
Print edition ISSN 2615-5109 Electronic edition ISSN 2621-0541
Upload
khangminh22Category
view
0download
0
Print ISSN: 2395 - 1400
Journal of Basic and Clinical Research
Chief Patron
Sri Kamineni Suryanarayana
Patron
Dr. Kamineni Shashidhar
Chairman
Dr. Shruti Mohanty
Advisory Board
Dr. N.N. Samanta
Dr. M. Dasaradha Rami Reddy
Editorial Board
Editor-in-chief
Dr. K. Nagaraj
Associate Editors
Dr. Suresh R. J. Thomas Dr. M. Arun Kumar Dr. N. Madhavi
Assistant Editors
Dr. T. Venkatramanaiah Dr. K. Sateesh Malkappa
Dr. P. Karuna Sree Dr. N. Rajya Lakshmi Dr. P. Sai Krishna
Assistant Managing Editors
Dr. V.G Prasad Dr. J. Kishore Yadav Dr. Varun Malhotra
Editorial Committee
Dr. Md. Sikinder Hayath Dr. M Dattatrey Dr. K Venu
Dr. S. Mohd. Ali Dr. M. Subrahmanyam Dr. P. V Sai Satyanarayana
Dr. V. Satyanarayana Dr. M. Anantha Reddy Dr. Y. Venkata Rao
Dr. K. Saileela Dr. G.V.S.N Prasad Dr. Chapay Soren
Dr. A.D Archana
iJournal of Basic and Clinical Research 2014; 1(1) i
Correspondence : Address for correspondence regarding submission of articles
Dr. K. Nagaraj Editor-in-chief
Journal of Basic and Clinical Research
Kamineni Institute of Medical Sciences
Sreepuram, Narketpally, Nalgonda (Dist.), Telangana State.
Email ID: [email protected]
Copy Right: Without written permission from editor in chief/publisher, any part of this journal should not be
reproduced or transmitted in any form or by any means, electronic or print including photocopying.
All rights reserved
Disclaimer:
Views expressed by authors are not those of the Journal of Basic and Clinical Research. All statements,
opinions expressed in the manuscript are those of the authors and not of the editor(s) or publishers. The
editor(s) and publishers disclaim any responsibillity for such material. The editor(s) and publishers also do
not guarantee, warrant or endorse any product or service advertised in the journal nor do they guarantee
any claim made by the manufacturer of such product or service.
Subscription: (Only for Print Format of the Journal)
Annual Subscription: vPersonal : Rs. 500/- within India / USD 50 $ outside India vInstitutional : Rs. 3000/- within India / USD 200 $ outside India
Publisher : Kamineni Education Society (KES)
Flat No.103, Kanchanjunga Complex,
King Koti Road, Abids,
Hyderabad, Telangana State - 500 001.
Tel: 040 – 24785511
Fax: 040 – 24758999
Email: [email protected]
Printer : Imperial Printmatics Pvt. Ltd.
H.No.10-2-35-/5/2, A. Battery Lane,
Bazar Ghat, Hyderabad- 500 057, T.S., India.
ii Journal of Basic and Clinical Research 2014; 1(1)
Journal of Basic and Clinical Research
Journal of Basic and Clinical Research 2014; 1(1) 1
Journal of Basic and Clinical Research
EditoRial 03
oRiginal aRtiClEs
Comparative study of obstructive sleep apnea among obese and non-obese adults: A hospital based study 05 Venu Kandala, Srikar Darisetty, Raghudeep Palla, Divyesh Kishen Waghray
Evaluation of Mass Drug Administration against ilariasis in Nalgonda district, Telangana State 10 Varun Malhotra, Prasad VG, Suguna D, Kishore Yadav J, Nagaraj K, S Bhayya.
Effect of facilitated self directed learning on poor performers among medical students 17 Shruti Mohanty, Sunitha N, Pragna Rao
REviEw aRtiClEs
Applications of Nanobiotechnology 21 RR Rao
Role of systematic reviews and meta-analysis in evidence based health care 25 Sreekumaran Nair N, Ravishankar, Melissa Glenda Lewis
CasE REpoRts
Pain Management in Chest Trauma: Intrapleural Analgesia 31 Vishwa Reddy Gankidi, Sai Satyanarayana Pelluri, Anjani Priya Vemula
A case of palpable purpura due to leukocytoclastic vasculitis 34 Nayeem Sadath Haneef, Ramachandra S, Arun Kumar M, Grace Swarupa Charles B
Adult Respiratory Distress Syndrome in dengue fever 37 Kanni YS, Rathod BH, Satya Srinivas A, Nithin Kumar
Recurrent massive hemorrhagic pleural effusion with pseudopancreatic cyst due to pancreatico-pleural istula : A case report 39 Venu Kandala, Venkat Kishan Tatikonda, Mateenuddin Saleem, Srikar Darisetty,
Raghudeep Palla, Syed Abdul Aleem
Quiz
Paediatric photo quiz 43 Dasaradha Rami Reddy M, Suresh R J Thomas, Sailaja K
Radiology quiz 44 Venkat Kishan Tatikonda, Kusuma Kumar K, RS Moorthy, Chethan BS, Yugandhara M Shaw
instRuCtions to authoRs 50
Volume: 1 / Issue: 1 July - December 2014Contents
Journal of Basic and Clinical Research 2014; 1(1) 2
Kamineni Education society
Kamineni institute of Medical sciences
Kamineni institute of dental sciences
Kamineni institute of paramedical
sciences
Kamineni institute of Medical sciences
College of nursing
Kamineni institute of Medical sciences
school of nursing
sree vidya peeth
KIDS
KIPS
KIMS-CON
KIMS-SON
Journal of Basic and Clinical Research 2014; 1(1) 3
Editorial
Currently Life style model of non-communicable
diseases is mainly concentrating on adulthood
risk factors like unhealthy diet, physical inactivity
and smoking. But adult risk factors are not able
to explain the social and geographical variation
of these diseases (MONICA study).1 The large
MONICA study (WHO MONICA project 1994) with
standardized data from 26 countries reveals weak
association between prevalence of conventional
adult risk factors and mortality from Coronary
Heart Disease (CHD). The study also shows that
only 25% of geographical variation in the disease
can be explained by smoking, blood pressure, and
total cholesterol.1 This has led to importance of life
cycle approach in prevention of non- communicable
diseases.
Today there is more literature on tracking of
conventional risk factors from childhood to
adulthood. The “fetal origins hypothesis” proposes
that non-communicable diseases including coronary
heart disease, Type II Diabetes and Hypertension
result from responses of fetus to undernutrition that
permanently change the structure and function of
the body.2 Early life model assumes that adult
diseases are programmed in fetal and adult life.
The term programming means adaptive responses
of the organisms to speciic conditions or insults such as undernutrition,chemical metabolites, drugs
etc. This programming may only occur during
narrow period of individual’s life. It is proposed
that programmed behavior is never forgotten.3
There are two distinct categories of programming
Biological (eg., maternal and fetal genotype, growth
hormones, glucocorticoids) and Environmental
(fetal and maternal nutrition, maternal psycho-social
and life style factors).3 Fetal nutrition is assumed
to be the most important. Fetal nutrition depends
on two factors, maternal nutrition and supply line
which carries nutrients from mother to fetus.3
Fetal undernutrition may fail to fuel the growth
process. Early nutrient environment may
Life cycle approach in prevention of non-communicable diseases
permanently alter gene expression, alter the clonal
selection of certain types of cells leading to alteration
of organ structure and may have permanent effect
on cell number which may affect the metabolism.
All these mechanisms may explain nutritional
programming.
A study conducted by Stein CE et al in South India
reveals that In India as in UK , coronary heart disease
is associated with small size at birth, suggesting
that its pathogenesis is inluenced by undernutrition in utero.4 The consistency of association between
fetal undernutrition and different adult outcomes
have been conirmed in different countries.The drawback of fetal origin hypothesis is that it did not
take into account confounding socio-economic
factors.Unlike early life model, life course approach
does not rely on assumptions regarding whether or
not critical period occurs early or later in life. Life
style model emerged as an attempt to integrate
both early life and adult life style risk factors in a
wider framework. Early life events are taken as irst stage along a pathway that determines risk later in
life. Social class at birth is related to childhood and
adult risk factors of non-communicable dieases.
Epidemiological basis of life style approach needs to
look at relative importance of inluences in different stages of life, which may vary according to type of
disease investigated. Pathways of risk have to be
studied to see the relationship between biological
and social factors that occur during life and their
association with health risks of non-communicable
diseases. Identifying pathways of risk involves use
of new epidemiological and statistical modeling
approaches.
Case study from Kerala reveals that there is a strong
reason to follow life course approach in India. Kerala
has highest prevalence of non-communicable
diseases and their risk factors in India. Survival
of Low Birth Weight (LBW) babies is substanially
high in Kerala than rest of India and these babies
: 3-4

Journal of Basic and Clinical Research 2014; 1(1) 4
are exposed to obesogenic environment. The ratio
of incidence of acute coronary syndrome in men
and women has decreased from 23:1 in 1967
to 4:1 in 2007 in Kerala.5 This may be explained
by restricted outdoor activity by girls and women
which decreases endogenous vitamin D synthesis
and imparts low skeletal mass and high body fat
composition.5 This study indicates the need for
life course approach targeting adolescents and
women.
The major biological risk factors of non-
communicable diseases emerge and act in early
life and continue throughout the life course and
they can affect the health of next generation.The
underlying socio-economic and environmental
factors have to be taken into consideration to
develop appropriate strategies.6 There is a need to
strategize through life course approach by focusing
on adult risk factors, societal change and targeted
approach (adolescents and women).
References:
1. WHO MONICA Project. MONICA Quality assessment
reports. Monia web publications 2-18. 12 June 2014.
Available from URL :http://www.kti.i/publications/monica/index.html (Accessed 12 June 2014).
2. Barker DJP. Fetal origins of coronary heart disease. BMJ
1995;311:171-4.
3. Harding JE. The nutritional basis of the fetal origins of
adult disease. Int J Epidemiol. 2001;30:15-23.
4. Stein CE, Fall CHD, Kunaran K, Osmond C, Cox V,
Barker DJP, Fetal growth and coronary disease in South
India. Lancet 1996;348:1269-73.
5. Sivasankaran S, Thankappa KR. Prevention of
non-communicable diseases requires a life course
approach: A case study from Kerala. Indian J Med Res.
2013;137:874-7.
6. Aboderin I, Kalache, Ben Shlomo Y, Lynch JW, Yajnik CS,
Kuh D, Yach D. Life course perspectives on Coronary
Heart disease, Stroke and Diabetes: Key issues and
implications for Policy and Research. Geneva: World
Health Organization 2002 (Document WHO/NMH/
NPH/02.1).
Dr. K. NagarajEditor-in-Chief
Professor & Head
Department of Community Medicine
Kamineni Institute of Medical Sciences,
Narketpally, Nalgonda District,
Telangana State - 508 254
phone : 08682 272018 Ext-314
E-mail : [email protected]
: 3-4
Journal of Basic and Clinical Research 2014; 1(1) 5
AbStRACt
Objective: This study was designed to know the relationship between Obstructive Sleep Apnea (OSA) and
Body Mass Index (BMI) and to identify the contributory factors of OSA in non-obese subjects.
Materials and Methods: A Cross-Sectional study was conducted in 30 subjects with history of snoring
and Epworth Sleepiness Scale (ESS) >10 by polysomnography. Out of 30 subjects 23 were diagnosed
as obstructive sleep apnea (OSA) [Apnoea Hypopnoea Index (AHI)>5]. These 23 subjects classiied into non-obese and obese groups based on BMI, <30 and ≥30 respectively. ESS, Anthropometric measurements [BMI,Neck Circumference (NC), Waist Circumference (WC), Hip Circumference (HC), Thyromental distance
(TMD) and Modiied Mallampati Score (MMS)] and polysomnographic recordings were scored and compared between the obese and non-obese subjects of OSA along with their life style habits. Student 't' test and
chi-square test was used to compare and assess statistical signiicance of difference in study variables between obese and non-obese subjects.
Results: Total number of cases with OSA were 23 (13 obese and 10 non-obese). No difference with reference to
mean age and sex distribution was observed between obese and non-obese subjects. Difference in mean BMI,
anthropometric measurements (NC, WC, HC, TMD), ESS, Arousal index, Oxygen desaturation parameters
[(Oxygen Desaturation Index (ODI), T % < SaO2] between obese and non-obese subjects was found to be
statistically signiicant. Mean value of lowest oxygen saturation was signiicantly lower in obese subjects as compared to non-obese subjects. Total sleep time, sleep eficiency, N3 stage and Rapid Eye Movement (REM) stage was signiicantly decreased in obese than non-obese patients.
Conclusion: OSA severity increased with obesity. Non-obese patients with OSA had structural abnormalities
(decreased TMD and MMS class 3) and life style factors which include smoking and alcohol consumption may
contribute to OSA.
Key words: Body Mass index, Epworth sleepiness scale, Modiied Mallampati score, Obstructive sleep apnea.
Comparative study of obstructive sleep apnea among obese and
non-obese adults: A hospital based study
Introduction:
Obstructive sleep apnea is age old disease and
is not a new one, is characterized by repetitive
episodes of upper airway collapse with air low limitation resulting in disruptive sleep, snoring and
*Corresponding Author :
Dr. Venu K, Department of Pulmonary Medicine,
Kamineni Institute of Medical Sciences, Narketpally,
Nalgonda District, Telangana State - 508 254,
Venu Kandala1, Yugaveer Kalagani2, Laxman babu V2, Srikar Darisetty3, Raghudeep Palla3,
Divyesh Kishen Waghray3
1Professor & Head, 2Assistant Professor, 3Post Graduate, Department of Pulmonary Medicine, Kamineni Institute of Medical Sciences,
Narketpally.
original article
oxygen desaturation. This disease is suspected
by snoring, excessive daytime sleepiness and
conirmed by polysomnography. Obstructive sleep apnea syndrome is deined as obstructive sleep apnea associated with excessive daytime
sleepiness. The OSA syndrome, characterized
by both an Apnoea Hypopnoea Index (AHI) ≥5 along with excessive daytime sleepiness was
present in 2% of women and 4% of men.1 Obesity
is a well recognized risk factor for a variety of
medical conditions such as obstructive sleep
: 5-9

Journal of Basic and Clinical Research 2014; 1(1) 6
apnea, type 2 diabetes mellitus, cardiovascular
diseases, hyperlipidemia, metabolic syndrome,
and nonalcoholic fatty liver disease.2 Nearly 60-
90% of patients with OSA were obese.3,4 Non-
obese people also get OSA and the occurrence of
OSA in non-obese patients may exhibit different
craniofacial abnormalities than obese patients.5,6
Materials and Methods:
Institutional Ethics committee approval and
informed consent from the study subjects was
obtained. This cross-sectional study was conducted
in 30 subjects, who attended the department of
pulmonary medicine, Kamineni Institute of Medical
Sciences (KIMS), Narketpally during October
2011 to September 2012. Age, sex, co-morbidity,
objective measurement for sleepiness (Epworth
Sleepiness Scale - ESS) and anthropometric
measurements [BMI, neck circumference, Waist
Circumference (WC), Hip Circumference (HC),
thyromental distance, Mallampati’s score] were
recorded. Neck circumference was measured
with a tape measure at the level of cricothyroid
membrane. Waist Circumference was measured at
a level midway between the lowest rib and the iliac
crest. Hip circumference was measured at a plane
which passes over the maximum circumference of
the buttocks. Thyromental distance was measured
from the thyroid prominence to a perpendicular
dropped from the soft tissue mentum. Mallampati’s
score was measured with mouth wide open,
tongue maximally protruded without phonation,
and classiied into Grades I-IV. Epworth Sleepiness Scale(ESS) is a scale which measures the day time
sleepiness by using a questionnaire which is based
on measurements of the sleep inducing potential of
certain routine diurnal activities. Snoring index(SI)
was deined as number of snores per hour of sleep. These patients were selected based on the
following criteria:
Inclusion criteria: Both genders, age > 15 years,
Body Mass Index (BMI) ≥ 18.5, patients who were having history of snoring, Epworth Sleepiness
Scale (ESS): ≥10, Apnea Hypopnea Index (AHI): ≥ 5)
Exclusion criteria: Pulmonary tuberculosis,
Chronic Obstructive Pulmonary Disease (COPD),
bronchial asthma, interstitial lung disease,
neuromuscular disorders, drug abuse, chronic
renal failure, congestive heart failure, pregnancy
and patients who were on treatment with sedatives
and hypnotics.
Overnight polysomnography was performed in
our sleep lab center and the polysomnographic
data including sleep stages, ODI, total sleep time
spent with oxygen saturation <90%, lowest oxygen
saturation and sleep eficiency were calculated. Oxygen Desaturation Index (ODI) is deined as number of instances per hour of sleep during which
blood oxygen saturation drops by 3% or more
from the baseline value. Oxygen saturation time
<90% (T%) is the duration of sleep during which
the oxygen saturation falls below 90% (expressed
as percentage of the total sleep time). Sleep
Eficiency is the ratio between total sleep time and total recording time. Severity of OSA diagnosed
by apnea hypopnea index(AHI) and classiied as mild OSA with AHI of 5 to 15, moderate OSA with
AHI of 16 to 30,and severe OSA with AHI > 30.7
NREM sleep has 3 stages . N1 stage of NREM
(Non rapid eye movement) sleep characterized by
transition of wakefulness and sleep, with a EEG
waveform transition from alpha rhythm to theta
rhythm. N2 stage of NREM sleep is characterized
by presence of abrupt electrical activity in the brain
which manifests itself on the EEG in the form of K
complexes and sleep spindles, with a background
theta rhythm. N3 stage of NREM consists of delta
rhythm, also referred to as slow wave sleep.
Rapid Eye Movement (REM) stage percentage
is the duration of REM sleep which is expressed
as a percentage of the total sleep time. After
polysomnography, 23 subjects were diagnosed
as OSA i.e. AHI ≥5, these subjects were classiied non-obese and obese based on BMI classiication. (BMI <30 non-obese and ≥30 were obese)8
and comparison was done between non-obese
and obese patients of obstructive sleep apnea.
Venu et al: Obstructive sleep Apnea among obese and non-obese adults
: 5-9
Journal of Basic and Clinical Research 2014; 1(1) 7
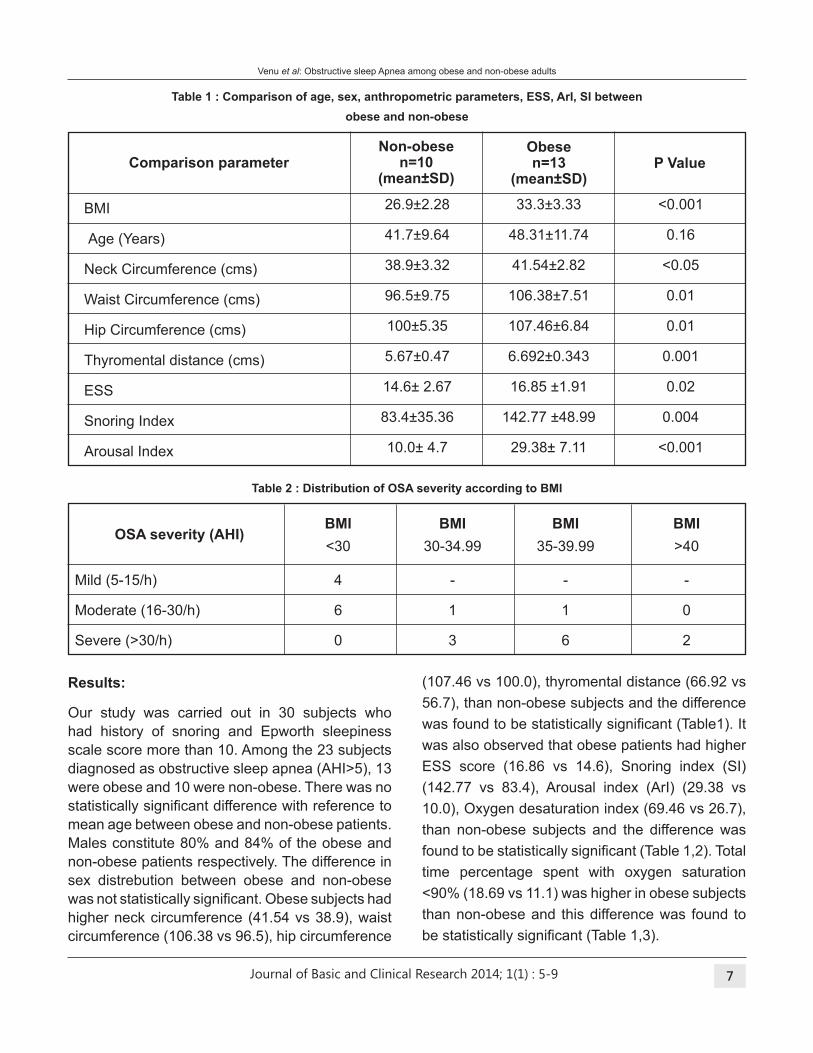
table 1 : Comparison of age, sex, anthropometric parameters, ESS, ArI, SI between
obese and non-obese
table 2 : Distribution of OSA severity according to bMI
Comparison parameter
BMI
Age (Years)
Neck Circumference (cms)
Waist Circumference (cms)
Hip Circumference (cms)
Thyromental distance (cms)
ESS
Snoring Index
Arousal Index
26.9±2.28
41.7±9.64
38.9±3.32
96.5±9.75
100±5.35
5.67±0.47
14.6± 2.67
83.4±35.36
10.0± 4.7
33.3±3.33
48.31±11.74
41.54±2.82
106.38±7.51
107.46±6.84
6.692±0.343
16.85 ±1.91
142.77 ±48.99
29.38± 7.11
<0.001
0.16
<0.05
0.01
0.01
0.001
0.02
0.004
<0.001
Non-obesen=10
(mean±SD)
Obese n=13
(mean±SD)P Value
bMI bMI bMI bMI
<30 30-34.99 35-39.99 >40
Mild (5-15/h) 4 - - -
Moderate (16-30/h) 6 1 1 0
Severe (>30/h) 0 3 6 2
OSA severity (AHI)
Results:
Our study was carried out in 30 subjects who
had history of snoring and Epworth sleepiness
scale score more than 10. Among the 23 subjects
diagnosed as obstructive sleep apnea (AHI>5), 13
were obese and 10 were non-obese. There was no
statistically signiicant difference with reference to mean age between obese and non-obese patients.
Males constitute 80% and 84% of the obese and
non-obese patients respectively. The difference in
sex distrebution between obese and non-obese
was not statistically signiicant. Obese subjects had higher neck circumference (41.54 vs 38.9), waist
circumference (106.38 vs 96.5), hip circumference
(107.46 vs 100.0), thyromental distance (66.92 vs
56.7), than non-obese subjects and the difference
was found to be statistically signiicant (Table1). It was also observed that obese patients had higher
ESS score (16.86 vs 14.6), Snoring index (SI)
(142.77 vs 83.4), Arousal index (ArI) (29.38 vs
10.0), Oxygen desaturation index (69.46 vs 26.7),
than non-obese subjects and the difference was
found to be statistically signiicant (Table 1,2). Total time percentage spent with oxygen saturation
<90% (18.69 vs 11.1) was higher in obese subjects
than non-obese and this difference was found to
be statistically signiicant (Table 1,3).
Venu et al: Obstructive sleep Apnea among obese and non-obese adults
: 5-9
Journal of Basic and Clinical Research 2014; 1(1) 8
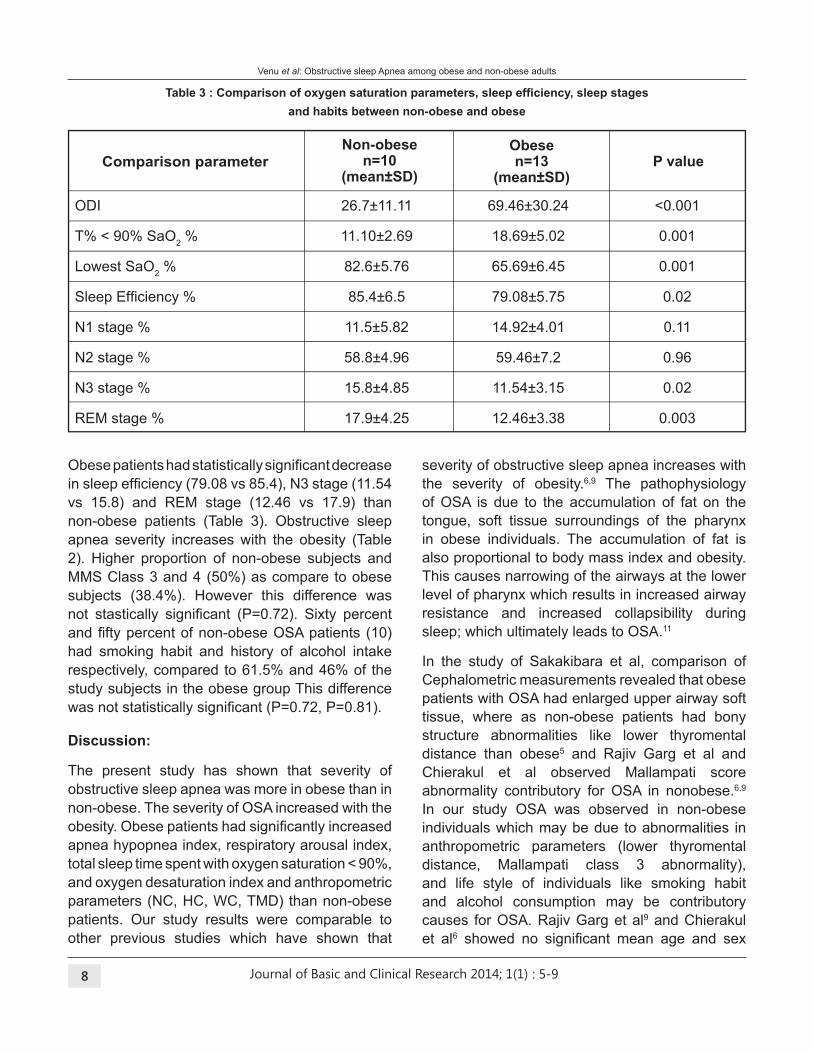
Table 3 : Comparison of oxygen saturation parameters, sleep eficiency, sleep stages and habits between non-obese and obese
Discussion:
The present study has shown that severity of
obstructive sleep apnea was more in obese than in
non-obese. The severity of OSA increased with the
obesity. Obese patients had signiicantly increased apnea hypopnea index, respiratory arousal index,
total sleep time spent with oxygen saturation < 90%,
and oxygen desaturation index and anthropometric
parameters (NC, HC, WC, TMD) than non-obese
patients. Our study results were comparable to
other previous studies which have shown that
severity of obstructive sleep apnea increases with
the severity of obesity.6,9 The pathophysiology
of OSA is due to the accumulation of fat on the
tongue, soft tissue surroundings of the pharynx
in obese individuals. The accumulation of fat is
also proportional to body mass index and obesity.
This causes narrowing of the airways at the lower
level of pharynx which results in increased airway
resistance and increased collapsibility during
sleep; which ultimately leads to OSA.11
In the study of Sakakibara et al, comparison of
Cephalometric measurements revealed that obese
patients with OSA had enlarged upper airway soft
tissue, where as non-obese patients had bony
structure abnormalities like lower thyromental
distance than obese5 and Rajiv Garg et al and
Chierakul et al observed Mallampati score
abnormality contributory for OSA in nonobese.6,9
In our study OSA was observed in non-obese
individuals which may be due to abnormalities in
anthropometric parameters (lower thyromental
distance, Mallampati class 3 abnormality),
and life style of individuals like smoking habit
and alcohol consumption may be contributory
causes for OSA. Rajiv Garg et al9 and Chierakul
et al6 showed no signiicant mean age and sex
ODI 26.7±11.11 69.46±30.24 <0.001
T% < 90% SaO2 % 11.10±2.69 18.69±5.02 0.001
Lowest SaO2 % 82.6±5.76 65.69±6.45 0.001
Sleep Eficiency % 85.4±6.5 79.08±5.75 0.02
N1 stage % 11.5±5.82 14.92±4.01 0.11
N2 stage % 58.8±4.96 59.46±7.2 0.96
N3 stage % 15.8±4.85 11.54±3.15 0.02
REM stage % 17.9±4.25 12.46±3.38 0.003
Comparison parameter P valueNon-obese
n=10(mean±SD)
Obese n=13
(mean±SD)
Obese patients had statistically signiicant decrease in sleep eficiency (79.08 vs 85.4), N3 stage (11.54
vs 15.8) and REM stage (12.46 vs 17.9) than
non-obese patients (Table 3). Obstructive sleep
apnea severity increases with the obesity (Table
2). Higher proportion of non-obese subjects and
MMS Class 3 and 4 (50%) as compare to obese
subjects (38.4%). However this difference was
not stastically signiicant (P=0.72). Sixty percent and ifty percent of non-obese OSA patients (10) had smoking habit and history of alcohol intake
respectively, compared to 61.5% and 46% of the
study subjects in the obese group This difference
was not statistically signiicant (P=0.72, P=0.81).
Venu et al: Obstructive sleep Apnea among obese and non-obese adults
: 5-9
Journal of Basic and Clinical Research 2014; 1(1) 9
difference in non-obese and obese patients of
OSA and also observed that AHI, ODI and T% with
SaO2<90% were signiicantly increased in obese
than non-obese and lowest oxygen saturation
was signiicantly decreased in obese than non-obese. Our study also had similar indings. YK Gupta et al10 showed decreased sleep eficiency in obese than non-obese which was not statistically
signiicant (80.15 vs 85.51± 11.48, p=0.42). J. Antczak et al12 observed N1 stage was signiicantly increased in obese than in non-obese, and also
observed signiicantly decreased N3 stage and REM stage in obese than non-obese. In our study
N1 stage was increased in obese than non-obese
but not signiicant and also observed signiicantly decreased N3 and REM stage in obese than non-
obese.
There are multiple imaging techniques available
to evaluate the upper airway in patients with OSA
such as Cephalometric radiography, CT, MRI,
luoroscopy and somnoluoroscopy but these methods are cumbersome and expensive.10 In this
study we used thyromental distance and Mallampati
score to evaluate the structural abnormalities.
Conclusion:
OSA is more common in obese than in non-obese
and the severity of OSA increased with the obesity.
Decreased thyromental distance, Mallampati score
abnormalities, smoking and alcohol habits are
contributory factors for obstructive sleep apnea
in non-obese. Proper evaluation of contributory
factors helps in appropriate treatment plan.
References:
1. Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr
S. The occurrence of sleep-disordered breathing among
middle-aged adults. N Engl J Med 1993; 328: 1230-5.
2. Haslam DW, James WP. Obesity Lancet 2005; 366:1197–
209.
3. Strohl KP, Redline S. Recognition of obstructive sleep
apnea. Am J Respir Crit Care Med 1996;154:279– 86.
4. Guilleminault C, Tikian A, Dement W. The sleep apnea
syndromes. Annu Rev Med 1976;27:465–84.
5. Sakakibara H, Tong M, Matsushita K, Hirata M, Konishi
Y, Suetsugu S. Cephalometric abnormalities in non-
obese and obese patients with obstructive sleep apnea.
Eur Respir J 1999;13:403-10.
6. Chierakul N, Chaipattarapol C, Ruttanaumpawan P,
Nana A, Naruman C, Tangchityongsiva S. Comparision
of clinical and polysomnographic characteristics of non
obese and obese patients with obstructive sleep apnea.
J Med Assoc Thai 2007; 90:48-53.
7. Roche F, Gaspoz JM, Court-Fortune I, et al: Screening
of obstructive sleep apnea syndrome by heart rate
variability analysis. Circulation 1999; 100:1411-5.
8. Obesity: preventing and managing the global epidemic:
report of a WHO Consultation on obesity, Geneva, June
3–5, 1997. Geneva: World Health Organization; 1998.
9. Garg R, Singh A, Prasad R, Saheer S, Jabeed P,
Verma R.A comparative study on the clinical and
polysomnographic pattern of obstructive sleep apnea
among obese and non-obese subjects. Ann Thorac Med.
2012; 7:26-30.
10. Gupta YK, Jaiswal A, Gupta R, Jain AK, Kumar D,
Behera D. Pattern of Sleep disordered breathing
in obese Indians. Indian J Sleep Med 2009; 4(1):
19-31.
11. Rollheim J, Osnes T, Miljeteig H. The relationship
between obstructive sleep apnoea and body mass index.
Clin Otolaryngol Allied Sci 1997; 22:419-22.
12. Antczak J, Horn B, Richter A, Jernajczyk W, Bodenschatz
R, W Schmidt EW. The inluence of obesity on sleep quality in male sleep apnea patients before and during
therapy. J Physiol Pharmacol. 2008;59(S6):123-34.
Venu et al: Obstructive sleep Apnea among obese and non-obese adults
: 5-9
Journal of Basic and Clinical Research 2014; 1(1) 10
AbStRACt
background : Lymphatic ilariasis is an important public health problem in India, and Nalgonda district of Telangana State is one of the endemic districts where mass drug administration programme is undertaken
every year to achieve the goal of elimination of the disease. The present study was undertaken to evaluate
the percentage coverage and compliance rates of the programme during 2014, and study reasons for non-
compliance.
Materials and Methods : The guidelines of National Vector Borne Disease Control Programme (NVBDCP)
were used to select a total of 130 households from four clusters (three rural and one urban). Each household
was visited by a team and data was recorded on pre-structured questionnaire available in operational guidelines
manual of NVBDCP.
Results : The study population consisted of 561 individuals from 130 households, out of which 537 were
eligible for mass drug administration. The study revealed that only 428 (79.70%) of the eligible individuals were
covered by the drug distributors. The overall compliance rates for diethylcarbamazine and albendazole were
67.78% and 64.43% respectively. ‘Fear of side effects’, ‘forgot to take medicines’ and dificulty in giving tablets to children were main reasons for non-compliance. Side effects were reported by only 1.35% of cases.
Conclusions : The study reveals that coverage rates are as important as compliance rates to achieve
elimination of lymphatic ilariasis, and efforts should be made to improve coverage rates by involving more human resources, supervision and incentive linked to work-output, and compliance rates by information,
education and communication activities.
Key words : Evaluation, Lymphatic Filariasis, Mass Drug Administration, Nalgonda District.
Evaluation of Coverage and Compliance of Mass Drug
Administration programme for elimination of lymphatic ilariasis in Nalgonda District of telangana State
Introduction:
Lymphatic ilariasis (LF), commonly known as elephantiasis, is a neglected tropical disease.
Infection is usually acquired in childhood causing
hidden damage to the lymphatic system.
The painful and profoundly disiguring visible manifestations of the disease, lymphoedema,
elephantiasis and scrotal swelling occur later in life
and lead to permanent disability. These patients
are not only physically disabled, but suffer mental,
social and inancial losses contributing to stigma and poverty. Currently, more than 1.4 billion people
in 73 countries are living in areas where lymphatic
ilariasis is transmitted and are at risk of being infected. Globally, an estimated 25 million men suffer
with genital disease and over 15 million people are
aflicted with lymphoedema. Eliminating lymphatic ilariasis can prevent unnecessary suffering and contribute to the reduction of poverty1.
*Corresponding author:
Dr. Varun Malhotra,
Dept of Community Medicine, Kamineni Institute of Medical
Sciences, Narketpally, Nalgonda District,
Telangana State - 508 254, [email protected]
Varun Malhotra1*, Prasad VG2, Suguna D1, Kishore Yadav J1,Nagaraj K3, S bhayya4
1Assistant Professor, 2Associate Professor, 3Professor & Head, 4Professor, Dept of Community Medicine, Kamineni Institute of Medical Sciences,
Narketpally.
original article
: 10-16
Journal of Basic and Clinical Research 2014; 1(1) 11
In 1997, the 50th World Health Assembly vide its
agenda item 20 urged Member States to take
advantage of recent advances in LF and develop
national plans that would lead to elimination of LF2.
In 2000, World Health Organization (WHO) initiated
the Global Programme to Eliminate Lymphatic
Filariasis (GPELF) with the goal to eliminate LF
as a public health problem by the year 2020 3.
Elimination means that LF ceases to be a public
health problem and will be measured by microilaria carrier state of less than 1%, and children born after
elimination to be free from circulating antigenaemia.
The National Health Policy of India (2002) has set
the goal of elimination of LF in India by 20154.
To achieve this goal the National Task Force has
recommended the strategy with two major thrust
areas i.e. (a) Transmission control by administration
of annual single dose of anti-ilarial drugs i.e. diethylcarbamazine (DEC) and albendazole called
Mass Drug Administration (MDA), and (b) Disability
prevention and management of individuals who
already suffer from the disease5.
The concept of MDA is to approach every
individual in the target community and administer
single dose of anti-ilarial drugs. As the longevity of adult worms is approximately 5 years, repetition
of annual dose for at least 5 years with minimum
85% actual dose compliance will achieve the
objective. Hence, the quality of MDA programme
in the community as measured by coverage and
compliance rates is important for success of the
elimination programme5.
The present study was undertaken to study the
overall coverage and compliance rates during the
annual MDA conducted during 2014 in Nalgonda,
an endemic district of Telangana State.
Material and Methods:
Annual MDA was undertaken in Nalgonda district
on 28th, 29th and 30th January 2014. As per the
directions, house to house visits were made by drug
distributors (DDs), and DEC and albendazole was
administered to the eligible population. Children
under 2 years, pregnant women and severely ill
persons were excluded from the MDA programme.
The DDs were instructed to persuade the eligible
population to consume tablets on the spot and
avoid taking tablet on empty stomach. The DDs
were provided with a note book to keep record of
name of head of the family, number of tablets given
and reason for not accepting the tablets.
The present study for evaluation of MDA was
carried out by the study team within a month after
the MDA activity. The evaluation was conducted
as per NVBDCP guidelines i.e. by selecting four
clusters; three from the rural and one from urban
area (each cluster having at least 30 households).
The clusters were selected by two stage random
sampling. In irst stage Primary Health Centres/ Urban Health Centre were selected, while second
stage was undertaken to select the village in
rural areas, and ward in urban area within the
jurisdiction of selected PHC/UHC. In each cluster,
the households were selected by systematic
sampling.
Data was collected by four teams, each team
consisting of a faculty of Department of Community
Medicine, one post graduate, and two interns.
Information was obtained from one individual,
preferably head of the family and recorded
on structured questionnaire as per NVBDCP
operational manual5. Data was compiled,
and analyzed using SPSS statistical package
version 19.
Results:
Total and Eligible Population : The study sample
consisted of 561 (425 rural and 136 urban)
individuals in 130 households (100 in rural and 30
in urban) in four clusters. The age distribution of the
population revealed that only 2.48% of population
was below 2 years of age, while maximum
population (70.41%) belonged to age group more
than 14 years. Distribution of population as per sex
revealed that 51.87% of study population was male
while 48.13% were females. As per the guidelines,
children below 2 years of the age, pregnant women
and seriously ill patients are not eligible to receive
MDA. Thus the individuals eligible to ingest the
drugs in four study clusters were 537 (95.72%) out
of 561(Table 1).
Malhotra et al: Mass Drug Administration programme for elimination of lymphatic ilariasis
: 10-16
Journal of Basic and Clinical Research 2014; 1(1) 12
Eligible Population
population covered by DDs
Kalavalapalli 131 116 88.55
Paddadevulapally 147 105 71.43
Kasarabad 131 114 87.02
Bhongir 128 93 72.66
Total 537 428 79.70
Village % coverage
table 2: Number of Households covered by Drug Distributor
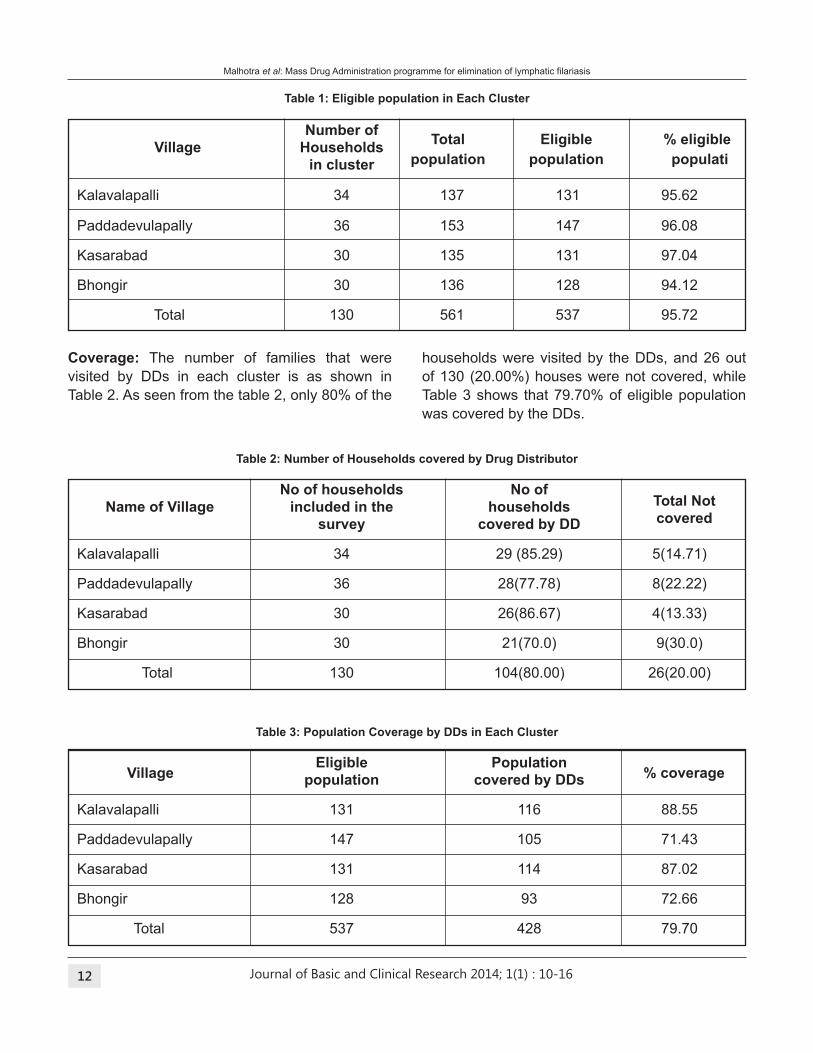
Coverage: The number of families that were
visited by DDs in each cluster is as shown in
Table 2. As seen from the table 2, only 80% of the
households were visited by the DDs, and 26 out
of 130 (20.00%) houses were not covered, while
Table 3 shows that 79.70% of eligible population
was covered by the DDs.
table 3: Population Coverage by DDs in Each Cluster
table 1: Eligible population in Each Cluster
Number of
Village Households
in cluster
Kalavalapalli 34 137 131 95.62
Paddadevulapally 36 153 147 96.08
Kasarabad 30 135 131 97.04
Bhongir 30 136 128 94.12
Total 130 561 537 95.72
total Eligible % eligible
population population populati
No of households No of
Name of Village included in the households
survey covered by DD
Kalavalapalli 34 29 (85.29) 5(14.71)
Paddadevulapally 36 28(77.78) 8(22.22)
Kasarabad 30 26(86.67) 4(13.33)
Bhongir 30 21(70.0) 9(30.0)
Total 130 104(80.00) 26(20.00)
total Not
covered
Malhotra et al: Mass Drug Administration programme for elimination of lymphatic ilariasis
: 10-16
Journal of Basic and Clinical Research 2014; 1(1) 13
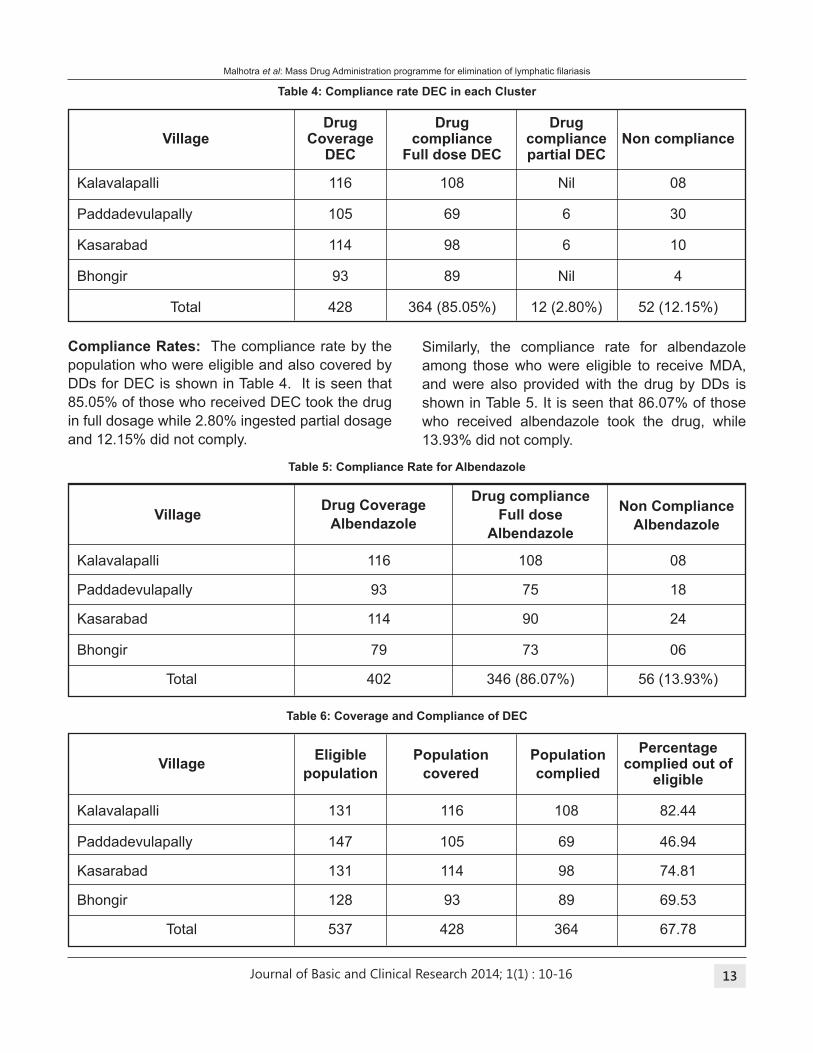
table 4: Compliance rate DEC in each Cluster
Compliance Rates: The compliance rate by the
population who were eligible and also covered by
DDs for DEC is shown in Table 4. It is seen that
85.05% of those who received DEC took the drug
in full dosage while 2.80% ingested partial dosage
and 12.15% did not comply.
Similarly, the compliance rate for albendazole
among those who were eligible to receive MDA,
and were also provided with the drug by DDs is
shown in Table 5. It is seen that 86.07% of those
who received albendazole took the drug, while
13.93% did not comply.
table 5: Compliance Rate for Albendazole
table 6: Coverage and Compliance of DEC
Drug Drug Drug Village Coverage compliance compliance Non compliance DEC Full dose DEC partial DEC
Kalavalapalli 116 108 Nil 08
Paddadevulapally 105 69 6 30
Kasarabad 114 98 6 10
Bhongir 93 89 Nil 4
Total 428 364 (85.05%) 12 (2.80%) 52 (12.15%)
Drug compliance
Village Full dose
Albendazole
Kalavalapalli 116 108 08
Paddadevulapally 93 75 18
Kasarabad 114 90 24
Bhongir 79 73 06
Total 402 346 (86.07%) 56 (13.93%)
Non Compliance
Albendazole
Drug Coverage
Albendazole
Percentage Village complied out of eligible
Kalavalapalli 131 116 108 82.44
Paddadevulapally 147 105 69 46.94
Kasarabad 131 114 98 74.81
Bhongir 128 93 89 69.53
Total 537 428 364 67.78
Eligible Population Population
population covered complied
Malhotra et al: Mass Drug Administration programme for elimination of lymphatic ilariasis
: 10-16
Journal of Basic and Clinical Research 2014; 1(1) 14
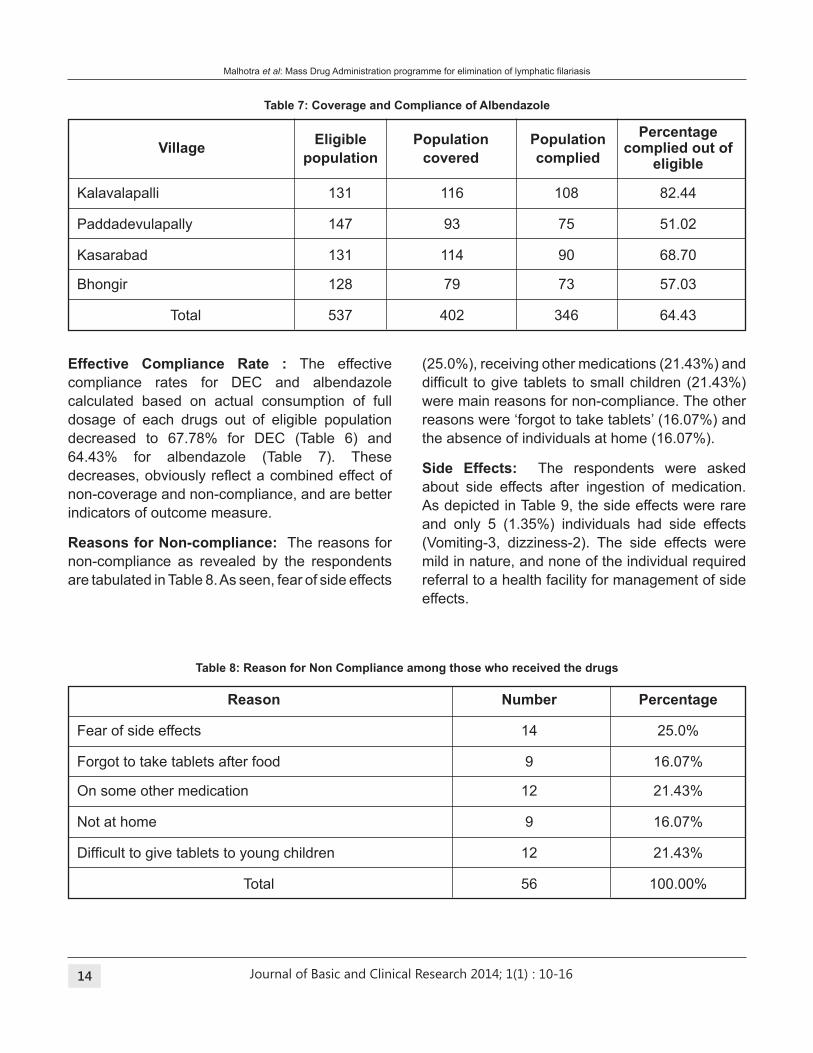
table 7: Coverage and Compliance of Albendazole
Effective Compliance Rate : The effective
compliance rates for DEC and albendazole
calculated based on actual consumption of full
dosage of each drugs out of eligible population
decreased to 67.78% for DEC (Table 6) and
64.43% for albendazole (Table 7). These
decreases, obviously relect a combined effect of non-coverage and non-compliance, and are better
indicators of outcome measure.
Reasons for Non-compliance: The reasons for
non-compliance as revealed by the respondents
are tabulated in Table 8. As seen, fear of side effects
table 8: Reason for Non Compliance among those who received the drugs
Reason Number Percentage
Fear of side effects 14 25.0%
Forgot to take tablets after food 9 16.07%
On some other medication 12 21.43%
Not at home 9 16.07%
Dificult to give tablets to young children 12 21.43%
Total 56 100.00%
(25.0%), receiving other medications (21.43%) and
dificult to give tablets to small children (21.43%) were main reasons for non-compliance. The other
reasons were ‘forgot to take tablets’ (16.07%) and
the absence of individuals at home (16.07%).
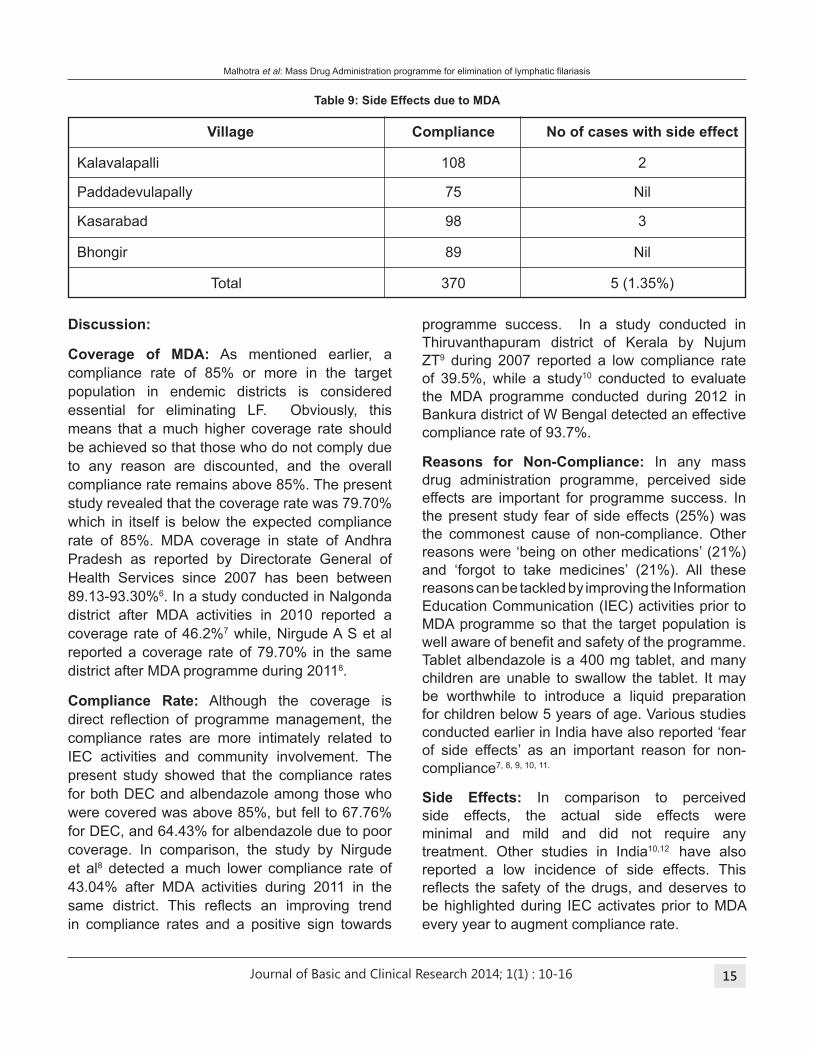
Side Effects: The respondents were asked
about side effects after ingestion of medication.
As depicted in Table 9, the side effects were rare
and only 5 (1.35%) individuals had side effects
(Vomiting-3, dizziness-2). The side effects were
mild in nature, and none of the individual required
referral to a health facility for management of side
effects.
Percentage Village complied out of eligible
Kalavalapalli 131 116 108 82.44
Paddadevulapally 147 93 75 51.02
Kasarabad 131 114 90 68.70
Bhongir 128 79 73 57.03
Total 537 402 346 64.43
Eligible Population Population
population covered complied
Malhotra et al: Mass Drug Administration programme for elimination of lymphatic ilariasis
: 10-16
Journal of Basic and Clinical Research 2014; 1(1) 15
Discussion:
Coverage of MDA: As mentioned earlier, a
compliance rate of 85% or more in the target
population in endemic districts is considered
essential for eliminating LF. Obviously, this
means that a much higher coverage rate should
be achieved so that those who do not comply due
to any reason are discounted, and the overall
compliance rate remains above 85%. The present
study revealed that the coverage rate was 79.70%
which in itself is below the expected compliance
rate of 85%. MDA coverage in state of Andhra
Pradesh as reported by Directorate General of
Health Services since 2007 has been between
89.13-93.30%6. In a study conducted in Nalgonda
district after MDA activities in 2010 reported a
coverage rate of 46.2%7 while, Nirgude A S et al
reported a coverage rate of 79.70% in the same
district after MDA programme during 20118.
Compliance Rate: Although the coverage is
direct relection of programme management, the compliance rates are more intimately related to
IEC activities and community involvement. The
present study showed that the compliance rates
for both DEC and albendazole among those who
were covered was above 85%, but fell to 67.76%
for DEC, and 64.43% for albendazole due to poor
coverage. In comparison, the study by Nirgude
et al8 detected a much lower compliance rate of
43.04% after MDA activities during 2011 in the
same district. This relects an improving trend in compliance rates and a positive sign towards
programme success. In a study conducted in
Thiruvanthapuram district of Kerala by Nujum
ZT9 during 2007 reported a low compliance rate
of 39.5%, while a study10 conducted to evaluate
the MDA programme conducted during 2012 in
Bankura district of W Bengal detected an effective
compliance rate of 93.7%.
Reasons for Non-Compliance: In any mass
drug administration programme, perceived side
effects are important for programme success. In
the present study fear of side effects (25%) was
the commonest cause of non-compliance. Other
reasons were ‘being on other medications’ (21%)
and ‘forgot to take medicines’ (21%). All these
reasons can be tackled by improving the Information
Education Communication (IEC) activities prior to
MDA programme so that the target population is
well aware of beneit and safety of the programme. Tablet albendazole is a 400 mg tablet, and many
children are unable to swallow the tablet. It may
be worthwhile to introduce a liquid preparation
for children below 5 years of age. Various studies
conducted earlier in India have also reported ‘fear
of side effects’ as an important reason for non-
compliance7, 8, 9, 10, 11.
Side Effects: In comparison to perceived
side effects, the actual side effects were
minimal and mild and did not require any
treatment. Other studies in India10,12 have also
reported a low incidence of side effects. This
relects the safety of the drugs, and deserves to be highlighted during IEC activates prior to MDA
every year to augment compliance rate.
table 9: Side Effects due to MDA
Village Compliance No of cases with side effect
Kalavalapalli 108 2
Paddadevulapally 75 Nil
Kasarabad 98 3
Bhongir 89 Nil
Total 370 5 (1.35%)
Malhotra et al: Mass Drug Administration programme for elimination of lymphatic ilariasis
: 10-16
Journal of Basic and Clinical Research 2014; 1(1) 16
Conclusions:
Mass drug administration is the backbone of
elimination of lymphatic ilariasis, a disease that causes disigurement, disability and discrimination. The world today has knowledge as well as
resources to eliminate the disease. The study
reveals that coverage rates are as important
as compliance rates to achieve elimination of
lymphatic ilariasis, and efforts should be made to improve coverage rates by involving more
human resources, supervision and incentive
linked to work-output. Similarly efforts should be
made to improve compliance by the community
by information, education and communication
activities and community involvement in planning
and implementation of MDA programme.
Conlict of interest: None declared
References:
1. Lymphatic Filariasis. Fact Sheet No 102. World Health
Organization, Media Centre. Available from www.who.
int/mediacentre/factsheets/fs102/ en/.
2. Elimination of lymphatic ilariasis as a public health problem. Resolution of the executive board of the
WHO. Available from www.who.int/lymphatic_ilariasis/resources/WHA_50%2029.pdf.
3. Lymphatic Filariasis. WHO. Progress report 2000-2009
and strategies 2010-2020. Available from Whqlibdoc.
who.int/publications/2010/ 97892415007 22_eng.
pdf?ua=1.
4. National Health Policy 2002 (India). Available from www.
childlineindia.org.in/CP-CR_Downloads/ National_
Health_Policy_2002.pdf.
5. Guidelines on ilariasis control in India and its elimi- nation (2009). Available on www.nvbdcp. gov.in/ Doc/
Guidelines-Filariasis-Elimination_ India.pdf.
6. MDA coverage since 2007. National Vector Borne
Disease Control Programme. DGHS. Ministry of Health
and Family Welfare. Available from http:// nvbdcp.gov.in/
il_mda.html .
7. Saiprasad GS, Takalkar Anant A, Prasad VG, Nir-
gude AS, Naik PR, Palve S. Evaluation of Mass Drug
Administration in Elimination of Lymphatic Filariasis in
Nalgonda District. Indian J Public Health 2010;54(4):
194-99.
8. Nirgude AS, Naik PR, Nagaraj K, Reshmi SS, Takalkar
AA, Prasad VG. Evaluation of coverage and compliance
of Mass Drug Administration programme 2011 for
Elimination of Lymphatic Filariasis in Nalgonda District of
Andhra Pradesh, India. National Journal of Community
Medicine 2012;3:288-93.
9. Nujum ZT. Coverage and compliance to mass drug
administration for lymphatic ilariasis elimination in a district of Kerala, India. Int Health 2011;3:22-6.
10. Ghosh S, Samanta A, Kole S. Mass drug administration
for elimination of lymphatic ilariasis: Recent experiences from a district of West Bengal, India. Trop Parasitol
2013;3:67-71.
11. Patel PK. Mass drug administration coverage evaluation
survey for lymphatic Filariasis in Bagalkot and Gulbarga
districts. Indian J Community Med 2012;37:101-6.
12. Chattopadhyay D, Bisoi S, Basu M, Dutta S, Chatterjee
T, Roy S. Annual mass drug administration to eliminate
lymphatic ilariasis: A study in Purba district of West Bengal. International Journal of Basic and Applied
Medical Sciences 2012;2:43-51.
Malhotra et al: Mass Drug Administration programme for elimination of lymphatic ilariasis
: 10-16
Journal of Basic and Clinical Research 2014; 1(1) 17
AbStRACt
background: First year MBBS students admitted to the medical college come from diverse background and
training. Some students are unable to cope with the pressure due to sudden change in the teaching methods
and examination pattern leading to poor performance in examinations. Since the MBBS course is of four and
half years duration, there was a need to design an intervention to enable and empower the students to adapt
to the change and encourage self learning.
Materials and Methods: Students who repeatedly scored less than 30% marks in written and viva voce
weekly assessment examinations were included in the study group. The study comprised of twenty two medical
students belonging to a batch of 100 students. A pre-study structured questionnaire, based on the feedback
of senior students, was administered to identify the dificult areas experienced by the students and post study questionnaire was given to assess any alteration in their dificulties. The outcome of the intervention was assessed by formative assessment. The intervention was in the form of facilitated active learning of 2 hours
each for two days in a week for six weeks period. During this period a faculty member was assigned to each
group, comprising of 11 students each, to facilitate learning.
Results: Commonest dificulty expressed was recalling the subject, though understanding the subject was not a major problem. In the post intervention internal assessment written test, each student in the study group
showed a marked improvement in his/her performance. Thirty two percent (32%) of the study group had an
improved score by at least 20%.
Conclusion: Early identiication of slow learners and introducing facilitated learning in early irst year will help them to overcome their learning dificulties.
Key words: Facilitated learning, self directed learning, slow learners.
Effect of facilitated self directed learning on poor
performers among medical students
Introduction:
Students with below average cognitive abilities
who are not disabled are called slow learners.
They struggle to cope with the traditional academic
demands of the regular classroom. Actually, they
are normal students but the problem with them
is that they are simply not interested in studying
under traditionally accepted system of education.1
While learning has many ends, teaching has only
one: to enable or cause learning.2 Educational
environment and training have a great impact
on students learning and performance outcome.
Although the study of learning has been given
considerable attention, the major shortcoming of
early theories was that the learner was viewed as
a passive receiver of information-an empty vessel
to be illed with good information by teachers. The history of learning theory has shown a shift from this
notion to one that accepts that the learner already
has considerable knowledge and understanding
about the world and takes an active part in creating
new knowledge. This shift, from an ‘instructivist’
*Corresponding Author :
Dr. Shruti Mohanty, Dept. of Biochemistry, Kamineni Institute of
Medical Sciences, Narketpally, Nalgonda District,
Telangana State - 508 254. [email protected]
Shruti Mohanty1*, Sunitha N2, Pragna Rao3
1Professor & Head of Biochemistry, 2Lecturer, Kamineni Institute of Medical Sciences, Narketpally, 3Professor & Head of Biochemistry, Kasturba
Medical College, Manipal.
original article
: 17-20

Journal of Basic and Clinical Research 2014; 1(1) 18
to a ‘constructivist’ approach, is the direction that
teaching has taken over the past several years.
This latter approach is an important concept in the
teaching of adolescents and adults.3
The present study was undertaken in a private
medical college in the rural district of Telangana
State that admits 60% students from state
common entrance test and 40% from management
quota. The students come from different medium
of instructions whereby it becomes dificult for some students to follow lectures, write answers
in English and answer viva-voce after admission
into the medical college. The syllabus being
vast and extensive the students have dificulty in differentiating the ‘must know’ and ‘desirable to
know’ areas resulting in insuficient preparation for examinations and improper time management.
Students must do more than just listen: They must
read, write, discuss, or engage in solving problems.
Most important, to be actively involved, students
must engage in such higher-order thinking tasks
as analysis, synthesis, and evaluation. Within this
context, it is proposed that strategies promoting
active learning be deined as instructional activities involving students in doing things and thinking
about what they are doing.4 Hence, the need to
introduce facilitated active learning that eventually
transforms them into independent self directed
lifelong learners.
Self Directed Learning (SDL) is deined as an approach where learners are motivated to assume
personal responsibility (Garrison, 1997.)
The present study was undertaken to assess
the effect of facilitated self directed learning
and eventually performance of slow learners in
Biochemistry.
Material and Methods
Institutional Ethics committee appproval and
informed consent from the study subjects was
obtained. The study was conducted among a group
of twenty two irst year medical students, which included 13 girls and 9 boys ( n =22) belonging
to a batch of 100 students who repeatedly scored
less than 30% marks in biochemistry written and
viva voce weekly assessment examination. The
students were randomly divided into two groups
of eleven students each, and a trained faculty
member was assigned to each group to act as a
facilitator and to assist in learning methodologies.
A pre study structured questionnaire, based on
the feedback of the previous batch students
was administered to identify the problem areas
in learning and performance in examinations in
Biochemistry.
Students attended two hours each of study
time twice a week for six weeks period during
the schedule tutorial timings. The facilitator
highlighted the importance of self planned learning
and instructed students about the self learning
techniques. Students selected speciic topics for preparation and were encouraged to use
question banks as a means to focus on learning
goals. The students were given assignments to
complete at home and submit to their facilitator.
The materials used were text books, class notes
and question banks. Brain storming sessions
in the form of clinical case solving exercises
followed by group discussions were undertaken
to inculcate higher order cognitive skills ability
and to emphasize the importance of application of
basic science in patient care. Seminar presentations
was introduced to help them overcome fear and
inhibition of public speaking. In order to evaluate
for recall and study completion, assessment was
done periodically by the facilitator by conducting
written tests, viva-voce, and quiz.
Post study questionnaire was administered to
determine the effect of the intervention on the
dificulties identiied before the study. The outcome of the study was evaluated by their performance in
the midterm examination along with others of their
batch. Their performance was compared with the
written test conducted before the study, based on
which the study group was selected. The difference
in marks in the two written tests was expressed in
percentage and analyzed for interpreting the extent
of improvement in performance.
Mohanty et al: Facilitators to promote self directed learning
: 17-20
Journal of Basic and Clinical Research 2014; 1(1) 19
Sl.
No.Questionnaire
Pre study
(n=22)
Agree Disagree Agree Disagree
n (%) n (%) n (%) n (%)
Biochemistry is easy to 14 8 20 2
understand (63.64%) (36.36%) (90.90%) (9.10%)
Topics are dificult to 17 5 5 17
recall (77.27%) (22.73%) (22.73%) (77.27%)
Require personal guidance 20 2 15 7
by a faculty member (90.90%) (9.10%) (68.18%) (31.82%)
Relevance of case 13 9 20 2
discussions in irst year (59.09%) (40.91%) (90.90%) (9.10%)
Repeated exam makes 16 6 20 2
me more conident (72.72%) (27.28%) (90.90%) (9.10%)
Feel inferior if isolated for 4 18 5 17
extra study hours (18.19%) 81.81%) (22.73%) (77.27%)
21 1 3 19
(95.45%) (4.55%) (13.63%) (86.37%)
1
2
3
4
5
6
7
Post study
(n=22)
Dificult to differentiate between
‘must know’ and
‘nice to know’ areas
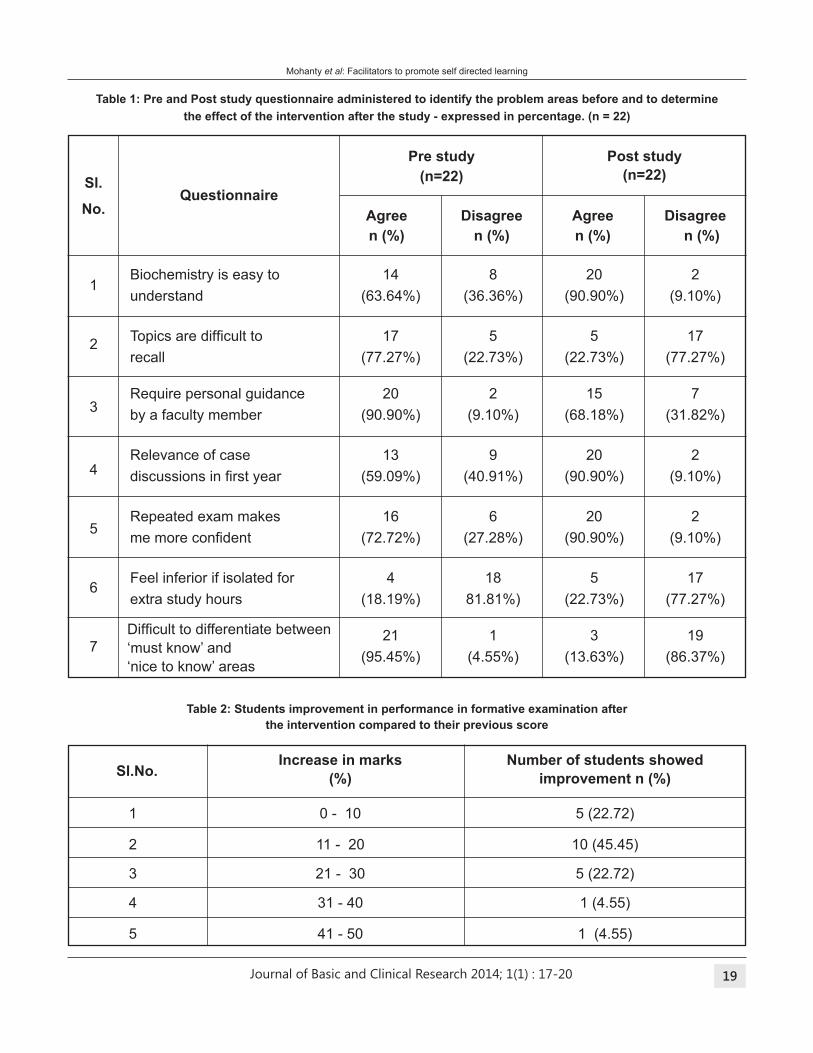
table 1: Pre and Post study questionnaire administered to identify the problem areas before and to determine
the effect of the intervention after the study - expressed in percentage. (n = 22)
table 2: Students improvement in performance in formative examination after
the intervention compared to their previous score
Increase in marks Number of students showed
(%) improvement n (%)
1 0 - 10 5 (22.72)
2 11 - 20 10 (45.45)
3 21 - 30 5 (22.72)
4 31 - 40 1 (4.55)
5 41 - 50 1 (4.55)
Sl.No.
Mohanty et al: Facilitators to promote self directed learning
: 17-20

Journal of Basic and Clinical Research 2014; 1(1) 20
Result and Discussion
Analysis of the pretest and posttest questionnaire
(Table 1) revealed that only 63% of the students
found the subject content easy to understand
before the intervention which markedly increased
to 91% after the intervention.
However, the scores reversed regarding
recalling the subject learnt earlier, where
77% of students expressed their dificulty in recalling the content studied earlier
before the study and only 23 % agreed after the
intervention. Majority (91%) of students could
appreciate the relevance of clinical case discussion
during biochemistry learning after the study in
comparison to 59% of students before the study.
Most of the students (95.5%) also had dificulty in identifying the core subject content ‘must know’
from ‘nice to know’ topics before intervention which
decreased noticeably to 13.6% after the study
period.
After the said intervention of facilitated self
directed learning, a signiicant increase in recall of the subject was observed when compared to
before study period. The percentage of students
requiring personal guidance from faculty member
also declined signiicantly, suggesting that students were more conident about independent learning. Secondly, the percentage of students not
comfortable with extra classes for poor performance
also increased signiicantly, endorsing the fact that they were conidant of learning through self study. In addition all students showed improvement
during post intervention test results, with 32.8 %
showing an improvement of more than 20% (Table
2). The above observations can be attributed to
the focused and need based support provided
by the facilitators during the intervention. The
facilitator helps deine the course objectives and goals. Secondly, intensive practice in writing and
speaking along with group discussions of clinical
case studies in small groups make the students
more comfortable and capable of expressing the
subject content.
Conclusion:
With minimal intervention and effective need based
facilitation, self directed study method can enable
and empower the students to overcome their
learning dificulties and score well in examination. This study also highlights that some students
are slow to learn but they do not have a learning
deiciency. What is essential is to customize the methodology for effective learning.
Conlict of interest: The authors declare no
conlict of interest.
References:
1. Borah RR. Slow Learners: Role of Teachers and
Guardians in Honing their Hidden skills. International
Journal of Educational Planning & Administration 2013;
3: 139-43.
2. Cross KP. In Search of Zippers. AAHE Bulletin 1988;
40(10):3-7.
3. Smith, Peter J, Blake, Damian. Facilitating learning
through effective teaching : at a glance, Adelaide, South
Australia: NCVER, 2005.
4. Bonwell, CC. Active Learning: Creating Excitement in
the Classroom. Available at https://www.ydae.purdue.
edu/lct/HBCU/documents/Active_Learning_Creating_
Excitement_in_the_Classroom.pdf (Last accessed 01
June 2014).
Mohanty et al: Facilitators to promote self directed learning
: 17-20
Journal of Basic and Clinical Research 2014; 1(1) 21
R.R.Rao*
*Professor & Head, Department of Microbiology, Kamineni Academy of Medical Sciences & Research Center, Hyderabad.
Applications of Nanobiotechnology
Nanotechnology encompasses many ields of Natural sciences and Nanobiotechnology refers
to the intersection of nanotechnology and biology.
Broadly speaking anything with a dimension of less
than 100 nm can be named as ‘nanostructured’ and
these days it also seems that anything that its into this deinition will be termed ‘nanostructured’.1 The
Physicist Richard Feynman in 1959, in his famous
speech mentioned the possibility of manipulating
and controlling them on a molecular scale in order
to achieve electronic and mechanical systems with
atomic sized components.2 He further made a remark
that the development of technologies to combat
such small systems would be inter disciplinary
combining the ields of Physics, Chemistry and Biology and could offer a new world of possibilities
that could radically change the technology that
is existing currently. Moore in 1965 noted that
the number of transistors on a chip had roughly
doubled every year since 1959 and predicted that
each new generation of micro systems would help
to develop the next generation at lower cost with
smaller components. To date the semiconductor
industry proved Moore’s law. The continuous down
scaling of systems will have a profound impact on
society and on lives and continues to open up new
frontiers and possibilities.
Fundamentals of Nanotechnology
Nevertheless, no exponential growth can continue
forever and the semiconductor industry will
eventually reach the atomic limit for downsizing
the transistors.
Interestingly the current trends in the development
indicate that atomic limit might not be the limiting
factor for technical development in near future
although it may take time to achieve it. As the
systems become more diverse and become so
small, quantum effects dominate. In addition
microbiology and biochemistry are becoming
important for applications of all the developments.
In early 1990's researchers got interest in
Feynman‘s observations probably because the
term ‘nanotechnology’ gained serious attention
just then following its use by K.Eric Drexier in
his book ‘Engines of creation: The coming Era of
nanotechnology’ which took Feynman’s concept of
billions of tiny factories and added the idea that
they can make more copies of themselves through
computer control instead of human operator.3 The
Japanese scientist Norio Tanaguchi of the Tokyo
University of Science was irst to use the term ‘nanotechnology’ in a conference in 1974. He deined “nanotechnology mainly consists of the processing
of separation, consolidation and deformation of
material by one atom or molecule”. In 1980s the
concept of nanotechnology was conceptually
explored in depth by K. Eric. Drexier and his 1991
PhD at MIT media lab was the irst doctoral degree on the topic of molecular nanotechnology for which
he received American publishers’ award for Best
Computer Science Book of 1992. Meanwhile
the advances in interface and colloid science
took place due to the scholarly work of Richard
Adolf Zsigmondy and Irvin Langmuir and both of
them received Nobel Prize for their contribution
to Chemistry. Harry Kroto, Richard Smalley and
Richard Curl discovered fullerenes in 1985 and
they shared Nobel Prize in Chemistry. Richard
*Corresponding author :
Dr. R.R.Rao, Department of Microbiology, Kamineni Academy
of Medical Sciences & Research Center, Hyderabad,
Telangana State. [email protected]
Review article
: 21-24

Journal of Basic and Clinical Research 2014; 1(1) 22
Smalley and Kroto collaborated and discovered
C60
and other fullerenes as a third allotropic form of
Carbon.4 Subsequently discoveries included
endohedral fullerenes and large form of fullerenes
in the following year. The discovery of carbon
nanotubes is largely attributed to Sumio lijima of
NEC in 1991. In the early 1990s Huffman and
Kraetschmer of the University of Arizona were
able to develop the technique of synthesizing and
purifying large quantities of fullerenes. A fullerene is
any molecule composed of entirely of carbon in the
form of a hallow sphere, ellipsoid or tube. Spherical
fullerenes are also called ‘buckyballs’ and the
cylindrical types are called carbon nanotubes or
‘buckytubes’. Fullerenes are similar to Graphite in
structure which is composed of staked grapheme
sheets of linked hexagonal rings. They can also
contain pentagonal or heptagonal rings). This
opened the doors for their characterization and
functionalization by hundreds of investigators.
Soon rubidium doped C60
was found to be a mid
temperature super conductor. Dr. T. Ebbsen at
a meeting of Material Research Society in 1992
described to a spell bound audience, his discovery
and characterization of carbon nanotubes. There
after hundreds of researchers further developed the
ield of nanotube-based nanotechnology. Today the visions of Richard Feynman are shared by many
others and nanotechnology is seen as general cross
disciplinary technology and it has the potential to
create an industrial revolution comparable or far
exceeding the impact of electricity and information
technology.5
Nanotechnology is not a new entity. It is old and
one can ind it in the sun screen that is used in summer and some paints as well as coatings can
also be called nanotech since they all contain
nanoparticles with unique optical properties.
Nanoparticles have been known in optics for
hundreds of years and they have been used to stain
and colour glasses for centuries.6 Catalysis which
is a major industrial process is highly dependent
on nanoscale catalytic particles. Nanoscale wires
and tubes have only recently really been given
attention with the advent of Carbon nanotubes and
Rao: Applications of Nanotechnology
semiconductor nanowires while nanoscale ilms are even present in anti-relecting coatings on the glasses and binoculars. Thin metal ilms have been used for sensitive detection with surface plasmons
for decades (Surface plasmons are excitations of
charges at surface).
Nano-components:7
The methods and components of nanotechnology
are constantly undergoing developments and each
generation is providing foundation for the next
one. The Scanning Tunnel Microscopy (STM) and
Atomic Force Microscopy (AFM) came into use
in1980s and opened up new ways to investigate
nanoscale materials. The transmission electron
microscopy (TEM) introduced in 1930s offered
the possibilities of images as well as created
nanodevices by electron beam lithography.
Several nanoscale structures were developed in
1990s such as Carbon 60 molecules and Carbon
nanotubes. In recent years more complex nano-
structures such as semiconductor nanowire
hetero-structures have proved to be useful as
building blocks or components in nanodevices.
Nano-components are useful in electronics optics /
photonics medical, biological as well as better and
smarter materials.
A main problem is reliable integration of the
nanoscale components into micro systems, since
production methods are often not compatible. Self-
assembly of devices in liquids is an expanding ield within nanotechnology but usually requires the
components to be covered with various surfactants
which usually also inluence the components’ properties. The current integration technique for
nanowire or tube systems seem to be Electron
beam lithography (EBL) of metal structures onto
substrates with randomly positioned nanowires
deposited from the liquid dispersion. By using low alignment or electrical ield the wire deposition from the liquids can be constructed to some extent.
The EBL method has allowed for systematic
investigation of ‘nanowires’ and ‘tubes’ for electrical
properties and creation of high performance
electronic components such as chemical sensors or
: 21-24

Journal of Basic and Clinical Research 2014; 1(1) 23
medical problems and reines their applications. Nanobiotechnology is also concerned in developing
new tools that are applicable to medical / biological
ields. The imaging of native biomolecules, biological membranes and tissues is also a major
area of Nanobiotechnology. Others include use of
Cantilevers array sensors (Cantilever is abeam
anchored only at one end) and applications of
nanophotonics for manipulating the molecular
processes in the living cells.
In simple language Nanobiotechnology is
miniatured biotechnology applied to biology or
medicine and Bionanotechnology is a speciic application of nanotechnology. A good example
of Bionanotechnology is DNA nanotechnology or
cellular engineering and conversely many new
medical technologies involving nanoparticles as
delivering systems or sensors fall under the term
Nanobiotechnology.9
Material properties and applications studied in
bionanoscience include mechanical (deformation,
adhesion and failure etc.), electrical / electronic
(electromechanical stimulation, capacitors and
storage batteries etc.), optical (absorption,
luminescence and photochemistry etc.), thermal
(thermo-mutability, thermal management etc.),
biological (the interaction of cells with nanoparticles,
nanodevices, molecular laws, defects and biosensing etc.), nanoscience of diseases (cancer,
organ or tissue failure etc.) and computing (e.g
DNA computin)
References:
1. Drexler KE. New era of nanotechnology. New York:
Anchor Press; 1986. Engines of creation: The coming
era of nanotechnology; 99–129.
2. Feynman RP. There's plenty of room at the bottom. Eng
Sci.1960;23:22–36.
3. Nano A. The A to Z of nanotechnology And nanomaterials.
The Institute of nanotechnology, Azom Co Ltd; 2003.
4. Freitas R., Jr Nanotechnology, nanomedicine and
nanosurgery. Int J Surg. 2005;3:243–6
5. Freitas RA., Jr Nanodentistry. J Am Dent Assoc.
2000;131:1559–66.
6. Reifman EM. Diamond teeth. In: Crandall BC, editor.
Rao: Applications of Nanotechnology
ield-effect transistors. Scanning probe microscopy has been used to create and study nanotube
junction properties.8
Materials reduced to nanoscale can show different
properties compared to what they exhibit on
macro scale enabling unique applications. For
example opaque substances become transparent,
stable material becomes combustible, insoluble
substances like gold becomes soluble. A material
such as gold which is chemically inert at normal
scales, can serve as potent chemical catalyst
at a nanoscale. Much of the fascination with
nanotechnology comes from these quantum
and surface phenomena that matter exhibits at
nanoscale. Material referred to as nanomaterials
generally fall into two categories: fullerenes
and inorganic nanoparticles. Nanoparticles or
nanocrystals made of metals, semiconductors or
oxides of particular interest for their mechanical,
electrical, magnetic, optical and chemical properties.
Nanoparticles have been used as quantum dots
and as chemical catalysts. Nanoparticles exhibit
a number of special properties relative to bulk
matter. Copper nanoparticles smaller than 50 nm
are considered super hard. Ferro electric materials
smaller than 10 nm can switch the magnetism
directly using room temperature thermal energy
thus making the material unsuitable for memory
storage. Suspensions of nanoparticles are possible
because of interaction of the particle surface with
the solvent is strong enough to overcome the
differences in density. Nanoparticles exhibit unique
optical properties because they are small enough to
conine their electrons to produce quantum effect. For example gold nanoparticles appear deep red
or black in solution.
Nanobiotechnology:
Nanobiotechnology indicates the merging
of biological research with various ields of nanotechnology. Biologically inspired
nanotechnology uses biological systems as the
inspiration for technologies not yet created. The
most important objective of Nanobiotechnology is
to involve applying nanotools to relevant biological/
: 21-24
Journal of Basic and Clinical Research 2014; 1(1) 24
Rao: Applications of Nanotechnology
Nanotechnology: Molecular speculations on global
abundance.Cambridge, Mass: MIT Press; 1996. 81–6.
7. Frietas RA., Jr Current status of nanomedicine and
medical nanorobotics. J Comut Ther Nanosci. 2005;
2:1-25.
8. Moghuni,SM,Hubter,AC, MurraymJC. Nanomedicine:
Current status and future prospects. FASEBJ
2005:19:311-30.
9. Fahy GM. Molecular nanotechnology and its possible
pharmaceutical implications. In: Bezold C, Halperin JA,
Eng JL, editors. 2020 visions: Health care information
standards and technologies. Rockville, MD: U.S
Pharmacopenial Convention; 1993. 152–9.
: 21-24

Journal of Basic and Clinical Research 2014; 1(1) 25
N.Sreekumaran Nair1*, Ravishankar2, Melissa Glenda Lewis2
1Professor of Biostatistics and Director, Public Health Evidence South Asia, Manipal University, Manipal, 2Research Scholar, Biostatistics,
Manipal University, Manipal.
Role of systematic reviews and meta-analysis in
evidence based health care
Introduction:
In broad sense, health care means prevention,
treatment and management of illness as well as
preservation of health of the people. This has been
achieved through various simple and complex
strategies and programmes jointly experimented
and implemented by multiple agencies and
professional organisations. In earlier days, the
health care system was dominated by eminence
based decision making in which expert opinion was
regarded as the ultimate evidence of effectiveness
of any programme. However, this approach
underwent major criticism during last two decades
mainly because of the chance of bias in the
approach and led to the emergence of evidence
based or evidence informed health care.
The evidence based health care relies on provision
for providing healthcare based on knowledge of a
combination of best available research indings, clinical experience & expertise, client needs and
preferences.1 This approach has been accepted
globally and at present almost all major healthcare
providing agencies have incorporated it in their
policy. The most dificult component in evidence informed health care is how to synthesise the
best available research indings? Looking at the magnitude of research articles getting published
every day, reading all these articles and targeting
the healthcare practice based on this knowledge
is almost an impossible task for any healthcare
provider. In this context it would be a great support,
irstly if there is a methodology which provides robust approach to pool all available evidence and
generate summary of evidence and secondly if
there can be a group/institution or an agency which
can conduct this synthesis and provide up to date
comprehensive research evidence for immediate
use to health care practitioners and policy makers.
Systematic review combined with meta-analysis
has been accepted as a potential robust method of
health care research evidence synthesis and there
are major international organisations exclusively
working for this purpose. The present article
sensitises the readers to the concept of systematic
reviews and meta-analysis, major organisations
involved in evidence synthesis and also the
historical development of meta-analysis.
Systematic Reviews
Reviews in health care are detailed reports related
to history, treatment strategies and outcomes
of intervention regarding a disease or a health
condition which are usually written by an expert
based on experience and available literature.
Even though these reviews are important, they are
proved not to be focussed on any speciic question and more prone to bias. To address this issue,
there emerged another concept called “Systematic
reviews”. These reviews are conducted to
answer a focussed research question based
on all available literature with a robust scientiic methodology. Systematic review methodology
involves scientiic processes to collect, combine, analyse and summarise all available evidences
*Corresponding author :
Dr. N Sreekumaran Nair,
Dept. of Biostatistics, Manipal University, Manipal,
Karnataka - 576 104, [email protected]
Review article
: 25-30
Journal of Basic and Clinical Research 2014; 1(1) 26
with minimum or no bias. Therefore systematic
reviews and meta-analysis occupy the top position
in the hierarchy of evidence.
Systematic reviews and meta-analysis are known
to produce highest form of evidence in medical
research.2 In a systematic review, a focussed
research question is formulated, all the procedures
of review are explicitly deined in advance, available research articles on the concerned question are
selected by a structured search strategy and
selected articles are assessed for quality with
standard quality evaluation tools. Results from
such selected articles are extracted with the help
of a predesigned data extraction tool and are
combined using a statistical method called meta-
analysis. Thus it helps to obtain a single concise
answer to every focussed research question,
enabling to arrive at a irm conclusion about the effectiveness of an intervention.
The steps involved in a systematic review process
are;3
1. Framing research question: the irst step in a systematic review process is to identify a
focused research question which is relevant and
answerable. The selection of an appropriate,
unique research question is the foundation of
the systematic review.
2. Protocol preparation: systematic review
requires an explicitly described protocol. The
protocol has a speciic structure and requires basic training for its preparation.
3. Literature search: systematic review involves
a structured and a rigorous literature search
so as to procure all the available and relevant
literature pertaining to the identiied research
question. The literature search strategy should
be extensive and must involve expert guidance
for its development. The aim of this process is
to gather all available literature pertaining to
the research question into one basket. This is
one of the crucial aspects that differentiate a
systematic review from a narrative review.
4. Data extraction: data (results) pertaining to
the pre-speciied outcomes are extracted in an objective manner from all collected studies by
means of a valid data extraction tool.
5. Quality assessment: The methodological
quality of the collected studies is assessed by
means of a pre-speciied scientiic technique.
6. Statistical analysis: the results of collected
individual studies are quantitatively combined
by robust statistical technique called “Meta-
analysis”.
7. Preparation of the review document: the
systematic review is prepared according to the
pre-decided criteria in a manner as stated in
the protocol. The limitations, existing biases,
strength of the evidence and recommendations
for further research are clearly stated.
8. Publication of the review: the developed
review is published in a suitable journal.
9. The above described rigorous procedures make
the systematic review evidence much distinct
from that of a narrative review.
Systematic review protocol
Every systematic review begins with a well
structured protocol, which describes all the
underlying systematic review processes explicitly.
Nair et al: Systematic reviews and meta-analysis
: 25-30
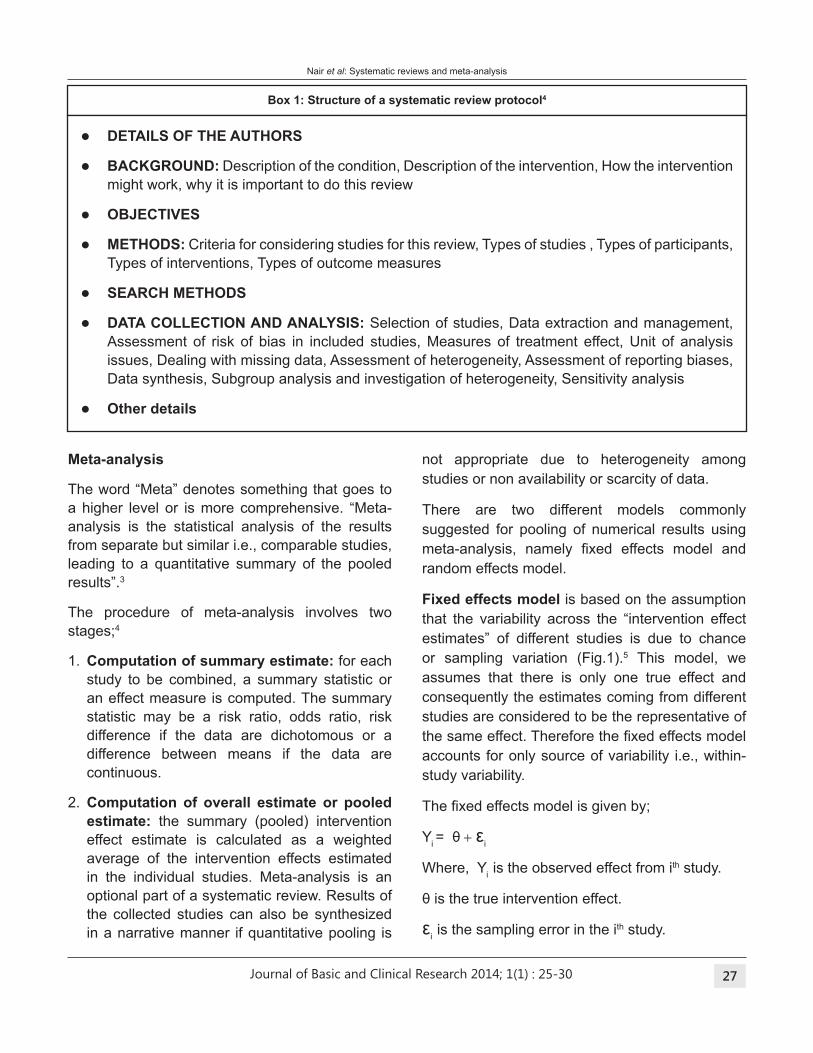
Journal of Basic and Clinical Research 2014; 1(1) 27
box 1: Structure of a systematic review protocol4
lDEtAILS OF tHE AUtHORS
lbACKGROUND: Description of the condition, Description of the intervention, How the intervention
might work, why it is important to do this review
lObJECtIVES
lMEtHODS: Criteria for considering studies for this review, Types of studies , Types of participants,
Types of interventions, Types of outcome measures
lSEARCH MEtHODS
lDAtA COLLECtION AND ANALYSIS: Selection of studies, Data extraction and management,
Assessment of risk of bias in included studies, Measures of treatment effect, Unit of analysis
issues, Dealing with missing data, Assessment of heterogeneity, Assessment of reporting biases,
Data synthesis, Subgroup analysis and investigation of heterogeneity, Sensitivity analysis
lOther details
Meta-analysis
The word “Meta” denotes something that goes to
a higher level or is more comprehensive. “Meta-
analysis is the statistical analysis of the results
from separate but similar i.e., comparable studies,
leading to a quantitative summary of the pooled
results”.3
The procedure of meta-analysis involves two
stages;4
1. Computation of summary estimate: for each
study to be combined, a summary statistic or
an effect measure is computed. The summary
statistic may be a risk ratio, odds ratio, risk
difference if the data are dichotomous or a
difference between means if the data are
continuous.
2. Computation of overall estimate or pooled
estimate: the summary (pooled) intervention
effect estimate is calculated as a weighted
average of the intervention effects estimated
in the individual studies. Meta-analysis is an
optional part of a systematic review. Results of
the collected studies can also be synthesized
in a narrative manner if quantitative pooling is
not appropriate due to heterogeneity among
studies or non availability or scarcity of data.
There are two different models commonly
suggested for pooling of numerical results using
meta-analysis, namely ixed effects model and random effects model.
Fixed effects model is based on the assumption
that the variability across the “intervention effect
estimates” of different studies is due to chance
or sampling variation (Fig.1).5 This model, we
assumes that there is only one true effect and
consequently the estimates coming from different
studies are considered to be the representative of
the same effect. Therefore the ixed effects model accounts for only source of variability i.e., within-
study variability.
The ixed effects model is given by;
Yi = θ + ε
i
Where, Yi is the observed effect from ith study.
θ is the true intervention effect.
εi is the sampling error in the ith study.
Nair et al: Systematic reviews and meta-analysis
: 25-30
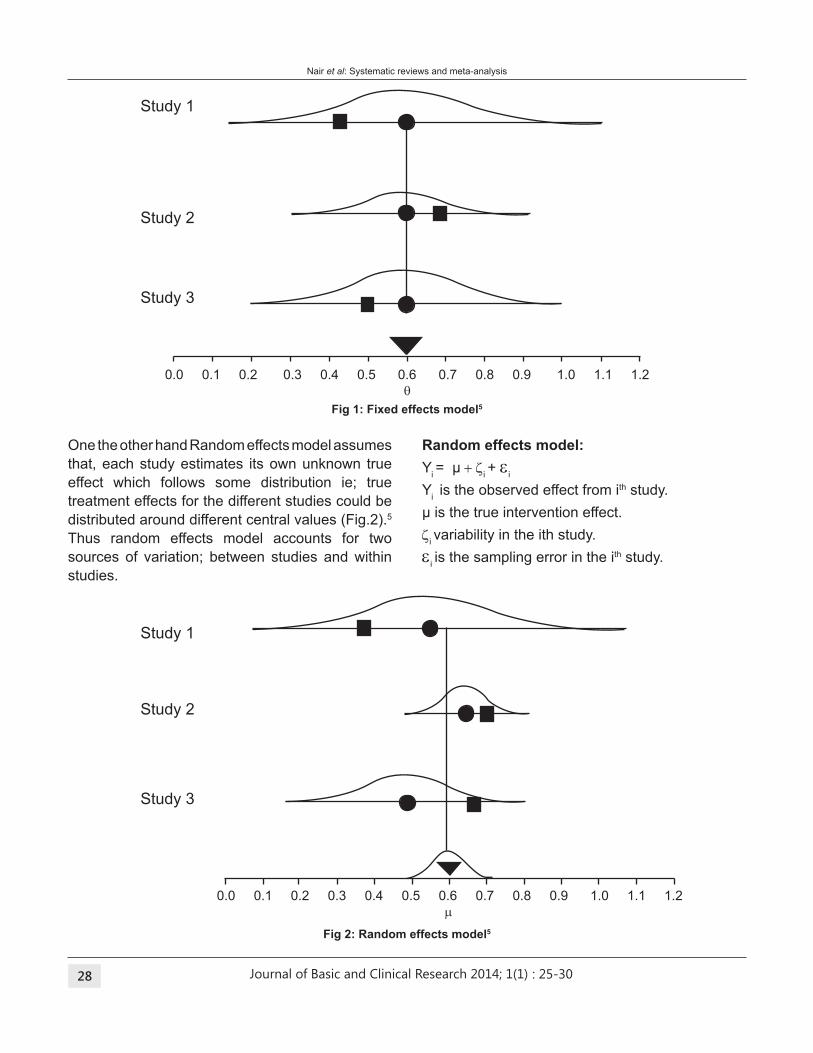
Journal of Basic and Clinical Research 2014; 1(1) 28
Fig 1: Fixed effects model5
Fig 2: Random effects model5
One the other hand Random effects model assumes
that, each study estimates its own unknown true
effect which follows some distribution ie; true
treatment effects for the different studies could be
distributed around different central values (Fig.2).5
Thus random effects model accounts for two
sources of variation; between studies and within
studies.
Random effects model:
Yi = μ + z
i + e
i
Yi is the observed effect from ith study.
μ is the true intervention effect.z
i variability in the ith study.
ei is the sampling error in the ith study.
0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0 1.1 1.2
m
Study 1
Study 2
Study 3
0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0 1.1 1.2
q
Study 1
Study 2
Study 3
Nair et al: Systematic reviews and meta-analysis
: 25-30
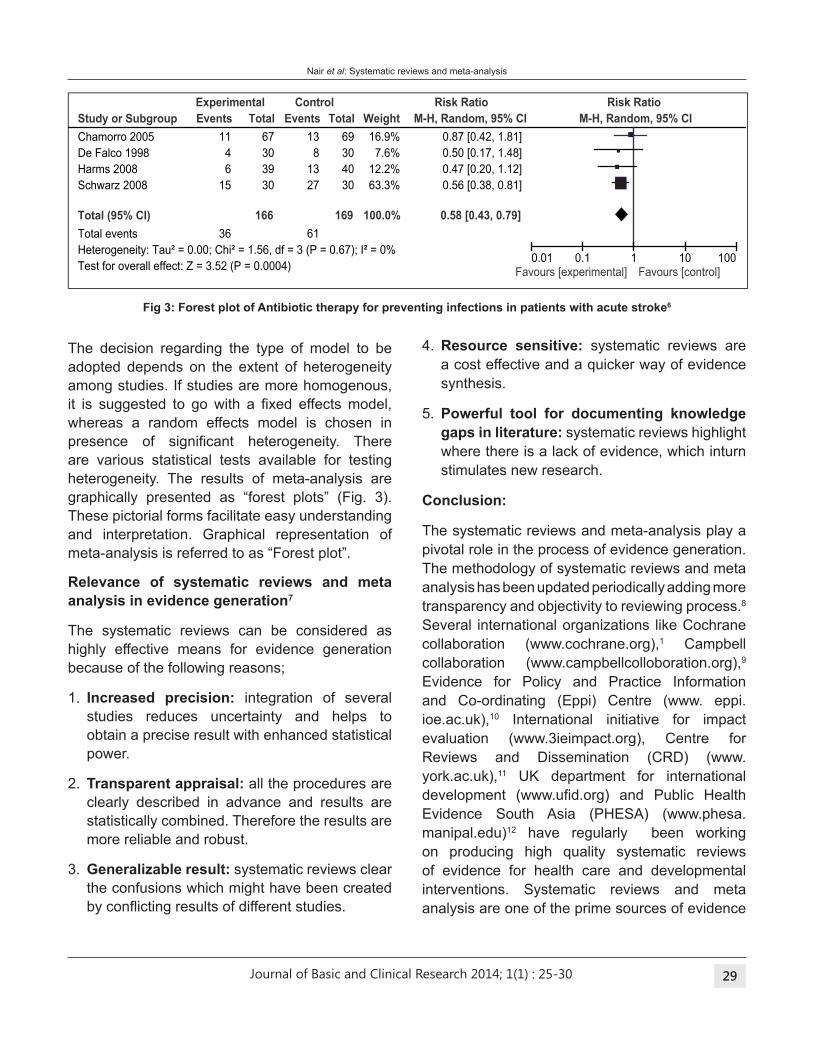
Journal of Basic and Clinical Research 2014; 1(1) 29
The decision regarding the type of model to be
adopted depends on the extent of heterogeneity
among studies. If studies are more homogenous,
it is suggested to go with a ixed effects model, whereas a random effects model is chosen in
presence of signiicant heterogeneity. There are various statistical tests available for testing
heterogeneity. The results of meta-analysis are
graphically presented as “forest plots” (Fig. 3).
These pictorial forms facilitate easy understanding
and interpretation. Graphical representation of
meta-analysis is referred to as “Forest plot”.
Relevance of systematic reviews and meta
analysis in evidence generation7
The systematic reviews can be considered as
highly effective means for evidence generation
because of the following reasons;
1. Increased precision: integration of several
studies reduces uncertainty and helps to
obtain a precise result with enhanced statistical
power.
2. transparent appraisal: all the procedures are
clearly described in advance and results are
statistically combined. Therefore the results are
more reliable and robust.
3. Generalizable result: systematic reviews clear
the confusions which might have been created
by conlicting results of different studies.
Fig 3: Forest plot of Antibiotic therapy for preventing infections in patients with acute stroke6
4. Resource sensitive: systematic reviews are
a cost effective and a quicker way of evidence
synthesis.
5. Powerful tool for documenting knowledge
gaps in literature: systematic reviews highlight
where there is a lack of evidence, which inturn
stimulates new research.
Conclusion:
The systematic reviews and meta-analysis play a
pivotal role in the process of evidence generation.
The methodology of systematic reviews and meta
analysis has been updated periodically adding more
transparency and objectivity to reviewing process.8
Several international organizations like Cochrane
collaboration (www.cochrane.org),1 Campbell
collaboration (www.campbellcolloboration.org),9
Evidence for Policy and Practice Information
and Co-ordinating (Eppi) Centre (www. eppi.
ioe.ac.uk),10 International initiative for impact
evaluation (www.3ieimpact.org), Centre for
Reviews and Dissemination (CRD) (www.
york.ac.uk),11 UK department for international
development (www.uid.org) and Public Health Evidence South Asia (PHESA) (www.phesa.
manipal.edu)12 have regularly been working
on producing high quality systematic reviews
of evidence for health care and developmental
interventions. Systematic reviews and meta
analysis are one of the prime sources of evidence
Nair et al: Systematic reviews and meta-analysis
Study or Subgroup
Chamorro 2005
De Falco 1998
Harms 2008
Schwarz 2008
total (95% CI)
Total events
Heterogeneity: Tau² = 0.00; Chi² = 1.56, df = 3 (P = 0.67); I² = 0%Test for overall effect: Z = 3.52 (P = 0.0004)
Events
11
4
6
15
36
total
67
30
39
30
166
Events
13
8
13
27
61
total
69
30
40
30
169
Weight
16.9%
7.6%
12.2%
63.3%
100.0%
M-H, Random, 95% CI
0.87 [0.42, 1.81]
0.50 [0.17, 1.48]
0.47 [0.20, 1.12]
0.56 [0.38, 0.81]
0.58 [0.43, 0.79]
Experimental Control Risk Ratio Risk Ratio
M-H, Random, 95% CI
0.01 0.1 1 10 100Favours [experimental] Favours [control]
: 25-30
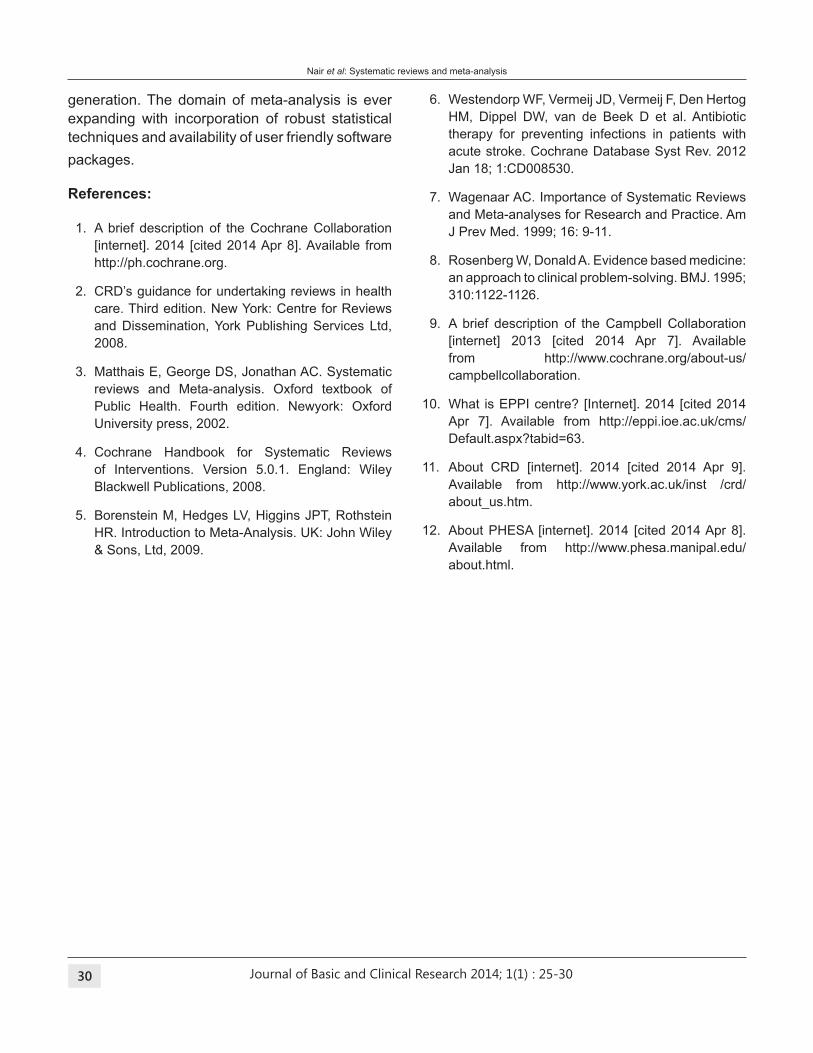
Journal of Basic and Clinical Research 2014; 1(1) 30
generation. The domain of meta-analysis is ever
expanding with incorporation of robust statistical
techniques and availability of user friendly software
packages.
References:
1. A brief description of the Cochrane Collaboration
[internet]. 2014 [cited 2014 Apr 8]. Available from
http://ph.cochrane.org.
2. CRD’s guidance for undertaking reviews in health
care. Third edition. New York: Centre for Reviews
and Dissemination, York Publishing Services Ltd,
2008.
3. Matthais E, George DS, Jonathan AC. Systematic
reviews and Meta-analysis. Oxford textbook of
Public Health. Fourth edition. Newyork: Oxford
University press, 2002.
4. Cochrane Handbook for Systematic Reviews
of Interventions. Version 5.0.1. England: Wiley
Blackwell Publications, 2008.
5. Borenstein M, Hedges LV, Higgins JPT, Rothstein
HR. Introduction to Meta-Analysis. UK: John Wiley
& Sons, Ltd, 2009.
6. Westendorp WF, Vermeij JD, Vermeij F, Den Hertog
HM, Dippel DW, van de Beek D et al. Antibiotic
therapy for preventing infections in patients with
acute stroke. Cochrane Database Syst Rev. 2012
Jan 18; 1:CD008530.
7. Wagenaar AC. Importance of Systematic Reviews
and Meta-analyses for Research and Practice. Am
J Prev Med. 1999; 16: 9-11.
8. Rosenberg W, Donald A. Evidence based medicine:
an approach to clinical problem-solving. BMJ. 1995;
310:1122-1126.
9. A brief description of the Campbell Collaboration
[internet] 2013 [cited 2014 Apr 7]. Available
from http://www.cochrane.org/about-us/
campbellcollaboration.
10. What is EPPI centre? [Internet]. 2014 [cited 2014
Apr 7]. Available from http://eppi.ioe.ac.uk/cms/
Default.aspx?tabid=63.
11. About CRD [internet]. 2014 [cited 2014 Apr 9].
Available from http://www.york.ac.uk/inst /crd/
about_us.htm.
12. About PHESA [internet]. 2014 [cited 2014 Apr 8].
Available from http://www.phesa.manipal.edu/
about.html.
Nair et al: Systematic reviews and meta-analysis
: 25-30
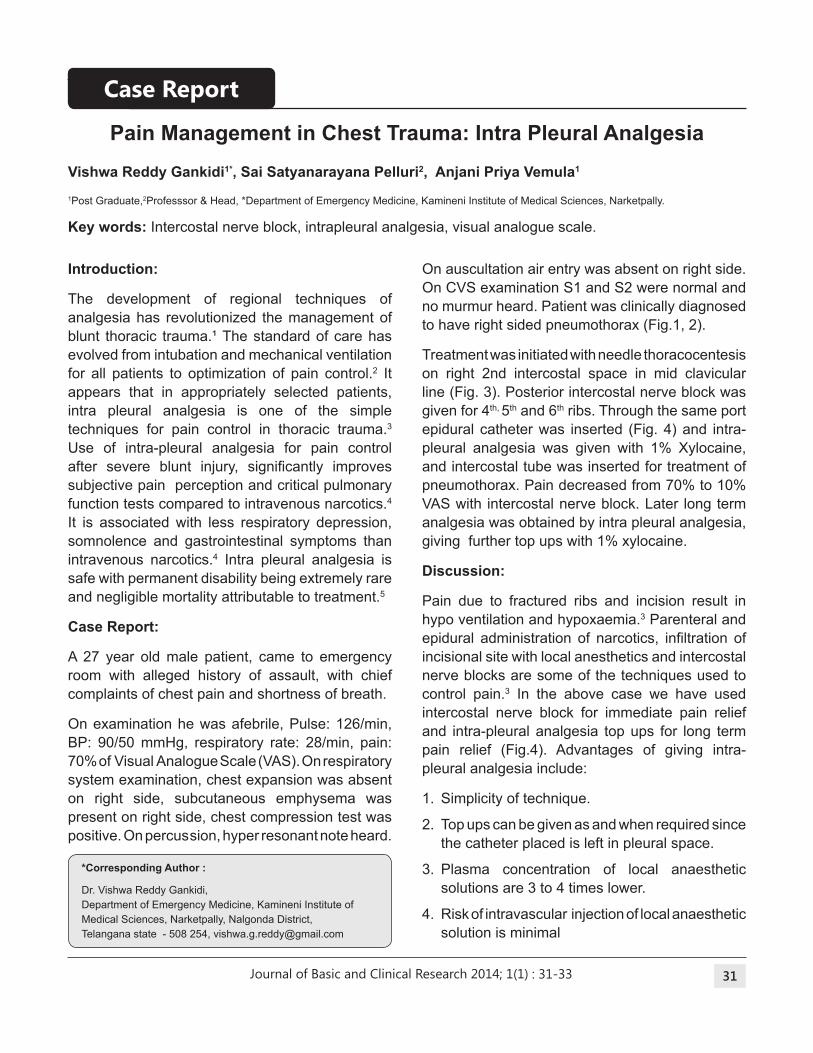
Journal of Basic and Clinical Research 2014; 1(1) 31
Vishwa Reddy Gankidi1*, Sai Satyanarayana Pelluri2, Anjani Priya Vemula1
1Post Graduate,2Professsor & Head, *Department of Emergency Medicine, Kamineni Institute of Medical Sciences, Narketpally.
Key words: Intercostal nerve block, intrapleural analgesia, visual analogue scale.
Pain Management in Chest trauma: Intra Pleural Analgesia
Introduction:
The development of regional techniques of
analgesia has revolutionized the management of
blunt thoracic trauma.¹ The standard of care has
evolved from intubation and mechanical ventilation
for all patients to optimization of pain control.2 It
appears that in appropriately selected patients,
intra pleural analgesia is one of the simple
techniques for pain control in thoracic trauma.3
Use of intra-pleural analgesia for pain control
after severe blunt injury, signiicantly improves subjective pain perception and critical pulmonary
function tests compared to intravenous narcotics.4
It is associated with less respiratory depression,
somnolence and gastrointestinal symptoms than
intravenous narcotics.4 Intra pleural analgesia is
safe with permanent disability being extremely rare
and negligible mortality attributable to treatment.5
Case Report:
A 27 year old male patient, came to emergency
room with alleged history of assault, with chief
complaints of chest pain and shortness of breath.
On examination he was afebrile, Pulse: 126/min,
BP: 90/50 mmHg, respiratory rate: 28/min, pain:
70% of Visual Analogue Scale (VAS). On respiratory
system examination, chest expansion was absent
on right side, subcutaneous emphysema was
present on right side, chest compression test was
positive. On percussion, hyper resonant note heard.
On auscultation air entry was absent on right side.
On CVS examination S1 and S2 were normal and
no murmur heard. Patient was clinically diagnosed
to have right sided pneumothorax (Fig.1, 2).
Treatment was initiated with needle thoracocentesis
on right 2nd intercostal space in mid clavicular
line (Fig. 3). Posterior intercostal nerve block was
given for 4th, 5th and 6th ribs. Through the same port
epidural catheter was inserted (Fig. 4) and intra-
pleural analgesia was given with 1% Xylocaine,
and intercostal tube was inserted for treatment of
pneumothorax. Pain decreased from 70% to 10%
VAS with intercostal nerve block. Later long term
analgesia was obtained by intra pleural analgesia,
giving further top ups with 1% xylocaine.
Discussion:
Pain due to fractured ribs and incision result in
hypo ventilation and hypoxaemia.3 Parenteral and
epidural administration of narcotics, iniltration of incisional site with local anesthetics and intercostal
nerve blocks are some of the techniques used to
control pain.3 In the above case we have used
intercostal nerve block for immediate pain relief
and intra-pleural analgesia top ups for long term
pain relief (Fig.4). Advantages of giving intra-
pleural analgesia include:
1. Simplicity of technique.
2. Top ups can be given as and when required since
the catheter placed is left in pleural space.
3. Plasma concentration of local anaesthetic
solutions are 3 to 4 times lower.
4. Risk of intravascular injection of local anaesthetic
solution is minimal
*Corresponding Author :
Dr. Vishwa Reddy Gankidi,
Department of Emergency Medicine, Kamineni Institute of
Medical Sciences, Narketpally, Nalgonda District,
Telangana state - 508 254, [email protected]
Case Report
: 31-33
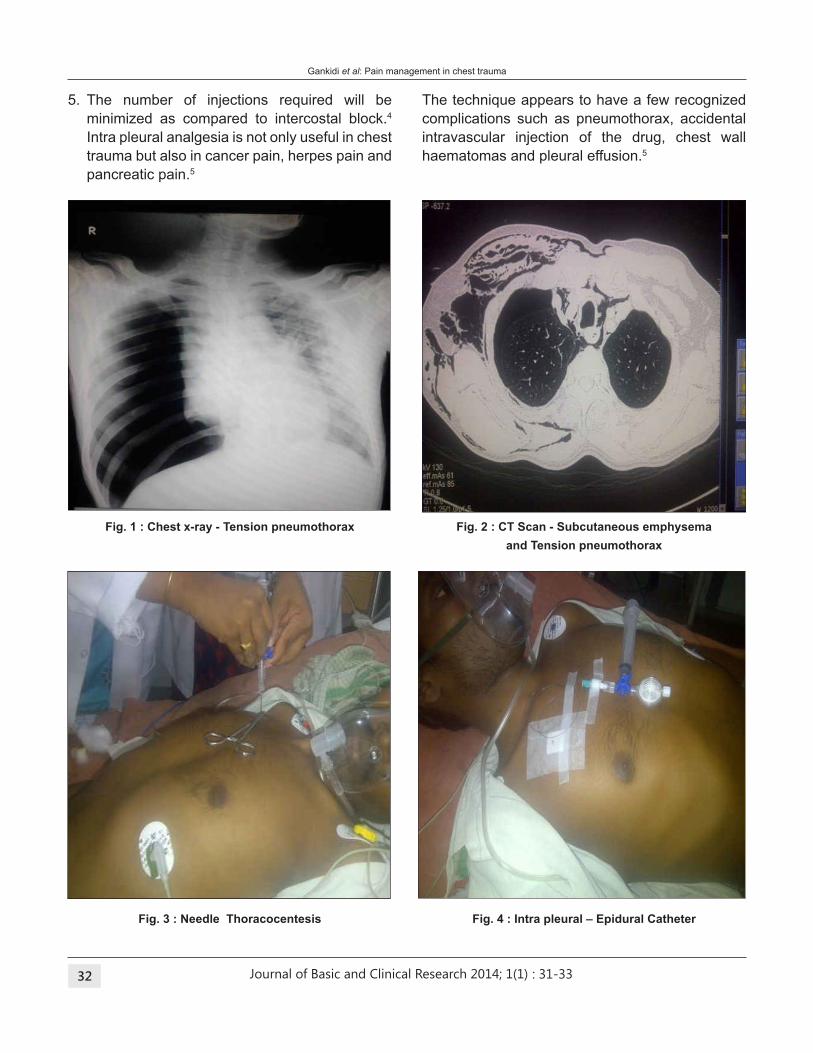
Journal of Basic and Clinical Research 2014; 1(1) 32
5. The number of injections required will be
minimized as compared to intercostal block.4
Intra pleural analgesia is not only useful in chest
trauma but also in cancer pain, herpes pain and
pancreatic pain.5
The technique appears to have a few recognized
complications such as pneumothorax, accidental
intravascular injection of the drug, chest wall
haematomas and pleural effusion.5
Fig. 1 : Chest x-ray - tension pneumothorax
Fig. 3 : Needle thoracocentesis
Fig. 2 : Ct Scan - Subcutaneous emphysema
and tension pneumothorax
Fig. 4 : Intra pleural – Epidural Catheter
Gankidi et al: Pain management in chest trauma
: 31-33

Journal of Basic and Clinical Research 2014; 1(1) 33
References:
1. Murphy DF. Interpleural analgesia. Br J Anaesth 1993;
71(13):426-434.
2. Gomez MN, Symreng T, Johnson B, Rossi NP, Chiang CK.
Intrapleural bupivacaine for intraoperative analgesia-a
dangerous technique. Anaesth Analg 1988;67:S78.
3. Murrell G. A new complication of the intrapleural catheter
method for postoperative analgesia. Anaesthesia and
Intensive Care 1988;16:499-500.
4. Lefever EB, Rosenthal RM, Ramamurthy S.
Intrapulmonary placement of a pleural catheter. Reg
Anesth. 1992;17(2):107-9.
5. Brockmeier V, Moen H, Karlsson BR, Fjeld
NB, Reiestad F, Steen PA. Interpleural or thoracic
epidural analgesia pain after thoracotomy. A double
blind study. Acta Anaesthesiol Scand. 1994;38(4):
317-21.
Gankidi et al: Pain management in chest trauma
: 31-33
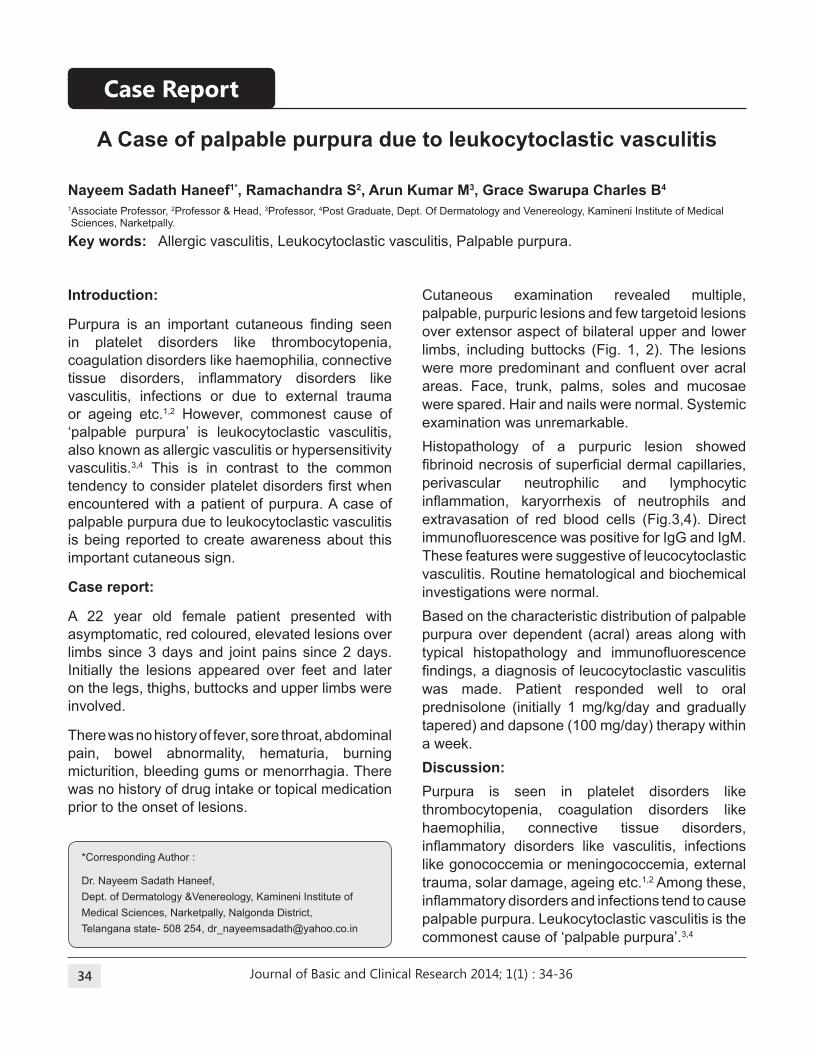
Journal of Basic and Clinical Research 2014; 1(1) 34
Nayeem Sadath Haneef1*, Ramachandra S2, Arun Kumar M3, Grace Swarupa Charles b4
1Associate Professor, 2Professor & Head, 3Professor, 4Post Graduate, Dept. Of Dermatology and Venereology, Kamineni Institute of Medical Sciences, Narketpally.
Key words: Allergic vasculitis, Leukocytoclastic vasculitis, Palpable purpura.
A Case of palpable purpura due to leukocytoclastic vasculitis
Introduction:
Purpura is an important cutaneous inding seen in platelet disorders like thrombocytopenia,
coagulation disorders like haemophilia, connective
tissue disorders, inlammatory disorders like vasculitis, infections or due to external trauma
or ageing etc.1,2 However, commonest cause of
‘palpable purpura’ is leukocytoclastic vasculitis,
also known as allergic vasculitis or hypersensitivity
vasculitis.3,4 This is in contrast to the common
tendency to consider platelet disorders irst when encountered with a patient of purpura. A case of
palpable purpura due to leukocytoclastic vasculitis
is being reported to create awareness about this
important cutaneous sign.
Case report:
A 22 year old female patient presented with
asymptomatic, red coloured, elevated lesions over
limbs since 3 days and joint pains since 2 days.
Initially the lesions appeared over feet and later
on the legs, thighs, buttocks and upper limbs were
involved.
There was no history of fever, sore throat, abdominal
pain, bowel abnormality, hematuria, burning
micturition, bleeding gums or menorrhagia. There
was no history of drug intake or topical medication
prior to the onset of lesions.
Cutaneous examination revealed multiple,
palpable, purpuric lesions and few targetoid lesions
over extensor aspect of bilateral upper and lower
limbs, including buttocks (Fig. 1, 2). The lesions
were more predominant and conluent over acral areas. Face, trunk, palms, soles and mucosae
were spared. Hair and nails were normal. Systemic
examination was unremarkable.
Histopathology of a purpuric lesion showed
ibrinoid necrosis of supericial dermal capillaries, perivascular neutrophilic and lymphocytic
inlammation, karyorrhexis of neutrophils and extravasation of red blood cells (Fig.3,4). Direct
immunoluorescence was positive for IgG and IgM. These features were suggestive of leucocytoclastic
vasculitis. Routine hematological and biochemical
investigations were normal.
Based on the characteristic distribution of palpable
purpura over dependent (acral) areas along with
typical histopathology and immunoluorescence indings, a diagnosis of leucocytoclastic vasculitis was made. Patient responded well to oral
prednisolone (initially 1 mg/kg/day and gradually
tapered) and dapsone (100 mg/day) therapy within
a week.
Discussion:
Purpura is seen in platelet disorders like
thrombocytopenia, coagulation disorders like
haemophilia, connective tissue disorders,
inlammatory disorders like vasculitis, infections like gonococcemia or meningococcemia, external
trauma, solar damage, ageing etc.1,2 Among these,
inlammatory disorders and infections tend to cause palpable purpura. Leukocytoclastic vasculitis is the
commonest cause of ‘palpable purpura’.3,4
*Corresponding Author :
Dr. Nayeem Sadath Haneef,
Dept. of Dermatology &Venereology, Kamineni Institute of
Medical Sciences, Narketpally, Nalgonda District,
Telangana state- 508 254, [email protected]
Case Report
: 34-36

Journal of Basic and Clinical Research 2014; 1(1) 35
positive C-ANCA or P-ANCA. Histopathology
shows characteristic swelling of endothelial cells,
ibrinoid necrosis of vessel wall, neutrophilic iniltration with leukocytoclasis and extravasation of RBCs.7 Direct immunoluorescence shows IgM or IgG with complement 3 (C3) deposits in
supericial dermal small vessels and perivascular area.7 Treatment is largely supportive in view of the
self-resolving nature of this disease. Avoidance of
triggering factors, compression stockings and limb
elevation for oedema, symptomatic treatment with
antihistaminics or NSAIDs when needed may be
suficient. Some patients may require systemic corticosteroid therapy, antineutrophilic drugs like
dapsone, colchicine, immunosuppressive drugs
like azathioprine, cyclosporine, cyclophosphamide,
methotrexate or newer biological drugs like
inliximab and rituximab. Establishment of exact etiology is an important aspect of management
of purpura. Leukocytoclastic vasculitis is the
commonest cause of palpable purpura. Thus
this case report of palpable purpura highlights
the importance of considering the other causes
apart from platelet disorders and leukocytoclastic
vasculitis as the common etiologic factor.
Fig. 1: Multiple, palpable, purpuric lesions and targetoid
lesions over upper limbs
Fig. 2: Multiple, palpable, purpuric lesions and targetoid
lesions over lower limbs
Haneef et al: Palpable purpura due to leucocytoclastic vasculitis
Leukocytoclastic vasculitis (also known as ‘allergic
vasculitis’ or ‘hypersensitivity vasculitis’) is a type
of small vessel vasculitis, especially affecting
post capillary venules.3 Drugs or infections are
the commonest causes besides others like
collagen vascular disorders and malignancies.5,6
The skin lesions typically arise as a crop of
palpable purpura over stasis prone areas like
feet and lower legs but sparing intertriginous
regions. Various other lesions such as papules,
nodules, plaques, vesicles, bullae, pustules, necrotic
ulceration, post-inlammatory hyper-pigmentation, oedema, livedo reticularis and urticaria may occur.
The lesions are mostly asymptomatic, though
pruritus, pain or burning may be present along
with constitutional symptoms like fever, arthralgia,
myalgia and anorexia. The lesions usually resolve
within few weeks or months.2,6
Diagnosis of this condition is mainly by exclusion,
and hence a thorough history, systemic examination
and investigations aimed at inding the aetiology or ruling out systemic involvement are essential.
It should be kept in mind that up to 50% of the
cases can be idiopathic. Some patients may show
: 34-36
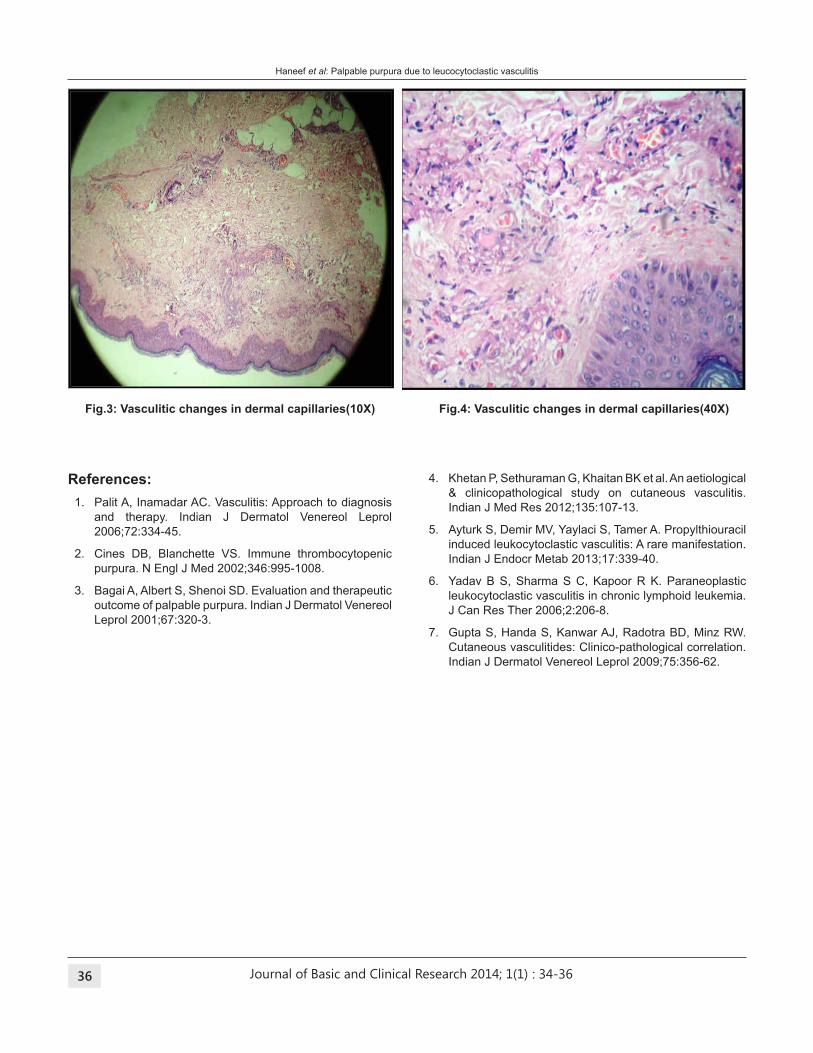
Journal of Basic and Clinical Research 2014; 1(1) 36
Fig.3: Vasculitic changes in dermal capillaries(10X) Fig.4: Vasculitic changes in dermal capillaries(40X)
References:
1. Palit A, Inamadar AC. Vasculitis: Approach to diagnosis
and therapy. Indian J Dermatol Venereol Leprol
2006;72:334-45.
2. Cines DB, Blanchette VS. Immune thrombocytopenic
purpura. N Engl J Med 2002;346:995-1008.
3. Bagai A, Albert S, Shenoi SD. Evaluation and therapeutic
outcome of palpable purpura. Indian J Dermatol Venereol
Leprol 2001;67:320-3.
4. Khetan P, Sethuraman G, Khaitan BK et al. An aetiological
& clinicopathological study on cutaneous vasculitis.
Indian J Med Res 2012;135:107-13.
5. Ayturk S, Demir MV, Yaylaci S, Tamer A. Propylthiouracil
induced leukocytoclastic vasculitis: A rare manifestation.
Indian J Endocr Metab 2013;17:339-40.
6. Yadav B S, Sharma S C, Kapoor R K. Paraneoplastic
leukocytoclastic vasculitis in chronic lymphoid leukemia.
J Can Res Ther 2006;2:206-8.
7. Gupta S, Handa S, Kanwar AJ, Radotra BD, Minz RW.
Cutaneous vasculitides: Clinico-pathological correlation.
Indian J Dermatol Venereol Leprol 2009;75:356-62.
Haneef et al: Palpable purpura due to leucocytoclastic vasculitis
: 34-36
Journal of Basic and Clinical Research 2014; 1(1) 37
Kanni.Y.S1*, Rathod.b.H2, Satyasrinivas A3, Nithin Kumar4
1Professor & Head, 2Associate Professor, 3Asst. Professor, 4Post Graduate, Department of General Medicine, Kamineni Institute of Medical
Sciences, Narketpally.
Key words: ARDS, Dengue fever.
Adult Respiratory Distress Syndrome in Dengue Fever
Introduction:
Today, dengue is one of the most important
emerging tropical viral diseases of humans in the
world. The World Health Organization [WHO]1
estimates that there are 50 to 100 million infections
yearly, including 50,000 Dengue Hemorrhagic
Fever [DHF] cases and 22,000 deaths, mostly
among children. Pulmonary manifestations are
rarely seen in DHF. Pleural effusion and pneumonitis
have been described as rare complication of DHF.
There are few case reports of dengue fever with
adult respiratory distress syndrome (ARDS)2,3,4
cited in literature. In the present article, we report a
similar case of dengue fever with ARDS.
Case Report:
A 27 year old female presented with history of high
grade fever since 2 days, shortness of breath since
1 day. Fever was associated with chills, rigors,
headache, myalgia and retro-orbital pain. There
was no history of rash or joint pain. Shortness of
breath was sudden in onset and progressive.
On examination, patient was febrile with tachycardia
(Pulse-110/min) and normotensive (BP-100/60 mm
Hg). Patient was tachypneic and had crepitations
bilaterally. There were no signs of meningeal
irritation. On abdominal examination, patient had
diffuse tenderness.
Investigations revealed thrombocytopenia
[Hemoglobin-11.4 g%, Total Leucocyte Count-3000
cells/cu.mm; neutrophils-56%, lymphocytes-38%,
Eosinophils-4%, Monocytes-1%, Basophils-1%;
Platelet count-60,000 cells/cu.mm, haematocrit-44]
Hepatic enzymes were normal. Prothrombin time
and activated partial thromboplastin time was
normal. Ultrasonography of the abdomen was
normal. In view of low platelets and leucopenia,
dengue fever was suspected and patient was
tested for dengue serology and IgM and IgG was
positive [Bio Standard Diagnostics, KIMS].
The Chest X ray showed bilateral luffy opacities, Serial arterial blood gas analysis showed
PaO2/FiO
2 ratio of 200 suggestive of ARDS.
The patient was intubated and was shifted under
intensive care. She was put on positive pressure
support ventilation and supportive medications.
Antibiotics were given to prevent secondary
nosocomial infections. Single donor platelet
transfusion was given. The patient improved over
the next 3 days after which she was extubated. The
patient was monitored in the ward till the patient
became asymptomatic and was discharged after
seven days of hospitalization.
Discussion:
The etiology for ARDS is varied and dengue is
reported as a rare cause for this condition. Wang
et al2 reported an incidence of 1.8% ARDS in their
study involving 606 dengue patients in China. All
these patients had concomitant DHF. Sen et al3
reported a patient of dengue hemorrhagic fever who
*Corresponding Author :
Dr. Kanni. Y. S, Department of General Medicine,
Kamineni Institute of Medical Siences, Narketpally, Nalgonda
District, Telangana State - 508 254, [email protected]
Case Report
: 37-38

Journal of Basic and Clinical Research 2014; 1(1) 38
progressed into ARDS. The patient recovered after
mechanical ventilation and supportive treatment.
Devarajan et al4 reported two cases of ARDS in
dengue from Chennai, India.
The exact pathophysiology of ARDS in dengue
is still unknown despite large scale research.
Wang et al reported from their study that sepsis
and upper gastrointestinal bleeding are the main
causes for these patients to progress in ARDS.
On univariate analysis bad prognosis in dengue
patients with ARDS was attributed to old age,
increases liver function tests, presence of urinary
albumin, increase in blood urea nitrogen, decrease
in GFR, development of bleeding (external and
internal) and bacterial co-infection.
Management of ARDS in dengue is similar to
ARDS of any other etiology. Initial therapy is
focused on maintaining adequate oxygenation and
tissue perfusion through mechanical ventilation
and luid management. Minimizing nosocomial complications, preventing multi organ dysfunction
syndrome and attenuating the inlammatory response also play important roles in ARDS
management5. The supportive management
for dengue also inluences the outcome of the condition. It involves hydration, and platelet
transfusion if required.
In the present case, the patient was diagnosed
to have dengue hemorrhagic fever conirmed by positive dengue serology, thrombocytopenia,
elevated hematocrit and signs of plasma leakage.
The aetiology for ARDS was assumed to be dengue
when a detailed evaluation for the known causes
of ARDS were ruled out. The good prognosis of
the patient could be attributed to patient’s younger
age, minimal delay in administering necessary
treatment and antibiotic therapy to prevent
nosocomial infections.
In conclusion, clinicians in endemic and hyper-
endemic areas need to be aware of this rare and
unusual complication of ARDS and an appropriate
therapy (hydration, platelet transfusion, positive
pressure ventilatory support) without delay results
in better outcome.
References:
1. World Health Organization Dengue haemorrhagic fever:
diagnosis, treatment, prevention and control. 2nd edition.
Geneva, Switzerland: World Health Organization: 1997.
2. Wang CC, Liu SF, Liao SC, Lee IK, Liu JW, Lin AS, et
al. Acute respiratory failure in adult patients with dengue
virus infection. Am J Trop Med Hyg 2007;77:151-8.
3. Sen MK, Ojha UC, Chakrabarti S, Suri JC. Dengue
hemorrhagic fever (DHF) presenting with ARDS. Indian J
Chest Dis Allied Sci 1999;41:115-9.
4. Devarajan TV, Prashant PS, Mani AK, Victor SM,
Khan PS. Dengue with ARDS. J Ind Acad Clin Med
2008;9:146-9.
5. Taylor MM. ARDS diagnosis and management:
implications for the critical care nurse. Dimens Crit Care
Nurs 2005;24:197-207
Kanni et al: Acute Respiratory Distress Syndrome in dengue fever
: 37-38
Journal of Basic and Clinical Research 2014; 1(1) 39
Venu Kandala1*, Venkat Kishan tatikonda2, Mateenuddin Saleem3, Srikar Darisetty4, Raghudeep
Palla4, Syed Abdul Aleem4
1Professor & Head, 3Professor, 4Post Graduates, Department of Pulmonary Medicine, 2Assistant Professor, Department of Radiology,
Kamineni Institute of Medical Sciences, Narketpally.
Key words : ERCP, octreotide, pancreatico-pleural istula, pancreatico-jejunostomy, pleural luid amylase, pseudocyst.
Recurrent massive hemorrhagic pleural effusion with
pseudopancreatic cyst due to
pancreatico-pleural istula : A case report
Introduction:
Pleural effusions are commonly encountered in
clinical practice by physicians. Pleural diseases
are often secondary to pulmonary diseases.
In most of the cases, thorough history taking,
examination, analysis, pleural biopsy and speciic diagnostic procedures clinch the diagnosis. In a
small percentage of cases (15-20%),1 the cause is
not established inspite of all the procedures.
Pleural effusions secondary to abdominal
conditions remain clinically silent. They are often
under-diagnosed or undiagnosed, particularly with
acute pancreatitis because of the predominant
respiratory symptoms. Pleural effusions in acute
pancreatitis can be left sided, bilateral, massive
and recurrent. Pancreatic pleural effusions with
pseudopancreatic cyst and pancreatico-pleural
istulas are rare.2
Case report:
A 42 year old male, chronic smoker and alcoholic
came to seek medical assistance in Pulmonary
Medicine department for dry cough, chest pain and
breathlessness of 2 weeks duration.
Chest pain was intractable, sharp, stabbing,
without any radiation. He has developed
progressive breathlessness. The patient had loss
of appetite and weight. There were no symptoms
of hemoptysis, paroxysmal nocturnal dyspnoea
or abdominal pain. He had no history of trauma,
but had history of chronic alcoholism and acute
pancreatitis.
Physical examination showed asthenic built,
cachexia, pallor, increased temperature, no icterus,
no clubbing or lymphadenopathy, with signs of left
sided pleural effusion. Abdominal examination did
not reveal any visceromegaly and ascites. There
were no complaints of abdominal discomfort, and
the abdomen was non tender on palpation.
Routine laboratory investigations showed
normocytic, normochromic anaemia with a blood
hemoglobin of 9.5 gm%.
Total leukocyte count was 8,000 cells/cu.mm;
Differential count : neutrophils – 70%, lymphocytes
– 24%, eosinophils – 3%, monocytes – 3%,
basophils - 0%. Blood urea, serum creatinine
and liver function tests were within normal limits.
Chest X ray revealed a left sided moderate pleural
effusion (Fig 1).
Ultrasound chest was done and showed the same
indings with no ascites. Pleural luid was aspirated on ten occasions, and about ten litres of luid was
*Corresponding Author :
Dr Venu K, Department of Pulmonary Medicine,
Kamineni Institute of Medical Sciences, Narketpally,
Nalgonda District, Telangana State - 508 254,
Case Report
: 39-42
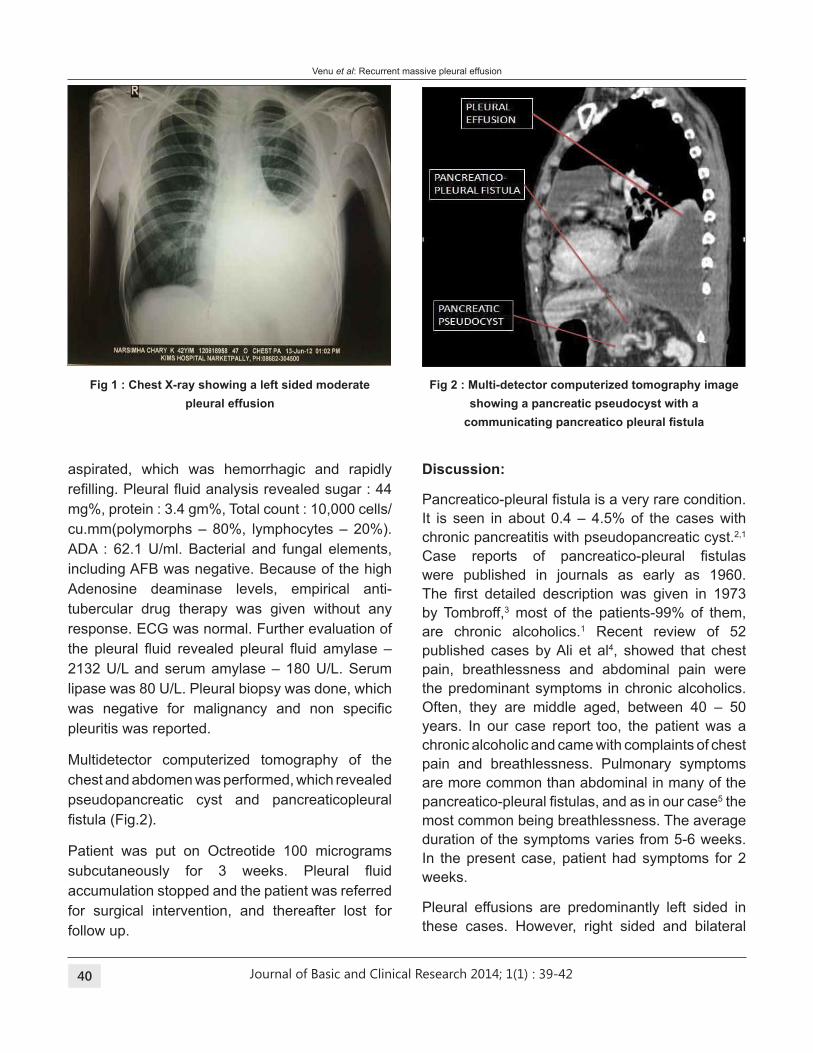
Journal of Basic and Clinical Research 2014; 1(1) 40
aspirated, which was hemorrhagic and rapidly
reilling. Pleural luid analysis revealed sugar : 44 mg%, protein : 3.4 gm%, Total count : 10,000 cells/
cu.mm(polymorphs – 80%, lymphocytes – 20%).
ADA : 62.1 U/ml. Bacterial and fungal elements,
including AFB was negative. Because of the high
Adenosine deaminase levels, empirical anti-
tubercular drug therapy was given without any
response. ECG was normal. Further evaluation of
the pleural luid revealed pleural luid amylase – 2132 U/L and serum amylase – 180 U/L. Serum
lipase was 80 U/L. Pleural biopsy was done, which
was negative for malignancy and non speciic pleuritis was reported.
Multidetector computerized tomography of the
chest and abdomen was performed, which revealed
pseudopancreatic cyst and pancreaticopleural
istula (Fig.2).
Patient was put on Octreotide 100 micrograms
subcutaneously for 3 weeks. Pleural luid accumulation stopped and the patient was referred
for surgical intervention, and thereafter lost for
follow up.
Discussion:
Pancreatico-pleural istula is a very rare condition. It is seen in about 0.4 – 4.5% of the cases with
chronic pancreatitis with pseudopancreatic cyst.2,1
Case reports of pancreatico-pleural istulas were published in journals as early as 1960.
The irst detailed description was given in 1973 by Tombroff,3 most of the patients-99% of them,
are chronic alcoholics.1 Recent review of 52
published cases by Ali et al4, showed that chest
pain, breathlessness and abdominal pain were
the predominant symptoms in chronic alcoholics.
Often, they are middle aged, between 40 – 50
years. In our case report too, the patient was a
chronic alcoholic and came with complaints of chest
pain and breathlessness. Pulmonary symptoms
are more common than abdominal in many of the
pancreatico-pleural istulas, and as in our case5 the
most common being breathlessness. The average
duration of the symptoms varies from 5-6 weeks.
In the present case, patient had symptoms for 2
weeks.
Pleural effusions are predominantly left sided in
these cases. However, right sided and bilateral
Fig 1 : Chest X-ray showing a left sided moderate
pleural effusion
Fig 2 : Multi-detector computerized tomography image
showing a pancreatic pseudocyst with a
communicating pancreatico pleural istula
Venu et al: Recurrent massive pleural effusion
: 39-42

Journal of Basic and Clinical Research 2014; 1(1) 41
effusions do occur in about 19% and 14% of cases
respectively.6 Most of the pleural effusions are
massive, recurrent, with or without hemorrhagic
effusion.7 They remain elusive diagnostically.
They often undergo detailed pulmonary evaluation
with less attention to abdominal symptoms.
Ultimately the pancreas would be the primary site
of pathology. These cases may be associated with
ascites (20%) and pericarditis (4%). The major
complication of these patients is superinfection
and ultimately sepsis, which is the cause of high
morbidity and mortality. Pseudopancreatic cyst
is more common with pancreatico-pleural istula than ascites. Recurrent, massive hemorrhagic
pleural effusions with minimal abdominal and
predominant respiratory symptoms puts the doctor
in a dilemma, and even increased serum amylase
and pleural luid amylase can also be found in gynecological cancers, lung cancer, metastatic
tumours, pneumonia, esophageal perforation,
lymphoma, leukemia and pulmonary tuberculosis.
In most of the cases, pleural luid amylase is very high; and serum amylase is moderately elevated.
In our case report, the pleural luid amylase was 2132 U/L but serum amylase was 180 U/L. All
other biochemical parameters were within normal
limits. This has given a high index of suspicion for
the presence of a pancreatico-pleural istula.
Further conirmation of the case was established by ultrasonography of the abdomen, which
demonstrated a pancreatic pseudocyst. CT scan
of the abdomen established the diagnosis of
chronic pancreatitis and pseudopancreatic cyst.
However some authors feel that endoscopic
retrograde cholangio pancreaticography should
be done along with magnetic resonance cholangio
pancreaticography, which would increase the
sensitivity for the detection of pancreatico-pleural
istula with pseudopancreatic cyst since it was effective for the diagnosis of istulas.3,4,8 The
abdominal ultrasound is not considered sensitive
for the diagnosis since the presence of stomach
and intestinal gas will interfere with the identiication of a pancreatico-pleural istula.9,2,4
A simple chest radiography is the irst line of investigation, which provides the evidence of
a massive pleural effusion.9,6 A computerized
tomography scan of the chest and abdomen
is valuable in the diagnosis. Currently, it
is the gold standard for the diagnosis of a
pleural effusion. Computerized tomography
scan may demonstrate the istula if obtained immediately after the endoscopic retrograde
cholangiopancreaticography. Magnetic resonance
cholangiopancreaticography is reported to be useful
in demonstrating the istula and pathology. This procedure helps in visualizing the duct anatomy,
small intra and extrapancreatic collections, and
pancreatico-pleural istulas where endoscopic retrograde cholangio pancreaticography fails10,5
since it may not be able to demonstrate the istula if there is a ductal rupture.9,6 Complete delineation
of the duct anatomy is necessary for surgical
management.
There are no speciic treatment guidelines for the management of pancreatico-pleural istulas based on earlier randomized controlled trials. Only a few
case reports are available.4
The treatment approach is classiied under
- Medical
- Surgical
- Non- invasive
- Invasive - Minimal invasive and complete
invasive
Medical treatment is conservative and includes
good nutrition, somatostatin analogues like
octreotide (50-150 ug) for 3 weeks to 6 months;
and chest tube drainage.2,4 The effectiveness of
conservative management varies from 30-60% in
some series, 0-33% in other series. In our case,
we have initially treated the patient conservatively
with nutritional support, octreotide (100 ug) via
subcutaneous route and repeated thoracentesis.
By this measure, only 50 – 60% of the cases
are beneited. Remaining cases may require endoscopic stenting after endoscopic retrograde
cholangio-pancreaticography, but where there is a
Venu et al: Recurrent massive pleural effusion
: 39-42
Journal of Basic and Clinical Research 2014; 1(1) 42
References:
1. Dixit R, Sharma S, Dave L. Massive haemothorax
in asymptomatic pseudocyst pancreas. Lung India
2008;25:126-8.
2. Ribeiro B, Gomes D, Rosa A, Amaro P, Tome L,
Leitao M, Freitas D. Derrame pleural recidivanteper
istula pancreatico-pleural. Journal Portugues de Gastroenterologia 2000;7:161-4.
3. Monteiro E, Terra JCA, Figueiredo LBP, Miranda LHS.
Pseudocisto de pancreas associado a derrame pleural
macico. J Pneumol 2002;28(3):159-62.
4. Ali T, Srinivasan N, Vu Le, Chimpiri R, Tiemey M.
Pancreatico-pleural istula. Pancreas 2009;38(1): 26-31.
5. Materne R, Vranckx P, Pauls C, Coche EE, Deprez P,
Van Beers B.E. Pancreatico-pleural istula : diagnosis with magnetic resonance pancreatography. Chest
2000;117(3):912-4.
6. Sut M, Gray R, Ramachandran M, Diamond T.
Pancreaticopleural istulas : a rare complication of ERCP induced pancreatitis. Ulster Medical Journal
2009;78(3):185-6.
7. Safadi BY, Marks JM. Pancreatico-pleural istula: the role of ERCP is diagnosis and treatment. Gastrointestinal
Endoscopy 2000;51:213-5.
8. Humphrey G, Stringer M. Pancreatico-pleural istula: A rare cause of massive pleural effusion. J Ped
gastroenterology and Nutrition 2003;36:134-7.\
9. Dhebri AR, Ferran N. Non surgical management of
pancreaticopleural istula. J. Pancreas 2005;6(2): 152-61.
10. Vyas S, Gogoi D, Sinha SK, Singh P, Yadav TD,
Khandewal N. Pancreaticopleural istula : an unusual complication of pancreatitis diagnosed with magnetic
resonance cholangiopancreatography. J. Pancreas
2009;10(6):671-3.
pseudopancreatic cyst and ductal rupture requires
repair of the duct and distal pancreatectomy,
internal drainage with pancreaticojejunostomy.2,4
In our case, the patient was managed conservatively
and was referred to department of surgery because
of pseudopancreatic cyst for further evaluation.
The case was then lost for follow up.
Conclusions:
1. Pleural effusion due to pancreaticopleural
istulas and pseudopancreatic cysts are very rare. (0.4 – 4.5%)
2. Pancreatic pleural effusion can be silent, and
present with massive, recurrent hemorrhagic
effusion and confuse with malignant effusion
and other causes of hemorrhagic effusion.
3. Serum amylase and pleural luid amylase should be done along with multidetector computerized
tomography for early detection.
4. 50 – 60 % of the cases respond to conservative
management.
5. Pseudocyst with disruption of the pancreatic
duct requires surgical intervention with stenting
and pancreaticojejunostomy.
Source of Support: Nil.
Conlict of Interest: None declared.
Venu et al: Recurrent massive pleural effusion
: 39-42
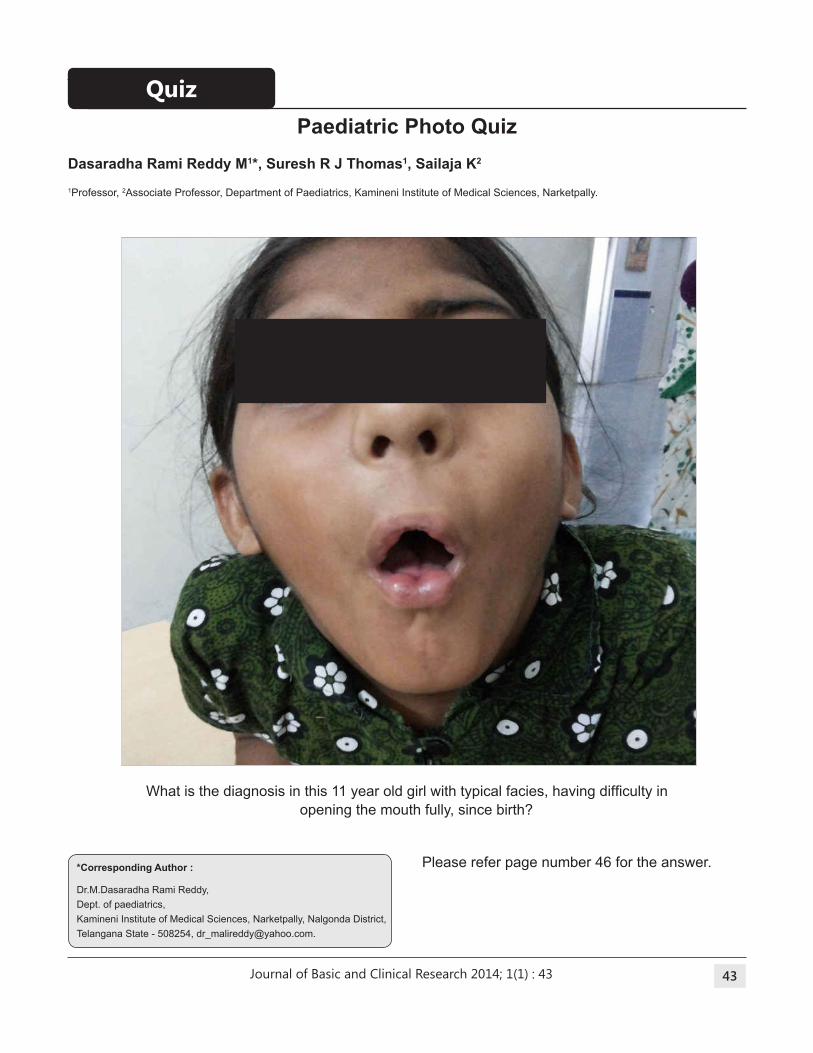
Journal of Basic and Clinical Research 2014; 1(1) 43
Dasaradha Rami Reddy M1*, Suresh R J thomas1, Sailaja K2
1Professor, 2Associate Professor, Department of Paediatrics, Kamineni Institute of Medical Sciences, Narketpally.
Paediatric Photo Quiz
What is the diagnosis in this 11 year old girl with typical facies, having dificulty in opening the mouth fully, since birth?
Please refer page number 46 for the answer.*Corresponding Author :
Dr.M.Dasaradha Rami Reddy,
Dept. of paediatrics,
Kamineni Institute of Medical Sciences, Narketpally, Nalgonda District,
Telangana State - 508254, [email protected].
Quiz
: 43
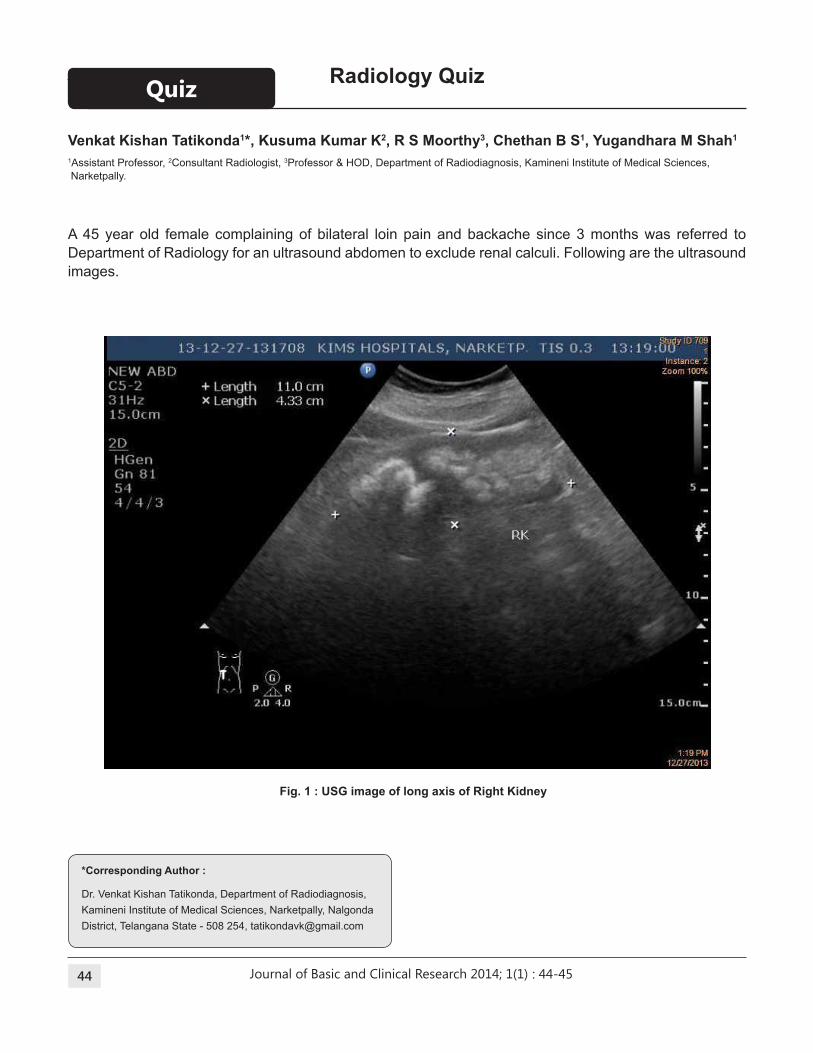
Journal of Basic and Clinical Research 2014; 1(1) 44
Venkat Kishan tatikonda1*, Kusuma Kumar K2, R S Moorthy3, Chethan b S1, Yugandhara M Shah1
1Assistant Professor, 2Consultant Radiologist, 3Professor & HOD, Department of Radiodiagnosis, Kamineni Institute of Medical Sciences,
Narketpally.
Radiology Quiz
A 45 year old female complaining of bilateral loin pain and backache since 3 months was referred to
Department of Radiology for an ultrasound abdomen to exclude renal calculi. Following are the ultrasound
images.
Fig. 1 : USG image of long axis of Right Kidney
*Corresponding Author :
Dr. Venkat Kishan Tatikonda, Department of Radiodiagnosis,
Kamineni Institute of Medical Sciences, Narketpally, Nalgonda
District, Telangana State - 508 254, [email protected]
Quiz
: 44-45
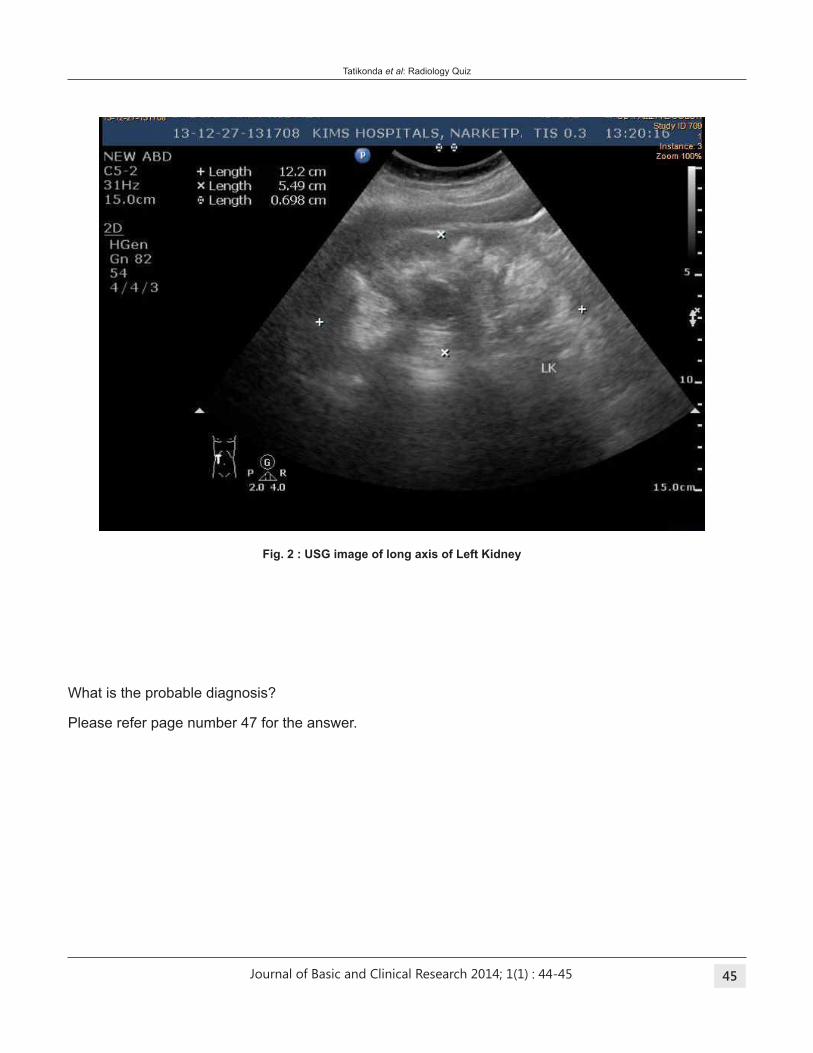
Journal of Basic and Clinical Research 2014; 1(1) 45
Fig. 2 : USG image of long axis of Left Kidney
What is the probable diagnosis?
Please refer page number 47 for the answer.
Tatikonda et al: Radiology Quiz
: 44-45
Journal of Basic and Clinical Research 2014; 1(1) 46
Answer: WHIStLING FACE SYNDROME
Whistling face syndrome is a disorder with
dysmorphic facies. It is also known as Freeman
Sheldon syndrome.1 It is characterized by small
mouth, and pursed lips (appears as if child is
whistling) and H shaped dimpling of chin. It is
due to contractures of facial muscles. It is one
of the multiple contracture syndromes. Usually
associated with Distal Arthrogryposis(DA).
Paediatric Photo Quiz
DA Syndrome
Distal arthrogryposis (DA) is the sub class
in arthrogryposis syndromes. It is a multiple
congenital contracture syndrome in contrast to an
isolated contracture syndrome. Arthrogryposis
is the term used by some, with non progressive
congenital contractures in two different body
areas. DA syndrome is characterized by
distal joint involvement, limited proximal joint
involvement, reduced dominant inheritance,
and variable expressivity.
Major manifestations of DA Syndrome
- Ulnar deviation of wrist and hands.
- Camptodactyly
- Hypoplastic/Absent lexion creases
- Overriding of ingers.
- Talipes equinovarus
- Calcaneovalgus
- Vertical talus
- Metatarsus varus
Freeman and Sheldon Syndrome (FSS)
types
FSS is characterised by two or more major
manifestations of DA syndrome and the following
features.2,3
- Small pinched mouth,
- Prominent nasolabial fold,
- H shaped dimpling of chin.
There aretwo types one with classical features and
other variant.
Cause
It is due to contractures of facial muscles. It can be
sporadic. Usually autosomal dominant inheritance
has been reported. Variant FSS may be associated
with mutations in genes TPM2, TNNI 2, TNNT
3 and MYH8. They encode isoforms of troponin I
and troponin T.
Precautions before surgery
Intubation is dificult in these cases because of small mouth.
They are more prone for malignant hyperthermia.
So inhalational induction without use of
neuromuscular blocking agents, laryngoscopy
assisted intubation, use of laryngeal mask airway
and non triggering anaesthetic techniques are
some of the measures beneicial to the patient.4,5
References:
1. Stevenson DA, Carey JC, Palumbos J, Rutherford
A, Dolcourt J, Bamshad MJ, Clinical Characteristics
And Natural History of Freeman-Sheldon Syndrome.
Pediatrics 2006;117:754-62.
2. Bamshad M, Jorde LB, Carey JC. A revised and extended
classiication of the distal arthrogryposis.Am J Med Genet 1996;65:277-81.
3. Krakowiak PA, O’Quinn JR, Bohnsack JF, Watkins WS,
Carey JC, Jorde LB et al. A variant of Freeman Sheldon
syndrome maps to 11p15.5-pter. Am J Hum Genet 1997;
60:426-32.
4. Cruickshanks GF, Brown S, Chitayat D. Anesthesia for
Freeman Sheldon syndrome using a laryngeal mask
airway. Can J Anaesth 1999; 46:783-7.
5. Agritmis A, Unlusoy O, Karaca S. Anesthetic management
of a patient with Freeman-Sheldon syndrome. Pediatr
Anesth 2004; 14:874-7.
Reddy et al: Paediatric photo quiz
: 46
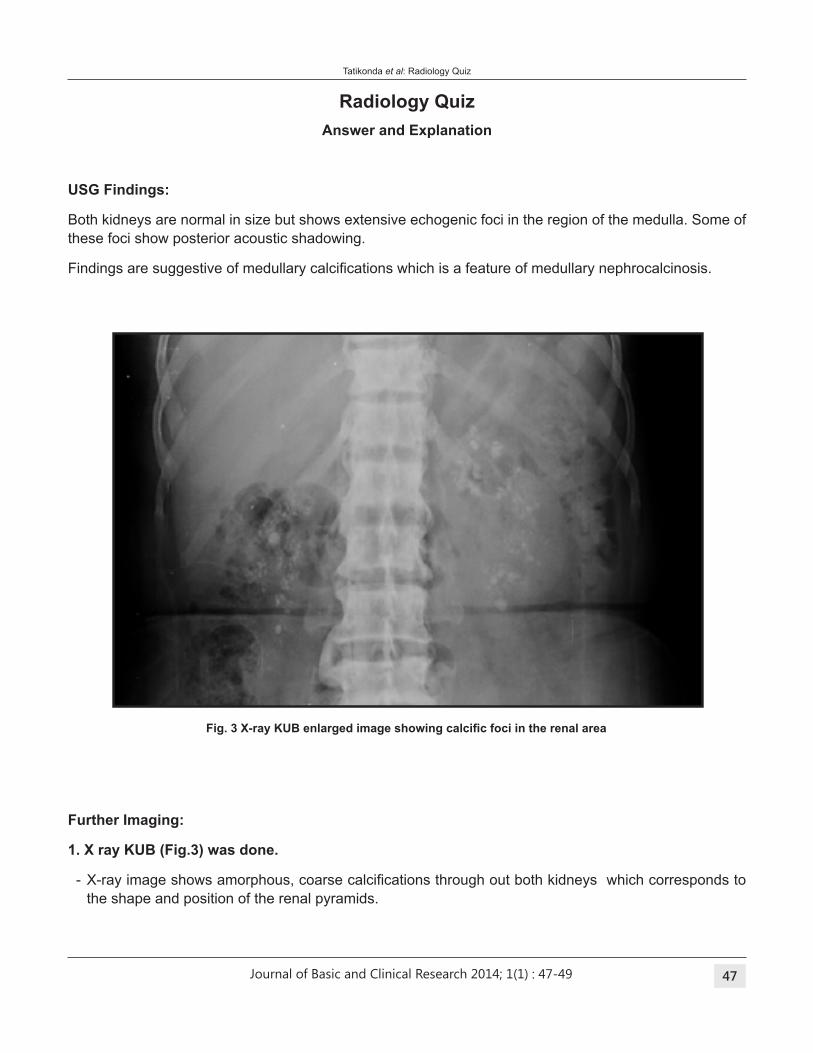
Journal of Basic and Clinical Research 2014; 1(1) 47
Fig. 3 X-ray KUB enlarged image showing calciic foci in the renal area
Radiology Quiz
Answer and Explanation
USG Findings:
Both kidneys are normal in size but shows extensive echogenic foci in the region of the medulla. Some of
these foci show posterior acoustic shadowing.
Findings are suggestive of medullary calciications which is a feature of medullary nephrocalcinosis.
Further Imaging:
1. X ray KUb (Fig.3) was done.
- X-ray image shows amorphous, coarse calciications through out both kidneys which corresponds to the shape and position of the renal pyramids.
Tatikonda et al: Radiology Quiz
: 47-49
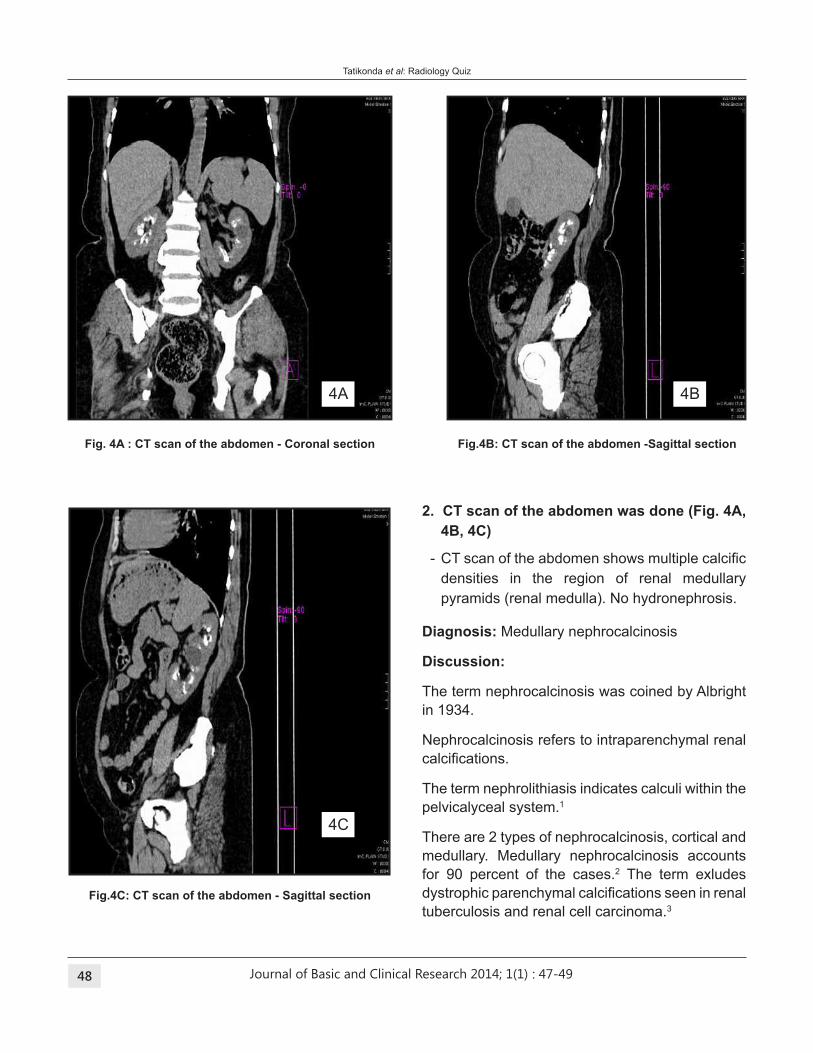
Journal of Basic and Clinical Research 2014; 1(1) 48
Diagnosis: Medullary nephrocalcinosis
Discussion:
The term nephrocalcinosis was coined by Albright
in 1934.
Nephrocalcinosis refers to intraparenchymal renal
calciications.
The term nephrolithiasis indicates calculi within the
pelvicalyceal system.1
There are 2 types of nephrocalcinosis, cortical and
medullary. Medullary nephrocalcinosis accounts
for 90 percent of the cases.2 The term exludes
dystrophic parenchymal calciications seen in renal tuberculosis and renal cell carcinoma.3
4A
4C
4B
2. Ct scan of the abdomen was done (Fig. 4A,
4b, 4C)
- CT scan of the abdomen shows multiple calciic densities in the region of renal medullary
pyramids (renal medulla). No hydronephrosis.
Fig. 4A : Ct scan of the abdomen - Coronal section Fig.4b: Ct scan of the abdomen -Sagittal section
Fig.4C: Ct scan of the abdomen - Sagittal section
Tatikonda et al: Radiology Quiz
: 47-49
Journal of Basic and Clinical Research 2014; 1(1) 49
Common causes of medullary nephrocalcinosis
are:4
- Hyperparathyroidism
- Medullary sponge kidney
- Renal tubular acidosis
- Immobilization
- Milk-alkali syndrome
- Sarcoidosis
- Hyperoxaluria
- Glucose-galactose malabsorption
- Chronic furosemide use
Imaging features:
Nephrocalcinosis can be demonstrated on plain
radiographs, ultrasonograms, or computed
tomography (CT) scans.
Plain radiographs can show both cortical and
medullary nephrocalcinosis.
Medullary nephrocalcinosis typically produces
clusters of stippled calciications, mainly within the regions of the renal pyramids.
Ultrasound reveals hyperechogenicity in renal
medullary pyramids.5
CT scanning is said to be the most sensitive imaging
modality in the diagnosis of nephrocalcinosis. CT
scans depict nephrocalcinosis at an early stage of
the disease, provide a better picture of the density
and extent of the nephrocalcinosis,
References:
1. Dahnert W, Radiology Review Manual.6th edition.
Philadelphia. Lippincott Williams and Wilkins, 2003; 893-
894.
2. David Sutton, Textbook of Radiology and Imaging. 7th ed.
Volume 2. Edinburgh. Churchill Livingstone. 2002; 976-
977.
3. Gary M. Glazer, Peter W. Callen, Roy A. Filly. Medullary
nephrocalcinosis: Sonologic Evaluation; AJR (1982)
138:55-57.
4. William E. Brant, Clyde A. Helms. Fundamentals of
Diagnostic Radiology, 2nd ed. : Philadelphia. Lippincott
Williams & Wilkins; 1999; 882-883.
5. N Reed Dunnik, Carl M Sandler, Jeffry H Newhouse,
Stephen Amis Jr. Text Book of Uroradiology, Third
edition: Philadelphia. Lippincott Williams & Wilkins, 2001;
179-182.
Tatikonda et al: Radiology Quiz
: 47-49
Journal of Basic and Clinical Research 2014; 1(1) 50
Journal of basic and Clinical Research (JbCR)
General
Manuscripts are accepted for publication with the
understanding that their contents, all or in part,
have not been published and will not be published
elsewhere, except in the Abstract form or with
the consent of the Editor. Material received for
consideration will be acknowledged. Manuscripts
will be initially reviewed by the Editor for suitability
for formal review and would then be reviewed
by peer Reviewers on originality, methodology,
scientiic content and quality, clinical importance and overall suitability for publication. Reviewer
comments will be sent to the corresponding author
for response, revision and resubmission within a
speciied time.
Authorship
All individuals designated as authors should qualify
for authorship.
An 'author' is considered to be someone who
has made substantive intellectual contributions
to a published study. Authorship credit should be
based on substantial contributions to conception
and design, acquisition of data, or analysis and
interpretation of data; drafting the article or revising
it critically for important intellectual content; and
inal approval of the version to be published. Authors should meet all the above conditions.
Participation solely in the acquisition of funding, for
the collection of data or data entry, and general
routine supervision does not justify authorship.
The order of authorship should be a joint decision
of all the co-authors. Once submitted, the order will
not be changed without written consent of all the
co-authors.
Conlicts of Interest
Authors should submit a conlict of interest statement which will be published with every
article. The purpose of the statement is to ensure
that any factors- personal relationships, inancial connections, sponsorships- that might bias the
author of an article, are declared so that readers
are aware of the potential conlict of interest and can include knowledge in the assessment of
information. Stating a conlict of interest does not disqualify an author from publication.
Plagiarism
Plagiarism is the wrongful appropriation or
purloining and publication as one's own, of the
ideas, or the expression of the ideas of another.
Plagiarism is considered by the journal as scientiic or professional misconduct and authors and
reviewers are advised to be careful to maintain
high ethical standards.
MANUSCRIPt
The manuscript should be typed in single space
throughout. Font size should be of English Arial 12
points. The identity of the author or institute should
not be revealed in the manuscript, except for the
title page. (For example, do not mention name of
institute in Methods, citing previous study as 'our
study', names on igure labels, name of institute in photographs etc).
The manuscript comprises (1) Title page, (2)
Abstract and keywords, (3) Text, (4) References,
(5) Tables, (6) Legends for illustrations and (7)
Illustrations. All these must start on separate pages
and in the above order.
(1) Title page - gives the title of the article, a short
title , type of article (original article, case report
etc), name(s) of the author(s), afiliations of author(s), place of work, names and addresses
of the authors and word count (excluding
abstract and references). Identify one author
as corresponding author and give his/her
postal address, direct telephone or mobile
number and email address. The title should
not exceed 60 characters. It should have no
abbreviations.
Guidelines for Authors: Manuscript preparation
: 50-56
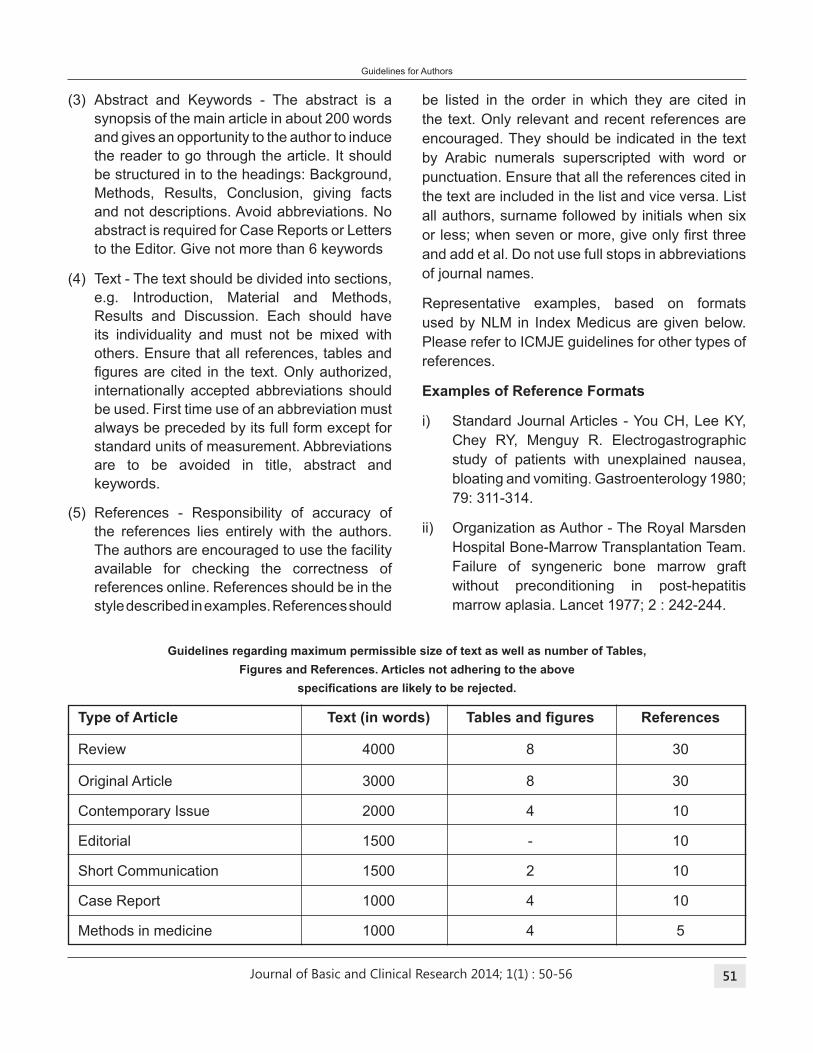
Journal of Basic and Clinical Research 2014; 1(1) 51
(3) Abstract and Keywords - The abstract is a
synopsis of the main article in about 200 words
and gives an opportunity to the author to induce
the reader to go through the article. It should
be structured in to the headings: Background,
Methods, Results, Conclusion, giving facts
and not descriptions. Avoid abbreviations. No
abstract is required for Case Reports or Letters
to the Editor. Give not more than 6 keywords
(4) Text - The text should be divided into sections,
e.g. Introduction, Material and Methods,
Results and Discussion. Each should have
its individuality and must not be mixed with
others. Ensure that all references, tables and
igures are cited in the text. Only authorized, internationally accepted abbreviations should
be used. First time use of an abbreviation must
always be preceded by its full form except for
standard units of measurement. Abbreviations
are to be avoided in title, abstract and
keywords.
(5) References - Responsibility of accuracy of
the references lies entirely with the authors.
The authors are encouraged to use the facility
available for checking the correctness of
references online. References should be in the
style described in examples. References should
be listed in the order in which they are cited in
the text. Only relevant and recent references are
encouraged. They should be indicated in the text
by Arabic numerals superscripted with word or
punctuation. Ensure that all the references cited in
the text are included in the list and vice versa. List
all authors, surname followed by initials when six
or less; when seven or more, give only irst three and add et al. Do not use full stops in abbreviations
of journal names.
Representative examples, based on formats
used by NLM in Index Medicus are given below.
Please refer to ICMJE guidelines for other types of
references.
Examples of Reference Formats
i) Standard Journal Articles - You CH, Lee KY,
Chey RY, Menguy R. Electrogastrographic
study of patients with unexplained nausea,
bloating and vomiting. Gastroenterology 1980;
79: 311-314.
ii) Organization as Author - The Royal Marsden
Hospital Bone-Marrow Transplantation Team.
Failure of syngeneric bone marrow graft
without preconditioning in post-hepatitis
marrow aplasia. Lancet 1977; 2 : 242-244.
Guidelines regarding maximum permissible size of text as well as number of tables,
Figures and References. Articles not adhering to the above
speciications are likely to be rejected.
Type of Article Text (in words) Tables and igures References
Review 4000 8 30
Original Article 3000 8 30
Contemporary Issue 2000 4 10
Editorial 1500 - 10
Short Communication 1500 2 10
Case Report 1000 4 10
Methods in medicine 1000 4 5
Guidelines for Authors
: 50-56
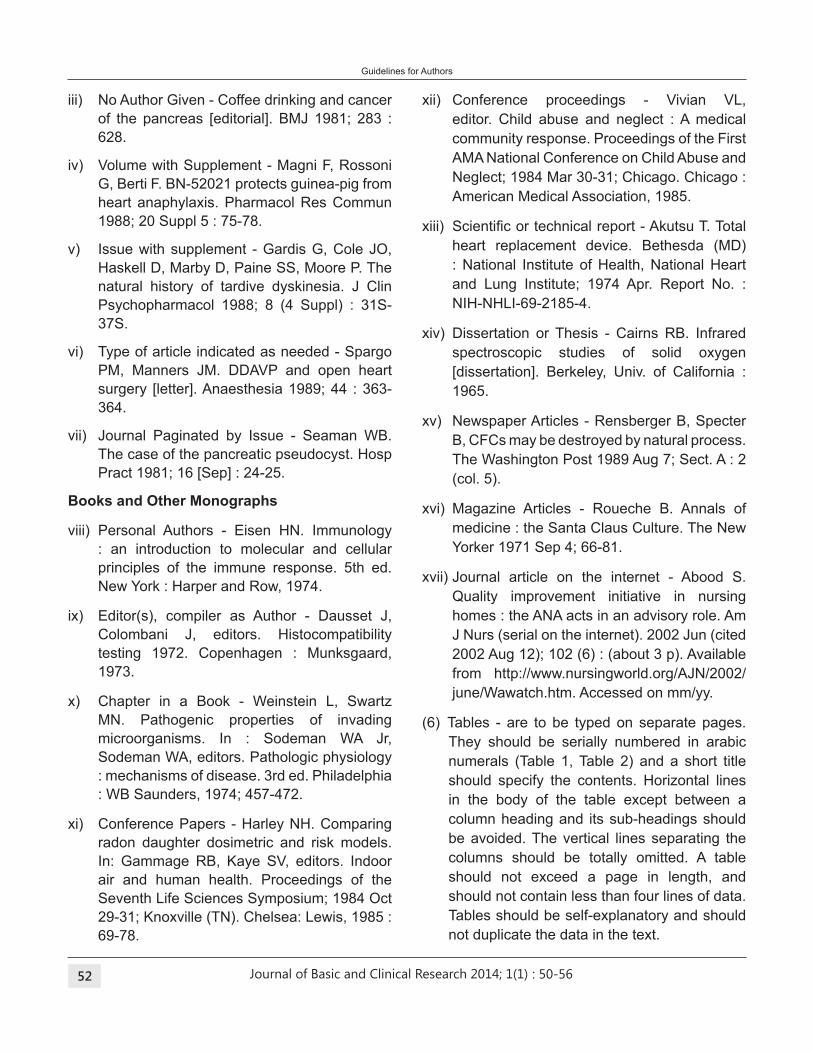
Journal of Basic and Clinical Research 2014; 1(1) 52
iii) No Author Given - Coffee drinking and cancer
of the pancreas [editorial]. BMJ 1981; 283 :
628.
iv) Volume with Supplement - Magni F, Rossoni
G, Berti F. BN-52021 protects guinea-pig from
heart anaphylaxis. Pharmacol Res Commun
1988; 20 Suppl 5 : 75-78.
v) Issue with supplement - Gardis G, Cole JO,
Haskell D, Marby D, Paine SS, Moore P. The
natural history of tardive dyskinesia. J Clin
Psychopharmacol 1988; 8 (4 Suppl) : 31S-
37S.
vi) Type of article indicated as needed - Spargo
PM, Manners JM. DDAVP and open heart
surgery [letter]. Anaesthesia 1989; 44 : 363-
364.
vii) Journal Paginated by Issue - Seaman WB.
The case of the pancreatic pseudocyst. Hosp
Pract 1981; 16 [Sep] : 24-25.
books and Other Monographs
viii) Personal Authors - Eisen HN. Immunology
: an introduction to molecular and cellular
principles of the immune response. 5th ed.
New York : Harper and Row, 1974.
ix) Editor(s), compiler as Author - Dausset J,
Colombani J, editors. Histocompatibility
testing 1972. Copenhagen : Munksgaard,
1973.
x) Chapter in a Book - Weinstein L, Swartz
MN. Pathogenic properties of invading
microorganisms. In : Sodeman WA Jr,
Sodeman WA, editors. Pathologic physiology
: mechanisms of disease. 3rd ed. Philadelphia
: WB Saunders, 1974; 457-472.
xi) Conference Papers - Harley NH. Comparing
radon daughter dosimetric and risk models.
In: Gammage RB, Kaye SV, editors. Indoor
air and human health. Proceedings of the
Seventh Life Sciences Symposium; 1984 Oct
29-31; Knoxville (TN). Chelsea: Lewis, 1985 :
69-78.
xii) Conference proceedings - Vivian VL,
editor. Child abuse and neglect : A medical
community response. Proceedings of the First
AMA National Conference on Child Abuse and
Neglect; 1984 Mar 30-31; Chicago. Chicago :
American Medical Association, 1985.
xiii) Scientiic or technical report - Akutsu T. Total heart replacement device. Bethesda (MD)
: National Institute of Health, National Heart
and Lung Institute; 1974 Apr. Report No. :
NIH-NHLI-69-2185-4.
xiv) Dissertation or Thesis - Cairns RB. Infrared
spectroscopic studies of solid oxygen
[dissertation]. Berkeley, Univ. of California :
1965.
xv) Newspaper Articles - Rensberger B, Specter
B, CFCs may be destroyed by natural process.
The Washington Post 1989 Aug 7; Sect. A : 2
(col. 5).
xvi) Magazine Articles - Roueche B. Annals of
medicine : the Santa Claus Culture. The New
Yorker 1971 Sep 4; 66-81.
xvii) Journal article on the internet - Abood S.
Quality improvement initiative in nursing
homes : the ANA acts in an advisory role. Am
J Nurs (serial on the internet). 2002 Jun (cited
2002 Aug 12); 102 (6) : (about 3 p). Available
from http://www.nursingworld.org/AJN/2002/
june/Wawatch.htm. Accessed on mm/yy.
(6) Tables - are to be typed on separate pages.
They should be serially numbered in arabic
numerals (Table 1, Table 2) and a short title
should specify the contents. Horizontal lines
in the body of the table except between a
column heading and its sub-headings should
be avoided. The vertical lines separating the
columns should be totally omitted. A table
should not exceed a page in length, and
should not contain less than four lines of data.
Tables should be self-explanatory and should
not duplicate the data in the text.
Guidelines for Authors
: 50-56
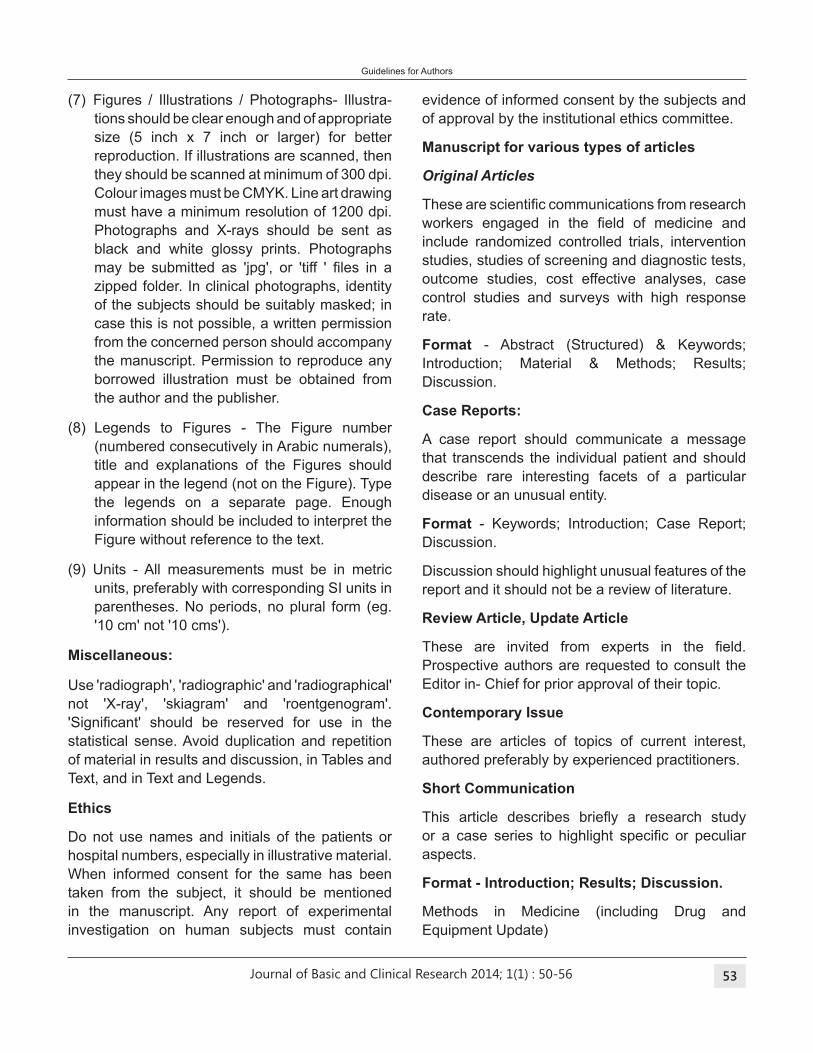
Journal of Basic and Clinical Research 2014; 1(1) 53
(7) Figures / Illustrations / Photographs- Illustra-
tions should be clear enough and of appropriate
size (5 inch x 7 inch or larger) for better
reproduction. If illustrations are scanned, then
they should be scanned at minimum of 300 dpi.
Colour images must be CMYK. Line art drawing
must have a minimum resolution of 1200 dpi.
Photographs and X-rays should be sent as
black and white glossy prints. Photographs
may be submitted as 'jpg', or 'tiff ' iles in a zipped folder. In clinical photographs, identity
of the subjects should be suitably masked; in
case this is not possible, a written permission
from the concerned person should accompany
the manuscript. Permission to reproduce any
borrowed illustration must be obtained from
the author and the publisher.
(8) Legends to Figures - The Figure number
(numbered consecutively in Arabic numerals),
title and explanations of the Figures should
appear in the legend (not on the Figure). Type
the legends on a separate page. Enough
information should be included to interpret the
Figure without reference to the text.
(9) Units - All measurements must be in metric
units, preferably with corresponding SI units in
parentheses. No periods, no plural form (eg.
'10 cm' not '10 cms').
Miscellaneous:
Use 'radiograph', 'radiographic' and 'radiographical'
not 'X-ray', 'skiagram' and 'roentgenogram'.
'Signiicant' should be reserved for use in the statistical sense. Avoid duplication and repetition
of material in results and discussion, in Tables and
Text, and in Text and Legends.
Ethics
Do not use names and initials of the patients or
hospital numbers, especially in illustrative material.
When informed consent for the same has been
taken from the subject, it should be mentioned
in the manuscript. Any report of experimental
investigation on human subjects must contain
evidence of informed consent by the subjects and
of approval by the institutional ethics committee.
Manuscript for various types of articles
Original Articles
These are scientiic communications from research workers engaged in the ield of medicine and include randomized controlled trials, intervention
studies, studies of screening and diagnostic tests,
outcome studies, cost effective analyses, case
control studies and surveys with high response
rate.
Format - Abstract (Structured) & Keywords;
Introduction; Material & Methods; Results;
Discussion.
Case Reports:
A case report should communicate a message
that transcends the individual patient and should
describe rare interesting facets of a particular
disease or an unusual entity.
Format - Keywords; Introduction; Case Report;
Discussion.
Discussion should highlight unusual features of the
report and it should not be a review of literature.
Review Article, Update Article
These are invited from experts in the ield. Prospective authors are requested to consult the
Editor in- Chief for prior approval of their topic.
Contemporary Issue
These are articles of topics of current interest,
authored preferably by experienced practitioners.
Short Communication
This article describes briely a research study or a case series to highlight speciic or peculiar aspects.
Format - Introduction; Results; Discussion.
Methods in Medicine (including Drug and
Equipment Update)
Guidelines for Authors
: 50-56
Journal of Basic and Clinical Research 2014; 1(1) 54
These are brief descriptions of a speciic technique or procedure, modiication of a technique, or equipment of interest and should be supported
by relevant diagrams and results of clinical and/or
ield trials.
book Review
Title of the book; name of the editor/authors; name
and address of the publisher; year of publication;
number of pages; number of illustrations; hard
bound or soft bound; price, ISBN number, text of
review. As a policy we do not encourage submission
of reviews of books that are more than a year old.
Others
These include Editorials, Guest Editorials and
Symposia, which are solicited by the Editorial
Board.
Guidelines for Authors
Undertaking by Authors
We, the undersigned, give an undertaking to the
following effect with regard to our article entitled
...............................................................................
...............................................................................
...............................................................................
...............................................................................
submitted for publication in the Journal of Basic
and Clinical Research:
1. The article mentioned above has not been
published or submitted to or accepted for
publication in any form, in any other journal.
2. We also vouchsafe that the authorship of this
article will not be contested by anyone whose
name(s) is/are not listed by us here.
3. I/We declare that I/We contributed signiicantly towards the research study i.e., (a) conception,
design and/or analysis and interpretation of
data and to (b) drafting the article or revising
it critically for important intellectual content
and on (c) inal approval of the version to be published.
4. I/We hereby acknowledge JBCRs conlict of interest policy requirement to scrupulously
avoid direct and indirect conlicts of interest and, accordingly, hereby agree to promptly inform
the editor or editor's designee of any business,
commercial, or other proprietary support,
relationships, or interests that I/We may have
which relate directly or indirectly to the subject
of the work.
5. Patient's written consent has been obtained
(strike off if not applicable)
6. I/We also agree to the authorship of the article
in the following sequence:
Authors' Names Nature of Signature of
Contribution Authors
(in sequence)
1.......................... ....................... ........................
2.......................... ....................... ........................
3.......................... ....................... ........................
4.......................... ....................... ........................
5.......................... ....................... ........................
6.......................... ....................... ........................
7.......................... ....................... ........................
8.......................... ....................... ........................
Important
(i) All the authors are required to sign independently
in this form in the sequence given above. In
case an author has left the institution/country
and whose whereabouts are not known, the
senior author may sign on his/her behalf taking
the responsibility.
(ii) No addition/deletion/ or any change in the
sequence of the authorship will be permissible
at a later stage, without valid reasons and
permission of the Editor.
(iii) If the authorship is contested at any stage,
the article will be either returned or will not
be processed for publication till the issue is
solved.
: 50-56
Journal of Basic and Clinical Research 2014; 1(1) 55
Guidelines for Authors
Copyright transfer Agreement Form
This document must be signed by all authors and
submitted with the manuscript.
COPYRIGHT TRANSFER AGREEMENT
The Journal of Basic and Clinical Research (JBCR)
is published half yearly by Kamineni Institute of
Medical Sciences Narketpally (India).
The JBCR and Authors hereby agree as follows:
In consideration of JBCR reviewing and editing the
following described work for irst publication on an exclusive basis:
Title of manuscript: .................................................
...............................................................................
...............................................................................
...............................................................................
...............................................................................
The undersigned author(s) hereby assigns,
conveys, and otherwise transfers all rights, title,
interest, and copyright ownership of said work for
publication. Work includes the material submitted
for publication and any other related material
submitted to JBCR. In the event that JBCR does not
publish said work, the author(s) will be so notiied and all rights assigned hereunder will revert to the
author(s).
The assignment of rights to JBCR includes but
is not expressly limited to rights to edit, publish,
reproduce,distribute copies, include in indexes
or search databases in print, electronic, or other
media, whether or not in use at the time of execution
of this agreement, and claim copyright in said work
throughout the world for the full duration of the
copyright and any renewals or extensions thereof.
All accepted works become the property of JBCR
and may not be published elsewhere without prior
written permission from JBCR. The author(s)
hereby represents and warrants that they are
sole author(s) of the work, that all authors have
participated in and agree with the content and
conclusions of the work,that the work is original,
and does not infringe upon any copyright, propriety,
or personal right of any third party, and that no part
of it nor any work based on substantially similar
data has been submitted to another publication.
Authors' Names (in sequence)
Signature of Authors
1.............................................................................
2.............................................................................
3.............................................................................
4.............................................................................
5.............................................................................
6.............................................................................
7.............................................................................
8.............................................................................
Patient Consent Form
Title of manuscript:
Name of the corresponding author:
I hereby give my consent for image(s) and clinical
information related to me to be reported in "Journal
of Basic and Clinical Research" (both in print and
electronic versions) with the understanding that
my name will not be mentioned. I was explained
about this in my mother tongue.
Signature of the patient
Date:
OR
Signature of the person giving consent on behalf
of the patient:
Relationship to the patient in case of other person
signing the consent:
(Strike off whichever is not applicable)
Name of patient:
Date of Birth (DD/MM/YY):
Address:
: 50-56
Journal of Basic and Clinical Research 2014; 1(1) 56
Guidelines for Authors
All editorial correspondence should be sent to
Dr. K. Nagaraj
Editor –in-Chief
Department of Community Medicine
Kamineni Institute of Medical Sciences
Sreepuram, Narketpally, Nalgonda District
Telangana State – 508 254
Phone : 08682 272018 Ext-314
E-mail : [email protected]
Manuscript Submission Check List
1. Covering letter
2. "Undertaking by Authors" signed by all authors
(form enclosed)
3. "Copyright Transfer Agreement Form" signed
by all authors (form enclosed)
4. Patient consent form, if necessary (form
enclosed)
5. Scientiic communication including
A. Title page
i. The complete manuscript title (max 125
characters including letters and spaces)
ii. A short title (max 45 characters including
letters and spaces)
iii. Full names (listed as irst name, middle initial, last name), afiliations and e-mails for all authors
iv. Corresponding Author's information (full
mailing address, oficial address phone and fax numbers, e-mail address)
v. 3-5 key words
vi. Disclosures
a. Financial support: indicate grants and
funds in support of the study. If none,
please state No.
b. Conlict of interest: state whether any Authors have conlict of interest or not
b. Abstract in structured format along with
key words (on a separate sheet)
C. Manuscript including acknowledgement,
references and tables
D. One set of illustrations
6. Scanned copy of duly illed in Undertaking by Authors signed by all authors, Copyright
Transfer Agreement Form signed by all authors
and Patient consent form signed by the patient
(wherever necessary)
7. Mode of communication: The soft copy of
covering letter, scientiic communication, scanned copy of undertaking by authors (1,
5 & 6) through e-mail ([email protected])
and / or CD posted to the editor-in-Chief. The
hard copies of "Undertaking by Authors" and
"Copyright Transfer Agreement Form" signed
by all authors and Patient consent form signed
by the patient (wherever necessary) (2, 3 & 4)
to be posted.
: 50-56

Journal of Basic and Clinical Research 2014; 1(1) 57
Notes

Journal of Basic and Clinical Research 2014; 1(1) 58

Copyright © 2022 FDOKUMEN

















![Starbucks Am Sci 2021;17(4):37-47]. ISSN 15451003 (print)](https://static.fdokumen.com/doc/165x107/6334af9f62e2e08d4902bbea/starbucks-am-sci-202117437-47-issn-15451003-print.jpg)


