Predicting Fetal Perchlorate Dose and Inhibition of Iodide Kinetics during Gestation: A...
21
Predicting Fetal Perchlorate Dose and Inhibition of Iodide Kinetics during Gestation: A Physiologically-Based Pharmacokinetic Analysis of Perchlorate and Iodide Kinetics in the Rat Rebecca A. Clewell,* ,1 Elaine A. Merrill,† Kyung O. Yu,‡ Deirdre A. Mahle,§ Teresa R. Sterner,† David R. Mattie,‡ Peter J. Robinson,§ Jeffrey W. Fisher‡ ,2 , and Jeffery M. Gearhart§ *Geo-Centers, Inc., Wright-Patterson AFB, Ohio 45433; †Operational Technologies Corp., Dayton, Ohio 45432; ‡AFRL/HEST, Wright-Patterson AFB, Ohio 45433; and §Mantech Environmental Technology, Inc., Dayton, Ohio 45437 Received November 20, 2002; accepted March 3, 2003 Perchlorate (ClO 4 – ) disrupts endocrine homeostasis by compet- itively inhibiting the transport of iodide (I – ) into the thyroid. The potential for health effects from human exposure to ClO 4 – in drinking water is not known, but experimental animal studies are suggestive of developmental effects from ClO 4 – induced iodide deficiency during gestation. Normal hormone-dependent develop- ment relies, in part, on synthesis of hormones in the fetal thyroid from maternally supplied iodide. Although ClO 4 – crosses the pla- centa, the extent of inhibition in the fetal thyroid is unknown. A physiologically-based pharmacokinetic (PBPK) model was devel- oped to simulate ClO 4 – exposure and the resulting effect on iodide kinetics in rat gestation. Similar to concurrent model development for the adult male rat, this model includes compartments for thyroid, stomach, skin, kidney, liver, and plasma in both mother and fetus, with additional compartments for the maternal mam- mary gland, fat, and placenta. Tissues with active uptake are described with multiple compartments and Michaelis-Menten (M-M) kinetics. Physiological and kinetic parameters were ob- tained from literature and experiment. Systemic clearance, pla- cental-fetal transport, and M-M uptake parameters were esti- mated by fitting model simulations to experimental data. The PBPK model is able to reproduce maternal and fetal iodide data over five orders of magnitude (0.36 to 33,000 ng/kg 131 I – ), ClO 4 – distribution over three orders of magnitude (0.01 to 10 mg/kg-day ClO 4 – ) and inhibition of maternal thyroid and total fetal I – uptake. The model suggests a significant fetal ClO 4 – dose in late gestation (up to 82% of maternal dose). A comparison of model-predicted internal dosimetrics in the adult male, pregnant, and fetal rat indicates that the fetal thyroid is more sensitive to inhibition than that of the adult. Key Words: PBPK model; pregnancy; perchlorate; iodide; thy- roid; inhibition; fetal dose. Recent findings of perchlorate (ClO 4 – ) contamination in groundwater and drinking water sources have resulted in wide- spread concern over the potential health effects from long-term ingestion of low-level perchlorate via drinking water (Motzer, 2001; Urbansky, 1998; Urbansky and Shock, 1999). Most drinking water sources reported to contain perchlorate appear to have concentrations less than 20 ppb, although concentra- tions as high as 3700 ppm have been reported in some Las Vegas ground water samples (Motzer, 2001). Perchlorate in- terferes with thyroidal iodide uptake by binding to the sodium iodide symporter (NIS) at the basolateral membrane of the thyroid follicular endothelial cell, resulting in decreased iodide uptake and decreased synthesis of thyroid hormones. However, hormone homeostasis is usually regained through upregulation of NIS via the hypothalamus-pituitary-thyroid (H-P-T) feed- back mechanism (Wolff, 1998). Nevertheless, due to the iden- tification of contaminated water sources, and the potential for interaction with thyroid iodide uptake in sensitive human sub- populations, the Environmental Protection Agency is currently in the process of evaluating human risk in order to recommend a safe water concentration of ClO 4 – (USEPA, 2002). The endocrine system maintains a delicate balance of hor- monal and inorganic iodide through the H-P-T feedback sys- tem, wherein the hypothalamus responds to diminished serum hormone levels by increasing production of thyrotropin releas- ing hormone (TRH). TRH then signals the pituitary to release thyroid stimulating hormone (TSH), which in turn increases NIS levels in the thyroid and downregulates hormone deiodi- nation by decreasing synthesis of thyroid peroxidase (TPO). The NIS is responsible for transporting inorganic iodide (I – ) into the thyroid follicular cell for the synthesis of thyroid hormones, particularly thyroxine (T 4 ) and triiodothyronine (T 3 ; Wolff, 1998). In an effort to quantitatively predict ClO 4 – ,I – , and inhibition kinetics in response to both acute and subchronic ClO 4 – expo- sure, we have developed a physiologically-based pharmacoki- netic (PBPK) model in the adult male rat (Merrill et al., 2003). Because the PBPK model is based on physiological, biochem- ical, and mechanistic data, it allows us to determine target site dosimetry and in vivo chemical interactions (inhibition) while 1 To whom correspondence should be addressed at CIIT Centers for Health Research, 6 Davis Drive, Research Triangle Park, NC 27709-2137. Fax: (919) 558-1300. E-mail: [email protected]. 2 Present address: The University of Georgia, Athens, GA 30602. TOXICOLOGICAL SCIENCES 73, 235–255 (2003) DOI: 10.1093/toxsci/kfg081 Copyright © 2003 by the Society of Toxicology 235 by guest on May 31, 2013 http://toxsci.oxfordjournals.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Predicting Fetal Perchlorate Dose and Inhibition of Iodide Kinetics during Gestation: A...

Predicting Fetal Perchlorate Dose and Inhibition of Iodide Kineticsduring Gestation: A Physiologically-Based Pharmacokinetic Analysis of
Perchlorate and Iodide Kinetics in the Rat
Rebecca A. Clewell,*,1 Elaine A. Merrill,† Kyung O. Yu,‡ Deirdre A. Mahle,§ Teresa R. Sterner,† David R. Mattie,‡Peter J. Robinson,§ Jeffrey W. Fisher‡,2, and Jeffery M. Gearhart§
*Geo-Centers, Inc., Wright-Patterson AFB, Ohio 45433; †Operational Technologies Corp., Dayton, Ohio 45432; ‡AFRL/HEST, Wright-Patterson AFB,Ohio 45433; and §Mantech Environmental Technology, Inc., Dayton, Ohio 45437
Received November 20, 2002; accepted March 3, 2003
Perchlorate (ClO4–) disrupts endocrine homeostasis by compet-
itively inhibiting the transport of iodide (I–) into the thyroid. Thepotential for health effects from human exposure to ClO4
– indrinking water is not known, but experimental animal studies aresuggestive of developmental effects from ClO4
– induced iodidedeficiency during gestation. Normal hormone-dependent develop-ment relies, in part, on synthesis of hormones in the fetal thyroidfrom maternally supplied iodide. Although ClO4
– crosses the pla-centa, the extent of inhibition in the fetal thyroid is unknown. Aphysiologically-based pharmacokinetic (PBPK) model was devel-oped to simulate ClO4
– exposure and the resulting effect on iodidekinetics in rat gestation. Similar to concurrent model developmentfor the adult male rat, this model includes compartments forthyroid, stomach, skin, kidney, liver, and plasma in both motherand fetus, with additional compartments for the maternal mam-mary gland, fat, and placenta. Tissues with active uptake aredescribed with multiple compartments and Michaelis-Menten(M-M) kinetics. Physiological and kinetic parameters were ob-tained from literature and experiment. Systemic clearance, pla-cental-fetal transport, and M-M uptake parameters were esti-mated by fitting model simulations to experimental data. ThePBPK model is able to reproduce maternal and fetal iodide dataover five orders of magnitude (0.36 to 33,000 ng/kg 131I–), ClO4
–
distribution over three orders of magnitude (0.01 to 10 mg/kg-dayClO4
–) and inhibition of maternal thyroid and total fetal I– uptake.The model suggests a significant fetal ClO4
– dose in late gestation(up to 82% of maternal dose). A comparison of model-predictedinternal dosimetrics in the adult male, pregnant, and fetal ratindicates that the fetal thyroid is more sensitive to inhibition thanthat of the adult.
Key Words: PBPK model; pregnancy; perchlorate; iodide; thy-roid; inhibition; fetal dose.
Recent findings of perchlorate (ClO4–) contamination in
groundwater and drinking water sources have resulted in wide-
spread concern over the potential health effects from long-termingestion of low-level perchlorate via drinking water (Motzer,2001; Urbansky, 1998; Urbansky and Shock, 1999). Mostdrinking water sources reported to contain perchlorate appearto have concentrations less than 20 ppb, although concentra-tions as high as 3700 ppm have been reported in some LasVegas ground water samples (Motzer, 2001). Perchlorate in-terferes with thyroidal iodide uptake by binding to the sodiumiodide symporter (NIS) at the basolateral membrane of thethyroid follicular endothelial cell, resulting in decreased iodideuptake and decreased synthesis of thyroid hormones. However,hormone homeostasis is usually regained through upregulationof NIS via the hypothalamus-pituitary-thyroid (H-P-T) feed-back mechanism (Wolff, 1998). Nevertheless, due to the iden-tification of contaminated water sources, and the potential forinteraction with thyroid iodide uptake in sensitive human sub-populations, the Environmental Protection Agency is currentlyin the process of evaluating human risk in order to recommenda safe water concentration of ClO4
– (USEPA, 2002).The endocrine system maintains a delicate balance of hor-
monal and inorganic iodide through the H-P-T feedback sys-tem, wherein the hypothalamus responds to diminished serumhormone levels by increasing production of thyrotropin releas-ing hormone (TRH). TRH then signals the pituitary to releasethyroid stimulating hormone (TSH), which in turn increasesNIS levels in the thyroid and downregulates hormone deiodi-nation by decreasing synthesis of thyroid peroxidase (TPO).The NIS is responsible for transporting inorganic iodide (I–)into the thyroid follicular cell for the synthesis of thyroidhormones, particularly thyroxine (T4) and triiodothyronine (T3;Wolff, 1998).
In an effort to quantitatively predict ClO4–, I–, and inhibition
kinetics in response to both acute and subchronic ClO4– expo-
sure, we have developed a physiologically-based pharmacoki-netic (PBPK) model in the adult male rat (Merrill et al., 2003).Because the PBPK model is based on physiological, biochem-ical, and mechanistic data, it allows us to determine target sitedosimetry and in vivo chemical interactions (inhibition) while
1 To whom correspondence should be addressed at CIIT Centers for HealthResearch, 6 Davis Drive, Research Triangle Park, NC 27709-2137. Fax: (919)558-1300. E-mail: [email protected].
2 Present address: The University of Georgia, Athens, GA 30602.
TOXICOLOGICAL SCIENCES 73, 235–255 (2003)DOI: 10.1093/toxsci/kfg081Copyright © 2003 by the Society of Toxicology
235
by guest on May 31, 2013
http://toxsci.oxfordjournals.org/D
ownloaded from

improving confidence in extrapolation between dose levels,exposure durations and routes. However, with ClO4
–, as withother potential endocrine disruptors, the primary concern is notnecessarily potential risk to the adult, but rather the possibledevelopmental effects resulting from perinatal exposure. Dur-ing gestation and early infancy, a critical window exists inwhich thyroid hormones are needed for normal physical andmental development (Bakke et al., 1976; Howdeshell, 2002;Myant, 1971; Porterfield, 1994). The most susceptible devel-opmental periods to thyroid perturbations are not known. How-ever, even short-term iodide deficiency in the perinatal periodcan result in lifelong consequences. In the human, gestationaliodide deficiency has been linked to increased incidence ofstillbirth, congenital abnormalities, lowered IQ, mental retar-dation, and impaired hearing (Delange, 2000; Haddow et al.,1999; Klein et al., 1972; Porterfield, 1994). In the rat, gesta-tional and neonatal hypothyroidism can result in brain celldisorganization and delayed onset of puberty and estrus (Bakkeet al., 1976; Clos et al., 1974).
Although the roles of maternal versus fetal hormone in fetaldevelopment are currently not well-defined, it appears that bothmaternal and fetal hormone production is necessary to carryout normal development (Howdeshell, 2002). As early as ges-tation day (GD) 9, before the onset of fetal thyroid function,maternal T3 and T4 have been detected in the rat fetus (Mor-reale de Escobar et al., 1985). The fetal thyroid begins tosequester iodide and synthesize and secrete hormones by ges-tation week 12 in the human (Roti et al., 1983) or GD 17–20in the rat (Eguchi et al., 1980; Geloso, 1961; Nataf and Sfez,1961), while the necessary iodide is obtained from the mothervia placental transport (Brown-Grant, 1961; Roti et al., 1983).Maturation of the fetal thyroid results in a significant increasein total thyroid hormone levels in the fetus between GD 18 andbirth (Howdeshell, 2002), indicating that fetal thyroid hormoneproduction may play a significant role in maintaining totalserum hormone levels in late gestation. Since thyroid hor-mones regulate various aspects of brain development through-out gestation (Howdeshell, 2002), it is important to determinepossible perturbation of thyroid activity, be it maternal or fetal.Because ClO4
– affects maternal hormone production, placentaliodide transfer, and fetal hormone production, it could presenta potential concern for fetal development at any time in ges-tation.
In order to determine the sensitivity of the developing fetusto perchlorate, it is necessary to associate an observed effectwith a measured fetal ClO4
– dose. However, the lack of data inboth rats and humans makes the calculation of a human fetalClO4
– dose from maternal drinking water measurements nearlyimpossible by classical methods. In this article, we propose theuse of a PBPK model to predict both fetal ClO4
– dose andsubsequent iodide kinetic changes in the dam and fetus aftermaternal exposure. The developed PBPK model accounts forchanging physiology and maternal-fetal transfer during gesta-tion and is able to predict both ClO4
– and radioiodide kinetics
in the pregnant and fetal rat, as well as ClO4– induced inhibi-
tion of iodide kinetics. Together with the model predictions formale rat kinetics (Merrill et al., 2003), this model allows for amore quantitative comparison of life stage differences (Clewellet al., 2001). Additionally, further extrapolation of this modelto human ClO4
– exposure could allow the fetal risk to beestimated in the absence of direct human data (Clewell et al.,2001).
MATERIALS AND METHODS
Supporting Experiments
All in-house experiments were performed with timed-pregnant dams of theSprague-Dawley strain (Crl: CD, Charles River Laboratory, Raleigh, NC). Theanimals used in in-house studies were handled in accordance with the princi-ples stated in the Guide for the Care and Use of Laboratory Animals, NationalResearch Council, 1996, and the Animal Welfare Act of 1966, as amended.GD 1 was verified by the presence of a vaginal plug. In all studies pregnant ratswere housed individually in light, heat, and humidity controlled cages. Ratswere kept on a 12 h light/dark cycle with access to food and water ad libitum.All rats from in-house studies (control and ClO4
–/I– dosed groups) were giventhe same diet (Purina #5000) containing 0.8 ppm iodine. Maternal drinkingwater consumption was measured daily and perchlorate drinking water levelswere adjusted when necessary to ensure the accuracy of dosing levels in thedrinking water studies. On GD 20, dams and fetuses were euthanized by CO2
asphyxiation.
Perchlorate drinking water study. Dams (n � 6 per dose group) wereexposed to drinking water treated with perchlorate from GD 2 through 20, atdoses of 0.0, 0.01, 0.1, 1.0, and 10.0 mg ClO4
–/kg-day. Two hours prior toeuthanization, dams were given an iv dose of 33 �g/kg 125I– with carrier (tracelevel radioiodide mixed with nonradiolabeld iodide). Maternal and fetal serumsamples were analyzed for free and total thyroxine (fT4 and tT4), T3, and TSH.ClO4
– was also analyzed in the maternal and fetal serum, skin and gastroin-testinal (GI) tract, as well as maternal thyroid, GI contents, and placentafollowing the methods described by Fisher et al. (2000). The same tissues werealso analyzed for 125I– with a gamma counter.
Radioiodide and inhibition kinetic studies. Timed-pregnant Sprague-Dawley dams were exposed via tail vein injection to a tracer dose of 125I–
(average dose � 2.19 ng/kg body weight [BW]) on GD 20. Dams (n � 6) wereeuthanized at 0.5, 1, 2, 4, 8, 12, and 24 h postdosing. Maternal and fetal serum,skin, and GI tract, as well as maternal thyroid, GI content, placenta, andmammary gland tissue were collected and analyzed for 125I– with a gammacounter. Fetal serum was pooled by litter due to small sample volume whilefetal skin and GI tract were analyzed individually. Inhibition kinetics wereexamined in this same manner; however, 2 h prior to the administration of 125I–
(average dose � 1.87 ng/kg BW), dams from the inhibition group were dosedwith 1.0 mg/kg BW ClO4
– via tail vein injection. This particular ClO4– dose
was chosen to be large enough dose to significantly affect iodide uptake, basedon inhibition in the male rat (Merrill et al., 2003), while being lower than thedose required to saturate the symporter, based on the drinking water studyresults (see Results section below). Euthanization was performed at 0.5, 1, 2,4, 8, 12, and 24 h post-125I– dosing.
Model structure. All model code was written in ACSL (Advanced Con-tinuous Simulation Language, Aegis Technologies Group, Inc., Huntsville,AL). Several classical mathematical models exist for iodine kinetics in bothhumans and rats (Berman et al., 1968; DiStefano et al., 1982; Hays andWegner, 1965). However, since these models are not physiologically based,they are limited in their usefulness for extrapolation across species and lifestage. The PBPK model proposed here supports these types of extrapolationsby accounting for physiological differences. The maternal models for both I–
and ClO4– consist of compartments for plasma, thyroid, skin, gut, kidney, liver,
236 CLEWELL ET AL.
by guest on May 31, 2013
http://toxsci.oxfordjournals.org/D
ownloaded from
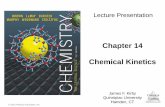
fat, mammary gland, and placenta, plus two lumped compartments for theremaining slowly and richly perfused tissues. The thyroid and gut are describedwith three subcompartments representing the stroma, follicle, and colloid in thethyroid, and the capillary bed, GI tract, and GI contents in the gut. Skin,placenta, and mammary gland are described with two subcompartments, rep-resenting the capillary bed and tissue. Active uptake into the thyroid follicleand colloid, as well as the skin tissue, mammary gland, GI contents, andplacenta, was described with Michaelis-Menten (M-M) terms for saturableprocesses (bold arrows in Fig. 1). Permeability area cross-products (PA) and
partition coefficients were used to describe the passive movement of the anions(I– and ClO4
–) between the capillary bed, tissue, and inner compartments(small arrows in Fig. 1), which results from the inherent electrochemicalgradients within these tissues (Chow et al., 1969). The flow-limited kidney,liver, and fat compartments were described using partition coefficients andblood flows. Urinary clearance and transfer of anions between the placenta andfetal serum were represented by first order clearance rates. Binding of ClO4
– toplasma proteins was described with a saturable term for association of theClO4
– anions to binding sites in the plasma and a first order clearance rate for
FIG. 1. Schematic of PBPK modelfor pregnant dam (left) and fetus (right).Note: plasma compartment includes pro-tein binding of ClO4
–, not I–.
237PBPK ClO4� MODEL FOR RAT GESTATION
by guest on May 31, 2013
http://toxsci.oxfordjournals.org/D
ownloaded from

dissociation from plasma binding sites. However, unlike ClO4– (Merrill et al.,
2003), the majority of iodide in the serum is not bound to proteins (Yu et al.,2002a,b). Thus, binding of I– to plasma proteins was not included in the model.
Given that the majority of thyroid iodide is organified shortly after transportinto the follicle, it was necessary include a simplified description of theincorporation of iodide into thyroid hormones and hormone precursors (mono-iodothyronine, diiodothyronine), as well as the secretion of these hormonesfrom the maternal thyroid. However, since the purpose of this present model isprimarily to determine perchlorate distribution and resulting inhibition of freeiodide transfer by NIS, it was possible to simplify the model by assuming thatthe radioiodine behaved as inorganic iodide in all compartments other than thethyroid, including serum. In the thyroid compartment, the partitioning andactive transport mechanisms account only for the movement of free iodide.Hormone production was modeled as a first order production rate from thethyroid follicle to an “incorporated iodine” compartment (ClProdi). Clearanceof this incorporated iodine from the thyroid was then described with a firstorder clearance rate from the incorporated iodide compartment into the serum(ClSecri). Due to the dynamic nature of the fetal thyroid, the uncertainty inhormone production kinetics, and the lack of supporting data, a description ofhormone production was not included in the fetal rat on GD 17–20. Rather,total iodine in the fetal thyroid was modeled using active uptake and diffusionfrom the serum.
The perchlorate anion was modeled in the same manner as inorganic iodide,based on the similar size and charge of the ions and their shared affinity forNIS. The thyroid, skin, GI, placenta, and mammary glands contain active NISand were therefore defined separately in the structure of the model (Kotani etal., 1998; Spitzweg et al., 1998). The thyroid, skin, and GI contents maintainhigher concentrations of ClO4
– and I– than the plasma (Brown-Grant andPethes, 1959; Chow et al., 1969; Halmi and Stuelke, 1959; Wolff, 1998;Zeghal et al., 1995), requiring active transport mechanisms to work against theconcentration gradient. Although other tissues, such as the salivary gland,ovary, and choroid plexus, are also known to sequester iodide and perchloratein the rat and human (Brown-Grant, 1961; Honour et al., 1952; Spitzweg et al.,1998), small amounts of the anions in these tissues do not affect plasmaconcentrations. Therefore, these tissues were lumped together with the richlyand slowly perfused compartments.
In addition to the reported presence of NIS, studies in our laboratory haveshown the uptake of iodide in placental tissue to be inhibited by ClO4
– (Mahleet al., 2002). Thus, it was necessary to include a description of NIS in theplacental compartment to account for ClO4
– and I– concentrations and themeasured ClO4
– induced inhibition of placental iodide uptake. The mammarygland has also been shown to concentrate both anions during lactation and isknown to contain NIS, which is regulated by hormones produced duringlactation (Tazebay et al., 2000). Intralaboratory studies found mammary gland:plasma ratios of less than one for ClO4
– and I– during gestation. However,time-course data indicate that mammary gland levels remain elevated well intothe clearance phase of the serum. In order to maintain these elevated tissueconcentrations, it was necessary to include symporter activity in the mammarygland of the pregnant rat.
The kidney and liver were also separately defined in the structure of themodel to describe the rapid urinary clearance of the anions and to allow futureelaboration of the model to address hormone metabolism in the liver. Acompartment was also included to account for the effect of changing fatvolume on the kinetics of hydrophilic anions during gestation. Since kidney,liver, and fat do not maintain tissue:plasma ratios greater than one for eitheranion, these tissues were described as single, flow-limited compartments anddo not contain terms for active uptake. Effective partitioning into thesecompartments is thought to result from the electrochemical gradient that movesClO4
– from serum to tissue, as in the thyroid (Chow and Woodbury, 1970).Plasma binding of perchlorate was included in the model, in order to
simulate the relatively high serum ClO4– concentrations observed in our
laboratory at low administered doses (Fig. 2). This binding has been measuredin human, bovine (Carr, 1952; Scatchard and Black, 1949), and rat serum(Merrill et al., 2003). At low serum concentrations (�100 �g/l), Fisherreported approximately 99% of the anion is bound to plasma proteins and athigher concentrations (�500 �g/l), 50% is bound (Fisher, 2002, as cited inMerrill et al., 2003). This plasma binding of perchlorate is also evidenced bythe ability of the anion to interfere with T4 binding to serum albumin andpre-albumin rats as it does in humans (Shishiba et al., 1970; Yamada, 1967).These studies suggest that perchlorate inhibits binding of T4 to albumin byreversibly binding to the albumin via weak covalent interactions.
The structure of the fetal perchlorate model is similar to that of the pregnantrat, with the exception of the mammary gland and placenta compartments. Inorder to simplify the model, all fetuses from a single litter were lumpedtogether within the model structure, essentially viewing all individual fetusesas one entity. Although there is evidence that delivered fetal dose of sometoxins may vary due to position within the uterine horn, the difficulty ofchemical analysis and the small sample volume obtained from the GD 20 fetuspreclude the possibility of analyzing serum for each individual fetus. Thus, themodel attempts to predict the available data, which consists of pooled fetalsamples. Though this may present a crude estimate of a particular individualfetus, the model is able to provide a reasonably accurate estimate of theaverage fetal dose, thereby enabling risk estimates to be made from dosimetryin the subject of interest, the fetus, rather than the less comparable but moreavailable adult rat. The model description of fetal dose is based on transfer ofthe anions between the placenta and fetal serum. Although a kidney compart-ment is included in the fetal model, urinary excretion is not used to identify theloss of perchlorate for the fetus, as the ability to produce urine is not welldeveloped until after parturition. Loss of ClO4
– and I– from the fetus wasdescribed as clearance from the fetal serum to the placenta. The anions are thenable to diffuse into the maternal serum and are, therefore, available forredistribution in the dam.
Perchlorate inhibition of iodide uptake was included in the maternal thyroidfollicle and colloid, GI contents, skin and placenta, as well as the fetal GIcontents and skin throughout gestation. Inhibition in the fetal thyroid follicleand colloid was also included from the onset of fetal thyroid iodide accumu-lation (GD 17) through parturition, based on the observation that perchloratewas present in the fetal blood and could, therefore, inhibit fetal NIS transportof iodide into the thyroid. Placental inhibition was observed in studies in ourlaboratory (Mahle et al., 2002) and was included in the model in order topredict the effect on iodide transfer to the fetus. Literature sources havereported inhibition in gastric juice of the male rat (Halmi and Stuelke, 1959)and intralaboratory studies showed consistent evidence of significant (�60%)inhibition of iodide uptake in both the fetal GI and skin, and slight inhibitionin the maternal skin (Mahle et al., 2002). Since the release of iodide from theseextrathyroidal tissues could affect the serum levels and the amount of storediodide in the fetus, it was necessary to include iodide inhibition in the tissueswith active uptake.
An additional description of thyroid perchlorate inhibition by iodide wasdetermined to be unnecessary, as it would not affect perchlorate thyroid levels.Although both anions are transported with NIS and would therefore inhibit theother’s ability to bind to the symporter, the fact that the Km for ClO4
– is anorder of magnitude lower than that of I– indicates that ClO4
– has a much greateraffinity for NIS. Additionally, even when considering dietary iodide, therelative intake of perchlorate in the drinking water dosing scenarios (on theorder of mg/kg-day) is much greater than that of the trace element iodide (onthe order of �g/kg-day). Competitive inhibition of ClO4
– by I– would bemodeled by adjusting the Kmp by one plus the ratio of serum iodide concen-tration to the Km for iodide. Because the Kmi is large (4 � 106 ng/l) and theendogenous serum iodide concentration (roughly 4000 ng/l) is approximately
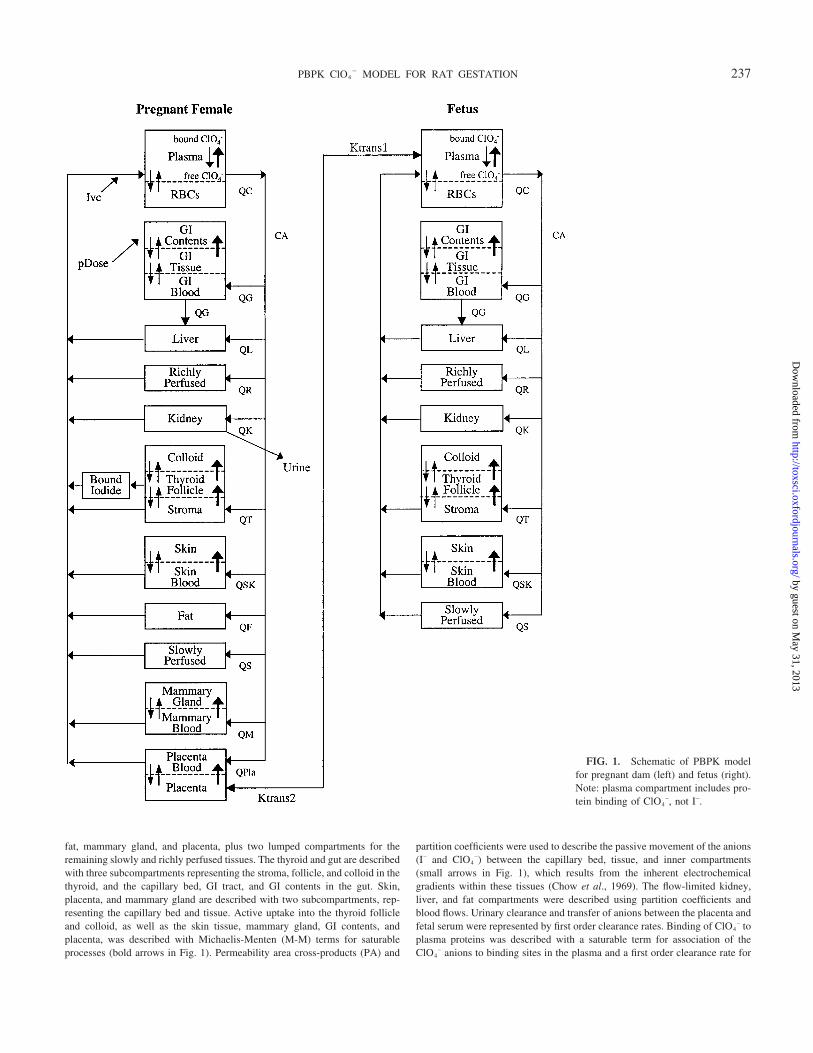
FIG. 2. Perchlorate concentration in maternal (a) serum (Clewell et al., 2001), (b) thyroid (upregulated), (c) GI contents, and (d) skin as well as fetal (e)serum (Clewell et al., 2001) and (f) skin at the 0.01, 0.1, 1.0, and 10.0 mg/kg-day dose on GD 20.
238 CLEWELL ET AL.
by guest on May 31, 2013
http://toxsci.oxfordjournals.org/D
ownloaded from
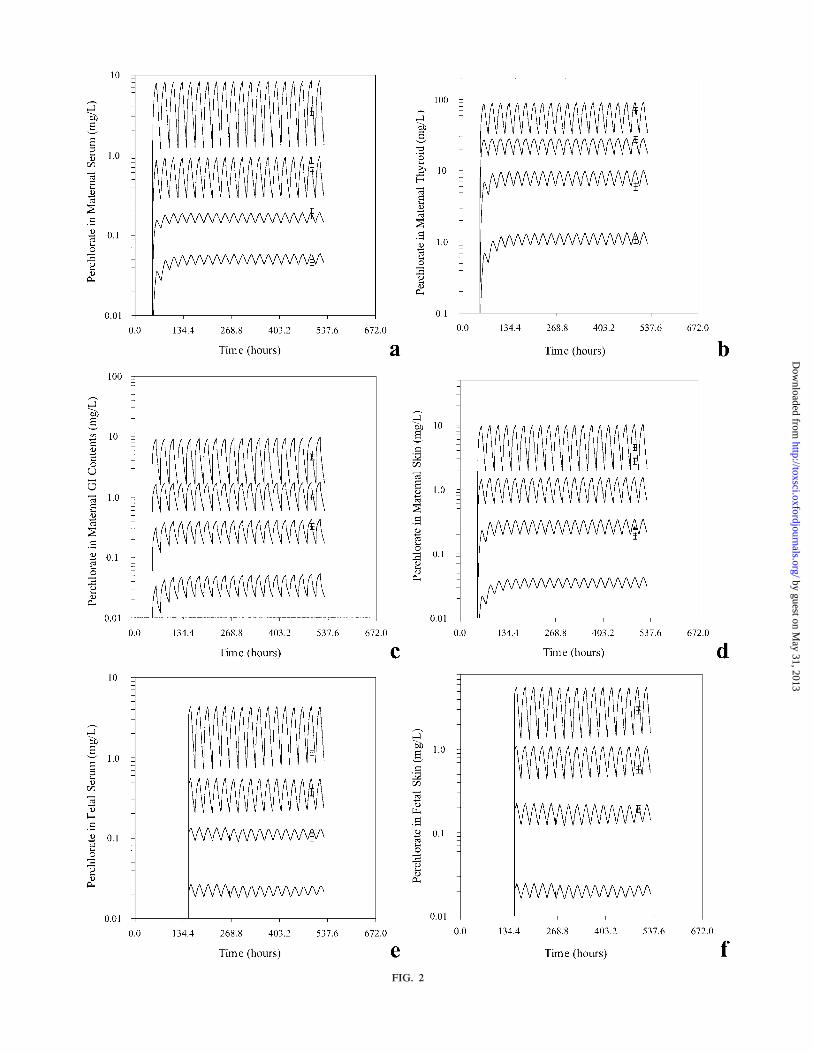
FIG. 2
by guest on May 31, 2013
http://toxsci.oxfordjournals.org/D
ownloaded from
1000 times smaller than Km, it is apparent that the effect of iodide on thyroidClO4
– will be negligible.
Dosing procedures. In order to simulate the daily dosing regimen of thedrinking water experiment, rats were modeled as drinking at a constant rate for12 of the 24 h per day (1800 to 0600 hours). A pulse function in ACSL wasused to introduce drinking water to the GI contents of the dam for the first 12 hof each 24-h period. Intravenous dosing was introduced into the venous bloodcompartment of the maternal model.
Model parameters. Whenever possible, physiological and kinetic param-eters were obtained from literature or experiments. Allometric scaling wasemployed when needed to account for differences in parameters due to vari-ations in body weight of male, female, and fetal rats. Tissue volumes werescaled linearly by body weight. Blood flows, maximum velocities, permeabil-ity area cross products (PA), and clearance values were scaled by BW0.75. Fetalvalues were scaled in a similar manner to the maternal parameters; however,it was necessary to scale the individual fetal values first and then adjust for thetotal number of fetuses in the litter.
Physiological parameters. The physiological description of maternal andfetal rats during gestation is based on O’Flaherty et al. (1992), Gentry et al.(2002), and Fisher et al. (1989). The model is able to incorporate differencesin gestation time, pup birth weight, and litter size between experiments and
strains of rats. Physiological parameters and the sources from which they wereobtained are listed in Table 1.
The maternal body weight (BW) increases significantly during the relativelyshort gestation time in the rat (21 days), with the majority of weight resultingfrom increasing volumes of the placenta, mammary gland, fat, and total fetalvolume. Therefore, the total change in maternal body weight was described asthe sum of the changes in these four tissue volumes and the initial (prepreg-nancy) body weight (BWinit). All other maternal organs were assumed to remainconstant throughout gestation.
Mammary tissue (VM) growth was described as a linear process, reaching amaximum volume of 4.6% BW at GD 21 (Hanwell and Linzell, 1973; Knightand Peaker, 1982). Maternal fat (VF) was also modeled with a linear increaseduring gestation (Naismith et al., 1982), with a 40% increase from thenonpregnant value (7.0% BW) for Sprague-Dawley rats (Brown et al., 1997).Placental volume (VPl) was described in the model as a sum of three stages ofgrowth, involving changes in both the yolk sac and chorioallantoic placenta,based on the model of O’Flaherty et al. (1992) and data from Buelke-Sam etal. (1982) and Sikov and Thomas (1970).
A three-stage description of fetal growth was also described in O’Flaherty etal. (1992) to mathematically reproduce several data sets (Beaton et al., 1954;Buelke-Sam et al., 1982; Goedbloed, 1972; Sikov and Thomas, 1970). In the
TABLE 1Physiological Parameters
Physiological parameters
Pregnancy
SourceDam Fetus
Tissue volumes (% BW)Body weight BW and V1fet (kg) 0.280–0.361 0.0–0.0045 O’Flaherty et al., 1992Slowly perfused VSc (% BW) 74.6 74.6 Brown et al., 1997Richly perfused VRc (% BW) 11 16 Schneidereit, 1985Fat VFc (% BW) 10.0–11.0 0.0 Naismith et al., 1982Kidney VKc (% BW) 1.7 0.3–0.44 Schneidereit, 1985Liver VLc (% BW) 3.4 8.5–7.2 Schneidereit, 1985GI tract VGIc (% BW) 3.60 2.0–3.0 Schneidereit, 1985GI contents VGIJc (% BW) 7.20 0.8–6.2 Proportional to difference in adult/fetal GIGI blood VGIBc (% VG) 2.9 2.9 Altman and Dittmer, 1971Skin tissue VSkc (% BW) 19.0 8.8–19.3 Brown et al., 1997; Palou et al., 1983Skin blood VSkBc (% VSk) 2.0 2.0 Brown et al., 1997Thyroid total VTc (% BW) 0.0105 0.058–0.038 Malendowicz and Bednarek, 1986; Schneidereit, 1985Thyroid follicle VTFc (% VT) 45.9 61.4 Conde et al., 1991; Malendowicz and Bednarek, 1986Thyroid colloid VTLc (% VT) 45 18.3 Conde et al., 1991; Malendowicz and Bednarek, 1986Thyroid blood VTSc (% VT) 9.1 20.3 Conde et al., 1991; Malendowicz and Bednarek, 1986Plasma VPlasc (% BW) 4.7 4.7 Brown et al., 1997; Altman and Dittmer, 1971Red blood cells VRBCc (% BW) 2.74 2.74 Altman and Dittmer, 1971; Brown et al., 1997Placenta VPlc (% BW) 0.0–2.57 — O’Flaherty et al., 1992Mammary gland VMc (% BW) 1.0–5.5 — Knight et al., 1984; O’Flaherty et al., 1992
Blood flows (% QC)Cardiac output QCc (l/h/kg) 14 67.8 Buelke-Sam et al., 1982; Gotshall et al., 1987;
O’Flaherty et al., 1992Slowly perfused QSc (% QC) 24.0 24.0 Brown et al., 1997Richly perfused QRc (% QC) 76.0 76.0 Brown et al., 1997Fat QFc (% QC) 7–8.1 — Brown et al., 1997Kidney QKc (% QC) 14.0 3.6 Brown et al., 1997, Rakusan and Marcinek, 1973Liver QLc (% QC) 18.0 4.5 Brown et al., 1997, Rakusan and Marcinek, 1973GI QGc (% QC) 13.6 4.6 Brown et al., 1997, Rakusan and Marcinek, 1973Thyroid QTc (% QC) 1.6 1.6 Brown et al., 1997Skin QSkc (%QC) 5.8 10.4 Brown et al., 1997, Rakusan and Marcinek, 1973Mammary QMc (% QC) 0.2–1.2 — Hanwell and Linzell, 1973Placenta QPlc (% QC) 0.0–12.3 — O’Flaherty et al., 1992
240 CLEWELL ET AL.
by guest on May 31, 2013
http://toxsci.oxfordjournals.org/D
ownloaded from
absence of data for fetal volumes before GD 11, an exponential growth curvewas used to approximate early embryonic growth, starting at zero liters andintercepting the first available data points at GD 11. The final equation for fetalgrowth is dependent on the weight of the pup at the time of birth (PupBW),allowing the model to be adjusted for variations in birth weight of different ratstrains.
Fetal GI, liver, kidney, and thyroid weights given for the Wistar rat (Schnei-dereit, 1985) on days 17 through 21 of gestation and skin volumes given fordays GD 19 through PND 1 (Palou et al., 1983) were fit to exponentialfunctions. These equations were then used in the model to describe organgrowth versus fetal body weight over the course of gestation. Since organweights are not available for earlier time points in gestation, the best-fitexponential curve to the above data was used to extrapolate to earlier timepoints in fetal development.
In accordance with the reported values of Schneidereit (1985), the fetal GIand kidney increased from 2.0 and 0.3 to 3.0 and 0.44% BW, respectively,from GD 17–21. In the same time period, the relative volumes of the fetal liverand thyroid decreased (with respect to body weight) from 8.5 and 0.058 to 7.15and 0.038% BW. Fetal skin relative volume increased more than threefold inthe last three days of gestation, comprising 8.8, 13.6, and 19.3% of the bodyweight on GD 19, 21, and PND 1 (Palou et al., 1983). Volume fractions of fetalstroma (VTSfet), follicle (VTFfet), and colloid (VTLfet) were also significantlydifferent than those of the dam (see Table 1) and were given values reportedfor the rat at birth (Conde et al., 1991). Fetal body fat (VFfet) was assumed tobe negligible for the purpose of the model, based on the work of Naismith etal. (1982), who found that two-day-old rats contained only 0.16% fat and thatbody fat quickly increased in the neonatal period.
Temporal changes in maternal cardiac output during gestation are describedin the model as the sum of initial cardiac output (Brown et al., 1997) and thechange in blood flow to the placenta, mammary and fat tissues, per theapproach of O’Flaherty et al. (1992), which employs changing blood flows inthe placenta, mammary gland, and fat. The fraction of maternal cardiac outputto the mammary gland, fat, and yolk sac change proportionally to the changein tissue volumes. Blood flow to the chorioallantoic placenta increases morerapidly than the tissue volume.
Fetal blood flow was assumed to operate independently from the mother,increasing with fetal volume. Since regional blood flow and cardiac output datawere not available for the rat fetus, the measured values could not be extrap-olated back through gestation with certainty. Therefore, the values for regionalblood flow to the fetal tissues were scaled allometrically (tissue weight0.75)from the earliest available time point in the pup and cardiac output was scaledby BW0.75 from the value given by Gotshall et al. (1987) at PND 1. Fractionalblood flows to fetal GI, skin, liver, and kidney (as % cardiac output) were givenfor the PND 1 rat in Rakusan and Marcinek (1973) and were significantlydifferent from those of the adult rat (4.6, 10.4, 4.5, and 3.6% vs. 13.6, 5.8, 18.3,and 14.0% of the cardiac output, respectively). These changing fractions are inagreement with the time-line for maturation of organ function in the develop-ing rat. For example, the liver and kidney are not fully functional duringgestation. In fact, the kidneys do not reach full function until well after birth(glomeruli levels increase up to day 100; Bengele and Solomon, 1974). Thus,the increasing trend seen in the fractional blood flows to the fetal liver andkidney with age may, at least in part, be due to their increasing functionalcapability.
Chemical-specific parameters. Chemical-specific parameters for per-chlorate and iodide are listed in Table 2. Binding of I– to human NIS wasdetermined to have an average Km of 4.0 � 106 ng/l (Gluzman and Niepom-niszcze, 1983). A similar value (4.4 � 106 ng/l) was measured by Kosugi andcoauthors (1996). This value for the follicular Km (KmTFi) remained constantacross species (Gluzman and Niepomniszcze, 1983) and tissues (Wolff, 1998)and was therefore applied to all compartments in the model with active uptakeby NIS. Golstein et al. (1992) measured a Km value of approximately 4.0 � 109
ng/l for iodide for the second thyroid transport mechanism at the apicalmembrane (KmTLi) in bovine thyroid. In the model, a slightly lower value thanthat measured by Golstein et al. of 1.0 � 109 was used for KmTLi, based on
the ability of the model to fit the later (�8 h) time-points. Like the NIS, thisapical channel is also inhibited by ClO4
–.The affinity of ClO4
– for NIS was not available in literature nor was itdetermined by experiment in our laboratory. However, since this anion com-petitively inhibits iodide uptake by NIS, the value for Km should be equal to itsKi. Wolff and Maurey (1963) and Kosugi et al. (1996) measured the Ki forClO4
– at 0.4 � 105 and 1.5 � 105 ng/l, respectively. Thus the Km value forbinding of ClO4
– to NIS (KmTFp) was set between these two values (1.0 � 105
ng/l) in the model. This value is further supported by various literature sourcessuggesting that ClO4
– actually has as much as an order of magnitude greateraffinity for NIS than I– itself (Chow et al., 1969; Halmi and Stuelke, 1959;Harden et al., 1968; Lazarus et al., 1974). The Km for the second transportmechanism in the thyroid colloid (KmTLp) was set to 1.0 � 108 ng/l, approx-imately a factor of 10 lower than the Km values used for iodide. This value forthe colloid Vmax is supported by the data of Chow and Woodbury (1970), whoreported saturation of this transport mechanism at 1.0 � 108 ng/l ClO4
–.Unlike Km, values for Vmax vary significantly between different species
and tissues with NIS (Wolff, 1998). Therefore, values for Vmax in the thyroid,GI, and skin were determined by the fit of the model to available data in thepregnant rat on GD 20. The nonlinear behavior of the ClO4
– uptake in tissueswith NIS suggested that the symporter was saturated between the 1.0 and 10.0mg/kg-day doses in the perchlorate drinking water study. The model fit to datafrom the lower dose groups (0.01 through 1.0 mg/kg-day) in the drinking waterstudy were used to set Vmax values for ClO4
– uptake, since nonsaturableprocesses dominate at higher doses (10 mg ClO4
–/kg-day). Kinetic data wereavailable for radioiodide in the maternal and fetal rat; the experiments wereperformed at tracer doses so as to stay well below saturation of NIS. Thus, theuptake and clearance of radioiodide as measured in the kinetic study were usedto determine values for Vmax in tissues with active uptake.
The ClO4– and I– anions are not expected to partition into tissues in the
classical understanding of the process. Rather, these anions are thought torespond to the electrochemical potential present across tissue membranes.Chow and Woodbury (1970) explored the relationship of these electrochemicalpotentials to ClO4
– concentrations in the stroma, follicle, and lumen in the malerat thyroid at three different doses of ClO4
–. Theoretical effective partitioncoefficients can be calculated (Kotyk and Janacek, 1977) from the measureddifferences in electrical potentials between the thyroid stroma and follicle. Theapproximately equal and opposite potential from the follicle to the colloidenhances passage of negatively charged species into the colloid and indicatesan effective partition coefficient of greater than one. From Chow and Wood-bury (1970), the potential difference for the stroma:follicle interface rangesfrom –58 to –51 mV; for a monovalent negatively charged ion, the resultingeffective partition coefficient (PTFp) is between 0.114 and 0.149. Similarly, thefollicle:lumen interface has a calculated effective partition coefficient (PTLp)between 6.48 and 8.74 (See Merrill et al., 2003, for calculation details).Thyroid effective partition coefficients for iodide were assigned within therange calculated for ClO4
–, based on the fact that iodide and perchlorate havethe same ionic charge and similar ionic radii.
Partition coefficients for ClO4– were estimated from the drinking water
study, since it contained the most complete ClO4– data sets for pregnant and
fetal rats. Whereas the values for Vmax were determined from the lower doses(prior to saturation of the symporter), partition parameters were determinedfrom the fit of the model to the highest dose (10.0 mg/kg-day). At this level ofperchlorate exposure, all measured tissues appeared to have saturated themechanism of active uptake and would therefore primarily be influenced bypartition coefficients and PA values. In the cases of muscle (slowly perfused),liver (richly perfused), kidney, and red blood cells, data were not available inthe pregnant rat but were calculated in this laboratory for the adult male rat foruse in the male rat PBPK model (Merrill et al., 2003). The partition coefficientfor perchlorate in fat was estimated from measured tissue:blood ratios in thelaying hen (Pena et al., 1976). Although measured in a different species,several other tissues were also found to have comparable values to the rat.
Iodide partition coefficients were calculated from the tissue:blood ratiosmeasured during the clearance phase (24 h postdosing) of data for the tissue of
241PBPK ClO4� MODEL FOR RAT GESTATION
by guest on May 31, 2013
http://toxsci.oxfordjournals.org/D
ownloaded from

interest either from literature or experimental data in the rat and PA valueswere visually optimized to measured data. The partitioning parameters for themuscle (slowly perfused), liver (richly perfused), kidney, and red blood cellswere again taken from corresponding male rat parameters (Merrill et al., 2003)and the values for the fat and mammary gland tissues were given the samevalues as ClO4
–, due to the lack of I– data and the similar polarity of the anions.
Binding of perchlorate in the serum was described as a saturable processwith a first order release of perchlorate from serum proteins. Because data werenot available for free versus bound serum ClO4
– in the pregnant or fetal rat,parameters for binding were determined by fitting the model to data at 0.01 and0.1 mg/kg-day ClO4
– from the drinking water study, since serum binding wasmost relevant at these lower doses. Urinary clearance of perchlorate was
TABLE 2Chemical-Specific Parameters
Parameters
Perchlorate Iodide
Dam Fetus Dam Fetus
Partition coefficients (unitless)Slowly perfused/plasma PS 0.31 0.31 0.21 0.21Rapidly perfused/plasma PR 0.56 0.56 0.40 0.40Fat/plasma PF 0.05 — 0.05 —Kidney/plasma PK 0.99 0.99 1.09 1.09Liver/plasma PL 0.56 0.56 0.44 0.44Gastric tissue/gastric blood PGI 0.50 1.80 1.00 1.00Gastric juice/gastric tissue PGIJ 1.30 2.30 2.00 2.00Skin tissue/skin blood PSk 1.15 1.15 0.70 0.70Thyroid tissue/thyroid blood PTF 0.15 0.15a 0.15 0.15Thyroid lumen/thyroid tissue PTL 7.0 7.0 7.0 7.0Red blood cells/plasma PRBC 0.73 0.73 1.00 1.00Placenta/plasma PPl 0.56 — 0.40 —Mammary/plasma PM 0.66 — 0.66 —
Max capacity, Vmaxc (ng/h/kg)Thyroid follicle VmaxcTF 2.6 � 103 0–2.25 � 103 4.4 � 104 0–5.0 � 104
Thyroid colloid VmaxcTL 1.0 � 104 1.0 � 104b 4.0 � 106 4.0 � 106b
Skin VmaxcSk 6.0 � 105 4.0 � 105 6.0 � 104 7.0 � 105
Gut VmaxcGI 8.0 � 105 1.0 � 105 1.0 � 106 2.0 � 106
Mammary VmaxcM 2.2 � 104 — 4.0 � 104 —Placenta VmaxcP 6.0 � 104 — 5.5 � 104 —
Affinity constants, Km (ng/l)Thyroid follicle KmTF 1.0 � 105 1.0 � 105 4.0 � 106 4.0 � 106
Thyroid colloid KmTL 1.0 � 108 1.0 � 108 1.0 � 109 1.0 � 109
Skin KmSk 1.0 � 105 1.0 � 105 4.0 � 106 4.0 � 106
Gut KmGI 1.0 � 105 1.0 � 105 4.0 � 106 4.0 � 106
Mammary KmM 1.0 � 105 — 4.0 � 106 —Placenta KmP 1.0 � 105 — 4.0 � 106 —
Permeability area cross-products (l/h-kg)Gastric blood to gastric tissue PAGIc 1.00 1.00 0.80 0.10Gastric tissue to gastric juice PAGIJc 1.00 1.00 0.60 0.30Thyroid stroma to follicle PATFc 6.0 � 10–5 6.0 � 10–5 1.0 � 10–4 1.0 � 10–4
Thyroid follicle to colloid PATLc 0.01 0.01b 4.0 � 10�7 4.0 � 10–4
Skin blood to skin tissue PASkc 1.00 1.00 0.10 0.02Mammary blood to mammary tissue PAMc 0.04 — 0.01 —Placenta blood to placenta tissue PAPc 0.1 — 0.005 —Plasma to red blood cells PARBCc 1.00 1.00 1.00 1.00
Clearance values (l/h-kg)Urinary excretion ClUc 0.07 — 0.03 —Incorporation of iodide into hormones ClProdc — — 0.03 —Incorporated iodine secretion to serum CSecrC — — 1.0 � 10–6 —Transfer from placenta to fetus ClTrans1c 0.065 0.06Transfer from fetus to placenta ClTrans2c 0.12 0.12
Binding constantsAssociation to binding sites VmaxcB 4.0 � 103 1.5 � 103 — —Affinity for binding sites KmB 1.0 � 104 1.5 � 104 — —Dissociation from plasma binding sites ClUnbc 0.034 0.01 — —
aParameters with two values indicate acute and drinking water parameters, respectively.bFetus was given maternal values for Vmax (scaled by fetal body weight) in the absence of data.
242 CLEWELL ET AL.
by guest on May 31, 2013
http://toxsci.oxfordjournals.org/D
ownloaded from

determined from the 10.0 mg/kg-day dose group, where binding had littleeffect on serum concentrations.
Upregulation of thyroid NIS activity. At the time of data collection in thedrinking water study, rats had been exposed to ClO4
– for 18 days. At this point,upregulation of the thyroid is evidenced by decreased T4 and elevated TSHlevels at all doses, as well as a lack of noticeable thyroid inhibition (Yu et al.,2001). Increased TSH compensates for the competitive inhibition of I– uptakeby increasing the number and activity of NIS at the basolateral membrane ofthe thyroid, while the affinity of iodide for the symporter remains constant(Wolff, 1998). Thus, the value for VmaxcTFi, which corresponds to themaximum capacity for active transport at the basolateral membrane, wasincreased to fit the measured radioiodide concentrations in the upregulatedthyroids for each dose. The resulting values for VmaxcTFi were then plottedversus the corresponding concentrations of serum-free ClO4
– and, since theability of the thyroid to be upregulated is finite, the data were fit to a M-Mequation. This equation was then used in the model to describe the inductionof NIS upregulation with time and dose, in a similar manner to the descriptionused by Andersen et al. (1984) to describe glutathione induction.
Upregulation of thyroidal NIS also affects thyroid ClO4– uptake, and hence
the measured thyroid ClO4– concentrations in the drinking water study, as both
ClO4– and I– are transported by the same symporter (Wolff, 1964, 1998). Thus,
increased thyroid ClO4– uptake was modeled in the same manner as I–,
increasing the value for Vmaxc_TFp with dose and applying the resulting M-Mfit to the model.
Sensitivity analysis of chemical-specific parameters. A sensitivity analy-sis was run after setting the model parameters as described above to explore theinfluence of the various parameters on model predictions. The model was runto determine the change in each of the two chosen dosimetrics, average serumClO4
– concentration (AUC: area under the curve) and total thyroid iodideuptake, resulting from a 1% change in the value of each kinetic parameter. Inan effort to determine the effect of NIS saturation on relative parameterimportance, the sensitivity analysis was performed at two ClO4
– doses, pre-sumably representing unsaturated and saturated symporter states. Thus sensi-tivity analysis for the serum ClO4
– AUC predictions were run at drinking waterdoses of 0.1 and 10.0 mg-kg-day. Because none of the iodide doses used in thismodel are expected to saturate the NIS, thyroid iodide sensitivity analysis wasrun only at the dose at which the experiments were run (1.87 ng/kg 125I–). Totalthyroid iodine concentration was measured at 8 h post-iodide dosing. Thefollowing equation shows the calculation of the sensitivity coefficient for eachparameter.
Sensitivity Coefficient ��A � B��B
�C � D��D
where A is the serum AUC with 1% increased parameter value, B is the serumAUC at the starting parameter value, C is the parameter value after 1%increase, and D is the original parameter value.
Model equations. The following equations represent the distribution ofiodide within the thyroid, in the absence of competitive inhibition. Perchlorateuptake into the thyroid is described similarly, but without the organification(ClProdi) and hormone secretion (ClSecri) terms.
RATSi � QT � �CAi � CTSi� � PATFi � �CTFi
PTFi� CTSi� � RupTFi
RATFi � RupTFi � PATFi � �CTSi �CTFi
PTFi� � RupTLi
� PATLi � �CTLi
PTLi� CTFi� � �Cl Pr odi � CTFi�
RATLi � RupTLi � PATLi � �CTFi �CTLi
PTLi�
RupTFi �V max TFi � CTSi
KmTi � CTSi
RupTLi �V max TLi � CTFi
KmTLi � CTFi
RAbndi � �Cl Pr odi � CTFi� � �ClSecri � CTFi�
RATSi, RATFi, RATLi, and RABndi are the rates of change in the amount ofinorganic iodide in the thyroid stroma, follicle, colloid (lumen) and the rate ofchange in the amount of organic or incorporated iodine in the total thyroid,respectively. PATFi, PATLi and PTFi, PTLi are the PAs and effective partitioncoefficients for the stroma:follicle and follicle:colloid membranes, respec-tively. RupTFi and RupTFi are the active uptake rates of iodide into the follicleand colloid. VmaxTFi, VmaxTLi and KmTFi, KmTLi are the maximum veloc-ities and affinity constants for transport of iodide into the follicle and colloid.QT represents fractional blood flow to the thyroid capillary bed. CAi, CTSi,CTi, and CTLi are the iodide concentrations in arterial plasma, thyroid stroma,follicle, and colloid.
The inhibited thyroid is described in the same manner as shown above,except that the M-M terms for active uptake are modified to account forcompetitive inhibition. The following equation gives an example of the de-scription of competitive inhibition of iodide uptake by perchlorate. As before,RupTFi represents the rate of active iodide uptake into the thyroid follicle. Thisrate is modified by the affinity of transport mechanism in the follicle for ClO4
–
(KmTFp) and the concentration of ClO4– in the stroma (CTSp). Inhibition of
iodide uptake in other tissues with NIS is described in the same manner as thethyroid follicle inhibition.
RupTFi �V max TFi � CTSi
KmTFi � � 1 �CTSp
KmTFp� � CTSi
The model description for active uptake of iodide into the GI contents withcompetitive inhibition by ClO4
– is given below. The skin compartment ismodeled in the same manner. Equations for perchlorate would be similar tothose of iodide without the terms for competitive inhibition. Here RAGBi RAGi
and RAGJi represent the rates of change in the gut capillary blood, GI tract, andGI contents, respectively. QG is the regional blood flow to the GI, RMR is therate of oral dosing, and CGBi CGi and CGJi are the total iodide concentrationin the GI blood, tract and contents. Finally, partitioning of iodide between theGI blood and tract and the GI tract and contents is described using the partitioncoefficients (PGi and PGJi) and permeability area cross products (PAGi andPAGJi).
RAGBi � QG � �CAi � CVGBi� � PAGi � �CGi �PGi � CVGBi�
RAGi � PAGi � �CVGBi � CGi �PGi�
� PAGJi � �CGJi �PGJi � CGi� � RupGJi
RAGJi � RupGJi � PAGJi � �CGi � CGJi �PGJi� � RMRi
RupGJi �V max GJi � CGi
KmGi � � 1 �CGp
KmGp� � CGi
Model equations for compartments without active uptake (shown for theliver, below) were modeled in the as flow-limited, using only partitioning andblood flow to control tissue iodide and perchlorate concentrations. In thefollowing equations, RALi is the rate of change in the amount of total iodide inthe liver, QL is the fractional blood flow to the liver, CLi is the concentration
243PBPK ClO4� MODEL FOR RAT GESTATION
by guest on May 31, 2013
http://toxsci.oxfordjournals.org/D
ownloaded from

of iodide in the liver and PLi is the blood:liver partition coefficient. The kidneyand fat are modeled similarly.
RALi � QL � �CAi � CLi �PLi�
RESULTS
Model Parameterization
Perchlorate data from the drinking water distribution studywere used to determine kinetic parameters for ClO4
– in thepregnant and fetal rat. Upregulation of NIS transport of ClO4
–
into the thyroid was accounted for as described in the Materialsand Methods section. Figure 2 shows the resulting modelpredictions for maternal serum, thyroid, skin, and GI contentClO4
– concentrations, as well as the fetal serum and skin ClO4–
concentrations, together with measured data from the drinkingwater study on GD 20 at 0.01, 0.1, 1.0, and 10.0 mg ClO4
–/kg-day. In the case of maternal GI contents, fetal serum, andfetal skin, the perchlorate levels in the 0.01 mg ClO4
–/kg-daywere below analytical detection. In these and subsequent plots,solid lines indicate the model prediction and cross-bars indicatethe mean � SD of measured data.
Maternal mammary gland and GI tract concentrations, aswell as the fetal total GI (tract plus contents), were available atthe 10 mg/kg-day dose only. Placental ClO4
– concentrationswere detectable only at the 1.0 and 10 mg/kg-day dose. TheClO4
– levels in these tissues from all other dose groups werebelow analytical detection limits. Therefore, these data wereused to verify the applicability of assigned partition coeffi-cients to the model. Figure 3 demonstrates that the PBPKmodel adequately simulates the data in these tissues.
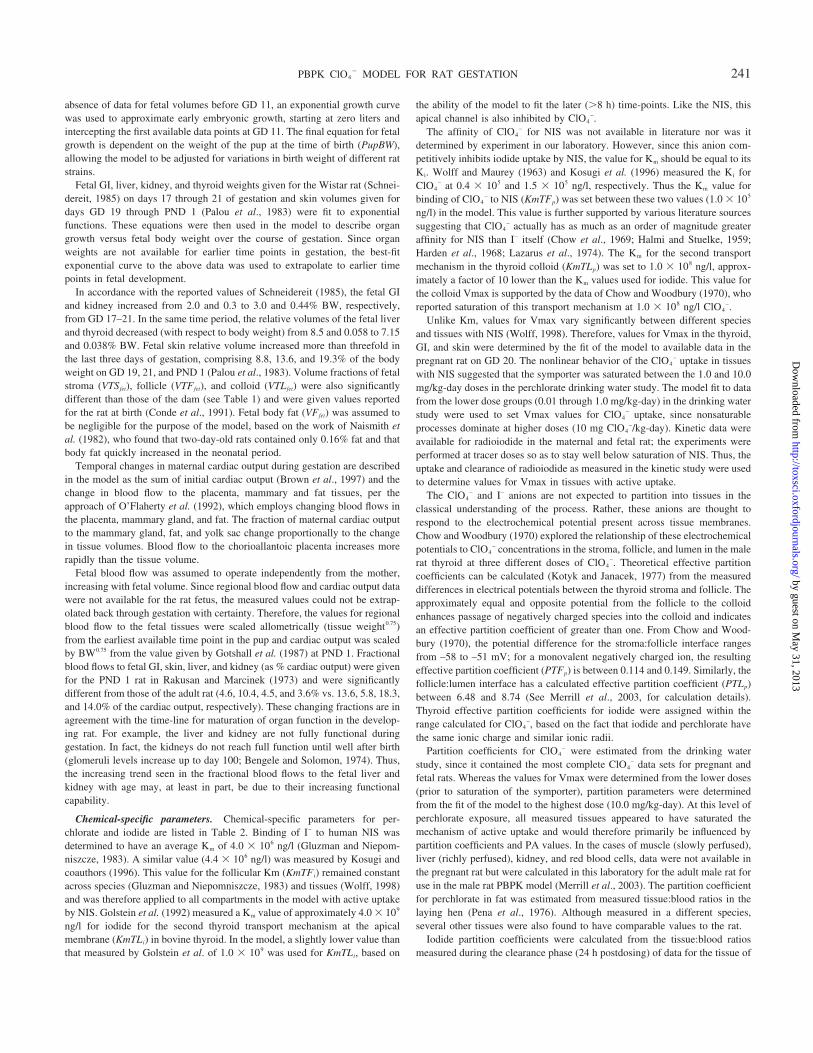
Iodide parameters were determined by fitting the model todata from the iv radiolabeled iodide kinetic study. PA valueswere adjusted to describe the behavior of iodide data, whereincreasing PA values toward 1.0 l/h-kg generally increased therate at which uptake and clearance in a particular tissue oc-curred, and decreasing PA slowed uptake and clearance. Clear-ance values for incorporation of inorganic iodide into hor-mones (ClProdCi) and clearance of the hormonal iodine(ClSecrCi) were determined from the fit of the model simulatedincorporated iodine concentrations in the thyroid versus kineticdata after an iv injection of inorganic radioiodide. Figure 4shows the simulations for various maternal tissues versus mea-sured 125I– data.
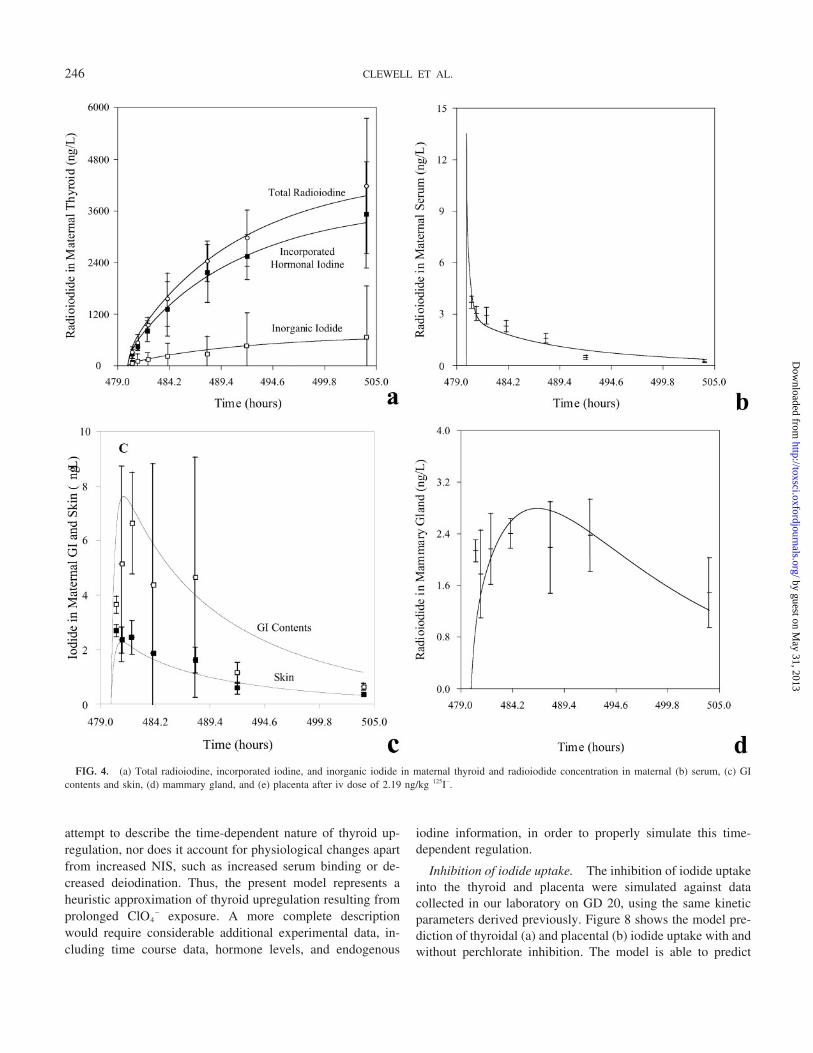
Clearance values for the transfer of iodide between theplacenta and fetal blood were determined by visually optimiz-ing the fit of the fetal serum prediction to the data, whilemaintaining the fit of the maternal blood, placenta, and fetaltissue data simulations. Figure 5 shows the model simulationversus fetal 125I– data. Fetal thyroid iodide uptake increasesrapidly in the final days of gestation (Carpenter, 1959; Feldmanet al., 1961). In order to describe this uptake, the modelsimulation was fit to fetal thyroid uptake data reported inFeldman et al. (1961) 24 h after administration of 131I– to the
dam on days 17, 18, and 19 of gestation (Fig. 5d). Thetime-dependent parameters were then incorporated into themodel using simple linear interpolation between data points toestimate the value of the parameter at any point in time.
Model Validation
Model simulations were tested against data sets collectedunder different conditions than the data used for model param-eterization to test the predictive capability of the model. Modelpredictions for iodide kinetics were tested against data col-lected in other laboratories and in different strains of rats fromthe literature. Although the limited data do not allow testing ofthe entire acute kinetic time course, they do allow validation oftissue iodide concentrations at specific time points (e.g., 2 and24 h postdosing). Finally, the model’s ability to describe bothacute perchlorate and iodide kinetics and the interaction be-tween the anions (inhibition of thyroidal iodide uptake) wastested against acute inhibition data collected in our laboratoryand in literature after iv dosing with both ClO4
– and radioio-dide.
Data of Versloot et al. (1997). A simulation was performedwith the model, using the exposure conditions of Versloot et al.(1997; an iv injection of 10 �Ci or 1.74 ng/kg carrier free 125I–
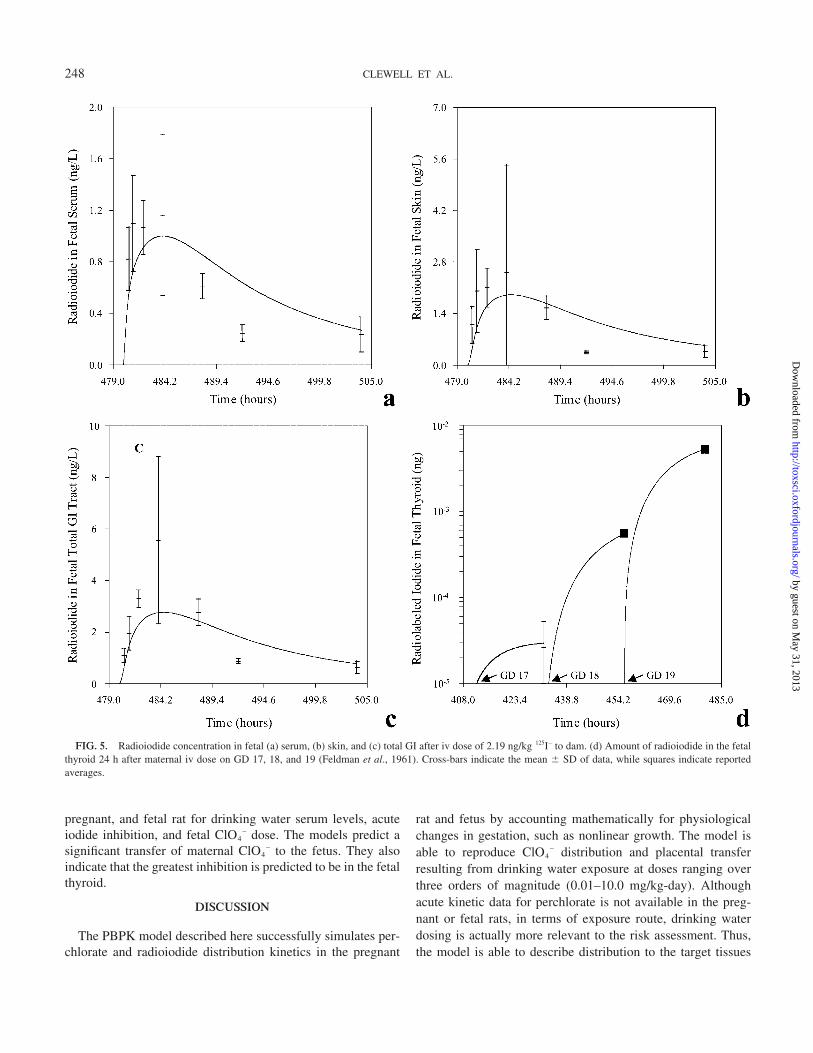
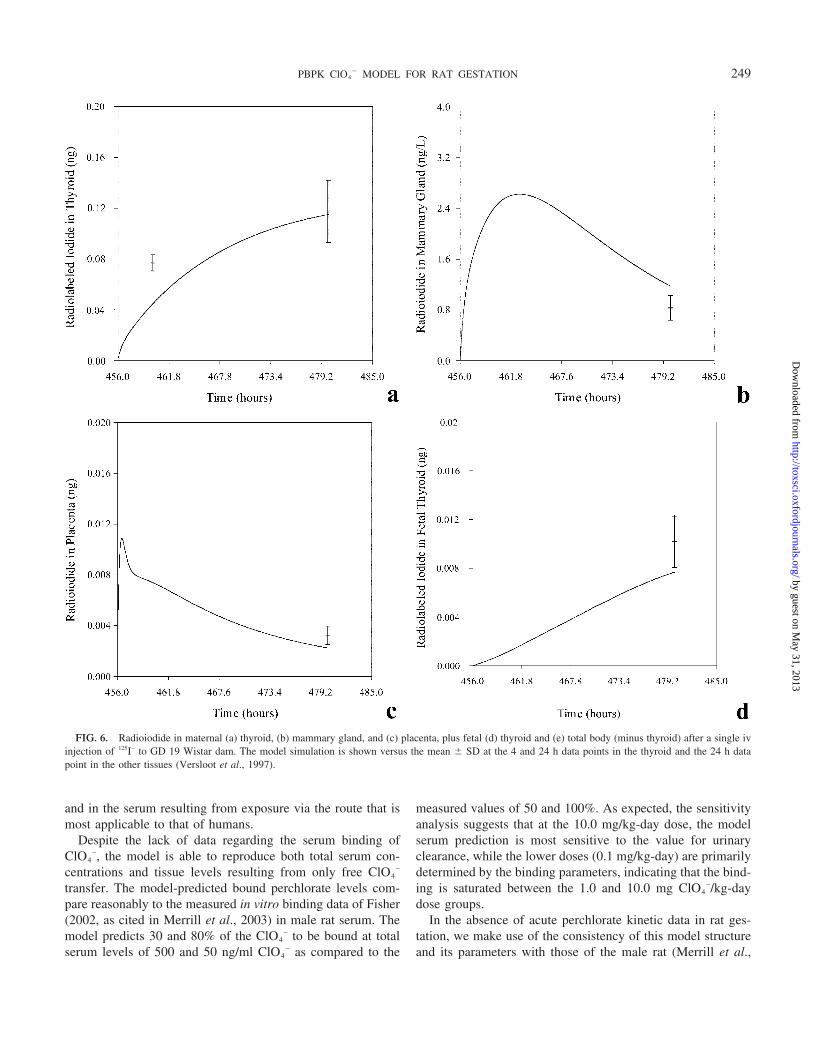
in pregnant Wistar rats on GD 19). This study provided a dataset on an additional day of gestation (GD 19 vs. GD 20), aswell as an additional time point (24 h) and included measure-ments of the total fetal burden, which had not previously beendetermined. The model was able to simulate the data in thematernal thyroid, mammary gland, and placenta, and fetalthyroid (Figs. 6a–6d). The model prediction of total bodyburden (Fig. 6e) underpredicted the rest of body iodide contentin the fetus after removal of the thyroid. However, the modelsimulation is within a factor of two from the measured data.
Data of Sztanyik and Turai (1988). A simulation of datareported in Sztanyik and Turai (1988) was performed with themodel to test the ability of the model to predict I– distributionfrom a lower dose than was used in model parameterization, aswell as a different species of radiolabeled iodide (131I– vs. 125I–).Sztanyik and Turai administered an ip injection of 0.36 ng/kgcarrier free 131I– to pregnant CFY albino rats on GD 20 andmeasured tissues at 24 h postdosing. The model reproduced theplacenta data well at 24 h postdosing without changing anykinetic parameters. The model prediction of the total fetal bodyburden was slightly high, but was within a factor of two fromthe measured data. Figure 7 shows the model simulation versusthe measured values of 131I– in the placenta and total fetal body.
Drinking water inhibition data. Inhibition of thyroid io-dide uptake as well as iodide distribution in several maternaland fetal tissues were measured in the perchlorate drinkingwater study after maternal exposure to levels of 0.0, 0.01, 0.1,1.0, and 10.0 mg ClO4
–/kg-day for 18 days (see Materials andMethods). Due to upregulation, none of the thyroid iodideconcentrations measured after 18 days of perchlorate dosing
244 CLEWELL ET AL.
by guest on May 31, 2013
http://toxsci.oxfordjournals.org/D
ownloaded from

were significantly different from the control levels. However,iodide data from the control group (0.0 mg/kg-day ClO4
–) wereuseful for testing model predictions at 125I– doses more thanfour orders of magnitude greater than those used to parame-terize the model (33,000 ng/kg vs. 2.19 ng/kg). Table 3 illus-trates the ability of the model to predict iodide uptake inseveral tissues in the dam and fetus on GD 20.
Upregulation of thyroid NIS activity was modeled as de-scribed in the Materials and Methods section. Using this equa-
tion, it was possible to describe the increase in iodide uptakebased on the perchlorate dose in chronic exposure scenarios.Neither the measured data nor the model showed any inhibitionin iodide concentrations in the maternal thyroid 2 h postdosingwith 125I– after 18 days of exposure to 0.01, 0.1, 1.0, and 10.0mg/kg ClO4
– in drinking water. Thus, the model was able toreproduce the upregulation of thyroid NIS activity resultingfrom subchronic perchlorate exposures in a semiempiricalmanner. Due to the lack of necessary data, this model does not
FIG. 3. Perchlorate concentration in maternal (a) GI tract and (b) mammary gland at 10.0 mg ClO4–/kg-day, (c) placenta at 10.0 and 1.0 mg ClO4
–/kg-day,and (d) fetal total GI (tract plus contents) at 10.0 mg ClO4
–/kg-day dose on GD 20. Perchlorate concentrations at the lower doses were below the analyticaldetection limit.
245PBPK ClO4� MODEL FOR RAT GESTATION
by guest on May 31, 2013
http://toxsci.oxfordjournals.org/D
ownloaded from
attempt to describe the time-dependent nature of thyroid up-regulation, nor does it account for physiological changes apartfrom increased NIS, such as increased serum binding or de-creased deiodination. Thus, the present model represents aheuristic approximation of thyroid upregulation resulting fromprolonged ClO4
– exposure. A more complete descriptionwould require considerable additional experimental data, in-cluding time course data, hormone levels, and endogenous
iodine information, in order to properly simulate this time-dependent regulation.
Inhibition of iodide uptake. The inhibition of iodide uptakeinto the thyroid and placenta were simulated against datacollected in our laboratory on GD 20, using the same kineticparameters derived previously. Figure 8 shows the model pre-diction of thyroidal (a) and placental (b) iodide uptake with andwithout perchlorate inhibition. The model is able to predict
FIG. 4. (a) Total radioiodine, incorporated iodine, and inorganic iodide in maternal thyroid and radioiodide concentration in maternal (b) serum, (c) GIcontents and skin, (d) mammary gland, and (e) placenta after iv dose of 2.19 ng/kg 125I–.
246 CLEWELL ET AL.
by guest on May 31, 2013
http://toxsci.oxfordjournals.org/D
ownloaded from

inhibition in the thyroid gland up to 24 h after dosing withiodide. The ability of the model to predict perchlorate-inducedinhibition of thyroid iodide uptake is dependent on accuratesimulations of both iodide and perchlorate kinetics. Thus, theappropriateness of the model perchlorate and iodide parametersis supported by the fit of the model simulation to these inhi-bition data.
Inhibition data of Sztanyik and Turai (1988). Further val-idation of model-predicted inhibition was validated againstadditional perchlorate dose levels (3.0 and 6.0 mg/kg KClO4)by testing the model-predicted fetal iodide uptake with andwithout ClO4
– against data from Sztanyik and Turai (1988). Inthis study, GD 20 pregnant rats were given an ip tracer dose of131I–. At 20, 60, or 120 min post-131I dosing, an ip dose ofKClO4 (either 3.0 or 6.0 mg) was administered to the dams.The uptake of radioiodide in the whole fetus was then mea-sured 24 h after the 131I– dose. The model was able to accu-rately predict the measured inhibition of fetal uptake in two ofthe three studied groups on GD 20. The third group showedonly slightly less inhibition than the model predicted. Table 4shows the model predicted inhibition of iodide uptake in thewhole fetus versus the ranges (mean � 1 SD) of measuredvalues given in Sztanyik and Turai (1988). Mean values aregiven in parentheses. The ability of the model to simulate thesedata supports its usefulness in predicting inhibition of placentaltransfer and fetal thyroid uptake.
Data of Brown-Grant (1966). Brown-Grant (1966) admin-istered 0.25 and 1% potassium perchlorate solution (approxi-mately 200 and 800 mg/kg respectively) by oral gavage for oneto five days (GD 2 to 8) in Wistar rats, and observed 131I
thyroid:plasma ratios of between 1.8 and 4.1. Since these largeperchlorate doses are sufficient to effectively swamp the NIS,the measured thyroid:plasma ratios primarily reflect the extentto which thyroid iodide uptake is dependent upon partitioning.As described previously, the PBPK model describes partition-ing based on the measured electrochemical potentials of Chowand Woodbury (1970). Using these previously calculated par-tition coefficients and permeability area cross products, themodel predicts thyroid: plasma ratios of 3.9 and 3.6, which arewithin the range of measured values reported by Brown-Grant(1966), thus supporting the validity of the method for calcu-lating partition parameters.
Sensitivity analysis. Sensitivity analysis performed at 0.1and 10.0 mg ClO4
–/kg-day drinking water revealed a dose-dependent difference in model sensitivity to various parame-ters. At 0.1 mg/kg-day, the maternal serum is primarily depen-dent on serum binding and urinary clearance parameters with agreater sensitivity to the serum binding. Sensitivity coefficientsfor all other parameters were less than 0.1. At the 10.0 mg/kg-day dose, however, only the urinary clearance remained sig-nificant, with a sensitivity coefficient of –0.84. Fetal serum isinfluenced by several model parameters at the 0.1 mg/kg-daydose, including placental transfer, placental active uptake, pla-cental diffusion, fetal serum binding, and maternal urinaryclearance parameters. At the higher dose (10.0 mg/kg-day),where active placental uptake and serum binding are likelysaturated, only the placental transfer, placental diffusion, andmaternal urinary clearance maintain significant sensitivity co-efficients. Figure 9 shows the calculated sensitivity coefficientsfor maternal and fetal serum ClO4
– AUC on GD 20. Results ofthe sensitivity analysis for thyroid iodide uptake (not shown)were similar, in that all of the parameter sensitivities were lessthan one in absolute values; however, model predictions of thismetric were sensitive to a much larger number of input param-eters. This result is not unexpected due to the fact that theuptake prediction is for a specific point in time after adminis-tration of the radioiodide, and the rate of distribution into alltissues can affect the time-dependent result (as compared to anaverage, or AUC, measure, which reflects steady-state behav-ior). Thus the validation of the model with data on thyroidiodine uptake and inhibition provides a stringent test of themodel parameterization.
Internal dosimetrics. The validated model was used tocalculate internal dosimetrics corresponding to perchloratedosing in the pregnant rat. These internal measures of ClO4
–
dose include the AUC for ClO4– in the maternal serum and
relative fetal dose after repeated drinking water exposure, aswell as inhibition of iodide uptake in the thyroid after acutedosing. These internal dosimetrics were then compared to theClO4
– serum AUC and iodide percent inhibition in the male rat(calculated from the model of Merrill et al., 2003) to provideinsight on relative exposure at different life stages. Tables 5and 6 show the dosimetric comparisons among the adult male,
FIG. 4.—Continued
247PBPK ClO4� MODEL FOR RAT GESTATION
by guest on May 31, 2013
http://toxsci.oxfordjournals.org/D
ownloaded from
pregnant, and fetal rat for drinking water serum levels, acuteiodide inhibition, and fetal ClO4
– dose. The models predict asignificant transfer of maternal ClO4
– to the fetus. They alsoindicate that the greatest inhibition is predicted to be in the fetalthyroid.
DISCUSSION
The PBPK model described here successfully simulates per-chlorate and radioiodide distribution kinetics in the pregnant
rat and fetus by accounting mathematically for physiologicalchanges in gestation, such as nonlinear growth. The model isable to reproduce ClO4
– distribution and placental transferresulting from drinking water exposure at doses ranging overthree orders of magnitude (0.01–10.0 mg/kg-day). Althoughacute kinetic data for perchlorate is not available in the preg-nant or fetal rats, in terms of exposure route, drinking waterdosing is actually more relevant to the risk assessment. Thus,the model is able to describe distribution to the target tissues
FIG. 5. Radioiodide concentration in fetal (a) serum, (b) skin, and (c) total GI after iv dose of 2.19 ng/kg 125I– to dam. (d) Amount of radioiodide in the fetalthyroid 24 h after maternal iv dose on GD 17, 18, and 19 (Feldman et al., 1961). Cross-bars indicate the mean � SD of data, while squares indicate reportedaverages.
248 CLEWELL ET AL.
by guest on May 31, 2013
http://toxsci.oxfordjournals.org/D
ownloaded from
and in the serum resulting from exposure via the route that ismost applicable to that of humans.
Despite the lack of data regarding the serum binding ofClO4
–, the model is able to reproduce both total serum con-centrations and tissue levels resulting from only free ClO4
–
transfer. The model-predicted bound perchlorate levels com-pare reasonably to the measured in vitro binding data of Fisher(2002, as cited in Merrill et al., 2003) in male rat serum. Themodel predicts 30 and 80% of the ClO4
– to be bound at totalserum levels of 500 and 50 ng/ml ClO4
– as compared to the
measured values of 50 and 100%. As expected, the sensitivityanalysis suggests that at the 10.0 mg/kg-day dose, the modelserum prediction is most sensitive to the value for urinaryclearance, while the lower doses (0.1 mg/kg-day) are primarilydetermined by the binding parameters, indicating that the bind-ing is saturated between the 1.0 and 10.0 mg ClO4
–/kg-daydose groups.
In the absence of acute perchlorate kinetic data in rat ges-tation, we make use of the consistency of this model structureand its parameters with those of the male rat (Merrill et al.,
FIG. 6. Radioiodide in maternal (a) thyroid, (b) mammary gland, and (c) placenta, plus fetal (d) thyroid and (e) total body (minus thyroid) after a single ivinjection of 125I– to GD 19 Wistar dam. The model simulation is shown versus the mean � SD at the 4 and 24 h data points in the thyroid and the 24 h datapoint in the other tissues (Versloot et al., 1997).
249PBPK ClO4� MODEL FOR RAT GESTATION
by guest on May 31, 2013
http://toxsci.oxfordjournals.org/D
ownloaded from

2003), which successfully describes such data. Having ac-counted for differences in physiology due to gestation, mostchemical-specific parameters remain essentially unchangedfrom those of the adult male rat. Therefore, we can assumethat, like the male rat model, this model is also able to ade-quately predict acute perchlorate kinetics. This is further sup-ported by the ability of the model to predict acute iodideinhibition kinetics, as inhibition of thyroid uptake is dependenton free serum perchlorate levels.
The PBPK model was able to predict the ClO4– induced
inhibition of iodide uptake in the maternal thyroid and the totalfetus after acute ClO4
– exposures in the pregnant rat by linkingthe perchlorate and iodide models via competitive inhibition atthe symporter. Although some authors have suggested thatClO4
– may not be translocated into the thyroid cell via NIS(Riedel et al., 2001a,b), the weight of evidence suggests thatthe anion is a true competitive inhibitor of iodide uptake(Clewell and Gearhart, 2002). Based on electrogenicity studiesshowing that the addition of 500 �M ClO4
– to a bathingmedium containing I– abolished the existing inward current inan oocyte with NIS (Eskandari et al., 1997), Riedel and coau-thors (2001a,b) suggested two potential mechanisms for ClO4
–
action on the thyroid: (1) that ClO4– blocks I– transport, but is
not transferred into the cell, and (2) ClO4– competes with I– and
is transferred into the cell by NIS at a 1:1 ratio with Na. In ourmodel, we utilize the latter proposed mechanism, in whichClO4
– competes for binding sites on the NIS and is transferredinto the follicle in place of iodide. This assumption is based onmeasured radiolabeled and cold perchlorate thyroid concentra-tions with tissue to blood ratios greater than one (Chow andWoodbury, 1970; Yu et al., 2002b), the consistency of ClO4
–
accumulation in tissues with NIS, and studies showing that
ClO4– affects the internal thyroid iodide as well as the external
uptake of iodide by NIS (Hildebrandt and Halmi, 1981). Theability of the model to reproduce experimental perchlorate,iodide, and inhibition data from different exposure scenarios(acute vs. drinking water) and over a wide range of dosessupports the use of this mode of action as the foundation for thepharmacokinetic models.
The iodide model was simplified by assuming that radiola-
FIG. 6—Continued
FIG. 7. Radioiodide concentration in (a) placenta and (b) total fetus afteran iv injection to the GD 20 CFY albino dam (0.36 ng/kg). The modelsimulation is shown versus the mean � SD of the data at 24 h after exposure(Sztanyik and Turai, 1988).
250 CLEWELL ET AL.
by guest on May 31, 2013
http://toxsci.oxfordjournals.org/D
ownloaded from

beled iodide could be described as free iodide in all compart-ments other than the maternal thyroid. Simulations wereperformed against total radioiodide concentrations in extrathy-roidal tissues and against inorganic and incorporated iodide inthyroid. Despite this simplification of the model structure, thekinetic behavior of radioiodide in the naıve rat (no ClO4
–
exposure) was accurately simulated in all measured maternaland fetal tissues over a range of doses spanning nearly fiveorders of magnitude (0.36 to 33,000 ng/kg) 24 h after a singleadministration of radiolabeled iodide. Intralaboratory studiesfound that approximately 80% of serum iodide is in the inor-ganic form in the pregnant rat as much as 12 h after dosing withradioiodide (Yu et al., 2002a). Thus, the model description ofextrathyroidal tissue iodide uptake based on the transfer ofinorganic iodide via NIS predicts the data reasonably wellwithout significant contribution from the uptake of incorpo-rated iodine.
This PBPK model describes the dosimetry, distribution,kinetic behavior, and interaction between administered radio-iodide and perchlorate. As such, a description of dietary iodideand interactions of endogenous and dosed iodide have not beenincluded in the present version of the model. For the purpose ofextrapolation of this animal model to human exposure scenar-ios, the influence of variations in dietary iodide intake willneed to be included, in order to make the human predictionsmore applicable across populations. However, in the rat, iodideintake is easily controlled through the animal’s diet, and giventhat iodide is an essential nutrient, the mineral is tightly con-trolled by regulatory mechanisms. Therefore, slight variationsin laboratory rat chow are not expected to affect model pre-dictions of distribution or even perchlorate-induced inhibition.Although the mechanism for iodide transfer (NIS) is saturable,the high value for Km dictates that very large doses of iodidewould be required to inhibit its own uptake, as opposed to moreeffective inhibition by the higher affinity ClO4
–. In fact, instudies by Wolff and Chaikoff (1948), it was found that theuptake of iodide into the thyroid is linear up to serum iodidelevels of 250 �g/l, which is more than six times higher than
serum levels of the highest dose groups used in our studies andmore than 60 times greater than would be expected from dailyiodide intake from a normal rat chow. Thus, this model isuseful for predicting tissue dosimetry and inhibition in the ratand for extrapolation to the average human with normal iodidediet. In order to address intraspecies variability and suscepti-bility to hormone effects due to variations in diet, futureelaborations of the model should include endogenous iodide, as
TABLE 3Model-Predicted Radioiodide Concentration in Maternal and
Fetal Tissues versus Measured Data (mean � SD)
Tissue
Radioiodide concentration (ng/l)
Model predicted Measured (mean � SD)
Maternal serum 4.5 � 104 4.1 � 0.6 � 104
Maternal thyroid 1.8 � 107 1.1 � 0.5 � 107
Maternal GI contents 1.3 � 105 1.3 � 0.6 � 105
Placenta 4.9 � 104 5.0 1.0 � 104
Fetal serum 1.8 � 104 2.3 � 1.7 � 104
Fetal GI (tract contents) 4.7 � 104 4.0 � 2.0 � 104
Fetal skin 3.5 � 104 4.0 � 2.0 � 104
Note. Two h after an iv dose of 33,000 ng/kg 125I– to the dam on GD 20.
FIG. 8. Iodide concentration in (a) maternal thyroid and (b) placenta withand without 1.0 mg/kg ClO4
– iv dose 2 h prior to an iv dose of 1.87 ng/kg 125I–
to the dam (Clewell et al., 2001). The top simulation (solid line) and data (solidbox) indicates the control group. The lower simulation (dotted line) and data(open circle) indicate the perchlorate-dosed inhibition group.
251PBPK ClO4� MODEL FOR RAT GESTATION
by guest on May 31, 2013
http://toxsci.oxfordjournals.org/D
ownloaded from

well as a more detailed description of hormone distribution,homeostasis, and regulation.
This model currently includes only a highly simplified de-scription of the hormone feedback system that controls iodideuptake and upregulation of the inhibited thyroid in order topredict the dose-dependent change in thyroid iodide uptakeafter long-term exposure to ClO4
– in the rat. However, it isimportant to note that the rat thyroid has a much greatersensitivity to perturbations in the pituitary-thyroid axis than thehuman. In fact, evidence of upregulation is seen as early as12 h after administration of ClO4
– to a male rat (Merrill et al.,2003), whereas human studies have found that after two weeksof ClO4
– exposure, TSH levels were not yet elevated andthyroidal iodide uptake showed inhibition similar to that of thecontrol subjects (Brabant et al., 1992; Greer et al., 2002).Although the human shows similar inhibition to the rat (Greeret al., 2002) at equal perchlorate doses, the human system doesnot respond by upregulating thyroid activity. This speciesdifference is most likely due to the fact that the human has agreater thyroid hormone storage capacity than the rat, resultingfrom increased thyroid colloid volume and serum binding
(thyroxine binding globulin; Brown et al., 1986; Dohler et al.,1979). Therefore, small perturbations in iodide uptake do notappear to affect hormone balance to the same extent in humansas in rats. Since stable serum ClO4
– levels cannot be estab-lished in rats for more than a few hours without inducingupregulation of NIS, it is not possible to use rats directly as ananimal model for human drinking water ClO4
– exposure. How-ever, by using the rat PBPK models to extrapolate to humans,we can mathematically bridge this gap by using the existing ratdata and incorporating a longer time course for upregulation inthe human model.
Together with a concurrent model developed by Merrill etal. (2003), the present PBPK model is able to define andquantify kinetic differences in the male, pregnant, and fetal rat.The models account for kinetic differences through the descrip-tion of physiological differences. Most of the kinetic parame-ters are nearly identical between the male rat and pregnant rat,with the exception of those for thyroid and skin uptake andurinary clearance of iodide. Where different kinetic parameterswere necessary in the two models, literature studies were ableto provide a justification for these differences. For example,
TABLE 4Model-Predicted Inhibition of Iodide Uptake in Total Fetus
versus Data of Sztanyik and Turai (1988)
KClO4 dose(mg)
Time of ClO4– dose
(after 131I– dose) (min)
% Inhibition in fetus(% control)
Modelpredicted Measured
6.0 20 13 8.1–15.1 (12)3.0 60 18 14.2–19.8 (17)3.0 120 20 24.2–34.6 (30)
FIG. 9. Calculated sensitivity coef-ficients for model parameters with re-spect to serum perchlorate AUC at drink-ing water doses of 0.1 and 10.0 mg/kg-day.
TABLE 5Model-Predicted Internal Dosimetrics: Fetal Dose and Serum
AUC in Male, Pregnant, and Fetal Rat from Drinking WaterPerchlorate Exposure
ClO4– dose
(mg/kg-day)
Serum ClO4– AUC (mg/l)
Fetal dose(% maternal dose)Male rat Pregnant rat Fetal rat
0.01 0.045 0.0510 0.0243 820.1 0.157 0.167 0.103 631.0 0.598 0.613 0.320 26
10.0 1.520 1.560 0.622 18
252 CLEWELL ET AL.
by guest on May 31, 2013
http://toxsci.oxfordjournals.org/D
ownloaded from

Brown-Grant and Pethes (1959) found that the adult male andneonatal rat possess a greater iodide reserve in the skin than thepregnant dam. This difference in life stage kinetics is reflectedin the parameters for skin iodide uptake in the pregnant andmale rat models (e.g., VmaxcSi � 6.0 � 104 vs. 5.0 � 105,respectively; Merrill et al., 2003). This information providedby the models, concerning the variation in perchlorate andiodide kinetics across gender and life stages in the rat, shouldimprove the accuracy of predictions for human perchlorateexposures during gestation (Clewell et al., 2001).
A comparison of model-predicted internal dosimetrics pro-vides important information on ClO4
– distribution and inhibi-tion kinetics across life stages. It is apparent that the fetusreceives a significant portion of the maternal ClO4
– dose, whilethe serum AUCs are similar between the male and pregnantrats. Comparison of thyroid iodide inhibition suggests that thethyroid of the pregnant rat may be somewhat more sensitive toinhibition than that of the male rat. This may be due to theincreased loss of iodine during pregnancy, resulting from lossto the fetus and increased urinary output (Versloot et al., 1997).The predicted fetal thyroid inhibition was even greater thanthat of the male and pregnant female, possibly due to thecombined effect of inhibition at both the placenta and fetalthyroid. Inhibition in the fetal thyroid is partially offset by theincreased fetal serum iodide levels resulting from inhibition inthe fetal skin and GI contents. However, the actual risk to thefetus may be better characterized by looking at the effect ofperchlorate on iodide levels in the total fetus, due to the factthat fetal iodide stores in extra-thyroidal tissues (e.g., skin) areimportant in maintaining the needed iodide supply during thetransition from intra- to extra-uterine life.
A potentially informative use of this PBPK model is in thecorrelation of predicted internal dosimetrics to periods in ges-tation where perchlorate exposure and/or iodide deficiency hasbeen associated with developmental effects. The model can beused to predict tissue dosimetry in effects studies and to pin-point specific times in gestation when fetal iodide uptake ismost critical. A lactation exposure model is currently in devel-opment for use with the gestation model to provide a completekinetic description of the developmental period. When usedtogether, these developmental models could be used to help
answer questions concerning susceptible time points and pri-mary routes of exposure during development.
ACKNOWLEDGMENTS
The authors would like to thank Tammie Covington, Harvey Clewell, andDr. Melvin Andersen for their modeling advice; Latha Narayanan and GerryButtler for sample analyses; Charles Goodyear for performing statistical anal-yses of the data; and Dick Godfrey, Peggy Parish, Susan Young, TSgt ToddLigman, MSgt Jim McCafferty, Tim Bausman, SSgt Paula Todd, and MSgtRick Black for technical support. The authors would like to acknowledgeAnnie Jarabek, LtCol Dan Rogers, Dr. Richard Stotts and the U.S. Air Forcefor their support of this project and the U.S. Navy for financial support.
REFERENCES
Altman, P. L., and Dittmer, D. S. (1971). Volume of blood in tissue: Verte-brates. In Respiration and Circulation, pp. 383–387. Federation of Ameri-can Societies for Experimental Biology, Bethesda, MD.
Andersen, M. E., Gargas, M. L., and Ramsey, J. C. (1984). Inhalation phar-macokinetics: Evaluating systemic extraction, total in vivo metabolism, andthe time course of enzyme induction for inhaled styrene in rats based onarterial blood:inhaled air concentration ratios. Toxicol. Appl. Pharmacol.73(1), 176–187.
Bakke, J. L., Lawrence, N. L., Robinson, S., and Bennett, J. (1976). Lifelongalterations in endocrine function resulting from brief perinatal hypothyroid-ism in the rat. J. Lab. Clin. Med. 88, 3–13.
Beaton, G. H., Beare, H., Ryu, M. H., and McHenry, E. W. (1954). Proteinmetabolism in the pregnant rat. J. Nutr. 54, 291–304.
Bengele, H. H., and Solomon, S. (1974). Devlopment of renal response toblood volume expansion in the rat. Am. J. Physiol. 227(2), 364–368.
Berman, M., Hoff, E., Barandes, M., Becker, D. B., Sonenberg, M., Benua, R.,and Koutras, D. A. (1968). Iodine kinetics in man—a model. J. Clin.Endocrinol. Metab. 28(1), 1–14.
Brabant, G., Bergmann, P., Kirsch, C. M., Kohrle, J., Hesch, R. D., and von zurMuhlen, A. (1992). Early adaptation of thyrotropin and thyroglobulin se-cretion to experimentally decreased iodine supply in man. Metabolism 41,1093–1096.
Brown, R. A., Al-Moussa, M., and Beck, J. (1986). Histometry of normalthyroid in man. J. Clin. Pathol. 39, 475–482.
Brown, R. P., Delp, M. D., Lindstedt, S. L., Rhomberg, L. R., and Beliles, R. P.(1997). Physiological parameter values for physiologically based pharma-cokinetic models. Toxicol. Ind. Health 13, 407–484.
Brown-Grant, K. (1961). Extrathyroidal iodide concentrating mechanisms.Physiol. Rev. 41, 189–213.
Brown-Grant, K. (1966). Failure of orally administered perchlorate to affectdeciduoma formation or pregnancy in the rat. J. Reprod. Fertil. 12(2),353–357.
Brown-Grant, K., and Pethes, G. (1959). Concentration of radioiodine in theskin of the rat. J. Physiol. 148, 683–693.
Buelke-Sam, J., Holson, J. F., and Nelson, C. J. (1982). Blood flow duringpregnancy in the rat: II. Dynamics of and litter variability in uterine flow.Teratology 26, 279–288.
Carpenter, E. (1959). Development of the fetal rat thyroid with special refer-ence to the uptake of radioactive iodine. J. Exp. Zool. 142, 247–257.
Carr, C. W. (1952). Studies on the binding of small ions in protein solutionswith the use of membrane electrodes. I. The binding of the chloride ion andother inorganic anions in solutions of serum albumin. Arch. Biochem.Biophys. 40, 286–294.
Chow, S. Y., Chang, L. R., and Yen, M. S. (1969). A comparison between the
TABLE 6Model-Predicted Internal Dosimetrics: % Inhibition of Thyroid
Iodide Uptake in Male, Pregnant, and Fetal Rat from AcutePerchlorate Exposure
ClO4– dose (mg/kg)
% Inhibition
Male rat Pregnant rat Fetal rat
0.01 1.7 2.5 4.10.1 17.9 25.4 36.01.0 76.0 87.1 88.8
10.0 90.6 93.4 95.7
253PBPK ClO4� MODEL FOR RAT GESTATION
by guest on May 31, 2013
http://toxsci.oxfordjournals.org/D
ownloaded from

uptakes of radioactive perchlorate and iodide by rat and guinea pig thyroidglands. J. Endocrinol. 45, 1–8.
Chow, S. Y., and Woodbury, D. M. (1970). Kinetics of distribution of radio-active perchlorate in rat and guinea-pig thyroid glands. J. Endocrinol. 47,207–218.
Clewell, R. A., and Gearhart, J. M. (2002). Proposed PBPK model to predictinfant exposure: Clewell and Gearhart’s Response. Environ. Health Per-spect. 110(11), A15–A16.
Clewell, R. A., Merrill, E. A., and Robinson, P. J. (2001). The use ofphysiologically based models to integrate diverse data sets and reduceuncertainty in the prediction of perchlorate kinetics across life stages andspecies. Toxicol. Ind. Health 17, 210–222.
Clos, J., Crepel, F., Legrand, C., Legrand, J., Rabie, A., and Vigouroux, E.(1974). Thyroid physiology during the postnatal period in the rat: A study ofthe development of thyroid function and of the morphogenetic effects ofthyroxine with special reference to cerebellar maturation. Gen. Comp. En-docrinol. 23, 178–192.
Conde, E., Martin-Lacave, I., Godalez-Campora, R., and Galera-Davidson, H.(1991). Histometry of normal thyroid glands in neonatal and adult rats.Am. J. Anat. 191, 384–390.
Delange, F. (2000). The role of iodine in brain development. Proc. Nutr. Soc.59, 75–79.
DiStefano, J. J., III, Malone, T. K., and Jang, M. (1982). Comprehensivekinetics of thyroxine distribution and metabolism in blood and tissue poolsof the rat from only six blood samples: Dominance of large, slowly ex-changing tissue pools. Endocrinology 111(1), 108–117.
Dohler, K. D., Wong, C. C., and von zur Muhlen, A. (1979). The rat model forthe study of drug effects on thyroid function: Consideration of methodolog-ical problems. Pharmacol. Ther. 5, 305–318.
Eguchi, Y., Fukiishi, Y., and Hasegawa, Y. (1980). Ontogeny of the pituitary-thyroid system in fetal rats: Observations on the fetal thyroid after maternaltreatment with goitrogen. Anat. Rec. 198, 637–642.
Eskandari, S., Loo, D. D., Dai, G., Levy, O., Wright, E. M., and Carrasco, N.(1997). Thyroid Na/I� symporter: Mechanism, stoichiometry, and speci-ficity. J. Biol. Chem. 272, 2730–2738.
Feldman, J. D., Vazquez, J. J., and Kurtz, S. M. (1961). Maturation of the fetalthyroid. J. Biophys. Biochem. Cytol. 11, 365–383.
Fisher, J., Todd, P., Mattie, D., Godfrey, D., Narayanan, L., and Yu, K. (2000).Preliminary development of a physiological model for perchlorate in theadult male rat: A framework for further studies. Drug Chem. Toxicol. 23,243–258.
Fisher, J. W., Whittaker, T. A., Taylor, D. H., Clewell, H. J., and Andersen,M. E. (1989). Physiologically based pharmacokinetic modeling of the preg-nant rat: A multiroute exposure model for trichloroethylene and its metab-olite, trichloroacetic acid: Toxicol. Appl. Pharmacol. 99, 395–414.
Geloso, J. P. (1961). Date de l’entree en fonction do la thyroide chez lel foetusde rat. C. R. Soc. Biol. (Paris) 155, 1239–1244.
Gentry, P. R., Covington, T. R., Andersen, M. E., and Clewell, H. J. (2002).Application of a physiologically-based pharmacokinetic model for isopro-panol in the derivation of an RfD/RfC. Reg. Toxicol. Pharmacol. 36, 51–68.
Gluzman, B. E., and Niepomniszcze, H. (1983). Kinetics of the iodide trappingmechanism in normal and pathological human thyroid slices. Acta Endocri-nol. 103, 34–39.
Goedbloed, J. F. (1972). The embryonic and postnatal growth of rat andmouse. I. The embryonic and early postnatal growth of the whole embryo.A model with exponential growth and sudden changes in growth rate. ActaAnat. 82, 305–306.
Golstein, P., Abramow, M., Dumont, J. E., and Beauwens, R. (1992). Theiodide channel of the thyroid: A membrane vesicle study. Am. J. Physiol.263, C590–C597.
Gotshall R. W., Breay-Pilcher J. C., and Boelcskevy B. D. (1987). Cardiacoutput in adult and neonatal rats utilizing impedance cardiography. Am. J.Physiol. 253(5 Pt. 2), H1298–H1304.
Greer, M. A., Goodman, G., Pleus, R. C., and Greer, S. E. (2002). Healtheffects assessment for environmental perchlorate contamination: The doseresponse for inhibition of thyroidal radioiodide uptake in humans. Environ.Health Perspect. 110, 927–937.
Haddow, J. E., Palomaki, G. E., Allan, W. C., Williams, J. R., Knight, G. J.,Gagnon, J., O’Heir, C. E., Mitchell, M. L., Hermos, R. J., Waisbren, S. E.,et al. (1999). Maternal thyroid deficiency during pregnancy and subsequentneuropsychological development of the child. N. Engl. J. Med. 341, 549–555.
Halmi, N. S., and Stuelke, R. G. (1959). Comparison of thyroidal and gastriciodide pumps in rats. Endocrinology 64, 103–109.
Hanwell, A., and Linzell, J. L. (1973). The time course of cardiovascularchanges in the rat. J. Physiol. 233, 99–109.
Harden, R. G., Alexander, W. D., Shimmins, J., and Robertson, J. W. (1968).A comparison between the inhibitory effect of perchlorate on iodide andpertechnetate concentrations in saliva in man. Q. J. Exp. Physiol. Cogn.Med. Sci. 3, 227–238.
Hays, M. T., and Wegner, L. H. (1965). A mathematical and physical modelfor early distribution of radioiodide in man. J. Appl. Physiol. 20, 1319–1328.
Hildebrandt, J. D., and Halmi, N. S. (1981). Intrathyroidally generated iodide:The role of transport in its utilization. Endocrinology 108, 842–849.
Honour, A. J., Myant, N. B., and Rowlands, E. N. (1952). Secretion ofradioiodine in digestive juices and milk in man. Clin. Sci. 11, 447–463.
Howdeshell, K. L. (2002). A model of the development of the brain as aconstruct of the thyroid system. Environ. Health Perspect. 110(3), 337–348.
Klein, A. H., Meltzer, S., and Kenny, F. M. (1972). Improved prognosis incongenital hypothyroidism treated before age three months. J. Pediatr. 81,912–915.
Knight, C. H., Docherty, A. H., and Peaker, M. (1984). Milk yield in the rat inrelation to activity and size of the mammary secretory cell population. J.Dairy Res. 51, 29–35.
Knight, C. H., and Peaker, M. (1982). Mammary cell proliferation in miceduring pregnancy and lactation in relation to milk yield. Q. J. Exp. Phys. 67,165–177.
Kosugi, S., Sasaki, N., Hai, N., Sugawa, H., Aoki, N., Shigemass, C., Mori, T.,and Yoshida, A. (1996). Establishment and characterization of a Chinesehamster ovary cell line, CHO-4J, stably expressing a number of Na/I-symporters. Biochem. Biophys. Res. Commun. 227(1), 94–101.
Kotani, T., Ogata, Y., Yamamoto, I., Aratake, Y., Kawano, J. I., Suganuma, T.,and Ohtaki, S. (1998). Characterization of gastric Na/I- symporter of therat. Clin. Immunol. Immunopathol. 89, 271–278.
Kotyk, A., and Janacek, K. (1977). Transport of ions. In Membrane Transport:An Interdisciplinary Approach, pp. 243–247. Plenum Press, New York.
Lazarus, J. H., Harden, R. M., and Robertson, J. W. K. (1974). Quantitativestudies of the inhibitory effect of perchlorate on the concentration of36ClO4
–, 125I–, and 99mTcO4– in salivary glands of male and female mice.Arch. Oral. Biol. 19, 493–498.
Mahle, D. A., Godfrey, R. J., McCafferty, J. D., Bausman, T. A., Narayanan,L., Parish, M. A., Todd, P. N., Ligman, T. A., Mattie, D. R., and Yu, K. O.(2002). Kinetics of perchlorate and iodide in lactating S-D rats and pups atpostnatal day 10. Toxicol. Sci, 66(1-S), 139 (Abstract).
Malendowicz, L. K., and Bednarek, J. (1986). Sex dimorphism in the thyroidgland. Acta Anat. 127, 115–118.
Merrill, E. A., Clewell, R. A., Gearhart, J. M., Robinson, P. J., Sterner, T. R.,Yu, K. O., and Fisher, J. W. (2003). PBPK model for perchlorate-inducedradioiodide inhibition in the male rat. Toxicol. Sci. 73, 256–269.
254 CLEWELL ET AL.
by guest on May 31, 2013
http://toxsci.oxfordjournals.org/D
ownloaded from

Morreale de Escobar, G., Pastor, R., Obregon, M. J., and Escobar del Rey, F.(1985). Effect of maternal hypothyroidism on the weight and thyroid hor-mone content of rat embryonic tissues, before and after onset of fetal thyroidfunction. Endocrinology 117(5), 1890–1900.
Motzer, W. E. (2001). Perchlorate: Problems, detection, and solutions. Envi-ron. Foren. 2, 301–311.
Myant, N. B. (1971). The role of thyroid hormone in the fetal and postnataldevelopment of mammals. In Hormones in Development (M. Hamburgh andE. J. W. Barrington, Eds.), pp. 465–471. Appleton-Century-Crofts, NewYork.
Naismith, D. J., Richardson, D. P., and Pritchard, A. E. (1982). The utilizationof protein and energy during lactation in the rat, with particular regard to theuse of fat accumulated during pregnancy. Br. J. Nutr. 48, 433–441.
Nataf, B., and Sfez, M. (1961). Debut du fonctionement de la thyroide foetaledu rat. C. R. Soc. Biol. 55, 1235–1238.
O’Flaherty, E. J., Scott, W., Schreiner, C., and Beliles, R. P. (1992). Aphysiologically based kinetic model of rat and mouse gestation: Dispositionof a weak acid. Toxicol. Appl. Pharmacol. 112, 245–256.
Palou, A., Remesar, X., Arola, L., and Alemany, M. (1983). Body and organsize and composition during late fetal and postnatal development of rat.Comp. Biochem. Physiol. A 75, 597–601.
Pena, H. G., Kessler, W. V., Christian, J. E., Cline, T. R., and Plumlee, M. P.(1976). A comparative study of iodine and potassium perchlorate metabo-lism in the laying hen. 2. Uptake, distribution, and excretion of potassiumperchlorate. Poult. Sci. 55, 188–201.
Porterfield, S. P. (1994). Vulnerability of the developing brain to thyroidabnormalities: Environmental insults to the thyroid system. Environ. HealthPerspect. 102(Suppl. 2), 125–130.
Rakusan, K., and Marcinek, H. (1973). Postnatal development of the cardiacoutput distribution in rat. Biol. Neonate. 22, 58–63.
Riedel, C., Dohan, O., De la Vieja, A., Ginter, C. S., and Carrasco, N. (2001a).Journey of the iodide transporter NIS: From its molecular identification to itsclinical role in cancer. Trends Biochem. Sci. 26, 490–496.
Riedel, C., Levy, O., and Carrasco, N. (2001b). Post-transcriptional regulationof the sodium/iodide symporter by thyrotropin. J. Biol. Chem. 276, 21458–21463.
Roti, E., Gnudi, A., and Braverman, L. E. (1983). The placental transport,synthesis and metabolism of hormones and drugs which affect thyroidfunction. Endocr. Rev. 4, 131–149.
Scatchard, G., and Black, E. S. (1949). The effects of salts on the isoionic andisoelectric points of proteins. J. Phys. Colloid Chem. 53, 88–99.
Schneidereit, M. (1985). Study of fetal organ growth in Wistar rats from day17 to 21. Lab. Anim. Lond. 19, 240–244.
Shishiba, Y., Shimizu, T., Yoshimura, S., and Shimizu, K. (1970). [Effect ofthiocyanate and perchlorate on free thyroxine fraction]. Nippon. Naibunpi.Gakkai. Zasshi. 46, 16–19.
Sikov, M. R., and Thomas, J. M. (1970). Prenatal growth of the rat. Growth 34,1–14.
Spitzweg, C., Joba, W., Eisenmenger, W., and Heufelder, A. E. (1998).Analysis of human sodium iodide symporter gene expression in extrathy-roidal tissues and cloning of its complementary deoxyribonucleic acids fromsalivary gland, mammary gland, and gastric mucosa. J. Clin. Endocrinol.Metab. 83, 1746–1751.
Sztanyik, L. B., and Turai, I. (1988). Modification of radioiodine incorporationin the fetus and newborn rats by the thyroid blocking agents. Acta Phys.Hungaria 72, 343–354.
Tazebay, U. H., Wapnir, I. L., Levy, O., Dohan, O., Zuckier, L. S., Zhao,Q. H., Deng, H. F., Amenta, P. S., Fineberg, S., Pestell., R. G., et al. (2000).The mammary gland iodide transporter is expressed during lactation and inbreast cancer. Nat. Med. 6, 871–878.
Urbansky, E. T. (1998). Perchlorate chemistry: Implications for analysis andremediation. Bioremediation Journal 2, 81–95.
Urbansky, E. T., and Schock, M. R. (1999). Issue in managing risks associatedwith perchlorate in drinking water. J. Environ. Manag. 56, 79–95.
USEPA. (2002). Report on the Peer Review of the U.S. EnvironmentalProtection Agency’s Draft External Review Document. USEPA EPA/635/R-02/003. 01 Jun 2002. U.S. Environmental Protection Agency, Washing-ton, DC, 412.
Versloot, P. M., Schroder-van der Elst, J. P., van der Heide, D., and Boogerd,L. (1997). Effects of marginal iodine deficiency during pregnancy: Iodideuptake by the maternal and fetal thyroid. Am. J. Physiol. 273, E1121–E1126.
Wolff, J. (1964). Transport of iodide and other anions in the thyroid gland.Physiol. Rev. 44, 45–90.
Wolff, J. (1998). Perchlorate and the thyroid gland. Pharmacolog. Rev. 50,89–105.
Wolff, J., and Chaikoff, I. L. (1948). Plasma inorganic iodide as a homeostaticregulator of thyroid function. J. Biol. Chem. 174, 555–564.
Wolff, J., and Maurey, J. R. (1963). Thyroidal iodide transport: IV. The role ofion size. Biochim. Biophys. Acta 69, 48–58.
Yamada, T. (1967). Effects of perchlorate and other anions on thyroxinmetabolism in the rat. Endocrinology 81, 1285–1290.
Yu, K., Mahle, D., Narayanan, L., Godfrey, D., Todd, P., Parish, M., McCaf-ferty, J., Ligman, T., Sterner, T., and Buttler, G. (2001). Tissue distributionand inhibition of iodide uptake by perchlorate in pregnant and lactating ratsin drinking water studies. Toxicol. Sci. 60(1-S), 291 (Abstract).
Yu, K. O., Mahle, D. A., Narayanan, L., Buttler, G. W., Todd, P. N., Parish,P. N., McCafferty, J. D., Ligman, T. A., Sterner, T. R., and Bausman, T. A.(2002a). Kinetics of perchlorate-induced inhibition of iodide uptake intissues of the pregnant rat and fetus. Toxicol. Sci. 66(1-S), 139 (Abstract).
Yu, K. O., Narayanan, L., Mattie, D. R., Godfrey, R. J., Todd, P. N., Sterner,T. R., Mahle, D. A., Lumpkin, M. H., and Fisher, J. W. (2002b). Thepharmacokinetics of perchlorate and its effect on the hypothalamus/pitu-itary-thyroid axis in the male rat. Toxicol. Appl. Pharmacol. 182(2), 148–159.
Zeghal, N., Redjem, M., Gondran, F., and Vigouroux, E. (1995). Analysis ofiodine compounds in young rat skin in the period of suckling and in theadult. Effect of perchlorate. Arch. Physiol. Biochem. 103, 502–511.
255PBPK ClO4� MODEL FOR RAT GESTATION
by guest on May 31, 2013
http://toxsci.oxfordjournals.org/D
ownloaded from