Muscarinic Toxidrome - Ohio ACEP
97
01/29/2014 1 Basic Training Diagnoses Killer Foils Associations Book of Commons Lyte Notes Complications Causes Paul de Saint Victor M.D., F.A.C.E.P., M.H.A., C.P.E., F.I.M. Associate Director, Emergency Medicine Residency Program St Vincent Mercy Medical Center Assistant Clinical Professor Department of Surgery University of Toledo, College of Medicine Toledo, Ohio Friday, February 7 2 Muscarinic Toxidrome Excess acetylcholine (ACh) at muscarinic parasympathetic end organ receptors • Diarrhea • Urination • Miosis • Bradycardia, • Bronchorrhea, Bronchospasm • Emesis • Lacrimation • Salivation, sweating, Secretion D U M B B E L S Nicotinic Toxidrome Excess ACh at central autonomic receptors Can be mixed sympathetic and parasympathetic presentation • Mydriasis • Tachycardia • Weakness • Hypertension, Hyperglycemia • Fasciculation • Seizures MTWHFS (days of the week) More severe toxicity: - seizures - respiratory depression - hyperthermia No specific antidote Supportive care Benzos
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Muscarinic Toxidrome - Ohio ACEP
01/29/2014
1
Basic Training
Diagnoses
Killer Foils
AssociationsBook of Commons
Lyte Notes
Complications
Causes
Paul de Saint Victor M.D., F.A.C.E.P., M.H.A., C.P.E., F.I.M.
Associate Director, Emergency Medicine Residency Program
St Vincent Mercy Medical Center
Assistant Clinical Professor
Department of Surgery
University of Toledo, College of Medicine
Toledo, OhioFriday, February 7
2
Muscarinic ToxidromeExcess acetylcholine (ACh) at muscarinic
parasympathetic end organ receptors
• Diarrhea
• Urination
• Miosis
• Bradycardia,
• Bronchorrhea, Bronchospasm
• Emesis
• Lacrimation
• Salivation, sweating, Secretion
D
U
M
B
B
E
L
S
Nicotinic ToxidromeExcess ACh at central autonomic receptors
Can be mixed sympathetic and parasympathetic presentation
• Mydriasis
• Tachycardia
• Weakness
• Hypertension, Hyperglycemia
• Fasciculation
• Seizures
MTWHFS (days of the week)
More severe toxicity:
- seizures
- respiratory depression
- hyperthermia
No specific antidote
Supportive care
Benzos
01/29/2014
2
www.ohacep.org/emrlectures
Trauma in Pregnancy and Fetal Death
• The most common cause of fetal death in
trauma is maternal shock and death.
• When the mother survives, abruption is the
next leading cause of fetal mortality
followed by uterine rupture
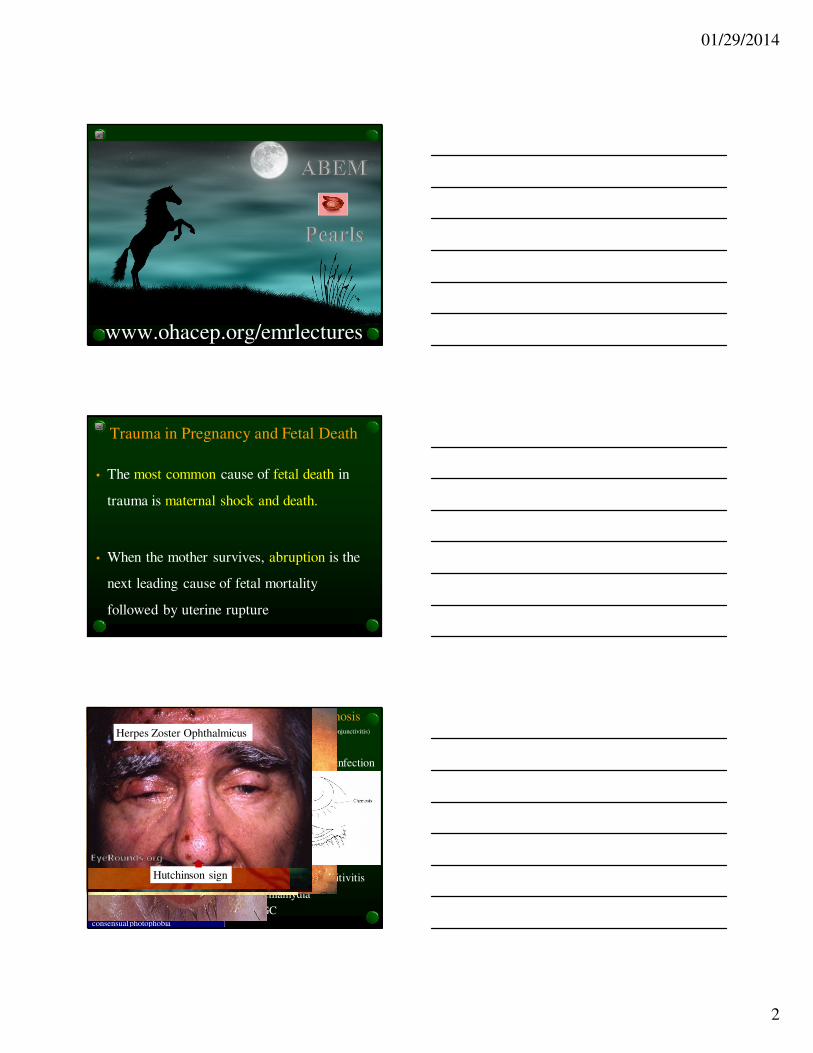
Match the following red eyes with the diagnosis
With preauricular adenopathy
With discharge and a cough
Painful with mild mucoserous
discharge for 5 d then spread
With cobblestone papillae under
upper lid
With hypopeon in contact wearer
After eye surgery
With diffuse punctate keratopathy
With cup:disc ratio > 1:2
Dendridic pattern (dumbells)
Cells in the vitreous cavity
Ciliary flush, flare in anterior chamber,
consensual photophobia
•EKC (epidemic keratoconjunctivitis)
•Uveitis
•Herpes simplex infection
•UV keratitis
•Pseudomonas
•Glaucoma
•Iritis
•Endophthalmitis
•Viral conjunctivitis
•Allergic conjuncitivitis
•Chlamydia
•GC
Herpes Zoster Ophthalmicus
Hutchinson sign

01/29/2014
3
ToxidromesAMS, Resp Alk,
Met Acid, tinnitus,
hyperpnea, diaphoresis
Salicylate
toxidrome
Agitation, mydriasis,
diphoresis, tachy, HTN,
hyperthermia, normal BS
Sympathomimetic
toxidrome
CNS depression,
miosis, resp depression
Opioid toxidrome
AMS, incr muscle tone,
hypereflexia, hypertherm
Serotonin
toxidrome
Sal, Lacr, urination, N/V,
diaphoresis, diarrhea,
muscle fasciculation,
bronchorhea, weakness
Cholinergic
toxidrome
AMS, mydriasis, dry mm
& skin, urinary retention,
BS, hyperthermia
Anticholinergic
toxidrome
WET/BS+
DRY/noBS
Sudden Loss of Vision
• Central retinal artery occlusion
• Central retinal vein occlusion
• Retinal detachment
• Temporal arteritis
• Multiple sclerosis
• Vitreous hemorrhage
• Amaurosis Fugax
Pale retina, cherry
red spot
squashed tomatoes
Blood and thunder
Sand dunes, flashes of light, floaters,
lowering curtain, visual field defect
Polymyalgia rheumatica, 50, CRP, prednisone, blindness, jaw claudication
Optic neuritis, Bilateral internuclear ophthalmoplegia, red desaturation test
Associations
Ocular TIA
Diabetic with visual floaters, loss of red reflex, with/without retinal detachment
3Fs
01/29/2014
4
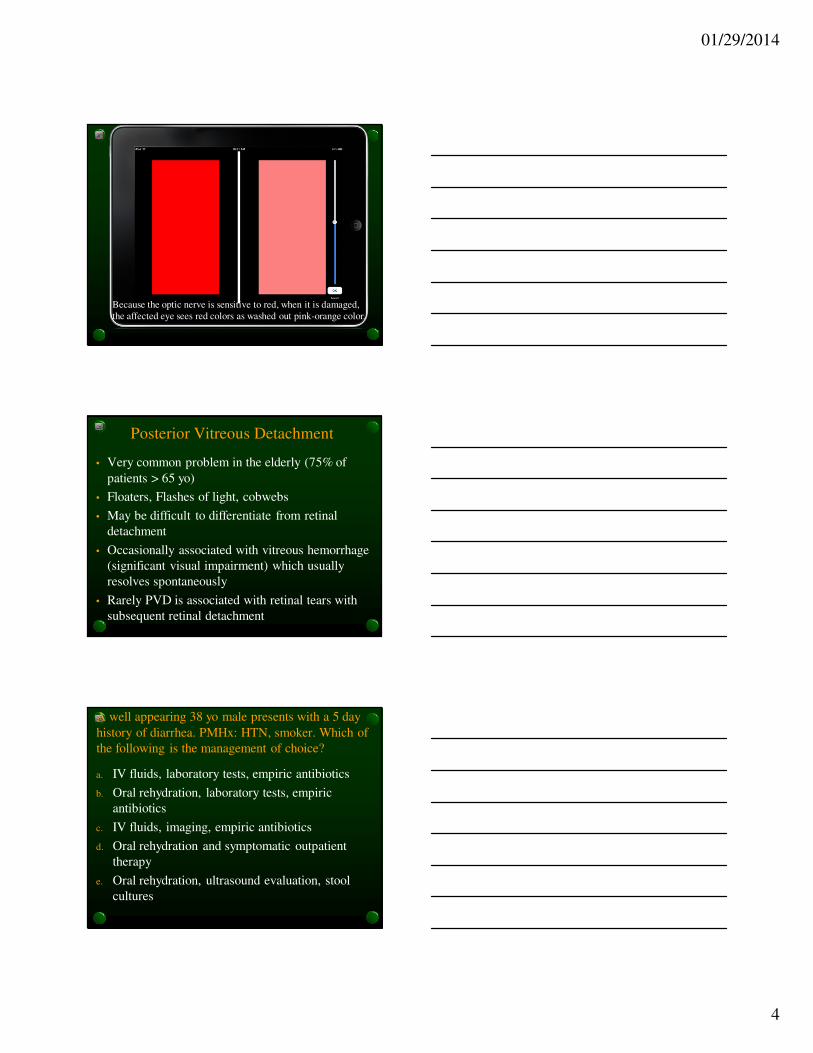
Because the optic nerve is sensitive to red, when it is damaged,
the affected eye sees red colors as washed out pink-orange color.
Posterior Vitreous Detachment
• Very common problem in the elderly (75% of
patients > 65 yo)
• Floaters, Flashes of light, cobwebs
• May be difficult to differentiate from retinal
detachment
• Occasionally associated with vitreous hemorrhage
(significant visual impairment) which usually
resolves spontaneously
• Rarely PVD is associated with retinal tears with
subsequent retinal detachment
A well appearing 38 yo male presents with a 5 day
history of diarrhea. PMHx: HTN, smoker. Which of
the following is the management of choice?
a. IV fluids, laboratory tests, empiric antibiotics
b. Oral rehydration, laboratory tests, empiric
antibiotics
c. IV fluids, imaging, empiric antibiotics
d. Oral rehydration and symptomatic outpatient
therapy
e. Oral rehydration, ultrasound evaluation, stool
cultures

01/29/2014
5
Seizing pt w diarrhea
Diarrhea w anxiety and heat intoleranceDiarrhea w paresthesiasand reverse temperature sensation Elderly pt with bloody diarrhea and abd POOP
Diarrhea , crampy abd pain, fever, antecedent Hx of Abiotic use
Diarrhea c Pneumonia
Cholera like diarrhea
Shigellosis, Theo Tox
Thyrotoxicosis
Pseudomembranous colitis
Mesenteric ischemia
Legionella Pneumonia
Ciguatera
Arsenic Poisoning
Toxin producing C diffFever, toxic, profuse diarrheaStop Abx, No antidiarrhealVanco, Metronidazole
Diarrhea, pet turtle or eggs,
Sickle cell pts get septic
Salmonella
All of the following are intrinsic (Contact
Activation Pathway) factors of the
clotting cascade EXCEPT:• Factor 8
• Factor 9
• Factor 10
• Factor 11
• Factor 12
The Clotting Cascade
9-118- -12VII
INtrinsicExtrinsic
1, 2, 5, 10, 13Common pathway
Heparin, PTTProtamine zinc
Warfarin, INR (PT)Vit K
Vit K dependent factors: II, VII, IX, X
On 9/11 we
were Contacted
by outsiders
How it works (in a minute)
Contact Activation
Pathway
Tissue Activation
Pathway
3, 4, 6 are out

01/29/2014
6
Hematology: Match the Following
1. CAP Factors (intrinsic)
2. Common pathway
factors
3. TAP factors (extrinsic)
4. Vitamin K
dependent factors
a. Factors I, II, V,
X, XII
b. II, VII, IX, X
c. Factors 9-11 and
8 and 12
d. Factors VII
Sore Throat2 – 7yo appears ill, dysphagia
drooling , distress, muffled
voice, PE findings except for
high fever normal, pain hyoid
Epiglottitis
6 mo – 3 yo, URI that worsens, worse at night, mildly ill, barky cough, stridor, dyspnea, subglotticinflammation, viral
Croup
Severe croup pt not
responding to racemic epi,
pus from ET tube
Bacterial
Tracheitis
6mo – 3yo (<4yo) severe airway obstruction, retropharyngeal lymph nodes, dysphagia, ill appearing tripod, muffled voice
Retropharyngeal
abscess
> 8 yo, dysphagia, trouble swallowing, trismus, deviated uvula
Peritonsilar
abscess
Peds: systemic
OR for direct exam
Adult: localized
Diarrheal disease: Match’em
• RLQ pain, little diarrhea
• Camper, gay, flatulence
• Shellfish, alcoholic incr
morbidity mortality
• Liver cysts
• Tuna, (looks like allergic Rx),
peppery taste, facial flushing,
palp, abd cramps
Vibrio
Vulnificus
Yersinia
Scombroid
Amebiasis
Giardia
Looks like appendicitis
Invasive dz of terminal ileum
and cecum –MC in children

01/29/2014
7
Peritonsillar Abscess
• Polymicrobial infections are the rule
• Fusopbacterium
• GABH strep
• Streptococcus
• Staphylococcus
• Numerous anaerobes
• Rx
• Needle aspiration + antibiotics
Withdrawal Syndrome
• Clinical Presentation
• Mydriasis
• Tachycardia looks sympathomimetic
• Hypertension
• Diarrhea
• Hallucinations
• Piloerection
• Lacrimation
• Crampy abdominal pain
• Yawning
• Seizures – only EtOH, BZ, barb, propoxyphene
Alcoholics drink cheap
D-CHEaPLY
these indicate withdrawal
01/29/2014
8
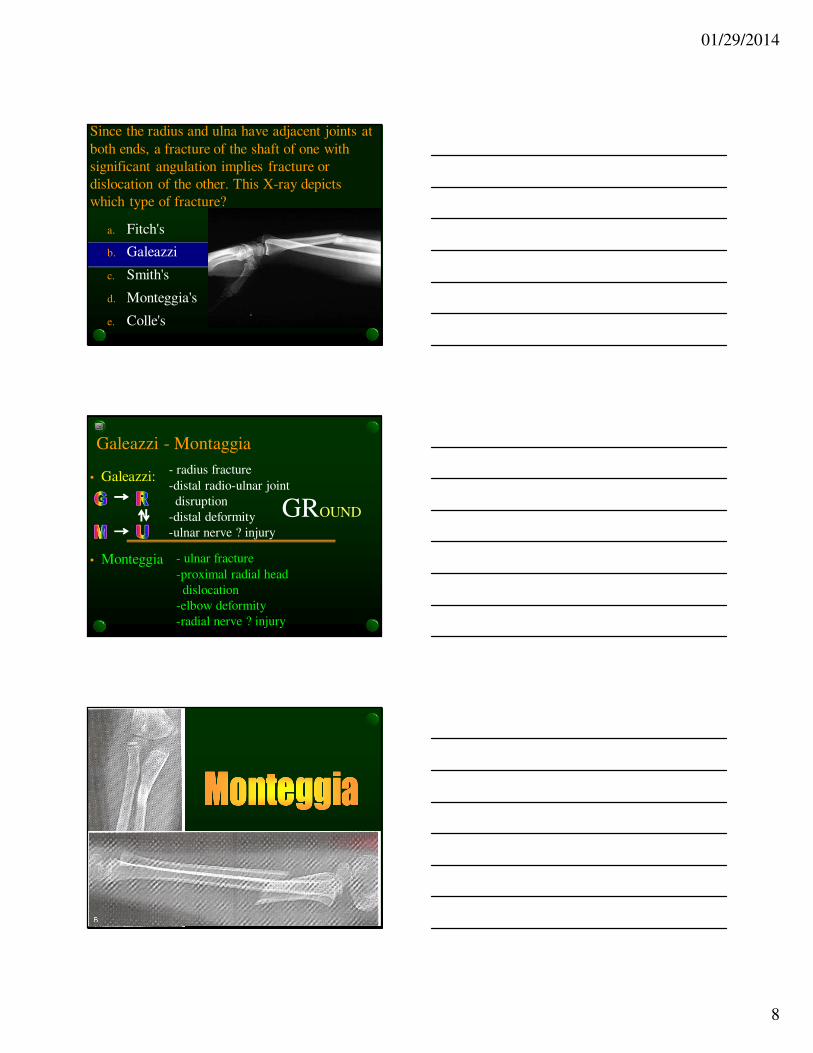
Since the radius and ulna have adjacent joints at
both ends, a fracture of the shaft of one with
significant angulation implies fracture or
dislocation of the other. This X-ray depicts
which type of fracture?
a. Fitch's
b. Galeazzi
c. Smith's
d. Monteggia's
e. Colle's
Galeazzi - Montaggia
• Galeazzi:
• Monteggia
- radius fracture
-distal radio-ulnar joint
disruption
-distal deformity
-ulnar nerve ? injury
- ulnar fracture
-proximal radial head
dislocation
-elbow deformity
-radial nerve ? injury
GROUND
01/29/2014
9
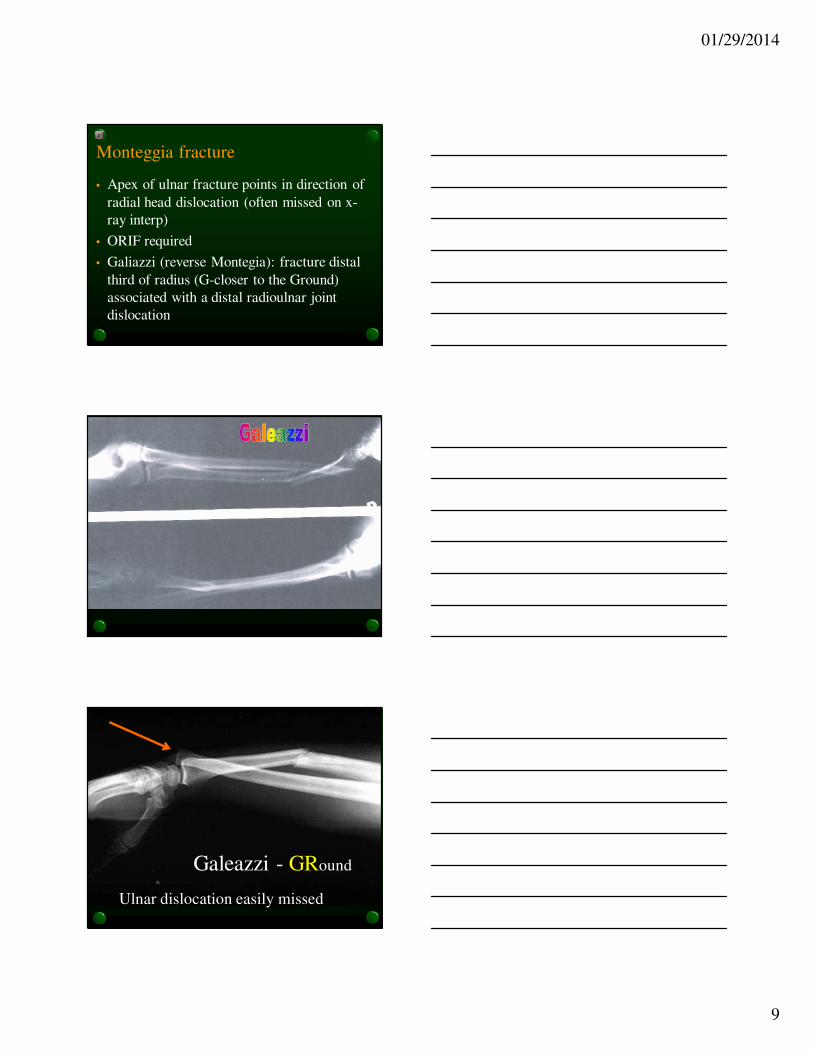
Monteggia fracture
• Apex of ulnar fracture points in direction of
radial head dislocation (often missed on x-
ray interp)
• ORIF required
• Galiazzi (reverse Montegia): fracture distal
third of radius (G-closer to the Ground)
associated with a distal radioulnar joint
dislocation
Galeazzi - GRound
Ulnar dislocation easily missed
01/29/2014
10
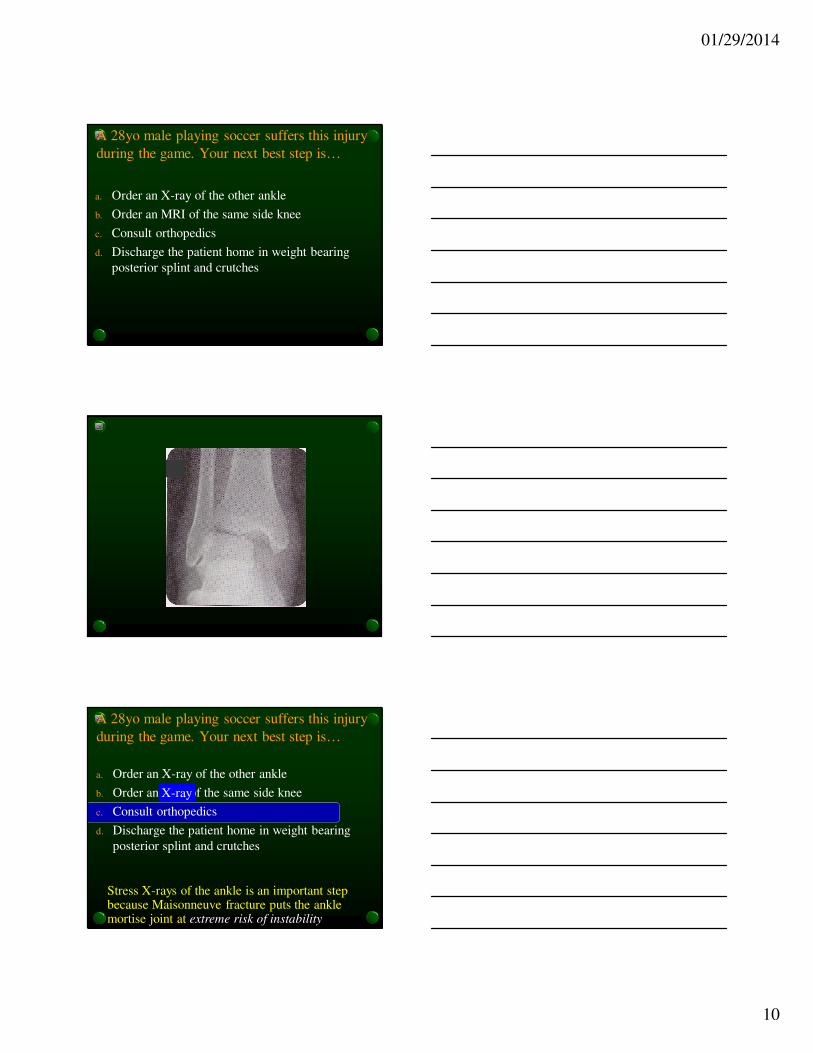
A 28yo male playing soccer suffers this injury
during the game. Your next best step is…
a. Order an X-ray of the other ankle
b. Order an MRI of the same side knee
c. Consult orthopedics
d. Discharge the patient home in weight bearing
posterior splint and crutches
A 28yo male playing soccer suffers this injury
during the game. Your next best step is…
a. Order an X-ray of the other ankle
b. Order an MRI of the same side knee
c. Consult orthopedics
d. Discharge the patient home in weight bearing
posterior splint and crutches
Stress X-rays of the ankle is an important step because Maisonneuve fracture puts the ankle mortise joint at extreme risk of instability
X-ray

01/29/2014
11
Maisonneuve Fracture
Associations• Proximal fibular fracture
• Deltoid ligament disruption
• and ankle joint instability
• (stress views of the ankle)
• Peroneal nerve injury• Motor: foot dorsiflexion
• Sensory: dorsum of foot
• With deep peroneal n injury
• only: sensory dorsum between
• big toe and second toes
• May get Maisonneuve with bad ankle sprain only so must look for fibular fracture
01/29/2014
12
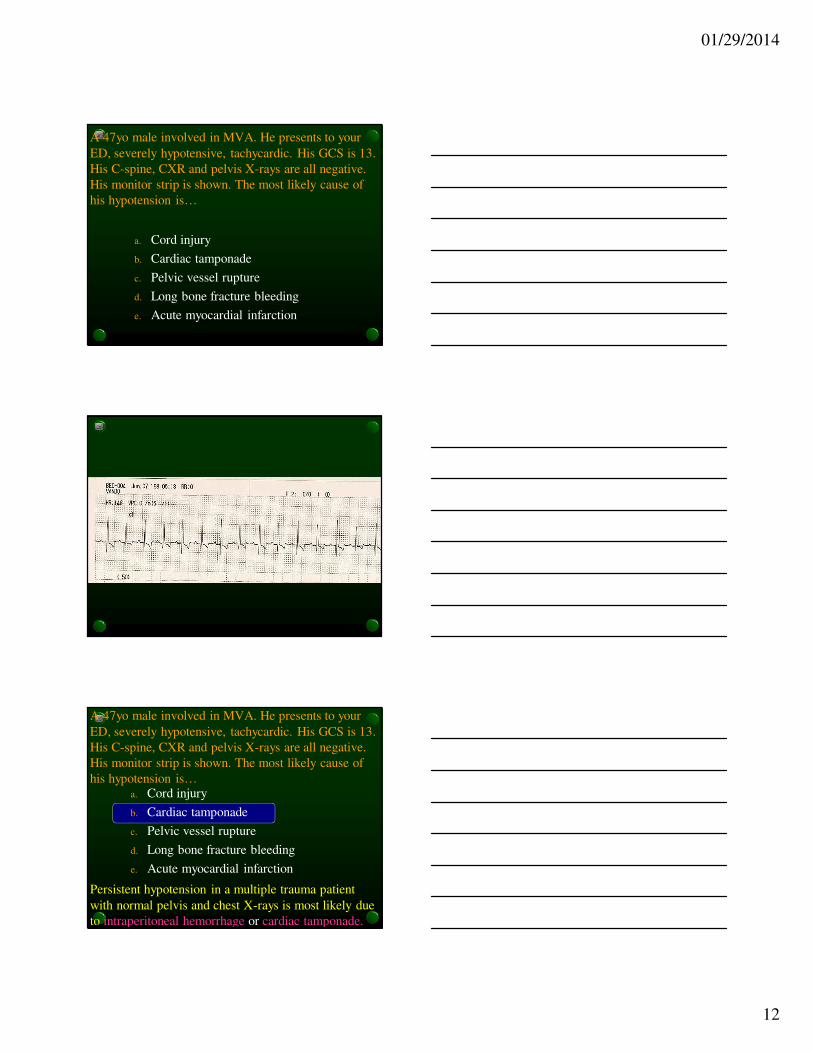
A 47yo male involved in MVA. He presents to your
ED, severely hypotensive, tachycardic. His GCS is 13.
His C-spine, CXR and pelvis X-rays are all negative.
His monitor strip is shown. The most likely cause of
his hypotension is…
a. Cord injury
b. Cardiac tamponade
c. Pelvic vessel rupture
d. Long bone fracture bleeding
e. Acute myocardial infarction
A 47yo male involved in MVA. He presents to your
ED, severely hypotensive, tachycardic. His GCS is 13.
His C-spine, CXR and pelvis X-rays are all negative.
His monitor strip is shown. The most likely cause of
his hypotension is…a. Cord injury
b. Cardiac tamponade
c. Pelvic vessel rupture
d. Long bone fracture bleeding
e. Acute myocardial infarction
Persistent hypotension in a multiple trauma patient
with normal pelvis and chest X-rays is most likely due
to intraperitoneal hemorrhage or cardiac tamponade.
01/29/2014
13
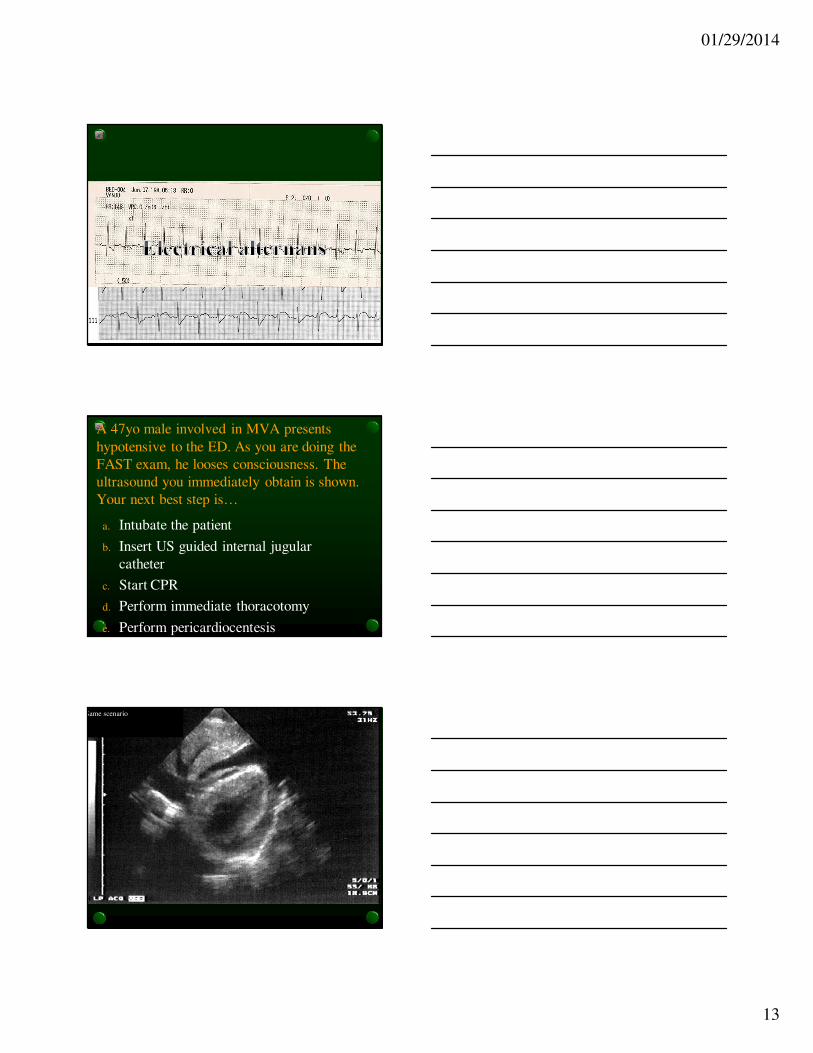
A 47yo male involved in MVA presents
hypotensive to the ED. As you are doing the
FAST exam, he looses consciousness. The
ultrasound you immediately obtain is shown.
Your next best step is…
a. Intubate the patient
b. Insert US guided internal jugular
catheter
c. Start CPR
d. Perform immediate thoracotomy
e. Perform pericardiocentesis
Pericardial Window:
Pericardial Tamponade
Same scenario

01/29/2014
14
A 47yo male involved in MVA presents
hypotensive to the ED. As you are doing the
FAST exam, he loses consciousness. The
ultrasound you immediately obtain is shown.
Your next best step is…
a. Intubate the patient
b. Insert US guided internal jugular
catheter
c. Start CPR
d. Perform immediate thoracotomy
e. Perform pericardiocentesis US guided
Beck’s triad…
• Hypotension
• Muffled heart sounds
• JVD
Removal of ______ cc may result in
immediate improvement
20 - 30
Pericardial Window:
Pericardial Tamponade
Rt Ventricular collapse consistent with tamponade
Pericardial fluid
L ventricle
Same scenario
Identify what arrows point to

01/29/2014
15
Tricuspid v
Mitral v
Liver
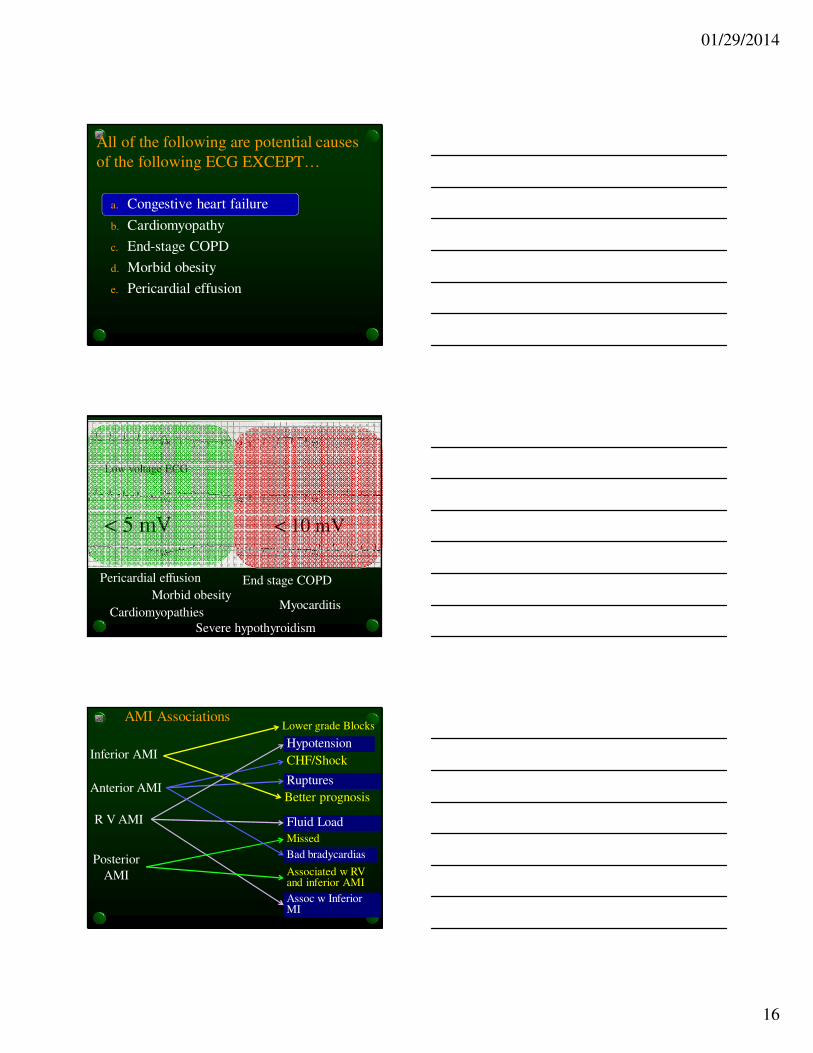
All of the following are potential causes
of the following ECG EXCEPT…
a. Congestive heart failure
b. Cardiomyopathy
c. End-stage COPD
d. Morbid obesity
e. Pericardial effusion
01/29/2014
16
All of the following are potential causes
of the following ECG EXCEPT…
a. Congestive heart failure
b. Cardiomyopathy
c. End-stage COPD
d. Morbid obesity
e. Pericardial effusion
Pericardial effusion
Morbid obesityEnd stage COPD
MyocarditisCardiomyopathies
Severe hypothyroidism
Low voltage ECG
< 5 mV < 10 mV
AMI Associations
Inferior AMI
Anterior AMI
R V AMI
Posterior
AMI
Lower grade Blocks
Better prognosis
Assoc w Inferior MI
Ruptures
Fluid Load
Associated w RV and inferior AMI
Bad bradycardias
Missed
Hypotension
CHF/Shock

01/29/2014
17
A 32 yo male involved in a roll-over MVA
presents with neck pain. Based on X-ray you
suspect…
a. A ligamentous disruption
b. An unstable fracture
c. A subluxation
d. A unilateral facet dislocation
e. A stable fracture
01/29/2014
18
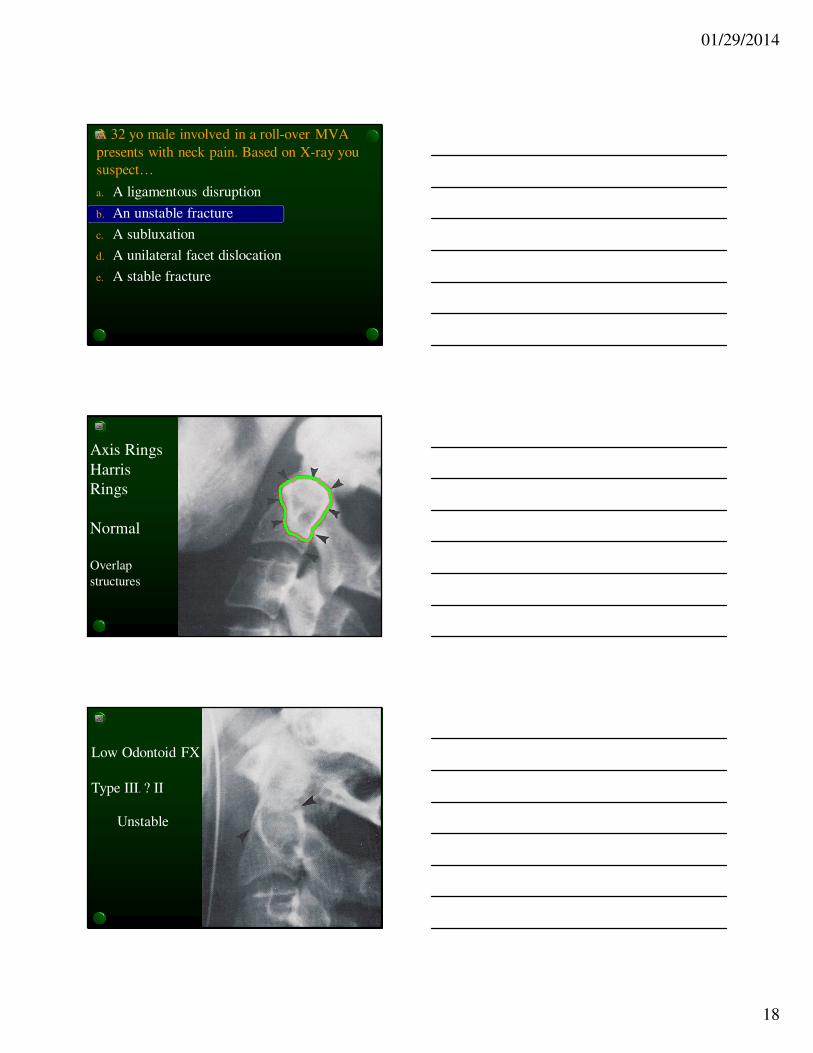
A 32 yo male involved in a roll-over MVA
presents with neck pain. Based on X-ray you
suspect…
a. A ligamentous disruption
b. An unstable fracture
c. A subluxation
d. A unilateral facet dislocation
e. A stable fracture
Axis Rings
Harris
Rings
Normal
Overlap
structures
Low Odontoid FX
Type III. ? II
Unstable
01/29/2014
19
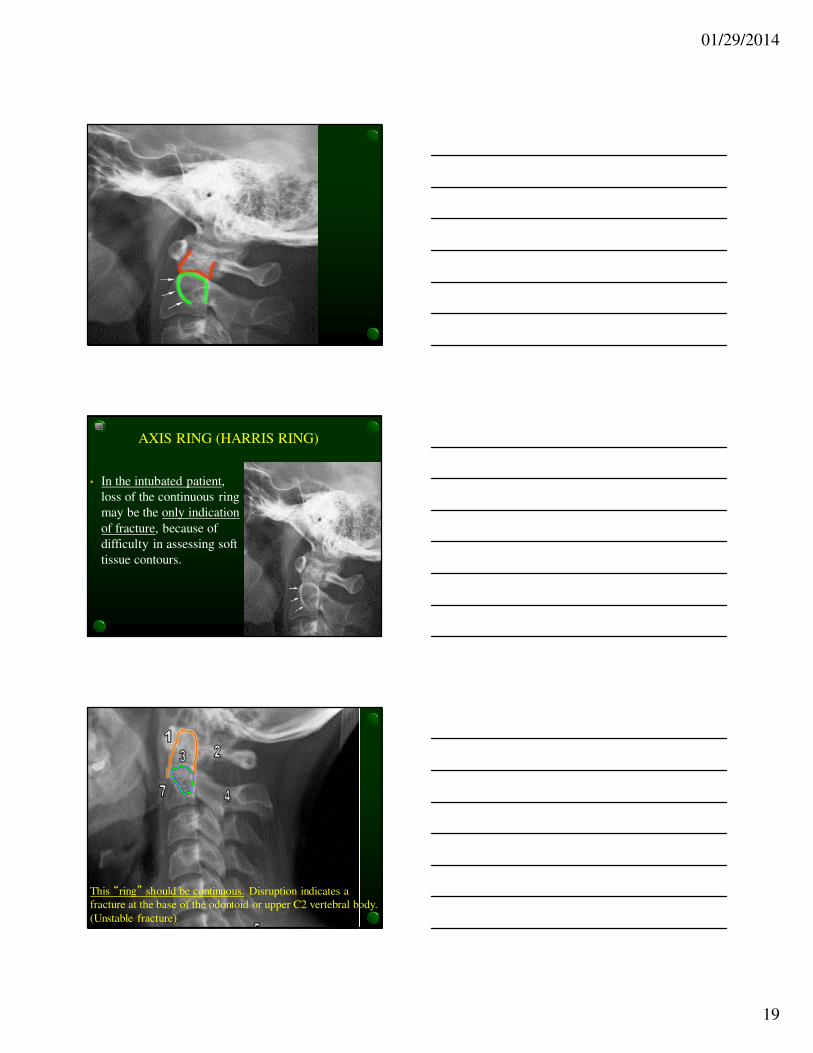
AXIS RING (HARRIS RING)
• In the intubated patient,
loss of the continuous ring
may be the only indication
of fracture, because of
difficulty in assessing soft
tissue contours.
This “ring” should be continuous. Disruption indicates a
fracture at the base of the odontoid or upper C2 vertebral body.
(Unstable fracture)

01/29/2014
20
Most Common
Most unstable
Unstable Cervical Spine Fractures –
Jefferson bit off a hangman’s thumb
• Jefferson
• Bilateral facet dislocation
• Odontoid II and III
• Any fracture dislocation
• Hangman’s
• Tear drop fracture
Stable Fractures
- spinous fracture
- transverse process #
- wedge fracture
- unilateral facet dislocation
- vertebral burst fracture
(except Jefferson)
A 5 yo male presents to the ED after falling into a hay stack from 5 feet up. He complains of neck pain. His X-ray is shown. You suspect…
a. Unilateral facet dislocation
b. Bilateral facet dislocation
c. Pseudosubluxation
d. Fracture/dislocation of C2
e. Axis fracture

01/29/2014
21
A 5 yo male presents to the ED after falling into a hay stack from 5 feet up. He complains of neck pain. His X-ray is shown. You suspect…
a. Unilateral facet dislocation
b. Bilateral facet dislocation
c. Pseudosubluxation
d. Fracture/dislocation of C2
e. Axis fracture
Pediatric Pseudosubluxation
•Usually C2 on C3
•Sometimes C3 on C4
•Check the spinolaminar line
•(Swischuk line)
•The spinolaminar line connecting
the anterior portions of the spinous
processes of C1 and C3 is within 2
mm of the C2 spinous process
01/29/2014
22
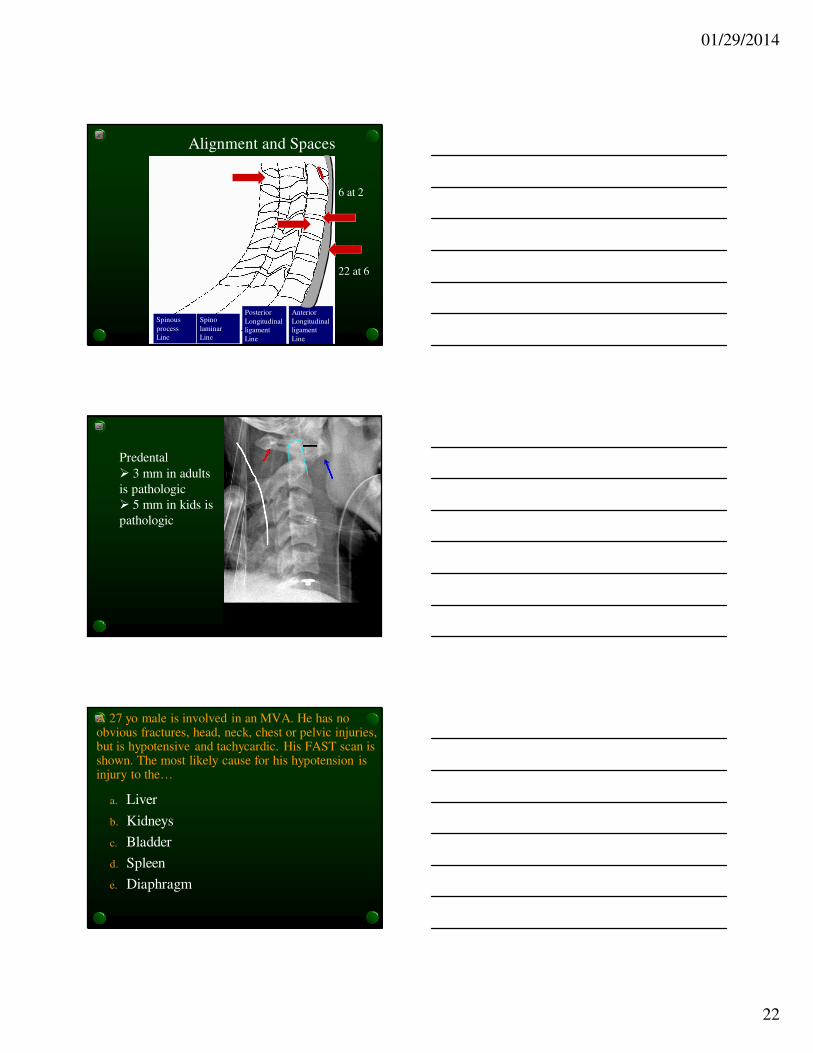
Alignment and Spaces
Spinous
process
Line
Spino
laminar
Line
Posterior
Longitudinal
ligament
Line
Anterior
Longitudinal
ligament
Line
6 at 2
22 at 6
Predental
� 3 mm in adults
is pathologic
� 5 mm in kids is
pathologic
A 27 yo male is involved in an MVA. He has no obvious fractures, head, neck, chest or pelvic injuries, but is hypotensive and tachycardic. His FAST scan is shown. The most likely cause for his hypotension is injury to the…
a. Liver
b. Kidneys
c. Bladder
d. Spleen
e. Diaphragm

01/29/2014
23
A 27 yo male is involved in an MVA. He has no obvious fractures, head, neck, chest or pelvic injuries, but is hypotensive and tachycardic. His FAST scan is shown. The most likely cause for his hypotension is injury to the…
a. Liver
b. Kidneys
c. Bladder
d. Spleen
e. Diaphragm
Spleen is MC organ injured, followed by:- liver- kidney- small bowel- bladder- colon- diaphragm- pancreas- retroperitoneal duodenum
01/29/2014
24
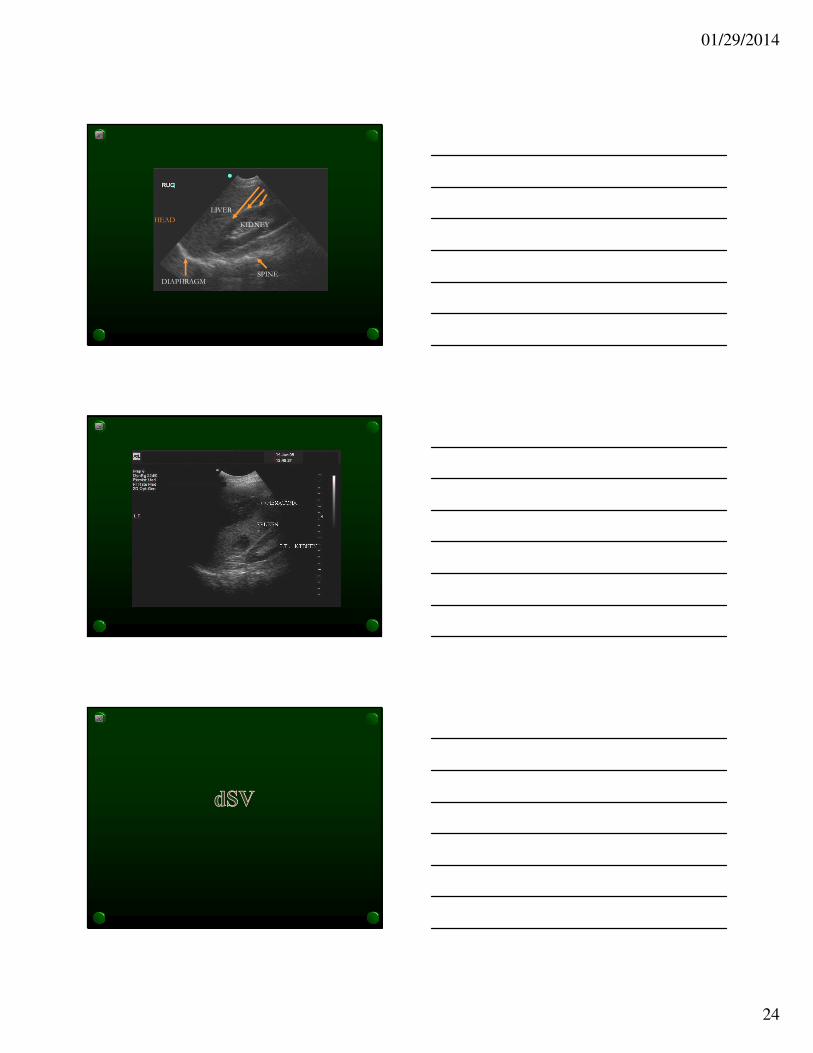
LIVER
KIDNEY
DIAPHRAGM
HEAD
SPINE

01/29/2014
25
Disseminated GC
Rocky Mountain Spotted Fever
Kawasaki
Muliforme (erythema)
Meningococcal Meningitis
Secondary syphilis
Scabies
Norwegian scabies
diSSeminated GC
hand Foot and mouth
Rash palms and soles – RKMSF
• Rocky Mountain Spotted Fever
• Kawasaki (sloughing)
• Multiforme (erythema), Meningococcal
Meningitis (petichiae)
• Scabies, Syphilis, diSSeminated GC
• Foot: hand foot and mouth disease
01/29/2014
26
Associate the bugs with the wound
• Cat bite…………………...
• PW through tennis shoe.…
• Osteo from above ………
• Dog bite………………….
• Human bite……………….
• Bat bite……………………
• Rat urine……………………
Pasteurella multocida
Staph, Strep MC
Bacteroides MC anaerobe
Eikenella corrodens (chronic/abscess)
Staph, Strep
Pseudomonas Aeruginosa
Alpha hemolytic strep, eik
corr pasteurella multocida
Rabies25%
50%
usually early infection after cat bite
Staph, Strep MCAlso consider: Hep B &C, Syph, TB, HIV
Leptospirosis
Associate the bugs with the wound
• Salt water abrasion infection…..
• Fish tank granuloma.…
• Rose thorn injury ………
• Reptile bites and exposures.
• Fish monger’s hand…….
• Cat-scratch fever………………
Vibrio Vulnificus
Erysipelothrix rhusiopathae
Mycobacterium marinum
Sporothrix schenckii
Salmonella (non typhi)
Bortonella henselaeBuboes in arm pit with
large lymph nodes
(Fungus)(skin lesions going up arm)
Which of the following vasopressors have
been shown to improve mortality in the setting
of shock (excluding anaphylaxis)?
a. Dobutamine
b. Vasopressin
c. Norepinephrine
d. Epinephrine
e. None of the above
Dose of norepinephrine: 1 – 20 mcg/min
01/29/2014
27
What is the most common mode of
completed suicide?
a. Medication overdose
b. Hanging
c. Firearms
d. Wrist slashing
e. Carbon monoxide
Completed Suicide• Most common method is firearms and presence of
firearms in the home is a independent risk factor
for completed suicide and patients should be asked
about presence of firearms in their home
• Medication is most MC of suicide attempt
• Hanging is 2nd MC method of completed suicide in
men
• Women attempt more, men succeed more
• Wrist slash and CO uncommon
Suicide
• Nearly half a million visits per year
• 9th leading cause of death
• 3rd leading cause of death in 10 - 24 yo
• Attempt to complete ratio 40:1
• Majority of attempts: drug OD

01/29/2014
28
S
A
D
P
E
R
S
O
N
S
Sex: male > female
Age < 19 or > 45
Depression S&S
Previous attempt or psych
ETOH or drug Excess
Rational thought loss
Separated/divorces/widow/single
Organized attempt
No social support
Stated future intent
� > 8 High
�6 – 8 Intermediate
� < 6 Low
In
S
A
D
C
A
G
E
S
Interest
Sleep
Appetite
Depression
Concentration
Affect
Guilt
Energy
Suicide
Plan
Means
Family Hx
completed
Diarrhea - Chinese
restaurant or fried rice
Bacillus Cereus
Secretory diarrhea in kids
6mo – 2yo in winter
Rotavirus
Froathy foul smelling
Giardia
Travellers’ diarrhea
ETEC
Diarrhea: then HUS
E-coli 0157:H7
Most common cause of bacterial diarrhea
Campylobacter
Most common cause of
chronic diarrhea in AIDS
Cryptosporidium
Rice water stool
Vibrio cholera
Diarrhea assoc with Guillain-Barre Syndalso Reiter’s, HUS
No antibiotics
MCC of HUS which is
MCC of ARF in kids
E-coli is MC
2nd MC is shigella
3rd viral/protozoa
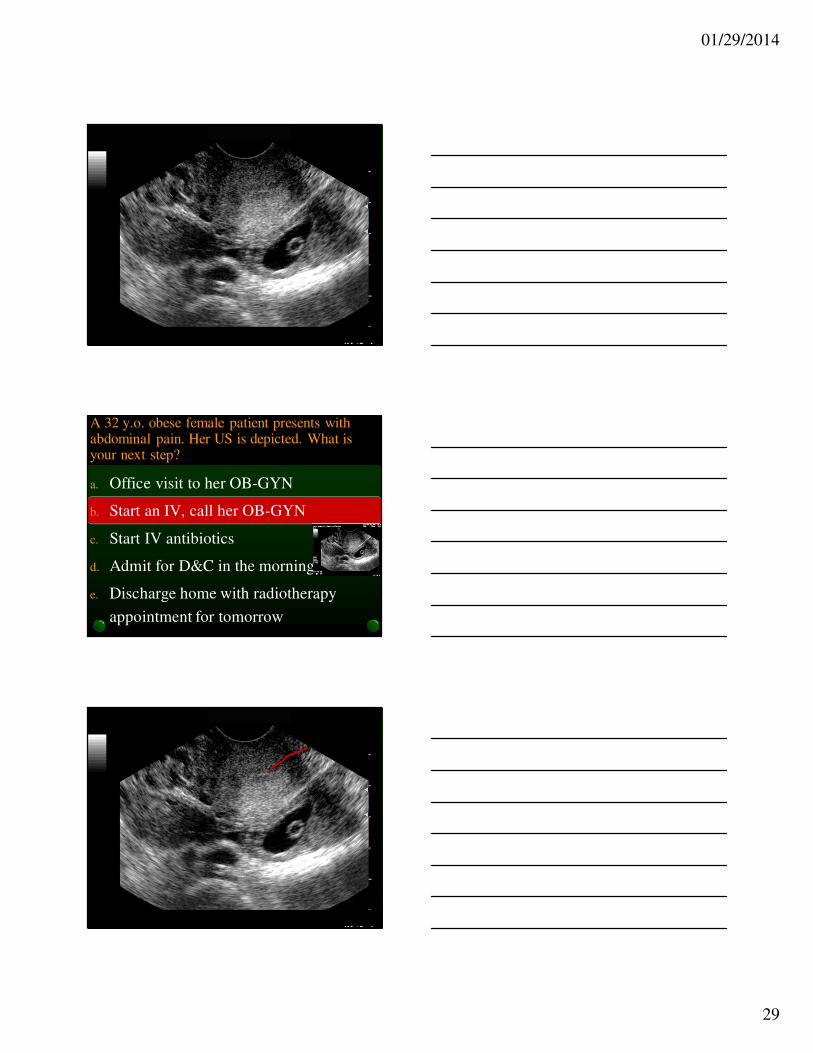
A 32 y.o. obese female patient presents with abdominal pain. Her US is depicted. What is your next step?
a. Office visit to her OB-GYN
b. Start an IV, call her OB-GYN
c. Start IV antibiotics
d. Admit for D&C in the morning
e. Discharge home with radiotherapy
appointment for tomorrow
01/29/2014
29
A 32 y.o. obese female patient presents with abdominal pain. Her US is depicted. What is your next step?
a. Office visit to her OB-GYN
b. Start an IV, call her OB-GYN
c. Start IV antibiotics
d. Admit for D&C in the morning
e. Discharge home with radiotherapy
appointment for tomorrow

01/29/2014
30
Ectopic Pregnancy – Keycepts
• Second leading cause of death of maternal death
• 50% missed diagnosis first office visit
• 36% missed diagnosis first ED visit
• Risk Factors: previous ectopic (7x), PID (6x),
IUD, recent elective abortion, older age, infertility
treatment, smoker
• Unilateral adnexal tenderness +/-
Ectopic Pregnancy - Keycepts
• Syncope = rupture (also BP, tachycardia)
• No blood on culdocentesis is non diagnostic
• B-hCG should double every 1 – 3 days (first 6 wks)
• B-hCG discriminatory zone for US (1500 TV,
6500 TA)
• Methotrexate treatment for stable patient with
unruptured ectopic < 4cm; can present one week
later with pelvic pain – but could be ectopic
progression
• Laparoscopy for definitive diagnosis

01/29/2014
31
The CDC states that all major criteria and one
minor criteria be present if the diagnosis of
PID is to be established. All of the following
are major criteria for the diagnosis of PID
EXCEPT…
a. Abdominal pain
b. Vaginal discharge
c. Adnexal tenderness
d. Cervical motion tenderness
Diagnosis of PID based on major and minor
criteria. All major criteria must be present and
at least on minor criteria• Minimal Criteria
• Abdominal (pelvic) pain
• Uterine/adnexal tenderness
• Cervical motion tenderness
• Additional Criteria
• Temp > 100 F
• Abnormal cervical/vaginal discharge
• Elevated ESR/CRP
• Positive cervical cultures for N gon or C. trachomatis,
anearobes
The most common
clear cut risk for
ectopic pregnancy
>25% of patients
admitted for PID
will develop TOA
Risk Factors for PID
• Young women (15 – 25)
• Multiple sex partners
• Smoking
• Bacterial vaginosis
Peak time is within 1st week of menses

01/29/2014
32
Who gets admitted
• Adnexal mass
• Pregnant
• IUD
• Peritonitis
• Immunocompromised
• OP Failure
• Unable to tolerate PO
• Concerns about future fertility
Treatment of PID
• Inpatient: • Cefoxitin 2 gm QID or Cefotetan 2 gm IV
BID + Doxy 100 mg BID or
• Clindamycin 900 mg IV Q8H + Gentamycin
• Augmentin 3 gms IV Q6H + Doxy
• Outpatient: • Ceftriaxone 250 mg IM x 1
• + Doxy 100 BID for 14 days
• +/- Flagyl 500 mg BID x 14 d
• NO quinolones – too much resistance
PID Morbidity
• Ectopic pregnancy is 6 times more likely in
women who have had PID
• Infertility 8 % with first episode
• Chronic pelvic pain in up to 18% of women
after PID had resolved

01/29/2014
33
What about IUDs in patients with PID
• The risk of PID assoc with IUD is confined
to the first 3 weeks after insertion and
uncommon thereafter. No evidence suggests
that IUD should be removed in women
diagnosed with acute PID, but close follow
up is mandatory
Fitz-Hugh-Curtis
MCC is…..………........
Occurs in 4% - 14% of patients with PID,
more common in adolescents with PID
Patient with PID
RUQ pain worse with deep breathing or cough
Radiation to Right Shoulder
Perihepatitis (LFT: N or minimally elevated)
“Violin string” adhesions on laparoscope
Chlamydia >>> GC
01/29/2014
34
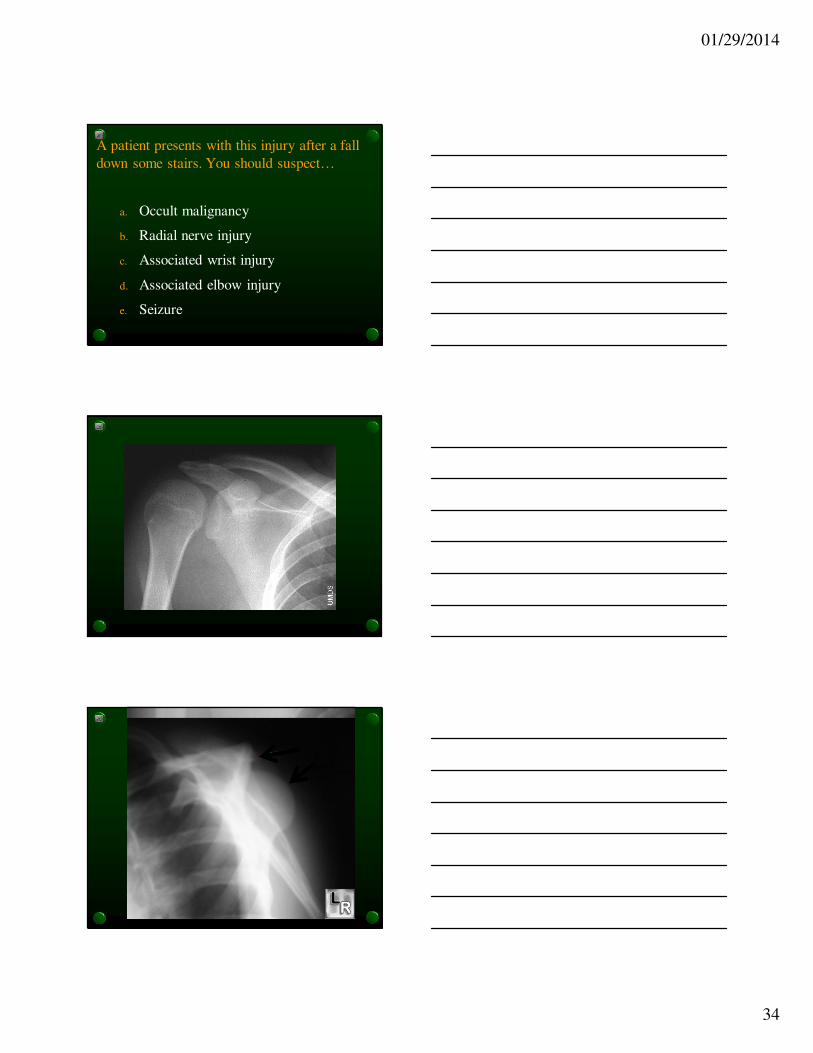
A patient presents with this injury after a fall
down some stairs. You should suspect…
a. Occult malignancy
b. Radial nerve injury
c. Associated wrist injury
d. Associated elbow injury
e. Seizure
01/29/2014
35
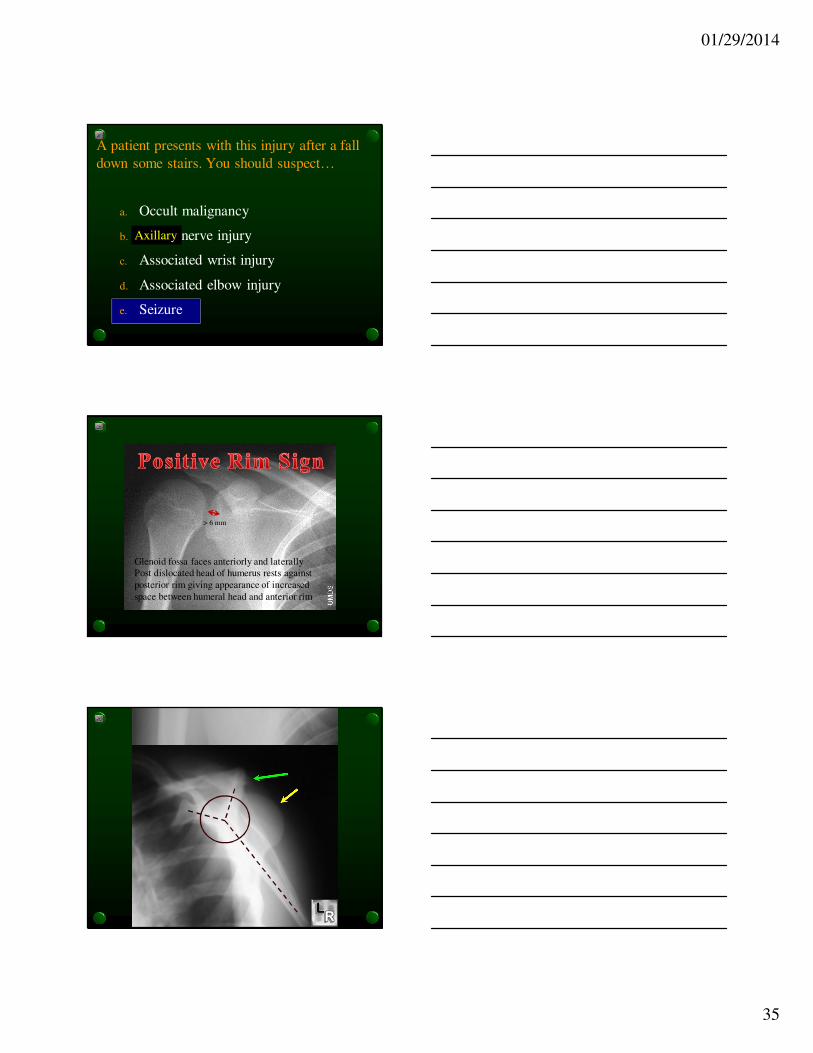
A patient presents with this injury after a fall
down some stairs. You should suspect…
a. Occult malignancy
b. Radial nerve injury
c. Associated wrist injury
d. Associated elbow injury
e. Seizure
Axillary
> 6 mm
Glenoid fossa faces anteriorly and laterally
Post dislocated head of humerus rests against
posterior rim giving appearance of increased
space between humeral head and anterior rim

01/29/2014
36
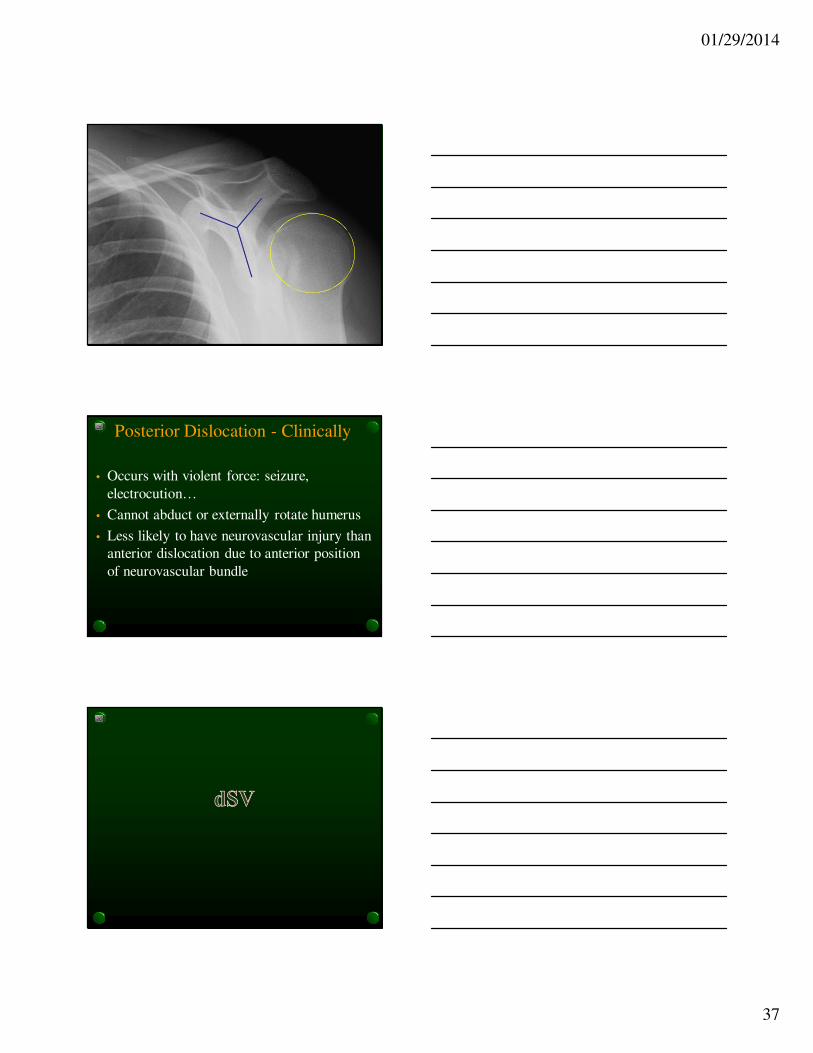
The lightbulb sign
01/29/2014
37
Posterior Dislocation - Clinically
• Occurs with violent force: seizure,
electrocution…
• Cannot abduct or externally rotate humerus
• Less likely to have neurovascular injury than
anterior dislocation due to anterior position
of neurovascular bundle
01/29/2014
38
Causes of Eosinophilia
• N Neoplasm
• A Allergy
• A Addison’s
• C Chlamydia
• P Parasites
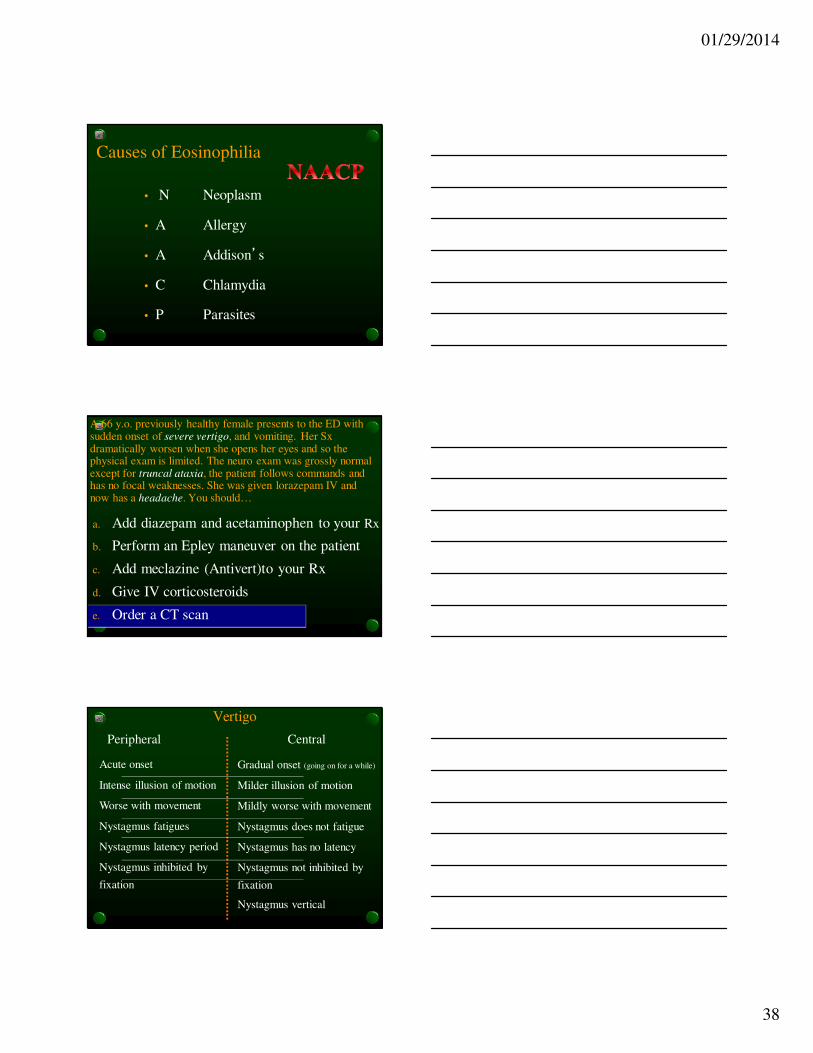
A 66 y.o. previously healthy female presents to the ED with sudden onset of severe vertigo, and vomiting. Her Sx dramatically worsen when she opens her eyes and so the physical exam is limited. The neuro exam was grossly normal except for truncal ataxia, the patient follows commands and has no focal weaknesses. She was given lorazepam IV and now has a headache. You should…
a. Add diazepam and acetaminophen to your Rx
b. Perform an Epley maneuver on the patient
c. Add meclazine (Antivert)to your Rx
d. Give IV corticosteroids
e. Order a CT scan
Vertigo
Peripheral Central
Acute onset
Intense illusion of motion
Worse with movement
Nystagmus fatigues
Nystagmus latency period
Nystagmus inhibited by
fixation
Gradual onset (going on for a while)
Milder illusion of motion
Mildly worse with movement
Nystagmus does not fatigue
Nystagmus has no latency
Nystagmus not inhibited by
fixation
Nystagmus vertical

01/29/2014
39
Illusion of motion
Vestibular System
Peripheral System Central System
BPPV
Labyrinthitis
Vestibular neuronitis
Meuniere’s
85% 15%
Cerebellar (infarct, infection, hem)
CNS infection
Brainstem (infarct, hem, tumor)
Multiple sclerosis
Vertebrobasilar dz
ETOHic cerebellar
degeneration
Cerebellar hemorrhage
• Neurosurgical emergency
• Headache
• Acute vertigo
• Vomiting
• Marked truncal ataxia
• Inability to walk
• Gaze palsies (6th Cr.N.),
• Increasing stupor. Romberg +ve.
Consider CT/MRI in any:
- Unable to ambulate
- Associated H/A
- Physical findings
suggestive of
central cause
- abn VS
- Cr N findings
- Truncal ataxia
V
II, III ,IV
VIVIIVIII
IX, X,XI, XII
Brainstem Fx:
RAS
Vital signs
Cranial nerve
01/29/2014
40
Cerebellar hemorrhage
• Neurosurgical emergency
• Headache
• Acute vertigo
• Vomiting
• Marked truncal ataxia
• Inability to walk
• Gaze palsies (6th Cr.N.),
• Increasing stupor. Romberg +ve.
Consider CT/MRI in any:
- Unable to ambulate
- Associated H/A
- Physical findings
suggestive of
central cause
- abn VS
- Cr N findings
- Truncal ataxia
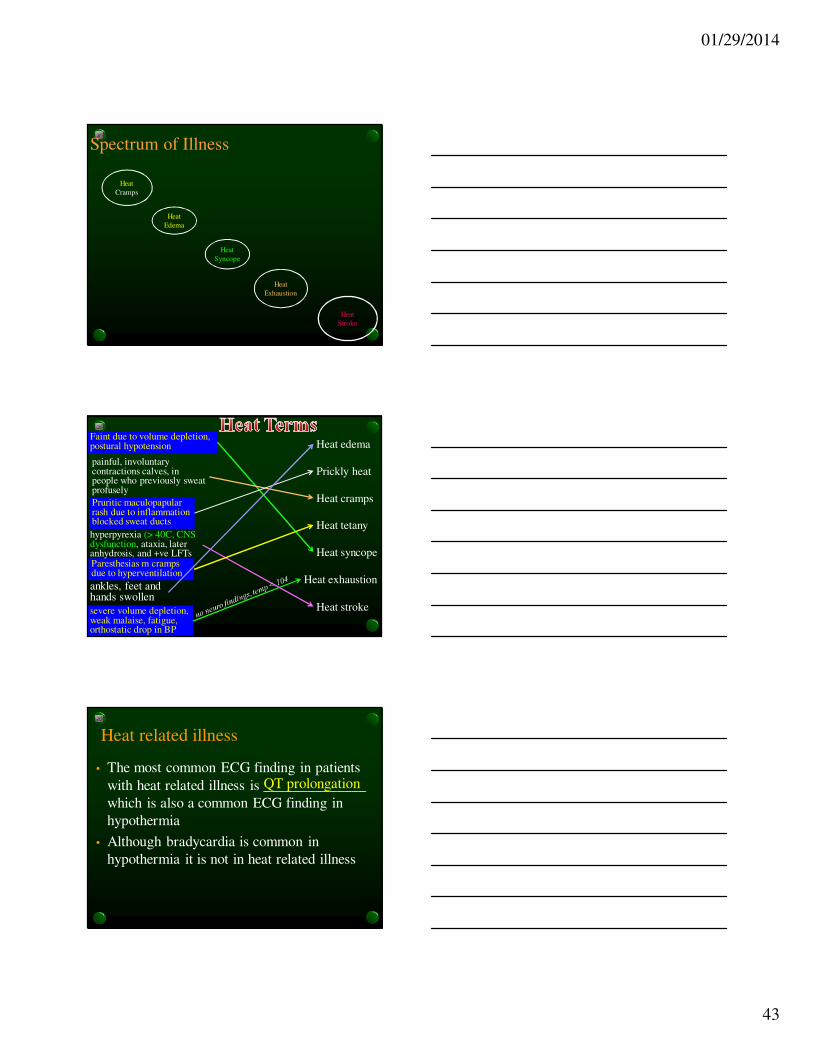
It’s all about the 4th ventricle
• All patients with cerebellar hemorrhage may
deteriorate rapidly due to obstructive
hydrocephalus (4th ventricle becomes compressed)
or progressive brainstem compression – both
of which require emergent operative
intervention
It’s all about the 4th ventricle
• Cerebellar infarcts can also progress to
impingement on the 4th ventricle with
subsequent hydrocephalus requiring
operative intervention and should all be
admitted to the ICU.
• Patients with vertebrobasilar insufficiency
(TIA) should be admitted because of
potential 4th ventricle compromise
01/29/2014
41
Steroids and Cerebellar infarct
• Although corticosteroids help reduce
vasogenic edema associated with tumors
they do not help in the cytotoxic edema
associated with infarction
With hemorrhage or edema from infarction, fourth ventricle gets compressed causing
obstructive hydrocephalus which requires immediate neurosurgical interventionn
A 26 yo fell of his bicycle when he hit a lamp post.
You are about to clear his C-spine. All of the
following must be met prior to clearing the C-spine
(NEXUS) EXCEPT:
a. No drugs or alcohol
b. No neck tenderness
c. No neurologic findings
d. No distracting injury
e. Clear sensorium
No midline neck tenderness

01/29/2014
42
Clearance of C-Spine
• Clinical• No neck pain
• No neck tenderness(midline) - *
• No neurologic signs/ symptoms - *
• Reliable• Clear sensorium - *
• No drugs/ ETOH - *
• No distracting injury - *
• Age > 4 years
• Lack of mechanism
* = NEXUS
All of the following are true about heat
stroke EXCEPT:
1. Classic heat stroke is associated with
temperature > 40.5 C
2. Classic heat stroke is associated with sweating
3. The hallmark of heat stroke is altered mental
status
4. Classic heat stroke may be associated with
coagulopathy
5. Classic heat stroke may be associated with mild
lactic acidosis
Heat Stroke – requires CNS dysfunction
• Elderly, debilitated
• Sedentary
• Associated with heat waves
• Anhidrosis common
• Normal glucose
• Mild coagulopathy
• CK mildly increased
• Oliguria
• Mild lactic acidosis
Classic Heat Stroke Exertional Heat Stroke
• Young healthy
• Extreme exertion
• Occurrence sporadic
• Sweating preserved
• Hypoglycemia
• Severe coagulopathy /DIC
• Rhabdomyolysis
• Acute renal failure
• Severe lactic acidosis
01/29/2014
43
Spectrum of Illness
Heat
Edema
Heat
Syncope
Heat
Cramps
Heat
Exhaustion
Heat
Stroke
Heat edema
Prickly heat
Heat cramps
Heat tetany
Heat syncope
Heat exhaustion
Heat stroke
ankles, feet and hands swollen
Pruritic maculopapular rash due to inflammation blocked sweat ducts
painful, involuntary contractions calves, in people who previously sweat profusely
Paresthesias m cramps due to hyperventilation
Faint due to volume depletion, postural hypotension
severe volume depletion, weak malaise, fatigue, orthostatic drop in BP
hyperpyrexia (> 40C, CNS dysfunction, ataxia, later anhydrosis, and +ve LFTs
Heat related illness
• The most common ECG finding in patients
with heat related illness is ______________
which is also a common ECG finding in
hypothermia
• Although bradycardia is common in
hypothermia it is not in heat related illness
QT prolongation

01/29/2014
44
A 17 yo male presents to the ED after a temporary and brief
interruption of neurologic function after hitting the goal post
with his head while playing soccer. He is feeling fine in
your ED. All of the following are true regarding this
condition EXCEPT…
a. Patients may be amnesic for the event
b. Patients may have insomnia after the event
c. Patients may have difficulty concentrating after
the event
d. Patients may have transient ataxia after the event
e. Patients may have headaches after the event
Which of the following regarding concussion
is correct?
a. It does not necessarily require a loss of
consciousness
b. Retrograde amnesia is more common than and
longer in duration than antegrade amnesia
c. Otherwise well patients may not be able to recall
their name or date of birth
d. Skull fractures is a strong predictor of brain
hemorrhage
e. Postconcussion syndrome (headache, dizziness, memory problems,
neuropsych complaints) is common in young children
malingering

01/29/2014
45
Head Trauma: Post Concussive Syndrome
• Headache: For weeks to years
• Dizziness
• Insomnia
• Anxiety
• Decreased concentration
• Any change in mental function
No ataxia, no focal neurologic signs
2011 Concussion Guidelines
• 1. Rest until asymptomatic ( physical, mental)
• 2. Light aerobic exercise ( exercise bike)
• 3. Sport- specific exercise
• 4. Non-contact training drills ( wt lifting or sleds)
• 5. Full contact training (after medical clearance)
• 6. Return to competition( game play)
� Each stage can be 24 hrs or longer
� and return to stage one if symptoms re-occur
What we are trying to avoid
• Second impact syndrome: The sudden death
that may result with a second concussion
before complete recovery from the first one.

01/29/2014
46
Head injury in kids – Who avoids a CT brain
• < 2yrs old
• Normal neuro exam
• No scalp hematoma except frontal
• No LOC or LOC < 5 seconds
• Consider mechanism
• No palpable skull fracture
• Acting normally
• > 2yrs old
• Normal mental status
• Normal neuro exam
• No LOC
• No severe headache
• No vomiting
• No signs of basilar skull fracture
• Consider mechanism
Bottom line for concussion guidelines
in children and adolescents
• No comprehensive return-to-play guidelines have
been adapted for the young athlete, and the
majority of current and past studies were
performed with older athletes.
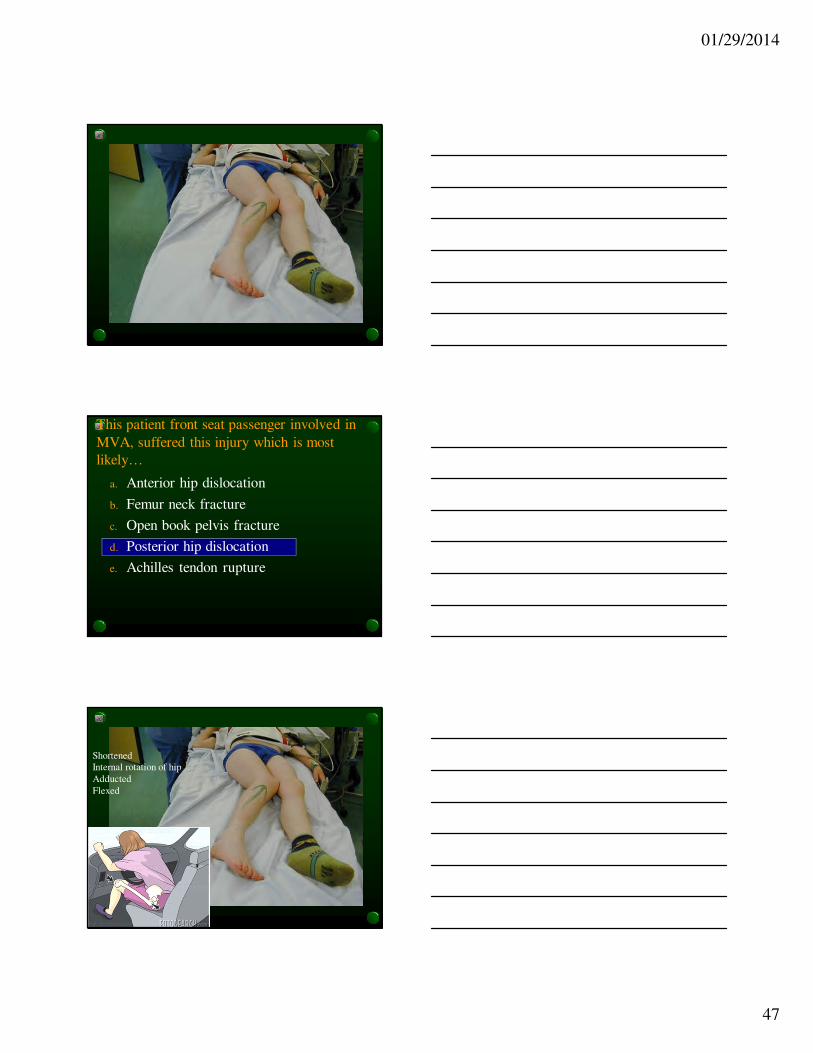
This patient front seat passenger involved in
MVA, suffered this injury which is most
likely…
a. Anterior hip dislocation
b. Femur neck fracture
c. Open book pelvis fracture
d. Posterior hip dislocation
e. Achilles tendon rupture
01/29/2014
47
This patient front seat passenger involved in
MVA, suffered this injury which is most
likely…
a. Anterior hip dislocation
b. Femur neck fracture
c. Open book pelvis fracture
d. Posterior hip dislocation
e. Achilles tendon rupture
Shortened
Internal rotation of hip
Adducted
Flexed
01/29/2014
48
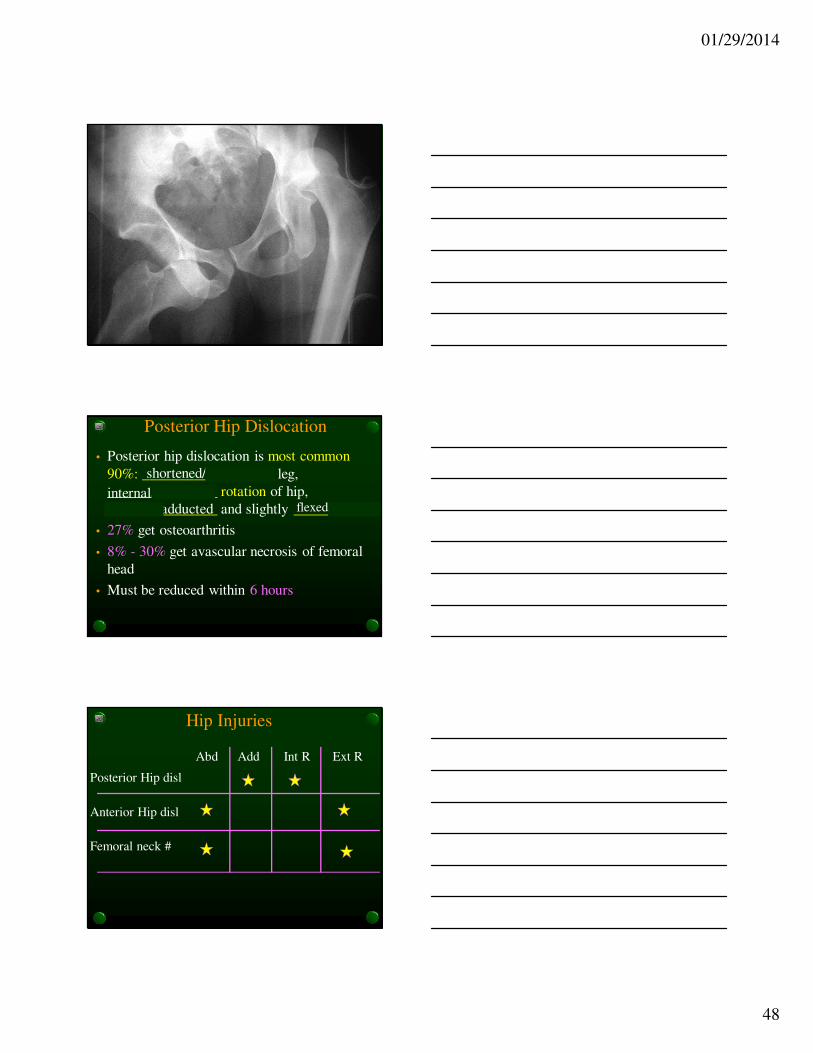
Posterior Hip Dislocation
• Posterior hip dislocation is most common
90%: __________________ leg,
_______________ rotation of hip,
_______________ and slightly __________
• 27% get osteoarthritis
• 8% - 30% get avascular necrosis of femoral
head
• Must be reduced within 6 hours
internal/external
shortened/lengthened
abducted/adducted flexed/extended
Hip Injuries
Posterior Hip disl
Anterior Hip disl
Femoral neck #
Abd Add Int R Ext R

01/29/2014
49
Aortic Dissection
2 lumens in aorta. Suspect dissection, you might
see it by scanning abdominal aorta.
75 yo male with abdominal pain
Upper extremity pulse deficit is the most specific
physical exam finding but its sensitivity is < 15%
50% do not survive to make it to the ED – of those who do
mortality increases 1% per minute
Heart
Belly
Back
Feet
Celiac
Aorta
SMA
Acute Thoracic Aortic Dissection
• Widened mediastinum is the most common abnormal finding
• 12% of patients have normal CXR
• 21% of patients have a normal mediastinum and aortic contour
• Non specific findings may be very subtle and not typically picked up by the ED physician
• Abnormal aortic contour in 50%
• Abnormal cardiac contour in 25%
• Pleural effusion in 19%
• Displacement or abnormal calcification of aorta in 14%

01/29/2014
50
There has been a radiation accident at your local nuclear power plant. A patient present at the site at the time of the accident presents to your ED with complaints of nausea and vomiting. She is now, 48 hours after the event, worried about this exposure. Her absolute lymphocyte count is 1600/mcL. You should explain to her that…
a. That her exposure will require intensive and aggressive therapy for her to survive
b. That her lab value suggests that she has a 50:50 chance of survival
c. That she requires no treatment and is expected to recover from her exposure without significant complications
d. That it is to early to tell and that her ALC will have to be re-taken in 24 hours
e. That she has likely suffered a lethal dose of radiation
Absolute lymphocyte counts at 48 hours
after exposure as a prognostic factor
• > 1200/mcL means it is unlikely that the
patient has received a clinically significant
dose of radiation
• 500 – 1200/mcL serial counts especially
if symptomatic
• 100 - 500 /mcL possibility of exposure to
a lethal dose of radiation should be
suspected

01/29/2014
51
All of the following are true regarding
radiation exposure EXCEPT:
a. Alpha rays are the most penetrating
b. GI syndrome (N/V/D) occurs at 1 Gy (gray)
c. Survival is unlikely with a exposure of greater than 800 rads
d. The GI tract is one of the tissues most affected by radiation
e. The absolute lymphocyte count (ALC) at 48 hours of 1200 indicates a 50% mortality
Types of Radiation
Alpha
0000−1−1−1−1ββββ−−−−
44442222α α α α ++++++++
00γ
Beta
Gamma and X-rays
Neutron
Paper Plastic Lead Concrete
10n
Geiger counter
Skin burns
Primary cause of acute radiation syndrome
Stopped neutrons are captured and cause
previously stable atoms to become
radioactive – source of radioactive fallout
? need alpha counter
a. Ciguatoxin
b. Scombroid fish poisoning
c. Bacillus cereus
d. Cyclospora cayentnenensis
e. E-coli 0157:H7
A 28 y.o. male presents to the ED with throbbing headache, palpitations and abdominal pain after eating at the Golden Lobster, where he states they put too much pepper on their fish. You note marked facial and neck flushing, conjunctival injection and scattered urticaria on his trunk. His BP 150/100, P 110, R 24, T N. What is the most likely cause?

01/29/2014
52
Scombroid• Multiple patients with ‘allergic reaction’ –
due to excessive histamine levels in the fish
due to inadequate refrigeration
• Tuna, mackerel, mahi-mahi
• Peppery taste
• Sx occur within minutes of eating the fish
• Facial flushing, throbbing H/A, abd cramps,
diarrhea, palpitations, burning sensation in
the mouth, pruritus
• Rx: antihistamines, H-2 blockers
Multiple patients
Facial flushing
allergic reaction
Tuna, mackerel, mahi-mahi
Peppery taste
38 y.o. female presents to ED with acute onset of N/V, watery diarrhea, diaphoresis and cramping abdominal pain that woke her up from sleep. Also c/o tingling tongue and around mouth. She refused a cold drink of water saying if felt like hot water. She had dinner at the “Fish House” 5 hours earlier. The most likely cause is:
a. Ciguatoxin
b. Scombroid fish poisoning
c. Bacillus cereus
d. Cyclospora cayentnenensis
e. E-coli 0157:H7
Ciguatera Fish Poisoning: neurotoxin
• Common cause of fish poisoning diarrhea
• Ciguatoxin produced by marine dinoflagellate –
Gambierdiscus toxicus; mostly in South Pacific
• Fish: grouper, barracuda, sea bass, red snapper
• Odorless and tasteless
• Incubation: 2 – 6 hrs; Duration: 12 – 30 hrs
• GI and neuro Sx
• Rx: symptomatic, ? Mannitol
• Common cause of fish poisoning diarrhea
• Ciguatoxin produced by marine dinoflagellate –
Gambierdiscus toxicus; mostly in South Pacific
• Fish: grouper, barracuda, sea bass, red snapper
• Odorless and tasteless
• Incubation: 2 – 6 hrs; Duration: 12 – 30 hrs
• GI and neuro Sx
• Rx: symptomatic, ? Mannitol

01/29/2014
53
Fish PoisoningCiguatera
- Produced by marine dinoflagylate
- Perioral paresthesia “loose teeth”
- Hot cold reversal
- Ataxia, weakness, vertigo
- Sx worse with ETOH
- Rx: Supportive, manitol (neuro
Sx)
- Antihistamines, H2-bl
- May be permanent
Scombroid
- Inadequate refrigeration
(excess histamine)
- Peppery taste
- Facial flushing
- Multiple patients –
allergic reaction
- Red meat fish
- Rx: Antihistamines, H-1,
H2-blockers, beta-2
agonists for bronchospasm
Parvovirus B-19• In pregnant patients
• Hydrops faetalis (due to severe fetal anemia) leading to miscarriage or stillbirth
• Risk of fetal loss is 10% if contracted before 20 wks gestation but minimal after that
• Patients with hemolytic anemias (incl SCDz)• Can cause aplastic crisis
• In AIDS patient• Can trigger an inflammatory reaction on patients
started on antiretroviral therapy
• Causes chronic anemia – frequently overlooked
• Adults• Seronegative arthritis, resolves by 1- 3 wks
• In kids• Erythema infectiosum – slapped cheek syndrome
Ciguatera Poisoning
• Perioral paresthesia, feels like loose painful teeth, burning hands/feet
• Hot cold reversal
• Ataxia, weakness, vertigo, visual hallucinations
• Abdominal pain, vomiting, profuse diarrhea (occur earlier)
• Fish eat dinoflagellates that contain toxins
• Sxtic treatment, lasts 1 – 2 wks (50% Sx at 8 wks)
• Sx may get worse with ETOH
• Sx may be permanent
• Perioral paresthesia, feels like loose painful teeth, burning hands/feet
• Hot cold reversal
• Ataxia, weakness, vertigo, visual hallucinations
• Abdominal pain, vomiting, profuse diarrhea (occur earlier)
• Fish eat dinoflagellates that contain toxins
• Sxtic treatment, lasts 1 – 2 wks (50% Sx at 8 wks)
• Sx may get worse with ETOH
• Sx may be permanent

01/29/2014
54
All of the following are true regarding
pancreatic injuries EXCEPT…a. They are more common in penetrating trauma
b. Although the pancreatic injury itself in blunt trauma may be subtle, pancreatic injuries usually occur in more severely injured patients
c. Classically the physical exam initially worsens and over the first 6 hours the patient looks and feels better
d. Serum amylase is elevated in only 27% of penetrating injuries to the pancreas
e. Release of pancreatic enzymes more commonly cause mild tenderness to palpation (rather than peritoneal signs)
Classically, physical exam improves initially and then worsens over the first six hours
All of the following are more consistent with
delirium than dementia EXCEPT…
a. Onset is acute (days to weeks)
b. It is usually reversible
c. Hallucinations
d. Consciousness is clear
e. Fluctuating course
Features Delirium Dementia
Onset
Course
Duration
Consciousness
Attention
Reversibility
Hallucinations
Delusions
Additional Info
Acute Insidious
Disorganized thoughtFlight of ideas Global disorder of cognition and attentionSleep/wake cycle disturbmeds, lytes, infection, liver fail
Mortality 20% - 30%
Fluctuating Progressive
Days to weeks Months to years
Clear – awake/alertAltered LOC
Poor attention Pays attention
Usually Rarely
Yes No
Fleeting delusions None until very late
50% of pts > 85Alzheimer’s accounts for 70% of dementia ptsImpaired memory and judgment ‘Sundowning’

01/29/2014
55
Treatable Causes of Dementia
Drugs
Electrolytes
Metabolic
Emotional
Nutritional/Normal pressure hydrocephalus
Trauma/Tumor
Inflammation (SLE,/infection)
Alcohol
Keycepts: Dementia
• Before diagnosing dementia R/O treatable Dz:
• Normal Pressure Hydrocephalus:
• dementia, ataxia, incontinence
• Wernicke-Korsakoff Syndrome:
• ataxia, ocular abn, confusion
• Pseudodimentia (depression):
• severely depressed patient
• Disturbed sleep pattern
• Sudden onset ppted by emotional event
• Mental status improves with encouragement
• Medical problem: drugs, lytes, metabolic dz
PSYCHO-BEHAVIORAL 165
Delirium
Frequency: 10-15% of admissions to
hospitals (but usually not primary diagnosis)
Mortality: 20-30%
Race: more common in Caucasians
Age: elderly, (20-40’s think toxic/withdrawal)
Sex: female > male

01/29/2014
56
166
Dementia
• Incidence: 50% over 85
• Alzheimer’s accounts for 70%
• Vascular dementia is 10-20%
• Earlier stages are subtle and may be concealed by the pt.
• Stuttering course points to multi-infarct
Transient Global Amnesia
• Patient working in garage all of a
sudden gets confused as to where he is,
and does not know how to get home
from where he is.
• Restricted memory loss
• Only 5% relapse
• What it is not:
• Not a stroke
• Not delirium
Terms
• Gray (Gy) is the international unit of
absorbed radiation dose of ionizing radiation
(IR) defined as absorption of one joule of IR
by 1Kg of matter
• Seivert is an international unit of equivalent
dose which for X-rays is numerically equal
to a Gy
• One Rad (old term) = 0.01Gy (1Gy = 100 rad)
• Roentgen equivalent man (REM) = 1 rad

01/29/2014
57
A patient presents to the ED with the
following injury. You tell him he has…
a. A fractured triquetrum
b. A perilunate dislocation
c. A Smith fracture
d. A Rolando fracture
e. A lunate dislocation
01/29/2014
58
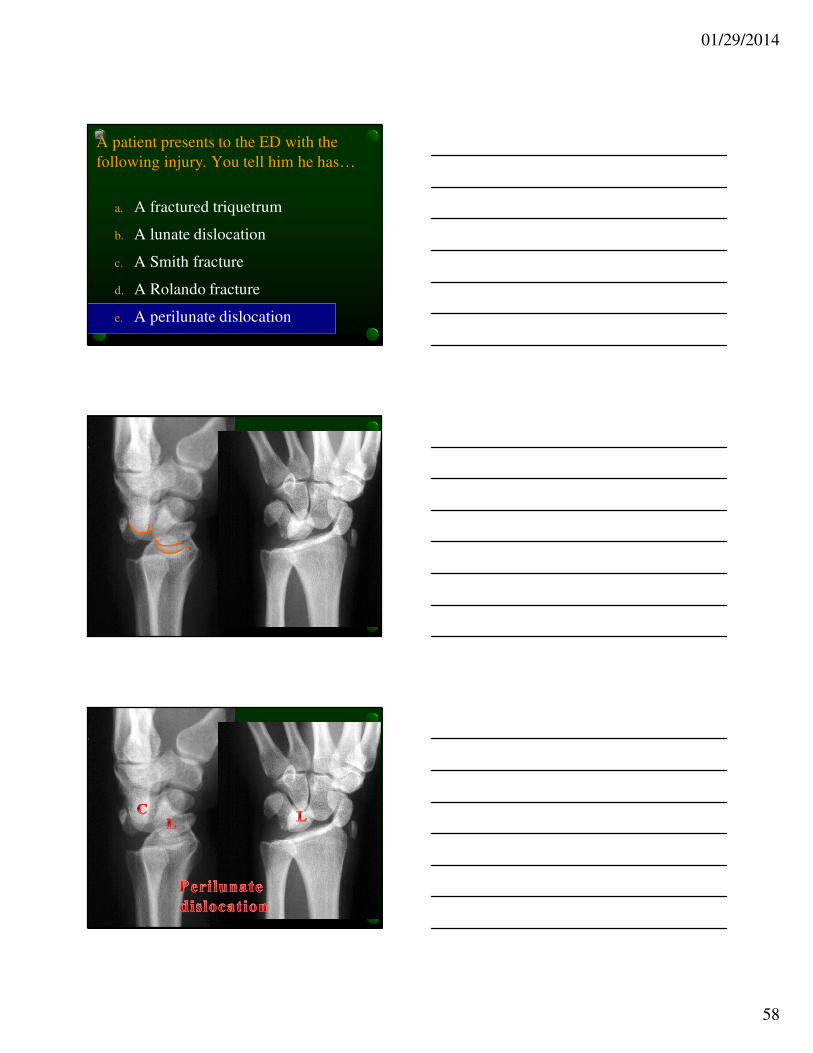
A patient presents to the ED with the
following injury. You tell him he has…
a. A fractured triquetrum
b. A lunate dislocation
c. A Smith fracture
d. A Rolando fracture
e. A perilunate dislocation
01/29/2014
59
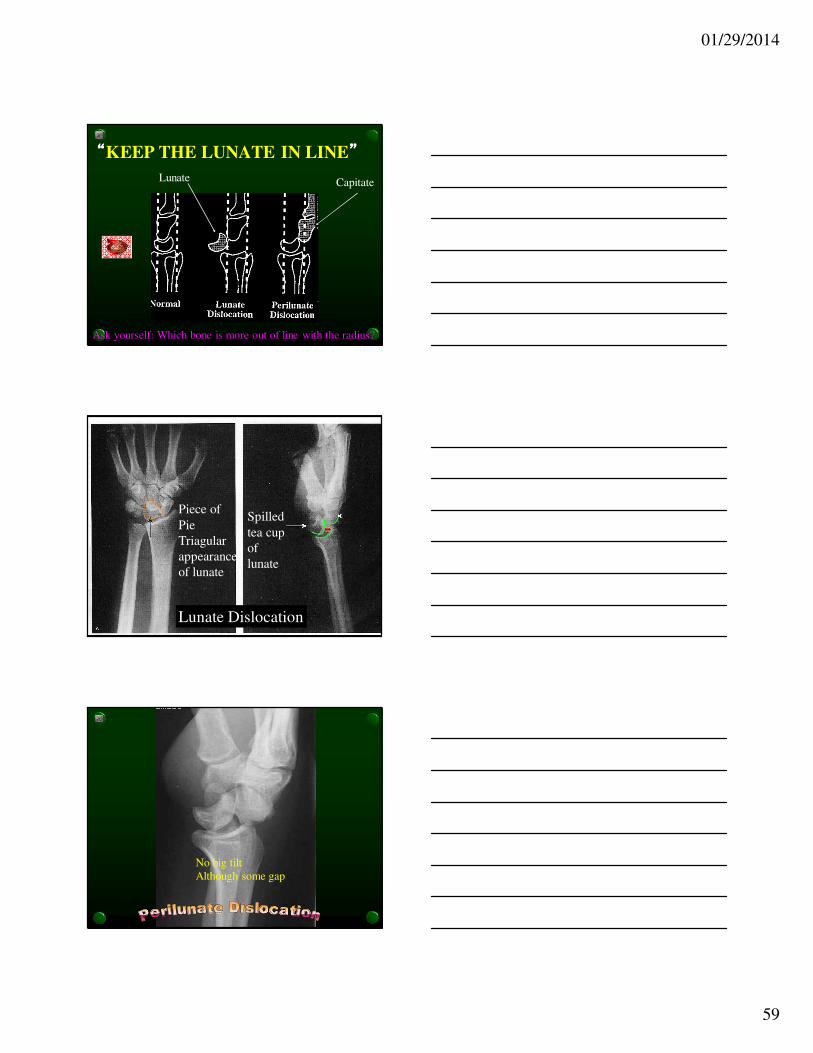
““““KEEP THE LUNATE IN LINE””””
Lunate Capitate
Ask yourself: Which bone is more out of line with the radius?
Piece of
Pie
Triagular
appearance
of lunate
Spilled
tea cup
of
lunate
Lunate Dislocation
No big tilt
Although some gap
01/29/2014
60
Ortho
Renal Ca
A patient presents with this lesion. The
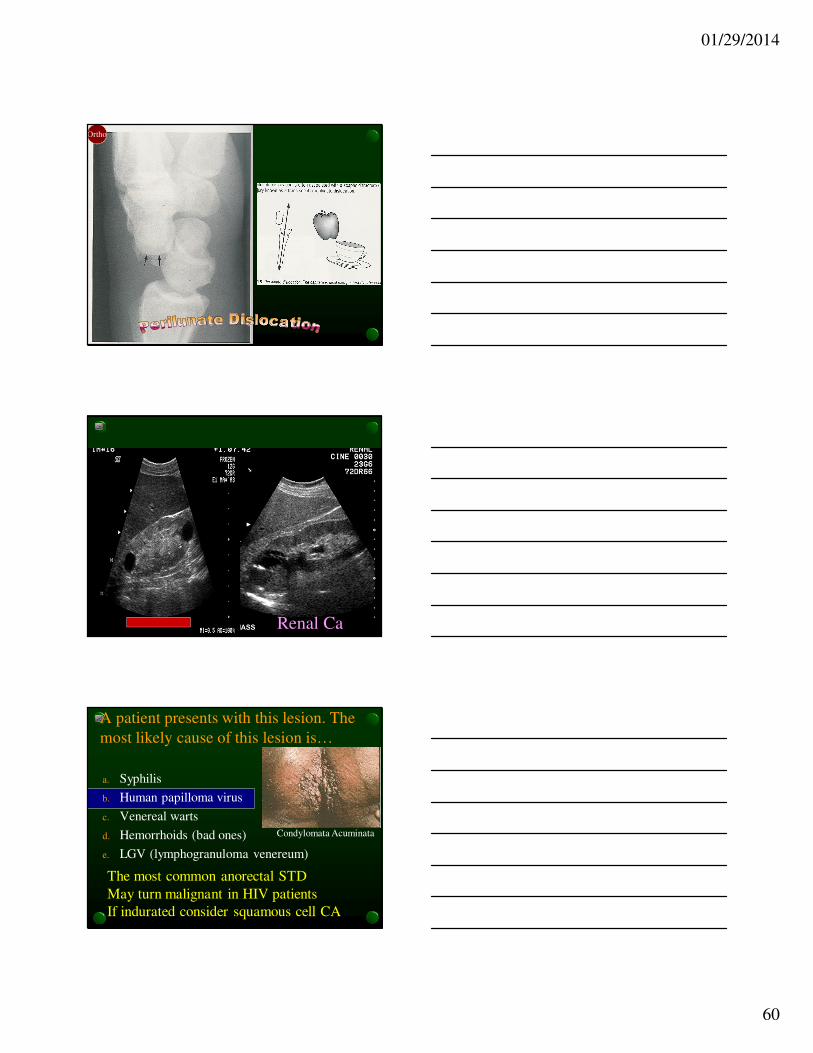
most likely cause of this lesion is…
a. Syphilis
b. Human papilloma virus
c. Venereal warts
d. Hemorrhoids (bad ones)
e. LGV (lymphogranuloma venereum)
The most common anorectal STD
May turn malignant in HIV patients
If indurated consider squamous cell CA
Condylomata Acuminata

01/29/2014
61
Condylomata acuminata
From secondary syphilis
Flat weeping warts on genitalia
Emits foul odor
Look also for diffuse maculo
papular rash all over body
including palm and soles
Loss of lateral 1/3 of eyebrow
Patchy alopecia
Benz pen 2.4 if greater than 1 yr
give weekly for 3 weeks
Human papilloma virusPedunculated papulesDevelop into cauliflower like massesDry, keratinized surfaceRx: Cryotherapy
A patient presents to the ED after he fell 20feet to the ground off a scaffolding landing on his feet. He comes in with the injury seen on this X-ray. His contrasted CT shows a non enhanced kidney on the left side. The most likely diagnosis is…
a. Acute traumatic hydronephrosis
b. Renal artery thrombosis
c. Acute renal contusion
d. Acute renal rupture
e. Patient only has one kidney

01/29/2014
62
A patient presents to the ED after he fell 15 feet to the ground off a scaffolding. He comes in with the injury seen on this X-ray. His contrasted CT shows a non enhanced kidney on the left side. The most likely diagnosis is…
a. Acute traumatic hydronephrosis
b. Renal artery thrombosis
c. Acute renal contusion
d. Acute renal rupture
e. Patient only has one kidney
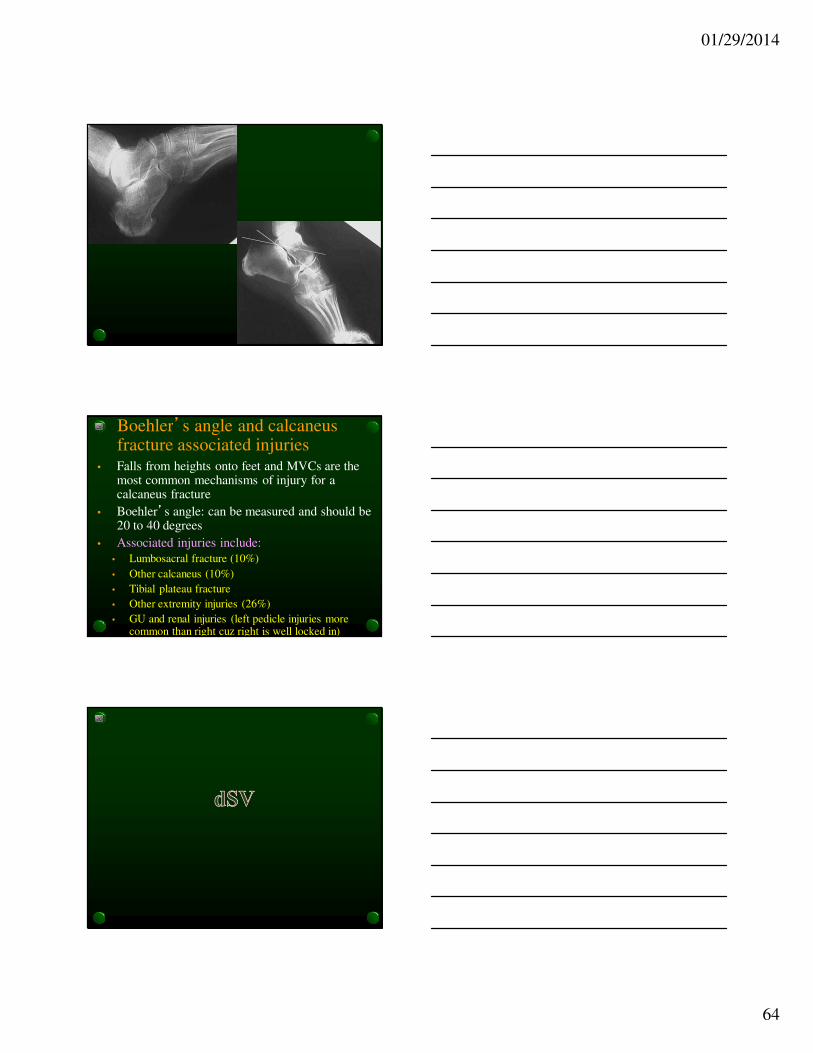
3415
o
Apex of anterior
process
Apex of
posterior
facet
Posterior
calcaneal
tuberosity
01/29/2014
63
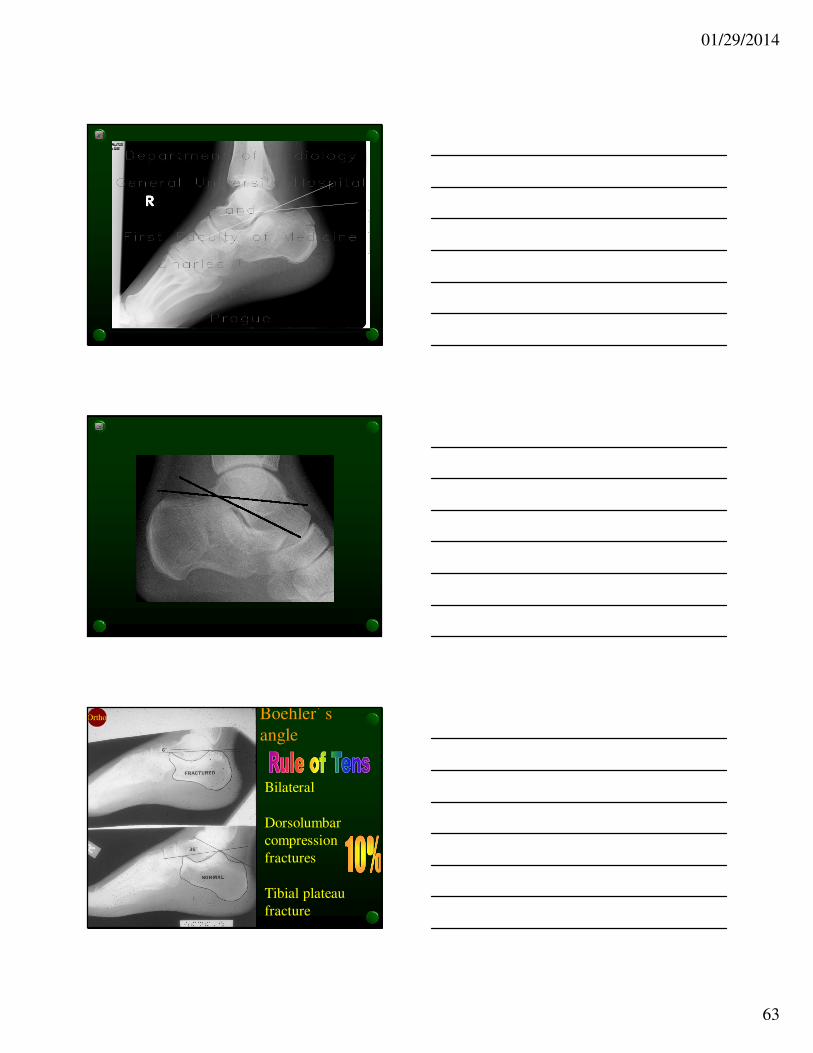
Boehler’s
angle
Bilateral
Dorsolumbar
compression
fractures
Tibial plateau
fracture
Ortho
01/29/2014
64
Boehler’s angle and calcaneus fracture associated injuries
• Falls from heights onto feet and MVCs are the most common mechanisms of injury for a calcaneus fracture
• Boehler’s angle: can be measured and should be 20 to 40 degrees
• Associated injuries include:
• Lumbosacral fracture (10%)
• Other calcaneus (10%)
• Tibial plateau fracture
• Other extremity injuries (26%)
• GU and renal injuries (left pedicle injuries more common than right cuz right is well locked in)

01/29/2014
65
AAA
� Definition > 3cm
� 90% begin below renal arteries
� 4 – 5 cm 50% are palpable
� 5cm are palpable, but pulsatileabdominal mass is felt in < 50%
� Grow at 4mm per year
� > 5cm requires vascular surgeon
� Audible bruit is rare
A 43yo male presents to the ED with altered mental
status. His wife says he just got over a “bad sore
throat” a few days ago. VS BP 90/60, P 110, RR 24,
T 39C. On exam you note a anisocoria (R >L), a
drooping L eyelid. You also note some tongue
deviation. Which of the following is the most likely
diagnosis?
a. Peritonsillar abscess
b. Epiglottitis
c. Ludwig’s angina
d. Parapharyngeal abscess
e. Tracheitis
Parapharyngeal Abscess leading to sepsis
• These patients typically present after resolution of
sore throat
• Can encroach of adjacent tissues:
• Cervical sympathetic chain (Horner’s)
• Carotid artery and jugular vein (causing sepsis)
• Patients with this complication will present in severe sepsis• Organ hypoperfusion (AMS in this case)
• Two of the following 4 (for dx of SIRS)• Fever > 38 or < 36
• Pulse rate > 90
• RR > 20 or PCO2 < 32
• WBC count > 12,000 or > 4,000 or > 10% bands
01/29/2014
66
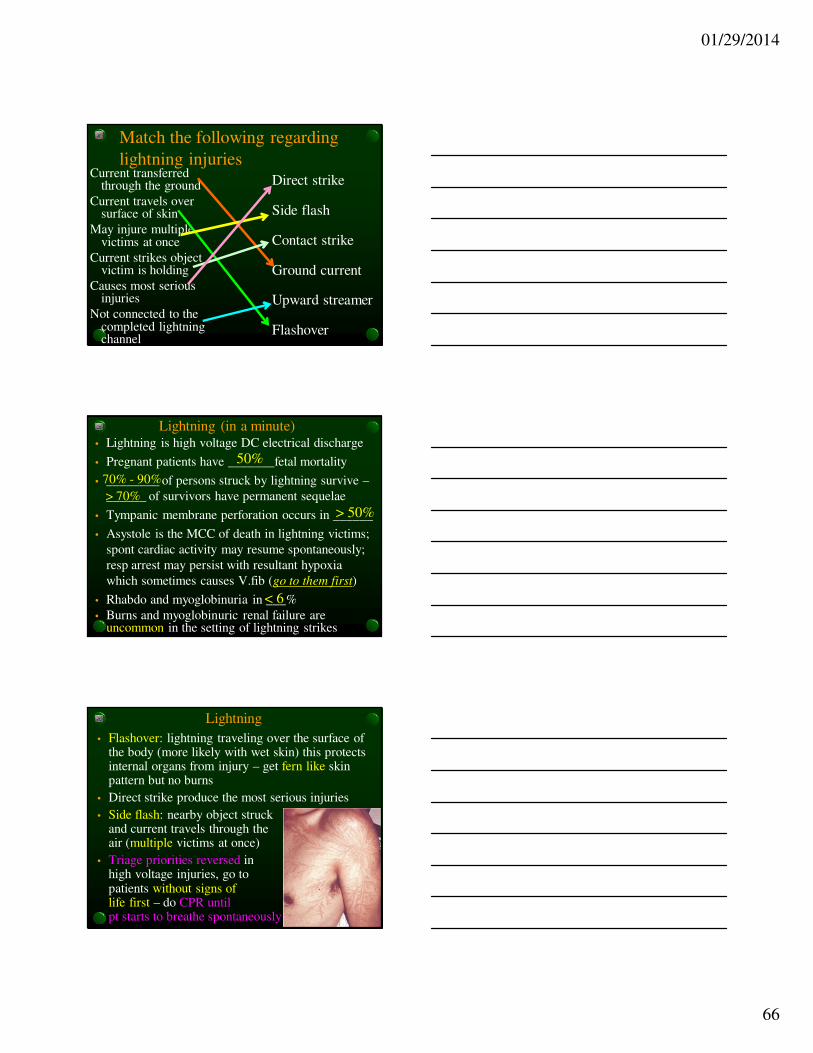
Match the following regarding
lightning injuriesDirect strike
Side flash
Contact strike
Ground current
Upward streamer
Flashover
Current transferred through the ground
Current travels over surface of skin
May injure multiple victims at once
Current strikes object victim is holding
Causes most serious injuries
Not connected to the completed lightning channel
Lightning (in a minute)• Lightning is high voltage DC electrical discharge
• Pregnant patients have _______fetal mortality
• ________ of persons struck by lightning survive –
______ of survivors have permanent sequelae
• Tympanic membrane perforation occurs in ______
• Asystole is the MCC of death in lightning victims;
spont cardiac activity may resume spontaneously;
resp arrest may persist with resultant hypoxia
which sometimes causes V.fib (go to them first)
• Rhabdo and myoglobinuria in ___%
• Burns and myoglobinuric renal failure are uncommon in the setting of lightning strikes
50%
70% - 90%
> 50%
< 6
> 70%
Lightning
• Flashover: lightning traveling over the surface of the body (more likely with wet skin) this protects internal organs from injury – get fern like skin pattern but no burns
• Direct strike produce the most serious injuries
• Side flash: nearby object struck and current travels through the air (multiple victims at once)
• Triage priorities reversed in high voltage injuries, go to patients without signs of life first – do CPR until pt starts to breathe spontaneously

01/29/2014
67
Keraunoparalysis
• Caused by lightning strike
• Typically occurs in the lower extremities
• Characterized by:
• Transient paralysis
• Mottled, cool, blue, pulseless extremities
• Typically resolves on its own within minutes
to hours
AC/DC (in a minute)• AC > danger than DC
• AC causes tetany once “let go current” is
exceeded
• Impossible to predict degree of underlying damage
by looking at extent of cutaneous burn
• ……. % of patients who suffer low voltage injury
have cardiac dysrhythmia and most common is
………………………..
• High-voltage electrical injuries (>1000V) =
increased risk of spinal injuries (immobilize)
• ECG changes or LOC requires 24 hrs monitoring.
< 10
ventricular fibrillation
01/29/2014
68
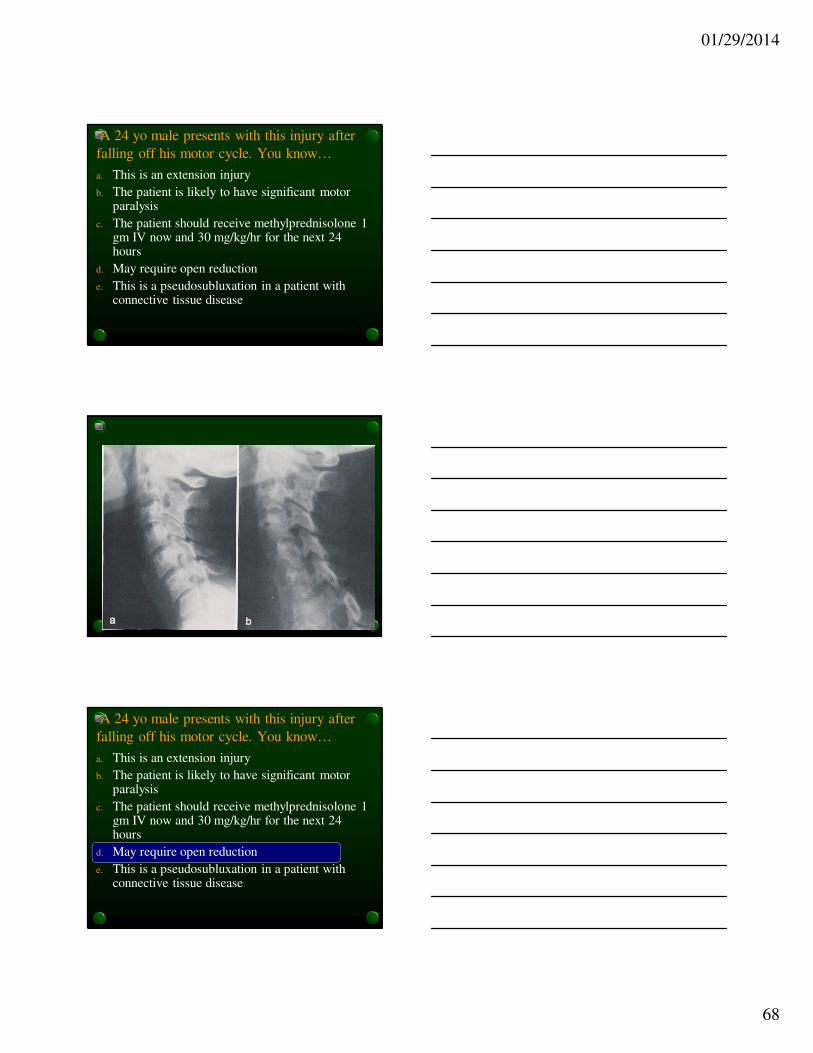
A 24 yo male presents with this injury after
falling off his motor cycle. You know…
a. This is an extension injury
b. The patient is likely to have significant motor paralysis
c. The patient should receive methylprednisolone 1 gm IV now and 30 mg/kg/hr for the next 24 hours
d. May require open reduction
e. This is a pseudosubluxation in a patient with connective tissue disease
A 24 yo male presents with this injury after
falling off his motor cycle. You know…
a. This is an extension injury
b. The patient is likely to have significant motor paralysis
c. The patient should receive methylprednisolone 1 gm IV now and 30 mg/kg/hr for the next 24 hours
d. May require open reduction
e. This is a pseudosubluxation in a patient with connective tissue disease

01/29/2014
69
Unilateral Facet Dislocation

01/29/2014
70
Anterior Subluxation
Injury
Hyperflexion Sprain
Delayed instability
Forced flexion disrupts
posterior ligaments
Often missed
Flexion Injury
Bilateral Facet
Hyperflexion
NOT perched
One facet in front of the other

01/29/2014
71
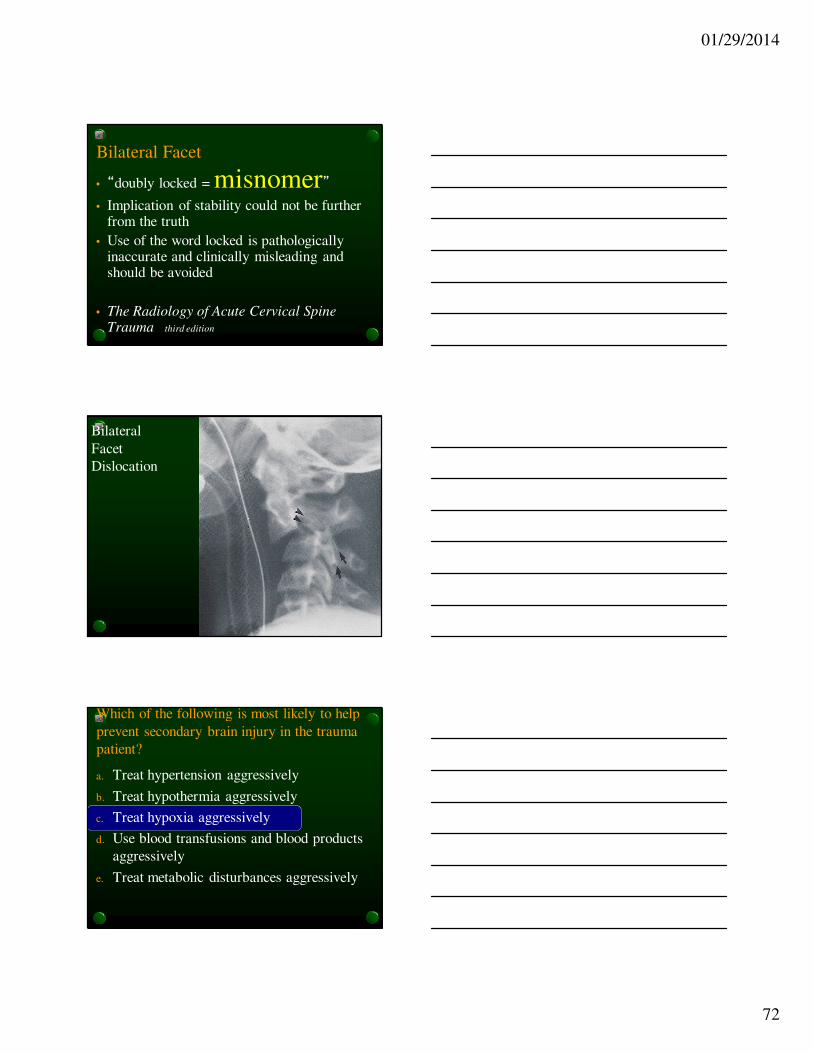
Bilateral Facet Dislocation
• Severe Flexion with distraction and
disruption of posterior ligaments
• Both inferior facets jump over the
corresponding superior facets
• > 50% subluxation of vert. body width
• Cord injury very common
• HIGHLY UNSTABLE
bilateralperched
01/29/2014
72
Bilateral Facet
• “doubly locked = misnomer”• Implication of stability could not be further
from the truth
• Use of the word locked is pathologically inaccurate and clinically misleading and should be avoided
• The Radiology of Acute Cervical Spine Trauma third edition
Bilateral
Facet
Dislocation
Which of the following is most likely to help
prevent secondary brain injury in the trauma
patient?
a. Treat hypertension aggressively
b. Treat hypothermia aggressively
c. Treat hypoxia aggressively
d. Use blood transfusions and blood products
aggressively
e. Treat metabolic disturbances aggressively
01/29/2014
73
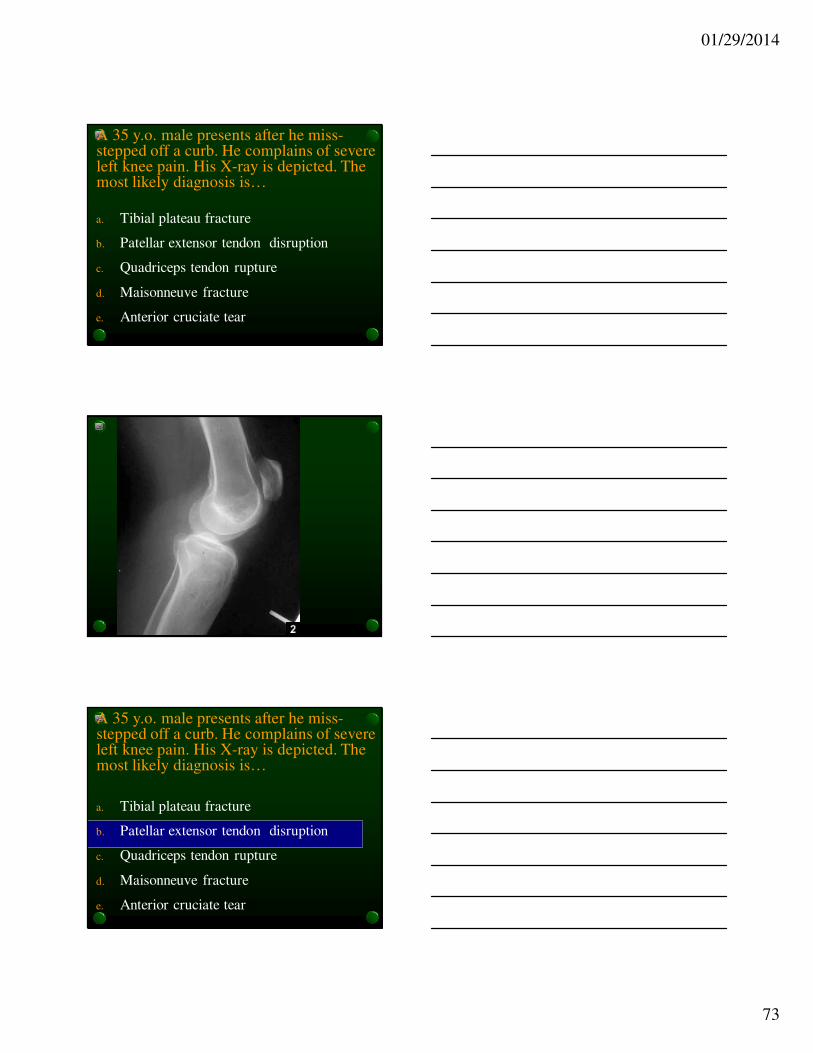
A 35 y.o. male presents after he miss-stepped off a curb. He complains of severe left knee pain. His X-ray is depicted. The most likely diagnosis is…
a. Tibial plateau fracture
b. Patellar extensor tendon disruption
c. Quadriceps tendon rupture
d. Maisonneuve fracture
e. Anterior cruciate tear
A 35 y.o. male presents after he miss-stepped off a curb. He complains of severe left knee pain. His X-ray is depicted. The most likely diagnosis is…
a. Tibial plateau fracture
b. Patellar extensor tendon disruption
c. Quadriceps tendon rupture
d. Maisonneuve fracture
e. Anterior cruciate tear

01/29/2014
74
Insall and Salvati Method
A
B
B/A =1
< 1 = patella alta
Greatest diagonal length measured
Lower pole of patella to tibial tubercle
A
B
A/B < 0.8
Blackburn
A
B
B/A =1
< 1 = patella alta
Insall and Salvati Method
Greatest diagonal length measured

01/29/2014
75
High riding patella – Patella Alta
• 80% of knee extensor disruptions in < 40
y.o. will be patellar extensor tendon that
will be affected
• 80% of knee extensor disruptions in > 40
y.o. will be the quadriceps tendon that will
be affected
• No trauma then chronic patella alta (not
expected at ABEM General)
A patient presents in coma after minor
traumatic event. You inject cold water into the
patient’s left ear and the eyes slowly move to
the left. This means
a. His cerebral cortex is intact
b. His brainstem is not functioning
c. His brainstem and cerebral cortex are not
functioning
d. His brainstem is functioning
e. His brainstem and cerebral cortex is intact
Cold calorics (Oculovestibular reflex)
• If you inject cold water into the left ear and the
eyes slowly move towards the left ear, this means
the brainstem is intact
• If then the eyes move with fast movement
(nystagmus) towards the opposite ear this means
the cerebral cortex is intact
• If both of the above occur, the patient is faking it
• If there is no movement then nothing is working
Corneal stimulation will cause eye to blink if Cr V and VII
are intact which is another way to check brainstem function

01/29/2014
76
Doll’s eyes (oculocephalic reflex)
• When you turn a doll’s head to one side, the eyes follow
slowly after the head is turned
• When you do this to a comatose patient (not a trauma pt)
and his eyes lag behind (as if the patient is maintaining
fixation on a single point in space). The eyes thus appear
to be moving relative to the head in the direction opposite
to the head movement (this means normal functioning
brainstem).
• The absence of this reflex suggests brainstem dysfunction
in a comatose patient.
• This reflex is suppressed in the conscious patient but is
normal in the unconscious patient without brainstem
injury
A 74 yo male known diabetic and hypertensive presents to the ED with sudden onset of left eye pain. He also complains of blurred vision, headache, abdominal pain and nausea. His VA is 20/200 OS and 20/40 OD. Exam of the eye shows conjunctival injection and pupil is mid position and non reactive to light. Funduscopic exam is shown. Your next best step
a. Order a sedimentation rate
b. Give prednisone 60 mg
c. Perform tonometry
d. Order a CTA brain
e. Order an ultrasound of L eye

01/29/2014
77
A 74 yo male known diabetic and hypertensive presents to the ED with sudden onset of left eye pain. He also complains of blurred vision, headache, abdominal pain and nausea. His VA is 20/200 OS and 20/40 OD. Exam of the eye shows conjunctival injection and pupil is mid position and non reactive to light. Funduscopic exam is shown. Your next best step
a. Order a sedimentation rate
b. Give prednisone 60 mg
c. Perform tonometry
d. Order a CTA brain
e. Order an ultrasound of L eye
Glaucoma: Associations
• Red painful eye
• ‘Steamy cornea’
• Blurred vision
• Nausea/headache
• Abdominal pain
• Mid dilated pupil
poorly reactive
• Cup/disc > 1:2
• Risks:
• Hypertension
• Vascular disease
• Familial
• IOP
• Diabetes mellitus
01/29/2014
78
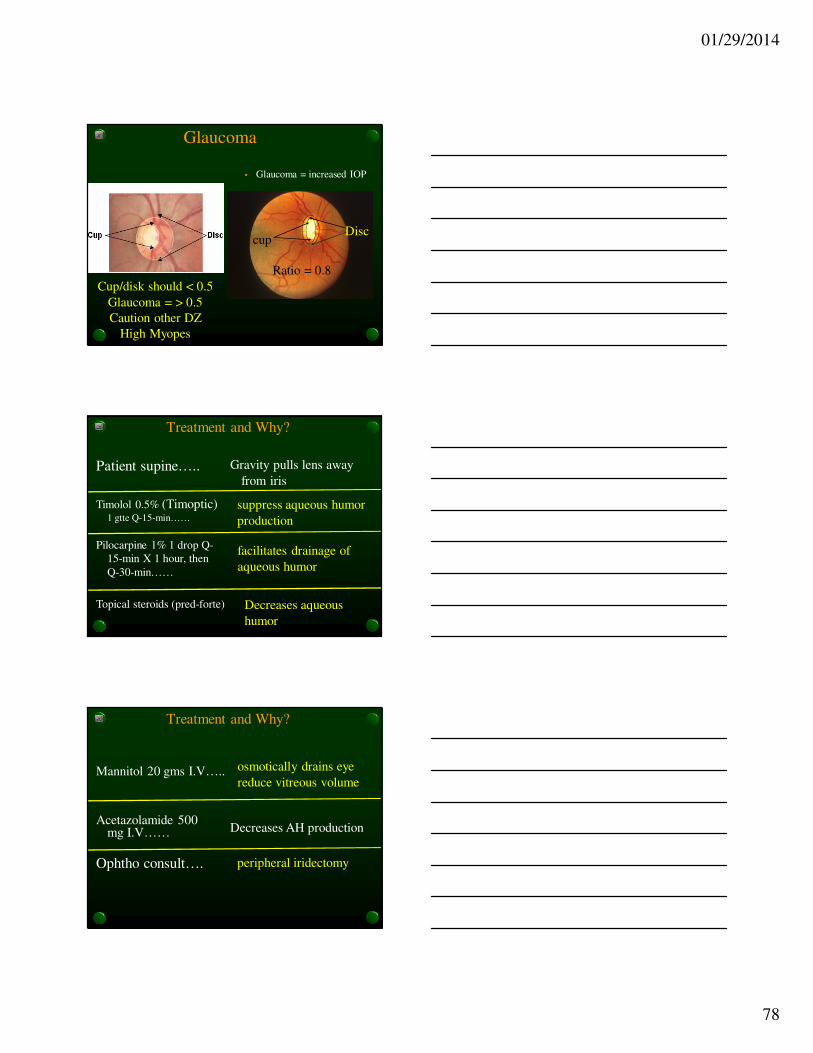
Glaucoma
• Glaucoma = increased IOP
Cup/disk should < 0.5
Glaucoma = > 0.5
Caution other DZ
High Myopes
cupDisc
Ratio = 0.8
Treatment and Why?
Patient supine….. Gravity pulls lens away
from iris
Timolol 0.5% (Timoptic)1 gtte Q-15-min……
suppress aqueous humor
production
Pilocarpine 1% 1 drop Q-
15-min X 1 hour, then
Q-30-min……
facilitates drainage of
aqueous humor
Topical steroids (pred-forte) Decreases aqueous
humor
Treatment and Why?
Acetazolamide 500 mg I.V…… Decreases AH production
Ophtho consult…. peripheral iridectomy
osmotically drains eye
reduce vitreous volumeMannitol 20 gms I.V…..
01/29/2014
79
Which of the following is true regarding
fetal exposure to radiationa. A single CXR in a women who is 6 weeks
pregnant could increase the risk of fetal
malformation by 20%
b. A CT of the abdomen of a 20 week pregnant
female gives more radiation to the fetus that is
considered a safe level of radiation exposure to
any fetus
c. During the nine months in utero the fetus is
exposed to an average of 50 – 100 mrads
d. The highest risk of radiation to the fetus occurs at
fetal age 8 to 16 weeks
Fetal exposure to radiation
• _______ is considered to be safe
• During the 9 months in utero the fetus is
exposed to ____________
• _______ increases the risk of childhood
cancer but does not increase the risk of:
• Fetal malformation
• Spontaneous abortion
• Growth retardation
< 5 rads
50 – 100 mrads
>10 rads
Fetal exposure to radiation
• Maternal plain films of the head, C-spine, T-
spine, extremities or CXR exposes the fetus
to _________
• X-rays of the LS spine, hips or pelvis expose
the fetus to ________
• CT of the abdomen exposes the fetus to
______
< 5 mrads (1000 times less than safe threshold)
> 5 mrads
2.5 rads

01/29/2014
80
Fetal exposure to radiation
• Maternal abdominal lead shielding decreases
radiation to the fetus by 50%
• The highest risk of radiation to the fetus is
__________ gestation 2 – 7 weeks organogenesis
53yo male presents to the ED with sudden
SOB. He is a smoker and has COPD and has
renal insufficiency. His dimer is +ve. A CXR
shows evidence of COPD but no PTX. What is
the most appropriate diagnostic test?
a. Alveolar dead space determination
b. PET Scan
c. VQ scan
d. Spiral CT scan
e. Pulmonary angiography
01/29/2014
81
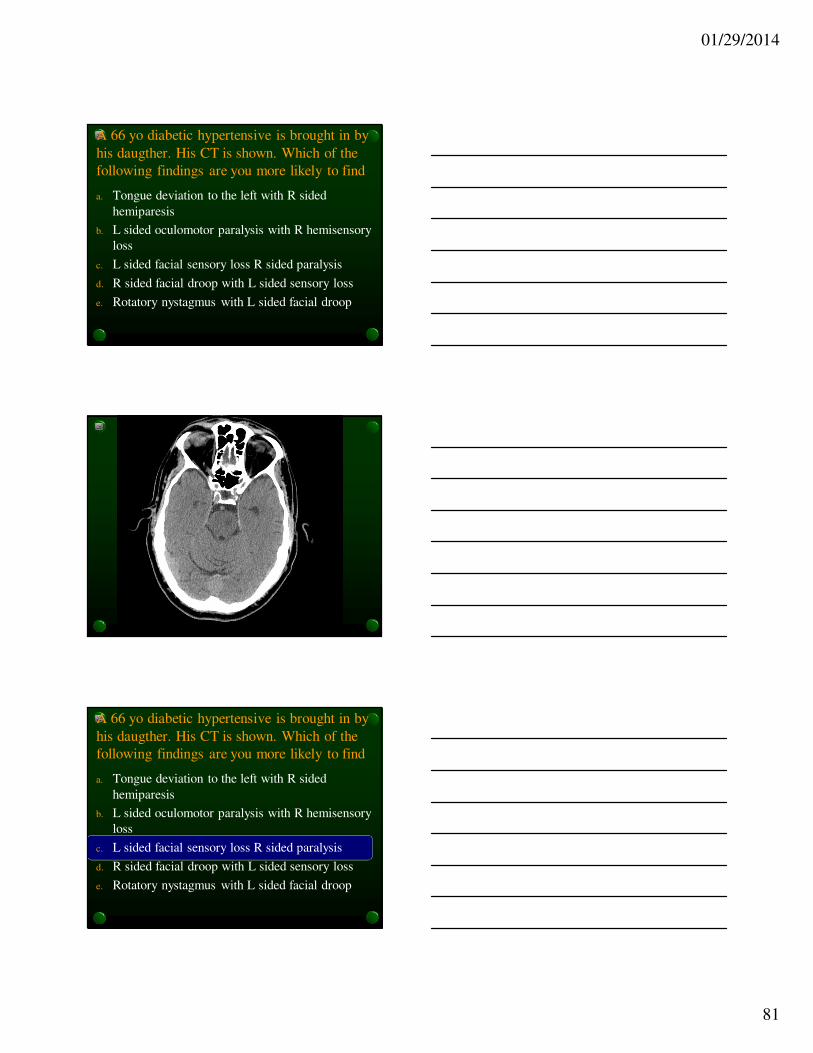
A 66 yo diabetic hypertensive is brought in by
his daugther. His CT is shown. Which of the
following findings are you more likely to find
a. Tongue deviation to the left with R sided
hemiparesis
b. L sided oculomotor paralysis with R hemisensory
loss
c. L sided facial sensory loss R sided paralysis
d. R sided facial droop with L sided sensory loss
e. Rotatory nystagmus with L sided facial droop
A 66 yo diabetic hypertensive is brought in by
his daugther. His CT is shown. Which of the
following findings are you more likely to find
a. Tongue deviation to the left with R sided
hemiparesis
b. L sided oculomotor paralysis with R hemisensory
loss
c. L sided facial sensory loss R sided paralysis
d. R sided facial droop with L sided sensory loss
e. Rotatory nystagmus with L sided facial droop

01/29/2014
82
V
II, III ,IV
VIVIIVIII
IX, X,XI, XII
Brainstem Fx:
RAS
Vital signs
Cranial nerve
Pontomedullary
junction

01/29/2014
83
Match’ em
Vertigo, N/V, nystagmus, drop ataxia, (fatal gastroenteritis)
Cerebellar infarct
Circumoral paresthesia, ipsiCr N contra hemi-loss, HTN
Brainstem stroke
Vertigo, dysarthria, syncope, diplopia, ipsilateral CN deficits, contralat motor dfts
Vertibrobasilar stroke
Contralateral paralysis: Leg > Arm, distal weakness > prox weakness, perseverates, responds slowly, abulia
Contralateral paralysis: , Face/Arm > Leg, homonoms hemianopsia, conj gaze impair
Middle cerebral artery stroke
Anterior cerebral
stroke
Homonomous hemianopsia, visual agnosia, memory loss, cortical blindness, minimal motor involvment, ipsi CN 3
Posterior cerebral
stroke
Coma, miosis, apneustic breathing, only up eye mvt
Pontine stroke
Significant edema
KEYCEPT
• The hallmark of a brainstem stroke is
crossed findings
• Think about this diagnosis in patients
with perioral paresthesia
• Ipsilateral cranial nerve findings with
contralateral hemi – findings (paresis or
sensory loss
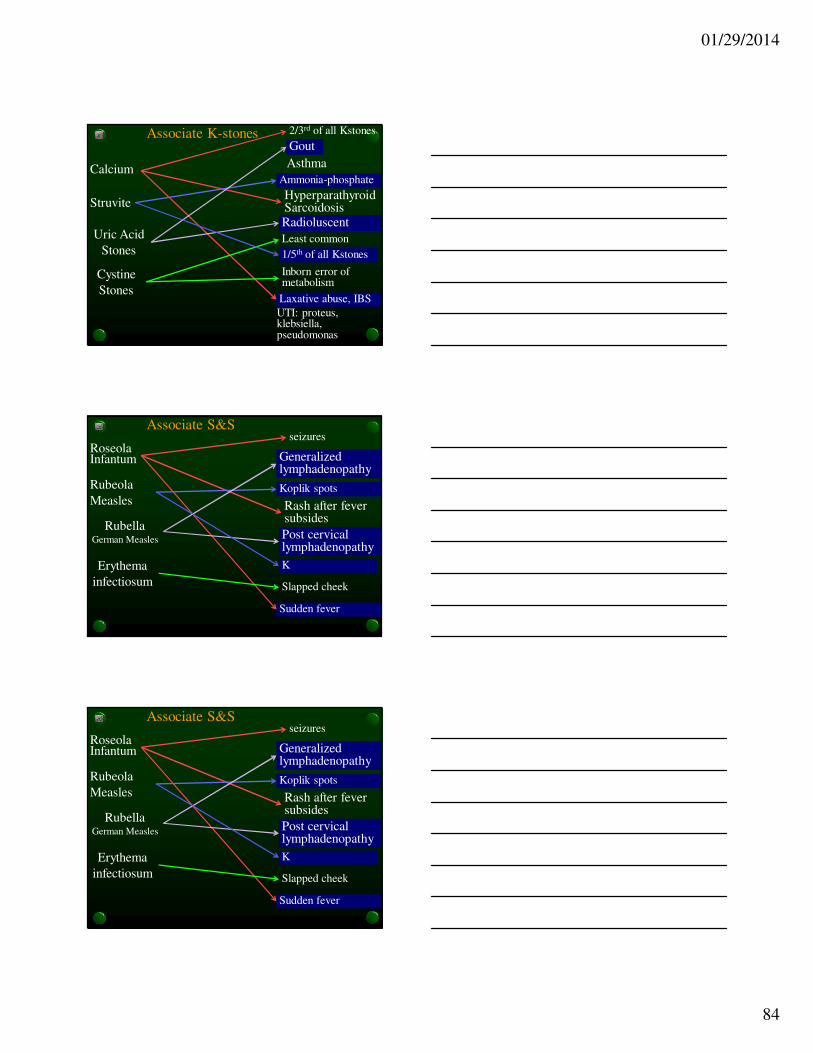
Associate K-stones
Calcium
Struvite
Uric Acid
Stones
Cystine
Stones
2/3rd of all Kstones
HyperparathyroidSarcoidosis
Laxative abuse, IBS
Ammonia-phosphate
Radioluscent
Inborn error of metabolism
1/5th of all Kstones
Least common
Gout
UTI: proteus, klebsiella, pseudomonas
01/29/2014
84
Associate K-stones
Calcium
Struvite
Uric Acid
Stones
Cystine
Stones
2/3rd of all Kstones
HyperparathyroidSarcoidosis
Laxative abuse, IBS
Ammonia-phosphate
Radioluscent
Inborn error of metabolism
1/5th of all Kstones
Least common
Gout
Asthma
UTI: proteus, klebsiella, pseudomonas
Associate S&S
Roseola Infantum
Rubeola
Measles
Rubella German Measles
Erythema
infectiosum
seizures
Rash after fever subsides
Sudden fever
Koplik spots
Post cervical lymphadenopathy
Slapped cheek
K
Generalized lymphadenopathy
Associate S&S
Roseola Infantum
Rubeola
Measles
Rubella German Measles
Erythema
infectiosum
seizures
Rash after fever subsides
Sudden fever
Koplik spots
Post cervical lymphadenopathy
Slapped cheek
K
Generalized lymphadenopathy
01/29/2014
85
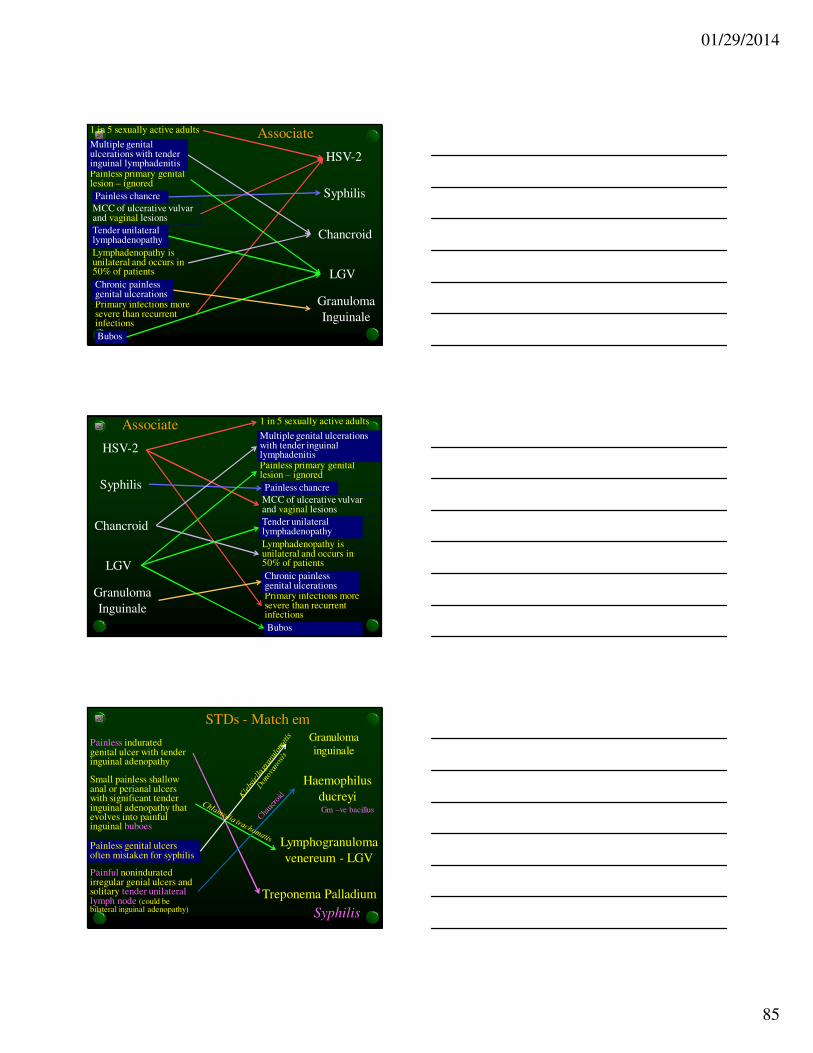
Associate
HSV-2
Syphilis
Chancroid
LGV
1 in 5 sexually active adults
MCC of ulcerative vulvarand vaginal lesions
Primary infections more severe than recurrent infections
Painless chancre
Lymphadenopathy is unilateral and occurs in 50% of patients
Painless primary genital lesion – ignored
Bubos
Multiple genital ulcerations with tender inguinal lymphadenitis
Tender unilateral lymphadenopathy
Granuloma
Inguinale
Chronic painless genital ulcerations
Associate
HSV-2
Syphilis
Chancroid
LGV
1 in 5 sexually active adults
MCC of ulcerative vulvarand vaginal lesions
Primary infections more severe than recurrent infections
Painless chancre
Lymphadenopathy is unilateral and occurs in 50% of patients
Painless primary genital lesion – ignored
Bubos
Multiple genital ulcerations with tender inguinal lymphadenitis
Tender unilateral lymphadenopathy
Granuloma
Inguinale
Chronic painless genital ulcerations
STDs - Match em
Painless indurated genital ulcer with tender inguinal adenopathy
Treponema Palladium
Small painless shallow anal or perianal ulcers with significant tender inguinal adenopathy that evolves into painful inguinal buboes
Lymphogranuloma
venereum - LGVPainless genital ulcers often mistaken for syphilis
Granuloma
inguinale
Painful nonindurated irregular genial ulcers and solitary tender unilateral lymph node (could be bilateral inguinal adenopathy)
Haemophilus
ducreyi
Syphilis
Gm –ve bacillus
01/29/2014
86
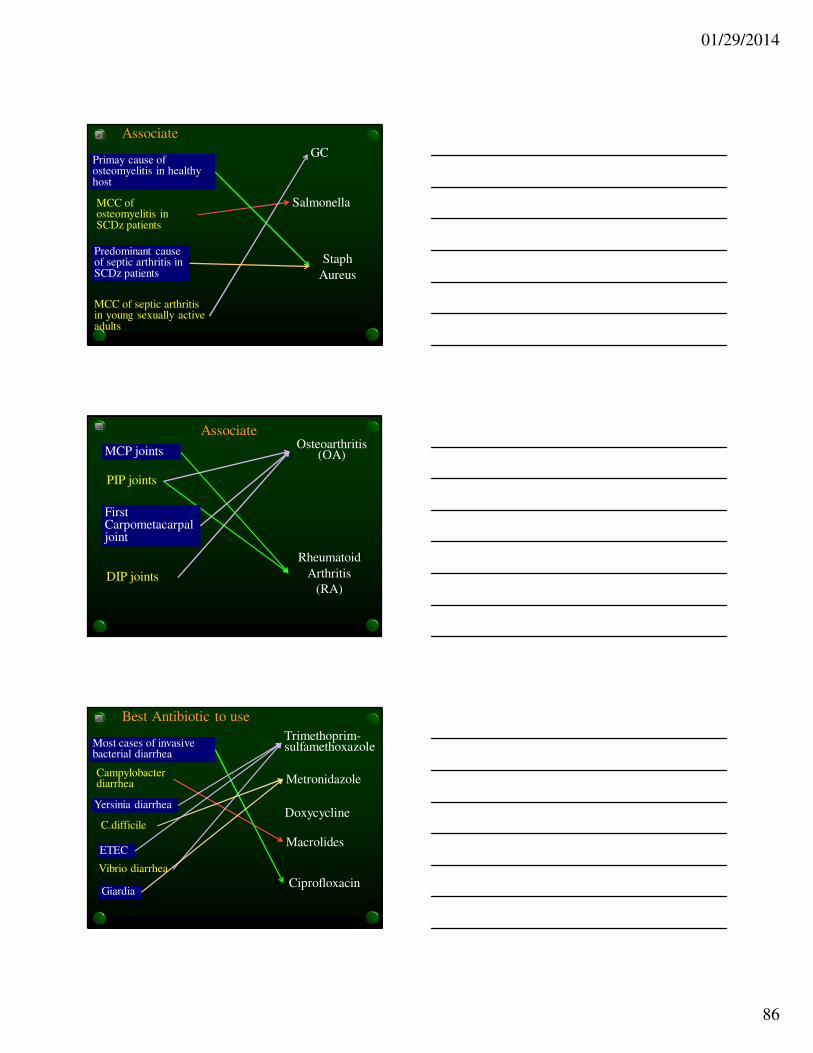
Associate
GC
Salmonella
Staph
Aureus
MCC of septic arthritis in young sexually active adults
MCC of osteomyelitis in SCDz patients
Primay cause of osteomyelitis in healthy host
Predominant cause of septic arthritis in SCDz patients
AssociateOsteoarthritis
(OA)
Rheumatoid
Arthritis
(RA)DIP joints
PIP joints
MCP joints
First Carpometacarpal joint
Best Antibiotic to use
Trimethoprim-sulfamethoxazole
Macrolides
Ciprofloxacin
C.difficile
Campylobacter diarrhea
Most cases of invasive bacterial diarrhea
Yersinia diarrhea
Vibrio diarrhea
ETEC
Giardia
Metronidazole
Doxycycline
01/29/2014
87
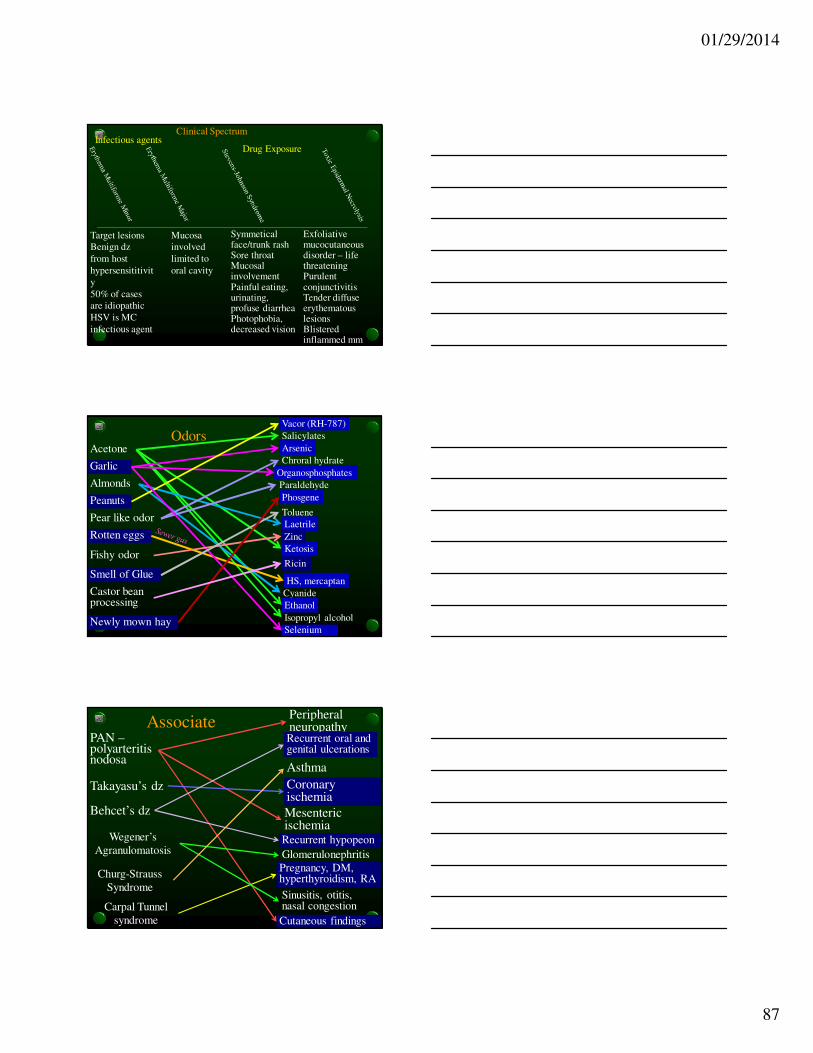
Clinical Spectrum
Target lesions
Benign dz
from host
hypersensititivit
y
50% of cases
are idiopathic
HSV is MC
infectious agent
Mucosa
involved
limited to
oral cavity
Symmetical face/trunk rashSore throatMucosal involvementPainful eating, urinating, profuse diarrheaPhotophobia, decreased vision
Exfoliative mucocutaneous disorder – life threateningPurulent conjunctivitisTender diffuse erythematous lesionsBlistered inflammed mm
Infectious agentsDrug Exposure
Odors
Laetrile
Cyanide
Arsenic
Organosphosphates
Ethanol
Salicylates
Acetone
Garlic
Almonds
Peanuts
Pear like odor
Rotten eggs
Isopropyl alcohol
Ketosis
Vacor (RH-787)
Chroral hydrate
Paraldehyde
HS, mercaptan
Selenium
Zinc
Toluene
Fishy odor
Smell of Glue
Phosgene
Ricin
Newly mown hay
Castor bean processing
AssociatePAN –polyarteritis nodosa
Takayasu’s dz
Behcet’s dz
Wegener’s
Agranulomatosis
Churg-Strauss
Syndrome
Peripheral neuropathy
Mesenteric ischemia
Cutaneous findings
Coronary ischemia
Recurrent hypopeon
Sinusitis, otitis, nasal congestion
Pregnancy, DM, hyperthyroidism, RA
Glomerulonephritis
Recurrent oral and genital ulcerations
Carpal Tunnel
syndrome
Asthma

01/29/2014
88
Associate
Medical cause of
Psychosis
Psychiatric
cause of
Psychosis
Acute onset
Older patient
Visual hallucinations
Disorientation
Gradual onsetFlat affect
Aphasia, ataxia
Auditory hallucinations
Young adult
Impaired consciousness
Abnormal VS
You are working in Nome, Alaska. A 15 yo fell 7 feet and hit his head. He was initially unconscious then woke up for a while and now is unconscious again and while you are attending to him his R pupil dilates and he no longer moves his L side and then crashes.Your next best step is…
a. Hyperventilate, manitol, call neurosurgeon in
Fairbanks for transfer
b. Elevated head of bed, manitol, decadron
c. Burr hole on the R if unsuccessful, burr hole on L
d. Burr hole on the L if unsuccessful bur hole on R
e. Call the neurosurgeon in Fairbanks
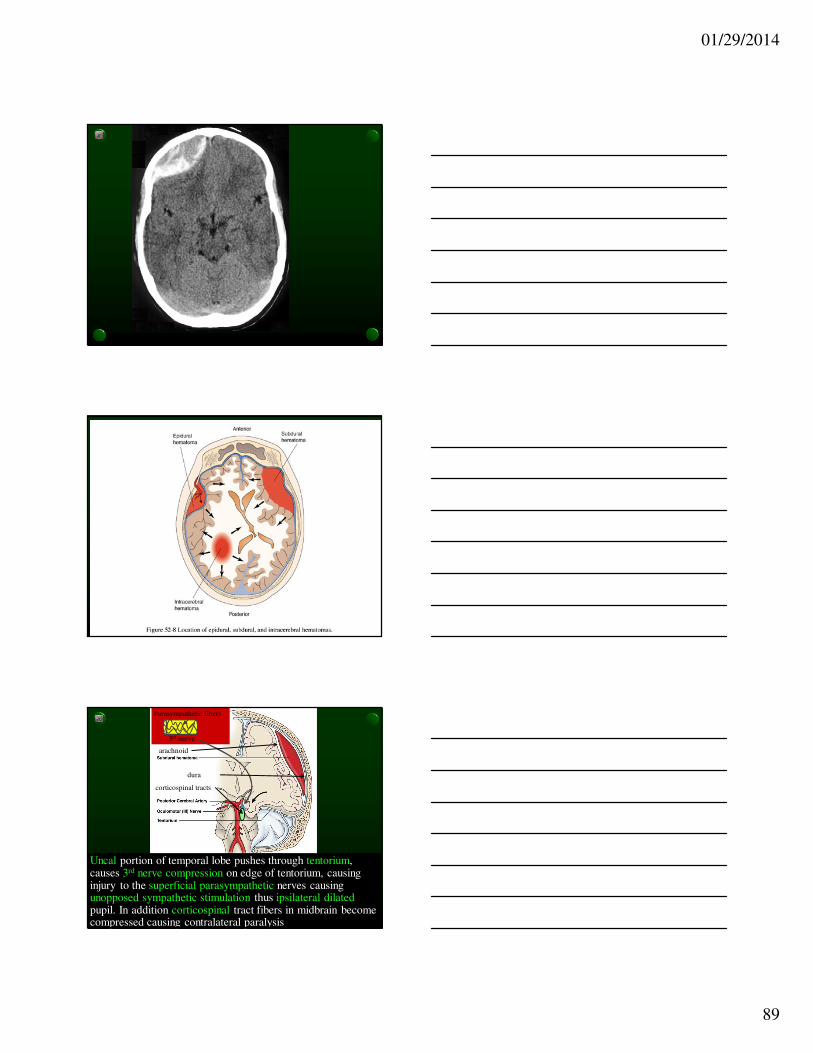
Epidural
• Classic: Brief LOC, then lucid interval, then LOC
• Decrease LOC, ipsilateral pupillary dilatation (due to compression of CN III and its superficial parasympathetic fibers), contralateral hemiparesis (due to compression of ipsilateral cerebral peduncle – motor fibers cross below this level)
• Lenticular (football) shape lesion on CT
• Mortality rate 0% - 20%
• Middle meningeal artery injury
01/29/2014
89
Uncal portion of temporal lobe pushes through tentorium, causes 3rd nerve compression on edge of tentorium, causing injury to the superficial parasympathetic nerves causing unopposed sympathetic stimulation thus ipsilateral dilatedpupil. In addition corticospinal tract fibers in midbrain become compressed causing contralateral paralysis
3rd nerve
Parasympathetic fibers
arachnoid
dura
corticospinal tracts

01/29/2014
90
Transtentorial (Uncal) herniation syndrome
• In 20% of cases
hematoma
compresses opposite
side of midbrain
against tentorium
edge resulting in
contralat pupil
dilatation and ipsilateral paralysis
• This is why bilateral burr holes is necessary
in ipsilateral burr hole does not work
Collection of blood below inner table of dura but
external to the brain (between cortex and venous
sinuses – dissects the arachnoid away from the dura)
Occurs in 33% of patients with severe head injury
Subdural
• H/A
• Decreased LOC
• Bridging veins
• 25% are bilateral
• Crescent shape lesion on CT
• 30% - 60% mortality
• Acute, subacute (isodense, coumadin), chronic
6X more common than epidural
Below inner layer of dura
External to arachnoid
subacute
acute
01/29/2014
91
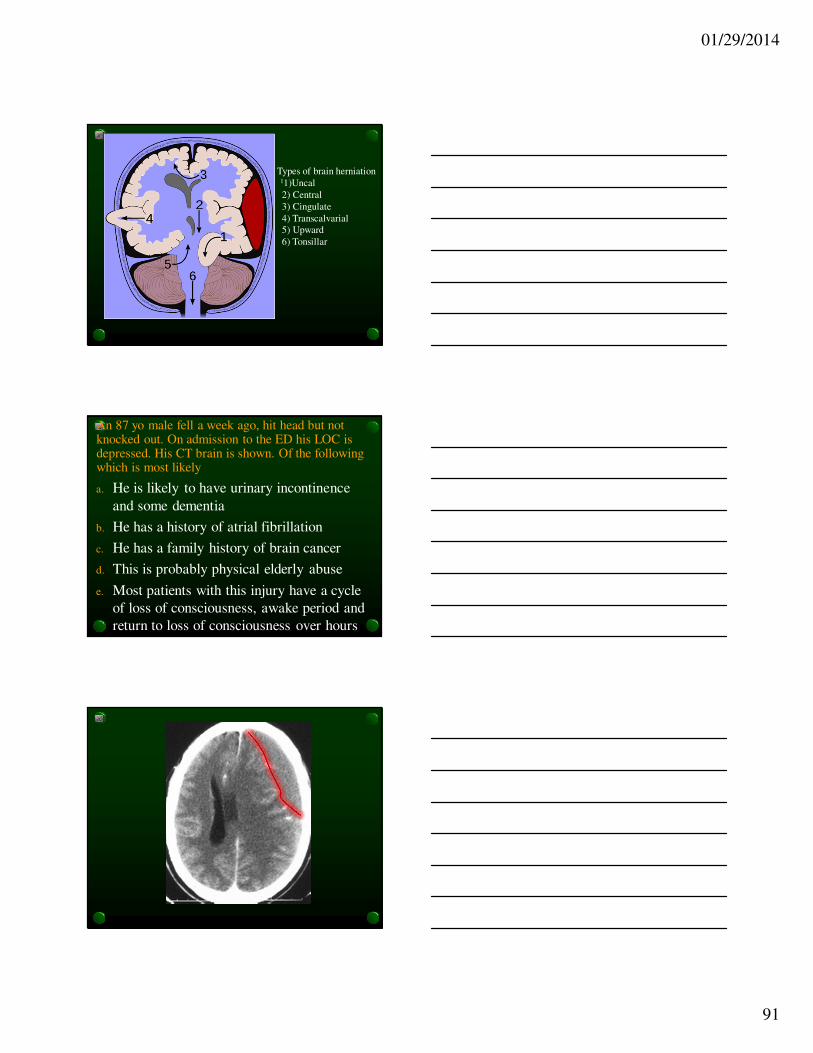
Types of brain herniation11)Uncal
2) Central
3) Cingulate
4) Transcalvarial
5) Upward
6) Tonsillar
An 87 yo male fell a week ago, hit head but not knocked out. On admission to the ED his LOC is depressed. His CT brain is shown. Of the following which is most likely
a. He is likely to have urinary incontinence
and some dementia
b. He has a history of atrial fibrillation
c. He has a family history of brain cancer
d. This is probably physical elderly abuse
e. Most patients with this injury have a cycle
of loss of consciousness, awake period and
return to loss of consciousness over hours

01/29/2014
92
An 87 yo male fell a week ago, hit head but not knocked out. On admission to the ED his LOC is depressed. His CT brain is shown. Of the following which is most likely
a. His LOC has been disturbed for at least 2
weeks
b. He has a history of atrial fibrillation
c. He has a family history of brain cancer
d. This is probably physical elderly abuse
e. Most patients with this injury have a cycle
of loss of consciousness, awake period and
return to loss of consciousness over hours

01/29/2014
93
An 87 yo male fell a week ago, hit head but not knocked out. On admission to the ED his LOC is depressed. His CT brain is shown. Of the following which is most likely
a. He is likely to have urinary incontinence
and some dementia
b. He has a history of atrial fibrillation
c. He has a family history of brain cancer
d. This is probably physical elderly abuse
e. Most patients with this injury have a cycle
of loss of consciousness, awake period and
return to loss of consciousness over hours

01/29/2014
94
An 87 yo male fell a week ago, hit head but not knocked out. On admission to the ED his LOC is depressed. His CT brain is shown. Of the following which is most likely
a. His LOC has been disturbed for at least 2
weeks
b. He has a history of atrial fibrillation
c. He has a family history of brain cancer
d. This is probably physical elderly abuse
e. Most patients with this injury have a cycle
of loss of consciousness, awake period and
return to loss of consciousness over hours

01/29/2014
95
Subdural
• H/A
• Decreased LOC
• Bridging veins
• 25% are bilateral
• Crescent shape lesion on CT
• 30% - 60% mortality
• Acute, subacute (isodense, coumadin), chronic
6X more common than epidural
Below inner layer of dura
External to arachnoid
subacute
acute
Collection of blood below inner table of dura but
external to the brain (between cortex and venous
sinuses – dissects the arachnoid away from the dura)
Occurs in 33% of patients with severe head injury

01/29/2014
96
Epidural
• Classic: Brief LOC, then lucid interval, then LOC
• Decrease LOC, ipsilateral pupillary dilatation (due to compression of CN III and its superficial parasympathetic fibers), contralateral hemiparesis (due to compression of ipsilateral cerebral peduncle – motor fibers cross below this level)
• Lenticular (football) shape lesion on CT
• Mortality rate 0% - 20%
• Middle meningeal artery injury

01/29/2014
97
You are working in Nome, Alaska. A 15 yo fell 7 feet and hit his head. He is unconscious and while you are attending to him his R pupil dilates and he no longer moves his L side and then crashes.Your next best step is…
a. Hyperventilate, manitol, call neurosurgeon in
Fairbanks for transfer
b. Elevated head of bed, manitol, decadron
c. Burr hole on the R if unsuccessful, burr hole on L
d. Burr hole on the L if unsuccessful bur hole on R
e. Call the neurosurgeon in Fairbanks
Transtentorial (Uncal) herniation syndrome
• In 20% of cases
hematoma
compresses opposite
side of midbrain
against tentorium
edge resulting in
contralat pupil
dilatation and ipsilateral paralysis
• This is why bilateral burr holes is necessary
in ipsilateral burr hole does not work
Match the following red eyes with the diagnosis
With preauricular adenopathy
With discharge and a cough
Painful with mild mucoserous
discharge for 5 d then spread
With cobblestone papillae under
upper lid
With hypopeon in contact wearer
After eye surgery
With diffuse punctate keratopathy
With cup:disc ratio > 1:2
Dendridic pattern (dumbells)
Cells in the vitreous cavity
Ciliary flush, flare in anterior chamber,
consensual photophobia
•EKC (epidemic keratoconjunctivitis)
•Uveitis
•Herpes simplex infection
•UV keratitis
•Pseudomonas
•Glaucoma
•Iritis
•Endophthalmitis
•Viral conjunctivitis
•Allergic conjuncitivitis
•Chlamydia
•GC