
Potential management of resistant microbial infections with a novel non-antibiotic: the...
8
International Journal of Antimicrobial Agents 30 (2007) 242–249 Potential management of resistant microbial infections with a novel non-antibiotic: the anti-inflammatory drug diclofenac sodium Noton Kumar Dutta a , Subramanian Annadurai b , Kaushiki Mazumdar c , Sujata G. Dastidar b , Jette E. Kristiansen d , Joseph Molnar e , Marta Martins f , Leonard Amaral f,∗ a Institute of Laboratory Animal Resources, Laboratory Animal Medicine, College of Veterinary Medicine, 85-Dong, 733-Ho, Seoul National University, San 56-1, Sillim 9 Dong, Gwanakgu, Seoul, South Korea b Division of Microbiology, Department of Pharmaceutical Technology, Jadavpur University, Calcutta 700032, India c Department of Microbiology and Immunology, College of Medicine, Seoul National University, 28 Yongon-Dong, Jongno-Gu, Seoul 110-799, South Korea d Department of Clinical Microbiology, Sønderborg, Southern Danish University, Sydvang 1, 6400 Sønderborg, Denmark e Institute of Medical Microbiology and Immunology, University of Szeged, H-6720 Szeged, Dom ter 10, Hungary f Mycobacteriology Unit, UPMM, Instituto de Higiene e Medicina Tropical, Universidade Nova de Lisboa, Rua da Junqueira 96, 1349-008 Lisbon, Portugal Received 10 November 2006; accepted 30 April 2007 Abstract Diclofenac sodium (Dc), an anti-inflammatory agent, has remarkable inhibitory action both against drug-sensitive and drug-resistant clinical isolates of various Gram-positive and Gram-negative bacteria. The aim of this study was to determine the ability of Dc to protect mice from a virulent Salmonella infection. Dc injected at 1.5 g/g and 3.0 g/g mouse body weight significantly protected animals from the lethality of Salmonella infection. As was the case for the in vitro interaction, Dc in combination with streptomycin was even more effective. The non-antibiotic drug Dc has potential for the management of problematic antibiotic-resistant bacterial infections. © 2007 Elsevier B.V. and the International Society of Chemotherapy. All rights reserved. Keywords: Resistant microbial infections; Diclofenac; Non-antibiotics; Antimicrobial activity; In vitro; In vivo 1. Introduction There is a serious, as yet unmet, medical need for new antimicrobial agents to treat drug-resistant infections [1]. In this context, successful identification and development of novel and efficient antibacterial agents to solve this problem is essential. A variety of compounds employed in the management of pathological conditions of a non-infectious aetiology have been shown to exhibit broad-spectrum antimicrobial activity in vitro and in vivo against a variety of Gram-positive and Gram-negative bacteria; such compounds are called ‘non- antibiotics’ [2]. Non-antibiotics such as promethazine [3], ∗ Corresponding author. Tel.: +351 21 365 2600; fax: +351 21 363 2105. E-mail address: [email protected] (L. Amaral). chlorpromazine [4] and thioridazine [5,6] have been shown to have in vitro activity against several strains of Gram-positive and Gram-negative bacteria. This activity required concen- trations that are beyond those clinically achievable. However, such non-antibiotics may be concentrated more than 100-fold by macrophages that have phagocytosed bacteria [7,8]. In this manner, clinically acceptable dosing of an infected patient with non-antibiotics might result in an inhibitory effect in situ (intracellular) similar to that observed in vitro. This sug- gests that such drugs might be used as adjuvants in current regimens used for the management of bacterial infections. Of the non-antibiotics reported so far, several have been found to enhance the activity of certain antibiotics and even non-antibiotics against specific bacteria, e.g. methdi- lazine in combination with streptomycin (STR), kanamycin and gentamicin showed enhancement of their antibac- 0924-8579/$ – see front matter © 2007 Elsevier B.V. and the International Society of Chemotherapy. All rights reserved. doi:10.1016/j.ijantimicag.2007.04.018
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Potential management of resistant microbial infections with a novel non-antibiotic: the...

A
iaon©
K
1
atni
pbiGa
0d
International Journal of Antimicrobial Agents 30 (2007) 242–249
Potential management of resistant microbial infections with a novelnon-antibiotic: the anti-inflammatory drug diclofenac sodium
Noton Kumar Dutta a, Subramanian Annadurai b, Kaushiki Mazumdar c, Sujata G. Dastidar b,Jette E. Kristiansen d, Joseph Molnar e, Marta Martins f, Leonard Amaral f,∗
a Institute of Laboratory Animal Resources, Laboratory Animal Medicine, College of Veterinary Medicine, 85-Dong,733-Ho, Seoul National University, San 56-1, Sillim 9 Dong, Gwanakgu, Seoul, South Korea
b Division of Microbiology, Department of Pharmaceutical Technology, Jadavpur University, Calcutta 700032, Indiac Department of Microbiology and Immunology, College of Medicine, Seoul National University,
28 Yongon-Dong, Jongno-Gu, Seoul 110-799, South Koread Department of Clinical Microbiology, Sønderborg, Southern Danish University, Sydvang 1, 6400 Sønderborg, Denmark
e Institute of Medical Microbiology and Immunology, University of Szeged, H-6720 Szeged, Dom ter 10, Hungaryf Mycobacteriology Unit, UPMM, Instituto de Higiene e Medicina Tropical, Universidade Nova de Lisboa,
Rua da Junqueira 96, 1349-008 Lisbon, Portugal
Received 10 November 2006; accepted 30 April 2007
bstract
Diclofenac sodium (Dc), an anti-inflammatory agent, has remarkable inhibitory action both against drug-sensitive and drug-resistant clinicalsolates of various Gram-positive and Gram-negative bacteria. The aim of this study was to determine the ability of Dc to protect mice fromvirulent Salmonella infection. Dc injected at 1.5 �g/g and 3.0 �g/g mouse body weight significantly protected animals from the lethality
f Salmonella infection. As was the case for the in vitro interaction, Dc in combination with streptomycin was even more effective. Theon-antibiotic drug Dc has potential for the management of problematic antibiotic-resistant bacterial infections.2007 Elsevier B.V. and the International Society of Chemotherapy. All rights reserved.
eywords: Resistant microbial infections; Diclofenac; Non-antibiotics; Antimicrobial activity; In vitro; In vivo
chatsbmwsg
. Introduction
There is a serious, as yet unmet, medical need for newntimicrobial agents to treat drug-resistant infections [1]. Inhis context, successful identification and development ofovel and efficient antibacterial agents to solve this problems essential.
A variety of compounds employed in the management ofathological conditions of a non-infectious aetiology haveeen shown to exhibit broad-spectrum antimicrobial activity
n vitro and in vivo against a variety of Gram-positive andram-negative bacteria; such compounds are called ‘non-ntibiotics’ [2]. Non-antibiotics such as promethazine [3],
∗ Corresponding author. Tel.: +351 21 365 2600; fax: +351 21 363 2105.E-mail address: [email protected] (L. Amaral).
r
fela
924-8579/$ – see front matter © 2007 Elsevier B.V. and the International Societyoi:10.1016/j.ijantimicag.2007.04.018
hlorpromazine [4] and thioridazine [5,6] have been shown toave in vitro activity against several strains of Gram-positivend Gram-negative bacteria. This activity required concen-rations that are beyond those clinically achievable. However,uch non-antibiotics may be concentrated more than 100-foldy macrophages that have phagocytosed bacteria [7,8]. In thisanner, clinically acceptable dosing of an infected patientith non-antibiotics might result in an inhibitory effect in
itu (intracellular) similar to that observed in vitro. This sug-ests that such drugs might be used as adjuvants in currentegimens used for the management of bacterial infections.
Of the non-antibiotics reported so far, several have been
ound to enhance the activity of certain antibiotics andven non-antibiotics against specific bacteria, e.g. methdi-azine in combination with streptomycin (STR), kanamycinnd gentamicin showed enhancement of their antibac-of Chemotherapy. All rights reserved.

l of An
thfdccacmoa
deHtiaa
2
2
a(ii
2
rpC
2
(iLsMi1
2
PadbsDnts
2c
Ld
2SK
w2snwta
2
SwNwaha
N.K. Dutta et al. / International Journa
erial effects, resulting in synergism [9–15]. Synergismas also been noted between two non-antibiotic drugs,or example between methdilazine and bromodiphenhy-ramine, diphenhydramine and m-DOPA [16] and betweenhlorpromazine and thioridazine [17]. These studies haveollectively led to the recognition that, as a group, non-ntibiotics such as phenothiazines are agents that must beonsidered either for immediate use when the manage-ent of the bacterial infection is problematic [8,18–24],
r as lead compounds for new and effective antibacterialgents [8].
Among the non-antibiotics is the anti-inflammatory agenticlofenac sodium (Dc), which possesses moderate to pow-rful antibacterial activity both in vitro and in vivo [25].owever, because the interaction of Dc with antibiotics and
he combined effects in vivo and ex vivo have not been stud-ed, we investigated the antimicrobial action of Dc in vitrond in vivo alone and in combination with an antibiotic andnother non-antibiotic drug.
. Materials and methods
.1. Bacteria
Bacterial strains were obtained from various hospitalsnd reference centres (American Type Culture CollectionATCC) and National Collection of Type Cultures (NCTC))n India and abroad. Bacteria were identified and preservedn freeze-dried condition until later use.
.2. Drugs
All agents were obtained as pure dry powder from theirespective manufacturers in India and stored at 4 ◦C. Thehenylacetic acid derivative Dc was obtained from Hindustaniba-Geigy (Mumbai, India) (Fig. 1).
.3. Media
The liquid media used in the study were peptone waterPW) (1.0% bacteriological peptone (Oxoid Ltd., Bas-ngstoke, UK) plus 0.5% NaCl), nutrient broth (NB) (Oxoidtd.) and Mueller–Hinton broth (MHB) (Oxoid Ltd.). The
olid media were peptone agar (PA), nutrient agar (NA) andueller–Hinton agar (MHA), which were prepared by solid-fying PW, NB and MHB, respectively, by the addition of.5% agar (Oxoid No. 3).
Fig. 1. Structure of diclofenac sodium.
s7sTm
daps[Sc
timicrobial Agents 30 (2007) 242–249 243
.4. Inoculum
All bacterial strains were grown overnight (24 h) inA/NA/MHA at 37 ◦C and harvested during the station-ry growth phase. From these cultures, the organisms wereirectly suspended in 5 mL of sterile distilled water. The tur-idity of each suspension was adjusted to 0.5 McFarlandtandard [26] using a spectrophotometer (Chemito UV 2600ouble Beam UV-Vis Spectrophotometer; Chemito Tech-ologies Pvt. Ltd., Mumbai, India) at 625 nm, correspondingo 2.4 × 108 colony-forming units (CFU)/mL. The suspen-ion was further diluted 1:100 with sterile distilled water.
.5. Determination of the minimum inhibitoryoncentration (MIC) of the drugs
The agar dilution method approved by the Clinical andaboratory Standards Institute (CLSI) was employed toetermine the MIC of antimicrobial agents [27].
.6. Determination of the mode of action of Dc ontaphylococcus aureus NCTC 6571 and Escherichia coli12C600
Staphylococcus aureus NCTC 6571 and E. coli K12C600ere grown overnight in NB at 37 ◦C. From each culture,mL was added to 4 mL of fresh NB and incubated for 2 h
o that the culture could reach logarithmic growth phase. Theumber of viable cells (CFU) was then determined and Dcas added at a concentration higher than the MIC value of
he test bacterium. CFU counts were determined at 0, 2, 4, 6nd 18 h [28].
.7. Animal experiments
The animals used in this study were 4-week-old, inbred,wiss albino male mice weighing 8–20 g. Systemic infectionsere produced in groups of 20 mice in accordance with theational Institutes of Health ethical guidelines [29]. Animalsere maintained in a certified animal house under supervision
nd standard conditions of 21 ± 1 ◦C and 50–60% relativeumidity with a photoperiod of 14 h:10 h light:dark. Waternd a dry pellet diet were given ad libitum. The test bacterialtrain was Salmonella enterica serotype Typhimurium NCTC4, as it is naturally virulent to mice. The virulence of thetrain was enhanced after repeated passage through mice.his strain is termed the ‘step-up mutant’ and represents theost virulent strain employed in this study.The median lethal dose (MLD) of the passaged strain was
etermined by injecting graded challenges in batches of micend recording the mortality up to 100 h. The MLD of theassaged strain, corresponding to 0.95 × 109 CFU/mouse,
uspended in 0.5 mL of NB served as the challenge dose30]. Standardising its optical density at 640 nm (Klett-ummerson colorimeter) ensured reproducibility of thehallenge dose.
2 l of An
2
1fa
2
eowfwea
agIIsgCIf[
2a
[S1cootcesepTdbTeTfidtti
dwf(awud
2
bcaEm9cruTwMtr
2
T[(ast(dTd
2
mwwwDoDD
44 N.K. Dutta et al. / International Journa
.8. Determination of the toxicity of Dc
Groups of 20 mice were injected intraperitoneally with5, 30 and 60 �g of Dc. Mice were kept under observationor up to 100 h. Mortality was the single criterion employeds a measure of toxicity.
.9. Determination of the protective capacity of Dc
Sixty mice were divided into three groups of 20 animalsach. Groups I, II and III were injected with 15, 30 and 60 �gf Dc, respectively. Three hours post injection, each animalas challenged with 50 MLD of S. Typhimurium NCTC 74. A
ourth group of 60 animals was similarly infected and injectedith 0.1 mL of sterile saline in place of Dc. The protective
ffect of the drug was assessed by recording the mortality ofnimals in different groups within 100 h of treatment.
Four additional groups of mice, each consisting of sixnimals, were employed as follows: Groups I and III wereiven 15 �g of Dc 3 h prior to infection, whilst GroupsI and IV were injected with sterile saline. Groups I andI were sacrificed 2 h after the challenge, their livers andpleens were removed aseptically, homogenised in sterilelass homogenisers and aliquots taken for determination ofFU. The same procedures were also followed for Groups
II and IV after 18 h. Statistical analysis of the data was per-ormed according to the method of Bhattacharya and Johnson31].
.10. Determination of in vitro synergism between Dcnd STR or trifluoperazine (Tf)
The disk diffusion technique, as described by the CLSI32], was used to determine the combined effects of Dc andTR or Tf. Sterile filter paper disks (7.25 mm, Whatman No.) were prepared according to Cruickshank et al. [33]. Forombination tests using STR and Dc, 100 �g of Dc and 10 �gf STR were added to the disks for determination of the effectf STR/Dc, and for the determination of the effect of Tf/Dche disks contained 200 �g of Tf and 200 �g of Dc. Individualontrol disks containing Dc, STR or Tf allowed the separateffects of each drug to be quantified. The selected bacterialtrains were grown in liquid media for 18 h and 100 �L ofach culture was uniformly spread in triplicate onto appro-riate solid media. The plates were dried at 37 ◦C for 45 min.he disks containing each drug and combinations of eachrug were placed on the surface of the agar containing theacterium and the plates were incubated at 37 ◦C for 18 h.he average diameter of the zone of inhibition produced byach drug was obtained from three different zone diameters.he individual inhibitory effects of Dc, STR and Tf wererst determined. The data obtained allowed the placement of
isks containing combinations of drugs in such a manner thathe predicted marginal edge of the zones of inhibition wouldouch each other tangentially. The diameters of the zones ofnhibition produced due to individual and mutual effects ofodtc
timicrobial Agents 30 (2007) 242–249
rugs were recorded. The interaction, if any, when two drugsere used in combination was assessed as follows: (i) indif-
erence, when both zones of inhibition remained unaffected;ii) antagonism, when the zones of inhibition receded andssumed a kidney shape; and (iii) synergism, in which thereas an enlargement of the inhibition zones. Statistical eval-ation of the increase in surface area (�r2) of a zone, if any,ue to a combination of effects was performed by the χ2 test.
.11. Checkerboard assessment
The degree of synergism was confirmed by the checker-oard method with 96-well microplates containing varyingoncentrations of the agents studied in MHB [27] alonend in combination. Staphylococcus aureus NCTC 6571 and. coli K12C600 were added to each well. Dispensing ofedia, drugs and bacteria to each well was conducted with a
6-channel dispenser. In tests with STR and Dc, the con-entrations of STR and Dc were 0–50 �g and 0–200 �g,espectively, whilst in tests with Tf and Dc each drug wassed at concentrations of 0–200 �g. In the first row, STR orf alone was distributed, whilst in the first column only Dcas dispensed. In each well, the inoculum was adjusted to 0.5cFarland standard and applied using a multipoint inocula-
or. The trays were incubated aerobically for 24 h. For eachun, ATCC reference strains served as controls.
.12. Data analysis
Determination of the interaction between Dc and STR orf can be done by the method of Eliopoulos and Moellering
34]. This method yields a fractional inhibitory concentrationFIC) index whose value corresponds to the degree of inter-ction. FIC indices <0.5 suggest synergy; a FIC of 0.5–0.75uggests partial synergy; a FIC of 0.76–1.0 indicates an addi-ive effect; a FIC of 1.0–4.0 is considered to be indifferentno interaction); and FIC > 4.0 is demonstrative of increasingegrees of antagonism (the effects of each drug are reduced).he degree of significance between any two comparisons wasetermined by χ2 analysis.
.13. In vivo synergistic effect
A total of 24 mice were divided into four groups of 6 ani-als. On the basis of standard pharmacological data [35], Dcas administered intraperitoneally at a dose of 1.5 �g/g bodyeight, STR at 3 �g/g body weight and Tf at 1.5 �g/g bodyeight. Each animal in Group I was injected with 30 �g ofc; animals in Group II received 60 �g of STR or 30 �gf Tf; animals in Group III were given a combination ofc and STR (30 �g Dc + 60 �g STR) or Dc and Tf (30 �gc + 30 �g Tf); and animals in Group IV received 0.5 mL
f sterile saline in place of the drugs. After 3 h, a challengeose of S. Typhimurium NCTC 74 was injected intraperi-oneally into each mouse. At 18 h after administration of thehallenge, all the mice were autopsied. Blood (0.2–0.4 mL)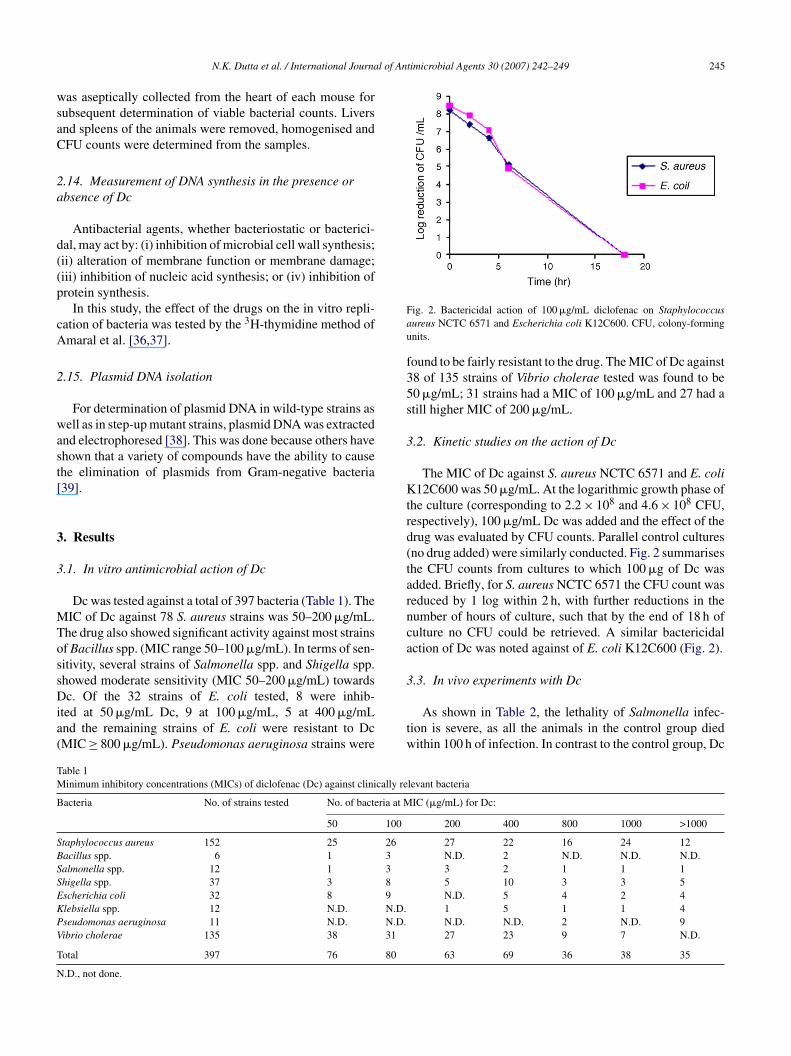
l of Antimicrobial Agents 30 (2007) 242–249 245
wsaC
2a
d((p
cA
2
wast[
3
3
MTossDia(
Fau
f35s
3
Ktrd(tarnca
3
TM
B
SBSSEKPV
T
N
N.K. Dutta et al. / International Journa
as aseptically collected from the heart of each mouse forubsequent determination of viable bacterial counts. Liversnd spleens of the animals were removed, homogenised andFU counts were determined from the samples.
.14. Measurement of DNA synthesis in the presence orbsence of Dc
Antibacterial agents, whether bacteriostatic or bacterici-al, may act by: (i) inhibition of microbial cell wall synthesis;ii) alteration of membrane function or membrane damage;iii) inhibition of nucleic acid synthesis; or (iv) inhibition ofrotein synthesis.
In this study, the effect of the drugs on the in vitro repli-ation of bacteria was tested by the 3H-thymidine method ofmaral et al. [36,37].
.15. Plasmid DNA isolation
For determination of plasmid DNA in wild-type strains asell as in step-up mutant strains, plasmid DNA was extracted
nd electrophoresed [38]. This was done because others havehown that a variety of compounds have the ability to causehe elimination of plasmids from Gram-negative bacteria39].
. Results
.1. In vitro antimicrobial action of Dc
Dc was tested against a total of 397 bacteria (Table 1). TheIC of Dc against 78 S. aureus strains was 50–200 �g/mL.
he drug also showed significant activity against most strainsf Bacillus spp. (MIC range 50–100 �g/mL). In terms of sen-itivity, several strains of Salmonella spp. and Shigella spp.howed moderate sensitivity (MIC 50–200 �g/mL) towards
c. Of the 32 strains of E. coli tested, 8 were inhib-ted at 50 �g/mL Dc, 9 at 100 �g/mL, 5 at 400 �g/mLnd the remaining strains of E. coli were resistant to DcMIC ≥ 800 �g/mL). Pseudomonas aeruginosa strains were
tw
able 1inimum inhibitory concentrations (MICs) of diclofenac (Dc) against clinically re
acteria No. of strains tested No. of bacteria at M
50 100
taphylococcus aureus 152 25 26acillus spp. 6 1 3almonella spp. 12 1 3higella spp. 37 3 8scherichia coli 32 8 9lebsiella spp. 12 N.D. N.D.seudomonas aeruginosa 11 N.D. N.D.ibrio cholerae 135 38 31
otal 397 76 80
.D., not done.
ig. 2. Bactericidal action of 100 �g/mL diclofenac on Staphylococcusureus NCTC 6571 and Escherichia coli K12C600. CFU, colony-formingnits.
ound to be fairly resistant to the drug. The MIC of Dc against8 of 135 strains of Vibrio cholerae tested was found to be0 �g/mL; 31 strains had a MIC of 100 �g/mL and 27 had atill higher MIC of 200 �g/mL.
.2. Kinetic studies on the action of Dc
The MIC of Dc against S. aureus NCTC 6571 and E. coli12C600 was 50 �g/mL. At the logarithmic growth phase of
he culture (corresponding to 2.2 × 108 and 4.6 × 108 CFU,espectively), 100 �g/mL Dc was added and the effect of therug was evaluated by CFU counts. Parallel control culturesno drug added) were similarly conducted. Fig. 2 summariseshe CFU counts from cultures to which 100 �g of Dc wasdded. Briefly, for S. aureus NCTC 6571 the CFU count waseduced by 1 log within 2 h, with further reductions in theumber of hours of culture, such that by the end of 18 h ofulture no CFU could be retrieved. A similar bactericidalction of Dc was noted against of E. coli K12C600 (Fig. 2).
.3. In vivo experiments with Dc
As shown in Table 2, the lethality of Salmonella infec-ion is severe, as all the animals in the control group diedithin 100 h of infection. In contrast to the control group, Dc
levant bacteria
IC (�g/mL) for Dc:
200 400 800 1000 >1000
27 22 16 24 12N.D. 2 N.D. N.D. N.D.3 2 1 1 15 10 3 3 5N.D. 5 4 2 41 5 1 1 4N.D. N.D. 2 N.D. 927 23 9 7 N.D.
63 69 36 38 35
246 N.K. Dutta et al. / International Journal of Antimicrobial Agents 30 (2007) 242–249
Table 2Effect of diclofenac (Dc) on groups of mice infected with Salmonellaenterica serotype Typhimurium NCTC 74 (0.95 × 109 colony-formingunits/0.5 mL of nutrient broth)
Dc (�g/mouse) Number of dead mice/group
0 60/6015 7/20*
30 6/20**
6 **
al
mfc
3
diftDbFD2
ftT
3
tfbi(T
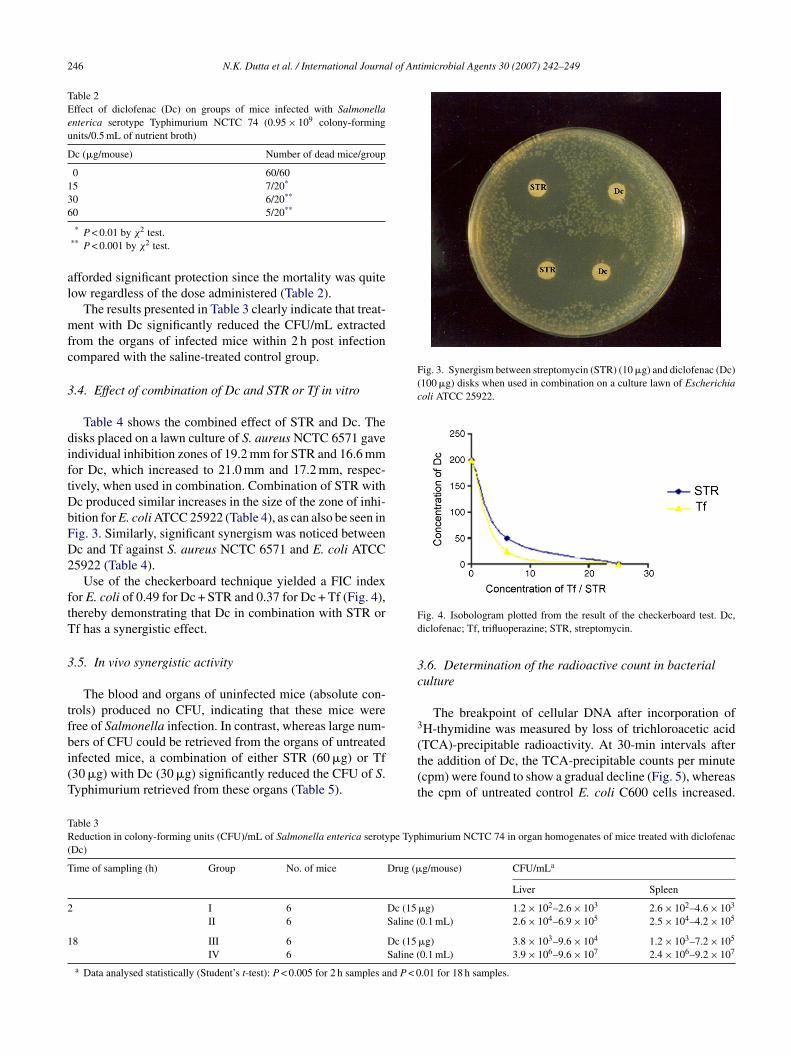
Fig. 3. Synergism between streptomycin (STR) (10 �g) and diclofenac (Dc)(100 �g) disks when used in combination on a culture lawn of Escherichiacoli ATCC 25922.
Fd
3c
3
TR(
T
2
1
0 5/20
* P < 0.01 by χ2 test.** P < 0.001 by χ2 test.
fforded significant protection since the mortality was quiteow regardless of the dose administered (Table 2).
The results presented in Table 3 clearly indicate that treat-ent with Dc significantly reduced the CFU/mL extracted
rom the organs of infected mice within 2 h post infectionompared with the saline-treated control group.
.4. Effect of combination of Dc and STR or Tf in vitro
Table 4 shows the combined effect of STR and Dc. Theisks placed on a lawn culture of S. aureus NCTC 6571 gavendividual inhibition zones of 19.2 mm for STR and 16.6 mmor Dc, which increased to 21.0 mm and 17.2 mm, respec-ively, when used in combination. Combination of STR withc produced similar increases in the size of the zone of inhi-ition for E. coli ATCC 25922 (Table 4), as can also be seen inig. 3. Similarly, significant synergism was noticed betweenc and Tf against S. aureus NCTC 6571 and E. coli ATCC5922 (Table 4).
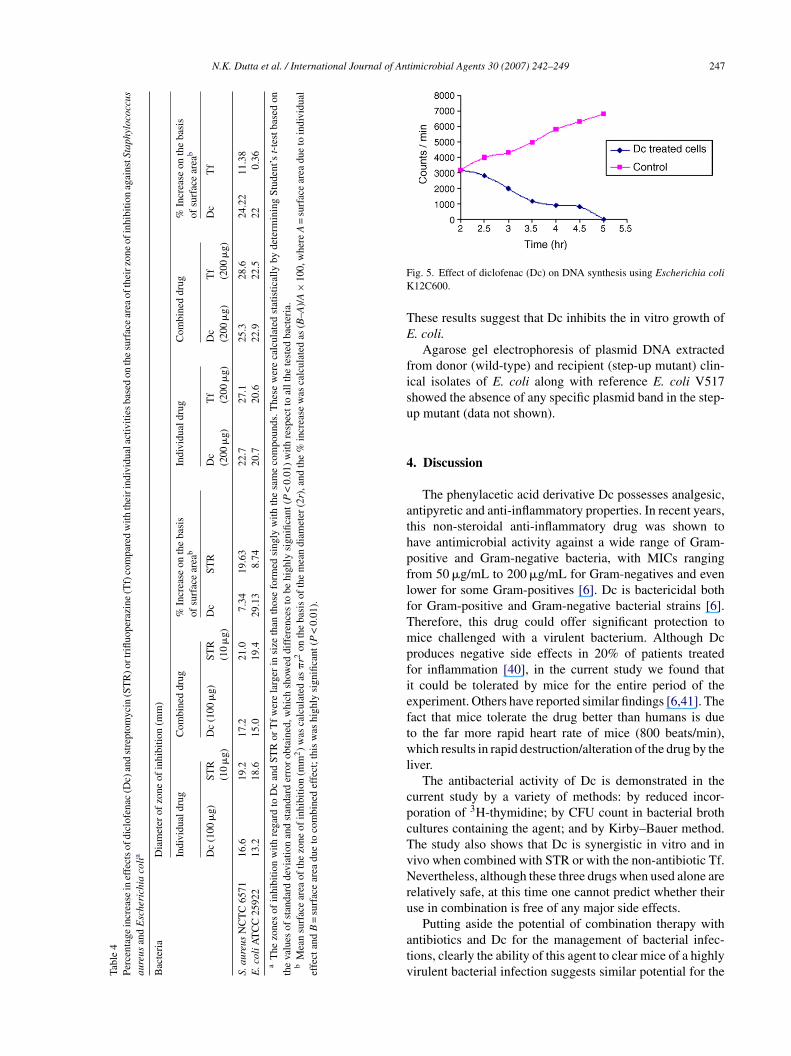
Use of the checkerboard technique yielded a FIC indexor E. coli of 0.49 for Dc + STR and 0.37 for Dc + Tf (Fig. 4),hereby demonstrating that Dc in combination with STR orf has a synergistic effect.
.5. In vivo synergistic activity
The blood and organs of uninfected mice (absolute con-rols) produced no CFU, indicating that these mice wereree of Salmonella infection. In contrast, whereas large num-
ers of CFU could be retrieved from the organs of untreatednfected mice, a combination of either STR (60 �g) or Tf30 �g) with Dc (30 �g) significantly reduced the CFU of S.yphimurium retrieved from these organs (Table 5).(t(t
able 3eduction in colony-forming units (CFU)/mL of Salmonella enterica serotype Typ
Dc)
ime of sampling (h) Group No. of mice Drug (�
I 6 Dc (15II 6 Saline (
8 III 6 Dc (15IV 6 Saline (
a Data analysed statistically (Student’s t-test): P < 0.005 for 2 h samples and P < 0
ig. 4. Isobologram plotted from the result of the checkerboard test. Dc,iclofenac; Tf, trifluoperazine; STR, streptomycin.
.6. Determination of the radioactive count in bacterialulture
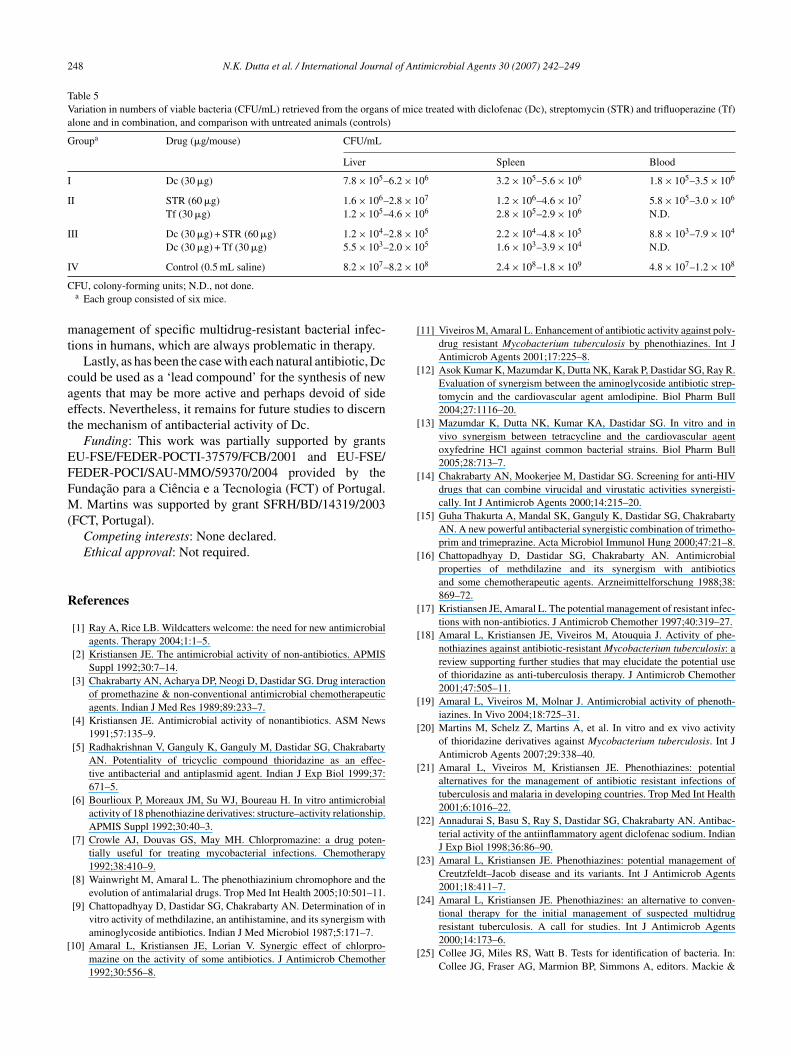
The breakpoint of cellular DNA after incorporation ofH-thymidine was measured by loss of trichloroacetic acidTCA)-precipitable radioactivity. At 30-min intervals after
he addition of Dc, the TCA-precipitable counts per minutecpm) were found to show a gradual decline (Fig. 5), whereashe cpm of untreated control E. coli C600 cells increased.himurium NCTC 74 in organ homogenates of mice treated with diclofenac
g/mouse) CFU/mLa
Liver Spleen
�g) 1.2 × 102–2.6 × 103 2.6 × 102–4.6 × 103
0.1 mL) 2.6 × 104–6.9 × 105 2.5 × 104–4.2 × 105
�g) 3.8 × 103–9.6 × 104 1.2 × 103–7.2 × 105
0.1 mL) 3.9 × 106–9.6 × 107 2.4 × 106–9.2 × 107
.01 for 18 h samples.
N.K. Dutta et al. / International Journal of Antimicrobial Agents 30 (2007) 242–249 247
Tabl
e4
Perc
enta
gein
crea
sein
effe
cts
ofdi
clof
enac
(Dc)
and
stre
ptom
ycin
(ST
R)o
rtri
fluop
eraz
ine
(Tf)
com
pare
dw
ithth
eiri
ndiv
idua
lact
iviti
esba
sed
onth
esu
rfac
ear
eaof
thei
rzon
eof
inhi
bitio
nag
ains
tSta
phyl
ococ
cus
aure
usan
dE
sche
rich
iaco
lia
Bac
teri
aD
iam
eter
ofzo
neof
inhi
bitio
n(m
m)
Indi
vidu
aldr
ugC
ombi
ned
drug
%In
crea
seon
the
basi
sof
surf
ace
area
bIn
divi
dual
drug
Com
bine
ddr
ug%
Incr
ease
onth
eba
sis
ofsu
rfac
ear
eab
Dc
(100
�g)
STR
(10
�g)
Dc
(100
�g)
STR
(10
�g)
Dc
STR
Dc
(200
�g)
Tf
(200
�g)
Dc
(200
�g)
Tf
(200
�g)
Dc
Tf
S.au
reus
NC
TC
6571
16.6
19.2
17.2
21.0
7.34
19.6
322
.727
.125
.328
.624
.22
11.3
8E
.col
iAT
CC
2592
213
.218
.615
.019
.429
.13
8.74
20.7
20.6
22.9
22.5
220.
36a
The
zone
sof
inhi
bitio
nw
ithre
gard
toD
can
dST
Ror
Tf
wer
ela
rger
insi
zeth
anth
ose
form
edsi
ngly
with
the
sam
eco
mpo
unds
.The
sew
ere
calc
ulat
edst
atis
tical
lyby
dete
rmin
ing
Stud
ent’s
t-te
stba
sed
onth
eva
lues
ofst
anda
rdde
viat
ion
and
stan
dard
erro
rob
tain
ed,w
hich
show
eddi
ffer
ence
sto
behi
ghly
sign
ifica
nt(P
<0.
01)
with
resp
ectt
oal
lthe
test
edba
cter
ia.
bM
ean
surf
ace
area
ofth
ezo
neof
inhi
bitio
n(m
m2)
was
calc
ulat
edas
�r2
onth
eba
sis
ofth
em
ean
diam
eter
(2r)
,and
the
%in
crea
sew
asca
lcul
ated
as(B
–A)/
A×
100,
whe
reA
=su
rfac
ear
eadu
eto
indi
vidu
alef
fect
and
B=
surf
ace
area
due
toco
mbi
ned
effe
ct;t
his
was
high
lysi
gnifi
cant
(P<
0.01
).
FK
TE
fisu
4
athpflfTmpfieftwl
cpcTvNru
atv
ig. 5. Effect of diclofenac (Dc) on DNA synthesis using Escherichia coli12C600.
hese results suggest that Dc inhibits the in vitro growth of. coli.
Agarose gel electrophoresis of plasmid DNA extractedrom donor (wild-type) and recipient (step-up mutant) clin-cal isolates of E. coli along with reference E. coli V517howed the absence of any specific plasmid band in the step-p mutant (data not shown).
. Discussion
The phenylacetic acid derivative Dc possesses analgesic,ntipyretic and anti-inflammatory properties. In recent years,his non-steroidal anti-inflammatory drug was shown toave antimicrobial activity against a wide range of Gram-ositive and Gram-negative bacteria, with MICs rangingrom 50 �g/mL to 200 �g/mL for Gram-negatives and evenower for some Gram-positives [6]. Dc is bactericidal bothor Gram-positive and Gram-negative bacterial strains [6].herefore, this drug could offer significant protection toice challenged with a virulent bacterium. Although Dc
roduces negative side effects in 20% of patients treatedor inflammation [40], in the current study we found thatt could be tolerated by mice for the entire period of thexperiment. Others have reported similar findings [6,41]. Theact that mice tolerate the drug better than humans is dueo the far more rapid heart rate of mice (800 beats/min),hich results in rapid destruction/alteration of the drug by the
iver.The antibacterial activity of Dc is demonstrated in the
urrent study by a variety of methods: by reduced incor-oration of 3H-thymidine; by CFU count in bacterial brothultures containing the agent; and by Kirby–Bauer method.he study also shows that Dc is synergistic in vitro and inivo when combined with STR or with the non-antibiotic Tf.evertheless, although these three drugs when used alone are
elatively safe, at this time one cannot predict whether theirse in combination is free of any major side effects.
Putting aside the potential of combination therapy withntibiotics and Dc for the management of bacterial infec-ions, clearly the ability of this agent to clear mice of a highlyirulent bacterial infection suggests similar potential for the
248 N.K. Dutta et al. / International Journal of Antimicrobial Agents 30 (2007) 242–249
Table 5Variation in numbers of viable bacteria (CFU/mL) retrieved from the organs of mice treated with diclofenac (Dc), streptomycin (STR) and trifluoperazine (Tf)alone and in combination, and comparison with untreated animals (controls)
Groupa Drug (�g/mouse) CFU/mL
Liver Spleen Blood
I Dc (30 �g) 7.8 × 105–6.2 × 106 3.2 × 105–5.6 × 106 1.8 × 105–3.5 × 106
II STR (60 �g) 1.6 × 106–2.8 × 107 1.2 × 106–4.6 × 107 5.8 × 105–3.0 × 106
Tf (30 �g) 1.2 × 105–4.6 × 106 2.8 × 105–2.9 × 106 N.D.
III Dc (30 �g) + STR (60 �g) 1.2 × 104–2.8 × 105 2.2 × 104–4.8 × 105 8.8 × 103–7.9 × 104
Dc (30 �g) + Tf (30 �g) 5.5 × 103–2.0 × 105 1.6 × 103–3.9 × 104 N.D.
I 8.2 × 1
C
mt
caet
EFFM(
R
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
V Control (0.5 mL saline) 8.2 × 107–
FU, colony-forming units; N.D., not done.a Each group consisted of six mice.
anagement of specific multidrug-resistant bacterial infec-ions in humans, which are always problematic in therapy.
Lastly, as has been the case with each natural antibiotic, Dcould be used as a ‘lead compound’ for the synthesis of newgents that may be more active and perhaps devoid of sideffects. Nevertheless, it remains for future studies to discernhe mechanism of antibacterial activity of Dc.
Funding: This work was partially supported by grantsU-FSE/FEDER-POCTI-37579/FCB/2001 and EU-FSE/EDER-POCI/SAU-MMO/59370/2004 provided by theundacao para a Ciencia e a Tecnologia (FCT) of Portugal.. Martins was supported by grant SFRH/BD/14319/2003
FCT, Portugal).Competing interests: None declared.Ethical approval: Not required.
eferences
[1] Ray A, Rice LB. Wildcatters welcome: the need for new antimicrobialagents. Therapy 2004;1:1–5.
[2] Kristiansen JE. The antimicrobial activity of non-antibiotics. APMISSuppl 1992;30:7–14.
[3] Chakrabarty AN, Acharya DP, Neogi D, Dastidar SG. Drug interactionof promethazine & non-conventional antimicrobial chemotherapeuticagents. Indian J Med Res 1989;89:233–7.
[4] Kristiansen JE. Antimicrobial activity of nonantibiotics. ASM News1991;57:135–9.
[5] Radhakrishnan V, Ganguly K, Ganguly M, Dastidar SG, ChakrabartyAN. Potentiality of tricyclic compound thioridazine as an effec-tive antibacterial and antiplasmid agent. Indian J Exp Biol 1999;37:671–5.
[6] Bourlioux P, Moreaux JM, Su WJ, Boureau H. In vitro antimicrobialactivity of 18 phenothiazine derivatives: structure–activity relationship.APMIS Suppl 1992;30:40–3.
[7] Crowle AJ, Douvas GS, May MH. Chlorpromazine: a drug poten-tially useful for treating mycobacterial infections. Chemotherapy1992;38:410–9.
[8] Wainwright M, Amaral L. The phenothiazinium chromophore and theevolution of antimalarial drugs. Trop Med Int Health 2005;10:501–11.
[9] Chattopadhyay D, Dastidar SG, Chakrabarty AN. Determination of in
vitro activity of methdilazine, an antihistamine, and its synergism withaminoglycoside antibiotics. Indian J Med Microbiol 1987;5:171–7.10] Amaral L, Kristiansen JE, Lorian V. Synergic effect of chlorpro-mazine on the activity of some antibiotics. J Antimicrob Chemother1992;30:556–8.
[
08 2.4 × 108–1.8 × 109 4.8 × 107–1.2 × 108
11] Viveiros M, Amaral L. Enhancement of antibiotic activity against poly-drug resistant Mycobacterium tuberculosis by phenothiazines. Int JAntimicrob Agents 2001;17:225–8.
12] Asok Kumar K, Mazumdar K, Dutta NK, Karak P, Dastidar SG, Ray R.Evaluation of synergism between the aminoglycoside antibiotic strep-tomycin and the cardiovascular agent amlodipine. Biol Pharm Bull2004;27:1116–20.
13] Mazumdar K, Dutta NK, Kumar KA, Dastidar SG. In vitro and invivo synergism between tetracycline and the cardiovascular agentoxyfedrine HCl against common bacterial strains. Biol Pharm Bull2005;28:713–7.
14] Chakrabarty AN, Mookerjee M, Dastidar SG. Screening for anti-HIVdrugs that can combine virucidal and virustatic activities synergisti-cally. Int J Antimicrob Agents 2000;14:215–20.
15] Guha Thakurta A, Mandal SK, Ganguly K, Dastidar SG, ChakrabartyAN. A new powerful antibacterial synergistic combination of trimetho-prim and trimeprazine. Acta Microbiol Immunol Hung 2000;47:21–8.
16] Chattopadhyay D, Dastidar SG, Chakrabarty AN. Antimicrobialproperties of methdilazine and its synergism with antibioticsand some chemotherapeutic agents. Arzneimittelforschung 1988;38:869–72.
17] Kristiansen JE, Amaral L. The potential management of resistant infec-tions with non-antibiotics. J Antimicrob Chemother 1997;40:319–27.
18] Amaral L, Kristiansen JE, Viveiros M, Atouquia J. Activity of phe-nothiazines against antibiotic-resistant Mycobacterium tuberculosis: areview supporting further studies that may elucidate the potential useof thioridazine as anti-tuberculosis therapy. J Antimicrob Chemother2001;47:505–11.
19] Amaral L, Viveiros M, Molnar J. Antimicrobial activity of phenoth-iazines. In Vivo 2004;18:725–31.
20] Martins M, Schelz Z, Martins A, et al. In vitro and ex vivo activityof thioridazine derivatives against Mycobacterium tuberculosis. Int JAntimicrob Agents 2007;29:338–40.
21] Amaral L, Viveiros M, Kristiansen JE. Phenothiazines: potentialalternatives for the management of antibiotic resistant infections oftuberculosis and malaria in developing countries. Trop Med Int Health2001;6:1016–22.
22] Annadurai S, Basu S, Ray S, Dastidar SG, Chakrabarty AN. Antibac-terial activity of the antiinflammatory agent diclofenac sodium. IndianJ Exp Biol 1998;36:86–90.
23] Amaral L, Kristiansen JE. Phenothiazines: potential management ofCreutzfeldt–Jacob disease and its variants. Int J Antimicrob Agents2001;18:411–7.
24] Amaral L, Kristiansen JE. Phenothiazines: an alternative to conven-
tional therapy for the initial management of suspected multidrugresistant tuberculosis. A call for studies. Int J Antimicrob Agents2000;14:173–6.25] Collee JG, Miles RS, Watt B. Tests for identification of bacteria. In:Collee JG, Fraser AG, Marmion BP, Simmons A, editors. Mackie &

l of An
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
N.K. Dutta et al. / International Journa
McCartney’s practical medical microbiology. 14th ed. New York, NY:Churchill Livingstone; 1996. p. 131–49.
26] McFarland J. The nephelometer: an instrument for estimating the num-ber of bacteria in suspensions used for calculating the opsonic indexand for vaccines. J Am Med Assoc 1907;49:1176–8.
27] National Committee for Clinical Laboratory Standards. Methods fordilution in antimicrobial susceptibility tests. Approved standard M2-A5. Villanova, PA: NCCLS; 1993.
28] Krogstad DJ, Moellering RC. Combinations of antibiotics, mecha-nisms of interaction against bacteria. In: Lorian V, editor. Antibioticsin laboratory medicine. Baltimore, MD: Williams and Wilkins; 1980.p. 298–341.
29] National Institutes of Health. Guide for the Care and Use of LaboratoryAnimals. 7th ed. Washington, DC: National Academy Press; 1996.
30] Reed LV, Muench H. A simple method for estimating fifty per centendpoints. Am J Hyg 1938;27:493–7.
31] Bhattacharya GK, Johnson RA. Statistical concepts and methods. NewYork, NY: John Wiley and Sons; 1977.
32] National Committee for Clinical Laboratory Standards. Performancestandards for antimicrobial disk susceptibility tests. Approved standardM2-A8. Wayne, PA: NCCLS; 2003.
33] Cruickshank R, Duguid JP, Marmion BP, Swain RHA, editors. Medicalmicrobiology. London, UK: Churchill Livingstone; 1989. p. 201–8.
[
timicrobial Agents 30 (2007) 242–249 249
34] Eliopoulos GM, Moellering RC. Antimicrobial combinations. In:Lorian V, editor. Antibiotics in laboratory medicine. 4th ed. Baltimore,MD: Williams and Wilkins; 1996. p. 330–96.
35] Lewis AJ, Furst DW. Nonsteroidal anti-inflammatory drugs: mecha-nisms and clinical use. New York, NY: Marcel Dekker; 1987.
36] Amaral L, Trigenis B, Viano I. A rapid radioactive method for antibioticsusceptibility testing. J Clin Lab Automation 1981;1:179–84.
37] Amaral L, Trigenis B, Atkinson B. The radioactive thymidine incor-poration method for the determination of antibiotic susceptibility ofgram-negative bacilli. Eur J Clin Microbiol 1982;1:149–54.
38] Maniatis T, Fritsch EF, Sambrook TJ. Molecular cloning: a labora-tory manual. 9th ed. Cold Spring Harbor, NY: Cold Spring HarborLaboratory Press; 1984.
39] Spengler G, Molnar AM, Schelz Z, Amaral L, Sharples D, MolnarJ. The mechanism of plasmid curing in bacteria. Curr Drug Targets2006;7:823–41.
40] Dastidar SG, Ganguly K, Chaudhuri K, Chakrabarty AN. The anti-bacterial action of diclofenac shown by inhibition of DNA synthesis.
Int J Antimicrob Agents 2000;14:249–51.41] Annadurai S, Guha-Thakurta A, Sa B, Dastidar SG, Ray R, ChakrabartyAN. Experimental studies on synergism between aminoglycosidesand the antimicrobial antiinflammatory agent diclofenac sodium. JChemother 2002;14:47–53.




















