Practical management of hyperinsulinism in infancy
10
HYPERINSULINISM Practical management of hyperinsulinism in infancy A Aynsley-Green, K Hussain, J Hall, J M Saudubray, C Nihoul-Fékété, P De Lonlay-Debeney, F Brunelle, T Otonkoski, P Thornton, K J Lindley Abstract Hyperinsulinism in infancy is one of the most diYcult problems to manage in con- temporary paediatric endocrinology. Al- though the diagnosis can usually be achieved without diYculty, it presents the paediatrician with formidable day to day management problems. Despite recent advances in understanding the patho- physiology of hyperinsulinism, the neuro- logical outcome remains poor, and there is often a choice of unsatisfactory treat- ments, with life long sequelae for the child and his or her family. This paper presents a state of the art overview on management derived from a consensus workshop held by the European network for research into hyperinsulinism (ENRHI). The consensus is presented as an educational aid for pae- diatricians and children’s nurses. It oVers a practical guide to management based on the most up to date knowledge. It presents a proposed management cascade and focuses on the clinical recognition of the disease, the immediate steps that should be taken to stabilise the infant during diagnostic investigations, and the princi- ples of definitive treatment. (Arch Dis Child Fetal Neonatal Ed 2000;82:F98–F107) Keywords: hyperinsulinism; treatment; hypoglycaemia; neurological damage; cation channels Hyperinsulinism is the most common cause of persistent or recurrent hypoglycaemia in infancy. 1 It is a major cause of neurological damage and life long handicap, and the fact that the incidence of such damage (in up to 20% of survivors) has changed little during the past 20 years 23 reflects the major diYculties in managing the disease. Until recently, the pathogenesis of hyperin- sulinism remained an enigma, 4 but during the past five years there has been an explosion of knowledge concerning the molecular genetics and the membrane physiology of the condition, which has given not only new insights into its cause, 5 but has also opened up new concepts of treatment. 67 It is now clear that the uncontrolled release of insulin is the final manifestation of a number of diVerent processes that either alter intra- cellular biochemical pathways of the pancreatic cell (thereby generating abnormal signals for the secretion of insulin 8 ), or alter the transport of cations across the cell membrane. These abnormalities perturb the stimulus–secretion coupling mechanisms that normally ensure that the amount of insulin secreted is directly related to the ambient blood glucose concentration. 8 Therefore, hyperinsulinism is characterised by the presence of insulin concentrations that are inappropriately high for the concentration of blood glucose. A “normal” insulin concen- tration for normoglycaemia is inappropriate in the presence of hypoglycaemia! Despite the new knowledge of pathogenesis, the management of the disease still presents the paediatrician with a choice of unsatisfactory treatments that have major long term implica- tions for the child and his or her family. Because of the urgent need to improve prog- nosis, the European network for research into hyperinsulinism (ENRHI) was created in 1997 through the support of the European Union. The network brings together leading basic and clinical scientists from seven European coun- tries to encourage collaboration, generate new scientific data, and from these, to define a con- sensus guide to management. A workshop was held in Finland in May 1999 to consider the latter, and this paper reflects the debate that occurred. As in any other area of medicine, consensus was achieved for many of the components of the manage- ment cascade. Nonetheless, controversy still surrounds other aspects, and these are defined and considered below. Further areas of clinical research that need to be developed are also highlighted. Background Hyperinsulinaemic hypoglycaemia has previ- ously masqueraded under a variety of diVerent descriptive names, including “idiopathic” hy- poglycaemia of childhood, leucine sensitive hypoglycaemia, neonatal insulinoma, pancre- atic microadenomatosis, nesidioblastosis, per- sistent hyperinsulinaemic hypoglycaemia of infancy, and congenital hyperinsulinism. Both sporadic and familial forms of the disease are recognised, the former having an estimated incidence in western Europe of one in 50 000 Arch Dis Child Fetal Neonatal Ed 2000;82:F98–F107 F98 The London Centre for Paediatric Endocrinology and Metabolism, Great Ormond Street Hospital for Children NHS Trust, London WC1N 3JH and the Institute of Child Health, University College, London WC1N 1EH, UK A Aynsley-Green K Hussain K J Lindley The Institute of Molecular Physiology and Department of Biomedical Science, University of SheYeld, SheYeld S10 2TN, UK J Hall The Metabolic Unit of Pediatrics and Departments of Radiology and Surgery, Hospital Necker Enfants Malades, 75015 Paris, France J M Saudubray C Nihoul-Fékété P De Lonlay-Debeney F Brunelle Hospital for Children and Adolescents and the Hartman Institute Transplantation Laboratory, 000140 University of Helsinki, Finland T Otonkoski The National Centre for Inherited Metabolic Disorders, The Children’s Hospital, Temple Street, Dublin 1, Ireland P Thornton On behalf of the European Network for Research into Hyperinsulinism (ENRHI) Correspondence to: Professor A Aynsley-Green, The Institute of Child Health, University College London, 30 Guilford Street, London WC1N 1EH, UK
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Practical management of hyperinsulinism in infancy

HYPERINSULINISM
Practical management of hyperinsulinism ininfancy
A Aynsley-Green, K Hussain, J Hall, J M Saudubray, C Nihoul-Fékété,P De Lonlay-Debeney, F Brunelle, T Otonkoski, P Thornton, K J Lindley
AbstractHyperinsulinism in infancy is one of themost diYcult problems to manage in con-temporary paediatric endocrinology. Al-though the diagnosis can usually beachieved without diYculty, it presents thepaediatrician with formidable day to daymanagement problems. Despite recentadvances in understanding the patho-physiology of hyperinsulinism, the neuro-logical outcome remains poor, and there isoften a choice of unsatisfactory treat-ments, with life long sequelae for the childand his or her family. This paper presentsa state of the art overview on managementderived from a consensus workshop heldby the European network for research intohyperinsulinism (ENRHI). The consensusis presented as an educational aid for pae-diatricians and children’s nurses. It oVersa practical guide to management based onthe most up to date knowledge. It presentsa proposed management cascade andfocuses on the clinical recognition of thedisease, the immediate steps that shouldbe taken to stabilise the infant duringdiagnostic investigations, and the princi-ples of definitive treatment.(Arch Dis Child Fetal Neonatal Ed 2000;82:F98–F107)
Keywords: hyperinsulinism; treatment; hypoglycaemia;neurological damage; cation channels
Hyperinsulinism is the most common cause ofpersistent or recurrent hypoglycaemia ininfancy.1 It is a major cause of neurologicaldamage and life long handicap, and the factthat the incidence of such damage (in up to20% of survivors) has changed little during thepast 20 years2 3 reflects the major diYculties inmanaging the disease.
Until recently, the pathogenesis of hyperin-sulinism remained an enigma,4 but during thepast five years there has been an explosion ofknowledge concerning the molecular geneticsand the membrane physiology of the condition,which has given not only new insights into itscause,5 but has also opened up new concepts oftreatment.6 7
It is now clear that the uncontrolled releaseof insulin is the final manifestation of a numberof diVerent processes that either alter intra-
cellular biochemical pathways of the pancreaticâ cell (thereby generating abnormal signals forthe secretion of insulin8), or alter the transportof cations across the cell membrane. Theseabnormalities perturb the stimulus–secretioncoupling mechanisms that normally ensurethat the amount of insulin secreted is directlyrelated to the ambient blood glucoseconcentration.8
Therefore, hyperinsulinism is characterisedby the presence of insulin concentrations thatare inappropriately high for the concentrationof blood glucose. A “normal” insulin concen-tration for normoglycaemia is inappropriate inthe presence of hypoglycaemia!
Despite the new knowledge of pathogenesis,the management of the disease still presents thepaediatrician with a choice of unsatisfactorytreatments that have major long term implica-tions for the child and his or her family.
Because of the urgent need to improve prog-nosis, the European network for research intohyperinsulinism (ENRHI) was created in 1997through the support of the European Union.The network brings together leading basic andclinical scientists from seven European coun-tries to encourage collaboration, generate newscientific data, and from these, to define a con-sensus guide to management.
A workshop was held in Finland in May1999 to consider the latter, and this paperreflects the debate that occurred. As in anyother area of medicine, consensus was achievedfor many of the components of the manage-ment cascade. Nonetheless, controversy stillsurrounds other aspects, and these are definedand considered below. Further areas of clinicalresearch that need to be developed are alsohighlighted.
BackgroundHyperinsulinaemic hypoglycaemia has previ-ously masqueraded under a variety of diVerentdescriptive names, including “idiopathic” hy-poglycaemia of childhood, leucine sensitivehypoglycaemia, neonatal insulinoma, pancre-atic microadenomatosis, nesidioblastosis, per-sistent hyperinsulinaemic hypoglycaemia ofinfancy, and congenital hyperinsulinism. Bothsporadic and familial forms of the disease arerecognised, the former having an estimatedincidence in western Europe of one in 50 000
Arch Dis Child Fetal Neonatal Ed 2000;82:F98–F107F98
The London Centre forPaediatricEndocrinology andMetabolism, GreatOrmond StreetHospital for ChildrenNHS Trust, LondonWC1N 3JH and theInstitute of ChildHealth, UniversityCollege, LondonWC1N 1EH, UKA Aynsley-GreenK HussainK J Lindley
The Institute ofMolecular Physiologyand Department ofBiomedical Science,University of SheYeld,SheYeld S10 2TN, UKJ Hall
The Metabolic Unit ofPediatrics andDepartments ofRadiology andSurgery, HospitalNecker EnfantsMalades, 75015 Paris,FranceJ M SaudubrayC Nihoul-FékétéP De Lonlay-DebeneyF Brunelle
Hospital for Childrenand Adolescents andthe Hartman InstituteTransplantationLaboratory, 000140University of Helsinki,FinlandT Otonkoski
The National Centrefor InheritedMetabolic Disorders,The Children’sHospital, TempleStreet, Dublin 1,IrelandP Thornton
On behalf of theEuropean Network forResearch intoHyperinsulinism(ENRHI)
Correspondence to:Professor A Aynsley-Green,The Institute of ChildHealth, University CollegeLondon, 30 Guilford Street,London WC1N 1EH, UK

births.9 In isolated European communities,including parts of Finland, the disease inci-dence is much higher10; the highest incidence isfound in societies with high rates ofconsanguinity.11 In these cultures, particularlyin the Arabian peninsular, the incidence maybe as high as one in 2500 births.10 11
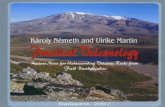
Clinical presentation and immediatemanagementMost infants with hyperinsulinism presentduring the 1st postnatal days, with others dur-ing the 1st year. Rarely, older children presentde novo with symptoms of hypoglycaemia. Fig-ure 1 shows the age distribution in one largeseries of cases.12
Hyperinsulinism can be associated with welldefined clinical conditions.13–16 Thus, theBeckwith-Wiedemann syndrome manifests atransient hyperinsulinism and these babieshave pathognomonic physical signs includingexomphalos, macroglossia, and transversecreases of the ear lobes. This disease and thehyperinsulinism caused by maternal diabetes,rhesus incompatibility, perinatal asphyxia,13
and maternal glucose and drug treatment dur-ing delivery will not be considered further inthis paper.
Infants with hyperinsulinism might have acharacteristic appearance with macrosomia,strongly resembling the infant of a diabeticmother. The appearance suggests the occur-rence of prenatal hyperinsulinism. However,not all infants have this appearance, and someof the most diYcult management problemsarise in infants born of normal or low birthweight, including preterm infants.17
The first clinical manifestations of hyperin-sulinism include non-specific features such as“floppiness”, “jitteriness”, poor feeding, andlethargy. More dramatically, the infants mayhave seizures, coma, and even averted neonataldeath.18
The importance of accurately measuringblood glucose in the presence of any of thesesymptoms cannot be overemphasised.
Considerable controversy surrounds thedefinition of neonatal and infantilehypoglycaemia.19–21 Pragmatically, any infantwith a persistent measurement of bloodglucose less than 2.6 mmol/litre (as measuredby an accurate laboratory method and not abedside screening test), particularly when
accompanied by symptoms, should be thefocus of particular attention, and the diagnosisof hyperinsulinism considered. Any persistenthypoglycaemia, whether symptomatic or not,needs investigation and treatment
Blood must be drawn and saved at the timeof hypoglycaemia (together with the next urinesample passed) for assay of the substanceslisted in table 1.
A baby who cannot maintain normoglycae-mia despite frequent enteral feeds (if necessaryvia a nasogastric feeding tube) needs to havethe support of an intravenous glucose infusionto prevent neuroglycopenia. It should com-mence at the normal neonatal and infantilehepatic production rate of glucose; namely,between 4–6 mg/kg/min. The infusion rateshould then be titrated upwards as necessary tomaintain the blood glucose value above 2.6–3.0 mmol/litre.
The definition of glucose requirement tomaintain normoglycaemia is a key diagnostic aswell as therapeutic step. The demonstration ofan increased glucose requirement is a powerfulindicator of underlying hyperinsulinism.
Many children require infusion rates inexcess of 15–20 mg/kg/min. Clearly, it is essen-tial to document that the infant actually needsthat high infusion rate. Infants are oftenreferred to regional centres with alleged highglucose requirements, but on being challengedby a cautious decrease are found not to be sodependent. It is, of course, possible that theglucose dependency may change dramaticallyfor the better in the 1st postnatal days, particu-larly in infants who may have experienced mildbirth asphyxia.
The need to assess carefully and regularlythe glucose infusion requirement withoutcausing severe hypoglycaemia, symptomatic ornot, is a key aspect of the initial managementprocess.
In infants who are dependent on high ratesof glucose infusion, the insertion of a centralvenous catheter through the umbilicus or via aperipheral vein is mandatory. This is becausethe sudden loss of a peripheral venous cannulain a child who has had multiple venepuncturescan cause a rapid onset of dramatic sympto-matic hypoglycaemia during attempts to re-sitethe line.
The need for early referral to a specialistcentreParticipants at the consensus workshop unani-mously criticised the current practice of late
Figure 1 Hyperinsulinism: age at presentation andsurgery.
80
70
60
50
40
30
20
10
0
Age
Number of childrenNumber going to surgery
Nu
mb
er o
f ch
ildre
n0–1
months2–6
months7–12
months1–2
years2–5
years6–9
years
Table 1 Intermediary metabolites and hormones to bemeasured at the point of hypoglycaemia
Blood Urine
Glucose KetonesLactate/pyrutate Reducing substancesKetone bodies Organic acidsFree fatty acidsAmino acidsAmmoniaTotal/free carnitineAcyl-carnitine profileInsulin/C peptideCortisol/growth hormone
Management of hyperinsulinism in infancy F99

referral to a centre experienced in the manage-ment of hyperinsulinism, and urged earliertransfer.
Practitioners should not underestimate thepractical diYculties of managing infants withhyperinsulinism, not least because of the vola-tility of glucose control and the vulnerability tounexpected and unpredictable severe hypogly-caemic episodes, but also because of the risks offluid overload and sepsis contributing to theconsiderable morbidity encountered by theseinfants.
Of central importance is the need fordedicated nursing support delivered in a unitthat has the infrastructure, quality standards,and training for rapid and repeated accurateblood glucose measurement. Protocols for theemergency management of the hypoglycaemicepisodes need to be in place, and staV shouldhave the experience and the knowledge toimpart confidence to parents at a time of majoremotional stress.
Members of ENRHI argue that late referralto a specialist centre after days or even weeks offruitless attempts to make a diagnosis andestablish eVective treatment is one of the mainreasons why the neurological morbidity re-mains so high. Indeed, because of the propen-sity of this disease to cause neural damage, itcould be deemed negligent not to transfer early.
The transfer process itself needs to becarefully orchestrated, as outlined in table 2.Transfer without a secure intravenous line anda trained nursing or medical escort is not anacceptable practice.
Establishing the diagnosis and the causeof hyperinsulinismFigure 2 outlines the consensus model for thenormal control of insulin secretion, and the lociat which abnormalities can occur. Knowledgeof this simple schematic is essential to under-stand the rationale for the diagnostic and man-agement cascades.
Three components of the diagnostic cascadeneed to be considered; namely, the biochemicaldiagnosis, the genotype and clinical phenotype,and the role of pancreatic imaging.
THE BIOCHEMICAL DIAGNOSIS
There is now a well established consensus onthe primary and secondary diagnostic indica-tors for hyperinsulinism, as shown in table 3. Inmany children, the diagnosis depends on theaggregation of several components, particularlybecause in the neonate the normal tight associ-ation seen in older children and adults betweenplasma insulin and blood glucose concentra-tions is not present.23 24 Attention is drawn tothe following:+ The characteristic metabolic profile of
hypoketonaemic hypofattyacidaemic hypo-glycaemia arises from the anabolic eVects ofinsulin preventing metabolic counter regula-tion as the blood glucose concentration falls.
+ The presence of any measurable insulinduring hypoglycaemia is strongly indicativeof a defect in regulating basal insulin secre-tion in the face of a falling blood glucoseconcentration. The interpretation of theresults depends on the sensitivity andspecificity of the local insulin assay.
+ Hyperinsulinism can occur in the absence offlorid hyperinsulinaemia—a normal insulinconcentration for normoglycaemia is inap-propriate in the presence of hypoglycaemia.
+ Insulin release is pulsatile and measurementof C peptide might be more helpful than asingle measurement of insulin because itreflects overall insulin production; there islittle extra value gained from measuringproinsulin concentrations.25
Table 2 Recommended guidelines to referring hospitals for transfer of babies withhyperinsulinism (transfer of babies/children with hypoglycaemia, regardless of aetiology)
(1) Before transfer discuss the case with the endocrine registrar/consultant on call(2) Must have secure intravenous access at all times before transfer (even if not requiring
intravenous fluids at time of transfer)(3) Baby/child must be transferred with nurse and doctor escort(4) Before transfer ensure you have:
10% dextrose (preferably 500 ml bag)Hypostop/sugary drinkGlucagon intramuscular/intravenous 0.1 mg/kg up to 1 mg maximumBlood glucose monitoring equipment
(5) Monitoring:Check blood glucose before leaving, then hourly if stable, or 15–30 minutes if unstableAim to keep blood glucose above 3.0 mmol/litre
(6) Hypoglycaemic event during journey (blood glucose < 2.6 mmol/litre)Recommendations: 2 ml/kg of 10% dextrose bolus over three minutes, start maintenance
infusion 6–8 mg/kg/min, which approximately equals 5 ml/kg/hour of 10% dextroseRecheck blood glucose 15 minutes later. If still low increase infusion by 1 mg/kg/min until
normoglycaemia attainedIf intravenous access lost give:
(a) Hypostop and repeat blood glucose in children > 2 years(b) Give one dose of glucagon and repeat blood glucose measurement for infants
Figure 2 The sequence of events leading to the release of insulin from a pancreatic â cell.In brief, SUR1 and KIR6.2 constitute the ATP sensitive potassium (KATP) channel. Thesetwo proteins are encoded by genes located on chromosome 11p15.1. Mutations in these genesaccount for some cases of hyperinsulinism. The KATP channel is normally kept openmaintaining a membrane resting potential of about –70 mV. When glucose enters the cell itraises the concentration ratio of ATP to ADP, which in turn causes the closure of the KATP
channel. Once closed, the cell membrane becomes depolarised, allowing the influx of calciumthrough specific voltage gated calcium channels. This is the trigger for insulin exocytosis.Mutations have also been described in the genes for glutamate dehydrogenase (GDH) andin the glucokinase (GK) system. These defects increase the intracellular ATP to ADP ratio,thereby initiating insulin secretion. In these conditions, there is no abnormality in thepotassium or calcium channel function. PHHI, persistent hyperinsulinaemic hypoglycaemiaof infancy; glucose-6-P, glucose-6-phosphate. (Reproduced with permission from Shepherd etal22)
Voltage gated Ca2+ channel
Control
Ca2+
Ca2+
Augmentation
ATP
–30 mV
–70 mVADP
Glucose-6-P
Glucose
ATP sensitiveK+ channel
K+
Depolarisation+
+Kir6.2SUR1 –
PHHISUR1 gene defects*
Kir6.2 gene defects*
Ca2+
Ca2+
–30 mV
–30 mV
*K+
Depolarisation+
+Kir6.2SUR1
Table 3 The diagnostic criteria for hyperinsulinism
Glucose requirements > 6–8 mg/kg/min to maintain bloodglucose above 2.6–3 mmol/litre
Laboratory blood glucose < 2.6 mmol/litreDetectable insulin at the point of hypoglycaemia with raised C
peptideInappropriately low blood free fatty acid and ketone body
concentrations at the time of hypoglycaemiaGlycaemic response after the adminstration of glucagon when
hypoglycaemicAbsence of ketonuria
F100 Aynsley-Green, Hussain, Hall, Saudubray, Nihoul-Fékété, De Lonlay-Debeney, et al

+ Very high glucose infusions rates (greaterthan 20 mg/kg/min) might be needed tosecure normoglycaemia. Titration of theinfusion rate against the blood glucose con-centration achieved allows the impact ofchanges in treatment to be assessed.
+ Progressive hepatic enlargement, presum-ably as a result of glycogen deposition, mightoccur during high infusion rates of glucose,but also secondary to fluid retention as aresult of high fluid infusion rates anddiazoxide treatment.
+ Babies show a glycaemic response to gluca-gon injection when hypoglycaemic becauseof the mobilisation of glycogen depositsfrom the liver. This phenomenon can be ofdiagnostic as well as therapeutic benefit.There is a lack of consensus over the dose ofglucagon used in diVerent centres, rangingfrom 0.1 mg/kg to a single overall dose of1.0 mg.26 In general, a positive response canbe said to occur when there is a clear incre-ment in blood glucose despite severe hy-poglycaemia. The injection of glucagon canbe useful at times of emergency, such as there-siting of a venous cannula. Glucagonshould be administered with caution be-cause of its insulin stimulatory eVect and thepropensity to cause rebound hypoglycaemia.
+ Other markers of hyperinsulinism includinglow circulating levels of branched chainamino acids at the time of hypoglycaemiaare of research interest only.27 The measure-ment of blood ammonia concentration isnow mandatory in view of the recentdescription of the syndrome of hyperammo-naemic hyperinsulinism.28 This condition islikely to be the explanation of the so called“leucine sensitive” hyperinsulinism in whichchildren show sensitivity to proteiningestion.29
+ Plasma concentrations of cortisol andgrowth hormone might not be consistentlyraised during episodes of even severe symp-tomatic hypoglycaemia.30 Nonetheless, con-genital hypopituitarism is an importantdiVerential diagnosis to consider; in thisdiagnosis, however, the plasma insulin con-centration should be undetectable, andthere may be other stigmata of the conditionincluding mid line defect and, in boys,micropenis. If in doubt, specific pituitarystimulation tests should be performed at thetertiary referral centre.
+ An increase in the blood glucose concentra-tion after somatostatin injection is sugges-tive of hyperinsulinism, but it is not recom-mended as a routine diagnostic criterion.
ESTABLISHING THE GENOTYPE AND CLINICAL
PHENOTYPE
Advances in the molecular genetics of the dis-ease have shown hyperinsulinism to be caused,in about 30–50% of patients, by abnormalitiesin either genes controlling intracellular meta-bolic pathways or membrane cation transport.Most abnormalities described to date relate tothe genes controlling the sulphonylurea recep-tor (SUR1) and the inward rectifier potassiumchannel (Kir6.2), proteins that together form
the functional ATP dependent potassiumchannel (KATP) in the â cell membrane. Over 40diVerent mutations have been reported, mostof which are recessively inherited.31 Domi-nantly expressed abnormalities have also beendescribed.32 Although the molecular genetics ofsome of these cases are now known,33 there isno information on the pancreatic lesion inthese patients because most patients with auto-somal dominant hyperinsulinism do not re-quire surgery.
Recently, a further twist has been added tothe story of the genetics of hyperinsulinism,with the discovery that “focal” hyperplasia inthe endocrine pancreas is the result of a uniquecombination of events: somatic loss of thematernal allele on the short arm of chromo-some 11, in a patient harbouring an SUR1mutation on the paternal allele.34 35 Thejuxtaposition of SUR1 and several imprintedgenes on chromosome 11p15 appears to beresponsible for this unique genetic mechanismof disease.
Gene mutations that cause abnormal activa-tion of glucose signalling of insulin secretion byaltering the enzyme kinetics of glutamatedehydrogenase or of glucokinase have beendescribed recently.28 36 Other loci have yet to bedefined in rare patients who present withhyperinsulinism in association with lacticacidosis.37 Because these abnormalities are notassociated with abnormal KATP channels, mostpatients with these defects respond to diazox-ide.
Despite these recent developments, less than50% of patients studied to date have adefinable genetic abnormality. Therefore, it islikely that other abnormalities will be revealedas the search continues for new defects in thesecretory apparatus, including defects in theintracellular control of calcium signalling ofexocytosis.38 For a more detailed description ofthe genetics of hyperinsulinism see Glaser et alelsewhere in this issue.39
Unfortunately it is not yet possible to usegenetic analysis routinely to screen for muta-tions except in specific populations withunique and characteristic abnormalities usuallyassociated with consanguinity.40
There is considerable variation in the clinicalphenotype of severity in hyperinsulinism. Ingeneral, children with hyperinsulinism born toconsanguineous parents, particularly those ofJewish or Arabic ancestry, have a severe form ofthe disease that is usually resistant to medicaltreatment. This also applies to patients fromparticular regions in Finland. It should be pre-dicted that these patients are likely to requireearly surgery to control the hypoglycaemia.Siblings are also at risk of the disease andshould be screened for the onset of neonatalhypoglycaemia.
In most European and white children, how-ever, there is no family history of intermarriageor aZicted members. Moreover, with theexception of hyperammonaemic hyperinsulin-ism it is not possible to predict at presentationwhich infants will respond dramatically to dia-zoxide treatment, although in general, neonatespresenting with severe hypoglycaemia in the 1st
Management of hyperinsulinism in infancy F101

postnatal days have the most unresponsiveform. It is equally impossible to predict whichinfants will have “transient” as opposed to“persistent” hyperinsulinism. In general, chil-dren with hyperammonaemic hyperinsulinismand upregulation of glucokinase have a milderdisease phenotype, which usually respondsrapidly to moderate doses of diazoxide, but agenetic heterozygosity certainly exists.
IMAGING OF THE PANCREAS
The need for methods to identify “focal” areasof hyperplasia has been given new impetusthrough the reports that preoperative percuta-neous trans-hepatic pancreatic venous sam-pling can identify “hot spots” of insulinhypersecretion.41 In children, preoperative pan-creatic venous sampling should be performedunder general anaesthesia in an interventionalangiographic room. Care should be taken tomaintain blood glucose concentrations atbetween 2.5 and 3 mmol/litre. The right portalvein is punctured with a 21 gauge catheter nee-dle. Specially shaped 3F catheters are thenexchanged over a guide wire. Multiple venoussamples are taken in the splenic, mesenteric,and portal veins but also in the small pancreaticveins draining the head, the body, and the tailof the pancreas. The concentrations of insulin,glucose, and C peptide are mapped accordingto the venous anatomy of the pancreas. A focalform is diagnosed when a single or twocontiguous veins have high amounts of insulin.The C peptide to insulin ratio is close to one inthose veins in that setting. A diVuse form isdiagnosed when several non-contiguous veinshave high concentrations of insulin. In cases ofhigh concentrations of glucose the mapping isnon-contributive. In a few patients, despite agood control of glucose below 3 mmol/litre, allthe sampled veins show low or normal concen-trations of insulin. These patients correspondto focal forms in which the draining vein of thelesion has not been selectively sampled. Whenfollowed by meticulous intraoperative micro-dissection, aided by immediate histologicalconfirmation of hyperplasia, there is evidencethat the long term prognosis is much betterthan in patients subjected to blind 95% partialpancreatectomy.41 Furthermore, focal diseasemight occur only in the head of the pancreas,and this may not be resected with blind partialpancreatectomy.
The ability to identify focal endocrinehyperplasia is a new and major advance indiagnosis and management. However, thelogistic aspects of this approach are substantialin terms of the availability of staV experiencedin interventional radiology and in pancreatichistology. Moreover, expert nursing care isneeded because the infants are at serious risk ofhypoglycaemia because medical treatmentsneed to be discontinued for several days beforethe procedure. In addition, the imaging proce-dure requires that the infant’s blood glucose bebrought as close as possible to hypoglycaemicvalues for up to several hours. The techniquerequires further evaluation before it can be rec-ommended for general use. Moreover, becauseof the logistic problems, the consensus work-
shop recommended that the use of thetechnique should be restricted to one or twonational centres in each country that have thecomprehensive resources needed to managethe children competently.
Alternative means have been proposed foridentifying focal disease. These include theintra-arterial calcium stimulation test, which isbased on the insulin stimulatory eVect of rapidselective injection of calcium into the branchesof the coeliac arteries supplying the diVerentparts of the pancreas.42 This technique alsorequires further evaluation, with members ofthe consensus workshop expressing concernover the potential for infarction of the coeliacarteries.
Other techniques, including preoperativeand intraoperative direct pancreatic ultra-sonography, computed tomography, magneticresonance imaging, and coeliac angiographyhave been used by many investigators. Thelimited published information has not shownthese techniques to be of value, particularly inthe neonate.43 However, imaging should beconsidered in the older child in whom thepossibility of the presence of an isolatedadenoma is high.1
The consensus workshop participantsagreed that currently available imaging tech-niques were not of value in the routine investi-gation of neonatal and early infantile hyperin-sulinism; they should only be considered in thesearch for an insulinoma in an older child pre-senting with recent onset of hypoglycaemia.
ManagementIt is important at the outset to identify theobjectives of management. They are to: (1)prevent hypoglycaemic brain damage and allownormal psychomotor development; (2) estab-lish normal feed volume, content, and fre-quency for the age of the child; (3) ensure nor-mal tolerance to fasting for age withoutdeveloping hypoglycaemia; and (4) maintainfamily integrity.
A regimen cannot be said to be successful ifit does not fulfil these objectives. However, inpractice it might be very diYcult to achievethem.
MEDICAL TREATMENT
Initial stabilisationThe mainstay of initial medical treatment is theprovision of adequate carbohydrate to maintainblood glucose concentrations above 2.6–3.0 mmol/litre. Very high infusion rates of glu-cose (> 20 mg/kg/min) in addition to frequententeral feeds may be required. This mightdemand the insertion of a central venous cath-eter to allow the administration of glucose inhigh concentrations, together with a nasogas-tric feeding tube for regular feeds. Glucosepolymer can be added to the enteral feed toincrease the carbohydrate intake. However, it isimportant not to cause too great an osmolarload in the gastrointestinal tract that mightpredispose to the onset of necrotising entero-colitis. Because of the immaturity of intestinalamylase during the 1st year of life, the admin-istration of cornstarch might not be eVective.
F102 Aynsley-Green, Hussain, Hall, Saudubray, Nihoul-Fékété, De Lonlay-Debeney, et al

When the blood glucose concentration hasbeen stabilised, pharmacological agents needto be introduced to try to decrease insulinsecretion and normalise the carbohydrateintake. The impact of their introduction can betested by the definition of a change in glucoserequirement. It is recommended that thesemanoeuvres be attempted only in referral cen-tres experienced in their use.
Pharmacological treatmentsA logical progression through the availabletreatments is proposed (table 4), which allows aclear definition of the clinical phenotype. Theessential principle of management is to intro-duce only one change in dose or treatment at atime and to assess the impact before moving onto the next change.
The drugs of first choice are those that canbe given orally, because some children mayrespond very well, even if they require ongoingtreatment for several months or years. It is rea-sonable to argue that it is essential to prove thata child will not respond to such agents beforeintroducing more powerful hormones.
Diazoxide (10–20 mg/kg/day in two to threedivided doses) and chlorothiazide (7–10 mg/kg/day in two divided doses) are recommendedfor initial treatment and should always be giventogether. Both these agents activate potassiumchannels by diVerent mechanisms,6 the diureticalso being given concurrently for its ability toovercome the fluid retaining eVects of diazox-ide. There is controversy over the frequencywith which infants respond fully to these drugs,with reports ranging from 15% to 60%, ormore.12 41 44 This diVerence in responsivenesscould perhaps reflect the selection of casesbeing referred to the centres. There is littleinformation on the pharmacodynamics orpharmacokinetics of diazoxide in childhood.Children who fail to respond to a dose of15–20 mg/kg/day might have pancreata thatwill respond in vitro to higher concentrations.In practice, the limit of clinical tolerance is
determined by the magnitude of side eVects, inparticular fluid retention and cardiac failure,and most children who will respond do so atdoses up to 15 mg/kg/day.
It is logical, in addition to activatingpotassium channels by diazoxide and chloro-thiazide, to try to decrease voltage dependentcalcium channel activity by blocking agents,such as the slow release form of nifedipine at adose of 0.25–2.5 mg/kg/day.17 The clinicalresponse to this drug is highly variable, anobservation that has now been explained bystudies performed in vitro on â cells frompatients with persistent hyperinsulinaemic hy-poglycaemia of infancy.38 Thus, some childrenwith KATP channel abnormalities might have aconcurrent defect in voltage gated calciumchannels. It is not possible to predict whichchildren will respond without trying the drug.The drug has not proved as useful as was firsthoped, yet nifedipine may still have a role as anadjuvant, although the long term eVects ofcontinuous treatment are unknown. The drugis light sensitive and there are practical diYcul-ties in its formulation when used in small chil-dren. Further research is needed to define theprecise value and role of calcium channelblocking drugs; nonetheless, their use is onetangible benefit that has arisen from a betterunderstanding of the pathophysiology of the âcells in this condition.
The side eVects of these drugs are impor-tant. Diazoxide causes fluid retention that canprecipitate cardiac failure. Rarely, it causes ablood dyscrasia. The most distressing eVectfrom the parental viewpoint is the stimulationof generalised hypertrichosis. Nifedipine ap-pears to be remarkably safe in the doses used,but blood pressure monitoring is mandatory.
Second line agents are those that need to begiven by infusion or injection. Ideally, theyshould be given when the orally administereddrugs have been shown not to be eVective, par-ticularly if the child remains glucose infusiondependent. In practice, however, there may be
Table 4 Drugs used in the medical management of hyperinsulinism
Drug DiazoxideIndication Hyperinsulinaemic hypoglycaemiaMechanism of action Opens KATP channels, increases adrenaline (epinephrine) secretion, increases gluconeogenesisDose 5–20 mg/kg/day orally 8 hourlySide eVects Fluid retention (chlorothiazide + diazoxide used together), hypertrichosis, hyperuricaemia, facial changes,
hypotension, rarely leucopenia, thrombocytopenia
Drug Chlorothiazide (act synergistically with diazoxide by activating non-KATP channels)Dose 7–10 mg/kg/day in 2 divided dosesSide eVects Hyponatraemia, hypokalaemia
Drug Nifedipine (slow release preparation)Indication Hyperinsulinaemic hypoglycaemiaMechanism of action Calcium channel antagonist, inhibits insulin releaseDose 0.25–2.5mg/kg/day orally 8 hourlyResponse rate Limited experienceSide eVects Hypotension
Drug GlucagonMechanism of action Increased glycogenolysis/gluconeogenesisDose 1–10 µg/kg/hour intravenous infusion, 1 mg bolus dose intramuscular or intravenousSide eVects Nausea, vomiting, increases growth hormone concentrations, increases myocardial contractility, decreases
gastric acid/pancreatic enzymes
Drug OctreotideIndication Hyperinsulinaemic hypoglycaemiaMechanism of action Activates G protein coupled rectifier K channel, hence inhibiting insulin releaseDose 5–20 µg/kg/day intravenous or subcutaneous infusionSide eVects Suppression of growth hormone, TSH, ACTH. Steatorrhea, cholelithiasis, abdominal distension,
decreases growth rate
ACTH, adrenocorticotrophin; KATP, ATP sensitive potassium channel; TSH, thyroid stimulating hormone.
Management of hyperinsulinism in infancy F103

compelling reasons to begin them because ofthe enormity of the management problems incontrolling the hypoglycaemia.
The two most important substances are glu-cagon and somatostatin. There is a consensusthat both hormones are of value, but contro-versy over the doses used and the need to givethem singly or in combination. Both hormoneswhen given in high doses cause tachyphylaxis.
Glucagon has a powerful eVect on mobilisingglucose from hepatic glycogen.1 Its administra-tion by means of a continuous intravenousinfusion at rates of between 5 and 10 µg/kg/hour can help reduce the infusion rate ofglucose needed to maintain normoglycaemia.Some authorities recommend its early use togain rapid stabilisation of blood glucoseconcentrations; others argue that it is a power-ful insulin secretagogue, and its administrationin theory will maintain a drive to insulin hyper-secretion. For this reason, they propose usingglucagon only with the concurrent administra-tion of somatostatin.
The somatostatin analogue, octreotide, acti-vates potassium channels in the â cell mem-brane, and may also aVect the intracellulartranslocation of calcium.7 The doses proposedfor initiating combination treatment are 1.0µg/kg/hour of glucagon together with 10 µg/kg/day of octreotide.6 7 It should be noted thatthese doses are less than those advocated forsingle hormone infusion. Further systematicresearch is needed to define the eVects and roleof these powerful hormones.
The use of steroids remains a controversialissue. In general, high doses of steroids havebeen contraindicated. However, the recentdemonstration of cortisol unresponsivenessduring hyperinsulinaemic hypoglycaemia30
raises important questions for further research,not only on the mechanism of this observation,but also on the impact of introducing cortisolsubstitution. Somatostatin administrationleads to the inhibition of a number of otherhormone systems,45 and in some centres suchchildren are given hydrocortisone replacement,particularly during surgical procedures. Thisapproach also needs further investigation andvalidation.
FURTHER MANAGEMENT IN MEDICALLY
RESPONSIVE CHILDREN
The overall aim of medical treatment is to pre-vent hypoglycaemia while allowing a normalfeeding pattern to be established. Children whorespond rapidly to diazoxide treatment (asdemonstrated by an ability to withdraw glucosesupport) should be maintained on their initialdose with repeated systematic attempts towithdraw the diazoxide during the next fewmonths. Some children, particularly those withhyperammonaemic hyperinsulinism, might re-quire treatment for many years. Others,without hyperammonaemia, might also remaindiazoxide dependent until adulthood. At-tempts to withdraw diazoxide should only bemade in hospital.
In severe early onset hyperinsulinism, thereis a tendency for gradual improvement in theclinical severity of the defect with the passage
of time. This observation led Glaser et al toadopt an aggressive medical treatment strategycomprising long term subcutaneous glucagonand octreotide infusions and continuous over-night gastrostomy feeds.46 The approach hasbeen used with some success in children withthe Ashkenazi Jewish and Palestinian Arabphenotype of hyperinsulinism.47 The part thatthis approach should play in treating otherpopulations is still to be defined, and the shortand long term eVects of this powerful hormo-nal treatment need further evaluation. Manyfamilies find the intensity of the regimenimpossible to cope with in their daily lives.
FAILURE OF MEDICAL TREATMENT: SURGICAL
TREATMENT
Children who fail to respond to medical treat-ment should be managed in a centre wherethere is the closest of collaboration anddialogue between the medical and surgicalteams. Some experts recommend that aggres-sive medical treatment should be continued forat least four to six weeks in early onset hyperin-sulinism. Hypoglycaemia must be preventedduring this period, through a combination ofhigh carbohydrate administration rates anddrugs, as described above. The rationale is thatan improvement in the severity of the hyperin-sulinism may be seen during this period; how-ever, there are no published studies that evalu-ate the change in the need for surgery in infantsin whom medical treatment is initially unsuc-cessful at two to three weeks compared withfive to six weeks. The criteria for successfulmedical management are a feeding regimenacceptable to the family, with normal bloodglucose concentrations during reasonable peri-ods of fasting. If an acceptable regimen forhome oral feeding cannot be established with-out hypoglycaemia, a surgical approach tomanagement should be considered.
Because of the risk of major managementrelated complications, including central linesepsis, venous thrombosis, hepatic dysfunction,bleeding diatheses, impaired nutrition, andhypoglycaemic encephalopathy, the consensusview expressed by the workshop was that chil-dren should be subjected to surgery soonerrather than later.
The absolute indications for surgery are: (1)demonstration of focal hyperplasia in childrenunresponsive to medical treatment; and (2)glucose infusion dependency despite maxi-mum doses of diazoxide, chlorothiazide, nifed-ipine, glucagon, and somatostatin.
Infants with diVuse disease will normallyrequire a 95% pancreatectomy to control thehyperinsulinism. After this procedure there is ahigh incidence of pancreatic endocrine andexocrine insuYciency. In infants with focalforms of the disease, an opportunity exists for apartial pancreatectomy, preserving the normalpancreatic tissue. The focal areas of abnormalpancreas are usually not macroscopically appar-ent at surgery and their resection requiresskilled microdissection aided by immediate his-tological examination of the resected tissue.41
Confirmation of the histological diagnosis is byfrozen section, the distinction between focal
F104 Aynsley-Green, Hussain, Hall, Saudubray, Nihoul-Fékété, De Lonlay-Debeney, et al

and diVuse forms being made on the basis ofnuclear size and nuclear crowding.48
The routine performance of 95% pancreate-ctomy in all cases of persistent hyperinsulinae-mic hypoglycaemia of infancy coming tosurgery is no longer justifiable. The new stand-ards in treatment will require the centralisationof management to a small number of desig-nated centres with the necessary resources andexpertise.
POSTOPERATIVE MANAGEMENT
Early postoperative glucose intoleranceA reduction in glucose requirement is normallyevident during surgery. Infants will frequentlybecome hyperglycaemic during the immediatepostoperative period. To avoid massive swingsin blood glucose concentrations, these infantsshould be changed to 5% dextrose infusions,with insulin being given with a sliding scaleregimen. These infants are usually exquisitelysensitive to exogenous insulin. The insulinrequirement will normally diminish early in thepostoperative course, and the optimum out-come is to be able to discontinue all treatment.The ability to do so is greatest in children withfocal disease.41
Postoperative diabetesThe risk of developing diabetes mellitus lateron in childhood after a 95% pancreactectomyis high.49 50 Interestingly, these children exhibitsome unusual characteristics in comparisonwith children who have type 1 juvenile diabetesmellitus.51 For example, they have strikingresistance to hyperketonaemia and diabeticketoacidosis. Management of the secondarydiabetes involves using either an intermediateacting insulin or using a combination of shortand long acting insulins in conjunction withdietary advice. Furthur studies are needed tofind out whether these children have a similarchance of developing the serious complicationsof diabetes to children with “ordinary”diabetes and whether the magnitude of thesecomplications is the same or diVerent.
Postoperative pancreatic exocrine insuYciencyStudies of exocrine pancreatic function ininfants who have undergone 95% pancreatec-tomy suggest that exocrine function is compro-mised from the early postoperative period,although malnutrition suYcient to causegrowth failure may not be apparent for avariable period (Lindley K, unpublished,1999). Evidence of impaired pancreatic exo-crine function is sought by measurement ofstool elastase. Infants with decreased concen-trations should have pancreatic enzyme re-placement.
Feeding managementForegut dysmotility and gastro-oesophagealreflux is common in hyperinsulinism.52 Thepathophysiology is yet to be determined.Infants may show poor sucking and swallow-ing, retching, vomiting, and intestinal dilata-tion; feeding problems are compounded by theuse of nasogastric or gastrostomy feeds, whichdelays the establishment of normal feeding
patterns, taste, and “orality”. In severe cases,the deprivation of oral stimulation may requiremonths of rehabilitation with skilled speechand language therapists. Infants in whomsevere gastro-oesophageal reflux is demon-strated preoperatively should undergo anantireflux surgical procedure at the same timeas having pancreatic surgery (Nihoul-Fekete C,personal communication, 1999). This ap-proach and the use of gut motility agonistsincluding erythromycin requires formal evalu-ation. The intestinal dysmotility problems areespecially diYcult to manage in children fromthe Arabian peninsular, many of whom requiremonths of hospital management.
Neurological managementIt is unfortunate that so many infants withhyperinsulinism develop evidence of neurologi-cal damage, ranging from the subtle to thesevere.2 3 53 54 Careful repeated documentationof neurological status is mandatory; this mightrequire expert paediatric neurological investi-gation, including magnetic resonance imagingand management of complex disabilities.
Other aspectsIn children subjected to pancreatic surgery,postoperative imaging of the spleen is neededto document splenic integrity and the absenceof the need for long term penicillin prophylaxisagainst pneumococcal infections.
Further hypoglycaemiaA small number of infants remain severelyhypoglycaemic despite 95% pancreatectomy.Possible reasons include the presence of focallesions in the head of the pancreas or diVusedisease that is medically unresponsive. Themanagement of this circumstance demandsfurther sequential introduction of medicaltreatment, and consideration of total pancre-atic resection. After an initial period of goodcontrol, some infants develop hypoglycaemiaafter weeks or months. This is usually a resultof regeneration of the pancreatic remnant forreasons that are not fully understood.
Psychosocial dimensionsThe management of hyperinsulinism imposesintolerable burdens on the families of the chil-dren as they witness weeks of diYcult treat-ment and the infliction of pain on their infants.It is hardly surprising that many fail to copeand disintegrate under the strain. Managementdemands skilled psychological and social sup-port.
As the children become older, they may rebelagainst the need for insulin treatment andbecome highly manipulative in the face of sub-stantial if not dominating family preoccupa-tions with the risk of hypoglycaemia.
Natural historyStudies of predominantly Ashkenazi Jewishchildren with hyperinsulinism suggest that thenatural history of the disease is one of progres-sive glucose intolerance and clinical diabetes.By undertaking both glucose tolerance testsand hypoglycaemic clamp studies it has been
Management of hyperinsulinism in infancy F105

shown that individuals with frankly diabeticglucose tolerance tests have evidence ofpersistent inappropriate insulin secretion in theface of hypoglycaemia.44 This suggests thatsuch individuals are diabetic by virtue of havinga reduced mass of functionally abnormal âcells. The diabetic phenotype might be theresult of enhanced apoptosis in hyperinsulinae-mic â cells.
The futureThe important distinction between focal anddiVuse disease has been highlighted through-out this commentary. Current methods ofdiagnostic evaluation are cumbersome and dif-ficult. The search for other techniques that areless invasive must be of high priority. The roleof genetic analysis and improvements in identi-fying the genome in the diagnostic investiga-tion are also areas for further reasearch, notleast because so many children at present havenot been shown to possess a known mutation.
New pharmacological agents with which toinhibit insulin secretion are urgently needed.Long acting octreotide and insulin specificanalogues are available from pharmaceuticalcompanies, but are either not licensed forhuman use, or only for adults.
Finally, the proof of principle that â cellsfrom some resected pancreata continue to rep-licate in tissue culture, coupled with the abilityto aVect gene therapy in vitro, oVers a tantalis-ing future prospect of reimplanting the pa-tient’s own genetically modified cells that haveregained normal glucose dependency of insulinsecretion.55
The European network for research into hyperinsulinism issupported by a concerted action grant (Biomed 2 programme:grant number BMH4-CT98–3284) from the European Com-mission. Some of this work was undertaken by Great OrmondStreet Hospital for Children NHS Trust who received aproportion of its funding from the NHS Executive; the viewsexpressed in this publication are those of the authors and are notnecessarily those of the NHS Executive.
1 Soltesz G, Aynsley-Green A. Hyperinsulinism in infancyand childhood. Ergeb Inn Med Kinderheilkd 1984;51:115–202.
2 Aynsley-Green A, Soltesz G, Jenkins PA. Hyperinsulinaemichypoglycaemia in infancy and childhood-a practicalapproach to diagnosis and treatment based on experienceof 18 cases. Acta Paediatr Hung 1984;25:319–32.
3 Meissner T, Brune W, Mayatepak E. Persistent hyperinsuli-naemic hypoglycaemic of infancy: therapy, clinical out-come and mutational analysis. Eur J Pediatr1997;156:754–7.
4 Milner RDG. Nesidoblastosis unravelled. Arch Dis Child1996;74:369–72.
5 Kane C, Shepherd RM, Squires PE, et al. Loss of functionalKatp channels in B-cells causes persistent hyperinsulinae-mic hypoglycaemia on infancy. Nat Med 1996;2:1344–7.
6 Aynsley-Green A, Dunne MJ, James RFL, Lindley KJ. Ionsand genes in persistent hyperinsulinaemic hypoglycaemiain infancy: a commentary on the implications for tailoringtreatment to disease pathogenesis. J Pediatr EndocrinolMetab 1998;11:121–9.
7 Kane C, Lindley KJ, Johnstone PRV, et al. Therapy for per-sistent hyperinsulinaemic hypoglycaemia of infancy. J ClinInvest 1997;100:1888–93.
8 Dunne MJ, Peterson OH. Potassium selective ion channelsin insulin secreting cells: physiology, pharmacology andtheir role in stimulus secretion coupling. Biochem BiophysActa 1991;1071:67–82.
9 Bruninig GJ. Recent advances in hyperinsulinism and thepathogenesis of diabetes mellitus. Curr Opin Pediatr1990;2:758–65.
10 Otonkoski T, Ammala C, Huopio H, et al. A point mutationinactivating the sulphonylurea receptor causes the severeform of persistent hyperinsulinaemic hypoglycaemia ofinfancy in Finland. Diabetes 1999;48:408–15.
11 Mathew PM, Young JM, Abu YK, et al. Persistent neonatalhyperinsulinism. Clin Pediatr (Phila) 1988;27:148–51.
12 Aynsley-Green A. Hyperinsulinism in infancy and chidhoodfrom genotype to clinical management. In: S O’Rahilly, DDunger, eds. Genetic insights into paediatric endocrinologyand metabolism. Bristol: Bioscientifica [In press.]
13 Collins JE, Leonard JVL. Hyperinsulinism in asphyxiatedand small for dates infants with hypoglycaemia. Lancet,1984;ii:311–13.
14 Brown G, Brown R, Hey E. Foetal hyperinsulinism in rhesusisoimmunisation. Am J Obstet Gynecol 1978;131:682–6.
15 Lucas A, Adrian TE, Bloom SR, Aynsley-Green A.Iatrogenic hyperinsulinism at birth. Lancet 80;i:144–5.
16 MoncrieV MM, Lacey KA, Malleson PN. Management ofprolonged hypoglycaemia in Beckwith syndrome. PostgradMed J 1977;53:159–61.
17 Lindley KJ, Dunne MJ, Kane C, et al. Ionic control of theB-cell function in nesidioblastosis, a possible role forcalcium channel blockade. Arch Dis Child 1996;74:373–8.
18 Aynsley-Green A, Pollak JM, Keeling J, Gough MH, BaumJD. Averted neonatal death due to pancreatic nesidioblas-tosis [letter]. Lancet 1978;i:550–1.
19 Koh THH, Eyre JA, Aynsley-Green A. Neonatalhypoglycaemia—the controversy regarding definition.Arch Dis Child 1988;63:1386–9.
20 Koh THHG, Eyre JA, Aynsley-Green A. Neural dysfunc-tion during hypoglycaemia. Arch Dis Child 1988;63:1353–8.
21 Cornblath M, Schwartz R, Aynsley-Green A, Lloyd JK.Hypoglycaemia in infancy: the need for a rationaldefinition. Pediatrics 1990;85:834–7.
22 Shepherd RM, Cosgrove KE, O’Brien RE, et al. Hyperin-sulinism in infancy: towards an understanding of unregu-lated insulin release. Arch Dis Child Fetal Neonatal Ed2000;82:F87–97.
23 Hawdon JM, Aynsley-Green A, Alberti KGMM, Ward PlattMP. The role of pancreatic insulin secretion in neonatalglucoregulation. 1. Healthy term and preterm infants. ArchDis Child 1993;68:274–9.
24 Hawdon JM, Aynsley-Green A, Ward Platt MP. The role ofpancreatic insulin secretion in neonatal glucoregulation. 2.Infants with disordered glucose homeostasis. Arch DisChild 1993;68:280–5.
25 Aynsley-Green A, Jenkins PA, Tronier B, Heding LG.Plasma proinsulin and C-peptide concentrations inchildren with hyperinsulinaemic hypoglycaemia. Acta Pae-diatr Scand 1984;73:359–63.
26 Finegold DN, Stanley CA, Baker L. Glycaemic response toglucagon during fasting hypoglycaemia: an aid in the diag-nosis of hyperinsulinism. J Pediatr 1980;96:257.
27 Levitt-Katz LE, Satin-Smith M, Collett-Solberg P, et al.Insulin like growth factor binding protein-1 levels in thediagnosis of hypoglycaemia caused by hyperinsulinism. JPediatr 1997;131:193–9.
28 Stanley CA, Lieu YK, Hsu BY, et al. Hyperinsulinism andhyperammonaemia in infants with regulatory mutations ofthe glutamate dehydrogenase gene. N Engl J Med1998;338:1352–7.
29 Sener A, Malaisse-Lagae F, Malassie WJ. Stimulation ofpancreatic islet metabolism and insulin release bynon-metabolizable amino acid. Proc Natl Acad Sci USA1981;78:5460–4.
30 Morris AAM, Thekekara A, Wilks Z, Clayton P, LeonardJVL, Aynsley-Green A. Evaluation of fasts for investigatinghypoglycaemia or suspected metabolic disease. Arch DisChild 1996;75:115–19.
31 Anguilar-Bryan L, Bryan J. The molecular biology of ATPsensitive K+ channels. Endocr Rev 1999;20:101–35.
32 Thornton PS, Martha S, Smith S, et al. Familial hyperin-sulinism with apparent autosomal dominant inheritance:clinical and genetic diVerences from the autosomal reces-sive variant. J Pediatr 1998;132:9–14.
33 Glaser B, Thornton PS, Herold K, Stanley CA. Clinical andmolecular heterogeneity of familial hyperinsulinism. JPediatr 1998;133:801.
34 Delonlay P, Fournet JC, Rashier J, et al. Somatic deletion ofthe imprinted 11p15.1 region in sporadic persistenthyperinsulinaemic hypoglycaemia of infancy is specific offocal adenomatous hyperplasia and endorses partialpancreatectomy. J Clin Invest 1997;100:802–7.
35 Ryan F, Devaney D, Joyce C, et al. Hyperinsulinism: themolecular aetiology of focal disease. Arch Dis Child1998;79:445–7.
36 Glaser B, Kesavan P, Heyman M, et al. Familial hyperin-sulinism caused by activating glucokinase mutation. NEngl J Med 1998;338:226–30.
37 Aynsley-Green A, Wiendling AM, Soltesz G, Jenkins PA.Transient lactic acidaemia and hyperalaninaemia associ-ated with neonatal hyperinsulinaemic hypoglycaemia:eVect of dichloroacetate. Eur J Pediatr 1983;141:114–17.
38 Cosgrove KE, Shepherd RM, Hashmi MN, et al. The role ofcalcium ions in determining insulin hypersecretion inpatients with PHHI [abstract]. Horm Res 1999;51(suppl2):29.
39 Glaser B, Thornton P, Otonkoski T, Junien C. Genetics ofneonatal hyperinsulinism. Arch Dis Child Fetal Neonatal Ed2000;82:F79–86.
40 Glaser B, Furth J, Stanley CA, et al. Intragenic single nucle-otide polymorphism haplotype analysis of SUR 1 muta-tions in familial hyperinsulinism. Hum Mutat 1999;14:23–9.
41 DeLonlay-Debeney P, Poggi-Trovert F, Fournet JC, et al.Clinical features of 52 neonates with hyperinsulinism. NEngl J Med 1999;340:1169–75.
42 Abernethy LJ, Davidson DC, Lamont GL, Shepherd RM,Dunne MJ. Intra-arterial calcium stimulation test in the
F106 Aynsley-Green, Hussain, Hall, Saudubray, Nihoul-Fékété, De Lonlay-Debeney, et al

investigation of hyperinsulinaemic hypoglycaemia. ArchDis Child 1998;78:359–63.
43 Nihoul-Fekete C, Delonlay-Debenay P, Brunelle F, RahierJ, Saudubray JM. Partial pancreatectomy as a curativetreatment in neonatal persistent hyperinsulinaemic hy-poglycaemia of infancy. In: Herausgegeben von, WolfgangRabl, K Mohnike, eds. Nesidoblastose, von der molekularen,Pathophysiologie zur Therapie. Heidelberg: Johann Ambri-ous Barth 1998:64–9.
44 Touati G, Poggi-Travaer F, Ogier de Baulney H, et al. Longterm treatment of persistent hyperinsulinaemic hypogly-caemia of infancy with diazoxide: a retrospective review of77 cases and analysis of eYcacy predicting criteria. Eur JPediatr 1998;157:628–33.
45 Aynsley-Green A, Barnes ND, Adrian TE, et al. EVect ofsomatostatin infusion on intermediary metabolism andentero-insular hormone release in infants with hyperinsuli-naemic hypoglycaemia. Acta Paediatr Scand 1981;70:889–95.
46 Glaser B, Hirsch HJ, Landau H. Persistent hyperinsulinae-mic hypoglycaemia of infancy: long term treatmentwithout pancreatectomy. J Pediatr 1993;123:644–50.
47 Rahier J, Falt K, Muntefering H, Becker K, Gepts W, Falk-mer S. The basic structural lesion in persistent neonatalhypoglycaemia with hyperinsulinism: deficiency of pancre-atic D cells or hyperactivity of B-cells? Diabetelogia1984;26:282–9.
48 Landau H, Glaser B. Conservative treatment and long termfollow-up of persistent hyperinsulinism of infancy (HI).Second international conference on ATP sensitive potas-sium channels and disease, St Charles, USA, 1998.Houston: Giovanni Lorenzini Medical Foundation:33–8.
49 Leibowitz G, Glaser B, Higazi AA, Salamah M, Cesari E,Landau H. Hyperinsulinaemic hypoglycaemia of infancy(nesidioblastosis) in clinical remission: high incidence ofdiabetes mellitus and persistent B-cell dysfunction at longterm follow up. J Clin Endocrinol Metab 1995;80:386–92.
50 Labrune P, Lechevallie S, Rault M, Odievre M. Diabetesmellitus 14 years after subtotal pancreatectomy for neona-tal hyperinsulinism. J Pediatr Surg 1990;25:1246–7.
51 Greene SA, Aynsley-Green A, Soltesz G, Baum JD.Management of secondary diabetes mellitus after pancrea-tectomy in infancy. Arch Dis Child 1984;59:356–9.
52 Lindley KJ, Knafelz D, St Louis D, Dunne MJ, Aynsley-Green A, Milla PJ. Surface electrogastrographic evidenceof forgut dysmotility in persistent hyperinsulinaemichypoglycaemia of infancy (PHHI). J Physiol (Lond)1997;499:108p.
53 Aynsley-Green A, Dunne MJ, James RF, Lindley KJ,Docherty K. Persistent hyperinsulinaemic hypoglycaemiaof infancy—an enigma only now being unravelled. In:Herausgegeben von, Wolfgang Rabl, Klaus Mohnike, eds.Nesidioblastose, von der molekularen, Pathophysiologie zurtherapie. Heidelberg: Johann Ambrosius Barth, 1998:57–65.
54 Gross-Tsur V, Shalev RS, Wertman-Elad R, Landau H,Amir N. Neurobehavioural profile of children with persist-ent hyperinsulinaemic hypoglycaemia of infancy. Dev Neu-ropsychol 1994;10:153–63.
55 Macfarlane WM, Chapman JC, Shepherd RM, et al.Engineering a glucose-responsive human insulin-secretingcell line from islets of Langerhans from a patient with per-sistent hyperinsulinaemic hypoglycaemia of infancy(PHHI). J Biol Chem 1999;274:34059–66.
Management of hyperinsulinism in infancy F107