Diagnosis and Management of Pleural Effusions: A Practical Approach
10
Diagnosis and Management of Pleural Effusions: A Practical Approach ENRIQUE DIAZ-GUZMAN, AND RAED A. DWEIK Department of Pulmonary, Allergy and Critical Care Medicine, Cleveland Clinic, Cleveland, OH, USA ORIGINAL ARTICLE Pleural effusion is defined as an abnormal amount of pleural fluid accumulation in the pleural space and is the result of an imbalance between excessive pleural fluid formation and pleural fluid absorption. Although the list of causes of pleural effusions is extensive, the great majority of the cases are caused by pneumonia, congestive heart failure, and malig- nancy. In this article, we provide an overview of the most common causes of pleural effusions likely to be encountered by the general practitioner, and a practical approach to the diagnosis and management of this common condition. Pleural effusion is defined as an abnormal amount of pleural fluid that accumulates in the pleural space. The pleural space is located between the visceral pleura covering the lung and the parietal pleura covering the chest wall. In healthy individuals, the pleural space con- tains approximately 5–10 ml of pleural fluid (0.1 mg/kg body weight) (1). Pleural effusion is a common problem in both the inpatient and the outpatient setting; the incidence of a pleural effusion in the general population is difficult to estimate given that this condition may be associated with an extensive list of pulmonary and nonpulmonary diseases, although reports have suggested an incidence of 0.3% in the general population with as many as 800,000 cases of pleural effusions in the USA annually (2). Pleural effusions result from an imbalance between excessive pleural fluid formation (i.e., pleural inflamma- tion) and pleural fluid absorption (i.e., obstruction of the lymphatic system) (3). Although the list of causes of pleural effusions is extensive, the great majority of the cases are caused by few disorders (4). Prompt recogni- tion of a pleural effusion, as well as an expedited diagnostic approach, is crucial to avoid long-term complications associated with an untreated pleural effusion such as empyema, loculation, and a trapped lung. In this article, we will provide an overview of the most common causes of pleural effusions likely to be encountered by the general practitioner. We will also CORRESPONDENCE Raed A. Dweik, MD, Department of Pulmonary, Allergy and Critical Care Medicine, Cleveland Clinic, Cleveland, OH, USA. E-mail: [email protected] Submitted for publication: August 15, 2007. Accepted: August 17, 2007. Comprehensive Therapy, vol. 33, no. 4, Winter 2007 ! The American Society of Contemporary Medicine and Surgery All rights of any nature whatsoever reserved. 0098-8243/07/33:237–246/$30.00 (Online) 1559–1190 COMP THER. 2007;33(4) ................................................................... 237
Transcript of Diagnosis and Management of Pleural Effusions: A Practical Approach

Diagnosis and Management of PleuralEffusions: A Practical Approach
ENRIQUE DIAZ-GUZMAN, AND RAED A. DWEIKDepartment of Pulmonary, Allergy and CriticalCare Medicine, Cleveland Clinic,Cleveland, OH, USA
O R I G I N A L A R T I C L E
Pleural effusion is defined as an abnormal amount ofpleural fluid accumulation in the pleural space andis the result of an imbalance between excessivepleural fluid formation and pleural fluid absorption.Although the list of causes of pleural effusions isextensive, the great majority of the cases are causedby pneumonia, congestive heart failure, and malig-nancy. In this article, we provide an overview of themost common causes of pleural effusions likely to beencountered by the general practitioner, and apractical approach to the diagnosis and managementof this common condition.
Pleural effusion is defined as an abnormal amount ofpleural fluid that accumulates in the pleural space.The pleural space is located between the visceral pleuracovering the lung and the parietal pleura covering thechest wall. In healthy individuals, the pleural space con-tains approximately 5–10 ml of pleural fluid (0.1 mg/kgbody weight) (1). Pleural effusion is a common problemin both the inpatient and the outpatient setting; theincidence of a pleural effusion in the general populationis difficult to estimate given that this condition may beassociated with an extensive list of pulmonary andnonpulmonary diseases, although reports have suggestedan incidence of 0.3% in the general population with asmany as 800,000 cases of pleural effusions in the USAannually (2).Pleural effusions result from an imbalance between
excessive pleural fluid formation (i.e., pleural inflamma-tion) and pleural fluid absorption (i.e., obstruction of thelymphatic system) (3). Although the list of causes ofpleural effusions is extensive, the great majority of thecases are caused by few disorders (4). Prompt recogni-tion of a pleural effusion, as well as an expediteddiagnostic approach, is crucial to avoid long-termcomplications associated with an untreated pleuraleffusion such as empyema, loculation, and a trappedlung. In this article, we will provide an overview of themost common causes of pleural effusions likely to beencountered by the general practitioner. We will also
CORRESPONDENCERaed A. Dweik, MD, Department of Pulmonary, Allergy and Critical CareMedicine, Cleveland Clinic, Cleveland, OH, USA.E-mail: [email protected]
Submitted for publication: August 15, 2007. Accepted: August 17, 2007.
Comprehensive Therapy, vol. 33, no. 4, Winter 2007! The American Society of Contemporary Medicine and SurgeryAll rights of any nature whatsoever reserved.0098-8243/07/33:237–246/$30.00 (Online) 1559–1190
COMP THER. 2007;33(4) ................................................................... 237

outline a practical approach to the diagnosis and man-agement of this common condition.
ETIOLOGY AND CLINICAL FINDINGSThe first step in the evaluation of a patient with a pleuraleffusion is to perform a thorough history and a fullphysical exam. The symptoms may or not be related topulmonary conditions, and in many cases are dictated bythe underlying process causing the effusion. Althoughdisease virtually in any organ system can be the cause ofa pleural effusion, the physician must remember thatmost cases are associated with common conditions suchas congestive heart failure, pneumonia, cancer, andpulmonary embolism (5). A list of different causes ofpleural effusions according to its frequency can be seenin Table 1.
SymptomsSymptoms associated with pleural effusions are neithersensitive nor specific for its diagnosis. Depending on itssize and the underlying lung function, pleural effusionsmay cause variable degrees of shortness of breath.Dyspnea is a consequence of different effects includinga restrictive lung defect and a reduction in the lung
capacity (6). Moreover, by inducing areas of atelectasis,pleural effusions may also be associated with ventilation-perfusion mismatches that cause hypoxemia. Largepleural effusions may also induce diastolic dysfunctionand a concomitant decrease in the cardiac output (7).Other common symptoms associated with pleural effu-sions include pleuritic chest pain, fever and cough.Constitutional symptoms such as weight loss, nightsweats, anorexia and malaise may occur in associationwith empyema, malignancy or tuberculous pleurisy (8).
Physical ExaminationPhysical exam findings associated with pleural effusionsinclude asymmetric chest expansion, absence of tactilefremitus, dullness to percussion, decreased breathsounds, egophonism, and a pleural rub (9). The physicalexam may reveal some clues to the etiology of a pleuraleffusion. Important clues to look for include the presenceof lower extremity edema and jugular venous distensionsuggestive of congestive heart failure, the presence ofascites suggestive of hepatic hydrothorax, lymphadenop-athy and organomegaly suggestive of neoplastic disease,arthropathy and cutaneous findings suggestive of rheu-matoid arthritis or other autoimmune process, etc. An
TABLE 1Causes of pleural effusions
Frequency Transudates Exudates
Common Congestive heart failure MalignancyHepatic hydrothorax PneumoniaNephrotic syndrome Pulmonary embolism
PancreatitisTuberculosisCollagen vascular diseasePost-cardiac injury syndrome
Less common Urinothorax ChylothoraxPeritoneal dialysis Esophageal perforationAtelectasis Asbestos related diseaseMyxedema Drug-induced reactionsPulmonary embolism Uremia
SarcoidosisRare Amyloidosis Parasitic infections
Vascular erosion by central line Radiation pleuritisTransudative chylothorax Trapped LungFontan procedure Yellow nail syndrome
COMP THER. 2007;33(4) ................................................................... 238

uncommon but almost pathognomonic finding is thepresence of yellow nails, the classical finding present inpatients with yellow nail syndrome.
DIAGNOSTIC APPROACHExcept in cases of large or massive pleural effusions, theinitial approach must involve the use of imaging toconfirm and evaluate the size and characteristics of the
pleural space. The amount of pleural fluid can estimatedbased on standard frontal and lateral radiographs.Although not commonly seen, studies have suggestedthat as little as 75 ml can be detected in the posteriorcostophrenic sulcus, whereas a minimum of 175 ml isnecessary to obscure the lateral costophrenic sulcus (10).In general practice, however, at least 500 ml of fluid arepresent when obscuring the diaphragm and up to
Approach to Pleural Effusion
History Physical Exam CXR
CHF, DVT/PE, Cancer, Pneumonia,
Medications
Look for dull percussion,
Absent breath sounds Rub
Small effusion, supine,Suspect complicated
effusion
No evidence of CHFModerate to large
Effusion.
Ultrasonography Thoracentesis Computed tomography
Initial Tests: Light’s Criteria
Exudate Transudate
Cytology, Microbiology
CHF, Cirrhosis Nephrotic
Parapneumonic Non parapneumonic
pH < 7.2 Malignancy
PE, Post Cardiac Surgery, Collagen vascular,
Drugs, Lipid effusion, Uremic, Asbestos
Follow Cultures, AFB, Antibiotics
Chest Tube, Surgery
Diuresis, follow up
Fig. 1. Algorithm for evaluating pleural effusions
COMP THER. 2007;33(4) ................................................................... 239

1,000 ml are present if effusion is close to the fourthanterior rib (11).When evaluating a patient with a standard chest
radiograph, the physician must remember two importantconsiderations:
(a) Patients in the supine position may have moderate tolarge effusions without changes in the diaphragm orpleural edges. In such cases, obscuring of thevascular markings and presence of haziness or a“pleural veil” over the normal aerated lung highlysuggests the presence of an effusion.
(b) Loculated pleural effusions may be confused withlung masses or areas of atelectasis. The addition of alateral decubitus view helps to differentiate areas offree fluid from loculated fluid.
What is the Role of Ultrasonography andComputed Tomography of the Chest?Ultrasonography is superior in clarifying the solid orfluid nature of a pleural opacity and it can detect smallereffusions compared to conventional radiology andphysical exam. Studies have found effusions as small as5 ml with careful ultrasonography of the costophrenicangle (12). Despite all its advantages, not all the patientsshould be evaluated with an ultrasound, particularly ifthis test would delay performance of further diagnostic ortherapeutic maneuvers. A particularly challenging situa-tion is in the intensive care unit (ICU), where supineposition and the use of mechanical ventilation complicatethe approach. In this setting, studies have suggested thatthe use of the ultrasound and computed tomographyfrequently adds useful information and helps to minimizecomplications (13). Computed tomography also detectsvery small pleural effusions, but more importantly,provides the physician with a thorough evaluation ofthe pleura (thickness, irregularity, masses, etc.) anddetects underlying parenchymal pathology frequentlymissed on the chest radiograph.
When to Perform a Thoracentesis?A diagnostic thoracentesis should always be performedin patients with pleural effusion of unknown origin.Experts in the field have suggested that unless there isevidence that the effusion is caused only by congestiveheart failure, the procedure is indicated in all patients ifthe thickness of the fluid is more than 10-mm height onan standard lateral decubitus chest radiograph (Fig. 1)(5). Chest radiograph is not indicated after a thoracent-esis but it should be done in high-risk patients or whencomplications arise during the procedure (14).
REEXPANSION PULMONARY EDEMA
The list of complications associated with a thoracentesisinclude vasovagal reaction, pneumothorax, pleural infec-tion, hemothorax, and reexpansion pulmonary edema.The later is described as the development of unilateralpulmonary edema after a period of lung collapsefollowed by rapid reinflation of the lung (15). Thisphenomenon is thought to be secondary to increasedpermeability of the pulmonary vasculature or secondaryto reperfusion injury (3). It is associated with therapeuticthoracentesis, generally when large amounts of pleuralfluid are withdrawn (16), although it can also be seenafter a pneumothorax. The inicidence of this complica-tion is probably very low (17), nevertheless, the clinicianmust consider limiting the amount of pleural fluidremoved to less than 1,500 ml unless pleural pressuremonitoring is performed during the procedure. Whensymptoms develop, the physician must have a high indexof suspicion since this complication can be associatedwith severe hypoxemia, hypotension and even death.
Biochemical AnalysisThe first step consists in establishing the transudative(due to hydrostatic forces, and with a low proteincontent) or exudative (due to increased permeability ofthe pleural surfaces and blood vessels, with a relativelyhigh protein content) nature of the fluid. If the fluid is atransudate, the differential diagnosis is narrowed, where-as an exudate almost requires additional testing. Specificcause of a pleural effusion can be definitively identifiedin a limited number of entities (Table 2).Since its original publication, Light’s criteria (18)
continue to be the most useful to separate exudates andtransudates. Perhaps the only limitation of this criteria isthe need of a concomitant blood draw for measurementof serum levels of LDH and protein. Other alternativemarkers have been proposed since then (Table 3),although several different reports have failed to showany significant advantage of using other markers (19). Byusing Light’s criteria, the physician can be confident incorrectly diagnosing almost all exudative effusions; aspecific problem using Light’s criteria occurs in patientswith congestive heart failure that are being treated withdiuretics, where the LDH levels can be significantlyelevated and give the false impression of an exudativeeffusion. In such cases, the physician must calculate thepleural fluid to serum protein gradient; if the gradient ismore than 3.1 g/dl the patient may be diagnosed with atransudative effusion (20). Another option, particularlyhelpful when serum levels of LDH and protein are notavailable, is to measure levels of cholesterol; a
COMP THER. 2007;33(4) ................................................................... 240
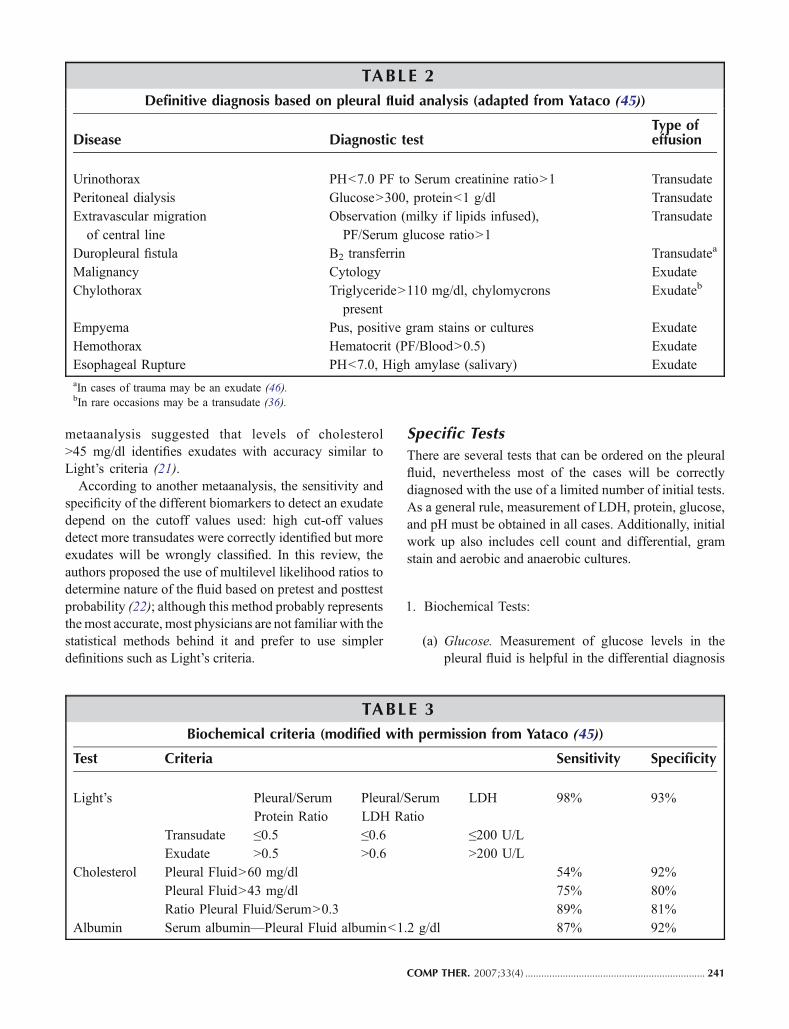
metaanalysis suggested that levels of cholesterol>45 mg/dl identifies exudates with accuracy similar toLight’s criteria (21).According to another metaanalysis, the sensitivity and
specificity of the different biomarkers to detect an exudatedepend on the cutoff values used: high cut-off valuesdetect more transudates were correctly identified but moreexudates will be wrongly classified. In this review, theauthors proposed the use of multilevel likelihood ratios todetermine nature of the fluid based on pretest and posttestprobability (22); although this method probably representsthemost accurate, most physicians are not familiar with thestatistical methods behind it and prefer to use simplerdefinitions such as Light’s criteria.
Specific TestsThere are several tests that can be ordered on the pleuralfluid, nevertheless most of the cases will be correctlydiagnosed with the use of a limited number of initial tests.As a general rule, measurement of LDH, protein, glucose,and pH must be obtained in all cases. Additionally, initialwork up also includes cell count and differential, gramstain and aerobic and anaerobic cultures.
1. Biochemical Tests:
(a) Glucose. Measurement of glucose levels in thepleural fluid is helpful in the differential diagnosis
TABLE 2Definitive diagnosis based on pleural fluid analysis (adapted from Yataco (45))
Disease Diagnostic testType ofeffusion
Urinothorax PH<7.0 PF to Serum creatinine ratio>1 TransudatePeritoneal dialysis Glucose>300, protein<1 g/dl TransudateExtravascular migrationof central line
Observation (milky if lipids infused),PF/Serum glucose ratio>1
Transudate
Duropleural fistula B2 transferrin Transudatea
Malignancy Cytology ExudateChylothorax Triglyceride>110 mg/dl, chylomycrons
presentExudateb
Empyema Pus, positive gram stains or cultures ExudateHemothorax Hematocrit (PF/Blood>0.5) ExudateEsophageal Rupture PH<7.0, High amylase (salivary) ExudateaIn cases of trauma may be an exudate (46).bIn rare occasions may be a transudate (36).
TABLE 3Biochemical criteria (modified with permission from Yataco (45))
Test Criteria Sensitivity Specificity
Light’s Pleural/SerumProtein Ratio
Pleural/SerumLDH Ratio
LDH 98% 93%
Transudate ≤0.5 ≤0.6 ≤200 U/LExudate >0.5 >0.6 >200 U/L
Cholesterol Pleural Fluid>60 mg/dl 54% 92%Pleural Fluid>43 mg/dl 75% 80%Ratio Pleural Fluid/Serum>0.3 89% 81%
Albumin Serum albumin—Pleural Fluid albumin<1.2 g/dl 87% 92%
COMP THER. 2007;33(4) ................................................................... 241

of exudative effusions. When the levels of glucoseare <60 mg/dl, the differential diagnosis is nar-rowed to a few conditions: parapneumonic, malig-nancy, rheumatoid arthritis, and tuberculosis. Otherless frequent causes include hemothorax, lupuspleuritis, paragonimiasis, and Churg-Strauss syn-drome (4).
(b) pH. Bicarbonate normally accumulates in thepleural space giving the pleural fluid a relativelyhigh pH∼7.6. Conditions that increase metabolicactivity (i.e., multiplying bacteria in parapneumo-nic effusions or cancer) decrease the glucose levelsin the fluid and decrease the pH (by increasing
production of lactic acid). Measurement of the pHis helpful in several ways. The presence of a lowpH helps to narrow the differential diagnosis;common conditions associated with low pHinclude parapneumonic effusions and malignancy(see Table 4). An important exception in para-pneumonic effusions is the infection with Proteus,organism that produces ammonia and typicallyelevates the pleural fluid pH. Assesment of pH isalso helpful to guide management of parapneumo-nic effusions; pH<7.0 warrants complete removalof the effusion by therapeutic thoracentesis or tubethoracostomy (23). Finally, pH has prognostic
TABLE 4Additional tests
Biochemical test Considerations Conditions associated
PH Systemic Acidosis may lower pH inpleural fluid.
Parapneumonic effusion, Malignancy,Rheumatoid Pleuritis, Tuberculosis,Hemothorax, Urinothorax, EsophagealPerforation.
Must be measured by a blood gasmachine.
LDH Isoenzyme LDH-1 elevated Bloody pleural effusionLDH>1000 U/L Complicated pleural effusion, Tuberculosis
Lipid Studies Centrifugation with milky supernatant Lipid effusionTriglycerides TG>110 mg/dl ChylothoraxChylomycrons Chylomycron screen+in Lipoprotein fluid
analysis.Chylothorax
Cholesterol Pleural fluid to serum cholesterol ratio>1 Cholesterol pleural effusion(Pseudochylothorax)
PF cholesterol>200 mg/dlCholesterol crystals
Cell count anddifferential
RBC>100,000 cells/mm3 HemothoraxWBC>10,000 cells/mm3 Complicated effusion, empyemaEosinophils>10% Blood or air in pleural space
Parasitic, Drug related, EosinophilicPneumonia, Churg-Strauss
Optional Tests (indicated only when clinical suspicion high)Amylase Higher than upper limit of normal
(serum amylase)Pancreatic disease, malignant tumor oresophageal rupture
Adenosinedeaminase(ADA)
>60 U/l Tuberculous pleuritisLower levels (<45 U/l) Empyema, Parapneumonic effusions,
Rheumatoid pleuritis.IFN-gamma >200 pg/ml Tuberculous pleuritisLE cells, ANA SLE effusion Not recommended
COMP THER. 2007;33(4) ................................................................... 242

implications in patients with malignant pleuraleffusions; patients that have a low pH do notrespond favorably to pleurodesis and have shorterlife expectancy (24). Unfortunately, measurementof pH is infrequently done following the righttechnique (25); the sample must be processed in anarterial blood gas machine, and the fluid must becollected into an anaerobic heparinized syringewith the same care as an arterial blood gas (contactof fluid with room air will let CO2 escape and thepH will be falsely high) (26).
(c) LDH and protein are used to differentiate transu-dative from exudative effusions by Light’s criteria.Measurement of LDH isoenzymes of little helpexcept in cases of transudates associated withbloody effusions (total LDH elevated suggestingan exudate, but if isoenzyme LDH-1 elevated thisindicates red blood cell source).
(d) Lipid studies particularly indicated when the pleuralfluid is milky or opalescent; an elevated WBC incases of empyema can also give the fluid a similarappearance. Centrifugation of the fluid will show amilky supernatant only in lipid effusions. The testsmost commonly ordered when suspect a lipid effusionare triglycerides, chylomycron screen, and cholesterol(see Table 4).
2. Cell Count and Differential: The fluid should becollected in a tube with anticoagulant (EDTA tube).RBC count is of little value except when >100,000/mm3 when physician should obtain a hematocrit to ruleout presence of hemothorax. Same applies to totalWBC count, with most transudates having a WBCcount <1,000/mm3, whereas parapneumonic effusionstypically have counts >10,000/mm3. Although theWBC differential can be helpful, rarely is specific of adiagnosis. In general, neutrophils predominate in recenteffusions whereas lymphocytes in chronic effusions.Eosinophils are generally considered markers for lesscommon diseases such as parasitic infections, Churg-Strauss syndrome, Eosinophilic Pneumonia, drug relat-ed effusion, etc., but in general, the most commoncauses of eosinophilia are air and blood in the pleuralspace (27).
3. Microbiologic Stains and Cultures: These must beobtained in all patients with a suspected exudativeeffusion. Fluid must be sent for aerobic, anaerobic,fungal, and when indicated, mycobacteria cultures.Some studies have suggested that inoculation of theculture media done at the bedside and not in thelaboratory since increases the yield (28). Obtainingcultures from chest tube drainages is not
recommended since this is associated with inaccurateresults (3).
4. Cytology: This test should be ordered always when thedifferential diagnosis includes malignancy. When pos-itive gives a definitive diagnosis of malignancy involv-ing the pleura. The sensitivity of the tests varies between40–87% depending on the expertise of the cytologist aswell as other factors such as tumor type and extent of thedisease (29).
Other Invasive Testing
(a) Bronchoscopy. The role for flexible bronchoscopy isvery limited and it should be considered only when anobstructing endobronchial lesion is suspected and thephysician cannot be certain of its presence based on aComputed Tomography (CT) scan.
(b) Pleural Biopsy. Consists in obtaining a small piece ofthe parietal pleura for microscopic and microbiologicexamination. Current recommendations for pleuralbiopsy include suspicion of tuberculous pleuritis andmalignancy. The procedure can be done blindly usinglocal anesthesia; it is recommended to obtain at leastfour samples with one dedicated for Mycobacteriumtuberculosis culture. Use of ultrasound or CT guid-ance increases the yield in cases of malignant pleuraleffusions. This procedure is currently used less oftendue to the development and wide availability ofmedical and surgical thoracoscopy.
(c) Thoracoscopy. Involves the passage of an endo-scope through the chest wall for direct visualizationand sampling of the pleura. There are two types ofthoracoscopy procedures: medical thoracoscopy andvideo-assisted thoracic surgery (VATS). Medicalthorascopy is performed under conscious sedationand local anesthesia in a procedure room, whereasVATS requires general anesthesia and is performedin an operating room. During both procedures, theentire surface of the lung can be examined andbiopsies from both the parietal and the visceralpleura can be obtained; VATS offers the addedadvantage of therapeutic intervention.
Specific Causes of Pleural EffusionsPARAPNEUMONIC EFFUSION
These are pleural effusions associated with pneumonia,lung abscess or bronchiectasis. Pneumonia is the mostcommon cause of exudative effusions in young patients.This type of effusion should be suspected in all cases ofpneumonia that do not respond to appropriate antibiotictherapy. When present, a diagnostic thoracentesis is
COMP THER. 2007;33(4) ................................................................... 243

indicated, and rapid analysis of the fluid is warranted toidentify all patients with empyema.Empyema is defined as thick purulent effusion (pus) in
the pleural space and is associated with a pH<7.2. Anapproach to the management of parapneumonic effusionsis shown in Table 5.
MALIGNANCY
The most common cause of exudative effusion in olderadults (>60 years old). Malignant pleural effusion can beprimary or secondary (metastatic). Metastatic cancer ofthe lung is the most common (43%), followed bycarcinoma of the breast (25%), lymphoma (8%), andovarian cancer (4%) (30). Between 5 to 10% of thepatients will have an unknown primary cancer. Malignantmesothelioma is the most common primary tumor of thepleura and is related to prior exposure to asbestos (notrelated to smoking tobacco) (31). The disease must besuspected in any patient with remote history of asbestosexposure and CT of chest with findings compatible withasbestos related lung disease: pleural plaques, calcifica-tion and parenchymal asbestosis. Diagnosis of mesothe-lioma almost always requires a thoracoscopic biopsy.
PLEURAL EFFUSION ASSOCIATED WITH HEART DISEASE
Congestive Heart Failure. Probably the most commoncause of pleural effusion worldwide. Typically a transu-dative effusion, although may be meet exudative criteriaby an elevated LDH in cases of excessive diuretic use.The diagnosis is frequently suspected based on clinicalgrounds: cardiomegaly, bilateral pleural effusions, ele-vated jugular venous pressure, cardiac gallop, etc.Post-Coronary Artery Bypass Surgery. Pleural effu-
sions are frequently seen in the immediate postoperative
period, and series have reported a frequency up to 40–70% 1 week after the surgery. Although the effusions canbe large, most of the times these are small, exudative,unilateral, and preferentially located in the left side of thechest (32). The characteristics of the fluid may also varydepending on the time to presentation, being typicallybloody exudates when developing less than 30 days aftersurgery, and nonbloody lymphocytic exudates whenpresenting after 30 days postoperatively (33).Dressler’s Syndrome was described 1 to 3 weeks after
myocardial infarction, cardiac surgery, chest trauma, orany other invasive procedure to the heart. IT wascharacterized by presence of fever, chest pain, andpleuro-pericarditis. The effusion is typically an exudateand may be unilateral or bilateral (34).
Lipid EffusionsChylothorax was defined as the presence of chyle in thepleural space, generally associated with disruption of thethoracic duct. This type effusion should be suspected inthe presence of a milky or turbid pleural fluid. Mostcommon causes are direct trauma to the thoracic duct(i.e., surgery) or malignancy (i.e., Lymphoma) (35);chylous effusions are characteristically exudative, al-though nontraumatic causes such as cirrhosis, nephroticsyndrome, or congestive heart failure can be associatedwith a transudative chylothorax (36) (see Table 4).Pseudochylothorax is also known as Chyliform pleural
effusions or Cholesterol effusions. This effusions are notassociated with trauma to the thoracic duct, typicallyresult from long standing untreated pleural effusions inpatients with rheumatoid or tuberculosis pleuritis. Path-ogenesis is not known and the diagnosis is established
TABLE 5Suggested approach to classification and management of parapneumonic pleural effusions
(it is not necessary to have a proven bacterial pneumonia: clinical diagnosis is enough; adaptedfrom Colice et al. (23))
Risk of pooroutcome Pleural space anatomy pH Microbiology
Drainageindicated
Very low Minimal free-flowing (<10 mm on lateraldecubitus)
AND >7.2 AND Negative orunknown
No
Low Small to moderate free-flowing effusion(>10 mm and <1/2 hemithorax)
AND ≥7.2 AND Negative NOa
Moderate Large free-flowing or loculated effusion(≥1/2 hemithorax)
OR <7.2 OR Positive YES
High Pus YESaIf clinical condition deteriorates, repeating thoracentesis and drainage should be considered.
COMP THER. 2007;33(4) ................................................................... 244

with high levels of cholesterol (>200 mg/dl), presence ofcholesterol crystals, and absence of chylomicrons (37).
TuberculosisAlthough the incidence of tuberculous pleuritis in theUSA is thought to be low (1,000 cases annually) (38),this disease continues to be a leading cause of pleuraleffusions in many other areas of the world. Clinically, thedisease manifests as an acute illness that mimics abacterial pneumonia, it is usually unilateral, and only19% of the patients present with evidence of parenchy-mal disease of standard radiographs (39). The effusion isdescribed as an exudate of lymphocytic predominance.The diagnosis can be difficult to establish and is based ondemonstration of acid fast bacilli in pleural fluid or abiopsy specimen. Pleural fluid cultures are positive onlyin 25% of the cases, while biopsy increases the yield to55% (39). Other helpful tests include measurement ofadenosine deaminase (ADA) isoenzymes. Two isoen-zymes exist: ADA1 (ubiquitous in all cells includinglymphocytes) and ADA2 (found only in monocytes,elevated in tuberculosis). Sensitivity and specificity ofthe test depends on the cut off level used, but studieshave suggested both are around 92% (40). ADA levels>70 U/l are almost diagnostic of tuberculosis, whereaslevels <40 U/l are helpful to rule out the disease. Anewer test, interferon-gamma, has been proposed as moresensitive and specific than ADA. Using cut-off levels of3.7 IU/ml, the test yields a sensitivity and specificity of98% (41). Given higher cost and similar accuracy,currently, measurement of IFN-y instead of ADA is notrecommended (3).
ManagementIn general, the key consists in identifying the cause andtreating the underlying disease process. Transudativeeffusions generally resolve, whereas exudative effusionsrequire therapeutic drainage. Except in cases of effusionsassociated with congestive heart failure, a diagnosticthoracentesis should be performed in all cases. Thera-peutic procedures include:
(a) Therapeutic thoracentesis. The main indicationsinclude drainage of fluid in patients with parapneu-monic effusions or empyema and relief of symptomsin patients with large effusions. In general, no morethan 1,000 to 1,500 ml of fluid should be removed atone time.
(b) Tube thoracostomy refers to the insertion of a chesttube to allow large volume drainage from the pleuralspace. Indications to place a chest tube in the
management of a pleural effusion includehemothorax, penetrating chest trauma, complicatedparapneumonic effusion or empyema, chylothorax,and pleurodesis. The size of the chest tube variesdepending of the viscosity of the fluid that needs tobe drained: 20–24 Fr for malignant effusions andpleurodesis, 28–36 Fr for parapneumonic effusionsand empyema, and 32–40 Fr for hemothorax. Inpatients with complicated effusions and loculations,a contrast CT of the chest is necessary to guide theappropriate placement of the chest tube.
(c) Pleurodesis consists of instillation of a sclerosingagent into the pleural cavity via a tube thoracostomy(chemical pleurodesis) or obliteration of the pleuralspace by abrasion during thoracoscopy or thoracot-omy (mechanical pleurodesis). Chemical pleurodesisis indicated to reduce recurrence in patients withmalignant pleural effusions (42). Several chemicalagents have been used (i.e., bleomycin, tetracycline,doxycyline, etc.), although studies have consistentlysuggested that talc is probably the most effectiveagent (42).
(d) Surgical Management, currently, is almost alwaysperformed via Video Assisted Thoracoscopic Sur-gery (VATS). With this technique loculations andother debris present in the pleural space can beemptied under direct visualization. In cases ofempyema with significant fibrosis and adhesions, apartial pleurectomy can be performed via thoraco-scopy, while in severe cases, a total pleurectomy viathoracotomy is sometimes necessary.
(e) Other indwelling catheters: In patients with malig-nant pleural effusions, a newer silicone rubbercatheter (PleurX catheter) can be used to allowpatients with recurrent effusions to have a drainagesystem that allows them to drain the effusion in theoutpatient setting obviating the need for hospitaliza-tion and repeated thoracentesis (43). The catheter issmall (15.5 F) and can be placed under localanesthesia in the outpatient setting by a pulmonolo-gist or a thoracic surgeon. Studies have shownexcellent results in symptomatic relief, low morbid-ity, and lower costs compared to chest tube place-ment and hospitalization (44).
REFERENCES1. Noppen M, et al. Volume and cellular content of normal pleural fluid
in humans examined by pleural lavage. Am J Respir Crit Care Med2000;162(3 Pt 1):1023–6.
2. Marel M, et al. The incidence of pleural effusion in a well-definedregion. Epidemiologic study in central Bohemia. Chest 1993;104(5):1486–9.
COMP THER. 2007;33(4) ................................................................... 245

3. Light RW. Pleural diseases. 5th ed. Philadelphia: Lippincott Williams& Wilkins; 2007. xiii, p. 427.
4. Bouros D, Pleural disease. Lung biology in health and disease; v. 186.New York: Marcel Dekker; 2004. xxxi, p. 1044.
5. Light RW. Clinical practice. Pleural effusion. N Engl J Med 2002;346(25):1971–7.
6. Gilmartin JJ, Wright AJ, Gibson GJ. Effects of pneumothorax orpleural effusion on pulmonary function. Thorax 1985;40(1):60–5.
7. Traylor JJ, et al. Large pleural effusions producing signs of cardiactamponade resolved by thoracentesis. Am J Cardiol 2002;89(1):106–8.
8. Rahman NM, Chapman SJ, Davies RJ. Pleural effusion: a structuredapproach to care. Br Med Bull 2004;72:31–47.
9. Kalantri S, et al. Accuracy and reliability of physical signs in thediagnosis of pleural effusion. Respir Med 2007;101(3):431–8.
10. Lange S, Stark P. Radiology of chest diseases. Stuttgart; New York:G. Thieme; Thieme Medical Publishers. 1990; viii, p. 293.
11. Moskowitz H, et al. Roentgen visualization of minute pleuraleffusion. An experimental study to determine the minimum amountof pleural fluid visible on a radiograph. Radiology 1973;109(1):33–5.
12. Gryminski J, Krakowka P, Lypacewicz G. The diagnosis of pleuraleffusion by ultrasonic and radiologic techniques. Chest 1976;70(1):33–7.
13. Azoulay E. Pleural effusions in the intensive care unit. Curr OpinPulm Med 2003;9(4):291–7.
14. Doyle JJ, et al. Necessity of routine chest roentgenography afterthoracentesis. Ann Intern Med 1996;124(9):816–20.
15. Tarver RD, Broderick LS, Conces DJ Jr. Reexpansion pulmonaryedema. J Thorac Imaging 1996;11(3):198–209.
16. Jackson RM, et al. Re-expansion pulmonary edema. A potential rolefor free radicals in its pathogenesis. Am Rev Respir Dis 1988;137(5):1165–71.
17. Jones PW, et al. Ultrasound-guided thoracentesis: is it a safer method?Chest 2003;123(2):418–23.
18. Light RW, et al. Pleural effusions: the diagnostic separation oftransudates and exudates. Ann Intern Med 1972;77(4):507–13.
19. Romero S, et al. Evaluation of different criteria for the separation ofpleural transudates from exudates. Chest 1993;104(2):399–404.
20. Romero-Candeira S, et al. Influence of diuretics on the concentrationof proteins and other components of pleural transudates in patientswith heart failure. Am J Med 2001;110(9):681–6.
21. Heffner JE, Brown LK, Barbieri CA. Diagnostic value of tests thatfdiscriminate between exudative and transudative pleural effusions.Primary Study Investigators. Chest 1997;111(4):970–80.
22. Heffner JE, Sahn SA, Brown LK. Multilevel likelihood ratios foridentifying exudative pleural effusions(*). Chest 2002;121(6):1916–20.
23. Colice GL, et al. Medical and surgical treatment of parapneumoniceffusions : an evidence-based guideline. Chest 2000;118(4):1158–71.
24. Rodriguez-Panadero F, Lopez Mejias J. Low glucose and pH levelsin malignant pleural effusions. Diagnostic significance and prog-nostic value in respect to pleurodesis. Am Rev Respir Dis 1989;139(3):663–7.
25. Chandler TM, et al. Comparison of the use and accuracy of methodsfor determining pleural fluid pH. South Med J 1999;92(2):214–7.
26. Cheng DS, et al. Comparison of pleural fluid pH values obtainedusing blood gas machine, pH meter, and pH indicator strip. Chest1998;114(5):1368–72.
27. Adelman M, et al. Diagnostic utility of pleural fluid eosinophilia. AmJ Med 1984;77(5):915–20.
28. Everts RJ, Reller LB. Pleural space infections: microbiology andantimicrobial therapy. Semin Respir Infect 1999;14(1):18–30.
29. Jarvi OH, et al. The accuracy and significance of cytologic cancerdiagnosis of pleural effusions. (A followup study of 338 patients).Acta Cytol 1972;16(2):152–8.
30. Spriggs AI, Boddington MM. The cytology of effusions: pleural,pericardial, andperitoneal and of cerebrospinalfluid, byA.I. Spriggs andM.M. Boddington. 2nd ed. New York: Grune & Stratton; 1968. p. 174.
31. Hendrick DJ. Occupational disorders of the lung: recognition,management and prevention. London: W. B. Saunders; 2002. xiv,p. 638.
32. Light RW, et al. Large pleural effusions occurring after coronaryartery bypass grafting. Cardiovascular Surgery Associates, PC. AnnIntern Med 1999;130(11):891–6.
33. Sadikot RT, et al. Pleural fluid characteristics of patients withsymptomatic pleural effusion after coronary artery bypass graftsurgery. Arch Intern Med 2000;160(17):2665–8.
34. Engle MA, et al. Postpericardiotomy syndrome. A new look at an oldcondition. Mod Concepts Cardiovasc Dis 1975;44(11):59–64.
35. Doerr CH, et al. Etiology of chylothorax in 203 patients. Mayo ClinProc 2005;80(7):867–70.
36. Diaz-Guzman E, Culver DA, Stoller JK. Transudative chylothorax:report of two cases and review of the literature. Lung 2005;183(3):169–75.
37. Garcia-Zamalloa A, et al. Pseudochylothorax. Report of 2 cases andreview of the literature. Medicine (Baltimore) 1999;78(3):200–7.
38. Baumann MH, et al. Pleural tuberculosis in the United States:incidence and drug resistance. Chest 2007;131(4):1125–32.
39. Valdes L, et al. Tuberculous pleurisy: a study of 254 patients. ArchIntern Med 1998;158(18):2017–21.
40. Goto M, et al. Diagnostic value of adenosine deaminase intuberculous pleural effusion: a meta-analysis. Ann Clin Biochem2003;40(Pt 4):374–81.
41. Villena V, et al. Interferon gamma levels in pleural fluid for thediagnosis of tuberculosis. Am J Med 2003;115(5):365–70.
42. Shaw P, Agarwal R. Pleurodesis for malignant pleural effusions.Cochrane Database Syst Rev 2004;1:CD002916.
43. Putnam JB Jr, et al. Outpatient management of malignant pleuraleffusion by a chronic indwelling pleural catheter. Ann Thorac Surg2000;69(2):369–75.
44. Tremblay A, Michaud G. Single-center experience with 250 tunnelledpleural catheter insertions for malignant pleural effusion. Chest2006;129(2):362–8.
45. Yataco JC, Dweik RA. Pleural effusions: evaluation and management.Cleve Clin J Med 2005;72(10):854–6, 858, 862–4 passim.
46. Lloyd C, Sahn SA. Subarachnoid pleural fistula due to penetratingtrauma: case report and review of the literature. Chest 2002;122(6):2252–6.
COMP THER. 2007;33(4) ................................................................... 246