
No evidence for protective erythropoietin alpha signalling in rat hepatocytes

Cancer Therapy: Clinical
Prospective Phase II Study on 5-Days Azacitidine forTreatment of Symptomatic and/or ErythropoietinUnresponsive Patients with Low/INT-1–RiskMyelodysplastic Syndromes
Carla Fil��1, Michele Malagola1, Matilde Y. Follo2, Carlo Finelli3, Ilaria Iacobucci3, Giovanni Martinelli3,Federica Cattina1, Cristina Clissa3, Anna Candoni4, Renato Fanin4, Marco Gobbi5, Monica Bocchia6,Marzia Defina6, Pierangelo Spedini7, Cristina Skert1, Lucia Manzoli2, Lucio Cocco2, and Domenico Russo1
AbstractPurpose: This phase II prospective study aimed to evaluate the efficacy and safety of 5-days azacytidine
(5d-AZA) in patients with low-risk myelodysplastic syndromes (MDS). Second, single-nucleotide poly-
morphism (SNP) genetic profile and phosphoinositide-phospholipase C (PI-PLC) b1 levels were studied to
evaluate possible biologic markers able to predict the hematologic response.
Experimental Design: The study tested a lower intensity schedule of azacytidine. The treatment plan
consisted of 75 mg/sqm/d subcutaneous administered for 5 days every 28 days, for a total of 8 cycles.
Results: Thirty-two patients were enrolled in the study. The overall response rate was 47% (15 of 32) on
intention-to-treat and 58% (15 of 26) for patients completing the treatment program. In this latter group,
5 (19%) achieved complete remission (CR) and 10 (38%) had hematologic improvement, according to the
International Working Group (IWG) criteria. Three patients have maintained their hematologic improve-
ment after 37, 34, and 33 months without other treatments. Moreover, 21 and 2 of 26 cases completing
8 cycles were transfusion-dependent for red blood cells and platelets at baseline, respectively. Of these,
7 (33%) and 2 (100%) became transfusion-independent at the end of the treatment program, respectively.
Grade 3–4 neutropenia occurred in 28% of patients and 4 patients died early due to infections or
hemorrhage. SNP results were not significantly correlated to the clinical outcome, whereas PI-PLCb1 level
anticipated either positive or negative clinical responses.
Conclusions: 5d-AZA is safe and effective in a proportion of patients with low-risk MDS. PI-PLCb1 gene
expression is a reliable and dynamic marker of response that can be useful to optimize azacytidine therapy.
Clin Cancer Res; 19(12); 3297–308. �2013 AACR.
IntroductionDuring the last years, the most relevant progress in
biology and treatment of myelodysplastic syndromes
(MDS) has been marked by results of epigenetic studies(1, 2).
Aberrant DNA methylation in the CpG sites of severaltumor suppressor genes (TSG), even in the absence of LOH,is considered one of the dominant pathogenetic mechan-isms in MDS and one of the main causes of progression toacute myelogenous leukemia (AML). Furthermore, clinicalresponses of MDS to drugs that reverse aberrant hyper-methylation, such as deoxycytidine or azacitidine, stronglysuggest that aberrant hypermethylation plays a causativerole in disease and not just a side effect resulting from aderegulated proliferation or DNA damage (3, 4).
Hypomethylating agents significantly modified the ther-apeutic approach to MDS, primarily in older patients withhigh-risk disease for whom intensive chemotherapy andallogeneic stemcell transplantation are not anoption (5, 6).At a molecular level, the mechanisms underlying the effectof epigenetic therapy are not completely understood,although it is well known that DNA methyltransferaseinhibitors can induce the expression of the methylation-
Authors' Affiliations: 1Chair of Hematology, Unit of Blood Disease andStem Cell Transplantation, University of Brescia, Brescia; 2Cellular Signal-ling Laboratory, Department of Human Anatomical Sciences, University ofBologna; 3Institute of Hematology and Medical Oncology "L. and A.Ser�agnoli", University of Bologna, Bologna; 4Chair and Division of Hema-tology, Stem Cell Transplantation Unit "Carlo Melzi", University Hospital ofUdine, Udine; 5Department of Hematology and Oncology, University ofGenova,Genova; 6Chair ofHematology,Hospital "SantaMaria alleScotte,"University of Siena, Siena; and 7Division of Hematology, Hospital "IstitutiOspitalieri" of Cremona, Cremona, Italy
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
Corresponding Author: Domenico Russo, Chair of Hematology, Unit ofBlood Diseases and Bone Marrow Transplantation, University of Brescia,AO Spedali Civili Brescia, P.le Spedali Civili 1, 25100 Brescia, Italy. Phone:39-030-3996811; Fax: 39-030-3996021; E-mail: [email protected]
doi: 10.1158/1078-0432.CCR-12-3540
�2013 American Association for Cancer Research.
ClinicalCancer
Research
www.aacrjournals.org 3297
on April 30, 2016. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst April 17, 2013; DOI: 10.1158/1078-0432.CCR-12-3540

silenced gene products (7). For instance, epigenetic regula-tion of phosphoinositide-phospholipase C (PI-PLC) b 1promoter, which affects keymolecules involved in cell cycleand differentiation (8, 9) such as cyclinD3, seems to play animportant role in the demethylating activity of azacytidine(10–12). Indeed, PI-PLCb1 is a central molecule in normalcell proliferation and differentiation (13, 14), as well as inhematologic malignancies, such as MDS (15, 16). In fact,MDS showing a PI-PLCb1 monoallelic deletion are associ-atedwith ahigher risk of AMLevolution (17), andPI-PLCb1deregulation affects both myeloid and erythroid differen-tiation of low-risk MDS cells (18, 19).
Clinically, in high-riskMDS, azacytidine has been thefirstand only agent able to induce a survival benefit as comparedwith conventional care regimens. In this setting, themedianoverall survival (OS) was 24.5 months in azacytidine-trea-ted cases versus 15 months in those treated with conven-tional care regimens (P ¼ 0.0001; refs. 20, 21).
In low-risk MDS, the role of hypomethylating agents isless understood. The main goals of hypomethylating ther-apy in low-risk disease should be to reduce transfusiondependency (22), improve quality of life (23), and hope-fully the survival, but it is still unclear if this therapeuticapproach would be cost-effective. Most data on the use ofazacytidine in low-risk MDS are retrospective and comefrom studies mainly conducted in larger cohorts of patientswith high-risk disease. In the prospective phase III study[Cancer andLeukemiaGroupB (CALGB)9221], 23patientswith low-risk MDS treated with azacytidine, at a dose of 75mg/d for 7 days monthly, achieved an overall response rate(ORR) of 59% and a longer OS, as compared with thepatients receiving only supportive care (24, 25). In anotherindependent study, including 23 to 65 patients with low-risk MDS across 3 azacytidine alternate dosing cohorts, theORR ranged between 44% and 56% and the rate of eryth-
rocyte transfusion independence was 46% to 60% (26).More recently, a multicenter retrospective analysis con-ducted on 74 patients with MDS with International Prog-nostic Scoring System (IPSS) risk low or Int-1 treated withazacytidine at a dose of 75 mg/sqm for 7 to 10 days for amedian of 7 cycles, reported 50% to 77%of responses, witha median duration of 6 months (27).
Altogether, these experiences suggest that azacytidineseem useful also for patients with low-risk MDS. However,the CALGB study 9221 included both high- and low-riskpatients and the other cited studies were retrospective.Therefore, they suffer from relevant biases derived fromthe heterogeneity of enrolled patients, the different sched-ule and duration of treatments and, moreover, from theabsence of biologic studies focused on identification offactors possibly correlated with sensitivity or drugresistance.
In this study, we prospectively evaluated the efficacy andsafety of azacytidine, administered at a lower cumulativemonthly dose [5-days azacytidine (5d-AZA); 75mg/sqm/dfor 5 days monthly], in patients with IPSS low- or Int-1–risk MDS who were symptomatic and/or unresponsive toprevious treatments. Furthermore, we studied the geneticprofile by single-nucleotide polymorphism (SNP) arraysand the molecular effects of azacytidine on PI-PLCb1promoter methylation and gene expression, to identifybiologic factors possibly correlated with response toazacytidine.
Materials and MethodsStudy plan
The study is a phase II prospective, multicenter, single-arm trial. It was approved by the Ethical Committee ofSpedali Civili University Hospital of Brescia (Brescia, Italy;EudraCT Number 2007-003943-55) and registered at Clin-icalTrial.gov as NCT00897130.
Azacytidine was administered at a dose of 75 mg/sqm/daily s.c. for 5 consecutive days every 28 days for a total of 8cycles. Response was firstly assessed after the first 4 cyclesand in case of any hematologic response or stable disease,patients received additional 4 cycles. Final response waschecked at the end of the eighth cycle.
Azacytidine dose was adjusted according to absoluteneutrophil count (ANC) and platelets values. In particular,in case of ANCbetween 0.5 and 1.5� 109/L and/or plateletsbetween 25 and 50 � 109/L the dose was reduced to 75%.WhenANCandplatelet countswere less than0.5� 109/L or25 � 109/L, respectively, dose reduction was of 50%. Thefirst cycle of 5d-AZA was administered in all the patients, atthe planned dose, independently of the peripheral bloodcounts.
Erythropoiesis-stimulating agents (ESA) were avoidedduring the study; however, granulocyte or granulocytemacrophage colony-stimulating factors (G-CSF or GM-CSF) were allowed in case of severe neutropenia (<0.2 �109/L) and/or systemic infection. Redblood cell (RBC)weretransfused in case of hemoglobin (Hb) level < 8 g/dL, orwhenever clinically indicated. Platelets supportwas allowed
Translational RelevanceIn this article, we prospectively evaluated the efficacy
of low-intensity 5-days azacytidine schedule in terms offrequency and duration of hematologic responses inInternational Prognostic Scoring System low/Int-1 mye-lodysplastic syndromes (MDS). We also showed thatthe quantification of phosphoinositide-phospholipaseC b1 (PI-PLCb1) gene expression is a reliable anddynamic marker of azacytidine activity, being correlatedwith the achievement and the loss of hematologicresponse, therefore contributing to the early identifica-tion of patients who can benefit from treatment withazacytidine. We think that our study provides usefulinformation on the efficacy, safety, and biologic activityof azacytidine in a specific setting of patients with low/Int-1 MDS. This information can be relevant for plan-ning new clinical studies and for the optimization oftreatment with azacytidine in patients with low-riskMDS.
Fil�� et al.
Clin Cancer Res; 19(12) June 15, 2013 Clinical Cancer Research3298
on April 30, 2016. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst April 17, 2013; DOI: 10.1158/1078-0432.CCR-12-3540

if platelet count was less than 20 � 109/L, or wheneverindicated. Antibiotics and antifungal prophylaxis were giv-en if neutrophils were less than 0.5 � 109/L. Systemicantibioticswere given in case of fever (>38�C for>24hours),whereas systemic antifungals were given in case of feverpersisting for more than 5 days on antibiotics or wheneverindicated. Other experimental drugs or agents were notallowed and if another experimental drug or agent wasadministered, the patient discontinued azacytidine, andwent off-study.Physical examination, peripheral blood count, and bio-
chemical assessment were carried out every 2weeks ormoreoften, depending on patients’ conditions. Bone marrowaspirate samples for SNPmicroarray analysis were collectedat study entry and after the fourth and eighth cycles. Periph-eral blood samples for PI-PLCb1 gene expression analysiswere collected monthly during the treatment. Adverseevents were graded according to the National Cancer Insti-tute-Common Toxicity Criteria for Adverse Events (NCI-CTCAE) andwere assessed at each patient visit. A TreatmentAdvisory Committee (TAC), made by investigators of theWriting Committee, was established to support decision-making and to check any relevant problem about the studyprotocol.Student t test was used to compare continuous values
and Fisher exact test was used to compare differences inpercentage.
Inclusion criteriaPatients could be enrolled if 18 years or older and if they
had IPSS low- or Int-1–risk MDS and one or more of thefollowing: (i) symptomatic anemia requiring RBC transfu-sion-supportive therapy, previously unresponsive to eryth-ropoietin (EPO) or not expected to respond to EPO (i.e.,with baseline serum EPO > 500), (ii) thrombocytopeniarequiring platelet transfusion with or without muco-cuta-neous hemorrhagic syndrome, (iii) persistent (>3 months)ANC less then 1.5 � 109/L, with or without infections,requiring or notmyeloid growth factor therapy. In addition,a performance status [EasternCooperativeOncologyGroup(ECOG)] of 0–2, an estimated life expectancy of at least 3months, and a serumbilirubin level� 1.5 upper limit of thenormal (ULN), serum aspartate aminotransferase (AST) oralanine aminotransferase (ALT) � 2 � ULN, and serumcreatinine level � 1.5 � ULN were required. A negativeserum b-human chorionic gonadotropin pregnancy test 24hours before beginning of therapy with azacytidine wasrequested for fertile women. All patients provided writteninformed consent.
Objective of the studyThe main objective of the study was to evaluate the
efficacy (hematologic response) and toxicity of azacytidinein patients with low-risk MDS (IPSS 0–1).Second, we investigated the molecular genetic profile by
SNP microarray and the effects of 5d-AZA on PI-PLCb1 forevaluating possible biologic markers able to predict thehematologic response.
Definition of hematologic responseThe response to treatment was assessed according to
International Working Group (IWG) criteria as reportedbyCheson and colleagues (28), 1month after the end of theeighth cycle of treatment. Briefly, we considered the follow-ing: (i) response criteria for altering the natural history ofMDS, such as complete or partial remission (CR/PR), mar-row remission, cytogenetic response, stable disease, failure,disease progression, or relapse after CR or PR; (ii) responsecriteria for hematologic improvement (HI), including ery-throid response (HI-E), platelet response (HI-P), neutrophilresponse (HI-N), progression, or relapse after any hemato-logic improvement. Patients were considered to be respon-ders if they had response duration of 8 weeks or more.
PI-PLCb1 methylation and gene expression analysisPI-PLCb1 promoter methylation and gene expression
were quantified in patients with MDS at baseline andmonthly during azacytidine treatment. Genomic DNA andtotal RNA were extracted from peripheral blood mononu-clear cells collected within 48 hours from the last azacyti-dine administration, by the DNeasy and RNeasy Mini Kits(Qiagen), according to the manufacturer’s protocol. DNAwas subjected to bisulfitemodification and PI-PLCb1meth-ylation was assessed as previously described (11). RNA wasretro-transcribed and PI-PLCb1b (Hs01001939_m1;Applied Biosystems) mRNA was quantified by a TaqManReal-Time PCR method, using the GAPDH gene(Hs99999905_m1; Applied Biosystems) as the internalreference and a pool of 15 healthy subjects as the calibrator(29). Data were statistically analyzed by the GraphPadPrism software (v.3.0). Baseline levels were calculated asa percentage ratio of PI-PLCb1 compared with healthysubjects, whereas the amount of PI-PLCb1 during treatmentwas calculated as a percentage ratio of PI-PLCb1 duringazacytidine treatment compared with baseline. Statistically,a difference of at least 20% compared with baseline wasconsidered significant, according to the Dunnett test post-ANOVA. Therefore, patients showing an increase in PI-PLCb1 expression of at least 20%as comparedwith baselineat a specific cycle of azacytidine treatment were consideredas having a positive "molecular response" at that cycle.
SNP microarray analysisGenomic DNA was extracted using the DNA Blood Mini
Kit (Qiagen) from mononuclear cells isolated from bonemarrow aspirate samples before treatmentwith azacytidine.DNA was quantified using the NanoDrop Spectrophotom-eter and quality was assessed using the NanoDrop and byagarose gel electrophoresis. DNA samples were genotypedwith Genome-Wide Human SNP 6.0 array microarrays(Affymetrix Inc.) following the manufacturer’s instructionsand as previously described (30). Briefly, copy numberaberrations (CNA) and LOHwere analyzed using Genotyp-ing Console v4.1 (Affymetrix Inc.) by a comparison with aset of 794 HapMap normal individuals and a set of 25normal samples run in our laboratory to reduce the noise ofraw copy number data. Affymetrix CNCHP files were also
Azacitidine in Low-Risk Myelodysplastic Syndromes
www.aacrjournals.org Clin Cancer Res; 19(12) June 15, 2013 3299
on April 30, 2016. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst April 17, 2013; DOI: 10.1158/1078-0432.CCR-12-3540

imported and analyzed by Chromosome Analysis Suite(ChAS) Software v1.2 (Affymetrix Inc.) using the followingsegment filters: minimum number of markers 25 and min-imum size of 50 kbp for both gain and loss. LOH wasdefined as a region greater than 5 Mbps.
ResultsPatients’ characteristics
Between September 2008 and February 2010, 7 ItalianHaematological Centres recruited 32 patients with IPSSlow- or Int-1–risk MDS (31) who met the eligibility criteriaand gave their informed consent to be enrolled into thestudy (32–34).
The main characteristics of these 32 patients are reportedin Table 1. Briefly, the median age was 71 years (range, 56–84) and according to World Health Organization (WHO)classification, 15 (47%) patients had refractory anemia(RA), 6 (19%) RA with ringed sideroblasts (RARS), 6(19%) refractory cytopenia with multilinear dysplasia(RCMD), and 5 (16%) RA with excess of blasts (RAEB-1).Most patients had a good-risk karyotype (72%) by conven-tional cytogenetics, were RBC transfusion-dependent(81%), receiving a median of 4 RBC U/mo (range, 0–8),and were previously unresponsive to treatment with ESAs
(77%). Only 4 patients (12%) were platelet transfusion-dependent.
Hematologic response to 5d-AZAAll patients started azacytidine at a dose of 75 mg/sqm/
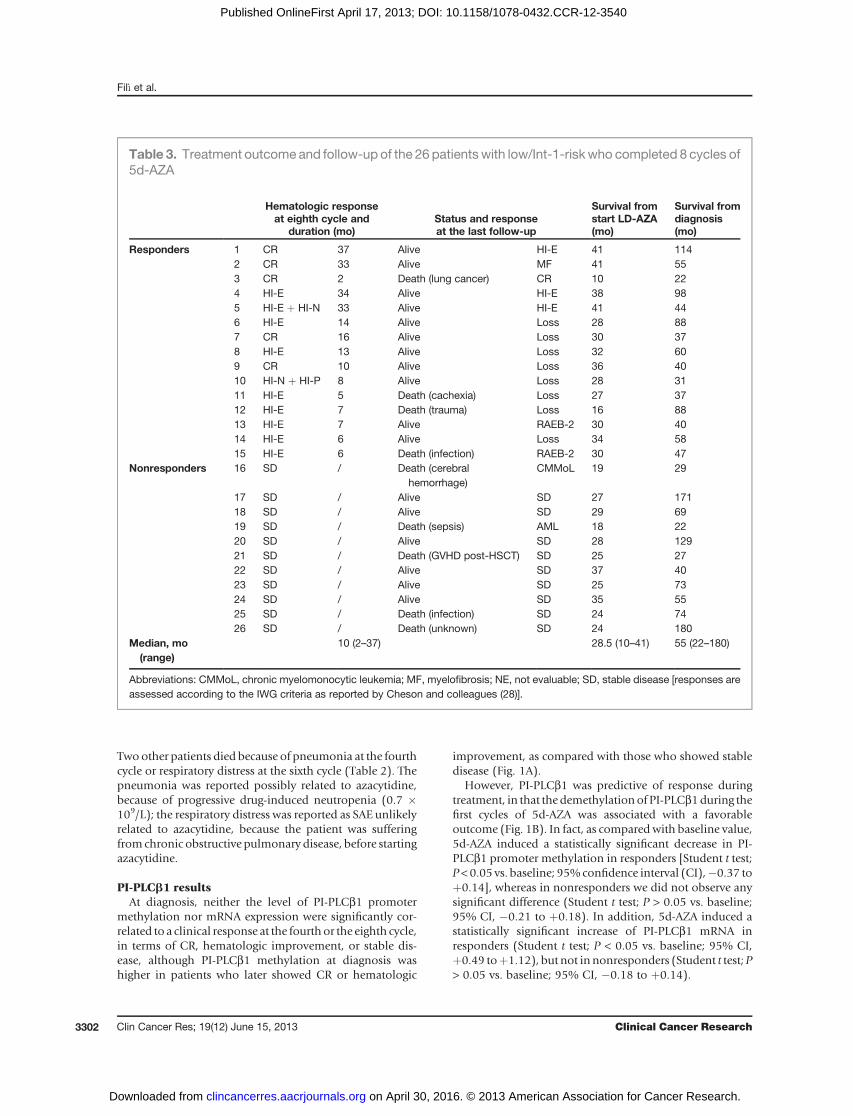
daily s.c. for 5 consecutive days and their response isreported in Table 2. Out of the 32 enrolled patients, 2 diedafter the first cycle, 1 withdrew the informed consent afterthe second cycle, and 29 (90%) completed the first 4 cycles.At this time, 10 (35%) patients achieved hematologicimprovement (HI-E in 7 and HI-N or HI-P in 3 cases),19 (65%) had stable disease. Among the 29 patients eligiblefor therapy continuation after the fourth cycle, 1 withdrewthe informed consent after the fourth cycle and 2 died afterthe fourth and sixth cycle, respectively. Therefore, 26patients (81%) completed the treatment plan (8 cycles)and out of them: 5 (19%) achieved CR, 10 (38%) achievedhematologic improvement (HI-E in 8 cases and HI-N/P inthe other 2 cases), and 11 (42%)maintained stable disease.Among the 5 patients who achieved CR after the eighthcycle, 3 had previously achieved hematologic improvementat the fourth cycle, whereas the other 2 had stable disease(Table 2). From a clinical point of view, out of the 26patients completing 8 cycles, 21 and 2 were transfusion-dependent for RBCandplatelets at baseline, respectively.Ofthem, 7 (33%) and 2 (100%) became transfusion-indepen-dent at the end of the treatment program, respectively. Nopatient progressed to high-risk MDS or AML during thetreatment period. Thus, on an intention-to-treat, the ORRwas 47% (15 of 32 cases), whereas assessing the data on thepatients who completed the 8 planned cycles, the ORR was58% (15 of 26 cases). As reported in Table 3, in the 15responsive patients, the median duration of hematologicresponse assessed 1 month after the eighth cycle was 10months (range, 2–37). At the time of the last follow-up, 17(65%) of the 26 patients who completed 8 cycles are alive.Three patients have maintained their response achievedwithin the 8 cycles, after 37, 34, and 33 months, withoutother treatments or supportive therapy; 6 patients are alive,but lost their hematologic response; 8 patients maintainedstable disease; 3 patients progressed to RAEB-2or developedmyelofibrosis. At the last follow-up, the median survivalfrom the start of 5d-AZA and from diagnosis was 28.5months (range, 10–41) and 55 months (range, 22–180),respectively. Nine of the 26 patients completing 8 cyclesdied. We did not find a correlation between response andthe following baseline variables: age, sex, type and durationof MDS, karyotype, type and duration of previous treat-ments, or supportive therapies (data not shown).
Furthermore, the median survival from the start of aza-cytidine for responders was not different from nonrespon-ders, including patients with stable disease (data notshown).
Hematologic and nonhematologic toxicityAzacytidine was generally well tolerated. As shown
in Table 4, the most common hematologic toxicity wasneutropenia, observed in 15 of 32 patients (47%) and 9
Table 1. Clinical features of the 32 patients withIPSS low/Int-1-risk MDS enrolled in theprospective 5d-AZA study
Number of enrolled patients 32Median age, y (range) 71 (56–84)Sex: M/F 22/10WHO classification: no. of cases, %RA 15 (47%)RARS 6 (19%)RCMD 6 (19%)RAEB-1 5 (16%)
IPSS: no. of cases, %0 15 (47%)0.5 8 (25%)1 9 (28%)
Karyotype: no. of cases, %Good (normal, �Y) 23 (72%)Intermediate [þ8, þ18, i(14q10)] 5 (16%)Poor (complex) 2 (6%)Nonevaluable 2 (6%)
Median time diagnosis/therapy, mo (range) 20 (1–101)Prior therapies: no. of cases, % 22 (69%)ESA 17 (77%)ESA þ G-CSF 4 (18%)Other (cyclosporine/danazole/thalidomide) 1 (5%)
RBC transfusion dependent: no. of cases, % 26 (81%)Median RBC U/mo, (range) 4 (0–8)PLT transfusion-dependent: no. of cases, % 4 (12%)
Abbreviation: PLT, platelets.
Fil�� et al.
Clin Cancer Res; 19(12) June 15, 2013 Clinical Cancer Research3300
on April 30, 2016. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst April 17, 2013; DOI: 10.1158/1078-0432.CCR-12-3540

(28%) of them had a grade� 3WHO neutropenia. Throm-bocytopenia occurred in 6 of 32 cases (19%) andwas severe(� 3 WHO) in 4 of 6 (12%) of them. The hematologictoxicity was transient and in these cases azacytidine dosewas adjusted according to the previously reportedrecommendations.Nonhematologic toxicitywas predominantlymild (grade
� 1) andmainly consisted of cutaneous erythema at the siteof injection (62%), asthenia (31%), diarrhea/constipation(28%), and fever (9%).Only 5 patients had grade� 3WHO
nonhematologic toxicities, who were reported as seriousadverse events (SAE), and had favorable outcome in 3 of 5cases (Table 4).
Out of the 32 enrolled patients, 2 patients died after thefirst cycle due to septic shockor gastrointestinal hemorrhageand these events were reported as SAE unlikely related to thestudydrug (Table 2). In thefirst case, theANCwas>2�109/Lat the time of death, and in the second case the patient hada severe thrombocytopenia (platelets < 10 � 109/L) atbaseline and had previously undergone a gastro-resection.
Table 2. Hematologic response to 5d-AZA in the 32 IPSS low/Int-1–risk MDS patients
Pt Age Sex WHO IPSS Karyotype
Timefromdiagnosisto LD-AZA(mo)
Priortherapy
SupportN RBC/mo
Hematologicresponse atfourth cycle
Hematologicresponse ateighth cycle
Responders 1 61 F RAEB-1 0.5 i(4q10) 73 ESAþG-CSF 8 HI-E CR2 77 M RA 0 N 14 ESA 4 SD CR3 69 M RAEB-1 1 N 12 No 8 SD CR4 69 F RAEB-1 1 N 60 ESAþCyAþ
danazolþTal1 HI-E HI-E
5 76 M RA 1 þ18 3 No 2 SD HI-E þ HI-N6 84 F RARS 0 �Y 60 ESA 4 SD HI-E7 67 M RCMD 0.5 N 7 No 0 HI-P CR8 64 M RARS 0 N 28 ESA 4 HI-E HI-E9 70 M RA 0 N 4 No 0 HI-N CR10 65 M RA 0.5 N 3 No 0 HI-N HI-N þ HI-P11 80 M RARS 1 þ8 10 No 4 SD HI-E12 76 F RCMD 0 N 72 ESA 2 HI-E HI-E13 67 M RA 0.5 N 10 ESA 2 HI-E HI-E14 69 M RA 0 N 24 ESA 0 HI-E HI-E15 77 F RA 0.5 þ8 17 ESA 0 HI-E HI-E
Nonresponders 16 56 M RAEB-1 0.5 N 10 ESA 4 SD SD17 76 M RARS 0 N 144 ESAþG-CSF 3 SD SD18 74 M RAEB-1 0 N 40 ESA þ G-CSF 8 SD SD19 72 M RA 0.5 N 4 No 3 SD SD20 72 F RA 0 N 101 ESA 6 SD SD21 56 M RA 1 Complex 2 No 6 SD SD22 80 M RA 0 �Y 20 ESA 4 SD SD23 67 M RCMD 0 N 48 ESA 6 SD SD24 59 M RA 0 NE 20 ESA 2 SD SD25 71 F RCMD 0.5 N 60 ESA 6 SD SD26 70 F RA 0 N 156 ESA 5 SD SD
Early discontinuation 27 69 M RARS 1 NE 10 ESA 4 SD NEa
28 71 M RA 0 �Y 2 No 0 SD NEb
29 71 F RARS 0 N 60 ESA 4 SD NEc
30 82 M RCMD 1 þ8 16 ESA 8 NEd /31 71 F RA 1 Complex 1 No 0 NEe /32 69 M RCMD 0.5 N 83 ESAþG-CSF-
danazol6 NEf /
Abbreviations: CyA, cyclosporine A; N, normal karyotype; NE: not evaluable; SD: stable disease [responses are assessed according tothe IWG criteria as reported by Cheson and colleagues (28)].aPt n� 27: died after the fourth cycle due to pneumonia.bPt n� 28: died after the sixth cycle due to respiratory distress.cPt n� 29: withdrew consent after the fourth cycle.dPt n� 30: died after the first cycle due to septic shock.ePt n� 31: withdrew consent after the second cycle.fPt n� 32: died after the first cycle due gastro-intestinal hemorrhage.
Azacitidine in Low-Risk Myelodysplastic Syndromes
www.aacrjournals.org Clin Cancer Res; 19(12) June 15, 2013 3301
on April 30, 2016. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst April 17, 2013; DOI: 10.1158/1078-0432.CCR-12-3540
Two other patients died because of pneumonia at the fourthcycle or respiratory distress at the sixth cycle (Table 2). Thepneumonia was reported possibly related to azacytidine,because of progressive drug-induced neutropenia (0.7 �109/L); the respiratory distress was reported as SAE unlikelyrelated to azacytidine, because the patient was sufferingfromchronic obstructive pulmonary disease, before startingazacytidine.
PI-PLCb1 resultsAt diagnosis, neither the level of PI-PLCb1 promoter
methylation nor mRNA expression were significantly cor-related to a clinical response at the fourth or the eighth cycle,in terms of CR, hematologic improvement, or stable dis-ease, although PI-PLCb1 methylation at diagnosis washigher in patients who later showed CR or hematologic
improvement, as compared with those who showed stabledisease (Fig. 1A).
However, PI-PLCb1 was predictive of response duringtreatment, in that the demethylationof PI-PLCb1during thefirst cycles of 5d-AZA was associated with a favorableoutcome (Fig. 1B). In fact, as compared with baseline value,5d-AZA induced a statistically significant decrease in PI-PLCb1 promoter methylation in responders [Student t test;P<0.05 vs. baseline; 95%confidence interval (CI),�0.37 toþ0.14], whereas in nonresponders we did not observe anysignificant difference (Student t test; P > 0.05 vs. baseline;95% CI, �0.21 to þ0.18). In addition, 5d-AZA induced astatistically significant increase of PI-PLCb1 mRNA inresponders (Student t test; P < 0.05 vs. baseline; 95% CI,þ0.49 toþ1.12), but not innonresponders (Student t test;P> 0.05 vs. baseline; 95% CI, �0.18 to þ0.14).
Table 3. Treatment outcome and follow-up of the 26 patientswith low/Int-1-riskwho completed 8 cycles of5d-AZA
Hematologic responseat eighth cycle and
duration (mo)Status and responseat the last follow-up
Survival fromstart LD-AZA(mo)
Survival fromdiagnosis(mo)
Responders 1 CR 37 Alive HI-E 41 1142 CR 33 Alive MF 41 553 CR 2 Death (lung cancer) CR 10 224 HI-E 34 Alive HI-E 38 985 HI-E þ HI-N 33 Alive HI-E 41 446 HI-E 14 Alive Loss 28 887 CR 16 Alive Loss 30 378 HI-E 13 Alive Loss 32 609 CR 10 Alive Loss 36 4010 HI-N þ HI-P 8 Alive Loss 28 3111 HI-E 5 Death (cachexia) Loss 27 3712 HI-E 7 Death (trauma) Loss 16 8813 HI-E 7 Alive RAEB-2 30 4014 HI-E 6 Alive Loss 34 5815 HI-E 6 Death (infection) RAEB-2 30 47
Nonresponders 16 SD / Death (cerebralhemorrhage)
CMMoL 19 29
17 SD / Alive SD 27 17118 SD / Alive SD 29 6919 SD / Death (sepsis) AML 18 2220 SD / Alive SD 28 12921 SD / Death (GVHD post-HSCT) SD 25 2722 SD / Alive SD 37 4023 SD / Alive SD 25 7324 SD / Alive SD 35 5525 SD / Death (infection) SD 24 7426 SD / Death (unknown) SD 24 180
Median, mo(range)
10 (2–37) 28.5 (10–41) 55 (22–180)
Abbreviations: CMMoL, chronic myelomonocytic leukemia; MF, myelofibrosis; NE, not evaluable; SD, stable disease [responses areassessed according to the IWG criteria as reported by Cheson and colleagues (28)].
Fil�� et al.
Clin Cancer Res; 19(12) June 15, 2013 Clinical Cancer Research3302
on April 30, 2016. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst April 17, 2013; DOI: 10.1158/1078-0432.CCR-12-3540

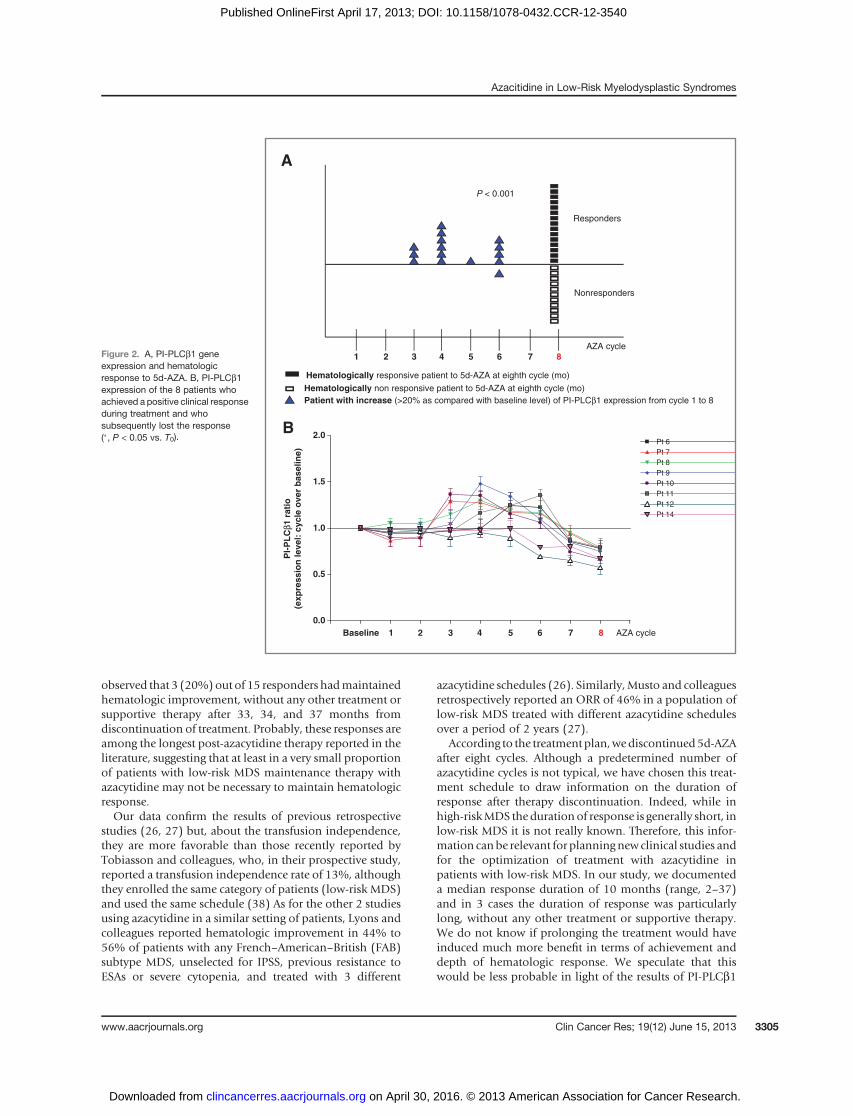
As for the 6 patientswhowent off-study during treatment,PI-PLCb1 mRNA increased in 1 case and decreased in 3cases, whereas the 2 remaining subjects died after the firstcycle.As reported in Fig. 2A, PI-PLCb1 molecular response
preceded the hematologic response in all but one of theresponders (14 of 15; 90%) and in only one of the non-responders (1 of 11; 9%; P < 0.001). In 9 of 14 (64%)responsive patients, the firstmolecular increase in PI-PLCb1level was observed between the third and fourth cycle,therefore anticipating the clinical evaluation. In addition,the 8 caseswho showed the loss of the response after the endof therapy (eighth cycle) displayed a significant reduction ofPI-PLCb1 levels, below the pretreatment values, alreadybefore the clinical loss of the response (Fig. 2B).
SNP array resultsTo overcome the technical limitations of metaphase
cytogenetics, such as its relatively low resolution and theneed for dividing cells, and to reveal all unbalanced genedefects as well as LOH, a whole-genome scanning by SNParrays (Affymetrix Genome-Wide Human SNP 6.0) wassuccessfully conducted in 26 of 32 patients with (81%)MDS. In 6 of 32 (19%) patients, the analysis failed for lackof sufficient DNA or for bad quality of the extracted DNA.SNP array karyotyping identified genomic abnormalities inall analyzed patients (100%), compared with only 9 of 26(35%) with metaphase cytogenetics, showing that SNParray analysis is more sensitive in identifying genetic altera-tions (P¼ 0.02; Fisher exact test; Supplementary Table S1).CNAs ranged from loss or gain of complete chromosomearms to focal deletions and gains targeting one or few genes(median size for loss was 123 kb, range, 51–76,763 kb;median size for gain was 100 kb, range, 50–146,091 kb).Overall, the median number of abnormalities per samplewas 12 (range, 5–57) and gains outnumbered deletionsalmost 2:1. Macroscopic alterations affecting a completechromosome or its armswere detected in 6 of 26 (23%) andincluded trisomy of chromosome 8 in 3 cases (12%), lossesof the long armsof the chromosomes 5 and7 in a single case
(4%) and a gain of chromosome 14q, that was not previ-ously identified by metaphase cytogenetics analysis, inanother case (4%). Moreover, a patient showed a complexkaryotype (defined as more than 3 macroscopic CNAs)including the gains of chromosomes 3q, 9p24-23 and lossesof chromosomes 6p and 7q. Importantly, SNP array anal-ysis of 17 patients with normal or unsuccessful metaphasecytogenetics enabled the detection of genetic lesions in all ofthese cases. Many new abnormalities detected by SNP arrayanalysis weremicroscopic genomic gains and deletions andcopy-neutral LOH (>5Mbps) affecting the chromosomes 2,3, 4, 6, 9, 10, and 15 (Supplementary Fig. S2).
Microscopic CNAs were not clusterized in specific geno-mic regions but were spread through the genome, suggest-ing a general genomic instability rather than a specificpathogenetic mechanism generating alterations. Notewor-thy, in more than 25% of MDS cases we found amplifica-tions of the small nucleolar RNA, C/D box 115-12 gene(SNORD115-12) on chromosome 15q12 involved in theregulation of alternative splicing andof the defender againstcell death 1 (DAD1) on chromosome 14q11, a negativeregulator of programmed cell death.
To investigate whether the findings from SNPs array maybe correlated with an early response to 5d-AZA (hemato-logic improvement/CR) or stable disease at fourth cycle, wefirst stratified the patients according to the presence ofmacroscopic copy number changes or LOH alterations(Supplementary Table S1). Among the 6 patients withMDS(23%) with macroscopic CNAs, 2 (33%) achieved HI/CR,whereas 8 of 20 (40%) without alterations (P ¼ 1.0; Fisherexact test), suggesting that macroscopic CNAs are not asso-ciatedwith response to 5d-AZA.More interestingly, patientswith LOH (n ¼ 5; 19%) have a trend for worse response interms of stable disease (80% vs. 57% of patients withoutLOH), even if this does not reach a statistically significantresult (P ¼ 0.61; Fisher exact test), mainly due to the smallnumber of analyzed patients. Taking advantage of the SNParray analysis, we subsequently stratified patients withMDSbased on the number of microscopic CNAs choosing ascutoff of their median number (n ¼ 12). However, we did
Table 4. Toxicity during the 8 cycles of 5d-AZA
Hematologic toxicity No. of patients Grade 1–2 WHO Grade 3–4 WHO
Neutropenia 15/32 (47%) 6/32 (19%) 9/32 (28%)Thrombocytopenia 6/32 (18%) 2/32 (6%) 4/32 (12%)Anemia 2/32 (6%) 2/32 (6%) 0Nonhematologic toxicityCutaneous erythema 20/32 (62%) 20/32 (62%) 0Asthenia 10/32 (31%) 10/32 (31%) 0Diarrhea/constipation 9/32 (28%) 8/32 (25%) 1/32 (3%)Nausea 4/32 (12%) 4/32 (12%) 0Fever 3/32 (9%) 3/32 (9%) 0Pneumonitis 2/32 (6%) 0 2/32 (6%)Respiratory distress 1/32 (3%) 0 1/32 (3%)Gastrointestinal bleeding 1/32 (3%) 0 1/32 (3%)
Azacitidine in Low-Risk Myelodysplastic Syndromes
www.aacrjournals.org Clin Cancer Res; 19(12) June 15, 2013 3303
on April 30, 2016. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst April 17, 2013; DOI: 10.1158/1078-0432.CCR-12-3540

not find differences in the response (HI/CR) to azacytidinebetween patientswithCNAs� 12 and thosewithCNAs<12(39% vs. 38%, respectively; P ¼ 1.0; Fisher exact test).
DiscussionIn patients with low-risk MDS, azacytidine has been
reported to induce transfusion independence and/or hema-tologic responses in 40% to 70%of cases (25–27). This highvariability probably reflects the fact that the low-risk MDSpatients’ population is clinically and biologically heteroge-neous (35–37) and explains why the effects of azacytidinein this setting of patients are less known and why dose andduration of treatment and profile of patients with low-riskMDS who can benefit of azacytidine are still undetermined.
To contribute to answer some of these questions, weconducted a prospective phase II study, to assess the clinical
and biologic effects of a 5d-AZA in patients with IPSS low/Int-1–risk MDS who were unresponsive to prior therapieswith ESAs or who were not appropriate candidates for ESAs(i.e., serum erythropoietin > 500 mUI/mL) in presence ofanemia, with or without other cytopenias. Therefore, thepatients selected for our studyhadanunfavorableprognosisand no alternative approach to supportive care, excepthypomethylating agents.
The hematologic response was assessed according to theIWG criteria (28): the ORRwas 58% (15 of 26 patients whocompleted eighth azacytidine cycles) and the rate of RBCtransfusion-independence after the eighth cycle was 33%.As observed in previous experiences, mainly conducted inpatients with high-risk MDS, the response rate increasedwith increasing cycles, from 38% after the first 4 cycles to58% after the eighth cycle but, more interestingly, we
BCR HI SD
MethylationGene expression
MethylationGene expression
0
1
2
3
00 1 2 3 4 5 6 7 8 0 1 2 3 4 5 6 7 8
1
2
3
4
P > 0.05
*P < 0.05 vs. T0P > 0.05 vs. T0
PI-
PL
β1re
lati
ve q
uan
tifi
cati
on
PI-
PL
Cβ1
rela
tive
qu
anti
fica
tio
n
0
1
2
3
PI-
PL
Cβ1
rela
tive
qu
anti
fica
tio
nCR HI SD
0
1
2
3
4
P > 0.05
PI-
PL
Cβ1
rela
tive
qu
anti
fica
tio
n
HI SD0
1
2
3
4
P > 0.05
PI-
PL
Cβ1
rela
tive
qu
anti
fica
tio
n
HI SD0
1
2
3
4
P > 0.05
PI-
PL
Cβ1
rela
tive
qu
anti
fica
tio
n
PI-PLCβ1 baseline expression vs.
5d-AZA responder patient: HI
5d-AZA (mo) 5d-AZA (mo)
5d-AZA nonresponder patient: SD
hematological response at the eighth cyclePI-PLCβ1 baseline methylation vs.hematological response at the eighth cycle
PI-PLCβ1 baseline expression vs.hematological response at the fourth cycle
PI-PLCβ1 baseline methylation vs.hematological response at the fourth cycle
A
Figure 1. A, PI-PLCb1 promoter methylation and gene expression at baseline, in correlation with hematologic response to 5d-AZA at the fourth and the eighthcycle of therapy (horizontal bars represent the median values; P > 0.05). B, representative results of PI-PLCb1 promoter methylation and gene expression atbaseline and during 5d-AZA treatment in a responder patient and in a patient refractory to 5d-AZA (�, P < 0.05 vs. T0). SD, stable disease.
Fil�� et al.
Clin Cancer Res; 19(12) June 15, 2013 Clinical Cancer Research3304
on April 30, 2016. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst April 17, 2013; DOI: 10.1158/1078-0432.CCR-12-3540
observed that 3 (20%)out of 15 responders hadmaintainedhematologic improvement, without any other treatment orsupportive therapy after 33, 34, and 37 months fromdiscontinuation of treatment. Probably, these responses areamong the longest post-azacytidine therapy reported in theliterature, suggesting that at least in a very small proportionof patients with low-risk MDS maintenance therapy withazacytidine may not be necessary to maintain hematologicresponse.Our data confirm the results of previous retrospective
studies (26, 27) but, about the transfusion independence,they are more favorable than those recently reported byTobiasson and colleagues, who, in their prospective study,reported a transfusion independence rate of 13%, althoughthey enrolled the same category of patients (low-risk MDS)and used the same schedule (38) As for the other 2 studiesusing azacytidine in a similar setting of patients, Lyons andcolleagues reported hematologic improvement in 44% to56% of patients with any French–American–British (FAB)subtype MDS, unselected for IPSS, previous resistance toESAs or severe cytopenia, and treated with 3 different
azacytidine schedules (26). Similarly,Musto and colleaguesretrospectively reported an ORR of 46% in a population oflow-risk MDS treated with different azacytidine schedulesover a period of 2 years (27).
According to the treatmentplan,wediscontinued5d-AZAafter eight cycles. Although a predetermined number ofazacytidine cycles is not typical, we have chosen this treat-ment schedule to draw information on the duration ofresponse after therapy discontinuation. Indeed, while inhigh-riskMDS the durationof response is generally short, inlow-risk MDS it is not really known. Therefore, this infor-mation canbe relevant for planningnewclinical studies andfor the optimization of treatment with azacytidine inpatients with low-risk MDS. In our study, we documenteda median response duration of 10 months (range, 2–37)and in 3 cases the duration of response was particularlylong, without any other treatment or supportive therapy.We do not know if prolonging the treatment would haveinduced much more benefit in terms of achievement anddepth of hematologic response. We speculate that thiswould be less probable in light of the results of PI-PLCb1
Figure 2. A, PI-PLCb1 geneexpression and hematologicresponse to 5d-AZA. B, PI-PLCb1expression of the 8 patients whoachieved a positive clinical responseduring treatment and whosubsequently lost the response(�, P < 0.05 vs. T0).
765432 8
Responders
Nonresponders
Hematologically responsive patient to 5d-AZA at eighth cycle (mo)
Hematologically non responsive patient to 5d-AZA at eighth cycle (mo)Patient with increase (>20% as compared with baseline level) of PI-PLCβ1 expression from cycle 1 to 8
AZA cycle
P < 0.001
1
0.0
0.5
1.0
1.5
2.0
7654321 8 AZA cycleBaseline
Pt 6Pt 7Pt 8Pt 9Pt 10Pt 11Pt 12Pt 14
PI-
PL
Cβ1
rat
io(e
xpre
ssio
n le
vel:
cyc
le o
ver
bas
elin
e)
A
B
Azacitidine in Low-Risk Myelodysplastic Syndromes
www.aacrjournals.org Clin Cancer Res; 19(12) June 15, 2013 3305
on April 30, 2016. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst April 17, 2013; DOI: 10.1158/1078-0432.CCR-12-3540

promoter methylation and gene expression during treat-ment. In fact, although PI-PLCb1 methylation was unableto clearly distinguish between responders (CR/HI) andnonresponders (stable disease) at diagnosis, all patientswho responded to 5d-AZA showed an early decrease ofPI-PLCb1 methylation and an early increase of PI-PLCb1mRNA during the therapy, as compared with the pretreat-ment values, whereas only one of the nonrespondersshowed the same feature. Furthermore, in 9 of 14 (64%)responders the increase of PI-PLCb1 mRNA occurred earlyduring treatment (within the fourth cycle of therapy). Ademethylation of PI-PLCb1 promoter, which induces geneexpression, has been correlatedwith response to azacytidinein high-risk MDS (10–12). Here, we showed that PI-PLCb1promoter is demethylated also in low-risk cases, where itcan be used for monitoring the effect of 5d-AZA duringtreatment. This contributes to elucidate the mechanismsunderlying the effect of azacytidine and confirms the role ofPI-PLCb1 as a key molecule in hematologic malignanciesandmyeloid differentiation. Indeed, PI-PLCb1 increase hasbeen specifically associated not only with expression ofcyclin D3 (12), but also with the recruitment of MZF-1transcription factor (39), therefore confirming the hypoth-esis of a contribution of PI-PLCb1 in azacytidine-inducedmyeloid differentiation (18).
Taken together, our results strongly suggest that the earlyevaluation of PI-PLCb1 expression could be a reliabledynamic marker of response to azacytidine. Indeed, amongthe responsive patients, a significant decrease of PI-PLCb1expression was observed in those patients that lost theclinical response after the end of treatment, but not in thepatients maintaining a durable hematologic response. Asfor this last point, the long-lasting responses that weobserved may shed some light on the potential activity ofazacytidine in terms of controlling disease progression andsuggest that, at least in a restricted number of patients withlow-risk MDS, survival could also be a possible therapeuticgoal, besides improvement in transfusion dependence andquality of life.
On the other hand, SNP array analysis, did not allowus toclearly identify those patients who achieved a benefit from5d-AZA. To identify genetic surrogate markers for responseand survival in patients with MDS following azacytidinetherapy, we applied SNP array technology. This approachwas more sensitive than conventional cytogenetics in iden-tifying genomic abnormalities, including both copy num-ber changes and LOH, in all analyzed patients (100%).However, the type and the number of CNAs did not cor-relate with the response (HI/CR) to azacytidine. Interest-ingly, a trend for worse response in terms of stable diseasehas been found in patients with LOH (80% vs. 57% ofpatients without LOH). Whether the lesions detected bySNP-array have a prognostic value on clinical outcome isstill controversial in MDS (40). In Gondek and colleagues’report with 141 patients withMDS andMDS/MPN, survivalduration was not affected by abnormal CNAs (41), bycontrast, in Yi and colleagues’ study the presence of abnor-mal SNP lesions correlated with lower CR and PR rate
following decitabine therapy and with worse OS even if itwas not confirmed in the multivariate analysis (42).
It must be considered that azacytidine, although effectiveand generally well tolerated, is not without toxicity. There-fore, the early identification of patients who could benefitmost from azacytidine would be useful to select thosepatients for whom the treatment may prove cost-effective-ness. Earlier discontinuation of azacytidine may avoid orreduce the risk of administering an ineffective drug for aprolonged period and to expose patients to unnecessarytoxicity in absence of clinical and hematologic benefit. Inour study, the most relevant toxicity was hematologic.Azacytidine may worsen preexisting neutropenia andthrombocytopenia and consequently may increase the riskof developing additional complications. It should be under-lined that we observed 4 early deaths, which were related toinfections in 3 cases and hemorrhage in 1 case. From aclinical point of view, it is very probable that these deathswere related to the underlying hematologic disease orcomorbidities and not due to azacytidine.
In conclusion, in this prospective phase II study, weobserved that a lower intensity schedule of azacytidine iseffective in about 60% of patients with low-risk MDS,refractory to ESAs or with severe cytopenia. Extreme cautionmust be adopted, particularly in elderly patients withcomorbidity. Because of hemato-toxicity associated withthe drug, risks of death due to bleeding and infection are notnegligible, especially during the initial cycles of therapy. Asfor the biologic studies, SNP array analysis showed that low-risk MDS is a very heterogeneous group of diseases, but itwas unable to identify genetic alterations possibly correlat-ed with hematologic response to azacytidine. On the otherhand, our results showed that the evaluation of PI-PLCb1gene expression during treatment with azacytidinemay be areliable and earlymarker of response to azacytidine and cancontribute to early identification of responsive patients,even though it does not predict the depth and duration ofresponse. That is why further studies are needed to validatethese data on larger series of patients. If confirmed, ourresults could also be useful to optimize the treatment withazacytidine and to design further investigational studiesboth in low- and high-risk MDS.
Disclosure of Potential Conflicts of InterestG.Martinelli has honoraria from Speakers Bureau ofNovartis and Bristol-
Myers Squibb and is a consultant/advisory board member of Roche andPfizer. No potential conflicts of interest were disclosed by the other authors.
Authors' ContributionsConception and design: M. Malagola, D. RussoDevelopment of methodology: C. Fil��, M.Y. Follo, C. Finelli, F. Cattina, C.Skert, L. Manzoli, L. Cocco, D. RussoAcquisitionofdata (provided animals, acquired andmanagedpatients,provided facilities, etc.): C. Fil��, M. Malagola, M.Y. Follo, C. Finelli, F.Cattina, C. Clissa, A. Candoni, R. Fanin, M. Gobbi, M. Bocchia, M. Defina, P.Spedini, L. Manzoli, L. CoccoAnalysis and interpretation of data (e.g., statistical analysis, biosta-tistics, computational analysis): C. Fil��, M.Y. Follo, C. Finelli, I. Iacobucci,G. Martinelli, C. Skert, L. Manzoli, L. Cocco, D. RussoWriting, review, and/or revision of the manuscript: C. Fil��, M. Malagola,M.Y. Follo, C. Finelli, R. Fanin, M. Bocchia, L. Cocco, D. RussoStudy supervision: M. Gobbi, D. Russo
Fil�� et al.
Clin Cancer Res; 19(12) June 15, 2013 Clinical Cancer Research3306
on April 30, 2016. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst April 17, 2013; DOI: 10.1158/1078-0432.CCR-12-3540

Grant SupportThis work was supported in part by PRIN-Cofin 2007, ItalianMIUR-FIRB,
Celgene, and Lions Bassa Bresciana Association.The costs of publication of this article were defrayed in part by the
payment of page charges. This article must therefore be hereby marked
advertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received November 15, 2012; revised March 13, 2013; accepted April 10,2013; published OnlineFirst April 17, 2013.
References1. Issa JP. Epigenetic changes in the myelodysplastic syndrome. Hema-
tol Oncol Clin North Am 2010;24:317–30.2. Taby R, Issa JP. Cancer epigenetics. CA Cancer J Clin 2010;60:
376–92.3. Nolte F, Hofmann WK. Molecular mechanisms involved in the pro-
gression of myelodysplastic syndrome. Future Oncol 2010;6:44555.4. Garcia-Manero G, Fenaux P. Hypomethylating agents and other novel
strategies in myelodysplastic syndromes. J Clin Oncol 2011;29:516–23.
5. Jain NE, Rossi A, Garcia-Manero G. Epigenetic therapy of leukaemia:an update. Int J Biochem Cell Biol 2009;41:72–80.
6. GarciaManeroG. Treatment of higher-riskmyelodysplastic syndrome.Semin Oncol 2011;38:673–81.
7. Quintas-Cardama A, Santos FP, Garcia-Manero G. Therapy withazanucleosides for myelodysplastic syndromes. Nat Rev Clin Oncol2010;7:433–44.
8. FolloMY, Faenza I, FiumeR, Ramazzotti G,McCubrey JA,Martelli AM,et al. Revisiting nuclear phospholipase C signalling in MDS. AdvEnzyme Regul 2012;52:2–6.
9. Cocco L, Follo MY, Faenza I, Fiume R, Ramazzotti G, Weber G, et al.Physiology andpathologyof nuclear phospholipaseCb1. AdvEnzymeRegul 2011;51:2–12.
10. FolloMY, Finelli C, BosiC,Martinelli G,Mongiorgi S, BaccaraniM, et al.PI-PLCbeta-1 and activatedAkt levels are linked to azacitidine respon-siveness in high-risk myelodysplastic syndromes. Leukemia 2008;22:198–200.
11. Follo MY, Finelli C, Mongiorgi S, Clissa C, Bosi C, Testoni N, et al.Reduction of phosphoinositide-phospholipase C beta 1 methylationpredicts the responsiveness to azacitidine in high-risk MDS. Proc NatlAcad Sci U S A 2009;106:16811–6.
12. Follo MY, Finelli C, Mongiorgi S, Clissa C, Chiarini F, Ramazzotti G,et al. Synergistic induction of PI-PLCbeta1 signaling by azacitidine andvalproic acid in high-risk myelodysplastic syndromes. Leukemia2011;25:271–80.
13. Martelli AM, Fiume R, Faenza I, Tabellini G, Evangelista C, Bortul R,et al. Nuclear phosphoinositide specific phospholipase C (PI-PLC)-beta 1: a central intermediary in nuclear lipid-dependent signal trans-duction. Histol Histopathol 2005;20:1251–60.
14. Faenza I, Billi AM, Follo MY, Fiume R, Martelli AM, Cocco L, et al.Nuclear phospholipase C signaling through type 1 IGF receptor and itsinvolvement in cell growth and differentiation. Anticancer Res 2005;25:2039–41.
15. Ramazzotti G, Faenza I, FiumeR,Matteucci A, PiazziM, FolloMY, et al.The physiology and pathology of inositide signaling in the nucleus.J Cell Physiol 2011;226:14–20.
16. FolloMY,Mongiorgi S, Finelli C, Clissa C, Ramazzotti G, FiumeR, et al.Nuclear inositide signaling in myelodysplastic syndromes. J Cell Bio-chem 2010;109:1065–71.
17. Follo MY, Finelli C, Clissa C, Mongiorgi S, Bosi C, Martinelli G, et al.Phosphoinositide-phospholipase C beta1 mono-allelic deletion isassociated with myelodysplastic syndromes evolution into acutemyeloid leukemia. J Clin Oncol 2009;27:782–90.
18. Follo MY, Russo D, Finelli C, Mongiorgi S, Clissa C, Fili C, et al.Epigenetic regulation of nuclear PI-PLCbeta1 signaling pathway inlow-risk MDS patients during azacitidine treatment. Leukemia2012;26:943–50.
19. Follo MY, Mongiorgi S, Clissa C, Paolini S, Martinelli G, Martelli AM,et al. Activation of nuclear inositide signalling pathways during eryth-ropoietin therapy in low-risk MDS patients. Leukemia 2012;26:2474–82.
20. Fenaux P, Mufti GJ, Hellstrom-Lindberg E, Santini V, Finelli C, Gia-gounidis A, et al. Efficacy of azacitidine compared with that of con-ventional care regimens in the treatment of higher-riskmyelodysplasticsyndromes: a randomised, open-label, phase III study. Lancet Oncol2009;10:223–32.
21. Fenaux P, Ades L. Review of azacitidine trials in intermediate-2-andhigh-risk myelodysplastic syndromes. Leuk Res 2009;33(Suppl 2):S7–11.
22. Hellstr€om-Lindberg E, Malcovati L. Supportive care and use ofhematopoietic growth factors in myelodysplastic syndromes. SeminHematol 2008;45:14–22.
23. Oliva EN, Finelli C, Santini V, Poloni A, Liso V, Cilloni D, et al. Quality oflife and physicians' perception in myelodysplastic syndromes. Am JBlood Res 2012;2:136–47.
24. Silverman LR, Demakos EP, Peterson BL, Kornblith AB, Holland JC,Odchimar-Reissig R, et al. Randomized controlled trial of azacitidine inpatients with themyelodysplastic syndrome: a study of the cancer andleukemia group B. J Clin Oncol 2002;20:2429–40.
25. Silverman LR, McKenzie DR, Peterson BL, Holland JF, Backstrom JT,Beach CL, et al. Further analysis of trials with azacitidine in patientswith myelodysplastic syndrome: studies 8421, 8921, and 9221 by theCancer and Leukemia Group B. J Clin Oncol 2006;24:3895–903.
26. Lyons RM, Cosgriff TM,Modi SS, Gersh RH, Hainsworth JD, Cohn AL,et al. Hematologic response to three alternative dosing schedules ofazacitidine in patients with myelodysplastic syndromes. J Clin Oncol2009;27:1850–56.
27. Musto P, Maurillo L, Spagnoli A, Gozzini A, Rivellini F, Lunghi M, et al.Azacitidine for the treatment of lower riskmyelodysplastic syndromes:a retrospective study of 74 patients enrolled in an Italian named patientprogram. Cancer 2010;116:1485–94.
28. Cheson BD, Greenberg PL, Bennet JM, Lowenberg B, Wijermans P,Nimer S , et al. Clinical application and proposal for modification of theInternational Working Group (IWG) response criteria in myelodyspla-sia. Blood 2006;108:419–25.
29. FolloMY, Bosi C, Finelli C, FiumeR, Faenza I, Ramazzotti G, et al. Real-time PCR as a tool for quantitative analysis of PI-PLCbeta1 geneexpression in myelodysplastic syndrome. Int J Mol Med 2006;18:267–71.
30. Iacobucci I, Storlazzi CT, Cilloni D, Lonetti A, Ottaviani E, Soverini S,et al. Identification and molecular characterization of recurrent geno-mic deletions on 7p12 in the IKZF1 gene in a large cohort of BCR-ABL1-positive acute lymphoblastic leukemia patients: on behalf ofGruppo Italiano Malattie Ematologiche dell'Adulto Acute LeukemiaWorking Party (GIMEMA AL WP). Blood 2009;114:2159–67.
31. Greenberg P, Cox C, LeBeau MM, Fenaux P, Morel P, Sanz G, et al.International scoring system for evaluating prognosis in myelodys-plastic syndromes. Blood 2009;114:937–51.
32. Fil�� C, Gobbi M, Martinelli G, Finelli C, Iacobucci I, Ottaviani E, et al.Azacitidine low-dose schedule in symptomatic low-risk (IPSS:0-1)myelodysplastic patients. Clin Biol Eff Haematol 2012;95(Suppl 3):S32–33.
33. Fil�� C, Finelli C, Gobbi M, Martinelli G, Iacobucci I, Ottaviani E, et al.Azacitidine low-dose schedule in low-risk myelodysplastic syn-dromes. Preliminary results of a multicenter phase II study [abstract].In: Proceedings of the 53rd ASH Annual Meeting and Exposition; 2011Dec 10–13; Orlando, FL: Orange County Convention Center; 2011. p.116. Abstract nr 4029.
34. Fil�� C, Finelli C, Gobbi M, Martinelli G, Iacobucci I, Ottaviani E, et al.Clinical results of a multicenter phase II study. Leuk Res 2011;35(Suppl 1):S84–85.
Azacitidine in Low-Risk Myelodysplastic Syndromes
www.aacrjournals.org Clin Cancer Res; 19(12) June 15, 2013 3307
on April 30, 2016. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst April 17, 2013; DOI: 10.1158/1078-0432.CCR-12-3540

35. JaderstenM, Hellstrom-Lindberg E.Myelodysplastic syndromes: biol-ogy and treatment. J Intern Med 2009;265:307–28.
36. Komrokji RS, Sekeres MA, List AF. Management of lower-risk mye-lodysplastic syndrome: the art and evidence. Curr Hematol Malig Rep2011;6:145–53.
37. Novotna B, Neuwirtova R, Siskova M, Bagryantseva Y. DNA insta-bility in low-risk myelodysplastic syndromes: refractory anemiawith or without ring sideroblasts. Hum Mol Genet 2008;17:2144–9.
38. TobiassonM,Brandefors L,Dybedal I,GareliusH,GrovdalM,Dufva IH,et al. Evaluation of Azacitidine in transfusion-dependent, epo-refrac-tory patients with lower-risk myelodysplastic syndrome [abstract]. In:Proceedings of the 53rd ASH Annual Meeting and Exposition; 2011Dec 10–13; San Diego, CA: San Diego Convention Center; 2011. p.118. Abstract nr 3798.
39. Morris JF, Rauscher FJ III, Davis B, KlemszM, XuD, TenenD, et al. Themyeloid zinc finger gene,MZF-1, regulates the CD34 promoter in vitro.Blood 1995;86:3640–7.
40. Mohamedali A, Gaken J, Twine NA, Ingram W, Westwood N, Lea N,et al. Prevalence and prognostic significance of allelic imbalance bysingle-nucleotide polymorphism analysis in low-risk myelodysplasticsyndromes. Blood 2007;110:3365–73.
41. Gondek LP, Tiu R, O'Keefe CL, SekeresMA, Theil KS, Maciejewski JP.Chromosomal lesions and uniparental disomy detected by SNP arraysinMDS,MDS/MPD, andMDS-derivedAML.Blood2008;111:1534–42.
42. Yi JH, Huh J, Kim HJ, Kim S, Kim SH, Kim KH, et al. Genome-widesingle-nucleotide polymorphism array-based karyotyping in myelo-dysplastic syndrome and chronic myelomonocytic leukemia and itsimpact on treatment outcomes following decitabine treatment. AnnHematol 2012:1635–7.
Fil�� et al.
Clin Cancer Res; 19(12) June 15, 2013 Clinical Cancer Research3308
on April 30, 2016. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst April 17, 2013; DOI: 10.1158/1078-0432.CCR-12-3540

2013;19:3297-3308. Published OnlineFirst April 17, 2013.Clin Cancer Res Carla Filì, Michele Malagola, Matilde Y. Follo, et al.
Risk Myelodysplastic Syndromes−Low/INT-1 Symptomatic and/or Erythropoietin Unresponsive Patients with
Prospective Phase II Study on 5-Days Azacitidine for Treatment of
Updated version
10.1158/1078-0432.CCR-12-3540doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2013/04/17/1078-0432.CCR-12-3540.DC1.html
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/19/12/3297.full.html#ref-list-1
This article cites 39 articles, 14 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/19/12/3297.full.html#related-urls
This article has been cited by 1 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
To request permission to re-use all or part of this article, contact the AACR Publications Department at
on April 30, 2016. © 2013 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst April 17, 2013; DOI: 10.1158/1078-0432.CCR-12-3540
Copyright © 2022 FDOKUMEN




















