PROFILE OF HUMAN LEPTOSPIROSIS _updated_ - CiteSeerX
125
ARTICLE 1 LEPTOSPIROSIS IN CHENNAI – CHANGING CLINICAL PROFILE In a recent article, M. Jayakumar et al from Chennai have stated that acute renal failure (ARF) due to Leptospirosis in Chennai has significantly declined from 31% in 1987 – 91 to 7.5% in 1995 – 2004 1 . Of the 120 cases of leptospiral ARF during the period 1987 –91, the highest numbers of 45 cases were reported in 1990 2 . Since 1992, there has been a decline in leptospiral ARF cases and during a 10 years period from 1995 – 2004, only 84 cases were reported. Our experience also suggests that though severe Leptospirosis has declined, mild Leptospirosis has increased. In a study of 57 cases in 1990 – 91, Jaundice occurred in 84% and renal failure occurred in 72%. Serogroup Automnalis was the most common serogroup encountered. 26 patients were dialysed and two patients died 3 . In a recent study of 106 cases of Leptospirosis from North Chennai, Jaundice occurred in 17.8% and renal failure occurred in 10.3% showing a decline in complications. Fever, headache and Myalgia were the common presentations. Only 2 patients were dialysed and there were no deaths. Contaminated environment (95%) and rainfall (50%) were the important epidemiological risk factors. Icterohemorrhagiae was the most common serogroup and Autumnalis was not detected. The reasons for decline of severe Leptospirosis suggested were greater awareness of the disease, availability of better diagnostic facilities and widespread use of antibiotics. In addition, serogroup Autumnalis, a virulent serogroup causing severe Leptospirosis has also declined since 1995. The seropositive prevalence rate in Chennai was 32.9% in1993. The increase in mild Leptospirosis suggests that the environmental risk factors (Infected rodents and domestic animals, contaminated environment and rainfall) play an important role in the JAPI · VOL. 54 · DECEMBER 2006 964 – 965
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of PROFILE OF HUMAN LEPTOSPIROSIS _updated_ - CiteSeerX
ARTICLE 1
LEPTOSPIROSIS IN CHENNAI – CHANGING CLINICAL PROFIL E
In a recent article, M. Jayakumar et al from Chennai have stated that
acute renal failure (ARF) due to Leptospirosis in Chennai has significantly
declined from 31% in 1987 – 91 to 7.5% in 1995 – 20041. Of the 120 cases of
leptospiral ARF during the period 1987 –91, the highest numbers of 45 cases were
reported in 19902. Since 1992, there has been a decline in leptospiral ARF cases
and during a 10 years period from 1995 – 2004, only 84 cases were reported.
Our experience also suggests that though severe Leptospirosis has
declined, mild Leptospirosis has increased. In a study of 57 cases in 1990 – 91,
Jaundice occurred in 84% and renal failure occurred in 72%. Serogroup
Automnalis was the most common serogroup encountered. 26 patients were
dialysed and two patients died3. In a recent study of 106 cases of Leptospirosis
from North Chennai, Jaundice occurred in 17.8% and renal failure occurred in
10.3% showing a decline in complications. Fever, headache and Myalgia were the
common presentations. Only 2 patients were dialysed and there were no deaths.
Contaminated environment (95%) and rainfall (50%) were the important
epidemiological risk factors. Icterohemorrhagiae was the most common serogroup
and Autumnalis was not detected.
The reasons for decline of severe Leptospirosis suggested were greater
awareness of the disease, availability of better diagnostic facilities and widespread
use of antibiotics. In addition, serogroup Autumnalis, a virulent serogroup causing
severe Leptospirosis has also declined since 1995. The seropositive prevalence
rate in Chennai was 32.9% in1993. The increase in mild Leptospirosis suggests
that the environmental risk factors (Infected rodents and domestic animals,
contaminated environment and rainfall) play an important role in the
JAPI · VOL. 54 · DECEMBER 2006 964 – 965
Profile of Human Leptospirosis
2
persistence and spread of the disease. Intensive surveillance for early detection of
mild Leptospirosis with appropriate therapy would definitely play an important
role in reducing the incidence of severe Leptospirosis. Since diagnostic tests
become positive only after 5 days, it would be appropriate to start empiric therapy
in suspect cases of Leptospirosis with Doxycycline or other appropriate
antibiotics.
S.Shivakumar Professor of Medicine, Department of Medicine, Stanley Medical College and Hospital, Chennai.
REFERENCES:
1. Jayakumar M, Ram Prabakar H, Edwin Fernando M, et al. Epidemiologic
trend changes in acute renal failure – A tertiary center experience from
south India. Renal Failure 2006; 28: 405-10.
2. Muthusethupathi MA, Shivakumar S, Jayakumar M, et al. Renal
involvement in Leptospirosis – our experience in Madras City J. Postgrad
Med 1994;40:127-31
3. Muthusethupathi MA, Shivakumar S, Jayakumar M, et al. Leptospirosis in
Madras – A clinical and serological study. J. Assoc phys India
1995;43:456-8.
JAPI · VOL. 54 · DECEMBER 2006 964 – 965

3
ARTICLE 2
LEPTOSPIROSIS – EVALUATION OF CLINICAL CRITERIA
I read the article “Evaluation of Clinical Criteria for the Diagnosis of
Leptospirosis” with interest1. I would like to make the following comments.
1. Leptospirosis can be diagnosed only by serological tests, as the clinical
features are non-specific. By this criteria, only 22 of 118 (18%) patients had
Leptospirosis. By Faine’s criteria, 44 out of 118 patients were diagnosed to have
Leptospirosis. The positive predictive value of this test is 40.9%. This value can
be increased by modification of Faine’s criteria (Part B). History of animal
contact (Part B) is not essential for diagnosis of Leptospirosis in developing
countries. The more important epidemiological factors in our country are 1. Rain
fall 2. Contact with contaminated environment. During rainfall, those who come
into contact with water contaminated with infected rodents (or other animals)
urine are prone to develop Leptospirosis which is facilitated by environmental
factors.2 It is impossible to trace the source of infection and any person can be
infected, irrespective of direct contact with animals.
The following factors have to be introduced in Part B of Faine’s criteria
(which is more relevant to India).
1. Rainfall
2. Outdoor activities leading to contact with contaminated environment.
These factors should be given appropriate scores.
JAPI · VOL. 51 · MARCH 2003 329 – 330
Profile of Human Leptospirosis
4
One hundred and eighteen patients with PUO in this study were seen
during a one-year period (Jan – Dec 1998). It would be interesting to note whether
the 22 Leptospirosis cases occurred during monsoon months (monthly breakup of
these cases would be useful). What was the diagnosis in those cases in whom
Faine’s criteria was positive, but MAT was negative? The group constituted
nearly 59% of the cases.
2. Leptospirosis was diagnosed by Micro Agglutination Test (MAT).
MAT is considered the gold standard test for serodiagnosis of Leptospirosis. This
is a complicated test and can be done only in specialized laboratories. Therefore,
ELISA IgM and Slide Agglutination Test (SAT) are considered to be more
sensitive, simpler and adequate for diagnosis of current leptospiral infection.2-4 In
fact they can replace MAT for diagnosis of current infection. But all these tests
become positive only after five days.
Thus, in the early stages of infection (5 days), clinical features are very
important to suspect Leptospirosis utilizing Faine’s criteria (Part A). But the
diagnosis should always be confirmed by ELISA (or) SAT.
I recommend that Leptospirosis diagnosis can be done by making the
following modification of Faine’s criteria.
Faine’s Criteria PART A No modification PART B (Include the following) SCORE
1. Rainfall – 5 2. Outdoor contact with
Contaminated environment – 4
3. Animal contact – 1
(The score of 10 in Part B has been split)
PART C (> 5 days)
a) Positive ELISA/SAT b) MAT – Rising titres/High titres
JAPI · VOL. 51 · MARCH 2003 329 – 330

5
It should be realized that clinical data on milder (Anicteric) forms of
Leptospirosis are inadequate in our country and this can be made available only if
simpler tests are done in small laboratories.
S. Shivakumar Additional Professor of Medicine, Government Stanley Medical College and Hospital, Chennai
REFERENCES:
1. Bal AM, Kakrani AL, Bharadwaj RS, Kagal AS, Joshi SA, Wadkar VP,
Evaluation of clinical criteria for diagnosis of Leptospirosis. J Assoc
Physicians India 2002;50:394-6.
2. Muthusethupathi MA, Shivakumar S, Suguna R, Jayakumar M,
Vijayakumar R, Everard COR, Carrington DG. Leptospirosis in Madras –
A clinical and serology study. J Assoc Physicians India 1995;43:456-8.
3. Chinari KS, Sumathi G, Vimala Ranga Rao A, Shiva Kumar S.
Leptospirosis laboratory, Chennai Medical College – A three year
experience in Serodiagnosis (1995-1997). Indian J Med Microbiol
1999;717:50-7.
4. Sumathi G, Chinari KS, Shiva Kumar S, MSAT-A Screening test for
Leptospirosis. Indian J Med Microbiol 1997;15:84.
JAPI · VOL. 51 · MARCH 2003 329 – 330

Profile of Human Leptospirosis
6
ARTICLE 3
DIAGNOSIS OF LEPTOSPIROSIS UTILIZING MODIFIED
FAINE’s CRITERIA
In a letter published in JAPI 2003, I had stated that certain modification to
be made on Faine’s criteria (WHO guidelines) to diagnose current leptospiral
infection in Indian institutions.1 A prospective study done in patients with
Leptospirosis is presented by us utilizing the modified Faine’s criteria. Faine had
evolved a criteria for diagnosis of Leptospirosis on the basis of clinical,
epidemiological and laboratory data (A+B+C).2 The modifications in the Faine’s
criteria has been made by us in the epidemiological and laboratory criteria
(Table1). No modifications have been made in the clinical aspects of Leptospirosis
(Part A). A score of 26 or more when using PART A, PART A+B or 25 or more
using PART A+B+C can be considered as current Leptospirosis.
The reasons for the modifications are:
(1) Most of the cases of Leptospirosis are reported in the monsoon and post
Monsoon seasons. Therefore, factors such as rainfall and contact with
contaminated environment have been incorporated with appropriate
scores (Part B).
(2) Laboratory tests are very essential for diagnosis of Leptospirosis. ELISA
IgM and Slide agglutination tests (SAT) are simple, sensitive tests and
can be used to diagnose current Leptospirosis. They have been included
with appropriate scores (Part C). Microscopic agglutination tests (MAT)
is the Gold standard test, but it is complicated and less sensitive
compared to ELISA and SAT.
JAPI · VOL. 52 · AUGUST 2004 678 – 679
7
The difficulties in utilizing MAT are due to the following factors:
a) The antibody titers rise and peak only in 2nd or 3rd week, making it a less
sensitive test.
b) The high titers of past infection persist for a long time (1-5years) and therefore
interfere with the diagnosis of current leptospirosis. A Positive titer may
represent a rising titer of current infection or declining titer of past infection.
c) The cut off titer for diagnosis of current infection depends in whether the area
is endemic or non-endemic, for example the cut off titer varies from 1/80 to
1/400. Therefore a second sample is usually required (to demonstrate 4 fold
rise in titer) to diagnose current infection. Sero-epidemiological studies are
required for determining the cutoff value.
d) The test is complicated requiring dark field microscopy and cultures of various
live serovars, which may not be available in small laboratories.
As Elisa and SAT measures IgM antibodies become positive by 5th day, they
are the tests of choice for diagnosis of current infection and more over a single
sample is adequate. A repeat sample is necessary, if the first sample is negative.
High titers and rising titers of MAT have been given appropriate scores (Part C).
This study has been undertaken to compare the standard and modified
Faine’s criteria. The original Faiane’s criteria (WHO guidelines) have been
designated as Standard Faine’s criteria in this study. One hundred and fifty patients
admitted with fever were taken up for the study from April 2002 to March 2003.
Leptospirosis was diagnosed by positive macroscopic slide agglutination test
(confirmed by MAT). Malaria, enteric fever, UTI, pneumonia and TB was excluded
by appropriate tests. Thirty-one of 150 patients (20.7%) were diagnosed to have
Leptospirosis. All these patients had both standard and modified Faine’s criteria
positive (A+B+C > 25). It is observed that 38% (22/57) of the patients with fever
had Leptospirosis during monsoon when compared to 9% in the non-monsoon season
(9/93).
JAPI · VOL. 52 · AUGUST 2004 678 – 679
Profile of Human Leptospirosis
8
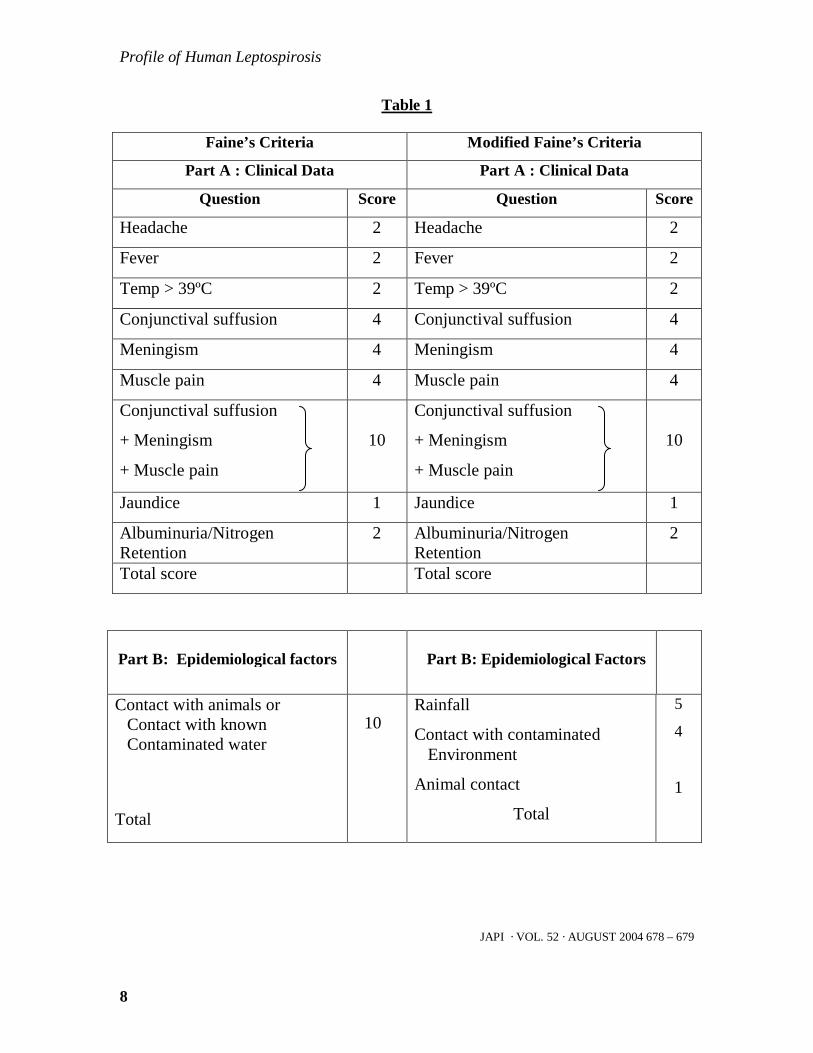
Table 1
Faine’s Criteria Modified Faine’s Criteria
Part A : Clinical Data Part A : Clinical Data
Question Score Question Score
Headache 2 Headache 2
Fever 2 Fever 2
Temp > 39ºC 2 Temp > 39ºC 2
Conjunctival suffusion 4 Conjunctival suffusion 4
Meningism 4 Meningism 4
Muscle pain 4 Muscle pain 4
Conjunctival suffusion
+ Meningism
+ Muscle pain
10
Conjunctival suffusion
+ Meningism
+ Muscle pain
10
Jaundice 1 Jaundice 1
Albuminuria/Nitrogen Retention
2 Albuminuria/Nitrogen Retention
2
Total score Total score
Part B: Epidemiological factors
Part B: Epidemiological Factors
Contact with animals or Contact with known Contaminated water
Total
10
Rainfall
Contact with contaminated Environment
Animal contact
Total
5
4 1
JAPI · VOL. 52 · AUGUST 2004 678 – 679

9
Part C: Bacteriological and Lab
Findings
Part C: Bacteriological and Lab
Findings
Isolation of leptospira in culture – Diagnosis certain
Isolation of leptospira in culture – Diagnosis certain
Positive Serology (MAT) Leptospirosis Endemic
Positive Serology
Single positive – Low titre Single positive – High titre Leptospirosis Non Endemic Single positive – Low titre Single positive – High titre Rising titre (Paired sera) Total Score
2 10 5 15 25
ELISA IgM Positive * SAT – Positive MAT – Single High titre * Rising titre (Paired sera) Total Score
15 15 15 25
* Any one of the tests only should be scored
Table 2
(PART A+B) Seropositive Seronegative
Standard Faine’s Criteria
Faine’s positive
Faiane’s negative
Modified Faine’s Criteria
Faine’s positive
Faine’s negative
13
18
31
18
13
31
18
101
119
3
116
119
JAPI · VOL. 52 · AUGUST 2004 678 – 679

Profile of Human Leptospirosis
10
Table 3
(PART A+B) Sensitivity Specificity PPV NPV Standard Faine’s criteria Modified Faine’s criteria Statistical significance
41.9%
58%
NS
84.9
97.4
p value <0.001
41.9%
85.7%
p value <0.001
84.9%
89.9%
NS
As Leptospirosis tests become positive only after the fifth day, the
diagnosis of Leptospirosis has to be done only by clinical and epidemiological
criteria during this period. Hence the clinical and epidemiological criteria (A+B)
only have been compared between standard and modified Faine’s criteria
(Table 2). The standard Faine’s criteria had a sensitivity of 41.9%, specificity of
84.9% and a positive predictive value of 41.9%. It was observed that the positive
features (A+B>26) were more in seronegative leptospirosis compared to
seropositive Leptospirosis. In contrast, modified Faine’s criteria had a sensitivity
of 58%, Specificity of 97.4% and positive predictive value (PPV) of 85.7%. By
modifying the epidemiological factors a significantly better PPV and specificity
was obtained in the modified Faine’s criteria. (Table 3). A study conducted by
AM Bal et al utilizing Faine’s criteria had observed that the sensitivity and PPV to
be 81.8% and 40.9% respectively3. In our study the PPV was much higher
utilizing modified Faine’s criteria though the sensitivity was low. An important
observation in the study has been the importance of laboratory tests. If clinical
and epidemiological criteria (A+B) along were utilized, only 18 cases were
diagnosed by modified Faine’s criteria (sensitivity – 58%), but if lab criteria was
incorporated 31 cases were diagnosed (A+B+C). This is because if A+B alone
JAPI · VOL. 52 · AUGUST 2004 678 – 679
11
were utilized, the score should be > 26, but if C is available, A+B can be just 11
(A+B=11+C=15 TOTAL=26). If lab criteria are included, the score in PART A
(Clinical features) can be just 2, PART B (epidemiological factors) 9 and PART C
(Laboratory test) 15 (TOTAL=26). Thus milder cases can be diagnosed if
laboratory tests are available. In addition, the modified Faine’s criteria makes it
more difficult to diagnose Leptospirosis in the non monsoon months as the
epidemiological factors would be minimal (PART A=10, PART B=0, PART
C=15).4
We would like to emphasize that the study has been done in symptomatic
patients only (A+B+C) to diagnose current Leptospirosis. It can be argued that a
score of 25 or more can be obtained from B+C along in asymptomatic patients.
This would be relevant only for epidemiological studies to evaluate the prevalence
rates of Leptospirosis in high-risk group and general population. This study has
been done to evaluate a simple method to diagnose current leptospiral infection,
with necessary modification of Faine’s criteria. Though other criteria are utilized,
this criteria is most useful because it utilizes clinical, epidemiological and lab
features.
To conclude, modified Faine’s criteria is a more a practical methods to
diagnose current Leptospirosis. Availability of simple diagnostic tests (ELISA –
IgM or SAT) should help in diagnosis of milder forms (Anicteric) of
Leptospirosis, which is more common (90%) than severe Leptospirosis (10%).
S. Shivakumar*, PS Shareek** *Professor; ** Post Graduate; Department of Medicine, Government Stanley Medical College and Hospital, Chennai
JAPI · VOL. 52 · AUGUST 2004 678 – 679

Profile of Human Leptospirosis
12
REFERENCES:
1. Shivakumar S. Leptospirosis evaluation. J Assoc Phys India 2003;51:
329-30
2. Faine.S. Guidelines for the control of Leptospirosis. WHO offset
publication 1982:67.
3. Bal AM, Kalkarni AL, Bharadwaj RS, Kagal AS, Joshi SA, Wadkov VP.
Evaluation of clinical criteria for diagnosis of Leptospirosis. J Assoc Phys
India 2002;50:394-6
4. Shivakumar S. Approach to Leptospirosis in India. Bhattacharya PK(Ed);
Medicine Update – APICON, Assam, 2003;7:699 – 703.
JAPI · VOL. 52 · AUGUST 2004 678 – 679

13
ARTICLE 4
DIAGNOSIS OF LEPTOSPIROSIS – ROLE OF MAT
We read the article by Dutta et al on “Leptospirosis – An Overview” with
interest.1 The problem in utilizing Microscopic Agglutination Test (MAT) has
been highlighted and we shall discuss briefly the current status of MAT.
MAT is considered the gold standard test for diagnosis of Leptospirosis.
It has unsurpassed specificity, but its sensitivity is low compared to ELISA/SAT
(Slide agglutination test). Angelo P Brendo et al from Brazil in their study of 108
cases of Leptospirosis have stated that 65% of first sample where positive by SAT
compared to 44% by MAT.2
A four-fold rise in titer or seroconversion is the most definitive criteria
for diagnosis of Leptospirosis. Therefore, a second sample is mandatory, which is
difficult to obtain. In such circumstances, a single high titer in MAT can be taken
as diagnostic criteria. As MAT titers peak and persist for a long time (5 – 10 yrs),
they would interfere with current diagnosis. Therefore, many workers use
different criteria.3 A titer of 1:100 is taken as significant criteria, but there is
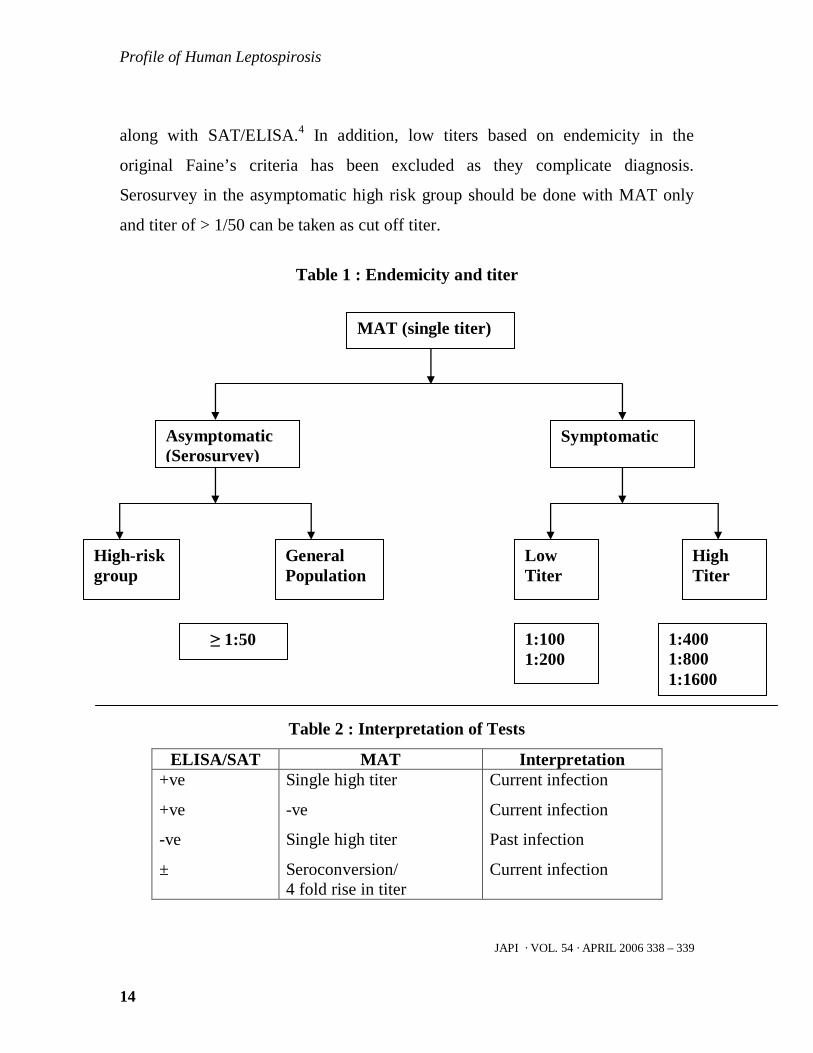
controversy on the single diagnostic titer as they depend on endemicity (Table 1).
In endemic areas, a titer of 1/100 or 1/200 is considered low; while high titer is
usually > 1/400 (some consider 1/800 or 1/1600 as diagnostic criteria). In non-
endemic areas, 1/100 titer is taken as diagnostic criteria. It is preferable to do
SAT/ELISA along with single high titers. Positive SAT/ELISA with high titers
suggest current infection, while negative SAT/ELISA is probably due to past
infection (Table 2). Therefore in the modified Faine’s criteria, a four-fold rise in
MAT has been given 25 points, while single high titer has been given 15 points
JAPI · VOL. 54 · APRIL 2006 338 – 339
Profile of Human Leptospirosis
14
along with SAT/ELISA.4 In addition, low titers based on endemicity in the
original Faine’s criteria has been excluded as they complicate diagnosis.
Serosurvey in the asymptomatic high risk group should be done with MAT only
and titer of > 1/50 can be taken as cut off titer.
Table 1 : Endemicity and titer
Table 2 : Interpretation of Tests
ELISA/SAT MAT Interpretation +ve
+ve
-ve
±
Single high titer
-ve
Single high titer
Seroconversion/ 4 fold rise in titer
Current infection
Current infection
Past infection
Current infection
JAPI · VOL. 54 · APRIL 2006 338 – 339
MAT (single titer)
Asymptomatic (Serosurvey)
Symptomatic
High-risk group
General Population
≥ 1:50
Low Titer
High Titer
1:100 1:200
1:400 1:800 1:1600

15
Table 3 : Approach to diagnosis of Leptospirosis
Confirm (If available)
JAPI · VOL. 54 · APRIL 2006 338 – 339
Clinical features suggestive of current Leptospirosis
Leptospiremic phase < 7days Immune phase > 7 days
Negative MAT Positive
Positive Negative
Repeat (if low titer)
Rising titer
Repeat (> 3 days)
Blood culture
PCR ELISA / MSAT
Repeat
Seroconversion High titer

Profile of Human Leptospirosis
16
During an epidemic, the microbiology laboratories would be burdened
with large number of samples (about 25 or more). It would be impossible to do
MAT as it is complicated test. In addition the laboratories need to have all the 24
serogroups; otherwise, a negative MAT does not exclude current Leptospirosis if
the considered serogroup is not available. Therefore, ELISA/SAT are adequate
for current diagnosis. If facilities for MAT are available, then the test should be
done to confirm the diagnosis and identify serovars (Table 3).
To conclude there is an urgent need to study the prevalence and incidence
of Leptospirosis in India. This can be done by
1. Sero-survey of asymptomatic high risk groups utilizing MAT.
2. Diagnosis of current infection utilizing ELISA/SAT.
3. Evaluating the cut off titers of single high titer and determine the
serogroups utilizing MAT in samples with positive ELISA/SAT.
S Shivakumar*, B Krishnakumar** * Professor of Medicine; **Postgraduate in General Medicine; Department of Medicine, Stanley Medical College, Chennai REFERENCES:
1. Dutta TK, Christopher M. Leptospirosis – An overview. Assoc Physicians
India 2005;53:545-51.
2. Brendo AP, Camargo ED, De Silva ED et al. Macroscopic agglutination
test for rapid diagnosis of Heman Leptospirosis. J Clin Microbiol
1998;36:3138-42.
3. Katz AR, Ansell VE, Effler PV, et al. Assessment of the clinical
presentation and treatment of 353 cases of laboratory confirmed
Leptospirosis in Hawaii, 1974-1998. Clini Infect Dis 2001;33:1834-41.
4. Shivakumar S, Shareek PS. Diagnosis of Leptospirosis – Utilizing
modified Faine;s criteria. J Assoc Physicians India 2004;52:678-9.
JAPI · VOL. 54 · APRIL 2006 338 – 339

17
ARTICLE 5
LEPTOSPIROSIS IN MADRAS –
A CLINICAL AND SEROLOGICAL STUDY
(1990 – 91)
MA MUTHUSETHUPATHI*, S SHIVAKUMAR*, R SUGUNA*,
M JAYAKUMAR*, R VIJAYAKUMAR*, COR EVERARD +,
DG CARRINGTON +
ABSTRACT
Leptospirosis was confirmed by Microscopic Agglutination Test (MAT) and/or ELISA in 57 patients admitted to the Government General Hospital, Madras, India, during November and December of 1990 and 1991 with symptomatology suggestive of the disease. Fifty (88%) of the 57 cases were males; the mean age of all the cases was 39.6 years (range 17 – 72). The main clinical features were: fever 100%, Jaundice 84%, Myalgia 82%, Acute Renal Failure 72% and Conjunctival Suffusion 58%. Non azotemic jaundice occurred in 19% of cases. Renal failure was non-oliguric in 24% of cases. 3.5% of patients died. 23 patients underwent peritoneal and/or hemodialysis. ELISA IgM titres ranged from1:80 to 1:10240 (geometric mean tire 911). MAT titres > 1:1600 and > 1:800 occurred in 39 of 54 and 51 of 54 cases respectively. Autumnalis was the serogroup most commonly recorded serologically, and Leptospira interrogans serovar autumnalis was isolated from one patient. This study shows that Leptospirosis is a significant health problem in Madras, though normally grossly underestimated due to the absence of routine laboratory diagnostic facilities for the disease. Gross under-reporting is also likely in other high rainfall third world areas.
* Department of Nephrology, Madras Medical College, Madras, India + Formerly of the Leptospira, Bridgetown, Barbados
JAPI · 1995, VOL. 43 · NO.7 456 – 458

Profile of Human Leptospirosis
18
INTRODUCTION
Leptospirosis had long been considered a rare zoonotic disease in India,
with only sporadic cases being recorded. Recently, however, the disease was
reported from Madras during the monsoon months in mini-epidemic proportions.1-3
Leptospiral infection is now recognized as a common cause of acute renal failure
in Madras.4
Leptospirosis has been under-diagnosed and under-reported from India
due to a lack of awareness of the disease, a lack of appropriate laboratory
diagnostic facilities in most parts of the country, and a reliance on indigenous
remedies to treat jaundice. Combining clinical expertise and awareness with
confirmatory laboratory backup dramatically increases the recognition of patients
with Leptospirosis.
PATIENTS AND METHODS
Single, paired or triple serum samples were obtained from patients with
clinical symptoms of Leptospirosis admitted o the Government General Hospital,
Madaras, during November-December of 1990 and 1991. The sera were
lyophilized and sent with ice packs to the Leptospira Laboratory, Bridgetown,
Barbados, where they were examined by the Microscopic Agglutination Test
(MAT)and/or the Enzyme-linked Immunosorbent Assay (ELISA). The ELISA
was undertaken using Leptospira biflexa, serovar patoc as an antigen to detect
specific IgM and IgG anatibodies.5 A patient was considered to have current
Leptospirosis if he had an ELISA IgtM titre of > 1:80 coupled with confirmatory
MAT serology and vice versa. The MAT was performed with 22 live culture
antigens using standard microtitre methodology6,7. The sera were initially
screened at dilutions of 1:50 and 1:100 and those that were positive were titrated
further to the end-point. The serogroup reacting at the highest titre was presumed
to be the infecting one. Where two or more serogroups reacted at the same
JAPI · 1995, VOL. 43 · NO.7 456 – 458

19
(highest) titre the result was recorded a “mixed equal”. Using EMJH medium
according to the standard methodology of Sulzer & Jones. Attempts were made to
culture leptospires from the blood of a few of these patients7.
The following data were noted for patients considered to have current
Leptospirosis: age, gender, occupation, residence, and clinical features including
fever, myalgia, jaundice, conjunctival suffusion, oliguria, volume depletion,
bleeding diathesis, gastrointestinal and neurologicval symptoms. The relevant
hematological and biochemical tests (liver and renal function) were also done.
Patients were started on a conservative treatment including maintenance of fluid
and electrolyte balance and administration of one million units i.v. of Benzyl
Penicillin four times a day. Peritoneal dialysis (PD) was instituted if patients had
severe renal failure (plasma Creatinine > 440uMol/L), acute pulmonary oedema,
severe metabolic acidosis or hyperkalemia. Hemodialysis (HD) was undertaken if
there was a contraindication to PD, or if the patient was in hypercatabolic renal
failure.
RESULTS
Current Leptospirosis was confirmed in 57 of the 70 patients whose sera
were examined by the MAT and ELISA. 31 patients provided single serum
samples, and 26 provided repeat samples. On average, the first, second and third
serum samples were taken 12.3 days (all 57 cases), 20.9 days (26 cases), and 28.5
days (7 cases) following onset of illness. The mean age of the 57 cases was 39.6
years (range 17-72); 50 (88%) were males. Occupation varied though not
surprisingly 28 (49%) cases were outdoor manual workers (Table 1). The
pataients came from various parts of the city, and no geographical clustering of
cases was evident.
JAPI · 1995, VOL. 43 · NO.7 456 – 458

Profile of Human Leptospirosis
20
The important clinical features and abnormal biochemical reports of those
57 patients are shown in Tables 2 and 3. All patients had fever. 48 of the 57
(84%) patients were icteric (serum bilirubin 17 uMol/L); the mean serum bilirubin
was 231.5 ± 159 uMol/L, with the highest value being 646 uMol/L. Jaundice
without renal failure occurred in 11 patients. The transminase levels were only
moderately elevated (4-fold). Renal failure occurred in 41 patients (Per >180
uMol/L), and was severe in 12 cases. 31 (76%) of renal failure patients were
oliguric. Anicteric renal failure occurred in four (9.7%) patients. Myalgia (82%),
conjunctival suffusion (58%) and volume depletion (39%) were the other major
clinical features noted. Thrombocytopenia occurred in 13 patients. Of the 23
patients who needed dialytic support, 18 (78%) were managed by peritoneal
dialysis. 4 patients were switched from peritoneal dialysis to haemodialysis and
only one patient needed haemodialysis from the beginning. Two patients died
(3.5%).
Of the 57 cases, only two had ELISA IgM titres of 1:80, four had 1:160,
and 51 had > 1:320. The highest value was 1:10240, and the geometric mean titre
(GMT) was 911. The IgG values ranged from 1:80 to 1:20480 (GMT 922). MAT
titres were not available for three patients; three patients had MAT titres in the
range 1:100 – 1:400; while the remaining 51 cases all had MAT titres > 1:800 (39
patients had titres > 1:1600). Of the 31 patients who provided single samples,
only one had an IgM value < 1:160 and another had a MAT valaue < 1:800.
considering the 26 repeat samples, nine showed rising titres, nine had stable titres
and eight had declining titres, particularly with regard to IgM but also to the IgG
and MAT values.
Serogroup Automnalis predominated in 40 of the 54 patients for whom
MAT results were available, with titres ranging from 1:100 to 1:51200 (GMT
2557). 38 of the 40 patients had titres > 1:800. In the “mixed equal” group, eight
JAPI · 1995, VOL. 43 · NO.7 456 – 458

21
patients had titres in the range 1:800 – 1:3200 to Autumnalis and Australis (GMT
1234). The presumptive infecting serogroups in the remaining 6 cases were
Icterohaemorrhagiae (2), Cynopteri (2), Australis (1) and Canicola (1). A single
isolate obtained was identified by the Leptospira reference Laboratory in
Amsterdam as Leptospira interrogans serovar autumnalis.
Table 1: Occupations of 57 cases of Leptospirosis in Madras City
Work Category No. %
Outdoor manual workers Indoor/outdoor artisans Outdoor non/manual workers Indoor non manual workers Housewives Unemployed Retired Unknown
28 7 5 6 7 1 1 2
49.0 12.3 8.8 10.5 12.3 1.8 1.8 3.5
Table 2 : Clinical features (n = 57)
N % Fever Jaundice Myalgia Oliguria Conjunctival Suffusion Vomiting Altered Sensorium Volume Depletion Gastrointestinal Bleed Diarrhoea Headache Abdominal Pain Hemoptysis Meningitis Epistaxis
57 48 47 41 33 33 24 22 15 15 15 10 5 4 2
100 84 82 72 58 58 42 39 26 26 26 18 9 7 3
JAPI · 1995, VOL. 43 · NO.7 456 – 458

Profile of Human Leptospirosis
22
Table 3 : Abnormal biochemical reports
PARAMETER n MEAN ± S.D RANGE
Plasma Urea (mmol/L)
Plasma Creatinine (uMol/L)
Plasma Bilirubin (uMol/L)
AAST (IU/L)
ALT (IU/L)
Platelets (105/c.mm)
41
41
48
25
27
13
23.5 ± 9.1
362.56 ± 119.9
231.46 ± 159
58.4 ± 24.4
70.4 ± 20.4
0.84 ± 0.2
15.0 – 49.0
204 – 661
20 – 646
20 – 125
24 – 132
0.2 – 0.98
DISCUSSION
Everard and Everard point out that where leptospires are widespread in
the environment, and where the disease is endemic, infection will be related to a
way of life as well as to specific occupations8. Thus, where there are large
numbers of rodents, stray dogs and wild animals, where people drink or bathe in
untreated water, where sewerage and drainage are inadequate, and where open
shoes or none at all are worn, leptospiral infection can be common. In such places
occupational risk factors are so inextricably linked with lifestyle risk factors that
investigations of sources of infection in individuals are inappropriate. In Madras
the general truth applies – that maleness, high rainfall and outdoor manual
occupation encourage higher incidence rates of Leptospirosis and that more
specific sources cannot be pinpointed with certainty.
Leptospira can survive outside the hosts vertebrate body more easily
under conditions of warmth and adequate rainfall (or in riverine areas) and if
looked for can be readily detected in man and other mammals (domestic,
peridomestic or wild) throughout the tropical belt. Long term environmental
JAPI · 1995, VOL. 43 · NO.7 456 – 458

23
changes are usually not sudden and dramatic and the increase in hospital
admissions with Leptospirosis from 9 cases in the 6 year period 1979 – 1984 to
159 cases in the 5 years 1987 – 1991 can be attributed to improved clinical
expertise and laboratory confirmation.
A simple, rapid diagnostic laboratory test is needed to confirm suspected
mild and severe cases, and as importantly, to eliminate non-cases. At this time,
ELISA should be the test of choice for the diagnosis of current illness. ELISA
(IgM) is more sensitive than the MAT and simpler to perform in a routine hospital
diagnostic laboratory, but it cannot determine the infecting serogroup. The
detection of specific IgM, which usually develops a few days after the onset of
fever, helps in the fairly rapid diagnosis of current infection. A high IgM titre in a
single blood sample can be diagnostic, though taking repeat samples should be
made mandatory to compare changes in titre. In the 31 single sample results, IgM
alone was just about adequate to diagnose nearly all the current infections. If a
MAT titre of 1:1600 is taken as diagnostic, they only 20 of 29 (two cases not
tested by MAT) would have been confirmed. At a MAT diagnostic level of 1:800,
the number of confirmed cases would have been 28. However, particularly in
endemic areas, evidence of previous infection, whether mild or severe, can be
common, and an elevated MAT from a single sample would inevitably result in a
false positive. (In some individuals MAT titres of 1:1600 have been known to
persist for a few years). Thus for single samples, ELISA IgM and MAT must be
combined. Because of the delay in antibody development (7 – 10 days after onset
of first symptoms) single early blood samples may not have any detectable
antibody and the negative result could be equally misleading. Thus at least two
serum samples taken at least 3 to 4 days apart should be examined before a
negative result can be confirmed.
JAPI · 1995, VOL. 43 · NO.7 456 – 458

Profile of Human Leptospirosis
24
Although the MAT is the test for choice for serological surveys, it is
complicated, has to be permanently established, and uses numerous serovars
which must be maintained aseptically in stock culture. Normally it is used daily or
weekly. Its main advantage is that it gives a good indication of infecting
serogroup, especially late in illness or in surveys, since it detects serovar specific
antibodies which tend to peak later. Repeat samples (ideally demonstrating a four
fold rise in titre) are usually necessary to confirm or disprove current illness.
MAT titres may take several years to decline. This of considerable value in
epidemiological studies, but it complicates the diagnosis of current illness,
particularly where recent asymptomatic or mild reexposure had resulted in
misleading anamnestic rise in titre.
Of the 57 Leptospirosis cases studied, 48 had jaundice and 41 renal
failure. By comparison, about 97% of all hospital cases of Leptospirosis on
Barbados were icteric. The jaundice was cholestatic in type as characterized by
high bilirubin levels with moderately elevated transaminases. Non azotemic
hepatitis occurred in 19% of patients. Renal failure was severe in 21% and was
non-oliguric in 24%. All patients received intravenous benzyl penicillin, though
its effectiveness in late Leptospirosis is controversial.9,10 Peritoneal disalysis was
adequate for most patients. Only two patients (3.5%) died.
A serosurvey recently undertaken by Ratnam et al, among conservancy
workers in Madras (using MAT) revealed a seropositive prevalence rate of 32.9%
(range 17.8% to 40.5%).11 The predominating serogroup was Autumnalis.
Autumnalis was also the most commonly recorded serogroup (serologically and
bacterilogically) in the present study.
JAPI · 1995, VOL. 43 · NO.7 456 - 458
25
ACKNOWLEDGEMENTS
The authors are indebted to the UK Medical Research Council, British
Council and Overseas Development Administration for their support and
assistance. We are also most grateful to the staff of the Barbados Leptospira
(particularly Carol Whitington) and staff of the Department of Nephrology,
Madras Medical College, for their help; and to Hans Korver of the WHO
Leptospirosis Reference Laboratory at the N.H. Swellengrebel Labaoratory for
Tropical Hygiene, Royal Tropical Institute, Amsterdam, for identifying our
isolate.
REFERENCES:
1. Krishnamurthi MV, Madanagopalan N, Hussain AT. Leptospirosis in
Madras. J Assoc Phys India 1965; 13: 737-740.
2. Muthusethupathi MA, Shivakumar S. Acute renal failure due to
Leptospirosis. J Assoc Phys India 1987;35: 631-633.
3. Muthusethupathi MA, Shivakumar S, Suguna Rajendran, Vijayakumar R,
Jayakumar M. Leptospiral renal failure in Madras City. Ind J. Neph. (New
Series). 1991; 1: 151-17.
4. Muthusethupathi MA, Shivakumar S, Jayakuamar M, Rajenderan S. Acute
renal failure in Madras City – Changing Profile. Ind J. Neph. (New
Series).1993; 3: 66 – 70.
5. Terpstra WJ, Lingthart TS, Schooner GJ. ELISA for the detection of
specific IgM and IgG in human Leptospirosis. Journal of General
Microbiology 1985; 131: 377-385.
6. Cole JR, Sulzer CR, Pursell AR. Improved Microtechnique for the
leptospiral microscopic agglutination test. Applied Microbiology 1973; 25:
976.
JAPI · 1995, VOL. 43 · NO.7 456 - 458

Profile of Human Leptospirosis
26
7. Sulzer CR & Jones WL. (1978) Leptospirosis; methods in laboratory
diagnosis. (Revised edition – reprinted.) US Department of Health,
Education and Welfare, Public Health Service, Centers for Disease Control,
Atlanta, Georgia, HEW Publication No.(CDC) 79 – 8275.
8. Everard JD, Everard COR. Leptospirosis in the Caribbean. Reviews in
Medical Microbiology 1993; 4: 114-122.
9. Watt G, Tuazom MA, Santiago LE. Placebo controlled trial of intravenous
penicillin for severe and late Leptospirosis. Lancet 1988; 1: 433-435.
10. Edwards CN, Nicholson GD, Hassell TA, Everard COR. & Calendar J.
Penicillin therapy in Icteric Leptospirosis. Am J Trop Med Hyg. 1988; 39
(4): 388-390.
11. Ratnam S, Everard COR, Alex JC, Suresh B, Thangaraju P.Prevalence of
leptospiral agglutinins among conservancy workers in Madras City, India.
Journal of Tropical Medicine and Hygiene 1993; 96: 41-45.
JAPI · 1995, VOL. 43 · NO.7 456 - 458

27
ARTICLE 6
RENAL INVOLVEMENT IN LEPTOSPIROSIS –
OUR EXPERIENCE IN MADRAS CITY
(1987 – 93)
MA MUTHUSETHUPATHI, S SHIVAKUMAR, R VIJAYAKUMAR,
M JAYAKUMAR
INTRODUCTION
Leptospirosis is now recognized as one of the important causes of Acute
Renal Failure (ARF) in Madras city.1-3 It has been under diagnosed in other parts
of the country probably due to lack of diagnostic facilities. In Thailand and
Singapore, it is the leading cause of ARF.4 In this article, we shall discuss the
various aspects of Leptospirosis and give our experience over the past few years.
EPIDEMIOLOGY Leptospirosis is an infectious disease caused by leptospira interrogans
complex which has over 20 sero groups and more than 200 serovars. The major
vectors to humans are rodents, though other animals such as cattle, dogs and pigs
can also transmit the illness.
These organisms are excreted in the urine of the animals and they affect
man when he comes into contact with the urine of infected animals directly or
indirectly when he is exposed to an environment contaminated by the urine of the
infected animals such as soil or surface water following monsoon rains.
Therefore, this illness commonly occurs during the monsoon. These organisms
survive for 6 hours in dry soil and for 6 months in flooded conditions. They enter
the host through abrasions of the skin (of the feet when they come into contact
with infected water) or intact mucus membranes of the eye, throat and gut, when
From: Department of Nephrology, Government General Hospital, Madras
J POSTGRAD MED 1994; 40(3) : 127 - 31
Profile of Human Leptospirosis
28
contaminated food is ingested. In urban areas of developing countries, a
contaminated environment due to various factors such as – overcrowded slums,
inadequate drainage and sanitation facilities for both man and animals, presence of
stray dogs, cattle, pigs and domestic rats and bandicoots, poor condition of
slaughter houses and people walking barefooted, contributes to the spread of this
illness.5,6
In rural areas, high-risk groups are workers in rice fields, can fields and
other agricultural crops and animals husbandry staff. In addition, workers in
sewers, mines and military operations are also at risk. Though Leptospirosis is
considered an occupational disease, a contaminated environment makes any
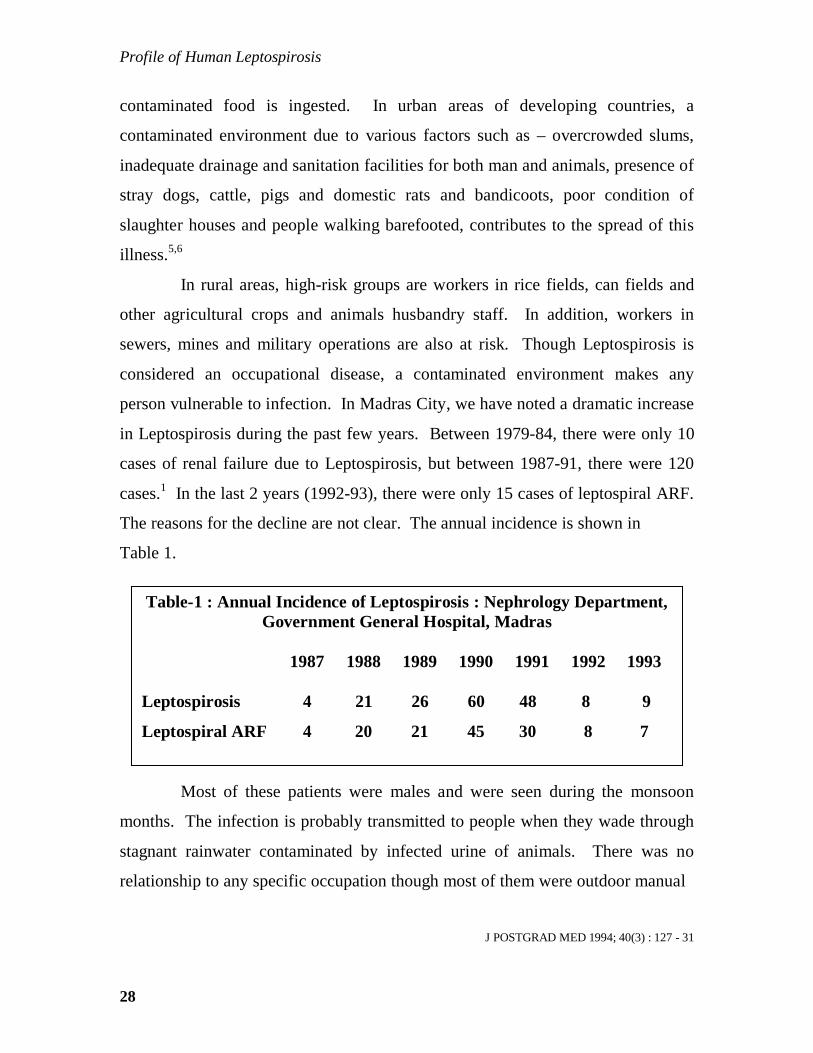
person vulnerable to infection. In Madras City, we have noted a dramatic increase
in Leptospirosis during the past few years. Between 1979-84, there were only 10
cases of renal failure due to Leptospirosis, but between 1987-91, there were 120
cases.1 In the last 2 years (1992-93), there were only 15 cases of leptospiral ARF.
The reasons for the decline are not clear. The annual incidence is shown in
Table 1.
Most of these patients were males and were seen during the monsoon
months. The infection is probably transmitted to people when they wade through
stagnant rainwater contaminated by infected urine of animals. There was no
relationship to any specific occupation though most of them were outdoor manual
J POSTGRAD MED 1994; 40(3) : 127 - 31
Table-1 : Annual Incidence of Leptospirosis : Nephrology Department, Government General Hospital, Madras
1987 1988 1989 1990 1991 1992 1993 Leptospirosis 4 21 26 60 48 8 9
Leptospiral ARF 4 20 21 45 30 8 7

29
laborers. These patients were seen from various parts of the city and there was no
geographical clustering. This emphasizes the epidemiological important of a
contaminated environment in the spread of Leptospirosis. A sero survey
conducted among conservancy workers in Madras City has revealed a prevalence
rate of about 33%.7
The common reservoirs appear to be rodents such as bandicoots, though it
has been reported in domestic animals such as dogs, cattle, goat, sheep and
buffaloes.8,9 Studies have revealed that the common serogroup is L. autumnalis
though other groups such as L. icterohaemorrhagia, L. canicola and L. Pomona
have been reported.1,2
CLINICAL FEATURES
The clinical features vary from a mild anicteric illness characterized by
fever, Myalgia and Conjunctival suffusion, to a severe illness in which jaundice,
renal failure, bleeding diathesis, meningitis and Myocarditis (Weil’s syndrome or
Icteric Leptospirosis) occur. The incubation period is 7 – 14 days but ranges from
2 to 21 days. Ninety percent or more of all cases of Leptospirosis are anicteric.11
Most patients noted by us presented with fever, Myalgia, conjunctival
suffusion, jaundice and renal failure. The comparisons of various clinical studies
are shown in Table 2.
J POSTGRAD MED 1994; 40(3) : 127 - 31

Profile of Human Leptospirosis
30
Although, the clinical course of leptospiral infection may vary in
individual cases, in general, it is predictable in that both anicteric and icteric cases
follow a biphasic course. The initial or “septicemic phase” is characterized by
development of fever, Myalgia, conjunctival suffusion, headache and vomiting.
Termination of this phase occurs after 4 to 7 days, with defervescence of fever and
symptomatic improvement coincident with the disappearance of leptospires from
the blood, cerebrospinal fluid and all other tissues with the exception of the
aqueous humor and renal parenchyma.
Circulating antibody titres leptospires develop rapidly and this immune
response ushers in the second or “Immune stage” of the illness, which varies in
duration from 4 to 30 days or longer. The “Immune stage” is characterized by
manifestations of the immune response of the host to the infecting
J POSTGRAD MED 1994; 40(3) : 127 - 31
Table – 2: Clinical features – comparison of various studies Barbados United States Korea India (Edwards) (Heath) (Park) (Muthusethupathi) Reference (12) (13) (14) (1987-91) Patient No. 88 345 93 159 Fever 85 100 97 100 Renal Failure 49 26 15 75 Jaundice 95 43 16 85 Conjunctival 54 33 58 42 Suffusion Myalgia 49 68 88 80 Bleeding 2 4 40 2 Diathesis CNS 2 21 6 43 Manifestations
(Figures represent %)

31
microorganisms. Leptospires are found only in renal and ocular tissue during this
phase. Leptospiruria, a hallmark of this stage, generally continues for 1 to 3
weeks, but rarely longer than 1 month, and is unaffected by antimicrobial therapy.
Meningitis and Uveitis become apparent and reach ‘peak’ intensity during this
stage of the disease.
The demarcation between the first and second stages is rarely as distinct
in patients with severe icteric illness as it is in anicteric cases. In the former, the
biphasic course of disease often is obscured. Although many authors have
regarded the onset of jaundice as the beginning of immune phase, it is not always a
reliable index because some investigators have been able to isolate organisms
from the blood of patients who have been icteric for 24 to 48 hours.11 It is
considered that jaundice, renal failure and other features of Weil’s syndrome are
“first stage” features and are due to leptospiremia, rather than to immune
mechanisms.
Data on anicteric illness have not been adequately reported from our
country probably due to lack of awareness. Available data only reveal a high
incidence of severe Leptospirosis with jaundice and renal failure.
Renal involvement is the most serious complication and is the commonest
cause of death. Renal manifestations range from urinary sediment changes
(pyuria, hematuria and granular casts) to renal failure. Renal manifestations are
observed commonly in all forms of Leptospirosis regardless of severity of disease
or of the infecting serogroup. In anicteric patients, proteinuria, microscopic
hematuria and azotemia have been noted. Proteinuria is mild and is due to the
febrile state. Hematuria may be due to hemorrhagic diathesis rather than
glomerular injury.
J POSTGRAD MED 1994; 40(3) : 127 - 31
Profile of Human Leptospirosis
32
Azotemia has been divided into two groups.15,16 The first is characterized
by decreased renal perfusion with diagnostic indices suggestive of pre renal
azotemia, with a good response to fluid administration. The second is
characterized by features consistent with tubular necrosis with no respose to fluid
challenge. It has been emphasized that hemodynamic alterations (Hypotension,
volume depletion) responsible for the former, may result in acute tubular necrosis
if uncorrected. In addition, acute interstitial nephritis may account for renal failure
regardless of the hemodynamic state. Renal failure occurs in the second week but
it can occur as early as the fourth day. It may be short lived or prolonged for upto
two weeks.
The pathogenesis of renal failure in Leptospirosis is multifactorial and
may include a) Hypoxia secondary to hypovolemia/Hypotension b) direct
nephrotoxicity due to toxic by products of leptospires. The possible causes of
hypovolemia and Hypotension must be considered. Body fluid loss due to
vomiting, increased insensible water losses, and diminished intake of fluid are
responsible for hypovolemia and Hypotension in some cases. Decreased
intravascular volume secondary to a shift in fluid from the intra – to extra vascular
space as a result of severe endothelial injury has been suggested, which result in
Hypotension and shock. Massive gastrointestinal hemorrhage is an important
cause of hypovolemia. Adrenal insufficiency secondary to adrenal hemorrhage is
a rare cause of Hypotension.
Hypo perfusion may also be the result of cardiac dysfunction. Cytotoxic
factors may be responsible for toxic tubular injury though nosuch toxin has been
isolated so far. In the kidney, leptospires initially cause glomerular injury and by
hematogenous spread, the organisms reach peritubular capillaries and migrate to
the interstitium, renal tubules and tubular lumen causing interstitial nephritis and
tubular necrosis.17
J POSTGRAD MED 1994; 40(3) : 127 - 31
33
The kidneys are greatly swollen with pale cortex and congested medulla.
Glomerular changes are mesangial proliferation with polymorphonuclear
infiltration. On immunofluorescence staining, nonspecific C3 uptake is reported
in the mesangial area and occasionally in the affected arterioles. C1q and IgM
deposition may be noted occasionally in the mesangial area. On electron
microscopy, occasional dense deposits are seen in the mesangial, paramesangial
and intramembranous location. Vascular changes in the kidney consist of
endothelial swelling and necrosis with platelet aggregation, especially in the
cortico- medullary region. Interstitial nephritis is the basic renal lesion
characterized by mononuclear cells infiltration.17
Renal failure in Leptospirosis is primarily the result of tubular damage.
Though some investigators have emphasized that interstitial nephritis is the
fundamental renal lesion of Leptospirosis others have found that it occurs only
inpatients who have survived until inflammation has had an opportunity to
develop.17,18 Evidence of interstitial nephritis frequently is absent in patients
whose disease is characterized by a rapid, fulminant course. Sequential
observations of histologic, enzymatic and functional renal changes in both animal
and human Leptospirosis suggest that the initial and most prominent renal lesion
is tubular and that in many cases it is unaccompanied by interstitial inflammatory
infiltrates. These tubular lesions are similar to acute tubular necrosis of other
causes.18
We did not do biopsy in most of our patients as serology was adequate for
diagnosis and there are no pathognomonic changes in Leptospirosis. In addition,
as bleeding diathesis is an important component of this illness we did not take the
risk of renal biopsy. In an earlier study, we did biopsy in a few patients and they
revealed acute interstitial nephritis.
J POSTGRAD MED 1994; 40(3) : 127 - 31

Profile of Human Leptospirosis
34
Most patients with renal failure also have significant hepatic involvement.
Jaundice occurs between the fourth and sixth day but may occur as early as the
second day or as late as the 9th day. Jaundice is partly due to hepatocellular
damage. However, hepatocellular necrosis is usually mild and additional factors
include intrahepatic cholestasis and increased billirubin load from absorption of
blood from tissue haemorrhage. Death is rarely due to hepatic failure. In our
patients, marked elevation of serum billirubin with near normal or mildly elevated
SGOT and SGPT levels were characteristic.
DIAGANOSIS
Laboratory diagnosis involves the isolation of leptospira in culture of
blood and urine and serological tests.
ISOLATION PROCEDURES
Isolation of leptospires from blood or cerebrospinal fluid generally can be
achieved only during the first 10 days of clinical illness. Leptospires usually
appear in the urine during the 2nd week of disease and may persist for 30 days or
longer. In general, other than blood, urine or cerebrospinal fluid, only tissue
sections obtained by biopsy or at necropsy serve as sources from which organisms
can be isolated. Fletcher’s semisolid medium or EMJH semisolid mediums are the
media often used.
SEROLOGICAL TESTS
a) Microscopic agglutination test (MAT) – MAT is considered the comer
stone of serodiagnosis.19 Rising titres or initial high titres are diagnostic of
leptospiral infection. The main advantage of MAT is that the serovars can be
identified which is of epidemiological importance. The main disadvantage is that
the titres rise late and peak about the third or fourth week. The high titres of MAT
take a much longer time to decline, which is of value for epidemiological studies,
but the presence of high titres from previous infection complicate the diagnosis of
current infection.6
J POSTGRAD MED 1994; 40(3) : 127 - 31

35
b) ELISA – The ELISA is now the test of choice for the diagnosis of current
infection. It detects specific IgM and IgG antibodies. Detection of specific IgM
antibodies helps in the rapid diagnosis of current infection.6,20 This test detects
genus specific antibodies which tend to become positive early in the disease and
also revert early. It is a relatively simple test as the antigen used is genus specific.
This test cannot determine the infecting serogroup. A high titre in a single sample
can be diagnostic though repeat samples may be necessary if initial titres are low.
Recently, a collaborative study done with Leptospira laboratory
Barbados, using ELISA for estimating elevated specific IgM titres has confirmed
the diagnosis of current leptospiral infection in Madras city.10 In addition, MAT
study revealed L. autumnalis tobe the commonest serogroup. L. auatumnaalis was
isolated from the blood of one of our patients at the Royal Tropical Institute,
Amsterdam.
MANAGEMENT
The conservative treatment of Leptospirosis consists of giving antibiotics
(Penicillin, Doxycycline) and adequate hydration. The efficacy of antibiotics in
the treatment of Leptospirosis remains controversial because of conflicting
data.22,23 It is generally believed that antibiotics are effective only if given early in
the course of disease and their efficacy in unknown in late or severe disease. Watt
et al22 conducted a placebo controlled trial of intravenous penicillin for severe
(S.Cr > 177 micromoles/L) and late (symptoms > 4 days) Leptospirosis in 42
patients and included that antibiotic therapy was definitely useful in these patients.
Fever lasted more in the placebo group compared to the treated group (11.6 vs 4.7
days) Creatinine rises persisted more than thrice as long in the patients receiving
only placebo (8.3 vs 2.7 days) Penicillin also shortened the hospital stay and
prevented leptospiruria.22 However, Edwards et al in a prospective controlled
study in 70 patients concluded that penicillin therapy has no effect in severe
J POSTGRAD MED 1994; 40(3) : 127 - 31

Profile of Human Leptospirosis
36
Leptospirosis. In animal studies, fewer deaths and less severe course of the
disease among penicillin treated, jaundiced puppies compared to untreated
controls were noted by Yoder et al.24 Hamsters severely ill with Leptospirosis
survived when given penicillin 1 – 2 days before the expected time of death.22
The overall impression thus seems to be that antibiotics are useful even in severe
or late Leptospirosis. It has been our policy to treat all patients with intravenous
crystalline penicillin. Of primary importance is the meticulous attention, which
must be paid, to fluid and electrolyte balance. Hypovolemia and Hypotension
needs prompt and specific treatment with intravenous fluids. In patients with
oliguria, if prerenal azotemia is suspected, prompt diuresis should be attempted
with fluid therapy. In patients who have no response to such therapy, they should
be managed as for ARF.
Peritoneal dialysis has been found to be a safe, simple and effective
procedure in the management of leptospiral ARF. Peritoneal dialysis was
adequate for most of our patients who needed dialysis (Table 3).
The overall mortality was 20.8% in our experience.
J POSTGRAD MED 1994; 40(3) : 127 – 31
Table – 3 : Dialysis and mortality data of leptospiral ARF (1987 – 91)
No. : 120 Mean age (Yrs) : 40.1 Males : 108 Peritoneal dialysis : 56 Haemodialysis : 14 Mortality No. : 25 % : 20.8 ----- Total No. of Leptospirosis : 159 -----

37
REFERENCES:
1. Muthusethupathi MA, Shivakumar S, Jayakumar M, Rajendran S. Acute
Renal failure in Madras City – Changing profile. Ind J Nephrol (New
series) 1993 ; 3 : 66-70.
2. Muthusethupathi MA, Shivakumar S, Suguna Rajenderan, Vijayakumar R,
Jayakumar M. Leptospiral Renal Failure in Madras City. Ind J Nephrol
1991; 1 : 15 – 7.
3. Muthusethupathi MA, Shivakumar S. Acute Renal Failure due to
Leptospirosis. J Assoc Phys India. 1987 ; 35 : 631 – 3.
4. Rastegar A, Sitprija V, Rocha R. Tropical Nephrology. In:Schrier RW,
Gottschalk CW (Es.,) Diseases of the Kidney – Fourth Edition. Boston.
Little. Brown and Company 1988; 2583 – 613.
5. Faine S. Guidelines for the control of Leptospirosis. WHO offset
Publications 1982; 67 : 151 – 3.
6. Everard JD, Everard COR Leptospirosis in the Caribbean. Reviews in
Medical Microbiology 1993; 4 : 114-22
7. Ratnam S, Everard COR, Alex JC, Suresh B, Thangaraju P. Prevalence of
Leptospiral agglutinins among conservancy workers in Madras City, India.
J Trop Med and Hygiene 1993; 96 : 41 – 5.
8. Ratnam S, Sundararaj T, Subramaniam S : Role of bandicoots in human
Leptospirosis in Madras City – An epidemiological approach. Ind J Pub
Health 1986; 30 : 167-8
9. Ratnam S, Subramaniam S, Sundararaj T : Evidence of Leptospiral
antibodies among domestic animals in Madras City. Cherion 1983; 12 :
176 – 9.
J POSTGRAD MED 1994; 40(3) : 127 - 31

Profile of Human Leptospirosis
38
10. Shivakumar S, Muthusethupathi MA, Everard COR et al. Leptospirosis in
Madras City – A collaborative study (abstract). V Asian Pacific Congress
of Nephrology 1992; 44.
11. Folgin RD, Anderson DC. Human Leptospirosis. CRC Crit Rev Clin Lab
Sci 19175; 5 : 413 – 67.
12. Edwards CN, Nicholson GD, Hassell TA, Everard COR Callender J.
Leptospirosis in Barbados – A clinical study. W I Med J 1990; 39 : 27 –
34.
13. Heath CW, Alexander AD, Galton MM. Leptospirosis in the United
States. N Engl J Med 1965; 273 : 857.
14. Park YK, Park SK, Rhee YK, Kang SK. Leptospirosis in the Chonbuk
province of Korea in 1987. Korean J Intern Med 1990; 5 : 34 – 43.
15. Sitprija V. Renal Involvement in human Leptospirosis. Br Med J 1968; 2
: 656 – 8
16. Nicholson GD, Edwards CN, Hassell TA, Everard COR, Callender J.
Urinary Diagnostic Indices in the Management of Leptospirosis –
Selection of patients for Dialysis Therapy. W I Med J 1989; 38 : 33 – 8.
17. Sitprija V, Pipalangul V, Metrowidjoji K. Pathogenesis of Renal disease
in Leptospirosis – Clinical and experimental studies. Kidney Int 1980;
17 : 827 – 36.
18. Arean VM. The pathologic anatomy and pathogenesis of fatal human
Leptospirosis (Wells disease). Am J Pathol 1962; 40 : 393 – 6.
19. Cole JR, Sulzer CR, Pursell AR. Improved micro technique for the
leptospiral microscopic agglutination test. Applied Microbiology 1973;
25 : 976.
J POSTGRAD MED 1994; 40(3) : 127 - 31

39
20. Terpstra W.J. Ligthart GS, Schooner GJ. ELISA for the detection of
specific IgM and IgG inhuman Leptospirosis. Journal of General
Microbiology 1985; 131 : 377 – 85.
21. Alexander AD, Rule PI. Penicillin, Cephalosporins and Tetracyclines in
treatment of hamsters with fetal Leptospirosis. Antimicrob Ag Chemother
1986; 30 : 835-39
22. Watt G, Tuazom MA, Santiago LE. Placebo Controlled trial of
intravenous penicillin for severe and late Leptospirosis. Lancet 1988;1 :
433 – 5
23. Edward CN, Nicholson GD, Hassell TA, Everard COR, Callendar J.
Penicillin therapy in icteric Leptospirosis. Am J Trop Med Hyg 1988;
39(4) : 388-90
24. Yoder HW, Bergman HN, Glener CA. Experimental Canine Leptospirosis
IV. Evaluation of selection antibiotics in the therapy of acute experimental
leptospira icterohaemorrhagic infections in immature dogs. J Infect Dis
1957; 100 : 257 – 67
J POSTGRAD MED 1994; 40(3) : 127 - 31

Profile of Human Leptospirosis
40
ARTICLE 7
LEPTOSPIROSIS – NEED FOR URGENT ACTION
Leptospirosis is an important cause of acute renal failure (ARF) in
Madras City, especially during and after the monsoon rains, when it assumes
near epidemic proportions1. In 1988, like in previous years, many cases of
leptospiral renal failure were treated at several large hospitals in Madras City;
in the Government General Hospital alone 21 cases of leptospiral renal failure
were encountered.
Leptospirosis is a public health problem of great importance since (a)
it has a predilection for people following certain occupations (e.g. workers in
rice or cane fields, veterinarians, sewage workers) causing loss of considerable
man-hours in a vital section of our economy (b) it affects domestic and farm
animals causing abortion and (c) it can be prevented by taking appropriate
public health measures. In view of these facts, the World Health Organization
(WHO) has done considerable work in this field and has laid down excellent
guidelines for the diagnosis and control of Leptospirosis2.
We have been interested in and are working on this problem since
1985. In the light of our experience, we would like to point out some
important facts and problems pertaining to diagnosis, management and
prevention of this condition in our country.
JAPI 1989, VOL. 37, NO.7 477

41
1. Diagnosis: Leptospirosis has a variety of clinicala manifestations;
once suspected, it can be confirmed by (a) isolation of pathogenic leptospira
from urine or blood (b) demonstrating a rising titre of leptospiral antibodies by
agglutination tests or (c) demonstration of leptospira in blood or urine by dark
field microscopy. Of these, (c) is the least reliable, since artifacts can easily be
mistaken for the organism; (a) is the most specific but needs a special
laboratory and trained personnel; it is not a sensitive test and several cases may
be missed, (b) comprises macroscopic agglutination test as a screening
procedure and microscopic agglutination test to determine the serogroup.
Overall, the best screening test is the macroscopic agglutination test, which can
be easily performed and is inexpensive.
The problem is that even this test is not readily available in
microbiology laboratories in our country. From the reports of our colleagues,
we are convinced that Leptospirosis occurs in many places in Tamil Nadu,
Kerala and elsewhere. Physicians are unable to get the diagnosis confirmed
due to lack of laboratory facilities. We have been helped in all our studies by
the Department of Veterinary Preventive Medicine, Madras, but for the
majority of our colleagues, no such help is available.
2. Epidemiology: Before control measures are started, it is essential
that we have relevant data on the problem. Since it is not transmitted by
humans and is initially confined to the animal reservoir, a thorough study
should involve animals in the locality also.
JAPI 1989, VOL. 37, NO.7 477

Profile of Human Leptospirosis
42
The principles of epidemiological investigations are (i) Identification
of cases (human and animals) (ii) Search for the source of individual
infections, and of epidemic and epizootic waves. (iii) Establishment of a level
of endemic and enzootic infection. (iv) Advice on implementation of a control
programme.
These data are useful to clinicians, veterinarians, microbiologists,
epidemiologists and public health staff. None of these groups can operate
independently to control Leptospirosis and they have to act as a team.
It is clear from the above that four steps should be immediately taken
if we are to study and control this infection (1) facilities for macroscopic
agglutination test should be made available in all medical college microbiology
laboratories. (2) A central Leptospirosis reference laboratory should be set up
(3) Leptospirosis should be made a ‘notifiable’ disease and (4) public health
officials should be actively associated in detection/control programmes.
MA Muthusethupathi Shivakumar S Department of Nephrology, Madras Medical College & Government General Hospital, Madras 600 003
REFERENCES
1. Muthusethupathi MA, Shivakumar S, Acute renal failure due to
Leptospirosis. J Assoc Phys India 1987 : 35 : 631 – 3.
2. Faine S, Guidelines for the control of Leptospirosis. WHO offset
Publication 1982 : 67 : 151 – 3.
JAPI 1989, VOL. 37, NO.7 477

43
ARTICLE 8
MSAT – A SCREENING TEST FOR LEPTOSPIROSIS
Microscopic agglutination test (MAT) and IgM ELISA are the important
tests used for serodiagnosis of Leptospirosis. But these tests can be done only in
specialized microbiological laboratories. Therefore, there is a need for a simple
screening test for diagnosis of current infection. We have evaluated the
Macroscopic Slide Agglutination Test (MSAT) as a screening test and shall
discuss out experience with it.
At the Institute of Microbiology, Chennai Medical College, serum
samples obtained from patients with clinical features suggestive of Leptospirosis
during the period Jan – Dec. 1995 were tested by a) Macroscopic slide
Agglutination Test (MSAT) using Patoc, Icterohaemorrhagiae and Autumnalis
antigens, b) IgM ELISA and c) Microscopic Agglutination Test (MAT). The
diagnosis of current leptospiral infection was made by a titre of > 40 by IgM
ELISA. MSAT was compared with IgM ELISA and MAT.
MAT and IgM ELISA were done by standard procedures as reported by
us earlier.1 MSAT was done using a dense suspension of killed Leptospirosis was
mixed with a drop of serum on a slide and rotated on a rotator (120 rpm) for 4
min. It was then examined by naked eye for presence of agglutination. A 4+
agglutination titre was considered significant.2-4
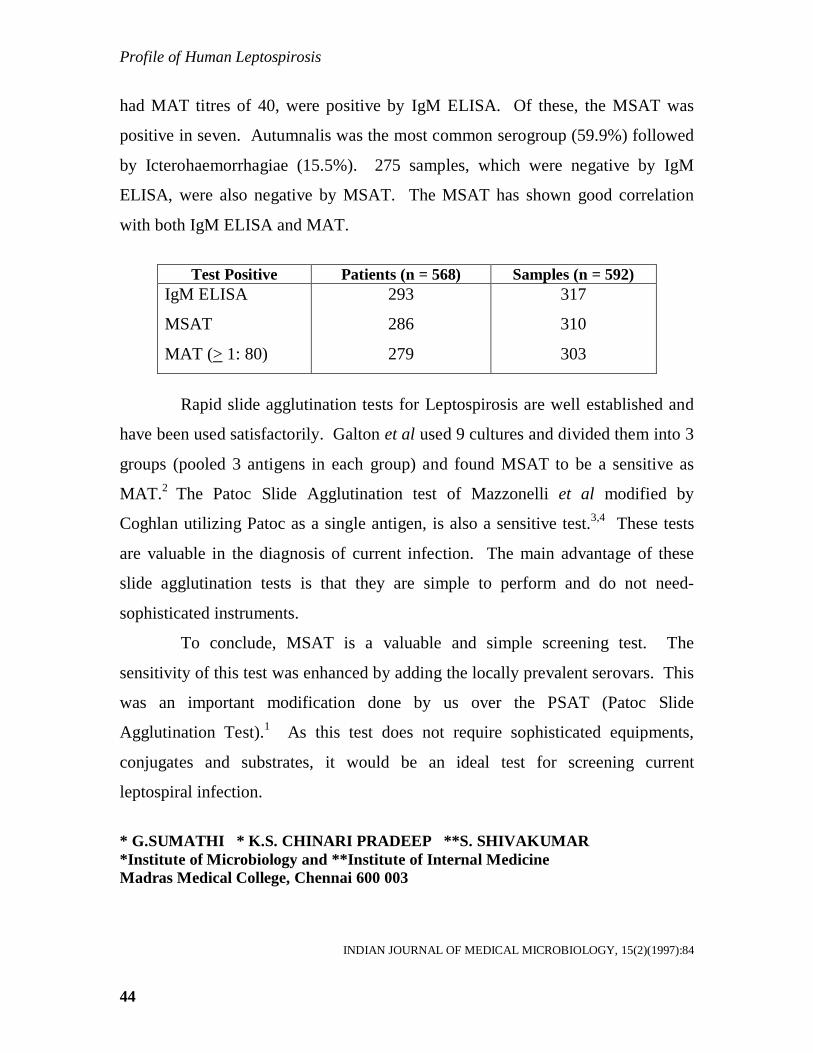
Of the 592 samples received, 317 were positive by IgM ELISA. Among
these, MSAT was positive in 310. (Sensitivity 97.8%). 303 samples had MAT
titres of > 80. In all these patients, the MSAT was positive. 14 samples, which
INDIAN JOURNAL OF MEDICAL MICROBIOLOGY, 15(2)(1997):84
Profile of Human Leptospirosis
44
had MAT titres of 40, were positive by IgM ELISA. Of these, the MSAT was
positive in seven. Autumnalis was the most common serogroup (59.9%) followed
by Icterohaemorrhagiae (15.5%). 275 samples, which were negative by IgM
ELISA, were also negative by MSAT. The MSAT has shown good correlation
with both IgM ELISA and MAT.
Test Positive Patients (n = 568) Samples (n = 592)
IgM ELISA
MSAT
MAT (> 1: 80)
293
286
279
317
310
303
Rapid slide agglutination tests for Leptospirosis are well established and
have been used satisfactorily. Galton et al used 9 cultures and divided them into 3
groups (pooled 3 antigens in each group) and found MSAT to be a sensitive as
MAT.2 The Patoc Slide Agglutination test of Mazzonelli et al modified by
Coghlan utilizing Patoc as a single antigen, is also a sensitive test.3,4 These tests
are valuable in the diagnosis of current infection. The main advantage of these
slide agglutination tests is that they are simple to perform and do not need-
sophisticated instruments.
To conclude, MSAT is a valuable and simple screening test. The
sensitivity of this test was enhanced by adding the locally prevalent serovars. This
was an important modification done by us over the PSAT (Patoc Slide
Agglutination Test).1 As this test does not require sophisticated equipments,
conjugates and substrates, it would be an ideal test for screening current
leptospiral infection.
* G.SUMATHI * K.S. CHINARI PRADEEP **S. SHIVAKU MAR *Institute of Microbiology and **Institute of Inter nal Medicine Madras Medical College, Chennai 600 003
INDIAN JOURNAL OF MEDICAL MICROBIOLOGY, 15(2)(1997):84
45
REFERENCES:
1. Sumathi G, Subudhi CPK, Manuel HPS, shivakumar KS, Rajendran S and
Muthusethupathi MA. Serodiagnosis of Leptospirosis. Indian J of Med.
Microbiol (1995) 13(4): 192-195.
2. Galton MM, Powers DK, Hall AD and Cornell RG. A rapid macroscopic
slide screening test for the serodiaganosis of Leptospirosis. Am J Vet Res
(1958) 19:505-512.
3. Mazzonelli J, Dorta de Mazzonelli G and Mailloux M. Possibilite de de
diagnostic serologique macroscopique des leptospires a Paide d;un
antigene unique. Medecine et Maladies Infectieuses (1974) 4:252-254.
4. Coghlan JD, Leptospira, Borrelia, Mackie and McCartney. Practical
Medical Microbiology, Thirteenth Edition (Churchill Livingstone,
London) (1989) 671.
INDIAN JOURNAL OF MEDICAL MICROBIOLOGY, 15(2)(1997):84

Profile of Human Leptospirosis
46
ARTICLE 9
LEPTOSPIROSIS LABORATORY, CHENNAI MEDICAL COLLEGE
– A THREE YEAR EXPERIENCE IN SERODIAGNOSIS (1995 – 1997)
The Leptospirosis laboratory was established in July 1994 at the Institute
of Microbiology, Chennai Medical College. We present our experience on
serodiagnosis of Leptospirosis during the period 1995 – 1997.
Blood samples were received from both public and private institutions for
the diagnosis of current Leptospirosis. The following tests were done:
Microscopic agglutination test (MAT), IgM ELISA and Macroscopic slide
agglutination test (MSAT) utilizing preparations of Patoc, Autumnalis and
Icterohaemorrhagiae serogroups. The diagnosis of Leptospirosis was made by the
standard criteria.1,2
A total number of 5614 samples were received of which 1764 (31.4%)
were positive for current infection (Table 1). The number of samples showed a
dramatic increase during the three-year period probably due to increased
awareness of the illness. Mostly single samples were received. The declining
percentage of positive cases is probably due to the fact that samples were sent
early (5 days of illness) and second samples were not available.
Table 1. Annual data of total and positive blood samples
Year Total samples Positive (%) 1995 592 317 (53.5) 1996 1461 581 (39.7) 1997 3561 866 (24.3) Total 5614 1764 (31.4)
INDIAN JOURNAL OF MEDICAL MICROBIOLOGY, (1999)17(1):50-51

47
During 1995, IgM ELISA, MSAT and MAT were done for serodiagnosis.
IgM ELISA was positive in 317 out of 592 samples. Among these MSAT was
positive in 310 (Sensitivity 97.8%). Three hundred and three samples had MAT
titres of > 1:80. During 1996, MSAT and MAT were done for serodiagnosis, the
IgM ELISA could not be done due to non-availability of reagents, the results are
shown in Table-2. As MSAT had shown good correlation with MAT and IgM
ELISA earlier in 1995, this was utilized as the screening test for current leptospiral
infection. One thousand four hundred and sixty one samples were received during
1996, of which 581 were positive by MSAT and 509 were positive by MAT.
MAT revealed the predominant serovars to be Autumnalis (48.3%) and
Icterohaemorrhagiae (31.1%) during 1995 and 19963. Since these two serovars
were incorporated along with Patoc in the MSAT, the sensitivity of this test was
enhanced. During 1997, MSAT along was used for serodiagnosis. Of the 3561
samples received during 1997, 866 were positive.
Table 2. The findings with three different leptospiral serological tests
No. Test Positive (%) Year
No.
Samples IgM ELISA MSAT MAT 1995 592 317(53.5) 310 (52.4) 303 (51.2) 1996 1461 -- 581 (39.8) 509 (34.8) 1997 3561 -- 866 (24.3) --
The microscopic agglutination test (MAT) is considered to be the gold
standard test for diagnosis of Leptospirosis. MAT was valuable in identifying the
serogroup. A tire of > 1:80 was used for diagnosis and it correlated with IgM
ELISA.1,3 The observation of a significant titre in a single sample does not
necessarily indicate current disease as it may be attributed to persistent antibodies
INDIAN JOURNAL OF MEDICAL MICROBIOLOGY, (1999)17(1):50-51

Profile of Human Leptospirosis
48
of past infection. We recommend genus specific test in addition (MSAT or IgM
ELISA) to confirm the diagnosis of current infection. For performing the MAT,
stock cultures of various antigens have to be maintained. In addition, poor growth
and subsequent loss of Leptospirosis used for antigens in the MAT, contamination
of culture medium are also other important problems encountered. Unless,
international Leptospira reference laboratories supply stock cultures to National
Laboratories, it would be impossible to perform the test. There is an urgent need
to establish a National reference laboratory to help the regional laboratories to
identify the predominant local serogroups which could not be utilized for the test.
As there is inter observer variation in cut off titres, standardization of this test
between various workers is essential. Therefore, MAT is a complicated test and
can be performed only in established Microbiology laboratories with trained
personnel.
The IgM ELISA test is a very sensitive test for the diagnosis of current
infection when appropriately developed in the laboratory. It is an expensive test,
kits are becoming commercially available but their sensitivity has to be evaluated
before use.
The MSAT is a simple, rapid and sensitive diagnostic test for current
Leptospirosis.2 The improved sensitivity was due to addition of locally prevalent
serovars. This test has become the test of choice in our laboratory for diagnosis of
current infection.
INDIAN JOURNAL OF MEDICAL MICROBIOLOGY, (1999) 17(1):50-51

49
To conclude, there is an urgent need to establish a National reference
laboratory in collaboration with international reference laboratories. This
laboratory should collate the information from various regional laboratories in our
country and also help them with supply of antigens and materials for diagnostic
purposes. We recommend that MSAT be made as the screening test of choice for
diagnosis of current leptospiral infection till other reliable tests become available.
CHINARI PRADEEP KS* SUMATHI G* VIMALA RANGA RAO G* SHIVAKUMAR S** *Institute of Microbiology *Institute of Internal Medicine Madras Medical College, Chennai 600 003
REFERENCES:
1. Sumathi G, Pradeep Kumar Subudhi Ch, Helen PS, Manuel, Kalpana,
Shiva Kumar S, Suguna Rajendran and Muthusethupathi MA,
Serodiagnosis of Leptospirosis – A Madras Study, Indian J Med Microbiol
(1995) 13 : 192 – 195.
2. Sumathi G, Chinari Pradeep KS and Shiva Kumar S. MSAT – A screening
test for Leptospirosis. Indian J Med Microbiol (1997) – 15 : 84.
3. Chinari Pradeep KS. A two year study on serodiagnosis of Leptospirosis.
M.D. (Thesis). The Tamil Nadu Dr. M.G.R. Medical University, March
1998.
INDIAN JOURNAL OF MEDICAL MICROBIOLOGY, (1999)17(1):50-51
Profile of Human Leptospirosis
50
ARTICLE 10
ACUTE RENAL FAILURE DUE TO LEPTOSPIROSIS
(1984 – 85)
*MA MUTHUSETHUPATHI, **S SHIVAKUMAR
SUMMARY
Nineteen patients with acute renal failure due to Leptospirosis were
encountered during a two year period, from January 1984 to December 1985. All
had positive agglutination tests for Leptospirosis. In seven patients, leptospira
were demonstrated in blood. Kidney biopsy in two patients showed acute tubulo-
interstitial nephritis. Marked seasonal and geographical “clustering” were evident.
Penicillin and conservative measures were the cornerstone of therapy,
supplemented by peritoneal or haemodialysis. Fifteen patients recovered. Severe
haemorrhage and uraemia resulted in four deaths. Leptospirosis thus appears to be
an important cause of acute renal failure in Madras.
INTRODUCTION
Leptospirosis is an infectious disease caused by the various serovars of
leptospira interrogans and is characterized by fever, conjunctival suffusion and
Myalgia; in severe cases, jaundice, renal failure and central nervous system
involvement may occur. In our country this condition was first reported from
Calcutta in 1938.1 In Thailand, 40 per cent of cases of acute renal failure (ARF)
are caused by leptospira.2 In this article, we report our experience with this
condition.
* Professor of Nephrology, **Tutor in Nephrology, Madras Medical College and Government General Hospital, Madras.
JAPI, 1987, VOL. 35, NO.9 631 – 633

51
MATERIAL AND METHODS
Leptospiral acute renal failure (L-ARF) was diagnosed according to the
following criteria; 1. Abrupt decline in glomerular filtration rate (GFR) shows by
progressive elevation of plasma urea (> 40 mg/dl) and plasma creatinine
(> 2 mg/dl). 2. Absence of pre renal (hypovolaemia) and post renal (obstructive)
factors. 3. Presence of jaundice. 4. Presence of any one of the following:
(a) Leptospira in blood (b) Positive micro-agglutination test for leptospira in
significant or rising titre. Dark field microscopy of blood for leptospira and the
micro agglutination test for leptospira were done by the method of Turner at the
department of Veterinary Preventive Medicine, Madras Veterinary College or the
Institute of Basic Medical Sciences, Taramani.3 Percutaneous kidney biopsy was
done in two patients. In 5 patients, the fractional excretion of sodium (FE Na) was
calculated according to the
Urine sodium Plasma Creatinine Formula FE Na = ------------------ X ------------------------- X 100 Plasma sodium Urine Creatinine After establishing the diagnosis, patients were started on conservative
treatment including maintenance of fluid and electrolyte balance, provision of high
carbohydrate calories and administration of Benzyl Penicillin 1 million units 4
times daily intramuscularly. Because of severe uraemia, peritoneal dialysis (PD)
was considered necessary in 4 patients. Haemodialysis was done in one patient.
RESULTS
Out of 80 patients of acute renal failure seen from January 1984 to
December 1985, 19 patients had leptospiral renal failure. Only one patient was a
female. The age distribution of these cases is given in Table 1. The clinical
features at presentation and hospital stay are tabulated separately (Table 2).
JAPI, 1987, VOL. 35, NO.9 631 – 633

Profile of Human Leptospirosis
52
Important biochemical parameters and agglutination titres are given in Table 3. A
characteristic feature was the association of high serum bilirubin with normal or
mildly elevated oxaloacetic and pyruvate transaminase levels in 10 of 19 patients.
Serum alkaline phosphatase was elevated in four patients. In 3 patients
microscopic haematuria was a prominent feature. Plasma creatinine was > 5
mg/dl in 13 of 19 patients. Dark-field microscopy of blood revealed leptospira in
7 of 19 cases. In the micro agglutination test all the 19 patients had a positive titre
of 1/10 or greater; 13 had a positive titre of 1/80 or more (Table 3). The FE Na
was available in five patients only in three of whom it was less than 1 per cent.
Renal biopsy in two patients showed tubular necrosis, interstitial edema
and diffuses interstitial infiltration.
Fifteen of 19 cases were seen during the three-month period, November
to January. Since October and November are the rainy months in Madras, it is
obvious that these cases occurred during or following monsoon rains. Eight of 19
cases came from T.Nagar, West Mambalam, Ashoknagar and Vadapalani,
contiguous divisions of Madras city.
Conservative management was adequate in 15 of 19 patients and
peritoneal dialysis was done in 4 patients because of severe renal failure and
oliguria. Of these, one patient subsequently needed haemodialysis because of
hypercatabolic renal failure, which could not be managed by PD alone. Fifteen of
19 patients recovered. In these patients, renal failure lasted 4 – 55 days, the mean
duration being 15.3 days. 4 patients died; two of them due to severe haemorrhage
and two died of uraemia before dialysis could be started.
JAPI, 1987, VOL. 35, NO.9 631 – 633

53
TABLE 1: AGE DISTRIBUTION
Age group No.
21 – 30 31 – 40 41 – 50 51 – 60 61 – 70
2 5 7 4 1
Total 19
TABLE 2: CLINICAL FEATURES
Clinical features No. of
patients GENERAL Fever Conjunctival suffusion haemorrhage Myalgia GI TRACT Vomiting diarrhoea, abdominal pain Hepatomegaly NEUROLOGIC Disorientation Seizures, coma Muscle Tenderness CARDIOVASCULAR Tachycardia Hypertension Hypotension BLEEDING Haematuria Petechiae GI Bleed Vaginal bleeding Epistaxis
17 10 6
17 12 7 1 2
18 3 8 3 2 2 1 1
JAPI, 1987, VOL. 35, NO.9 631 – 633

Profile of Human Leptospirosis
54
DISCUSSION
Leptospirosis is characterized by fever, severe Myalgia, conjunctival
suffusion, jaundice and acute renal failure. Since the first description by Weil in
1886, over 130 serotypes of the pathogenic leptospira interrogans and the disease
severity varying from a mild, self limiting, febrile illness to a life threatening
syndrome of hepatic and renal failure have been reported.4
TABLE 3
Parameter Mean SD Range Blood Urea (mg/dl)
Plasma Creatinine (mg/dl)
Serum Bilirubin (mg/dl)
SGOT (I.U)
SGPT (I.U)
Alkaline Phosphatase (KA Units)
Leptospiral agglutination titre
228.2
6.7
19.9
107.4
51.4
10.8
186.3
106.6
3.3
11.1
92.9
38.4
5.6
199.5
80 – 390
2.5 - 16
3.2 – 42.2
32 – 380
14 – 150
4.2 – 24.2
10 – 640
Ooi et al reported renal histological changes consisting of interstitial
infiltration and tubular necrosis inhuman Leptospirosis from Singapore.5 Inspite of
the close geographical similarity between Thailand and parts of India, viz. large
areas of paddy fields, stagnant water and the ubiquitous rodents, leptospiral renal
failure which is known to occur frequently in Thailand2, was not documented in
our country till 1965 when Krishnamurthy et al published the first case report of
leptospiral hepato renal syndrome in two patients seen in Government Royapettah
Hospital, Madras.6 Leptospirosis accounted for 19 of a total of 80 cases of ARF
seen by us over a two year period, thus accounting for 23.5 per cent of all cases of
ARF.
JAPI, 1987, VOL. 35, NO.9 631 – 633

55
Certain epidemiological features of this disease are worth noting. There
is a definite seasonal “clustering” since 15 of these 19 cases occurred during the
period, November to January. Also, 8 of 19 cases occurred in contiguous, low-
lying areas of Madras city following heavy monsoon rains in which several streets
were flooded. This is in keeping with a water-borne infectious disease. Identical
epidemiological features have been noted in USA and elsewhere.4,7
Only one out of 19 patients was a female (Table 1). The difference is
likely to be due to the greater exposure of males while wading through the
monsoon floods. The male preponderance has been noted by others.4,6
All the 19 patients had jaundice and acute renal failure. It is seen from
Table 2 that fever, abdominal pain, vomiting and diarrhoea were almost constant
features of this disease. This combination occurred in 17 of 19 patients (89%) and
has been reported in 95% of cases by MeCrumb and in 50% of cases by Edwards
and Domm.4 Abdominal pain is probably due to involvement of abdominal
muscles; subserosal haemorrhages, pancratitis and hepatitis are other factors
contributing to abdominal pain. Nausea and vomiting probably represent hepatic
dysfunction. Conjunctival suffusion or haemorrhage occurred in 10 of 19 patients
(52%). This is rather low as compared to 73% reported by Edwards and Domm.4
Since conjunctival injection is an early feature of this disease occurring in the
“Septicaemic” stage, it is possible that it had already resolved in many of our
patients, who were seen later in the course of the illness. The infrequency of
Myalgia (6/19) probably has a similar explanation. Liver was enlarged in12 of 19
patients. Its incidence was much lower (3/16) in the series of Edwards and
Domm.4 Other notable feature is a bleeding tendency, shown by Epistaxis,
gastrointestinal haemorrhage, haematuria and vaginal bleeding.
JAPI, 1987, VOL. 35, NO.9 631 – 633

Profile of Human Leptospirosis
56
Disorientation occurred in 7 of 19 patients. Severe central nervous
system involvement giving rise to seizures and coma was rare (1/19). Features of
meningitis like neck rigidity were also rare, as compared to other series.4
Biochemically, there were some characteristic features. Marked elevation
of serum bilirubin with near normal or minimally elevated SGOT and SGPT levels
occurred in 10 of 19 patients. Serum alkaline phosphatase was elevated in only 4
patients. Others have reported raised alkaline phosphatase levels in most patients.2
Renal failure was severe (Creatinine > 5 mg/dl) in 13 patients. The
fractional excretion of sodium (FE Na) is one of the most useful urinary indices in
diagnosing tubular injury. Since FE Na was available in only a small number of
cases its usefulness in this situation cannot be commented on.
Laboratory diagnosis of Leptospirosis involves the isolation of leptospiras
in culture of body fluids and serological tests. Leptospira in the blood was
demonstrated in 7 of 19 patients in this series. Macroscopic or microscopic
agglutination test was positive in all cases. Identification of the serogroup in 9
cases showed Leptospira autumnalis, L. Canicola and L. icterohaemorrhagic
species. Some studies have shown L. Autumnalis to be the commnest serotype in
this area.7,8
Renal failure could be managed by conservative measures along in14
patients; only 4 were dialysed peritoneally and one required haemodialysis. This
is consistent with our general experience.9
JAPI, 1987, VOL. 35, NO.9 631 – 633

57
Four patients in this series died. The mortality in L-ARF is about the
same as seen in the overall group of ARF in our series of 187 patients (21% vs
24%) (Unpublished data). The notable feature is the frequency of gastro-intestinal
bleeding as the cause of death in two of four patients.
In conclusion, Leptospirosis is responsible for nearly a quarter of our
cases of ARF. The diagnosis is often missed chiefly because of a lack of
awareness of the condition and inadequate facilities for confirmation of the
diagnosis.
JAPI, 1987, VOL. 35, NO.9 631 – 633

Profile of Human Leptospirosis
58
REFERENCE:
1. Das Gupta BM: Further observation of leptospiral infection in Calcutta.
Indian Med Gaz 1939; 74 : 31-2.
2. Sitprija V: Benyajatic. Tropical disease and acute renal failure. Ann Acad
Med (Supple) 1975; 4 : 112-4.
3. Turner LH, Leptospirosis LL. Trans R Sec Trop Med Hyg 1968; 62 : 880
4. Edwards GA Domm BM Human Leptospirosis. Medicine 1960; 39 : 117-
56.
5. Ooi BS, Beatrice TM, Chen TM et al. Human renal Leptospirosis. AM JI
Trop Med Hyg 21 : 336-41.
6. Krishnamurthy MV, Madanagopalan N, Tajmal Hussain A. Leptospirosis
in Madras. J Assoc Physicians India 1965; 13 : 737-40.
7. Ratnam S, Subramaniam S, Madanagopalan N, Sundaraj T, Jayanthi V.
Isolation of leptospiras and demonstration of antibodies in human
Leptospirosis in Madras, India. Transaction of the Royal Society of
Tropical Medicine and Hygiene 1983; 77 : 455-8.
8. Jayanthi V, Ratnam S, Madanagopalan N, Ramachandran MS,
Subramaniam S. Clinical Profile of Leptospirosis. Tropical
gastroenterology 1983; 4 : 100-3.
9. Muthusethupathi MA, Shivakumar S, Damodaran K. Management of renal
failure in India. J Assoc Physicians India 1985; 33 : 647-9.
JAPI, 1987, VOL. 35, NO.9 631 - 633

59
ARTICLE 11
LEPTOSPIRAL RENAL FAILURE IN MADRAS CITY (1988)
M.A. MUTHUSETHUPATHI, S. SHIVAKUMAR, SUGUNA RAJENDE RAN,
R. VIJAYAKUMAR, M. JAYAKUMAR
Madras Medical College & Government General Hospital, Madras.
Abstract
Eighteen patients with acute renal failure due to Leptospirosis were
encountered in November – December 1988. All patients had fever, Myalgia and
jaundice. The levels of blood urea and serum creatinine (mean ± SD) were 149.06
± 53.58 mg/dl and 4.8 ± 2.05 mg/dl respectively. Marked elevation of bilirubin
with near normal transaminases was characteristic. All patients had a positive
microscopic agglutination test for Leptospirosis. In five patients, leptospira were
isolated from urine by culture. L. icterohaemorrhagiae was the commonest
serogroup observed. Penicillin and conservative measures were adequate in 8
patients. Ten patients needed dialysis. Three patients (16.6%) died.
Key Words : Leptospirosis, Acute renal failure.
INTRODUCTION
Leptospirosis is an important cause of acute renal failure (ARF) in
Madras City.1 It usually occurs during and after the monsoon. This is a public
health problem of great importance as it affects people of various occupations and
can be prevented by taking appropriate measures.2 In this article, we report our
experience with leptospiral is ARF which occurred in November – December
1988.
INDIAN JOURNAL OF NEPHROLOGY NEW SERIES VOL 1 NO.1 JAN-MARCH 1991 15 - 17

Profile of Human Leptospirosis
60
MATERIAL AND METHODS
Leptospiral ARF was diagnosed according to the following criteria:
1. Abrupt decline in glomerular filtration rate (GFR) shown by progressive
elevation of plasma urea (> 40mg/dl) and plasma creatinine (> 2mg/dl),
2. Presence of jaundice,
3. Presence of any one of the following:
a. Positive leptospiral culture from blood or urine
b. Positive micro-agglutination test for leptospira in significant or
rising titre. These tests were done by the method of Turner.3-5
After establishing the diagnosis, patients were started on conservative
treatment, including maintenance of fluid and electrolyte balance and
administration of benzyl penicillin one million units four times a day. Peritoneal
dialysis (PD) was done in severe renal failure. Hemodialysis was done if there
was a contraindication to PD or if the patient was in hyper catabolic ARF.
RESULTS
18 patients had leptospiral ARF. There were 13 males. Mean age was 39
years (range 15 – 70 yrs). The clinical features are shown in Table I. Important
biochemical parameters and agglutination titres are given in Table II.
Renal failure was severe (plasma creatinine > 5mg/dl) in 9 patients.
Jaundice was characterized by high serum bilirubin with normal or mildly elevated
oxaloacetic and pyruvate transaminase levels. Positive urine culture for leptospira
was obtained in 5 patients. All patients demonstrated significant and rising
agglutination titres. The serogroups isolated are shown in Tamble III. All patients
were seen during the monsoon months (November – December). There was no
relationship to any specific occupation. Peritoneal dialysis was done in 10
patients, one of whom needed hemodialysis. Three patients (16.6%) died.
INDIAN JOURNAL OF NEPHROLOGY NEW SERIES VOL 1 NO.1 JAN-MARCH 1991 15 – 17

61
TABLE I
Symptoms and Signs of 18 patients with leptospiral ARF
No PERCENT Fever 18 100 Jaundice 18 100 Myalgia 18 100 Oliguria 14 77.7 Conjunctival suffusion 13 72.2 Vomiting 13 72.2 Hypovolemia 8 44.4 Altered Sensorium 8 44.4 Hematuria 6 33.3 Meningeal irritation 4 22.2 Diarrhoea 4 22.2 Arthralgia 4 22.2 Hypotension 4 22.2 Anuria 1 5.5 Pleural Effusion 1 5.5 Splenomegaly 1 5.5
TABLE II
Biochemical parameters and agglutination titres
Mean SD
Blood Urea (mg/dl) 149.06 53.58 Plasma creatinine (mg/dl) 4.8 2.05 S.Bilirubin (mg/dl) 16.87 8.17 Direct 11.78 5.46 SGOT (IU) 41.13 20.69 SGPT (IU) 28.13 19.4 Alk. Phosphatase (KA units) 16.65 10.57 Leptospiral agglutination titre Initial Repeat
480.00 1536.00
389.4
712.67
INDIAN JOURNAL OF NEPHROLOGY NEW SERIES VOL 1 NO.1 JAN-MARCH 1991 15 –1 7

Profile of Human Leptospirosis
62
TABLE III
Microbiology
Urine Culture Microscopic agglutination test (MAT) L. Icterohaemorrhagiae - 4 L. Icterohaemorrhagiae - 12 L. Autumnalis - 1 L. Canicola - 4 L. Autumnalis - 2
DISCUSSION Leptospirosis is a zoonosis caused by Leptospira interrogans. There are
19 serogroups6. The clinical features vary from a mild anicteric illness
characterized by fever, Myalgia and Conjunctival suffusion, to a severe illness in
which jaundice, renal failure and meningitis occur. It is transmitted to man by
contact with infected urine or water contaminated with infected urine.
In Madras City, Leptospirosis is commonly observed during the monsoon
months and is transmitted by rodents such as bandicoots7. It has also been
reported in domestic animals, such as dogs, cattle, goat, sheep and buffaloes8,9.
Studies have revealed that the common serogroups are L. autumnalis and L.
icterohaemorrhagiae though other groups such as L.Pomona and L. canicola are
also known to occur.10-12 India is predominantly an agricultural country which
provides the most important factors necessary for survival of leptospira, namely,
animals and water. It has been reported from other parts of the country such as
Kerala, Calcutta and Bombay.13-17 But it has not been well documented in other
regions because of lack of facilities for diagnosis.18
Renal involvement is the most serious complication and is the commonest
cause of death. Renal manifestations range from urinary sediment changes
(pyuria, hematuria and granular casts) to renal failure. Renal failure occurs in 44 –
67% of cases. Proteinuria is usually less than 1 gm/day. Leptospira by
INDIAN JOURNAL OF NEPHROLOGY NEW SERIES VOL 1 NO.1 JAN-MARCH 1991 15 -17
63
hematogenous spread reach the peritubular capillaries and migrate to interstitium,
renal tubules and tubular lumen causing interstitial nephritis and tubular necrosis19.
The pathogenesis of impaired renal function is both toxic and ischemic in origin.
Cytotoxic factors are responsible for the toxic injury. Hypovolemia in
Leptospirosis is due to decreased fluid intake, increased fluid loss and increased
vascular permeability caused by chemical mediators released during inflammation.
In addition, increased blood viscosity and low-grade intravascular coagulation
occur. Hypoperfusion may also result from cardiac dysfunction. Renal failure
occurs in the 2nd week but it can occur as early as the 4th day. It may be short lived
or prolonged for up to two weeks.
All the 18 patients in this study had fever, jaundice, Myalgia and ARF.
Oliguria occurred in 14 patients and 6 patients had hematuria. We have
documented in our earlier study that two patients with leptospiral ARF had acute
interstitial nephritis on kidney biopsy1. We have not thought it necessary to do
kidney biopsy in this series because the diagnosis was confirmed by other means
and because of the risk of bleeding.
Most patients with renal failure also have significant hepatic
involvement6. Jaundice occurs between the fourth and sixth day but may occur as
early as second day or as late as the 9th day. Jaundice is partly due to
hepatocellular damage. However, hepatocellular necrosis is usually mild and
additional factors include intrahepatic cholestasis and increased bilirubin load
from absorption of blood from tissue hemorrhage. Death is rarely due to hepatic
failure. In our patients, marked elevation of serum bilirubin with near normal or
mildly elevated SGOT and SGPT levels were characteristic. Serum alkaline
phosphatase was elevated in 7 patients.
INDIAN JOURNAL OF NEPHROLOGY NEW SERIES VOL 1 NO.1 JAN-MARCH 1991 15 – 17

Profile of Human Leptospirosis
64
Laboratory diagnosis involves the isolation of leptospira in culture of
blood and urine and serological tests. Leptospira were isolated in urine culture in
5 patients. Micro agglutination test was positive in significant and rising titres in
all patients. L.icterohaemorrhagiae was the common serogroup in this study
followed by L. canicola and L. autumnalis.
Renal failure could be managed by conservative measures alone in 8
patients. Ten patients were dialysed peritoneally and only one patient required
haemodialysis. This is consistent with out general experience20. Three patients
(16.6%), died which was less than the overall mortality of 27.8% of ARF in our
experience21.
In conclusion, Leptospirosis is an important cause of ARF in Madras
City. The diagnosis is often missed because of inadequate facilities for
confirmation of diagnosis. Establishment of a Central Leptospirosis Reference
Laboratory and making a screening test (microscopic agglutination test) available
in all microbiological laboratories should be taken up urgently to tackle this
problem.
Acknowledgement We express our grateful thanks to both Dr.N.Raghavan, MVSc., DVSM.,
Ph.D. (Edin), Professor and Head, Department of Preventive Medicine and
Mr.K.S.Venkataraman, Ph.D. student of the Madras Veterinary College, Madras
for their valuable help in doing microbiological investigations.
INDIAN JOURNAL OF NEPHROLOGY NEW SERIES VOL 1 NO.1 JAN-MARCH 1991 15 – 17

65
REFERENCES:
1. Muthusethupathi MA, Shivakumar S : Acute renal failure due to
Leptospirosis J Assoc Phys India 35 : 631-3, 1987.
2. Faine S: Guidelines for the control of Leptospirosis. WHO offset
publication 67 : 151-3, 1982
3. Turner LH: Leptospirosis I. Trans R Soc Trop Med Hyg 61 : 842-854,
1967.
4. Turner LH: Leptospirosis II. Trans R Soc Trop Med Hyg 62 : 880, 1968.
1967.
5. Turner LH: Leptospirosis III. Trans R Soc Trop Med Hyg 64 : 623-644,
1970.
6. Sitprija V: Leptospirosis, in Weatherall DJ, Ledingham JGG, Warrell DA
Eds. Oxford Text Book of Medicine, Oxford University Press 1987 : 5 :
327-5 : 331.
7. Ratnam S, Sundararaj T, Subramaniam S : Role of bandicoots in human
Leptospirosis in Madras City – An epidemiological approach. Ind J Pub
Health 30 : 167-168, 1986.
8. Ratnam S, Subramaniam S, Sundararaj T : Evidence of Leptospiral
antibodies among domestic animals in Madras City. Cherion 12 :
176-179, 1983.
9. Ratnam S, Sundararaj T, Subramaniam S: Serological evidence of
Leptospirosis in a human population following an outbreak of the disease in
cattle. Trans R Soc Trop Med Hyg 77: 94-98, 1983.
10. Ratnam S, Sundararaj T, Thiagarajan SP et al: Serological evidence of
Leptospirosis in jaundice and pyrexia of unknown origin. Ind. J Med Res.
77 : 427-430, 1983.
INDIAN JOURNAL OF NEPHROLOGY NEW SERIES VOL 1 NO.1 JAN-MARCH 1991 15 –17
Profile of Human Leptospirosis
66
11. Ratnam S, Subramaniam S, Madanagopalan N : Isolation of Leptospirosis
and demonstration of antibodies in human Leptospirosis in Madras, India.
Trans R Soc Trop Med Hyg 77 : 455-458, 1983.
12. Jayanthi V, Ratnam S, Madanagopalan N et al : Clinical profile of
Leptospirosis. Trop Gastroenterol 4 : 100-3, 1983.
13. Dalal PM : Leptospirosis in Bombay. Ind J Med Sci. 14 : 285-290, 1960.
14. Bhatnagar RK, Sant MC, Jhala H : Prevalence of Leptospirosis in Bombay
– Studies in man and animals. Ind J Path Bact 10 : 324-331, 1967.
15. Joseph KM, Kalra SL : Leptospirosis in India. J Med Res 54 : 611-614,
1966.
16. Das Gupta BM : Further observation of leptospiral infection in Calcutta.
Ind Med Gaz 74 : 31-2, 1939.
17. Kumar RS, Varghese PK, Ravindran M, Paulose K : Analysis of mortality
in Leptospirosis in central Kerala. J Assoc Phys India 37 : 7, 1989.
18. Muthusethupathi MA, Shivakumar S : Leptospirosis – need for urgent
action. J Assoc Phys India 37 : 477, 1989.
19. Sitprija V, Pipalanagul V, Metrowidjojo K, et al : Pathogenesis of renal
disease in Leptospirosis – Clinical and experimental studies. Kidney Int
17: 827-836, 1980.
20. Muthusethupathi MA, Shivakumar S, Damodaran : Management of renal
failure in India. J Assoc Phys India 33 : 647-9, 1985.
21. Muthusethupathi MA, Shivakumar S : Acute renal failure in South India. J
Assoc Phys India 36 : 504-506, 1987.
INDIAN JOURNAL OF NEPHROLOGY NEW SERIES VOL 1 NO.1 JAN-MARCH 1991 15 – 17
67
ARTICLE 12
SERODIAGNOSIS OF LEPTOSPIROSIS – A MADRAS STUDY (1994 – 95)
G. SUMATHI, CH.PRADEEP KUMAR SUBUDHI, HELEN P.S. MA NUEL,
KALPANA, S.SHIVAKUMAR, SUGUNA RAJENDRAN AND
M.A.MUTHUSETHUPATHI
Institute of Microbiology and Department of Nephrology, Madras Medical
College, Madras 600 003
ABSTRACT
Sera from patients with clinical suspicion of Leptospirosis during October
1994 to February 1995 were examined by a) Microscopic agglutination test
(MAT) b) Enzyme linked Immunosorbent Assay (ELISA) c) Patoc Slide
agglutination test (PSAT). The diagnosis of current Leptospirosis was may be
a) initial titre of > 1:80 or a four fold rise in the titre of MAT, b) a tire of > 1:40
IgM and above by ELISA, c) a 4+ agglutination titre by PSAT. 66 of 158 patients
showed significant MAT titre – 1:80 in 15, > 1:160 in 48 and 1:40 in 3 patients.
IgM ELISA was positive in all these 66 patients. Only 52 patients (79%) had
positive PSAT.
Key words: Leptospirosis, Microscopic Agglutination Test, ELISA, Patoc Slide Agglutination Test. Leptospirosis is an important zoonosis occurring in Madras City. It
usually occurs during the monsoon months (Oct – Dec).1-3 It has also been
reported from Kerala, Maharashtra, U.P. and Andaman.4 It has probably been
under-reported and under-diagnosed from other parts of the country due to lack of
diagnostic facilities. Laboratory diagnosis involved the isolation of Leptospira in
INDIAN JOURNAL OF MEDICAL MICROBIOLOGY, 13(4)(1995):192-195

Profile of Human Leptospirosis
68
culture of blood and urine and serological tests. The common serological tests
done are genus specific tests (ELISA and PSAT) and serovar specific test (MAT).
The presence of leptospiral antibiotics from previous infections (usually
mild or subclinical) in large proportion of people living in endemic areas
complicates laboratory diagnosis of current illness. Genus specific tests tend to
become positive early in the disease and also revert to negative relatively early;
and are of value in diagnosing current infection. As published data on all these 3
tests together are inadequate, this study has been done to evaluate their efficacy in
the diagnosis of human Leptospirosis.
MATERIALS AND METHODS
One hundred and fifty eight serum samples obtained from patients with
clinical features suggestive of Leptospirosis received at the Microbiology
Department, Madras Medical College during October 1994 – February 1995 were
examined by (a) MAT (b) ELISA (IgM) (c) PSAT.
The MAT was performed with 8 live culture antigens (Autumnalis,
Australis, Canicola, Javanica, Pomona, Icterohaemorrhagiae, Sejroe and Patoc)
using standard microtitre methodology.5-7 The sera were initially screened at
dilutions of 1:20 and those that were positive, were titrated further to the endpoint.
The highest dilution of serum which agglutinated 50% of leptospires under dark
field microscopy was presumed to represent the titre of antibody specific for the
particular serogroup used. When two or more serogroups reacted at the same
(highest) titre, the result was recorded as ‘mixed equal’. Controls were put up for
each one of the batteries of antigens used in the test.
INDIAN JOURNAL OF MEDICAL MICROBIOLOGY, 13(4)(1995): 192-195
69
The ELISA was undertaken using Leptospiraicterohaemorrhagiae
serovar copenhagani, reference strain Wijnberg as antigen to detect specific IgM
antibodies.8-9 The sera were initially screened at 1:20 dilution and if positive were
titrated upto 1:40 and 1:80. Negative and positive controls were put up. It was
read by naked eye. Colour change to a deep purple red was noted for positive
samples.
PSAT was done by mixing a drop of dense suspension of leptospires
(Leptospira biflexa serovar Patoc) with a drop of serum on a slide and rotated on a
rotator (120/min) for 4 minutes.10-11 It was then examined by naked eye for
presence of agglutination. Negative and positive controls were put up.
The following were considered as significant titres, diagnostic of
leptospiral infection.
a. An initial titre of > 1:80 or a four-fold rise in titre of MAT.
b. A titre of > 1:40 IgM by ELISA
c. A 4 + agglutination titre by PSAT
RESULTS
Antibody titres suggestive of current Leptospirosis was obtained in 66 of
the 158 patients. Of these 45 patients provided single serum samples and 21
provided paired sera. The mean age of the patients was 36 years (range 6 – 74
years) and 50 were males (76%). Most of the patients were outdoor manual
workers. The important clinical features are shown on Table 1.
INDIAN JOURNAL OF MEDICAL MICROBIOLOGY, 13(4)(1995):192-195
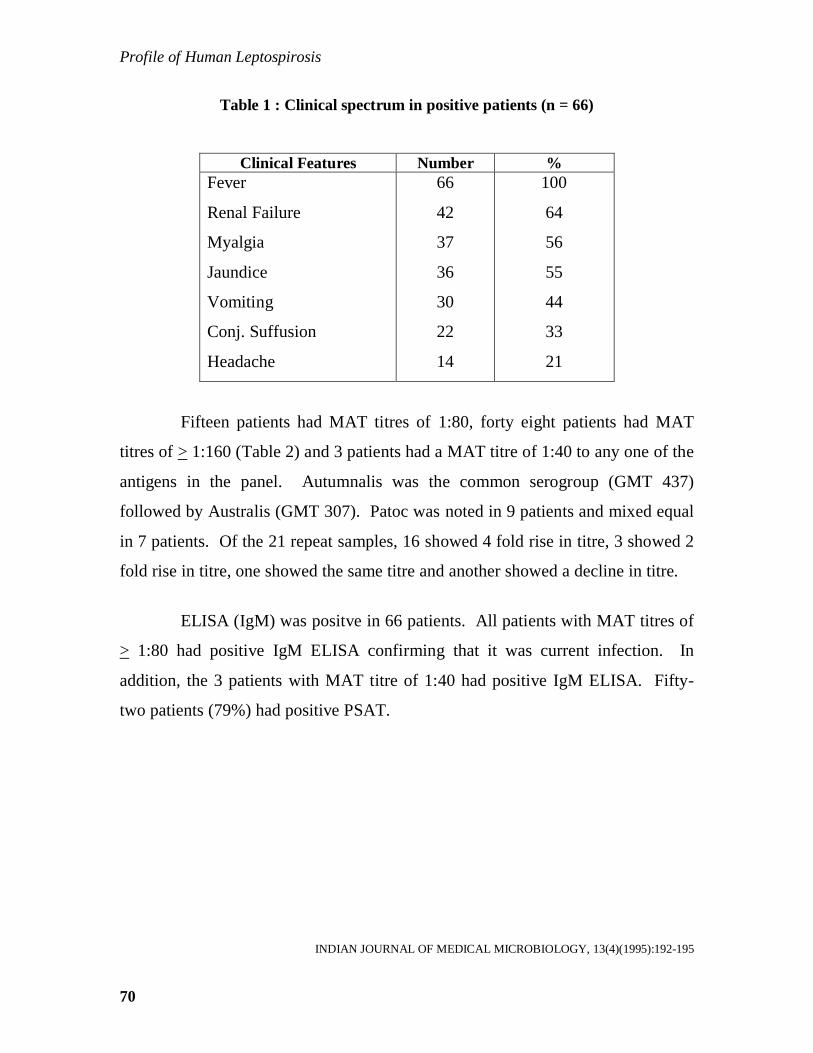
Profile of Human Leptospirosis
70
Table 1 : Clinical spectrum in positive patients (n = 66)
Clinical Features Number % Fever
Renal Failure
Myalgia
Jaundice
Vomiting
Conj. Suffusion
Headache
66
42
37
36
30
22
14
100
64
56
55
44
33
21
Fifteen patients had MAT titres of 1:80, forty eight patients had MAT
titres of > 1:160 (Table 2) and 3 patients had a MAT titre of 1:40 to any one of the
antigens in the panel. Autumnalis was the common serogroup (GMT 437)
followed by Australis (GMT 307). Patoc was noted in 9 patients and mixed equal
in 7 patients. Of the 21 repeat samples, 16 showed 4 fold rise in titre, 3 showed 2
fold rise in titre, one showed the same titre and another showed a decline in titre.
ELISA (IgM) was positve in 66 patients. All patients with MAT titres of
> 1:80 had positive IgM ELISA confirming that it was current infection. In
addition, the 3 patients with MAT titre of 1:40 had positive IgM ELISA. Fifty-
two patients (79%) had positive PSAT.
INDIAN JOURNAL OF MEDICAL MICROBIOLOGY, 13(4)(1995):192-195

71
Table 2 : Antibody titre in micro agglutination test
Serogroup
40
80
160
320
640
1280
2560
5120
*GM
T
TO
TA
L %
Autumnalis -- 4 6 1 12 3 -- 3 437 29 43.9
Australis -- 2 7 2 4 1 -- 1 307 17 25.7
Canicola -- 3 -- -- -- -- -- -- 80 3 4.5
Javanica -- -- -- 1 -- -- -- -- 320 1 1.5
Patoc 2 4 1 2 -- -- -- -- 101 9 13.6
Icterohaemorrhagiae -- -- -- -- -- -- -- -- -- -- --
Sejroe -- -- -- -- -- -- -- -- -- -- --
Pomona -- -- -- -- -- -- -- -- -- -- --
Mixed 1 2 -- -- 4 -- -- -- 238 7 10.6
Total 3 15 14 6 20 4 -- 4 66 100
DISCUSSION
All patients presented with fever. Anicteric Leptospirosis was noted in
only 45% of patients. It has been reported that 90% or more of all cases of
Leptospirosis are anicteric.12 This is probably because the clinical features of
Leptospirosis varies widely and can differ in different geographic regions. Renal
failure was noted in 64% of patients. In Madras City Leptospirosis is an important
cause of renal failure.13
INDIAN JOURNAL OF MEDICAL MICROBIOLOGY, 13(4)(1995):192-195

Profile of Human Leptospirosis
72
MAT is the cornerstone of serodiagnosis. The main advantage is that the
serovar can be identified which is of epidemiological importance. The test is
complicated as it involves the use of a battery of leptospires of widely differing
antigenic structure to cover the spectrum of leptospiral infection and therefore
requires maintenance of stock cultures. Rising titres or initial high titres are
diagnostic of leptospiral infection. These titres begin to rise by end of first week
and peak about third or four week. The high titres of MAT take much longer time
to decline, which is of value for epidemiological surveys. In endemic areas
persisting antibodies may be found in a large proportion of the population, which
may complicate the diagnosis of current infection.14
Autumnalis was the most common serogroup observed in this study.
Mixed equal serogroups suggest the presence of heterologous antibodies. Repeat
titres may have revealed the probable infecting serogroup. Patoc was observed in
9 patients. It is presumed that a serogroup has not been identified by the panel of
MAT. Culture of blood and urine samples will help in identifying the local
serovars which can be subsequently used in the panel for MAT. Autumnalis was
the most common serogroup observed in a seroepidemiological study done in
Madras.15-16
ELISA IgM is now the test of choice for the diagnosis of current
infection. The test detects genus specific antibodies, which tend to become
positive early in the disease (5th day) and also reverts early (60 days). It measures
specific IgM antibodies. Detection of specific IgM antibodies helps in the rapid
diagnosis of current infection. It is a relatively simple test and the antigens can be
prepared from pathogenic leptospires (L. icterohaemorrhagiae) or saprophytic
leptospira (L. biflexa). This test cannot determine the infecting serogroup. A high
titre in a single sample can be diagnostic, though repeat samples may be necessary
if initial titres are low.
INDIAN JOURNAL OF MEDICAL MICROBIOLOGY, 13(4)(1995):192-195

73
ELISA was positive in all the 66 patients. In 45 single samples ELISA
was positive and confirmed the diagnosis of current infection. In all these patients
the MAT titres were > 1:80. In 3 patients ELISA (IgM) was more sensitive in the
diagnosis of current infection. ELISA IgM should be the test of choice for the
diagnosis of current infection.16
PSAT is a simple, satisfactory and quick screening test for those
laboratories which do not have other facilities. In this study PSAT was positive in
52 patients (79%).
It is preferable to have repeat serum samples for diagnosis of
Leptospirosis. If single samples only are available it is essential to do both ELISA
(IgM) and MAT. ELISA (IgM) will help in the diagnosis of current infection and
MAT will give the serogroup. If facilities for ELISA are not available, PSAT
should be done to reveal the current infection.
From the results of this study, it can be concluded that a combination of at
least two serological tests should be carried out for diagnosis of human
Leptospirosis, especially when only single serum samples are available.
INDIAN JOURNAL OF MEDICAL MICROBIOLOGY, 13(4)(1995):192-195

Profile of Human Leptospirosis
74
REFERENCES:
1. Krishnamurthy MV, Madanagopalan N, Tajmal Hussain AT. Leptospirosis
in Madras. J Assoc Physicians India 1965; 13 : 737-40.
2. Muthusethupathi MA, and Shivakumar S. Acute renal failure due to
Leptospirosis. J. Assoc. Phy India (1987) 35:631-633.
3. Muthusethupathi MA, Shivakumar S, Rajendran S, Vijayakumar R and
Jayakumar M. Leptospirala renal failure in Madras City. Ind J Neph (New
series) (1991)1:15-17.
4. South Asian Workshop on Diagnostic methods in Leptospirosis (Madras)
(1995):49-80.
5. Cole JR, Sulzer CR, Pursell AR. Improved micro technique for the
leptospiral microscopic agglutination test. Applied Microbiology.
(1973)25:976.
6. Sulzer CR and Jones WL. Leptospirosis: methods in laboratory diagnosis
(Revised edition – reprinted) U.S.Department of Health,education and
welfare, Public Health Service, Centres for Disease Control, Atlanta,
Georgia HEW Publications No(CDC)(1978):79-8275.
7. Wolff JW. The laboratory diagnosis of Leptospirosis. (Thomas,
Springfield, Illinois, USA)(1954).
8. Terpstra WJ, Ligthart GS and Schooner GJ. ELISA for detection of
specific IgM and IgG in human Leptospirosis. Journalof General
Microbiology (1985) 131:377-385.
9. Terpstra WJ, Ligthart GS and Schooner GJ. Serodiagnosis of human
Leptospirosis by ELISA, Zbl. Bakt. Hgy. I Abt. Orig. A (1980)247:400-405.
INDIAN JOURNAL OF MEDICAL MICROBIOLOGY, 13(4)(1995): 192-195
75
10. WHO. Guideline for the control of Leptospirosis. Faine S (ed) WHO offset
publication No.67, Geneva (1982).
11. Joyce D and Coghlan. Leptospira, Borrelia, Mackie and MeCartney
Practical Medical Microbiology, Thirteenth Edition, (Churchill
Livingstone, London) 671.
12. Ralph D. Fegin, Donald C and Anderson. Human Leptospirosis Crit Rev.
Cl Lab. Sci 5:413-467.
13. Muthusethupathi MA, Shivakumar S, Jayakumar M and Rajendran S.
Acute Renal failure in Madras City – Changing profile. Ind J Nehp (New
series) (1993)3:66-70.
14. Everard JD and Everard COR. Leptospirosis in the Caribbean. Reviews in
Medical Microb. (1993)4:114-122.
15. Ratnam S, Everard COR, Alex JC, Suresh B and Thangarju P. Prevalence
of leptospiral agglutinins among conservancy workers in Madras City,
India. Journal of Tropical Medicine and Hygiene (11993)96:41-45.
16. Muthusethupathi MA, Shivakumar S, Suguna R, Jayakumar M,
Vijayakumar R, Everard COR and Carrington DG. Leptospirosis in
Madras – A clinical and Serological study. J Assoc Phy. India
(1995)43:456-458.
INDIAN JOURNAL OF MEDICAL MICROBIOLOGY, 13(4)(1995):192-195

Profile of Human Leptospirosis
76
ARTICLE 13
APPROACH TO LEPTOSPIROSIS IN INDIA S. SHIVAKUMAR INTRODUCTION Leptospirosis has long been considered a rare zoonotic disease where
only sporadic cases being recorded. Since 1980’s the disease has been reported
from various states during the monsoon months in mini epidemic proportions.
Cases have been reported from Kerala, Tamil Nadu, Gujarat, Andamans,
Kartnataka, Maharashtra, Orissa and Bihar.1,2
Leptospirosis has been under reported and under diagnosed from India
due to a lack of awareness of the disease and a lack of appropriate laboratory
diagnostic facility in most parts of the country. Combining clinical expertise and
awareness with confirmatory laboratory back up dramatically increases the
recognition of patients with Leptospirosis. In this article I shall discuss the
Epidemiology, clinical features, diagnosis and management of Leptospirosis.
EPIDEMIOLOGY
Leptospirosis is an infectious disease caused by leptospira interrogans
complex which has over 20 sero groups and more than 200 serovars. Rodents,
domestic and wild animals, form the reservoir of infection where domestic animals
such as cattle, dogs, pigs may act as carriers for several months (temporary
carrier), rodents usually remain carrier throughout their life (permanent carrier).
Thus rodents are considered the major reservoir of infection.3 Leptospirosis are
MEDICINE UPDATE 699 - 703
77
excreted in the urine of the animals and they affect man when he comes into
contact with urine of infected animals, directly or indirectly, when he is exposed to
an environment contaminated by the urine of the infected animals such as soil and
surface water following monsoon rains. Therefore the illness commonly occurs
during the monsoon. The infection is probably transmitted when they wade
through stagnant rainwater contaminated by infected urine of animals.
These organisms survive for 6 hours in dry soil and for 6 months in
flooded condition. They enter the host through abrasion of the skin (of the feet
when they come into contact with infected water) or intact mucous membranes of
eye, throat, and gut.
Leptospirosis can occur in both urban and rural areas. In urban areas of
developing countries, a contaminated environment due o various factors such as
overcrowded slums, inadequate drainage and sanitation facilities for both man and
animals, presence of stray dogs, cattle pigs, domestic rats, bandicoots, poor
condition of slaughter houses and people walking bare footed, contribute to the
spread of the illness.4,5 In rural areas, high risk groups are workers in rice fields,
cane fields and other agricultural crops and animal husbandry staff. In addition,
workers in sewers mines and military personnel are also at risk.
Person of all ages and races are susceptible. Adult men however are more
frequently infected because they tend to work in high-risk jobs. The number of
cases in a region often fluctuates from year to year due to various factors such as
rainfall, flooding and animal infections. Leptospirosis infections tend to occur as
MEDICINE UPDATE 699 - 703
Profile of Human Leptospirosis
78
individual/small cluster of cases or large outbreaks/epidemics. In India, urban
Leptospirosis has been reported from Chennai and Mumbai, while rural
Leptospirosis has been reported from Gujarat, Kerala and Andamans. Non
reporting of Leptospirosis from other states parts of India does not mean that it is
absent in those parts.
CLINICAL FEATURES
Leptospirosis can manifest in many ways. The various syndromes of
presentation are as follows:3,4
1. Anicteric Leptospirosis
2. Icteric Leptospirosis (Weil’s disease)
3. Haemorrhagic fever with renal syndrome
4. Atypical pneumonia syndrome
5. Myocarditis
6. Aseptic meningo-encephalitis
7. Ocular manifestations
The incubation period is 7 – 14 days, but ranges from 2 – 21 days. 90%
or more of all cases of Leptospirosis are anicteric. In general both anicteric and
icteric cases follow a biphasic course ‘septicaemia’ or ‘leptospiremic’ phase.
I. ANICTERIC LEPTOSPIROSIS This can be mild with fever, headache, and body pains or more severe
which is a biphasic illness. The onset is abrupt with chills, rigor, fever
(temperature 30 - 40˚C), severe headache and body pain. The body aches are
severe and most marked in the lower limbs especially thighs and calves. The pain
and weakness make walking difficult. Severe pain in the back, neck, abdomen and
MEDICINE UPDATE 699 - 703

79
upper limbs are frequent. The headache is throbbing and often severe. Anorexia,
nausea and vomiting are frequent and may be associated with constipation or
diarrhoea. Epistaxis may occur during the early stage. Chest pain, dry cough and
haemoptysis may occur. Mental symptoms such as restlessness, confusion,
delirium, hallucination and occasional psychotic behavior may occur. Abdominal
pain and vomiting are frequent. The most characteristic findings on examination
are conjunctival suffusion and severe myalgia. A transient rash can occur. The
‘septicaemia’ phase subsides after 4 – 7 days. The temperature than becomes
normal and the patient feels well. The second or immune phase is characterized
by severe headache due to meningeal involvement, uveitis and low grade fever.
This lasts from 4 to 30 days longer. The biphasic course may not be seen in all
patients.
II. ICTERIC LEPTOSPIROSIS
In some patients, the septicaemic phase instead of subsiding progresses to
a severe icteric illness with renal failure. Meningeal symptoms are frequent, but
are overshadowed by hepatic or renal features. Severe bleeding, hypotension,
cardiac and pulmonary complications are frequent. Death occurs usually due to
renal failure. Sudden death may occur due to massive bleeding, arrhythmias or
cardiac and respiratory failure. In those who are not severely ill, diuresis occurs
and renal failure improves. The fever subsides and the general condition gradually
improves. Some of the important clinical features are:
Kidneys: Renal involvement is the most serious complication and is the
commonest cause of death. Renal manifestations range from urinary sediment
changes (pyuria, haematuria and granular casts) to severe renal failure. Renal
MEDICINE UPDATE 699 - 703

Profile of Human Leptospirosis
80
manifestations are observed commonly in all forms of Leptospirosis regardless of
the severity of disease or of the infecting sero-group. In anicteric patients,
proteinuria, microscopic haematuria and azotaemia have been noted. Proteinuria
is mild and is due to the febrile state. Haematuria may be due to hemorrhagic
diathesis rather than glomerular injury. Azotaemia has been divided into two
groups. The first is characterized by decreased renal perfusion with diagnostic
indices suggesting pre-renal azotaemia, with a good response to fluid
administration. The second is characterized by features consistent with tubular
necrosis, with no response to fluid challenge and has been emphasized that
hemodynamic alterations, (hypotension, volume depletion) responsible for the
former may result in acute tubular necrosis, if uncorrected. In addition, acute
interstitial nephritis may account for renal failure regardless of hemodynamic
state. Renal failure occurs in the second week but it can occur as early as the
fourth day. It may be short lived or prolonged for up to two weeks.
Hypotension: Hypotension is an important complication, noted in patients with
severe Leptospirosis. The causes of hypotension are 1) hypovolaemia secondary
to vomiting, increased insensible water losses and diminished fluid intake; 2)
massive haemorrhage most often gastrointestinal; 3) unidentified vasoactive
endotoxin; 4) widespread vascular injury leading to fluid shifts from intravascular
to extra vascular fluid spaces; 5) myocardial dysfunction and 6) rarely adrenal
haemorrhage.
Liver: Jaundice is the most important clinical feature of the severity of illness.
Jaundice occurs between the fourth to sixth day but may occur as early as the
second day or as late as the ninth day, deepens rapidly, reaching a peak within a
week. The liver is often enlarged and tender. Jaundice is mainly due to
hepatocellular damage. However, hepatocellular necrosis is usually mild and
MEDICINE UPDATE 699 - 703
81
additional factors include intrahepatic cholestasis and increased bilirubin load
from absorption of tissue haemorrhage. Marked elevation of serum bilirubin with
mildly elevated transaminases is characteristic. Death is rarely due to hepatic
failure.
III. HAEMORRHAGIC FEVER WITH RENAL SYNDROME
Bleeding is a constant feature of Leptospirosis and is due to vascular
damage. It is usually mild in anicteric cases but more common is a severe icteric
patient. Bleeding may occur from respiratory, alimentary, renal and genital tracts
and occasionally into sub arachnoid space and adrenal glands. Death may occur
from massive bleeding usually gastrointestinal or into internal organs. This may
be associated with renal failure.
IV. ATYPICAL PNEUMONIA SYNDROME
Severe hemorrhagic pneumonitis may occur usually in the second week,
but occasionally as early as 24 – 48 hours after onset. This may present with
haemoptysis, chest pain, respiratory distress and cyanosis. Massive haemoptysis
may cause asphyxiation. Radiological abnormalities range from single ill-defined
opacity, multiple areas of infiltration to a large area of consolidation. This clears
up within 2 weeks without any residual damage.
V. MYOCARDITIS
Cardiac complications are frequent in severe Leptospirosis. They are
usually mild and are observed as electrocardiographic abnormalities ranging from
low voltage complexes, non specific ST and T wave changes, conduction defects
MEDICINE UPDATE 699 - 703

Profile of Human Leptospirosis
82
and arrhythmias. Atrial fibrillation is the most common arrhythmia observed.
Severe manifestations such as cardiomegaly, cardiac failure and severe
arrhythmias due to hemorrhagic myocarditis are observed. Sudden death may
occur from cardiac failure or arrhythmias. All cardiac abnormalities revert to
normal within 2 to 3 weeks.
VI. ASEPTIC MENINGOENCEPHALITIS
This usually occurs in the immune phase and may present with signs of
meningeal irritation. The CSF shows lymphocyte pleocytosis, raised proteins
(1 – 2 gm/L) and normal sugar. Convulsions, focal neurological deficits, myelitis,
polyneuritis, encephalitis are rare. Prognosis in meninigitic illness is excellent.
VII. OCULAR MANIFESTATIONS
Conjunctival suffusion is a common feature of the septicaemic phase and
is usually associated with conjunctival haemorrhage. There is no inflammatory
exudates and true conjunctivitis does not occur. It usually occurs in the first three
days and lasts for one day to more than a week. It subsides within a week without
any complications. More important is the late complication of anterior uveal tract
inflammation and presents clinically as iritis, iridocyclitis, and rarely as
chorioretinitis. This may occur as early as the second week or may be delayed up
to a year but are more frequent in the first 6 months. Uveitis may be unilateral or
bilateral and the course is variable (i.e. acute benign episode, recurrent episodes or
a chronic process). The ultimate prognosis is good but chronic Uveitis may cause
blindness from cataract formation and hypopyon in the anterior chamber.
MEDICINE UPDATE 699 - 703

83
DIFFERENTIAL DIAGNOSIS Leptospirosis with its varied manifestations may mimic a large number of
diseases processes.
Anicteric leptospirosis is usually misdiagnosed as pyrexia of unknown
origin, viral fever, malaria, enteric fever, influenza or pyelonephritis.
Severe Icteric leptospirosis may be confused with febrile icteric illness such
as a) viral hepatitis, b) septicemia with jaundice and c) malaria. In Leptospirosis the
onset is abrupt. Severe headache, myalgia and conjunctival suffusion are constant
features, and proteinuria is common, whereas in viral hepatitis, onset is gradual,
headache and myalgia are mild and proteinuria and conjunctival suffusion are absent.
Jaundice also occurs in malaria and sepsis.
MEDICINE UPDATE 699 - 703
Jau
ndic
e
R
enal
Fai
lure
Fev
er
Hyp
oten
sion
Con
junc
tival
B
leed
ing
Mya
lgia
Pne
umon
ia
Hea
dach
e
M
yoca
rditi
s
Men
ingi
tis
Uve
itis
SUMMARY OF CLINICAL FEATURES
MILD IMMUNE LEPTOSPIREMIC PHASE SEVERE

Profile of Human Leptospirosis
84
Leptospiral renal failure must be differentiated from renal failure due to
malaria, sepsis and hanta virus.
Hemorrhagic manifestations are noted in infection due to hanta virus. The
diagnosis can be confirmed by microbiological investigations.
In those presenting with Meningitis, leptospirosis has to be differentiated
from bacterial and viral meningitis and encephalitis. Bacterial meningitis can be
confirmed by spinal fluid examinations. Viral meningitis is indistinguishable from
leptospiral meningitis.
Conjunctival suffusion, myalgia and evidence of bleeding suggest the
diagnosis of Leptospirosis and this can be confirmed by the serological tests. In
children, clinical features that are not seen or are rare in adults such as hypertension,
acalculus cholecystitis and pancreatitis can occur.
DIAGNOSIS OF LEPTOSPIROSIS Culture: The isolation of Leptospirosis by culture of blood, CSF and urine is the
most definite way of confirming the diagnosis of Leptospirosis. Unfortunately,
culture of blood does not contribute to an early diagnosis as results come late, weeks
or even months after inoculation of culture medium.
PCR is promising on both sensitivity and specificity, but is complicated and
expensive.
Serology: The serological tests from diagnosis of Leptospirosis have been classified
as serovar specific tests and genus specific tests.
MEDICINE UPDATE 699 - 703
85
Serovar specific tests: Microscopic agglutination test (MAT): MAT is the gold
standard test for diagnosis of Leptospirosis. The main advantage is that serovar can
be identified which is of epidemiological importance. The test is complicated as it
involves the use of a battery of leptospira of widely differing antigenic structure to
cover the spectrum of leptospiral infection. Therefore, it requires the maintenance of
stock cultures. Rising titres or an initial high titre is diagnostic of leptospiral
infection. These titres begin to rise by the end of the first week, peak about the third
or fourth week, therefore are not valuable for the diagnosis of current infection. The
high titres take a much longer time to decline, which is of value for epidemiological
surveys, but the presence of high titres from previous infection complicate the
diagnosis of recent infection.
Genus specific tests: The two common tests are the ELISA & Macroscopic slide
agglutination tests (MSAT). The other tests are latex agglutination test, complement
fixation test and haemagglutination tests. The genus specific tests are the test of
choice for the diagnosis of current infection. These tests are simple, more sensitive
and become positive earlier than MAT. In India ELISA SAT is available. MAT is
available in specialaized microbiological centers.
ELISA : The test detects genus specific antibodies, which tend to become positive
early in the disease (4th and 5th day). Detection of specific IgM antibodies helps in
rapid diagnosis of current infection. Commercial kits are available in India, but they
are expensive.
MSAT : The slide agglutination test is a simple macroscopic test is a simple
macroscopic test in which a drop of the dense suspension of leptospira is mixed with
drop of serum on a slide is examined by the naked eye from agglutination.
MEDICINE UPDATE 699 - 703
Profile of Human Leptospirosis
86
The physicians has to rely on clinical features, characteristic of Leptospirosis for
early diagnosis and start treatment, but should be confirmed by serological tests. At
present, it is adequate to ELISA/SAT to diagnose current Leptospirosis. If MAT is
available, rising titres will help confirm the diagnosis.
MANAGEMENT Chemotherapy: The aims of chemotherapy are to eradicate Leptospirosis and to
prevent complications. Leptospirosis are sensitive to most antibiotics.
Penicillin is the most effective antibiotic when given early. In severe illness large
doses (6 – 8 million units per day) of benzyl penicillin may be given in divided doses,
preferably by IV route, for 5 – 7 days. Fever subsides in 24 – 36 hours.
Ampicillin I g IV qid in severe illness or 500 – 750 mg quid PO in mild illness.
Doxycyline 200 mg / day, Amoxicillin 500 mg qid and Erythromycin 250 mg
quid are effective. Quinolones and Cefotaxime are also effective against
leptospira. Recently there is evidence to suggest that antibiotics are useful even in
the late stages of illness.
Symptomatic and supportive treatment: Of primary importance is the
meticulous attention to fluid and electrolyte balance. Hypovolaemia and
hypotension need prompt and specific treatment with intravenous luids. In patient
With oliguria, if pre renal azotaemia is suspected, prompt diuresis should be
attempted with fluid therapy. Patients who have no response to therapy should be
managed as established renal failure. Headache and myalgia are treated with
analgesics; fever with anti pyretics, restlessness and anxiety with sedatives and
anaemia with blood transfusion.
MEDICINE UPDATE 699 - 703
87
Peritoneal dialysis has been found to be safe, simple and effective procedure for
management of Leptospiral renal failure. If there is contraindication to peritoneal
dialysis, haemodialysis can be done.
PROGNOSIS
Most patients recover. Overall mortality used to be about 15 – 40% and
has been reduced to about 5% with better management. Death is usually due to
renal failure but it can also occur due to massive bleeding or cardiac
complications.
Faine’s Criteria
Faine has evolved criteria for diagnosis of Leptospirosis on the basis of
clinical, epidemiological and laboratory data. Certain necessary modifications
have been made by us to make the diagnosis more practical in Indian institutions.9
The modifications have been made in the epidemiological and laboratory criteria.
The reasons of the modifications are:
1. Laboratory tests are essential for diagnosis. ELISA IgM/SAT are adequate for
the diagnosis of current infection. In MAT is available, rising titres would
confirm the diagnosis and identify the serovars.
2. Epidemiological factors such as rainfall and contact with contaminated
environment are important for diagnosis. Most of the cases of Leptospirosis
are reported in the monsoon or post monsoon season.
3. Clinical features if combined with epidemiological and laboratory data
confirm the diagnosis of Leptospirosis.
Presumptive diagnosis of Leptospirosis is made of: Part A or part A & part B score : 26 or more Part A, B, C (Total): 25 or more A score between 20 and 25 suggests Leptospirosis as possible but unconfirmed
diagnosis.
MEDICINE UPDATE 699 – 703
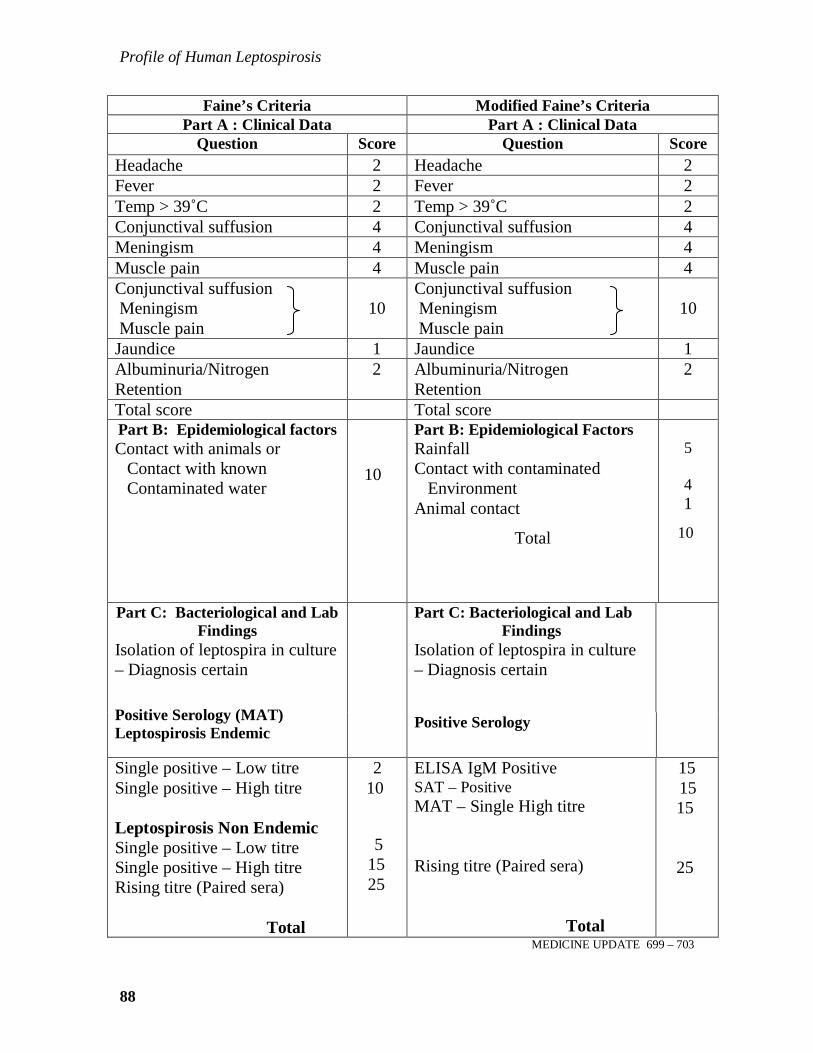
Profile of Human Leptospirosis
88
Faine’s Criteria Modified Faine’s Criteria Part A : Clinical Data Part A : Clinical Data
Question Score Question Score Headache 2 Headache 2 Fever 2 Fever 2 Temp > 39˚C 2 Temp > 39˚C 2 Conjunctival suffusion 4 Conjunctival suffusion 4 Meningism 4 Meningism 4 Muscle pain 4 Muscle pain 4 Conjunctival suffusion Meningism Muscle pain
10
Conjunctival suffusion Meningism Muscle pain
10
Jaundice 1 Jaundice 1 Albuminuria/Nitrogen Retention
2 Albuminuria/Nitrogen Retention
2
Total score Total score Part B: Epidemiological factors Contact with animals or
Contact with known Contaminated water
10
Part B: Epidemiological Factors Rainfall Contact with contaminated Environment Animal contact
Total
5 4 1
10
Part C: Bacteriological and Lab Findings
Isolation of leptospira in culture – Diagnosis certain
Part C: Bacteriological and Lab
Findings Isolation of leptospira in culture – Diagnosis certain
Positive Serology (MAT) Leptospirosis Endemic
Positive Serology
Single positive – Low titre Single positive – High titre Leptospirosis Non Endemic Single positive – Low titre Single positive – High titre Rising titre (Paired sera) Total
2 10 5 15 25
ELISA IgM Positive SAT – Positive MAT – Single High titre Rising titre (Paired sera) Total
15 15 15 25
MEDICINE UPDATE 699 – 703

89
The Faine’s criteria is valuable for diagnosis of anicteric Leptospirosis.
Severe Leptospirosis can be diagnosed by the presence of fever, jaundice and renal
failure. This is the pattern commonly seen in Kerala, Tamil Nadu and Gujarat.
Atypical pneumonia has been reported from Andamans. To conclue, Leptospirosis is
a common cause of fever during monsoon month. There is an urgent need to develop
diagnostic facilities in the country10. By combining clinical, epidemiology and
laboratory data, I hope the clinician would able to diagnose Leptospirosis without
difficulty.
EXAMPLES UTILISING MODIFICED FAINE’s CRITERIA
1. A Patient with fever during the monsoon month with positive ELISA IgM
A Fever 2 B Rain Fall + Contact with
contaminated environment 9
Score
C ELISA IgM positive 15 Score = 2+9+15 = 26 Diagnosis Leptospirosis (confirmed)
2(a) A patient with fever, myalgia and headache in the month of April (Non monsoon period) without contact with contaminated environment
A Fever, Headache, Myalgia 2 + 2 + 4 = 8 B No contact with contaminated
environment 0
Score
C ELISA 1gM positive 15 Score = 8 + 15 = 23
Diagnosis Possible Leptospirosis (Confirm by MAT – raising titres)
MEDICINE UPDATE 699 – 703

Profile of Human Leptospirosis
90
2(b) A patient with fever, myalgia and headache in the month of April (Non monsoon period) with contact with contaminated environment is positive for Leptospirosis ELISA IgM:
A Fever, Headache, Myalgia 2 + 2 + 4 = 8 B Contact with contaminated
environment +(e.g. Infected dog at home) animal contact
4 + 1
Score
C ELISA IgM positive 15 Score = 8 + 5+15 = 28
Diagnosis Leptospirosis (definite)
3. A patient with fever, myalgia and headache in the monsoon and contact with contaminated environment is negative by SAT.
A Fever, Headache, Myalgia 2 + 2 + 4 = 8 B Rainfall + Contact with contaminated
environment 4 + 5 = 9
Score
C SAT – Negative 0 Score = 8 + 9 = 17
Diagnosis Leptospirosis – Negative
MEDICINE UPDATE 699 - 703

91
REFERENCES:
1. Singh J & Sokhey J. Epidemiology, Presentation & Control of Leptospirosis.
Proceedings of the third round table conference. Series-Leptospirosis.
Ranbaxy science foundation(3);1998: 17-31
2. Verma R & Srivastava SK. Leptospirosis in Animals. Prevalence &
Distribution. Proceedings of the third round table conference. Series-
Leptospirosis. Ranbaxy science foundation (3);1998: 49-64
3. Faine S. guidelines for the control of Leptospirosis. WHO offset publication.
1982; 67
4. Everard JD, Everard CM; Leptospirosis in the Caribbean. Reviews in Medical
Microbiology, 1993; 4: 114-22
5. Muthusethupathi MA, Shivakumar S, et al. Leptospirosis in Chennai. A
clinical & serological study. J. Assoc. phys. India. 1995; 43: 450-58
6. Feigin RD, Anderson DC. Human Leptospirosis. CRC Cri Rev lab sci. 1975;
5: 413-67
7. Sumathi G, Chinari Pradeep KS & Shivakumar S MSAT – A screening test for
Leptospirosis .Indian J Med Microbiol(1997) 15:84
8. Chinari Pradeep KS, Sumathi G, Vimala RangaRao G, Shivakumar S
Leptospirosis laboratory. Chennai Medical College – A three year experience
in sero- diagnosis (1995-1997). Indian J Med Microbiol (1999) 17(10): 50-51.
9. Shivakumar S Leptospirosis –Evaluation of clinical criteria J.Assoc Phys India
2003,51:329-330
10. Kamath SA, Joshi SR. Re-emerging of infections in urban India – Focus
Leptospirosis. .J.Assoc Phys India 2003,51:247-248
MEDICINE UPDATE 699 – 703

Profile of Human Leptospirosis
92
ARTICLE 14
LEPTOSPIROSIS IN MADRAS, INDIA – A STUDY OF 206 CASES
(1987 – 95)
M.A. MUTHUSETHUPATHI, S.SHIVAKUMAR
Department of Nephrology, Madras Medical College and Government General Hospital, Madras.
OBJECTIVE:
To study the epidemiological factors, clinical features, diagnosis,
management and prognosis of patients with Leptospirosis admitted in Government
General Hospital, Madras.
PATIENTS & METHODS:
A retrospective analysis of patients admitted with Leptospirosis during
the period 1987 – 1995 was undertaken. Microscopic Agglutination Test (MAT),
ELISA (IgM) and Patoc Agglutination Test (PSAT) were utilized for diagnosis.
RESULTS
206 patients with Leptospirosis were studied. There were 171 males
(83%). Most of them were outdoor manual workers. No specific occupational
risk groups could be identified and there was no geographical clustering. 178
(86%) patients were admitted during the “monsoon” months (Nov. - Dec.). The
important clinical features noted were a) Fever – 100% b) Jaundice – 83%
c) Renal Failure – 79% d) Myalgia – 79% e) Conjunctival suffusion – 43%
f) CNS – 43% g) Bleeding – 28%. Autumnalis was the common serogroup.
First Meeting of the International Leptospirosis Society, Nantes (France) 9 – 13 September 1996

93
Lcterohaemorrhagiae, Canicola, Australis were the other serogroups noted. 102
patients (49.5%) needed dialysis. Peritoneal dialysis was adequate for 83 patients
and 19 patients needed Haemodialysis. 32 patients died (mortality – 15.5%).
CONCLUSIONS:
1. Most patients with Leptospirosis were seen during the “monsoon” months.
2. No specific occupational risk – groups were observed.
3. Jaundice, Renal failure and Myalagia were the common clinical features
noted.
4. Autumnalis was the most common serogroup.
5. Peritoneal dialysis was adequate for most patients with renal failure.
6. The mortality was 15.5%.
LEPTOSPIROSIS CASES DATA (1987 – 1995)
Total cases = 206 Males = 171 (83%)
ANNUAL INCIDENCE
1987 1988 1989 1990 1991 1992 1993 1994 1995 Total 4 21 26 60 48 8 9 6 24 206
MONTHLY INCIDENCE (1987 – 1995)
Jan Feb Mar Apr May June July Aug Sept Oct Nov Dec Total
7 3 -- -- 3 2 1 -- 8 4 110 68 206
First Meeting of the International Leptospirosis Society, Nantes (France) 9 – 13 September 1996

Profile of Human Leptospirosis
94
CLINICAL FEATURES
Fever 100% Jaundice 83%
Renal Failure 79% Myalgia 79%
Conjunctival Suffusion 43% CNS dysfunction 43%
Bleeding 28%
DIALAYSIS DONE
Total = 102 (49.5%)
Peritoneal dialysis = 83
Hemodialysis = 19
MORTALITY = 32 (15.5%)
First Meeting of the International Leptospirosis Society, Nantes (France) 9 – 13 September 1996

95
ARTICLE 15
LEPTOSPIROSIS - CURRENT SCENARIO IN INDIA
S. SHIVAKUMAR
INTRODUCTION Leptospirosis has long been considered a rare zoonotic disease in India with
only sporadic cases being recorded1,2. Since 1980’s the disease has been reported
from various states during monsoon months in mini epidemic proportions. The
disease is endemic in Kerala Tamilnadu, Gujarat, Andamans, Karnataka,
Maharashtra. It has also been reported from Andhra Pradesh, Orissa, West Bengal,
Uttar Pradesh, Delhi & Puducherry.3,4
Leptospirosis has been under reported and under diagnosed from India due to
a lack of awareness of the disease and lack of appropriate laboratory diagnostic
facilities in most parts of the country. Combining clinical expertise and awareness
with confirmatory laboratory back up dramatically increases the recognition of
patients with leptospirosis. Clinical features of leptospirosis vary from mild illness to
severe life threatening illness. Leptospirosis can be diagnosed only by laboratory tests
as the clinical features are nonspecific. But the laboratory tests are complex and hence
definite guidelines for diagnosis of human leptospirosis is necessary. In this article,
the current scenario of leptospirosis in various endemic states of India will be
highlighted and the problems in diagnosis and management will be discussed.
EPIDEMIOLOGY Leptospirosis is an infectious disease caused by leptospira interrogans
complex, which has over 20 serogroups and more than 200 serovars. Rodents,
Medicine Update 2008 Vol. 18 799 – 809

Profile of Human Leptospirosis
96
domestic & wild animals form the reservoir of infection where domestic animals such
as cattle, dogs, and pigs may act as carriers for several months (temporary carrier)
while rodents usually remain carrier throughout their life (permanent carrier). Rodents
are therefore considered as the major reservoir of infection. Leptospires are excreted
in the urine of the animals and they affect man when he comes into contact with urine
of infected animals, directly or indirectly, when he is exposed to an environment
contaminated by the urine of the infected animals such as soil and surface water
following monsoon rains. Therefore this illness commonly occurs during the monsoon
months. The infection is probably transmitted when they wade through stagnant
rainwater contaminated by infected urine of animals. These organisms can survive for
6 hours in dry soil and for 6 months in flooded condition. They enter the host through
the abrasions of the skin of the feet or intact mucous membranes of eye, throat and
gut5.
Leptospirosis can occur in both urban and rural areas. In urban areas of
developing countries, a contaminated environment due to various factors such as
overcrowded slums, inadequate drainage and sanitation facilities for man and animals,
presence of stray dogs, cattle, pigs, domestic rats, bandicoots, poor condition of
slaughter houses and people walking bare foot contribute to the spread of the illness.
In rural areas, high-risk groups are workers in rice fields, cane fields and other
agricultural crops and animal husbandry staff. In addition, workers in sewers mines
and military personnel are also at risk. History of animal contact is not essential for
diagnosis for leptospirosis in developing countries. It is impossible to trace the source
of infection and any person can be infected, irrespective of direct contact with
animals, due to contaminated environment. Therefore the more important
epidemiological factors are rainfall and contact with contaminated environment5.
Medicine Update 2008 Vol. 18 799 – 809

97
Persons of all ages and races are susceptible. Adult men however are more
frequently infected because they tend to work in high-risk jobs. The number of cases
in a region often fluctuates from year to year due to various factors such as rainfall,
flooding and animal infections. Leptospiral infections tend to occur as
individual/small cluster of cases or large outbreaks/epidemics. In India, urban
leptospirosis has been reported from Chennai & Mumbai while rural leptospirosis has
been reported from Gujarat, Kerala and Andamans. Non-reporting of leptospirosis
from other states of India does not mean that it is absent in those parts.
CLINICAL FEATURES Leptospirosis can manifest in many ways.6 The various syndromes of
presentation are as follows.
1. Acute febrile illness
2. Weil’s syndrome characterized by jaundice, renal failure and Myocarditis
with cardiac arrhythmias
3. Pulmonary Haemorrhage with respiratory failure
4. Meningitis / Meningo encephalitis
The incubation period is 7—14 days, but ranges from 2—21 days.
The incidence rate ranges from 0.1 – 1/100,000 per year in temperate climates
to 10- 100/100,000 in tropical countries. During outbreak the incidence may reach
over 100/100,000. Hospital based data on clinical manifestations confirmed by
laboratory tests (Rapid tests / MAT) are usually needed to obtain the incidence rates.
Mild cases may not be admitted to hospitals and hence these data may result in a bias
towards severity in assessing the public health importance of leptospirosis.6
Medicine Update 2008 Vol. 18 799 – 809

Profile of Human Leptospirosis
98
The prevalence rates are obtained from asymptomatic individuals of selected
high risk groups. Sero surveillance provides data on infection rather than as a disease.
MAT is required for sero surveys.
INDIAN SCENARIO The current scenario of leptospirosis in various endemic states will be
discussed. Data from other states will also be analyzed. In addition, the problems in
diagnosis and management will be highlighted.
ANDAMAN AND NICOBAR ISLANDS Andaman and Nicobar Islands are endemic for leptospirosis since early part
of the 20th century. Outbreaks of Andaman Haemorrhagic Fever (AHF) were reported
since 1988.3,7,8 This was proved to be leptospirosis in 1994. 524 cases of AHF
(leptospirosis) were reported from 1988 - 97. The disease presented as febrile illness
with pulmonary haemorrhage during post monsoon periods. As the disease presented
with predominant pulmonary involvement, a Leptospiral etiology was never
considered. In addition, absence of diagnostic facilities were responsible for not
diagnosing leptospirosis7.
During 2000-04, 544 cases were reported in Andamans by disease
surveillance system. There were total of 93 deaths with the highest incidence in
2002.3 At present, Andaman islands has probably the highest incidence rates of
leptospirosis in the country with figures ranging between 50 - 65 cases / 100,000 per
year7.
Medicine Update 2008 Vol. 18 799 – 809

99
In 2005, 58 cases of confirmed leptospirosis were admitted and 14 patients
died [Case Fatality Rate (CFR) - 24.1%]. Majority of deaths were due to pulmonary
haemorrhage and occurred within 48 hours. Rural urban ratio was 46:12 with
exposure to agriculture being 69% and history of contact with animals being 72.4%3.
In 2004, 322 of 611 sera samples from different high risk populations were
positive giving an overall sero prevalence of 52.7%. The sero prevalence was highest
among agricultural workers (62.5 %) followed by sewage workers (39.4%), animal
handlers (37.5%), butchers (30%) and forest workers (27.3%). Among the control
group the sero prevalence was 14.7%. Grippotyphosa followed by Australis were the
common sero groups identified.9
These studies were done at the Regional Medical Research Centre (ICMR),
WHO Collaborating Centre for Diagnosis Reference, Research and training in
leptospirosis which is situated in Andaman and Nicobar Islands.
GUJARAT The disease is endemic in south Gujarat since 1994.3,10,11 The endemic
districts are Valsad, Navsari and Surat. Cases are seen during the monsoon months.
The annual data of leptospirosis in Gujarat are shown in Table 1 which shows yearly
fluctuations in numbers with the highest CFR in 2005 (20.6 %).3,11
TABLE 1 : Year wise cases & deaths due to leptospirosis in South Gujarat
Year 1997 1998 1999 2000 2001 2002 2003 2004 2005
Cases 657 515 357 156 4 37 373 630 392
Death 76 40 32 16 0 6 40 92 81
CFR % 11.5 7.77 8.96 10.26 0 16.2 10.7 14.6 20.66
Medicine Update 2008 Vol. 18 799 – 809

Profile of Human Leptospirosis
100
In the year 2005, 392 cases and 81 deaths due to leptospirosis were reported
from various districts of south Gujarat (Table 2). There were 310 males and 82
females, mostly in the age group of 26 - 45 year.11 Jaundice, renal failure and
haemorrhagic pneumonitis were the common complications noted.
TABLE 2: Summary of Leptospirosis cases and associated deaths in the year 2005
Districts Cases Deaths CFR Taluks PHCs Villages
Surat 185 43 23.24 10 41 123
Navsari 114 26 22.80 5 31 70
Valsad 88 11 12.50 5 25 58
Bharuch 2 0 0 2 2 2
Gandhinagar 2 1 50 2 2 2
Others 1 0 0 1 1 1
Total 392 81 20.66 25 102 256
Based on extensive studies conducted in Gujarat, it was highlighted that
agro-climatic conditions for south Gujarat favour endemicity for leptospirosis.
These include heavy rainfall, clay soil and high water table3.
Public health control measures have been directed towards source
reduction to begin with followed by case reduction and then subsequent reduction
in case mortality. This is achieved through a mulitsectoral approach involving
collaborative work between Department of health, Irrigation, Agriculture, Animal
Husbandry, Tribal Development and Public works3.
Gujarat has a well organized leptospirosis control programme extending
from primary health centre to district hospital / medical college hospitals in
endemic areas. A medical officer at PHC can treat any febrile illness during
Medicine Update 2008 Vol. 18 799 – 809

101
monsoon months with chloroquine and doxycycline. If leptospirosis is suspected,
I.V Penicillin is given. If there is organ dysfunction, he refers them to the nearest
hospital for laboratory diagnosis and management.11
Chemoprophylaxis is given to all persons working in agricultural farms
and those involved in animal husbandry. They are given doxycycline 200 mg once
a week for a period of 6 weeks, during the period of maximum rains and water
stagnation in a particular district. Public awareness is created by Television and
pamphlets at PHCs.11
MAHARASHTRA: Leptospirosis has been reported regularly since 1998.3,12,13 The annual
data from 1998 - 2005 is shown in table 3.
TABLE 3: Year wise cases and deaths due to leptospirosis (1998 - 2005) Year 1998 1999 2000 2001 2002 2003 2004 2005
Cases 197 120 324 860 53 350 225 2355
Deaths 7 3 59 111 5 24 18 167
2355 cases and 167 deaths were reported in 2005, mainly due to large
outbreak during the post monsoon floods. The number of districts in Maharashtra
reporting leptospirosis has expanded from two in 1998 to ten districts in 2005. The
important districts are Mumbai, Thane, Kolhapur, Sangli and Sindhudurg which
are affected by leptospirosis. The serovars isolated were L. icterhaemorrhagie
(rats), L. canicola (canines) and L. australis (cattle).
Medicine Update 2008 Vol. 18 799 – 809
Profile of Human Leptospirosis
102
In a study of 74 cases, haemorrhagic pneumonitis occurred in 35.1 %
cases. Of the 11 deaths (14.8%), 9 were due to pulmonary haemorrhage.14
Autopsy findings of 62 cases of leptospirosis revealed pulmonary intra alveolar
hemorrhage in 48 cases and renal acute tubular necrosis / acute interstitial
nephritis in 45 cases15.
In a study of ICU admissions, 7.2% of cases were due to leptospirosis
(60/834). Mortality due to leptospirosis was 52% and 95% of these patients needed
ventilatory support for respiratory failure16.
KERALA Leptospirosis is endemic in many areas of Kerala. Kolenchery is in the
midlands of Kerala. In this area leptospirosis was rarely diagnosed before 1987.
Since then a yearly increase in incidence was observed. In a study of 976 cases of
leptospirosis confirmed by culture and / or serological tests, a mortality rate of 5.32
% was observed. Autumnalis, Australis and Icterohaemorrhagiae were the common
serogroups identified17.
In study of 282 cases of leptospirosis from Calicut, hepatic (69.8%), renal
(56.3%) involvement and thrombocytopenia (65.8%) were the common
complications noted. The mortality was 6.03%.18 Sero prevalence in Calicut among
high risk groups was 38.1% (Fishermen – 52.8%, Sanitary workers – 56.2 %,
Agricultural workers - 30 %, and sewarage workers was 28.2%). The rate in healthy
control was 24 %. Pomona, Shermani, Canicola were the common serogroups
identified19.
In a study of leptospirosis from kottayam of 900 cases treated over 10
years, Jaundice - (80%), renal failure (59%), hypotension (20%) were the common
Medicine Update 2008 Vol. 18 799 – 809
103
complications noted. The disease was commonly seen in agricultural workers,
fishermen and oyster shell catchers (82%). 74% were seen during the monsoon
months with a male/female ratio 7:1.20
A model leptospirosis control programme has been formulated by Kerala
state and is awaiting implementation. A state level diagnostic and epidemiology
centre at each district has been established to provide technical leadership with the
aim to reduce the incidence/prevalence of leptospirosis. This is not a separate
programme to control leptospirosis but is integrated with other illness at the district
levels.21
TAMILNADU: Leptospirosis has been reported from Chennai since 1980’s.22,23 The
leptospirosis laboratory at Institute of Microbiology, Madras Medical College was
established in 1994.24 This laboratory receives samples from both government and
private hospitals. Data on leptospirosis from government hospitals during the period
2004 – 2006 is given in Table 4.
TABLE 4: Leptospirosis: Annual data of public sector hospitals - Chennai
(2004-2006):
Year 2004 2005 2006 Leptospirosis 963 1724 2765
There has been a dramatic increase in the number of leptospirosis cases &
during 2006, 2765 cases were reported. The data on leptospirosis from various
major public sector hospitals from Chennai city is given in Table 5.
TABLE 5: Year 2006 - Government hospital data - Chennai ( No. 2765 cases):
Hospital General Hospital
Stanley hospital
Kilpauk MC Hospital
Royapettah Hospital
Children’s Hospital
Leptospirosis 965 511 563 169 557 Medicine Update 2008 Vol. 18 799 – 809

Profile of Human Leptospirosis
104
All the Chennai city government hospitals reported cases of leptospirosis.
Data on leptospirosis in private sector hospitals are not available and therefore the
incidence of leptospirosis is under reported.
During the period 1987 – 91, there were 159 cases of leptospirosis at the
General Hospital, Chennai. There were 108 males and the mean age was 40.1 years.
136 (85%) had jaundice and 120 (75%) had renal failure. 70 patients were dialyzed
and 25 patients died (15.6%).25
In the recent past, acute renal failure due to leptospirosis at general hospital
Chennai has significantly declined from 31% in 1987 – 91 to 7.5% in 1995 – 2004.26
Of the 120 cases of leptospiral ARF during the period 1987 - 91, the highest number
of 45 cases were reported in 1990. Since 1992 there has been a decline in
leptospiral renal failure cases and during a 10 year period from 1995 - 2004 only 84
cases were reported.27
Though severe leptospirosis has declined, mild leptospirosis has increased.
In a collaborative study with Leptospirosis Laboratory, Barbados of 57 cases in
1990 - 91 Jaundice occurred in 84 %, and acute renal failure occurred in 72%. Sero
group Autumnalis was the most common sero group encountered. 26 patients were
dialyzed and 2 patients died.28 In a recent study of 106 cases of leptospirosis from
north Chennai, Jaundice occurred in 17.8% and renal failure occurred in 10.3%
showing a decline in complications. Only two patients were dialyzed and there were
no deaths. Fever, headache, myalgia were the common presentations. Contaminated
environment (95%) and rainfall (50%) were the important epidemiological risk
factors. Icterohaemorrhagiae was the most common serogroup and Autumnalis was
not detected.27
Medicine Update 2008 Vol. 18 799 – 809

105
The reasons for the decline in severe leptospirosis suggested were greater
awareness of disease, availability of better diagnostic facilities and wide spread use
of antibiotics. In addition, serogroup Autumnalis, a virulent serogroup causing
severe leptospirosis has also declined since 1995. The increase in mild leptospirosis
suggest that contaminated environment plays an important role in the persistence
and spread of the disease.27
Leptospirosis is an important cause of acute febrile illness. In a recent study
of 500 cases of fever at government Stanley hospital, leptospirosis was the second
common cause of fever contributing to 17%, following malaria which was 27%. Co-
infection of leptospirosis (48 cases) with malaria (220 cases) occurred in 22% of
cases.29 Co-infection of Malaria and Leptospirosis has been reported from
Chandigarh.30
A sero survey in Chennai revealed a seroprevalence rate of 32.9% (Range
17.8% - 40.5%).31 Uveitis due to leptospirosis has been reported from Madurai.32 A
majority of 73 cases had panuveitis (95.5%), retinal phlebitis (51.4%) and hypopyon
(12.6%).
PUDUCHERRY
In a study of 33 icteric patients from Puducherry, 22 had altered sensorium
and 20 had multiorgan failure and thrombocytopenia. 13 patients died (39.3%).33
KARNATAKA Leptospirosis outbreaks have been reported from 15 districts of Karnataka.
The highest incidence of cases have occurred in Bangalore city, Uttara kannada,
Shimoga, Bidar, Gulbarga, Udupi and dakshina kannada districts. During the year
2004, 152 cases and 11 deaths were reported and during 2005, 224 cases and 19
deaths were reported. Patients responded to treatment with amoxicillin and
paracetamol3.
Medicine Update 2008 Vol. 18 799 – 809
Profile of Human Leptospirosis
106
In study of 733 patients suspected of leptospirosis, 84 (11.45%) were found
positive by ELISA. The important complications noted were hepatic (65%) and renal
failure (63%).
Diarrhoea occurred in 24% of cases. 54.7% were agriculture workers and
55.9% gave history of contact with animals.34
ORISSA: After the cyclone during the October-November 1999, 142 patients with
febrile illness and haemorrhagic manifestations were evaluated. 28 (19.2%) had
evidence of leptospirosis which was confirmed by MAT. 6 were positive by
culture/PCR.35
143 people suspected of leptospirosis in a remote village of Mayurbhanj
district in north Orissa was evaluated by the Orissa Multi-disease Surveillance
System (OMDSS) during the period June - July 2002. The attack rate was 5.95%
(143/2404) and the CFR was 7.69% (11/143). There was exposure to infected water
in a canal which was probably the source of infection.36
OTHER STATES Data from Andhra Pradesh, Uttar Pradesh, West Bengal and Delhi are
becoming available. Evaluation of acute febrile patients in Uttar Pradesh revealed
that 7% had leptospirosis (25/346). 17 of the 25 patients had jaundice.37 In a study
of 55 cases of leptospirosis in Hyderabad, 52% had renal failure and jaundice
occurred in 42%.38 Out of 42 persons with jaundice who were evaluated in Calcutta,
10 (23.8% ) were found positive for leptospirosis.39 75 patients from Delhi with
symptoms of leptospirosis were evaluated, 32 were found positive for leptospirosis
and 5 died.40 180 febrile patients from urban slums of Delhi were evaluated and 27
(15%) were positive for leptospirosis.41
Medicine Update 2008 Vol. 18 799 – 809

107
All the available evidence from endemic states suggests that the disease is
now emerging in India as an important public health problem. Inspite of adequate
knowledge, we do not have an accurate estimate of the disease burden in the
country, as data from many other states is not available probably because of lack of
diagnostic facilities. The importance of early diagnosis and case management should
be emphasized and appropriate modification in approach is essential.3
This should include,
a. Guidelines for simple case definition and empiric therapy in small rural hospitals,
where diagnostic facilities are not available.
b. Diagnosis of leptospirosis utilizing Modified Faine’s Criteria for in patients
admitted to district / teaching hospitals where diagnostic facilities are available.3
DIAGNOSIS OF LEPTOSPIROSIS Laboratory support is needed: 1. To confirm the diagnosis 2. For epidemiological and public health reasons, to determine which serovar caused the infection, the likely source of infection, potential reservoir and its location.
The tests depend on the phase of the infection. During leptospiremic phase
(< 7days) leptospires can be isolated by blood culture and PCR, while in the immune
phase, rising antibodies can be detected by serological tests.
Culture
The isolation of leptospirosis by culture of blood, CSF and urine is the most
definite way of confirming the diagnosis of leptospirosis. Unfortunately, culture of
blood does not contribute to an early diagnosis as results come late, weeks or even
months after inoculation of culture medium, however it is valuable in critically ill
patients who might die in the first week before the development of antibodies.
Medicine Update 2008 Vol. 18 799 – 809

Profile of Human Leptospirosis
108
PCR is promising on both sensitivity and specificity, but is complicated and
expensive. Its value for rapid diagnosis is being evaluated and is used in higher
centres.42,43
Serology
The serological tests for diagnosis of leptospirosis have been classified as
serovar specific tests and genus specific tests.
SEROVAR SPECIFIC TESTS
Microscopic Agglutination Test (MAT)
MAT is the gold standard test for diagnosis of leptospirosis because of its
unsurpassed diagnostic specificity. The main advantage is that serovars can be
identified which is of epidemiological importance. The difficulties in utilizing MAT
are due to the following factors.44
a. The antibody titers rise and peak only in 2nd or 3rd week, making it a less
sensitive test. A study of 108 cases of leptospirosis from Brazil have revealed
that 65% of the first sample were positive by SAT compared to 44% by
MAT.45
b. A four fold rise in titer or seroconversion is the most definitive criteria for
diagnosis of leptospirosis. Therefore a second sample is mandatory, which is
difficult to obtain. In such circumstances, a single high titer in MAT can be
taken as diagnostic criteria. As MAT titers peak and persist for a long time (5 -
10 years), they would interfere with current diagnosis. Therefore many
workers use different criteria.
A titer of 1:100 is taken as significant criteria, but there is controversy on the
single diagnostic titer as they depend on endemicity. In endemic areas, a titer
of 1/100 or 1/200 is considered low; while high titer is usually > 1/400 (some
consider 1/800 or 1/1600 as diagnostic criteria). In non- endemic areas, 1/100
Medicine Update 2008 Vol. 18 799 – 809

109
titer is taken as the diagnostic criteria. It is preferable to do rapid tests along
with single high titers. Positive rapid tests with high titers suggest current
infection while negative rapid tests is probably due to past infection. In
Andamans, a titer of 1/200 is taken as diagnostic titer. Serosurvey in the
asymptomatic high risk group should be done with MAT only and a titer of
> 1/50 can be taken as cut off titer.
c. The test is complicated requiring dark field microscopy and cultures of various
live serovars. This may not be available in small laboratories.
Genus specific tests (Rapid tests)
The common tests are the ELISA, Macroscopic slide agglutination test
(MSAT), latex agglutination test, Dipstick tests (Lepto dipstick, Lepto Tek lateral
flow) and Lepto Tek Dri-Dot test.6,11,44,46,47 The genus specific tests are the tests of
choice for the diagnosis of current infection. These tests are simple, more sensitive
and become positive earlier than MAT. These tests detect genus specific antibodies,
which are shared by pathogenic and saprophytic leptospira. These test become
positive early in the disease (5-6th day) as they detect specific IgM antibodies and
help in the rapid diagnosis of current infection.
LABARATORY CRITERIA FOR DIAGNOSIS OF CURRENT LEPTOS PIROSIS CONFIRMED
1. CULTURE: Positive
2. MAT: a) Seroconversion / 4 fold rise in the titer
PROBABLE
1. Rapid tests: Positive
2. MAT: High titer (Single sample)
The approach to diagnostic tests for leptospirosis is given in Table 6. Medicine Update 2008 Vol. 18 799 – 809
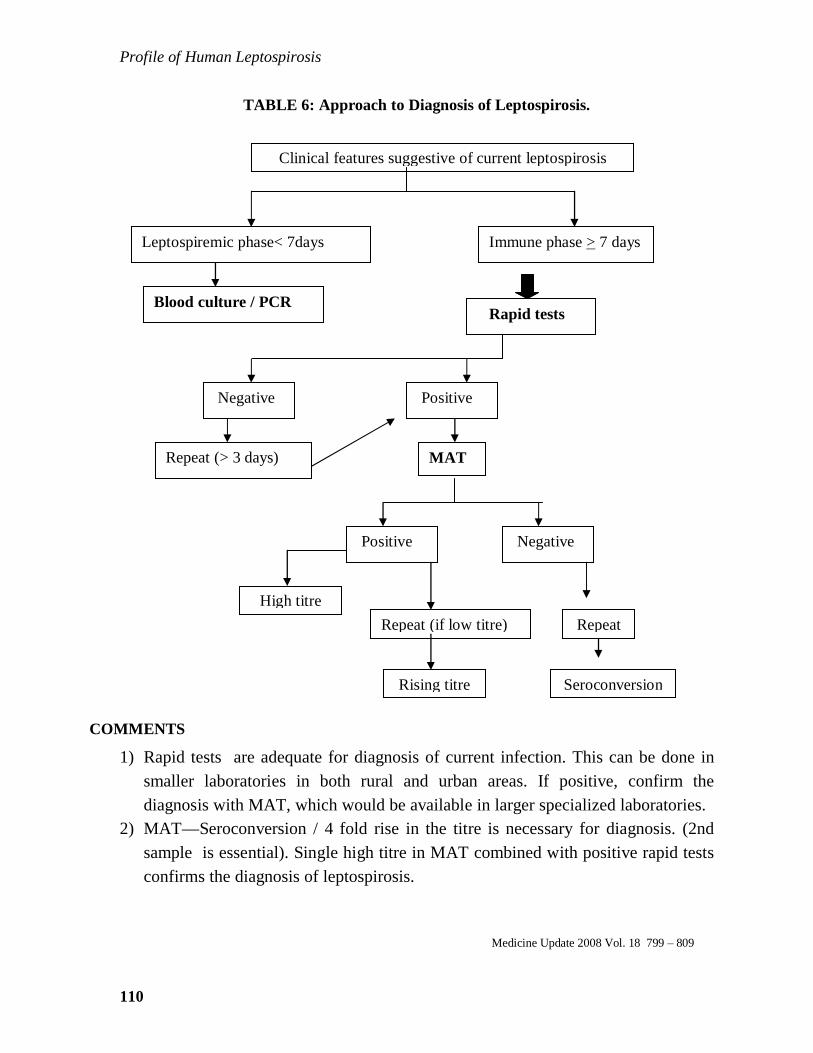
Profile of Human Leptospirosis
110
TABLE 6: Approach to Diagnosis of Leptospirosis.
COMMENTS
1) Rapid tests are adequate for diagnosis of current infection. This can be done in smaller laboratories in both rural and urban areas. If positive, confirm the diagnosis with MAT, which would be available in larger specialized laboratories.
2) MAT—Seroconversion / 4 fold rise in the titre is necessary for diagnosis. (2nd sample is essential). Single high titre in MAT combined with positive rapid tests confirms the diagnosis of leptospirosis.
Medicine Update 2008 Vol. 18 799 – 809
Clinical features suggestive of current leptospirosis
Leptospiremic phase< 7days Immune phase > 7 days
Negative Positive
Positive Negative
Repeat (if low titre)
Rising titre
Repeat (> 3 days)
Blood culture / PCR Rapid tests
Repeat
Seroconversion
High titre
MAT

111
3) Blood culture - not sensitive but can be done in critically ill patient. (As they may
not survive to produce antibodies).
MODIFIED FAINE’S CRITERIA
Faine has evolved criteria for diagnosis of leptospirosis on the basis of
clinical, epidemiological and laboratory data (WHO guidelines).Certain necessary
modifications have been made by us in the epidemiological (Part B) and the
laboratory criteria (Part C) of original Faine’s criteria to make the diagnosis more
practical in Indian institutions. (Shown in Table 7). In the Modified Faine’s Criteria
rapid tests (ELISA / SAT) have been introduced in Part C and Rainfall has been
included in Part B to make the diagnosis early and simple.48,49 This criteria can be
utilized for diagnosis of leptospirosis in district / teaching institutes.3
Medicine Update 2008 Vol. 18 799 – 809
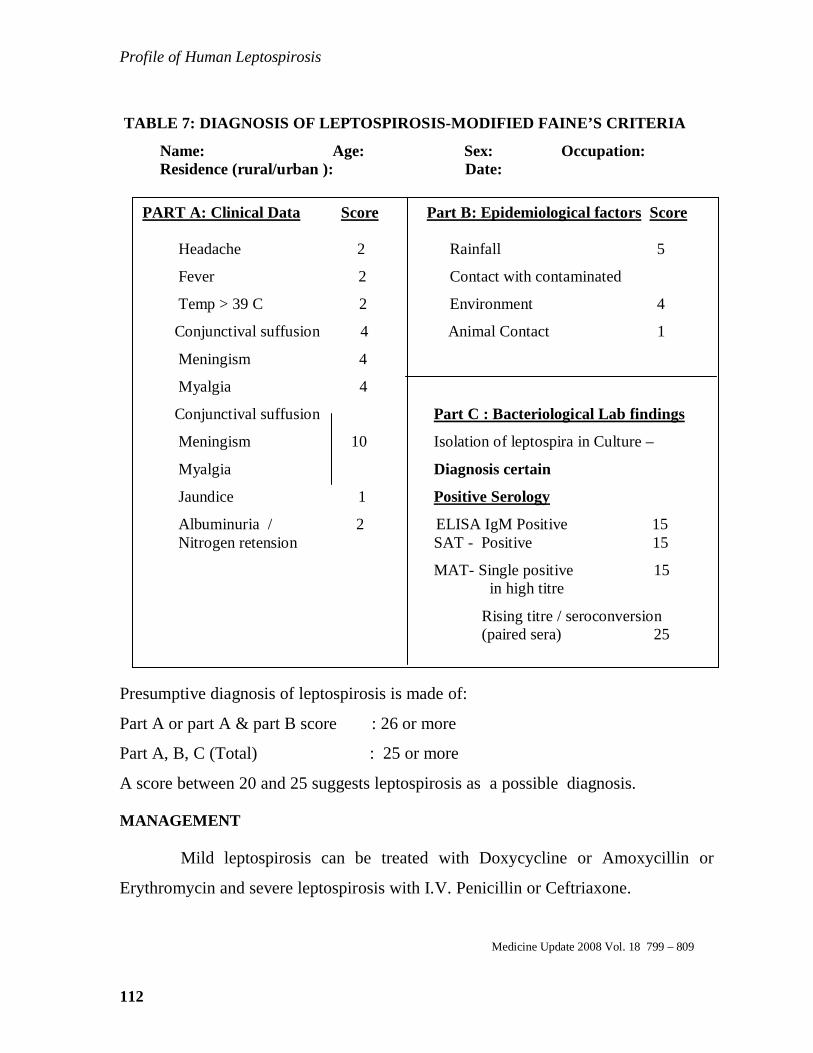
Profile of Human Leptospirosis
112
TABLE 7: DIAGNOSIS OF LEPTOSPIROSIS-MODIFIED FAINE’ S CRITERIA
Name: Age: Sex: Occupation: Residence (rural/urban ): Date:
Presumptive diagnosis of leptospirosis is made of:
Part A or part A & part B score : 26 or more
Part A, B, C (Total) : 25 or more
A score between 20 and 25 suggests leptospirosis as a possible diagnosis. MANAGEMENT Mild leptospirosis can be treated with Doxycycline or Amoxycillin or
Erythromycin and severe leptospirosis with I.V. Penicillin or Ceftriaxone.
Medicine Update 2008 Vol. 18 799 – 809
PART A: Clinical Data Score Part B: Epidemiological factors Score Headache 2 Rainfall 5
Fever 2 Contact with contaminated
Temp > 39 C 2 Environment 4
Conjunctival suffusion 4 Animal Contact 1
Meningism 4
Myalgia 4
Conjunctival suffusion Part C : Bacteriological Lab findings
Meningism 10 Isolation of leptospira in Culture –
Myalgia Diagnosis certain
Jaundice 1 Positive Serology
Albuminuria / 2 ELISA IgM Positive 15 Nitrogen retension SAT - Positive 15
MAT- Single positive 15 in high titre
Rising titre / seroconversion (paired sera) 25

113
RECOMMENDATIONS FOR MANAGEMENT BASED ON THE AVAILAB ILITY OF DIAGNOSTIC FACILITIES In centers where no diagnostic facilities are available (Rural areas) The common causes of acute febrile illnesses are Malaria, Leptospirosis,
Dengue and Viral respiratory diseases. It is difficult to diagnose these illness without
laboratory facilities. It is recommended that all febrile patients can be treated with
doxycycline and chloroquine which is the empiric therapy for Malaria &
Leptospirosis. If there is organ dysfunction and / or fever persists, they should be
transferred to higher centres for further management. This is being implemented in
the state of Gujarat11.
In centres where diagnostic facilities are available
Even in centres with laboratory facilities, empiric therapy is recommended
for leptospirosis where the disease is endemic, since serological tests become positive
only after one week (unless PCR is available). Mild cases can be treated with
chloroquine and doxycycline and severe cases with I.V. crystalline penicillin /
quinine or artemisinin and doxycycline50.If they are admitted later (after a week),
rapid tests would confirm leptospirosis and appropriate treatment can be given. It is
essential that all febrile patients are investigated for leptospirosis, Malaria and
Dengue fever as co-infection can occur29. In addition, dialysis and ventilatory support
for renal and respiratory failure would definitely decrease mortality.
To conclude, data on leptospirosis is urgently needed from all states of the
country. This can be done by making rapid tests available at all district / teaching
hospitals. The National Institute of Communicable Diseases (NICD) utilizing the
Integrated Disease Surveillance Programme (IDSP) should organize the availability
of rapid tests.3 Appropriate guidelines for management should be implemented to
reduce the morbidity and mortality of leptospirosis.
Medicine Update 2008 Vol. 18 799 – 809

Profile of Human Leptospirosis
114
REFERENCES
1. Singh J & Sokhey J. Epidemiology, Presentation & Control of leptospirosis.
Proceedings of the third round table conference. Series-leptospirosis. Ranbaxy
science foundation(3);1998: 17-31
2. Rao RS, Gupta N, Bhalla P et al. Leptospirosis in India and the rest of the world.
Braz J infec Dis 2003; 7(3) 178-193.
3. Report of the Brainstorming meeting on Leptospirosis Prevention and
control.Mumbai, 16- 17 February 2006. Joint Publication by Office of WHO,
Representative to India, New Delhi and Regional Medical Research Centre
(ICMR), WHO Collaborating Centre for Diagnosis, Research, Reference and
Training in Leptospirosis.
4. Kamath SA, Joshi SR. Re-emerging infections in urban India – Focus
Leptospirosis. J.Assoc Phys India 2003,51:247-248
5. Faine S. guidelines for the control of Leptospirosis. WHO offset publication.
1982; 67
6. Terepstra et al. Human Leptospirosis: Guidelines for Diagnosis, Surveillance &
Control {WHO} 2003:1-109
7. SehgalSC, Emergence of leptospirosis as a public health problem. Proceedings of
the third round table conference.Series-leptospirosis.Ranbaxy science
foundation(3);1998: 7-12.
8. Singh SS, Vijayachari P,Sinha A et al. Clinical- Epidemiological study of
hospitalized cases of severe leptospirosis. Indian J Med Research 1999.109:94-9
9. Sharma S, Vijayachari P. Sugunan AP et al. Seroprevalence of leptospirosis
among high risk population of Andaman Islands, India. Am J Trop Med Hyg 74
(2) 2006: 278-283.
10.Clerke AM,Leuva AC, Joshi C et al. Clinical profile of leptospirosis in south
Gujarat. J Post Grad Med 2002. 48: 117-118.
Medicine Update 2008 Vol. 18 799 – 809

115
11.Patel BK, Gandhi SJ, Desai DC. Clinico-epidemiological aspects of leptospirosis
in south Gujarat. .Indian J Med Microbiol 2006 24(4). 322-326.
12.Karande S, Kulkarni H, Kulkarni M et al. Leptospirosis in children in Mumbai
slums. (2002). Indian Journal of Pediatrics 69, 855-858.
13.Karande S, Bhatt M, Kelkar A et al. An observational study to detect
leptospirosis in Mumbai , India 2000. Archieves of disease in childhood.2003.
88( 12) 1070-1075.
14.Bharadwaj R, Bal AM, Joshi SA. An Urban Outbreak of leptospirosis in
Mumbai, India. Jpn J Infect Dis 2002:55.194-196.
15.Saikada AP, Divale S, Deshpande. A study of autopsy findings in 62 cases of
leptospirosis in a Metropolitan city in India. J Post Grad Med 2005. 51: 169-
173.
16.Chawla V , Trivedi TH, Yeolkar. Epidemic of leptospirosis- An ICU experience.
J.Assoc Phys India 2004:32:619-622.
17.Kuriakose M,EapenCK, Paul R. Leptospirosis in Kolenchery, Kerala,India.
Epidemiology, Prevalent local serogroups and serovars and a new serovar.
European Journal of Epidemiology.1997. 13 (6). 691-697.
18.Pappachan MJ,Mathew S,Aravindan KP et al. Risk factors for mortality in
patients with leptospirosis during an epidemic in Northern Kerala. Nat Med J
India 2004; 17:240-2.
19.Swapna RN, Tuteja U, Nair L et al.Seroprevalence of leptospirosis in high risk
groups in calicut, North Kerala, India. .Indian J Med Microbiol 2006 24(4).
349-352.
20.Vimala A , Kasi Visweswaran . Leptospirosis in kottayam. South Asian Work
shop on Diagnostic Methods in Leptospirosis (SAWDIL). Madras.1995:61
Medicine Update 2008 Vol. 18 799 – 809

Profile of Human Leptospirosis
116
21.John TJ. The prevention and control of Human leptospirosis. J Post Grad Med
2005.57: 205-209.
22.Ratnam S, Sundararaj T, Thiagarajan SP et al. Serological evidence of
leptospirosis in Jaundice and Pyrexia of unknown origin. Ind J Med Res. 1983.
77:427-430.
23.Ratnam S, Suramaniam S, Madanagopalan T. Isolation of leptospirosis and
demonstration of antibodies in Human leptospirosis in Madras, India. Trans R
Soc Trop Med Hyg 1983. 77:455-458.
24.Chinari Pradeep KS, Sumathi G, Vimala RangaRao G, Shivakumar S
Leptospirosis laboratory. Chennai Medical College – A three year experience in
sero- diagnosis (1995-1997). Indian J Med Microbiol (1999) 17(10): 50-51.
25.Muthusethupati MA, Shivakumar S, Vijaykumar R et al. Renal involvement in
Leptospirosis- Our Experience in Madras City. J Post Grad
Med1994;40(3):127-31.
26.Jayakumar M, Ram Prabakar H, Edwin Fernando M et al. Epidemiologic trend
changes in acute renal failure – A tertiary centre experience from South India.
Renal Failure 2006; 28:405-10.
27.Shivakumar S. Leptospirosis in Chennai- Changing clinical Profile. J.Assoc Phys
India 2006,54:964-965.
28.Muthusethupathi MA, Shivakumar S, et al. Leptospirosis in Chennai. A clinical
& serological study. J. Assoc. phys. India. 1995; 43: 450-58
29.Loganathan N, Shivakumar S, Ravishankar D.Co-infection of Malaria and
Leptospirosis – A Study of 48 cases (Abstract).62nd Annual Conference of
Association of Physicians of India 2007.Goa.
30.Srinivas R, Agarwal R, Gupta D. Severe sepsis due to severe Falciparum Malaria
and leptospirosis co-infection treated with activated Protein C. Malaria Journal
2007.6:42.
Medicine Update 2008 Vol. 18 799 – 809
117
31.Ratnam S, Evarard COR, Alex JC et al. Prevalence of leptospiral agglutinins
among conservancy workers in Madras City, India. Journal Of Tropical
Medicine and Hygiene 1993; 96:41-45.
32.Rathinam SR, Rathinam S, Selvaraj D et al. Uveitis associated with an epidemic
outbreak of leptospirosis. Am J Ophthalmol 1997;124:71-9.
33.Dutta TK, Christopher M, Leptospirosis – An Overview. J.Assoc Phys India
2005,52:545-551.
34.Jagadishchandra K,Prathb AG, Rao SP. Clinical and epidemiological correlation
of leptospirosis among patients attending KMCH. Indian J Med Sci
2003;57:101-104.
35.Sehgal SC, Sugunan AP, Vijayalakshmi P. Outbreak of leptospirosis after the
cyclone in Orissa. Nat Med J India. 2002.15, 22-23.
36.Jena AB, Mohanty KC, Devadasan N. An outbreak of leptospirosis in Orissa,
India: the importance of surveillance.Tropical Medicine and International
Health 2004.9(9).1016-1021.
37.Manocha H, Gushal V, Singh SK et al. Frequency of leptospirosis in patients of
acute febrile illness in Uttar Pradesh. J.Assoc Phys India 2004,52:623-625.
38.Velineni S,Asuthkar S, Umabala P et al. Serological evaluation of leptospirosis
in Hyderabad,Andhra Pradesh: A retrospective hospital – based study. Indian J
Med Microbiol 2007; 25:24-27.
39.Debnath C, Pal NK, Pramanik AK et al. A serological study of leptospirosis
among hospitalized jaundice patients in around Kolkata. . Indian J Med
Microbiol 2005; 23:68.
40.Chaudhry R, Premalatha MM, Mohanty S et al. Emerging leptospirosis, North
India. Emerging Infectious Disease 2002. 8 (12): 1526-1527.
Medicine Update 2008 Vol. 18 799 – 809

Profile of Human Leptospirosis
118
41.Kaur I, Sachdeva R, Arora V et al. Preliminary survey of leptospirosis among
febrile patients from Urban slums of E.Delhi. J.Assoc Phys India 2003,51:249-
251.
42.Baburaj P, Nandakumar VS, Khanna LV.PCR in the diagnosis of leptospiral
infection. . J.Assoc Phys India 2006,54:339-340.
43.Nizamuddin M, Tuteja V, Shukla J. Early diagnosis of Human leptospirosis by
Antigen Detection in Blood. Indian J Med Microbiol 2006.24 (4):342-345.
44.Shivakumar S, Krishnakumar B. Diagnosis of Leptospirosis- Role of MAT.
J.Assoc Phys India 2006,54:338-339.
45.Angelo P. Brendo et al. Macroscopic agglutination test for Rapid diagnosis of
Human Leptospirosis. Journal of Clinical Microbiology {1998}; 36(11): 3138-
3142
46.Sumathi G, Chinari Pradeep KS & Shivakumar S MSAT – A screening test for
Leptospirosis .Indian J Med Microbiol(1997) 15:84
47.Maskey M, Shastri JS, Saraswathi K. Leptospirosis in Mumbai. Post deluge
outbreak. Indian J Med Microbiol 2006.24: 337-338
48.Shivakumar S Leptospirosis –Evaluation of clinical criteria J.Assoc Phys India
2003,51:329-330
49.Shivakumar S, Shareek PS. Diagnosis of Leptospirosis –Utilizing modified
faine’s criteria.J.Assoc Phys India 2004,52:678-679
50.Kothari MV, Karnad DR,Bichile LS. Tropical infection in ICU. J.Assoc Phys
India 2006,54:291-8.
Medicine Update 2008 Vol. 18 799 – 809
119
Foreword
When Dr. Bichile asked me to write the Foreword to API Medicine Update
2008, I went down the memory lane. When the first meeting of API took place in
1945 I was a 17 years old second year student at the Osmania Medical College in
Hyderabad where Urdu was the medium of instruction. Mine was the last batch of
students who wrote the final MBBS examination papers in 1949 in Urdu. Eleven
years after my graduation my first participation was in APICON 1960 in New Delhi
where I presented a paper on “Sensory Dissociation”. In the APICON 1979 at Chenni
I delivered the Netaji Oration “Never Vistas in Nuclear Medicine” with Dr.BK Naik,
previously my teacher at the Osmania Hospital, as President. During APICON 1984
at Hyderabad, my home-town, my first book “Principles & Practice of Nuclear
Medicine” was released by Dr.BB Tripathy as President. He said he always
remembered my guest lecture at APICON 1968 at Cuttack organized by him, on
Nuclear Medicine and Radio immuno assay. APICON 2008 marks my 48th active
participation, on the verge of my 80th birthday on 16th January 2008. My Guest
Lecture in the CME is on “Information and Communication Technology (ICT) in day-
today clinical practice”.
When the API Medicine Update was started in 1990, the impact of the
Internet was neither felt not anticipated. Today every API member has access to the
Internet by just a click on the mouse. Searching the Internet is now part of my daily
routine. I also have on my table the latest edition of Harrison’s Principles of Internal
Medicine as well as the API Text Book of Medicine, whose utility for me, in
competition with Harrison’s, is determined by how much incremental Indian
experience it provides to me. The legitimate expectation from API Medicine Update
is that it necessarily provides incremental Indian experience. This does not apply to
new concepts, new diagnostic and therapeutic innovations introduced in Medicine.
Every one is always eager to know all about them.
Profile of Human Leptospirosis
120
Medicine Update 2008 Vol. 18 799 – 809
I went through the last 8 API Medicine Updates (2000 to 2007), about 6800
pages produced by 8 editors and over 2000 contributors. I found only about 20%
articles with great incremental value. Another 10% articles had some Indian data
in the text and 1 – 3 Indian references which have marginal incremental value.
Over 65% articles neither had any Indian content in the text nor a single Indian
reference; hence these have zero incremental value. This is “redundant recycling
of information”. Some 5% of the articles represent “futile recycling of
information”, reminding one of the limerick: “The cow kicked Nelly in the belly in
the barn : did not do her any good, did not do her any harm”.
I do not claim my personal assessment to be representative of the
consensus of the API readership. If any editors or contributors are hurt or
offended by my candid appraisal, I offer my sincere apology.
Applying my touch-stone to Medicine Update 2008, again I find 20%
articles with high incremental value. To give a few examples – BM Hegde :
Wavelength analysis of heart rate variability – new method of studying the heart’s
function; S. Shivakumar : Leptospirosis – Current Indian Scenario; M. Ganu
& AS Ganu : Chikungunya an overview : Siddharth Das : Lean T2DM, Profile,
Peculiarities and paradox; SG Godbole : Breaking bad news.
Articles published in JAPI are available on the Internet while articles
published in Medicine Update are not. My suggestion to Dr.Bichile is that during
his tenure as President he initiates steps to bring all high value Update articles
published so far on the Internet. I give below a sample list.
Model Concept articles
� Neuronal control of Aging : Hormonal Signaling and Metabolic pathways
(JS Bajaj 2007)
� Deadly Quartet Revisited (Prakash Deedwania 2000)
Medicine Update 2008 Vol. 18 799 – 809

121
Model Indian Work
� Metabolic Bone Disease. Past present and future challenges (SNA Rizvi
2007)
� Rising prevalence of diabetes in India and the implications of ADA-EASD
concensus on management (R.Ramachandran 2007).
Articles with high Indian Content
� Hyperhomocysteinemia and its implications in atherosclerosis – the Indian
Scenario (GS Sainani et al 2007)
� Epidemiology of Hypertension in India (Rajeev Gupta 2006)
� Emerging Trends and unsolved issues in the management of HCV-Indian
perspective (SN Arya 2006).
� Five decades of nephrology (KS Chugh 2004)
� Falciparum malaria – complications and management (BB Thakur 2001).
� CAD in the young – Indian scenario (Satyawan Sharma 2001)
� Telemedicine at the turn of Millenium (Rissam HS 2000).
Thought provoking articles
� Genes, dreams and realities (BM Hegde 2001)
� Cardiopulmonary manifestations of tobacco : Physician’s role in their
prevention (RS Bhatia 2001)
� National TB control program – involvement of Physician (KJR Murthy
2006)
� Economic burden of Diabetes (Siddharth Shah 2001)
� Changing doctor – patient relationship in 21st Century (YP Munjal 2001)
� Chloroquin in HBV and HCV Hepatitis (M. Chandramohan 2004)
� Demise of the physical examination (Jain & Ingole 2007).
Medicine Update 2008 Vol. 18 799 – 809

Profile of Human Leptospirosis
122
A provocative question – After 18 years of experience should future API
Medicine Updates continue in the present form or can we do better? All of us
appreciate that “The cow is as eager to suckle as the calf is eager to suck”.
Henceforth, if the cow is eager to suckle she should make it worthwhile for the
calf to suck, since the calf has the better option of clicking the mouse!
Dr. R.D. Lele M.B.B.S. (OSM), DTM & H(Eng.), MRCP(Edin.), FRCP(London), FNAMS Hon.DSc. Hon. Chief Physician & Director Nuclear Medicine Dept. Jaslok Hospital & Research Centre Hon. Director of Nuclear Medicine & RIA Dept. Lilavati Hospital & Research Centre Emeritus Professor of Medicine (for life) & Ex-Dean, GMC & Sir J.J.Hospitals, Mumbai Emeritus Professor of the National Academy of Medical Sciences (India)
Medicine Update 2008 Vol. 18 799 – 809

123
ARTICLE 16
LEPTOSPIROSIS LABORATORY, MADRAS MEDICAL COLLEGE:
REVIEW OF OUR EXPERIENCE (2004 – 2006)
G. Sumathi, R Narayanan, S Shivakumar
The Leptospira Laboratory in Madras Medical College at Chennai was
established in 1994. We have already published our experience during the period
1995 – 19971. In this article, we discuss our experience during the period 2004 –
2006, with the samples received from public hospitals in Chennai. There has been
a dramatic increase in the numbers of both samples and of positive cases, probably
because of increased awareness of the illness (Table 1). These samples were from
patients suffering from fever. During 2006, 2765 positive cases were reported
from public sector hospitals. The data of numbers of samples and positive
samples from city hospitals are shown in Table 2. Government Stanley Hospital
(GSH) caters to patients from North Chennai while Government Royapettah
Hospital (GRH) caters to patients from south Chennai. Government General
Hospital (GGH) and Kilpauk Medical College and Hospital (KMC) cater to
patients from central Chennai and the surrounding areas. The Institute of Child
Health (ICH) caters to children from all areas.
Table 1: Year wise distribution of leptospirosis in Chennai (2004-6)
Year No. of samples Postives (%)
2004
2005
2006
Total
6,512
6,909
8,537
21,958
963 (14.7%)
1724 (24.9%)
2765 (32.3%)
5452 (24.8%)
Indian Journal of Medical Microbiology Vol.26. No.2 April-June 2008 p.206 – 207
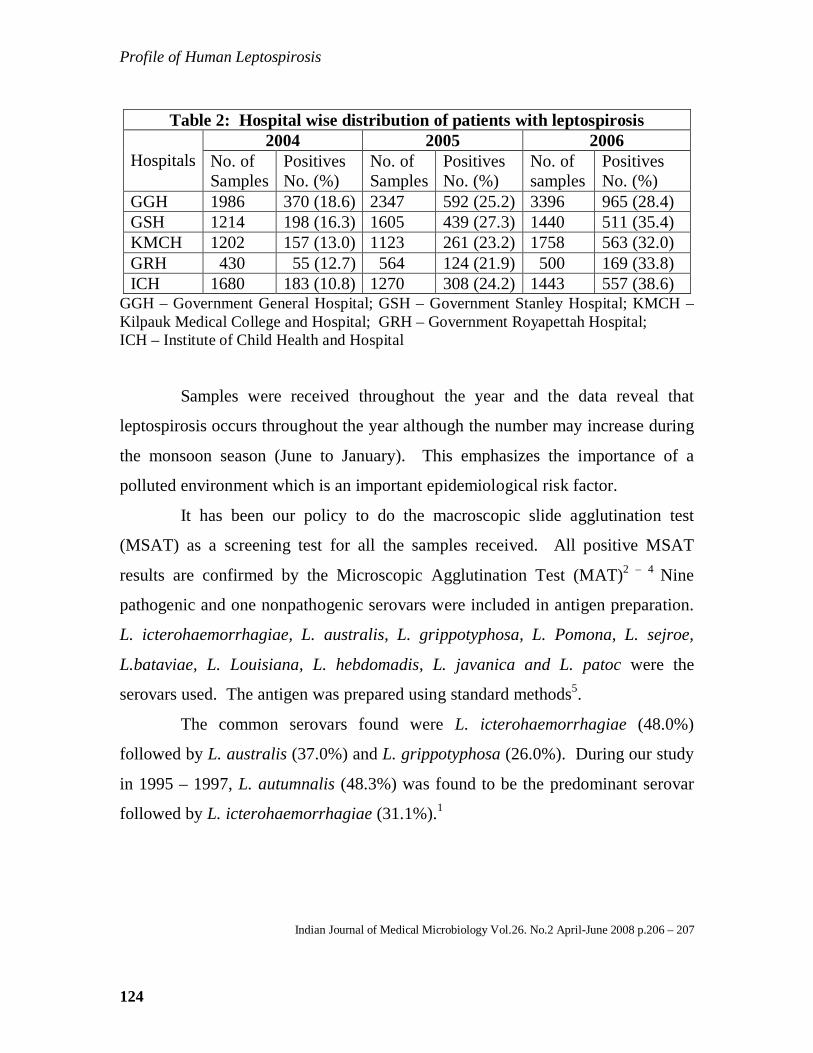
Profile of Human Leptospirosis
124
Table 2: Hospital wise distribution of patients with leptospirosis 2004 2005 2006
Hospitals No. of Samples
Positives No. (%)
No. of Samples
Positives No. (%)
No. of samples
Positives No. (%)
GGH 1986 370 (18.6) 2347 592 (25.2) 3396 965 (28.4) GSH 1214 198 (16.3) 1605 439 (27.3) 1440 511 (35.4) KMCH 1202 157 (13.0) 1123 261 (23.2) 1758 563 (32.0) GRH 430 55 (12.7) 564 124 (21.9) 500 169 (33.8) ICH 1680 183 (10.8) 1270 308 (24.2) 1443 557 (38.6)
GGH – Government General Hospital; GSH – Government Stanley Hospital; KMCH – Kilpauk Medical College and Hospital; GRH – Government Royapettah Hospital; ICH – Institute of Child Health and Hospital
Samples were received throughout the year and the data reveal that
leptospirosis occurs throughout the year although the number may increase during
the monsoon season (June to January). This emphasizes the importance of a
polluted environment which is an important epidemiological risk factor.
It has been our policy to do the macroscopic slide agglutination test
(MSAT) as a screening test for all the samples received. All positive MSAT
results are confirmed by the Microscopic Agglutination Test (MAT)2 – 4 Nine
pathogenic and one nonpathogenic serovars were included in antigen preparation.
L. icterohaemorrhagiae, L. australis, L. grippotyphosa, L. Pomona, L. sejroe,
L.bataviae, L. Louisiana, L. hebdomadis, L. javanica and L. patoc were the
serovars used. The antigen was prepared using standard methods5.
The common serovars found were L. icterohaemorrhagiae (48.0%)
followed by L. australis (37.0%) and L. grippotyphosa (26.0%). During our study
in 1995 – 1997, L. autumnalis (48.3%) was found to be the predominant serovar
followed by L. icterohaemorrhagiae (31.1%).1
Indian Journal of Medical Microbiology Vol.26. No.2 April-June 2008 p.206 – 207

125
Therefore, we conclude that there has been a dramatic increase in the
number of leptospirosis cases reported in our laboratory during the period 2004 –
2006 and the common serovars are L. icterohaemorrhagiae, L. australis and L.
grippotyphosa. We also conclude that leptospirosis in Chennai occurs throughout
the year.
References:
1. Pradeep KS, Sumathi G, Rao GV, Kumar SS. Leptospirosis laboratory,
Chennai Medical College: A three year experience in serodiagnosis (1995
– 1997). Indian J Med Microbiol 1999; 17:50 – 1.
2. Shivakumar S, Krishnakumar B. Diagnosis of leptospirosis: Role of mat. J
Assoc Physicians India 2006;54:338 – 9.
3. Sumathi G, Pradeep KS, Subudhi CH, Helen PS, Kalpana, Shivakumar S,
et al. Serodiagnosis of leptospirosis: A Madras study. Indian J Med
Microbiol 1995;13:192 – 5.
4. Sumathi G, Shivakumar S, Chinari Pradeep KS. MSAT: A screening test
for leptospirosis. Indian J Med Microbiol 1997;15:84.
5. Faine s, editor. WHO Guidelines for the control of leptospirosis. Geneva;
WHO Offset publication No.67; 1982.
Indian Journal of Medical Microbiology Vol.26. No.2 April-June 2008 p.206 – 207