
Perfectionism in depression, obsessive-compulsive disorder and eating disorders
10
This article appeared in a journal published by Elsevier. The attached copy is furnished to the author for internal non-commercial research and education use, including for instruction at the authors institution and sharing with colleagues. Other uses, including reproduction and distribution, or selling or licensing copies, or posting to personal, institutional or third party websites are prohibited. In most cases authors are permitted to post their version of the article (e.g. in Word or Tex form) to their personal website or institutional repository. Authors requiring further information regarding Elsevier’s archiving and manuscript policies are encouraged to visit: http://www.elsevier.com/copyright
-
Upload
studicognitivi -
Category
Documents
-
view
3 -
download
0
Transcript of Perfectionism in depression, obsessive-compulsive disorder and eating disorders

This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/copyright

Author's personal copy
Behaviour Research and Therapy 46 (2008) 757–765
Shorter communication
Perfectionism in depression, obsessive-compulsivedisorder and eating disorders
Sandra Sassarolia,b,�, Leonor J. Romero Lauroa,c, Giovanni Maria Ruggieroa,b,Massimo C. Maurid, Piergiuseppe Vinaia, Randy Froste
a‘‘Studi Cognitivi’’ Cognitive Psychotherapy School, Foro Buonaparte 57, 20121 Milano, Italyb‘‘Psicoterapia Cognitiva e Ricerca’’ Cognitive Psychotherapy School, Milano, Italy
cDepartment of Psychology, University of Milano-Bicocca, Milan, ItalydMood Disorders Unit, Clinica Psichiatrica ‘‘Guardia II’’, Policlinico Ospedale Maggiore Milano e Universita degli Studi di Milano, Italy
eSmith College, Clark Science Center, Northampton, MA, USA
Received 12 November 2007; received in revised form 22 February 2008; accepted 25 February 2008
Abstract
High levels of perfectionism have been observed in major depression, anxiety disorders and eating disorders. Though few
studies have compared levels of perfectionism across these disorders, there is reason to believe that different dimensions of
perfectionism may be involved in eating disorders than in depression or anxiety [Bardone-Cone, A. M. et al. (2007).
Perfectionism and eating disorders: Current status and future directions. Clinical Psychology Review, 27, 84–405]. The
present study compared patients with major depression, obsessive-compulsive disorder, and eating disorders on
dimensions of perfectionism. Concern over Mistakes was elevated in each of the patient groups while Pure Personal
Standards was only elevated in the eating disorder sample. Doubts about Actions was elevated in both patients with
obsessive-compulsive disorder and eating disorders, but not in depressed patients. Analyses of covariance indicated that
Concern over Mistakes accounted for most of the variance in the relationship of perfectionism to these forms of
psychopathology.
r 2008 Elsevier Ltd. All rights reserved.
Keywords: Perfectionism; Depression; Eating disorders; Obsessive-compulsive disorder
Introduction
Dimensions of perfectionism
Perfectionism has emerged as an important construct with respect to the etiology and maintenance ofvarious types of psychopathology (Flett & Hewitt, 2002). Research on perfectionism has supported two basic
ARTICLE IN PRESS
www.elsevier.com/locate/brat
0005-7967/$ - see front matter r 2008 Elsevier Ltd. All rights reserved.
doi:10.1016/j.brat.2008.02.007
�Corresponding author at: ‘‘Studi Cognitivi’’ Cognitive Psychotherapy School, Foro Buonaparte 57, 20121 Milano, Italy.
Tel.: +39024 150998; fax: +39 023 6505866.
E-mail address: [email protected] (S. Sassaroli).

Author's personal copy
dimensions corresponding to maladaptive evaluative concerns (MEC) and achievement striving (AS), thoughthe titles for these dimensions vary somewhat depending in part on the measure being used (Bieling, Israeli, &Antony, 2004; Blankstein & Dunkley, 2002; Cox, Enns, & Clara, 2002; Dunkley, Blankstein, Masheb, &Grilo, 2006; Frost, Heimberg, Holt, Mattia, & Neubauer, 1993). On the Frost Multidimensional PerfectionismScale (FMPS; Frost, Marten, Lahart, & Rosenblate, 1990) the Concern over Mistakes subscale appears to bethe central feature of MEC (Dunkley, Zuroff, & Blankstein, 2006; Frost & DiBartolo, 2002), though thisdimension also reflects to a lesser degree Doubts about Actions, Parental Expectations, and ParentalCriticism. The Personal Standards subscale of the FMPS most closely corresponds to the AS dimension ofperfectionism. However, DiBartolo, Frost, Chang, La Sota, and Grills (2004) identified several items on thissubscale that measured not only high personal standards, but also evaluative self-worth. Reanalysis ofdatasets and additional data confirmed that removing these items from the scale provided a purer measure ofpersonal standards.
Concern over Mistakes has been found to correlate with measures of psychopathology among nonclinicalpopulations (see Frost & DiBartolo, 2002 for a review) and to be significantly higher among clinicalpopulations including most anxiety disorders, depression, and eating disorders (see Bardone-Cone et al., 2007;Frost & DiBartolo, 2002 for reviews).
Though it is clear that Concern over Mistakes is associated with psychopathology and maladaptivecharacteristics, debate has ensued as to whether the achievement striving perfectionism might be considered‘‘positive’’ or ‘‘adaptive’’ (Bieling et al., 2004; Flett & Hewitt, 2006; Greenspon, 2000; Slade & Owens, 1998;Stober & Otto, 2006). The Personal Standards scale of the FMPS has been found to correlate with positivemood, conscientiousness, and other ‘‘adaptive’’ qualities (Bieling et al., 2004; Frost et al., 1990; Stober, 1998),and some have argued this may be a form of ‘‘healthy’’ perfectionism (Parker, 1997). In a comprehensivereview of this area, Stober and Otto (2006) concluded that perfectionistic strivings, as measured by scales likethe Personal Standards scale, are associated with adaptive behaviors rather than pathology. However, otherstudies have found small but significant correlations between Personal Standards and indices of anxiety anddepression in nonclinical samples (Brown et al., 1999; Cheng, Chong, & Wong, 1999; Frost et al., 1990; Lynd-Stevenson & Hearne, 1999; Stober, 1998). DiBartolo et al. (2004) have suggested that these correlations maybe due to some items on the Personal Standards subscale that pair meeting high standards with self-worth.When these items were removed from the scale, the more pure personal standards scale correlated withmeasures of adaptive outcome and not with measures of distress. On the other hand, DiBartolo, Li, and Frost(in press) still found a significant positive correlation between this Pure Personal Standards measure and socialanxiety, though it was no longer significant when the association with Concern over Mistakes was partialledout.
Enns, Cox, and Borger (2001) have suggested that associations between Personal Standards and depressionmay be specific to analogue populations and therefore less relevant for clinical disorders. Among clinicalsamples no studies have found anxiety disordered or depressed patients to have higher Personal Standardsscores than nonclinical controls (Bardone-Cone et al., 2007). For eating disorders, however, the evidencereveals a different pattern. In reviewing the literature, Bardone-Cone et al. (2007) concluded that patients withanorexia nervosa scored higher than nonclinical controls on Personal Standards as well as Concern overMistakes from the FMPS. Some evidence using the Hewitt and Flett Multidimensional Perfectionism Scale(Hewitt & Flett, 1991) is consistent with these findings. Cockell et al. (2002) found higher levels of both Self-Oriented and Socially Prescribed Perfectionism among anorexia patients compared to a mixed group of mooddisorder patients and nonclinical controls. In addition, among studies of anorexia nervosa patients, scores onthe Personal Standards subscale appeared to be higher than Personal Standards scores reported ininvestigations involving anxious and depressed patients (Bardone-Cone et al., 2007). Only one study hasdirectly compared depressed, anxious, and eating disorder patients on these dimensions of perfectionism(Bulik et al., 2003). In a large twin study, Concern over Mistakes was associated with a higher odds ratio foreating disorders but not for major depression and anxiety disorders; Doubts about Actions was associatedwith a higher odds ratio for both eating disorders and anxiety disorders but not for major depression; PersonalStandards was not associated with an elevated odds ratio for any of the disorders. However, it is difficult tointerpret these findings in light of the numerous studies that have found higher levels of Concern overMistakes and Doubts about Actions in anxiety disorders and depression (Antony, Purdon, Huta, & Swinson,
ARTICLE IN PRESSS. Sassaroli et al. / Behaviour Research and Therapy 46 (2008) 757–765758
Author's personal copy
1998; Enns & Cox, 1999; Frost & Steketee, 1997; Juster et al., 1996; Saboonchi & Lundh, 1997; Shafran &Mansell, 2001).
Of all the anxiety disorders, obsessive-compulsive disorder has had the longer recognized association withperfectionism. Early theories of obsessive-compulsive disorder regarded perfectionism as an attempt tomaintain control over threats (Guidano & Liotti, 1983; Janet, 1909; Mc Fall & Wollersheim, 1979; Salzman,1968; Straus, 1948). Studies of perfectionism in anxiety disorders have suggested that MEC perfectionism maybe greatest among patients with obsessive-compulsive disorder (Antony et al., 1998; Frost & Steketee, 1997;Shafran & Mansell, 2001; Tolin, Worhunsky, & Maltby, 2006). However, not all of the MEC subscales appearto be equally important in obsessive-compulsive disorder. Both Antony et al. (1998) and Frost and Steketee(1997) found that Concern over Mistakes and Doubts about Actions subscales were significantly higheramong patients with obsessive-compulsive disorder than nonclinical controls, but the Parental Expectationsand Parental Criticism subscales were not.
Aims of the study
The present study aimed to compare patients with major depression, obsessive-compulsive disorder, andeating disorders on the FMPS dimensions. It was expected that Concern over Mistakes and Doubts aboutActions would be elevated in each of the three clinical groups, but that pure Personal Standards would beelevated in only the sample with eating disorders. Furthermore, based on the review by Bardone-Cone et al.(2007), it was predicted that participants with eating disorders would display higher scores on both Concernover Mistakes and Pure Personal Standards than the other clinical groups. Finally, based on the findings ofDiBartolo et al. (2004), differences among the clinical groups involving Pure Personal Standards wereexpected to disappear when Concern over Mistakes was covaried out.
Methods
Participants
Thirty-seven individuals with obsessive-compulsive disorder, 25 individuals with major depression, 39individuals with eating disorders, and 44 individuals without obsessive-compulsive disorder, depression, oreating disorder diagnoses were recruited for the study. The sample was 92% female with an average age of32.7 (s.d. ¼ 10.4).1 Patients with anorexia or bulimia nervosa were combined into a single group for analysessince recent work on both the transdiagnostic model and on the instability of diagnoses highlights thesimilarities among eating disorders (Fairburn, Cooper, & Shafran, 2003; Milos, Spindler, & Schnyder, 2005).
All participants were interviewed using the Structural Clinical Interview for DSM-IV (SCID-I, First,Spitzer, Gibbon, & Williams, 1997; Italian version by Mazzi, Morosini, De Girolamo, Lussetti, & DeGuaraldi, 2000). Patients with obsessive-compulsive disorder and with eating disorders were recruited in the‘‘Studi Cognitivi’’ Psychoterapy Center of Milano. Individuals with major depression were recruited in themood disorders unit of the Policlinico Ospedale Maggiore di Milano. Within the sample with eating disorders15 patients were diagnosed with anorexia and 24 with bulimia. Twenty-one patients with eating disorders wereco-morbid for depression, obsessive-compulsive disorder, or both. None of the participants with depression orobsessive-compulsive disorder were co-morbid for eating disorders, and no one in the depressed group was co-morbid for obsessive-compulsive disorder. Three patients with obsessive-compulsive disorder were co-morbidfor depression. Nine depressed patients and two patients with obsessive-compulsive disorder were co-morbidfor generalized anxiety disorder.2
Fourteen of the controls were students in the ‘‘Studi Cognitivi’’ Psychotherapy School of Milano. Thirtycontrols were recruited from the ‘‘Michelin’’ firm in Cuneo. Nonclinical individuals were matched for age,gender, education and marital status of the clinical groups. There were no significant differences among the
ARTICLE IN PRESS
1The results of analyses including only female participants were identical to those including both males and females. Therefore, both
genders were included in the analyses reported here.2The results of analyses not including the 3 OCD participants co-morbid for depression were identical to those including them.
S. Sassaroli et al. / Behaviour Research and Therapy 46 (2008) 757–765 759

Author's personal copy
groups on age, F(3, 141) ¼ 1.60, p4.05; gender, chi square (3, N ¼ 145) ¼ .4, p4.05; education, chi square(6, N ¼ 145) ¼ 11.3, p4.05; and marital status, chi square (6, N ¼ 145) ¼ 8.38, p4.05.
Psychologists trained in cognitive therapy conducted the interviews and administered the FMPS. Criteriafor inclusion included a minimum age of 18 years, and the ability to adequately comprehend written Italian.
This study was approved by the Institutional Review Board of the ‘‘Studi Cognitivi’’ and of the PoliclinicoOspedale Maggiore di Milano. All participants provided informed consent. The study participants received nocompensation.
Instruments
The Frost Multidimensional Perfectionism Scale (FMPS; Frost et al., 1990) is a 35-item self-reportquestionnaire which includes six subscales: Concern over Mistakes, Doubts about Actions, PersonalStandards, Parental Expectations, Parental Criticism, and Organization. Concern over Mistakes is consideredas the feature of perfectionism most closely associated with psychopathology (e.g., anxiety, depression) (Frost& DiBartolo, 2002). It consists on a negative reaction to mistakes and a perception of even minor ones as afailure. Doubts about Actions refers to a over repeated doubting about the quality of one’s performance.Personal Standards reflects the tendency to set excessively high standards. Parental Expectations and ParentalCriticism refer to perceiving one’s parents as having high expectations or being excessively critical (Frost et al.,1990).
The Pure Personal Standards subscale (DiBartolo et al., 2004) was used for this investigation instead of thePersonal Standards scale since it includes only items that capture the tendency to strive for excellence withoutany component of negative self-evaluation in case these standards are not met. The FMPS was translated intoItalian and then re-translated into English by a person from the USA who was unfamiliar with the tool. Oneof the authors of the FMPS (R.O.F.) compared the original version and the re-translated version of the FMPSand did not find any meaningful differences. The Italian version of the FMPS has adequate reliability andvalidity (Ruggiero, Levi, Ciuna, & Sassaroli, 2003). The reliability coefficients for the FMPS subscales used inthe present study ranged from .71 to .92.
Procedures
One-way analyses of variance were used to compare groups on each perfectionism subscale. Tukey’s B post-hoc analyses were used for individual comparisons. Analyses of covariance were used to test predictions aboutthe independence of Concern over Mistakes and Pure Personal Standards.
Results
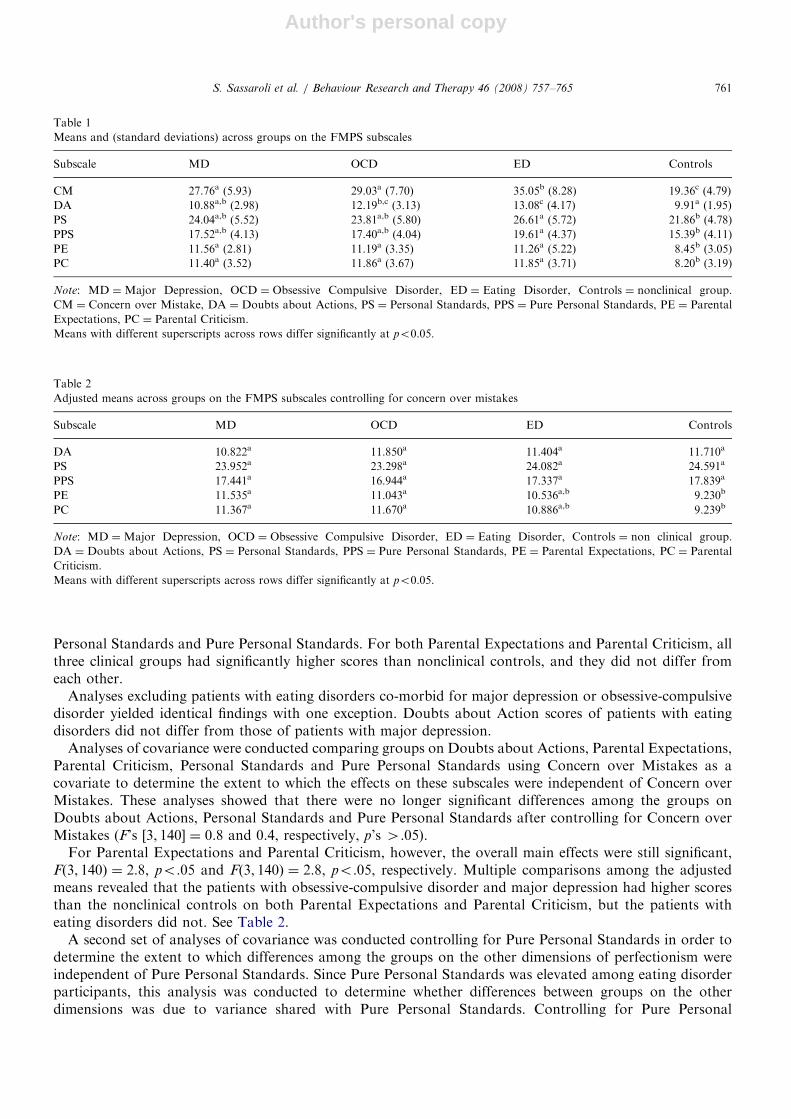
Analyses of variance revealed significant differences among the groups on each of the FMPS subscales(Concern over Mistakes, F[3, 141] ¼ 39.4; Doubts about Actions, F[3, 141] ¼ 8.2; Pure Personal Standards,F[3, 141] ¼ 8.5; Parental Expectations, F[3, 141] ¼ 7.8; Parental Criticism, F[3, 141] ¼ 9.8; all p’so.001). SeeTable 1 for means and standard deviations.
Multiple comparisons among the groups revealed that for Concern over Mistakes, all three clinical groupsscored significantly higher than the nonclinical controls, and as predicted the group with eating disordersscored significantly higher than the group with obsessive-compulsive disorder and with major depression, whodid not differ from each other. For Doubts about Actions, only the groups with eating disorders andobsessive-compulsive disorder differed significantly from the nonclinical controls, but not from each other.The group with eating disorders had significantly higher scores than the depressed group, but did not differfrom the group with obsessive-compulsive disorder.
As expected, both Personal Standards and Pure Personal Standards scores of the patients with obsessive-compulsive disorder and major depression did not differ from the nonclinical controls. Also as predicted, boththe Personal Standards and the Pure Personal Standards scores of the group with eating disorders weresignificantly higher than the nonclinical controls. Contrary to predictions, however, the group with eatingdisorders did not differ from the patients with obsessive-compulsive disorder or major depression on either
ARTICLE IN PRESSS. Sassaroli et al. / Behaviour Research and Therapy 46 (2008) 757–765760
Author's personal copy
Personal Standards and Pure Personal Standards. For both Parental Expectations and Parental Criticism, allthree clinical groups had significantly higher scores than nonclinical controls, and they did not differ fromeach other.
Analyses excluding patients with eating disorders co-morbid for major depression or obsessive-compulsivedisorder yielded identical findings with one exception. Doubts about Action scores of patients with eatingdisorders did not differ from those of patients with major depression.
Analyses of covariance were conducted comparing groups on Doubts about Actions, Parental Expectations,Parental Criticism, Personal Standards and Pure Personal Standards using Concern over Mistakes as acovariate to determine the extent to which the effects on these subscales were independent of Concern overMistakes. These analyses showed that there were no longer significant differences among the groups onDoubts about Actions, Personal Standards and Pure Personal Standards after controlling for Concern overMistakes (F’s [3, 140] ¼ 0.8 and 0.4, respectively, p’s 4.05).
For Parental Expectations and Parental Criticism, however, the overall main effects were still significant,F(3, 140) ¼ 2.8, po.05 and F(3, 140) ¼ 2.8, po.05, respectively. Multiple comparisons among the adjustedmeans revealed that the patients with obsessive-compulsive disorder and major depression had higher scoresthan the nonclinical controls on both Parental Expectations and Parental Criticism, but the patients witheating disorders did not. See Table 2.
A second set of analyses of covariance was conducted controlling for Pure Personal Standards in order todetermine the extent to which differences among the groups on the other dimensions of perfectionism wereindependent of Pure Personal Standards. Since Pure Personal Standards was elevated among eating disorderparticipants, this analysis was conducted to determine whether differences between groups on the otherdimensions was due to variance shared with Pure Personal Standards. Controlling for Pure Personal
ARTICLE IN PRESS
Table 1
Means and (standard deviations) across groups on the FMPS subscales
Subscale MD OCD ED Controls
CM 27.76a (5.93) 29.03a (7.70) 35.05b (8.28) 19.36c (4.79)
DA 10.88a,b (2.98) 12.19b,c (3.13) 13.08c (4.17) 9.91a (1.95)
PS 24.04a,b (5.52) 23.81a,b (5.80) 26.61a (5.72) 21.86b (4.78)
PPS 17.52a,b (4.13) 17.40a,b (4.04) 19.61a (4.37) 15.39b (4.11)
PE 11.56a (2.81) 11.19a (3.35) 11.26a (5.22) 8.45b (3.05)
PC 11.40a (3.52) 11.86a (3.67) 11.85a (3.71) 8.20b (3.19)
Note: MD ¼Major Depression, OCD ¼ Obsessive Compulsive Disorder, ED ¼ Eating Disorder, Controls ¼ nonclinical group.
CM ¼ Concern over Mistake, DA ¼ Doubts about Actions, PS ¼ Personal Standards, PPS ¼ Pure Personal Standards, PE ¼ Parental
Expectations, PC ¼ Parental Criticism.
Means with different superscripts across rows differ significantly at po0.05.
Table 2
Adjusted means across groups on the FMPS subscales controlling for concern over mistakes
Subscale MD OCD ED Controls
DA 10.822a 11.850a 11.404a 11.710a
PS 23.952a 23.298a 24.082a 24.591a
PPS 17.441a 16.944a 17.337a 17.839a
PE 11.535a 11.043a 10.536a,b 9.230b
PC 11.367a 11.670a 10.886a,b 9.239b
Note: MD ¼Major Depression, OCD ¼ Obsessive Compulsive Disorder, ED ¼ Eating Disorder, Controls ¼ non clinical group.
DA ¼ Doubts about Actions, PS ¼ Personal Standards, PPS ¼ Pure Personal Standards, PE ¼ Parental Expectations, PC ¼ Parental
Criticism.
Means with different superscripts across rows differ significantly at po0.05.
S. Sassaroli et al. / Behaviour Research and Therapy 46 (2008) 757–765 761
Author's personal copy
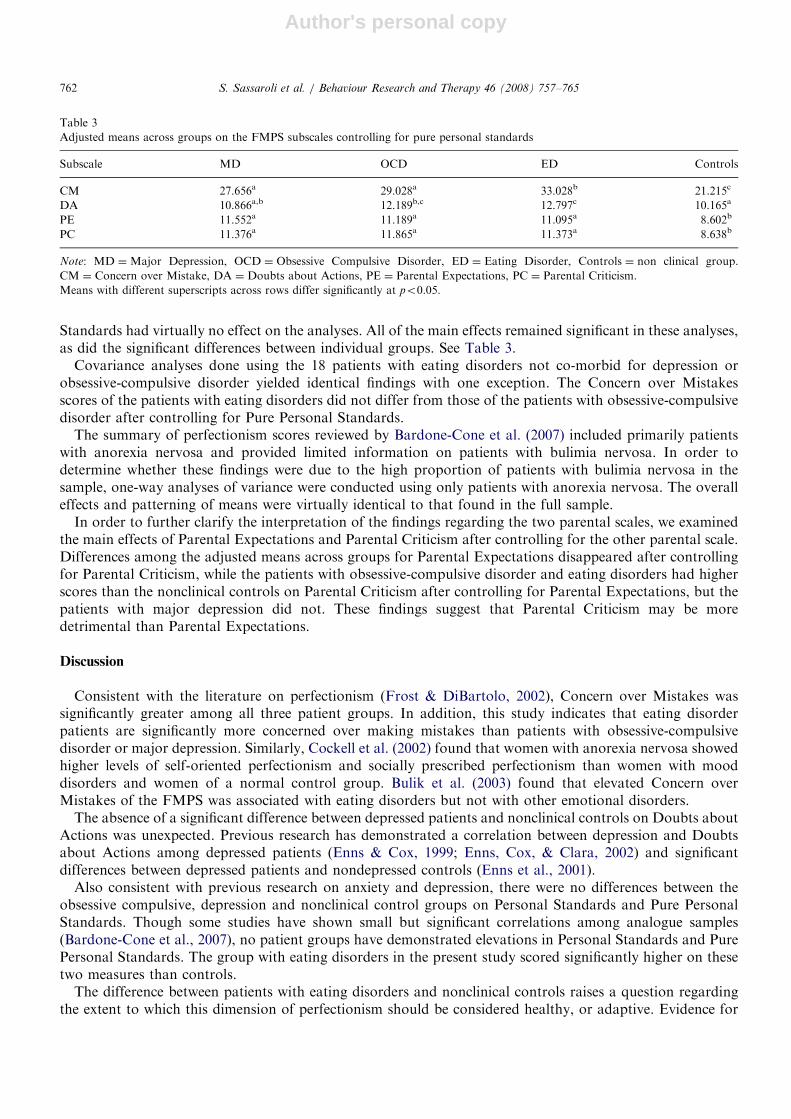
Standards had virtually no effect on the analyses. All of the main effects remained significant in these analyses,as did the significant differences between individual groups. See Table 3.
Covariance analyses done using the 18 patients with eating disorders not co-morbid for depression orobsessive-compulsive disorder yielded identical findings with one exception. The Concern over Mistakesscores of the patients with eating disorders did not differ from those of the patients with obsessive-compulsivedisorder after controlling for Pure Personal Standards.
The summary of perfectionism scores reviewed by Bardone-Cone et al. (2007) included primarily patientswith anorexia nervosa and provided limited information on patients with bulimia nervosa. In order todetermine whether these findings were due to the high proportion of patients with bulimia nervosa in thesample, one-way analyses of variance were conducted using only patients with anorexia nervosa. The overalleffects and patterning of means were virtually identical to that found in the full sample.
In order to further clarify the interpretation of the findings regarding the two parental scales, we examinedthe main effects of Parental Expectations and Parental Criticism after controlling for the other parental scale.Differences among the adjusted means across groups for Parental Expectations disappeared after controllingfor Parental Criticism, while the patients with obsessive-compulsive disorder and eating disorders had higherscores than the nonclinical controls on Parental Criticism after controlling for Parental Expectations, but thepatients with major depression did not. These findings suggest that Parental Criticism may be moredetrimental than Parental Expectations.
Discussion
Consistent with the literature on perfectionism (Frost & DiBartolo, 2002), Concern over Mistakes wassignificantly greater among all three patient groups. In addition, this study indicates that eating disorderpatients are significantly more concerned over making mistakes than patients with obsessive-compulsivedisorder or major depression. Similarly, Cockell et al. (2002) found that women with anorexia nervosa showedhigher levels of self-oriented perfectionism and socially prescribed perfectionism than women with mooddisorders and women of a normal control group. Bulik et al. (2003) found that elevated Concern overMistakes of the FMPS was associated with eating disorders but not with other emotional disorders.
The absence of a significant difference between depressed patients and nonclinical controls on Doubts aboutActions was unexpected. Previous research has demonstrated a correlation between depression and Doubtsabout Actions among depressed patients (Enns & Cox, 1999; Enns, Cox, & Clara, 2002) and significantdifferences between depressed patients and nondepressed controls (Enns et al., 2001).
Also consistent with previous research on anxiety and depression, there were no differences between theobsessive compulsive, depression and nonclinical control groups on Personal Standards and Pure PersonalStandards. Though some studies have shown small but significant correlations among analogue samples(Bardone-Cone et al., 2007), no patient groups have demonstrated elevations in Personal Standards and PurePersonal Standards. The group with eating disorders in the present study scored significantly higher on thesetwo measures than controls.
The difference between patients with eating disorders and nonclinical controls raises a question regardingthe extent to which this dimension of perfectionism should be considered healthy, or adaptive. Evidence for
ARTICLE IN PRESS
Table 3
Adjusted means across groups on the FMPS subscales controlling for pure personal standards
Subscale MD OCD ED Controls
CM 27.656a 29.028a 33.028b 21.215c
DA 10.866a,b 12.189b,c 12.797c 10.165a
PE 11.552a 11.189a 11.095a 8.602b
PC 11.376a 11.865a 11.373a 8.638b
Note: MD ¼Major Depression, OCD ¼ Obsessive Compulsive Disorder, ED ¼ Eating Disorder, Controls ¼ non clinical group.
CM ¼ Concern over Mistake, DA ¼ Doubts about Actions, PE ¼ Parental Expectations, PC ¼ Parental Criticism.
Means with different superscripts across rows differ significantly at po0.05.
S. Sassaroli et al. / Behaviour Research and Therapy 46 (2008) 757–765762

Author's personal copy
considering high personal standards as healthy comes from correlations with other positive attributes such astask focus, vulnerability to negative affect, positive affect, school performance, work habits (Bieling et al.,2004; Stober & Otto, 2006). Evidence that it is associated with eating disorders must be evidence againstconsidering it healthy. In the first study using the FMPS, Frost et al. (1990) concluded that Personal Standardswas associated with both healthy and unhealthy experiences. It is probably reasonable to conclude that incertain contexts or under certain conditions high personal standards are adaptive, and under othercircumstances they are not.
The fact that Doubts about Actions was no longer elevated among obsessive-compulsive disorder andeating disorder patients after controlling for Concern over Mistakes warrants further discussion. This findingmay suggest that there is redundancy among certain indicators of the broader MEC dimension ofperfectionism. This result supports the suggestion that the maladaptive dimension of perfectionism might beassessed more efficiently with fewer measures (Dunkley, Zuroff et al., 2006)
Although Personal Standards was significantly greater among patients with eating disorders, when thevariance in common with Concern over Mistakes was covaried out, the difference between groups on bothPersonal Standards and Pure Personal Standards disappeared. The variance that these two scales shared withConcern over Mistakes was the feature setting patients with eating disorders apart from nonclinical controls.
Despite the fact that two items of the Personal Standards scale were removed from the Pure PersonalStandards scale to make it more ‘‘pure’’, this latter scale still shares some variance with Concern overMistakes. This suggests that high personal standards could be maladaptive in some situations. As suggested inone of the early definitions of perfectionism, ‘‘Perfectionism involves high standards of performance which areaccompanied by tendencies for overly critical evaluations of one’s own behavior’’ (Frost et al., 1990, p. 450).Perhaps the self-critical component related to maladaptive perfectionism can be found in the items ‘‘I sethigher goals than most people’’ and ‘‘I expect higher performance in my daily tasks than most people’’, wherethe person is asked to evaluate the tendency to compare himself or herself with other people.
The analysis of covariance controlling for Pure Personal Standards did not change the results for Concernover Mistakes, however. The overall main effects for each of the subscales were still significant and thedifferences between the individual groups remained the same. Therefore, Concern over Mistakes was morecritical in explaining the differences among these groups than Pure Personal Standards. This is consistent withother conclusions that the MEC dimensions of perfectionism are more relevant for psychopathology than highpersonal standards.
As would be expected from their association with the other MEC dimensions, Parental Expectations andParental Criticism were higher among the clinical groups than in the nonclinical group. The findings that theoverall effects for Parental Expectations and Parental Criticism remained significant after controlling forConcern over Mistakes were unexpected. Multiple comparisons indicated that the differences betweennonclinical controls and patients who were depressed or had obsessive-compulsive disorder remained aftercontrolling for Concern over Mistakes while patients with an eating disorder did not. Parental Expectationsand Parental Criticism appear to operate in depression and obsessive-compulsive disorder independent ofConcern over Mistakes and warrant further investigation as potential etiological factors. However, they donot appear to provide any unique variance in eating disorders beyond that provided by Concern overMistakes.
The strength of this study is that it is one of the few direct comparisons of eating disorder patients withother patient groups and fills a gap in the literature of perfectionism and psychopathology. One limitation wasthe fact that the sample was 92% female. This was partly due to the fact that eating disorders occurpredominantly among women. However, this feature raises a concern about whether the findings wouldgeneralize to male samples. A second limitation was the relatively small number of participants and limitednumber of clinical groups examined. Including additional anxiety disorder groups would have providedstronger evidence of the relative contributions of these dimensions of perfectionism. In addition, using othermeasures of perfectionism would have added to the strength of these findings. Finally, future research shouldclarify the unexpected findings of higher levels of Parental Expectations and Parental Criticism across theclinical groups.
In summary, eating disorder patients displayed higher levels of Concern Over Mistakes than depressed orOCD patients. They also displayed higher levels of Personal Standards and Pure Personal Standards than
ARTICLE IN PRESSS. Sassaroli et al. / Behaviour Research and Therapy 46 (2008) 757–765 763

Author's personal copy
controls while depressed and OCD patients did not. Different patterns of perfectionism across types ofpsychopathology may have important implications for understanding and treating them.
References
Antony, M. M., Purdon, C. L., Huta, V., & Swinson, R. P. (1998). Dimensions of perfectionism across the anxiety disorders. Behaviour
Research and Therapy, 36, 1143–1154.
Bardone-Cone, A. M., Wonderlich, S. A., Frost, R. O., Bulik, C. M., Mitchell, J. E., Uppala, S., et al. (2007). Perfectionism and eating
disorders: Current status and future directions. Clinical Psychology Review, 27, 84–405.
Bieling, P. J., Israeli, A. L., & Antony, M. M. (2004). Is perfectionism good, bad, or both? Examining models of the perfectionism
construct. Personality and Individual Differences, 36, 373–1385.
Blankstein, K. R., & Dunkley, D. M. (2002). Evaluative concerns, self-critical, and personal standards perfectionism: A structural
equation modeling strategy. In G. L. Flett, & P. L. Hewitt (Eds.), Perfectionism, theory, research and treatment (pp. 33–62).
Washington, DC: American Psychological Association.
Brown, E. J., Heimberg, R. G., Frost, R. O., Makris, S. G., Juster, H. R., & Leung, A. W. (1999). Relationship of perfectionism to affect,
expectations, attributions and performance in the classroom. Journal of Social and Clinical Psychology, 18, 98–120.
Bulik, C. M., Tozzi, F., Anderson, C., Mazzeo, S. E., Aggen, S., & Sullivan, P. F. (2003). The relation between eating disorders and
components of perfectionism. American Journal of Psychiatry, 160, 366–368.
Cheng, S. K., Chong, G. H., & Wong, C. W. (1999). Chinese frost multidimensional perfectionism scale: A validation and prediction of
self-esteem and psychological distress. Journal of Clinical Psychology, 55, 1051–1061.
Cockell, S. J., Hewitt, P. L., Seal, B., Sherry, S., Goldner, E. M., Flett, G. L., et al. (2002). Trait and self-presentational dimensions of
perfectionism among women with anorexia nervosa. Cognitive Therapy and Research, 26, 745–758.
Cox, B. J., Enns, M. W., & Clara, I. P. (2002). The multidimensional structure of perfectionism in clinically distressed and college student
samples. Psychological Assessment, 14, 365–373.
DiBartolo, P. M., Frost, R. O., Chang, P., La Sota, M., & Grills, A. E. (2004). Shedding light on the relationship between personal
standards and psychopathology: The case for contingent self-worth. Journal of Rational-Emotive & Cognitive-Behavior Therapy, 22,
37–250.
DiBartolo, P. M., Li, C. Y., & Frost, R. O. (in press). How do the dimensions of perfectionism relate to psychopathology? Cognitive
Therapy and Research. /http://www.springerlink.com/content/h525140v3j88183x/S.
Dunkley, D. M., Blankstein, K. R., Masheb, R. M., & Grilo, C. M. (2006). Personal standards and evaluative concerns dimensions of
‘‘clinical’’ perfectionism: A reply to Shafran et al. (2002, 2003) and Hewitt et al. (2003). Behaviour Research and Therapy, 44, 63–84.
Dunkley, D. M., Zuroff, D. C., & Blankstein, K. R. (2006). Specific perfectionism components versus self-criticism in predicting
maladjustment. Personality and Individual Differences, 40, 665–676.
Enns, M. W., & Cox, B. J. (1999). Perfectionism and depression symptom severity in major depressive disorder. Behaviour Research and
Therapy, 37, 783–794.
Enns, M. W., Cox, B. J., & Borger, S. C. (2001). Correlates of analogue and clinical depression: A further test of the phenomenological
continuity hypothesis. Journal of Affective Disorders, 66, 175–183.
Enns, M. W., Cox, B. J., & Clara, I. P. (2002). Adaptive and maladaptive perfectionism: Developmental origins and association with
depression. Personality and Individual Differences, 33, 921–935.
Fairburn, C. G., Cooper, Z., & Shafran, R. (2003). Cognitive behaviour therapy for eating disorders: A ‘‘transdiagnostic’’ theory and
treatment. Behaviour Research and Therapy, 41, 509–528.
First, M. B., Spitzer, R. L., Gibbon, M., & Williams, J. B. W. (1997). Structured clinical interview for DSM-IV axis I disorders—Clinician
version (SCID-CV). Washington, DC: American Psychiatric Press.
Flett, G. L., & Hewitt, P. L. (2002). Perfectionism: Theory and research. Washington, DC: American Psychological Association.
Flett, G. L., & Hewitt, P. L. (2006). Positive versus negative perfectionism in psychopathology. A comment on Slade and Owens’s dual
process model. Behavior Modification, 30, 472–495.
Frost, R. O., & DiBartolo, P. M. (2002). Perfectionism, anxiety, and obsessive compulsive disorder. In G. L. Flett, & P. L. Hewitt (Eds.),
Perfectionism: Theory, research, and treatment (pp. 341–371). Washington, DC: American Psychological Association.
Frost, R. O., Heimberg, R. G., Holt, C. S., Mattia, J. I., & Neubauer, A. L. (1993). A comparison of two measures of perfectionism.
Personality and Individual Differences, 14, 119–126.
Frost, R. O., Marten, P., Lahart, C., & Rosenblate, R. (1990). The dimensions of perfectionism. Cognitive Therapy and Research, 14,
449–468.
Frost, R. O., & Steketee, G. (1997). Perfectionism in obsessive compulsive disorder patients. Behaviour Research and Therapy, 35, 291–296.
Greenspon, T. S. (2000). ‘‘Healthy perfectionism’’ is an oxymoron! reflections on the psychology of perfectionism and the sociology of
science. Journal of Secondary Gifted Education, 11, 197–208.
Guidano, V. F., & Liotti, G. (1983). Cognitive processes and emotional disorders. New York: Guilford.
Hewitt, P. L., & Flett, G. L. (1991). Perfectionism in the self and social context: Conceptualization, assessment, and association with
psychopathology. Journal of Personality and Social Psychology, 60, 456–470.
Janet, P. (1909). Les Nevroses. Paris: Flamarion.
ARTICLE IN PRESSS. Sassaroli et al. / Behaviour Research and Therapy 46 (2008) 757–765764

Author's personal copy
Juster, H. R., Heimberg, R. G., Frost, R. O., Holt, C. S., Mattia, J. I., & Faccenda, K. (1996). Social phobia and perfectionism.
Personality and Individual Differences, 21, 403–410.
Stevenson, L. R. M., & Hearne, C. M. (1999). Perfectionism and depressive affect: The pros and cons of being a perfectionist. Personality
and Individual Differences, 26, 549–562.
Mazzi, F., Morosini, P., De Girolamo G., Lussetti M., & De Guaraldi, G. P. (2000). SCID-I. Structured clinical interview for DSM– IV
axis I disorders (Italian version), OS-Organizzazioni Speciali, Firenze.
Mc Fall, M. E., & Wollersheim, J. P. (1979). Obsessive compulsive neurosis: A cognitive behavioural formulation and approach to
treatment. Cognitive Therapy and Research, 3, 333–348.
Milos, G., Spindler, A., & Schnyder, U. (2005). Instability of eating disorder diagnoses: Prospective study. British Journal of Psychiatry,
187, 573–578.
Parker, W. D. (1997). An empirical typology of perfectionism in academically talented children. American Educational Research Journal,
34, 545–562.
Ruggiero, G. M., Levi, D., Ciuna, A., & Sassaroli, S. (2003). Stress situation reveals an association between perfectionism and drive for
thinness. International Journal of Eating Disorders, 34, 220–226.
Saboonchi, F., & Lundh, L. G. (1997). Perfectionism, self-consciousness and anxiety. Personality and Individual Differences, 22, 921–928.
Salzman, L. (1968). The obsessive personality. New York: Science House.
Shafran, R., & Mansell, W. (2001). Perfectionism and psychopathology: A review of research and treatment. Clinical Psychology Review,
21, 879–906.
Slade, P. D., & Owens, R. G. (1998). A dual process model of perfectionism based on reinforcement theory. Behavior Modification, 22,
372–390.
Straus, E. (1948). On obsession: A clinical and methodological study. New York, NY: Nervous Mental Diseases Monography.
Stober, J. (1998). The frost multidimensional perfectionism scale: More perfect with four (instead of six) dimensions. Personality and
Individual Differences, 24, 481–491.
Stober, J., & Otto, K. (2006). Positive conceptions of perfectionism: Approaches, evidence, challenges. Personality and Social Psychology
Review, 10, 295–319.
Tolin, D. F., Worhunsky, P., & Maltby, N. (2006). Are ‘‘obsessive’’ beliefs specific to OCD?: A comparison across anxiety disorders.
Behaviour Research and Therapy, 44, 469–480.
ARTICLE IN PRESSS. Sassaroli et al. / Behaviour Research and Therapy 46 (2008) 757–765 765




















