
Waterlogging risk assessment: An undervalued disaster risk in ...
Upload
georgetownCategory
view
0download
0
ORIGINAL PAPER
Perceived risk of breast cancer among Latinas attendingcommunity clinics: risk comprehension and relationshipwith mammography adherence
Kristi D. Graves Æ Elmer Huerta Æ Jennifer Cullen Æ Elizabeth Kaufman ÆVanessa Sheppard Æ George Luta Æ Claudine Isaacs Æ Marc D. Schwartz ÆJeanne Mandelblatt
Received: 23 October 2007 / Accepted: 8 July 2008 / Published online: 15 August 2008
� Springer Science+Business Media B.V. 2008
Abstract
Objective To describe breast cancer risk perceptions,
determine risk comprehension, and evaluate mammogra-
phy adherence among Latinas.
Methods Latina women age C35, primarily from Central
and South America, were recruited from community-based
clinics to complete in-person interviews (n = 450). Risk
comprehension was calculated as the difference between
numeric perceived risk and Gail risk score. Based on rec-
ommended guidelines from the year data were collected
(2002), mammography adherence was defined as having a
mammogram every one to two years for women C40 years
of age.
Results Breast cancer risk comprehension was low, as
81% of women overestimated their risk and only 6.9% of
women were high risk based on Gail risk scores. Greater
cancer worry and younger age were significantly associated
with greater perceived risk and risk overestimation. Of
women age eligible for mammography (n = 328), 29.0%
were non-adherent to screening guidelines. Adherence was
associated with older age, (OR = 2.99, 95% CI = 1.76–
5.09), having insurance (OR = 1.81, 95% CI = 1.03–
3.17), greater acculturation (OR = 1.18, 95% CI =
1.02–1.36), and higher breast cancer knowledge
(OR = 2.03, 95% CI = 1.21–3.40).
Conclusions While most Latinas over-estimated their
breast cancer risk, older age, having insurance, being more
acculturated, and having greater knowledge were associ-
ated with greater screening adherence in this Latino
population. Perceived risk, risk comprehension, and cancer
worry were not associated with adherence. In Latinas,
screening interventions should emphasize knowledge and
target education efforts at younger, uninsured, and less
acculturated mammography-eligible women.
Keywords Latina � Breast cancer � Risk perception �Risk comprehension � Mammography adherence �Acculturation
Introduction
The rapid growth and aging of the Latino population, along
with acculturation to US lifestyles that increase the risk of
breast cancer [1], will increase the absolute number of Latino
women (hereafter referred to as Latinas) at risk for breast
Supported by Grants U01CA86114, U01CA114593, K05CA96940
(JM), and K07CA131172 (KG) from the National Cancer Institute.
K. D. Graves (&) � E. Huerta � E. Kaufman � V. Sheppard �M. D. Schwartz � J. Mandelblatt
Department of Oncology, Cancer Control Program, Lombardi
Comprehensive Cancer Center, Georgetown University,
3300 Whitehaven Street, NW, Suite 4100, Washington,
DC 20007, USA
e-mail: [email protected]
E. Huerta
Washington Hospital Center, Washington, DC 20010, USA
J. Cullen
American Legacy Foundation, Washington, DC 20036, USA
G. Luta
Department of Biostatistics, Bioinformatics, and
Biomathematics, Lombardi Comprehensive Cancer Center,
Georgetown University, Washington, DC 20007, USA
C. Isaacs
Clinical Breast Cancer Program, Lombardi Comprehensive
Cancer Center, Georgetown University, Washington, DC 20057,
USA
123
Cancer Causes Control (2008) 19:1373–1382
DOI 10.1007/s10552-008-9209-7

cancer over the coming decades. Although breast cancer
incidence rates remain lower among Latinas compared to
non-Hispanic Whites and African-American women [2],
Latinas are more likely to be diagnosed with advanced breast
cancer compared to non-Hispanic White women [3]. Despite
these trends, rates of mammography adherence remain
suboptimal in the Latina population [4–7].
There are several possible reasons for low screening
adherence in Latinas, including low breast cancer knowl-
edge, lack of insurance/access to care, and low education [5,
7–10]. Results have been equivocal for the impact of
acculturation (and English ability) on screening adherence
[8, 11–15]. These reasons for non-adherence map onto the
predisposing, enabling, and need factors described in the
Behavioral Model for Vulnerable Populations [16]. Spe-
cifically, the predisposing and enabling factors that likely
impact mammography behavior include sociodemograph-
ics, insurance, knowledge, access to care, and acculturation,
while need factors could include perceived breast cancer
risk, comprehension of risk, and breast cancer worry.
In other populations, perceptions of breast cancer risk
appear to impact screening behaviors [17, 18]. For instance,
research conducted with African American women indi-
cates a non-linear relationship between perceived risk and
screening adherence [19]. However, we know little about
the impact of perceived risk on screening in Latinas. We are
aware of only one study that has examined perceived risk
and mammography adherence in Latinas [10]. In that study,
perceived risk was measured as comparative risk (likeli-
hood of getting cancer compared to other people their age)
and was unrelated to mammography outcomes. Moreover,
the construct of breast cancer risk comprehension, repre-
senting how closely a woman’s perceived risk matches her
objective risk (based on family history, reproductive his-
tory, and prior biopsies) has only been explored with
predominately Caucasian samples [20–22]. To our knowl-
edge, other types of perceived risk (e.g., absolute risk,
numerical risk), risk comprehension, and cancer worry have
not been assessed in prior work with Latinas. Thus, con-
structs associated with perceived breast cancer risk remain
under explored in broad groups of Latinas, particularly as
these factors may relate to mammography adherence.
The purpose of this study is to describe the correlates of
perceived risk and comprehension of risk as well as to assess
the degrees of association between risk and a related risk
construct—cancer worry—on adherence to mammography
guidelines after considering covariates (e.g., predisposing
factors) in a sample of Central and South American Latinas
attending community health clinics. We hypothesized that
younger age and a more significant family history would be
associated with greater perceived risk [23]. We also hypoth-
esized that Latina women, similar to other women [20, 22],
would overestimate their actual risk of breast cancer. In
addition, we hypothesized that adherence to mammography
recommendations would be associated with higher perceived
risk for breast cancer, greater (more accurate) risk compre-
hension, and more cancer worry. Finally, we explored the
impact of level of acculturation on adherence to mammog-
raphy guidelines, hypothesizing that greater acculturation
would be associated with higher levels of adherence.
Materials and methods
Setting
In the Washington DC metropolitan area, Latinos make up
15% of the total population. Many Latinos in the area are
recently immigrated and typically come to the US from
Central and South American countries. The predominant
countries of origin for the DC Latino population are El Sal-
vador, Ecuador, Peru, and Columbia [24]. Data were
collected from women recruited from three community-
based clinics in the DC area that provide services at no cost to
primarily uninsured Latino individuals. The three commu-
nity clinics are non-federally funded and the majority of the
staff at the clinics is bilingual, English- and Spanish-speak-
ing. Non-physician staff at each clinic served as
interviewers. The clinics are part of the Latin American
Cancer Research Coalition, a National Cancer Institute
Community Network Program.
The present study was part of an IRB-approved larger
trial investigating an intervention to educate Latina patients
about a breast cancer prevention trial (Study of Tamoxifen
and Raloxifene; STAR trial) [24]. During the larger trial
women were screened for STAR eligibility and in a base-
line interview answered questions about willingness to
participate in clinical trials, use of screening, and their
perceptions of risk of breast cancer. The present study used
data from the baseline interviews of the larger trial.
Sample
The sample consisted of 450 Latinas who were 35 years of
age and older and were seen for a medical appointment at
one of the three clinics. More than half of patients served at
these clinics are women (Range: 55–83% of clinic popu-
lation). The average age of the women served at these
clinics is 57 years, and El Salvador is the country of origin
for the largest segment of clinic patients (Range: 42–51%
of clinic populations). In addition, most patients are
monolingual in Spanish and on average, have completed
eight years of education. The women served at the three
clinics are similar in terms of demographics, education,
country of origin, and language abilities to women at the
other clinics within the Latin American Cancer Research
Coalition [25].
1374 Cancer Causes Control (2008) 19:1373–1382
123

Of the 450 women who completed interviews, three
were missing data related to either actual and/or perceived
breast cancer risk. Thus, the final sample consisted of 447
women; for analyses related to mammogram adherence, we
included the 328 women who were 43 years or older, as
described below.
Recruitment and survey procedures
Using appointment logs and medical records, clinic staff
determined women’s eligibility prior to scheduled clinic
appointments. Women were eligible if they were 35 years of
age and older and attended an appointment at one of the three
clinics. Study staff approached all potentially eligible women
during their scheduled appointment for consent to participate.
A small number of women were missed during appointment
sessions due to administrative delays or other clinic flow
issues unrelated to the study questions. Of the eligible women
approached, 96% consented to participate. The IRB-approved
consent procedures and interviews were conducted in a pri-
vate area while women waited for their appointment. In-
person interviews were conducted in the language of the
patient’s choice using a computer-assisted format. Almost all
women elected to have their interview conducted in Spanish
(97.5%), and 95% agreed to the computer-assisted format.
The remaining 5% of responses were recorded on a hard copy
of the study questionnaire. The interview took *30 min to
complete. All interviewers were bilingual, completed exten-
sive training, and engaged in mock interviews.
Measures
We first piloted a brief version of the study interview in a
separate sample of 79 Latinas, assessing sociodemograph-
ics, acculturation, family history of cancer, medical history,
and perceived risk [26]. Women were able to understand
the questions and reported relatively high perceived risk
(e.g., 19% of pilot sample rated their risk for breast cancer
as ‘‘high’’).
Using our pilot results and following the factors outlined
in The Behavioral Model for Vulnerable Populations [16],
we assessed the following variables in the present study.
Predisposing and enabling factors
Sociodemographics
Information was collected on age, marital status, education,
insurance status, and employment. Variables were catego-
rized as follows: age (\50 years vs. C50 years), marital
status (married vs. not married), education (\High School
vs. CHigh School), insurance status (yes vs. no), and
employment (yes vs. no). We created a binary variable for
age (\50 years vs. C50 years) to account for the increase
in risk of breast cancer for women age 50 and over.
Acculturation
We assessed acculturation with three questions related to
language use [27]. Women were asked to identify the
language they (a) spoke at home, (b) thought in, and (c)
spoke outside the home with the following options: (1)
Only Spanish, (2) Spanish better than English, (3) Both
equally, (4) English better than Spanish, or (5) Only Eng-
lish. Level of acculturation was determined by summing
responses to these questions. Higher scores represent
higher levels of acculturation.
Cancer worry
We measured breast cancer worry with two questions used
in prior research [28, 29]. Specifically, we asked partici-
pants, ‘‘In the past month, how often have you thought
about your own chances of getting breast cancer?’’ and ‘‘In
the past month, how often have these thoughts affected
your mood?’’ Responses to both questions were on a Likert
scale (not at all or rarely, sometimes, often to a lot) and
were summed to create an overall cancer worry score.
Breast cancer knowledge
We used a 13-item scale to measure breast cancer knowl-
edge [24]. Response options were true, false, or unsure, and
questions assessed knowledge related to the etiology of
breast cancer, screening recommendations, population-
level rates of breast cancer, how age relates to risk for
breast cancer, and screening and treatment. Sample items
included ‘‘A hard blow to the breast may cause a woman to
get cancer later in life,’’ ‘‘Mammography can detect lumps
that can’t be felt,’’ and ‘‘If a woman gets regular mam-
mography, she does not need to do breast self exams or
have physical examinations.’’ Scores were calculated as
percent of correct responses, ranging from 0% to 100%.
Responses of unsure were coded as incorrect. In order to
account for a bimodal distribution of knowledge scores, we
created a binary breast cancer knowledge score with a
median split to represent low and high knowledge.
Need factors
Perceived risk
Perceived risk was assessed with three distinct items. First,
an absolute estimate of perceived risk was obtained
through responses on a 3-point Likert scale (‘‘not at all’’ to
‘‘definitely’’) to the question, ‘‘How likely do you think it is
Cancer Causes Control (2008) 19:1373–1382 1375
123

that you will develop breast cancer?’’ To assess compar-
ative risk, participants were asked ‘‘How do you think your
risk of dying from breast cancer compares to an average
women your own age?’’ on a 3-point Likert scale (‘‘lower
than average’’ to ‘‘higher than average’’) [30]. For numeric
risk, participants were asked to rate their likelihood of
developing breast cancer on a scale from 0 (definitely will
not get breast cancer) to 20 (definitely will get breast
cancer). The items were not combined into scales.
Medical history/Gail model risk
We used the Gail risk model to estimate objective risk [31],
with scores determined by age at menarche (e.g., \12,
12–13, and C14), biopsy history (calculated separately for
women \50 and women C50 by number of biopsies),
pregnancy history (age at first live birth), history of
atypical hyperplasia, number of first degree relatives
(mother, daughter, sister) with breast or ovarian cancer, and
current age. High (C1.7%) and low (\1.7%) objective risk
were categorized as the 5-year risk of disease, with high
risk scores being equal to or greater than the 5-year risk of
disease among the average 60-year old woman [31, 32].
Risk comprehension
Based on prior research, we calculated risk comprehension
as the difference between subjective numeric risk estimates
and objective Gail score percentage risk [20]. We converted
numeric risk and Gail scores to a common metric. Specifi-
cally, numeric risk was multiplied by five, so that the original
scale (0–20) became a 0–100 scale (Range = 5–100) and
5-year Gail model risk scores were multiplied by 10 to pro-
vide percentages between 1.0 and 100 (Range = 1.66–38.3).
We then subtracted objective risk from perceived numeric
risk. We categorized risk comprehension as accurate if the
difference between subjective and objective risk estimates
was B10 points in either direction, an underestimate if the
difference was [10 points below objective risk, and an
overestimate if[10 points above objective risk. Only 2% of
the sample (n = 9) underestimated risk, so the underesti-
mation and accurate risk categories were collapsed, as done
in prior research [22].
Health behavior outcomes
Adherence to mammography recommendations
Mammography use was classified as never, ever, and recent
(B2 years). Specifically, women were asked if they had
ever had a mammogram (yes/no), when they had their most
recent mammogram (within 1–2 years, [2 years but
\3 years ago, or [3 years ago), and whether they had a
mammogram during the two years before the most recent
mammogram (yes/no). For these analyses, we only inclu-
ded women age 43 or older (n = 328) to match guidelines
outlined by the National Cancer Institute for mammogra-
phy in 2002, the year in which the data were collected [33].
Women age 43 and older were considered adherent if they
reported having a recent mammogram (B2 years). Women
age 45 and older were considered adherent if they reported
having a recent mammogram (B2 years) and having a
mammogram prior to the most recent mammogram.
Analysis
After generating descriptive statistics to characterize the
sample, we conducted bivariate analyses using v2 tests, t tests,
and Pearson correlation coefficients to determine associations
between study variables and perceived risk, risk comprehen-
sion, and adherence to mammography guidelines.
Depending on the scale of each outcome variable—
continuous, or binary—and the scale of the independent
variable—categorical or continuous—we used ANOVAs,
linear regression, and logistic regression to identify vari-
ables that were associated with each outcome. Specifically,
we entered significant (p \ .05) bivariate predictors of our
outcomes (perceived risk, risk comprehension, and adher-
ence) as well as predictors associated with the
predisposing, enabling, and need factors from our con-
ceptual model, into the multivariate analyses. We used
logistic regression models for our statistical analyses
investigating predictors of risk comprehension and adher-
ence to mammography. The final models were selected
using backward elimination procedures. This approach
allowed us to control for relevant sociodemographics (e.g.,
education, insurance status, clinic site) while assessing the
effect of the main predictors. In subsequent sensitivity
analyses we evaluated the effect of potential correlation of
the outcomes within clinic by using related logistic
regression models based on Generalized Estimating
Equations (GEE) with an exchangeable working correla-
tion structure. The estimated within-clinic correlations
were practically null; and the overall results were not
changed. Thus, we elected to report the results from the
previously described logistic regression models.
Results
Sample characteristics
In the final sample of 447 women, the mean age was 50.5
(SD = 10.5) and the majority of women were married
(64%), had less than a high school education (73%), and
1376 Cancer Causes Control (2008) 19:1373–1382
123
were uninsured (68%). Fewer women had experienced a
breast biopsy (12%) or had a family history of breast
cancer (5%). The largest number of participants (n = 172;
38.2%) were born in El Salvador, and the mean level of
acculturation was low (see Table 1).
Rates of perceived risk and risk comprehension
Based on absolute estimates of perceived risk, one-quarter
(26.2%) of the sample considered themselves to be at high
risk for breast cancer, meaning that they rated their risk as
3, or ‘‘definitely’’ will get breast cancer. For comparative
risk estimates, 24.4% reported their risk of breast cancer as
higher than the average woman’s risk. The average
numeric estimate of perceived risk was 9.0 (SD = 4.8). All
estimates of risk (absolute, comparative, numeric) were
statistically significantly correlated (r’s ranging from .22 to
.38, all p’s \ .0001).
For objective risk, only 6.9% of the sample was high
risk as defined by the eligibility requirements for the STAR
Trial (i.e., 5-year Gail score of C1.7%). Based on differ-
ences between objective and subjective (i.e., perceived
numeric risk) estimates, more than three-quarters (81%,
n = 362) of the sample overestimated their breast cancer
risk.
Variables associated with perceived breast cancer risk
We examined bivariate associations among our three per-
ceived risk variables (absolute, comparative, and numeric)
and predisposing/enabling (age, education, race, insurance,
marital status, clinic site, acculturation, cancer worry, breast
cancer knowledge), and need (Gail score) factors. The three
perceived risk variables were all significantly associated
with cancer worry, with higher levels of cancer worry
associated with higher perceived risk. In addition, clinic site
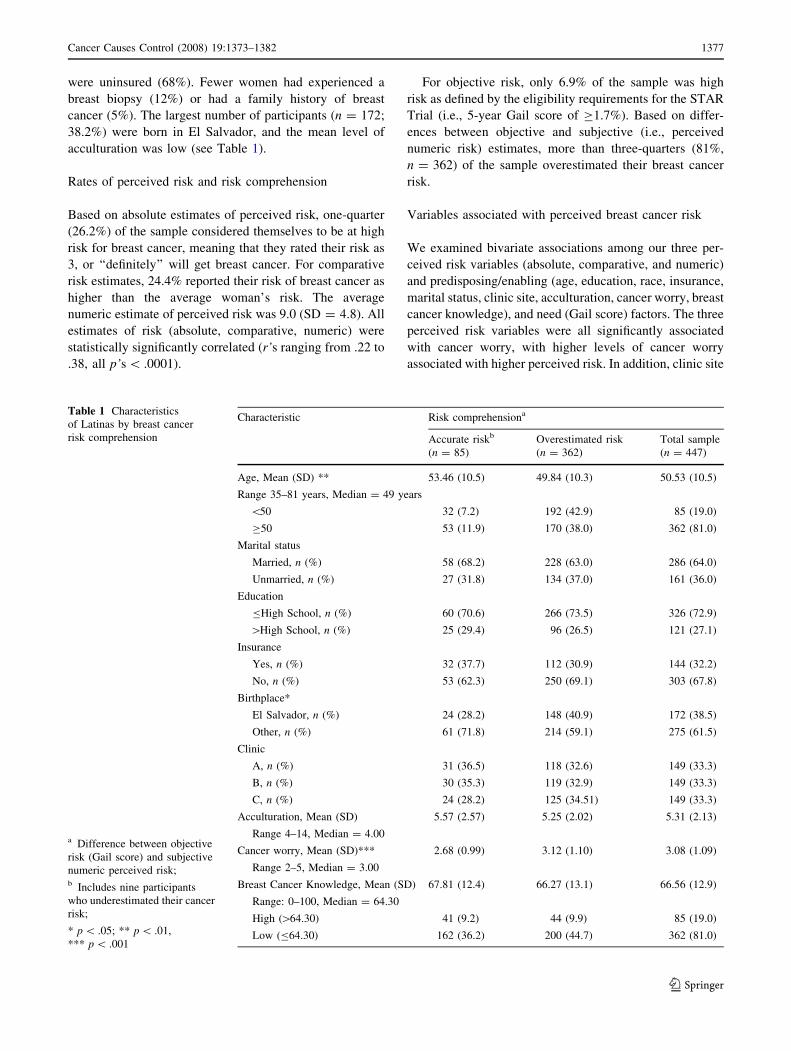
Table 1 Characteristics
of Latinas by breast cancer
risk comprehension
a Difference between objective
risk (Gail score) and subjective
numeric perceived risk;b Includes nine participants
who underestimated their cancer
risk;
* p \ .05; ** p \ .01,
*** p \ .001
Characteristic Risk comprehensiona
Accurate riskb
(n = 85)
Overestimated risk
(n = 362)
Total sample
(n = 447)
Age, Mean (SD) ** 53.46 (10.5) 49.84 (10.3) 50.53 (10.5)
Range 35–81 years, Median = 49 years
\50 32 (7.2) 192 (42.9) 85 (19.0)
C50 53 (11.9) 170 (38.0) 362 (81.0)
Marital status
Married, n (%) 58 (68.2) 228 (63.0) 286 (64.0)
Unmarried, n (%) 27 (31.8) 134 (37.0) 161 (36.0)
Education
BHigh School, n (%) 60 (70.6) 266 (73.5) 326 (72.9)
[High School, n (%) 25 (29.4) 96 (26.5) 121 (27.1)
Insurance
Yes, n (%) 32 (37.7) 112 (30.9) 144 (32.2)
No, n (%) 53 (62.3) 250 (69.1) 303 (67.8)
Birthplace*
El Salvador, n (%) 24 (28.2) 148 (40.9) 172 (38.5)
Other, n (%) 61 (71.8) 214 (59.1) 275 (61.5)
Clinic
A, n (%) 31 (36.5) 118 (32.6) 149 (33.3)
B, n (%) 30 (35.3) 119 (32.9) 149 (33.3)
C, n (%) 24 (28.2) 125 (34.51) 149 (33.3)
Acculturation, Mean (SD) 5.57 (2.57) 5.25 (2.02) 5.31 (2.13)
Range 4–14, Median = 4.00
Cancer worry, Mean (SD)*** 2.68 (0.99) 3.12 (1.10) 3.08 (1.09)
Range 2–5, Median = 3.00
Breast Cancer Knowledge, Mean (SD) 67.81 (12.4) 66.27 (13.1) 66.56 (12.9)
Range: 0–100, Median = 64.30
High ([64.30) 41 (9.2) 44 (9.9) 85 (19.0)
Low (B64.30) 162 (36.2) 200 (44.7) 362 (81.0)
Cancer Causes Control (2008) 19:1373–1382 1377
123

was associated with absolute perceived risk (see Table 2).
No other variables were significantly associated with the
perceived risk measures. In adjusted ANOVA models for
our two categorical perceived risk outcomes (absolute and
comparative risk), clinic site (F = 6.3, p = .01; F = 4.7,
p = .03), and cancer worry (F = 11.8, p \ .001; F = 5.2,
p = .02) were independently associated with absolute risk
and comparative risk, respectively. In a multiple regression
model, cancer worry was independently associated with
numeric perceived risk (t = 5.3, p \ .001; b = 0.3), with
greater worry associated with greater perceived risk.
Variables associated with risk comprehension
Overall, 85 participants held accurate estimates of breast
cancer risk and 362 overestimated risk. Risk overestima-
tion was associated with being born in El Salvador,
younger age, and higher breast cancer worry (Table 2). No
other variables were associated with risk comprehension.
In the logistic regression model with backward elimination
of variables, older age (OR = 1.84, 95% CI = 1.13, 3.01),
and lower cancer worry (OR = 0.64, 95% CI = 0.50–
0.82) were independent predictors of accurate risk com-
prehension (Table 3). Thus, risk overestimation was more
likely to occur in younger women and in women with
greater cancer worry.
Adherence to mammography recommendations
Of women age 43 and older, 29% (n = 95) were classified
as not adherent to mammography guidelines. Women from
different countries had varying rates of non-adherence to
mammography guidelines, with women from Guatemala
reporting the highest rates of non-adherence (50.0%), fol-
lowed by Bolivia (41.2%), Peru (38.1%), El Salvador
(30.0%), Nicaragua (23.5%), Columbia (18.2%), Honduras
(18.2%), and Ecuador (15.4%).
Variables associated with adherence at the bivariate and
multivariate levels included age 50 years or older,
(OR = 2.99, 95% CI = 1.76–5.09), having insurance
(OR = 1.81, 95% CI = 1.03–3.17), greater acculturation
(OR = 1.18, 95% CI = 1.02–1.36), and higher breast
cancer knowledge (OR = 2.03, 95% CI = 1.21–3.40; see
Tables 4 and 5). Country of birth, level of education,
cancer worry, and risk comprehension were not associated
with adherence. Women at high-risk for breast cancer
based on Gail scores (n = 31) had the same rate of non-
adherence to mammography guidelines (29%) as women in
the entire sample.
Discussion
To our knowledge, this is the first study to evaluate the
relationships among perceived risk, risk comprehension,
cancer worry, and mammography adherence while consid-
ering demographics, acculturation, and breast cancer
knowledge in Latinas. Overall, Latinas significantly over-
estimated their cancer risk. Interestingly, risk perceptions
and cancer worry were not associated with adherence,
although age, insurance status, acculturation, and knowledge
were independently associated with screening behavior.
Latinas’ overestimation of their breast cancer risk is
consistent with findings among Caucasian women [20, 22].
Similarly, the significant relationship between cancer
Table 2 Correlates of risk perception and risk comprehension
Characteristic Perceived risk variables
Absolute
risk
Comparative
risk
Numeric
risk
Risk
comprehension
Age -0.07 -0.002 -0.02 -0.14**
Marital status -0.05 -0.03 -0.05 0.04
Education -0.02 -0.05 -0.07 -0.03
Insurance
status
0.01 -0.07 -0.04 -0.06
Birth place 0.06 0.02 0.08 0.10*
Clinic site 0.11* -0.08 0.001 0.04
Acculturation 0.01 -0.05 -0.03 -0.05
5-year Gail
risk
-0.07 -0.01 -0.07 –
Cancer worry 0.20*** 0.13** 0.28*** 0.17***
Breast cancer
knowledge
0.02 0.03 -0.03 -0.05
* p \ .05; ** p \ .01; *** p \ .001
Note: Values in the table represent the Pearson-Product Correlation
Coefficients for continuous variables (age, education, acculturation,
5-year Gail risk, Cancer worry, Breast cancer knowledge) and Point-
biserial correlation coefficients for dichotomous variables [insurance
status (yes/no), marital status (yes/no), birth place (El Salvador/
other)]. Dashes indicate that the correlation between the 5-year Gail
risk score and the Risk comprehension score was not evaluated
because the Gail risk score was used to create the Risk comprehension
score
Table 3 Variables associated with risk comprehension
Variable Accurate risk comprehension
OR (95%CI)
Age (C50 years vs. \50 years) 1.84 (1.13, 3.01)*
Cancer worrya 0.64 (0.50, 0.82)**
a Cancer worry measured as a continuous variable; higher scores
represent greater cancer worry
* p \ .05; ** p \ .001
Note: Odds Ratios calculated from parameter estimates of the logistic
regression models with backward elimination of the following vari-
ables: education (v2 = 0.03, p [ .05), acculturation (v2 = 0.25,
p [ .05), insurance status (v2 = 1.08, p [ .05), clinic (v2 = 0.80,
p [ .05), knowledge (v2 = 1.86, p [ .05), and country of origin
(v2 = 3.51, p [ .05)
1378 Cancer Causes Control (2008) 19:1373–1382
123

worry and perceived risk is also consistent with prior
research indicating a strong and significant relationship
between these two variables [30, 34]. In these prior studies,
cancer worry has been treated as both an independent
predictor of perceived risk and as an outcome of perceived
risk. Thus, the direction and nature of this relationship
among Latina women warrants further evaluation in studies
with prospective research designs.
Slightly less than one-third (29%) of Latinas were non-
adherent to mammography guidelines. Consistent with
prior research with Latinas who identified as Cuban,
Mexican, Puerto Rican, and Central American [10], breast
cancer knowledge was significantly associated with
screening adherence in our population of both Central and
South American Latinas, with lower knowledge associated
with lower rates of adherence. Women from the various
Central and South American countries reported differing
rates of adherence. Due to low sample sizes of women from
certain countries, we were not able to evaluate these dif-
ferences statistically; however, future research with Latinas
could explore whether individual cultural differences
account for these discrepancies. Similar to prior research,
sociodemographic characteristics including younger age
and not having insurance were associated with non-
adherence to mammography guidelines [5, 7–10]. Our
findings of the positive association between acculturation
and adherence may clarify equivocal results in prior stud-
ies. Women who were less acculturated reported lower
rates of adherence. Other culturally relevant factors that
may be associated with adherence include cancer fatalism
and medical mistrust, as these constructs may influence risk
perception and mammography adherence in Latinas [35].
Examination of these pathways will be important to
explore in future research.
Our finding that Latinas between ages 43 and 50 were
less likely to adhere to mammography screening guidelines
than women age 50 and older is consistent with cancer
screening research conducted with Latinas [5] and other
populations [36]. These results indicate that women eligi-
ble for mammography may not be initiating this screening
behavior at the appropriate time. Although the Latina
population in the present study had access to community
health clinics, actual access to free or reduced-cost mam-
mography services was not assessed.
Unlike predictors of mammography adherence in pre-
dominately non-Hispanic White samples and contrary to
expectation in the present study, perceived risk, risk
Table 4 Unadjusted associations between variables of interest and
adherence to screening guidelines (n = 328)
Variable Adherent
(n = 233)
Non-adherent
(n = 95)
Age**
Mean (SD) 55.3 (8.3) 53.7 (9.9)
\50, n (%) 61 (18.6) 44 (13.4)
C50, n (%) 172 (52.4) 51 (15.6)
Marital status
Married, n (%) 163 (49.7) 63 (19.2)
Unmarried, n(%) 70 (21.3) 32 (9.8)
Education**
BHigh School, n (%) 171 (52.1) 76 (23.2)
[High School, n (%) 62 (18.9) 19 (5.8)
Insurance **
Yes, n (%) 85 (25.9) 23 (7.0)
No, n (%) 148 (45.1) 72 (22.0)
Birthplace
El Salvador, n (%) 84 (25.6) 36 (11.0)
Other, n (%) 149 (45.4) 59 (18.0)
Clinic
A, n (%) 67 (20.4) 35 (10.7)
B, n (%) 85 (25.9) 29 (8.8)
C, n (%) 81 (24.7) 31 (9.5)
Acculturation, Mean (SD)** 5.3 (2.3) 4.8 (1.5)
Cancer worry, Mean (SD) 3.02 (1.07) 3.08 (1.10)
Breast cancer knowledge,
Mean (SD)*
68.8 (10.4) 62.7 (17.1)
High, n (%) 122 (37.2) 35 (10.7)
Low, n (%) 111 (33.8) 60 (18.3)
Risk comprehension
Accurate, n (%) 55 (16.7) 14 (4.3)
Overestimate, n (%) 178 (54.3) 81 (24.7)
* p \ .05; ** p \ .001
Note: Percents calculated as the percent of the total 328 participants
included in these analyses
Table 5 Variables associated with adherence to mammography
guidelines
Variable Adherence to mammography
guidelinesa
OR (95% CI)
Age (C50 years vs. \50 years) 2.99 (1.76, 5.09)***
Insurance(Yes vs. No) 1.81 (1.03, 3.17)*
Acculturationb 1.18 (1.02, 1.36)*
Breast cancer knowledge (High
vs. Low)
2.03 (1.21, 3.40)**
a n = 328b Acculturation measured as a continuous variable; higher scores
represent greater acculturation
* p \ .05; ** p \ .01; *** p \ .001
Note: Odds Ratios calculated from parameter estimates of the logistic
regression models with backward elimination of the following vari-
ables: cancer worry (v2 = 0.06, p [ .05), country of origin
(v2 = 1.02, p [ .05), education (v2 = 1.51, p [ .05), clinic
(v2 = 1.33, p [ .05), and risk comprehension (v2 = 1.48, p [ .05)
Cancer Causes Control (2008) 19:1373–1382 1379
123

comprehension and cancer worry were not associated with
adherence in Latinas, whereas breast cancer knowledge
was associated with adherence. Thus, for Latinas, educa-
tion about breast cancer and mammography may be more
valuable intervention targets than efforts to improve risk
comprehension, particularly among newly immigrated
and/or mono-lingual Latinas. Moreover, these interventions
may be particularly useful in younger Latinas who are
appropriate candidates for mammography, but have not yet
initiated screening.
Study strengths and limitations
Strengths of this study include the focus on an understudied
and primarily uninsured Latina population recruited from
community health clinics. Latinas in our sample were from
predominately Central American countries, whereas prior
research has often focused on women from Mexico and
Puerto Rico. Our inclusion of multiple risk perception
measures allowed us to evaluate the relationship of each
measure with adherence. Although the measurement
approaches (absolute, comparative, and numeric perceived
risk) were associated with one another, none were associ-
ated with mammography adherence. Finally, we had a very
high participation rate, likely due to our use of bilingual
study interviewers and conduct of the survey within clinics
that were trusted by our study population [37, 38].
Limitations to the present study should be noted, includ-
ing use of a clinic-based convenience sample and assessment
of mammography adherence through self-report. Our clinic-
based sample may differ from non-clinic based samples
regarding both perceived risk and mammography adherence,
and thus results may not generalize to Latina women who do
not seek care through community health clinics. For exam-
ple, women seen through community health clinics may be
more likely to engage in breast cancer screening behaviors
compared to women who do not regularly seek health care. In
contrast, patients at community clinics may engage in less
cancer prevention behavior than women who are seen reg-
ularly by a primary care physician. In terms of self-report of
mammography adherence, some evidence indicates women
over-report adherence [39], whereas other evidence suggests
women are able to report mammography adherence with
acceptable sensitivity and specificity [40, 41]. If women in
the present study over-reported adherence, then an even
greater proportion of this population may have been non-
adherent to screening.
Adherence to mammography screening guidelines in the
present study followed 2002 recommendations of the
National Cancer Institute, which at the time advised
women 40 years of age and older to have a mammogram
every 1–2 years. Other agencies (e.g., American Cancer
Society) had different recommendations in 2002, such that
women over age 50 should have a mammogram every year
[42]. As such, our data reflect a conservative estimate of
the number of women who were non-adherent to mam-
mography screening guidelines. In addition, the current
sample consisted of a small number of women at high risk
of breast cancer based on objective criteria, thus limiting
our power to detect significant relationships within this
sub-sample. Use of the Gail model in a population of La-
tinas could also be considered a limitation as few studies
have used this model in racial and ethnic minority popu-
lations [43, 44]. Moreover, even less is known about how
the Gail model applies to particular subgroups of Latinas
(e.g., Salvadoran women).
This study has important implications for primary care
providers and clinics treating Latinas. Our high participa-
tion rate indicates that Latinas are willing to engage in
dialog about breast cancer screening [24]. The key finding
from this research stresses the importance of education to
improve breast cancer knowledge in this population—
teaching Latinas more about breast cancer, including
symptoms (and lack thereof), screening/early detection
recommendations, and risk factors—may be an effective
approach to improve mammography adherence. These
education efforts may not benefit from any focus on
improving the risk comprehension in Latinas, as our data
indicate that risk comprehension is not associated with
screening behavior. Future research would be strengthened
by use of prospective designs, ascertainment of actual
mammography behaviors, and inclusion of larger numbers
of high-risk Latinas. Finally, future work should build on
and expand existing efforts to intervene with Latinas so
that cultural influences are appropriately considered when
educating these women about breast cancer and breast
screening behaviors [45].
Conclusion
While most Latinas over-estimated their breast cancer risk,
older age, having insurance, being more acculturated, and
having greater knowledge were associated with greater
screening adherence in this Latino population. Perceived
risk, risk comprehension, and cancer worry were not
associated with adherence. In Latinas, screening interven-
tions should emphasize knowledge and target education
efforts at younger, uninsured, and less acculturated mam-
mography-eligible women.
Acknowledgments We would like to thank all the women who
participated in this study, as well as Susan Marx for assistance with
manuscript preparation. Our sincere appreciation also goes to Janet
Canar, Jyl Pomeroy, and Yosselyn Rodriguez for data collection at
each of the clinics; and to Michael Sanchez, Maria Lopez-Class, and
Barbara Kreiling for information about the LACRC clinics.
1380 Cancer Causes Control (2008) 19:1373–1382
123
References
1. John EM, Phipps AI, Davis A, Koo J (2005) Migration history,
acculturation, and breast cancer risk in Hispanic women. Cancer
Epidemiol Biomarkers Prev 14:2905–2913. doi:10.1158/1055-
9965.EPI-05-0483
2. Carozza SE, Howe HL (2006) Patterns of cancer incidence
among US Hispanics/Latinos, 1995–2000. Cancer Causes Control
17:1067–1075. doi:10.1007/s10552-006-0045-3
3. Howe HL, Wu X, Ries LA, Cokkinides V, Ahmed F, Jemal A
et al (2006) Annual report to the nation on the status of cancer,
1975–2003, featuring cancer among U.S. Hispanic/Latino popu-
lations. Cancer 107:1711–1742. doi:10.1002/cncr.22193
4. Abraido-Lanza AF, Chao MT, Gammon MD (2004) Breast and
cervical cancer screening among Latinas and non-Latina whites.
Am J Public Health 94:1393–1398
5. Gorin SS, Heck JE (2005) Cancer screening among Latino sub-
groups in the United States. Prev Med 40:515–526. doi:10.1016/
j.ypmed.2004.09.031
6. Mandelblatt JS, Gold K, O’Malley AS, Taylor K, Cagney K,
Hopkins JS et al (1999) Breast and cervix cancer screening
among multiethnic women: role of age, health, and source of
care. Prev Med 28:418–425. doi:10.1006/pmed.1998.0446
7. Thompson B, Coronado GD, Solomon CC, McClerran DF,
Neuhouser ML, Feng Z (2002) Cancer prevention behaviors and
socioeconomic status among Hispanics and non-Hispanic whites
in a rural population in the United States. Cancer Causes Control
13:719–728. doi:10.1023/A:1020280427712
8. Abraido-Lanza AF, Chao MT, Gates CY (2005) Acculturation
and cancer screening among Latinas: results from the National
Health Interview Survey. Ann Behav Med 29:22–28.
doi:10.1207/s15324796abm2901_4
9. Brown WM, Consedine NS, Magai C (2006) Time spent in the
United States and breast cancer screening behaviors among
ethnically diverse immigrant women: evidence for accultura-
tion? J Immigr Minor Health 8:347–358. doi:10.1007/s10903-
006-9005-y
10. Ramirez AG, Suarez L, Laufman L, Barroso C, Chalela P (2000)
Hispanic women’s breast and cervical cancer knowledge, atti-
tudes, and screening behaviors. Am J Health Promot 14:292–300
11. Echeverria SE, Carrasquillo O (2006) The roles of citizenship
status, acculturation, and health insurance in breast and cervical
cancer screening among immigrant women. Med Care 44:788–
792. doi:10.1097/01.mlr.0000215863.24214.41
12. O’Malley AS, Kerner J, Johnson AE, Mandelblatt J (1999)
Acculturation and breast cancer screening among Hispanic
women in New York City. Am J Public Health 89:219–227
13. Peragallo NP, Fox PG, Alba ML (2000) Acculturation and breast
self-examination among immigrant Latina women in the USA.
Int Nurs Rev 47:38–45. doi:10.1046/j.1466-7657.2000.00005.x
14. Ruiz MS, Marks G, Richardson JL (1992) Language accultura-
tion and screening practices of elderly Hispanic women. The role
of exposure to health-related information from the media. J Aging
Health 4:268–281. doi:10.1177/089826439200400206
15. Zambrana RE, Breen N, Fox SA, Gutierrez-Mohamed ML (1999)
Use of cancer screening practices by Hispanic women: analyses by
subgroup. Prev Med 29:466–477. doi:10.1006/pmed.1999.0566
16. Gelberg L, Andersen RM, Leake BD (2000) The Behavioral
Model for Vulnerable Populations: application to medical care
use and outcomes for homeless people. Health Serv Res 34:
1273–1302
17. Katapodi MC, Lee KA, Facione NC, Dodd MJ (2004) Predictors
of perceived breast cancer risk and the relation between perceived
risk and breast cancer screening: a meta-analytic review. Prev
Med 38:388–402. doi:10.1016/j.ypmed.2003.11.012
18. Moser RP, McCaul K, Peters E, Nelson W, Marcus SE (2007)
Associations of perceived risk and worry with cancer health-
protective actions: data from the Health Information National
Trends Survey (HINTS). J Health Psychol 12:53–65.
doi:10.1177/1359105307071735
19. Calvocoressi L, Stolar M, Kasl SV, Claus EB, Jones BA (2005)
Applying recursive partitioning to a prospective study of factors
associated with adherence to mammography screening guide-
lines. Am J Epidemiol 162:1215–1224. doi:10.1093/aje/kwi337
20. Daly MB, Lerman CL, Ross E, Schwartz MD, Sands CB, Masny
A (1996) Gail model breast cancer risk components are poor
predictors of risk perception and screening behavior. Breast
Cancer Res Treat 41:59–70. doi:10.1007/BF01807037
21. Kelly K, Leventhal H, Marvin M, Toppmeyer D, Much J, Der-
mody J et al (2004) Subjective and objective risk of breast cancer
in Ashkenazi Jewish individuals at risk for BRCA1/2 mutations.
Genet Test 8:139–147
22. Lerman C, Lustbader E, Rimer B, Daly M, Miller S, Sands C et al
(1995) Effects of individualized breast cancer risk counseling: a
randomized trial. J Natl Cancer Inst 87:286–292. doi:10.1093/
jnci/87.4.286
23. Li R, Gilliland FD, Baumgartner KB, Samet J (2001) Family
history and risk of breast cancer in Hispanic and non-Hispanic
women: the New Mexico Women’s Health Study. Cancer Causes
Control 12:747–753. doi:10.1023/A:1011285205870
24. Mandelblatt J, Kaufman E, Sheppard VB, Pomeroy J, Kavanaugh
J, Canar J et al (2005) Breast cancer prevention in community
clinics: will low-income Latina patients participate in clinical
trials? Prev Med 40:611–618. doi:10.1016/j.ypmed.2004.09.004
25. Kreling BA, Canar J, Catipon E, Goodman M, Pallesen N,
Pomeroy J et al (2006) Latin American Cancer Research Coali-
tion. Community primary care/academic partnership model for
cancer control. Cancer 107:2015–2022. doi:10.1002/cncr.22145
26. Sheppard VB, Kaufman E, Pomeroy J, Kavanaugh J, O’Malley
A, Pallandre L et al (2004) Latina’s willingness to participate in
chemoprevention trials. Int J Cancer Prev 1:391–396
27. Marin G, Marin BV (1991) Research with Hispanic populations
(Applied Social Research Methods Series, vol. 23). Sage Publi-cations, Newbury Park, CA
28. Armstrong K, Micco E, Carney A, Stopfer J, Putt M (2005)
Racial differences in the use of BRCA1/2 testing among women
with a family history of breast or ovarian cancer. JAMA
293:1729–1736. doi:10.1001/jama.293.14.1729
29. Lerman C, Trock B, Rimer BK, Boyce A, Jepson C, Engstrom PF
(1991) Psychological and behavioral implications of abnormal
mammograms. Ann Intern Med 114:657–661
30. Lipkus IM, Kuchibhatla M, McBride CM, Bosworth HB, Pollak
KI, Siegler IC et al (2000) Relationships among breast cancer
perceived absolute risk, comparative risk, and worries. Cancer
Epidemiol Biomarkers Prev 9:973–975
31. Gail MH, Costantino JP, Bryant J, Croyle R, Freedman L, Hel-
zlsouer K et al (1999) Weighing the risks and benefits of
tamoxifen treatment for preventing breast cancer. J Natl Cancer
Inst 91:1829–1846. doi:10.1093/jnci/91.21.1829
32. McTiernan A, Kuniyuki A, Yasui Y, Bowen D, Burke W, Culver
JB et al (2001) Comparisons of two breast cancer risk estimates
in women with a family history of breast cancer. Cancer Epi-
demiol Biomarkers Prev 10:333–338
33. National Cancer Institute (2002) NCI statement on mammography
screening. http://www.cancer.gov/newscenter/mammstatement31
jan02. Accessed 29 March 2007]
34. McGregor BA, Bowen DJ, Ankerst DP, Andersen MR, Yasui Y,
McTiernan A (2004) Optimism, perceived risk of breast cancer,
and cancer worry among a community-based sample of women.
Health Psychol 23:339–344. doi:10.1037/0278-6133.23.4.339
Cancer Causes Control (2008) 19:1373–1382 1381
123

35. Luquis RR, Villanueva-Cruz IJ (2006) Knowledge, attitudes, and
perceptions about breast cancer and breast cancer screening
among Hispanic women residing in South Central Pennsylvania. J
Community Health 31:25–42. doi:10.1007/s10900-005-8187-x
36. O’Malley AS, Forrest CB, Mandelblatt J (2002) Adherence of
low-income women to cancer screening recommendations. J Gen
Intern Med 17:144–154. doi:10.1046/j.1525-1497.2002.10431.x
37. Sheppard VB, Zambrana RE, O’Malley AS (2004) Providing
health care to low-income women: a matter of trust. Fam Pract
21:484–491. doi:10.1093/fampra/cmh503
38. Sheppard VB, Cox LS, Kanamori MJ, Canar J, Rodriguez Y,
Goodman M et al (2005) Brief report: if you build it, they will
come: methods for recruiting Latinos into cancer research. J Gen
Intern Med 20:444–447. doi:10.1111/j.1525-1497.2005.0083.x
39. Armstrong K, Long JA, Shea JA (2004) Measuring adherence to
mammography screening recommendations among low-income
women. Prev Med 38:754–760. doi:10.1016/j.ypmed.2003.12.023
40. McPhee SJ, Nguyen TT, Shema SJ, Nguyen B, Somkin C, Vo P
et al (2002) Validation of recall of breast and cervical cancer
screening by women in an ethnically diverse population. Prev
Med 35:463–473. doi:10.1006/pmed.2002.1096
41. Tumiel-Berhalter LM, Finney MF, Jaen CR (2004) Self-report
and primary care medical record documentation of mammogra-
phy and Pap smear utilization among low-income women. J Natl
Med Assoc 96:1632–1639
42. Smith RA, Saslow D, Sawyer KA, Burke W, Costanza ME,
Evans WPIII et al (2003) American Cancer Society guidelines
for breast cancer screening: update 2003. CA Cancer J Clin 53:
141–169
43. Abu-Rustum NR, Herbolsheimer H (2001) Breast cancer risk
assessment in indigent women at a public hospital. Gynecol
Oncol 81:287–290. doi:10.1006/gyno.2001.6160
44. Grann VR, Jacobson JS, Troxel AB, Hershman D, Karp J, Myers
C et al (2005) Barriers to minority participation in breast carci-
noma prevention trials. Cancer 104:374–379. doi:10.1002/
cncr.21164
45. Thompson B, Coronado G, Chen L, Islas I (2006) Celebremos la
salud! a community randomized trial of cancer prevention
(United States). Cancer Causes Control 17:733–746. doi:10.1007/
s10552-006-0006-x
1382 Cancer Causes Control (2008) 19:1373–1382
123
Copyright © 2022 FDOKUMEN




















