Propensity-Matched, Longitudinal Outcomes Analysis of Complications and Cost Comparing Abdominal...
36
Accepted Manuscript Propensity-Matched, Longitudinal Outcomes Analysis of Complications and Cost Comparing Abdominal Free Flaps and Implant-Based Breast Reconstruction John P. Fischer, MD Ari M. Wes, BA Jonas A. Nelson, MD Marten Basta, BA Jeffrey I. Rohrbach, MSN Liza C. Wu, MD FACS Joseph M. Serletti, MD FACS Stephen J. Kovach, MD PII: S1072-7515(14)00306-8 DOI: 10.1016/j.jamcollsurg.2014.02.028 Reference: ACS 7364 To appear in: Journal of the American College of Surgeons Received Date: 31 October 2013 Revised Date: 14 February 2014 Accepted Date: 17 February 2014 Please cite this article as: Fischer JP, Wes AM, Nelson JA, Basta M, Rohrbach JI, Wu LC, Serletti JM, Kovach SJ, Propensity-Matched, Longitudinal Outcomes Analysis of Complications and Cost Comparing Abdominal Free Flaps and Implant-Based Breast Reconstruction, Journal of the American College of Surgeons (2014), doi: 10.1016/j.jamcollsurg.2014.02.028. This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Propensity-Matched, Longitudinal Outcomes Analysis of Complications and Cost Comparing Abdominal...

Accepted Manuscript
Propensity-Matched, Longitudinal Outcomes Analysis of Complications and CostComparing Abdominal Free Flaps and Implant-Based Breast Reconstruction
John P. Fischer, MD Ari M. Wes, BA Jonas A. Nelson, MD Marten Basta, BA JeffreyI. Rohrbach, MSN Liza C. Wu, MD FACS Joseph M. Serletti, MD FACS Stephen J.Kovach, MD
PII: S1072-7515(14)00306-8
DOI: 10.1016/j.jamcollsurg.2014.02.028
Reference: ACS 7364
To appear in: Journal of the American College of Surgeons
Received Date: 31 October 2013
Revised Date: 14 February 2014
Accepted Date: 17 February 2014
Please cite this article as: Fischer JP, Wes AM, Nelson JA, Basta M, Rohrbach JI, Wu LC, Serletti JM,Kovach SJ, Propensity-Matched, Longitudinal Outcomes Analysis of Complications and Cost ComparingAbdominal Free Flaps and Implant-Based Breast Reconstruction, Journal of the American College ofSurgeons (2014), doi: 10.1016/j.jamcollsurg.2014.02.028.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service toour customers we are providing this early version of the manuscript. The manuscript will undergocopyediting, typesetting, and review of the resulting proof before it is published in its final form. Pleasenote that during the production process errors may be discovered which could affect the content, and alllegal disclaimers that apply to the journal pertain.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
Propensity-Matched, Longitudinal Outcomes Analysis of Complications and Cost
Comparing Abdominal Free Flaps and Implant-Based Breast Reconstruction
John P Fischer, MD1, Ari M Wes, BA1, Jonas A Nelson, MD1, Marten Basta, BA1, Jeffrey I
Rohrbach, MSN2, Liza C Wu, MD1, FACS, Joseph M Serletti, MD1, FACS, Stephen J Kovach,
MD1
1Division of Plastic Surgery, Perelman School of Medicine at the Hospital of the University of
Pennsylvania, Philadelphia, PA.
2Division of Finance, Perelman School of Medicine at the Hospital of the University of
Pennsylvania, Philadelphia, PA.
Disclosure: None of the authors listed have any conflicts of interest to report.
Disclosure Information: Nothing to disclose.
Correspondence address: John P. Fischer, MD University of Pennsylvania Division of Plastic Surgery 3400 Spruce Street Philadelphia, PA 19104 [email protected]
Running head: Matched Modality Outcomes Study

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
2
Abstract
Background
Choosing a breast reconstructive modality after mastectomy is an important step in the
reconstructive process. The authors hypothesize that autologous tissue is associated with greater
success rates and cost-efficacy over time, relative to implant reconstructions.
Study Design
A retrospective review of patients undergoing free tissue (FF) transfer and expander
implant (E/I) reconstruction between 2005-2011 was performed. Variables evaluated included:
co-morbidities, surgical timing, complications, overall outcome, unplanned reoperations, and
costs. A propensity-matching technique was used to account for the non-randomized selection of
modality.
Results
A total of 310 propensity-matched patients underwent 499 reconstructions. No
statistically significant differences in preoperative variables were noted between propensity-
matched cohorts. Operative characteristics were similar between FF and E/I reconstructions. E/I
reconstruction was associated with a significantly higher rate of reconstructive failure (5.6% vs.
1.2%, P<0.001). E/I reconstructions were associated with higher rates of seroma (P=0.009),
lower rates of medical complications (P=0.02), but overall significantly higher rates of
unplanned operations (15.5% vs. 5.8%, P=0.002). The total cost of reconstruction did not differ
significantly between groups ($23,120.49±$6,969.56 vs. $22,739.91±$9,727.79, P=0.060), but
E/I reconstruction was associated with higher total cost for secondary procedures
($10,157.89±$8,741.77 vs. $3,200.71±$4,780.64, P<0.0001) and a higher cost of unplanned
revisions over time (P<0.05).

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
3
Conclusions
Our matched outcomes analysis does demonstrate a higher overall, 2-year success rate
using FF reconstruction and a significantly lower rate of unplanned surgical revisions and cost.
Although autologous reconstruction is not ideal for every patient, these findings can be used to
enhance preoperative discussions when choosing a reconstructive modality.
Level of Evidence: prognostic/risk category, level III

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
4
Introduction
Breast reconstruction is known to provide a significant psychosocial and aesthetic benefit
for patients following mastectomy [1-4], yet complications can impact recovery[4],
satisfaction[5], and generate added reconstructive cost[6]. Free tissue (FF) transfer and expander
implant (E/I) reconstruction have established benefits and downsides. To date there is limited
data on the comparative surgical risk profiles, long-term outcomes, and costs associated with
these two common reconstructive modalities [7-12].
Through a deeper understanding of long-term, modality-specific risk, and outcomes, cost-
conscious and efficacious breast reconstruction can be performed. Longitudinal outcomes data
can be employed by reconstructive surgeons to assist patients better navigate the modality
selection process. The authors hypothesis that autologous tissue reconstruction (FF) is associated
with higher success rates and cost-efficacy over time, relative to implant-based breast
reconstructions.
Methods
(i.) Study Design
We performed a retrospective review of our prospectively maintained breast
reconstruction database and identified patients from June 2005 through May 2011 who
underwent either abdominally-based free autologous breast reconstruction (FF) or E/I
reconstruction at the Hospital of the University of Pennsylvania. Breast reconstruction was
performed by three surgeons (JMS, LCW, and SJK).
E/I reconstructions were uniformly performed as two-staged procedures with sub-
muscular coverage of tissue expanders using pectoralis majorand serratus muscle/fascia flaps

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
5
with a secondary staged implant exchange. We compared overall outcomes and cost between the
two modalities over the study period. This study was approved by our institutional review board.
(ii.) Data collection
A detailed review of hospital and office records included the following: preoperative
history and physical, operative reports, anesthesia records, postoperative nursing records,
discharge summaries, and outpatient clinic notes. Additionally, the institutional hospital database
was queried for institutional costs associated with each patient’s reconstructive hospitalization,
subsequent operative course, and unplanned admissions or operations. Revenue generated from
breast reconstruction related to surgeon professional fees was not collected or reported.
Similarly, downstream revenue from cancer care, such as chemotherapy or radiation treatment,
was not included in this analysis.
Specific variables examined included baseline patient characteristics such as age, body
mass index (BMI), hypertension (HTN), chronic obstructive pulmonary disease (COPD),
hyperlipidemia (HL), smoking (active or previous), and coronary artery disease (CAD).
Variables indicating patient demographics, comorbidities, and perioperative risk factors were
selected for analysis. These included baseline health characteristics, past medical and surgical
history, and American Society of Anesthesiologists (ASA) physical status. The World Health
Organization definition of obesity was used to classify patients with a BMI <30 kg/m2 as non-
obese, class I obese (BMI = 30.0-34.9 kg/m2), class II obese (BMI=34.9-39.9 kg/m2), and class
III obese (BMI ≥ 40 kg/m2)[13].
We characterized oncologic factors (mastectomy type, pre- and postoperative
chemotherapy and radiation), reconstructive details (immediate versus delayed, unilateral versus
bilateral, and flap type), and directly comparable complications (hematoma, seroma, delayed

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
6
breast healing, cellulitis, and reconstructive failure). Specific complication rates were expressed
on a per reconstruction basis unless otherwise noted (failure, mastectomy flap necrosis, seroma,
etc.). Overall complications defined throughout the reconstruction process were defined on a per
patient basis. Modality-specific complications related to donor-site morbidity and fat necrosis in
FF and implant-related complications in the E/I cohort were also reported.
Reconstructive failure was defined as total flap loss or tissue expander/implant removal
secondary to either infection or exposure. Capsular contraction requiring revision or implant
exchange was defined as an unplanned surgical revision procedure as opposed to a reconstructive
failure. Delayed wound healing at the abdominal donor site and mastectomy flap were defined as
skin necrosis or wound breakdown necessitating topical care or dressing changes for more than
three weeks. Fat necrosis was defined as a palpable firmness on clinical examination greater than
1 cm in diameter present at follow-up but not related to cancer recurrence. Superficial infection
was defined as incisional cellulitis at either the donor site or breast that occurred within 30 days
of surgery, only involving skin and subcutaneous tissue structures, treated with antibiotics, and
was documented by a physician.
We also evaluated the incidence of nipple areolar reconstruction, overall complications
(major and minor), total hospital days, number of clinic visits, and unplanned surgical revisions.
Major unplanned operative complications included any operative intervention for a postoperative
complication. Specifically, in the FF cohort such complications included postoperative
thrombotic events, flap loss, hematoma, major wound breakdown, or hernia, whereas those for
E/I were implant replacement for infection or exposure, hematoma, seroma, or wound
complications requiring operative interventions. Minor complications included non-operative
complications. Unplanned surgical revisions were separately defined as surgical interventions

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
7
related to postoperative complications following the initial reconstructive period, specifically
after the initial discharge from the primary reconstructive procedure.
(iii.) Cost analysis
Financial data were obtained from the Department of Finance at the Hospital of the
University of Pennsylvania to characterize the hospital, institution-specific cost. These data were
used to derive costs associated with the completion of breast reconstruction using E/I or FF
within our health system. Specifically, we obtained all cost data for each patient in the post-
operative period by characterizing the cost of each episode of care related to reconstruction. Cost
was defined for the complete reconstructive course as “all”, or for events of care and operations
following the initial completion of reconstruction “subsequent” (i.e., everything after the initial
reconstruction). We obtained several cost figures for each patient, including: total hospital cost,
total direct variable cost, and operative room costs. Direct variable cost represents the
institutional cost without overhead or labor, essentially representing the opportunity cost of
doing one more procedure. Operating room costs reflect the cost of operating room utilization,
implants and devices, and the use of other equipment. These cost figures did not include
professional service fees or charges, nor did we attempt to obtain any downstream revenue
created by performing breast reconstruction.
(iv.) Propensity matching
Propensity scores were incorporated into this analysis to reduce the risk of selection bias
due to the non-randomized assignment of modality and retrospective nature of this study [14-16].
A propensity score for modality selection (autologous reconstruction) was calculated by
assessing perioperative factors associated with autologous reconstruction (yes or no) in a
multivariate logistic regression. Specifically, the propensity score represented the probability of

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
8
having an autologous reconstruction based on preoperative patient characteristics. The
propensity score ranged from 0, representing the lowest probability of autologous reconstruction,
to 1, representing the highest probability of autologous reconstruction. Patients were matched
using a caliper of 0.005.
(v.) Statistical analysis
Bivariate analysis was performed using Pearson Chi Square for categorical variables and
Wilcoxon rank-sum test for continuous variables. All tests were two-sided, with statistical
significance set at a probability value of ≤0.05. Analyses were performed using STATA IC 10.0
(StataCorp, College Station, Texas).
Results
A total of 1,083 patients (1,634 reconstructions) were identified; 842 patients underwent
FF reconstruction and 241 patients underwent E/I reconstruction with an average follow-up of
21±16 months and 25±17 months, respectively (P=0.001). The overall rate of successful
reconstruction was 98.3%. A summary of reconstructive modality and number by year is found
in Figure 1. A multivariate regression analysis of preoperative factors associated with FF
reconstruction was performed (Table 1). Independent factors associated with FF reconstruction
were age (P<0.001), BMI (P<0.001), preoperative radiation (P=0.006), Surgeon C (P=0.011),
and laterality (P=0.002). Propensity-matched FF’s (N=155) and E/I’s (N=155) were compared
with respect to preoperative characteristics, operative variables, and postoperative outcomes and
cost. A total of 310 patients who underwent 499 reconstructions were matched through a
propensity analysis. No statistically significant preoperative variables differed between

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
9
propensity-matched FF and E/I (Table 2). Matched patients were of similar age (P=0.454), BMI
(P=0.357), ASA physical status (P=0.693), and smoking status (P=0.301). A higher rate of
postoperative radiation was noted in FF patients (P=0.012). Reconstructions were predominantly
immediate – FF (89.7%) and E/I (90.3%). Operative characteristics were similar between FF and
E/I reconstructions, with a higher rate of simple mastectomies in E/I (P=0.002). The most
commonly used FF was the TRAM (unilateral: 28.4%; bilateral: 34.2%)(Table 3).
Procedure-specific complications are summarized in Table 4. Major surgical
complications in matched patients were significantly higher in E/I reconstructions (20.0% vs.
11.0%, P=0.028), but overall complications were higher in FF reconstructions (63.9% vs. 32.9%,
P<0.001). The incidence of donor-site morbidity in the FF cohort was 25.6%. The rate of
unplanned operative complications of E/I reconstrictions over-time tended to increase at
significantly greater rate compared to FF (Fig. 2). The overall rate of unplanned surgical
interventions was higher for E/I at <6 months (3.9% vs. 5.2%) (P=0.562), <12 months (4.5% vs.
11.0%) (P=0.017), <24 months (4.5% vs.13.5%)(P=0.003), and overall (5.8% vs. 15.5%)
(P=0.006) (Figure 2). E/I reconstruction was associated with a significantly higher rate of
reconstructive failure (5.6% vs. 1.2% P<0.001). Kaplan-Meier curve demonstrated earlier and
less frequent failures with FF and more frequent, but delayed device failures with prosthetic
reconstructions over time (Fig. 3).
E/I reconstructions were associated with lower rates of medical complications (P=0.02),
but higher rates of seroma (P=0.009). Patients receiving FF reconstruction more frequently
received nipple areolar reconstruction (74.2% vs. 54.8%, P<0.001) and did so sooner (9.8±6.8
vs. 13.8±9.2 months, P<0.001) (Table 4). FF patients required longer total hospital length of stay

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
10
(4.5±1.8 vs. 2.1±0.9 days, P<0.0001), but significantly fewer postoperative clinic visits (9.8±4.9
vs. 19.0±8.4, P<0.0001) (Table 5).
Cost differences between propensity-matched E/I and FF patients are summarized in
Table 5. E/I reconstruction was associated with higher total direct variable operative costs (“all”)
($1,332.98±$1,143.04 vs. $3,767.63±$1,838.36, P<0.0001) and total direct variable costs for
reconstruction (“all”) ($2,485.72±$1,288.62 vs. $5,652.97±$2,258.40, P<0.0001). The total cost
(“all”) of reconstruction did not differ significantly between groups ($23,120.49±$6,969.56 vs.
$22,739.91±$9,727.79, P=0.060), but E/I reconstruction was associated with higher total cost for
“subsequent” procedures ($3,200.71±$4,780.64 vs. $10,157.89±$8,741.77, P<0.0001). The
overall cost of unplanned operative revisions was significantly higher after one year for E/I
reconstructions (Fig. 4).
Discussion
Comprehensive outcomes and cost data examining reconstructive modalities is lacking in
the current literature [7, 8, 17-20]. This study is the first longitudinal, propensity-matched, multi-
surgeon outcome and cost analysis of two breast reconstructive modalities (FF and E/I). Our
study focuses on modality performance and hospital-associated cost between two common
reconstructive modalities, and includes more than 1,000 patients who underwent over 1,600
reconstructions with an average follow-up period of 2 years. Propensity-matching techniques
provided a useful statistical tool which mitigated modality selection bias. Data derived from this
analysis can be employed to guide perioperative decision-making, optimize informed consent,
and better counsel patients. Our findings demonstrate time-dependent modality-specific risk and
cost profiles, such that autologous tissue reconstructions are associated with higher rates of 2-

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
11
year reconstructive success and lower rates of cumulative, unplanned surgical reoperation and
cost. These data are relatively early postoperative endpoints, since device-related complications
and implant maintenance will inevitably accrue over time and further contribute to the notable
early cost divergence presented herein[21]. Additionally, prosthetic-based reconstructive
techniques used by the surgeons at our institutional use a sub-muscular only technique rarely, if
ever, using ADM which would otherwise create significantly greater cost[22]. Several findings
merit further discussion.
Our group recently reported the outcomes of a 3-year experience by our senior surgeon
(JMS) which demonstrated higher rates of reconstructive success in FF, but this study did not
include a matched analysis nor did it include as many patients[7]. Recent work by Mioton et al
(2013) attempted to compare perioperative outcomes between autologous reconstruction and
implant reconstruction using a large, national database, National Surgical Quality Improvement
Dataset (NSQIP), and demonstrated higher rates of prosthesis/flap failure in autologous
reconstruction (3.13% vs. 0.85%, P<0.001)[20]. However, there are clear limitations of these
data due to the clustering of autologous reconstructions (pedicled and microsurgical flaps) and
the short-term follow-up (30-day) which creates significant selection bias favoring lower rates of
complications in the implant cohort. Our current analysis directly compares, matched FF and E/I
patients with respect to complications and cost. Important to note is that our current study is only
on average 2 years follow-up and likely does not capture the longer term complications and
associated cost linked to implant reconstruction both related to device complications and needed
implant maintenance over time.
Addressing some of the limitations of using national datasets and our prior study, our
current analysis provides a propensity-matched, homogeneous, generalizable comparison of two

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
12
commonly used modalities—the abdominally-based free flap and the two-staged implant
reconstruction. In performing this analysis, we were able to control for multiple preoperative
variables which may impact reconstructive modality selection. The ultimate result following
propensity-matching was two cohorts of patients which are virtually identical as demonstrated by
the lack of significant differences in preoperative characteristics. Our current analysis allows for
a more accurate comparison of outcomes and overall generalizable outcomes.
The rate of tissue expander loss has been reported to occur at a rate of 0.9-2.7% in the
current literature[9, 23-26], and these figures compare favorably with our overall 5.6% rate of
two-stage implant reconstruction loss at an average of two years. Few studies cite an overall rate
of reconstructive success, such that the outcome variable represents successful breast
reconstruction with the initially planned modality, as in our current study does. Thus, there is a
2-year 94.4% reconstructive success rate with E/I patients and a 98.8% success rate with free
tissue transfer with regards to the initial chosen modality at just less than two years of follow-up.
These findings underscore the reliability of both the two-stage implant based breast
reconstruction and free flap breast reconstruction at a high-volume center, but also show that
autologous tissue is superior over time. Furthermore, unplanned reoperation rates were lower in
FF reconstruction (5.8% vs.16.8%, P=0.002), with the rate of implant revisions comparing
favorably with published results from Spear et al. (2008) at 11.3%[27]. Unplanned reoperations
for this analysis were defined specifically as surgical interventions that occurred after the initial
discharge for primary reconstruction that were performed due to a complication. Additionally,
the authors report an overall operative complication variable (“major surgical complications”)
which is inclusive of all operative complications and demonstrates a higher risk of complications
in E/I reconstructions (11.0% vs 20.0%, P=0.028).. Second stage implant exchanges, nipple

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
13
reconstruction, and planned aesthetic refinements were not considered unplanned reoperations.
Additionally, minor revisions to scars performed in conjunction with planned procedures
(implant exchange or nipple reconstruction) were not included in the analysis of complications.
Procedure-specific complications for FF included, hernia, wound complications, fat necrosis,
partial flap excision, hematoma, and seroma were considered for FF. Wound complications,
hematoma, seroma, device loss, capsular contracture, and device malposition were considered
for E/I. Of note our analysis demonstrated a significant rise in the rate of unplanned surgical
interventions over time for E/I relative to FF, which also mirror the rate of unplanned cost over
time (Fig. 2 and 4). Furthermore, FF reconstructions tended to experience failure early, whereas
device losses for E/I reconstructions tended to occur statistically more frequent and later during
the study period (Fig. 3). These findings underscore the fact the autologous reconstruction,
although associated with a greater upfront operation, surgical risk, and cost, tends to perform
better over time and is likely more cost-efficient.
The down side of FF reconstruction can be appreciated by the significantly higher overall
complication profile in the matched cohort (63.9% vs. 32.9%, P<0.001). The higher rate of
surgical complications likely relates to wound complications and donors-site complications
which occurred in 25.4% of the FF matched cohort [28, 29]. These data provide important
information for counseling patients regarding expected risk of minor wound complications and
donor-site complications including a risk of hernia/bulge in upwards of 4% of our cohort[30].
The importance of meticulous donor-site closure and management has been established in the
literature, and remains an important consideration in preoperative risk counseling, particularly in
the obese patient [29-34].

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
14
Autologous tissue reconstruction, and specifically free tissue transfer, represents a larger
upfront operation with a greater risk of complications related to donor-site morbidity, early
microsurgical complication, and medical complications[6]. Previous work from our institution
has shown a higher rate of perioperative medical morbidity related to autologous reconstruction
and this larger, matched analysis confirms these findings[7]; FF patients experienced higher rates
of postoperative medical complications (5.8% vs. 0.6%, P=0.02). These data are useful in
preoperative risk discussions, informed consent, expectation management, and in planning and
discussing the anticipated time course and reconstruction-specific risk profiles of these two
modalities.
Our analysis also assessed reconstructive course and follow-up between the two
modalities and revealed that patients undergoing E/I reconstructions required longer follow-up
(P=0.0025) and more postoperative clinic visits (P<0.0001), likely due to longer follow-up
length (P=0.001). These findings are intuitive but the ability to explain preoperatively that an
implant reconstruction will require more visits for a longer period of time can provide useful
information in the informed consent process to assist with modality selection.
This study also incorporates a cost analysis, which revealed that the 2 year reconstructive
cost does not statistically differ between modalities (P=0.06). A more in-depth analysis however,
reveals that E/I reconstruction was associated with higher total direct variable operative costs of
approximately $2,400 per patient (P<0.0001) and a higher total direct variable costs for
reconstruction of approximately $3,400 per patient (P<0.0001). The “subsequent” cost of E/I
reconstruction was associated with higher total cost of approximately $7,000 per patient which
included the staged procedure and all subsequent procedures (P<0.0001).

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
15
Another important consideration is that TRAM is cost efficient and profitable for
hospitals (19) (20). We report that although the total cost for the upfront hospitalization for the
two reconstructive modalities are similar (P=0.06), the direct variable cost, a reliable marker of
efficiency, and opportunity cost demonstrate that FF were less expensive by about $2,400
(P<0.0001). Other studies have shown a greater cost associated with two-stage implant based
reconstructions compared to TRAMs (21), especially over time (22). The current study enabled
an average of just less than two years of follow up. It is likely that many of the implant
reconstructions would eventually require further procedures including implant exchange and
conversion to autologous reconstruction[35]. Such long term procedures were not captured in
this analysis, but should be kept in mind when critically thinking about the results we
demonstrate.
Important differences in the matched cohorts which should be noted since there was a
higher rate of modified radical mastectomy and postoperative radiation in FF patients. These
differences may contribute to higher postoperative complications in FFs, but recent work has
shown that postoperative radiation does not increase the reoperation rate in autologous breast
reconstruction [36].
Despite the large number of patients included in our study, there remain several
limitations. First, we are comparing two different techniques of breast reconstruction with
inherently different patient selection criteria and bias which cannot be controlled despite
matching. We attempted to reconcile this by using a propensity-matching technique to find
patients from both cohorts that exhibited similar preoperative features. We concede that at our
institution we tend to utilize abdominally-based free tissue transfer more than I/E which
inevitably has generated a degree of selection bias. Additionally, our cost data is based on the

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
16
one health system’s cost figures and direct variable cost, which does not include labor or
overhead costs. Several other important factors related to cost are worth noting. First, this
analysis did not attempt to define or compare professional fees related to reconstruction, as this
did not fall within the scope of cost, rather revenue. Similarly no downstream revenue for the
large referall base created by a busy reconstructive center for radiation or chemotherapy was
quantified. Second, our practice does not routinely use ADM which would have further increase
the cost of E/I reconstruction. Furthermore, the outcome variables assessed in this study are all
objective and do not account for the more subjective patient variables such as ultimate
satisfaction with reconstruction. However, we believe the strengths of our study design and
rigorous analysis, alongside with the strong relevance to patient care and perioperative decision-
making, outweigh these limitations.
Conclusion
Autologous reconstruction is an efficacious and cost-effective reconstructive modality
that is associated with favorable 2-year outcomes and cost relative to E/I reconstruction. Overall
the performance of free flaps appears to be stable over time, be associated with lower
reconstructive failures, and fewer unplanned operative interventions compared to E/I.
Acknowledgment: We would like to acknowledge and thank Nancy Folsom, BSN for her
assistance in the organization and preparation of the IRB for this study.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
17
References
1. Alderman A, Wilkins E, Lowery J, et al. Determinants of patient satisfaction in
postmastectomy breast reconstruction. Plast Reconstr Surg 2000;106:769-776.
2. McCarthy CM, Klassen AF, Cano SJ, et al. Patient satisfaction with postmastectomy
breast reconstruction: a comparison of saline and silicone implants. Cancer 2010;116:5584-5591.
3. Pusic AL, Klassen AF, Scott AM, et al. Development of a new patient-reported outcome
measure for breast surgery: the BREAST-Q. Plast Reconstr Surg 2009;124:345-353.
4. Zhong T, McCarthy C, Min S, et al. Patient satisfaction and health-related quality of life
after autologous tissue breast reconstruction: a prospective analysis of early postoperative
outcomes. Cancer 2012;118:1701-1709.
5. Alderman AK, Wilkins EG, Lowery JC, et al. Determinants of patient satisfaction in
postmastectomy breast reconstruction. Plast Reconstr Surg 2000;106:769-776.
6. Fischer JP, Sieber B, Nelson JA, et al. Comprehensive outcome and cost analysis of free
tissue transfer for breast reconstruction: an experience with 1303 flaps. Plast Reconstr Surg
2013;131:195-203.
7. Fischer JP, Nelson JA, Cleveland E, et al. Breast reconstruction modality outcome study:
a comparison of expander/implants and free flaps in select patients. Plast Reconstr Surg
2013;131:928-934.
8. Alderman AK, Wilkins EG, Kim HM, Lowery JC. Complications in postmastectomy
breast reconstruction: two-year results of the Michigan Breast Reconstruction Outcome Study.
Plast Reconstr Surg 2002;109:2265-2274.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
18
9. Cordeiro PG, McCarthy CM. A single surgeon's 12-year experience with tissue
expander/implant breast reconstruction: part I. A prospective analysis of early complications.
Plast Reconstr Surg 2006;118:825-831.
10. Gart MS, Smetona JT, Hanwright PJ, et al. Autologous options for postmastectomy
breast reconstruction: a comparison of outcomes based on the American College of Surgeons
National Surgical Quality Improvement Program. J Am Coll Surg 2013;216:229-238.
11. Mehrara BJ, Santoro TD, Arcilla E, et al. Complications after microvascular breast
reconstruction: experience with 1195 flaps. Plast Reconstr Surg 2006;118:1100-1109; discussion
1010-1011.
12. Vega S, Smartt JM Jr, Jiang S, et al. 500 Consecutive patients with free TRAM flap
breast reconstruction: a single surgeon's experience. Plast Reconstr Surg 2008;122:329-339.
13. Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of obesity in the United States,
2009-2010. NCHS Data Brief 2012:1-8.
14. Sturmer T, Schneeweiss S, Rothman KJ, et al. Performance of propensity score
calibration--a simulation study. Am J Epidemiol 2007;165:1110-1118.
15. Baser O. Too much ado about propensity score models? Comparing methods of
propensity score matching. Value Health 2006;9:377-385.
16. Gu S, Rosenbaum, PR. Comparison of multivariate matching methods: structure,
distances, and algorithms. J Comput Graph Stat 1993;2:405-420.
17. Fischer JP, Nelson JA, Au A, Ct T 3rd, et al. Complications and morbidity following
breast reconstruction - a review of 16,063 cases from the 2005-2010 NSQIP datasets. J Plast
Surg Hand Surg 2013 Jul 18.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
19
18. Garvey PB, Villa MT, Rozanski AT, et al. The advantages of free abdominal-based flaps
over implants for breast reconstruction in obese patients. Plast Reconstr Surg 2012;130:991-
1000.
19. Hanwright PJ, Davila AA, Hirsch EM, et al. The differential effect of BMI on prosthetic
versus autogenous breast reconstruction: A multivariate analysis of 12,986 patients. Breast 2013
Jun 12.
20. Mioton LM, Smetona JT, Hanwright PJ, et al. Comparing thirty-day outcomes in
prosthetic and autologous breast reconstruction: A multivariate analysis of 13,082 patients? J
Plast Reconstr Aesthet Surg 2013;66:917-925.
21. Lista F, Ahmad J. Evidence-based medicine: augmentation mammaplasty. Plast Reconstr
Surg 2013;132:1684-1696.
22. Bank J, Phillips NA, Park JE, Song DH. Economic analysis and review of the literature
on implant-based breast reconstruction with and without the use of the acellular dermal matrix.
Aesthetic Plast Surg 2013;37:1194-1201.
23. Fischer JP, Nelson JA, Serletti JM, Wu LC. Peri-operative risk factors associated with
early tissue expander (TE) loss following immediate breast reconstruction (IBR): a review of
9305 patients from the 2005-2010 ACS-NSQIP datasets. J Plast Reconstr Aesthet Surg
2013;66:1504-1512.
24. Fischer JP, Wes AM, Tuggle CT 3rd, et al. Risk analysis of early implant loss after
immediate breast reconstruction: a review of 14,585 patients. J Am Coll Surg 2013;217:983-990.
25. Disa JJ, Ad-El DD, Cohen SM, et al. The premature removal of tissue expanders in breast
reconstruction. Plast Reconstr Surg 1999;104:1662-1665.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
20
26. McCarthy CM, Mehrara BJ, Riedel E, et al. Predicting complications following
expander/implant breast reconstruction: an outcomes analysis based on preoperative clinical risk.
Plast Reconstr Surg 2008;121:1886-1892.
27. Spear SL, Newman MK, Bedford MS, et al. A retrospective analysis of outcomes using
three common methods for immediate breast reconstruction. Plast Reconstr Surg 2008;122:340-
347.
28. Vyas RM, Dickinson BP, Fastekjian JH, et al. Risk factors for abdominal donor-site
morbidity in free flap breast reconstruction. Plast Reconstr Surg 2008;121:1519-1526.
29. Fischer JP, Nelson JA, Sieber B, et al. Free tissue transfer in the obese patient: an
outcome and cost analysis in 1258 consecutive abdominally based reconstructions. Plast
Reconstr Surg 2013;131:681e-692e.
30. Cleveland EC, Fischer JP, Nelson JA, et al. Optimizing the fascial closure: an analysis of
1261 abdominally based free flap reconstructions. Ann Plast Surg 2013;71:255-260.
31. Fischer JP, Nelson JA, Kovach SJ, et al. Impact of obesity on outcomes in breast
reconstruction: analysis of 15,937 patients from the ACS-NSQIP datasets. J Am Coll Surg
2013;217:656-664.
32. Fischer JP, Wes AM, Tuggle CT, et al. Risk analysis and stratification of surgical
morbidity after immediate breast reconstruction. J Am Coll Surg 2013;217:780-787.
33. Ozturk CN, Kundu N, Bernard S, et al. Breast reconstruction with abdominal-based free
flaps in high body mass index population: postoperative complications and impact of weight
loss. Ann Plast Surg 2013 Mar 28.
34. Jandali S, Nelson JA, Sonnad SS, et al. Breast reconstruction with free tissue transfer
from the abdomen in the morbidly obese. Plast Reconstr Surg 2011;127:2206-2213.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
21
35. Tadiparthi S, Staley H, Collis N, O'Donoghue JM. An analysis of the motivating and risk
factors for conversion from implant-based to total autologous breast reconstruction. Plast
Reconstr Surg 2013;132:23-33.
36. Albino FP, Koltz PF, Ling MN, Langstein HN. Irradiated autologous breast
reconstructions: effects of patient factors and treatment variables. Plast Reconstr Surg
2010;126:12-16.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
22
Table 1. Multivariate Regression Analysis of Perioperative Factors Associated with Autologous
Reconstruction
Odds Ratio Confidence Interval p Value
Age 1.04 1.02 – 1.06 <0.001
Diabetes 0.84 0.33 – 2.13 0.715
Body mass index 1.21 1.16 – 1.27 <0.001
ASA physical status 0.69 0.44 – 1.06 0.09
Hypertension 0.92 0.56 – 1.53 0.76
Preoperative radiation 2.06 1.23 – 3.47 0.006
Preoperative
chemotherapy 1.39 0.92 – 2.12 0.122
Surgeon B 1.35 0.95 – 1.93 0.099
Surgeon C 0.44 0.24 – 0.83 0.011
Laterality 0.57 0.40 – 0.81 0.002
Reconstructive timing 1.32 0.82 – 2.11 0.254

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
23
Table 2. Bivariate Analysis of Preoperative Difference between Propensity-Matched Free Flaps
and Implant Reconstructions
Abdominal free flap,
n=155
Tissue
expander,
n=155 p Value
Age, y (SD) 48.5 (9.1) 47.9 (11.6) 0.454
Body mass index, kg/m2 (SD) 25.4 (4.2) 25.4 (5.4) 0.357
Chronic obstructive pulmonary
disease, % 1.3 1.3 1
Diabetes, % 5.2 4.5 1
Obesity, % 0.376
Non-obese 83.9 84.5
Class I 12.9 10.3
Class II 2.6 1.9
Class III 0.6 3.2
ASA physical status, % 0.693
1 5.8 7.7
2 78.1 78.1
3 16.1 13.5
4 0.0 0.6
Hypertension, % 18.7 16.1 0.549
Coronary artery disease, % 0.6 2.6 0.371

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
24
Smoking, % 0.301
Never 64.5 60.6
Current 12.3 9.0
Quit 23.2 30.3
Preoperative radiation, % 16.8 16.8 1
Postoperative radiation, % 28.4 16.8 0.012
Preoperative chemotherapy, % 25.2 30.3 0.31
Postoperative chemotherapy, % 40.0 47.7 0.202

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
25
Table 3. Bivariate analysis of preoperative difference between propensity-matched free flaps and
implant reconstructions.
Abdominal free
flap, n=155, %
Tissue expander,
n=155, % p Value
Surgeon 0.959
A 54.8 54.2
B 37.4 38.7
C 7.7 7.1
Laterality 0.727
Unilateral 38.1 40.0
Bilateral 61.9 60.0
Flap timing 0.089
Immediate 89.7 90.3
Delayed 10.3 7.1
Mixed 0.0 2.6
Ipsilateral mastectomy defect 0.002
Simple 58.7 75.5
Modified radical 32.9 15.5
Nipple sparing 1.3 3.2
Unknown 7.1 5.8
Contralateral mastectomy defect 0.063
Simple 57.4 54.8

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
26
Modified radical 0.0 3.2
Nipple sparing 2.6 3.9
Unknown 0.6 0.0
Acellular dermal matrix n/a 3.7 n/a
Flap type, unilateral n/a
TRAM 28.4 n/a
DIEP 9.0 n/a
SIEA 0.6 n/a
Flap type, bilateral n/a
TRAM/TRAM 34.2 n/a
TRAM/DIEP 13.5 n/a
DIEP/DIEP 6.5 n/a
TRAM/SIEA 4.5 n/a
DIEP/SIEA 2.6 n/a
SIEA/SIEA 0.6 n/a

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
27
Table 4. Bivariate analysis of complications between propensity-matched free flaps and implant
reconstructions.
Abdominal free
flap, n=155
Tissue
expander,
n=155 p Value
Flap specific complications n/a
Thrombosis 2.0% n/a
Flap loss 1.2% n/a
Fat necrosis 4.8% n/a
Donor-site cellulitis 5.6% n/a
Delayed donor healing 14.8% n/a
Donor hernia/bulge 3.9% n/a
Donor seroma 1.3% n/a
Any donor site complication 25.6% n/a
Implant specific complications n/a
Implant exposure n/a 3.6
Implant infection n/a 7.3
Implant rupture n/a 3.2
Nipple areolar reconstruction 74.2% 54.8% <0.001
Time to nipple areolar reconstruction,
mo (SD) 9.8 (6.8) 13.8 (9.2) <0.001
Major surgical complication 11.0% 20.0% 0.028
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
28
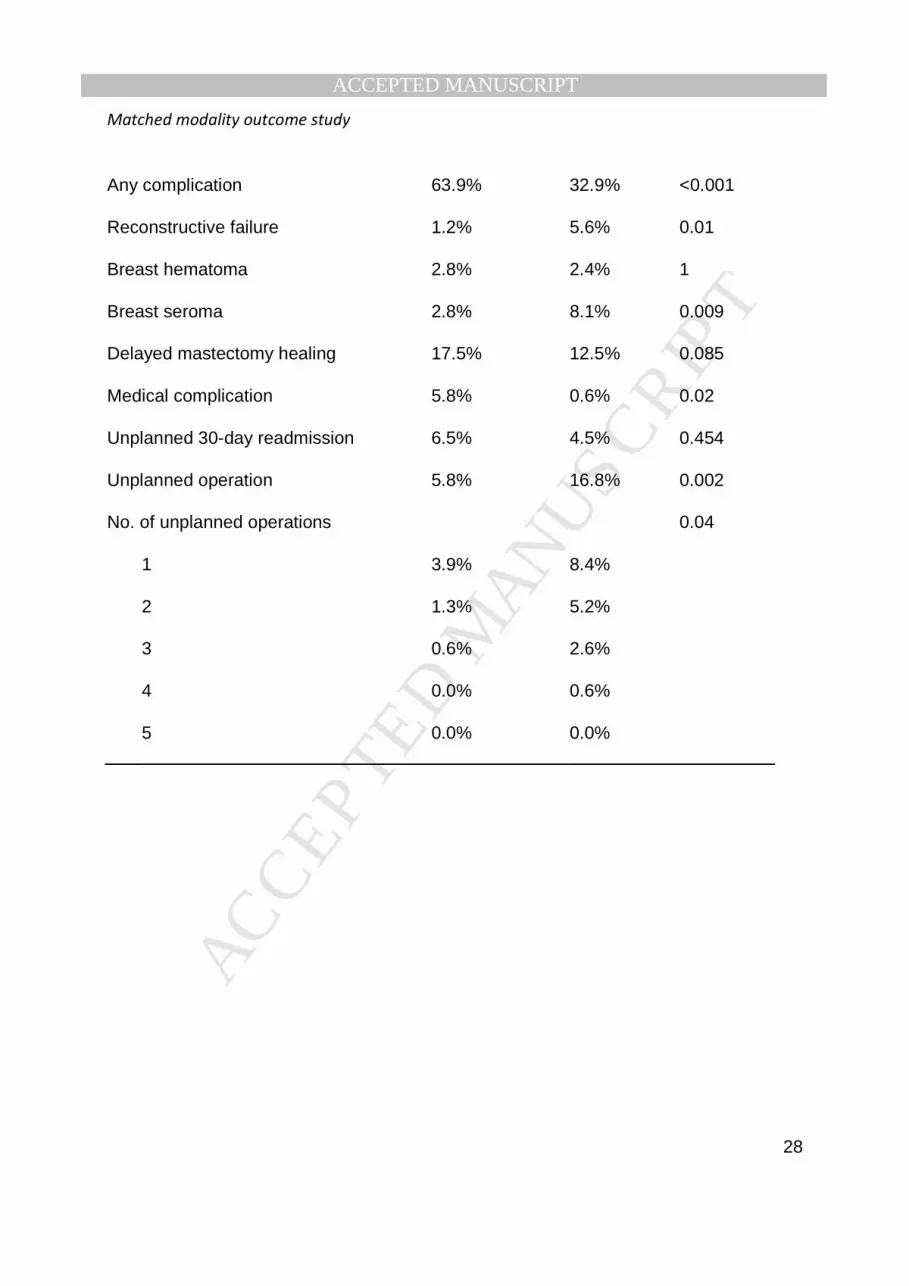
Any complication 63.9% 32.9% <0.001
Reconstructive failure 1.2% 5.6% 0.01
Breast hematoma 2.8% 2.4% 1
Breast seroma 2.8% 8.1% 0.009
Delayed mastectomy healing 17.5% 12.5% 0.085
Medical complication 5.8% 0.6% 0.02
Unplanned 30-day readmission 6.5% 4.5% 0.454
Unplanned operation 5.8% 16.8% 0.002
No. of unplanned operations 0.04
1 3.9% 8.4%
2 1.3% 5.2%
3 0.6% 2.6%
4 0.0% 0.6%
5 0.0% 0.0%

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
29
Table 5. Bivariate analysis of cost differences between propensity-matched free flaps and
implant reconstructions.
Abdominal free
flap, n=155
Tissue expander,
n=155 p Value
Total hospital stay, d (SD) 4.5 (1.8) 2.1 (0.9) <0.0001
Follow-up, d (SD) 624 (479) 780 (509) 0.0025
No. of postoperative visits
(SD) 9.8 (4.9) 19.0 (8.4) <0.0001
OR direct variable cost, all
(SD)
$1,332.98
($1,143.04)
$3,767.63
($1,838.36) <0.0001
OR direct variable cost,
subsequent (SD)
$217.01
($714.11)
$1,386.47
($1,669.26) <0.0001
Total direct variable cost, all
(SD)
$2,485.72
($1,288.62)
$5,652.97
($2,258.40) <0.0001
Total direct variable cost,
subsequent (SD)
$402.76
($873.87)
$2,651.91
($1,759.51) <0.0001
Total cost, all (SD)
$23,120.49
($6,969.56)
$22,739.91
($9,727.79) 0.0603
Total cost, subsequent (SD)
$3,200.71
($4,780.64)
$10,157.89
($8,741.77) <0.0001

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
30
FIGURE LEGENDS
Figure 1. Number of patients receiving either free tissue transfer reconstruction or expander
implant reconstruction, by year. Data for the calendar year 2011 were not complete and thus not
included. Blue bar, free tissue transfer reconstruction; red bar, expander implant reconstruction;
green bar, total reconstructions.
Figure 2. Total cumulative incidence of unplanned reoperations between modalities. *p<0.05.
Blue bar, autologous; red bar, expander/implant.
Figure 3. Kaplan-Meier curve estimates of flap and device failure over time, days.
Figure 4. Cumulative added cost of unplanned reoperations between modalities. *p<0.05. Red
bar, autologous; blue bar, expander/implant.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTMatched modality outcome study
31
Precis
Our matched outcomes analysis demonstrates a higher overall, 2-year success rate using free
tissue transfer reconstruction and a significantly lower rate of unplanned surgical revisions and
cost. Although autologous reconstruction is not ideal for every patient, these findings can be used
to enhance preoperative discussions when choosing a reconstructive modality.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
0
50
100
150
200
250
300
2005 2006 2007 2008 2009 2010
Nu
mb
er o
f p
atie
nts
rec
eivi
ng
rec
on
stru
ctio
ns
Year of Reconstruction
Figure 1.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Figure 2.
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
<6 months<12 months*
<24 monthsTotal course*
3.9% 4.5%4.5%
5.8%
5.2%
11.0%
13.5%
15.5%
Inci
den
ce o
f O
per
ativ
e C
om
plic
atio
ns

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
0.00
0.25
0.50
0.75
1.00
0 100 200 300analysis time
Kaplan-Meier survival estimates
Implants (5.6%, N=14)
Free flaps (1.2%, N=3)
P<0.001
Figure 3.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Figure 4.
$303
$533
$710
$883
$528
$984
$1,239
$1,524
$0.00
$200.00
$400.00
$600.00
$800.00
$1,000.00
$1,200.00
$1,400.00
$1,600.00
$1,800.00
<6 Months <12 Months* <24 Months* Total Course*
Co
st (
US
do
llars
)Cost divergence at 1-year