Toward a Puerto Rican Popular Nosology: Nervios and Ataque de Nervios
28
PETER J. GUARNACCIA, ROBERTO LEWIS-FERN ´ ANDEZ, AND MELISSA RIVERA MARANO TOWARD A PUERTO RICAN POPULAR NOSOLOGY: NERVIOS AND ATAQUE DE NERVIOS ABSTRACT. This paper is about naming illnesses—about who determines what cate- gories are used and the implications of these determinations. The central concerns of medi- cal/psychiatric anthropology have been to understand popular categories of and systems for classification of illness, to examine the relationship of illness categories to cultural under- standings of the body, and to interpret the role of categories of illness in mediating between the personal and social spheres. At the same time, the paper also discusses the interplay of popular categories and psychiatric diagnoses. This paper examines the multiple experi- ences of nervios among Puerto Ricans in Puerto Rico and New York City. Our contention is that nervios is more than a diffuse idiom of distress, and that there are different cate- gories and experiences of nervios which provide insights into how distress is experienced and expressed by Puerto Ricans and point to different social sources of suffering. The data in this paper come from the responses to a series of open-ended questions which tapped into people’s general conceptions of nervios and ataques de nervios. These questions were incorporated into follow-up interviews to an epidemiological study of the mental health of adults in Puerto Rico. The results suggest ways to incorporate these different categories of nervios into future research and clinical work with different Latino groups in the United States and in their home countries. KEY WORDS: ataques de nervios, culture and diagnosis, nervios, Puerto Ricans, social sources of suffering All men have the stars, ... but they are not the same things for different people. For some, who are travelers, the stars are guides. For others, they are no more than little lights in the sky. For others, who are scholars, they are problems. For my businessman they were wealth. But all these stars are silent. The Little Prince, Antoine de Saint Exup´ ery, 1971 (104). This paper is about naming illnesses—about who determines what categories are used and the implications of these determinations. The central concerns of med- ical/psychiatric anthropology have been to understand popular categories of and systems for classification of illness, to examine the relationship of illness categories to cultural understandings of the body, and to interpret the role of categories of illness in mediating between the personal and social spheres (Scheper-Hughes and Lock 1987; Good 1994). Medical anthropologists have examined the relationship between popular categories of illness and biomedical categories of disease, both in terms of the different understandings of experience incorporated in these different Culture, Medicine and Psychiatry 27: 339–366, 2003. C 2003 Kluwer Academic Publishers.
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Toward a Puerto Rican Popular Nosology: Nervios and Ataque de Nervios

P1: IAZPP940-medi-469946 MEDI.cls August 11, 2003 11:42
PETER J. GUARNACCIA, ROBERTO LEWIS-FERNANDEZ,
AND MELISSA RIVERA MARANO
TOWARD A PUERTO RICAN POPULAR NOSOLOGY:NERVIOSAND ATAQUE DE NERVIOS
ABSTRACT. This paper is about naming illnesses—about who determines what cate-gories are used and the implications of these determinations. The central concerns of medi-cal/psychiatric anthropology have been to understand popular categories of and systems forclassification of illness, to examine the relationship of illness categories to cultural under-standings of the body, and to interpret the role of categories of illness in mediating betweenthe personal and social spheres. At the same time, the paper also discusses the interplayof popular categories and psychiatric diagnoses. This paper examines the multiple experi-ences ofnerviosamong Puerto Ricans in Puerto Rico and New York City. Our contentionis thatnerviosis more than a diffuse idiom of distress, and that there are different cate-gories and experiences ofnervioswhich provide insights into how distress is experiencedand expressed by Puerto Ricans and point to different social sources of suffering. The datain this paper come from the responses to a series of open-ended questions which tappedinto people’s general conceptions ofnerviosandataques de nervios. These questions wereincorporated into follow-up interviews to an epidemiological study of the mental health ofadults in Puerto Rico. The results suggest ways to incorporate these different categories ofnerviosinto future research and clinical work with different Latino groups in the UnitedStates and in their home countries.
KEY WORDS: ataques de nervios, culture and diagnosis, nervios, Puerto Ricans, socialsources of suffering
All men have the stars,. . .but they are not the same things for differentpeople. For some, who are travelers, the stars are guides. For others,they are no more than little lights in the sky. For others, who arescholars, they are problems. For my businessman they were wealth.But all these stars are silent.
The Little Prince, Antoine de Saint Exup´ery, 1971 (104).
This paper is about naming illnesses—about who determines what categories areused and the implications of these determinations. The central concerns of med-ical/psychiatric anthropology have been to understand popular categories of andsystems for classification of illness, to examine the relationship of illness categoriesto cultural understandings of the body, and to interpret the role of categories ofillness in mediating between the personal and social spheres (Scheper-Hughes andLock 1987; Good 1994). Medical anthropologists have examined the relationshipbetween popular categories of illness and biomedical categories of disease, both interms of the different understandings of experience incorporated in these different
Culture, Medicine and Psychiatry27: 339–366, 2003.©C 2003Kluwer Academic Publishers.

P1: IAZPP940-medi-469946 MEDI.cls August 11, 2003 11:42
340 P.J. GUARNACCIA, R. LEWIS-FERNANDEZ, AND M.R. MARANO
kinds of category systems and in terms of the different social consequences ofunderstanding distress and suffering through these different schemata (Kleinman1988; Rubel et al. 1984).
In this paper, we examine the multiple experiences ofnerviosamong PuertoRicans in Puerto Rico and New York City. Although we are concerned aboutdelineating the specificity of these experiences ofnervios, we also contend thatour approach is applicable across syndromes and cultural groups. Our contentionis thatnervios is more than a diffuse idiom of distress; that there are differentcategories and experiences ofnervioswhich provide insights into how distress isexperienced and expressed by Puerto Ricans and point to different social sourcesof suffering (Kleinman et al. 1997). We propose that these different ways of talkingaboutnerviosare systematized, not into discrete Linnaean classification schemata,but rather into “fuzzy sets” (White 1982:74–75). We propose calling this schemaa “popular nosology of suffering,” for we contend that this kind of schema is notjust important for analytic purposes, but may also provide the basis for alternativepraxis in mental health and other social arenas to alleviate the distress of thosewho experiencenerviosin its varied forms.
We also want to clarify that the experiences ofnervioswe discuss are notuniquely Puerto Rican, but are shared among many Latin American cultures. Atthe same time, theremaybe particular inflections tonerviosamong Puerto Ricansand other Latinos from the Caribbean, which distinguish them from the experiencesof nerviosamong Mexicans and Central and South Americans (Guarnaccia andFarıas 1988). However, as we illustrate with our discussion of the emergence ofthe term “Puerto Rican Syndrome” in the psychiatric literature of the 1960s, notall attempts to identify cultural issues in mental health are benign. Our purpose inthis paper is to propose a popular nosology based on our research among PuertoRicans which could serve as a model for cross-cultural mental health research andpractice.
The study of how cultural groups categorize illness has long been a central con-cern in anthropology (Evans-Pritchard 1937; Frake 1961). There is a widespreadhuman tendency to use classification systems as a way to both understand and actin the world. Our work was influenced by Geertz’s argument that a major goal ofanthropology is to describe experience from “the native’s point of view” (Geertz1983). We see our research as contributing to the development of a Puerto Ricanethnopsychiatry. We draw methodological support from Gaines’ (1992) culturalconstructivist approach to studying folk/popular and professional psychiatrieswhich argues that all these systems are equally cultural and should be consideredequivalent “ethnopsychiatries.” Given that no system has an inherent claimto greater ontological reality, Gaines argues that the focus of analysis shouldbe on experience-near realities in experience-near terms such as suffering. Inaddition, each ethnopsychiatry is understood to express its respective culture. In

P1: IAZPP940-medi-469946 MEDI.cls August 11, 2003 11:42
TOWARD A PUERTO RICAN POPULAR NOSOLOGY 341
this view, ethnopsychiatric nosologies are products of cultural processes whichchange over time as human interactions create and recreate ethnopsychiatricrealities. More specifically, our approach takes Good’s (1994) interpretive andcritical approach to studying illness categories across cultures as its startingpoint.
[I]llness categories can be understood as images which condense fields of experience,particularly of stressful experience. And they can be understood as core symbols in a seman-tic network, a network of words, situations, symptoms, and feelings which are associatedwith an illness and give it meaning for the sufferer. The meaning of an illness term is gener-ated socially as it is used by individuals to articulate their experiences of conflict and stress,thus becoming linked to typical syndromes of stresses in the society. (Good 1977:39–40)
In analyzing these categories ofnervios, we start with experience-near descrip-tions of these categories and then discuss the larger frameworks of social andcultural meanings which surround them. We utilize the frameworks provided byGood and Gaines to propose a way of linking Puerto Rican popular terms foremotional distress into a schema that can inform anthropology and mental healthpractice.
PREVIOUS WORK ON LATINO ILLNESS CLASSIFICATION
The development of a Puerto Rican popular nosology builds on previous work onLatino cultural models of mental health problems. Over twenty years ago, Newton(1978) proposed a Mexican-American emic model of mental illness based on qual-itative interviews with 23 subjects who were part of a larger study to investigateMexican Americans’ underutilization of mental health services. Newton system-atized the families’ understandings of mental illness into a model (see Table I).
He argued that the first major distinction was between an emotional problem,where emotional control and the persistence of problems are key factors, and amental problem, where mental functioning and violent behavior determine thedegrees of severity of the problem. Problems ofnerviosfigured prominently onboth sides of this divide. Unfortunately, the model was never developed furtheron larger or more diverse Latino samples, nor were the clinical implications ofusing this system with Mexican American clients developed. However, this schemaprovides a useful reference point for our work.
Harwood (1977) provided another schema for diagnosis within the frameworkof espiritismo, a form of religious healing and practice among Puerto Ricans bothon the Island and the mainland (see also Garrison 1977). Harwood’s study ofespiritismoin New York City was explicitly carried out under the sponsorshipof a community health center whose directors sought to make the center respon-sive to the needs of the surrounding Latino community. Thus, the developmentof ethnopsychiatric knowledge was directly relevant to the clinical practice of

P1: IAZPP940-medi-469946 MEDI.cls August 11, 2003 11:42
342 P.J. GUARNACCIA, R. LEWIS-FERNANDEZ, AND M.R. MARANO
TABLE IMexican American Emic Model of Mental Illness
Condition Degree Symptoms Treatment
Minor: Worries, hurt Self-helptemporary, feelings, tensionscan be endured,can be handled
Emotional Nervous (nervioso) Seek help;Problem worried, jittery talk it out with a(Problema mildly depressed relative, friend,Emocional) maybe a
severe depression, physiciandesperation(desesperado),or hysteria
Serious: No emotional control See a physician,persistent cannot cope, perhaps then apervasive feel like exploding psychotherapistcannot solvealone
Mentally ill Mind “snaps/clicks,” “Mental help”suicide attempt, psychotherapist“nervous crisis”(crisis nerviosa)“attack of nerves”(ataque de nervios)
MentalDisorder Crazy (loco) Psychotherapist(Problema harmless medication;Mental) partial cure
Insane Violent, bizarre, Institutionalization;homicidal behavior no hope of curecomplete withdrawal
Note: N = 23 Mexican Americans.Adapted from: Newton, Frank. 1978. The Mexican American Emic System of Mental Illness:An Exploratory Study. InFamily and Mental Health in the Mexican American Community(Monograph 7), J.M. Casas and S.E. Keefe, eds., p. 82. Los Angeles: Spanish Speaking MentalHealth Research Center.
providers at the center. Of particular relevance to our paper is Harwood’s delin-eation of the etiological categories of Spiritist diagnosis (see Table II).
In contrast to the kinds of diagnostic categories presented by the Mexican-American informants which describe certain kinds of feelings and behaviors, theSpiritist categories are based on different spiritual causes of illness.
Comparing these two nosological systems provides several insights. Whereassome diagnostic categories are based on certain core symptoms and aredescriptiveof particular types of experiences, others are based on shared causes of illness and

P1: IAZPP940-medi-469946 MEDI.cls August 11, 2003 11:42
TOWARD A PUERTO RICAN POPULAR NOSOLOGY 343
TABLE IIEtiological Categories in Spiritist Diagnosis
Etiological Category Implied Spiritual Cause
1. Envidia(envy) The unexpressed envy of incarnate spirits in close association withthe victim
2. Brujerıa (sorcery) A disembodied spirit sent to harm the victim by an enemy workingin league with a spiritist
3. Mala influencia A disembodied spirit of low rank seeking to be “given light”(evil influence)
4. Facultades(faculties) Spirits of various ranks who possess the body of a personinsufficiently trained in controlling such seizures
5. Prueba(test or trial) a. Protective spirits who test a person while he or she isdeveloping faculties
b. God-predestined trials in a person’s life6. Cadena(chain) The spirit of a deceased relative or other associate from the past
who has done some misdeed7. Castigo(punishment) Misguided spirits allowed to beset a victim who has neglected his
relationship with his spiritual protectors
From: Harwood, Alan. 1977.Rx: Spiritist as Needed. p. 94. New York: Wiley-Interscience
areetiological in nature (Guimera 1978; Bibeau 1981; Good and Good 1982).Some diagnoses focus on internal experiences of the person, whereas others markthe interactions between the person and important others in the society or withthe spiritual world. Some ethnopsychiatric categories reflect reactions to stressfulexperiences which can be resolved by the person him/herself or with the help ofclose others, whereas other experiences are more enduring and less controllable(see also Rogler and Hollingshead 1985; Koss-Chioino 1992). These dimensionsare useful in thinking about different kinds ofnerviosand in understanding theirrelationship to biomedical categories and we refer to them in our discussions of ourown study. The Spiritist diagnostic framework also reminds us that even within acultural group such as Puerto Ricans, there are multiple popular nosologies whichexist in relation to each other and to the frameworks of biomedicine.
THE MISUSE OF POPULAR CATEGORIES: THE CASE OF THE “PUERTO
RICAN SYNDROME”
The use of popular categories does not always provide a more culturally meaningfulperspective on illness and suffering in a culture. The history of the discussionof ataques de nerviosin the psychiatric literature illustrates this point. Early inthe writing on ataques denervios the label of “Puerto Rican Syndrome” wasused to refer to these phenomena, usually by military psychiatrists attached toUS Army recruiting and training stations in Puerto Rico (Roberts de Ram´ırez deArellano et al. 1954; Rubio et al. 1955). Puerto Rican and American psychiatrists

P1: IAZPP940-medi-469946 MEDI.cls August 11, 2003 11:42
344 P.J. GUARNACCIA, R. LEWIS-FERNANDEZ, AND M.R. MARANO
responding to the growing professional use of the label in the 1960s reacheddiverse opinions about its appropriateness. But the majority concluded that theseexpressions of distress denoted something uniquely Puerto Rican, which renderedthem worthy of serious attention (Fern´andez-Marina 1961; Rothenberg 1964).The more disturbing implication of this label, however, was that there was somedefect in Puerto Rican character which led Puerto Ricans to express distress in thisfashion (De la Cancela et al. 1986). Unfortunately, both the label and the focuson the problem lying in Puerto Rican character have continued to the present inthe responses of medical personnel in urban US contexts to these expressions ofdistress by Puerto Ricans and other Latinos, as well as in the informal diagnosticpractice of some psychiatrists and psychologists in Puerto Rico.
Ironically, one setting where the label seems to survive today is among mentalhealth professionals on the Island, in the form of the spoken acronym “PRS,” invari-ably pronounced in English—“pea are ess”—even when speaking in Spanish. Thisexpression is especially popular among residents in psychiatry training programsin Puerto Rico, but it is also employed by some established psychiatrists and psy-chologists, whose use of the term sanctions it for the next generation of clinicians.The settings in which it emerges are strictly informal, verbal and extra-official.The expression signals the existence of a kind of conspiratorial familiarity amongparticipants, an understanding that formal categories have been transcended andmore basic understandings are being discussed which perhaps do not conform tostrict professional standards. Although superficially derogatory and condemning,the label is not infrequently applied with some degree of affection for the behaviorreferred to, and even a sense of kinship, especially when the speaker is also PuertoRican. Implied is the notion of a shared weakness between the labeler and theone labeled, which the latter has had the misfortune, ignorance, mischievousness,or obduracy to succumb to, a meaning highlighted by the tone of irony or hu-mor that typically underlines the comment. An accompanying notion is that thebehavior denoted is somehow inevitable, in that there is something about beingPuerto Rican that predisposes one to the appearance of “el PRS.” Additionally,the term can even evoke a judgment of the behavior as maliciously funny, con-stituting a kind of resistance against an overly serious and ordered view of theworld.
We would argue that these labels say more about the reactions of the labelers tobehavior from which they seek to divorce themselves (with poignant ambivalencein the case of the Puerto Rican clinicians), than they do to help to explain thephenomena they describe on their own terms or in relation to biomedical categories.The use of the term “Puerto Rican Syndrome” and its modern equivalent “PRS”has impeded development of an understanding of these phenomena by researchersand health professionals and has led to a justifiable defensiveness among manyPuerto Ricans concerning studies which explore the differences in the ways Puerto

P1: IAZPP940-medi-469946 MEDI.cls August 11, 2003 11:42
TOWARD A PUERTO RICAN POPULAR NOSOLOGY 345
Ricans and other Latinos express distress compared to Anglo populations on themainland. For the Puerto Rican clinicians who employ it, the term unfortunatelysignals the additional burden of having to struggle with an internalization of thenotion of defective Puerto Rican character, which tars them with the same brushas their patients. As such, the label and its use constitute part of the colonialdomination of the Island by the United States, as evidenced by the fact that theoriginal formulation of the concept of “Puerto Rican Syndrome” occurred in thecontext of the forced incorporation of young Puerto Rican men into the US military,and that the label is in English and has no Spanish equivalent.
The early psychiatric writings onataque de nervios, and the clinical labelsthat resulted from them, clearly fit what Thompson (1995) characterizes as the“othering” of Puerto Ricans. Turningataquesinto the “Puerto Rican Syndrome”effected a transformation from the anger and resistance implicit in the experiencesof the young Puerto Rican army recruits who invoked this idiom of distress intoa proposed defective feature of Puerto Ricanness. In fact, the culturally appropri-ate labels ofataque de nerviosandmal de pelea(“fighting sickness,” denotingataques particularly characterized by outwardly aggressive behavior) are nearlyabsent from the initial descriptions of the phenomenon (for a notable exception,see Roberts de Ram´ırez de Arellano et al. 1954). One of the goals of this paper isto start from the categories people in Puerto Rico use to communicate their emo-tional distress and build a nosological system from them, rather than imposing orinventing categories. We seek to take seriously both the local categorizations ofemotion and the social experiences which produce them.
METHODS OF ANALYSIS
The genesis of the research on different experiences ofnerviosreported in thispaper began with the inclusion of a single question identifying those who hadexperienced anataque de nerviosin an epidemiological study of the mental healthof the Puerto Rican population. The details of this study and the inclusion of thequestion onataques de nerviosare provided in a previous paper by Guarnaccia andcolleagues (1993). Briefly, after preliminary work onataques de nervioswith theBehavioral Sciences Research Institute at the University of Puerto Rico MedicalSchool, we added a question to identify people who had experienced anataquede nerviosto the Diagnostic Interview Schedule (DIS), a standardized psychiatricdiagnostic interview (Robins et al. 1981) being used in the Puerto Rico DisasterStudy (Canino et al. 1987). The question was added to the Somatization section ofthe DIS, and people were asked whether they had experienced anataque, and if theyhad, to briefly describe the symptoms and context to the interviewer. This studywas based on a sampling frame which included the entire population of PuertoRico, thus making it representative of the Island. Of the 912 people interviewed,

P1: IAZPP940-medi-469946 MEDI.cls August 11, 2003 11:42
346 P.J. GUARNACCIA, R. LEWIS-FERNANDEZ, AND M.R. MARANO
TABLE IIIRelationship Between Reports ofataque de nerviosand Socio-demographic Variables
Demographic No Ataque deVariables Ataque Nervios
N = 912 767 (84%) 145 (16%)Sex
Male 348 (45%) 41 (28%)∗∗Female 419 (55) 104 (72)
Age17–24 189 (25%) 22 (15%)∗∗25–44 344 (45) 61 (42)45–68 234 (30) 62 (43)
Education< High school 372 (48%) 96 (66%)∗∗High school+ 395 (52) 49 (34)
Marital StatusMarried 379 (49%) 67 (46%)∗∗Formerly married 134 (18) 43 (30)Never married 254 (33) 35 (25)
Employment StatusOut of Labor Force 392 (52%) 91 (63%)∗Unemployed 140 (18) 26 (18)Employed 225 (30) 28 (19)
Chi-square was used to establish if differences were significant for eachdemographic variable.∗ p < 0.05.∗∗ p < 0.01.
145 people, or 16 percent, reported having had anataque de nerviosduring theirlifetime (see Table III).
Experiencing anataque de nervioswas strongly associated with meeting criteriafor a range of anxiety and depression diagnoses (Guarnaccia et al. 1993) (seeTable IV).
Given the large number of people who reported anataque de nerviosand therepresentative nature of the sample, we saw this as a valuable opportunity to ex-plore the experiences ofataquesandnerviosmore broadly and thoroughly. Wedeveloped a detailed follow-up interview (structured on the Explanatory ModelInterview Catalogue [EMIC] designed by Weiss and colleagues [1992] on the basisof Kleinman’s [1980] Explanatory Model framework) to explore the experiencesof ataque de nerviosamong Puerto Ricans. This follow-up interview containedsections which discussed general ideas about various forms ofnervios(being anervous person, suffering from nerves, and having anataque de nervios). We hadalready identified these ways of talking aboutnervios in clinical ethnographicwork that Guarnaccia and Lewis-Fern´andez had previously carried out in com-munity mental health programs in the Boston area. The follow-up interview alsocollected descriptions of specific experiences ofataques de nervios, help-seeking

P1: IAZPP940-medi-469946 MEDI.cls August 11, 2003 11:42
TOWARD A PUERTO RICAN POPULAR NOSOLOGY 347
TABLE IVRelationship Between Reports ofataque de nerviosand Psychiatric Diagnoses
Psychiatric No Ataque de OddsDiagnoses Ataque Nervios Ratio
N = 912 767 (84%) 145 (16%)Depression (5%) 19 (2%) 29 (20%) 9.84Dysthymia (12%) 67 (9%) 40 (28%) 3.63Generalized Anxiety (18%) 108 (14%) 55 (38%) 3.73Panic Disorder (2%) 3 (0.4%) 13 (9%) 25.08Posttraumatic Stress Disorder (6%) 29 (4%) 25 (17%) 5.30Any Affective Disorder 49 (6%) 43 (30%) 6.18Any Anxiety Disorder 109 (14%) 58 (40%) 4.02Any DIS Disorder 214 (28%) 91 (63%) 4.35
for ataques, evaluations of the severity ofataques, and perceived causes of theseexperiences (Guarnaccia et al. 1996).
In the follow-up study, we attempted to interview all of the people who hadreported anataque de nerviosin the Puerto Rico Disaster Study (N = 145). We alsoadded a comparison sample which consisted of either people who had experienceda panic attack but not anataque de nervios(N = 17) or people who had not hadeither of these experiences (N = 13). The follow-up sample included people fromthe entire island of Puerto Rico, both from large cities and small towns. Giventhe social characteristics of those experiencingataques de nervios, the follow-upsample over-represented women over 45 with less than a high school education whowere divorced or widowed (Guarnaccia et al. 1993). We interviewed 121 people inthe follow-up study, 79 of whom reported having experienced at least oneataquede nerviosand 42 who reported not having this experience (see Table V).
The data in this paper come from the responses to a series of open-ended ques-tions which tapped into people’s general conceptions ofnerviosandataques denervios. These questions are detailed in Appendix A in Spanish, followed bytheir English equivalents. The interview was developed in Spanish by the firsttwo authors of this paper and their collaborators at the Behavioral Sciences Re-search Institute. The interview team included the first author and three PuertoRican interviewers with long research experience in community studies of mentalhealth. The questions focus on three categories ofnervioswhich we had identifiedas important through preliminary clinical ethnography (Guarnaccia et al. 1989;Lewis-Fernandez 1995):ser nervioso(being a nervous person);padecer de losnervios(suffering from nerves); andtener ataques de nervios(having nervous at-tacks). We consistently asked all respondents, both those with and withoutataques,to describe a person who fit these categories, to speculate on the causes of theseexperiences, and to discuss what kinds of help a person with these experiencesmight receive.

P1: IAZPP940-medi-469946 MEDI.cls August 11, 2003 11:42
348 P.J. GUARNACCIA, R. LEWIS-FERNANDEZ, AND M.R. MARANO
TABLE VSocial Characteristics ofataque de nerviosStudy Sample
Social Characteristics No Ataque Ataque
N = 121 N = 42 N = 79Sex
Male 15 (36%) 65 (20%)∗∗Female 27 (64) 63 (80)
Age< 29 11 (25%) 9 (12%)∗∗30–49 19 (43) 31 (40)> 50 12 (32) 39 (48)
Education< High School 19 (46%) 48 (61%)∗∗High School 23 (54) 31 (39)
Chi-square was used to establish if differences were significantfor each demographic variable.∗ p < 0.05.∗∗ p < 0.01.
Responses to these questions were grouped according to the different categoriesof nerviosusing a text analysis package. These were read by two trained, bilin-gual/bicultural research assistants (including the third author), who provided sum-maries of the responses for all respondents, for men and women separately, and forthose who had and had not had anataque de nervios. Thus we were able to look atoverall understanding ofnerviosas well as examine differences in understandingsof these categories by gender and by degree of experience withnervios.
WAYS OF BEING NERVOUS: EXPERIENCES OFNERVIOSAND ATAQUE DE NERVIOS
The different kinds ofnerviosrepresent complex physical, emotional, and socialexperiences that occur simultaneously on multiple levels.Nerviosoccur in responseto stressful social events and are commentaries on a social world out of control.Although much of this section focuses on distinguishing among “being a nervousperson,” “suffering from nerves,” and having “nervous attacks,” there are also keysimilarities among these experiences. No one feature of any of these experiencesuniquely defines it; rather it is the sum total of the experience which distinguishesit from other experiences. Whereas these kinds of “somatopsychosocial” experi-ences occur throughout the world in different forms, the particular configurationof experiences makes them fit within specific sociocultural contexts.
These expressions and the experiences which they describe are not universal inPuerto Rico. They are powerful idioms invoked much more frequently by workingclass and poor individuals, although they are familiar to most Puerto Ricans. Theyare also particularly prominent forms of expression for the generation of Puerto

P1: IAZPP940-medi-469946 MEDI.cls August 11, 2003 11:42
TOWARD A PUERTO RICAN POPULAR NOSOLOGY 349
Ricans who lived through the transition from an agrarian to an industrial societyand who came of age in the post-World War II period. This is also the generationthat migrated in large numbers to New York City. We will return to these issuesafter describing the different forms ofnerviosand identifying the social sourcesof these experiences.
These experiences ofnerviosalso span the range from expected responses toupsetting life events, to signs of vulnerability to emotional problems, to expressionsof mental illness. The terms “normal” and “abnormal” complicate as much asthey illuminate this discussion. It is clear that these terms are relative ones thatmust be understood within their cultural context, and that they carry strong moraljudgments as well (Benedict 1934; Good 1994). These different expressions ofnerviosare often responses to significant pain, suffering, and social loss—in thissense they are responses to extreme and exceptional occurrences. But that does notnecessarily make them “abnormal,” because these responses may be the way oneshould respond to suffering within the culture. What could be considered abnormalinstead, for example, may be controlling one’s emotions in the face of tragedy ordeath.
The “normality” or appropriateness of these expressions has always been con-tested within Puerto Rican culture according to the positions taken by participantsaround issues of class, gender roles, and the influence of education on behavior.What may be considered normal in a working class woman in her ruralbarrio—such as, prototypically, having anataque de nerviosduring her husband’s funeral—may be judged as the sign of impending mental imbalance in a wealthy man froma prominent family in a similar setting of acute grief. Given the particular socialexpectations determining such a person’s behavior, the dramatic expressiveness oftheataquemay appear quite outside the normal.
What seems to us more important is how to judge when the suffering marked bydifferent types ofnerviosis beyond the expected or “normative,” which may serveas a better term here. One measure may be when the pain is significant enough thatit requires outside help, particularly professional help. Even this determination is asmuch social as clinical, as the growing literature on the increasing medicalizationof social life indicates.
“BEING A NERVOUS PERSON” (SER NERVIOSO)
“Being a nervous person” (ser nervioso) usually starts in childhood, sometimes asa result of suffering or traumatic experiences, or as an inherited vulnerability thatmakes the person more prone to being affected by the normal stresses of everydaylife. In this latter sense, nervousness can run in families or is said to be hereditary,and the affected child is said to “llevarlo en la sangre” (“carry it in the blood”) orto “ser nervioso de nacion” (“be nervous by constitution,” lit. nation, race). This
P1: IAZPP940-medi-469946 MEDI.cls August 11, 2003 11:42
350 P.J. GUARNACCIA, R. LEWIS-FERNANDEZ, AND M.R. MARANO
explanation is especially evoked in the absence of any clearly identifiable socialprecipitants for nervousness in a child and the presence of other family memberssuffering from some form ofnervios.
Respondents reported that severe family traumas, such as deaths in the familyor abusive parents, could cause someone to becomenervioso. Some felt that ner-vousness could develop in the womb, even in the absence of affected relatives.Although people often referred to this as “hereditary,” what they described wasthat if the mother suffered physical or emotional abuse while she was pregnant,drank excessively, or used drugs, or experienced severe nutritional deprivation, thiscould result in the child becoming a “nervous person.” Once someone isnerviosothey tend to remain so for the rest of their lives, although most people can controlthis condition with the help and support of family members and others. However,people who arenerviosoare vulnerable to upsetting events and more likely torespond to them in severe ways.
People who arenerviosohave more life problems, what Finkler (1994) hasreferred to as “life’s lesions,” than others, and often have great difficulty in solvingtheir problems. They worry more than others. The common symptoms that goalong with “being a nervous person” include trembling and crying more thanothers, talking and moving one’s hands rapidly, and biting one’s nails a lot. Peoplewho arenerviosoare more prone to headaches and stomachaches. They startlemore easily than others and are also quicker to lose their tempers. Men were morelikely than women to see someone who isnerviosoas more prone to anger andviolence. Men also associated becomingnerviosowith the traumas of war. Womenwere more apt to see serious family and economic problems as sources of becomingnerviosoin adulthood.
Family members were seen as the primary source of help for someone who isnervioso, but it was also clear that “being a nervous person” has become med-icalized in Puerto Rico. The key thing family members can do is to help theperson lead a calm life (una vida tranquila), which is highly valued in PuertoRico (Lewis-Fern´andez 1998). The major gender difference in help-seeking wasthat women knew and recommended a wide range of home remedies, particularlyherbal teas, which men did not report at all. Spiritual help was also viewed asuseful, again because it aided the person in finding tranquility. Interestingly, re-spondents both recommended and sought help more from priests and ministersthan fromespiritistasor santeros, who have received much more anthropologicalattention in studying spiritual healing in Puerto Rico (Garrison 1977; Harwood1977; Koss-Chioino 1992). People strongly recommended professional help andfelt that therapy and counseling from psychologists or psychiatrists would bevaluable. They also felt that medications would be helpful. People who sufferedfrom some kind ofnervioswere even more likely to recommend professionalhelp.

P1: IAZPP940-medi-469946 MEDI.cls August 11, 2003 11:42
TOWARD A PUERTO RICAN POPULAR NOSOLOGY 351
In general, “being a nervous person” is viewed as a chronic condition that eitherone is born with or that occurs as the result of childhood traumas. Although beingnerviosois difficult to control, it can be controlled through family support andoutside help. However, people who arenerviosoare more vulnerable to stressfullife events and more likely to break down under the weight of accumulating lifeproblems. It is thisenhanced vulnerabilitythat is a critical aspect of “being anervous person.”
“SUFFERING FROM NERVES” (PADECER DE LOS NERVIOS)
Padecer de los nerviosis more of an illness thanser nervioso, and was mostfrequently associated with depression by our respondents. It affects the body andmind and is seen as more debilitating. Whereas “suffering from nerves” is morelikely to develop in adulthood as the result of an overburdening series of “life’slesions,” many respondents felt that the vulnerability to suffering from nerves washereditary or congenital, much in the same way that people described “being anervous person.”
People who suffer from nerves experience a sense of having too many thoughtsthat overwhelm them. They cannot stay still and are always moving and trembling,and they talk very fast. Their personalities are affected as well; people who sufferfrom nerves are described as erratic, very sensitive to stressors, often nervous andfearful, and more prone to explosive anger. This constellation of experiences sharesfeatures with the evolving psychiatric diagnosis of atypical depression (Liebowitzet al. 1984).
In many ways, the causes ofpadecer de los nerviosare similar toser nervioso.The differences are that the stressful events occur more in adulthood, are moresevere, and particularly come together in an overwhelming way. The feeling thatone cannot find a solution to one’s problems was also a key aspect of suffering fromnerves. Women prominently mentioned marital difficulties, as well as concernsabout and conflicts with children. Men and women both mentioned the effects ofwar, although for men it was more often the effects of having gone to war and forwomen concerns over a family member serving in the military. Instead of beingable to “control” their reactions to life’s lesions, a valued attitude of equanimityin most Puerto Rican communities (Lewis-Fern´andez 1998),nerviossufferers feltfrequently “out of control” when faced with significant stressors, displaying morethan the normal share of irritability, sadness, or anxiety.
The seriousness ofpadecer de los nerviosis reflected in the kinds of help respon-dents recommended for someone who suffers from nerves. Whereas respondentssaw support from close family and friends as helpful, the overwhelming major-ity thought that someone who suffered from nerves should get professional help.Doctors can help with the physical damage to the nerves, whereas a psychologist

P1: IAZPP940-medi-469946 MEDI.cls August 11, 2003 11:42
352 P.J. GUARNACCIA, R. LEWIS-FERNANDEZ, AND M.R. MARANO
or psychiatrist can provide therapy and medication to deal with the psychologicalproblems. Respondents also recommended that activities which occupied the per-son would be helpful to keep them from worrying and thinking too much. Sufferingnerves is very difficult to control on one’s own; it requires outside help to manageone’snervios. These recommendations indicate that once someone “suffers fromnerves,” he or she has crossed over into the realm of mental illness; in Newton’s(1978) terms, they have crossed the line from an emotional to a mental disorder.
“NERVOUS ATTACKS” (ATAQUES DE NERVIOS)
Ataques de nerviosare acute, dramatic episodes which occur as the result of amajor stressful event, particularly in the family sphere (for a fuller discussion ofataques de nerviossee Guarnaccia et al. 1996 and Lewis-Fern´andez 1996).Ataquescan happen to anyone who experiences a stressful enough event, although peoplewho are nervous or suffer from nerves are more prone to experience an ataque.Although women are more likely to experience anataque de nervios, men do havethem in the face of upsetting or frightening situations.
Ataquesusually occur directly in response to an upsetting situation and beginwith uncontrollable crying and screaming; people become “hysterical.” Sufferersmay throw things or strike out at others; at this point they are seen as “out of control”both in terms of the intentionality of their behavior and their actual actions. Theataquealso reflects a social world out of control. During theataque de nervios,sufferers may fall to the ground and lie there “as if dead,” or shake as if experiencinga seizure. The whole episode is relatively brief, with a rapid return to the pre-ataquestate, although a period of post-ataqueexhaustion or depression is not uncommon.Afterwards, the person frequently reports little memory of what happened duringtheataque. In severe cases, people may contemplate or even attempt suicide duringtheataquein response to the despair they feel as a result of the event that provokedthe episode.
The classic event which provokes anataqueis unexpected news of the deathof a family member. Both the tragedy of the death and the unexpected nature ofthe news are seen to have a physical as well as emotional force within PuertoRican ethnopsychology. Other events include conflicts between spouses, particu-larly when they threaten divorce, and conflicts between parents and older children,particularly when the children no longer share the same values of family relationsas their parents. In severe cases, the dramatic nature of theataquereflects violencein the relationship.
The appropriate source of help depends greatly on the cause of theataque denerviosand the class and religious characteristics of the person’s social network.When anataqueoccurs at a rural Catholic funeral, the appropriate helpers are fam-ily members, who will protect the person when she falls and then pray over her and

P1: IAZPP940-medi-469946 MEDI.cls August 11, 2003 11:42
TOWARD A PUERTO RICAN POPULAR NOSOLOGY 353
rub her face withalcoholado(alcohol with herbs) to bring her back to conscious-ness. When family conflicts are the source ofataques, both religious counselingand mental health treatments are seen as useful by many Puerto Ricans. If theataquesare thought to have a spiritual cause, several help options are available.An espiritistamay be consulted to mediate with the spirit of a deceased relativewho is bothering the person. Alternatively, in Pentecostal circles the episode maybe seen as a demonic intrusion, and rebuking of the spirit (reprender) in the nameof Jesus Christ may be the preferred course of action. If theataquemarks the wors-ening of a more chronic problem ofnervios, the person may seek or be brought tomental health treatment. For both assessing the relation of theataque de nerviosto mental illness and for deciding on appropriate helpers, social context is critical.
THE SOCIAL SOURCES OF NERVIOS
All the forms ofnerviosare powerful idioms employed primarily by working classand poor Puerto Rican women and men to express personal distress, crises in thefamily, and social deprivation. Describing someone as suffering from the varioustypes of “nerves” simultaneously recognizes bodily pain, interpersonal tensions,and social dislocation. Using the different categories ofnerviosis not only a wayto label certain illnesses in Puerto Rico, it is also a way to talk about certain kindsof persons, their social relationships, and their place in society.
People’s discussions ofnerviosmake clear their recognition of the social sourcesof these conditions while acknowledging the interaction between life experienceand bodily vulnerability. Although the language of heredity is often invoked intalking about the sources ofnervios, it signifies equally a recognition of a socialinheritance as of the influence of genes. Puerto Ricans recognize that physical andemotional deprivation of the developing child takes its toll in a number of ways,including the development ofnervios.
The language ofnerviosalso recognizes the emotional and physical force ofsocial relations to alter one’s nervous system. At another level, people recog-nize that many of life’s lesions, such as family losses, abusive and violent fam-ily relationships, lack of economic resources, and the traumas of sending lovedone’s off to or going to war, can produce major alterations in one’snervios(Finkler 1994). When one talks about one’snervios, one is talking as much aboutone’s life circumstances and need for help as about bodily pains and emotionaldistress.
Nervioshave also become a potent form of commentary for a generation ofPuerto Ricans who have lived through major social transformations of the Islandfrom a more agrarian and rural society to a more industrial and urban one. Much ofthis transformation occurred starting in the late 1940s, during Operation Bootstrap.

P1: IAZPP940-medi-469946 MEDI.cls August 11, 2003 11:42
354 P.J. GUARNACCIA, R. LEWIS-FERNANDEZ, AND M.R. MARANO
Operation Bootstrap was the major program of rapid industrialization of the Islandin the interests of American corporations and Puerto Rican elites, associated witha far-reaching populist campaign of “modernization” (Lewis 1968). The resultantdestruction of the agricultural base of Puerto Rican society led to massive migrationto the cities of San Juan and New York.
On breaking the communicative ties which served him as a means of orientation in thecountry, the migrant dwelling in the slums of San Juan or the ghettos of New York findshimself without points of references for the orientation of his behavior. The result is thephenomenon of alienation: a feeling of impotence and fatalism in the face of the surroundingworld. (Maldonado-Denis 1972:161)
Operation Bootstrap also significantly altered the shape and function of the PuertoRican family. Although the authors do not want to overly romanticize the traditionalPuerto Rican family, the traditional rural family provided important complemen-tary resources to its members, both emotional and instrumental. The destructionof those social networks by the dual processes of industrialization and migrationled to the increase of family dissolution and family violence. One avenue for thisgeneration’s expression of their losses and crises was the various forms ofnervios,which continues as a potent idiom of distress for working class and poor PuertoRicans now in their fifties, sixties, and seventies.
This generation also lived through the significant involvement of Puerto Ricanmen in both the Korean War and the Vietnam War, in which Puerto Ricans servedin much higher proportions than their percentage of the US population. Both thedirect experiences of participation in these wars and the fears for family memberssent overseas to fight were expressed through people’snervios.
Thus the various forms ofnervioshave emerged as multivocal idioms of distressfor a generation of Puerto Ricans affected by particular historical events and trans-formations, both on the Island and more globally. Clearly, not all Puerto Ricans ofthis generation, not even those who are working class or poor, experiencednerviosas a result of these major social changes. Nervios serve to mark a constellation ofvulnerabilities—physical, emotional, social, economic, and political.
AN EXPLORATION OF THE POPULAR NOSOLOGY APPROACH
We illustrate the benefits of linking popular and medical/psychiatric nosologiesin two case histories ofnerviosfrom clinical research at the Hispanic TreatmentProgram of the Anxiety Disorder Clinic at the New York State Psychiatric In-stitute. The Hispanic Treatment Program started in 1990 to serve the large andgrowing Latino community which surrounds the Psychiatric Institute in northernManhattan. Previous studies by Liebowitz and colleagues (Leibowitz et al. 1994;Salman et al. 1998) of the interplay among cultural syndromes, psychiatric disorder

P1: IAZPP940-medi-469946 MEDI.cls August 11, 2003 11:42
TOWARD A PUERTO RICAN POPULAR NOSOLOGY 355
and important life experiences had already made clear that leaving any one of theseaspects out of clinical work distorts understanding significantly. This particular re-search project provided a unique opportunity to look at the complex and interwovennature of these experiences in a systematic fashion. It provides the best evidenceto date of incorporating perspectives from a popular nosology into clinical work.
We developed these case histories from a series of interviews that were part of theresearch program of the Hispanic Treatment Program. The study was designed toprovide a multi-dimensional perspective on the experience ofataques de nerviosand its relationship to anxiety disorders. Subjects were recruited from personsseeking treatment in the Hispanic Treatment Program for anxiety and/or depressionwho were then screened for having had anataque de nervios. New subjects werealso recruited specifically for help with theirataques de nervios; recruitment wasdone through fliers and through referrals from other mental health and medicalservices within the large Columbia University medical system that surrounds thePsychiatric Institute. Overall there were 92 subjects recruited into the study, ofwhom 66 reported having had at least oneataque de nervios. Of this group, 48(70 percent) were Dominican and 18 (30 percent) Puerto Rican, reflecting thechanging Latino mix of Washington Heights (see Lewis-Fern´andez et al. 2002 formore detail on the sample).
The results of three different interviews were used to assess the experiences ofnerviosand develop the profiles we present below. The first was the ExplanatoryModel Interview Catalogue (EMIC), which the authors adapted specifically forthis study of the broad range ofnerviosamong Puerto Ricans and other Latinos.The second interview was the Structured Clinical Interview for Diagnosis (SCID).The SCID is a structured clinical interview designed to standardize clinicians’psychiatric assessments of patients according to DSM criteria. The interviewerswho conducted the EMIC and the SCID were blind to the results of each other’sassessments. The final interview was an integrative interview which took the resultsof both the EMIC and SCID, developed the sequencing and interaction of thecultural experiences with the episodes of psychiatric disorder, and placed them inthe context of important events in the person’s life.
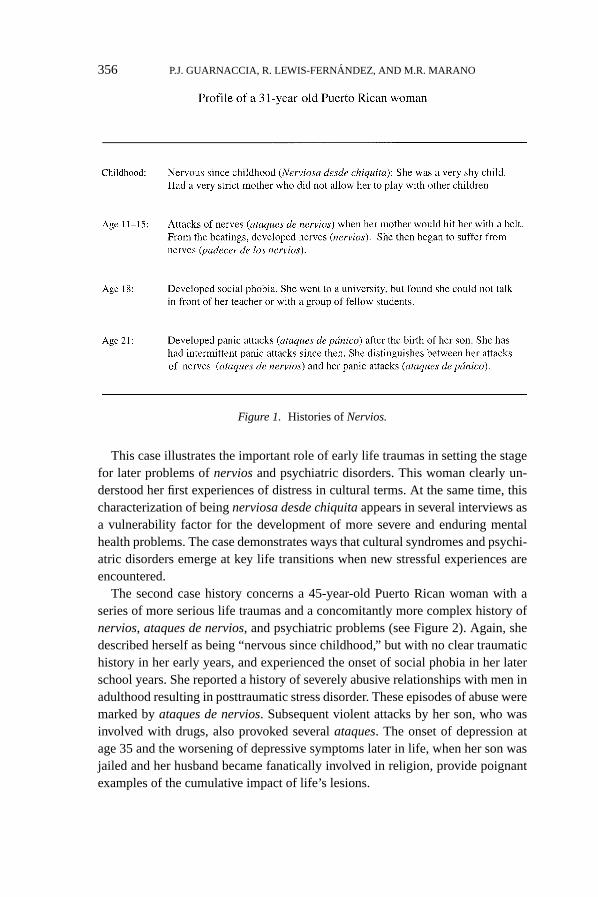
The first case history is of a 31-year-old Puerto Rican woman who had a historyof nervios, ataques de nervios, and anxiety disorders (see Figure 1). She describedherself as “nervous since childhood” because of shyness and because her motherforbade her to play with other children. This cultural identification ofnerviosadesde chiquitaappears to signal vulnerability to later traumas and mental healthproblems. Herataquesbegan in adolescence as the result of beatings from hermother. Her anxiety problems emerged in early adulthood, first appearing as socialphobia during her university studies and then as panic attacks after the birth of herfirst child at age 21. She was quite clear about the differences between herataquesde nerviosand panic attacks.
P1: IAZPP940-medi-469946 MEDI.cls August 11, 2003 11:42
356 P.J. GUARNACCIA, R. LEWIS-FERNANDEZ, AND M.R. MARANO
Figure 1. Histories ofNervios.
This case illustrates the important role of early life traumas in setting the stagefor later problems ofnerviosand psychiatric disorders. This woman clearly un-derstood her first experiences of distress in cultural terms. At the same time, thischaracterization of beingnerviosa desde chiquitaappears in several interviews asa vulnerability factor for the development of more severe and enduring mentalhealth problems. The case demonstrates ways that cultural syndromes and psychi-atric disorders emerge at key life transitions when new stressful experiences areencountered.
The second case history concerns a 45-year-old Puerto Rican woman with aseries of more serious life traumas and a concomitantly more complex history ofnervios, ataques de nervios, and psychiatric problems (see Figure 2). Again, shedescribed herself as being “nervous since childhood,” but with no clear traumatichistory in her early years, and experienced the onset of social phobia in her laterschool years. She reported a history of severely abusive relationships with men inadulthood resulting in posttraumatic stress disorder. These episodes of abuse weremarked byataques de nervios. Subsequent violent attacks by her son, who wasinvolved with drugs, also provoked severalataques. The onset of depression atage 35 and the worsening of depressive symptoms later in life, when her son wasjailed and her husband became fanatically involved in religion, provide poignantexamples of the cumulative impact of life’s lesions.

P1: IAZPP940-medi-469946 MEDI.cls August 11, 2003 11:42
TOWARD A PUERTO RICAN POPULAR NOSOLOGY 357
Figure 2. Histories ofNervios.
This case illustrates the important role ofataques de nerviosin highlightingepisodes of severe distress and trauma within key social relationships. Theseataquesneed to be recognized as clear cries for help in a social world that isprogressively spiraling out of control (Guarnaccia et al. 1996; Lewis-Fernandez1998). Surrounding both of these case histories are larger clusters of social ad-versities which many Puerto Rican and other Latino migrants to New York Cityface: discrimination, poverty, neighborhood violence, unstable employment, andhousing. These broader problems linked to the biographies of these women createthe context for these histories ofnerviosand psychiatric problems.
As a result of our research and clinical experience, we have expanded our un-derstanding of the different experiences ofnerviosinto the following categoriesreflected in the questions in Appendix B. “Being a nervous person since childhood”(ser nervioso desde chiquito) has emerged in a number of the clinical research casesas signaling a particular vulnerability to social distress and psychiatric disorderlater in life. Thus we have added the qualifier “since childhood” to the originalcategory of “being a nervous person” (ser nervioso). We have also distinguishedbetween “suffering from nerves” (padecer de los nervios) as a more chronic expe-rience and “being sick from nerves” (estar enfermo de los nervios) as a more acuteand more serious condition. As an example, these distinctions would parallel thepsychiatric distinction between dysthymia, a chronic and lower intensity form ofdepression lasting two years or longer, and major depressive episode, an acute and

P1: IAZPP940-medi-469946 MEDI.cls August 11, 2003 11:42
358 P.J. GUARNACCIA, R. LEWIS-FERNANDEZ, AND M.R. MARANO
intense depressive episode occurring over a two-week period of intense sadnessand disability.
Finally, we have distinguished betweenataques de nervios, which occur onceor twice in a person’s life, taking place during funerals or other culturally ap-propriate events, andataqueswhich happen frequently. The first kind ofataque,while marking a period of intense suffering, is much less likely to be associatedwith psychiatric disorder. Frequentataques, particularly when accompanied bydissociative experiences and/or suicidal gestures, are much more likely signs ofpsychiatric disorder and people suffering them may benefit significantly from clin-ical intervention. This refinement of our proposal for a popular nosology ofnerviosgrows out of the interaction between epidemiological, clinical and anthropologicalresearch and direct clinical work with people who seek help from the sufferingexpressed through theirnervios. At the same time, we want to emphasize thatthis is a preliminary proposal for further research both to continue to develop thispopular nosology ofnerviosand to test its clinical applicability.
TOWARD A PUERTO RICAN POPULAR NOSOLOGY
I have serious reason to believe that the planet from which the lit-tle prince came is the asteroid known as B-612. This asteroid hasonly once been seen through the telescope. That was by a Turkishastronomer, in 1909. On making his discovery, the astronomer hadpresented it to the International Astronomical Congress in a greatdemonstration. But he was in Turkish costume, and so nobody wouldbelieve what he said.. . .Fortunately, however for the reputation ofAsteroid B-612, a Turkish dictator made a law that his subjects, un-der pain of death, should change to European costume. So in 1920the astronomer gave his demonstration all over again, dressed withimpressive style and elegance. And this time everybody accepted hisreport.
The Little Prince, Antoine de Saint Exup´ery, 1971 (15–16).
In a time when biological psychiatry continues to outpace psychotherapy as a formof clinical practice and social psychiatry as the focus of research, developing analternative mental health nosology built on cultural idioms of distress may be aquixotic proposal. Yet our research and clinical experiences make clear that thesevarious forms ofnerviosare still widely used by some people in Puerto Rican toexpress a range of personal and social suffering.
Much of this suffering is healed in the family context and is most appropriatelyhandled in that realm. However, because of the multiple strains on families, both in-ternally and externally produced, some significant portion ofnerviossufferers need

P1: IAZPP940-medi-469946 MEDI.cls August 11, 2003 11:42
TOWARD A PUERTO RICAN POPULAR NOSOLOGY 359
the help of people outside the family. Religious help, within mainstream Catholicand Protestant churches, in the newer charismatic and Pentecostal churches, andfrom those with spiritual faculties who practice asespiritistasandsanteros, servesas one broad set of resources. Medical and mental health professionals are anotherset of resources widely consulted by and seen as relevant for help withnerviosbya wide range of Puerto Ricans.
We want to end this paper with several arguments for the value of a popularnosology ofnerviosboth for clinical practice and for mental health research. Oneargument for a Puerto Rican popular nosology is that it more closely reflects the“local knowledge” (Geertz 1983) of those who seek care and provides for a form ofcommunication about suffering more immediate to their concerns than psychiatricdiagnoses. By developing and elucidating this popular nosology, researchers andclinicians can more accurately and effectively translate between these cultural id-ioms of distress and medical/psychiatric diagnoses which guide clinical action andintervention (for a fuller discussion of an approach to examining the interface be-tween cultural idioms and psychiatric diagnoses, see Guarnaccia and Rogler 1999).In particular, “psycho-educational” approaches, geared at providing patients withinformation about their diagnoses and treatments in order to maximize treatmentadherence, would clearly benefit from knowledge about local categories of distress.
A corollary of this improved understanding of the translation process betweenthe popular and professional classification systems is a potential reduction in themisdiagnosis of Puerto Rican and other Latino patients presenting withnerviosandataquesto mainstream medical services.Ataquesin particular, due to their seizure-like character, can be confused with various medical conditions with paroxysmicpresentations, such as syncope (loss of consciousness brought on by various causes,including cardiac conduction abnormalities) or epilepsy. In addition, the distinctionbetweenataqueand the psychiatric diagnosis of panic disorder can be subtle—involving clarification of the exact phenomenology of the episode and the issue ofwhether the attack was or was not precipitated—but essential to the proper man-agement of either condition (Liebowitz et al. 1994; Lewis-Fern´andez et al. 2002).Finally,nerviosandataquescan be associated with reports of perceptual distortions(such as hearing one’s name being called when alone or experiencing presences),which are common non-psychotic experiences among Puerto Ricans but whichcan become more frequent and distressing in the context ofnerviosconditions.These distortions can be easily misdiagnosed by clinicians as psychotic processesrequiring unnecessarily drastic interventions, such as intramuscular medication orpsychiatric hospitalization (Lewis-Fern´andez 1996).
Another value of the popular nosology is that it expands therapeutic concernsfrom a narrow focus on lesions in organ systems to a broader focus on life’s lesionsin their personal and social context. Medications and individual therapy can oftenbe quite useful in helping people cope with the pains and sorrows reflected in

P1: IAZPP940-medi-469946 MEDI.cls August 11, 2003 11:42
360 P.J. GUARNACCIA, R. LEWIS-FERNANDEZ, AND M.R. MARANO
different experiences ofnervios. By paying attention tonerviosin the ways wehave defined and described here, it becomes immediately clear that internal andindividual interventions will not suffice, but that clinical interventions will alsoneed to deal with the social sources of suffering, and particularly with the waysthese are mediated through family relationships and interactions. This links clinicalwork to social and community practice on the one hand, and to family interventionson the other. These links are often theoretically recognized but less frequentlyimplemented in practice. A comprehensive therapeutic model fornerviosandataquesshould ideally have access to a wide range of interventions that can beimplemented in diverse combinations and sequences.
A final value of developing a popular nosology is that it stands as a challenge toa narrow medical/psychiatric model (Kleinman 1988). Popular nosologies are onestrategy for challenging the medical/psychiatric hegemony which has developedfor naming and healing human suffering. In contrast to current dominant medicalnosologies, which focus attention on the internal and biological sources of distress,popular nosologies focus on the interpersonal, social, political, economic, andspiritual sources of distress. They present a dynamic, contextual alternative tothe highly bounded, descriptive medical approach. A key characteristic of thePuerto Rican popular nosology we have described is that it defines the realms ofhealth and pathology in the interaction between the coping skills of the person andthe amount of suffering endured, as lying in the borderland between resilience,support, and stress. The full concept ofnerviosencapsulates this tension, playingout its thematic variations in the subtleties of the classification system we haveoutlined. This basic contextuality enables a popular nosology such as the one wehave proposed for Puerto Rican mental health to provide an alternative languageand framework for understanding human suffering and thereby suggest differentforms of intervention to alleviate that suffering.
APPENDIX A
Questions onNerviosandAtaque de Nerviosfrom the EMIC
CREENCIAS GENERALES SOBRE NERVIOS Y ATAQUES DE NERVIOS
(GENERAL CONCEPTIONS OF “NERVES” AND “NERVOUS ATTACKS”)
1. Para Ud., ¿cu´al es la diferencia entre ser nerviosa(o), tener ataques de nervios, ypadecer de losnervios? For you, what is the difference between being “nervous,”having “nervous attacks,” and “suffering from nerves”?
a. ser nerviosa(o)/being “nervous”b. tener ataques de nervios/having “nervous attacks”c. padecer de los nervios/suffering from “nerves”

P1: IAZPP940-medi-469946 MEDI.cls August 11, 2003 11:42
TOWARD A PUERTO RICAN POPULAR NOSOLOGY 361
2. ¿Como describir´ıa Ud. a la persona que . . .How would you describe a personthat. . .
a. es nerviosa?is “nervous”?b. tiene un ataque de nervios?has a “nervous attack”?c. padece de los nervios?suffers from “nerves”?
3. ¿Cual piensa Ud. que es la causa m´as probable de . . .What do you think is themost probable cause of. . .
a. ser nervioso?being “nervous”?b. tener un ataque de nervios?having a “nervous attack”?c. padecer de los nervios?suffering from “nerves”?
9. ¿Una persona que . . .deber´ıa recibir algun tipo de atenci´on? SI DICE SI, ¿Qu´etipo de ayuda debe recibir?Should a person that . . . receive some type of help? IFTHEY SAY YES, What type of help should be received?
a. es nerviosa/is “nervous”b. tiene un ataque de nervios/has “nervous attacks”c. padece de los nervios/suffers from “nerves”
10. ¿Un doctor, un psiquiatra, un psic´ologo, u otro profesional de salud puedeayudar a una persona que . . .Can a doctor, a psychiatrist, a psychologist, or otherhealth professional help a person that. . .
a. es nerviosa?is “nervous”?b. tiene un ataque de nervios?has “nervous attacks”?c. padece de los nervios?suffers from “nerves”?
APPENDIX B
Proposed Questions for AssessingNerviosandAtaques de Nerviosin Clinical andResearch Settings
1. ¿Ha sido usted una persona nervioso(a) desde ni˜no(a)?Have you been “nervous” since childhood?
2. ¿Es usted una persona nerviosa?Are you a “nervous” person?
3. ¿Ha padecido de los nervios alguna vez en la vida?Have you ever suffered from “nervios” in your life?3a. SI DICE SI: ¿Padece de los nervios todav´ıa?
IF YES: Do you still suffer from “nervios” now?4. ¿Ha tenido alguna vez un ataque de nervios?
Have you ever had an “ataque de nervios”?

P1: IAZPP940-medi-469946 MEDI.cls August 11, 2003 11:42
362 P.J. GUARNACCIA, R. LEWIS-FERNANDEZ, AND M.R. MARANO
4a. ¿Cu´antos ataques de nervios ha tenido en su vida?How many “ataques de nervios” have you had in your life?Especifique el n´umero de ataques de nervios:Specify the number of “ataques de nervios”[77= “too many to count”; 88= don’t know; 99=denied, refused]
5. Ultimamente, ¿ha estado enfermo(a) de los nervios?Recently, have you been “ill with nervios”?
(Developed by Roberto Lewis-Fern´andez for use in clinical practice and research.)
ACKNOWLEDGMENTS
The research for this paper was supported by a FIRST Award to Dr. Guarnacciafrom the Division of Biometry and Epidemiology of the National Institute of Men-tal Health [MH45789]. Dr. Guarnaccia was a Visiting Scholar at the Russell SageFoundation, New York, NY, during the conceptual development of this paper. Dr.Lewis-Fernandez was supported by grants from the MacArthur Foundation Mind-Body Network and the Nathan Cummings Foundation. Dr. Rivera was supportedby Project L/EARN at the Institute for Health, Health Care Policy and Aging Re-search and by a Supplement for Underrepresented Minorities in Biomedical andBehavioral Research from the National Institute of Mental Health. The authorswould like to thank Angel Lopez, Project L/EARN intern, for his help in codingthe data for this paper. The cases in this paper come from interviews carried outby Dr. Michael Liebowitz, Professor of Clinical Psychiatry, Columbia Univer-sity College of Physicians and Surgeons, and Director, Anxiety Disorders Clinic,New York State Psychiatric Institute.
REFERENCES
Benedict, Ruth1934 Anthropology and the Abnormal. Journal of General Psychology 10: 59–82.
Bibeau, Gilles1981 The Circular Semantic Network in Ngbandi Disease Nosology. Social Science and
Medicine 15B: 295–307.Canino, Glorisa, H´ector Bird, Patrick Shrout, Matiza Rubio-Stipec, Milagros Bravo, RuthMartınez, Myrna Sesman, Luz M. Guevara
1987 The Prevalence of Specific Psychiatric Disorders in Puerto Rico. Archives of Gen-eral Psychiatry 44: 727–735.
De la Cancela, Victor, Peter Guarnaccia and Emilio Carrillo1986 Psychosocial Distress Among Latinos: A Critical Analysis of Ataques de Nervios.
Humanity and Society 10: 431–447.Evans-Pritchard, E.E.
1937 Witchcraft, Oracles, and Magic among the Azande. Oxford: Oxford UniversityPress.

P1: IAZPP940-medi-469946 MEDI.cls August 11, 2003 11:42
TOWARD A PUERTO RICAN POPULAR NOSOLOGY 363
Fernandez-Marina, R.1961 The Puerto Rican Syndrome. Psychiatry 24: 79–82.
Finkler, Kaja1994 Women in Pain: Gender and Morbidity in Mexico. Philadelphia: University of
Pennsylvania Press.Frake, Charles O.
1961 The Diagnosis of Disease among the Subanun of Mindanao. American Anthropol-ogist 63: 113–132.
Gaines, Atwood D.1992 Ethnopsychiatry. Albany: SUNY Press.
Garrison, Vivian1977 The “Puerto Rican Syndrome” in Psychiatry andEspiritismo. In Case Studies in
Spirit Possession. Vincent Crapanzano and Vivian Garrison, eds., pp. 383–449.New York: Wiley-Interscience.
Geertz, Clifford1983 “From the Native’s Point of View”: On the Nature of Anthropological Understand-
ing. In Local Knowledge: Further Essays in Interpretive Anthropology, pp. 55–70.New York: Basic Books.
Good, Byron J.1977 The Heart of What’s the Matter: The Semantics of Illness in Iran. Culture, Medicine
and Psychiatry 1: 25–58.1994 Medicine, Rationality and Experience: An Anthropological Perspective.
Cambridge: Cambridge University Press.Good, Byron J., and Mary-Jo DelVecchio Good
1982 Toward a Meaning-Centered Analysis of Popular Illness Categories: “Fright Ill-ness” and “Heart Distress” in Iran.In Cultural Conceptions of Mental Health andTherapy. A. J. Marsella and G. M. White, eds., pp. 141–166. Dordrecht, Holland:D. Reidel Publishing.
Guarnaccia, Peter J., and Pablo Far´ıas1988 The Social Meanings of Nervios: A Case Study of a Cen-
tral American Woman. Social Science and Medicine 26: 1223–1231.
Guarnaccia, Peter J., Victor DeLaCancela and Emilio Carrillo1989 The Multiple Meanings of Ataques de Nervios in the Latino Community. Medical
Anthropology 11: 47–63.Guarnaccia, Peter J., Glorisa Canino, Martiza Rubio-Stipec, and MilagrosBravo
1993 The Prevalence of Ataques de Nervios in the Puerto Rico Disaster Study: TheRole of Culture in Psychiatric Epidemiology. The Journal of Nervous and MentalDisease 181: 157–165.
Guarnaccia, Peter J., Melissa Rivera, Felipe Franco, and Charlie Neighbors1996 The Experiences of Ataques de Nervios: Towards an Anthropology of
Emotion in Puerto Rico. Culture, Medicine and Psychiatry 20: 343–367.
Guarnaccia, Peter J., and Lloyd H. Rogler1999 Research on Culture-Bound Syndromes: New Directions. The American Journal
of Psychiatry156: 1322–1327.Guimera, Louis Mallart
1978 Witchcraft Illness in the Evuzok Nosological System. Culture, Medicine andPsychiatry 2:374.
Harwood, Alan1977 Rx: Spiritist as Needed: A Study of a Puerto Rican Community Mental Health
Resource. New York: Wiley-Interscience.

P1: IAZPP940-medi-469946 MEDI.cls August 11, 2003 11:42
364 P.J. GUARNACCIA, R. LEWIS-FERNANDEZ, AND M.R. MARANO
Kleinman, Arthur1980 Patients and Healers in the Context of Culture: An Exploration of the Borderland be-
tween Anthropology, Medicine and Psychiatry. Berkeley: University of CaliforniaPress.
1988 Rethinking Psychiatry: From Cultural Category to Personal Experience. New York:Free Press.
Kleinman, Arthur, Veena Das and Margaret Lock, eds.1997 Social Suffering. Berkeley: University of California Press.
Koss-Chioino, Joan1992 Women as Healers, Women as Patients: Mental Health Care and Traditional Healing
in Puerto Rico. Boulder: Westview Press.Lewis, Gordon K.
1968 Puerto Rico: Freedom and Power in the Caribbean. New York: Harper and Row.Lewis-Fernandez, Roberto
1995 Puerto Rico, los nervios, y “la nueva psiquiatr´ıa transcultural.” Revista de Siquiatr´ıa2(5–6): (5): 5–19; (6): 21–24.
1996 Diagnosis and Treatment of Nervios and Ataques in a Female Puerto Rican Migrant.Culture, Medicine and Psychiatry 20: 155–163.
1998 “Eso no estaba en m´ı . . . nopude controlarme”: El control, la identidad y las emo-ciones en Puerto Rico. Revista de Ciencias Sociales 4: 268–299.
Lewis-Fernandez, Roberto, Peter Guarnaccia, Igda Martinez, Ester Salman, AndrewSchmidt, and Michael Liebowitz
2002 Comparative Phenomenology ofAtaque de Nervios, Panic Attacks and Panic Dis-order. Culture, Medicine and Psychiatry 26(2): 199–223.
Liebowitz, Michael R., F.M. Quitkin, J.W. Stewart, P.J. McGrath, W. Harrison, J.G. Rabkin,E. Tricamo, J.S. Markowitz, and D.F. Klein
1984 Psychopharmacologic Validation of Atypical Depression. Journal of ClinicalPsychiatry 45: 22–25.
Liebowitz, Michael R, Ester Salm´an, Carlos Jusino, Robin Garfinkel, Linda Street, Dora L.Cardenas, Jo˜ao Silvestre, Abby J. Fyer, Jos´e L. Carrasco, Sharon Davies, Peter Guarnaccia,and Donald F. Klein
1994 Ataque de Nervios and Panic Disorder. American Journal of Psychiatry 151: 871–875.
Maldonado-Denis, Manuel1972 Puerto Rico: A Socio-Historic Interpretation. New York: Vintage.
Newton, Frank1978 The Mexican-American Emic System of Mental Illness: An Exploratory Study.
In Family and Mental Health in the Mexican American Community. Monograph7.J. M. Casa and S.E. Keefe, eds., pp. 69–90. Los Angeles: Spanish SpeakingMental Health Research Center.
Roberts de Ram´ırez de Arellano, M.I., Max Ram´ırez de Arellano, Leopoldo Garc´ıa,Jorge J. Dieppa, Mercedes Rodrigo Bellido, Carmen A. Rodr´ıguez, Estela M. Lanauze,Marıa del Carmen Cruz de Garc´ıa, and Aida T. Moylan
1954 “Ataques,” Hyperkinetic Type: The so-called “Puerto Rican Syndrome,” its med-ical, psychological and social implications. Paper presented at the Annual Meet-ing of the Puerto Rico Medical Association. San Juan, Puerto Rico. December,1954.
Robins, L.N., J.E. Helzer, J. Croughan, and K.S. Ratcliffe1981 National Institute of Mental Health Diagnostic Interview Schedule. Archives of
General Psychiatry 38: 281–289.Rogler, Lloyd, and August B. Hollingshead
1985 Trapped: Puerto Rican Families and Schizophrenia. Maplewood, NJ: WaterfrontPress.

P1: IAZPP940-medi-469946 MEDI.cls August 11, 2003 11:42
TOWARD A PUERTO RICAN POPULAR NOSOLOGY 365
Rothenberg, Albert1964 Puerto Rico and Aggression. American Journal of Psychiatry 120: 962–
970.Rubel, Arthur, Carl W. O’Nell, and Rolando Collado-Ardon
1984 Susto: A Folk Illness. Berkeley: University of California Press.Rubio, Mauricio, Mario Urdaneta, and John L. Doyle
1955 Psychopathologic Reaction Patterns in the Antilles Command. United States ArmedForces Medical Journal 6: 1767–1772.
Saint Exupery, Antoine de1971 The Little Prince. New York: Harbrace Paperbound Library.
Salman, Ester, Michael R. Liebowitz, Peter J. Guarnaccia, Carlos M. Jusino, RobinGarfinkle, Linda Street, Dora L. C´ardenas, Jo˜ao Silvestre, Abby J. Fyer, Jos´e L. Carrasco,Sharon O. Davies, and Donald F. Klein
1998 Subtypes of Ataques de Nervios: The Influence of Coexisting Psychiatric Diag-noses. Culture, Medicine and Psychiatry 22: 231–244.
Scheper-Hughes, Nancy, and Margaret Lock1987 The Mindful Body: A Prolegomenon to Future Work in Medical Anthropology.
Medical Anthropology Quarterly 1: 6–41.Thompson, Lanny
1995 Nuestra isla y su gente: La constucc´ıon del “otro” puertorrique˜no en Our Islands andTheir People. R´ıo Piedras, P.R.: Centro de Investigaciones Sociales y Departamentode Historia de la Universidad de Puerto Rico.
Weiss, Mitchell, D.R. Doongaji, S. Siddhartha, D. Wypij, S. Pathare, M. Bhatawdekar,A. Bhave, A. Seth, and R. Fern´andes
1992 The Explanatory Model Interview Catalogue (EMIC): Contribution to Cross-Cultural Research Methods from a Study of Leprosy and Mental Health. BritishJournal of Psychiatry 160: 819–830.
White, Geoffrey1982 The Ethnographic Study of Cultural Knowledge of “Mental Disorder.”In Cultural
Conceptions of Mental Health and Therapy. A.J. Marsella and G. M. White, eds.,pp. 69–95. Dordrecht, Holland: D. Reidel Publishing Company.
Peter J. GuarnacciaInstitute for Health, Health Care Policy, and Aging Research30 College AvenueRutgers UniversityNew Brunswick, NJ 08901-1293
Roberto Lewis-Fern´andezAnxiety Disorders Clinic and Hispanic Treatment ProgramNew York State Psychiatric Institute and Columbia UniversityNew York, NY

P1: IAZPP940-medi-469946 MEDI.cls August 11, 2003 11:42
366 P.J. GUARNACCIA, R. LEWIS-FERNANDEZ, AND M.R. MARANO
Melissa Rivera MaranoGraduate School of Applied and Professional Psychology, andInstitute for Health, Health Care Policy, and Aging ResearchRutgers UniversityNew Brunswick, NJ