Prevention Across the Lifespan: A Review of Evidence-Based ...
293
Editors Ann Eshenaur Spolarich • Fotinos S. Panagakos Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions Supported through an educational grant from
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Prevention Across the Lifespan: A Review of Evidence-Based ...
EditorsAnn Eshenaur Spolarich • Fotinos S. Panagakos
Prevention Across the Lifespan: A Review of
Evidence-Based Interventions for Common Oral Conditions
Supported through an educational grant from

Prevention Across the Lifespan: A Review of Evidence-Based Interventions
for Common Oral Conditions
Ann Eshenaur Spolarich, RDH, PhD, FSCDHProfessor and Director of Research
Arizona School of Dentistry and Oral HealthA.T. Still UniversityMesa, AZ, USA
Fotinos S. Panagakos, DMD, PhDGlobal Director, Scientific AffairsColgate-Palmolive CompanyPiscataway, NJ, USA
i
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
Copyright © 2017 by the Colgate-Palmolive Company. All rights reserved.
No part of this publication may be used or reproduced in any form or by any means,or stored in a database or retrieval system, without prior written permission of theColgate-Palmolive Company. Making copies of any part of this book for any purposeother than your own personal use is a violation of United States copyright laws.
ISBN-10: 0966284917ISBN-13: 978-0-9662849-1-1
Published by …
Professional Audience Communications, Inc.PO Box 39486Charlotte, North Carolina 28278 USA
Editorial Quality Control/Proofreading: Teri S. SiegelCopyediting: Donna FrassettoLayout and Design: Horizons Advertising & Graphic DesignCover Design: Horizons Advertising & Graphic DesignIndexing: Allegheny Writing & Publishing Services, LLCPublisher: Stephen M. Siegel
Printed in the United States of America
Last digit is the print number: 6 5 4 3 2 1
iiii
P. Mark Bartold, BDS, BScDent(Hons)PhD, DDSc, FRACDS(Perio)Professor of Periodontology, Director, Colgate Australian Clinical Dental Research CentreUniversity of Adelaide Department of DentistryAdelaide, South Australia
Sharon M. Compton, DipDH, BSc, MA(Ed), PhDProfessor and DirectorDental Hygiene Undergraduate and Graduate ProgramsSchool of Dentistry, Faculty of Medicineand DentistryUniversity of AlbertaAlberta, Canada
Louis G. DePaola, DDS, MSAssistant Dean of Clinical AffairsProfessor, Department of Oncology and Diagnostic Sciences University of Maryland School of DentistryBaltimore, Maryland, USA
Zameera Fida, DMDDepartment of Dentistry, Boston Children’s HospitalDirector of Predoctoral Pediatric DentistryInstructor, Developmental BiologyHarvard School of Dental MedicineBoston, Massachusetts, USA
Jacquelyn L. Fried, RDH, BA, MSAssociate Professor and Director of Interprofessional InitiativesAssociate Faculty, Schools of Nursing and PharmacyDepartment of Periodontics, Division of Dental HygieneUniversity of Maryland School of DentistryBaltimore, Maryland, USA
JoAnn R. Gurenlian, RDH, MS, PhDProfessor and Graduate Program DirectorDepartment of Dental HygieneDivision of Health SciencesIdaho State UniversityPocatello, Idaho, USA
Phuu P. Han, DDS, PhDDiplomate of the American Board of Orofacial PainAssistant Professor of Clinical DentistryDivision of Dental Public Health and Pediatric DentistryHerman Ostrow School of Dentistry of USCLos Angeles, California, USA
Yiming Li, DDS, MSD, PhDAssociate Dean for ResearchProfessor and Director, Center for Dental ResearchLoma Linda University School of DentistryLoma Linda, California, USA
Mark S. Montana, DDSCertificate in ProsthodonticsPrivate practice, Tempe, Arizona, USA
Antonio J. Moretti, DDS, MSAssociate Professor and Graduate Program DirectorDepartment of PeriodontologyUniversity of North Carolina School of DentistryChapel Hill, North Carolina, USA
Roseann Mulligan, DDS, MSFellow of the Gerontological Society of AmericaDirector of the Online Programs in Geriatric DentistryCharles M. Goldstein Professor of Community DentistryAssociate Dean, Community Health Programs and Hospital Affairs Chair of the Division of Dental PublicHealth and Pediatric Dentistry Herman Ostrow School of Dentistry of USCProfessor, USC Davis School of GerontologyLos Angeles, California, USA
CONTRIBUTORS
iii
Fotinos S. Panagakos, DMD, PhDGlobal Director, Scientific AffairsColgate-Palmolive CompanyPiscataway, New Jersey, USA
Philip M. Preshaw, BDS, FDS RCSEd, PhDProfessor of PeriodontologySchool of Dental Sciences and Institute of Cellular MedicineNewcastle UniversityNewcastle upon Tyne, United Kingdom
Professor Iain A. Pretty Dental Health Unit, University of ManchesterManchester, England
Michael P. Rethman, DDS, MSAssociate Professor (adjunct), BaltimoreCollege of Dental Surgery, University of MarylandAssistant Professor (adjunct), College ofDentistry, The Ohio State UniversityPrescott, Arizona, USA
Erik R. Roskam, DDSTandartsenpraktijk Santpoort NoordThe Netherlands
S.D. Shanti, DDS, MPH, PhD, CPH Associate Professor of Public Health Arizona School of Dentistry and Oral HealthCollege of Graduate Health Studies A.T. Still University of Health SciencesMesa, Arizona, USA
Harlan Shiau, DDS, DMedScDiplomate, American Board of Periodontology Clinical Associate Professor, Department of Periodontology University of Maryland School of DentistryBaltimore, Maryland, USA
Marc Shlossman, DDS, MSAssistant Professor and Interim Director,Periodontics Director, Clinical Research Arizona School of Dentistry and Oral HealthA.T. Still UniversityMesa, Arizona, USA
Ann Eshenaur Spolarich, RDH, PhD, FSCDHProfessor and Director of ResearchArizona School of Dentistry and Oral HealthA.T. Still UniversityMesa, Arizona, USA
Piedad Suarez-Durall, DDSSection Chair, Geriatric and Special Patients ClinicCo-director of the Special Patients ClinicAssociate Professor of Clinical DentistryDivision of Dental Public Health and Pediatric DentistryHerman Ostrow School of Dentistry of USCLos Angeles, California, USA
J.M. (‘Bob’) ten Cate, PhD, DrhcEmeritus Professor of Preventive DentistryAcademic Center for Dentistry Amsterdam(ACTA)The Netherlands
Rebecca S. Wilder, BSDH, MSProfessor and Director of Faculty DevelopmentOffice of Academic AffairsDirector, Graduate Dental Hygiene EducationUniversity of North Carolina-Chapel HillChapel Hill, North Carolina, USA
iv
CONTRIBUTORS

Mark S. Wolff, DDS, PhDAssociate Dean for Predoctoral Clinical EducationAssociate Dean for DevelopmentProfessor and Chair, Cariology and Comprehensive Care New York University College of DentistryNew York, New York, USA
Minn N. Yoon, PhDAssistant Professor, School of DentistryFaculty of Medicine and DentistryUniversity of AlbertaEdmonton, Alberta, Canada
v
CONTRIBUTORS
Dear Reader:
We are delighted to present the textbook Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions. It is very appropriate that this book is beingpublished at a time when prevention is front and center within oral healthcare, both in educa-tion and professional practice.
In this textbook, we have structured the material so that it can be used by those early in theireducational journey as well as seasoned practitioners. It will provide the reader with practicalinformation regarding the prevention of the most common oral health indications, with a spe-cial emphasis on age-related considerations. This text focuses on the current best evidence avail-able to support decision making for recommended preventive interventions.This book is notintended to be a comprehensive review of the science around diagnosis and treatment for eachof these indications – there are numerous resources available from experts in the field if one isinterested in diving deeper in areas such as caries, periodontal disease, or dry mouth. Rather,it is our intention to emphasize how practitioners can help patients prevent disease from oc-curring, recurring, or progressing.
This book is the result of a 12-month process based on the most contemporary thinking behindwhat the literature suggests regarding prevention of oral disease. A unique feature in many ofthe chapters is the addition of case reviews that bring to life the content in the chapter. Thereader will be able to use these cases to reinforce what they just read. Students will find thesecases useful in incorporating the content into the broader learning process in which they areengaged. Finally, dental faculty will find these cases useful in their respective courses.
We would like to express our deep appreciation to the chapter authors. It was through theirknowledge of these vitally important subjects, their professional relationships with the two ofus, and their backgrounds as highly regarded researchers and educators in dentistry, that weare able to bring you this significant work.
Since the launch of its first toothpaste in 1873, the Colgate-Palmolive Company has been aworld leader in oral care, both through cutting-edge therapeutics, as well as important educa-tional services to the dental professions.This book, Prevention Across the Lifespan: A Reviewof Evidence-Based Interventions for Common Oral Conditions, which has been produced anddistributed through an educational grant from the company (by which the company providedfunding to the publisher), is a prime example of Colgate’s continuing commitment to ensuringeducation for dental professionals.
vi
From the Editors
Ann E. Spolarich Fotinos A. Panagakos

vii
CHAPTER 1Adopting an Evidence-Based Philosophy of PracticeAnn Eshenaur Spolarich and Fotinos Panagakos . . . . . . . . . . . . . . . . . . . . . . .1
CHAPTER 2Behavioral ScienceS.D. Shanti . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
CHAPTER 3Risk AssessmentJoAnn R. Gurenlian . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .37
CHAPTER 4Dental CariesJ.M. (“Bob”) ten Cate and Erik R. Roskam . . . . . . . . . . . . . . . . . . . . . . . 57
CHAPTER 5Gingival DiseasesRebecca Wilder and Antonio Moretti . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71
CHAPTER 6Preventing Damage to Oral Hard and Soft TissuesMarc Shlossman and Mark Montana . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .97
CHAPTER 7Head and Neck CancersJacquelyn Fried . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .121
CHAPTER 8Oral MalodorP. Mark Bartold . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .146
CONTENTS
viii
CHAPTER 9Dentin HypersensitivityYiming Li . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .160
CHAPTER 10Dry MouthSharon Compton and Minn Yoon . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .175
CHAPTER 11Orofacial InjuriesZameera Fida . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .192
CHAPTER 12Prevention in the Context of Oral–Systemic HealthPhilip M. Preshaw . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .207
CHAPTER 13Preventive Considerations in Special Care DentistryRoseann Mulligan, Phuu Pwint Han, and Piedad Suarez-Durall . . . . . . . . .221
CHAPTER 14FluoridesI. A. Pretty . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .235
CHAPTER 15Non-Fluoride Remineralization TherapiesMark S. Wolff and Michael P. Rethman . . . . . . . . . . . . . . . . . . . . . . . . . . .246
CHAPTER 16Chemotherapeutic AgentsHarlan J. Shiau and Louis G. DePaola . . . . . . . . . . . . . . . . . . . . . . . . . . . . .257
INDEX . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .272
CONTENTS
Evidence-based dentistry (EBD) is a philosophi-cal approach to practice that facilitates the clini-cian’s decision making about patient care.Decisions should be patient centered, tailoringcare to each individual’s treatment needs, whiletaking into consideration the clinician’s expertiseand experiences, as well as the patient’s needs,preferences, and desires. Clinical decisions arebased on knowledge of current best evidenceobtained by accessing and critically appraisingpublished studies in the scientific literature. Theclinician must carefully weigh the patient’s generaland oral healthcare needs and determine how theevidence may be applied to address those needs.Clinicians must also help patients make treatmentdecisions utilizing this knowledge when consider-
ing options for care, while taking into account thepatient’s values, expectations, and unique clinicalcircumstances. Social, cultural, and behavioralfactors may influence the patient’s willingness toaccept the proposed plan of treatment as well ascompliance with professional recommendations.Practicing with this type of philosophy is not easyand demands certain skills and due diligence tobe successful. Ultimately, the goal is to improvethe consistency and quality of care deliveredwhile improving patient outcomes1–3 (see Figure 1).
Since the evidence-based decision-making(EBDM) discussion began, there has been astronger emphasis on the strength of the sciencethan on the clinician and on the patient. There is amystical view that evidence is “all knowing” andthat the evidence alone is the most critical factorthat drives decision making. However, the objec-tive of EBDM is to improve the probability ofmaking the “best” decision. In a true evidence-based model of care, the clinician’s judgmentshould be regarded as being at least as, if notmore, important as the science. Clinicians are theend-users of this information and must be able tointerpret and apply that knowledge to the best oftheir abilities with the best of intentions for a suc-cessful outcome. In this chapter, we explore thechallenges encountered when trying to incorpo-rate this model of care into daily practice.
1
Adopting an Evidence-Based Philosophy of Practice
Chapter 1
Ann Eshenaur Spolarich and Fotinos Panagakos
Figure 1. Evidence-Based Practice Model
Source:Adapted fromhttp://www.lonestar.edu/departments/libraries/kingwood-library/ebp_illus.jpg.
ImprovedPatientOutcomes
IndividualClinicalExpertise
Patient’s Values &
Expectations
Best Available Clinical Evidence
CHALLENGES IN ADOPTING AN EVIDENCE-BASED
PHILOSOPHY OF PRACTICEKeeping Up with the LiteratureClinicians may face many challenges when choos-ing to adopt an evidence-based philosophy of prac-tice. It can be overwhelming to learn how tonavigate the sheer volume of information that isavailable to clinicians in the scientific literature.More than two million articles are published annu-ally, including over 500 clinical trials publishedacross 50 journals representing all the dental spe-cialties.4,5 The challenge of finding time to read onlythose papers that are most relevant to the clinician’sarea of expertise is daunting. Most clinicians find itdifficult to keep up with the latest findings fromresearch because of the lack of time needed toread. Thus, clinicians may be tempted to read onlythose publications to which they subscribe, andthen may briefly peruse the article or simply readthe abstract and conclusions of the paper. Readers
should know that abstracts do not always accurate-ly portray the content of the paper, leading them tomiss important nuances about the study design oradditional results that may influence how the studyoutcomes may be interpreted. Conclusions statedin the abstract are often too limited to reflect all thathas been learned from reported results.
Accessing InformationDifficulty in gaining access to information is also acommon frustration. The lack of access to full textarticles discourages clinicians’ attempts to locate bestevidence. Some publishers offer access to full textarticles for a fee, which is collected for downloadingindividual papers online or for electronic access to alljournals within the publisher’s library with paymentof an annual subscription fee. Professional organiza-tions offer access to articles published in their respec-tive journals—print or electronic format, orboth—as a benefit of membership. Studies that arepublicly funded through the National Institutes of
CHAPTER 1 Adopting an Evidence-Based Philosophy of Practice
2
Database Web Address
http://www.cochranelibrary.com
http://www.york.ac.uk/crd
http://www.tripdatabase.com
https://www.ncbi.nlm.nih.gov/pubmed
https://www.ncbi.nlm.nih.gov/pubmedhealth
https://www.ncbi.nlm.nih.gov/pubmed/clinical
https://scholar.google.com
https://www.nlm.nih.gov/nichsr
http://www.dimdi.de/static/en/db/dbinfo/inahta.htm
https://www.elsevier.com/solutions/embase-biomedical-research
http://www.apa.org/pubs/databases/psycinfo/index.aspx
https://health.ebsco.com/products/the-cinahl-database/allied-health-nursing
http://lilacs.bvsalud.org/en
http://www.scielo.org/php/index.php
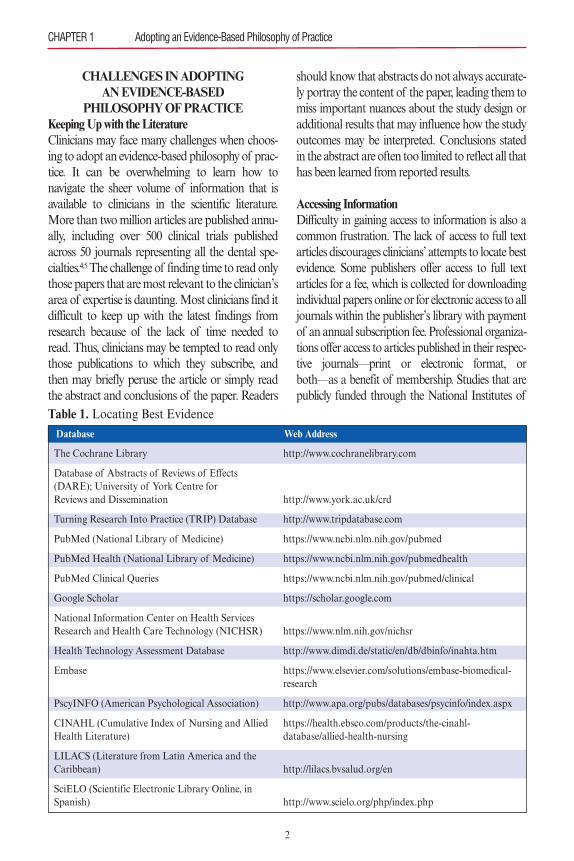
Table 1. Locating Best Evidence
The Cochrane Library
Database of Abstracts of Reviews of Effects(DARE); University of York Centre for Reviews and Dissemination
Turning Research Into Practice (TRIP) Database
PubMed (National Library of Medicine)
PubMed Health (National Library of Medicine)
PubMed Clinical Queries
Google Scholar
National Information Center on Health Services Research and Health Care Technology (NICHSR)
Health Technology Assessment Database
Embase
PscyINFO (American Psychological Association)
CINAHL (Cumulative Index of Nursing and AlliedHealth Literature)
LILACS (Literature from Latin America and theCaribbean)
SciELO (Scientific Electronic Library Online, inSpanish)

Health (NIH) are available through an open-accessmechanism after 1 year. There are an increasingnumber of open-access journals, but as with all jour-nals, the reader must be able to critically evaluate thestudies that appear in these publications.
Locating Best EvidenceClinicians must learn how to locate the informa-tion that is needed to guide their decision making.Skills necessary for navigating electronic databasesto locate best evidence can be developed throughpractice or may be obtained through participationin a training program. Numerous databases areavailable to clinicians to assist with informationretrieval (see Table 1). While developing gooddatabase searching skills may help improve theclinician’s confidence in locating information, pos-sessing these skills alone is not enough to answerthe many questions that arise in daily practice. Cli-nicians must also possess the necessary skills tocritically appraise the literature, which requires anunderstanding of research methodology and crite-ria used to determine the quality of the evidence.
Understanding Research MethodologyTo practice with an evidence-based philosophy,clinicians must possess at least some basic knowl-edge about research design. Lack of training inresearch methods while in school significantlychallenges many clinicians when reading andinterpreting a published study. The following sec-tion is intended to introduce the reader to somebasic elements for consideration of various studydesigns. This section is not intended to be a com-prehensive review; the reader is referred elsewherefor more detailed information about specific studydesigns. There is a hierarchy of research designsreflecting the levels of evidence (see Figure 2).
INTRODUCTION TO STUDY DESIGNS Self-Reported Data: Surveys and InterviewsSurveys are used to collect self-reported data fromindividual participants using questionnaires or aninterview. Surveys provide an easy, cost-effective, andtime-efficient way to gather information, especiallywhen information is needed from a large number of
people. Interviews allow for gathering more detailedinformation, which can later be verified by patientrecords, including laboratory tests. An importantlimitation is that self-reported data are subject torecall bias, meaning that participants may not alwaysaccurately report their answers. An advantage ofconducting interviews is that trained interviewersrecord participants’ responses, which helps ensurethat answers are accurate and complete. Surveys canalso be used to gather sensitive information that oth-erwise might not be disclosed, especially when par-ticipant identity can remain anonymous.
Self-reported data may be supplemented withanthropometric measures, such as height, weight,waist/hip circumference, mid-/upper arm circum-ference, or body fat percentage. Physiologicalmeasures may include vital signs or tests of bio-logical specimens, such as urinalysis, blood tests,salivary tests, or tests of physical fitness. Othermeasures may be obtained from a clinical exami-nation or diagnostic imaging.6
For example, individuals may be asked tocomplete a survey about their perceptions abouttheir own oral health status and oral hygienehabits. These responses could then be supplement-ed with findings from dental and radiographicexaminations. A response to a question about
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
3
Figure 2.Hierarchy of Research Designs
Source: http://valueanalysismag.com/wp-content/up-loads/2013/04/use-this-one-now.jpg with permission.
whether the person believes that he or she has peri-odontal disease could be verified using pocketdepths and clinical attachment loss measures, aswell as radiographic evidence of bone loss. Theadditional measures give greater insight about theself-reported information on the survey.
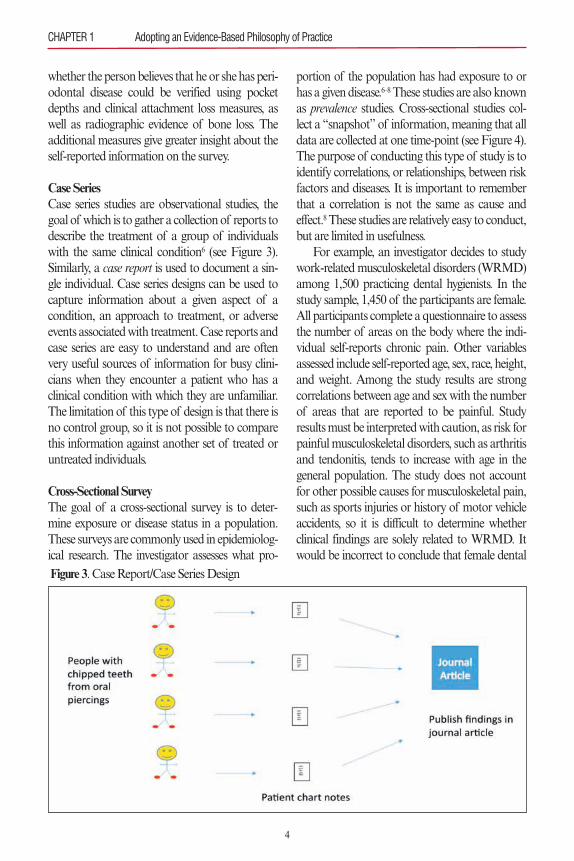
Case SeriesCase series studies are observational studies, thegoal of which is to gather a collection of reports todescribe the treatment of a group of individualswith the same clinical condition6 (see Figure 3).Similarly, a case report is used to document a sin-gle individual. Case series designs can be used tocapture information about a given aspect of acondition, an approach to treatment, or adverseevents associated with treatment. Case reports andcase series are easy to understand and are oftenvery useful sources of information for busy clini-cians when they encounter a patient who has aclinical condition with which they are unfamiliar.The limitation of this type of design is that there isno control group, so it is not possible to comparethis information against another set of treated oruntreated individuals.
Cross-Sectional SurveyThe goal of a cross-sectional survey is to deter-mine exposure or disease status in a population.These surveys are commonly used in epidemiolog-ical research. The investigator assesses what pro-
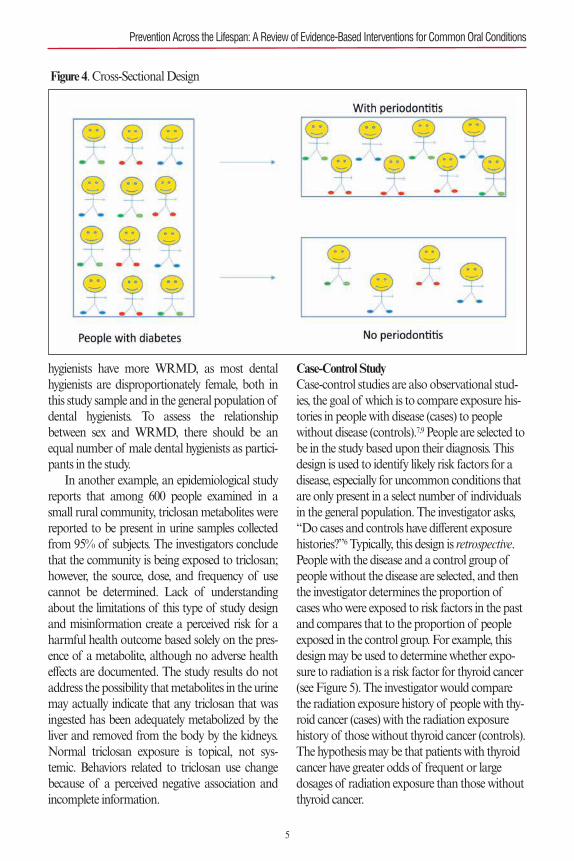
portion of the population has had exposure to orhas a given disease.6–8 These studies are also knownas prevalence studies. Cross-sectional studies col-lect a “snapshot” of information, meaning that alldata are collected at one time-point (see Figure 4).The purpose of conducting this type of study is toidentify correlations, or relationships, between riskfactors and diseases. It is important to rememberthat a correlation is not the same as cause andeffect.8 These studies are relatively easy to conduct,but are limited in usefulness.
For example, an investigator decides to studywork-related musculoskeletal disorders (WRMD)among 1,500 practicing dental hygienists. In thestudy sample, 1,450 of the participants are female.All participants complete a questionnaire to assessthe number of areas on the body where the indi-vidual self-reports chronic pain. Other variablesassessed include self-reported age, sex, race, height,and weight. Among the study results are strongcorrelations between age and sex with the numberof areas that are reported to be painful. Studyresults must be interpreted with caution, as risk forpainful musculoskeletal disorders, such as arthritisand tendonitis, tends to increase with age in thegeneral population. The study does not accountfor other possible causes for musculoskeletal pain,such as sports injuries or history of motor vehicleaccidents, so it is difficult to determine whetherclinical findings are solely related to WRMD. Itwould be incorrect to conclude that female dental
CHAPTER 1 Adopting an Evidence-Based Philosophy of Practice
4
Figure 3. Case Report/Case Series Design
hygienists have more WRMD, as most dentalhygienists are disproportionately female, both inthis study sample and in the general population ofdental hygienists. To assess the relationshipbetween sex and WRMD, there should be anequal number of male dental hygienists as partici-pants in the study.
In another example, an epidemiological studyreports that among 600 people examined in asmall rural community, triclosan metabolites werereported to be present in urine samples collectedfrom 95% of subjects. The investigators concludethat the community is being exposed to triclosan;however, the source, dose, and frequency of usecannot be determined. Lack of understandingabout the limitations of this type of study designand misinformation create a perceived risk for aharmful health outcome based solely on the pres-ence of a metabolite, although no adverse healtheffects are documented. The study results do notaddress the possibility that metabolites in the urinemay actually indicate that any triclosan that wasingested has been adequately metabolized by theliver and removed from the body by the kidneys.Normal triclosan exposure is topical, not sys-temic. Behaviors related to triclosan use changebecause of a perceived negative association andincomplete information.
Case-Control StudyCase-control studies are also observational stud-ies, the goal of which is to compare exposure his-tories in people with disease (cases) to peoplewithout disease (controls).7,9 People are selected tobe in the study based upon their diagnosis. Thisdesign is used to identify likely risk factors for adisease, especially for uncommon conditions thatare only present in a select number of individualsin the general population. The investigator asks,“Do cases and controls have different exposurehistories?”6 Typically, this design is retrospective.People with the disease and a control group ofpeople without the disease are selected, and thenthe investigator determines the proportion ofcases who were exposed to risk factors in the pastand compares that to the proportion of peopleexposed in the control group. For example, thisdesign may be used to determine whether expo-sure to radiation is a risk factor for thyroid cancer(see Figure 5). The investigator would comparethe radiation exposure history of people with thy-roid cancer (cases) with the radiation exposurehistory of those without thyroid cancer (controls).The hypothesis may be that patients with thyroidcancer have greater odds of frequent or largedosages of radiation exposure than those withoutthyroid cancer.
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
5
Figure 4. Cross-Sectional Design
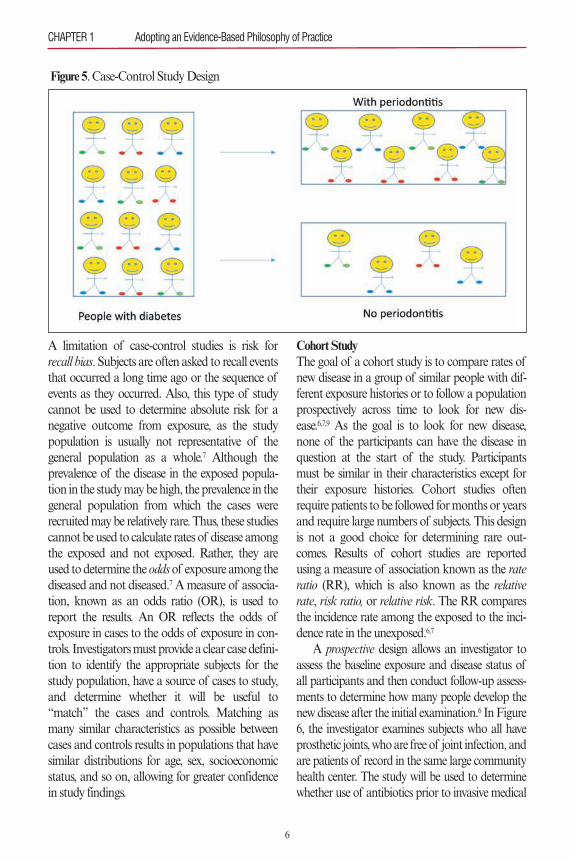
A limitation of case-control studies is risk forrecall bias. Subjects are often asked to recall eventsthat occurred a long time ago or the sequence ofevents as they occurred. Also, this type of studycannot be used to determine absolute risk for anegative outcome from exposure, as the studypopulation is usually not representative of thegeneral population as a whole.7 Although theprevalence of the disease in the exposed popula-tion in the study may be high, the prevalence in thegeneral population from which the cases wererecruited may be relatively rare. Thus, these studiescannot be used to calculate rates of disease amongthe exposed and not exposed. Rather, they areused to determine the oddsof exposure among thediseased and not diseased.7 A measure of associa-tion, known as an odds ratio (OR), is used toreport the results. An OR reflects the odds ofexposure in cases to the odds of exposure in con-trols. Investigators must provide a clear case defini-tion to identify the appropriate subjects for thestudy population, have a source of cases to study,and determine whether it will be useful to“match” the cases and controls. Matching asmany similar characteristics as possible betweencases and controls results in populations that havesimilar distributions for age, sex, socioeconomicstatus, and so on, allowing for greater confidencein study findings.
Cohort StudyThe goal of a cohort study is to compare rates ofnew disease in a group of similar people with dif-ferent exposure histories or to follow a populationprospectively across time to look for new dis-ease.6,7,9 As the goal is to look for new disease,none of the participants can have the disease inquestion at the start of the study. Participantsmust be similar in their characteristics except fortheir exposure histories. Cohort studies oftenrequire patients to be followed for months or yearsand require large numbers of subjects. This designis not a good choice for determining rare out-comes. Results of cohort studies are reportedusing a measure of association known as the rateratio (RR), which is also known as the relativerate, risk ratio, or relative risk. The RR comparesthe incidence rate among the exposed to the inci-dence rate in the unexposed.6,7
A prospective design allows an investigator toassess the baseline exposure and disease status ofall participants and then conduct follow-up assess-ments to determine how many people develop thenew disease after the initial examination.6 In Figure6, the investigator examines subjects who all haveprosthetic joints, who are free of joint infection, andare patients of record in the same large communityhealth center. The study will be used to determinewhether use of antibiotics prior to invasive medical
CHAPTER 1 Adopting an Evidence-Based Philosophy of Practice
6
Figure 5. Case-Control Study Design

and dental procedures influences the developmentof prosthetic joint infection. For this study, patientsare not randomly assigned to receive prophylacticantibiotics or not; the investigator does not controlthe exposure history (antibiotic use). Patients reportwhether they take prophylactic antibiotics when theinvestigator tracks the patients every 6 months asthey undergo a variety of invasive procedures over3 years. At the end of the study period, the investi-gator can sort the patients who develop prostheticjoint infection by reported prophylactic antibioticuse or not, as well as identify when an infectionoccurred during the study period, and type of inva-sive procedures performed prior to the onset of theinfection. In this illustrated example, the outcomeof prosthetic joint infection did not differ amongparticipants, regardless of antibiotic use. The inci-dence rate was the same in the exposed and unex-posed; this means that the exposure was notassociated with the disease (RR = 1). Limitationsof this design include risk for dropouts or informa-tion bias (e.g., examining patients who did not takeprophylactic antibiotics more vigorously to checkfor signs of infection). To reduce risk for informa-tion bias, subjects should undergo the same exami-nation procedures at baseline and at all follow-upappointments.
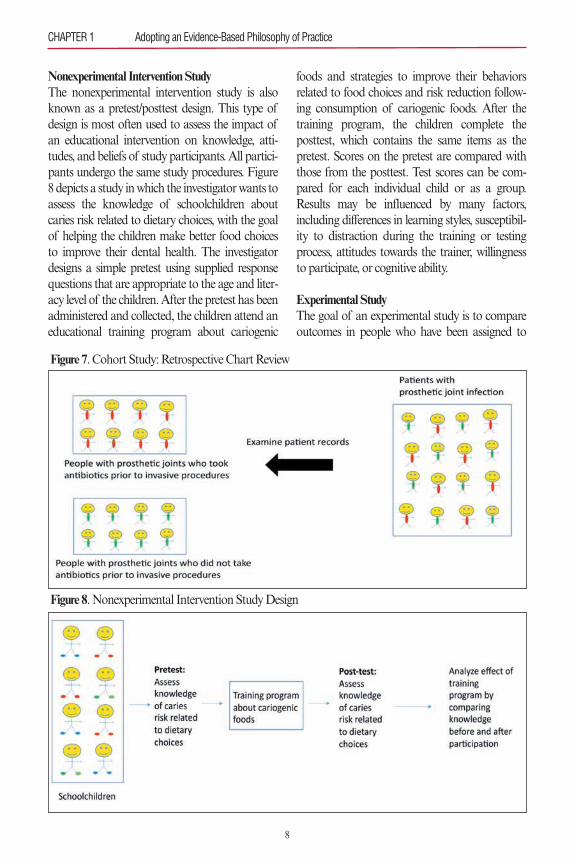
A cohort study may also be retrospective, when asource of individuals with the disease is alreadyavailable and the investigator is trying to learn about
the events (risks) that may have contributed to devel-opment of the disease.6,7,10 Retrospective studies usedocumented information to establish baseline statusand track members of the cohort to a point in thepast or to the present. A critical consideration is thatthe outcome of interest is not present at baseline inany members of the cohort.10 In Figure 7, the investi-gator already has access to a group of subjects withprosthetic joint infection. The investigator conductsa chart review to identify risk factors that may havecontributed to the development of prosthetic jointinfection going back to the time of prosthetic place-ment. Limitations of this design include missingdata from incomplete documentation and missingrecords. In this illustrated example, the investigatorsorts the cases, identifying those who took prophy-lactic antibiotics prior to invasive procedures fromthose who did not.11,12
Longitudinal cohort studies also follow agroup of people across time. However, membersof the cohort are recruited because they belong toa well-defined population pool, which differs froma prospective study, where recruitment is based onparticipant exposure status. At baseline, partici-pants are assessed for many exposures and dis-eases and are tracked across time to determine theincidence rate for new disease(s).11,12 There are sev-eral variations in design themes for longitudinalstudies using different measurement schemes atdifferent time-points.7,10
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
7
Figure 6. Cohort Study: Prospective Design
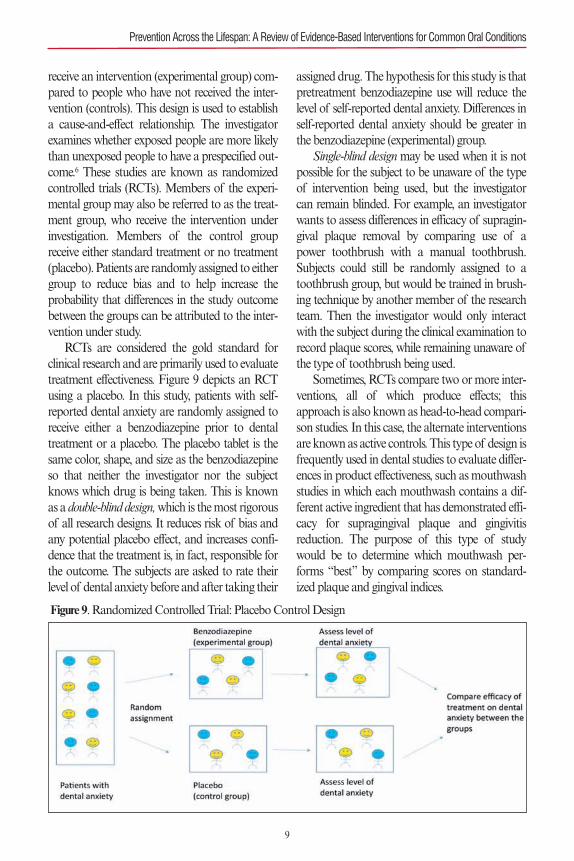
Nonexperimental Intervention StudyThe nonexperimental intervention study is alsoknown as a pretest/posttest design. This type ofdesign is most often used to assess the impact ofan educational intervention on knowledge, atti-tudes, and beliefs of study participants. All partici-pants undergo the same study procedures. Figure8 depicts a study in which the investigator wants toassess the knowledge of schoolchildren aboutcaries risk related to dietary choices, with the goalof helping the children make better food choicesto improve their dental health. The investigatordesigns a simple pretest using supplied responsequestions that are appropriate to the age and liter-acy level of the children. After the pretest has beenadministered and collected, the children attend aneducational training program about cariogenic
foods and strategies to improve their behaviorsrelated to food choices and risk reduction follow-ing consumption of cariogenic foods. After thetraining program, the children complete theposttest, which contains the same items as thepretest. Scores on the pretest are compared withthose from the posttest. Test scores can be com-pared for each individual child or as a group.Results may be influenced by many factors,including differences in learning styles, susceptibil-ity to distraction during the training or testingprocess, attitudes towards the trainer, willingnessto participate, or cognitive ability.
Experimental StudyThe goal of an experimental study is to compareoutcomes in people who have been assigned to
CHAPTER 1 Adopting an Evidence-Based Philosophy of Practice
8
Figure 7. Cohort Study: Retrospective Chart Review
Figure 8. Nonexperimental Intervention Study Design
receive an intervention (experimental group) com-pared to people who have not received the inter-vention (controls). This design is used to establisha cause-and-effect relationship. The investigatorexamines whether exposed people are more likelythan unexposed people to have a prespecified out-come.6 These studies are known as randomizedcontrolled trials (RCTs). Members of the experi-mental group may also be referred to as the treat-ment group, who receive the intervention underinvestigation. Members of the control groupreceive either standard treatment or no treatment(placebo). Patients are randomly assigned to eithergroup to reduce bias and to help increase theprobability that differences in the study outcomebetween the groups can be attributed to the inter-vention under study.
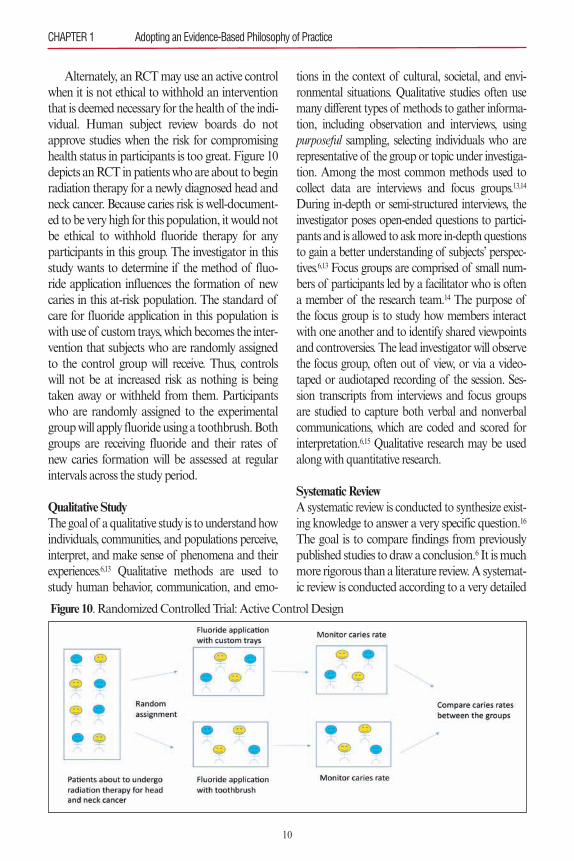
RCTs are considered the gold standard forclinical research and are primarily used to evaluatetreatment effectiveness. Figure 9 depicts an RCTusing a placebo. In this study, patients with self-reported dental anxiety are randomly assigned toreceive either a benzodiazepine prior to dentaltreatment or a placebo. The placebo tablet is thesame color, shape, and size as the benzodiazepineso that neither the investigator nor the subjectknows which drug is being taken. This is knownas a double-blind design,which is the most rigorousof all research designs. It reduces risk of bias andany potential placebo effect, and increases confi-dence that the treatment is, in fact, responsible forthe outcome. The subjects are asked to rate theirlevel of dental anxiety before and after taking their
assigned drug. The hypothesis for this study is thatpretreatment benzodiazepine use will reduce thelevel of self-reported dental anxiety. Differences inself-reported dental anxiety should be greater inthe benzodiazepine (experimental) group.
Single-blind designmay be used when it is notpossible for the subject to be unaware of the typeof intervention being used, but the investigatorcan remain blinded. For example, an investigatorwants to assess differences in efficacy of supragin-gival plaque removal by comparing use of apower toothbrush with a manual toothbrush.Subjects could still be randomly assigned to atoothbrush group, but would be trained in brush-ing technique by another member of the researchteam. Then the investigator would only interactwith the subject during the clinical examination torecord plaque scores, while remaining unaware ofthe type of toothbrush being used.
Sometimes, RCTs compare two or more inter-ventions, all of which produce effects; thisapproach is also known as head-to-head compari-son studies. In this case, the alternate interventionsare known as active controls. This type of design isfrequently used in dental studies to evaluate differ-ences in product effectiveness, such as mouthwashstudies in which each mouthwash contains a dif-ferent active ingredient that has demonstrated effi-cacy for supragingival plaque and gingivitisreduction. The purpose of this type of studywould be to determine which mouthwash per-forms “best” by comparing scores on standard-ized plaque and gingival indices.
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
9
Figure 9. Randomized Controlled Trial: Placebo Control Design
Alternately, an RCT may use an active controlwhen it is not ethical to withhold an interventionthat is deemed necessary for the health of the indi-vidual. Human subject review boards do notapprove studies when the risk for compromisinghealth status in participants is too great. Figure 10depicts an RCT in patients who are about to beginradiation therapy for a newly diagnosed head andneck cancer. Because caries risk is well-document-ed to be very high for this population, it would notbe ethical to withhold fluoride therapy for anyparticipants in this group. The investigator in thisstudy wants to determine if the method of fluo-ride application influences the formation of newcaries in this at-risk population. The standard ofcare for fluoride application in this population iswith use of custom trays, which becomes the inter-vention that subjects who are randomly assignedto the control group will receive. Thus, controlswill not be at increased risk as nothing is beingtaken away or withheld from them. Participantswho are randomly assigned to the experimentalgroup will apply fluoride using a toothbrush. Bothgroups are receiving fluoride and their rates ofnew caries formation will be assessed at regularintervals across the study period.
Qualitative StudyThe goal of a qualitative study is to understand howindividuals, communities, and populations perceive,interpret, and make sense of phenomena and theirexperiences.6,13 Qualitative methods are used tostudy human behavior, communication, and emo-
tions in the context of cultural, societal, and envi-ronmental situations. Qualitative studies often usemany different types of methods to gather informa-tion, including observation and interviews, usingpurposeful sampling, selecting individuals who arerepresentative of the group or topic under investiga-tion. Among the most common methods used tocollect data are interviews and focus groups.13,14
During in-depth or semi-structured interviews, theinvestigator poses open-ended questions to partici-pants and is allowed to ask more in-depth questionsto gain a better understanding of subjects’ perspec-tives.6,13 Focus groups are comprised of small num-bers of participants led by a facilitator who is oftena member of the research team.14 The purpose ofthe focus group is to study how members interactwith one another and to identify shared viewpointsand controversies. The lead investigator will observethe focus group, often out of view, or via a video-taped or audiotaped recording of the session. Ses-sion transcripts from interviews and focus groupsare studied to capture both verbal and nonverbalcommunications, which are coded and scored forinterpretation.6,15 Qualitative research may be usedalong with quantitative research.
Systematic ReviewA systematic review is conducted to synthesize exist-ing knowledge to answer a very specific question.16
The goal is to compare findings from previouslypublished studies to draw a conclusion.6 It is muchmore rigorous than a literature review. A systemat-ic review is conducted according to a very detailed
CHAPTER 1 Adopting an Evidence-Based Philosophy of Practice
10
Figure 10. Randomized Controlled Trial: Active Control Design

process, which the authors disclose in their pub-lished review. This disclosure helps the reader tounderstand which articles have been included inthe review and why.
The first step in conducting a systematic reviewis to identify a very narrow and focused question.The investigators then define criteria as part of thestrategy that is used to search the literature. Thismay include the use of specific search terms, timeframes during which the papers were published,studies with specific types of research designs, andstudies with a minimum number of subjects.6 Stud-ies that do not meet these criteria are automaticallyexcluded. The investigators then systematicallysearch multiple databases to locate possible studiesfor inclusion. Each article is read in its entirety todetermine eligibility for inclusion. A systematicreview is also unique in that investigators may alsochoose to include unpublished data if it meets thecriteria and is relevant to the question. Afterward,the investigators identify a count of the final num-ber of papers included for review.
The investigators then critically appraise eachof the included articles, and results from the indi-vidual studies are combined for analysis. Studiesthat find no statistically significant findings arealso included with those that do not. These resultsare also disclosed in the review. For example, theinvestigators may report that, “Of the 150 articlesthat were identified in the search, 30 studies metthe criteria for inclusion. Of those 30 studies, 13studies show that use of Drug A significantlyreduced the level of postoperative dental pain
while 17 studies found that there were no differ-ences between using Drug A and placebo ondegree of postoperative dental pain.”
In the context of a systematic review, the quali-ty of the included articles reflects the degree ofconfidence that the estimates of the treatmenteffect are correct. Systematic reviews are at risk forpublication bias, meaning that articles that demon-strate statistically significant findings are morelikely to be published than those that do not.6,17,18
There is also a risk that a systematic review isbased on only a small number of studies due to alimited number of available published papers onthe topic. The reader must also be mindful of thetime frame used for study inclusion. A systematicreview may influence a reader to believe that anintervention is not appropriate for a given patientpopulation, when in fact many other studies thatsupport the intervention as a favorable choice havebeen published after the time frame for inclusionhas ended. Clinicians should be aware that otherpublications, speakers, and marketing materialsfrequently cite findings from a systematic reviewlong after the review has become outdated, espe-cially if the review can be used to endorse a partic-ular product. As with all studies, as newinformation becomes available, systematic reviewsneed to be continuously updated.19
Meta-AnalysisA meta-analysis is also conducted to synthesizeexisting knowledge, but with a different strategyfrom a systematic review.6,20A meta-analysis merges
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
11
Figure 11. Meta-Analysis

the results from previously published studies pool-ing the statistics to obtain an estimate of treatmenteffectiveness (see Figure 11). Data are typicallyfrom RCTs, although data can also be combinedfrom case control and cohort studies.20,21
Only results from studies with the sameresearch design, similar statistics used for analysis,and those using the same intervention, type ofcontrol, and study populations may be pooled.Similar studies are known as homogeneous studies.Studies that are too different (heterogeneous) arenot appropriate for inclusion. The investigatorsare responsible for demonstrating that the resultsfrom studies are comparable and therefore appro-priate for inclusion.
Meta-analyses answer questions not posed byindividual studies. As with systematic reviews,
there is also risk for publication bias with this typeof study.22,23 Quality of the findings of the meta-analysis is based on the quality of the design ofthe included studies. Meta-analyses should reflectthe highest level of evidence available to supportclinical decision making.
Registering Systematic Reviews and Meta-AnalysesThere has been a widespread effort to encourage inves-tigators to register their protocols for systematicreviews to promote collaboration and to avoid dupli-cation of efforts by multiple research teams who areinterested in answering the same question. These reg-istries include the Campbell Collaboration, which pro-duces systematic reviews of the effects of socialinterventions (https://www.campbellcollaboration.org);
CHAPTER 1 Adopting an Evidence-Based Philosophy of Practice
12
Resource
http://www.casp-uk.net/checklists
http://www.agreetrust.org/wp-content/uploads/2013/12/AGREE-II-GRS-Instument.pdf
http://www.unisa.edu.au/Research/Sansom-Institute-for-Health-Research/Research/Allied-Health-Evidence/Resources/CAT
http://www.cebm.net/critical-appraisal
http://www.consort-statement.org
http://www.equator-network.org/reporting-guidelines/stard
http://www.strobe-statement.org/index.php?id=strobe-home
https://www.editorialmanager.com/jognn/account/MOOSE.pdf
http://cdn.elsevier.com/promis_misc/ISSM_COREQ_Check-list.pdf
http://www.record-statement.org/
http://inspiresim.com/simreporting
http://www.cdc.gov/trendstatement/Index.html
http://prisma-statement.org
https://www.cebma.org/resources-and-tools/what-is-critical-appraisal
[Textbook] London, England: Quintessence Publishing Company; 2008. ISBN: 13:978-1-85097-126-9
[Textbook] Chicago, IL: Quintessence Publishing Company;2014. ISBN: 978-0-86715-646-1
Table 2. Resources to Assist with Critically Appraising the Literature
Critical Appraisal Skills Programme (CASP)
Appraisal of Guidelines Research and Evaluation (AGREE)
University of South Australia Critical Appraisal Tools
University of Oxford Critical Appraisal Tools
CONSORT
STARD
STROBE
MOOSE
COREQ
RECORD
INSPIRE
TREND
PRISMA
Stichting Center for Evidence-Based Management (CEBMa)
Richards D, Clarkson J, Matthews D, Nieder-man R. Evidence-based Dentistry: ManagingInformation for Better Practice.
Frantsve-Hawley J. Evidence-Based Dentistryfor the Dental Hygienist.
the Cochrane Collaboration, an international groupthat produces and disseminates systematic reviews ofhealthcare interventions (http://www.cochrane.org);and PROSPERO, an international prospective regis-ter of systematic reviews (http://www.crd.york.ac.uk/prospero).24–26
Guidelines for Reporting Guidelines have been developed to improve thequality of reporting study methods and results inthe literature. The purpose of these guidelines is tohelp the reader better understand how the studieswere designed and conducted and to aid with inter-pretation of the results.27 Use of these guidelines ishelpful when clinicians critically appraise publishedpapers to determine relevancy and usefulness tohelp answer clinical questions. There are guidelinesto authors for reporting RCTs (CONSORT), diag-nostic tests (STARD), observational studies(STROBE), meta-analyses of observational studies(MOOSE), qualitative studies (COREQ), observa-tional routinely collected health data (RECORD),healthcare simulation research (INSPIRE), non-randomized designs (TREND), and systematicreviews and meta-analyses (PRISMA).28–38 TheInternational Committee of Medical Journal Edi-tors (ICMJE) also has requirements for authors tofollow when submitting papers for publication tobiomedical journals.39 Clinicians are encouraged touse available resources, found in Table 2, to assistwith critically appraising a published paper.
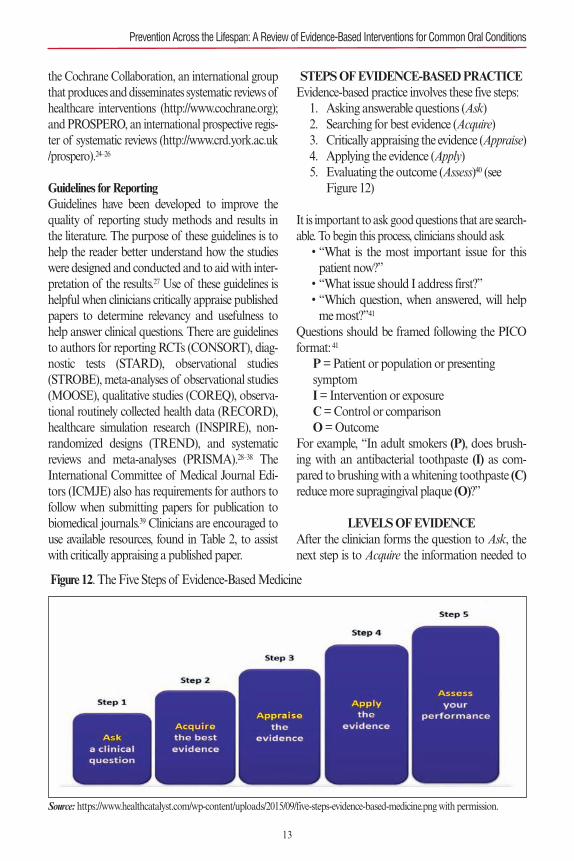
STEPS OF EVIDENCE-BASED PRACTICEEvidence-based practice involves these five steps:1. Asking answerable questions (Ask)2. Searching for best evidence (Acquire)3. Critically appraising the evidence (Appraise)4. Applying the evidence (Apply)5. Evaluating the outcome (Assess)40 (see
Figure 12)
It is important to ask good questions that are search-able. To begin this process, clinicians should ask• “What is the most important issue for thispatient now?”• “What issue should I address first?”• “Which question, when answered, will helpme most?”41
Questions should be framed following the PICOformat:41
P= Patient or population or presenting symptomI= Intervention or exposureC= Control or comparisonO= Outcome
For example, “In adult smokers (P), does brush-ing with an antibacterial toothpaste (I) as com-pared to brushing with a whitening toothpaste (C)reduce more supragingival plaque (O)?”
LEVELS OF EVIDENCEAfter the clinician forms the question to Ask, thenext step is to Acquire the information needed to
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
13
Figure 12. The Five Steps of Evidence-Based Medicine
Source: https://www.healthcatalyst.com/wp-content/uploads/2015/09/five-steps-evidence-based-medicine.png with permission.
CHAPTER 1 Adopting an Evidence-Based Philosophy of Practice
answer the question. With so many publishedpapers to choose from, clinicians may strugglewith deciding which type of information is mostcurrent and most useful. As previously discussed,the ability to both search and locate the informa-tion that is being sought are skills unto themselvesthat can directly impact which papers the clinicianaccesses to read. Further, a decision must be madeabout whether the information is truly useful,which largely depends on the methodology of thestudy. As can be seen from the preceding discus-sion, not all methodology is equally reliable.Today, it is rare for a clinician to seek sources fromprimary research, meaning the original, individualstudies about a topic of interest. Many cliniciansalso depend upon expert opinion, which is consid-ered the lowest level of evidence. Primary sourcesinclude the laboratory, observational, experimen-tal, and qualitative studies that have been pub-lished, which are the important building blocks for
what is known as secondary, or preappraised,research.
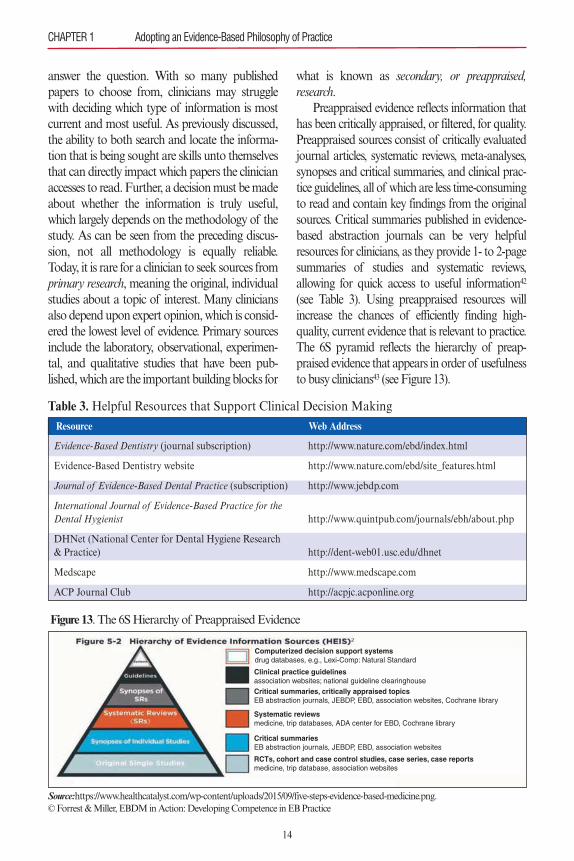
Preappraised evidence reflects information thathas been critically appraised, or filtered, for quality.Preappraised sources consist of critically evaluatedjournal articles, systematic reviews, meta-analyses,synopses and critical summaries, and clinical prac-tice guidelines, all of which are less time-consumingto read and contain key findings from the originalsources. Critical summaries published in evidence-based abstraction journals can be very helpfulresources for clinicians, as they provide 1- to 2-pagesummaries of studies and systematic reviews,allowing for quick access to useful information42
(see Table 3). Using preappraised resources willincrease the chances of efficiently finding high-quality, current evidence that is relevant to practice.The 6S pyramid reflects the hierarchy of preap-praised evidence that appears in order of usefulnessto busy clinicians43 (see Figure 13).
14
Source:https://www.healthcatalyst.com/wp-content/uploads/2015/09/five-steps-evidence-based-medicine.png.© Forrest & Miller, EBDM in Action: Developing Competence in EB Practice
Figure 13. The 6S Hierarchy of Preappraised Evidence
Computerized decision support systemsdrug databases, e.g., Lexi-Comp: Natural Standard
RCTs, cohort and case control studies, case series, case reportsmedicine, trip database, association websites
Critical summariesEB abstraction journals, JEBDP, EBD, association websites
Systematic reviewsmedicine, trip databases, ADA center for EBD, Cochrane library
Critical summaries, critically appraised topicsEB abstraction journals, JEBDP, EBD, association websites, Cochrane library
Clinical practice guidelinesassociation websites; national guideline clearinghouse
Resource Web Address
http://www.nature.com/ebd/index.html
http://www.nature.com/ebd/site_features.html
http://www.jebdp.com
http://www.quintpub.com/journals/ebh/about.php
http://dent-web01.usc.edu/dhnet
http://www.medscape.com
http://acpjc.acponline.org
Table 3. Helpful Resources that Support Clinical Decision Making
Evidence-Based Dentistry (journal subscription)
Evidence-Based Dentistry website
Journal of Evidence-Based Dental Practice (subscription)
International Journal of Evidence-Based Practice for theDental Hygienist
DHNet (National Center for Dental Hygiene Research & Practice)
Medscape
ACP Journal Club

CLINICAL PRACTICE GUIDELINESClinical practice guidelines (CPGs) are among theeasiest of resources for clinicians to locate and useto support their practice. Guidelines represent bestavailable evidence, preferably obtained from sys-tematic reviews and meta-analyses. Informationcontained within the guidelines has usually under-gone the first three steps of the evidence-basedprocess (Ask, Acquire, Appraise), and some guide-lines include recommendations about when andhow they should be applied and how the usershould assess outcomes, reflecting the last twosteps of the process (Apply, Assess).40
Use of CPGs promotes consistency of careand best practices. The recommendations includ-ed in CPGs are often broad enough to allow clini-cians to deviate within an “acceptable frameworkof variation.”44 Variation occurs for a variety ofreasons, encouraging clinicians to exercise theirjudgment, tailor interventions to a patient’s indi-vidual needs, and weigh risks versus benefits.These actions reflect the underlying premise ofpracticing with an evidence-based philosophy: sci-entific evidence alone is not sufficient to support
clinical decision making.45,46 From this perspective,CPGs should not be viewed as a “one-size-fits-all”approach to care, but instead as a guide to pro-mote the delivery of quality, patient-centered care.Patients, too, may access information about CPGson the Internet, empowering them to engage indiscussions with their care providers to participatein the planning and evaluation of their treatmentand expected outcomes.47 CPGs should not bemisconstrued as rules or as legal documents,although if widely adopted and endorsed by keystakeholders in dentistry, they may reflect the cur-rent standard of care. Finally, CPGs help to iden-tify additional needs for research using bettermethodologies to answer clinical questions.44Table4 provides a list of resources for locating clinicalpractice guidelines.
GRADING SCIENTIFIC EVIDENCE(APPRAISE)
One of the most challenging aspects of reviewingand interpreting the scientific evidence is assigningor ascribing some sort of value to the evidence.Putting aside personal bias, it is often challenging
Organization Web Address
http://www.guideline.gov
http://www.effectivehealthcare.ahrq.gov/index.cfm/search-for-guides-reviews-and-reports/
https://www.acponline.org/clinical-information/guidelines
https://www.cma.ca/En/Pages/clinical-practice-guide-lines.aspx
http://ebd.ada.org
http://www.aapd.org/policies
http://www.cdc.gov/oralhealth/guidelines.htm
https://www.uspreventiveservicestaskforce.org/BrowseRec/Index/browse-recommendations
http://www.sign.ac.uk/guidelines/published/index.html#Dentistry
http://www.sdcep.org.uk
https://www.nice.org.uk
Table 4. Locating Clinical Practice Guidelines
National Guideline Clearinghouse (part of AHRQ)
AHRQ Search for Research Summaries, Reviews,and Reports
American College of Physicians
Canadian Medical Association Infobase: ClinicalPractice Guidelines Database
American Dental Association Center for Evidence-Based Dentistry
American Academy of Pediatric Dentistry
Centers for Disease Control and Prevention: OralHealth Home
U.S. Preventive Services Task Force
Scottish Intercollegiate Guidelines Network (SIGN)
Scottish Dental Clinical Effectiveness Programme(SDCEP)
National Institute for Health and Care Excellence(NICE)
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
15
for the clinician, who is not directly involved withreviewing the science, to determine the quality ofthe information contained in the article he or shejust read. Fortunately, there are groups that focuson evaluating and grading the scientific literature.These groups are a superb resource when the clini-cian is searching for quality evidence regarding aclinical question. These groups are well establishedand respected, and the reviews they create areoften used by policy makers and others in the pro-vision of care. Understanding the grading systemsused by these groups allows any clinician to applyone of these approaches to the scientific informa-tion under review and determine the strength ofthe evidence.
Centre for Evidence-Based Medicine(http://www.cebm.net)The Centre for Evidence-Based Medicine (CEBM)is located on the campus of the University of
Oxford, UK. CEBM is a nonprofit organizationthat focuses on three important areas related to evi-dence-based medicine: research, teaching, andinformation dissemination. CEBM has a largestaff, who work with a wide variety of individualsthroughout the world, producing high-quality sys-tematic reviews meant to improve clinical practice.The Centre also teaches courses in evidence-basedmedicine at all levels—from undergraduate stu-dents to seasoned clinicians—via workshops andcourses. Finally, the Centre also publishes its find-ings in a publicly accessible database.
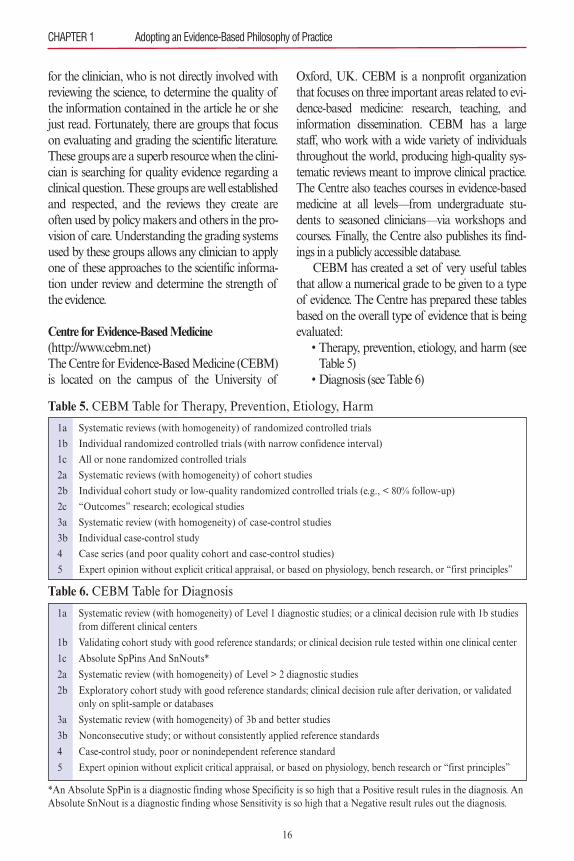
CEBM has created a set of very useful tablesthat allow a numerical grade to be given to a typeof evidence. The Centre has prepared these tablesbased on the overall type of evidence that is beingevaluated: • Therapy, prevention, etiology, and harm (seeTable 5) • Diagnosis (see Table 6)
Table 5. CEBM Table for Therapy, Prevention, Etiology, Harm
1a Systematic reviews (with homogeneity) of randomized controlled trials
1b Individual randomized controlled trials (with narrow confidence interval)
1c All or none randomized controlled trials
2a Systematic reviews (with homogeneity) of cohort studies
2b Individual cohort study or low-quality randomized controlled trials (e.g., < 80% follow-up)
2c “Outcomes” research; ecological studies
3a Systematic review (with homogeneity) of case-control studies
3b Individual case-control study
4 Case series (and poor quality cohort and case-control studies)
5 Expert opinion without explicit critical appraisal, or based on physiology, bench research, or “first principles”
Table 6. CEBM Table for Diagnosis
1a Systematic review (with homogeneity) of Level 1 diagnostic studies; or a clinical decision rule with 1b studiesfrom different clinical centers
1b Validating cohort study with good reference standards; or clinical decision rule tested within one clinical center
1c Absolute SpPins And SnNouts*
2a Systematic review (with homogeneity) of Level > 2 diagnostic studies
2b Exploratory cohort study with good reference standards; clinical decision rule after derivation, or validated only on split-sample or databases
3a Systematic review (with homogeneity) of 3b and better studies
3b Nonconsecutive study; or without consistently applied reference standards
4 Case-control study, poor or nonindependent reference standard
5 Expert opinion without explicit critical appraisal, or based on physiology, bench research or “first principles”
*An Absolute SpPin is a diagnostic finding whose Specificity is so high that a Positive result rules in the diagnosis. AnAbsolute SnNout is a diagnostic finding whose Sensitivity is so high that a Negative result rules out the diagnosis.
CHAPTER 1 Adopting an Evidence-Based Philosophy of Practice
16
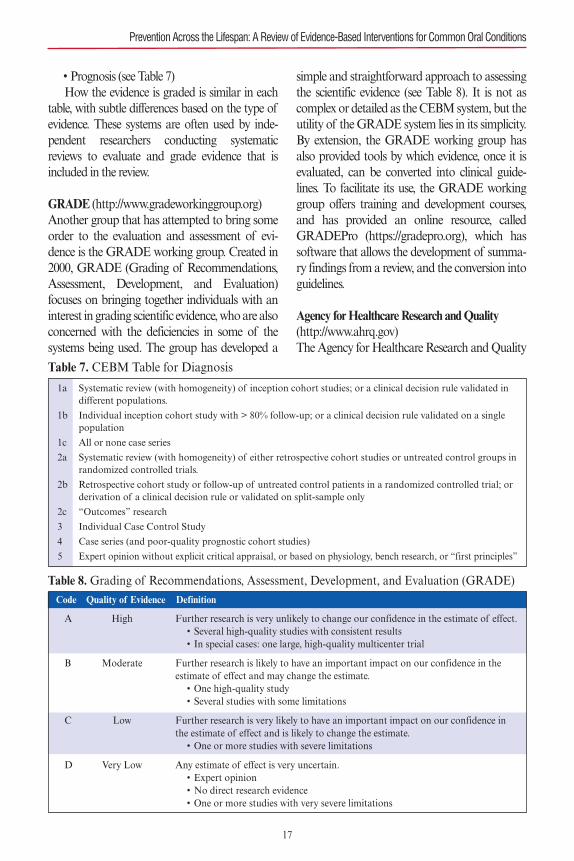
• Prognosis (see Table 7)How the evidence is graded is similar in each
table, with subtle differences based on the type ofevidence. These systems are often used by inde-pendent researchers conducting systematicreviews to evaluate and grade evidence that isincluded in the review.
GRADE (http://www.gradeworkinggroup.org)Another group that has attempted to bring someorder to the evaluation and assessment of evi-dence is the GRADE working group. Created in2000, GRADE (Grading of Recommendations,Assessment, Development, and Evaluation)focuses on bringing together individuals with aninterest in grading scientific evidence, who are alsoconcerned with the deficiencies in some of thesystems being used. The group has developed a
simple and straightforward approach to assessingthe scientific evidence (see Table 8). It is not ascomplex or detailed as the CEBM system, but theutility of the GRADE system lies in its simplicity.By extension, the GRADE working group hasalso provided tools by which evidence, once it isevaluated, can be converted into clinical guide-lines. To facilitate its use, the GRADE workinggroup offers training and development courses,and has provided an online resource, calledGRADEPro (https://gradepro.org), which hassoftware that allows the development of summa-ry findings from a review, and the conversion intoguidelines.
Agency for Healthcare Research and Quality(http://www.ahrq.gov)The Agency for Healthcare Research and Quality
Table 7. CEBM Table for Diagnosis
1a Systematic review (with homogeneity) of inception cohort studies; or a clinical decision rule validated indifferent populations.
1b Individual inception cohort study with > 80% follow-up; or a clinical decision rule validated on a single population
1c All or none case series
2a Systematic review (with homogeneity) of either retrospective cohort studies or untreated control groups in randomized controlled trials.
2b Retrospective cohort study or follow-up of untreated control patients in a randomized controlled trial; or derivation of a clinical decision rule or validated on split-sample only
2c “Outcomes” research
3 Individual Case Control Study
4 Case series (and poor-quality prognostic cohort studies)
5 Expert opinion without explicit critical appraisal, or based on physiology, bench research, or “first principles”
Code Quality of Evidence Definition
Table 8. Grading of Recommendations, Assessment, Development, and Evaluation (GRADE)
A High Further research is very unlikely to change our confidence in the estimate of effect.• Several high-quality studies with consistent results• In special cases: one large, high-quality multicenter trial
B Moderate Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.• One high-quality study• Several studies with some limitations
C Low Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.• One or more studies with severe limitations
D Very Low Any estimate of effect is very uncertain.• Expert opinion• No direct research evidence• One or more studies with very severe limitations
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
17

(AHRQ) is a United States federal organization,part of the United States Department of Healthand Human Services, which conducts researchabout healthcare evidence, with the goal of makingcare safer and of better quality. A main focus ofAHRQ is to evaluate, measure, and track the UShealthcare system, providing data to health profes-sionals and policy makers on the performance ofthe system. AHRQ also has an important missionof producing high-quality resources that can beused to educate health professionals to improve thequality of care for their patients. AHRQ has adapt-ed evidence-based approaches into its system ofevidence reviews and how recommendationsshould be graded (see Tables 9 and 10).
Cochrane Collaboration(http://www.cochrane.org)Finally, the entity that is likely most recognizableto the reader is the Cochrane Collaboration,which was established in 1993 by Sir IainChalmers, a British health services researcher. Thisindependent, nonprofit, and nongovernmentalorganization evolved in response to Dr. Archibald
(Archie) Cochrane’s advocacy for using RCTs toenhance the effectiveness and efficiency of medi-cine. Cochrane’s book, Effectiveness and Efficien-cy: Random Reflections on Health Service, remainsa staple for those in the field of evidence-basedmedicine.48
The Cochrane Collaboration was formed toreview and organize medical research informationusing a systematic approach so that health profes-sionals, policy makers, and even patients, canmake informed decisions regarding health treat-ments and interventions according to establishedprinciples of evidence-based medicine. Thestrength of the organization comes from the morethan 37,000 volunteers in over 130 countries whoform the core that conducts the systematic reviewsfor which the Collaboration is famous. TheCochrane Collaboration publishes the resultsfrom these reviews in the Cochrane Library.Details about the Collaboration, how it is organ-ized, and access to reviews can be found at theorganization’s website, listed earlier. Table 11 pro-vides a succinct summary of the organization’sguiding principles.
Level Type of Scientific Evidence (SE)
Table 9. AHRQ Levels of Scientific Evidence
Ia SE obtained from meta-analyses of randomized clinical trials.
Ib SE obtained from at least one randomized clinical trial
IIa SE obtained from at least one well-designed, nonrandomized controlled prospective study
IIb SE obtained from at least one well-designed, quasi-experimental study
III SE obtained from well-designed observational studies, such as comparative studies, correlation study, or case-control studies
IV SE obtained from documents or opinions of expert committees, or clinical experiences of renowned opinion leaders, or both
Grade Recommendation
Table 10. AHRQ Grades of Recommendation
A It requires at least one randomized clinical trial as part of the scientific evidence,(Levels of SE Ia, Ib) with overall good quality and consistency in terms of the specific recommendation.
B It requires methodologically correct clinical trials that are not randomized clinical (Levels of SE IIa, IIb, III) trials on the topic of recommendation. It includes studies that do not meet Criteria
A or C.
C It requires documents or opinions of expert committees or clinical experiences of (Level of SE IV) renowned opinion leaders, or both. It indicates the absence of high-quality, directly
applicable clinical studies.
SE, scientific evidence.
CHAPTER 1 Adopting an Evidence-Based Philosophy of Practice
18
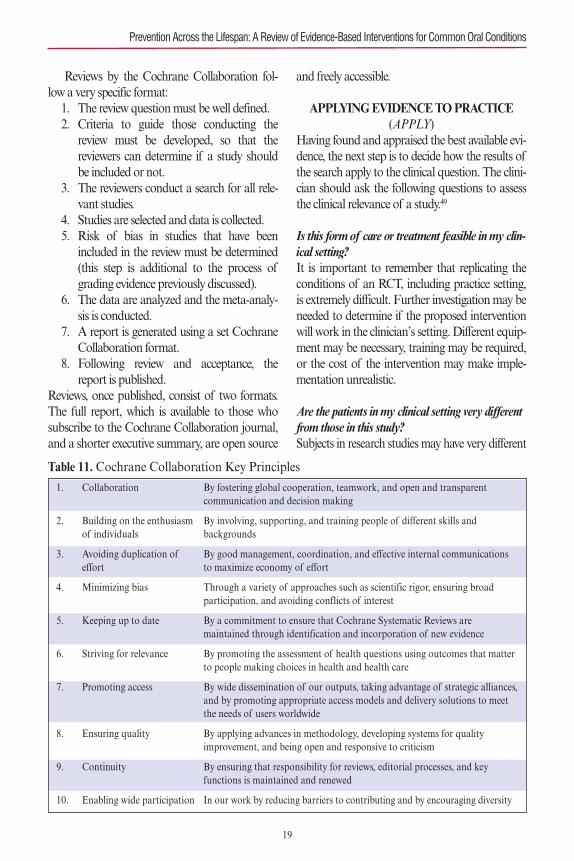
Reviews by the Cochrane Collaboration fol-low a very specific format:1. The review question must be well defined.2. Criteria to guide those conducting the
review must be developed, so that thereviewers can determine if a study shouldbe included or not.
3. The reviewers conduct a search for all rele-vant studies.
4. Studies are selected and data is collected.5. Risk of bias in studies that have been
included in the review must be determined(this step is additional to the process ofgrading evidence previously discussed).
6. The data are analyzed and the meta-analy-sis is conducted.
7. A report is generated using a set CochraneCollaboration format.
8. Following review and acceptance, thereport is published.
Reviews, once published, consist of two formats.The full report, which is available to those whosubscribe to the Cochrane Collaboration journal,and a shorter executive summary, are open source
and freely accessible.
APPLYING EVIDENCE TO PRACTICE(APPLY)
Having found and appraised the best available evi-dence, the next step is to decide how the results ofthe search apply to the clinical question. The clini-cian should ask the following questions to assessthe clinical relevance of a study.49
Is this form of care or treatment feasible in my clin-ical setting?It is important to remember that replicating theconditions of an RCT, including practice setting,is extremely difficult. Further investigation may beneeded to determine if the proposed interventionwill work in the clinician’s setting. Different equip-ment may be necessary, training may be required,or the cost of the intervention may make imple-mentation unrealistic.
Are the patients in my clinical setting very differentfrom those in this study?Subjects in research studies may have very different
Table 11. Cochrane Collaboration Key Principles1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
Collaboration
Building on the enthusiasmof individuals
Avoiding duplication of effort
Minimizing bias
Keeping up to date
Striving for relevance
Promoting access
Ensuring quality
Continuity
Enabling wide participation
By fostering global cooperation, teamwork, and open and transparent communication and decision making
By involving, supporting, and training people of different skills and backgrounds
By good management, coordination, and effective internal communicationsto maximize economy of effort
Through a variety of approaches such as scientific rigor, ensuring broad participation, and avoiding conflicts of interest
By a commitment to ensure that Cochrane Systematic Reviews are maintained through identification and incorporation of new evidence
By promoting the assessment of health questions using outcomes that matterto people making choices in health and health care
By wide dissemination of our outputs, taking advantage of strategic alliances,and by promoting appropriate access models and delivery solutions to meetthe needs of users worldwide
By applying advances in methodology, developing systems for quality improvement, and being open and responsive to criticism
By ensuring that responsibility for reviews, editorial processes, and key functions is maintained and renewed
In our work by reducing barriers to contributing and by encouraging diversity
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
19

characteristics than the patients seen in the clini-cian’s work setting.Compliance with the proposedintervention may have been easier for the subjects,especially if they were closely monitored orrewarded in some way for their participation.Compliance is a critical consideration when ask-ing any individual to try something new or “differ-ent” from what is currently being used.
Will my patient benefit more or less than the peoplein the study?Ultimately, the clinician must decide if his or herpatients will benefit more or less than those whowere studied. Clinicians must look carefully atwhat was actually being tested in the study. In thecase of an oral care product, it is important toknow whether the study evaluated the actualproduct formulation or just an ingredient found inthis and many other products. Clinicians shouldbeware of statements such as “45 studies supportthe efficacy of this product.” Ask to see a refer-ence list of these cited studies.
Other important questions to ask include• What was the duration of the study? Twenty-four hours? One week? One month? Threemonths?• How long is “long enough?”• Is the strength, dose, or concentration of theproduct the same as the product I will usewith my patients?• How big was the study sample?• Are these pilot data?
Is there evidence of harm? A particular challenge is that it is not easy to findinformation about possible harmful effects associat-ed with an intervention. As previously mentioned,publication bias has resulted in a preponderance ofpublished studies with positive outcomes. Cliniciansneed to know whether something is contraindicatedor not the best choice for certain individuals. Poten-tial harm is also an important consideration inweighing risk versus benefit and identifying alterna-tive options when obtaining informed consent fortreatment. Doing nothing may also be an optionshould no good alternative exist.
Will the potential benefits outweigh the potentialharms of this form of care (or treatment) for mypatients?Clinicians need to be informed of both risks andbenefits in order to make good decisions. Thisinformation is also needed to inform patients aboutreasonable, anticipated outcomes and what poten-tial risks are involved if the proposed treatment isaccepted. Clinicians are cautioned not to becomeoverly affected by marketing claims made by prod-uct competitors, who may exaggerate benefits orsuggest risk if the clinician chooses a product otherthan theirs. Clinicians should always refer back topublished data that support product claims.
CONCLUSIONS Adopting an evidence-based philosophy of prac-tice requires a commitment to skill development inaccessing, critically appraising, and applying thebest information to support clinical decision mak-ing, lifelong learning, and professional develop-ment. Using research in daily practice may bechallenging for the clinician; however, many onlinetools and resources are available to help withimplementation. Keeping current with newresearch findings is of major importance in thedelivery of quality patient care. Clinicians shouldbe aware of interventions that are beneficial, aswell as harmful, to patients so they can assist theirpatients with making choices about treatmentoptions. Further, knowledge about the ineffective-ness of interventions is also helpful, so that clini-cians can seek better alternatives for their patientsand themselves. Finally, if there is no evidenceavailable to answer a clinical question, clinicianscan rely on their experience and judgment to guidetheir decision making.
REFERENCES1. Sackett DL, Straus SE, Richardson WS, et al. Evidence-
Based Medicine: How to Practice and Teach EBM. 2nded. Edinburgh, Scotland: Churchill Livingstone; 2000.
2. Sackett DL, Rosenberg WM, Gray JA, Haynes RB,Richardson WS. Evidence based medicine: what it is andwhat it isn’t. BMJ. 1996;312:71–72.
3. Haynes RB, Devereaux PJ, Guyatt GH. Clinical expert-ise in the era of evidence-based medicine and patientchoice. Evid Based Med. 2002;7:36–38.
CHAPTER 1 Adopting an Evidence-Based Philosophy of Practice
20
4. Haines A, Donald A. Getting Research Findings intoPractice. London, England: BMJ Publishing Group;1998.
5. Niederman R. Evidence-based dentistry finds a newforum: Exelauno. J Am Dent Assoc. 2009;140:272–274.
6. Jacobsen KJ. Introduction to Health Research Methods.A Practical Guide. Sudbury, MA: Jones & BartlettLearning; 2012.
7. Mann CJ. Observational research methods. Researchdesign II: cohort, cross sectional, and case-control stud-ies. Emerg Med J. 2003;20:54–60.
8. Lucas RM, McMichael AJ. Association or causation:evaluating links between “environment and disease.”Bull World Health Org. 2005;83:792–795.
9. Black N. Why we need observational studies to evaluatethe effectiveness of health care. BMJ. 1996;312(7040):1215–1218.
10. Rochon PA, Gurwitz JH, Sykora K, et al. Reader’sguide to critical appraisal of cohort studies: 1. Role anddesign. BMJ. 2005;330(7496):895–897.
11. Mamdani M, Sykora K, Li P, et al. Reader’s guide tocritical appraisal of cohort studies: 2. Assessing potentialfor confounding. BMJ. 2005;330(7497):960–962.
12. Normand SL, Sykora K, Li P, Mamdani M, RochonPA, Anderson GM. Reader’s guide to critical appraisalof cohort studies: 3. Analytical strategies to reduce con-founding. BMJ. 2005;330(7498):1021–1023.
13. Sofaer S. Qualitative research methods. Int J QualHealth Care. 2002;14:329–336.
14. Krueger RA, Casey MA. Focus Groups. A PracticalGuide for Applied Research. Thousand Oaks, CA: SagePublications; 2000.
15. Dixon-Woods M, Shaw RL, Agarwal S, et al. The prob-lem of appraising qualitative research. Qual Saf HealthCare. 2004;13:223–225.
16. Agency for Healthcare Research and Quality. Trainingmodules for the systematic reviews methods guide. Avail-able at: https://www.effectivehealthcare.ahrq.gov/search-for-guides-reviews-and-reports/?pageaction=displayproduct&productID=2351. Accessed December 3, 2016.
17. Dwan K, Gamble C, Williamson PR, Kirkham JJ,Reporting Bias Group: Systematic review of the empiri-cal evidence of study publication bias and outcomereporting bias—an updated review. PLoS ONE2013,8(7):e66844.
18. Page MJ, McKenzie JE, Kirkham J, et al. Bias due to selec-tive inclusion and reporting of outcomes and analyses insystematic reviews of randomised trials of healthcare inter-ventions. Cochrane Lib. 2014;(10):Art No.:MR000035. doi:10.1002/14651858.MR000035.pub2.
19. Moher D, Tsertsvadze A. Systematic reviews: when is anupdate an update? Lancet. 2006;367:881–883.
20. Sacks HS, Reitman D, Pagano D, Kupelnick B. Meta-analysis: an update. Mt Sinai J Med. 1996;63:216–224.
21. Stewart LA, Clarke MJ. Practical methodology of meta-analyses (overviews) using updated individual patient
data. Cochrane Working Group. Stat Med.1995;14:2057–2079.
22. Sutton AJ. Evidence concerning the consequences ofpublication and related biases. In: Rothstein HR, SuttonAJ, Borenstein M, eds. Publication Bias in Meta-Analy-sis—Prevention, Assessment and Adjustments. Chich-ester, England: John Wiley; 2005:175–192.
23. Dickersin K. Publication bias: recognizing the problem,understanding its origins and scope, and preventingharm. In: Rothstein HR, Sutton AJ, Borenstein M, eds.Publication Bias in Meta-Analysis—Prevention, Assess-ment and Adjustments. Chichester, England: John Wiley;2005:11–33.
24. Straus S, Moher D. Registering systematic reviews.CMAJ. 2010,182:13–14. doi: 10.1503/cmaj.081849.
25. Booth A, Clarke M, Ghersi D, Moher D, Petticrew M,Stewart L. An international registry of systematic-reviewprotocols. Lancet. 2011;377(9760):108–109.
26. Booth A, Clarke M, Dooley G, Ghersi D, Moher D,Petticrew M, Stewart L: The nuts and bolts of PROS-PERO: an international prospective register of systemat-ic reviews. Syst Rev. 2012;1:2.
27. Sarkis-Onofre R, Cenci MS, Demarco FF, et al. Use ofguidelines to improve the quality and transparency ofreporting oral health research. J Dent. 2015;43:397–404.
28. Moher D, Schultz KF, Altman D. The CONSORTstatement: revised recommendations for improving thequality of reports of parallel-group randomized trials.JAMA. 2001;285:1987–1991.
29. Rennie D. Improving reports of studies of diagnostictests: the STARD initiative. JAMA. 2003;289:89–90.
30. Bossuyt PM, Cohen JF, Gatsonis CA, Korevaar DA;STARD group. STARD 2015: updated reporting guide-lines for all diagnostic accuracy studies. Ann Transl Med.2016;4:85. doi: 10.3978/j.issn.2305–5839.2016.02.06.
31. Vandenbroucke JP, von Elm E, Altman DG, et al.STROBE Initiative. Strengthening the Reporting ofObservational Studies in Epidemiology (STROBE):explanation and elaboration. Ann Intern Med.2007;147(8):W163–194.
32. von Elm E, Altman DG, Egger M, et al. STROBE Ini-tiative. Strengthening the Reporting of ObservationalStudies in Epidemiology (STROBE) Statement: guide-lines for reporting observational studies. Int J Surg.2014;12:1495–1499.
33. Stroup DF, Berlin JA, Morton SC, et al. Meta-analysisof observational studies in epidemiology: a proposal forreporting Meta-analysis of Observational Studies in Epi-demiology (MOOSE) group. JAMA. 2000;283:2008–2012.
34. Nicholls SG, Quach P, von Elm E, et al. The Reportingof Studies Conducted Using Observational Routinely-Collected Health Data (RECORD) statement: methodsfor arriving at consensus and developing reportingguidelines. PLoS One. 2015;10:e0125620.
35. Cheng A, Kessler D, Mackinnon R, et al. International
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
21
Network for Simulation-based Pediatric Innovation,Research, and Education (INSPIRE) reporting guide-lines investigators. Reporting guidelines for health caresimulation research: extensions to the CONSORT andSTROBE statements. Simul Healthc. 2016;11:238–248.
36. Des Jarlais DC, Lyles C, Crepaz N. TREND Group.Improving the reporting quality of nonrandomized eval-uations of behavioral and public health interventions:the TREND statement. Am J Public Health.2004;94:361–366.
37. Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMAGroup. Preferred reporting items for systematic reviewsand meta-analyses: the PRISMA statement. BMJ.2009;339:b2535.
38. Moher D, Shamseer L, Clarke M, et al. PRISMA-PGroup. Preferred reporting items for systematic reviewand meta-analysis protocols (PRISMA-P) 2015 state-ment.Syst Rev. 2015;4:1.
39. International Committee of Medical Journal Editors.Recommendations for the conduct, reporting, editing,and publication of scholarly work in medical journals.Available at: http://www.icmje.org/recommendations.Accessed December 3, 2016.
40. Richards D, Clarkson J, Matthews D, Niederman R.Evidence-based guidelines. In: Evidenced-Based Den-tistry: Managing Information for Better Practice. Lon-don, England: Quintessence Publishing Co. 2008.
41. Richardson WS, Wilson MC, Nishikawa J, Hayward
RS. The well-built clinical question: a key to evidence-based decisions. ACP J Club. 1995;123(3):A12–A13.
42. Abt E, Bader JD, Bonetti D. A practitioner’s guide todeveloping critical appraisal skills: translating researchinto clinical practice. J Am Dent Assoc. 2012;143:386–390.
43. DiCenso A, Bayley L, Haynes RB. ACP Journal Club.Editorial: Accessing preappraised evidence: fine-tuningthe 5S model into a 6S model. Ann Intern Med.2009;151(6):JC3-2, JC3-3.
44. Sutherland SE, Matthews DC, Fendrich P. Clinical prac-tice guidelines in dentistry. Part I. Navigating new waters.J Can Dent Assoc. 2001;67:379–383.
45. Kay E, Nuttall N. Clinical decision making—an art or ascience? Part III: To treat or not to treat? Br Dent J.1995;178:153–155.
46. Kay E, Nuttall N. Clinical decision making—an art or ascience? Part II: Making sense of treatment decisions. BrDent J. 1995;178:113–116.
47. Sutherland SE. Evidence-based dentistry: Part III: Search-ing for answers to clinical questions. Finding evidence onthe Internet. J Can Dent Assoc. 2001;67:320–323.
48. Cochrane AL. Effectiveness and Efficiency: RandomReflections on Health Service. London, England:Nuffield Provincial Hospitals Trust; 1972.
49. Clinical Information Access Portal. Module 4: Integrat-ing evidence into practice. Available at:http://www.ciap.health.nsw.gov.au/education/learningmodule4/intro.html. Accessed December 3, 2016.
CHAPTER 1 Adopting an Evidence-Based Philosophy of Practice
22

THE BIOPSYCHOSOCIAL APPROACH TO PATIENT CARE
Dentistry originated with a focus on biologicalaspects of illness and health. This “biomedical”model of disease offered a limited perspective forunderstanding patient health. To expand this per-spective Engel proposed the “biopsychosocial”approach, which takes into consideration the psy-chological, behavioral, and social aspects alongwith the biological aspects of health.1 This con-ceptualization offers clinicians a deeper under-standing of their patients’ orientation towardhealth and wellness and the numerous factors thatinfluence their health behaviors. Thus, this modelcan help illuminate why a patient might choose anaction that differs from what the clinician recom-mends. For instance, a dental professional mightsuggest that the patient have root canal therapyand a crown, but if the patient is accustomed toextractions and this is the norm in his or her envi-ronment, he or she may not wish to spend themoney on retaining the tooth. Similarly, if it iscommon for most children in a community tohave extensive caries in primary teeth, parents maycome to see this oral disease condition asinevitable and not accept recommendations forcaries prevention. It is important to bear in mind that patient
behavior is a major determinant of oral health. Interms of general health, it is estimated that 40% ofpremature deaths can be attributed to behavioralpatterns, putting patient behavior ahead of othercauses such as genetic vulnerability, social circum-stances, and experiences within the healthcare sys-tem.2 Although this statistic applies to generalhealth, one can extrapolate the implications fororal health. All dental professionals have encoun-
tered situations in which behavioral issues such aslack of self-care, improper diet, and tobacco con-tributed to oral disease. The behavioral sciences offer instruments to help
patients achieve optimal oral health; these instru-ments are in the form of theories. Theories areintended to serve as a guide or means of explainingphenomena and offer two major benefits:3
• A way to understand patients and the con-text of their actions (or inaction)• A means to effectively intervene, either topromote a healthy behavior or to stop anunhealthy oneDental clinicians often share health informa-
tion with patients in the hopes of persuading themto adopt recommended behaviors. However, infor-mation alone is not enough to make a personchange his or her behavior. If it were so, then mostsmokers would stop smoking, as they alreadyknow that it is harmful to their health. Simply giv-ing patients more information and telling themwhat to do is an authoritarian way of interactingwith patients and is not likely to bring about last-ing change. Rather, patients must be encouragedto take responsibility for their own self-care. Bycommunicating well with their patients, clinicianscan help to identify barriers to behavioral change,such as a low level of health literacy or inability orunwillingness to engage in a behavior. The goal isto promote self-efficacy so that patients do notplace the burden of their well-being entirely upontheir clinicians. Successful behavioral changethrough improved partnerships between cliniciansand patients are crucial for long-term health.Health behavior is complex and varies among
individuals. Clinicians may feel overwhelmed andfrustrated when patients do not adopt their rec-ommendations, and may be tempted to stop try-ing to help their patients change their behaviors.This chapter offers a means to help clinicians bet-ter understand patient behavior and to supportclinicians in their quest to have patients adopthealthy behaviors.
KEY CONSIDERATIONS Social Determinants of Health Social determinants of health are the variables out-side the healthcare system that exert an influence
23
Behavioral Science
Chapter 2
S. D. Shanti

on a person’s health and well-being.4 Also termed“the cause of causes,” social determinants includeincome, education, and the social and political con-ditions under which people live. Clinicians mayoffer well-intended advice about optimal oralhealth, but when doing so, it is important to consid-er the social context of the patient’s life and itsimpact on his or her health behavior.
Socioeconomic Gradient and PovertyPoverty and related financial pressures are ubiq-uitous. In wealthier countries, there are poor peo-ple; in poorer countries, there are relativelywealthy people. The distribution of wealth anddifferences between members of a society arereferred to as the social gradient, and theseinequalities are manifested in differences inhealth status.5 The higher a person is on the gra-dient, the more likely it is that he or she will behealthy as compared to someone at the lower endof the gradient.Poverty is the single most important social
determinant of health, affecting over a billion peo-ple.6 Poverty limits access to resources and restrictsthe range of options for interventions related tohealth. Poverty is stressful because limitedresources, often linked with marginalization insociety, present a multitude of challenges relatedto basic necessities such as food, water, shelter, andhealth care.7 Disease prevention is relevant toeveryone, but is especially poignant when peopleat greatest risk for experiencing disease have diffi-culty affording a simple product such as tooth-paste with fluoride.8
Quality of Life Disease prevention and timely treatment are self-evident goals in patient care. However, the individ-ual’s subjective experience of health (or illness)and ability to function influences quality of life(QOL). Within dentistry, oral health is also meas-ured as the patient’s perceived oral health-relatedquality of life (OHRQOL).9,10 The concept ofOHRQOL encompasses such things as thepatient’s ability to chew, speak, eat foods withoutrestrictions, and be free from pain and infections.
OHRQOL provides a means of understandingthe patient’s perspective on how he or she experi-ences oral health. As OHRQOL is a subjective experience,
patients present with a range of perceptions. Yet,what is evident from research across differentcountries is that people report poorer quality oflife when their oral health is suffering.11–13Negativelife events can have an adverse effect on a person’sOHRQOL.14 Lower levels of parental educationare also associated with lower levels of OHRQOLamong children.15 Taking a proactive stancetoward one’s oral health, as characterized byengaging in positive health behaviors and seekingregular dental care, have been found to increase aperson’s OHRQOL.16
Health Literacy Health literacy encompasses basic literacy (i.e., theability to read and write simple text) and addition-ally the ability to understand, evaluate, and applyhealth information.17 Levels of health literacy varywidely, depending on age, education, attitudestoward health issues, and life experiences. Healthliteracy should not be underestimated in light ofdata indicating that half the adults in the UnitedStates lack the skills to understand print materialsfor everyday tasks.18 The European Health Litera-cy Survey also found that half the Europeans inthe study had “inadequate or problematic healthliteracy.”19 Lower levels of health literacy increasethe likelihood that patients may not follow instruc-tions and may fail to understand the importanceof disease preventive practices.
Common Risk Factor Approach In recent years, there has been a call in the dentalprofession for taking a “common risk factorapproach” to preventing oral diseases.20,21 Thisapproach focuses on three major pathogenic ele-ments—poor diet, alcohol misuse, and tobaccouse—and seeks to place oral health within the larg-er context of overall health. These three elementsare associated not only with oral disease, but alsowith diabetes and cardiovascular disease—whichare among the leading chronic diseases throughout
CHAPTER 2 Behavioral Science
24
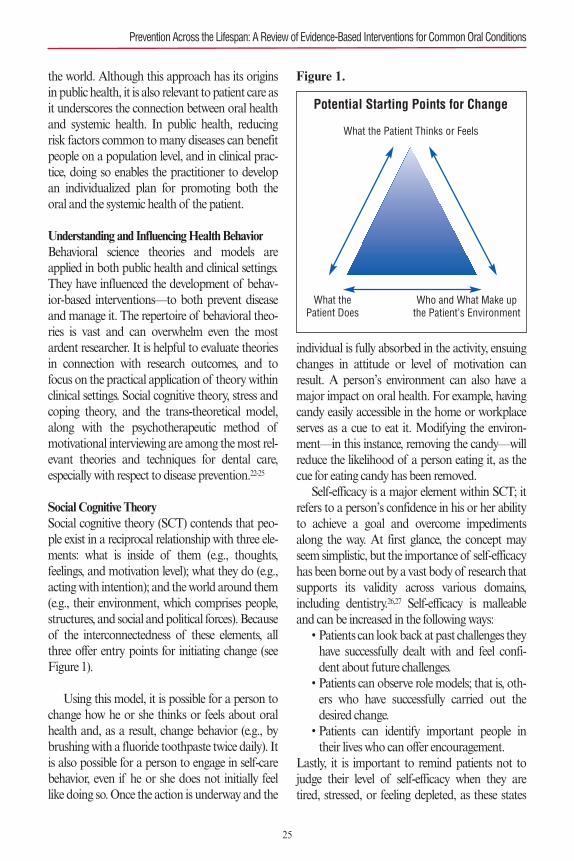
the world. Although this approach has its originsin public health, it is also relevant to patient care asit underscores the connection between oral healthand systemic health. In public health, reducingrisk factors common to many diseases can benefitpeople on a population level, and in clinical prac-tice, doing so enables the practitioner to developan individualized plan for promoting both theoral and the systemic health of the patient.
Understanding and Influencing Health Behavior Behavioral science theories and models areapplied in both public health and clinical settings.They have influenced the development of behav-ior-based interventions—to both prevent diseaseand manage it. The repertoire of behavioral theo-ries is vast and can overwhelm even the mostardent researcher. It is helpful to evaluate theoriesin connection with research outcomes, and tofocus on the practical application of theory withinclinical settings. Social cognitive theory, stress andcoping theory, and the trans-theoretical model,along with the psychotherapeutic method ofmotivational interviewing are among the most rel-evant theories and techniques for dental care,especially with respect to disease prevention.22-25
Social Cognitive Theory Social cognitive theory (SCT) contends that peo-ple exist in a reciprocal relationship with three ele-ments: what is inside of them (e.g., thoughts,feelings, and motivation level); what they do (e.g.,acting with intention); and the world around them(e.g., their environment, which comprises people,structures, and social and political forces). Becauseof the interconnectedness of these elements, allthree offer entry points for initiating change (seeFigure 1).
Using this model, it is possible for a person tochange how he or she thinks or feels about oralhealth and, as a result, change behavior (e.g., bybrushing with a fluoride toothpaste twice daily). Itis also possible for a person to engage in self-carebehavior, even if he or she does not initially feellike doing so. Once the action is underway and the
individual is fully absorbed in the activity, ensuingchanges in attitude or level of motivation canresult. A person’s environment can also have amajor impact on oral health. For example, havingcandy easily accessible in the home or workplaceserves as a cue to eat it. Modifying the environ-ment—in this instance, removing the candy—willreduce the likelihood of a person eating it, as thecue for eating candy has been removed. Self-efficacy is a major element within SCT; it
refers to a person’s confidence in his or her abilityto achieve a goal and overcome impedimentsalong the way. At first glance, the concept mayseem simplistic, but the importance of self-efficacyhas been borne out by a vast body of research thatsupports its validity across various domains,including dentistry.26,27 Self-efficacy is malleableand can be increased in the following ways:• Patients can look back at past challenges theyhave successfully dealt with and feel confi-dent about future challenges.• Patients can observe role models; that is, oth-ers who have successfully carried out thedesired change. • Patients can identify important people intheir lives who can offer encouragement.
Lastly, it is important to remind patients not tojudge their level of self-efficacy when they aretired, stressed, or feeling depleted, as these states
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
Potential Starting Points for Change
What the Patient Thinks or Feels
What the Patient Does
Who and What Make upthe Patient’s Environment
Figure 1.
25

hinder an accurate self-assessment of their capaci-ty for change. Goal setting, done in a collaborative manner,
encompasses not only clear definitions of the goal,but also the necessary steps toward the goal (i.e.,the subgoals). Often clinicians focus on the goalbut do not address the subgoals. However, it isnecessary to attend to subgoals, because what mayseem like a simple request to the clinician can beexperienced as something complex by the patient.Patients may be embarrassed or hesitant to admitthat they cannot actually do what is asked of thembecause they lack the skills to do so. Taking timewith patients to elaborate upon the subgoals helpsthem break down a complex task into small unitsthat they can more readily take on. Eating fewer sweets and flossing daily are
common health recommendations made in den-tal settings. The likelihood of behavior change isincreased by breaking each of these recommen-dations into small steps that are necessary forreaching the desired goal. Subgoals relevant tohealthy eating include identifying healthy snacksto substitute for high sugar ones, writing a gro-cery list that includes healthy items and omitsusual purchases of cookies or candy, structuringthe patient’s home and work environment toremove easily accessible sweets, and preparing aplan for refusing sweets when offered by others.Subgoals for flossing include discovering whichkind of floss best suits the patient’s situation;knowing how to floss correctly; making adapta-tions for physical limitations; identifying a time inthe patient’s day when the desired behavior canbe implemented; linking the flossing to an exist-ing habit such as toothbrushing, so the new habitcan be tied to another behavior; and placing flossin a prominent area so it serves as a visual cue forthe desired action. Environments play an important role in influ-
encing behaviors. While it is beyond the scope ofthe dental clinician to address major environ-mental factors, such as social and politicalprocesses that influence a patient’s life, it is possi-ble to address the patient’s physical environ-ment—in terms of the modifications that can be
made in the home and workplace—in order tosupport the desired behavior. Previouslydescribed measures, such as omitting sweets inthe home and placing floss where it is readily visi-ble, are examples of how patients can modifytheir environment to support their behaviors.Other people in the patient’s life are also a part ofthe environment that surrounds the individualand can influence his or her actions. For instance,a sleep-deprived parent who has to go to workearly in the morning may insist that the otherparent give a bottle at night to soothe a cryingchild. Friends who continue to smoke in the pres-ence of the individual who is attempting to quitor friends who offer sweets to someone who isdiabetic exemplify how behavior change effortscan be undermined by environmental factors,including other people.
Stress and CopingStress is something that every human being expe-riences, but when it is persistent or overwhelming,it has the potential to affect people’s health inadverse ways.28 Stress exerts direct physical effectson the body. People may also cope with stress inunhealthy ways—such as eating unhealthy foods,smoking, or drinking—and may forgo healthyhabits during stressful times. Stress is defined as a situation in which the
demands placed on an individual exceed his or herresources. The process of evaluating the resourcesat hand and deciding how to respond to the stres-sors is referred to as appraisal, and it influences thecoping process.29 Events such as job loss and thedeath of a family member are categorized asmajor stressors. It is important not to underesti-mate what are called microstressors or daily has-sles, as these are important in their own right andhave been shown to have an impact on well-being.Microstressors include recurring events, such asproblems with paying bills, difficulties with trans-portation, and neighborhood annoyances beyondone’s control.30
Broadly speaking, there are two ways of copingwith stress: emotion-focused coping and action-focused coping (also called problem-focused
CHAPTER 2 Behavioral Science
26

coping). Emotion-focused coping refers to thesoothing of emotions associated with stress andencompasses such things as empathy and reas-surance. Action-focused coping refers to activeproblem solving, and taking steps to deal withthe stressor and ease the burden. These twoforms of coping are not mutually exclusive, andthe dental professional can draw upon bothforms of coping to support patients. Forinstance, a father may have a job that preventshim from supervising his child’s nightly tooth-brushing. In such a situation, the clinician can beempathic toward the parent’s dilemma and alsobrainstorm alternatives to direct supervision. Per-haps there are other adults who might be able tosupervise brushing in such situations. Or, perhapsthe parent can phone the child from work tocheck on the brushing behavior. Other people in the patient’s life can offer
social support and, in doing so, help reduce thepatient’s stress. They can offer reassurance tosoothe the individual or offer practical assistancewith stressful tasks. Family members, friends, andother caring individuals can offer social supportand can become involved in supporting thepatient’s healthy behaviors.
Transtheoretical Model The transtheoretical model (TTM) arose out ofProchaska and DiClemente’s examination of theprocess of change within the context of variouspsychological theories.23 It offers a way of under-standing patient behaviors—and underscores thatpeople do not reach their desired goals in one step.Rather, before overt behavior change is visible,there are underlying steps that set the stage for car-rying out the new behavior, or the ceasing ofunwanted behaviors. Additionally, people do notsimply move forward through stages of change ina linear manner, as they may also go back andforth among the stages. The stages of change according to the TTM are• Precontemplation: The person is neitheraware of the need to change nor has plans tochange, even if he or she knows that there is aneed to change. Examples of this stage
include a parent giving a child a bottle filledwith milk at bedtime because he or she isunaware of the potential harm it can cause;or a smoker who is aware of the dangers oftobacco use but has no plans to quit. • Contemplation: The person is thinkingabout changing his or her behavior but isweighing the cost versus the benefit of thenew behavior. Using the earlier examples,this stage includes a parent who is thinkingabout stopping the child’s bottle use at bed-time but doubts whether he or she can dealwith the child crying when refused the bot-tle; or a smoker who is thinking about quit-ting reflects on the effort involved incessation, and doubts whether he or she canbe successful. • Preparation: The person creates a plan ofaction to reach the desired goal. At this stage,individuals may acquire skills if needed tocarry out the desired behavior. For example,the parent comes up with a list of responsesto opposition from the child when not giventhe bottle; or the smoker identifies ways tomodify his or her home environment so thatcues for smoking are eliminated. • Action: The person finally undertakes thedesired behavior, and repetition of the behav-ior helps to strengthen the change. Examplesinclude the parent not giving a milk-filledbottle to the child at bedtime; or the smokerrefraining from smoking. • Termination (or Maintenance): This is thestage where action has taken hold andbecome a long-term habit. For example, theparent no longer feeds the child milk in a bot-tle at bedtime and has established a new rou-tine, replacing the old one; or the smoker hasstopped smoking, and furthermore hasstopped craving cigarettes and no longer hasthe desire to smoke.
The TTM led to efforts to match interventionswith the patient’s stage in the change process.Although this approach appears logical, studieshave shown that for patients enrolled in smoking
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
27

cessation programs, the mere fact of being offeredassistance with quitting was beneficial, even if thecessation intervention did not match the patient’sparticular stage of readiness.31
Motivational Interviewing Motivational interviewing (MI) is a technique tohelp resolve ambivalence about the changeprocess, and seeks to draw forth the patient’sintrinsic motivation to help reach the goal. Keyelements that contribute to its success includecombining empathy with evoking the patient'sown desire to change his or her behaviors. MI hasemerged in the literature as a promising interven-tion in dental settings both for patients and forparents of pediatric patients.32,33 This techniquehas also been found to be useful in addressingalcohol misuse and smoking cessation.34,35Howev-er, the originators of the method, Miller and Roll-nick, caution against adopting a simplisticapproach to MI.36 Although free resources on theInternet offer training in MI, and various continu-ing education courses teach this technique, theyadvise that this technique be approached withcaution. It is a sensitive intervention that needs tobe carried out by people with proper training inthe method. Without extensive training, it is diffi-cult for dental professionals to replicate the precisemethods used in research studies of MI; therefore,clinicians may not achieve the same results asreported in the scientific literature. An important lesson from the body of work on
MI is that it is natural for patients who are “stuck”to have ambivalence about the process of change.The best response in such situations is to reflect backto the patient with empathy while also striving topromote self-efficacy. For instance, if a patient says,“I’m not sure about quitting smoking; it’s really diffi-cult,” the dental professional could respond by say-ing, “Tell me more about that. I’d like to understandwhat’s going on.” After the patient elaborates on thesituation and feels understood, the clinician mightreply, “I realize that it’s not easy to quit, but it is pos-sible. If you would like me to, I can share resourceswith you that you may find useful.” Such a responsefrom the clinician, couched in empathy and curiosi-
ty, invites dialogue and potential partnership. This isin contrast to an authoritarian response, such as,“You have to quit smoking, otherwise your gum dis-ease will continue to progress and you also risk get-ting cancer.” Often strong emotions, such asambivalence, that surround a behavior change (e.g.,quitting smoking) can override rational factors (e.g.,that smoking is harmful to the patient’s health).Therefore, it is necessary to address emotions inorder to facilitate change.
APPLICATION TO CLINICAL PRACTICE The Process of Disease Prevention Despite advances in medical and dental research,it is not possible to entirely prevent disease. Onemay speak of disease prevention and predict theefficacy of a preventive measure on a populationlevel. However, in clinical terms, it is impossible topredict with accuracy whether a person will devel-op a disease. As a result, while one can prevent dis-ease on a population level, on a clinical level thedental professional can only reduce risk of diseaseoccurrence for each individual. Nevertheless, by adopting healthy behaviors
and ending unhealthy ones, individuals can greatlyincrease their odds of being disease free. Sporadicbehaviors have little to no impact in terms ofimproving a patient’s health. In order to exertmaximum benefits, healthy behaviors must be car-ried out on a regular basis. Making a behavior ahabit and integrating the desired behavior into thepatient’s lifestyle are best. If the patient hasunhealthy habits, such as tobacco use or improperdiet, then these behaviors need to be eliminatedfrom the patient’s routines and replaced withhealthy alternatives.
Disease Prevention Across the LifespanChildren are dependent upon parents or othercaregivers for their well-being. Thus, it is impor-tant to include both the child and the parent orcaregiver when offering oral hygiene instructions.Many parents experience difficulty in motivatingtheir children to brush their teeth regularly. Thebest way to encourage children to brush is tomodel the desired behavior.37
CHAPTER 2 Behavioral Science
28

If parents or caregivers are stressed, they areless able to attend to the oral health needs of theirchild.38 Depending on their social norms, parentsmay not view primary teeth as important, andthus may not be concerned about a healthy pri-mary dentition. In such situations, the importanceof primary teeth in the child’s overall health andwell-being should be explained to the parents,given that if left untreated, decayed primary teethcan lead to pain and potentially life-threateninginfections. Progression from childhood to adolescence is
marked by the emergence of autonomy, which attimes may lead patients to resist guidance aboutself-care. In such instances, the dental professionalcan attempt to establish rapport and take a collab-orative approach with the patient. Additionally, itcan be helpful to connect with the values andgoals of the adolescent and his or her family. Forinstance, if the patient values looking good, onecan link oral hygiene to appearances; or, if thepatient values being a good son or daughter, thenself-care can be linked to being virtuous. This isalso a period when individuals begin experiment-ing with tobacco and alcohol use. Thus, it is neces-sary to inquire about substance use—and offerassistance in linking patients with resources tosupport responsible drinking and tobacco avoid-ance. Additional strategies for communicatingwith youth about alcohol and tobacco use includeaddressing ways to resist peer pressure to partakeof these substances. It can be challenging to coun-sel an adolescent not to smoke, especially when hisor her parents are smoking. In such instances, it isbest to emphasize the health benefits of smokingcessation, and offer to help both the patient andhis parents in stopping tobacco use. Older adults may experience difficulty with
oral hygiene because of physical limitations suchas arthritis, neurodegenerative diseases or motordisorders, or mental challenges due to cognitiveimpairment. These situations impair the olderadult’s ability to effectively complete self-care,including oral care. Along with exploring how toadapt oral self-care behaviors according to theindividual’s ability, it is equally important to vali-
date the person’s expression of independence. When caring for elderly patients who are not
living independently, it becomes necessary toinvolve caregivers in oral hygiene instructions. Insituations where patients present with complexmedical conditions or cognitive impairment, it isnecessary to use a collaborative, interdisciplinaryapproach to inform other healthcare providersand family members about the individual’s oralhealthcare needs.39,40 Patients affected by dementiamay engage fully in conversation, but may notrecall health-related instructions later on. Visualcues and written instructions may provideprompts that allow the individual to participate inself-care, with assistance from others to ensure efficacy.
Common Risk Factors and Links to Systemic Health The dental appointment presents an opportunityto link oral health with systemic health and toemphasize this connection to patients. It is a wayof approaching oral health that underscores thefact that the mouth is situated within the body,and that what a patient does to his or her mouth(e.g., consumption of tobacco or sugar-sweetenedbeverages) has far-reaching effects beyond cariesand aesthetics. These are sensitive issues forpatients, and a nonjudgmental approach wheninquiring about them is less likely to elicit a defen-sive response. If a patient indicates that he or shehas a problem in one of these areas, it is beneficialto offer practical suggestions to stop the habit. Ifthe patient expresses a desire to change but doesnot know how, he or she can be referred to onlineresources and in-person programs, for instance,for smoking cessation.
From Trying New Behaviors to EstablishingHealthy HabitsFor optimal health, it is necessary to regularlyengage in health-promoting behavior. Introducingpatients to new behavior is only the first step, andthe greatest benefits are obtained when the behav-ior becomes a habit. A habit can be defined assomething the patient does automatically in
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
29

response to external cues.41 For example, a redtraffic light is an external cue to stop at an intersec-tion, and likewise the process of getting dressed inthe morning for school or work can become a cuefor brushing one’s teeth. The following elements are helpful in turning a
new or sporadic behavior into a lasting habit: • Defining the desired behavior and goal clearly • Stating an intention to carry out the behavior,or committing to the goal• Bolstering the patient’s self-efficacy• Learning the desired behavior• Repeating the desired behavior so it becomesautomatic• Integrating the behavior into existing routinesso it becomes part of the patient’s lifestyle• Monitoring the repetition of the behavior bytracking the frequency with which the desiredbehavior is carried out• Anticipating impediments in advance andplanning ways to deal with them• Rewarding efforts, especially through internalrewards such as feelings of accomplishment(versus external rewards such as gifts)• Attending to the patient’s environment tomake modifications so that the environmentis conducive to carrying out the new behavior • Identifying people in the patient’s life whocan support and encourage the adoption ofthe new behavior. (It may also be necessary toidentify people who might undermine thepatient’s efforts at behavior change, anddevelop a plan to address that challenge.)
These processes can be used not only to acquire apositive health behavior, but also to eliminate neg-ative health habits. For example, a patient maystate “not smoking cigarettes” as a goal.
Integrating Desired Behavior into Patient LifestylesAny change from a person’s norms and routineshas the potential to create discomfort. Patientsmay intellectually understand the benefits of dis-ease-preventing behavior, such as eating less sugarand not smoking. However, asking them to
change long-term habits can elicit stress and con-flicting feelings, resulting in ambivalence. On theone hand, the patient may desire health, but onthe other hand he or she may find it difficult to dowhat is required and thus dread the effort involvedin behavior change. What may seem like an obvi-ous choice of action for a dental professional canbe experienced as a major stressor by the patient,or the parent of a child patient—for instance,when asking the parent not to feed the child with abottle at bedtime. Patients may experienceambivalence and express doubts about their abili-ty to adopt new behaviors or to let go of long-last-ing ones. Respectful inquiry can illuminate reasons for
the patient’s reluctance to adopt the recommend-ed behavior. It is important to keep in mind thatnot all patients are ready to change behaviorsimmediately. Additionally, individuals who areexperiencing stressful life situations, such as caringfor a severely ill family member or dealing withunemployment, may hesitate to adopt a newbehavior because they perceive it as yet anotherstressor, even if the benefits are apparent. In suchinstances, clinicians can let their patients knowthat they are available to help whenever they areready to change, and offer to connect patients withsupportive resources.
Interpersonal Communication Interpersonal communication is a fundamentalelement of all dental appointments. It is the vehi-cle through which the psychological and socialaspects of the appointment are manifested. It isimportant to maintain a caring and empathic tonewhen striving to build a partnership with patients,as they are sensitive to nuances of the clinician’svoice. A study of surgeons and their tone of voice
found that it was possible to differentiate betweenthose who had a history of malpractice and thosewho did not, solely on the basis of listening to 10-second snippets of conversations with theirpatients.42 Surgeons who used a harsh tone ofspeech were more likely to have been sued for mal-practice compared with those who used a warmer
CHAPTER 2 Behavioral Science
30

tone. Interpersonal communication also touchesupon health literacy as it influences how onespeaks and the words one uses.
Health Literacy in the Context of the Dental Appointment In practical terms, attending to a patient’s abilityto comprehend and utilize medical informationwill yield better patient outcomes, and reduce frus-tration for both the patient and the clinician.Patients may not admit that they do not under-stand medical terms or instructions fully. Theymight be embarrassed to let the clinician knowthat they have not understood what they havebeen told. Even patients who hold advanceddegrees may lack the capacity to understand med-ical and dental terminology, especially if theirdegrees are in another field. Health literacy is closely linked with patient
communication, and the following suggestionsoffer strategies to increase the likelihood thatpatients will more fully comprehend what is beingsaid:
Respectful Patient Communication• Do not “talk down” to the patient when heor she does not understand dental terminolo-gy, or has misconceptions.• Be sensitive to the patient’s gender, age, andculture.• Engage in a dialogue and establish a partner-ship with the patient rather than speakingwith an authoritarian tone.
Simplified Communication• Use straightforward language to explain situ-ations to patients.• Avoid use of technical terms.• Explain concepts using short sentences thatallow the patient to closely follow what isbeing said.
Use the Teach-Back Method• Ask the patient to repeat back in his or herwords what the healthcare provider has said(e.g., details about a medication regimen).
• Ask the patient to demonstrate the self-caretechnique (e.g., flossing) to ensure that thepatient has the necessary skills to carry outthe behavior at home.
Common Psychological Conditions Depression is one of the leading causes of disabili-ty around the world.43 Although its manifestationcan vary across cultures, the most common ele-ments include feelings of hopelessness and dimin-ished ability to engage in and enjoy life. It may alsomanifest as complaints of feeling unwell. One canthink of depression as existing on a spectrumfrom mild to intense distress. From a practicalpoint of view, it is important to consider whetherthe distress is interfering with the patient’s func-tioning and whether a referral to a mental healthprofessional might be indicated. Often depressionis found as a comorbid condition among patientswith chronic illnesses, such as heart disease anddiabetes, and is associated with diminished self-care.44
In many cultures, there are negative attitudestoward depression and other psychological condi-tions. Unfortunately, these conditions are viewedas personal weaknesses rather than as an illness. Itis important to be open-minded toward patientswho may be depressed and make appropriatereferrals for further care. Depression is associatedwith increased risk for suicide; thus, a timely men-tal health referral can benefit the patient greatly. Interms of preventing dental disease, it is importantto explore ways of supporting the patient’s self-care and draw upon individuals in the patient’s lifewho might be able to help encourage compliancewith recommended self-care regimens. Anxiety is also a common psychological con-
dition experienced around the world.45 It canoccur in a generalized form or as a specific phobia(e.g., dental phobia); it can also occur as post-trau-matic stress disorder following a traumatic experi-ence. Anxiety disorders vary in presentation andtend to be characterized by feelings of vulnerabili-ty, threat, or lack of a sense of safety. It is veryimportant for care providers to reassure patientsand not dismiss their concerns, or brand the
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
31

patients as “excessive worriers.” If the patientappears to be experiencing difficulty because ofanxiety, referral to a mental health care profes-sional may be beneficial. In situations where amental health professional is not accessible, thedental professional might consider referring thepatient to a primary care physician.
Supporting Patients in the Clinical Setting: A Chairside ChecklistThe Chairside Checklist (Appendix 1) presented inthis chapter draws upon theoretical constructs fromthe social and behavioral sciences, and aims to trans-late them into a practical instrument that dental pro-fessionals can use to enhance patient outcomes. It ishoped that this checklist will lessen dental profes-sionals’ frustration with patient challenges, andthereby enhance enjoyment of their work. TheChairside Checklist is intended to facilitate the appli-cation of the information presented in this chapter.It is a guide to help dental professionals supporttheir patients in the adoption and maintenance ofhealthy behaviors. Additionally, it can also beapplied to help patients stop unhealthy behaviors. The checklist integrates practitioner and
patient variables and can be used to enrich thepatient appointment. Some items on the checklistmay not be relevant to each patient or eachappointment. The nature of the clinical encounterwill dictate which items might be most applicableto a patient, and the clinician can choose those ele-ments that are most relevant. Another value of thechecklist is in understanding challenging patients,who might be variously referred to as “difficult,”“uncooperative,” “resistant,” or “stubborn.” In anideal situation, the checklist can enhance theappointment. But in a difficult situation, thechecklist can help to identify problems and identi-fy potential solutions. Lastly, the checklist can beviewed as an instrument to help foster an atmos-phere of patient-centered care.
SUMMARY Good oral health is a component of overall well-being, and disease prevention is a goal shared bydental professionals around the world. What peo-
ple eat and drink, and whether or not they usetobacco, will influence their oral health status.Convincing patients to develop health-promotinghabits and eliminate harmful behavior is a chal-lenge frequently encountered by dental profes-sionals. Patients cannot be kept free of diseasesolely through biomedical agents, nor can healthbe guaranteed solely on the basis of procedurescarried out in the clinical setting. Patients need toactively engage in self-care in an ongoing way. Inmany instances, clinicians give their patients healthinformation with the expectation that patients willimmediately adopt the recommended behavior.However, providing information is but one stepwithin the larger process of eliciting and maintain-ing healthy behavior. Information alone is notenough to change behavior.The behavioral sciences contain numerous the-
ories that can explain patient behavior. Patientbehavior must be understood in terms of internalinfluences (i.e., thoughts, feelings, motivations), aswell as external influences (i.e., the environment,which comprises other people, physical structures,cultural norms, economics, and sociopolitical fac-tors). Owing to practical considerations, it is notpossible to explore all theories of potential rele-vance in this chapter. The theories and constructsdiscussed were selected because of the strong basisof support from research, and for their utility inthe clinical setting and relevance to patients fromvaried cultures and socioeconomic levels. The authoritarian approach to patient educa-
tion is outmoded; it leads to frustration (for boththe clinician and the patient) and hampers inter-personal communication. Dental professionalsshould not merely inform patients about strategiesfor disease prevention and hope that patients willautomatically adopt their recommendations. Thewealth of information from the behavioral sci-ences informs dental professionals about how tocreate an efficacious and meaningful partnershipthat facilitates the process of change. It is possiblefor patients to adopt new behavior leading to last-ing habits; it is also possible to eliminate harmfulbehavior in the long term. The partnershipbetween clinician and patient is the vehicle
CHAPTER 2 Behavioral Science
32
through which the process of change is facilitated,and the contents of this chapter, including theChairside Checklist, are intended to guide thereader in supporting his or her patients in theirquest for optimal oral health.
1. Interpersonal Communication • What is the provider’s tone of voice? • Is it warm, expressing empathy and concern? • Is the manner of speaking authoritarian orcollaborative? • Are messages framed to motivate the patientby emphasizing the benefits of disease pre-vention, rather than evoking fear of disease? • Does the provider seek to promote thepatient’s self-efficacy by offering encourage-ment and identifying role models, and build-ing upon past successes?
2. Expectations for Treatment• What are the provider’s expectations fortreatment, and how might these differ fromthose of the patient? • What is the patient’s perception of his or heroral health quality of life, and does this needto be reconciled with the expectations of thecare provider?
3. Defining Goals and Identifying Resources Needed to Reach and Maintain Them• What are the desired preventive goals, andare they clearly defined? • What are the subgoals (i.e., steps along theway that must be reached on the way toachieving the main goal)? • What resources and skills are needed to reachthe goals? • What are potential barriers to achieving thegoals and how might the patient plan ways toaddress these barriers? • Is the patient aware that repetition of thedesired behavior will lead to mastery and sup-port the long-term maintenance of the goals? • How will the patient monitor his or her
progress toward the goals? • How can the patient connect with the inter-nal rewards of success, such as feeling pridein one’s accomplishment? • How can the goals be integrated into thepatient’s lifestyle so they become automatic?
4. Lifespan Considerations• Are the goals and recommendations ageappropriate and realistic in terms of thepatient’s level of comprehension and motorskills? • Is there a caregiver in addition to the patient?• Is this caregiver included in important con-versations?
5. Environmental Factors that Influence thePatient’s Behavior • What kinds of cultural norms might be influ-encing the patient’s behavior? • Are there economic constraints that imposelimitations on the patient’s ability to care forhim- or herself, or purchase health necessitiessuch as toothbrush and toothpaste?• Who are the important people in thepatient’s life who can be sources of supportand encouragement? • Might there be people in the patient’s life whocan potentially sabotage the patient’s efforts forbehavior change? If so, how might the patientmake a plan for dealing with this situation?
6. Barriers to Preventive Care• What are potential barriers to self-care, andhow can the patient cope or overcome the bar-riers? Has the patient anticipated barriers andidentified strategies to overcome the barriers? • Are there unsupportive people who detract
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
Acknowledgments: The author is grateful to Ms. A. Brodie, Mr.H. Bright, and Mr. V. Tedeschi, librarians at A.T. Still Universi-ty of Health Sciences in Mesa, Arizona, USA, for their assis-tance in retrieving documents; and Ms. B.J. LeBaron for herassistance in preparing the manuscript.
Appendix 1: Chairside Checklist
33
from the desired goals? How can the patientbe assertive and navigate around these people? • If finances are a barrier, are there alternatepaths to the goals? Can the patient andprovider brainstorm and arrive at creativesolutions? • If the patient is experiencing stress, whichpeople in the patient’s life can assist with bothemotion-focused coping and action-focusedcoping?
7. Basic Literacy • Can the person read and write and, if so, atwhat level of literacy? How might the clini-cian adapt communication to optimizepatient engagement in the conversation?• Do the consent forms, educational materials,and appointment reminders need to beadapted to the patient’s literacy level? • Is the patient being treated respectfully, evenif his or her literacy level is low? • Might the teach-back method enhancepatient understanding of his or her situation?
8. Health Literacy • Is communication with the patient respectful,free of jargon, and clearly understood? • Has the patient been asked to “teach back”to demonstrate his or her level of under-standing of critical concepts?
9. Resources to Support the Patient in Self-Care• Which person or people in the patient’s lifecan be a source of encouragement, support,and stress reduction? • Which resources, such as Internet sites andeducational materials and guides, might be ofuse to the patient? • Are there smartphone applications (apps) orother technologies that the patient can use toset up reminders and to track progresstoward a goal?
10. Stressors and Coping Resources• What are the demands that the patient (orparent of child patient) is experiencing that
interfere with carrying out health behavior? • What kinds of emotional support might helpthe patient to achieve his or her goals? • What kinds of practical support might helpthe patient to achieve his or her goals? • Are there individuals in the patient’s life whomight be recruited to support the patient inthe pursuit of his or her health behavior?
11. Patient’s Self-Dialogue• Is the patient speaking in a manner that con-notes hopelessness or helplessness? If so, howmight the clinician increase the patient’s self-efficacy? • How might the clinician respectfully counterthe patient’s negative self-talk? • Does the patient need additional help if he orshe is expressing a degree of helplessness orhopelessness that prevents achievement ofthe goal? • Are there family members and friends whocan be recruited to encourage and supportthe patient?
12. Medical Referral • Does the patient have unhealthy habits thathave implications for poor oral health, and isthere a need for medical consultation?• Does the patient present with medical condi-tions that impede self-care?• Might the patient have a systemic conditionsuch as diabetes that interferes with achievinggood oral health? • If the patient’s medication is exerting a nega-tive side effect on the oral cavity, are therealternatives that have fewer side effects?
13. Referral to a Behavioral Health Provider• Does the patient engage in unhealthy behav-iors, such as unhealthy diet, tobacco use, andalcohol misuse, and might he or she benefitfrom a referral for counseling? • Does the patient present with signs of depres-sion, anxiety, substance use, or other psycho-logical problems? If so, might the patientbenefit from a psychological referral?
CHAPTER 2 Behavioral Science
34
• If the patient is having trouble establishinghealthy habits, would a psychological referralbe beneficial?
14. Structures and Resources to Help the PatientMaintain Lasting Habits• What kinds of stressors might be occurringin the patient’s life that prevent him or herfrom maintaining a healthy behavior? • What kinds of environmental barriers might
be influencing the patient’s behavior? • What are ways to promote the patient’s self-efficacy—especially if the patient is express-ing loss of hope? • Is the patient adequately connected with therewards and benefits of the healthy behavior,rather than focused on the efforts to achievethe goal? • What kinds of internal rewards might boostthe patient’s motivation?
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
REFERENCES 1. Engel GL. The need for a new medical model: a chal-
lenge for biomedicine. Science. 1977;196:129–136. 2. Schroeder SA. We can do better—improving the health
of the American people. N Engl J Med. 2007;357:1221–1228.
3. Glanz K, Bishop DB. The role of behavioral science the-ory in development and implementation of public healthinterventions. Annu Rev Public Health. 2010;31:399–418.
4. Braverman P, Gottleib L. The social determinants ofhealth: it’s time to consider the causes of the causes. Pub-lic Health Rep. 2014;129(suppl 2):19–31.
5. Kawachi I, Subramanian SV, Almeida-Filho N. A glos-sary for health inequalities. J Epidemiol CommunityHealth. 2002;56:647–652.
6. World Health Organization. Dying for Change: PoorPeople’s Experience of Health and Ill Health. Report no.33125. Geneva, Switzerland: World Health Organiza-tion; 2005.
7. Haushofer J, Fehr E. On the psychology of poverty. Sci-ence. 2014;344(6186):862–867.
8. Goldman AS, Yee R, Holmgren CJ, Benzian H. Globalaffordability of fluoride toothpaste. Global Health.2008;4:7.
9. WHOQOL Group. The World Health OrganizationQuality of Life Assessment (WHOQOL). Developmentand psychometric properties. Soc Sci Med.1998;46:1569–1585.
10. Bennadi D, Reddy CVK. Oral health related quality oflife. J Int Soc Prev CommunityDent. 2013;3:1–6.
11. Vettore MV, Aqeeli A. The roles of contextual and indi-vidual social determinants of oral health-related qualityof life in Brazilian adults. Qual Life Res. 2015; Sep 5.[Epub ahead of print.]
12. Yiengprugsawan V, Somkotra T, Seubsman SA, SleighAC; Thai Cohort Study Team. Oral health-related quali-ty of life among a large national cohort of 87,134 Thaiadults. Health Qual Life Outcomes. 2011;9:42.
13. Enoki K, Ikebe K, Matsuda KI, Yoshida M, Maeda Y,Thomson WM. Determinants of change in oral health-related quality of life over 7 years among older Japanese.J Oral Rehabil. 2013;40:252–257.
14. Brennan DS, Spencer JA. Life events and oral-health-related quality of life among young adults. Qual LifeRes. 2009;18:557–565.
15. Khatri SG, Acharya S, Srinivasan SR. Mother’s sense ofcoherence and oral health related quality of life of pre-school children in Udupi Taluk. Comm Dental Health.2014;31:32–36.
16. Almozino G, Aframian DJ, Sharav Y, Sheftel Y,Mzabaev A, Zini A. Lifestyle and dental attendance aspredictors of oral health-related quality of life. Oral Dis.2015;21:659–666.
17. World Health Organization. Health Promotion Glossary.Geneva, Switzerland: World Health Organization; 1998.
18. Nouri S, Rudd RE. Health literacy in the “oralexchange”: an important element of patient-providercommunication. Patient Educ Couns. 2015;98:565–571.
19. Kickbusch I, Pelikan JM, Apfel F, Tsouros AD, eds.Health Literacy: The Solid Facts. Geneva, Switzerland:World Health Organization; 2012.
20. Watt RG, Sheiham A. Integrating the common risk fac-tor approach into a social determinants framework.Comm Dent Oral Epidemiol. 2012;40:289–296.
21. Heilmann A, Sheiham A, Watt RG, Jordan RA. Thecommon risk factor approach—an integrated popula-tion- and evidence-based approach for reducing socialinequalities in health [in German]. Gesundheitswesen.2015; Sep 3. [Epub ahead of print.]
22. Bandura A. Social Foundations of Thought and Action:A Social Cognitive Theory. Englewood Cliffs, NJ: Pren-tice-Hall; 1986.
23. Prochaska JO, DiClemente CC, Norcross JC. In searchof how people change. Applications to addictive behav-iors. Am Psychol. 1992;47:1102–1114.
24. Lazarus RS, Folkman S. Stress, Appraisal and Coping.New York, NY: Springer Publishing; 1984.
25. Miller WR, Rose GS. Toward a theory of motivationalinterviewing. Am Psychol. 2009;64(6):527-37
26. Askelson AM, Chi DL, Momany ET, et al. The impor-tance of efficacy: Using the extended parallel processmodel to examine factors related to preschool-age chil-dren enrolled in Medicaid receiving preventive dental vis-its. Health Educ Behav. 2015;42:805–813.
35

CHAPTER 2 Behavioral Science
27. Gholami M, Knoll N, Schwarzer R. A brief self-regula-tory intervention increases dental flossing in adolescentgirls. Int J Behav Med. 2015;22:645–651.
28. Thoits PA. Stress and health: major findings and policyimplications. J Health Soc Behav. 2010;51(suppl):S41–S53.
29. Folkman S, Lazarus RS, Dunkel-Schetter C, DeLongisA, Gruen RJ. Dynamics of a stressful encounter: cogni-tive appraisal, coping, and encounter outcomes. J PersSoc Psychol. 1986;50:992–1003.
30. DeLongis A, Folkman S, Lazarus RS. The impact ofdaily stress on health and mood: psychological andsocial resources as mediators. J Pers Soc Psychol.1988;54:486–495.
31. Cahill K, Lancaster T, Green N. Stage-based interven-tions for smoking cessation. Cochrane Database SystRev. 2010;(11):CD004492.
32. Gao, X, Lo EC, Chan KC. Motivational interviewing inimproving oral health: a systematic review of random-ized clinical trials. J Periodontol. 2014;85:426–437.
33. Borrelli B, Tooley EM, Scott-Sheldon LA. Motivationalinterviewing for parent-child health interventions: a sys-tematic review and meta-analysis. Pediatr Dent.2015;37:254–265.
34. Foxcroft DF, Coombes L, Wood S, Allen D, AlmeidaSantimano NM. Motivational interviewing for alcoholmisuse in young adults. Cochrane Database Syst Review.2014;(8):CD007025.
35. Lindson-Hawley N, Thompson TP, Begh R. Motiva-tional interviewing for smoking cessation. CochraneDatabase Syst Rev. 2015;(3):CD006936.
36. Miller WR, Rollnick S. Ten things that motivational
interviewing is not. Behav Cogn Psychother.2009;37:129–140.
37. Collett BR, Huebner CE, Seminario AL, Wallace E,Gray KE, Speltz ML. Observed child and parent tooth-brushing behaviors and child oral health. Int J PaediatrDent. 2015; Jul 4. [Epub ahead of print.]
38. Tiwari T, Albino J, Batliner TS. Challenges faced inengaging American Indian mothers in an early child-hood caries preventive trial. Int J Dent.2015;2015:179189.
39. Wang TF, Huang CM, Chou C, Yu S. Effect of oralhealth education programs for caregivers on oral hygieneof the elderly: a systematic review and meta-analysis. IntJ Nurs Studies. 2015;52:1090–1096.
40. Brennan L, Strauss J. Cognitive impairment in olderadults and oral health considerations: treatment andmanagement. Dent Clin North Am. 2014;58:815–828.
41. Lally P, Gardner B. Promoting habit formation. HealthPsychol Rev. 2013;7(suppl):S137–S158.
42. Ambady N, LaPlante D, Nguyen MA, Rosenthal R,Chaumeton N, Levinson W. Surgeon’s tone of voice: aclue to malpractice history. Surgery. 2002;132:5–9.
43. Kessler RC, Bromet EJ. The epidemiology of depressionacross cultures. Annu Rev Public Health. 2013;34:119–138.
44. Chan HL, Lin CK, Chau YL, Chang CM. The impactof depression on self-care activities and health care uti-lization among people with diabetes in Taiwan. DiabetesRes Clin Pract. 2012;98:e4–7.
45. Baxter AJ, Scott KM, Vos T, Whiteford HA. Globalprevalence of anxiety disorders: a systematic review andmeta-regression. Psychol Med. 2013;43:897–910.
36

As each patient completes a comprehensive oral evalu-ation or assessment, the data collected must bereviewed to determine whether the patient can partici-pate in the planned dental or dental hygiene treatment.This process, referred to as a risk assessment, is used todetermine if treatment outweighs the potential risks tothe patient.Risk assessment has been defined in various ways.
Little and colleagues1 described risk assessment asinvolving the following four components: (1) thenature, severity, control, and stability of the patient’smedical condition; (2) functional capacity of thepatient; (3) emotional status of the patient; and (4) typeand magnitude of the planned procedure. In Standardsfor Clinical Dental Hygiene Practice of the AmericanDental Hygienists’ Association, risk assessment isdescribed as the “qualitative and quantitative evalua-tion gathered from the assessment process to identifyany risks to general and oral health.”2 These data “pro-vide the clinician with the information to develop anddesign strategies for preventing or limiting disease andpromoting health.”2Within this standard, risk is classi-fied as high, moderate, or low. Examples include fluo-ride exposure, smoking, systemic diseases, xerostomia,age, gender, family history, physical disability, and psy-chological and social considerations.This chapter discusses risk assessment for both sys-
temic health and oral health conditions. Risk assess-ment tools to support clinical practice are addressed toaid dental professionals in creating accurate risk pro-files for their patients as a means of preventing medicalcomplications and oral diseases to the extent possible.
RISK ASSESSMENT FOR SYSTEMIC HEALTH
Dental professionals assess the general health status oftheir patients as part of the comprehensive health his-
tory obtained during an initial appointment. Thishealth history should be updated routinely at subse-quent patient appointments. One purpose of complet-ing a health history is to identify risk factors that maybe present, placing the patient at risk for a potentialmedical emergency during the dental or dental hygieneappointment. Another purpose is to identify possiblerisks for health conditions not yet identified. In thissection, risk assessment is demonstrated through dis-cussion of the systemic conditions of cardiovasculardisease and stroke, diabetes mellitus, and sleep-relatedbreathing disorders.
Cardiovascular Disease and StrokeKey ConsiderationsEach year, the American Heart Association (AHA), theCenters for Disease Control and Prevention (CDC), theNational Institutes of Health (NIH), and other govern-ment agencies join together to identify current statisticsrelated to cardiovascular, cerebrovascular, and metabol-ic diseases, and present them as a statistical update.3 TheAHA statistical update titled “Heart Disease andStroke Statistics—2015 Update: A Report from theAmerican Heart Association” appears in the journalCirculation (downloadable from http://circ.ahajour-nals.org) and serves as the basis for a fact sheet thatappears on the joint website of the AHA and theAmerican Stoke Association (ASA).3 From thisresource, it is apparent that cardiovascular disease(CVD) remains the leading cause of death globally andin the United States, and among both men and women.Approximately 787,000 Americans died from heart dis-ease, stroke, and other CVD in 2011, accounting forone of every three deaths in the United States (see Fig-ure 1). Considered another way, one person dies fromCVD every 40 seconds. CVD is also the leading causeof death worldwide, representing 31% of all globaldeaths in 2012. Of these deaths, approximately 7.4 mil-lion were due to coronary heart disease.4 Although thedeath rate from heart disease continues to fall, the bur-den and risk factors remain alarmingly high. In particu-lar, almost 735,000 Americans have myocardialinfarctions each year, and approximately 120,000 die.3
Stroke is the fifth leading cause of death in theUnited States, killing someone once every 4 min-utes, and is the leading preventable cause of disabil-ity.3 Approximately 795,000 people have a strokeevery year, equating to one every 40 seconds.
37
RiskAssessment
Chapter 3
JoAnn R. Gurenlian
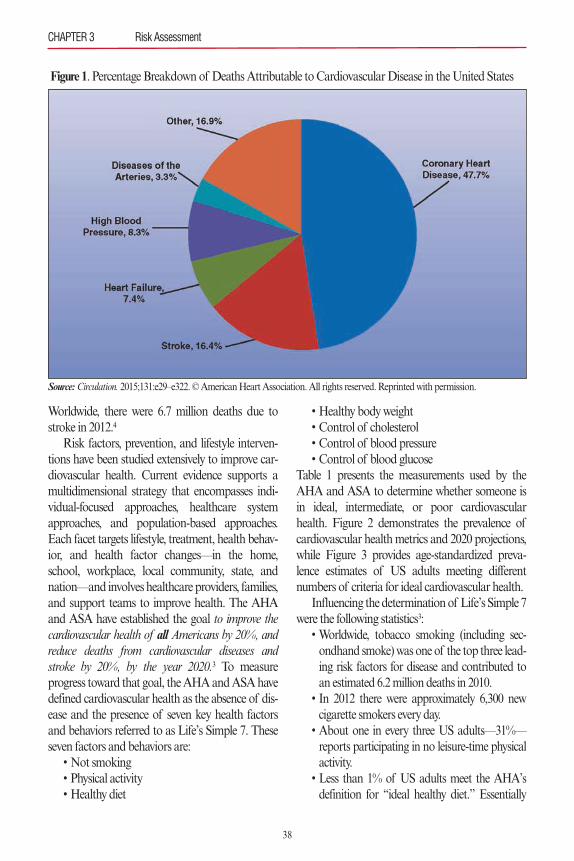
Worldwide, there were 6.7 million deaths due tostroke in 2012.4
Risk factors, prevention, and lifestyle interven-tions have been studied extensively to improve car-diovascular health. Current evidence supports amultidimensional strategy that encompasses indi-vidual-focused approaches, healthcare systemapproaches, and population-based approaches.Each facet targets lifestyle, treatment, health behav-ior, and health factor changes—in the home,school, workplace, local community, state, andnation—and involves healthcare providers, families,and support teams to improve health. The AHAand ASA have established the goal to improve thecardiovascular health of all Americans by 20%, andreduce deaths from cardiovascular diseases andstroke by 20%, by the year 2020.3 To measureprogress toward that goal, the AHA and ASA havedefined cardiovascular health as the absence of dis-ease and the presence of seven key health factorsand behaviors referred to as Life’s Simple 7. Theseseven factors and behaviors are:• Not smoking• Physical activity• Healthy diet
• Healthy body weight• Control of cholesterol• Control of blood pressure• Control of blood glucose
Table 1 presents the measurements used by theAHA and ASA to determine whether someone isin ideal, intermediate, or poor cardiovascularhealth. Figure 2 demonstrates the prevalence ofcardiovascular health metrics and 2020 projections,while Figure 3 provides age-standardized preva-lence estimates of US adults meeting differentnumbers of criteria for ideal cardiovascular health.Influencing the determination of Life’s Simple 7
were the following statistics3:• Worldwide, tobacco smoking (including sec-ondhand smoke) was one of the top three lead-ing risk factors for disease and contributed toan estimated 6.2 million deaths in 2010.• In 2012 there were approximately 6,300 newcigarette smokers every day.• About one in every three US adults—31%—reports participating in no leisure-time physicalactivity.• Less than 1% of US adults meet the AHA’sdefinition for “ideal healthy diet.” Essentially
CHAPTER 3 Risk Assessment
38
Source:Circulation. 2015;131:e29–e322. © American Heart Association. All rights reserved. Reprinted with permission.
Figure 1. Percentage Breakdown of Deaths Attributable to Cardiovascular Disease in the United States
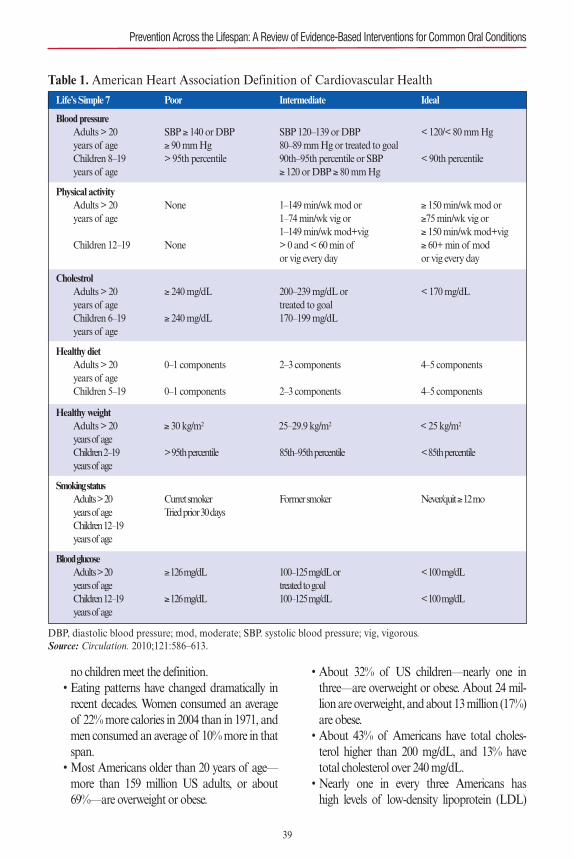
no children meet the definition.• Eating patterns have changed dramatically inrecent decades. Women consumed an averageof 22% more calories in 2004 than in 1971, andmen consumed an average of 10% more in thatspan.• Most Americans older than 20 years of age—more than 159 million US adults, or about69%—are overweight or obese.
• About 32% of US children—nearly one inthree—are overweight or obese. About 24 mil-lion are overweight, and about 13 million (17%)are obese.• About 43% of Americans have total choles-terol higher than 200 mg/dL, and 13% havetotal cholesterol over 240 mg/dL.• Nearly one in every three Americans has high levels of low-density lipoprotein (LDL)
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
39
Life’s Simple 7 Poor Intermediate Ideal
Blood pressureAdults > 20 SBP ≥ 140 or DBP SBP 120–139 or DBP < 120/< 80 mm Hgyears of age ≥ 90 mm Hg 80–89 mm Hg or treated to goalChildren 8–19 > 95th percentile 90th–95th percentile or SBP < 90th percentileyears of age ≥ 120 or DBP ≥ 80 mm Hg
Physical activityAdults > 20 None 1–149 min/wk mod or ≥ 150 min/wk mod oryears of age 1–74 min/wk vig or ≥75 min/wk vig or
1–149 min/wk mod+vig ≥ 150 min/wk mod+vigChildren 12–19 None > 0 and < 60 min of ≥ 60+ min of mod
or vig every day or vig every day
CholestrolAdults > 20 ≥ 240 mg/dL 200–239 mg/dL or < 170 mg/dLyears of age treated to goalChildren 6–19 ≥ 240 mg/dL 170–199 mg/dLyears of age
Healthy dietAdults > 20 0–1 components 2–3 components 4–5 componentsyears of ageChildren 5–19 0–1 components 2–3 components 4–5 components
Healthy weightAdults > 20 ≥ 30 kg/m2 25–29.9 kg/m2 < 25 kg/m2
years of ageChildren 2–19 > 95th percentile 85th–95th percentile < 85th percentileyears of age
Smoking statusAdults > 20 Curret smoker Former smoker Never/quit ≥ 12 moyears of age Tried prior 30 daysChildren 12–19years of age
Blood glucoseAdults > 20 ≥ 126 mg/dL 100–125 mg/dL or < 100 mg/dLyears of age treated to goalChildren 12–19 ≥ 126 mg/dL 100–125 mg/dL < 100 mg/dLyears of age
Table 1. American Heart Association Definition of Cardiovascular Health
DBP, diastolic blood pressure; mod, moderate; SBP. systolic blood pressure; vig, vigorous.Source: Circulation. 2010;121:586–613.
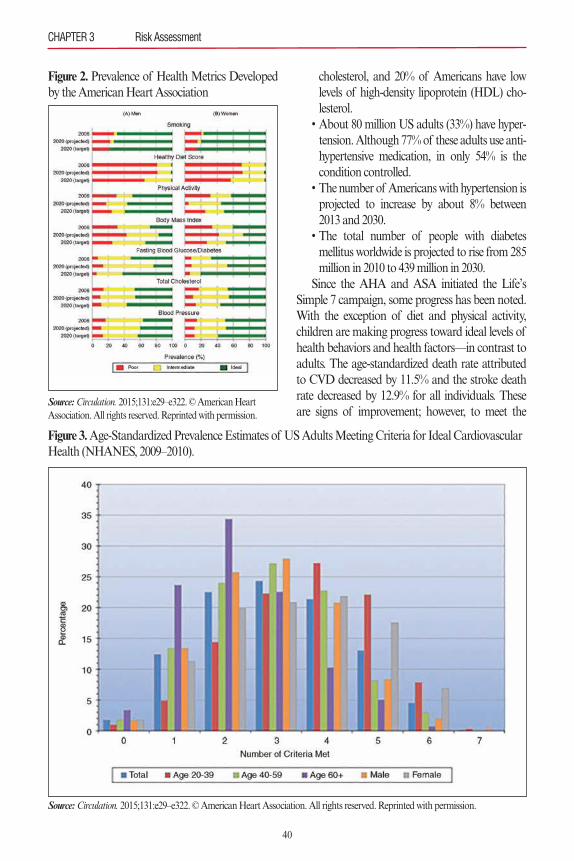
cholesterol, and 20% of Americans have lowlevels of high-density lipoprotein (HDL) cho-lesterol.• About 80 million US adults (33%) have hyper-tension. Although 77% of these adults use anti-hypertensive medication, in only 54% is thecondition controlled.• The number of Americans with hypertension isprojected to increase by about 8% between2013 and 2030.• The total number of people with diabetes mellitus worldwide is projected to rise from 285million in 2010 to 439 million in 2030. Since the AHA and ASA initiated the Life’s
Simple 7 campaign, some progress has been noted.With the exception of diet and physical activity,children are making progress toward ideal levels ofhealth behaviors and health factors—in contrast toadults. The age-standardized death rate attributedto CVD decreased by 11.5% and the stroke deathrate decreased by 12.9% for all individuals. Theseare signs of improvement; however, to meet the
CHAPTER 3 Risk Assessment
40
Figure 2. Prevalence of Health Metrics Developedby the American Heart Association
Source:Circulation. 2015;131:e29–e322. © American Heart Association. All rights reserved. Reprinted with permission.
Figure 3.Age-Standardized Prevalence Estimates of US Adults Meeting Criteria for Ideal CardiovascularHealth (NHANES, 2009–2010).
Source:Circulation. 2015;131:e29–e322. © American Heart Association. All rights reserved. Reprinted with permission.

target goal, diet quality, physical activity, and bodyweight metrics will need to change significantly, andall metrics will continue to require a major focus.The AHA and ASA emphasize the need for treat-ment of acute cardiovascular events as well as sec-ondary prevention through management of riskfactors and health behaviors.
Application to Clinical PracticeTo reduce the risk of medical emergencies in thedental office setting, it is recommended that dentalprofessionals obtain vital signs for all patients ateach appointment, including blood pressure, respi-rations, temperature, and pulse.5 If patients presentwith obvious signs of medical emergency (chestpain, shortness of breath, significantly elevatedpulse or hypertension, unilateral numbness, speechdisturbance, etc.), oral treatment should be deferredand immediate medical care sought, using emer-gency medical services (EMS) as needed. Heightand weight are additional forms of vital signs thatshould be measured, and cardiovascular healthassessment should be clearly addressed. Smokingshould also be assessed as part of the health history.If these factors raise concern, the next step inassessment is to perform the AHA/ASA My LifeCheckTM–Life’s Simple 7 risk assessment with thepatient. The assessment, which evaluates the riskfactors and health behaviors discussed earlier, takesapproximately 5 minutes to complete. The patientreceives a score from 1 to 10, with 10 representingan ideal heart score. The assessment can be per-formed in English or Spanish. Recommendationsare then made concerning next steps and goals forthe future, and patients are encouraged to repeatthe assessment to see if progress is made over time.The My Life CheckTM–Life’s Simple 7 assessmentcan be found online at www.heart.org/mylifecheck.Another assessment model, advocated in the
European Guidelines on Cardiovascular DiseasePrevention in Clinical Practice (version 2012), is theHeartScore® electronic risk assessment system.6
This system evolved from the earlier Systemic Coro-nary Risk Evaluation (SCORE) project used to pre-dict and manage risk of heart attack and stroke inEurope.7 The tool is based on the 2007 European
Guidelines on CVD Prevention and offers twoEuropean versions based on low-risk and high-riskmodels and risk charts. It is designed to provide agraphic picture of absolute CVD risk to helpaddress the benefits of preventive interventions. Theclinician can then discuss the impact of modifiablerisk factors and tailor health advice based on theindividual risk profile of the patient. HeartScore®can be accessed at www.heartscore.org.The dental professional can complete the Life’s
Simple 7 assessment or HeartScore® with thepatient and provide education about oral health,particularly periodontal health and its relationshipwith cardiovascular health. For example, a system-atic review conducted by the AHA Committee onRheumatic Fever, Endocarditis, and Kawasaki Dis-ease found that observational studies support a con-sistent association between periodontal disease andatheromatous diseases independent of known con-founders.8 Meta-analyses have been conducted per-taining to the association between atherosclerosisand periodontal disease. Meurman and colleaguesfound a 20% increase in the risk for CVD amongpatients with periodontal disease (95% confidenceinterval [CI]: 1.08–1.32) and a higher risk ratio forstroke, varying from 2.85 (95% CI: 1.78–4.56) to1.75 (95% CI: 1.08–2.81).9 Khader and associates10
reported relative risk estimates of 1.19 (95% CI: 1.08–1.32) whereas Vettore11 noted 1.15 (95%CI: 1.06–1.25). Helping patients appreciate that aconnection exits between cardiovascular and strokehealth and oral health, particularly periodontalhealth, is an important step in empowering them totake charge of their lifestyle behaviors and homeefforts to improve their general and oral health.
Diabetes MellitusKey ConsiderationsThe National Diabetes Statistics Report, 2014 esti-mate of diabetes prevalence in the United Statesnoted that 29.1 million people have diabetes, and 8.1million of these individuals do not know they havethe disease.12 Figure 4 illustrates the percentages ofindividuals diagnosed and undiagnosed with dia-betes and those whose condition is well managedversus uncontrolled. Further demonstrating the
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
41
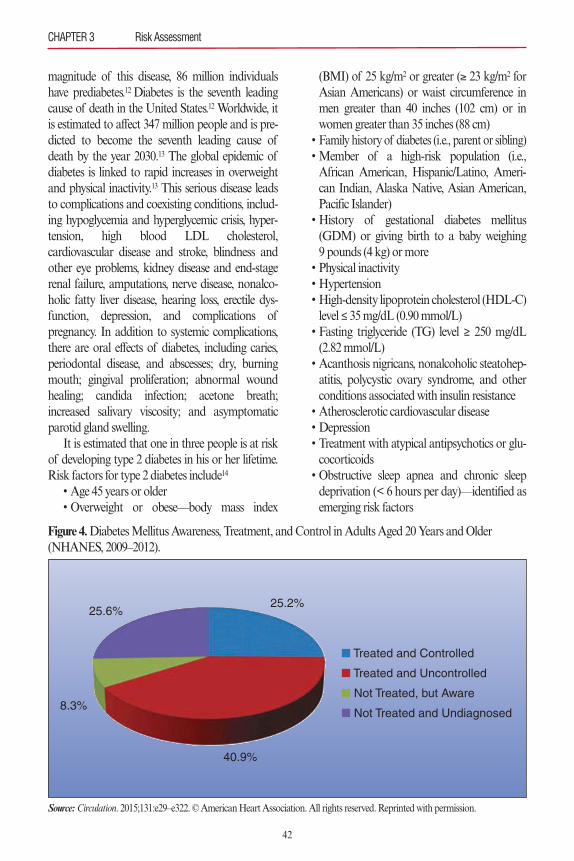
magnitude of this disease, 86 million individualshave prediabetes.12 Diabetes is the seventh leadingcause of death in the United States.12 Worldwide, itis estimated to affect 347 million people and is pre-dicted to become the seventh leading cause ofdeath by the year 2030.13 The global epidemic ofdiabetes is linked to rapid increases in overweightand physical inactivity.13 This serious disease leadsto complications and coexisting conditions, includ-ing hypoglycemia and hyperglycemic crisis, hyper-tension, high blood LDL cholesterol,cardiovascular disease and stroke, blindness andother eye problems, kidney disease and end-stagerenal failure, amputations, nerve disease, nonalco-holic fatty liver disease, hearing loss, erectile dys-function, depression, and complications ofpregnancy. In addition to systemic complications,there are oral effects of diabetes, including caries,periodontal disease, and abscesses; dry, burningmouth; gingival proliferation; abnormal woundhealing; candida infection; acetone breath;increased salivary viscosity; and asymptomaticparotid gland swelling.It is estimated that one in three people is at risk
of developing type 2 diabetes in his or her lifetime.Risk factors for type 2 diabetes include14
• Age 45 years or older• Overweight or obese—body mass index
(BMI) of 25 kg/m2 or greater (≥ 23 kg/m2 forAsian Americans) or waist circumference inmen greater than 40 inches (102 cm) or inwomen greater than 35 inches (88 cm)• Family history of diabetes (i.e., parent or sibling)• Member of a high-risk population (i.e.,African American, Hispanic/Latino, Ameri-can Indian, Alaska Native, Asian American,Pacific Islander)• History of gestational diabetes mellitus(GDM) or giving birth to a baby weighing 9 pounds (4 kg) or more • Physical inactivity• Hypertension• High-density lipoprotein cholesterol (HDL-C)level ≤ 35 mg/dL (0.90 mmol/L)• Fasting triglyceride (TG) level ≥ 250 mg/dL(2.82 mmol/L)• Acanthosis nigricans, nonalcoholic steatohep-atitis, polycystic ovary syndrome, and otherconditions associated with insulin resistance • Atherosclerotic cardiovascular disease• Depression• Treatment with atypical antipsychotics or glu-cocorticoids• Obstructive sleep apnea and chronic sleepdeprivation (< 6 hours per day)—identified asemerging risk factors
CHAPTER 3 Risk Assessment
42
Figure 4.Diabetes Mellitus Awareness, Treatment, and Control in Adults Aged 20 Years and Older(NHANES, 2009–2012).
Source: Circulation. 2015;131:e29–e322. © American Heart Association. All rights reserved. Reprinted with permission.
25.6%
8.3%
40.9%
25.2%
n Treated and Controlled
n Treated and Uncontrolled
n Not Treated, but Aware
n Not Treated and Undiagnosed
To address and reverse the high incidence andprevalence of type 2 diabetes, the National Dia-betes Education Program (NDEP) created “Guid-ing Principles for the Care of People With or atRisk for Diabetes” for healthcare professionals, keystakeholders, and patients. These principles arebriefly presented in Table 2, and can be reviewed indetail at http://ndep.nih.gov/hcp-businesses-and-schools/guiding-principles.15 These principlesdemonstrate that all healthcare providers, includingdentists and dental hygienists, can have a moreactive role in the detection and management ofpatients with diabetes, particularly type 2 diabetesmellitus.Further, the American Medical Association
(AMA) and the CDC partnered to create a toolkittitled “Prevent Diabetes STAT” (Screen, Test, Act-Today) as an immediate action because peoplewith prediabetes who are overweight are at risk fordeveloping type 2 diabetes within 5 years unlessthey lose weight. This toolkit is a guide for physi-cians and other healthcare providers as to the bestmethods to screen and refer high-risk patients todiabetes prevention programs in their communities.Dentists and dental hygienists interested in adopt-ing this program for patients with prediabetes canaccess the toolkit at www.cdc.gov/diabetes/preven-tion/pdf/STAT_toolkit.pdf. Online screening toolsare also available at www.preventdiabetesstat.org(patient screening) and www.cdc.gov/diabetes (pre-diabetes screening), the latter as part of the CDC’sNational Diabetes Prevention Program.Other risk-scoring algorithms have been devel-
oped for estimating diabetes risk and are summa-rized in the toolkit titled “Take Action to PreventDiabetes: A Toolkit for the Prevention of Type 2Diabetes in Europe.” This document is available atwww.idh.org. One of the featured risk assessmentsin this document—and highlighted in the “Guide-lines on Diabetes, Prediabetes, and CardiovascularDiseases: Executive Summary”16—is the FinnishDiabetes Risk Score (FINDRISC). This screeningdevice examines predictive variables such as age;BMI; waist circumference; use of antihypertensivetherapy; history of high blood glucose; physicalactivity; consumption of fruits, vegetables, and
berries; and family history of diabetes. The toolpredicts a 10-year risk of type 2 diabetes with 85%accuracy and detects current asymptomatic dia-betes and abnormal glucose tolerance.17–19 Individu-als screened and identified to be at high risk shouldhave subsequent glucose testing.
Application to Clinical PracticeTo reduce the risk of hypoglycemia or a hyper-glycemic crisis in the dental office, appointments forpatients with a known history of diabetes mellitusshould begin with a glucometer reading. Levels lessthan 70 mg/dL indicate hypoglycemia; commonsigns and symptoms include perspiration, confu-sion, anxiety, mood changes, tachycardia, hunger,and nausea. If the patient is conscious, a sugarsource such as candy, 4 ounces of fruit juice, or aglucose tablet can be offered. If the patient losesconsciousness, the dental provider should callEMS, provide basic life support, and administerintravenous 50% dextrose or intramuscularglucagon (1 mg). The best way to prevent hypo-glycemia is to remind patients to eat after takingtheir diabetes medication and to monitor their glu-cose before their appointment. If the patient is tak-ing insulin, it is important to inquire when the peakeffect of the specific insulin being used is likely tooccur and avoid scheduling appointments aroundthat time. For patients presenting with a glucometerreading of 300 mg/dL or greater, representing dangerous hyperglycemia, the dental provider isadvised to defer treatment, contact EMS, providebasic life support, and allow the EMS personnel togive necessary medication and treatment. Treat-ment can be resumed when the patient’s blood glu-cose is better controlled.Because diabetes and CVD are closely associat-
ed, a risk factor assessment is recommended foradult patients. The risk factors described earlier canbe generated into a screening form and used toidentify level of risk for type 2 diabetes. Patients canbe counseled to seek further evaluation with a med-ical specialist if multiple risk factors are identified.In addition, for patients unaware of their predia-betes or diabetes status, a screening test can beimplemented while the patient is in the reception
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
43
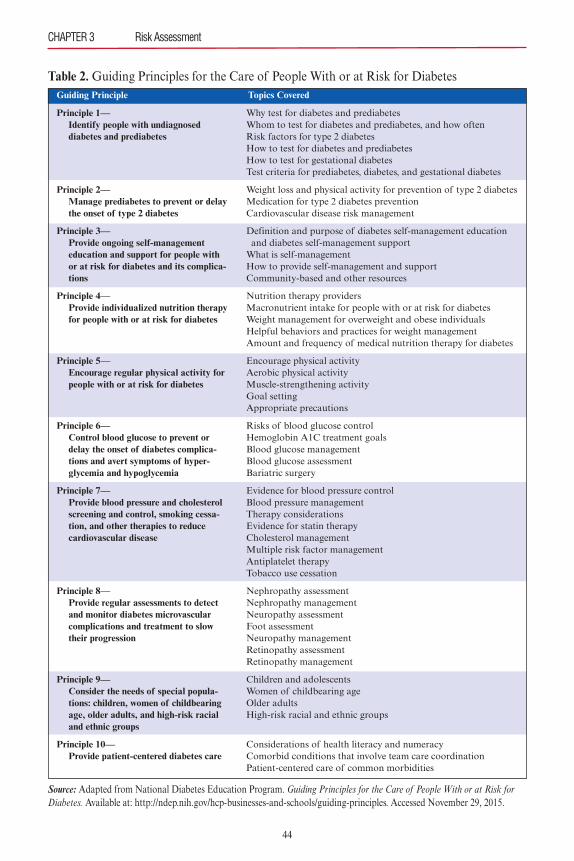
CHAPTER 3 Risk Assessment
44
Why test for diabetes and prediabetesWhom to test for diabetes and prediabetes, and how oftenRisk factors for type 2 diabetesHow to test for diabetes and prediabetesHow to test for gestational diabetesTest criteria for prediabetes, diabetes, and gestational diabetes
Weight loss and physical activity for prevention of type 2 diabetesMedication for type 2 diabetes preventionCardiovascular disease risk management
Definition and purpose of diabetes self-management education and diabetes self-management supportWhat is self-managementHow to provide self-management and supportCommunity-based and other resources
Nutrition therapy providersMacronutrient intake for people with or at risk for diabetesWeight management for overweight and obese individualsHelpful behaviors and practices for weight managementAmount and frequency of medical nutrition therapy for diabetes
Encourage physical activityAerobic physical activityMuscle-strengthening activityGoal settingAppropriate precautions
Risks of blood glucose controlHemoglobin A1C treatment goalsBlood glucose managementBlood glucose assessmentBariatric surgery
Evidence for blood pressure controlBlood pressure managementTherapy considerationsEvidence for statin therapyCholesterol managementMultiple risk factor managementAntiplatelet therapyTobacco use cessation
Nephropathy assessmentNephropathy managementNeuropathy assessmentFoot assessmentNeuropathy managementRetinopathy assessmentRetinopathy management
Children and adolescentsWomen of childbearing ageOlder adultsHigh-risk racial and ethnic groups
Considerations of health literacy and numeracyComorbid conditions that involve team care coordinationPatient-centered care of common morbidities
Principle 1—Identify people with undiagnosed diabetes and prediabetes
Principle 2—Manage prediabetes to prevent or delay the onset of type 2 diabetes
Principle 3—Provide ongoing self-management education and support for people with or at risk for diabetes and its complica-tions
Principle 4—Provide individualized nutrition therapy for people with or at risk for diabetes
Principle 5—Encourage regular physical activity for people with or at risk for diabetes
Principle 6—Control blood glucose to prevent or delay the onset of diabetes complica-tions and avert symptoms of hyper-glycemia and hypoglycemia
Principle 7—Provide blood pressure and cholesterol screening and control, smoking cessa-tion, and other therapies to reduce cardiovascular disease
Principle 8—Provide regular assessments to detect and monitor diabetes microvascular complications and treatment to slow their progression
Principle 9—Consider the needs of special popula-tions: children, women of childbearing age, older adults, and high-risk racial and ethnic groups
Principle 10—Provide patient-centered diabetes care
Guiding Principle Topics Covered
Table 2. Guiding Principles for the Care of People With or at Risk for Diabetes
Source: Adapted from National Diabetes Education Program. Guiding Principles for the Care of People With or at Risk forDiabetes. Available at: http://ndep.nih.gov/hcp-businesses-and-schools/guiding-principles. Accessed November 29, 2015.
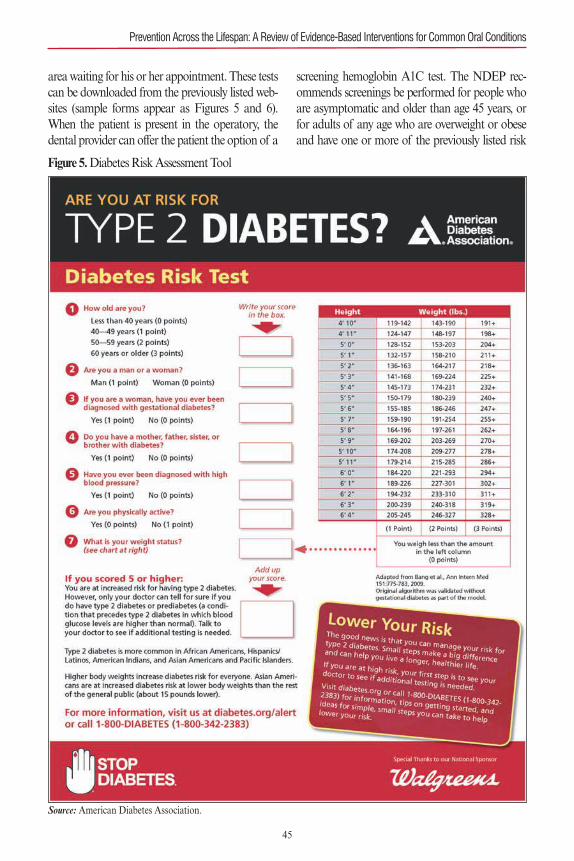
area waiting for his or her appointment. These testscan be downloaded from the previously listed web-sites (sample forms appear as Figures 5 and 6).When the patient is present in the operatory, thedental provider can offer the patient the option of a
screening hemoglobin A1C test. The NDEP rec-ommends screenings be performed for people whoare asymptomatic and older than age 45 years, orfor adults of any age who are overweight or obeseand have one or more of the previously listed risk
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
45
Figure 5.Diabetes Risk Assessment Tool
Source: American Diabetes Association.
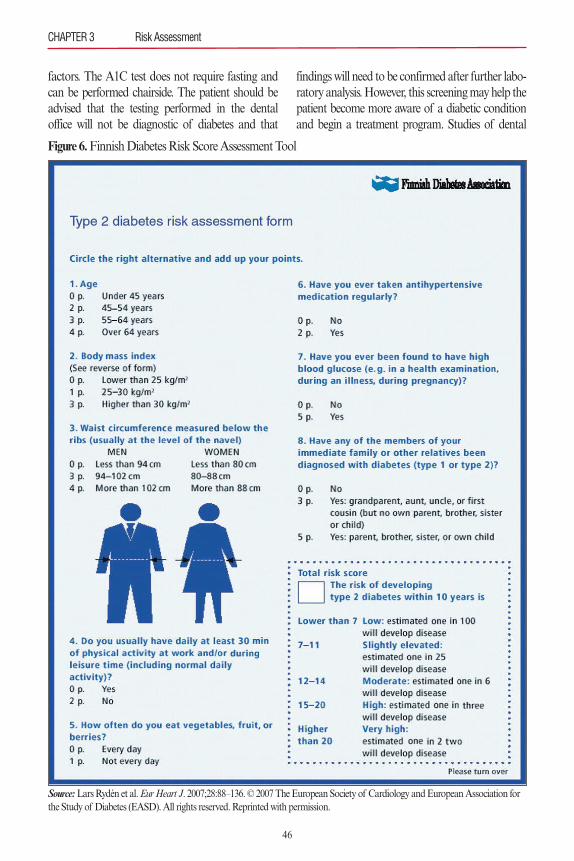
factors. The A1C test does not require fasting andcan be performed chairside. The patient should beadvised that the testing performed in the dentaloffice will not be diagnostic of diabetes and that
findings will need to be confirmed after further labo-ratory analysis. However, this screening may help thepatient become more aware of a diabetic conditionand begin a treatment program. Studies of dental
CHAPTER 3 Risk Assessment
46
Figure 6.Finnish Diabetes Risk Score Assessment Tool
Source:Lars Rydén et al. Eur Heart J. 2007;28:88–136. © 2007 The European Society of Cardiology and European Association forthe Study of Diabetes (EASD). All rights reserved.Reprinted with permission.
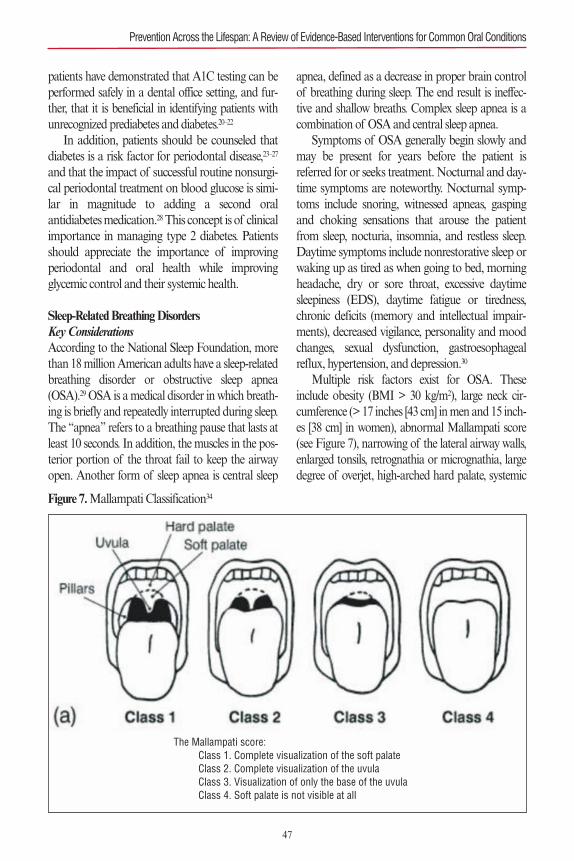
patients have demonstrated that A1C testing can beperformed safely in a dental office setting, and fur-ther, that it is beneficial in identifying patients withunrecognized prediabetes and diabetes.20–22
In addition, patients should be counseled thatdiabetes is a risk factor for periodontal disease,23–27
and that the impact of successful routine nonsurgi-cal periodontal treatment on blood glucose is simi-lar in magnitude to adding a second oralantidiabetes medication.28This concept is of clinicalimportance in managing type 2 diabetes. Patientsshould appreciate the importance of improvingperiodontal and oral health while improvingglycemic control and their systemic health.
Sleep-Related Breathing DisordersKey ConsiderationsAccording to the National Sleep Foundation, morethan 18 million American adults have a sleep-relatedbreathing disorder or obstructive sleep apnea(OSA).29 OSA is a medical disorder in which breath-ing is briefly and repeatedly interrupted during sleep.The “apnea” refers to a breathing pause that lasts atleast 10 seconds. In addition, the muscles in the pos-terior portion of the throat fail to keep the airwayopen. Another form of sleep apnea is central sleep
apnea, defined as a decrease in proper brain controlof breathing during sleep. The end result is ineffec-tive and shallow breaths. Complex sleep apnea is acombination of OSA and central sleep apnea.Symptoms of OSA generally begin slowly and
may be present for years before the patient isreferred for or seeks treatment. Nocturnal and day-time symptoms are noteworthy. Nocturnal symp-toms include snoring, witnessed apneas, gaspingand choking sensations that arouse the patientfrom sleep, nocturia, insomnia, and restless sleep.Daytime symptoms include nonrestorative sleep orwaking up as tired as when going to bed, morningheadache, dry or sore throat, excessive daytimesleepiness (EDS), daytime fatigue or tiredness,chronic deficits (memory and intellectual impair-ments), decreased vigilance, personality and moodchanges, sexual dysfunction, gastroesophagealreflux, hypertension, and depression.30
Multiple risk factors exist for OSA. Theseinclude obesity (BMI > 30 kg/m2), large neck cir-cumference (> 17 inches [43 cm] in men and 15 inch-es [38 cm] in women), abnormal Mallampati score(see Figure 7), narrowing of the lateral airway walls,enlarged tonsils, retrognathia or micrognathia, largedegree of overjet, high-arched hard palate, systemic
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
47
Figure 7.Mallampati Classification34
The Mallampati score:Class 1. Complete visualization of the soft palateClass 2. Complete visualization of the uvulaClass 3. Visualization of only the base of the uvulaClass 4. Soft palate is not visible at all

arterial hypertension (in approximately 50% ofpatients), congestive heart failure, pulmonary hyper-tension, stroke, metabolic syndrome, type 2 diabetesmellitus, alcohol consumption, smoking, and nasalcongestion.30–32 Further, due to increased risk forEDS, individuals with OSA are at increased risk formotor vehicle accidents.33
In their review of the literature on OSA, Korne-gay and Brame report that OSA is linked to multi-ple systemic diseases, most notably cardiovascularconditions such as hypertension, stroke, congestiveheart failure, cardiac arrhythmias, and myocardialinfarction.34 Further, OSA is associated with dia-betes mellitus, and with diminished quality of lifeand neurocognitive function.34Recent research sug-gests that the blood-brain barrier becomes morepermeable in OSA, which could contribute to braininjury and enhance or accelerate damage affectingmemory, mood, and cardiovascular risk, likely dueto reduction in oxygen from repeated breathinginterruptions. Although this study was conductedon a small sample, it suggests that treatment needsto focus on improving breathing in patients withOSA as well as repairing and improving blood-brain barrier function.35
Application to Clinical PracticeSeveral screening tools exist to assess patients forOSA. The STOP questionnaire36 is a brief tool thatcan easily be administered in the dental office set-ting (see Table 3). Patients who answer “yes” to twoor more questions are considered to be at high risk.Analysis of this screening tool revealed a moderate-ly high sensitivity and specificity.36 Another screen-ing tool is the STOP-Bang questionnaire, aneight-item instrument (see Table 4) that has a highprobability of OSA detection. If a patient answers“yes” to three or more items, he or she is consideredat high risk for OSA.37
As patients are evaluated for risk factors andeither of the above screening tools is completed, theyshould be counseled that research demonstrates anassociation between OSA and periodontitis37–39;therefore, a thorough periodontal evaluation is war-ranted. In light of the oral health concerns and sys-temic health risks, patients should give serious
consideration to seeking treatment for OSA andimproving their quality of life.
RISK ASSESSMENT FOR ORAL HEALTHOnce the comprehensive health history is complet-ed, the oral professional continues with a dentalhistory and evaluates the patient for oral diseaserisks. This section focuses on risks for oral healthdiseases, including oral cancer, caries, periodontaldisease, and xerostomia. Many of these problemsshare risk factors. Available screening tools are pre-sented so that oral professionals can utilize meas-ures to help their patients become aware of the riskfor serious oral conditions that impact their healthand quality of life, as well as ways to prevent orminimize risk.
Oral CancerKey ConsiderationsAccording to the American Cancer Society, an esti-mated 48,330 new cases of oral and pharyngeal
CHAPTER 3 Risk Assessment
48
Snoring Do you snore loudly?
Tired Do you often feel tired, fatigued, orsleepy during the daytime?
Observed Has anyone observed you stop breathing during your sleep?
Blood Pressure Do you have or are you being treated forhigh blood pressure?
Table 3.STOP Questionnaire36
Snoring Do you snore loudly?
Tired Do you often feel tired, fatigued,or sleepy during the daytime?
Observed Has anyone observed you stopbreathing during your sleep?
Blood Pressure Do you have or are you beingtreated for high blood pressure?
Basal Metabolic Index Is your BMI > 35 kg/m2?(BMI)
Age Are you older than 50 years?
Neck circumference Is your neck circumference > 40 cm?
Gender Are you male?
Table 4.STOP-Bang Questionnaire37
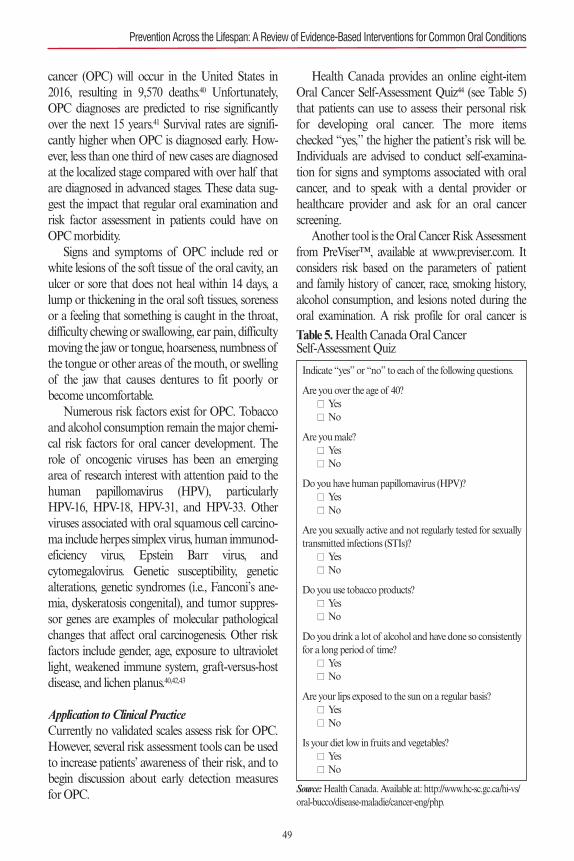
cancer (OPC) will occur in the United States in2016, resulting in 9,570 deaths.40 Unfortunately,OPC diagnoses are predicted to rise significantlyover the next 15 years.41 Survival rates are signifi-cantly higher when OPC is diagnosed early. How-ever, less than one third of new cases are diagnosedat the localized stage compared with over half thatare diagnosed in advanced stages. These data sug-gest the impact that regular oral examination andrisk factor assessment in patients could have onOPC morbidity.Signs and symptoms of OPC include red or
white lesions of the soft tissue of the oral cavity, anulcer or sore that does not heal within 14 days, alump or thickening in the oral soft tissues, sorenessor a feeling that something is caught in the throat,difficulty chewing or swallowing, ear pain, difficultymoving the jaw or tongue, hoarseness, numbness ofthe tongue or other areas of the mouth, or swellingof the jaw that causes dentures to fit poorly orbecome uncomfortable.Numerous risk factors exist for OPC. Tobacco
and alcohol consumption remain the major chemi-cal risk factors for oral cancer development. Therole of oncogenic viruses has been an emergingarea of research interest with attention paid to thehuman papillomavirus (HPV), particularly HPV-16, HPV-18, HPV-31, and HPV-33. Otherviruses associated with oral squamous cell carcino-ma include herpes simplex virus, human immunod-eficiency virus, Epstein Barr virus, andcytomegalovirus. Genetic susceptibility, geneticalterations, genetic syndromes (i.e., Fanconi’s ane-mia, dyskeratosis congenital), and tumor suppres-sor genes are examples of molecular pathologicalchanges that affect oral carcinogenesis. Other riskfactors include gender, age, exposure to ultravioletlight, weakened immune system, graft-versus-hostdisease, and lichen planus.40,42,43
Application to Clinical PracticeCurrently no validated scales assess risk for OPC.However, several risk assessment tools can be usedto increase patients’ awareness of their risk, and tobegin discussion about early detection measuresfor OPC.
Health Canada provides an online eight-itemOral Cancer Self-Assessment Quiz44 (see Table 5)that patients can use to assess their personal riskfor developing oral cancer. The more itemschecked “yes,” the higher the patient’s risk will be.Individuals are advised to conduct self-examina-tion for signs and symptoms associated with oralcancer, and to speak with a dental provider orhealthcare provider and ask for an oral cancerscreening.Another tool is the Oral Cancer Risk Assessment
from PreViser™, available at www.previser.com. Itconsiders risk based on the parameters of patientand family history of cancer, race, smoking history,alcohol consumption, and lesions noted during theoral examination. A risk profile for oral cancer is
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
49
Indicate “yes” or “no” to each of the following questions.
Are you over the age of 40?n Yesn No
Are you male?n Yesn No
Do you have human papillomavirus (HPV)?n Yesn No
Are you sexually active and not regularly tested for sexuallytransmitted infections (STIs)?
n Yesn No
Do you use tobacco products?n Yesn No
Do you drink a lot of alcohol and have done so consistentlyfor a long period of time?
n Yesn No
Are your lips exposed to the sun on a regular basis?n Yesn No
Is your diet low in fruits and vegetables?n Yesn No
Table 5.Health Canada Oral Cancer Self-Assessment Quiz
Source:Health Canada. Available at: http://www.hc-sc.gc.ca/hi-vs/oral-bucco/disease-maladie/cancer-eng/php.

50
created based on a scale of 1 to 5 (less risk to morerisk), and preventive treatment options the patientshould consider—pertaining to visits to the dentist,oral cancer screening examinations, alcohol use,and family cancer history—are provided. Addi-tional online cancer resources are included as partof the risk assessment for patients seeking moreinformation.Philips has created the CARE (Customizable
Assessment and Risk Evaluator) Tools to help den-tal professionals identify patients at risk for oral dis-eases and develop plans for preventing andmanaging oral conditions across the lifespan.Among these is the six-step Oral Pathology CARETool. Step 1 is a patient interview that includes asection related to disease indicators, a section focus-ing on risk factors, and a section on protective fac-tors. Step 2 is an assessment of risk, which rangesfrom low to moderate, high, or extreme. Step 3involves review of clinical guidelines based on theidentified risk category. In step 4, the clinicianselects a protocol based on the risk profile of thepatient. A customized protocol is created anddownloaded for the patient in step 5. Topics to bediscussed may include biopsy, HPV susceptibilitytesting, routine screenings, additional follow-up,other instructions, counseling, and lifestyle habits.Step 6 encompasses any other product recommen-dations, questions, and answers. Additional infor-mation about the Oral Pathology CARE Tool canbe found at www.philipsoralhealthcare.com.
CariesKey ConsiderationsDental caries remains one of the most seriouschronic oral health conditions across the lifespan.At epidemic proportions, caries is the most chronicinfection of children.45 The National Institute ofDental and Craniofacial Research provides sum-maries of the National Health and NutritionExamination Survey (NHANES) data collectedbetween 1999 and 2004. Key findings for dentalcaries follow.46
• Among children 2 to 11 years of age, 42%have had dental caries in their primary teeth,and 23% have untreated dental caries.
• Among children 6 to 11 years of age, 21%have had dental caries in their permanentteeth, and 8% have untreated dental caries.• Among adolescents 12 to 19 years of age, 59%have had dental caries in their permanentteeth, and 20% have untreated caries.• Among adults 20 to 64 years of age, 92% havehad dental caries in their permanent teeth,and 26% have untreated caries.• Among seniors 65 years of age and older, 93%have had dental caries in their permanentteeth, and 15% have untreated caries.• Black and Hispanic subgroups and those withlower incomes and less education have hadmore caries and more untreated primary andpermanent teeth.
Signs and symptoms of dental caries include pain,sensitivity, visible pits in tooth surfaces, and brownor white lesions on tooth surfaces. Risk factors fordental caries have been studied in developed anddeveloping countries. A systematic review of the lit-erature and pediatric clinical practice guidelineshave identified the following risk factors for dentalcaries in children and adolescents: diet, fluorideexposure, microflora (Streptococcus mutans, Lacto-bacillus), level of education, a susceptible host, oralhygiene, parental oral health, enamel hypoplasia,and social, cultural, and behavioral factors.47,48
Applications to Clinical PracticeThe American Academy of Pediatric Dentistry’sClinical Practice Guidelines include risk assessmenttools for children from birth to 3 years of age forphysicians and other nondental healthcareproviders, a caries-risk assessment tool for thosefrom birth through 5 years of age for dentalproviders (see Table 6), and a caries risk assessmentform for children 6 years of age and older for dentalprofessionals (see Table 7).48 These forms were devel-oped based on available evidence and incorporatebiological risk factors, protective factors, and clinicalfindings from examination. Risk is classified as low,moderate, and high. Caries management protocolsare provided within the Clinical Practice Guidelinesfor each risk category pertaining to diagnostics, pre-ventive interventions, and restorative care. These
CHAPTER 3 Risk Assessment
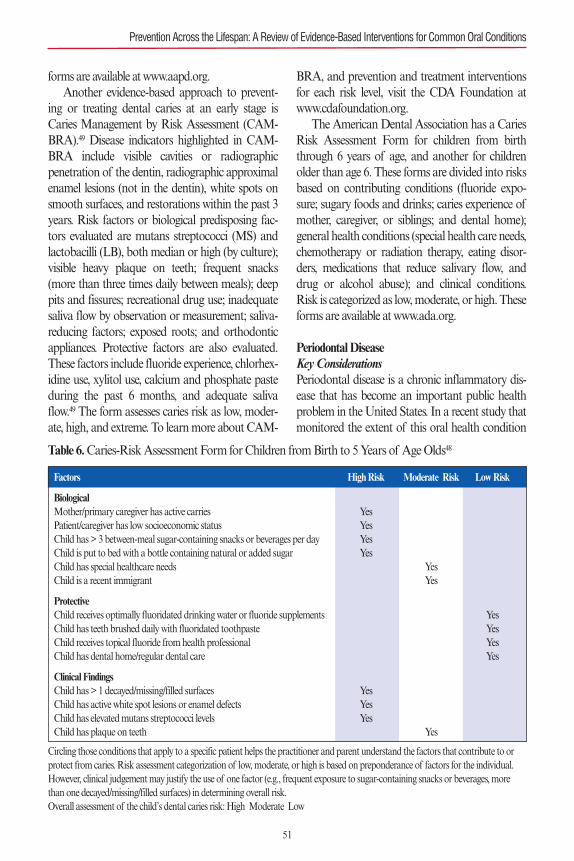
forms are available at www.aapd.org.Another evidence-based approach to prevent-
ing or treating dental caries at an early stage isCaries Management by Risk Assessment (CAM-BRA).49 Disease indicators highlighted in CAM-BRA include visible cavities or radiographicpenetration of the dentin, radiographic approximalenamel lesions (not in the dentin), white spots onsmooth surfaces, and restorations within the past 3years. Risk factors or biological predisposing fac-tors evaluated are mutans streptococci (MS) andlactobacilli (LB), both median or high (by culture);visible heavy plaque on teeth; frequent snacks(more than three times daily between meals); deeppits and fissures; recreational drug use; inadequatesaliva flow by observation or measurement; saliva-reducing factors; exposed roots; and orthodonticappliances. Protective factors are also evaluated.These factors include fluoride experience, chlorhex-idine use, xylitol use, calcium and phosphate pasteduring the past 6 months, and adequate salivaflow.49 The form assesses caries risk as low, moder-ate, high, and extreme. To learn more about CAM-
BRA, and prevention and treatment interventionsfor each risk level, visit the CDA Foundation atwww.cdafoundation.org.The American Dental Association has a Caries
Risk Assessment Form for children from birththrough 6 years of age, and another for childrenolder than age 6. These forms are divided into risksbased on contributing conditions (fluoride expo-sure; sugary foods and drinks; caries experience ofmother, caregiver, or siblings; and dental home);general health conditions (special health care needs,chemotherapy or radiation therapy, eating disor-ders, medications that reduce salivary flow, anddrug or alcohol abuse); and clinical conditions.Risk is categorized as low, moderate, or high. Theseforms are available at www.ada.org.
Periodontal DiseaseKey ConsiderationsPeriodontal disease is a chronic inflammatory dis-ease that has become an important public healthproblem in the United States. In a recent study thatmonitored the extent of this oral health condition
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
51
Factors High Risk Moderate Risk Low Risk
BiologicalMother/primary caregiver has active carries YesPatient/caregiver has low socioeconomic status YesChild has > 3 between-meal sugar-containing snacks or beverages per day YesChild is put to bed with a bottle containing natural or added sugar YesChild has special healthcare needs YesChild is a recent immigrant Yes
ProtectiveChild receives optimally fluoridated drinking water or fluoride supplements YesChild has teeth brushed daily with fluoridated toothpaste YesChild receives topical fluoride from health professional YesChild has dental home/regular dental care Yes
Clinical FindingsChild has > 1 decayed/missing/filled surfaces YesChild has active white spot lesions or enamel defects YesChild has elevated mutans streptococci levels YesChild has plaque on teeth Yes
Table 6.Caries-Risk Assessment Form for Children from Birth to 5 Years of Age Olds48
Circling those conditions that apply to a specific patient helps the practitioner and parent understand the factors that contribute to orprotect from caries. Risk assessment categorization of low, moderate, or high is based on preponderance of factors for the individual.However, clinical judgement may justify the use of one factor (e.g., frequent exposure to sugar-containing snacks or beverages, morethan one decayed/missing/filled surfaces) in determining overall risk. Overall assessment of the child’s dental caries risk: High Moderate �Low
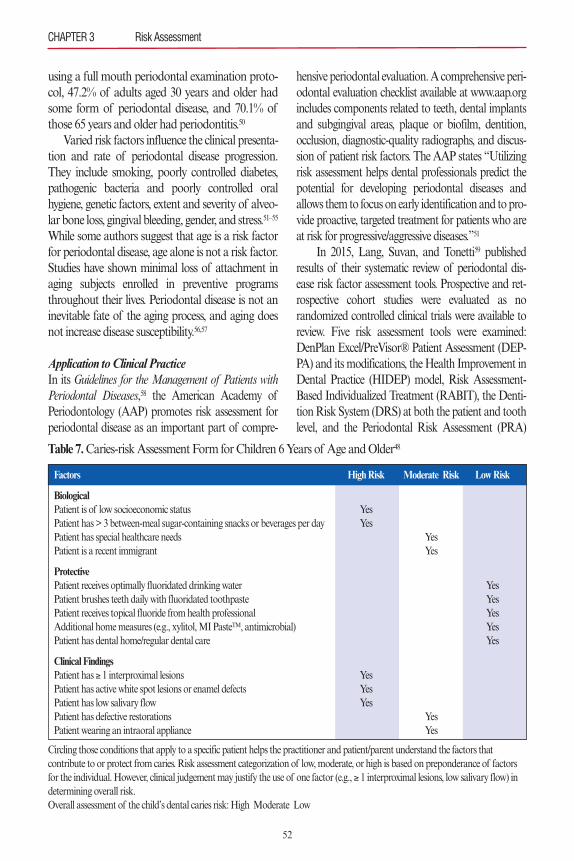
using a full mouth periodontal examination proto-col, 47.2% of adults aged 30 years and older hadsome form of periodontal disease, and 70.1% ofthose 65 years and older had periodontitis.50
Varied risk factors influence the clinical presenta-tion and rate of periodontal disease progression.They include smoking, poorly controlled diabetes,pathogenic bacteria and poorly controlled oralhygiene, genetic factors, extent and severity of alveo-lar bone loss, gingival bleeding, gender, and stress.51–55
While some authors suggest that age is a risk factorfor periodontal disease, age alone is not a risk factor.Studies have shown minimal loss of attachment inaging subjects enrolled in preventive programsthroughout their lives. Periodontal disease is not aninevitable fate of the aging process, and aging doesnot increase disease susceptibility.56,57
Application to Clinical PracticeIn its Guidelines for the Management of Patients withPeriodontal Diseases,58 the American Academy ofPeriodontology (AAP) promotes risk assessment forperiodontal disease as an important part of compre-
hensive periodontal evaluation. A comprehensive peri-odontal evaluation checklist available at www.aap.orgincludes components related to teeth, dental implantsand subgingival areas, plaque or biofilm, dentition,occlusion, diagnostic-quality radiographs, and discus-sion of patient risk factors. The AAP states “Utilizingrisk assessment helps dental professionals predict thepotential for developing periodontal diseases andallows them to focus on early identification and to pro-vide proactive, targeted treatment for patients who areat risk for progressive/aggressive diseases.”51
In 2015, Lang, Suvan, and Tonetti59 publishedresults of their systematic review of periodontal dis-ease risk factor assessment tools. Prospective and ret-rospective cohort studies were evaluated as norandomized controlled clinical trials were available toreview. Five risk assessment tools were examined:DenPlan Excel/PreVisor® Patient Assessment (DEP-PA) and its modifications, the Health Improvement inDental Practice (HIDEP) model, Risk Assessment-Based Individualized Treatment (RABIT), the Denti-tion Risk System (DRS) at both the patient and toothlevel, and the Periodontal Risk Assessment (PRA)
52
CHAPTER 3 Risk Assessment
Factors High Risk Moderate Risk Low Risk
BiologicalPatient is of low socioeconomic status YesPatient has > 3 between-meal sugar-containing snacks or beverages per day YesPatient has special healthcare needs YesPatient is a recent immigrant Yes
ProtectivePatient receives optimally fluoridated drinking water YesPatient brushes teeth daily with fluoridated toothpaste YesPatient receives topical fluoride from health professional YesAdditional home measures (e.g., xylitol, MI PasteTM, antimicrobial) YesPatient has dental home/regular dental care Yes
Clinical Findings Patient has ≥ 1 interproximal lesions YesPatient has active white spot lesions or enamel defects YesPatient has low salivary flow YesPatient has defective restorations YesPatient wearing an intraoral appliance Yes
Table 7.Caries-risk Assessment Form for Children 6 Years of Age and Older48
Circling those conditions that apply to a specific patient helps the practitioner and patient/parent understand the factors that contribute to or protect from caries. Risk assessment categorization of low, moderate, or high is based on preponderance of factorsfor the individual. However, clinical judgement may justify the use of one factor (e.g., ≥ 1 interproximal lesions, low salivary flow) indetermining overall risk. Overall assessment of the child’s dental caries risk: High Moderate Low �

and its modifications. The authors noted that themajority of these tools are variations of the Periodon-tal Risk Calculator (PRC) and the PRA. Findingsshowed that periodontitis progression and tooth lossmight be predicted based on risk using these tools;however, no data were available on the impact of riskassessment and patient management. The authorsreported that the PRA and its modifications have beenvalidated on multiple occasions and that this tool hasapplicability for clinical practice.Lang and Tonetti60 introduced the PRA in 2003. It
uses six vectors weighted equally to evaluate thepatient’s risk for susceptibility and progression of peri-odontal disease. These parameters are percentage ofbleeding on probing, prevalence of pockets greaterthan 4 mm, loss of teeth from a total of 28 teeth, lossof periodontal support in relation to the patient’s age,systemic and genetic conditions, and environmentalfactors such as smoking. Each parameter has its ownscale for minor-, moderate-, and high-risk profiles. Thediagram is shaped like a spider web and the shape ofthe web changes as specific areas of risk increase. ThePRA can be accessed at www.perio-tools.com.The Periodontal Assessment Tool, part of the Oral
Health Information Suite from www.previser.com, isan online tool designed to create a periodontal diagno-sis and risk score for future disease. A report is pre-pared for the clinician’s documentation and for thepatient. Parameters reviewed include history of smok-ing, diabetes status, prior periodontal treatment, prob-ing depth and bleeding in each quadrant, and estimateof bone loss. Risk scores range from 1 (lowest risk) to5 (highest risk). The disease state score ranges from 1(health) to 100 (severe periodontitis).61 Studies havevalidated that the risk scores calculated by the Peri-odontal Assessment Tool predicted future periodontalstatus with a high level of accuracy.62,63
XerostomiaKey ConsiderationsSaliva plays an important role in oral health. Itserves as a lubricant for the oral cavity and offersprotective functions, providing antimicrobial activi-ty, control of pH, and remineralization, and main-taining the integrity of the oral mucosa. Inaddition, saliva has a mechanical cleansing action.
Without these actions, individuals would be at anincreased risk for developing oral diseases such ascaries, periodontal disease, and fungal infections.Hyposalivation is the decreased flow of saliva
that may result in xerostomia (dry mouth). Xeros-tomia is often referred to as a subjective sensation.64
Current estimates of xerostomia and hyposaliva-tion based on epidemiological studies are unavail-able, but older studies emphasize widespreadcomplaints of oral dryness among the general pop-ulation with increases among the elderly.65Negativeconsequences of hyposalivation with xerostomia, inaddition to increased risk for oral diseases, includedifficulty eating, swallowing, speaking, sleeping,and wearing prostheses; impaired social function;and decreased quality of life.65
Multiple risk factors are associated with hypos-alivation with xerostomia. The primary risk factoris the use of prescription and nonprescription med-ications. Other risk factors include sex (more com-mon in women versus men), smoking, diabetes,autoimmune disorders (Sjögren’s syndrome),radioactive iodine treatment for thyroid malignan-cy, and anxiety.43
Application to Clinical PracticeThere are currently no validated risk assessmenttools for xerostomia. However, the ADHA has cre-ated a Screening Tool for Hyposalivation withXerostomia66 (see Figure 8) designed to help detectthe presence of disease and its nature. The screen-ing tool comprises a questionnaire and clinicalexamination by which the practitioner identifies arisk level of low, moderate, or high. Planning andimplementation options are provided for each levelof risk.66 Further evaluation of this instrument iswarranted to establish its validity and utility as ascreening tool.
SUMMARYRisk assessment provides dental professionals anopportunity to strengthen their understanding ofthe patient’s health profile prior to providingplanned interventions. As this chapter emphasizes,multiple tools are available that can be used toassess systemic and oral health. Some of these
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
53
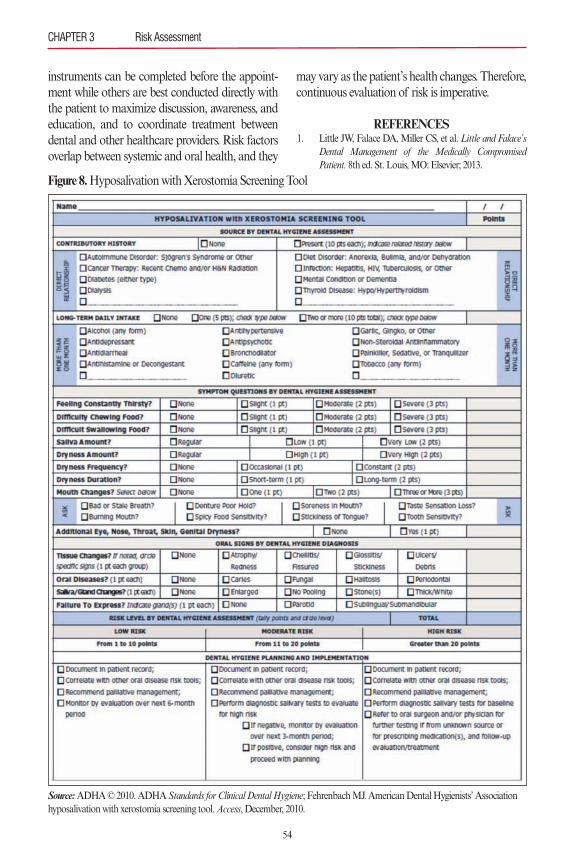
instruments can be completed before the appoint-ment while others are best conducted directly withthe patient to maximize discussion, awareness, andeducation, and to coordinate treatment betweendental and other healthcare providers. Risk factorsoverlap between systemic and oral health, and they
may vary as the patient’s health changes. Therefore,continuous evaluation of risk is imperative.
REFERENCES1. Little JW, Falace DA, Miller CS, et al. Little and Falace’s
Dental Management of the Medically CompromisedPatient. 8th ed. St. Louis, MO: Elsevier; 2013.
54
CHAPTER 3 Risk Assessment
Figure 8.Hyposalivation with Xerostomia Screening Tool
Source:ADHA © 2010. ADHA Standards for Clinical Dental Hygiene; Fehrenbach MJ. American Dental Hygienists’ Associationhyposalivation with xerostomia screening tool. Access, December, 2010.
2. American Dental Hygienists’ Association. Standards forClinical Dental Hygiene Practice. Chicago, IL: AmericanDental Hygienists’ Association; 2008.
3. Mozaffarian D, Benjamin EJ, Go AS, et al. on behalf ofthe American Heart Association Statistics Committeeand Stroke Statistics Committee. Heart disease and strokestatistics—2015 update: a report from the AmericanHeart Association. Circulation. 2015;131:e29–e322.
4. World Health Organization. Cardiovascular disease(CVDs). Fact sheet No. 317. Available at:http://www.who.int/mediacentre/factsheets/fs317/en/.Accessed February 27, 2016.
5. Pickett FA, Gurenlian JR. Preventing Medical Emergen-cies: Use of the Medical History in Dental Practice. 3rd ed.Baltimore, MD: Wolters Kluwer Health; 2015.
6. Perk J, Backer GD, Gohike H, et al. European Guidelineson cardiovascular disease prevention in clinical practice(version 2012). Eur Heart J. 2012;33:1635–1701.
7. Conroy RM, Pyörälä K, Fitzgerald AP, et al. Estimationof a ten-year risk of fatal cardiovascular disease inEurope: The SCORE project. Eur Heart J. 2003;24:987–1003.
8. Lockhart PB, Bolger AF, Papapanou PN, et al. AmericanHeart Association Rheumatic Fever, Endocarditis, andKawasaki Disease Committee of the Council on Cardio-vascular Disease in the Young, Council on Epidemiologyand Prevention, Council on Peripheral Vascular Disease,and Council on Clinical Cardiology. Periodontal diseaseand atherosclerotic vascular disease: does the evidencesupport an independent association? A scientific state-ment from the American Heart Association. Circulation.2012;125:2520–2544.
9. Meurman JF, Sanz M, Janket SJ. Oral health, atheroscle-rosis and cardiovascular disease. Crit Rev Oral Biol Med.2004;15:403–413.
10. Khader YS, Albashaiereh ZS, Alomari MA. Periodontaldiseases and the risk of coronary heart and cerebrovasculardiseases: a meta-analysis. J Periodontol. 2004;75:1046–1053.
11. Vettore MS. Periodontal disease and cardiovascular dis-ease. Evid Based Dent. 2004;5:69.
12. Centers for Disease Control and Prevention. NationalDiabetes Statistics Report: Estimates of Diabetes and ItsBurden in the United States, 2014. Atlanta, GA: U.S.Department of Health and Human Services; 2014.
13. World Health Organization. 10 facts about diabetes.Available at: http://ww.who.int/features/factfiles/diabetes/facts/en/. Accessed February 27, 2016.
14. National Diabetes Education Program. Risk factors fortype 2 diabetes. Available at: http://ndep.nih.gov/hcp-busi-nesses-and-schools/guiding-principles/principles-01-idenify-undiagnosed-diabetes-and-prediabetes-aspx.Accessed November 29, 2015.
15. National Diabetes Education Program. Guiding princi-ples for the care of people with or at risk for diabetes.Available at: http://ndep.nih.gov/hcp-businesses-and-schools/guiding-principles. Accessed November 29, 2015.
16. Rydén L, Standl E, Bartnik M, et al. Guidelines on dia-betes, prediabetes, and cardiovascular diseases: executivesummary. Eur Heart J. 2007;28:88–136.
17. Lindstrom J, Tuomilehto J. The diabetes risk score: a prac-tical tool to predict type 2 diabetes risk. Diabetes Care.2003;26:725–731.
18. Saaristo T, Peltonen M, Lindstrom J, et al. Cross-sectionalevaluation of the Finnish Diabetes Risk Score: a tool toidentify undetected type 2 diabetes, abnormal glucose tol-erance and metabolic syndrome. Diab Vasc Dis Res.2005;2:67–72.
19. De Berardis G, Pellegrini F, Franciosi M, et al. Longitudi-nal assessment of quality of life in patients with type 2diabetes and self-reported erectile dysfunction. DiabetesCare. 2005;28:2637–2643.
20. Lalla E, Kunzel C, Burkett S, et al. Identification ofunrecognized diabetes and prediabetes in a dental setting.J Dent Res. 2011:29;90:855–860.
21. Genco R, Schifferle R, Dunford R, et al. Screening fordiabetes mellitus in dental practices: a field trial. J AmDent Assoc. 2014:145:57–64.
22. Wolff R, Wolff L, Michalowicz B. A pilot study of glyco-sylated hemoglobin levels in periodontitis cases andhealthy controls. J Clin Periodontol. 2009:80:1057–1061.
23. Bossart M, Calley KH, Gurenlian JR, et al. HBA1Cchairside screening for diabetes in patients with chronicperiodontitis. Int J Dent Hyg. Mar 2015; Mar 23. [Epubahead of print.]
24. Mealey BL, Ocampo GL. Diabetes mellitus and peri-odontal disease. Periodontol 2000. 2007;44:127–153.
25. Lamster IB, Lalla E, Borgnakke WS, et al. The relation-ship between oral health and diabetes mellitus. J Am DentAssoc. 2008;139(suppl):19S–24S.
26. Taylor GW, Borgnakke WS. Periodontal disease associa-tions with diabetes, glycemic control and complications.Oral Dis. 2008;14:191–203.
27. Taylor GW, Manz MC, Borgnakke WS. Diabetes, peri-odontal diseases, dental caries, and tooth loss: a review ofthe literature. Compend Contin Educ Dent. 2004;24:179–184, 186–178, 190.
28. Bornakke WS. Hyperglycemia/diabetes mellitus and peri-odontal infection adversely affect each other. In: GencoRJ, Williams RC, eds. Periodontal Disease and OverallHealth: A Clinician’s Guide. 2nd ed. Yardley, PA: Profes-sional Audience Communication, Inc; 2014:99–122.
29. National Sleep Foundation. Sleep apnea. Available at:http://sleepfoundation.org/sleepdosrders-problems/sleep-apnea. Accessed December 5, 2015.
30. Downey R. Obstructive sleep apnea. Available at:http://emedicine.medscape.com/article295807. AccessedDecember 5, 2015.
31. Lee W, Nagubadi S, Kryger MD, et al. Epidemiology ofobstructive sleep apnea: a population-based perspective.Expert Rev Respir Med. 2008;2:349–364.
32. Seo WH, Cho ER, Thomas RJ, et al. The associationbetween periodontitis and obstructive sleep apnea: a pre-
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
55
liminary study. J Periodontal Res. 2012;48:500–506.33. Levendowski DJ, Olmstead R, Popovic D, et al. Assess-
ment of obstructive sleep apnea risk and severity in truckdrivers: validation of a screening questionnaire. SleepDiagnosis Ther. 2007;2(2):20–26.
34. Kornegay EC, Brame JL. Obstructive sleep apnea and therole of dental hygienists. J Dent Hyg. 2015;89:286–292.
35. Palomares JS, Tummala S, Wang D, et al. Water exchangeacross the blood-brain barrier in obstructive sleep apnea:an MRI diffusion-weighted pseudo-continuous arterialspin labeling study. J Neuroimaging. 2015;25:900–905.
36. Chung F, Yegneswaran B, Lia P, et al. STOP question-naire: a tool to screen patients for obstructive sleep apnea.Anesthesiology. 2008;108:812–821.
37. Ahmad NE, Sanders AE, Sheats R, et al. Obstructivesleep apnea in association with periodontitis: a case-con-trol study. J Dent Hyg. 2013;87:188–199.
38. Gunaratnam K, Taylor B, Curtis B, et al. Obstructivesleep apnea and periodontitis: a novel association? SleepBreath. 2009;13:233–239.
39. Seo W, Cho ER, Thomas RJ, et al. The associationbetween periodontitis and obstructive sleep apnea: a pre-liminary study. J Periodont Res. 2012;48:500–506.
40. American Cancer Society. Cancer Facts & Figures 2016.Atlanta, GA: American Cancer Society; 2016.
41. Laronde DM. Oral cancer and the dental hygienist: mak-ing a difference and saving lives. Can J Dent Hyg.2014;48:5–6.
42. Ram H, Sarkar J, Kumar H, et al. Oral cancer: risk factorsand molecular pathogenesis. J Maxillofac Oral Surg.2011;10:132–137.
43. Regezi JA, Sciubba JJ, Jordan RCK. Oral Pathology: Clini-cal Pathologic Correlations. 5th ed. St. Louis, MO: Saun-ders; 2008.
44. Health Canada. Healthy living. Oral health. Oral diseases.Available at: http://www.hc-sc.gc.ca/hi-vs/oral-bucco/ dis-ease-maladie/cancer-eng/php. Accessed December 6, 2015.
45. Colak H, Dülgergil CT, Dalli M, Hamidi MM. Earlychildhood caries update: A review of causes, diagnoses, andtreatments. J Nat Sci Biol Med. 2013;4:29–38.
46. National Institute of Dental and Craniofacial Research.Dental caries. Available at http://www.nidc.nih.gov/DataS-tatistics/FindDataByTopic/DentalCaries/htm. AccessedDecember 9, 2015.
47. Harris R, Nicoll AD, Adair PM, et al. Risk factors for den-tal caries in young children: a systematic review. Communi-ty Dental Health. 2004;21(suppl):71–85.
48. American Academy of Pediatric Dentistry, Council onClinical Affairs. Guidelines on caries-risk assessment andmanagement for infants, children, and adolescents. PediatrDent. 2014;37(6):132–139.
49. Featherstone JD, Domejean-Orliaguet S, Jenson L, et al.Caries risk assessment in practice for age 6 through adult. JCalif Dent Assoc. 2007;35:703–713.
50. Eke PI, Dye BA, Wei L, et al. Prevalence of periodontitis inadults in the United States: 2009 and 2010. J Dent Res.2012;91:914–920.
51. American Academy of Periodontology. American Acade-my of Periodontology statement on risk assessment. Avail-able at: http://www.aap.org. Accessed December 9, 2015.
52. van Winkelhoff AJ, Bosch-Tijhof CJ, Winkel EG, et al.Smoking affects the subgingival microflora in periodontitis.J Periodontol. 2001;72:666–671.
53. Demmer RT, Jacobs DR Jr, Desvarieux M. Periodontaldisease and incident type 2 diabetes: results from the firstNational Health and Nutrition Examination Survey andits epidemiologic follow-up survey. Diabetes Care.2008;31:1371–1379.
54. Michalowicz BS, Diehl SR, Gonsolley JC, et al. Evidenceof a substantial genetic basis for risk of adult periodontitis.J Periodontol. 2000;71;1699–1707.
55. Linden GJ, Mullally BH, Freeman R. Stress and the pro-gression of periodontal disease. J Clin Periodontol.1996;23:675–680.
56. Brown LJ, Oliver RC, Loe H. Evaluating periodontal sta-tus of US employed adults. J Am Dent Assoc.1990;121:226–232.
57. Novak KF, Novak MJ. Clinical risk assessment. In: New-man MG, Takei HN, Klokkevold PE, et al. Carranza’s Clin-ical Periodontology. 12th ed. St. Louis, MO: Elsevier; 2015.
58. American Academy of Periodontology. Guidelines for themanagement of patients with periodontal diseases. J Peri-odontol. 2006;77:1607–1611.
59. Lang NP, Suvan JE, Tonetti MS. Risk factor assessmenttools for the prevention of periodontitis progression a system-atic review. J Clin Periodontol. 2015:42(suppl 16):S59–S70.
60. Lang NP, Tonetti MS. Periodontal risk assessment (PRA)for patients in supportive periodontal therapy (SPT). OralHealth Prev Dent. 2003;1:7–16.
61. Page RC, Martin JA, Loeb CF. The Oral Health Informa-tion Suite (OHIS): its use in the management of periodon-tal disease. J Dent Ed. 2005:69:509–520.
62. Page RC, Krall EA, Martin JA, et al. Validity and accuracyof a risk calculator in predicting periodontal disease. J AmDent Assoc. 2002;133:569–576.
63. Page RC, Martin JA, Krall EA, et al. Longitudinal valida-tion of a risk calculator for periodontal disease. J Clin Peri-odontol. 2003;30:819–827.
64. Fehrenbach MJ, Phelan JA, Ibsen OAC. Immunity andimmunologic oral lesions. In: Ibsen OAC, Phelan JA. OralPathology for the Dental Hygienist. 6th ed. St. Louis, MO:Elsevier; 2014:78–113.
65. Turner MD, Ship JA. Dry mouth and its effects on the oralhealth of elderly people. J Am Dent Assoc.2007;138(suppl):15S–20S.
66. Fehrenbach MJ. American Dental Hygienists’ Associationhyposalivation with xerostomia screening tool. Access.December 22–25, 2010.
CHAPTER 3 Risk Assessment
56

Dental caries has an interesting association withwealth. Human skulls from various periods in histo-ry show tooth decay when the subject could affordluxury foods. More specifically, diets with a highintake of refined sugars were associated with toothdecay. Today, this pattern is noticed in emergingeconomies. Improving economics may lead to ashift in dietary patterns and allow opportunities toconsume a healthier diet, but often the diet is alsomore cariogenic. Additionally, the necessaryimprovement in attention to oral health often lagsbehind. This may result in a dramatic increase indental caries in youngsters. (See Box 1.) However,increasing wealth also enables people to affordproper dental care, and gradually this drives thedesire to keep a dentition that is “worth being seen.”Generally speaking, a society and its role models setthe norms that dictate the behavior of individuals.
Without question this applies to choices in dentistry,such as the choice of orthodontics based on aesthet-ics rather than functionality, a wish to bleach teeth,and a preference for white fillings and porcelain-coated crowns and bridges.
Several decades ago, a full denture was the treat-ment option preferred by many patients, as keepingone’s own teeth was considered neither feasible noraffordable. In a population where most individualsover a particular age were edentulous, having a den-ture was not a stigma, as it probably is today. Theexpectation of keeping one’s teeth in a functionaland aesthetically acceptable state spread graduallyamong the population. This development wasimportant in setting the research priorities for pre-ventive dentistry. It meant that prevention becamean issue for all age groups, expanding beyond chil-dren and young adults to include the elderly.
A pivotal question still concerns the preferredscheme for caries prevention in patients older than30 years of age. Toothbrushing—more specificallytoothbrushing with a fluoridated toothpaste—developed as the norm over the past 50 years. How-ever, few data evaluating successful additional toolsfor caries prevention in middle-aged and olderadults are available as most efficacy studies involvedschoolchildren. Although it is tempting to general-ize these findings to older patients, it should benoted that oral physiology changes with age. Thisapplies in particular to elderly patients, who general-ly take multiple forms of medication or suffer from
57
Dental Caries
Chapter 4
J.M. (“Bob”) ten Cate and Erik R. Roskam
A B
Box 1.Dental Caries: Still a Worldwide Problem
Figures 1A and B show two examples of extreme tooth decay in the primary dentition: one fromSouth America, the other from Europe. One is from an area with high living standards and easilyaccessible, properly funded dental care. The other is from an area with poor dietary habits and ade-quate dental care only for the happy few. Can you see a difference?
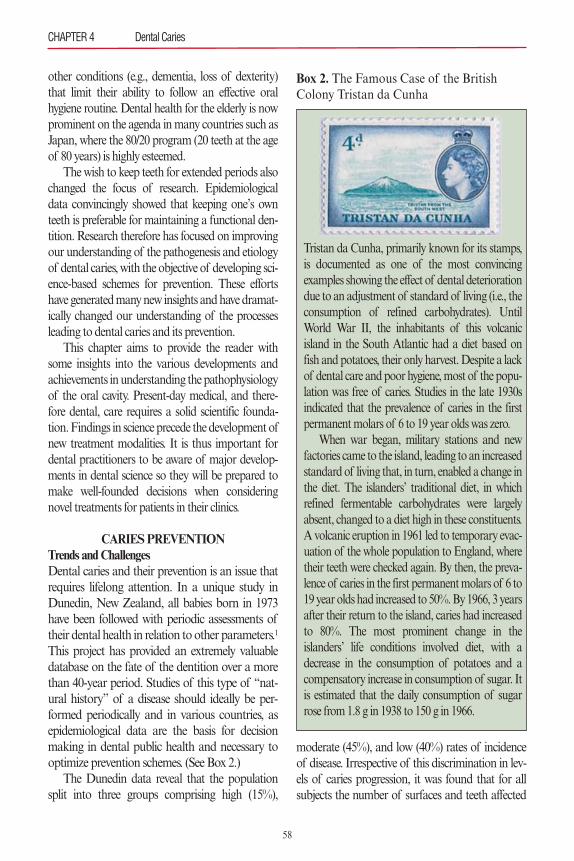
other conditions (e.g., dementia, loss of dexterity)that limit their ability to follow an effective oralhygiene routine. Dental health for the elderly is nowprominent on the agenda in many countries such asJapan, where the 80/20 program (20 teeth at the ageof 80 years) is highly esteemed.
The wish to keep teeth for extended periods alsochanged the focus of research. Epidemiologicaldata convincingly showed that keeping one’s ownteeth is preferable for maintaining a functional den-tition. Research therefore has focused on improvingour understanding of the pathogenesis and etiologyof dental caries, with the objective of developing sci-ence-based schemes for prevention. These effortshave generated many new insights and have dramat-ically changed our understanding of the processesleading to dental caries and its prevention.
This chapter aims to provide the reader withsome insights into the various developments andachievements in understanding the pathophysiologyof the oral cavity. Present-day medical, and there-fore dental, care requires a solid scientific founda-tion. Findings in science precede the development ofnew treatment modalities. It is thus important fordental practitioners to be aware of major develop-ments in dental science so they will be prepared tomake well-founded decisions when consideringnovel treatments for patients in their clinics.
CARIES PREVENTIONTrends and ChallengesDental caries and their prevention is an issue thatrequires lifelong attention. In a unique study inDunedin, New Zealand, all babies born in 1973have been followed with periodic assessments oftheir dental health in relation to other parameters.1
This project has provided an extremely valuabledatabase on the fate of the dentition over a morethan 40-year period. Studies of this type of “nat-ural history” of a disease should ideally be per-formed periodically and in various countries, asepidemiological data are the basis for decisionmaking in dental public health and necessary tooptimize prevention schemes. (See Box 2.)
The Dunedin data reveal that the populationsplit into three groups comprising high (15%),
moderate (45%), and low (40%) rates of incidenceof disease. Irrespective of this discrimination in lev-els of caries progression, it was found that for allsubjects the number of surfaces and teeth affected
CHAPTER 4 Dental Caries
58
Box 2. The Famous Case of the BritishColony Tristan da Cunha
Tristan da Cunha, primarily known for its stamps,is documented as one of the most convincingexamples showing the effect of dental deteriorationdue to an adjustment of standard of living (i.e., theconsumption of refined carbohydrates). UntilWorld War II, the inhabitants of this volcanicisland in the South Atlantic had a diet based onfish and potatoes, their only harvest. Despite a lackof dental care and poor hygiene, most of the popu-lation was free of caries. Studies in the late 1930sindicated that the prevalence of caries in the firstpermanent molars of 6 to 19 year olds was zero.
When war began, military stations and newfactories came to the island, leading to an increasedstandard of living that, in turn, enabled a change inthe diet. The islanders’ traditional diet, in whichrefined fermentable carbohydrates were largelyabsent, changed to a diet high in these constituents.A volcanic eruption in 1961 led to temporary evac-uation of the whole population to England, wheretheir teeth were checked again. By then, the preva-lence of caries in the first permanent molars of 6 to19 year olds had increased to 50%. By 1966, 3 yearsafter their return to the island, caries had increasedto 80%. The most prominent change in theislanders’ life conditions involved diet, with adecrease in the consumption of potatoes and acompensatory increase in consumption of sugar. Itis estimated that the daily consumption of sugarrose from 1.8 g in 1938 to 150 g in 1966.

by or treated for caries increased with time. Thisrate of increase was obviously lowest in the lowcaries subgroup. These data also prove that caries isnot a disease limited to childhood or adolescence.On this point it should be noted that with progress-ing age many surfaces received new restorations,which presumably were larger (i.e., included addi-tional surfaces) than the original restorations. In thehigh caries group, by the age of 38 years, the aver-age value on the Decayed, Missing, Filled Surfaces(DMFS) Index was 50, compared with 8 in the lowcaries group.1
For various reasons it is of interest to furtherconsider these findings. The studied populationgrew up in a period when fluoride toothpastes hadjust become widely available and were, in fact, wide-ly used. However, the prevailing procedures in den-tal practice were largely still oriented to earlyrestoration. It is interesting to speculate what thedata would have shown if a more restrictive surgicaltreatment policy had been followed.
From clinical trials on fluoride efficacy, such asthe Tiel-Culemborg drinking water fluoride studyperformed in the 1960s and 1970s, we know thatlesions are arrested or even reversed as a result ofusing fluoride.2 The fact that early lesions may rem-ineralize or be arrested requires that practitionersmaintain a policy of “watchful waiting” and bevery restrictive in placing restorations. This “mod-ern” type of operative dentistry focusing on nonop-erative interventions (often referred to as anonoperative caries treatment program [NOCTP])is still not common practice throughout the world.A large-scale clinical study was very successfullyperformed at the Danish municipality of Nexo;since then this method is often referred to as theNexo approach.3 The NOCTP approach evaluatedat Nexo is based on four pillars: (1) dental educa-tion of children and caretakers; (2) intensive train-ing of these individuals in maintaining oral hygiene,with a focus on the quality of hygienic practice; (3)early nonrestorative interventions based on earlydetection of signs of disease; and (4) individuallydetermined recall schemes based on caries riskassessment. This approach has many similaritieswith minimally invasive dentistry.
Dental caries is more than just cavities. Numer-ous studies have identified the stages that precede theformation of a cavity. In particular, when fluoride isavailable it takes several years before a sound surfaceis cavitated. During this period both patient anddentist should be made aware of surfaces in the den-tition that appear to be at particular risk. The studyof the pathogenesis of dental caries has demonstrat-ed that the early stages of caries are characterized bya preferential dissolution of tooth mineral fromweak spots in the tissue, at both the microscopic andmacroscopic level. During an average day, when apatient consumes sugars, several periods of dissolu-tion of the teeth occur. When, at the end of such aspecific episode, all sugars are fermented and acidsare neutralized by saliva, the physiology returns to astable situation with calcium phosphates being rede-posited from saliva into the damaged areas. Thisremineralization process is enhanced in the presenceof fluoride. However, it should be noted that thisremineralization is typically up to 10 times slowerthan the preceding demineralization. Practically, thisimplies that about 5 hours of remineralization areneeded to repair a 30-minute demineralizationepisode. It is also clear that a pattern of continuousconsumption of cariogenic food will impair the pos-sibility for a fluoride-enhanced “natural” repair.Simply stated, there is a limit to fluoride efficacy incaries prevention. This is important to remember aspatients (and dentists) often think that brushing witha fluoride toothpaste makes the teeth strong andable to withstand cariogenic snacking.
A focus on early caries prevention and reversalis also reflected in novel methods of early detectionof caries, both to assess the state of disease in thehard tissue (level of demineralization of enameland dentin) and characteristics of the dental plaquethat might result in caries. Using such methods,caries can be detected long before it has progressedinto a cavity, or can even be identified in the averagedental practice. Firstly, it is possible to see earlycaries as white spot lesions after removal of plaque,drying the surface, and proper illumination of thesites at risk. Secondly, more advanced techniquesinvolving a change in the optical properties ofenamel have been developed. One of these optical
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
59
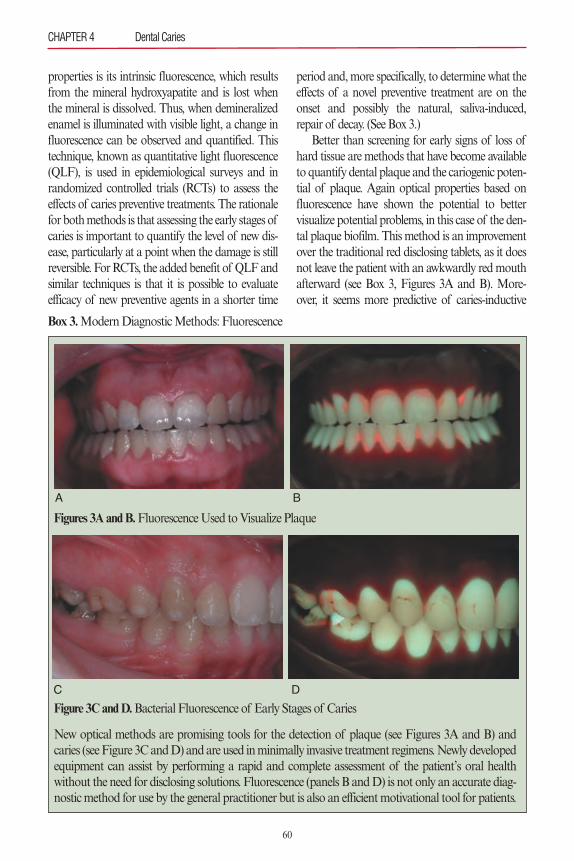
properties is its intrinsic fluorescence, which resultsfrom the mineral hydroxyapatite and is lost whenthe mineral is dissolved. Thus, when demineralizedenamel is illuminated with visible light, a change influorescence can be observed and quantified. Thistechnique, known as quantitative light fluorescence(QLF), is used in epidemiological surveys and inrandomized controlled trials (RCTs) to assess theeffects of caries preventive treatments. The rationalefor both methods is that assessing the early stages ofcaries is important to quantify the level of new dis-ease, particularly at a point when the damage is stillreversible. For RCTs, the added benefit of QLF andsimilar techniques is that it is possible to evaluateefficacy of new preventive agents in a shorter time
period and, more specifically, to determine what theeffects of a novel preventive treatment are on theonset and possibly the natural, saliva-induced,repair of decay. (See Box 3.)
Better than screening for early signs of loss ofhard tissue are methods that have become availableto quantify dental plaque and the cariogenic poten-tial of plaque. Again optical properties based onfluorescence have shown the potential to bettervisualize potential problems, in this case of the den-tal plaque biofilm. This method is an improvementover the traditional red disclosing tablets, as it doesnot leave the patient with an awkwardly red mouthafterward (see Box 3, Figures 3A and B). More-over, it seems more predictive of caries-inductive
CHAPTER 4 Dental Caries
60
A B
C D
Box 3.Modern Diagnostic Methods: Fluorescence
New optical methods are promising tools for the detection of plaque (see Figures 3A and B) andcaries (see Figure 3C and D) and are used in minimally invasive treatment regimens. Newly developedequipment can assist by performing a rapid and complete assessment of the patient’s oral healthwithout the need for disclosing solutions. Fluorescence (panels B and D) is not only an accurate diag-nostic method for use by the general practitioner but is also an efficient motivational tool for patients.
Figures 3A and B.Fluorescence Used to Visualize Plaque
Figure 3C and D.Bacterial Fluorescence of Early Stages of Caries

plaque. It is foreseeable that this optical phenome-non can be employed in smart tools to be used bydentists, and patients, as motivation for better oralhygiene.4
The Dunedin study, a new classic in oral epi-demiology, is very informative about changes inoral health in an age cohort as it passes throughstages in life. Other interesting data are obtainedfrom cohorts at a given age in time. The WorldHealth Organization has chosen particular agegroups for this purpose. Using this database,countries may be compared and their respectivesuccess in implementing oral care improvementprograms can be evaluated. The past 40 yearshave, by and large, shown a significant improve-ment in oral health: average levels of diseasedecreased, and the number of individuals withoutdisease increased. Despite the overall success ofreduced caries levels, there are indications thatimprovements in oral health have halted and mayhave been somewhat reversed.5 This trend hasbeen reported for countries that initially showedthe largest reductions in caries. It is unknownwhether this pattern will continue or spread toother countries. Additional data are needed to fur-ther our understanding of what contributed toslowing of improvement in the caries rate.
Paradigm Shifts in EtiologyOral bacteria have been the subject of study foralmost four centuries. In 1674, Antony vanLeeuwenhoek used one of the first microscopes toobserve dental plaque. Some later findings werealready hinted at in his early correspondence withthe Royal Society of Medicine, such as the acid sus-ceptibility of the small “creatures” he was observ-ing. The role of acids produced by bacteria wasalso the basis for the theories on dental caries thatwere described by W.D. Miller in the last decade ofthe nineteenth century. Still, the study of bacteriol-ogy and oral microbiology remained very similar interms of the methods used to identify bacteria: bac-teria were cultured on various types of agar mediathat enabled a phenotypic discrimination betweenspecies. The discovery of antibiotics obviously ledto a major improvement in health, as infectious dis-
eases were no longer the most common cause ofdeath early in life.
A major breakthrough in microbiology tookplace a few decades ago with the introduction ofvarious methods enabling manipulation of DNA,and the development of techniques to analyze andcharacterize the genomes of species. Around thetime that the human genome was decoded, the firstDNA sequences of bacteria were reported. Thismade it possible to link specific genes to physiologi-cal properties, and allowed a more comprehensiveapproach to understanding the bacterial world. Astriking finding was that numerous bacteria identi-fied by their DNA had never been isolated usingthe traditional culturing method. A practical conse-quence was that bacteria could be assessed “deador alive.” Even in prehistoric samples it becamepossible to search for traces of life, including bacte-ria. As a result of these DNA methods, the taxono-my (“name giving”) of bacteria changed: bacteriathat were previously considered to be related wererepositioned in the phylogenic tree of life. As it wasnow possible to study specific genes, the research ofstructure and function of bacterial communitiescould go to a higher, “supra-species,” level.
Bacteria provide vital components of thehuman physiology. It takes courage to accept that90% of the cells in our body are bacterial cells. Wewould never survive without bacteria living in asymbiotic relationship with us and inside us. Thepivotal survival strategy for humans is withoutquestion to encourage and cherish the beneficialbacteria and to fight the pathogenic ones! Still, themost prevalent diseases in the oral cavity are causedby bacteria. These diseases could be classified asinfectious diseases—although typically infectiousdiseases are caused by pathogenic bacteria that arenot part of the normal, commensal bacterial flora.
Various hypotheses have been proposed overtime to explain the etiology of dental caries. In the1970s, the intellectual fight was between groups ofscientists who supported the specific versus thenonspecific plaque hypothesis. Briefly, they asked:Is it the volume of plaque or the presence of certainbacteria in the plaque that is responsible for the dis-solution of the dental hard tissues? A decade later,
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
61

Marsh and Bradshaw (reviewed in 1993) formulat-ed a compromise in the now widely accepted eco-logical plaque hypothesis.6 The essence of thistheory is that ecological changes, in particular theconsumption of large amounts of fermentable car-bohydrates (sugars), lead to an intense acidificationof dental plaque. This, in turn, results in a shift inmicrobial composition of dental plaque with anincrease of those bacteria that survive periods ofhigh acidity (i.e., low pH). These so-called aciduricbacteria usually also form high amounts of acid.Collectively this implies that changes in bacterialcomposition shift the natural balance betweendemineralization (dissolution) and remineralization(repair) to an overall loss of tooth tissue, eventuallyleading to cavitation. A similar reasoning can bemade to explain the enrichment of plaque withbacteria that are associated with infections of thegingival tissues.
Although the ecological plaque hypothesisfocused research efforts to better understand thecauses of oral disease, several points merit mentionand remain the topics of current investigations. Itwas found that species other than the “arch-crimi-nal of caries,” Streptococcus mutans, were able toform large amounts of acids and, more important-ly, survive in the acidic environment they create.With DNA-based methods, the oral cavity wasstudied in great detail and thousands of differentbacterial species were identified in a group of about100 people.7 A separate study showed that varioussites in the mouth differ in bacterial composition,with notable differences seen among saliva, soft tis-sues of the tongue and gingiva, and tooth surfaces.A quick analysis of saliva, therefore, is not a goodindicator of the bacterial load at various sites thatare at risk for caries or periodontal disease. Themicrobial variability is far greater than the classical-ly reported difference between supra- and subgingi-val plaque.
The oral cavity also provided nine sites that weresampled in the large Human Microbiome Project,in which an inventory was made of the bacterialflora of the total human body.8 A consequence ofthis generic approach to study bacteria andbiofilms was that the oral cavity as habitat for bac-
terial communities was chosen to address funda-mental research issues by colleagues from outsidethe traditional oral/dental research field. The oralbiofilms of dental plaque are very similar in struc-ture and function when compared with otherbiofilms. This finding holds promise because dis-coveries derived from biofilms in nature may haveapplicability to the prevention of oral diseases.
Our deepened understanding of the livingmicroscopic world in our mouths has alreadyresulted in paradigm shifts in caries etiology thathave implications for practical prevention. Forinstance, it is now accepted that, beyond the use ofchemotherapeutic agents, preventive efforts shouldconsider routes to attain a healthy microbiome.Research groups that study the microbiome from amore foundational perspective should be able todevise creative approaches that hit “bad” bacteriaat their weakest spots and encourage “good” bacte-ria that help to foster health. Another insight con-cerns the interplay between bacteria and othermicroscopic species, such as fungi and viruses, aswell as interactions with the host. This microworld,which is now slowly being disclosed, is governed bycomplex signaling systems between the variouscomponents. As described later in this chapter, thisinformation has translational potential.
Evidence for Efficacy: Focus on FluorideFor the past 40 years, prevention of dental carieshas centered around fluoride, in various forms ofapplication. The discovery of fluoride was a classicexample of serendipity. Dentist Frederick McKay,a careful observer, noticed that although the teethof his patients were stained, they also had lower lev-els of tooth decay when compared with patients insimilar communities elsewhere in the country. Ittook several decades before the cause of this “fluo-rosis” and the associated reduced levels of dentalcaries was unravelled and effective caries preventionagents were formulated. In the early 1970s, fluoridetoothpastes became available, marking the onset ofsignificant reductions in tooth decay.
Numerous RCTs were completed to quantifythe effects of various preventive products. Thesestudies focused on the type of fluoride in a paste or
CHAPTER 4 Dental Caries
62

rinse, the fluoride level, and the effects of otheradditives. As is generally done, the results of thesestudies were combined in meta-analyses in whichdata from individual studies were critically recon-sidered and combined. This procedure is followedto overcome the risk of accidentally positive or neg-ative outcomes. The conclusions are then oftendocumented in the Cochrane CollaborationLibrary. This comprehensive evaluation confirmedthat fluoride toothpastes are highly effective incaries prevention. Additional benefits were foundfrom using fluoride gels and rinses.9 Theoreticalconsiderations led to a consensus that fluoride ismainly active though a localized effect in the oralcavity. This implied that fluoride, brought into themouth during toothbrushing, is most effectivewhen given with “high” frequency—that is, prefer-ably at least twice daily. This mode of action speaksagainst the use of fluoride tablets and other formsof fluoride administration in which fluoride is pres-ent only transiently in the oral cavity. Understand-ing how a treatment works is essential, given thecurrent emphasis on evidence-based treatments or,in general, evidence-based medicine. For any typeof medical, and thus dental, treatment, rigorousand scrutinized data should be available before it isused in patients.
CARIES RISK ASSESSMENT AND NON-FLUORIDE INTERVENTIONS
In recent years there has been increasing supportfor a more restrictive, truly conserving, approachin restorative dentistry. The rationale is that plac-ing a filling is the irreversible start of a series of re-restorations that, in time, increase the risk oflosing the whole tooth. A decision to place arestoration means having “lost the battle” as aresult of inadequate prevention to safeguard therespective tooth against decay. The Dunedin studycited earlier in this chapter provides irrefutabledata that invasive treatment gradually leads tomore surfaces being restored or teeth being lost.With this in mind, research has focused on evalu-ating nonoperative anticaries approaches in con-junction with a caries risk assessment. One of thepromising approaches has been the Caries Man-
agement by Risk Assessment (CAMBRA) initia-tive. Based on this principle, several clinical studieshave now been reported. In high-risk adults, Chaf-fee and colleagues studied three types of anticariesagents.10 The study design encompassed separategroups in which the protocol followed a single orrepeated delivery of agents, and a no-additionscontrol group. The three treatments chosen were0.12% chlorhexidine gluconate, 5,000 ppm fluo-ride toothpaste or varnish, and xylitol products.The study revealed that the one-time deliverygroup had similar caries scores as the controlgroup that followed the basic dental care. Howev-er, the group that received the repeated, spaceddelivery showed a significantly higher anticariesbenefit, with on average one additional restorationbeing prevented in every three subjects during the18 months of the study.
Encouraged by the success of fluoride, consid-erable efforts were taken to find other agents thatcould positively influence the demineralization–remineralization balance. Remineralization isenhanced by low levels of fluoride in the oral flu-ids. However, calcium and phosphate also arerequired to form new hydroxyapatite. Calciumand phosphate additions have been researched inseveral chemical forms, notably tricalcium phos-phate, calcium glycerophosphate, and nanopartic-ulate hydroxyapatite. Currently, information islimited and none of these additions has reachedthe level of a thorough Cochrane review with apositive recommendation. Of particular interesthave been products based on casein phosphopep-tide–amorphous calcium phosphate (CPP-ACP).The rationale for developing this compound wasthat the milk-derived CPP binds high levels of cal-cium and phosphate in an amorphous form.Accumulation of CPP-ACP in dental plaqueincreases the calcium and phosphate levels, whichmay then be expected to increase mineral deposi-tion as a remineralization of enamel. Numerouspapers have focused on elucidating the mode ofaction of CPP-ACP and, more recently, determin-ing the clinical efficacy of CPP-ACP–based prod-ucts. In spite of this extensive research, a reviewrecently concluded that there is a lack of evidence
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
63

to support the use of products based on this tech-nology at this time.11 The authors suggest that fur-ther, well-designed RCTs are needed before thereis widespread recommendation of these productsfor the prevention and treatment of early dentalcaries in the general population.
NOVEL APPROACHES: A FOCUS ON THE PLAQUE BIOFILM
The stagnation in the improvement of oral health,mentioned earlier, has intensified efforts in cariolo-gy research to find new antimicrobial agents. Suchcompounds should have an effect additive to fluo-ride. The rationale is that fluoride is primarilyeffective in enhancing the remineralization of earlycaries lesions and, in general, the mineral–tissuereactions. For patients with a cariogenic lifestyle(i.e., too-frequent snacking), the deleterious effectof numerous acid attacks on the teeth cannot becounteracted by remineralization. Various studieshave confirmed that no more than about six cario-genic meals or snacks can still be repaired by (fluo-ride-enhanced) remineralization from saliva.12
The new information about the dental plaquebiofilm, and bacteria in general, has led to promis-ing new approaches for interfering with the bacte-rial etiology of caries.13 In general, theseencompass the new insights of biofilm properties.Some of these routes are described in the nextparagraphs. One of the perplexing questions inunderstanding life in a biofilm has been how it ispossible for so many different bacteria to livetogether in a crowded environment. From studieson individual species it is evident that bacteria arevery different in terms of optimal growth condi-tions and growth rates. Why, then, is dental plaquenot dominated by a particular species that out-grows all the others? One explanation is that bac-teria possess smart signaling systems. Amongthese, the quorum sensing system is vital to enablebacteria to sense neighboring species. When acolony begins to exceed a particular density, thebacteria adjust their physiology in a way thatallows all to survive—a very intelligent approachthat humans can only dream about! With ourknowledge of the quorum sensing system, and
more specifically the tools to control (shut off) thissystem, we could upset the balanced bacterial lifein a biofilm. Initial experiments have shown thatthis will result in reduced overall bacterial growthin the treated biofilms. Bacteria also shareadvanced metabolic networks. The metabolicwaste of one species is food for another. Again, ifreactions in this network are impaired, it will leadto a buildup of intermediate products and a meta-bolic congestion with effects similar to overloadedhighways on Friday afternoon!
Another possible approach centers on the ques-tion, can we modify the bacterial composition ofour biofilms? In principle this is difficult as thebiofilm composition is the result of a long historicevolution. Fortunately, a bacterial invader, often apathogen, is not easily accepted in a bacterial com-munity. This so-called colonization resistance servesan important purpose for the host (us, in this case):Without it, we would be more often struck bypathogens and the resultant bacterial infections.Despite this protective mechanism, selected bacte-ria may be taken up in biofilms and assume a rolein the overall physiology. (See Box 4.)
The role of probiotics in affecting the bacterialflora in the gut is a classic example. Probiotics aremicroorganisms that are believed to providehealth benefits when consumed. Commonlyclaimed benefits include a decrease in potentiallyharmful gastrointestinal microorganisms, reduc-tion of gastrointestinal discomfort, and strength-ening of the immune system. There is anecdotalevidence that individuals who regularly take pro-biotics have a higher life expectancy. With respectto oral diseases, some studies have shown a limitedbenefit when schoolchildren drank milk withadded probiotics, or used probiotics in anotherform. As there have also been negative study out-comes, the final verdict for probiotics in oralhealth is still pending. Of historic interest is therelated Replacement Theory, which was first pro-posed in the 1970s. Hillman and colleagues modi-fied Streptococcus mutans to reduce its acidogenicpotential and added other features to the genometo give it an ecological advantage.14 Eventually thisapproach was abandoned as the many legal
CHAPTER 4 Dental Caries
64

restrictions for this type of genetic modificationmade it too difficult to pursue. Other investigatorshave studied bacteria that selectively eliminatepathogens, which might be called “predator bacte-ria.” The discovery that bacteria can now be man-ufactured by introducing selected genes hasundoubtedly great potential but is, in terms of itsapplications, still in the realm of science fiction.
A potentially more promising approachinvolves prebiotics. Prebiotics are chemicals thatinduce the growth or activity of bacteria and fungithat contribute to the well-being of their host.Stated more simply, these are not bacteria butrather food for bacteria. Dental caries is caused byacids formed in the dental plaque; therefore, ifbacteria could either break down or neutralizethese acids it would be advantageous. In thesearch for such bacteria, arginolytic bacteria werefound: Various streptococci (e.g., Streptococcusgordonii and sanguinis) catabolise arginine or ureato form ammonium, and thereby elevate the pHof the medium. Although a first patent to include
arginine in oral care products dates from 1978, ittook almost 30 years before a toothpaste with flu-oride and arginine was introduced.15 The firststudies with arginine in toothpastes and confec-tionary have shown the great potential of thisapproach, with outcomes similar to fluoride con-trol groups. Recent clinical trials in Thailand andChina confirmed that the addition of arginineprovided an additional anticaries benefit of about25% compared with a fluoride control paste.16
This is a significant development as the search forother active substances that would significantlyboost fluoride has so far not been successful.
In the search for chemical formulations thathave antimicrobial properties, researchers haveinvestigated many types of compounds. The ration-ale for this comprehensive research is the need toalso search for a medication that might be a next-generation antibotic agent. Avenues that have beenresearched include both active compounds andvehicles that would specifically target pathogenswith antimicrobial agents. If the medicament could
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
65
When we examine members of the same family, we often observe the same health trends in differentgenerations. For example, when parents present with multiple decayed teeth, most likely, their chil-dren will present with the same problem. Conversely, parents with excellent oral health often havechildren with healthy mouths as well. This prompts an important question: What role does natureplay in caries risk, and which part is nurture?
Genetics has an impact on several oral risk factors: the composition and quantity of saliva, theshape of the teeth, and whether the enamel is in “good shape.” The position of the teeth, crowding,and bite issues are also important variables when considering a predisposition to caries. Good dentalhygiene and careful maintenance may help overcome these negative factors. However, patients withmore risk factors will have to be more committed to performing their best oral hygiene.
What are the “nurture” factors that require extra vigilance on the part of dental professionals?Bacteria that cause caries and periodontal disease were not present in the oral cavity at birth. Unfa-vorable bacterial flora are acquired, passed from person to person, and thrive with an unhealthy diet.Sharing utensils, drinks, and even kissing can result in the sharing of “bad” bacteria among all mem-bers of the family.
Encourage adult patients to set the right example for their children. The numbers of sugarydrinks and in-between snacks ingested each day are crucial determinants in the caries debate. Drink-ing plain water, maintaining thorough brushing and flossing habits, and seeing a dental professionalregularly are helpful in reducing caries risk. As a practitioner, keep a keen eye on arising problems.Use of current oral care products, methods, and technologies—such as dental sealants and intercep-tive orthodontics—can help patients keep their smiles healthy and beautiful.
Box 4.Nature versus Nurture

be made to actively search for pathogens, a reduceddose would probably suffice to kill the pathogen.Such selective targeted antimicrobial peptides(STAMPs) have shown promise, although for den-tal caries it is now clear that the disease does notresult from a mono-infection. In general, develop-ments in nanotechnology and nanoparticulatematerials offer numerous opportunities. Forinstance, nano-sized calcium phosphate particlescan penetrate deeply into biofilms, serving assources of calcium and phosphate, and in additioncan carry a “load” of an antimicrobial to bereleased at the site where it is most needed.17
SUMMARYMajor paradigm shifts in all issues related to dentalcaries have occurred in recent decades. First andforemost is probably the changed perceptionregarding the importance of oral health in relationto general health. The following editorial plea inThe Lancet is a clear and important message to awide readership, from general medical practitionersto insurance companies and policy makers: “Politi-cally, commitment is needed to integrate oral diseaseprevention into programmes to prevent chronic dis-eases and into public-health systems. Good oralhealth should be everyone’s business.”18
Secondly, the notion has spread that it is doableto keep one’s teeth for a lifetime, but that it is not aneasy task to achieve. As part of the collaborationbetween patient and dental professional, preven-tion-oriented schemes should be set and followed.Maintaining a functional dentition is primarily thepatient’s responsibility, and this should be acknowl-edged. However, dental practitioners should startor continue to change their focus from a restorativeapproach to a prevention-oriented one. The deci-sion to place a restoration should only be madewhen all other options have failed. Althoughtoday’s dental restorations are acceptable fromboth aesthetic and functional perspectives, they areinferior to the original tooth. Similarly, it should bestressed that dentures are not really an acceptablealternative to one’s natural dentition.
In terms of dental public health, the searchshould continue for the most effective and cost-
effective programs for caries prevention. This dis-cussion and outcome will depend on the econom-ic conditions of the groups under study. Thefinding that caries is still highly prevalent amongeconomically deprived individuals demands areconsideration of available schemes. This requiresnot only evaluating products for oral care, but alsonumerous food types that are components of thecausative diets. Overweight, obesity, and dentalcaries often go hand in hand; therefore, we shouldjoin forces with colleagues working in foodresearch or as dietary consultants. A dietary evalu-ation is the task of dental practitioners during thedental visit.
Numerous agents and products are on thedrawing board and it is conceivable that promisingnew products will become available in the nextdecade. It is the task of the dental community,including manufacturers of oral care products, tomake these products available to and affordablefor the consumer at large.
The argument that good oral health is vital for general health should help to remove the bor-ders between the respective disciplines. The mostprevalent human diseases are, or originate from,infectious diseases. Our improved understandingof the importance of bacteria in the body andinsights regarding their functions should induce amore rational approach to controlling them.Undoubtedly this is the most appealing, challeng-ing, and potentially most rewarding facet of thedental care agenda for the future.
CASE 1: Caries in Adolescent Patients
Despite careful instructions regarding dentalhygiene, the absence of responsibility often seenamong adolescents may lead to a lack of dentalhygiene for extended periods of time. As seen in Fig-ures 4A and 4B, a stable, caries-free dentition maydeteriorate if the patient does not follow instructions.This case depicts the need for enhanced oral atten-tion during orthodontic treatment. Observationssuch as these are, unfortunately, rather common ingeneral practice and could result in heated discus-sions with parents or caretakers about responsibility,
CHAPTER 4 Dental Caries
66
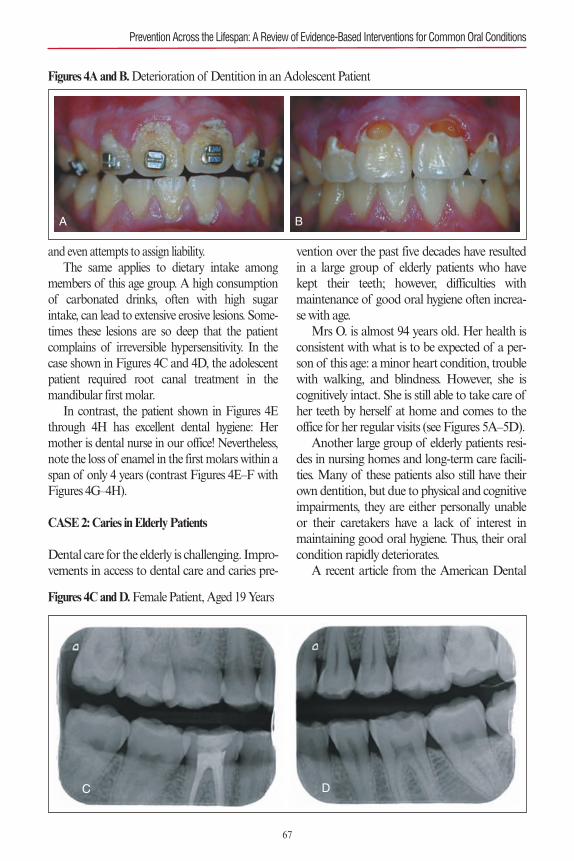
and even attempts to assign liability. The same applies to dietary intake among
members of this age group. A high consumptionof carbonated drinks, often with high sugarintake, can lead to extensive erosive lesions. Some-times these lesions are so deep that the patientcomplains of irreversible hypersensitivity. In thecase shown in Figures 4C and 4D, the adolescentpatient required root canal treatment in themandibular first molar.
In contrast, the patient shown in Figures 4Ethrough 4H has excellent dental hygiene: Hermother is dental nurse in our office! Nevertheless,note the loss of enamel in the first molars within aspan of only 4 years (contrast Figures 4E–F withFigures 4G–4H).
CASE 2: Caries in Elderly Patients
Dental care for the elderly is challenging. Impro-vements in access to dental care and caries pre-
vention over the past five decades have resultedin a large group of elderly patients who havekept their teeth; however, difficulties with maintenance of good oral hygiene often increa-se with age.
Mrs O. is almost 94 years old. Her health isconsistent with what is to be expected of a per-son of this age: a minor heart condition, troublewith walking, and blindness. However, she iscognitively intact. She is still able to take care ofher teeth by herself at home and comes to theoffice for her regular visits (see Figures 5A–5D).
Another large group of elderly patients resi-des in nursing homes and long-term care facili-ties. Many of these patients also still have theirown dentition, but due to physical and cognitiveimpairments, they are either personally unableor their caretakers have a lack of interest inmaintaining good oral hygiene. Thus, their oralcondition rapidly deteriorates.
A recent article from the American Dental
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
67
A B
Figures 4A and B.Deterioration of Dentition in an Adolescent Patient
C D
Figures 4C and D.Female Patient, Aged 19 Years
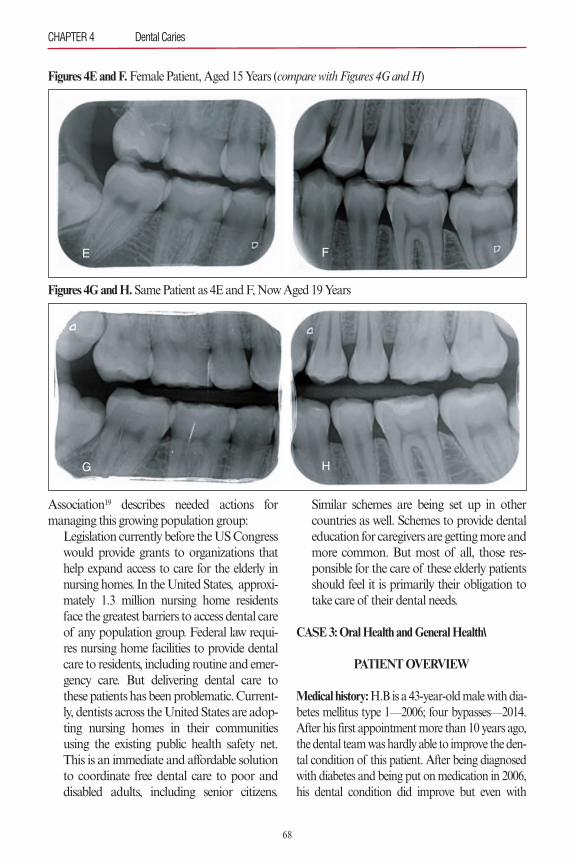
Association19 describes needed actions formanaging this growing population group:
Legislation currently before the US Congresswould provide grants to organizations thathelp expand access to care for the elderly innursing homes. In the United States, approxi-mately 1.3 million nursing home residentsface the greatest barriers to access dental careof any population group. Federal law requi-res nursing home facilities to provide dentalcare to residents, including routine and emer-gency care. But delivering dental care tothese patients has been problematic. Current-ly, dentists across the United States are adop-ting nursing homes in their communitiesusing the existing public health safety net.This is an immediate and affordable solutionto coordinate free dental care to poor anddisabled adults, including senior citizens.
Similar schemes are being set up in othercountries as well. Schemes to provide dentaleducation for caregivers are getting more andmore common. But most of all, those res-ponsible for the care of these elderly patientsshould feel it is primarily their obligation totake care of their dental needs.
CASE 3: Oral Health and General Health\
PATIENT OVERVIEW
Medical history:H.B is a 43-year-old male with dia-betes mellitus type 1—2006; four bypasses—2014.After his first appointment more than 10 years ago,the dental team was hardly able to improve the den-tal condition of this patient. After being diagnosedwith diabetes and being put on medication in 2006,his dental condition did improve but even with
CHAPTER 4 Dental Caries
68
G H
Figures 4G and H.Same Patient as 4E and F, Now Aged 19 Years
E F
Figures 4E and F.Female Patient, Aged 15 Years (compare with Figures 4G and H)
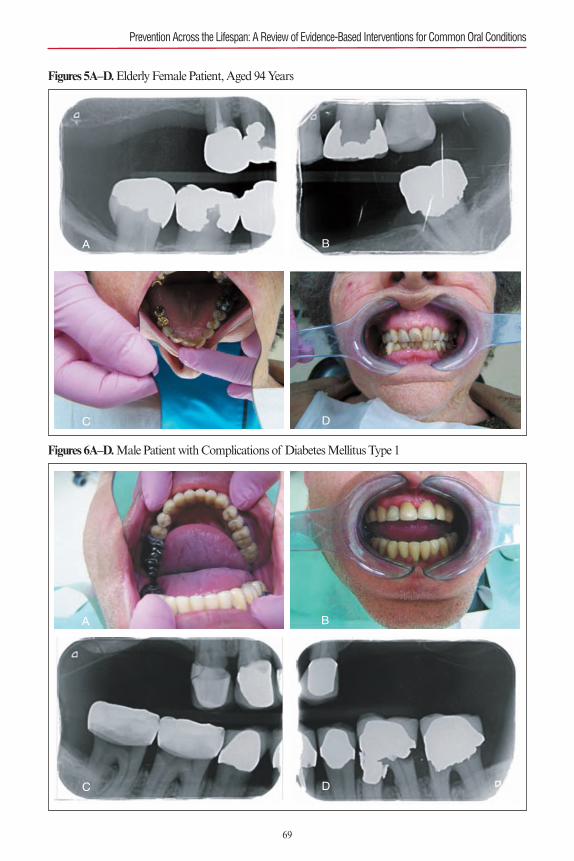
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
69
A B
C D
Figures 5A–D.Elderly Female Patient, Aged 94 Years
C D
A B
Figures 6A–D.Male Patient with Complications of Diabetes Mellitus Type 1

70
maximal support from the dental hygienist stillstayed at a rather poor level. But after coronary sur-gery in 2014 his overall condition as well as his den-tal condition improved markedly.Risk Assessment/Risk Factors: As dental practi-tioners we know it all too well. On the intakeexamination we see poor dentition, poorly main-tained oral hygiene, and a long history of dentalwork (see Figures 6A–D). For the medical anam-neses, we then typically expect the same: a highlycompromised history with many medical issues.
It was previously known that poor oral hygienesubstantially increases the risk for cardiovasculardisease. But recently, poor dentition and poor oralhygiene have been suspected of having links tonumerous systemic diseases, such as diabetes,osteoporosis, rheumatoid arthritis, pneumonia,and chronic obstructive pulmonary disease. Stud-ies have also linked obesity to gum disease.Researchers are investigating the possible role oforal health during pregnancy. Infection andinflammation in general seem to interfere with thedevelopment of a fetus in the womb. General anddental health are possibly already affected by thedevelopment of immune responses at that stage(see Chapter 12).
AcknowledgmentsThe authors are indebted to Drs. Catherine Chaussain, RitaVillena, Monique van der Veen, and Janneke Krikken forallowing the use of case information as illustrations for thischapter.
REFERENCES1. Broadbent JM, Foster Page LA, Thomson WM, Poul-
ton R. Permanent dentition caries through the first halfof life. Br Dent J. 2013;215:E12.
2. Groeneveld A. Longitudinal study of prevalence ofenamel lesions in a fluoridated and non-fluoridated area.Community Dent Oral Epidemiol. 1985;13:159–163.
3. Ekstrand KR, Christiansen ME. Outcomes of a non-operative caries treatment programme for children andadolescents. Caries Res. 2005;39:455–467.
4. van der Veen MH. Detecting short-term changes in theactivity of caries lesions with the aid of new technologies.Curr Oral Health Rep. 2015;2:102–109.
5. Bagramian RA, Garcia-Godoy F, Volpe AR. The globalincrease in dental caries. A pending public health crisis.Am J Dent. 2009;22:3–8.
6. Marsh PD, Bradshaw DJ. Microbiological effects of newagents in dentifrices for plaque control. Int Dent J.1993;43(4 suppl 1):399–406.
7. Keijser BJ, Zaura E, Huse SM, et al. Pyrosequencinganalysis of the oral microflora of healthy adults. J DentRes. 2008;87:1016–1020.
8. Human Microbiome Project Consortium. Structure,function and diversity of the healthy human microbio-me. Nature. 2012;486:207–214.
9. Marinho VC. Cochrane reviews of randomized trials offluoride therapies for preventing dental caries. Eur ArchPaediatr Dent. 2009;10:183–191.
10. Chaffee BW, Cheng J, Featherstone JD. Non-operativeanti-caries agents and dental caries increment amongadults at high caries risk: a retrospective cohort study.BMC Oral Health. 2015;15:111.
11. Raphael S, Blinkhorn A. Is there a place for ToothMousse® in the prevention and treatment of early den-tal caries? A systematic review. BMC Oral Health.2015;15:113.
12. Duggal MS, Toumba KJ, Amaechi BT, Kowash MB,Higham SM. Enamel demineralization in situ with vari-ous frequencies of carbohydrate consumption with andwithout fluoride toothpaste. J Dent Res. 2001;80:1721–1724.
13. ten Cate JM, Zaura E. The numerous microbial speciesin oral biofilms: how could antibacterial therapy be effec-tive? Adv Dent Res. 2012;24:108–111.
14. Hillman JD, Brooks TA, Michalek SM, Harmon CC,Snoep JL, van Der Weijden CC. Construction and char-acterization of an effector strain of Streptococcus mutansfor replacement therapy of dental caries. Infect Immun.2000;68:543–549.
15. Kleinberg I. A mixed-bacteria ecological approach tounderstanding the role of the oral bacteria in dentalcaries causation: an alternative to Streptococcus mutansand the specific-plaque hypothesis. Crit Rev Oral BiolMed. 2002;13:108–125.
16. Li X, Zhong Y, Jiang X, et al. Randomized clinical trialof the efficacy of dentifrices containing 1.5% arginine, aninsoluble calcium compound and 1450 ppm fluorideover two years. J Clin Dent. 2015;26:7–12.
17. Zhou C, Weir MD, Zhang K, Deng D, Cheng L, XuHH. Synthesis of new antibacterial quaternary ammoni-um monomer for incorporation into CaP nanocompos-ite. Dent Mater. 2013;29:859–870.
18. Editorial. Oral health: prevention is key. Lancet.2009;373(9657):1.doi: http://dx.doi.org/10.1016/S0140-6736(08)61933-9.
19. American Dental Association. Action for Dental Health.Provide Care Now to People Suffering with UntreatedDental Disease. Chicago, IL: ADA; 2015. Available at:http://www.ada.org/en/public-programs/action-for-dental-health. Accessed May 4, 2016.
CHAPTER 4 Dental Caries

PART 1: OVERVIEW OF THE CONDITIONThis chapter focuses on gingivitis and chronicperiodontitis associated with dental plaque, whichare the most common forms of periodontal dis-eases. Topics covered are classification, epidemiol-ogy, etiology and pathogenesis, risk assessment,and interventional and preventative measures. Inaddition, the chapter reports on the emerging evi-dence of similar inflammatory conditions affect-ing peri-implant tissues.
PERIODONTAL DISEASES: DEFINITIONSAND CLASSIFICATION
Gingivitis is inflammation of the gingiva (gums)surrounding the teeth, with no radiographic evi-dence of bone loss. Periodontitis is inflammationof the supporting tissues of the teeth. Periodonti-tis is usually a progressively destructive processleading to the loss of the surrounding structures ofthe teeth. It is, in fact, an extension of inflamma-tion from the gingiva into the adjacent structures(i.e., alveolar bone and periodontal ligament).1
Periodontitis is clinically characterized by gingivalpocket formation or gingival recession, or both.One can normally observe the presence of biofilm(bacterial plaque) and calculus. Radiographically,one can notice alveolar bone loss, especially inmoderate to severe cases.The last comprehensive Classification System
for Periodontal Diseases and Conditions was pub-lished in 1999 by the American Academy of Peri-odontology (AAP).2 This was based on theknowledge and consensus report of approximate-ly 60 periodontist clinicians and researchers fromaround the world who participated in the Interna-tional Workshop for a Classification of Periodon-tal Diseases and Conditions.2 Table 1 summarizes
the main conditions discussed and presented tothe dental profession approximately 17 years ago.More recently, the AAP published a Task
Force Report on the update to the 1999 Classifica-tion of Periodontal Disease and Conditions.3 TheAcademy also announced that a comprehensiveupdate to the 1999 Classification would com-mence in 2017. Meanwhile, minor modificationshave been introduced, which are discussed below.Formulation of a diagnosis of periodontitis is
based on multiple clinical and radiographicparameters, all of which may not be required. Ingeneral, a patient has periodontitis when one ormore sites have inflammation exhibiting bleedingon probing (BOP), radiographic alveolar boneloss, and increased probing pocket depth (PPD)or clinical attachment loss (CAL).3 Table 2 sum-marizes the most recent guidelines for determiningthe severity of periodontitis in patients.
Chronic and Aggressive PeriodontitisChronic periodontitis is the most common form ofperiodontitis seen in the adult population. It hasbeen recommended as a descriptor to denote theslowly progressive nature of the condition. Howev-er, there are, in some patients, short periods of rapiddestruction of the periodontal structures.3 Aggres-sive periodontitis is a rare condition that occurs inpatients who otherwise are clinically healthy (exceptfor periodontal disease). Common features includerapid attachment and alveolar loss; familial aggre-gation is also common. Normally, the amounts ofmicrobial deposits (biofilm) and calculus are incon-sistent with the severity of the disease. Phagocyteabnormalities are observed, as well as elevated pro-portions of Aggregatibacter actinomycetemcomi-tans and, in some populations, Porphyromonasgingivalis.1 The recent AAP Task Force Report hasrecommended that patient age younger than 25years at the time of the disease onset be used, alongwith other signs or criteria, to support the diagnosisof aggressive periodontitis.3 Currently, there are nodefinitive biomarkers that can differentiate betweenaggressive and chronic periodontitis or between gen-eralized and localized forms of aggressive periodon-titis. The clinician must base diagnostic decisions onthe patient history and clinical and radiographicsigns.3 Additional information on classification of
71
GingivalDiseases
Chapter 5
Rebecca Wilder and Antonio Moretti
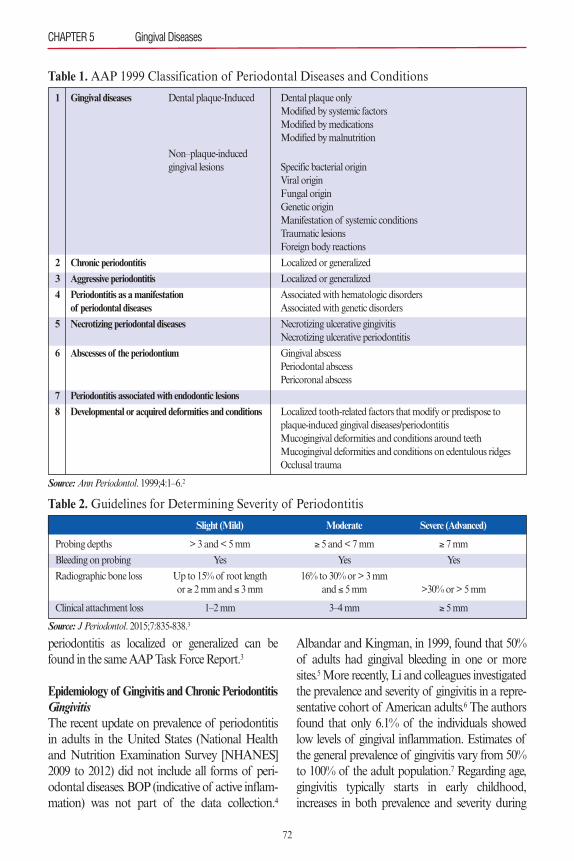
periodontitis as localized or generalized can befound in the same AAP Task Force Report.3
Epidemiology of Gingivitis and Chronic PeriodontitisGingivitisThe recent update on prevalence of periodontitisin adults in the United States (National Healthand Nutrition Examination Survey [NHANES]2009 to 2012) did not include all forms of peri-odontal diseases. BOP (indicative of active inflam-mation) was not part of the data collection.4
Albandar and Kingman, in 1999, found that 50%of adults had gingival bleeding in one or moresites.5More recently, Li and colleagues investigatedthe prevalence and severity of gingivitis in a repre-sentative cohort of American adults.6 The authorsfound that only 6.1% of the individuals showedlow levels of gingival inflammation. Estimates ofthe general prevalence of gingivitis vary from 50%to 100% of the adult population.7 Regarding age,gingivitis typically starts in early childhood,increases in both prevalence and severity during
CHAPTER 5 Gingival Diseases
72
Table 1. AAP 1999 Classification of Periodontal Diseases and Conditions
1 Gingival diseases Dental plaque-Induced Dental plaque onlyModified by systemic factorsModified by medicationsModified by malnutrition
Non–plaque-inducedgingival lesions Specific bacterial origin
Viral originFungal originGenetic originManifestation of systemic conditionsTraumatic lesionsForeign body reactions
2 Chronic periodontitis Localized or generalized
3 Aggressive periodontitis Localized or generalized
4 Periodontitis as a manifestation Associated with hematologic disordersof periodontal diseases Associated with genetic disorders
5 Necrotizing periodontal diseases Necrotizing ulcerative gingivitisNecrotizing ulcerative periodontitis
6 Abscesses of the periodontium Gingival abscessPeriodontal abscessPericoronal abscess
7 Periodontitis associated with endodontic lesions
8 Developmental or acquired deformities and conditions Localized tooth-related factors that modify or predispose to plaque-induced gingival diseases/periodontitisMucogingival deformities and conditions around teethMucogingival deformities and conditions on edentulous ridgesOcclusal trauma
Source:Ann Periodontol. 1999;4:1–6.2
Table 2. Guidelines for Determining Severity of Periodontitis
Slight (Mild) Moderate Severe (Advanced)
Probing depths > 3 and < 5 mm ≥ 5 and < 7 mm ≥ 7 mm
Bleeding on probing Yes Yes Yes
Radiographic bone loss Up to 15% of root length 16% to 30% or > 3 mmor ≥ 2 mm and ≤ 3 mm and ≤ 5 mm >30% or > 5 mm
Clinical attachment loss 1–2 mm 3–4 mm ≥ 5 mm
Source: J Periodontol. 2015;7:835-838.3

adolescence, and remains stable in the seconddecade of life.7 There is a small increase in theprevalence of gingival bleeding with age, but with amore marked increase in the extent of gingivalbleeding. In addition, the prevalence and extent ofgingival bleeding have been reported to be signifi-cantly higher in males than in females.5
Chronic PeriodontitisPeriodontitis affects almost 50% of the US adultpopulation aged 30 years and older. The preva-lence is higher in Hispanics followed by non-His-panic blacks. Non-Hispanic Asians are the thirdmost affected group followed by non-Hispanicwhites. Other important factors that can negative-ly affect the prevalence of periodontitis are (1)being a current smoker, (2) sex (males are moreaffected than females), and (3) lower socioeco-nomic status (including either poverty or educa-tion).4 Eke and associates noted that US estimatesappear to be much lower than those reported forcertain European populations.4Around the world,epidemiological studies show a large variationwhen defining and classifying periodontal dis-eases. More importantly, the great disparityamong populations makes it difficult to compiledata from the various sources. Nevertheless,chronic periodontitis is a very significant health-care problem. Severe periodontitis is the sixthmost prevalent disease in humans.8
Etiology and Pathogenesis of Periodontal DiseasesGingivitis and periodontitis are best viewed as acontinuum of a chronic inflammatory diseaseentity, with periodontitis representing a perturba-tion of host–microbial homeostasis in susceptibleindividuals that leads to irreversible destruction oftissues.9 Bacterial plaque or biofilm has long beenrecognized as a major factor contributing to theinitiation and persistence of gingival inflamma-tion.10 The bacterial challenge elicits the innateimmune system with the production of cytokinesand chemokines in the gingival tissues, leading tothe expression of adhesion molecules, increasedpermeability of gingival capillaries, and chemo-taxis of polymorphonuclear neutrophils andmacrophages. As the process continues, the adap-
tive immune system brings other critical partici-pants such as T and B lymphocytes and plasmacells. These have both protective and nonprotec-tive features. A great number of proinflammatorymediators (e.g., prostaglandin E2, interleukin-1b�[IL-1b], tumor necrosis factor-�, and matrix metal-loproteinases), microorganisms other than bacte-ria (i.e., viruses and fungi), and additional eventsand conditions are involved in this very complexprocess. The poor and imbalanced interactionbetween the host and the microbial challengeleads to irreversible pathological alveolar boneresorption, mostly of slow progression, that even-tually, if untreated, may lead to tooth loss.
Diagnostic Testing of Periodontal DiseasesOver the past two to three decades, both cliniciansand scientists have been focused on the importantgoals of early diagnosis and treatment of peri-odontal diseases, preventing the irreversible loss ofstructures. The destructive nature of chronic peri-odontitis makes early detection and interventionparticularly important. There is still much to belearned in this field. Despite tremendous develop-ment in both basic and clinical sciences, clinicianscontinue to rely primarily on clinical and radi-ographic findings to diagnose, prevent, and treatperiodontal diseases.Several diagnostic biomarkers exist that might
help the clinician. These molecular markers of tis-sue destruction can be present in the gingivalcrevicular fluid, saliva, and serum. However,Buduneli and Kinane concluded that there is nosingle or combination of biomarkers than can dis-close periodontal tissue destruction adequately.11
Microbial sampling has also been considered oflimited value. In a systematic review, Listgartenand Loomer concluded that for chronic periodon-titis, there is lack of strong evidence that microbialidentification is a valuable adjunct to its manage-ment.12 Another more recent systematic reviewthat explored the association of susceptible geno-types to periodontal disease concluded that IL-1–positive genotypes increase the risk for tooth loss.13
Regarding imaging, Aljehani reviewed the diag-nostic application of cone-beam computed tomog-raphy (CBCT) in the field of periodontology.14 It
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
73
was concluded that bony defects, craters, and furca-tion involvement seem to be better depicted onCBCT, whereas bone quality and periodontal lig-ament space scored better on conventional intrao-ral radiography. The author concluded thatCBCT does not offer a significant advantage overconventional radiography for assessing periodon-tal bone levels.
Periodontal Prognosis and Risk AssessmentIt is well-known that periodontal diseases have acomplex and multifactorial etiology. For the clini-cian, it is important to determine the relative riskfor disease progression in a once-treated patient.15
Although periodontal prognosis relates to treat-ment outcome for the tooth or dentition, or both,risk assessment is more global and involves a morethorough understanding of the patient and his orher future oral health. Both prognosis and riskassessment are integral parts of practice. However,according to Kwok and Caton, there is limiteddirect evidence in the literature regarding theassignment of periodontal prognosis.16 It thusremains a nonscientific aspect of the professionalroutine. Conversely, a recent systematic review byLang and coworkers identified five available peri-odontal risk assessment tools in the literature.15
The various assessment tools and multiple publi-cations associated with their methods support thepossibility that periodontitis progression andtooth loss can be predicted in a treated populationbased on risk segmentation. The authors also stat-ed that there are no data yet to determine theimpact that risk assessments may have on patientmanagement.The frequency of periodontal maintenance
recalls has been discussed, along with the idea thatit may help in treatment planning; however, thesuggestion remains unsubstantiated. One riskassessment tool in the public domain was intro-duced by Lang and Tonetti in 2003.17 The toolmay be accessed from the website at the Universityof Bern School of Dental Medicine, Switzerland(www.perio-tools.com/pra/en/). (Chapter 3, RiskAssessment, includes additional informationabout periodontal risk assessment.)
PERI-IMPLANT DISEASESPeri-implant diseases can be divided into peri-implant mucositis and peri-implantitis. Very similarto the bacterial plaque–induced inflammatoryprocess that occurs surrounding natural teeth, peri-implant mucositis affects the mucosal tissues adja-cent to the implants without loss of thesupporting alveolar bone. Conversely, peri-implantitis involves both inflammation of themucosa and the irreversible loss of alveolar bone.From a clinical and radiographic standpoint,when tracing a parallel between natural teeth anddental implants, peri-implant mucositis is theequivalent of gingivitis and peri-implantitis is theequivalent of periodontitis.According to the 2013 paper published by the
AAP Task Force on Peri-Implantitis, peri-implant mucositis includes BOP or suppuration,or both, which is usually associated with probingdepths of 4 mm or greater and no evidence ofradiographic loss of bone beyond bone remodel-ing.18 When the same parameters are present withany degree of detectable bone loss following ini-tial bone remodeling after implant placement, adiagnosis of peri-implantitis is made.18 This diag-nostic threshold can only be applied in cases inwhich a baseline radiograph has been taken atthe time of placement of the prosthesis. Sanz andChapple have recommended use of a thresholdvertical distance of 2 mm from the expected mar-ginal bone level following remodeling post-implant placement as the threshold for thediagnosis of peri-implantitis in cases where abaseline radiograph is absent.19
EpidemiologyThe frequency of peri-implant diseases has beenstudied.20,21 Both scientists and clinicians still havearduous work ahead to understand the etiology,pathogenesis, and especially the magnitude ofthese conditions affecting the global population.In a systematic review, the estimated frequency ofperi-implant mucositis has been reported inapproximately 64% of individuals and 31% ofimplants.21 In addition, peri-implantitis frequencyhas been estimated to affect approximately 19% of
CHAPTER 5 Gingival Diseases
74

individuals and 10% of implants.21 Atieh and col-leagues concluded that high-risk groups shouldreceive planned long-term maintenance care toreduce risk of peri-implantitis. They also stronglysuggested that informed consent is needed, includ-ing the commitment to long-term maintenancetherapy, when planning for implant therapy.21
PathogenesisIn 2014, Belibasakis described how peri-implantmucositis and peri-implantitis involve a sequence ofinflammatory events and qualitative compositionof the immune cells similar to gingivitis and peri-odontitis but of greater magnitude.22 The authoralso stated that the molecular events that governthese processes are not yet fully characterized. Nospecific genotype or systemic inflammatory markerexists that can reliably indicate peri-implant diseaseprogression or susceptibility. When analyzing thedifferences in peri-implant microbiota between fullyand partially edentulous patients, it was concludedthat partially edentulous patients harbor a poten-tially more pathogenic peri-implant microflorathan fully edentulous patients.23
Risk AssessmentWhen assessing risk for dental implant patients, theliterature includes levels of oral hygiene, cigarettesmoking, history of periodontitis, and diabetes aspotentially relevant factors. In addition, other con-siderations include genetic traits, osteoporosis, typeof implant design or surface, and occlusion. To date,there have been numerous prospective studies toguide the clinician in addressing this matter withaccuracy. Nevertheless, the clinician is expected toadvise patients who need tooth replacement therapy.A meta-analysis revealed that smoking led to a rateof implant bone loss of 0.164 mm per year. Expo-sure to smoking had a negative impact on implantalveolar bone loss.24 The correlation betweenimplant failure and marginal bone loss due to a his-tory of periodontitis has been reported to be ofmoderate level of evidence in at least two systematicreviews and meta-analyses.25,26 Finally, the effect ofocclusal overload and bone implant loss was system-atically reviewed by Naert and coworkers in 2012.27
The authors concluded that there is little or no evi-dence to support a cause-and-effect relationship.
PART 2: PATIENT MANAGEMENT ANDINTERVENTIONSMaintaining low levels of biofilm is essential tothe prevention of most gingival and periodontaldiseases, including natural teeth and implants.28
Fifty years of experimental research and clinicaltrials have confirmed the importance of effectiveplaque removal to periodontal health.10 Methodsinvestigated to remove or prevent oral biofilm pro-duction have included those rendered in an oralhealthcare setting by clinicians, as well as thoseperformed by patients at home. Following is areview of evidence-based strategies to prevent dis-ease or disease progression of the gingival diseases.
IN-OFFICE PREVENTIVE TREATMENTSAND STRATEGIES FOR THE
PREVENTION OF GINGIVAL DISEASESAlthough the evidence supports care by a clinicianfor reduction or prevention of gingival diseases,there is little evidence for the traditional 6-monthrecare appointment typically recommended topatients.29–31 More importantly, it is the quality ofbiofilm removal along with other indicators oforal–systemic health or risk for disease that shouldbe considered when determining recare appoint-ment intervals.In-office preventive strategies should be per-
formed based on the evidence available. Preventiveand therapeutic methods should include mechani-cal and adjunctive treatments to reduce biofilmand its byproducts for the prevention of periodon-tal diseases, including gingivitis, chronic periodon-titis, peri-implant mucositis, and peri-implantitis.
Mechanical TherapyScaling and root planing (SRP) is considered themainstay of periodontal therapy, reversing micro-bial shifts associated with disease and reestablish-ing microbiota seen in periodontal health.32
Mechanical therapy using SRP is an essentialcomponent in the removal of plaque biofilm andcalculus deposits.33,34 Considered the gold standard
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
75

of periodontal therapy, its efficacy is well docu-mented in the literature.33–36 SRP has been shownto result in gains in clinical attachment loss (CAL)between 0.55 mm and 1.29 mm, reductions inprobing pocket depth (PPD) between 1.29 mmand 2.16 mm, and reduction of BOP.34While clini-cians should try to remove as much of thedeposits as possible, investigators have shown thatas PPD depth increases it becomes difficult for cli-nicians to thoroughly remove deposits.37–40 In addi-tion, success in deposit removal is highlydependent on the skill of the clinician and his/herattention to detail.41,42
Hand instruments and powered instrumenta-tion have been shown to be equally effective in theremoval of deposits and disruption of the biofilm,although power-driven instruments remove calculusat a faster rate.33,34,43,44 Influencing factors in the suc-cess of mechanical therapy include the pocketdepth, furcations, and bony lesions, as well as patienthabits, such as use of tobacco and adherence tohome care instructions for biofilm reduction.34
New therapies have been proposed and investi-gated for prevention and reduction of plaquebiofilm, and, in some cases, calculus removal.These include laser technologies, full-mouth disin-fection, subgingival air abrasive systems withglycine powder air polishing (GPAP), dentalendoscopy, and others.
Laser TechnologyLasers have been used as an adjunctive treatmentto SRP. Potential therapeutic benefits includereduction in inflammation and enhancement ofthe healing process.45 Lasers are categorizedaccording to the wavelength of emitted light. In2012, Sanz and coworkers reported on the currentevidence for nonsurgical treatment of periodonti-tis. The authors concluded that soft tissue lasersare not indicated in periodontal therapy as they donot remove dental biofilm or calculus.34 In addi-tion, they reported that although the Er:YAG(erbium–yttrium aluminium garnet) laser hasshown efficacy as a monotherapy, it does notdemonstrate superiority when used as an adjunctto conventional periodontal instrumentation.34
Additional clinical research is needed in this field.In 2015, Smiley and colleagues reported on
evidence-based treatments for chronic periodonti-tis by means of SRP with and without adjuncts.46
The group of expert reviewers, convened by theADA Council on Scientific Affairs, conducted asystematic review of randomized controlled trialsthat were at least 6 months in duration. They alsoselected CAL as the sole measure to assess treat-ment effectiveness as it is routinely reported in thescientific literature as a valid measurement of dis-ease progression and is considered the mostimportant outcome in arresting or reversing peri-odontal disease onset and progression. The use oflasers was reviewed as an adjunctive treatment toSRP. Compared with SRP alone, the Nd:YAG(neodymium–yttrium aluminium garnet) laserresulted in a 0.41-mm mean gain in CAL (95%confidence interval [CI], −0.12 to 0.94). TheEr:YAG, resulted in a 0.18-mm mean gain inCAL (95% CI, −0.63 to 0.98). Both were judgedto have an overall low level of certainty in the evi-dence on the basis of the evidence profile. Basedon the review, a clinical practice guideline wasdeveloped by the ADA that provides treatmentrecommendations to clinicians using a scale ofstrong, in favor, weak, expert opinion for, expertopinion against, and against.47,48 Expert opinionagainst is the recommendation for use of lasers forpatients with moderate to severe chronic peri-odontitis because the “current evidence shows nonet benefit when used as an adjunct to SRP.”46
The authors noted that lasers have no defined andaccepted protocol for standard usage and thatlarger clinical trials are needed to properly evaluatethe benefits of utilizing lasers as an adjunct toSRP. The photodynamic therapy diode (PDT)laser was the only laser that the reviewers noted ashaving a “moderate” level of certainty as anadjunctive treatment to SRP. The PDT has showna 0.53-mm CAL (95% CI, 0.06 to 1.00) gain overSRP alone.46
Full-Mouth DisinfectionFull-mouth scaling and root planing (FMSRP) isa mode of periodontal therapy that consists of
CHAPTER 5 Gingival Diseases
76

SRP (with hand or ultrasonic instrumentation) ofall pockets within a 24-hour time frame. Full-mouth disinfection (FMD) is SRP of all pocketsin combination with topical application ofchlorhexidine within 24 hours. The rationale forthis therapy is that it avoids bacterial transmissionto other parts of the oral cavity, such as thetongue, mucosa, and untreated periodontal pock-ets.34 Although early studies showed significantimprovements in clinical outcomes, other studieshave shown no benefits as compared with conven-tional staged debridement (CSD), or SRP overseveral weeks. Eberhard and coworkers, in a sys-tematic review, reported that FMD resulted inhigher PPD reductions in 5- to 6-mm pockets ascompared with CSD. However, they concludedthat all three interventions (FMD, FMSRP, CSD)could result in improvements in clinical out-comes.49Recently two papers have reported on theclinical and microbiological effects of FMSRPcompared with CSD. Zijnge and associatesreported no differences in PPD or BOP after 3months.50 Similarly, after a 12-month randomizedcontrolled trial, Knöfler and colleagues reportedthat FMSRP and CSD were similar in targetingperiodontal pathogens.51 Fang and colleaguespublished a systematic review and meta-analysiscomparing FMD, FMSRP, and quadrant scalingand root planing (Q-SRP). FMD showed anadditional effect in PPD reduction (0.25 mm) andCAL gain (0.33 mm) versus Q-SRP in studieslonger than 3 months. The authors reported nodifferences in patient discomfort post-treatment,and less time was needed to complete treatmentwith FMD. However, the authors concluded thatFMD, FMSRP, and Q-SRP are all effective in thetreatment of chronic periodontitis.52 Since conven-tional treatment, FMD, and FMSRP are all clini-cally effective, clinicians should make treatmentdecisions based on their judgment and clinicianand patient preferences.
Dental EndoscopyA fiber-optic endoscopic system was introducedto dentistry in the late 1990s to assist clinicians inviewing the subgingival area. Used as an adjunct
to SRP, the technology produces a real-time videoshowing the subgingival environment, thus allow-ing the clinician to see the tooth structure, gingivalattachment, and sulcus wall, as well as residualcalculus remaining on the root surface at a magni-fication of 24 to 48 times their actual size.53 A ran-domized controlled trial conducted by Geisingerand coworkers reported significantly less residualcalculus in deeper probing depths when cliniciansused the dental endoscope for detection but nodifference in shallower probing depths. In addi-tion, differences in PPD at treated sites were signif-icant only at deeper sites greater than 4 mm forbuccal and lingual surfaces and greater than 6 mmfor interproximal surfaces.54 In a subsequent study,the same investigators reported that the endo-scope showed no significant improvement in cal-culus removal in multirooted molar teeth.55 Asmaller but more recent study reported that clini-cians were able to detect more calculus when usingthe dental endoscope versus a dental explorer inpatients with moderate periodontitis.56 More stud-ies are needed to determine how using the peri-odontal endoscope results in improved clinicalparameters.
Subgingival Air PolishingAir polishing devices were first introduced in the1940s for tooth restorative preparation.57 Using anabrasive slurry of particles, the powder inside thechamber is stirred up by pressurized air allowingair and water to be transported to the top of thedevice. Plaque and stain can be removed while thedevice tip is held 3 to 4 mm from the enamel sur-face and moved in a circular motion. Although airpolishing with sodium bicarbonate (mean particlesize up to 250 µm) has been utilized since the1980s as a treatment for removal of oral biofilmsand stains, safety concerns regarding damage toexposed root surfaces, gingival tissues, and restora-tive materials have limited its use.32 Recently, fine-grain glycine powder has been investigated forsubgingival removal of biofilm. Glycine is 80%lower in abrasiveness (45- to 60-µm particle size)when compared with air polishing using sodiumbicarbonate powder.58 Many studies have been
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
77

conducted to investigate the efficacy, safety, andpatient perceptions of glycine powder air polish-ing (GPAP) as compared with traditional meth-ods of SRP.57–61
A nozzle is available for supra- and subgingivalGPAP, depending on the pocket depth. Subgingi-val GPAP has been shown to reach pocket depthsup to 9 mm. In one study by Flemmig andcoworkers, subgingival GPAP was more effica-cious in removing subgingival biofilm in 4- to 9-mm pockets than SRP.59 In addition, time forbiofilm removal was shown to be less with subgin-gival GPAP (10 seconds per site) than with ultra-sonic debridement (30 seconds per site). The timedid not include calculus removal as subgingivalGPAP does not remove hard deposits.60,61
In 2012, a consensus conference on mechani-cal biofilm management was conducted duringthe Europerio 7 Congress in Vienna. Specifically,the conference experts were charged with review-ing the current evidence from the peer-reviewed lit-erature on the clinical relevance of subgingival useof air polishing and to make practical recommen-dations for clinicians.62 The consensus was that airpolishing devices are efficient in removing bothsub- and supragingival biofilm and stains. Thesubgingival nozzles provide better access to sub-gingival and interdental areas, and when com-pared with hand curettes, air polishing removessignificantly more biofilm in shallow and deeperpockets. GPAP is faster than hand or ultrasonicinstrumentation and is perceived by patients asbeing more comfortable.62
Subgingival GPAP has been investigated inpatients presenting with peri-implantitis.57 Arecent study reported on the biofilm removal andsurface roughness of 10 instruments on implantsurfaces. Biofilm on titanium disks was cleanedusing nine mechanical implant cleaning instru-ments or an erbium laser. Cleaning methodsincluded plastic instruments, carbon curettes, tra-ditional prophylaxis, powered instrumentation,and an air polishing device using glycine powderparticles of less than 63 µm. The best cleaningwith the least amount of damage resulted with theGPAP method and the sonic-driven polyether
ether ketone (PEEK) plastic tip.63
Protocol for use of subgingival GPAP includesusing the glycine air polishing prior to using pow-ered or hand instruments for stain and calculusremoval. High-volume evacuation should be usedwith air polishing. Although a traditional air pol-ishing device should never be directed into the gin-gival sulcus, subgingival GPAP uses anapplication tip designed for subgingival tissue andis required to reach depths of up to 10 mm in apocket (see Figure 1). Although the risk is low,facial emphysema can occur. Flemmig andcoworkers estimated the probability of this condition occurring from subgingival GPAP as 1in 666,666.59
Given the available evidence, subgingivalGPAP is safe and effective for biofilm removal andmay reduce clinician time.
Supra- and Subgingival IrrigationSeveral devices have been used by clinicians to irri-gate periodontal pockets. These include syringes, ajet irrigator with a cannula, and an ultrasonic unit.Many studies have been conducted to determinethe efficacy of in-office subgingival irrigation toimprove the parameters of gingivitis and periodon-titis.64 Currently there are limited data to supportthe benefits of a single episode of subgingival irri-gation while the patient is receiving professionaltreatment.64 Although data are very limited, the
CHAPTER 5 Gingival Diseases
78
Figure 1.Glycine Powder Air Polishing
Source: AIR-FLOW® Perio, used with permission from Hu-Friedy, Chicago, IL, USA).

exception may be with multiple irrigations in-officeusing antimicrobials to treat sites that do notrespond to traditional therapies. The lack of effica-cy for a one-time irrigation treatment may be relat-ed to the quick elimination of subgingivally placedfluids.64 However, at-home irrigation by patients hasbeen shown to be beneficial for the reduction ofgingivitis and is discussed later in this chapter.
Local and Systemic Therapies, Including Antimicrobials and AntibioticsIn-office treatments for gingivitis control typicallyconsist of debridement and scaling or debride-ment of the biofilm and calculus. For chronic peri-odontitis, other therapies, adjunctive to SRP, havebeen developed and proposed in recent years.Although patients with chronic periodontitisshould see improved results from SRP, some sitesand patients may not respond adequately. SRP ofdeep pockets has its limitations, such as clinicianinability to reach the depth of the pocket and diffi-culty with SRP of furcations. Certain pathogensare resistant to SRP, oral niches make SRP verydifficult, and clinicians may be limited due to time,patient sensitivity, and other factors. In addition,recolonization of subgingival biofilm is a concernand dependent to some degree on good daily oralhygiene by the patient. With poor supragingivalplaque control, bacteria may reestablish them-selves in a short period following SRP. For exam-ple, Sbordone and coworkers reported that after asingle episode of SRP and in the absence of oralhygiene, recolonization of subgingival sites withperiodontal pathogens may occur at 3 weeks.They also reported that at 60 days, there was nosignificant variation in any clinical and microbio-logical parameters as compared with pretreatmentlevels. Conclusions were that for patients withoutgood oral hygiene who are at risk for periodontaldisease, more frequent recare visits may be neces-sary.65 For all of these reasons, adjunctive treat-ments may be necessary for the control andtreatment of chronic periodontitis and to preventfurther destruction.Adjunctive treatments to SRP, such as systemic
antibiotics and locally delivered antimicrobials and
antibiotics, have been used in recent years by clini-cians. As the focus of this chapter is on the preven-tion of gingivitis and periodontitis, we provide onlya brief discussion of the treatments.
Locally Delivered Antimicrobials and AntibioticsSite-specific, locally delivered, controlled-releaseantimicrobials and antibiotics have been availablein dentistry since the 1980s. These agents, used asadjuncts to SRP, deliver an antimicrobial orantibiotic to the base of the periodontal pocketwith the goals of improving PPD and CAL gains,and reducing BOP. One benefit of using a locallydelivered antimicrobial is substantivity, or the abil-ity of an agent to remain in an area or site withoutbecoming diluted or washed away by gingivalcrevicular fluid or salivary action.66 Agents deliv-ered in this way slowly release active ingredients ata high minimal inhibitory concentration (MIC)level required to inhibit growth of a planktonicbacterial population. The premise for use of site-specific locally delivered agents is that due to high-er and longer substantivity, the MIC is maintainedat a level needed to significantly reduce the level ofpathogens over what can be achieved by SRPalone, with the intended outcome being improve-ments in periodontal parameters. Substantivityvaries from approximately 7 days for the chlorhex-idine chip and doxycycline hyclate gel to about 14to 21 days for minocycline microspheres.67–70
As mentioned earlier, the ADA Council onScientific Affairs conducted a systematic reviewand meta-analysis of nonsurgical treatments ofchronic periodontitis utilizing SRP with or with-out adjuncts.46 Using CAL as the outcome meas-ure, the authors assessed the overall level ofcertainly in the body of evidence as high, moder-ate, or low. SRP alone resulted in a 0.49-mm gainin CAL and was judged to be moderate on thebasis of the evidence profile. When comparedwith SRP alone, the chlorhexidine chip plus SRPresulted in a 0.40-mm mean gain in CAL (95%CI, 0.24 to 0.56) and was judged moderate basedon the evidence profile. Doxycycline hyclate gelresulted in a 0.64-mm gain in CAL (95% CI, 0.00to 1.28), and minocycline microspheres resulted in
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
79

a 0.24-mm gain in CAL (95% CI, −0.06 to 0.55),and both were judged to be low based on the evi-dence profile. A clinical practice guideline wasdeveloped by the ADA based on the review andprovided recommendations for these treatmentsbased on a scale of strong, in favor, weak, expertopinion for, expert opinion against, and against.47
Regarding locally delivered antimicrobials andantibiotics, the chlorohexidine chip was ratedweak, and doxycycline hyclate gel and minocyclinemicrospheres received expert opinion for. Expertsemphasized that “expert opinion for” does notimply endorsement but signifies that evidence islacking and the level of certainty in the evidence islow. Clinicians should determine use based on theirprofessional judgment and the patient’s needs andpreferences. A chairside guide is available for clini-cians on the ADA Center for Evidence-Based Den-tistry website (http://ebd.ada.org/en/).48
Systemic AntibioticsSystemic antibiotics have been utilized for the treat-ment of chronic periodontitis as adjunctive therapyto SRP. The rationale is that they can affect peri-odontal pathogens in saliva and gingival crevicularfluid. They can also reduce the microbial load inmultiple subgingival areas and at extracrevicularsites that have been insufficiently treated by SRP.71
Frequently used antibiotics are amoxicillin,metronidazole, erythromycin, tetracycline, doxycy-cline, and others. Sgolastra and colleagues reportedon a systematic review and meta-analysis of combi-nation amoxicillin (AMX) and metronidazole(MET) as an adjunctive treatment to SRP.71 Theselection process included four randomized clinicaltrials. They concluded that there was overall effec-tiveness of AMX/MET as an adjunct to SRP com-pared with SRP alone in the treatment of chronicperiodontitis. Six major groups of antibiotics werereported in the systematic review and meta-analysisconducted by Smiley and others at the ADA.46
Compared with SRP alone, SRP plus systemicantimicrobials resulted in a 0.35-mm mean gain inCAL (95% CI, 0.20 to 0.51). Experts judged theoverall level of certainty in the evidence to be mod-erateon the basis of the evidence profile.
Another systemic antibiotic has been used forthe adjunctive treatment of chronic periodontitissince the late 1990s and is considered a host mod-ulating agent. Systemic subantimicrobial dosedoxycycline (SDD) is provided at low doses (20mg), which may be taken twice a day up to 9months. It is sold in the United States as generic 20mg doxycycline tablets. Systemic levels do notreach inhibitory concentrations against bacteria.The drug inhibits collagenase activity in vitro andmay prevent further breakdown of connective tis-sue and alveolar bone. Compared with SRPalone, Smiley and colleagues reported that SDDresulted in a 0.35-mm gain in CAL (95% CI, 0.15to 0.56). The overall level of certainty in the evi-dence is moderate based on the evidence profile.The experts concluded that for patients with mod-erate to severe chronic periodontitis, cliniciansmay consider SSD (20 mg twice daily) for 3 to 9months as an adjunct to SRP, with a small netbenefit expected. The strength is in favor.46,47
Maintenance and RecallMost clinicians would agree that a combinationof professional care and oversight coupled withexcellent home care by the patient is ideal to pre-vent or control most forms of gingivitis andchronic periodontitis.29 However, patient recalland periodontal maintenance intervals have beendebated for many years. Traditionally, a 6-monthrecall system has been advocated by dentistry,but other intervals have been recommended,including 2 weeks, 2 to 3 months, 3 months, 3 to4 months, 3 to 6 months, and 12 to 18 months.72
A systematic review published by Beirne andcoworkers in 2007 revealed that there is insuffi-cient evidence from randomized controlled trialsto make any evidence-based recommendationson the benefits or harm of altering the recallinterval between dental checkups.30 Farooqi andassociates published a systematic review onappropriate recall intervals for periodontal main-tenance. Eight cohort studies met the inclusioncriteria. The authors concluded that there isweak evidence for a specific recall interval forpatients following periodontal therapy. They also
CHAPTER 5 Gingival Diseases
80
suggested that the merits of a risk-based recom-mendation over fixed recall interval regimensshould be investigated.72
Worthington and others conducted a system-atic review to determine the level of evidence forroutine SRP for periodontal health in adults.73
They concluded that some statistically significantevidence favored SRP at more frequent intervals,particularly between 3- and 12-month visits forgingivitis reduction (evaluated at 24 months).There was also some evidence for reduced calcu-lus with more frequent recalls. Needleman andcoworkers reported that more frequent profes-sional mechanical plaque control can improveplaque, bleeding, and attachment loss; however,the strength of the evidence is low.74 Both reviewsstressed the lack of high-quality clinical trials inthis area of prevention. As there is little evidenceto guide the frequency of mechanical plaque con-trol, clinicians are advised to make professionaljudgments based on a needs and risk assessmentfor each patient, including the patient’s adherenceto oral hygiene biofilm removal.75
A recent study conducted by Giannobile andcolleagues investigated how risk for periodontaldisease and number of preventive visits per yearimpacted tooth loss.76 The retrospective studyinvolved more than 5,000 patients over a 16-yearperiod. The authors investigated how smoking,diabetes, and the IL-1 genotype influenced toothloss in patients who had preventive visits eitheronce or twice per year. Patients were deemed highrisk if they had one or more of the conditions.Patients at low risk did not experience a signifi-cant difference in tooth loss rates whether theyhad one or two visits a year. High-risk patientshad better periodontal outcomes if they attendedtwo preventive visits a year. These results supportthe use of risk-based assessment as one methodof determining maintenance intervals.76
The prevention of gingivitis and chronic peri-odontitis is of concern in fixed prosthodontics aswell as implant-borne restorations. Recently, theAmerican College of Prosthodontists (ACP)convened a panel of experts to critically evaluateand debate recently published findings from two
systematic reviews. After consensus, the panelpublished “Clinical Practice Guidelines forRecall and Maintenance of Patients with Tooth-Borne and Implant-Borne Dental Restora-tions.”77 The ACP experts noted that to theirknowledge, these are the first clinical practiceguidelines addressing patient recall regimen, pro-fessional maintenance regimen, and at-homemaintenance regimen for these patients (seeTables 3 and 4). Although the recommendationsare intended for healthy adult patients and notthose with peri-implant disease or periodontaldisease, the authors noted that the recall andmaintenance regimen guidelines may be helpfulto patients with these diseases.77
AT-HOME PREVENTIVE TREATMENTSAND STRATEGIES
Previous studies have reported that patients retainmore teeth over time if they brush more than oncea day, perform interdental cleaning, and obtainprofessional dental care.29,78 A 2015 systematicreview found that there is likely little value in pro-viding professional mechanical plaque control(PMPC) without oral hygiene instruction.79
PMPC consists of supragingival and subgingivalplaque and calculus removal using hand or pow-ered instruments. PMPC plus oral hygiene instruc-tion results in the greatest benefit. In fact, theauthors emphasized that oral hygiene instructionis as influential as PMPC for periodontal health.79
Since most individuals are unable to accomplishcomplete disruption and removal of biofilm atand below the gingival margin, professional inter-vention is required.9 Tonetti and coworkers report-ed on expert consensus regarding effectiveprevention of periodontal and peri-implant dis-eases. Opinions and recommendations from thegroup included9
• repeated and individually tailored oralhygiene instruction is the key element inachieving gingival health;• patients should have professional supervisionfor PMPC and have appropriate oral hygieneinstruction tailored to their needs and moni-tored for efficacy; and
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
81
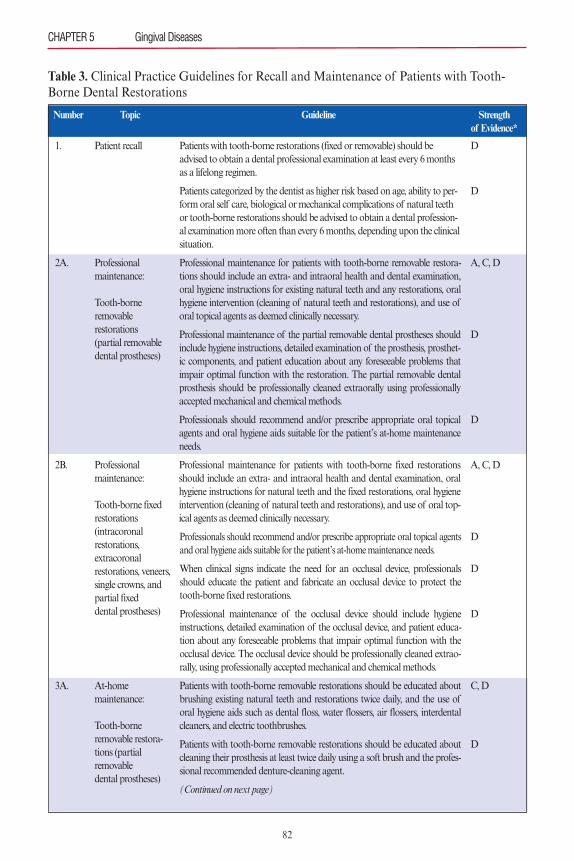
CHAPTER 5 Gingival Diseases
82
Table 3. Clinical Practice Guidelines for Recall and Maintenance of Patients with Tooth-Borne Dental Restorations
Patient recall
Professional maintenance:
Tooth-borne removablerestorations (partial removabledental prostheses)
Professional maintenance:
Tooth-borne fixedrestorations (intracoronalrestorations, extracoronalrestorations, veneers,single crowns, andpartial fixed dental prostheses)
At-home maintenance:
Tooth-borne removable restora-tions (partial removable dental prostheses)
1.
2A.
2B.
3A.
D
D
A, C, D
D
D
A, C, D
D
D
D
C, D
D
Patients with tooth-borne restorations (fixed or removable) should beadvised to obtain a dental professional examination at least every 6 monthsas a lifelong regimen.
Patients categorized by the dentist as higher risk based on age, ability to per-form oral self care, biological or mechanical complications of natural teethor tooth-borne restorations should be advised to obtain a dental profession-al examination more often than every 6 months, depending upon the clinicalsituation.
Professional maintenance for patients with tooth-borne removable restora-tions should include an extra- and intraoral health and dental examination,oral hygiene instructions for existing natural teeth and any restorations, oralhygiene intervention (cleaning of natural teeth and restorations), and use oforal topical agents as deemed clinically necessary.
Professional maintenance of the partial removable dental prostheses shouldinclude hygiene instructions, detailed examination of the prosthesis, prosthet-ic components, and patient education about any foreseeable problems thatimpair optimal function with the restoration. The partial removable dentalprosthesis should be professionally cleaned extraorally using professionallyaccepted mechanical and chemical methods.
Professionals should recommend and/or prescribe appropriate oral topicalagents and oral hygiene aids suitable for the patient’s at-home maintenanceneeds.
Professional maintenance for patients with tooth-borne fixed restorationsshould include an extra- and intraoral health and dental examination, oralhygiene instructions for natural teeth and the fixed restorations, oral hygieneintervention (cleaning of natural teeth and restorations), and use of oral top-ical agents as deemed clinically necessary.
Professionals should recommend and/or prescribe appropriate oral topical agentsand oral hygiene aids suitable for the patient’s at-home maintenance needs.
When clinical signs indicate the need for an occlusal device, professionalsshould educate the patient and fabricate an occlusal device to protect thetooth-borne fixed restorations.
Professional maintenance of the occlusal device should include hygieneinstructions, detailed examination of the occlusal device, and patient educa-tion about any foreseeable problems that impair optimal function with theocclusal device. The occlusal device should be professionally cleaned extrao-rally, using professionally accepted mechanical and chemical methods.
Patients with tooth-borne removable restorations should be educated aboutbrushing existing natural teeth and restorations twice daily, and the use oforal hygiene aids such as dental floss, water flossers, air flossers, interdentalcleaners, and electric toothbrushes.
Patients with tooth-borne removable restorations should be educated aboutcleaning their prosthesis at least twice daily using a soft brush and the profes-sional recommended denture-cleaning agent.
(Continued on next page)
Number Topic Guideline Strength of Evidence*
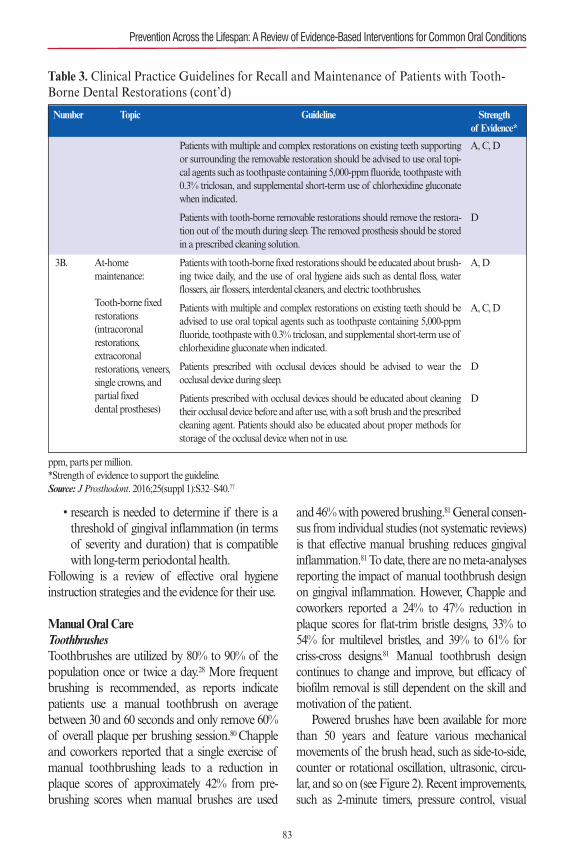
• research is needed to determine if there is athreshold of gingival inflammation (in termsof severity and duration) that is compatiblewith long-term periodontal health.
Following is a review of effective oral hygieneinstruction strategies and the evidence for their use.
Manual Oral CareToothbrushesToothbrushes are utilized by 80% to 90% of thepopulation once or twice a day.28 More frequentbrushing is recommended, as reports indicatepatients use a manual toothbrush on averagebetween 30 and 60 seconds and only remove 60%of overall plaque per brushing session.80 Chappleand coworkers reported that a single exercise ofmanual toothbrushing leads to a reduction inplaque scores of approximately 42% from pre-brushing scores when manual brushes are used
and 46% with powered brushing.81General consen-sus from individual studies (not systematic reviews)is that effective manual brushing reduces gingivalinflammation.81 To date, there are no meta-analysesreporting the impact of manual toothbrush designon gingival inflammation. However, Chapple andcoworkers reported a 24% to 47% reduction inplaque scores for flat-trim bristle designs, 33% to54% for multilevel bristles, and 39% to 61% forcriss-cross designs.81 Manual toothbrush designcontinues to change and improve, but efficacy ofbiofilm removal is still dependent on the skill andmotivation of the patient.Powered brushes have been available for more
than 50 years and feature various mechanicalmovements of the brush head, such as side-to-side,counter or rotational oscillation, ultrasonic, circu-lar, and so on (see Figure 2). Recent improvements,such as 2-minute timers, pressure control, visual
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
83
Table 3. Clinical Practice Guidelines for Recall and Maintenance of Patients with Tooth-Borne Dental Restorations (cont’d)
At-home maintenance:
Tooth-borne fixedrestorations (intracoronalrestorations, extracoronalrestorations, veneers,single crowns, andpartial fixed dental prostheses)
3B.
A, C, D
D
A, D
A, C, D
D
D
Patients with multiple and complex restorations on existing teeth supportingor surrounding the removable restoration should be advised to use oral topi-cal agents such as toothpaste containing 5,000-ppm fluoride, toothpaste with0.3% triclosan, and supplemental short-term use of chlorhexidine gluconatewhen indicated.
Patients with tooth-borne removable restorations should remove the restora-tion out of the mouth during sleep. The removed prosthesis should be storedin a prescribed cleaning solution.
Patients with tooth-borne fixed restorations should be educated about brush-ing twice daily, and the use of oral hygiene aids such as dental floss, waterflossers, air flossers, interdental cleaners, and electric toothbrushes.
Patients with multiple and complex restorations on existing teeth should beadvised to use oral topical agents such as toothpaste containing 5,000-ppmfluoride, toothpaste with 0.3% triclosan, and supplemental short-term use ofchlorhexidine gluconate when indicated.
Patients prescribed with occlusal devices should be advised to wear theocclusal device during sleep.
Patients prescribed with occlusal devices should be educated about cleaningtheir occlusal device before and after use, with a soft brush and the prescribedcleaning agent. Patients should also be educated about proper methods forstorage of the occlusal device when not in use.
Number Topic Guideline Strength of Evidence*
ppm, parts per million.*Strength of evidence to support the guideline.Source: J Prosthodont. 2016;25(suppl 1):S32–S40.77
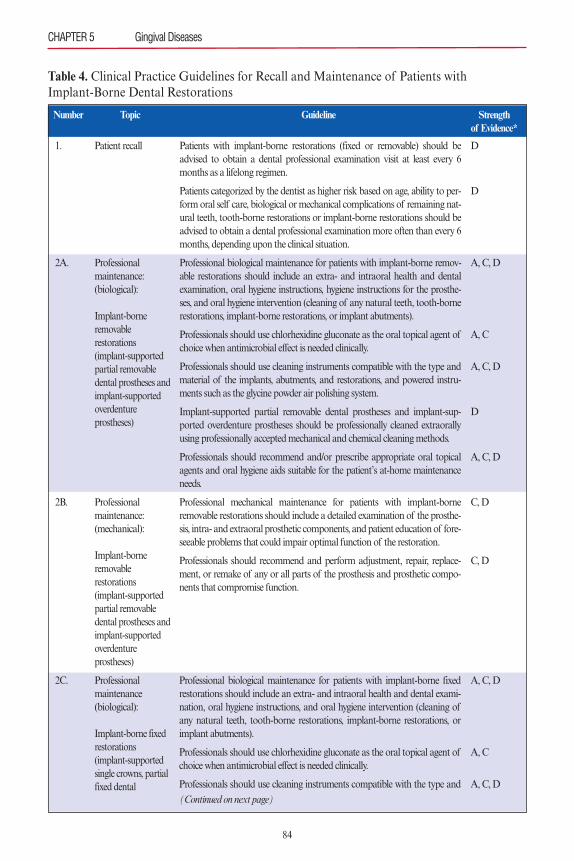
84
CHAPTER 5 Gingival Diseases
Table 4. Clinical Practice Guidelines for Recall and Maintenance of Patients with Implant-Borne Dental Restorations
Patient recall
Professional maintenance:(biological):
Implant-borneremovable restorations(implant-supportedpartial removabledental prostheses andimplant-supportedoverdenture prostheses)
Professional maintenance:(mechanical):
Implant-borneremovable restorations(implant-supportedpartial removabledental prostheses andimplant-supportedoverdenture prostheses)
Professional maintenance (biological):
Implant-borne fixedrestorations(implant-supportedsingle crowns, partialfixed dental
1.
2A.
2B.
2C.
D
D
A, C, D
A, C
A, C, D
D
A, C, D
C, D
C, D
A, C, D
A, C
A, C, D
Patients with implant-borne restorations (fixed or removable) should beadvised to obtain a dental professional examination visit at least every 6months as a lifelong regimen.
Patients categorized by the dentist as higher risk based on age, ability to per-form oral self care, biological or mechanical complications of remaining nat-ural teeth, tooth-borne restorations or implant-borne restorations should beadvised to obtain a dental professional examination more often than every 6months, depending upon the clinical situation.
Professional biological maintenance for patients with implant-borne remov-able restorations should include an extra- and intraoral health and dentalexamination, oral hygiene instructions, hygiene instructions for the prosthe-ses, and oral hygiene intervention (cleaning of any natural teeth, tooth-bornerestorations, implant-borne restorations, or implant abutments).
Professionals should use chlorhexidine gluconate as the oral topical agent ofchoice when antimicrobial effect is needed clinically.
Professionals should use cleaning instruments compatible with the type andmaterial of the implants, abutments, and restorations, and powered instru-ments such as the glycine powder air polishing system.
Implant-supported partial removable dental prostheses and implant-sup-ported overdenture prostheses should be professionally cleaned extraorallyusing professionally accepted mechanical and chemical cleaning methods.
Professionals should recommend and/or prescribe appropriate oral topicalagents and oral hygiene aids suitable for the patient’s at-home maintenanceneeds.
Professional mechanical maintenance for patients with implant-borneremovable restorations should include a detailed examination of the prosthe-sis, intra- and extraoral prosthetic components, and patient education of fore-seeable problems that could impair optimal function of the restoration.
Professionals should recommend and perform adjustment, repair, replace-ment, or remake of any or all parts of the prosthesis and prosthetic compo-nents that compromise function.
Professional biological maintenance for patients with implant-borne fixedrestorations should include an extra- and intraoral health and dental exami-nation, oral hygiene instructions, and oral hygiene intervention (cleaning ofany natural teeth, tooth-borne restorations, implant-borne restorations, orimplant abutments).
Professionals should use chlorhexidine gluconate as the oral topical agent ofchoice when antimicrobial effect is needed clinically.
Professionals should use cleaning instruments compatible with the type and
Number Topic Guideline Strength of Evidence*
(Continued on next page)
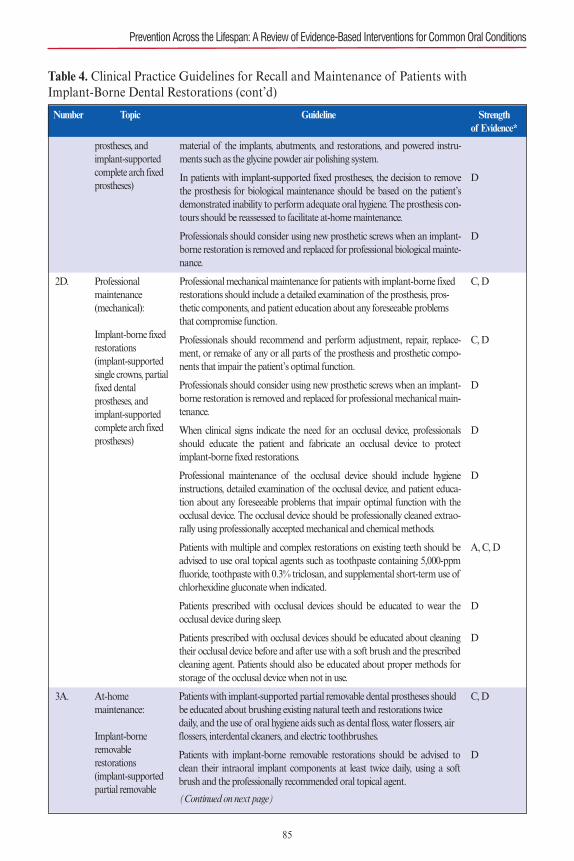
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
85
Table 4. Clinical Practice Guidelines for Recall and Maintenance of Patients with Implant-Borne Dental Restorations (cont’d)
prostheses, andimplant-supportedcomplete arch fixedprostheses)
Professional maintenance(mechanical):
Implant-borne fixedrestorations(implant-supportedsingle crowns, partialfixed dental prostheses, andimplant-supportedcomplete arch fixedprostheses)
At-home maintenance:
Implant-borneremovable restorations(implant-supportedpartial removable
2D.
3A.
material of the implants, abutments, and restorations, and powered instru-ments such as the glycine powder air polishing system.
In patients with implant-supported fixed prostheses, the decision to removethe prosthesis for biological maintenance should be based on the patient’sdemonstrated inability to perform adequate oral hygiene. The prosthesis con-tours should be reassessed to facilitate at-home maintenance.
Professionals should consider using new prosthetic screws when an implant-borne restoration is removed and replaced for professional biological mainte-nance.
Professional mechanical maintenance for patients with implant-borne fixedrestorations should include a detailed examination of the prosthesis, pros-thetic components, and patient education about any foreseeable problemsthat compromise function.
Professionals should recommend and perform adjustment, repair, replace-ment, or remake of any or all parts of the prosthesis and prosthetic compo-nents that impair the patient’s optimal function.
Professionals should consider using new prosthetic screws when an implant-borne restoration is removed and replaced for professional mechanical main-tenance.
When clinical signs indicate the need for an occlusal device, professionalsshould educate the patient and fabricate an occlusal device to protectimplant-borne fixed restorations.
Professional maintenance of the occlusal device should include hygieneinstructions, detailed examination of the occlusal device, and patient educa-tion about any foreseeable problems that impair optimal function with theocclusal device. The occlusal device should be professionally cleaned extrao-rally using professionally accepted mechanical and chemical methods.
Patients with multiple and complex restorations on existing teeth should beadvised to use oral topical agents such as toothpaste containing 5,000-ppmfluoride, toothpaste with 0.3% triclosan, and supplemental short-term use ofchlorhexidine gluconate when indicated.
Patients prescribed with occlusal devices should be educated to wear theocclusal device during sleep.
Patients prescribed with occlusal devices should be educated about cleaningtheir occlusal device before and after use with a soft brush and the prescribedcleaning agent. Patients should also be educated about proper methods forstorage of the occlusal device when not in use.
Patients with implant-supported partial removable dental prostheses shouldbe educated about brushing existing natural teeth and restorations twicedaily, and the use of oral hygiene aids such as dental floss, water flossers, airflossers, interdental cleaners, and electric toothbrushes.
Patients with implant-borne removable restorations should be advised toclean their intraoral implant components at least twice daily, using a softbrush and the professionally recommended oral topical agent.
Number Topic Guideline Strength of Evidence*
D
D
C, D
C, D
D
D
D
A, C, D
D
D
C, D
D
(Continued on next page)
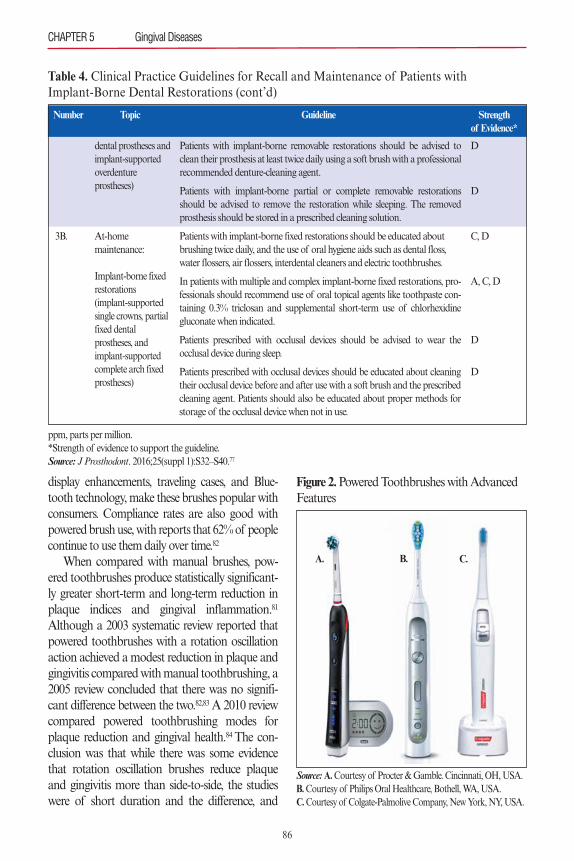
display enhancements, traveling cases, and Blue-tooth technology, make these brushes popular withconsumers. Compliance rates are also good withpowered brush use, with reports that 62% of peoplecontinue to use them daily over time.82
When compared with manual brushes, pow-ered toothbrushes produce statistically significant-ly greater short-term and long-term reduction inplaque indices and gingival inflammation.81
Although a 2003 systematic review reported thatpowered toothbrushes with a rotation oscillationaction achieved a modest reduction in plaque andgingivitis compared with manual toothbrushing, a2005 review concluded that there was no signifi-cant difference between the two.82,83 A 2010 reviewcompared powered toothbrushing modes forplaque reduction and gingival health.84 The con-clusion was that while there was some evidencethat rotation oscillation brushes reduce plaqueand gingivitis more than side-to-side, the studieswere of short duration and the difference, and
86
CHAPTER 5 Gingival Diseases
Table 4. Clinical Practice Guidelines for Recall and Maintenance of Patients with Implant-Borne Dental Restorations (cont’d)
dental prostheses andimplant-supportedoverdenture prostheses)
At-home maintenance:
Implant-borne fixedrestorations(implant-supportedsingle crowns, partialfixed dental prostheses, andimplant-supportedcomplete arch fixedprostheses)
3B.
Patients with implant-borne removable restorations should be advised toclean their prosthesis at least twice daily using a soft brush with a professionalrecommended denture-cleaning agent.
Patients with implant-borne partial or complete removable restorationsshould be advised to remove the restoration while sleeping. The removedprosthesis should be stored in a prescribed cleaning solution.
Patients with implant-borne fixed restorations should be educated aboutbrushing twice daily, and the use of oral hygiene aids such as dental floss,water flossers, air flossers, interdental cleaners and electric toothbrushes.
In patients with multiple and complex implant-borne fixed restorations, pro-fessionals should recommend use of oral topical agents like toothpaste con-taining 0.3% triclosan and supplemental short-term use of chlorhexidinegluconate when indicated.
Patients prescribed with occlusal devices should be advised to wear theocclusal device during sleep.
Patients prescribed with occlusal devices should be educated about cleaningtheir occlusal device before and after use with a soft brush and the prescribedcleaning agent. Patients should also be educated about proper methods forstorage of the occlusal device when not in use.
Number Topic Guideline Strength of Evidence*
ppm, parts per million.*Strength of evidence to support the guideline.Source: J Prosthodont. 2016;25(suppl 1):S32–S40.77
D
D
C, D
A, C, D
D
D
Figure 2.Powered Toothbrushes with AdvancedFeatures
Source: A.Courtesy of Procter & Gamble. Cincinnati, OH, USA.B.Courtesy of Philips Oral Healthcare, Bothell, WA, USA. C.Courtesy of Colgate-Palmolive Company, New York, NY, USA.
A. B. C.
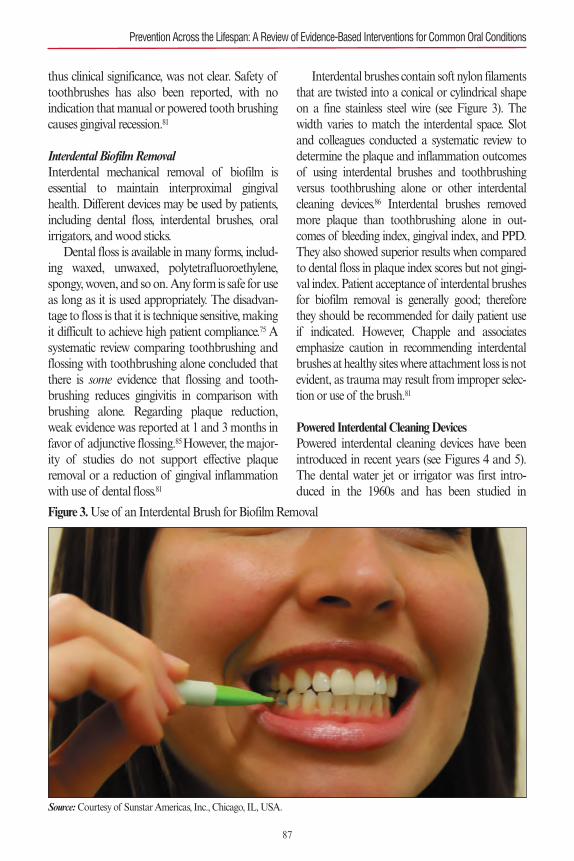
thus clinical significance, was not clear. Safety oftoothbrushes has also been reported, with no indication that manual or powered tooth brushingcauses gingival recession.81
Interdental Biofilm RemovalInterdental mechanical removal of biofilm isessential to maintain interproximal gingivalhealth. Different devices may be used by patients,including dental floss, interdental brushes, oralirrigators, and wood sticks.Dental floss is available in many forms, includ-
ing waxed, unwaxed, polytetrafluoroethylene,spongy, woven, and so on. Any form is safe for useas long as it is used appropriately. The disadvan-tage to floss is that it is technique sensitive, makingit difficult to achieve high patient compliance.75 Asystematic review comparing toothbrushing andflossing with toothbrushing alone concluded thatthere is some evidence that flossing and tooth-brushing reduces gingivitis in comparison withbrushing alone. Regarding plaque reduction,weak evidence was reported at 1 and 3 months infavor of adjunctive flossing.85 However, the major-ity of studies do not support effective plaqueremoval or a reduction of gingival inflammationwith use of dental floss.81
Interdental brushes contain soft nylon filamentsthat are twisted into a conical or cylindrical shapeon a fine stainless steel wire (see Figure 3). Thewidth varies to match the interdental space. Slotand colleagues conducted a systematic review todetermine the plaque and inflammation outcomesof using interdental brushes and toothbrushingversus toothbrushing alone or other interdentalcleaning devices.86 Interdental brushes removedmore plaque than toothbrushing alone in out-comes of bleeding index, gingival index, and PPD.They also showed superior results when comparedto dental floss in plaque index scores but not gingi-val index. Patient acceptance of interdental brushesfor biofilm removal is generally good; thereforethey should be recommended for daily patient useif indicated. However, Chapple and associatesemphasize caution in recommending interdentalbrushes at healthy sites where attachment loss is notevident, as trauma may result from improper selec-tion or use of the brush.81
Powered Interdental Cleaning DevicesPowered interdental cleaning devices have beenintroduced in recent years (see Figures 4 and 5).The dental water jet or irrigator was first intro-duced in the 1960s and has been studied in
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
87
Figure 3.Use of an Interdental Brush for Biofilm Removal
Source: Courtesy of Sunstar Americas, Inc., Chicago, IL, USA.
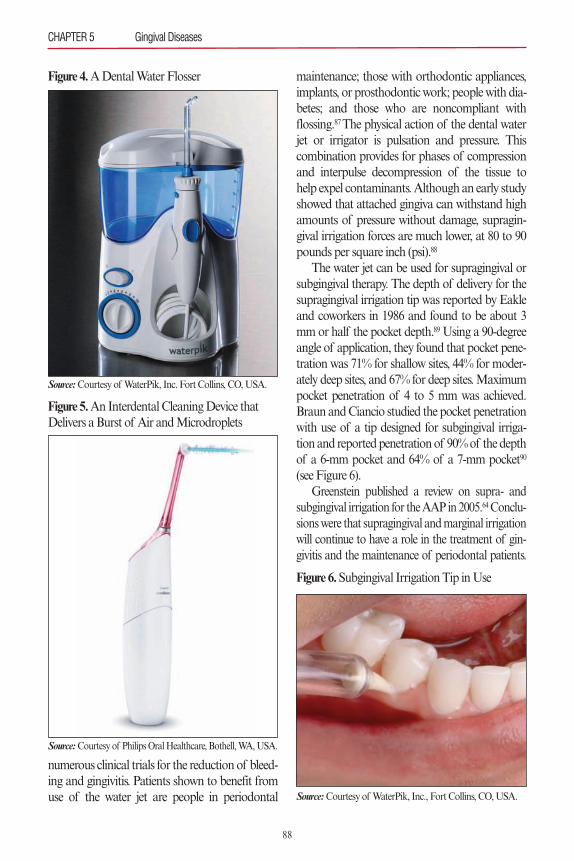
numerous clinical trials for the reduction of bleed-ing and gingivitis. Patients shown to benefit fromuse of the water jet are people in periodontal
maintenance; those with orthodontic appliances,implants, or prosthodontic work; people with dia-betes; and those who are noncompliant withflossing.87 The physical action of the dental waterjet or irrigator is pulsation and pressure. Thiscombination provides for phases of compressionand interpulse decompression of the tissue tohelp expel contaminants. Although an early studyshowed that attached gingiva can withstand highamounts of pressure without damage, supragin-gival irrigation forces are much lower, at 80 to 90pounds per square inch (psi).88
The water jet can be used for supragingival orsubgingival therapy. The depth of delivery for thesupragingival irrigation tip was reported by Eakleand coworkers in 1986 and found to be about 3mm or half the pocket depth.89 Using a 90-degreeangle of application, they found that pocket pene-tration was 71% for shallow sites, 44% for moder-ately deep sites, and 67% for deep sites. Maximumpocket penetration of 4 to 5 mm was achieved.Braun and Ciancio studied the pocket penetrationwith use of a tip designed for subgingival irriga-tion and reported penetration of 90% of the depthof a 6-mm pocket and 64% of a 7-mm pocket90
(see Figure 6).Greenstein published a review on supra- and
subgingival irrigation for the AAP in 2005.64Conclu-sions were that supragingival and marginal irrigationwill continue to have a role in the treatment of gin-givitis and the maintenance of periodontal patients.
88
CHAPTER 5 Gingival Diseases
Figure 4.A Dental Water Flosser
Source: Courtesy of WaterPik, Inc. Fort Collins, CO, USA.
Figure 5.An Interdental Cleaning Device thatDelivers a Burst of Air and Microdroplets
Source: Courtesy of Philips Oral Healthcare, Bothell, WA, USA.
Figure 6.Subgingival Irrigation Tip in Use
Source: Courtesy of WaterPik, Inc., Fort Collins, CO, USA.

The author noted that one of the advantages of self-administered subgingival irrigation is that it allowspatients to participate in maintaining the bacterialreduction achieved by mechanical therapy.A systematic review that was published in 2008
reported on the adjunctive effect of oral irrigationin addition to toothbrushing on plaque and clinicalparameters of periodontal inflammation. Theauthors reported that as an adjunct to brushing,oral irrigation does not visibly reduce plaque buttends to improve gingival health, as evidenced byimproved gingival index, bleeding scores, and pock-et depth compared with toothbrushing alone. Inaddition, the periodontal index of the toothbrushonly group worsened over time, but that of theoral irrigation group did not.91
Clinicians should always instruct patients inthe proper use of the water jet for at-home use,reinforcing proper force and placement of the tip.The supragingival tip should be directed at a 90-degree angle to the long axis of the tooth andabout 3 mm away from the gingival margin.Patient adherence is vital to efficacy of treatment.(See Chapter 2, Behavioral Science.)
Antimicrobial DentifriceSystematic reviews have shown evidence for signif-icant improvements in plaque and gingivitis scoreswhen chemical antiplaque agents are used in addi-tion to toothbrushing.81 Since most individualsclaim to brush their teeth at least once or twice aday, an antimicrobial dentifrice is an easy and effi-cient way to provide additional plaque and gin-givitis benefit to patients.Dentifrice formulations available include stan-
nous fluoride/sodium hexametaphosphate, aminefluoride/stannous fluoride, triclosan (2 �́-hydroxy-2,4,4 �́-tricholordiphenyl ether), essential oils, sodi-um bicarbonate, quaternary ammoniumcompounds, zinc citrate, or zinc chloride.29 Fewsystematic reviews have been reported to provideevidence for use of the different formulations.However, systematic reviews have been publishedand reported evidence for the use of triclosan forreducing supragingival plaque and gingivitis.92–94
Gunsolley also reported on positive plaque and
gingivitis reduction with dentifrices containingstannous fluoride.94 (See Chapter 16, Chemother-apeutic Agents.)
Antimicrobial MouthrinsesMechanical biofilm removal is difficult for somepatients making the use of antimicrobial rinsesappealing. They are easy and quick to use and arerelatively inexpensive. Therapeutic mouthrinseshave been widely investigated for plaque and gin-givitis reduction and control. The most studiedmouthrinses are those containing chlorhexidinegluconate (CHX), essential oils, and cetylpyridini-um chloride (CPC). Systematic reviews havereported substantial plaque and gingivitis reduc-tion.94,95 Gunsolley concluded that there is strongevidence supporting the efficacy of CHX andessential oils as antiplaque, antigingivitismouthrinses.94 (See Chapter 16, Chemotherapeu-tics in Prevention.)Use of antimicrobial rinses has been studied as
an adjunct to mechanical plaque control. Whencompared with adjunctive flossing or flossingalone, essential oils had a significant effect as anantigingivitis and antiplaque treatment and, insome cases, performed better than floss alone.96
Currently, a combination of daily toothbrushing,interdental cleaning, and antimicrobial rinsing isrecommended by clinicians throughout the world.Other factors that may influence patient accept-
ance of daily use of a mouthrinse include the poten-tial for taste alteration, staining, burning, increase incalculus formation, and cost.97 However, the advan-tages are many; among them, mouthrinses arequick and easy to use and inexpensive in most cases.CHX 0.12% mouthrinse requires a prescription inthe United States, but other formulations are avail-able elsewhere over the counter. The 0.12% formula-tion available in the United States is recommendedas a 15-mL rinse. In Europe, the formulation is 0.2%and recommended as a 10-mL rinse. The two con-centrations have equal efficacy and should be usedfor 20 seconds twice a day.98 Essential oil rinsesshould be used undiluted (20 mL) for 30 secondstwice daily. Another consideration with potential to impact
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
89

efficacy and compliance with the use of antimicro-bial mouthrinses is the adverse interaction reportedbetween dentifrice ingredients and CHX or CPC.Sheen and colleagues reported that a dentifrice mayadversely affect the activity of CHX and CPC ifused immediately after the rinse.99 Kolahi andSoolari reported on a systematic review that foundCHX and dentifrice ingredients such as sodium lau-rel sulfate and sodium fluoride were not compatible,“although the evidence does not allow for a defini-tive conclusion.”100 Recommendations for use fromthe review are that the interval between brushingand rinsing with CHX should be at least 30 minutesand perhaps close to 2 hours after brushing.100 Nointeraction effect between essential oils and denti-frice has been reported.Patient adherence to oral health instruction is
vital to efficacy of treatment, and an evidence-basedrecommendation by clinicians is important to pre-venting disease. Considerations for daily use of anantimicrobial rinse include patient acceptance oftaste and potential for staining.
New TherapiesProbiotics, an herbal patch, and antioxidants are allin various phases of investigation as adjunctiveproducts for the treatment of gingivitis, periodonti-tis, and peri-implant diseases. A recent systematicreview by Yanine and colleagues concluded that theeffectiveness of probiotics on the prevention andtreatment of periodontal diseases is questionable.101
An herbal patch is available to relieve the signsand symptoms of inflammation caused by gingivi-tis and periodontitis. It has two layers, with theouter layer composed of a nonabsorptive matrixthat allows for slow dissolution of an inner layer.The patch provides a protective seal over inflamedgingival and oral mucosa while promoting woundhealing by absorbing the local inflammatory exu-date from the inflamed tissue.102 Recently, theherbal patch has been investigated for the adjunc-tive management of chronic periodontitis andshown to have efficacy (R. Wilder, personal com-munication).Antioxidants are also of interest to clinicians.
San Miguel and coworkers studied the in vitro
effects of antioxidants in human oral fibroblastsand concluded that they may have beneficialeffects on gingival healing and periodontalrepair.103 However, a 2015 systematic review con-cluded that while the use of some antioxidants hasthe potential to improve periodontal clinicalparameters, more investigation is needed.104
PATIENT LIFESTYLE AND EFFECT ONPREVENTION OF GINGIVAL DISEASESThe most important risk factor for gingivitis andperiodontitis is the accumulation and maturationof plaque biofilm at and below the gingival mar-gin. However, patient lifestyle factors may alsocontribute to the incidence and severity of gingivi-tis and periodontitis.81
Tobacco UseTobacco use is an undeniable risk factor for peri-odontal disease. Numerous studies have been pub-lished on the effect of smoking on the periodontaltissues and on the outcomes of treatment. As a pre-ventive measure, clinicians may consider providingcounseling for tobacco cessation in the dental set-ting. Rosa and colleagues reported on the effect ofsmoking cessation on nonsurgical periodontal thera-py after 24 months.105 Subjects received nonsurgicalperiodontal therapy and a concurrent smoking ces-sation intervention. Periodontal maintenance wasperformed every 3 months. The subjects who quitsmoking showed significantly better improvementin CAL than subjects who did not quit.105Ramseierand Suvan published a systematic review support-ing the use of brief interventions in the dental set-ting to increase the smoking cessation rate. Six ofthe eight studies in the review were conducted indental offices.106
Patients appreciate and expect involvementfrom clinicians regarding smoking cessation.9
Even though dental clinicians may not feel com-fortable with conducting a full tobacco cessationprogram with a patient, most professionals canlearn to provide a “brief intervention,” which is ashort conversation with the patient of up to 5 min-utes to provide advice and limited counseling.9
In their consensus report on prevention of
CHAPTER 5 Gingival Diseases
90
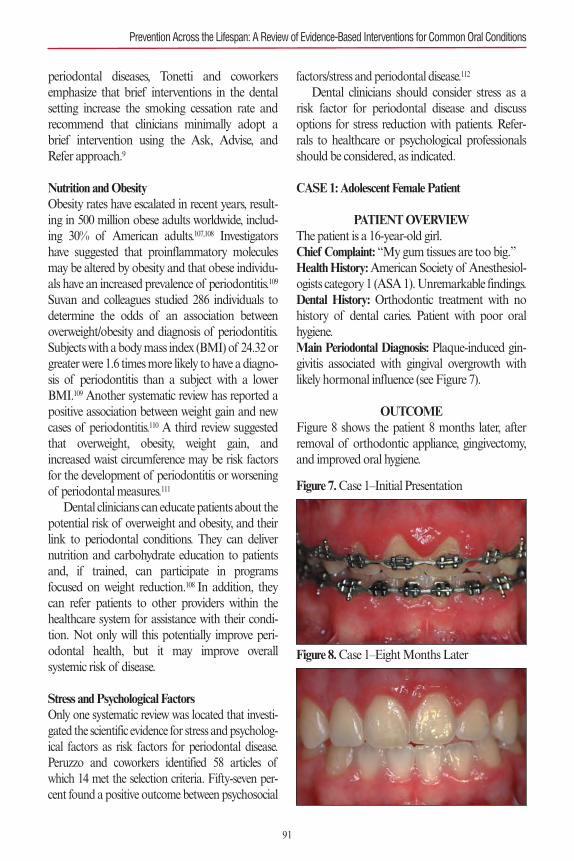
periodontal diseases, Tonetti and coworkersemphasize that brief interventions in the dentalsetting increase the smoking cessation rate andrecommend that clinicians minimally adopt abrief intervention using the Ask, Advise, andRefer approach.9
Nutrition and ObesityObesity rates have escalated in recent years, result-ing in 500 million obese adults worldwide, includ-ing 30% of American adults.107,108 Investigatorshave suggested that proinflammatory moleculesmay be altered by obesity and that obese individu-als have an increased prevalence of periodontitis.109
Suvan and colleagues studied 286 individuals todetermine the odds of an association betweenoverweight/obesity and diagnosis of periodontitis.Subjects with a body mass index (BMI) of 24.32 orgreater were 1.6 times more likely to have a diagno-sis of periodontitis than a subject with a lowerBMI.109 Another systematic review has reported apositive association between weight gain and newcases of periodontitis.110 A third review suggestedthat overweight, obesity, weight gain, andincreased waist circumference may be risk factorsfor the development of periodontitis or worseningof periodontal measures.111
Dental clinicians can educate patients about thepotential risk of overweight and obesity, and theirlink to periodontal conditions. They can delivernutrition and carbohydrate education to patientsand, if trained, can participate in programsfocused on weight reduction.108 In addition, theycan refer patients to other providers within thehealthcare system for assistance with their condi-tion. Not only will this potentially improve peri-odontal health, but it may improve overallsystemic risk of disease.
Stress and Psychological FactorsOnly one systematic review was located that investi-gated the scientific evidence for stress and psycholog-ical factors as risk factors for periodontal disease.Peruzzo and coworkers identified 58 articles ofwhich 14 met the selection criteria. Fifty-seven per-cent found a positive outcome between psychosocial
factors/stress and periodontal disease.112
Dental clinicians should consider stress as arisk factor for periodontal disease and discussoptions for stress reduction with patients. Refer-rals to healthcare or psychological professionalsshould be considered, as indicated.
CASE 1: Adolescent Female Patient
PATIENT OVERVIEWThe patient is a 16-year-old girl.Chief Complaint: “My gum tissues are too big.”Health History:American Society of Anesthesiol-ogists category 1 (ASA 1). Unremarkable findings.Dental History: Orthodontic treatment with nohistory of dental caries. Patient with poor oralhygiene.Main Periodontal Diagnosis: Plaque-induced gin-givitis associated with gingival overgrowth withlikely hormonal influence (see Figure 7).
OUTCOMEFigure 8 shows the patient 8 months later, afterremoval of orthodontic appliance, gingivectomy,and improved oral hygiene.
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
91
Figure 7.Case 1–Initial Presentation
Figure 8.Case 1–Eight Months Later
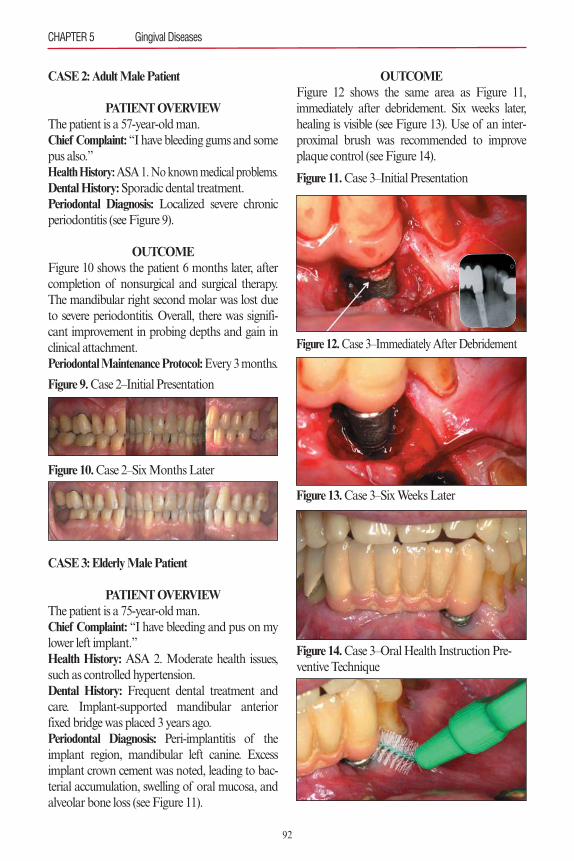
CASE 2: Adult Male Patient
PATIENT OVERVIEWThe patient is a 57-year-old man.Chief Complaint: “I have bleeding gums and somepus also.”Health History:ASA 1. No known medical problems.Dental History:Sporadic dental treatment.Periodontal Diagnosis: Localized severe chronicperiodontitis (see Figure 9).
OUTCOMEFigure 10 shows the patient 6 months later, aftercompletion of nonsurgical and surgical therapy.The mandibular right second molar was lost dueto severe periodontitis. Overall, there was signifi-cant improvement in probing depths and gain inclinical attachment.Periodontal Maintenance Protocol:Every 3 months.
CASE 3: Elderly Male Patient
PATIENT OVERVIEWThe patient is a 75-year-old man.Chief Complaint: “I have bleeding and pus on mylower left implant.”Health History: ASA 2. Moderate health issues,such as controlled hypertension.Dental History: Frequent dental treatment andcare. Implant-supported mandibular anteriorfixed bridge was placed 3 years ago.Periodontal Diagnosis: Peri-implantitis of theimplant region, mandibular left canine. Excessimplant crown cement was noted, leading to bac-terial accumulation, swelling of oral mucosa, andalveolar bone loss (see Figure 11).
OUTCOMEFigure 12 shows the same area as Figure 11,immediately after debridement. Six weeks later,healing is visible (see Figure 13). Use of an inter-proximal brush was recommended to improveplaque control (see Figure 14).
CHAPTER 5 Gingival Diseases
92
Figure 9.Case 2–Initial Presentation
Figure 10.Case 2–Six Months Later
Figure 12.Case 3–Immediately After Debridement
Figure 11.Case 3–Initial Presentation
Figure 14.Case 3–Oral Health Instruction Pre-ventive Technique
Figure 13.Case 3–Six Weeks Later
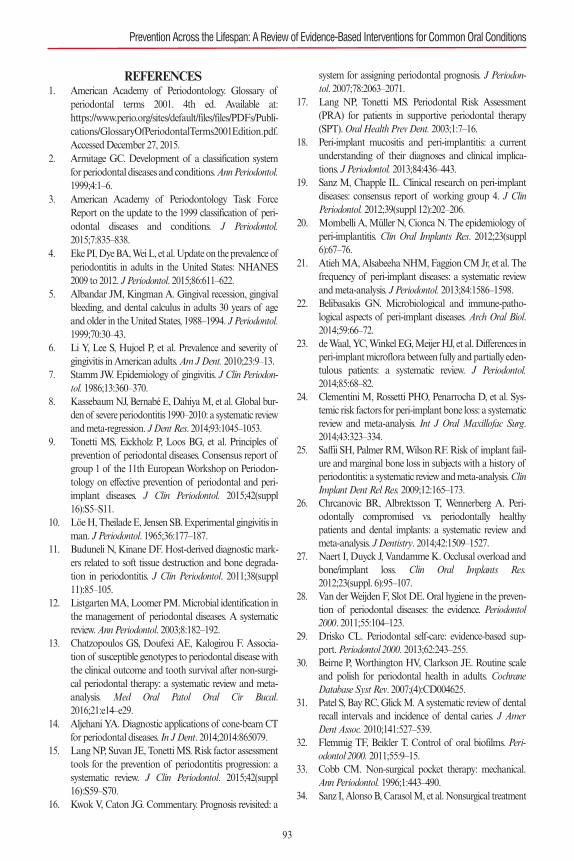
REFERENCES1. American Academy of Periodontology. Glossary of
periodontal terms 2001. 4th ed. Available at:https://www.perio.org/sites/default/files/files/PDFs/Publi-cations/GlossaryOfPeriodontalTerms2001Edition.pdf.Accessed December 27, 2015.
2. Armitage GC. Development of a classification systemfor periodontal diseases and conditions. Ann Periodontol.1999;4:1–6.
3. American Academy of Periodontology Task ForceReport on the update to the 1999 classification of peri-odontal diseases and conditions. J Periodontol.2015;7:835–838.
4. Eke PI, Dye BA, Wei L, et al. Update on the prevalence ofperiodontitis in adults in the United States: NHANES2009 to 2012. J Periodontol. 2015;86:611–622.
5. Albandar JM, Kingman A. Gingival recession, gingivalbleeding, and dental calculus in adults 30 years of ageand older in the United States, 1988–1994. J Periodontol.1999;70:30–43.
6. Li Y, Lee S, Hujoel P, et al. Prevalence and severity ofgingivitis in American adults. Am J Dent. 2010;23:9–13.
7. Stamm JW. Epidemiology of gingivitis. J Clin Periodon-tol. 1986;13:360–370.
8. Kassebaum NJ, Bernabé E, Dahiya M, et al. Global bur-den of severe periodontitis 1990–2010: a systematic reviewand meta-regression. J Dent Res. 2014;93:1045–1053.
9. Tonetti MS, Eickholz P, Loos BG, et al. Principles ofprevention of periodontal diseases. Consensus report ofgroup 1 of the 11th European Workshop on Periodon-tology on effective prevention of periodontal and peri-implant diseases. J Clin Periodontol. 2015;42(suppl16):S5–S11.
10. Löe H, Theilade E, Jensen SB. Experimental gingivitis inman. J Periodontol. 1965;36:177–187.
11. Buduneli N, Kinane DF. Host-derived diagnostic mark-ers related to soft tissue destruction and bone degrada-tion in periodontitis. J Clin Periodontol. 2011;38(suppl11):85–105.
12. Listgarten MA, Loomer PM. Microbial identification inthe management of periodontal diseases. A systematicreview. Ann Periodontol. 2003;8:182–192.
13. Chatzopoulos GS, Doufexi AE, Kalogirou F. Associa-tion of susceptible genotypes to periodontal disease withthe clinical outcome and tooth survival after non-surgi-cal periodontal therapy: a systematic review and meta-analysis. Med Oral Patol Oral Cir Bucal.2016;21:e14–e29.
14. Aljehani YA. Diagnostic applications of cone-beam CTfor periodontal diseases. In J Dent. 2014;2014:865079.
15. Lang NP, Suvan JE, Tonetti MS. Risk factor assessmenttools for the prevention of periodontitis progression: asystematic review. J Clin Periodontol. 2015;42(suppl16):S59–S70.
16. Kwok V, Caton JG. Commentary. Prognosis revisited: a
system for assigning periodontal prognosis. J Periodon-tol. 2007;78:2063–2071.
17. Lang NP, Tonetti MS. Periodontal Risk Assessment(PRA) for patients in supportive periodontal therapy(SPT). Oral Health Prev Dent. 2003;1:7–16.
18. Peri-implant mucositis and peri-implantitis: a currentunderstanding of their diagnoses and clinical implica-tions. J Periodontol. 2013;84:436–443.
19. Sanz M, Chapple IL. Clinical research on peri-implantdiseases: consensus report of working group 4. J ClinPeriodontol. 2012;39(suppl 12):202–206.
20. Mombelli A, Müller N, Cionca N. The epidemiology ofperi-implantitis. Clin Oral Implants Res. 2012;23(suppl6):67–76.
21. Atieh MA, Alsabeeha NHM, Faggion CM Jr, et al. Thefrequency of peri-implant diseases: a systematic reviewand meta-analysis. J Periodontol. 2013;84:1586–1598.
22. Belibasakis GN. Microbiological and immune-patho-logical aspects of peri-implant diseases. Arch Oral Biol.2014;59:66–72.
23. de Waal, YC, Winkel EG, Meijer HJ, et al. Differences inperi-implant microflora between fully and partially eden-tulous patients: a systematic review. J Periodontol.2014;85:68–82.
24. Clementini M, Rossetti PHO, Penarrocha D, et al. Sys-temic risk factors for peri-implant bone loss: a systematicreview and meta-analysis. Int J Oral Maxillofac Surg.2014;43:323–334.
25. Saffii SH, Palmer RM, Wilson RF. Risk of implant fail-ure and marginal bone loss in subjects with a history ofperiodontitis: a systematic review and meta-analysis. ClinImplant Dent Rel Res. 2009;12:165–173.
26. Chrcanovic BR, Albrektsson T, Wennerberg A. Peri-odontally compromised vs. periodontally healthypatients and dental implants: a systematic review andmeta-analysis. J Dentistry. 2014;42:1509–1527.
27. Naert I, Duyck J, Vandamme K. Occlusal overload andbone/implant loss. Clin Oral Implants Res.2012;23(suppl. 6):95–107.
28. Van der Weijden F, Slot DE. Oral hygiene in the preven-tion of periodontal diseases: the evidence. Periodontol2000. 2011;55:104–123.
29. Drisko CL. Periodontal self-care: evidence-based sup-port. Periodontol 2000. 2013;62:243–255.
30. Beirne P, Worthington HV, Clarkson JE. Routine scaleand polish for periodontal health in adults. CochraneDatabase Syst Rev. 2007;(4):CD004625.
31. Patel S, Bay RC, Glick M. A systematic review of dentalrecall intervals and incidence of dental caries. J AmerDent Assoc. 2010;141:527–539.
32. Flemmig TF, Beikler T. Control of oral biofilms. Peri-odontol 2000. 2011;55:9–15.
33. Cobb CM. Non-surgical pocket therapy: mechanical.Ann Periodontol. 1996;1:443–490.
34. Sanz I, Alonso B, Carasol M, et al. Nonsurgical treatment
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
93
of periodontitis. J Evid Based Dent Pract. 2012;12:76–86.35. Van der Weijden GA, Timmerman MF. A systematic
review on the clinical efficacy of subgingival debride-ment in the treatment of chronic periodontitis. J ClinPeriodontol. 2002;29(suppl 3):55–71.
36. Hallmon WW, Rees TD. Local anti-infective therapy:mechanical and physical approaches. A systematicreview. Ann Periodontol. 2003;8:99–114.
37. Rabbani GM, Ash MM Jr, Caffesse RG. The effective-ness of subgingival scaling and root planing in calculusremoval. J Periodontol. 1981;52:119–123.
38. Stambaugh RV, Dragoo M, Smith DM, et al. The limitsof subgingival scaling. Int J Periodontics RestorativeDent. 1981;1:30–41.
39. Waerhaug J. Healing of the dento-epithelial junction fol-lowing subgingival plaque control. II: as observed onextracted teeth. J Periodontol. 1978;49:119–134.
40. Sherman PR, Hutchens LH, Jewson LG. The effective-ness of subgingival scaling and root planing II. Clinicalresponses related to residual calculus. J Periodontal.1990;61:16–20.
41. Baderstein A, Nilveus R. Egelberg J. Effect of nonsurgi-cal periodontal therapy. Moderately advanced periodon-titis. J Clin Periodontol. 1981;8:57–72.
42. Drisko, CH. Nonsurgical periodontal therapy. Periodon-tol 2000. 2001;25:77–88.
43. Tunkel J, Heinecke A, Flemmig TF. A systematic reviewof efficacy of machine-driven and manual subgingivaldebridement in the treatment of chronic periodontitis. JClin Periodontol. 2002;29:72–81.
44. Walmsley AD, Lea SC, Landini G, Moses AJ. Advancesin power driven pocket/root instrumentation. J Clin Peri-odontol. 2008;35:22–28.
45. Aykol G, Baser U, Maden I, et al. The effect of low-levellaser therapy as an adjunct to non-surgical periodontaltreatment. J Periodontol. 2011;82:481–488.
46. Smiley CJ, Tracy SL, Abt E, et al. Systematic review andmeta-analysis on the nonsurgical treatment of chronicperiodontitis by means of scaling and root planing withor without adjuncts. J Am Dent Assoc. 2015;146:508–524.
47. Smiley CJ, Tracy SL, Michalowicz BS, et al. Evidence–based clinical practice guideline on the nonsurgical treat-ment of chronic periodontitis by means of scaling androot planing with or without adjuncts. J Am Dent Assoc.2015;146:525–535.
48. ADA Center for Evidence Based Dentistry. Clinical prac-tice guidelines. Available at: http://ebd.ada.org/en/evi-dence/guidelines/nonsurgical-treatment-of-chronic-periodontitis. Accessed January 9, 2016.
49. Eberhard J, Jervoe-Storm PM, Needleman I, et al. Full-mouth treatment concepts for chronic periodontitis: asystematic review. J Clin Periodontol. 2008;35:591–604.
50. Zijnge V, Meijer HF, Lie M-A, et al. The recolonizationhypothesis in a full-mouth or multiple-session treatmentprotocol: a blinded, randomized clinical trial. J Clin Peri-odontol. 2010;37:518–525.
51. Knöfler GU, Purschwitz RE, Eick S, et al. Microbiolog-ic findings 1 year after partial- and full-mouth scaling inthe treatment of moderate chronic periodontitis. Quin-tessence Int. 2011;42:e107–e117.
52. Fang H, Han M, Li QL, et al. Comparison of full-mouth disinfection and quadrant-wise scaling in thetreatment of adult chronic periodontitis: a systematicreview and meta-analysis. J Periodontal Res. 2015 Oct19. doi: 10.1111/jre.12326. [Epub ahead of print.]
53. Stambaugh RV, Myers G, Ebling W, et al. Endoscopicvisualization of the submarginal gingiva dental sulcusand tooth root surfaces. J Periodontol. 2002;73:374–382.
54. Geisinger ML, Mealey BL, Schoolfield J, et al. The effec-tiveness of subgingival scaling and root planing: an eval-uation of therapy with and without the use of theperiodontal endoscope. J Periodontol. 2007;78:22–28.
55. Michaud RM, Schoolfield J, Mellonig JT, et al. The effi-cacy of subgingival calculus removal with endoscopy-aided scaling and root planing: a study on multirootedteeth. J Periodontol. 2007;78:2238–2245.
56. Osborn JB, Lenton PA, Lunos SA, et al. Endoscopic vs.tactile evaluation of subgingival calculus. J Dent Hyg.2014;88:229–236.
57. Petersilka GJ. Subgingival air-polishing in the treatmentof periodontal biofilm infections. Periodontol 2000.2011;55;124–142.
58. Petersilka GJ, Bell M, Haberlein I, et al. In vitro evalua-tion of novel low abrasive air polishing powders. J ClinPeriodontal. 2003; 30:9–13.
59. Flemmig TF, Arushanov D, Daubert D, et al. Random-ized controlled trial assessing efficacy and safety ofglycine powder air polishing in moderate to deep peri-odontal pockets. J Periodontol . 2012;83:444–452.
60. Wennström JL, Dahlén G, Ramberg P. Subgingivaldebridement of periodontal pockets by air polishing incomparison with ultrasonic instrumentation during main-tenance therapy. J Clin Periodontol. 2011;38:820–827.
61. Moëne R, Décaillet F, Andersen E, et al. Subgingivalplaque removal using a new air-polishing device. J Peri-odontol. 2010;81:79–88.
62. Sculean A, Bastendorf ,KD, Becker C, et al. A para-digm shift in mechanical biofilm management? Subgin-gival air polishing: a new way to improve mechanicalbiofilm management in the dental practice. QuintessenceInt. 2013;44:475–477.
63. Schmage P, Thielemann J, Nergiz I, et al. Effects of 10cleaning instruments on four different implant surfaces.Int J Oral Maxillofac Implants. 2012;27:308–317.
64. Greenstein G. Research, Science and Therapy Commit-tee of the American Academy of Periodontology. Posi-tion paper: the role of supra- and subgingival irrigationin the treatment of periodontal diseases. J Periodontol2005:76:2015–2027.
65. Sbordone L, Ramaglia L, Guletta W, et al. Recoloniza-tion of the subgingival microflora after scaling and rootplaning in human periodontitis. J Periodontol.
CHAPTER 5 Gingival Diseases
94
1990;61:579–584.66. Elworthy A, Greenman J, Doherty FM, et al. The sub-
stantivity of a number of oral hygiene products deter-mined by the duration of effects on salivary bacteria. JPeriodontol. 1996;76:572–576.
67. Jeffcoat MK, Bray KS, Ciancio SG, et al. Adjunctive useof a subgingival controlled-release chlorhexidine chipreduces probing depth and improves attachment levelcompared with scaling and root planing along. J Peri-odontol. 1998;69:989–997.
68. Stoller NH, Johnson LR, Trapnell S, et al. The pharma-cokinetic profile of a biodegradable controlled releasedelivery system containing doxycycline compared to sys-temically delivered doxycycline in gingival crevicular fluid,saliva, and serum. J Periodontol. 1998;69:1085–1091.
69. Christersson LA. Tissue Response and Release of Minocy-cline After Subgingival Deposition by Use of a ResorbablePolymer. Warminster, PA: OraPharma Inc; 1988.
70. Finkelman RD, Polson AM. Evidence-based considera-tions for the clinical use of locally delivered, controlled-release antimicrobials in periodontal therapy. J DentHyg. 2013;87:249–264.
71. Sgolastra F, Gatto R, Petrucci A, et al. Effectiveness ofsystemic amoxicillin/metronidazole as adjunctive thera-py to scaling and root planing in the treatment of chron-ic periodontitis: a systematic review and meta-analysis. JPeriodontol. 2012;83:1257–1269.
72. Farooqi OA, Wehler CJ, Gibson G, et al. Appropriaterecall interval for periodontal maintenance: a systematicreview. J Evid Based Dent Pract. 2015;15:171–181.
73. Worthington HV, Clarkson JE, Bryan G, et al. Routinescale and polish for periodontal health in adults.Cochrane Database Syst Rev. 2013;(11):CD004625.
74. Needleman I, Nibali L, Di Iorio A. Professionalmechanical plaque removal for prevention of periodon-tal diseases in adults—systematic review update. J ClinPeriodontol. 2015;42(suppl 16):S12–S35.
75. Wilder RS, Bray KS. Improving periodontal outcomes:merging clinical and behavioral science. Periodontol2000. 2016;71:65–81.
76. Giannobile WV, Braun TM, Caplis AK, et al. Patientstratification for preventive care in dentistry. J Dent Res2013;92:694–701.
77. Bidra AS, Daubert DM, Garcia LT, et al. Clinical prac-tice guidelines for recall and maintenance of patientswith tooth-borne and implant-borne dental restorations.J Prosthodont. 2016;25(suppl 1):S32–S40.
78. Van der Weijden GA, Hioe KP. A systematic review ofthe effectiveness of self-performed mechanical plaqueremoval in adults with gingivitis using a manual tooth-brush. J Clin Periodontol. 2005;32:214–228.
79. Needleman I, Nibali L, Di Iorio A. Professionalmechanical plaque removal for prevention of periodon-tal diseases in adults—systematic review update. J ClinPeriodontol. 2015;42(suppl 16):S12–S35.
80. Beals D, Ngo T, Feng Y, et al. Development and labora-
tory evaluation of a new toothbrush with a novel brushhead design. Am J Dent. 2000;13:5A–14A.
81. Chapple IL, Van der Weijden F, Doerfer C, et al. Pri-mary prevention of periodontitis: managing gingivitis. JClin Periodontol. 2015;42(suppl 16):S71–S76.
82. Heanue M, Deacon SA, Deery C, et al. Manual versuspowered toothbrushing for oral health. Cochrane Data-base Syst Rev. 2003;(1):CD002281.
83. Robinson PG, Deacon SA, Deery C, et al. Manual ver-sus powered toothbrushing for oral health. CochraneDatabase Syst Rev. 2005;(2):CD002281.
84. Deacon SA, Glenny AM, Deery C, et al. Different pow-ered toothbrushes for plaque control and gingival health.Cochrane Database Syst Rev. 2010;(12):CD004971.
85. Sambunjak D, Nickerson JW, Poklepovic T, et al. Floss-ing for the management of periodontal diseases anddental caries in adults. Cochrane Database Syst Rev.2011;(12):CD008829.
86. Slot DE, Dörfer CE, Van der Weijden GA. The efficacyof interdental brushes on plaque and parameters of peri-odontal inflammation: a systematic review. Int J DentHyg. 2008;6:253–264.
87. Jahn CA. The dental water jet: a historical review of theliterature. J Dent Hyg. 2010;84:114–120.
88. Bhaskar SN, Cutright DE, Frisch J. Effect of high pres-sure water jet on oral mucosa of varied density. J Peri-odontol. 1969; 40:593-598.
89. Eakle WS, Ford C, Boyd RL. Depth of penetration inperiodontal pockets with oral irrigation. J Clin Periodon-tol. 1986;13:39–44.
90. Braun RE, Ciancio SG. Subgingival delivery by an oralirrigation device. J Periodontol. 1992;63:469–472.
91. Husseini A, Slot DE, Van der Weijden GA. The efficacyof oral irrigation in addition to a toothbrush on plaqueand the clinical parameters of periodontal inflammation:a systematic review. Int J Dent Hyg. 2008;6:304–314.
92. Hioe KP, van der Weijden GA. The effectiveness of self-performed mechanical plaque control with triclosancontaining dentifrices. Int J Dent Hyg. 2005;3:192–204.
93. Davies RM, Ellwood RP, Davies GM. The effectivenessof a toothpaste containing triclosan and polyvinyl-methyl ether maleic acid copolymer in improving plaquecontrol and gingival health: a systematic review. J ClinPeriodontol. 2004;31:1029–1033.
94. Gunsolley JC. A meta-analysis of six-month studies ofantiplaque and antigingivitis agents. J Am Dent Assoc.2006;137:1649–1657.
95. Van Strydonck DA, Slot DE, Van der Velden U, et al.Effect of a chlorhexidine mouthrinse on plaque, gingivalinflammation and staining in gingivitis patients: a sys-tematic review. J Clin Periodontol. 2012;39:1042–1055.
96. Sharma N, Charles CH, Lynch MC, et al. Adjunctivebenefit of an essential oil-containing mouthrinse inreducing plaque and gingivitis in patients who brush andfloss regularly: a six-month study. J Am Dent Assoc.2004;135:496–504.
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
95
97. Addy M. Oral hygiene products: potential for harm to oraland systemic health? Periodontol 2000. 2008;48:54–65.
98. Rath SK, Singh M. Comparative clinical and microbio-logical efficacy of mouthwashes containing 0.2% and0.12% chlorhexidine. Dent Res J. 2013;10:364–369.
99. Sheen S, Owens J, Addy M. The effect of toothpaste onthe propensity of chlorhexidine and cetylpyridiniumchloride to produce staining in vitro: a possible predictorof inactivation. J Clin Periodontol. 2001;28:46–51.
100. Kolahi J, Soolari A. Rinsing with chlorhexidine glu-conate solution after brushing and flossing teeth: a sys-tematic review of effectiveness. Quintessence Int.2006;37:605–612.
101. Yanine N, Ayaya I, Brignardello-Petersen R, et al.Effects of probiotics in periodontal diseases: a systematicreview. Clin Oral Investig. 2013;17:1627–1634.
102. Chaushu L, Weinreb M, Beitlitum I, et al. Evaluation ofa topical herbal patch for soft tissue wound healing: ananimal study. J Clin Periodontol. 2015;42:288–293.
103. San Miguel SM, Opperman LA, Allen EP, et al. Bioac-tive antioxidant mixtures promote proliferation andmigration on human oral fibroblasts. Arch Oral Biol.2011;56:812–822.
104. Muniz FW, Nogueira SB, Mendes FL. The impact ofantioxidant agents complimentary to periodontal thera-py on oxidative stress and periodontal outcomes: a sys-tematic review. Arch Oral Biol. 2015;60:1203–1214.
105. Rosa EF, Corraini P, Inoue G, et al. Effect of smokingcessation on non-surgical periodontal therapy: resultsafter 24 months. J Clin Periodontol. 2014;41:1145–1153.
106. Ramseier CA, Suvan JE. Behaviour change counsellingfor tobacco use cessation and promotion of healthylifestyles: a systematic review. J Clin Periodontol.2015;42(suppl 16):S47–S58.
107. Wang YC, McPherson K, Marsh T, et al. Health andeconomic burden of the projected obesity trends in theUSA and the UK. Lancet. 2011;378:815–825.
108. Lamster IB, Eaves K. A model for dental practice in the21st century. Am J Pub Health. 2011;101:1825–1830.
109. Suvan J, D’Aiuto F, Moles DR, et al. Associationbetween overweight/obesity and periodontitis in adults.A systematic review. Obesity Reviews. 2011;12:3381–3404.
110. Nascimento GG, Leite FR, Do LG, et al. Is weight gainassociated with the incidence of periodontitis? A system-atic review and meta-analysis. J Clin Periodontol.2015;42:495–505.
111. Keller A, Rohde JF, Raymond K, et al. Associationbetween periodontal disease and overweight and obesity:a systematic review. J Periodontol. 2015;86:766–776.
112. Peruzzo DC, Benatti BB, Ambrosano GM, et al. A sys-tematic review of stress and psychological factors as pos-sible risk factors for periodontal disease. J Periodontol.2007;78:1491–1504.
96

PART 1: DAMAGE TO ORAL SOFT TISSUES
EPIDEMIOLOGYWear and tear is damage that naturally, inevitablyoccurs with normal wear or aging but can beaccelerated by various etiologic factors. Trauma ofthe marginal gingiva may result from different eti-ologies and clinical manifestations, causing apicalmigration of the gingiva that exposes root sur-faces. Loss of soft tissue can be rapid and acute orslow and chronic. Both preventative measures toreduce damage and corrective procedures areavailable to improve esthetics or function.
The American Academy of Periodontology(AAP) 1999 Classification of Periodontal Diseaseincludes a section on nonplaque-induced gingivaldisease, listing traumatic gingival lesions as a sub-category.1 These lesions may result from self-inflict-ed (factitious), accidental, or iatrogenic injuries.They may present as localized gingival recession,abrasions, ulcerations, or burns. Traumatic lesionsalso may be induced by gingival exposure to chemi-cals or medication. Physical injury may result froman accident, ill-fitting appliance, or inappropriateoral hygiene procedures or agents. Self-inflictedlesions are also termed gingivitis artefacta. Self-inflicted gingival injuries in children and adoles-cents can result from accidental trauma,premeditated infliction, or chronic habits such asfingernail biting, digit sucking, or sucking onobjects such as pens, pencils, or pacifiers.2
Very few studies discuss the epidemiology oftrauma to gingiva, and they are primarily casereports. One recent case series presents a samplingof traumatic gingival lesions resulting from chemi-
cal, physical, and thermal insult.3 Another paperdescribes 13 cases with chemical, physical, andthermal injuries to the oral tissues.4 Several othercase reports document trauma resulting from oralpiercings. Another report presents unusual gingi-val recession caused by lip piercing.5,6
In one study, 52 adults with tongue piercingswere examined for gingival recession on the lin-gual aspect of the 12 anterior teeth and for toothchipping anywhere in the mouth. The authorsreported that long-term use of a tongue barbellincreased the prevalence of these complications.Tongue piercing was also associated with lingualrecession of mandibular anterior teeth and chip-ping of posterior teeth. This paper also included areport of an 18-year-old man who developed gin-gival recession on the facial aspect of themandibular right central incisor associated withlip piercing. A concurrent recession along the lin-gual aspects of the mandibular left lateral and cen-tral incisors plus the mandibular right lateralincisor were attributed to an unusually large-diam-eter tongue barbell the patient wore.7
Intraoral and perioral jewelry may be associatedwith the development of significant mucogingivaldeformities. Most periodontal lesions reported withoral piercings involved tongue jewelry (64.3%) andlip jewelry (35.7%). The site of gingival recessionmost frequently recorded with tongue piercing wasthe lingual aspect of the lower central incisors.Injuries caused by lip jewelry, when specified, werelocalized to the facial aspect of the mandibularright central incisor in 58.3% of the reported casesand to the mandibular central incisors in 41.7% ofthe reported cases8 (see Figure 1).
The AAP Classification also recognizes devel-opmental or acquired conditions that can lead toa localized tooth-related position that may predis-pose to plaque accumulation and inflammatorychanges or mucogingival abnormalities. Preva-lence and severity of gingival recession defects areassociated with periodontitis. Unfortunately, thereare few epidemiological studies dealing with gingi-val recession. A review of cross-sectional epidemi-ological studies of gingival recession correlatesrecession to trauma, gender, malpositioned teeth,tobacco consumption, and inflammation (see Fig-ure 2). Gingival recession was found in patients
Preventing Damage to Oral Hard and Soft Tissues
Chapter 6
Marc Shlossman and Mark Montana
97
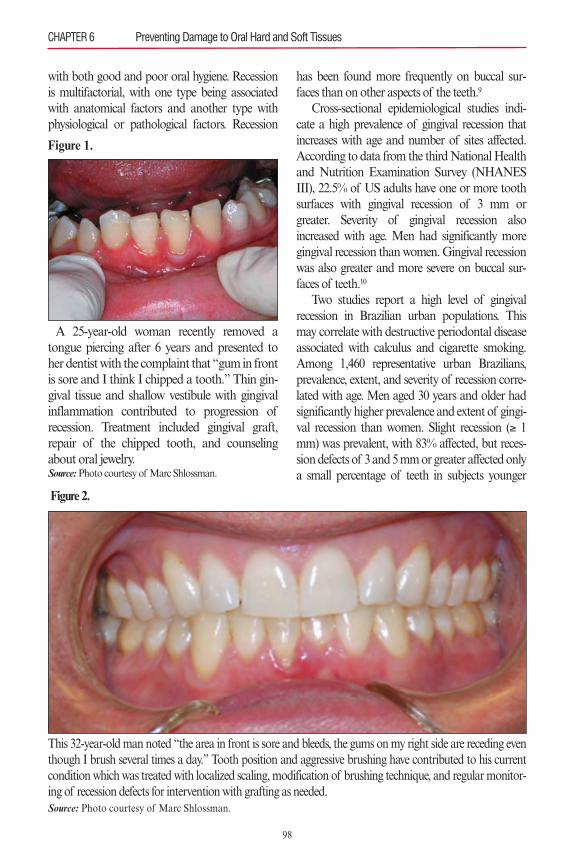
with both good and poor oral hygiene. Recessionis multifactorial, with one type being associatedwith anatomical factors and another type withphysiological or pathological factors. Recession
has been found more frequently on buccal sur-faces than on other aspects of the teeth.9
Cross-sectional epidemiological studies indi-cate a high prevalence of gingival recession thatincreases with age and number of sites affected.According to data from the third National Healthand Nutrition Examination Survey (NHANESIII), 22.5% of US adults have one or more toothsurfaces with gingival recession of 3 mm orgreater. Severity of gingival recession alsoincreased with age. Men had significantly moregingival recession than women. Gingival recessionwas also greater and more severe on buccal sur-faces of teeth.10
Two studies report a high level of gingivalrecession in Brazilian urban populations. Thismay correlate with destructive periodontal diseaseassociated with calculus and cigarette smoking.Among 1,460 representative urban Brazilians,prevalence, extent, and severity of recession corre-lated with age. Men aged 30 years and older hadsignificantly higher prevalence and extent of gingi-val recession than women. Slight recession (≥ 1mm) was prevalent, with 83% affected, but reces-sion defects of 3 and 5 mm or greater affected onlya small percentage of teeth in subjects younger
CHAPTER 6 Preventing Damage to Oral Hard and Soft Tissues
Figure 1.
A 25-year-old woman recently removed atongue piercing after 6 years and presented toher dentist with the complaint that “gum in frontis sore and I think I chipped a tooth.” Thin gin-gival tissue and shallow vestibule with gingivalinflammation contributed to progression ofrecession. Treatment included gingival graft,repair of the chipped tooth, and counselingabout oral jewelry.Source:Photo courtesy of Marc Shlossman.
Figure 2.
This 32-year-old man noted “the area in front is sore and bleeds, the gums on my right side are receding eventhough I brush several times a day.” Tooth position and aggressive brushing have contributed to his currentcondition which was treated with localized scaling, modification of brushing technique, and regular monitor-ing of recession defects for intervention with grafting as needed.Source: Photo courtesy of Marc Shlossman.
98
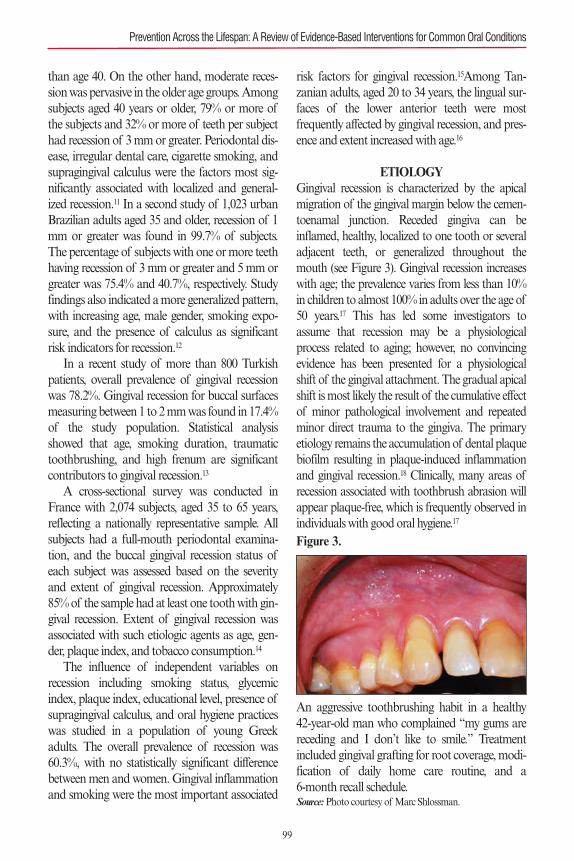
than age 40. On the other hand, moderate reces-sion was pervasive in the older age groups. Amongsubjects aged 40 years or older, 79% or more ofthe subjects and 32% or more of teeth per subjecthad recession of 3 mm or greater. Periodontal dis-ease, irregular dental care, cigarette smoking, andsupragingival calculus were the factors most sig-nificantly associated with localized and general-ized recession.11 In a second study of 1,023 urbanBrazilian adults aged 35 and older, recession of 1mm or greater was found in 99.7% of subjects.The percentage of subjects with one or more teethhaving recession of 3 mm or greater and 5 mm orgreater was 75.4% and 40.7%, respectively. Studyfindings also indicated a more generalized pattern,with increasing age, male gender, smoking expo-sure, and the presence of calculus as significantrisk indicators for recession.12
In a recent study of more than 800 Turkishpatients, overall prevalence of gingival recessionwas 78.2%. Gingival recession for buccal surfacesmeasuring between 1 to 2 mm was found in 17.4%of the study population. Statistical analysisshowed that age, smoking duration, traumatictoothbrushing, and high frenum are significantcontributors to gingival recession.13
A cross-sectional survey was conducted inFrance with 2,074 subjects, aged 35 to 65 years,reflecting a nationally representative sample. Allsubjects had a full-mouth periodontal examina-tion, and the buccal gingival recession status ofeach subject was assessed based on the severityand extent of gingival recession. Approximately85% of the sample had at least one tooth with gin-gival recession. Extent of gingival recession wasassociated with such etiologic agents as age, gen-der, plaque index, and tobacco consumption.14
The influence of independent variables onrecession including smoking status, glycemicindex, plaque index, educational level, presence ofsupragingival calculus, and oral hygiene practiceswas studied in a population of young Greekadults. The overall prevalence of recession was60.3%, with no statistically significant differencebetween men and women. Gingival inflammationand smoking were the most important associated
risk factors for gingival recession.15Among Tan-zanian adults, aged 20 to 34 years, the lingual sur-faces of the lower anterior teeth were mostfrequently affected by gingival recession, and pres-ence and extent increased with age.16
ETIOLOGYGingival recession is characterized by the apicalmigration of the gingival margin below the cemen-toenamal junction. Receded gingiva can beinflamed, healthy, localized to one tooth or severaladjacent teeth, or generalized throughout themouth (see Figure 3). Gingival recession increaseswith age; the prevalence varies from less than 10%in children to almost 100% in adults over the age of50 years.17 This has led some investigators toassume that recession may be a physiologicalprocess related to aging; however, no convincingevidence has been presented for a physiologicalshift of the gingival attachment. The gradual apicalshift is most likely the result of the cumulative effectof minor pathological involvement and repeatedminor direct trauma to the gingiva. The primaryetiology remains the accumulation of dental plaquebiofilm resulting in plaque-induced inflammationand gingival recession.18 Clinically, many areas ofrecession associated with toothbrush abrasion willappear plaque-free, which is frequently observed inindividuals with good oral hygiene.17
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
Figure 3.
An aggressive toothbrushing habit in a healthy 42-year-old man who complained “my gums arereceding and I don’t like to smile.” Treatmentincluded gingival grafting for root coverage, modi-fication of daily home care routine, and a 6-month recall schedule.Source:Photo courtesy of Marc Shlossman.
99
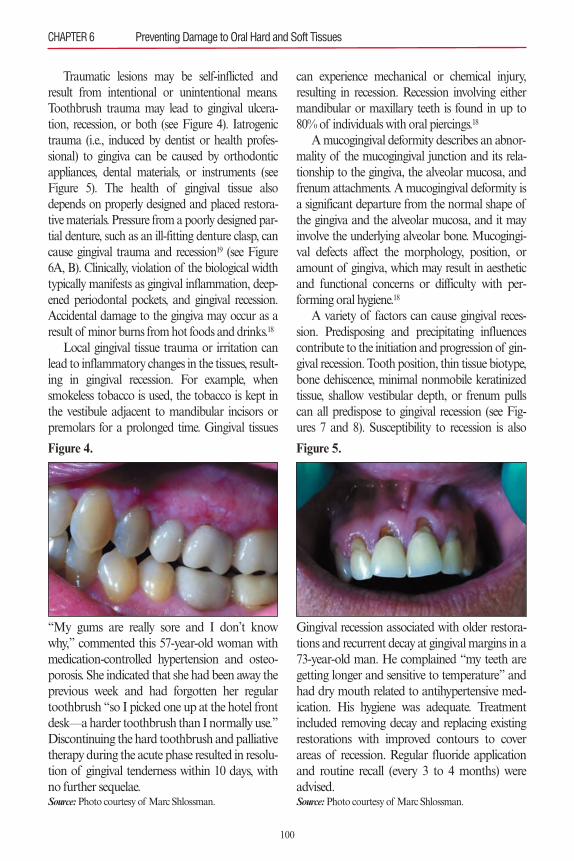
Traumatic lesions may be self-inflicted andresult from intentional or unintentional means.Toothbrush trauma may lead to gingival ulcera-tion, recession, or both (see Figure 4). Iatrogenictrauma (i.e., induced by dentist or health profes-sional) to gingiva can be caused by orthodonticappliances, dental materials, or instruments (seeFigure 5). The health of gingival tissue alsodepends on properly designed and placed restora-tive materials. Pressure from a poorly designed par-tial denture, such as an ill-fitting denture clasp, cancause gingival trauma and recession19 (see Figure6A, B). Clinically, violation of the biological widthtypically manifests as gingival inflammation, deep-ened periodontal pockets, and gingival recession.Accidental damage to the gingiva may occur as aresult of minor burns from hot foods and drinks.18
Local gingival tissue trauma or irritation canlead to inflammatory changes in the tissues, result-ing in gingival recession. For example, whensmokeless tobacco is used, the tobacco is kept inthe vestibule adjacent to mandibular incisors orpremolars for a prolonged time. Gingival tissues
can experience mechanical or chemical injury,resulting in recession. Recession involving eithermandibular or maxillary teeth is found in up to80% of individuals with oral piercings.18
A mucogingival deformity describes an abnor-mality of the mucogingival junction and its rela-tionship to the gingiva, the alveolar mucosa, andfrenum attachments. A mucogingival deformity isa significant departure from the normal shape ofthe gingiva and the alveolar mucosa, and it mayinvolve the underlying alveolar bone. Mucogingi-val defects affect the morphology, position, oramount of gingiva, which may result in aestheticand functional concerns or difficulty with per-forming oral hygiene.18
A variety of factors can cause gingival reces-sion. Predisposing and precipitating influencescontribute to the initiation and progression of gin-gival recession. Tooth position, thin tissue biotype,bone dehiscence, minimal nonmobile keratinizedtissue, shallow vestibular depth, or frenum pullscan all predispose to gingival recession (see Fig-ures 7 and 8). Susceptibility to recession is also
CHAPTER 6 Preventing Damage to Oral Hard and Soft Tissues
Figure 4.
“My gums are really sore and I don’t knowwhy,” commented this 57-year-old woman withmedication-controlled hypertension and osteo-porosis. She indicated that she had been away theprevious week and had forgotten her regulartoothbrush “so I picked one up at the hotel frontdesk—a harder toothbrush than I normally use.”Discontinuing the hard toothbrush and palliativetherapy during the acute phase resulted in resolu-tion of gingival tenderness within 10 days, withno further sequelae.Source:Photo courtesy of Marc Shlossman.
Figure 5.
Gingival recession associated with older restora-tions and recurrent decay at gingival margins in a73-year-old man. He complained “my teeth aregetting longer and sensitive to temperature” andhad dry mouth related to antihypertensive med-ication. His hygiene was adequate. Treatmentincluded removing decay and replacing existingrestorations with improved contours to coverareas of recession. Regular fluoride applicationand routine recall (every 3 to 4 months) wereadvised.Source:Photo courtesy of Marc Shlossman.
100
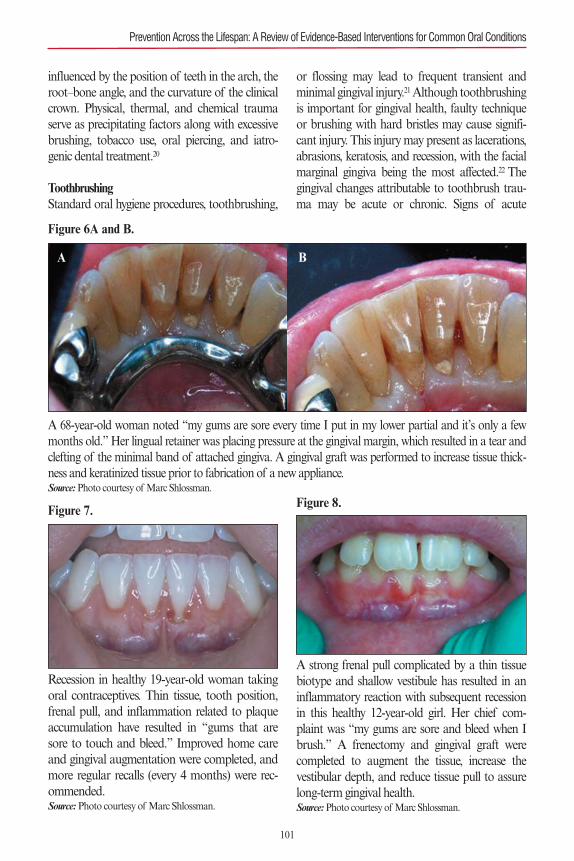
influenced by the position of teeth in the arch, theroot–bone angle, and the curvature of the clinicalcrown. Physical, thermal, and chemical traumaserve as precipitating factors along with excessivebrushing, tobacco use, oral piercing, and iatro-genic dental treatment.20
ToothbrushingStandard oral hygiene procedures, toothbrushing,
or flossing may lead to frequent transient andminimal gingival injury.21Although toothbrushingis important for gingival health, faulty techniqueor brushing with hard bristles may cause signifi-cant injury. This injury may present as lacerations,abrasions, keratosis, and recession, with the facialmarginal gingiva being the most affected.22 Thegingival changes attributable to toothbrush trau-ma may be acute or chronic. Signs of acute
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
Figure 6A and B.
A 68-year-old woman noted “my gums are sore every time I put in my lower partial and it’s only a fewmonths old.” Her lingual retainer was placing pressure at the gingival margin, which resulted in a tear andclefting of the minimal band of attached gingiva. A gingival graft was performed to increase tissue thick-ness and keratinized tissue prior to fabrication of a new appliance.Source:Photo courtesy of Marc Shlossman.
A B
Figure 7.
Recession in healthy 19-year-old woman takingoral contraceptives. Thin tissue, tooth position,frenal pull, and inflammation related to plaqueaccumulation have resulted in “gums that aresore to touch and bleed.” Improved home careand gingival augmentation were completed, andmore regular recalls (every 4 months) were rec-ommended.Source:Photo courtesy of Marc Shlossman.
Figure 8.
A strong frenal pull complicated by a thin tissuebiotype and shallow vestibule has resulted in aninflammatory reaction with subsequent recessionin this healthy 12-year-old girl. Her chief com-plaint was “my gums are sore and bleed when Ibrush.” A frenectomy and gingival graft werecompleted to augment the tissue, increase thevestibular depth, and reduce tissue pull to assurelong-term gingival health.Source:Photo courtesy of Marc Shlossman.
101
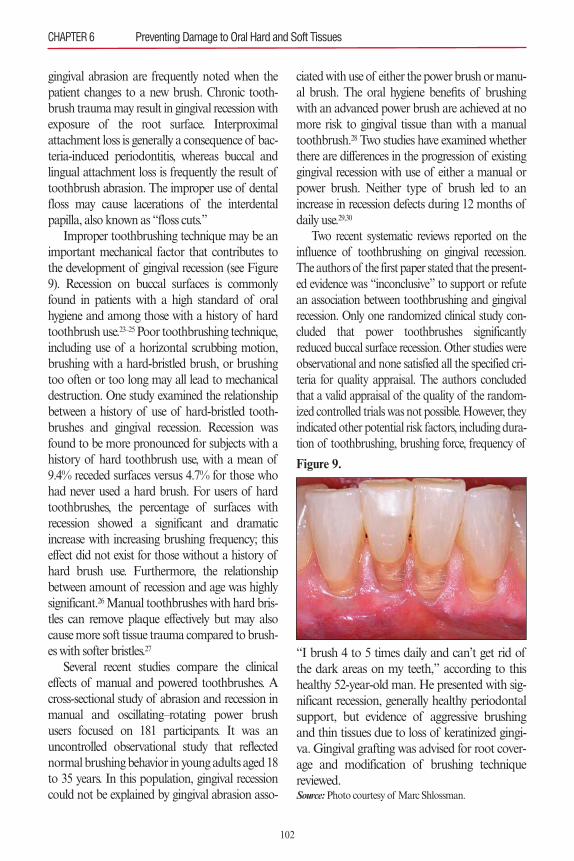
gingival abrasion are frequently noted when thepatient changes to a new brush. Chronic tooth-brush trauma may result in gingival recession withexposure of the root surface. Interproximalattachment loss is generally a consequence of bac-teria-induced periodontitis, whereas buccal andlingual attachment loss is frequently the result oftoothbrush abrasion. The improper use of dentalfloss may cause lacerations of the interdentalpapilla, also known as “floss cuts.”
Improper toothbrushing technique may be animportant mechanical factor that contributes tothe development of gingival recession (see Figure9). Recession on buccal surfaces is commonlyfound in patients with a high standard of oralhygiene and among those with a history of hardtoothbrush use.23–25 Poor toothbrushing technique,including use of a horizontal scrubbing motion,brushing with a hard-bristled brush, or brushingtoo often or too long may all lead to mechanicaldestruction. One study examined the relationshipbetween a history of use of hard-bristled tooth-brushes and gingival recession. Recession wasfound to be more pronounced for subjects with ahistory of hard toothbrush use, with a mean of9.4% receded surfaces versus 4.7% for those whohad never used a hard brush. For users of hardtoothbrushes, the percentage of surfaces withrecession showed a significant and dramaticincrease with increasing brushing frequency; thiseffect did not exist for those without a history ofhard brush use. Furthermore, the relationshipbetween amount of recession and age was highlysignificant.26Manual toothbrushes with hard bris-tles can remove plaque effectively but may alsocause more soft tissue trauma compared to brush-es with softer bristles.27
Several recent studies compare the clinicaleffects of manual and powered toothbrushes. Across-sectional study of abrasion and recession inmanual and oscillating–rotating power brushusers focused on 181 participants. It was anuncontrolled observational study that reflectednormal brushing behavior in young adults aged 18to 35 years. In this population, gingival recessioncould not be explained by gingival abrasion asso-
ciated with use of either the power brush or manu-al brush. The oral hygiene benefits of brushingwith an advanced power brush are achieved at nomore risk to gingival tissue than with a manualtoothbrush.28 Two studies have examined whetherthere are differences in the progression of existinggingival recession with use of either a manual orpower brush. Neither type of brush led to anincrease in recession defects during 12 months ofdaily use.29,30
Two recent systematic reviews reported on theinfluence of toothbrushing on gingival recession.The authors of the first paper stated that the present-ed evidence was “inconclusive” to support or refutean association between toothbrushing and gingivalrecession. Only one randomized clinical study con-cluded that power toothbrushes significantlyreduced buccal surface recession. Other studies wereobservational and none satisfied all the specified cri-teria for quality appraisal. The authors concludedthat a valid appraisal of the quality of the random-ized controlled trials was not possible. However, theyindicated other potential risk factors, including dura-tion of toothbrushing, brushing force, frequency of
CHAPTER 6 Preventing Damage to Oral Hard and Soft Tissues
Figure 9.
“I brush 4 to 5 times daily and can’t get rid ofthe dark areas on my teeth,” according to thishealthy 52-year-old man. He presented with sig-nificant recession, generally healthy periodontalsupport, but evidence of aggressive brushingand thin tissues due to loss of keratinized gingi-va. Gingival grafting was advised for root cover-age and modification of brushing techniquereviewed.Source:Photo courtesy of Marc Shlossman.
102
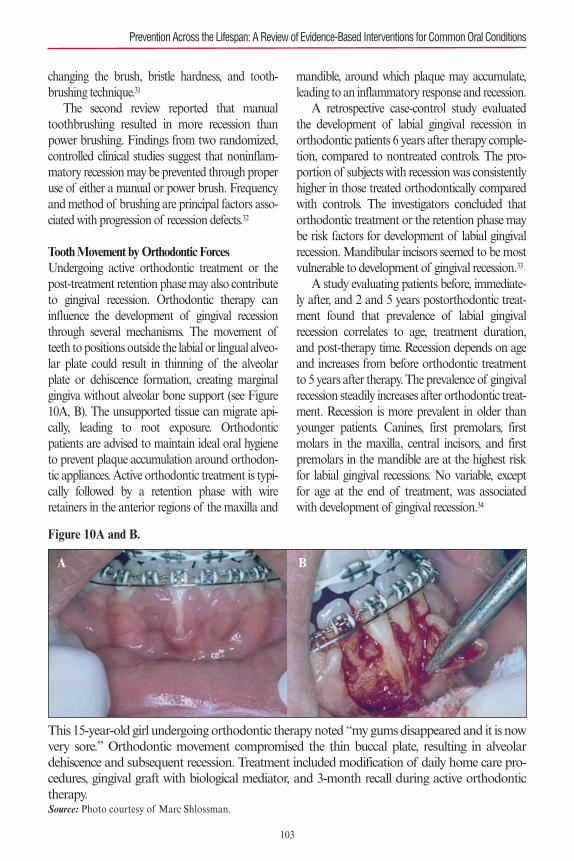
changing the brush, bristle hardness, and tooth-brushing technique.31
The second review reported that manualtoothbrushing resulted in more recession thanpower brushing. Findings from two randomized,controlled clinical studies suggest that noninflam-matory recession may be prevented through properuse of either a manual or power brush. Frequencyand method of brushing are principal factors asso-ciated with progression of recession defects.32
Tooth Movement by Orthodontic ForcesUndergoing active orthodontic treatment or thepost-treatment retention phase may also contributeto gingival recession. Orthodontic therapy caninfluence the development of gingival recessionthrough several mechanisms. The movement ofteeth to positions outside the labial or lingual alveo-lar plate could result in thinning of the alveolarplate or dehiscence formation, creating marginalgingiva without alveolar bone support (see Figure10A, B). The unsupported tissue can migrate api-cally, leading to root exposure. Orthodonticpatients are advised to maintain ideal oral hygieneto prevent plaque accumulation around orthodon-tic appliances. Active orthodontic treatment is typi-cally followed by a retention phase with wireretainers in the anterior regions of the maxilla and
mandible, around which plaque may accumulate,leading to an inflammatory response and recession.
A retrospective case-control study evaluatedthe development of labial gingival recession inorthodontic patients 6 years after therapy comple-tion, compared to nontreated controls. The pro-portion of subjects with recession was consistentlyhigher in those treated orthodontically comparedwith controls. The investigators concluded thatorthodontic treatment or the retention phase maybe risk factors for development of labial gingivalrecession. Mandibular incisors seemed to be mostvulnerable to development of gingival recession.33
A study evaluating patients before, immediate-ly after, and 2 and 5 years postorthodontic treat-ment found that prevalence of labial gingivalrecession correlates to age, treatment duration,and post-therapy time. Recession depends on ageand increases from before orthodontic treatmentto 5 years after therapy. The prevalence of gingivalrecession steadily increases after orthodontic treat-ment. Recession is more prevalent in older thanyounger patients. Canines, first premolars, firstmolars in the maxilla, central incisors, and firstpremolars in the mandible are at the highest riskfor labial gingival recessions. No variable, exceptfor age at the end of treatment, was associatedwith development of gingival recession.34
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
Figure 10A and B.
This 15-year-old girl undergoing orthodontic therapy noted “my gums disappeared and it is nowvery sore.” Orthodontic movement compromised the thin buccal plate, resulting in alveolardehiscence and subsequent recession. Treatment included modification of daily home care pro-cedures, gingival graft with biological mediator, and 3-month recall during active orthodontictherapy.Source: Photo courtesy of Marc Shlossman.
A B
103

Studies about effects of orthodontic treatmenton gingival recession typically suggest an inci-dence of 10% to 20% in patients evaluated for aslong as 5 years after the completion of orthodon-tic therapy.35 These rates of occurrence, consideredrelative to the overall high prevalence found inadults, suggest that orthodontic tooth movementmay contribute minimally to the overall preva-lence of gingival recession. Several recent studieseven suggest that postorthodontic recession mayaffect only 10% of patients, with most cases beingreadily treatable as Miller class I lesions.36
Frenal PullFrenal pull is frequently cited as a predisposing fac-tor to gingival recession. When the frenum attach-ment is proximate to the gingival margin,repetitious frenum stretch during oral functioncould exert forces that compromise mucosal tissuemargins, leading to gingival recession. Plaqueremoval along affected marginal gingiva may alsobe impeded. However, cross-sectional studies failedto demonstrate an association of recession withhigh frenum attachment.20 Previous studies examin-ing the influence of frenal pull on recession areinconclusive. Only one study reported a correlationbetween high frenum and gingival recession, andthis involved male participants in Turkey.13
Traumatic Lesions (Factitious, Iatrogenic, and Accidental)Traumatic lesions may be accidental or result frominappropriate oral hygiene procedures, inadequatedental restorations, poorly designed dental appli-ances, or orthodontic bands and devices. Deficien-cies in dental restorations or prostheses may alsoeffect gingival inflammation and periodontaldamage. Inadequate dental procedures that con-tribute to deterioration of periodontal tissues arereferred to as iatrogenic factors. Laceration of thegingiva may result from the use of rubber damclamps, matrix bands, and burs. Although suchtransient injuries generally heal, they are unneces-sary patient discomforts. Orthodontic therapymay affect the periodontium by directly injuringthe gingiva as a result of overextended bands or
loose wires.37 Maintenance of periodontal healthfocuses on specific characteristics of dentalrestorations and removable partial dentures. Theyinclude location of the gingival margin for therestoration, space between restorative margin andunprepared tooth, contour of restoration, occlu-sion, materials used in the restoration, type ofrestorative procedure, and design of the removablepartial denture.
Chemical, physical, and thermal injuries in theoral, gingival, or palatal mucosa of iatrogenic ori-gin can exhibit various clinical features. Manage-ment of traumatic injuries is dependent on theseverity of involved periodontal tissues. Thirteencases of chemical (ferric sulfate and formocresol),physical (due to orthodontic wires and appli-ances), and thermal (due to electrosurgery)injuries to the oral tissues have been reported. Inmost cases, elimination of the offending agent andsymptomatic therapy are sufficient to allow for tis-sue repair; in severe cases, or when injury results inpermanent defects, periodontal surgery and regen-erative therapy may be necessary.3,38
Iatrogenic injuries are often acute and are gen-erally self-limiting, whereas factitious injuries tendto be more chronic in nature. Patients may beunaware of self-inflicted injurious habits that mayimpact the initiation and progression of periodon-tal pathology. Mechanical forms of trauma canstem from the improper use of a toothbrush,toothpicks and other interdental aids between theteeth, dental floss, fingernail pressure, pizza burns,and other causes (see Figure 11). Sources ofchemical irritation include the topical applicationof caustic agents, such as aspirin (see Figure 12) orcocaine; accidental contact with drugs, such asphenol or silver nitrate; allergic reactions to com-ponents in toothpaste and chewing gum; or theuse of chewing tobacco, betel nut, bleachingagents, and concentrated mouthrinse.37
Use of smokeless tobacco is an important eti-ologic factor that can lead to gingival recession.Snuff and chewing tobacco constitute the twomain forms of smokeless tobacco. Snuff is a fine-cut form of tobacco that is available looselypacked or in small sachets. Chewing tobacco is a
CHAPTER 6 Preventing Damage to Oral Hard and Soft Tissues
104
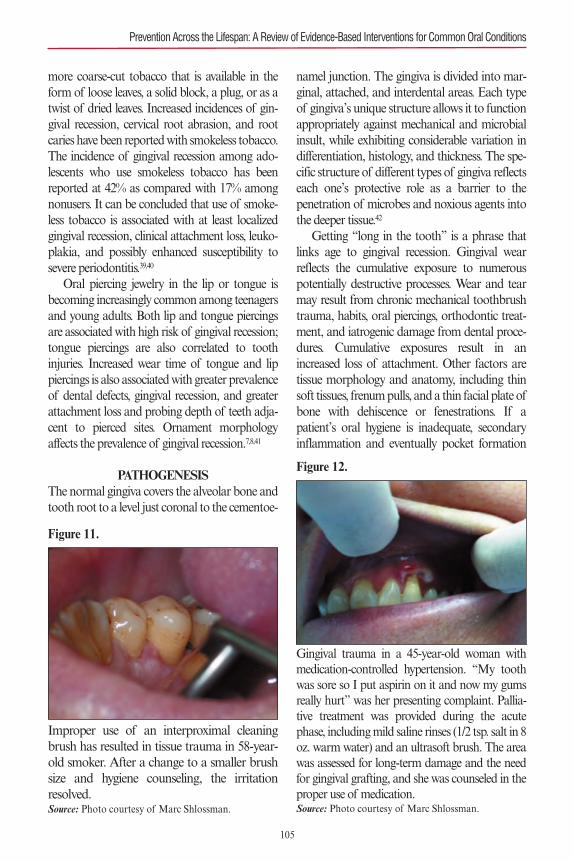
more coarse-cut tobacco that is available in theform of loose leaves, a solid block, a plug, or as atwist of dried leaves. Increased incidences of gin-gival recession, cervical root abrasion, and rootcaries have been reported with smokeless tobacco.The incidence of gingival recession among ado-lescents who use smokeless tobacco has beenreported at 42% as compared with 17% amongnonusers. It can be concluded that use of smoke-less tobacco is associated with at least localizedgingival recession, clinical attachment loss, leuko-plakia, and possibly enhanced susceptibility tosevere periodontitis.39,40
Oral piercing jewelry in the lip or tongue isbecoming increasingly common among teenagersand young adults. Both lip and tongue piercingsare associated with high risk of gingival recession;tongue piercings are also correlated to toothinjuries. Increased wear time of tongue and lippiercings is also associated with greater prevalenceof dental defects, gingival recession, and greaterattachment loss and probing depth of teeth adja-cent to pierced sites. Ornament morphologyaffects the prevalence of gingival recession.7,8,41
PATHOGENESISThe normal gingiva covers the alveolar bone andtooth root to a level just coronal to the cementoe-
namel junction. The gingiva is divided into mar-ginal, attached, and interdental areas. Each typeof gingiva’s unique structure allows it to functionappropriately against mechanical and microbialinsult, while exhibiting considerable variation indifferentiation, histology, and thickness. The spe-cific structure of different types of gingiva reflectseach one’s protective role as a barrier to the penetration of microbes and noxious agents intothe deeper tissue.42
Getting “long in the tooth” is a phrase thatlinks age to gingival recession. Gingival wearreflects the cumulative exposure to numerouspotentially destructive processes. Wear and tearmay result from chronic mechanical toothbrushtrauma, habits, oral piercings, orthodontic treat-ment, and iatrogenic damage from dental proce-dures. Cumulative exposures result in anincreased loss of attachment. Other factors aretissue morphology and anatomy, including thinsoft tissues, frenum pulls, and a thin facial plate ofbone with dehiscence or fenestrations. If apatient’s oral hygiene is inadequate, secondaryinflammation and eventually pocket formation
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
Figure 11.
Improper use of an interproximal cleaningbrush has resulted in tissue trauma in 58-year-old smoker. After a change to a smaller brushsize and hygiene counseling, the irritationresolved.Source: Photo courtesy of Marc Shlossman.
Figure 12.
Gingival trauma in a 45-year-old woman withmedication-controlled hypertension. “My toothwas sore so I put aspirin on it and now my gumsreally hurt” was her presenting complaint. Pallia-tive treatment was provided during the acutephase, including mild saline rinses (1/2 tsp. salt in 8oz. warm water) and an ultrasoft brush. The areawas assessed for long-term damage and the needfor gingival grafting, and she was counseled in theproper use of medication.Source: Photo courtesy of Marc Shlossman.
105

may result. Five to ten percent of all periodontalattachment loss is termed “classical” recession.18
Despite gingival margin recession, the interdentalpapillae usually fill the entire embrasure area inyounger patients. The periodontal supportingstructures in teeth exhibiting classical gingivalrecession generally have excellent health and min-imal mobility.43
PREVENTION AND THERAPYWith scrupulous and proper oral hygiene, reces-sion can be halted. Proper technique must bestressed for all patients who have preexistingdefects or are more prone to recession. Manualand power brushes that carry the American Den-tal Association seal should be recommended.Chronic floss tearing requires educating patientsin proper flossing technique to avoid furtherdamage. Additional damage to soft and hard tis-sues from oral jewelry can only be prevented byeducating patients who do not regard oral pierc-ings as health hazards or who may be reluctantto remove them. Chewing tobacco has directeffects on the gingiva, so habit cessation and edu-cation efforts are critical. The potential for malig-nant change to the tissues must also be stressed(see Chapter 7).
Every effort by dental practitioners to avoidiatrogenic soft tissue damage during dental treat-ment is vital. Proper tissue isolation duringendodontic and restorative procedures can mini-mize mechanical and chemical trauma. Use ofappropriate retraction during surgical therapy canavoid tissue trauma and protect adjacent struc-tures. Care must be taken not to violate the biolog-ical width during preparation of tooth surfaces.Despite efforts to prevent gingival recession, severetypes of recession may require mucogingival sur-gery. Surgical correction of gingival recession isoften considered when (1) a patient raises a con-cern about esthetics or tooth hypersensitivity(which cannot be managed using professional orconsumer products that reduce dentin hypersensi-tivity), or when (2) evidence of ongoing active gin-gival recession persists despite other interventions.Successful treatment of recession-type defects is
based on the use of predictable periodontal plasticsurgery procedures.20 Subepithelial connective tis-sue grafts, coronally advanced flaps, either aloneor associated with other biomaterial, and guidedtissue regeneration may be used as root coverageprocedures for the treatment of localized reces-sion-type defects.44 Treatment options are dis-cussed in detail in several recent workshopproceedings.
A comprehensive assessment of the relevantliterature, performed as part of the 2014 Ameri-can Academy of Periodontology Workshop onPeriodontal Regeneration and Tissue Engineer-ing, revealed a sizable volume of publications sup-porting most root coverage procedures. From thiscomprehensive assessment of the root coverageliterature, a “decision tree” was generated. Theensuing consensus report should help clinicians intheir daily practice to determine the best treatmentmodality to satisfy their patients’ needs.45 Thescope of this consensus report was to assess thestrength of the scientific evidence and make clini-cal and research recommendations for surgicalinterventions to cover exposed root surfaces andenhance soft tissues at implants. Emerging dataindicate that it is possible to obtain complete rootcoverage at sites with some interdental attachmentloss. The consensus of the report is that periodon-tal plastic procedures are complex, technique-sen-sitive interventions that require advanced skillsand expertise.46
PART 2: DAMAGE TO ORAL HARD TISSUESDamage to oral hard tissues may be categorizedas biocorrosive (caries), impact trauma, and non-carious tooth surface loss, also known as toothwear. Three processes result in tooth wear: attri-tion, abrasion, and erosion.47 Tooth wear, which isthe focus of this discussion, may be defined asphysiological or pathological, and is typicallydependent upon subjective interpretation as noclear set of criteria is currently available to assistthe clinician. This section addresses several causesof damage to the hard tissues, with related discus-sions of etiology, pathogenesis, risk factors, andpreventive strategies.
CHAPTER 6 Preventing Damage to Oral Hard and Soft Tissues
106
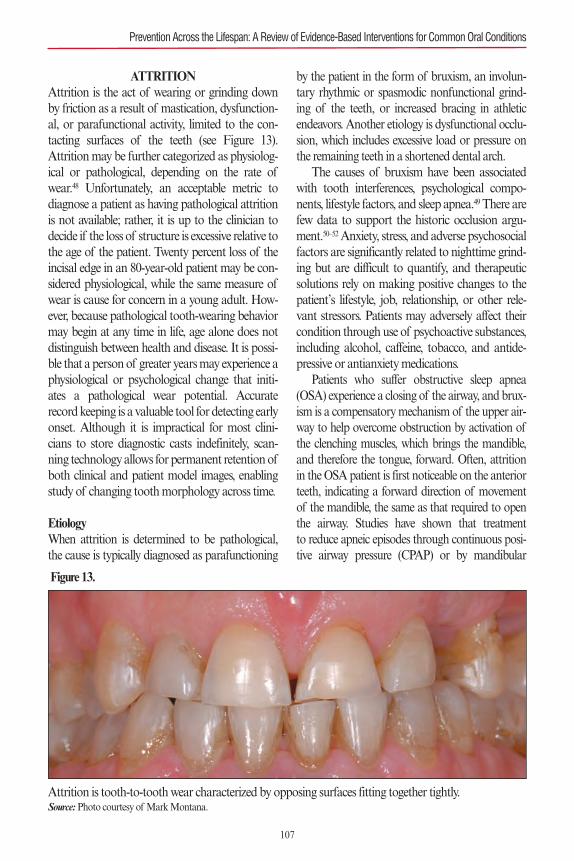
ATTRITIONAttrition is the act of wearing or grinding downby friction as a result of mastication, dysfunction-al, or parafunctional activity, limited to the con-tacting surfaces of the teeth (see Figure 13).Attrition may be further categorized as physiolog-ical or pathological, depending on the rate ofwear.48 Unfortunately, an acceptable metric todiagnose a patient as having pathological attritionis not available; rather, it is up to the clinician todecide if the loss of structure is excessive relative tothe age of the patient. Twenty percent loss of theincisal edge in an 80-year-old patient may be con-sidered physiological, while the same measure ofwear is cause for concern in a young adult. How-ever, because pathological tooth-wearing behaviormay begin at any time in life, age alone does notdistinguish between health and disease. It is possi-ble that a person of greater years may experience aphysiological or psychological change that initi-ates a pathological wear potential. Accuraterecord keeping is a valuable tool for detecting earlyonset. Although it is impractical for most clini-cians to store diagnostic casts indefinitely, scan-ning technology allows for permanent retention ofboth clinical and patient model images, enablingstudy of changing tooth morphology across time.
EtiologyWhen attrition is determined to be pathological,the cause is typically diagnosed as parafunctioning
by the patient in the form of bruxism, an involun-tary rhythmic or spasmodic nonfunctional grind-ing of the teeth, or increased bracing in athleticendeavors. Another etiology is dysfunctional occlu-sion, which includes excessive load or pressure onthe remaining teeth in a shortened dental arch.
The causes of bruxism have been associatedwith tooth interferences, psychological compo-nents, lifestyle factors, and sleep apnea.49 There arefew data to support the historic occlusion argu-ment.50–52Anxiety, stress, and adverse psychosocialfactors are significantly related to nighttime grind-ing but are difficult to quantify, and therapeuticsolutions rely on making positive changes to thepatient’s lifestyle, job, relationship, or other rele-vant stressors. Patients may adversely affect theircondition through use of psychoactive substances,including alcohol, caffeine, tobacco, and antide-pressive or antianxiety medications.
Patients who suffer obstructive sleep apnea(OSA) experience a closing of the airway, and brux-ism is a compensatory mechanism of the upper air-way to help overcome obstruction by activation ofthe clenching muscles, which brings the mandible,and therefore the tongue, forward. Often, attritionin the OSA patient is first noticeable on the anteriorteeth, indicating a forward direction of movementof the mandible, the same as that required to openthe airway. Studies have shown that treatment to reduce apneic episodes through continuous posi-tive airway pressure (CPAP) or by mandibular
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
Figure 13.
Attrition is tooth-to-tooth wear characterized by opposing surfaces fitting together tightly.Source:Photo courtesy of Mark Montana.
107

advancement appliance therapy decreased or elimi-nated nocturnal bruxism. Once the patient is able tobreathe, the body’s need to protect the airwaythrough posturing the jaw forward is reduced.53
PreventionPrevention of pathological wear of the contactingsurfaces of teeth resulting from nighttime bruxismis achieved through the reduction of apneaepisodes by CPAP or a mandibular advancementappliance. By understanding that snoring is a signof a body in distress, clinical intervention mayoccur before wear of teeth is exhibited. The conse-quences of OSA are serious and may affect youngand old, slim and heavy alike.
Traditional nighttime appliance therapy forbruxism using a single arch occlusal splint may beeffective for non-OSA patients but is not recom-mended for those with airway obstruction, as itmay worsen the scenario by allowing the mandibleto slide backward.54Diagnosis of the etiology of apatient’s bruxism is crucial to determine if it isbreathing related; consequently, an appropriatesleep study is required.
Wear from bruxism in the non-OSA patient isprevented through interference using a plasticocclusal splint or a soft mouthguard in the case ofathletes who clench and grind during their activity.The goal is not to stop the grinding, but rather toavoid damage to the teeth.
For patients who have a reduced number ofteeth and therefore wear away the remaining den-tition at an accelerated rate, treatment consists ofreplacing proper masticatory function with har-monious bilateral contact to the first molar, if pos-sible. Studies show that a reduction in thefunctional arch length increases pressure on theremaining dentition, often manifesting in wear tothese teeth.55 Prevention of this occurrence is ofcourse best achieved by preserving the naturaldentition, repairing it when damaged, and replac-ing it with dental implants when repair is unlikely.
ABRASIONAbrasion is the wearing away of tooth structurethrough some unusual or mechanical process other
than mastication. In other words, something otherthan an opposing tooth is causing frictional wear.56
Suspects include highly abrasive foods, contamina-tion of food with abrasive particles, inhalation ofabrasive particles, and iatrogenic abrading by theindividual or by a dental professional.
EtiologyHistorically, teeth were abraded by tough, fibrousdiets and by eating food contaminated by grittysubstances. Most wear occurred on the buccalcusps of the lower molars and the palatal cusps ofthe upper molars. These functional cusps oftenhad scooped-out anatomy where the exposeddentin was worn away below the surface of thesurrounding enamel by fibrous food or foreignparticles. Interestingly, interstitial wear betweenteeth was a common finding as well, caused byteeth moving against each other with grit trappedbetween them. Modernization of food processingin industrialized society softened diets, dramatical-ly reducing this cause of abrasion.57,58
People employed in historically dusty occupa-tions, such as farmers, experienced acceleratedwear of the chewing surfaces of their teeth due tothe constant intake of ambient dust. The grittyfeeling likely induced grinding, creating effectivemilling of the opposing surfaces. The result wascharacteristically flattened teeth. Abrasion mayalso be caused by habitual behavior, such as chew-ing on objects like pencils, nail biting, opening hairpins, or biting thread or fishing line, and by play-ing wind instruments. Abrasion may also occur asa result of dentally related actions, such as restora-tion of teeth with abrasive materials and purpose-ful sanding of dental structures.
The introduction of feldspathic porcelaincrowns, starting in the mid-1960s, providedpatients with an esthetically pleasing alternative togold or silver-black restorations. Unfortunately,the surface of dental porcelain is extremely abra-sive, resembling sandpaper when viewed underextreme magnification. The longer these crownsstay in the mouth, the more abrasive they becomeas the finer grains and glassy surface wear away,leaving behind the most abrasive particles. When
CHAPTER 6 Preventing Damage to Oral Hard and Soft Tissues
108
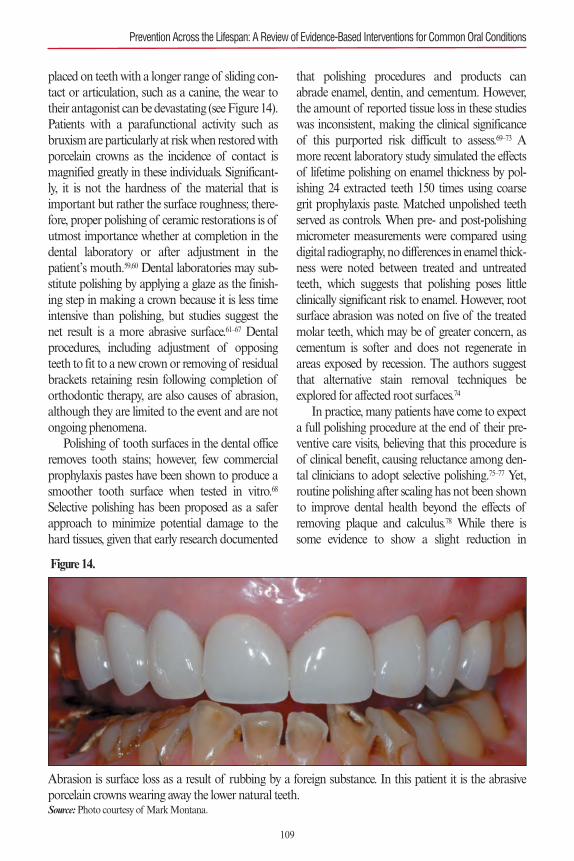
placed on teeth with a longer range of sliding con-tact or articulation, such as a canine, the wear totheir antagonist can be devastating (see Figure 14).Patients with a parafunctional activity such asbruxism are particularly at risk when restored withporcelain crowns as the incidence of contact ismagnified greatly in these individuals. Significant-ly, it is not the hardness of the material that isimportant but rather the surface roughness; there-fore, proper polishing of ceramic restorations is ofutmost importance whether at completion in thedental laboratory or after adjustment in thepatient’s mouth.59,60 Dental laboratories may sub-stitute polishing by applying a glaze as the finish-ing step in making a crown because it is less timeintensive than polishing, but studies suggest thenet result is a more abrasive surface.61–67 Dentalprocedures, including adjustment of opposingteeth to fit to a new crown or removing of residualbrackets retaining resin following completion oforthodontic therapy, are also causes of abrasion,although they are limited to the event and are notongoing phenomena.
Polishing of tooth surfaces in the dental officeremoves tooth stains; however, few commercialprophylaxis pastes have been shown to produce asmoother tooth surface when tested in vitro.68
Selective polishing has been proposed as a saferapproach to minimize potential damage to thehard tissues, given that early research documented
that polishing procedures and products canabrade enamel, dentin, and cementum. However,the amount of reported tissue loss in these studieswas inconsistent, making the clinical significanceof this purported risk difficult to assess.69–73 Amore recent laboratory study simulated the effectsof lifetime polishing on enamel thickness by pol-ishing 24 extracted teeth 150 times using coarsegrit prophylaxis paste. Matched unpolished teethserved as controls. When pre- and post-polishingmicrometer measurements were compared usingdigital radiography, no differences in enamel thick-ness were noted between treated and untreatedteeth, which suggests that polishing poses littleclinically significant risk to enamel. However, rootsurface abrasion was noted on five of the treatedmolar teeth, which may be of greater concern, ascementum is softer and does not regenerate inareas exposed by recession. The authors suggestthat alternative stain removal techniques beexplored for affected root surfaces.74
In practice, many patients have come to expecta full polishing procedure at the end of their pre-ventive care visits, believing that this procedure isof clinical benefit, causing reluctance among den-tal clinicians to adopt selective polishing.75–77 Yet,routine polishing after scaling has not been shownto improve dental health beyond the effects ofremoving plaque and calculus.78 While there issome evidence to show a slight reduction in
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
Figure 14.
Abrasion is surface loss as a result of rubbing by a foreign substance. In this patient it is the abrasiveporcelain crowns wearing away the lower natural teeth.Source:Photo courtesy of Mark Montana.
109
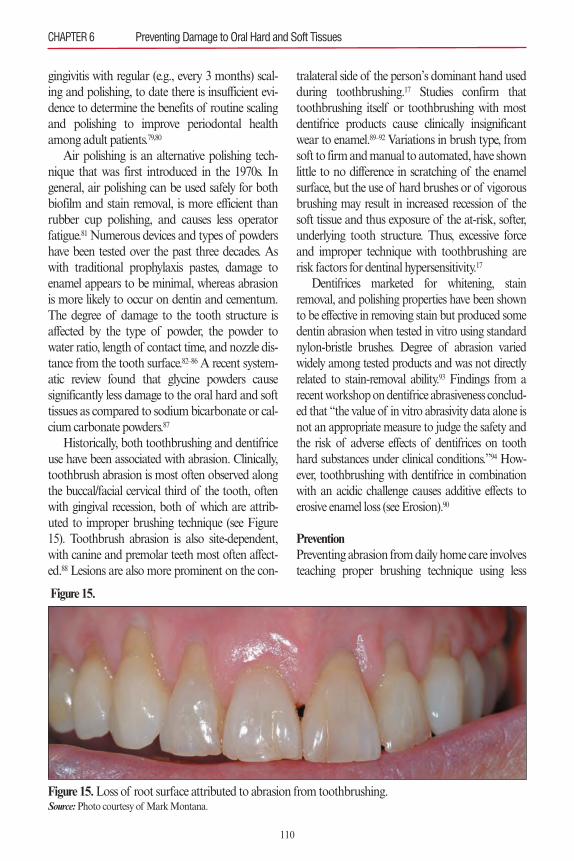
CHAPTER 6 Preventing Damage to Oral Hard and Soft Tissues
gingivitis with regular (e.g., every 3 months) scal-ing and polishing, to date there is insufficient evi-dence to determine the benefits of routine scalingand polishing to improve periodontal healthamong adult patients.79,80
Air polishing is an alternative polishing tech-nique that was first introduced in the 1970s. Ingeneral, air polishing can be used safely for bothbiofilm and stain removal, is more efficient thanrubber cup polishing, and causes less operatorfatigue.81 Numerous devices and types of powdershave been tested over the past three decades. Aswith traditional prophylaxis pastes, damage toenamel appears to be minimal, whereas abrasionis more likely to occur on dentin and cementum.The degree of damage to the tooth structure isaffected by the type of powder, the powder towater ratio, length of contact time, and nozzle dis-tance from the tooth surface.82–86 A recent system-atic review found that glycine powders causesignificantly less damage to the oral hard and softtissues as compared to sodium bicarbonate or cal-cium carbonate powders.87
Historically, both toothbrushing and dentifriceuse have been associated with abrasion. Clinically,toothbrush abrasion is most often observed alongthe buccal/facial cervical third of the tooth, oftenwith gingival recession, both of which are attrib-uted to improper brushing technique (see Figure15). Toothbrush abrasion is also site-dependent,with canine and premolar teeth most often affect-ed.88 Lesions are also more prominent on the con-
tralateral side of the person’s dominant hand usedduring toothbrushing.17 Studies confirm thattoothbrushing itself or toothbrushing with mostdentifrice products cause clinically insignificantwear to enamel.89–92 Variations in brush type, fromsoft to firm and manual to automated, have shownlittle to no difference in scratching of the enamelsurface, but the use of hard brushes or of vigorousbrushing may result in increased recession of thesoft tissue and thus exposure of the at-risk, softer,underlying tooth structure. Thus, excessive forceand improper technique with toothbrushing arerisk factors for dentinal hypersensitivity.17
Dentifrices marketed for whitening, stainremoval, and polishing properties have been shownto be effective in removing stain but produced somedentin abrasion when tested in vitro using standardnylon-bristle brushes. Degree of abrasion variedwidely among tested products and was not directlyrelated to stain-removal ability.93 Findings from arecent workshop on dentifrice abrasiveness conclud-ed that “the value of in vitro abrasivity data alone isnot an appropriate measure to judge the safety andthe risk of adverse effects of dentifrices on toothhard substances under clinical conditions.”94 How-ever, toothbrushing with dentifrice in combinationwith an acidic challenge causes additive effects toerosive enamel loss (see Erosion).90
PreventionPreventing abrasion from daily home care involvesteaching proper brushing technique using less
Figure 15.
Figure 15.Loss of root surface attributed to abrasion from toothbrushing.Source:Photo courtesy of Mark Montana.
110

force, a soft toothbrush, and a nonabrasive denti-frice.17,95 Proper brushing technique should beassessed and reinforced at regular recare appoint-ments. Clinicians should select the least abrasiveprophylaxis paste or powder when polishing isdeemed necessary for stain removal and use atechnique that helps to prevent damage to thedentin and cementum.
EROSIONDental erosion is the progressive loss of tooth sub-stance by chemical processes that do not involvebacterial action. Erosion is divided into twocausative categories: endogenic (intrinsic), fromrefluxed gastric juices; and exogenic (extrinsic),from dietary, medicinal, occupational, and recre-ational sources.96 Teeth undergoing dissolutionfrom acid may exhibit subtle external changesbefore diagnosis is finally made. Early signsinclude a dulling or matte appearance of theenamel followed by a noticeable smoothing of thecontours.97 The affected sites may begin to appearmore yellow as the thinning enamel no longermasks the underlying dentin shade. If penetrationthrough the enamel occurs, dimpling or deep cup-ping at these sights may follow as the exposeddentin will degrade at a faster rate than the sur-rounding enamel. The areas of the mouth mostaffected as well as the surfaces of the teethinvolved are clinically helpful signs to aid in diag-nosis. An endogenic etiology will manifest inchanges to the lingual and possibly occlusal aspectof teeth while extrinsic erosion attacks the labialand buccal surfaces first. Sustained or repeateddirect contact of the teeth by acidic substances(those with a pH below 5.5) is the common factorin all cases of dental erosion.
ENDOGENIC EROSIONEtiologyEndogenic erosion is due to bathing teeth in stom-ach acids through passive or active means. Passiveintroduction of digestive acid to the oral cavity canoccur with gastroesophageal reflux disease(GERD), during which gastric and duodenal regur-gitation may erode the teeth. Gastroesophageal
reflux (GER) is considered normal and is character-ized by physiological retrograde flow of gastric con-tents into the esophagus that occurs after meals foraround 1 hour per day. In healthy individuals,esophageal reflux is cleared by esophageal peristalsisand saliva within 1 to 2 minutes.
When GER progresses to cause troublesomesymptoms or complications, it is classified asGERD. This disease state can occur during bothsleep and waking stages, but most patients whosuffer from GERD report that it occurs duringsleep. It is during this cycle that the body is ill pre-pared to offset the acid intrusion; the saliva in themouth is reduced, diminishing the buffering effect,and swallowing is infrequent. The acid strips awaythe protective biofilm of the teeth, and the chemi-cal action causes rapid dissolution of exposedtooth surfaces. As the person is in a supine posi-tion, it is typical and expected that the teeth mostaffected are those closest to the esophagus, thelower molars (see Figure 16).
GERD is a potentially dangerous conditionthat may manifest as Barrett’s esophagus, a low-grade and high-grade dysplasia, and is thestrongest risk factor for esophageal adenocarcino-ma. Dentists may be the first professionals to diag-nose the possibility of GERD, particularly whenobserving unexplained instances of tooth erosion,which might be accompanied by coexisting hypos-alivation. The appearance is generally a smooth-ing of the tooth surface and potential exposure ofunderlying dentin, even where no antagonist artic-ulates. Existing restorations, particularly amalgamfillings, are not affected by the acid washing andtherefore may appear as islands protruding abovethe eroded surrounding tooth surface.98–101
The dental practitioner who is suspicious thata patient may be experiencing GERD should dis-cuss his or her findings with the patient and referto or consult with the patient’s primary care physi-cian for appropriate investigation. Evaluation ofthe patient for OSA is also advised.
Bulimia nervosa is an eating disorder charac-terized by frequent vomiting resulting in the disso-lution of the tooth surface by gastric acid.102,103
Because the action is violent, in contrast to GER,
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
111
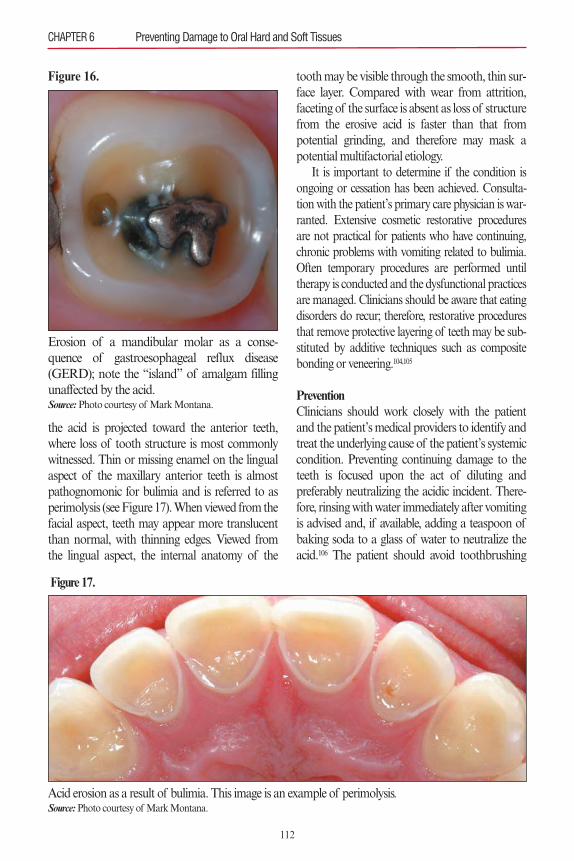
the acid is projected toward the anterior teeth,where loss of tooth structure is most commonlywitnessed. Thin or missing enamel on the lingualaspect of the maxillary anterior teeth is almostpathognomonic for bulimia and is referred to asperimolysis (see Figure 17). When viewed from thefacial aspect, teeth may appear more translucentthan normal, with thinning edges. Viewed fromthe lingual aspect, the internal anatomy of the
tooth may be visible through the smooth, thin sur-face layer. Compared with wear from attrition,faceting of the surface is absent as loss of structurefrom the erosive acid is faster than that frompotential grinding, and therefore may mask apotential multifactorial etiology.
It is important to determine if the condition isongoing or cessation has been achieved. Consulta-tion with the patient’s primary care physician is war-ranted. Extensive cosmetic restorative proceduresare not practical for patients who have continuing,chronic problems with vomiting related to bulimia.Often temporary procedures are performed untiltherapy is conducted and the dysfunctional practicesare managed. Clinicians should be aware that eatingdisorders do recur; therefore, restorative proceduresthat remove protective layering of teeth may be sub-stituted by additive techniques such as compositebonding or veneering.104,105
PreventionClinicians should work closely with the patientand the patient’s medical providers to identify andtreat the underlying cause of the patient’s systemiccondition. Preventing continuing damage to theteeth is focused upon the act of diluting andpreferably neutralizing the acidic incident. There-fore, rinsing with water immediately after vomitingis advised and, if available, adding a teaspoon ofbaking soda to a glass of water to neutralize theacid.106 The patient should avoid toothbrushing
CHAPTER 6 Preventing Damage to Oral Hard and Soft Tissues
Figure 16.
Erosion of a mandibular molar as a conse-quence of gastroesophageal reflux disease(GERD); note the “island” of amalgam fillingunaffected by the acid.Source:Photo courtesy of Mark Montana.
Figure 17.
Acid erosion as a result of bulimia. This image is an example of perimolysis.Source:Photo courtesy of Mark Montana.
112
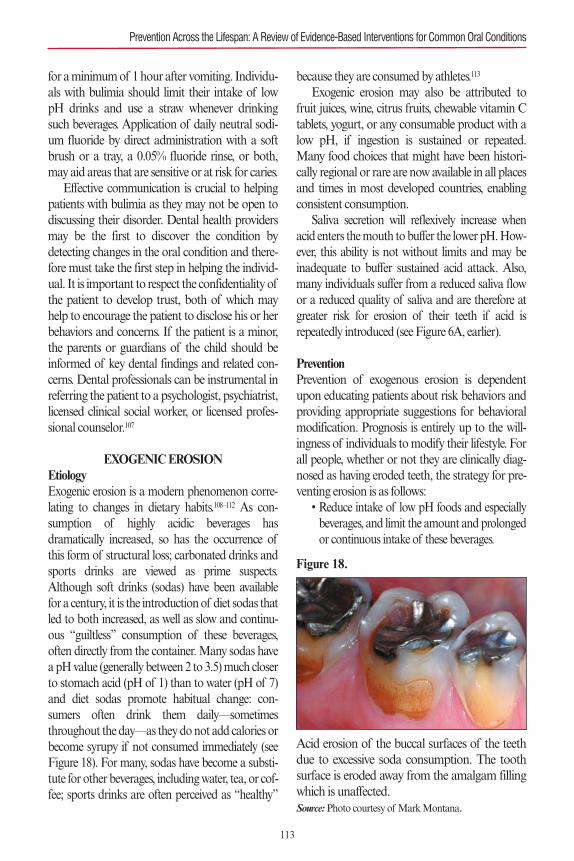
for a minimum of 1 hour after vomiting. Individu-als with bulimia should limit their intake of lowpH drinks and use a straw whenever drinkingsuch beverages. Application of daily neutral sodi-um fluoride by direct administration with a softbrush or a tray, a 0.05% fluoride rinse, or both,may aid areas that are sensitive or at risk for caries.
Effective communication is crucial to helpingpatients with bulimia as they may not be open todiscussing their disorder. Dental health providersmay be the first to discover the condition bydetecting changes in the oral condition and there-fore must take the first step in helping the individ-ual. It is important to respect the confidentiality ofthe patient to develop trust, both of which mayhelp to encourage the patient to disclose his or herbehaviors and concerns. If the patient is a minor,the parents or guardians of the child should beinformed of key dental findings and related con-cerns. Dental professionals can be instrumental inreferring the patient to a psychologist, psychiatrist,licensed clinical social worker, or licensed profes-sional counselor.107
EXOGENIC EROSIONEtiologyExogenic erosion is a modern phenomenon corre-lating to changes in dietary habits.108–112 As con-sumption of highly acidic beverages hasdramatically increased, so has the occurrence ofthis form of structural loss; carbonated drinks andsports drinks are viewed as prime suspects.Although soft drinks (sodas) have been availablefor a century, it is the introduction of diet sodas thatled to both increased, as well as slow and continu-ous “guiltless” consumption of these beverages,often directly from the container. Many sodas havea pH value (generally between 2 to 3.5) much closerto stomach acid (pH of 1) than to water (pH of 7)and diet sodas promote habitual change: con-sumers often drink them daily—sometimesthroughout the day—as they do not add calories orbecome syrupy if not consumed immediately (seeFigure 18). For many, sodas have become a substi-tute for other beverages, including water, tea, or cof-fee; sports drinks are often perceived as “healthy”
because they are consumed by athletes.113
Exogenic erosion may also be attributed tofruit juices, wine, citrus fruits, chewable vitamin Ctablets, yogurt, or any consumable product with alow pH, if ingestion is sustained or repeated.Many food choices that might have been histori-cally regional or rare are now available in all placesand times in most developed countries, enablingconsistent consumption.
Saliva secretion will reflexively increase whenacid enters the mouth to buffer the lower pH. How-ever, this ability is not without limits and may beinadequate to buffer sustained acid attack. Also,many individuals suffer from a reduced saliva flowor a reduced quality of saliva and are therefore atgreater risk for erosion of their teeth if acid isrepeatedly introduced (see Figure 6A, earlier).
PreventionPrevention of exogenous erosion is dependentupon educating patients about risk behaviors andproviding appropriate suggestions for behavioralmodification. Prognosis is entirely up to the will-ingness of individuals to modify their lifestyle. Forall people, whether or not they are clinically diag-nosed as having eroded teeth, the strategy for pre-venting erosion is as follows:
• Reduce intake of low pH foods and especiallybeverages, and limit the amount and prolongedor continuous intake of these beverages.
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
Figure 18.
Acid erosion of the buccal surfaces of the teethdue to excessive soda consumption. The toothsurface is eroded away from the amalgam fillingwhich is unaffected.Source:Photo courtesy of Mark Montana.
113
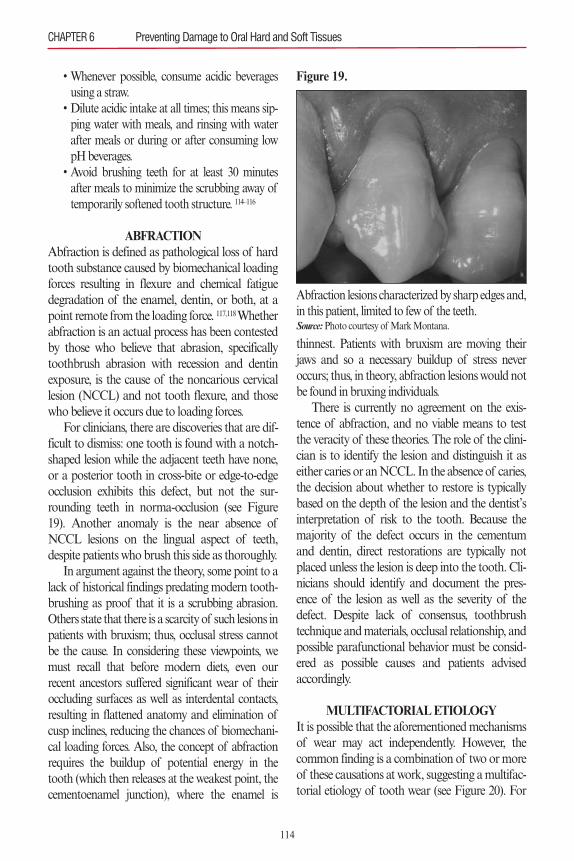
• Whenever possible, consume acidic beveragesusing a straw.
• Dilute acidic intake at all times; this means sip-ping water with meals, and rinsing with waterafter meals or during or after consuming lowpH beverages.
• Avoid brushing teeth for at least 30 minutesafter meals to minimize the scrubbing away oftemporarily softened tooth structure. 114–116
ABFRACTIONAbfraction is defined as pathological loss of hardtooth substance caused by biomechanical loadingforces resulting in flexure and chemical fatiguedegradation of the enamel, dentin, or both, at apoint remote from the loading force. 117,118 Whetherabfraction is an actual process has been contestedby those who believe that abrasion, specificallytoothbrush abrasion with recession and dentinexposure, is the cause of the noncarious cervicallesion (NCCL) and not tooth flexure, and thosewho believe it occurs due to loading forces.
For clinicians, there are discoveries that are dif-ficult to dismiss: one tooth is found with a notch-shaped lesion while the adjacent teeth have none,or a posterior tooth in cross-bite or edge-to-edgeocclusion exhibits this defect, but not the sur-rounding teeth in norma-occlusion (see Figure19). Another anomaly is the near absence ofNCCL lesions on the lingual aspect of teeth,despite patients who brush this side as thoroughly.
In argument against the theory, some point to alack of historical findings predating modern tooth-brushing as proof that it is a scrubbing abrasion.Others state that there is a scarcity of such lesions inpatients with bruxism; thus, occlusal stress cannotbe the cause. In considering these viewpoints, wemust recall that before modern diets, even ourrecent ancestors suffered significant wear of theiroccluding surfaces as well as interdental contacts,resulting in flattened anatomy and elimination ofcusp inclines, reducing the chances of biomechani-cal loading forces. Also, the concept of abfractionrequires the buildup of potential energy in thetooth (which then releases at the weakest point, thecementoenamel junction), where the enamel is
thinnest. Patients with bruxism are moving theirjaws and so a necessary buildup of stress neveroccurs; thus, in theory, abfraction lesions would notbe found in bruxing individuals.
There is currently no agreement on the exis-tence of abfraction, and no viable means to testthe veracity of these theories. The role of the clini-cian is to identify the lesion and distinguish it aseither caries or an NCCL. In the absence of caries,the decision about whether to restore is typicallybased on the depth of the lesion and the dentist’sinterpretation of risk to the tooth. Because themajority of the defect occurs in the cementumand dentin, direct restorations are typically notplaced unless the lesion is deep into the tooth. Cli-nicians should identify and document the pres-ence of the lesion as well as the severity of thedefect. Despite lack of consensus, toothbrushtechnique and materials, occlusal relationship, andpossible parafunctional behavior must be consid-ered as possible causes and patients advisedaccordingly.
MULTIFACTORIAL ETIOLOGYIt is possible that the aforementioned mechanismsof wear may act independently. However, thecommon finding is a combination of two or moreof these causations at work, suggesting a multifac-torial etiology of tooth wear (see Figure 20). For
CHAPTER 6 Preventing Damage to Oral Hard and Soft Tissues
Figure 19.
Abfraction lesions characterized by sharp edges and,in this patient, limited to few of the teeth.Source:Photo courtesy of Mark Montana.
114
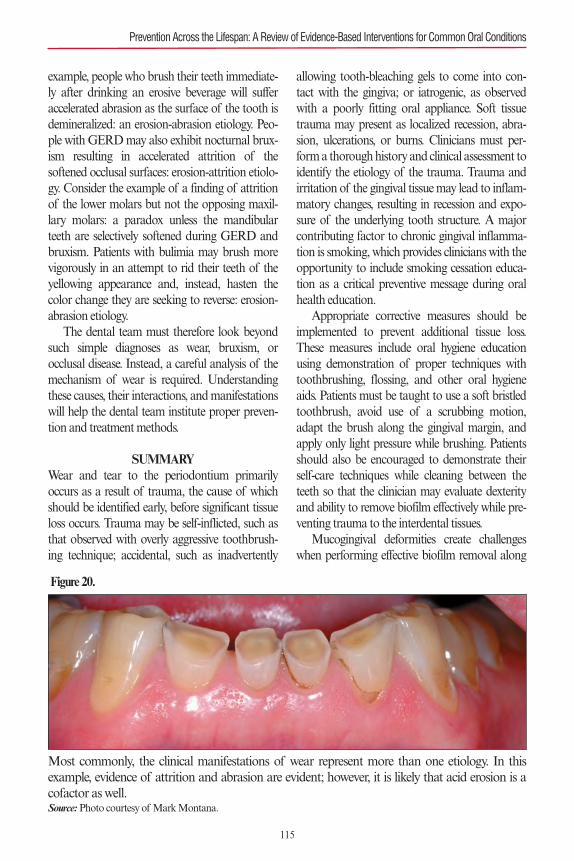
example, people who brush their teeth immediate-ly after drinking an erosive beverage will sufferaccelerated abrasion as the surface of the tooth isdemineralized: an erosion-abrasion etiology. Peo-ple with GERD may also exhibit nocturnal brux-ism resulting in accelerated attrition of thesoftened occlusal surfaces: erosion-attrition etiolo-gy. Consider the example of a finding of attritionof the lower molars but not the opposing maxil-lary molars: a paradox unless the mandibularteeth are selectively softened during GERD andbruxism. Patients with bulimia may brush morevigorously in an attempt to rid their teeth of theyellowing appearance and, instead, hasten thecolor change they are seeking to reverse: erosion-abrasion etiology.
The dental team must therefore look beyondsuch simple diagnoses as wear, bruxism, orocclusal disease. Instead, a careful analysis of themechanism of wear is required. Understandingthese causes, their interactions, and manifestationswill help the dental team institute proper preven-tion and treatment methods.
SUMMARYWear and tear to the periodontium primarilyoccurs as a result of trauma, the cause of whichshould be identified early, before significant tissueloss occurs. Trauma may be self-inflicted, such asthat observed with overly aggressive toothbrush-ing technique; accidental, such as inadvertently
allowing tooth-bleaching gels to come into con-tact with the gingiva; or iatrogenic, as observedwith a poorly fitting oral appliance. Soft tissuetrauma may present as localized recession, abra-sion, ulcerations, or burns. Clinicians must per-form a thorough history and clinical assessment toidentify the etiology of the trauma. Trauma andirritation of the gingival tissue may lead to inflam-matory changes, resulting in recession and expo-sure of the underlying tooth structure. A majorcontributing factor to chronic gingival inflamma-tion is smoking, which provides clinicians with theopportunity to include smoking cessation educa-tion as a critical preventive message during oralhealth education.
Appropriate corrective measures should beimplemented to prevent additional tissue loss.These measures include oral hygiene educationusing demonstration of proper techniques withtoothbrushing, flossing, and other oral hygieneaids. Patients must be taught to use a soft bristledtoothbrush, avoid use of a scrubbing motion,adapt the brush along the gingival margin, andapply only light pressure while brushing. Patientsshould also be encouraged to demonstrate theirself-care techniques while cleaning between theteeth so that the clinician may evaluate dexterityand ability to remove biofilm effectively while pre-venting trauma to the interdental tissues.
Mucogingival deformities create challengeswhen performing effective biofilm removal along
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
Figure 20.
Most commonly, the clinical manifestations of wear represent more than one etiology. In thisexample, evidence of attrition and abrasion are evident; however, it is likely that acid erosion is acofactor as well.Source:Photo courtesy of Mark Montana.
115

the gingival margin. For these patients, correctivesurgery may be warranted to help prevent addi-tional tissue loss. Poorly constructed dentalrestorations, crowns, or both, need to be replacedto help restore tissue health and cleansibility. Cor-rection of habits, such as fingernail biting or suck-ing on pens, should also be addressed with thepatient, and the wearing of intraoral jewelry dis-couraged.
The loss of hard tooth structure may be attrib-uted to one or more mechanisms, including attri-tion, abrasion, erosion, and abfraction. Mostcommonly, it is a combination of two or more ofthese factors. An accurate differential diagnosis istherefore essential to provide effective preventionand treatment. Because abrasion and exogenicerosion are largely preventable conditions requir-ing changes in habit and lifestyle, the emphasisfrom the dental community should be educationand instruction of clinicians, patients, and thepopulation at large.
Extrinsic erosion, in particular, plays a majorsynergistic role when combined with abrasion andattrition and is, without doubt, the most easily pre-vented. Simply making healthier beverage choicesis a profound step, and when an acidic beverage isdesired, patients should be taught to limit the num-ber consumed and to drink quickly or use a strawto reduce the duration of acid attack. Drinkingwater with meals and alternating sips with anadjoining acidic beverage will dilute the acid andraise the pH in the oral cavity. Remembering torinse with water after meals instead of brushing willremove acid and lingering sugars and allow timefor dental structures to remineralize.
Abrasion may be reduced if as noted, erosion isprevented. Further, changing the schedule ofbrushing, choosing soft brushes, and using appro-priate toothbrush technique are all simple and inex-pensive steps to reducing this form of wear.
For patients suffering damage from abrasionand erosion, cessation of causation is of greaterimportance than restoration; it is more importantto preserve what remains. Restoration without ces-sation caries a poorer prognosis as even the best fit-ting crown or filling margins are potential sites for
breakdown, particularly from acids. Those patientswho present with a history of oral damage resultingfrom GERD, bulimia, bruxism, alcoholism, andother nondental conditions require coordination ofcare with medical, physical, or psychosocial thera-pists to provide effective treatment.
The loss of tooth structure has been shown tobe consistent with human history; however, thenature of wear today differs greatly from that inthe past. Wearing away of enamel, dentin, andcementum are no longer consequences of the actof survival but commonly result from a marriageof poor choices, bad habits, and misinformation.Fortunately, prevention of most wear is simple,inexpensive, and available to everyone, requiringno painful sacrifices. By encouraging only limitedconsumption of acidic beverages, neutralization ofthe effects of acids by rinsing the mouth withwater, and proper, nondestructive oral self-care, thedental team can negate the risk of most causes oftooth structure loss. Identifying the characteristicsof the different causes of wear and the likelihoodthat more than one is at work in an individualenhances early diagnosis, and therefore manage-ment through prevention.
REFERENCES1. Armitage GC. Development of a classification system
for periodontal diseases and conditions. Ann Periodontol.1999;4:1–6.
2. Holmstrup P. Non-plaque-induced gingival lesions. AnnPeriodontol. 1999;4:20–29.
3. Rawal SY, Claman LJ, Kalmar JR, Tatakis DN. Trau-matic lesions of the gingiva: a case series. J Periodontol.2004;75:762–769.
4. Onur OM, Haytac C, Akkaya M. Iatrogenic trauma tooral tissues. J Periodontol. 2005;76:1793–1797.
5. Chambrone LI, Chambrone LA. Gingival recessionscaused by lip piercing: case report. J Can Dent Assoc.2003;69:505–508.
6. Dibart SI, De Feo P, Surabian G, Hart A, Capri D, SuMF. Oral piercing and gingival recession: review of theliterature and a case report. Quintessence Int.2002;33:110–112.
7. Campbell AI, Moore A, Williams E, Stephens J, TatakisDN. Tongue piercing: impact of time and barbell stemlength on lingual gingival recession and tooth chipping.J Periodontol. 2002;73:289–297.
8. Brooks JK, Hooper KA, Reynolds MA. Formation ofmucogingival defects associated with intraoral and peri-
CHAPTER 6 Preventing Damage to Oral Hard and Soft Tissues
116
oral piercing. J Am Dent Assoc. 2003;134:837–843.9. Kassab MM, Cohen RE. The etiology and prevalence
of gingival recession. J Am Dent Assoc. 2003;134:220–225.
10. Albandar JM, Kingman A. Gingival recession, gingivalbleeding, and dental calculus in adults 30 years of ageand older in the United States. J Periodontol.1999;70:1988–1994.
11. Susin C, Haas AN, Oppermann RV, Haugejorden O,Albandar JM. Gingival recession: epidemiology and riskindicators in a representative urban Brazilian popula-tion. J Periodontol. 2004;75:1377–1386.
12. Rios FS, Costa RSA, Moura MS, Jardim JJ, Maltz M,Haas AN. Estimates and multivariable risk assessmentof gingival recession in the population of adults fromPorto Alegre, Brazil. J Clin Periodontol. 2014;41:1098–1107. doi: 10.1111/jcpe.12303.
13. Toker H, Ozdemir H. Gingival recession: epidemiologyand risk indicators in a university dental hospital inTurkey. Int J Dent Hyg. 2009;7:115–120.
14. Alexandre S, Bourgeois D, Katsahian S, et al. Riskassessment for buccal gingival recession defects in anadult population. J Periodontol. 2010;81:1419–1425.
15. Chrysanthakopoulos NA. Prevalence and associatedfactors of gingival recession in Greek adults. J Invest ClinDent. 2013;4:178–185.
16. Pradeep K, Rajababu P, Satyanarayana D, Sagar, V.Gingival recession: review and strategies in treatment ofrecession. Case Rep Dent. 2012;2012:563421. doi:10.1155/2012/563421.
17. Dababneh RH, Khouri AT, Addy M. Dentine hyper-sensitivity—an enigma? A review of terminology, epi-demiology, mechanisms, aetiology and management. BrDent J. 1999;187:606–611.
18. Hinrichs, JE, Kotsakis G. Classification of diseases andconditions affecting the periodontium. In: NewmanMG, Takei H, Klokkevold PR, Carranza FA, eds. Car-ranza’s Clinical Periodontology. 12th ed. St Louis, MO:Elsevier/Saunders; 2015:45–67.
19. Zlataric DK, Celebic A, Valentic-Peruzovic M. Theeffect of removable partial dentures on periodontalhealth of abutment and non-abutment teeth. J Periodon-tol. 2002;73:137.
20. Chan HL, Chun YP, MacEachern M, Oates TW. Doesgingival recession require surgical treatment? Dent ClinNorth Am. 2015;59:981–996.
21. Danser MM, Timmerman MF, IJzerman Y, et al: Eval-uation of the incidence of gingival abrasion as a result oftoothbrushing. J Clin Periodontol. 1998;25:701.
22. Offenbacher S, Barros SP, Singer RE, et al: Periodontaldisease at the biofilm-gingival interface. J Periodontol.2007;78:1911.
23. Serino G, Wennstrom JL, Lindhe J, Eneroth L. Theprevalence and distribution of gingival recession in sub-jects with a high standard of oral hygiene. J Clin Peri-odontol. 1994;21:57–63.
24. Carlos MC, Muyco MM, Caliwag ML, Fajardo JA, UyHG. The prevalence and distribution of gingival reces-sion among U.E. dental students with a high standard oforal hygiene. J Philipp Dent Assoc. 1995;47:27–48.
25. Goutoudi P, Koidis PT, Konstantinidis A. Gingivalrecession: a cross-sectional clinical investigation. Eur JProsthodont Rest Dent. 1997;5:57–61.
26. Khocht A, Simon G, Person P, Denepitiya JL. Gingivalrecession in relation to history of hard toothbrush use. JPeriodontol.1993;64:900–905.
27. Zimmer S, Öztürk M, Barthel CR, Bizhang M, JordanRA. Cleaning efficacy and soft tissue trauma after use ofmanual toothbrushes with different bristle stiffness. JPeriodontol. 2011;82:267–271.
28. Rosema NA, Adam R, Grender JM, Van der Sluijs E,Supranoto SC, Van der Weijden GA. Gingival abrasionand recession in manual and oscillating–rotating powerbrush users. Int J Dent Hyg. 2014;12:257–266.
29. McCracken GI, Heasman L, Stacey F, et al. The impactof powered and manual toothbrushing on incipient gin-gival recession. J Clin Periodontol. 2009;36:950–957.
30. Sälzer S, Graetz C, Plaumann A, et al. Effect of a multi-directional power and a manual toothbrush in subjectssusceptible to gingival recession: a 12-month randomizedcontrolled clinical study. J Periodontol. 2016;16:1–15.
31. Rajapakse PS, McCracken GI, Gwynnett E, Steen ND,Guentsch A, Heasman PA. Does tooth brushing influ-ence the development and progression of non-inflam-matory gingival recession? A systematic review. J ClinPeriodontol. 2007;34:1046–1061.
32. Heasman PA, Holliday R, Bryant A, Preshaw PM. Evi-dence for the occurrence of gingival recession and non-carious cervical lesions as a consequence of traumatictoothbrushing. J Clin Periodontol. 2015;42(suppl16):S237–S255. doi: 10.1111/jcpe.12330.
33. Renkema AM, Fudalej PS, Renkema AAP, Abbas F,Bronkhorst E, Katsaros C. Gingival labial recessions inorthodontically treated and untreated individuals—apilot case–control study. J Clin Periodontol. 2013;40:631–637. doi: 10.1111/jcpe.12105.
34. Renkema AM, Fudalej PS, Renkema A, Kiekens R,Katsaros C. Development of labial gingival recessions inorthodontically treated patients. Am J Ortho DentofacOrthop. 2013;143:206–212.
35. Aziz T, Flores-Mir C. A systematic review of the associa-tion between appliance-induced labial movement ofmandibular incisors and gingival recession. Aust OrthodJ. 2011;27:33–39.
36. Joss-Vassalli I, Grebenstein C, Topouzelis N, et al:Orthodontic therapy and gingival recession: a systematicreview. Orthod Craniofac Res. 2010;13:127–141.
37. Hinrichs JE, Math VT. The role of dental calculus andother local predisposing factors. In: Newman MG, TakeiH, Klokkevold PR, Carranza FA, eds. Carranza’s Clini-cal Periodontology. 12th ed. St. Louis, MO:Elsevier/Saunders; 2015:116–131.
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
117
38. Ozcelik, O, Haytac MC, Akkaya M. Iatrogenic traumato oral tissue. J Periodontol. 2005;76:1793-1797.
39. Monten U, Wennstrom JL, Ramberg P. Periodontalconditions in male adolescents using smokeless tobacco(moist snuff). J Clin Periodontol. 2006;33:863–868.
40. Tomar SL, Winn DM. Chewing tobacco use and dentalcaries among U.S. men. J Am Dent Assoc.1999;130:1601–1610.
41. Plessas, A, Pepelassi E. Dental and periodontal compli-cations of lip and tongue piercing: prevalence and influ-encing factors. Aust Dent J. 2012;57:71–78. doi:10.1111/j.1834-7819.2011.01647.x.
42. Fiorellini JP, Stathopoulou PG. Anatomy of the peri-odontium. In: Newman MG, Takei H, Klokkevold PR,Carranza FA, eds. Carranza’s Clinical Periodontology.12th ed. St. Louis, MO: Elsevier/Saunders; 2015:9–39.
43. Wolf HF, Hassell TM. Color Atlas of Dental Hygiene.Stuttgart, Germany: Thieme; 2006:155–164.
44. Chambrone L, Sukekava F, Araújo MG, Pustiglioni FE,Chambrone LA, Lima LA. Root coverage proceduresfor the treatment of localised recession-type defects.Cochrane Database Syst Rev. 2009(2):CD007161. doi:10.1002/14651858.CD007161.pub2.
45. Richardson CR, Allen EP, Chambrone L, et al., Peri-odontal soft tissue root coverage procedures: practicalapplications from the AAP regeneration workshop. ClinAdv Perio. 2015;5:1,2–10.
46. Tonetti MS, Jepsen S. Clinical efficacy of periodontalplastic surgery procedures: consensus report of group 2of the 10th European Workshop on Periodontology. JClin Periodontol. 2014;41(suppl 15):S36–S43.doi:10.1111/jcpe.12219.
47. Addy M, Shellis RP. Interaction between attrition, abra-sion and erosion in tooth wear. Monogr Oral Sci.2006;20:17–31.
48. Kaidonis, JA. Tooth wear: the view of the anthropolo-gist. Clin Oral Investig. 2008;12(suppl 1):21–26.
49. Bader G, Lavigne G. Sleep bruxism; an overview of anoromandibular sleep movement disorder. Sleep MedRev. 2000;4:27–43.
50. Butler JH. Occlusal adjustment. Dent Dig. 1970;76422–426.
51. Frumker SC. Occlusion and muscle tension. Basal Facts.1981;4:85–87.
52. Holmgren K, Sheikholeslam A. Occlusal adjustmentand myoelectric activity of the jaw elevator muscles inpatients with nocturnal bruxism and craniomandibulardisorders. Scand J Dent Res. 1994;102:238–243.
53. Landry ML, Rompré PH, Manzini C, Guitard F, deGrandmont P, Lavigne GJ. Reduction of sleep bruxismusing a mandibular advancement device: an experimen-tal controlled study. Int J Prosthodont. 2006;19:549–556.
54. Clark GT, Beemsterboer PL, Solberg WK, Rugh JD.Nocturnal electromyographic evaluation of myofascialpain dysfunction in patients undergoing occlusal splinttherapy. J Am Dent Assoc. 1979;99:607–611.
55. Sarita PTN, Kreulen CM, Witter DJ, van’t Hof M,Creugers NHC. A study on occlusal stability in short-ened dental arches. Int J Prosthodont. 2003;16:375–380.
56. Smith BGN, Knight JK. Toothwear: aetiology and diag-nosis. Dent Update. 1989;16:204–212.
57. Benazzi S, Nguyen HN, Schulz D, et al. The evolution-ary paradox of tooth wear: simply destruction orinevitable adaptation? PLoS ONE. 2013;8:e62263.
58. Eliasson S, Richter S. Tooth wear in medieval Icelanders.The XXth Nordic Medical Congress, ProgramAbstracts, pp. 49, Abstract 32, 2005.
59. Seghi RR, Rosenstiel SF, Bauer P. Abrasion of humanenamel by different dental ceramics in vitro. J DentRes.1991;70:221–225.
60. Dahl BL, Oilo G. In vivo wear ranking of some restora-tive materials. Quintessence Int. 1994;25:561–565.
61. Janyavula S, Lawson N, Cakir D, Beck P, Ramp LC,Burgess JO. The wear of polished and glazed zirconiaagainst enamel. J Prosthet Dent. 2013;109:22–29.
62. Park JH, Park S, Lee K, Yun KD, Lim HP. Antagonistwear of three CAD/CAM anatomic contour zirconiaceramics. J Prosthet Dent. 2014;111:20–29.
63. Luangruangrong P, Cook NB, Sabrah AH, Hara AT,Bottino MC. Influence of full-contour zirconia surfaceroughness on wear of glass-ceramics. J Prosthodont.2014;23:198–205.
64. Hmaidouch R, Weigl P. Tooth wear against ceramiccrowns in posterior region: a systematic literature review.Int J Oral Sci. 2013;5:183–190.
65. Miyazaki T, Nakamura T, Matsumura H, Ban S,Kobayashi T. Current status of zirconia restoration. JProsth Res. 2013;57:236–261.
66. Olivera AB, Matson E, Marques MM. The effect ofglazed and polished ceramics on human enamel wear.Int J Prosthodont. 2006;19:547–548.
67. Jagger DC, Harrison A. An in vitro investigation intothe wear effects of unglazed, glazed, and polished porce-lain on human enamel. J Prosthetic Dent.1994;72:320–323.
68. Avey KD, DeBiase CB, Gladwin MA, Kao EC, BagbyMD. Development of a standardized abrasive scale: ananalysis of commercial prophylaxis pastes. J Dent Hyg.2006;80:21.
69. Biller IR, Hunter EL, Featherstone MJ, Silverstone LM.Enamel loss during a prophylaxis polish in vitro. J IntAssoc Dent Child. 1980;11:7–12.
70. Rühling A, Wulf J, Schwahn C, Kocher T. Surface wearon cervical restorations and adjacent enamel and rootcementum caused by simulated long-term maintenancetherapy. J Clin Periodontol. 2004;31:293–298.
71. Stookey GK. In vitro estimates of enamel and dentinabrasion associated with a prophylaxis. J Dent Res.1978;57:36.
72. Christensen RP, Bangerter VW. Immediate and long-term in vivo effects of polishing on enamel and dentin. JProsthet Dent. 1987;57:150–160.
CHAPTER 6 Preventing Damage to Oral Hard and Soft Tissues
118
73. Thompson RE, Way DC. Enamel loss due to prophy-laxis and multiple bonding/debonding of orthodonticattachments. Am J Orthod. 1981;79:282–295.
74. Pence SD, Chambers DA, van Tets IG, Wolf RC, Pfeif-fer DC. Repetitive coronal polishing yields minimalenamel loss. J Dent Hyg. 2011;85:348–357.
75. Barnes CM. The science of polishing. Dimensions ofDental Hygiene. 2009;7(11):18–20.
76. Nagel Beebe S. To polish or not to polish: understandingthe principle and the pros and cons of selective polishing.Dimensions of Dental Hygiene. 2009;7(3):32–35.
77. Frame PS, Sawai R, Bowen WH, Meyerowitz C. Preven-tive dentistry: practitioner’s recommendations for low-risk patients compared with scientific evidence andpractice guidelines. Am J Prev Med. 2000;18:159–162.
78. Zanatta FB, Pinto TMP, Kantorski KZ, Rösing CK.Plaque, gingival bleeding and calculus formation aftersupragingival scaling with and without polishing: a ran-domised clinical trial. Oral Health Prev Dent.2011;9:275–280.
79. Worthington HV, Clarkson JE, Bryan G, Beirne PV.Routine scale and polish for periodontal health in adults.Cochrane Database Syst Rev. 2013;(11):CD004625.doi:10.1002/14651858.CD004625.pub4.
80. Slot DE. Insufficient evidence to determine the effects ofroutine scale and polish treatments. Evid Based Dent.2014;15:74–75.
81. Graumann SJ, Sensat ML, Stoltenberg JL. Air polish-ing: a review of current literature. J Dent Hyg.2013;87:173–180.
82. Petersilka GJ, Bell M, Mehl A, Hickel R, Flemming TF.Root defects following air polishing. An in vitro study onthe effects of working parameters. J Clin Periodontol.2003;30:165–170.
83. Agger MS, Hörsted-Bindslev P, Hovgaard O. Abrasive-ness of an air-powder polishing system on root surfacesin vitro. Quintessence Int. 2001;32:407–411.
84. Pikdoken ML, Ozcelik C. Severe enamel abrasion due tomisuse of an air polishing device. Int J Dent Hyg.2006;4:209–212.
85. Tada K, Kakuta K, Ogura H, Sato S. Effect of particlediameter on air polishing of dentin surfaces. Odontology.2010;98:31–36.
86. Tada K, Wiroj S, Inatomi M, Sato S. The characteriza-tion of dentin defects produced by air polishing, Odon-tology. 2012;100:41–46.
87. Bühler J, Amato M, Weiger R, Walter C. A systematicreview on the effects of air polishing devices on oral tis-sues. Int J Dent Hyg. 2015;14:15–28.
88. Addy M, Griffiths G, Dummer P, Kingdon A, ShawWC. The distribution of plaque and gingivitis and theinfluence of brushing hand in a group of 11-12 year oldschool children. J Clin Periodontol. 1987;14:564–572.
89. Addy M. Tooth brushing, tooth wear and dentinehypersensitivity—are they associated? Int Dent J.2005;55(suppl 1):261–267.
90. Addy M, West NX. The role of toothpaste in the aetiol-ogy and treatment of dentine hypersensitivity. MonogrOral Sci. 2013;23:75–87.
91. Abrahamsen TC. The worn dentition pathognomonicpatterns of abrasion and erosion. Int Dent J.2005;55:268–276.
92. Grippo JO, Simring M, Schreiner S. Attrition, abrasion, cor-rosion and abfraction revisited: a new perspective on toothsurface lesions. J Am Dent Assoc. 2004;135:1109–1118.
93. Schemelhorn BR, Moore MH, Putt MS. Abrasion, pol-ishing, and stain removal characteristics of various com-mercial dentifrices in vitro. J Clin Dent. 2011;22:11–18.
94. Dörfer CE, Hefferren J, Gonz�lez-Cabezas C, Imfeld T,Addy M. Methods to determine dentifrice abrasiveness.Summary proceedings of a workshop in Frankfurt, Ger-many. J Clin Dent. 2010;21(suppl):S1–S16. Available at:http://www.gaba-dent.de/data/docs/en/6848/JCD-21-Suppl-RDA-Suppl.pdf.
95. Wiegand A, Egert S, Attin T. Toothbrushing before orafter an acidic challenge to minimize tooth wear? An insitu/ex vivo study. Am J Dent. 2008;21:13–16.
96. ten Cate JM, Imfeld T. Dental erosion, summary. Eur JOral Sci. 1996;104(part 2):241–244.
97. Johansson AK, Omar R, Carlsson GE, Johansson A.Dental erosion and its growing importance in clinicalpractice: from past to present. Int J Dent.2012;2012.632907.
98. Wang GR, Zhang H, Wang ZG, Jiang GS, Guo CH.Relationship between dental erosion and respiratorysymptoms in patients with gastro-oesophageal reflux dis-ease. J Dent. 2010;38:892–898.
99. Schlueter N, Hardt M, Klimek J, Ganss C. Influence ofthe digestive enzymes trypsin and pepsin in vitro on theprogression of erosion in dentine. Arch Oral Biol.2010;55:294–299.
100. Bartlett DW, Evans DF, Anggiansah A, Smith BG. Astudy of the association between gastro-oesophagealreflux and palatal dental erosion. Br Dent J.1996;181:125–131.
101. Ranjitkar S, Kaidonis JA, Smales RJ. Gastroesophagealreflux disease and tooth erosion. Int J Dent.2012;2012:479850.
102. Öhrn R, Enzell K, Angmar-Månsson B. Oral status of81 subjects with eating disorders. Eur J Oral Sci.1999;107:157–163.
103. Johansson AK, Norring C, Unell L, Johansson A. Eat-ing disorders and oral health: a matched case-controlstudy. Eur J Oral Sci. 2012;120:61–69.
104. Briggs P, Bishop K, Kelleher M. Case report: the use ofindirect composite for the management of extensive ero-sion. Eur J Prosthodont Rest Dent. 1994;3:51–54.
105. Burke FJ, Kelleher MG, Wilson N, Bishop K. Introduc-ing the concept of pragmatic esthetics, with special refer-ence to the treatment of tooth wear. J Esthetic RestDent. 2011;23:277–293.
106. Messias DC, Turssi CP, Hara AT, Serra MC. Sodium
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
119
bicarbonate solution as an anti-erosive agent againstsimulated endogenous erosion. Eur J Oral Sci.2010;118:385–388.
107. Burkhart NW. Bulimia: decreasing the damage to enam-el. Available at: http://www.rdhmag.com/articles/print/volume-31/issue-1/columns/bulimia-decreasing-the-damage-to-enamel.html. Accessed August 10, 2016.
108. Khan F, Young WG, Law V, Priest J, Daley TJ. Cuppedlesions of early onset dental erosion in young southeastQueensland adults. Aust Dent J. 2001;46:100–107.
109. Hemingway CA, Parker DM, Addy M, Barbour ME.Erosion of enamel by non-carbonated soft drinks withand without toothbrushing abrasion. Br Dent J.2006;201:447–450.
110. Jacobson MF. Liquid candy: how soft drinks are harm-ing Americans’ health. 2005. Available at:http://www.cspinet.org/new/pdf/liquid_candy_final_w_new_supplement.pdf. Accessed August 10, 2016.
111. Harnack L, Stang J, Story M. Soft drink consumptionamong US children and adolescents: nutritional conse-quences. J Am Dietetic Assoc. 1999;99:436–441.
112. Messer LB, Young WG. Childhood diet and dental ero-
sion. In:Khan F, Young WG, eds. Tooth Wear. The ABCof the Worn Dentition. Chichester, UK: Wiley-Blackwell;2011:34–49.
113. Milosevic A. Sports drinks hazard to teeth. Br J SportsMed. 1997;31:28–30.
114. Jaeggi T, Lussi A. Toothbrush abrasion of erosivelyaltered enamel after intraoral exposure to saliva: an insitu study. Caries Res. 1999;33:455–461.
115. Rios D, Honorio HM, Magalhães AC, et al. Influenceof toothbrushing on enamel softening and abrasive wearof eroded bovine enamel: an in situ study. Braz Oral Res.2006;20:148–154.
116. Johansson AK, Lingstrom P, Imfeld T, Birkhed D. Influ-ence of drinking method on tooth-surface pH in relationto dental erosion. Eur J Oral Sci. 2004;112:484–489.
117. Grippo JO. Abfraction: a new classification of hard tis-sue lesions of teeth. J Esth Dent. 1991;3:14–18.
118. Aubry M, Maffart B, Donat B, Brau JJ. Brief communi-cation: study of noncarious cervical tooth lesions in sam-ples of prehistoric, historic and modern populationsfrom the South of France. Am J Phys Anthropol.2003;121:10–14.
CHAPTER 6 Preventing Damage to Oral Hard and Soft Tissues
120

Oral health professionals have a responsibility tohelp reduce the morbidity and mortality associatedwith head and neck cancers (HNCs). Globally, headand neck carcinomas are the sixth most commoncancer in developed countries.1,2 In the United States,HNCs rank eighth among men, with men experi-encing twice as many cases as women.3 Survival ratesfor oral cancers have been relatively unchanged forthree decades. Early detection remains elusive. In theUnited States, between 2005 and 2011, only 62.5%of all patients with HNCs survived for 5 years.4
Oropharyngeal cancers (OPCs) associated with thehuman papillomavirus (HPV) have shown morepromising survival rates than HPV-negative oralcancers, but early detection is difficult because a pre-malignant state is as yet unidentifiable and lesionsites are less accessible visually.Oral health professionals must understand the
threats posed by HNCs, take positive actions tocombat them, and strive to educate other healthcareproviders about the importance of screening forHNCs and referring, when appropriate. HNC is acondition that affects many aspects of a patient’s life.Ensuring a patient’s ability to eat, speak, realize psy-chosocial well-being, and maintain strength fallswithin the purview of many healthcare providers.Speech pathologists, oncologists, nurses, dentists,dietitians, and dental hygienists are healthcareproviders who can work together to make basicpatient needs attainable. Through awareness, educa-tion, and action, the collaborative healthcare teamcan help address and prevent HNCs. This chapterprovides a comprehensive framework to guide oraland nonoral health professionals as they strive toreduce the incidence and prevalence of HNCs andtheir associated morbidity and mortality.
EPIDEMIOLOGYHNCs are a broad grouping of malignanciesthat include cancers of the oral cavity and can-cers of the oropharynx (OPCs). The latter arecommonly associated with HPV. Since the etio-logic pathways for “traditional” carcinogen-induced oral cancers and HPV-driven OPCs aredifferent, some researchers have designated themas two different disease entities.5 While the inci-dence of oral cavity cancers in the United Stateshas decreased over the past 15 years, the numberof new OPCs has risen at an alarming rate.6 Anincidence of approximately 15,500 new cases ofHPV-associated oropharynx cancer is anticipat-ed in the United States per year.4 Between 1988and 2004, in the United States, oral cancersdeclined by 50% while OPCs increased by225%.7 These statistical findings have been attrib-uted to changes in lifestyle, decreased tobaccouse, and increased practices of high-risk sexualbehaviors (see Figure 1). In 2012, an estimated 291,108 people were
living with oral cavity and pharyngeal cancer inthe United States.4 Oral and oropharyngeal can-cer rates are higher for men than for women.Hispanic and black men suffer more oral can-cers than do whites. Oral cancers have long beenassociated with African-American elderly menof low socioeconomic status who use tobaccoand alcohol, whereas the typical HPV-OPCpatient is a white man, in his early 50s, of themiddle-income bracket, with little to no historyof alcohol and tobacco use.5 Although HNCrates increase with age, the median age for HPV-OPCs is lower than that for “traditional” car-cinogen-induced oral cancers. Additionally,comorbidities such as tobacco use do lessen sur-vival rates for HPV-induced HNCs.8 Figure 2and Table 1 show the number of new casesbetween 2008 and 2012 by age and ethnicity,while Figure 3 displays mortality rates by age forthe same time period.OPC rates have risen dramatically in eco-
nomically developed countries, including Cana-da, England, Sweden, and Australia.7 OPC is the11th most common cancer worldwide.9 In lightof the rampant increase in OPCs with noplateau in sight, the late stage of HNC detection,
121
Head and Neck Cancers
Chapter 7
Jacquelyn Fried
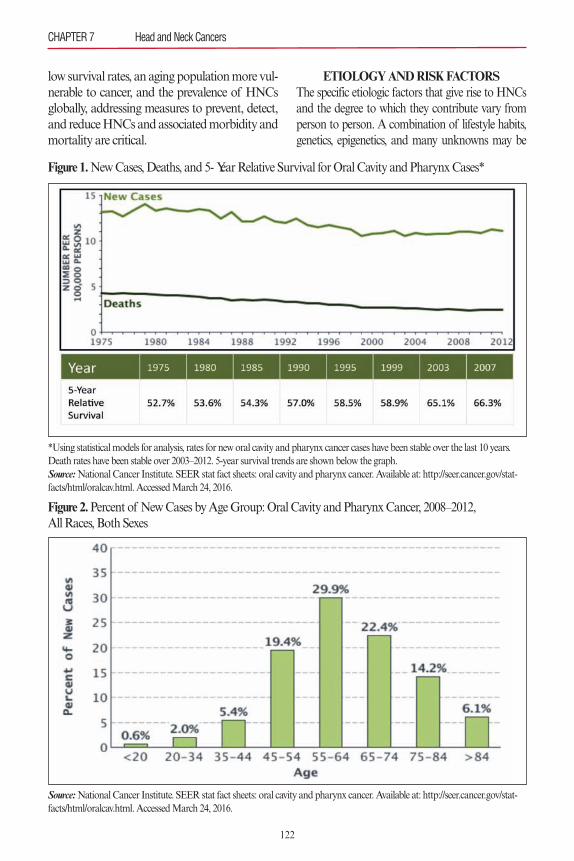
low survival rates, an aging population more vul-nerable to cancer, and the prevalence of HNCsglobally, addressing measures to prevent, detect,and reduce HNCs and associated morbidity and mortality are critical.
ETIOLOGY AND RISK FACTORSThe specific etiologic factors that give rise to HNCsand the degree to which they contribute vary fromperson to person. A combination of lifestyle habits,genetics, epigenetics, and many unknowns may be
CHAPTER 7 Head and Neck Cancers
122
Figure 1. New Cases, Deaths, and 5- Year Relative Survival for Oral Cavity and Pharynx Cases*
*Using statistical models for analysis, rates for new oral cavity and pharynx cancer cases have been stable over the last 10 years.Death rates have been stable over 2003–2012. 5-year survival trends are shown below the graph. Source:National Cancer Institute. SEER stat fact sheets: oral cavity and pharynx cancer. Available at: http://seer.cancer.gov/stat-facts/html/oralcav.html. Accessed March 24, 2016.
Figure 2.Percent of New Cases by Age Group: Oral Cavity and Pharynx Cancer, 2008–2012, All Races, Both Sexes
Source:National Cancer Institute. SEER stat fact sheets: oral cavity and pharynx cancer. Available at: http://seer.cancer.gov/stat-facts/html/oralcav.html. Accessed March 24, 2016.
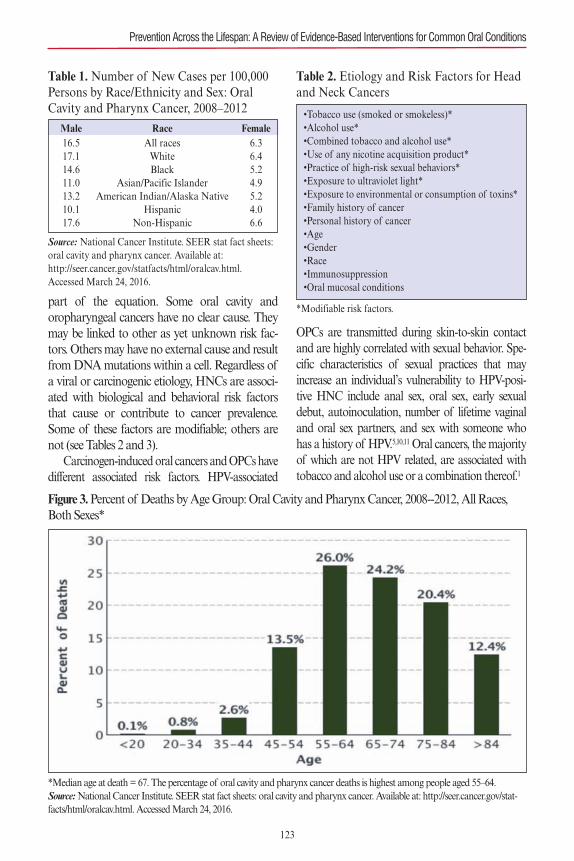
part of the equation. Some oral cavity andoropharyngeal cancers have no clear cause. Theymay be linked to other as yet unknown risk fac-tors. Others may have no external cause and resultfrom DNA mutations within a cell. Regardless ofa viral or carcinogenic etiology, HNCs are associ-ated with biological and behavioral risk factorsthat cause or contribute to cancer prevalence.Some of these factors are modifiable; others arenot (see Tables 2 and 3).Carcinogen-induced oral cancers and OPCs have
different associated risk factors. HPV-associated
OPCs are transmitted during skin-to-skin contactand are highly correlated with sexual behavior. Spe-cific characteristics of sexual practices that mayincrease an individual’s vulnerability to HPV-posi-tive HNC include anal sex, oral sex, early sexualdebut, autoinoculation, number of lifetime vaginaland oral sex partners, and sex with someone whohas a history of HPV.5,10,11 Oral cancers, the majorityof which are not HPV related, are associated withtobacco and alcohol use or a combination thereof.1
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
123
Figure 3. Percent of Deaths by Age Group: Oral Cavity and Pharynx Cancer, 2008--2012, All Races,Both Sexes*
*Median age at death = 67. The percentage of oral cavity and pharynx cancer deaths is highest among people aged 55–64. Source:National Cancer Institute. SEER stat fact sheets: oral cavity and pharynx cancer. Available at: http://seer.cancer.gov/stat-facts/html/oralcav.html. Accessed March 24, 2016.
Table 1. Number of New Cases per 100,000Persons by Race/Ethnicity and Sex: OralCavity and Pharynx Cancer, 2008–2012
Source: National Cancer Institute. SEER stat fact sheets:oral cavity and pharynx cancer. Available at:http://seer.cancer.gov/statfacts/html/oralcav.html. Accessed March 24, 2016.
Male Race Female16.5 All races 6.317.1 White 6.414.6 Black 5.211.0 Asian/Pacific Islander 4.913.2 American Indian/Alaska Native 5.210.1 Hispanic 4.017.6 Non-Hispanic 6.6
Table 2. Etiology and Risk Factors for Headand Neck Cancers
*Modifiable risk factors.
•Tobacco use (smoked or smokeless)*•Alcohol use*•Combined tobacco and alcohol use*•Use of any nicotine acquisition product*•Practice of high-risk sexual behaviors*•Exposure to ultraviolet light*•Exposure to environmental or consumption of toxins*•Family history of cancer•Personal history of cancer•Age•Gender•Race•Immunosuppression•Oral mucosal conditions
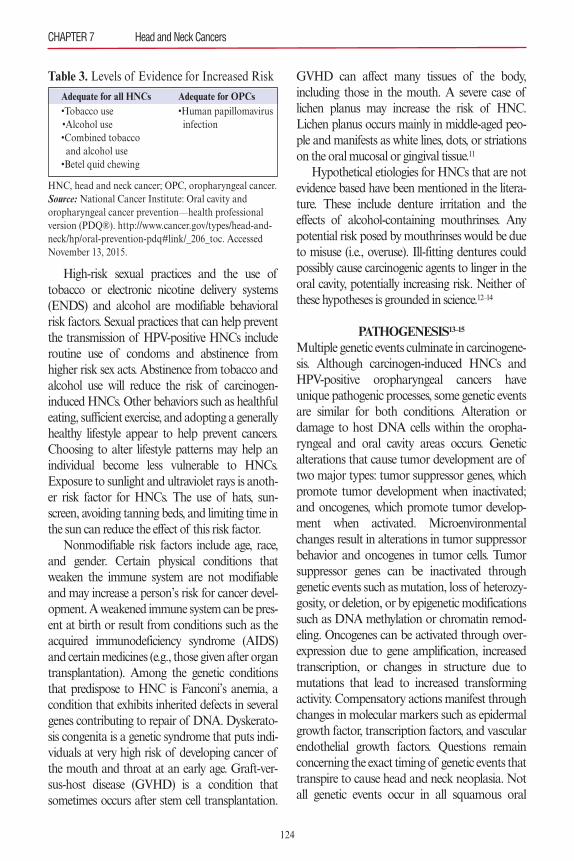
High-risk sexual practices and the use oftobacco or electronic nicotine delivery systems(ENDS) and alcohol are modifiable behavioralrisk factors. Sexual practices that can help preventthe transmission of HPV-positive HNCs includeroutine use of condoms and abstinence fromhigher risk sex acts. Abstinence from tobacco andalcohol use will reduce the risk of carcinogen-induced HNCs. Other behaviors such as healthfuleating, sufficient exercise, and adopting a generallyhealthy lifestyle appear to help prevent cancers.Choosing to alter lifestyle patterns may help anindividual become less vulnerable to HNCs.Exposure to sunlight and ultraviolet rays is anoth-er risk factor for HNCs. The use of hats, sun-screen, avoiding tanning beds, and limiting time inthe sun can reduce the effect of this risk factor.Nonmodifiable risk factors include age, race,
and gender. Certain physical conditions thatweaken the immune system are not modifiableand may increase a person’s risk for cancer devel-opment. A weakened immune system can be pres-ent at birth or result from conditions such as theacquired immunodeficiency syndrome (AIDS)and certain medicines (e.g., those given after organtransplantation). Among the genetic conditionsthat predispose to HNC is Fanconi’s anemia, acondition that exhibits inherited defects in severalgenes contributing to repair of DNA. Dyskerato-sis congenita is a genetic syndrome that puts indi-viduals at very high risk of developing cancer ofthe mouth and throat at an early age. Graft-ver-sus-host disease (GVHD) is a condition thatsometimes occurs after stem cell transplantation.
GVHD can affect many tissues of the body,including those in the mouth. A severe case oflichen planus may increase the risk of HNC.Lichen planus occurs mainly in middle-aged peo-ple and manifests as white lines, dots, or striationson the oral mucosal or gingival tissue.11
Hypothetical etiologies for HNCs that are notevidence based have been mentioned in the litera-ture. These include denture irritation and theeffects of alcohol-containing mouthrinses. Anypotential risk posed by mouthrinses would be dueto misuse (i.e., overuse). Ill-fitting dentures couldpossibly cause carcinogenic agents to linger in theoral cavity, potentially increasing risk. Neither ofthese hypotheses is grounded in science.12–14
PATHOGENESIS13–15Multiple genetic events culminate in carcinogene-sis. Although carcinogen-induced HNCs andHPV-positive oropharyngeal cancers haveunique pathogenic processes, some genetic eventsare similar for both conditions. Alteration ordamage to host DNA cells within the oropha-ryngeal and oral cavity areas occurs. Geneticalterations that cause tumor development are oftwo major types: tumor suppressor genes, whichpromote tumor development when inactivated;and oncogenes, which promote tumor develop-ment when activated. Microenvironmentalchanges result in alterations in tumor suppressorbehavior and oncogenes in tumor cells. Tumorsuppressor genes can be inactivated throughgenetic events such as mutation, loss of heterozy-gosity, or deletion, or by epigenetic modificationssuch as DNA methylation or chromatin remod-eling. Oncogenes can be activated through over-expression due to gene amplification, increasedtranscription, or changes in structure due tomutations that lead to increased transformingactivity. Compensatory actions manifest throughchanges in molecular markers such as epidermalgrowth factor, transcription factors, and vascularendothelial growth factors. Questions remainconcerning the exact timing of genetic events thattranspire to cause head and neck neoplasia. Notall genetic events occur in all squamous oral
CHAPTER 7 Head and Neck Cancers
124
Table 3. Levels of Evidence for Increased Risk
HNC, head and neck cancer; OPC, oropharyngeal cancer.Source: National Cancer Institute: Oral cavity andoropharyngeal cancer prevention—health professionalversion (PDQ®). http://www.cancer.gov/types/head-and-neck/hp/oral-prevention-pdq#link/_206_toc. AccessedNovember 13, 2015.
Adequate for all HNCs Adequate for OPCs•Tobacco use •Human papillomavirus•Alcohol use infection•Combined tobacco and alcohol use•Betel quid chewing
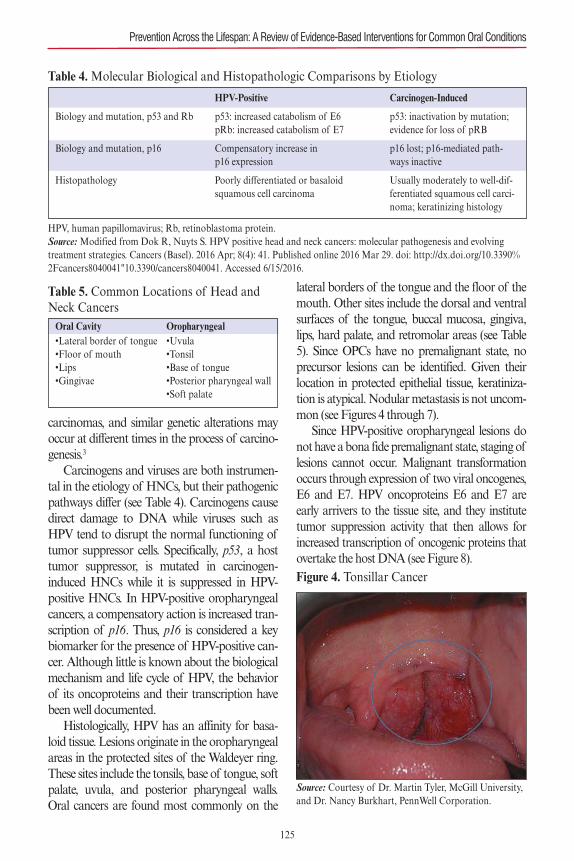
carcinomas, and similar genetic alterations mayoccur at different times in the process of carcino-genesis.3
Carcinogens and viruses are both instrumen-tal in the etiology of HNCs, but their pathogenicpathways differ (see Table 4). Carcinogens causedirect damage to DNA while viruses such asHPV tend to disrupt the normal functioning oftumor suppressor cells. Specifically, p53, a hosttumor suppressor, is mutated in carcinogen-induced HNCs while it is suppressed in HPV-positive HNCs. In HPV-positive oropharyngealcancers, a compensatory action is increased tran-scription of p16. Thus, p16 is considered a keybiomarker for the presence of HPV-positive can-cer. Although little is known about the biologicalmechanism and life cycle of HPV, the behaviorof its oncoproteins and their transcription havebeen well documented.Histologically, HPV has an affinity for basa-
loid tissue. Lesions originate in the oropharyngealareas in the protected sites of the Waldeyer ring.These sites include the tonsils, base of tongue, softpalate, uvula, and posterior pharyngeal walls.Oral cancers are found most commonly on the
lateral borders of the tongue and the floor of themouth. Other sites include the dorsal and ventralsurfaces of the tongue, buccal mucosa, gingiva,lips, hard palate, and retromolar areas (see Table5). Since OPCs have no premalignant state, noprecursor lesions can be identified. Given theirlocation in protected epithelial tissue, keratiniza-tion is atypical. Nodular metastasis is not uncom-mon (see Figures 4 through 7).Since HPV-positive oropharyngeal lesions do
not have a bona fide premalignant state, staging oflesions cannot occur. Malignant transformationoccurs through expression of two viral oncogenes,E6 and E7. HPV oncoproteins E6 and E7 areearly arrivers to the tissue site, and they institutetumor suppression activity that then allows forincreased transcription of oncogenic proteins thatovertake the host DNA (see Figure 8).
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
125
Table 4. Molecular Biological and Histopathologic Comparisons by Etiology
HPV, human papillomavirus; Rb, retinoblastoma protein.Source: Modified from Dok R, Nuyts S. HPV positive head and neck cancers: molecular pathogenesis and evolvingtreatment strategies. Cancers (Basel). 2016 Apr; 8(4): 41. Published online 2016 Mar 29. doi: http://dx.doi.org/10.3390%2Fcancers8040041"10.3390/cancers8040041. Accessed 6/15/2016.
HPV-Positive Carcinogen-Induced
Biology and mutation, p53 and Rb p53: increased catabolism of E6 p53: inactivation by mutation; pRb: increased catabolism of E7 evidence for loss of pRB
Biology and mutation, p16 Compensatory increase in p16 lost; p16-mediated path-p16 expression ways inactive
Histopathology Poorly differentiated or basaloid Usually moderately to well-dif-squamous cell carcinoma ferentiated squamous cell carci-
noma; keratinizing histology
Table 5. Common Locations of Head andNeck CancersOral Cavity•Lateral border of tongue•Floor of mouth•Lips•Gingivae
Oropharyngeal•Uvula•Tonsil•Base of tongue•Posterior pharyngeal wall•Soft palate
Figure 4. Tonsillar Cancer
Source: Courtesy of Dr. Martin Tyler, McGill University,and Dr. Nancy Burkhart, PennWell Corporation.
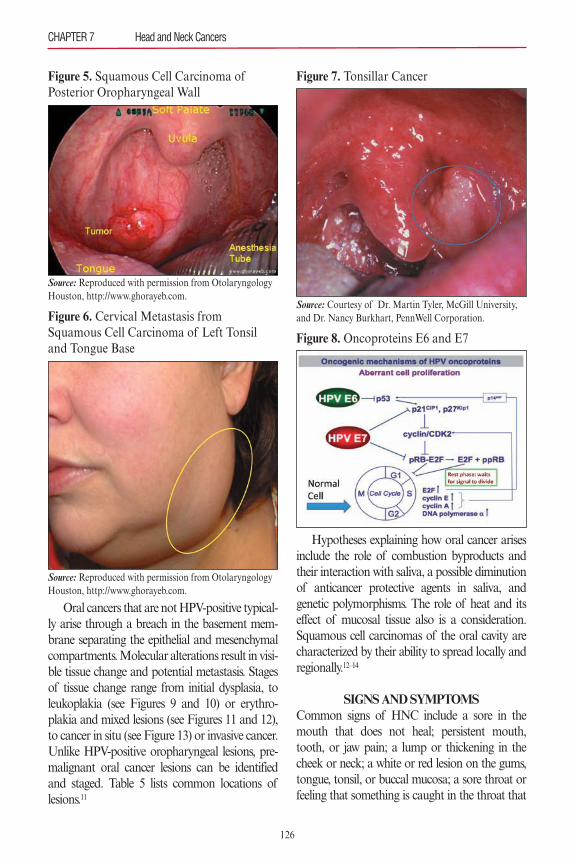
Oral cancers that are not HPV-positive typical-ly arise through a breach in the basement mem-brane separating the epithelial and mesenchymalcompartments. Molecular alterations result in visi-ble tissue change and potential metastasis. Stagesof tissue change range from initial dysplasia, toleukoplakia (see Figures 9 and 10) or erythro-plakia and mixed lesions (see Figures 11 and 12),to cancer in situ (see Figure 13) or invasive cancer.Unlike HPV-positive oropharyngeal lesions, pre-malignant oral cancer lesions can be identifiedand staged. Table 5 lists common locations oflesions.11
Hypotheses explaining how oral cancer arisesinclude the role of combustion byproducts andtheir interaction with saliva, a possible diminutionof anticancer protective agents in saliva, andgenetic polymorphisms. The role of heat and itseffect of mucosal tissue also is a consideration.Squamous cell carcinomas of the oral cavity arecharacterized by their ability to spread locally andregionally.12–14
SIGNS AND SYMPTOMSCommon signs of HNC include a sore in themouth that does not heal; persistent mouth,tooth, or jaw pain; a lump or thickening in thecheek or neck; a white or red lesion on the gums,tongue, tonsil, or buccal mucosa; a sore throat orfeeling that something is caught in the throat that
CHAPTER 7 Head and Neck Cancers
126
Figure 5. Squamous Cell Carcinoma of Posterior Oropharyngeal Wall
Source: Reproduced with permission from OtolaryngologyHouston, http://www.ghorayeb.com.
Figure 6. Cervical Metastasis from Squamous Cell Carcinoma of Left Tonsiland Tongue Base
Source: Reproduced with permission from OtolaryngologyHouston, http://www.ghorayeb.com.
Figure 7. Tonsillar Cancer
Source: Courtesy of Dr. Martin Tyler, McGill University,and Dr. Nancy Burkhart, PennWell Corporation.
Figure 8. Oncoproteins E6 and E7
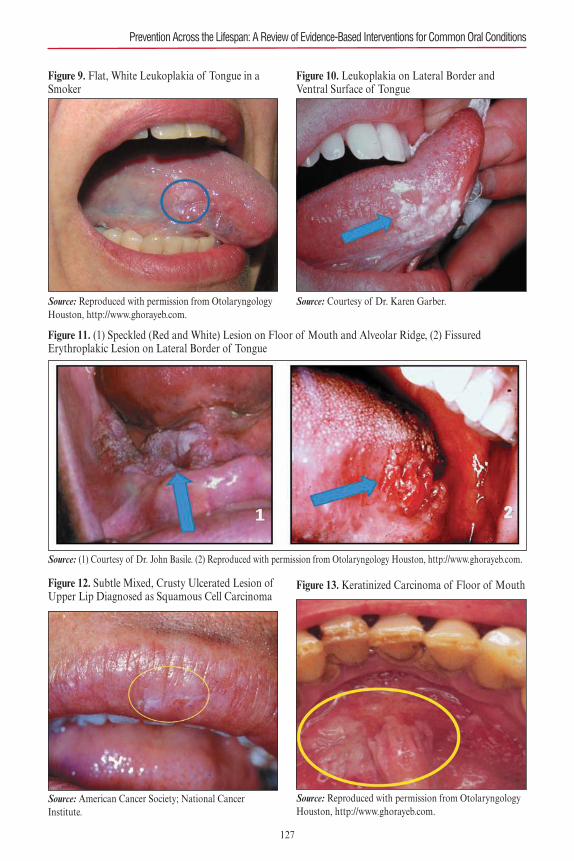
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
127
Figure 9. Flat, White Leukoplakia of Tongue in aSmoker
Source: Reproduced with permission from OtolaryngologyHouston, http://www.ghorayeb.com.
Figure 10. Leukoplakia on Lateral Border and Ventral Surface of Tongue
Source: Courtesy of Dr. Karen Garber.
Figure 11. (1) Speckled (Red and White) Lesion on Floor of Mouth and Alveolar Ridge, (2) Fissured Erythroplakic Lesion on Lateral Border of Tongue
Source: (1) Courtesy of Dr. John Basile. (2) Reproduced with permission from Otolaryngology Houston, http://www.ghorayeb.com.
Figure 12. Subtle Mixed, Crusty Ulcerated Lesion ofUpper Lip Diagnosed as Squamous Cell Carcinoma
Source: American Cancer Society; National Cancer Institute.
Figure 13. Keratinized Carcinoma of Floor of Mouth
Source: Reproduced with permission from OtolaryngologyHouston, http://www.ghorayeb.com.

does not go away; difficulty swallowing, chewing,or moving the jaw or tongue; numbness of thetongue or elsewhere in the mouth; jaw swelling;loosening of the teeth; hoarseness or voicechanges; weight loss; and persistent bad breath(see Table 6). Although many of the signs andsymptoms of HNCs are shared, OPCs are specifi-cally characterized by odynophagia (painful swal-lowing), dysphagia (difficulty swallowing), andotalgia (ear pain). Bleeding, decreased tonguemobility, and trismus may be accompanying signs.Base of tongue cancers are associated with sub-mucosal spread. Table 7 shows clinical differencesby etiology.Carcinogen-induced precancerous or cancer-
ous lesions may be described as leukoplakic, ery-throplakic, or speckled. Leukoplakic lesions havethe lowest conversion rates and clinically mayappear flat and white. As the lesions increase insize, terms such as exophytic, pedunculated, verru-cous, and sessile are used to describe them. Neo-plasms may appear keratinized, nodular, warty,
fissured, or ulcerated (see Figures 11 through 14).
DIAGNOSTIC TESTSSurvival rates for OPC vary depending on thetumor’s stage when it is detected.4 A thorough andaccurate diagnosis is the first step in developing atargeted and effective patient care plan. Manydiagnostic tests and techniques are available toassess the presence of HNCs. Some are conductedclinically but most require laboratory analysis.Only a handful of diagnostic tests are evidencebased, but several are used in dental practices andclinics.A comprehensive head and neck examination
and screening must be a component part of rou-tine risk assessment. It is considered a standard ofcare for detecting early HNCs and premalignantlesions, yet no evidence supports its role in reduc-ing mortality in the general population.16 Allintraoral and extraoral head and neck structures,including all lymph nodes and lymph nodechains, must be palpated manually and visually
CHAPTER 7 Head and Neck Cancers
128
Table 6. Symptoms of Oral and Oropharyngeal Cancer
•Fatigue•Difficulty chewing, swallowing, or moving jaws or tongue•Loss of appetite•Unexplained weight loss•Trismus•Red or white patch•Lump or thickening in cheek•Headaches
HPV, human papillomavirus; Rb, retinoblastoma protein.Source: Modified from: Cantrell et al. (2013); Dufour et al. (2012). National Cancer Institute; Centers for Disease Control.
Table 7. Comparison of Head and Neck Cancers by Etiology
Source: Courtesy of Dr. John Basile.
HPV-Positive Carcinogen-Induced
Incidence Increasing Decreasing
Age Younger (~ 50s) Older (~ 60+)
Sex Male Male (smoking)
Risk factors Sexual: number of partners, early Alcohol and smoking, otherfirst sexual encounters, smoking, and host factorsimmunosuppression may play role
Prognosis Good Poor
Vaccine Yes (for some types) No
•Ear or jaw pain, or both•Chronic bad breath•Changes in speech•Loose teeth or toothache•Dentures that no longer fit•Sore that does not heal •Hoarseness•Numbness of mouth or tongue•Pain or bleeding in mouth
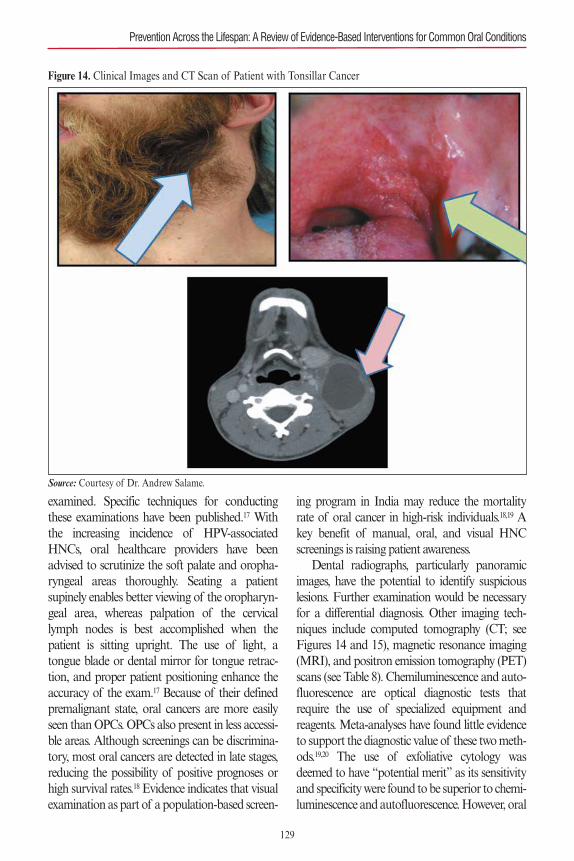
examined. Specific techniques for conductingthese examinations have been published.17 Withthe increasing incidence of HPV-associatedHNCs, oral healthcare providers have beenadvised to scrutinize the soft palate and oropha-ryngeal areas thoroughly. Seating a patientsupinely enables better viewing of the oropharyn-geal area, whereas palpation of the cervicallymph nodes is best accomplished when thepatient is sitting upright. The use of light, atongue blade or dental mirror for tongue retrac-tion, and proper patient positioning enhance theaccuracy of the exam.17 Because of their definedpremalignant state, oral cancers are more easilyseen than OPCs. OPCs also present in less accessi-ble areas. Although screenings can be discrimina-tory, most oral cancers are detected in late stages,reducing the possibility of positive prognoses orhigh survival rates.18 Evidence indicates that visualexamination as part of a population-based screen-
ing program in India may reduce the mortalityrate of oral cancer in high-risk individuals.18,19 Akey benefit of manual, oral, and visual HNCscreenings is raising patient awareness.Dental radiographs, particularly panoramic
images, have the potential to identify suspiciouslesions. Further examination would be necessaryfor a differential diagnosis. Other imaging tech-niques include computed tomography (CT; seeFigures 14 and 15), magnetic resonance imaging(MRI), and positron emission tomography (PET)scans (see Table 8). Chemiluminescence and auto-fluorescence are optical diagnostic tests thatrequire the use of specialized equipment andreagents. Meta-analyses have found little evidenceto support the diagnostic value of these two meth-ods.19,20 The use of exfoliative cytology wasdeemed to have “potential merit” as its sensitivityand specificity were found to be superior to chemi-luminescence and autofluorescence. However, oral
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
129
Figure 14. Clinical Images and CT Scan of Patient with Tonsillar Cancer
Source: Courtesy of Dr. Andrew Salame.
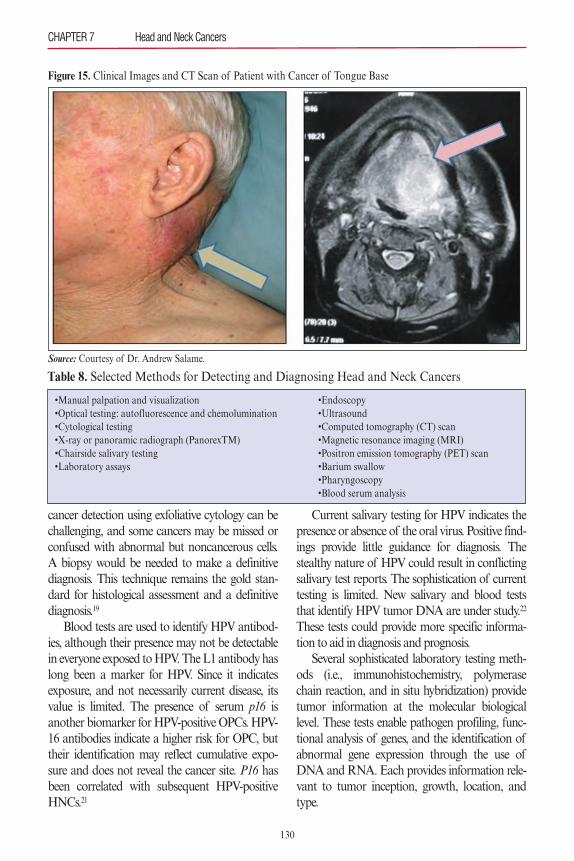
cancer detection using exfoliative cytology can bechallenging, and some cancers may be missed orconfused with abnormal but noncancerous cells.A biopsy would be needed to make a definitivediagnosis. This technique remains the gold stan-dard for histological assessment and a definitivediagnosis.19
Blood tests are used to identify HPV antibod-ies, although their presence may not be detectablein everyone exposed to HPV. The L1 antibody haslong been a marker for HPV. Since it indicatesexposure, and not necessarily current disease, itsvalue is limited. The presence of serum p16 isanother biomarker for HPV-positive OPCs. HPV-16 antibodies indicate a higher risk for OPC, buttheir identification may reflect cumulative expo-sure and does not reveal the cancer site. P16 hasbeen correlated with subsequent HPV-positiveHNCs.21
Current salivary testing for HPV indicates thepresence or absence of the oral virus. Positive find-ings provide little guidance for diagnosis. Thestealthy nature of HPV could result in conflictingsalivary test reports. The sophistication of currenttesting is limited. New salivary and blood teststhat identify HPV tumor DNA are under study.22
These tests could provide more specific informa-tion to aid in diagnosis and prognosis.Several sophisticated laboratory testing meth-
ods (i.e., immunohistochemistry, polymerasechain reaction, and in situ hybridization) providetumor information at the molecular biologicallevel. These tests enable pathogen profiling, func-tional analysis of genes, and the identification ofabnormal gene expression through the use ofDNA and RNA. Each provides information rele-vant to tumor inception, growth, location, andtype.
CHAPTER 7 Head and Neck Cancers
130
Table 8. Selected Methods for Detecting and Diagnosing Head and Neck Cancers
•Manual palpation and visualization•Optical testing: autofluorescence and chemolumination•Cytological testing•X-ray or panoramic radiograph (PanorexTM)•Chairside salivary testing•Laboratory assays
•Endoscopy•Ultrasound•Computed tomography (CT) scan•Magnetic resonance imaging (MRI)•Positron emission tomography (PET) scan•Barium swallow•Pharyngoscopy•Blood serum analysis
Figure 15. Clinical Images and CT Scan of Patient with Cancer of Tongue Base
Source: Courtesy of Dr. Andrew Salame.

Other medical tests diagnose tumors. Bariumswallows stain suspicious areas. Endoscopy, directand indirect pharyngoscopy, and laryngoscopypermit visualization of the patient in real time.During indirect pharyngoscopy, small mirrors areplaced at the most posterior portion of the throatto clearly examine the throat, the base of tongue,and part of the larynx. Direct scoping requires afiber-optic source directed to the site of interest.Scalpel biopsy and subsequent histological assess-ment is still the gold standard for diagnosing oralcancers, but more advanced imaging and labora-tory diagnostic tests may be necessary to identifyless obvious lesions or those that manifest no pre-malignant state (see Table 8).
PATIENT MANAGEMENT AND INTERVENTIONS
Preventive StrategiesOral health professionals are well-positioned toprevent HNCs. It is one of the most importantservices they can provide. Regardless of age andpopulation served, certain preventive strategiesand provider services that target HNCs are univer-sal. Others may be more age specific. Communi-cation techniques and the delivery of educationalcontent will depend on the recipient of the mes-sages. Regardless of the scenario, patients must befully engaged in all discussions. By personalizingrisk factors, patients may become more inquisitiveabout signs and symptoms of disease and preven-tive behaviors. All patients must become familiarwith the appearance of their oral cavities throughself-screening; if changes should occur, they thenmay have a better chance of noticing them.Patients must become their own advocates andmake certain that they receive HNC screeningswhenever they visit their oral health professionals.For all patients and target populations, behav-
ioral and biological risk factors for HNCs must beassessed and addressed. These include tobacco ornicotine dependence, excessive use of alcohol, andtheir combination, and engagement in high-risksexual practices. Health education topics withalmost universal applicability include preventionof HNCs, tobacco and nicotine use prevention
and cessation (see Table 9), measured consump-tion of alcohol, the oral–systemic link, and theadoption of healthy lifestyle behaviors related tonutrition and weight control. Individuals of anyage must know that tobacco use not only increasestheir risk for most cancers, but negatively affectstheir abilities to engage in physical activity,whether it be playing on a sports team, dancing,or climbing stairs. Individuals with family historiesof cancers and those with conditions associatedwith cancer must understand the cumulative effectof additional risk factors. Those who areimmunocompromised or may have genetic orclinical conditions associated with HNCs mustreceive tailored messages related to their status.Manual and visual screenings and radiographicimaging are routine assessment tools for all agegroups. If a suspicious lesion is detected, follow-upor referral to a specialist for biopsy and furthertesting is warranted.Primary and middle school curricula typically
include sex education and content on misuse ofdrugs, alcohol, and tobacco. Echoing and rein-forcing concepts learned in school is appropriateand needed. However, young students may notlearn that high-risk sexual behaviors can promotethe acquisition and transmission of HPV. Theyalso may not be told that timely vaccinationagainst HPV will prevent it. Oral health profes-sionals may need to broach topics such as risk fac-tors for HPV (which could include discussions of
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
131
Table 9. Levels of Evidence for Interventionsto Reduce Risk
HNC, head and neck cancer; OPC, oropharyngeal cancer.Source: National Cancer Institute: Oral cavity andoropharyngeal cancer prevention—health professionalversion (PDQ®). http://www.cancer.gov/types/head-and-neck/hp/oral-prevention-pdq#link/_206_toc. AccessedNovember 13, 2015.
Adequate for all HNCs: Tobacco cessation
Inadequate for all HNCs:Cessation of alcohol consumption
Inadequate for OPCs:Vaccination against HPV-16 and other high risk subtypes

safe sex) and the importance of HPV vaccinationfor prevention. Conversations related to sensitivetopics can be seamlessly raised in the context ofthe risks they pose for HNCs. Since children asyoung as 9 years of age are encouraged to be vac-cinated against HPV, these conversations shouldbegin at an early age. Likewise, tobacco preventionand cessation counseling should begin when chil-dren are young, as most individuals begin smok-ing before the age of 18 years.Parents or caretakers must be made aware of
age-appropriate HNC prevention strategies. Sig-nificant others often make choices for theirinfants, toddlers, children, and adolescents. Care-takers must be shown how important their rolesare in shaping an individual’s growth and develop-ment. Providers should encourage caretakers torole model and promote healthy lifestyles thatinclude nutritious food plans, exercise, and avoid-ance of cancer risk factors. Older children andteenagers with concerns about their appearancesmust be advised to limit their sun exposure, avoidtanning beds, use sunscreen, and wear hats andvisors for protection if outdoors. Similar rulesmust be enforced with young children to ensurecompliance.Other issues may facilitate behavioral change
in adults. In the context of aesthetics, providersmay be able to help adults make lifestyle changes.Tobacco use has been associated with prematureskin wrinkling, low sperm counts, spontaneousabortion, and difficulties conceiving. Oral effectsinclude halitosis, staining, and calculus buildup.Cumulative years of sun exposure may cause pre-malignant or cancerous skin lesions, necessitatinga dermatologist’s care. The HPV vaccine is posit-ed to be effective in individuals up to the age of 26years. A discussion of the vaccine is thus relevantto young adults and adults. Pregnant womenshould be aware that HPV can be transmitted toan infant during delivery through the birth canal.They should also understand that good prenatalnutrition and abstinence from tobacco and alco-hol use during pregnancy may favorably shapetheir child’s development.Adults may have a better understanding of the
host–response relationship and its relevance totheir risk of HNC. Individuals with long historiesof tobacco and alcohol use, those who areimmunocompromised, and others with geneticconditions associated with HNCs must under-stand that they are at increased risk for disease.Oral conditions such as lichen planus also havebeen associated with oral cancer. The most impor-tant preventive behavior a healthcare provider canassume is advocacy for prevention of HNCs,patient wellness, and public awareness. A verysmall percentage of the public is aware of HNC,and few recognize its relationship to sexual behav-iors. Only a small percentage of younger aged chil-dren are being vaccinated against HPV. Manyadults may not understand the value of vaccina-tion, fear immunizations in general, or think thatvaccination promotes sexual behaviors. Oralhealth professionals must endorse HPV vaccina-tion and promulgate the message that HNCs canbe prevented through adherence to healthylifestyles and the adoption of judicious healthbehaviors.
Therapeutic Interventions Prior to TreatmentTherapeutic interventions may help preventHNCs from developing. Aside from tailored andpoignant preventive educational messages, thera-peutic interventions for tobacco prevention andcessation and for assisting recovering alcoholicsare available. Much research has considered inter-ventions for cessation of tobacco use. Some areevidence based while others may work effectivelyfor certain individuals. An evidence-basedapproach to tobacco cessation, referred to as the 5A’s, is endorsed by the Agency for HealthcareResearch and Quality. In this approach, patientsare asked about tobacco use, advised to stop, theirreadiness to abstain is assessed, they are assisted intheir attempts to refrain, and follow-up isarranged.23 Advising is a critical piece of the 5 A’s.During this phase of the five-step process, patientsare shown the effects of their tobacco habits intheir mouths, enabling their ownership of theproblem. The 5 A’s also advocates the use ofpharmacological adjuncts to assist the patient in
CHAPTER 7 Head and Neck Cancers
132
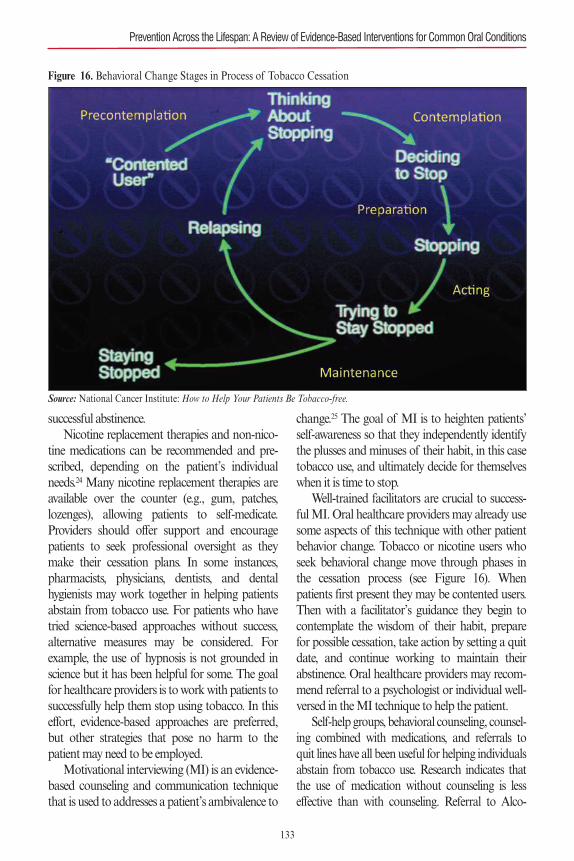
successful abstinence.Nicotine replacement therapies and non-nico-
tine medications can be recommended and pre-scribed, depending on the patient’s individualneeds.24 Many nicotine replacement therapies areavailable over the counter (e.g., gum, patches,lozenges), allowing patients to self-medicate.Providers should offer support and encouragepatients to seek professional oversight as theymake their cessation plans. In some instances,pharmacists, physicians, dentists, and dentalhygienists may work together in helping patientsabstain from tobacco use. For patients who havetried science-based approaches without success,alternative measures may be considered. Forexample, the use of hypnosis is not grounded inscience but it has been helpful for some. The goalfor healthcare providers is to work with patients tosuccessfully help them stop using tobacco. In thiseffort, evidence-based approaches are preferred,but other strategies that pose no harm to thepatient may need to be employed.Motivational interviewing (MI) is an evidence-
based counseling and communication techniquethat is used to addresses a patient’s ambivalence to
change.25 The goal of MI is to heighten patients’self-awareness so that they independently identifythe plusses and minuses of their habit, in this casetobacco use, and ultimately decide for themselveswhen it is time to stop. Well-trained facilitators are crucial to success-
ful MI. Oral healthcare providers may already usesome aspects of this technique with other patientbehavior change. Tobacco or nicotine users whoseek behavioral change move through phases inthe cessation process (see Figure 16). Whenpatients first present they may be contented users.Then with a facilitator’s guidance they begin tocontemplate the wisdom of their habit, preparefor possible cessation, take action by setting a quitdate, and continue working to maintain theirabstinence. Oral healthcare providers may recom-mend referral to a psychologist or individual well-versed in the MI technique to help the patient.Self-help groups, behavioral counseling, counsel-
ing combined with medications, and referrals toquit lines have all been useful for helping individualsabstain from tobacco use. Research indicates thatthe use of medication without counseling is lesseffective than with counseling. Referral to Alco-
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
133
Figure 16. Behavioral Change Stages in Process of Tobacco Cessation
Source: National Cancer Institute: How to Help Your Patients Be Tobacco-free.

134
holics Anonymous might be appropriate for prob-lem drinkers who need or request assistance. The12-step programs have successfully aided individu-als with addictions. Other in-patient programs orself-help groups are available through local hospitalsand the American Cancer Society.All of the detection tests previously mentioned
in this chapter offer the therapeutic benefit ofmaking patients more aware. If a patient has hadgenital HPV or has had sexual relationships withsomeone who is HPV positive, education will helpthat individual monitor himself or herself. Fre-quent Pap smears may be required, which couldbe beneficial in diminishing patient anxiety or dis-covering an early-stage malignancy. Other bloodserum markers can indicate the presence of HPVantibodies. Although the time from their identifi-cation to the development of a carcinoma couldtake decades,21 the patient and his or her providerswill be vigilant and could detect a lesion at an earlystage.Members of the oral healthcare team should
work together to endorse a practice or clinic phi-losophy that promotes cancer prevention. Healthprofessionals who collaborate on interprofessionalteams should reinforce positive messages for pre-vention of disease and promotion of wellness.When more providers work together, the chancesfor patient success are greater.
Therapeutic Interventions26–28Oral health professionals are instrumental in ther-apeutic interventions prior to, during, and follow-ing surgery, radiation, or chemotherapy.Treatments for HNCs often have oral ramifica-tions, reinforcing the need to educate patients andprovide therapy during all phases of care. Somerecommended therapies, such as practicing goodoral hygiene, are universal, regardless of treatmentrendered. Other protocols and therapeutic inter-ventions must be based on the patient’s level oftolerance, medical status, type of cancer, treatmentrendered, and response to treatment.Prior to treatment, all patients should receive
thorough clinical examinations. The dentist anddental hygienist should examine the soft tissues to
identify inflammation or infection, assess plaquelevels and dental caries, review oral hygiene andoral care protocols, and prescribe antimicrobialtherapy as indicated. Implementing periodontaldebridement and the use of adjunctive therapiescan help reduce the patient’s oral bacterial load.Therapeutic interventions can help minimize theseverity of a patient’s pain and oral infection,thereby preventing a disruption or termination oftreatment.Treatment interventions for HNCs include sur-
gery, chemotherapy, radiation therapy, combina-tion therapies, and biological and targetedtherapies. Oral healthcare providers should beaware of the side effects associated with eachapproach so that individualized patient therapeu-tic interventions can be designed and implement-ed. Most patients with HNC present with locallyadvanced stage III or IV disease. These stages typ-ically require a combination of chemotherapy,radiation, or surgery. For patients who presentwith early stage I or II disease, radiation or surgeryis the commonly recommended course of care.These patients have an excellent prognosis.Side effects of surgical procedures may include
swelling, loss of voice, speech impairment, difficul-ty chewing or swallowing, ear numbness, impairedmovement in lower lip, limited ability to raise thearms over the head, and facial disfigurement.Reconstructive surgery may be needed if largemasses of tissue are removed. Healthy tissue andbone may be taken from other parts of the bodyto compensate. Prosthodontists may design andfabricate artificial dental and facial parts andobturators to improve aesthetics. In theseinstances, oral health professionals may be work-ing collaboratively with speech pathologists andregistered dieticians who, respectively, will helppatients relearn speech patterns and design accept-able and healthy food plans.Radiation therapy may be the primary form of
treatment or used following surgery to furtherensure the complete destruction of the cancercells. Radiation therapy remains a mainstay ofcurative therapy for oropharyngeal cancer. Sideeffects of radiation therapy can include skin red-
CHAPTER 7 Head and Neck Cancers

ness, xerostomia, difficulty swallowing or speak-ing, mucositis and oral lesions, loss of appetite,bone pain or dental problems (e.g., osteora-dionecrosis), nausea, fatigue, ear wax buildup, andhearing loss. Chemotherapy is an integral part oftreating locally advanced HNC. Side effects ofchemotherapy may include fatigue, nausea, loss ofappetite, hair loss, xerostomia, difficulty eating,mucositis, infection, and diarrhea.Patients and their caretakers must understand
the importance of working to maintain good oralhygiene to minimize infection and reduce patientdiscomfort throughout any type of cancer treat-ment. Basic oral self-care should include brushingin a nontraumatic fashion with a soft brush andflossing or other interdental cleansing as tolerated.Oral health professionals must provide patientswith recommendations for treating dry mouth,such as sipping water frequently, sucking on icechips or sugar-free candy, using moisturizingagents, chewing sugar-free gum with xylitol, andusing a saliva substitute spray or gel or a pre-scribed saliva stimulant. For caries prevention, theuse of fluorides may be warranted. The strengthand delivery agent should be adjusted to meet thepatient’s comfort level. Prescribing topical anes-thetics or analgesics for oral pain may be neces-sary. The Cochrane Oral Health Groupconsidered interventions for preventing and reduc-ing the severity of oral mucositis in cancerpatients. Agents and therapeutic interventionswere evaluated in patients with different forms ofcancer, undergoing different types of treatment, sobenefits may pertain to only the disease and treat-ment combinations evaluated.27 Cryotherapy (icechips) and keratinocyte growth factor (palifermin)showed some benefit in preventing mucositis, andsucralfate was deemed effective in reducing theseverity of mucositis. Seven additional interven-tions—aloe vera, amifostine, intravenous gluta-mine, granulocyte colony-stimulating factor(G-CSF), honey, laser, and antibiotic lozengescontaining polymyxin/tobramycin/amphotericin(PTA)—showed weaker evidence of benefit.27 TheMultinational Association of Supportive Care inCancer and International Society of Oral Oncolo-
gy (MASCC/ISOO), in a more recent systematicreview, established no guidelines regarding the useof these seven interventions due to insufficient orconflicting findings.28 The use of sucralfate alsowas not recommended for the prevention or treat-ment of chemotherapeutic or radiation-inducedmucositis, as opposed to the earlier Cochranereport. Based on the evidence supporting theMASCC/ISOO Guidelines, the following inter-ventions were deemed most effective, given thespecific circumstances indicated: oral cryotherapy,palifermin, and low-level laser therapy. (SeeAppendix 1.) To help reduce the risk of oral andpotentially systemic infection, essential surgical orrestorative dental care should be completed priorto treatment. Patients with lichen planus or othertreatable risk factors may require prescriptiontherapy.The goal of any treatment is to prolong life,
but quality of life, preservation of function, andappearance must be considered. Treatments arecontinually being researched and refined to mini-mize invasiveness. Surgical techniques have con-tinued to evolve, with greater focus on minimallyinvasive procedures where appropriate. Currentresearch suggests that therapies less intensive thanthose used for HPV-negative HNCs may be effec-tive for HPV-positive tumors. HPV-positive can-cers tend to be more sensitive to radiation,chemotherapy, and combined therapies, prompt-ing some researchers to suggest a reexaminationof prescribing similar treatments regardless of eti-ology.29 Survival rates, in general, are higher andrelapse rates lower for HPV-positive HNCs.Recurring cancers also may require modifiedapproaches to treatment.
Patient Management ConsiderationsThroughout treatment, a team approach topatient care is essential. Dentists, oncologists, den-tal hygienists, speech pathologists, dieticians, andothers must be aware of the potential oral sideeffects of surgery, radiation, and chemotherapyand work together to minimize them. Patientsneed to understand that side effects are treatableand that reconstructive surgery and rehabilitation
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
135

can help with facial disfigurements and speech orswallowing difficulties. When delivering preventivemessages or communicating with patients diag-nosed with HNCs, receiving treatment, recover-ing, or seeking palliative care, variations inapproach are necessary. Patients diagnosed withHNCs of different etiologies should receive tai-lored educational messages regarding risk factorsand management of the condition. Demographicfactors such as ethnicity, health literacy level, andsocioeconomic status will influence dialogues.Some cultural and religious groups hold healthbeliefs that may conflict with those of the provider,and they should be met with respect. The emo-tional impact of a cancer diagnosis can be pro-found. Oral health professionals can provideessential psychosocial support to patients withnew diagnoses or to those experiencing side effects.Helping patients identify support systems may beanother provider role.Patients should be closely monitored post-
treatment with periodic dental evaluations andprophylaxes as a mainstay of therapeutic interven-tions. Thorough examinations must be included atall recall appointments. Subsequent visits and fol-low-up should be based on patient need. Oralcomplications can continue or emerge long afterradiation therapy has ended. High-dose radiationtreatment carries a lifelong risk of xerostomia,dental caries, and osteonecrosis. Lifelong daily flu-oride application, good nutrition, and conscien-tious oral hygiene are especially important forpatients with salivary gland dysfunction. At anystage of diagnosis, patients remain at high risk forrecurrence and second primary tumors. Oralhealth professionals should be mindful of thesepossibilities and remain proactive when treatingpatients who have had HNCs.30
Special ConsiderationsChildren who have received radiation to craniofa-cial and dental structures should be monitored forabnormal growth and development. Develop-mental disturbances in children treated before age12 years generally affect craniofacial development,including the size, shape, and eruption patterns of
teeth. Common manifestations may includeabnormal tooth formation, such as decreasedcrown size, shortened and conical shaped roots,and microdontia; delayed tooth eruption, includ-ing increased frequency of impacted maxillarycanines; and diminished alveolar processes thatlead to decreased occlusal vertical dimension.These changes tend to be symmetrical, so theymay not be clinically evident. The child’s age at thetime of cancer therapy and the protocol followedinfluence the extent and location of dental andcraniofacial anomalies. For children younger than5 or 6 years of age at the time of treatment (partic-ularly those who undergo treatment that involvesconcomitant chemotherapy and head and neckradiation), a higher incidence of dental and cran-iofacial anomalies tends to occur as compared toolder children or those who undergo onlychemotherapy. Managing oral complications inpediatric patients is challenging, as limited researchaddresses oral toxicities.31,32
FUTURE EPIDEMIOLOGICAL TRENDSFuture epidemiological trends will vary by globalregion. Based on current data, carcinogen-induced cancers will continue to decline or remainrelatively stable in the United States and in selectwestern European countries.2,3 High tobacco userates persist in areas of Eastern Europe, SouthAsia, and the Middle East.2 Unless usage ratesdecline, the incidence, prevalence, and mortalityrates for HNCs will not change substantially. Theuse of betel quid in India remains a significant riskfactor for HNC, a disease that is the second lead-ing cause of death in that country.2,33
Trends indicate that the rise in HPV-associatedOPCs will remain unabated in the United States,Canada, Sweden, Great Britain, and other devel-oped western European countries.6 It is suggestedthat by 2020, the incidence of HPV-positive HNCscould reach epidemic proportions.34 In Australia,where HPV vaccination is mandated, a reductionin HPV-positive HNCs is anticipated.35 Despitelower compliance rates in the United States, arecent analysis of National Health and NutritionExamination Survey (NHANES) data indicates a
136
CHAPTER 7 Head and Neck Cancers

lower prevalence of certain HPV strains amonggirls who have been vaccinated.36 To increase thevaccination rate in the United States, adolescentsand adults must become more aware and bettereducated about the value of the vaccine and under-stand that already-contracted genital infectionsincrease the risk of transmission when high-risksexual behaviors are practiced. Greater dissemina-tion of information related to HPV transmissioncould alter the practice of high-risk sexual behav-iors, thereby decreasing transmission rates.More public health campaigns and health pro-
fessionals’ advocacy is needed to enlighten societyabout the cancer threats that genital and oralHPV infections pose.37 All health professionalsshould be educated about the genital–oral linkassociated with HPV, and they should promoteearly vaccination against HPV during patient care.Preventing and diminishing tobacco use and nico-tine dependence must remain a high priority.Although tobacco rates have decreased in somecountries, they remain high in others.2 It behoovesall professionals to stay engaged in the war ontobacco and nicotine addiction.Epidemiological trends will also depend on the
use of other, less traditional smoked products suchas hookah, clove cigarettes (Bidi, Kretek), andmarijuana. Unsmoked products such as spittobacco also pose harm. ENDS may also affectthe incidence and prevalence of HNCs. The long-term effect of these products on the developmentof HNCs is unknown.38 It also is unknown if theiruse encourages or discourages smoking. The Food& Drug Administration recently developed regula-tions for e-cigarettes and other alternative nicotineproducts..39 The legalization of recreational mari-juana, an agricultural substance that could containtobacco products and does produce combustion,may become more widespread in the UnitedStates.40Little research has examined the long-termeffects of marijuana on the oral cavity or theoropharyngeal areas. The relationship betweenmarijuana use and subsequent or concomitantadoption of a tobacco habit is also unclear.Another consideration that could affect futuretrends will be the oral health professional’s philos-
ophy on harm reduction versus total abstinencefrom tobacco and nicotine acquisition products.
FUTURE RESEARCH EFFORTSNew scientific discoveries and technologicalchange will influence the screening, detection, andtreatment of HNCs. Advances could improvescreening methods and boost early detection,thereby increasing survival rates. More sophisticat-ed salivary and serum blood tests under studymay help identify HPV tumor DNA when the dis-ease is in an incipient stage, also potentiallyimproving survival rates.22 The use of chairsidesalivary diagnostics is expected to grow, whichcould prove beneficial for screening, detection,and treatment.41 With personalized genomic map-ping, at-risk individuals could be identified beforea malignancy develops.42 Studies looking at theeffectiveness of the current HPV vaccine againstHPV oral infection have been undertaken, and theresults appear promising. For some individuals,dosages lower than the three prescribed adminis-trations proved effective.43 Developing a vaccinethat prevents oral HPV infection will occur.In the area of treatment, research on minimal-
ly invasive surgical techniques continues.44 Transo-ral endoscopic and robotic surgeries allow accessto the tumor through the mouth, thereby avoidingincisions through the neck or face. Recentadvances in radiotherapy have focused on frac-tionation schedules and the use of intensity-mod-ulated radiation therapy, a form of high-precisionradiotherapy that delivers radiation more preciselyto the tumor while relatively sparing the surround-ing normal tissues. Reconstruction and free-tissue-transfer techniques have also improved, resultingin better function and aesthetics. Biological(immunotherapy) and targeted therapies are rela-tively new and are still being researched. Biologicaltherapies include drugs that boost the body’simmune system.42 Targeted therapies kill cancercells and not healthy cells. An example would beantibodies against epidermal growth factor usedwith radiation therapy (EGFR). Another newertherapy is radiofrequency thermal ablation(RFA). RFA uses heat to destroy cancer cells. It is
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
137
a minimally invasive treatment option that may beuseful for localized tumors that cannot beremoved with surgery.45
Advancements in science and research are dif-ficult to predict. Given the global morbidity andmortality associated with HNCs, their late stagedetection, and the rise in HPV-associated HNCs,one can assume that more answers will be foundand more successful strategies will be developed.
CONCLUSIONSOral health professionals must continue to main-tain a proactive, visible, and relevant role in thefight against HNC. Dentists and dental hygienistshave many opportunities to engage with patientsand reduce the morbidity and mortality associat-ed with these cancers. As preventive health educa-tors, oral health professionals have an ethicalobligation to inform their patients about HNCs,the associated risk factors, and the measures toprevent them. They must be advocates for tobaccocessation and prevention and for the administra-tion of the HPV vaccine. They must talk to theirpatient populations but also to the community atlarge about HNCs.A critical role for oral health professionals is
the screening for and detection of HNCs. Allpatients must receive routine head and neck oraland visual cancer screenings. Patients must betaught how to conduct self-examinations and beadvised to request a screening when they presentfor routine care.The oral health professional may be the first
provider to come in contact with a patient whopresents with a suspicious finding. Patient monitor-ing and triage with other specialists often follows.Oral health professionals must value their own con-tributions to the patient’s well-being and maintainopen communication with other involved health-care providers. Therapeutic roles for oral healthprofessionals are many and essential throughoutthe patient’s treatment. Psychosocial support, pal-liative care, necessary interventions, and assistancewith oral side effects help patients maintain theirstrength and continue their courses of treatment.In summary, dentists and dental hygienists are
leaders in preventing and combatting HNCs. Oralhealth professionals know best the head and neckregions and can help educate other healthcareproviders about HNCs and the relationshipbetween oral and systemic well-being. In interpro-fessional collaborations, oral healthcare providersshould share their expertise and maintain keypositions in discussions addressing patient care,the oral side effects of treatments, the need forpossible oral health interventions, and the impor-tance of maintaining good oral hygiene practicesduring treatment. Oral health professionals areneeded in the preventive, therapeutic, and inter-vention phases of patient care. They mustembrace and value their contributions.
In the next section, patient cases are included.They highlight information related to risk assess-ment, risk behaviors, and potential preventive and therapeutic interventions. Thoughts on howto interact with patients are presented.
CASE 1: Adolescent Patient Who Uses Spit Tobacco
PATIENT OVERVIEWJames S. is a 16-year-old Caucasian male. He hasbeen a patient since he was 5 years old.Chief Complaint: “A white area on my gum.”Medical History: Broken arm in 2014 while play-ing basketball on the high school varsity team. Allelse, within normal limits.Risk Assessment/Risk Factors: Uses spit tobacco(ST) in sachet form; places sachet in the mandibu-lar labial vestibule where lesion is located; usesduring basketball season (October to March) butat no other time. Believes ST helps his concentra-tion and improves his playing. Parents areunaware of his habit. Patient claims he does notengage in high-risk behaviors other than the occa-sional beer with his “buddies on the weekends.”If patient continues habit, he is at moderate
risk for oral cancer and periodontal disease. If thecurrent brand contains sugar or silicate particles,or both, the risk for caries, abrasion, and reces-sion, respectively, is increased.
138
CHAPTER 7 Head and Neck Cancers
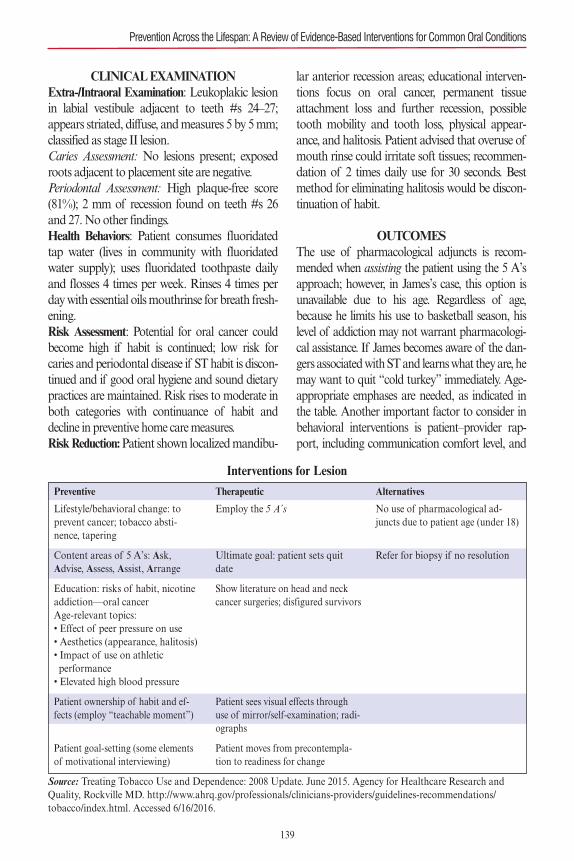
CLINICAL EXAMINATIONExtra-/Intraoral Examination: Leukoplakic lesionin labial vestibule adjacent to teeth #s 24–27;appears striated, diffuse, and measures 5 by 5 mm;classified as stage II lesion.Caries Assessment: No lesions present; exposedroots adjacent to placement site are negative.Periodontal Assessment: High plaque-free score(81%); 2 mm of recession found on teeth #s 26and 27. No other findings.Health Behaviors: Patient consumes fluoridatedtap water (lives in community with fluoridatedwater supply); uses fluoridated toothpaste dailyand flosses 4 times per week. Rinses 4 times perday with essential oils mouthrinse for breath fresh-ening.Risk Assessment: Potential for oral cancer couldbecome high if habit is continued; low risk forcaries and periodontal disease if ST habit is discon-tinued and if good oral hygiene and sound dietarypractices are maintained. Risk rises to moderate inboth categories with continuance of habit anddecline in preventive home care measures.Risk Reduction:Patient shown localized mandibu-
lar anterior recession areas; educational interven-tions focus on oral cancer, permanent tissueattachment loss and further recession, possibletooth mobility and tooth loss, physical appear-ance, and halitosis. Patient advised that overuse ofmouth rinse could irritate soft tissues; recommen-dation of 2 times daily use for 30 seconds. Bestmethod for eliminating halitosis would be discon-tinuation of habit.
OUTCOMESThe use of pharmacological adjuncts is recom-mended when assisting the patient using the 5 A’sapproach; however, in James’s case, this option isunavailable due to his age. Regardless of age,because he limits his use to basketball season, hislevel of addiction may not warrant pharmacologi-cal assistance. If James becomes aware of the dan-gers associated with ST and learns what they are, hemay want to quit “cold turkey” immediately. Age-appropriate emphases are needed, as indicated inthe table. Another important factor to consider inbehavioral interventions is patient–provider rap-port, including communication comfort level, and
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
Preventive
Lifestyle/behavioral change: toprevent cancer; tobacco absti-nence, tapering
Content areas of 5 A’s: Ask, Advise, Assess, Assist, Arrange
Education: risks of habit, nicotineaddiction—oral cancerAge-relevant topics:• Effect of peer pressure on use• Aesthetics (appearance, halitosis)• Impact of use on athletic performance• Elevated high blood pressure
Patient ownership of habit and ef-fects (employ “teachable moment”)
Patient goal-setting (some elementsof motivational interviewing)
Therapeutic
Employ the 5 A’s
Ultimate goal: patient sets quitdate
Show literature on head and neckcancer surgeries; disfigured survivors
Patient sees visual effects throughuse of mirror/self-examination; radi-ographs
Patient moves from precontempla-tion to readiness for change
Alternatives
No use of pharmacological ad-juncts due to patient age (under 18)
Refer for biopsy if no resolution
Interventions for Lesion
Source: Treating Tobacco Use and Dependence: 2008 Update. June 2015. Agency for Healthcare Research andQuality, Rockville MD. http://www.ahrq.gov/professionals/clinicians-providers/guidelines-recommendations/tobacco/index.html. Accessed 6/16/2016.
139
the length and depth of the relationship.Ethical considerations also must be weighed.
Since James’s parents are unaware of his habit,should the provider keep the findings confidentialuntil the 2-week follow-up appointment? If no res-olution is apparent, is that the time to engage theparents? Should informing the parents be used asan impetus for cessation?James struggled with abstinence initially but at
his follow-up appointment 2 weeks after the lesionidentification, resolution had occurred. James wasrelieved to see the tissue change. He is aware that ifhe returns to his habit, a reversion to his formerstate will occur and dysplasia and malignancycould follow. Given his level of motivation,James’s prognosis is good.
FUTURE CONSIDERATIONSAfter his 2-week follow-up, James will be called toensure he has maintained abstinence and notrelapsed. Relapse is common when patients have anicotine addiction. If he has adhered to the absti-nence regimen, James will be rescheduled for a 3-month follow-up to reinforce his abstinence andreassess his tissue health. He will receive an interimcall for support. If he remains tobacco-free andhis lesion resolves, he will be placed on a 6-monthmaintenance schedule.
CASE 2: Young Adult Female Patient with Historyof E-Cigarette and Marijuana Use, Irregular PapSmear, and Low Health Literacy
PATIENT OVERVIEWAmanda B. is a 21-year-old Caucasian femalewho is new to the practice. She presents for herdental hygiene appointment.Chief Complaint: “I want the stain removed frommy teeth.”Health History:Takes birth control pills and mul-tivitamins; has not seen her general physician for 2years; saw OB/GYN 3 months ago.Past Medical History: Irregular Pap smear lastyear—mild dysplasia noted; OB/GYN is moni-toring condition; cryosurgery may be necessary.History of genital herpes.
Family History: Parents both alive, divorced;father has history of gout; mother uses tobaccobut has no medical conditions.Social History:Uses marijuana on weekends; occa-sional e-cigarette use; attends local community col-lege; employed as legal secretary in large law firm.Physical Assessment: Of average weight and size;pierced nose and obvious tattoo on right shoulder;hair color is purple.Risk Assessment/Risk Factors: Marijuana use;sporadic use of e-cigarettes; irregular Pap smear;possibility of high-risk sexual behaviors; lowhealth literacy regarding relationship betweenhuman papillomavirus (HPV) and head and necksquamous cell carcinomas (HNSCCs); no knowl-edge of HPV vaccine.
CLINICAL ASSESSMENTExtra-/Intraoral Examination:Xerostomia; coatedtongue.Periodontal Assessment: Hyperplastic gingiva;minimal bleeding; localized moderate periodontaldisease; generalized health.Accretions:Generalized heavy stain; moderate cal-culus localized.Plaque-Free Score: 52%.Home Care Regimen: Patient brushes once dailywith hard toothbrush; rinses 4 times per day withessential oils mouth rinse; uses water irrigator forinterdental cleansing 2 times per week.No diagnostic tests indicted.
RISK REDUCTIONSee table on next page.
OUTCOMESAmanda is at an age when many young people donot have well-shaped identities. These individualssometimes exhibit edgy appearances and engage inrisky behaviors. What is marked is Amanda’s gyne-cological history and her marijuana and e-cigaretteuse. She also presents with low health literacy, soeducating her is critical. Using motivational inter-viewing (MI) techniques may be helpful, butAmanda is defensive and it may take time for her todecide to abstain from her risky behaviors.
CHAPTER 7 Head and Neck Cancers
140
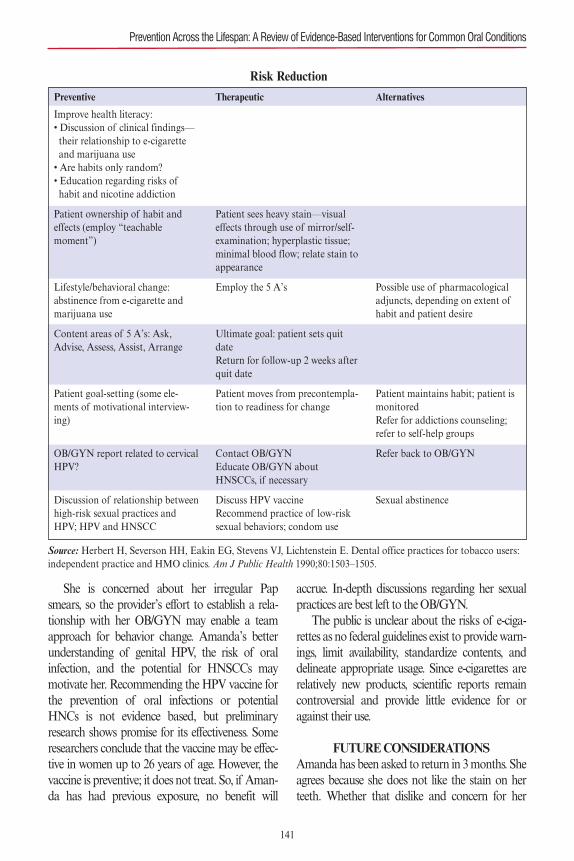
She is concerned about her irregular Papsmears, so the provider’s effort to establish a rela-tionship with her OB/GYN may enable a teamapproach for behavior change. Amanda’s betterunderstanding of genital HPV, the risk of oralinfection, and the potential for HNSCCs maymotivate her. Recommending the HPV vaccine forthe prevention of oral infections or potentialHNCs is not evidence based, but preliminaryresearch shows promise for its effectiveness. Someresearchers conclude that the vaccine may be effec-tive in women up to 26 years of age. However, thevaccine is preventive; it does not treat. So, if Aman-da has had previous exposure, no benefit will
accrue. In-depth discussions regarding her sexualpractices are best left to the OB/GYN.The public is unclear about the risks of e-ciga-
rettes as no federal guidelines exist to provide warn-ings, limit availability, standardize contents, anddelineate appropriate usage. Since e-cigarettes arerelatively new products, scientific reports remaincontroversial and provide little evidence for oragainst their use.
FUTURE CONSIDERATIONSAmanda has been asked to return in 3 months. Sheagrees because she does not like the stain on herteeth. Whether that dislike and concern for her
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
Preventive
Improve health literacy:• Discussion of clinical findings—their relationship to e-cigarette and marijuana use• Are habits only random?• Education regarding risks of habit and nicotine addiction
Patient ownership of habit and effects (employ “teachable moment”)
Lifestyle/behavioral change: abstinence from e-cigarette andmarijuana use
Content areas of 5 A’s: Ask, Advise, Assess, Assist, Arrange
Patient goal-setting (some ele-ments of motivational interview-ing)
OB/GYN report related to cervicalHPV?
Discussion of relationship betweenhigh-risk sexual practices andHPV; HPV and HNSCC
Therapeutic
Patient sees heavy stain—visual effects through use of mirror/self-examination; hyperplastic tissue;minimal blood flow; relate stain toappearance
Employ the 5 A’s
Ultimate goal: patient sets quitdateReturn for follow-up 2 weeks afterquit date
Patient moves from precontempla-tion to readiness for change
Contact OB/GYNEducate OB/GYN aboutHNSCCs, if necessary
Discuss HPV vaccineRecommend practice of low-risksexual behaviors; condom use
Alternatives
Possible use of pharmacologicaladjuncts, depending on extent ofhabit and patient desire
Patient maintains habit; patient ismonitoredRefer for addictions counseling;refer to self-help groups
Refer back to OB/GYN
Sexual abstinence
Risk Reduction
141
Source: Herbert H, Severson HH, Eakin EG, Stevens VJ, Lichtenstein E. Dental office practices for tobacco users:independent practice and HMO clinics. Am J Public Health 1990;80:1503–1505.
appearance will translate into behavior change isunknown. The fact that she is willing to return is apositive sign. Employing MI techniques during hervisits and suggesting that she join a self-help groupor see an addiction counselor if she needs help torefrain from marijuana and e-cigarette use will con-tinue. Dialogue with the OB/GYN provider will bemaintained as it may provide insight into future dis-cussions with Amanda about her risk for HPV.
REFERENCES1. National Institute of Dentistry and Craniofacial Research
(NIDCR). Oral cancer. NIH Fact sheet. Available at:http://report.nih.gov/nihfactsheets/ViewFactSheet.aspx?csid=106. Accessed October 30, 2015.
2. Bray F, Ren J-S, Masuyer E, Ferlay J. Global estimatesof cancer prevalence for 27 sites in the adult popula-tion in 2008. Int J Cancer 2013;132:1133–1145.doi: 10.1002/ijc.27711. (Cited in International Agencyfor Research on Cancer. Globocan 2012: EstimatedCancer Incidence, Mortality and Prevalence Worldwidein 2012. Lyon, France: IARC; 2012. World HealthOrganization; 2013.
3. American Cancer Society. Cancer Facts & Figures 2015.Atlanta, GA: American Cancer Society; 2015.
4. National Comprehensive Cancer Network. NCCN clini-cal practice guidelines in oncology: head and neck can-cers. Vol 1. 2012. Available at: http://www.nccn.org/professionals/physician_gls/pdf/head-and-neck.pdf.Accessed October 2015.
5. Gillison ML, D’Souza G, Westra W, et al. Distinct riskfactor profiles for human papillomavirus type 16-positiveand human papillomavirus type 16-negative head andneck cancers. J Natl Cancer Inst. 2008;100:407–420.
6. Chaturvedi AK, Anderson WF, Lortet-Tieulent J, et al.Worldwide trends in incidence rates for oral cavity andoropharyngeal cancers. J Clin Oncol. 2013;31:1–10.
7. Chaturvedi AK, Engels EA, Anderson WF, Gillison ML.Incidence trends for human papillomavirus-related andunrelated oral squamous cell carcinomas in the UnitedStates. J Clin Oncol. 2008;26:612–619.
8. Gillison ML, Zhang Q, Jordan R, et al. Tobacco smokingand increased risk of death and progression for patientswith p16-positive and p16-negative oropharyngeal cancer.J Clin Oncol. 2012;30:2202–2211.
9. Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, etal. Globocan 2012 v1.0, Cancer Incidence and MortalityWorldwide: IARC CancerBase No. 11 (Internet). Lyon,France: International Agency for Research on Cancer;2013. Available from: http://globocan.iarc.fr, accessed15/6/2016. (Cited in International Agency for Research onCancer. Globocan 2012: Estimated Cancer Incidence, Mor-tality and Prevalence Worldwide in 2012. Lyon, France:
IARC; 2012. World Health Organization; 2013.)10. D’Souza G, Kreimer AR, Viscidi R, et al. Case-control
study of human papillomavirus and oropharyngeal can-cer. N Engl J Med. 2007;356:1944–1956.
11. Vigneswaran N, Williams MD. Epidemiological trends inhead and neck cancer and aids in diagnosis.Oral Maxillo-fac Surg Clin North Am. 2014;26:123–141.
12. Oral Cancer Foundation. Risk factors. Available from:http://www.oralcancerfoundation.org/cdc/cdc_chapter3.php. Accessed November 19, 2015.
13. Choi I, Myers JN. Molecular pathogenesis of oral squa-mous cell carcinoma: implications for therapy. J Dent Res.2008;87:14–32.
14. Lassen P. The role of human papillomavirus in head andneck cancer and the impact on radiotherapy outcome.Radiother Oncol. 2010;95:371–380.
15. Ram H, Sarkar J, Kumar H, Konwar R, Bhatt MLB,Mohammed S. Oral cancer: risk factors and molecularpathogenesis. J Maxillofac Oral Surg. 2011;10:132–137.
16. Brocklehurst P, Kujan O, O’Malley LA, Ogden G, Shep-herd S, Glenny AM. Screening programmes for the earlydetection and prevention of oral cancer. Cochrane Data-base Syst Rev. 2013;(11):CD004150.
17. National Institute of Dentistry and Craniofacial Research(NIDCR). Detecting oral cancer: a guide for health care pro-fessionals. [Poster.] Available at: http://www.nidcr.nih.gov/oralhealth/Topics/OralCancer/Documents/DetectingOral-CancerPoster_100313_508C.pdf. Accessed February 27,2016.
18. Ford PJ, Farah CS. Early detection and diagnosis of oralcancer: strategies for improvement. J Canc Policy.2013;1:e2–e7.
19. Liu JLY, Walsh T, Kerr A, et al. Diagnostic tests for oralcancer and potentially malignant disorders in patients pre-senting with clinically evident lesions. Cochrane DatabaseSyst Rev. 2012;(12):CD010276, 1–19.
20. Olson CM, Burda BU, Beil T, Whitlock EP. Screening forOral Cancer: A Targeted Evidence Update for the U.S.Preventive Services Task Force. Evidence Synthesis No.102. AHRQ Publication No. 13-05186-EF-1. Rockville,MD: Agency for Healthcare Research and Quality; April2013.
21. Kreimer AR, Johansson M, Waterboer T, et al. Evaluationof human papillomavirus antibodies and risk of subsequenthead and neck cancer. J Clin Oncol. 2013;31:2708–2715.
22. Agarawal N, VanHook A. Science Translational Medi-cine. Podcast. American Association for the Advancementof Science; June 24, 2015;7(293):293pc1. Available at:http://podcasts.aaas.org/science_transl_med/Sci-TranslMed_150624.mp3. Accessed November 30, 2015.
23. Fiore M, Bailey W, Cohen SJ, et al. Treating Tobacco Useand Dependence: Clinical Practice Guideline:2008 Update.Rockville, MD: U.S. Department of Health and HumanServices, Agency for Healthcare Research and Quality;June 2015. Available at: http://www.ahrq.gov/profession-
CHAPTER 7 Head and Neck Cancers
142
als/clinicians-providers/guidelines-recommendations/tobacco/index.html. Accessed February 27, 2016.
24. Boyce JH, Stead, LF, Cahill K, Lancaster T. Efficacy ofinterventions to combat tobacco addiction: Cochraneupdate of 2013 reviews. Addiction. 2014;109:414–425.
25. Lindson-Hawley N, Thompson TP, Begh R. Motivation-al interviewing for smoking cessation. Cochrane DatabaseSyst Rev. 2015;(3):CD006936.
26. National Institute of Dentistry and Craniofacial Research(NIDCR). Oral complications of cancer treatment: what thedental team can do. Available at: http://www.nidcr.nih.gov/oralhealth/Topics/CancerTreatment/OralComplication-sCancerOral.htm. Accessed November 15, 2015.
27. Worthington HV, Clarkson JE, Bryan G, et al. Interven-tions for preventing oral mucositis for patients with cancerreceiving treatment. Cochrane Database Syst Rev.2011;(4):CD000978.
28. Lalla RV, Bowen J, Barasch A, et al. MASCC/ISOO Clin-ical practice guidelines for the management of mucositissecondary to cancer therapy. Cancer. 2014;120:1453–1461.
29. Ramqvist T, Grün N, Dalianis T. Human papillomavirusand tonsillar and base of tongue cancer. Virus-es. 2015;7(3);1332–1343.
30. Gregoire V, Lefebvre JL, Licitra L, Felip E; EHNS-ESMO-ESTRO Guidelines Working Group. Squamouscell carcinoma of the head and neck: EHNS–ESMO–ESTRO Clinical Practice Guidelines for diagnosis, treat-ment and follow-up. Ann Oncol. 2010;21(suppl5):v184–v186.
31. Carrillo CM, Correa FN, Lopes NN, Fava M, Filho VO.Dental anomalies in children submitted to antineoplastictherapy. Clinics. 2014;69:433–437.
32. National Cancer Institute. Oral complication ofchemotherapy and head/neck radiation–health profes-sional version (PDQ®). Updated April 2014. Available at:http://www.cancer.gov/about-cancer/treatment/side-effects/mouth-throat/oral-complications-hp-pdq#section/_207. Accessed November 17, 2015.
33. Coelho KR. Review article: challenges of the oral cancerburden in India. J Cancer Epidemiol. 2012;(2012):701932.
34. Ramqvist T, Dalianis T. Oropharyngeal cancer epidemicand human papillomavirus. Emerg Infect Dis.
2010;16:1671–1677.35. Cancer Council of Australia. HPV vaccine. Has the pro-
gram been successful? Available at: http://www.hpvvac-cine.org.au/the-hpv-vaccine/has-the-program-been-successful.aspx. Accessed February 27, 2016.
36. Markowitz LE, Liu G, Harairi S, Steinau M, Denne EF,Unger E. Prevalence of HPV after introduction of thevaccination program in the United States. Pediatrics.2016;137(2):e20151968.
37. President’s Cancer Panel. Accelerating HPV VaccineUptake: Urgency for Action to Prevent Cancer. Bethesda,MD: National Cancer Institute; 2014.
38. National Cancer Institute. Health risks of e-cigarettes,smokeless tobacco, and waterpipes. Available at:http://www.cancer.net/navigating-cancer-care/prevention-and-healthy-living/tobacco-use/health-risks-e-cigarettes-smokeless-tobacco-and-waterpipes. Accessed February27, 2016.
39. http://www.fda.gov/TobaccoProducts/Labelling/RulesRegulationsGuidance/ucm394909.htm.
40. Lopes CFB, de Angelis BB, Prudente HM, et al. Con-comitant consumption of marijuana, alcohol and tobac-co in oral squamous cell carcinoma development andprogression: recent advances and challenges. Arch OralBiol. 2012;57:1026–1033.
41. Guerra ENS, Acevedo AC, Leite AF, et al. Diagnosticcapability of salivary biomarkers in the assessment ofhead and neck cancer: a systematic review and meta-analysis. Oral Oncol. 2015;51:805–818.
42. Dorsey K, Agulnik M. Promising new molecular targetedtherapies in head and neck cancer. Drugs. 2013;73:315–325.
43. Kreimer AR, Gonzalez P, Katki HA, Porras C, Schiff-man M. Efficacy of a bivalent HPV 16/18 vaccine againstanal HPV 16/18 infection among young women: a nestedanalysis within the Costa Rica Vaccine Trial. LancetOncol. 2011;12:862–870.
44. Lawson G, Matar N, Remacle M, Jamart J, Bachy V.Transoral robotic surgery for the management of headand neck tumors: learning curve. Eur Arch Otorhinolaryn-gol. 2011;268:1795–1801.
45. Chu KF, Dupuy DE. Thermal ablation of tumours: bio-logical mechanisms and advances in therapy. Nat RevCancer. 2014;14:199–208.
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
143
RECOMMENDATIONS IN FAVOR OF AN INTERVENTION (i.e., strong evidence supports effectiveness in the treatment setting listed):1. The panel recommends that 30 minutes of oralcryotherapy be used to prevent oral mucositisin patients receiving bolus 5-fluorouracilchemotherapy (II).
2. The panel recommends that recombinanthuman keratinocyte growth factor-1 (KGF-1/palifermin) be used to prevent oral mucositis(at a dose of 60 mcg/kg per day for 3 daysprior to conditioning treatment and for 3 daysafter transplant) in patients receiving high-dose chemotherapy and total body irradia-tion, followed by autologous stem celltransplantation, for a hematological malig-nancy (II).
3. The panel recommends that low-level lasertherapy (wavelength at 650 nm, power of 40mW, and each square centimeter treated withthe required time to a tissue energy dose of 2J/cm2), be used to prevent oral mucositis inpatients receiving HSCT conditioned withhigh-dose chemotherapy, with or withouttotal body irradiation (II).
4. The panel recommends that patient-controlledanalgesia with morphine be used to treat paindue to oral mucositis in patients undergoingHSCT (II).
5. The panel recommends that benzydaminemouthwash be used to prevent oral mucositisin patients with head and neck cancer receiv-ing moderate dose radiation therapy (up to 50Gy), without concomitant chemotherapy (I).
SUGGESTIONS IN FAVOR OF AN INTERVENTION (i.e., weaker evidence supportseffectiveness in the treatment setting listed):1. The panel suggests that oral care protocols beused to prevent oral mucositis in all agegroups and across all cancer treatmentmodalities (III).
2. The panel suggests that oral cryotherapy beused to prevent oral mucositis in patients
receiving high-dose melphalan, with or with-out total body irradiation, as conditioning forHSCT (III).
3. The panel suggests that low-level laser therapy(wavelength around 632.8 nm) be used to pre-vent oral mucositis in patients undergoingradiotherapy, without concomitant chemother-apy, for head and neck cancer (III).
4. The panel suggests that transdermal fentanylmay be effective to treat pain due to oralmucositis in patients receiving conventionalor high-dose chemotherapy, with or withouttotal body irradiation (III).
5. The panel suggests that 2% morphine mouth-wash may be effective to treat pain due tooral mucositis in patients receiving chemora-diation for head and neck cancer (III).
6. The panel suggests that 0.5% doxepin mouth-wash may be effective to treat pain due tooral mucositis (IV).
7. The panel suggests that systemic zinc supple-ments administered orally may be of benefitto prevent oral mucositis in oral cancerpatients receiving radiation therapy orchemoradiation (III).
RECOMMENDATIONS AGAINST AN INTERVENTION (i.e., strong evidence indicateslack of effectiveness in the treatment setting listed):1. The panel recommends that PTA (polymyxin,tobramycin, amphotericin B) and BCoG (bac-itracin, clotrimazole, gentamicin) antimicrobiallozenges and PTA paste not be used to preventoral mucositis in patients receiving radiationtherapy for head and neck cancer (II).
2. The panel recommends that iseganan antimi-crobial mouthwash not be used to prevent oralmucositis in patients receiving high-dosechemotherapy, with or without total body irra-diation, for HSCT (II), or in patients receivingradiation therapy or concomitant chemoradia-tion for head and neck cancer (II).
3. The panel recommends that sucralfatemouthwash not be used to prevent oral
Appendix 1: MASCC/ISOO Clinical Practice Guidelines for Oral Mucositis*
CHAPTER 7 Head and Neck Cancers
144
mucositis in patients receiving chemotherapyfor cancer (I), or in patients receiving radia-tion therapy (I) or concomitant chemoradia-tion (II) for head and neck cancer.
4. The panel recommends that sucralfatemouthwash not be used to treat oral mucosi-tis in patients receiving chemotherapy forcancer (I), or in patients receiving radiationtherapy (II) for head and neck cancer.
5. The panel recommends that intravenous glut-amine not be used to prevent oral mucositisin patients receiving high-dose chemotherapy,with or without total body irradiation, forHSCT (II).
SUGGESTIONS AGAINST AN INTERVENTION (i.e., weaker evidence indicateslack of effectiveness in the treatment setting listed):1. The panel suggests that chlorhexidine mouth-wash not be used to prevent oral mucositis inpatients receiving radiation therapy for headand neck cancer (III).
2. The panel suggests that granulocyte-macrophage colony-stimulating factor mouth-wash not be used to prevent oral mucositis inpatients receiving high-dose chemotherapy, for
autologous or allogeneic stem cell transplanta-tion (II).
3. The panel suggests that misoprostol mouth-wash not be used to prevent oral mucositis inpatients receiving radiation therapy for headand neck cancer (III).
4. The panel suggests that systemic pentoxifylline,administered orally, not be used to prevent oralmucositis in patients undergoing bone marrowtransplantation (III).
5. The panel suggests that systemic pilocarpine,administered orally, not be used to prevent oralmucositis in patients receiving radiation thera-py for head and neck cancer (III), or in patientsreceiving high-dose chemotherapy, with orwithout total body irradiation, for HSCT (II).
Source:© Multinational Association of Supportive Care in Can-cer (MASCC) and The International Society of Oral Oncology(ISOO). All rights reserved worldwide. Publication/adaptationof these guidelines in any form requires prior permission from theMASCC/ISOO Mucositis Study Group. http://www.mascc.org Abbreviations: Gy, grays; HSCT, hematopoietic stem cell trans-plantation; MASCC/ISOO, Multinational Association of Sup-portive Care in Cancer and International Society of OralOncology; mW, milliwatt; nm, nanometers.*Level of evidence for each guideline is in brackets after theguideline statement.
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
145
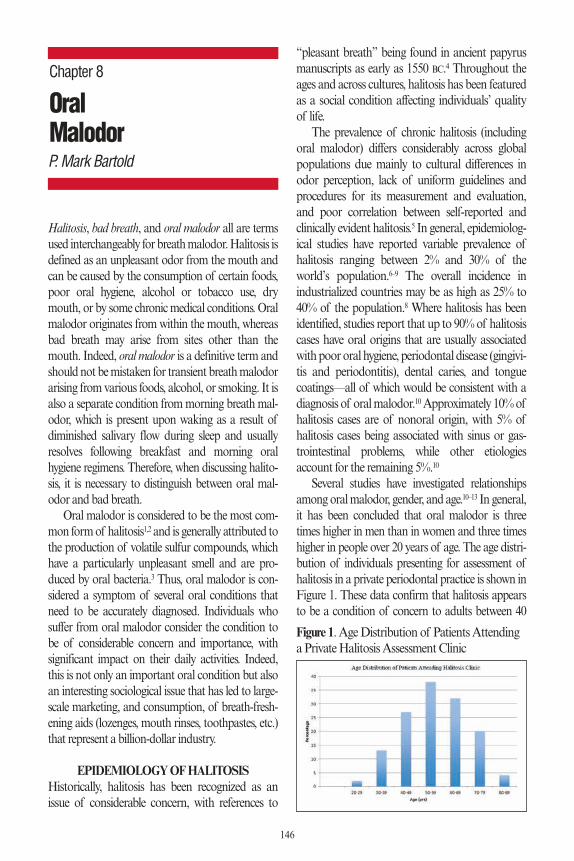
Halitosis, bad breath, and oral malodor all are termsused interchangeably for breath malodor. Halitosis isdefined as an unpleasant odor from the mouth andcan be caused by the consumption of certain foods,poor oral hygiene, alcohol or tobacco use, drymouth, or by some chronic medical conditions. Oralmalodor originates from within the mouth, whereasbad breath may arise from sites other than themouth. Indeed, oral malodor is a definitive term andshould not be mistaken for transient breath malodorarising from various foods, alcohol, or smoking. It isalso a separate condition from morning breath mal-odor, which is present upon waking as a result ofdiminished salivary flow during sleep and usuallyresolves following breakfast and morning oralhygiene regimens. Therefore, when discussing halito-sis, it is necessary to distinguish between oral mal-odor and bad breath.
Oral malodor is considered to be the most com-mon form of halitosis1,2 and is generally attributed tothe production of volatile sulfur compounds, whichhave a particularly unpleasant smell and are pro-duced by oral bacteria.3 Thus, oral malodor is con-sidered a symptom of several oral conditions thatneed to be accurately diagnosed. Individuals whosuffer from oral malodor consider the condition tobe of considerable concern and importance, withsignificant impact on their daily activities. Indeed,this is not only an important oral condition but alsoan interesting sociological issue that has led to large-scale marketing, and consumption, of breath-fresh-ening aids (lozenges, mouth rinses, toothpastes, etc.)that represent a billion-dollar industry.
EPIDEMIOLOGY OF HALITOSISHistorically, halitosis has been recognized as anissue of considerable concern, with references to
“pleasant breath” being found in ancient papyrusmanuscripts as early as 1550 BC.4 Throughout theages and across cultures, halitosis has been featuredas a social condition affecting individuals’ qualityof life.
The prevalence of chronic halitosis (includingoral malodor) differs considerably across globalpopulations due mainly to cultural differences inodor perception, lack of uniform guidelines andprocedures for its measurement and evaluation,and poor correlation between self-reported andclinically evident halitosis.5 In general, epidemiolog-ical studies have reported variable prevalence ofhalitosis ranging between 2% and 30% of theworld’s population.6–9 The overall incidence inindustrialized countries may be as high as 25% to40% of the population.8 Where halitosis has beenidentified, studies report that up to 90% of halitosiscases have oral origins that are usually associatedwith poor oral hygiene, periodontal disease (gingivi-tis and periodontitis), dental caries, and tonguecoatings—all of which would be consistent with adiagnosis of oral malodor.10Approximately 10% ofhalitosis cases are of nonoral origin, with 5% ofhalitosis cases being associated with sinus or gas-trointestinal problems, while other etiologiesaccount for the remaining 5%.10
Several studies have investigated relationshipsamong oral malodor, gender, and age.10–13 In general,it has been concluded that oral malodor is threetimes higher in men than in women and three timeshigher in people over 20 years of age. The age distri-bution of individuals presenting for assessment ofhalitosis in a private periodontal practice is shown inFigure 1. These data confirm that halitosis appearsto be a condition of concern to adults between 40
146
OralMalodor
Chapter 8
P. Mark Bartold
Figure 1. Age Distribution of Patients Attendinga Private Halitosis Assessment Clinic
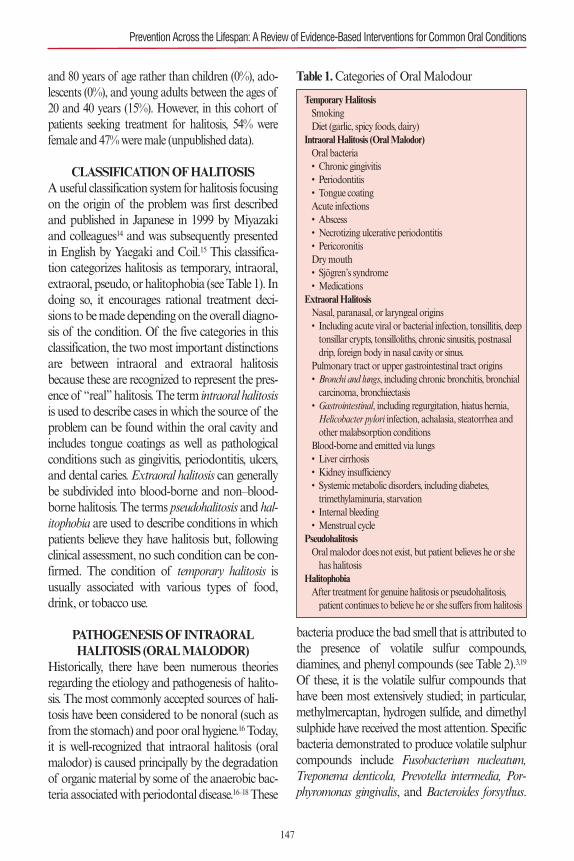
and 80 years of age rather than children (0%), ado-lescents (0%), and young adults between the ages of20 and 40 years (15%). However, in this cohort ofpatients seeking treatment for halitosis, 54% werefemale and 47% were male (unpublished data).
CLASSIFICATION OF HALITOSISA useful classification system for halitosis focusingon the origin of the problem was first describedand published in Japanese in 1999 by Miyazakiand colleagues14 and was subsequently presentedin English by Yaegaki and Coil.15 This classifica-tion categorizes halitosis as temporary, intraoral,extraoral, pseudo, or halitophobia (see Table 1). Indoing so, it encourages rational treatment deci-sions to be made depending on the overall diagno-sis of the condition. Of the five categories in thisclassification, the two most important distinctionsare between intraoral and extraoral halitosisbecause these are recognized to represent the pres-ence of “real” halitosis. The term intraoral halitosisis used to describe cases in which the source of theproblem can be found within the oral cavity andincludes tongue coatings as well as pathologicalconditions such as gingivitis, periodontitis, ulcers,and dental caries. Extraoral halitosis can generallybe subdivided into blood-borne and non–blood-borne halitosis. The terms pseudohalitosis and hal-itophobia are used to describe conditions in whichpatients believe they have halitosis but, followingclinical assessment, no such condition can be con-firmed. The condition of temporary halitosis isusually associated with various types of food,drink, or tobacco use.
PATHOGENESIS OF INTRAORAL HALITOSIS (ORAL MALODOR)
Historically, there have been numerous theoriesregarding the etiology and pathogenesis of halito-sis. The most commonly accepted sources of hali-tosis have been considered to be nonoral (such asfrom the stomach) and poor oral hygiene.16 Today,it is well-recognized that intraoral halitosis (oralmalodor) is caused principally by the degradationof organic material by some of the anaerobic bac-teria associated with periodontal disease.16–18These
bacteria produce the bad smell that is attributed tothe presence of volatile sulfur compounds,diamines, and phenyl compounds (see Table 2).3,19
Of these, it is the volatile sulfur compounds thathave been most extensively studied; in particular,methylmercaptan, hydrogen sulfide, and dimethylsulphide have received the most attention. Specificbacteria demonstrated to produce volatile sulphurcompounds include Fusobacterium nucleatum,Treponema denticola, Prevotella intermedia, Por-phyromonas gingivalis, and Bacteroides forsythus.
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
147
Table 1. Categories of Oral Malodour
Temporary HalitosisSmokingDiet (garlic, spicy foods, dairy)
Intraoral Halitosis (Oral Malodor)Oral bacteria• Chronic gingivitis• Periodontitis• Tongue coatingAcute infections• Abscess• Necrotizing ulcerative periodontitis• PericoronitisDry mouth• Sjögren’s syndrome• Medications
Extraoral HalitosisNasal, paranasal, or laryngeal origins• Including acute viral or bacterial infection, tonsillitis, deeptonsillar crypts, tonsilloliths, chronic sinusitis, postnasaldrip, foreign body in nasal cavity or sinus.
Pulmonary tract or upper gastrointestinal tract origins• Bronchi and lungs, including chronic bronchitis, bronchialcarcinoma, bronchiectasis
• Gastrointestinal, including regurgitation, hiatus hernia,Helicobacter pylori infection, achalasia, steatorrhea andother malabsorption conditions
Blood-borne and emitted via lungs• Liver cirrhosis• Kidney insufficiency• Systemic metabolic disorders, including diabetes,trimethylaminuria, starvation
• Internal bleeding• Menstrual cycle
PseudohalitosisOral malodor does not exist, but patient believes he or shehas halitosis
HalitophobiaAfter treatment for genuine halitosis or pseudohalitosis,patient continues to believe he or she suffers from halitosis
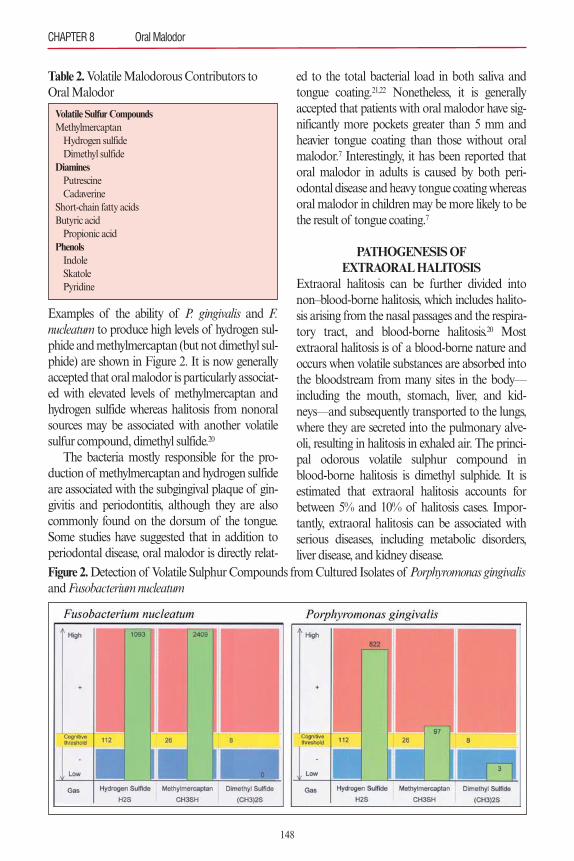
Examples of the ability of P. gingivalis and F.nucleatum to produce high levels of hydrogen sul-phide and methylmercaptan (but not dimethyl sul-phide) are shown in Figure 2. It is now generallyaccepted that oral malodor is particularly associat-ed with elevated levels of methylmercaptan andhydrogen sulfide whereas halitosis from nonoralsources may be associated with another volatilesulfur compound, dimethyl sulfide.20
The bacteria mostly responsible for the pro-duction of methylmercaptan and hydrogen sulfideare associated with the subgingival plaque of gin-givitis and periodontitis, although they are alsocommonly found on the dorsum of the tongue.Some studies have suggested that in addition toperiodontal disease, oral malodor is directly relat-
ed to the total bacterial load in both saliva andtongue coating.21,22 Nonetheless, it is generallyaccepted that patients with oral malodor have sig-nificantly more pockets greater than 5 mm andheavier tongue coating than those without oralmalodor.7 Interestingly, it has been reported thatoral malodor in adults is caused by both peri-odontal disease and heavy tongue coating whereasoral malodor in children may be more likely to bethe result of tongue coating.7
PATHOGENESIS OF EXTRAORAL HALITOSIS
Extraoral halitosis can be further divided intonon–blood-borne halitosis, which includes halito-sis arising from the nasal passages and the respira-tory tract, and blood-borne halitosis.20 Mostextraoral halitosis is of a blood-borne nature andoccurs when volatile substances are absorbed intothe bloodstream from many sites in the body—including the mouth, stomach, liver, and kid-neys—and subsequently transported to the lungs,where they are secreted into the pulmonary alve-oli, resulting in halitosis in exhaled air. The princi-pal odorous volatile sulphur compound inblood-borne halitosis is dimethyl sulphide. It isestimated that extraoral halitosis accounts forbetween 5% and 10% of halitosis cases. Impor-tantly, extraoral halitosis can be associated withserious diseases, including metabolic disorders,liver disease, and kidney disease.
CHAPTER 8 Oral Malodor
148
Figure 2.Detection of Volatile Sulphur Compounds from Cultured Isolates of Porphyromonas gingivalisand Fusobacterium nucleatum
Table 2. Volatile Malodorous Contributors toOral Malodor
Volatile Sulfur CompoundsMethylmercaptanHydrogen sulfideDimethyl sulfide
DiaminesPutrescineCadaverine
Short-chain fatty acidsButyric acidPropionic acid
PhenolsIndoleSkatolePyridine

HOW CAN HALITOSIS BE ASSESSED?A thorough history, both medical and dental, is anessential starting point when assessing for halito-sis. The medical history should include questionsrelating to current medications, nasal and sinusconditions, snoring and sleep apnea, mouthbreathing, throat infections, tonsilloliths, and anassessment of ingestion of foods that may con-tribute to bad odor.
The dental history should focus on generaldental care through regular dental visits; oralhygiene practices, including frequency of tooth-brushing; and use of other oral hygiene aids suchas dental floss, interdental cleaning aids,mouthrinses, and tongue cleaning/scraping. Spe-cific questions relating to the oral malodor mustalso be addressed, such as how long the problemhas been present, whether it is worse at any partic-ular time of day, and if anyone has commented onthe problem. Following the initial interview, bothan oral evaluation and breath analysis arerequired.23
The oral evaluation should include an assess-ment of the following: tonsils, oral debris, caries,exposed pulps, extraction wounds, interdentalfood impaction, gingivitis, periodontitis, necrotiz-ing periodontal conditions, peri-implantitis, peri-coronitis, and recurrent oral ulcerations.
An assessment of tongue coating is also anintegral part of the oral assessment for halitosis.An index (Winkel Tongue Coating Index) forassessing tongue coatings has been used in whichthe dorsum of the tongue is divided into six sec-tions (see Figure 3).24 The presence of any tonguecoating is then graded and recorded for each ofthe sextants. No coating is given a score of 0, alight–thin coating is given a score of 1 and aheavy–thick coating is given a score of 2 (see Fig-ure 4). A score is then calculated by adding all sixscores, thus obtaining a total score within a rangeof 0 to 12.
It is also important to assess the quantity andquality of saliva and any relationship this has tothe presence of a dry mouth. An important conse-quence of reduced saliva and dry mouth isincreased bacterial growth due to the absence or
reduction in the antibacterial properties of saliva.With the increased bacterial load, there is an asso-ciated increase in release of volatile sulfur com-pounds and thus an increase in oral malodor.
Following the oral examination, breath odorshould be evaluated. There are numerous ways inwhich this can be done, including organolepticmethods (smelling patients’ exhaled breath) or useof purpose-built instruments (Halimeter®,Breathtron® or OralChromaTM).
Organoleptic Measurement of HalitosisOrganoleptic measurement of halitosis requires atrained clinician to sniff and smell the patient’sexpired air and score the level of odor. This is con-sidered the gold standard for assessing oral mal-odor. An intensity of odor range has beenproposed based on the clinical rating of the odorand subsequently slightly modified (see Table3).25,26 However, there are a number of concernswith this very subjective approach to breathassessment. One concern is the potential for differ-ences in scoring between different assessors. Thiscan somewhat be overcome by using multipleassessors who have been calibrated in their scoringand assessment. Clearly the biggest problem withthis form of assessment is that it is an unpleasant
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
149
Figure 3.Winkel Tongue Coating ScoreThe dorsum of the tongue is divided into sextants, and theamount of tongue coating is subjectively graded for each sex-tant. The score is calculated by adding the scores for all sex-tants (0 to 2) for a total score within a range of 0 to 12.
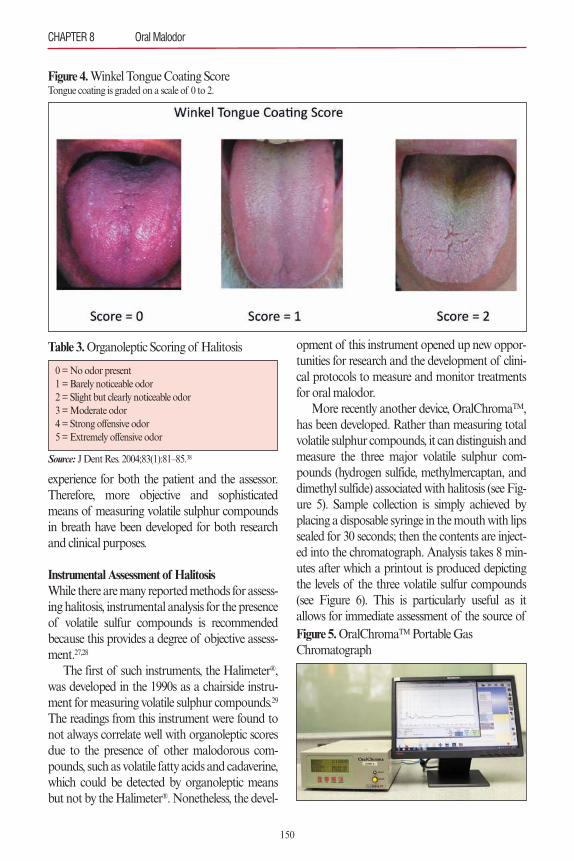
experience for both the patient and the assessor.Therefore, more objective and sophisticatedmeans of measuring volatile sulphur compoundsin breath have been developed for both researchand clinical purposes.
Instrumental Assessment of HalitosisWhile there are many reported methods for assess-ing halitosis, instrumental analysis for the presenceof volatile sulfur compounds is recommendedbecause this provides a degree of objective assess-ment.27,28
The first of such instruments, the Halimeter®,was developed in the 1990s as a chairside instru-ment for measuring volatile sulphur compounds.29
The readings from this instrument were found tonot always correlate well with organoleptic scoresdue to the presence of other malodorous com-pounds, such as volatile fatty acids and cadaverine,which could be detected by organoleptic meansbut not by the Halimeter®. Nonetheless, the devel-
opment of this instrument opened up new oppor-tunities for research and the development of clini-cal protocols to measure and monitor treatmentsfor oral malodor.
More recently another device, OralChromaTM,has been developed. Rather than measuring totalvolatile sulphur compounds, it can distinguish andmeasure the three major volatile sulphur com-pounds (hydrogen sulfide, methylmercaptan, anddimethyl sulfide) associated with halitosis (see Fig-ure 5). Sample collection is simply achieved byplacing a disposable syringe in the mouth with lipssealed for 30 seconds; then the contents are inject-ed into the chromatograph. Analysis takes 8 min-utes after which a printout is produced depictingthe levels of the three volatile sulfur compounds(see Figure 6). This is particularly useful as itallows for immediate assessment of the source of
CHAPTER 8 Oral Malodor
150
Figure 4.Winkel Tongue Coating ScoreTongue coating is graded on a scale of 0 to 2.
Table 3. Organoleptic Scoring of Halitosis
0 = No odor present1 = Barely noticeable odor2 = Slight but clearly noticeable odor3 = Moderate odor4 = Strong offensive odor5 = Extremely offensive odor
Source: J Dent Res. 2004;83(1):81–85.38
Figure 5.OralChromaTMPortable Gas Chromatograph
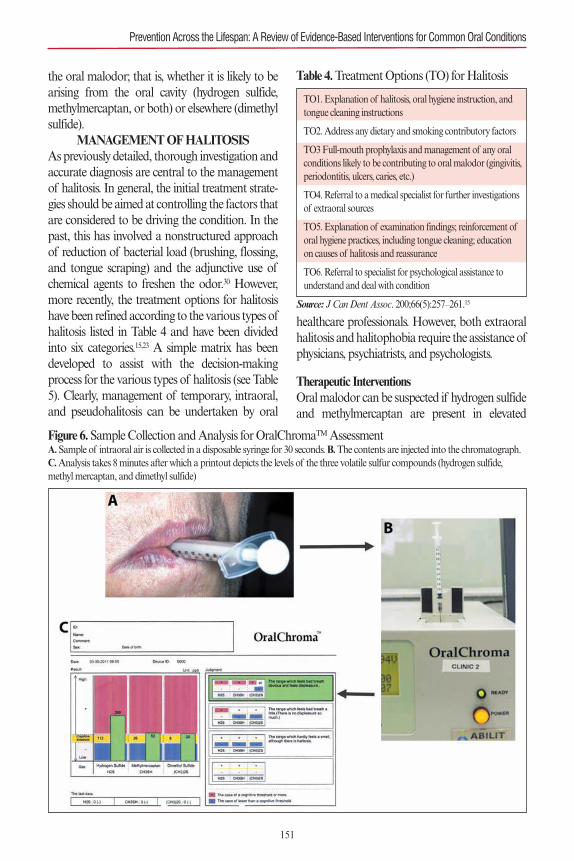
the oral malodor; that is, whether it is likely to bearising from the oral cavity (hydrogen sulfide,methylmercaptan, or both) or elsewhere (dimethylsulfide).
MANAGEMENT OF HALITOSISAs previously detailed, thorough investigation andaccurate diagnosis are central to the managementof halitosis. In general, the initial treatment strate-gies should be aimed at controlling the factors thatare considered to be driving the condition. In thepast, this has involved a nonstructured approachof reduction of bacterial load (brushing, flossing,and tongue scraping) and the adjunctive use ofchemical agents to freshen the odor.30 However,more recently, the treatment options for halitosishave been refined according to the various types ofhalitosis listed in Table 4 and have been dividedinto six categories.15,23 A simple matrix has beendeveloped to assist with the decision-makingprocess for the various types of halitosis (see Table5). Clearly, management of temporary, intraoral,and pseudohalitosis can be undertaken by oral
healthcare professionals. However, both extraoralhalitosis and halitophobia require the assistance ofphysicians, psychiatrists, and psychologists.
Therapeutic InterventionsOral malodor can be suspected if hydrogen sulfideand methylmercaptan are present in elevated
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
151
Figure 6.Sample Collection and Analysis for OralChromaTMAssessmentA.Sample of intraoral air is collected in a disposable syringe for 30 seconds. B.The contents are injected into the chromatograph.C.Analysis takes 8 minutes after which a printout depicts the levels of the three volatile sulfur compounds (hydrogen sulfide,methyl mercaptan, and dimethyl sulfide)
Table 4. Treatment Options (TO) for Halitosis
TO1. Explanation of halitosis, oral hygiene instruction, andtongue cleaning instructions
TO2. Address any dietary and smoking contributory factors
TO3 Full-mouth prophylaxis and management of any oralconditions likely to be contributing to oral malodor (gingivitis,periodontitis, ulcers, caries, etc.)
TO4. Referral to a medical specialist for further investigationsof extraoral sources
TO5. Explanation of examination findings; reinforcement oforal hygiene practices, including tongue cleaning; educationon causes of halitosis and reassurance
TO6. Referral to specialist for psychological assistance tounderstand and deal with condition
Source: J Can Dent Assoc. 200;66(5):257–261.15
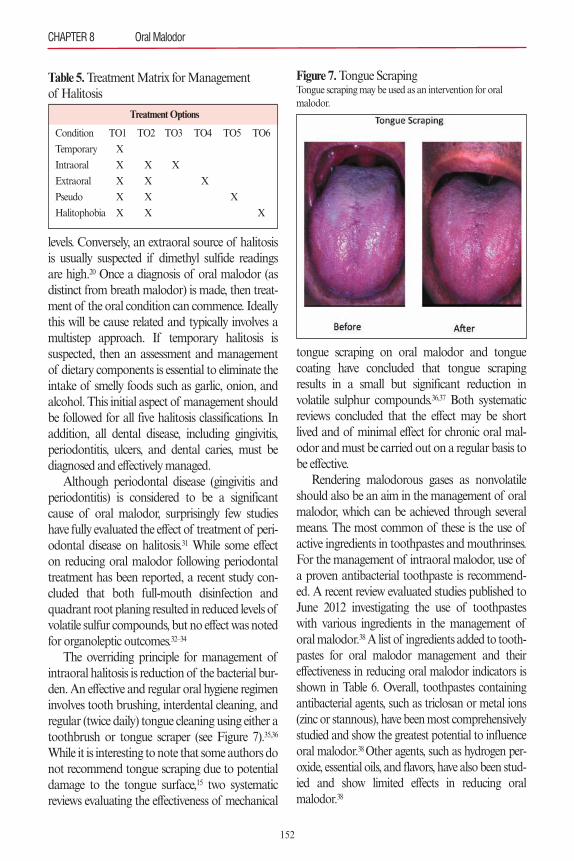
levels. Conversely, an extraoral source of halitosisis usually suspected if dimethyl sulfide readingsare high.20 Once a diagnosis of oral malodor (asdistinct from breath malodor) is made, then treat-ment of the oral condition can commence. Ideallythis will be cause related and typically involves amultistep approach. If temporary halitosis is suspected, then an assessment and managementof dietary components is essential to eliminate theintake of smelly foods such as garlic, onion, andalcohol. This initial aspect of management shouldbe followed for all five halitosis classifications. Inaddition, all dental disease, including gingivitis,periodontitis, ulcers, and dental caries, must bediagnosed and effectively managed.
Although periodontal disease (gingivitis andperiodontitis) is considered to be a significantcause of oral malodor, surprisingly few studieshave fully evaluated the effect of treatment of peri-odontal disease on halitosis.31 While some effecton reducing oral malodor following periodontaltreatment has been reported, a recent study con-cluded that both full-mouth disinfection andquadrant root planing resulted in reduced levels ofvolatile sulfur compounds, but no effect was notedfor organoleptic outcomes.32–34
The overriding principle for management ofintraoral halitosis is reduction of the bacterial bur-den. An effective and regular oral hygiene regimeninvolves tooth brushing, interdental cleaning, andregular (twice daily) tongue cleaning using either atoothbrush or tongue scraper (see Figure 7).35,36
While it is interesting to note that some authors donot recommend tongue scraping due to potentialdamage to the tongue surface,15 two systematicreviews evaluating the effectiveness of mechanical
tongue scraping on oral malodor and tonguecoating have concluded that tongue scrapingresults in a small but significant reduction involatile sulphur compounds.36,37 Both systematicreviews concluded that the effect may be shortlived and of minimal effect for chronic oral mal-odor and must be carried out on a regular basis tobe effective.
Rendering malodorous gases as nonvolatileshould also be an aim in the management of oralmalodor, which can be achieved through severalmeans. The most common of these is the use ofactive ingredients in toothpastes and mouthrinses.For the management of intraoral malodor, use ofa proven antibacterial toothpaste is recommend-ed. A recent review evaluated studies published toJune 2012 investigating the use of toothpasteswith various ingredients in the management oforal malodor.38A list of ingredients added to tooth-pastes for oral malodor management and theireffectiveness in reducing oral malodor indicators isshown in Table 6. Overall, toothpastes containingantibacterial agents, such as triclosan or metal ions(zinc or stannous), have been most comprehensivelystudied and show the greatest potential to influenceoral malodor.38 Other agents, such as hydrogen per-oxide, essential oils, and flavors, have also been stud-ied and show limited effects in reducing oralmalodor.38
CHAPTER 8 Oral Malodor
152
Table 5. Treatment Matrix for Management of Halitosis
Treatment Options
Condition TO1 TO2 TO3 TO4 TO5 TO6
Temporary X
Intraoral X X X
Extraoral X X X
Pseudo X X X
Halitophobia X X X
Figure 7.Tongue ScrapingTongue scraping may be used as an intervention for oral malodor.
The adjunctive use of antiseptic mouthrinses isessential to a satisfactory outcome in the manage-ment of oral malodor.39,40 While chlorhexidineremains the gold standard for chemical plaque con-trol, its long-term use cannot be recommended.Therefore, formulations with cetylpyridinium chlo-ride or zinc ions have been recommended.41–43
According to studies, these formulations work byreducing the overall bacterial load and also have adiluting effect on the volatile sulphur compoundsresponsible for malodor.41–43 The use of agents con-taining zinc is particularly interesting as zinc appearsto have both an antibacterial effect and an ability toneutralize volatile sulfur compounds.44 For these rea-sons, mouthrinses and also toothpastes containingzinc are gaining acceptance as useful adjuncts in themanagement of oral halitosis.
A recent systematic review evaluated the effective-ness of mouthrinses in the management of oral mal-odor and reported that mouthrinses containingchlorhexidine (CHX) + cetylpyridinium chloride(CPC) + zinc (Zn) and those containing zinc chloride(ZnCl) + cetylpyridinium chloride (CPC) have themost evidence to support a beneficial outcome.45 Fol-lowing application of the Grading of Recommenda-tions Assessment, Development, and Evaluation(GRADE) system,46 the evidence emerging from thissystematic review was graded. Specifically, risk ofbias of the individual studies, consistency and preci-sion among the study outcomes, directness of thestudy results, detection of publication bias, and mag-nitude of the effect were assessed by the authors. For
this assessment, grading was possible for the combi-nation of ingredients CHX + CPC + Zn and ZnCl +CPC mouthwashes. When taken together, theGRADE assessment resulted in the authors con-cluding that the strength for a recommendationregarding their use in the management of oral mal-odor was “weak.” Another “interesting” mouthrinseis water. Simply by increasing oral hydration, the sol-ubility of volatile sulfur compounds is increased andcan lead to some reduction in malodor. For these rea-sons, it is suggested that frequent water intake canreduce malodor for an hour.47
For some time, probiotics have been proposedas a useful adjunct in the management of bothintraoral and extraoral halitosis.48,49 The use of pro-biotics for oral malodor is based on the bacterialorigin of this condition.3 Thus, controlling thereappearance of bacteria capable of producingoral malodor through the selective introduction ofnon–odor-producing, commensal bacteria to colo-nize the oral cavity is an attractive proposal. Earlystudies demonstrated that by introducing Strepto-coccus salivarius K12 following mechanical peri-odontal debridement, volatile sulfur compoundscould be reduced.48–51 However, two studies investi-gating morning bad breath failed to show anyeffect of probiotic use on volatile sulphur com-pounds.52,53 It should be noted that morning badbreath is usually a transient condition and is mostlikely a different condition than oral malodor.Therefore, to date, the results of studies investigat-ing the use of probiotics as an adjunctive aid formanagement of oral malodor have been equivocaland are not universally accepted as a provenmethod to control oral malodor.49–55
It is important to recognize that the use of agentsthat merely mask the offensive smell of oral malodorare generally of limited value. These agents includemouthrinses, sprays, lozenges, and chewing gums.While these products will most likely produce short-term effects, they are not a treatment per se and maydelay correct diagnosis.
As stated earlier, it is generally accepted thataround 10% of all halitosis cases arise from extrao-ral sources. An extraoral source of halitosis is usual-ly suspected if dimethyl sulfide readings are high.20
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
153
Source: J Clin Periodontol. 2014;40(5):505–513.38
Table 6. Toothpaste Additives Evaluated for Management of Halitosis
Additive Reduction in Malodor(%)
Hydrogen peroxide 59
Sodium bicarbonate 29–50
Flavors 24–70
Sodium lauryl sulfate 33–38
Essential oils 37–40
Stannous fluoride 14–59
Zinc ions 35–68
Triclosan 24–88

In these cases, additional assessment and tests arerequired. If deemed appropriate, referral to anappropriate physician specializing in the manage-ment of nasal, throat, or gastrointestinal abnormal-ities may be required. The specialist may alsorecommend blood tests to assess for kidney insuffi-ciency, liver insufficiency or dysfunction, and meta-bolic diseases. Although good oral hygiene is likelyto be of general benefit to the patient suffering fromextraoral halitosis, it is unlikely to have any signifi-cant impact on this specific condition.
Prevention of Oral MalodorSurprisingly, there is very little scientific literaturepublished about primary prevention of oral mal-odor before it develops. Nearly all studies havefocused on the treatment and subsequent preven-tion of recurrence of the problem. Nonetheless, itseems intuitive that prevention of recurrenceshould be the same as prevention of development.Accordingly, preventive measures for patientsshould be directed at preventing malodor-formingsituations, such as dental and periodontal disease,and the development of tongue coatings. Clearlythis will involve (as described above for the man-agement of intraoral malodor) regular dentalcheckups, as well as good oral hygiene regimens,including toothbrushing, flossing, and tonguescraping, and use of toothpastes and mouthrinsesscientifically validated to be effective in the man-agement of oral malodor. Of the few studies pub-lished on prevention of oral malodor, one reportsthat an effective preventive measure for this condi-tion is to continually reinforce to patients the riskof halitosis through an education program utiliz-ing oral malodor as a motivational tool.56
CONCLUSIONSWhile perhaps not the most glamorous facet of den-tistry, management of oral malodor is a fascinatingand important aspect of clinical practice and patientcare. For many patients, this is a very distressingproblem. Through the use of developing aids todetect oral malodor and recognition of the role ofcertain bacteria in oral malodor, the management ofthis condition is becoming more predictable.
CASE1: Intraoral Halitosis (Oral Malodor)
PATIENT OVERVIEW Gender: Male.Age: 46 years.Chief Complaint and Duration: Wife complains hehas bad breath. Present for over 12 months.Oral Hygiene: Brushes once daily with manualtoothbrush; does not use dental floss ormouthrinses.Do Gums Bleed After Brushing/Flossing?Yes.Bad Taste in Mouth?Yes.Dry Mouth:Yes; drinks 1 liter of water daily.Last Prophylaxis: 2 months ago.Diet: Wife vegetarian, low in dairy foods, other-wise no abnormality detected.Smoking History: Never a smoker.Medical History: Slight high blood pressure; nomedication for this condition. Otherwise no abnor-mality detected.
CLINICAL EXAMINATIONExtra-/Intraoral ExaminationOral Hygiene:Fair, poor interproximally.Bleeding on Probing:All molars.Periodontal Assessment: Generalized 4- to 5-mmpockets. Minimal radiographic evidence of boneloss. No furcations, no mobility.Caries:None.Winkel Tongue Coating:Score 6.Periodontal Diagnosis: Mild/moderate chronicperiodontitis in otherwise healthy 46-year-oldmale.Breath Analysis:An OralChromaTMbreath analysiswas undertaken and the results are shown in Figure8. Hydrogen sulfide and methylmercaptan levelswere high and above the cognitive threshold. Thelevel of dimethyl sulphide was elevated but notabove the cognitive threshold.Halitosis Assessment:Overt oral malodor detected.
TREATMENT PLAN• Oral hygiene instruction: twice daily brush-ing, daily flossing.
• Recommend daily tongue scraping.• Use of therapeutic mouthrinse twice daily.
CHAPTER 8 Oral Malodor
154
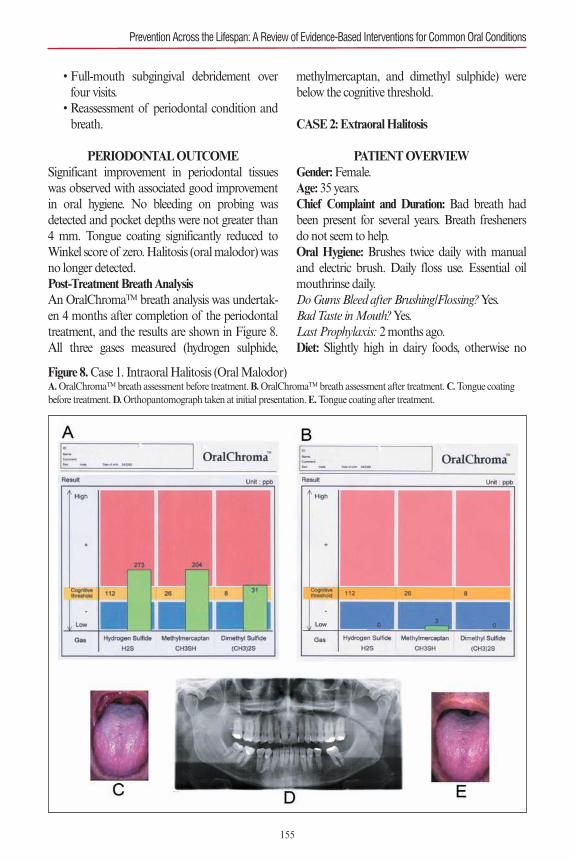
• Full-mouth subgingival debridement overfour visits.
• Reassessment of periodontal condition andbreath.
PERIODONTAL OUTCOMESignificant improvement in periodontal tissueswas observed with associated good improvementin oral hygiene. No bleeding on probing wasdetected and pocket depths were not greater than4 mm. Tongue coating significantly reduced toWinkel score of zero. Halitosis (oral malodor) wasno longer detected.Post-Treatment Breath AnalysisAn OralChromaTM breath analysis was undertak-en 4 months after completion of the periodontaltreatment, and the results are shown in Figure 8.All three gases measured (hydrogen sulphide,
methylmercaptan, and dimethyl sulphide) werebelow the cognitive threshold.
CASE2: Extraoral Halitosis
PATIENT OVERVIEWGender: Female.Age: 35 years.Chief Complaint and Duration: Bad breath hadbeen present for several years. Breath freshenersdo not seem to help.Oral Hygiene: Brushes twice daily with manualand electric brush. Daily floss use. Essential oilmouthrinse daily.Do Gums Bleed after Brushing/Flossing?Yes.Bad Taste in Mouth?Yes.Last Prophylaxis: 2 months ago.Diet: Slightly high in dairy foods, otherwise no
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
155
Figure 8.Case 1. Intraoral Halitosis (Oral Malodor)A.OralChromaTMbreath assessment before treatment. B.OralChromaTMbreath assessment after treatment. C.Tongue coatingbefore treatment. D.Orthopantomograph taken at initial presentation. E.Tongue coating after treatment.
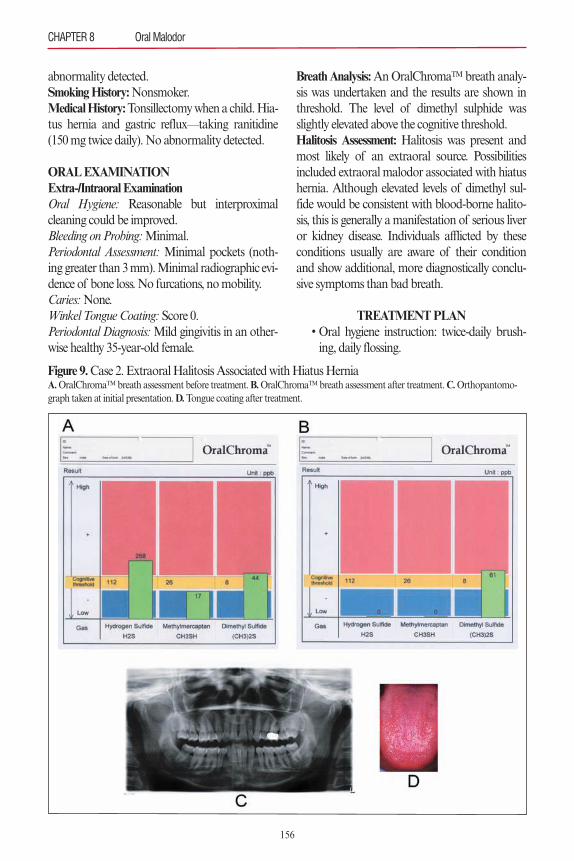
abnormality detected.Smoking History:Nonsmoker. Medical History: Tonsillectomy when a child. Hia-tus hernia and gastric reflux—taking ranitidine(150 mg twice daily). No abnormality detected.
ORAL EXAMINATIONExtra-/Intraoral ExaminationOral Hygiene: Reasonable but interproximalcleaning could be improved.Bleeding on Probing:Minimal.Periodontal Assessment: Minimal pockets (noth-ing greater than 3 mm). Minimal radiographic evi-dence of bone loss. No furcations, no mobility.Caries:None.Winkel Tongue Coating:Score 0.Periodontal Diagnosis:Mild gingivitis in an other-wise healthy 35-year-old female.
Breath Analysis:An OralChromaTM breath analy-sis was undertaken and the results are shown inthreshold. The level of dimethyl sulphide wasslightly elevated above the cognitive threshold.Halitosis Assessment: Halitosis was present andmost likely of an extraoral source. Possibilitiesincluded extraoral malodor associated with hiatushernia. Although elevated levels of dimethyl sul-fide would be consistent with blood-borne halito-sis, this is generally a manifestation of serious liveror kidney disease. Individuals afflicted by theseconditions usually are aware of their conditionand show additional, more diagnostically conclu-sive symptoms than bad breath.
TREATMENT PLAN• Oral hygiene instruction: twice-daily brush-ing, daily flossing.
CHAPTER 8 Oral Malodor
156
Figure 9.Case 2. Extraoral Halitosis Associated with Hiatus HerniaA.OralChromaTMbreath assessment before treatment. B.OralChromaTMbreath assessment after treatment. C.Orthopantomo-graph taken at initial presentation. D.Tongue coating after treatment.
• Recommend daily tongue scraping.• Use of a therapeutic mouthrinse twice daily.• Referral for further medical follow up withregard to better management of hiatus her-nia, as well as possible source of blood-bornevolatile sulfur compounds associated withliver or kidney disease.
• Continue to monitor oral hygiene and halitosison 6-month basis and provide general full-mouth fine scale and prophylaxis at these visits.
PERIODONTAL OUTCOMEPeriodontal condition remained stable. No bleed-ing on probing was observed, and pocket depthswere not greater than 3 mm. Tongue coating sig-nificantly remained at Winkel score of zero. Hali-tosis (oral malodor) still not detected.Medical OutcomeHiatus hernia managed by keyhole surgery andappropriate postoperative care. Patient is nolonger reporting bad breath.Post-Treatment Breath AnalysisAn OralChromaTM breath analysis was undertaken12 months after initial consultation, and the resultsare shown in Figure 9. All three gasses measured(hydrogen sulphide, methylmercaptan, and dimethylsulphide) were below the cognitive threshold. Halito-sis (extraoral malodor) was no longer detected.
SUMMARY OF CASE REPORTSThese two cases illustrate how with correct diag-nosis based on clinical and other diagnostic aids,halitosis of both intraoral and extraoral sourcescan be successfully managed. It is important toremember that the vast majority of halitosis caseshave an intraoral source, which can be easily man-aged by oral health professionals. Extraoral halito-sis is uncommon, affecting around 5% to 10% ofall halitosis cases. Nonetheless, it is very importantto distinguish between intraoral and extraoral hal-itosis as treatments differ considerably.
AcknowledgmentParts of this chapter are based on the following publication:Bartold PM. Oral malodor—a review. Dimensions of DentalHygiene (January Issue, 56–61, 2015). Approval for the use ofthis material has been obtained from the publisher.
REFERENCES1. Delanghe G, Ghyselen J, Feenstra L, van Steenberghe D.
Experiences of a Belgian multidisciplinary breath odourclinic. Acta Otorhinolaryngol Belg. 1997;51(1):43–48.
2. Delanghe G, Ghyselen J, van Steenberghe D, Feenstra L.Multidisciplinary breath-odour clinic. Lancet. 1997;350(9072):187.
3. Tonzetich J. Production and origin of oral malodor: areview of mechanisms and methods of analysis. J Peri-odontol. 1977;48(1):13–20.
4. Elias MS, Ferriani MD. Historical and social aspects ofhalitosis. Rev Lat Am Enfermagem. 2006;14(5):821–823.
5. Akaji EA, Folaranmi N, Ashiwaju O. Halitosis: a reviewof the literature on its prevalence, impact and control.Oral Health Prev Dent. 2014;12(4):297–304.
6. Söder B, Johansson B, Söder PO. The relation betweenfoetor ex ore, oral hygiene and periodontal disease. SwedDent J. 2000;24(3):73–82.
7. Miyazaki H, Sakao S, Katoh Y, Takehara T. Correlationbetween volatile sulphur compounds and certain oralhealth measurements in the general population. J Peri-odontol. 1995;66(8):679–684.
8. Liu XN, Shinada K, Chen XC, Zhang BX, Yaegaki K,Kawaguchi Y. Oral malodor related parameters in theChinese general population. J Clin Periodontol.2006;33(1):31–36.
9. Nadanovsky P, Carvalho LB, Ponce de Leon A. Oralmalodour and its association with age and sex in a gener-al population in Brazil. Oral Dis. 2007;13(1):105–109.
10. Zalewska A, Zatoñski M, Jabłonka-Strom A, Parad-owska A, Kawala B, Litwin A. Halitosis—a commonmedical and social problem. A review on pathology,diagnosis and treatment. Acta Gastroenterol Belg.2012;75(3):300–309.
11. Nalçaci R, Dülgergil T, Oba AA, Gelgör IE. Prevalenceof breath malodour in 7- to 11-year-old children living inMiddle Anatolia, Turkey. Community Dent Health.2008;25(3):173–177.
12. Patil PS, Pujar P, Poornima S, Subbareddy VV. Preva-lence of oral malodour and its relationship with oralparameters in Indian children aged 7–15 years. Eur ArchPaediatr Dent. 2014;15(4):251–258.
13. Villa A, Zollanvari A, Alterovitz G, Cagetti MG,Strohmenger L, Abati S. Prevalence of halitosis in chil-dren considering oral hygiene, gender and age. Int J DentHyg. 2014;12(3):208–212.
14. Miyazaki H, Arao M, Okamura K, et al. Tentative clas-sification of halitosis and its treatment needs (Japanese).Niigata Dent J. 1999;32:7–11.
15. Yaegaki K, Coil JM. Examination, classification, andtreatment of halitosis; clinical perspectives. J Can DentAssoc. 2000;66(5):257–261.
16. Loesche WJ, Kazor C. Microbiology and treatment ofhalitosis. Periodontol 2000. 2002;28:256–279.
17. Persson S, Edlund MB, Claesson R, Carlsson J. The
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
157
formation of hydrogen sulfide and methyl mercaptan byoral bacteria. Oral Microbiol Immunol. 1990;5(4):195–201.
18. McNamara TF, Alexander JF, Lee M. The role ofmicroorganisms in the production of oral malodor. OralSurg Oral Med Oral Pathol. 1972;34(1):41–48.
19. Scully C, Greenman J. Halitology (breath odour:aetiopathogenesis and management). Oral Dis.2012;18(4):333–345.
20. Tangerman A, Winkel EG. Volatile sulfur compoundsas the cause of bad breath: a review. Phosphorous Sulfurand Silicon and the Related Elements. 2013;188:396–402.
21. Tonzetich J, Kestenbaum RC. Odour production byhuman salivary fractions and plaque. Arch Oral Biol.1969;14(7):815–827.
22. De Boever EH, Loesche WJ. Assessing the contributionof anaerobic microflora of the tongue to oral malodor. JAm Dent Assoc. 1995;126(10):1384–1393.
23. Seemann R, Conceicao MD, Filippi A, et al. Halitosismanagement by the general dental practitioner—resultsof an international consensus workshop. J Breath Res.2014;8(1):017101. doi: 10.1088/1752 7155/8/1/017101.[Epub Feb 24 2014.]
24. Winkel EG, Roldán S, Van Winkelhoff AJ, Herrera D,Sanz M. Clinical effects of a new mouthrinse containingchlorhexidine, cetylpyridinium chloride and zinc-lactateon oral halitosis. A dual-center, double-blind placebo-controlled study. J Clin Periodontol. 2003;30(4):300–306.
25. Rosenberg M, McCulloch CA. Measurement of oralmalodor: current methods and future prospects. J Peri-odontol. 1992;63(9):776–782.
26. Greenman J, Duffield J, Spencer P, et al. Study on theorganoleptic intensity scale for measuring oral malodor.J Dent Res. 2004;83(1):81–85.
27. Dadamio J, Laleman I, De Geest S, et al. Usefulness of anew malodour-compound detection portable device inoral malodour diagnosis. J Breath Res.2013;7(4):046005. doi: 10.1088/1752-7155/7/4/046005.[Epub Nov 1 2013.]
28. Laleman I, Dadamio J, De Geest S, Dekeyser C, Quiry-nen M. Instrumental assessment of halitosis for the gen-eral dental practitioner. J Breath Res. 2014;8(1):017103.doi: 10.1088/1752-7155/8/1/017103. [Epub Feb 24 2014.]
29. Rosenberg M, Septon I, Eli I, et al. Halitosis measure-ment by an industrial sulphide monitor. J Periodontol.1991;62(8):487–489.
30. Yaegaki K, Coil JM, Kamemizu T, Miyazaki H. Tonguebrushing and mouth rinsing as basic treatment measuresfor halitosis. Int Dent J. 2002;52(suppl 3):192–196.
31. Soares LG, Tinoco EMB. Prevalence and relatedparameters of halitosis in general population and peri-odontal patients. OA Dentistry. 2014;2(1):1–7.
32. Pham TA, Ueno M, Zaitsu T, et al. Clinical trial of oralmalodor treatment in patients with periodontal diseases.J Periodontal Res. 2011;46(6):722–729.
33. Apatzidou DA, Kinane DF. Quadrant root planing ver-
sus same-day full-mouth root planing. I. Clinical find-ings. J Clin Periodontol. 2004;31(2):132–140.
34. Soares LG, Castagna L, Weyne SC, Silva DG, FalabellaMEV, Tinoco EMB. Effectiveness of full- and partial-mouth disinfection on halitosis in periodontal patients. JOral Sci. 2015;57(1):1–6.
35. van den Broek AM, Feenstra L, de Baat C. A review ofthe current literature on management of halitosis. OralDis. 2008;14(1):30–39.
36. Outhouse TL, Al-Alawi R, Fedorowicz Z, Keenan JV.Tongue scraping for treating halitosis. Cochrane Data-base SystRev. 2006;2:CD005519.
37. Van der Sleen MI, Slot DE, Van Trijffel E, Winkel EG,Van der Weijden GA. Effectiveness of mechanicaltongue cleaning on breath odour and tongue coating: asystematic review. Int J Dent Hyg. 2010;8(4):258–268.
38. Dadamio J, Laleman I, Quirynen M. The role of tooth-pastes in oral malodour management. Monogr Oral Sci.2013;23:45–60.
39. Quirynen M, Zhao H, Soers C, et al. The impact of peri-odontal therapy and the adjunctive effect of antiseptics onbreath odor-related outcome variables: a double-blind ran-domized study. J Periodontol. 2005;76(5):705–712.
40. Quirynen M, Zhao H, van Steenberghe D. Review ofthe treatment strategies for oral malodour. Clin OralInvestig. 2002;6(1):1–10.
41. Young A, Jonski G, Rölla G. Combined effect of zincions and cationic antibacterial agents on intraoralvolatile sulphur compounds (VSC). Int Dent J.2003;53(4):237–242.
42. Winkel EG, Roldán S, Van Winkelhoff AJ, Herrera D,Sanz M. Clinical effects of a new mouthrinse containingchlorhexidine, cetylpyridinium chloride and zinc-lactateon oral halitosis. A dual-center, double-blind placebo-controlled study. J Clin Periodontol. 2003;30(5):300–306.
43. van Steenberghe D, Avontroodt P, Peeters W, et al. Effectof different mouthrinses on morning breath. J Periodon-tol. 2001;72:1183–1191.
44. Dadamio J, Van Tournout M, Teughels W, Dekeyser C,Coucke W, Quirynen M Efficacy of differentmouthrinse formulations in reducing oral malodour: arandomized clinical trial. J Clin Periodontol. 2013;40(5):505–513.
45. Slot DE, De Geest S, van der Weijden FA, Quirynen M.Treatment of oral malodour. Medium-term efficacy ofmechanical and/or chemical agents: a systematic review.J Clin Periodontol. 2015;42(suppl 16):S303–316.
46. Guyatt GH, Oxman AD, Kunz R, et al. GRADEWorking Group. Incorporating considerations ofresources use into grading recommendations. BMJ.2008;336:1170–1173.
47. Van der Sluijs E, Slot DE, Bakker E, Van der Weijden GA.The effect of water on morning bad breath: a randomizedclinical trial. Int J Dent Hyg. 2016;14(2):124–134.
48. Burton JP, Chilcott CN, Moore CJ, Speiser G, Tagg JR.A preliminary study of the effect of probiotic
CHAPTER 8 Oral Malodor
158
159
Streptococcus salivarius K12 on oral malodour parame-ters. J Appl Microbiol. 2006;100(4):754–764.
49. Teughels W, Van Essche M, Sliepen I, Quirynen M. Pro-biotics and oral healthcare. Periodontol 2000.2008;48:111–147.
50. Iwamoto T, Suzuki N, Tanabe K, Takeshita T, HirofujiT. Effects of probiotic Lactobacillus salivariusWB21 onhalitosis and oral health: an open-label pilot trial. OralSurg Oral Med Oral Pathol Oral Radiol Endod.2010;110(2):201–208.
51. Suzuki N, Yoneda M, Tanabe K, et al. Lactobacillus sali-variusWB21–containing tablets for the treatment of oralmalodor: a double-blind, randomized, placebo-con-trolled crossover trial. Oral Surg Oral Med Oral PatholOral Radiol. 2014;117(4):462–470.
52. Keller MK, Bardow A, Jensdottir T, Lykkeaa J, Twet-man S. Effect of chewing gums containing the probiotic
bacterium Lactobacillus reuteri on oral malodour. ActaOdontol Scand. 2012;70(3):246–250.
53. Sutula J, Coulthwaite LA, Thomas LV, Verran J. Theeffect of a commercial probiotic drink containing Lacto-bacillus casei strain Shirota on oral health in healthy den-tate people. Microb Ecol Health Dis. 2013 Oct 29;24. doi:10.3402/mehd.v24i0.21003.
54. Masdea L, Kulik EM, Hauser-Gerspach I, RamseierAM, Filippi A, Waltimo T. Antimicrobial activity ofStreptococcus salivariusK12 on bacteria involved in oralmalodour. Arch Oral Biol. 2012;57(8):1041–1047.
55. Laleman I, Teughels W. Probiotics in the dental practice:a review. Quintessence Int. 2015;46(3):255–264.
56. Ueno M, Shinada K, Zaitsu T, Yokoyama S, KawaguchiY. Effects of an oral health education program targetingoral malodor prevention in Japanese senior high schoolstudents. Acta Odontol Scand. 2012;70(5):426–431.
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions

OVERVIEW OF THE CONDITIONEpidemiologyDentinal hypersensitivity is commonly known astooth sensitivity to most patients; it has also beentermed cervical hypersensitivity, root hypersensi-tivity, and cemental hypersensitivity.1 Dentinalhypersensitivity is one of the most encounteredcomplaints by patients seeking dental treatment.2
Strassler and coworkers called tooth sensitivity the“common cold of dentistry.”3
The reported prevalence of dentinal hypersen-sitivity ranges from 3% to 74%, with an average of57% among dental patients of different lifestylesand cultures.2,4–14 Females are affected more thanmales, with a peak occurrence between 20 and 40years of age. Women between the ages of 20 and40 years who have meticulous oral hygiene aremost likely to develop dentin hypersensitivity.15
In general, canines and premolars are mostoften affected, and the buccal cervical area is also
a commonly affected site.16 Among patients whoreceived periodontal treatment, the reportedprevalence of postoperative dentinal hypersensi-tivity ranged from 60% to as high as 98%.5,17,18
EtiologySignificant efforts have been made to understandthe etiology and mechanisms involved in thedevelopment of dentinal hypersensitivity. A com-mon key characteristic is the exposed dentin sur-face. Loss of enamel and root surface denudationresult in the exposure of underlying dentinaltubules. It is believed that these exposed dentinaltubules allow various stimuli to disturb the denti-nal tubular fluid, which consequently activates thepulpal nerves. This activation is then perceived aspain by the patient. The hydrodynamic theory wasfirst proposed by Kramer in 1955 and later con-firmed and developed by Brännström in 1962,who correlated in vivo studies on tooth sensitivityassociated with applied pressure, air blasts, andchemical stimuli to in vitro measurements ofdentinal fluid shifts in response to these stimuli.19,20
(See Figure 1.) Results of further research suggestthat the pain sensation is caused by the activationof mechanoreceptors in intratubular nerves or inthe superficial pulp due to changes of the flow orvolume of fluid within dentinal tubules, orboth.18,21 These findings help explain the observa-tion that for sensitivity caused by a tooth wearlesion, symptoms become more difficult to resolve
160
DentinHypersensitivity
Chapter 9
Yiming Li
Figure 1.Brännström’s Theory
Source: Image courtesy of the Colgate-Palmolive Company.

by normal methods, largely due to more exposedtubules and wider tubule diameter.22
Tooth bleaching using peroxide-based materi-als is also known to cause tooth sensitivity, whichmay or may not be associated with exposeddentin.23–25 In most cases, the sensation is mild tomoderate and usually transient, dissipating spon-taneously without specific treatment.
Risk FactorsRisk factors are primarily those that cause dentinexposure (see Table 1). A number of factors,including gingival recession, periodontal disease,deep tooth cracks, and loss of enamel, cementum,and dentin due to mechanical abrasion, chemicalerosion, and chipped or broken cusps, have beenidentified.5,18 Gingival recession, resulting fromabrasion or periodontal disease, is the primaryroute through which the underlying dentinbecomes exposed, and acid erosion is an importantfactor in opening exposed dentinal tubules.2,26,27
Once a patient has exposed dentin with opentubules, any external stimulus can cause discom-fort or dentinal hypersensitivity for the patient.
Attrition, abrasion, or erosion causes enamelloss (see Table 2). Attrition is the wear of teeth at
sites of direct contact between teeth, which is asso-ciated with occlusal function and may be aggra-vated by habits and bruxism.28 The latter has beenreported to be responsible for pathological toothwear in 11% of referred tooth wear cases and is acontributing factor in two-thirds of cases of com-bined etiology.29
Abrasion is tooth wear caused by objects otherthan another tooth, such as toothbrushing andpipe smoking. While a toothbrush itself causes lit-tle or no effects on enamel and dentin, certaintypes of abrasive dentifrices can remove mineralcontent of enamel, leaving dentinal tubulesexposed.30,31 When combined with erosive agents,toothbrushing is capable of causing enormousenamel and dentin loss.32 Abfraction occurs as aresult of eccentric loading that causes cusp flexure,resulting in compressive and tensile forces in thecervical area of a tooth. Abfraction may potenti-ate the effects of abrasion and erosion.33
Erosion, which can be extrinsic or intrinsic inorigin, is considered to be a growing cause ofdentin exposure. Extrinsic factors include acidicfoods and beverages, chemical exposure, orimproper tooth bleaching. There have beenreports of significant enamel erosion caused bytooth bleaching products of poor quality.34 Gastric
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
161
Table 1.Frequently Encountered ConditionsAssociated with Tooth Sensitivity
Primary Origin Etiological Condition
Tooth • Dental caries • Erosion, attrition, or abrasion • Chipped or broken tooth • Cracked tooth syndrome • Pulp inflammation • Trauma • Palato-gingival grooves and other anatomical defects
Restoration • Broken or failing restorations, or both • Marginal leakage • Nanoshrinkage of restorative polymer materials
Periodontal tissues • Gingival recession • Chronic periodontal disease
Dental procedure • Tooth whitening • Restoration placement • Scaling and root planing or periodontal surgery
Table 2.Questions for Patients ExperiencingDentin Hypersensitivity
Etiology Questions
Erosion • How often do you drink acidic beverages such as soda, citrus juice, wine, etc.?
• How often do you drink beverages other than water between meals?
• Are you currently experiencing any medical conditions that cause acid reflux?
Abrasion • What kind of toothpaste do you use at home?
• How often do you brush and for how long?
• How often do you replace your manual or power brush head?
• Do you use light, moderate, or heavy pressure when brushing?
Attrition • Do you have a history of clenching or grinding your teeth?
• Do you currently have a night guard or has one been recommended previously?
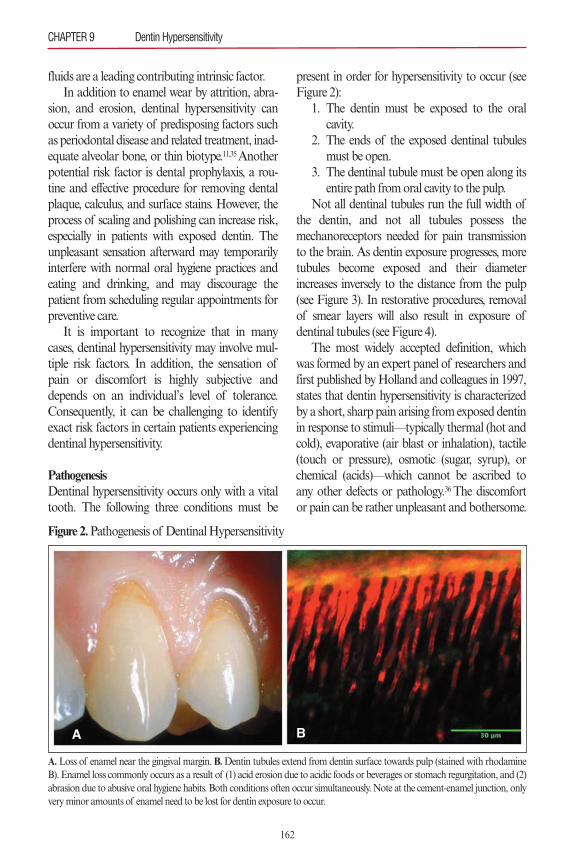
fluids are a leading contributing intrinsic factor.In addition to enamel wear by attrition, abra-
sion, and erosion, dentinal hypersensitivity canoccur from a variety of predisposing factors suchas periodontal disease and related treatment, inad-equate alveolar bone, or thin biotype.11,35 Anotherpotential risk factor is dental prophylaxis, a rou-tine and effective procedure for removing dentalplaque, calculus, and surface stains. However, theprocess of scaling and polishing can increase risk,especially in patients with exposed dentin. Theunpleasant sensation afterward may temporarilyinterfere with normal oral hygiene practices andeating and drinking, and may discourage thepatient from scheduling regular appointments forpreventive care.
It is important to recognize that in manycases, dentinal hypersensitivity may involve mul-tiple risk factors. In addition, the sensation ofpain or discomfort is highly subjective anddepends on an individual’s level of tolerance.Consequently, it can be challenging to identifyexact risk factors in certain patients experiencingdentinal hypersensitivity.
PathogenesisDentinal hypersensitivity occurs only with a vitaltooth. The following three conditions must be
present in order for hypersensitivity to occur (seeFigure 2):
1. The dentin must be exposed to the oral cavity.2. The ends of the exposed dentinal tubules must be open.3. The dentinal tubule must be open along its entire path from oral cavity to the pulp.Not all dentinal tubules run the full width of
the dentin, and not all tubules possess themechanoreceptors needed for pain transmissionto the brain. As dentin exposure progresses, moretubules become exposed and their diameterincreases inversely to the distance from the pulp(see Figure 3). In restorative procedures, removalof smear layers will also result in exposure ofdentinal tubules (see Figure 4).
The most widely accepted definition, whichwas formed by an expert panel of researchers andfirst published by Holland and colleagues in 1997,states that dentin hypersensitivity is characterizedby a short, sharp pain arising from exposed dentinin response to stimuli—typically thermal (hot andcold), evaporative (air blast or inhalation), tactile(touch or pressure), osmotic (sugar, syrup), orchemical (acids)—which cannot be ascribed toany other defects or pathology.36 The discomfortor pain can be rather unpleasant and bothersome.
CHAPTER 9 Dentin Hypersensitivity
162
Figure 2.Pathogenesis of Dentinal Hypersensitivity
A.Loss of enamel near the gingival margin. B.Dentin tubules extend from dentin surface towards pulp (stained with rhodamineB). Enamel loss commonly occurs as a result of (1) acid erosion due to acidic foods or beverages or stomach regurgitation, and (2)abrasion due to abusive oral hygiene habits. Both conditions often occur simultaneously. Note at the cement-enamel junction, onlyvery minor amounts of enamel need to be lost for dentin exposure to occur.
A B

In severe cases, dentin hypersensitivity may have asignificant negative impact on an individual’s dailylife, as it may cause difficulties with eating anddrinking, especially hot and cold items, and eveninterfere with speaking under certain circum-stances.37 Normal hygiene maintenance may alsobecome more difficult, which increases risks ofcaries, gingivitis, and periodontal problems.
The sensation of dentin hypersensitivity ishighly subjective, and its occurrence and severitycan be episodic and sporadic. Consequently, itcan be challenging to define exact signs andsymptoms in certain patients experiencing dentinhypersensitivity.
PATIENT MANAGEMENT AND INTERVENTIONS
DiagnosisThe general approach to the diagnosis of dentinalhypersensitivity includes the following fouraspects:
1. Patient history2. Oral examination3. Testing of patient response to stimuli4. Differential diagnosisWhen diagnosing dentinal hypersensitivity, it is
important to take into consideration the followingfour specific elements:
1. The nature of the pain
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
163
Figure 3.Odontoblast and Dentinal Tubules
A.Relationship of odontoblasts and the odontoblast processes to nerve fibers. Not all processes are in proximity to a nerve fiber,and not all tubules run the entire width of the dentin. B.The seal closes off the tubule ends and prevents dentinal fluid movementand thus stimulation of the mechanoreceptors adjacent to the odontoblasts, eliminating the sensation of dentin hypersensitivity.Source: Image courtesy of the Colgate-Palmolive Company.
Figure 4. Scanning Electron Micrograph Images
A.Dentin surface with a smear layer covering the dentin tubules below. B. Exposed dentin surface with no smear layer showingopen ends of dentin tubules. Low-pH foods and beverages and some oral hygiene products can remove the smear layer.

2. The occurrence in areas of exposed dentin3. An identified stimulus4. The exclusion of any other possible causes for the pain
Patient HistoryDuring review of the patient’s history, the individ-ual should be asked whether his or her tooth painoccurs when eating or drinking hot, cold, sweet, oracidic foods or beverages; during toothbrushing;or after a dental procedure. If so, attempts shouldbe made to obtain a specific description of thepain, including onset, severity, and duration. Adetailed dietary history and oral hygiene habits,including frequency, duration, and timing ofbrushing, is helpful for assessing potential risk fac-tors. The patient should be asked to identify thelocation of the pain, which can help confirmwhether dentin exposure is present during the den-tal examination. When the patient reports under-going a recent dental procedure, he or she shouldbe questioned about the nature of the procedureto help determine whether the procedure itself oroutcomes from the treatment may be possiblesources for the pain.
Oral ExaminationA comprehensive oral examination is critical forcorrect diagnosis and differential diagnosis ofdentinal hypersensitivity. A thorough examinationwill also help identify etiological and predisposingfactors, particularly with respect to erosion andabrasion, which will be essential for formulatingthe strategies for intervention and management.The oral examination should include both theteeth and surrounding gingival tissues, with specialattention directed toward exclusion of possibledifferential diagnoses, including
• Dental or root caries• Traumatic occlusion• Fractured restoration• New restoration for possible postoperative sensitivity
• Marginal integrity of a restoration for possi-ble leakage
• Pulpitis
• Gingival inflammation• Signs of tooth bleaching• Atypical odontalgia
Any dentin exposure observed should be charac-terized by its location, size, and severity. Whenindicated, radiographs may also be considered.
Testing of Patient Response to StimuliA number of clinical tests have been developed forevaluating dentinal hypersensitivity; however, theyare all subjective to a certain extent and requirepatient responses to applied stimuli. As pain sensa-tion is highly dependent on an individual’s disposi-tion, its perception may be influenced bypsychological factors, past experience, anxiety, eth-nic differences, gender, and potential social impacts.
Current clinical methods for detection anddiagnosis of dentinal hypersensitivity essentiallyrely on delivering a mechanical or thermal stimu-lus to the suspected tooth, and judgment is madebased on the patient’s response describing theconsequential sensation.11,38–40 The tactile methodcommonly used in the dental clinic producesmechanical stimuli; it typically involves running asharp-tipped dental probe on the exposed dentinsurface. Such a tactile procedure, though clinical-ly feasible and easy to perform, is difficult todeliver using a consistent, standardized forcewhich may affect the reliability of the response.Specialized electromagnetic devices, such as theYeaple Electronic Pressure Sensitive Probe(www.yeapleprobe.com), are capable of produc-ing standardized mechanical pressure to thetooth surface. The Yeaple probe delivers pressurein increments of 5 g each progressively until thepatient reports the onset of pain; a tooth that sus-tains pressure of 70 g with no pain is considerednonsensitive.38,41 The Yeaple probe offers advan-tages of controllable force delivery and more con-sistent diagnostic outcomes, but requires thepurchase of the device and more clinical time; todate, it has primarily been used in clinicalresearch. (See Figure 5.)
The air blast method is commonly used in den-tal clinics to produce thermal stimuli for evaluatingdentinal hypersensitivity. The tooth to be examined
CHAPTER 9 Dentin Hypersensitivity
164
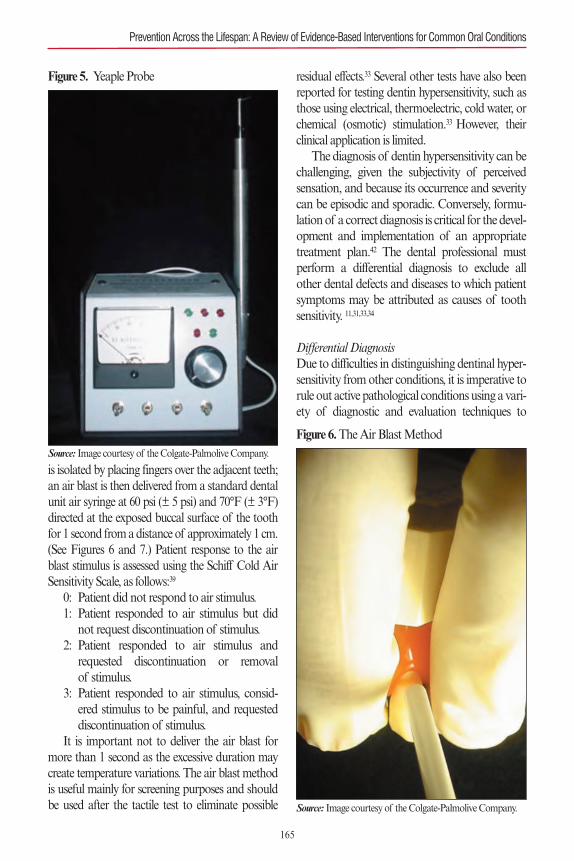
is isolated by placing fingers over the adjacent teeth;an air blast is then delivered from a standard dentalunit air syringe at 60 psi (± 5 psi) and 70°F (± 3°F)directed at the exposed buccal surface of the toothfor 1 second from a distance of approximately 1 cm.(See Figures 6 and 7.) Patient response to the airblast stimulus is assessed using the Schiff Cold AirSensitivity Scale, as follows:39
0: Patient did not respond to air stimulus.1: Patient responded to air stimulus but did not request discontinuation of stimulus.2: Patient responded to air stimulus and requested discontinuation or removal of stimulus.3: Patient responded to air stimulus, consid- ered stimulus to be painful, and requested discontinuation of stimulus.It is important not to deliver the air blast for
more than 1 second as the excessive duration maycreate temperature variations. The air blast methodis useful mainly for screening purposes and shouldbe used after the tactile test to eliminate possible
residual effects.33 Several other tests have also beenreported for testing dentin hypersensitivity, such asthose using electrical, thermoelectric, cold water, orchemical (osmotic) stimulation.33 However, theirclinical application is limited.
The diagnosis of dentin hypersensitivity can bechallenging, given the subjectivity of perceivedsensation, and because its occurrence and severitycan be episodic and sporadic. Conversely, formu-lation of a correct diagnosis is critical for the devel-opment and implementation of an appropriatetreatment plan.42 The dental professional mustperform a differential diagnosis to exclude allother dental defects and diseases to which patientsymptoms may be attributed as causes of toothsensitivity. 11,31,33,34
Differential DiagnosisDue to difficulties in distinguishing dentinal hyper-sensitivity from other conditions, it is imperative torule out active pathological conditions using a vari-ety of diagnostic and evaluation techniques to
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
165
Figure 5. Yeaple Probe
Source: Image courtesy of the Colgate-Palmolive Company.
Figure 6.The Air Blast Method
Source: Image courtesy of the Colgate-Palmolive Company.
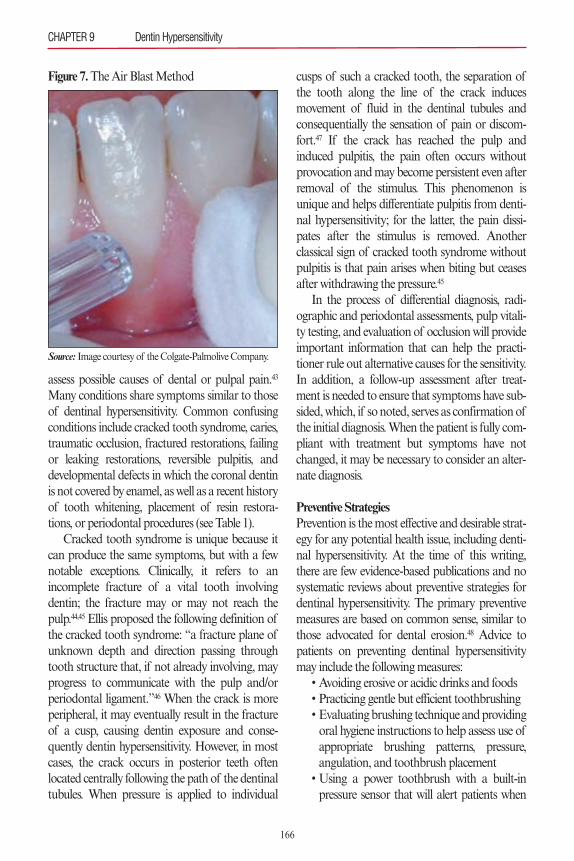
assess possible causes of dental or pulpal pain.43
Many conditions share symptoms similar to thoseof dentinal hypersensitivity. Common confusingconditions include cracked tooth syndrome, caries,traumatic occlusion, fractured restorations, failingor leaking restorations, reversible pulpitis, anddevelopmental defects in which the coronal dentinis not covered by enamel, as well as a recent historyof tooth whitening, placement of resin restora-tions, or periodontal procedures (see Table 1).
Cracked tooth syndrome is unique because itcan produce the same symptoms, but with a fewnotable exceptions. Clinically, it refers to anincomplete fracture of a vital tooth involvingdentin; the fracture may or may not reach thepulp.44,45 Ellis proposed the following definition ofthe cracked tooth syndrome: “a fracture plane ofunknown depth and direction passing throughtooth structure that, if not already involving, mayprogress to communicate with the pulp and/orperiodontal ligament.”46 When the crack is moreperipheral, it may eventually result in the fractureof a cusp, causing dentin exposure and conse-quently dentin hypersensitivity. However, in mostcases, the crack occurs in posterior teeth oftenlocated centrally following the path of the dentinaltubules. When pressure is applied to individual
cusps of such a cracked tooth, the separation ofthe tooth along the line of the crack inducesmovement of fluid in the dentinal tubules andconsequentially the sensation of pain or discom-fort.47 If the crack has reached the pulp andinduced pulpitis, the pain often occurs withoutprovocation and may become persistent even afterremoval of the stimulus. This phenomenon isunique and helps differentiate pulpitis from denti-nal hypersensitivity; for the latter, the pain dissi-pates after the stimulus is removed. Anotherclassical sign of cracked tooth syndrome withoutpulpitis is that pain arises when biting but ceasesafter withdrawing the pressure.45
In the process of differential diagnosis, radi-ographic and periodontal assessments, pulp vitali-ty testing, and evaluation of occlusion will provideimportant information that can help the practi-tioner rule out alternative causes for the sensitivity.In addition, a follow-up assessment after treat-ment is needed to ensure that symptoms have sub-sided, which, if so noted, serves as confirmation ofthe initial diagnosis. When the patient is fully com-pliant with treatment but symptoms have notchanged, it may be necessary to consider an alter-nate diagnosis.
Preventive StrategiesPrevention is the most effective and desirable strat-egy for any potential health issue, including denti-nal hypersensitivity. At the time of this writing,there are few evidence-based publications and nosystematic reviews about preventive strategies fordentinal hypersensitivity. The primary preventivemeasures are based on common sense, similar tothose advocated for dental erosion.48 Advice topatients on preventing dentinal hypersensitivitymay include the following measures:
• Avoiding erosive or acidic drinks and foods• Practicing gentle but efficient toothbrushing• Evaluating brushing technique and providingoral hygiene instructions to help assess use ofappropriate brushing patterns, pressure,angulation, and toothbrush placement
• Using a power toothbrush with a built-inpressure sensor that will alert patients when
CHAPTER 9 Dentin Hypersensitivity
166
Figure 7.The Air Blast Method
Source: Image courtesy of the Colgate-Palmolive Company.
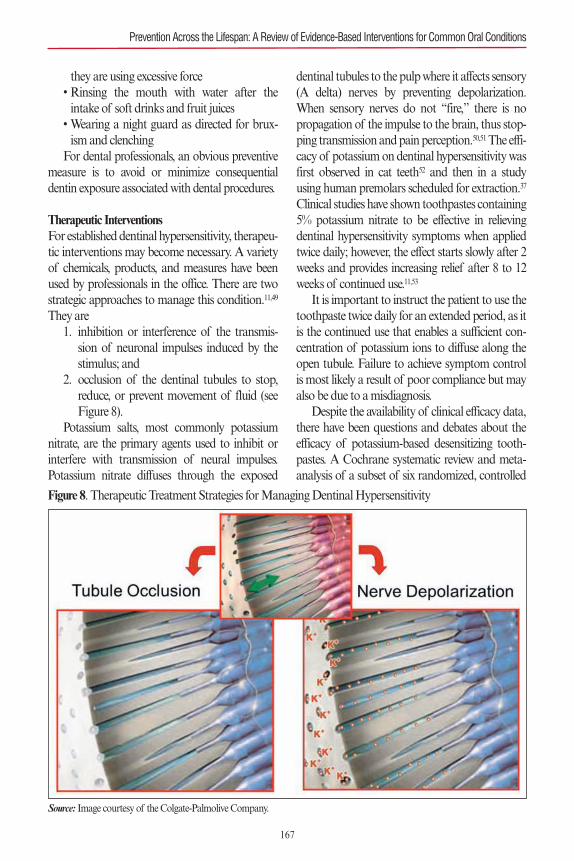
they are using excessive force• Rinsing the mouth with water after theintake of soft drinks and fruit juices
• Wearing a night guard as directed for brux-ism and clenching
For dental professionals, an obvious preventivemeasure is to avoid or minimize consequentialdentin exposure associated with dental procedures.
Therapeutic InterventionsFor established dentinal hypersensitivity, therapeu-tic interventions may become necessary. A varietyof chemicals, products, and measures have beenused by professionals in the office. There are twostrategic approaches to manage this condition.11,49
They are1. inhibition or interference of the transmis- sion of neuronal impulses induced by the stimulus; and2. occlusion of the dentinal tubules to stop, reduce, or prevent movement of fluid (see Figure 8).Potassium salts, most commonly potassium
nitrate, are the primary agents used to inhibit orinterfere with transmission of neural impulses.Potassium nitrate diffuses through the exposed
dentinal tubules to the pulp where it affects sensory(A delta) nerves by preventing depolarization.When sensory nerves do not “fire,” there is nopropagation of the impulse to the brain, thus stop-ping transmission and pain perception.50,51The effi-cacy of potassium on dentinal hypersensitivity wasfirst observed in cat teeth52 and then in a studyusing human premolars scheduled for extraction.37
Clinical studies have shown toothpastes containing5% potassium nitrate to be effective in relievingdentinal hypersensitivity symptoms when appliedtwice daily; however, the effect starts slowly after 2weeks and provides increasing relief after 8 to 12weeks of continued use.11,53
It is important to instruct the patient to use thetoothpaste twice daily for an extended period, as itis the continued use that enables a sufficient con-centration of potassium ions to diffuse along theopen tubule. Failure to achieve symptom controlis most likely a result of poor compliance but mayalso be due to a misdiagnosis.
Despite the availability of clinical efficacy data,there have been questions and debates about theefficacy of potassium-based desensitizing tooth-pastes. A Cochrane systematic review and meta-analysis of a subset of six randomized, controlled
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
167
Figure 8. Therapeutic Treatment Strategies for Managing Dentinal Hypersensitivity
Source: Image courtesy of the Colgate-Palmolive Company.

clinical studies led its authors to conclude that theclinical efficacy of potassium-containing tooth-pastes in reducing dentin hypersensitivity is equiv-ocal.51
To reduce or prevent fluid movement in opendentinal tubules, the most commonly employedtechnologies include protein precipitants, calciumand phosphate precipitating agents, various crys-tallizing agents, bonding agents, laser therapy, andsurgical grafting of gingival tissue.11,33 Varnishesand pastes of high fluoride concentration havebeen reported to be effective in promoting mineraldeposition and consequential tubule occlusionleading to symptom relief. However, the evidencesupporting fluoride in toothpaste as a desensitiz-ing agent is minimal.
To date, there has been little research into useof lasers for reducing dentinal hypersensitivity.54,55
Two systematic reviews comparing laser therapywith desensitizing agents suggest that lasers seemto have a slight clinical and immediate advantageover topically applied medicaments.56,57 Similarly, asystematic review58 and meta-analysis59 found noevidence of benefits from treating dentinal hyper-sensitivity with oxalates beyond a placebo effectand consequently concluded that available evi-dence did not support the recommendation ofusing oxalates for treatment, with the possibleexception of 3% monohydrogen monopotassiumoxalate. The use of professional treatments, suchas resin sealers, bonding agents, and gingival sur-gery, is limited to certain patients due to cost andneed for an office visit.
A protein precipitant, casein phosphopeptide(CPP), has been incorporated in oral hygieneproducts with an intention to reduce dentinalhypersensitivity. CPP is a casein derivative and iscapable of stabilizing amorphous calcium phos-phate (ACP), which is usually insoluble, in a stateforming a CPP-ACP complex.60 A commercialproduct containing CPP-ACP has been designedto promote remineralization through depositionof fluoride-containing calcium-phosphate precipi-tates, which has been suggested for reducing risksof dental caries and dentinal hypersensitivity (MIPaste Plus®, GC America). However, results from
published studies are inconsistent.61–64 A systemat-ic review of the literature concludes that “there isinsufficient clinical trial evidence (in quantity,quality, or both) to make a recommendationregarding the long-term effectiveness of caseinderivatives, specifically CPP-ACP, in preventingcaries in vivo and in treating dentin hypersensitivi-ty or dry mouth.”65 The authors questioned thepotential possibility of interactions between fluo-ride and ACP that may precipitate out as calciumfluoride, rendering both inorganic componentsineffective, and expressed their concerns with the900 ppm fluoride dose in the product, and thusrecommended against its use in children youngerthan 6 years of age.
Approximately 50 years ago, before the wide-spread adoption of potassium as a desensitizer,strontium chloride was incorporated into tooth-paste because it was believed to treat tooth sensi-tivity by occluding dentinal tubules. More recently,strontium acetate has been used in toothpastesbecause of its compatibility with fluoride.66 How-ever, data on the clinical efficacy of strontium-based toothpaste for dentinal hypersensitivity havebeen inconsistent and equivocal, at best.11,67–69 Aliterature review of clinical studies on effects ofstrontium-based toothpastes used for periods of 4to 12 weeks determined that many of the double-blind, controlled studies showed no significantbenefit for 10% strontium chloride or 8% stron-tium acetate toothpastes as compared with regu-lar fluoride toothpaste.70
More recently, a novel technology using argi-nine, an amino acid naturally found in saliva, andcalcium carbonate has been introduced to controldentinal hypersensitivity.26,69 The arginine in salivaitself is incapable of providing quick plugging andsealing of open dentinal tubules; however, a newtechnology delivering arginine and calcium car-bonate in dental prophylaxis paste and toothpastehas research that supports its efficacy. The tech-nology of 8% arginine was extensively investigatedusing atomic force microscopy, confocal laserscanning microscopy, electron spectroscopy, andhigh-resolution scanning electron microscopy.Results show that the formed sealing plugs are
CHAPTER 9 Dentin Hypersensitivity
168
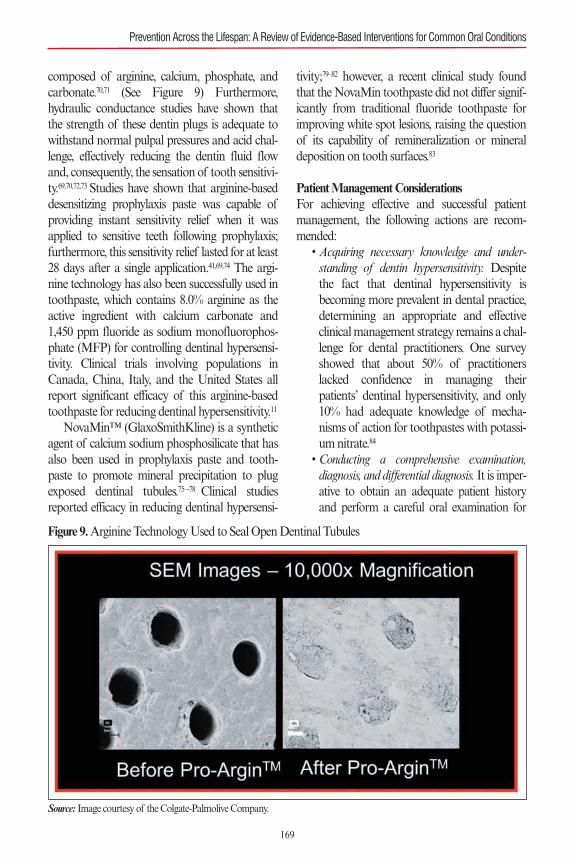
composed of arginine, calcium, phosphate, andcarbonate.70,71 (See Figure 9) Furthermore,hydraulic conductance studies have shown thatthe strength of these dentin plugs is adequate towithstand normal pulpal pressures and acid chal-lenge, effectively reducing the dentin fluid flowand, consequently, the sensation of tooth sensitivi-ty.69,70,72,73 Studies have shown that arginine-baseddesensitizing prophylaxis paste was capable ofproviding instant sensitivity relief when it wasapplied to sensitive teeth following prophylaxis;furthermore, this sensitivity relief lasted for at least28 days after a single application.41,69,74 The argi-nine technology has also been successfully used intoothpaste, which contains 8.0% arginine as theactive ingredient with calcium carbonate and1,450 ppm fluoride as sodium monofluorophos-phate (MFP) for controlling dentinal hypersensi-tivity. Clinical trials involving populations inCanada, China, Italy, and the United States allreport significant efficacy of this arginine-basedtoothpaste for reducing dentinal hypersensitivity.11
NovaMin™ (GlaxoSmithKline) is a syntheticagent of calcium sodium phosphosilicate that hasalso been used in prophylaxis paste and tooth-paste to promote mineral precipitation to plugexposed dentinal tubules.75–-78 Clinical studiesreported efficacy in reducing dentinal hypersensi-
tivity;79–82 however, a recent clinical study foundthat the NovaMin toothpaste did not differ signif-icantly from traditional fluoride toothpaste forimproving white spot lesions, raising the questionof its capability of remineralization or mineraldeposition on tooth surfaces.83
Patient Management ConsiderationsFor achieving effective and successful patientmanagement, the following actions are recom-mended:
• Acquiring necessary knowledge and under-standing of dentin hypersensitivity. Despitethe fact that dentinal hypersensitivity isbecoming more prevalent in dental practice,determining an appropriate and effectiveclinical management strategy remains a chal-lenge for dental practitioners. One surveyshowed that about 50% of practitionerslacked confidence in managing theirpatients’ dentinal hypersensitivity, and only10% had adequate knowledge of mecha-nisms of action for toothpastes with potassi-um nitrate.84
• Conducting a comprehensive examination,diagnosis, and differential diagnosis. It is imper-ative to obtain an adequate patient historyand perform a careful oral examination for
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
169
Figure 9.Arginine Technology Used to Seal Open Dentinal Tubules
Source: Image courtesy of the Colgate-Palmolive Company.
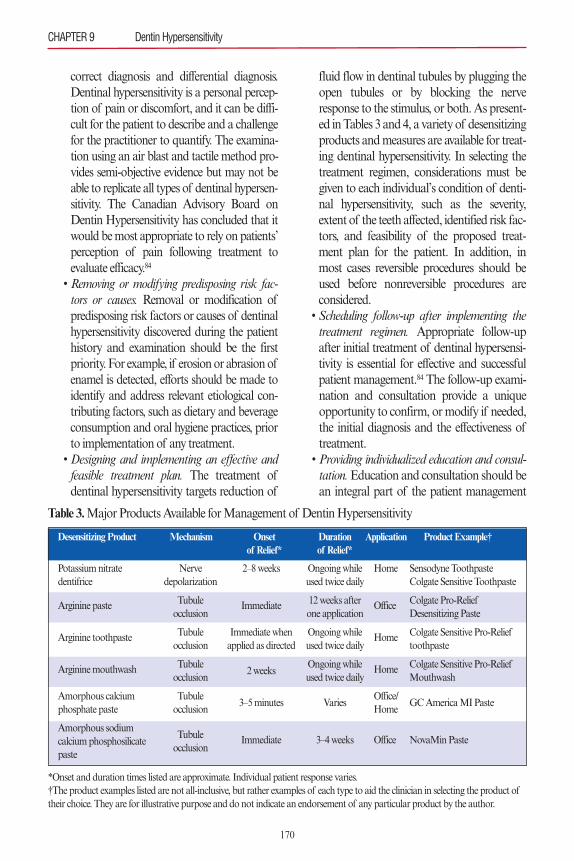
correct diagnosis and differential diagnosis.Dentinal hypersensitivity is a personal percep-tion of pain or discomfort, and it can be diffi-cult for the patient to describe and a challengefor the practitioner to quantify. The examina-tion using an air blast and tactile method pro-vides semi-objective evidence but may not beable to replicate all types of dentinal hypersen-sitivity. The Canadian Advisory Board onDentin Hypersensitivity has concluded that itwould be most appropriate to rely on patients’perception of pain following treatment toevaluate efficacy.84
• Removing or modifying predisposing risk fac-tors or causes. Removal or modification ofpredisposing risk factors or causes of dentinalhypersensitivity discovered during the patienthistory and examination should be the firstpriority. For example, if erosion or abrasion ofenamel is detected, efforts should be made toidentify and address relevant etiological con-tributing factors, such as dietary and beverageconsumption and oral hygiene practices, priorto implementation of any treatment.
• Designing and implementing an effective andfeasible treatment plan. The treatment ofdentinal hypersensitivity targets reduction of
fluid flow in dentinal tubules by plugging theopen tubules or by blocking the nerveresponse to the stimulus, or both. As present-ed in Tables 3 and 4, a variety of desensitizingproducts and measures are available for treat-ing dentinal hypersensitivity. In selecting thetreatment regimen, considerations must begiven to each individual’s condition of denti-nal hypersensitivity, such as the severity,extent of the teeth affected, identified risk fac-tors, and feasibility of the proposed treat-ment plan for the patient. In addition, inmost cases reversible procedures should beused before nonreversible procedures areconsidered.
• Scheduling follow-up after implementing thetreatment regimen. Appropriate follow-upafter initial treatment of dentinal hypersensi-tivity is essential for effective and successfulpatient management.84 The follow-up exami-nation and consultation provide a uniqueopportunity to confirm, or modify if needed,the initial diagnosis and the effectiveness oftreatment.
• Providing individualized education and consul-tation. Education and consultation should bean integral part of the patient management
CHAPTER 9 Dentin Hypersensitivity
170
*Onset and duration times listed are approximate. Individual patient response varies.†The product examples listed are not all-inclusive, but rather examples of each type to aid the clinician in selecting the product oftheir choice. They are for illustrative purpose and do not indicate an endorsement of any particular product by the author.
Table 3.Major Products Available for Management of Dentin Hypersensitivity
Desensitizing Product Mechanism Onset Duration Application Product Example†of Relief* of Relief*
Potassium nitrate dentifrice
Arginine paste
Arginine toothpaste
Arginine mouthwash
Amorphous calcium phosphate paste
Amorphous sodium calcium phosphosilicate paste
Nerve depolarization
Tubule occlusion
Tubule occlusion
Tubule occlusion
Tubule occlusion
Tubule occlusion
2–8 weeks
Immediate
Immediate whenapplied as directed
2 weeks
3–5 minutes
Immediate
Ongoing whileused twice daily
12 weeks afterone application
Ongoing whileused twice daily
Ongoing whileused twice daily
Varies
3–4 weeks
Home
Office
Home
Home
Office/Home
Office
Sensodyne ToothpasteColgate Sensitive Toothpaste
Colgate Pro-Relief Desensitizing Paste
Colgate Sensitive Pro-Relieftoothpaste
Colgate Sensitive Pro-ReliefMouthwash
GC America MI Paste
NovaMin Paste
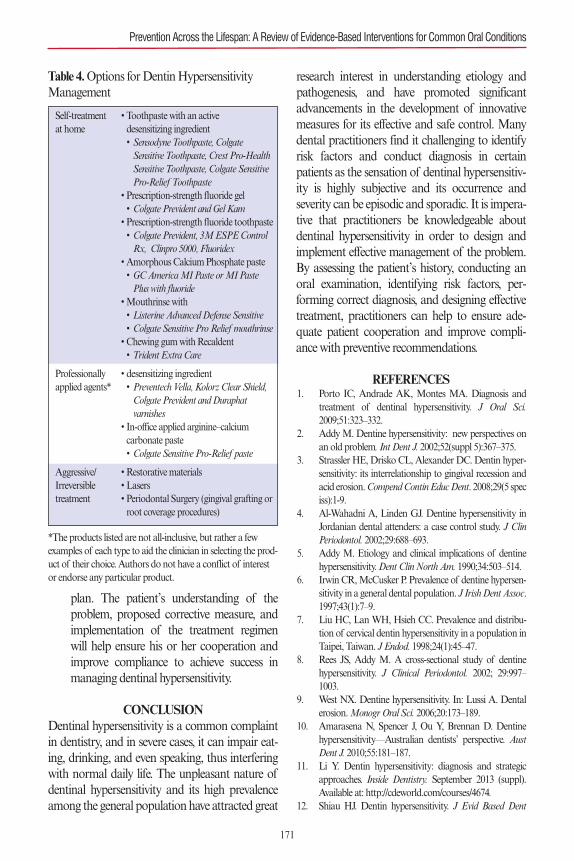
plan. The patient’s understanding of theproblem, proposed corrective measure, andimplementation of the treatment regimenwill help ensure his or her cooperation andimprove compliance to achieve success inmanaging dentinal hypersensitivity.
CONCLUSION Dentinal hypersensitivity is a common complaintin dentistry, and in severe cases, it can impair eat-ing, drinking, and even speaking, thus interferingwith normal daily life. The unpleasant nature ofdentinal hypersensitivity and its high prevalenceamong the general population have attracted great
research interest in understanding etiology andpathogenesis, and have promoted significantadvancements in the development of innovativemeasures for its effective and safe control. Manydental practitioners find it challenging to identifyrisk factors and conduct diagnosis in certainpatients as the sensation of dentinal hypersensitiv-ity is highly subjective and its occurrence andseverity can be episodic and sporadic. It is impera-tive that practitioners be knowledgeable aboutdentinal hypersensitivity in order to design andimplement effective management of the problem.By assessing the patient’s history, conducting anoral examination, identifying risk factors, per-forming correct diagnosis, and designing effectivetreatment, practitioners can help to ensure ade-quate patient cooperation and improve compli-ance with preventive recommendations.
REFERENCES1. Porto IC, Andrade AK, Montes MA. Diagnosis and
treatment of dentinal hypersensitivity. J Oral Sci.2009;51:323–332.
2. Addy M. Dentine hypersensitivity: new perspectives onan old problem. Int Dent J. 2002;52(suppl 5):367–375.
3. Strassler HE, Drisko CL, Alexander DC. Dentin hyper-sensitivity: its interrelationship to gingival recession andacid erosion. CompendContin Educ Dent. 2008;29(5 speciss):1-9.
4. Al-Wahadni A, Linden GJ. Dentine hypersensitivity inJordanian dental attenders: a case control study. J ClinPeriodontol. 2002;29:688–693.
5. Addy M. Etiology and clinical implications of dentinehypersensitivity. Dent Clin North Am. 1990;34:503–514.
6. Irwin CR, McCusker P. Prevalence of dentine hypersen-sitivity in a general dental population. J Irish Dent Assoc.1997;43(1):7–9.
7. Liu HC, Lan WH, Hsieh CC. Prevalence and distribu-tion of cervical dentin hypersensitivity in a population inTaipei, Taiwan. J Endod. 1998;24(1):45–47.
8. Rees JS, Addy M. A cross-sectional study of dentinehypersensitivity. J Clinical Periodontol. 2002; 29:997–1003.
9. West NX. Dentine hypersensitivity. In: Lussi A. Dentalerosion. Monogr Oral Sci. 2006;20:173–189.
10. Amarasena N, Spencer J, Ou Y, Brennan D. Dentinehypersensitivity—Australian dentists’ perspective. AustDent J. 2010;55:181–187.
11. Li Y. Dentin hypersensitivity: diagnosis and strategicapproaches. Inside Dentistry. September 2013 (suppl).Available at: http://cdeworld.com/courses/4674.
12. Shiau HJ. Dentin hypersensitivity. J Evid Based Dent
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
171
Table 4.Options for Dentin HypersensitivityManagement
Self-treatment • Toothpaste with an activeat home desensitizing ingredient
• Sensodyne Toothpaste, Colgate Sensitive Toothpaste, Crest Pro-Health Sensitive Toothpaste, Colgate Sensitive Pro-Relief Toothpaste
• Prescription-strength fluoride gel • Colgate Prevident and Gel Kam
• Prescription-strength fluoride toothpaste • Colgate Prevident, 3M ESPE Control Rx, Clinpro 5000, Fluoridex
• Amorphous Calcium Phosphate paste • GC America MI Paste or MI Paste Plus with fluoride
• Mouthrinse with • Listerine Advanced Defense Sensitive• Colgate Sensitive Pro Relief mouthrinse
• Chewing gum with Recaldent • Trident Extra Care
Professionally • desensitizing ingredientapplied agents* • Preventech Vella, Kolorz Clear Shield,
Colgate Prevident and Duraphat varnishes
• In-office applied arginine–calcium carbonate paste • Colgate Sensitive Pro-Relief paste
Aggressive/ • Restorative materialsIrreversible • Laserstreatment • Periodontal Surgery (gingival grafting or
root coverage procedures)
*The products listed are not all-inclusive, but rather a fewexamples of each type to aid the clinician in selecting the prod-uct of their choice. Authors do not have a conflict of interestor endorse any particular product.
Practice. 2012;12(3 suppl);220–228.13. Scaramucci T, de Almeida Anfe TE, da Silva Ferreira S,
Frias AC, Sobral MAP. Investigation of the prevalence,clinical features, and risk factors of dentin hypersensitivi-ty in a selected Brazilian population. Clin Oral Investig.2014;18:651–657.
14. Haneet RK, Vandana LK. Prevalence of dentinalhypersensitivity and study of associated factors: a cross-sectional study based on the general dental populationof Davangere, Karnataka, India. Int Dent J. 2015 Nov19. doi: 10.1111/idj.12206. [Epub ahead of print.]
15. Daniel SJ, Harfst SA, Wilder RS. Dental Hygiene Con-cepts, Cases, and Competencies. 2nd ed. St. Louis, MO:Mosby Elsevier; 2008:623–637.
16. Addy M, Mostafa P, Newcombe RG. Dentine hypersen-sitivity: the distribution of recession, sensitivity andplaque. J Dent. 1987;15:242–248.
17. Drisko CH. Dentine hypersensitivity—dental hygieneand periodontal considerations. Int Dent J. 2002;52:385–393.
18. Pashley DH, Tay FR, Haywood VB, Collins MA,Drisko CL. Consensus-based recommendations for thediagnosis and management of dentin hypersensitivity.Inside Dentistry. 2008;4(special issue):1–7.
19. Kramer IRH. The relationship between dentine sensitiv-ity and movements in the contents of dentinal tubules.Br Den J. 1955; 98:391–392.
20. Brännström M. The elicitation of pain in human den-tine and pulp by chemical stimuli. Arch Oral Biol.1962;7:59–62.
21. Matthews B, Vongsavan N. Interactions between neuraland hydrodynamic mechanisms in dentine and pulp.Arch Oral Biol. 1994;39(suppl):87S–95S.
22. Brännström M. In: Anderson DJ, ed. Sensory Mecha-nisms in Dentine. Oxford, England: Pergamon Press;1963.
23. Leonard RH Jr, Bentley C, Eagle JC, Garland GE,Knight MC, Phillips C. Nightguard vital bleaching: along-term study on efficacy, shade retention, side effects,and patients’ perceptions. J Esthet Restor Dent.2001;13:357–369.
24. Li Y. The safety of peroxide-containing at-home toothwhiteners. Compend Contin Educ Dent. 2003;24:384–389.
25. Li Y. Safety controversies in tooth bleaching. Dent ClinNorth Am. 2011;55:255–263.
26. Cummins D. Dentin hypersensitivity: from diagnosis toa breakthrough therapy for everyday sensitivity relief. JClin Dent. 2009;20(special issue):1–9.
27. Drisko C. Oral hygiene and periodontal considerationsin preventing and managing dentine hypersensitivity. IntDent J. 2007;57:399–393.
28. Smith BGN. Toothwear: aetiology and diagnosis. DentUpdate. 1989;16:204–212.
29. Smith BGN, Knight JK. A comparison of patterns oftoothwear with the etiological factors. Br Dent J.
1984;157:16–19.30. Absi EG, Addy M, Adams D. Dentine hypersensitivi-
ty—the effect of toothbrushing and dietary compoundson dentine in vitro: an SEM study. J Oral Rehabil.1992;19:101–110.
31. Wolff M. Science behind the sensitivity: science-support-ed therapy for the effective relief of dentin hypersensitivi-ty. J Clin Dent. 2009;20(special issue):23–31.
32. Davis WB, Winter PJ. The effect of abrasion on enameland dentine after exposure to dietary acids. Br Dent J.1980;148:253–256.
33. Trushkowsky RD, Garcia-Godoy F. Dentin hypersensi-tivity: differential diagnosis, tests, and etiology. CompendContin Educ Dent. 2014:99–103.
34. Li Y, Greenwall L. Safety issues of tooth whitening usingperoxide-based materials. Br Dent J. 2013;215:29–34.
35. West NX, Lussi A, Seong J, Hellwig E. Dentin hypersen-sitivity: pain mechanisms and aetiology of exposed cer-vical dentin. Clin Oral Investig. 2013;17(suppl 1):S9–S19.
36. Holland GR, Narhi MN, Addy M, Gangarosa L,Orchardson R. Guidelines for the design and conduct ofclinical trials on dentine hypersensitivity. J Clin Periodon-tol. 1997;24:808–813.
37. Ajcharanukul O, Kraivaphan P, Wanachantararak S,Vongsavan N, Matthews B. Effects of potassium ions ondentine sensitivity in man. Arch Oral Biol. 2007;52:632–639.
38. Clark GE, Troullos ES. Designing hypersensitivity stud-ies. Dent Clin North Am. 1990;34:531–533.
39. Schiff T, Dotson M, Cohen S, De Vizio W, McCool J,Volpe A. Efficacy of a dentifrice containing potassiumnitrate, soluble pyrophosphate, PVM/MA copolymer,and sodium fluoride on dentinal hypersensitivity: atwelve-week clinical study. J Clin Dent. 1994;5(specialissue):87–92.
40. Gillam DG, Bulman JS, Jackson RJ, Newman HN. Effi-cacy of a potassium nitrate mouthwash in alleviatingcervical dentine. J Clin Periodontol. 1996;23:993–997.
41. Li Y, Lee S, Mateo LR, Delgado E, Zhang YB. Com-parison of clinical efficacy of three professionally appliedpastes on immediate and sustained reduction of dentinhypersensitivity. Compend Contin Educ Dent. 2013;34:1–7.
42. Ide M. The differential diagnosis of sensitive teeth. DentUpdate. 1998;25:462–466.
43. Gernhardt C. How valid and applicable are current diag-nostic criteria and assessment methods for dentin hyper-sensitivity? An overview. Clin Oral Investig. 2013;17(suppl 1):S31–S40.
44. Cameron CE. Cracked-tooth syndrome. J Am DentAssoc. 1964;68:405–411.
45. Ehrmann EH, Tyas MT. Cracked tooth syndrome: diag-nosis, treatment and correlation between symptoms andpost-extraction findings. Aust Dent J. 1990;35:105–112.
46. Ellis SG. Incomplete tooth fracture-proposal for a newdefinition. Br Dent J. 2001;190:424–428.
CHAPTER 9 Dentin Hypersensitivity
172
173
47. Rosen H. Cracked tooth syndrome. J Prosthet Dent.1982;47:36–43.
48. Twetman S. The evidence base for professional and self-care prevention—caries, erosion and sensitivity. BMCOral Health. 2015;15(suppl 1):S4.
49. Mantzourani M, Sharma D. Dentine sensitivity: past,present and future. J Dent. 2013;41(suppl 4):S3–S17.
50. Peacock JM, Orchardson R. Action potential conduc-tion block of nerves in vitro by potassium citrate, potas-sium tartrate and potassium oxalate. J Clin Periodontol.1999; 26:33–37.
51. Poulsen S, Errboe M, Lescay Mevil Y, Glenny AM.Potassium containing toothpastes for dentine hypersen-sitivity. Cochrane Database Syst Rev. 2006;3:CD001476.
52. Markowitz K, Bilotto G, Kim S. Decreasing intradentalnerve activity in the cat with potassium and divalentcations. Arch Oral Biol. 1991;36:1–7.
53. Nagata T, Ishida H, Shinohara H, et al. Clinical evalua-tion of a potassium nitrate dentifrice for the treatment ofdentinal hypersensitivity. J Clin Periodontol. 1994;21:217–221.
54. Schwarz F, Arweiler N, Georg T, Reich E. Desensitizingeffects of an Er:YAG laser on hypersensitive dentine. JClin Periodontol. 2002;29:211–215.
55. Birang R, Poursamimi J, Gutknecht N, Lampert F, MirM. Comparative evaluation of the effects of Nd:YAGand Er:YAG laser in dentin hypersensitivity treatment.Lasers Med Sci. 2007;22:21–24.
56. Sgolastra F, Petrucci A, Severino M, Gatto R, MonacoA. Lasers for the treatment of dentin hypersensitivity: ameta-analysis. J Dent Res. 2013;92:492–499.
57. Douglas de Oliveira DW, Oliveira-Ferreira F, FlechaOD, Gonçalves PF. Is surgical root coverage effective forthe treatment of cervical dentin hypersensitivity? A sys-tematic review. J Periodontol. 2013;84:295–306.
58. Cunha-Cruz J, Stout JR, Heaton LJ, Wataha JC; North-west PRECEDENT.Dentin hypersensitivity and oxalates:a systematic review. J Dent Res. 2011;90:304–310.
59. Poulsen S. Available evidence does not support use ofoxalates for dentine hypersensitivity. Evid Based Dent.2011;12:47.
60. Reynolds EC, Cain CJ, Webber FL, et al. Anticario-genicity of calcium phosphate complexes of trypticcasein phosphopeptides in the rat. J Dent Res.1995;74:1272–2379.
61. Reynolds EC. Anticariogenic complexes of amorphouscalcium phosphate stabilized by casein phosphopep-tides: a review. Spec Care Dentist. 1998;18:8–16.
62. Suge T, Ishikawa K, Kawasaki A, et al. Calcium phos-phate precipitation method for the treatment of dentinhypersensitivity. Am J Dent. 2002;15:220–226.
63. Kowalczyk A, Botuli�ski B, Jaworska M, et al. Evalua-tion of the product based on Recaldent technology inthe treatment of dentin hypersensitivity. Adv Med Sci.2006;51(suppl 1):40–42.
64. Martinez-Mier EA. Casein phosphopeptide used in
toothpaste suggests an efficacy similar to toothpastecontaining sodium monofluorophosphate for caries pre-vention. J Evid Based Dent Pract. 2010;10:154–155.
65. Azarpazhooh A, Limeback H. Clinical efficacy of caseinderivatives: a systematic review of the literature. J AmDent Assoc. 2008;139:915–924.
66. Markowitz K. The original desensitizers: strontium andpotassium salts. J Clin Dent. 2009;20(special issue):145–151.
67. Zappa U. Self-applied treatments in the management ofdentine hypersensitivity. Arch Oral Biol. 1994;39(suppl):107S–112S.
68. Jackson RJ. Potential treatment modalities for dentinehypersensitivity: home use products. In: Addy M,Embery G, Edgar WM, Orchardson R, eds. Tooth Wearand Sensitivity. Clinical Advances in Restorative Dentistry.London, England: Martin Dunitz, 2000;327–338.
69. Cummins D. Recent advances in dentin hypersensitivity:Clinically proven treatments for instant and lasting sensi-tivity relief. Am J Dent. 2010;23(special issue A):3A–13A.
70. Petrou I, Heu R, Stranick M, et al. A breakthrough ther-apy for dentin hypersensitivity: how dental products con-taining 8% arginine and calcium carbonate work todeliver effective relief of sensitive teeth. J Clin Dent.2009;20(special issue):23–31.
71. Lavender SA, Petrou I, Heu R, et al. Mode of actionstudies on a new desensitizing dentifrice containing 8.0%arginine, a high cleaning calcium carbonate system and1450 ppm fluoride. Am J Dent. 2010;23(special issueA):14A–19A.
72. Hamlin D, Williams KP, Delgado E, Zhang YP, DeVi-zio W, Mateo LR. Clinical evaluation of the efficacy of adesensitizing paste containing 8% arginine and calciumcarbonate for the in-office relief of dentin hypersensitivi-ty associated with dental prophylaxis. Am J Dent.2009;22(special issue A):16A–20A.
73. Panagakos F, Schiff T, Guignon A. Dentin hypersensi-tivity: effective treatment with an in-office desensitizingpaste containing 8% arginine and calcium carbonate.Am J Dent. 2009;22(special issue A):3A–7A.
74. Kleinberg I. Sensistat. A new saliva-based compositionfor simple and effective treatment of dentinal sensitivitypain. Dent Today. 2002:21:42–47.
75. Earl JS, Leary RK, Muller KH, Langford RM,Greenspan DC. Physical and chemical characterizationof dentin surface following treatment with NovaMintechnology. J Clin Dent. 2011;22:62–67.
76. Layer TM. Development of a fluoridated, daily-usetoothpaste containing NovaMin technology for thetreatment of dentin hypersensitivity. J Clin Dent.2011;22:59–61.
77. Chen CL, Parolia A, Pau A, Celerino de Moraes PortoIC. Comparative evaluation of the effectiveness of desen-sitizing agents in dentine tubule occlusion using scanningelectron microscopy. Aust Dent J. 2015;60:65–72.
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions

78. Jena A, Shashirekha G. Comparison of efficacy of threedifferent desensitizing agents for in-office relief of dentinhypersensitivity: A 4 weeks clinical study. J ConservDent. 2015;18:389–393.
79. Litkowski L, Greenspan DC. A clinical study of theeffect of calcium sodium phosphosilicate on dentinhypersensitivity—proof of principle. J Clin Dent.2010;21:77–81.
80. Salian S, Thakur S, Kulkarni S, LaTorre G. A random-ized controlled clinical study evaluating the efficacy oftwo desensitizing dentifrices. J Clin Dent. 2010;21:82–87.
81. Sharma N, Roy S, Kakar A, Greenspan DC, Scott R. Aclinical study comparing oral formulations containing7.5% calcium sodium phosphosilicate (NovaMin), 5%potassium nitrate, and 0.4% stannous fluoride for the
management of dentin hypersensitivity. J Clin Dent.2010;21:88–92.
82. Gendreau L, Barlow AP, Mason SC. Overview of theclinical evidence for the use of NovaMin in providingrelief from the pain of dentin hypersensitivity. J ClinDent. 2011;22:90–95.
83. Hoffman DA, Clark AE, Rody WJ Jr, McGorray SP,Wheeler TT. A prospective randomized clinical trial intothe capacity of a toothpaste containing NovaMin toprevent white spot lesions and gingivitis during ortho-dontic treatment. Prog Orthod. 2015;16:25.
84. Canadian Advisory Board on Dentin Hypersensitivity.Consensus-based recommendations for the diagnosisand management of dentin hypersensitivity. J Can DentAssoc. 2003;69:221–226.
CHAPTER 9 Dentin Hypersensitivity
174

PART 1: OVERVIEW OF DRY MOUTH
The importance of saliva in our daily activities ofliving is often taken for granted. Saliva performs amyriad of functions essential to oral and systemichealth and well-being. When the quality or quan-tity of saliva is altered, it is likely that individualsexperience dry mouth. Dry mouth can have aprofound impact on both quality of life and oralhealth status.1–3 Saliva is pivotal to maintainingoverall function of the oral cavity, which can becategorized into three key areas: (1) swallowing,enjoyment, and digestion of food; (2) maintain-ing and protecting the function and physicalstructures of the oral cavity; and (3) maintainingthe equilibrium of the oral microflora.4 Patientsexperiencing dry mouth often show signs of taste disturbances (dysgeusia); difficulties withchewing, swallowing (dysphagia), and speaking(dysarthria);5 and a range of oral diseases, includ-ing ill-fitting dentures,6 dental caries, oral candidi-asis, periodontal disease, halitosis, and burningmouth syndrome.7 This chapter provides anoverview of dry mouth and associated etiologies,and discusses evidence-based prevention andmanagement strategies.
PATHOGENESIS OF DRY MOUTHWhat Is Dry Mouth?Dry mouth is a complex condition. Clinical diag-nosis would be straightforward if, in fact, a person’sreport of dry mouth paralleled his or her physicalsalivary output. However, much research hasshown that the two are not necessarily concurrent.8
Dry mouth presents in two forms. Xerostomia is thesubjective self-reported sensation of dry mouth,and salivary gland hypofunction (SGH) is the clini-cally observed condition of lower-than-normal sali-vary output, which is typically assessed usingsialometry. Alterations in the salivary compositionfurther add to the complexity of dry mouth.9
The bulk (~90%) of salivary secretion is pro-duced by three bilateral pairs of major salivaryglands (parotid, submandibular, and sublingual).The remaining salivary secretion (~10%) is pro-duced in the hundreds of minor salivary glandslocated throughout the mucosal surfaces of theoral cavity, which are important for lubrication andprotection of the oral mucosa due to their mucoussecretions. The major and minor salivary glands aremade of acinar cells, which are responsible for gen-erating fluid and transporting electrolytes and pro-teins. Each gland makes a compositionally distinctcontribution to the saliva (see Figure 1).Healthy adults produce between 0.5 and 1.5 L
of saliva per day.10 Salivary secretion occurs inresponse to autonomic stimulation primarily underthe parasympathetic pathway (see Figure 2).Parasympathetic (cholinergic) simulation results inhigh-volume, watery saliva. Sympathetic (adrener-gic) stimulation results in small-volume, highly vis-cous saliva. When salivary fluid production isdecreased by about 50%, a person begins to experi-ence symptoms of dry mouth.11
175
Dry Mouth
Chapter 10
Sharon Compton and Minn Yoon
Figure 1. Control of Salivary Secretion
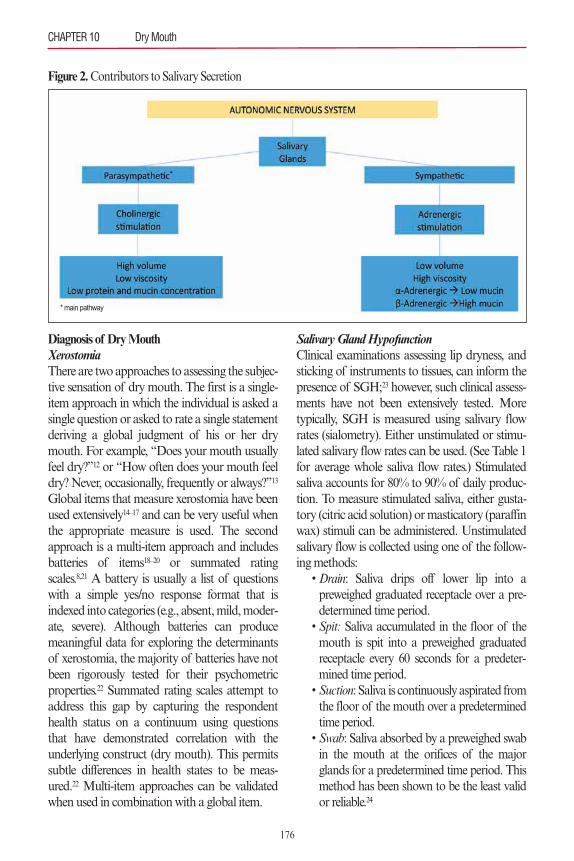
Diagnosis of Dry MouthXerostomiaThere are two approaches to assessing the subjec-tive sensation of dry mouth. The first is a single-item approach in which the individual is asked asingle question or asked to rate a single statementderiving a global judgment of his or her drymouth. For example, “Does your mouth usuallyfeel dry?”12 or “How often does your mouth feeldry? Never, occasionally, frequently or always?”13
Global items that measure xerostomia have beenused extensively14–17 and can be very useful whenthe appropriate measure is used. The secondapproach is a multi-item approach and includesbatteries of items18–20 or summated ratingscales.8,21 A battery is usually a list of questionswith a simple yes/no response format that isindexed into categories (e.g., absent, mild, moder-ate, severe). Although batteries can producemeaningful data for exploring the determinantsof xerostomia, the majority of batteries have notbeen rigorously tested for their psychometricproperties.22 Summated rating scales attempt toaddress this gap by capturing the respondenthealth status on a continuum using questionsthat have demonstrated correlation with theunderlying construct (dry mouth). This permitssubtle differences in health states to be meas-ured.22 Multi-item approaches can be validatedwhen used in combination with a global item.
Salivary Gland HypofunctionClinical examinations assessing lip dryness, andsticking of instruments to tissues, can inform thepresence of SGH;23 however, such clinical assess-ments have not been extensively tested. Moretypically, SGH is measured using salivary flowrates (sialometry). Either unstimulated or stimu-lated salivary flow rates can be used. (See Table 1for average whole saliva flow rates.) Stimulatedsaliva accounts for 80% to 90% of daily produc-tion. To measure stimulated saliva, either gusta-tory (citric acid solution) or masticatory (paraffinwax) stimuli can be administered. Unstimulatedsalivary flow is collected using one of the follow-ing methods:
• Drain: Saliva drips off lower lip into apreweighed graduated receptacle over a pre-determined time period.
• Spit: Saliva accumulated in the floor of themouth is spit into a preweighed graduatedreceptacle every 60 seconds for a predeter-mined time period.
• Suction: Saliva is continuously aspirated fromthe floor of the mouth over a predeterminedtime period.
• Swab: Saliva absorbed by a preweighed swabin the mouth at the orifices of the majorglands for a predetermined time period. Thismethod has been shown to be the least validor reliable.24
CHAPTER 10 Dry Mouth
176
Figure 2. Contributors to Salivary Secretion
* main pathway

EPIDEMIOLOGY OF DRY MOUTHObtaining a representative picture of xerostomiaor SGH prevalence is difficult because ofmethodological discrepancies and variances indiagnostic criteria. Further, xerostomia and SGHare not concurrent, only occurring in approxi-mately one-sixth of those with either condition or6% of the population.8 The prevalence of xeros-tomia is approximately 20% overall,25 increasingto approximately 30% of the population aged 65years and older.26 The population most studiedfor dry mouth is older adults. A limited numberof studies have assessed the prevalence of drymouth in younger populations.27 In the olderadult population, as health becomes more com-promised, a higher prevalence of dry mouth isexperienced as compared with the general pub-lic.28 (See Table 2 for prevalence rates.)
ETIOLOGY OF DRY MOUTHAgeThe deleterious effects of dry mouth are most fre-quently seen in the older adult population. Thepaucity of reports on the prevalence of xerosto-mia and SGH in younger populations createschallenges in distinguishing the true impact of ageon dry mouth.27 A cross-sectional study of stimu-lated whole saliva from three different age groupsfound that older adults (> 70 years) did have a sig-nificantly decreased flow.29,30 No differences werefound between young (20 to 30 years) and mid-dle-aged (40 to 50 years) adults, but significantdifferences between the young and old and the
middle-aged and old were found.30 Therefore,much of the literature currently promotes the ideathat the prevalence of xerostomia and SGHincreases with age but this may be more stronglyassociated with medication use and health status.Physiologically, with aging, the number of aci-
nar cells is reduced and replaced by fibrous andfatty tissue, altering the composition of saliva.There is a 30% to 40% decrease in the number ofacinar cells within salivary glands between ages 34and 75+ years.31The primary effect of this changeis thought to result from disruption of theparasympathetic pathway (see Figure 2).29 Thispathway is also the one most affected bypolypharmacy (via anticholinergics).
MedicationOne of the most common causes of dry mouth isthe use of xerogenic medications. As people age, itis common for them to be taking multiple med-ications, of which over 1,000 are known to con-tribute to dry mouth.32 The primary path ofaction is through anticholinergic activity, resultingin a reduction of salivary flow. Increasing thenumber and dosage of anticholinergic drugsbeing taken (anticholinergic burden) was found toincrease the likelihood and severity of drymouth.33,34 In a longitudinal study, it was foundthat the prevalence and incidence of xerostomiawas strongly associated with medication expo-sure.35 Furthermore, there is a strong correlationbetween number of diseases, medications, andxerostomia.36,37
Systemic DisordersMany systemic conditions are known to cause orare associated with varying degrees of dry mouth;however, one of the most common autoimmunediseases, Sjögren’s syndrome, almost alwaysresults in both xerostomia and SGH. In the Unit-ed States, an estimated 0.4 million to 3.1 millionadults are living with Sjögren’s syndrome.38 Dis-turbances in salivary output arising from this syn-drome can cause difficulty chewing or swallowingand increase the risk for oral infections.39
Other systemic conditions frequently associat-ed with dry mouth symptoms include diabetes
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
177
Table 1. Flow Rates of Whole Saliva
Normal Hyposalivation
Unstimulated 0.3–0.5 mL/min < 0.12-0.16 mL/min
Stimulated 1.0–3.0 mL/min < 0.5 mL/min
Source: Adapted from Oral Surg Oral Med Oral PatholOral Radiol Endod. 2012;114:52–60.28
Table 2. Prevalence of Xerostomia and Salivary Gland Hypofunction (SGH)
Population Xerostomia SGH
General public 5.5–39% —Community dwelling 17–40% 15–23%Institutionalized 20–72% 17–50%
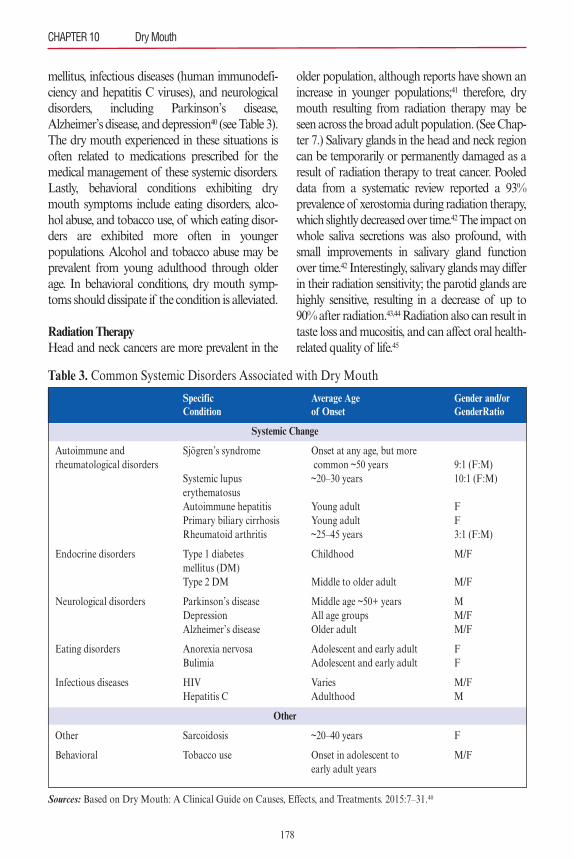
mellitus, infectious diseases (human immunodefi-ciency and hepatitis C viruses), and neurologicaldisorders, including Parkinson’s disease,Alzheimer’s disease, and depression40 (see Table 3).The dry mouth experienced in these situations isoften related to medications prescribed for themedical management of these systemic disorders.Lastly, behavioral conditions exhibiting drymouth symptoms include eating disorders, alco-hol abuse, and tobacco use, of which eating disor-ders are exhibited more often in youngerpopulations. Alcohol and tobacco abuse may beprevalent from young adulthood through olderage. In behavioral conditions, dry mouth symp-toms should dissipate if the condition is alleviated.
Radiation TherapyHead and neck cancers are more prevalent in the
older population, although reports have shown anincrease in younger populations;41 therefore, drymouth resulting from radiation therapy may beseen across the broad adult population. (See Chap-ter 7.) Salivary glands in the head and neck regioncan be temporarily or permanently damaged as aresult of radiation therapy to treat cancer. Pooleddata from a systematic review reported a 93%prevalence of xerostomia during radiation therapy,which slightly decreased over time.42The impact onwhole saliva secretions was also profound, withsmall improvements in salivary gland functionover time.42 Interestingly, salivary glands may differin their radiation sensitivity; the parotid glands arehighly sensitive, resulting in a decrease of up to90% after radiation.43,44Radiation also can result intaste loss and mucositis, and can affect oral health-related quality of life.45
CHAPTER 10 Dry Mouth
178
Table 3. Common Systemic Disorders Associated with Dry Mouth
Sources: Based on Dry Mouth: A Clinical Guide on Causes, Effects, and Treatments. 2015:7–31.40
Specific Average Age Gender and/or Condition of Onset GenderRatio
Systemic Change
Autoimmune and Sjögren’s syndrome Onset at any age, but morerheumatological disorders common ~50 years 9:1 (F:M)
Systemic lupus ~20–30 years 10:1 (F:M)erythematosusAutoimmune hepatitis Young adult FPrimary biliary cirrhosis Young adult FRheumatoid arthritis ~25–45 years 3:1 (F:M)
Endocrine disorders Type 1 diabetes Childhood M/Fmellitus (DM)Type 2 DM Middle to older adult M/F
Neurological disorders Parkinson’s disease Middle age ~50+ years MDepression All age groups M/FAlzheimer’s disease Older adult M/F
Eating disorders Anorexia nervosa Adolescent and early adult FBulimia Adolescent and early adult F
Infectious diseases HIV Varies M/FHepatitis C Adulthood M
Other
Other Sarcoidosis ~20–40 years F
Behavioral Tobacco use Onset in adolescent to M/Fearly adult years

PART 2: PATIENT MANAGEMENT
AND INTERVENTIONSWhen considering an approach to patient man-agement and prevention for patients experiencingdry mouth, the clinician must determine whetherany salivary gland function remains. If there issome salivary gland function, the next step wouldbe to determine the underlying cause of drymouth. The dominant contributors to dry mouthare medications, systemic or behavioral condi-tions, and radiation therapy. Once the cliniciandetermines the underlying cause, a managementstrategy can be devised. The management strategymay include changing the contributing factors orpreventing the intensification of the dry mouthcondition, or both. This section addresses thethree main areas of care for patients with drymouth, namely (1) preventive strategies, (2) thera-peutic interventions, and (3) patient managementstrategies.
PREVENTIVE STRATEGIESPreventive Strategies in Dry Mouth Resulting from Radiation TherapyUntil the more recent widespread use of intensity-modulated radiation therapy (IMRT), patientstreated for head and neck cancer (HNC) with radi-ation therapy experienced severe damage to thesalivary glands, which often resulted in permanentdry mouth. When patients are about to undergoradiation therapy for HNC treatment, a few pre-ventive strategies exist that may limit or decreasethe likelihood of extreme postradiation dry mouth.The strategies include IMRT, three-dimensional(3D) conformal radiation therapy, and sub-mandibular gland transfer surgical procedures.46,47
An overarching process as a preventive strategywith HNC patients is for the dental practitioner towork with the patient’s oncology care team in orderto advocate for gland sparing or gland transfertechniques for the patient’s cancer care.
Intensity-Modulated Radiation Therapy or 3DConformal Radiation TherapyIn the past 10 years, IMRT use for HNC hasincreased considerably in the United States,48
United Kingdom,49,50 and Canada.51 IMRT and3D conformal radiation therapy techniques areable to more specifically target the delivery of radi-ation to the affected area and consequently haveproduced results that decrease the destructiveimpact on salivary glands.42,46 Studies have shownthat IMRT and 3D conformal radiation therapieswere able to better preserve salivary gland func-tion in comparison to conventional radiation ther-apy processes that were not able to deliverradiation therapy to the tissues in a focused andspecific manner.32,42 Better results in decreasing drymouth have been reported with use of IMRT ver-sus 3D conformal radiation therapy.47,52,53
Salivary Gland TransferA substantial preventive approach for reducingthe risk of developing radiation-induced drymouth is the salivary gland transfer (SGT) proce-dure described and implemented in 2000, andknown as the Seikaly Jha procedure (SJP).46,53,54 Inan appropriate patient, this surgical procedure pre-serves the submandibular gland by moving itaway from the intended path of radiation, therebyeliminating or minimizing detrimental effects tothe salivary gland. Studies show very encouragingresults related to minimizing dry mouth when theSJP is used in HNC patients.53,55 In both a system-atic review and meta-analysis, subjects who hadreceived the SJP maintained their stimulated andunstimulated salivary flow rates at near-normallevels pre–cancer treatment.53 Furthermore, overtime, post-treatment, the subjects who receivedSJP continued to report improvement in salivaryflow rates.53
Preventive Strategies in Dry Mouth Resulting from MedicationsIn the case of medication-induced dry mouth,prevention strategies include consulting with med-ical practitioners to review the patient’s medica-tions and assessing whether alterations could bemade in medication number, dose or formulation,and type. There is minimal evidence to supportany relief of symptoms from altering medications,and the process is very much a time-consuming,
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
179

trial-and-error approach.32 Although studies haveshown that taking multiple medications or differ-ent doses, formulations, or brands of drug canresult in more or less xerostomic effects, situationsin which any aspect of a person’s medication regi-men can be altered are limited, and the evidence isminimal to support its effectiveness for decreasingdry mouth.56
Preventive Strategies in Dry Mouth Resulting fromSystemic or Behavioral ConditionsIn patients whose dry mouth is the result of a sys-temic change, there is little to nothing that can bedone preventively to change the condition. Oncethe diagnosis has been made, the process focuseson therapies and management protocol, as appro-priate. If the condition contributing to dry mouthis systemic, such as an eating disorder or alcoholabuse, the patient should be referred to an appro-priate health practitioner to provide support, treat-ment, and a management program. In situationsof dry mouth resulting from behavioral condi-tions, the dry mouth should resolve and normalsalivary function return if the behavior is greatlymodified or eliminated.
THERAPEUTIC INTERVENTIONSWhen considering therapeutic approaches to alle-viating the effects of dry mouth in any of thesethree dominant contributing situations, the clini-cian should determine if the salivary glands haveany remaining function.56 The following sectionsdescribe therapeutic interventions for patients withand without salivary gland function. Although a2011 Cochrane review found no strong evidenceto support any topical therapies for stimulating orsubstituting saliva,57 patients have reportedresponding to topical therapies and receivingsome relief from dry mouth symptoms.58 Thetherapeutic interventions are included here so cli-nicians will be versed in the various topical thera-py options patients may want to discuss.
Salivary Glands Remain FunctioningWhen some salivary flow remains, two groups oftherapeutic interventions can be considered for
patients with dry mouth: (1) saliva stimulants (sial-agogues), and (2) saliva substitutes.
Saliva StimulantsSaliva stimulants commonly used and readily avail-able include chewing gum, oral lozenges, topical orsystemic pilocarpine, acupuncture, and electrostim-ulation.59 Studies of each of these forms of stimu-lants have demonstrated some efficacy formanaging the symptoms of dry mouth; however,available evidence is weak, and no specific interven-tion has any strong evidence to support its efficacyfor relieving dry mouth.57,59,60 The dental practition-er must assess the individual’s condition and con-sider the etiology, as well as patient acceptance,willingness to try, and level of compliance, as all willinfluence the degree of effectiveness and relief expe-rienced by patients for any of these interventions.
Chewing Agents. Chewing gumshave shown effec-tiveness in stimulating salivary flow; however, thepatient must continue the chewing action as therelief of dry mouth symptoms comes from thechewing function.57,61 Studies have not shownwhether chewing gums are more or less effectivethan any salivary substitute, but patients havereported a preference for chewing agents over sali-vary substitutes.57 To preserve and protect the den-tition, the chewing gum should be sugar-free orsweetened with xylitol or sorbitol.32
Lozenges. Similar to chewing gums, lozenges haveproduced some relief of symptoms while theagent is being consumed and possibly for a shorttime after it dissolves; however, long-term relief isnot apparent with any lozenge. Additionally, thelozenges should be sugar-free or sweetened with asugar substitute to protect the dentition fromcaries. Lozenge use may be more appealing thanchewing gum to older adults, both as a moresocially acceptable action and because their useavoids possible discomfort of chewing associatedwith arthritis or wearing of dentures.32
Prescription Medications. Pilocarpine, in bothtopical and systemic forms, has shown some
CHAPTER 10 Dry Mouth
180

effectiveness in relieving the effects of dry mouth.This agent is a muscarinic receptor agonist andstimulates the secretion of saliva; however, acommon side effect is stimulation of sweatglands, resulting in excessive sweating by users.Pilocarpine is contraindicated in people withasthma, acute iritis, and certain types of glauco-ma, and patients should be closely monitored ifthey have cardiovascular or pulmonary dis-eases.62 Dental professionals should consult withthe patient’s physician before prescribing pilo-carpine to ensure compatibility with concurrentsystemic conditions and medication use. Pilo-carpine has been most effective in people whohave some remaining salivary gland function andsalivary flow; however, patients do reportimprovement in the subjective sensation of drymouth.32 The positive effects cease when pilo-carpine is discontinued; therefore, continued useis necessary for ongoing relief of symptoms.32
Topical preparations of pilocarpine includelozenges, sprays, and mouthwashes. Studies haveshown the most effective form of topical pilo-carpine is the lozenge, in both the 5 mg59 and 10mg formulations. Systemic preparations are inthe form of tablets.Cevimeline is a muscarinic acetylcholine
receptor agonist that has a longer half-life andduration of action than pilocarpine, and has alsobeen shown to have fewer adverse effects on car-diovascular and respiratory conditions. Cevime-line is approved by the U.S. Food and DrugAdministration for use in people with Sjögren’ssyndrome and for treatment of radiation thera-py-induced salivary hypofunction.59,63
Nonpharmacological Interventions for SalivaryStimulation. Other processes being researched orused to stimulate salivary flow with some demon-strated positive effect on reducing dry mouthsymptoms are acupuncture and electrostimula-tion. Studies of acupuncture as a therapy to stim-ulate salivary flow reported varied outcomes foreffectiveness, and it is clear that more research isneeded to determine if acupuncture is an effec-tive therapy for dry mouth. In studies showing
some positive effect, the patients had someremaining salivary gland function.32,59,64,65
Electrostimulation is a newer technique beingstudied to stimulate salivary flow.59 An intraoralelectrostimulating appliance, which was studiedin a multicenter, randomized control trial, wasfound to reduce dry mouth symptoms and stim-ulate salivary flow.66,67 However, a Cochranereview published in 2013 concluded that therewas limited evidence to determine the effective-ness of electrostimulation; therefore, moreresearch studies are needed before making anyrecommendations for therapeutic use.65
Saliva SubstitutesSaliva substitutes contain lubricating macromol-ecules as a substitute for salivary glycoproteins,whereas stimulants increase the salivary flow rateresulting in an increasing level of protein secretedper minute.59 The salivary substitute should beneutral pH and should contain fluoride to aid inprotecting the dentition. Patients must be cau-tioned about using any products with higheracidity due to the damaging effect on the denti-tion. Different agents have been developed in theform of gels, lubricants, sprays, and lozenges.32,64
A short list of products and home remedies isprovided in Table 4. Most of the substances usedfor moisturizing or coating the tissues need to beapplied many times during the day, which maylimit patient compliance. Therefore, some formof a sugar-free or sugar-substitute lozenge maybe best for providing relief of dry mouth symp-toms, as it is easy to use and may be more accept-able in work or social settings.
Sprays. Sprays may be effective for some people.The product is sprayed into the mouth, coatingthe oral tissues in an attempt to provide moistureand lubrication. Sprays must also be used fre-quently, and therefore must be kept on hand forease of use, both of which may limit compliance.Rinses. Rinses with antimicrobial and caries-pre-ventive properties should be recommended fortheir action of decreasing the oral bacterial loadand for reducing the incidence of new carious
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
181
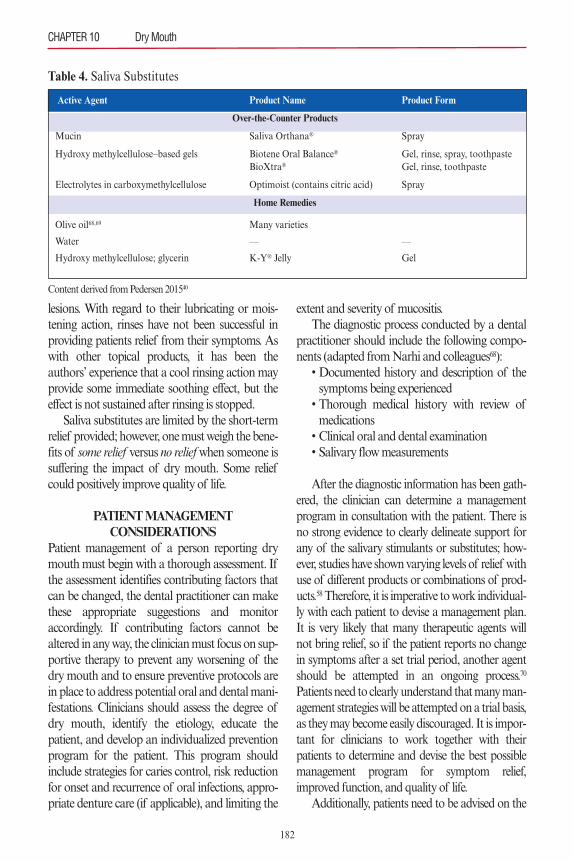
lesions. With regard to their lubricating or mois-tening action, rinses have not been successful inproviding patients relief from their symptoms. Aswith other topical products, it has been theauthors’ experience that a cool rinsing action mayprovide some immediate soothing effect, but theeffect is not sustained after rinsing is stopped.Saliva substitutes are limited by the short-term
relief provided; however, one must weigh the bene-fits of some relief versus no reliefwhen someone issuffering the impact of dry mouth. Some reliefcould positively improve quality of life.
PATIENT MANAGEMENT CONSIDERATIONS
Patient management of a person reporting drymouth must begin with a thorough assessment. Ifthe assessment identifies contributing factors thatcan be changed, the dental practitioner can makethese appropriate suggestions and monitoraccordingly. If contributing factors cannot bealtered in any way, the clinician must focus on sup-portive therapy to prevent any worsening of thedry mouth and to ensure preventive protocols arein place to address potential oral and dental mani-festations. Clinicians should assess the degree ofdry mouth, identify the etiology, educate thepatient, and develop an individualized preventionprogram for the patient. This program shouldinclude strategies for caries control, risk reductionfor onset and recurrence of oral infections, appro-priate denture care (if applicable), and limiting the
extent and severity of mucositis.The diagnostic process conducted by a dental
practitioner should include the following compo-nents (adapted from Narhi and colleagues68):• Documented history and description of thesymptoms being experienced• Thorough medical history with review ofmedications• Clinical oral and dental examination• Salivary flow measurements
After the diagnostic information has been gath-ered, the clinician can determine a managementprogram in consultation with the patient. There isno strong evidence to clearly delineate support forany of the salivary stimulants or substitutes; how-ever, studies have shown varying levels of relief withuse of different products or combinations of prod-ucts.58 Therefore, it is imperative to work individual-ly with each patient to devise a management plan.It is very likely that many therapeutic agents willnot bring relief, so if the patient reports no changein symptoms after a set trial period, another agentshould be attempted in an ongoing process.70
Patients need to clearly understand that many man-agement strategies will be attempted on a trial basis,as they may become easily discouraged. It is impor-tant for clinicians to work together with theirpatients to determine and devise the best possiblemanagement program for symptom relief,improved function, and quality of life.Additionally, patients need to be advised on the
CHAPTER 10 Dry Mouth
182
Table 4. Saliva Substitutes
Active Agent Product Name Product Form
Over-the-Counter Products
Mucin Saliva Orthana® Spray
Hydroxy methylcellulose–based gels Biotene Oral Balance® Gel, rinse, spray, toothpasteBioXtra® Gel, rinse, toothpaste
Electrolytes in carboxymethylcellulose Optimoist (contains citric acid) Spray
Home Remedies
Olive oil68,69 Many varieties
Water — —
Hydroxy methylcellulose; glycerin K-Y® Jelly Gel
Content derived from Pedersen 201540

following professional recommendations andhome remedies that in some cases have providedrelief of symptoms for some periods of time. Theyinclude (1) increasing hydration with water;70 (2)using a room humidifier;70 (3) avoiding coffee,alcohol, and any other dehydrating beverages;61,70
(4) avoiding or preferably quitting tobacco use;61,70
(5 ) avoiding oral irritants such as spicy, sour, andacidic foods and sweetened beverages;70 (6) prac-ticing optimal oral hygiene;70 (7) using fluorideproducts;70 and (8) maintaining regular care with a professional dental office (dentist, dental hygienist).70
During the clinical examination, the dentist ordental hygienist must assess for new carious lesionsand treat accordingly. If the patient has dentures,the denture and the oral tissues need to be exam-ined as the likelihood of oral candidiasis increaseswith dry mouth. Furthermore, since saliva is vitallyimportant to the fit and stability of dentures,patients need to understand how their denture fitmay increasingly decline to the point of not beingable to wear dentures if salivary flow is extremelycompromised. In addition to the treatments forthese oral and dental issues, patients need to beclearly informed and supported to follow a strictoral hygiene protocol; however, even with optimaloral hygiene, it may not be possible to preventsome oral conditions from deteriorating. Salivahas many important functions in the oral cavityand without it, oral status is compromised.Some specific recommendations to maintain
oral health include (1) use of home and profession-ally applied fluoride therapies, (2) following dietaryrecommendations to decrease sugar intake, and (3)increasing the number of professional office visitsfor monitoring and maintenance. Patients withdentures should be advised to wear dentures onlyduring the day, to clean dentures daily, and to soakdentures overnight in an appropriate solution.Rinsing twice daily with an antiseptic mouthrinsehas been shown to be beneficial for edentulouspatients to reduce the bacterial load and to preventdenture stomatitis.71,72
Lastly, it is imperative that dentists and dentalhygienists work collaboratively with other health-
care providers to determine the most effectivestrategies for managing patients suffering with drymouth.
Therapeutic Interventions Specific to Radiation-Induced Dry MouthThere is new and ongoing research on therapeuticinterventions to address damage to the salivaryglands after radiation therapy and the severe drymouth associated with Sjögren’s syndrome.42,73–75
Some of these therapeutic interventions includestem cell therapy, gene therapy, and hyperbaric oxy-gen therapy.
Stem Cell ResearchResearch investigating the use of mesenchymalstem cells to regenerate salivary production anddecrease dry mouth has shown some promise.However, a systematic review published in 2014reported a lack of conclusive evidence and calledfor future research to substantiate the possibilitiesof this therapy to regenerate salivary glands andrestore salivary flow.74
Gene TherapyResults are favorable from a human clinical trialinvolving salivary gland gene transfer to repairdamaged salivary glands after radiation therapy. Itis expected that this research will initiate furtherefforts to determine whether gene transfer may bean effective therapy to aid in relief from dry mouthafter radiation therapy to the salivary glands.75
Hyperbaric Oxygen TherapyHyperbaric oxygen therapy delivers oxygen to irra-diated tissues. A recent study of hyperbaric oxygenshowed a decrease in dry mouth symptoms result-ing from radiation therapy; however, this was asmall pilot study and further research is recom-mended to assess the effectiveness of these interven-tions.73 Similarly, a 2010 systematic review reporteda decrease in dry mouth symptoms after varyingregimens of hyperbaric oxygen treatment; however,the results were reported with high caution notingthe potential of many confounding variables thatcould have influenced the positive results.42
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
183
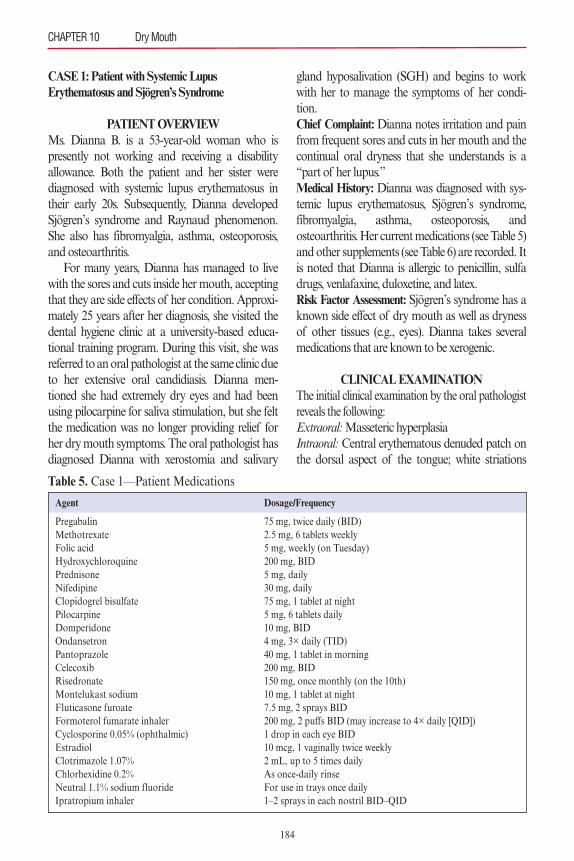
CASE 1: Patient with Systemic Lupus Erythematosus and Sjögren’s Syndrome
PATIENT OVERVIEWMs. Dianna B. is a 53-year-old woman who ispresently not working and receiving a disabilityallowance. Both the patient and her sister werediagnosed with systemic lupus erythematosus intheir early 20s. Subsequently, Dianna developedSjögren’s syndrome and Raynaud phenomenon.She also has fibromyalgia, asthma, osteoporosis,and osteoarthritis.For many years, Dianna has managed to live
with the sores and cuts inside her mouth, acceptingthat they are side effects of her condition. Approxi-mately 25 years after her diagnosis, she visited thedental hygiene clinic at a university-based educa-tional training program. During this visit, she wasreferred to an oral pathologist at the same clinic dueto her extensive oral candidiasis. Dianna men-tioned she had extremely dry eyes and had beenusing pilocarpine for saliva stimulation, but she feltthe medication was no longer providing relief forher dry mouth symptoms. The oral pathologist hasdiagnosed Dianna with xerostomia and salivary
gland hyposalivation (SGH) and begins to workwith her to manage the symptoms of her condi-tion.Chief Complaint: Dianna notes irritation and painfrom frequent sores and cuts in her mouth and thecontinual oral dryness that she understands is a“part of her lupus.”Medical History: Dianna was diagnosed with sys-temic lupus erythematosus, Sjögren’s syndrome,fibromyalgia, asthma, osteoporosis, andosteoarthritis. Her current medications (see Table 5)and other supplements (see Table 6) are recorded. Itis noted that Dianna is allergic to penicillin, sulfadrugs, venlafaxine, duloxetine, and latex.Risk Factor Assessment: Sjögren’s syndrome has aknown side effect of dry mouth as well as drynessof other tissues (e.g., eyes). Dianna takes severalmedications that are known to be xerogenic.
CLINICAL EXAMINATIONThe initial clinical examination by the oral pathologistreveals the following:Extraoral:Masseteric hyperplasiaIntraoral:Central erythematous denuded patch onthe dorsal aspect of the tongue; white striations
CHAPTER 10 Dry Mouth
184
Table 5. Case 1—Patient Medications
Agent Dosage/Frequency
Pregabalin 75 mg, twice daily (BID)Methotrexate 2.5 mg, 6 tablets weeklyFolic acid 5 mg, weekly (on Tuesday)Hydroxychloroquine 200 mg, BIDPrednisone 5 mg, dailyNifedipine 30 mg, dailyClopidogrel bisulfate 75 mg, 1 tablet at nightPilocarpine 5 mg, 6 tablets dailyDomperidone 10 mg, BIDOndansetron 4 mg, 3× daily (TID)Pantoprazole 40 mg, 1 tablet in morningCelecoxib 200 mg, BIDRisedronate 150 mg, once monthly (on the 10th)Montelukast sodium 10 mg, 1 tablet at nightFluticasone furoate 7.5 mg, 2 sprays BIDFormoterol fumarate inhaler 200 mg, 2 puffs BID (may increase to 4× daily [QID])Cyclosporine 0.05% (ophthalmic) 1 drop in each eye BIDEstradiol 10 mcg, 1 vaginally twice weeklyClotrimazole 1.07% 2 mL, up to 5 times dailyChlorhexidine 0.2% As once-daily rinseNeutral 1.1% sodium fluoride For use in trays once dailyIpratropium inhaler 1–2 sprays in each nostril BID–QID
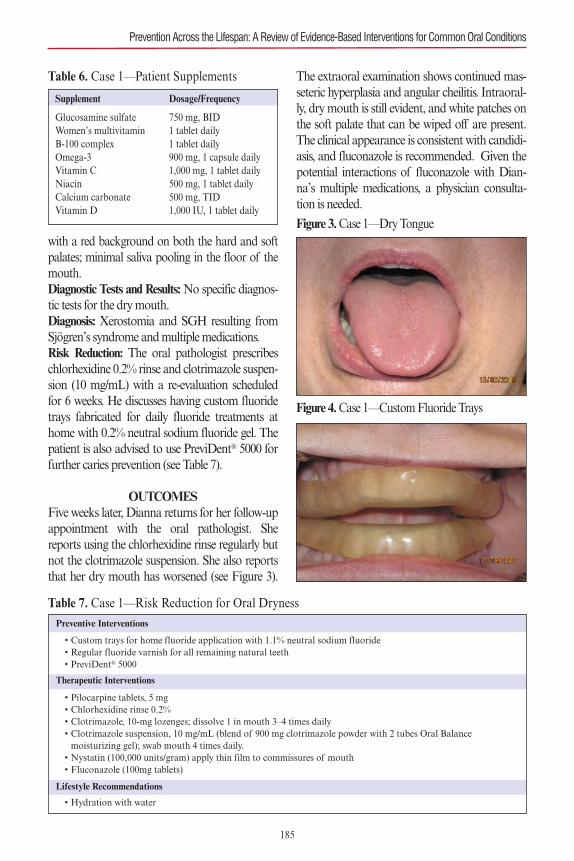
with a red background on both the hard and softpalates; minimal saliva pooling in the floor of themouth.Diagnostic Tests and Results: No specific diagnos-tic tests for the dry mouth.Diagnosis: Xerostomia and SGH resulting fromSjögren’s syndrome and multiple medications.Risk Reduction: The oral pathologist prescribeschlorhexidine 0.2% rinse and clotrimazole suspen-sion (10 mg/mL) with a re-evaluation scheduledfor 6 weeks. He discusses having custom fluoridetrays fabricated for daily fluoride treatments athome with 0.2% neutral sodium fluoride gel. Thepatient is also advised to use PreviDent® 5000 forfurther caries prevention (see Table 7).
OUTCOMESFive weeks later, Dianna returns for her follow-upappointment with the oral pathologist. Shereports using the chlorhexidine rinse regularly butnot the clotrimazole suspension. She also reportsthat her dry mouth has worsened (see Figure 3).
The extraoral examination shows continued mas-seteric hyperplasia and angular cheilitis. Intraoral-ly, dry mouth is still evident, and white patches onthe soft palate that can be wiped off are present.The clinical appearance is consistent with candidi-asis, and fluconazole is recommended. Given thepotential interactions of fluconazole with Dian-na’s multiple medications, a physician consulta-tion is needed.
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
185
Table 6. Case 1—Patient Supplements
Supplement Dosage/Frequency
Glucosamine sulfate 750 mg, BIDWomen’s multivitamin 1 tablet dailyB-100 complex 1 tablet dailyOmega-3 900 mg, 1 capsule dailyVitamin C 1,000 mg, 1 tablet dailyNiacin 500 mg, 1 tablet dailyCalcium carbonate 500 mg, TIDVitamin D 1,000 IU, 1 tablet daily
Table 7. Case 1—Risk Reduction for Oral DrynessPreventive Interventions
• Custom trays for home fluoride application with 1.1% neutral sodium fluoride• Regular fluoride varnish for all remaining natural teeth• PreviDent® 5000
Therapeutic Interventions
• Pilocarpine tablets, 5 mg• Chlorhexidine rinse 0.2%• Clotrimazole, 10-mg lozenges; dissolve 1 in mouth 3–4 times daily• Clotrimazole suspension, 10 mg/mL (blend of 900 mg clotrimazole powder with 2 tubes Oral Balance moisturizing gel); swab mouth 4 times daily.• Nystatin (100,000 units/gram) apply thin film to commissures of mouth• Fluconazole (100mg tablets)
Lifestyle Recommendations
• Hydration with water
Figure 3. Case 1—Dry Tongue
Figure 4. Case 1—Custom Fluoride Trays
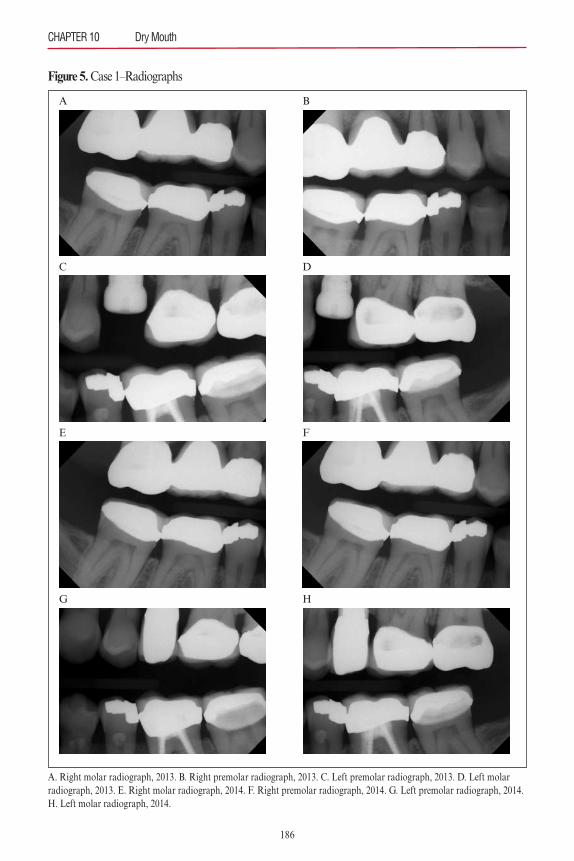
CHAPTER 10 Dry Mouth
186
Figure 5. Case 1–Radiographs
A. Right molar radiograph, 2013. B. Right premolar radiograph, 2013. C. Left premolar radiograph, 2013. D. Left molar radiograph, 2013. E. Right molar radiograph, 2014. F. Right premolar radiograph, 2014. G. Left premolar radiograph, 2014.H. Left molar radiograph, 2014.
A
C
E
G
B
D
F
H
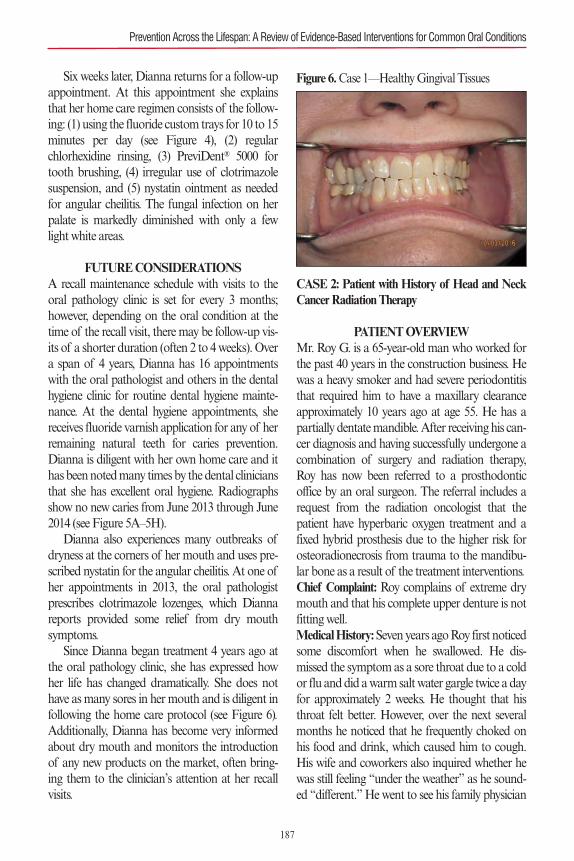
Six weeks later, Dianna returns for a follow-upappointment. At this appointment she explainsthat her home care regimen consists of the follow-ing: (1) using the fluoride custom trays for 10 to 15minutes per day (see Figure 4), (2) regularchlorhexidine rinsing, (3) PreviDent® 5000 fortooth brushing, (4) irregular use of clotrimazolesuspension, and (5) nystatin ointment as neededfor angular cheilitis. The fungal infection on herpalate is markedly diminished with only a fewlight white areas.
FUTURE CONSIDERATIONSA recall maintenance schedule with visits to theoral pathology clinic is set for every 3 months;however, depending on the oral condition at thetime of the recall visit, there may be follow-up vis-its of a shorter duration (often 2 to 4 weeks). Overa span of 4 years, Dianna has 16 appointmentswith the oral pathologist and others in the dentalhygiene clinic for routine dental hygiene mainte-nance. At the dental hygiene appointments, shereceives fluoride varnish application for any of herremaining natural teeth for caries prevention.Dianna is diligent with her own home care and ithas been noted many times by the dental cliniciansthat she has excellent oral hygiene. Radiographsshow no new caries from June 2013 through June2014 (see Figure 5A–5H).Dianna also experiences many outbreaks of
dryness at the corners of her mouth and uses pre-scribed nystatin for the angular cheilitis. At one ofher appointments in 2013, the oral pathologistprescribes clotrimazole lozenges, which Diannareports provided some relief from dry mouthsymptoms.Since Dianna began treatment 4 years ago at
the oral pathology clinic, she has expressed howher life has changed dramatically. She does nothave as many sores in her mouth and is diligent infollowing the home care protocol (see Figure 6).Additionally, Dianna has become very informedabout dry mouth and monitors the introductionof any new products on the market, often bring-ing them to the clinician’s attention at her recallvisits.
CASE 2: Patient with History of Head and NeckCancer Radiation Therapy
PATIENT OVERVIEWMr. Roy G. is a 65-year-old man who worked forthe past 40 years in the construction business. Hewas a heavy smoker and had severe periodontitisthat required him to have a maxillary clearanceapproximately 10 years ago at age 55. He has apartially dentate mandible. After receiving his can-cer diagnosis and having successfully undergone acombination of surgery and radiation therapy,Roy has now been referred to a prosthodonticoffice by an oral surgeon. The referral includes arequest from the radiation oncologist that thepatient have hyperbaric oxygen treatment and afixed hybrid prosthesis due to the higher risk forosteoradionecrosis from trauma to the mandibu-lar bone as a result of the treatment interventions.Chief Complaint: Roy complains of extreme drymouth and that his complete upper denture is notfitting well.Medical History: Seven years ago Roy first noticedsome discomfort when he swallowed. He dis-missed the symptom as a sore throat due to a coldor flu and did a warm salt water gargle twice a dayfor approximately 2 weeks. He thought that histhroat felt better. However, over the next severalmonths he noticed that he frequently choked onhis food and drink, which caused him to cough.His wife and coworkers also inquired whether hewas still feeling “under the weather” as he sound-ed “different.” He went to see his family physician
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
187
Figure 6. Case 1—Healthy Gingival Tissues
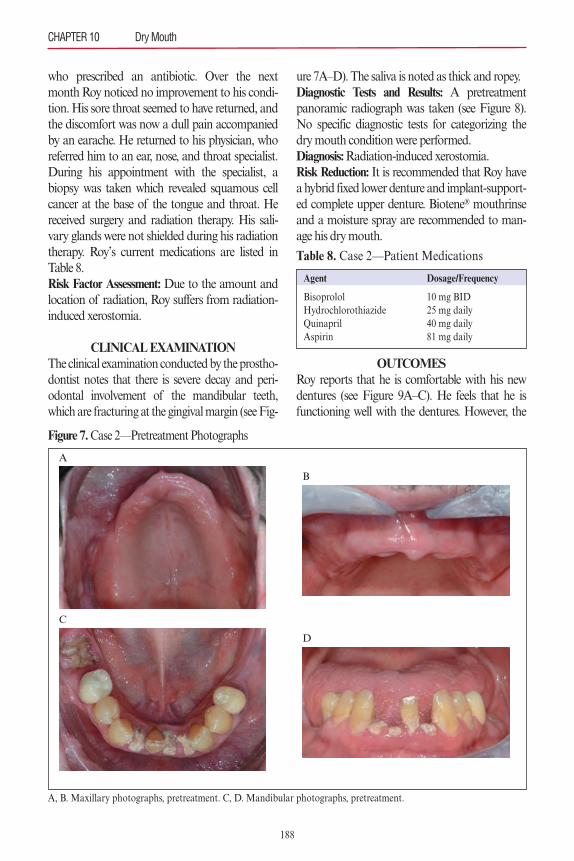
188
who prescribed an antibiotic. Over the nextmonth Roy noticed no improvement to his condi-tion. His sore throat seemed to have returned, andthe discomfort was now a dull pain accompaniedby an earache. He returned to his physician, whoreferred him to an ear, nose, and throat specialist.During his appointment with the specialist, abiopsy was taken which revealed squamous cellcancer at the base of the tongue and throat. Hereceived surgery and radiation therapy. His sali-vary glands were not shielded during his radiationtherapy. Roy’s current medications are listed inTable 8.Risk Factor Assessment: Due to the amount andlocation of radiation, Roy suffers from radiation-induced xerostomia.
CLINICAL EXAMINATIONThe clinical examination conducted by the prostho-dontist notes that there is severe decay and peri-odontal involvement of the mandibular teeth,which are fracturing at the gingival margin (see Fig-
ure 7A–D). The saliva is noted as thick and ropey.Diagnostic Tests and Results: A pretreatmentpanoramic radiograph was taken (see Figure 8).No specific diagnostic tests for categorizing thedry mouth condition were performed.Diagnosis: Radiation-induced xerostomia.Risk Reduction: It is recommended that Roy havea hybrid fixed lower denture and implant-support-ed complete upper denture. Biotene® mouthrinseand a moisture spray are recommended to man-age his dry mouth.
OUTCOMESRoy reports that he is comfortable with his newdentures (see Figure 9A–C). He feels that he isfunctioning well with the dentures. However, the
CHAPTER 10 Dry Mouth
Table 8. Case 2—Patient Medications
Agent Dosage/Frequency
Bisoprolol 10 mg BIDHydrochlorothiazide 25 mg dailyQuinapril 40 mg dailyAspirin 81 mg daily
Figure 7. Case 2—Pretreatment Photographs
A, B. Maxillary photographs, pretreatment. C, D. Mandibular photographs, pretreatment.
A
C
B
D
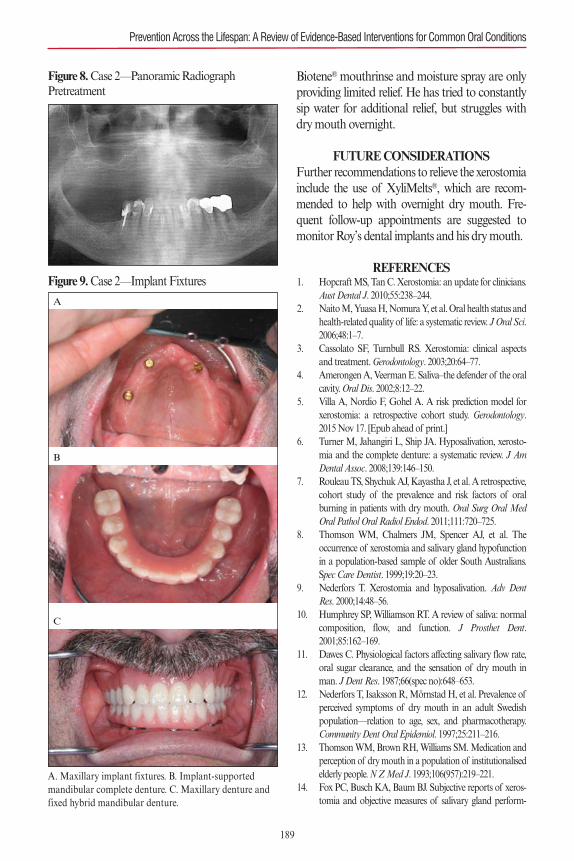
Biotene® mouthrinse and moisture spray are onlyproviding limited relief. He has tried to constantlysip water for additional relief, but struggles withdry mouth overnight.
FUTURE CONSIDERATIONSFurther recommendations to relieve the xerostomiainclude the use of XyliMelts®, which are recom-mended to help with overnight dry mouth. Fre-quent follow-up appointments are suggested tomonitor Roy’s dental implants and his dry mouth.
REFERENCES1. Hopcraft MS, Tan C. Xerostomia: an update for clinicians.
Aust Dental J. 2010;55:238–244.2. Naito M, Yuasa H, Nomura Y, et al. Oral health status and
health-related quality of life: a systematic review. J Oral Sci.2006;48:1–7.
3. Cassolato SF, Turnbull RS. Xerostomia: clinical aspectsand treatment. Gerodontology. 2003;20:64–77.
4. Amerongen A, Veerman E. Saliva–the defender of the oralcavity. Oral Dis. 2002;8:12–22.
5. Villa A, Nordio F, Gohel A. A risk prediction model forxerostomia: a retrospective cohort study. Gerodontology.2015 Nov 17. [Epub ahead of print.]
6. Turner M, Jahangiri L, Ship JA. Hyposalivation, xerosto-mia and the complete denture: a systematic review. J AmDental Assoc. 2008;139:146–150.
7. Rouleau TS, Shychuk AJ, Kayastha J, et al. A retrospective,cohort study of the prevalence and risk factors of oralburning in patients with dry mouth. Oral Surg Oral MedOral Pathol Oral Radiol Endod. 2011;111:720–725.
8. Thomson WM, Chalmers JM, Spencer AJ, et al. Theoccurrence of xerostomia and salivary gland hypofunctionin a population-based sample of older South Australians.Spec Care Dentist. 1999;19:20–23.
9. Nederfors T. Xerostomia and hyposalivation. Adv DentRes. 2000;14:48–56.
10. Humphrey SP, Williamson RT. A review of saliva: normalcomposition, flow, and function. J Prosthet Dent.2001;85:162–169.
11. Dawes C. Physiological factors affecting salivary flow rate,oral sugar clearance, and the sensation of dry mouth inman. J Dent Res. 1987;66(spec no):648–653.
12. Nederfors T, Isaksson R, Mörnstad H, et al. Prevalence ofperceived symptoms of dry mouth in an adult Swedishpopulation—relation to age, sex, and pharmacotherapy.Community Dent Oral Epidemiol. 1997;25:211–216.
13. Thomson WM, Brown RH, Williams SM. Medication andperception of dry mouth in a population of institutionalisedelderly people. N Z Med J. 1993;106(957):219–221.
14. Fox PC, Busch KA, Baum BJ. Subjective reports of xeros-tomia and objective measures of salivary gland perform-
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
189
Figure 8. Case 2—Panoramic Radiograph Pretreatment
Figure 9. Case 2—Implant Fixtures
A. Maxillary implant fixtures. B. Implant-supported mandibular complete denture. C. Maxillary denture andfixed hybrid mandibular denture.
A
B
C
ance. J Am Dent Assoc. 1987;115:581–584.15. Fure S, Zickert I. Salivary conditions and cariogenic
microorganisms in 55, 65, and 75�year�old Swedish individ-uals. Eur J Oral Sci. 1990;98:197–210.
16. Närhi TO. Prevalence of subjective feelings of dry mouthin the elderly. J Dent Res. 1994;73:20–25.
17. Locker D. Subjective reports of oral dryness in an olderadult population. Community Dent Oral Epidemiol.1993;21:165–168.
18. Locker D. Dental status, xerostomia, and the oralhealth�related quality of life of an elderly institutionalizedpopulation. Spec Care Dentist. 2003;23:86–93.
19. Osailan SM, Pramanik R, Shirlaw P, et al. Clinical assess-ment of oral dryness: development of a scoring system relat-ed to salivary flow and mucosal wetness. Oral Surg Oral MedOral Pathol Oral Radiol Endod. 2012;114:597–603.
20. Pai S, Ghezzi EM, Ship JA. Development of a visual ana-logue scale questionnaire for subjective assessment of sali-vary dysfunction. Oral Surg Oral Med Oral Pathol OralRadiol Endod. 2001;91:311–316.
21. Thomson WM, Chalmers JM, Spencer AJ, et al. Thexerostomia inventory: a multi-item approach to measuringdry mouth. Community Dent Health. 1999;16:12–17.
22. Thomson WM. Subjective aspects of dry mouth. In: Car-penter G, ed. Dry Mouth: A Clinical Guide on Causes,Effects, and Treatments. New York, NY: Springer-Verlag;2015:103–115.
23. Navazesh M, Christensen C, Brightman V. Clinical criteriafor the diagnosis of salivary gland hypofunction. J DentRes. 1992;71:1363–1369.
24. Navazesh M, Christensen C. A comparison of wholemouth resting and stimulated salivary measurement proce-dures. J Dent Res. 1982;61:1158–1162.
25. Thomson WM. Issues in the epidemiological investigationof dry mouth. Gerodontology. 2005;22:65–76.
26. Ship JA, Pillemer SR, Baum BJ. Xerostomia and the geri-atric patient. J Am Geriatr Soc. 2002;50:535–543.
27. Orellana MF, Lagravere MO, Boychuk DG, et al. Preva-lence of xerostomia in population-based samples: a system-atic review. J Public Health Dent. 2006;66:152–158.
28. Liu B, Dion MR, Jurasic MM, et al. Xerostomia and sali-vary hypofunction in vulnerable elders: prevalence and eti-ology. Oral Surg Oral Med Oral Pathol Oral Radiol Endod.2012;114:52–60.
29. Nagler RM, Hershkovich O. Relationships between age,drugs, oral sensorial complaints, and salivary profile. ArchOral Biol. 2005;50:7–16.
30. Smith CH, Boland B, Daureeawoo Y, et al. Effect of agingon stimulated salivary flow in adults. J Am Geriatr Soc.2013;61:805–808.
31. Navazesh M. Salivary gland hypofunction in elderlypatients. J Calif Dent Assoc. 1994;22:62–68.
32. Han P, Suarez-Durall P, Mulligan R. Dry mouth: a criticaltopic for older adult patients. J Prosthodont Res. 2015;59:6–19.
33. Chew ML, Mulsant BH, Pollock BG, et al. Anticholinergicactivity of 107 medications commonly used by older adults.
J Am Geriatr Soc. 2008;56:1333–1341.34. Desoutter A, Soudain-Pineau M, Munsch F, et al. Xeros-
tomia and medication: A cross-sectional study in long-termgeriatric wards. J Nutr Health Aging. 2012;16:575–579.
35. Murray Thomson W, Chalmers JM, John Spencer A, et al.A longitudinal study of medication exposure and xerosto-mia among older people. Gerodontology. 2006;23:205–213.
36. Smidt D, Torpet LA, Nauntofte B, et al. Associationsbetween oral and ocular dryness, labial and whole salivaryflow rates, systemic diseases and medications in a sample ofolder people. Community Dent Oral Epidemiol.2011;39:276–288.
37. Pajukoski H, Meurman JH, Halonen P, et al. Prevalence ofsubjective dry mouth and burning mouth in hospitalizedelderly patients and outpatients in relation to saliva, med-ication, and systemic diseases. Oral Surg Oral Med OralPathol Oral Radiol Endod. 2001;92:641–649.
38. Helmick CG, Felson DT, Lawrence RC, et al. Estimates ofthe prevalence of arthritis and other rheumatic conditions inthe United States: Part I. Arthritis Rheum. 2008;58:15–25.
39. Mavragani CP, Moutsopoulos HM. Sjögren’s syndrome.Can Med Assoc J. 2014;186:E579–E586.
40. Pedersen AML. Diseases causing oral dryness. In: CarpenterG, ed. Dry Mouth: A Clinical Guide on Causes, Effects, andTreatments.New York, NY: Springer-Verlag; 2015:7–31.
41. Chaturvedi AK, Engels EA, Pfeiffer RM, et al. Humanpapillomavirus and rising oropharyngeal cancer incidencein the United States. J Clin Oncol. 2011;29:4294–4301.
42. Jensen SB, Pedersen AM, Vissink A, et al. A systematicreview of salivary gland hypofunction and xerostomiainduced by cancer therapies: prevalence, severity, andimpact on quality of life. Support Care Cancer.2010;18:1039–1060.
43. Wijers OB, Levendag PC, Braaksma MMJ, et al. Patientswith head and neck cancer cured by radiation therapy: asurvey of the dry mouth syndrome in long-term survivors.Head Neck. 2002;24:737–747.
44. Eisbruch A, Ship JA, Kim HM, Ten Haken RK. Partialirradiation of the parotid gland. Semin Radiat Oncol.2001;11:234–239.
45. Kielbassa AM, Hinkelbein W, Hellwig E, et al. Radiation-related damage to dentition. Lancet Oncol. 2006;7:326–335.
46. Seikaly H, Jha N, Harris JR, et al. Long-term outcomes ofsubmandibular gland transfer for prevention of postradia-tion xerostomia. Arch Otolaryngol Head Neck Surg.2004;130:956–961.
47. Zhang B, Mo Z, Du W, et al. Intensity-modulated radia-tion therapy versus 2D-RT or 3D-CRT for the treatment ofnasopharyngeal carcinoma: a systematic review and meta-analysis. Oral Oncol. 2015 Aug 18. PMID: 26296274.
48. Mell LK, Mehrotra AK, Mundt AJ. Intensity�modulatedradiation therapy use in the US, 2004. Cancer.2005;104:1296–1303.
49. Mayles W. Survey of the availability and use of advancedradiotherapy technology in the UK. Clin Oncol.2010;22:636–642.
190
CHAPTER 10 Dry Mouth
50. Mayles W, Cooper T, Mackay R, et al. Progress with inten-sity-modulated radiotherapy implementation in the UK.Clin Oncol. 2012;24:543–544.
51. AlDuhaiby EZ, Breen S, Bissonnette J-P, et al. A nationalsurvey of the availability of intensity-modulated radiationtherapy and stereotactic radiosurgery in Canada. RadiatOncol. 2012;7:18.
52. Klein J, Livergant J, Ringash J. Health related quality of lifein head and neck cancer treated with radiation therapywith or without chemotherapy: a systematic review. OralOncol. 2014;50:254–262.
53. Sood AJ, Fox NF, O’Connell BP, et al. Salivary glandtransfer to prevent radiation-induced xerostomia: a system-atic review and meta-analysis. Oral Oncol. 2014;50:77–83.
54. Jha N, Seikaly H, McGaw T, et al. Submandibular salivarygland transfer prevents radiation-induced xerostomia. Int JRadiat Oncol Biol Phys. 2000;46:7–11.
55. Rieger J, Seikaly H, Jha N, et al. Submandibular glandtransfer for prevention of xerostomia after radiation thera-py: swallowing outcomes. Arch Otolaryngol Head NeckSurg. 2005;131:140–145.
56. Villa A, Wolff A, Aframian D, et al. World Workshop onOral Medicine VI: a systematic review of medication-induced salivary gland dysfunction: prevalence, diagnosis,and treatment. Clin Oral Investig. 2015;19:1563–1580.
57. Furness S, Worthington HV, Bryan G, et al. Interventionsfor the management of dry mouth: topical therapies.Cochrane Database Syst Rev. 2011(12):CD008934.
58. Davies A, Bagg J, Laverty D, et al. Salivary gland dysfunc-tion (�dry mouth�) in patients with cancer: a consensusstatement. Eur J Cancer Care (Engl). 2010;19:172–177.
59. Lovelace TL, Fox NF, Sood AJ, et al. Management ofradiotherapy-induced salivary hypofunction and conse-quent xerostomia in patients with oral or head and neckcancer: meta-analysis and literature review. Oral Surg OralMed Oral Pathol Oral Radiol Endod. 2014;117:595–607.
60. Wolff A, Fox PC, Porter S, et al. Established and novelapproaches for the management of hyposalivation andxerostomia. Curr Pharm Des. 2012;18:5515–5521.
61. Visvanathan V, Nix P. Managing the patient presenting withxerostomia: a review. Int J Clin Pract. 2010;64:404–407.
62. Dirix P, Nuyts S, Van den Bogaert W. Radiation-inducedxerostomia in patients with head and neck cancer: a litera-ture review. Cancer. 2006;107:2525–2534.
63. Spolarich AE. Risk management strategies for reducingoral adverse drug events. J Evid Based Dent Pract. 2014;(14suppl):87–94.
64. Hanchanale S, Adkinson L, Daniel S, et al. Systematic lit-erature review: xerostomia in advanced cancer patients.Support Care Cancer. 2015;23:881–888.
65. Furness S, Bryan G, McMillan R, et al. Interventions forthe management of dry mouth: non-pharmacologicalinterventions. Cochrane Database Syst Rev.2013;(8):CD009603.
66. Strietzel FP, Lafaurie GI, Mendoza GR, et al. Efficacy andsafety of an intraoral electrostimulation device for xerosto-mia relief: a multicenter, randomized trial. Arthritis Rheum.2011;63:180–190.
67. Strietzel FP, Martin-Granizo R, Fedele S, et al. Electros-timulating device in the management of xerostomia. OralDis. 2007;13:206–213.
68. Narhi TO, Meurman JH, Ainamo A. Xerostomia andhyposalivation—causes, consequences, and treatment inthe elderly. Drugs Aging. 1999;15:103–116.
69. Dost F, Farah CS. Stimulating the discussion on saliva sub-stitutes: a clinical perspective. Aust Dent J. 2013;58:11–17.
70. Napenas JJ, Brennan MT, Fox PC. Diagnosis and treat-ment of xerostomia (dry mouth). Odontology. 2009;97:76–83.
71. DePaola L, Minah G, Leupold R, et al. The effect of anti-septic mouthrinses on oral microbial flora and denturestomatitis. Clin Prevent Dent. 1985;8:3–8.
72. DePaola LG, Minah GF, Elias SA, et al. Clinical andmicrobial evaluation of treatment regimens to reduce den-ture stomatitis. Int J Prosthodont. 1990;3:369–374.
73. Forner L, Hyldegaard O, von Brockdorff AS, et al. Doeshyperbaric oxygen treatment have the potential to increasesalivary flow rate and reduce xerostomia in previously irra-diated head and neck cancer patients? A pilot study. OralOncol. 2011;47:546–551.
74. Jensen DH, Oliveri RS, Trojahn Kølle SF, et al. Mesenchy-mal stem cell therapy for salivary gland dysfunction andxerostomia: a systematic review of preclinical studies. OralSurg Oral Med Oral Pathol Oral Radiol Endod. 2014;117:335–342.
75. Baum BJ, Alevizos I, Chiorini JA, et al. Advances in sali-vary gland gene therapy—oral and systemic implications.Expert Opin Biol Ther. 2015;15:1443–1454.
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
191
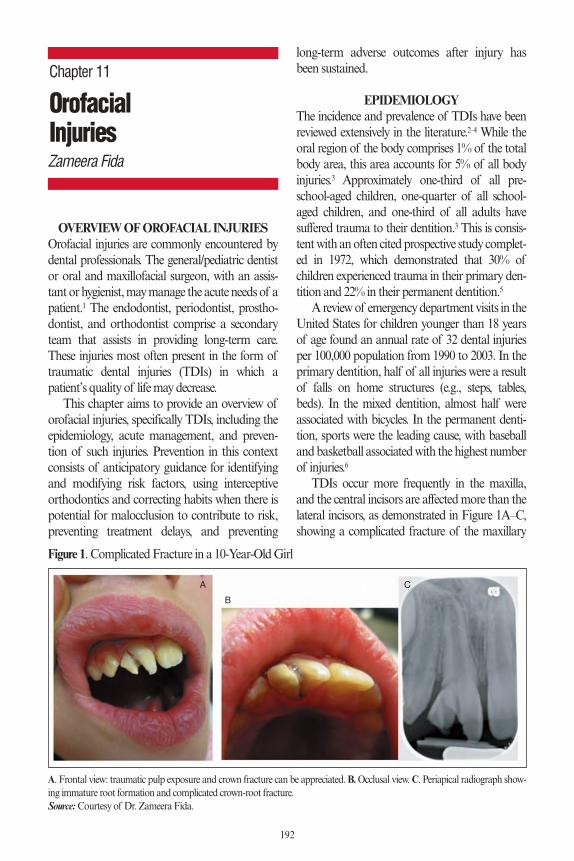
OVERVIEW OF OROFACIAL INJURIESOrofacial injuries are commonly encountered bydental professionals. The general/pediatric dentistor oral and maxillofacial surgeon, with an assis-tant or hygienist, may manage the acute needs of apatient.1 The endodontist, periodontist, prostho-dontist, and orthodontist comprise a secondaryteam that assists in providing long-term care.These injuries most often present in the form oftraumatic dental injuries (TDIs) in which apatient’s quality of life may decrease.
This chapter aims to provide an overview oforofacial injuries, specifically TDIs, including theepidemiology, acute management, and preven-tion of such injuries. Prevention in this contextconsists of anticipatory guidance for identifyingand modifying risk factors, using interceptiveorthodontics and correcting habits when there ispotential for malocclusion to contribute to risk,preventing treatment delays, and preventing
long-term adverse outcomes after injury hasbeen sustained.
EPIDEMIOLOGYThe incidence and prevalence of TDIs have beenreviewed extensively in the literature.2–4 While theoral region of the body comprises 1% of the totalbody area, this area accounts for 5% of all bodyinjuries.3 Approximately one-third of all pre-school-aged children, one-quarter of all school-aged children, and one-third of all adults havesuffered trauma to their dentition.3 This is consis-tent with an often cited prospective study complet-ed in 1972, which demonstrated that 30% ofchildren experienced trauma in their primary den-tition and 22% in their permanent dentition.5
A review of emergency department visits in theUnited States for children younger than 18 yearsof age found an annual rate of 32 dental injuriesper 100,000 population from 1990 to 2003. In theprimary dentition, half of all injuries were a resultof falls on home structures (e.g., steps, tables,beds). In the mixed dentition, almost half wereassociated with bicycles. In the permanent denti-tion, sports were the leading cause, with baseballand basketball associated with the highest numberof injuries.6
TDIs occur more frequently in the maxilla,and the central incisors are affected more than thelateral incisors, as demonstrated in Figure 1A–C,showing a complicated fracture of the maxillary
192
OrofacialInjuries
Chapter 11
Zameera Fida
Figure 1. Complicated Fracture in a 10-Year-Old Girl
A. Frontal view: traumatic pulp exposure and crown fracture can be appreciated. B.Occlusal view.C. Periapical radiograph show-ing immature root formation and complicated crown-root fracture.Source:Courtesy of Dr. Zameera Fida.
A
B
C
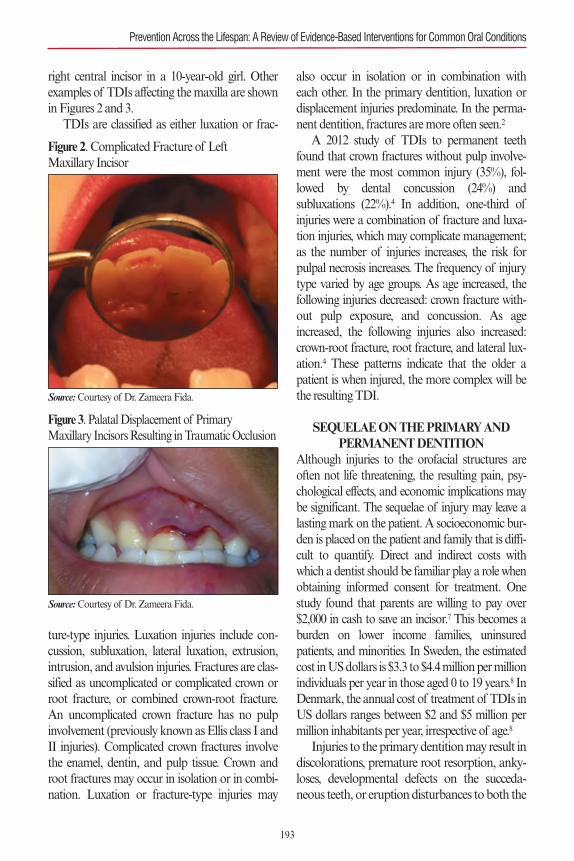
right central incisor in a 10-year-old girl. Otherexamples of TDIs affecting the maxilla are shownin Figures 2 and 3.
TDIs are classified as either luxation or frac-
ture-type injuries. Luxation injuries include con-cussion, subluxation, lateral luxation, extrusion,intrusion, and avulsion injuries. Fractures are clas-sified as uncomplicated or complicated crown orroot fracture, or combined crown-root fracture.An uncomplicated crown fracture has no pulpinvolvement (previously known as Ellis class I andII injuries). Complicated crown fractures involvethe enamel, dentin, and pulp tissue. Crown androot fractures may occur in isolation or in combi-nation. Luxation or fracture-type injuries may
also occur in isolation or in combination witheach other. In the primary dentition, luxation ordisplacement injuries predominate. In the perma-nent dentition, fractures are more often seen.2
A 2012 study of TDIs to permanent teethfound that crown fractures without pulp involve-ment were the most common injury (35%), fol-lowed by dental concussion (24%) andsubluxations (22%).4 In addition, one-third ofinjuries were a combination of fracture and luxa-tion injuries, which may complicate management;as the number of injuries increases, the risk forpulpal necrosis increases. The frequency of injurytype varied by age groups. As age increased, thefollowing injuries decreased: crown fracture with-out pulp exposure, and concussion. As ageincreased, the following injuries also increased:crown-root fracture, root fracture, and lateral lux-ation.4 These patterns indicate that the older apatient is when injured, the more complex will bethe resulting TDI.
SEQUELAE ON THE PRIMARY AND PERMANENT DENTITION
Although injuries to the orofacial structures areoften not life threatening, the resulting pain, psy-chological effects, and economic implications maybe significant. The sequelae of injury may leave alasting mark on the patient. A socioeconomic bur-den is placed on the patient and family that is diffi-cult to quantify. Direct and indirect costs withwhich a dentist should be familiar play a role whenobtaining informed consent for treatment. Onestudy found that parents are willing to pay over$2,000 in cash to save an incisor.7 This becomes aburden on lower income families, uninsuredpatients, and minorities. In Sweden, the estimatedcost in US dollars is $3.3 to $4.4 million per millionindividuals per year in those aged 0 to 19 years.8 InDenmark, the annual cost of treatment of TDIs inUS dollars ranges between $2 and $5 million permillion inhabitants per year, irrespective of age.8
Injuries to the primary dentition may result indiscolorations, premature root resorption, anky-loses, developmental defects on the succeda-neous teeth, or eruption disturbances to both the
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
193
Figure 2. Complicated Fracture of Left Maxillary Incisor
Source:Courtesy of Dr. Zameera Fida.
Figure 3. Palatal Displacement of Primary Maxillary Incisors Resulting in Traumatic Occlusion
Source:Courtesy of Dr. Zameera Fida.
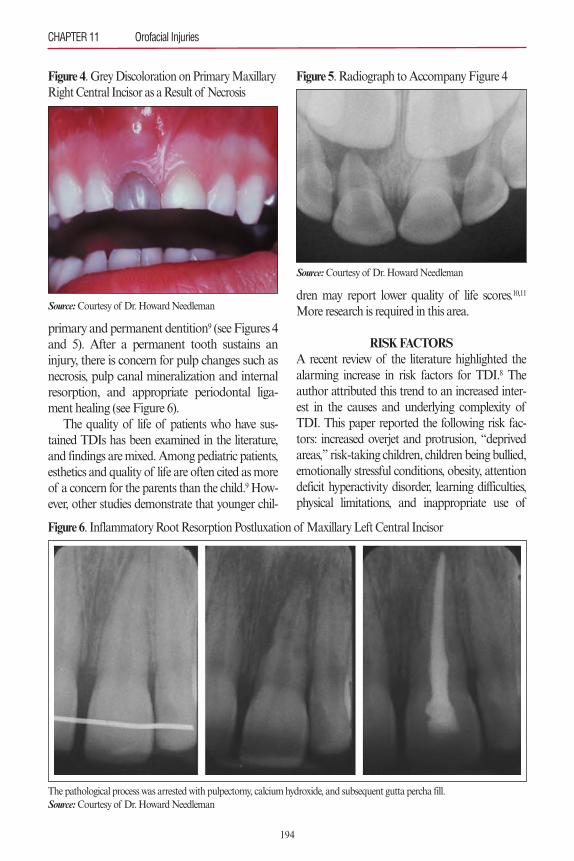
primary and permanent dentition9 (see Figures 4and 5). After a permanent tooth sustains aninjury, there is concern for pulp changes such asnecrosis, pulp canal mineralization and internalresorption, and appropriate periodontal liga-ment healing (see Figure 6).
The quality of life of patients who have sus-tained TDIs has been examined in the literature,and findings are mixed. Among pediatric patients,esthetics and quality of life are often cited as moreof a concern for the parents than the child.9 How-ever, other studies demonstrate that younger chil-
dren may report lower quality of life scores.10,11
More research is required in this area.
RISK FACTORSA recent review of the literature highlighted thealarming increase in risk factors for TDI.8 Theauthor attributed this trend to an increased inter-est in the causes and underlying complexity ofTDI. This paper reported the following risk fac-tors: increased overjet and protrusion, “deprivedareas,” risk-taking children, children being bullied,emotionally stressful conditions, obesity, attentiondeficit hyperactivity disorder, learning difficulties,physical limitations, and inappropriate use of
CHAPTER 11 Orofacial Injuries
194
Figure 4. Grey Discoloration on Primary MaxillaryRight Central Incisor as a Result of Necrosis
Source:Courtesy of Dr. Howard Needleman
Figure 6. Inflammatory Root Resorption Postluxation of Maxillary Left Central Incisor
The pathological process was arrested with pulpectomy, calcium hydroxide, and subsequent gutta percha fill.Source:Courtesy of Dr. Howard Needleman
Figure 5. Radiograph to Accompany Figure 4
Source:Courtesy of Dr. Howard Needleman
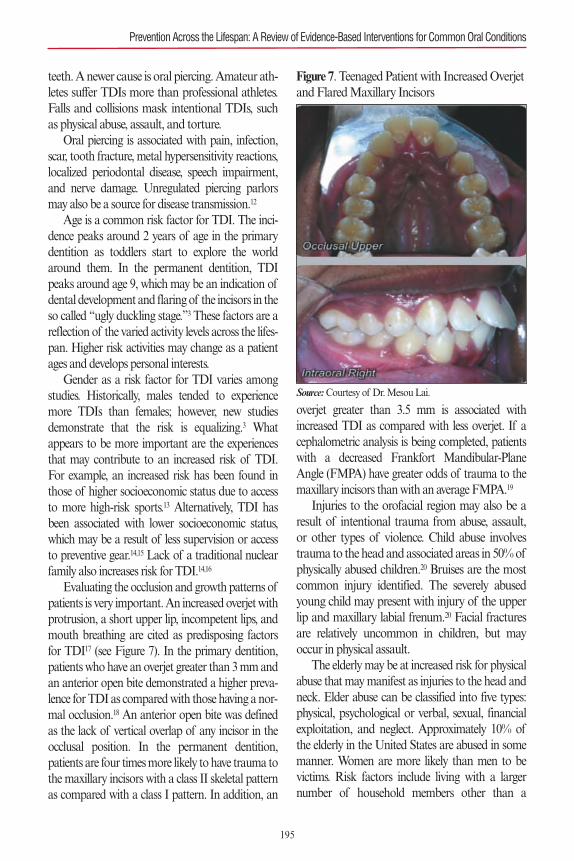
teeth. A newer cause is oral piercing. Amateur ath-letes suffer TDIs more than professional athletes.Falls and collisions mask intentional TDIs, suchas physical abuse, assault, and torture.
Oral piercing is associated with pain, infection,scar, tooth fracture, metal hypersensitivity reactions,localized periodontal disease, speech impairment,and nerve damage. Unregulated piercing parlorsmay also be a source for disease transmission.12
Age is a common risk factor for TDI. The inci-dence peaks around 2 years of age in the primarydentition as toddlers start to explore the worldaround them. In the permanent dentition, TDIpeaks around age 9, which may be an indication ofdental development and flaring of the incisors in theso called “ugly duckling stage.”3 These factors are areflection of the varied activity levels across the lifes-pan. Higher risk activities may change as a patientages and develops personal interests.
Gender as a risk factor for TDI varies amongstudies. Historically, males tended to experiencemore TDIs than females; however, new studiesdemonstrate that the risk is equalizing.3 Whatappears to be more important are the experiencesthat may contribute to an increased risk of TDI.For example, an increased risk has been found inthose of higher socioeconomic status due to accessto more high-risk sports.13 Alternatively, TDI hasbeen associated with lower socioeconomic status,which may be a result of less supervision or accessto preventive gear.14,15 Lack of a traditional nuclearfamily also increases risk for TDI.14,16
Evaluating the occlusion and growth patterns ofpatients is very important. An increased overjet withprotrusion, a short upper lip, incompetent lips, andmouth breathing are cited as predisposing factorsfor TDI17 (see Figure 7). In the primary dentition,patients who have an overjet greater than 3 mm andan anterior open bite demonstrated a higher preva-lence for TDI as compared with those having a nor-mal occlusion.18 An anterior open bite was definedas the lack of vertical overlap of any incisor in theocclusal position. In the permanent dentition,patients are four times more likely to have trauma tothe maxillary incisors with a class II skeletal patternas compared with a class I pattern. In addition, an
overjet greater than 3.5 mm is associated withincreased TDI as compared with less overjet. If acephalometric analysis is being completed, patientswith a decreased Frankfort Mandibular-PlaneAngle (FMPA) have greater odds of trauma to themaxillary incisors than with an average FMPA.19
Injuries to the orofacial region may also be aresult of intentional trauma from abuse, assault,or other types of violence. Child abuse involvestrauma to the head and associated areas in 50% ofphysically abused children.20 Bruises are the mostcommon injury identified. The severely abusedyoung child may present with injury of the upperlip and maxillary labial frenum.20 Facial fracturesare relatively uncommon in children, but mayoccur in physical assault.
The elderly may be at increased risk for physicalabuse that may manifest as injuries to the head andneck. Elder abuse can be classified into five types:physical, psychological or verbal, sexual, financialexploitation, and neglect. Approximately 10% ofthe elderly in the United States are abused in somemanner. Women are more likely than men to bevictims. Risk factors include living with a largernumber of household members other than a
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
195
Figure 7. Teenaged Patient with Increased Overjetand Flared Maxillary Incisors
Source:Courtesy of Dr. Mesou Lai.

spouse, lower income, being isolated, and having alack of social support. With the exception ofdementia, specific diseases have not been identifiedas increasing risk for abuse.21
Another risk factor for orofacial injury is silenttrauma, which is a well-known complication ofgeneral anesthesia during endotracheal intubationand extubation. Although the incidence reportedin the literature is very low, varying from 0.01% to0.1%, preexisting dental and periodontal damageare risk factors. Silent trauma may occur in abroad range of surgical specialties.22 Promptassessment by a dental specialist is required uponoccurrence.
Finally, the lack of a dental home may increasethe risk for orofacial injuries. In this circumstance,a patient may not have access to appropriate pre-ventive care, as defined earlier (i.e., anticipatoryguidance for identifying and modifying risk fac-tors, using interceptive orthodontics and correct-ing habits when there is potential for malocclusionto contribute to risk, preventing treatment delays,and preventing long-term adverse outcomes afterinjury has been sustained).
MANAGEMENT OF OROFACIALINJURIES
A growing body of literature supports the man-agement of traumatic dental injuries. The Interna-tional Association of Dental Traumatology(IADT) most recently updated its guidelines fortreatment in 2012.23–25 In addition, the interactivewebsite created by the IADT provides a real-time
resource for clinicians.26 Interested dental careproviders are able to join the IADT and haveaccess to Dental Traumatology, which is a Med-line-indexed scientific journal and the official pub-lication of the IADT. It provides the latestresearch in the field of traumatology. Moreresearch is needed in the area of management ofTDI as it is difficult to perform randomized clini-cal studies with traumatic injuries. The researchthat has been completed in animal models may bedifficult to extrapolate or not applicable tohumans. One important factor to consider is pre-venting delay in treatment. For this reason, prepa-ration is critical when addressing TDI (see Figure8 and Table 1).
Treatment may differ between primary andpermanent teeth as the health of the developingpermanent dentition plays a role in decision mak-ing when primary teeth are injured.27The ability torecognize what constitutes an injury requiringacute, emergent care is key and will be discussed in
CHAPTER 11 Orofacial Injuries
196
Table 1. Sample Contents of a Trauma Bin
Examination Anesthetic Splinting Material Pulp Treatment Miscellaneous
GauzeCotton rollsSlow- and high-
vacuum suctionAir/water syringe tipMirrorExplorerPeriodontal probeEndo-Ice®
Topical lidocaine
Restorative Material High- and low-
speed handpiecesBursGlass ionomer linerTopical lidocaine
Extraction ForcepsUpper, lower
Acid etchBondFlowable compositeFishing line as
alternative to orthodontic wire
Flexible orthodontic wire
Anterior rubber dam clamp
Rubber dam Endodontic files and
broachesIrrigation liquidCalcium hydroxide,
formocresol, MTA
Suture materialIce packOver-the-counter pain
control medicationsNitrous oxide nasal
hoodPeriodontal dressingTopical fluorideChlorhexidine
Figure 8. Example of a Trauma Bin
Source:Courtesy of Dr. Howard Needleman.
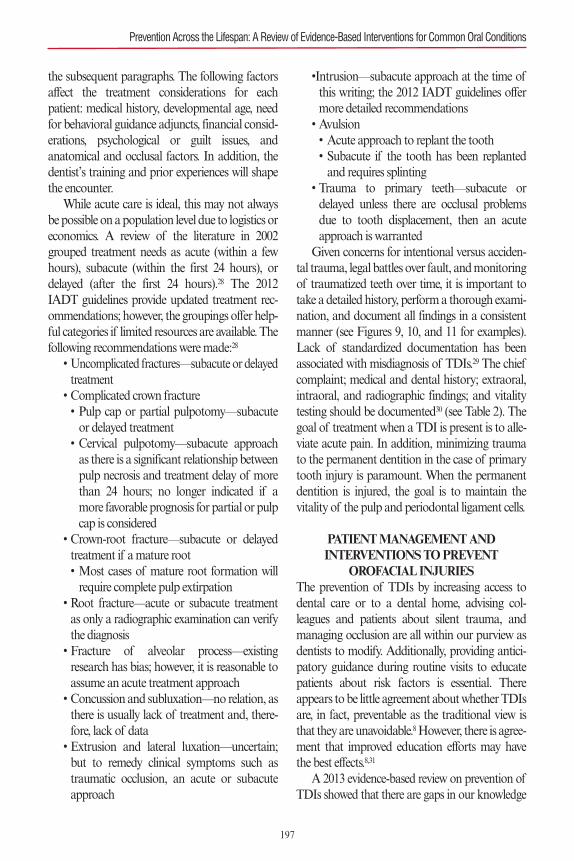
the subsequent paragraphs. The following factorsaffect the treatment considerations for eachpatient: medical history, developmental age, needfor behavioral guidance adjuncts, financial consid-erations, psychological or guilt issues, andanatomical and occlusal factors. In addition, thedentist’s training and prior experiences will shapethe encounter.
While acute care is ideal, this may not alwaysbe possible on a population level due to logistics oreconomics. A review of the literature in 2002grouped treatment needs as acute (within a fewhours), subacute (within the first 24 hours), ordelayed (after the first 24 hours).28 The 2012IADT guidelines provide updated treatment rec-ommendations; however, the groupings offer help-ful categories if limited resources are available. Thefollowing recommendations were made:28
• Uncomplicated fractures—subacute or delayedtreatment
• Complicated crown fracture• Pulp cap or partial pulpotomy—subacute or delayed treatment
• Cervical pulpotomy—subacute approach as there is a significant relationship between pulp necrosis and treatment delay of more than 24 hours; no longer indicated if a more favorable prognosis for partial or pulp cap is considered
• Crown-root fracture—subacute or delayedtreatment if a mature root• Most cases of mature root formation will require complete pulp extirpation
• Root fracture—acute or subacute treatmentas only a radiographic examination can verifythe diagnosis
• Fracture of alveolar process—existingresearch has bias; however, it is reasonable toassume an acute treatment approach
• Concussion and subluxation—no relation, asthere is usually lack of treatment and, there-fore, lack of data
• Extrusion and lateral luxation—uncertain;but to remedy clinical symptoms such astraumatic occlusion, an acute or subacuteapproach
•Intrusion—subacute approach at the time ofthis writing; the 2012 IADT guidelines offermore detailed recommendations
• Avulsion• Acute approach to replant the tooth• Subacute if the tooth has been replanted and requires splinting
• Trauma to primary teeth—subacute ordelayed unless there are occlusal problemsdue to tooth displacement, then an acuteapproach is warranted
Given concerns for intentional versus acciden-tal trauma, legal battles over fault, and monitoringof traumatized teeth over time, it is important totake a detailed history, perform a thorough exami-nation, and document all findings in a consistentmanner (see Figures 9, 10, and 11 for examples).Lack of standardized documentation has beenassociated with misdiagnosis of TDIs.29 The chiefcomplaint; medical and dental history; extraoral,intraoral, and radiographic findings; and vitalitytesting should be documented30 (see Table 2). Thegoal of treatment when a TDI is present is to alle-viate acute pain. In addition, minimizing traumato the permanent dentition in the case of primarytooth injury is paramount. When the permanentdentition is injured, the goal is to maintain thevitality of the pulp and periodontal ligament cells.
PATIENT MANAGEMENT AND INTERVENTIONS TO PREVENT
OROFACIAL INJURIESThe prevention of TDIs by increasing access todental care or to a dental home, advising col-leagues and patients about silent trauma, andmanaging occlusion are all within our purview asdentists to modify. Additionally, providing antici-patory guidance during routine visits to educatepatients about risk factors is essential. Thereappears to be little agreement about whether TDIsare, in fact, preventable as the traditional view isthat they are unavoidable.8However, there is agree-ment that improved education efforts may havethe best effects.8,31
A 2013 evidence-based review on prevention ofTDIs showed that there are gaps in our knowledge
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
197
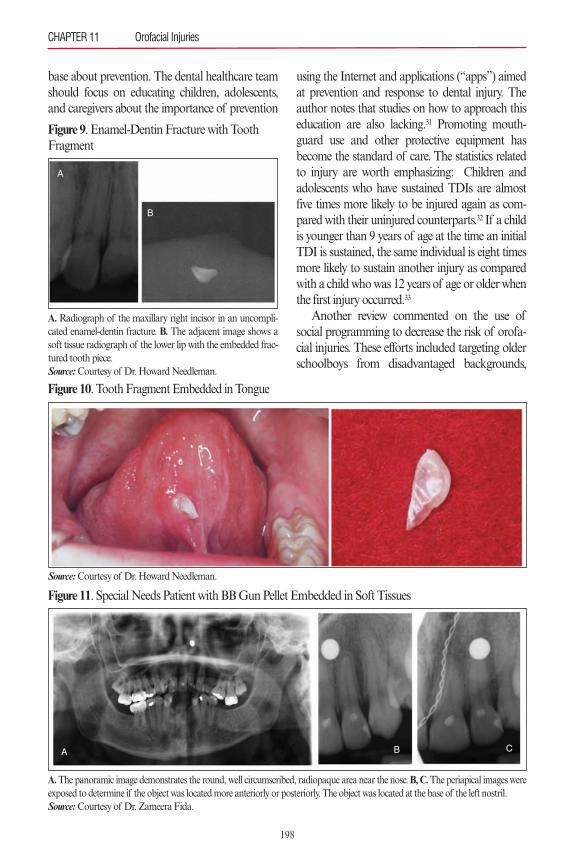
base about prevention. The dental healthcare teamshould focus on educating children, adolescents,and caregivers about the importance of prevention
using the Internet and applications (“apps”) aimedat prevention and response to dental injury. Theauthor notes that studies on how to approach thiseducation are also lacking.31 Promoting mouth-guard use and other protective equipment hasbecome the standard of care. The statistics relatedto injury are worth emphasizing: Children andadolescents who have sustained TDIs are almostfive times more likely to be injured again as com-pared with their uninjured counterparts.32 If a childis younger than 9 years of age at the time an initialTDI is sustained, the same individual is eight timesmore likely to sustain another injury as comparedwith a child who was 12 years of age or older whenthe first injury occurred.33
Another review commented on the use ofsocial programming to decrease the risk of orofa-cial injuries. These efforts included targeting olderschoolboys from disadvantaged backgrounds,
CHAPTER 11 Orofacial Injuries
198
Figure 9. Enamel-Dentin Fracture with ToothFragment
A. Radiograph of the maxillary right incisor in an uncompli-cated enamel-dentin fracture. B. The adjacent image shows asoft tissue radiograph of the lower lip with the embedded frac-tured tooth piece.Source:Courtesy of Dr. Howard Needleman.
B
A
Figure 11. Special Needs Patient with BB Gun Pellet Embedded in Soft Tissues
A.The panoramic image demonstrates the round, well circumscribed, radiopaque area near the nose. B, C.The periapical images wereexposed to determine if the object was located more anteriorly or posteriorly. The object was located at the base of the left nostril.Source:Courtesy of Dr. Zameera Fida.
A B C
Figure 10. Tooth Fragment Embedded in Tongue
Source:Courtesy of Dr. Howard Needleman.
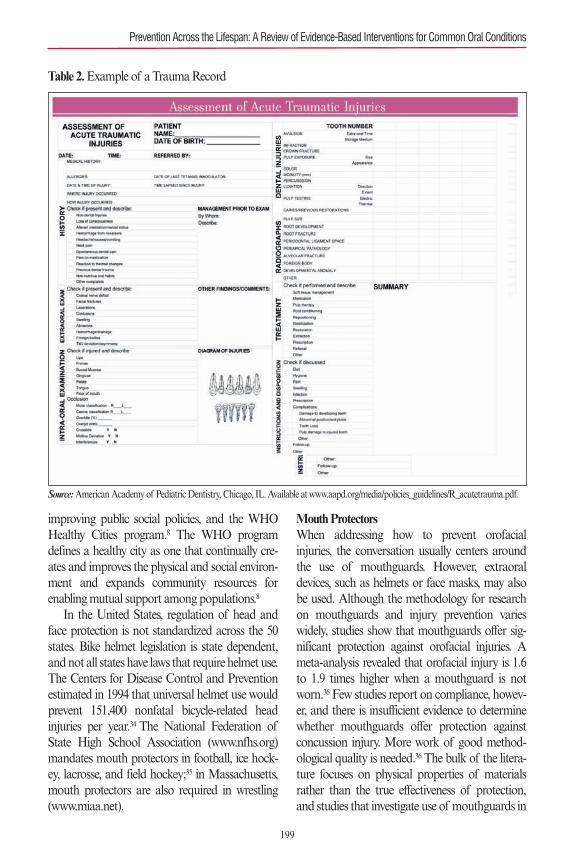
improving public social policies, and the WHOHealthy Cities program.8 The WHO programdefines a healthy city as one that continually cre-ates and improves the physical and social environ-ment and expands community resources forenabling mutual support among populations.8
In the United States, regulation of head andface protection is not standardized across the 50states. Bike helmet legislation is state dependent,and not all states have laws that require helmet use.The Centers for Disease Control and Preventionestimated in 1994 that universal helmet use wouldprevent 151,400 nonfatal bicycle-related headinjuries per year.34 The National Federation ofState High School Association (www.nfhs.org)mandates mouth protectors in football, ice hock-ey, lacrosse, and field hockey;35 in Massachusetts,mouth protectors are also required in wrestling(www.miaa.net).
Mouth ProtectorsWhen addressing how to prevent orofacialinjuries, the conversation usually centers aroundthe use of mouthguards. However, extraoraldevices, such as helmets or face masks, may alsobe used. Although the methodology for researchon mouthguards and injury prevention varieswidely, studies show that mouthguards offer sig-nificant protection against orofacial injuries. Ameta-analysis revealed that orofacial injury is 1.6to 1.9 times higher when a mouthguard is notworn.36 Few studies report on compliance, howev-er, and there is insufficient evidence to determinewhether mouthguards offer protection againstconcussion injury. More work of good method-ological quality is needed.36 The bulk of the litera-ture focuses on physical properties of materialsrather than the true effectiveness of protection,and studies that investigate use of mouthguards in
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
199
Table 2. Example of a Trauma Record
Source:American Academy of Pediatric Dentistry, Chicago, IL. Available at www.aapd.org/media/policies_guidelines/R_acutetrauma.pdf.

real time are lacking due to ethical concerns.Three types of mouthguards are in use. The
first is a stock appliance that is the least expensiveoption. This appliance is held in place by clench-ing the teeth together. It is available in only a fewsizes. Patients may find that it obstructs speechand breathing and, therefore, may decide not towear it. The second is a mouth-formed, or “boiland bite,” type appliance (see Figure 12). This isan inexpensive and disposable alternative to pur-chasing a custom-made mouthguard. This appli-ance is heated and adapted for a better fit, whichcan be done by a dentist in-office during a clinicvisit. It may be a good option for the mixed denti-tion or during orthodontic therapy.
The custom-made appliance has two versions:(1) a single layer, which is a vacuum-formed appli-ance (see Figure 13), and (2) laminate of multiplelayers (see Figure 14). Again, more research in thearea of mouthguard laminating is needed. Com-puter models have been studied, but there is a lackof standardization in these models and the find-ings may not be translated into clinical practice.36
The more common materials used in mouth-guard fabrication are polyvinylacetate-polyethyleneor ethylene vinyl acetate (EVA) copolymer,polyvinylchloride, latex rubber, acrylic resin, andpolyurethane. EVA copolymers are the most popu-
lar because of their ease of use in custom fabrica-tion. Polyvinylchloride has been criticized for pre-sumed links with certain chronic conditions. EVAappears to be the most studied material. Studieshave demonstrated that an increase in EVA increas-es the shock-absorbing capability, but after 4 to 5mm of thickness, there is little additional improve-ment. The inclusion of systematic air cells in EVAcopolymers also improves shock absorbency.36
A 2007 review on mouthguard use addressedthe physical properties of mouthguards and theireffectiveness in prevention of injuries.36Many vari-ables influence the effectiveness of the mouth-guard: material, thickness, manner of fabrication,area of coverage over teeth and gingiva, character-istics of the protected tissue (teeth, bone, gingiva),and direction or force and nature of impact. Thephysical properties of mouthguards (shock-absorbing capability, hardness, stiffness, tearstrength, tensile strength, and water absorption)are measured differently in different studies. Theshock, hardness, and stiffness indicate protectivecapability. The tensile and tear strength indicatedurability, as the appliance will likely be bitten andchewed by the user. Water absorption suggests sta-bility in the aqueous environment of the mouth,and a high water absorption indicates the appli-ance is likely to retain saliva and oral bacteria.36
CHAPTER 11 Orofacial Injuries
200
Figure 12. Examples of Mouth-Formed, “Boil and Bite” Mouthguards
Source:Courtesy of Dr. Howard Needleman.

The following recommendations on mouth-guard construction have been made:36
• A custom-made appliance of EVA results inless tooth deflection and fewer fractured teeththan a “boil and bite” type appliance.
• Custom-made laminate appliances mayinclude a stainless steel arch or foil in an innerlayer to assist in distributing forces, but thismay cause additional injury if the appliance isbroken. Further investigation is needed here.
• Mouthguards may lose their thickness dur-ing fabrication, so the final thickness shouldbe measured and controlled.
• Use of a large occlusal surface area is recom-mended to decrease mandibular distortionand possibility of mandibular fracture. Thisalso results in a faster decay rate of theimpact, which suggests more dispersion of
the impact forces.• Material in use should be moderately stiff orhard. If it is too hard, then high forces may betransmitted to underlying tissues. If it is toosoft, then the appliance itself may compressand deliver forces to a small area of tissue.
• The object causing the impact should be con-sidered in mouthguard fabrication (hard orsoft).
• The patient-specific oral characteristicsshould also be considered in mouthguardfabrication. These include• the occlusal surface available to distribute forces. A softer material with good shock-absorbing capability should be used here.
• the position and periodontal support around incisors, as they are exposed to forces that can be concentrated in a small area. A material with moderate stiffness and shock-absorbing capability should be used to assist in redistributing forces and absorbing shock.
• the gingiva is a soft tissue capable of absorbing force and may need a stiffer material to assist in force redistribution.
The literature is limited regarding whethermouthguards can decrease the rate of brain concussion. The studies that advocated this werecompleted in the 1960s.31 A recent review con-cludes there is no strong evidence for protection ofbrain injuries and that manufacturers may makeunsubstantiated claims.37 Face masks also havelimited evidence regarding prevention of injuries.It has been speculated that spinal injuries may beincreased when young adults use face masks asthey may take unwarranted risks from a falsesense of security.38 Nevertheless, the AmericanDental Association encourages dentists to educatetheir patients on risk of oral injury in sports, fabri-cate properly fitted mouthguards, and provideappropriate guidance on mouthguard types, costs,and benefits.39 Mouthguard use is recommendedanytime there is a risk for orofacial injury.36
Interceptive OrthodonticsAs issues related to occlusion may increase the risk
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
201
Figure 13. Single-Layer Custom-Made Mouthguard.
Source:Courtesy of Dr. Howard Needleman.
Figure 14. Custom-Made Laminate Mouthguard
Source:Courtesy of Dr. Howard Needleman.

for orofacial injuries, it is reasonable to considerwhether orthodontic treatment may decrease thisrisk. An increased overjet, short upper lip, andincompetent lips are known predisposing factors.This occlusal pattern may be the result of a dentalor skeletal issue.
Nonnutritive habits—such as pacifier or digitsucking, tongue thrust swallow, and abnormaltongue position—that are of sufficient frequency,duration, and intensity may be associated withincreased overjet, reduced overbite, posteriorcrossbite, or long facial height.40 Nonnutritivehabits are normal in infants and young children.Dentoalveolar changes resulting from suckinghabits may persist after the habit stops. Part of theanticipatory guidance of early dental visits shouldbe to encourage parents to help children stop thesehabits by the age of 36 months.40
Management of an oral habit should be con-sidered if there is an adverse effect on dentofacialdevelopment. Treatment must be appropriate forthe child’s development and ability to cooperate.40
Treatment modalities include patient–parentcounseling, behavior modification, myofunctionaltherapy, appliance therapy, or referral to otherproviders, such as orthodontists or speech thera-pists. Appliance therapy should only be consid-ered if the child wants to stop the habit and wouldbenefit from a reminder.40
The research to pursue orthodontic appliancetherapy as a modality to decrease overjet has onlybeen completed in children. A 2003 clinical trialshowed no difference in the incidence of trauma ifan overjet of greater than 7 mm was treated earlywith phase 1 orthodontic therapy.41 However, aCochrane review in 2013 provided evidence sug-gesting that early orthodontic treatment (phase 1)for children younger than 16 years of age withprominent upper incisors is more effective inreducing the incidence of incisal trauma than pro-viding one course of orthodontic treatment whenthe child is in early adolescence. This review alsonoted that there appears to be no other advantagefor providing early phase 1 treatment as comparedwith a single phase of treatment in adolescence.42
INTENTIONAL ABUSEDentists are able to prevent orofacial injuries byrecognizing patterns that are indicative of inten-tional trauma. The goal is to prevent furtherinjury by bringing appropriate services to thepatient or family. In the United States, dental pro-fessionals are considered mandated reporters incases of suspected head and neck abuse. If onesuspects intentional abuse, the following questionsshould be considered:20
• Is the injury consistent with the history?• Is there a history of or signs of repeated trau-ma?
• Are there cutaneous manifestations thatstrongly suggest abuse?
• Does the parent, patient, or caretaker exhibitunusual behaviors that may indicate abuse?
• Is there any evidence of neglect or poorsupervision of the patient—specifically, achild or elderly patient?
An increasing body of literature has beenpublished on abuse in the elderly population. Arecent review demonstrated that studies haveuncovered high rates of interpersonal violenceand aggression toward older adults, in particularby other residents in long-term care facilities,rather than by staff in these facilities.21 In general,the victims of elder abuse have some functionalimpairment and are in poor physical health.21
Studies to identify risk factors for becoming aperpetrator in elder abuse are limited. However,limited evidence shows that perpetrators aremore likely to be adult children or spouses of theelder; to be male; to have histories that includesubstance abuse, mental health issues, and trou-ble with police; to be socially isolated; to beunemployed; or to experience financial problemsor major stress.21
The importance of recognizing victims ofabuse cannot be overstated. These patients maybe isolated and their interactions with healthcareproviders may be rare.21 The dental care team hasan opportunity to recognize warning signs andmake referrals to the appropriate specialists forcare.
CHAPTER 11 Orofacial Injuries
202
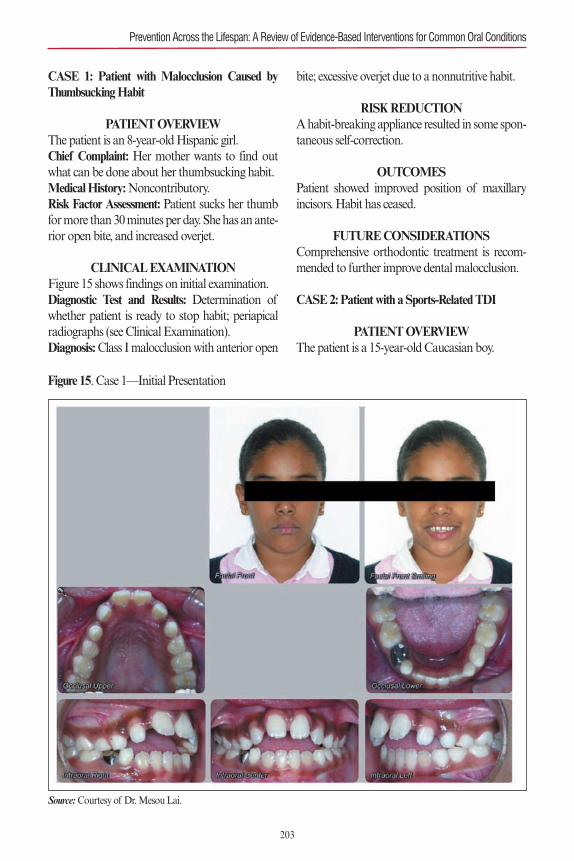
CASE 1: Patient with Malocclusion Caused byThumbsucking Habit
PATIENT OVERVIEWThe patient is an 8-year-old Hispanic girl.Chief Complaint: Her mother wants to find outwhat can be done about her thumbsucking habit.Medical History:Noncontributory.Risk Factor Assessment: Patient sucks her thumbfor more than 30 minutes per day. She has an ante-rior open bite, and increased overjet.
CLINICAL EXAMINATIONFigure 15 shows findings on initial examination.Diagnostic Test and Results: Determination ofwhether patient is ready to stop habit; periapicalradiographs (see Clinical Examination). Diagnosis:Class I malocclusion with anterior open
bite; excessive overjet due to a nonnutritive habit.
RISK REDUCTIONA habit-breaking appliance resulted in some spon-taneous self-correction.
OUTCOMESPatient showed improved position of maxillaryincisors. Habit has ceased.
FUTURE CONSIDERATIONSComprehensive orthodontic treatment is recom-mended to further improve dental malocclusion.
CASE 2: Patient with a Sports-Related TDI
PATIENT OVERVIEWThe patient is a 15-year-old Caucasian boy.
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
203
Figure 15. Case 1—Initial Presentation
Source:Courtesy of Dr. Mesou Lai.
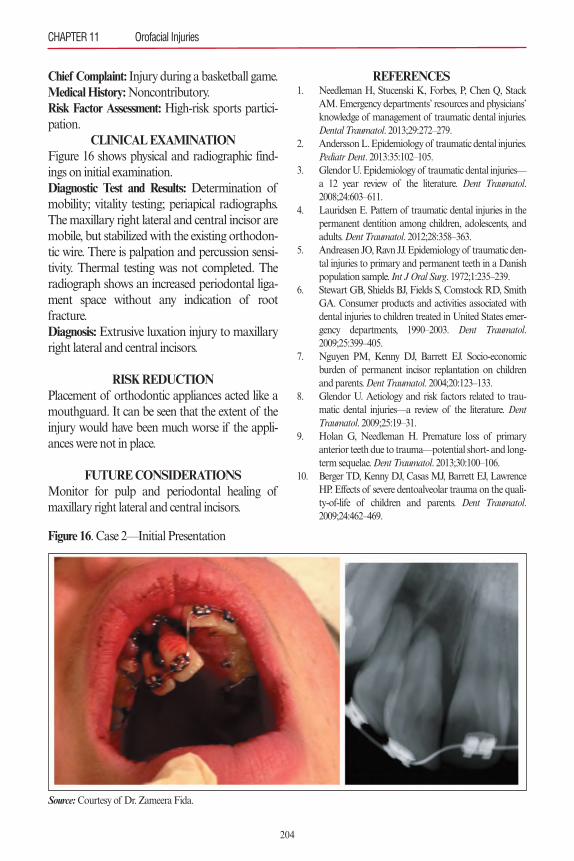
Chief Complaint: Injury during a basketball game.Medical History:Noncontributory.Risk Factor Assessment: High-risk sports partici-pation.
CLINICAL EXAMINATIONFigure 16 shows physical and radiographic find-ings on initial examination.Diagnostic Test and Results: Determination ofmobility; vitality testing; periapical radiographs.The maxillary right lateral and central incisor aremobile, but stabilized with the existing orthodon-tic wire. There is palpation and percussion sensi-tivity. Thermal testing was not completed. Theradiograph shows an increased periodontal liga-ment space without any indication of root fracture.Diagnosis: Extrusive luxation injury to maxillaryright lateral and central incisors.
RISK REDUCTIONPlacement of orthodontic appliances acted like amouthguard. It can be seen that the extent of theinjury would have been much worse if the appli-ances were not in place.
FUTURE CONSIDERATIONSMonitor for pulp and periodontal healing ofmaxillary right lateral and central incisors.
REFERENCES1. Needleman H, Stucenski K, Forbes, P, Chen Q, Stack
AM. Emergency departments’ resources and physicians’knowledge of management of traumatic dental injuries.Dental Traumatol. 2013;29:272–279.
2. Andersson L. Epidemiology of traumatic dental injuries.Pediatr Dent. 2013:35:102–105.
3. Glendor U. Epidemiology of traumatic dental injuries—a 12 year review of the literature. Dent Traumatol.2008;24:603–611.
4. Lauridsen E. Pattern of traumatic dental injuries in thepermanent dentition among children, adolescents, andadults. Dent Traumatol. 2012;28:358–363.
5. Andreasen JO, Ravn JJ. Epidemiology of traumatic den-tal injuries to primary and permanent teeth in a Danishpopulation sample. Int J Oral Surg. 1972;1:235–239.
6. Stewart GB, Shields BJ, Fields S, Comstock RD, SmithGA. Consumer products and activities associated withdental injuries to children treated in United States emer-gency departments, 1990–2003. Dent Traumatol.2009;25:399–405.
7. Nguyen PM, Kenny DJ, Barrett EJ. Socio-economicburden of permanent incisor replantation on childrenand parents. Dent Traumatol. 2004;20:123–133.
8. Glendor U. Aetiology and risk factors related to trau-matic dental injuries—a review of the literature. DentTraumatol. 2009;25:19–31.
9. Holan G, Needleman H. Premature loss of primaryanterior teeth due to trauma—potential short- and long-term sequelae. Dent Traumatol. 2013;30:100–106.
10. Berger TD, Kenny DJ, Casas MJ, Barrett EJ, LawrenceHP. Effects of severe dentoalveolar trauma on the quali-ty-of-life of children and parents. Dent Traumatol.2009;24:462–469.
CHAPTER 11 Orofacial Injuries
204
Figure 16. Case 2—Initial Presentation
Source:Courtesy of Dr. Zameera Fida.
205
11. Traebert J, Lacerda JT, Foster Page LA, Thomson WM,Bortoluzzi MC. Impact of traumatic dental injuries onthe quality of life of schoolchildren. Dent Traumatol.2012;28:423–428.
12. Council on Clinical Affairs, American Academy ofPediatric Dentistry. Policy on intraoral/perioral piercingand oral jewelry/accessories, revised 2011. Available at:http://www.aapd.org/media/Policies_Guidelines/P_Pierce.pdf. Accessed March 30, 2016.
13. Marcenes W, Zabot NE, Traebert J. Socio-economiccorrelates of traumatic injuries to the permanent incisorsin schoolchildren aged 12 years in Blumenau, Brazil.Dent Traumatol. 2001;17:222–226.
14. Lalloo R. Risk factors for major injuries to the face andteeth. Dent Traumatol. 2003;19:12–14.
15. Jorge KO, Moysés SJ, Ferreira e Ferreira E, Ramos-Jorge ML, de Aranjo Zarzar PM. Prevalence and fac-tors associated to dental trauma in infants 1-3 years ofage. Dent Traumatol. 2009;25:185–189.
16. Nicolau B, Marcenes W, Sheiham A. Prevalence, causesand correlates of traumatic dental injuries among 13-year-olds in Brazil. Dent Traumatol. 2001;17:213–217.
17. Güngör HC. Management of crown-related fractures inchildren: an update review. Dent Traumatol. 2014;30:88–99.
18. Bonini GC, Bönecker M, Braga MM, Mendes FM.Combined effect of anterior malocclusion and inade-quate lip coverage on dental trauma in primary teeth.Dent Traumatol. 2012;28:437–440.
19. Bozabadi-Farahani A, Bozabadi-Farahani A,Eslamipour F. An investigation into the associationbetween facial profile and maxillary incisor trauma, aclinical non-radiographic study. Dent Traumatol.2010;26:403–408.
20. Needleman HL. Orofacial trauma in child abuse: types,prevalence, management and the dental profession’sinvolvement. Pediatr Dent. 1986;8:(special issue 1):71–80.
21. Lach MS, Pillemer KA. Elder abuse. N Engl J Med.2015; 373:1947–1956.
22. Adolphs N, Kessler B, von Heymann C, et al. Den-toalveolar injury related to general anesthesia: a 14 yearsreview and a statement from the surgical point of viewbased on a retrospective analysis of the documentationof a university hospital. Dent Traumatol. 2011;27:10–14.
23. Diangelis AJ, Andreasen JO, Ebeleseder KA, et al. Inter-national Association of Dental Traumatology guidelinesfor the management of traumatic dental injuries. I. Frac-tures and luxations of permanent teeth. Dent Traumatol.2012;28:2–12.
24. Andersson L, Andreasen JO, Day P, et al. InternationalAssociation of Dental Traumatology guidelines for themanagement of traumatic dental injuries. II. Avulsion ofpermanent teeth. Dent Traumatol. 2012;28:88–96.
25. Malmgren B, Andreasen JO, Flores MT, et al. Interna-tional Association of Dental Traumatology guidelines
for the management of traumatic dental injuries. III.Injuries in the primary dentition. Dent Traumatol.2012;28:174–182.
26. University Hospital of Copenhagen. The dental traumaguide, updated 2014. Available at: http://www.dental-traumaguide.org._Accessed April 18, 2016.
27. Needleman HL. The art and science of managing trau-matic injuries to primary teeth. Dent Traumatol.2011;27:295–299.
28. Andreasen JO, Andreasen FM, Skeie A, Hjørting-HansenE, Schwartz O. Effect of treatment delay upon pulp andperiodontal healing of traumatic dental injuries—a reviewarticle. Dent Traumatol. 2002;18:116–128.
29. Andreasen FM, Kahler B. Diagnosis of acute dentaltrauma: the importance of standardized documentation:a review. Dent Traumatol. 2015;31:340–349.
30. American Academy of Pediatric Dentistry. Assessmentof acute traumatic injuries. Available from:http://www.aapd.org/media/Policies_Guidelines/R_AcuteTrauma.pdf. Accessed March 30, 2016.
31. Sigurdsson A. Evidence-based review of prevention ofdental injuries. Pediatr Dent. 2013:35;184–190.
32. Ramos-Jorge ML, Peres MA, Traebert J, et al. Incidenceof dental trauma among adolescents: a prospectivecohort study. Dent Traumatol. 2008;24:159–163.
33. Glendor U, Koucheki B, Halling A. Risk evaluation andtype of treatment of multiple dental trauma episodes topermanent teeth. Endod Dent Traumatol. 2000;16:205–210.
34. Centers for Disease Control and Prevention. Injury con-trol recommendations: Bicycle helmets. 1995;44(RR-1);1–18. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/00036941.htm. Accessed March 30, 2016.
35. American Academy of Pediatric Dentistry. Policy onprevention of sports-related orofacial injuries, revised2013. Available from: http://www.aapd.org/media/Poli-cies_Guidelines/P_Sports.pdf. Accessed March 30, 2016.
36. Knapik JJ, Marshall SW, Lee RB, et al. Mouthguards insports activities: history, physical properties and injuryprevention effectiveness. Sports Med. 2007;37(2):117–144.
37. Benson BW, Hamilton GM, Meeuwisse WH, et al. Isprotective equipment useful in preventing concussion? Asystematic review of the literature. Br J Sports Med.2009;43(suppl 1):i56–67.
38. Murray TM, Livingston LA. Hockey helmets, facemasks, and injurious behavior. Pediatrics. 1995;95:419–421.
39. ADA Council on Access, Prevention and Interprofes-sional Relations, ADA Council on Scientific Affairs.Using mouthguards to reduce the incidence and severityof sports-related oral injuries. J Am Dent Assoc.2006;137:1712–1720.
40. Clinical Affairs Committee–Developing Dentition Sub-committee. Guideline on management of the developingdentin and occlusion in pediatric dentistry. Availablefrom: http://www.aapd.org/media/Policies_Guidelines/
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions

G_DevelopDentition.pdf. Accessed March 30, 2016.41. Koroluk LD, Tulloch JF, Phillips C. Incisor trauma and
early treatment for Class II Division 1 malocclusion. AmJ Orthod Dentofacial Orthop. 2003;123:117–126.
42. Thiruvenkatachari B, Harrison JE, Worthington HV,O’Brien KD. Orthodontic treatment for prominentupper front teeth (Class II malocclusion) in children.Cochrane Database Syst Rev. 2013;(11):CD003452.
ADDITIONAL READINGS A. Andreasen JO, Andreasen FM and Andersson, L. Text-
book and Color Atlas of Traumatic Injuries to the Teeth.4th ed. Munksgaard, Cogenhagen: 2007.
B. Dental Traumatology—Official publication of the Inter-national Association of Dental Traumatology and Acad-emy of Sports Medicine (http://interscience.wiley.com/journal/dt).
CHAPTER 11 Orofacial Injuries
206

Since the late 1980s, there has been a steady accu-mulation of scientific evidence linking poor oralhealth (specifically the presence of periodontitis)with a number of systemic diseases, notably dia-betes and cardiovascular disease. Potential linksbetween adverse pregnancy outcomes and pres-ence of maternal periodontitis have also beenextensively investigated. While many of the indi-vidual studies that have evaluated links betweenoral health and systemic health have been relative-ly small and of short duration, sufficient numbershave now been published to enable systematicreviews and meta-analyses to be performed. Thesepermit researchers to combine data from differentstudies to create much larger datasets and there-fore allow analyses to be performed with increasedstatistical power.
These studies have led to a resurgence of inter-est into the links between periodontal health andgeneral health. Given the huge increases in preva-lence rates of noncommunicable diseases (such asdiabetes and cardiovascular disease) currentlybeing observed in many populations around theworld, in parallel with increases in obesity, theimportance of optimizing oral health and pre-venting development or progression of periodon-tal disease is likely to become increasingly relevant.Dental professionals will find they have anincreasingly important role to play in the overallhealth management of their patients. This repre-sents a paradigm shift in the way the dental profes-sion has operated in recent times. For many years,the dental profession has been functioning quitedistinctly from the broader medical profession, tothe detriment of our patients. This separation ofmedicine and dentistry became particularly evi-
dent in the latter half of the twentieth century,driven partly by differences in clinical care path-ways and remuneration systems between the med-ical and dental professions, and partly also bytechnical advances in dental surgical and restora-tive techniques and materials that were used exclu-sively by the dental profession to treat (i.e., repair)the consequences of diseases such as dental caries.However, in the twenty-first century, we now rec-ognize the importance of moving away from arestorative/reparative paradigm that focused onrestoring damaged, diseased, or missing teethtoward a disease prevention paradigm within thecontext of overall systemic health.
While it may appear that the expansion in thenumbers of studies investigating oral–systemiclinks is a relatively recent phenomenon, the con-cept is not new. Indeed, in the late 1800s, followingthe publication of Robert Koch’s germ theory ofdisease, a number of authors were linking oral dis-eases with a wide range of systemic diseases anddisorders.1 In broad terms, it was believed thatmicroorganisms from the mouth would translo-cate to other regions of the body, thereby causingdisease at those distant locations. Thus, Miller, inhis 1891 publication, considered a wide range ofsystemic disorders to be caused by bacteria fromthe teeth and mouth (see Table 1).2
Numerous publications and prominentspeakers of that time expounded upon anddeveloped this theme, leading to the concept of
207
Prevention in the Contextof Oral–Systemic Health
Chapter 12
Philip M. Preshaw
Source: Based on Dental Cosmos. 1891;33:689–713.2
Table 1. Systemic Diseases and ConditionsAttributable to Oral Bacteria
Actinomycosis
Diphtheria
Encephalitis
Meningitis
Noma
Osteomyelitis
Pneumonia
Pyemia
Septicemia
Sinusitis
Syphilis
Tonsillitis
Tuberculosis

“focal infection,” which stated that infections anddisease could be caused by the dissemination ofbacteria or bacterial products from a focus ofinfection at one location in the body to anothersite in the body via the circulatory or lymphaticsystems.3 The primary foci of infection were con-sidered to be the teeth, tonsils, and sinuses, andthis concept was particularly attractive forexplaining the cause of various diseases for whichthere was, at that time, no other known etiology.This led to patients undergoing procedures suchas dental clearances and tonsillectomies as amanagement strategy for systemic diseases, pro-cedures that clearly would not be indicated todayaccording to our modern understanding of vari-ous disease etiologies.
Fortunately, the more rigorous application ofscientific methods in the early parts of the twenti-eth century began to reverse this trend. For exam-ple, a study of different treatments for rheumatoidarthritis (tonsillectomy, dental clearance, and notreatment) found no benefit from the surgicalinterventions, with the authors questioning thevalidity of the focal infection theory.4 A 1940 edi-torial in the Journal of the American MedicalAssociation vigorously discredited the concept offocal infection, bringing this era of clinical andresearch activity to an end.5 Although this wasappropriate, given that the focal infection theorywas not supported by scientific or clinical evi-dence, one consequence was that for the next 50years or so, medicine and dentistry went their sep-arate ways.
The study that rekindled interest in the linksbetween oral health and systemic disease in morerecent times was a case-control study of patientswho had experienced acute myocardial infarction,published in 1989.6 Poor oral health, as assessedusing a dental index that was calculated based onthe numbers of caries lesions, missing teeth, peri-apical lesions, probing depths, and presence ofpericoronitis, was found to be significantly associ-ated with acute myocardial infarction, independ-ent of other cardiac risk factors that included age,social class, smoking, serum lipid concentrations,and presence of diabetes. Since then, numerous
studies have investigated links between oral healthand a range of systemic conditions; this chapterconsiders current knowledge in this area.
KEY CONSIDERATIONSThe term periodontal disease refers to a range ofconditions that affect the supporting structures ofthe teeth, including the gingiva, connective tissueand alveolar bone. Gingivitis refers to inflamma-tion that affects the gingiva only, whereas peri-odontitis refers to inflammation that also affectsthe periodontal ligament and alveolar bone, lead-ing to breakdown of the attachment between theteeth and the bone, alveolar bone resorption, andultimately tooth mobility and tooth loss (seeChapter 5). Our understanding of periodontalpathogenesis has evolved over the years: in themid-twentieth century, periodontitis was consid-ered to be ubiquitous, with dental plaque beingthe sole etiological factor. However, our modernconcept of disease pathogenesis focuses on therole of inflammation as a response to the subgin-gival microbiota in driving periodontal tissuebreakdown, and hence, the development of clini-cal signs and symptoms of disease. Thus, we con-sider that the subgingival microbiota initiates andperpetuates the chronic inflammatory response inthe gingival and periodontal tissues, yet it is theinflammation that is primarily responsible for thetissue destruction that characterizes disease. Thereare variations in disease susceptibility between dif-ferent individuals, likely derived from variations inthe inflammatory response profile, which in turn isinfluenced by a wide variety of genetic, epigenetic,microbial, and environmental factors.7 The com-mon end point is the tissue damage that dentalprofessionals recognize clinically as periodontitis.
The inflammatory response in the gingival andperiodontal tissues is characterized by infiltrationof the tissues by circulating host defense cells (neu-trophils, monocytes/macrophages, and lympho-cytes), together with increasing concentrations ofinflammatory mediators such as cytokines,prostaglandins, and matrix metalloproteinases(MMPs). Key cytokines include interleukin-1b�(IL-1b), IL-6, tumor necrosis factor-a (TNF-a),
CHAPTER 12 Prevention in the Context of Oral–Systemic Health
208

T-cell regulatory cytokines, chemokines (such asIL-12 and IL-18), and cytokines that mediatebone metabolism, such as receptor activator ofNF-kB ligand (RANKL) and osteoprotegerin(OPG). Cytokines do not function in isolation,but interact functionally in complex networks inthe periodontium, with regulatory control exertedat a number of levels and involving infiltratingimmune cells as well as resident cells in the peri-odontium.8 Periodontitis can be regarded as acomplex chronic disease in which the inflamma-tion is ineffective in eliminating the initiatingpathogens, the persistence of which leads tochronic inflammation and concomitant progres-sive tissue destruction.9
In broad terms, there are two main potentialpathways in which the microbiota-inducedinflammation in the periodontal tissues may havean impact on overall health.10 One mechanism isvia translocation of bacteria and bacterial prod-ucts across the pocket or junctional epitheliuminto the circulation, leading to bacteremia and sys-temic inflammatory responses. It is noteworthythat the surface area of inflamed and ulceratedpocket epithelium in a patient with generalizedperiodontitis has been estimated as being approxi-mately 20 cm2, presenting clear opportunity forpassage of bacteria and their products into the cir-culation.11 The second mechanism is via passageof inflammatory mediators produced locally inthe periodontal tissues into the circulation, leadingto increased systemic inflammation and acutephase responses from the liver. Both pathways arelikely to play a role in the links between periodon-tal and systemic diseases, and the precise mecha-nisms are the focus of considerable research effortscurrently. Whereas many systemic diseases andconditions have been linked to periodontitis, thosethat have been the subject of most research activi-ty are diabetes, cardiovascular disease, and adversepregnancy outcomes.
PERIODONTAL DISEASE AND DIABETESIn considering all the systemic diseases that havebeen associated with periodontal disease, thestrongest evidence exists for the links between peri-
odontal disease and diabetes. A large number ofepidemiological studies and population-based sur-veys have confirmed that the risk of periodontitisis significantly increased in people with diabetes,with the level of glycemic control being a key fac-tor in determining risk. It has been estimated thatpeople with poorly controlled diabetes have anapproximately threefold increased risk of peri-odontitis compared with those who do not havediabetes.12 In the US National Health and Nutri-tion Examination Survey III (NHANES III),patients with glycated hemoglobin (HbA1c)greater than 9% (> 75 mmol/mol) had a signifi-cantly higher prevalence of severe periodontitiscompared with those who did not have diabetes(odds ratio [OR]: 2.90; 95% confidence interval[CI]: 1.40–6.03) after controlling for age, smoking,gender, and ethnicity.13 Most studies of the epi-demiological links between the two conditionshave tended to focus on type 2 diabetes, becausehistorically, type 2 diabetes and chronic periodon-titis tended to present in patients in their 40s and50s. The risk of periodontitis is increased in type 1diabetes also, with the level of glycemic controlappearing to be the key factor in determining risk.Therefore, all people with diabetes should be con-sidered to be at increased risk of periodontitis,particularly if they have poor glycemic control.14
The pathogenesis of periodontal disease is char-acterized by the development of chronic (i.e., per-sisting) and dysregulated inflammatory responsesin the periodontal tissues as a defense mechanismagainst the subgingival microbiota, which results inthe tissue damage that we identify clinically as dis-ease. Key inflammatory mediators were listed earli-er and have been extensively reviewed elsewhere.8
Dysregulated immune responses also contribute tothe pathogenesis of type 1 and type 2 diabetes, andare associated with hyperglycemia, hyperlipidemia,and other metabolic and physiological changes.Hyperglycemia drives the formation of advancedglycation end products (AGEs), a process in whichnonenzymatic glycation of structural proteins ofthe body (including collagens) leads to altered cellu-lar function and proinflammatory effects involvinginteractions between AGEs and the receptor for
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
209

advanced glycation end products (RAGE), result-ing in activation of proinflammatory genes. As aresult of increased numbers of RAGE ligands indiabetes (because of hyperglycemia), this receptor isconsidered to have a causative role in many of thecomplications of diabetes. Elevated circulating lev-els of cytokines, such as IL-6 and TNF-a, arefound in diabetes, and increased serum levels of IL-6 and C-reactive protein (CRP) have been linked tofuture occurrence of type 2 diabetes.15–17 Inflamma-tion is of central importance to the pathogenesis ofboth periodontitis and diabetes, and mechanistical-ly links the pathogenesis of both conditions. Thisarea has been extensively reviewed: IL-1b, TNF-a,IL-6, OPG, and RANKL mediate periodontitis inpatients with diabetes, with the AGE-RAGE axisalso being an important pathway of periodontaltissue destruction in people with diabetes.18
Inflammation clearly drives the increased sus-ceptibility to periodontitis that is observed in peo-ple with diabetes, similar to many of thecomplications of diabetes. There is also evidencethat periodontal inflammation has a negativeimpact on glycemic control and complications ofdiabetes, thus suggesting a potential benefit ofperiodontal disease prevention and treatment onthe diabetic state. The potential negative impact ofperiodontitis on diabetes outcomes was initiallydescribed in studies in which severe periodontitiswas associated with increased risk of poorerglycemic control (defined as HbA1c ≥ 9%, or 75mmol/mol) in individuals from the Gila RiverIndian community, a population with a very highprevalence of periodontitis, who were monitoredlongitudinally over 2 years.19 Further studies in thesame population identified that the presence ofsevere periodontitis was associated with a morethan twofold increased risk of development ofnephropathy (macroalbuminuria and end-stagerenal disease) in individuals with diabetes com-pared with diabetic individuals who did not havesevere periodontitis, after adjusting for potentialconfounders such as age, sex, smoking, diabetesduration, and body mass index.20 In a long-termstudy of Pima Indians with type 2 diabetes inwhich the impact of periodontitis on cardiovascu-
lar disease mortality was assessed, the presence ofsevere periodontitis was a statistically significantpredictor of deaths from ischemic heart diseasesand diabetic nephropathy, and, after adjusting forknown risk factors (age, sex, smoking, diabetesduration, body mass index, HbA1c macroalbu-minuria, cholesterol, hypertension), subjects withsevere periodontitis and diabetes had a three timesincreased risk of cardiorenal mortality (ischemicheart disease and diabetic nephropathy combined)compared with those who did not have severeperiodontitis.21
The impact of periodontitis on HbA1c levelsin individuals who did not have diabetes has beenstudied in a 5-year longitudinal follow-up study.22
After adjustment for risk factors (age, sex, smok-ing, family history of diabetes, obesity), those indi-viduals who had the most advanced periodontitisat study commencement experienced a five timesgreater increase in HbA1c over the 5-year studyperiod (DHbA1c = 0.11%) compared with thosewho had no periodontitis at baseline (DHbA1c =0.02%), suggesting that severe periodontitis possi-bly increases risk for incidence of diabetes. In across-sectional study of periodontitis and predia-betes (defined according to American DiabetesAssociation criteria for impaired fasting glucoseand impaired glucose tolerance), presence ofsevere periodontitis was associated with a 93%increase in the odds of having impaired glucosetolerance, after adjusting for confounders, suggest-ing a role for periodontitis in the etiology ofimpaired glycemic regulation and risk for develop-ment of diabetes.23
In a systematic review of studies that have eval-uated the effects of periodontal disease on dia-betes control, complications, and incidentdiabetes, it was concluded that, although few stud-ies have addressed this topic, current evidence sug-gests that compared with individuals who areperiodontally healthy, those who have poor peri-odontal health and no diabetes have a greater riskof developing diabetes, and those who have poorperiodontal health and diabetes have a greater riskfor developing diabetes complications and devel-oping poorer glycemic control.24 If these findings
CHAPTER 12 Prevention in the Context of Oral–Systemic Health
210
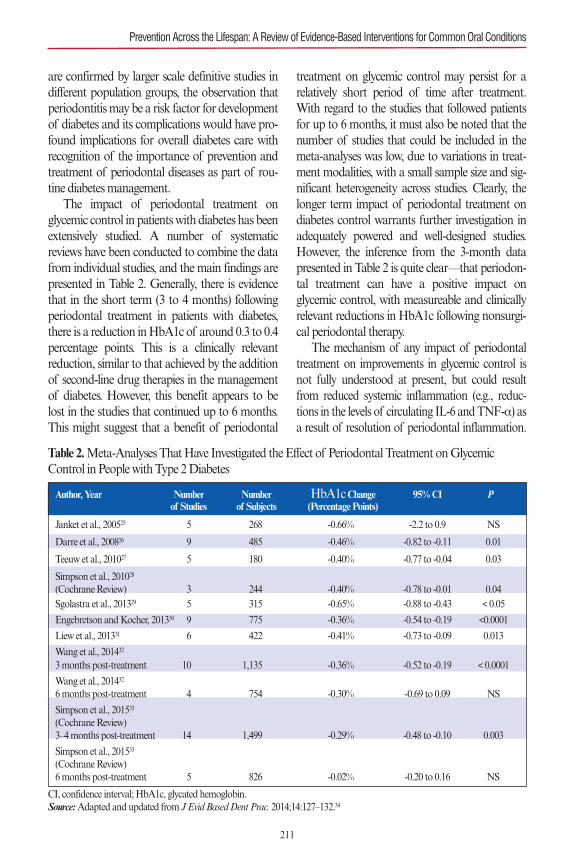
are confirmed by larger scale definitive studies indifferent population groups, the observation thatperiodontitis may be a risk factor for developmentof diabetes and its complications would have pro-found implications for overall diabetes care withrecognition of the importance of prevention andtreatment of periodontal diseases as part of rou-tine diabetes management.
The impact of periodontal treatment onglycemic control in patients with diabetes has beenextensively studied. A number of systematicreviews have been conducted to combine the datafrom individual studies, and the main findings arepresented in Table 2. Generally, there is evidencethat in the short term (3 to 4 months) followingperiodontal treatment in patients with diabetes,there is a reduction in HbA1c of around 0.3 to 0.4percentage points. This is a clinically relevantreduction, similar to that achieved by the additionof second-line drug therapies in the managementof diabetes. However, this benefit appears to belost in the studies that continued up to 6 months.This might suggest that a benefit of periodontal
treatment on glycemic control may persist for arelatively short period of time after treatment.With regard to the studies that followed patientsfor up to 6 months, it must also be noted that thenumber of studies that could be included in themeta-analyses was low, due to variations in treat-ment modalities, with a small sample size and sig-nificant heterogeneity across studies. Clearly, thelonger term impact of periodontal treatment ondiabetes control warrants further investigation inadequately powered and well-designed studies.However, the inference from the 3-month datapresented in Table 2 is quite clear—that periodon-tal treatment can have a positive impact onglycemic control, with measureable and clinicallyrelevant reductions in HbA1c following nonsurgi-cal periodontal therapy.
The mechanism of any impact of periodontaltreatment on improvements in glycemic control isnot fully understood at present, but could resultfrom reduced systemic inflammation (e.g., reduc-tions in the levels of circulating IL-6 and TNF-a) asa result of resolution of periodontal inflammation.
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
211
Table 2. Meta-Analyses That Have Investigated the Effect of Periodontal Treatment on Glycemic Control in People with Type 2 Diabetes
CI, confidence interval; HbA1c, glycated hemoglobin.Source: Adapted and updated from J Evid Based Dent Prac. 2014;14:127–132.34
Author, Year Number Number HbA1cChange 95% CI Pof Studies of Subjects (Percentage Points)
Janket et al., 200525 5 268 -0.66% -2.2 to 0.9 NS
Darre et al., 200826 9 485 -0.46% -0.82 to -0.11 0.01
Teeuw et al., 201027 5 180 -0.40% -0.77 to -0.04 0.03
Simpson et al., 201028
(Cochrane Review) 3 244 -0.40% -0.78 to -0.01 0.04 Sgolastra et al., 201329 5 315 -0.65% -0.88 to -0.43 < 0.05
Engebretson and Kocher, 201330 9 775 -0.36% -0.54 to -0.19 <0.0001
Liew et al., 201331 6 422 -0.41% -0.73 to -0.09 0.013
Wang et al., 201432
3 months post-treatment 10 1,135 -0.36% -0.52 to -0.19 < 0.0001
Wang et al., 201432
6 months post-treatment 4 754 -0.30% -0.69 to 0.09 NS
Simpson et al., 201533
(Cochrane Review)3–4 months post-treatment 14 1,499 -0.29% -0.48 to -0.10 0.003
Simpson et al., 201533
(Cochrane Review)6 months post-treatment 5 826 -0.02% -0.20 to 0.16 NS

Both of these cytokines induce the production ofacute phase proteins, including CRP, and evidenceindicates that these cytokines can impair insulin sig-naling.35–37 Reduction of periodontal inflammationcould thus lead to reductions in systemic inflamma-tion, with a potential benefit of improved glycemiccontrol. However, more research is necessary to testthis hypothesis. Whereas elevated CRP levels are aconsistent finding in patients with periodontitiscompared with healthy controls,38 evidence that hasconsistently demonstrated elevated circulatingcytokine levels in patients with periodontitis com-pared with controls is lacking.18 Further research inthis area is required, but clearly optimizing oral andperiodontal health is an important aspect of con-tributing to good general health, and preventionand treatment of periodontitis should form part ofthe overall healthcare management of all patients,including those with diabetes.
PERIODONTAL DISEASE AND CARDIOVASCULAR DISEASE
Cardiovascular diseases include conditions suchas coronary heart disease (myocardial infarction,angina); peripheral artery disease; and cerebrovas-cular disease (stroke, transient ischemic attack).Bacteria, including those from the oral cavity, havebeen implicated in the etiology of cardiovasculardiseases, and it is clear that periodontal bacteriacan enter the circulation, particularly followingany form of trauma to the gingival tissues (such asfollowing toothbrushing, chewing, flossing, anddental procedures), causing a bacteremia.39 Tran-sient bacteremias involving periodontal bacteriaappear, therefore, to be a regular occurrence.There is also clear evidence that periodontal bacte-ria can be found in atheromatous tissues, andspecies such as Porphyromonas gingivalis andAggregatibacter actinomycetemcomitanshave beendemonstrated to live in atheromas.40 In a review ofthe literature, evidence was identified to support aprocess by which periodontal bacteria enter thecirculation and disseminate to systemic vasculartissues, where they can live in sites affected byatheromas. Periodontal bacteria can also invadeaffected cell types in vitro and induce atherosclero-
sis in animal models of disease.40The bacteria acti-vate host inflammatory responses at these distantsites, and the host immune–inflammatoryresponse favors atheroma formation, maturation,and exacerbation.41 Although it is difficult to dif-ferentiate the direct role of bacteria from theresultant inflammatory response, taken collective-ly these findings support the concept that peri-odontal bacteria can contribute to atherosclerosis.
Epidemiological studies have reported anincreased risk for cardiovascular disease inpatients with periodontal disease compared withthose who do not have periodontal disease. In asystematic review of cohort and case-control stud-ies on the association between periodontal diseaseand cardiovascular disease, it was identified thatincidence (i.e., new cases) of cardiovascular dis-ease (specifically incident coronary heart disease,cerebrovascular disease, and peripheral artery dis-ease) is higher in patients who had periodontaldisease or more advanced periodontal diseasecompared with patients who did not have peri-odontal disease or had better periodontal status,independent of many cardiovascular disease riskfactors.42 In other words, periodontal disease wasfound to impart a statistically significant excessrisk for incident cardiovascular disease, independ-ent of other risk factors. The level of excess riskvaried across populations and was greater in cere-brovascular disease than coronary heart disease, inmales, and in younger individuals. There was noevidence for an association between periodontaldisease and incident cardiovascular disease inpatients older than 65 years.
Clearly, many potential confounding variablescan affect associations between periodontal diseaseand cardiovascular disease. The studies that wereincluded in the systematic review routinely con-trolled for smoking, and excess risk for cardiovascu-lar disease in patients with periodontal disease wasalso reported in never-smokers in a number of thestudies. Excess risk associated with periodontitiswas also reported in studies that controlled for dia-betes as a confounder. It is quite possible that theassociation between periodontal disease and car-diovascular disease could be affected by as yet
CHAPTER 12 Prevention in the Context of Oral–Systemic Health
212

unrecognized confounders, such as shared proin-flammatory phenotypes that result from commongenetically controlled pathways of inflammationthat influence the nature of the host inflammatoryresponses to bacterial challenge. The importance ofinflammation in the pathogenesis of cardiovasculardisease is well established, and several mechanismshave been reported by which periodontal bacteriamay cause increased inflammatory responses asso-ciated with atheroma lesions.43 More research isrequired in this area, particularly prospective clini-cal trials and studies to identify causal relationshipsas opposed to associations.
A number of intervention studies have beenconducted to evaluate the effect of periodontaltreatment on cardiovascular disease. Many areassociation studies, for example, a population-based national survey identified that as patient-reported frequency of toothbrushing increased,prevalence of hypertension decreased, afteradjusting for confounders such as presence ofperiodontitis, age, sex, smoking, body fat, alcoholconsumption, exercise, education, and income.44
When considering intervention studies, periodon-tal treatment has been reported to induce a short-term acute inflammatory response (characterizedby increases in systemic inflammatory markerssuch as CRP, IL-6, TNF-a, and endothelial dys-function),45 followed by progressive reductions insystemic inflammation and improvements inendothelial function.46 A systematic review con-cluded that there is moderate evidence for a reduc-tion in systemic inflammation followingperiodontal treatment as evidenced by reductionsin serum CRP levels and improvements inendothelial function.46 Both of these parameters(elevated CRP and impaired endothelial function)have been associated with risk for cardiovasculardisease. The review also identified moderate evi-dence that periodontal treatment has no effect onlipid profiles and serum IL-6 levels, and limitedevidence that periodontal treatment results inreductions of other biomarkers for cardiovasculardisease (markers of inflammation, coagulation,and biomarkers of endothelial cell activation), aswell as limited evidence that periodontal treatment
reduces arterial blood pressure.46 Clearly, interven-tion studies are indicated to investigate the impactof periodontal treatment on primary preventionof cardiovascular disease (i.e., prevention of firstischemic event) and secondary prevention of car-diovascular disease (i.e., prevention of subsequentischemic events), although these are very challeng-ing to design and implement.
To summarize, there is consistent and strongepidemiological evidence that periodontal diseaseimparts an excess risk for cardiovascular disease,after controlling for the impact of other risk fac-tors. From a mechanistic perspective, the impactof periodontitis on cardiovascular diseases is bio-logically plausible, relating to periodontal bacteriagaining access to the circulation and, both directlyand indirectly (by inducing systemic inflamma-tion), affecting the pathogenesis of atheroma for-mation. Although intervention and animal studiesreport reductions in the levels of specific inflam-matory biomarkers that are associated with car-diovascular disease risk following periodontaltreatment, more research is required in this area toinvestigate the impact of prevention and treat-ment of periodontal diseases on primary and sec-ondary prevention of cardiovascular diseases.41
PERIODONTAL DISEASE AND ADVERSEPREGNANCY OUTCOMES
Pregnancy is a physiological process that usuallyproceeds normally but sometimes has adverseoutcomes, including low birthweight (defined as < 2,500 g), preterm birth (defined as < 37 weeks ofgestation), and other complications such asgrowth restriction, preeclampsia, miscarriage, andstillbirth. Adverse pregnancy outcomes are associ-ated with several risk factors, including environ-mental exposures (e.g., smoking), medicalconditions and treatments, genetic susceptibility,and individual behavioral and psychosocial fac-tors. Adverse pregnancy outcomes are thought tomainly originate from ascending infections fromthe vagina or cervix, or from hematogenous (i.e.,blood-borne) spread from known or unknownnongenital sources of infection. The presence ofperiodontitis in the mother represents a potential
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
213

source of microorganisms that are known to enterthe circulation and thus may have both direct andindirect effects on the developing fetal–placentalunit.47
A systematic review of epidemiological studiesconcluded that maternal periodontitis is signifi-cantly, but modestly, associated with low birth-weight and preterm birth.48 However, the strengthof the associations was influenced by factors suchas the case definition employed in individual stud-ies to describe whether or not a participant hadperiodontitis. Indeed, studies that used a categori-cal assessment of the presence of periodontitis(e.g., based on a case definition defined dichoto-mously according to the presence of variablenumbers of teeth and sites with specific probingdepth or attachment loss thresholds) were morelikely to report significant positive associationsbetween maternal periodontitis and adverse preg-nancy outcomes than studies (including someconducted in the same populations) that used con-tinuous variables (e.g., mean probing depths) asthe outcome measure for periodontitis in the sta-tistical analyses. Further limitations in the studiesthat have been conducted include highly variablestudy designs, differing case definitions for peri-odontitis, and inadequate and varying manage-ment of potential confounders such associoeconomic status, race and ethnicity, andsmoking. Other potential exposures that mayaffect risk for adverse pregnancy outcomesinclude maternal age and weight, weight gain dur-ing pregnancy, behavioral factors (e.g., alcoholconsumption, nutrition, exercise, and stress), andmedical conditions (e.g., diabetes).
Regarding the possible mechanistic linksbetween maternal periodontitis and adverse preg-nancy outcomes, two major pathways have beenproposed that could trigger an immune–inflam-matory response in the fetal–placental unit. Theseinclude
1. A direct pathway by which periodontal ororal bacteria and bacterial products enterthe circulation in the oral cavity and reachthe fetal–placental unit by means of the cir-culation, or alternatively, oral bacteria reach
the fetal–placental unit by an ascendingroute through the genitourinary tract.
2. An indirect pathway by which inflammatorymediators (e.g., prostaglandin E2, TNF-a)produced locally in the periodontal tissuesenter the circulation and affect the fetal–pla-cental unit, or microbial products or inflam-matory mediators enter the circulation fromthe periodontal tissues and circulate to theliver, resulting in acute-phase proteinresponses (e.g., production of CRP) andrelease of cytokines such as IL-6, which thenaffect the fetal–placental unit.
The evidence from animal and human studiesis strongest to support the direct pathway, in whichhematogenous spread of periodontal bacteria andtheir products leads to effects on the fetal–placen-tal unit. These include various outcomes that aredependent on the nature and the timing of theexposure. For example, lower exposures may leadto increased risk of prematurity by causing hyper-contractility of the uterus, cervical dilation, andloss of membrane integrity. Higher exposurespotentially could lead to abortion, miscarriage,and stillbirth.49
Given the associations that have been reportedbetween maternal periodontitis and adverse preg-nancy outcomes, several clinical trials have beenconducted in which periodontal treatment hasbeen provided to pregnant mothers and outcomeshave been assessed. These studies have consistentlyreported that periodontal therapy (root surfacedebridement) is safe to perform during pregnancyand results in improved periodontal status in thepregnant women, but there is no clear or consis-tent evidence of any impact of the periodontaltherapy in reducing overall rates of low birth-weight or preterm birth.50 Nonetheless, the posi-tive outcomes reported in some clinical trialssuggest that specific patient populations may ben-efit more from periodontal treatment than otherpopulations. More research is required to investi-gate this area further, but clearly prevention andtreatment of periodontal conditions in pregnantwomen is important for optimizing oral health,just as it is in nonpregnant individuals.47
CHAPTER 12 Prevention in the Context of Oral–Systemic Health
214

APPLICATION TO CLINICAL PRACTICEDental clinicians have long been aware that pre-vention of disease is better than cure. We have hada tendency, however, to focus specifically on themouth, and our role in preventing and treatingoral and dental diseases has naturally been placedprimarily within the context of the oral cavity. Wewould all agree, also, that good oral health is inte-gral to good general health and life quality, andthat optimizing oral health and preventing oraldisease should be a part of overall healthcaremanagement strategies.51
Now we have a further extension of this con-cept; namely, that the prevention and treatment ofperiodontal disease may have a benefit on the gen-eral health and systemic disease states of ourpatients. This opens up the potential for the dentalteam to play a broader role in the overall generalhealth management of our patients. For example,the importance of optimized oral hygiene in theprevention of systemic disease has been demon-strated in the context of hospital-acquired pneu-monias in institutionalized elderly and nursinghome residents,52 and the use of oral antiseptics hasbeen shown to significantly reduce the risk of venti-lator-associated pneumonia.53 Clearly, improve-ments in oral hygiene achieved by routinepreventive strategies for periodontal disease areimportant in the prevention of pneumonia in sus-ceptible populations, emphasizing the importanceof oral and dental care as part of overall medicalmanagement.
It is noteworthy that there are similaritiesbetween the management strategies required forsuccessful treatment of periodontitis and those forother chronic diseases such as diabetes and cardio-vascular diseases. For example, the managementof diabetes requires lifestyle changes by thepatient, achieved by a process of patient educationabout aspects such as exercise, diet, and use ofmedications, as well as self-management and self-monitoring. A key concept is that patients musttake responsibility (assisted by their medical clini-cians in this task) for the management of their dia-betes if successful outcomes are to be achieved.These principles are instantly recognizable to den-
tal clinicians who manage patients with periodon-titis. Lifestyle changes by periodontal patients aresimilarly important, such as optimizing oralhygiene, compliance with the periodontal mainte-nance care plan, and smoking cessation, allachieved by patient education and regular andrepeated interactions with dental clinicians. Struc-tured educational programs exist for the manage-ment of diabetes,54,55 and similar initiatives havealso been reported for the management of peri-odontitis.56,57 The unifying concept behind theseeducational programs is the emphasis on develop-ing self-efficacy for managing disease, achieved bypatient education to effect lifelong behaviorchange, supported by the clinical team as theyprogress toward this goal (see Chapter 2).
Patient education and self-efficacy are funda-mental to the management of chronic diseasessuch as diabetes and periodontitis, and it is cer-tainly the case that dental clinicians are adept atinfluencing behavior change in their patients.Given the evidence of links between periodontaldisease and systemic diseases such as diabetes, aswell as the potential systemic health benefits fol-lowing periodontal treatment that have beenobserved, it is likely that decisions about preven-tive strategies and oral disease management will beinfluenced by the dental clinician’s knowledge ofthe patient’s general health status. The rising tideof obesity and increasing prevalence of diabetes inpopulations throughout the world, coupled withthe already high prevalence of periodontal dis-eases, make this topic highly relevant to both den-tal and medical professionals. Dentalprofessionals will have an increasingly importantrole to play in overall healthcare management,alongside our medical colleagues, in preventingand managing periodontitis (and other oral condi-tions) so as to have a positive impact on generalhealth status and life quality. As dental profession-als, we can now recognize that we have importantcontributions to make in improving the overallhealth care of our patients.
The results of a recent study conducted in theUnited States exemplify the roles that dental profes-sionals may have in the future. The researchers eval-
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
215

uated 239 dental patients with risk factors for dia-betes who were screened in a dental clinic; of these,101 were identified as having HbA1c greater than5.7%, or 39 mmol/mol.58 These individuals werethen randomized to two groups. Participants in thefirst group were told about their diabetes risk fac-tors and blood test results and advised to see aphysician; those in the second group were given adetailed explanation of the findings together with awritten report for the physician, and were then fol-lowed up. Whereas no significant differences in out-comes between the two groups were recorded at 6months after the intervention, 84% of all thepatients reported having seen a physician and 49%reported at least one positive lifestyle change as aresult of the intervention in the dental clinic.
In a study conducted in various dental clinicalsettings, including general dental practices in theUK, 166 patients were screened for diabetes risk.59
All patients were given written advice on healthylifestyles by the dental team, and those at moderateor high risk for diabetes were referred to their med-ical practitioner for further investigation, resultingin 30% of the moderate-risk and 20% of the high-risk patients visiting their medical professional.The patients welcomed the opportunity to discusstheir general health in the dental practice, and thedental clinicians also enjoyed the additional train-ing and skills that they acquired. Whereas the mainchallenge was the time taken for the diabetesassessment (adding approximately 20 minutes toeach dental appointment), this study suggests thatpeople at risk of developing type 2 diabetes can beidentified in primary, community, and secondarydental care settings. The use of blood collectedfrom the gingival crevice for the purpose of meas-uring HbA1c has also been evaluated, andresearchers identified a very high degree of correla-tion between HbA1c values derived from gingivalcrevice blood and those derived from standard fin-gerstick blood samples.60 This finding suggests thatthe dental team, with appropriate equipment andtraining, could use gingival crevicular fluid bloodcollected at the time of routine dental appoint-ments to screen for presence of diabetes.
The prevention and treatment of periodontal
disease is fundamentally important in patientswith diabetes, not only because of the increasedrisk for periodontitis in patients with diabetes (par-ticularly if glycemic control is poor), but alsobecause of the potential negative impacts of peri-odontitis on glycemic control and diabetes compli-cations. Patients with diabetes should therefore beinformed about their increased risk for periodonti-tis. It should also be explained that the presence ofperiodontitis may make glycemic control moredifficult, and may increase the risk for other dia-betes complications such as cardiovascular diseaseand kidney disease.61 Patients with diabetes shouldreceive an appropriate periodontal examinationand if periodontitis is diagnosed, it should beproperly managed. Other potential oral complica-tions of diabetes should also be evaluated, such asdry mouth, burning mouth, and candidal infec-tions. People with diabetes who do not have peri-odontitis should receive appropriate preventivecare, including optimized oral hygiene and profes-sional mechanical plaque removal as required,and regular monitoring of periodontal status.Patients who do not have a diagnosis of diabetes,but who present with other obvious risk factorsfor diabetes together with signs of periodontitisshould be informed about their risk of having dia-betes and referred to their medical physician forassessment, with the results of a chairside HbA1ctest, if available, provided.61
As described earlier, the presence of peri-odontitis has also been associated with increasedrisk for incident cardiovascular disease after con-trolling for known cardiovascular risk factors.Clearly, it is important to treat periodontal dis-ease to improve oral health and prevent progres-sion of disease, and the association withcardiovascular disease further underscores theimportance of primary and secondary preven-tion of periodontal disease. Given the consistentepidemiological evidence that periodontitisimparts increased risk for cardiovascular disease,it is important for the dental clinician to be awareof this evidence and to communicate it topatients when necessary. In particular, patientswith periodontitis who also have other risk
CHAPTER 12 Prevention in the Context of Oral–Systemic Health
216

factors for cardiovascular disease (e.g., smoking,hypertension, overweight, obesity) should bemade aware of shared disease risks and advisedto see their medical practitioner. Modifiable riskfactors associated with both conditions (e.g.,smoking) should routinely be addressed in thedental setting, and patients should be encouragedto take action to manage these risks (e.g., throughreferral to smoking cessation services).41
Procedures to improve periodontal health aresafe during pregnancy, and these procedures areusually effective in improving and maintaining oraland periodontal health.48 In accordance with rou-tine clinical practice, elective procedures should beavoided in the first trimester of pregnancy to avoidstress to the fetus and generally should be under-taken in the second trimester. Preventive treatmentregimens are important during pregnancy, and rec-ommendations have been published regarding pre-ventive care in pregnant women with varyingperiodontal disease presentations.47 Thus, forwomen with a healthy periodontium, health educa-tion about preventing periodontal diseases isimportant for their own health and that of theirchildren. This includes explanation of transientchanges to the gingival tissues during pregnancy(such as increased bleeding and possible gingivalenlargement as a result of increased vascularity ofthe tissues), as well as advice and instruction in oralhygiene techniques. For pregnant women with gin-givitis, the same health promotion measures shouldbe undertaken, together with professional interven-tion to treat the gingivitis to reduce the bacterialload and reduce inflammation. For those with peri-odontitis, in addition to the same health promotionadvice, nonsurgical periodontal therapy should beprovided to disrupt and reduce the subgingivalbiofilm and to reduce inflammation. The currentlack of evidence to indicate that treatment ofmaternal periodontitis has a beneficial effect onreducing adverse pregnancy outcomes50 suggeststhat such preventive and therapeutic regimens dur-ing pregnancy have their primary efficacy in treat-ing periodontal disease and reducing periodontaldisease progression rather than having an effect onthe outcomes of the pregnancy.
CONCLUSIONSThis chapter has reviewed the evidence for thelinkage between periodontal disease and systemicdiseases such as diabetes and cardiovascular dis-ease, and also adverse pregnancy outcomes. Theplausibility of the biological links between peri-odontitis and diabetes and cardiovascular diseaseis based on the finding that periodontal inflamma-tion that develops in response to the challengefrom the subgingival microbiota contributes to thecumulative systemic inflammatory burden in thehost.24 Furthermore, blood-borne spread of peri-odontal bacteria and their products can haveeffects throughout the body, contributing to sys-temic inflammation and risk for disease.
Associations between a number of differentsystemic diseases and periodontitis have beenreported in the periodontal literature. Some of thesystemic conditions that have been associated withperiodontitis include chronic obstructive pul-monary disease, pneumonia, osteoporosis, chronickidney disease, rheumatoid arthritis, cognitiveimpairment, obesity, metabolic syndrome, andcancer, and the interested reader is referred to textsthat have dealt with these topics in greater detail.62
However, it is recognized that research into possi-ble associations between periodontitis and manysystemic conditions has been hampered by theinherent difficulties in controlling for common riskfactors or confounders such as smoking andsocioeconomic status. Furthermore, by necessityof cost and practicality, most studies have been ofrelatively short duration and have relied on surro-gate disease markers to assess outcomes. Furtherproblems, such as inconsistent use of case defini-tions for periodontitis, have hampered our effortsto advance knowledge in this area.63
Research into the links between periodontaldisease and various systemic diseases will thereforecontinue. Clearly, it is important to prevent andtreat periodontal disease for the oral health andquality of life benefits that such treatments areknown to achieve. Prevention of periodontal dis-eases requires the combined efforts of the patientin achieving effective oral hygiene and reducingrisk factors with those of the clinician in providing
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
217
professionally delivered therapies for mechanicalplaque removal and root surface debridement.Repeated and individually tailored oral hygieneinstruction is fundamental to achieving gingivaland periodontal health, together with profession-ally delivered mechanical plaque removal bothsupra- and subgingivally to disrupt and reduce thebiofilm and remove hard deposits.64 As our under-standing of the mechanisms that underpin thelinks between periodontal disease and systemicconditions improves, and if causality is clearlydemonstrated, then a new paradigm for care willbe warranted, with closer collaboration betweenmedical and dental healthcare providers and newstandards for prevention and management of sys-temic diseases such as diabetes.24 Periodontal dis-eases are largely preventable, and the preventionand treatment of periodontitis is warranted notonly to establish and optimize oral health, butpotentially to have positive effects on generalhealth and well-being and quality of life.
REFERENCES1. Williams RC. Understanding and managing periodontal
diseases: a notable past, a promising future. J Periodon-tol. 2008;79:1552–1559.
2. Miller WD. The human mouth as a focus of infection.Dental Cosmos. 1891;33:689–713.
3. Billings FA. Chronic focal infections and their etiologicrelations to arthritis and nephritis. Arch Int Med.1912;9:484–498.
4. Cecil RL, Angevine DM. Clinical and experimentalobservations on focal infection, with an analysis of 200cases of rheumatoid arthritis. Ann Intern Med.1938;12:577–584.
5. Reimann HA, Havens WP. Focal infection and systemicdisease: a critical appraisal. JAMA. 1940;114:1–6.
6. Mattila KJ, Nieminen MS, Valtonen VV, et al. Associa-tion between dental health and acute myocardial infarc-tion. BMJ. 1989;298:779–781.
7. Kinane DF, Preshaw PM, Loos BG. Host-response:understanding the cellular and molecular mechanisms ofhost-microbial interactions-consensus of the SeventhEuropean Workshop on Periodontology. J Clin Peri-odontol. 2011;38(suppl 11):44–48.
8. Preshaw PM, Taylor JJ. How has research into cytokineinteractions and their role in driving immune responsesimpacted our understanding of periodontitis? J ClinPeriodontol. 2011;38(suppl 11):60–84.
9. Chapple ILC. Periodontal diagnosis and treatment—where does the future lie? Periodontol 2000. 2009;51:9–24.
10. Williams RC, Barnett AH, Claffey N, et al. The potentialimpact of periodontal disease on general health: a con-sensus view. Curr Med Res Opin. 2008;24:1635–1643.
11. Hujoel PP, White BA, Garcia RI, et al. The dentogingi-val epithelial surface area revisited. J Periodontal Res.2001;36:48–55.
12. Mealey BL, Ocampo GL. Diabetes mellitus and peri-odontal disease. Periodontol 2000. 2007;44:127–153.
13. Tsai C, Hayes C, Taylor GW. Glycemic control of type 2diabetes and severe periodontal disease in the US adultpopulation. Community Dent Oral Epidemiol.2002;30:182–192.
14. Preshaw PM, Bissett SM. Periodontitis: oral complica-tion of diabetes. Endocrinol Metab Clin North Am.2013;42:849–867.
15. Brownlee M. The pathobiology of diabetic complica-tions: a unifying mechanism. Diabetes. 2005;54:1615–1625.
16. Dandona P, Aljada A, Bandyopadhyay A. Inflamma-tion: the link between insulin resistance, obesity and dia-betes. Trends Immunol. 2004;25:4–7.
17. Schmidt MI, Duncan BB, Sharrett AR, et al. Markersof inflammation and prediction of diabetes mellitus inadults (Atherosclerosis Risk in Communities study): acohort study. Lancet. 1999;353:1649–1652.
18. Taylor JJ, Preshaw PM, Lalla E. A review of the evi-dence for pathogenic mechanisms that may link peri-odontitis and diabetes. J Clin Periodontol. 2013;40(suppl.14):S113–S134.
19. Taylor GW, Burt BA, Becker MP, et al. Severe periodon-titis and risk for poor glycemic control in patients withnon-insulin-dependent diabetes mellitus. J Periodontol.1996;67:1085–1093.
20. Shultis WA, Weil EJ, Looker HC, et al. Effect of peri-odontitis on overt nephropathy and end-stage renal dis-ease in type 2 diabetes. Diabetes Care. 2007;30:306–311.
21. Saremi A, Nelson RG, Tulloch-Reid M, et al. Periodon-tal disease and mortality in type 2 diabetes. DiabetesCare. 2005;28:27–32.
22. Demmer RT, Desvarieux M, Holtfreter B, et al. Peri-odontal status and A1C change: longitudinal resultsfrom the study of health in Pomerania (SHIP). DiabetesCare. 2010;33:1037–1043.
23. Arora N, Papapanou PN, Rosenbaum M, et al. Peri-odontal infection, impaired fasting glucose and impairedglucose tolerance: results from the Continuous NationalHealth and Nutrition Examination Survey 2009–2010. JClin Periodontol. 2014;41:643–652.
24. Borgnakke WS, Ylostalo PV, Taylor GW, et al. Effect ofperiodontal disease on diabetes: systematic review of epi-demiologic observational evidence. J Clin Periodontol.2013;40(suppl. 14):S135–S152.
25. Janket SJ, Wightman A, Baird AE, et al. Does periodon-tal treatment improve glycemic control in diabeticpatients? A meta-analysis of intervention studies. J DentRes. 2005;84:1154–1159.
CHAPTER 12 Prevention in the Context of Oral–Systemic Health
218
26. Darre L, Vergnes JN, Gourdy P, et al. Efficacy of peri-odontal treatment on glycaemic control in diabeticpatients: A meta-analysis of interventional studies. Dia-betes Metab. 2008;34:497–506.
27. Teeuw WJ, Gerdes VEA, Loos BG. Effect of periodon-tal treatment on glycemic control of diabetic patients: asystematic review and meta-analysis. Diabetes Care.2010;33:421–427.
28. Simpson TC, Needleman I, Wild SH, et al. Treatment ofperiodontal disease for glycaemic control in people with dia-betes. Cochrane Database Syst Rev. 2010;(5):CD004714.doi: 10.1002/14651858.CD004714. pub2.
29. Sgolastra F, Severino M, Pietropaoli D, et al. Effective-ness of periodontal treatment to improve metabolic con-trol in patients with chronic periodontitis and type 2diabetes: a meta-analysis of randomized clinical trials. JPeriodontol. 2013;84:958–973.
30. Engebretson S, Kocher T. Evidence that periodontaltreatment improves diabetes outcomes: a systematicreview and meta-analysis. J Clin Periodontol.2013;40(suppl 14):S153–S163.
31. Liew AK, Punnanithinont N, Lee YC, et al. Effect ofnon-surgical periodontal treatment on HbA1c: a meta-analysis of randomized controlled trials. Aust Dent J.2013;58:350–357.
32. Wang X, Han X, Guo X, et al. The effect of periodontaltreatment on hemoglobin a1c levels of diabetic patients:a systematic review and meta-analysis. PLoS One.2014;9:e108412. doi: 10.1371/journal.pone.0108412.
33. Simpson TC, Weldon JC, Worthington HV, et al. Treat-ment of periodontal disease for glycaemic control inpeople with diabetes mellitus. Cochrane Database SystRev. 2015;(11):CD004714. doi: 10.1002/14651858.CD004714.pub3.
34. Borgnakke WS, Chapple ILC, Genco RJ, et al. Themulti-center randomized controlled trial (RCT) pub-lished by the Journal of the American Medical Associa-tion (JAMA) on the effect of periodontal therapy onglycated hemoglobin (HbA1c) has fundamental prob-lems. J Evid Based Dent Prac. 2014;14:127–132.
35. Hotamisligil GS. Molecular mechanisms of insulinresistance and the role of the adipocyte. Int J Obes RelatMetab Disord. 2000;24(suppl 4):S23–S27.
36. Hotamisligil GS. Inflammation and metabolic disorders.Nature. 2006;444:860–867.
37. Rotter V, Nagaev I, Smith U. Interleukin-6 (IL-6)induces insulin resistance in 3T3-L1 adipocytes and is,like IL-8 and tumor necrosis factor-a, overexpressed inhuman fat cells from insulin-resistant subjects. J BiolChem. 2003;278:45777–45784.
38. Loos BG. Systemic markers of inflammation in peri-odontitis. J Periodontol. 2005;76:2106–2115.
39. Tomas I, Diz P, Tobias A, et al. Periodontal health statusand bacteraemia from daily oral activities: systematicreview/meta-analysis. J Clin Periodontol. 2012;39:213–228.
40. Reyes L, Herrera D, Kozarov E, et al. Periodontal bacte-
rial invasion and infection: contribution to atherosclerot-ic pathology. J Clin Periodontol. 2013;40(suppl 14):S30–S50.
41. Tonetti MS, Van Dyke TE. Periodontitis and atheroscle-rotic cardiovascular disease: consensus report of theJoint EFP/AAP Workshop on Periodontitis and Sys-temic Diseases. J Clin Periodontol. 2013;40(suppl14):S24–S29.
42. Dietrich T, Sharma P, Walter C, et al. The epidemiologi-cal evidence behind the association between periodonti-tis and incident atherosclerotic cardiovascular disease. JClin Periodontol. 2013;40(suppl 14):S70–S84.
43. Schenkein HA, Loos BG. Inflammatory mechanismslinking periodontal diseases to cardiovascular diseases. JClin Periodontol. 2013;40(suppl 14):S51–S69.
44. Choi HM, Han K, Park YG, et al. Associations amongoral hygiene behavior and hypertension prevalence andcontrol: the 2008 to 2010 Korea National Health andNutrition Examination Survey. J Periodontol.2015;86:866–873.
45. Tonetti MS, D’Aiuto F, Nibali L, et al. Treatment ofperiodontitis and endothelial function. N Engl J Med.2007;356:911–920.
46. D’Aiuto F, Orlandi M, Gunsolley JC. Evidence that peri-odontal treatment improves biomarkers and CVD out-comes. J Clin Periodontol. 2013;40(suppl 14):S85–S105.
47. Sanz M, Kornman K. Periodontitis and adverse preg-nancy outcomes: consensus report of the JointEFP/AAP Workshop on Periodontitis and SystemicDiseases. J Clin Periodontol. 2013;40(suppl 14):S164–S169.
48. Ide M, Papapanou PN. Epidemiology of associationbetween maternal periodontal disease and adverse preg-nancy outcomes systematic review. J Clin Periodontol.2013;40(suppl 14):S181–S194.
49. Madianos PN, Bobetsis YA, Offenbacher S. Adversepregnancy outcomes (APOs) and periodontal disease:pathogenic mechanisms. J Clin Periodontol. 2013;40(suppl 14):S170–S180.
50. Michalowicz BS, Gustafsson A, Thumbigere-Math V, etal. The effects of periodontal treatment on pregnancyoutcomes. J Clin Periodontol. 2013;40(suppl 14):S195–S208.
51. Oral health: prevention is key. Lancet. 2009;373:1.52. Sjogren P, Nilsson E, Forsell M, et al. A systematic
review of the preventive effect of oral hygiene on pneu-monia and respiratory tract infection in elderly people inhospitals and nursing homes: effect estimates andmethodological quality of randomized controlled trials.J Am Geriatr Soc. 2008;56:2124–2130.
53. Labeau SO, Van de Vyver K, Brusselaers N, et al. Pre-vention of ventilator-associated pneumonia with oralantiseptics: a systematic review and meta-analysis.Lancet Infect Dis. 2011;11:845–854.
54. Davies MJ, Heller S, Khunti K, et al. The DESMONDeducational intervention. Chronic Illn. 2008;4:38–40.
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
219
220
55. Gillett M, Dallosso HM, Dixon S, et al. Delivering thediabetes education and self management for ongoingand newly diagnosed (DESMOND) programme forpeople with newly diagnosed type 2 diabetes: cost effec-tiveness analysis. BMJ. 2010;341:c4093.
56. Jonsson B, Ohrn K, Oscarson N, et al. The effectivenessof an individually tailored oral health educational pro-gramme on oral hygiene behaviour in patients with peri-odontal disease: a blinded randomized-controlledclinical trial (one-year follow-up). J Clin Periodontol.2009;36:1025–1034.
57. Jonsson B, Ohrn K, Oscarson N, et al. An individuallytailored treatment programme for improved oralhygiene: introduction of a new course of action in healtheducation for patients with periodontitis. Int J Dent Hyg.2009;7:166–175.
58. Lalla E, Cheng B, Kunzel C, et al. Six-month outcomes indental patients identified with hyperglycaemia: a random-ized clinical trial. J Clin Periodontol. 2015;42:228–235.
59. Wright D, Muirhead V, Weston-Price S, et al. Type 2 dia-betes risk screening in dental practice settings: a pilot
study. Br Dent J. 2014;216:E15.60. Strauss SM, Rosedale MT, Pesce MA, et al. The poten-
tial for glycemic control monitoring and screening fordiabetes at dental visits using oral blood. Am J PublicHealth. 2015;105:796–801.
61. Chapple IL, Genco R. Diabetes and periodontal dis-eases: consensus report of the Joint EFP/AAP Work-shop on Periodontitis and Systemic Diseases. J ClinPeriodontol. 2013;40(suppl 14):S106–S112.
62. Genco RJ, Williams RC, eds. Periodontal Disease andOral Health: A Clinician’s Guide. 2nd ed. Yardley, PA:Professional Audience Communications, Inc.; 2014.
63. Linden GJ, Lyons A, Scannapieco FA. Periodontal sys-temic associations: review of the evidence. J Clin Peri-odontol. 2013;40(suppl 14):S8–S19.
64. Tonetti MS, Eickholz P, Loos BG, et al. Principles in pre-vention of periodontal diseases: Consensus report ofgroup 1 of the 11th European Workshop on Periodon-tology on effective prevention of periodontal and peri-implant diseases. J Clin Periodontol. 2015;42(suppl16):S5–S11.
CHAPTER 12 Prevention in the Context of Oral–Systemic Health
SPECIAL NEEDS PATIENTS AND DENTAL HEALTH
The increase in the number of individuals withdisabilities is a worldwide phenomenon, in partdue to growth in the number of people who areliving into chronologically older ages and in partdue to premature aging and the resulting suscepti-bility to aging diseases experienced by many peo-ple with disabilities, especially those of thedevelopmental type.1 Individuals with disabilitiesare likely to have poorer health as a result of barri-ers to care that can include physical impediments,prohibitive costs, and limited availability.1 In den-tistry, the care of people with disabilities is thatbranch of dentistry that provides oral care servicesfor people with physical, medical, developmental,or cognitive conditions that limit their ability toreceive routine dental care.2
ORAL DISEASE BURDEN AND BARRIERSTO CARE IN SPECIAL NEEDS PATIENTSAs noted in the US Surgeon General’s report onoral health, people with special needs have dispro-portionately high levels of oral disease due to thenature and limitations of access to care.3 Fre-quently, patients with special care needs, especiallythose with developmental disabilities, are caredfor by pediatric dentists with whom they continuetheir treatment even after entering adulthood. Yetthese patients often have comorbidities, second-ary health conditions, and age-related ailmentsthat are not within the purview of the pediatricdentist. For them, an adult-centered dental homewould be much more appropriate.4 Because of
the all-inclusive definition of special care needs,the increasing population of the United States,and the disproportionately high level of oral dis-ease in patients with special healthcare needs, alldental care providers need to be willing and com-petent to treat patients in the primary care set-ting.5,6 This situation is true for all countries, eventhose where special care dentistry is considered adental specialty.7
In the best of situations and even when apatient with special needs has access to care, his orher ability to cooperate in receiving dental caremay be a huge barrier to receiving preventive orcurative treatments for dental diseases.8 The mosteffective and efficient way to reduce the dental dis-ease burden is by prevention, which in the past hasbeen provided to the general population mainlyby water fluoridation, the widespread use of fluo-ride-containing toothpastes and mouthrinses,9
and regular dental care according to the patient’srisk for dental disease.10 However, patients withspecial healthcare needs have extra barriers toreceiving routine care. This is especially true ofthose patients presenting with a variety of cogni-tive and physical disabilities that may impede theirability to understand the importance of preventivecare or how to access it and to safely tolerate den-tal care delivery without the use of a sedative.6,11
With new and better diagnostic and interventionalmedical procedures, people are living longer, eventhose diagnosed with multiple medical conditions,thus necessitating a manageable lifelong preven-tive care approach to reach and maintain a posi-tive level of oral health.
IMPORTANCE OF PREVENTIVE CAREOF ORAL HEALTH
When discussing preventive dentistry it is impossi-ble to describe the one best approach, as everypatient is different. Announcements of new dentalmaterials and technologies occur almost daily.12
However evidence-based articles on the best tech-niques to be used for people with certain disabilitiesare not readily available. The alternative is to reviewthe basic principles of preventive dentistry andextrapolate those concepts to the preventive care ofindividuals with special needs. DePaola andCheney described two basic preventive principles
221
Preventive Considerations in Special Care Dentistry
Chapter 13
Roseann Mulligan, Phuu Pwint Han, andPiedad Suarez-Durall

that should serve as the foundation of preventiveprograms: (1) an accurate diagnosis that allowsdevelopment of a detailed treatment plan reflectiveof the patient’s needs; and (2) reinforcement of theprevention program at various steps, with theunderstanding that the patient or caregiver, orboth, would be able to accomplish each of thosesteps.13 In order to accomplish this outcome,knowledge of behavioral guidance methods is vitalfor the entire prevention team.
BEHAVIOR AND PSYCHOLOGICALINTERVENTIONS
Behavior guidance techniques have been widelyused in pediatric dental care because they modelappropriate coping behavior during dental treat-ment.6,14 Such techniques can be used to reduce thepatient’s anxiety, and to promote positive dentalcare experiences and attitudes, thus allowing thedental healthcare provider to perform safe and effi-cient oral healthcare services.14 These same behav-ioral guidance techniques can be useful for allpatients, including those with limited cooperativeability (e.g., patients with high fear and dental anxi-ety) and some older adult patients with cognitiveimpairment.15,16
The American Academy of Pediatric Dentistry(AADP) identifies 11 different approaches to non-pharmacological behavioral guidance: communi-cation and communicative guidance, positiveprevisit imagery, direct observation, tell-show-do,ask-tell-ask, voice control, nonverbal communica-tion, positive reinforcement and descriptive praise,distraction, memory restructuring, and parentalpresence or absence.14 Different strategies describedby other resources include modeling, shaping, flexi-bility, visualization, relaxation, consistency, desensi-tization and repetitive tasking, contingent andnoncontingent escape, hypnosis, and escape extinc-tion.6 These behavioral strategies have overlappingprinciples and as one becomes more comfortableusing the techniques and appreciating the principlesthat drive them, multiple techniques can be com-bined. For example, hypnosis is a formalizedprocess of suggestion, visualization, and distrac-tion, whereas tell-show-do utilizes similar compo-
nents of suggestion and visualization.16 If treat-ment failure occurs using one type of therapeuticapproach, an alternative approach may lead to suc-cess. When used consistently over time, theseapproaches can assist the patient in developingbehavioral responses that are conducive to receiv-ing preventive and curative dental care without theneed for sedation modalities.
Systematic DesensitizationKemp defined desensitization as the gradual expo-sure of the patient to the feared object or situation,with the concurrent training of and reinforcementof relaxation as a response that was incompatiblewith anxiety or fear.17 Desensitization can be con-ducted systematically in one’s imagination, byvideo or computer program, or by clinical simula-tion.17,18 The goal is to increase compliance or toreduce the amount of behavioral support, restraint,or sedation needed by the patient in order to receivedental care.6The desensitization process for patientswith special needs often involves repeating moresteps to reach the end goal of actual treatmentmore gradually.17 This strategy can become costlyas it often requires more visits to the dental office,and predicting when the end point will be achievedmay be difficult due to individual variability. Cre-ative approaches to dental visits that involve a fewminutes’ visit with a staff member rather than theclinician to assess how home care is going and pro-vide feedback help keep costs down and takeadvantage of the engagement of the entire clinicalstaff in a preventive focus.For many people with special needs, the foun-
dation of desensitization is heavily dependent oncaregivers—in partnership with the oral healthcareteam—teaching tolerance of daily toothbrushingor flossing in incremental steps. Repetitive tasksthat involve prompting or shaping of cooperativebehavior consistent with actions necessary toachieve the target goal behavior are a componentof the desensitization.6 Positive reinforcementthrough use of small tangible rewards and verbalpraise for achieving each step of desensitization willfacilitate success. This technique is especially helpfulfor patients whose behavior is influenced by fear
CHAPTER 13 Preventive Considerations in Special Care Dentistry
222

and anxiety.
Shaping Through Successive ApproximationThe tell-show-do method is the most widely usedbehavioral management method of successiveapproximation.19For individuals who have receptivelanguage capabilities, the provider first explains theprocedure verbally, in language appropriate to thedevelopmental level of the patient. Descriptions aregiven of what is about to happen, what instrumentswill be used, and the reason (the “tell” component),followed by demonstrations of the sensory cues ofthe procedures in a carefully defined, nonthreaten-ing setting (the “show”); then, the actual procedureis completed (the “do”).6,14,18,19 “Foreshadowing”and visualization are similar concepts to tell-show-do.6,18 Successive approximation can be used to gainpatient acceptance of operative or other, more inva-sive, procedures as well.19
If the patient has an intellectual disability orcognitive impairment, oral hygiene techniquesmust be broken down into simple, multiple, dis-crete steps. Steps should be addressed one at atime, making sure the patient understands andmasters each step before advancing to the next.Instructions should be short and simple. Writtenor recorded reminders can be given to the patientor the caregiver, or both. The technique should bemonitored and reinforced, with encouragement(and perhaps some brightly colored new tooth-brushes or other attractive oral hygiene aids) serv-ing as positive reinforcement until the patient orcaregiver can adequately incorporate the newbehaviors into the patient’s daily routine.
Contingent and Noncontingent EscapeIt is not a surprise that individuals with specialneeds would be eager to escape from a dentalappointment that can prove difficult to tolerate evenfor patients without special needs.20,21 Neurobiologi-cal changes in certain brain regions of special needspatients can trigger the “flight or fight” reaction thatmanifests as fighting or attempts to escape fromwhat is perceived as threatening or uncomfortablebehaviors.Contingent escape offers the opportunity to stop
the immediate activity after a period of acceptablebehavior is achieved. An example might be a restperiod after a treatment interval in which the patientdid not engage in any mouth closing or strugglingactivity. This is positive reinforcement of the target-ed behavior.6 On the other hand, noncontingentescape provides breaks from demands in relation toa prescribed period of time and is not related to theindividual’s compliance. For example, the providercould include a rest period after a quadrant ofsealants is placed before moving on to anotherquadrant, whether or not the patient’s behavior wasconducive to the treatment. These temporaryescape periods can give the patient some degree ofcontrol over the situation and the ability to commu-nicate with the provider when rest is needed.16 Infearful and anxious patients, pausing the procedurecan allow patients to calm down, and the providershould initiate the rest breaks.18 It is important thatthese rest breaks be initiated before the tolerancelevel of the patient has been exceeded and the breakbeing called due to lack of cooperation.When seen in demented patients, such care-resis-
tant behavior (CRB) is likely to progress over timeas the severity of the dementia increases, due tocausative neurological deterioration.22 Methods toovercome CRB in individuals with dementia impactthe effectiveness of caregivers in providing adequatecaregiving interventions23 and will be discussed in alater section.
Consistency and Role ModelingWhen a message or situation is regularly and repeat-edly presented, patients with special healthcareneeds can adapt, learn, and function more pre-dictably. This sensitization can help make what waspreviously an intolerable situation, tolerable. Thenecessity for familiarity may translate to the sameoperatory, same dentist and dental assistant, samecheck-in protocol at the front desk, and so on. Toencourage the impression of “sameness,” it can helpimmeasurably to allow the attendant from the facili-ty or a family caregiver to accompany the patientinto the operatory and possibly stay there duringcare provision.Role modeling involves having patients observe
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
223

the positive behavior of someone being treated,either in a video or in vivo. It could be watching thecare delivery of a relative or of another patient fromthe same setting or facility. The important compo-nent of this strategy is being certain that the modelwill demonstrate positive behavior when engaged inthe same or a similar task that is planned for thepatient with special needs. While role modeling hasbeen shown to be effective for children and manypatients who have special needs, with increasingseverity of the patient’s disabilities, the likelihood ofsuccess lessens.6
Escape ExtinctionWhen patients become physically resistant and thusrequire the cessation of dental treatment, the successof their disruptive behavior at escaping the threat(dental care) reinforces the resistive behavior andsets the stage for future episodes of disruption. It isimportant to prevent or address escape; however,escape extinction utilizes medical immobilization orphysical guidance, or both, in order to proceed withdental care. Providers should be very careful inusing these techniques and ideally need to have aplan that shows how these initial strategies will beused less often in the future. These techniques aremainly used for patients for whom other behavioralguidance techniques cannot be employed and whensedative techniques are not available. Nationalguidelines16 and the laws of individual jurisdictionsshould be consulted relative to the interpretation ofthese types of interventions within the political andgeographical boundaries of the dental delivery sitewhere they are to be utilized.
CLASSIFICATIONS OF PREVENTIVE DENTISTRY FOR
THE GERIATRIC PATIENTWhen discussing preventive dentistry, it is impossi-ble to describe the one best approach since everypatient is different and announcements of new den-tal materials and technologies occur almost daily.12
Historically few evidence-based articles have beenpublished on the best preventive techniques to beused for people with certain disabilities. There arealso few national guidelines. One that we were able
to locate, authored by Johnson and Chalmers(2011), focused on the care of older adults who arefunctionally dependent; have cognitive impair-ments; have intraoral conditions that negativelyimpact the oral milieu, resulting in dry mouth; orhave lesions associated with diabetes, anticancertherapy, and so on.24 This guideline identifies riskfactors, provides an instrument for assessing base-line and ongoing oral health status, helps to lay outan oral health plan, and discusses specific approach-es to mitigating individual findings, including dis-ruptive behavior, cognitive impairment, andmedication use.In order to develop a preventive program for
each individual patient, the dental office needs to beaware of the latest scientific findings related to theprevention of oral disease in general and map outthe roles of each member on the prevention team:the patient or patient helper, the dental staff mem-ber, and the dentist or dental hygienist. When noresources relative to a specific condition are discov-erable, the alternative is to review the two basic prin-ciples of preventive dentistry recommended byDePaola and Cheney, as mentioned earlier, andextrapolate those concepts into the preventive careof individuals with special needs.13
For the most part, few dental problems arelinked to only one specific condition. Therefore, it iscritically important to determine the nature of thepatient’s medical conditions, including whether theyare progressive, and whether they involve the centralnervous system, sensory organs, cognition, orfrailty—for all of these factors will influence the ulti-mate preventive strategy chosen for each patient.However, determining the individual’s ability toaccomplish or tolerate oral hygiene proceduresrelates far more to his or her functional capabilitiesthan to the number or type of medical diagnoses.A dental office team can provide information
about prevention with an enthusiastic commitmentfrom the entire staff to be an active part of thepatient’s preventive oral health team. One size orstyle does not fit all offices; each clinic needs to devel-op a strategy that works in that setting and for thepersonnel who will attempt to motivate the patientmember of the preventive team.25 Providing training
CHAPTER 13 Preventive Considerations in Special Care Dentistry
224

and an understanding of behavioral techniques,motivational methods, and prevention strategies forthe entire dental team is critical to achieving success.In developing a treatment plan, the preventive
aspect of care cannot be an afterthought, the lastitem in the list of “things to do,” or relegated only toactions that are described by a procedural code. Pre-vention should be an important part of everypatient interaction. DePaola and Cheney describefive types of prevention that should occur in thedental office, with the first occurring at the initialencounter.26
Predictive Prevention26
In predictive prevention, the patient is observed ashe or she comes into the dental office. Aspects suchas how the patient ambulates and transfers or sits inthe dental chair (with or without assistance) canprovide clues to his or her functionality. For exam-ple, a patient’s gait could suggest the amount ofmotor ability remaining for a patient with Parkin-son’s disease. This could then translate into a moreinformed assessment and discussion about thepatient’s ability to manage dentures now and in thefuture. Or, if a patient has consistent repetitivemovements of the mandible, this could be a possibleindicator of dystonia or bruxism and the need for anight guard. The flexed arm and circumduction ofthe leg seen in the hemiplegic gait of a patient fol-lowing a stroke alerts to possible problems not onlywith prostheses but overall oral hygiene skills. Somepatients may present with multiple bruises of thelegs and arms that could be indicative of anticoagu-lant medication use or possible elder abuse; swollenankles may be a sign of heart disease; and a patientwho is short of breath and unable to lie back in thedental chair may have chronic obstructive pul-monary disease. The observation of these conditionsor signs and a good review of the medical history inthis first appointment are important first steps indeveloping not only successful treatment but also asuccessful prevention plan.
Clinical Prevention26
It is important to delay or arrest problems with inter-ceptive or corrective actions at chairside. Consulting
with the patient’s physician is highly appropriate incertain circumstances, such as when intraoral mani-festations occur as a result of medication side effectsor due to chronic disease comorbidities that affectthe oral cavity. The dentist has the responsibility tounderstand and differentiate changes in the oral cav-ity due to aging from pathology in older adults.Gaining a better understanding of chronic diseaseswill assist dental professionals in providing appropri-ate preventive care to all patients to help promoteand preserve a healthy mouth for their lifetimes.When treating older adults, adherence to the threeR’s in dentistry serves as a guide: Repair, Remove,and Replace, utilizing chemotherapeutic preventiveagents to minimize further damage. In patients whoare chronically ill and debilitated or terminally ill,these three R’s are modified to RRI—Repair,Reline, and Ignore—as in some complex cases, thebest treatment could be not to perform any proce-dure and just observe or maintain the status quo.
Empirical Prevention26
The empirical method of trial and error is often nec-essary when dealing with patients who have com-plex intraoral and disability issues, present with rareconditions, or may not be able to tolerate a complexdental treatment protocol, or because of uncertain-ty about the etiology of the disease. At this time,instituting a practical, palliative treatment strategycould be of value.
Conservative Prevention26
When the goal is limited to preserving healthy tis-sue and removing the foci of infection, conserva-tive prevention principles are invoked. Such actionmight be confined to eliminating calculus or overtperiodontal disease, active decay, or teeth with apoor prognosis. Conservative prevention is likelyto be considered for the older adult who is unableto tolerate dental care due to significant medicalissues, has poor oral tissue tolerance, has a verylimited life expectancy, could cooperate with carebut is unwilling to do so, or has no way to fund hisor her care. Taking this approach will, at a mini-mum, allow the patient to regain comfort andmany times restore nutritional support.
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
225

Aggressive PreventionGood oral health is an important component ofquality of life for the older adult. Being aggressivein applying a preventive strategy before diseaseand destruction occur will help maintain thehealth of the dentition and periodontium. Suchhealth will have a significant effect on a variety ofcomponents that make up the psychological andemotional well-being of the individual, as reflectedin his or her oral health-related quality of life pro-file.27 Beyond the impact that oral health can playon nutrition, mastication, digestion, and estheticappearance, enjoyment of food and the socializa-tion that occurs at mealtimes are also important.28
Self-esteem is significantly linked to quality of lifeand is a contributor to socialization. An olderadult with a lot of calculus, missing teeth, or badbreath is not socially acceptable. Communicationand social interaction decline, leaving the individ-ual feeling lonely and depressed. Once teeth arelost, there may be many impediments that pre-clude getting proper treatment, ranging from aninability to tolerate care to lack of financialresources to pay for it.29 If aggressive preventionwere introduced early into the care regimen, thesehighly negative outcomes could be forestalled.Examples of aggressive prevention include regularrecare appointments for prophylaxis and exami-nation scheduled at short intervals, and applica-tion of chlorhexidine varnish or fluoride varnishevery 3 months, depending upon a patient’s needs.
PREVENTIVE DENTAL CARE CONSIDERATIONS
First Visit and Annual VisitsOne of the main goals of prevention is to havezero or minimal oral problems, especially thoserelated to dental plaque, caries, and periodontaldisease. Therefore, to be optimally effective, anyprevention program must focus on intervening atincipient stages of these developing conditions.This approach will allow the dental professional tomove from what has typically been a traditionalemphasis on secondary and tertiary preventivedentistry to primary preventive care.30 Critical tothis process is determining the follow-up visit
interval, consideration of which actually starts atthe first visit in the reception area as the patient iscompleting the medical history questionnaire.Before the clinical examination, the dental profes-sional should review in detail the patient’s medicalhistory information for both evidence of trans-missible disease and systemic conditions withpotential for oral manifestations. For example,patients with depression and hypertension whoare taking medications may experience drymouth, putting them at risk for a higher incidenceof caries. The initial and subsequent annual examsshould include not only the detailed intraoralexamination findings, but also the disabilities ofthe patient. This information will help determinethe level of prevention needed by the patient. Den-tal professionals should have the knowledge andexperience to develop an appropriate preventivetreatment plan, including use of behavior modifi-cation and related strategies.31
Periodic Preventive MaintenanceThe timing of preventive maintenance appoint-ments should be individualized and should reflectthe patient’s or caregiver’s ability to successfullyperform oral hygiene procedures at home. Whiledevelopment of the preventive plan should occurat the initial visit, during each follow-up or recareappointment, that plan should be reviewed to seeif it has been successful at preventing oral disease.If not, both the frequency of the recare intervaland the components of the preventive plan shouldbe reconsidered. Often, medically compromisedpatients are on fixed or limited incomes and havedifficulty financing their oral health care, includingtheir preventive visits. While some are eligible forgovernment insurance plans, they may have littleaccess to clinics accepting such plans. Manypatients with disabilities rely on family memberswho can, once educated about the importance ofpreventive care, assist the patient with performingself-care at home.31
Adjuvant InterventionsOlder adults are retaining their natural teeth longer.However, the prevalence of gingival recession and
CHAPTER 13 Preventive Considerations in Special Care Dentistry
226

the exposure of root surfaces increases susceptibili-ty to root caries. Since root caries develops morerapidly in dentin than in enamel due to the presenceand the pH of the surrounding dental biofilm, pre-ventive interventions are critical for reducing risk ofthis disease.32,33 In 2015, Wierichs and Meyer-Lueckel performed a systematic review of noninva-sive treatment of root caries lesions, summarizingthe results of clinical studies investigating profes-sional or home use of chemical agents.34 Manystudies included in their review reported that regu-lar dental prophylaxis and motivation of patientsimproves and intensifies patient oral hygiene care.Findings also supported regular control of plaqueas the first choice among interventions to manageroot caries lesions.34 This systematic review alsoidentified different agents that can be used to keeproot caries from forming or to inactivate them ifthey do, such as daily use of dentifrices containing5,000 ppm fluoride, professionally appliedchlorhexidine varnish (1% or 10%), or silverdiamine fluoride varnish (38%). However, Wierichsand Meyer-Lueckel recommended interpretingthese results with caution because the clinical trialswere few and had both high potential for bias andlower levels of evidence.
Impact of Systemic or Psychological DeclinesRecently, chronic periodontitis (CP), a prevalentinflammatory disease, has become a focus ofincreasing interest in relation to other chronicinflammatory conditions in the body.35 CP is high-ly prevalent in adults and is associated with life-threatening systemic disorders, such asatherosclerosis, autoimmune diseases, neurode-generative and neuroprogressive conditions, andaspiration pneumonia. CP is characterized bychronic immune activation, oxidative andnitrosative stress, and systemic inflammation.36
However, there is a lack of consensus amongexperts about the nature of these associations andconfusion among healthcare providers and thepublic on how to interpret this rapidly growingbody of science.37
The geriatric literature includes little writtenabout the concept of psychological frailty encom-
passing cognitive, mood, and motivational com-ponents. The concept considers brain changes thatare beyond normal aging, but not necessarilyinclusive of disease. Most studies exploring theinterface among cognition, mood, and physicalfrailty have demonstrated a bidirectional associa-tion between the domains. Psychological symp-toms or deficits have been described as eitherworsening the degree of physical frailty, or physi-cal frailty has been viewed as a risk to worseningcognition or depression.38
Anxiety associated with a potential or actualdiagnosis of dementia is common among olderadults. Patients with Alzheimer’s disease tend toexpress fear of further cognitive decline.39–42 Men-tal and physical well-being are intrinsic compo-nents in the dialogue of the concerned olderadults. Well-being studies support that some indi-viduals are motivated to maintain mental andphysical health by implementation of compensa-tory or preventative strategies to impede furthercognitive decline. Evidence supports the need forphysical exercise, healthy diet, and maintenance ofsocial interactions as early preventive strategies fora range of diseases, including cognitive decline.43–45
All of these topics are very important to considerwhen formulating the best prevention plan for ourpatients, especially the involvement of familymembers or caregivers. As cognitive impairmentincreases, an individual may experience anincrease in tooth loss, dental decay, gum disease,and denture-related problems, all of which nega-tively affect nutrition.28,46,47
Dietary Considerations31,48For some patients with special needs, foods high insugar are distributed throughout the day asrewards for having been compliant. In a studydone by Fure in 2004, it was found that the fre-quency of daily carbohydrate intake increasedwith age, from around five times per day in the 55-year-old to seven times per day in the 85-year-old.49 No difference was found between men andwomen. A significantly higher caries incidence wasfound in those who had a carbohydrate intake ofsix times or more per day. With patients who have
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
227

decreased neuromuscular coordination, decreasedsalivary flow, or both, it may be difficult to ade-quately clean the mouth of food debris. Food mayremain in the buccal vestibule and interproximallyuntil the next brushing. To decrease the risk ofcaries, we often tell patients that it is necessary torestrict between-meal snacking and limit the use ofhighly cariogenic food. Yet, some are encouragedto eat multiple small meals a day for a variety ofmedical reasons and encouraged to eat high-carbo-hydrate foods to keep their weight up.31 We knowthat if sweets are to be consumed, they should beconsumed at mealtime, when salivary flow is best.If bedtime snacking cannot be avoided, the patientshould be encouraged to brush immediately aftereating.
Home Care Need for Parent and Family InvolvementIt is extremely important for dental clinicians tocollaborate with other healthcare professionals aswell as with family members or caregivers who areresponsible for the care of the patient. A high andconsistent quality of care can only be providedwith the cooperation of primary caregivers andthe full knowledge of the personal and social lifeof the patient and environment. Often the futurehealth of the older adult with physical or mentaldisability is uncertain. Caregivers and patients aresometimes so overwhelmed in dealing with med-ical or social challenges that oral health concernsare given lesser priority, which can lead to neglectof dental problems. An additional challengeoccurs when dental treatment is sought: patientsand their caregivers may be unable to find dentistswho are trained in the unique issues of olderadults.50
CARE DELIVERY PROBLEMS SPECIFICTO PATIENTS WITH SPECIAL NEEDS
Patients with Neurodegenerative DiseasesPatients with neurodegenerative diseases shouldhave preventive care and aggressive treatment inpreparation for the classic progressive nature ofthese conditions that result in functional decline.These disorders—including stroke, multiple scle-
rosis, amyotrophic lateral sclerosis (ALS),Alzheimer’s disease, Parkinson’s disease, andHuntington’s disease—are among the most chal-lenging and devastating illnesses. Dental profes-sionals who are treating patients affected by any ofthese disorders are confronted with major chal-lenges of cognitive decline, mobility losses, andbehavioral changes, as well as the physical limita-tions that preclude being able to manage regulardental homecare and professional dental visits.51
The dental problems associated with these condi-tions mainly include poor oral hygiene; difficultyin wearing, cleaning, and retaining dentures; androot caries and recurrent decay as a result of med-ication-induced hyposalivation.51
Daily oral hygiene care with toothbrushingand flossing requires fine motor skills and dexteri-ty of the small muscles of the fingers and hands aswell as the gross motor skills of the larger musclegroups in the upper extremities.52 Either hypoac-tive or hyperactive muscles and nerves of the head,neck, and upper extremities affected by neurode-generative conditions will influence dexterity,motor skills, and range of motion of the bonesand joints.It is important to assess the functional capacity
of the patient and his or her ability to perform oralhygiene. A modified device, power device, or care-giver assistance may be needed to compensate forthe patient’s limitations. The gross motor skillsneeded to grasp a toothbrush handle and movethe brush to the mouth can be improved with theuse of orthotic devices such as splints and bracesto support a deformed, constricted, or weakenedlimb (arm or shoulder). However, the skill anddexterity needed to apply fine vibratory brushingmotions and properly utilize dental floss typicallycannot be enhanced with orthotics or physicalmedicine modalities.31 In such cases, modifiedpower toothbrushes or flossing devices may bebeneficial.
Patients with Sensory DisordersPatients with sensory disorders that impair hear-ing, vision, or speech will have communicationbarriers. Those with significant visual impairment
CHAPTER 13 Preventive Considerations in Special Care Dentistry
228

may need to be escorted to the operatory. Suchindividuals may be carrying a cane, arrive with anescort (human or animal), or have no obvious out-ward signs of visual impairment except the inabili-ty to read a treatment consent form. If a patientrequests that a companion be allowed in the treat-ment area, such a request should be accommodat-ed. While a human escort may be involved inlearning about oral hygiene instructions and partic-ipating in demonstrations, animal companionsmay be equally as important to keep the patientcalm so that he or she can pay attention to instruc-tions. Dental professionals must ensure that theirpatients are able to fully participate in their care.They can do so by using appropriate communica-tion strategies so that patients understand theirdental treatment needs, are able to provideinformed consent, and commit to proposed pre-ventive homecare recommendations. Custom-tai-lored instruction sheets with large black letters ofat least 12-point font size, typed onto white paper,53
and use of oversized dental models and oversizedtoothbrushes for demonstrations can be helpful.Colored floss and magnifying mirrors can be usedto help patients observe the effectiveness of theiroral hygiene skills. Other recommendations includechecking to be sure that all demonstrations are per-formed within the patient’s visual field and pre-venting possible discomfort from the glare of thedental light by carefully focusing and positioningthe operatory light. If a patient is blind, he or shecan be taught to feel how to perform self-careusing an individualized training technique in thepatient’s mouth, and sensitizing the patient to the“feeling” and “smell” of a clean mouth to ensurethe success of oral hygiene measures.54
Patients with hearing impairments can be nega-tively impacted by the sound of dental equipment,background noises from music and televisions, andstreet noises. Ideally these noises should besilenced; if that is not possible, noise should beminimized so that it does not interfere with thecommunication going on in the dental operatory.The individual who is communicating with thepatient with a hearing impairment needs to loweror remove his or her face mask and stay directly in
front of the patient at the same eye level to allowthe patient to lip read and take cues from thespeaker’s facial expression and body posture.55
Speaking distinctly and slightly slower in a well-modulated voice can facilitate communication.56
Shouting at the person is not recommended.Patients who have hearing aids may prefer toremove them or turn them off prior to dental treat-ment to avoid the electronic feedback that fre-quently results in noxious sounds. Ensuring thatthe hearing aids are in place and turned back onfor postoperative instructions is critical. If thepatient with a hearing impairment communicatesthrough sign language, the dentist must retain andpay for a sign language interpreter's services if, infact, an interpreter is needed to achieve the same“effective communication” for the patient as wouldoccur for a patient without hearing impairment.57
Patients with Speech and Language ImpairmentSeveral motor or cognitive impairment disorderscan affect a patient’s speech or language ability.The patient with cerebral palsy may have a speechimpairment due to central nervous systeminvolvement affecting the muscle movementsneeded for speech. Patients with neuromusculardiseases such as Parkinson’s or ALS may havesevere weakness of the muscles, resulting in aninability to articulate sounds (dysarthria). Apatient may experience a language disorder suchas aphasia (an inability to express or understandspeech) following a stroke. In these circumstances,it is helpful for the patient’s caregiver or familymember, who is attuned to “reading” the patient’sneeds, to be readily available to help interpret thepatient’s nonverbal actions. Aphasia may presentdifferently in affected individuals, with retention ofsome speech, although the actual words used maynot be appropriate. Listening to the emphasis thepatient places on the words spoken frequentlyhelps to clarify his or her intent.
Patients with Autism Spectrum DisordersThe number of patients who present with autismspectrum disorders (ASD) continues to grow. Anincreased prevalence of ASD over the past decade
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
229

requires familiarity with this diagnosis and itspotential impact on oral health.58 Patients withASD have an overly sensitive nervous system59
and, as a result, exhibit extreme and peculiarresponses to visual, auditory, tactile, olfactory, andgustatory signals, all of which invariably occur aspart of a dental appointment.60 Thus, sensoryoverload during a dental appointment can quicklylead to overstimulation and subsequent challeng-ing behaviors, including noncompliance, hyperac-tivity, sensory hypersensitivity, and self-injuriousbehavior.59,60
Communicating with patients who have ASDcan be difficult due to language deficits, poor com-prehension of speech, or difficulties reading socialcues. Moreover, many patients with ASD insist onsameness, adhere to strict routines, demonstraterigid thinking patterns, and may react adversely toeven minor changes in their daily routine.61 Theseimpediments to care can be overcome in somepatients with ASD using traditional approachesor basic behavioral guidance strategies. Uniquestrategies have been developed for approachingthe dental care of the individual with ASD. Non-traditional approaches of behavior guidance, suchas visual pedagogy (a strategy that takes advan-tage of the ability of patients with autism torespond better to pictures than words), social sto-ries, and video modeling have been used in con-junction with traditional behavior guidanceapproaches.59,62More recent successes in the dentaloffice have been found when a sensory-adapteddental environment (SADE) is provided for thepatient with ASD.63
Patients with ASD may present with hypersen-sitivity to the oral region, and in fact, oral defen-siveness has been reported to be evident in 50% ofchildren with this condition.64 Experimental intro-duction of relaxing light conditions, rhythmicmusic, and deep pressure applications in the den-tal setting,65 together with using the shortest possi-ble duration of the dental visit and minimumsensory stimulation, can reduce the patient’s anxi-ety and enhance positive participation in the den-tal care visit. Parental input regarding thebehaviors and preferences of the patient can be of
tremendous value to the success of the oral health-care appointment. Parents can bring the child’sfavorite music, video, movie, or toy to help encour-age the patient to relax. Treating the patient in thesame operatory with the same dentist and dentalassistant, and designating a separate waiting areafor patients with ASD, are recommended.59
Preventive Dental Care for Geriatric PatientsOlder adults are the fastest growing segment ofthe population in the United States; populationprojections indicate that by 2030, more than 20%of US residents will be aged 65 years and older.66
Dentists are challenged with treating communitydwelling older adults who have chronic stable sys-temic diseases as well as with caring for the dentalneeds of frail homebound or institutionalizedolder adults. Preventive dental care for geriatricpatients is complicated by the presence of systemicdiseases, medications taken for these comorbidconditions, and disease- and drug-induced adverseeffects on the oral tissues.67 Oral problems in den-tate or partially edentulous geriatric patientsinclude dental caries, periodontal disease, chronicfacial pain or temporomandibular dysfunction,and benign or malignant lesions of the oralmucosa or the jaws. Medications taken for med-ical conditions may result in decreased salivaryflow that impairs the patient’s ability to chew,swallow, or clean the oral cavity. Some medica-tions and systemic conditions, such as orthostatichypotension68 and medication-related osteonecro-sis of the jaw,69 can have significant effects on thewell-being of older adults.In vulnerable older adults, oral infections can
cause significant morbidity and mortality. Aspira-tion pneumonia is the most common infection innursing home residents, who are particularly atrisk for dysphagia secondary to neurological dis-ease.70Aspiration pneumonia is the most commonreason for hospitalization and is the leading causeof death from infection in these frail olderpatients.71
Residents of nursing homes are prone to poororal health and present with increased periodontaland dental disease burden due to lack of oral
CHAPTER 13 Preventive Considerations in Special Care Dentistry
230

hygiene care. Although the complex nature ofperiodontal disease and aspiration pneumoniamake direct cause-and-effect connections chal-lenging, many studies suggest an associationbetween poor oral hygiene and respiratorypathogens. In one National Institutes of Healthstudy, poor oral hygiene was implicated as a com-mon risk factor for aspiration, accounting for 21%of such cases.72 A decrease in the incidence of res-piratory complications was noted when patientswere provided with chemical or mechanical inter-ventions to improve oral conditions.70 Clearly, reg-ular oral hygiene care for this population is ofprime importance. However as previously dis-cussed, brain-related changes often cause CRB inthese patients, so much so that 80% of the certifiednursing assistants (CNAs) report experiencingCRB from elderly patients with whom they haveworked.73
CNAs may benefit from instructional programsabout behavioral management strategies that can beused with patients while providing oral hygiene care.Such strategies include approaching the patient ateye level and within the patient’s visual field to avoidstartling the patient, smiling, providing positive rein-forcements such as compliments, engaging in simplepositive conversations, and accompanying interac-tions with gentle touches. These strategies work bestwhen performed in a relaxing, quiet environmentwith minimal disruptions.22
For those who are not bedbound, engaging inoral healthcare behavior in the patient’s bathroomin front of a sink can serve as cue to similar behav-ior from past memories. Having the CNA standbehind the patient and having both in front of thebathroom mirror can prompt mouth openingwhen oral hygiene aids are placed in sight. Hand-ing the toothbrush to the patient and cueing himor her to begin brushing is especially helpful tothose who have lost language ability. Hand-over-hand prompting can serve as gentle reminders ofthe task to be accomplished.Respectful communication and delivery of
simple, one-step commands, as well as the elimi-nation of disrespectful “baby talk,” have beenshown to be helpful in promoting self-care and
eliminating CRB.23 Distraction techniques suchas singing or talking can be uniquely helpful orcause negative reactions, depending on the indi-vidual patient with whom they are used. Whenvarious techniques are not successful and CRBsbegin to occur, a rescue strategy should beinvoked, wherein one caregiver is replaced withanother in an attempt to rescue the oral health-care effort.74 Such a tradeoff is often successful insalvaging the experience.
PROVIDERS’ READINESS TO CONSIDERUNIQUE NEEDS OF SPECIAL PATIENTSIt should not be presumed that it is only thepatient or caregiver who may or may not have thecapability and motivation to improve the oralhealth of the patient with special needs. The prac-titioner must also be willing and able to develophis or her skills with communication, motivation,planning, and patient management. Watching apatient with a disability progress from being virtu-ally unapproachable in the dental office to beingable to maintain his or her home care at an accept-able level, and smiling with self-satisfaction whencomplimented on these efforts, brings a sense ofsatisfaction and accomplishment to the clinicianas well.Individuals with special healthcare needs have
disproportionate amounts of oral disease and aremore likely to have barriers when attempting toreceive oral healthcare services. Studies show thatdentists who feel that they were adequately edu-cated in how to manage patients with specialneeds are more likely to treat these patients aftergraduation. The dental educational system has animportant role to play in ensuring that futurehealthcare professionals are well-educated to meetthe complex needs and overcome the healthcaredisparities experienced by these patients.75
Dental education must address developing theappropriate attitudes and skill required to providecare as a part of an interprofessional team in avariety of settings.5 Adequate educational prepa-ration is essential to support the delivery of effec-tive and efficient preventive care to meet theunique needs of special patient populations.
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
231
REFERENCES1. World Health Organization. Disability and health. Fact
sheet No. 352. Available at: http://www.who.int/media-centre/factsheets/fs352/en/.
2. Special Care Dentistry Association. SCDA definition.Available at: http://www.scdaonline.org/?SCDA Defi-nitions.
3. Oral Health in America: A Report of the Surgeon Gener-al. Rockville, MD: U.S. Department of Health andHuman Services, National Institutes of Health, Nation-al Institute of Dental and Craniofacial Research; 2000.
4. Council of Clinical Affairs, American Academy of Pedi-atric Dentistry. Policy on transitioning from a pediatric-centered to an adult-centered dental home forindividuals with special health care needs. In: AmericanAcadamy of Pediatric Dentistry Reference Manual. Vol37. Chicago, IL: American Academy of Pediatric Den-tistry; 2011:108–110.
5. Albino JE, Ingelhart MR, Tedesco LA. Dental educa-tion and changing oral health care needs: dispartities anddemands. J Dent Educ. 2012;76:75–88.
6. Lyons RA. Understanding basic behavioral supporttechniques as an alterative to sedation and anesthesia.Spec Care Dentist. 2009;29:39–50.
7. Greig V, Sweeney P. Special care dentistry for generaldental practice. Dental Update. 2012;40:452–454.
8. Gordon SM, Dionne RA, Snyder J. Dental fear andanxiety as a barrier to accessing oral health care amongpatients with special health care needs. Spec Care Den-tist. 1998;18:88–92.
9. Bansal A, Ingle NA, Kaur N, Ingle E. Recent advance-ments in fluoride: a systematic review. J Int Soc PrevCommunity Dent. 2015;5:341–346.
10. Giannobile WV, Braun TM, Caplis AK, Doucette-Stamm L, Duff GW, Kornman KS. Patient stratificationfor preventive care in dentistry. J Dent Res. 2013;92:694–701.
11. Horner-Johnson W, Dobbertin K, Beilstein-Wedel E.Disparities in dental care associated with disability andrace and ethnicity. J Am Dent Assoc. 2015;146:366–374.
12. Scheller-Sheridan C. Basic Guide to Dental Materials.Chichester, UK: Wiley-Blackwell; 2010:2.
13. DePaola DP, Cheney HG. Commentary on preventivedentistry for the individual. In: Preventive Dentistry. Lit-tleton, CO: PSG Publishing Company; 1979:37.
14. American Academy of Pediatric Dentistry ClinicalAffairs Committee–Subcommittee on Behavior Man-agement. Guideline on behavior guidance for the pedi-atric dental patient. In: Clinical Practice GuidelinesReference Manual.Vol 37. Chicago, IL: American Acad-emy of Pediatric Dentistry; 2015:180–192.
15. Newton T., et al. The management of dental anxiety:time for a sense of proportion? Br Dent J. 2012;213(6)271–274.
16. Oliver K, Manton DJ. Contemporary behavior manage-
ment techniques in clinical pediatric dentistry: out withthe old and in with the new? J Dent Child. 2015;82:22–28.
17. Kemp F. Alternatives: a review of non-pharmacologicapproaches to increasing the cooperation of patientswith special needs to inherently unpleasant dental proce-dures.Behavior Analyst Today. 2005;6:88–108.
18. Armfield JM, Heaton LJ. Management of fear and anx-iety in the dental clinic. Aust Dent J. 2013;58:390–407.
19. Law CS, Blain S. Approaching the pediatric dentalpatient: a review of nonpharmacologic behavior man-agement strategies. CDA J. 2003;31:703–713.
20. Do C. Applying the social learning theory to childrenwith dental anxiety. J Contemp Dent Pract. 2004;5:1–8.
21. Allen KD, Wallace DP. Effectiveness of using noncon-tingent escape for general behavior managment in apediatric dental clinic. J Appl Behav Anal. 2013;46:723–737.
22. Jablonski RA, Therrien B, Kolanowski A. No morefighting and biting during mouth care: applying thetheroretical contructs of threat perception to clinicalpractice.Res Theory Nurs Pract. 2011;25:163–175.
23. Jablonski RA, Therrien B, Mahoney EK, KolanowskiA, Gabello M, Brock A. An intervention to reduce care-resistant behavior in persons with dementia during oralhygiene: a pilot study. Spec Care Dentist. 2011;31:77–87.
24. Johnson VB, Chalmers J. Oral Hygiene Care for Func-tionally Dependent and Cognitively Imparied OlderAdults. Iowa City, IA: University of Iowa College ofNursing, John A. Hartford Foundation Center of Geri-atric Excellence; 2011. Available from the NationalGuideline Clearinghouse (NGC), Agency for Health-care Research and Quality at: http://www.guideline.gov/content.aspx?id=34447&search=oral+health.
25. Mobley CC, Rugh J, Karotkin JW, Bhatt AA. Enhancingpatient adherence to preventive programs. In: MobleyCC, Cappelli DP, eds. Prevention in Clinical Oral HealthCare. St. Louis, MO: Mosby; 2008:chap 11, p. 140.
26. Freedman KA. Geriatric oral health care. In: DePaolaDP, Cheney HG, eds. Preventive Dentistry. Littleton, CO:PSG Publishing Company; 1979:chap 11, pp. 199–200.
27. Jensen PM, Saunders RL, Thierer T, Friedman B. Fac-tors associated with oral health-related quality of life incommunity-dwelling elderly persons with disabilities. JAm Geriatr Soc. 2008;56:711–717.
28. Daly B, Smith K. Promoting good dental health in olderadults: role of community nurse.Br J Community Nurs.2015;20:431–436.
29. Freedman KA. Geriatric oral health care. In: DePaolaDP, Cheney HG, eds. Preventive Dentistry. Littleton, CO:PSG Publishing Group; 1979:chap 11, p. 208.
30. Freedman KA. Geriatric oral health care. In: DePaolaDP, Cheney HG, eds. Preventive Dentistry. Littleton, CO:PSG Publishing Company; 1979:chap 11, p. 196.
CHAPTER 13 Preventive Considerations in Special Care Dentistry
232
31. Mulligan R, Sobel S. Preventive oral health care forcompromised individuals. In: Garcia-Godoy F, HarrisNO, eds. Primary Preventive Dentistry. 6th ed. Engle-wood Cliffs, NJ: Prentice-Hall; 2003:559–588.
32. Peters MC. Strategies for noninvasive demineralized tis-sue repair. Dent Clin North Am. 2010;54:507–525.
33. Schiffner U, Hoffmann T, Kerschbaum T, Micheelis W.Oral health in German children, adolescents, adults andsenior citizens in 2005. Community Dent Health.2009;26:18–22.
34. Wierichs RJ, Meyer-Lueckel H. Systematic review onnoninvasive treatment of root caries lesions. J Dent Res.2015;94:261–271.
35. Thornton-Evans G, Eke P, Wei L, et al. Centers for Dis-ease Control and Prevention (CDC). Periodontitisamong adults aged ≥ 30 years—United States, 2009–2010. MMWR Suppl. 2013;62(3):129–135.
36. Hajishengallis G. Periodontitis from microbial immunesubversion to systemic inflammation.Nat Rev Immunol.2015;15:30–44.
37. Otomo-Corgel J, Pucher JJ, Rethman MP, ReynoldsMA. State of the science: chronic periodontitis and sys-temic health. J Evid Based Dent Pract. 2012;12(suppl3):20–28.
38. Fitten LJ. Psychological frailty in the aging patient.Nes-tle Nutr Inst Workshop Ser. 2015;83:45–53.
39. Begum A, Whitley R, Banerjee S, Matthews D, StewartR, Morgan C. Help-seeking response to subjective mem-ory complaints in older adults: toward a conceptualmodel. Gerontologist. 2013;53:462–473.
40. Lingler JH, Nightingale MC, Erlen JA, et al. Makingsense of mild cognitive impairment: a qualitative explo-ration of the patient’s experience. Gerontologist.2006;46:791–800.
41. Lawrence V, Samsi K, Banerjee S, Morgan C, Murray J.Threat to valued elements of life: the experience ofdementia across three ethnic groups. Gerontologist.2011;51:39–50.
42. Sabat SR. Voices of Alzheimer’s disease sufferers: a callfor treatment based on personhood. J Clin Ethics.1998;9:35–48.
43. Stathi A, Fox KR, McKenna J. Physical activity anddimensions of subjective well-being in older adults. JAging Phys Act. 2002;10:76–92.
44. Corner L, Bond J. Being at risk of dementia: fears and anx-ieties of older adults. J Aging Studies. 2004;18:143–155.
45. Friedman DB, Laditka JN, Hunter R, et al. Getting themessage out about cognitive health: a cross-culturalcomparison of older adults’ media awareness and com-munication needs on how to maintain a healthy brain.Gerontologist. 2009;49(suppl 1):S50–60.
46. Chalmers JM, Hodge C, Fuss JM, Spencer AJ, CarterKD. The prevalance and experience of oral diseases inAdelaide nursing home residents. Aust Dent J.2002;47:123–130.
47. Zimmerman S, Solane PD, Cohen LW, Barrick AL.
Changing the culture of mouth care: mouth care with-out a battle. Gerontologist. 2014;54(suppl 1):S25–34.
48. Hayes M, Allen E, da Mata C, McKenna G, Burke F.Minimal intervention dentistry and older patients. Part1: Risk assessment and caries prevention. Dent Update.2014 Jun;41(5):406-8, 411-2.
49. Fure S. Ten-year cross-sectional and incidence study ofcoronal and root caries and some related factors in elder-ly Swedish individuals. Gerodontology. 2004;21(3):130–140.
50. Freedman KA. Geriatric oral health care. In: DePaolaDP, Cheney HG, eds. Preventive Dentistry.Littleton, CO: PSG Publishing Company; 1979:chap 11,pp. 212–214, 223.
51. Kieser J, Jones G, Borlase G, MacFadyen E. Dentaltreatment of patients with neurodegenerative disease. NZ Dent J. 1999;95:130–134.
52. Mulligan R, Wilson S. Design characteristics of flossholding devices for persons with upper extremity disabil-ities.Spec Care Dent. 1984;4:168–172.
53. American Dental Association. Patients with physicaland mental disabilities. In: Oral Health Care Guidelines.Chicago, IL: American Dental Association; 1991:19.
54. Morsey S. Communicating with and treating the blindchild.Dent Hygiene. 1980;54:288–290.
55. Cherney LR. The effects of aging on communication.In: Lewis BC, ed. Aging: The Health Care Challenge.Philadelphia, PA: FA Davis; 1996:103.
56. Lange BM, Entwistle BM, Lipson LF. Dental Manag-ment of the Handicapped: Approaches for Dental Auxil-iaries. Philadelphia, PA: Lee & Febiger; 1983.
57. Sfikas PM. Treating hearing-impaired people. J AmDent Assoc. 2000;131:108–110.
58. Perou R, Bitsko RH, Blumberg SJ, et al. Centers for Dis-ease Control and Prevention (CDC). Mental health sur-veillance among children—United States, 2005–2011.MMWR Suppl. 2013;62(2):1–35.
59. Gandhi RP, Klein U. Autism spectrum disorders: Anupdate on oral health managment. J Evid Base DentPract. 2014;14S:115–126.
60. Delli K, Reichart PA, Bornstein MM, Livas C. Manage-ment of children with autism spectrum disorder in thedental setting: concerns, behavioural approaches andrecommendations. Med Oral Patol Oral Cir Bucal.2013;18:e862–868.
61. American Psychiatric Association. Diagnostic and Statis-tical Manual of Mental Disorders. 5th ed. Arlington, VA:American Psychiatric Association; 2013.
62. Pilebro C, Backman B. Visual pedagogy in dentistry forchildren with autism. ASDC J Dent Child. 1999;66:325–331.
63. Cermak SA, Stein Duker LI, Williams ME, et al. Feasi-bility of a sensory-adapted dental environment for chil-dren with autism. Am J Occup Ther. 2014;69:6903220020p1–10.
64. DeMattei R, Cuvo A, Maurizio S. Oral assessment of
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
233

234
children with an autism spectrum disorder. J Dent Hyg.2007;81:65.
65. Shapiro M, Sgan-Cohen HD, Parush S, Melmed RN.Influence of adapted environment on the anxiety ofmedically treated children with developmental disability.J Pediatr. 2009;154:546–550.
66. Ortman JM, Velkoff VA, Hogan H. An Aging Nation:The Older Population in the United States. PopulationEstimates and Projections. Washington, DC: US CensusBureau; 2014:25–1140.
67. Schreiber A, Glickman R. Geriatric dentistry: maintain-ing oral health in the geriatric population. In: Fillit HM,Rockwood K, Woodhouse K, eds. Brocklehurst’s Text-book of Geriatric Medicine and Gerontology.Philadelphia,PA: Elsevier Health Sciences; 2010:chap 75, pp. 599–607.
68. Figueroa JJ, Basford JR, Low PA. Preventing and treat-ing orthostatic hypotension: as easy as A, B, C. CleveClin J Med. 2010;77:298–306.
69. McClung M, Harris ST, Miller PD, et al. Bisphospho-nate therapy for osteoporosis: benefits, risks, and drug
holiday. Am J Med. 2013;126:13–20.70. Pace CC, McCullogh GC. The association between oral
micororganisms and aspiration penumonia in the insti-tutionalized elderly: review and recommendations. Dys-phagia. 2010;25:307–322.
71. Oh E, Weintraub N, Dhanani S. Can we prevent aspira-tion pneumonia in the nursing home? J Am Med DirAssoc. 2004;5:174–179.
72. Quagliarello V, Ginter S, Han L, Van Ness P, Allore H,Tinetti M. Modifiable risk factors for nursing home-acquired pneumonia.Clin Infect Dis. 2005;40:1–6.
73. Frenkel HF. Behind the screens: care staff observationson delivery of oral health care in nursing homes.Gerodontology. 1999;16:75–80.
74. Chalmers JM. Behavior management and communica-tion strategies for dental professionals when caring forpatients with dementia.Spec Care Dent. 2000;20:147–154.
75. Dao LP, Zwetchkenbaum S, Inglehart MR. Generaldentists and special needs patients: does dental educationmatter? J Dent Educ. 2005;69:1107–1115.
CHAPTER 13 Preventive Considerations in Special Care Dentistry

Fluoride has been employed in dentistry for over100 years for the prevention and treatment of den-tal caries.1 Despite this long history there has beenconsiderable debate over its mode of action, theoptimal way of delivering fluoride to differentpatient groups, and risks associated with its use.2
This chapter examines the background, history,and current application of fluorides for individualpatients, considering the life course and risk as acontext for determining optimal fluoride therapiesfor individual patients as well as populations.
HISTORY OF FLUORIDESSince the late nineteenth century, fluoride has beenemployed by those concerned with the preventionand treatment of dental caries. The first use of fluo-rides was as powders, often calcium or potassiumfluoride, and it was Denninger whose early clinicaltrials suggested that children and expectant moth-ers would benefit from their use.3
It is paradoxical that the benefit of fluoridewas first established from studies that assessed itsdetrimental effects. A Colorado dentist, Dr. Fred-
erick McKay, had observed that many of hispatients had a unique appearance to their teeth—an appearance that became known as “Coloradobrown stain,” now referred to as enamel fluorosis.(See Figure 1.) The presence of the stain was asso-ciated with patients who had had exposure to nat-urally fluoridated water.3 Norman Ainsworth, anEnglish dentist, subsequently found that patientswho presented with enamel fluorosis had fewercaries—approximately half the decay of patientswithout enamel mottling.
These initial findings, of a relationshipbetween mottled enamel and reduced caries, werefurther investigated in a series of landmark epi-demiological studies by H. Trendley Dean. Deanfound that children between the ages of 12 and 14years who were living in communities with waterfluoridation had roughly half the caries experi-ence of children living in areas where the watersupply had low levels of fluoride.4 Encouraged bythese findings, the “21 Cities” study was under-taken that aimed to determine the optimal level offluoride needed to reduce caries while reducingthe risk of enamel fluorosis.4 This study estab-lished 1.0 to 1.2 mg of fluoride (F)/L as the opti-mal level, which has remained largely unchangeduntil recently by, among others, the Irish and USregulators to 0.7 mg F/L.
What Is Fluoride?Fluoride is the ionic form of the trace element fluo-rine and is commonly found in the natural environ-ment. Most individuals acquire fluoride fromdietary sources such as foodstuffs and beverages;however, this can vary from individual to individ-ual. The accidental swallowing of dental productscontaining fluoride (such as toothpaste in youngchildren) can exceed that consumed throughdietary intake.
Benefits of Fluoride?Fluoride is used for the prevention and treatment(arrest) of both enamel and dentin (root) caries. Inthe early part of the twentieth century, fluorida-tion of public water supplies was the main focus of fluoride applications. Use of fluoridated toothpaste is now the most common means ofdelivering fluoride and has been largely credited
235
FluoridesChapter 14
I. A. Pretty
Figure 1. Enamel Mottling (now known as dental fluorosis)
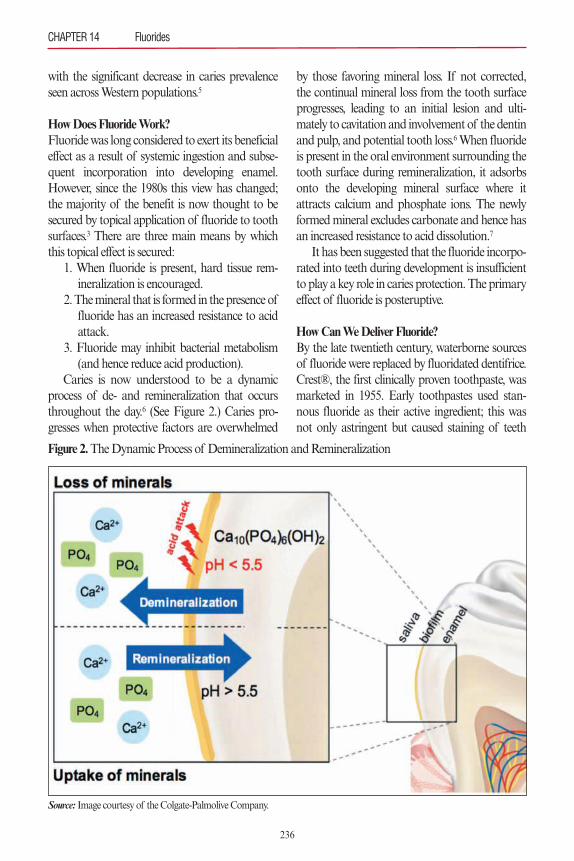
with the significant decrease in caries prevalenceseen across Western populations.5
How Does Fluoride Work?Fluoride was long considered to exert its beneficialeffect as a result of systemic ingestion and subse-quent incorporation into developing enamel.However, since the 1980s this view has changed;the majority of the benefit is now thought to besecured by topical application of fluoride to toothsurfaces.3 There are three main means by whichthis topical effect is secured:
1. When fluoride is present, hard tissue rem-ineralization is encouraged.
2. The mineral that is formed in the presence offluoride has an increased resistance to acidattack.
3. Fluoride may inhibit bacterial metabolism(and hence reduce acid production).
Caries is now understood to be a dynamicprocess of de- and remineralization that occursthroughout the day.6 (See Figure 2.) Caries pro-gresses when protective factors are overwhelmed
by those favoring mineral loss. If not corrected,the continual mineral loss from the tooth surfaceprogresses, leading to an initial lesion and ulti-mately to cavitation and involvement of the dentinand pulp, and potential tooth loss.6When fluorideis present in the oral environment surrounding thetooth surface during remineralization, it adsorbsonto the developing mineral surface where itattracts calcium and phosphate ions. The newlyformed mineral excludes carbonate and hence hasan increased resistance to acid dissolution.7
It has been suggested that the fluoride incorpo-rated into teeth during development is insufficientto play a key role in caries protection. The primaryeffect of fluoride is posteruptive.
How Can We Deliver Fluoride?By the late twentieth century, waterborne sourcesof fluoride were replaced by fluoridated dentifrice.Crest®, the first clinically proven toothpaste, wasmarketed in 1955. Early toothpastes used stan-nous fluoride as their active ingredient; this wasnot only astringent but caused staining of teeth
CHAPTER 14 Fluorides
236
Figure 2.The Dynamic Process of Demineralization and Remineralization
Source: Image courtesy of the Colgate-Palmolive Company.

and silicone-based restorative materials. Modernfluorides, sodium fluoride and sodium monofluo-rophosphate, were introduced in the 1970s and1980s.
While dentifrices remain the main source offluoride, there are supplemental or adjunct sourcesthat include rinses, tablets, drops, varnishes, gels,and foodstuffs such as salt, milk, and juices.Restorative filling materials were developed thatclaimed to release fluorides with the potential toreduce the incidence of secondary caries. Theseinclude glass ionomer, compomers, and resin-modified glass-ionomer cements.8
Risks of Fluoride UseEarly water fluoridation studies demonstrated thatvery high levels of fluoride can be detrimental. Themain risk of fluoride ingestion, for levels seen inpopulations with optimally fluoridated water, isenamel fluorosis. This results from the ingestion ofsufficiently high levels of fluoride over a prolongedperiod during tooth development.9Those who haveall of their adult teeth developed are not at risk offluorosis. Fluorosis at the levels seen within the nor-mal therapeutic use of fluorides is typically mildand generally not of aesthetic concern.10
Optimal DeliveryGiven the risk of fluorosis for children (generallythose younger than 6 years old) and the mechanismof fluoride action, topical fluoride systems that areeasily ingested or are designed to be swallowed aregenerally discouraged. For example, fluoride tabletsare rapidly ingested and hence have little benefit,but they increase the risk of fluorosis. Therefore, itis not surprising that the main contemporary deliv-ery methods of fluoride are toothpaste, mouthrins-es, gels, and varnishes.
The rest of this chapter describes the evidencebase for use of these products within the context ofthe life course.
A LIFE COURSE APPROACHCaries is a lifelong disease experienced by individu-als of all ages that is characterized by periods ofhigher and lower risk at both an individual patient
level and a population level. For example, youngchildren are regarded as being at high risk for cariesdue to difficulties with toothbrushing, dietary chal-lenges, and erupting teeth. Older adults, who have asimilar level of caries incidence as children, faceother challenges such as loss of manual dexterity,cognitive impairment, and polypharmacy that canlead to a dry mouth and hence loss of the protec-tive effect of saliva.
Individual patients present with their own riskprofiles. These include
• Previous caries experience• Diet and, in particular, sugar consumptionand grazing behaviors
• Presence of restorations and plaque-retentiveareas
• Level of oral health literacy• Medical conditions and special care needs• Prescribed medicines• Dental-attending behavior• Oral hygiene behavior and individual fluoride use
• Bacterial composition of plaque biofilm• Socioeconomic status• Education levelThere are many tools available to assess caries
risk, and it is beyond the scope of this chapter toexamine these in detail. The reader is referred toChapter 3, “Risk Assessment.”
When considering either populations or individ-ual patients, it is useful to consider the life course,11
as shown in Figure 3. A “typical” life course pro-vides a framework to understand opportunities forcaries prevention among patients as they age. Peri-ods of vulnerability have a higher risk for cariesthat are associated with events in the life course.These include birth and early childhood, a recog-nized period of risk, and later life, where increasedgeneral vulnerability, often referred to as frailty,increases caries risk.
The consideration of life course encourages clini-cians to assess their patients’ risk factors, not only atthe time of presentation, but for the future. In partic-ular, clinicians can introduce preventive strategies ina timely manner and improve the likelihood of effectiveness. Considering risk, age, and level of vul-
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
237
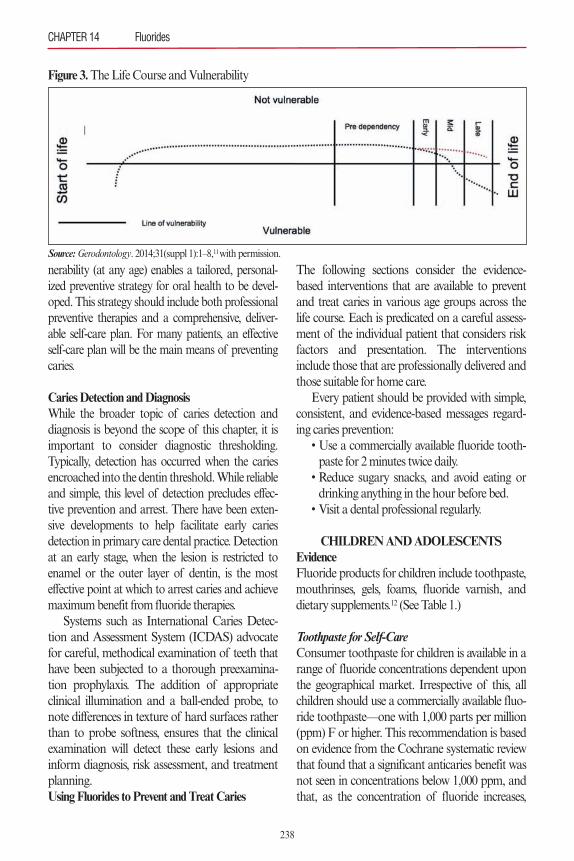
nerability (at any age) enables a tailored, personal-ized preventive strategy for oral health to be devel-oped. This strategy should include both professionalpreventive therapies and a comprehensive, deliver-able self-care plan. For many patients, an effectiveself-care plan will be the main means of preventingcaries.
Caries Detection and DiagnosisWhile the broader topic of caries detection anddiagnosis is beyond the scope of this chapter, it isimportant to consider diagnostic thresholding.Typically, detection has occurred when the cariesencroached into the dentin threshold. While reliableand simple, this level of detection precludes effec-tive prevention and arrest. There have been exten-sive developments to help facilitate early cariesdetection in primary care dental practice. Detectionat an early stage, when the lesion is restricted toenamel or the outer layer of dentin, is the mosteffective point at which to arrest caries and achievemaximum benefit from fluoride therapies.
Systems such as International Caries Detec-tion and Assessment System (ICDAS) advocatefor careful, methodical examination of teeth thathave been subjected to a thorough preexamina-tion prophylaxis. The addition of appropriateclinical illumination and a ball-ended probe, tonote differences in texture of hard surfaces ratherthan to probe softness, ensures that the clinicalexamination will detect these early lesions andinform diagnosis, risk assessment, and treatmentplanning.Using Fluorides to Prevent and Treat Caries
The following sections consider the evidence-based interventions that are available to preventand treat caries in various age groups across thelife course. Each is predicated on a careful assess-ment of the individual patient that considers riskfactors and presentation. The interventionsinclude those that are professionally delivered andthose suitable for home care.
Every patient should be provided with simple,consistent, and evidence-based messages regard-ing caries prevention:
• Use a commercially available fluoride tooth-paste for 2 minutes twice daily.
• Reduce sugary snacks, and avoid eating ordrinking anything in the hour before bed.
• Visit a dental professional regularly.
CHILDREN AND ADOLESCENTSEvidenceFluoride products for children include toothpaste,mouthrinses, gels, foams, fluoride varnish, anddietary supplements.12 (See Table 1.)
Toothpaste for Self-CareConsumer toothpaste for children is available in arange of fluoride concentrations dependent uponthe geographical market. Irrespective of this, allchildren should use a commercially available fluo-ride toothpaste—one with 1,000 parts per million(ppm) F or higher. This recommendation is basedon evidence from the Cochrane systematic reviewthat found that a significant anticaries benefit wasnot seen in concentrations below 1,000 ppm, andthat, as the concentration of fluoride increases,
CHAPTER 14 Fluorides
238
Figure 3. The Life Course and Vulnerability
Source:Gerodontology. 2014;31(suppl 1):1–8,11 with permission.
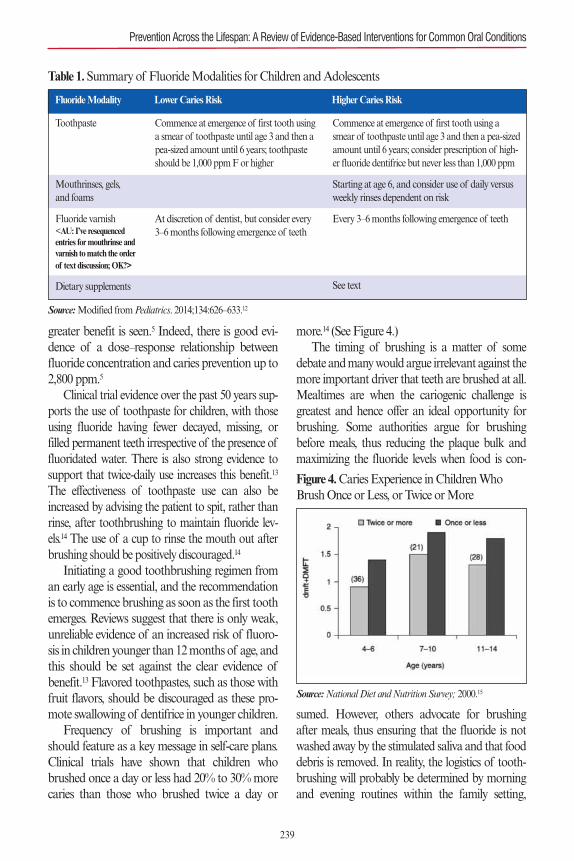
greater benefit is seen.5 Indeed, there is good evi-dence of a dose–response relationship betweenfluoride concentration and caries prevention up to2,800 ppm.5
Clinical trial evidence over the past 50 years sup-ports the use of toothpaste for children, with thoseusing fluoride having fewer decayed, missing, orfilled permanent teeth irrespective of the presence offluoridated water. There is also strong evidence tosupport that twice-daily use increases this benefit.13
The effectiveness of toothpaste use can also beincreased by advising the patient to spit, rather thanrinse, after toothbrushing to maintain fluoride lev-els.14 The use of a cup to rinse the mouth out afterbrushing should be positively discouraged.14
Initiating a good toothbrushing regimen froman early age is essential, and the recommendationis to commence brushing as soon as the first toothemerges. Reviews suggest that there is only weak,unreliable evidence of an increased risk of fluoro-sis in children younger than 12 months of age, andthis should be set against the clear evidence ofbenefit.13 Flavored toothpastes, such as those withfruit flavors, should be discouraged as these pro-mote swallowing of dentifrice in younger children.
Frequency of brushing is important andshould feature as a key message in self-care plans.Clinical trials have shown that children whobrushed once a day or less had 20% to 30% morecaries than those who brushed twice a day or
more.14 (See Figure 4.)The timing of brushing is a matter of some
debate and many would argue irrelevant against themore important driver that teeth are brushed at all.Mealtimes are when the cariogenic challenge isgreatest and hence offer an ideal opportunity forbrushing. Some authorities argue for brushingbefore meals, thus reducing the plaque bulk andmaximizing the fluoride levels when food is con-
sumed. However, others advocate for brushingafter meals, thus ensuring that the fluoride is notwashed away by the stimulated saliva and that fooddebris is removed. In reality, the logistics of tooth-brushing will probably be determined by morningand evening routines within the family setting,
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
239
Table 1.Summary of Fluoride Modalities for Children and Adolescents
Toothpaste
Mouthrinses, gels, and foams
Fluoride varnish<AU: I’ve resequencedentries for mouthrinse andvarnish to match the orderof text discussion; OK?>
Dietary supplements
Commence at emergence of first tooth usinga smear of toothpaste until age 3 and then apea-sized amount until 6 years; toothpasteshould be 1,000 ppm F or higher
At discretion of dentist, but consider every 3–6 months following emergence of teeth
Commence at emergence of first tooth using asmear of toothpaste until age 3 and then a pea-sizedamount until 6 years; consider prescription of high-er fluoride dentifrice but never less than 1,000 ppm
Starting at age 6, and consider use of daily versusweekly rinses dependent on risk
Every 3–6 months following emergence of teeth
See text
Fluoride Modality Lower Caries Risk Higher Caries Risk
Source:Modified from Pediatrics. 2014;134:626–633.12
Figure 4. Caries Experience in Children WhoBrush Once or Less, or Twice or More
Source:National Diet and Nutrition Survey; 2000.15

although the low saliva rate during sleeping lendssome credibility to the recommendation that thelast activity before sleep should be toothbrushing.
The amount of toothpaste to be used is lessimportant than the frequency of exposure andfluoride content. Clinical trials have found noassociation with amount of toothpaste used andanticaries efficacy, but the amount of paste on thebrush is important in relation to fluorosis risk andrecommendations for smear and pea-sizedamounts for younger children. Using appropriateconcentrations, twice daily, with spitting and norising will maximize the anticaries benefit andminimize the fluorosis risk.14
In summary, good toothbrushing advice forpatients, parents, and caregivers would be the useof fluoride toothpaste with no less than 1,000ppm F, twice daily, once after or before a meal andonce before bed with no rinsing.
Fluoride MouthrinsesMouthrinses are most commonly available asdaily (227 ppm F) and weekly (909 ppm F) prod-ucts, and typical use consists of rinsing with 10mL of solution for approximately 1 minute.Mouthrinses offer an excellent risk–benefit profilewhen used appropriately as they maximize topicalexposure and minimize the risk of fluorosis. Clini-cal trials demonstrate caries reductions of around30%,16 although the differences in those areasserved by water fluoridation are lower. ACochrane review of evidence for the use ofmouthrinses found that at either strength (daily orweekly), their use was associated with a clearreduction (23% to 30%) in caries.17
Patients and parents should be advised to usemouthrinses and toothpaste at different times ofthe day to maximize efficacy.18 Use of mouthrinsesfor children younger than age 6 years is not recom-mended due to risk of swallowing and ingestion.
Fluoride Gels and FoamsIn many parts of the world, fluoride gels andfoams are available as either self-care or profes-sionally applied products. They typically have flu-oride concentrations similar to those found in
mouthrinses, although some may have up to 5,000ppm. They are generally highly viscous and areplaced in either custom or preformed trays. ACochrane review found moderate-quality evi-dence to support a large caries-inhibiting effect(approximately 28%) from clinical studies thatwere largely school based, making gels and foamssimilar in efficacy to mouthrinsing.19 It is interest-ing to note that the use of chlorhexidine in gels (orindeed varnishes) was not shown to have anyeffect.20
Fluoride Dietary SupplementsFluoride tablets were introduced in the 1940s toact as an alternative to water fluoridation, anddosage was based on delivering the equivalent of 1ppm based on average water consumption. Thiscalculation is fundamentally flawed as it shouldhave been based on the dose per kilogram weightof the child—as for any other drug. As previouslydescribed, the action of fluoride is now under-stood to be topical and posteruptive; therefore,any ingestion of fluoride will have little impact oncaries but will significantly increase the risk of flu-orosis. Despite this risk, many professional dentalorganizations recommend the use of supplementsin areas without water fluoridation. Use oflozenges that are chewed or sucked (and provide atopical effect) is preferable to tablets or drops thatare swallowed. Evidence from clinical trials sup-ports the use of lozenges and suggests a 20% to28% reduction in caries.21,22 However, one shouldconsider the continuing risk from fluoride inges-tion versus the use of professional products suchas fluoride varnish prior to advising patients to usesupplements of this kind.
Professional Fluoride Interventions for Children and AdolescentsIn addition to a custom-tailored self-care plan,patients can also benefit from professional preven-tion, which should be considered as active treat-ment within the treatment planning process. Theneed for a professionally applied fluoride treatmentshould also be informed by the clinical examinationand risk assessment process and should be
CHAPTER 14 Fluorides
240

reassessed on a regular basis. Recall intervals forsuch patients should reflect their higher risk.
Fluoride VarnishThe popularity of fluoride varnish for the treat-ment and prevention of caries has increased overthe past decade with increasing use and a widerprofessional team involved in its application.Across healthcare systems, physicians, nurses, andthe dental team have all been involved in the deliv-ery of fluoride varnish, both in the private settingand in community-based health programs.
Fluoride varnish is used in a targeted fashion onspecific risk sites, or applied on a whole mouthbasis for those at greatest risk. Varnishes are appliedusually every 3 to 6 months and contain high levelsof sodium fluoride (22,600 ppm F). These fluorideproducts are designed to be highly retentive in theoral environment by hardening on the tooth sur-face after application following contact with saliva.(See Figure 5.) It is thought that the local deliveryof high levels of fluoride produces local areas ofcalcium fluoride that acts as a reservoir for subse-quent slow release of fluoride.23 There is strong evi-dence for the use of fluoride varnish in children andadolescents, with a Cochrane systematic reviewconcluding that there is a substantial caries-inhibit-ing effect of fluoride varnish in both permanent(43% reduction) and primary teeth (37%).24 Fluo-ride varnish represents an important, cost-effective,and easily applied mechanism for the managementand prevention of caries in children and adoles-cents.
Fluoride varnish application is simple, non–
operator sensitive, and well-tolerated by patients.Early carious lesions, especially those restricted toenamel, are especially suitable for varnish applica-tion, but it appears that whole mouth treatmentsare an effective means of prevention.24A systematicreview examining the evidence base for profession-ally applied fluoride treatments, including silicontetrafluoride, fluoride gel, and traditional sodiumfluoride varnishes, found that only sodium fluoridegel and silver diamine fluoride (not widely used inWestern populations) have significant benefit.25
Toothpaste: Professional PrescriptionsChildren and adolescents at higher risk of carieswill benefit from toothpastes with higher concen-trations of fluoride. The available levels of higherfluoride pastes vary between markets. For example,in Europe products with 2,800 ppm and 5,000 ppmare available, whereas in North America, only a5,000 ppm product is available. There is a well-rec-ognized dose–response relationship between theconcentration of fluoride and caries prevention,and the evidence to support the use of fluoridatedtoothpastes is described by Cochrane as unequivo-cal.13 A recent Cochrane review examined the useof fluoride toothpastes containing up to 2,800 ppmand described a dose–response effect up to thislevel, but stated that this was not always statisticallysignificant. The review found that the highest prob-ability of caries preventive benefits was found inthose toothpastes containing greater fluoride con-centrations.5 In comparisons to placebos, low-con-centration pastes (400 to 550 ppm) demonstratedno significant benefit, those with “standard” levelsof fluoride having a median prevented fraction of25%, and those with the highest levels of fluorideone of 45%. These findings were mirrored in anearlier review by Ammari and colleagues that con-sidered differences between pastes ranging from alow of 250 ppm up to 1,055 ppm.26
Toothpastes with higher concentrations of fluo-ride should therefore be considered for those athigher risk of caries and may be prescribed forthose with transitory increased risk—for example,adolescents wearing fixed orthodontic appliancesas well as patients with special needs. The decision
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
241
Figure 5. Application of Fluoride Varnish to aTooth Surface
Source: Image courtesy of the Colgate-Palmolive Company.

to prescribe these toothpastes should be revisitedon a regular basis and should reflect the currentrisk assessment of the patient.
ADULTS AND OLDER ADULTSEvidenceEvidence for the use of fluoride products in adultsis relatively scarce. This is largely due to the fact thatthe caries studies are traditionally undertaken inschool settings where large numbers of study par-ticipants are easily reached and assessed. Studiesundertaken using long-term care and nursing homeresidents have largely examined the use of profes-sional fluoride applications to prevent and arrestroot caries.27 However, large-scale trials of fluoridesin adults are not available; thus, professionals mustalso rely on their judgment to make the best deci-sions for their patients.
For nonfrail, nonvulnerable adults, self-care andprofessional interventions are broadly similar tothose for children and adolescents. This reflects thefact that caries is a lifelong disease and that the eti-ology of the disease is constant across the lifecourse. Treatment planning should reflect changesin risk and risk factors of the adult population.27
Sugar consumption, for example, can change witha reduced intake of candies but an increased con-sumption of carbonated drinks, contributing notonly to caries but also erosion risk. The presence ofrestorations, both extra- and intracoronal, needs tobe considered with respect to secondary caries anddiagnosis of early lesions, and the assessment oftheir activity can be complicated by the presence ofdietary and other habitual stains.27
The responsibility of the dental professional isto assess when the patient is at a life stage where,owing to a range of internal and external factors,that risk may increase.28 (See Figure 3, earlier.) Thisincreased vulnerability is often, but not exclusively,associated with older adults, can occur at any time,and may be manifested by physical or cognitiveimpairment, or both.28 Although the research basefor older adults largely comprises long-term careand nursing home residents, it should be recognizedthat this is a function of clinical trial efficiencyrather than population-specific interventions. The
nursing home setting largely mirrors that of theschool—an accessible population for interventions.It is crucial that the predependency stage be identi-fied and that care plans that reflect the increasingrisk of caries in this group be put in place for bothprofessional care and self-care.28
Older adults with predependency and earlydependency have a range of risk factors that differfrom those of children or nondependent adults.These include
• Cognitive impairment: This can manifest assimply forgetting to brush the teeth or can leadto combative behavior, preventing caregiversfrom undertaking oral hygiene procedures.29
• Manual dexterity: Toothbrushing requires ahigh degree of manual dexterity, which isslowly lost with aging and may be adverselyaffected by conditions such as rheumatoidarthritis or Parkinson’s disease.30
• Polypharmacy: The number of medicationsprescribed increases with age. Either as indi-vidual agents or as a function of their collec-tive physiological effects, medications cancause decreased salivary flow, reducing theprotective effect of saliva and also encourag-ing behaviors to stimulate saliva that furtherincrease caries risk.31
• Finances and access to care: Older adultsserved by insurance-based dental care mayfind financial barriers to continuing access toservices, and there is evidence to suggest thatdental professionals in primary care settingsare reluctant to treat patients with extensive,complex medical histories or conditions.
Published in 2014, “The Seattle Care Pathwayfor Securing Oral Health in Older Patients”describes an evidence-based approach to managingolder adults with increased dependency. Providedas an open access document, it is recommended forall practitioners who serve older patients.28
Therapies available for older adults are the sameas those for children and adolescents. The provisionof a detailed and achievable self-care plan (whichmay include the prescription of a high-fluoridedentifrice) and professional application of fluoride(typically in the form of varnish) are recommend-
CHAPTER 14 Fluorides
242

ed.7 Both sodium fluoride and silver diamine fluo-ride varnishes have significant levels of trial evi-dence to support efficacy.32 Dental professionalsshould also consider how they can help to mediatethe risk factors associated with increased vulnera-bility by undertaking a personalized assessment ofthe patient’s needs. This may involve recommenda-tions for toothbrush modifications (e.g., powerbrushes) or consultation with the patient’s physi-cian to alter an existing medication to one thatcauses less xerostomia.28
Using Skill Mix to Deliver Fluoride-Based PreventionThere is a growing trend to extend the applicationof fluoride beyond the traditional dental practicemodel to expand the reach of this effective preven-tive intervention.32 The use of midlevel providers,while not without its detractors, presents an oppor-tunity for both dental practice–based and popula-tion-based fluoride interventions to be delivered inan effective and efficient manner. By using the prin-ciple of “every contact counts,” pediatricians andnurse practitioners are now applying fluoride var-nish to patients seen in their practice settings, as areother healthcare professionals in school-based pro-grams. The simple, safe and effective technique offluoride varnish means that it can be adoptedacross populations rather than just individuals, andfor those areas where water fluoridation is eitherlogistically or politically impossible, it offers analternative strategy.33
Population-Based Fluoride InterventionsCommunity (or population) prescriptions forhigh-fluoride toothpastes are being considered,whereby a lead dentist will undertake to prescribenot to an individual, but to a defined population.This could enable, for example, all long-term careor nursing home residents to be provided with5,000 ppm toothpaste. While such populationinterventions should not be seen as negating theneed for dental attendance and personalized care,this approach may help in areas where access tocare is restricted.
Community-based water fluoridation remains
the population fluoride intervention of choice, butit is not always physically possible (e.g., due to thewater provision infrastructure) or may be problem-atic due to regulatory or legislative issues.34 Dietaryfluorides, such as those in salt or milk, are consid-ered as alternatives,35,36 although their evidence baseis weaker.
The integration of fluoride into public healthsystems and population interventions is bestachieved in a holistic manner. By working withinwider public health concerns, such as childhoodobesity, the integration of dental prevention isaligned to other work streams and program effi-ciency is increased. Dental professionals have animportant advocacy role to ensure that oral healthis featured in community health plans and thatemphasis that is placed, quite correctly, on youngchildren, is not at the expense of older adults whohave similar needs for oral health improvement.
FUTURE DIRECTIONS AND BEST PRACTICE
Fluoride remains the mainstay of caries preventionand, in the case of early lesions, treatment.Although other technologies show promise (e.g.,arginine and casein phosphopetides-amorphouscalcium phosphate [CP-ACP]), the use of fluoridein toothpaste, gels, and varnishes will continue to bethe therapy of choice for consumers, professionals,and populations.37,38
Technologies for delivering fluoride remainlargely unchanged since the introduction of var-nishes to supplement dentifrices. The incorporationof fluoride into restorative materials continues andnew-generation materials may offer the potentialfor slower fluoride release and improved rechargeproperties.8 There has been considerable interest inthe development of further slow-release materials,possibly using degradable glass beads bonded to atooth surface that then release fluoride over a longperiod. Despite initial promise, concerns about thebeads being swallowed (and risk for toxicity or fluo-rosis in appropriately aged children) and a lack ofevidence of efficacy persist.39 It is likely that the bestmeans of improving the efficacy of fluoride will beensuring that compliance is optimized; concentra-
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
243

tion levels are appropriate to risk; and simple, con-sistent messages regarding rinsing, timing, andamount are provided.
SUMMARYCaries is a lifelong condition that is characterizedby periods of increased risk, but it should beremembered that some individuals will be consid-ered at high risk throughout life.11 Caries risk isassociated with a number of physical and psy-chosocial factors, and risk assessment is the cor-nerstone of any preventive treatment program,which should include consideration for self-careand professional interventions.40 Caries is adynamic process in which alternate periods ofdemineralization and remineralization occur, andcaries lesions can be prevented and, if detected inearly stages, reversed.41
Fluoride is the main therapeutic agent for theprevention and arrest of dental caries and can bedelivered through population, professional, orindividual routes using a range of delivery sys-tems.42 Evidence is clear that fluoride exerts itscaries-preventive effects topically, and there is littlejustification for the use of fluoride delivery sys-tems based on systemic use. For population pre-vention, water fluoridation remains theintervention of choice, whereas the vast majorityof fluoride is delivered by means of fluoridateddentifrices.43,44 The efficacy of such pastes, whichremain the mainstay of preventive self-care plansfor adults and children, can be increased by simplemessages on utilization, including avoidance ofrinsing, using twice daily for 2 minutes, and appro-priate dosage and concentration based on age, riskof fluorosis, and caries risk.44 The risk of fluorosisin younger children should always be balancedagainst the risk of dental caries.45
Professional application of fluorides, usingvarnishes, gels, or foams has a strong and soundevidence base established by systematic reviews.25
Their use is to be encouraged within a wider pre-ventive plan that considers physical barriers suchas pit and fissure sealants. The effectiveness ofboth the self-care plan and any professional appli-cation of fluorides is predicated on the detection
of early caries lesions (those limited to enamel orthe very outer aspects of dentin). Dental profes-sionals should recognize members of the widerhealthcare team for fluoride delivery and advocatefor population-based programs within integratedpublic health programs.
REFERENCES1. Rugg-Gunn A. Dental caries: strategies to control this
preventable disease. Acta Med Acad. 2013;42:117–130.2. Buzalaf MA, Pessan JP, Honório HM, ten Cate JM.
Mechanisms of action of fluoride for caries control.Monogr Oral Sci. 2011;22:97–114.
3. McGrady MG, Ellwood RP, Pretty IA. Why fluoride?Dent Update. 2010;37:595–598, 601–602.
4. Dean H. Nutriton classics. Public Health Reports, Vol-ume 56, 1941, pages 761–792. In: Dean HT, Jay P,Arnold FA Jr, Elvove E, eds. Domestic water and dentalcaries. II. A study of 2,832 white children, aged 12–14years, of 8 suburban Chicago communities, includingLactobacillus acidophilus studies of 1,761 children. NutrRev. 1976;34:116–118.
5. Walsh T, Worthington HV, Glenny AM, Appelbe P,Marinho VC, Shi X. Fluoride toothpastes of differentconcentrations for preventing dental caries in childrenand adolescents. Cochrane Database Syst Rev.2010(1):CD007868.
6. Featherstone JD. The continuum of dental caries—evi-dence for a dynamic disease process. J Dent Res.2004;83(special no. C):C39–42.
7. Wierichs RJ,. Meyer-Lueckel H. Systematic review onnoninvasive treatment of root caries lesions. J Dent Res.2015;94:261–271.
8. Raggio DP, Tedesco TK, Calvo AF, Braga MM. Doglass ionomer cements prevent caries lesions in marginsof restorations in primary teeth?: A systematic reviewand meta-analysis. J Am Dent Assoc. 2016;147:177–185.
9. Iheozor-Ejiofor Z, Worthington HV, Walsh T, et al.Water fluoridation for the prevention of dental caries.Cochrane Database Syst Rev. 2015;(6):CD010856.
10. Whelton HP, Ketley CE, McSweeney F, O’MullaneDM. A review of fluorosis in the European Union:prevalence, risk factors and aesthetic issues. CommunityDent Oral Epidemiol. 2004;32(suppl 1):9–18.
11. Pretty IA. The life course, care pathways and elements ofvulnerability. A picture of health needs in a vulnerablepopulation. Gerodontology. 2014;31(suppl 1):1–8.
12. Clark MB, Slayton RL, Section on Oral Health. Fluo-ride use in caries prevention in the primary care setting.Pediatrics. 2014;134:626–633.
13. Wong MC, Clarkson J, Glenny AM, et al. Cochranereviews on the benefits/risks of fluoride toothpastes. JDent Res. 2011;90:573–579.
14. Chesters RK, Huntington E, Burchell CK, Stephen
CHAPTER 14 Fluorides
244
KW. Effect of oral care habits on caries in adolescents.Caries Res. 1992;26:299–304.
15. Walker A. National Diet and Nutrition Survey: Young Peo-ple Aged 4–18 Years. Volume 2. Report of the Oral HealthSurvey. London, England: Stationery Office; 2000.
16. Ripa LW. A critique of topical fluoride methods (denti-frices, mouthrinses, operator-, and self-applied gels) in anera of decreased caries and increased fluorosis preva-lence. J Public Health Dent. 1991;51:23–41.
17. Marinho VC, Higgins JP, Logan S, Sheiham A. Fluoridemouthrinses for preventing dental caries in children and ado-lescents. Cochrane Database Syst Rev. 2003;(3):CD002284.
18. Blinkhorn AS, Holloway PJ, Davies TG. Combinedeffects of a fluoride dentifrice and mouthrinse on theincidence of dental caries. Community Dent Oral Epi-demiol. 1983;11:7–11.
19. Marinho VC, Worthington HV, Walsh T, Chong LY.Fluoride gels for preventing dental caries in children andadolescents. Cochrane Database Syst Rev.2015;(6):CD002280.
20. Walsh T, Oliveira-Neto JM, Moore D. Chlorhexidinetreatment for the prevention of dental caries in childrenand adolescents. Cochrane Database Syst Rev.2015;(4):CD008457.
21. Driscoll WS, Heifetz SB, Korts DC, Meyers RJ,Horowitz HS. Effect of acidulated phosphate-fluoridechewable tablets in schoolchildren: results after 55months. J Am Dent Assoc. 1977;94:537–543.
22. DePaola PF, Lax M. The caries-inhibiting effect of acidu-lated phosphate-fluoride chewable tablets: a two-yeardouble-blind study. J Am Dent Assoc. 1968;76:554–557.
23. Ripa LW. An evaluation of the use of professional (oper-ator-applied) topical fluorides. J Dent Res. 1990;69(spe-cial no.):786–796; discussion 820–823.
24. Marinho VC, Worthington HV, Walsh T, Clarkson JE.Fluoride varnishes for preventing dental caries in chil-dren and adolescents. Cochrane Database Syst Rev.2013;(7):CD002279.
25. Gao SS, Zhang S, Mei ML, Lo EC, Chu CH. Cariesremineralisation and arresting effect in children by pro-fessionally applied fluoride treatment—a systematicreview. BMC Oral Health. 2016;16:12.
26. Ammari AB, Bloch-Zupan A, Ashley PF. Systematicreview of studies comparing the anti-caries efficacy ofchildren’s toothpaste containing 600 ppm of fluoride orless with high fluoride toothpastes of 1,000 ppm orabove. Caries Res. 2003;37:85–92.
27. Pretty I. The Seattle Care Pathway: defining dental carefor older adults. J Calif Dent Assoc. 2015;43:429–437.
28. Pretty IA, Ellwood RP, Lo EC, et al. The Seattle CarePathway for securing oral health in older patients.Gerodontology. 2014;31(suppl 1):77–87.
29. Chen X, Clark JJ, Naorungroj S. Oral health in olderadults with dementia living in different environments: apropensity analysis. Spec Care Dentist. 2013;33:239–247.
30. Marchini L, Vieira PC, Bossan TP, Montenegro FL,Cunha VP. Self-reported oral hygiene habits amonginstitutionalised elderly and their relationship to the con-dition of oral tissues in Taubate, Brazil. Gerodontology.2006;23:33–37.
31. Närhi TO, Vehkalahti MM, Siukosaari P, Ainamo A.Salivary findings, daily medication and root caries in theold elderly. Caries Res. 1998;32:5–9.
32. Gluzman R, Katz RV, Frey BJ, McGowan R. Preventionof root caries: a literature review of primary and secondarypreventive agents. Spec Care Dentist. 2013;33:133–140.
33. Brocklehurst P, Macey R. Skill-mix in preventive dentalpractice—will it help address need in the future? BMCOral Health. 2015;15(suppl 1):S10.
34. Melbye ML, Armfield JM. The dentist’s role in promot-ing community water fluoridation: a call to action for den-tists and educators. J Am Dent Assoc. 2013;144:65–75.
35. Marthaler TM. Salt fluoridation and oral health. ActaMed Acad. 2013;42:140–155.
36. Yeung CA, Chong LY, Glenny AM. Fluoridated milkfor preventing dental caries. Cochrane Database SystRev. 2015;(9):CD003876.
37. Cummins D. Dental caries: a disease which remains apublic health concern in the 21st century—the explo-ration of a breakthrough technology for caries preven-tion. J Clin Dent. 2013;24(special no. A):A1–14.
38. Reema SD, Lahiri PK, Roy SS. Review of casein phos-phopeptides-amorphous calcium phosphate. Chin JDent Res. 2014;17:7–14.
39. Chong LY, Clarkson JE, Dobbyn-Ross L, Bhakta S.Slow-release fluoride devices for the control of dentaldecay. Cochrane Database Syst Rev. 2014;(11):CD005101.
40. Senneby A, Mejàre I, Sahlin NE, Svensäter, Rohlin M.Diagnostic accuracy of different caries risk assessmentmethods. A systematic review. J Dent. 2015;43:1385–1393.
41. Fejerskov O. Changing paradigms in concepts on dentalcaries: consequences for oral health care. Caries Res.2004;38:182–191.
42. Lenzi TL, Montagner AF, Soares FZ, de Oliveira RochaR. Are topical fluorides effective for treating incipientcarious lesions?: A systematic review and meta-analysis.J Am Dent Assoc. 2016;147:84–91 e1.
43. McGrady MG, Ellwood RP, Maguire A, Goodwin M,Boothman N, Pretty IA. The association between socialdeprivation and the prevalence and severity of dentalcaries and fluorosis in populations with and withoutwater fluoridation. BMC Public Health. 2012;12:1122.
44. McGrady MG, Ellwood RP, Pretty IA. Water fluorida-tion as a public health measure. Dent Update.2010;37:658–660, 662–664.
45. Goodwin M, Sanders C, Davies G, Walsh T, Pretty IA.Issues arising following a referral and subsequent waitfor extraction under general anaesthetic: impact on chil-dren. BMC Oral Health. 2015;15:3.
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
245

The utilization of low concentrations of the fluo-ride ion as a caries prevention tactic is well estab-lished and has been in wide use for nearly 60 years.Contemporary approaches include a number offluoride delivery regimens that are well supportedby research. Fluoride-containing dentifrices, high-concentration fluoride compounds, and low-con-centration fluoride in community water supplieshave all had significant beneficial effects on thepublic’s oral health. Nevertheless, all dental clini-cians are aware that the use of fluoride-containingproducts alone does not prevent or arrest all toothdecay.1–3 Indeed, caries remains a problem formany patients despite widespread utilization offluoride-containing products.4 This chapter exam-ines the notion that patients with high caries risk,such as those with xerostomia or poor diets, mayfare better if fluoride-based therapeutics are sup-plemented with other non-fluoride-based regi-mens aimed at countering the etiology of caries orby making the teeth more resistant to cavitation.
Utilizing an individualized caries risk assess-ment facilitates a customized approach to oralhealth based on an individual’s specific needs (seeChapter 3, Risk Assessment). As noted, the use ofnon-fluoride preventive interventions and rem-ineralization agents may help prevent or bettermitigate caries in some patients. However, thecost-effectiveness of these agents has been ques-tioned, particularly for patients with low cariesrisk. This is because such individuals are unlikelyto develop caries with or without these interven-tions. It is for this reason that non-fluoride cariespreventive and remineralization agents are notappropriate for every patient. On the other hand,
higher risk individuals may benefit from theseagents. The bottom line is that a customized anti-caries regimen for every patient (that may beadjusted as risks change over time) is consideredoptimal.5
As clinicians consider using or recommendingnon-fluoride preventive interventions or reminer-alization agents, they should keep in mind thatfluoridated community water supplies (or supple-mental systemic fluoride if community water sup-plies are fluoride-free), good home oral hygiene,limited dietary intake of fermentable carbohy-drates, local application of high-concentration flu-oride compounds (when or where indicated), andthe consistent use of fluoride-containing denti-frices are the pillars of any well-reasoned anti-caries program.5 Thus, non-fluoride preventiveand remineralization agents should be consideredadjunctive.
BEYOND FLUORIDES: FINDING OTHERMETHODS TO REDUCE CARIES
Dental biofilm, also known as dental plaque, haslong been implicated in the etiology of caries. In1973, Miller proposed a two-step process of cariesdevelopment. The first step involves tooth-adherentoral bacteria that produce acids when exposed tofermentable carbohydrates. In the second step, theacids act on tooth structure to dissolve mineralcomponents of teeth (hydroxyapatite), eventuallycausing cavitation.6 The production of bacterialacids within plaque in response to fermentable car-bohydrates and the subsequent slow recoverytoward a neutral plaque pH was demonstrated byStephan.7,8 The consumption of dietary carbohy-drates (especially sugars), even if only thin layers ofdental biofilm are present, results in significant bac-terial acid production. Such acid acts immediatelyto begin dissolving the mineral components of theteeth. The amount and duration of the pH dropare related to the amount of dissolution and are tosome degree mitigated by the natural acid–basebuffering capabilities of saliva and nearby dentalplaque.9,10 Dental plaque is a highly diverse, tempo-rally dynamic, three-dimensional communityembedded in a polymeric matrix of bacterial andsalivary origins.11 Marsh demonstrated that thenature of this bacterial community is dependent, in
246
Non-Fluoride Remineralization Therapies
Chapter 15
Mark S. Wolff and Michael P. Rethman
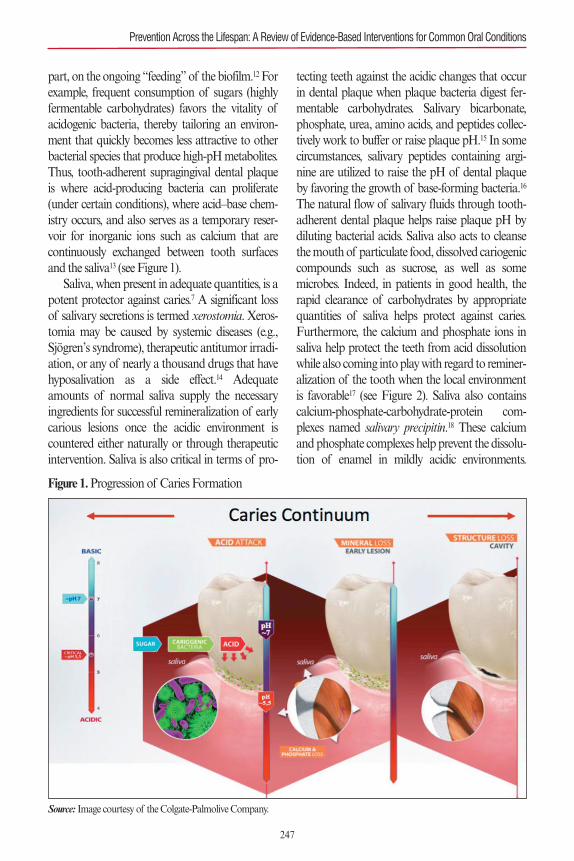
part, on the ongoing “feeding” of the biofilm.12 Forexample, frequent consumption of sugars (highlyfermentable carbohydrates) favors the vitality ofacidogenic bacteria, thereby tailoring an environ-ment that quickly becomes less attractive to otherbacterial species that produce high-pH metabolites.Thus, tooth-adherent supragingival dental plaqueis where acid-producing bacteria can proliferate(under certain conditions), where acid–base chem-istry occurs, and also serves as a temporary reser-voir for inorganic ions such as calcium that arecontinuously exchanged between tooth surfacesand the saliva13 (see Figure 1).
Saliva, when present in adequate quantities, is apotent protector against caries.7 A significant lossof salivary secretions is termed xerostomia. Xeros-tomia may be caused by systemic diseases (e.g.,Sjögren’s syndrome), therapeutic antitumor irradi-ation, or any of nearly a thousand drugs that havehyposalivation as a side effect.14 Adequateamounts of normal saliva supply the necessaryingredients for successful remineralization of earlycarious lesions once the acidic environment iscountered either naturally or through therapeuticintervention. Saliva is also critical in terms of pro-
tecting teeth against the acidic changes that occurin dental plaque when plaque bacteria digest fer-mentable carbohydrates. Salivary bicarbonate,phosphate, urea, amino acids, and peptides collec-tively work to buffer or raise plaque pH.15 In somecircumstances, salivary peptides containing argi-nine are utilized to raise the pH of dental plaqueby favoring the growth of base-forming bacteria.16
The natural flow of salivary fluids through tooth-adherent dental plaque helps raise plaque pH bydiluting bacterial acids. Saliva also acts to cleansethe mouth of particulate food, dissolved cariogeniccompounds such as sucrose, as well as somemicrobes. Indeed, in patients in good health, therapid clearance of carbohydrates by appropriatequantities of saliva helps protect against caries.Furthermore, the calcium and phosphate ions insaliva help protect the teeth from acid dissolutionwhile also coming into play with regard to reminer-alization of the tooth when the local environmentis favorable17 (see Figure 2). Saliva also containscalcium-phosphate-carbohydrate-protein com-plexes named salivary precipitin.18 These calciumand phosphate complexes help prevent the dissolu-tion of enamel in mildly acidic environments.
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
247
Figure 1.Progression of Caries Formation
Source: Image courtesy of the Colgate-Palmolive Company.
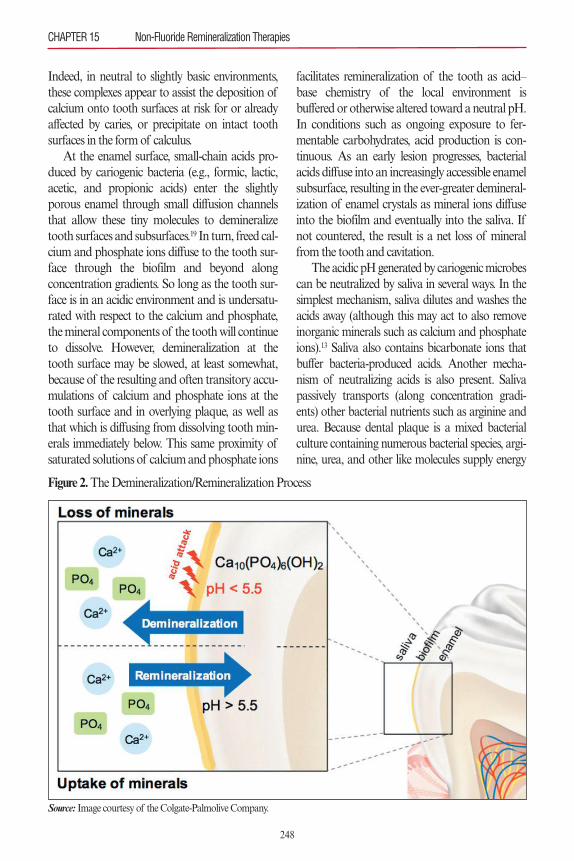
Indeed, in neutral to slightly basic environments,these complexes appear to assist the deposition ofcalcium onto tooth surfaces at risk for or alreadyaffected by caries, or precipitate on intact toothsurfaces in the form of calculus.
At the enamel surface, small-chain acids pro-duced by cariogenic bacteria (e.g., formic, lactic,acetic, and propionic acids) enter the slightlyporous enamel through small diffusion channelsthat allow these tiny molecules to demineralizetooth surfaces and subsurfaces.19 In turn, freed cal-cium and phosphate ions diffuse to the tooth sur-face through the biofilm and beyond alongconcentration gradients. So long as the tooth sur-face is in an acidic environment and is undersatu-rated with respect to the calcium and phosphate,the mineral components of the tooth will continueto dissolve. However, demineralization at thetooth surface may be slowed, at least somewhat,because of the resulting and often transitory accu-mulations of calcium and phosphate ions at thetooth surface and in overlying plaque, as well asthat which is diffusing from dissolving tooth min-erals immediately below. This same proximity ofsaturated solutions of calcium and phosphate ions
facilitates remineralization of the tooth as acid–base chemistry of the local environment isbuffered or otherwise altered toward a neutral pH.In conditions such as ongoing exposure to fer-mentable carbohydrates, acid production is con-tinuous. As an early lesion progresses, bacterialacids diffuse into an increasingly accessible enamelsubsurface, resulting in the ever-greater demineral-ization of enamel crystals as mineral ions diffuseinto the biofilm and eventually into the saliva. Ifnot countered, the result is a net loss of mineralfrom the tooth and cavitation.
The acidic pH generated by cariogenic microbescan be neutralized by saliva in several ways. In thesimplest mechanism, saliva dilutes and washes theacids away (although this may act to also removeinorganic minerals such as calcium and phosphateions).13 Saliva also contains bicarbonate ions thatbuffer bacteria-produced acids. Another mecha-nism of neutralizing acids is also present. Salivapassively transports (along concentration gradi-ents) other bacterial nutrients such as arginine andurea. Because dental plaque is a mixed bacterialculture containing numerous bacterial species, argi-nine, urea, and other like molecules supply energy
CHAPTER 15 Non-Fluoride Remineralization Therapies
248
Figure 2.The Demineralization/Remineralization Process
Source: Image courtesy of the Colgate-Palmolive Company.

to arginolytic bacteria that, in turn, produce high-pH metabolites that serve to neutralize the plaqueacids produced by cariogenic bacteria.16
It is noteworthy that if the enamel surfaceremains intact, bacteria have no way of invadingthe dentin because enamel diffusion channels aretoo small to permit bacterial invasion. This is trueeven though radiography may reveal significantdecreases in enamel radiodensity. This observationof an early enamel-only lesion provides the ration-ale for therapies aimed at chemical remineraliza-tion of partially demineralized enamel. This is inlieu of traditional surgical interventions (i.e.,preparing the site for a dental restoration) for earlycarious lesions. Indeed, a remineralizationapproach is usually indicated when bacterial acidshave penetrated but not completely destroyed theenamel.20 However, clinicians would do well toremember that remineralization is a microscopicphenomenon and will not macroscopicallyreplace tooth structure. Once frank cavitationoccurs, surgical restoration is often indicated.13
NON-FLUORIDE STRATEGIES FOR MANAGING CARIOGENIC BIOFILMS
Traditional ApproachesThree strategies have dominated the history ofmodern dentistry, namely (1) brush one’s teethwith fluoride toothpaste, (2) use dental floss everyday, and (3) decrease the consumption of fer-mentable carbohydrates (“cut down on sweets”).Combinations of these strategies have beenresponsible for substantial reductions in the ratesof dental caries.
Oral hygiene education has been shown toreduce bacterial counts but not reduce the bacteri-al burden by clinically significant amounts.21
Plaque elimination by toothbrushing has beenwell documented. A review of the literature relat-ed to flossing revealed that self-flossing failed toproduce effective reductions in caries.22However, itmust be remembered that comparative studiesreport average responses in what are thought to besufficiently large groups of patients selected toreflect the population as a whole. No one is aver-age. This means that while flossing (or perhaps
brushing using a non-fluoride dentifrice) may notproduce dramatic population effects in terms ofreducing caries, toothbrushing and daily flossingstill make sense for individuals. Furthermore,when reviewing studies related to toothbrushingeffectiveness and caries, it is difficult to separateout the beneficial effects of frequent toothbrush-ing using fluoride-containing dentifrices—anintervention that has been repeatedly demonstrat-ed to reduce caries rates. Incremental reduction incaries increases with the concentration of fluoridein the dentifrice and the frequency of its use. Notsurprising, such benefits are more noticeable inthose patients most prone to caries.23
Attempts to decrease the rate of dental cariesby lowering the consumption of sugars have metwith less success. The Vipeholm studies of themid-20th century demonstrated that the nature ofsugar exposures affects the risk of caries, withsticky foods and frequent consumption increasingcaries rates.24–26 Despite this information, cariesmanagement by dietary control of sugar hasremained difficult. Draconian decreases in sugarconsumption, such as that which occurred in post-World War II Japan and later in trade-embargoedIraq, demonstrated that dramatic reductions inthe consumption of sugars could decrease cariesincidence.27,28 However, voluntary dietary restric-tions that largely eliminate the consumption ofdietary sugars necessitate lifelong changes inhabits that are seldom sustainable.29
Targeted Antimicrobial TherapiesModifying the dental plaque to be less cariogenic is amore recent and logical strategy. Multiple method-ologies have been suggested to manage the bacterialconstituents of dental biofilms. Stannous fluorideand amine fluoride (as well as numerous metallicions) have demonstrated antimicrobial effective-ness.30,31Naturally high levels of tin, zinc, copper, andother ions dissolved in community water supplieshave demonstrated antimicrobial effects, but none ofthese ions have demonstrated anticaries effectiveness.Taste, safety, and lack of clinical trials make any rec-ommendation difficult.32,33 Essential oils (a mixtureof thymol, eucalyptol, methyl salicylate, and
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
249

menthol) have been demonstrated to be effective inlimiting accumulations of supragingival plaque,acid-producing Streptococcus mutans, and gingivi-tis,34–37 but have failed to demonstrate effectivenessagainst caries. Triclosan/copolymer has demonstrat-ed clinical effectiveness in reducing plaque and gin-givitis. Research conducted by several groups hasdemonstrated that the addition of triclosan/copoly-mer enhances the caries-preventative effect of fluo-ride.38–40 A recent Cochrane Collaboration review ofthe body of evidence for the clinical benefit of tri-closan/copolymer toothpaste confirmed a 5% reduc-tion in caries above what was seen in toothpastesthat contain fluoride alone.41 Certain silver com-pounds, especially diamine fluoride, have demon-strated effectiveness in arresting active caries,although they are not considered non-fluoride rem-ineralizing agents.42,43
Chlorhexidine, a bisguanide, is a broad-spec-trum antimicrobial that functions by disturbing thecell membrane of bacteria. It is available in combi-nation with thymol in a varnish, a 0.12% or 0.2%mouthrinse, and a 10% to 40% varnish in manyparts of the world. Studies have demonstrated thatchlorhexidine, administered frequently enough andin high enough doses, can reduce Streptococcalbioburden in the mouth.44 Unfortunately, clinicalstudies assessing caries reduction have been equivo-cal, especially in high-risk cases where beneficialeffects would be most likely detected.45,46 One usefor which there is positive evidence is for adults andelderly people prone to root caries. In this popula-tion, a 1:1 chlorhexidine:thymol varnish producedsignificant reductions in caries and should be con-sidered as adjunctive therapy.47–49
Polyol-sweetened chewing gums, candies, andpastes have been suggested as methods of prefer-entially altering the bacterial contents of thebiofilm. Xylitol is a low-calorie polyol that is afive-carbon sugar alcohol. Xylitol is widely avail-able in lozenges, gum, and other foods. Polyols aremetabolized by plaque bacteria slowly and do notresult in a decrease in plaque pH.50 Multiple stud-ies have also demonstrated that xylitol reduces thegrowth of S. mutans.51 It has been suggested thatthe consumption of 6 to 10 grams of xylitol per
day may reduce dental caries.52 However, in stud-ies, reductions in caries incidence have been con-founded by the effects of supplemental fluorides,the effects of fluoride dentifrices, or the positiveeffects of chewing gums on saliva production.53
Nevertheless, many low-evidence-quality studieshave reported positive effects on caries rates withsubstantial daily amounts of xylitol delivered insyrups, gums, and confections.45,54–57 Unfortunate-ly, low doses of xylitol have failed to demonstratesimilar positive effects.58,59 Data on other polyolsare equivocal.44
Multiple modifiers to the activity and viabilityof specific biofilm bacteria have been suggested.Koo (2009) suggested the utilization of naturallyoccurring molecules, such as apigenin, a potentinhibitor of insoluble-glucan synthesis, and tt-far-nesol, a disrupter of S. mutans cell membranes,aimed at reducing counts of this cariogenicspecies in dental biofilms.60,61 These methods haveyet to yield commercial products. Others have rec-ommended the introduction of antimicrobialpeptides that can kill target organisms by attach-ing to and altering electrostatic charges on bacter-ial cell walls. Combined peptide–cetylpyridiniumchloride combinations have shown promise inregulating S. mutans in the biofilm but to datehave not achieved clinical utility.62 Anotherantimicrobial peptide, termed specifically targetedantimicrobial peptide (STAMP), targets apheromone produced by S. mutans.63 STAMP isnow being investigated in vivo for its effectivenessin the reduction of S. mutans within the mixedecology of dental plaque. Results are promising,but STAMP has thus far not been evaluated withregard to its effects on caries.64
The microenvironment of supragingival plaquehas a tendency to become increasingly acidic, there-by favoring overpopulation of the biofilm with aci-dogenic bacteria such as S. mutans andLactobacillus species.9,11,12 Other commensal bacter-ial species in the plaque, such as Streptococcus san-guinis, are suppressed in an acidic biofilm.65
However, S. sanguinis metabolizes the amino acidarginine that is naturally found in saliva, producingammonia and carbon dioxide.16,66 Supplemental
CHAPTER 15 Non-Fluoride Remineralization Therapies
250

arginine, when provided to the mixed ecology ofplaque, promotes the reproduction of arginolyticbacteria, such as S. sanguinis. Ammonia productionis thereby enhanced. Ammonia in aqueous solutionis basic. It neutralizes the acids produced by cario-genic bacteria and alters the acid–base balance ofplaque toward a more neutral pH.66,67 A new acid-neutralizing toothpaste containing arginine is nowavailable in much of the world (Colgate MaximumCavity Protection plus Sugar Acid Neutralizer™).This dentifrice also contains typical concentrationsof fluoride ion. The new dentifrice has demonstrat-ed greater caries prevention capabilities than a con-trol dentifrice that contains fluoride ion alone.67–70
However, the new dentifrice also contains insolublecalcium that might also have a beneficial effect oncaries rates. The observed improvement over fluo-ride-containing dentifrice is likely due, at least inpart, to the ability of ammonia to neutralize acidsproduced by cariogenic bacteria.71
Stimulating Salivary FlowThe concept of stimulating salivary flow as ameans to reduce caries seems notionally sound.Saliva has many properties that are beneficial interms of reducing caries. Saliva contains bicarbon-ate, a potent buffer to acidic challenges, and alsocontains calcium and phosphate ions, both ofwhich are useful in terms of remineralizing earlycarious lesions. Saliva also has a slightly basic pHof 7.4. Saliva washes away sugar-containing foods,serves to dilute and neutralize cariogenic acids,and stocks the dental biofilm with calcium andphosphate ions that help prevent tooth demineral-ization while encouraging remineralization.
Chewing gum can produce and sustain up to a
10- to 12-fold increase in salivary flow comparedwith unstimulated salivary flow.72–74 Stimulatedsalivary flow has been demonstrated to neutralizeacids, clear debris, and return the plaque pH toneutrality.75–77 Both experimental evidence andexpert opinions recommend that sugarless chew-ing gums, particularly those containing polyols, beutilized multiple times per day in patients at highrisk of caries.45,78,79
Calcium-Based RemineralizationRemineralization of the tooth utilizing calcium isnot a new concept. A classic chemistry equation (seeFigure 3) describes the relationship between bacteri-al acids and the eventual release of calcium andphosphate ions into the plaque and eventually thesaliva. Increasing calcium and phosphate ion con-centrations proximate to the tooth helps preventdemineralization and may force remineralization bythe law of mass action.80 Calcium-containing prod-ucts have been recommended for decades in thewake of in vitrodata that demonstrated the filling ofexposed dentinal tubules treated with calciumhydroxide.81 A key problem associated with localapplication of calcium hydroxide is its high solubili-ty in water and saliva.
In more recent decades, numerous calcium-based desensitizing products have appeared. In theearly 1990s, an amorphous calcium phosphate(ACP)–based dentifrice became commerciallyavailable. It contained sodium fluoride, calciumsalts, and phosphate salts. Calcium hydroxide wasseparated from the phosphate and fluoride by aplastic divider inside the tube to prevent chemicalinteractions while stored. In an 8-week clinicaltrial, the product was shown to reduce sensitivity
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
251
Figure 3.Relationship of Bacterial Acids to Calcium and Phosphate Ions
Source: Image courtesy of the Colgate-Palmolive Company.

about as well as nondentifrice products available atthe time.82 ACP has recently been incorporatedinto a commercially available dentifrice that alsocontains bicarbonate. ACP is also included in anumber of prophylactic polishing pastes and den-tal varnishes.
In the late 1990s, a calcium-based remineraliz-ing product was introduced that demonstrateddesensitization capabilities as both a toothpasteand a prophylaxis paste. This product is an argi-nine bicarbonate/calcium carbonate compound(formally known as Cavistat™, Ortek Therapeu-tics, Garden City, NY, USA) that can be incorpo-rated into multiple delivery platforms to assist inmineralization. It is currently available on the mar-ket in many countries in dentifrice form (ColgateMaximum Cavity Protection Plus Sugar AcidNeutralizer™, Colgate-Palmolive Company, NewYork, NY, USA). The mechanism of action isdescribed as follows:
The highly soluble arginine bicarbonate com-ponent surrounds, or is surrounded by, particlesof less soluble calcium carbonate, and becauseof the adhesive qualities of this composition,forms a paste-like plug that not only fills butalso adheres to the dentinal tubule walls.Because of its alkalinity, the arginine bicarbon-ate/calcium carbonate also reacts with the calci-um and phosphate ions of the dentinal fluid tomake the plug chemically contiguous with thedentinal walls.83
Twice-daily self-application of the dentifricecontaining arginine bicarbonate/calcium carbonateachieved similar results in clinical trials. Two stud-ies, including one double-blind, placebo-controlledstudy utilizing a chewable mint and a cohort-con-trolled study of a Cavistat™-containing dentifrice,demonstrated reductions in new decayed, missing,filled surfaces (DMFS), as well as reversals of earlycarious lesions.84,85 Subsequently, a similar 1.5%arginine carbonate/insoluble calcium carbonatecompound has been incorporated into a commer-cial dentifrice and has demonstrated both reminer-alization of early lesions and caries-preventivecapabilities.69,70
Also in late 1990s, another calcium-based rem-
ineralizing technology became available. This tech-nology addressed the problem of stabilizing amor-phous calcium phosphate under neutral oralkaline conditions in an effort to increase theplaque content of calcium and phosphate. Thisgoal was achieved by the development of a caseinphosphopeptide linked to amorphous calciumphosphate (CPP-ACP; RecaldentTM, CadburyEnterprises Pte Ltd, Parsippany, NJ, USA).86 Thisproduct, in a series of in situ studies, has demon-strated the ability to remineralize enamel that waspreviously demineralized.87 The effectiveness ofthe CPP-ACP product in reducing dentin hyper-sensitivity was demonstrated utilizing a dentifricedelivery system. In a small study of patients withSjögren’s syndrome, a casein derivative coupledwith calcium phosphate was used to slightlyreduce the caries incidence without a statisticallysignificant difference being noted.88 A 2,720-patient, 2-year, double-blind clinical study useddigital bitewing radiographs to assess the progres-sion or regression of interproximal caries in ado-lescent subjects chewing a sugar-free gumcontaining CPP-ACP. Caries progression orregression was analyzed and, for subjects chewingthe CPP-ACP gum, the odds of a surface experi-encing caries progression were 18% less than forthose chewing a control gum.89 In 2010, a studyusing light-induced fluorescence analyzed theeffects of CPP-ACP on demineralized white spotsafter orthodontic treatment. No apparent differ-ences in remineralization were observed whencompared with controls.90 Another study foundthat patients with xerostomia who used a supersat-urated Ca2+/PO4
(3−) and fluoride-containing rinsedemonstrated significantly fewer caries than thosewho did not use a fluoride-containing rinse.Unfortunately fluoride usage was a confoundingvariable in this study.91
CONCLUSIONDecisions related to reducing caries risk must be simple, cost-effective, and individualized. Allrecommendations start with an understanding ofwhat causes the disease. The consistent use of afluoride-containing dentifrice, professionally
CHAPTER 15 Non-Fluoride Remineralization Therapies
252

applied high-concentration fluoride applications(e.g., fluoride varnishes), and at-home supplemen-tal fluorides (e.g., 5,000 ppm sodium fluoride) arethe cornerstones of most evidence-based oralhealth recommendations. This includes propertoothbrushing technique and regular brushinghabits. Dietary issues must also be considered byencouraging patients to tightly limit the frequencyof highly fermentable carbohydrate intake. Thismay require major and lifelong changes to familialhabits.
Patients at high risk for developing cariesshould substitute polyols, particularly xylitol (at aminimum of 6 grams per day), for sugar wherepossible so as to gain the benefits of decreasedbacterial acids as well as the inhibitory effects ofxylitol on cariogenic bacteria. Antimicrobial rins-es, such as those that contain chlorhexidine,should be approached with caution because evi-dence for anticaries effectiveness is weak andbecause chlorhexidine rinses are expensive andcan cause side effects such as tooth staining andtaste alteration. However, for patients who havedeveloped or are at risk for root caries, the use ofchlorhexidine-containing varnishes should be con-sidered. The use of calcium-containing pastesshould only be considered in patients who are atthe highest risk and neveras a substitute for a fluo-ride-containing dentifrice. Unfortunately, theincorporation of calcium into fluoride dentifricesmay alter the anticaries capabilities of the fluorideions. These dentifrices should undergo additionalclinical studies to support the hypothesis that cal-cium compounds do not reduce the effectivenessthe fluorides.
In closing, clinicians need to fully appreciatethat non-fluoride anticaries preventive interven-tions or remineralization agents should almostalways be considered as adjunctive to therapiesaimed at patients for whom quality self-care andthe full use of a wide range of fluoride-containingproducts does not seem to be enough to eliminateor otherwise control dental caries.
REFERENCES1. Marinho VC, Higgins JP, Sheiham A, Logan S. Combi-
nations of topical fluoride (toothpastes, mouthrinses,gels, varnishes) versus single topical fluoride for prevent-ing dental caries in children and adolescents. CochraneDatabase Syst Rev. 2004;(1):CD002781.
2. Marinho VC, Worthington HV, Walsh T, Clarkson JE.Fluoride varnishes for preventing dental caries in chil-dren and adolescents. Cochrane Database Syst Rev.2013;(7):CD002279.
3. Featherstone JD. Delivery challenges for fluoride,chlorhexidine and xylitol. BMC Oral Health.2006;6(suppl 1):S8.
4. Beltran-Aguilar ED, Barker LK, Canto MT, et al. Sur-veillance for dental caries, dental sealants, tooth reten-tion, edentulism, and enamel fluorosis—United States,1988–1994 and 1999–2002. MMWR Surveill Summ.2005;54(3):1–43.
5. Twetman S. Treatment protocols: nonfluoride manage-ment of the caries disease process and available diagnos-tics. Dent Clin North Am. 2010;54:527-–540.
6. Miller WD. The Micro-Organisms of the Human Mouth;the Local and General Diseases Which Are Caused byThem. Basel, Switzerland: S. Karger; 1973.
7. Stephan RM. Changes in hydrogen ion concentration ortooth surfaces and in carious lesions. J Am Dent Assoc.1940;27:718–723.
8. Stephan RM. Intra oral hydrogen ion concentrationsassociated with dental caries activity. J Dent Res.1944;23:257–266.
9. Kleinberg I. Formation and accumulation of acid on thetooth surface. J Dent Res. 1970;49:1300–1317.
10. Kleinberg I, Jenkins GN, Chatterjee R, Wijeyeweera L.The antimony pH electrode and its role in the assessmentand interpretation of dental plaque pH. J Dent Res.1982;61:1139–1147.
11. Marsh P, Martin M. Oral Microbiology. 3rd ed. Lon-don, England: Chapman & Hall; 1992.
12. Marsh PD, Bradshaw DJ. Dental plaque as a biofilm. JInd Microbiol. 1995;15:169–175.
13. Wolff MS, Larson C. The cariogenic dental biofilm:good, bad or just something to control? Braz Oral Res.2009;23(suppl 1):31–38.
14. Sreebny LM, Schwartz SS. A reference guide to drugsand dry mouth—2nd edition. Gerodontology.1997;14:33–47.
15. Mandel ID. The functions of saliva. J Dent Res.1987;66(special no.):623–627.
16. Kleinberg I, Kanapka J, Chatterjee R, et al. Metabolismof nitrogen by mixed bacteria. In: Kleinberg I, EllisonSA, Mandel ID, eds. Proceedings: Saliva and Caries.Special Supplement, Microbiology Abstracts. New York,NY: Information Retrieval; 1979:357–377.
17. Kleinberg I, Chatterjee R, Denepetya L. Effects of salivaand dietary eating habits on the pH and demineralisa-tion-remineralisation potential of dental plaque. In:
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
253
Dr. Mark Wolff is a paid consultant, lecturer, and researcherfor the Colgate-Palmolive Company and C3-Jian, Inc. Dr. Michael Rethman is a paid consultant for the Colgate-Palmolive Company and Interleukin Genetics Inc.
Demineralisation-Remineralisation of the Teeth. Oxford,England: IRL Press; 1983:25–50.
18. Kleinberg I, Kaufman HW, Wolff M. Measurement oftooth hypersensitivity and oral factors involved in itsdevelopment. Arch Oral Biol. 1994;39(suppl):63S–71S.
19. Featherstone JD, Holmen L, Thylstrup A, Fredebo L,Shariati M. Chemical and histological changes duringdevelopment of artificial caries. Caries Res. 1985;19:1–10.
20. Featherstone JD, Cutress TW, Rodgers BE, DennisonPJ. Remineralization of artificial caries-like lesions invivo by a self-administered mouthrinse or paste. CariesRes. 1982;16:235–242.
21. Smiech-Slomkowska G, Jablonska-Zrobek J. The effectof oral health education on dental plaque developmentand the level of caries-related Streptococcus mutans andLactobacillus spp. Eur J Orthod. 2007;29:157–160.
22. Hujoel PP, Cunha-Cruz J, Banting DW, Loesche WJ.Dental flossing and interproximal caries: a systematicreview. J Dent Res. 2006;85:298–305.
23. Marinho VC, Higgins JP, Sheiham A, Logan S. Fluoridetoothpastes for preventing dental caries in children andadolescents. Cochrane Database Syst Rev.2003;(1):CD002278.
24. Gustafsson BE, Quensel CE, Lanke LS, et al. TheVipeholm dental caries study; the effect of different levelsof carbohydrate intake on caries activity in 436 individu-als observed for five years. Acta Odontol Scand.1954;11:232–264.
25. Krasse B. The Vipeholm Dental Caries Study: recollec-tions and reflections 50 years later. J Dent Res.2001;80:1785–1788.
26. Newbrun E. Frequent sugar intake—then and now:interpretation of the main results. Scand J Dent Res.1989;97:103–109.
27. Moynihan PJ, Kelly SA. Effect on caries of restrictingsugars intake: systematic review to inform WHO guide-lines. J Dent Res. 2014;93:8–18.
28. Sheiham A, James WP. A new understanding of therelationship between sugars, dental caries and fluorideuse: implications for limits on sugars consumption. Pub-lic Health Nutr. 2014;17:2176–2184.
29. Sheiham A, James WP. Diet and dental caries: The piv-otal role of free sugars reemphasized. J Dent Res.2015;94:1341–1347.
30. Gaffar A, Afflitto J, Nabi N. Chemical agents for thecontrol of plaque and plaque microflora: an overview.Eur J Oral Sci. 1997;105(5 pt 2):502–507.
31. Scheie AA, Fejerskov O, Assev S, Rolla G. Ultrastructur-al changes in Streptococcus sobrinus induced by xylitol,NaF and ZnCl2. Caries Res. 1989;23:320–327.
32. Glass RL, Rothman KJ, Espinal F, Velez H, Smith NJ.The prevalence of human dental caries and water-bornetrace metals. Arch Oral Biol. 1973;18:1099–1104.
33. Navia JM. Evaluation of nutritional and dietary factorsthat modify animal caries. J Dent Res. 1970;49:1213–1228.
34. Walker CB. Microbiological effects of mouthrinses con-
taining antimicrobials. J Clin Periodontol. 1988;15:499–505.35. Charles CH, Vincent JW, Borycheski L, et al. Effect of an
essential oil-containing dentifrice on dental plaque microbialcomposition. Am J Dent. 2000;13(special no.):26C–30C.
36. Fine DH, Furgang D, Barnett ML, et al. Effect of anessential oil-containing antiseptic mouthrinse on plaqueand salivary Streptococcus mutans levels. J Clin Periodon-tol. 2000;27:157–161.
37. Lobo PL, Fonteles CS, Marques LA, et al. The efficacyof three formulations of Lippia sidoides Cham. essentialoil in the reduction of salivary Streptococcus mutans inchildren with caries: a randomized, double-blind, con-trolled study. Phytomedicine. 2014;21:1043–1047.
38. Gjermo P, Saxton CA. Antibacterial dentifrices. Clinicaldata and relevance with emphasis on zinc/triclosan. JClin Periodontol. 1991;18:468–473.
39. Mann J, Vered Y, Babayof I, et al. The comparative anti-caries efficacy of a dentifrice containing 0.3% triclosanand 2.0% copolymer in a 0.243% sodium fluoride/silicabase and a dentifrice containing 0.243% sodium fluo-ride/silica base: a two-year coronal caries clinical trial onadults in Israel. J Clin Dent. 2001;12:71–76.
40. Vered Y, Zini A, Mann J, et al. Comparison of a denti-frice containing 0.243% sodium fluoride, 0.3% triclosan,and 2.0% copolymer in a silica base, and a dentifricecontaining 0.243% sodium fluoride in a silica base: athree-year clinical trial of root caries and dental crownsamong adults. J Clin Dent. 2009;20:62–65.
41. Riley P, Lamont T. Triclosan/copolymer containingtoothpastes for oral health. Cochrane Database Syst Rev.2013;(12):CD010514.
42. Rosenblatt A, Stamford TC, Niederman R. Silverdiamine fluoride: a caries “silver-fluoride bullet”. J DentRes. 2009;88:116–125.
43. Zhang W, McGrath C, Lo EC, Li JY. Silver diamine fluor-ide and education to prevent and arrest root caries amongcommunity-dwelling elders. Caries Res. 2013;47:284–290.
44. Ribeiro LG, Hashizume LN, Maltz M. The effect of dif-ferent formulations of chlorhexidine in reducing levels ofmutans streptococci in the oral cavity: A systematicreview of the literature. J Dent. 2007;35:359–370.
45. Rethman MP, Beltran-Aguilar ED, Billings RJ, et al.Nonfluoride caries-preventive agents: executive summa-ry of evidence-based clinical recommendations. J AmDent Assoc. 2011;142:1065–1071.
46. Petti S, Hausen H. Caries-preventive effect of chlorhexi-dine gel applications among high-risk children. CariesRes. 2006;40:514–521.
47. Baca P, Clavero J, Baca AP, Gonzalez-Rodriguez MP,Bravo M, Valderrama MJ. Effect of chlorhexidine-thy-mol varnish on root caries in a geriatric population: arandomized double-blind clinical trial. J Dent.2009;37:679–685.
48. Brailsford SR, Fiske J, Gilbert S, Clark D, Beighton D.The effects of the combination of chlorhexidine/thymol-and fluoride-containing varnishes on the severity of root
CHAPTER 15 Non-Fluoride Remineralization Therapies
254
caries lesions in frail institutionalised elderly people. JDent. 2002;30:319–324.
49. Tan HP, Lo EC, Dyson JE, Luo Y, Corbet EF. A ran-domized trial on root caries prevention in elders. J DentRes. 2010;89:1086–1090.
50. Dodds MW. The oral health benefits of chewing gum. JIrish Dent Assoc. 2012;58:253–261.
51. Van Loveren C. Sugar alcohols: what is the evidence forcaries-preventive and caries-therapeutic effects? CariesRes. 2004;38:286–293.
52. Milgrom P, Ly KA, Roberts MC, Rothen M, Mueller G,Yamaguchi DK. Mutans streptococci dose response toxylitol chewing gum. J Dent Res. 2006;85:177–181.
53. Maguire A, Rugg-Gunn AJ. Xylitol and caries preven-tion—is it a magic bullet? Br Dent J. 2003;194:429–436.
54. Alanen P, Isokangas P, Gutmann K. Xylitol candies incaries prevention: results of a field study in Estonian chil-dren. Community Dent Oral Epidemiol. 2000;28:218–224.
55. Honkala E, Honkala S, Shyama M, Al-Mutawa SA.Field trial on caries prevention with xylitol candiesamong disabled school students. Caries Res.2006;40:508–513.
56. Isokangas P, Soderling E, Pienihakkinen K, Alanen P.Occurrence of dental decay in children after maternalconsumption of xylitol chewing gum, a follow-up from 0to 5 years of age. J Dent Res. 2000;79:1885–1889.
57. Riley P, Moore D, Ahmed F, Sharif MO, WorthingtonHV. Xylitol-containing products for preventing dentalcaries in children and adults. Cochrane Database SystRev. 2015;(3):CD010743.
58. Kovari H, Pienihakkinen K, Alanen P. Use of xylitol chew-ing gum in daycare centers: a follow-up study in Savonlin-na, Finland. Acta Odontol Scand. 2003;61:367–370.
59. Oscarson P, Lif Holgerson P, Sjostrom I, Twetman S,Stecksen-Blicks C. Influence of a low xylitol-dose onmutans streptococci colonisation and caries develop-ment in preschool children. Eur Arch Paediatr Dent.2006;7:142–147.
60. Jeon JG, Klein MI, Xiao J, Gregoire S, Rosalen PL, KooH. Influences of naturally occurring agents in combina-tion with fluoride on gene expression and structuralorganization of Streptococcus mutans in biofilms. BMCMicrobiol. 2009;9:228.
61. Koo H, Jeon JG. Naturally occurring molecules as alter-native therapeutic agents against cariogenic biofilms. AdvDent Res. 2009;21:63–68.
62. Leung KP, Abercrombie JJ, Campbell TM, et al.Antimicrobial peptides for plaque control. Adv DentRes. 2009;21:57–62.
63. Eckert R, He J, Yarbrough DK, Qi F, Anderson MH,Shi W. Targeted killing of Streptococcus mutans by apheromone-guided “smart” antimicrobial peptide.Antimicrob Agents Chemother. 2006;50:3651–3657.
64. Guo L, McLean JS, Yang Y, et al. Precision-guidedantimicrobial peptide as a targeted modulator of humanmicrobial ecology. Proc Natl Acad Sci U S A.
2015;112:7569–7574.65. Caufield PW, Dasanayake AP, Li Y, Pan Y, Hsu J,
Hardin JM. Natural history of Streptococcus sanguinisin the oral cavity of infants: evidence for a discrete win-dow of infectivity. Infect Immun. 2000;68:4018–4023.
66. Cummins D. Dental caries: a disease which remains apublic health concern in the 21st century—the explo-ration of a breakthrough technology for caries preven-tion. J Clin Dent. 2013;24(special no. A):A1–14.
67. Wolff M, Corby P, Klaczany G, et al. In vivo effects of anew dentifrice containing 1.5% arginine and 1450 ppmfluoride on plaque metabolism. J Clin Dent.2013;24(special no. A):A45–54.
68. Kleinberg I. A new saliva-based anticaries composition.Dent Today. 1999;18:98–103.
69. Yin W, Hu DY, Fan X, et al. A clinical investigation usingquantitative light-induced fluorescence (QLF) of the anti-caries efficacy of a dentifrice containing 1.5% arginineand 1450 ppm fluoride as sodium monofluorophosphate.J Clin Dent. 2013;24(special no. A):A15–22.
70. Hu DY, Yin W, Li X, et al. A clinical investigation of theefficacy of a dentifrice containing 1.5% arginine and1450 ppm fluoride, as sodium monofluorophosphate ina calcium base, on primary root caries. J Clin Dent.2013;24(special no. A):A23–31.
71. ten Cate JM, Cummins D. Fluoride toothpaste contain-ing 1.5% arginine and insoluble calcium as a new stan-dard of care in caries prevention. J Clin Dent.2013;24:79–87.
72. Dawes C. The unstimulated salivary flow rate after pro-longed gum chewing. Arch Oral Biol. 2005;50:561–563.
73. Dawes C, Kubieniec K. The effects of prolonged gumchewing on salivary flow rate and composition. ArchOral Biol. 2004;49:665–669.
74. Dawes C, Macpherson LM. Effects of nine differentchewing-gums and lozenges on salivary flow rate andpH. Caries Res. 1992;26:176–182.
75. Dodds MW, Hsieh SC, Johnson DA. The effect ofincreased mastication by daily gum-chewing on salivarygland output and dental plaque acidogenicity. J DentRes. 1991;70:1474–1478.
76. Fu Y, Li X, Ma H, et al. Assessment of chewing sugar-free gums for oral debris reduction: a randomized con-trolled crossover clinical trial. Am J Dent. 2012;25:118–122.
77. Jenkins GN, Edgar WM. The effect of daily gum-chew-ing on salivary flow rates in man. J Dent Res.1989;68:786–790.
78. Deshpande A, Jadad AR. The impact of polyol-contain-ing chewing gums on dental caries: a systematic review oforiginal randomized controlled trials and observationalstudies. J Am Dent Assoc. 2008;139:1602–1614.
79. Mickenautsch S, Leal SC, Yengopal V, Bezerra AC, Cru-vinel V. Sugar-free chewing gum and dental caries: a sys-tematic review. J Appl Oral Sci. 2007;15:83–88.
80. Voit EO, Martens HA, Omholt SW. 150 years of the
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
255
mass action law. PLoS Comput Biol. 2015;11:e1004012.81. Brannstrom M, Isacsson G, Johnson G. The effect of
calcium hydroxide and fluorides on human dentine. ActaOdontol Scand. 1976;34:59–67.
82. Kaufman HW, Wolff MS, Winston AE, Triol CW. Clin-ical evaluation of the effect of a remineralizing tooth-paste on dentinal sensitivity. J Clin Dent. 1999;10(1special no.):50–54.
83. Kleinberg I. SensiStat. A new saliva-based compositionfor simple and effective treatment of dentinal sensitivitypain. Dent Today. 2002;21:42–47.
84. Acevedo AM, Machado C, Rivera LE, Wolff M, Klein-berg I. The inhibitory effect of an argininebicarbonate/calcium carbonate CaviStat-containing den-tifrice on the development of dental caries in Venezuelanschool children. J Clin Dent. 2005;16:63–70.
85. Acevedo AM, Montero M, Rojas-Sanchez F, et al. Clin-ical evaluation of the ability of CaviStat in a mint confec-tion to inhibit the development of dental caries inchildren. J Clin Dent. 2008;19:1–8.
86. Reynolds EC. Anticariogenic complexes of amorphouscalcium phosphate stabilized by casein phosphopep-tides: a review. Spec Care Dentist 1998;18:8–16.
87. Cai F, Shen P, Morgan MV, Reynolds EC. Remineral-ization of enamel subsurface lesions in situ by sugar-freelozenges containing casein phosphopeptide-amorphouscalcium phosphate. Aust Dent J. 2003;48:240–243.
88. Hay KD, Thomson WM. A clinical trial of the anti-caries efficacy of casein derivatives complexed with calci-um phosphate in patients with salivary glanddysfunction. Oral Surg Oral Med Oral Pathol Oral Radi-ol Endod. 2002;93:271–275.
89. Morgan MV, Adams GG, Bailey DL, Tsao CE, Fis-chman SL, Reynolds EC. The anticariogenic effect ofsugar-free gum containing CPP-ACP nanocomplexeson approximal caries determined using digital bitewingradiography. Caries Res. 2008;42:171–184.
90. Beerens MW, van der Veen MH, van Beek H, ten CateJM. Effects of casein phosphopeptide amorphous calci-um fluoride phosphate paste on white spot lesions anddental plaque after orthodontic treatment: a 3-monthfollow-up. Eur J Oral Sci. 2010;118:610–617.
91. Singh ML, Papas AS. Long-term clinical observation ofdental caries in salivary hypofunction patients using asupersaturated calcium-phosphate remineralizing rinse.J Clin Dent. 2009;20:87–92.
CHAPTER 15 Non-Fluoride Remineralization Therapies
256

At the patient level, prevention of the majororal maladies, caries and periodontitis, re-quires clinician-inspired health literacy andinstruction in essential home care. The pre-vention of dental caries seeks to stem the de-velopment of incipient lesions. Primaryprevention of periodontal diseases, includinggingivitis, focuses on thwarting their clinicalonset. Secondary prevention, especially in thecontext of chronic periodontitis, aims toavoid progression or exacerbation of the con-ditions. At the individual level, oral hygiene isthe single most effective means for preventionof periodontal disease, and it also has a cru-cial role in dental caries prevention. Chemotherapeutics is a general term often
used to designate the application of an activecompound or agent with intended beneficialclinical effects. For example, in the treatment ofperiodontal diseases, such as aggressive orchronic periodontitis, this entails adjunctive useof antimicrobials or antibiotics.1 Chemothera-peutics, in the context of prevention, refers to astrategy of employing active compounds tocounter disease onset or recurrence. The termchemotherapeutics is also used to contrast me-chanical approaches to oral disease preven-tion. Specifically, plaque biofilm is anetiologic agent of both caries and periodontaldiseases; mechanical removal or reduction ofsupragingival and subgingival plaque,whether professionally or by the individual,is the intervention target. With that same endgoal in mind, chemical plaque-control agentsare commonly used in the management ofcaries and periodontal disease—whether forprevention or treatment. As discussed later in
this chapter, targeting the etiology is but oneof the available approaches in preventivechemotherapeutics.
KEY CONSIDERATIONSClinical Evaluation of Preventive Chemotherapeutics Published studies in the 1960s bolstered theview that routine removal of plaque was es-sential to establish and maintain oral health.Mechanical toothbrushing and flossing wasuniversally accepted by the profession to thisend; when properly and precisely performed,mechanical practices proved sufficient.2 How-ever, most patients do not adequately brushand floss effectively and do not remove dentalplaque on a daily basis. An amount of manualdexterity is needed to achieve qualitatively ac-ceptable results for mechanical therapy, as wellas a patient commitment to the necessary timeto achieve acceptable results. Furthermore,physical removal of plaque biofilm is oftenchallenging in difficult-to-access regions ofthe mouth, and in the presence of anatomicalcontributing factors (furcations, malposi-tioned teeth, developmental grooves, cervicalenamel projections, etc.) or iatrogenic factors(poorly contoured restorations, overhangingcrown margins, etc.). A final consideration isthat beyond the hard surfaces of teeth—thecustomary target of mechanical home care—there exist additional sites of bacterial colo-nization in the mouth, such as the dorsum ofthe tongue and oral mucosal sites.3
In the early 1980s, chemotherapeuticagents were introduced as adjuncts to brush-ing and flossing. It should be noted, however,that these agents, often dispensed in the vehi-cle of an oral rinse, had historically been inuse for centuries; only in modern history haveattempts been made to adjudicate clinicalclaims in a systematic manner. In fact, the his-toric formulations in many instances wereperhaps reasonable in their concept but ques-tionable in their intended biological activity.In the early twentieth century, some advo-cated use of compounds, such as sulfuricacid, mercuric chloride, and formaldehyde,
257
ChemotherapeuticAgents
Chapter 16
Harlan J. Shiau and Louis G. DePaola
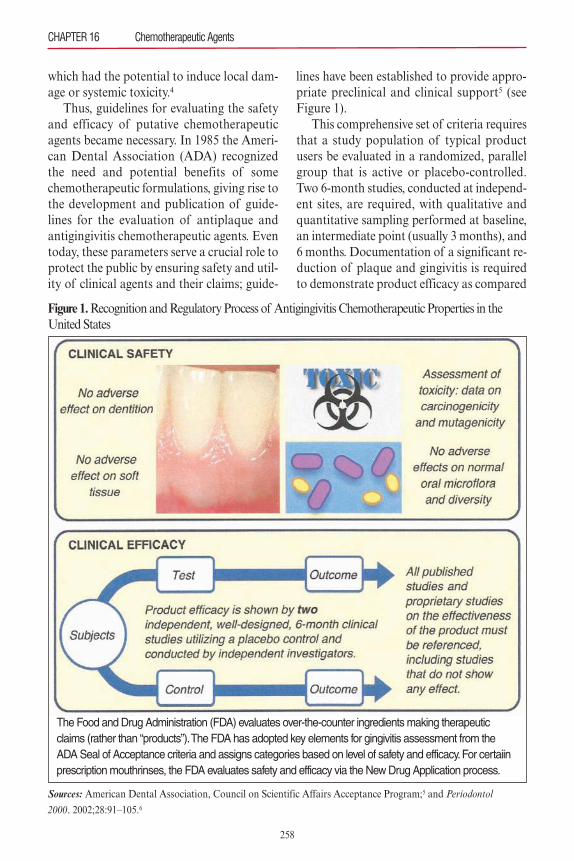
which had the potential to induce local dam-age or systemic toxicity.4
Thus, guidelines for evaluating the safetyand efficacy of putative chemotherapeuticagents became necessary. In 1985 the Ameri-can Dental Association (ADA) recognizedthe need and potential benefits of somechemotherapeutic formulations, giving rise tothe development and publication of guide-lines for the evaluation of antiplaque andantigingivitis chemotherapeutic agents. Eventoday, these parameters serve a crucial role toprotect the public by ensuring safety and util-ity of clinical agents and their claims; guide-
lines have been established to provide appro-priate preclinical and clinical support5 (seeFigure 1).This comprehensive set of criteria requires
that a study population of typical productusers be evaluated in a randomized, parallelgroup that is active or placebo-controlled.Two 6-month studies, conducted at independ-ent sites, are required, with qualitative andquantitative sampling performed at baseline,an intermediate point (usually 3 months), and6 months. Documentation of a significant re-duction of plaque and gingivitis is requiredto demonstrate product efficacy as compared
CHAPTER 16 Chemotherapeutic Agents
258
Figure 1.Recognition and Regulatory Process of Antigingivitis Chemotherapeutic Properties in theUnited States
The Food and Drug Administration (FDA) evaluates over-the-counter ingredients making therapeuticclaims (rather than “products”). The FDA has adopted key elements for gingivitis assessment from theADA Seal of Acceptance criteria and assigns categories based on level of safety and efficacy. For certaiinprescription mouthrinses, the FDA evaluates safety and efficacy via the New Drug Application process.
Sources: American Dental Association, Council on Scientific Affairs Acceptance Program;5 and Periodontol 2000. 2002;28:91–105.6

with a control. In addition to efficacy, eachagent has to establish safety of the formula-tion, which mandates microbiological profilesto evaluate possible adverse shifts in micro-bial populations and resistance, as well astoxicological testing. Notably in the UnitedStates, the Food and Drug Administrationhas accepted the ADA guidelines for determi-nation of over-the-counter products that re-duce or prevent dental plaque and gingivitis.6
Overview of Active Agents of ChemotherapeuticsConceptually, active agents target the etiologicagent—plaque bacteria—or confer a defensiveadvantage to the host. The former approachdescribes the majority of prevalently used orprescribed preventive chemotherapeutics. Ashas been described earlier in the chapter, thisis not surprising given the established patho-genesis paradigms of caries, gingivitis, and de-structive periodontal disease. Table 1 presentsthe major strategies employed by chemother-apeutic agents. Note that some groups, such asantibiotics or the host-modulation approach,are not used in preventive applications.7 Otherstrategic approaches, such as antiadhesiveagents, lack any relevant examples with robustclinical support for efficacy. The majority ofcommercially available preventive chemother-apeutic products, to date, follow an antisepticapproach. Some preclinical data exist indicat-ing that these chemotherapeutics exhibit addi-tional properties—such as anti-inflammatoryproperties or the ability to interfere with
plaque colonization—that might contribute tooverall efficacy.8
By definition, antimicrobials that are anti-septic in nature aim to kill or prevent prolifer-ation of bacteria within the plaque biofilm.There are, of course, many antiseptic agents orspecific formulations of agents in existence notappropriated for intraoral use. The literatureis replete with applications such as surgicalwound management, patient perioperativeskin preparation, standard hand washing, andgeneral hard-surface asepsis. Antiseptics arean indispensable part of infection controlpractices and help in the prevention of noso-comial infections.9 In spite of their usage, lessis known about antiseptics relative to antibi-otics. In the United States, a recent Food andDrug Administration advisory committee cau-tiously seeks more scientific data on safety andeffectiveness of active ingredients of antisep-tics present in hand soaps in response to con-cerns. Because of the inherent biologicalactivity of these chemotherapeutics, the con-ventional wisdom is that evidence-based safetyin the context of oral application must be es-tablished.
Safety of Active Agents in Preventive ChemotherapeuticsIn the context of intraoral chemotherapeutics,investigations have addressed the safety andcompatibility of long-term use. Pragmaticsafety concerns include effect on existing bio-materials in the mouth, whether aesthetic orfunctional, and generation of xerostomia-like
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
259
Table 1. Major Strategies for Effective Chemotherapeutic Agents
Host Modulation: Antimicrobials: Target the Biofilm Attenuates Disease
Pathogenesis
Antiseptic
Broad-spectrumchemical agentsthat slow or stopthe growth of microorganisms
Antibiotic
Agents capable ofkilling and inhibitinggrowth of specificmicroorganisms,such as infectiousbacteria and fungi
Enzyme or Dispersal Agent
Alters the structureor the metabolic activity of plaquebiofilm
Antiadhesive
Interferes with bacteria attachmentto aquired pellicle orbacterial coaggregation
Antiproteinase, anti-inflammatory orbone sparing strategies
Agent provides interference to keycomponents of diseasepathogenesis
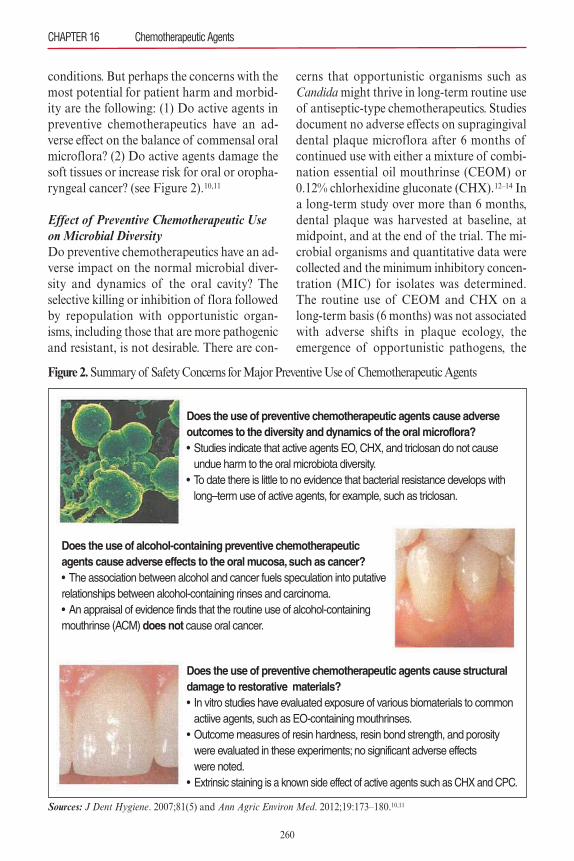
conditions. But perhaps the concerns with themost potential for patient harm and morbid-ity are the following: (1) Do active agents inpreventive chemotherapeutics have an ad-verse effect on the balance of commensal oralmicroflora? (2) Do active agents damage thesoft tissues or increase risk for oral or oropha-ryngeal cancer? (see Figure 2).10,11
Effect of Preventive Chemotherapeutic Useon Microbial DiversityDo preventive chemotherapeutics have an ad-verse impact on the normal microbial diver-sity and dynamics of the oral cavity? Theselective killing or inhibition of flora followedby repopulation with opportunistic organ-isms, including those that are more pathogenicand resistant, is not desirable. There are con-
cerns that opportunistic organisms such asCandidamight thrive in long-term routine useof antiseptic-type chemotherapeutics. Studiesdocument no adverse effects on supragingivaldental plaque microflora after 6 months ofcontinued use with either a mixture of combi-nation essential oil mouthrinse (CEOM) or0.12% chlorhexidine gluconate (CHX).12–14 Ina long-term study over more than 6 months,dental plaque was harvested at baseline, atmidpoint, and at the end of the trial. The mi-crobial organisms and quantitative data werecollected and the minimum inhibitory concen-tration (MIC) for isolates was determined.The routine use of CEOM and CHX on along-term basis (6 months) was not associatedwith adverse shifts in plaque ecology, theemergence of opportunistic pathogens, the
CHAPTER 16 Chemotherapeutic Agents
260
Figure 2. Summary of Safety Concerns for Major Preventive Use of Chemotherapeutic Agents
Sources: J Dent Hygiene. 2007;81(5) and Ann Agric Environ Med. 2012;19:173–180.10,11
Does the use of preventive chemotherapeutic agents cause adverseoutcomes to the diversity and dynamics of the oral microflora?• Studies indicate that active agents EO, CHX, and triclosan do not cause undue harm to the oral microbiota diversity.• To date there is little to no evidence that bacterial resistance develops with long– term use of active agents, for example, such as triclosan.
Does the use of preventive chemotherapeutic agents cause structuraldamage to restorative materials?• In vitro studies have evaluated exposure of various biomaterials to common actiive agents, such as EO-containing mouthrinses.• Outcome measures of resin hardness, resin bond strength, and porosity were evaluated in these experiments; no significant adverse effects were noted.• Extrinsic staining is a known side effect of active agents such as CHX and CPC.
Does the use of alcohol-containing preventive chemotherapeuticagents cause adverse effects to the oral mucosa, such as cancer?• The association between alcohol and cancer fuels speculation into putativerelationships between alcohol-containing rinses and carcinoma.• An appraisal of evidence finds that the routine use of alcohol-containingmouthrinse (ACM) does not cause oral cancer.

emergence of resistance strains, or changes inmicrobial susceptibility.14
Triclosan is an antimicrobial agent used inconsumer preventive products to reduce dentalplaque, gingivitis, and oral malodor. Thisbroad-spectrum chemotherapeutic has utilityagainst gram-positive and gram-negative bac-teria, fungi, and yeasts. Triclosan has beenused in oral preventive applications since the1980s in Europe and subsequently beginningin the 1990s in the United States. Notably, thebody of science evaluating triclosan safety issubstantial because of applications in nonoralconsumer products for skincare, cosmetics, de-odorants/antiperspirants, and even productssuch as clothing, utensils, trash bags, andtoys.15 With its prolific use, one area of concernraised is the development of bacterial resist-ance; there have been studies related to thisconcern in oral preventive applications. Mul-tiple clinical trials 6 months in duration16–18
and a long-term community assessment, withplaque samples collected over 19 years,19 havefound no evidence of unfavorable shifts in bac-teria and no evidence of development of bac-terial resistance to the active agent, triclosan.Plaque samples collected from participants ina 5-year clinical, randomized control trial havealso yielded similar conclusions.20 The use ofthe triclosan dentifrice does not increase tri-closan MICs for oral bacteria and does not re-sult in triclosan-resistant oral bacteria.Potential toxicity of triclosan is a second-
ary safety concern raised, as the mechanismof triclosan is to disrupt cell cytoplasmicmembranes. Reviewed human safety studieson the use of triclosan-containing dentifriceor rinses, measuring hematological and clini-cal chemistry, reveal no difference comparedwith controls.21 Rodricks and colleagues con-firm safety of triclosan, and present a com-prehensive review detailing acute and chronictoxicity studies, issues of pharmacokinetics,and effects on carcinogenesis.21 Furthermore,triclosan has not been found to be a dermalor oral mucosal irritant.22
Available research does not support thenotion that the CEOM group of antisepticagents can induce significant bacterial resist-ance.23 The potential for a selective increaseof Streptococcus mutans, with a possible neg-ative impact on caries rate, was addressed byFine and colleagues.24 In this randomizedcrossover study, 29 adults with recoverablesalivary S. mutans levels were evaluated afterrinsing with CEOM-containing mouthrinseversus placebo. Recoverable S. mutans countsfrom interproximal spaces were reduced by75.4% with the essential oil compared withthe control. Total streptococci in interproxi-mal plaque were reduced by 69.9%, and ac-tivity of the essential oil was 37.1% greateragainst S. mutans than against other strepto-cocci.24 The data clearly document a reduc-tion rather than an increase of S. mutans.While there is no intentional claim of anticar-iogenicity of CEOM rinses, there certainlyappears to be no increase in caries risk withroutine use. Interestingly, recent clinical re-search has proposed the alternative use ofCEOM-type antiseptics in response to trendsof increasing drug-resistant bacteria. Thecombination of phytochemicals, such as es-sential oils, with traditional systemic antibi-otics has been proposed; in vitro studies haveshown synergism or additive effects whenthese combinations are used together. 23 Fur-ther research is needed to build on the possi-bility of essential oils being used in anadjunctive manner. Opportunistic infections, such as fungal
overgrowth during long-term antiseptic use,would seem to be a possibility given analogoustrends with traditional antibiotic use. Yet,studies seem to indicate the contrary. Antisep-tic mouthrinses appear to decrease the levelsof viable Candida species, for example. In anin vitro investigation, five species of Candida(albicans, dubliniensis, krusei, glabrata, andtropicalis) were grown and treated with CEOMand 0.12% CHX. Antifungal activity wasmeasured, and both agents were found to be
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
261
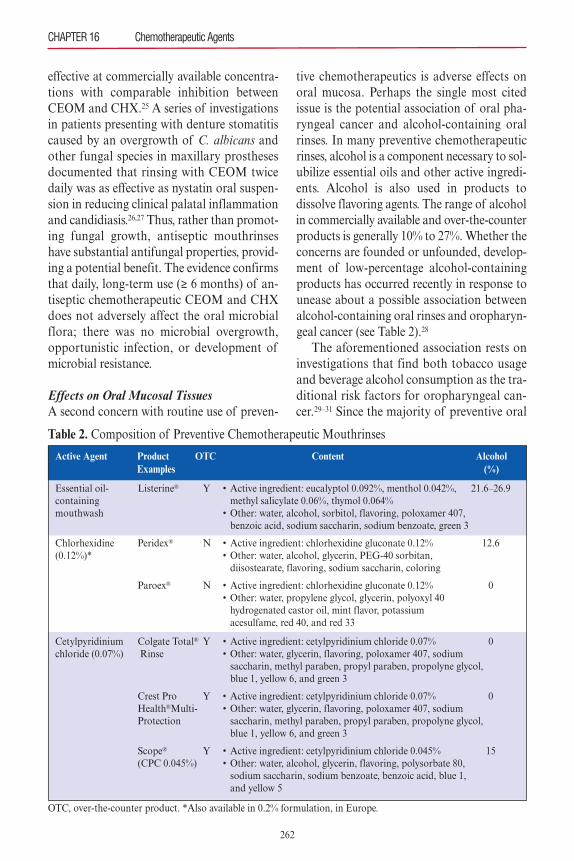
effective at commercially available concentra-tions with comparable inhibition betweenCEOM and CHX.25 A series of investigationsin patients presenting with denture stomatitiscaused by an overgrowth of C. albicans andother fungal species in maxillary prosthesesdocumented that rinsing with CEOM twicedaily was as effective as nystatin oral suspen-sion in reducing clinical palatal inflammationand candidiasis.26,27 Thus, rather than promot-ing fungal growth, antiseptic mouthrinseshave substantial antifungal properties, provid-ing a potential benefit. The evidence confirmsthat daily, long-term use (≥ 6 months) of an-tiseptic chemotherapeutic CEOM and CHXdoes not adversely affect the oral microbialflora; there was no microbial overgrowth, opportunistic infection, or development ofmicrobial resistance.
Effects on Oral Mucosal TissuesA second concern with routine use of preven-
tive chemotherapeutics is adverse effects onoral mucosa. Perhaps the single most citedissue is the potential association of oral pha-ryngeal cancer and alcohol-containing oralrinses. In many preventive chemotherapeuticrinses, alcohol is a component necessary to sol-ubilize essential oils and other active ingredi-ents. Alcohol is also used in products todissolve flavoring agents. The range of alcoholin commercially available and over-the-counterproducts is generally 10% to 27%. Whether theconcerns are founded or unfounded, develop-ment of low-percentage alcohol-containingproducts has occurred recently in response tounease about a possible association betweenalcohol-containing oral rinses and oropharyn-geal cancer (see Table 2).28
The aforementioned association rests oninvestigations that find both tobacco usageand beverage alcohol consumption as the tra-ditional risk factors for oropharyngeal can-cer.29–31 Since the majority of preventive oral
CHAPTER 16 Chemotherapeutic Agents
262
Table 2. Composition of Preventive Chemotherapeutic Mouthrinses
Active Agent Product OTC Content Alcohol Examples (%)
Essential oil- Listerine® Y • Active ingredient: eucalyptol 0.092%, menthol 0.042%, 21.6–26.9containing methyl salicylate 0.06%, thymol 0.064%mouthwash • Other: water, alcohol, sorbitol, flavoring, poloxamer 407, benzoic acid, sodium saccharin, sodium benzoate, green 3
Chlorhexidine Peridex® N • Active ingredient: chlorhexidine gluconate 0.12% 12.6(0.12%)* • Other: water, alcohol, glycerin, PEG-40 sorbitan, diisostearate, flavoring, sodium saccharin, coloring
Paroex® N • Active ingredient: chlorhexidine gluconate 0.12% 0 • Other: water, propylene glycol, glycerin, polyoxyl 40 hydrogenated castor oil, mint flavor, potassium acesulfame, red 40, and red 33
Cetylpyridinium Colgate Total® Y • Active ingredient: cetylpyridinium chloride 0.07% 0chloride (0.07%) Rinse • Other: water, glycerin, flavoring, poloxamer 407, sodium saccharin, methyl paraben, propyl paraben, propolyne glycol, blue 1, yellow 6, and green 3
Crest Pro Y • Active ingredient: cetylpyridinium chloride 0.07% 0 Health®Multi- • Other: water, glycerin, flavoring, poloxamer 407, sodium Protection saccharin, methyl paraben, propyl paraben, propolyne glycol, blue 1, yellow 6, and green 3
Scope® Y • Active ingredient: cetylpyridinium chloride 0.045% 15 (CPC 0.045%) • Other: water, alcohol, glycerin, flavoring, polysorbate 80, sodium saccharin, sodium benzoate, benzoic acid, blue 1, and yellow 5
OTC, over-the-counter product. *Also available in 0.2% formulation, in Europe.

rinses contain alcohol, the logical assumptionwould be that they potentially increase riskfor oropharyngeal cancer as well. Gandiniand colleagues identified epidemiologicalstudies of mouthwash and oralcancer/oropharyngeal cancer, and conducteda quantitative meta-analysis.11 They con-cluded from the 18 studies that routinemouthwash use and risk of oral cancer hadno statistically significant association, or anytrend in risk with increasing daily use.Currie and colleagues reviewed 15 case-
control studies evaluating the existence orlack of an association between the use of al-cohol-containing mouthrinses and the devel-opment of oral squamous cell carcinoma(OSCC).32 A solid consensus is lackingamong these investigations, with six studiesindicating positive and statistically significantassociations, and nine reporting nonsignifi-cant positive, none, or negative correlationsbetween alcohol-containing mouthwash useand OSCC.Other important considerations must also
be weighed in building any substantial case foralcohol-containing rinses and associationswith cancer.33,34 Evidence-based appraisal ofthe literature should turn a critical eye to thefollowing issues. First, available studies needto show a dose-response based on frequencyor duration of mouthrinse use, or both. Sec-ond, studies need to offer a scientific or bio-logical basis for inconsistent findings betweenmen and women. Investigations may need tocorrect for combined alcoholic beverage inges-tion and tobacco use. Finally, population datashould exclude or at least separate the pharyn-geal cancer and other head and neck carcino-mas, lymphomas, and sarcomas that occur inregions with no regular oral rinse contact.
APPLICATION TO CLINICAL PRACTICE
This section focuses on the major commer-cially available or prescription preventivechemotherapeutics, reviewing their mecha-
nism and claims to efficacy. Published system-atic reviews are useful when taking steps toconsider a particular active agent’s effective-ness. Clinicians should be judicious in han-dling the “bottom line” results of thesestudies by considering magnitude of the ef-fect, number of available studies, consistencyof the results, and heterogeneity.
ChlorhexidineChlorhexidine (CHX 0.12%) is a cationic bis-biguanide antiseptic with a broad antimicro-bial spectrum, demonstrating efficacy againsta wide range of gram-positive and gram-neg-ative organisms.35 CHX 0.2% is also availableas an over-the-counter product in Europe.The cationic property of CHX allows favor-able interactions—that is, a strong binding—with anionic cell membrane and wallcomponents. As such, CHX demonstrates in-hibitory effects on a wide range of bacteriaassociated with periodontal disease andcaries.36 CHX also exhibits antiviral activityagainst herpes simplex viruses 1 and 2, HIV-1, cytomegalovirus, influenza A, humanparainfluenza, and hepatitis B.37,38 Finally,CHX has been shown to demonstrate anti-fungal properties, of note, against severalCandida species and others.39,40 In fact, CHXis often used either alone or in combinationwith other antifungal medications to reduceopportunistic infections in at-risk popula-tions.41 CHX binds to cell membranes anddisrupts the bacterial cell membrane, cata-strophically altering cell permeability.42 In ad-dition, CHX prevents colonization of plaquebacteria by binding to salivary mucins, whichresults in a reduced acquired pellicle forma-tion.43 CHX has high substantivity by bindingtightly to tooth structure, dental plaque, andoral soft tissues; high substantivity greatly en-hances its antibacterial properties.44
Long-term studies (≥ 6 months) haveshown CHX is effective in reducing plaqueand reducing gingivitis, as has been con-firmed in systematic reviews.45–47 In several
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
263
controlled trials for periods of 6 months orlonger, CHX demonstrated reduction inplaque ranging from 16% to 49%. In anothersystematic review on the efficacy of CHX inplaque reduction in gingivitis patients, the au-thors include studies as short as 4 weeks induration, the rationale being that this durationrepresents the majority of CHX applications.In this investigation, when used as an adjunctto normal home care, an average of 33%plaque reduction was confirmed as comparedwith controls.48 With respect to gingival health,as measured by gingival index, CHX use re-sults in significant improvement.47 A system-atic review of randomized controlled clinicaltrials lasting 4 weeks or longer and comparingCHX to placebo or control found significantimprovement in gingival health, as measuredby gingival index scores.48 The aforementionedtrends in plaque and gingivitis reduction asso-ciated with CHX use have elevated the statusof CHX, which is now considered the goldstandard and is used as a positive control inmany clinical investigations.
Cetylpyridinium ChlorideCetylpyridinium chloride (CPC) is an anti-septic agent with evidence supporting effec-tiveness in preventing supragingival plaqueaccumulation and reducing signs of gingivitis.CPC is a quaternary ammonium compoundthat has broad-spectrum antimicrobial prop-erties. In clinical studies, CPC has been pri-marily evaluated in an oral rinse format. CPCfunctions by disrupting the bacterial cellmembrane, causing leakage of intracellularcontents and ultimately cell death. A 2006 review of long-term (≥ 6 months)
studies on CPC efficacy produced equivocalconclusions.45 A portion of the included stud-ies, four of the seven, reported a statisticallysignificant benefit over the control. A chal-lenge in drawing strong conclusions was theheterogeneity in the type of CPC formulationused and the results. A second systematic review, which included
clinical trials as short as 4 weeks, found thatCPC-containing mouthrinses provided a smallbut significant additional benefit—reducingplaque and gingival inflammation—when com-pared with toothbrushing only or toothbrush-ing followed by a placebo rinse.49 A recentreview on oral rinses notes that the limitednumber of controlled clinical trials investigat-ing the same CPC formulations presents a chal-lenge to issuing clinical recommendations.50
Combination Essential OilAntiseptics containing essential oils act by dis-rupting the microorganism cell wall and in-hibiting enzymatic activity. Essential oils havebeen shown to prevent bacterial aggregationand slow bacterial multiplication. Commer-cially available CEOM is a mixture of thymol0.063%, eucalyptol 0.091%, and menthol0.042%, with other ingredients such as methylsalicylate 0.0660%.51 Phenolic compounds ex-hibit anti-inflammatory properties by inhibit-ing prostaglandin synthetase, an enzymeinvolved in the formation of prostaglandins,which are primary inflammatory mediators.The anti-inflammatory effect occurs at con-centrations lower that those needed for anti-bacterial activity.52 Phenols, especially thymol,also reduce inflammation by altering neu-trophil function, specifically by suppressingthe formation of and scavenging existing freeradicals generated in neutrophils, and by alter-ing neutrophil chemotaxis.53
CEOM bactericidal activity has beendemonstrated in situ to penetrate the bacterialbiofilm.51,54,55 CEOM kills a wide variety of aer-obic and anaerobic bacteria associated withplaque and gingivitis, including Actinobacillusactinomycetemcomitans, Actinomyces viscosus,Streptococcus sanguis, S. mutans, and Bac-teroides species.56 Efficacy against gram-positiveand gram-negative organisms occurs even atconcentrations that are less than fullstrength.56,57 A single 30-second rinse penetratesand exerts an antibacterial effect interproxi-mally; this is an important consideration, given
CHAPTER 16 Chemotherapeutic Agents
264

that periodontal disease and caries patterns ini-tiate interproximally, and that patients usuallydemonstrate inadequate mechanical interprox-imal plaque control. The total recovered bacteria from proximal tooth surfaces was43.8% lower following a single 30-second rinse of CEOM compared with a control (P = 0.001).58 Rinsing twice daily with CEOMas an adjunct to brushing for 11 days reducedtotal recoverable streptococci in interproximalplaque by 69.9% (P < 0.001), with CEOM pro-ducing a 37.1% greater activity against S. mu-tans than other streptococci. A significantreduction of 75.4% in total recoverable S. mu-tans count was observed (P < 0.001).24
Essential oil antiseptic mouthrinses are ableto reduce bacterial plaque and gingivitis, as ev-idenced in long-term studies. In a systematicreview and meta-analysis, the majority oflong-term studies investigating efficacy ofCEOM-containing rinses found significant re-duction in plaque.45 There exists some hetero-geneity in comparisons made within clinicaltrials. In these investigations, CEOM has beenfound superior in plaque reduction to negativecontrol/placebo; also, studies find essential oil-containing mouthrinses to be as good or supe-rior to positive controls (CHX).46 Similarly, theantigingivitis effects of CEOM have been sub-stantiated by systematic reviews. Again, the ev-idence supports, when used as an adjunct toat-home oral hygiene measures, that CEOMprovide benefit in reduction of plaque and gin-givitis compared with controls.45,46
The combined effectiveness of daily me-chanical methods with CEOM was demon-strated in a study by Araujo and colleagues.52
This meta-analysis demonstrated clinically sig-nificant, site-specific benefit of adjunctive es-sential oil mouthrinse application in subjectsbetween routine 6-month dental visits.
Stannous Fluoride with Sodium HexametaphosphateStannous fluoride is a broad-spectrum an-timicrobial agent and had previously been
identified for its plaque-control properties.59
The mechanism of action of this active agentinvolves inhibition and reduction of bacterialplaque biomass, virulence, and metabolism.It is the formulation of stannous fluoridewith sodium hexametaphosphate (SnF2) thathas enabled the active agent to overcome un-desirable properties of extrinsic staining andunpalatable taste.60 SnF2 can be delivered invehicles such as a dentifrice or gel, amouthrinse, or even a regimen of combina-tion dentifrice and mouthrinse. The use of a stabilized 0.454% SnF2 den-
tifrice over a 6-month period provided statis-tically significant improvements in gingivitis,gingival bleeding, and plaque levels whencompared with a negative control dentifrice.61
Specifically, with 6 months of SnF2 usage, theexperimental group had 21.7% less gingivitis(P < 0.001), 57.1% less bleeding (P < 0.001),and 6.9% less plaque (P = 0.01) on averagecompared with the negative control group. Asimilar 6-month controlled trial producedcomparable improvements, with the experi-mental arm showing significant long-term re-ductions in gingival bleeding and gingivalinflammation relative to a negative control.62
In this analysis, the use of SnF2 dentifriceproduced a 16.9% reduction in gingivitis (P < 0.001), a 40.8% reduction (P < 0.001) ingingival bleeding, and an 8.5% reduction inplaque levels compared with negative control.Paraskevas and colleagues addressed the
effects of SnF2-containing dentifrices orrinses on gingival health parameters in a sys-tematic review/meta-analysis.63 Randomizedor controlled clinical trials having a minimum6-month duration were considered. Therewere, overall, insufficient studies with regardto the effect of SnF2 mouthrinses as well asthe combined (dentifrice/mouthrinse) regi-men on gingivitis and plaque. SnF2 in denti-frice vehicles, however, yielded a significantalbeit small improvement in plaque levels andgingivitis compared with control sodium flu-oride dentifrices.
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
265

Triclosan and PVM/MAAs described previously, triclosan has been stud-ied as an active agent for preventive chemother-apeutics owing to its antibacterial properties.First, at bacteriostatic concentrations, triclosaninhibits uptake of essential amino acids. Athigher bactericidal levels, triclosan disrupts thebacterial cellular membrane causing fatal leak-age of contents. In this scenario, the bacterialenzyme enoyl-acyl carrier protein reductase isthe target of triclosan; this reductase is neces-sary for fatty acid synthesis, a process involvedin bacterial cell membrane formation. Polyvinyl-methyl ether/maleic acid copolymer (PVM/MA)is the carrier copolymer that enhances the deliv-ery of triclosan.64 Studies indicate that triclosanwith PVM/MA (triclosan/PVM/MA) has en-hanced binding to enamel surfaces and buccalepithelial cells compared with triclosan alone.Triclosan has demonstrated preclinical efficacyin altering levels of viable plaque, which is rep-resentative of both gram-positive bacteria andgram-negative periodontal pathogens.Triclosan, in addition to actions on the bac-
terial plaque, may also exert clinical effects bymodulation of host inflammatory response.There are preliminary in vitro and animalmodel data documenting the anti-inflamma-tory properties of triclosan. In vitro studieshave shown triclosan provides inhibition ofproinflammatory mediators and cytokines, in-cluding prostaglandin E2, leukotriene, and in-terferon-� pathways when challenged withlipopolysaccharide (LPS).65–67 Finally, tri-closan has been shown to be a potent inhibitorof oral epithelial cell LPS-induced proinflam-matory responses by inducing mitochondrialRNA regulation of the toll-like receptor-sig-naling pathway.68
A substantial body of controlled long-termtrials evaluated triclosan/PVM/MA–contain-ing dentifrice in comparison to negative con-trol or placebo. The effect of triclosan/PVM/MA on supragingival plaque accumula-tion and gingivitis development was meas-ured.8 With respect to plaque levels, on average
these studies showed 25% (range, 12% to 59%)efficacies relative to the placebo control. Long-term clinical studies also support the efficacyof triclosan/PVM/MA in reducing gingivitis.8
A Cochrane review found a 49% reduction inthe proportion of sites with bleeding, when tri-closan was compared with control fluoridedentifrice.69 On average these studies showed25% (range, 19% to 32%) efficacies relative tothe placebo control. Triclosan use, as a preven-tive chemotherapeutic, may have considerablevalue in the maintained chronic periodontitispopulation of practices. Rosling and col-leagues recruited maintenance patients show-ing signs of disease recurrence.70 Specifically,the subjects were given either triclosan/PVM/MA or placebo dentifrice, and moni-tored up to 36 months. The triclosan arm ex-hibited quantitative and qualitative reductionin subgingival bacteria, and prevalence of re-current periodontitis sites was reduced.
CONCLUSIONThe supplemental use of chemotherapeutics,in concert with mechanical control, confersmarked advantages in terms of aiding plaquebiofilm control and the reduction of gingivalinflammation. The current available evidencesupports various applications, though to dif-fering degrees (see Table 3).71–78 The clinicianshould embrace a personalized medicine ap-proach to disease prevention and treatment;this accounts for differences in people’s genes,environments, and lifestyles—and from thisassessment select an appropriate preventivechemotherapeutic approach. For example, al-though xerostomia is a concern when alcohol-containing mouthrinses are used, the clearpreventive benefit of these agents would usu-ally still not preclude their use in the majorityof our patient population. Perhaps only in themost profoundly xerostomic patient cohortwould alcohol not be a desired constituent ofthe preventive chemotherapeutic agent. Thedelivery format of the active agent might alsobe an important consideration. Selecting a
CHAPTER 16 Chemotherapeutic Agents
266
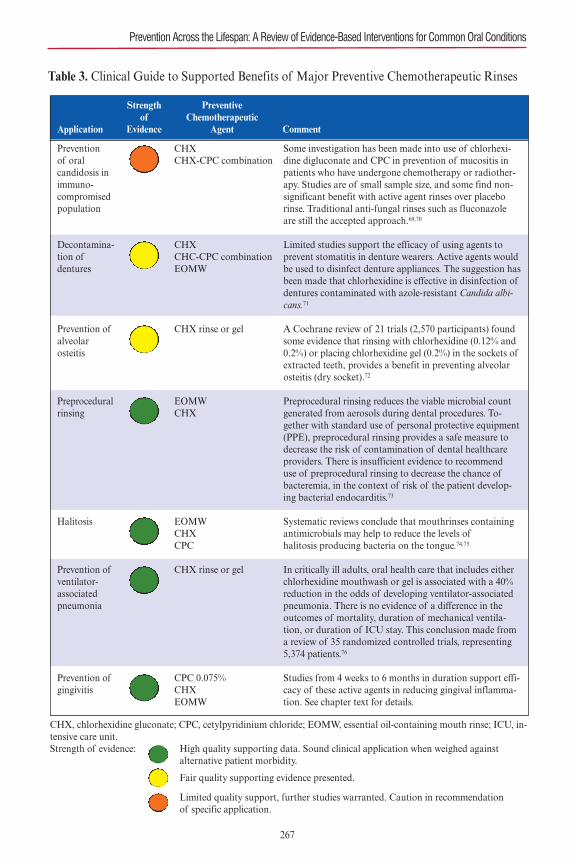
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
Table 3. Clinical Guide to Supported Benefits of Major Preventive Chemotherapeutic Rinses
CHX, chlorhexidine gluconate; CPC, cetylpyridinium chloride; EOMW, essential oil-containing mouth rinse; ICU, in-tensive care unit.Strength of evidence: High quality supporting data. Sound clinical application when weighed against
alternative patient morbidity.
Fair quality supporting evidence presented.
Limited quality support, further studies warranted. Caution in recommendation of specific application.
Strength Preventive of Chemotherapeutic
Application Evidence Agent Comment
Prevention of oral candidosis inimmuno-compromisedpopulation
Decontamina-tion of dentures
Prevention ofalveolar osteitis
Preproceduralrinsing
Halitosis
Prevention ofventilator-associatedpneumonia
Prevention ofgingivitis
CHXCHX-CPC combination
CHXCHC-CPC combinationEOMW
CHX rinse or gel
EOMWCHX
EOMWCHXCPC
CHX rinse or gel
CPC 0.075%CHXEOMW
Some investigation has been made into use of chlorhexi-dine digluconate and CPC in prevention of mucositis inpatients who have undergone chemotherapy or radiother-apy. Studies are of small sample size, and some find non-significant benefit with active agent rinses over placeborinse. Traditional anti-fungal rinses such as fluconazoleare still the accepted approach.69,70
Limited studies support the efficacy of using agents toprevent stomatitis in denture wearers. Active agents wouldbe used to disinfect denture appliances. The suggestion hasbeen made that chlorhexidine is effective in disinfection ofdentures contaminated with azole-resistant Candida albi-cans.71
A Cochrane review of 21 trials (2,570 participants) foundsome evidence that rinsing with chlorhexidine (0.12% and0.2%) or placing chlorhexidine gel (0.2%) in the sockets ofextracted teeth, provides a benefit in preventing alveolarosteitis (dry socket).72
Preprocedural rinsing reduces the viable microbial countgenerated from aerosols during dental procedures. To-gether with standard use of personal protective equipment(PPE), preprocedural rinsing provides a safe measure todecrease the risk of contamination of dental healthcareproviders. There is insufficient evidence to recommend use of preprocedural rinsing to decrease the chance ofbacteremia, in the context of risk of the patient develop-ing bacterial endocarditis.73
Systematic reviews conclude that mouthrinses containingantimicrobials may help to reduce the levels ofhalitosis�producing bacteria on the tongue.74,75
In critically ill adults, oral health care that includes eitherchlorhexidine mouthwash or gel is associated with a 40%reduction in the odds of developing ventilator-associatedpneumonia. There is no evidence of a difference in theoutcomes of mortality, duration of mechanical ventila-tion, or duration of ICU stay. This conclusion made froma review of 35 randomized controlled trials, representing5,374 patients.76
Studies from 4 weeks to 6 months in duration support effi-cacy of these active agents in reducing gingival inflamma-tion. See chapter text for details.
267
dentifrice delivery vehicle for the active agent,as it is linked to “traditional” and “routine”mechanical toothbrushing, might be the ap-propriate route for our general patient cohortin maintaining reasonable compliance. The lit-erature supports the efficacy of mouthrinses,and these products might be appropriate forat-risk or “downhill” periodontal maintenancepatients, or in other similar clinical scenarios.All in all, achieving success at patient-level pre-vention requires clinicians to assess a patient’slevel of compliance and degree of motivationto attain his or her healthcare goals. In this re-gard, the use of preventive chemotherapeuticsis a welcome addition to the complete arma-mentarium available to care for our patients.With knowledge of preventive chemother-
apeutics’ established safety and efficacy, theoral healthcare team can suggest routine use—that is, applied in a truly preventive capacity. Alarge proportion of the general populace en-gages dentistry only on an urgent care basis, inresponse to oral disease and associated mor-bidity. This is diametrically opposed to the oralhealthcare practitioner’s value of preventivedentistry. The clinician and patient might dowell to view appropriate chemotherapeutics aspreventive, and not only for use after the ap-pearance of disease. If we consider the overalldisease mechanism of plaque-caused and in-flammatory-driven diseases, this makes all themore sense. The clinical onset of disease (de-tection) lags behind the subclinical diseaseprocess that has already begun. Furthermore,preventive chemotherapeutics can serve as abuffer against poor patient compliance and theoccasional below-standard mechanical oralhygiene measures. Preventive chemotherapeu-tics can augment existing oral hygiene meas-ures, with an end goal of keeping the biofilmburden below a threshold for disease initiation.
REFERENCES1. Feres M, Figueiredo LC, Soares GM, Faveri M.
Systemic antibiotics in the treatment of periodon-titis. Periodontol 2000. 2015;67:131–186.
2. Lang WP, Ronis DL, Farghaly MM. Preventive be-
haviors as correlates of periodontal health status. JPublic Health Dent. 1995;55:10–17.
3. Paster BJ, Olsen I, Aas JA, Dewhirst FE. Thebreadth of bacterial diversity in the human peri-odontal pocket and other oral sites. Periodontol2000. 2006;42:80–87.
4. Addy M, Moran JM. Evaluation of oral hygieneproducts: science is true; don’t be misled by thefacts. Periodontol 2000. 1997;15:40–51.
5. American Dental Association Council on ScientificAffairs, ed. Acceptance Program Guidelines:Chemotherapeutic Products for Control of Gingivitis.Chicago, IL: American Dental Association; 2011.
6. Wu CD, Savitt ED. Evaluation of the safety and ef-ficacy of over-the-counter oral hygiene products forthe reduction and control of plaque and gingivitis.Periodontol 2000. 2002;28:91–105.
7. Mandel ID. Chemotherapeutic agents for control-ling plaque and gingivitis. J Clin Periodontol.1988;15:488–498.
8. Panagakos FS, Volpe AR, Petrone ME, DeVizio W,Davies RM, Proskin HM. Advanced oral antibac-terial/anti-inflammatory technology: a comprehen-sive review of the clinical benefits of atriclosan/copolymer/fluoride dentifrice. J ClinDent. 2005;16(suppl):S1–19.
9. Siani H, Maillard JY. Best practice in healthcare en-vironment decontamination. Eur J Clin MicrobiolInfect Dis. 2015;34:1–11.
10. DePaola LG, Spolarich AE. Safety and efficacy ofantimicrobial mouthrinses in clinical practice. JDental Hyg. 2007;81(5).
11. Gandini S, Negri E, Boffetta P, La Vecchia C, BoyleP. Mouthwash and oral cancer risk quantitativemeta-analysis of epidemiologic studies. Ann AgricEnviron Med. 2012;19:173–180.
12. Emilson CG, Fornell J. Effect of toothbrushing withchlorhexidine gel on salivary microflora, oral hygiene,and caries. Scand J Dent Res. 1976;84:308–319.
13. Schiott CR, Briner WW, Loe H. Two year oral useof chlorhexidine in man. II. The effect on the sali-vary bacterial flora. J Periodontal Res.1976;11:145–152.
14. Minah GE, DePaola LG, Overholser CD, et al. Ef-fects of 6 months use of an antiseptic mouthrinseon supragingival dental plaque microflora. J ClinPeriodontol. 1989;16:347–352.
15. Jones RD, Jampani HB, Newman JL, Lee AS. Tri-closan: A review of effectiveness and safety inhealth care settings. Am J Infect Control.2000;28:184–196.
16. Zambon JJ, Reynolds HS, Dunford RG, Bonta CY.Effect of a triclosan/copolymer/fluoride dentifriceon the oral microflora. Am J Dent. 1990;(3 specno.):S27–34.
17. Walker C, Borden LC, Zambon JJ, Bonta CY, De-
CHAPTER 16 Chemotherapeutic Agents
268
Vizio W, Volpe AR. The effects of a 0.3% triclosan-containing dentifrice on the microbial compositionof supragingival plaque. J Clin Periodontol.1994;21:334–341.
18. Zambon JJ, Reynolds HS, Dunford RG, et al. Mi-crobial alterations in supragingival dental plaquein response to a triclosan-containing dentifrice.Oral Microbiol Immunol. 1995;10:247–255.
19. Haraszthy VI, Sreenivasan PK, Zambon JJ. Com-munity-level assessment of dental plaque bacteriasusceptibility to triclosan over 19 years. BMC OralHealth. 2014;14:61.
20. Cullinan MP, Bird PS, Heng NC, West MJ, Sey-mour GJ. No evidence of triclosan-resistant bacte-ria following long-term use of triclosan-containingtoothpaste. J Periodontal Res. 2014;49:220–225.
21. Rodricks JV, Swenberg JA, Borzelleca JF, Maron-pot RR, Shipp AM. Triclosan: a critical review ofthe experimental data and development of marginsof safety for consumer products. Crit Rev Toxicol.2010;40:422–484.
22. Barkvoll P, Rolla G. Triclosan protects the skinagainst dermatitis caused by sodium lauryl sulphateexposure. J Clin Periodontol. 1994;21:717–719.
23. Langeveld WT, Veldhuizen EJ, Burt SA. Synergybetween essential oil components and antibiotics:a review. Crit Rev Microbiol. 2014;40:76–94.
24. Fine DH, Furgang D, Barnett ML, et al. Effect ofan essential oil-containing antiseptic mouthrinse onplaque and salivary Streptococcus mutans levels. JClin Periodontol. 2000;27:157–161.
25. Meiller TF, Kelley JI, Jabra-Rizk MA, DepaolaLG, Baqui AA, Falkler WA, Jr. In vitro studies ofthe efficacy of antimicrobials against fungi. OralSurg Oral Med Oral Pathol Oral Radiol Endod.2001;91:663–670.
26. DePaola LG, Minah GE, Leupold RJ, FaraoneKL, Elias SA. The effect of antiseptic mouthrinseson oral microbial flora and denture stomatitis. ClinPrev Dent. 1986;8:3–8.
27. DePaola LG, Minah GE, Elias SA, Eastwood GW,Walters RA. Clinical and microbial evaluation oftreatment regimens to reduce denture stomatitis. IntJ Prosthodont. 1990;3:369–374.
28. White DJ. An alcohol-free therapeutic mouthrinsewith cetylpyridinium chloride (CPC)—the latestadvance in preventive care: Crest pro-health rinse.Am J Dent. 2005;18(spec no.):3A–8A.
29. Johnson N. Tobacco use and oral cancer: a globalperspective. J Dent Educ. 2001;65:328–339.
30. Sturgis EM, Cinciripini PM. Trends in head andneck cancer incidence in relation to smoking preva-lence: an emerging epidemic of human papillo-mavirus-associated cancers? Cancer. 2007;110:1429–1435.
31. Lopes CF, de Angelis BB, Prudente HM, de Souza
BV, Cardoso SV, de Azambuja Ribeiro RI. Con-comitant consumption of marijuana, alcohol andtobacco in oral squamous cell carcinoma develop-ment and progression: recent advances and chal-lenges. Arch Oral Biol. 2012;57:1026–1033.
32. Currie S, Farrah C. Alcohol-containing mouth-wash and oral cancer risk: a review of current evi-dence. OA Alcohol. 2014;10:1–4.
33. Ciancio S. Alcohol in mouthrinse: lack of associa-tion with cancer. Biol Ther Dent. 1993;9:1–2.
34. Silverman S Jr, Wilder R. Antimicrobial mouthrinseas part of a comprehensive oral care regimen. Safetyand compliance factors. J Am Dent Assoc. 2006;137(suppl):22S–26S.
35. Van Leeuwen MP, Slot DE, Van der Weijden GA.The effect of an essential-oils mouthrinse as com-pared to a vehicle solution on plaque and gingivalinflammation: a systematic review and meta-analy-sis. Int J Dent Hyg. 2014;12:160–167.
36. Haffajee AD, Yaskell T, Socransky SS. Antimicro-bial effectiveness of an herbal mouthrinse com-pared with an essential oil and a chlorhexidinemouthrinse. J Am Dent Assoc. 2008;139:606–611.
37. Bernstein D, Schiff G, Echler G, Prince A, FellerM, Briner W. In vitro virucidal effectiveness of a0.12%-chlorhexidine gluconate mouthrinse. J DentRes. 1990;69:874–876.
38. Baqui AA, Kelley JI, Jabra-Rizk MA, DepaolaLG, Falkler WA, Meiller TF. In vitro effect of oralantiseptics on human immunodeficiency virus-1and herpes simplex virus type 1. J Clin Periodontol.2001;28:610–616.
39. Giuliana G, Pizzo G, Milici ME, Musotto GC, Gi-angreco R. In vitro antifungal properties ofmouthrinses containing antimicrobial agents. J Pe-riodontol. 1997;68:729–733.
40. Giuliana G, Pizzo G, Milici ME, Giangreco R. Invitro activities of antimicrobial agents against can-dida species. Oral Surg Oral Med Oral Pathol OralRadiol Endod. 1999;87:44–49.
41. Ellepola AN, Samaranayake LP. Oral candidal in-fections and antimycotics. Crit Rev Oral Biol Med.2000;11:172–198.
42. Ciancio SG. Nonsurgical chemical periodontaltherapy. Periodontol 2000. 1995;9:27–37.
43. Auschill TM, Hein N, Hellwig E, Follo M, SculeanA, Arweiler NB. Effect of two antimicrobial agentson early in situ biofilm formation. J Clin Periodon-tol. 2005;32:147–152.
44. Quintas V, Prada-Lopez I, Donos N, Suarez-Quin-tanilla D, Tomas I. In situ neutralisation of the an-tibacterial effect of 0.2% chlorhexidine on salivarymicrobiota: quantification of substantivity. ArchOral Biol. 2015;60:1109–1116.
45. Gunsolley JC. A meta-analysis of six-month studiesof antiplaque and antigingivitis agents. J Am Dent
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
269
Assoc. 2006;137:1649–1657.46. Stoeken JE, Paraskevas S, van der Weijden GA.
The long-term effect of a mouthrinse containing es-sential oils on dental plaque and gingivitis: a sys-tematic review. J Periodontol. 2007;78:1218–1228.
47. Serrano J, Escribano M, Roldan S, Martin C, Her-rera D. Efficacy of adjunctive anti-plaque chemicalagents in managing gingivitis: a systematic reviewand meta-analysis. J Clin Periodontol.2015;42(suppl 16):S106–S138.
48. Van Strydonck DA, Slot DE, Van der Velden U,Van der Weijden F. Effect of a chlorhexidinemouthrinse on plaque, gingival inflammation andstaining in gingivitis patients: a systematic review.J Clin Periodontol. 2012;39:1042–1055.
49. Haps S, Slot DE, Berchier CE, Van der WeijdenGA. The effect of cetylpyridinium chloride-con-taining mouth rinses as adjuncts to toothbrushingon plaque and parameters of gingival inflamma-tion: a systematic review. Int J Dent Hyg.2008;6:290–303.
50. Gunsolley JC. Clinical efficacy of antimicrobialmouthrinses. J Dent. 2010;38(suppl 1):S6–10.
51. Ouhayoun JP. Penetrating the plaque biofilm: im-pact of essential oil mouthwash. J Clin Periodontol.2003;30(suppl 5):10–12.
52. Araujo MW, Charles CA, Weinstein RB, et al.Meta-analysis of the effect of an essential oil-con-taining mouthrinse on gingivitis and plaque. J AmDent Assoc. 2015;146:610–622.
53. Kuehl FA, Jr, Humes JL, Egan RW, Ham EA, Bev-eridge GC, Van Arman CG. Role of prostaglandinendoperoxide PGG2 in inflammatory processes.Nature. 1977;265(5590):170–173.
54. Pan P, Barnett ML, Coelho J, Brogdon C,Finnegan MB. Determination of the in situ bacte-ricidal activity of an essential oil mouthrinse usinga vital stain method. J Clin Periodontol.2000;27:256–261.
55. Fine DH, Furgang D, Barnett ML. Comparativeantimicrobial activities of antiseptic mouthrinsesagainst isogenic planktonic and biofilm forms ofActinobacillus actinomycetemcomitans. J Clin Peri-odontol. 2001;28:697–700.
56. Ross NM, Charles CH, Dills SS. Long-term effectsof Listerine antiseptic on dental plaque and gingivi-tis. J Clin Dent. 1989;1(4):92–95.
57. Whitaker EJ, Pham K, Feik D, Rams TE, BarnettML, Pan P. Effect of an essential oil-containing an-tiseptic mouthrinse on induction of platelet aggre-gation by oral bacteria in vitro. J Clin Periodontol.2000;27:370–373.
58. Charles CH, Pan PC, Sturdivant L, Vincent JW. Invivo antimicrobial activity of an essential oil-con-taining mouthrinse on interproximal plaque bacte-ria. J Clin Dent. 2000;11:94–97.
59. Tinanoff N. Progress regarding the use of stannousfluoride in clinical dentistry. J Clin Dent.1995;6(spec no.):37–40.
60. Walters PA, Biesbrock AR, Bartizek RD. Benefitsof sodium hexametaphosphate-containing chewinggum for extrinsic stain inhibition. J Dent Hyg.2004;78:8.
61. Mankodi S, Bartizek RD, Winston JL, BiesbrockAR, McClanahan SF, He T. Anti-gingivitis efficacyof a stabilized 0.454% stannous fluoride/sodiumhexametaphosphate dentifrice. J Clin Periodontol.2005;32:75–80.
62. Mallatt M, Mankodi S, Bauroth K, Bsoul SA, Bar-tizek RD, He T. A controlled 6-month clinical trialto study the effects of a stannous fluoride dentifriceon gingivitis. J Clin Periodontol. 2007;34:762–767.
63. Paraskevas S, van der Weijden GA. A review of theeffects of stannous fluoride on gingivitis. J Clin Pe-riodontol. 2006;33:1–13.
64. Nabi N, Mukerjee C, Schmid R, Gaffar A. In vitroand in vivo studies on triclosan/PVM/MA copoly-mer/NaF combination as an anti-plaque agent. AmJ Dent. 1989;(2 spec no.):197–206.
65. Modeer T, Bengtsson A, Rolla G. Triclosan reducesprostaglandin biosynthesis in human gingival fi-broblasts challenged with interleukin-1 in vitro. JClin Periodontol. 1996;23:927–933.
66. Mustafa M, Bakhiet M, Wondimu B, Modeer T.Effect of triclosan on interferon-gamma produc-tion and major histocompatibility complex class IIexpression in human gingival fibroblasts. J Clin Pe-riodontol. 2000;27:733–737.
67. Mustafa M, Wondimu B, Yucel-Lindberg T, Kats-Hallstrom AT, Jonsson AS, Modeer T. Triclosan re-duces microsomal prostaglandin E synthase-1expression in human gingival fibroblasts. J Clin Pe-riodontol. 2005;32:6–11.
68. Wallet MA, Calderon N, Alonso TR, et al. Triclosanalters antimicrobial and inflammatory responses ofepithelial cells. Oral Dis. 2013;19:296–302.
69. Davies RM, Ellwood RP, Davies GM. The effec-tiveness of a toothpaste containing triclosan andpolyvinyl-methyl ether maleic acid copolymer inimproving plaque control and gingival health: asystematic review. J Clin Periodontol. 2004;31:1029–1033.
70. Rosling B, Dahlen G, Volpe A, Furuichi Y, Ram-berg P, Lindhe J. Effect of triclosan on the subgin-gival microbiota of periodontitis-susceptiblesubjects. J Clin Periodontol. 1997;24:881–887.
71. Lanzos I, Herrera D, Santos S, et al. Mucositis inirradiated cancer patients: effects of an antisepticmouthrinse. Med Oral Patol Oral Cir Bucal.2010;15:e732–738.
72. Worthington HV, Clarkson JE, Bryan G, et al. In-terventions for preventing oral mucositis for pa-
CHAPTER 16 Chemotherapeutic Agents
270

tients with cancer receiving treatment. CochraneDatabase Syst Rev. 2011;(4):CD000978.
73. Salim N, Silikas N, Satterthwaite JD, Moore C, Ra-mage G, Rautemaa R. Chlorhexidine-impregnatedPEM/THFM polymer exhibits superior activity tofluconazole-impregnated polymer against Candidaalbicans biofilm formation. Int J AntimicrobAgents. 2013;41:193–196.
74. Daly B, Sharif MO, Newton T, Jones K, Worthing-ton HV. Local interventions for the management ofalveolar osteitis (dry socket). Cochrane DatabaseSyst Rev. 2012;(12):CD006968.
75. Wilson W, Taubert KA, Gewitz M, et al. Preventionof infective endocarditis: guidelines from the Ameri-can Heart Association: a guideline from the AmericanHeart Association Rheumatic Fever, Endocarditis,
and Kawasaki Disease Committee, Council on Car-diovascular Disease in the Young, and the Council onClinical Cardiology, Council on Cardiovascular Sur-gery and Anesthesia, and the Quality of Care andOutcomes Research Interdisciplinary WorkingGroup. Circulation. 2007;116:1736–1754.
76. Fedorowicz Z, Aljufairi H, Nasser M, OuthouseTL, Pedrazzi V. Mouthrinses for the treatment ofhalitosis. Cochrane Database Syst Rev.2008;(4):CD006701.
77. Loesche WJ, Kazor C. Microbiology and treatmentof halitosis. Periodontol 2000. 2002;28:256–279.
78. Shi Z, Xie H, Wang P, et al. Oral hygiene care forcritically ill patients to prevent ventilator-associatedpneumonia. Cochrane Database Syst Rev.2013;(8):CD008367.
Prevention Across the Lifespan: A Review of Evidence-Based Interventions for Common Oral Conditions
271
Please note: tables, figures, and boxes are indicated byan italicized “t“, “f“, or “b“, respectively.
A
A1C test/levels, 44t, 45–47, 209–211, 211t, 216AAP Task Force Report, 71–72, 74abfraction, 114, 114f, 116, 161abrasiondefined, 108etiology, 108–110examples, 109f, 110fprevention, 110–111role in dentin hypersensitivity, 161, 161t
abuse, recognizing and reporting, 202ACP (amorphous calcium phosphate), 168, 251acquired immunodeficiency syndrome (AIDS), 124Actinobacillus actinomycetemcomitans, 264Actinomyces viscosus, 264ADA Seal of Acceptance criteria, 258fadverse pregnancy outcomes, evidence supporting oral-systemic link, 213–214Agency for Healthcare Research and Quality (AHRQ),17–18grades of recommendation, 18tlevels of scientific evidence, 18t
Aggregatibacter actinomycetemcomitans, 71, 212AGREE (Appraisal of Guidelines Research and Evaluation), 12tAHA/ASA My Life Check–Life’s Simple 7, 41AHA Committee on Rheumatic Fever, Endocarditis,and Kawasaki Disease, 41AHRQ (Agency for Healthcare Research and Quality).See Agency for Healthcare Research and QualityAIDS (acquired immunodeficiency syndrome), 124American Academy of Pediatric Dentistry’s ClinicalPractice Guidelines, 50–51American Academy of Periodontology Workshop onPeriodontal Regeneration and Tissue Engineering, 106amorphous calcium phosphate (ACP), 168, 251amoxicillin (AMX), 80anticholinergic drugs, 177antimicrobials/antibioticsantimicrobial dentifrice, 89antimicrobial mouthrinses, 89–90locally delivered, 79–80systemic, 80
antioxidants, 90Appraisal of Guidelines Research and Evaluation(AGREE), 12targinine, 65arginine-based desensitizing prophylaxis paste, 169ASD (autism spectrum disorders), 229–230attrition
defined, 107etiology, 107–108examples, 107fprevention, 108role in dentin hypersensitivity, 161, 161t
autism spectrum disorders (ASD), 229–230autoimmune diseases, 177, 183, 184–187
B
bacterial fluorescence, 60–61, 60bBacteroides forsythus, 147Bacteroides species, 264bad breath, 146behavior and psychological interventions. Seebiopsychosocial patient care; special care dentistrybiofilmsecological plaque hypothesis, 62inflammatory response to, 208–210. See alsooral-systemic healthinterdental biofilm removal, 87–89, 87fmodifying composition of, 64, 65bnon-fluoride management strategies, 249–252powered interdental cleaning devices, 87–89, 88fprebiotics and, 65probiotics and, 64–65quantifying, 60–61role of nature vs. nurture in, 65bselective targeted antimicrobial peptides, 66smart signaling systems in, 64
biomedical model of disease, 23biopsychosocial patient care, 23–35application to clinical practicecommon psychological conditions, 31–32common risk factors and links to systemichealth, 29disease prevention across the lifespan, 28health literacy in the context of dental appointments, 31integrating desired behavior into patientlifestyles, 30interpersonal communication, 30–31process of disease prevention, 28respectful patient communication, 31simplified communication, 31trying new behaviors vs. establishing healthyhabits, 29–30using teach-back method, 31
benefits of, 32–33Chairside Checklist, 32, 33–35defined, 23goal of, 23key considerationscommon risk factor approach, 24–25health literacy, 24motivational interviewing, 28quality of life, 24social cognitive theory, 25–26, 25fsocial determinants of health, 23–24socioeconomic gradient and poverty, 24stress and coping, 26–27
INDEX
272
273
transtheoretical model, 27–28understanding and influencing health behavior, 25
See also special care dentistryBradshaw, D. I., 62bulimia nervosa, 111–113, 112f
C
calcium glycerophosphate, 63calcium sodium phosphosilicate, 169CAMBRA (Caries Management by Risk Assessment),51, 63Campbell Collaboration, 12Candid. albicans, 262Candida species, 260–262, 263cardiovascular disease and strokeage-standardized prevalence estimates for ideal cardiovascular health, 40fAHA definition of cardiovascular health, 39tAHA prevalence of health metrics, 40fdeaths in U.S., 38fevidence supporting oral-systemic link, 212–213incidence, symptoms and risk factors, 37–41risk assessment, 41
CARE (Customizable Assessment and Risk Evaluator)Tools, 50care-resistant behavior (CRB), 223cariescase studies inadolescent patients, 66–67deterioration of dentition in adolescent patients, 67–68fdiabetes mellitus complications, 69felderly patients, 67–68, 69foral-systemic health, 68–70, 69f
demineralization and remineralization process, 236,236fdiagnosis and detection, 238fluoride therapies, 62–63, 238incidence and symptoms of, 50lifestyles promoting, 64non-fluoride interventions, 63–64paradigm shifts in etiology, 61–62risk assessment, 50–51, 63–64for birth to 5 years of age, 51tCaries Management by Risk Assessment(CAMBRA), 51, 63for children 6 and older, 52t
risk factors for, 50, 57, 57b, 58–59, 58brole of biofilms, 64–66nature vs. nurture, 65b
role of prevention, 57–58, 66trends and challenges in preventionDunedin, New Zealand study, 58–59, 63early detection of caries, 59–60, 60fnonoperative caries treatment programs, 59pathogenesis of caries, 59quantification of dental plaque, 60–61WHO database conclusions, 61
Caries Management by Risk Assessment (CAMBRA),51, 63case-control study design, 5–6, 6fcasein phosphopeptide (CPP), 168casein phosphopeptide–amorphous calcium phosphate(CPP-ACP), 63–64case report/case series studies, 4, 4fCASP (Critical Appraisal Skills Programme), 12tCavistat toothpaste, 252CBCT (cone-beam computed tomography), 73–74CDA Foundation, 51Centre for Evidence-Based Medicine, 12t, 16–17CEBM table for diagnosis, 16tCEBM table for prognosis, 17tCEBM table for therapy, prevention, etiology,harm, 16t
CEOM (combination essential oil mouthrinse)application to clinical practice, 264–265composition of preventive chemotherapeuticmouthrinses, 262tefficacy of, 89, 260–262
cetylpyridinium chloride (CPC), 89, 264cevimeline, 180Chairside Checklist (for biopsychosocial patient care),32, 33–35chemotherapeutic agents, 257–268application to clinical practicecetylpyridinium chloride (CPC), 264chlorhexidine (CHX), 263–264combination essential oil, 264–265stannous fluoride with sodium hexametaphosphate, 265triclosan and PVM/MA, 266
benefits of, 266–268strength of supporting evidence, 267t
clinical evaluation of, 257–259, 258fdefined, 257effect on microbial diversity, 260–262effect on oral mucosal tissues, 262–263composition of preventive chemotherapeuticmouthrinses, 262t
overview of active agents, 259major strategies for effective chemotherapeuticagents, 259t
safety of active agents, 259–260, 260fchewing tobacco, 104–105children and adolescentscaries risk assessment, for children 6 and older, 52tfluoride use inbenefits of professional interventions, 240–241caries experience in children who brush once orless vs. twice or more, 239fdietary supplements, 240fluoride varnish, 241, 241fgels and foams, 240mouthrinses, 240products available, 238, 239ftoothpaste prescriptions, 242
INDEX
toothpastes, 238–239mouthrinses for, 239f, 240toothbrushing in, 239toothpastes for, 238–239, 239f
chlorhexidine gluconate (CHX)application to clinical practice, 263–264composition of preventive chemotherapeuticmouthrinses, 262tefficacy of, 79–80, 89–90, 260–262in root caries prevention, 250
CINAHL (Cumulative Index of Nursing and AlliedHealth Literature), 2tclinical decision making, 14
See also evidence-based practiceclinical practice guidelines (CPGs), 15, 15tCochrane Collaboration, 2t, 13, 18–19, 19t, 63cohort studies, 6–7, 7f, 8fColgate Maximum Cavity Protection Plus Sugar AcidNeutralizer, 251–252Colgate Pro-Relief, 170fColgate Sensitive Toothpaste, 170fColgate Total Rinse, 262tcombination essential oil mouthrinse (CEOM)application to clinical practice, 264–265composition of preventive chemotherapeuticmouthrinses, 262tefficacy of, 89, 260–262
common risk factor approach, 24–25communication, role in patient care, 30–31cone-beam computed tomography (CBCT), 73–74consistency, 223–224CONSORT, 12t, 13contingent/noncontingent escape, 223conventional staged debridement (CSD), 77COREQ, 12t, 13CPC (cetylpyridinium chloride), 89, 264CPGs (clinical practice guidelines), 15, 15tCPP (casein phosphopeptide), 168CPP-ACP (casein phosphopeptide–amorphous calcium phosphate), 63–64, 168, 252CRB (care-resistant behavior), 223Crest Pro Health Multi-Protection, 262tCritical Appraisal Skills Programme (CASP), 12tcross-sectional study design, 4–5, 5fCSD (conventional staged debridement), 77Cumulative Index of Nursing and Allied Health Literature (CINAHL), 2tCustomizable Assessment and Risk Evaluator (CARE)Tools, 50
D
damage prevention. See oral tissue damageDARE (Database of Abstracts of Reviews of Effects), 2tDean, H. Trendley, 235Decayed, Missing, Filled Surfaces (DMFS) Index, 59demineralization/remineralization process, 59, 236,236f, 247–249DenPlan Excel/PreVisor Patient Assessment (DEPPA),
52dental caries. See cariesdental endoscopy, 77dental floss, 87dental fluorosis (enamel mottling), 235, 235fDental Traumatology (journal), 196dentin hypersensitivity, 160–171diagnosisair blast stimuli response, 165f, 166faspects and elements of, 163–164differential diagnosis, 165–166oral examination, 164patient history, 164stimuli response testing, 164–165Yeaple probe stimuli response, 165f
epidemiology, 160etiology, 160–161Brännström’s Theory, 160f
overview of, 171pathogenesis, 162–163enamel loss, 162fodontoblast and dentinal tubules, 163fscanning electron micrograph images, 163f
patient management and interventionsarginine technology sealing of dentinal tubules,169fconsiderations for, 169–171major products available for, 170toptions for, 171tpreventive strategies, 166–167therapeutic interventions, 167–169, 167f
risk factors, 161–162frequently encountered conditions associatedwith tooth sensitivity, 161tquestions for patients experiencing dentin hypersensitivity, 161t
Dentition Risk System (DRS), 52DEPPA (DenPlan Excel/PreVisor Patient Assessment),52diabetes mellitusawareness, treatment and control in adults, 42fcase studies in, 68–70, 69fevidence supporting oral-systemic link, 209–212,211tguiding principles for care, 44tincidence, symptoms and risk factors, 41–43risk assessment, 43–47, 70ADA assessment tool, 45fFinnish Diabetes Risk Score, 46f
DMFS (Decayed, Missing, Filled Surfaces) Index, 59double-blind study design, 9doxycycline, 79–80DRS (Dentition Risk System), 52dry mouth (xerostomia)case studies infemale with autoimmune diseases, 184–187,184t, 185f, 185t, 186f, 187fmale receiving radiation therapy, 187–189, 188f,
274
INDEX
188t, 189fdiagnosisflow rates of whole saliva, 177tsalivary gland hypofunction, 176xerostomia, 176
epidemiology, 177prevalence of xerostomia and salivary gland hypofunction, 177t
etiologyage, 177common systemic disorders associated with drymouth, 178tmedication, 177radiation therapy, 178systemic disorders, 177–178
incidence, symptoms and risk factors, 53overview, 175pathogenesis, 175contributors to salivary secretion, 176fcontrol of salivary secretion, 175f
patient management considerations, 182–183prevention, 179–180saliva substitutes, 181–182, 182t
risk assessment, 53hyposalivation with xerostomia screening tool,54f
role in caries progression, 247–248therapeutic interventions, saliva stimulants, 180–181
Dunedin, New Zealand prevention study, 58–59, 63dyskeratosis congenita, 124
E
EBD (evidence-based dentistry), 1See also evidence-based practice
EBDM (evidence-based decision-making), 1See also evidence-based practice
ecological plaque hypothesis, 62EDS (excessive daytime sleepiness), 47
See also sleep-related breathing disordersEffectiveness and Efficiency: Random Reflections onHealth Service (Cochrane), 18electronic nicotine delivery systems (ENDS), 124Ellis class I and II injuries, 193Embase, 2tenamel mottling (dental fluorosis), 235, 235fendogenic erosiondue to bulimia, 112fdue to GERD, 112fetiology, 111–112prevention, 112–113
ENDS (electronic nicotine delivery systems), 124Engel, G. L., 23erbium–yttrium aluminium garnet (Er:YAG) laser, 76erosiondefined, 111endogenic, 111–113, 112fexogenic, 113–114, 113f
role in dentin hypersensitivity, 161, 161tEr:YAG (erbium–yttrium aluminium garnet) laser, 76erythromycin, 80escape extinction, 224essential oil rinses. See combination essential oilmouthrinseEuropean Health Literacy Survey, 24evidence-based decision-making (EBDM), 1
See also evidence-based practiceevidence-based dentistry (EBD), 1
See also evidence-based practiceEvidence-Based Dentistry for the Dental Hygienist(Frantsve-Hawley), 12t
Evidence-based Dentistry: Managing Information forBetter Practice (Richards, et. al.), 12tevidence-based practice, 1–20applying evidence to practice, 19–20challenges in adoptingaccessing information, 2–3keeping up with literature, 2locating best evidence, 3resources to assist with critical appraisal, 12tunderstanding research methodology, 3
clinical practice guidelines, 15, 15tdefined, 1grading scientific evidenceAgency for Healthcare Research and Quality,17–18AHRQ grades of recommendation, 18tAHRQ levels of scientific evidence, 18tCEBM table for therapy, prevention, etiology,harm, 16tCEBM tables for diagnosis, 16t, 17tCentre for Evidence-Based Medicine, 16–17Cochrane Collaboration, 18–19Cochrane collaboration key principles, 19tGRADE system, 17, 17toverview of, 15–16
levels of evidence, 13–14hierarchy of preappraised evidence, 14fresources supporting clinical decision making,14t
locating best evidence, 2tmodel, 1foverview of, 20steps of, 13, 13fstudy designscase-control, 5–6, 6fcase report/case series, 4, 4fcohort studies, 6–7cohort studies: prospective, 7fcohort studies: retrospective chart review, 8fcross-sectional, 4–5, 5fexperimental studies, 8–10guidelines for reporting, 13hierarchy of, 3fmeta-analyses, 11–12, 11fnonexperimental intervention, 8, 8f
275
INDEX
276
qualitative studies, 10randomized controlled trial: active control, 10frandomized controlled trial: placebo control, 9fregistering systematic reviews and meta-analyses, 12–13surveys and interviews, 3–4systematic reviews, 10–11
excessive daytime sleepiness (EDS), 47See also sleep-related breathing disorders
exogenic erosionetiology, 113examples, 113fprevention, 113–114
experimental studies, 8–10extraoral halitosis, 147case studies in, 155–157, 156fclassification, categories of oral malodor, 147tpathogenesis, 148See also oral malodor
F
Fanconi’s anemia, 124Finnish Diabetes Risk Score (FINDRISC), 43fluorescence, 60–61, 60bfluoridesin adults and older adultsevidence for use, 238f, 242–243midlevel providers and, 243population-based interventions, 243
benefits of, 235–236in children and adolescentsbenefits of professional interventions, 240–241caries experience in children who brush once orless vs. twice or more, 239fdietary supplements, 240fluoride varnish, 241, 241fgels and foams, 240mouthrinses, 240products available, 238, 239ftoothpaste prescriptions, 241–242toothpastes, 238–239
delivery methods, 236–237dietary intake of, 235efficacy of, 59, 62–63future directions and best practices, 243–244history of, 235enamel mottling (dental fluorosis), 235, 235f
life course approach to, 237–238, 238fcaries detection and diagnosis, 238using fluorides to prevent and treat caries, 238
optimal delivery, 237optimal level, 235overview of, 244risks of use, 237topical effect of, 236demineralization and remineralization, 236f
fluorosis, 239FMD (full-mouth disinfection), 77
FMPA (Frankfort Mandibular-Plane Angle), 195FMSRP (full-mouth scaling and root planing), 76–77focal infections, 208foreshadowing, 223Frankfort Mandibular-Plane Angle (FMPA), 195frenal pull, influence on gingival recession, 104full-mouth disinfection (FMD), 77full-mouth scaling and root planing (FMSRP), 76–77Fusobacterium nucleatum, 147–148, 148f
G
gastroesophageal reflux disease (GERD), 111–112, 112fGC America MI Paste, 170fGERD (gastroesophageal reflux disease), 111–112, 112fgeriatric patientsaggressive prevention, 226clinical prevention, 225conservative prevention, 225empirical prevention, 225fluoride use in, 242–243guidelines for preventive dentistry, 224influence of medical condition, 224oral physiology changes in, 57–58predictive prevention, 225preventive care considerations, 230–231team approach to preventive care, 224–225
gingival recessioneffects of oral piercings, 105effects of tobacco use, 104–105epidemiology, 97–99etiology, 99–101examples, 98f, 99f, 100f, 101fpathogenesis, 105–106prevention and therapy, 106role in dentin hypersensitivity, 161, 161t
gingivitiscase studies in, 91, 91fclassification, 72tdefined, 71, 208epidemiology, 72–74etiology and pathogenesis, 73See also periodontal diseases
gingivitis artefacta, 97glycated hemoglobin. See A1C test/levelsglycine powder air polishing (GPAP), 77–78, 78fGoogle Scholar, 2tGRADE (Grading of Recommendations, Assessment,Development, and Evaluation) system, 17, 17tgraft-versus- host disease (GVHD), 124Guidelines for the Management of Patients with Periodontal Diseases (AAP), 52
H
habits, establishing, 29–30Halimeter, 150halitophobia, 147, 147t
INDEX
277
halitosis, 146See also oral malodor
hard tissue damage. See under oral tissue damageHbA1c. See A1C test/levelshead and neck cancers (HNCs)case studies inadolescent male using tobacco, 138–140young female with low health literacy, 140–141
diagnostic tests, 128–131images and CT scan of tongue cancer, 130fimages and CT scan of tonsillar cancer, 129fselected methods for detection and diagnosis,130t
epidemiology, 121–122new cases, deaths, and 5-year relative survival,122fnumber of new cases by race/ethnicity and sex,123tpercent of deaths by age group, 123fpercent of new cases by age group, 122f
etiology and risk factors, 122–124, 123tlevels of evidence for increased risk, 124t
future epidemiological trends, 136–137future research efforts, 137–138incidence of, 121MASCC/ISOO practice guidelines, 144–145pathogenesis, 124–126cancer in situ, 127fcervical metastasis of left tonsil and tonguebase, 126fcommon locations of head/neck cancers, 125terythroplakia and mixed lesions, 127fHPV oncoproteins E6 and E7, 126fleukoplakia of tongue, 127fmolecular biological and histopathologic comparisons, 125tSCC of posterior oropharyngeal wall, 126fSCC of upper lip, 127ftonsillar cancer, 125f, 126f
patient management and interventionsbehavioral change stages in tobacco cessation,133fconsiderations for, 135–136interventions prior to treatment, 132–134levels of evidence for interventions to reducerisk, 131tpreventive strategies, 131–132special considerations, 136therapeutic interventions, 134–135
role in dry mouth, 179role of oral health professionals, 121, 138signs and symptoms, 126–128comparison of HNCs by etiology, 128tsymptoms of OPCs, 128t
See also oral and pharyngeal cancerHealth Improvement in Dental Practice (HIDEP), 52health literacydefined, 24
role in interpersonal communication, 31role in patient care, 24, 31
Health Technology Assessment Database, 2tHeartScore electronic risk assessment system, 41herbal patches, 90heterogeneous studies, 12HIDEP (Health Improvement in Dental Practice), 52HNCs (head and neck cancers). See head and neckcancershomogeneous studies, 12HPV-associated cancerdiagnosis, 129–131etiology and risk factors, 123–124comparison of HNCs by etiology, 128tmolecular biological and histopathologic comparisons, 125t
future directions and best practices, 136–137future research efforts, 137–138HPV susceptibility testing, 50pathogenesis, 125HPV oncoproteins E6 and E7, 126f
risk reduction, 141tsurvival rates, 121therapeutic interventions, 134–135vaccination against, 131–132, 136–137viruses included, 49See also head and neck cancers; oral and pharyngeal cancer
Human Microbiome Project, 62hydrodynamic theory (of dentin hypersensitivity), 160hydroxyapatite, 60hypersensitivity. See dentin hypersensitivity
I
IADT (International Association of Dental Traumatology), 196–197ICMJE (International Committee of Medical JournalEditors), 13implants. See peri-implant diseasesIMRT (intensity modulated radiation therapy), 179INSPIRE, 12t, 13intentional abuse, recognition and reporting, 202International Association of Dental Traumatology(IADT), 196–197International Committee of Medical Journal Editors(ICMJE), 13interpersonal communication, role in patient care, 30–31intraoral chemotherapeutics, 259
See also chemotherapeutic agentsintraoral halitosiscase studies in, 154–155, 155fclassification, categories of oral malodor, 147tdefined, 147pathogenesis, 147–148detection of volatile sulphur compounds fromP. gingivalis and F. nucleatum, 148fvolatile malodorous contributors to, 148t
INDEX
278
See also oral malodorintrinsic fluorescence, 60, 60birrigation, supra- and subgingival, 78–79, 88f
L
Lactobacillus species, 250laser technology, 76LILACS (Literature from Latin America and theCaribbean), 2tListerine, 262tlocal and systemic therapies, 79longitudinal study design, 7
M
maintenance and recall, 80–81for implant-borne restorations, 84–86tfor tooth-borne restorations, 82–83t
malodor. See oral malodorMarsh, P. D., 62MASCC/ISOO practice guidelines for oral mucositis,144–145McKay, Frederick, 62mechanical therapy, 75–76meta-analyses, 11–13, 11fmetronidazole (MET), 80MFP (sodium monofluorophosphate), 169MI (motivational interviewing), 28, 133MIC (minimal inhibitory concentration) level, 79, 260minimally invasive dentistry, 59minocycline, 79–80MOOSE, 12t, 13motivational interviewing (MI), 28, 133mouth protectors, 199–201, 200f, 201fmouthrinsesantimicrobial, 89–90arginine-based desensitizing prophylaxis, 169ffor children and adolescents, 239f, 240oral malodor and, 153
My Life Check–Life’s Simple 7, 41
N
nanoparticulate hydroxyapatite, 63nanotechnology/nanoparticulate materials, 66National Diabetes Education Program (NDEP), 43, 44tNational Information Center on Health Services Research and Health Care Technology (NICHSR), 2tNational Institutes of Health, accessing informationthrough, 2–3NCCL (noncarious cervical lesions), 114Nd:YAG (neodymium–yttrium aluminium garnet)laser, 76neurodegenerative diseases, 228Nexo approach, 59NICHSR (National Information Center on HealthServices Research and Health Care Technology), 2tNOCTP (nonoperative caries treatment program), 59noncarious cervical lesions (NCCL), 114nonexperimental intervention study design, 8, 8f
non-fluoride remineralizationbenefits of, 246calcium-based remineralization, 251–252, 251fcasein phosphopeptide–amorphous calcium phos-phate, 63–64demineralization/remineralization process, 59, 248–249, 248foverview of, 252–253patient assessment, 246progression of caries formation, 246–247, 247frole of dental plaque in caries, 246–247stimulating salivary flow, 251targeted antimicrobial therapies, 249–251traditional approaches, 249
nonoperative caries treatment program (NOCTP), 59NovaMin toothpaste, 169, 170fnutrition, 91
O
obesity, 91obstructive sleep apnea (OSA), 47, 107–108, 111
See also sleep-related breathing disordersodds ratio (OR), 6OHRQOL (oral health-related quality of life), 24OPC (oral and pharyngeal cancer). See oral and pharyngeal canceroral and pharyngeal cancer (OPC)diagnosis, 129–131epidemiology, 121incidence, symptoms and risk factors, 48–49, 128, 128tmouthrinses and, 263risk assessment, 49–50CARE (Customizable Assessment and RiskEvaluator) Tools, 50Health Canada self-assessment quiz, 49tPreViser Oral Cancer Risk Assessment, 49
See also head and neck cancersOralChroma portable gas chromatograph, 150f, 151f,155f, 156fOral Health Information Suite, 53oral health-related quality of life (OHRQOL), 24oral malodor, 146–157assessmentHalimeter, 150history and evaluation, 149instrumental assessment, 150–151OralChroma portable gas chromatograph, 150f,151f, 155f, 156forganoleptic measurement, 149–150, 150tsaliva quantity and quality, 149Winkel Tongue Coating Index, 149, 149f, 150f
case studies infemale with extraoral halitosis, 155–157, 156fmale with intraoral halitosis, 154–155, 155f
classification, 147categories of oral malodor, 147t
defined, 146
INDEX
279
epidemiology, 146–147age distribution of patients attending privatehalitosis assessment clinic, 146f
management and treatmentmasking odor, 153mouthrinses, 153multistep approach to, 152options for, 151, 151tprevention, 154probiotics, 153referral to specialists, 154tongue scraping, 152, 152ftoothpaste additives, 152, 153ttreatment matrix, 152t
pathogenesis of extraoral halitosis, 148pathogenesis of intraoral halitosis, 147–148detection of volatile sulphur compounds fromP. gingivalis and F. nucleatum, 148fvolatile malodorous contributors to, 148t
oral mucositis, MASCC/ISOO practice guidelines, 144–145Oral Pathology CARE Tool, 50oral piercings, 97–98, 98f, 100–101, 105–106, 116, 195oral-systemic health, 207–218adverse pregnancy outcomes, 213–214application to clinical practice, 215–217cardiovascular disease, 212–213diabetes, 209–212effect of periodontal treatment on glycemiccontrol, 211, 211t
evidence supporting oral-systemic links, 207–208, 207tkey considerations, 208–209overview of, 217–218
oral tissue damage, 97–116hard tissuesabfraction, 114, 114fabrasion, 108–111, 109f, 110fattrition, 107–108, 107fendogenic erosion, 111–113, 112ferosion, 111exogenic erosion, 101f, 113–114, 113fmultifactorial etiology, 114–115, 115foral piercings, 98foverview of, 106–107
overview of, 115–116soft tissuesappliance-related recession, 100f, 101f, 103fchemical irritation, 105fepidemiology, 97–99etiology, 99–105gingival recession, 98f, 99f, 101fiatrogenic damage, 106pathogenesis, 105prevention and therapy, 106toothbrush trauma, 98f, 100f, 102ftraumatic lesions, 105f
orofacial injuries, 192–204
case studies insports-related TDI, 203–204, 204fthumbsucking, 203, 203f
epidemiology, 192–193complicated fracture in 10-year-old girl, 192fcomplicated fracture of left maxillary incisor,193fpalatal displacement resulting in traumatic occlusion, 193f
intentional abuse, 202management, 196–197BB gun pellet embedded in soft tissues, 198fenamel-dentin fracture with tooth fragment,198ftooth fragment embedded in tongue, 198ftrauma bin contents, 196ttrauma bin example, 196ftrauma record example, 199t
overview, 192preventioninterceptive orthodontics, 201–202mouth protectors, 199–201, 200f, 201foverview of, 197–199
risk factors, 194–196increased overjet and flared maxillary incisors,195f
sequelae, 193–194inflammatory root resorption, 194fresults of necrosis, 194f
orthodontic treatment, influence on gingival recession,103–104OSA (obstructive sleep apnea). See obstructive sleepapnea
P
p53 tumor suppressor, 125Paroex, 262tpatient behavior. See biopsychosocial patient care; special care dentistrypatient lifestylecariogenic lifestyles, 64integrating desired behavior into, 30periodontal diseases andnutrition and obesity, 91stress and psychological factors, 91tobacco use, 90–91
PDT (photodynamic therapy diode), 76pediatric dentistry. See children and adolescentspeptide–cetylpyridinium chloride combinations, 250Peridex, 262tperi-implant diseasescase studies in, 92, 92fclassification, 74defined, 74diagnosis, 74epidemiology, 74–75pathogenesis, 75risk assessment, 75
INDEX
280
subgingival air polishing, 78Periodontal Assessment Tool, 53periodontal diseasescase studies ingingivitis in adolescent female, 91, 91fperi-implantitis in geriatric male, 92, 92fperiodontitis in adult male, 92, 92f
defined, 208diagnostic testing of, 73–74etiology and pathogenesis, 73gingivitiscase studies in, 91, 91fclassification, 72tdefined, 71, 208epidemiology, 72–74etiology and pathogenesis, 73
incidence, symptoms and risk factors, 51–52patient lifestyle andnutrition and obesity, 91stress and psychological factors, 91tobacco use, 90–91
peri-implant diseasescase studies in, 92, 92fclassification, 74defined, 74diagnosis, 74epidemiology, 74–75pathogenesis, 75risk assessment, 75subgingival air polishing, 78
periodontitiscase studies in, 92, 92fchronic vs. aggressive, 71–72Classification System for Periodontal Diseasesand Conditions (AAP), 71, 72tdefined, 71, 208diagnosis, 71epidemiology of chronic, 73etiology and pathogenesis, 73guidelines for determining severity, 72tInternational Workshop for a Classification ofPeriodontal Diseases and Conditions, 71Task Force Report (AAP), 71–72
prognosis and risk assessment, 74risk assessment, 52–53DenPlan Excel/PreVisor Patient Assessment(DEPPA), 52Dentition Risk System (DRS), 52Health Improvement in Dental Practice(HIDEP), 52Periodontal Risk Assessment (PRA), 52Periodontal Risk Calculator (PRC), 53Risk Assessment-Based Individualized Treatment (RABIT), 52
treatments and strategies, at-homeantimicrobial dentifrice, 89antimicrobial mouthrinses, 89–90antioxidants, 90
herbal patches, 90interdental biofilm removal, 87, 87fpowered interdental cleaning devices, 87–89, 88fprobiotics, 90recommendations for, 81–83toothbrushes, 83–87, 86f
treatments and strategies, in-officedental endoscopy, 77full-mouth disinfection, 76–77laser technology, 76local and systemic therapies, 79locally delivered antimicrobials/antibiotics, 79–80maintenance and recall, 80–81maintenance and recall for implant-bornerestorations, 84–86tmaintenance and recall for tooth-borne restorations, 82–83tmechanical therapy, 75–76subgingival air polishing, 77–78, 78fsupra- and subgingival irrigation, 78–79, 88fsystemic antibiotics, 80
Periodontal Risk Assessment (PRA), 52Periodontal Risk Calculator (PRC), 53periodontitis. See under periodontal diseasesphotodynamic therapy diode (PDT), 76PICO format, 13piercings. See oral piercingspilocarpine, 180polyvinylmethyl ether/maleic acid copolymer(PVM/MA), 266
Porphyromonas gingivalis, 71, 147–148, 148f, 212poverty, as determinant of health, 24
See also biopsychosocial patient carePRA (Periodontal Risk Assessment), 52PRC (Periodontal Risk Calculator), 53preappraised research, 14, 14fprebiotics, 65predator bacteria, 65pregnancy outcomes, evidence supporting oral-systemiclink, 213–214prevalence studies, 4Prevent Diabetes STAT toolkit, 43prevention across the lifespanbiopsychosocial patient care, 23–35caries, 57–70chemotherapeutic agents, 257–268dentin hypersensitivity, 160–171dry mouth (xerostomia), 175–189evidence-based practice, 1–20fluorides, 235–244head and neck cancers, 121–142MASCC/ISOO oral mucositis guidelines, 144–145non-fluoride remineralization, 246–253oral malodor, 146–157oral-systemic health, 207–218oral tissue damage, 91–116orofacial injuries, 192–204
INDEX
281
periodontal diseases, 71–92risk assessment, 37–54special care dentistry, 221–231
PreViser Oral Cancer Risk Assessment, 49Prevotella intermedia, 147primary research, 14PRISMA, 12t, 13probiotics, 64–65, 90, 153prospective study design, 6–7PROSPERO, 13PscyINFO, 2tpseudohalitosis, 147, 147tpsychological conditions, effect on patient care, 31–32publication bias, 11PubMed, 2tPVM/MA (polyvinylmethyl ether/maleic acid copolymer), 266
Q
QLF (quantitative light fluorescence), 60–61QOL (quality of life), 24quadrant scaling and root planing (Q-SRP), 77qualitative studies, 10quality of life (QOL), 24quantitative light fluorescence (QLF), 60–61
R
RABIT (Risk Assessment-Based Individualized Treatment), 52radiation therapyrole in dry mouth, 178, 179therapeutic interventions, 183
RAGE (receptor for advanced glycation end products),209–210randomized controlled trials (RCTs), 9–10, 12, 13active control design, 10fplacebo control design, 9f
rate ratio (RR), 6recall. See maintenance and recallrecall bias, 6receptor for advanced glycation end products (RAGE),209–210RECORD, 12t, 13red disclosing tablets, 60relative rate, 6relative risk, 6remineralization therapies. See fluorides; non-fluorideremineralizationReplacement Theory, 64retrospective study design, 5, 7risk assessment, 37–54defined, 37for oral healthcaries, 50–51, 51t, 52t, 63–64oral cancer, 48–50, 49tperi-implant diseases, 75periodontal disease, 51–53, 74
xerostomia, 53, 54foverview of, 53–54for systemic healthcardiovascular disease and stroke, 37–41, 38f,39t, 40fdiabetes mellitus, 41–47, 42f, 44t, 45f, 46f, 70goals of, 37sleep-related breathing disorders, 47–48, 47f, 48t
Risk Assessment-Based Individualized Treatment(RABIT), 52risk ratio, 6role modeling, 223–224RR (rate ratio), 6
S
salivary gland hypofunction (SGH)case studies in, 184–187defined, 175diagnosis, 176epidemiology, 177, 177tetiology, 177–178
salivary gland transfer (SGT), 179salivary precipitin, 247scaling and root planing (SRP)adjunct therapies, 76efficacy of, 75–76FMSRP (full-mouth scaling and root planing), 76–77
SciELO (Scientific Electronic Library Online, in Spanish), 2tscientific evidenceapplying to practice, 19–20gradingAgency for Healthcare Research and Quality,17–18AHRQ grades of recommendation, 18tAHRQ levels of scientific evidence, 18tCEBM table for therapy, prevention, etiology,harm, 16tCEBM tables for diagnosis, 16t, 17tCentre for Evidence-Based Medicine, 16–17Cochrane Collaboration, 18–19Cochrane collaboration key principles, 19tGRADE system, 17, 17toverview of, 15–16
levels of, 13–14hierarchy of preappraised evidence, 14fresources supporting clinical decision making,14t
Scope, 262tSCORE (Systemic Coronary Risk Evaluation), 41Screening Tool for Hyposalivation with Xerostomia,53–54, 54fSCT (social cognitive theory), 25–26, 25fSDD (subantimicrobial dose doxycycline), 80secondary research, 14Seikaly Jha procedure (SJP), 179selective targeted antimicrobial peptides (STAMPs),
INDEX
282
66, 250self-efficacy, 25Sensodyne Toothpaste, 170fsensory disorders, 228–229SGH (salivary gland hypofunction). See salivary gland hypofunctionSGT (salivary gland transfer), 179shaping, 223single-blind study design, 96S Hierarchy of Preappraised Evidence, 14, 14fSjögren’s syndrome, 177, 183, 184–187SJP (Seikaly Jha procedure), 179sleep-related breathing disordersincidence, symptoms and risk factors, 47–48Mallampati Classification, 47frisk assessment, 48STOP-Bang questionnaire, 48, 48tSTOP questionnaire, 48, 48t
smokeless tobacco, 104–105SnF2 (stannous fluoride with sodium hexametaphosphate), 265snuff, 104–105social cognitive theory (SCT), 25–26, 25fsocial determinants of health, 23–24
See also biopsychosocial patient caresoda beverages, 113–114sodium monofluorophosphate (MFP), 169soft tissue damage. See under oral tissue damagespecial care dentistry, 221–231application to clinical practice, 231barriers to care in special needs patients, 221behavior and psychological interventionsapproaches to, 222benefits of, 222consistency and role modeling, 223–224contingent and noncontingent escape, 223escape extinction, 224shaping through successive approximation, 223systematic desensitization, 222–223
care delivery problemspatients with autism spectrum disorders, 229–230patients with neurodegenerative diseases, 228patients with sensory disorders, 228–229patients with speech and language impairments, 229
geriatric patientsaggressive prevention, 226clinical prevention, 225conservative prevention, 225empirical prevention, 225guidelines for preventive dentistry, 224influence of medical condition, 224predictive prevention, 225preventive care considerations, 230–231team approach to preventive care, 224–225
importance of preventive care, 221–222populations included, 221
preventive care considerationsadjuvant interventions, 226–227dietary considerations, 227–228first and annual visits, 226home care and family involvement, 228impact of systemic or psychological declines, 227periodic preventive maintenance, 226
speech and language impairments, 229SRP (scaling and root planing). See scaling and rootplaningSTAMPs (selective targeted antimicrobial peptides), 66, 250stannous fluoride with sodium hexametaphosphate(SnF2), 265STARD, 12t, 13Stichting Center for Evidence-Based Management(CEBMa), 12tSTOP-Bang questionnaire, 48, 48tSTOP questionnaire, 48, 48tStreptococcus gordonii, 65Streptococcus mutans, 62, 64, 250, 261, 264–265Streptococcus salivarius K12, 153Streptococcus sanguinis, 65, 250–251, 264stress and coping, effect on health, 26–27, 91STROBE, 12t, 13study designscase-control, 5–6, 6fcase report/case series, 4, 4fcohort, 6–7prospective, 7fretrospective, 8f
cross-sectional, 4–5, 5fexperimental, 8–10hierarchy of, 3fmeta-analyses, 11–12, 11fnonexperimental intervention, 8, 8fqualitative, 10randomized controlled trials (RCTs)active control, 10fplacebo control, 9f
registering systematic reviews and meta-analyses,12–13surveys and interviews, 3–4systematic reviews, 10–11
subantimicrobial dose doxycycline (SDD), 80subgingival air polishing, 77–78, 78fsuccessive approximation, 223supra- and subgingival irrigation, 78–79, 88fsurveys and interviews, 3–4systematic desensitization, 222–223systematic reviews, 10–11, 12–13Systemic Coronary Risk Evaluation (SCORE), 41
T
Take Action to Prevent Diabetes: A Toolkit for the Prevention of Type 2 Diabetes in Europe, 43TDIs (traumatic dental injuries). See traumatic dental
INDEX
283
injuriesteach-back method, 31tell-show-do method, 223temporary halitosis, 147, 147ttetracycline, 803D conformal radiation therapy, 179Tiel-Culemborg study, 59tissue damage. See oral tissue damagetobacco use, 90–91, 104–105, 132–133, 133ftongue scraping, oral malodor and, 152, 152ftoothbrushes, 83–87, 86ftoothbrushingin children and adolescents, 239effects of improper technique, 102gingival injury due to, 101–102influence on gingival recession, 102–103recommendations for, 106
toothpastesacid-neutralizing, 251arginine-based desensitizing prophylaxis paste, 169, 170farginine bicarbonate/calcium carbonate, 252for children and adolescents, 238–239, 239foral malodor and, 152, 153tprescription fluoride, 242
transtheoretical model (TTM), 27–28traumatic dental injuries (TDIs)case studies in, 203–204, 204fepidemiology, 192–193management, 196–197BB gun pellet embedded in soft tissues, 198fenamel-dentin fracture with tooth fragment, 198ftooth fragment embedded in tongue, 198f
trauma bin contents, 196ttrauma bin example, 196ftrauma record example, 199t
overview of, 192prevention, 197–202interceptive orthodontics, 201–202mouth protectors, 199–201, 200f, 201f
risk factors, 194–196sequelae, 193–194
traumatic lesions, 104–105TREND, 12t, 13Treponema denticola, 147tricalcium phosphate, 63triclosan/copolymer, 250, 261, 266TRIP (Turning Research Into Practice), 2tTristan da Cunha (British colony), 58bTTM (transtheoretical model), 27–2821 Cities study, 235
U
University of Oxford Critical Appraisal Tools, 12tUniversity of South Australia Critical Appraisal Tools, 12t
V
visualization, 223
W
Winkel Tongue Coating Index, 149, 149f, 150f
X
xerostomia. See dry mouth
INDEX

Oral diseases affect people of all ages. Prevention is the best strategy to reduce risksfor disease and to minimize and/or eliminate the need for invasive procedures to correct or arrest the disease process. This book is a collection of preventive interventions that are evidence-based and reflect current best practices. We hopethat readers will find this book to be a valuable resource to guide clinical decision-making and recommendations for their patients. Together, we can strive toeliminate oral disease through effective preventive efforts, at home, in the dentaloffice, and in the community.
—Ann E.Spolarich, Fotinos S. Panagakos