Performance of the Diagnostic Interview Schedule for Children Version 2.3 (DISC‐2.3) in an...
9
Performance of the Diagnostic Interview Schedule for Children Version 2.3 (DISC-2.3) in an Informal Settlement Area in South Africa BRIANA. ROBERTSON, M.D., KARIN ENSINK, M.A., CHARLES D.H. PARRY, PH.D., AND DEREK CHALTON, PH.D. ABSTRACT Objective: To investigate the performance of the Xhosa Diagnostic Interview Schedule for Children Version 2.3 (DISC- 2.3) in a community study of African children and adolescents in Khayelitsha, a largely informal settlement area in Cape Town, South Africa. Method: A cross-sectional community study of 500 youths aqed 6 to 16 years was undertaken using a systematic sampling strategy based on random starting points in the community. Three trained Xhosa-speaking lay interviewers administered the DISC-2.3 to youths and their parents in their homes. Additional questions included degree of impairment, selected risk factors, and service use. Results: The administration of the Xhosa DISC-2.3 in an informal settlement area was both feasible and acceptable to respondents. Psychiatric disorder with impairment was recorded for 76 (15.2%) of the children and adolescents. Consultation had been sought in only 20 cases, mostly from medical doctors, except for 3 who had attended indigenous healers. Rates of disorder were significantly higher among respondents who were living in unserviced areas or who came from homes where food was needed. Conclusions: The DISC is a potentially useful instrument even in the presence of major constraints on conducting epidemiological research. J. Am. Acad. Child Ado/esc. Psychiatry, 1999, 38(9):1156-1164. Key Words: mental health, epidemiology, psychiatric disorder, Africa. Recent years have seen significant methodological improvements in studies investigating the epidemiology of psychiatric disorders (Robins and Regier, 1991). The Methods for the Epidemiology of Child and Adolescent Mental Disorders (MECA) study examined the per- formance of the lay-administered Diagnostic Interview Schedule for Children Version 2.3 (DISC-2.3) and con- cluded that the instrument "could be especiallyvaluable in settings where there is limited availability of skilled Accepted February 23, 1999. From the Department of Psychiatry, University of Cape Town (Dr. Robertson and Ms. Ensink), the National Urbanisation and Health Research Programme of the Medical Research Council (Dr. Parry), and the Department of Statistics, University of the western Cape (Dr. Chalton), Cape Town, SouthAfrica. This study wassupported bygrants from the SouthAfrican Medical Research Council and the Centre for Science Development of theHuman Sciences Research Council of SouthAfrica. The authors acknowledge the helpfUl comments of Dr. A. Flisher on the manuscript. Correspondence to Dr. Robertson, Department of Psychiatry, Groote Schuur Hospital Observatory 1925, SouthAfrica; e-mail: [email protected]. 0890-8567/99/3809-1156© 1999by the American Academy of Child and Adolescent Psychiatry. clinicians or when clinicians' time is at a premium" (Shaffer et al., 1996, p. 876). The relative lack of skilled clinicians in low-income countries, combined with an increasing prevalence rate of mental health problems (Desjarlais et al., 1995), suggests that such an instru- ment might be appropriate for Africa and other areas of the developing world where resources are limited and essentialservices can be made available for priority needs only. With this goal in mind, we decided to investigate the performance of the DISC-2.3 in Khayelitsha, an informal settlement area in South Africa where the pre- dominant language is Xhosa. Khayelitsha is a rapidly expanding township on the outskirts of Cape Town, with a population of at least 300,000. Approximately equal proportions of residents live in 3 different types of housing: formal housing in areaswhere services such aspiped water and water-borne or bucket-sewerage are supplied; informal housing or shackswith the above services; and informal housing or shacks on unserviced land. Khayelitsha experiences high levels of violence. The infant mortality rate is 31.4 to 1156 J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 38:9, SEPTEMBER 1999
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Performance of the Diagnostic Interview Schedule for Children Version 2.3 (DISC‐2.3) in an...

Performance of the Diagnostic Interview Schedule forChildren Version 2.3 (DISC-2.3) in an Informal
Settlement Area in SouthAfricaBRIANA. ROBERTSON,M.D., KARINENSINK, M.A., CHARLES D.H. PARRY, PH.D.,
AND DEREKCHALTON, PH.D.
ABSTRACTObjective: To investigate the performance of the Xhosa Diagnostic Interview Schedule for Children Version 2.3 (DISC-2.3) in a community study of African children and adolescents in Khayelitsha, a largely informal settlement area in CapeTown, South Africa. Method: A cross-sectional community study of 500 youths aqed 6 to 16 years was undertakenusing a systematic sampling strategy based on random starting points in the community. Three trained Xhosa-speakinglay interviewers administered the DISC-2.3 to youths and their parents in their homes. Additional questions includeddegree of impairment, selected risk factors, and service use. Results: The administration of the Xhosa DISC-2.3 inan informal settlement area was both feasible and acceptable to respondents. Psychiatric disorder with impairment wasrecorded for 76 (15.2%) of the children and adolescents. Consultation had been sought in only 20 cases, mostly frommedical doctors, except for 3 who had attended indigenous healers. Rates of disorder were significantly higher amongrespondents who were living in unserviced areas or who came from homes where food was needed. Conclusions:The DISC is a potentially useful instrument even in the presence of major constraints on conducting epidemiologicalresearch. J. Am. Acad. Child Ado/esc. Psychiatry, 1999, 38(9):1156-1164. KeyWords: mental health, epidemiology,psychiatric disorder, Africa.
Recent years have seen significant methodologicalimprovements in studies investigating the epidemiologyof psychiatric disorders (Robins and Regier, 1991). TheMethods for the Epidemiology of Child and AdolescentMental Disorders (MECA) study examined the per-formance of the lay-administered Diagnostic InterviewSchedule for Children Version 2.3 (DISC-2.3) and con-cluded that the instrument "could be especiallyvaluablein settings where there is limited availability of skilled
AcceptedFebruary 23, 1999.From theDepartment of Psychiatry, University ofCape Town (Dr. Robertson
andMs. Ensink), theNational Urbanisation andHealth Research Programme ofthe Medical Research Council (Dr. Parry), and the Department of Statistics,University ofthewestern Cape (Dr. Chalton), Cape Town, SouthAfrica.Thisstudy wassupported bygrants from theSouthAfrican Medical Research
Counciland theCentrefor Science Development of theHumanSciences ResearchCouncil of SouthAfrica. Theauthors acknowledge thehelpfUl comments of Dr.A. Flisher on themanuscript.
Correspondence to Dr. Robertson, Department of Psychiatry, Groote SchuurHospital Observatory 1925, SouthAfrica; e-mail: [email protected]/99/3809-1156©1999by theAmerican Academy of Child and
Adolescent Psychiatry.
clinicians or when clinicians' time is at a premium"(Shafferet al., 1996, p. 876). The relative lack of skilledclinicians in low-income countries, combined with anincreasing prevalence rate of mental health problems(Desjarlais et al., 1995), suggests that such an instru-ment might be appropriate for Africa and other areas ofthe developing world where resources are limited andessentialservices can be made available for priority needsonly.With this goal in mind, we decided to investigatethe performance of the DISC-2.3 in Khayelitsha, aninformal settlement area in South Africawhere the pre-dominant language isXhosa.Khayelitsha is a rapidly expanding township on the
outskirts of Cape Town, with a population of at least300,000. Approximately equal proportions of residentslive in 3 different types of housing: formal housing inareaswhere services such as piped water and water-borneor bucket-sewerage are supplied; informal housing orshackswith the above services; and informal housing orshacks on unserviced land. Khayelitsha experienceshighlevels of violence. The infant mortality rate is 31.4 to
1156 J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 38:9, SEPTEMBER 1999

50.3 per 1,000 (62.9 in unserviced areas), and 25% to50% of preschool children are chronically malnourished(Harrison and McQueen, 1992). Youths in Khayelitshaare considered to be at high risk for psychiatric disorder(United Nations Children's Fund and National Children'sRights Committee, 1993) , yet no psychiatric epidemio-logical studies of youths in Khayelitsha or anywhere inSouthMrica have been published in peer-reviewed jour-nals (Parry, 1996; Robertson and Berger, 1994).Conditions in periurban communities in Africa (and
in many parts of the developing world) place significantconstraints on undertaking psychiatric epidemiologicalresearch. Particular constraints include high populationmobility, population density, spatial layout of commu-nities (including unavailability of street names, housenumbers, telephones, and mail delivery), low literacy ratesand poor fluency in official (or main) languages, socialinstability, and unavailability of mental health profes-sionals (Parry, 1995). In addition, budgetary and infra-structural constraints are likely to make large-scaleEpidemiologic Catchment Area-type studies less feasiblein most African countries. The standardization of instru-ments and criterion validity and test-retest reliabilitystudies of imported instruments are daunting undertak-ings for the same reasons.Cultural differences and the translation process pose
major threats to the validity of psychiatric epidemiologi-cal research when instruments imported from othercountries are used, and ethnographic studies to exploreindigenous forms of expression and classification ofmental illness are (Kleinman, 1988; Parry,1996). Such a study among Xhosa-speaking children andadolescents in Khayelitsha identified 5 indigenous syn-dromes (Ensink and Robertson, 1996). An investigationinto the performance of a combined DISC-IndigenousSyndrome Questionnaire among children and adoles-cents attending a community health center in Guguletutownship showed that (1) the Xhosa version of the DISCWaS well understood by the respondents, (2) the longadministration time of the DISC (on average, 2-3 hours)was not acceptable to respondents, and (3) the DISC-2.3yielded adequate response rates in this population(Robertson et al., unpublished manuscript, 1993, Uni-versity of Cape Town). However, it became evident thatit was not possible to inquire directly about indigenoussyndromes: respondents became anxious and reluctant toparticipate, as they were afraid to openly discuss phe-nomena involving possible bewitchment.
DISC-2.3 STUDY IN SOUTH AFRICA
A further constraint on psychiatric epidemiologicalresearch is the difficulty of comparing prevalence ratesbecause ofmethodological differences (Bird et al., 1988).A review of major diagnosis-based epidemiologicalstudies carried out in different cultural settings over thepast 2 decades found rates varying between 6% and 19%when measures of impairment or severity were included(Bird, 1996). The recent multisite MECA study foundthat, when impairment of functioning was included inthe determination of caseness, 21% of children met theDSM-III-R ( American Psychiatric Association, 1987)criteria for one or more disorder (Shaffer et al., 1996). Astudy in a rural area of the United States, which includeda federal reservation of the Cherokee Nation, reported a3-month prevalence rate of 20%, or 4% to 8% whenusing impairment criteria (Costello et al., 1996a). Thefew community-based studies in sub-Saharan Africareviewed by Nikapota (1991) found prevalence rates ofpsychiatric disorder in Sudan and Ethiopia between 3%and 11%.It was felt that the results of an investigation into the
local. performance of the DISC-2.3 would have rel-evance for the use of the DISC and similar instrumentseven in Western countries. First, increasing numbers ofcommunities in Western countries share some of thesimilarities of informal settlements in South Africa, suchas foreign-language ghettos, refugee camps, war-tornpopulations, and very low-income areas. If the DISCcan be administered to children living in informal settle-ments in SouthAfrica and be shown to be useful and rel-evant, it will encourage investigators to conduct studiesin other high-risk but "difficult to research" areas .Second, such studies will shed light on the extent towhich the same expressions of distress can be elicited indifferent cultures.The aims of this study were (1) to determine the
feasibility of conducting a large epidemiological studyin an informal settlement area, (2) to document therates of psychiatric disorders in this population, (3) todocument the screening properties of the ReportingQuestionnaire for Children (RQC), (4) to investigatethe association between psychiatric disorder and selectedpotential correlates, and (5) to inquire about serviceutilization.
METHODTo address the above aims, a cross-sectional study was undertaken
in Khayelitsha.
] . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 38:9, SEPTEMBER 1999 1157

ROBERTSON ET AL.
InstrumentsDISC-2.3.A Xhosa translation of the DISC-2.3, which is based
on the DSM-III-R, was administered to children and parents in thesample. A full description of the development of the DISC-2.3 andits validation is given by Schwab-Stone et al. (1996) and Shafferet al.(1996). It has not been validated in a South African population. Inthis study both child (DISC-C) and parent (DISC-P) interviewswere used for children aged 10 to 16 years, and parent-only inter-views for children aged 6 to 9 years, as suggested by the reliabilitystudy of Schwab-Stone et al. (1994). The translation of the DISC-2.3 into Xhosa, its back-translation, and its pilot study are fullydescribed in the Guguletu study (Robertson et al., unpublished man-uscript, 1993, University of Cape Town). The interviewers were thesame as those used in the Guguletu study, which was completedshortly before this study was undertaken, and their training isdescribed in that study. The interviewers were 3 Xhosa-speakingwomen with a secondaty school education (completed grade 12)whowere residents of Khayelitsha.As the administration time of the DISC was found by many
respondents in the Guguletu study to be too long, we decided toomit modules that were expected to yield low prevalencerates amongchildren and adolescents in the community. Thus the schizophrenia,mania, and hypomania modules were omitted. The alcohol and sub-stance abuse modules were also omitted because experience in theGuguletu study showed that lack of privacy in township dwellingsmade children and adolescents unwilling to disclose informationabout substance use at home interview.RQC The World Health Organization's RQC has demonstrated
satisfactory sensitivity and specificity as a screening instrument forepidemiological studies among various language groups in devel-oping countries (Giel et al., 1988). The RQC is a IO-item question-naire, administered to the child's caretaker, and a score of onepositive response is regarded as suggestive of a psychiatric disorder(Giel et al., 1988). Its Xhosa translation, back-translation, and pilot-testing is described in the Guguletu study (Robertson et al., unpub-lished manuscript, 1993, University of Cape Town). We decided todocument its screening properties in relation to the DISC-2.3.ImpairmentScale. We instituted a simple 5-point rating scale for
estimating the perceiveddegree of impairment: whenever the DISC-P required respondents to indicate whether a defined behavior ormood caused impairment of functioning at school, at home, or withpeers, respondents were also asked to rate the degree of impairmenton a 5-point rating scale (0 = no impairment, 5 = severe impairment).Correlates and Service Use. We added questions to relevant sections
of the DISC-2.3 in order to investigate certain putative correlates ofpsychiatric disorder and to elicit service use, with regard to indige-nous African healers. In the Introduction module, it was recordedwhether the dwelling was in a serviced or unserviced area; parentswere asked whether they had enough food, and their response wascorroborated by the observations of the interviewer. Inquiry wasmade into the urbanization history of the child and parents and thenumber of siblings living in the family's traditional rural homesteador elsewhere. In the psychiatric disorder modules, at the point whenquestions were asked about consultation with mental health profes-sionals, we inserted an additional question about consultation withindigenous African healers.
SampleDistance and transport considerations made it necessary to con-
fine the study to sites Band C in Khayelitsha. These sites have atotal estimated population of 92,211 and are comparable with
Khayelitsha as a whole, in terms of the mixture of serviced andunserviced dwellings.A sample of 500 children aged 6 to 16 yearswas selected from an
equal number of serviced (n = 249) and unserviced (n = 251) dwell-ings. When a child was not living with a biological or adoptiveparent, a caretaker who had cared for the child for at least 6 monthswas interviewed for the DISC-P.
ProcedureA systematic sampling strategy was used to select dwellings; 18
routes were determined using aerial photographs and street maps,and a random sample of one third of the routes was then selected.Every fifth dwelling was visited, using a random starting point oneach block. If no reliable adult informant was present, interviewersmade 3 return visits before removing the dwelling from the sample.Interviewers introduced themselvesand the purpose of the study andrequested consent for participation of the respondents. In house-holds with more than one child between the ages of 6 and 16 yearsliving in the dwelling, selection for participation in the study wasmade using a table of random numbers. Appointments to completethe interviewswere then set and a participation payment was offeredto each family. Interviews were conducted at the child's home; thechild was interviewed privately, with the consent of the parents.Interviewers frequently required more than one visit to completeinterviews. No institutions were included in the study.
Data AnalysisThe data were analyzedusing a StatisticalAnalysisSystempackage
from the Division of Child and Adolescent Psychiatry, ColumbiaUniversity (New York).The construction of the algorithms leadingto diagnosis is described in the report of the MECA study (Shafferet al., 1996). The rates of disorder reported reflect combined parent-child diagnoses, that is, a diagnostic criterion is considered met ifreported present by either the parent or the child. Similarly, impair-ment criteria are met if reported by either parent orchild.Since the sample is a systematic one, the variance of prevalence
cannot be estimated. However, on the assumption that there was noperiodicity in the dwellings selected, the sample can be regarded as asimple random sample (Raj, 1968). This assumption was made forthe computation of the confidence intervals for the prevalence rates.
RESULTS
Description of the Sample
The interviewers visited 814 dwellings to obtain asample of 500 subjects. There was 1 refusal; at 3 dwell-ings a respondent was not found during 3 return visits; at102 dwellings there were no children aged 6 to 16 years;and at an additional 208 dwellings there were no childrenat all. At the 810 households sampled there were 1,451children younger than age 17, but 229 (15.8%) livedelsewhere, usually in the rural areas (86.4%). Only 2 chil-dren were sent to live in rural areas because of behaviorproblems or mental handicap. Of the total 1,222 chil-dren (aged 0-16 years) living at the 810 dwellings, 362(30%) were younger than 6 and 860 (70.4%) werebetween the ages of 6 and 16 years.
1158 ]. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 38:9, SEPTEMBER 1999

Of the sample of 500 children, 272 (54.5%) werefemale and 227 (45.5%) were male; 280 (56%) were aged6 to 9 and 217 (44%) were aged 10 to 16. One hundredeight children (21.6%) were not attending school, and58.8% had been born in rural areas. Biologicalor adoptiveparents constituted 90% of the caretakers interviewed, theremainder being aunts, grandparents, and other relatives.Of the caretakers, 33.4% had been in Cape Town for 5years or less, 33.8% for 5 to 10years.The majority of care-takers (94%) had been born in rural areas, and 52% spentfewer than 7 months a year in Cape Town. Seventeen per-cent of the caretakers had had no formal education. In asignificant percentage of households (19%) there was noincome, and in 21% food was needed urgently.
Feasibility of Conducting a Large Epidemiological Study inan Informal Settlement Area
The use of aerial photographs made it possible to planand successfully implement a random sampling strategydespite the lack of formal streets and systematic housenumbering. The fact that the interviewers lived inKhayelitsha themselves meant that they could moreeasily find their way around, were less likely to put them-selves in dangerous situations, and did not engender theusual distrust of strangers.Respondents were often not at home when appoint-
ments had been made; all the DISC interviewswere com-pleted because of the willingness of the interviewers to goback in the evenings and weekends if necessary. Fivehun-dred of an identified 501 eligible children and their care-takers agreed to participate and completed the study. The
DISC-2.3 STUDY IN SOUTH AFRICA
use of financial incentives was an essential component toensure the full cooperation of some respondents.No significant problems were experienced by the inter-
viewers with regard to the language, concepts, format, oradministration time (on average, 1-2 hours) of the DISC-2.3, although explanations and encouragement had to begiven about the importance of responding to all the ques-tions despite their apparent repetitive nature.
Rates of Psychiatric Disorders According to DISC-2.3
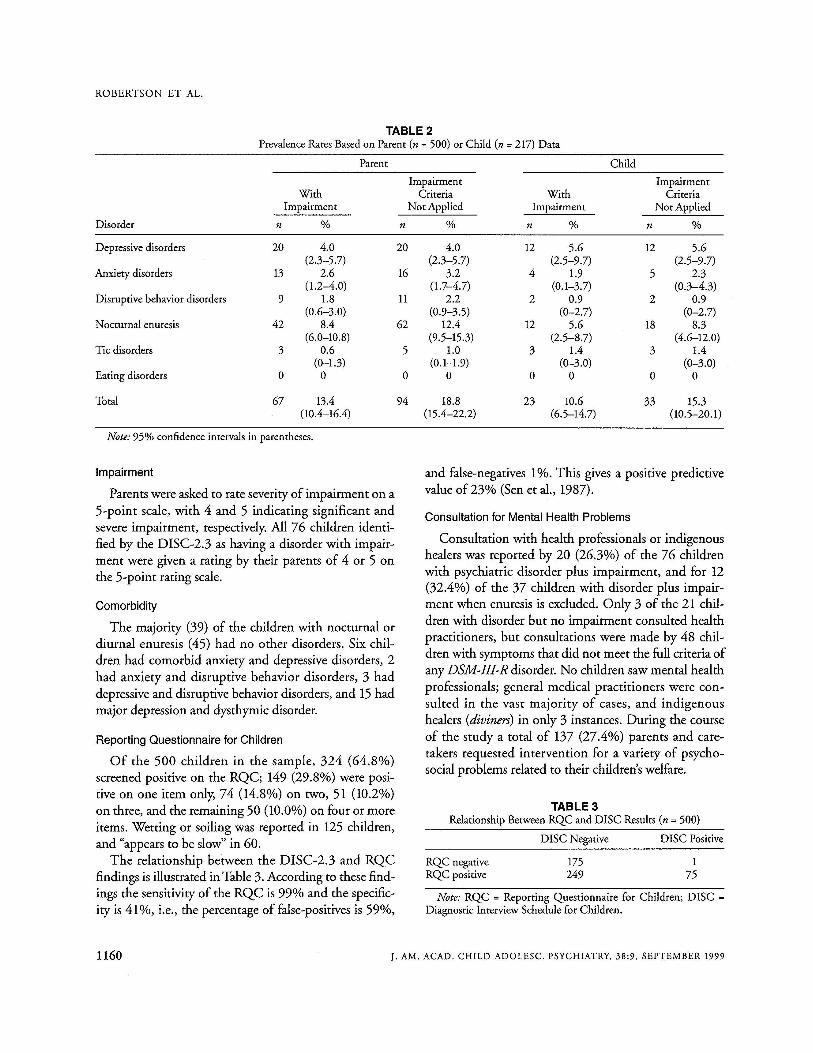
These data are provided to give an indication of theperformance of the DISC-2.3 in Xhosa-speaking re-spondents in an informal settlement area in SouthAfrica.The prevalence rates reported are not viewed as indicativeof the actual rates in the population studied or ofAfricancommunities generally. All rates presented are 6-monthperiod prevalence rates and are for disorders which metimpairment criteria (unmodified) in at least one area (atschool, at home, or among friends) (Table 1). Rates arealso provided for children who met DSM-III-R symp-tom, onset, and duration criteria only, and in Table 2 fordiagnoses derived from parent and child data separately.Seventy-six (15.2%) had one or more psychiatric dis-
order with impairment (Table 1). When children or ado-lescentswith enuresis only are excluded, 37 or 7.4% of thesample had one or more psychiatric disorder. After noctur-nal enuresis (8.8%), dysthymic disorder (4.0%) was themost prevalent, followed by major depressive disorder(3.4%). None of the children had obsessive-compulsivedisorder (OCD), and only 2 children met criteria forattention-deficit hyperactivity disorder.
TABLE 1PrevalenceRates (n = 500)
With Impairment Impairment Criteria Not AppliedDisorder n % n %
Depressive disorders 22 4.4 22 4.4(2.6- 6.2) (2.6-6.2)
Anxiety disorders 14 2.8 18 3.6(1.4-4.2) (2.0-5.2)
Disruptive behavior disorders 10 2.0 11 2.2(0.8- 3.2) (0.9-3.5)
Nocturnal enuresis 44 8.8 64 12.8(6.3- 11.3) (9.9-15.7)
Tic disorders 3 0.6 5 1.0Eating disorders 0 0 0 0
Total 76 15.2 97 19.4(12.1-18.3) (15.9-22.9)
Note: 95% confidence intervals in parentheses.
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 38:9, SEPTEMBER 1999 1159
ROBERTSON ET AL.
TABLE 2PrevalenceRates Basedon Parent (n = 500) or Child (n = 217) Data
Parent
WithImpairment
Disorder n %
Depressivedisorders 20 4.0(2.3-5.7)
Anxiety disorders 13 2.6(1.2-4.0)
Disruptive behavior disorders 9 1.8(0.6-3.0)
Nocturnal enuresis 42 8.4
Tic disorders(6.0-10.8)
3 0.6
Eating disorders(0-1.3)
0 0
Total 67 13.4(10.4-16.4)
ImpairmentCriteria With
Not Applied Impairmentn % n %
20 4.0 12 5.6(2.3-5.7) (2.5-9.7)
16 3.2 4 1.9(1.7-4.7) (0.1-3.7)
11 2.2 2 0.9(0.9-3.5) (0-2.7)
62 12.4 12 5.6(9.5-15.3) (2.5-8.7)
5 1.0 3 1.4(0.1-1.9) (0-3.0)
0 0 0 0
94 18.8 23 10.6(15.4-22.2) (6.5-14.7)
ChildImpairmentCriteria
Not Appliedn %
12 5.6(2.5-9.7)
5 2.3(0.3-4.3)
2 0.9(0-2.7)
18 8.3(4.6-12.0)
3 1.4(0-3.0)
0 0
33 15.3(10.5-20.1)
Note: 95% confidence intervals in parentheses.
TABLE 3Relationship Between RQC and DISC Results (n = 500)
Note: RQC = Reporting Questionnaire for Children; DISC =Diagnostic Interview Schedule for Children.
and false-negatives 1%. This gives a positive predictivevalue of 23% (Sen et al., 1987).
Consultation for Mental Health Problems
Consultation with health professionalsor indigenoushealers was reported by 20 (26.3%) of the 76 childrenwith psychiatric disorder plus impairment, and for 12(32.4%) of the 37 children with disorder plus impair-ment when enuresis is excluded. Only 3 of the 21 chil-dren with disorder but no impairment consulted healthpractitioners, but consultations were made by 48 chil-dren with symptoms that did not meet the full criteria ofanyDSM-III-R disorder. No children sawmental healthprofessionals; general medical practitioners were con-sulted in the vast majority of cases, and indigenoushealers (diviners) in only 3 instances. During the courseof the study a total of 137 (27.4%) parents and care-takers requested intervention for a variety of psycho-social problems related to their children'swelfare.
175
175249
DISC Negative DISC Positive
RQC negativeRQC positive
Reporting Questionnaire for Children
Of the 500 children in the sample, 324 (64.8%)screened positive on the RQC; 149 (29.8%) were posi-tive on one item only, 74 (14.8%) on two, 51 (10.2%)on three, and the remaining 50 (10.0%) on four or moreitems. Wetting or soiling was reported in 125 children,and "appears to be slow" in 60.The relationship between the DISC-2.3 and RQC
findings is illustrated in Table 3. According to these find-ings the sensitivity of the RQC is 99% and the specific-ity is 41%, i.e., the percentage of false-positives is 59%,
Comorbidity
The majority (39) of the children with nocturnal ordiurnal enuresis (45) had no other disorders. Six chil-dren had comorbid anxiety and depressive disorders, 2had anxiety and disruptive behavior disorders, 3 haddepressive and disruptive behavior disorders, and 15hadmajor depression and dysthymic disorder.
Impairment
Parentswere asked to rate severityof impairment on a5-point scale, with 4 and 5 indicating significant andsevere impairment, respectively. All 76 children identi-fied by the DISC-2.3 as having a disorder with impair-ment were given a rating by their parents of 4 or 5 onthe 5-point rating scale.
1160 J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 38:9, SEPTEMBER 1999

Correlates of Psychiatric Disorder
The rates of disorder, both including and excludingenuresis, were higher in boys than in girls, children olderthan 12 years of age, children from families where foodwas needed , children in unserviced areas, and childrenwith a history of either hospitalization, chronic physicalproblems, "fits," head inju ry, or serious physical illness(Table 4). All correlates of disorder, except gender andage, reached statistical significance in both groups at alevel greater than .05, using the X2 test, with 1df
DISCUSSION
The study shows that it is feasible to obtain completediagnostic information from indigenous African youthsand their adult caretakers living in informal settlementsusing an unfamiliar, highlystructured interview schedule.With careful but inexpensive planning, random samplescan be drawn in informal settlement areas, and a satisfac-tory rate of participant recruitment can be achieved.The omission of several modules of the DISC-2.3
made the administration time acceptable, and generallyparticipants felt more positive at the end of the inter-
DISC-2 .3 STUDY IN SOUTH AFRICA
view when they had a better understanding of psychiat-ric disorders. Effective enlightenment about mentalhealth and about psychiatric disorders in young peoplewas an unexpected benefit of this study. The almost100% participation rate in this study was achieved bythe persistence and flexibility of the interviewers andtheir being members of the same community, aided bythe use of financial incentives.The reason for the larger number ofyounger children
in the sample is not known. The interviewers believe asignificant number of older children were among thosesent away to the traditional homesteads in the rural areas,but corroboratory information is lacking. As Khayelitshais a rapidly developing area, it may be that familieswithyoung children outnumber those with older children,but again data for the specific age groups designated inthis study, and their gender distribution, are lacking.Although the prevalence rates reported cannot be
assumed to reflect accurately the actual rates in the com-munity, the DISC·2.3 elicited DSM-III-R criteria formost psychiatric disorders included in the study. Theindividual rates raise some interesting questions forfuture research. To our knowledge a similarly high rate
GenderMale (n = 227)Female (n = 272)
Age6-11 yr (n = 357)12-16 yr (n = 143)
Need ing foodYes (n = 104)No (n = 295)
UnservicedYes (n = 251)No (n = 249)
History of illness"Yes (n = 169)No (n = 331)
TABLE 4Correlates of Disorder (n = 500)
Disordern (%)
41 (18.1)34 (12.5)P=.08 (X2 =2.997)
51 (14.3)25 (17.5)P = .37 (X2 = 0.810)
28 (26.9)40 (13.6)P = .002 (X2 = 9.7 13)
50 (19.9)26 (1004)P=.003 (X2 =8.713)
35 (20.7)41 (1204)P=.01 (X2 =6.013)
Disorder Excluding Enuresisn (%)
21 (9.2)16 (5.9)
P=.153 (X2 =2.045)
18 (5.0)19 (13.3)
P = .001 (X2 = 10.128)
19 (18.3)16 (SA)p = .001 (X2 = 15.855)
27 (10.8)10 (4.0)p =.004 (x2=8.289)
22 (13.0)IS (4.5)
P = .001 (X2 = 11.757)
Note: Totals less than the expected n reflect missing responses.a Includes history of hospitalization , chronic physical problems , "fits," head injury, or serious physical illness.
] . AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 38:9, SEPTEMBER 1999 1161

ROBERTSON ET AL.
of nocturnal enuresis (more than half the total rate ofdisorder with impairment) has not been reported inother epidemiological studies, although a comparison ofSwedish and African children found higher rates of noc-turnal enuresis in African children older than 7 years ofage (Cederblad, 1988). Major factors considered likelyto contribute to this finding are (1) that nocturnal enure-sis, unlike many psychiatric disorders in young people, iswell recognized by African communities as it manifestsphysically and is linked to particular traditional beliefsand practices (Reynolds, 1989); (2) the preponderanceof younger children in the sample; (3) the possibility ofa relatively higher rate ofmental handicap in the sample(there were no measures to corroborate this directly, but108 youths were not attending school and according tothe RQC, 60 were reported as "slow"); and (4) inade-quate toilet training in this population (an opinionexpressed by the interviewers), leading to higher rates ofnocturnal enuresis.The rate of disorder with impairment (excluding
enuresis) is considerably less than that found in theMECA study, but similar to the rates for serious emo-tional disturbance in the Great Smoky Mountains Study,in which a 3-month time frame was used (Costello et al.,1996a; Shaffer et al., 1996). We expected higher rates,given the experience of past and present adversity byyoung people in Khayelitsha, especially for the anxietyand disruptive behavior disorders.The possibility that theDISC-2.3 has a lower identification rate for some dis-orders in this population has been confirmed for posttrau-matic stressdisorder (PTSD) (Ensink et al., 1997b). A lowidentification rate may be due to problems with the valid-ity of part or all of the DISC-2.3, its translation intoXhosa, or cultural factors such as unfamiliarity with thepsychological concepts underpinning the DSM nosology.Different cultural groups are likely to have some uniqueconstructs of psychological distress and dysfunction andsome unique modes of expressing them (Kleinman,1988). On the one hand, for instance, somatoform anddissociative mechanisms have been cited as common inAfrican society (Ensink and Robertson, 1996; Guinness,1992), but the DISC-2.3 does not have modules forsomatoform or dissociativedisorders. On the other hand,eating disorders and OCD appear to be virtuallyunknown in traditional African communities (German,1987; Ilechukwu, 1991; Minde and Nikapora, 1993).It is also possible that the overall prevalence rate of
psychiatric disorder reported in this study may reflect
lower actual rates among Khayelitsha young people thanexpected. Possible reasons for lower actual rates includeconstitutional factors aswell as higher thresholds for sub-jective feelings of stress (or, in parents, higher thresholdsfor labeling behavior as pathological). Higher stressthresholds may have been shaped by cultural expecta-tions, traditional beliefs, or early continuous exposure tostress (Cederblad, 1988). Higher stress thresholds couldbe expected to result in proportionately more seriousand less mild psychiatric disorders, with higher levels ofimpairment and comorbidity, for which there is someevidence in this study (seebelow).The low rate of anxiety disorders reported is due par-
tially to the lack of a PTSD data analysisprogram in theDISC-2.3 and also to the absence of OCD in this popu-lation. The rate of disruptive behavior disorderswas lowerthan expected, and most of the cases were of conduct dis-order.The absence of eating disorderswas expected.If parents' ratings of impairment were true, none of
the disorders were mild. As reported in other studies(Costello et al., 1996a; Shaffer et al., 1996), depressiveand disruptive behavior disorders produced more impair-ment than other disorders. Approximately halfof the dis-order categories were comorbid with other categories,and the majority of youths with depressivedisorders haddouble depression. This rate of comorbidity is higherthan in the Great Smoky Mountains Study (Costelloet al., 1996b) and could partially account for the highratings of impairment among Khayelitsha youths.If a sensitivity of 99% is confirmed by future studies
of the RQC, considerable time could be saved by usingit as a screening instrument and administering the DISConly to screen positives.The finding of a low rate of consultation for mental
health problems which increased when psychiatric dis-order or impairment was present is in accordwith findingsof other studies (Costello et al., 1996a; Leaf et al., 1996).The lack of contact with mental health professionals con-firms the findings ofpreviousstudies that specialistservicesare relatively inaccessible to this population (Ensink et al.,1997a). Given the apparent severity of psychiatric dis-orders reported in this study, the situation warrants urgentattention. The limited consultation with indigenoushealersdoes not match the more substantial rates reportedin other local studies, although these studies usually inves-tigate consultation by adults with mental health problems(Ensink and Robertson, 1999;McIntyre et al., 1994).Thelow rate reported in this study may reflect the preponder-
1162 J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY. 38:9. SEPTEMBER 1999

ance of young children and the fact that dissociative andpsychotic disorderswere not investigated.The nonrepresentativeness of the sample precludes
definitive conclusions being drawn from the findingsabout the correlatesofpsychiatricdisorder,although all arein the expected direction (Bird er al., 1989; Buckner andBassuk, 1997; Gortrnaker et al., 1990; Velez et al., 1989).There are likelyto be many factors contributing indirectlyto the strong associationbetween poverty ("needing food")and psychiatric disorder, such as single-parent families,lack of social support, and physical and mental ill-health,but it is alsopossiblethat the distress of these parents led tomagnification ofsymptoms in their children.The majorityof Khayelitsha families are recently urbanized, but it wasnot possible to analyze any association between recenturbanization and psychiatric disorder because of thefrequent movement of parents and children between theirurban and rural homesteads. Probably both poverty andrecent urbanization contribute to the association betweenpsychiatricdisorder and living in an unserviced dwelling.
Clinical Implications
Although validation of the DISC in this population isnecessary before prevalence rates of psychiatric disordercan be accepted with confidence, the study points to thepresence of severe psychiatric disorders in youths whohave little access to specialized mental health services.The findings suggest the prioritization of youths livingin unserviced dwellings who have no food, but the kindof service which will be appropriate, effective, and sus-tainable in this context requires careful consideration.The pattern of individual disorders elicited by the
DISC in this study raises several questions for futureresearch, for instance: Does PTSD occur in this popula-tion? Are attention-deficit hyperactivity disorder andOCD rare in African children, or are they underdiag-hosed? We hope that the recent publication of theDISC-4, compatible with both the DSM-IVand theICD-Ill.}yill facilitate improvements in the methodol-ogy of epidemiological studies in Africa.
REFERENCESAmerican PsychiatricAssociation (1987), Diagnostic and StatisticalManualof
.Mental Disorders, 3rd edition-revised (DSM-III-R). Washington, DC:American Psychiatric Association
Bird HR (1996), Epidemiology of childhood disorders in a cross-culturalcontext. ] Child PsycholPsychiatry 37:35-49
Bird HR, Canino G, Rubio-Stipec M et al. (1988), Estimates of the prev-alenceof childhood maladjustment in a community surveyin Puerto Rico.ArchGen Psychiatry 45:1120-1126
DISC-2 .3 STUDY IN SOUTH AFRICA
Bird HR, Gould MS, YagerT, Staghezza B, Canino G (1989), Risk factorsfor maladjustment in Puerto Rican children. JAm Acad ChildAdolescP.rychiatry 28:847-850
Buckner ]C. Bassuk EL (1997) , Mental disorders and service utilizationamong youths from homeless and low-income housed families. JAmAcadChildAdolesc Psychiatry 36:890-900
Cederblad M (1988). Behavioural disorders in children from different cul-tures. ActaPsychiatr ScandSuppI344:85-92
Costello ]E, Angold A, Burns B], Erkanli A, Stangl DK, Tweed DL (1996a),The Great Smoky Mountains Study of Youth: functional impairmentand serious emotional disturbance. ArchGen Psychiatry 53:1137-1143
. Costello ]E, AngoldA, Bums B] er al, (1996b), The Great Smoky MountainsStudy ofYouth: goals, design, methods, and the prevalenceof DSM-III-Rdisorders. ArchGenP.rychiatry 53:1129-1136
Desjarlais R, Eisenberg1, Good B, Kleinman A (1995), WorldMentalHealth:Problems andPriorities in Low-Income Countries. New York:Oxford Uni-versity Press
Ensink K, Leger PH, Robertson BA (1997a), Mental health services in theWestern Cape, 2: review of public sector services, 1992/93. SAftMedJ87:1196-1200
Ensink K, Robertson B (1996), Indigenous categories of distress and dys-function in South African Xhosa children and adolescents as described byindigenous healers. Transcult Psycbiatr Res Rev 33:137-172
Ensink K, Robertson B (1999), Patient and family experiences of psychiatricservices and African indigenous healers. Transcult P.rychiatry36:23-43
Ensink K, Robertson BA, Zissis C, Leger P (1997b), Post-traumatic stressdisorder in children exposed to violence. SAftMedJ 87:1526-1530
German GA (1987). Mental health in Africa, II: the nature of mental disor-der in Africatoday.Some clinical observations.BrJ Psychiatry 151:440-446
Giel R, Harding TW, Ten Hom GHMM et al. (1988), The detection ofchildhood mental disorders in primary care in some developing coun-tries. In: Handbook ofSocial P.rychiatry, Henderson AS, Burrows GS, eds.New York:Elsevier Science Publishers, pp 233-244
Gortmaker SL. Walker DK, Weitzman M, Sobol AM (1990). Chronic con-ditions, socioeconomic risks, and behavioral problems in children andadolescents. Pediatrics 85:267-276
Guinness EA (1992), Relationship between the neuroses and brief reactivepsychosis: descriptive case studies in Africa. Br J Psychiatry SupplApril:12-23
Harrison D , McQueen A (1992), An OverviewofKhayelitsha: ImplicationsforHealth Policy and Planning. Parow. South Mrica: Medical ResearchCouncil
Ilechukwu STC (1991), Psychiatry in Mrica: special problems and uniquefeatures. Transcult PsychiatrResRev28:169-218
Kleinman A (1988). RethinkingPsychiatry: From Cultural Category toPersonalExperience. New York: Free Press
LeafPJ, Alegria M, Cohen P ecaI. (1996), Mental health service use in thecommunity and schools: results from the four-community MECA study.JAm AcadChildAdolesc P.rychiatry 35:889-897
McIntyre D, Chetty K, Ensink K (1994), TheUtilisation ofHealth Services inSite C, Khayelitsha (Working Paper No.8). Cape Town, South Mrica:Health Economics Unit, University of Cape Town
Minde K, Nikapota AD (1993), Child psychiatry and the developing world:recent developments. Transcult P.rychiatrRes Rev 30:315-346
Nikapota AD (1991), Child psychiatry in developing countries. BrJ Psychi-atry 158:743-751
Parry CDH (1995), Quantitative measurement of mental health problems inurban areas: opportunities and constraints. In: Urbanisation andMentalHealth in Developing Countries, Harpham T, Blue I, eds. Aldershot,England: Avery, pp 193-224
Parry CDH (1996), A reviewof psychiatric epidemiology in Mri ca: strategiesfor increasing validity when using instruments transculturally. TranscultPsycbiatr Res Rev33: 173-188
Raj D (1968), Sampling Theory. New York:McGraw-HillReynolds P (1989), Childhood in Crossroads. Cape Town, South Africa: David
PhilipRobertson B, Berger S (1994), Child psychopathology in South Africa. In:
Childhood andAdversity, Dawes A, Donald D, eds, Cape Town, SouthMrica: David Philip
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 38:9, SEPTEMBER 1999 1163

ROBERTSON ET AL.
Robins LN, Regier DA (1991), PsychiatricDisorders in America. New York:Free Press
Schwab-Stone M, Fallon T, Briggs M, Crowther B (1994), Reliability ofdiagnostic reporting for children aged 6-11 yeats: a test-retest srudy ofthe Diagnostic Interview Schedule for Children-Revised.Am]Psychiatry151:1048-1054
Schwab-Stone M, ShafferD, Dulcan MK et al. (1996), Criterion validity ofthe NIMH Diagnostic Int erview Schedule for Ch ildren Version 2.3(DISC-2.3) . ] Am Acad Child.Molesc Psychiatry35:878-888
Sen B.Wilkinson G,Mari JJ (1987), Psychiatricmorbidity in primary healthcare. A two-stage screening procedure in developing countries: choice ofinstruments and cost-effectiveness.BrJPsychiatry151:33-38
Shaffer D , Fisher P, Dulc an MK et al. (1996), The NIMH DiagnosticInterview Schedule for Children Version 2.3 (DISC-2.3): description,acceptability. prevalence rates. and performance in the MECA study. ]AmAcad ChildAdolesc Psychiatry35:865-877
United Nations Children's Fund and National Children's Rights Committee(1993) , Children and WOmen in South Africa: A Situation Analysis.Johannesburg, South Africa: United Nations Children's Fund andNational Children'sRights Committee
Velez CN . Johnson J, Cohen P (1989), A longitudinal analysis of selectedrisk factors for childhood psychopathology. ] Am Acad Child AdolescPsychiatry28:861-864
1164
Unnatural Sudden Infant Death. Roy Meadow
Aim:To identify features to help paediatr icians differen tiate between natural and unnatural infant death s.Method:Clinical featuresof 81 children judged by criminal and family courts to have been killed by their paren ts were studied. Health and social service rec-ords, court documents, and records from meetings with paren ts, relatives, and social workers were studied. Results: Initial ly, 42 chil-dren had been cert ified as dying from sudden infant death syndrome (SIDS), and 29 were given another cause of natural death . In24 families, more than one child died; 58 died before the age of 6 months and most died in the afternoon or evening . Seventy per-cent had experienced unexplained illnesses; over half were admi tted to hospital within the previous month, and 15 had been dis-charged withi n 24 hours of death . The mother, father, or both were responsible for death in 43, five, and two families, respectively.Most homes were disadvantaged-no regular income, receiving income support-and mothers smoked. Half the perpetrators hada history of somatising or factitious disorder. Death was usually by smothering and 43% of children had bruises, petech iae, Otblood on the face. Conclusions: Although certain featur es are indicative of unnarural infant death, some are also associated withSIDS. Despite the recent reduction in numbers of infants dying suddenly, inadequacies in the assessment of their deaths exist. Untila thorough postmortem examination is combined with evaluation of the history and circumstances of death by an experienced pae-diatrician, most cases of covert fatal abuse will go und etected . The term SIDS requires revision or abandonment . Arch Dis Child1999;80:7-14. Reproduced with permission from the BMJ Publishing Group.
J. AM. ACAD. CH ILD ADOLESC. PSYCHIATRY, 38 :9, SEPTEMBER 1999