
Period Problems: From Puberty to the Post-Menopause
31
7/4/19 1 Period Problems: From Puberty to the Post-Menopause Jody Steinauer, MD, MAS No Disclosures, July 4 th , 2019 • I have nothing to disclose
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Period Problems: From Puberty to the Post-Menopause
7/4/19
1
!
Period Problems: From Puberty to the Post-Menopause
JodySteinauer,MD,MAS
!
No Disclosures, July 4th, 2019• Ihavenothingtodisclose

7/4/19
2
!
Objectives• Whatisnewwiththeperiod• Workupandtreatmentofuterinebleeding• Treatmentofabnormalbleedingduetocontraceptives
1:Periods
3:Fibroids
2:PerimenopausalAUB
4:ContraceptiveSideEffects
!
Case 1A23year-oldwomantellsyouaboutanappsheisusingtotrackhercycleandwondersifitiseffectiveasnaturalcontraception.Shealsowonderswhatyouthinkofthemenstrualcuporthenewdiscshereadabout– dotheyworkaswellastampons?
7/4/19
3
!
What’s new with the period? • Mail-orderproducts
– Manywithdonationstolow-resourcesettings• Products
– Menstrualcupsanddiscs– Combotampon+liner– Organiccottontampons– Underwear– Washablepads
!
Menstrual Cups• Highacceptability• Higheracceptabilitythantampons
• Lowercostanddecreasedwaste
Howard,FLOW,CFP,2011.Liswood,ObGynm1959.

7/4/19
4
!
Menstrual Cycle Apps!• Systematicreviewoffreeapps• Of108only20wereaccurate(19%)• 80%conception/50%contraception• Only1/8womenhavea28daycycle
• Accuracy:averaged4ofpriorcycles,includingoutsideofusualrange
Moglia,ObGyn,2016
!Vox.com
• Collectdata,fewprivacypolicies• Advertising• Mostfertilityoriented• Incorrectlymarketedaseffectivebc• Assumptionsaboutgender/sexuality,oddemojis/images
7/4/19
5
!
Free App by Planned Parenthood
Plannedparenthood.org
This one from Planned Parenthood is “Spot On”!
• Includesbirthcontrolinformationandreminders
• Noassumptionsaboutgenderorsexuality
• “Nopinkflowersorbutterflies”• Allowslimitedimportfromotherapps
!
Case 2A46year-oldwomanreportsherperiodshavebecomeincreasinglyirregularandheavyoverthelast6-8months.Sometimestheycome2timespermonthandsometimesthereare2monthsbetween.Shebleeds10dayswithclotsandfrequentlybleedsthroughpadstoherclothes.Shealsohasdiabetesandisobese.HerLMPwas2monthsago.

7/4/19
6
!
1. FSH2. Testosterone&DHEAS3. Urinehcg4. TSH5. Transvaginal Ultrasound(TVUS)6. EndometrialBiopsy(EMB)
Q1: Which is the first test should you order in this patient?
!
Step 1: Pregnant?Pregnant• Ectopic• SpontaneousAbortion• ThreatenedAbortion• (MolarPregnancy)• (Trauma)• (Othercauses)
NotPregnant• Anovulation***• Anatomic/structural**• Neoplastic*• Infectious• Iatrogenic• Non-gynecologic
* = Most likely for this patient

7/4/19
7
!
Terminology: What is abnormal?• Normal:Cycle=28days+- 7d(21-35);Length=2-7days;Heaviness=self-defined
• Toolittlebleeding:amenorrheaoroligomenorrhea• Toomuchbleeding:Menorrhagia(regulartimingbutheavy(accordingtopatientor>80cc)ORlongflow(>7days)
• Irregularbleeding:Metrorrhagia,intermenstrual orpost-coitalbleeding
• IrregularandExcessive:Menometrorrhagia
Preferredtermfornon-pregnantheavyand/orirregularbleeding=AbnormalUterineBleeding(AUB)
!
Pathophysiology: AnovulatoryBleeding
Bricks&MortarEstrogen=Bricks,buildendometriumProgesterone(P)=Mortar,stabilizes,onlyhavePifovulateNormalmenses:WithdrawalofPcauseswalltofalldown,allatonce(heavywhenhemostatic&vaso-constrictionnotworking,highPG)
Anovulation: NoPsowhenwallgrowstootall,itfalls–irregularly,irregular(Fibroids: Un-steady vasculature, abnlcontraction)

7/4/19
8
!
Abnormal Uterine Bleeding
Bradley,AJOG,2016
!
History and Physical Examination• Hx:bleedingpattern,symptomsofanemia,sexual&reproductivehistory,chronicmedicalillness,meds
• Acutev.chronic• PE:signsofanemia,thyroidexamination,abd andgyn exam,(cervicaldysplasia/STIscreening?)

7/4/19
9
!
Initial Work-up: Menometrorrhagia• Always:Urinepregnancy• Usually:TSH• Maybe:Hct,r/ocoagulopathy• Maybe:EMB(EndometrialBiopsy)• Maybebutlater:Transvaginal Ultrasound• Usuallynotnecessary:FSH,LH,Testost,Estradiol
!
ACOG, July 2012
ACOGPracticeBulletin128,DiagnosisofAUBinReproductive-AgedWomen

7/4/19
10
!
Perimenopause
• Averages4years
•12%suddenlystopmenstruating
•18%havelonger,heaviermenses
•70%haveshort,irregularmenses
ShouldwethereforeperformEMB onallbut12%ofwomen?
!
A Rational Approach to EMB• Naturalhistory:Endometrialcatakesyearstodevelop- noatypia→atypia →invasion.
• Bleedingpatterncues:Cancer&hyperplasiacommonlypresentwithmenometrorrhagia,sometimeswithintermenstrualbleeding,rarelywithregularly-timedmenses.

7/4/19
11
!
A Rational Approach to EMBPost-Menopause:ALLwomenWITHANY BLEEDING(except4-6months
afterstartingHT)
Recentonsetirregularbleeding: Considertreatingfirstandifbleedingnormalizes,noneedforEMB
>50: Allwomenwithrecurrent,irregular bleeding(considernotdoingifperiodslightandspacingout)
45-50: Recurrentirregularbleedingplus>1riskfactorOR>6mosmenometrorrhagia (considernotdoingifperiodslightandspacingout)
<45:Longhistory(>2yr?)ofuntreatedanovulatory bleedingorfailedmedicalmanagement
!
Otherreasons:Papwithatypicalglandularcellsorendometrialcells(ifnotdoneattimeofmenses).
EMB isnotperfectlysensitivesofurtherevaluationmandatoryif:
1.PersistentAUB afternegativeEMB2.PersistentAUB after3-6monthsofmedicaltherapy
A Rational Approach to EMB

7/4/19
12
!
Do all women with AUB need an ultrasound?AlthoughTVUSisthebestimagingchoiceforpelvicpathology(betterthanMR,CT)….• 80%withheavymenstrualbleedinghavenoanatomicpathology
• Incidentalfindingssuchasfunctionalovariancystsandsmallfibroids(~50%)areoftenfoundleadingtoanxietyandunnecessarytreatments
• SO….treatfirst,TVUSiftreatmentfails
!
What about U/S instead of EMB for post-menopausal bleeding?Transvaginal Ultrasound
• Measureendometrialstripe• Abnormal=>4mm(or5)• Non-specific:myomas,polypsalsocausethickEM• Operatorskillmandatory• NOTUSEFULPRE-MENOPAUSE

7/4/19
13
!
!!!!!!TVUS! ! !!!!!!!!!!EMB!
96%! Sensitivity! 94%!
61%! Specificity! 99%!
99%! NPV! 99%!
40;50%! Further!w/u!necessary!
?!<5%!!
!
CanofferpatientchoiceaslongaseitherisquicklyavailableandpatientunderstandsshemayneedEMBafterU/S
TVUS vs EMB to detect cancer (in post-menopausal women)
!
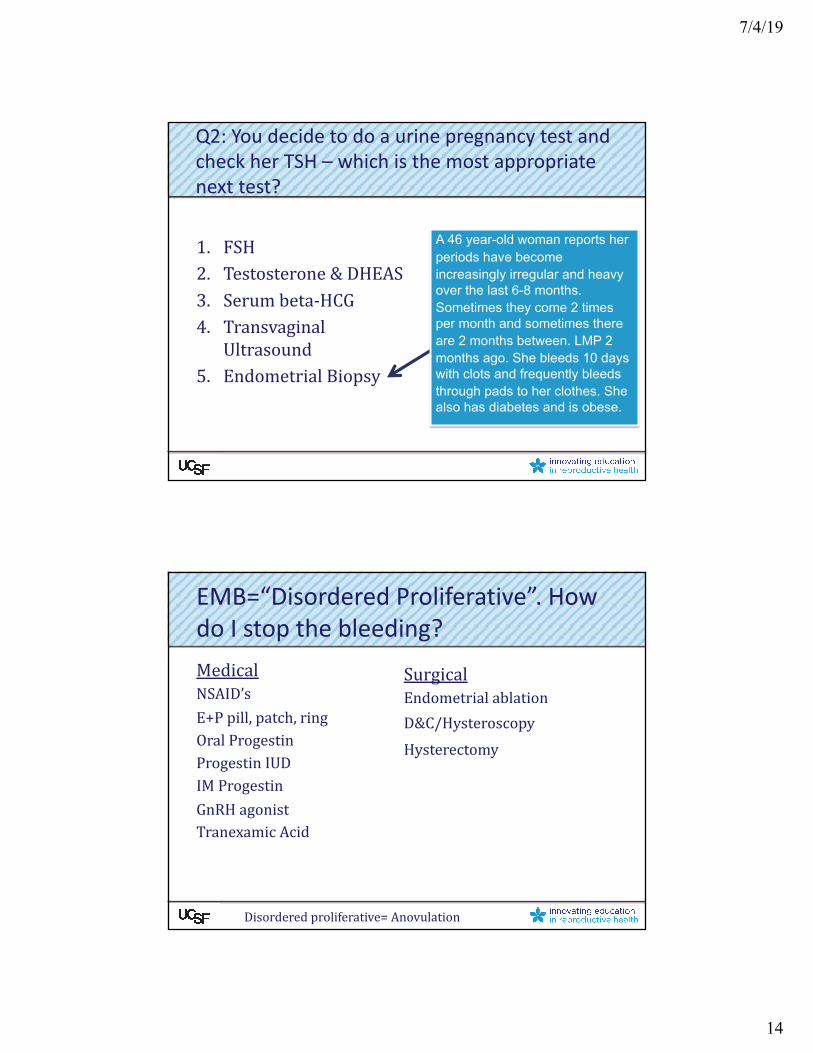
Q2: You decide to do a urine pregnancy test and check her TSH – which is the most appropriate next test?1. FSH2. Testosterone&DHEAS3. Serumbeta-HCG4. Transvaginal Ultrasound5. EndometrialBiopsy
7/4/19
14
!
1. FSH2. Testosterone&DHEAS3. Serumbeta-HCG4. Transvaginal
Ultrasound5. EndometrialBiopsy
A 46 year-old woman reports her periods have become increasingly irregular and heavy over the last 6-8 months. Sometimes they come 2 times per month and sometimes there are 2 months between. LMP 2 months ago. She bleeds 10 days with clots and frequently bleeds through pads to her clothes. She also has diabetes and is obese.
Q2: You decide to do a urine pregnancy test and check her TSH – which is the most appropriate next test?
!
EMB=“Disordered Proliferative”. How do I stop the bleeding?MedicalNSAID’sE+Ppill,patch,ringOralProgestinProgestinIUDIMProgestinGnRH agonistTranexamic Acid
SurgicalEndometrialablationD&C/HysteroscopyHysterectomy
Disorderedproliferative=Anovulation
7/4/19
15
!
Treatment of AUB: NSAIDs• Suppressprostaglandinsynthesis,increasesplateletaggregation,andreducesmenstrualbloodloss
• Reducesbloodlossby40%• Usealoneorwithothertreatments• Prescribe5daysATC
– Ibuprofen,mefenamic acid,naproxen
!
Treatment of AUB: Estrogen• CHC– pill,patch,ring– improvecyclecontrol,decreasemenstrualbloodloss,decreaseirregularbleeding,whenusedtraditionallyorcontinuously– OneapprovedbyFDAforheavymenstrualbleeding– OftenusedtotreatacuteandchronicAUB– despitelimited(butsome)evidencetosupportit

7/4/19
16
!
Treatment of AUB: Progestins• Oralprogestin
– IfovulatoryAUB:daily progestindecreasesbloodloss(MPA2.5-10mgqd,norethindrone 2.5-5mgqd)
– Ifanovulatory:cyclicprogestin-12-14d/monthimprovesmensesinhalfofwomen
• Injectableprogestin– 50%amenorrheaafter1year,irreg.bleedinginfirstfewmonthsand50%atoneyear
• Intrauterineprogestin– Significantdecreaseinbloodloss,superiortootherprogestins andCHCs
!
First Line Hormonal Treatments• Firstchoice:Levonorgestrel IUD
– >80%reductioninbloodloss,decreasedcramping,prevents/treatshyperplasia,highlyeffectivebirthcontrol
– Veryfewcontraindicationstousing– Bloodlosscomparabletoablation,satisfactioncomparabletohyst.
• 2nd choice:combinedcontraceptives(pill,patch,ring)ororalprogestin(cyclicv.daily)orprogestininjection– Proventodecreaseirregularperi-menopausalbleeding– Anytypeok,20mcgpreferredforwomen>40– Estrogencontraindications:smokers>35,HTN,complicatedDM,multipleRFforCAD,h/oDVT,migraines

7/4/19
17
!
Treatment of AUB: Tranexamic Acid• Preventsplasmaformation,fibrindegradation,andclotdegradation
• Moreeffectivethanplacebo,NSAID,cyclicprogestin
• Dose:1gto1.3gevery6-8hoursduringmenses• Risks:TheoreticriskofVTE,noincreaseinlargestudies.Contraindicatedwithhistoryof/riskfactorsforVTE.ProbablysafeinconjunctionwithCHC.
• Sideeffects:Minimal
!
Surgical Treatments• D&C,Hysteroscopy:
– Temporaryreductioninbleeding.Curativeiffibroidorpolypremoved.
• EndometrialAblation– Reducesbutdoesn’teliminatemenses– ~25%repeatablationorhyst in5years– Mustruleoutcancerfirst– Can’tbedonein>12weekuteriorforwomenwhowantfertility

7/4/19
18
!
Perimenopausal / Anovulatory Bleeding: SummaryR/opregnancy,thyroiddz
EMBifmeetscriteria
Treatfirstasifanovulatory bleeding:– NSAID’s+– Hormones(Levo IUD,CHC,DMPA)
Ifpersists:– U/Stor/oanatomiccauses(andEMBifnotalreadydone)– Discusssurgicaloptionsifrefractorytomedicalmanagement.
!
Case 3: Is it the fibroids?SamehistoryasCase2exceptshehasfibroids….Onexaminationheruterusis16weeks’size.• Verycommonà 80%ofhysterectomyspecimens(doneforanyreason)and~75%haveonU/Satage50.
• About50%areasymptomatic• Growslowlyuntilmenopauseandthendecreaseby~50%(canstillcausebleedingpost-menopause)

7/4/19
19
!
AUB with Known Fibroids: Work-up and Treatment• R/ocancer(using“rationalemb algorithm”andpregnancy(don’tblamefibroidsforthebleeding)
• NSAID’sandLNGIUD,CHC,tranexamicacid
• Ifnobetter,blamethefibroids
• +/- Lupron--asabridgetomenopauseorpre-optoshrinktoobtainlessinvasiverouteofhysterectomy
• Othertx (hysteroscopic resectionif<3cm,myomectomy,MR-guidedfocusedu/s,RFA,UAE,hysterectomy)
!
Case 4: Because of her contraceptive…• A32year-oldwomanhasrecentlyinitiatedthebirthcontrolpill.
• Shehashadspottingfor30straightdays!Sheisannoyed.

7/4/19
20
!
Case 4: Because of the injection…• A32year-oldwomanhasrecentlyinitiatedthecontraceptiveinjection.
• Shehashadspottingfor30straightdays!Sheisannoyed.
!
Case 4: Because of the implant…• A32year-oldwomanhasrecentlyinitiatedthecontraceptiveimplant.
• Shehashadspottingfor30straightdays!Sheisannoyed.
7/4/19
21
!
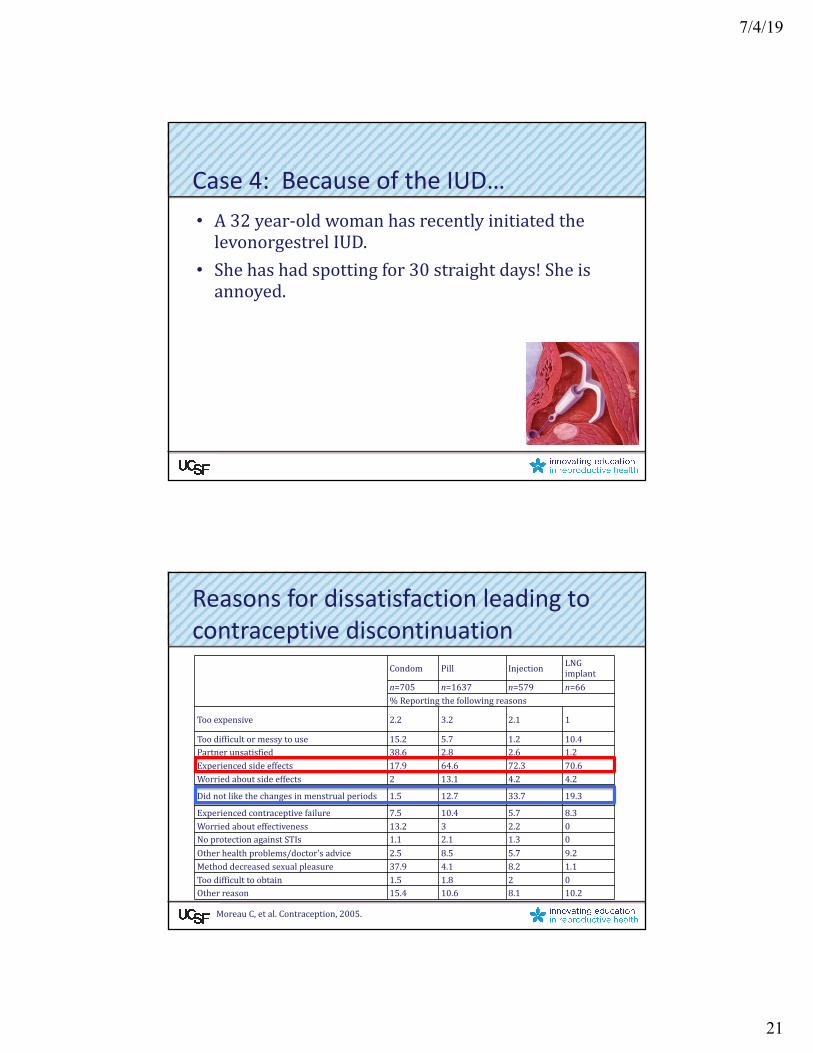
Case 4: Because of the IUD…• A32year-oldwomanhasrecentlyinitiatedthelevonorgestrel IUD.
• Shehashadspottingfor30straightdays!Sheisannoyed.
!
Condom Pill Injection LNGimplant
n=705 n=1637 n=579 n=66%Reportingthefollowingreasons
Tooexpensive 2.2 3.2 2.1 1
Toodifficultormessytouse 15.2 5.7 1.2 10.4Partnerunsatisfied 38.6 2.8 2.6 1.2Experiencedsideeffects 17.9 64.6 72.3 70.6Worriedaboutsideeffects 2 13.1 4.2 4.2
Didnotlikethechangesinmenstrualperiods 1.5 12.7 33.7 19.3
Experiencedcontraceptivefailure 7.5 10.4 5.7 8.3Worriedabouteffectiveness 13.2 3 2.2 0NoprotectionagainstSTIs 1.1 2.1 1.3 0Otherhealthproblems/doctor'sadvice 2.5 8.5 5.7 9.2Methoddecreasedsexualpleasure 37.9 4.1 8.2 1.1Toodifficulttoobtain 1.5 1.8 2 0Otherreason 15.4 10.6 8.1 10.2
Reasons for dissatisfaction leading to contraceptive discontinuation
MoreauC,etal.Contraception,2005.

7/4/19
22
!
Mechanism for Abnormal Bleeding with Hormonal Contraceptives
Irregularbleeding
Transitionfromthicktothinendometrium
Fragileandsuperficial
bloodvesselsinendometrium
Unstableendometrialstromaandglands
Alteredendometrialremodeling
!
Abnormal Bleeding from Contraceptives
Settingexpectations
Bleedingsideeffects Treatment

7/4/19
23
!
COCs: Setting Expectations
• Ratesofunscheduledbleeding– 10-30%inthefirstmonth– Lessthan10%bythethirdmonth
• Ratesofamenorrhea– Lessthan2%inthefirstyear– Upto5%after1year
1. Speroff L, Darney PD. Clinical Guide for Contraception. 4th Ed. 2011
!
COCs: General Counseling
• Takepillatthesametimeeachday– Inconsistentpilluseassociatedwithincreasedriskofunscheduledbleeding1
• Stopsmoking!– Smokersmorelikelytoexperienceunscheduledbleeding/spotting1
– Amongsmokers,bleedingmorelikelytopersistthroughsubsequentcycles
1. Rosenberg WJ et al. Contraception, 1996.
7/4/19
24
!
COCs: Regimens
• CyclicUse • ExtendedCycle
!
Treating Bleeding on Cyclic COCs• Supplementalestrogen1
– OralCEE1.25mgx7days– Oralestradiol2mgx7days
• IncreasedoseofestrogenifwomanusingCOCwith< 20mcgestrogen– SeveralCOCscontaining20mcgethinylestradiolresultedin:
• Higherratesofearlytrialdiscontinuation• Increasedriskofbleedingdisturbances2
• Switchtovaginalring1.SperoffL,DarneyPD.ClinicalGuideforContraception.4th Ed.2011.
2.Gallo,MF.CochraneDatabaseofSystematicReviews,2013.
Double or triple the birth control pill?

7/4/19
25
!
Treating Bleeding on Extended COCs
• DiscontinuetheCOCsfor3-4consecutivedays1– A3-dayhormonefreeintervalwasassociatedwithgreaterresolutioninbreakthroughbleeding/spottingincomparisontocontinuingactivepills2
– Afterthefirst21daysofthehormone
1. Godfrey EM et al. Contraception, 201; 2. Sulak PJ et al. AJOG, 2006
!
DMPA: Setting Expectations• Abnormalbleedingiscommoninthefirstyear• Ratesofunscheduledbleeding1
– Upto70%inthefirstyear– Approximately10%afterthefirstyear
• Amenorrheaismorelikelyovertime1
Within3months After1year At5years
Rateofamenorrhea 12% 46% 80%
1. Speroff L, Darney PD. Clinical Guide for Contraception. 4th Ed. 2011

7/4/19
26
!
Treating Injection Bleeding
EnhancedCounseling• Bleedingpatterns• Reassurance
ContinueDMPA• Moreinjections,lessbleeding
TREAT• NSAIDsx5-7days
• Estrogen(COCsorsupplementalestrogenx10-20days)
• Tranexamicacid
!
Etonogestrel Implant: Setting Expectations• Mostwomenexperienceareductionofmenstrualbleeding1
• Bothersomebleedingreportedin25%ofpatients2– 6.7%reportedfrequentbleeding– 17.7%prolongedbleeding
• Ratesofamenorrhea3– Approximately20%infirstyear– 30-40%after1year
1. Mansour D. Contraception, 2011.2. Mansour D. European Journal of
Contraception & Reproductive Health Care, 2008
3. Speroff L, Darney PD. Clinical Guide for Contraception. 4th Ed. 2011

7/4/19
27
!
Contraceptive Implant: Bleeding Patterns
• Numberofunscheduledbleedingdays:– IsHIGHESTinthefirst3months
– DECREASESoverthefirstyear
– PLATEAUSinthesecondandthirdyear
1 Flores JB, International Journal of Gynecology & Obstetrics, 2005.
!
Contraceptive Implant: Bleeding Patterns
• Moreunpredictablebleedingpattern1– Amenorrheamaynotbesustainedifachieved
– “Favorable”patterninthefirst3monthspredictsacontinuedfavorablepattern
– Forthosewithan“unfavorable”bleedingpattern,50%reportimprovementovertime
1 Mansour D, European Journal of Contraception & Reproductive Health Care, 2008.

7/4/19
28
!
Treating Implant Bleeding
EXPECTANTMANAGEMENT
for6-12months
Supplementalestrogen
COCs-10-20days
Oralestrogen-1.25mgCEE-2mgestradiol
Transdermalestrogen-0.1mg/day
NSAIDsx5-7days
USSelectedPracticeRecommendationfor
ContraceptiveUse,2013
!
LNG IUS: Setting Expectations• Unscheduledspottingorlightbleedingiscommon,especiallyduringthefirst3–6months
• ForLNG52/5,spottingwaspresentin25%oftheusersat6monthsanddecreasedovertime.1
1. Hidalgo M et al. Contraception, 2002.

7/4/19
29
!
LNG IUS: Setting Expectations
• 79-97%reductioninbleeding• 33%developedoligo/amenorrheainfirst3months,70%at2yrs
• Amenorrheaat1yr:20%• Amenorrheaat2yrs:30-40%
• Amenorrheaat1yr:6%• Amenorrheaat2yrs:12%
LNG 52/5
LNG13.5/3
!
Treating LNG IUS Bleeding
• Pre-insertioncounseling– Discussbleeding/spottinginfirst3-6months
– Discussamenorrhea
• Providereassuranceasbleedinglikelytoimprove
• CheckIUDlocation• NSAIDsATCq4wks mayhelp,noevidenceforestrogen

7/4/19
30
!
Irregular Bleeding by Contraceptive Ratesofirregularbleeding
COCs • 10-30%infirstmonthofuse• <10%bythethirdmonthofuse
VaginalRing • Lesscommonin comparisontoCOCs• Upto6%infirstyear
Patch • SimilartoCOCs exceptslightlyhigherrateofspottinginfirst2cycles
Injectable • 70%in first year• 10% afterthefirstyear
Implant • Upto25% infirst2years
Cu-IUD • Lessirregularbleedingcompared toLNG-IUS
LNG-IUS • Upto25% at6months• 8-11%at18-24months
!
Amenorrhea by ContraceptiveRATESOFAMENORRHEAWithin 1st year At1year Beyond
COCs <2% Upto5%
VaginalRing SimilartoCOCs
Patch SimilartoCOCs
Injectable 12% 46% 80%at5yrs
Implant 21% 30-40%
Cu-IUD 0% 0% 0%
LNG-20 20% 30-40% at2yrs
LNG-14 6% 12%at2years

7/4/19
31
!
US Selected Practice Recommendation for Contraceptive Use, 2013
!
Conclusions• Abnormaluterinebleeding – thinkofanovulation• Work-up:Alwaysruleoutpregnancy.Usually:TSH,PLN,PossibleHCT,EMB,TVUSifinitialtx fails.
• Treatment:allbleedingtreatedsimilarly• NSAID’splushormones.Persistentrequirescontinuedwork-upevenifEMBand/orultrasoundarenegative.
• Hormonalorcopperbirthcontrol:setexpectations
ThankyoutoRebeccaJacksonandSaraWhetstoneforsharingslides!




















