Leptospirosis: An ignored cause of acute renal failure in Taiwan
6
Leptospirosis: An Ignored Cause of Acute Renal Failure in Taiwan Chih-Wei Yang, MD, Ming-Jeng Pan, PhD, Mai-Szu Wu, MD, Yu-Ming Chen, MD, Yu-Tang Tsen, MD, Chun-Liang Lin, MD, Cheng-Hung Wu, MD, and Chiu-Ching Huang, MD 0 Leptospirosis, caused by a spirochete, is the most common zoonosis in domestic or wild animals. Animals excrete infected urine in soil or water and may cause human infections through abrased wound, mucosa, conjunc- tiva, or by swallowing contaminated water. Clinical presentations of leptospirosis are mostly subclinical. Five to ten percent of leptospirosis are fatal, causing fever, hemorrhage, jaundice, and acute renal failure @Veil’s syndrome). Leptospirosis has been ignored as a cause of acute renal failure in Taiwan. We report two patients with lep- tospirosis who presented with high fever, abdominal pain, jaundice, and acute renal failure. Patient 1 died on day 12 of admission of multiple organ failure associated with pancytopenia, hypogammaglobulinemia, and reactive hemophagocytosis. Leptospirosis was recognized after death. Patient 2 was admitted with similar presentations 2 weeks later. Penicillin and doxycycline were given early in the course, and azotemia, jaundice, respiratory failure, and aseptic meningitis gradually improved. Renal biopsy showed interstitial nephritis. Several tubular clearance tests showed proximal tubular defect with severe bicarbonate wasting (FeHCO,- 20.9%) and incomplete type II renal tubular acidosis without affecting the distal nephron. After 80 days of treatment, this patient was discharged with recovery of conscious level and renal function. This is the first leptospirosis patient with detailed tubular functional and morphological studies of the kidney. Diagnosis of leptospirosis was made by microscopic agglutina- tion test (MAT) for antibody to leptospira and by polymerase chain reaction (PCR) for leptospira DNA in blood and urine (interrogans serogroup australis in case 1 and Leptospira borgpetersenii serogroup ballum in case 2). Because active surveillance has resulted in 13 cases diagnosed as leptospirosis islandwide thereafter, underesti- mation and ignorance of leptospirosis as a cause of acute renal failure may occur in Taiwan. Therefore, an area with a low leptospirosis incidence may actually have a very high incidence. Leptospirosis should be suspected in febrile patients with jaundice and renal failure when pathogens cannot be identified by traditional culture for microorganisms. 0 1997 by the National Kidney Foundation, Inc. INDEX WORDS: Leptospirosis; acute renal failure; interstitial nephritis. EPTOSPIROSIS is considered to be the most L widespread spirochetal zoonosis in the world, infecting humans particularly in regions with humid climates. It causes a broad spectrum of clinical manifestations in humans when trans- mitted from animals. The clinical syndromes vary from subclinical infection, self-limited anic- teric febrile illness, to severe and potentially fatal disease. Well’s syndrome, a most severe form of the infection, consists of febrile illness with hemorrhagic tendency, hepatic dysfunction, and acute renal failure. l-3 Risk factors of the infection include occupational exposures, recreational ac- tivities, and household environment with close contacts with animals. Its diagnosis depends on serologic methods, polymerase chain reaction (PCR), and culture of organism from patient’s From the Division of Nephrology, Chang Gung Memorial Hospital, Department of Veterinary Medicine, National Tai- wan University, Taipei, Taiwan, Republic of China. Received February 8, 1997; accepted in revisedform May 23, 1997. Address reprint requests to Chih- Wei Yang, MD, Associate Professor, Division of Nephrology, Chang Gung Memorial Hospital, 199, Tun-Hwa North Rd, Taipei, 105, Taiwan. E- mail: [email protected] 0 1997 by the National Kidney Foundation, Inc. 0272.6386/97/3006-0017$3.00/O blood, urine, or body fluid. Penicillin is the drug of choice for moderate to severe leptospirosis. Oral doxycycline can be used for mild cases.? The kidney is the major target organ, and renal involvement is very common in both icteric and anicteric leptospirosis, but the symptoms are seen only in patients with icterus. Azotemia, oliguria, and anuria commonly occur during the second week of the illness but may appear as early as 3 to 4 days after the onset.3 Despite adequate ther- apy, the cured patients may become carriers or shedders of the pathogens from their urine for several months.’ Both oliguric or nonoliguric forms of acute renal failure have been reported to be associated with high frequencies of hypoka- lemia.4 The cause of hypokalemia is thought to be attributable to the proximal tubular lesion, leading to the decrease in sodium and water reab- sorption. The increase in distal sodium and water delivery may enhance potassium secretion.4*5 In Taiwan, leptospirosis has not been thought of as a common infectious disease, although the first cases were reported 20 years ago.6 The rea- son for the absence of diagnostic cases for the last 20 years was that the diagnostic facilities had not been established for human study. Recently, we have encountered two patients infected by leptospira presented by acute renal failure, which 840 American Journal of Kidney Diseases, Vol 30, No 6 (December), 1&7: pp 640-845
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Leptospirosis: An ignored cause of acute renal failure in Taiwan

Leptospirosis: An Ignored Cause of Acute Renal Failure in Taiwan Chih-Wei Yang, MD, Ming-Jeng Pan, PhD, Mai-Szu Wu, MD, Yu-Ming Chen, MD,
Yu-Tang Tsen, MD, Chun-Liang Lin, MD, Cheng-Hung Wu, MD, and Chiu-Ching Huang, MD
0 Leptospirosis, caused by a spirochete, is the most common zoonosis in domestic or wild animals. Animals excrete infected urine in soil or water and may cause human infections through abrased wound, mucosa, conjunc- tiva, or by swallowing contaminated water. Clinical presentations of leptospirosis are mostly subclinical. Five to ten percent of leptospirosis are fatal, causing fever, hemorrhage, jaundice, and acute renal failure @Veil’s syndrome). Leptospirosis has been ignored as a cause of acute renal failure in Taiwan. We report two patients with lep- tospirosis who presented with high fever, abdominal pain, jaundice, and acute renal failure. Patient 1 died on day 12 of admission of multiple organ failure associated with pancytopenia, hypogammaglobulinemia, and reactive hemophagocytosis. Leptospirosis was recognized after death. Patient 2 was admitted with similar presentations 2 weeks later. Penicillin and doxycycline were given early in the course, and azotemia, jaundice, respiratory failure, and aseptic meningitis gradually improved. Renal biopsy showed interstitial nephritis. Several tubular clearance tests showed proximal tubular defect with severe bicarbonate wasting (FeHCO,- 20.9%) and incomplete type II renal tubular acidosis without affecting the distal nephron. After 80 days of treatment, this patient was discharged with recovery of conscious level and renal function. This is the first leptospirosis patient with detailed tubular functional and morphological studies of the kidney. Diagnosis of leptospirosis was made by microscopic agglutina- tion test (MAT) for antibody to leptospira and by polymerase chain reaction (PCR) for leptospira DNA in blood and urine (interrogans serogroup australis in case 1 and Leptospira borgpetersenii serogroup ballum in case 2). Because active surveillance has resulted in 13 cases diagnosed as leptospirosis islandwide thereafter, underesti- mation and ignorance of leptospirosis as a cause of acute renal failure may occur in Taiwan. Therefore, an area with a low leptospirosis incidence may actually have a very high incidence. Leptospirosis should be suspected in febrile patients with jaundice and renal failure when pathogens cannot be identified by traditional culture for microorganisms. 0 1997 by the National Kidney Foundation, Inc.
INDEX WORDS: Leptospirosis; acute renal failure; interstitial nephritis.
EPTOSPIROSIS is considered to be the most L widespread spirochetal zoonosis in the world, infecting humans particularly in regions with humid climates. It causes a broad spectrum of clinical manifestations in humans when trans- mitted from animals. The clinical syndromes vary from subclinical infection, self-limited anic- teric febrile illness, to severe and potentially fatal disease. Well’s syndrome, a most severe form of the infection, consists of febrile illness with hemorrhagic tendency, hepatic dysfunction, and acute renal failure. l-3 Risk factors of the infection include occupational exposures, recreational ac- tivities, and household environment with close contacts with animals. Its diagnosis depends on serologic methods, polymerase chain reaction (PCR), and culture of organism from patient’s
From the Division of Nephrology, Chang Gung Memorial Hospital, Department of Veterinary Medicine, National Tai- wan University, Taipei, Taiwan, Republic of China.
Received February 8, 1997; accepted in revisedform May 23, 1997.
Address reprint requests to Chih- Wei Yang, MD, Associate Professor, Division of Nephrology, Chang Gung Memorial Hospital, 199, Tun-Hwa North Rd, Taipei, 105, Taiwan. E- mail: [email protected]
0 1997 by the National Kidney Foundation, Inc. 0272.6386/97/3006-0017$3.00/O
blood, urine, or body fluid. Penicillin is the drug of choice for moderate to severe leptospirosis. Oral doxycycline can be used for mild cases.?
The kidney is the major target organ, and renal involvement is very common in both icteric and anicteric leptospirosis, but the symptoms are seen only in patients with icterus. Azotemia, oliguria, and anuria commonly occur during the second week of the illness but may appear as early as 3 to 4 days after the onset.3 Despite adequate ther- apy, the cured patients may become carriers or shedders of the pathogens from their urine for several months.’ Both oliguric or nonoliguric forms of acute renal failure have been reported to be associated with high frequencies of hypoka- lemia.4 The cause of hypokalemia is thought to be attributable to the proximal tubular lesion, leading to the decrease in sodium and water reab- sorption. The increase in distal sodium and water delivery may enhance potassium secretion.4*5
In Taiwan, leptospirosis has not been thought of as a common infectious disease, although the first cases were reported 20 years ago.6 The rea- son for the absence of diagnostic cases for the last 20 years was that the diagnostic facilities had not been established for human study. Recently, we have encountered two patients infected by leptospira presented by acute renal failure, which
840 American Journal of Kidney Diseases, Vol 30, No 6 (December), 1&7: pp 640-845

LEPTOSPIROSIS AND ACUTE RENAL FAILURE 841
was diagnosed with the help of a veterinary diag- nostic facility. Patient 1 died of severe multiple organ failure associated with reactive hemopha- gocytosis, and patient 2 was rescued by the timely diagnosis and treatment. A complete renal functional and morphological study was carried out for patient 2, and the results are reported herein. This is the first report of leptospirosis with detailed tubular clearance studies that may help in understanding the mechanism of tubu- lointerstitial kidney injury by this organism.
CASE REPORT
Case 1: Leptospirosis Associated With Hypogammaglobulinemia, Reactive Hemophagocytosis, and Acute Renal Failure
On May 15, 1996, a 61.year-old homemaker was hospital- ized after 4 days of malaise, gradual onset of abdominal pain, diarrhea, and intermittent fever. She had type II diabetes mellitus for 4 years and had been treated with oral hypoglyce- mic agents irregularly. She also used topical steroid for psori- asis vulgaris for years. She was quite well until 1 week before admission, when fatigue and flulike symptoms appeared.
On admission, she was acutely ill-looking but was con- scious. Body temperature was 39.2”C with mild tachycardia 88 beats/min and normal blood pressure at 130/80 mm Hg. Physical examination showed pale conjunctiva, icteric sclera, abdominal tenderness, splenomegaly, and bilateral pretibial edema. Laboratory test at admission showed a picture of pancytopenia. She was anemic with hemoglobin 10.1 g/dL, and a leukopenia with left shift appearance was found (white blood cell count, 1,300/cm3; 54% segment form neutrophil, 9% band form neutrophil, 22% lymphocyte, 8% monocyte, 2% atypical lymphocyte, 2% myelocyte, and 2% metamyelo- cyte). Thrombocytopenia (platelet count, 41,000/cm3) and prolonged activated partial thrombin time (39.2 s&30.1 set of control) were also noted. Blood chemistry showed the following: blood urea nitrogen/creatinine 86/9.5 mg/dL, aspartate aminotransferase (AST)/alanine aminotransferase (ALT) 190/78 IU/L, and bilirubin direct/total 2.7/4.3 mg/dL with a high alkaline phosphatase 232 mg/dL and gamma- glutamyl transferase 268 mg/dL. The uric acid level also increased to 16.8 mg/dL. In addition, high levels of lactate dehydrogenase (1,516 IU/L), triglyceride (414 mg/dL), and ferritin (9,152 ng/mL) were also noted. Creatinine clearance was 5 ml/mm at admission, and the total urine protein was 0.58 g/day. Urine analysis showed a mild microscopic hema- turia. An increased fractional excretion of sodium (FeNa) to 18% was found. Arterial blood gas showed metabolic acidosis with respiratory compensation (pH: 7.36, pCOZ: 24.5 mEq/ L, pOZ: 73.8 mEq/L, HCO,: 13.8 mEq/L). After admission, intravenous ceftriaxone and metronidazole were given under the impression of sepsis from intraabdominal infection. How- ever, no definite source of intraabdominal infection was found, because the abdominal sonography and computed to- mography showed only mild splenomegaly and suspected infiltrating liver disease. Large and swollen kidneys (left, 12.3 cm; right, 13.2 cm) were detected by renal sonography. Because of the oliguria and severe azotemia, hemodialysis
was started on the day of admission and intermittently there- after. Despite the administration of various therapies, oliguria, nausea, dizziness, severe abdominal pain, and intermittent high fever persisted.
This patient received a series of microbiological, immuno- logic, and virological studies. Blood and urine cultures for aerobic or anaerobic bacteria were negative. Immunologic examinations showed negative results for Venereal Disease Research Laboratory (VDRL) test, Widal test, cold hemag- glutinin, antinuclear antibody (ANA), rheumatic factor, anti- mitochondria antibody, and anti-smooth muscle antibody. Hypogammaglobulinemia was found with concerted low lev- els of serum immunoglobulin (Ig) A (< 7.1 mg/dL), IgG (1.24 mg/dL), IgM (< 7.2 mg/dL), and IgE (< 32.7 IU/mL). The complement levels were normal. Bone marrow biopsy on day 4 of admission showed normal cellularity but with an increased monohistiocytes with hemophagocytic picture compatible with hemophagocytosis. Virological tests were negative for acute hepatitis viruses (A, B, and C), human immunodeficiency virus (HIV), Epstein-Barr virus (EBV), cytomegalovirus (CMV), and herpes simplex virus (HSV). Stool culture was negative for salmonella and shigella.
Because of the worsening jaundice and renal failure, the patient’s urine and blood were sent to the National Institute of Preventive Medicine and the Department of Veterinary Medicine, National Taiwan University, for examinations for the Hanta virus, Ricketsia tsutsugamushi, and Leptospiua on day 7. Oral doxycyclin was supplemented on the same day. Deteriorating general condition, including consciousness, liver function, and hemodynamic status, developed in the following days. On May 26, the 1 lth hospital day, this patient had generalized seizure and became comatose. The blood pressure dropped to 77/40 mm Hg associated with Kuss- maul’s respiration. Despite the intensive treatment, this pa- tient died on day 12 of admission before being diagnosed as leptospirosis. Cerebrospinal fluid study was not done because of the late onset of disturbed consciousness and rapidly devel- oping downhill condition of this patient.
Case 2: Leptospirosis Associated With Interstitial Nephritis, Proximal Tubular Defect, and Acute Renal Failure
A 77-year-old man was admitted on June 7, 1996,2 weeks after the death of the first patient, because of fever, abdominal pain, and consciousness disturbance for a week. He had a history of hypertension and atria1 fibrillation for several years, An episode of right hemispheric infarct occurred 4 years ago and resulted in left hemiparesis. One week before the admission, he began to suffer from progressive abdominal pain, fullness, moderate fever, and delirium with disturbed consciousness that fluctuated with fever. Two days before admission, turbid urine and tarry stool started to appear, and he became oliguric 1 day before admission. Impaired renal function and jaundice were noticed in emergency service, and gastric ulcer bleeding was shown by panendoscopy. On admission, his blood pressure measured 140/92 mm Hg; pulse rate, 105 beats/mm; respiratory rate, 26 breaths/mm; and body temperature was 39.O”C. On examination, he appeared acutely ill, lethargic, and disoriented. Physical examination showed pale conjunctiva, icteric sclera, tender abdomen, and irregular heartbeat.
842 YANG ET AL
Laboratory tests showed the following results: blood leuko- cyte count, 17,000/cm3; hemoglobin, 13.5 g/dL; blood urea nitrogen, 44 mg/dL; creatinine, 1.5 mg/dL; total bilirubin, 6.6 mg/dL; serum sodium, 137 mEq/L; potasium, 3.9 mEq/L. The coagulation profile was normal. Under the impression of sepsis and upper gastrointestinal tract bleeding, he was given intravenous gentamycin and cephalosporin treatment. The an- tibiotics were changed to the third-generation cephalosporin on day 4 because the spiking high fever and disturbed con- sciousness did not improve. Abdominal sonogram showed parenchymal liver disease and a normal spleen size. When a nephrologist was consulted on day 7, the blood urea nitrogen increased to 107 mg/dL and serum creatinine to 8.3 mg/dL. Creatinine clearance was 7.4 mL/min on admission, and urine total protein was 2.8 g/day. Hemodialysis was prescribed because of acute renal failure. Because of the similarity be- tween the two patients, leptospirosis was suspected, and he was immediately given treatments with aqua penicillin 3 mil- lion units every 6 hours intravenously and doxycyclin 100 mg per OS twice daily. This patient’s blood and urine were also examined for Leptospiru in addition to Hanta virus and Rickettsia tsutsugnmushi on day 7. Swollen and markedly enlarged kidneys (left, 14.1 cm; right, 14.2 cm) were found by renal sonography. After the penicillin treatment, however, his general condition did not improve immediately, and he became comatose in consciousness the following day, and respiratory failure developed. He was then transferred to the intensive care unit for ventilatory support. Fever subsided after 4 days of penicillin treatment, and the patient’s general condition gradually improved.
CF+GM
-2 CR0 PCN TC 2
,
10 20 30 40 60 60 70 60
Admission Day
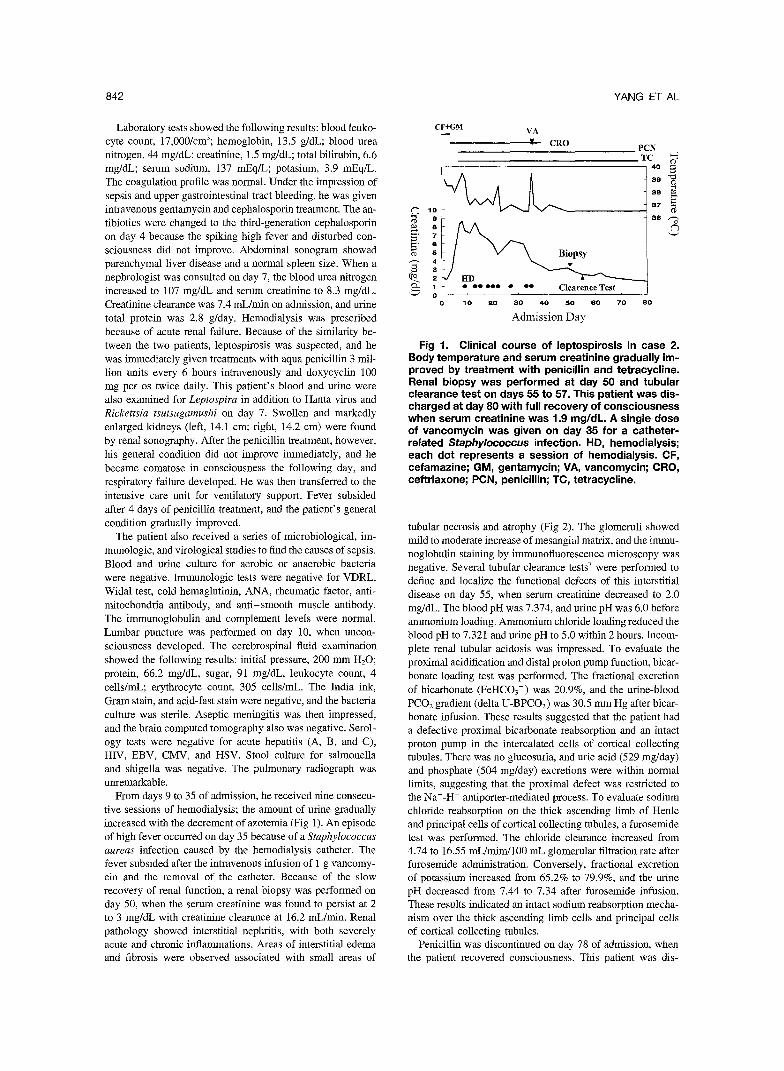
Fig 1. Clinical course of leptospirosis in case 2. Body temperature and serum creatinine gradually im- proved by treatment with penicillin and tetracycline. Renal biopsy was performed at day 50 and tubular clearance test on days 55 to 57. This patient was dis- charged at day 80 with full recovery of consciousness when serum creatinine was 1 .g mg/dL. A single dose of vancomycin was given on day 35 for a catheter- related Staphylococcus infection. HD, hemodialysis; each dot represents a session of hemodialysis. CF, cefamazine; GM, gentamycin; VA, vancomycin; CRO, ceftriaxone; PCN, penicillin; TC, tetracycline.
The patient also received a series of microbiological, im- munologic, and virological studies to find the causes of sepsis. Blood and urine culture for aerobic or anaerobic bacteria were negative. Immunologic tests were negative for VDRL, Widal test, cold hemaglutinin, ANA, rheumatic factor, anti- mitochondria antibody, and anti-smooth muscle antibody. The immunoglobulin and complement levels were normal. Lumbar puncture was performed on day 10, when uncon- sciousness developed. The cerebrospinal fluid examination showed the following results: initial pressure, 200 mm H,O; protein, 66.2 mg/dL, sugar, 91 mg/dL, leukocyte count, 4 cells/ml; erythrocyte count, 305 cells/ml. The India ink, Gram stain, and acid-fast stain were negative, and the bacteria culture was sterile. Aseptic meningitis was then impressed, and the brain computed tomography also was negative. Serol- ogy tests were negative for acute hepatitis (A, B, and C), HIV, EBV, CMV, and HSV. Stool culture for salmonella and shigella was negative. The pulmonary radiograph was unremarkable.
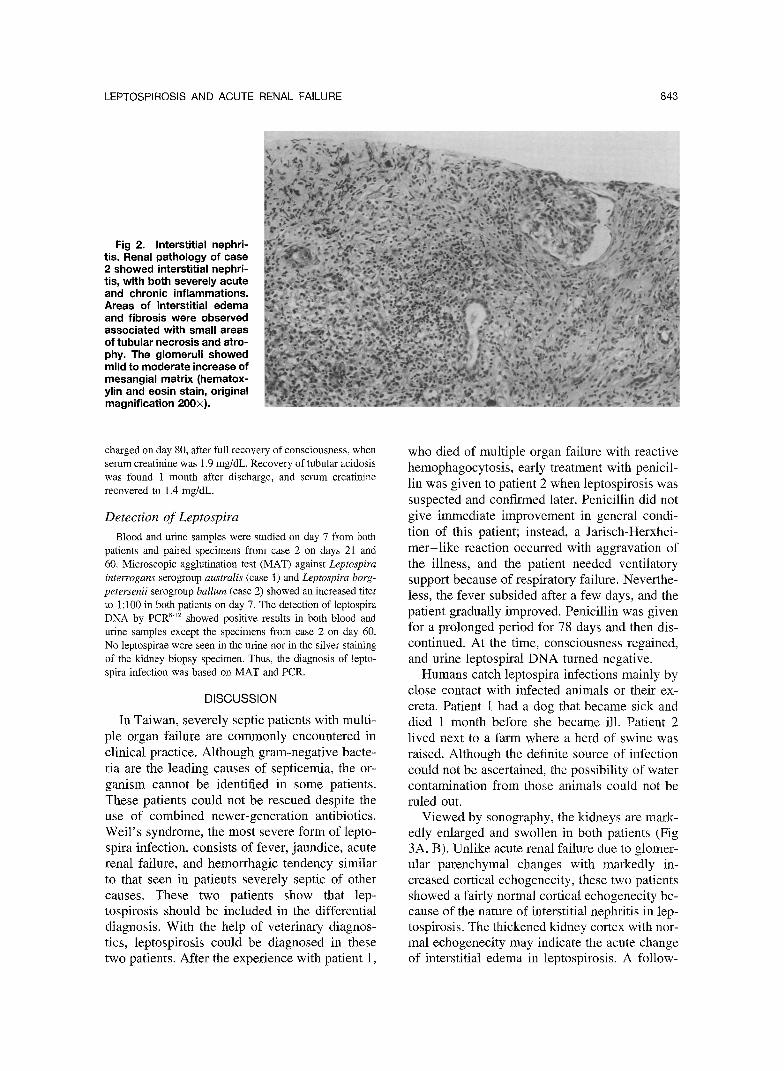
From days 9 to 35 of admission, he received nine consecu- tive sessions of hemodialysis; the amount of urine gradually increased with the decrement of azotemia (Fig 1). An episode of high fever occurred on day 35 because of a Staphylococcus aureas infection caused by the hemodialysis catheter. The fever subsided after the intravenous infusion of 1 g vancomy- tin and the removal of the catheter. Because of the slow recovery of renal function, a renal biopsy was performed on day 50, when the serum creatinine was found to persist at 2 to 3 mg/dL with creatinine clearance at 16.2 mL/min. Renal pathology showed interstitial nephritis, with both severely acute and chronic inflammations. Areas of interstitial edema and fibrosis were observed associated with small areas of
tubular necrosis and atrophy (Fig 2). The glomeruli showed mild to moderate increase of mesangial matrix, and the immu- noglobulin staining by immunofluorescence microscopy was negative. Several tubular clearance tests7 were performed to define and localize the functional defects of this interstitial disease on day 55, when serum creatinine decreased to 2.0 mg/dL. The blood pH was 7.374, and urine pH was 6.0 before ammonium loading. Ammonium chloride loading reduced the blood pH to 7.321 and urine pH to 5.0 within 2 hours. Incom- plete renal tubular acidosis was impressed. To evaluate the proximal acidification and distal proton pump function, bicar- bonate loading test was performed. The fractional excretion of bicarbonate (FeHCOS-) was 20.9%, and the urine-blood PC02 gradient (delta U-BPC02) was 30.5 mm Hg after bicar- bonate infusion. These results suggested that the patient had a defective proximal bicarbonate reabsorption and an intact proton pump in the intercalated cells of cortical collecting tubules. There was no glucosuria, and uric acid (529 mg/day) and phosphate (504 mg/day) excretions were within normal limits, suggesting that the proximal defect was restricted to the Na+-H+ antiporter-mediated process. To evaluate sodium chloride reabsorption on the thick ascending limb of Henle and principal cells of cortical collecting tubules, a furosemide test was performed. The chloride clearance increased from 4.74 to 16.55 mL/mim/lOO mL glomerular filtration rate after furosemide administration. Conversely, fractional excretion of potassium increased from 65.2% to 79.9%, and the urine pH decreased from 7.44 to 7.34 after furosemide infusion. These results indicated an intact sodium reabsorption mecha- nism over the thick ascending limb cells and principal cells of cortical collecting tubules.
Penicillin was discontinued on day 78 of admission, when the patient recovered consciousness. This patient was dis-
LEPTOSPIROSIS AND ACUTE RENAL FAILURE a43
Fig 2. Interstitial nephri- tis. Renal pathology of case 2 showed interstitial nephri- tis, with both severely acute and chronic inflammations. Areas of interstitial edema and fibrosis were observed associated with small areas of tubular necrosis and atro- phy. The glomeruli showed mild to moderate increase of mesangial matrix (hematox- ylin and eosin stain, original magnification 200x).
charged on day 80, after full recovery of consciousness, when serum creatinine was 1.9 mg/dL. Recovery of tubular acidosis was found 1 month after discharge, and serum creatinine recovered to 1.4 mg/dL.
Detection of Leptospira Blood and urine samples were studied on day 7 from both
patients and paired specimens from case 2 on days 21 and 60. Microscopic agglutination test (MAT) against Leptospiru interrogans serogroup australis (case 1) and Leptospira borg- petersenii serogroup ballum (case 2) showed an increased titer to 1:lOO in both patients on day 7. The detection of leptospira DNA by PCR’.” showed positive results in both blood and urine samples except the specimens from case 2 on day 60. No leptospirae were seen in the urine nor in the silver staining of the kidney biopsy specimen. Thus, the diagnosis of lepto- spira infection was based on MAT and PCR.
DISCUSSION
In Taiwan, severely septic patients with multi- ple organ failure are commonly encountered in clinical practice. Although gram-negative bacte- ria are the leading causes of septicemia, the or- ganism cannot be identified in some patients. These patients could not be rescued despite the use of combined newer-generation antibiotics. Weil’s syndrome, the most severe form of lepto- spira infection, consists of fever, jaundice, acute renal failure, and hemorrhagic tendency similar to that seen in patients severely septic of other causes. These two patients show that lep- tospirosis should be included in the differential diagnosis. With the help of veterinary diagnos- tics, leptospirosis could be diagnosed in these two patients. After the experience with patient 1,
who died of multiple organ failure with reactive hemophagocytosis, early treatment with penicil- lin was given to patient 2 when leptospirosis was suspected and confirmed later. Penicillin did not give immediate improvement in general condi- tion of this patient; instead, a Jarisch-Herxhei- mer-like reaction occurred with aggravation of the illness, and the patient needed ventilatory support because of respiratory failure. Neverthe- less, the fever subsided after a few days, and the patient gradually improved. Penicillin was given for a prolonged period for 78 days and then dis- continued. At the time, consciousness regained, and urine leptospiral DNA turned negative.
Humans catch leptospira infections mainly by close contact with infected animals or their ex- creta. Patient 1 had a dog that became sick and died 1 month before she became ill. Patient 2 lived next to a farm where a herd of swine was raised. Although the definite source of infection could not be ascertained, the possibility of water contamination from those animals could not be ruled out.
Viewed by sonography, the kidneys are mark- edly enlarged and swollen in both patients (Fig 3A, B). Unlike acute renal failure due to glomer- ular parenchymal changes with markedly in- creased cortical echogenecity, these two patients showed a fairly normal cortical echogenecity be- cause of the nature of interstitial nephritis in lep- tospirosis. The thickened kidney cortex with nor- mal echogenecity may indicate the acute change of interstitial edema in leptospirosis. A follow-

844 YANG ET AL
Fig 3. Renal sonography. The kidneys at acute re- nal failure are markedly enlarged in both patients. Shown are left kidney size 12.3 cm in case 1 (A); 14.1 cm in case 2 (B). Kidney cortex thickened with low echogenecity indicates marked interstitial edema in leptospirosis. A follow-up renal sonography in case 2 (C) shows a reduction of kidney size (left kidney, 10.8 cm) and appearance of irregular kidney contour after 6 weeks.
up renal sonography in case 2 showed a marked reduction in kidney size (left, 10.8 cm; right, 9.6 cm), and irregular kidney contour was observed during the recovery phase after 6 weeks of treat- ment (Fig 3C). Although it needs to be confirmed by more observations, the characteristic feature of enlarged kidneys with low echogenecity may be an early sign of tubulointerstitial involvement in leptospira infection.
Hemophagocytic syndrome is a group of clini- cal, laboratory, and pathological findings among which hemophagocytosis is prominent in the bone marrow.13 It was first proposed by Risdall et a1,14 who inaugurated the term “virus-associated hemophagocytic syndrome.“14 A multitude of diseases other than viral infections have subse- quently been shown to be associated with this syndrome, which include bacterial, mycobacteria tuberculosis, fungal, and parasitic infections; au- toimmune diseases, and T-cell neoplasm. Reac- tive hemophagocytic syndrome (RHS) is pro-
posed and used broadly later, because of its emphasis on the reactive nature as well as key pathological features.13’15 The common cause of RHS in the Western population is viral infection or malignant lymphoma. On the contrary, the bacterial infection is the major cause of RHS in the Oriental locality.16 In case 1, severe infection associated with leptospira-induced hypogam- maglobulinemia and reactive hemophagocytosis may occur. This is the first case of reactive hemo- phagocytosis associated with leptospirosis.
From animal studies, it is known that the spiro- chetes lodge in the kidney, mainly in the proxi- mal tubular areas.17 In case 2, the cellular infil- tration was diffuse in the tubulo-interstitium; therefore, several simple tubular clearance tests7 were used to verify the integrity of each nephron segment. Proximal bicarbonate reabsorption, which indirectly indicates the proximal sodium- hydrogen exchanger function, was defective in this patient, as suggested by the increased

LEPTOSPIROSIS AND ACUTE RENAL FAILURE 845
FeHC03- after bicarbonate loading. The in- creased chloride clearance after furosemide infu- sion indicated an intact furosemide-sensitive so- dium-potassium-chloride co-transporter located on the thick ascending limb of Henle. The proton pump function on intercalated cells of cortical collecting tubules was normal, as indicated by a normal gradient between urine and blood PCO, after bicarbonate loading. Sodium-dependent po- tassium and proton excretion were increased after furosemide administration. These results indi- cated the presence of functional principal cells on cortical collecting tubules. Taken together, patient 2 had a defect on bicarbonate reabsorp- tion in proximal tubules without affecting the distal nephron, including the thick ascending limb of Henle and collecting tubules. This defect might explain the incomplete proximal renal tu- bular acidosis in this patient. One may question that the defect might come from the residual tu- bular necrosis and is not specific to the lep- tospirosis. We believed that the proximal tubular defect is unique to the leptospirosis, because the sodium-potassium-chloride cotransporter on the thick ascending cells, which is the most fragile segment in acute tubular insults, remained in- tact.” To our knowledge, this is the first report of leptospirosis in which complete tubular func- tional and morphological studies have been con- ducted that may explain the clinical pictures.
After we reported the cases in the monthly meeting of the Infectious Disease Society, Re- public of China, in October 1996 and in the an- nual meeting of the Nephrology Society, Repub- lic of China, in December 1996,19 11 more patients have been diagnosed with leptospirosis with acute renal failure from hospitals around the island by sending specimens to the Department of Veterinary Medicine, National Taiwan Uni- versity. The growing number of leptospirosis cases indicates underestimation and ignorance of the disease in this country. As shown in Hawaii, active surveillance may result in a fivefold in- crease in the incidence of the disease2’; therefore, an area with a low leptospirosis incidence may actually have a very high incidence. Lep- tospirosis should be suspected in febrile patients with jaundice and renal failure even if the patho- gens cannot be identified. Favorable outcome may be anticipated even with severe multiple organ failure if adequate treatment is initiated early.
REFERENCES
1. Alston JM, Broom JC: Leptospirosis in Man and Ani- mals. Edinburgh and London, E & S Livingstone LTD, 1958, pp 4-12
2. Fame S: Leptospira and Leptospirosis. Boca Raton, FL, CRC Press, 1994
3. Farr RW: Leptospirosis. Clin Infect Dis 21: 1-6, 1995 4. Seguro AC, Lomar AV, Rocha AS: Acute renal failure
of leptospirosis: Nonoliguric and hypokalemic forms. Neph- ron 55:146-151, 1990
5. Magaldi AJ, Yasuda PN, Kudo LH, Seguro AC, Rocha AS: Renal involvement in leptospirosis: A pathophysiologic study. Nephron 62:332-339, 1992
6. Lin KC, Fong MS, Lee LD: Leptospirosis in Taiwan. China Med .I 23:204-216, 1976
7. Wu MS, Hong JJ, Lin JL, Yang CW, Chien HC: Multi- ple tubular dysfunction induced by mixed Chinese herbal medicines containing cadmium. Nephrol Dial Transplant 11:867-870, 1996
8. Brown PD, Gravekamp C, Carrington DG, van de Kemp H, Hartskeerl RA, Everard CO, Terpstra WJ, Levett PN: Evaluation of the polymerase chain reaction for early diagno- sis of leptospirosis. .I Med Microbial 43: 110-l 14, 1995
9. Bal AE, Gravekamp C, Hartskeerl RAT De Meza-Brew- ster J, Korver H: Detection of leptospires in urine by PCR for early diagnosis of leptospirosis. J Clin Microbial 32: 1894. 1898, 1994
10. Kee SH, Kim IS, Choi MS, Chang WH: Detection of leptospiral DNA by PCR. J Clin Microbial 32:1035-1039, 1994
Il. Merien F, Baranton G, Perolat P: Comparison of poly- merase chain reaction with microagglutination test and culture for diagnosis of leptospirosis. J Infect Dis 172:281-285, 1995
12. Merien F, Amouriaux P, Perolat P, Baranton G, Saint Girons I: Polymerase chain reaction for detection of Lepto- spira spp. in clinical samples. J Clin Microbial 30:2219-2224, 1992
13. Wong KF, Chan JKC: Hemophagocytic syndrome: A review. Hematol Rev 5:335-337, 1991
14. Risdall RJ, McKenna RW, Nesbit ME, Krivit W, Bal- four HH Jr, Simmons RL, Brunning RD: Virus-associated hemophagocytic syndrome: A benign histiocytic proliferation distinct from malignant histiocytosis. Cancer 44:993-1002, 1979
15. Arya S, Hong R, Gilbert EF: Reactive hemophagocytic syndrome. Pediatr Path01 3:129-141, 1985
16. Wong KF, Chan JK: Reactive hemophagocytic syn- drome: A clinicopathologic study of 40 patients in an Oriental population. Am J Med 93:177-180, 1992
17. Thompson JC, Manktelow BW: Pathogenesis of renal lesions in haemoglobinaemic and non-haemoglobinaemic leptospirosis. J Comp Path01 101:201-214, 1989
18. Lake EW, Dumes D: Acute renal failure including cortical necrosis, in Massry SG, Glassock RJ: Textbook of Nephrology (ed 3). Baltimore, MD, Williams & Wilkins, 1995, pp 984-1003
19. Tsen YT, Yang CW, Pan MJ, Wu MS, Chen YM, Lin CL, Wu CH, Huang CC: Leptospirosis: An ignored cause of acute renal failure in Taiwan. Annual Meeting of Society of Nephrology, ROC, Taipei 1996 (abstr)
20. Sasaki DM, Pang L, Minette HP, Wakida CK, Fuji- moto WJ, Manea SJ, Middleton CR: Active surveillance and risk factors for leptospirosis in Hawaii. Am J Trop Med Hyg 48:35-43, 1993