
Prevention of cisplatin-induced acute and delayed emesis by the selective neurokinin-1 antagonists,...
10
Prevention of Cisplatin-Induced Acute and Delayed Emesis by the Selective Neurokinin-1 Antagonists, L-758,298 and MK-869 A Randomized Controlled Trial Simon Van Belle, M.D., Ph.D. 1 Michael R. Lichinitser, M.D., Ph.D. 2 Rudolph M. Navari, M.D. 3 August M. Garin, M.D., Ph.D. 4 Marc L. A. Decramer, M.D., Ph.D. 5 Alain Riviere, M.D. 6 Myo Thant, M.D. 7 Elmer Brestan, M.D. 8 Binh Bui, M.D. 9 Krista Eldridge, B.S.N. 10 Marina De Smet, Pharm.D., Ph.D. 11 Nicole Michiels 11 Rick R. Reinhardt, M.D., Ph.D. 12 Alexandra D. Carides, Ph.D. 13 Judith K. Evans, M.D. 14 Barry J. Gertz, M.D., Ph.D. 15 1 Oncologisch Centrum, Universitair Ziekenhuis, Gent, Belgium. 2 Department of Combined Therapy, Cancer Re- search Center, Moscow, Russia. 3 College of Science and Walther Cancer Research Center, University of Notre Dame, Notre Dame, Indiana. 4 Department of Clinical Pharmacology and Che- motherapy, Cancer Research Center, Moscow, Russia. 5 Department of Respiratory Diseases, University Hospitals KU Leuven, UZ Gasthuisberg, Leuven, Belgium. 6 Centere Regional F. Baclesse, Caen, France. 7 Baltimore, Maryland. 8 Baptist Hospital Cancer Support Services, Pensacola, Florida. 9 Institut Bergonie, Bordeaux Cedex, France. 10 Clinical Research, Merck and Company, Inc., Blue Bell, Pennsylvania. 11 Clinical Pharmacology Europe, MSD Europe, Inc., Brussels, Belgium. 12 Novo Nordisk Pharmaceuticals, Inc., Princeton, New Jersey. 13 Clinical Biostatistics, Merck and Company, Inc., Blue Bell, Pennsylvania. 14 Medical Communications, Merck and Company, Inc., Blue Bell, Pennsylvania. 15 Clinical Pharmacology, Merck and Company, Inc., Rahway, New Jersey. Presented in abstract form at the 35th annual meeting of the American Society of Clinical Oncol- ogy, Atlanta, Georgia, May 14 –18, 1999. Supported by Merck and Company, Inc., manufac- turers of L-758,298 and MK-869. Drs. De Smet, Reinhardt, Carides, Evans, Gertz, Nurse Eldridge, and Ms. Michiels are employees of Merck and Company, Inc., at the time the study was conducted, and may potentially own stock and/or hold stock options in the company. Dr. Decramer is a consultant for Merck and Com- pany, Inc. All other authors are compensated consultants for Merck and Company, Inc. Address for reprints: Barry J. Gertz, M.D., Ph.D., Clinical Pharmacology, Merck and Company, Inc., Rahway, NJ 07065; Fax: (732) 594-7310; E-mail: [email protected] Received September 17, 2001; revision received December 19, 2001; accepted December 26, 2001. BACKGROUND. Recent studies have suggested that antiemetic therapy with a triple combination of the neurokinin-1 receptor antagonist MK-869, a serotonin (5-HT 3 ) antagonist, and dexamethasone provides enhanced control of cisplatin-induced emesis compared with standard therapy regimens. The authors compared the antiemetic activity of a dual combination of MK-869 and dexamethasone with that of a standard dual combination of ondansetron and dexamethasone to character- ize further the efficacy and tolerability profile of MK-869. METHODS. This was a multicenter, double-blind, randomized, active agent-con- trolled study of 177 cisplatin-naı ¨ve patients with malignant disease. On Day 1, MK-869 was given intravenously as its water-soluble prodrug, L-758,298. Patients were randomized to one of three groups as follows. Group I received L-758,298 100 mg intravenously (i.v.), then dexamethasone 20 mg i.v., and cisplatin 70 mg/m 2 on Day 1 followed by 300 mg MK-869 (tablet) orally on Days 2–5; Group II received L-758,298 100 mg i.v., then dexamethasone 20 mg i.v., and cisplatin 70 mg/m 2 on Day 1 followed by placebo on Days 2–5; and Group III received ondansetron 32 mg i.v., then dexamethasone 20 mg i.v., and cisplatin 70 mg/m 2 on Day 1 followed by placebo on Days 2–5. Emesis was recorded over Days 1–5 in a diary. Nausea was assessed every 24 hours by visual analog scale. Additional medication was available for emesis or nausea at any time. The primary efficacy parameters of interest were the proportion of patients without emesis and the proportion without emesis or rescue therapy on Day 1 (acute phase) and on Days 2–5 (delayed phase). 3032 © 2002 American Cancer Society
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Prevention of cisplatin-induced acute and delayed emesis by the selective neurokinin-1 antagonists,...
Prevention of Cisplatin-Induced Acute and DelayedEmesis by the Selective Neurokinin-1 Antagonists,L-758,298 and MK-869A Randomized Controlled Trial
Simon Van Belle, M.D., Ph.D.1
Michael R. Lichinitser, M.D., Ph.D.2
Rudolph M. Navari, M.D.3
August M. Garin, M.D., Ph.D.4
Marc L. A. Decramer, M.D., Ph.D.5
Alain Riviere, M.D.6
Myo Thant, M.D.7
Elmer Brestan, M.D.8
Binh Bui, M.D.9
Krista Eldridge, B.S.N.10
Marina De Smet, Pharm.D., Ph.D.11
Nicole Michiels11
Rick R. Reinhardt, M.D., Ph.D.12
Alexandra D. Carides, Ph.D.13
Judith K. Evans, M.D.14
Barry J. Gertz, M.D., Ph.D.15
1 Oncologisch Centrum, Universitair Ziekenhuis,Gent, Belgium.
2 Department of Combined Therapy, Cancer Re-search Center, Moscow, Russia.
3 College of Science and Walther Cancer ResearchCenter, University of Notre Dame, Notre Dame,Indiana.
4 Department of Clinical Pharmacology and Che-motherapy, Cancer Research Center, Moscow,Russia.
5 Department of Respiratory Diseases, UniversityHospitals KU Leuven, UZ Gasthuisberg, Leuven,Belgium.
6 Centere Regional F. Baclesse, Caen, France.
7 Baltimore, Maryland.
8 Baptist Hospital Cancer Support Services,Pensacola, Florida.
9 Institut Bergonie, Bordeaux Cedex, France.
10 Clinical Research, Merck and Company, Inc.,Blue Bell, Pennsylvania.
11 Clinical Pharmacology Europe, MSD Europe,Inc., Brussels, Belgium.
12 Novo Nordisk Pharmaceuticals, Inc., Princeton,New Jersey.
13 Clinical Biostatistics, Merck and Company, Inc.,Blue Bell, Pennsylvania.
14 Medical Communications, Merck and Company,Inc., Blue Bell, Pennsylvania.
15 Clinical Pharmacology, Merck and Company,Inc., Rahway, New Jersey.
Presented in abstract form at the 35th annualmeeting of the American Society of Clinical Oncol-ogy, Atlanta, Georgia, May 14–18, 1999.
Supported by Merck and Company, Inc., manufac-turers of L-758,298 and MK-869.
Drs. De Smet, Reinhardt, Carides, Evans, Gertz,Nurse Eldridge, and Ms. Michiels are employees ofMerck and Company, Inc., at the time the studywas conducted, and may potentially own stockand/or hold stock options in the company.
Dr. Decramer is a consultant for Merck and Com-pany, Inc.
All other authors are compensated consultants forMerck and Company, Inc.
Address for reprints: Barry J. Gertz, M.D., Ph.D.,Clinical Pharmacology, Merck and Company, Inc.,Rahway, NJ 07065; Fax: (732) 594-7310; E-mail:[email protected]
Received September 17, 2001; revision receivedDecember 19, 2001; accepted December 26, 2001.
BACKGROUND. Recent studies have suggested that antiemetic therapy with a triple
combination of the neurokinin-1 receptor antagonist MK-869, a serotonin (5-HT3)
antagonist, and dexamethasone provides enhanced control of cisplatin-induced
emesis compared with standard therapy regimens. The authors compared the
antiemetic activity of a dual combination of MK-869 and dexamethasone with that
of a standard dual combination of ondansetron and dexamethasone to character-
ize further the efficacy and tolerability profile of MK-869.
METHODS. This was a multicenter, double-blind, randomized, active agent-con-
trolled study of 177 cisplatin-naı̈ve patients with malignant disease. On Day 1,
MK-869 was given intravenously as its water-soluble prodrug, L-758,298. Patients
were randomized to one of three groups as follows. Group I received L-758,298 100
mg intravenously (i.v.), then dexamethasone 20 mg i.v., and cisplatin � 70 mg/m2
on Day 1 followed by 300 mg MK-869 (tablet) orally on Days 2–5; Group II received
L-758,298 100 mg i.v., then dexamethasone 20 mg i.v., and cisplatin � 70 mg/m2 on
Day 1 followed by placebo on Days 2–5; and Group III received ondansetron 32 mg
i.v., then dexamethasone 20 mg i.v., and cisplatin � 70 mg/m2 on Day 1 followed
by placebo on Days 2–5. Emesis was recorded over Days 1–5 in a diary. Nausea was
assessed every 24 hours by visual analog scale. Additional medication was available
for emesis or nausea at any time. The primary efficacy parameters of interest were
the proportion of patients without emesis and the proportion without emesis or
rescue therapy on Day 1 (acute phase) and on Days 2–5 (delayed phase).
3032
© 2002 American Cancer Society

RESULTS. No serious adverse events were attributed to L-758,298 or MK-869. On
Day 1, the proportions of patients with no emesis and no use of rescue medication
were 44% of patients in Group I, 36% of patients in Group II, 40% of patients in
Groups I and II combined, and 83% of patients in Group III (P � 0.001 for Group
III vs. the combined Groups I and II). The proportions of patients with no emesis
and no use of rescue medication on Days 2–5 were 59% of patients in Group I, 46%
of patients in Group II, and 38% of patients in Group III (P � 0.05 for Group I vs.
Group III). The proportions of patients who were without emesis on Day 1 were
49% of patients in Group I, 47% of patients in Group II, and 84% of patients in
Group III (P � 0.01 for Group I or II vs. Group III). On Days 2-5, however, the
proportions of patients who were without emesis on Days 2–5 were 65% of patients
in Group I, 61% of patients in Group II, and 41% of patients in Group III (P � 0.05
for Group I or II vs. Group III). Nausea scores in the acute phase were lower for
Group III than for Group I, Group II, or Groups I and II combined (P � 0.05),
although there was no significant difference among groups either for the delayed
phase or overall for Days 1–5.
CONCLUSIONS. Although the L-758,298 and dexamethasone combination reduced
acute (Day 1) emesis compared with historic rates, dual therapy with ondansetron
and dexamethasone was superior in controlling acute emesis. Continued dosing
with MK-869 may enhance control of other measures of delayed emesis, such as
the use of rescue medication, although confirmation is required before a definitive
conclusion may be drawn. MK-869 given as dual therapy with dexamethasone was
superior to ondansetron with dexamethasone for the control of delayed emesis
(Days 2–5) and control of the need for rescue medication on Days 2–5. Cancer
2002;94:3032– 41. © 2002 American Cancer Society.
DOI 10.1002/cncr.10516
KEYWORDS: antiemetic, cancer, substance P, neurokinin, clinical trial.
Patients with cancer consistently report that che-motherapy-induced emesis and associated nausea
are among the most unpleasant and distressing as-pects of treatment; in fact, patients may even delay orrefuse potentially curative therapy because of severechemotherapy-induced emesis.1,2 It has been shownthat the specific chemotherapy, dose, and regimen ofadministration influence the severity and pattern ofchemotherapy-induced emesis,3 with cisplatin mostcommonly associated with profound nausea and eme-sis. These symptoms tend to occur in a distinct, bi-phasic pattern. The acute phase generally is consid-ered the first 24 hours (or Day 1) after theadministration of chemotherapy, and the delayedphase is considered to be Days 2–5 postchemo-therapy.4 Virtually all patients who receive cisplatin indoses � 50 mg/m2 without prophylactic antiemeticsexperience severe acute-phase emesis,5 whereas 57–89% of patients experience delayed emesis,6 – 8 whichoccurs with maximal intensity on Days 2 and 3 aftercisplatin chemotherapy.9,10
The best control of acute emesis has beenachieved with the combination of a serotonin (5-HT3)antagonist and dexamethasone, a regimen on which48 –91% of patients report no acute emesis.11–13 Al-
though this therapy represents a significant advancein the control of acute nausea and emesis, room forimprovement still exists. Furthermore, the 5-HT3 an-tagonists are not highly effective in preventing delayedemesis,14,15 for which the most effective therapy cur-rently available is the combination of a 5-HT3 antag-onist or metoclopramide with dexamethasone (52–69% of patients report no delayed emesis).8,16 Thiscombination of medications is disadvantageous inthat it requires multiple doses per day and carries arisk of sedation and extrapyramidal side effects asso-ciated with metoclopramide.17 Therefore, a need re-mains for improved therapy for the prevention of bothacute and delayed emesis.
The neurokinin 1 (NK1) receptor antagonists are anew class of antiemetic compounds. L-758,298 is theintravenous (i.v.) prodrug of MK-869 (previouslyknown as L-754,030), a potent, selective, orally active,nonpeptide NK1 receptor antagonist. Previous publi-cations have reported the efficacy of MK-869 in pre-clinical models as well as in patients when given asmonotherapy and as part of triple-combination ther-apy with dexamethasone and a 5HT3 antagonist.17–19
Monotherapy on Day 1 with L-758,298 was less effec-tive numerically than monotherapy with ondansetron
Trial of MK-869 for Prevention of CIE/Van Belle et al. 3033

for the prevention of acute emesis, but there was asignificant reduction in delayed emesis after the initialtreatment with L-758,298 on Day 1.19 The triple com-bination was superior to the current standard dualtherapy with a 5HT3 antagonist and dexamethasonefor the prevention of both acute emesis and delayedemesis;18 in addition, continued dosing with the NK1
antagonist had a favorable impact on certain mea-sures of delayed emesis, such as nausea ratings. How-ever, although triple-combination therapy was shownto be more effective than standard dual therapy, itremained unclear whether the NK1 antagonist shouldbe combined with both dexamethasone and the 5HT3
antagonist to achieve maximum reduction of acuteemesis, or whether a dual combination of the NK1
antagonist and dexamethasone would suffice. Thisdual combination (using an oral formulation of theNK1 antagonist) was assessed preliminarily in the con-text of an additional triple-therapy study, the results ofwhich suggested that the NK1 antagonist plus dexa-methasone combination was superior to standarddual therapy in the prevention of delayed emesis butnot acute emesis.20 The dual therapy study describedhere was designed to confirm those earlier results byassessing the tolerability and benefits of an NK1 an-tagonist (in i.v. formulation) in combination withdexamethasone for the prevention of acute and de-layed cisplatin-induced emesis, as well as to evaluatethe benefit of continued dosing with the oral formu-lation.
MATERIALS AND METHODSStudy DesignThis multicenter, double-blind, randomized, activeagent-controlled (ondansetron plus dexamethasone)study was conducted in cisplatin-naı̈ve male and fe-male patients with cancer. The local ethical commit-tee in each of the participating centers approved thestudy protocol. Patients, all of whom signed an in-formed consent form, were assigned to one of threetreatment groups according to a computer-generated,randomized allocation schedule. Randomization wasstratified both for gender and for treatment with ad-ditional highly emetogenic therapy based on a pub-lished categorization.21
It is important to note that when this study wasdesigned and performed (with the first patient in thestudy in June, 1997 and the last patient out of thestudy in March, 1998), consensus guidelines had notyet been established regarding the use of prophylaxisfor chemotherapy-induced nausea and emesis. It isacknowledged that at the time these data are pub-lished, such guidelines have been incorporated intothe conduct of oncology research23 and include rec-
ommendations either for a 5HT3 antagonist and dexa-methasone or for metoclopramide and dexametha-sone in the delayed phase after patients receive high-dose cisplatin.
Patient EligibilityPatients � 18 years old who were scheduled to receivetheir first course of cisplatin-based chemotherapy (�70 mg/m2) were enrolled in the study. Female patientsof reproductive potential demonstrated a serum � hu-man chorionic gonadotropin level negative for preg-nancy at the prestudy visit. Primary criteria for exclu-sion included a Karnofsky score � 60, allergy orintolerance to dexamethasone or ondansetron, cur-rent abuse of alcohol or use of illicit drugs, use ofanother antiemetic agent within 72 hours of Day 1 ofthe study (serotonin antagonists, phenothiazines, bu-tyrophenones, cannabinoids, metoclopramide, corti-costeroids, or lorazepam), an episode of emesis orretching within 24 hours prior to the start of the cis-platin infusion on Day 1 of the study, severe concur-rent illness other than neoplasia, gastrointestinal ob-struction or an active peptic ulcer, radiation therapy tothe abdomen or pelvis within 1 week before or afterDay 1 of the study, or one of the following laboratorymeasurements: hemoglobin � 8.5 g/dL; white bloodcell (WBC) count � 3500/�L; platelets � 100,000/�L;alanine aminotransferase, aspartate aminotransferase,bilirubin, or alkaline phosphatase levels � 2 � theupper limit of normal; albumin � 3 g/dL; or serumcreatinine � 2.0 mg/dL.
TreatmentsThe schedule of treatments for each group is outlinedin Table 1. On Day 1, patients in Groups I and IIreceived L-758,298 (100 mg i.v.) infused over 15 min-utes beginning 1 hour prior to cisplatin infusion. Pa-tients in Group III received ondansetron (32 mg i.v.)infused over 15 minutes beginning 1 hour prior tocisplatin infusion. All patients received dexametha-sone 20 mg i.v. 30 minutes prior to cisplatin (� 70mg/m2).
An oral formulation of MK-869 (for whichL-758,298 is an i.v. prodrug) was used in the delayedphase, when patients were taking study medication ontheir own. On Days 2–5, patients in Group I receivedoral doses of MK-869 (300 mg tablet) once daily. OnDay 2, the dose of MK-869 was taken approximately 24hours after the initiation of the cisplatin infusion, andon subsequent days, the dose of MK-869 was takenbetween 8:00 AM and 10:00 AM.
Patients in Groups II and III received placebo onDays 2–5. Rescue therapy was available on an as-needed basis at any time for all patients.
3034 CANCER June 1, 2002 / Volume 94 / Number 11

AssessmentsBeginning immediately after infusion of chemother-apy and continuing for a total of 5 days, episodes ofemesis or retching (date, time, and number of epi-sodes) were recorded by the patients on diary cards.An emetic episode was defined as a single vomit orretch or any number of continuous vomits or retches.Distinct episodes were defined as those separated byat least 1 minute.
Nausea was assessed every 24 hours (from Day 1to Day 5) by the patients and was recorded as a verticalmark in the diary on a 100-mm horizontal visual an-alogue scale (VAS) headed as follows: How much nau-sea have you had over the last 24 hours?, with 0 mmlabeled on this scale as no nausea and 100 mm labelednausea as bad as it could be.
Using a different 100-mm VAS, patients reportedglobal satisfaction with their antiemetic treatment onthe morning of Day 2 and the morning of Day 6postcisplatin. The scale for Day 2 was headed as fol-lows: How satisfied are you with your antiemetic treat-ment over the past 24 hours? The scale for Day 6 washeaded as follows: How satisfied are you with yourantiemetic treatment over the entire study period? Oneach scale, 0 mm was labeled not at all satisfied, and100 mm was labeled completely satisfied. The VAS fornausea and the VAS for global satisfaction with anti-emetic treatment were translated into the native lan-guages of the participating centers and were validatedbefore use.
Safety was evaluated by physical examinations,electrocardiograms, and laboratory safety studies (he-matology, serum chemistry, and urinalysis) performedfor each patient prior to chemotherapy, once duringthe interval between Day 6 and Day 8, and once againduring the interval between Day 17 and Day 29. Ad-verse events other than episodes of emesis and nauseawere recorded by the patients on diary cards from Day1 to Day 5. Patients also recorded any adverse events,
including episodes of emesis and nausea, from Day 6to their poststudy visit (Days 17–29).
Statistical AnalysisThe analysis approach was intent to treat. All random-ized patients who received at least one dose of studydrug and had at least one post-treatment assessmentwere included in the efficacy analyses. For compari-sons involving the incidence of emesis, the Fisherexact test was used, and frequencies were rounded tothe nearest percent. A nominal 95%, exact, two-sidedconfidence interval was calculated for each of the rel-evant comparisons.
For comparison of the effect of the NK1 antagonistand dexamethasone combination with the ondanse-tron and dexamethasone combination on delayedemesis, a response rate of 35% for ondansetron anddexamethasone followed by 4 days of placebo wasassumed, with sample sizes projected at 50 patientsreceiving L-758,298 on Day 1 followed by 4 days ofMK-869, 50 patients receiving L-758,298 on Day 1 fol-lowed by 4 days of placebo, and 50 patients receivingondansetron on Day 1 followed by 4 days of placebo.The study had 80% power to detect a 28 percentagepoint increase or a 24 percentage point decrease foreither of the NK1 antagonist groups compared with thestandard dual-therapy group in the percentage of pa-tients with no emesis in the delayed phase. Specifi-cally, the efficacy analyses focused on the followingend points: the proportions of patients with no emesisand no use of rescue medication and the proportionsof patients with no emesis in both the acute phase andthe delayed phase; the proportions of patients withone or two emetic episodes in the delayed phase; andpatients with three or more emetic episodes in thedelayed phase.
In addition, patient self-assessment of nausea wasevaluated as a secondary efficacy parameter. Non-parametric analyses were performed on the ranked
TABLE 1Treatment Plan
Group
Day 1
Days 2–5One hourprechemotherapy
Thirty minutesprechemotherapy Chemotherapy
I L-758,298 (100 mg i.v.a) Dexamethasone (20 mg i.v.) Cisplatin (� 70 mg/m2 i.v.b) MK-869 (300 mg orally q.d.)II L-758,298 (100 mg i.v.a) Dexamethasone (20 mg i.v.) Cisplatin (� 70 mg/m2 i.v.b) Placebo (orally q.d.)III Ondansetron (32 mg i.v.a) Dexamethasone (20 mg i.v.) Cisplatin (� 70 mg/m2 i.v.b) Placebo (orally q.d.)
i.v.: intravenously; q.d.: daily.a Infused over 15 minutes.b Infused over � 3 hours.
Trial of MK-869 for Prevention of CIE/Van Belle et al. 3035

scores for nausea ratings due to a non-normal distri-bution of values in each treatment group. An analysisfor Day 1 used the VAS value recorded on Day 1, anda similar analysis for Day 2 used the VAS value re-corded for that day. For analysis of the delayed phase(Days 2–5) and the overall cumulative interval of Days1–5, an average score was computed for each patientusing the VAS values recorded over those intervals.The Kruskal–Wallis chi-square test was used to com-pare the distributions of these average scores amongthe treatment groups for the two intervals, and themedian values for these distributions are reported.The Wilcoxon test was used to perform pairwise com-parisons. The Fisher exact test was used to make pair-wise comparisons of the proportions of patients withno nausea or minimal nausea (defined post hoc as aVAS rating that averaged � 5 mm over the entire giveninterval) for Day 2, for the delayed phase (Days 2–5),and for the overall cumulative interval of Days 1–5.
Patient global satisfaction with antiemetic therapywas evaluated as an exploratory parameter. Due to anon-normal distribution of values, nonparametricanalyses were performed for Hour 24 and Day 6 usingthe ranked VAS global satisfaction scores for the cor-responding time points. The distributions were com-pared among the three treatment groups using theKruskal–Wallis chi-square test. In addition, pairwisecomparisons were performed using the Wilcoxon test.
Safety analyses were performed by examination oflaboratory parameters outside the normal range andby examination of between-group differences in theincidence of clinical adverse events. Summary statis-tics (the mean and standard deviation for each treat-ment group by time point) were calculated for relevantlaboratory analytes, vital signs, and PR interval andQTc, and an analysis of variance was used to comparemean changes in laboratory values between groups.
In addition, at the end of the study, the numbersand proportions of patients in each treatment groupwith laboratory value changes from baseline outsidepredefined limits were tabulated. National Cancer In-stitute toxicity criteria guidelines23 were used to tab-ulate the frequency with which laboratory values ofinterest fell into each toxicity grade per treatmentgroup, and the numbers and proportions of patientsin each group at each time point were reported. Noformal statistical tests were performed on either ofthese tabulations.
RESULTSPatient Characteristics and Inclusion in the AnalysisA total of 177 patients received an allocation number,and all patients received either L-758,298 with dexa-methasone or ondansetron with dexamethasone. The
baseline characteristics of the patients were similaracross treatment groups (Table 2). Two patients wereexcluded from both the acute phase and the delayedphase efficacy analyses. One of these patients (fromGroup I) expired and the diary was lost, and the otherpatient (from Group I) discontinued due to an adverselaboratory experience that occurred after the patientreceived L-758,298 and dexamethasone; this patientdid not receive cisplatin and did not complete thestudy. Two additional patients (one each in Groups Iand II) were excluded from the delayed-phase analysisbecause they discontinued after the acute phase dueto lack of efficacy, and incomplete data were collectedfor them. All 177 patients were included in the safetyanalysis.
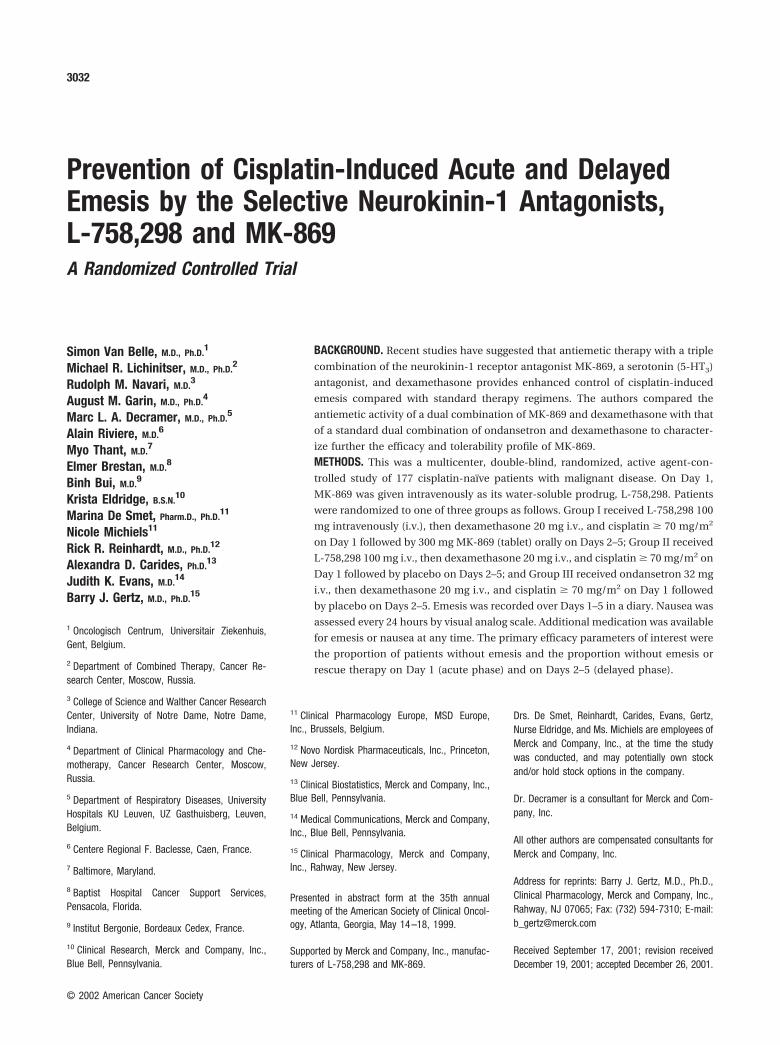
EmesisAcute phase (Day 1)The proportion of patients without emesis or use ofrescue medication in Group III (83%) was higherthan in either Group I (44%), Group II (36%), or thecombined group (I and II), which received L-758,298and dexamethasone (40%) on Day 1 (P � 0.001 forIII vs. the combined group) (Fig. 1). The differencebetween Group III and the combined group was 43percentage points (95% exact confidence interval,28 –57%). Furthermore, more patients in the com-
TABLE 2Patient Characteristicsa
Characteristic
Group I(n � 61patients)
Group II(n � 58patients)
Group III(n � 58patients)
Male:female (%) 62:38 67:33 60:40Mean � SD age (yrs) 59 � 13 56 � 13 59 � 15Alcohol drinks per week (%)
0–4 75 83 885–10 16 7 11�11 7 10 2
Mean � SD cisplatin dose(mg/m2) 90 � 15 87 � 15 86 � 16
Additional emetogenicchemotherapy (%)b 26 28 28
Type of cancer (%)Lung 41 34 44Gastrointestinal 21 17 19Head and neck 20 21 21Genitourinary 8 21 7Other 10 7 9
SD: standard deviation.a Group I received L-758,298 and dexamethasone on Day 1 and received MK-869 on Days 2–5; Group
II received L-758,298 and dexamethasone on Day 1 and received placebo on Days 2–5; and Group III
received ondansetron and dexamethasone on Day 1 and received placebo on Days 2–5.b The use of additional emetogenic chemotherapy was classified according to Hesketh et al.22
3036 CANCER June 1, 2002 / Volume 94 / Number 11
bined group (38%) took rescue medication in theacute phase compared with Group III (9%) (P� 0.001).
Likewise, the proportion of patients without eme-sis in the acute phase (regardless of use of rescuemedication) was significantly higher in Group III(84%) compared with Group I (49%), with Group II(47%), and with Groups I and II combined (48%; P� 0.001 for Group III vs. the combined group) (Table
3). The difference between Group III and the com-bined group was 36 percentage points (95% exact con-fidence interval, 22–52%).
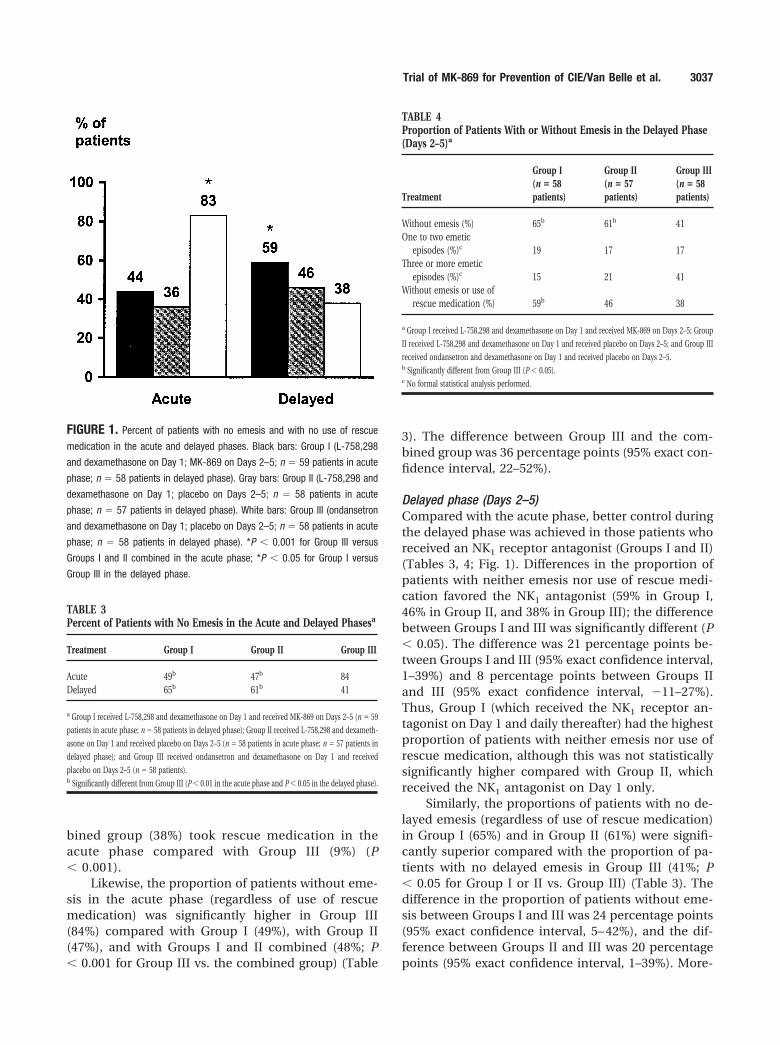
Delayed phase (Days 2–5)Compared with the acute phase, better control duringthe delayed phase was achieved in those patients whoreceived an NK1 receptor antagonist (Groups I and II)(Tables 3, 4; Fig. 1). Differences in the proportion ofpatients with neither emesis nor use of rescue medi-cation favored the NK1 antagonist (59% in Group I,46% in Group II, and 38% in Group III); the differencebetween Groups I and III was significantly different (P� 0.05). The difference was 21 percentage points be-tween Groups I and III (95% exact confidence interval,1–39%) and 8 percentage points between Groups IIand III (95% exact confidence interval, �11–27%).Thus, Group I (which received the NK1 receptor an-tagonist on Day 1 and daily thereafter) had the highestproportion of patients with neither emesis nor use ofrescue medication, although this was not statisticallysignificantly higher compared with Group II, whichreceived the NK1 antagonist on Day 1 only.
Similarly, the proportions of patients with no de-layed emesis (regardless of use of rescue medication)in Group I (65%) and in Group II (61%) were signifi-cantly superior compared with the proportion of pa-tients with no delayed emesis in Group III (41%; P� 0.05 for Group I or II vs. Group III) (Table 3). Thedifference in the proportion of patients without eme-sis between Groups I and III was 24 percentage points(95% exact confidence interval, 5– 42%), and the dif-ference between Groups II and III was 20 percentagepoints (95% exact confidence interval, 1–39%). More-
FIGURE 1. Percent of patients with no emesis and with no use of rescue
medication in the acute and delayed phases. Black bars: Group I (L-758,298
and dexamethasone on Day 1; MK-869 on Days 2–5; n � 59 patients in acute
phase; n � 58 patients in delayed phase). Gray bars: Group II (L-758,298 and
dexamethasone on Day 1; placebo on Days 2–5; n � 58 patients in acute
phase; n � 57 patients in delayed phase). White bars: Group III (ondansetron
and dexamethasone on Day 1; placebo on Days 2–5; n � 58 patients in acute
phase; n � 58 patients in delayed phase). *P � 0.001 for Group III versus
Groups I and II combined in the acute phase; *P � 0.05 for Group I versus
Group III in the delayed phase.
TABLE 3Percent of Patients with No Emesis in the Acute and Delayed Phasesa
Treatment Group I Group II Group III
Acute 49b 47b 84Delayed 65b 61b 41
a Group I received L-758,298 and dexamethasone on Day 1 and received MK-869 on Days 2–5 (n � 59
patients in acute phase; n � 58 patients in delayed phase); Group II received L-758,298 and dexameth-
asone on Day 1 and received placebo on Days 2–5 (n � 58 patients in acute phase; n � 57 patients in
delayed phase); and Group III received ondansetron and dexamethasone on Day 1 and received
placebo on Days 2–5 (n � 58 patients).b Significantly different from Group III (P � 0.01 in the acute phase and P � 0.05 in the delayed phase).
TABLE 4Proportion of Patients With or Without Emesis in the Delayed Phase(Days 2–5)a
Treatment
Group I(n � 58patients)
Group II(n � 57patients)
Group III(n � 58patients)
Without emesis (%) 65b 61b 41One to two emetic
episodes (%)c 19 17 17Three or more emetic
episodes (%)c 15 21 41Without emesis or use of
rescue medication (%) 59b 46 38
a Group I received L-758,298 and dexamethasone on Day 1 and received MK-869 on Days 2–5; Group
II received L-758,298 and dexamethasone on Day 1 and received placebo on Days 2–5; and Group III
received ondansetron and dexamethasone on Day 1 and received placebo on Days 2–5.b Significantly different from Group III (P � 0.05).c No formal statistical analysis performed.
Trial of MK-869 for Prevention of CIE/Van Belle et al. 3037

over, numerically fewer patients took rescue medica-tion in Group I (26%) compared with Group III (36%),and the percentage of patients with 0 –2 emetic epi-sodes was significantly lower in Group I (84%) and inGroup II (79%) compared with Group III (59%; P� 0.03 for Group I or II vs. Group III).
To assess whether effects in the delayed phasewere related to efficacy in the acute phase, a post hocanalysis was performed, which showed that the per-centage of patients who were without emesis in thedelayed phase despite having had emesis in the acutephase was greater in the L-758,298 groups than in theondansetron group (13 patients [22%] in Group I, 15patients [26%] in Group II, and 0 patients in GroupIII). To check the consistency of this finding, the pro-portions of patients who reported no acute emesis butthen experienced emesis in the delayed phase werealso tabulated: Patients who had emesis only in thedelayed phase were least common in Group I (thedaily MK-869 group; 4 patients), whereas 7 such pa-tients were noted in Group II (the single-doseL-758,298 group), and 25 such patients were noted inGroup III (the ondansetron group).
NauseaFor the acute phase, the distribution of nausea scoreswas lower in Group III (acute phase median VAS 1)compared with either Group I, Group II, or Groups Iand II combined (acute phase median VAS 11; P� 0.05). However, for both the delayed phase and theoverall cumulative interval, no significant difference inthe distribution of nausea scores was observed amongthe three treatment groups (delayed-phase medianVAS � 5 for Group I, 4 for Group II, and 1 for Group III;overall median VAS for Days 1–5 � 5 for Group I, 6 forGroup II, and 1 for Group III). In considering patientswho reported no nausea or minimal nausea (VAS av-erage rating � 5 mm) in the delayed phase, the relativefrequencies across treatment groups were 38% inGroup I, 46% in Group II, and 50% in Group III, withno significant differences observed among groups. Ex-ploratory analysis of the overall cumulative interval(Days 1–5) showed frequencies of no nausea or mini-mal nausea of 33% in Group I, 37% in Group II, and46% in Group III, with no significant difference seenamong groups.
Global SatisfactionThe median global satisfaction ratings 24 hours aftercisplatin were 91 mm for Groups I and II combinedand 99 mm for Group III (P � 0.05 for Group III vs.Groups I and II combined). Day 6 global satisfactionrating medians were 92 mm for Group I, 88 mm forGroup II, and 96 mm for Group III, with no significant
differences noted among the distribution of the scoresin the 3 groups.
TolerabilityAll 177 patients who received study medication wereincluded in the tolerability analysis. A total of 30 seri-ous clinical adverse events were reported, of whichnone was considered by any investigator to be relatedto study drug. Table 5 lists the most common adverseevents (occurring in � 10% of patients in at least 1treatment group) reported through Day 7, includingvarious gastrointestinal symptoms, headache, dizzi-ness, hiccups, abdominal pain, and asthenia. No sig-nificant differences were seen in the incidence ofthese adverse events among the treatment groups ex-cept for a higher incidence of diarrhea in Groups I andII (which did not receive ondansetron on Day 1).
No significant differences in laboratory measureswere observed among the treatment groups. Amongpatients who had normal or above-normal baselinevalues, fewer than 10% had transient decreases inWBC count (defined as WBC � 1.9 � 109/L and neu-trophils/bands � 0.9 � 109/L; National Cancer Insti-tute Grade 3 or 424). Similarly, fewer than 10% ofpatients had transient increases in transaminases (de-fined as at least 2.6 times the upper limit of the normalrange in patients who had normal or below-normalbaseline values; National Cancer Institute toxicityGrade 2, 3, or 423).
DISCUSSIONThe introduction of NK1 antagonists as a novel class ofantiemetic has shown promising initial results, espe-
TABLE 5Number (%) of Patients with the Most Common Clinical AdverseEventsa
Adverse eventb
Group I(n � 61patients)
Group II(n � 58patients)
Group III(n � 58patients)
Anorexia 6 (10) 7 (12) 5 (9)Constipation 5 (8) 4 (7) 8 (14)Diarrhea 14 (23) 13 (23) 3 (5)Nausea 7 (11) 11 (19) 3 (5)Dizziness 5 (8) 6 (11) 3 (5)Headache 8 (13) 11 (19) 7 (12)Hiccups 5 (8) 6 (11) 2 (4)Asthenia 10 (16) 11 (19) 7 (12)Pain, abdominal 5 (8) 4 (7) 6 (11)
a Group I received L-758,298 and dexamethasone on Day 1 and received MK-869 on Days 2–5; Group
II received L-758,298 and dexamethasone on Day 1 and received placebo on Days 2–5; and Group III
received ondansetron and dexamethasone on Day 1 and received placebo on Days 2–5.b The list shows adverse events reported in � 10% of patients from study Days 1–7, regardless of the
event’s relationship to the study drug.
3038 CANCER June 1, 2002 / Volume 94 / Number 11

cially in the prevention of delayed emesis. A compar-ison of L-758,298 and ondansetron given as mono-therapies prior to cisplatin showed that L-758,298 wasactive against cisplatin-induced acute emesis and wassuperior to the 5HT3 antagonist in the prevention ofdelayed emesis.19 Two previous trials also demon-strated the superiority of the triple combination of theNK1 antagonist with a 5HT3 antagonist and dexameth-asone,17,20 but it was not clear from those trialswhether the dual combination of L-758,298 and dexa-methasone required the addition of a 5HT3 antagonistfor maximum effect. The present dual-therapy trialnot only evaluated the NK1 antagonist versus a 5HT3
antagonist when each was given in combination withdexamethasone, but it also assessed the potential ben-efit of continued dosing with an NK1 antagonist beyondDay 1.
The results of the dual-therapy trial reported herereinforce the findings of previous studies19,20 by show-ing that patients who received L-758,298/L754,030 anddexamethasone had significantly better reduction ofdelayed emesis (in terms of complete response, whichwas defined as no emesis and no use of rescue ther-apy, and in terms of no emesis) compared with pa-tients who received ondansetron and dexamethasoneon Day 1. Consistent with previously observedtrends,17,19,20 L-758,298 and dexamethasone also ap-peared to be active against acute emesis, although notto the same extent as the 5-HT3 antagonist and dexa-methasone; the percentage of patients protected fromacute emesis in the ondansetron and dexamethasonegroup (84%) was comparable to that found in previoustrials24 –26 and was superior to that observed in GroupsI and II. In the delayed phase, however, L-758,298followed by once-daily oral doses of MK-869 improvedthe proportion of patients who achieved completeresponse (59%) by 21 percentage points comparedwith the patients who received parallel treatment withondansetron and dexamethasone followed by placebo(38%). In addition, L-758,298 followed by daily MK-869 improved the proportion of patients without eme-sis (65%) by 24 percentage points compared with pa-tients who received ondansetron and dexamethasonefollowed by placebo (41%), results similar to the bestreported results for delayed emesis with a complexdual-therapy regimen (5-HT3 antagonists or metoclo-pramide with dexamethasone, 52– 69%).8,16
Given the comparatively modest efficacy ofL-758,298 and dexamethasone in preventing acuteemesis, its more pronounced efficacy in preventingdelayed emesis is notable and cannot be attributedmerely to carry-over effects from the acute phase.Moreover, it has been shown that the plasma half-lifeof MK-869 is in the range of 10 –17 hours (data on file),
suggesting that the delayed-phase efficacy findingscannot be explained on a pharmacokinetic basis. Posthoc analyses lend additional support to these asser-tions by revealing a numeric trend toward better con-trol of delayed emesis despite less control of acuteemesis in patients who received MK-869 comparedwith patients who received ondansetron. In addition,analysis of the proportions of patients who reportedno acute emesis but then experienced emesis in thedelayed phase found the fewest of such patients in thedaily MK-869 group (4 patients), whereas 7 such pa-tients were noted in the single-dose L-758,298 group,and 25 such patients were noted in the ondansetrongroup. These findings, combined with the evidence ofthe superiority of the NK1 antagonist in the delayedphase despite lesser efficacy in the acute phase, sug-gest that control of acute emesis and control of de-layed emesis do not necessarily represent a straight-forward predictive relationship; this, in turn, issuggestive of different pathophysiologic mechanismsfor acute and delayed emesis.
If, in fact, the mechanisms that mediate acute-phase and delayed-phase emesis are different, and,because an initial dose of the NK1 antagonist appearsparticularly useful in the prevention of delayed eme-sis, it follows that continued dosing with the NK1
antagonist into the delayed phase may provide evengreater efficacy. In support of this reasoning, datafrom the first triple-therapy study have shown thatpatients who received an initial dose of MK-869 400mg orally followed by daily doses of MK-869 300 mgorally in the delayed phase appeared to experiencegreater relief of delayed emesis compared with pa-tients who received an initial dose of MK-869 400 mgorally followed by placebo in the delayed phase.18
Likewise, in the present dual-therapy study, the pro-portion of patients in Group I (initial L-758,298 100 mgi.v. followed by daily MK-869 300 mg orally in thedelayed phase) who reported no emesis in the delayedphase was numerically greater than the proportion inGroup II (initial L-758,298 100 mg i.v. followed by dailyplacebo in the delayed phase). Considered in the con-text of a serial comparison of the three treatmentgroups, these data reveal a trend toward further im-provement of delayed emesis with continued dosingwith MK-869: The lowest proportion of patients withno delayed emesis was observed in Group III (initialondansetron and daily placebo); the proportion inGroup II (initial L-758, 298 and daily placebo) wassignificantly higher, and the percentage in Group I(initial L-758,298 and daily MK-869) was higher still. Inboth studies, this trend may have been even strongerif patients had not been given such a high initial doseof L-758,298 on Day 1. The possibility that the true
Trial of MK-869 for Prevention of CIE/Van Belle et al. 3039

magnitude of this enhancing effect may have beensomewhat obscured in this study by the high initialdose suggests that the potential benefit of continueddosing may be more pronounced in studies usinglower initial oral doses of MK-869.
A 13 percentage point numerical advantage alsowas observed in this study for the daily MK-869 groupcompared with the single-dose L-758,298 group interms of the proportion of patients with completeresponse in the delayed phase; moreover, in terms ofthe number of patients who took rescue medication,the superiority of the daily MK-869 group approachedstatistical significance (26% in Group I vs. 42% inGroup II; P � 0.1). Although the results of this studyare not definitive, the trends in the data are supportiveof the results of the triple-therapy trial18 regarding thebenefit of continued dosing with an NK1 antagonist inthe delayed phase, a regimen that will be incorporatedinto future trials with MK-869.
Although emesis was the primary end point of thisstudy, control of nausea also was examined. Because itis widely believed that response to treatment in thedelayed period is determined to some extent by re-sponse in the acute period, patients in Groups I and IImight be expected to have had worse nausea in thedelayed phase than patients in Group III. However,although patients in Group III started out in the first24 hours with better control of nausea compared withpatients in Groups I and II, no such difference intreatment groups was observed in the delayed phase.This similarity of nausea ratings in the delayed phaseacross all groups indicates that the NK1 antagonistreduced nausea in the delayed phase despite its lessereffect on nausea in the acute phase. The use of MK-869, therefore, may result in an improvement in pa-tient reported outcomes associated with improvedcontrol of delayed nausea, because nausea has super-seded emesis as the most unpleasant and distressingaspect of chemotherapy.1
MK-869 administered as an oral prodrug was gen-erally well tolerated: Except for a higher incidence ofdiarrhea, the adverse events seen in Group III weresimilar to those seen in the groups that did not receiveondansetron (Groups I and II). This result likely re-flects the loss of the constipating influence of a 5HT3
antagonist in patients who did not receive ondanse-tron; in the absence of antiemetics, it has been shownthat cisplatin causes diarrhea in up to 60% of pa-tients,27 whereas prophylactic administration of a5-HT3 antagonist has been associated with a lowerincidence of cisplatin-related diarrhea.28 In normalvolunteer studies, administration of MK-869 has notresulted in diarrhea (data on file; Merck Research Lab-oratories, Blue Bell, PA).
The findings of the dual-therapy study presentedhere support the use of MK-869 as a particularly ef-fective agent for the control of delayed emesis in pa-tients receiving highly emetogenic chemotherapy.These results also confirm that MK-869 combinedsolely with dexamethasone exerts suboptimal efficacyin the acute phase compared with standard therapy.This finding is consistent with and emphasizes theimportance of previously published results showingthat the triple combination of MK-869, a 5-HT3 recep-tor antagonist, and dexamethasone was more effectivethan dual combinations consisting of dexamethasoneand one other agent.17,20 The results of the currentstudy, combined with the results obtained from otherstudies of MK-869,17,19,20 suggest that the likely differ-ent underlying mechanisms of acute and delayedemesis may be addressed most effectively by admin-istering triple therapy (NK1 antagonist, 5-HT3 antago-nist, and dexamethasone) prior to initiation of chemo-therapy for control of acute emesis, with control ofdelayed symptoms most likely optimized by contin-ued dosing with an NK1 antagonist after Day 1.
REFERENCES1. Griffin AM, Butow PN, Coates AS, et al. On the receiving end
V: patient perceptions of the side effects of cancer chemo-therapy. Ann Oncol. 1997;7:189 –195.
2. Laszlo J, Lucas VSJ. Emesis as a critical problem in chemo-therapy. N Engl J Med. 1981;305:948 –949.
3. Gralla RJ. Controlling emesis in patients receiving can-cer chemotherapy. Recent Results Cancer Res. 1991;121:68 – 82.
4. Gralla RJ, Tyson LB, Kris MG, Clark RA. The management ofchemotherapy-induced nausea and vomiting. Med ClinNorth Am. 1987;71:289 –301.
5. Kris MG, Cubeddu LX, Gralla RJ, et al. Are more antiemetictrials with a placebo necessary? Report of patient data fromrandomized trials of placebo antiemetics with cisplatin.Cancer. 1996;78:2193–2198.
6. Passalacqua R, Cocconi G, Bella M, et al. Double-blind,randomized trial for the control of delayed emesis in pa-tients receiving cisplatin: comparison of placebo vs. adre-nocorticotropic hormone (ACTH). Ann Oncol. 1992;3:481–485.
7. Gandara DR, Harvey WH, Monaghan GG, Perez EA, HeskethPJ. Delayed emesis following high-dose cisplatin: a double-blind randomized comparative trial of ondansetron (GR38032F) versus placebo. Eur J Cancer. 1993;29A(Suppl 1):S35–S38.
8. Kris MG, Gralla RJ, Tyson LB, Clark RA, Cirrincione C, Gro-shen S. Controlling delayed vomiting: double-blind, ran-domized trial comparing placebo, dexamethasone alone,and metoclopramide plus dexamethasone in patients re-ceiving cisplatin. J Clin Oncol. 1989;7:108 –114.
9. Kris MG, Gralla RJ, Clark RA, et al. Incidence, course, andseverity of delayed nausea and vomiting following the ad-ministration of high-dose cisplatin. J Clin Oncol. 1985;3:1379 –1384.
3040 CANCER June 1, 2002 / Volume 94 / Number 11

10. Navari RM, Madajewicz S, Anderson N, et al. Oral ondanse-tron for the control of cisplatin-induced delayed emesis: alarge, multicenter, double-blind, randomized comparativetrial of ondansetron versus placebo. J Clin Oncol. 1995;13:2408 –2416.
11. Roila F, Tonato M, Cognetti F, et al. Prevention of cisplatin-induced emesis: a double-blind multicenter randomizedcrossover study comparing ondansetron and ondansetronplus dexamethasone. J Clin Oncol. 1991;9:675– 678.
12. Smith DB, Newlands ES, Rustin GJ, et al. Comparison ofondansetron and ondansetron plus dexamethasone as an-tiemetic prophylaxis during cisplatin-containing chemo-therapy. Lancet. 1991;338:487– 490.
13. Hesketh PJ, Harvey WH, Harker WG, et al. A randomized,double-blind comparison of intravenous ondansetron aloneand in combination with intravenous dexamethasone in theprevention of high-dose cisplatin-induced emesis. J ClinOncol. 1994;12:596 – 600.
14. Roila F, Bracarda S, Tonato M, et al. Ondansetron in theprophylaxis of acute and delayed cisplatin-induced emesis.Clin Oncol. 1990;2:268 –272.
15. Hesketh P. Management of cisplatin-induced delayed eme-sis. Oncology. 1996;53(Suppl 1):78 – 85.
16. Gralla RJ, Rittenberg C, Peralta M, Lettow L, Cronin M.Cisplatin and emesis: aspects of treatment and a new trialfor delayed emesis using oral dexamethasone plus ondan-setron beginning at 16 hours after cisplatin. Oncology. 1996;53(Suppl 1):86 –91.
17. Navari R, Reinhardt R, Gralla RJ, et al. Reduction of cispla-tin-induced emesis by a selective neurokinin-1 receptor an-tagonist. N Engl J Med. 1999;340:190 –195.
18. Tattersall FD, Rycroft W, Cumberbatch M, et al. The novelNK1 receptor antagonist MK-0869 (L-754,030) and its watersoluble phosphoryl prodrug, L-758,298, inhibit acute anddelayed cisplatin-induced emesis in ferrets. Neuropharma-cology. 2000;39:652– 663.
19. Cocquyt V, Van Belle S, Reinhardt R, et al. L-758,298, a
prodrug for the selective neurokinin-1 antagonist,L-754,030, compared to ondansetron for the prevention ofcisplatin-induced emesis. Eur J Cancer. 2001;37:835– 842.
20. Campos D, Pereira JR, Reinhardt R, et al. Prevention ofcisplatin-induced emesis by the oral neurokinin-1 antago-nist, MK-869, in combination with granisetron and dexa-methasone or with dexamethasone alone. J Clin Oncol.2001;19:1759 –1767.
21. Hesketh PJ, Kris MG, Grunberg SM, et al. Proposal for clas-sifying the acute emetogenicity of cancer chemotherapy.J Clin Oncol. 1997;15:103–109.
22. Antiemetic Subcommittee of the Multinational Associationof Supportive Care in Cancer. Prevention of chemotherapy-and radiotherapy-induced emesis: results of Perugia Con-sensus Conference. Ann Oncol. 1998;9:811– 819.
23. National Cancer Institute. Cancer therapy evaluation pro-gram. Common toxicity criteria, version 2.0. Bethesda, MD:National Cancer Institute, National Institutes of Health, De-partment of Health and Human Services, 1998.
24. Italian Group For Antiemetic Research. Ondansetron� dexamethasone vs metoclopramide � dexamethasone� diphenhydramine in prevention of cisplatin-inducedemesis. Lancet. 1992;340:96 –99.
25. Kris MG, Baltzer L, Pisters KMW, Tyson LB. Enhancing theeffectiveness of the specific serotonin antagonists. Cancer.1993;72:3436 –3442.
26. Perez EA. Comparative efficacy of oral and intravenousgranisetron for the prevention of acute chemotherapy-in-duced emesis. Clin Therapeutics. 1996;18:578 –590.
27. Gralla RJ, Itri LM, Pisko SE, et al. Antiemetic efficacy of high-dose metoclopramide: randomized trials with placebo andprochlorperazine in patients with chemotherapy-inducednausea and vomiting. N Engl J Med. 1981;305:905–909.
28. Medical Economics Company. Physician’s desk reference.52nd ed. Montvale: Medical Economics Company, 1998:2836 –2838.
Trial of MK-869 for Prevention of CIE/Van Belle et al. 3041




















