
Prevalence of the fibrinogen β-chain, angiotensin-converting enzyme and plasminogen activator...
18
For Peer Review Prevalence of the Fibrinogen β-chain, Angiotensin- Converting Enzyme and Plasminogen Activator Inhibitor-1 polymorphisms in Costa Rican young adults with thrombotic disease. Journal: Cell Biochemistry & Function Manuscript ID: CBF-09-0155.R1 Wiley - Manuscript type: Research Article Date Submitted by the Author: Complete List of Authors: Hidalgo, Andrea; University of Costa Rica, CIHATA Salazar-Sanchez, Lizbeth; University of Costa Rica, cihata Cartin, Mayra; University of Costa Rica, Public Healthy School Arauz, Jorge; San Juan de Dios, Hospital, Cardiology Keywords: polymorphisms, , Fibrinogen, &amp;amp;amp;amp;nbsp;plasminogen activator inhibitor-1, thrombosis, &amp;amp;nbsp;angiotensin-converting enzyme Abstract: Thrombotic disease is a multifactorial condition that involves both classical and genetic risk factors. We studied the association between the classical risk factors of hypertension and smoking, and polymorphisms on the genes of the Angiotensin-Converting Enzyme (ACE), the β-chain of Fibrinogen (FG) and the Plasminogen Activator Inhibitor-1 (PAI-1) in patients with venous thrombosis, myocardial infarction and stroke. The present investigation is a retrospective case-control study. A total of 340 participants were analyzed, including 162 patients and 178 healthy controls. Hypertension and smoking showed a significant association with thrombotic disease (p < 0.05). Significant differences between groups were found for the levels of FG in plasma (p = 0.013), and for polymorphisms of ACE (p = 0.04) and PAI-1 (p < 0.001). For both fibrinogen β–chain gene polymorphisms, none of the molecular analyses showed a positive sample for any mutating allele (p > 0.05). PAI-1 polymorphism showed the most significant association with thrombotic disease. http://mc.manuscriptcentral.com/cbf Cell Biochemistry & Function
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Prevalence of the fibrinogen β-chain, angiotensin-converting enzyme and plasminogen activator...
For Peer Review
Prevalence of the Fibrinogen β-chain, Angiotensin-Converting Enzyme and Plasminogen Activator Inhibitor-1 polymorphisms in Costa Rican young adults with thrombotic
disease.
Journal: Cell Biochemistry & Function
Manuscript ID: CBF-09-0155.R1
Wiley - Manuscript type: Research Article
Date Submitted by the Author:
Complete List of Authors: Hidalgo, Andrea; University of Costa Rica, CIHATA Salazar-Sanchez, Lizbeth; University of Costa Rica, cihata Cartin, Mayra; University of Costa Rica, Public Healthy School Arauz, Jorge; San Juan de Dios, Hospital, Cardiology
Keywords: polymorphisms, , Fibrinogen, &amp;amp;amp;amp;nbsp;plasminogen activator inhibitor-1, thrombosis, &amp;amp;nbsp;angiotensin-converting enzyme
Abstract:
Thrombotic disease is a multifactorial condition that involves both classical and genetic risk factors. We studied the association between the classical risk factors of hypertension and smoking, and polymorphisms on the genes of the Angiotensin-Converting Enzyme (ACE), the β-chain of Fibrinogen (FG) and the Plasminogen Activator Inhibitor-1 (PAI-1) in patients with venous thrombosis, myocardial infarction and stroke. The present investigation is a retrospective case-control study. A total of 340 participants were analyzed, including 162 patients and 178 healthy controls. Hypertension and smoking showed a significant association with thrombotic disease (p < 0.05). Significant differences between groups were found for the levels of FG in plasma (p = 0.013), and
for polymorphisms of ACE (p = 0.04) and PAI-1 (p < 0.001). For both fibrinogen β–chain gene polymorphisms, none of the molecular analyses showed a positive sample for any mutating allele (p > 0.05). PAI-1 polymorphism showed the most significant association with thrombotic disease.
http://mc.manuscriptcentral.com/cbf
Cell Biochemistry & Function

For Peer Review
Page 1 of 16
http://mc.manuscriptcentral.com/cbf
Cell Biochemistry & Function
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
1
Prevalence of the Fibrinogen β-chain, Angiotensin-Converting Enzyme and Plasminogen Activator Inhibitor polymorphisms in Costa Rican
young adults with thrombotic disease.
Introduction
According to the World Health Organization (WHO), cardiovascular disease
(CVD) is one of the major causes of death worldwide and it is responsible for 12
million deaths per year [1]. In Costa Rica, it has been the main cause of death since
1970. In 2007, a total of 4.992 circulatory system-related cases were reported
nationwide [2].
Thrombotic disease is a multifactorial condition which involves both classical
risk factors like: hypertension, obesity, smoking, sedentary life style, age,
hyperlipidemias, Diabetes Mellitus (DM), and also genetic factors.
Many investigations have addressed the association between genetic
polymorphisms and the classical risk factors. The aim of the present study was to
determine the possible association between two classical risk factors: hypertension and
smoking, the -455 G > A and -148 C > T polymorphisms located on the β-chain gene of
Fibrinogen (FG), the Insertion/Deletion of the Angiotensin Converting Enzyme (ACE)
and the -675 4G > 5G polymorphism of the Plasminogen Activator Inhibitor-1 (PAI-1),
and thrombotic disease in the young population of Costa Rica.
Fibrinogen is a plasmatic protein produced by hepatocytes which has a half-life
of 3 to 5 days. It participates in different coagulation processes: first, it is part of the
final coagulation cascade as a fibrin precursor; second, it contributes to platelet
aggregation; and third, it is the main determinant of plasma viscosity and interacts with
Endothelial Cells (EC) to produce cell migration and proliferation [3, 4, 5].
The most frequently studied FG polymorphisms are located in the β-chain gene.
Both, the -455 G > A (HaeIII) and the -148 C > T (HindIII) polymorphisms are located
on the gene promoter region. Experimental studies have shown an up-regulation of the
β-chain gene transcription which has therefore been related with higher FG levels in
plasma [6, 7]. Polymorphism -148 C > T is related to an increased stimulus exerted by
IL-6 on the gene transcription [8]. This factor joins specific promoting region sequences
between approximately -150 and -82 base pairs (bp) and increases the levels of FG in
plasma [9].
Page 2 of 16
http://mc.manuscriptcentral.com/cbf
Cell Biochemistry & Function
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
2
The Angiotensin-Converting Enzyme is a zinc transmembrane enzyme which is
part of the Renin-Angiotensin-Aldosterone System (RAAS). The latter regulates sodium
homeostasis, arterial pressure and vascular tone [10, 11]. The ACE also plays a
fundamental role in the Kallicrein–Kininogen System (KKS) which catalyzes the
conversion of angiotensin I into the powerful vasoconstrictor: angiotensin II, and at the
same time, deactivates bradikinin, a powerful vasodilator [12, 13].
The National Center for Biotechnology Information (NCBI) database contains
more than 160 ACE gene polymorphisms [14]. The polymorphism most frequently
studied, described by Rigat and collaborators in 1990 [15], consists of the presence
(Insertion, I) or the absence (Deletion, D) of a 287 bp Alu sequence on intron 16. Such
an insertion on the gene has been linked to a protective effect for myocardial infarction
since its presence (allele I) reduces angiotensin II levels [16].
The Plasminogen Activator Inhibitor-1 is part of the serine protease inhibitor
super-family (Serpine). With an endothelial origin, it is also present in platelets and
hepatocytes [17]. PAI-1 participates on the fibrinolysis process, inhibiting the tissue
Plasminogen Activator (t-PA). This prevents activation of plasminogen and, therefore,
plasmin is not formed, and the fibrin clot is not destroyed.
Approximately nine polymorphisms have been identified for the PAI-1 gene.
The most widely studied is -675 4G > 5G; the genotype lacking the mutation (allele 5G)
creates a link site for an inhibitor, leading to a down-regulation of the gene product, and
thus, PAI-1 levels are low [17, 19]. Individuals with a 4G4G genotype exhibit an increase
on PAI-1 concentration in plasma of up to 25 times greater than individuals with a
5G5G genotype [17].
Materials and Methods
Patients
This retrospective case-control study included a total of 340 subjects, consisting
of 162 cases and 178 healthy controls. The cases were males and females, ages 18 to 50
years old, with the diagnosis of Myocardial Infarction (MI), Stroke, Deep Venous
Thrombosis (DVT) and Pulmonary Embolism (PE), with or without a family history for
these diseases, and admitted to Social Security Hospitals of Costa Rica. The controls
were healthy individuals, males and females, ages 18 to 50 years old, which had not
Page 3 of 16
http://mc.manuscriptcentral.com/cbf
Cell Biochemistry & Function
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
3
suffered any cardiovascular disease and were unrelated to the studied patients. Genetic
and protein quantification assays were conducted at the Center for Research on
Hematology and Related Disorders (CIHATA) of the University of Costa Rica. All
participants gave informed consent according to a protocol approved by the University
of Costa Rican Bioethics on Human Subjects Research Committee and participating
hospitals.
Coagulation assays
Blood samples were obtained by venipuncture and collected in plastic tubes
containing 0.109M trisodium citrate (9:1 vol/vol). The samples were spun at 5000 rpm
for 10 min. Plasma was isolated and stored at -70ºC until use. The amount of FG in
plasma was determined using the Fibri-Prest kit and the semi-auto coagulation analyzer
STart4 (Diagnostica Stago, Asnieres, France), according to the method described by
Clauss [3, 20].
DNA extraction and polymorphism determination
For extraction of genomic DNA and polymorphism analysis, DNA was isolated
from blood samples collected into tubes containing 1.7mM EDTA-K3. DNA was
isolated from peripheral blood according to standardized protocols [21]. Then, we used
polymerase chain reaction (PCR) [22] carried out in an Applied Biosystems (9700)
thermal cycler, with master mix (Fermentas, California, USA), for polymorphism
characterization.
Polymorphism within intron 16 of the ACE gene was analyzed according to the
description by Rigat et al. [15]. To prevent mistyping of the DD genotype, a second PCR
with insertion-specific primers was performed as described by Odawara et al. [23].
Polymorphisms of FG β-chain -455G > A and -145 C > T were analyzed by
amplification of a 1301 bp fragment and its digestion with HaeIII and HindIII [9, 24].
Primers and amplification conditions for polymorphisms -675 4G > 5G of the
PAI-1 gene have previously been described by Margaglione et al. [25]. The
amplification fragment was digested with BslI.
Statistical analysis
Statistical analysis was performed using SSPS 13.0 (SSPS Inc., USA). To
determine the association between the classic risk factors and the genetic risk factors
Page 4 of 16
http://mc.manuscriptcentral.com/cbf
Cell Biochemistry & Function
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
4
between cases and controls, we used a χ2-test for qualitative variables. The t-student
analysis was applied for quantitative variables (age), as well as an ANOVA to compare
age differences between the disease groups.
To determine the risk of developing thrombosis we calculated the Odds Ratios
(OR) with a 95% confidence interval (CI) and χ2-test. Finally, allele frequencies of each
polymorphism were determined according to the Hardy-Weinberg law, with χ2-test.
Results
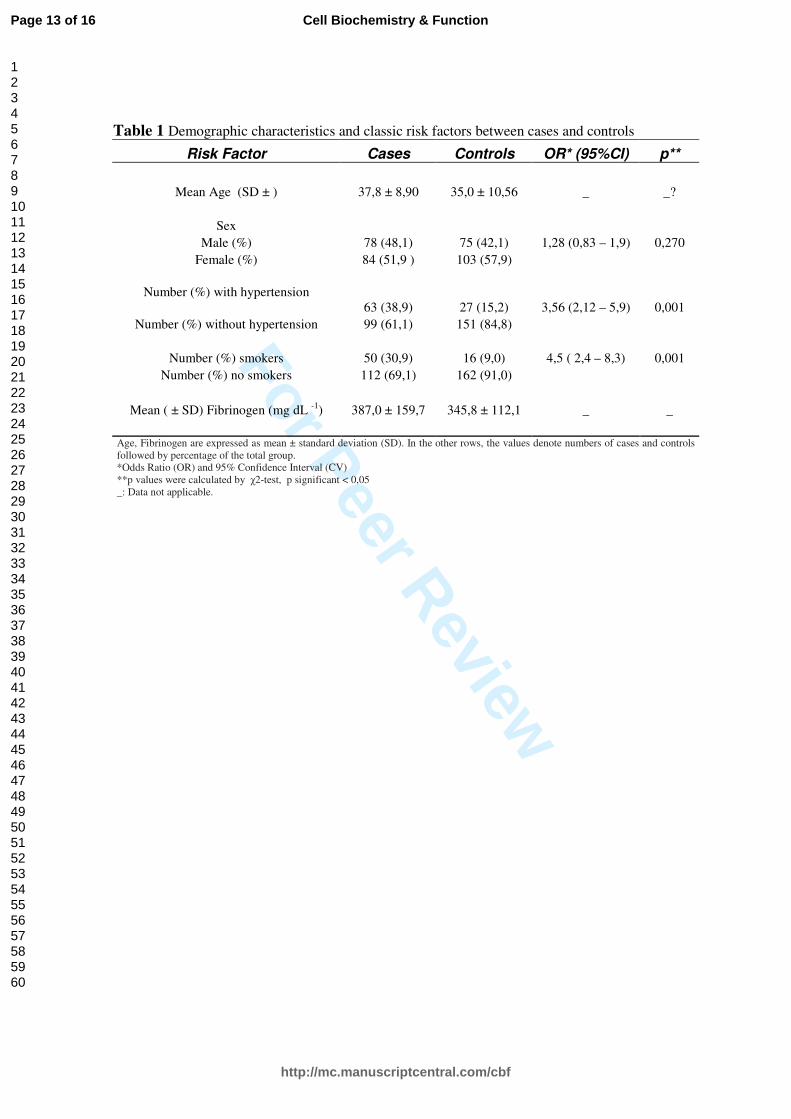
Demographic and clinical characteristics and the prevalence of risk factors are
summarized in Table 1. The average age was 37, 4 years for the cases and 35, 0 years
for the controls. Hypertension and smoking showed a significant association to
thrombotic disease (p < 0, 05 for both). Between smokers and non-smokers, OR was 4.5
(95% IC 2,4 – 8,3, p = 0,001). A significant difference was found for FG plasma levels
between patients and control samples as well (p = 0,013).
Prevalence of genetic polymorphisms
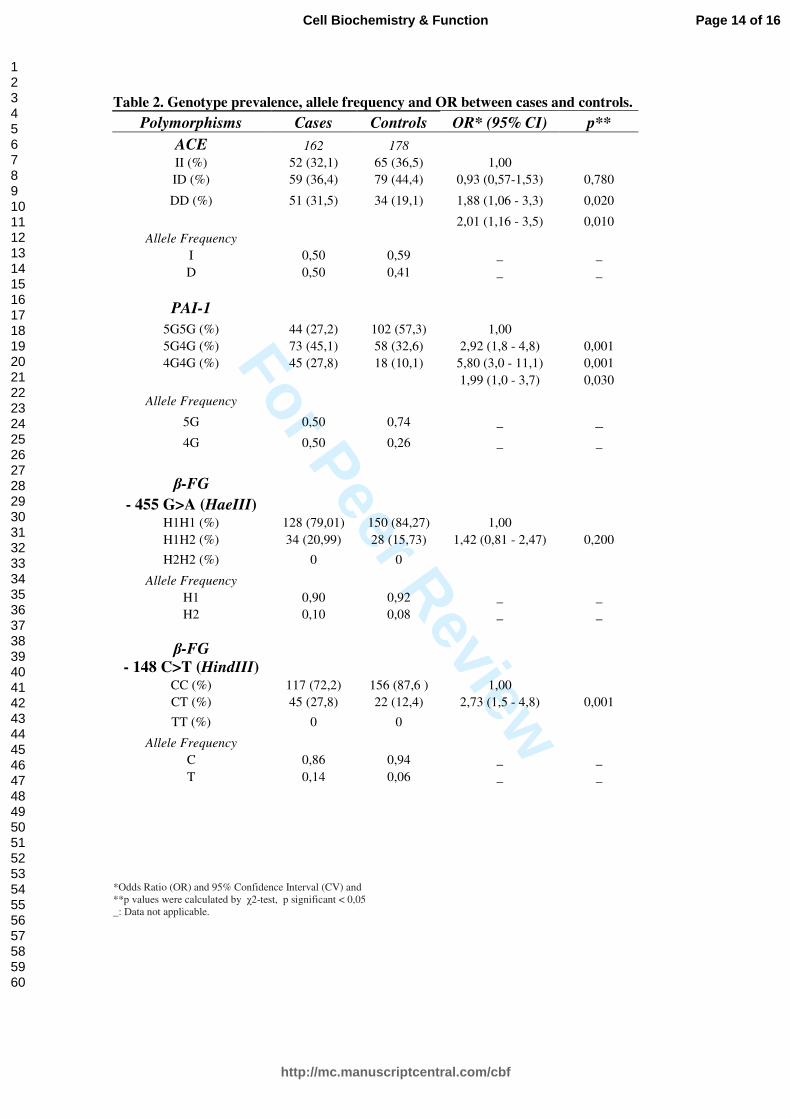
The ACE polymorphism (p = 0,04) and PAI-1 (p = 0,001) showed a significant
difference between cases and controls (Table 2). Individuals with the DD genotype had
a 1,88 risk of suffering the disease in comparison with people having genotype II.
Presence of 4G4G PAI-1 polymorphism conferred a 5,80 risk of suffering the disease as
compared to those with the wild homozygote (5G5G). For FG β–chain gene
polymorphisms (HindIII and HaeIII), none of the molecular analyses showed a positive
sample for any mutating allele (p > 0,05).
Allele frequency distribution of the four polymorphisms studied in the control
group were in Hardy–Weinberg (H-W) equilibrium. Among the patient samples, only
the ACE polymorphism’s allele frequency was not in H-W equilibrium (χ2 = 11,95, gl 2,
p = 0,0025).
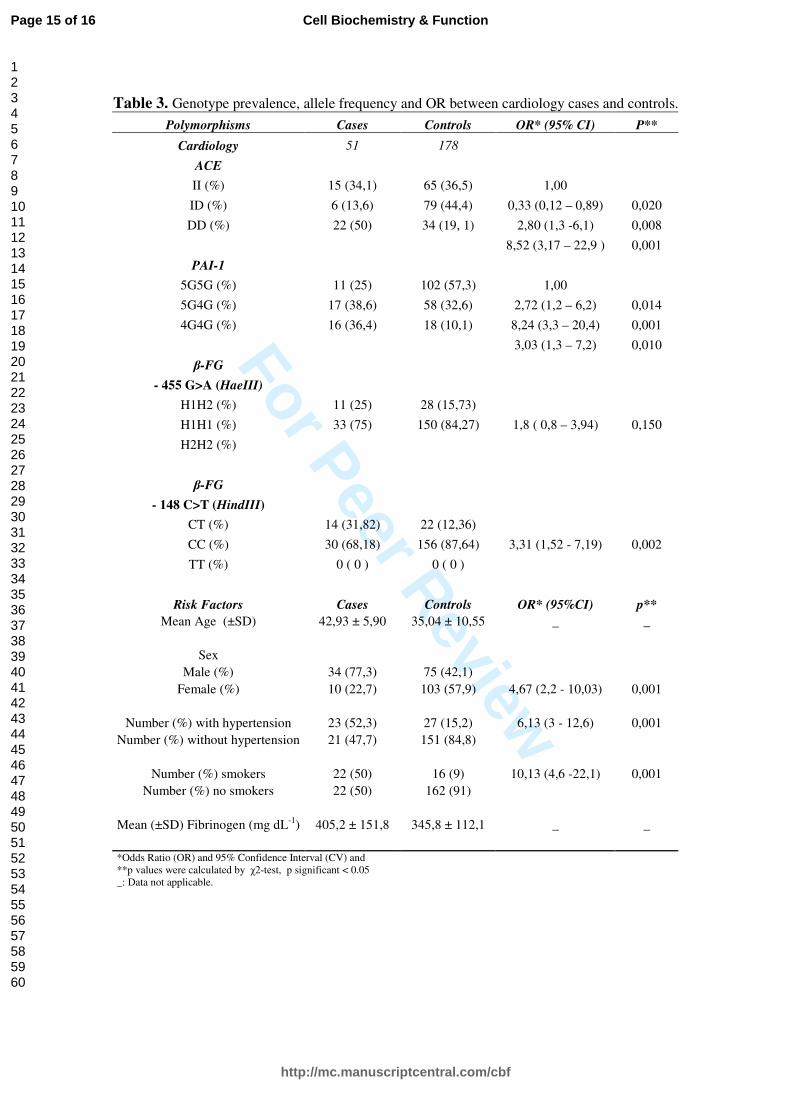
The group with the highest incidence of classic risk factors (HTA and smoking)
and polymorphisms associated to the risk of developing disease were the cardiology
patients, having 8 out of 9 positive parameters (age, sex, smoking, hypertension, FG in
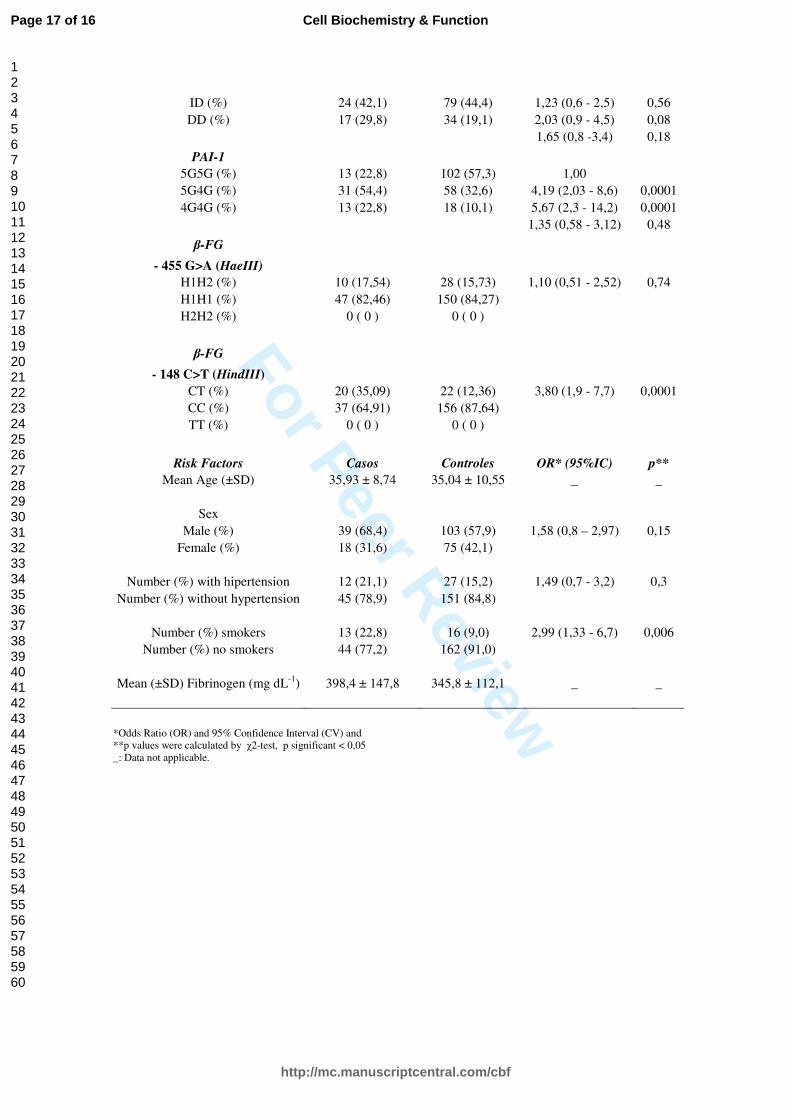
plasma, PAI-1, ACE, HindIII) (Table 3). The thrombosis group ranked second, with 4
significant parameters (smoke, FG in plasma, PAI-1, HindIII) (Table 4). And lastly
Page 5 of 16
http://mc.manuscriptcentral.com/cbf
Cell Biochemistry & Function
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
5
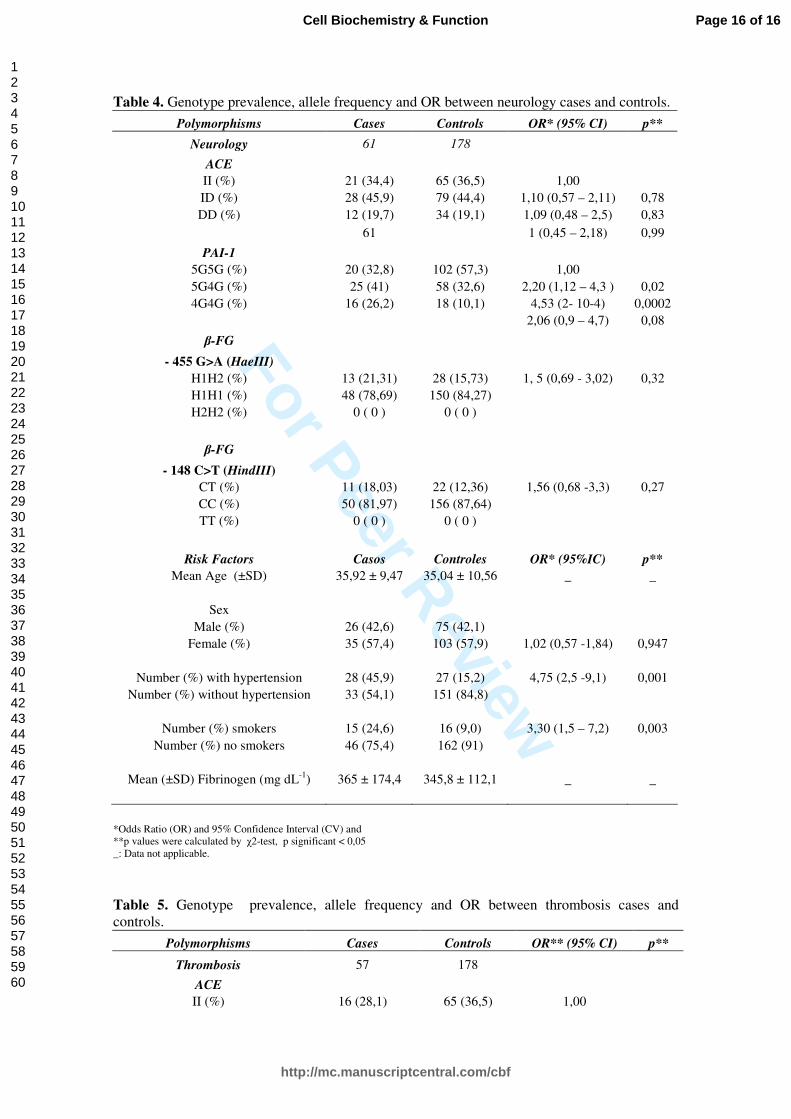
comes the neurology group, with three significant parameters (smoking, hypertension,
PAI-1) (Table 5).
The PAI-1 polymorphism showed the most significant association among those
studied, with an OR of 5,80 (95 % IC 3,0-11,1, p < 0,001), cardiology patients showing
the greatest risk (OR 8,24; 95 % IC 3,3-20,4, p < 0,001).
Discussion
Regarding classical risk factors, hypertension and smoking, analyzed in this
study, they show once again a strong link with thrombotic pathologies. Also, a
significant difference was found for the levels of FG in plasma between patients and
controls which agrees with numerous epidemiological studies where plasma fibrinogen
has been associated with thrombotic disease, atherosclerotic disease and an increased
risk of cardiovascular disorders, including ischemic heart disease, stroke and other
thromboembolisms [6].
Molecular analysis reveals that polymorphisms on ACE and PAI-1 differ significantly
between cases and controls. In the analysis between disease groups, polymorphisms for
ACE were only significantly associated with the cardiology group, with a higher
frequency of the DD genotype. These data agree with a similar study by Mata et al.,
2004 [26], done in Spanish population. It is described that ACE activity levels in DD
carriers were approximately twice those found in individuals carrying the II genotype.
Subjects with the ID genotype had intermediate levels indicating codominance [12, 15].
Several reports demonstrate the relationship between the ID polymorphism and
high blood pressure [12], atherosclerosis, coronary heart disease [13, 26], stroke [27,
28] and disorders like diabetic nephropathy and Alzheimer's disease. The wide
distribution and multifunctional properties of these peptides suggest that ACE could be
involved in various pathophysiological conditions. Nevertheless, association studies on
the ID polymorphism and clinical outcomes continue to be performed, mostly with
conflicting results. Genotypic and phenotypic misclassifications, insufficient statistical
power in some studies, and the presence of interaction with other genes or
environmental factors are possible explanations for contradictory findings. [29, 30, 31,
32].
After the analyses between patients and controls, the - 675 4G > 5G PAI-1
polymorphism showed the most significant association with disease among those
studied. The 4G allele was significantly associated with higher plasma PAI-1
Page 6 of 16
http://mc.manuscriptcentral.com/cbf
Cell Biochemistry & Function
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
6
concentrations, and it was the most strongly associated as risk factor of CVD [17]. The
cardiology patient group showed the greatest risk in comparison with neurology and
thrombosis groups. These data are in accordance with several studies [18, 35, 36, 37],
where the prevalence of the 4G4G genotype is higher in people with CVD than healthy
controls. This suggests that polymorphisms within the fibrinolytic system, specifically
on PAI-1, play an important role on the development of coronary artery disease. This is
supported by the biologic characteristics of PAI-1 and the association between high
plasma PAI-1 concentrations and other cardiovascular risk factors [17, 38]. Subjects
who are homozygous for the 4G allele have plasma PAI-1 concentrations that are
approximately 25% higher than those of subjects who are homozygous for the 5G allele
[17]. The – 675 bp polymorphism at PAI-1 has been linked to some conditions as
dyslipidemias, arterial thrombosis in antiphospholipid syndrome, insulin resistance
syndrome, type 2 diabetic nephropathy, atherosclerosis, myocardial infarction, coronary
artery disease, venous thrombosis in Factor V Leiden carriers and rheumatoid arthritis
[17, 19, 25, 39]. Also, in one Mexican study, the genetic variability of the – 675 bp
polymorphism at the PAI-1 promoter in healthy subjects from a Mexican population
was correlated with clinical parameters [39].
Finally, the two polymorphisms of the β-FG chain could not be significantly
associated with any condition, in the studied group. Many investigations demonstrate
the positive relationship between the genetic background and the increase of FG plasma
levels that could participate on the development of CVD [6, 9, 33]. The influence of the
β-FG chain gene has been more extensively studied, because the synthesis of this chain
is the limiting step for the production of the mature protein. Similarly, it has been
demonstrated that the – 455 G > A as other polymorphisms of the β-FG gene have a
significant impact on plasma concentration [34,39].
In general, there is still a wide controversy on FG polymorphisms and their role
on CVD. There is much debate on whether FG is a consequence or a cause of the
thrombotic event, because FG is also an acute response protein. Also, the differences
within our results could be influenced by the study's case-control design, which allowed
only to process post-event patient samples. It would be interesting to develop a
prospective cohort study to confirm the difference on FG plasma levels.
Individual genetic variability may play a determinant role on thrombotic disease,
especially among patients with one or more classic risk factors and/or family history.
Moreover, the levels of ACE, PAI-1 and FG can be altered by many factors like:
Page 7 of 16
http://mc.manuscriptcentral.com/cbf
Cell Biochemistry & Function
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
7
smoking, HTA, obesity, age, hypertriglyceridemia, gender, and hereditary factors. This
supports the study of genetic polymorphisms and their association with CVD clinical
risk and disease course, in order to be able to better understand their role.
In summary, HTA and smoking are classical risk factors found strongly linked
with thrombotic disease. Molecular analysis of ACE polymorphisms revealed that the
DD genotype showed the most significant association with disease among our
cardiology patients. Polymorphism of PAI-1 was the most significantly associated with
vascular disease. Moreover, this polymorphism showed the highest OR within the
cardiology group. Further studies are necessary to determine the exact impact of this
polymorphism on the disease risk, including quantitative analysis of ACE and PAI-1
proteins and determination of its correlation with their respective polymorphisms.
This is the first report which studies the relationship of these classical factors
and four genetic polymorphisms in the Costa Rican population, and these data show the
importance of continuing with this kind of research in order to analyze the possible use
of genetics as a preventive screening for CVD in our population.
References
1. Araya M, Guzmán S (2004) Evolución de la Mortalidad por Enfermedad Isquémica del Corazón e Infarto Agudo del Miocardio en Costa Rica, 1970-2001. Rev Panam Sal Public 16: 295-301
2. Ministerio de Salud, Costa Rica. http://www.ministeriodesalud.go.cr. Accessed July 7, 2008 3. Sáenz G. Hematología Analítica (2003). Tomo II. Cuarta edición. Editorial Nacional de Salud y Seguridad social (EDNASSS). San José, Costa Rica 4. Reinhart W (2003) Fibrinogen-marker or mediator of vascular disease? Vasc Med 8: 211-216 5. Stec J, Silbershatz H, Tofler G, Matheney T, Sutherland P, Lipinska I, Massaro J, Wilson P, Muller J and D’ Agostino R (2000) Association of Fibrinogen with cardiovascular Risk factors and Cardiovascular Disease in the Framingham Offspring Population. Circul 102: 1634-1638
Page 8 of 16
http://mc.manuscriptcentral.com/cbf
Cell Biochemistry & Function
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
8
6. Iacoviello L, Vischetti M, Zito F, Benedetta M (2001) Genes Encoding Fibrinogen and Cardiovascular Risk. Hypert 38: 1199-1203 7. Maat M, Kastelein J, Jukema W, Zwinderman A, Jansen H, Groenemeier B, Bruschke A, Kluft C (1998) –455G/A Polymorphism of the β-Fibrinogen Gene is Associated with the progression of Coronary Atherosclerosis in Symptomatic Men. Arterioscler Thromb Vasc Biol 18: 265-271 8. Arocha C, Campos C, Pereira A. Enciclopedia Iberoamericana de Hematología (1992) Tomo III. Primera edición. Edición Universal Salamanca. Salamanca, España 9. Thomas A, Green F, Kelleher C, Wilkes H, Brennan P, Meade T, Humphries S (1991) Variation in the Promotor Region of the β Fibrinogen Gene is Associated with plasma Fibrinogen Levels in Smokers and Non-Smokers. Thromb Haemost 65: 487-490 10. Carluccio M, Soccio M, De Caterina R (2001) Aspects of Gene Polymorphisms in Cardiovascular Disease: the Renin-Angiotensin System. Eur J Clin Invest 31: 476-488 11. Buraczynska M, Pijanowski Z, Spasiewicz D, Nowicka T, Sodolski T, Widomska T, Ksiazek A (2003) Renin-Angiotensin System Gene Polymorphisms: Assessments of the Risk on Coronary Heart Disease. Kardiol Pol. 58: 1- 4 12. Sayed F, Oostra B, Isaacs A, van Duijn C, Witteman J (2006) ACE Polymorphism. Circ Res 98: 1123-1133 13. Niu T, Chen Xiu, Xu X (2002) Angiotensin Coverting Enzyme gene Insertion/Deletion Polymorphism and Cardiovascular Disease. Drugs 62: 977-993 14. National Center for Biotechnology Information (NCBI), http://www.ncbi.nlm.nih.gov. Accessed March 17, 2008 15. Rigat B, Humbert C, Corvol P, Soubrier F (1992) PCR detection of the insertion/deletion polymorphism of the human angiotensin converting enzyme gene (DCP 1) (dipeptidyl carboxipeptidase 1). Nucl Acids Res 20: 1433 16. Cambien F, Costerousse O, Tiret L, Poirier O, Lecert L, Gonzáles M, Evans A, Arvelier D, Cambou J,Luc G, Rakotovao R, Ducimetiere P, Soubrier F, Althenc-Gelas F (1994) Plasma Level and Gene Polymorphism of Angiotensin-Coverting Enzyme in Relation to Myocardial Infarction. Circul 90: 669-676 17. Kohler H, Grant P (2000) Plasminogen-Activator Inhibitor Type 1 and Coronary Artery Disease. N Engl J Med 342: 1792-1801 18. Hoekstra T, Geleijnse J, Schouten E, Kluft C (2004) Plasminogen activator inhibitor I: it´s plasma determinants and relation with cardiovascular risk. Tromb Haemost 91: 861-72 19. Catto A, Carter A, Barrett J, Stickland M, Bamford J, Davies A. Grant P. (1997) Plasminogen-Activator Inhibitor-1 (PAI-1) 4G/5G Promotor Polymorphism and Levels in Subjects with Cerebrovascular Disease. Throm Haemost 77: 730- 734
Page 9 of 16
http://mc.manuscriptcentral.com/cbf
Cell Biochemistry & Function
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
9
20. Clauss A (1957) Rapid Physiological Coagulation Method in Determination of Fibrinogen. Acta Haematol 17: 237 21. Miller S, Dykes D, Polesky H (1988) A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acids Res 16: 1215 22. Mullis, K., F. Faloona, S. Scharf, R. Saiki, G. Horn & H. Erlich (1986) Specific enzymatic amplification of DNA in vitro: the polymerase chain reaction. Cold Spring Harb Symp Quant Biol 51: 263-273 23. Odawara M, Matsunuma A, Yamashita K (1997) Mistyping frequency of the Angiotensin Coverting Enzyme Gene Polymorphism and an improved method for its avoidance. Hum Genet 100: 163-166 24. van´t Hooft F, von Barh A, Silveira A, Iliadou A, Erikson P, Hansten A (1999) Two Common Functional Polymorphisms in the Promoter Region of the β-Fibrinogen Gene Contribute to the Regulation of plasma Fibrinogen Concentrations. Arterioscler Thromb Vasc Biol 19: 3063-3070 25. Margalione M, Grandone E, Cappucci G, Colaizzo D, Giuliani N, Vecchione G, dÁddedda M, Minno G Di (1997) An alternative method for PAI-1 promoter polymorphism (4G/5G) typing, Tromb Haemost 77: 605–606 26. Mata T, Herrán R, Ruiz C, Ruiz M, Garrido M, Ruiz F (2004) Angiotensin-Covering Enzyme and p22phox polymorphisms and the risk of coronary heart disease in a low risk Spanish population. Inter J Cardiol 95: 145-151 27. Jackson A, Brown K, Langdown J, Luddington R, Baglin T (2000) Effect of the Angiotensin-Coverting Enzyme Gene Deletion Polymorphism on the Risk of Venous Trombo-Embolism. British J Haemat 111: 562-564 28. Catto A, Carter A, Barrett J, Stickland M, Bamford J, Davies A, Grant P (1996) Angiotensin-Coverting Enzyme Insertion/Deletion Polymorphism and Cerebrovascular Disease. Stroke 27: 435-440 29. Kammerer C, Gouin N, Samollow P, VandeBerg J, Hixson J, Cole S, MacCluer J, Atwood L (2004) Two quantitative trait loci affect ACE activities in Mexican-Americans. Hypert 43: 466-470 30. Ledru F, Blanchard D, Battalglia S, Jeunemaitre X, Courbon D, Guize L, Guermonprez J. Ducimetiere P, Diebold B (1998) Relation Between severity of Coronary Artery Disease, Left Ventricular function, and Myocardial Infarction, and influence of The ACE I/D Gene Polymorphism. Am J Cardiol 82: 160-165 31. Sharma P (1998) Meta-analysis of the ACE gene in ischaemic stroke. J Neurol Neurosurg Psychiatry 64: 227-230 32. Vidal P, Bongard V, Ruidavets J, Fauvel J, Perret B, Ferrieres J (2003) Effect of Apoliprotein E Alleles and Angiotensin-Coverting Enzyme Insertion/Deletion
Page 10 of 16
http://mc.manuscriptcentral.com/cbf
Cell Biochemistry & Function
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
1
Polymorphism on Lipid and Lipoprotein Markers in Middle-Age Men and Patient with stable Angina Pectoris or Healed Myocardial Infarction. Am J Cardiol 92: 1102-1105 33. Thomas A, Lamlum H, Green F. Humphries S (1994) Linkage Disequilibrium Across the Fibrinogen Locus as shown by five genetic polymorphism, G/A-455 (Hae III), C/T-148 (HindIII/AluI), T/G+1689 (AvaII) and BclI (β-Fibrinogen) and TaqI (α-fibrinogen), and Their Detection by PCR. Human Mutat 3: 79-81 34. Acevedo M, Foody J, Pearce G, Sprecher D (2002) Fibrinogen: Association with Cardiovascular Events in an Outpatient Clinic. Am Heart J 143: 277-82 35. Eriksson P, Kallin B, van´t Hooft F, Bavenholm P, Hamsten A (1995) Allele-specific increase in basal transcription of the plasminogen-activator inhibitor 1 gene is associated with myocardial infarction. Proc Natl Acad Sci 92: 1851-1855 36. Eriksson P, Nilsson L, Karpe F, Hamsten A (1998) Very-low-density lipoprotein responsen element in the promoter region of the human plasminogen activator inhibitor-1 gene implicated in the impaired fibrinolysis of hypertriglyceridemia. Arterioscler Thromb Vasc Biol 18: 20-6 37. Endler G, Lalouschek W, Exner M, Mitterbauer G, Haring D, Mannhalter C (2000) The 4G/5G Genotype at Nucleotide Position –675 in the Promotor Region of the Plasminogen-Activator Inhibitor 1 (PAI-1) gene is less Frequent in Young Patients with Minor Stroke than in Controls. British J Haemat 110: 469-471 38. Wiklund P, Nilsson L, Nilsson S, Eriksson P, Johansson L, Stegmayr B, Hamsten A, Holmberg D, Asplund K (2005) Plasminogen Activator Inhibitor-1 4G/5G Polymorphism and Risk of Stroke. Replicated findings in two nested case-control studies based on independent cohorts. Stroke 36: 1661-1665 39. Ruiz S, Vázquez M, Parra I, Rangel H, Best C, Sánchez L, Muñoz J (2004) Genotype and allele frequency of PAI-1 promoter polymorphism in healthy subjects from the west of Mexico. Association with biochemical and hematological parameters. Annales de Génétique 47: 155-162.
Page 11 of 16
http://mc.manuscriptcentral.com/cbf
Cell Biochemistry & Function
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
1
Acknowledgements This study was supported by the Vicerrectoría de Investigación, University of Costa Rica, with the project code number 807-A4 307, and by the National Council for Scientific and Technological Research, No. 7-367-05.
Page 12 of 16
http://mc.manuscriptcentral.com/cbf
Cell Biochemistry & Function
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
Table 1 Demographic characteristics and classic risk factors between cases and controls
Risk Factor Cases Controls OR* (95%CI) p**
Mean Age (SD ± ) 37,8 ± 8,90 35,0 ± 10,56 _ _?
Sex
Male (%) 78 (48,1) 75 (42,1) 1,28 (0,83 – 1,9) 0,270
Female (%) 84 (51,9 ) 103 (57,9)
Number (%) with hypertension
63 (38,9) 27 (15,2) 3,56 (2,12 – 5,9) 0,001
Number (%) without hypertension 99 (61,1) 151 (84,8)
Number (%) smokers 50 (30,9) 16 (9,0) 4,5 ( 2,4 – 8,3) 0,001
Number (%) no smokers 112 (69,1) 162 (91,0)
Mean ( ± SD) Fibrinogen (mg dL -1
) 387,0 ± 159,7 345,8 ± 112,1 _ _
Age, Fibrinogen are expressed as mean ± standard deviation (SD). In the other rows, the values denote numbers of cases and controls
followed by percentage of the total group.
*Odds Ratio (OR) and 95% Confidence Interval (CV)
**p values were calculated by χ2-test, p significant < 0,05
_: Data not applicable.
Page 13 of 16
http://mc.manuscriptcentral.com/cbf
Cell Biochemistry & Function
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
Table 2. Genotype prevalence, allele frequency and OR between cases and controls.
*Odds Ratio (OR) and 95% Confidence Interval (CV) and
**p values were calculated by χ2-test, p significant < 0,05
_: Data not applicable.
Polymorphisms Cases Controls OR* (95% CI) p**
ACE 162 178
II (%) 52 (32,1) 65 (36,5) 1,00
ID (%) 59 (36,4) 79 (44,4) 0,93 (0,57-1,53) 0,780
DD (%) 51 (31,5) 34 (19,1) 1,88 (1,06 - 3,3) 0,020
2,01 (1,16 - 3,5) 0,010
Allele Frequency
I 0,50 0,59 _ _
D 0,50 0,41 _ _
PAI-1
5G5G (%) 44 (27,2) 102 (57,3) 1,00
5G4G (%) 73 (45,1) 58 (32,6) 2,92 (1,8 - 4,8) 0,001
4G4G (%) 45 (27,8) 18 (10,1) 5,80 (3,0 - 11,1) 0,001
1,99 (1,0 - 3,7) 0,030
Allele Frequency
5G 0,50 0,74 _ _
4G 0,50 0,26 _ _
β-FG
- 455 G>A (HaeIII)
H1H1 (%) 128 (79,01) 150 (84,27) 1,00
H1H2 (%) 34 (20,99) 28 (15,73) 1,42 (0,81 - 2,47) 0,200
H2H2 (%) 0 0
Allele Frequency
H1 0,90 0,92 _ _
H2 0,10 0,08 _ _
β-FG
- 148 C>T (HindIII)
CC (%) 117 (72,2) 156 (87,6 ) 1,00
CT (%) 45 (27,8) 22 (12,4) 2,73 (1,5 - 4,8) 0,001
TT (%) 0 0
Allele Frequency
C 0,86 0,94 _ _
T 0,14 0,06 _ _
Page 14 of 16
http://mc.manuscriptcentral.com/cbf
Cell Biochemistry & Function
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
Table 3. Genotype prevalence, allele frequency and OR between cardiology cases and controls.
Polymorphisms Cases Controls OR* (95% CI) P**
Cardiology 51 178
ACE
II (%) 15 (34,1) 65 (36,5) 1,00
ID (%) 6 (13,6) 79 (44,4) 0,33 (0,12 – 0,89) 0,020
DD (%) 22 (50) 34 (19, 1) 2,80 (1,3 -6,1) 0,008
8,52 (3,17 – 22,9 ) 0,001
PAI-1
5G5G (%) 11 (25) 102 (57,3) 1,00
5G4G (%) 17 (38,6) 58 (32,6) 2,72 (1,2 – 6,2) 0,014
4G4G (%) 16 (36,4) 18 (10,1) 8,24 (3,3 – 20,4) 0,001
3,03 (1,3 – 7,2) 0,010
β-FG
- 455 G>A (HaeIII)
H1H2 (%) 11 (25) 28 (15,73)
H1H1 (%) 33 (75) 150 (84,27) 1,8 ( 0,8 – 3,94) 0,150
H2H2 (%)
β-FG
- 148 C>T (HindIII)
CT (%) 14 (31,82) 22 (12,36)
CC (%) 30 (68,18) 156 (87,64) 3,31 (1,52 - 7,19) 0,002
TT (%) 0 ( 0 ) 0 ( 0 )
Risk Factors Cases Controls OR* (95%CI) p**
Mean Age (±SD) 42,93 ± 5,90 35,04 ± 10,55 _ _
Sex
Male (%) 34 (77,3) 75 (42,1)
Female (%) 10 (22,7) 103 (57,9) 4,67 (2,2 - 10,03) 0,001
Number (%) with hypertension 23 (52,3) 27 (15,2) 6,13 (3 - 12,6) 0,001
Number (%) without hypertension 21 (47,7) 151 (84,8)
Number (%) smokers 22 (50) 16 (9) 10,13 (4,6 -22,1) 0,001
Number (%) no smokers 22 (50) 162 (91)
Mean (±SD) Fibrinogen (mg dL-1
) 405,2 ± 151,8 345,8 ± 112,1 _ _
*Odds Ratio (OR) and 95% Confidence Interval (CV) and
**p values were calculated by χ2-test, p significant < 0.05
_: Data not applicable.
Page 15 of 16
http://mc.manuscriptcentral.com/cbf
Cell Biochemistry & Function
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
Table 4. Genotype prevalence, allele frequency and OR between neurology cases and controls.
Polymorphisms Cases Controls OR* (95% CI) p**
Neurology 61 178
ACE
II (%) 21 (34,4) 65 (36,5) 1,00
ID (%) 28 (45,9) 79 (44,4) 1,10 (0,57 – 2,11) 0,78
DD (%) 12 (19,7) 34 (19,1) 1,09 (0,48 – 2,5) 0,83
61 1 (0,45 – 2,18) 0,99
PAI-1
5G5G (%) 20 (32,8) 102 (57,3) 1,00
5G4G (%) 25 (41) 58 (32,6) 2,20 (1,12 – 4,3 ) 0,02
4G4G (%) 16 (26,2) 18 (10,1) 4,53 (2- 10-4) 0,0002
2,06 (0,9 – 4,7) 0,08
β-FG
- 455 G>A (HaeIII)
H1H2 (%) 13 (21,31) 28 (15,73) 1, 5 (0,69 - 3,02) 0,32
H1H1 (%) 48 (78,69) 150 (84,27)
H2H2 (%) 0 ( 0 ) 0 ( 0 )
β-FG
- 148 C>T (HindIII)
CT (%) 11 (18,03) 22 (12,36) 1,56 (0,68 -3,3) 0,27
CC (%) 50 (81,97) 156 (87,64)
TT (%) 0 ( 0 ) 0 ( 0 )
Risk Factors Casos Controles OR* (95%IC) p**
Mean Age (±SD) 35,92 ± 9,47 35,04 ± 10,56 _ _
Sex
Male (%) 26 (42,6) 75 (42,1)
Female (%) 35 (57,4) 103 (57,9) 1,02 (0,57 -1,84) 0,947
Number (%) with hypertension 28 (45,9) 27 (15,2) 4,75 (2,5 -9,1) 0,001
Number (%) without hypertension 33 (54,1) 151 (84,8)
Number (%) smokers 15 (24,6) 16 (9,0) 3,30 (1,5 – 7,2) 0,003
Number (%) no smokers 46 (75,4) 162 (91)
Mean (±SD) Fibrinogen (mg dL-1
) 365 ± 174,4 345,8 ± 112,1 _ _
*Odds Ratio (OR) and 95% Confidence Interval (CV) and
**p values were calculated by χ2-test, p significant < 0,05
_: Data not applicable.
Table 5. Genotype prevalence, allele frequency and OR between thrombosis cases and
controls.
Polymorphisms Cases Controls OR** (95% CI) p**
Thrombosis 57 178
ACE
II (%) 16 (28,1) 65 (36,5) 1,00
Page 16 of 16
http://mc.manuscriptcentral.com/cbf
Cell Biochemistry & Function
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review
ID (%) 24 (42,1) 79 (44,4) 1,23 (0,6 - 2,5) 0,56
DD (%) 17 (29,8) 34 (19,1) 2,03 (0,9 - 4,5) 0,08
1,65 (0,8 -3,4) 0,18
PAI-1
5G5G (%) 13 (22,8) 102 (57,3) 1,00
5G4G (%) 31 (54,4) 58 (32,6) 4,19 (2,03 - 8,6) 0,0001
4G4G (%) 13 (22,8) 18 (10,1) 5,67 (2,3 - 14,2) 0,0001
1,35 (0,58 - 3,12) 0,48
β-FG
- 455 G>A (HaeIII)
H1H2 (%) 10 (17,54) 28 (15,73) 1,10 (0,51 - 2,52) 0,74
H1H1 (%) 47 (82,46) 150 (84,27)
H2H2 (%) 0 ( 0 ) 0 ( 0 )
β-FG
- 148 C>T (HindIII)
CT (%) 20 (35,09) 22 (12,36) 3,80 (1,9 - 7,7) 0,0001
CC (%) 37 (64,91) 156 (87,64)
TT (%) 0 ( 0 ) 0 ( 0 )
Risk Factors Casos Controles OR* (95%IC) p**
Mean Age (±SD) 35,93 ± 8,74 35,04 ± 10,55 _ _
Sex
Male (%) 39 (68,4) 103 (57,9) 1,58 (0,8 – 2,97) 0,15
Female (%) 18 (31,6) 75 (42,1)
Number (%) with hipertension 12 (21,1) 27 (15,2) 1,49 (0,7 - 3,2) 0,3
Number (%) without hypertension 45 (78,9) 151 (84,8)
Number (%) smokers 13 (22,8) 16 (9,0) 2,99 (1,33 - 6,7) 0,006
Number (%) no smokers 44 (77,2) 162 (91,0)
Mean (±SD) Fibrinogen (mg dL-1
) 398,4 ± 147,8 345,8 ± 112,1 _ _
*Odds Ratio (OR) and 95% Confidence Interval (CV) and
**p values were calculated by χ2-test, p significant < 0,05
_: Data not applicable.
Page 17 of 16
http://mc.manuscriptcentral.com/cbf
Cell Biochemistry & Function
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960




















