Primary Sjögren Syndrome in Spain
10
Primary Sjo ¨gren Syndrome in Spain Clinical and Immunologic Expression in 1010 Patients Manuel Ramos-Casals, MD, PhD, Roser Solans, MD, PhD, Jose Rosas, MD, PhD, Marı ´a Teresa Camps, MD, PhD, Antonio Gil, MD, PhD, Javier del Pino-Montes, MD, PhD, Jaime Calvo-Alen, MD, PhD, Juan Jime ´nez-Alonso, MD, PhD, Maria-Luisa Mico ´, MD, PhD, Juan Beltra ´n, MD, Rafael Belenguer, MD, PhD, Lucio Pallare ´s, MD, PhD, and the GEMESS Study Group* Abstract: We conducted the current study to characterize the clinical presentation of primary Sjo ¨gren syndrome (SS) in a large cohort of Spanish patients and to determine whether epidemiologic, clinical, and analytical features modulate disease expression. Patients were from the GEMESS Study group, which was formed in 2005 and included 12 Spanish reference centers. By March 2007, the database included 1010 consecutive patients, recruited since 1994, both incident and prevalent cases. The cohort included 937 women and 73 men (ratio, 13:1), with a mean age of 53 years at diagnosis and 59 years at inclusion in the registry. Multivariate analysis showed that male patients had a lower frequency of thyroiditis, Raynaud phenomenon, and antinu- clear antibodies. Young-onset patients had a low degree of sicca involvement (xerostomia and parotid enlargement) and a high frequency of immunologic markers (anti-Ro/SS-A and low C4 levels). Patients with disease duration of more than 10 years had a higher prevalence of xerophthalmia, parotid enlargement, lung involvement, and peripheral neuropathy in comparison with incident cases. The subset of patients with anti-Ro/La antibodies had the highest prevalence of most systemic, hematologic, and immunologic alterations (higher frequency of Raynaud phenome- non, altered parotid scintigraphy, positive salivary gland biopsy, peripheral neuropathy, thrombocytopenia, and rheumatoid factor). Hypocomplementemia was associated with a higher frequency of vasculitis and lymphoma, and cryoglobulins with a higher frequency of parotid enlargement, vasculitis, and leukopenia. Epidemiologic, clinical, and analytical features have a significant impact on the clinical presentation of primary SS, influencing the results of the main diagnostic tests, the prevalence and diversity of extraglandular involvement, and the frequency of the main immunologic markers. Primary SS should be considered as a systemic autoimmune disease that can express in many guises beyond sicca involvement. (Medicine 2008;87:210–219) INTRODUCTION S jo ¨gren syndrome (SS) is a systemic autoimmune disease that presents with sicca symptomatology of the main mucosa surfaces 15 . The main sicca features (xerophthalmia and xerostomia) are detected by specific ocular (Rose Bengal staining, Schirmer test) and oral (salivary flow measurement, parotid scintigraphy) tests. The histologic hallmark is a focal lymphocytic infiltration of the exocrine glands, determined by a biopsy of the minor labial salivary glands 22 . Patients with SS present a broad spectrum of serologic features (cytopenias, hypergammaglobulinemia, high erythrocyte sedimentation rate) and autoantibodies, of which antinuclear antibodies (ANA) are the most frequently detected, anti-Ro/ SS-A the most specific, and cryoglobulins and hypocomple- mentemia the main prognostic markers 34 . The disease spectrum extends from sicca syndrome to systemic involve- ment (extraglandular manifestations) 37 . SS is a heterogeneous disease that can be expressed in many guises 17 . The variability of its presentation may significantly delay the diagnosis after the onset of symptoms 15 . In addition, the epidemiologic characteristics, systemic involvement, or immunologic profile at diagnosis may have a significant influence on the presentation of SS. Researchers have analyzed these factors in various studies 18,23,33,41 with differing results, which may be due to the small number of patients included and the different sets of classification criteria used. We conducted the current study to characterize the clinical presentation of primary SS in a large cohort of Spanish patients and to Abbreviations: ANA = antinuclear antibodies, CNS = central nervous system, RF = rheumatoid factor, SS = Sjo ¨gren syndrome. 210 Medicine Volume 87, Number 4, July 2008 From Laboratory of Autoimmune Diseases ‘‘Josep Font,’’ Department of Autoimmune Diseases, IDIBAPS, Hospital Clı ´nic (MRC), Barcelona; Department of Internal Medicine, Hospital Vall d’Hebron (RS), Barcelona; Rheumatology Unit, Hospital de Villajoyosa (JR), Alicante; Department of Internal Medicine, Hospital Carlos Haya (MTC), Malaga; Department of Internal Medicine, Hospital La Paz (AG), Madrid; Department of Internal Medicine and Rheumatology, Hospital Universitario de Salamanca (JdPM), Salamanca; Rheumatology Section, Hospital de Sierrallana (JCA), Torrelavega; Department of Internal Medicine, Hospital Virgen de las Nieves (JJA), Granada; Department of Internal Medicine, Hospital La Fe (MLM), Valencia; Rheumatology Unit, Hospital General de Castello ´n (JB), Castello ´n; Rheumatology Unit, Hospital 9 d’Octubre (RB), Valencia; Department of Internal Medicine, Hospital de Son Dureta (LP), Palma de Mallorca; Spain. *The members of the GEMESS Study Group are listed in the Appendix. Supported by Grant 071810 La Marato ´ de TV3 2006. Address reprint requests to: Dr. Manuel Ramos-Casals, Servei de Malalties Autoimmunes Siste `miques, Hospital Clı ´nic, C/Villarroel, 170, 08036- Barcelona, Spain. Fax: 34-93-2275774; e–mail: [email protected]. Copyright n 2008 by Lippincott Williams & Wilkins ISSN: 0025-7974/08/8704-0210 DOI: 10.1097/MD.0b013e318181e6af Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Transcript of Primary Sjögren Syndrome in Spain

Primary Sjogren Syndrome in SpainClinical and Immunologic Expression in 1010 Patients
Manuel Ramos-Casals, MD, PhD, Roser Solans, MD, PhD, Jose Rosas, MD, PhD,
Marıa Teresa Camps, MD, PhD, Antonio Gil, MD, PhD, Javier del Pino-Montes, MD, PhD,
Jaime Calvo-Alen, MD, PhD, Juan Jimenez-Alonso, MD, PhD, Maria-Luisa Mico, MD, PhD,
Juan Beltran, MD, Rafael Belenguer, MD, PhD, Lucio Pallares, MD, PhD,
and the GEMESS Study Group*
Abstract: We conducted the current study to characterize the
clinical presentation of primary Sjogren syndrome (SS) in a large
cohort of Spanish patients and to determine whether epidemiologic,
clinical, and analytical features modulate disease expression.
Patients were from the GEMESS Study group, which was formed
in 2005 and included 12 Spanish reference centers. By March 2007,
the database included 1010 consecutive patients, recruited since
1994, both incident and prevalent cases.The cohort included 937 women and 73 men (ratio, 13:1), with a
mean age of 53 years at diagnosis and 59 years at inclusion in the
registry. Multivariate analysis showed that male patients had a
lower frequency of thyroiditis, Raynaud phenomenon, and antinu-
clear antibodies. Young-onset patients had a low degree of sicca
involvement (xerostomia and parotid enlargement) and a high
frequency of immunologic markers (anti-Ro/SS-A and low C4
levels). Patients with disease duration of more than 10 years had a
higher prevalence of xerophthalmia, parotid enlargement, lung
involvement, and peripheral neuropathy in comparison with
incident cases. The subset of patients with anti-Ro/La antibodies
had the highest prevalence of most systemic, hematologic, and
immunologic alterations (higher frequency of Raynaud phenome-
non, altered parotid scintigraphy, positive salivary gland biopsy,
peripheral neuropathy, thrombocytopenia, and rheumatoid factor).
Hypocomplementemia was associated with a higher frequency of
vasculitis and lymphoma, and cryoglobulins with a higher
frequency of parotid enlargement, vasculitis, and leukopenia.
Epidemiologic, clinical, and analytical features have a
significant impact on the clinical presentation of primary SS,
influencing the results of the main diagnostic tests, the prevalence
and diversity of extraglandular involvement, and the frequency of
the main immunologic markers. Primary SS should be considered as
a systemic autoimmune disease that can express in many guises
beyond sicca involvement.
(Medicine 2008;87:210–219)
INTRODUCTION
S jogren syndrome (SS) is a systemic autoimmune diseasethat presents with sicca symptomatology of the main
mucosa surfaces15. The main sicca features (xerophthalmiaand xerostomia) are detected by specific ocular (Rose Bengalstaining, Schirmer test) and oral (salivary flow measurement,parotid scintigraphy) tests. The histologic hallmark is a focallymphocytic infiltration of the exocrine glands, determinedby a biopsy of the minor labial salivary glands22. Patientswith SS present a broad spectrum of serologic features(cytopenias, hypergammaglobulinemia, high erythrocytesedimentation rate) and autoantibodies, of which antinuclearantibodies (ANA) are the most frequently detected, anti-Ro/SS-A the most specific, and cryoglobulins and hypocomple-mentemia the main prognostic markers34. The diseasespectrum extends from sicca syndrome to systemic involve-ment (extraglandular manifestations)37.
SS is a heterogeneous disease that can be expressedin many guises17. The variability of its presentation maysignificantly delay the diagnosis after the onset ofsymptoms15. In addition, the epidemiologic characteristics,systemic involvement, or immunologic profile at diagnosismay have a significant influence on the presentation of SS.Researchers have analyzed these factors in variousstudies18,23,33,41 with differing results, which may be dueto the small number of patients included and the differentsets of classification criteria used. We conducted thecurrent study to characterize the clinical presentation ofprimary SS in a large cohort of Spanish patients and to
Abbreviations: ANA = antinuclear antibodies, CNS = central nervoussystem, RF = rheumatoid factor, SS = Sjogren syndrome.
210 Medicine � Volume 87, Number 4, July 2008
From Laboratory of Autoimmune Diseases ‘‘Josep Font,’’ Department ofAutoimmune Diseases, IDIBAPS, Hospital Clınic (MRC), Barcelona;Department of Internal Medicine, Hospital Vall d’Hebron (RS),Barcelona; Rheumatology Unit, Hospital de Villajoyosa (JR), Alicante;Department of Internal Medicine, Hospital Carlos Haya (MTC), Malaga;Department of Internal Medicine, Hospital La Paz (AG), Madrid;Department of Internal Medicine and Rheumatology, HospitalUniversitario de Salamanca (JdPM), Salamanca; RheumatologySection, Hospital de Sierrallana (JCA), Torrelavega; Department ofInternal Medicine, Hospital Virgen de las Nieves (JJA), Granada;Department of Internal Medicine, Hospital La Fe (MLM), Valencia;Rheumatology Unit, Hospital General de Castellon (JB), Castellon;Rheumatology Unit, Hospital 9 d’Octubre (RB), Valencia; Departmentof Internal Medicine, Hospital de Son Dureta (LP), Palma de Mallorca;Spain.
*The members of the GEMESS Study Group are listed in the Appendix.Supported by Grant 071810 La Marato de TV3 2006.Address reprint requests to: Dr. Manuel Ramos-Casals, Servei de Malalties
Autoimmunes Sistemiques, Hospital Clınic, C/Villarroel, 170, 08036-Barcelona, Spain. Fax: 34-93-2275774; e–mail: [email protected].
Copyright n 2008 by Lippincott Williams & WilkinsISSN: 0025-7974/08/8704-0210DOI: 10.1097/MD.0b013e318181e6af
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
define epidemiologic, clinical, and immunologic subsets ofpatients with a more homogeneous expression in order tofacilitate earlier diagnosis.
METHODS
PatientsThe GEMESS Study Group was formed in 2005 with the
aim of collecting a large series of Spanish patients withprimary SS, and included 12 Spanish reference centers withsubstantial experience in the management of SS patients. ByMarch 2007, the database included 1010 consecutive patients,recruited since 1994, both incident and prevalent cases.Incident cases were classified as those diagnosed during thefirst study visit or within the previous 12 months. All patientsfulfilled 4 or more of the preliminary diagnostic criteria for SSproposed by the European Community Study Group in 199344
and underwent a complete history and physical examination.Diagnostic tests for SS (Rose Bengal staining, Schirmer test,parotid scintigraphy, and salivary gland biopsy) were appliedaccording to the recommendations of the European Commu-nity Study Group44. Clinical and laboratory data werecollected and computerized according to a standard protocoldesigned by the GEMESS Study Group and based on previousmulticenter studies17,35. Salient features included in theprotocol were 1) age at diagnosis, defined as the age whenthe patient fulfilled the classification criteria; 2) age atinclusion, defined as the age when the patient was included inthe registry; and 3) cumulative clinical and immunologicfeatures during disease evolution (from the diagnosis untilprotocol inclusion). Exclusion criteria were chronic viralinfections (negative test for anti-hepatitis C virus antibodiesby ELISA), previous lymphoproliferative processes, andassociated systemic autoimmune diseases defined accordingto previous studies17,30.
Definition of Clinical FeaturesClinical features were defined as follows: Xerostomia
and xerophthalmia were defined according to the EuropeanCommunity Study Group44.
Articular involvement included arthralgia (joint painwithout inflammatory signs) and arthritis (tenderness, swell-ing, and/or joint effusion).
Raynaud phenomenon: intermittent attacks of digitalpallor followed by cyanosis and/or rubor of the fingers, toes,ears, nose, or tongue, induced by exposure to cold, stress, orboth, in the absence of any associated disease or anatomicalabnormality.
Vasculitis was defined according to previous studies29.Vasculitides related to drugs, neoplasia, or infectiousprocesses were excluded.
Lung involvement: persistent cough and/or dyspnea,with chronic diffuse interstitial infiltrates on X-ray, alteredpattern on pulmonary function studies, and/or evidence ofpulmonary alveolitis/fibrosis in computed tomography scans.
Nephropathy: persistent proteinuria >0.5 g/d, alteredurinalysis (hematuria, pyuria, red blood cell casts), renaltubular acidosis, interstitial nephritis, or glomerulonephritis.
Pancreatic involvement: clinical signs of pancreatitiswith raised levels of pancreatic enzymes.
Peripheral neuropathy: paresthesia, numbness, and/ormotor defects of the lower/upper extremities confirmed byelectromyography.
Involvement of the central nervous system (CNS):including demyelinating disorders, asymptomatic whitematter lesions in magnetic resonance examination, and/ormyelopathy.
Autoimmune thyroiditis: altered thyroid function withpositive antithyroidal autoantibodies.
Lymphoma: histologic diagnosis of lymphoprolifera-tive disorders was performed according to the World HealthOrganization (WHO) classification of tumors of hematopoi-etic and lymphoid tissues21.
Immunologic StudiesImmunologic tests included ANA determined by
indirect immunofluorescence using triple tissue cryostatsections (liver-stomach-kidney), precipitating antibodies tothe extractable nuclear antigens Ro/SS-A and La/SS-Bdetected by ELISA, and rheumatoid factor (RF) detectedby nephelometry. Serum cryoglobulins were determinedas previously described42. Complement measurementconsisted of the determination of C3 and C4 levels bynephelometry.
Statistical AnalysisCategorical data were compared using the chi-square
and Fisher exact tests. Continuous variables were analyzedwith the Student t-test in large samples of similar varianceand with the nonparametric Mann-Whitney U-test for smallsamples, with results indicated as mean ± standard error ofthe mean. A 2-tailed value of p < 0.05 was taken to indicatestatistical significance. We compared the main cumulative,clinical, and immunologic SS data of the total cohortaccording to the following dichotomized variables: sex(male/female), age at diagnosis (< or > 35 yr, < or > 70 yr),incident/prevalent case, fulfillment of the 2002 criteria(yes/no)43, systemic involvement (presence of extraglandularfeatures), and presence of immunologic markers (ANA, RF,anti-Ro/La, hypocomplementemia, and cryoglobulinemia). Amultiple logistic regression analysis adjusted for age, sex,length of follow-up, and the variables that were statisticallysignificant (p < 0.05) in the univariate analysis was performed.The statistical analysis was performed with the 12.0 SPSSprogram (SPSS, Chicago, IL).
RESULTSThe cohort consisted of 1010 patients, including 937
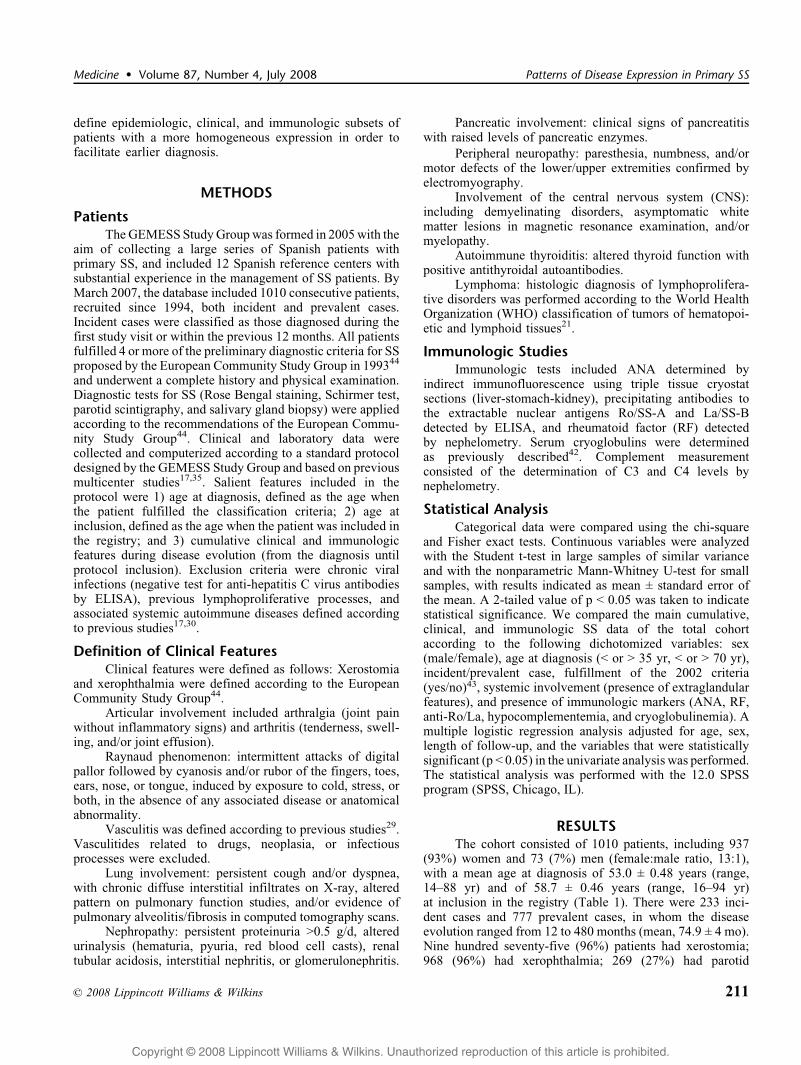
(93%) women and 73 (7%) men (female:male ratio, 13:1),with a mean age at diagnosis of 53.0 ± 0.48 years (range,14–88 yr) and of 58.7 ± 0.46 years (range, 16–94 yr)at inclusion in the registry (Table 1). There were 233 inci-dent cases and 777 prevalent cases, in whom the diseaseevolution ranged from 12 to 480 months (mean, 74.9 ± 4 mo).Nine hundred seventy-five (96%) patients had xerostomia;968 (96%) had xerophthalmia; 269 (27%) had parotid
n 2008 Lippincott Williams & Wilkins 211
Medicine � Volume 87, Number 4, July 2008 Patterns of Disease Expression in Primary SS
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

enlargement; 898/956 (94%) had abnormal ocular diagnostictests (Schirmer test and/or Rose Bengal staining); 580/759(76%) had altered salivary flows and/or parotid scintigraphy;and 449/561 (79%) had a salivary gland biopsy showinglymphocytic infiltrates grade 3 or 4. The main extraglandularfeatures were arthralgia in 490 (48%) patients, Raynaudphenomenon in 187 (18%), arthritis in 150 (15%), pulmonaryinvolvement in 112 (11%), peripheral neuropathy in 110(11%), vasculitis in 91 (9%), renal involvement in 48 (5%),CNS involvement in 21 (2%) and pancreatitis in 5 (0.5%).
Two hundred eighty-seven (28%) patients had cytopenias,including anemia (18%), leukopenia (16%), and thrombocy-topenia (13%). The main immunologic features were ANA �1/80 in 859/1005 (85%) patients, anti-Ro/SS-A in 518/1002(52%), RF in 467/982 (48%), anti-La/SS-B in 343/1000(34%), low C3 levels in 67/753 (9%), low C4 levels in 66/747(9%), and cryoglobulinemia in 62/628 (10%).
EPIDEMIOLOGIC SUBSETS
SS in MenOf the 1010 patients with primary SS, 73 (7%) were
men. A lower frequency of altered ocular tests, positiveANA, Raynaud phenomenon, and thyroiditis was found inmen compared with women in the univariate analysis. Theadjusted multivariate analysis identified altered ocular tests(p = 0.004), Raynaud phenomenon (p = 0.025), autoimmunethyroiditis (p = 0.034), and ANA (p = 0.037) as independentvariables (Table 2).
Age at Diagnosis <35 Years (Young-Onset SS)In 137 (14%) patients, primary SS was diagnosed
before the age of 35 years. A lower frequency of xerostomia,positive ocular tests, and thyroiditis and a higher prevalenceof parotid enlargement, vasculitis, leukopenia, and immuno-logic markers (RF, anti-Ro/SS-A, anti-LaSS-B, low C3 andlow C4 levels) were found in patients aged <35 years atdiagnosis, compared with those aged >35 years in theunivariate analysis. The adjusted multivariate analysisidentified length of follow-up (p=0.002), xerostomia(p=0.008), altered ocular tests (p = 0.03), anti-Ro/SS-Aantibodies (p < 0.001), low C3 (p = 0.018), and low C4 levels(p = 0.017) as independent variables (Table 3).
Age at SS Diagnosis >70 Years (Elderly-Onset SS)In 156 (15%) patients, primary SS was diagnosed after
the age of 70 years. A lower frequency of parotidenlargement, arthralgia, Raynaud phenomenon, and anti-Ro/SS-A antibodies and a higher prevalence of pulmonaryinvolvement and anemia were found in patients aged > 70years at diagnosis, compared with those aged < 70 years inthe univariate analysis. The adjusted multivariate analysisidentified length of follow-up (p < 0.001), arthralgia (p =0.006), lung involvement (p < 0.001), anemia (p = 0.017),and anti-Ro/SS-A antibodies (p = 0.035) as independentvariables (Table 4).
TABLE 2. Univariate and Multivariate Analysis of the Main Demographic, Clinical, and Immunologic Features in Patients WithPrimary SS, According to Sex
Variable
Female No. (%)
(n = 937)
Male No. (%)
(n = 73)
Univariate Analysis
(2-Tailed p Value)
Multivariate
Analysis*
Altered ocular test 840/888 (95%) 58/68 (85%) 0.006 0.004
Raynaud phenomenon 182 (19%) 5 (7%) 0.007 0.025
Thyroiditis 148 (16%) 4 (5%) 0.016 0.034
ANA �1/80 805/933 (86%) 54/72 (75%) 0.014 0.037
*Adjusted by age and duration of follow-up.
TABLE 1. Demographic, Clinical, and Immunologic Featuresof 1010 Spanish Patients With Primary Sjogren Syndrome
Feature* No. (%) (n = 1010)
Sex (female) 937 (93)
Age at onset (yr)y 53.0 ± 0.48
Age at protocol (yr)y 58.7 ± 0.46
Xerostomia 975 (96%)
Xerophthalmia 968 (96%)
Parotid enlargement 269 (27%)
Abnormal ocular tests 898/956 (94%)
Abnormal parotid scintigraphy/salivary flow 580/759 (76%)
Positive salivary gland biopsy 449/561 (79%)
Arthralgia 490 (48%)
Raynaud phenomenon 187 (18%)
Arthritis 150 (15%)
Pulmonary involvement 112 (11%)
Peripheral neuropathy 110 (11%)
Vasculitis 91 (9%)
Renal involvement 48 (5%)
CNS involvement 21 (2%)
Pancreatitis 5 (0.5%)
ANA 859/1005 (85%)
Anti-Ro/SS-A 518/1002 (52%)
RF 467/982 (48%)
Anti-La/SS-B 343/1000 (34%)
Low C3 67/753 (9%)
Low C4 66/747 (9%)
Cryoglobulins 62/628 (10%)
*See definitions of clinical features in Methods section.yMean ± standard error of the mean (SEM).
212 n 2008 Lippincott Williams & Wilkins
Ramos-Casals et al Medicine � Volume 87, Number 4, July 2008
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight

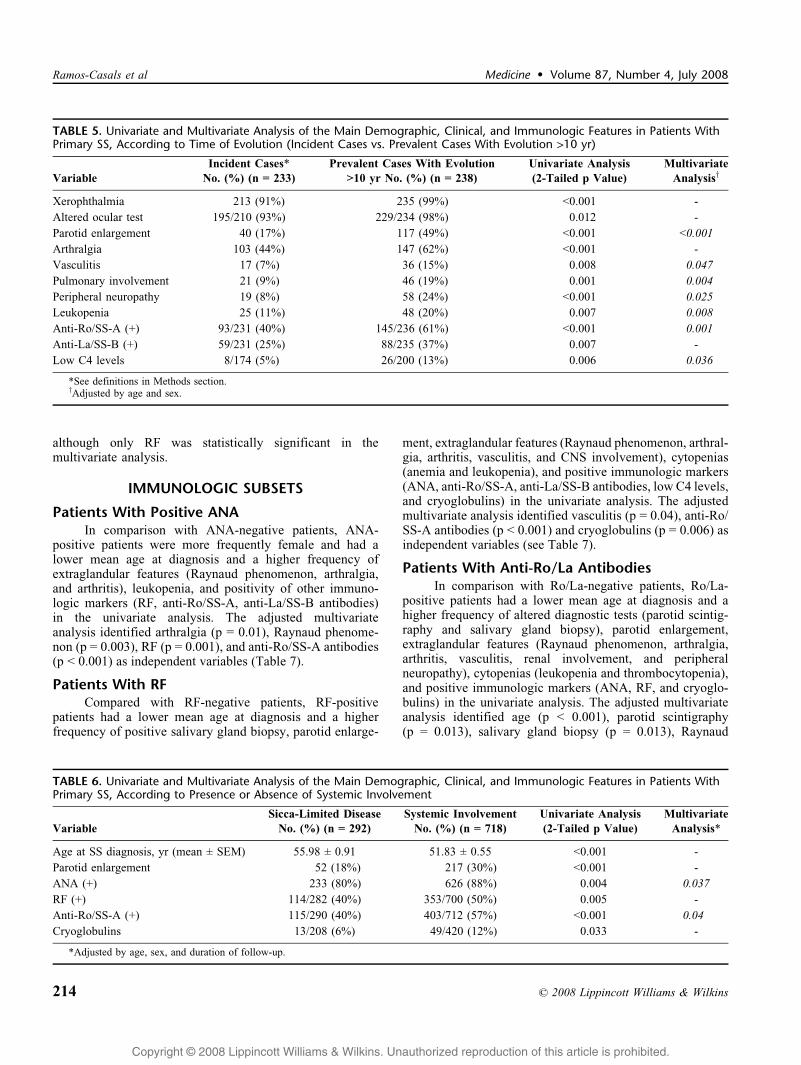
Long-Term Evolution (>10 Years)Two hundred thirty-eight patients had an evolution of
more than 10 years from diagnosis until inclusion in theregistry. Compared with the incident cases, these patientshad a lower mean age at diagnosis, a higher prevalence ofxerophthalmia, positive ocular tests, anti-Ro/SS-A and anti-La/SS-B antibodies, parotid enlargement, arthralgia, vascu-litis, lung involvement, peripheral neuropathy, leukopenia,and low C4 levels in the univariate analysis. The adjustedmultivariate analysis identified age (p < 0.001), parotidenlargement (p < 0.001), lung involvement (p = 0.044),vasculitis (p = 0.047), peripheral neuropathy (p = 0.025),leukopenia (p = 0.008), anti-Ro/SS-A antibodies (p = 0.001),and low C4 levels (p = 0.036) as independent variables(Table 5).
CLINICAL SUBSETS
Sicca-Limited DiseaseTwo hundred ninety-two (29%) patients presented only
sicca symptomatology (without extraglandular features),
while the remaining 718 (71%) presented a systemic processwith diverse extraglandular manifestations. When SSpatients were compared according to the presence ofextraglandular involvement, those with a sicca-limiteddisease had a higher mean age at diagnosis and a lowerfrequency of parotid enlargement and immunologic markers(ANA, RF, anti-Ro/SS-A antibodies, and cryoglobulins) inthe univariate analysis. The adjusted multivariate analysisidentified length of follow-up (p = 0.003), ANA (p = 0.037),and anti-Ro/SS-A (p = 0.04) as independent variables(Table 6).
Fulfillment of the 2002 American-EuropeanCriteria
All diagnostic tests included in the 2002 criteria wereperformed in 766 patients: 707 (92%) fulfilled the 2002criteria, and 59 (8%) fulfilled only the 1993 criteria. WhenSS patients were compared according to the criteria fulfilled,those who fulfilled only the 1993 criteria showed a lowerprevalence of arthritis, pulmonary involvement, peripheralneuropathy, RF, and cryoglobulins in the univariate analysis,
TABLE 4. Univariate and Multivariate Analysis of the Main Demographic, Clinical, and Immunologic Features in Patients WithPrimary SS, According to Age at Diagnosis (<70 or >70 yr)
Variable
Age at Diagnosis >70 yr
No. (%) (n = 156)
Age at Diagnosis <70 yr
No. (%) (n = 854)
Univariate Analysis
(2-Tailed p Value)
Multivariate
Analysis*
Parotid enlargement 28 (18%) 241 (28%) 0.008 -
Raynaud phenomenon 19 (12%) 168 (20%) 0.025 -
Arthralgia 57 (36%) 463 (54%) <0.001 0.006
Pulmonary involvement 26 (17%) 86 (10%) 0.025 0.01
Anemia 39 (25%) 141 (16%) 0.012 0.017
Anti-Ro/SS-A (+) 61/156 (39%) 457/846 (54%) 0.001 0.035
*Adjusted by sex and duration of follow-up.
TABLE 3. Univariate and Multivariate Analysis of the Main Demographic, Clinical, and Immunologic Features in Patients WithPrimary SS, According to Age at Diagnosis (<35 or >35 yr)
Variable
Age at Diagnosis <35 yr
No. (%) (n = 137)
Age at Diagnosis >35 yr
No. (%) (n = 873)
Univariate Analysis
(2-Tailed p Value)
Multivariate
Analysis*
Xerostomia 125 (91%) 850 (97%) 0.001 0.008
Altered ocular test 117/131 (89%) 781/825 (95%) 0.028 0.03
Parotid enlargement 52 (38%) 217 (25%) 0.002 -
Thyroiditis 11 (8%) 141 (16%) 0.014 -
Vasculitis 21 (15%) 70 (8%) 0.009 -
Leukopenia 33 (24%) 127 (15%) 0.008 -
RF �25 UI/L 83/132 (63%) 384/850 (45%) <0.001 -
Anti-Ro/SS-A (+) 101/135 (75%) 417/867 (48%) <0.001 <0.001
Anti-La/SS-B (+) 68/135 (50%) 275/865 (32%) <0.001 -
Low C3 levels 18/100 (18%) 49/653 (7%) 0.002 0.018
Low C4 levels 22/99 (22%) 44/648 (7%) <0.001 0.017
*Adjusted by sex and duration of follow-up.
n 2008 Lippincott Williams & Wilkins 213
Medicine � Volume 87, Number 4, July 2008 Patterns of Disease Expression in Primary SS
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
although only RF was statistically significant in themultivariate analysis.
IMMUNOLOGIC SUBSETS
Patients With Positive ANAIn comparison with ANA-negative patients, ANA-
positive patients were more frequently female and had alower mean age at diagnosis and a higher frequency ofextraglandular features (Raynaud phenomenon, arthralgia,and arthritis), leukopenia, and positivity of other immuno-logic markers (RF, anti-Ro/SS-A, anti-La/SS-B antibodies)in the univariate analysis. The adjusted multivariateanalysis identified arthralgia (p = 0.01), Raynaud phenome-non (p = 0.003), RF (p = 0.001), and anti-Ro/SS-A antibodies(p < 0.001) as independent variables (Table 7).
Patients With RFCompared with RF-negative patients, RF-positive
patients had a lower mean age at diagnosis and a higherfrequency of positive salivary gland biopsy, parotid enlarge-
ment, extraglandular features (Raynaud phenomenon, arthral-gia, arthritis, vasculitis, and CNS involvement), cytopenias(anemia and leukopenia), and positive immunologic markers(ANA, anti-Ro/SS-A, anti-La/SS-B antibodies, low C4 levels,and cryoglobulins) in the univariate analysis. The adjustedmultivariate analysis identified vasculitis (p = 0.04), anti-Ro/SS-A antibodies (p < 0.001) and cryoglobulins (p = 0.006) asindependent variables (see Table 7).
Patients With Anti-Ro/La AntibodiesIn comparison with Ro/La-negative patients, Ro/La-
positive patients had a lower mean age at diagnosis and ahigher frequency of altered diagnostic tests (parotid scintig-raphy and salivary gland biopsy), parotid enlargement,extraglandular features (Raynaud phenomenon, arthralgia,arthritis, vasculitis, renal involvement, and peripheralneuropathy), cytopenias (leukopenia and thrombocytopenia),and positive immunologic markers (ANA, RF, and cryoglo-bulins) in the univariate analysis. The adjusted multivariateanalysis identified age (p < 0.001), parotid scintigraphy(p = 0.013), salivary gland biopsy (p = 0.013), Raynaud
TABLE 6. Univariate and Multivariate Analysis of the Main Demographic, Clinical, and Immunologic Features in Patients WithPrimary SS, According to Presence or Absence of Systemic Involvement
Variable
Sicca-Limited Disease
No. (%) (n = 292)
Systemic Involvement
No. (%) (n = 718)
Univariate Analysis
(2-Tailed p Value)
Multivariate
Analysis*
Age at SS diagnosis, yr (mean ± SEM) 55.98 ± 0.91 51.83 ± 0.55 <0.001 -
Parotid enlargement 52 (18%) 217 (30%) <0.001 -
ANA (+) 233 (80%) 626 (88%) 0.004 0.037
RF (+) 114/282 (40%) 353/700 (50%) 0.005 -
Anti-Ro/SS-A (+) 115/290 (40%) 403/712 (57%) <0.001 0.04
Cryoglobulins 13/208 (6%) 49/420 (12%) 0.033 -
*Adjusted by age, sex, and duration of follow-up.
TABLE 5. Univariate and Multivariate Analysis of the Main Demographic, Clinical, and Immunologic Features in Patients WithPrimary SS, According to Time of Evolution (Incident Cases vs. Prevalent Cases With Evolution >10 yr)
Variable
Incident Cases*
No. (%) (n = 233)
Prevalent Cases With Evolution
>10 yr No. (%) (n = 238)
Univariate Analysis
(2-Tailed p Value)
Multivariate
Analysisy
Xerophthalmia 213 (91%) 235 (99%) <0.001 -
Altered ocular test 195/210 (93%) 229/234 (98%) 0.012 -
Parotid enlargement 40 (17%) 117 (49%) <0.001 <0.001
Arthralgia 103 (44%) 147 (62%) <0.001 -
Vasculitis 17 (7%) 36 (15%) 0.008 0.047
Pulmonary involvement 21 (9%) 46 (19%) 0.001 0.004
Peripheral neuropathy 19 (8%) 58 (24%) <0.001 0.025
Leukopenia 25 (11%) 48 (20%) 0.007 0.008
Anti-Ro/SS-A (+) 93/231 (40%) 145/236 (61%) <0.001 0.001
Anti-La/SS-B (+) 59/231 (25%) 88/235 (37%) 0.007 -
Low C4 levels 8/174 (5%) 26/200 (13%) 0.006 0.036
*See definitions in Methods section.yAdjusted by age and sex.
214 n 2008 Lippincott Williams & Wilkins
Ramos-Casals et al Medicine � Volume 87, Number 4, July 2008
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

phenomenon (p = 0.014), peripheral neuropathy (p =0.001), thrombocytopenia (p = 0.017), and RF (p <0.001) as independent variables (see Table 7).
Patients With HypocomplementemiaCompared with patients with normal C3/C4 levels,
those with hypocomplementemia had a lower mean age atdiagnosis and a higher frequency of extraglandular features(vasculitis), lymphoma, cytopenias (anemia, leukopenia, andthrombocytopenia) and positivity of other immunologicmarkers (RF and cryoglobulins) in the univariate analysis.The adjusted multivariate analysis identified the age atdiagnosis (p < 0.001), vasculitis (p = 0.001), lymphoma (p =0.01), and cryoglobulins (p < 0.001) as independent variables(see Table 7).
Patients With CryoglobulinemiaIn comparison with patients without cryoglobulins,
those with cryoglobulinemia had a lower mean age atdiagnosis and a higher frequency of parotid enlargement,extraglandular features (Raynaud phenomenon, vasculitis,renal involvement, and peripheral neuropathy), cytopenias(anemia, leukopenia, and thrombocytopenia), and positivityof other immunologic markers (RF, anti-Ro/SS-A antibodies,low C3 and low C4 levels) in the univariate analysis. The
multivariate analysis identified parotid enlargement (p =0.034), vasculitis (p < 0.001), leukopenia (p = 0.003), andlow C4 levels (p < 0.001) as independent variables (seeTable 7).
DISCUSSIONSS is a systemic autoimmune disease that affects
mainly the exocrine glands and usually presents as persistentdryness of the mouth and eyes due to functional impairmentof the salivary and lacrimal glands15. Although most patientspresent with sicca symptoms, SS is a disease that can beexpressed in many guises, depending on the specificepidemiologic, clinical, or immunologic features. In thecurrent study we evaluated the clinical and immunologicexpression of primary SS in 1010 consecutive Spanishpatients, the largest series analyzed to date, to ourknowledge. We confirmed that, epidemiologically, primarySS is a systemic autoimmune disease that overwhelminglyaffects women of middle age, with xerostomia, xerophthal-mia, ANA, anti-Ro/SS-A, and RF being the most frequentfeatures. However, several other manifestations not includedin the current classification criteria such as arthralgia (48%),cytopenia (28%), parotid enlargement (27%), Raynaudphenomenon (18%), and arthritis (15%) were frequently
TABLE 7. Univariate and Multivariate Analysis of the Main Demographic, Clinical, and Immunologic Features in Patients WithPrimary SS, According to Presence or Absence of the Main Immunologic Markers
Variable
ANA (+) No. (%)
(n = 859)
RF (+) No. (%)
(n = 467)
Ro/La (+) No. (%)
(n = 534)
Low C3/C4 No. (%)
(n = 102)
Cryoglobulins
No. (%) (n = 62)
Sex (female) 805 (94%) - - - -
Age at diagnosis, yr(mean ± SEM)
52.6 ± 0.5 50.7 ± 0.7 49.6 ± 0.7* 47.2 ± 1.6* 49.8 ± 1.9
Parotid scintigraphy III/IV - - 266/363 (75%)* - -
Salivary gland biopsy (+) - 152/182 (83%) 181/214 (85%)* - -
Parotid enlargement - 141 (30%) 168 (31%) - 25 (40%)*
Raynaud phenomenon 177 (21%)* 110 (24%) 126 (24%)* - 18 (29%)
Arthralgia 465 (54%)* 266 (57%) 297 (56%) - -
Vasculitis - 64 (14%)* 65 (12%) 22 (22%)* 21 (34%)*
Renal involvement - - 33 (6%) - 8 (13%)
Peripheral neuropathy - - 74 (14%)* - 11 (18%)
CNS involvement - - 5 (1%) - -
Lymphoma - - - 10 (10%)* -
Anemia - 101 (22%) - 35 (34%) 35 (40%)
Leukopenia 147 (17%) 106 (23%) 113 (21%) 30 (29%) 21 (34%)*
Thrombocytopenia - - 86 (16%)* 20 (20%) 21 (34%)
ANA (+) NA 430/466 (92%) 490 (92%) - -
RF (+) 430/838 (51%)* NA 340/523 (65%)* 59 (58%) 37 (61%)
Anti-Ro/SS-A (+) 478/855 (56%)* 335/465 (72%)* NA - 36 (59%)
Anti-La/SS-B (+) 313/853 (37%) 243/464 (52%) NA - -
Low C3 levels - - - NA 14/46 (30%)
Low C4 levels - 40/342 (12%) - NA 19/45 (42%)*
Cryoglobulins - 37/260 (14%)* 39/300 (13%) 23/76 (30%)* NA
*Statistically significant in the multivariate analysis adjusted by age, sex, and duration of follow-up.
n 2008 Lippincott Williams & Wilkins 215
Medicine � Volume 87, Number 4, July 2008 Patterns of Disease Expression in Primary SS
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight

found. These figures are similar to those found in the 2largest reported series that we know of, from Greece20 (723patients) and Sweden40 (484 patients).
The expression of SS in males was less pronouncedthan in females, and was characterized by a lower frequencyof altered ocular tests and a lower prevalence of someextraglandular and immunologic features. All previousstudies4,5,8,10,13,27,38 except one12 have described a lesserautoimmune expression (whether clinical, histologic, sialo-graphic, and/or immunologic) in male patients. This is in linewith one of the generally accepted ideas in autoimmunity,namely, that women have higher levels of autoimmuneprocesses (both clinical and serologic) than men. Variousreports have demonstrated this higher rate of autoimmunealterations in female patients, including a higher frequencyof autoantibodies in healthy females16, higher levels ofserum immunoglobulins9 and stronger humoral and cell-mediated immune responses14. These differences are espe-cially marked in patients with autoimmune diseasescharacterized by B-cell hyperreactivity, such as systemiclupus erythematosus or primary SS32. This less-pronouncedautoimmune expression in men may make early diagnosis ofthe disease difficult.
We found that the age at SS diagnosis plays asignificant role in the clinical and immunologic expressionof the disease. There was a specific pattern in the clinicalexpression of primary SS in young-onset patients (lowdegree of sicca involvement, high degree of systemicinvolvement). The identification of this specific presentationpattern may aid earlier diagnosis of these patients, in whomthe diagnosis may be complicated by the less pronouncedexpression of sicca features. In addition, this subset ofpatients had a high frequency of immunologic features thatmay also facilitate the diagnosis. This confirms results inchildren and adolescents6,13 and other young-onset SSpopulations18,41. The clinical presentation of primary SS inelderly patients was diametrically opposite, with a lowerprevalence of some systemic and immunologic features. Thisless pronounced autoimmune expression in older-onsetpatients may reflect senescence of the immune system36.However, no differences in the results of diagnostic tests(including salivary gland biopsy) were observed betweenolder and younger patients, suggesting that the tests have thesame diagnostic validity in older patients.
Positive autoantibodies are 1 of the 6 currentclassification criteria for SS and are the only analytical dataincluded. The 1993 European Criteria44 include the presenceof 1 or more of 4 antibodies (ANA, RF, Ro/SS-A, and/or La/SS-B), while the 2002 Criteria include only anti-Ro/SS-Aand/or anti-La/SS-B antibodies43. ANA is the most frequent-ly detected antibody in primary SS (85% in the currentstudy), and is closely associated with various extraglandularand analytical SS features, as is RF, which was associatedwith the main extraglandular, histopathologic, hematologic,and immunologic SS features5,39,45. In light of this evidence,we believe that a patient with sicca syndrome, positive oculartests and parotid scintigraphy, and positive ANA and/or RFshould be classified as having SS, even when Ro/La
antibodies are negative. ANA and RF determinations mayplay a central role in differentiating SS from nonautoimmunecauses of sicca syndrome, and their role in the diagnosis ofpatients with suspected SS should be reconsidered. Our andother results suggest an important diagnostic role for ANA/RF determination and support their possible inclusion infuture classification criteria.
The subset of patients with anti-Ro/La antibodies hadthe highest prevalence of most systemic, hematologic, andimmunologic alterations, confirming previous reports insmaller series which found a close correlation between theseautoantibodies and extraglandular manifestations2,3,11,19,28,serologic markers11,19,24,28, and a higher focus score in thesalivary gland biopsy25,45. This suggests that anti-Ro/Laantibodies should not be considered per se as a mandatorycriterion for primary SS, since that characteristic identifies aspecific subset of patients who probably have the mostclinically and immunologically ‘‘active’’ SS presentation.The inclusion of positive anti-Ro/La antibodies as amandatory criterion limits the diagnosis of primary SS,since some subsets, such as males, patients with late-onsetSS, and those with sicca-limited disease, had a lowerprevalence of anti-Ro/La antibodies, and therefore a lowerprobability of fulfilling the 2002 criteria.
The current study found a close association betweenhypocomplementemia/cryoglobulinemia and several epide-miologic, clinical, and immunologic features, such as a lowermean age and a higher frequency of vasculitis, lymphoma,and RF. Previous studies have prospectively confirmed thatpatients with hypocomplementemia and cryoglobulins atdiagnosis have a higher risk of developing vasculitis and B-cell lymphoma during follow-up20,30,40. These studies alsofound that the presence of these immunologic markers atdiagnosis have a key prognostic value in the survival ofpatients with primary SS. To our knowledge, Ioannidis andcolleagues20 were the first to suggest the prognostic role oflow C4 levels, and this was confirmed, together with low C3levels, by Theander et al40. We have recently confirmed theprognostic role for low C4 levels at diagnosis and identifiedcryoglobulins as a new prognostic marker in primary SS.However, cryoglobulins, but not C4 levels, were indepen-dently associated with mortality in the multivariate analysis,suggesting that the negative association between hypocom-plementemia and survival found in previous studies20,30,40
may be due to the complement activation caused bycryoglobulinemia. These data, all coming from large,prospective series of patients, confirm that complement andcryoglobulin measurement should be considered as the keyimmunologic markers in the follow-up of patients withprimary SS (as complement and anti-DNA are for systemiclupus erythematosus), and their inclusion in the classificationcriteria of SS should be strongly suggested.
We found some differences in the main features of thecurrent 1010 patients compared with those of the 400patients described 7 years ago17. These included a higherfrequency of xerophthalmia, parotid enlargement, articularinvolvement, and the main autoantibodies (ANA, RF, anti-Ro/La) (Table 8)1,20,40. Overall, the 4 studies have analyzed
216 n 2008 Lippincott Williams & Wilkins
Ramos-Casals et al Medicine � Volume 87, Number 4, July 2008
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
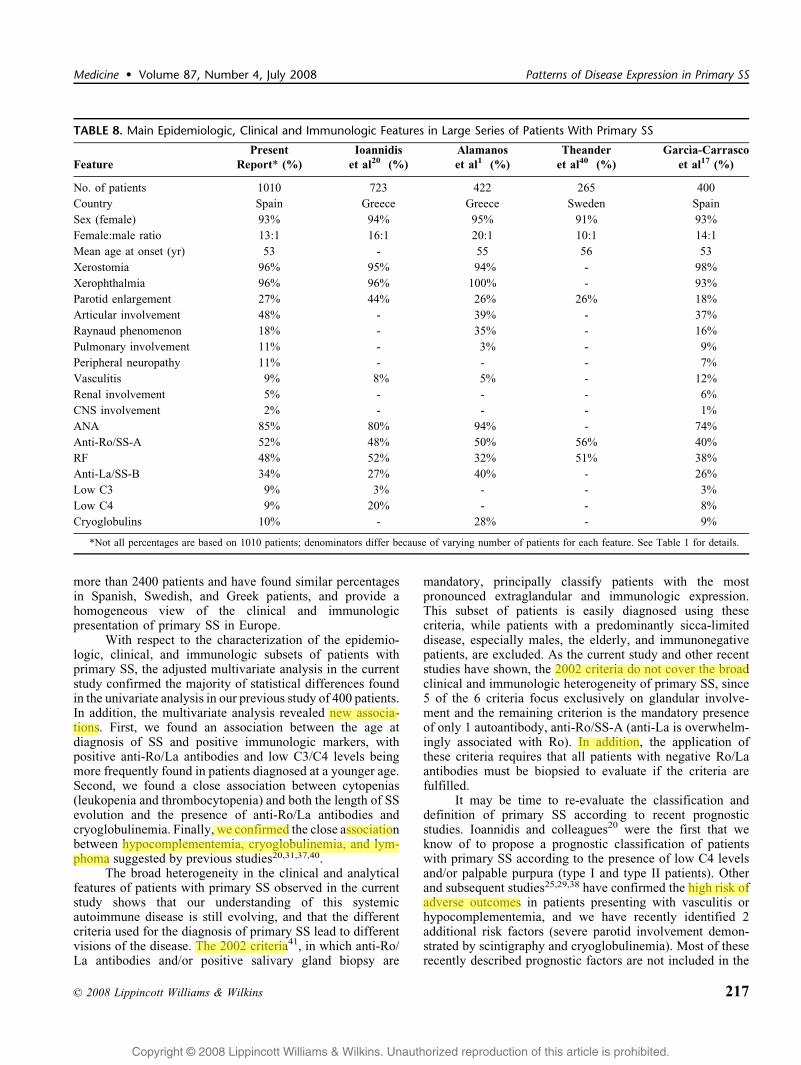
more than 2400 patients and have found similar percentagesin Spanish, Swedish, and Greek patients, and provide ahomogeneous view of the clinical and immunologicpresentation of primary SS in Europe.
With respect to the characterization of the epidemio-logic, clinical, and immunologic subsets of patients withprimary SS, the adjusted multivariate analysis in the currentstudy confirmed the majority of statistical differences foundin the univariate analysis in our previous study of 400 patients.In addition, the multivariate analysis revealed new associa-tions. First, we found an association between the age atdiagnosis of SS and positive immunologic markers, withpositive anti-Ro/La antibodies and low C3/C4 levels beingmore frequently found in patients diagnosed at a younger age.Second, we found a close association between cytopenias(leukopenia and thrombocytopenia) and both the length of SSevolution and the presence of anti-Ro/La antibodies andcryoglobulinemia. Finally, we confirmed the close associationbetween hypocomplementemia, cryoglobulinemia, and lym-phoma suggested by previous studies20,31,37,40.
The broad heterogeneity in the clinical and analyticalfeatures of patients with primary SS observed in the currentstudy shows that our understanding of this systemicautoimmune disease is still evolving, and that the differentcriteria used for the diagnosis of primary SS lead to differentvisions of the disease. The 2002 criteria41, in which anti-Ro/La antibodies and/or positive salivary gland biopsy are
mandatory, principally classify patients with the mostpronounced extraglandular and immunologic expression.This subset of patients is easily diagnosed using thesecriteria, while patients with a predominantly sicca-limiteddisease, especially males, the elderly, and immunonegativepatients, are excluded. As the current study and other recentstudies have shown, the 2002 criteria do not cover the broadclinical and immunologic heterogeneity of primary SS, since5 of the 6 criteria focus exclusively on glandular involve-ment and the remaining criterion is the mandatory presenceof only 1 autoantibody, anti-Ro/SS-A (anti-La is overwhelm-ingly associated with Ro). In addition, the application ofthese criteria requires that all patients with negative Ro/Laantibodies must be biopsied to evaluate if the criteria arefulfilled.
It may be time to re-evaluate the classification anddefinition of primary SS according to recent prognosticstudies. Ioannidis and colleagues20 were the first that weknow of to propose a prognostic classification of patientswith primary SS according to the presence of low C4 levelsand/or palpable purpura (type I and type II patients). Otherand subsequent studies25,29,38 have confirmed the high risk ofadverse outcomes in patients presenting with vasculitis orhypocomplementemia, and we have recently identified 2additional risk factors (severe parotid involvement demon-strated by scintigraphy and cryoglobulinemia). Most of theserecently described prognostic factors are not included in the
TABLE 8. Main Epidemiologic, Clinical and Immunologic Features in Large Series of Patients With Primary SS
Feature
Present
Report* (%)
Ioannidis
et al20 (%)
Alamanos
et al1 (%)
Theander
et al40 (%)
Garcıa-Carrasco
et al17 (%)
No. of patients 1010 723 422 265 400
Country Spain Greece Greece Sweden Spain
Sex (female) 93% 94% 95% 91% 93%
Female:male ratio 13:1 16:1 20:1 10:1 14:1
Mean age at onset (yr) 53 - 55 56 53
Xerostomia 96% 95% 94% - 98%
Xerophthalmia 96% 96% 100% - 93%
Parotid enlargement 27% 44% 26% 26% 18%
Articular involvement 48% - 39% - 37%
Raynaud phenomenon 18% - 35% - 16%
Pulmonary involvement 11% - 3% - 9%
Peripheral neuropathy 11% - - - 7%
Vasculitis 9% 8% 5% - 12%
Renal involvement 5% - - - 6%
CNS involvement 2% - - - 1%
ANA 85% 80% 94% - 74%
Anti-Ro/SS-A 52% 48% 50% 56% 40%
RF 48% 52% 32% 51% 38%
Anti-La/SS-B 34% 27% 40% - 26%
Low C3 9% 3% - - 3%
Low C4 9% 20% - - 8%
Cryoglobulins 10% - 28% - 9%
*Not all percentages are based on 1010 patients; denominators differ because of varying number of patients for each feature. See Table 1 for details.
n 2008 Lippincott Williams & Wilkins 217
Medicine � Volume 87, Number 4, July 2008 Patterns of Disease Expression in Primary SS
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight
usuario
Highlight

current 2002 classification criteria, an additional reason forrevisiting the diagnosis and classification of primary SS.
ACKNOWLEDGMENTS
The authors thank David Buss for his editorialassistance.
APPENDIXThe members of the GEMESS Study Group are listed
below:M. Ramos-Casals (Coordination), P. Brito-Zeron
(Laboratorio de Enfermedades Autoinmunes ‘‘Josep Font,’’Servicio de Enfermedades Autoinmunes, IDIBAPS, HospitalClınic, Barcelona); R. Solans, J. A. Bosch, M. Vilardell(Servicio de Medicina Interna, Hospital Vall d’Hebron,Barcelona); J. Rosas, G. Santos, R. Martın (Seccion deReumatologıa, Hospital de Villajoyosa, Alicante); A. Gil, P.Lavilla, I. Perez (Servicio de Medicina Interna, Hospital LaPaz, Madrid); M. T. Camps (Servicio de Medicina Interna,Hospital Carlos Haya, Malaga); J. Del Pino, C. A. Montilla(Servicio de Reumatologıa, Hospital Universitario deSalamanca, Salamanca); L. Pallares (Servicio de MedicinaInterna, Hospital de Son Dureta, Palma de Mallorca); J.Calvo-Alen (Seccion de Reumatologıa, Hospital de Sierral-lana, Torrelavega); M. L. Mico (Servicio de MedicinaInterna, Hospital La Fe, Valencia); J. Beltran (Seccion deReumatologıa, Hospital General de Castellon, Castellon); C.Hidalgo-Tenorio, J. M. Sabio, J. Jimenez-Alonso (Serviciode Medicina Interna, Hospital Virgen de las Nieves,Granada); R. Belenguer (Unidad de Reumatologıa, Hospital9 de Octubre, Valencia).
REFERENCES
1. Alamanos Y, Tsifetaki N, Voulgari PV, Venetsanopoulou AI, Siozos C,Drosos AA. Epidemiology of primary Sjogren’s syndrome in north-westGreece, 1982–2003. Rheumatology (Oxford). 2006;45:187–191.
2. Alexander E, Arnett F, Provost T, Stevens M. Sjogren’s syndrome:association of anti-Ro(SS-A) antibodies with vasculitis, hematologicabnormalities, and serologic hyperreactivity. Ann Intern Med. 1983;98:155–159.
3. Alexander E, Provost T, Stevens M, Alexander G. Neurologiccomplications of primary Sjogren’s syndrome. Medicine (Baltimore).1982;61:247–257.
4. Anaya J, Liu G, D’Souza E, Ogawa N, Luan X, Talal N. PrimarySjogren’s syndrome in men. Ann Rheum Dis. 1995;54:748–751.
5. Asmussen K, Andersen V, Bendixen G, Schiodt M, Oxholm P. A newmodel for classification of disease manifestations in primary Sjogren’ssyndrome: evaluation in a retrospective long-term study. J Intern Med.1996;239:475–482.
6. Bartunkova J, Sediva A, Vencovsky J, Tesar V. Primary Sjogren’ssyndrome in children and adolescents: proposal for diagnostic criteria.Clin Exp Rheumatol. 1999;17:381–386.
7. Brennan M, Fox P. Sex differences in primary Sjogren’s syndrome.J Rheumatol. 1999;26:2373–2376.
8. Brennan M, Sankar V, Leakan R, Kleiner D, Atkinson J, Wilkinson W,Baum B, Pillemer S. Risk factors for positive minor salivary glandbiopsy findings in Sjogren’s syndrome and dry mouth patients. ArthritisRheum. 2002;47:189–195.
9. Butterworth M, McClellan B, Allansmith M. Influence of sex inimmunoglobulin levels. Nature. 1967;214:1224–1225.
10. Cervera R, Font J, Ramos-Casals M, Garcia-Carrasco M, Rosas J, MorlaR, Munoz F, Artigues A, Pallares L, Ingelmo M. Primary Sjogren’s
syndrome in men: clinical and immunological characteristics. Lupus.2000;9:61–64.
11. Davidson B, Kelly C, Griffiths I. Primary Sjogren’s syndrome in theNorth East of England: a long-term follow-up study. Rheumatology(Oxford). 1999;38:245–253.
12. Diaz-Lopez C, Geli C, Corominas H, Malat N, Diaz-Torner C, Llobet J,De La Serna A, Laiz A, Moreno M, Vazquez G. Are there clinical orserological differences between male and female patients with primarySjogren’s syndrome? J Rheumatol. 2004;31:1352–1355.
13. Drosos A, Tsiakou E, Tsifetaki N, Politi E, Siamopoulou-Mavridou A.Subgroups of primary Sjogren’s syndrome. Sjogren’s syndrome inmale and paediatric Greek patients. Ann Rheum Dis. 1997;56:333–335.
14. Eidinger D, Garrett T. Studies of the regulatory effects of the sexhormones on antibody formation and stem cell differentiation. J ExpMed. 1972;136:1098–1116.
15. Fox R. Sjogren’s syndrome. Lancet. 2005;366:321–331.16. Fritzler M, Pauls J, Kinsella T, Bowen T. Antinuclear, anticytoplasmic,
and anti-Sjogren’s syndrome antigen A (SS-A/Ro) antibodies in femaleblood donors. Clin Immunol Immunopathol. 1985;36:120–128.
17. Garcia-Carrasco M, Ramos-Casals M, Rosas J, Pallares L, Calvo-Alen J,Cervera R, Font J, Ingelmo M. Primary Sjogren syndrome: clinical andimmunologic disease patterns in a cohort of 400 patients. Medicine(Baltimore). 2002;81:270–280.
18. Haga H, Jonsson R. The influence of age on disease manifestations andserological characteristics in primary Sjogren’s syndrome. Scand JRheumatol. 1999;28:227–232.
19. Harley J, Alexander E, Bias W, Fox O, Provost T, Reichlin M,Yamagata H, Arnett F. Anti-Ro (SS-A) and anti-La (SS-B) in patientswith Sjogren’s syndrome. Arthritis Rheum. 1986;29:196–206.
20. Ioannidis J, Vassiliou V, Moutsopoulos H. Long-term risk of mortalityand lymphoproliferative disease and predictive classification of primarySjogren’s syndrome. Arthritis Rheum. 2002;46:741–747.
21. Jaffe ES, Harris NL, Stein H, Vardiman JW. World Health OrganizationClassification of Tumors. Pathology and Genetics of Tumors ofHematopoietic and Lymphoid Tissues. Lyon: IARC Press; 2001.
22. Kassan S, Moutsopoulos H. Clinical manifestations and early diagnosisof Sjogren syndrome. Arch Intern Med. 2004;164:1275–1284.
23. Kraus A, Alarcon-Segovia D. Primary juvenile Sjogren’s syndrome.J Rheumatol. 1988;15:803–806.
24. Manoussakis M, Tzioufas A, Pange P, Moutsopoulos H. Serologicalprofiles in subgroups of patients with Sjogren’s syndrome. Scand JRheumatol. 1986; Suppl 61: 89–92.
25. Markusse H, Veldhoven C, Swaak A, Smeenk R. The clinicalsignificance of the detection of anti-Ro/SS-A and anti-La/SS-Bautoantibodies using purified recombinant proteins in primary Sjogren’ssyndrome. Rheumatol Int. 1993;13:147–150.
26. Martens P, Pillemer S, Jacobsson L, O’Fallon W, Matteson E.Survivorship in a population based cohort of patients with Sjogren’ssyndrome, 1976-1992. J Rheumatol. 1999;26:1296–1300.
27. Molina R, Provost T, Arnett F, Bias W, Hochberg M, Wilson R,Alexander E. Primary Sjogren’s syndrome in men. Clinical, serologic,and immunogenetic features. Am J Med. 1986;80:23–31.
28. Moutsopoulos H, Zerva L. Anti-Ro (SSA)/La (SSB) antibodies andSjogren’s syndrome. Clin Rheumatol. 1990;9(1 Suppl 1):123–130.
29. Ramos-Casals M, Anaya J, Garcia-Carrasco M, Rosas J, Bove A, ClaverG, Diaz L, Herrero C, Font J. Cutaneous vasculitis in primary Sjogrensyndrome: classification and clinical significance of 52 patients.Medicine (Baltimore). 2004;83:96–106.
30. Ramos-Casals M, Brito-Zeron P, Garcia-Carrasco M, Font J. Sarcoid-osis or Sjogren syndrome? Clues to defining mimicry or coexistence in59 cases. Medicine (Baltimore). 2004;83:85–95.
31. Ramos-Casals M, Brito-Zeron P, Yague J, Akasbi M, Bautista R, RuanoM, Claver G, Gil V, Font J. Hypocomplementaemia as an immunolog-ical marker of morbidity and mortality in patients with primarySjogren’s syndrome. Rheumatology (Oxford). 2005;44:89–94.
32. Ramos-Casals M, Cervera R, Font J. Do male patients withprimary Sjogren’s syndrome have a higher frequency of autoanti-bodies? J Rheumatol. 2005;32:1634–1635.
33. Ramos-Casals M, Cervera R, Font J, Garcia-Carrasco M, Espinosa G,Reino S, Pallares L, Ingelmo M. Young onset of primary Sjogren’s
218 n 2008 Lippincott Williams & Wilkins
Ramos-Casals et al Medicine � Volume 87, Number 4, July 2008
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

syndrome: clinical and immunological characteristics. Lupus. 1998;7:202–206.
34. Ramos-Casals M, Font J. Primary Sjogren’s syndrome: current andemergent aetiopathogenic concepts. Rheumatology (Oxford). 2005;44:1354–1367.
35. Ramos-Casals M, Font J, Garcia-Carrasco M, Brito M, Rosas J, Calvo-Alen J, Pallares L, Cervera R, Ingelmo M. Primary Sjogren syndrome:hematologic patterns of disease expression. Medicine (Baltimore). 2002;81:281–292.
36. Ramos-Casals M, Garcia-Carrasco M, Brito M, Lopez-Soto A, Font J.Autoimmunity and geriatrics: clinical significance of autoimmunemanifestations in the elderly. Lupus. 2003;12:341–355.
37. Ramos-Casals M, Tzioufas A, Font J. Primary Sjogren’s syndrome: newclinical and therapeutic concepts. Ann Rheum Dis. 2005;64:347–354.
38. Saito T, Sato J, Kondo K, Horikawa M, Ohmori K, Fukuda H. Lowprevalence of clinicopathologic and sialographic changes in salivaryglands of men with Sjogren’s syndrome. J Oral Pathol Med. 1999;28:312–316.
39. Shah F, Rapini R, Arnett F, Warner N, Smith C. Association of labialsalivary gland histopathology with clinical and serologic features ofconnective tissue diseases. Arthritis Rheum. 1990;33:1682–1687.
40. Theander E, Manthorpe R, Jacobsson L. Mortality and causes of death
in primary Sjogren’s syndrome: a prospective cohort study. ArthritisRheum. 2004;50:1262–1269.
41. Tishler M, Yaron I, Shirazi I, Yaron M. Clinical and immunologicalcharacteristics of elderly onset Sjogren’s syndrome: a comparison withyounger onset disease. J Rheumatol. 2001;28:795–797.
42. Trejo O, Ramos-Casals M, Garcia-Carrasco M, Yague J, Jimenez S, dela Red G, Cervera R, Font J, Ingelmo M. Cryoglobulinemia: study ofetiologic factors and clinical and immunologic features in 443 patientsfrom a single center. Medicine (Baltimore). 2001;80:252–262.
43. Vitali C, Bombardieri S, Jonsson R, Moutsopoulos H, Alexander E,Carsons S, Daniels T, Fox P, Fox R, Kassan S, Pillemer S, Talal N,Weisman M. Classification criteria for Sjogren’s syndrome: a revisedversion of the European criteria proposed by the American-EuropeanConsensus Group. Ann Rheum Dis. 2002;61:554–558.
44. Vitali C, Bombardieri S, Moutsopoulos H, Balestrieri G, Bencivelli W,Bernstein R, Bjerrum K, Braga S, Coll J, de Vita S. Preliminary criteriafor the classification of Sjogren’s syndrome. Results of a prospectiveconcerted action supported by the European Community. ArthritisRheum. 1993;36:340–347.
45. Wise C, Woodruff R. Minor salivary gland biopsies in patientsinvestigated for primary Sjogren’s syndrome. A review of 187 patients.J Rheumatol. 1993;20:1515–1518.
n 2008 Lippincott Williams & Wilkins 219
Medicine � Volume 87, Number 4, July 2008 Patterns of Disease Expression in Primary SS
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.