Talk, Tools, and Tensions: Observing biological talk over time
Upload
khangminh22Category
view
2download
0
4/21/15
1
Antibiotics: The Talk You Always
Wanted
Umang Sood, MD Washington University Saint Louis Division of Hospitalist Medicine
l I have no financial disclosures l Off-‐label uses of certain an7microbials will be discussed
l Chemical names will be used primarily (brand names when relevant)
Overall goals of talk • “The talk I wanted in nursing school”
• The goals of this talk is to provide a: – Review of basic understanding as to how antibiotics work – Practical approach to choosing an empiric antibiotic regimen – Deeper understanding of antibiotic resistance – Good balance of inpatient and outpatient antibiotics
Three Ways to Learn An7bio7cs
• Antibiotic classes – penicillins, cephalosporins, macrolides,…
• Which drugs kill a particular bacteria – “Which antibiotics have pseudomonas coverage?”
• Disease based – “Which antibiotics are recommended for AOM?”
Outline l History of an7bio7cs l Overview of how an7bio7cs work l Things to consider when choosing an an7bio7c l Bacterial resistance and beta-‐lactamases l Overview of specific an7bio7cs
n organisms covered n various uses in pediatrics n resistance mechanisms n pharmacological considera7ons and side effects
l Case discussions intermixed l Feel free to interrupt with ques1ons!
Sir Alexander Fleming-‐ 1929

4/21/15
2
History of An7bio7cs 1910 -‐ arsenic (Salvarsan) 1935 -‐ sulfanilamide (Prontosil) 1942 -‐ benzylpenicillin 1944 -‐ streptomycin 1949 -‐ chloramphenicol 1952 -‐ erythromycin 1955 -‐ tetracycline 1955 -‐ vancomycin 1960 -‐ methicillin 1961 -‐ ampicillin 1961 -‐ TMP / SMX 1964 -‐ gentamicin
1968 - clindamycin 1971 - cefazolin 1972 - amoxicillin 1975 - ticarcillin 1977 - cefuroxime 1982 - ceftriaxone 1983 - ceftazidime 1985 - imipenem 1987 - ciprofloxacin 1988 - azithromycin 1994 - cefepime 2000 - linezolid
Review and Overview of Bacterial Targets
1) Cell Wall 2) Protein Synthesis 3) Metabolic Inhibitors 4) Nucleic Acid Synthesis and thus DNA replica7on
Review and Overview of Bacterial Targets: Bacterial Cell Walls
• Except for Mycoplasma and rela7ves, all bacteria possess pep7doglycan – Provides shape and structural support to bacterial cells
– Structure contributes to its func7on • Polysaccharide chains composed of 2 alterna7ng sugars, N-‐acetylglucosamine (NAG) and N-‐acetylmuramic acid (NAM)
• Cross-‐linked in 3 dimensions with amino acid chains • A breach in pep7doglycan endangers the bacterium
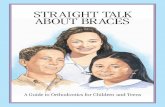
Pep7doglycan Molecule Bacterial Cell Walls
• Bacterial cytoplasm is generally hypertonic compared to their environment • Net flow of water: into
cell • Wall under high
osmo7c pressure
There is no molecule similar to peptidoglycan in humans, making drugs that target cell wall synthesis
very selective in their toxicity against bacteria.

4/21/15
3
Gram posi7ve & Gram Nega7ve • Gram posi7ve bacteria have a thick cell wall
– Pep7doglycan directly accessible from environment • Gram nega7ve bacteria have a different wall
– Thin layer of pep7doglycan – Surrounded by an outer membrane composed of lipopolysaccharide, phospholipids, and proteins
– Outer membrane is a barrier to diffusion of molecules including many an7bio7cs
• Some hydrophobic an7bio7cs may diffuse in. • Porins allow passage of only some an7bio7cs
Gram posi7ve & Gram Nega7ve
Bacteriosta7c vs. Bactericidal
• An7bio7cs differ by mode of ac7on • Bacteriosta1c compounds inhibit the growth of
bacteria – Holds invaders in check; host immune system does the killing
• Bactericidal compounds directly kill the bacteria • Loca7on and severity of infec7on affect choice of
an7bio7c – E.g. CNS infec7on calls for bactericidal treatment.
Case #1
16 yo p/w sore throat and has a posi7ve rapid strep test. The best an7bio7c choice is:
A. Amoxicillin 40-‐50 mg/kg/day div BID B. Amoxicillin 80-‐90 mg/kg/day div BID C. Azithromycin 12 mg/kg/day x 5 days D. Penicillin VK
Case #1
16 yo p/w sore throat and has a posi7ve rapid strep test. The best an7bio7c choice is:
A. Amoxicillin 40-‐50 mg/kg/day div BID B. Amoxicillin 80-‐90 mg/kg/day div BID C. Azithromycin 12 mg/kg/day x 5 days D. Penicillin VK

4/21/15
4
1-‐Inhibi7on of cell wall synthesis
l Mechanism: n binds to penicillin binding proteins (PBPs)àprevents cross linkage between pep7de chains in cell walls (especially gram +) and therefore cannot syntehesize reinforced cell wallàs7mulates endogenous autoly7c systemsà lysis when they try to grow
l Time dependent bacteriocidal killing • All of these only kill growing bacteria
Penicillin backbone
Beta-‐lactam structure
Beta Lactams
are poorly lipid soluble and do not cross the blood-‐brain barrier in appreciable concentra7ons unless it is inflamed (so they are effec7ve in meningi7s)
• They are ac7vely excreted unchanged by the kidney, but the dose should be reduced in severe renal failure
Two ways bacteria develop resistance to beta-‐lactams
1. Alteration of the penicillin binding protein (PBP) – Pneumococcus – Staph aureus resistance to methicillin
2. Production of beta-lactamases (>200 identified) – Hydrolyze penicillin only (“penicillinase”) – Hydrolyze 3rd gen cephalosporins, but not cefepime – Hydrolyze all beta-lactams other than carbapenems – Hydrolyze all beta-lactams including carbapenems

4/21/15
5
Important Beta-‐lactamases • AmpC beta-‐lactamases
– SPACE organisms (Serra7a, Providencia, Pseudomonas, Acinetobacter, Citrobacter, Enterobacter)
– resistant to 3rd gen. cephs and beta-‐lactamase inhibitors
– use cefepime or carbapenems
• Extended spectrum beta-‐
lactamases (ESBLs) – Hydrolyze all beta-‐lactams
but carbapenems – E. coli, Klebsiella, Proteus,
others
Beta-‐lactams: Penicillin
(acid labile) (acid stable) (mod. serum levels for 12H)
(low serum levels for 3-‐4 weeks)
l Ager ~70 years of penicillin use, GAS and GBS are exquisitely sensi7ve
Beta-‐lactams: penicillin
l S7ll drug of choice for: n Group A and B streptococcus n Rou7ne dental infec7ons n Pasteurella multocida n Rat bite fever n Treponema pallidum n Pneumococcal prophylaxis in HbSS
Case #2 You see a 4 yo in your office with a PMH significant for autism. He presents with fever to 101 F and sore throat. Exam shows tonsillar erythema and exudate. Rapid strep is positive. Mom says he won’t take oral meds well. They are leaving for Disney World tomorrow. You prescribe:
A. IM ceftriaxone x 1 B. IM ampicillin C. IM penicillin aqueous G D. IM Bicillin CR (procaine and benzathine
penicillin)
Case #2 You see a 4 yo in your office with a PMH significant for autism. He presents with fever to 101 F and sore throat. Exam shows tonsillar erythema and exudate. Rapid strep is positive. Mom says he won’t take oral meds well. They are leaving for Disney World tomorrow. You prescribe:
A. IM ceftriaxone x 1 B. IM ampicillin C. IM penicillin aqueous G D. IM Bicillin CR (procaine and benzathine
penicillin)
Case #3 21 mo old presents with fever to 102.5F and obvious bilateral AOM. His only other illness was 12 months ago and it was AOM treated with successfully with amoxicillin. The best antibiotic choice is:
A. amoxicillin 40-50 mg/kg/day div BID B. amoxicillin 80-90 mg/kg/day div BID C. azithromycin D. amoxicillin / clavulanic acid (Augmentin) E. cefdinir (Omnicef)

4/21/15
6
Case #3 21 mo old presents with fever to 102.5F and obvious bilateral AOM. His only other illness was 12 months ago and was AOM treated with successfully with amoxicillin. The best antibiotic choice is:
A. amoxicillin 40-50 mg/kg/day div BID B. amoxicillin 80-90 mg/kg/day div BID C. azithromycin D. amoxicillin / clavulanic acid (Augmentin) E. cefdinir (Omnicef)
Beta lactams -‐ aminopenicillins
l More GN coverage than PCN, with same GP coverage l E. Coli, Klebsiella, Proteus. H. Flu,
l Aminopenicillins are popular in pediatrics because:
n Amoxicillin is so palatable (Yum!) n AOM n Community acquired pneumonia n UTI (some7mes) n Neonatal sepsis to cover Listeria, GBS, enterococci
S. pneumoniae and H. influenzae B • 1940-1975
– S. pneumo and H. flu B common – Penicillin resistance in both uncommon
• 1985 – Hib B vaccine – Leads to significant decline in invasive disease – Non-typable H. flu less virulent
• 1980-2000 – Rise in penicillin-resistant pneumococcus
• 2001 – Prevnar 7 • 2001-2010
– Rise of emerging serotypes (i.e. 19 A) – Emerging serotypes often had high penicillin resistance
S. pneumoniae and H. influenzae b • 2004-2006
– AAP: increase amoxicillin to 80-100mg/kg/day • 2010 – Prevnar 13
– included 19A and other emerging serotypes in vaccine • 2010-2013
– Decrease in penicillin-resistance serotypes! (prelim data) – CAP guidelines recommend ampicillin monotherapy! – Some increase in resistant NT H.flu (some beta-lactamase
negative)
• Do we still need high-dose amoxicillin? • Should we be using a beta-lactamase inhibitor or
cephalosporin more often to cover NT H. flu?
Case #4
2.5 yo p/w 4 days of fever and cough. RR=30, SpO2 is 93% on 1L. CXR shows RLL consolida7on You admit to the floor and start:
A. IV ampicillin B. IV cefuroxime C. IV cegriaxone D. azithromycin
Case #4
2.5 yo p/w 4 days of fever and cough. RR=30, SpO2 is 93% on 1L. CXR shows RLL consolida7on You admit to the floor and start:
A. IV ampicillin B. IV cefuroxime C. IV cegriaxone D. azithromycin

4/21/15
7
The penicillinase-resistant penicillins
– Resistant to S. aureus’s beta-lactamase
– Still drug of choice for MSSA infections
• Unfortunately, S. aureus is smart – Methicillin
resistance first seen in 1961
An7-‐pseudomonal penicillins
l Higher affinity for PBPs + beqer GN penetra7on l Broad GN coverage
(including Pseudomonas) while retaining gram posi7ve coverage
l Ampicillin beqer for S.
pneumo + enterococci l Pipercillin > 7carcillin in GN
and enterococci l Piperacillin has worse renal
effects
Case #5 14 mo old male with fever to 103F, bilateral otitis media on exam. He appears non-toxic but miserable. This is his third episode of otitis media and he has been treated with amoxicillin at 80mg/kg/day each time, most recently 2 weeks ago.
You decide to treat with: A. amoxicillin at 80-90 mg/kg/day B. amoxicillin / clavulanic acid (Augmentin) C. Cefixime (Suprax) D. azithromycin
Case #5 14 mo old male with fever to 103F, bilateral otitis media on exam. He appears non-toxic but miserable. This is his third episode of otitis media and he has been treated with amoxicillin at 80mg/kg/day each time, most recently 2 weeks ago.
You decide to treat with: A. amoxicillin at 80-90 mg/kg/day B. amoxicillin / clavulanic acid (Augmentin) C. Cefixime (Suprax) D. azithromycin
Beta-‐lactam/beta-‐lactamase inhibitors
• Activity against MSSA, most GNs, anaerobes
Amoxicillin / clavulanic acid (Augmen7n)
• Amox:clavulanic acid ratio varies on dosing schedule • Covers MSSA and beta-lactamase producing strains
l H. flu, M. catarrhalis l E. coli, Proteus, Klebsiella l Anaerobes
• Not effective against resistant pneumococcus
• Indications: PNA, AOM, UTI, SSTI, bite wounds • Clavulanic acid causes diarrhea (~9%)

4/21/15
8
Dosage forms Amox (mg) Clav (mg) Ratio
Suspension 125 31.25 4:1 250 62.5 4:1 200 28.5 7:1 400 57 7:1 600ES 42.9 14:1
Chewables 125 31.25 4:1 250 62.5 4:1 200 28.5 7:1 400 57 7:1
Tabs (film coated)
250 125 2:1 500 125 4:1 875 125 7:1 1000XR 62.5 16:1
Augmentin dosing can be confusing
l Above concentra7ons appropriate for 80-‐90 mg/kg/day dosing l BID sufficient in most cases, but consider TID for pneumonia
Dosage forms Amox (mg) Clav (mg) Ratio
Suspension
200 28.5 7:1 400 57 7:1 600ES 42.9 14:1
Chewables
200 28.5 7:1 400 57 7:1
Augmentin Dosing
Case #6 l 4 yo male p/w fever and significant swelling/redness
around his right eye. He is non-‐toxic appearing. l You want to admit for IV an7bio7cs.
The best an7bio7c regimen is: A. Ampicillin / sulbactam (Unasyn) B. Vancomycin + ampicillin/sulbactam (Unasyn) C. Clindamycin + cegriaxone D. Vancomycin + cegriaxone E. Clindamycin monotherapy
Case #6 l 4 yo male p/w fever and significant swelling/redness
around his right eye. He is non-‐toxic appearing. l You want to admit for IV an7bio7cs.
The best an7bio7c regimen is: A. Ampicillin / sulbactam (Unasyn) B. Vancomycin + ampicillin/sulbactam (Unasyn) C. Clindamycin + cegriaxone D. Vancomycin + cegriaxone E. Clindamycin monotherapy
Ampicillin / sulbactam (Unasyn)
l IV equivalent to Augmen7n
l Excellent MSSA/GAS coverage
l Good gram nega7ve/anaerobe coverage
l Used for SSTIs, UTIs, head and neck infec7ons
l No ac7vity against ESBLs and MRSA
Ticarcillin / clavulanic acid (Timen7n)
l Broad GP, GN, anaerobic coverage (including Pseudo.)
l Misses: MRSA, some enterococci, resistant S. pnuemo
l Indica7ons: intraabdominal infec7ons, F+N, SSTIs, UTIs
l Na7onal shortage as of 2012-‐2013

4/21/15
9
Pipercillin / tazobactam (Zosyn) l Broad GP, GN + anaerobic
coverage (including Pseudo.) l Slightly broader GN and beqer
enterococci coverage when compared to Timen7n
l Misses: MRSA, some enterococci, resistant S. pnuemo
l Indica7ons: intraabdominal infec7ons, F+N, SSTIs, UTIs
l Beware of renal side effects (esp with vanco/IV contrast)
Beta-‐lactams -‐ cephalosporins
S
Cephalosporin backbone
Cephalosporins Spectrum
Cephalosporins
• All have activity against MSSA
• Increased GN coverage with higher generations
• ALWAYS miss enterococci, Listeria, MRSA
• 1st generation - poor CSF penetration
• 3rd and 4th generation - good CSF penetration
• Renal excretion except for ceftriaxone
1st genera7on cephalosporins
l Good GP (including MSSA) and some GN l Not effec7ve against H. flu or M. catarrhalis
-‐ pre-‐op, osteo, MSSA
-‐ SSTI, UTI
-‐ QD for GAS
*All the PH ones! Excpet Cefazolin… don’t let this PHaze you J

4/21/15
10
2nd genera7on cephalosporins
• Think: 1st gen ceph PLUS H. flu, M. cat. coverage
- used for AOM, CAP, early Lyme
- same as above
- serum sickness
– no longer 1st line for CAP
2nd Gen. Ceph. -‐ the cephamycins
• Cefoxitin (IV) and cefotetan (IV)
• “Cefuroxime + anaerobic coverage”
• Indications: – intraabdominal infx (better
options now avail.) – Abdominal surgery
perioperative prophylaxis – PID: “cefoxy / doxy”
• 25% B. fragilis are resistant
3rd genera7on cephalosporins
– QD – Inferior to high-dose amoxicillin for S. pneumo CAP
– QD
- QD – Excellent gram negative (mildly better than cefdinir) – Only fair gram positive coverage – Very expensive
• cefdinir (Omnicef) 250 mg/5ml (60 ml) = $19.65 • cefixime (Suprax) 200 mg/5ml (50 ml) = $247.42
4th genera7on -‐ Cefepime
• Excellent GN – stability against GN beta-lactamases
• Good for AmpC-mediated resistant SPACE organisms
• Not recommended for ESBL, steno., burkholderia sp.
• Retains good gram positive coverage (MSSA and PRP)
• Covers ~90% of Pseudomonas
• Indications: F+N, serious GN infections
GPs Pseudomonas
Aztreonam
• Gram negative plus moderate Pseudomonas activity
• No gram positive activity • Used inhaled in CF
patients • Can be used in patients
with beta-lactam allergies • IV form in limited use
today
Carbapenems
(IV) – lowers seizure threshold (IV) - most widely used
(IV, IM) - QD dosing, misses Pseudomonas • Broadest activity of beta-lactams (GP+GN+anaerobes) • Good CSF penetration

4/21/15
11
Carbapenems
l Effec7ve against almost all Citrobacter, Enterobacter, E. coli, Klebsiella, Serra7a, Pseudomonas, B. frag.
l S7ll misses: n MRSA n some enterococci n Stenotrophomonas sp. n 10% of Pseudomonas strains n Metallo-‐beta-‐lactamases or carbapenemases
Case #7
5 yo previously well child presents with fever to 103F, meningismus, ill appearance. LP shows 1500 WBC/hpf, glucose 20, protein 500.
Your choice of empiric antibiotics should be:
a. ampicillin and ceftriaxone b. ceftriaxone c. vancomycin and ceftriaxone d. vancomycin and meropenem
Case #7
5 yo previously well child presents with fever to 103F, meningismus, ill appearance. LP shows 1500 WBC/hpf, glucose 20, protein 500.
Your choice of empiric antibiotics should be:
a. ampicillin and ceftriaxone b. ceftriaxone c. vancomycin and ceftriaxone d. vancomycin and meropenem
Vancomycin • Interferes with bacterial cell
wall production • Slowly bactericidal against
GP ONLY, NO GRAM NEGATIVE – Opposite of Meropenum
• Binds D-ala-D-ala moieties of cell wall (not PBP) so interferes in an earlier stage than PCN
• Resistance: – thicken cell wall (VISA) – Mutation leading to
altered binding- D-ala D-lac (VRSA)
• Vancomycin resistant enterococci still rare at SLCH
Vancomycin
l CSF penetra7on good with inflamed meninges l Indica7ons:
n MRSA n beta-‐lactam allergies n CONS, Enterococcus infec7ons (? with gent), n empiric meningi7s treatment (S. pneumo coverage) n C. diff
l Red man syndrome -‐ flushing, pruri7s, angioedema l Ototoxicity (peak over 50 mcg/ml) and nephrotoxicity l Trough levels 10-‐20 moderate infec7ons, 15-‐20 severe
Case #8 You are called to a delivery of a BG born vaginally to a GBS posi7ve mom who did not receive an7bio7c prophylaxis. Mom had fever in labor and the OB says there is evidence of chorioamnioni7s. The baby looks well.
You obtain a blood culture and start: A. cefotaxime B. ampicillin and cefotaxime C. ampicillin and gentamicin D. No an7bio7cs

4/21/15
12
Case #8 You are called to a delivery of a BG born vaginally to a GBS posi7ve mom who did not receive an7bio7c prophylaxis. Mom had fever in labor and the OB says there is evidence of chorioamnioni7s. The baby looks well.
You obtain a blood culture and start: A. cefotaxime B. ampicillin and cefotaxime C. ampicillin and gentamicin D. No an7bio7cs
2-‐ Inhibi7on of Protein Synthesis
(bactericidal):
(bacteriosta1c) • These act on the ribosome which
is the site of protein synthesis – Has two parts:
• Large Unit: 50S • Smaller Unit: 30S
Protein synthesis inhibitors
• Aminoglycosides (streptomycin, gentamicin) change shape of 30S ribosome subunit
• Tetracycline blocks access to A site of 30S subunit
Protein synthesis inhibitors
• Chloramphenicol block peptide bond formation from 50S subunit
• Macrolides (erythromycin) block 50S subunit action
Aminoglycosides
l Rapid, bacteriocidal, concentra7on dependent
l Bind to 30S subunit – so ini7a7on of protein synthesis can’t occur
l Covers: n Mostly GN organisms
(many Burkholderia and Pseudo)
n Some GP organisms (MSSA, many enterococci)
n Poorly lipid soluble so not given orally
Aminoglycosides
l Poor CSF penetra7on even if meninges are inflammed (killing dependent on high peaks)
l Excreted in urine unchangedà Urine concentra7on exceeds plasma 25-‐100Xà toxicity!! l QD dosing
l Indica1ons: neonatal sepsis, intraabdominal infec7ons, endocardi7s, complicated UTIs
l Aminoglycoside + cell wall agent = synergy for gram posi7ve bacteria (S. viridans, enterococci, S. aureus)
l Should not rou7nely be used as monotherapy l Allergy uncommon l Injures -‐ prox. renal tubules, cochlea, ves7b. apparatus

4/21/15
13
Tetracyclines
l Reversibly bind to 30S subunit l Resistance seen in GAS, H. flu, S. pneumo
l Resistant organisms develop an efflux pump and do not accumulate the drug.
l Indica7ons: n Doxy for RickeLsia, Ehrlichia, mycoplasma, Lyme dx, MRSA, anthrax, leptospirosis, Coxiella
n Minocycline for acne n They bind avidly to heavy metal ions and so absorption is
greatly reduced if taken with food, milk, antacids or iron tablets. Thus take 30 min before
Tetracyclines
• Adverse effects -‐ Destruc7on of normal intes7nal flora resul7ng in increased secondary infec7ons; GI upset, staining and impairment of the structure of bone and teeth, photosensi7vity,
Clindamycin
, although chemically dis1nct, is similar to erythromycin in mode of ac1on and spectrum.
l Binds 50S subunit l Gram posi7ve and anaerobes, NO GRAM NEG
n Covers ~85% CA-‐MRSA (careful if severe illness) n ~ 30% resistance in B. frag. n ~ 30% resistance in S. pnuemo
n Good oral absorp7on, but liquid tastes bad • It is rapidly absorbed and penetrates most 1ssues well, except
CNS. • Indica7ons: CA-‐MRSA, anaerobic infx, toxin suppression
Clindamycin (lincosamide class)
l Resistance by methyla7on of ribosomal subunit or efflux pump
l This methyla7on (erm gene) confers resistance to erythromycin and clindamycin
l Erm is inducible or cons7tu7ve l If inducible resistance, consider avoiding clindamycin
Macrolides
l Binds 50S subunit l Broad coverageà mainly for
gram + bugs l Many gram nega7ves resistant l Intracellular pathogens: l Distrubted well throughout the
body except brain and CSF. l Resistance is increasing l Penicillin resistant
pneumococcus are usually resistant to macrolides
Macrolides
• Indications: l Bartonella, Mycoplasma, Chlamydia, B. pertussis l AOM, GAS pharyngitis, pneumonia, sinusitis l H. pylori l Mycobacteria
• Azithromycin: long half life (QD x 5 days) • Pertussis and GAS require different dosing • Clinically inferior to amox/clav for AOM and sinusitis

4/21/15
14
Chloramphenicol
• Binds 50S • Broad – GP, GN, anaerobes,
mycoplasma, Rickettsia • Excellent CSF levels and oral
absorption • Adverse effects: Aplastic anemia, “gray baby” syndrome
• Indications: – Rickettsial disease with doxy
allergy – Brain abscess with resistant
B. frag • Use in underdeveloped
countries- useful as it is inexpensive
3-‐ Metabolic inhibitors-‐ Sulfa Drugs
• Sulfonamides (sulfanilamide) are structural analogs of PABA, a molecule crucial for Nucleic acid synthesis
• Humans do not synthesize dihydropteroic acid from PABA
• Trimethoprim interferes in next step DHF -‐> THF
Sulfa drugs
– Better known as Septra or Bactrim – Introduced together in1960’s due to synergy – TMP/SMX 1:5 ratio
• Broad coverage of gram positive and negative (IBD) (topical for seborrhea in 10% solution)
(toxoplasmosis) (Fansidar) - high
resistance
Sulfa drugs
l Indica7ons: l T(Tree): Respiratory tree-‐ pneumococcus, H.Flu therefore can be
used for PNA, OM, sinusi7s l M(Mouth): GI tract-‐ GN that cause diarrhea:Salmonella, Shigella,
E.Coli l P(PEE): Empiric UTI coverage; covers UTI and urethri7s caused by enterics
l SMX(Syndrome): PCP coverage in AIDS pa7ents. n CA-‐MRSA n Nocardia (if you see PNA and brain abscesses)
l Does NOT cover GAS (careful with SSTIs) l No longer recommended for AOM, sinusi7s, PNA
Case #9
9 yo with Grade IV urinary reflux and a history of multiple UTIs with many different gram negative organisms now presents with dysuria and urinalysis suggestive of UTI. Pt is AF and well appearing. Which of the following is the best empiric choice of oral antibiotics:
A. TMX/SMX B. amoxicillin C. ciprofloxacin D. cephalexin
Case #9
9 yo with Grade IV urinary reflux and a history of multiple UTIs with many different gram negative organisms now presents with dysuria and urinalysis suggestive of UTI. Pt is AF and well appearing. Which of the following is the best empiric choice of oral antibiotics:
A. TMX/SMX B. amoxicillin C. ciprofloxacin D. cephalexin

4/21/15
15
4-‐Interference with nucleic acid synthesis
• Bacterial DNA is nega7vely supercoiled – Supercoiling is maintained by gyrase, a type II topoisomerase. – Inhibi7on of gyrase and type IV topoisomerase interferes with DNA replica7on, causes cell death
– Eukaryo7c topoisomerases differ in structure
Fluoroquinolones
l Bind to A subunit of DNA gyrase (topoisomerase) and prevent supercoiling of DNA, thereby inhibi7ng DNA synthesis.
l Spectrum: GPCs and UTI’s l Rare use in pediatrics because of concern for tendon
rupture /car7lage problems l Good oral absorp7on (70% cipro and 95% levo)
and moxi have beqer GP coverage beqer has beqer GN coverage and Pseudomonas has broad coverage and anaerobic coverage
Fluoroquinolones
FDA approved indications 1. Complicated UTI / pyelonephritis 2. Exposure to anthrax Acceptable FQ uses in pediatrics may include: 1. Pseudomonas infections (OE, UTI, osteochondritis) 2. Mycobacterial infections 3. Bacterial enteritis (e.g. MDR Salmonella, Shigella) 4. Patients with life-threatening allergies to other classes
Metronidazole (Flagyl)
l Binds to DNA and prevents replica7on l It is widely distributed in the body (including into
abscess cavi7es) l Gold standard for anaerobic coverage l Best coverage for B. frag l Indica7ons:
n CSF penetra7on for brain abscess n Intraabdominal anaerobic coverage (Bacteroides, Clostrida)
n C. diff n Entameba histoly7ca, Giardia
Case #10
3 yo had prolonged close contact with a sibling with N. meningi7dis. She is asymptoma7c. Appropriate prophylaxis would be:
A. Rifampin B. Ciprofloxacin C. Azithromycin D. Penicillin VK
Case #10
3 yo had prolonged close contact with a sibling with N. meningi7dis. She is asymptoma7c. Appropriate prophylaxis would be:
A. Rifampin B. Ciprofloxacin C. Azithromycin D. Penicillin VK

4/21/15
16
Rifampin
l Inhibit DNA-‐dependent RNA polymerase l Excellent oral absorp7on and CSF penetra7on l Prophylaxis for contacts of H.flu and N. meningi7dis l Indica7ons:
n Shunt or catheter-‐related Staph infec7ons n S. aureus related hardware infec7ons, n Bartonella, atypical mycobacteria, TB
l Hepatotoxicity, discolora7on of body fluids
Spectrum of Ac7on of An7microbials
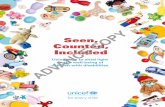
An7biograms • Developed by the micro lab based on isolated
strains • Only represents in-vitro susceptibility • MICs are used to determine susceptibility
– These can change over time – May vary based on location of infection (e.g.
CNS) • Ask: “Does this represent my patient
population?”
Case #1
48
Gram posi7ve an7biogram 22009 SLCH antibiogram
94
46
Considera7ons for empiric an7bio7cs
• What organisms do you want to cover? • Treating an active infection OR providing prophylaxis? • How do you want to administer the drug? • How sick is the patient? • Patient allergies? • Dosing schedule? • Palatability of oral medication? • Hepatic or renal problems? • What medications is the child already on? • Adverse reactions / toxicity of drug? • Bacteriocidal versus bacteriostatic? • Cost?

4/21/15
17
THE END! Resources
• Miller, Aaron. 'An7bio7cs I +II'. 2014. Lecture. Saint Louis Children’s Hospital
• Gladwin, Mark, and Bill Traqler. Clinical Microbiology Made Ridiculously Simple. Miami: MedMaster, Inc., 2007. Print.
• hqps://eis.hu.edu.jo/acuploads/10111/lecture%205-‐%20an1bio1cs.ppt
Copyright © 2022 FDOKUMEN