at an alarming
rate (Al-Turki 2006; Merdad et al. 2007; Al-Turki and
Al-Rowais 2008). In Riyadh, among a sample of 230 health
care providers, 29% of males and 11.6% of females
smoked cigarettes at the time of their study (Siddiqui and
Ogbeide 2001). Jarallah et al. (1999) surveyed Saudi
nationals in three regions of Saudi Arabia and reported that
the overall prevalence of current smoking was 21.1% for
males and 0.9% for females. Most smokers (78%) were
young to middle-aged (21–50 years). Smoking prevalence
T. T. Amin (&)
Family and Community Medicine Department, College
of Medicine-Al Hassa, King Faisal University, PO Box 400,
Al-Hassa 31982, Saudi Arabia
e-mail: [email protected]
T. T. Amin
Community Health Department, Faculty of Medicine,
Cairo University, Cairo, Egypt
M. A. M. Amr
Department of Clinical Neuroscience, College of Medicine-Al
Hassa, King Faisal University, Al-Hassa, Saudi Arabia
B. O. Zaza
School Health Program Technical Manager, Ministry
of Education, Local Directorate-Al Hassa, Al Hassa,
Saudi Arabia
123
J Behav Med (2011) 34:339–350
DOI 10.1007/s10865-011-9319-7
Author's personal copy

was higher among married, uneducated, and those in certain
occupations including manual workers, businessmen, army
officers, and office workers. Saudi Authorities banned
smoking based on religious backgrounds (Fatwa) since
1926. The existence of many social, cultural, and religious
inhibitions may prevent smokers from providing accurate
information about their smoking status (Bassiony 2009).
Several explanations for the increased trend of tobacco use
among Saudi population were provided. First, despite the
recent increase in tobacco taxes; cigarettes are still very
inexpensive in Saudi Arabia compared with other countries;
the average price for a pack of 20 cigarettes in Saudi Arabia
is $1.3 compared with about $3 in the United States and
$5.4 in Norway (Schultz et al. 1998). In Saudi Arabia
people on low income and young children can obtain cig-
arettes easily (Abdalla et al. 2009). Second, the increase in
tobacco use might represent a relief from psychological
distress that may be attributable to increased stress on Saudi
families undergoing rapid social and cultural transformation
(Al-Gelban 2007) and lastly, the incorrect beliefs about the
possible advantages of smoking might add to this high
prevalence. For instance, many Saudi smokers reported that
smoking calmed them down (Abolfotouh et al. 1998). Over
the past 30 years, the number of young Saudi smokers has
increased. The prevalence of regular smokers among male
secondary school students was 12% in 1987 (Rowlands and
Shipster 1987), 22% in 1993 (Saeed et al. 1993) and 29.8%
in 2004 (Al-Damegh et al. 2004). The prevalence of
smoking among females was much less; about 14% in 1993
(Saeed et al. 1993), 11.1% in 2006 (Abdalla et al. 2007) and
14.9% in 2009 (Abou-Zeid et al. 2009). Recent studies have
shown that peer smoking seemed to be the most important
factor influencing smoking behavior among young people
(Qidwai et al. 2010; Ferreira and Torgal 2010). In addition,
interviews with adolescents who have begun smoking
showed that a large majority (80%) of initial cigarette
smoking experimentation occurs in the presence of other
adolescents who are smoking (Friedman et al. 1985). In
fact, smoking is usually a shared activity with important
socialization functions for youth (McGraw et al. 1991).
Desire, Idleness, imitation, relief from psychological ten-
sion and improve self-esteem are among the motives to
smoke among Saudis (Al-Faris 1995). Smoking parents and
siblings seems to be important in the initiation as well as the
continuation of smoking behavior. Al-Mohamed and Amin
(2010) found that those aged 19–20 years whose relatives
‘especially parents and siblings’ currently smoke were
almost twice as likely to smoke as those whose relatives had
never smoked (Al-Mohamed and Amin 2010). In addition, a
study from Saudi Arabia reported that the average starting
age for current smokers was 13.8 years and the proportion
of adolescents smoke increases with age (Al Yousef and
Karim 2001).
A series of studies noted that cigarette smoking among
youth is a complex behavior with several identifiable
determinants including: interpersonal factors (such as fam-
ily and peer influence), intrapersonal factors (self-esteem),
individual motivational and attitudinal determinants as well
as cultural settings (Goddard 1990; O’Loughlin et al. 1998;
Kandel et al. 2007). Furthermore, there is an increasing body
of research demonstrating the presence of psychiatric dis-
orders among tobacco smokers compared with nonsmokers
(Sonntag et al. 2000; Griesler et al. 2008). For example, two
epidemiological studies found that cigarettes smoking to
be correlated significantly with depression (Nelson and
Wittchen 1998; Dierker et al. 2001). Similarly, Breslau and
Klein (1999) reported an association between tobacco
smoking and higher incidence of panic symptoms. In Egypt,
in a nationwide representative survey of general secondary
school students it was reported that smokers had signifi-
cantly more behavioral deviations and receiving psychiatric
treatment more often than nonsmokers (Soueif et al. 1990).
In Saudi Arabia, surprisingly little attention has been paid
to psychiatric morbidity, especially anxiety and depres-
sive symptoms among young smokers and considerable
researches have focused only on the smoking habits as well
as the related demographic and socioeconomic parameters.
To address the existing gap in the literature on smoking
among adolescents we have tested the following hypothe-
ses: First, older male adolescents are more likely to smoke
tobacco than younger and female adolescents. Second,
smoking among close relatives (environmental tobacco
exposure) and friends (peer pressure) would increase the
likelihood (risk) of being current smoker. Finally, certain
motives (socializing, imitation, outing, rather than relieve of
stress and pleasure) and the presence of depressive and/or
anxiety disorders may represent potential predictors for the
current smoking status among adolescents. To the best of the
authors’ knowledge, there are no previous studies in Saudi
Arabia that address the psychosocial predictors of smoking
status among this age group. In this study, we attempted to
provide baseline information on the psychosocial determi-
nants and prevalence of smoking among adolescents in
secondary school in Al Hassa, KSA, for proper design of
practical and effective intervention strategy.
Methods
A cross-sectional descriptive study carried out in Al-Hassa
Governorate, located in the Eastern Province of Saudi
Arabia, populated with nearly one million Saudis. Al-Hassa
is comprised of three areas; urban, populated by about 60%
of total population and consisted of five major districts,
rural, consisted of eight major villages and 15 other rural
collections, occupied by 35% and Hegar ‘‘Bedouin scattered
340 J Behav Med (2011) 34:339–350
123
Author's personal copy

communities’’ represented 5% ‘‘nearest Hegar is about
65 km distance’’.
Participants
The total students enrolled at secondary schools in Al
Hassa according to the local Directorate of Education year
2009 were 50,399, of which 24,466 were males distributed
in 52 schools in urban (N = 14,337) and rural (N =
10,129) areas. Females secondary schools (N = 51) with a
total population of 25,933; 16,753 in urban and 9,180 in
rural. Considering smoking prevalence of 30% (Abdalla
et al. 2007), the worst acceptable frequency of 27%, using
a confidence level of 95%; the minimum sample size would
be 1,490 students.
An additional 30% was added for the possible non-
response; subsequently, the total sample size would be
1,930: of which males would constitute 49% (N = 950).
Appropriate sampling fraction was used to calculate urban–
rural samples; 1,200 subjects were targeted from urban and
750 from rural schools. Secondary schools were randomly
assigned using an updated sampling frame, where 10 urban,
two from each urban district (5 males and 5 females) and
8 rural schools, one from each major village (4 male and
4 females) were selected. Proportionate sample size was
selected from each school according to the number of
enrolled students in the assigned schools. In the final phase
we employed a systematic technique using the academic
number from school roster to randomly select Saudi students.
Research protocols and data collection tools were approved
by our institution and the local Directorate of Education.
Consent forms were sent to students’ parents/guardians at
home following subjects’ selection a week before the data
collection phase. Those demonstrated parental/guardians’
approvals with signed consent forms were included. Assents
were obtained from the included students. Proper orientation
was carried out to explain the objectives of the study with
emphasis on the right of non participation. The data confi-
dentiality was preserved throughout.
Measures
Anonymous self-administered questionnaire was used for
data collection included the following:
Socio-demographic characteristics: age in years, gender,
residence, parental occupational and educational status,
family income in Saudi Riyals, the presence of any
co-morbid disease or chronic conditions ‘verified through
asking the teachers and revision of school files’.
The Arabic version of the Global Youth Tobacco Survey
2001 (GYTS 2001) developed by Centers for Diseases
Control (CDC, Atlanta, GA, USA) for smoking survey
among youth was used to determine pattern and prevalence
of smoking, similar questions were used to assess water-
pipe (WP) or shisha smoking. Those who had not smoked
in the previous 12 months or longer were asked to consider
themselves as former smokers. Ever smokers included both
current and former smokers while current smoker was
defined as those who smoked one or more cigarette(s) and/
or WP within the past 30 days.
Nicotine dependence: This item was measured using the
modified Fagerstorm test for nicotine dependence (FTND)
(Fagerstrom and Schneider 1989). A widely used and
validated 6-items questionnaire to assess severity of nico-
tine dependence with scores that ranges from 0 to 10. A
score of B4 suggests a low level of nicotine dependence,
while a score C6 usually indicates high dependence level.
A clinically validated screening instrument; the Patient
Health Questionnaire (PHQ) was administered to deter-
mine the prevalence of current depressive and anxiety
disorders: Depression was measured using the Patient
Health Questionnaire (PHQ-9) which is a nine-item
instrument based on the nine DSM-IV criteria for a major
depressive episode. This instrument asks the respondent to
indicate the frequency of various symptoms over the past
2 weeks. Following the standard algorithms for interpret-
ing the results of PHQ-9 (Spitzer et al. 1999), we catego-
rized students as screening positive for major depression,
other depressive disorders including mild depression, dys-
thymia and minor depression. This tool has been validated
as being highly correlated with diagnosis made by mental
health professionals and other depression assessment tools
(Diez-Quevedo et al. 2001; Henkel et al. 2004; Kroenke
et al. 2001) in a variety of populations. In the original
validation study, the sensitivity and specificity were 73%
and 98%, respectively, for major depression among pri-
mary care patients (Spitzer et al. 1999).
Anxiety was measured using items from the Patient-
Health-Questionnaire (PHQ). Items asked about symptoms
of panic and generalized anxiety disorders over the past
4 weeks. Standard algorithm was employed to categorize
students as screening positive for panic disorder, general-
ized anxiety disorder, both, or neither (Spitzer et al. 1999).
In the original validation study the sensitivity and speci-
ficity of the PHQ anxiety scale were 81 and 99%, respec-
tively, for panic disorder, and 63 and 97% for generalized
anxiety disorder (Spitzer et al. 1999).
Three questions from the National Comorbidity Survey
Replication (Kessler et al. 2005) were used to assess
suicidality in the past 4 weeks. These questions asked
whether in the past 4 weeks the respondent ever seriously
thought about committing suicide, made a plan for com-
mitting or attempted suicide.
School visits were carried out to conduct orientation
sessions for schools administration staff and selected
J Behav Med (2011) 34:339–350 341
123
Author's personal copy

students regarding the objectives, contents and data confi-
dentiality. With regards to female schools, female teachers
were assigned for procedures of orientation, and data col-
lection under the supervision of a female research assistant
and in response to the conservative nature of Saudi culture.
Questionnaire administration was carried out at school’s
library or computer laboratory in anonymous and solicited
setting after reading it loudly.
Pilot testing and reliability analysis: Initial data collec-
tion form was tested on 102 secondary school students
beyond the sample size, at a nearby school for convenience.
Pilot testing was used to identify the possible common
motives for smoking behavior and for reliability testing of
the used data collection tools. The reliability coefficients
(Cronbach’s a) for PHQ-9 were 0.79, PHQ selected anxiety
items was 0.76, and for suicidality it was (0.73).
Statistical analysis
Questionnaires with missing of more than two elements
were discarded (N = 71). The overall response rate was
89.3% and it was 66.8% among urban female secondary
schools.
Data entry and analysis was carried out using SPSS
version 13.0 (SPSS Inc., Chicago IL, USA). Categorical
data were reported in frequency, proportion and percent-
age, univariate analysis with estimation of Odds ratio and
95% confidence intervals, Chi-square, Fisher exact and
Z test for proportions tests of significance were used for
comparisons. Continuous data were expressed using mean,
median and standard deviation, student’s t and Mann–
Whitney tests of significance were used for comparisons.
Scores of the PHQ were classified according to the pro-
posed algorithm (Spitzer et al. 1999) into any depression,
major depression, panic and anxiety disorders.
Regression analysis: Hierarchical logistic regression
analysis was generated to determine whether socio-demo-
graphic variables (age, gender), exposure to environmental
tobacco (smoking among close relatives and friends), the
motives for smoking and the presence of psychiatric mor-
bidity in the form of depression or anxiety are potential
determinants for the adoption of the current smoking status.
Predictors were entered in three steps according to a
specified hierarchy (O’Loughlin et al. 1998; Jarallah et al.
1996): The first step included forced entry of demographic
variables (gender, age in years). The second step entailed
entry of smoking among close family members and close
friends. The final step entailed entry of possible psycho-
social predictors; motives for current smoking status
(socializing, outing, vs. relieving stress) and the presence
of depressive or anxiety disorders.
This procedure for constructing hierarchy was recom-
mended by (DeCoster 2006) to reduce potential problems
with multicollinearity. Odds ratio with 95% confidence
intervals, change in v2 were evaluated at the final step of
the regression equation when all variables were entered.
Because there are no agreed-upon measures for R2 contri-
butions to date in multilevel logistic regression, we ana-
lyzed the data as a single level model to obtain the
Nagelkerke R2 statistic (Nagelkerke 1991), which com-
pares the null model and fitted model likelihood functions
as a proportion of the maximum possible R2 value. The R2s
for all predictors and Chi-square statistic with its signifi-
cance were reported for the single-level logistic regression,
since there are no agreed-upon measures in hierarchical
logistic multivariate analysis. Dummy codes were used in
entering of dichotomous variables for the generation of
intercorrelation matrix (Pearson correlation coefficients)
and hierarchical models: Gender (1 = male, 0 = female),
smoking among close relatives (1 = father and/or brothers,
0 = others or none), smoking among friends (1 = All or
most of them, 0 = some or none), motives (1 = socializ-
ing, imitation, outing, 0 = relieve of stress, pleasure),
depression (1 = any depression, 0 = none), Anxiety dis-
orders (1 = present, 0 = none). Probability used for
inclusion in the regression model was 0.05 and for removal
was set at P = 0.10. Statistical significance was set at 0.05.
Results
The sample composed of 1,652 secondary school students,
of which 60.4% were males. Age ranged from 15 to
19 years with a mean of 17.5 ± 1.0 (males 17.4 ± 1.1 and
females 17.4 ± 1.0) years. Urban students represented
57.5% of the sample.
Prevalence of smoking: For any type of tobacco; 358
(21.7%) were considered as the current smokers (both
genders). The prevalence of current smokers was 30.3 and
8.5% among males and females, respectively. Of the total,
419 (25.4%) were ever smokers as 43 males and 18 females
reported as being former smokers (ever smokers were 34.6
and 11.3% among males and females, respectively), 1,233
were never smokers (74.6 and 88.7% among males and
females, respectively). Forms of tobacco use among cur-
rent smokers includes: cigarettes in 224 (62.6%) as the only
method of tobacco use (in 175/224 78.1% of current
smokers) or in combination with WP/shisha in 59/224
(26.3%). WP as a method of tobacco was mentioned by
193/358 (53.9%) of current tobacco users, while both
cigarettes and WP smoking were used by 59/358 (16.5%).
Table 1 demonstrates the socio-demographics of the
included students in relation to their current smoking sta-
tus: Male gender (Odds ratio ‘OR’ = 4.65), higher years at
secondary school (3rd grade, OR = 1.77, P = 0.001),
older age of students ([18 years, OR = 2.34, P = 0.001)
342 J Behav Med (2011) 34:339–350
123
Author's personal copy
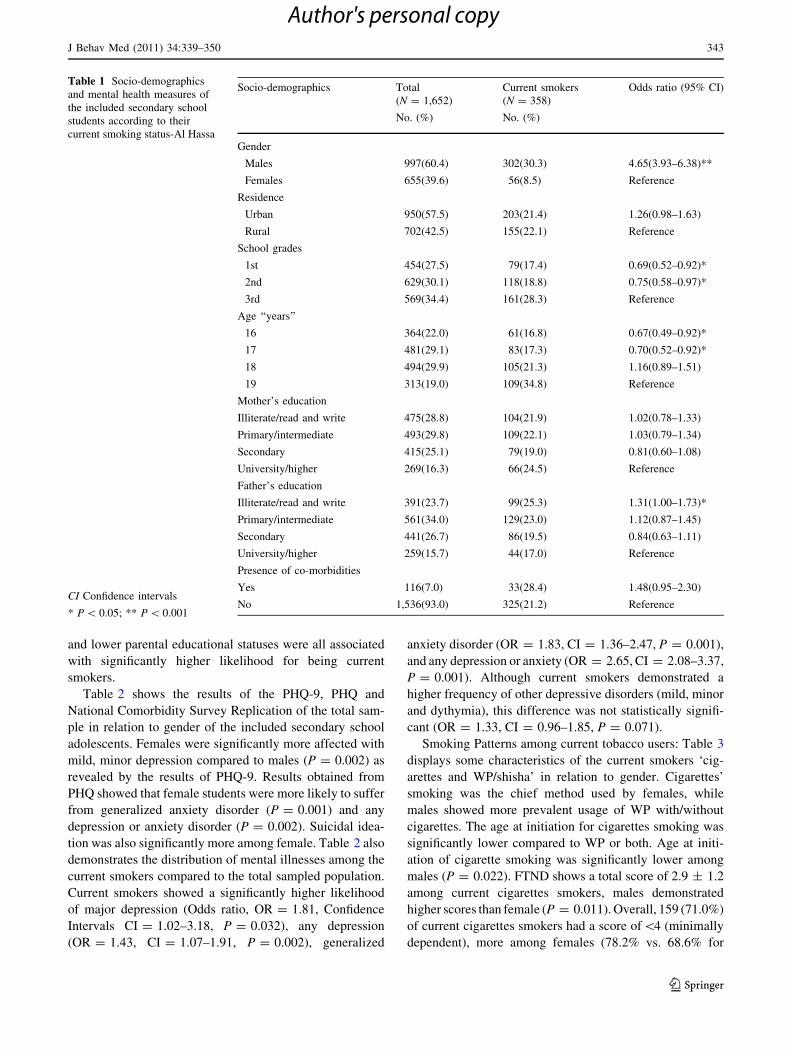
and lower parental educational statuses were all associated
with significantly higher likelihood for being current
smokers.
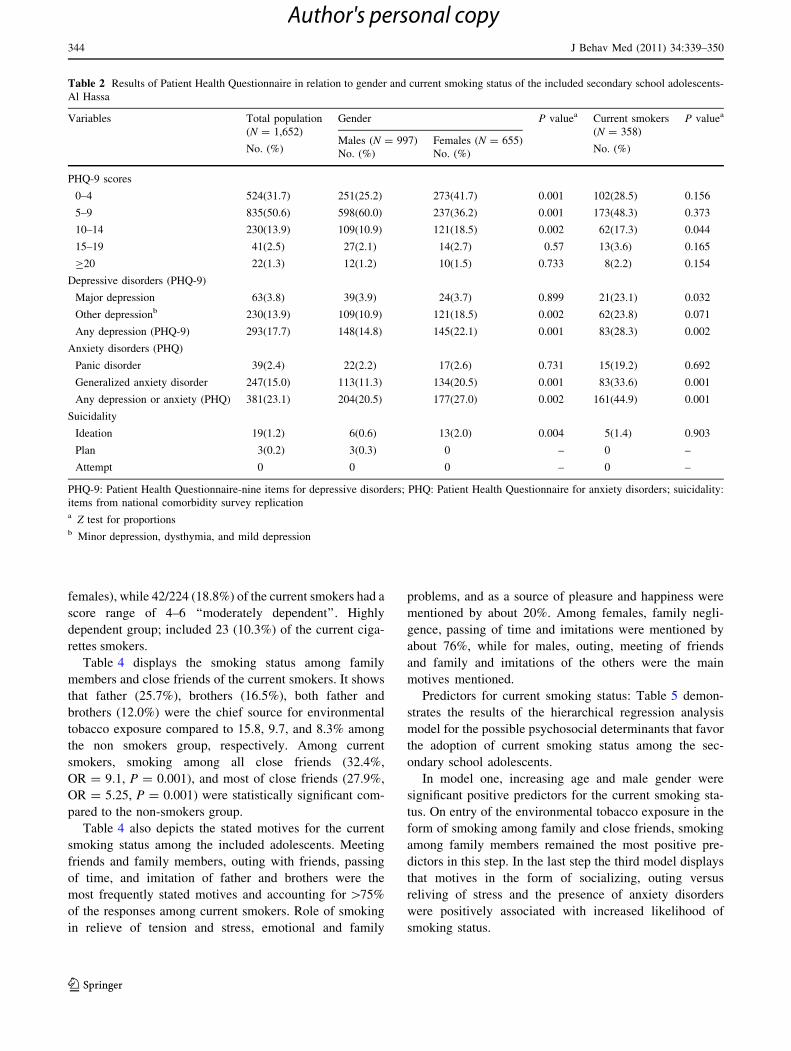
Table 2 shows the results of the PHQ-9, PHQ and
National Comorbidity Survey Replication of the total sam-
ple in relation to gender of the included secondary school
adolescents. Females were significantly more affected with
mild, minor depression compared to males (P = 0.002) as
revealed by the results of PHQ-9. Results obtained from
PHQ showed that female students were more likely to suffer
from generalized anxiety disorder (P = 0.001) and any
depression or anxiety disorder (P = 0.002). Suicidal idea-
tion was also significantly more among female. Table 2 also
demonstrates the distribution of mental illnesses among the
current smokers compared to the total sampled population.
Current smokers showed a significantly higher likelihood
of major depression (Odds ratio, OR = 1.81, Confidence
Intervals CI = 1.02–3.18, P = 0.032), any depression
(OR = 1.43, CI = 1.07–1.91, P = 0.002), generalized
anxiety disorder (OR = 1.83, CI = 1.36–2.47, P = 0.001),
and any depression or anxiety (OR = 2.65, CI = 2.08–3.37,
P = 0.001). Although current smokers demonstrated a
higher frequency of other depressive disorders (mild, minor
and dythymia), this difference was not statistically signifi-
cant (OR = 1.33, CI = 0.96–1.85, P = 0.071).
Smoking Patterns among current tobacco users: Table 3
displays some characteristics of the current smokers ‘cig-
arettes and WP/shisha’ in relation to gender. Cigarettes’
smoking was the chief method used by females, while
males showed more prevalent usage of WP with/without
cigarettes. The age at initiation for cigarettes smoking was
significantly lower compared to WP or both. Age at initi-
ation of cigarette smoking was significantly lower among
males (P = 0.022). FTND shows a total score of 2.9 ± 1.2
among current cigarettes smokers, males demonstrated
higher scores than female (P = 0.011). Overall, 159 (71.0%)
of current cigarettes smokers had a score of\4 (minimally
dependent), more among females (78.2% vs. 68.6% for
Table 1 Socio-demographics
and mental health measures of
the included secondary school
students according to their
current smoking status-Al Hassa
CI Confidence intervals
* P \ 0.05; ** P \ 0.001
Socio-demographics Total
(N = 1,652)
No. (%)
Current smokers
(N = 358)
No. (%)
Odds ratio (95% CI)
Gender
Males 997(60.4) 302(30.3) 4.65(3.93–6.38)**
Females 655(39.6) 56(8.5) Reference
Residence
Urban 950(57.5) 203(21.4) 1.26(0.98–1.63)
Rural 702(42.5) 155(22.1) Reference
School grades
1st 454(27.5) 79(17.4) 0.69(0.52–0.92)*
2nd 629(30.1) 118(18.8) 0.75(0.58–0.97)*
3rd 569(34.4) 161(28.3) Reference
Age ‘‘years’’
16 364(22.0) 61(16.8) 0.67(0.49–0.92)*
17 481(29.1) 83(17.3) 0.70(0.52–0.92)*
18 494(29.9) 105(21.3) 1.16(0.89–1.51)
19 313(19.0) 109(34.8) Reference
Mother’s education
Illiterate/read and write 475(28.8) 104(21.9) 1.02(0.78–1.33)
Primary/intermediate 493(29.8) 109(22.1) 1.03(0.79–1.34)
Secondary 415(25.1) 79(19.0) 0.81(0.60–1.08)
University/higher 269(16.3) 66(24.5) Reference
Father’s education
Illiterate/read and write 391(23.7) 99(25.3) 1.31(1.00–1.73)*
Primary/intermediate 561(34.0) 129(23.0) 1.12(0.87–1.45)
Secondary 441(26.7) 86(19.5) 0.84(0.63–1.11)
University/higher 259(15.7) 44(17.0) Reference
Presence of co-morbidities
Yes 116(7.0) 33(28.4) 1.48(0.95–2.30)
No 1,536(93.0) 325(21.2) Reference
J Behav Med (2011) 34:339–350 343
123
Author's personal copy
females), while 42/224 (18.8%) of the current smokers had a
score range of 4–6 ‘‘moderately dependent’’. Highly
dependent group; included 23 (10.3%) of the current ciga-
rettes smokers.
Table 4 displays the smoking status among family
members and close friends of the current smokers. It shows
that father (25.7%), brothers (16.5%), both father and
brothers (12.0%) were the chief source for environmental
tobacco exposure compared to 15.8, 9.7, and 8.3% among
the non smokers group, respectively. Among current
smokers, smoking among all close friends (32.4%,
OR = 9.1, P = 0.001), and most of close friends (27.9%,
OR = 5.25, P = 0.001) were statistically significant com-
pared to the non-smokers group.
Table 4 also depicts the stated motives for the current
smoking status among the included adolescents. Meeting
friends and family members, outing with friends, passing
of time, and imitation of father and brothers were the
most frequently stated motives and accounting for [75%
of the responses among current smokers. Role of smoking
in relieve of tension and stress, emotional and family
problems, and as a source of pleasure and happiness were
mentioned by about 20%. Among females, family negli-
gence, passing of time and imitations were mentioned by
about 76%, while for males, outing, meeting of friends
and family and imitations of the others were the main
motives mentioned.
Predictors for current smoking status: Table 5 demon-
strates the results of the hierarchical regression analysis
model for the possible psychosocial determinants that favor
the adoption of current smoking status among the sec-
ondary school adolescents.
In model one, increasing age and male gender were
significant positive predictors for the current smoking sta-
tus. On entry of the environmental tobacco exposure in the
form of smoking among family and close friends, smoking
among family members remained the most positive pre-
dictors in this step. In the last step the third model displays
that motives in the form of socializing, outing versus
reliving of stress and the presence of anxiety disorders
were positively associated with increased likelihood of
smoking status.
Table 2 Results of Patient Health Questionnaire in relation to gender and current smoking status of the included secondary school adolescents-
Al Hassa
Variables Total population
(N = 1,652)
No. (%)
Gender P valuea Current smokers
(N = 358)
No. (%)
P valuea
Males (N = 997)
No. (%)
Females (N = 655)
No. (%)
PHQ-9 scores
0–4 524(31.7) 251(25.2) 273(41.7) 0.001 102(28.5) 0.156
5–9 835(50.6) 598(60.0) 237(36.2) 0.001 173(48.3) 0.373
10–14 230(13.9) 109(10.9) 121(18.5) 0.002 62(17.3) 0.044
15–19 41(2.5) 27(2.1) 14(2.7) 0.57 13(3.6) 0.165
C20 22(1.3) 12(1.2) 10(1.5) 0.733 8(2.2) 0.154
Depressive disorders (PHQ-9)
Major depression 63(3.8) 39(3.9) 24(3.7) 0.899 21(23.1) 0.032
Other depressionb 230(13.9) 109(10.9) 121(18.5) 0.002 62(23.8) 0.071
Any depression (PHQ-9) 293(17.7) 148(14.8) 145(22.1) 0.001 83(28.3) 0.002
Anxiety disorders (PHQ)
Panic disorder 39(2.4) 22(2.2) 17(2.6) 0.731 15(19.2) 0.692
Generalized anxiety disorder 247(15.0) 113(11.3) 134(20.5) 0.001 83(33.6) 0.001
Any depression or anxiety (PHQ) 381(23.1) 204(20.5) 177(27.0) 0.002 161(44.9) 0.001
Suicidality
Ideation 19(1.2) 6(0.6) 13(2.0) 0.004 5(1.4) 0.903
Plan 3(0.2) 3(0.3) 0 – 0 –
Attempt 0 0 0 – 0 –
PHQ-9: Patient Health Questionnaire-nine items for depressive disorders; PHQ: Patient Health Questionnaire for anxiety disorders; suicidality:
items from national comorbidity survey replicationa Z test for proportionsb Minor depression, dysthymia, and mild depression
344 J Behav Med (2011) 34:339–350
123
Author's personal copy

Discussion
The prevalence rates of current and ever smoking among
secondary school students in Al-Hassa are accounted for
21.4 and 25.4%, respectively. Such prevalence are in
accordance with the findings of others conducted in many
parts of Saudi Arabia (Al Yousef and Karim 2001;
Al-Damegh et al. 2004; Abdalla et al. 2007) and in other
countries of the Arab gulf, Middle East, Africa, Europe,
Asia and Latin America (Al-Haddad and Hamadeh 2003;
Maziak and Mzayek 2000; Kwamanga et al. 2003; Golan
et al. 2004; Valdivia et al. 2004; Washio et al. 2003).
Our figures are higher than those reported 20 years earlier
in similar studies by Felimban and Jarallah (1994) and
Al-Faris (1995) (12 and 17%, respectively). However, the
ever smoking prevalence rate is lower than the preva-
lence of 43.7% among the corresponding students in
Tabuk at the Western region of Saudi Arabia (Abdalla
et al. 2009).
Although cigarettes were used by most smokers in both
males and females in Saudi Arabia, WP or shisha although
relatively unpopular among educated people, was smoked
by many regular smokers, being common in the Western
region of Saudi Arabia (Abolfotouh et al. 1998). Many
people consider that WP smoking is less harmful than
cigarettes because they believe that the water filters out
harmful substances (Zahran et al. 1985). Our study
revealed a higher percentage of current smokers used
WP (53.9%) than other studies in Saudi Arabia; 43.6%
(Abolfotouh et al. 1998), or other Arab countries; 24.6% in
Kuwait (Mohammed et al. 2006) and 25.5% in Syrian Arab
Republic (Maziak et al. 2004). This could be explained by
the increasing popularity of WP smoking. The widespread
attention focused on the dangers of cigarette smoking,
Table 3 Pattern of smoking among current tobacco users of the included secondary school students in relation to gender
Smoking characteristics Gender P value
Males
(N = 302)
No. (%)
Females
(N = 56)
No. (%)
Total
(N = 358)
No. (%)
Smoking type (regular smokers)
Cigarettes only 116(38.4) 49(87.5) 165(46.1)
Shsisha (water pipe/Maassel) only 133(44.0) 1(1.8) 134(37.4) 0.010a
Cigarettes and Shisha 53(17.5) 6(10.7) 59(16.5)
Age at initiation
Cigarettes
B10 years 29(25.0) 0 29(17.5)
11 to \ 14 years 50(43.1) 8(16.3) 58(35.2) 0.001a
C14 years 37(31.9) 41(83.7) 78(47.3)
Mean ± SD (median) 12.7 ± 2.8(13.0) 13.9 ± 3.6(14.0) 13.2 ± 2.9(13.0) 0.022b
Shisha ‘‘Maassel’’
B10 years 5(3.8) 0 5(3.7)
11 to \ 14 years 43(32.3) 0 43(32.1)
C14 years 85(63.9) 1(100.0) 86(64.2) –
Mean ± SD (median) 15.1 ± 2.1(15.0) – – –
Cigarettes/Shisha
B10 years 7(13.2) 0 7(11.9)
11 to \ 14 years 23(43.4) 0 23(39.0) –
C14 years 23(43.4) 6(100.0) 29(49.1)
Mean ± SD (median) 14.7 ± 3.3(15.0) 16.4 ± 1.7(16.0) 15.4 ± 2.7(15.0) 0.231b
Total FTND score (for cigarettes) 169(56.0) 55(98.2) 224(62.3)
3.01 ± 1.27 2.03 ± 0.44 2.90 ± 1.17 0.011c
FTND Fagerstorm Nicotine Dependence scorea Fisher exactb t testc Mann–Whitney test
J Behav Med (2011) 34:339–350 345
123
Author's personal copy

coupled with the stigma associated, might unintentionally
encourage WP smoking (Mohammed et al. 2006). Other
reasons for this increasing trend may be because WP use is a
cultural form of hospitality among adults of the Middle East
and as youth approach adulthood this behavior becomes
more and more acceptable (Kandela 2000). These findings
suggest that tobacco-control programs must address all
forms of tobacco use, not just cigarettes. Consistent with
Table 4 Stated motives among
current smokers and smoking
among close family members
and close friends among
secondary school students-Al
Hassa
CI Confidence intervals
** P = \0.001a Sisters, mothers, grand
parents and other resident
family membersb More than one response was
mentioned� Only currently smokers
Variables Total
(N = 1,652)
No. (%)
Smokers�
(N = 358)
No. (%)
Odds ratio (95% CI)
Smoking among close family
Father 296(17.9) 92(31.1) 1.85(1.38–2.74)**
Brothers 185(11.2) 59(31.9) 1.83(1.29–2.59)**
Father and brothers 151(9.1) 43(28.5) 1.50(1.01–2.21)**
Othersa 110(6.7) 23(20.9) 0.95(0.58–1.57)
None 910(55.1) 141(15.5) Reference
Smoking close friends
All of them 131(7.9) 116(88.5) 9.06(6.41–12.83)**
Most of them 139(8.4) 100(71.9) 5.25(3.78–7.28)**
Some of them 425(25.7) 78(18.4) 0.76(0.57–1.01)
None 957(57.9) 64(6.7) Reference
Primary motives for smokingb
Meeting friends and family – 269(75.1) –
Outing with friends and company – 291(81.4) –
Boredom/passing of time – 272(76.0) –
Negligence by the family – 171(47.8) –
Imitations of father and brothers – 199(55.6) –
Relieve of tension and stresses – 73(20.4) –
Emotional and family problems – 62(17.3) –
Pleasure and happiness – 32(8.9) –
Table 5 Hierarchical regression analysis for smoking predictors among current secondary school smoking adolescents
Steps Variables entered Odds ratio (95% confidence intervals)
Model 1 Model 2 Model 3
1. Socio-demographics Age 1.83(1.24–2.70)*** 1.62(1.13–2.32)** 1.23(1.15–2.58)**
Gender 3.4(1.46–8.35)*** 2.71(1.61–4.56)*** 1.79(1.17–2.74)*
2. Environmental tobacco exposure Close relatives 3.30(2.1–5.17)*** 2.09(1.22–3.58)**
Friends 2.78(1.28–6.07)** 1.51(0.62–1.94)
3. Motives and psychiatric morbidity Motives 1.98(1.34–2.93)**
Depression 1.39(0.83–2.33)
Anxiety 2.18(1.42–3.34)**
Constant 13.35 13.08 12.25
R2! 0.133 0.195 .216
Dv2 26.44 28.17 31.32
Significance 0.001 0.003 0.005
Gender (1 = male, 0 = female), age in years, smoking among close relatives (1 = father and brothers, 0 = others or none), smoking among
friends (1 = All or most of them, 0 = some or none), motives (1 = socializing, imitation, outing, 0 = relieve of stress, pleasure), depression
(1 = any depression, 0 = none), anxiety disorders (1 = present, 0 = none)
R2!: Using Nagelkerke likelihood ratio
* P \ 0.05; ** P \ 0.01; *** P \ 0.001
346 J Behav Med (2011) 34:339–350
123
Author's personal copy

previous studies from Saudi Arabia and other Arab cultures,
male adolescents were at a much higher risk for smoking
behavior than female adolescents (Saeed et al. 1993;
Abdalla et al. 2007; WHO–EMRO 2003). In Saudi com-
munity there is a social stigma against women smoking,
which is seen as shameful (Jarallah et al. 1999). Accord-
ingly, the relatively low smoking rates among females may
simply be a reflection of a cultural taboo, and may be an
underestimate of the true female prevalence, since many
young females may be reluctant to admit their smoking
status (Hassan 2003). In a study from Riyadh, Abdalla et al.
(2007) found that there were significant gender differences
among secondary school students with respect to source of
cigarettes, usual place of smoke, intensity of smoking,
knowledge on addiction of tobacco, exposure to education
on tobacco, attitudes, and exposure to tobacco smoke in
public places. However, there was no difference regarding
age of initiation, health hazards knowledge, media expo-
sure, quit motivations, and home exposure. In a recent study
among female university students in Jeddah, the prevalence
of cigarettes smoking was 5% while 8.7% were users of
WP/shisha (Merdad et al. 2007). Another recent study in
Riyadh found that 70% of female medical students were
smoking WP/shisha (Al-Turki and Al-Rowais 2008). While
in male medical students, 44% were smoking WP and 24%
were smoking both WP and cigarettes (Al-Turki 2006). A
much lower rate of WP use among females in our study may
be due to the fact that Al-Hassa, in Eastern region, is less
urbanized and people constitutes a traditional society which
less tolerates to female smoking and with little access to
places for WP smoking.
Data showed that the proportion of adolescents who
smoke increases with age (Bilir et al. 1997). Also, adoles-
cents who start to smoke early are more likely to continue
smoking as adults (Rend et al. 1995). In the present survey,
we found a positive association between smoking status and
age which support the first statement. Also, the mean age at
initiation of smoking cigarettes was 13 years; the mean age
of initiation for those smoke both WP and cigarettes was
15 years. These results were lower than those obtained by
similar study in Saudi Arabia where about 59% started
smoking at or above the age of 18 years (Abolfotouh et al.
1998), whereas another study conducted in secondary
schools found that 83.7% of the current smokers started at
age 15 years or below (Al-Damegh et al. 2004).
The interesting finding that emerges from this study is
that unlike Western adolescents, Saudi youth seem to be
more influenced by their parents’ smoking than peer
smoking. Although Western studies have shown that fam-
ily smoking increases the risk of smoking among adoles-
cents, peer smoking are consistently stronger risk factors
than family smoking (Goddard 1990; Kandel et al. 2007;
Gilpin and Pierce 2001).
This is not surprising since Saudi Arabia is a traditional
conservative society where the family unit is more
important than the individual or his peers (Al-Sabie 1989).
Young adults in the Eastern part of the world adopt a
collective identity. Children are encouraged through a
process of strict and consistent socialization to obey and
submit to their families hence the self is not differentiated
from family. One’s needs, manners, style of thinking,
attitudes, and beliefs are not distinct from those of the
family (Dewairy 1999).
To some degree this pattern of development acts as a
catalytic promoter of smoking among adolescents in their
milieu. This result is consistent with Bandore’s Cognitive
Social Theory which believes that through observational
learning or modeling of the behaviors of others, we adopt
these behaviors ourselves especially if the model is
someone respected like the father (Santrock 1995).
This study showed that father’s smoking habit is
strongly associated with student’s current smoking status
and remained so among Saudi Adolescents similar to that
found in studies conducted outside Saudi Arabia. Maziak
and Mzayek (2000) reported that among Syrian adolescents
parental and siblings smoking was the strongest predictor
of the smoking status (Odds ratio of 4.4) (Maziak and
Mzayek 2000). In Kuwait, another Arab country, among a
sample of 761 university students, 96.4% of WP smokers
smoked in their homes. Forty-three percent of the male WP
smokers and 74.1% of the female smokers reported two or
more other smokers living in their homes (Mohammed
et al. 2006). Also in Singapore, it was found that family
factors especially the father’s smoking habit and the pres-
ence of negative role models within the home were sig-
nificantly associated with current smoking habits among
secondary school students (Shamsuddin and Haris 2000).
In the present study, a higher prevalence of anxiety
disorders measured by the PHQ is associated with the
current smoking status. This finding is consistent with
previous research in developing and developed countries
(Soueif et al. 1990; Sonntag et al. 2000). Although in our
sample those with any depression or anxiety disorder were
found to be significantly higher in the smoker group, this
effect was attenuated when controlling for other factors and
demographic effects. Prospective analyses might reveal the
specific relation between anxiety and tobacco use and if
adolescents with prior anxiety disorders tend to smoke
more.
Limitations
Results of this study are based on cross-sectional data
rather than longitudinal, this limited the extent to which
conclusions about causality could be drawn. To develop a
J Behav Med (2011) 34:339–350 347
123
Author's personal copy

better understanding of the conditions under which these
variables operate as causal factors, more longitudinal study
designs are required. However, the influences of family
smoking and anxiety disorders on adolescent’s smoking
behavior cannot be explained by this reversal of causality
and remains an important risk factor that needs to be
addressed. Another limitation of is the lack of information
on the smoking behavior of the non-responders particularly
in females and those adolescents outside schools. It is
possible that non-responders had higher smoking preva-
lence than those surveyed which may have caused an
underestimation of the smoking prevalence rates in this
study. The results of smoking behavior in this study were
based on students’ self-reports. The use of self reported
measures may be unable to investigate the anxiety and
depressive disorders. It might be better to use more
objective measures of psychiatric comorbidity such as
standardized interviews. Although adolescents’ self-reports
of psychiatric morbidity obtained under similar conditions
in the United States have been shown to be quite accurate
across ethnic groups (Spitzer et al. 1999), it is not known
whether this is also true for Saudi adolescents. The results
of this study point to the notion that some of the smoking
risk factors associated with eastern adolescents’ smoking
behavior such as anxiety disorders and socializing moti-
vation might be addressed and appropriate prevention
programs should be tailored depending on the concerned
culture. The present results from a standardized question-
naire (PHQ) that depends on self-report to assess for the
depressive symptoms over the past 2 weeks and suicidality
in the past 4 weeks is very limited and is likely to pick up
only a small proportion of available diagnoses of depres-
sion and suicidal behavior, likewise for panic and gen-
eralized anxiety disorder over the past few weeks.
Moreover, unfortunately the PHQ do not include items for
the diagnosis of phobias.
Study implications
The results of this study provide important new informa-
tion about some of the psychosocial smoking risk factors in
Saudi adolescents. Smoking prevention programs aimed at
adolescents in Saudi Arabia, should be a collaborative
multidisciplinary involving schools, family, community
members and the media. Families and community adult
members should be made aware of the detrimental influ-
ence their smoking behavior has on their youth. Therefore,
smoking prevention programs aimed at Saudi adolescents
should go hand in hand with smoking cessation interven-
tions aimed at Saudi adults. The results of this study
show that it is necessary to pay attention to the levels of
anxiety among current adolescent smokers. Counseling and
preventive psychiatric services should be an integral part of
the clinical facilities caring for secondary school students
in Al-Hassa, Saudi Arabia.
Conflict of interest None.
References
Abdalla, A. M., Al-Kaabba, A. F., Saeed, A. A., Abdulrahman, B. M.,
& Raat, H. (2007). Gender differences in smoking behavior
among adolescents in Saudi Arabia. Saudi Medical Journal,28(7), 1102–1108.
Abdalla, A. M., Saeed, A. A., Abdulrahman, B. M., Al-Kaabba, A. F.,
& Raat, H. (2009). Correlates of ever-smoking habit among
adolescents in Tabuk, Saudi Arabia. Eastern MediterraneanHealth Journal, 15(4), 983–992.
Abolfotouh, M. A., Abdel Aziz, M., Badawi, I. A., & Alakija, W.
(1998). Smoking intervention program for male secondary-
school students in Saudi Arabia. Eastern Mediterranean HealthJournal, 3, 90–100.
Abou-Zeid, A. H., Hifnawy, T. M., & Abdel Fattah, M. (2009).
Health habits and behaviour of adolescent schoolchildren, Taif,
Saudi Arabia. Eastern Mediterranean Health Journal, 15(6),
1525–1534.
Al Yousef, M. A., & Karim, A. (2001). Prevalence of smoking among
high school students. Saudi Medical Journal, 22(10),
8723–8724.
Al-Damegh, S. A., Saleh, M. A., Al-Alfi, M. A., & Al-Hoqail, I. A.
(2004). Cigarette smoking behavior among male secondary
school students in the Central region of Saudi Arabia. SaudiMedical Journal, 25(2), 215–219.
Al-Faris, E. A. (1995). Smoking habits of secondary school boys in
rural Riyadh. Public Health, 109(1), 47–55.
Al-Gelban, K. S. (2007). Depression, anxiety and stress among Saudi
adolescent school boys. The Journal of the Royal Society for thePromotion of Health, 127(1), 33–37.
Al-Haddad, N., & Hamadeh, R. R. (2003). Smoking among second-
ary-school boys in Bahrain: Prevalence and risk factors. EasternMediterranean Health journal, 9(1–2), 78–86.
Al-Mohamed, H. I., & Amin, T. T. (2010). Pattern and prevalence of
smoking among students at King Faisal University, Al Hassa,
Saudi Arabia. Eastern Mediterranean Health Journal, 16(1),
56–64.
Al-Sabie, A. (1989). Psychiatry in Saudi Arabia: Cultural perspec-
tives. Trans-Cultural Psychiatric Research Review, 26, 245–262.
Al-Turki, Y. A. (2006). Smoking habits among medical students in
Central Saudi Arabia. Saudi Medical Journal, 27(5), 700–703.
Al-Turki, Y. A., & Al-Rowais, N. A. (2008). Prevalence of smoking
among female medical students in the College of Medicine,
Riyadh, Saudi Arabia. Saudi Medical Journal, 29(2), 311–312.
Bassiony, M. M. (2009). Smoking in Saudi Arabia. Saudi MedicalJournal, 11(7), 876–881.
Bilir, N., Dogan, B. G., & Yildis, A. N. (1997). Smoking behavior,publication no. 7. Ankara: Hacettepe Public Health Foundation
(in Turkish).
Breslau, N., & Klein, D. F. (1999). Smoking and panic attacks.
Archive General Psychiatry, 56, 1141–1147.
DeCoster, J. (2006). Applied linear regression notes set 1. http://
www.stathelp.com/notes.htm.
Dewairy, M. (1999). Toward psycho-cultural approach in Middle
Eastern societies. Clinical Psychology Review, 19(8), 909–915.
Dierker, L. C., Avenevoli, S., Merikangas, K. R., Flaherty, B. P., &
Stolar, M. (2001). Association between psychiatric disorders and
348 J Behav Med (2011) 34:339–350
123
Author's personal copy

the progression of tobacco use behaviors. Journal AmericanAcademic Child Adolescent Psychiatry., 40(10), 1159–1167.
Diez-Quevedo, C., Rangil, T., Sanchez-Planell, L., Kroenke, K., &
Spitzer, R. L. (2001). Validation and utility of the patient health
questionnaire in diagnosing mental disorders in 1003 general
hospital Spanish inpatients. Psychosomatic Medicine, 63(4),
679–686.
Fagerstrom, K. O., & Schneider, N. G. (1989). Measuring nicotine
dependence: A review of the Fagerstrom tolerance questionnaire.
Journal Behavioral Medicine, 12, 159–182.
Felimban, F. M., & Jarallah, J. S. (1994). Smoking habits of
secondary school boys in. Riyadh, Saudi Arabia. Saudi MedicalJournal, 15(6), 438–442.
Ferreira, M. M., & Torgal, M. C. (2010). Tobacco and alcohol
consumption among adolescents. Review Latin America Enfer-magem, 18(2), 255–261.
Friedman, L. S., Lichtenstein, E., & Biglan, A. (1985). Smoking onset
among teens: An empirical analysis of initial situations. Addic-tive Behavior, 10(1), 1–13.
Gilpin, E. A., & Pierce, J. P. (2001). Smoking initiation. Pulmonaryand critical care online update. Last Accessed October 4, 2009,
from
http://www.chestnet.org/education/pccu/vol12/lesson05.html.
Goddard, E. (1990). Why children start smoking? Office of populationcensus and surveys (social survey division). London: HMSO.
Golan, L., Lubanda, J. C., Netuka, M., Bosanska, L., Lubanda, H.,
Linhart, A., et al. (2004). Tobacco use amongst high school
students in the Czech Republic. Central European JournalPublic Health, 12(1), 32–35.
Griesler, P. C., Hu, M. C., Schaffran, C., & Kandel, D. B. (2008).
Comorbidity of psychiatric disorders and nicotine dependence
among adolescents: Findings from a prospective, longitudinal
study. Journal American Academy Child Adolescent Psychiatry,47(11), 1340–1350.
GYTS: Core Questionnaire. (2001). Centers for disease control andprevention. Accessed June 15, 2010, from http://www.cdc.gov/
tobacco/global/GYTS/questionnaire.htm.
Hassan, H. (2003). The economics of tobacco in Egypt: A newanalysis of demand. World Bank Publications. Last Accessed
January 15, 2010, from http://www.emro.who.int/tfi/Tobacco
Economics-Egypt.pdf.
Henkel, V., Mergl, R., Kohnen, R., Allgaier, A. K., Moller, H. J., &
Hegerl, U. (2004). Use of brief depression screening tools in
primary care: Consideration of heterogeneity in performance in
different patient groups. General Hospital Psychiatry, 26(3),
190.
Jarallah, J. S., al-Rubeaan, K. A., al-Nuaim, A. R., Al-Ruhaily, A. A.,
& Kalantan, K. A. (1999). Prevalence and determinants of
smoking in three regions of Saudi Arabia. Tobacco Control,8(1), 53–56.
Jarallah, J. S., Bamgboye, E. A., al-Ansary, L. A., & Kalantan, K. A.
(1996). Predictors of smoking among male junior secondary
school students in Riyadh, Saudi Arabia. Tobacco Control, 5(1),
26–29.
Jha, P., & Chaloupka, F. J. (Eds.). (2000). Tobacco control indeveloping countries. Oxford: Oxford United Press for the World
Bank and WHO.
Kandel, D. B., Hu, M. C., Griesler, P. C., & Schaffran, C. (2007). On
the development of nicotine dependence in adolescence. DrugAlcohol Dependence, 91(1), 26–39.
Kandela, P. (2000). Narghile smoking keeps Arabs in wonderland.
Lancet, 356(9236), 1175.
Kessler, R. C., Berglund, P., Borges, G., Nock, M., & Wang, P. S.
(2005). Trends in suicide ideation, plans, gestures, and attempts
in the United States, 1990–1992 to 2001–2003. JAMA, 293(20),
2487–2495.
Kroenke, K., Spitzer, R. L., & Williams, J. B. (2001). The PHQ-9:
Validity of a brief depression severity measure. Journal GeneralInternal Medicine, 16(9), 606–613.
Kwamanga, D., Odhiambo, J., & Amukoye, E. (2003). Prevalence and
risk factors of smoking among secondary school students in
Nairobi. East African Medical Journal, 80(4), 207–212.
Maziak, W., & Mzayek, F. (2000). Characterization of the smoking
habit among high school students in Syria. European JournalEpidemiology, 16(12), 1169–1176.
Maziak, W., Rastam, S., Eissenberg, T., et al. (2004). Gender and
smoking status based analysis of views regarding waterpipe and
cigarette smoking in Aleppo, Syria. Preventive Medicine, 38,
479–484.
McGraw, S. A., Smith, K. W., Schensul, J. J., & Carrillo, J. E. (1991).
Socio-cultural factors associated with smoking behavior by
Puerto Rican adolescents in Boston. Journal Social ScienceMedicine, 33(12), 1355–1364.
Merdad, L. A., Al-Zahrani, M. S., & Farsi, J. M. (2007). Smoking
habits among Saudi female university students: Prevalence,
influencing factors and risk awareness. Annals Saudi Medicine,27(5), 366–369.
Mohammed, H. R., Newman, I. M., & Tayeh, R. (2006). Shisha
smoking among a sample of future teachers in Kuwait. KuwaitMedical Journal, 38(2), 107–113.
Nagelkerke, N. J. D. (1991). A note on a general definition of the
coefficient of determination. Biometrika, 78(3), 691–692.
Nelson, C. B., & Wittchen, H. U. (1998). Smoking and nicotine
dependence: Results from a sample of 14- to 24-year-olds in
Germany. European Addictive Research, 4(1–2), 42–49.
O’Loughlin, J., Paradis, G., Renaud, L., & Sanchez Gomez, L. (1998).
One-year predictors of smoking initiation and of continued
smoking among elementary schoolchildren in multiethnic, low-
income, inner-city neighborhoods. Tobacco Control, 7(3),
268–275.
Peto, R., & Lopez, A. D. (2001). Future worldwide health effects of
current smoking patterns. In C. E. Koop, C. E. Pearson, & M.
R. Schwarz (Eds.), Critical issues in global health. San
Francisco, CA: Jossey-Bass.
Qidwai, W., Ishaque, S., Shah, S., & Rahim, M. (2010). Adolescent
lifestyle and behaviour: A survey from a developing country.
PLoS One, 5(9), e12914.
Rend, D. J., McNeill, A. D., & Glynn, T. J. (1995). Reducing the
prevalence of smoking in youth in Western countries: An
international overview. Tobacco Control, 4, 266–277.
Rowlands, D. F., & Shipster, P. J. (1987). Cigarette smoking amongst
Saudi schoolboys. Saudi Medical Journal, 8, 613–618.
Saeed, A. A., Al-Johali, E. A., & al-Shahry, A. H. (1993). Smoking
habits of students in secondary health institutes in Riyadh City,
Saudi Arabia. Journal Royal Social Health, 113(3), 132–135.
Santrock, J. W. (1995). Life span development (5th ed.). Madison:
Brown & Benchmark Publ.
Schultz, H., Ezzat, A., Allam, A., & Gray, A. (1998). Smoking and
health: New insights and recent developments. Annals SaudiMedicine, 18(1), 1–5.
Shamsuddin, K., & Haris, M. A. (2000). Family influence on current
smoking habits among secondary school children in Kota Bharu,
Kelantan. Singapore Medical Journal, 41(4), 167–171.
Siddiqui, S., & Ogbeide, D. O. (2001). Profile of smoking amongst
health staff in a primary care unit at a general hospital in Riyadh,
Saudi Arabia. Saudi Medical Journal, 22(12), 1101–1104.
Sonntag, H., Wittchen, H. U., Hofler, M., Kessler, R. C., & Stein, M.
B. (2000). Are social fears and DSM-IV social anxiety disorder
associated with smoking and nicotine dependence in adolescents
and young adults? European Psychiatry, 15(1), 67–74.
Soueif, M. I., Youssuf, G. S., Taha, H. S., Moneim, H. A., Sree, O. A.,
Badr, K. A., et al. (1990). Use of psychoactive substances among
J Behav Med (2011) 34:339–350 349
123
Author's personal copy

male secondary school pupils in Egypt: A study on a nationwide
representative sample. Drug Alcohol Dependence, 26(1), 63–79.
Spitzer, R. L., Kroenke, K., & Williams, J. B. (1999). Validation and
utility of a self-report version of PRIME-MD: The PHQ primary
care study. Primary care evaluation of mental disorders. Patient
health questionnaire. JAMA, 282(18), 1737–1744.
Valdivia, G., Simonetti, F., Cumsille, P., Ramırez, V., Hidalgo, C. G.,
& Palma, B. (2004). Smoking habit in school age children, in
Chile. Review Medicine Chile, 132(2), 171–182.
Washio, M., Kiyohara, C., Morioka, S., & Mori, M. (2003). The
experience of smoking in school children up to and including
high school ages and the current status of smoking habits; a
survey of male high students in Japan. Asian Pacific JournalCancer Prevention, 4(4), 344–351.
WHO. (1999). World No-Tobacco Day. (2010). Director-general of theworld health organization for world no-tobacco day. Last
Accessed February 1, 2010, from http://www.forces-nl.org/WHO/
ADVISORY98.PDF.
WHO–EMRO (Eastern Mediterranean Regional Office). (2003).
Country profiles, Egypt. WHO EMRO. Last Accessed December
25, 2009, from http://www.emro.who.int/emrinfo/Country
Profilesegy.html.
World Health Organization (WHO). (2001). Middle-East and NorthAfrica (MNA) regional office. Tobacco in Middle-East andNorthern Africa. WHO, Region Office for the Eastern Mediter-
ranean Publication, report # 23, Geneva.
Zahran, F. M., Ardawi, M. S., & Al Fayez, S. (1985). Carboxyhae-
moglobin concentration in smokers of shisha and cigarette in
Saudi Arabia. British Medical Journal, 291, 1768–1770.
350 J Behav Med (2011) 34:339–350
123
Author's personal copy




















