Prevalence and Treatment of Diagnosed Depression among Elderly Nursing Home Residents in Ohio
19
Prevalence and Treatment of Diagnosed Depression among Elderly Nursing Home Residents in Ohio Carrie A. Levin, PhD, Wenhui Wei, PhD, Ayse Akincigil, PhD, Judith A. Lucas, EdD, Scott Bilder, MS, and Stephen Crystal, PhD Foundation for Informed Medical Decision Making, Boston, MA (C.A.L.); Institute for Health, Health Policy, and Aging Research, Rutgers, The State University of New Jersey, New Brunswick, NJ (W.W., A.A., J.A.L., S.B., S.C.) Abstract Objectives—To examine the prevalence and treatment of diagnosed depression among elderly nursing home residents and determine the resident and facility characteristics associated with diagnosis and treatment. Design, Setting, and Participants—Documented depression, pharmacotherapy, psychotherapy, sociodemographics, and medical characteristics were obtained from Ohio's Minimum Data Set for 76 735 residents in 921 nursing homes. The data were merged with Online Survey Certification and Reporting System data to study the impact of facility characteristics. Chi- squared statistics were used to test group differences in depression diagnosis and treatment. Multiple logistic regressions were used to examine the prevalence of diagnosed depression, and among those diagnosed, of receiving any treatment. Results—There were 48% of residents who had an active depression diagnosis; among those diagnosed, 23% received no treatment; 74% received antidepressants; 0.5% received psychotherapy; and 2% received both. African Americans, the severely cognitively impaired, and those in government facilities were less likely to be diagnosed. Residents aged 85 and older, African Americans, individuals with severe mental illness, those with severe ADL or cognitive impairment, and individuals living in a facility with 4 or more deficiencies were less likely to receive treatment. Conclusion—Significant disparities exist both in diagnosis and treatment of depression among elderly residents. Disadvantaged groups such as African Americans and residents with physical and cognitive impairments are less likely to be diagnosed and treated. Our results indicate that work needs to be done in the nursing home environment to improve the quality of depression care for all residents. Keywords Nursing homes; antidepressant; psychotherapy Depression is the most burdensome and prevalent mental illness among nursing home (NH) residents.1 – 3 If untreated, inadequately treated, or unresponsive to treatment, depression can lead to a cascade of other adverse health outcomes such as malnutrition, poor hydration, weakening from physical inactivity, functional decline, decreased quality of life, and ultimately, death.1 – 6 Among NH residents, prior studies have reported estimates of the prevalence rate for depression (variously defined to include major depressive disorder, other depression diagnoses and/or depressive symptoms) to range from 11% to 78%. 7– 13 Rates in Address correspondence to Carrie A. Levin, PhD, Foundation for Informed Medical Decision Making, 40 Court Street, Suite 300, Boston, MA 02108. E-mail: [email protected]. NIH Public Access Author Manuscript J Am Med Dir Assoc. Author manuscript; available in PMC 2010 June 18. Published in final edited form as: J Am Med Dir Assoc. 2007 November ; 8(9): 585–594. doi:10.1016/j.jamda.2007.07.010. NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
Transcript of Prevalence and Treatment of Diagnosed Depression among Elderly Nursing Home Residents in Ohio
Prevalence and Treatment of Diagnosed Depression amongElderly Nursing Home Residents in Ohio
Carrie A. Levin, PhD, Wenhui Wei, PhD, Ayse Akincigil, PhD, Judith A. Lucas, EdD, ScottBilder, MS, and Stephen Crystal, PhDFoundation for Informed Medical Decision Making, Boston, MA (C.A.L.); Institute for Health, HealthPolicy, and Aging Research, Rutgers, The State University of New Jersey, New Brunswick, NJ(W.W., A.A., J.A.L., S.B., S.C.)
AbstractObjectives—To examine the prevalence and treatment of diagnosed depression among elderlynursing home residents and determine the resident and facility characteristics associated withdiagnosis and treatment.
Design, Setting, and Participants—Documented depression, pharmacotherapy,psychotherapy, sociodemographics, and medical characteristics were obtained from Ohio'sMinimum Data Set for 76 735 residents in 921 nursing homes. The data were merged with OnlineSurvey Certification and Reporting System data to study the impact of facility characteristics. Chi-squared statistics were used to test group differences in depression diagnosis and treatment. Multiplelogistic regressions were used to examine the prevalence of diagnosed depression, and among thosediagnosed, of receiving any treatment.
Results—There were 48% of residents who had an active depression diagnosis; among thosediagnosed, 23% received no treatment; 74% received antidepressants; 0.5% received psychotherapy;and 2% received both. African Americans, the severely cognitively impaired, and those ingovernment facilities were less likely to be diagnosed. Residents aged 85 and older, AfricanAmericans, individuals with severe mental illness, those with severe ADL or cognitive impairment,and individuals living in a facility with 4 or more deficiencies were less likely to receive treatment.
Conclusion—Significant disparities exist both in diagnosis and treatment of depression amongelderly residents. Disadvantaged groups such as African Americans and residents with physical andcognitive impairments are less likely to be diagnosed and treated. Our results indicate that work needsto be done in the nursing home environment to improve the quality of depression care for all residents.
KeywordsNursing homes; antidepressant; psychotherapy
Depression is the most burdensome and prevalent mental illness among nursing home (NH)residents.1–3 If untreated, inadequately treated, or unresponsive to treatment, depression canlead to a cascade of other adverse health outcomes such as malnutrition, poor hydration,weakening from physical inactivity, functional decline, decreased quality of life, andultimately, death.1–6 Among NH residents, prior studies have reported estimates of theprevalence rate for depression (variously defined to include major depressive disorder, otherdepression diagnoses and/or depressive symptoms) to range from 11% to 78%.7–13 Rates in
Address correspondence to Carrie A. Levin, PhD, Foundation for Informed Medical Decision Making, 40 Court Street, Suite 300, Boston,MA 02108. E-mail: [email protected].
NIH Public AccessAuthor ManuscriptJ Am Med Dir Assoc. Author manuscript; available in PMC 2010 June 18.
Published in final edited form as:J Am Med Dir Assoc. 2007 November ; 8(9): 585–594. doi:10.1016/j.jamda.2007.07.010.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
these NH studies were substantially higher than rates for community-dwelling elderlyindividuals.1,14–16 Despite this consistent evidence of high rates of underlying depressivesymptomatology, we lack sufficient understanding of the extent to which depression amongresidents is identified by facilities, the predictors of facility-identified depression, and theextent to which treatment is provided for identified depression. Generally, in prior studies,depression among NH residents has been reported to be substantially underdiagnosed8,11,15
and undertreated8,17–20 or inadequately treated.8,20–22 However, as there is rapid evolution ofdepression identification and treatment patterns among the community-dwelling near-elderlyand elderly,23,24 as well as disparities in such care, depression care in nursing homes may bea moving target. To inform efforts at quality improvement, it is important to examine recentpatterns of depression identification and treatment in routine care across the full spectrum ofnursing homes.
Improving care for depression among NH residents has been a widely acknowledged goaldating back to the 1987 Omnibus Budget Reconciliation Act (OBRA) nursing home reforms.25 In reviewing priorities for quality of care, improvement for vulnerable adults such as thosein nursing homes, an expert panel ranked improvement of depression care second only to theoverall issue of improved pharmacologic management among 78 conditions and problemsconsidered.26 Similar recommendations were highlighted in the first National HealthcareQuality Report, released by AHRQ in 200327 and in the 2003 American Geriatrics Society/American Association for Geriatric Psychiatry Consensus Statement on Improving the Qualityof Mental Health Care in US Nursing Homes.3 Yet many issues remain unresolved regardingadequacy of depression-related care in NHs such as unequal access to specialty care, length ofpersistent use of antidepressants and proper dosing of antidepressants,21,28 and information onmany topics is outdated.
Antidepressants have been shown to be safe and efficacious in the treatment of geriatricdepression1,3,9,29 and have been widely used in the nursing home population.3,21,29–36
Psychotherapy constitutes an alternative modality, particularly when antidepressant treatmentis not acceptable to residents or their families, a situation that may be more frequent for AfricanAmerican elders.37
One critical issue in the care of NH residents with depression is the role of mental healthspecialists such as psychiatrists or psychologists. Psychiatric evaluation can be important indifferential diagnosis and optimizing use of psychotropic treatment, including adjustment ofregimens and dosages for initially unresponsive residents, and decisions on need for psychiatrichospitalization. In their 2003 consensus statement, the American Geriatrics Society andAmerican Association for Geriatric Psychiatry recommended that residents who havedepression with psychotic features who have not responded to 6 or more weeks of treatmentbe referred to mental health professionals.3
Surprisingly little information is available about the extent and predictors of mental healthservices use for depressed NH residents; disparities in such care; and variations across facilities.18,19 Greater prevalence of identified depression among nursing home residents has beenshown to be associated with younger age, being female, having ever been married, white non-Hispanic ethnicity, higher cognitive function, heart disease, and Parkinson's disease,7 usingdata from the 1996 Medical Expenditure Panel Survey-Nursing Home Component.
Although dated, the few prior studies on this topic indicate low overall rates of specialty careuse; sharp disparities by race/ethnicity, age, and other socioeconomic factors; and very limitedaccess to care in rural areas.18,24,38 Residents 85 and older, those with severe cognitiveimpairment, and black residents were less likely to receive antidepressants once depressionhas been identified.8 Residents who receive care from mental health specialists tend to be
Levin et al. Page 2
J Am Med Dir Assoc. Author manuscript; available in PMC 2010 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
younger; live in the Northeast; and have schizophrenia, dementia, or other mental disorder.17 Other results report that residents with depression, schizophrenia, or psychosis are morelikely to receive specialist mental health services, while those with more ADL (activities ofdaily living) limitations, and older residents, as well as those residing in government NHs, orhomes run by chains, are less likely to receive specialist mental health services.18,19
While geriatric depression has traditionally been considered much underdiagnosed, Crystaland colleagues recently reported that the depression diagnosis rate more than doubled amongcommunity-dwelling elderly individuals between 1992 and 1998, increasing by 107%,23 withconcomitant increases in antidepressant use. Rapidly evolving patterns of depressionidentification and treatment in the NH setting create a critical need for more current analyses.In this study, we used a merged Minimum Data Set (MDS) and online Survey Certificationand Reporting (OSCAR) data set to assess the prevalence of diagnosed depression amongelderly nursing home residents, and subsequently, to examine the rate of treatments(pharmacotherapy and psychotherapy) they received. Additionally, we examined whetherdisparities in diagnosis and treatment exist and described how both resident-and facility-levelcharacteristics are associated with such differences.
Design And MethodsData
In this study, the 2000 Ohio Long-term Care MDS was used as the source of NH residentinformation. These data were merged with the OSCAR data to obtain nursing home facilitycharacteristics. The research protocol was approved by Rutgers, the State University of NewJersey's Institutional Review Board. The MDS is a nationally standardized 350-item summaryscreening and assessment tool designed to collect data on nursing home residents includingtheir physical, psychological, and psychosocial functioning, active clinical diagnoses, healthconditions, treatments and services received, demographics, payer source, and advancedirectives.39 All Medicare- and Medicaid-certified nursing facilities are required to use theMDS to assess each resident, first upon admission and then on a quarterly and annual basisand when there is “significant change” in the resident's health status and needs.40 OSCAR isa uniform computerized database maintained by the Centers for Medicaid and MedicareServices (CMS) containing information on all Medicare/Medicaid-certified NHs includingfacility characteristics and staffing data; aggregated resident characteristics; and surveydeficiencies. The information in OSCAR is collected by state licensure and certificationagencies as part of the yearly Medicare/Medicaid certification process.
In the current study, the sample includes all residents 65 or older who had been in an Ohio NHfor at least 3 months in 2000, but excluded those who were comatose or those living in ahospital-based NH, as research has suggested that hospital-based nursing homes might have adifferent case-mix than freestanding ones.41–43 When there was more than one assessment foreach resident within the year, we chose the assessment closest to the end of the year. Facilitycharacteristics were drawn from the OSCAR data closest to the MDS assessment date. Thefinal sample included 76 735 residents in 921 nursing homes.
MeasuresDepression Diagnosis and Treatment—A resident was considered to have diagnoseddepression on an MDS assessment (Section Iee. Disease Diagnoses: Depression) if there wasan “active” physician-documented depression diagnosis in the resident's clinical record usinga 7-day look-back period. An “active” diagnosis is defined as having “a relationship to currentADL status, cognitive status, mood and behavior status, medical treatments, nursingmonitoring, or risk of death.”40
Levin et al. Page 3
J Am Med Dir Assoc. Author manuscript; available in PMC 2010 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Our analysis showed that among residents without a depression diagnosis, 15% receivedantidepressant therapy and 1.3% received psychotherapy (data not shown). Some of theseindividuals may have unrecorded depression, but these treatments are also widely used forconditions or symptoms other than depression. Because the objective of the current study wasto examine the pattern of treatment among depressed residents, we focused on the treatment(antidepressant and/or psychotherapy) received by residents with diagnosed depression.Depression treatment was defined dichotomously as any antidepressant, psychosocial therapy,or group therapy received by the resident during the 7 days prior to the assessment. Our analysisshowed that among those who received depression treatment, less than 1% had psychotherapyas the sole mode of treatment. Given that such a small portion of the depressed elderly residentsreceived psychotherapy as their sole treatment, we determined that it is more meaningful tocombine antidepressant therapy and psychotherapy together to examine any treatment as ouroutcome of interest, rather than to conduct separate analyses of antidepressant therapy andpsychotherapy. Because of the low proportion of residents receiving psychotherapy only, ourfindings on predictors of treatment are dominated by variations in antidepressant use.
Resident Characteristics—Sociodemographic characteristics included resident's gender,age (categorized as 65 to 74, 75 to 84, and 85 or older to allow for nonlinear age effects), race/ethnicity (white, African American, and other), education level (less than high school, highschool graduate, and college graduate or above), and marital status at assessment (nevermarried, married, widowed, and separated/divorced).
Physical and mental comorbidities were extracted from the Disease Diagnoses section of theMDS. Individual physical comorbidities were summed to create a summary measure of burdenof physical comorbidity, which included arthritis, diabetes, hypertension, cancer, stroke,congestive heart failure, and chronic obstructive pulmonary disease (COPD). The number ofconditions was categorized into none, 1–2, 3–4, and 4+. Comorbid severe mental illness (SMI)was defined as having an active diagnosis of schizophrenia or bipolar disorder. Physicalfunction was measured using the hierarchical activities of daily living (ADL) scale developedand validated by Morris et al44 using 7 MDS ADL self-performance variables. Chroniccognitive impairment was constructed using the Cognitive Performance Scale, which assignsresidents into cognitive performance categories (from intact to severely impaired).
Facility Characteristics (from OSCAR)—Nursing home size was measured by numberof beds (categorized as less than 50, 50–99, 100–199, and 200+), occupancy rate (percentageof beds occupied on the day of the survey), and NH location (rural or urban). Ownership typewas classified into government, for profit, or not for profit, and Medicaid ratios represent theproportion of residents whose care was paid for by Medicaid. We also distinguished NHs thathad a multifacility chain affiliation from freestanding facilities. Another dichotomous controlvariable was provision of onsite mental health services. Staffing was measured as total nursinghours (RNs, LPNs, and NAs) per resident per day. Aggregate facility acuity level was measuredwith an acuity index that is a sum of an ADL index (proportion of residents dependent in eating,toileting, transferring, ambulation) and a special treatments index (proportion of residentsrequiring respiratory care, suctioning, IV therapy, tracheostomy care, or parenteral feeding).45–47 Since occupancy rates, total nursing hours, Medicaid ratios and the acuity index werenot distributed uniformly across their range, we categorized the rates into quartiles. Data onfacility deficiencies represent the number of deficiencies recorded in OSCAR across the 17major areas used in the survey process,48 categorized into 0–2, 3–4, and greater than 4deficiencies, to allow for nonlinear effects.
Levin et al. Page 4
J Am Med Dir Assoc. Author manuscript; available in PMC 2010 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

AnalysesBivariate group differences in rates of outcomes (diagnosis of depression and any treatmentamong those diagnosed with depression) were tested across resident and facility characteristicsusing chi-square analyses. Robust multiple logistic regressions were then performed todetermine the adjusted effects of the covariates on a resident's probability of receiving adepression diagnosis, and if depressed, on the probability of receiving any treatment(antidepressant only, psychotherapy only, or both antidepressant therapy and psychotherapy).Both the bivariate analysis and logistic regressions adjusted for clustering of residents withinfacilities and were done using SAS-callable SUDAAN V8.0.49
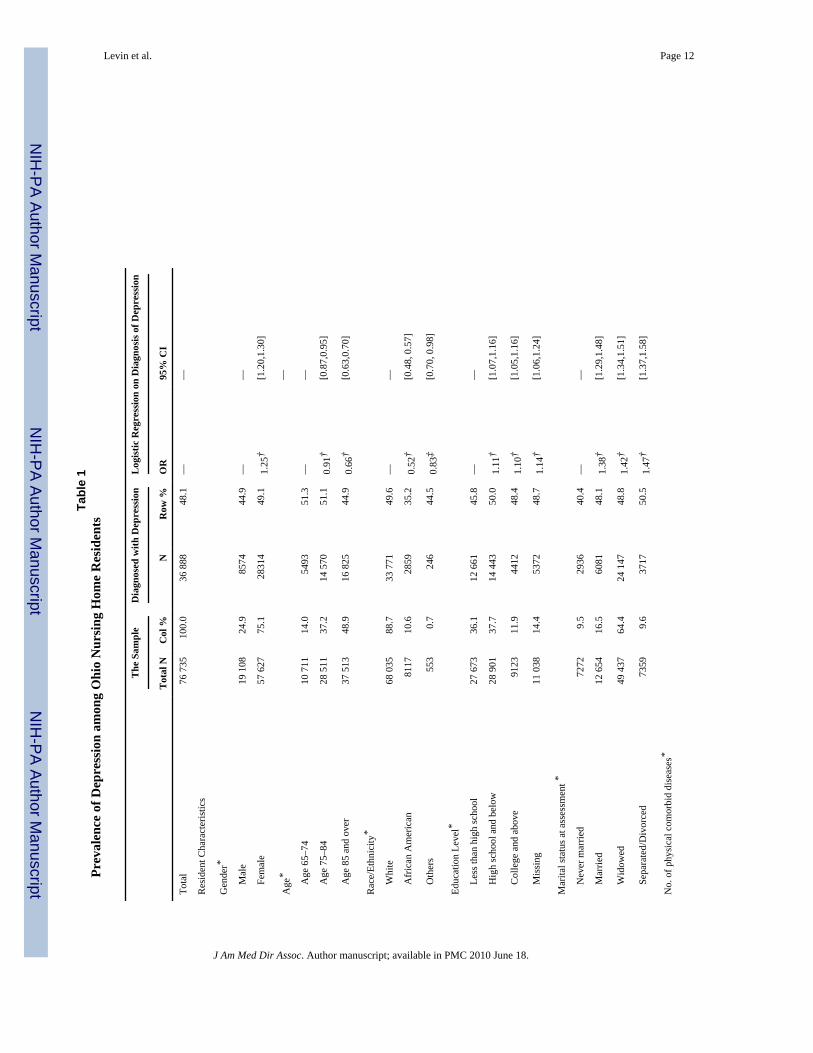
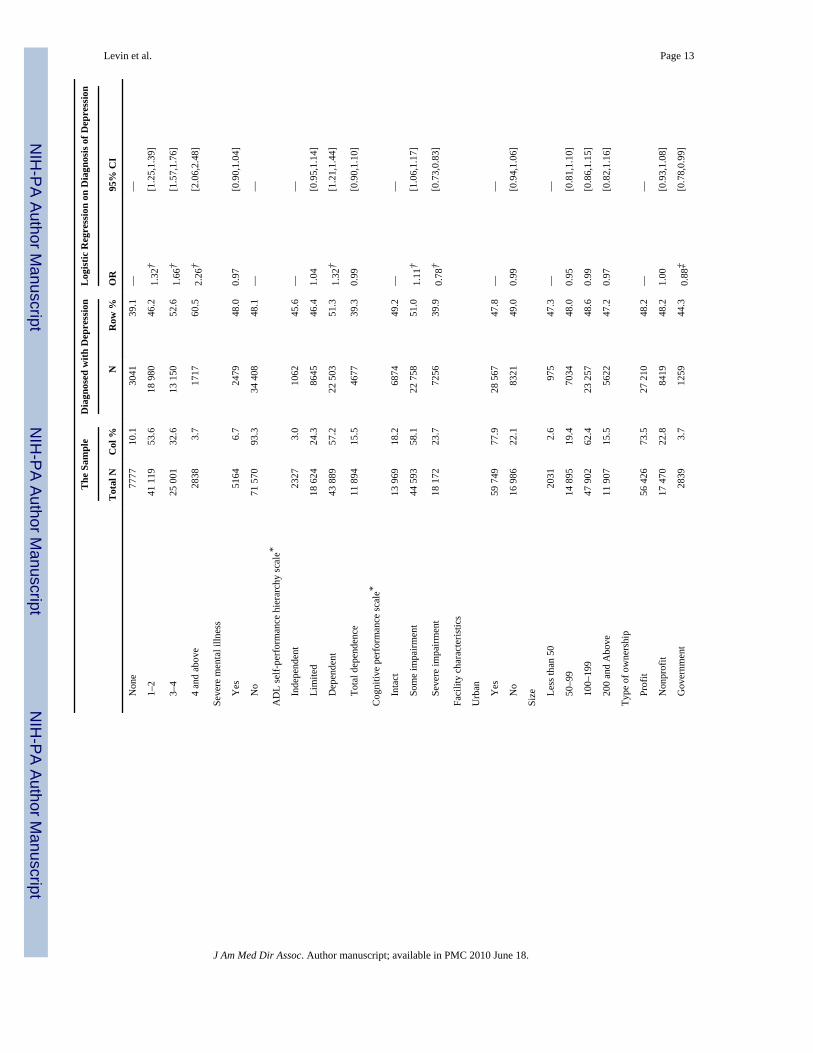
ResultsThe characteristics of Ohio elderly nursing home residents in 2000 are presented in the first 2columns of Table 1. Most were female (75%), white (89%), and widowed (64%). Physicalcomorbidity was prevalent, with 90% having at least 1 chronic physical illness. Over 75% weredependent in ADL activities, and 81% had at least some cognitive impairment. The modelresident lived in a for-profit (74%) facility in an urban area (78%) with 100 to 199 (62%)residents.
Diagnosis of DepressionTable 1 shows the prevalence of diagnosed depression among residents by sociodemographiccharacteristics as well as the characteristics of the facility in which they lived. Forty-eightpercent of the elderly residents (N = 36 888) were documented as having a depression diagnosis.Bivariate analyses showed that rates of depression diagnosis varied significantly by most ofthe resident characteristics including gender, age, race/ethnicity, education, marital status,presence of physical comorbid conditions, ADL status, and cognitive impairment status.However, only 2 facility characteristics (percentage of residents in the facility with Medicaidas the primary payer, and number of facility deficiencies) showed significant differences in thebivariate analyses. Results from the multiple logistic regression on diagnosis of depressionconfirmed the results from the bivariate analysis. When controlling for other factors, beingfemale, having higher education achievement, and ever being married were associated withsignificantly higher likelihood of being diagnosed with depression. African Americans wereabout half as likely as whites to have a depression diagnosis (OR = 0.52, 95% CI = [0.48,0.57]). Older age was also associated with lower likelihood of having a depression diagnosis(aged 75–84: OR = 0.91, 95% CI = [0.87, 0.95]; aged 85 and older: OR = 0.66, 95% CI = [0.63,0.70]). While physical comorbidity was associated with higher odds of being diagnosed withdepression, comorbid SMI did not have a significant impact. Compared to elderly residentsindependent in ADLs, those who were dependent, but not totally dependent, were more likelyto be diagnosed with depression (OR = 1.32, 95% CI = [1.21,1.44]). The impact of cognitiveimpairment on the odds of receiving a depression diagnosis was not monotonic, with odds ofdiagnosis highest among those with some impairment, lowest among those with severeimpairment, and intermediate among those with no impairment.
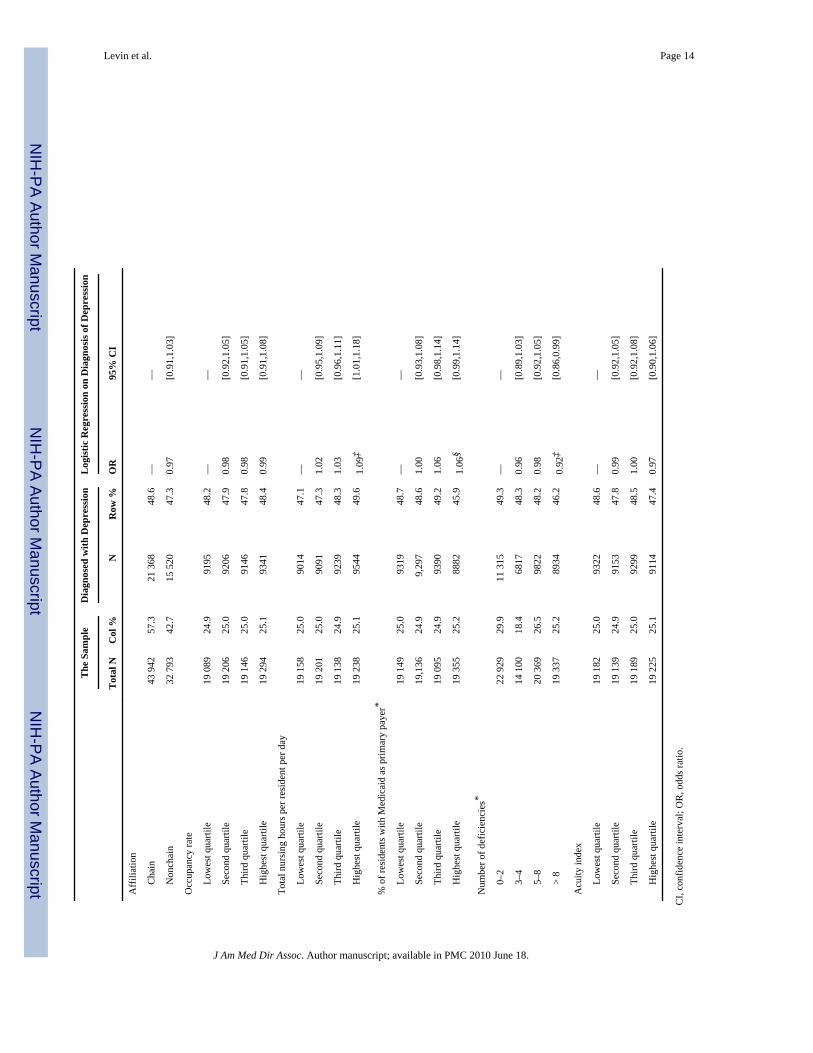
Similar to the results from the bivariate analyses, few facility characteristics had impact on theresident's likelihood of being diagnosed with depression. Residents in facilities with the highestquartile of total nursing hours per resident per day were more likely to have a depressiondiagnosis than those in the lowest quartile (OR = 1.09, 95% CI = [1.01, 1.18]). Residents livingin government-owned facilities were significantly less likely to be diagnosed with depressionthan those in for-profit facilities (OR = 0.88, 95% CI = [0.78, 0.99]). Residents in facilitieswith a high number of deficiencies (8+) were less likely to be diagnosed with depression thanthose in facilities with a very low number of deficiencies (0–2) (OR=0.92, 95% CI = [0.86,0.99]).
Levin et al. Page 5
J Am Med Dir Assoc. Author manuscript; available in PMC 2010 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
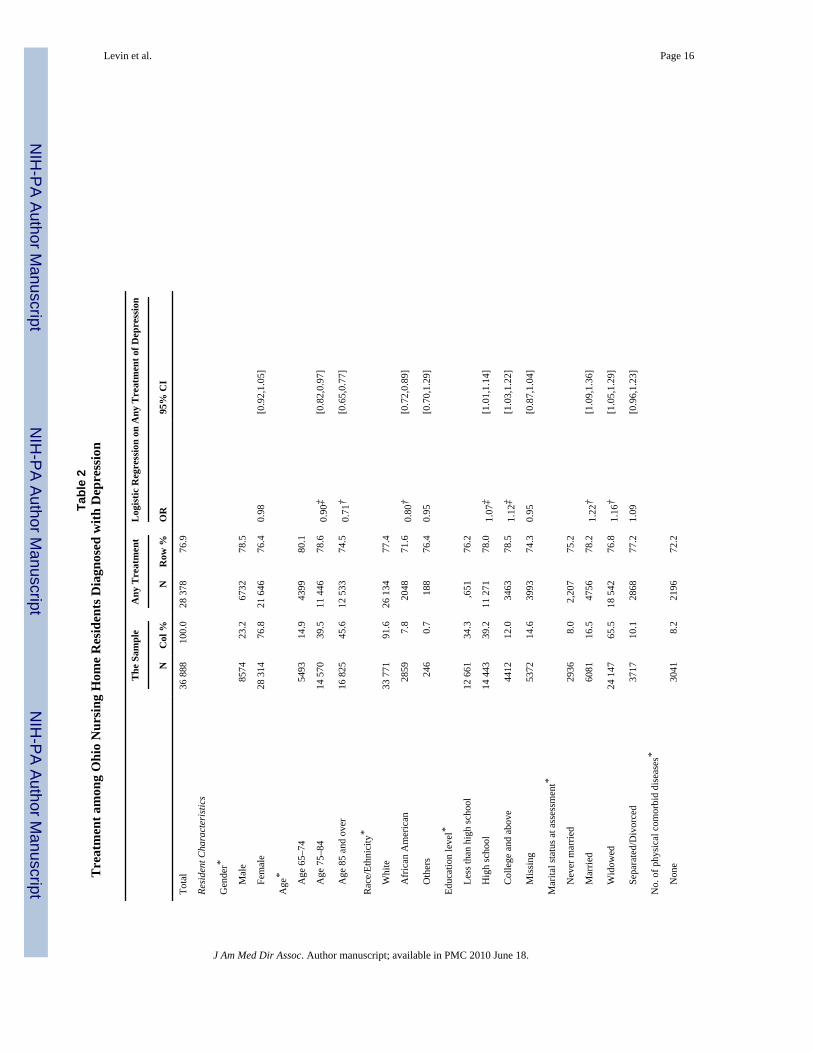
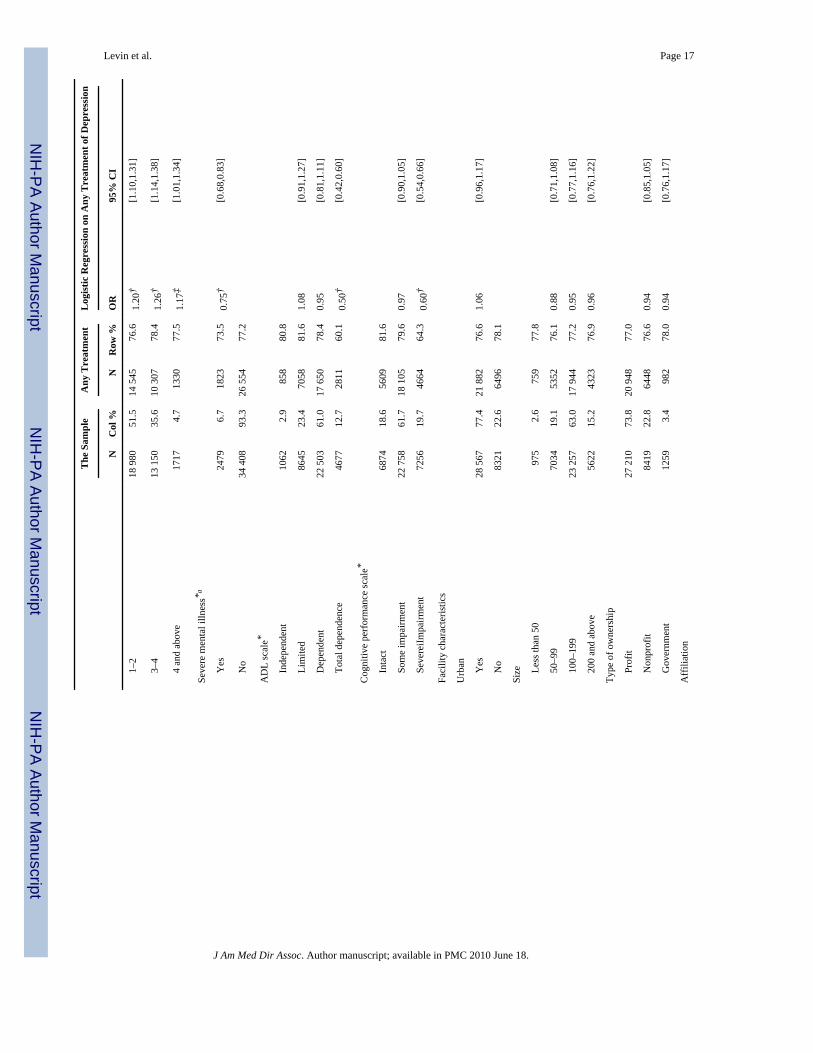
Treatment of DepressionTable 2 presents results on the rates of any depression treatment (antidepressant and/orpsychotherapy or group therapy) received by elderly residents diagnosed with depression. Ingeneral, 77% received either an antidepressant or psychotherapy within the 7 days prior to theassessment. The bivariate analyses of any treatment showed that significant subgroupdifferences exist for all of the resident variables. Older age, minority race/ethnicity, comorbidSMI, total ADL dependence, and severe cognitive impairment were associated withsignificantly lower rates of depression treatment, while higher educational achievement, everbeing married, and physical comorbidities were associated with significantly higher treatmentrates. Similar to the findings on the depression diagnosis, few facility characteristics, exceptfor percentage of residents with Medicaid as primary payer and number of deficiencies, hadsignificant impact on treatment rates.
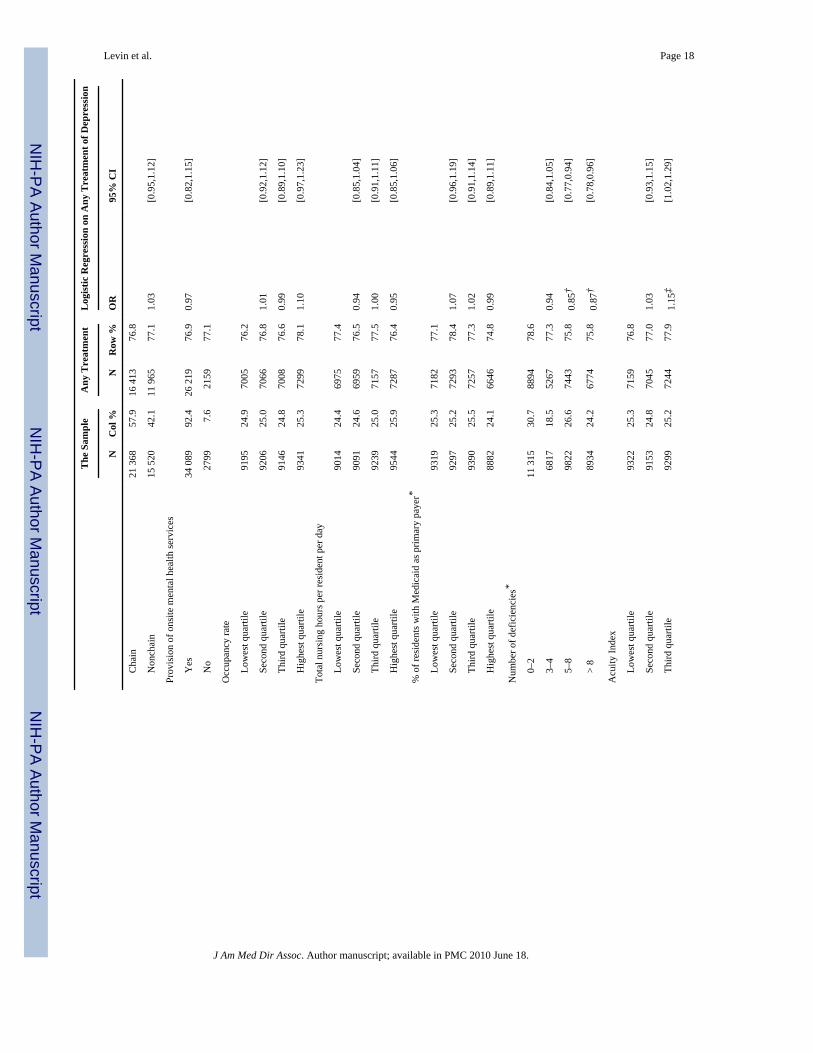
Multiple logistic regression results on any use were consistent with these findings. Whencontrolling for other factors, compared to their counterparts, older residents (aged 75–84: OR= 0.90, 95% CI = [0.82, 0.97]; aged 85 and oldr: OR = 0.71, 95%CI = [0.65, 0.77]), AfricanAmericans (OR = 0.80, 95% CI = [0.72, 0.89]), residents with SMI (OR = 0.75, 95% CI =[0.68, 0.93]), residents with total ADL dependence (OR = 0.50, 95% CI = [0.42, 0.60]), andresidents with severe cognitive impairment (OR = 0.60, 95% CI = [0.54, 0.66]) weresignificantly less likely to receive depression treatment, while residents with higher education(high school: OR = 1.07, 95% CI = [1.01, 1.14]; college and above: OR = 1.12, 95% CI = [1.03,1.22]), married or widowed residents (OR = 1.22, 95% CI = [1.09, 1.36], and OR = 1.16, 95%CI = [1.05, 1.29]), and more comorbid physical conditions were associated with significantlyhigher odds of receiving any treatment. The only facility characteristic that was significant inthe regression was the number of deficiencies. Compared with residents living in facilities with0 to 2 deficiencies, those living in facilities with 5 or more deficiencies were significantly lesslikely to be treated.
DiscussionIn this paper, we described patterns of identification of depression (diagnosis) and its treatmentamong long-stay nursing home residents aged 65 and older. We also determined characteristicsof residents and facilities that predict whether a resident received a depression diagnosis andsubsequent treatment.
Our results indicate that the oldest-old are approximately a third less likely than those age 65to 75 to be diagnosed; those with very severe cognitive impairment are a third less likely to bediagnosed than cognitively intact residents; and African Americans are half as likely as whitesto be diagnosed with depression. It is beyond the scope of this paper to determine the relativecontribution to these differences of differential underdiagnosis (or overdiagnosis), versusactual variations in rates of depression. Results also indicate that residents in facilities withmore than 4 deficiencies were less likely to be diagnosed with depression.
There are also significant disparities in the likelihood of treatment for identified depression,with those who are cognitively impaired, non-white, and those with more ADL dependencybeing less likely to receive treatment among persons diagnosed with depression. There is apressing need to better understand why those who are more physically and psychologicallydependent are less likely to receive treatment, and to address these disparities. What, forexample, are the roles of resident and family preferences; residents' physicians; nursing staff;consultant pharmacists; and other actors in decisions on treatment? What are the mostappropriate measures of depression care quality for use as benchmarks for qualityimprovement? Does depression manifest itself in different ways among African American
Levin et al. Page 6
J Am Med Dir Assoc. Author manuscript; available in PMC 2010 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

residents, and what other factors are involved in the lower rates of identified depression and,once identified, of depression treatment among these residents?
Much more research is needed on the identification and treatment of depression among nursinghome residents. Ideally, such research would use data that combine independent, structuredresearcher assessments of underlying depression symptoms with detailed information onfacility recognition and treatment; however, few such data are available on large, recent,generalizable populations of facilities. Existing data such as the MDS provide important clues,but are subject to significant limitations. One limitation of using the MDS as a data source isthat treatments (antidepressant and/or psychotherapy) received by the resident were examinedonly during the seven days prior to the assessment, and no detailed pharmaceutical data werereported, such as medication name and dosage. Among NH residents generally, both for thosediagnosed with depression and those who are not, psychotherapy was received ratherinfrequently. A possible explanation may be that antidepressant therapy is cheaper and easierto administer than psychotherapy. The low frequency of psychotherapy is not unexpected inthis population because many nursing homes do not directly employ or contract withpsychiatrists or other mental health professionals. Also, as psychotherapy was not likely to beprovided on a daily basis, the 7-day look-back period using MDS data limited our ability toidentify psychotherapy users.
Additionally, more information about the types of treatment that residents receive wouldimprove the study. The antidepressants as a class are recorded on the MDS, but we did nothave access to particular drug names and also did not know much about the type of or reasonsfor pharmacotherapy offered (whether it was to treat depression; whether a resident receivesan antidepressant because of sleep problems; whether a resident is prescribed a stimulant fordepressive symptoms; whether the resident is on hospice; whether a resident has been offeredtherapies other than antidepressants; and whether a resident has a strong social network). Weare able to identify the total number of medications that a resident is taking, but do not knowthe type of concomitant medications.
Depression is often underrecognized or undertreated because it occurs in the context of otherphysical and social problems9,29 especially when age is often accompanied by social isolation,withdrawal, prolonged bereavement, and economic problems.51 It is well established thatpsychiatric disorders such as depression tend to co-occur with chronic general medicalillnesses. Functional impairment and comorbidity, both physical and mental, are likely to havean effect on treatment and diagnosis of depression, although through opposing mechanisms.On the one hand, it is likely that patients with many comorbidities may have stronger ties tothe health care system and may be more likely to view psychological distress as a medicalproblem. They may be more likely to receive a depression diagnosis because of their morefrequent interaction with health care professionals. Conversely, depression may beundertreated because providers may be concerned about the side effects or interaction of theantidepressants with one or more other pharmacological treatments the patient is receiving forhis or her comorbid conditions.23
Another limitation of our study is the lack of specificity in the diagnosis and treatment ofdepression as indicated on the MDS. Our results indicate the prevalence of depression amongNH residents as documented in the MDS as 48%, which is fairly high, compared to a studythat found fewer than 20% of residents to have major depression (as measured through directresident interview via the Geriatric Depression Scale) or symptoms of depression.11 Ourrelatively high prevalence rate may be due to the way in which depression is measured in theMDS as our study relies on a documented depression diagnosis in the MDS assessment, butproviders may enter a diagnosis of depression on a resident's chart for a range of depressivedisorders from mild depression that may accompany other comorbid conditions afflicting
Levin et al. Page 7
J Am Med Dir Assoc. Author manuscript; available in PMC 2010 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
elderly nursing home residents to more serious cases of major depression. More detail on thetype and severity of the depression as well as the type of pharmacotherapy offered would beuseful, but since the MDS is our sole data source for resident variables and we did not haveaccess to MDS Section U (specific medication name and dose), our specification of bothdiagnosis and treatment is limited to that information that is captured in routine MDSassessments.
With systemwide automated reporting of MDS data now in place, new opportunities exist touse these data to address important research needs as well as for regulation and qualityimprovement of nursing facilities. The Center for Health Systems Research and Analysis(CHSRA) originally developed quality indicators for use by individual facilities for qualityimprovement efforts including 2 depression measures: the prevalence of symptoms ofdepression and the prevalence of depression without antidepressant therapy. These indicatorsare used in connection with the survey process and for internal quality improvement.Prevalence of symptoms of depression and prevalence of depression with no antidepressanttherapy have been used as 1 of 24 MDS quality indicators that individual facilities can havebeen using for quality improvement efforts since the late 1990s50; however, depressionmeasures were not included among the original publicly reported quality measures for nursinghome residents on the Centers for Medicare and Medicaid (CMS) Web page: Nursing HomeCompare (www.cms.gov). Following the National Quality Forum recommendations in 2003,percent of residents who have become more depressed or anxious was added to Nursing HomeCompare beginning in January 2004. The data used in this study are from 2000–2001 OhioMDS data when MDS data were newly automated and depression was not yet publicly reportedon the CMS Nursing Home Compare web site. Future research should address longitudinalchanges in documentation of depression throughout this period to assess whether changes inpublic reporting has an impact on the reliability and validity of the documentation of depressiondiagnoses and symptoms on individual resident MDS assessments.
Our finding that elderly depressed residents with some cognitive impairment were as likely toreceive psychotherapy as those with intact cognitive ability was consistent with findings fromAbraham et al,51 who reported that residents with mild to moderate cognitive impairment werelikely to benefit from psychotherapy. Nevertheless, further analyses linking the MDS toMedicaid or Medicare claims would certainly allow for more detailed exploration ofinitialization and persistence in pharmacotherapy and psychotherapy among nursing homeresidents.
The cross-sectional design is another limitation of this study. Data used in this analysis are asnapshot of long-stay residents and do not support analysis of longitudinal results. We do notknow whether a resident's depression is chronic, or if his or her depression diagnosis representsa new episode. Our analyses were limited to long-stay residents who had been in the facilityfor at least 3 months; short-stay residents were excluded. We made no attempt to compareresults between residents who were long versus short-stay. These are topics for future research.Finally, our results represent nursing home residents in only one state and therefore may notbe generalizable to the whole nation.
ConclusionDespite these limitations, our findings tend to dispel the longstanding belief that depression issubstantially underdiagnosed and undertreated among NH residents. Our findings indicate avery substantial rate both of depression identification and of antidepressant treatment fordepression among NH residents, perhaps as a result of general increases in awareness ofdepression among the elderly, and of the positive potential of available treatments. However,many questions are left unanswered. Do lower treatment rates for cognitively impaired
Levin et al. Page 8
J Am Med Dir Assoc. Author manuscript; available in PMC 2010 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
individuals signify appropriate treatment, or that this subpopulation of NH residents is beingundertreated? Is depression care quality related to other measures of quality, as suggested bythe association between number of deficiencies and lower treatment rates? And with relativelyhigh rates of depression, treatment now common in nursing home settings, how successful arethese treatments in improving outcomes for residents? Further work needs to be done to assessthe quality of depression care in nursing homes to determine the optimal treatment for all NHresidents.
AcknowledgmentsFunded by National Institute of Mental Health Grant 1-RO1 MH076206 and AHRQ Grant R24-HS011825.
References1. Blazer DG. Depression in late life: review and commentary. J Gerontol A Biol Sci Med Sci 2003;58
(3):249–265. [PubMed: 12634292]2. American Geriatrics Society and American Association for Geriatric Psychiatry. The American
Geriatrics Society and American Association for Geriatric Psychiatry recommendations for policiesin support of quality mental health care in U.S. nursing homes. J Am Geriatr Soc 2003b;51(9):1299–1304.
3. American Geriatrics Society and American Association for Geriatric Psychiatry. Consensus statementon improving the quality of mental health care in U.S. nursing homes: management of depression andbehavioral symptoms associated with dementia. J Am Geriatr Soc 2003a;51(9):1287–1298.
4. Koenig HG, Blazer DG. Epidemiology of geriatric affective disorders. Clin Geriatr Med 1992;8(2):235–251. [PubMed: 1600475]
5. Morley JE, Silver AJ. Nutritional issues in nursing home care. Ann Intern Med 1995;123(11):850–859. [PubMed: 7486469]
6. Wright BA. Weight loss and weight gain in a nursing home: A prospective study. Geriatr Nurs 1993;14(3):156–159. [PubMed: 8508975]
7. Jones RN, Marcantonio ER, Rabinowitz T. Prevalence and correlates of recognized depression in U.S.nursing homes. J Am Geriatr Soc 2003;51(10):1404–1409. [PubMed: 14511160]
8. Brown MN, Lapane KL, Luisi AF. The management of depression in older nursing home residents. JAm Geriatr Soc 2002;50(1):69–76. [PubMed: 12028249]
9. Diagnosis and treatment of depression in late life. JAMA; NIH consensus conference; 1992. p.1018-1024.
10. Parmelee PA, Katz IR, Lawton MP. Incidence of depression in long-term care settings. J Gerontol1992;47(6):M189–196. [PubMed: 1430853]
11. Rovner BW, German PS, Brant LJ, Clark R, Burton L, Folstein MF. Depression and mortality innursing homes. JAMA 1991;265(8):993–996. [PubMed: 1992213]
12. Schnelle JF, Wood S, Schnelle ER, Simmons SF. Measurement sensitivity and the Minimum DataSet depression quality indicator. Gerontologist 2001;41(3):401–405. [PubMed: 11405438]
13. Teresi J, Abrams R, Holmes D, Ramirez M, Eimicke J. Prevalence of depression and depressionrecognition in nursing homes. Soc Psychiatry Psychiatr Epidemiol 2001;36(12):613–620. [PubMed:11838834]
14. Katz IR, Parmelee PA, Beaston-Wimmer P, Smith BD. Association of antidepressants and othermedications with mortality in the residential-care elderly. J Geriatr Psychiatry Neurol 1994;7(4):221–226. [PubMed: 7826490]
15. Rovner BW. Depression and increased risk of mortality in the nursing home patient. Am J Med1993;94(5A):19S–22S. [PubMed: 8503476]
16. Snowdon J, Donnelly N. A study of depression in nursing homes. J Psychiatr Res 1986;20(4):327–333. [PubMed: 3806427]
17. Burns BJ, Wagner HR, Taube JE, Magaziner J, Permutt T, Landerman LR. Mental health service useby the elderly in nursing homes. Am J Public Health 1993;83(3):331–337. [PubMed: 8438968]
Levin et al. Page 9
J Am Med Dir Assoc. Author manuscript; available in PMC 2010 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
18. Shea DG, Streit A, Smyer MA. Determinants of the use of specialist mental health services by nursinghome residents. Health Serv Res 1994;29(2):169–185. [PubMed: 8005788]
19. Smyer MA, Shea DG, Streit A. The provision and use of mental health services in nursing homes:results from the National Medical Expenditure Survey. Am J Public Health 1994;84(2):284–287.[PubMed: 8296955]
20. Heston LL, Garrard J, Makris L, et al. Inadequate treatment of depressed nursing home elderly. J AmGeriatr Soc 1992;40(11):1117–1122. [PubMed: 1401696]
21. Datto CJ, Oslin DW, Streim JE, Scheinthal SM, DiFilippo S, Katz IR. Pharmacologic treatment ofdepression in nursing home residents: A mental health services perspective. J Geriatr PsychiatryNeurol 2002;15(3):141–146. [PubMed: 12230084]
22. Weintraub D, Datto CJ, Streim JE, Katz IR. Second-generation issues in the management ofdepression in nursing homes. J Am Geriatr Soc 2002;50(12):2100–2101. author reply 2101.[PubMed: 12473032]
23. Crystal S, Sambamoorthi U, Walkup JT, Akincigil A. Diagnosis and treatment of depression in theelderly Medicare population: Predictors, disparities, and trends. J Am Geriatr Soc 2003;51(12):1718–1728. [PubMed: 14687349]
24. Miller DK, Malmstrom TK, Joshi S, Andresen EM, Morley JE, Wolinsky FD. Clinically relevantlevels of depressive symptoms in community-dwelling middle-aged African Americans. J AmGeriatr Soc 2004;52:741–748. [PubMed: 15086655]
25. OBRA. Omnibus Budget Reconciliation Act of 1987. Annu Rev Popul Law 1987 December 22;198714:473–475. Public Law No. 100–203.
26. Sloss EM, Solomon DH, Shekelle PG, et al. Selecting target conditions for quality of careimprovement in vulnerable older adults. J Am Geriatr Soc 2000;48(4):363–369. [PubMed:10798460]
27. National Healthcare Quality Report. Agency for Healthcare Research and Quality. Rockville, MD:2003 [September 15, 2007]. Available at: http://www.ahrq.gov/qual/nhqr03/nhqr03.htm
28. Streim JE, Oslin D, Katz IR, Parmelee PA. Lessons from geriatric psychiatry in the long-term caresetting. Psychiatr Q 1997;68(3):281–307. [PubMed: 9237321]
29. Lebowitz BD, Pearson JL, Schneider LS, et al. Diagnosis and treatment of depression in late life.Consensus statement update. JAMA 1997;278(14):1186–1190. [PubMed: 9326481]
30. Reynolds CF 3rd. Depression: Making the diagnosis and using SSRIs in the older patient. Geriatrics1996;51(10):28–34. [PubMed: 8863755]
31. Snowden M, Sato K, Roy-Byrne P. Assessment and treatment of nursing home residents withdepression or behavioral symptoms associated with dementia: A review of the literature. J Am GeriatrSoc 2003;51(9):1305–1317. [PubMed: 12919245]
32. Friedrich MJ. Recognizing and treating depression in the elderly. JAMA 1999;282(13):1215.[PubMed: 10517408]
33. Katona C. Managing depression and anxiety in the elderly patient. Eur Neuropsychopharmacol2000;10 4:S427–432. [PubMed: 11114487]
34. Katz IR, Simpson GM, Curlik SM, Parmelee PA, Muhly C. Pharmacologic treatment of majordepression for elderly patients in residential care settings. J Clin Psychiatry 1990;51(Suppl):41–47.discussion 48. [PubMed: 2195013]
35. Koenig HG. Late-life depression: How to treat patients with comorbid chronic illness. Interview byAlice V. Luddington. Geriatrics 1999;54(5):56–61. quiz 62. [PubMed: 10365186]
36. Menting JE, Honig A, Verhey FR, et al. Selective serotonin reuptake inhibitors (SSRIs) in thetreatment of elderly depressed patients: A qualitative analysis of the literature on their efficacy andside-effects. Int Clin Psychopharmacol 1996;11(3):165–175. [PubMed: 8923095]
37. Cooper LA, Gonzales JJ, Gallo JJ, et al. The acceptability of treatment for depression among African-American, Hispanic, and white primary care patients. Med Care 2003;41(4):479–489. [PubMed:12665712]
38. Bureau of Health Professions (BHP). Supply and Distribution of Health Professions in Rural Ameirca.Chapel Hill, NC: North Carolina Health Research Program; 1993.
39. Morris JN, Hawes C, Fries BE, et al. Designing the national resident assessment instrument for nursinghomes. Gerontologist 1990;30(3):293–307. [PubMed: 2354790]
Levin et al. Page 10
J Am Med Dir Assoc. Author manuscript; available in PMC 2010 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
40. Centers for Medicare and Medicaid Services (CMS). RAI: Minimum Data Set (MDS). Version 2.0Manual. 2004 [September 15, 2007]. Available at:http://www.cms.hhs.gov/NursingHomeQualityInits/20_NHQIMDS20.asp
41. Burns, BJ.; Taube, CA. Mental health services in general medical care in nursing homes. In: Fogel,B.; Furino, A.; Gottieb, G., editors. Mental Health Policy for Older Americans: Protecting Minds atRisk. Washington, DC: American Psychiatric Press; 1984. p. 63-84.
42. Harrington C, Carrillo H, Mullan J, Swan JH. Nursing facility staffing in the states: The 1991 to 1995period. Med Care Res Rev 1998;55(3):334–363. [PubMed: 9727302]
43. Singh DA, Schwab RC. Retention of administrators in nursing homes: What can management do?Gerontologist 1998;38(3):362–369. [PubMed: 9640856]
44. Morris JN, Fries BE, Mehr DR, et al. MDS Cognitive Performance Scale. J Gerontol 1994;49(4):M174–182. [PubMed: 8014392]
45. Cowles, CME. 2002 Nursing Home Statistical Yearbook. Montgomery Village, MD: CowlesResearch Group; 2003.
46. Fries BE, Schneider DP, Foley WJ, Gavazzi M, Burke R, Cornelius E. Refining a case-mix measurefor nursing homes: Resource Utilization Groups (RUG-III). Med Care 1994;32(7):668–685.[PubMed: 8028403]
47. Johnson-Pawlson J, Infeld DL. Nurse staffing and quality of care in nursing facilities. J Gerontol Nurs1996;22(8):36–45. [PubMed: 8826283]
48. Harrington, C.; Carrillo, H.; Wellin, V. Nursing Facilities, Staffing, Residents, and FacilityDeficiencies, 1994 through 2000. San Francisco: Department of Social and Behavioral Science,University of California; 2001.
49. Research Triangle Institute. Sudaan User's Manual. 8.0. Research Triangle Park, NC: ResearchTriangle Institute; 2001.
50. Zimmerman DR, Karon SL, Arling G, et al. Development and testing of nursing home qualityindicators. Health Care Financ Rev 1995;16:107–127. [PubMed: 10151883]
51. Abraham IL, Neundorfer MM, Currie LJ. Effects of group interventions on cognition and depressionin nursing home residents. Nurs Res 1992;41(4):196–202. [PubMed: 1383947]
Levin et al. Page 11
J Am Med Dir Assoc. Author manuscript; available in PMC 2010 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Levin et al. Page 12
Tabl
e 1
Prev
alen
ce o
f Dep
ress
ion
amon
g O
hio
Nur
sing
Hom
e R
esid
ents
The
Sam
ple
Dia
gnos
ed w
ith D
epre
ssio
nL
ogis
tic R
egre
ssio
n on
Dia
gnos
is o
f Dep
ress
ion
Tot
al N
Col
%N
Row
%O
R95
% C
I
Tota
l76
735
100.
036
888
48.1
——
Res
iden
t Cha
ract
eris
tics
Gen
der*
M
ale
19 1
0824
.985
7444
.9—
—
Fe
mal
e57
627
75.1
2831
449
.11.
25†
[1.2
0,1.
30]
Age
*—
A
ge 6
5–74
10 7
1114
.054
9351
.3—
—
A
ge 7
5–84
28 5
1137
.214
570
51.1
0.91
†[0
.87,
0.95
]
A
ge 8
5 an
d ov
er37
513
48.9
16 8
2544
.90.
66†
[0.6
3,0.
70]
Rac
e/Et
hnic
ity*
W
hite
68 0
3588
.733
771
49.6
——
A
fric
an A
mer
ican
8117
10.6
2859
35.2
0.52
†[0
.48,
0.5
7]
O
ther
s55
30.
724
644
.50.
83‡
[0.7
0, 0
.98]
Educ
atio
n Le
vel*
Le
ss th
an h
igh
scho
ol27
673
36.1
12 6
6145
.8—
—
H
igh
scho
ol a
nd b
elow
28 9
0137
.714
443
50.0
1.11
†[1
.07,
1.16
]
C
olle
ge a
nd a
bove
9123
11.9
4412
48.4
1.10
†[1
.05,
1.16
]
M
issi
ng11
038
14.4
5372
48.7
1.14
†[1
.06,
1.24
]
Mar
ital s
tatu
s at a
sses
smen
t *
N
ever
mar
ried
7272
9.5
2936
40.4
——
M
arrie
d12
654
16.5
6081
48.1
1.38
†[1
.29,
1.48
]
W
idow
ed49
437
64.4
24 1
4748
.81.
42†
[1.3
4,1.
51]
Se
para
ted/
Div
orce
d73
599.
637
1750
.51.
47†
[1.3
7,1.
58]
No.
of p
hysi
cal c
omor
bid
dise
ases
*
J Am Med Dir Assoc. Author manuscript; available in PMC 2010 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Levin et al. Page 13
The
Sam
ple
Dia
gnos
ed w
ith D
epre
ssio
nL
ogis
tic R
egre
ssio
n on
Dia
gnos
is o
f Dep
ress
ion
Tot
al N
Col
%N
Row
%O
R95
% C
I
N
one
7777
10.1
3041
39.1
——
1–
241
119
53.6
18 9
8046
.21.
32†
[1.2
5,1.
39]
3–
425
001
32.6
13 1
5052
.61.
66†
[1.5
7,1.
76]
4
and
abov
e28
383.
717
1760
.52.
26†
[2.0
6,2.
48]
Seve
re m
enta
l illn
ess
Y
es51
646.
724
7948
.00.
97[0
.90,
1.04
]
N
o71
570
93.3
34 4
0848
.1—
—
AD
L se
lf-pe
rfor
man
ce h
iera
rchy
scal
e*
In
depe
nden
t23
273.
010
6245
.6—
—
Li
mite
d18
624
24.3
8645
46.4
1.04
[0.9
5,1.
14]
D
epen
dent
43 8
8957
.222
503
51.3
1.32
†[1
.21,
1.44
]
To
tal d
epen
denc
e11
894
15.5
4677
39.3
0.99
[0.9
0,1.
10]
Cog
nitiv
e pe
rfor
man
ce sc
ale*
In
tact
13 9
6918
.268
7449
.2—
—
So
me
impa
irmen
t44
593
58.1
22 7
5851
.01.
11†
[1.0
6,1.
17]
Se
vere
impa
irmen
t18
172
23.7
7256
39.9
0.78
†[0
.73,
0.83
]
Faci
lity
char
acte
ristic
s
Urb
an
Y
es59
749
77.9
28 5
6747
.8—
—
N
o16
986
22.1
8321
49.0
0.99
[0.9
4,1.
06]
Size
Le
ss th
an 5
020
312.
697
547
.3—
—
50
–99
14 8
9519
.470
3448
.00.
95[0
.81,
1.10
]
10
0–19
947
902
62.4
23 2
5748
.60.
99[0
.86,
1.15
]
20
0 an
d A
bove
11 9
0715
.556
2247
.20.
97[0
.82,
1.16
]
Type
of o
wne
rshi
p
Pr
ofit
56 4
2673
.527
210
48.2
——
N
onpr
ofit
17 4
7022
.884
1948
.21.
00[0
.93,
1.08
]
G
over
nmen
t28
393.
712
5944
.30.
88‡
[0.7
8,0.
99]
J Am Med Dir Assoc. Author manuscript; available in PMC 2010 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Levin et al. Page 14
The
Sam
ple
Dia
gnos
ed w
ith D
epre
ssio
nL
ogis
tic R
egre
ssio
n on
Dia
gnos
is o
f Dep
ress
ion
Tot
al N
Col
%N
Row
%O
R95
% C
I
Aff
iliat
ion
C
hain
43 9
4257
.321
368
48.6
——
N
onch
ain
32 7
9342
.715
520
47.3
0.97
[0.9
1,1.
03]
Occ
upan
cy ra
te
Lo
wes
t qua
rtile
19 0
8924
.991
9548
.2—
—
Se
cond
qua
rtile
19 2
0625
.092
0647
.90.
98[0
.92,
1.05
]
Th
ird q
uarti
le19
146
25.0
9146
47.8
0.98
[0.9
1,1.
05]
H
ighe
st q
uarti
le19
294
25.1
9341
48.4
0.99
[0.9
1,1.
08]
Tota
l nur
sing
hou
rs p
er re
side
nt p
er d
ay
Lo
wes
t qua
rtile
19 1
5825
.090
1447
.1—
—
Se
cond
qua
rtile
19 2
0125
.090
9147
.31.
02[0
.95,
1.09
]
Th
ird q
uarti
le19
138
24.9
9239
48.3
1.03
[0.9
6,1.
11]
H
ighe
st q
uarti
le19
238
25.1
9544
49.6
1.09
‡[1
.01,
1.18
]
% o
f res
iden
ts w
ith M
edic
aid
as p
rimar
y pa
yer*
Lo
wes
t qua
rtile
19 1
4925
.093
1948
.7—
—
Se
cond
qua
rtile
19,1
3624
.99,
297
48.6
1.00
[0.9
3,1.
08]
Th
ird q
uarti
le19
095
24.9
9390
49.2
1.06
[0.9
8,1.
14]
H
ighe
st q
uarti
le19
355
25.2
8882
45.9
1.06
§[0
.99,
1.14
]
Num
ber o
f def
icie
ncie
s*
0–
222
929
29.9
11 3
1549
.3—
—
3–
414
100
18.4
6817
48.3
0.96
[0.8
9,1.
03]
5–
820
369
26.5
9822
48.2
0.98
[0.9
2,1.
05]
>
819
337
25.2
8934
46.2
0.92
‡[0
.86,
0.99
]
Acu
ity in
dex
Lo
wes
t qua
rtile
19 1
8225
.093
2248
.6—
—
Se
cond
qua
rtile
19 1
3924
.991
5347
.80.
99[0
.92,
1.05
]
Th
ird q
uarti
le19
189
25.0
9299
48.5
1.00
[0.9
2,1.
08]
H
ighe
st q
uarti
le19
225
25.1
9114
47.4
0.97
[0.9
0,1.
06]
CI,
conf
iden
ce in
terv
al; O
R, o
dds r
atio
.
J Am Med Dir Assoc. Author manuscript; available in PMC 2010 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Levin et al. Page 15* Si
gnifi
cant
gro
up d
iffer
ence
(P <
.05)
in p
reva
lenc
e of
dep
ress
ion
diag
nosi
s by
chi-s
quar
e st
atis
tics.
†, ‡
, and
§ d
enot
e si
gnifi
cant
eff
ect i
n th
e lo
gist
ic re
gres
sion
, at 1
%, 5
%, a
nd 1
0% le
vel,
resp
ectiv
ely.
Bot
h ch
i-squ
are
test
s and
logi
stic
regr
essi
ons a
djus
ted
for c
lust
erin
g of
resi
dent
s with
in fa
cilit
ies.
J Am Med Dir Assoc. Author manuscript; available in PMC 2010 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Levin et al. Page 16
Tabl
e 2
Tre
atm
ent a
mon
g O
hio
Nur
sing
Hom
e R
esid
ents
Dia
gnos
ed w
ith D
epre
ssio
n
The
Sam
ple
Any
Tre
atm
ent
Log
istic
Reg
ress
ion
on A
ny T
reat
men
t of D
epre
ssio
n
NC
ol %
NR
ow %
OR
95%
CI
Tota
l36
888
100.
028
378
76.9
Resi
dent
Cha
ract
eris
tics
Gen
der*
M
ale
8574
23.2
6732
78.5
Fe
mal
e28
314
76.8
21 6
4676
.40.
98[0
.92,
1.05
]
Age
*
A
ge 6
5–74
5493
14.9
4399
80.1
A
ge 7
5–84
14 5
7039
.511
446
78.6
0.90
‡[0
.82,
0.97
]
A
ge 8
5 an
d ov
er16
825
45.6
12 5
3374
.50.
71†
[0.6
5,0.
77]
Rac
e/Et
hnic
ity*
W
hite
33 7
7191
.626
134
77.4
A
fric
an A
mer
ican
2859
7.8
2048
71.6
0.80
†[0
.72,
0.89
]
O
ther
s24
60.
718
876
.40.
95[0
.70,
1.29
]
Educ
atio
n le
vel*
Le
ss th
an h
igh
scho
ol12
661
34.3
,651
76.2
H
igh
scho
ol14
443
39.2
11 2
7178
.01.
07‡
[1.0
1,1.
14]
C
olle
ge a
nd a
bove
4412
12.0
3463
78.5
1.12
‡[1
.03,
1.22
]
M
issi
ng53
7214
.639
9374
.30.
95[0
.87,
1.04
]
Mar
ital s
tatu
s at a
sses
smen
t*
N
ever
mar
ried
2936
8.0
2,20
775
.2
M
arrie
d60
8116
.547
5678
.21.
22†
[1.0
9,1.
36]
W
idow
ed24
147
65.5
18 5
4276
.81.
16†
[1.0
5,1.
29]
Se
para
ted/
Div
orce
d37
1710
.128
6877
.21.
09[0
.96,
1.23
]
No.
of p
hysi
cal c
omor
bid
dise
ases
*
N
one
3041
8.2
2196
72.2
J Am Med Dir Assoc. Author manuscript; available in PMC 2010 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Levin et al. Page 17
The
Sam
ple
Any
Tre
atm
ent
Log
istic
Reg
ress
ion
on A
ny T
reat
men
t of D
epre
ssio
n
NC
ol %
NR
ow %
OR
95%
CI
1–
218
980
51.5
14 5
4576
.61.
20†
[1.1
0,1.
31]
3–
413
150
35.6
10 3
0778
.41.
26†
[1.1
4,1.
38]
4
and
abov
e17
174.
713
3077
.51.
17‡
[1.0
1,1.
34]
Seve
re m
enta
l illn
ess*
a
Y
es24
796.
718
2373
.50.
75†
[0.6
8,0.
83]
N
o34
408
93.3
26 5
5477
.2
AD
L sc
ale*
In
depe
nden
t10
622.
985
880
.8
Li
mite
d86
4523
.470
5881
.61.
08[0
.91,
1.27
]
D
epen
dent
22 5
0361
.017
650
78.4
0.95
[0.8
1,1.
11]
To
tal d
epen
denc
e46
7712
.728
1160
.10.
50†
[0.4
2,0.
60]
Cog
nitiv
e pe
rfor
man
ce sc
ale*
In
tact
6874
18.6
5609
81.6
So
me
impa
irmen
t22
758
61.7
18 1
0579
.60.
97[0
.90,
1.05
]
Se
vere
iImpa
irmen
t72
5619
.746
6464
.30.
60†
[0.5
4,0.
66]
Faci
lity
char
acte
ristic
s
Urb
an
Y
es28
567
77.4
21 8
8276
.61.
06[0
.96,
1.17
]
N
o83
2122
.664
9678
.1
Size
Le
ss th
an 5
097
52.
675
977
.8
50
–99
7034
19.1
5352
76.1
0.88
[0.7
1,1.
08]
10
0–19
923
257
63.0
17 9
4477
.20.
95[0
.77,
1.16
]
20
0 an
d ab
ove
5622
15.2
4323
76.9
0.96
[0.7
6,1.
22]
Type
of o
wne
rshi
p
Pr
ofit
27 2
1073
.820
948
77.0
N
onpr
ofit
8419
22.8
6448
76.6
0.94
[0.8
5,1.
05]
G
over
nmen
t12
593.
498
278
.00.
94[0
.76,
1.17
]
Aff
iliat
ion
J Am Med Dir Assoc. Author manuscript; available in PMC 2010 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Levin et al. Page 18
The
Sam
ple
Any
Tre
atm
ent
Log
istic
Reg
ress
ion
on A
ny T
reat
men
t of D
epre
ssio
n
NC
ol %
NR
ow %
OR
95%
CI
C
hain
21 3
6857
.916
413
76.8
N
onch
ain
15 5
2042
.111
965
77.1
1.03
[0.9
5,1.
12]
Prov
isio
n of
ons
ite m
enta
l hea
lth se
rvic
es
Y
es34
089
92.4
26 2
1976
.90.
97[0
.82,
1.15
]
N
o27
997.
621
5977
.1
Occ
upan
cy ra
te
Lo
wes
t qua
rtile
9195
24.9
7005
76.2
Se
cond
qua
rtile
9206
25.0
7066
76.8
1.01
[0.9
2,1.
12]
Th
ird q
uarti
le91
4624
.870
0876
.60.
99[0
.89,
1.10
]
H
ighe
st q
uarti
le93
4125
.372
9978
.11.
10[0
.97,
1.23
]
Tota
l nur
sing
hou
rs p
er re
side
nt p
er d
ay
Lo
wes
t qua
rtile
9014
24.4
6975
77.4
Se
cond
qua
rtile
9091
24.6
6959
76.5
0.94
[0.8
5,1.
04]
Th
ird q
uarti
le92
3925
.071
5777
.51.
00[0
.91,
1.11
]
H
ighe
st q
uarti
le95
4425
.972
8776
.40.
95[0
.85,
1.06
]
% o
f res
iden
ts w
ith M
edic
aid
as p
rimar
y pa
yer*
Lo
wes
t qua
rtile
9319
25.3
7182
77.1
Se
cond
qua
rtile
9297
25.2
7293
78.4
1.07
[0.9
6,1.
19]
Th
ird q
uarti
le93
9025
.572
5777
.31.
02[0
.91,
1.14
]
H
ighe
st q
uarti
le88
8224
.166
4674
.80.
99[0
.89,
1.11
]
Num
ber o
f def
icie
ncie
s*
0–
211
315
30.7
8894
78.6
3–
468
1718
.552
6777
.30.
94[0
.84,
1.05
]
5–
898
2226
.674
4375
.80.
85†
[0.7
7,0.
94]
>
889
3424
.267
7475
.80.
87†
[0.7
8,0.
96]
Acu
ity In
dex
Lo
wes
t qua
rtile
9322
25.3
7159
76.8
Se
cond
qua
rtile
9153
24.8
7045
77.0
1.03
[0.9
3,1.
15]
Th
ird q
uarti
le92
9925
.272
4477
.91.
15‡
[1.0
2,1.
29]
J Am Med Dir Assoc. Author manuscript; available in PMC 2010 June 18.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Levin et al. Page 19
The
Sam
ple
Any
Tre
atm
ent
Log
istic
Reg
ress
ion
on A
ny T
reat
men
t of D
epre
ssio
n
NC
ol %
NR
ow %
OR
95%
CI
H
ighe
st q
uarti
le91
1424
.769
3076
.01.
04[0
.94,
1.16
]
CI,
conf
iden
ce in
terv
al; O
R, o
dds r
atio
.
* Sign
ifica
nt g
roup
diff
eren
ce (P
< .0
5) in
the
type
s of t
reat
men
t am
ong
resi
dent
s dia
gnos
ed w
ith d
epre
ssio
n by
chi
-squ
are
stat
istic
s. C
hi-s
quar
e te
sts w
ere
adju
sted
for c
lust
erin
g of
resi
dent
s with
in fa
cilit
ies.
† an
d ‡
deno
te si
gnifi
cant
eff
ect i
n th
e lo
gist
ic re
gres
sion
, at 1
% a
nd 5
% le
vel,
resp
ectiv
ely.
Bot
h ch
i-squ
are
test
s and
logi
stic
regr
essi
ons a
djus
ted
for c
lust
erin
g of
resi
dent
s with
in fa
cilit
ies.
J Am Med Dir Assoc. Author manuscript; available in PMC 2010 June 18.