
Pitfalls of using microalbuminuria as a screening tool to ...
154
Pitfalls of using microalbuminuria as a screening tool to identify subjects with increased risk for kidney and cardiovascular disease Results of the Unreferred Renal Insufficiency (URI) study and the Early Renal Impairment and Cardiovascular Assessment in Belgium study (ERICABEL). Arjan van der Tol Promotor: Prof. dr. Wim Van Biesen Co-promotor: Prof. dr. Raymond Vanholder Thesis submitted in fulfillment of the requirements for the degree of ‘Doctor in Health Sciences’ 2014
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Pitfalls of using microalbuminuria as a screening tool to ...

Pitfalls of using microalbuminuria as a screening tool to
identify subjects with increased risk for kidney and
cardiovascular disease
Results of the Unreferred Renal Insufficiency (URI) study and the Early Renal
Impairment and Cardiovascular Assessment in Belgium study (ERICABEL).
Arjan van der Tol
Promotor: Prof. dr. Wim Van Biesen
Co-promotor: Prof. dr. Raymond Vanholder
Thesis submitted in fulfillment of the requirements for the degree of ‘Doctor in Health Sciences’ 2014


Contents
TABLE OF CONTENTS
LIST OF ABBREVIATIONS ....................................................................................................... 5
CHAPTER 1: INTRODUCTION ................................................................................................ 7
1.1 Preface ................................................................................................................................... 9
1.2. Normal renal handling of albuminuria ................................................................................. 11
1.3. Mechanisms of tubular and glomerular albuminuria ........................................................... 13
1.4. Albuminuria as a manifestation of chronic kidney disease ................................................. 18
1.5. Albuminuria as a manifestation of cardiovascular disease .................................................. 21
1.6. The prevalence of albuminuria ............................................................................................ 25
1.7. How to measure albuminuria ............................................................................................... 27
1.8. Outline and aims of the thesis .............................................................................................. 30
1.9. Participants and methods ..................................................................................................... 31
1.10. References ............................................................................................................................ 33
CHAPTER 2: RESULTS ............................................................................................................ 43
2.1. Screening for cardiovascular and renal markers in unselected subjects: results
from URI trial ...................................................................................................................... 43
2.1.1. Towards a rational screening strategy for albuminuria ............................................. 45
2.1.2. Microalbuminuria is more consistent in presence of risk factors ............................... 65
2.1.3. Should screening of renal markers be recommended in a working population ......... 78
2.2. Screening for kidney disease in selected hypertensive subjects: results from the
ERICABEL study ................................................................................................................ 96
2.2.1 Statin use and the presence of microalbuminuria ....................................................... 97
CHAPTER 3: GENERAL DISCUSSION AND CONCLUSIONS ....................................... 115
3.1. The prevalence of microalbuminuria and macroalbuminuria, and the associations
with traditional cardiovascular risk factors in a general population .................................. 118
3.2. Should we use microalbuminuria as a screening tool to identify subjects with unrecognized
cardiovascular risk factors in a presumably healthy population ........................................ 120

Contents
3.3. Conditions which could lead to false positive test results of microalbuminuria ............... 121
3.4. Can we prevent ESRD by screening for microalbuminuria in a general population ......... 123
3.4.1. The disease should be an obvious burden for the individual and the community
in terms of death, poor quality of life and socio-economic factors including
health care costs ........................................................................................................ 124
3.4.2. The natural course of disease should be well-known and the disease should go
through an initial latent stage or be determined by risk factors, which can be
detected by appropriate tests .................................................................................... 125
3.4.3. A suitable test is highly sensitive and specific for the disease as well as being
acceptable to the person screened ............................................................................ 126
3.4.4. Screening followed by diagnosis and interventions in an early stage of the disease
should provide a better prognosis than intervention after spontaneously sought
treatment ................................................................................................................... 127
3.4.5. Adequate treatment or other intervention possibilities are indispensable.
Adequacy is determined both by proven medical effect and ethical and legal
acceptability .............................................................................................................. 128
3.4.6. The cost of case-finding should be economically balanced in relation to possible
expenditure on medical care as a whole ................................................................... 129
3.4.7. Case-finding should be a continuing process and the interval of testing should be
known ....................................................................................................................... 130
3.5 Conclusions ........................................................................................................................ 132
3.6 References .......................................................................................................................... 135
3.7 Conclusies .......................................................................................................................... 143
3.8 References .......................................................................................................................... 146
Dankwoord .................................................................................................................................. 149
Curriculum Vitae ......................................................................................................................... 151

List of abbreviations
LIST OF ABBREVIATIONS
ACR urinary albumin creatinine ratio (mg/g)
ACE-I angiotensin concerting enzyme inhibitor
ADA American Diabetes Association
ADVANCE Preterax and Diamicron Modified Released Control Education study
AER albumin excretion rate (mg/24 h)
AKI acute kidney injury
ARB angiotensin receptor blocker
Aus Diab Kidney study Australian Diabetes, Obesity and Lifestyle Study
BMI body mass index
BP blood pressure
CGA CKD classification: Cause, Glomerular filtration rate, Albuminuria
CVD cardiovascular disease
CKD chronic kidney disease
CKD-EPI Chronic Kidney Disease Epidemiology Collaboration
DALY disability adjusted life year
DM diabetes mellitus
EPIC-Norfolk European Prospective Investigation into Cancer in Norfolk
ERA-EDTA European Renal Association-European Dialysis Transplantation Association
ERICABEL Early Renal Impairment and Cardiovascular Assessment in Belgium study
ESRD end stage renal disease
GDP gross domestic product
GFR glomerular filtration rate
HMG-CoA reductase 3-hydroxy-3-methylglutaryl-CoA reductase
HOPE Heart Outcomes and Prevention Evaluation Study
HPLC high performance liquid chromatography
HUNT Nord-Trøndelag Health Study
HT hypertension
IDMS isotope dilution mass spectrometry
IFCC International Federation of Clinical Chemistry
IGT impaired glucose tolerance
IMAU intermittent microalbuminuria

List of abbreviations
K/DOQI Kidney Disease Outcomes Quality Initiative
KDIGO Kidney Disease Improving Global Outcomes
KEAPS Kidney Evaluation and Awareness Program in Sheffield
NCEP National Cholesterol Education Program
NHANES National Health and Nutrition Examination Survey
NKF National Kidney Foundation
NPHS1/2 congenital nephrotic syndrome of Finnish type
MAU microalbuminuria
MDRD Modification of Diet in Renal Disease
OCRL-1 oculocerebrorenal locus 1
ONTARGET Ongoing Telmisartan Alone and in combination with Ramipril Global
Endpoint Trial
PCER physicochemical exposure risk
PCR protein creatinine ratio
PMAU persistent microalbuminuria
PolNef Early detection of chronic kidney disease in Poland
PREVEND Prevention of Renal and Vascular End Stage Disease Study Group
QALY Quality Adjusted Life Year
RAAS renin angiotensin aldosterone system
RCT randomized control trial
RENAAL Reduction of Endpoints in NIDDM with Angiotensin II Antagonist Losartan
ROADMAP Randomized Olmesartan and Diabetes Microalbuminuria Prevention
RRT renal replacement therapy
SGLT-2 sodium glucose co-transporter 2
SNP single nucleotide polymorphism
TRPC transient receptor potential canonical
UAC urinary albumin concentration (mg/l)
USRDS United States Renal Data System
URIS Unreferred Renal Insufficiency Study
WHO World Health Organization
Zo-1 Zona Occludens 1

CHAPTER 1: INTRODUCTION


CHAPTER 1: Introduction
9
1.1 Preface
Around 20-25% of the Belgian population has hypertension and 5% has diabetes mellitus (1, 2).
Patients with diabetes mellitus and/or hypertension have an increased risk for chronic kidney
disease (CKD), yet only a small proportion of these patients progresses to end stage renal disease
(ESRD) to a degree that renal replacement therapy (RRT) in the form of dialysis or kidney
transplantation is required (3, 4). The prevalence of RRT was 1200 per million persons in
Belgium at 31 December 2012 (5). Asymptomatic microalbuminuria might precede the
development of ESRD by years (6, 7). Timely detection of microalbuminuria in patients with
diabetes and hypertension, followed by administration of renal protective agents, might reduce
the number of patients with ESRD (8). Consequently, the American Diabetes Association (ADA)
recommends annual screening for microalbuminuria in diabetes patients (1). Yet, in only one fifth
of the Belgian RRT patients, renal failure was caused by diabetes (5). Additionally,
microalbuminuria is common in the general population and an independent predictor of
cardiovascular and renal outcome (7, 9). It has been suggested to organize mass screening using
microalbuminuria to identify subjects with increased risk for cardiovascular and renal events (3,
10, 11). Testing for microalbuminuria is easy to perform and does not cause inconvenience for
the tested person. In the present thesis, we measured cardiovascular risk factors and albuminuria
in a Belgian working cohort (URI: unreferred renal insufficiency study) and in a Belgian
hypertensive cohort (ERICABEL: Early Renal Impairment and Cardiovascular Assessment in
Belgium study). We investigated which parameters are associated with microalbuminuria in the
URI and ERICABEL study and whether screening for microalbuminuria is useful to identify
persons with cardiovascular and renal disease.

CHAPTER 1: Introduction
10
Figure 1: normal renal handling of albumin
Figure 1a. Normal glomerulus and proximal tubule. Figure 1b. The glomerular filtration barrier
comprises the innermost fenestrated glomerular endothelial cells, glomerular basement membrane and the
outermost podocytes. The endothelial cells synthesize a negatively charged glycocalyx that forms a plug
in the fenestrae. Podocytes attach to the outermost aspect of the glomerular filtration barrier by foot
processes, between which there is a protein layer comprising the size barrier slit diaphragm. Figure 1c.
Proximal tubular cell. Filtered albumin is taken up by the megalin/cubilin mediated endocytosis of
proximal tubular cells, is internalized by endosomes, and degradated by the lysozymes. Adapted from (12).
Cubilin Albumin
Proximal tubular cell
Parietal
epithelial cell
Glomerular basement membrane
Podocyte
Glomerular endothelial cell
Fenestrae
Parietal epithelial cell
me
galin

CHAPTER 1: Introduction
11
1.2 Normal renal handling of albuminuria
Under normal conditions, the glomerular filtration barrier is nearly impermeable for albumin. The
histologic components of the ’glomerular filtration barrier’ include the endothelial surface layer
of glomerular fenestrated capillaries; the glomerular basement membrane and the slit diaphragm
(fig. 1b). Albumin filtration is restricted by the negatively charged endothelial glycocalyx and the
glomerular basement membrane, and by the fine pores of the slit diaphragm (13-15). The slit
diaphragm is a dynamic junction between podocyte foot processes (16). These foot processes
form a scaffolding around the capillary loops that are anchored to the glomerular basement
membrane via α3β1 integrin and α-/β-dystroglycans (17). Although the diameter of the
glomerular slit pores is slightly smaller than the diameter of albumin (3.5 versus 3.6 nm), some
albumin molecules might pass through the slit diaphragm by the variation in diameter of the slit-
pores and the shape of albumin (14, 18). The flux of albumin across the glomerular filter is driven
by different forces: convection, diffusion and electrokinetic effects (19). Experimental research in
normal rats shows that the glomerular-sieving coefficient of albumin is 0.00062 (14). As the
filtration of albumin in humans is considered to be small too, the amount of albumin filtered per
day is significant because the glomerular filtration rate is so high (filtered albumin = glomerular
filtration rate x plasma albumin x glomerular sieving coefficient of albumin: thus daily filtered
albumin = 144 L/day (100 mL/min x 60 min. x 24h) x 37 g/l x 0.00062 = 3.3 g/day) (14). Most
part of the filtered albumin (fig. 1a) is reabsorbed by the proximal tubular cells (fig. 1c). The
tubular uptake of albumin is mediated by megalin and cubilin. Cubilin was originally identified
as the intestinal intrinsic factor-B12 receptor and megalin is a member of the LDL receptor
family (20).

CHAPTER 1: Introduction
12
Figure 2a shows a normally functioning proximal tubular cell with uptake of albumin, including
carrier albumin for hormones, calcium, folate and vitamin A, D, B12 (20). Following uptake and
degradation of albumin into albumin fragments, the compound is metabolized and/or returned to
the circulation (20).
Figure 2: Endocytic receptors in the proximal tubular renal cells
Figure 2a: Megalin and/or cubilin normally mediate the uptake of filtered proteins, including carrier
protein for vitamins and hormones. Following uptake and degradation of protein, the compound is
metabolized and/or returned to the circulation. 2b: Loss of functional receptor expression, as observed in
rare inherited disorders, leads to defective uptake and tubular proteinuria with the possible loss of
important nutrients and associated deficiencies. 2c: Tubular protein overload, leads to increased tubular
uptake of proteins causing tubular cell apoptosis and change of function with activation of
proinflammatory and profibrotic mediators. 2d: Shedding of receptors, as may be observed in diabetes,
leads to increased urinary excretion of receptors and possible tubular cell dysfunction. Adapted from (20).
a: Normal receptor
mediated uptake of
filtered proteins
b: Loss of receptor
function leading to
tubular proteinuria
c: Tubular protein
overload
d: Shedding of
receptors
Interstitial
inflammation and
fibrosis, nephron
loss
megalin cubilin albumin
vitamin binding protein
lumen
blood

CHAPTER 1: Introduction
13
1.3 Mechanisms of tubular and glomerular albuminuria
Albuminuria occurs by dysfunction of the glomerular filtration barrier and/or of the receptor
mediated endocytosis process of the proximal tubular cells. Figure 2b shows that dysfunction of
proximal tubular receptors results in albuminuria and loss of nutrients (20). Whether this
mechanism could lead to progressive CKD in humans has not been investigated yet. Mutations of
the megalin encoding gene occur in rare genetic disorders, such as Donnai-Barrow and Facio-
Oculo-Acustico-Renal Syndrome, characterized by multiple developmental anomalies and
asymptomatic tubular albuminuria (20). Mutations of the cubulin encoding gene occur in
Imerslund-Gräsebeck disease, characterized by asymptomatic tubular albuminuria and
megaloblastic anemia due to intestinal and tubular vitamin B12 malabsorption (20-22). A
missense variant (SNP) in the cubulin gene is associated with tubular albuminuria in the general
and diabetic populations (23). The presence of tubular albuminuria in Dent’s disease is related to
genetic mutations (CLCN5 or OCRL1) causing abnormal endosomal and lysosomal trafficking in
the proximal tubular cells (24, 25). The tubular dysfunction in Dent’s disease is associated with
Fanconi syndrome, albuminuria, hypercalciuria, nephrocalcinosis, nephrolithiasis and renal
failure (26).
Increased protein synthesis or glomerular albumin leakage might result in albuminuria as tubular
albumin receptor mediated endocytosis is oversaturated (figure 2c). Tubular overflow proteinuria
might be an expression of a hematological disorder, yet it might also occur by exposure of toxic
agents, such as Chinese herbs, mercury or cadmium (27, 28). Both cadmium and mercury
increase the liver synthesis of metallothionein. This heavy metal binding low molecular weight
protein is freely filtered and is excreted by the kidney as the tubular reabsorption is saturated (29).
Conceivably, albuminuria protects the body, including the kidneys against the accumulation of
toxic heavy metals. However, in case of glomerular induced nephrotic range albuminuria,
receptor mediated endocytosis acts as a biological Trojan horse, by reabsorption of toxic fatty
acids and lipoproteins bound to albumin, leading to activation of pro-inflammatory and pro-
fibrotic mediators, tubular cell apoptosis, interstitial inflammation, fibrosis and nephron loss (20,
30-32). These receptors could be a potential target for therapy. Adenoviral delivery of antisense
RNA leading to partial knockdown of cubilin was shown to protect against adriamycine-induced
glomerulosclerosis and tubulointerstitial renal damage in rats despite resulting in higher levels of

CHAPTER 1: Introduction
14
albuminuria (33). In patients with nephrotic range proteinuria, statins might abrogate the toxic
effects of modified albumin by inhibiting protein uptake via inhibition of HMG-CoA reductase
and reduced prenylation of proteins involved in the endocytosis of the proximal tubular cell (34-
37), while in subjects with no albuminuria, statins induce tubular albuminuria by the same
mechanism (38-40).
Figure 2d shows that a reduction of megalin expression on the proximal tubular cells and the
coinciding increase of urinary megalin excretion, results in albuminuria. Shedding of the
receptors has been observed in diabetic patients, yet the underlying mechanism remains to be
elucidated (41). Additionally, diabetic patients with poor glycemic control have a higher
proportion of glycated albumin in urine than in plasma, which has been attributed to lower
efficiency of tubular uptake of modified glycated albumin (42). Reduction of albuminuria is
observed after correcting hyperglycemia (43). In vitro, megalin expression is reduced by
activation of tubular angiotensin II type 1A receptors (44). In diabetic rats, angiotensin II
blockade restores megalin expression associated with a decrease in albuminuria (45).
Angiotensin II plays a key role in renal hemodynamic and molecular mechanisms which lead to
albuminuria. Angiotensin II decreases renal blood flow and increases glomerular filtration for
albumin by inducing vasoconstriction of the efferent glomerular arterioles (46). Besides,
angiotensin II upregulates the expression of sodium-glucose cotransporter-2 (SGLT-2) in the
proximal tubules of patients with diabetes (47). As sodium reabsorption increases, the
concentration of sodium in the distal tubules decreases (47). This results in an inhibition of the
tubuloglomerular feedback that causes hyperfiltration by vasodilatation of afferent arterioles and
rising intraglomerular pressure (47). Interestingly, in adults with obesity and essential
hypertension glomerular hyperfiltration is also associated with increased sodium reabsorption in
the proximal tubules of the kidney (48). Additionally, direct release of angiotensin II, insulin,
prostaglandins, glucagon and growth hormones increases the intraglomerular pressure (46).
These hemodynamic disturbances lead to shedding of the endothelial surface layer of the
glomerular fenestrated capillaries and subsequent leakage of albumin into the sub-podocyte space
(15, 49). This consequently exposes the glomerular basal membrane and the podocytes to the
deleterious effects of modified albumin, resulting in thickening of basal membrane and retraction
of podocyte foot processes that lead to increased glomerular permeability for albumin (50).

CHAPTER 1: Introduction
15
The accompanying structural abnormalities, such as glomerular endothelial injury, foot process
detachment and podocyte loss are more marked in diabetic patients with macroalbuminuria than
in those with microalbuminuria or normoalbuminuria (51, 52). Traditionally, the presence of
microalbuminuria in diabetic patients is considered as a sign of early nephropathy. In the eighties,
Mogensen et.al. published retrospective data (figure 3) of 20 type 1 diabetic males who had poor
metabolic control and hyperfiltration, and who subsequently developed microalbuminuria, overt
nephropathy and decline of renal function over years (53-56).
Figure 3
Figure 3 Landmark publication of the natural course of diabetic nephropathy in 20 male patients with
insulin dependent diabetes mellitus (GFR measured with iothalamate). Poor metabolic control is
associated with GFR > 150 mL/min. After 7-14 years of diabetes, microalbuminuria develops, followed
by clinically overt nephropathy. After 18 years of diabetes blood pressure rises, GFR starts to decline and
ESRD is reached after 25 years. Adapted from (56).

CHAPTER 1: Introduction
16
This hyperfiltration theory has been universally accepted as the natural cause of diabetic
nephropathy, and extended to individuals with impaired glucose tolerance, metabolic syndrome
and hypertension since glomerular hyperfiltration in these conditions also predicts de novo
microalbuminuria (56-60). For this reason, it is discussed whether a screening of
microalbuminuria in the general population to detect subjects with early nephropathy should be
recommended (11). Microalbuminuria is not only an early predictor for overt nephropathy, it
predicts independently also cardiovascular disease (CVD) and mortality (61, 62). Moreover,
whether the presence of microalbuminuria inevitably results in overt nephropathy is uncertain,
especially nowadays more and more patients are treated for their underlying risk factors (4, 63).
In primary kidney disease the pathophysiologic course of proteinuria might be different.
Mutations in molecular signaling pathways of the slit diaphragm or in podocyte genes have been
implicated in the susceptibility for idiopathic focal and segmental glomerulosclerosis, minimal
change nephropathy and membranous glomerulopathy (16, 64, 65). The sudden onset of overt
nephropathy in non-diabetic glomerular diseases, is conceivably not preceded by the presence of
longterm microalbuminuria in most cases. A mass screening for microalbuminuria will
consequently not be effective to detect these relatively rare disorders. Studies of podocyte
proteins, including nephrin (NPHS1), podocin (NPHS2), zona occludens-1 (ZO-1), α-actinin-4,
CD2 associated protein and transient receptor potential canonical (TRPC) channels, and their
mutation analysis have shed light on the pathogenesis of glomerular kidney disease and
manifestation of albuminuria and emphasized the critical role of the podocyte and the slit
diaphragm in maintaining the function of the glomerular barrier (17, 50). Beside genetic factors,
also drugs, immunologic mechanisms, and bacterial toxins might induce the expression of
podocyte co-stimulatory molecule B7-1 (also termed CD 80), leading to foot process effacement
and albuminuria (17, 66). It is unclear why molecule B7-1 is expressed on the podocyte, as it is
normally expressed on antigen presenting cells and B-cells (67). It is suggested that the disruption
of the glomerular filter by the expression of molecule B7-1 may help the innate immune system
in clearing the circulation from harmful agents through transient urinary albumin loss (68).
Noteworthy, the onset of nephrotic syndrome in minimal change nephropathy is often preceded
by an infection or allergic reaction (69). However, it is unknown whether screening for
albuminuria in presence of infectious or allergic symptoms would be effective, since the patho-
physiologic mechanisms in these diseases are entirely different from those leading to albuminuria

CHAPTER 1: Introduction
17
in metabolic disorders, including diabetes, hypertension and obesity. The main focus in this thesis
will be on cardiovascular risk factors, as the prevalence of these risk factors was high in the
populations we investigated.

CHAPTER 1: Introduction
18
1.4 Albuminuria as a manifestation of chronic kidney disease
To identify patients at risk for progressive kidney disease, the National Kidney Foundation’s -
Kidney Disease Outcomes Quality Initiative (NKF-K/DOQI) developed a definition and
classification for CKD that is updated by the Kidney Disease Improving Global Outcomes
(KDIGO) CKD recommendations in 2013 (70, 71). CKD is defined as abnormalities of kidney
structure or function, present for more than 3 months, with implications for health (71). The CGA
staging system classifies subjects with CKD based on the cause of CKD (C), renal dysfunction,
manifested by reduced glomerular filtration rate (G) and kidney damage, manifested by presence
of persistent albuminuria (A). Based on this subdivision, table 1 shows the risk for progressive
CKD (71).
GFR: glomerular filtration rate, adapted from (71).
Notice that the respective misnomers “normoalbuminuria”, “microalbuminuria” and
“macroalbuminuria” have been replaced by “normal to mildly increased albuminuria”,
“moderately increased albuminuria” (CKD stage A2) and “severely increased albuminuria”
(CKD stage A3). Throughout this manuscript, we will continue to use the terminology
“normoalbuminuria”, “microalbuminuria” and macroalbuminuria” as several of the publications
Table 1. Classification of chronic kidney disease (71)
ACR: urinary albumin creatinine ratio
A1 A2 A3
< 30 mg/g 30-300 mg/g >300mg/g
G
FR
cate
go
ries
(
ml/
min
/1.7
3m
²)
G1 ≥ 90 Normal Low High
G2 60-89 Normal Low High
G3a 45-59 Low High Very high
G3b 30-44 High Very high Very high
G4 15-29 Very high Very high Very high
G5 <15 or RRT Very high Very high Very high

CHAPTER 1: Introduction
19
included in the present thesis were submitted before the publication of the CGA staging system at
January 2013 (71).
The prevalence of CKD in the general population is estimated around 10-15% (72, 73). The
ageing of the population along with the growing global prevalence of diabetes, obesity and other
chronic non communicable diseases has led to a corresponding worldwide increase in prevalence
of CKD (74). The prevalence of all stages CKD is 35% in elderly (age > 60 years), 40% in
diabetes, 23% in hypertension, 17% in obesity and 41% in CVD, as estimated by the USRDS in
2013 (73). Yet, the majority of CKD patients is identified by ACR of 30-300 mg/g and/or
reduced estimated GFR of 30-60 ml/min/1.73m² while a minority (10%) has developed an ACR
higher than 300mg/g and/or an estimated GFR lower than 30 ml/min/1.73m² (73). Only 10% of
the latter subgroup progresses to a degree that RTT is required (75). Consequently, the incidence
rate for RRT is around 10-30 per 100,000 person-years and the prevalence of RRT in the general
population is around 0.1% (3, 72).
It is debatable whether an uniform CKD definition is valid and appropriate for implementing
patients into renal care (76, 77). One point of discussion is the physiological reduction of kidney
function with increasing age and consequently, whether a reduction of GFR of a certain degree
has the same pathophysiological meaning throughout different age strata (72, 73, 77). A
substantial part of patients with an eGFR < 60 ml/min/1.73m² did not have preceding albuminuria
and do not develop progressive CKD (78, 79).
Another concern is whether it is appropriate to include subjects with microalbuminuria in the
definition of CKD, as microalbuminuria is frequently associated with cardiovascular risk factors
(80). In addition, fluctuations in microalbuminuria occur commonly by temporary physiological
responses after strenuous exercise, meal, fever, extreme cold or standing (43, 81-84). For this
reason, repeated measurements of albuminuria should be obtained, and consequently persistent
microalbuminuria is required for diagnosing CKD stage 1 and 2. As most trials do not include
follow-up examinations, CKD stage 1 and 2 could not be identified directly. Therefore, the
prevalence rates of microalbuminuria were assumed to be 51% and 75% for persons with
eGFRs > 90 and, 60-90 ml/min/1.73m², respectively (85). This persistence ratio to define
microalbuminuria acts as self-fulfilling prophecy to establish microalbuminuria as marker for
progressive CKD, whereas macroalbuminuria has a higher specificity to detect renal damage and

CHAPTER 1: Introduction
20
decline of renal function (52, 86). Of note, diabetic patients with ACR > 3000 mg/g had an 8-fold
higher risk for ESRD than those with ACR < 1500 mg/g (figure 4).
Figure 4
Figure 4. Effect of baseline albuminuria on ESRD in the RENAAL study. Adjusted for baseline serum
creatinine, blood pressure, HbA1c, age and ethnicity. Adapted from (87).
CHAPTER 1: Introduction
21
1.5 Albuminuria as a manifestation of cardiovascular disease
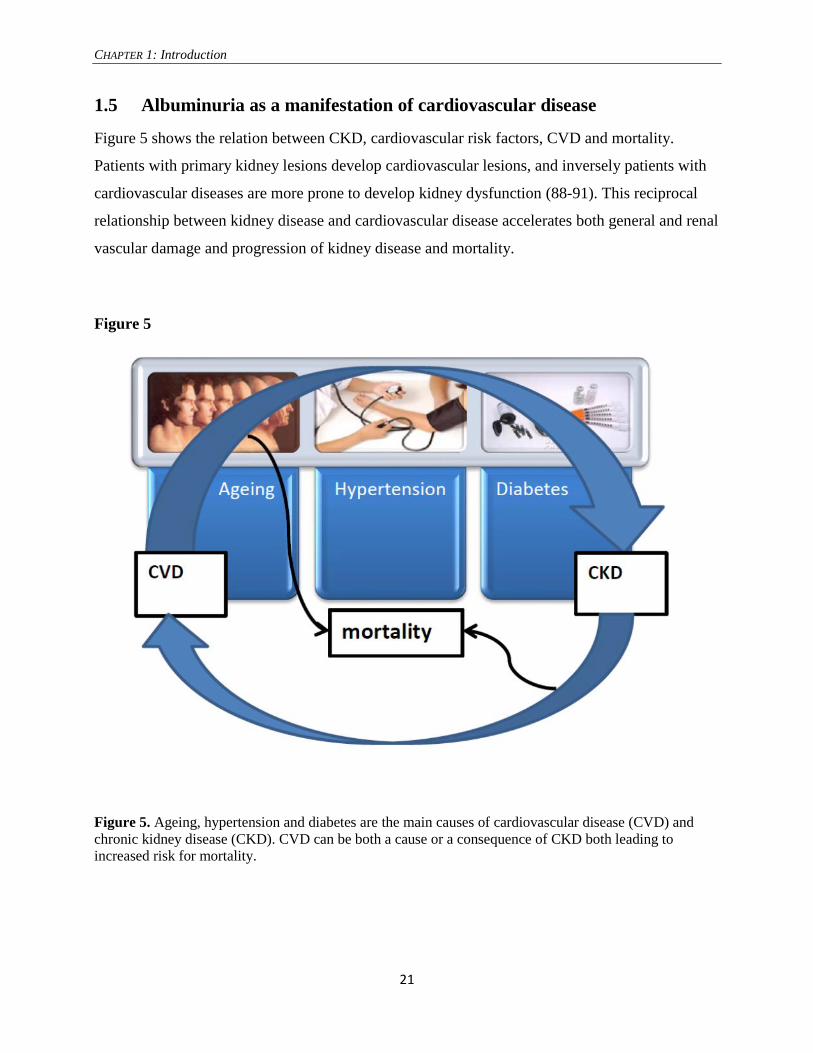
Figure 5 shows the relation between CKD, cardiovascular risk factors, CVD and mortality.
Patients with primary kidney lesions develop cardiovascular lesions, and inversely patients with
cardiovascular diseases are more prone to develop kidney dysfunction (88-91). This reciprocal
relationship between kidney disease and cardiovascular disease accelerates both general and renal
vascular damage and progression of kidney disease and mortality.
Figure 5
Figure 5. Ageing, hypertension and diabetes are the main causes of cardiovascular disease (CVD) and
chronic kidney disease (CKD). CVD can be both a cause or a consequence of CKD both leading to
increased risk for mortality.

CHAPTER 1: Introduction
22
In the 19th
century, James Goodhart observed albuminuria in sedentary and unhealthy subjects,
“bulky men or women complain of a certain amount of ill health, and it is found that they eat and
drink to much, they take no exercise, very possibly have gouty antecedents, they have a congested
state of the capillaries of the face, short breath, and are fat and unhealthy looking. The urine of
such as these is often of high specific gravity, and contains little albumen. Give these people
periodical purges, diet them, and make them live altogether more according to natural law, and
albumen disappears” (92). Nowadays, one third of the US population are identified with
“metabolic syndrome” clustering high blood pressure, abnormal lipid status, high glycaemia
and/or large waist circumference (93-95). It is suggested that the Western sedentary lifestyle is an
important cause of the metabolic syndrome (96). The metabolic syndrome is considered to be a
pre-diabetes condition with increased cardiovascular risk (96). Cardiovascular risk factors trigger
oxidative stress that upregulates the expression of inflammatory cytokines and induces
endothelial dysfunction, leading to concomitant kidney damage that might manifest as
microalbuminuria (50, 97-102). In a cross-sectional study of hypertensive patients, those with
microalbuminuria combined to inflammation had more obesity, metabolic syndrome, cardiac
hypertrophy and smokers, while patients with microalbuminuria in absence of inflammation had
no increased cardiovascular risk factors (102). However, prospective studies show that higher
levels of albuminuria are an independent prognostic predictor for cardiovascular morbidity and
mortality in patients with diabetes, metabolic syndrome, vascular disease, hypertension and even
in the general population (62, 103-108). The increased relative risk for CVD according to
microalbuminuria is approximately the same in different cohorts (106, 108-111), but the absolute
risk for CVD is much higher in diabetic versus non-diabetic cohorts (table 2). These findings are
important, as they indicate that a screening program will be more successful targeting specific
groups (such as diabetics and hypertensives). The panels of figure 6 shows Kaplan-Meier curves
for free survival of CVD according to microalbuminuria in different populations. Figure 6a
shows that slightly elevated levels of urinary albumin are already associated with CVD. Figure 6c
show that diabetic populations have a higher absolute risk for CVD than general cohorts (figure
6a and 6b).

CHAPTER 1: Introduction
23
Table 2: Relative risk and absolute risk for adverse outcomes according to microalbuminuria
(MAU) vs. no MAU in different studies.
Framingham(106): General population, no diabetes, no hypertension, no previous CVD at baseline, high
ACR ≥ 3.9 mg/g in men and ≥ 7.5 mg/g in women.
EPIC(108): General population, no previous CVD, 2% diabetes, 11% hypertension, high ACR > 20 mg/g.
CCHS(109): Copenhagen City Heart Study III: 100% hypertensive patients without previous CVD, 4%
diabetes, high UAE > 6.9 mg/day.
ADVANCE(110): Diabetic patients, history of previous CVD 32%, high ACR ≥ 30mg/g.
Diabetes(111): Diabetic patients without macroalbuminuria, high UAE; 30-300 mg/d.
Study: Relative risk according to MAU
vs. no MAU
Absolute risk (per 1000
person years)
RR 95% CI p No MAU MAU
Framingham (n= 1,568)
-Cardiovascular disease 2.9 1.6-5.4 <0.001 3 9
-All-cause mortality 1.8 1.0-3.2 0.08 3 7
EPIC (n=22,368)
-Cardiovascular disease 1.7 1.2-1.9 <0.001 4 7
-All-cause mortality 1.5 1.2-1.8 <0.001 5 9
-Cardiovascular mortality 2.0 1.6-2.7 <0.001 2 4
CCHS (n=1,734)
-Cardiovascular disease 2.0 1.4-2.9 <0.001 7 16
-All-cause mortality 1.5 1.2-1.8 <0.001 13 29
ADVANCE (n= 10,640)
-Cardiovascular disease 1.5 1.1-1.9 <0.001 15 22
-Cardiovascular mortality 1.7 1.2-2.6 <0.001 5 9
Diabetes (n=199)
-Cardiovascular disease 2.2 2.1-2.5 0.03 26 70
-All-cause mortality 2.5 0.7-8.4 0.15 NA NA

CHAPTER 1: Introduction
24
Figure 6. Kaplan-Meier survival curves for CVD in population-based cohorts (Framingham: fig.
6a. and EPIC: fig. 6b) and in type 2 diabetic cohort (fig. 6c) according to baseline ACR.
Median ACR = 3.9 mg/g in men
and = 7.5 mg/g in women
Figure 6a
Figure 6b Figure 6c
Years

CHAPTER 1: Introduction
25
1.6 The prevalence of albuminuria
The prevalence of microalbuminuria and macroalbuminuria ranged from 6 to 12% and 0.6 to
1.3% respectively, according to population cohorts (9, 72, 85, 112-115).
Table 3. Clinical studies reporting the prevalence of albuminuria in the general population
Study HUNT II EPIC KEAPS PolNef PREVEND NHANES AusDiab
Country Norway UK UK Poland Netherlands US Australia
Invited 92,703 77,630 2,199 9,700 85,421 All ?
Responded 65,181 25,112 1,208 2,501 40,856 13,233 11,247
Year 1995-97 93-97 04-05 04-05 1997 99-04 99-20
Age > 20 40-79 > 18 > 18 28-75 > 20 ?
THT 11 14.4 16.7 13.1 11.2 14 12
Diabetes 3.4 2.3 4.4 6.6 2.6 6.8 7
CVD 8 9.8 11.6 ? 3.6 15 0.8
Micro 7.1 11.8 7.1 11.9 7.2 8.2 6.0
Macro 0.8 0.9 0.7 1.3 0.6
Threshold 17-250/ 25-
355**
20-200* > 21/ > 30** > 20° 20-200° 30-300* 30-300*
Collection morning°° random morning random morning random morning
Table 3 shows the numbers of subjects who were invited and responded, year of enrollment, age of
inclusion, THT: prevalence of treated hypertension (%), prevalence diabetes (%), CVD: prevalence of
cardiovascular disease, prevalence of micro= microalbuminuria and macro= macroalbuminuria (%),
Threshold to define microalbuminuira: by (*): ACR = urinary albumin creatinine ratio (mg/g), by (°):
UAE = urinary albumin excretion (mg/l) or by (**): ACR gender specific thresholds: male/female.
Collection: how urine specimens were collected: first morning or random. (°°) in 9,598 subjects 3 first
morning urine specimens were collected.

CHAPTER 1: Introduction
26
The prevalence of micro- or macro-albuminuria varied in these cohorts as a result of the different
proportions of subjects with CVD, definitions of microalbuminuria and macroalbuminuria, age
range and timing of urinary sample collection (table 3). According to the NHANES cohort, the
prevalence of albuminuria was 34.2% in diabetes (microalbuminuria 28.1%, macroalbuminuria
6.1%), 14.5% in non-diabetic hypertension (microalbuminuria 12.8%, macroalbuminuria 1.7%),
and 5.1% in non-diabetes non-hypertension (microalbuminuria 4.8%, macroalbuminuria
0.3%)(116). Yet, the prevalence of albuminuria (micro- and macro-albuminuria) varied also
markedly between cohorts in the presence of diabetes (6-39%), hypertension (4-47%) and CVD
(15-59%) (6, 117).

CHAPTER 1: Introduction
27
1.7 How to measure albuminuria
Clinical guidelines on how to measure albuminuria are not uniform with regard to patient
preparation, timing of urine samples, units of reporting, thresholds to define micro- or macro-
albuminuria and the methods which are used to measure urinary albumin and creatinine (42).
Overnight urinary albumin excretion is considered as the golden standard, but is impractical in
clinical settings and in epidemiologic studies. A practical alternative is measurement of urinary
albumin creatinine ratio (ACR) in milligrams albumin per gram creatinine as the units of measure,
in early or first morning urine samples (42, 118). Yet, albuminuria is commonly measured in
random urine samples due to practical reasons. However, a higher within-subjects biological
variability for ACR has been reported with random urine samples compared with first morning
urine samples (119).
Preparation of the patient. Measuring albuminuria during circumstances of pyrexia, exposure to
cold, gout attacks, glycosuria, anemia, hematuria, urinary tract infections, alcohol excess, heart
failure, medication, after exercise and mental anxiety should be interpreted with caution as all
these conditions might affect the level of albuminuria (92, 120). To exclude postural albuminuria,
measuring albuminuria should be performed in a first morning sample, particularly in relatively
young subjects (42).
Molecular forms of albumin. Albumin is the most abundant plasma protein, serving multiple
functions as a carrier of metabolites (long-chain fatty acids, bilirubin…), ions (calcium..),
hormones (thyroxin), organic molecules, vitamins and drugs, as an acid/base buffer, as
antioxidant and by supporting the oncotic pressure and volume of the blood (121). Albumin can
be degraded into albumin fragments of 0.5-5kD by time, proximal tubular cells (cubilin-megalin),
proteolysis during passage through the urinary tract, oxidation in the urine and during specimen
storage (42). Mutations of the gene encoding albumin (<1/1000) might affect renal albumin
clearance, producing different proportions of modified albumin in urine compared to serum (122).
Methods for measuring urine albumin. Urinary albumin can be quantified with immunochemical
methods, such as radioimmunoassay (RIA), immunoturbidimetry and immunonephelometry (42,
123). These routine methods use either polyclonal or monoclonal antibodies. Immunoassays with
polyclonal antisera react with many modified albumins whereas immunoassays with monoclonal

CHAPTER 1: Introduction
28
antisera can only react with immunoreactively intact albumin (42). However, current
immunoassays have a considerable inter-assay coefficient of variation. Additionally, the
variability between-laboratory appears to be tremendous (124). Size exclusion high performance
liquid chromatography (HPLC) measures both immunoreactive and immunounreacive intact
albumin (125). Albuminuria can also be measured semiquantitatively with point of care methods
by colorimetric test strips (“dipsticks”), such as HemoCue Albumin 201 system (HemoCue®),
Clinitek Microalbumin Reagent strips (Bayer Health Care®) and the Chemstrip Micral Test strips
(Roche Diagnostic®) with a good sensitivity and specificity for urinary albumin excretion (24
hours)(126). Interestingly, a quantitative dye-binding based test strip analysis seems to be reliable
to detect microalbuminuria (127). Additionally, this test might be suitable to perform in a mass
screening as it is very cheap (2 Eurocent per test)(128). The National Kidney Disease Education
Program-International Federation of Clinical Chemistry (IFCC) Working Group is establishing
standardization of albumin measurements (42, 129).
Which threshold for microalbuminuria should be used. Microalbuminuria has been introduced as
a surrogate marker for early diabetic nephropathy based on a small retrospective study of 63
diabetic patients; seven of 8 patients with overnight albuminuria between 30-140 µg/min
developed overt nephropathy after 14 years (130). Another small study, defined early diabetic
nephropathy as an overnight urine albumin excretion between 30-140 µg/min, which was
predictive for the development of clinical proteinuria (131). These values are considered to be
approximately equivalent to an ACR of 20-100 mg/g in a random untimed urine sample. KDIGO
recommends to use a threshold for AER of 30-300 mg/24 hours (ACR of 30-300 mg/g) to
indicate microalbuminuria (71). This threshold is based on the “normal” values of the distribution
of ACR in apparently healthy young subjects and on the increased risk of all cause mortality,
cardiovascular mortality, acute kidney injury (AKI) and CKD progression once ACR exceeds 30
mg/g (6, 117). Also, the Scientific Advisory Board on the prevention of diabetic nephropathy of
the US National Kidney Foundation recommends to use an ACR risk-based cut off above 30
mg/g in random urine samples (132). This threshold can however be debated, as albuminuria is a
continuous parameter that over its entire range is related to cardiovascular events, even with
values below the threshold (133). In addition, such a cut-off of 30 mg/g does not give weight to
the prognostic values of substantially higher degrees of albuminuria (macroalbuminuria), which
carry a much higher risk to be associated with rapid decline of renal function than these relatively

CHAPTER 1: Introduction
29
modest values of 30 mg/g (86). Beside the amount of urinary albumin concentration, ACR
depends also on muscle mass as it is measured in 24 hour creatinine collection. Consequently,
ACR in females, elderly and in patients with muscle wasting overestimates true AER. Warram
et. al. found a lower threshold in men (ACR ≥ 17 mg/g) than in women (ACR ≥ 25 mg/g) with
serial specimens in 1,613 patients with diabetes mellitus type 1. These gender specific thresholds
corresponded to the 95th
percentiles of distribution of the ACR in 218 healthy control subjects
(134). Higher values of ACR in women than in men are caused by the lower muscle mass and
thus the lower urinary creatinine excretion. For that reason, we decided to use gender specific
thresholds as proposed by Warram et. al., as these values are equivalent to an albumin excretion
rate of 30 µg/min in men and 31 µg/min in women. As a matter of fact, thresholds of
approximately 30 µg/min were also the ones used in the first studies (130, 131).

CHAPTER 1: Introduction
30
1.8 Outline and aims of the thesis
The presence of microalbuminuria is considered to be an independent indicator for cardiovascular
and/or kidney disease in general populations (7, 88, 135). Microalbuminuria seems to be a
suitable screening tool in persons with diabetes, as treatment of microalbuminuria delays the
development of overt nephropathy (136). Although, screening for microalbuminuria in a general
population, followed by treatment did not improve renal and cardiovascular outcome (137, 138).
One reason for this disappointed result might be that microalbuminuria is an inappropriate test to
select persons with cardiovascular and renal risk. This thesis discusses the pitfalls of using
microalbuminuria to identify subjects with cardiovascular and renal events.
The aims of this thesis are:
1) To evaluate the prevalence of microalbuminuria and the associations with traditional
cardiovascular risk factors in a general population.
2) To evaluate whether we can use microalbuminuria as a screening tool to identify subjects
with unrecognized cardiovascular risk factors in a presumably healthy population.
3) To evaluate which conditions could lead to false positive test results of microalbuminuria.
4) Whether the risk of ESRD could be reduced by screening for microalbuminuria according
to the literature.

CHAPTER 1: Introduction
31
1.9 Participants and methods
The Unreferred Renal Insufficiency (URI) cohort and Early Renal Impairment and
Cardiovascular Assessment in Belgium (ERICABEL) cohort were applied for this thesis.
The URI study is a non-interventional prospective study that included 1,486 Causcasian workers
who presented at a routine yearly occupational check-up between January 2007 and December
2009. The first study; “towards a rational screening strategy for albuminuria”, excluded subjects
with hematuria, leucocyturia, known comorbidities as diabetes, cardiovascular disease, renal
disease, and on antihypertensive drugs and lipid lowering drugs, leaving a cross-sectional cohort
of 1,191 apparently healthy workers with a mean age of 38 ± 10 years. The second study,
“microalbuminuria is more consistent in presence of risk factors” included 341 workers of the
URI cohort who underwent at least two consecutive occupational heath care examinations.
Subjects with macroalbuminuria and those with incomplete data were excluded, leaving a
prospective cohort of 239 subjects with known and unknown cardiovascular risk factors. The
third study “screening for kidney disease in a presumed healthy working population” included all
screened workers with known and unknown cardiovascular risk factors. The presence of
hematuria and subjects with incomplete data were exclusion criteria for further analysis, leaving a
cross-sectional cohort of 1,398 workers.
Description of procedures: All subjects were investigated during their yearly check up by their
occupational physician. Body weight was recorded to the nearest 0.1 kg and height was measured
to the nearest centimeter. Waist circumference was measured by trained nurses following
recommendations by WHO(139). Body mass index (BMI) was calculated as body weight in kg
divided by height² (kg/m²). Blood pressure and resting heart rate were measured in sitting
position by a calibrated electronic device (OMRON®). A questionnaire about current cigarette
smoking, physical activity and prescribed medication was taken by an occupational physician in
each participant. A random blood and urine spot specimen was collected and analyzed on the
same day in one central laboratory (no frozen samples). Urinary albumin was measured by an
immune turbidimetric method with an inter-assay coefficient of variation of 11.2% at a mean
level of 82 mg/L and an inter-assay coefficient of variation of 4.9% at a mean level of 580 mg/l.
Serum creatinine was analyzed by a colorimetric assay (compensated Jaffe reaction), calibrated
by Isotope Dilution Mass Spectrometry (IDMS), with an inter-assay coefficient of variation of

CHAPTER 1: Introduction
32
1.75% at a mean level of 104 µmol/l (Roche). Serum cystatin C was determined by nephelometry
with an inter-assay coefficient of variation of 5.1% at a mean level of 0.95 mg/l (Siemens DII).
Serum CRP was measured with an immune turbidimetric method with an inter-assay coefficient
of variation of 4.6% at a mean level of 3.2 mg/l and inter-assay coefficient of variation of 2.5%
at a mean level of 5.5 mg/l.
The ERICABEL study included patients with hypertension, aged 40-70 years. We used the
baseline data of the ERICABEL cohort, a non-interventional epidemiological study with a follow
up of 5 years that included 1,076 Caucasian patients with hypertension, defined as systolic blood
pressure ≥140 mmHg and/or intake of at least one antihypertensive drug, recruited by 96 general
practitioners, between 2006 and 2007, in Belgium. Of the 1076 patients included in this cross-
sectional study, 420 patients had a missing value for at least one of the variables under
investigation. Multiple imputation techniques were used to account for the missing data, using
20 imputations (140). All characteristics and outcome (MAU) were simultaneously used in the
imputation model. The imputation was done using the R function aregImpute from the Hmisc
package (141).
Description of procedures: Each participating primary care physician was asked to include 10
consecutive hypertensive patients aged between 40-70 years, in a 1:1 sex ratio. The eligible
persons were evaluated at baseline and if eligible, sociodemographic information (age, sex, race,
and education level), personal and family medical history, smoking status and medication use
were collected prospectively in an online database. Body weight was recorded to the nearest 0.1
Kg and height was measured to the nearest centimeter. Body mass index (BMI) was calculated as
body weight in Kg divided by height² (kg/m²). Blood pressure was measured according to the
WHO criteria with a calibrated Omron HEM-907 device (average of 2 measurements, sitting,
with 5 minutes in between). All these measurements were done by the primary care physician.
After exclusion of a urinary infection or hematuria (negative Combur® test), MAU was screened
by a Micral® dipstick test. MAU was considered present if measured albuminuria was ≥ 20mg/l
on a morning midstream urine sample. Blood sampling was performed by the general practitioner
in fasting patients.

CHAPTER 1: Introduction
33
1.10 References
1. International Diabetes Federation. Available at http://www.idf.org/atlasmap/atlasmap.
2. Wolf M, Heuten HG, De Swaef A, de Falleur M, Verpooten GA. The evolution of hypertension
treatment in Belgium, a pharmacoepidemiological study. Acta Cardiol 2012; 67: 147-152. Available at
<Go to ISI>://WOS:000303851000001.
3. van der Velde M, Halbesma N, de Charro FT, Bakker SJL, de Zeeuw D, de Jong PE, Gansevoort RT.
Screening for Albuminuria Identifies Individuals at Increased Renal Risk. Journal of the American
Society of Nephrology 2009; 20: 852-862. Available at <Go to ISI>://000264831300023.
4. de Boer IH, Rue TC, Cleary PA, Lachin JM, Molitch ME, Steffes MW, Sun W, Zinman B, Brunzell
JD, Diabetes C, Complications Trial/Epidemiology of Diabetes I, Complications Study Research G,
White NH, Danis RP, Davis MD, Hainsworth D, Hubbard LD, Nathan DM. Long-term renal outcomes
of patients with type 1 diabetes mellitus and microalbuminuria: an analysis of the Diabetes Control and
Complications Trial/Epidemiology of Diabetes Interventions and Complications cohort. Arch Intern Med 2011; 171: 412-420. Available at http://www.ncbi.nlm.nih.gov/pubmed/21403038.
5. ERA-EDTA Registry: ERA-EDTA Registry 2011 Annual report. Academic Medical Center,
Amsterdam, the Netherlands, june 2011. Available at http://www.era-edta-
reg.org/files/annualreports/pdf/AnnRep2011.pdf.
6. Mahmoodi BK, Matsushita K, Woodward M, Blankestijn PJ, Cirillo M, Ohkubo T, Rossing P, Sarnak
MJ, Stengel B, Yamagishi K, Yamashita K, Zhang L, Coresh J, de Jong PE, Astor BC, Chronic Kidney
Disease Prognosis C. Associations of kidney disease measures with mortality and end-stage renal
disease in individuals with and without hypertension: a meta-analysis. Lancet 2012; 380: 1649-1661.
Available at http://www.ncbi.nlm.nih.gov/pubmed/23013600.
7. Gansevoort RT, Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, de Jong PE,
Coresh J, Chronic Kidney Disease Prognosis C. Lower estimated GFR and higher albuminuria are
associated with adverse kidney outcomes. A collaborative meta-analysis of general and high-risk
population cohorts. Kidney Int 2011; 80: 93-104. Available at
http://www.ncbi.nlm.nih.gov/pubmed/21289597.
8. Palmer AJ, Valentine WJ, Chen R, Mehin N, Gabriel S, Bregman B, Rodby RA. A health economic
analysis of screening and optimal treatment of nephropathy in patients with type 2 diabetes and
hypertension in the USA. Nephrology Dialysis Transplantation 2008; 23: 1216-1223. Available at <Go
to ISI>://WOS:000254472400024.
9. Hillege HL, Janssen WMT, Bak AAA, Diercks GFH, Grobbee DE, Crijns H, van Gilst WH, de Zeeuw
D, de Jong PE, Prevend Study G. Microalbuminuria is common, also in a nondiabetic, nonhypertensive
population, and an independent indicator of cardiovascular risk factors and cardiovascular morbidity.
Journal of Internal Medicine 2001; 249: 519-526. Available at <Go to ISI>://000169568600005.
10. Ozyilmaz A, Bakker SJ, de Zeeuw D, de Jong PE, Gansevoort RT. Selection on albuminuria enhances
the efficacy of screening for cardiovascular risk factors. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association 2010;
25: 3560-3568. Available at http://www.ncbi.nlm.nih.gov/pubmed/20702530.
11. de Jong PE, Hillege HL, Pinto-Sietsma SJ, de Zeeuw D. Screening for microalbuminuria in the general
population: a tool to detect subjects at risk for progressive renal failure in an early phase? Nephrology
Dialysis Transplantation 2003; 18: 10-13. Available at <Go to ISI>://000180293800002.
12. Jefferson JA, Shankland SJ, Pichler RH. Proteinuria in diabetic kidney disease: a mechanistic
viewpoint. Kidney International 2008; 74: 22-36. Available at
http://www.ncbi.nlm.nih.gov/pubmed/18418356.
13. Haraldsson B, Nystrom J, Deen WM. Properties of the glomerular barrier and mechanisms of
proteinuria. Physiol Rev 2008; 88: 451-487. Available at <Go to ISI>://000257595300005.
14. Tojo A, Kinugasa S. Mechanisms of glomerular albumin filtration and tubular reabsorption.
International journal of nephrology 2012; 2012: 481520. Available at
http://www.ncbi.nlm.nih.gov/pubmed/22685655.

CHAPTER 1: Introduction
34
15. Haraldsson B, Nystrom J. The glomerular endothelium: new insights on function and structure. Curr
Opin Nephrol Hypertens 2012; 21: 258-263. Available at
http://www.ncbi.nlm.nih.gov/pubmed/22388551.
16. Mundel P, Reiser J. Proteinuria: an enzymatic disease of the podocyte? Kidney Int 2010; 77: 571-580.
Available at http://www.ncbi.nlm.nih.gov/pubmed/19924101.
17. Reiser J, von Gersdorff G, Loos M, Oh J, Asanuma K, Giardino L, Rastaldi MP, Calvaresi N,
Watanabe H, Schwarz K, Faul C, Kretzler M, Davidson A, Sugimoto H, Kalluri R, Sharpe AH,
Kreidberg JA, Mundel P. Induction of B7-1 in podocytes is associated with nephrotic syndrome. J Clin Invest 2004; 113: 1390-1397. Available at http://www.ncbi.nlm.nih.gov/pubmed/15146236.
18. Solling K, Mogensen CE. Studies on the mechanism of renal tubular protein reabsorption. Proceedings
of the European Dialysis and Transplant Association European Dialysis and Transplant Association
1977; 14: 543-549. Available at http://www.ncbi.nlm.nih.gov/pubmed/341145.
19. Hausmann R, Grepl M, Knecht V, Moeller MJ. The glomerular filtration barrier function: new
concepts. Curr Opin Nephrol Hypertens 2012; 21: 441-449. Available at
http://www.ncbi.nlm.nih.gov/pubmed/22614627.
20. Christensen EI, Birn H, Storm T, Weyer K, Nielsen R. Endocytic receptors in the renal proximal tubule.
Physiology 2012; 27: 223-236. Available at http://www.ncbi.nlm.nih.gov/pubmed/22875453.
21. Imerslund O. Idiopathic chronic megaloblastic anemia in children. Acta paediatrica Supplementum
1960; 49(Suppl 119): 1-115. Available at http://www.ncbi.nlm.nih.gov/pubmed/13852753.
22. Broch H, Imerslund O, Monn E, Hovig T, Seip M. Imerslund-Grasbeck anemia. A long-term follow-up
study. Acta paediatrica Scandinavica 1984; 73: 248-253. Available at
http://www.ncbi.nlm.nih.gov/pubmed/6741523.
23. Boger CA, Chen MH, Tin A, Olden M, Kottgen A, de Boer IH, Fuchsberger C, O'Seaghdha CM,
Pattaro C, Teumer A, Liu CT, Glazer NL, Li M, O'Connell JR, Tanaka T, Peralta CA, Kutalik Z, Luan
J, Zhao JH, Hwang SJ, Akylbekova E, Kramer H, van der Harst P, Smith AV, Lohman K, de Andrade
M, Hayward C, Kollerits B, Tonjes A, Aspelund T, Ingelsson E, Eiriksdottir G, Launer LJ, Harris TB,
Shuldiner AR, Mitchell BD, Arking DE, Franceschini N, Boerwinkle E, Egan J, Hernandez D, Reilly
M, Townsend RR, Lumley T, Siscovick DS, Psaty BM, Kestenbaum B, Haritunians T, Bergmann S,
Vollenweider P, Waeber G, Mooser V, Waterworth D, Johnson AD, Florez JC, Meigs JB, Lu X,
Turner ST, Atkinson EJ, Leak TS, Aasarod K, Skorpen F, Syvanen AC, Illig T, Baumert J, Koenig W,
Kramer BK, Devuyst O, Mychaleckyj JC, Minelli C, Bakker SJ, Kedenko L, Paulweber B, Coassin S,
Endlich K, Kroemer HK, Biffar R, Stracke S, Volzke H, Stumvoll M, Magi R, Campbell H, Vitart V,
Hastie ND, Gudnason V, Kardia SL, Liu Y, Polasek O, Curhan G, Kronenberg F, Prokopenko I, Rudan
I, Arnlov J, Hallan S, Navis G, Consortium CK, Parsa A, Ferrucci L, Coresh J, Shlipak MG, Bull SB,
Paterson NJ, Wichmann HE, Wareham NJ, Loos RJ, Rotter JI, Pramstaller PP, Cupples LA, Beckmann
JS, Yang Q, Heid IM, Rettig R, Dreisbach AW, Bochud M, Fox CS, Kao WH. CUBN is a gene locus
for albuminuria. J Am Soc Nephrol 2011; 22: 555-570. Available at
http://www.ncbi.nlm.nih.gov/pubmed/21355061.
24. Devuyst O, Jouret F, Auzanneau C, Courtoy PJ. Chloride channels and endocytosis: new insights from
Dent's disease and ClC-5 knockout mice. Nephron Physiology 2005; 99: p69-73. Available at
http://www.ncbi.nlm.nih.gov/pubmed/15637424.
25. Hryciw DH, Ekberg J, Pollock CA, Poronnik P. ClC-5: a chloride channel with multiple roles in renal
tubular albumin uptake. The international journal of biochemistry & cell biology 2006; 38: 1036-1042.
Available at http://www.ncbi.nlm.nih.gov/pubmed/16226913.
26. Devuyst O, Thakker RV. Dent's disease. Orphanet journal of rare diseases 2010; 5: 28. Available at
http://www.ncbi.nlm.nih.gov/pubmed/20946626.
27. Kabanda A, Jadoul M, Lauwerys R, Bernard A, van Ypersele de Strihou C. Low molecular weight
proteinuria in Chinese herbs nephropathy. Kidney Int 1995; 48: 1571-1576. Available at
http://www.ncbi.nlm.nih.gov/pubmed/8544416.
28. Roels HA, Hoet P, Lison D. Usefulness of biomarkers of exposure to inorganic mercury, lead, or
cadmium in controlling occupational and environmental risks of nephrotoxicity. Ren Fail 1999; 21:
251-262. Available at http://www.ncbi.nlm.nih.gov/pubmed/10416202.

CHAPTER 1: Introduction
35
29. Vacca CV, Hines JD, Hall PW, 3rd. The proteinuria of industrial lead intoxication. Environ Res 1986;
41: 440-446. Available at http://www.ncbi.nlm.nih.gov/pubmed/3780642.
30. Abbate M, Zoja C, Remuzzi G. How does proteinuria cause progressive renal damage? J Am Soc Nephrol 2006; 17: 2974-2984. Available at http://www.ncbi.nlm.nih.gov/pubmed/17035611.
31. Caruso-Neves C, Pinheiro AAS, Cai H, Souza-Menezes J, Guggino WB. PKB and megalin determine
the survival or death of renal proximal tubule cells. P Natl Acad Sci USA 2006; 103: 18810-18815.
Available at <Go to ISI>://000242689800076.
32. Arici M, Chana R, Lewington A, Brown J, Brunskill NJ. Stimulation of proximal tubular cell apoptosis
by albumin-bound fatty acids mediated by peroxisome proliferator activated receptor-gamma. J Am
Soc Nephrol 2003; 14: 17-27. Available at http://www.ncbi.nlm.nih.gov/pubmed/12506134.
33. Liu J, Li K, He Y, Zhang J, Wang H, Yang J, Zhan J, Liang H. Anticubilin antisense RNA ameliorates
adriamycin-induced tubulointerstitial injury in experimental rats. Am J Med Sci 2011; 342: 494-502.
Available at http://www.ncbi.nlm.nih.gov/pubmed/22108171.
34. Verhulst A, D'Haese PC, De Broe ME. Inhibitors of HMG-CoA reductase reduce receptor-mediated
endocytosis in human kidney proximal tubular cells. Journal of the American Society of Nephrology :
JASN 2004; 15: 2249-2257. Available at http://www.ncbi.nlm.nih.gov/pubmed/15339974.
35. Sidaway JE, Davidson RG, McTaggart F, Orton TC, Scott RC, Smith GJ, Brunskill NJ. Inhibitors of 3-
hydroxy-3-methylglutaryl-CoA reductase reduce receptor-mediated endocytosis in opossum kidney
cells. Journal of the American Society of Nephrology : JASN 2004; 15: 2258-2265. Available at
http://www.ncbi.nlm.nih.gov/pubmed/15339975.
36. Douglas K, O'Malley PG, Jackson JL. Meta-analysis: the effect of statins on albuminuria. Annals of internal medicine 2006; 145: 117-124. Available at http://www.ncbi.nlm.nih.gov/pubmed/16847294.
37. Sandhu S, Wiebe N, Fried LF, Tonelli M. Statins for improving renal outcomes: a meta-analysis.
Journal of the American Society of Nephrology : JASN 2006; 17: 2006-2016. Available at
http://www.ncbi.nlm.nih.gov/pubmed/16762986.
38. Deslypere JP, Delanghe J, Vermeulen A. Proteinuria as Complication of Simvastatin Treatment.
Lancet 1990; 336: 1453-1453. Available at <Go to ISI>://A1990EL85100061.
39. Kostapanos MS, Milionis HJ, Saougos VG, Lagos KG, Christine K, Bairaktari ET, Elisaf MS. Dose-
dependent effect of rosuvastatin treatment on urinary protein excretion. J Cardiovasc Pharmacol Ther
2007; 12: 292-297. Available at <Go to ISI>://000251110600003.
40. Wehlou CMJ, Speeckaert MM, Fiers T, De Buyzere ML, Delanghe JR. alpha(1)-
Microglobulin/albumin ratio may improve interpretation of albuminuria in statin-treated patients.
Clinical Chemistry and Laboratory Medicine 2013; 51: 1529-1534. Available at <Go to
ISI>://WOS:000321104900031.
41. Thrailkill KM, Nimmo T, Bunn RC, Cockrell GE, Moreau CS, Mackintosh S, Edmondson RD,
Fowlkes JL. Microalbuminuria in Type 1 Diabetes Is Associated With Enhanced Excretion of the
Endocytic Multiligand Receptors Megalin and Cubilin. Diabetes Care 2009; 32: 1266-1268. Available
at <Go to ISI>://000267878300027.
42. Miller WG, Bruns DE, Hortin GL, Sandberg S, Aakre KM, McQueen MJ, Itoh Y, Lieske JC,
Seccombe DW, Jones G, Bunk DM, Curhan GC, Narva AS, Urine NKDEP-IWGSA. Current Issues in
Measurement and Reporting of Urinary Albumin Excretion. Clinical Chemistry 2009; 55: 24-38.
Available at <Go to ISI>://WOS:000262303900008.
43. Mogensen CE, Vestbo E, Poulsen PL, Christiansen C, Damsgaard EM, Eiskjaer H, Froland A, Hansen
KW, Nielsen S, Pedersen MM. Microalbuminuria and Potential Confounders - a Review and Some
Observations on Variability of Urinary Albumin Excretion. Diabetes Care 1995; 18: 572-581.
Available at <Go to ISI>://A1995QQ21600025.
44. Hosojima M, Sato H, Yamamoto K, Kaseda R, Soma T, Kobayashi A, Suzuki A, Kabasawa H,
Takeyama A, Ikuyama K, Iino N, Nishiyama A, Thekkumkara TJ, Takeda T, Suzuki Y, Gejyo F, Saito
A. Regulation of Megalin Expression in Cultured Proximal Tubule Cells by Angiotensin II Type 1A
Receptor- and Insulin-Mediated Signaling Cross Talk. Endocrinology 2009; 150: 871-878. Available at
<Go to ISI>://WOS:000262851200035.

CHAPTER 1: Introduction
36
45. Tojo A, Onozato ML, Kurihara H, Sakai T, Goto A, Fujita T. Angiotensin II blockade restores albumin
reabsorption in the proximal tubules of diabetic rats. Hypertens Res 2003; 26: 413-419. Available at
<Go to ISI>://WOS:000184027600009.
46. Wolf G. New insights into the pathophysiology of diabetic nephropathy: from haemodynamics to
molecular pathology. Eur J Clin Invest 2004; 34: 785-796. Available at
http://www.ncbi.nlm.nih.gov/pubmed/15606719.
47. Vallon V. The proximal tubule in the pathophysiology of the diabetic kidney. Am J Physiol-Reg I 2011;
300: R1009-R1022. Available at <Go to ISI>://000290149800001.
48. Semplicini A, Ceolotto G, Sartori M, Maresca A, Baritono E, De Toni R, Paparella I, Calo L.
Regulation of glomerular filtration in essential hypertension: Role of abnormal Na+ transport and atrial
natriuretic peptide. Journal of Nephrology 2002; 15: 489-496. Available at <Go to
ISI>://WOS:000179183400004.
49. Deckert T, Feldt-Rasmussen B, Borch-Johnsen K, Jensen T, Kofoed-Enevoldsen A. Albuminuria
reflects widespread vascular damage. The Steno hypothesis. Diabetologia 1989; 32: 219-226.
Available at http://www.ncbi.nlm.nih.gov/pubmed/2668076.
50. Garg P, Rabelink T. Glomerular proteinuria: a complex interplay between unique players. Advances in chronic kidney disease 2011; 18: 233-242. Available at
http://www.ncbi.nlm.nih.gov/pubmed/21782129.
51. Toyoda M, Najafian B, Kim Y, Caramori ML, Mauer M. Podocyte detachment and reduced glomerular
capillary endothelial fenestration in human type 1 diabetic nephropathy. Diabetes 2007; 56: 2155-2160.
Available at http://www.ncbi.nlm.nih.gov/pubmed/17536064.
52. Nakamura T, Ushiyama C, Suzuki S, Hara M, Shimada N, Ebihara I, Koide H. Urinary excretion of
podocytes in patients with diabetic nephropathy. Nephrol Dial Transplant 2000; 15: 1379-1383.
Available at http://www.ncbi.nlm.nih.gov/pubmed/10978394.
53. Mogensen CE, Christensen CK. Predicting diabetic nephropathy in insulin-dependent patients. N Engl
J Med 1984; 311: 89-93. Available at http://www.ncbi.nlm.nih.gov/pubmed/6738599.
54. Mogensen CE. Microalbuminuria, blood pressure and diabetic renal disease: origin and development
of ideas. Diabetologia 1999; 42: 263-285. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=10096778.
55. Mogensen CE, Schmitz A, Christensen CK. Comparative renal pathophysiology relevant to IDDM and
NIDDM patients. Diabetes/metabolism reviews 1988; 4: 453-483. Available at
http://www.ncbi.nlm.nih.gov/pubmed/3061756.
56. Mogensen CE. Prediction of clinical diabetic nephropathy in IDDM patients. Alternatives to
microalbuminuria? Diabetes 1990; 39: 761-767. Available at
http://www.ncbi.nlm.nih.gov/pubmed/2191882.
57. Jerums G, Premaratne E, Panagiotopoulos S, MacIsaac RJ. The clinical significance of hyperfiltration
in diabetes. Diabetologia 2010; 53: 2093-2104. Available at
http://www.ncbi.nlm.nih.gov/pubmed/20496053.
58. Melsom T, Mathisen UD, Ingebretsen OC, Jenssen TG, Njolstad I, Solbu MD, Toft I, Eriksen BO.
Impaired Fasting Glucose Is Associated With Renal Hyperfiltration in the General Population.
Diabetes Care 2011; 34: 1546-1551. Available at <Go to ISI>://WOS:000293261200020.
59. Premaratne E, Macisaac RJ, Tsalamandris C, Panagiotopoulos S, Smith T, Jerums G. Renal
hyperfiltration in type 2 diabetes: effect of age-related decline in glomerular filtration rate.
Diabetologia 2005; 48: 2486-2493. Available at http://www.ncbi.nlm.nih.gov/pubmed/16261309.
60. Palatini P, Mormino P, Dorigatti F, Santonastaso M, Mos L, De Toni R, Winnicki M, Dal Follo M,
Biasion T, Garavelli G, Pessina AC, Group HS. Glomerular hyperfiltration predicts the development of
microalbuminuria in stage 1 hypertension: the HARVEST. Kidney Int 2006; 70: 578-584. Available at
http://www.ncbi.nlm.nih.gov/pubmed/16788693.
61. Hallan SI. Chronic kidney disease: a new opportunity for better cardiovascular risk stratification.
Journal of Internal Medicine 2009; 266: 414-417. Available at <Go to ISI>://000269875100009.
62. Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, de Jong PE, Coresh J,
Gansevoort RT. Association of estimated glomerular filtration rate and albuminuria with all-cause and

CHAPTER 1: Introduction
37
cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet 2010; 375:
2073-2081. Available at http://www.ncbi.nlm.nih.gov/pubmed/20483451.
63. Perkins BA, Ficociello LH, Silva KH, Finkelstein DM, Warram JH, Krolewski AS. Regression of
microalbuminuria in type 1 diabetes. The New England Journal of Medicine 2003; 348: 2285-2293.
Available at http://www.ncbi.nlm.nih.gov/pubmed/12788992.
64. Williams ME. Diabetic nephropathy: the proteinuria hypothesis. Am J Nephrol 2005; 25: 77-94.
Available at http://www.ncbi.nlm.nih.gov/pubmed/15746541.
65. Henique C, Tharaux PL. Targeting signaling pathways in glomerular diseases. Curr Opin Nephrol Hypertens 2012; 21: 417-427. Available at http://www.ncbi.nlm.nih.gov/pubmed/22660552.
66. Wharram BL, Goyal M, Wiggins JE, Sanden SK, Hussain S, Filipiak WE, Saunders TL, Dysko RC,
Kohno K, Holzman LB, Wiggins RC. Podocyte depletion causes glomerulosclerosis: diphtheria toxin-
induced podocyte depletion in rats expressing human diphtheria toxin receptor transgene. J Am Soc
Nephrol 2005; 16: 2941-2952. Available at http://www.ncbi.nlm.nih.gov/pubmed/16107576.
67. Abbas AK, Sharpe AH. T-cell stimulation: an abundance of B7s. Nature medicine 1999; 5: 1345-1346.
Available at http://www.ncbi.nlm.nih.gov/pubmed/10581066.
68. Reiser J, Mundel P. Danger signaling by glomerular podocytes defines a novel function of inducible
B7-1 in the pathogenesis of nephrotic syndrome. J Am Soc Nephrol 2004; 15: 2246-2248. Available at
http://www.ncbi.nlm.nih.gov/pubmed/15339973.
69. Eddy AA, Schnaper HW. The nephrotic syndrome: from the simple to the complex. Semin Nephrol 1998; 18: 304-316. Available at http://www.ncbi.nlm.nih.gov/pubmed/9613871.
70. National Kidney F. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation,
classification, and stratification. Am J Kidney Dis 2002; 39: S1-266. Available at
http://www.ncbi.nlm.nih.gov/pubmed/11904577.
71. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical
Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. . Kidney Int 2013:
1-150. Available at http://www.nature.com/kisup/journal/v3/n1/index.html.
72. Hallan SI, Coresh J, Astor BC, Asberg A, Powe NR, Romundstad S, Hallan HA, Lydersen S, Holmen J.
International comparison of the relationship of chronic kidney disease prevalence and ESRD risk.
Journal of the American Society of Nephrology 2006; 17: 2275-2284. Available at <Go to
ISI>://000239449000029.
73. United States Renal Data System. USRDS Annual Data Report: Atlas of Chronic Kidney Disease and
End-Stage Renal Disease in US. . National Institute of Health, National Institute of Diabetes and Digestive and Kidney Disease. Available at www.usrds.org/adr.htm.
74. James MT, Hemmelgarn BR, Tonelli M. Early recognition and prevention of chronic kidney disease.
Lancet 2010; 375: 1296-1309. Available at http://www.ncbi.nlm.nih.gov/pubmed/20382326.
75. de Jong PE, van der Velde M, Gansevoort RT, Zoccali C. Screening for chronic kidney disease: Where
does Europe go? Clinical Journal of the American Society of Nephrology 2008; 3: 616-623. Available
at <Go to ISI>://000253709800041.
76. Glassock RJ, Winearls C. CKD--fiction not fact. Nephrol Dial Transplant 2008; 23: 2695-2696; author
reply 2696-2699. Available at http://www.ncbi.nlm.nih.gov/pubmed/18567889.
77. Hallan SI, Orth SR. The conundrum of chronic kidney disease classification and end-stage renal risk
prediction in the elderly--what is the right approach? Nephron Clin Pract 2010; 116: c307-316.
Available at http://www.ncbi.nlm.nih.gov/pubmed/20664285.
78. Hoerger TJ, Wittenborn JS, Segel JE, Burrows NR, Imai K, Eggers P, Pavkov ME, Jordan R, Hailpern
SM, Schoolwerth AC, Williams DE, Centers for Disease C, Prevention CKDI. A health policy model
of CKD: 1. Model construction, assumptions, and validation of health consequences. Am J Kidney Dis
2010; 55: 452-462. Available at http://www.ncbi.nlm.nih.gov/pubmed/20116911.
79. Retnakaran R, Cull CA, Thorne KI, Adler AI, Holman RR, Group US. Risk factors for renal
dysfunction in type 2 diabetes: U.K. Prospective Diabetes Study 74. Diabetes 2006; 55: 1832-1839.
Available at http://www.ncbi.nlm.nih.gov/pubmed/16731850.
80. Hillege HL, Janssen WM, Diercks GF, Pinto-Sietsma SJ, Bak AA, Van Gilst WH, De Zeeuw D, De
Jong PE. Microalbuminuria, a better predictor for clinical outcome than hypertension and/or
hypercholesterolemia? Circulation 2000; 102: 4113. Available at <Go to ISI>://000090072304104.

CHAPTER 1: Introduction
38
81. Rytand DA, Spreiter S. Prognosis in postural (orthostatic) proteinuria: forty to fifty-year follow-up of
six patients after diagnosis by Thomas Addis. N Engl J Med 1981; 305: 618-621. Available at
http://www.ncbi.nlm.nih.gov/pubmed/7266586.
82. Naderi ASA, Reilly RF. Primary Care Approach to Proteinuria. J Am Board Fam Med 2008; 21: 569-
574. Available at <Go to ISI>://000260721500014.
83. Poortmans JR, Vanderstraeten J. Kidney function during exercise in healthy and diseased humans. An
update. Sports medicine 1994; 18: 419-437. Available at
http://www.ncbi.nlm.nih.gov/pubmed/7886356.
84. Fink HA, Ishani A, Taylor BC, Greer NL, Macdonald R, Rossini D, Sadiq S, Lankireddy S, Kane RL,
Wilt TJ. Screening for, monitoring, and treatment of chronic kidney disease stages 1 to 3: a systematic
review for the u.s. Preventive services task force and for an american college of physicians clinical
practice guideline. Annals of internal medicine 2012; 156: 570-581. Available at
http://www.ncbi.nlm.nih.gov/pubmed/22508734.
85. Coresh J, Selvin E, Stevens LA, Manzi J, Kusek JW, Eggers P, Van Lente F, Levey AS. Prevalence of
chronic kidney disease in the United States. JAMA 2007; 298: 2038-2047. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=17986697.
86. Bakris GL, Williams M, Dworkin L, Elliott WJ, Epstein M, Toto R, Tuttle K, Douglas J, Hsueh W,
Sowers J, Diab NKFH. Preserving renal function in adults with hypertension and diabetes: A
consensus approach. American Journal of Kidney Diseases 2000; 36: 646-661. Available at <Go to
ISI>://000089227300027.
87. de Zeeuw D, Remuzzi G, Parving HH, Keane WF, Zhang Z, Shahinfar S, Snapinn S, Cooper ME,
Mitch WE, Brenner BM. Proteinuria, a target for renoprotection in patients with type 2 diabetic
nephropathy: lessons from RENAAL. Kidney Int 2004; 65: 2309-2320. Available at
http://www.ncbi.nlm.nih.gov/pubmed/15149345.
88. Astor BC, Matsushita K, Gansevoort RT, van der Velde M, Woodward M, Levey AS, Jong PE, Coresh
J, Chronic Kidney Disease Prognosis C, Astor BC, Matsushita K, Gansevoort RT, van der Velde M,
Woodward M, Levey AS, de Jong PE, Coresh J, El-Nahas M, Eckardt KU, Kasiske BL, Wright J,
Appel L, Greene T, Levin A, Djurdjev O, Wheeler DC, Landray MJ, Townend JN, Emberson J, Clark
LE, Macleod A, Marks A, Ali T, Fluck N, Prescott G, Smith DH, Weinstein JR, Johnson ES, Thorp
ML, Wetzels JF, Blankestijn PJ, van Zuilen AD, Menon V, Sarnak M, Beck G, Kronenberg F,
Kollerits B, Froissart M, Stengel B, Metzger M, Remuzzi G, Ruggenenti P, Perna A, Heerspink HJ,
Brenner B, de Zeeuw D, Rossing P, Parving HH, Auguste P, Veldhuis K, Wang Y, Camarata L,
Thomas B, Manley T. Lower estimated glomerular filtration rate and higher albuminuria are associated
with mortality and end-stage renal disease. A collaborative meta-analysis of kidney disease population
cohorts. Kidney Int 2011; 79: 1331-1340. Available at http://www.ncbi.nlm.nih.gov/pubmed/21289598.
89. Dickinson WH. The Croonian Lectures on the Pathology and Relations of Albuminuria. Br Med J 1876;
1: 467-469. Available at http://www.ncbi.nlm.nih.gov/pubmed/20748179.
90. Vanholder R, Massy Z, Argiles A, Spasovski G, Verbeke F, Lameire N, European Uremic Toxin Work
G. Chronic kidney disease as cause of cardiovascular morbidity and mortality. Nephrol Dial
Transplant 2005; 20: 1048-1056. Available at http://www.ncbi.nlm.nih.gov/pubmed/15814534.
91. Van Biesen W, De Bacquer D, Verbeke F, Delanghe J, Lameire N, Vanholder R. The glomerular
filtration rate in an apparently healthy population and its relation with cardiovascular mortality during
10 years. Eur Heart J 2007; 28: 478-483. Available at http://www.ncbi.nlm.nih.gov/pubmed/17223665.
92. Goodhart JF. Two Clinical Lectures on Albuminuria. Br Med J 1890; 1: 1121-1123. Available at
http://www.ncbi.nlm.nih.gov/pubmed/20753040.
93. Lorenzo C, Williams K, Hunt KJ, Haffner SM. The National Cholesterol Education Program - Adult
Treatment Panel III, International Diabetes Federation, and World Health Organization definitions of
the metabolic syndrome as predictors of incident cardiovascular disease and diabetes. Diabetes Care
2007; 30: 8-13. Available at http://www.ncbi.nlm.nih.gov/pubmed/17192325.
94. Expert Panel on Detection E, Treatment of High Blood Cholesterol in A. Executive Summary of The
Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection,

CHAPTER 1: Introduction
39
Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA
2001; 285: 2486-2497. Available at http://www.ncbi.nlm.nih.gov/pubmed/11368702.
95. Ervin RB. Prevalence of metabolic syndrome among adults 20 years of age and over, by sex, age, race
and ethnicity, and body mass index: United States, 2003-2006. National health statistics reports 2009:
1-7. Available at http://www.ncbi.nlm.nih.gov/pubmed/19634296.
96. Thomas G, Sehgal AR, Kashyap SR, Srinivas TR, Kirwan JP, Navaneethan SD. Metabolic Syndrome
and Kidney Disease: A Systematic Review and Meta-analysis. Clinical Journal of the American
Society of Nephrology 2011; 6: 2364-2373. Available at <Go to ISI>://WOS:000295657000008.
97. Karalliedde J, Viberti G. Proteinuria in diabetes: bystander or pathway to cardiorenal disease? J Am
Soc Nephrol 2010; 21: 2020-2027. Available at http://www.ncbi.nlm.nih.gov/pubmed/21051738.
98. Mimran A, Ribstein J, Du Cailar G. Microalbuminuria in essential hypertension. Curr Opin Nephrol Hypertens 1999; 8: 359-363. Available at http://www.ncbi.nlm.nih.gov/pubmed/10456269.
99. Bianchi S, Bigazzi R, Campese VM. Microalbuminuria in essential hypertension: Significance,
pathophysiology, and therapeutic implications. American Journal of Kidney Diseases 1999; 34: 973-
995. Available at <Go to ISI>://000084126000002.
100. Klausen KP, Parving HH, Scharling H, Jensen JS. The association between metabolic syndrome,
microalbuminuria and impaired renal function in the general population: impact on cardiovascular
disease and mortality. Journal of Internal Medicine 2007; 262: 470-478. Available at <Go to
ISI>://000249947500010.
101. Bohm M, Reil JC, Danchin N, Thoenes M, Bramlage P, Volpe M. Association of heart rate with
microalbuminuria in cardiovascular risk patients: data from I-SEARCH. Journal of Hypertension 2008;
26: 18-25. Available at <Go to ISI>://000252095900007.
102. Pedrinelli R, Dell'Omo G, Di Bello V, Pellegrini G, Pucci L, Del Prato S, Penno G. Low-grade
inflammation and microalbuminuria in hypertension. Arteriosclerosis, thrombosis, and vascular biology 2004; 24: 2414-2419. Available at http://www.ncbi.nlm.nih.gov/pubmed/15486313.
103. Hillege HL, Fidler V, Diercks GFH, van Gilst WH, de Zeeuw D, van Veldhuisen DJ, Gans ROB,
Janssen WMT, Grobbee DE, de Jong PE, Grp PS. Urinary albumin excretion predicts cardiovascular
and noncardiovascular mortality in general population. Circulation 2002; 106: 1777-1782. Available at
<Go to ISI>://000178385700010.
104. Hallan SI, Matsushita K, Sang Y, Mahmoodi BK, Black C, Ishani A, Kleefstra N, Naimark D,
Roderick P, Tonelli M, Wetzels JF, Astor BC, Gansevoort RT, Levin A, Wen CP, Coresh J, Chronic
Kidney Disease Prognosis C. Age and association of kidney measures with mortality and end-stage
renal disease. JAMA 2012; 308: 2349-2360. Available at
http://www.ncbi.nlm.nih.gov/pubmed/23111824.
105. Romundstad S, Holmen J, Kvenild K, Hallan H, Ellekjaer H. Microalbuminuria and all-cause mortality
in 2,089 apparently healthy individuals: A 4.4-year follow-up study. The Nord-Trondelag Health Study
(HUNT), Norway. American Journal of Kidney Diseases 2003; 42: 466-473. Available at <Go to
ISI>://000185518500004.
106. Arnlov J, Evans JC, Meigs JB, Wang TJ, Fox CS, Levy D, Benjamin EJ, D'Agostino RB, Vasan RS.
Low-grade albuminuria and incidence of cardiovascular disease events in nonhypertensive and
nondiabetic individuals: the Framingham Heart Study. Circulation 2005; 112: 969-975. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=16087792.
107. Yuyun MF, Khaw KT, Luben R, Welch A, Bingham S, Day NE, Wareham NJ. Microalbuminuria
independently predicts all-cause and cardiovascular mortality in a British population: The European
Prospective Investigation into Cancer in Norfolk (EPIC-Norfolk) population study. Int J Epidemiol
2004; 33: 189-198. Available at <Go to ISI>://000220615000034.
108. Yuyun MF, Khaw KT, Luben R, Welch A, Bingham S, Day NE, Wareham NJ. A prospective study of
microalbuminuria and incident coronary heart disease and its prognostic significance in a British
population: the EPIC-Norfolk study. Am J Epidemiol 2004; 159: 284-293. Available at
http://www.ncbi.nlm.nih.gov/pubmed/14742289.

CHAPTER 1: Introduction
40
109. Klausen KP, Scharling H, Jensen G, Jensen JS. New definition of microalbuminuria in hypertensive
subjects - Association with incident coronary heart disease and death. Hypertension 2005; 46: 33-37.
Available at <Go to ISI>://000230012700010.
110. Ninomiya T, Perkovic V, de Galan BE, Zoungas S, Pillai A, Jardine M, Patel A, Cass A, Neal B,
Poulter N, Mogensen CE, Cooper M, Marre M, Williams B, Hamet P, Mancia G, Woodward M,
Macmahon S, Chalmers J, Group AC. Albuminuria and kidney function independently predict
cardiovascular and renal outcomes in diabetes. J Am Soc Nephrol 2009; 20: 1813-1821. Available at
http://www.ncbi.nlm.nih.gov/pubmed/19443635.
111. Viana LV, Gross JL, Camargo JL, Zelmanovitz T, da Costa Rocha EP, Azevedo MJ. Prediction of
cardiovascular events, diabetic nephropathy, and mortality by albumin concentration in a spot urine
sample in patients with type 2 diabetes. J Diabetes Complications 2012; 26: 407-412. Available at
http://www.ncbi.nlm.nih.gov/pubmed/22677793.
112. Atkins RC, Polkinghorne KR, Briganti EM, Shaw JE, Zimmet PZ, Chadban SJ. Prevalence of
albuminuria in Australia: the AusDiab Kidney Study. Kidney Int Suppl 2004: S22-24. Available at
http://www.ncbi.nlm.nih.gov/pubmed/15485411.
113. Yuyun MF, Khaw KT, Luben R, Welch A, Bingham S, Day NE, Wareham NJ. Microalbuminuria,
cardiovascular risk factors and cardiovascular morbidity in a British population: The EPIC-Norfolk
population-based study. European Journal of Cardiovascular Prevention & Rehabilitation 2004; 11:
207-213. Available at <Go to ISI>://000222392100005.
114. Bello AK, Peters J, Wight J, El Nahas M. The Kidney Evaluation and Awareness Program in Sheffield
(KEAPS): a community-based screening for microalbuminuria in a British population. Nephron Clin Pract 2010; 116: c95-103. Available at http://www.ncbi.nlm.nih.gov/pubmed/20502045.
115. Krol E, Rutkowski B, Czarniak P, Kraszewska E, Lizakowski S, Szubert R, Czekalski S, Sulowicz W,
Wiecek A. Early Detection of Chronic Kidney Disease: Results of the PolNef Study. American Journal of Nephrology 2009; 29: 264-273. Available at <Go to ISI>://000261132000015.
116. Garg AX, Kiberd BA, Clark WF, Haynes RB, Clase CM. Albuminuria and renal insufficiency
prevalence guides population screening: results from the NHANES III. Kidney Int 2002; 61: 2165-
2175. Available at http://www.ncbi.nlm.nih.gov/pubmed/12028457.
117. Fox CS, Matsushita K, Woodward M, Bilo HJ, Chalmers J, Heerspink HJ, Lee BJ, Perkins RM,
Rossing P, Sairenchi T, Tonelli M, Vassalotti JA, Yamagishi K, Coresh J, de Jong PE, Wen CP,
Nelson RG, Chronic Kidney Disease Prognosis C. Associations of kidney disease measures with
mortality and end-stage renal disease in individuals with and without diabetes: a meta-analysis. Lancet 2012; 380: 1662-1673. Available at http://www.ncbi.nlm.nih.gov/pubmed/23013602.
118. Levin A, Rocco M. KDOQI clinical practice guidelines and clinical practice recommendations for
diabetes and chronic kidney disease. American Journal of Kidney Diseases 2007; 49: S10-S179.
Available at <Go to ISI>://000244490200001.
119. Witte EC, Lambers Heerspink HJ, de Zeeuw D, Bakker SJ, de Jong PE, Gansevoort R. First morning
voids are more reliable than spot urine samples to assess microalbuminuria. J Am Soc Nephrol 2009;
20: 436-443. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=19092125.
120. Johnson G. On the Etiology of Albuminuria. Br Med J 1873; 2: 112-113. Available at
http://www.ncbi.nlm.nih.gov/pubmed/20747168.
121. Birn H, Christensen EI. Renal albumin absorption in physiology and pathology. Kidney International
2006; 69: 440-449. Available at http://www.ncbi.nlm.nih.gov/pubmed/16514429.
122. Iwao Y, Hiraike M, Kragh-Hansen U, Mera K, Noguchi T, Anraku M, Kawai K, Maruyama T, Otagiri
M. Changes of net charge and alpha-helical content affect the pharmacokinetic properties of human
serum albumin. Biochimica et biophysica acta 2007; 1774: 1582-1590. Available at
http://www.ncbi.nlm.nih.gov/pubmed/18029235.
123. Viberti GC, Vergani D. Detection of Potentially Reversible Diabetic Albuminuria - a 3-Drop
Agglutination-Test for Urinary Albumin at Low Concentration. Diabetes 1982; 31: 973-975. Available
at <Go to ISI>://WOS:A1982PN97900007.

CHAPTER 1: Introduction
41
124. Jones GR. Laboratory reporting of urine protein and albumin. The Clinical biochemist Reviews /
Australian Association of Clinical Biochemists 2011; 32: 103-107. Available at
http://www.ncbi.nlm.nih.gov/pubmed/21611084.
125. Brinkman JW, Bakker SJL, Gansevoort RT, Hillege HL, Kema IP, Gans ROB, De Jong PE, De Zeeuw
D. Which method for quantifying urinary albumin excretion gives what outcome? A comparison of
immunonephelometry with HPLC. Kidney International 2004; 66: S69-S75. Available at <Go to
ISI>://WOS:000224751000020.
126. Sarafidis PA, Riehle J, Bogojevic Z, Basta E, Chugh A, Bakris GL. A comparative evaluation of
various methods for microalbuminuria screening. American Journal of Nephrology 2008; 28: 324-329.
Available at http://www.ncbi.nlm.nih.gov/pubmed/18046079.
127. Decavele AS, Fiers T, Penders J, Delanghe JR. A sensitive quantitative test strip based point-of-care
albuminuria screening assay. Clinical chemistry and laboratory medicine : CCLM / FESCC 2012; 50:
673-678. Available at http://www.ncbi.nlm.nih.gov/pubmed/22505559.
128. Tugirimana PL, Delanghe JR. Development of an affordable dye-stained microalbuminuria screening
test. Nephrol Dial Transplant 2009; 24: 1485-1490. Available at
http://www.ncbi.nlm.nih.gov/pubmed/19096085.
129. Speeckaert MM, Speeckaert R, Van De Voorde L, Delanghe JR. Immunochemically unreactive
albumin in urine: fiction or reality? Critical reviews in clinical laboratory sciences 2011; 48: 87-96.
Available at http://www.ncbi.nlm.nih.gov/pubmed/21871001.
130. Viberti GC, Hill RD, Jarrett RJ, Argyropoulos A, Mahmud U, Keen H. Microalbuminuria as a
predictor of clinical nephropathy in insulin-dependent diabetes mellitus. Lancet 1982; 1: 1430-1432.
Available at http://www.ncbi.nlm.nih.gov/pubmed/6123720.
131. Mogensen CE. Microalbuminuria predicts clinical proteinuria and early mortality in maturity-onset
diabetes. N Engl J Med 1984; 310: 356-360. Available at
http://www.ncbi.nlm.nih.gov/pubmed/6690964.
132. Bennett PH, Haffner S, Kasiske BL, Keane WF, Mogensen CE, Parving HH, Steffes MW, Striker GE.
Screening and management of microalbuminuria in patients with diabetes mellitus: recommendations
to the Scientific Advisory Board of the National Kidney Foundation from an ad hoc committee of the
Council on Diabetes Mellitus of the National Kidney Foundation. American journal of kidney diseases : the official journal of the National Kidney Foundation 1995; 25: 107-112. Available at
http://www.ncbi.nlm.nih.gov/pubmed/7810516.
133. Chase HP, Marshall G, Garg SK, Harris S, Osberg I. Borderline increases in albumin excretion rate
and the relation to glycemic control in subjects with type I diabetes. Clin Chem 1991; 37: 2048-2052.
Available at http://www.ncbi.nlm.nih.gov/pubmed/1764780.
134. Warram JH, Gearin G, Laffel L, Krolewski AS. Effect of duration of type I diabetes on the prevalence
of stages of diabetic nephropathy defined by urinary albumin/creatinine ratio. Journal of the American
Society of Nephrology 1996; 7: 930-937. Available at <Go to ISI>://A1996UT21600017.
135. van der Velde M, Matsushita K, Coresh J, Astor BC, Woodward M, Levey A, de Jong P, Gansevoort
RT, Chronic Kidney Disease Prognosis C, van der Velde M, Matsushita K, Coresh J, Astor BC,
Woodward M, Levey AS, de Jong PE, Gansevoort RT, Levey A, El-Nahas M, Eckardt KU, Kasiske
BL, Ninomiya T, Chalmers J, Macmahon S, Tonelli M, Hemmelgarn B, Sacks F, Curhan G, Collins AJ,
Li S, Chen SC, Hawaii Cohort KP, Lee BJ, Ishani A, Neaton J, Svendsen K, Mann JF, Yusuf S, Teo
KK, Gao P, Nelson RG, Knowler WC, Bilo HJ, Joosten H, Kleefstra N, Groenier KH, Auguste P,
Veldhuis K, Wang Y, Camarata L, Thomas B, Manley T. Lower estimated glomerular filtration rate
and higher albuminuria are associated with all-cause and cardiovascular mortality. A collaborative
meta-analysis of high-risk population cohorts. Kidney Int 2011; 79: 1341-1352. Available at
http://www.ncbi.nlm.nih.gov/pubmed/21307840.
136. Patel A, MacMahon S, Chalmers J, Neal B, Woodward M, Billot L, Harrap S, Poulter N, Marre M,
Cooper M, Glasziou P, Grobbee DE, Hamet P, Heller S, Liu LS, Mancia G, Mogensen CE, Pan CY,
Rodgers A, Williams B. Effects of a fixed combination of perindopril and indapamide on
macrovascular and microvascular outcomes in patients with type 2 diabetes mellitus (the ADVANCE
trial): a randomised controlled trial. Lancet 2007; 370: 829-840. Available at <Go to
ISI>://000249733300028.

CHAPTER 1: Introduction
42
137. Romundstad S, Holmen J, Kvenild K, Aakervik O, Hallan H. Clinical relevance of microalbuminuria
screening in self-reported non-diabetic/non-hypertensive persons identified in a large health screening-
-the Nord-Trondelag Health Study (HUNT), Norway. Clin Nephrol 2003; 59: 241-251. Available at
http://www.ncbi.nlm.nih.gov/pubmed/12708563.
138. Asselbergs FW, Diercks GF, Hillege HL, van Boven AJ, Janssen WM, Voors AA, de Zeeuw D, de
Jong PE, van Veldhuisen DJ, van Gilst WH. Effects of fosinopril and pravastatin on cardiovascular
events in subjects with microalbuminuria. Circulation 2004; 110: 2809-2816. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=15492322.
139. WHO STEPS Surveillance, part 3. Training and Practical Guides, section 3: guide to physical
Measurements. Available at http://www.who.int/chp/steps/Part3_Section3.pdf.
140. Rubin DB. multiple imputation for nonrespons in surveys. New York: John Wiley & Sons 1987.
141. Frank EH. Hmisc: Harrell Miscerllaneous. R package version 3.7-0. 2009. Available at CRAN.R-
project.org/package=Hmisc.

CHAPTER 2: RESULTS
2.1. SCREENING FOR CARDIOVASCULAR AND RENAL MARKERS IN UNSELECTED
SUBJECTS: RESULTS FROM URI TRIAL.


CHAPTER 2: Results
45
2.1.1 Towards a rational screening strategy for albuminuria: Results from the
Unreferred Renal Insufficiency Trial
Arjan van der Tol1, Wim Van Biesen
1, Francis Verbeke
1, Guy De Groote
2, Frans Vermeiren
3,
Kathleen Eeckhaut3, Raymond Vanholder
1
1 Renal Division, Department of Internal Medicine, University Hospital Gent
2 CRI laboratory, Gent
3 Occupational Health Care Adhesia, Belgium.
PLoS ONE October 2010; 5(10): e13328
Available at: http://www.plosone.org/article/info%3Adoi%2F10.1371%2Fjournal.pone.0013328

CHAPTER 2: Results
46
Abstract.
Background. There remains debate about the screening strategies for albuminuria. This study
evaluated whether a screening strategy in an apparently healthy population based on basic clinical
and biochemical parameters could be more effective than a strategy where screening for
albuminuria is performed unselectively.
Methodology/Principal Findings. The Unreferred Renal Insufficiency (URI) Study is a cross-
sectional study on the prevalence of metabolic risk factors in Belgian workers, volunteering to be
screened during a routine yearly occupational check-up. Subjects (n=295) with treated
hypertension, known diabetes, treated dyslipidaemia, cardiovascular and renal disease were
excluded. Among 1,191 apparently healthy subjects, 23% had unknown hypertension, 13% had
impaired glucose tolerance, 15.4% had normoalbuminuria, 4.2% had microalbuminuria and 0.4%
had macroalbuminuria. Subjects with resting heart rate ≥85 bpm, plasma glucose ≥5.6 mmol/L
and blood pressure ≥140/90mmHg were associated with albuminuria of any degree. A strategy
where only subjects with at least one of these risk factors (n=431) were screened for albuminuria,
would identify all subjects with macroalbuminuria (5/5), 64% of those with microalbuminuria
(32/50), and less than half of those with normoalbuminuria (81/183). An alternative strategy
whereby subjects were first screened for presence of albuminuria, and additional cardiovascular
risk factors were only measured in subjects positive for albuminuria (n=238), would identify only
27% (118/431) of the subjects with additional and potentially modifiable cardiovascular risk
factors. On the other hand, half of the subjects in this study with albuminuria (120/238, of which
102 had normoalbuminuria), had no additional cardiovascular risk factor at all.
Conclusions. Screening an apparently healthy population directly for albuminuria will result in a
high percentage of false positives, mostly measured in the normal range. Screening for
microalbuminuria and macroalbuminuria based on presence of additional, potentially modifiable
risk factors appears to be more beneficial.

CHAPTER 2: Results
47
Introduction
The number of patients with end stage renal disease (ESRD) in need of renal replacement therapy
has dramatically increased over the last decades (1). A substantial part of this increase is
attributable to the rising prevalence of diabetes and/or hypertension (2-4). Microalbuminuria
seems to be an important predictor of progressive renal disease and end stage renal disease in
diabetic and hypertensive subjects (5, 6). It has been demonstrated that in these populations,
preventive measures can delay the evolution to macroalbuminuria and potentially also the
progression to renal failure (7, 8). Consequently, it is advised to screen these high risk subjects
with diabetes and hypertension, in order to identify and eventually treat those at risk for
progressive renal disease. Extending this line of reasoning, some authors advocate to screen also
low risk groups, or even the general population, arguing that most persons with albuminuria
and/or reduced eGFR (<60 ml/min/1.73m²) are asymptomatic (9). Van der Velde et al e.g. found
that 45% of subjects with microalbuminuria were younger than 55 years and had no hypertension
or diabetes (9). It is debated whether such a large scale screening project should be advocated
(10, 11). Concerns are not only the cost of screening itself, but more importantly, the risk and the
cost of treating false positive subjects (12). In the study by van der Velde et al, out of 40,854
subjects screened, 7.8% (n=3,200) had at least microalbuminuria, but only 45 of those developed
ESRD over a 9 year follow up period (9). In addition, effective screening presumes that an
intervention to alter the course of the disease is available (13), which is not the case if the subject
only has albuminuria and no other modifiable risk factor. It would therefore be very useful to
develop a screening strategy based on additional, modifiable, risk factors to enhance the yield of
screening without having too much false positives, and to make interventions possible.
In this study, we used data collected in an apparently healthy working population, aged 17 to 65
years, to evaluate which easily obtainable parameters or combinations of them are associated
with albuminuria, and whether using these risk factors can be of help to increase the effectiveness
of a screening program.

CHAPTER 2: Results
48
Methods
Objectives: The primary aim was to determine the prevalence of different levels of albuminuria,
some (cardiovascular) risk factors and their associations, to develop a rational screening strategy
for albuminuria in the healthy population.
Participants: The Unreferred Renal Insufficiency (URI) is a cross sectional study that included
only Caucasian workers (n=1,486) who presented at a routine yearly occupational check-up
between January 2007 and December 2009, in Belgium. The presence of more than 100
leukocytes/μl (2.2%), and/or more than 50 erythrocytes/μl (2.4%) in the urinary sediment were
considered as confounders for reliable measurement of urinary albumin; these subjects and
subjects with incomplete data (1.8%) were consequently excluded from further analysis. Subjects
with known comorbid conditions or risk factors of which it is well established that they could
affect albuminuria, such as diabetes (1.2%), cardiovascular disease (0.3%), renal disease (0.4%),
subjects on antihypertensive drugs (8.3%) and on lipid lowering drugs (3.3%) were also
excluded, leaving a cohort of 1,191 apparently healthy subjects for analysis.
Description of procedures: All subjects were investigated during their yearly check up by their
occupational physician. Body weight was recorded to the nearest 0.1 kg and height was measured
to the nearest centimeter. Waist circumference was measured by trained nurses following
recommendations by WHO (14). Body mass index (BMI) was calculated as body weight in kg
divided by height² (kg/m²). Blood pressure and resting heart rate were measured in sitting
position by a calibrated electronic device (OMRON®). A questionnaire about current cigarette
smoking, physical activity and prescribed medication was taken by an occupational physician in
each participant. A random blood and urine spot specimen was collected and analyzed on the
same day in one central laboratory (no frozen samples). Urinary albumin was measured by an
immune turbidimetric method with an inter-assay coefficient of variation of 11.2% at a mean
level of 82 mg/L and an inter-assay coefficient of variation of 4.9% at a mean level of 580 mg/l.
Serum creatinine was analyzed by a colorimetric assay (compensated Jaffe reaction), calibrated
by Isotope Dilution Mass Spectrometry (IDMS), with an inter-assay coefficient of variation of
1.75% at a mean level of 104 µmol/l (Roche). Serum CRP was measured with an immune
turbidimetric method with an inter-assay coefficient of variation of 4.6% at a mean level of 3.2
mg/l and inter-assay coefficient of variation of 2.5% at a mean level of 5.5 mg/l.

CHAPTER 2: Results
49
Definitions: Gender specific urinary albumin creatinine ratio (uACR) cutoff values as proposed
by Warram et al. were used because men have a higher urinary excretion of creatinine than
women due to higher muscle mass. Normoalbuminuria was defined as uACR: 0.6-1.8 mg/mmol
(5-16 mg/g) in men and uACR 0.8-2.7 mg/mmol (7-24 mg/g) in women, microalbuminuria was
defined as uACR 1.9-27 mg/mmol (17-249 mg/g) in men and uACR 2.8-39 mg/mmol (25-354
mg/g) in women, macroalbuminuria was defined as uACR ≥ 28 mg/mmol (250 mg/g) in men and
uACR ≥ 40 mg/mmol (355mg/g) in women (15). The Modification of Diet in Renal disease
(MDRD) equation was used to assess the estimated GFR: eGFR= 175× standardized Scr −1.154
×
age−0.203
× 1.212 [if black] × 0.742 [if female](16). Impaired glucose tolerance (IGT) was defined
as a plasma glucose level ≥ 5.6 mmol/L (17). Hypertension was defined as diastolic blood
pressure ≥ 90 mmHg and/or systolic blood pressure ≥140 mmHg. Obesity was defined as BMI >
30 kg/m². Abdominal adiposity was defined according the National Cholesterol Education
Program (NCEP) criteria: waist circumference >102 cm in men and >88 cm in women.
Hypercholesterolemia was defined as serum total cholesterol >6.5 mmol/L.
Ethics: A written informed consent was obtained from all participants. The Ethics Committee of
University Hospital Ghent approved the study (2006-038).
Statistical methods: SPSS 15.0 was used for all calculations. Results are presented as percentages
or as mean ± standard deviation. The baseline characteristics of groups were compared by use of
ANOVA: post-hoc Scheffé test (continuous variables), Kruskal-Wallis (continuous variable with
a skewed distribution) and a Chi-square test (categorical variables). Ordinal regression analysis
was performed to select the associated risk factors with different categories of albuminuria, in a
random selection of 50% of the subjects. The significant continuous variables were
dichotomized. These risk factors were validated in the other 50% of the sample. The prevalence
and test characteristics, of normo-, micro- and macroalbuminuria were calculated, if at least one
of these risk factors was present. The sensitivity was defined as the number of subjects with true-
positive test results divided by the total number of subjects with albuminuria. The specificity was
defined as the number of true-negative test results divided by the total of number of subjects
without albuminuria. The positive predictive value was defined as the number of true-positive
test results divided by the total number of positive test results. The negative predictive value was
defined as the number of true negative test results divided by the total number of negative test

CHAPTER 2: Results
50
results. The positive likelihood ratio was defined as sensitivity divided by 1-specificity; the
negative likelihood ratio was defined as 1-sensitivity divided by specificity.

CHAPTER 2: Results
51
Results
Our cohort (n=1,191) of apparently healthy subjects, after excluding those with treated
hypertension, treated dyslipidaemia, known diabetes, cardiovascular or renal disease, still had a
high prevalence of unknown hypertension, dyslipidaemia and impaired glucose metabolism.
Table 1. Basic characteristics and metabolic risk factors of 1,191 apparently healthy subjects.
Unknown impaired glucose tolerance (IGT)/diabetes: plasma glucose ≥ 5.6 mmol/L.
Hypercholesterolemia: serum cholesterol >6.5 mmol/L. Hypertension: RR ≥140 and/or 90 mmHg.
Table 1 shows the basic characteristics and cardiovascular risk factors of the cohort.
Almost all subjects (98.9%) had an estimated GFR higher than 60 ml/min/1.73m² and none had
an estimated GFR lower than 50 ml/min/1.73m². As expected, the cohort was rather young (age
38.3 ± 9.7 years, range 17-64). Albumin was detected in the urine of one fifth. The large majority
of albuminuric subjects had normoalbuminuria, fewer subjects had microalbuminuria and
macroalbuminuria was only rarely observed (table 1).
Parameters N %
Male gender 998 83.8
Unknown hypertension 279 23.4
Unknown hypercholesterolemia 86 7.2
Unknown IGT/diabetes 150 13.3
Obesity (BMI>30kg/m²) 160 13.5
Abdominal adiposity (%) 168 16.0
No physical activity 491 49.2
Current smoking 370 32.4
Normoalbuminuria 183 15.4
Microalbuminuria 50 4.2
Macroalbuminuria 5 0.4

CHAPTER 2: Results
52
Table 2 shows the distribution of some measured clinical and biochemical parameters in
subgroups according to different levels of albuminuria.
Table 2. Metabolic risk factors in subjects with different level of albuminuria.
Unknown impaired glucose tolerance (IGT)/diabetes: plasma glucose ≥ 5.6 mmol/L.
Hypertension: RR ≥140 and/or 90 mmHg. *p<0.05, **p<0.01 versus no albuminuria.
In a randomly selected cohort (n=599), a multivariate ordinal regression model selected resting
heart rate, plasma glucose and hypertension as significant independent predictors for presence of
albuminuria at any degree (table 3).
Albuminuria no Normo- Micro- Macro-
n=1,191 (%) 953 183 (15.4) 50 (4.2) 5 (0.4)
Age (years) 38.2±9.6 38.7± 10.1 38.8± 10.7 39.0± 9.1
Men (%) 799 (83.8) 147 (80.3) 47 (94) 5 (100)
Systolic blood pressure (mmHg) 126.9± 13.8 129.8± 14.1 132.6± 18.3* 142.6± 11.2
Diastolic blood pressure (mmHg) 77.4± 9.9 79.9± 10.6* 80.8± 13.2 90± 8.9*
Unknown hypertension 199 (20.9) 55(30.1)* 20 (40)** 5(100)**
Resting heart rate 69.5± 10.3 72.6± 11.3** 75.9± 16.1** 78.8± 3.7
Total cholesterol (mmol/L) 5.0± 1.0 5.1± 1.0 4.9± 1.1 7.0± 1.0**
Plasma glucose (mmol/L) 4.8± 0.7 5.0± 1.2* 5.0± 0.9 5.2± 1.1
Unknown IGT/diabetes (%) 103 (11.5) 34(19.3)* 12(24)* 1(20)
Body mass index (kg/m²) 25.9± 3.9 25.5± 4.3 25.3± 5.3 27.5± 2.7
Abdominal adiposity (%) 135 (16.1) 21 (12.7) 11 (25.6) 1 (25)
Serum uric acid (µmol/L) 315± 71 315± 77 339± 77 482± 119**
White blood cell count (109/L) 7.0± 1.9 7.2± 1.9 7.9± 2.3** 8.0± 1.8
C-reactive protein (mg/L) 2.2± 4.8 2.5± 4.2 4.1± 1.0 3.4± 3.6
Current smoking (%) 283 (31) 64 (35.6) 20 (40) 3 (60)

CHAPTER 2: Results
53
Table 3. Multivariate regression analyses to predict different categories of albuminuria
Random sample n=599, R²=0.07 E St error P
Resting heart rate (beats per min) 0.026 0.009 0.006
Plasma glucose (mmol/L) 0.341 0.141 0.015
Unknown Hypertension 0.487 0.237 0.040
White blood cell count 0.079 0.053 0.132
Serum uric acid (µmol/L) 0.001 0.001 0.464
Total serum cholesterol (mmol/L) -0.106 0.104 0.310
The continuous variables were dichotomized (0 or 1) as follows: resting heart rate ≥85 bpm
(cutoff level according to the 90th
percentile); plasma glucose: ≥5.6 mmol/L (impaired glucose
tolerance). Consequently, the prevalence of normoalbuminuria, microalbuminuria and
macroalbuminuria in this randomly selected cohort, was higher in subjects with at least one risk
factor (n=206) than in subjects with no risk factors (n=393), respectively: 21.4 vs 14.1% (n=44 vs
58); 8.7 vs 3.1% (n=18 vs 12) and 1.5 vs 0% (n=3 vs 0), p<0.001. Our risk assessment was
validated in the other randomly selected cohort (n=592). The prevalence of normoalbuminuria,
microalbuminuria and macroalbuminuria in this validation cohort, was also higher in subjects
with at least one risk factor (n=225) than in subjects with no risk factors (n=367), respectively:
16.4 vs 12% (n=37 vs 44); 6.2 vs 1.6% (n=14 vs 6) and 0.9 vs 0% (n=2 vs 0), p=0.001. Table 4
shows the test characteristics for subjects with at least one risk factor, to identify
normoalbuminuria, microalbuminuria and macroalbuminuria in both randomly selected cohorts.

CHAPTER 2: Results
54
Table 4. Test characteristics to identify normo-, micro- and macroalbuminuria with at least one
risk factor in randomly selected populations and in the complete “healthy” population.
Population albuminuria sensitivity specificity PPV NPV LR+ LR-
random cohort
n=599
Normo- 43 70 24 85 1.4 0.8
Micro- 60 70 11 96 2.0 0.6
Macro- 100 70 2 100 3.3 ≈0
validation cohort
n=592
Normo- 46 65 18 88 1.3 0.8
Micro- 70 65 8 98 2.0 0.5
Macro- 100 65 1 100 2.9 ≈0
complete population
n=1191
Normo- 44 67 21 86 1.3 0.8
Micro- 64 67 9 97 1.9 0.6
Macro- 100 67 1 100 3.0 ≈0
PPV: positive predictive value; NPV: negative predictive value; LR+: positive likelihood and LR-:
negative likelihood ratio
Because our risk assessment fitted quite well in both cohorts, we applied it in the complete
population. The prevalence of normoalbuminuria, microalbuminuria and macroalbuminuria in the
complete population, was higher in subjects with at least one risk factor (n=431) than in subjects
with no risk factors (n=760), respectively; 18.8 vs 13.4% (n=81 vs 102); 7.4 vs 2.4% (n=32 vs
18) and 1.2 vs 0% (n=5 vs 0), p<0.001 (figure 1).

CHAPTER 2: Results
55
Figure 1. The prevalence of albuminuria in subjects with at least one vs. none risk factors
We evaluated two strategies for screening albuminuria in our population, one strategy where a set
of additional risk factors were screened as first line, with later screening for albuminuria only in
subjects with at least one of those additional risk factors and an alternative strategy where
albuminuria was screened as first line, and additional risk factors were measured only in those
with albuminuria.
A strategy where only subjects with at least one modifiable risk factor (n=431) were screened for
albuminuria, would identify all subjects with macroalbuminuria (5/5), 64% of subjects with
microalbuminuria (32/50), but less than half of those with normoalbuminuria (81/183), table 4
shows the corresponding likelihoods and predictive values.
An alternative strategy whereby subjects were first screened for presence of albuminuria, and
additional cardiovascular risk factors were only measured in subjects positive for albuminuria
(n=238), would identify only 27% (118/431) of the subjects with additional and potentially
modifiable cardiovascular risk factors. On the other hand, half of the subjects in this study with
albuminuria (120/238, of which 102 had normal range albuminuria), had no additional
cardiovascular risk factor at all.

CHAPTER 2: Results
56
Table 5 shows that subjects with no modifiable risk factor had also lower levels of risk factors
which were not included in our screening model.
Table 5. Cardiometabolic profile in subjects with none versus one or more risk factors.
Risk factors None ≥ 1 p
N 760 431
Age 37.0 ± 9.4 40.6 ± 9.8 <0.001
Male gender (%) 604 (79.5) 394 (91.48) <0.001
Resting heart rate (bpm) 67.7 ± 8.3 74.9 ± 13.1 <0.001
Systolic blood pressure (mmHg) 121.9± 10.4 137.9 ± 14.1 <0.001
Diastolic blood pressure (mmHg) 74.4 ± 8.3 84.3 ± 10.2 <0.001
Plasma glucose (mmol/L) 4.6 ±0.5 5.3 ±1.0 <0.001
White blood cell count (10*109/L) 6.9 ± 1.9 7.3 ± 1.9 <0.001
Body mass index (kg²/m) 25.2 ± 3.6 26.9 ± 4.4 <0.001
Abdominal obesity (%) 72 (10.8) 96 (24.8) <0.001
Obesity >30 kg/m² (%) 71 (9.4) 89 (20.6) <0.001
Total cholesterol (mmol/L) 4.9 ±0.9 5.3 ±1.0 <0.001
Serum uric acid (µmol/L) 305 ± 70 336 ± 77 <0.001
C-reactive protein (mg/L) 2.0 ± 3.4 3.0 ±7.0 <0.001
Current smoking 225 (30.7) 145 (34.9) 0.130
No physical activity 282 (44.3) 209 (57.9) <0.001

CHAPTER 2: Results
57
Discussion
Our data indicate that albuminuria, unknown hypertension and impaired glucose metabolism are
quite prevalent findings in an apparently healthy population. When present, albuminuria was
mostly measured in the normal range, and was frequently found in subjects without other
modifiable risk factors, making its relevance as a predictor of outcome questionable. A screening
strategy for albuminuria starting from assessment of simple and easy to obtain risk factors, such
as resting heart rate, blood pressure and plasma glucose level identified subjects at risk for micro-
and macroalbuminuria in a more effective way than a strategy of screening a healthy population
for albuminuria alone.
There is little debate that screening for albuminuria should be performed in patients with diabetes
and/or hypertension, where early intervention can slow down deterioration of renal function.
Whether it should also be performed in the general population remains ambigiuous (12, 18, 19).
There is heated debate whether screening the healthy population for presence of albuminuria is
fulfilling all conditions requested to define a successful screening program (13).
A first request is that the screened factor either relates to an important health risk, or is prevalent
in the population. In our healthy population, the prevalence of albuminuria was 20%. However,
many cases had normoalbuminuria without additional risk factors. Those in favor of screening
the general population argue that an urinary albumin excretion > 5µg/min is related with
increased risk of cardiovascular morbidity and mortality (20-22). In some of these studies, an
adjustment for presence of hypertension and diabetes was performed, indicating that albuminuria
is an independent risk factor on top of diabetes and hypertension, but it is not clear whether the
increased risk was also present in those with normal blood pressure and glucose levels (21). In
the PREVEND cohort, hypertension and diabetes were not actually assessed objectively, but
were based on “self declared” status (23). In our study, the prevalence of unknown hypertension
and impaired glucose levels was high, even after excluding subjects with known risk factors, so
most likely also in the PREVEND cohort a substantial part of “false negatives” for hypertension
and impaired glucose tolerance are present. Accordingly, the definition of “healthy population” in
the PREVEND cohort is probably not correct, making also the recommendation to screen the
healthy population incorrect, as most likely a substantial number of subjects in this “healthy
cohort” would have hypertension or elevated glucose levels if these would have been measured.

CHAPTER 2: Results
58
In other studies restricted to non-diabetic and non-hypertensive subjects, although the increased
risk for renal disease in those with microalbuminuria seems dramatic, the absolute risk remains
low, with less than 0.1% of persons with microalbuminuria ending up on renal replacement
therapy, or 0.6% developing cardiovascular disease over an 8 year period (9, 24). In the
PREVEND study, the relation between albuminuria and decline of renal function in subjects
without known risk factors, was only observed in those individuals with macroalbuminuria (9).
As mentioned, in our study, all subjects with macroalbuminuria would be detected if only
subjects with more than one risk factor were screened, as none of the subjects without risk factors
(the truly healthy population) had macroalbuminuria. In our cohort, the prevalence of
microalbuminuria, in subjects without risk factors, was 2.4%. A similar figure was found in a
New Zealand study (2.0%) in subjects without diabetes, impaired glucose tolerance, hypertension
or dyslipidaemia (25). In the Copenhagen City Heart Study, the prevalence of microalbuminuria
was also 2.0% in subjects without any feature of the metabolic syndrome, and these subjects had
no increased risk for cardiovascular disease and death, suggesting that microalbuminuria by itself
might not be an independent determinant of outcome without presence of associated risk factors
(26). It can be that this microalbuminuria is the equivalent of “exertional”(27) or “orthostatic”
albuminuria.
Another request for a screening program to be meaningful and effective, is that risk factors
should be modifiable. As a prospective trial to test the hypothesis that medical management of
microalbuminuria affects patient-centered events independent of blood pressure reduction is still
lacking (28), screening for microalbuminuria in subjects without measured additional risk factors,
appears not to be justified from a general health care perspective.
In our cohort of apparently healthy subjects, the likelihood of having albuminuria was related to
the well established and potentially modifiable risk factors blood pressure and plasma glucose
level, but also to resting heart rate. Two thirds of our cohort had none of these risk factors. Table
5 shows that those subjects had also much lower levels of other cardiovascular risk factors not
included in our risk score. Nevertheless, 13.4% of these subjects had normoalbuminuria, but none
had macroalbuminuria. Most likely, these subjects have thus a very low absolute risk for
cardiovascular or renal disease, and the potential benefit of a treatment should be considered very
low. Consequently, a strategy of screening only in those with at least one risk factor would miss
only few potentially relevant cases, at the same time avoiding many “false positives”, who

CHAPTER 2: Results
59
compose nearly 50% of albuminuric subjects when unrestricted screening for albuminuria is
performed first. However, testing for albuminuria in subjects with additional cardiovascular risk
factors is warranted, as a more aggressive treatment can be defended in subjects with additional
risk factors in presence of albuminuria compared to those with risk factors but without
albuminuria.
There is substantial evidence that reduction of blood pressure, decreases the progression of renal
disease and reduces cardiovascular events (29-31). Disturbed glucose metabolism, as indicated by
increased plasma glucose levels, is a condition with increased risk for the development of overt
diabetes. Life style modification, and the use of drugs such as metformin and acarbose can slow
down progression to overt diabetes and/or cardiovascular disease in these subjects (32). The
association of resting heart rate with albuminuria was previously mentioned (33, 34). An
explanation could be that a high resting heart rate may cause mechanical stress that might
contribute to renal endothelial dysfunction leading to albuminuria (35). Previous reports
mentioned that tachycardia as a sign of sympathetic overactivity, is an independent risk factor for
chronic kidney disease, cardiovascular and noncardiovascular mortality, even in an apparently
healthy population (34, 36-38). Reduction of sympathetic overactivity by regular physical activity
and smoking cessation appear to be beneficial in this patient group (39). Carvedilol appears to
reduce proteinuria to a higher degree than expected by the blood pressure lowering effect alone in
patients with hypertension, but it is unclear whether this effect is due to the reduction in heart rate
modification or to genuine metabolic effects (40).
A strength of this study is the nearly 100% participation rate of a relatively young and apparently
healthy occupational population. A limitation is that we only measured urinary albumin to
creatinine ratio at one occasion, guidelines recommend to have at least two positive albumin to
creatinine ratio’s in three consecutive first morning urine samples before labeling a person with
microalbuminuria(41). Furthermore, the prevalence of microalbuminuria was underestimated if
albumin to creatinine ratio was measured in morning urine samples (42), while an overestimation
was observed if random samples were obtained (43).Thus, the association between subjects with
albuminuria and additional risk factors could be confounded by measuring the urinary albumin to
creatinine ratio at only one random occasion.

CHAPTER 2: Results
60
In conclusion, our data provide evidence to support the concept that screening for albuminuria
should only be performed in subjects with additional and potentially modifiable risk factors, and
that this strategy is more beneficial than screening the general population. We identified 3
parameters that are easy and cheap to obtain: blood pressure, plasma glucose and resting heart
rate to identify subjects in whom further assessment of presence of albuminuria might be
relevant.
Acknowledgment We thank all concerned employees of Adhesia (Occupational Heath Care,
Ghent, Belgium) and the recruited participants who made this study possible.

CHAPTER 2: Results
61
References
1. Kramer A, Stel V, Zoccali C, Heaf J, Ansell D, Gronhagen-Riska C, Leivestad T, Simpson K, Palsson
R, Postorino M, Jager K. An update on renal replacement therapy in Europe: ERA-EDTA Registry
data from 1997 to 2006. Nephrol Dial Transplant 2009; 24: 3557-3566. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=19820003.
2. ERA-EDTA Registry: ERA-EDTA Registry 2009 Annual report. Academic Medical Center,
Amsterdam, the Netherlands, june 2009. Available at http://www.era-edta-
reg.org/files/annualreports/pdf/AnnRep2009_new.pdf.
3. ERA-EDTA Registry: ERA-EDTA Registry 1998 Annual Report. Academic Medical Center,
Amsterdam, The Netherlands, May 2003. Available at http://www.era-edta-
reg.org/files/annualreports/pdf/AnnRep1998.pdf.
4. The concise 2009 Annual Data Report Atlas of Chronic Kidney Disease & End-Stage Renal Disease in
the United States Available at www.usrds.org.
5. Bigazzi R, Bianchi S, Baldari D, Campese VM. Microalbuminuria predicts cardiovascular events and
renal insufficiency in patients with essential hypertension. Journal of Hypertension 1998; 16: 1325-
1333. Available at <Go to ISI>://000075719400014.
6. Mogensen CE. Microalbuminuria, blood pressure and diabetic renal disease: origin and development
of ideas. Diabetologia 1999; 42: 263-285. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=10096778.
7. Effects of ramipril on cardiovascular and microvascular outcomes in people with diabetes mellitus:
results of the HOPE study and MICRO-HOPE substudy. Heart Outcomes Prevention Evaluation Study
Investigators. Lancet 2000; 355: 253-259. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=10675071.
8. Keane WF, Zhang Z, Lyle PA, Cooper ME, de Zeeuw D, Grunfeld JP, Lash JP, McGill JB, Mitch WE,
Remuzzi G, Shahinfar S, Snapinn SM, Toto R, Brenner BM. Risk scores for predicting outcomes in
patients with type 2 diabetes and nephropathy: the RENAAL study. Clin J Am Soc Nephrol 2006; 1:
761-767. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=17699284.
9. van der Velde M, Halbesma N, de Charro FT, Bakker SJL, de Zeeuw D, de Jong PE, Gansevoort RT.
Screening for Albuminuria Identifies Individuals at Increased Renal Risk. Journal of the American
Society of Nephrology 2009; 20: 852-862. Available at <Go to ISI>://000264831300023.
10. Hallan SI, Dahl K, Oien CM, Grootendorst DC, Aasberg A, Holmen J, Dekker FW. Screening
strategies for chronic kidney disease in the general population: follow-up of cross sectional health
survey. Brit Med J 2006; 333: 1047-1050. Available at <Go to ISI>://000242229800016
http://www.bmj.com/cgi/reprint/333/7577/1047.pdf.
11. Fried L. Are we ready to screen the general population for microalbuminuria? J Am Soc Nephrol 2009;
20: 686-688. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=19279125.
12. Romundstad S, Holmen J, Kvenild K, Aakervik O, Hallan H. Clinical relevance of microalbuminuria
screening in self-reported non-diabetic/non-hypertensive persons identified in a large health screening -

CHAPTER 2: Results
62
The Nord-Trondelag Health Study (HUNT), Norway. Clin Nephrol 2003; 59: 241-251. Available at
<Go to ISI>://000181878200001.
13. Wilson JMG, Jungner G. principles and practice of screening for disease. public health papers, Geneva,
World Health Organization 1968; 34: . Available at http://whqlibdoc.who.int/php/WHO_PHP_34.pdf.
14. WHO STEPS Surveillance, part 3. Training and Practical Guides, section 3: guide to physical
Measurements. Available at http://www.who.int/chp/steps/Part3_Section3.pdf.
15. Warram JH, Gearin G, Laffel L, Krolewski AS. Effect of duration of type I diabetes on the prevalence
of stages of diabetic nephropathy defined by urinary albumin/creatinine ratio. Journal of the American
Society of Nephrology 1996; 7: 930-937. Available at <Go to ISI>://A1996UT21600017.
16. Levey AS, Coresh J, Greene T, Stevens LA, Zhang YL, Hendriksen S, Kusek JW, Van Lente F. Using
standardized serum creatinine values in the modification of diet in renal disease study equation for
estimating glomerular filtration rate. Ann Intern Med 2006; 145: 247-254. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=16908915.
17. Genuth S, Alberti KGMM, Bennett P, Buse J, DeFronzo R, Kahn R, Kitzmiller J, Knowler WC,
Lebovitz H, Lernmark A, Nathan D, Palmer J, Rizza R, Saudek C, Shaw J, Steffes M, Stern M,
Tuomilehto J, Zimmet P, Classificat ECD. Follow-up report on the diagnosis of diabetes mellitus.
Diabetes Care 2003; 26: 3160-3167. Available at <Go to ISI>://000186269100030.
18. Hallan SI, Stevens P. Screening for chronic kidney disease: which strategy? J Nephrol 2010; 23: 147-
155. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=20155721.
19. Nielen MM, Schellevis FG, Verheij RA. The usefulness of a free self-test for screening albuminuria in
the general population: a cross-sectional survey. BMC Public Health 2009; 9: 381. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=19818129.
20. Klausen KP, Scharling H, Jensen JS. Very low level of microalbuminuria is associated with increased
risk of death in subjects with cardiovascular or cerebrovascular diseases. Journal of Internal Medicine
2006; 260: 231-237. Available at <Go to ISI>://000239860200005.
21. Klausen K, Borch-Johnsen K, Feldt-Rasmussen B, Jensen G, Clausen P, Scharling H, Appleyard M,
Jensen JS. Very low levels of microalbuminuria are associated with increased risk of coronary heart
disease and death independently of renal function, hypertension, and diabetes. Circulation 2004; 110:
32-35. Available at <Go to ISI>://000222461800009.
22. Hillege HL, Fidler V, Diercks GFH, van Gilst WH, de Zeeuw D, van Veldhuisen DJ, Gans ROB,
Janssen WMT, Grobbee DE, de Jong PE, Grp PS. Urinary albumin excretion predicts cardiovascular
and noncardiovascular mortality in general population. Circulation 2002; 106: 1777-1782. Available at
<Go to ISI>://000178385700010.
23. Hillege HL, Janssen WMT, Bak AAA, Diercks GFH, Grobbee DE, Crijns H, van Gilst WH, de Zeeuw
D, de Jong PE, Prevend Study G. Microalbuminuria is common, also in a nondiabetic, nonhypertensive
population, and an independent indicator of cardiovascular risk factors and cardiovascular morbidity.
Journal of Internal Medicine 2001; 249: 519-526. Available at <Go to ISI>://000169568600005.
24. Arnlov J, Evans JC, Meigs JB, Wang TJ, Fox CS, Levy D, Benjamin EJ, D'Agostino RB, Vasan RS.
Low-grade albuminuria and incidence of cardiovascular disease events in nonhypertensive and
nondiabetic individuals: the Framingham Heart Study. Circulation 2005; 112: 969-975. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=16087792.

CHAPTER 2: Results
63
25. Metcalf PA, Scragg RK, Dryson E. Associations between body morphology and microalbuminuria in
healthy middle-aged European, Maori and Pacific Island New Zealanders. Int J Obes Relat Metab
Disord 1997; 21: 203-210. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=9080259.
26. Klausen KP, Parving HH, Scharling H, Jensen JS. The association between metabolic syndrome,
microalbuminuria and impaired renal function in the general population: impact on cardiovascular
disease and mortality. Journal of Internal Medicine 2007; 262: 470-478. Available at <Go to
ISI>://000249947500010.
27. Heathcote KL, Wilson MP, Quest DW, Wilson TW. Prevalence and duration of exercise induced
albuminuria in healthy people. Clin Invest Med 2009; 32: E261-265. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=19640328.
28. Weir MR, Bakris GL. Should Microalbuminuria Ever Be Considered as a Renal Endpoint in Any
Clinical Trial? American Journal of Nephrology 2010; 31: 469-470. Available at <Go to
ISI>://000277757300014.
29. Turnbull F. Effects of different blood-pressure-lowering regimens on major cardiovascular events:
results of prospectively-designed overviews of randomised trials. Lancet 2003; 362: 1527-1535.
Available at http://www.ncbi.nlm.nih.gov/pubmed/14615107.
30. Ruilope LM, Salvetti A, Jamerson K, Hansson L, Warnold I, Wedel H, Zanchetti A. Renal function
and intensive lowering of blood pressure in hypertensive participants of the hypertension optimal
treatment (HOT) study. Journal of the American Society of Nephrology : JASN 2001; 12: 218-225.
Available at http://www.ncbi.nlm.nih.gov/pubmed/11158211.
31. Walker WG, Neaton JD, Cutler JA, Neuwirth R, Cohen JD. Renal function change in hypertensive
members of the Multiple Risk Factor Intervention Trial. Racial and treatment effects. The MRFIT
Research Group. JAMA : the journal of the American Medical Association 1992; 268: 3085-3091.
Available at http://www.ncbi.nlm.nih.gov/pubmed/1433739.
32. Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10-year follow-up of intensive glucose
control in type 2 diabetes. N Engl J Med 2008; 359: 1577-1589. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=18784090.
33. Bohm M, Reil JC, Danchin N, Thoenes M, Bramlage P, Volpe M. Association of heart rate with
microalbuminuria in cardiovascular risk patients: data from I-SEARCH. Journal of Hypertension 2008;
26: 18-25. Available at <Go to ISI>://000252095900007.
34. Inoue T, Iseki K, Iseki C, Ohya Y, Kinjo K, Takishita S. Heart rate as a risk factor for developing
chronic kidney disease: longitudinal analysis of a screened cohort. Clin Exp Nephrol 2009; 13: 487-
493. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=19444548.
35. Facchini FS, Stoohs RA, Reaven GM. Enhanced sympathetic nervous system activity. The linchpin
between insulin resistance, hyperinsulinemia, and heart rate. Am J Hypertens 1996; 9: 1013-1017.
Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=8896654.
36. Gillman MW, Kannel WB, Belanger A, D'Agostino RB. Influence of heart rate on mortality among
persons with hypertension: the Framingham Study. Am Heart J 1993; 125: 1148-1154. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=9080259
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=9080259

CHAPTER 2: Results
64
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=8465742.
37. Palatini P. Elevated heart rate: a "new" cardiovascular risk factor? Prog Cardiovasc Dis 2009; 52: 1-5.
Available at http://www.ncbi.nlm.nih.gov/pubmed/19615486.
38. Jouven X, Empana JP, Escolano S, Buyck JF, Tafflet M, Desnos M, Ducimetiere P. Relation of heart
rate at rest and long-term (>20 years) death rate in initially healthy middle-aged men. The American
journal of cardiology 2009; 103: 279-283. Available at
http://www.ncbi.nlm.nih.gov/pubmed/19121452.
39. Ritz E, Ogata H, Orth SR. Smoking: a factor promoting onset and progression of diabetic nephropathy.
Diabetes Metab 2000; 26 Suppl 4: 54-63. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=10922974.
40. Bakris GL, Fonseca V, Katholi RE, McGill JB, Messerli FH, Phillips RA, Raskin P, Wright JT, Jr.,
Oakes R, Lukas MA, Anderson KM, Bell DS. Metabolic effects of carvedilol vs metoprolol in patients
with type 2 diabetes mellitus and hypertension: a randomized controlled trial. JAMA 2004; 292: 2227-
2236. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=15536109.
41. Clinical Practice Guidelines for Chronic Kidney Disease: Evaluation C, and Stratification, part 5.
Evaluation of laboratory measurements for clinical assessment of kidney disease, guidelines 5.
Assesment of proteinuria
Accessed March 10, 2012; . Available at
http://www.kidney.org/professionals/kdoqi/pdf/ckd_evaluation_classification_stratification.pdf.
42. Stehouwer CD, Fischer HR, Hackeng WH, den Ottolander GJ. Identifying patients with incipient
diabetic nephropathy. Should 24-hour urine collections be used? Arch Intern Med 1990; 150: 373-375.
Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=2302012.
43. Witte EC, Lambers Heerspink HJ, de Zeeuw D, Bakker SJ, de Jong PE, Gansevoort R. First morning
voids are more reliable than spot urine samples to assess microalbuminuria. J Am Soc Nephrol 2009;
20: 436-443. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=19092125.
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=8465742
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=8465742
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=2302012

CHAPTER 2: Results
65
2.1.2. Microalbuminuria is more consistent in presence of cardiovascular risk
factors: Results from the Unreferred Renal Insufficiency Trial
Arjan van der Tol1, Wim Van Biesen
1, Guy De Groote
2, Paul Verbeke
3, Frans Vermeiren
3,
Kathleen Eeckhaut3, Raymond Vanholder
1
1 Renal Division, Department of Internal Medicine, University Hospital Ghent
2 CRI laboratory, Ghent
3 Occupational Health Care Adhesia, Belgium
J Nephrol, May-Jun 2013, 26(3): 580-5.
Available at http://www.ncbi.nlm.nih.gov/pubmed/22865595

CHAPTER 2: Results
66
Abstract
Background. The use of microalbuminuria (MAU) to screen for cardiovascular and renal risk
might be hampered by its intermittent character. This prospective observational study assessed
traditional risk factors in presumed healthy workers with intermittent MAU (IMAU) compared to
persistent MAU (PMAU).
Methods. A cohort of 239 Belgian workers underwent at least two consecutive occupational
check-ups with a median time of 12 months. Hypertension (HT) was defined as blood pressure ≥
140/90 mmHg. Impaired glucose tolerance (IGT) was defined as plasma glucose ≥ 5.6 mmol/L.
MAU was defined as urinary albuminin to creatinine ratio of 17-249 mg/g in men and 25-354
mg/g in women. Workers with IMAU had one positive MAU and workers with PMAU had two
positive MAU during follow up.
Results. The mean age of this mainly male (95%) cohort was 41± 9 years. The prevalence of
persistent risk factors (HT and/or IGT) was higher in workers with PMAU than without MAU
(8/12[67%] vs. 55/210[26%], p= 0.005) while workers with IMAU had no increased risk
(5/17[29%]). The prevalence of PMAU was higher in workers with vs. without persistent risk
factors (8/68= 12% vs.4/171= 2%, p= 0.005) while the prevalence of IMAU was the same (5/68=
7% vs. 12/171= 7%, p= 0.93). The reproducibility of initial MAU at consecutive visits was
higher in workers with vs. without persistent risk factors (8/9[89%] vs.4/11[36%], p= 0.03).
Conclusions. The use of MAU as a first step screening strategy in an occupational health care
setting is hampered by false positives and low sensitivity to identify subjects with cardiovascular
and renal risk. Trial registration 2006 NCT00365911

CHAPTER 2: Results
67
Introduction
There is still debate whether a large scale screening starting from MAU (microalbuminuria) may
identify more accurately subjects at risk for cardiovascular and renal events than measuring
simple clinical index factors (1-4). Supporters of direct screening for MAU substantiate that the
presence of asymptomatic MAU can be measured easily in a simple urine spot whereas
opponents substantiate that the use of MAU might be hampered by its intermittent character,
leading to false positives (5-7). False positive measurements of MAU are provoked by temporary
inflammation, exercise, stature, diet, urinary tract infection, hematuria and medication (8, 9). The
HUNT study data revealed that subjects with persistent MAU (PMAU) had an increased
mortality whereas subjects with intermittent MAU (IMAU) had no increased risk (10).
Nevertheless, many outcome studies including MAU as a risk marker include only single
measurements, most likely for practical reasons (11-13). The primary aim of this study is to
assess the prevalence of traditional cardiovascular risk factors in workers with IMAU as
compared to PMAU to asses whether IMAU or PMAU are related to enhanced cardiovascular
risk.

CHAPTER 2: Results
68
Subjects and methods
The Unreferred Renal Insufficiency study is a non-interventional observational study that
included 1486 voluntary Caucasian workers in Belgium (14). Some of these subjects (n= 341)
underwent consecutive occupational check-ups between January 2007 and December 2009.
Subjects with urinary albumin creatinine ratio (ACR) > 300 mg/g (n=1) and subjects with
missing values of interest were excluded, leaving a cohort of 239 “presumed healthy” workers
with at least two measurements of ACR, blood pressure and plasma glucose. This small
subcohort (n=239) had approximately the same prevalence of hypertension and/or impaired
glucose tolerance as the original population (38 vs.39%).
All participants were investigated annually by their occupational physician. At every
investigation, body weight, height and waist circumference was measured by trained nurses
following WHO recommendations. Body mass index (BMI) was calculated as body weight in kg
divided by height² (kg/m²). Blood pressure and resting heart rate were measured in sitting
position by a calibrated electronic device (OMRON®) and a questionnaire about current cigarette
smoking, physical activity and prescribed medication was performed by a physician in each
participant. In addition, a random blood and urine spot specimen was collected and analyzed on
the same day in one laboratory, at every examination, to mimic a routine screening procedure.
Urinary albumin was measured by an immune turbid metric method with an inter-assay
coefficient of variation of 11.2% at a mean level of 82 mg/L and an inter-assay coefficient of
variation of 4.9% at a mean level of 580 mg/L. Serum creatinine was analyzed by a colorimetric
assay (compensated Jaffe reaction), calibrated by Isotope Dilution Mass Spectrometry, with an
inter-assay coefficient of variation of 1.75% at a mean level of 104 µmol/L. Serum CRP was
measured with an immune turbid metric method with an inter-assay coefficient of variation of
4.6% at a mean level of 3.2 mg/L and inter-assay coefficient of variation of 2.5% at a mean level
of 5.5 mg/L.
Definitions: MAU was defined as ACR between 17-249 mg/g in men and 25-354 mg/g in women
as proposed by Warram et al. (15). Subjects with only one positive MAU were determined as
IMAU and those with at least two positive measurements were labeled as PMAU. Hypertension
(HT) was defined as BP ≥ 140/90 mmHg. Persistent hypertension (PHT) was defined as at least
two measurements were positive. Less than half of the subjects (n=10) treated with

CHAPTER 2: Results
69
antihypertensive agents (n=26) had PHT. Impaired glucose tolerance (IGT) was defined as
plasma glucose ≥ 5.6 mmol/L. Persistent IGT (PIGT) was defined as at least two positive
measurements. All subject who were treated for diabetes (n=6) had PIGT. The Modification of
Diet in Renal disease (MDRD) equation was used to assess the estimated GFR: eGFR= 175 × Scr
−1.154 × age
−0.203 × 1.212 [if black] × 0.742 [if female] (16). Abdominal adiposity was defined
according the National Cholesterol Education Program criteria: waist circumference >102cm in
men and >88 cm in women (17). The Framingham risk score was calculated in every subject (18).
Institutional Review Board (IRB)/Ethics Committee approval was obtained at University
Hospital Ghent (2006-038). This study was in adherence with the Declaration of Helsinki A
written informed consent was obtained from all participants.
Statistical methods: SPSS Statistics 19 was used for all calculations. Results are presented as
percentages or as mean ± standard deviation. The baseline characteristics of groups were
compared by use of ANOVA: post-hoc Scheffé test (continuous variables), Kruskal-Wallis
(continuous variable with a skewed distribution) or a Chi-square test (categorical variables).

CHAPTER 2: Results
70
Results
We followed 239 workers during annual consecutive clinical occupational check-ups with a
median follow up of 12 months (range 8-35 months). Three examinations were performed on 38
subjects. In 220 of the 239 workers (92%) the time between the initial examination and the
confirmation test was within 3-13 months and in 20 subjects this time interval was within 14-26
months. The mean age of this mainly male cohort (95%) was 41.1 ± 9.3 years, range 21-61 years.
All workers had an estimated GFR higher than 60 ml/min/1.73m². At the first visit, 72 of 239
workers had hypertension (30%), 33 had impaired glucose tolerance (14%), 90 had hypertension
and/or impaired glucose tolerance (38%) and 20 had MAU (8%) which was reproducible in 50
(70%), 23 (70%), 68 (76%) and 12 (60%), respectively, at subsequent visits (table 1).
Table 1. Reproducibility of microalbuminuria (MAU), hypertension (HT), impaired glucose
tolerance (IGT) and HT and/or IGT at initial testing and during follow up.
Initial test (n) Follow-up (n)
MAU No MAU
MAU 20 12 8
No MAU 219 9 210
HT No HT
HT 72 50 22
No HT 167 27 140
IGT No IGT
IGT 33 23 10
No IGT 206 35 171
HT and/or IGT No risk
HT and/or IGT 90 68 22
No risk 149 47 102
HT = hypertension; IGT = impaired glucose tolerance; MAU is microalbuminuria. MAU is defined as
ACR 17-249 mg/g in men and 25-354 mg/g in women. HT was defined as BP ≥140/90 mmHg. IGT was
defined as plasma glucose ≥5.6 mmol/L.

CHAPTER 2: Results
71
Table 2. Cardiovascular risk factors in subjects with no microalbuminuria (MAU), intermittent
MAU (IMAU) and persistent MAU (PMAU).
No MAU IMAU PMAU p
N (%) 210 17 (7) 12 (5)
Male gender (%) 200 (95) 15 (88) 12 (100) 0.22
Age(yr) 41± 9 40± 12 45± 11 0.32
Heart rate (bpm) 70± 10 74± 16 72± 12 0.24
SBP (mmHg) 131± 14 129± 17 147± 30**°° 0.002
DBP (mmHg) 80± 10 76± 13 91± 16**°° <0.001
BMI (kg/m²) 26.4± 3.6 25.9± 5.5 29.1± 7.6 0.09
Cholesterol (mmol/l) 5.2± 0.9 5.1± 1.2 5.5± 1.0 0.58
C-Reactive protein (mg/L) 1.9± 2.4 3.0± 2.8 3.9± 5.8 0.03
WBC count (109/L) 7.0± 2.0 7.9± 1.5 7.4± 1.9 0.18
Glucose (mmol/l) 5.0± 1.4 5.1± 1.2 6.7± 4.4* 0.05
PHT and/or PIGT (%) 55 (26) 5 (29) 8 (67)*° 0.01
Adiposity (%) 37 (18) 3 (18) 4 (36) 0.32
Framingham score (%) 7± 5 7± 5 13± 11**°° <0.001
Current smoking (%) 68 (32) 6 (35) 4 (33) 0.97
No physical acitivity (%) 81 (39) 6 (37) 9 (75)* 0.05
MAU is defined as ACR 17-249 mg/g in men and 25-354 mg/g in women, SBP: systolic blood pressure,
DBP: diastolic blood pressure, BMI: body mass index, WBC: white blood cell count, PHT: persistent
hypertension was defined as BP ≥140/90 mmHg in at least two occasions, PIGT was defined as plasma
glucose ≥5.6 mmol/L in at least two occasions, adiposity defined by waist circumference >88 cm in
women and >102 cm in men.
*p < 0.05, **p<0.001 vs no albuminuria, °p<0.05, °°p< 0.005 vs IMAU
Approximately one quarter (n=68) of the 239 workers had persistent hypertension and/or
impaired glucose tolerance and only 5% of the workers (n=12) had MAU confirmed during
follow up.
Workers with PMAU had higher mean blood pressure, mean plasma glucose, Framingham risk
score and higher frequency of inactivity than workers without MAU, while workers with IMAU
had no increased cardiovascular risk (table 2).
The prevalence of persistent HT and/or IGT was higher in workers with PMAU (8/12 [67%])
than in those with IMAU (5/17 [29%], p= 0.05) or without MAU (55/210 [26%], p= 0.005, table

CHAPTER 2: Results
72
2). The prevalence of PMAU was higher in workers with risk factors (HT and/or IGT) than in
workers without persistent risk factors (8/68= 12% vs. 4/171= 2%, p= 0.005) while the
prevalence of IMAU was the same in workers with risk factors (HT and/or IGT) vs. those without
persistent risk factors (5/68= 7% vs. 12/171= 7%, p= 0.93). Workers with risk factors (HT and/or
IGT) had a higher reproducibility of initial MAU than workers without persistent risk factors
(8/9 [89%] vs. 4/11 [36%] p= 0.03, table 3).
Table 3. Reproducibility of microalbuminuria (MAU) at initial testing and during follow-up in
workers with and without persistent hypertension (PHT) and/or persistent impaired glucose
tolerance (PIGT).
Initial test (n) Follow-up (n)
MAU No MAU
With PHT and/or PIGT (n=68) MAU 9 8 1
No Mau 59 4 55
Without PHT and/or PIGT (n=171) MAU 11 4 7
No MAU 160 5 155
MAU is defined as ACR 17-249 mg/g in men and 25-354 mg/g in women, PHT: persistent hypertension
was defined as BP ≥140/90 mmHg in at least two occasions; PIGT was defined as plasma glucose ≥5.6
mmol/L in at least two occasions

CHAPTER 2: Results
73
Discussion
Our data indicate that in subjects with initial MAU, the presence of MAU should be confirmed,
to establish it as a renal and cardiovascular risk marker in an occupational screening programme.
Screening for modifiable risk factors, such as blood pressure and plasma glucose, will identify
proportionally more subjects who could benefit from available therapies than screening for MAU
(14). We now add that individuals with intermittent MAU have approximately the same
percentage of cardiovascular risk factors than subjects without MAU, and that subjects with
persistent MAU have higher cardiovascular risk (19). As a consequence, screening for
cardiovascular and/or renal risk in an occupational population should commence from traditional
risk factors rather than from MAU as a first step. In Addition, this study suggests that MAU is
more consistent in presence of cardiovascular risk factors; thus, screening for MAU in subjects
with persistent risk factors might be more effective than screening a presumed healthy
population for MAU. Of note, subjects with cardiovascular risk factors are more likely to be
screened for MAU as a surrogate marker for cardiovascular and renal outcome (20, 21).
According to our data, subjects with intermittent MAU were not associated with increased
established cardiovascular risk factors and thus should be considered as “false positives” in a
screening programme that uses MAU as first step to identify subjects with cardiovascular and
renal risk. Besides the low reproducibility of MAU in our population, the use of MAU was
further hampered by a low sensitivity to detect traditional risk factors. Only 13% (9/68) of the
cases with persistent HT and/or IGT were identified when MAU was used as a first step to screen
for cardiovascular and renal risk (table 3). The PREVEND trial also observed a low sensitivity of
12% to detect at least one traditional risk factor but the authors argued that the 10 years
cardiovascular disease incidence in hypertensive subjects in absence of MAU is sufficiently low
so as not to require treatment (22). However this claim is inconsistent with PREVEND data that
revealed that half of the subjects on renal replacement therapy and 77% of cardiovascular deaths,
had no MAU when they were screened (23, 24). Moreover, medical management in diabetes
and/or hypertension even without influencing MAU can slow down the clinical course of
progressive CKD, end stage renal disease, cardiovascular morbidity and mortality, whereas it is
unproven whether making MAU as such disappear without influencing other risk factors would
have a benefit on outcomes (25-27). When a screening program to detect cardiovascular and renal
risk starts from MAU another question also arises: how to handle subjects with MAU in the

CHAPTER 2: Results
74
absence of cardiovascular risk factors. According to our data, more than half of the subjects (n=
11) with initial MAU had no persistent cardiovascular risk factors. These subjects could be
considered as having masked or premature cardiovascular risk; however, MAU was only
confirmed in four subjects (36%). Some prospective trials showed that such subjects have a
higher risk of developing de novo hypertension and diabetes (11, 12, 28). However, it is unclear
whether preventive steps focusing on MAU would be effective to postpone this risk. More likely,
there is a high probability that such subjects would pay a price, that is, the side effects of life-long
medication and medical intimidation (1, 7).
Unfortunately, this small sample of young, white and mainly male subjects who were screened in
a working environment, is not entirely representative of the global population. However, as the
association between cardiovascular risk factors and MAU is weaker in women, the
reproducibility of MAU would have been even lower if a similar percentage of women and men
had been recruited (29, 30). Another limitation is that we could not exclude exercise-induced
MAU in this cohort as MAU was measured during working time. MAU might fluctuate more in
random urine samples than in early morning urine samples. Participants with only one positive
MAU in at least two examinations, were considered as false positive. Indeed this study confirmed
that at least two consecutive MAU measurements are necessary to identify subjects with an
increased risk for cardiovascular and renal disease .
In conclusion, a first line screening for MAU in an occupational health care setting as a whole as
an index for renal and cardiovascular risk appears inefficient because of low reproducibility of
MAU and low sensitivity to detect traditional cardiovascular risk factors. Screening for MAU in
subjects with modifiable risk factors might be more effective, because MAU seems to be more
consistent in these subjects than in those without risk factors.
Acknowledgments
We thank all concerned employees of Adhesia (Occupational Health Care, Ghent, Belgium) and
the recruited participants who made this study possible.

CHAPTER 2: Results
75
References
1. Romundstad S, Holmen J, Kvenild K, Aakervik O, Hallan H. Clinical relevance of microalbuminuria
screening in self-reported non-diabetic/non-hypertensive persons identified in a large health screening -
The Nord-Trondelag Health Study (HUNT), Norway. Clin Nephrol 2003; 59: 241-251. Available at
<Go to ISI>://000181878200001.
2. Hallan SI, Stevens P. Screening for chronic kidney disease: which strategy? J Nephrol 2010; 23: 147-
155. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=20155721.
3. Nielen MM, Schellevis FG, Verheij RA. The usefulness of a free self-test for screening albuminuria in
the general population: a cross-sectional survey. BMC Public Health 2009; 9: 381. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=19818129.
4. Haynes R, Winearls C. Screening for risk with albuminuria: should we start from here? Nephrology,
dialysis, transplantation : official publication of the European Dialysis and Transplant Association -
European Renal Association 2010; 25: 3463-3465. Available at
http://www.ncbi.nlm.nih.gov/pubmed/20855631.
5. Bottomley MJ, Kalachik A, Mevada C, Brook MO, James T, Harden PN. Single Estimated Glomerular
Filtration Rate and Albuminuria Measurement Substantially Overestimates Prevalence of Chronic
Kidney Disease. Nephron Clin Pract 2010; 117: c348-c352. Available at
http://www.ncbi.nlm.nih.gov/pubmed/20948233.
6. Weir MR, Bakris GL. Should Microalbuminuria Ever Be Considered as a Renal Endpoint in Any
Clinical Trial? American Journal of Nephrology 2010; 31: 469-470. Available at <Go to
ISI>://000277757300014.
7. Fink HA, Ishani A, Taylor BC, Greer NL, Macdonald R, Rossini D, Sadiq S, Lankireddy S, Kane RL,
Wilt TJ. Screening for, monitoring, and treatment of chronic kidney disease stages 1 to 3: a systematic
review for the u.s. Preventive services task force and for an american college of physicians clinical
practice guideline. Annals of internal medicine 2012; 156: 570-581. Available at
http://www.ncbi.nlm.nih.gov/pubmed/22508734.
8. Mogensen CE, Vestbo E, Poulsen PL, Christiansen C, Damsgaard EM, Eiskjaer H, Froland A, Hansen
KW, Nielsen S, Pedersen MM. Microalbuminuria and Potential Confounders - a Review and Some
Observations on Variability of Urinary Albumin Excretion. Diabetes Care 1995; 18: 572-581.
Available at <Go to ISI>://A1995QQ21600025.
9. van der Tol A, Van Biesen W, Van Laecke S, Bogaerts K, De Lombaert K, Warrinnier H, Vanholder R.
Statin Use and the Presence of Microalbuminuria. Results from the ERICABEL Trial: A Non-
Interventional Epidemiological Cohort Study. PloS one 2012; 7: e31639. Available at
http://www.ncbi.nlm.nih.gov/pubmed/22359611.
10. Romundstad S, Holmen J, Kvenild K, Hallan H, Ellekjaer H. Microalbuminuria and all-cause mortality
in 2,089 apparently healthy individuals: A 4.4-year follow-up study. The Nord-Trondelag Health Study
(HUNT), Norway. American Journal of Kidney Diseases 2003; 42: 466-473. Available at <Go to
ISI>://000185518500004.
11. Wang TJ, Evans JC, Meigs JB, Rifai N, Fox CS, D'Agostino RB, Levy D, Vasan RS. Low-grade
albuminuria and the risks of hypertension and blood pressure progression. Circulation 2005; 111:
1370-1376. Available at

CHAPTER 2: Results
76
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=15738353.
12. Halimi JM, Bonnet F, Lange C, Balkau B, Tichet J, Marre M. Urinary albumin excretion is a risk
factor for diabetes mellitus in men, independently of initial metabolic profile and development of
insulin resistance. The DESIR Study. J Hypertens 2008; 26: 2198-2206. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=18854761.
13. Yuyun MF, Khaw KT, Luben R, Welch A, Bingham S, Day NE, Wareham NJ. Microalbuminuria,
cardiovascular risk factors and cardiovascular morbidity in a British population: The EPIC-Norfolk
population-based study. European Journal of Cardiovascular Prevention & Rehabilitation 2004; 11:
207-213. Available at <Go to ISI>://000222392100005.
14. van der Tol A, Van Biesen W, Verbeke F, De Groote G, Vermeiren F, Eeckhaut K, Vanholder R.
Towards a rational screening strategy for albuminuria: results from the unreferred renal insufficiency
trial. PloS one 2010; 5: e13328. Available at http://www.ncbi.nlm.nih.gov/pubmed/20967254.
15. Warram JH, Gearin G, Laffel L, Krolewski AS. Effect of duration of type I diabetes on the prevalence
of stages of diabetic nephropathy defined by urinary albumin/creatinine ratio. Journal of the American
Society of Nephrology 1996; 7: 930-937. Available at <Go to ISI>://A1996UT21600017.
16. Levey AS, Coresh J, Greene T, Stevens LA, Zhang YL, Hendriksen S, Kusek JW, Van Lente F. Using
standardized serum creatinine values in the modification of diet in renal disease study equation for
estimating glomerular filtration rate. Annals of internal medicine 2006; 145: 247-254. Available at
http://www.ncbi.nlm.nih.gov/pubmed/16908915.
17. Cleeman JI, Grundy SM, Becker D, Clark LT, Cooper RS, Denke MA, Howard WJ, Hunninghake DB,
Illingworth DR, Luepker RV, McBride P, McKenney JM, Pasternak RC, Stone NJ, Van Horn L,
Brewer HB, Ernst ND, Gordon D, Levy D, Rifkind B, Rossouw JE, Savage P, Haffner SM, Orloff DG,
Proschan MA, Schwartz JS, Sempos CT, Shero ST, Murray EZ, Expe NCEP. Executive summary of
the Third Report of the National Cholesterol Education Program (NCEP) expert panel on detection,
evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III). Jama-Journal
of the American Medical Association 2001; 285: 2486-2497. Available at <Go to
ISI>://000168547600031.
18. Wilson PWF, D'Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB. Prediction of
coronary heart disease using risk factor categories. Circulation 1998; 97: 1837-1847. Available at <Go
to ISI>://000073519200014.
19. Van der Tol A, Van Biesen W, De Groote G, Verbeke P, Vermeiren F, Eeckhaut K, Vanholder R.
Mislabeling Cardiovascular Risk by One Single Measurement of Microalbuminuria. Acta Clin Belg
2011; 66: 171-171. Available at <Go to ISI>://000290931300089.
20. Degli Esposti L, Saragoni S, Buda S, Sturani A, Quintaliani G, Bartolucci S, Di Turi R, Lilli P, Didoni
G, Degli Esposti E. Awareness of albuminuria in an Italian population-based cohort of patients treated
with hypoglycemic drugs. J Nephrol 2011: 0. Available at
http://www.ncbi.nlm.nih.gov/pubmed/21748718.
21. Uchida J, Machida Y, Iwai T, Iguchi T, Kamada Y, Naganuma T, Kumada N, Kim T, Kawashima H,
Nakatani T. Low-grade albuminuria reduction with angiotensin II type 1 receptor blocker in renal
transplant recipients. J Nephrol 2011; 24: 515-521. Available at
http://www.ncbi.nlm.nih.gov/pubmed/21240871.
22. Ozyilmaz A, Bakker SJ, de Zeeuw D, de Jong PE, Gansevoort RT. Selection on albuminuria enhances
the efficacy of screening for cardiovascular risk factors. Nephrology, dialysis, transplantation : official

CHAPTER 2: Results
77
publication of the European Dialysis and Transplant Association - European Renal Association 2010;
25: 3560-3568. Available at http://www.ncbi.nlm.nih.gov/pubmed/20702530.
23. van der Velde M, Halbesma N, de Charro FT, Bakker SJL, de Zeeuw D, de Jong PE, Gansevoort RT.
Screening for Albuminuria Identifies Individuals at Increased Renal Risk. Journal of the American
Society of Nephrology 2009; 20: 852-862. Available at <Go to ISI>://000264831300023.
24. Hillege HL, Fidler V, Diercks GFH, van Gilst WH, de Zeeuw D, van Veldhuisen DJ, Gans ROB,
Janssen WMT, Grobbee DE, de Jong PE, Grp PS. Urinary albumin excretion predicts cardiovascular
and noncardiovascular mortality in general population. Circulation 2002; 106: 1777-1782. Available at
<Go to ISI>://000178385700010.
25. Effects of ramipril on cardiovascular and microvascular outcomes in people with diabetes mellitus:
results of the HOPE study and MICRO-HOPE substudy. Heart Outcomes Prevention Evaluation Study
Investigators. Lancet 2000; 355: 253-259. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=10675071.
26. Keane WF, Zhang Z, Lyle PA, Cooper ME, de Zeeuw D, Grunfeld JP, Lash JP, McGill JB, Mitch WE,
Remuzzi G, Shahinfar S, Snapinn SM, Toto R, Brenner BM. Risk scores for predicting outcomes in
patients with type 2 diabetes and nephropathy: the RENAAL study. Clin J Am Soc Nephrol 2006; 1:
761-767. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=17699284.
27. Asselbergs FW, Diercks GF, Hillege HL, van Boven AJ, Janssen WM, Voors AA, de Zeeuw D, de
Jong PE, van Veldhuisen DJ, van Gilst WH. Effects of fosinopril and pravastatin on cardiovascular
events in subjects with microalbuminuria. Circulation 2004; 110: 2809-2816. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=15492322.
28. Brantsma AH, Bakker SJ, Hillege HL, de Zeeuw D, de Jong PE, Gansevoort RT. Urinary albumin
excretion and its relation with C-reactive protein and the metabolic syndrome in the prediction of type
2 diabetes. Diabetes Care 2005; 28: 2525-2530. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=16186291.
29. Halimi JM, Forhan A, Balkau B, Novak M, Wilpart E, Tichet J, Marre M, Grp DS. Is
microalbuminuria an integrated risk marker for cardiovascular disease and insulin resistance in both
men and women? Journal of Cardiovascular Risk 2001; 8: 139-146. Available at <Go to
ISI>://000169768400004.
30. Verhave JC, Hillege HL, Burgerhof JGM, Navis G, De Zeeuw D, De Jong PE, Grp PS. Cardiovascular
risk factors are differently associated with urinary albumin excretion in men and women. Journal of the
American Society of Nephrology 2003; 14: 1330-1335. Available at <Go to ISI>://000182492900025.

CHAPTER 2: Results
78
2.1.3. Should screening of renal markers be recommended in a working
population?
Arjan van der Tol1, Wim Van Biesen
1, Guy De Groote
2, Paul Verbeke
3, Frans Vermeiren
3,
Kathleen Eeckhaut3, Raymond Vanholder
1
1 Renal Division, Department of Internal Medicine, University Hospital Ghent
2 CRI laboratory, Ghent
3 Occupational Health Care Adhesia, Belgium.
Int Urology Nephrology 2014 Aug 46(8): 1601-8
Available at: http://link.springer.com/article/10.1007%2Fs11255-014-0718-x

CHAPTER 2: Results
79
Abstract
Introduction. It is debated whether the general population should be screened for kidney disease.
This study evaluated whether screening of albuminuria and estimated glomerular filtration rate
(eGFR) in a working population should be recommended to detect subjects with CKD.
Methods. The Unreferred Renal Insufficiency (URI) study is a cross-sectional study in 1,398
workers aged 17-65. Markers of cardiovascular and renal disease were measured. Cardiovascular
risk (CVR) was defined by hypertension (n= 416), diabetes (n= 45), dyslipidemia (n= 159) and/or
history of a cardiovascular event (n= 10).
Results. In our population, 5% of the workers had microalbuminuria, 0.5% had
macroalbuminuria and < 0.1% had eGFR < 60 ml/min/1.73m². All workers with an eGFR < 60
ml/min/1.73m² and/or macroalbuminuria (8/8) had at least one cardiovascular risk factor whereas
this was the case in only half of workers with microalbuminuria (36/73, p= 0.007). In workers
without cardiovascular risk factors, the presence of microalbuminuria was associated with low
body mass index (BMI, p < 0.001) or physiochemical exposure risk (p < 0.001).
Conclusions. Screening of renal markers in a working population, identified only a few subjects
with an eGFR < 60 ml/min/1.73m² or macroalbuminuria. Although microalbuminuria was more
prevalent, it might not necessarily indicate kidney disease, as it may have a completely different
meanings depending of the phenotype of the screened subjects. Besides underlying
cardiovascular risk factors, microalbuminuria was also associated with low BMI in absence of
any risk factor, suggesting presence of benign postural proteinuria. In addition, microalbuminuria
also seemed to be related to physicochemical exposure. In view of the impossibility to further
analyse this finding in the present study, the meaning of this observation needs to be further
investigated.

CHAPTER 2: Results
80
Introduction
Chronic kidney disease (CKD) is increasingly considered as a prevalent and important condition
(1). Subjects with CKD are identified by presence urinary albumin creatinine ratio (ACR) > 30
mg/g and/or an estimated glomerular filtration rate (GFR) < 60 ml per minute per 1.73m² of body
surface area (2). Several epidemiologic studies suggested that CKD is an independent risk factor
for acute kidney injury, need for renal replacement therapy, cardiovascular events, all cause
mortality and increased health care costs (3-7). However, the thesis that screening for CKD
would improve clinical outcome is not established by interventional studies, and is thus still a
matter of debate (8-10). A systematic review on the effect of screening programs in the general
population, demonstrated that such programs detect large numbers of subjects with an eGFR < 60
ml/min/1.73m² and ACR > 30 mg/g, but that these subjects have a lower relative risk for
progressive kidney disease than patients in a clinical setting (11). Hence, there is lot of debate
whether the general population should be screened for CKD, even if it is considered as an
important prevalent health problem (8, 9, 11). Misclassification of CKD frequently occurs in
subjects with microalbuminuria, as a consequence of the high intra-individual variability of
albuminuria (8). Moreover, in many subjects microalbuminuria tends to regress to normal levels,
especially nowadays more and more patients are treated for their underlying risk factors (12). The
current study investigated whether screening of renal markers should be recommended in a
working population to detect CKD.

CHAPTER 2: Results
81
Methods
Aims: This study was performed to investigate whether screening for renal markers, such as
microalbuminuria or macroalbuminuria and eGFR < 60 ml/min/1.73m², is useful to detect CKD
in an unselected working population.
Participants: The Unreferred Renal Insufficiency (URI) study is a cross sectional evaluation
including only Caucasian workers (n=1486) who presented at a routine annual occupational
check-up between January 2007 and December 2009, in Belgium. The presence of more than
100 erythrocytes/µl in the urinary sediment was considered as a confounder for reliable
measurements of urinary albumin; subjects showing this degree of hematuria (n=17) and
subjects with incomplete data (n=71) were excluded from further analysis, leaving a cohort of
1,398 subjects. In our study, 351 (25%) workers were exposed to physicochemical hazard, such
as silica, heavy metals, solvents.
Ethics: A written informed consent was obtained from all participants. The Ethics Committee of
University Hospital Ghent approved the study (2006-038) (13).
Description of procedures
All subjects were investigated during their yearly check up by their occupational physician. Body
weight was recorded to the nearest 0.1 kg and height was measured to the nearest centimeter.
Waist circumference was measured by trained nurses following recommendations by WHO.
Body mass index (BMI) was calculated as body weight in kg divided by height² (kg/m²). Blood
pressure and resting heart rate were measured in sitting position by a calibrated electronic device
(OMRON®). A questionnaire about current cigarette smoking, physical activity and prescribed
medication was taken by an occupational physician in each participant. A random blood and
urine spot specimen was collected and analyzed on the same day in one central laboratory (no
frozen samples). Urinary albumin was measured by an immune turbidimetric method with an
inter-assay coefficient of variation of 11.2% at a mean level of 82 mg/L and an inter-assay
coefficient of variation of 4.9% at a mean level of 580 mg/l. Serum creatinine was analyzed by a
colorimetric assay (compensated Jaffe reaction), calibrated by Isotope Dilution Mass
Spectrometry (IDMS), with an inter-assay coefficient of variation of 1.75% at a mean level of
104 µmol/l (Roche). Serum CRP was measured with an immune turbidimetric method with an

CHAPTER 2: Results
82
inter-assay coefficient of variation of 4.6% at a mean level of 3.2 mg/l and inter-assay coefficient
of variation of 2.5% at a mean level of 5.5 mg/l (13).
Definitions: Gender specific urinary albumin creatinine ratio (ACR) cut-off values as proposed
by Warram et al. were used. Microalbuminuria was defined as ACR 17-250 in men and ACR
25-355 mg/g in women, macroalbuminuria as ACR > 250 in men and ACR > 355 mg/g in
women (14). GFR was estimated by the combined creatinine-cystatin C based CKD-EPI equation
(15). Abdominal adiposity was defined according to the National Cholesterol Education Program
(NCEP) criteria as a waist circumference > 102 cm in men and > 88 cm in women (16).
Hypertension was defined as blood pressure ≥140/90 or anti-hypertensive treatment. Diabetes
was defined as plasma glucose ≥ 126 mg/dl or glucose lowering treatment (17). Dyslipidemia
was defined as serum cholesterol ≥ 250 mg/dl or lipid lowering treatment.
Statistical methods: SPSS statistics 22 was used for all calculations. Results are presented as
percentages or as mean ± standard deviation. The baseline characteristics of more than 2 groups
were compared by use of ANOVA: post-hoc Scheffé test (continuous variables), Kruskal-Wallis
(continuous variable with a skewed distribution). The baseline characteristics of two groups were
compared by the use of t-test for continuous variables, Mann-Whitney for continuous variables
with a skewed distribution and Chi-square test for categorical variables. Multivariate logistic
regression analysis was performed for the association of microalbuminuria with other parameters.
Subjects were classified by < 10th
, 10-50th
, 50th
-90th
and >90th
percentile of BMI in presence of
physicochemical exposure risk (PCER), CVR or no risk factor (table 3, figure 1). Subjects were
classified according to median of age (17-39, 40-65 years) (table 4).

CHAPTER 2: Results
83
Results
In this population of 1,398 workers we found 416 subjects (30%) with hypertension (119 treated),
45 (3%) with diabetes (15 treated), 159 (11%) with dyslipidemia (44 treated) and 10 (0.7%) with
a history of cardiovascular event. Since sometimes some of these risk factors coincided in the
same patient, the total number of subjects with one or more cardiovascular risk factors (CVR)
was 512 (37%), of whom only 151 were treated for at least one risk factor, resulting in 361 (26%)
of this population having at least one untreated risk factor. In this cohort, 5% (n= 73) had
microalbuminuria, 0.5% (n= 7) had macroalbuminuria and 0.1% (n= 1) had eGFR< 60 ml per
minute per 1.73m² of body surface area in presence of microalbuminuria. Workers with vs.
without cardiovascular risk factors had higher prevalence of microalbuminuria (7.0 vs. 4.2%, p =
0.001) and macroalbuminuria (1.4 vs. 0, p = 0.001). The worker with an eGFR < 60
ml/min/1.73m² and all workers with macroalbuminuria (8/8) had at least one cardiovascular risk
factor whereas this was the case in only half of workers with microalbuminuria (36/73, p= 0.007).
Only, 15 of these 36 workers with microalbuminuria (42%) and one of 7 (14%) workers with
macroalbuminuria were treated for diabetes, hypertension and/or dyslipidemia.
In the overall cohort, workers with versus without physicochemical exposure risk (PCER) had a
higher prevalence of microalbuminuria (7.4 vs. 4.6%, p = 0.04), but not a higher percentage of
CVR (36 vs. 37%, p = 0.61). As cardiovascular risk factors confound the association between
microalbuminuria and PCER, we split our cohort in workers with and without CVR. As expected,
the workers with CVR had more additional risk factors than those without CVR (table 1). In the
population with CVR, workers with vs. without PCER were only more likely to be male. In the
population without CVR, workers with PCER (n= 226) had a higher prevalence of
microalbuminuria (p <0.001), were younger (p < 0.001) and were more likely to be male (p<
0.001) than those without any risk (n = 660) (table1).

CHAPTER 2: Results
84
Table 1. Characteristics according to without vs. with physicochemical exposure risk (PCER) in
workers without vs. with cardiovascular risk (CVR).
No CVR (n=886) CVR (n=512) P
No PCER PCER No PCER PCER
N 660 226 387 125
Age (years) 38 ± 10 36 ± 9° 44 ± 10 42 ± 9 <0.001
Female (%) 183 (28) 12 (5)° 57 (15) 5 (4)° <0.001
ACR (mg/g) 4 (3-5) 5 (3-6) 13 (4-22) 14 (0-27) 0.02
Microalbuminuria 18 (2.7) 19 (8.4)° 29 (7.5) 7 (5.6) 0.001
Macroalbuminuria 0 0 5 (1.3) 2 (1.6) 0.002
Smoking (%) 199 (31) 73 (36) 118 (31) 35 (30) 0.57
Adiposity (%) 69 (13) 18 (8) 115 (33) 39 (33) <0.001
Inactive (%) 245 (44) 98 (51) 192 (59) 60 (55) <0.001
BMI (kg/m²) 25.1 ± 3.7 25.2 ± 3.2 27.9 ± 4.72 27.8 ± 4.4 <0.001
SBP(mmHg) 122 ± 11 123 ± 10 139 ± 16 142 ± 14 <0.001
DBP (mmHg) 74 ± 9 75 ± 8 86 ± 11 88 ± 11 <0.001
Heart rate (bpm) 69 ± 9 68 ± 10 73 ± 12 72 ± 13 <0.001
Glucose (mg/dl) 85 ± 12 85 ± 12 94 ± 27 91 ± 22 <0.001
Cholesterol (mg/dl) 186 ± 31 186 ± 32 216 ± 45 206 ± 40 <0.001
CRP (mg/l) 2.2 ± 4.0 2.2 ± 4.2 2.9 ± 7.0 2.6 ± 3.7 <0.001
CVR: cardiovascular risk defined by hypertension, diabetes, dyslipidemia and/or cardiovascular event.
ACR (mg/g): urinary albumin creatinine ratio (95% CI of the mean) Microalbuminuria (MAU) is defined
as UACR 17-250 in men and 25-355 mg/g in women. Adiposity: waist circumference > 102 in men and >
88 cm in women. BMI: body mass index. SBP: systolic blood pressure. DBP: diastolic blood pressure,
CRP: C-reactive protein.
°p < 0.01 PCER vs. no PCER.

CHAPTER 2: Results
85
Table 2. Characteristics according to absence or presence of microalbuminuria (MAU) in
workers without vs. with physicochemical exposure risk (PCER) in absence vs. presence of
cardiovascular risk (CVR)
No CVR (n=886) No PCER (n=660) PCER (n=226)
No MAU MAU P No MAU MAU P
N 642 18 (3) 207 19 (8)
Age (years) 38 ± 9 37 ± 11 0.59 36 ± 9 35 ± 11 0.90
Female (%) 178 (28) 5 (28) 1 9 (4) 3 (16) 0.11
Smoking (%) 193 (31) 6 (33) 0.80 66 (36) 7 (37) 0.90
Adiposity (%) 68 (13) 1 (8) 0.60 17 (9) 1 (6) 0.70
Inactive (%) 236 (44) 9 (53) 0.47 87 (50) 11 (58) 0.53
Low BMI <10th
per. 62 (10) 10 (56) <0.001 18 (9) 4 (21) 0.18
High BMI >90th
per. 67 (11) 0 0.29 13(6) 1(5) 1
BMI (kg/m²) 25.2 ± 3.7 21.8 ± 3.2 <0.001 25.3 ± 3.2 23.7± 3.5 0.04
SBP(mmHg) 122 ± 11 120 ± 12 0.53 123 ± 10 121 ± 11 0.33
DBP (mmHg) 74 ± 9 70 ± 11 0.09 75 ± 8 75 ± 9 0.98
Heart rate (bpm) 69 ± 9 71 ± 15 0.57 68± 10 73 ± 12 0.04
Glucose (mg/dl) 85 ± 12 87 ± 11 0.40 85 ± 12 87 ± 16 0.46
Cholesterol (mg/dl) 186 ± 31 177 ± 31 0.25 187 ± 31 174 ± 39 0.46
CRP (mg/l) 2.2 ± 3.4 4.4 ± 1.4 0.48 2.1± 3.7 3.1± 8.0 0.32
CVR (n =505) No PCER (n=382) PCER (n=123)
No MAU MAU P No MAU MAU P
N 353 29 (7) 116 7 (6)
Age (years) 44 ± 10 44 ± 11 0.88 41 ± 9 50 ± 5 0.01
Female (%) 52 (15) 4 (14) 0.58 5 (4) 0 1
Smoking (%) 102 (30) 12(43) 0.15 32 (30) 2(29) 0.92
Adiposity (%) 97 (31) 15 (60) 0.005 35 (32) 3 (60) 0.19
Inactive (%) 170 (59) 15(60) 0.926 55 (54) 4(57) 0.89
Low BMI <10th
per. 30 (9) 1 (4) 0.34 7 (6) 1 (4) 0.39
High BMI >90th
per. 30 (9) 6 (21) 0.03 12 (10) 1 (14) 0.74
BMI (kg/m²) 27.7 ± 4.6 30.0 ± 5.3 0.01 27.6 ± 4.2 30.0 ± 5.8 0.16
SBP(mmHg) 138 ± 16 146 ± 19 0.02 142 ± 13 154 ± 27 0.29
DBP (mmHg) 85 ± 11 90 ± 11 0.03 88 ± 10 97 ± 14 0.02
Heart rate (bpm) 72 ± 11 81 ± 14 0.02 71 ± 12 85 ± 17 0.004
Glucose (mg/dl) 93 ± 21 110 ± 64 0.19 90 ± 21 108 ± 37 0.26
Cholesterol (mg/dl) 215 ± 45 216 ± 40 0.89 204 ± 40 224 ± 37 0.19
CRP (mg/l) 2.8 ± 6.6 6.2 ± 11.7 0.02 2.6 ± 3.8 2.9 ± 0.7 0.002
CVR: cardiovascular risk defined by hypertension, diabetes, dyslipidemia and/or cardiovascular events.
Microalbuminuria (MAU) is defined as UACR 17-250 in men and 25-355 mg/g in women. Adiposity:
waist circumference >102 in men and >88 cm in women. BMI: body mass index. SBP: systolic blood
pressure. DBP: diastolic blood pressure, CRP: C-reactive protein.

CHAPTER 2: Results
86
In the population without CVR, workers with microalbuminuria had a higher percentage of low
BMI (< 10th
percentile of BMI; 38 vs. 12%, p < 0.001) and PCER (51 vs. 25%, p < 0.001) as
compared to those without microalbuminuria. In the population without CVR in presence of
PCER (table 2), workers with microalbuminuria had a higher heart rate (p= 0.04), lower BMI
(p=0.04) but no higher percentage of low BMI (21 vs. 9%, p = 0.18) as compared to those
without microalbuminuria. In the population without CVR and low BMI (table 3), workers with
microalbuminuria had no higher percentage of PCER than those without microalbuminuria (29
vs. 23%, p = 0.62). In the population without any risk (table 2), workers with microalbuminuria
had a higher percentage of low BMI (56 vs. 10%, p< 0.001) as compared to those without
microalbuminuria. After a multivariate adjustment, high heart rate (p = 0.02) was retained as the
only significant predictor for microalbuminuria in workers with PCER, whereas low BMI (p <
0.001) was retained as the only significant predictor for microalbuminuria in workers without any
risk.
In the population with CVR (table 2), workers with microalbuminuria had a higher blood
pressure, heart rate and CRP as compared to those without microalbuminuria, independent of
PCER. After multivariate adjustment, high heart rate (p = 0.02) and CRP (p = 0.02) were retained
as significant predictors for microalbuminuria in workers without PCER, whereas older age was
retained as a significant predictor for microalbuminuria in workers with PCER.
Figure 1 shows the prevalence of microalbuminuria in lean (< 10th
percentile of BMI), normal
(between 10-50th
percentile of BMI), overweight (between 50-90th
percentile of BMI) and obese
workers (> 90th
percentile of BMI) according to no risk, PCER and CVR. In presence of CVR,
overweight or obese workers had a higher prevalence of microalbuminuria than normal or lean
workers (p < 0.05), whereas in absence of risk factors lean workers had a higher prevalence of
microalbuminuria than workers with BMI > 10th
percentile (p < 0.001, table 3). In the population
without CVR, microalbuminuria was not affected by different BMI groups in workers with PCER
(table 3).

CHAPTER 2: Results
87
Table 3. Prevalence of microalbuminuria (MAU) according to percentile of BMI in workers with
no risk, with physicochemical exposure risk (PCER) and cardiovascular risk (CVR).
BMI < 10th
percentile
BMI 10-50th
percentile
BMI 50-90th
percentile
BMI > 90th
percentile
P
No risk
(n=658)
BMI < 21 21-25 25-30 > 30
n 72 284 235 67
Age 34 ± 9 37 ± 10* 40 ± 9**° 38 ± 10* <0.001
MAU 10 (13.9) 5 (1.8)** 3 (1.3)** 0** <0.001
PCER
(n= 226)
n 22 86 104 14
Age 30 ± 7 35 ± 9 38 ± 9* 33 ± 9 0.002
MAU 4 (18.2) 9 (10.5) 5 (4.8) 1 (7.1) 0.17
CVR
(n=503)
BMI < 22 22-28 28-34 > 34
n 40 234 179 50
Age 38 ± 12 43 ± 10 45 ± 9* 46 ± 9* <0.001
MAU 2 (5) 10 (4.3) 16 (9)° 7 (14)° 0.01
CVR is defined by hypertension, diabetes, dyslipidemia and/or cardiovascular event. Microalbuminuria is
defined as UACR 17-250 in men and 25-355 mg/g in women. BMI = body mass index (kg/m²). *p< 0.05,
**p< 0.001 vs. BMI ≤ 10th percentile, °p = 0.01-0.05 vs. BMI 10-50
th percentile.

CHAPTER 2: Results
88
Figure 1. Prevalence of albuminuria in lean (BMI <10th
percentile), normal (BMI between 10-
50th
percentile, overweight (BMI between 50-90th
percentile) and obese workers (BMI > 90th
percentile) in absence of risk factors, in presence of physicochemical exposure risk (PCER) and
presence of cardiovascular risk factors (CVR).
0
5
10
15
20
BMI <10thpercentile BMI 10-50th
percentile BMI 50-90thpercentile BMI > 90th
percentile
pre
vale
nce
of
alb
um
inu
ria
no risk PCER CVR
Microallbuminuria is defined as UACR17-250 in men and 25-355 mg/g in women. CVR risk is defined by
hypertension, diabetes, dyslipidemia and/or cardiovascular event. BMI (body mass index).

CHAPTER 2: Results
89
The prevalence of CVR increased above the age of 40, from 24 to 49% (p < 0.001). We showed
that age is an effect modifier; the presence of microalbuminuria was associated with CVR and
PCER in workers above the age of 40 while it was associated with low BMI and PCER in
workers under the age of 40 years (table 4).
Table 4. Mean BMI (body mass index), the number of workers with cardiovascular risk factors
(CVR) and of physicochemical exposure risk (PCER) according to median of age in absence or
presence of microalbuminuria (MAU).
No MAU MAU
Age n n BMI n BMI P
17-39 682 649 25.3 ± 3.9 33 23.3 ± 4.4 0.004
40-65 705 666 26.9 ± 4.2 39 28.9 ± 5.6 0.04
CVR CVR
17-39 682 649 152 (23) 33 9 (27) 0.61
40-65 709 669 317 (47) 40 27 (68) 0.01
PCER PCER
17-39 511 487 134 (28) 24 12 (50) 0.02
40-65 358 345 73 (21) 13 7 (54) 0.01
CVR: cardiovascular risk defined by hypertension, diabetes, dyslipidemia and/or cardiovascular events.
Microalbuminuria (MAU) is defined as UACR 17-250 in men and 25-355 mg/g in women. BMI: body
mass index in kg/m².

CHAPTER 2: Results
90
Discussion
Screening for renal markers in a working population containing 1,398 workers, identified only
one subject with an eGFR < 60 ml/min/1.73m² (n= 1) and a few subjects with macroalbuminuria
(n= 7), all of whom had at least one traditional cardiovascular risk factor. More workers with
microalbuminuria were detected, but half of these had no modifiable traditional cardiovascular
risk factor (37/73). Microalbuminuria in these subjects was associated with low BMI or PCER.
Young workers had a lower BMI in presence vs. absence of microalbuminuria. Conceivably, a
substantial number of young workers had postural proteinuria and might be mislabeled as having
a risk for cardiovascular and/or renal disease. Whether the presence of microalbuminuria in
workers with PCER is related to early reversible kidney disease might be considered as
potentially possible but remains to be proven. On the other hand, only a limited number of
patients with traditional cardiac risk factors did already receive treatment for that risk factor.
Screening for renal markers in a healthy population might thus identify patients without
modifiable risk factors, whereas screening for and treating traditional cardiac risk factors in this
group might be more appropriate (13).
The presence of microalbuminuria in the general population is independently considered as a
renal and cardiovascular risk marker (18, 19). However, whether this simple marker can be easily
used to start uniform treatment to improve renal and cardiovascular outcome remains uncertain
(10, 20). Our data showed that the presence of microalbuminuria has completely different
meanings according to the population concerned. Microalbuminuria is associated with CVR or
PCER in workers above the age of 40, while it associated with low BMI or PCER in workers
under the age of 40. Consequently, a substantial number of young, healthy and lean workers with
microalbuminuria might have postural proteinuria. It has been suggested that postural
albuminuria commonly occurs in healthy lean adolescents (21, 22). Microalbuminuria might
develop in normal subjects by a physiological response after strenuous exercise or upon standing
(23, 24). Postural albuminuria might be a sign of renal congestion (25), due to the compression
of the left renal vein between the superior mesenteric artery and the abdominal aorta (nutcracker
syndrome) (26). Lean subjects are more likely to develop postural proteinuria as the left renal
vein is at higher risk to be compressed in the space between the aorta and the superior mesenterial
artery which is smaller than on the right side (27). Adolescents with postural proteinuria have an

CHAPTER 2: Results
91
excellent outcome (28). Mostly the problem disappears beyond the age of 30, pointing to an
irrelevant condition, rather than a risk factor (29).
Although it might be useful to know the potentially toxic conditions in a working population, in
our database we had not registered the type of work nor measured toxic agents. However, we
classified our patients into a subgroup with and without PCER. According to the literature,
subjects who are exposed to heavy metals, such as cadmium, mercury might develop tubular
overflow microalbuminuria (30-32). But, whether this microalbuminuria is an indicator for
kidney disease remains unknown. In our study, no worker with PCER had macroalbuminuria.
Thus, it seems unlikely that the presence of microalbuminuria in workers with PCER might
contribute to the development of progressive CKD. However, microalbuminuria was associated
with high heart rate in workers with PCER. Whether this might be related to CKD or CVD is
unknown. This finding underlines the need of prospective studies of the long-term effects of toxic
agents on markers of outcome in CKD and CVD.
One third of the workers had one or more traditional cardiovascular risk factor. Most of these
were however untreated. In terms of prevention and cost-effectiveness, it would thus be more
effective to screen for and treat traditional cardiovascular risk factors, rather than screening of
renal markers. However, as the prevalence of renal markers was much higher in those with
traditional cardiovascular risk factors, this patient group should be explored for presence of
chronic kidney disease, of course one of the problems is that most of these risk factors are
undetected or at least untreated. In this case the screening physician may remain unaware of the
patient’s condition, and not recognize the direct reason to do the appropriate screening test for
CKD. Therefore, traditional risk factors as fasting hyperglycemia and hypertension may be seen
as important part of basic screening that is often neglected.
A strength of this study is that we not only used a “self-declared” status of diabetes, hypertension
and dyslipidemia, but that we also measured plasma glucose, blood pressure and cholesterol, to
identify subjects with unknown traditional risk factors. A limitation is that all parameters in this
cohort were measured at one random occasion. Microalbuminuria might fluctuate more in
random urine samples than in early morning urine samples (33, 34).
We conclude that direct screening of renal markers is not useful in a working population, as half
of the subjects with microalbuminuria had no modifiable cardiovascular risk factors. The

CHAPTER 2: Results
92
presence of microalbuminuria in these workers might not be indicative for progressive CKD as
none of them had macroalbuminuria. The presence of microalbuminuria in these mainly young
workers was associated with low BMI or PCER. Consequently, young, healthy and lean workers
with microalbuminuria might have postural proteinuria and thus an irrelevant condition, rather
than that it would display a risk factor. The occurrence of microalbuminuria in workers with
PCER was unrelated to CVR and should be further investigated. Most likely intervention in this
population may engender medical frustration, unnecessary anxiety, harm, and worries in those
affected and excess of costs to society, employers and individuals. To reduce these false positive
results, a mass screening strategy to identify cardiovascular disease by using microalbuminuria
seems to make sense only when limiting inclusion to subjects above the age of 40. However,
screening for traditional cardiovascular risk factors identifies more subjects at risk for
cardiovascular and renal disease than screening for microalbuminuria for potential preventive
intervention (13).
Acknowledgment We thank all concerned employees of Adhesia (Occupational Heath Care,
Ghent, Belgium) and the recruited participants who made this study possible.

CHAPTER 2: Results
93
References
1. Couser WG, Remuzzi G, Mendis S, Tonelli M. The contribution of chronic kidney disease to the
global burden of major noncommunicable diseases. Kidney Int 2011; 80: 1258-1270. Available at
http://www.ncbi.nlm.nih.gov/pubmed/21993585.
2. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical
Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. . Kidney Int 2013:
1-150. Available at http://www.nature.com/kisup/journal/v3/n1/index.html.
3. Gansevoort RT, Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, de Jong PE,
Coresh J, Chronic Kidney Disease Prognosis C. Lower estimated GFR and higher albuminuria are
associated with adverse kidney outcomes. A collaborative meta-analysis of general and high-risk
population cohorts. Kidney Int 2011; 80: 93-104. Available at
http://www.ncbi.nlm.nih.gov/pubmed/21289597.
4. Van Biesen W, De Bacquer D, Verbeke F, Delanghe J, Lameire N, Vanholder R. The glomerular
filtration rate in an apparently healthy population and its relation with cardiovascular mortality during
10 years. Eur Heart J 2007; 28: 478-483. Available at http://www.ncbi.nlm.nih.gov/pubmed/17223665.
5. Vanholder R, Massy Z, Argiles A, Spasovski G, Verbeke F, Lameire N, European Uremic Toxin Work
G. Chronic kidney disease as cause of cardiovascular morbidity and mortality. Nephrol Dial Transplant
2005; 20: 1048-1056. Available at http://www.ncbi.nlm.nih.gov/pubmed/15814534.
6. Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, de Jong PE, Coresh J,
Gansevoort RT. Association of estimated glomerular filtration rate and albuminuria with all-cause and
cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet 2010; 375:
2073-2081. Available at http://www.ncbi.nlm.nih.gov/pubmed/20483451.
7. Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death,
cardiovascular events, and hospitalization. N Engl J Med 2004; 351: 1296-1305. Available at
http://www.ncbi.nlm.nih.gov/pubmed/15385656.
8. Fink HA, Ishani A, Taylor BC, Greer NL, Macdonald R, Rossini D, Sadiq S, Lankireddy S, Kane RL,
Wilt TJ. Screening for, monitoring, and treatment of chronic kidney disease stages 1 to 3: a systematic
review for the u.s. Preventive services task force and for an american college of physicians clinical
practice guideline. Annals of internal medicine 2012; 156: 570-581. Available at
http://www.ncbi.nlm.nih.gov/pubmed/22508734.
9. van der Velde M, Halbesma N, de Charro FT, Bakker SJL, de Zeeuw D, de Jong PE, Gansevoort RT.
Screening for Albuminuria Identifies Individuals at Increased Renal Risk. Journal of the American
Society of Nephrology 2009; 20: 852-862. Available at <Go to ISI>://000264831300023.
10. Romundstad S, Holmen J, Kvenild K, Aakervik O, Hallan H. Clinical relevance of microalbuminuria
screening in self-reported non-diabetic/non-hypertensive persons identified in a large health screening-
-the Nord-Trondelag Health Study (HUNT), Norway. Clin Nephrol 2003; 59: 241-251. Available at
http://www.ncbi.nlm.nih.gov/pubmed/12708563.
11. Black C, Sharma P, Scotland G, McCullough K, McGurn D, Robertson L, Fluck N, MacLeod A,
McNamee P, Prescott G, Smith C. Early referral strategies for management of people with markers of
renal disease: a systematic review of the evidence of clinical effectiveness, cost-effectiveness and
economic analysis. Health Technol Assess 2010; 14: 1-184. Available at
http://www.ncbi.nlm.nih.gov/pubmed/20441712.
12. Perkins BA, Ficociello LH, Silva KH, Finkelstein DM, Warram JH, Krolewski AS. Regression of
microalbuminuria in type 1 diabetes. The New England Journal of Medicine 2003; 348: 2285-2293.
Available at http://www.ncbi.nlm.nih.gov/pubmed/12788992.

CHAPTER 2: Results
94
13. van der Tol A, Van Biesen W, Verbeke F, De Groote G, Vermeiren F, Eeckhaut K, Vanholder R.
Towards a rational screening strategy for albuminuria: results from the unreferred renal insufficiency
trial. PloS one 2010; 5: e13328. Available at http://www.ncbi.nlm.nih.gov/pubmed/20967254.
14. Warram JH, Gearin G, Laffel L, Krolewski AS. Effect of duration of type I diabetes on the prevalence
of stages of diabetic nephropathy defined by urinary albumin/creatinine ratio. Journal of the American
Society of Nephrology 1996; 7: 930-937. Available at <Go to ISI>://A1996UT21600017.
15. Inker LA, Schmid CH, Tighiouart H, Eckfeldt JH, Feldman HI, Greene T, Kusek JW, Manzi J, Van
Lente F, Zhang YL, Coresh J, Levey AS, Investigators C-E. Estimating Glomerular Filtration Rate
from Serum Creatinine and Cystatin C. New Engl J Med 2012; 367: 20-29. Available at <Go to
ISI>://000305979400002.
16. Cleeman JI, Grundy SM, Becker D, Clark LT, Cooper RS, Denke MA, Howard WJ, Hunninghake DB,
Illingworth DR, Luepker RV, McBride P, McKenney JM, Pasternak RC, Stone NJ, Van Horn L,
Brewer HB, Ernst ND, Gordon D, Levy D, Rifkind B, Rossouw JE, Savage P, Haffner SM, Orloff DG,
Proschan MA, Schwartz JS, Sempos CT, Shero ST, Murray EZ, Expe NCEP. Executive summary of
the Third Report of the National Cholesterol Education Program (NCEP) expert panel on detection,
evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III). Jama-Journal
of the American Medical Association 2001; 285: 2486-2497. Available at <Go to
ISI>://000168547600031.
17. Genuth S, Alberti KGMM, Bennett P, Buse J, DeFronzo R, Kahn R, Kitzmiller J, Knowler WC,
Lebovitz H, Lernmark A, Nathan D, Palmer J, Rizza R, Saudek C, Shaw J, Steffes M, Stern M,
Tuomilehto J, Zimmet P, Classificat ECD. Follow-up report on the diagnosis of diabetes mellitus.
Diabetes Care 2003; 26: 3160-3167. Available at <Go to ISI>://000186269100030.
18. Hillege HL, Janssen WMT, Bak AAA, Diercks GFH, Grobbee DE, Crijns H, van Gilst WH, de Zeeuw
D, de Jong PE, Prevend Study G. Microalbuminuria is common, also in a nondiabetic, nonhypertensive
population, and an independent indicator of cardiovascular risk factors and cardiovascular morbidity.
Journal of Internal Medicine 2001; 249: 519-526. Available at <Go to ISI>://000169568600005.
19. Klausen K, Borch-Johnsen K, Feldt-Rasmussen B, Jensen G, Clausen P, Scharling H, Appleyard M,
Jensen JS. Very low levels of microalbuminuria are associated with increased risk of coronary heart
disease and death independently of renal function, hypertension, and diabetes. Circulation 2004; 110:
32-35. Available at <Go to ISI>://000222461800009.
20. Asselbergs FW, Diercks GF, Hillege HL, van Boven AJ, Janssen WM, Voors AA, de Zeeuw D, de
Jong PE, van Veldhuisen DJ, van Gilst WH. Effects of fosinopril and pravastatin on cardiovascular
events in subjects with microalbuminuria. Circulation 2004; 110: 2809-2816. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=15492322.
21. Hirschler V, Molinari C, Maccallini G, Aranda C. Is albuminuria associated with obesity in school
children? Pediatr Diabetes 2010; 11: 322-330. Available at
http://www.ncbi.nlm.nih.gov/pubmed/19968814.
22. Nguyen S, McCulloch C, Brakeman P, Portale A, Hsu CY. Being overweight modifies the association
between cardiovascular risk factors and microalbuminuria in adolescents. Pediatrics 2008; 121: 37-45.
Available at <Go to ISI>://000252096300006.
23. Robinson RR, Coggins CH, Shapiro K, Cohen JJ, Harrington JT, Kassirer JP. Isolated Proteinuria in
Asymptomatic Patients. Kidney International 1980; 18: 395-406. Available at <Go to
ISI>://WOS:A1980KK18700014.

CHAPTER 2: Results
95
24. Smithies O. Why the kidney glomerulus does not clog: a gel permeation/diffusion hypothesis of renal
function. Proc Natl Acad Sci U S A 2003; 100: 4108-4113. Available at
http://www.ncbi.nlm.nih.gov/pubmed/12655073.
25. Cho LS, Choi YM, Kang HH, Park SJ, Lim JW, Yoon TY. Diagnosis of nut-cracker phenomenon
using renal Doppler ultrasound in orthostatic proteinuria. Nephrology Dialysis Transplantation 2001;
16: 1620-1625. Available at <Go to ISI>://WOS:000170410000019.
26. Mazzoni MB, Kottanatu L, Simonetti GD, Ragazzi M, Bianchetti MG, Fossali EF, Milani GP. Renal
vein obstruction and orthostatic proteinuria: a review. Nephrol Dial Transplant 2011; 26: 562-565.
Available at http://www.ncbi.nlm.nih.gov/pubmed/20656752.
27. Milani G, Bianchetti MG, Bozzani S, Bettinelli A, Fossali EF. Body mass index modulates postural
proteinuria. International urology and nephrology 2010; 42: 513-515. Available at
http://www.ncbi.nlm.nih.gov/pubmed/19283505.
28. Rytand DA, Spreiter S. Prognosis in postural (orthostatic) proteinuria: forty to fifty-year follow-up of
six patients after diagnosis by Thomas Addis. N Engl J Med 1981; 305: 618-621. Available at
http://www.ncbi.nlm.nih.gov/pubmed/7266586.
29. Naderi ASA, Reilly RF. Primary Care Approach to Proteinuria. J Am Board Fam Med 2008; 21: 569-
574. Available at <Go to ISI>://000260721500014.
30. Roels HA, Hoet P, Lison D. Usefulness of biomarkers of exposure to inorganic mercury, lead, or
cadmium in controlling occupational and environmental risks of nephrotoxicity. Ren Fail 1999; 21:
251-262. Available at http://www.ncbi.nlm.nih.gov/pubmed/10416202.
31. Bernard A, Lauwerys RR. Proteinuria: changes and mechanisms in toxic nephropathies. Critical
reviews in toxicology 1991; 21: 373-405. Available at http://www.ncbi.nlm.nih.gov/pubmed/1741950.
32. Vacca CV, Hines JD, Hall PW, 3rd. The proteinuria of industrial lead intoxication. Environ Res 1986;
41: 440-446. Available at http://www.ncbi.nlm.nih.gov/pubmed/3780642.
33. Clinical Practice Guidelines for Chronic Kidney Disease: Evaluation C, and Stratification, part 5.
Evaluation of laboratory measurements for clinical assessment of kidney disease, guidelines 5.
Assesment of proteinuria Accessed March 10, 2012; . Available at
http://www.kidney.org/professionals/kdoqi/pdf/ckd_evaluation_classification_stratification.pdf.
34. Witte EC, Lambers Heerspink HJ, de Zeeuw D, Bakker SJ, de Jong PE, Gansevoort R. First morning
voids are more reliable than spot urine samples to assess microalbuminuria. J Am Soc Nephrol 2009;
20: 436-443. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=19092125.

CHAPTER 2: Results
96
2.2. Screening for kidney disease in selected hypertensive subjects: results
from the ERICABEL trial: a non interventional epidemiological cohort study.

CHAPTER 2: Results
97
2.2.1. Statin use and the presence of microalbuminuria.
Arjan van der Tol1, Wim Van Biesen
1, Steven Van Laecke
1, Kris Bogaerts
2, Koen De Lombaert
3,
Hans Warrinnier3 and Raymond Vanholder
1.
1 Renal Divison, Department of Internal Medicine, University Hospital Ghent, Belgium.
2 Interuniversity centre for biostatistics and statistical bioinformatics, Leuven, Belgium.
3 F. Hoffman-La Roche LTD, Brussels, Belgium.
PLoS ONE February 2012; 7 (2): e31639
Available at: http://www.plosone.org/article/info%3Adoi%2F10.1371%2Fjournal.pone.0031639

CHAPTER 2: Results
98
Abstract
Background. Microalbuminuria (MAU) is considered as a predictor or marker of cardiovascular
and renal events. Statins are widely prescribed to reduce cardiovascular risk and to slow down
progression of kidney disease. But statins may also generate tubular MAU. The current
observational study evaluated the impact of statin use on the interpretation of MAU as a predictor
or marker of cardiovascular or renal disease.
Methodology/Principal Findings. We used cross-sectional data of ERICABEL, a cohort with
1,076 hypertensive patients. MAU was defined as albuminuria ≥ 20mg/l. A propensity score was
created to correct for “bias by indication” to receive a statin. As expected, subjects using statins
vs. no statins had more cardiovascular risk factors, pointing to bias by indication. Statin users
were more likely to have MAU (OR: 2.01, 95% CI: 1.34-3.01). The association between statin
use and MAU remained significant after adjusting for the propensity to receive a statin based on
cardiovascular risk factors (OR: 1.82, 95% CI: 1.14-2.91). Next to statin use, only diabetes (OR:
1.92, 95% CI: 1.00-3.66) and smoking (OR: 1.49, 95% CI: 0.99-2.26) were associated with MAU.
Conclusions. Use of statins is independently associated with MAU, even after adjusting for bias
by indication to receive a statin. In the hypothesis that this MAU is of tubular origin, statin use
can result in incorrect labeling of subjects as having a predictor or marker of cardiovascular or
renal risk. In addition, statin use affected the association of established cardiovascular risk factors
with MAU, blurring the interpretation of multivariable analyses.

CHAPTER 2: Results
99
Introduction
Microalbuminuria (MAU) is considered as a predictor or marker of cardiovascular morbidity and
mortality, particularly in patients with other risk factors [1-4], and as a surrogate for early kidney
damage especially in subjects with diabetes and hypertension [5,6]. Statins are frequently
prescribed in patients with hypertension, diabetes and metabolic syndrome, to reduce
cardiovascular morbidity and mortality [7]. Statins can reduce existent proteinuria [8-10] through
a positive impact on endothelial dysfunction. In contrast, there is in vitro [11,12] and in vivo [13-
16] evidence that statins are associated with de novo albuminuria and proteinuria. It is of
importance to establish the association between statin use and MAU to correctly interpret
presence of MAU as a predictor or marker of cardiovascular or renal disease in observational
trials with a mixed population of subjects taking and not taking a statin. If statin use is associated
with MAU, there is a risk of incorrect labeling of subjects as having a predictor or marker of
cardiovascular or renal risk. The current study evaluated the association between statin use and
MAU, and used a propensity score analysis to adjust for bias by indication. For this goal, we used
the baseline data of the early renal impairment and cardiovascular assessment in Belgium
(ERICABEL) trial, a prospective cohort of hypertensive patients followed by primary care
physicians created to evaluate the impact of metabolic syndrome on cardiovascular and renal
endpoints.

CHAPTER 2: Results
100
Methods
Objectives. The primary aim of the ERICABEL study was to determine the effect of metabolic
risk factors on the evolution of renal function and cardiovascular outcome over 5 years, in
patients aged between 40 and 70 years with diagnosed hypertension, and followed by their
primary care physician. The current analysis was designed to evaluate 1° the association between
statin treatment and MAU and 2° the impact of statin treatment on the interpretation of the
association between individual cardiovascular risk factors and MAU in epidemiological studies.
Particpants. We used the baseline data of the ERICABEL cohort, a non-interventional
epidemiological study with a follow up of 5 years that included 1,076 Caucasian patients with
hypertension, defined as systolic blood pressure ≥140mmHg and/or intake of at least one
antihypertensive drug, recruited by 96 general practitioners, between 2006 and 2007, in Belgium.
Of the 1076 patients included in this cross-sectional study, 420 patients had a missing value for at
least one of the variables under investigation (see appendix table S1 for detailed list). Multiple
imputation techniques were used to account for the missing data, using 20 imputations [17]. All
characteristics and outcome (MAU) were simultaneously used in the imputation model. The
imputation was done using the R function aregImpute from the Hmisc package [18].
Description of procedures. Each participating primary care physician was asked to include 10
consecutive hypertensive patients aged between 40-70 years, in a 1:1 sex ratio. The eligible
persons were evaluated at baseline and if eligible, sociodemographic information (age, sex, race,
and education level), personal and family medical history, smoking status and medication use
were collected prospectively in an online database. Body weight was recorded to the nearest 0.1
Kg and height was measured to the nearest centimeter. Body mass index (BMI) was calculated as
body weight in Kg divided by height² (kg/m²). Blood pressure was measured according to the
WHO criteria with a calibrated Omron HEM-907 device (average of 2 measurements, sitting,
with 5 minutes in between). All these measurements were done by the primary care physician.
After exclusion of a urinary infection or hematuria (negative Combur® test), MAU was screened
by a Micral® dipstick test. MAU was considered present if measured albuminuria was ≥ 20mg/l
on a morning midstream urine sample. Blood sampling was performed by the general practitioner
in fasting patients.

CHAPTER 2: Results
101
Definitions. The metabolic syndrome was defined as three or more of the following criteria,
according to the National Cholesterol Education Program Third Adult Treatment Panel guidelines
ATP III criteria [19]: elevated blood pressure ≥ 130/85 mmHg and/or antihypertensive
medication (by definition 100% in this cohort), (2) high plasma triglycerides (> 1.7 mmol/l), low
HDL cholesterol (< 1.0 mmol/l in men and < 1.3 mmol/l in women), (4) abdominal adiposity
(waist circumference > 102/88 cm men/women) and/or impaired glucose tolerance (IGT)
(fasting plasma glucose ≥ 6.1 mmol/l and/or known diabetes).
Ethics. The study was approved by an independent ethics committee review board, protocol
number: ML 19208. A written informed consent was obtained from all participants.
Statistical methods. All analyses have been performed using SAS software (SAS software,
version 9.2 of the SAS System for Windows. Copyright © 2002 SAS Institute Inc.) or R Version
2.12.0 (R Foundation for Statistical Computing, Vienna, Austria. ISBN 3-900051-07-0, 2009)
[20]. MAU was considered as a dichotomic variable. Continuous variables were described by
their mean, standard deviation, median and interquartile range. Categorical variables were
summarised by frequencies and percentages.
A propensity score for statin use was created to correct for “bias by indication”. Propensity score
analysis is a well established method to adjust for confounding by indication in observational
trials [21,22]. Primarily, for the statistical analyses, 20 imputed samples were created. In a second
step, within each of the 20 samples separately, a propensity model was constructed and the
resulting propensity score was calculated for each of these patients. The propensity model
included the following variables that were deemed to be possibly related to statin use: age, gender,
BMI, waist circumference, SBP, previous CV event, CRP, fasting glucose, diabetes, serum uric
acid, HDL and LDL cholesterol, triglycerides, use of angiotensin converting enzyme
inhibitor/angiotensin receptor blocker (ACE-I/ARB) and smoking. Continuous variables in the
model were included using restricted cubic splines: each continuous variable was included in the
model using 3 dummy variables, called var1, var2 and var3. For the first 5 imputed samples, a
histogram of the propensity scores was presented by statin use (see appendix, table S2). In
addition, in order to check the ability of the propensity scores to balance the two statin groups for
baseline characteristics, tables were presented for the first 5 imputed samples, comparing the
baseline characteristics between the groups (see appendix, table S3). In this way, patients with the

CHAPTER 2: Results
102
same “likelihood” or “propensity” to receive a statin (i.e. in this setting mainly with comparable
cardiovascular risk factors), but in one case taking and in the other case not taking a statin, were
compared for presence of MAU.
For comparison of continuous variables, ANOVA was used, adjusted for propensity scores,
whereas for binary variables, logistic regression analyses, also adjusted for propensity scores,
were employed. Logistic regression analyses were used to assess the association between statin
use and MAU using the “GENMOD” procedure in SAS. The associations were assessed in each
of the 20 imputation samples separately and the results were combined using the SAS procedure
“MIANALYZE”. The following logistic regression models were used: 1°: Univariable model
only including statin use; 2° a model including statin use and propensity scores (using a restricted
cubic spline); 3° a model including statin use, propensity scores and all relevant variables
mentioned above. Since the linearity assumption was deemed appropriate for all continuous
variables in the model (p> 0.1 for the assessment of linearity in the full model), the final model
only included linear terms for all variables.

CHAPTER 2: Results
103
Results
The baseline characteristics of the population are provided in tables 1 and 2.
Table 1. Baseline characteristics (categorical variables)
MS: metabolic syndrome, MAU: microalbuminuria, ACE-I/ARB: angiotensin converting enzyme
inhibitor /angiotensin receptor blocker, CVevent: cardiovascular event
p*:p values between all three groups; p§: p value between users vs. non statin users
There was an equal distribution in gender (51.3% males) in the overall cohort. There was a high
prevalence of metabolic syndrome (44.5%), diabetes (19.8%), current smokers (36.5%) and
MAU (16.4%) in the overall cohort. ACE-I and/or ARB were the most commonly prescribed
antihypertensive agents (55.9%). History of a cardiovascular event was recorded in 11.3% of the
patients. Mean age of the cohort was 57.5 ± 7.5 years. One third (30.8%) of the patients used a
statin.
parameter No statins
(N=724)
Statins
(N=332)
Statin use
unknown (N=20)
Total
(N=1076)
P* P§
Female 384/724
(53%)
132/332
(39.8%)
7/19
(36.8%)
523/1075
(48.7%)
<.001 <.001
MS 239/624
(38.3%)
172/299
(57.5%)
2/4
(50.0%)
413/927
(44.6%)
<.001 <.001
Diabetes 98/700
(14.0%)
104/327
(31.8%)
2/5
(40.0%)
204/828
(19.8%)
<.001 <.001
Smoker 249/698
(35.7%)
123/325
(37.9%)
3/5
(60.0%)
375/653
(36.5%)
0.438 0.501
MAU 68/529
(12.9%)
60/248
(24.2%)
0/4
(0.0%)
128/653
(16.4%)
<.001 <.001
ACE-
ARB
358/724
(49.5%)
232/332
(69.9%)
590/1056
(55.9%)
<.001 <.001
CV event 38/693
(5.5%)
77/325
(23.7%)
1/5
(20.0%)
116/1023
(11.3%)
<.001 <.001

CHAPTER 2: Results
104
Table 2. Baseline characteristics (continuous variables)
Patient
Characteristic
Statistic No statin Statin Statin use
unknown
Total P* P§
Age (years) Mean±SD 56.8± 7.6 59.1± 7.1 58.2± 6.0 57.5± 7.5 < .001 < .001
Median 57.2 60.0 58.6 58.5
N 724 332 19 1075
BMI (kg/m²) Mean±SD 29.3± 5.4 30.6± 5.5 30.5± 4.4 29.7± 5.4 0.001 < .001
Median 28.5 29.7 31.7 28.8
N 689 326 5 1020
SBP (mmHg) Mean±SD 144± 15 143± 16 149± 11 143± 16 0.527 0.394
Median 142.5 140.0 152.0 142.0
N 704 331 5 1040
DBP (mmHg) Mean±SD 84± 10 83± 10 87± 6 84± 10 0.054 0.020
Median 84.5 82.0 86.5 83.5
N 704 331 5 1040
Glucose (mmol/l) Mean±SD 5.6± 2.9 6.3± 2.1 6.8± 1.4 5.9± 2.7 0.001 < .001
Median 5.2 5.7 6.9 5.3
N 644 311 4 959
Uric acid (µmol/l) Mean±SD 339± 89 357± 83 291± 83 345± 89 0.008 0.004
Median 333 357 286 339
N 629 306 4 939
Triglycerides
(mmol/l)
Mean±SD 1.6± 1.1 1.9± 1.1 2.0±1.7 1.7± 1.1 0.011 0.003
Median 1.3 1.6 1.4 1.4
N 638 316 4 958
LDL-Cholesterol
(mmol/l)
Mean±SD 3.2± 0.8 2.7± 1.0 2.9± 0.8 3.0± 0.9 < .001 < .001
Median 3.2 2.6 3.2 3.0
N 628 312 4 944
HDL-Cholesterol
(mmol/l)
Mean±SD 1.5± 0.5 1.4± 0.4 1.3± 0.4 1.5± 0.5 0.004 0.001
Median 1.4 1.3 1.4 1.4
N 637 315 4 956
CRP (mg/dl) Mean±SD 0.5± 0.8 0.4± 0.5 0.4± 0.4 0.5± 0.7 0.148 0.055
Median 0.3 0.2 0.4 0.3
N 608 291 4 903
BMI: body mass index, SBP: systolic blood pressure, DBP diastolic blood pressure, CRP: C-reactive
protein. p*:p values between all three groups; p§: p value between users vs. non statin users

CHAPTER 2: Results
105
Table 3. Association between statin use and microalbuminuria (MAU)
$ Pscore= propensity score; The propensity score was fit using a restricted cubic spline.
ACE-I/ARB: angiotensin converting enzyme inhibitor/angiotensin receptor blocker, CV event:
cardiovascular event, BMI: body mass index, BP: Blood pressure, CRP: C-reactive protein.
Odds Ratio
Logistic regression
model for presence of
MAU
Parameter Estimate 95% Confidence
Interval
P-value
A. Univariable
association
Statin use 2.01 (1.34;3.01) < 0.001
B. Association
adjusted for
propensity score
Statin use 1.82 (1.14; 2.91) 0.01
Pscore$ . 0.6
C. Association fully
adjusted
Statin use 1.90 (1.15; 3.11) 0.01
Pscore 7.92 (0.18; 357.3) 0.28
Age 1.02 (0.91; 1.14) 0.74
Diabetes 1.92 (1.004; 3.66) 0.05
Smoker 1.49 (0.99; 2.26) 0.06
ACE-I/ARB 1.47 (0.92; 2.34) 0.11
CV event 1.32 (0.59; 2.95) 0.50
BMI 1.03 (0.86; 1.24) 0.74
Mean BP 0.96 (0.89; 1.04) 0.35
Fasting glucose 0.97 (0.91; 1.04) 0.44
Uric acid 0.89 (0.50; 1.50) 0.61
Triglycerides 0.99 (0.98; 1.01) 0.44
Cholesterol 1.00 (0.98; 1.02) 0.77
CRP 1.49 (0.01; 359.73) 0.89

CHAPTER 2: Results
106
In univariable analysis, statin users were more likely to be male (p< 0.001), had a higher
frequency of metabolic syndrome (p< 0.001), diabetes type 2 (p< 0.001), MAU (p< 0.001), ACE-
i/ARB treatment (p< 0.001), and previous cardiovascular events (p< 0.001), were older (p<
0.001), had larger BMI (p< 0.001), lower diastolic blood pressure (p= 0.02), higher fasting
glucose (p< 0.001), serum uric acid (p= 0.004), and triglycerides (p= 0.003), had lower levels of
LDL (p< 0.001) and HDL cholesterol (p= 0.001) compared to patients not taking statins (tables 1
and 2). The univariable odds ratio of MAU in patients using vs. not using a statin was 2.01 (95%
CI: 1.34-3.01, p= 0.0009, table 3A).
After multivariable analysis including the propensity score for statin use, the odds of MAU was
still significantly higher in patients taking a statin (OR: 1.82, 95% CI: 1.14-2.91, p= 0.01, table
3B). When all other variables were forced into the model, use of statin still was independently
associated with a higher odds of MAU (OR: 1.90, 95% CI: 1.15-3.11, p= 0.01, table 3C). Next to
statin use, only diabetes (OR: 1.92, 95% CI: 1.00-3.66, p= 0.05) and smoking (OR: 1.49, 95% CI:
0.99-2.26, p= 0.06) were independently associated with MAU after adjusting for the likelihood
of receiving a statin, suggesting that prescription of a statin overrides the association between
cardiovascular risk factors, MAU and creates collinearity by acting as a surrogate.

CHAPTER 2: Results
107
Figure S1. Flow chart of hypotheses to explain the observation of higher prevalence of MAU in
statin users

CHAPTER 2: Results
108
Discussion
Our data create concern on the use of MAU as a predictor or marker of cardiovascular or renal
disease in cohorts with patients using statins. Statin use apparently could blur the interpretation of
MAU by two potential mechanisms: 1° higher prevalence of MAU in patients using a statin, even
after correction for bias by indication and 2° masking of cardiovascular risk factors in
multivariable analyses, as statin use behaves as a surrogate for these markers. In epidemiological
studies evaluating the association between cardiovascular risk factors and MAU, statin use can
induce incorrect labeling of patients as having a cardiovascular or renal risk factor, and
interpretation of other risk factors for cardiovascular or renal disease can be confounded by the
way the use of statins is handled in the analysis. In this cross-sectional analysis, we observed a
two-fold higher prevalence of MAU in subjects who use vs. those who do not use a statin.
However, part of this association (figure S1) can be attributed to bias by indication, as patients
are often prescribed statins because they have cardiovascular risk factors which are by themselves
associated with enhanced risk for MAU. Indeed, we observed a higher prevalence of
cardiovascular risk factors in patients taking vs. not taking a statin in our study. We tried to
exclude this bias by indication by the use of a propensity score analysis. Adjusting for the
propensity score allows to analyze the difference in occurrence of MAU between patients with a
comparable propensity to receive a statin, while one group does whereas the other does not
receive the drug. The technique of propensity score is well established to address confounding
and bias by indication in observational studies [23,24]. However, this increased odds ratio
remained present even after correcting for the fact that statins are usually prescribed in patients
with cardiovascular risk factors which by themselves are associated with MAU, using the robust
technique of propensity score. This observation can either be due to residual or unmeasured
confounding or there can really be an induction of MAU by statin use (figure S1). Our data stress
that statin use confounds the impact of the individual risk factors on MAU, as statin use behaves
as a surrogate for presence of cardiovascular risk factors. As a consequence, in studies where
MAU is either used as a marker or as a surrogate endpoint, the association between outcomes and
certain cardiovascular risk factors can be blurred, and this in an unpredictable and variable
fashion, depending upon the prevalence of statin use in the cohort. On the other hand, if statins
really induce MAU, theoretically it can be both of glomerular or of tubular origin (figure S1). We
did not find any publication, either human, animal or in vitro, indicating that statin associated

CHAPTER 2: Results
109
proteinuria is of glomerular origin, but at least three in vitro or animal studies demonstrated that
statins do inhibit tubular reabsorption of filtered albumin and in this way could generate MAU in
a dose-dependent manner and in absence of cytotoxicity [11,12,25]. There is also growing
evidence that also in other conditions MAU can be the consequence of tubular dysfunction, even
in presence of an entirely intact glomerulus [26,27]. One epidemiological study in humans also
coined statin induced proteinuria as being tubular in origin, and even demonstrated a dose-effect
relation with rosuvastatin [28]. This would explain why statins fail to consistently result in
reduction of MAU in subjects with low grade MAU, or why higher vs. lower doses of statin fail
to further reduce MAU [29,30], as the beneficial effect of statins on the glomerular MAU is
counterbalanced by the induction of tubular MAU. It is very unlikely that statin induced MAU is
associated with an increased cardiovascular risk, but its impact on the functional capacity and the
morphological integrity of the kidneys is unknown. Even when the tubular albuminuria induced
by statins is harmless [31], it interferes with the implication of MAU as predictor or marker of
cardiovascular and renal risk by incorrectly labeling a subject as having a risk factor. Of note, this
would imply that the prognostic impact of glomerular MAU (so not induced by statin use) in
populations with a high prevalence of statin use, would be underestimated. The hypothesis that
statin induced MAU is tubular in origin would also fit with the favorable effect of statins on
cardiovascular disease and on progression of renal disease, as these effects are related to the
reduction of glomerular MAU associated with the improvement of endothelial dysfunction
[32,33].
Limitations. This cross-sectional study could not prove a causal connection between statin use
and de novo MAU. Using the technique of propensity score we achieved “pseudo-
randomization”, which in fact obviates the drawbacks imposed by the method of the study, but
which is not free from unmeasured biases [24]. Unfortunately, although dose dependency and a
higher frequency of more potent inhibitors of HMG coA reductase could add further strength to
the association with MAU, the prescribed daily dose and type of statin were as per protocol not
registered in our study. Another limitation of our study is that MAU was measured in a single
morning urine, whereas guidelines recommend to have at least two positive MAU in three
consecutive first morning urine samples before labeling a person as having MAU [34]. However,
in view of the mechanism of inhibition of tubular endocytosis, it is unlikely that statin associated
MAU would disappear by repeated testing, unless the statin would be stopped temporarily to

CHAPTER 2: Results
110
confirm the diagnosis. Second, intermittent MAU should not be considered as a predictor or
marker of cardiovascular or renal risk, as it is not linked to endothelial dysfunction [35]. In line
with this, we demonstrated in another cohort, that patients with intermittent MAU have far less
cardiovascular risk factors as compared to patients with persisting MAU [36]. Our study shows
that, in addition to the problems caused by single vs. multiple sampling, the use of a statin can
also lead to an in incorrect labeling of subject as having MAU.
The strength of this study is that it reflects routine clinical practice in hypertensive patients. To
the best of our knowledge, this is the first study pointing to an independent association between
statin use and MAU, even after correction for bias by indication by the use of a propensity score,
underlining the potential consequences of confounding induced by statin use on the interpretation
of MAU as a predictor or marker of cardiovascular or renal disease in epidemiological trials.
According to our data, statins are independently associated with an increased prevalence of
MAU, even after correction for bias by indication. As this MAU is most likely of tubular origin,
it is uncertain and rather unlikely whether it has the same prognostic impact for renal and
cardiovascular disease as endothelial dysfunction induced glomerular MAU. As such, it can lead
to incorrect labeling of subjects as having a cardiovascular risk factor.

CHAPTER 2: Results
111
Acknowledgments
We thank the steering committee members: JM Billiouw, M Couttenye, J Donck, M Dratwa, A
Dufour, B Georges, M Henckes, M Jadoul, E. Lessafre, JM Krzesinski, N Lameire, P Leenaerts,
R Lins, Y Pirson, JC Stolear, C Tielemans, W Van Biesen, R Vanholder, Y Vanrenterghem, D
Verbeelen, G Verpooten and the investigators: F Bare, A Bernaers, I Bijnens, P Blondeel, L
Bonami, L Bostoen, N Boussemaere, I Buntinx, D Chevalier, A Cleys, H Cuypers, G D'Hont, E
De Ganck, J De Jaeger, A De Leeuw, K De Praeter, K De Schutter, JL Delattre, P Delhaye, A
Delvosalle, A Demeester, B Dewaele, M Dooms, B Englebienne, L Erpicum, P Feys, H Flamee,
R Follet, J Galot, K Geens, W Geerts, C Gilio, P Govaert, J Helincks, K Hendrickx, Y
Henoumont, G Hoogmartens, S Hoppenbrouwers, J Ingelaere, S Konings, G Lannoo, R
Leuridan, M Lootens, J Luyts, D Mebis, J Mestdagh, L Meyvis, B Morelle, D Mulkers, M
Nevelsteen, F Nollomont, L Phang, A Pollet, E Pycke, V Rémy, M Rombouts, P Schleich, E
Schoofs, H Symons, C Tack, L Tanghe, J Van Assche, J Van Boxem, O Van Damme, E Van der
Putte, H Van der Stockt, J Van Massenhove, N Van Mulders, M Vande Voorde, D Vanmansart, J
Vermaete, J Vernijns, L Vernijns, B Verstraete, A Villé, E Willekens, S Delville, M Deroubaix,
M Ferro, M Ghesquiere, L Rouvroy, P Soetaert, N Van Nieuwenhuyse, E Vanden Eynde
Funding: The funder of this study was F. Hoffmann-La Roche Ltd. The funder had a role in data
collection because the ERICABEL study was initiated by F. Hoffmann-La Roche Ltd. The funder
had no other role in the study design, analysis, decision to publish, or preparation of the
manuscript.

CHAPTER 2: Results
112
References
1. Gerstein HC, Mann JF, Yi Q, Zinman B, Dinneen SF, et al. (2001) Albuminuria and risk of
cardiovascular events, death, and heart failure in diabetic and nondiabetic individuals. JAMA 286:
421-426.
2. Hallan H, Romundstad S, Kvenild K, Holmen J (2003) Microalbuminuria in diabetic and hypertensive
patients and the general population - Consequences of various diagnostic criteria - The Nord-Trondelag
Health Study (HUNT). Scandinavian Journal of Urology and Nephrology 37: 151-158.
3. Klausen KP, Scharling H, Jensen G, Jensen JS (2005) New definition of microalbuminuria in
hypertensive subjects - Association with incident coronary heart disease and death. Hypertension 46:
33-37.
4. van der Tol A, Van Biesen W, Verbeke F, De Groote G, Vermeiren F, et al. (2010) Towards a rational
screening strategy for albuminuria: results from the unreferred renal insufficiency trial. PloS one 5.
5. Bigazzi R, Bianchi S, Baldari D, Campese VM (1998) Microalbuminuria predicts cardiovascular
events and renal insufficiency in patients with essential hypertension. Journal of Hypertension 16:
1325-1333.
6. Mogensen CE (1999) Microalbuminuria, blood pressure and diabetic renal disease: origin and
development of ideas. Diabetologia 42: 263-285.
7. Baigent C, Keech A, Kearney PM, Blackwell L, Buck G, et al. (2005) Efficacy and safety of
cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14
randomised trials of statins. Lancet 366: 1267-1278.
8. Douglas K, O'Malley PG, Jackson JL (2006) Meta-analysis: the effect of statins on albuminuria.
Annals of internal medicine 145: 117-124.
9. Sandhu S, Wiebe N, Fried LF, Tonelli M (2006) Statins for improving renal outcomes: a meta-analysis.
Journal of the American Society of Nephrology : JASN 17: 2006-2016.
10. Fried LF, Orchard TJ, Kasiske BL (2001) Effect of lipid reduction on the progression of renal disease:
a meta-analysis. Kidney International 59: 260-269.
11. Verhulst A, D'Haese PC, De Broe ME (2004) Inhibitors of HMG-CoA reductase reduce receptor-
mediated endocytosis in human kidney proximal tubular cells. Journal of the American Society of
Nephrology : JASN 15: 2249-2257.
12. Sidaway JE, Davidson RG, McTaggart F, Orton TC, Scott RC, et al. (2004) Inhibitors of 3-hydroxy-3-
methylglutaryl-CoA reductase reduce receptor-mediated endocytosis in opossum kidney cells. Journal
of the American Society of Nephrology : JASN 15: 2258-2265.
13. van Zyl-Smit R, Firth JC, Duffield M, Marais AD (2004) Renal tubular toxicity of HMG-CoA
reductase inhibitors. Nephrology, dialysis, transplantation : official publication of the European
Dialysis and Transplant Association - European Renal Association 19: 3176-3179.
14. Wolfe SM (2004) Dangers of rosuvastatin identified before and after FDA approval. Lancet 363: 2189-
2190.
15. Deslypere JP, Delanghe J, Vermeulen A (1990) Proteinuria as Complication of Simvastatin Treatment.
Lancet 336: 1453-1453.
16. Atthobari J, Brantsma AH, Gansevoort RT, Visser ST, Asselbergs FW, et al. (2006) The effect of
statins on urinary albumin excretion and glomerular filtration rate: results from both a randomized
clinical trial and an observational cohort study. Nephrology Dialysis Transplantation 21: 3106-3114.
17. Rubin DB (1987) multiple imputation for nonrespons in surveys. New York: John Wiley & Sons.
18. Frank EH (2009) Hmisc: Harrell Miscerllaneous. R package version 3.7-0.

CHAPTER 2: Results
113
19. Cleeman JI, Grundy SM, Becker D, Clark LT, Cooper RS, et al. (2001) Executive summary of the
Third Report of the National Cholesterol Education Program (NCEP) expert panel on detection,
evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III). Jama-Journal
of the American Medical Association 285: 2486-2497.
20. http://www.R-project.org (Accessed 2012 jan 18) The R project for statistical computing. .
21. Heinze G, Juni P (2011) An overview of the objectives of and the approaches to propensity score
analyses. European heart journal.
22. Zhehui L, Gardiner JC, Bradley CJ (2010) Applying propensity score methods in medical research:
pitfalls and prospects. Medical care research and review : MCRR 67: 528-554.
23. Barnieh L, James MT, Zhang J, Hemmelgarn BR (2011) Propensity score methods and their
application in nephrology research. Journal of nephrology.
24. Rosenbaum PR, Rubin DB (1983) The Central Role of the Propensity Score in Observational Studies
for Causal Effects. Biometrika 70: 41-55.
25. Corna D, Sangalli F, Cattaneo D, Carrara F, Gaspari F, et al. (2007) Effects of rosuvastatin on
glomerular capillary size-selectivity function in rats with renal mass ablation. American Journal of
Nephrology 27: 630-638.
26. Pollock CA, Poronnik P (2007) Albumin transport and processing by the proximal tubule: physiology
and pathophysiology. Current opinion in nephrology and hypertension 16: 359-364.
27. Jefferson JA, Shankland SJ, Pichler RH (2008) Proteinuria in diabetic kidney disease: a mechanistic
viewpoint. Kidney International 74: 22-36.
28. Kostapanos MS, Milionis HJ, Saougos VG, Lagos KG, Christine K, et al. (2007) Dose-dependent
effect of rosuvastatin treatment on urinary protein excretion. Journal of cardiovascular pharmacology
and therapeutics 12: 292-297.
29. Sorof J, Berne C, Siewert-Delle A, Jorgensen L, Sager P, et al. (2006) Effect of rosuvastatin or
atorvastatin on urinary albumin excretion and renal function in type 2 diabetic patients. Diabetes
Research and Clinical Practice 72: 81-87.
30. Rutter MK, Prais HR, Charlton-Menys V, Gittins M, Roberts C, et al. (2011) Protection Against
Nephropathy in Diabetes with Atorvastatin (PANDA): a randomized double-blind placebo-controlled
trial of high- vs. low-dose atorvastatin. Diabetic Medicine 28: 100-108.
31. http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/Drug
SafetyInformationforHeathcareProfessionals/PublicHealthAdvisories/UCM051756 (accessed 2012 jan
18) FDA Public Health Advisory for Crestor (Rosuvastatin).
32. Knight SF, Yuan J, Roy S, Imig JD (2010) Simvastatin and tempol protect against endothelial
dysfunction and renal injury in a model of obesity and hypertension. American journal of physiology
Renal physiology 298: F86-94.
33. Park JK, Mervaala EM, Muller DN, Menne J, Fiebeler A, et al. (2009) Rosuvastatin protects against
angiotensin II-induced renal injury in a dose-dependent fashion. Journal of Hypertension 27: 599-605.
34. http://www.kidney.org/professionals/kdoqi/guidelines_ckd/p5_lab_g5.htm (accessed 2012 jan 18)
KDOQI Clinical Practice Guidelines for Chronic Kidney Disease: Evaluation, Classification, and
Stratification, part 5. Evaluation of laboratory measurements for clinical assessment of kidney disease,
guidelines 5. Assesment of proteinuria
35. Romundstad S, Holmen J, Kvenild K, Hallan H, Ellekjaer H (2003) Microalbuminuria and all-cause
mortality in 2,089 apparently healthy individuals: A 4.4-year follow-up study. The Nord-Trondelag
Health Study (HUNT), Norway. American Journal of Kidney Diseases 42: 466-473.

CHAPTER 2: Results
114
36. Van der Tol A, Van Biesen W, De Groote G, Verbeke P, Vermeiren F, et al. (2011) Mislabeling
Cardiovascular Risk by One Single Measurement of Microalbuminuria. Acta Clinica Belgica 66: 171-
171.

CHAPTER 3: GENERAL DISCUSSION AND
CONCLUSIONS


CHAPTER 3: General discussion and conclusions
117
In this thesis we discuss whether cardiovascular risk factors and kidney damage could be
screened by measuring albuminuria. Our results are based on two prospective studies, one study
was performed in workers (URI study) and another study was performed in hypertensive subjects
(ERICABEL study). In what follows we will discuss the main questions raised at the start of this
thesis.

CHAPTER 3: General discussion and conclusions
118
3.1. The prevalence of microalbuminuria and the associations with
traditional cardiovascular risk factors in a general population.
In the URI study (n = 1,398), the prevalence of microalbuminuria was 5.2 and 0.5%. Only a
minority of the workers with microalbuminuria (14/73 = 19%) had known diabetes and/or
hypertension. In a Dutch population cohort (PREVEND), also a minority of the subjects with
microalbuminuria (644/2,918 = 22%) had self-reported diabetes and/or hypertension (1). After
exclusion of these known risk factors, the PREVEND trial reported a higher prevalence of
microalbuminuria than the URI study (6.6 vs. 4.2%, p < 0.001), conceivably as a consequence of
higher mean age (49.5 ± 12.9 y vs. 38.3 ± 9.7 y, p< 0.001), higher prevalence of smokers (42 vs.
31%, p < 0.001) and differences in methods to define microalbuminuria; urinary albumin
concentration (UAC): 20-200 mg/l in the PREVEND study vs. urinary albumin creatinin ratio
(ACR): 17-249 in men 25-354 mg/g in women in the URI study (2). The PREVEND study
concluded that the presence of microalbuminuria predicts cardiovascular morbidity and mortality,
even in subjects without recognized cardiovascular risk factors (2, 3). However, this association
might be confounded by inflammation, unrecognized cardiovascular risk factors and ‘borderline’
levels of cardiovascular risk factors, such as prehypertension or impaired glucose tolerance (4-6).
In this thesis, we described in chapter 2.1.1 based on data from the URI study, that ACR in
apparently healthy workers was positively associated with unrecognized hypertension (≥ 140/90
mmHg), plasma glucose (≥100 mg/dl) and resting heart rate (≥ 85 bpm). The prevalence of these
risk factors was high (36%) in this presumably healthy population. Moreover, as described in
chapter 2.1.3, one third of the workers of the overall URI population had at least one traditional
cardiovascular risk factor (hypertension, diabetes and/or dyslipidemia) of whom only one third
was known and treated. In the PREVEND study (n = 40,856) cardiovascular risk factors were
only measured in selected subjects with UAC > 10 mg/l (n= 6,000) and in a randomly selected
control group of the total study population with UAC < 10 mg/l (n = 2,592). Microalbuminuria as
defined by UAE > 30 mg/24h was only confirmed in 933 subjects (7). Two thirds of these
subjects (633/933) had hypertension, diabetes and/or a cardiovascular history, and one third
(300/933) was considered to have isolated microalbuminuria. Nevertheless, the subjects with
isolated microalbuminuria had associated additional cardiovascular risk factors, such as age, male
gender, smoking, obesity and dyslipidemia, ‘borderline’ levels of cardiovascular risk factors, and

CHAPTER 3: General discussion and conclusions
119
also an increased risk to develop diabetes, hypertension and cardiovascular diseases (7). Thus,
persistent microalbuminuria is rather a reflection of widespread vascular damage that is linked to
associated risk factors than an independent risk factor (8). In the URI study (chapter 2.1.1), two
thirds of the workers with microalbuminuria had associated cardiovascular risk factors. We
hypothesized that a subject with microalbuminuria in absence of any cardiovascular risk factor
could be considered as a false positive. The prevalence of these false positive results was 2.4%.
Similar figures were found in a New Zealand study (2.0%) and in the Copenhagen City Heart
Study (2%) (9, 10). In subjects without any feature of the metabolic syndrome, the presence of
microalbuminuria was not associated with increased risk for cardiovascular disease and death,
suggesting that microalbuminuria by itself might not be an independent determinant of outcome
(10).

CHAPTER 3: General discussion and conclusions
120
3.2. Should we use microalbuminuria as a screening tool to identify subjects
with unrecognized cardiovascular risk factors in a presumably healthy
population?
The authors of the PREVEND trial suggest that screening for albuminuria improves the detection
of unrecognized renal and cardiovascular risk factors (1, 11, 12). When this approach had been
implemented in the URI cohort, only 9% (37/431) of the workers with at least one unrecognized
risk factor would have been identified (chapter 2.1.1). The sensitivity of microalbuminuria to
detect a subject with at least one cardiovascular risk factor was low (12%) in the PREVEND
study as well, leaving most subjects (88%) with modifiable cardiovascular risk factors untreated
(12). According to the authors of the PREVEND trial, hypertensive patients without
microalbuminuria would not benefit from blood pressure lowering agents as the risk reduction for
cardiovascular events would be too low. It was estimated that more hypertensive patients without
vs. with microalbuminuria need to be treated (111 vs. 8) to prevent one cardiovascular event (13).
Yet, no RCT exists to test the hypothesis that medical management of microalbuminuria reduces
cardiovascular or renal events independent of blood pressure reduction (14). According to us, the
‘PREVEND’ approach might offer prospects for secondary prevention in high risk patients with
microalbuminuria while more subjects would be (earlier) identified by screening for
cardiovascular risk factors with more potential possibilities to reduce cardiovascular risk (chapter
2.1.1). The efficiency of interventions in patients with diabetes and/or hypertension is also
practically more easy to assess by measuring the plasma glucose and blood pressure levels than it
would be by controlling urinary albumin. Additionally, the interpretation of microalbuminuria is
hampered by the fluctuations which commonly occur.

CHAPTER 3: General discussion and conclusions
121
3.3. Conditions which could lead to false positive test results of
microalbuminuria
Another problem of using microalbuminuria as a screening tool is the high number of false
positive results. Biological variation and temporary conditions such as changes in blood pressure,
plasma glucose, fever, urinary tract infections, hematuria, exposure to cold and physical exercise
might result in false positive results (chapter 1). Microalbuminuria fluctuates more in random
urine samples than in early morning urine samples (15). Conceivably, the URI trial included a
substantial number of false positive test results as urine was collected randomly. The exact
number of false positive subjects in our trial is unknown as we did not perform an overnight or
24-h urine collection in all subjects.
In the URI study, we used gender specific cut-off values (ACR: 17-249 for males and 25-354
mg/g for females) in an urine spot to indicate microalbuminuria, because men have a higher
urinary excretion of creatinine than women due to higher muscle mass (16). According to the
PREVEND trial, the sensitivity, specificity and positive predictive value of these gender specific
cut-off values in an urinary spot, to predict microalbuminuria in subsequent 24-hours urine
collection was 65, 98 and 65%, respectively (17). However, the PREVEND trial used a lower
threshold to define microalbuminuria UAC > 10 mg/l during the prescreening, consequently
more subjects with microalbuminuria were identified (increased sensitivity) but simultaneously
also more subjects with a false positive result were included.
As described in chapter 2.1.2, within the URI study, a prospective analysis was designed to
evaluate the reproducibility of microalbuminuria. Of the overall URI population, 341 subjects
underwent consecutive occupational check-ups. Only 60% of the initially microalbuminuric
subjects tested positive for microalbuminuria at a subsequent visit. The reproducibility of initial
microalbuminuria was higher in subjects with vs. without traditional risk factors (89 vs. 36%, p =
0.03). In addition, subjects with persistent microalbuminuria had a higher cardiovascular risk
score than subjects with intermittent or without microalbuminuria. These findings corroborate the
data from the HUNT study that showed that intermittent microalbuminuria in presumably healthy
subjects might simply reflect biological variation, whereas persistent microalbuminuria more
likely explains a cardiovascular risk and/or disease (18). We assumed in chapter 2.1.1 that

CHAPTER 3: General discussion and conclusions
122
approximately 1 of 3 detected workers had a false positive test result, as one third of the workers
with microalbuminuria had no cardiovascular risk factor. In workers younger than 40 years, the
presence of microalbuminuria was not associated with cardiovascular risk factors (chapter 2.1.3).
In this group, the presence of microalbuminuria was associated with low BMI or with
physicochemical exposure risk (PCER). Conceivably, a substantial number of young workers had
postural proteinuria and might be mislabeled as having a risk for cardiovascular and/or renal
disease (19-21). The meaning of microalbuminuria in workers with PCER is unknown.
According to the literature, exposure to some heavy metals is associated to reversible tubular
overflow albuminuria by increased liver synthesis of metallothionein (22-24).
Another condition that affects urinary albumin excretion is use of statins. In chapter 2.2.1 we
showed that statin use is associated with microalbuminuria, even after adjusting for bias by
indication to receive a statin. Other studies confirmed that statin use generates tubular
albuminuria hence affecting the total excreted albumin (25-27). The effect of statins was maximal
after 3 hours and disappears after 24 hours in healthy subjects (27). The ERICABEL study did
not evaluate the timing of statin intake. The finding of an increased urinary α1-
microglobulin/albumin ratio might help to distinguish statin induced tubular albuminuria from
glomerular albuminuria (27). This might help to anticipate incorrect labeling of persons with an
increased risk for a cardiovascular or renal disease. In the ERICABEL study no marker for
tubular albuminuria was measured. Thus, whether microalbuminuria could be implemented in a
mass screening program is uncertain as it might have different underlying causes, and prognostic
meanings.

CHAPTER 3: General discussion and conclusions
123
3.4. Can we prevent ESRD by screening for microalbuminuria in a general
population?
The central idea of screening for albuminuria is early disease detection followed by adequate
treatment to reduce the risk of the disease or progression. KDIGO recommends to screen for
albuminuria in selected patients with hypertension, diabetes, and/or cardiovascular disease (28).
However, some authors advocate to screen for albuminuria in the general population as many
persons are not aware of the presence of cardiovascular risk factors (1). The criteria to select a
disease for screening have been reported by Wilson and Jungner and the Council of Europe and
are summarized in table 1 (29, 30). We discuss by means of these criteria whether a population
wide albuminuria screening followed by appropriate treatment might lead to benefits in terms of
prevention of end stage renal disease (ESRD).
Table 1. The Wilson-Jungner criteria (29) and recommendations of the Council of Europe
(30)
1) The disease should be an obvious burden for the individual and the community in terms of
death, poor quality of life and socio-economic factors including health care costs.
2) The natural course of the disease should be well known and the disease should go through an
initial latent stage or be determined by risk factors, which can be detected by appropriate tests.
3) A suitable test is highly sensitive and specific for the disease as well as being acceptable to the
person screened.
4) Screening followed by diagnosis and interventions in an early stage of the disease should
provide a better prognosis than intervention after spontaneously sought treatment.
5) Adequate treatment or other intervention possibilities are indispensable. Adequacy is
determined both by proven medical effect and ethical and legal acceptability.
6) The cost of case-finding should be economically balanced in relation to possible expenditure
on medical care as a whole.
7) Case-finding should be a continuing process and the interval of testing should be known.

CHAPTER 3: General discussion and conclusions
124
3.4.1 ‘The disease should be an obvious burden for the individual and the community in
terms of death, poor quality of life and socio-economic factors including health care costs’.
Although this condition seems to be fulfilled for ESRD (31-33), the incidence of ESRD might be
too low to justify a population screening for albuminuria. In the PREVEND study (n= 40,854)
only 13 subjects reached ESRD while 568 subjects experienced a CVD event in a follow-up
period of 7 years (34). The burden of disease for the community can be measured by disability
adjusted life year (DALY). DALYs are the sum of years of life lost due to premature death and
years lived with disability (prevalence of a disease sequel multiplied by the disability weight for
that sequel), compared to the standard life expectancy in full health (35). In the developed
countries, the major part of the DALYs in the general population is lost by cardiovascular
diseases whereas a negligible part is lost by ESRD (36). Conceivably, population-based screening
for albuminuria is only useful if CVD would be detected early and prevented.

CHAPTER 3: General discussion and conclusions
125
3.4.2 ‘The natural course of disease should be well-known and the disease should go through
an initial latent stage or be determined by risk factors, which can be detected by appropriate
tests’.
The precursor stage of diabetic kidney disease is detected by a sustained presence of
microalbuminuria, a long preclinical phase before the development of overt nephropathy (37, 38).
Consequently, one third of the diabetic patients have microalbuminuria (39). Prospective long
term studies observed that 40-60% of the diabetic patients with microalbuminuria regressed to
lower level of albuminuria spontaneously, or by improvement of glycaemia and blood pressure
control, while only 20-30% of microalbuminuric diabetic patients progressed to a higher level of
albuminuria (40-42). A major concern of using microalbuminuria as an early indicator for
nephropathy is that this potentially causal relation is confounded by hematuria, age, gender,
essential hypertension, hyperglycemia, obesity, inflammation, atherosclerosis and drugs (43-46).
The presence of microalbuminuria is also frequently found in hypertensive subjects, even in the
absence of diabetes (39). The prevalence of microalbuminuria was 16% in our Belgian
hypertensive cohort (ERICABEL). Large epidemiological studies in general and high risk
populations showed that microalbuminuria was independently associated with an increased
likelihood of renal events and mortality (47, 48). However, it seems unlikely that
microalbuminuria is part of the causal pathway for overt nephropathy in non-diabetic subjects, as
the presence of microalbuminuria might be rather a sign of systemic endothelial dysfunction or
underlying systemic disease (atherosclerosis, cancer, CVD...) than a (first) manifestation of
kidney disease (49). The positive predictive value of microalbuminuria to find a subject with a
primary kidney disease will be low as primary kidney diseases are rare. Moreover, in patients
with a primary kidney disease the occurrence of microalbuminuria will progress rapidly to
macroalbuminuria whereas diabetic patients with microalbuminuria slowly progress to
macroalbuminuria. Additionally, the causes of renal failure in RRT patients differ widely:
diabetes (18.3%), glomerulosclerosis (17.8%), polycystic kidney disease (9.6%), pyelonephritis
(7.6%), renovascular disease (7.6%), hypertension (6.8%), miscellaneous (23%) and unknown
(9%) in Belgium (50). Thus, unselected screening for microalbuminuria does not fulfill the
second request, as the natural course of diabetic microalbuminuria could not extrapolated to
other kidney diseases, where the initial latent stage is too short or absent.

CHAPTER 3: General discussion and conclusions
126
3.4.3 ‘A suitable test is highly sensitive and specific for the disease as well as being
acceptable to the person screened’.
Subjects with microalbuminuria have approximately a twofold relative risk for CVD or ESRD,
but the absolute risk is 40 fold higher for CVD than for ESRD (34, 51, 52). According to the
literature, the diagnostic performance of microalbuminuria to predict RRT is not satisfied,
especially the positive predictive value is too low (0.8%) (1). According to the results of the
PREVEND study, subjects with microalbuminuria in absence of cardiovascular risk factors had a
normal decline of renal function over time whereas subjects with macroalbuminuria had a rapid
decline of renal function (1). Collecting urine samples to measure albuminuria is clinically
acceptable for the general population (1, 53). However, a person with a positive test result should
be screened for a second time to confirm the diagnosis of microalbuminuria, whereas in subjects
with macroalbuminuria a second urine sample is not necessary as fluctuations in this range of
albuminuria are less prominent. Thus, screening for macroalbuminuria is more appropriate than
screening for microalbuminuria to predict ESRD.

CHAPTER 3: General discussion and conclusions
127
3.4.4 ‘Screening followed by diagnosis and interventions in an early stage of the disease
should provide a better prognosis than intervention after spontaneously sought treatment’.
There is no robust evidence to suggest that interventions that directly target microalbuminuria
result in a reduction of ESRD and CVD (14, 54). A randomized controlled trial (PREVEND-IT)
showed that detecting subjects with microalbuminuria in the general population, followed by the
initiation of an ACE-I vs. placebo was associated with a reduction in baseline albuminuria but
this was not translated in a significant reduction of renal and cardiovascular events (55). In
contrast, trials in patients with diabetes and/or hypertension who were treated with ACE-I vs.
placebo notably showed a reduction of albuminuria, and a decrease of cardiovascular events and
mortality (42, 56-62), although these trials are confounded by a reduction of blood pressure.
Only in post hoc analyses, a reduction in baseline albuminuria has been associated to a reduction
in cardiovascular morbidity and mortality, independent of blood pressure (63-66). In addition ,
reducing albuminuria is not always associated with improvement of clinical outcome. The
ONTARGET trial showed that ARB + ACE-I vs. ACE-I or ARB reduce blood pressure and
albuminuria but not the clinical outcome in patients with cardiovascular risk factors (67). The
ROADMAP trial showed that an ARB on top of antihypertensive medication in 4,447 diabetes
patients reduced blood pressure and albuminuria, but was associated with a higher cardiovascular
mortality (15 vs. 3 patients, p = 0.01) (60). No evidence exists that protective treatment in
patients with microalbuminuria avoids new cases of ESRD whereas ACE-I or ARB in patients
with macroalbuminuria showed a 25% reduction of ESRD (68-75). All these data suggest that
mainly screening for macroalbuminuria (and not microalbuminuria) followed by treatment could
be effective to reduce ESRD.

CHAPTER 3: General discussion and conclusions
128
3.4.5 ‘Adequate treatment or other intervention possibilities are indispensable. Adequacy is
determined both by proven medical effect and ethical and legal acceptability’.
Despite the use of ACE-I or ARB, some patients might develop macroalbuminuria and/or CKD
stage 4 or 5. These patients should be timely referred to renal care to delay the progress to ESRD
and to detect and manage associated conditions, such as anemia, hypertension, dyslipidaemia,
hyperkaliemia, hyperphophatemia, bone mineral disorders, cardiovascular disease and mental
health disturbances. The availability of renal care (including RRT) depends on macro-economic
parameters, such as gross domestic product (GDP) per capita, the percentage of GDP spent on
health care and dialysis reimbursement (76). In countries spending less on health care the need
for renal care is not being met, whereas in countries spending more on health care the need for
renal care is being created by patients who survive long enough to develop ESRD (76).
Paradoxically, a rise of RRT patients is expected by introducing interventions that reduce
cardiovascular mortality (77). Each 1-year increase in life expectancy at 60 years is associated
with a 12% increase in RRT incidence (76). In Belgium, half of the patients who start with RRT
is older than 75 (50). In the elderly population, the life expectancy is quite limited after the
initiation of RRT, many experience loss of functional status and independence, much of the time
gained will be spent in a health care setting, and one third of these elderly discontinue
maintenance dialysis prior to death (78). This shows that chronic dialysis should not be proposed
to patients with a short life expectancy as a necessity but as a choice, and that conservative
(nondialytic) care is a legimate option. In clinical practice, initiation and maintenance of chronic
dialysis is encouraged in patients even when the treatment burden outweights the medical and
psychosocial benefits (79). The most important reason for this malpractice is that many
nephrologists do not feel comfortable talking with patients about end-of-life treatment
preferences (78). The real challenge in nephrology with regards to the ageing problem is to force
back the increasing incidence of RRT in adults above the age of 75. We need more therapeutic
options and/or better guidelines to delay RRT in CKD patients, particularly in elderly.

CHAPTER 3: General discussion and conclusions
129
3.4.6 ‘The cost of case-finding should be economically balanced in relation to possible
expenditure on medical care as a whole’.
Screening followed by diagnosis and intervention at an early reversible stage of disease should be
cost-effective, which means that screening plus intervention should result in a more positive
socioeconomic balance than not screening and following the traditional approach. The costs of
screening contain not only the expenditure for the screening test, but also those of treating
because of false positive screening results and not treating because of false negatives (80). False
positive screening tests lead to increased medical visits with further tests, increased health care
costs and unnecessary treatment with in some cases adverse effects that further increase cost (80).
False negative test results provide false reassurance about the absence of disease and possibly
longer waiting before installing appropriate treatment which again may increase costs. Even, a
“truly positive test” has a psychological cost for the patient that comes from being labeled earlier
in the natural history of the process than would have occurred without screening (80). According
to the literature, screening for albuminuria (microalbuminuria and macroalbuminuria) in the
general population is not cost-effective, unless selectively directed toward high risk groups or
conducted at a ten-year interval (81-83). In addition, the beneficial effect of screening is to large
extent based on a delay in onset of ESRD or death. This delay is clearly illustrated in a modeling
analysis in patients with diabetes and hypertension that showed an increase of ESRD-free
survival from 10.8 to 11.2 years per patient (5 months) and a life expectancy from 10.7 to 11.0
years per patient (4 months) by screening for albuminuria (microalbuminuria and
macroalbuminuria) followed by optimized treatment versus no screening (84). However, these
modeling studies need to be confirmed in an RCT, whereby the outcome of subjects who are
invited for albuminuria screening should be compared to subjects who are not screened. In
addition, an RCT obviates a potentially prognostic selection bias that occurs in a population-
based screening program as volunteers are more likely to improve their health than those who
refuse to be screened (80). However, an RCT to jusitify screening might fail by contamination.
Contamination is the effect of opportunistic case-finding that commonly occurs in those who
were randomized not to be screened (the control group). The latter effect was one of the main
reasons why screening programs for diabetes and prostate cancer have failed (85-90). We suggest
that an RCT to justify screening for CKD might fail as well, as nowadays more and more patients
are already treated with ACE-I or ARB, irrespective of the presence of microalbuminuria.

CHAPTER 3: General discussion and conclusions
130
3.4.7 ‘Case-finding should be a continuing process and the interval of testing should be
known’.
A benchmark of US$50,000/QALY is often used for judging the cost-effectiveness of
interventions (91). Figure 1 shows that only in diabetic patients annual screening vs. no screening
is cost-effective. Decreasing the frequency of screening for microalbuminuria in patients with
diabetes or hypertension has little impact on QALYs or ESRD incidence while simultaneously
reducing the costs (82). As the lowest cost-effectiveness ratios were achieved when screening
was started in persons between 50 and 60 years old (figure 1), it was hypothesized that screening
for albuminuria (microalbuminuria and macroalbuminuria) beginning at the age of 50 years with
an interval of 2 years, was cost-effective in hypertensive patients (82). Screening for albuminuria
in subjects with neither diabetes nor hypertension is supposed to be cost-effective if it is started at
the age of 50 years only with an interval of 10 years (81, 82). By using such long interval for
testing albuminuria, patients with rapidly progressive kidney disease (such as glomerulonephritis)
would be hard to identify while subjects with slow disease progression (such as diabetes) would
be detected more frequently (length-bias sampling).

CHAPTER 3: General discussion and conclusions
131
Figure 1. Cost-effectiveness of universal annual albuminuria screening beginning at different
ages relative to no screening for the full population and subgroups with diabetes or hypertension,
adapted from (82).
Whether population screening for microalbuminuria to detect and treat new cases of
hypertension, diabetes and CVD might improve outcome is uncertain.

CHAPTER 3: General discussion and conclusions
132
3.5 Conclusions
This thesis explores the pitfalls of screening for microalbuminuria to detect persons with
cardiovascular and renal risk in an apparently healthy working (URI) and in a hypertensive
(ERICABEL) cohort.
A conducted microalbuminuria screening to detect subjects with cardiovascular and renal risk in
the URI population was not effective for two reasons. Firstly, only a small proportion (9%) of the
unrecognized cardiovascular risk factors was detected. When traditional cardiovascular risk
factors are taken into account to select candidates for screening, more subjects (36%) were
detected with possibilities to improve cardiovascular and renal outcome than was the case from a
population-based screening for microalbuminuria. Second, as the causes of microalbuminuria are
widely divergent, not all subjects with microalbuminuria had at least one cardiovascular risk
factor. In addition, the underlying condition of microalbuminuria determines the clinical outcome.
This is confirmed in the literature; subjects with orthostatic microalbuminuria have an excellent
prognosis, whereas diabetic patients with microalbuminuria have a high risk for overt
nephropathy (92, 93). In the cross-sectional URI study, healthy young workers with
microalbuminuria had a low BMI, suggesting orthostatic proteinuria. The presence of
microalbuminuria was also associated in workers with physicochemical exposure risk. A
longitudinal study is necessary to investigate the prognostic value of microalbuminuria in
workers with physicochemical exposure risk. Furthermore, a longitudinal study is lacking that
observes the outcomes in microalbuminuric subjects with different underlying conditions.
Conceivably, interventions in persons with microalbuminuria in absence of cardiovascular risk
factors engender medical frustration, unnecessary anxiety, harm, worries and lead to excess of
costs, whereas interventions in persons with microalbuminuria in presence of modifiable
cardiovascular risk factors may improve clinical outcome.
Microalbuminuria was associated with low BMI and physicochemical exposure risk in workers
under the age of 40, whereas microalbuminuria was associated with cardiovascular risk factors in
workers above the age of 40. Thus, if a mass screening for microalbuminuria to detect new
cardiovascular or renal risk factors is conducted, it should start above the age of 40. Moreover,
there is no direct evidence that treatment of microalbuminuria reduces cardiovascular disease.

CHAPTER 3: General discussion and conclusions
133
Screening for microalbuminurie might become useful as new therapeutic options become
available to prevent CVD.
According to the literature, the absolute risk to develop ESRD in patients with microalbuminuria
seems to be too low to justify a population-based screening for albuminuria (48).
The predictive value of micro- or macroalbuminuria to develop ESRD increases dramatically by
selecting subjects with an estimated GFR lower than 60 ml/min/1.73m² (94). It was estimated that
1.4% of a population (with an estimated GFR lower than 60 ml/min/1.73m² and micro- or
macroalbuminuria) had an increased risk for ESRD (94). As the prevalence of reduced GFR
increases with age, screening of renal markers to identify those with increased risk for ESRD has
been suggested to be performed in subjects who are older than 55 years (94). However, the URI
population was relatively young and we identified only one subject with microalbuminuria in
presence of an estimated GFR lower than 60 ml/min/1.73m². Thus, screening for
microalbuminuria in a relatively young population might not be useful to identify subjects with
increased risk for ESRD, as almost all subjects had an estimated GFR higher than 60
ml/min/1.73m².
According to the URI study, screening for microalbuminuria is more useful in adults with vs.
without cardiovascular risk factors to detect CKD. Screening for albuminuria in diabetic patients
is considered to be effective as treatment of an ACE-I or ARB reduces the level of albuminuria
and the number of ESRD in those with macroalbuminuria. However, screening is less effective as
more and more patients are already treated with ACE-I or ARB, irrespectively of the presence of
albuminuria (95). In addition, false positive test results might also occur in presence of
cardiovascular risk factors. In the ERICABEL cohort we observed that statin use was associated
with microalbuminuria in hypertensive patients, very likely related to the characteristics of statins
to induce tubular albuminuria by inhibition of albumin reabsorption. The presence of
microalbuminuria in statin users can lead to incorrect labeling of subjects as having an increased
risk for overt nephropathy. We need more prospective studies to investigate the prognostic value
of microalbuminuria in patients who are treated with statins.
The URI study showed that only persistent microalbuminuria is associated with increased
cardiovascular risk. Microalbuminuria should be confirmed in a subsequent urine sample, as a

CHAPTER 3: General discussion and conclusions
134
single measurement could be false positive due to a temporary condition. According to KDIGO,
all subjects with microalbuminuria for longer than 3 months have CKD stage A2. Consequently,
the prevalence of CKD (A2) is overestimated in most cohorts as mostly one single measurement
of microalbuminuria is performed. Moreover, microalbuminuria in half of diabetic patients
disappears according longitudinal studies. We showed that fluctuations of microalbuminuria
commonly occur in persons without cardiovascular risk factors. The fluctuations of
microalbuminuria generate a substantial bias if microalbuminuria is used as a screening tool or as
a surrogate for renal or cardiovascular outcome. In the ERICABEL cohort, the presence of
microalbuminuria fluctuated in hypertensive patients during a follow-up of 5 years. Thus,
doubts could also arise about the diagnostic performance of using microalbuminuria in this
population.
A rapid decline of renal function is more frequently observed in subjects with macroalbuminuria
than in presence of no albuminuria or microalbuminuria (1, 75). Thus, screening for progressive
kidney disease might be more effective by identifying subjects with macoralbuminuria (late or
overt nephropathy) than by identifying subjects with microalbuminuria (early or potential
nephropathy). Currently, no hard evidence exists whether screening for albuminuria is cost-
effective in the general population, even by using a ten-year screening interval. Such mass
screening might not be feasible as a substantial number of subjects may develop overt
nephropathy over a short period of time. Whether a population screening program that measures
albuminuria and estimates GFR (by serum creatinine and/or cystatin C) in subjects who are older
than 55 years could reduce the incidence of ESRD should be studied in a RCT.

CHAPTER 3: General discussion and conclusions
135
3.6 References
1. van der Velde M, Halbesma N, de Charro FT, Bakker SJL, de Zeeuw D, de Jong PE, Gansevoort RT.
Screening for Albuminuria Identifies Individuals at Increased Renal Risk. Journal of the American Society of Nephrology 2009; 20: 852-862. Available at <Go to ISI>://000264831300023.
2. Hillege HL, Janssen WMT, Bak AAA, Diercks GFH, Grobbee DE, Crijns H, van Gilst WH, de Zeeuw
D, de Jong PE, Prevend Study G. Microalbuminuria is common, also in a nondiabetic, nonhypertensive
population, and an independent indicator of cardiovascular risk factors and cardiovascular morbidity.
Journal of Internal Medicine 2001; 249: 519-526. Available at <Go to ISI>://000169568600005.
3. Hillege HL, Fidler V, Diercks GFH, van Gilst WH, de Zeeuw D, van Veldhuisen DJ, Gans ROB,
Janssen WMT, Grobbee DE, de Jong PE, Grp PS. Urinary albumin excretion predicts cardiovascular
and noncardiovascular mortality in general population. Circulation 2002; 106: 1777-1782. Available at
<Go to ISI>://000178385700010.
4. Brantsma AH, Bakker SJ, Hillege HL, de Zeeuw D, de Jong PE, Gansevoort RT. Urinary albumin
excretion and its relation with C-reactive protein and the metabolic syndrome in the prediction of type
2 diabetes. Diabetes Care 2005; 28: 2525-2530. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=16186291.
5. Jorgensen L, Jenssen T, Heuch I, Jacobsen BK. The combined effect of albuminuria and inflammation
on all-cause and cardiovascular mortality in nondiabetic persons. J Intern Med 2008; 264: 493-501.
Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=18624904.
6. Pedrinelli R, Dell'Omo G, Di Bello V, Pellegrini G, Pucci L, Del Prato S, Penno G. Low-grade
inflammation and microalbuminuria in hypertension. Arteriosclerosis, thrombosis, and vascular biology 2004; 24: 2414-2419. Available at http://www.ncbi.nlm.nih.gov/pubmed/15486313.
7. Scheven L, Van der Velde M, Lambers Heerspink HJ, De Jong PE, Gansevoort RT. Isolated
microalbuminuria indicates a poor medical prognosis. Nephrol Dial Transplant 2013; 28: 1794-1801.
Available at http://www.ncbi.nlm.nih.gov/pubmed/23493327.
8. Jensen JS, Borchjohnsen K, Jensen G, Feldtrasmussen B. Atherosclerotic Risk-Factors Are Increased
in Clinically Healthy-Subjects with Microalbuminuria. Atherosclerosis 1995; 112: 245-252. Available
at <Go to ISI>://A1995QH02000011.
9. Metcalf PA, Scragg RK, Dryson E. Associations between body morphology and microalbuminuria in
healthy middle-aged European, Maori and Pacific Island New Zealanders. Int J Obes Relat Metab
Disord 1997; 21: 203-210. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=9080259.
10. Klausen KP, Parving HH, Scharling H, Jensen JS. The association between metabolic syndrome,
microalbuminuria and impaired renal function in the general population: impact on cardiovascular
disease and mortality. Journal of Internal Medicine 2007; 262: 470-478. Available at <Go to
ISI>://000249947500010.
11. Brantsma AH, Bakker SJ, de Zeeuw D, de Jong PE, Gansevoort RT. Urinary albumin excretion as a
predictor of the development of hypertension in the general population. J Am Soc Nephrol 2006; 17:
331-335. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=16434504.
12. Ozyilmaz A, Bakker SJ, de Zeeuw D, de Jong PE, Gansevoort RT. Selection on albuminuria enhances
the efficacy of screening for cardiovascular risk factors. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association 2010;
25: 3560-3568. Available at http://www.ncbi.nlm.nih.gov/pubmed/20702530.
13. Boersma C, Postma MJ, Visser ST, Atthobari J, de Jong PE, de Jong-van den Berg LT, Gansevoort RT, Group PS. Baseline albuminuria predicts the efficacy of blood pressure-lowering drugs in preventing
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=9080259
CHAPTER 3: General discussion and conclusions
136
cardiovascular events. Br J Clin Pharmacol 2008; 65: 723-732. Available at
http://www.ncbi.nlm.nih.gov/pubmed/18241288.
14. Weir MR, Bakris GL. Should Microalbuminuria Ever Be Considered as a Renal Endpoint in Any
Clinical Trial? American Journal of Nephrology 2010; 31: 469-470. Available at <Go to
ISI>://000277757300014.
15. Witte EC, Lambers Heerspink HJ, de Zeeuw D, Bakker SJ, de Jong PE, Gansevoort R. First morning
voids are more reliable than spot urine samples to assess microalbuminuria. J Am Soc Nephrol 2009;
20: 436-443. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=19092125.
16. Warram JH, Gearin G, Laffel L, Krolewski AS. Effect of duration of type I diabetes on the prevalence
of stages of diabetic nephropathy defined by urinary albumin/creatinine ratio. Journal of the American
Society of Nephrology 1996; 7: 930-937. Available at <Go to ISI>://A1996UT21600017.
17. Gansevoort RT, Verhave JC, Hillege HL, Burgerhof JGM, Bakker SJL, de Zeeuw D, de Jong PE, Grp
PS. The validity of screening based on spot morning urine samples to detect subjects with
microalbuminuria in the general population. Kidney International 2005; 67: S28-S35. Available at <Go
to ISI>://WOS:000227251000007.
18. Romundstad S, Holmen J, Kvenild K, Hallan H, Ellekjaer H. Microalbuminuria and all-cause mortality
in 2,089 apparently healthy individuals: A 4.4-year follow-up study. The Nord-Trondelag Health Study
(HUNT), Norway. American Journal of Kidney Diseases 2003; 42: 466-473. Available at <Go to
ISI>://000185518500004.
19. Miller WG, Bruns DE, Hortin GL, Sandberg S, Aakre KM, McQueen MJ, Itoh Y, Lieske JC,
Seccombe DW, Jones G, Bunk DM, Curhan GC, Narva AS, Urine NKDEP-IWGSA. Current Issues in
Measurement and Reporting of Urinary Albumin Excretion. Clinical Chemistry 2009; 55: 24-38.
Available at <Go to ISI>://WOS:000262303900008.
20. Robinson RR, Coggins CH, Shapiro K, Cohen JJ, Harrington JT, Kassirer JP. Isolated Proteinuria in
Asymptomatic Patients. Kidney International 1980; 18: 395-406. Available at <Go to
ISI>://WOS:A1980KK18700014.
21. Rytand DA, Spreiter S. Prognosis in postural (orthostatic) proteinuria: forty to fifty-year follow-up of
six patients after diagnosis by Thomas Addis. N Engl J Med 1981; 305: 618-621. Available at
http://www.ncbi.nlm.nih.gov/pubmed/7266586.
22. Roels HA, Hoet P, Lison D. Usefulness of biomarkers of exposure to inorganic mercury, lead, or
cadmium in controlling occupational and environmental risks of nephrotoxicity. Ren Fail 1999; 21:
251-262. Available at http://www.ncbi.nlm.nih.gov/pubmed/10416202.
23. Bernard A, Lauwerys RR. Proteinuria: changes and mechanisms in toxic nephropathies. Critical
reviews in toxicology 1991; 21: 373-405. Available at http://www.ncbi.nlm.nih.gov/pubmed/1741950.
24. Vacca CV, Hines JD, Hall PW, 3rd. The proteinuria of industrial lead intoxication. Environ Res 1986;
41: 440-446. Available at http://www.ncbi.nlm.nih.gov/pubmed/3780642.
25. Deslypere JP, Delanghe J, Vermeulen A. Proteinuria as Complication of Simvastatin Treatment.
Lancet 1990; 336: 1453-1453. Available at <Go to ISI>://A1990EL85100061.
26. Kostapanos MS, Milionis HJ, Saougos VG, Lagos KG, Christine K, Bairaktari ET, Elisaf MS. Dose-
dependent effect of rosuvastatin treatment on urinary protein excretion. J Cardiovasc Pharmacol Ther
2007; 12: 292-297. Available at <Go to ISI>://000251110600003.
27. Wehlou CMJ, Speeckaert MM, Fiers T, De Buyzere ML, Delanghe JR. alpha(1)-
Microglobulin/albumin ratio may improve interpretation of albuminuria in statin-treated patients.
Clinical Chemistry and Laboratory Medicine 2013; 51: 1529-1534. Available at <Go to
ISI>://WOS:000321104900031.
28. Levey AS, Atkins R, Coresh J, Cohen EP, Collins AJ, Eckardt KU, Nahas ME, Jaber BL, Jadoul M,
Levin A, Powe NR, Rossert J, Wheeler DC, Lameire N, Eknoyan G. Chronic kidney disease as a
global public health problem: Approaches and initiatives - a position statement from Kidney Disease
Improving Global Outcomes. Kidney International 2007; 72: 247-259. Available at <Go to
ISI>://000248394300007.

CHAPTER 3: General discussion and conclusions
137
29. Wilson JMG, Jungner G. principles and practice of screening for disease. public health papers, Geneva,
World Health Organization 1968; 34: . Available at http://whqlibdoc.who.int/php/WHO_PHP_34.pdf.
30. Council of Europe. Recommendation no R(94))11 on screening as a tool of preventive medicine. 1994.
Available at
https://wcd.coe.int/com.instranet.InstraServlet?command=com.instranet.CmdBlobGet&InstranetImage
=534532&SecMode=1&DocId=514336&Usage=2.
31. de Jong PE, Curhan GC. Screening, monitoring, and treatment of albuminuria: Public health
perspectives. J Am Soc Nephrol 2006; 17: 2120-2126. Available at
http://www.ncbi.nlm.nih.gov/pubmed/16825331.
32. Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, de Jong PE, Coresh J,
Gansevoort RT. Association of estimated glomerular filtration rate and albuminuria with all-cause and
cardiovascular mortality in general population cohorts: a collaborative meta-analysis. Lancet 2010; 375:
2073-2081. Available at http://www.ncbi.nlm.nih.gov/pubmed/20483451.
33. Mahmoodi BK, Matsushita K, Woodward M, Blankestijn PJ, Cirillo M, Ohkubo T, Rossing P, Sarnak
MJ, Stengel B, Yamagishi K, Yamashita K, Zhang L, Coresh J, de Jong PE, Astor BC, Chronic Kidney
Disease Prognosis C. Associations of kidney disease measures with mortality and end-stage renal
disease in individuals with and without hypertension: a meta-analysis. Lancet 2012; 380: 1649-1661.
Available at http://www.ncbi.nlm.nih.gov/pubmed/23013600.
34. de Jong PE, van der Velde M, Gansevoort RT, Zoccali C. Screening for chronic kidney disease: Where
does Europe go? Clinical Journal of the American Society of Nephrology 2008; 3: 616-623. Available
at <Go to ISI>://000253709800041.
35. Collaborators USBoD. The state of US health, 1990-2010: burden of diseases, injuries, and risk factors.
JAMA 2013; 310: 591-608. Available at http://www.ncbi.nlm.nih.gov/pubmed/23842577.
36. Murray CJ, Richards MA, Newton JN, Fenton KA, Anderson HR, Atkinson C, Bennett D, Bernabe E,
Blencowe H, Bourne R, Braithwaite T, Brayne C, Bruce NG, Brugha TS, Burney P, Dherani M, Dolk
H, Edmond K, Ezzati M, Flaxman AD, Fleming TD, Freedman G, Gunnell D, Hay RJ, Hutchings SJ,
Ohno SL, Lozano R, Lyons RA, Marcenes W, Naghavi M, Newton CR, Pearce N, Pope D, Rushton L,
Salomon JA, Shibuya K, Vos T, Wang H, Williams HC, Woolf AD, Lopez AD, Davis A. UK health
performance: findings of the Global Burden of Disease Study 2010. Lancet 2013; 381: 997-1020.
Available at http://www.ncbi.nlm.nih.gov/pubmed/23668584.
37. Jerums G, Premaratne E, Panagiotopoulos S, MacIsaac RJ. The clinical significance of hyperfiltration
in diabetes. Diabetologia 2010; 53: 2093-2104. Available at
http://www.ncbi.nlm.nih.gov/pubmed/20496053.
38. Mogensen CE. Prediction of clinical diabetic nephropathy in IDDM patients. Alternatives to
microalbuminuria? Diabetes 1990; 39: 761-767. Available at
http://www.ncbi.nlm.nih.gov/pubmed/2191882.
39. Jones CA, Francis ME, Eberhardt MS, Chavers B, Coresh J, Engelgau M, Kusek JW, Byrd-Holt D,
Narayan KM, Herman WH, Jones CP, Salive M, Agodoa LY. Microalbuminuria in the US population:
third National Health and Nutrition Examination Survey. Am J Kidney Dis 2002; 39: 445-459.
Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=11877563.
40. Perkins BA, Ficociello LH, Silva KH, Finkelstein DM, Warram JH, Krolewski AS. Regression of
microalbuminuria in type 1 diabetes. The New England Journal of Medicine 2003; 348: 2285-2293.
Available at http://www.ncbi.nlm.nih.gov/pubmed/12788992.
41. Hovind P, Tarnow L, Rossing P, Jensen BR, Graae M, Torp I, Binder C, Parving HH. Predictors for
the development of microalbuminuria and macroalbuminuria in patients with type 1 diabetes: inception
cohort study. Bmj 2004; 328: 1105. Available at http://www.ncbi.nlm.nih.gov/pubmed/15096438.
42. de Boer IH, Rue TC, Cleary PA, Lachin JM, Molitch ME, Steffes MW, Sun W, Zinman B, Brunzell
JD, Diabetes C, Complications Trial/Epidemiology of Diabetes I, Complications Study Research G,
White NH, Danis RP, Davis MD, Hainsworth D, Hubbard LD, Nathan DM. Long-term renal outcomes
of patients with type 1 diabetes mellitus and microalbuminuria: an analysis of the Diabetes Control and

CHAPTER 3: General discussion and conclusions
138
Complications Trial/Epidemiology of Diabetes Interventions and Complications cohort. Arch Intern
Med 2011; 171: 412-420. Available at http://www.ncbi.nlm.nih.gov/pubmed/21403038.
43. Glassock RJ. Is the Presence of Microalbuminuria a Relevant Marker of Kidney Disease? Curr Hypertens Rep 2010; 12: 364-368. Available at <Go to ISI>://WOS:000283145900009.
44. Hallan SI, Orth SR. The conundrum of chronic kidney disease classification and end-stage renal risk
prediction in the elderly--what is the right approach? Nephron Clin Pract 2010; 116: c307-316.
Available at http://www.ncbi.nlm.nih.gov/pubmed/20664285.
45. Mogensen CE, Vestbo E, Poulsen PL, Christiansen C, Damsgaard EM, Eiskjaer H, Froland A, Hansen
KW, Nielsen S, Pedersen MM. Microalbuminuria and Potential Confounders - a Review and Some
Observations on Variability of Urinary Albumin Excretion. Diabetes Care 1995; 18: 572-581.
Available at <Go to ISI>://A1995QQ21600025.
46. Mogensen CE. Microalbuminuria and hypertension with focus on type 1 and type 2 diabetes. Journal
of Internal Medicine 2003; 254: 45-66. Available at <Go to ISI>://000183583600006.
47. Gansevoort RT, Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, de Jong PE,
Coresh J, Chronic Kidney Disease Prognosis C. Lower estimated GFR and higher albuminuria are
associated with adverse kidney outcomes. A collaborative meta-analysis of general and high-risk
population cohorts. Kidney Int 2011; 80: 93-104. Available at
http://www.ncbi.nlm.nih.gov/pubmed/21289597.
48. van der Velde M, Matsushita K, Coresh J, Astor BC, Woodward M, Levey A, de Jong P, Gansevoort
RT, Chronic Kidney Disease Prognosis C, van der Velde M, Matsushita K, Coresh J, Astor BC,
Woodward M, Levey AS, de Jong PE, Gansevoort RT, Levey A, El-Nahas M, Eckardt KU, Kasiske
BL, Ninomiya T, Chalmers J, Macmahon S, Tonelli M, Hemmelgarn B, Sacks F, Curhan G, Collins AJ,
Li S, Chen SC, Hawaii Cohort KP, Lee BJ, Ishani A, Neaton J, Svendsen K, Mann JF, Yusuf S, Teo
KK, Gao P, Nelson RG, Knowler WC, Bilo HJ, Joosten H, Kleefstra N, Groenier KH, Auguste P,
Veldhuis K, Wang Y, Camarata L, Thomas B, Manley T. Lower estimated glomerular filtration rate
and higher albuminuria are associated with all-cause and cardiovascular mortality. A collaborative
meta-analysis of high-risk population cohorts. Kidney Int 2011; 79: 1341-1352. Available at
http://www.ncbi.nlm.nih.gov/pubmed/21307840.
49. Weir MR. Microalbuminuria and cardiovascular disease. Clin J Am Soc Nephrol 2007; 2: 581-590.
Available at http://www.ncbi.nlm.nih.gov/pubmed/17699466.
50. ERA-EDTA Registry: ERA-EDTA Registry 2011 Annual report. Academic Medical Center,
Amsterdam, the Netherlands, june 2011. Available at http://www.era-edta-
reg.org/files/annualreports/pdf/AnnRep2011.pdf.
51. Hui X, Matsushita K, Sang Y, Ballew SH, Fulop T, Coresh J. CKD and cardiovascular disease in the
Atherosclerosis Risk in Communities (ARIC) study: interactions with age, sex, and race. Am J Kidney
Dis 2013; 62: 691-702. Available at http://www.ncbi.nlm.nih.gov/pubmed/23769137.
52. Hallan SI, Matsushita K, Sang Y, Mahmoodi BK, Black C, Ishani A, Kleefstra N, Naimark D,
Roderick P, Tonelli M, Wetzels JF, Astor BC, Gansevoort RT, Levin A, Wen CP, Coresh J, Chronic
Kidney Disease Prognosis C. Age and association of kidney measures with mortality and end-stage
renal disease. JAMA 2012; 308: 2349-2360. Available at
http://www.ncbi.nlm.nih.gov/pubmed/23111824.
53. de Jong PE, Hillege HL, Pinto-Sietsma SJ, de Zeeuw D. Screening for microalbuminuria in the general
population: a tool to detect subjects at risk for progressive renal failure in an early phase? Nephrology
Dialysis Transplantation 2003; 18: 10-13. Available at <Go to ISI>://000180293800002.
54. Karalliedde J, Viberti G. Proteinuria in diabetes: bystander or pathway to cardiorenal disease? J Am Soc Nephrol 2010; 21: 2020-2027. Available at http://www.ncbi.nlm.nih.gov/pubmed/21051738.
55. Asselbergs FW, Diercks GF, Hillege HL, van Boven AJ, Janssen WM, Voors AA, de Zeeuw D, de
Jong PE, van Veldhuisen DJ, van Gilst WH. Effects of fosinopril and pravastatin on cardiovascular
events in subjects with microalbuminuria. Circulation 2004; 110: 2809-2816. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=15492322.

CHAPTER 3: General discussion and conclusions
139
56. Gaede P, Vedel P, Larsen N, Jensen GVH, Parving H, Pedersen O. Multifactorial intervention and
cardiovascular disease in patients with type 2 diabetes. New Engl J Med 2003; 348: 383-393. Available
at <Go to ISI>://WOS:000180643800003.
57. Group AS, Cushman WC, Evans GW, Byington RP, Goff DC, Jr., Grimm RH, Jr., Cutler JA, Simons-
Morton DG, Basile JN, Corson MA, Probstfield JL, Katz L, Peterson KA, Friedewald WT, Buse JB,
Bigger JT, Gerstein HC, Ismail-Beigi F. Effects of intensive blood-pressure control in type 2 diabetes
mellitus. N Engl J Med 2010; 362: 1575-1585. Available at
http://www.ncbi.nlm.nih.gov/pubmed/20228401.
58. Patel A, MacMahon S, Chalmers J, Neal B, Woodward M, Billot L, Harrap S, Poulter N, Marre M,
Cooper M, Glasziou P, Grobbee DE, Hamet P, Heller S, Liu LS, Mancia G, Mogensen CE, Pan CY,
Rodgers A, Williams B. Effects of a fixed combination of perindopril and indapamide on
macrovascular and microvascular outcomes in patients with type 2 diabetes mellitus (the ADVANCE
trial): a randomised controlled trial. Lancet 2007; 370: 829-840. Available at <Go to
ISI>://000249733300028.
59. Gaede P, Vedel P, Parving HH, Pedersen O. Intensified multifactorial intervention in patients with type
2 diabetes mellitus and microalbuminuria: the Steno type 2 randomised study. Lancet 1999; 353: 617-
622. Available at http://www.ncbi.nlm.nih.gov/pubmed/10030326.
60. Haller H, Ito S, Izzo JL, Jr., Januszewicz A, Katayama S, Menne J, Mimran A, Rabelink TJ, Ritz E,
Ruilope LM, Rump LC, Viberti G, Investigators RT. Olmesartan for the delay or prevention of
microalbuminuria in type 2 diabetes. N Engl J Med 2011; 364: 907-917. Available at
http://www.ncbi.nlm.nih.gov/pubmed/21388309.
61. de Galan BE, Perkovic V, Ninomiya T, Pillai A, Patel A, Cass A, Neal B, Poulter N, Harrap S,
Mogensen CE, Cooper M, Marre M, Williams B, Hamet P, Mancia G, Woodward M, Glasziou P,
Grobbee DE, MacMahon S, Chalmers J, Group AC. Lowering blood pressure reduces renal events in
type 2 diabetes. Journal of the American Society of Nephrology 2009; 20: 883-892. Available at
http://www.ncbi.nlm.nih.gov/pubmed/19225038.
62. Effects of ramipril on cardiovascular and microvascular outcomes in people with diabetes mellitus:
results of the HOPE study and MICRO-HOPE substudy. Heart Outcomes Prevention Evaluation Study
Investigators. Lancet 2000; 355: 253-259. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=10675071.
63. Schmieder RE, Mann JF, Schumacher H, Gao P, Mancia G, Weber MA, McQueen M, Koon T, Yusuf
S, Investigators O. Changes in albuminuria predict mortality and morbidity in patients with vascular
disease. J Am Soc Nephrol 2011; 22: 1353-1364. Available at
http://www.ncbi.nlm.nih.gov/pubmed/21719791.
64. Ibsen H, Olsen MH, Wachtell K, Borch-Johnsen K, Lindholm LH, Mogensen CE, Dahlof B, Devereux
RB, de Faire U, Fyhrquist F, Julius S, Kjeldsen SE, Lederballe-Pedersen O, Nieminen MS, Omvik P,
Oparil S, Wan Y. Reduction in albuminuria translates to reduction in cardiovascular events in
hypertensive patients: losartan intervention for endpoint reduction in hypertension study. Hypertension
2005; 45: 198-202. Available at http://www.ncbi.nlm.nih.gov/pubmed/15655123.
65. Estacio RO, Dale RA, Schrier R, Krantz MJ. Relation of reduction in urinary albumin excretion to ten-
year cardiovascular mortality in patients with type 2 diabetes and systemic hypertension. Am J Cardiol 2012; 109: 1743-1748. Available at http://www.ncbi.nlm.nih.gov/pubmed/22440125.
66. Schrader J, Luders S, Kulschewski A, Hammersen F, Zuchner C, Venneklaas U, Schrandt G,
Schnieders M, Rangoonwala B, Berger J, Dominiak P, Zidek W, Group MS. Microalbuminuria and
tubular proteinuria as risk predictors of cardiovascular morbidity and mortality in essential
hypertension: final results of a prospective long-term study (MARPLE Study)*. J Hypertens 2006; 24:
541-548. Available at http://www.ncbi.nlm.nih.gov/pubmed/16467658.
67. Yusuf S, Teo KK, Pogue J, Dyal L, Copland I, Schumacher H, Ingelheim B, Dagenais G, Sleight P,
Anderson C, Investigators O. Telmisartan, ramipril, or both in patients at high risk for vascular events.
New Engl J Med 2008; 358: 1547-1559. Available at <Go to ISI>://WOS:000254783300004.
68. Jafar TH, Schmid CH, Landa M, Giatras I, Toto R, Remuzzi G, Maschio G, Brenner BM, Kamper A,
Zucchelli P, Becker G, Himmelmann A, Bannister K, Landais P, Shahinfar S, de Jong PE, de Zeeuw D,

CHAPTER 3: General discussion and conclusions
140
Lau J, Levey AS. Angiotensin-converting enzyme inhibitors and progression of nondiabetic renal
disease. A meta-analysis of patient-level data. Ann Intern Med 2001; 135: 73-87. Available at
http://www.ncbi.nlm.nih.gov/pubmed/11453706.
69. Randomised placebo-controlled trial of effect of ramipril on decline in glomerular filtration rate and
risk of terminal renal failure in proteinuric, non-diabetic nephropathy. The GISEN Group (Gruppo
Italiano di Studi Epidemiologici in Nefrologia). Lancet 1997; 349: 1857-1863. Available at
http://www.ncbi.nlm.nih.gov/pubmed/9217756.
70. Jerums G, Panagiotopoulos S, Premaratne E, Power DA, Maclsaac RJ. Lowering of proteinuria in
response to antihypertensive therapy predicts improved renal function in late but not in early diabetic
nephropathy: A pooled analysis. American Journal of Nephrology 2008; 28: 614-627. Available at
<Go to ISI>://000255896200011.
71. Brenner BM, Cooper ME, de Zeeuw D, Keane WF, Mitch WE, Parving HH, Remuzzi G, Snapinn SM,
Zhang Z, Shahinfar S, Investigators RS. Effects of losartan on renal and cardiovascular outcomes in
patients with type 2 diabetes and nephropathy. N Engl J Med 2001; 345: 861-869. Available at
http://www.ncbi.nlm.nih.gov/pubmed/11565518.
72. Lewis EJ, Hunsicker LG, Bain RP, Rohde RD. The effect of angiotensin-converting-enzyme inhibition
on diabetic nephropathy. The Collaborative Study Group. N Engl J Med 1993; 329: 1456-1462.
Available at http://www.ncbi.nlm.nih.gov/pubmed/8413456.
73. Lewis EJ, Hunsicker LG, Clarke WR, Berl T, Pohl MA, Lewis JB, Ritz E, Atkins RC, Rohde R, Raz I,
Collaborative Study G. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in
patients with nephropathy due to type 2 diabetes. N Engl J Med 2001; 345: 851-860. Available at
http://www.ncbi.nlm.nih.gov/pubmed/11565517.
74. Ruggenenti P, Perna A, Mosconi L, Matalone M, Garini G, Salvadori M, Zoccali C, Scolari F,
Maggiore Q, Tognoni G, Remuzzi G, Migone L, Marubini E, DelFavero A, Ideo G, Geraci E, Loi U,
Bracchi M, Costantino E, Scolari F, Maiorca R, Cofano F, Fellin G, DAmico G, Dissegna D,
Brendolan A, LaGreca G, Feriozzi A, Ancarani E, Gandini E, dAmato I, Giangrande A, Garneri G,
Giacchino F, Giannico G, Giotta N, Vitale O, Manno C, Mazzi A, Garini G, Borghetti A, Pisoni R,
Bertani T, Novelli R, Scanferla F, Bazzato G, Oliva E, Zoccali C, Pieri F, Sisca S, Maggiore Q,
Pignone E, Boero R, Piccoli G, Piperno R, Rosati A, Salvadori M, Arnoldi F, Gaspari F, Signorini O,
Ferrari S, Guerini E. Randomised placebo-controlled trial of effect of ramipril on decline in glomerular
filtration rate and risk of terminal renal failure in proteinuric, non-diabetic nephropathy. Lancet 1997;
349: 1857-1863. Available at <Go to ISI>://WOS:A1997XG41700007.
75. Bakris GL, Williams M, Dworkin L, Elliott WJ, Epstein M, Toto R, Tuttle K, Douglas J, Hsueh W,
Sowers J, Diab NKFH. Preserving renal function in adults with hypertension and diabetes: A
consensus approach. American Journal of Kidney Diseases 2000; 36: 646-661. Available at <Go to
ISI>://000089227300027.
76. Caskey FJ, Kramer A, Elliott RF, Stel VS, Covic A, Cusumano A, Geue C, Macleod AM, Zwinderman
AH, Stengel B, Jager KJ. Global variation in renal replacement therapy for end-stage renal disease.
Nephrol Dial Transplant 2011; 26: 2604-2610. Available at
http://www.ncbi.nlm.nih.gov/pubmed/21245131.
77. Orlando LA, Belasco EJ, Patel UD, Matchar DB. The chronic kidney disease model: a general purpose
model of disease progression and treatment. BMC medical informatics and decision making 2011; 11:
41. Available at http://www.ncbi.nlm.nih.gov/pubmed/21679455.
78. Williams AW, Dwyer AC, Eddy AA, Fink JC, Jaber BL, Linas SL, Michael B, O'Hare AM, Schaefer
HM, Shaffer RN, Trachtman H, Weiner DE, Falk RJ, Quality ASN. Critical and Honest Conversations:
The Evidence Behind the "Choosing Wisely" Campaign Recommendations by the American Society
of Nephrology. Clinical Journal of the American Society of Nephrology 2012; 7: 1664-1672. Available
at <Go to ISI>://WOS:000310036800018.
79. Tong A, Cheung KL, Nair SS, Kurella Tamura M, Craig JC, Winkelmayer WC. Thematic Synthesis of
Qualitative Studies on Patient and Caregiver Perspectives on End-of-Life Care in CKD. Am J Kidney Dis 2014. Available at http://www.ncbi.nlm.nih.gov/pubmed/24411716.
80. Rothman KJ. Epidemiology an introduction. Oxford university press 2002: 202-203.

CHAPTER 3: General discussion and conclusions
141
81. Boulware LE, Jaar BG, Tarver-Carr ME, Brancati FL, Powe NR. Screening for proteinuria in US
adults - A cost-effectiveness analysis. Jama-Journal of the American Medical Association 2003; 290:
3101-3114. Available at <Go to ISI>://WOS:000187277300029.
82. Hoerger TJ, Wittenborn JS, Segel JE, Burrows NR, Imai K, Eggers P, Pavkov ME, Jordan R, Hailpern
SM, Schoolwerth AC, Williams DE, Centers for Disease C, Prevention CKDI. A health policy model
of CKD: 2. The cost-effectiveness of microalbuminuria screening. Am J Kidney Dis 2010; 55: 463-473.
Available at http://www.ncbi.nlm.nih.gov/pubmed/20116910.
83. Kessler R, Keusch G, Szucs TD, Wittenborn JS, Hoerger TJ, Brugger U, Wieser S. Health economic
modelling of the cost-effectiveness of microalbuminuria screening in Switzerland. Swiss medical
weekly 2012; 142: w13508. Available at http://www.ncbi.nlm.nih.gov/pubmed/22307760.
84. Palmer AJ, Valentine WJ, Chen R, Mehin N, Gabriel S, Bregman B, Rodby RA. A health economic
analysis of screening and optimal treatment of nephropathy in patients with type 2 diabetes and
hypertension in the USA. Nephrology Dialysis Transplantation 2008; 23: 1216-1223. Available at <Go
to ISI>://WOS:000254472400024.
85. Simmons RK, Echouffo-Tcheugui JB, Sharp SJ, Sargeant LA, Williams KM, Prevost AT, Kinmonth
AL, Wareham NJ, Griffin SJ. Screening for type 2 diabetes and population mortality over 10 years
(ADDITION-Cambridge): a cluster-randomised controlled trial. Lancet 2012; 380: 1741-1748.
Available at http://www.ncbi.nlm.nih.gov/pubmed/23040422.
86. Griffin SJ, Borch-Johnsen K, Davies MJ, Khunti K, Rutten GE, Sandbaek A, Sharp SJ, Simmons RK,
van den Donk M, Wareham NJ, Lauritzen T. Effect of early intensive multifactorial therapy on 5-year
cardiovascular outcomes in individuals with type 2 diabetes detected by screening (ADDITION-
Europe): a cluster-randomised trial. Lancet 2011; 378: 156-167. Available at
http://www.ncbi.nlm.nih.gov/pubmed/21705063.
87. Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, Lachin JM, Walker EA, Nathan DM,
Diabetes Prevention Program Research G. Reduction in the incidence of type 2 diabetes with lifestyle
intervention or metformin. N Engl J Med 2002; 346: 393-403. Available at
http://www.ncbi.nlm.nih.gov/pubmed/11832527.
88. Tuomilehto J, Lindstrom J, Eriksson JG, Valle TT, Hamalainen H, Ilanne-Parikka P, Keinanen-
Kiukaanniemi S, Laakso M, Louheranta A, Rastas M, Salminen V, Uusitupa M, Finnish Diabetes
Prevention Study G. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with
impaired glucose tolerance. N Engl J Med 2001; 344: 1343-1350. Available at
http://www.ncbi.nlm.nih.gov/pubmed/11333990.
89. Chamnan P, Simmons RK, Khaw KT, Wareham NJ, Griffin SJ. Estimating the potential population
impact of stepwise screening strategies for identifying and treating individuals at high risk of Type 2
diabetes: a modelling study. Diabet Med 2012; 29: 893-904. Available at
http://www.ncbi.nlm.nih.gov/pubmed/22340130.
90. Glumer C, Carstensen B, Sandbaek A, Lauritzen T, Jorgensen T, Borch-Johnsen K, inter s. A Danish
diabetes risk score for targeted screening: the Inter99 study. Diabetes Care 2004; 27: 727-733.
Available at http://www.ncbi.nlm.nih.gov/pubmed/14988293.
91. Grosse SD. Assessing cost-effectiveness in healthcare: history of the $50,000 per QALY threshold.
Expert review of pharmacoeconomics & outcomes research 2008; 8: 165-178. Available at
http://www.ncbi.nlm.nih.gov/pubmed/20528406.
92. Springberg PD, Garrett LE, Jr., Thompson AL, Jr., Collins NF, Lordon RE, Robinson RR. Fixed and
reproducible orthostatic proteinuria: results of a 20-year follow-up study. Ann Intern Med 1982; 97:
516-519. Available at http://www.ncbi.nlm.nih.gov/pubmed/7125410.
93. Parving HH, Chaturvedi N, Viberti G, Mogensen CE. Does microalbuminuria predict diabetic
nephropathy? Diabetes Care 2002; 25: 406-407. Available at
http://www.ncbi.nlm.nih.gov/pubmed/11815526.
94. Hallan SI, Ritz E, Lydersen S, Romundstad S, Kvenild K, Orth SR. Combining GFR and Albuminuria
to Classify CKD Improves Prediction of ESRD. Journal of the American Society of Nephrology 2009;
20: 1069-1077. Available at <Go to ISI>://000265959800020
http://jasn.asnjournals.org/cgi/reprint/20/5/1069.pdf.

CHAPTER 3: General discussion and conclusions
142
95. Fink HA, Ishani A, Taylor BC, Greer NL, Macdonald R, Rossini D, Sadiq S, Lankireddy S, Kane RL,
Wilt TJ. Screening for, monitoring, and treatment of chronic kidney disease stages 1 to 3: a systematic
review for the u.s. Preventive services task force and for an american college of physicians clinical
practice guideline. Annals of internal medicine 2012; 156: 570-581. Available at
http://www.ncbi.nlm.nih.gov/pubmed/22508734.

CHAPTER 3: General discussion and conclusions
143
3.7 Conclusies
Deze thesis omvat twee studies waarbij het opsporen van cardiovasculaire en renale
risicofactoren met behulp van microalbuminurie ter discussie staat. In de URI studie werden
arbeiders geïncludeerd door arbeidsgeneeskundigen en in de ERICABEL studie werden
hypertensie patiënten geïncludeerd door huisartsen.
Een screeningsprogramma om arbeiders op te sporen met cardiovasculaire en renale
risicofactoren met behulp van een bepaling van albumine in een urinestaal leek niet zinvol
wegens de volgende redenen. Ten eerste, slechts een klein deel (9%) van de personen met
ongekende cardiovasculaire risicofactoren werd opgespoord met behulp van detectie van
microalbuminurie. Door traditionele cardiovasculaire risicofactoren (bloeddruk, hartslag,
bloedglucosespiegel) direct op te sporen, konden veel meer personen (36%) worden gedetecteerd
met meer mogelijkheden om nier-, hart- en vaatziekten te voorkomen dan door het opsporen van
microalbuminurie alleen. Ten tweede, zijn er ook andere onderliggende oorzaken van
microalbuminurie dan louter cardiovasculair risicofactoren. Bijvoorbeeld, de aanwezigheid van
orthostatische albuminurie heeft een goede prognose, daar waar de aanwezigheid van
albuminurie bij diabetici een hoog risico voor macroalbuminurie en vervolgens nierfalen heeft (1,
2). Arbeiders die blootgesteld werden aan fysisch-chemische agentia hadden een hogere
prevalentie van microalbuminuria, onafhankelijk van hun cardiovasculaire risicofactoren. Om de
prognostische waarde van microalbuminurie bij arbeiders met fysisch-chemische blootstelling te
investigeren is een longitudinale studie nodig. Eveneens ontbreekt er een studie waarbij de
prognose van personen met de verschillende onderliggende oorzaken van microalbuminurie met
elkaar worden vergeleken. Mogelijks zullen interventies bij personen met microalbuminurie in
afwezigheid van cardiovasculaire risicofactoren aanleiding geven tot frustratie, angst,
psychologische schade, neveneffecten van onnodig behandelingen en toename van medische
kosten, terwijl interventies bij patiënten met microalbuminurie in aanwezigheid van behandelbare
risicofactoren aanleiding zouden kunnen geven tot een verbetering van de klinische prognose.
De aanwezigheid van microalbuminurie was geassocieerd met een mager gestalte (orthostatische
albuminurie) en aan fysisch-chemische blootstelling in arbeiders jonger dan 40 jaar, terwijl de
aanwezigheid van microalbuminurie was geassocieerd met cardiovasculaire risicofactoren in
arbeiders ouder dan 40 jaar. Een populatiescreening voor microalbuminurie om cardiovasculaire

CHAPTER 3: General discussion and conclusions
144
en renale risicofactoren op te sporen lijkt dus pas zinvol vanaf het 40ste
levensjaar. Doch, er is
geen rechtstreeks bewijs dat het opsporen en vervolgens behandelen van microalbuminurie
geassocieerd is met een significante daling van hart- en vaatziekten (4, 5). Het opsporen van
microalbuminurie zou zinvol kunnen worden als nieuwe behandelingen ter beschikking worden
gesteld om hart- en vaatziekten te voorkomen. Alhoewel, personen met microalbuminurie een
verhoogd relatief risico vertonen om nierfalen te ontwikkelen, is het absolute risico te laag om
een populatiescreening te verantwoorden. De predictieve waarde van microalbuminurie of
macroalbuminurie om nierfalen te ontwikkelen stijgt aanzienlijk bij personen met een geschatte
eGFR < 60 ml/min/1.73m² (3). Omdat de prevalentie van een geschatte GFR < 60 ml/min/1.73m²
toeneemt met de leeftijd, zou een screening om personen met een verhoogd risico op ESRD te
identificeren zinvol kunnen zijn vanaf een bepaalde leeftijd (bv. 55 jaar). In de URI populatie,
waar bijna iedereen een geschatte GFR > 60 ml/min/1.73m² had (jonge arbeiders populatie) is de
predictieve waarde van microalbuminurie om nierfalen te ontwikkelen dus veel te zwak.
Volgens de URI studie is het opsporen van microalbuminurie effectiever bij arbeiders met versus
zonder cardiovasculaire risicofactoren om bijvoorbeeld nierschade te kunnen detecteren. Het
opsporen van microalbuminuria in aanwezigheid van risicofactoren kan invloed hebben op de
behandeling. Bij patiënten met diabetes is het opsporen van microalbuminurie zinvol omdat een
behandeling met ACE-I of ARB, de incidentie van macroalbuminurie en vervolgens nierfalen
reduceert (1). Alhoewel, het opsporen van microalbuminurie momenteel minder efficiënt is
omdat meer en meer patiënten reeds worden behandeld met een ACE-I of ARB, onafhankelijk
van de aanwezigheid van albuminurie (5). De afwezigheid van microalbuminurie bij patiënten die
behandeld worden met een ACE-I sluit nierschade niet uit, terwijl de aanwezigheid van
microalbuminurie in patiënten die behandeld worden met een statine niet altijd geassocieerd is
met nierschade. De ERICABEL cohorte observeerde dat het gebruik van een statine geassocieerd
was met microalbuminurie. Mogelijks doordat statines tubulaire proteinurie kunnen genereren
door inhibitie van tubulaire reabsorptie. De aanwezigheid van microalbuminurie bij patiënten die
een statine gebruiken zou aanleiding kunnen geven tot het incorrect vaststellen van een nierziekte.
Meer prospectieve studies zijn nodig om de prognostische waarde van microalbuminurie in
patiënten die worden behandeld met een statine in kaart te brengen.

CHAPTER 3: General discussion and conclusions
145
De URI studie toonde dat enkel personen met persisterend microalbuminurie geassocieerd waren
aan een verhoogd cardiovasculair risico. De aanwezigheid van microalbuminurie dient dus te
worden bevestigd in een nieuw urinestaal, omdat tijdelijke omstandigheden (zoals fysische
inspanning, koorts, stress e.a.) aanleiding kunnen geven tot een vals positieve meting. Volgens
KDIGO, heeft iedereen met microalbuminurie dat langer dan 3 maanden persisteert CKD stadium
A2. Hieruit volgt dat de prevalentie van CKD stadium A2 in cohorten overschat wordt wanneer
slechts éénmalig microalbuminurie wordt gemeten. Bovendien, zal bij de helft van de diabetici
met microalbuminurie “deze aandoening” verdwijnen in functie van de tijd (6). In de URI studie
werd bij personen zonder risicofactoren frequent fluctuerende microalbuminurie waargenomen.
Het fluctuerende karakter van microalbuminurie werd ook geobserveerd in de ERICABEL
cohorte (nog niet gepubliceerd).
Een vermindering van de nierfunctie wordt voornamelijk gezien bij personen met
macroalbuminurie terwijl dit minder het geval is bij personen met microalbuminurie. Hieruit, zou
men kunnen concluderen dat het opsporen van personen met macroalbuminurie effectiever is om
nierinsufficiëntie te detecteren dan het opsporen van personen met microalbuminurie. Echter de
kosten van een massascreening voor albuminurie worden hoger geschat dan de baten. De
screeningskosten kunnen worden gereduceerd door een screeningsinterval van 10 jaar te hanteren.
Echter, hierdoor zullen personen die macroalbuminurie ontwikkelen op enkele jaren niet
gedetecteerd kunnen worden. Of een screeningsprogramma aanleiding zou kunnen geven om de
incidentie van ESRD te reduceren door bepaling van albuminurie en een schatting van de GFR
(door serumcreatinine en/of Cystatine C te meten) in personen ouder dan bv. 55 jaar dient in de
toekomst onderzocht te worden.

CHAPTER 3: General discussion and conclusions
146
3.8 Referenties
1. Parving HH, Chaturvedi N, Viberti G, Mogensen CE. Does microalbuminuria predict diabetic
nephropathy? Diabetes Care 2002; 25: 406-407. Available at
http://www.ncbi.nlm.nih.gov/pubmed/11815526.
2. Springberg PD, Garrett LE, Jr., Thompson AL, Jr., Collins NF, Lordon RE, Robinson RR. Fixed and
reproducible orthostatic proteinuria: results of a 20-year follow-up study. Ann Intern Med 1982; 97:
516-519. Available at http://www.ncbi.nlm.nih.gov/pubmed/7125410.
3. Hallan SI, Ritz E, Lydersen S, Romundstad S, Kvenild K, Orth SR. Combining GFR and Albuminuria
to Classify CKD Improves Prediction of ESRD. Journal of the American Society of Nephrology 2009;
20: 1069-1077. Available at <Go to ISI>://000265959800020
http://jasn.asnjournals.org/cgi/reprint/20/5/1069.pdf.
4. Asselbergs FW, Diercks GF, Hillege HL, van Boven AJ, Janssen WM, Voors AA, de Zeeuw D, de
Jong PE, van Veldhuisen DJ, van Gilst WH. Effects of fosinopril and pravastatin on cardiovascular
events in subjects with microalbuminuria. Circulation 2004; 110: 2809-2816. Available at
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids
=15492322.
5. Fink HA, Ishani A, Taylor BC, Greer NL, Macdonald R, Rossini D, Sadiq S, Lankireddy S, Kane RL,
Wilt TJ. Screening for, monitoring, and treatment of chronic kidney disease stages 1 to 3: a systematic
review for the u.s. Preventive services task force and for an american college of physicians clinical
practice guideline. Annals of internal medicine 2012; 156: 570-581. Available at
http://www.ncbi.nlm.nih.gov/pubmed/22508734.
6. Perkins BA, Ficociello LH, Silva KH, Finkelstein DM, Warram JH, Krolewski AS. Regression of
microalbuminuria in type 1 diabetes. The New England Journal of Medicine 2003; 348: 2285-2293.
Available at http://www.ncbi.nlm.nih.gov/pubmed/12788992.



149
Dankwoord
Dit proefschrift is grotendeels gebaseerd op epidemiologisch onderzoek dat dankzij de volgende
enthousiaste protagonisten tot stand is gekomen.
Prof. Dr. Em. Raymond Vanholder en Prof. Dr. Van Biesen van de dienst nefrologie UZG, wil ik
bijzonder bedanken voor de mogelijkheden om de URI studie te initiëren. Dank voor jullie
engelengeduld en de investering die nodig bleek om mij tot het niveau te krijgen om A1
publicaties te schrijven. Het is jullie verdiensten geweest om de teksten van mijn chaotisch brein
te structuren tot een leesbaar en verstaanbaar geheel.
Dr. Frans Vermeiren, directeur van Adhesia en schoonpapa, wil ik graag bedanken voor de
opportuniteit om de URI studie uit te voeren in zijn bedrijf. Ook dient vermeld te worden dat veel
studiepersonen door hem zelf werden geïncludeerd. Zijn interesse in de geneeskunde uitte zich
door bespreking van individuele afwijkende resultaten die door de URI studie aan het licht
kwamen. Dr. Kathleen Eeckhaut, wil ik graag bedanken voor haar praktische inzicht, ijverige
inzet en enthousiaste betrokkenheid om de URI studie te initiëren en de arbeiders ook
daadwerkelijk te includeren. Eveneens, dank ik alle andere dokters en verpleegkundigen die
geholpen hebben om de arbeiders te includeren. Dr. Guy De Groote, directeur van CRI labo, wil
ik bedanken voor zijn wetenschappelijke kennis en inzicht bij het initiëren van de URI studie.
Prof. Dr. Kris Bogaerts, statisticus verbonden aan KULeuven, voor zijn bijdrage aan het
manuscript ‘microalbuminuria and statins”. Dr. Hans Warrinnier, medical director bij Hoffmann-
La Roche voor de samenwerking in kader van de ERICABEL studie.
De leden van examencommissie, Prof. Dr. Joris R. Delange, Prof. Dr. Jan De Maeseneer,
Prof. Dr. Johannes Ruige, Dr. Johan De Meester, Dr. Marijn Speeckaert en Dr. Kitty Jager, voor
het kritisch nalezen en hun constructieve suggesties.
Graag richt ik ook het woord aan mijn collega’s: Prof. Dr. Nic Veys, Katrien Blanckaert,
Prof. Dr. Annemie Dhondt, Dr. Patrick Peeters, Prof. Dr. Francis Verbeke en Prof. in spe
Dr. Van Laecke en Dr. Marijn Speeckaert, zijn ieder op zich een groot voorbeeld voor mij en
verrijking van de dienst nefrologie UZG. Idem dito voor Jill Vanmassenhove, Nathalie Neirynck
en Evi Nagler die binnenkort hun proefschrift succesvol zullen voltooien.

150
Een speciale dank voor Christel voor mijn vragen en te helpen met “WORD” en Chantal om er
een echt feest van te maken.
Last but not least, wil ik Vanessa, Dr., Prof., mama en mijn levensgezel bedanken voor je morele
steun. Aanvankelijk was ik voor jou een voorbeeld en met onze tijd keerde dit om, doch met
blijvend wederzijds respect. Ik dank je om mijn chaotische denkpaden te simplificeren tot een
beter verstaanbaar persoon, al blijven mijn gedachtenkronkels zoals de jouwe bestaan. Ik dank
mijn familie, voor hun steun aan hun ontwortelde zoon en broer. Ik dank tante Sonja om al die
jaren voor het huishouden te zorgen. Tenslotte is dit werk speciaal opgedragen aan mijn
belangrijkste creaturen: Laura en Arthur, zolang ik voor hen als voorbeeld kan dienen.
Mijn excuses aan hen die ik in bovenstaand dankwoord vergat; ik vraag hen om begrip voor de
vergetelheid.
Arjan 2014

151
CURRICULUM VITAE
Arjan van der Tol
1 PERSONALIA
SURNAME Van der Tol
FIRST NAME Arjan
PLACE of BIRTH Alphen a/d Rijn, The Netherlands
DATE of BIRTH July 22th, 1971
PROFESSIONAL ADRESS Renal Division, Department: Internal Medicine
Gent University Hospital
De Pintelaan 185
B-9000 Gent
Tel: +32-(0)9-3326665
2 QUALIFICATIONS
ACADEMIC STUDIES IN THE MEDICAL SCIENCES
Legal degree of Bachelor of Medicine, cum laude, granted by the State University Antwerp,
Belgium, 1995
Legal degree of Doctor of Medicine, Surgery and Obstetrics, cum laude, granted by the State
University of Antwerp, Belgium, 1999
Legal degree of Specialist in Internal Medicine recognized as such by the Department of Social
Affairs, Public Health and Environment of Belgium, 2004
Legal degree of Specialist in Nephrology recognized as such by the Department of Social Affairs,
Public Health and Environment of Belgium, 2005
Working in Renal Division, Ghent University Hospital, Belgium, since 2003

152
3 MEMBERSHIP
Renal Disaster Relief Task Force (RDRTF) as volunteer doctor in:
Kashmir earthquake (Islamabad October 2005)
Yogyakarta earthquake (Java May 2006)
Chicuan earthquake (Chengdu May 2008)
Padang earthquake (Sumatra October 2009)
EDTA-ERA: member
4 SCIENTIFIC PUBLICATIONS
ARTICLES IN INTERNATIONAL JOURNALS WITH REFEREE SYSTEM
Van der Tol A, Hussain A, Sever MS, Claus S, Van Biesen W, Hoste E, Khan S, Vanholder R.
Impact of local circumstances on outcome of renal casualties in major disasters. Nephrol Dial
Transplant. 2009 Mar;24(3):907-12. Epub 2008 Oct 8. Available at:
http://ndt.oxfordjournals.org/content/24/3/907.full.pdf+html
Van der Tol A, Van Biesen W, Verbeke F, De Groote G, Vermeiren F, Eeckhaut K, Vanholder R.
Towards a rational screening strategy for albuminuria: results from the unreferred renal
insufficiency trial. PLoS ONE. 13 Oct 2010. Available at:
http://www.plosone.org/article/info%3Adoi%2F10.1371%2Fjournal.pone.0013328
Van der Tol A, Van Biesen W, Bogaerts K, Van Laecke S, De Lombaert K, Warrinnier H and
Vanholder R (2012) Statin use and the presence of microalbuminuria. Results from the
ERICABEL trial: a non interventional epidemiological cohort study. PLoS ONE: 16 Feb 2012.
Available at: http://www.plosone.org/article/info%3Adoi%2F10.1371%2Fjournal.pone.0031639
Van der Tol A, Van Biesen W, De Groote G, Verbeke P, Vermeiren F, Eeckhaut K, Vanholder R.
Microalbuminuria is more consistent in presence of cardiovascular risk factors: Results from the
Unreferred Renal Insufficiency Trial..J Nephrol, May-Jun 2013, 26(3): 580-5. Available at:
http://www.ncbi.nlm.nih.gov/pubmed/22865595

153
Van der Tol A, Van Biesen W, De Groote G, Verbeke P, Vermeiren F, Eeckhaut K, Vanholder R.
Should screening of renal markers be recommended in a working population? Int. Urology
Nephrology 2014 Aug 46(8): 1601-8. Available at:
http://link.springer.com/article/10.1007%2Fs11255-014-0718-x
ARTICLES IN NATIONAL JOURNALS
Van der Tol A, E pelzers, G Wyffels, J Mareels, H Verbraeken. Non β-cel tumour induced
hypoglycemia. Tijdschrift voor Geneeskunde 2006; 62, p 299-305.
Van der Tol A, Dhondt A diabetische nefropathie. Tijdschrift voor Geneeskunde 2012; 68, p
1089-1094.
5 ABSTRACTS
Van der Tol A, Van Biesen W, De Groote G, Vermeiren F, Eeckhaut K, Vanholder R. High
prevalence of cardiovascular risk factors but not of CKD stage 3-5 in healthy worker. M302.
World Congress of Nephrology 2009, Milan, Italy
Van der Tol A, Van Biesen W, De Groote G, Vermeiren F, Eeckhaut K, Vanholder R. Do women
with CKD stage 3 as estimated by MDRD really have CKD? M272. World Congress of
Nephrology 2009, Milan, Italy
Van der Tol A, Van Biesen W, De Groote G, Paul Verbeke, Eeckhaut K, Vanholder R.
Mislabeling cardiovascular risk by one single measurement of microalbuminuria
ERA-EDTA, 2011, Praag, Czech.
Van der Tol, A, Van Biesen W, De Groote G, Vermeiren F, Verbeke P, Vanholder R.
Albuminuria is strongly associated with low BMI and only weakly to cardiovascular risk factors
in apparently healthy subjects younger than forty. ASN 2011, Philadelphia, VS.
Van der Tol A, Van Biesen W, De Groote G, Vermeiren F, Eeckhaut K, Vanholder R. Is Cystatin
C an independent biomarker to predict renal function in a general population? Annual Scientific
Meeting of the BVN/SBN, UCL Brussel, 23/04/2009





















