Passive smoking and lung cancer in nonsmoking women
6
Passive Smoking and Lung Cancer in Nonsmoking Women Ross C. Brownson, PhD, Michael C. R Alavanja, DrPH, Edward T. Hock, BS, and Tinothy S. Loy, MD Introduction Although most lung cancer occurs in smokers, approximately 9% to 13% of lung cancer cases in US women develop in lifetime nonsmokers.'-5 The causes of lung cancer in nonsmokers have not been widely studied, but probably comprise a diverse set of factors including genetics, occupational factors, radon exposure, diet, and a history of nonmalignant lung disease. In addition to these risk factors, the etiologic role of passive smoke exposure has received increasing scrutiny over the past decade. Numerous studies5-20 have suggested an elevation in lung cancer risk for nonsmoking females who live with a smoker, with a summary excess risk of approximately 30%.21,22 However, sev- eral recent studies'"23-27 have shown no increased lung cancer risk due to spousal smoking. Limited evidence7,26 also suggests that exposure to passive smoke in child- hood may increase risk of lung cancer. For example, a recent case-control study from New York found that household exposure to tobacco smoke during childhood of 25 or more smoker-years' duration was as- sociated with a doubling of lung cancer risk.36 Most previous studies of passive smoking and lung cancer, although sug- gestive of a positive effect, have had sev- eral deficiencies. These deficiencies in- clude sample sizes insufficient to singly demonstrate significant elevations in risk, limited data on passive smoke exposure in both childhood and adulthood, and lack of histologic review of cases to verify lung cancer diagnosis and to allow analyses by cell type. To more fully evaluate the relation- ship between lung cancer and passive smoke exposure in childhood and adult- hood, we conducted a large case-control study of lung cancer among nonsmoking women. Methods Case Group Case patients were identified through the Missouri Cancer Registry, which is maintained by the Missouri Department of Health. The Registry began collecting data on incident cancer cases from public and private hospitals in 1972, and hospital reporting was mandated by law in 1984. Registry reporting procedures have been discussed in more detail elsewhere.23 To ensure complete reporting of lung cancer cases in women for the current study, we had Registry staff complete special case ascertainment visits to participating hos- pitals. The case series included White Missouri women, aged 30 to 84 years, who were diagnosed with primary lung cancer between January 1986 and June 1991. Se- lection was limited to Whites because of small numbers of other racial/ethnic Ross C. Brownson is with the Division of Chronic Disease Prevention and Health Pro- motion, Missouri Department of Health, Co- lumbia, Mo. Michael C. R. Alavanja is with the Epidemiology and Biostatistics Program, Na- tional Cancer Institute, Rockville, Md. Edward T. Hock is with Information Management Ser- vices, Rockville, Md. Timothy S. Loy is with the Pathology Department, University of Mis- souri School of Medicine, Columbia, Mo. Requests for reprints should be sent to Ross C. Brownson, PhD, Division of Chronic Disease Prevention and Health Promotion, Missouri Department of Health, 201 Business Loop 70 West, Columbia, MO 65203. This paper was submitted to the Journal February 19, 1992, and accepted with revisions August 12, 1992. American Journal of Public Health 1525 I.......I.......I.......I...I...--.
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Passive smoking and lung cancer in nonsmoking women

Passive Smoking and Lung Cancer inNonsmoking Women
Ross C. Brownson, PhD, Michael C. R Alavanja, DrPH, Edward T. Hock, BS,and Tinothy S. Loy, MD
IntroductionAlthough most lung cancer occurs in
smokers, approximately 9% to 13% oflung cancer cases inUSwomen develop inlifetime nonsmokers.'-5 The causes oflung cancer in nonsmokers have not beenwidely studied, but probably comprise adiverse set of factors including genetics,occupational factors, radon exposure,diet, and a history of nonmalignant lungdisease.
In addition to these risk factors, theetiologic role of passive smoke exposurehas received increasing scrutiny over thepast decade. Numerous studies5-20 havesuggested an elevation in lung cancer riskfor nonsmoking females who live with asmoker, with a summary excess risk ofapproximately 30%.21,22 However, sev-eral recent studies'"23-27 have shown noincreased lung cancer risk due to spousalsmoking.
Limited evidence7,26 also suggeststhat exposure to passive smoke in child-hood may increase risk of lung cancer. Forexample, a recent case-control study fromNew York found that household exposureto tobacco smoke during childhood of 25or more smoker-years' duration was as-sociated with a doubling of lung cancerrisk.36
Most previous studies of passivesmoking and lung cancer, although sug-gestive of a positive effect, have had sev-eral deficiencies. These deficiencies in-clude sample sizes insufficient to singlydemonstrate significant elevations in risk,limited data on passive smoke exposure inboth childhood and adulthood, and lack ofhistologic review of cases to verify lungcancer diagnosis and to allow analyses bycell type.
To more fully evaluate the relation-ship between lung cancer and passive
smoke exposure in childhood and adult-hood, we conducted a large case-controlstudy of lung cancer among nonsmokingwomen.
Methods
Case GroupCase patients were identified through
the Missouri Cancer Registry, which ismaintained by the Missouri Department ofHealth. The Registry began collectingdata on incident cancer cases from publicand private hospitals in 1972, and hospitalreporting was mandated by law in 1984.Registry reporting procedures have beendiscussed in more detail elsewhere.23 Toensure complete reporting of lung cancercases in women for the current study, wehad Registry staff complete special caseascertainment visits to participating hos-pitals. The case series included WhiteMissouri women, aged 30 to 84 years, whowere diagnosed with primary lung cancerbetween January 1986 and June 1991. Se-lection was limited to Whites because ofsmall numbers of other racial/ethnic
Ross C. Brownson is with the Division ofChronic Disease Prevention and Health Pro-motion, Missouri Department of Health, Co-lumbia, Mo. Michael C. R. Alavanja is with theEpidemiology and Biostatistics Program, Na-tional Cancer Institute, Rockville, Md. EdwardT. Hock is with Information Management Ser-vices, Rockville, Md. Timothy S. Loy is withthe Pathology Department, University of Mis-souri School of Medicine, Columbia, Mo.
Requests for reprints should be sent toRoss C. Brownson, PhD, Division of ChronicDisease Prevention and Health Promotion,Missouri Department of Health, 201 BusinessLoop 70 West, Columbia, MO 65203.
This paper was submitted to the JournalFebruary 19, 1992, and accepted with revisionsAugust 12, 1992.
American Journal of Public Health 1525
I.......I.......I.......I... I...--.

BDiwuso et aL
groups. The case group included both life-time nonsmokers and ex-smokers whohad stopped smoking at least 15 years be-fore diagnosis orwho had smoked for lessthan 1 pack-year. From the 3475 cases oflung cancer in women reported for thestudy period, 650 eligible patients wereidentified. Physicians denied interviewpermission for 24 (4%) of these patientsand an additional 8women (1%) refused tobe interviewed. The final case group in-cluded 432 (70%) lifetime nonsmokers and186 (30%o) ex-smokers. Of the 618 caseinterviews, 216 were conducted with pa-tients themselves and 402were conductedwith surrogates because the patient wastoo ill tobe interviewed orhad died. Ofthesurrogate interviews, 105 (26%) were con-ducted with the patient's spouse and 297(74%) were conducted with another rela-tive (e.g., offspring or sibling).
Histologic Confirrnation ofCasesTissue slides were reviewed for his-
tologicverification for468 (76%) ofthe 618cases. Slides for these cases were exam-ined simultaneously by three pathologists(T.L., E.I., and J.M.) using a multiheadedmicroscope without knowledge of the re-ferring pathologist's diagnosis. In surgicalspecimens, consensus diagnoses were ob-tained with the criteria outlined in theWorld Health Organization classificationscheme.29 When only cytologic materialwas available, consensus was obtainedwith standard cytologic criteria.30
Contol GroupA population-based sample of con-
trol subjectswas ascertained bytwo meth-ods. Forwomen younger than 65 years, asample of state driver's license files wasprovided by the Missouri Department ofRevenue. Forwomen aged 65 to 84 years,control subjects were generated from theHealth Care Finance Administration'sroster ofMedicare recipients.31 On the ba-sis of age distnbution of lung cancer casespreviously reported to the Registry, thefinal control group was matched by agegroup to case patients at an approximate2.2 to 1 ratio. All control subjects wereinterviewed directly. Of the 1862 poten-tially eligible control subjects, 335 (18%)refused the initial screening interview and125 (7%) of those screened and found el-igible refused the full interview. The finalcontrol group numbered 1402.
Questionnaire Design andAdministration
Telephone interviews were con-ducted by trained interviewers. The first
phase of the interview consisted of ascreening questionnaire to verify the age,race, and smoking status of case patientsand control subjects. For subjects whowere screened and found eligible andwhoagreed to the full interview, the studyquestionnaire consisted ofsections on res-idential history, passive smoke exposure,personal health history, family health his-tory, reproductive history, occupationalexposure, and dietary factors.
Questions regarding passive smokingfocused on exposure in both childhood (17years and younger) and adulthood (18years and older). For each time period,respondents were questioned about thesource of exposure (e.g., a parent orspouse). After an individual source wasdetermined, a series of detailed questionswere asked on the ype of tobacco used,duration of exposure, intensity of expo-sure, and average number of hours perday exposed. These questions were par-'tially modeled after those developed byWynder et al.32 In addition to quantitativeestimates of exposure, respondents wereasked to estimate a perceived level of ex-posure during childhood and adulthood("During most ofyour adult years, wouldyou say that your average exposure tosmoke at home was light, moderate, orheavy?").
AnalysesOdds ratios (ORs) and 95% confi-
dence intervals (Cls) were calculated withmultiple logistic regression.33 The linear-ity of trends in risk according to level ofpassive smoke exposure was evaluatedwith Mantel's one-tailed test.34 We ini-tially exanmined numerous potential con-founding factors. These included age, ac-tive smoking (for ex-smokers), history ofprevious lung disease, dietary beta caro-tene, and dietary fat. Of these variables,only age, active smoking, and previouslung disease appeared to confound pas-sive smoking findings; therefore, the re-sults presented are adjusted for these fac-tors.
Histologic type-specific analyseswere conducted for cases for which con-sensus diagnoses were determined. Theseanalyses were undertaken because earlierstudies5.'8'w have shownvariations in riskby cell type, and biological mechanismshave been proposed that might accountfor these variations.20M
Sociodemographic and smoking-re-lated characteristics of case patients and
control subjects have been presented indetail elsewhere.36 In brief, the averageages of case patients and control subjectswere 71.5 years and 69.9 years, respec-tively. The two groups were also compa-rable on level of education and income.Among ex-smokers, the median intervalsince cessation was 24 years, and averagesmoking intensity was 16.4 cigarettes perday.
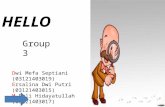
Therewas little evidence ofincreasedlung cancer risk associated with passivesmoke exposure in childhood (Table 1).This lack of association was apparent forboth the dichotomous variables (never vsever exposed) and quantitative measuressuch as pack-years. The only suggestionof elevated risk was noted for less quan-titative exposure variables (not shown intable). Among lifetime nonsmokers, an in-creased risk of lung cancer was shown forthose reporting moderate (OR = 1.7; 95%CI = 1.1, 2.5) and heavy (OR = 2.4; 95%CI = 1.3, 4.7) exposure to passive smokein childhood. Risk estimates for mostchildhood exposure variables wereslightly higher (approximately 20% to30%) when analyses included only directinterviews, although none achieved statis-tical signficance.
An elevated risk of lung cancer wasidentified for lifetime nonsmokers at thehighest quardle of passive smoke expo-sure in adulthood (Table 2). At an expo-sure level ofmore than 40 pack-years, life-time nonsmokers showed a 30%o increasein riskwhetherthe source ofexposurewasall household members or spouses only.Similarly, when the product ofpack-yearsand average number of hours exposed perday was considered, lung cancer risk forlifetime nonsmokers was elevated for thehighest exposure quartile whether thesource was all household members(OR = 1.3;95%CI = 1.0, 1.8)orspousesonly (OR = 1.3; 95% CI = 1.0, 1.7).Among lifetime nonsmokers, a positive in-creasing trend in risk was noted for pack-years (P = .06). Passive smoking-relatedrisk estimates for adulthood exposureswere slightly lower for all subjects (i.e.,both ex-smokers and lifetime nonsmok-ers) than for lifetime nonsmokers alone,although the same general elevations inriskwere noted. When analyses were lim-ited to direct interviews, no clear patternof increase or decrease in risk estimateswas apparent. Regarding less quantitativeexposure variables, elevated risk wasshown for all subjects (OR = 1.7; 95%CI = 1.1, 2.6) and for lifetime nonsmok-
1526 American Jounal of Public Health November 1992, Vol. 82, No. 11
Passive SMOking and I Al CaDw
ers (OR = 1.8; 95% CI = 1.1, 2.9) whoreported heavy exposure to passivesmoke.
In general, therewas no elevated lungcancer risk associated with passive smokeexposure in the workplace (not shown intable). Only lifetime nonsmokers showeda slight increase in risk at the highest quar-tile of workplace exposure (OR = 1.2;95% CI = 0.9, 1.7).
Among the 468 lung cancers that wereverified histolgally, the predminat ceil;tys were adeocarcinoma (62.4%), other/mixed celi ;tp (25.2%), squamous ceil car-cnoma (5.8%), bronchioalveolarcarcinoma(4.1%), and small cell carcinoma (2.5%).The other/mixed cell type category con-sisted mainly of large cell lung cancers,though these lacked sufficient pathologicevidence for precise classification. Table 3presents results of cell tye-specific analy-ses for adulthood exposures. Elevated riskwas shown for other/mixed cell types atmore than 40 pack-years of exposure(OR = 1.6; 95% CI = 1.0, 2.5). Although itwasbasedon small numbers, a riskestimateof1.7wasobserved for small cell carcinomaat the highest level of exposure.
We also examined risk amongwomen who had been exposed to passivesmoke in both childhood and adulthood,in childhood but not in adulthood, and inadulthood but not in childhood. Therewasno evidence of interaction between expo-sure during the two periods.
Diwussion
Our study suggests that eposure tohigh levels of environmental tobaccosmoke in adulthood increases the risk oflung cancer in nonsmokers. Exposure ofmore than 40 pack-years' duration in-creased the riskoflung canceramong non-smokers by approximately 30%o. This re-lationship was consistently demonstratedamong lifetime nonsmokers whether theexposure variable was pack-years or thetime-weighted product of pack-years andaverage number ofhours exposed per day.Our findings are similar to those ofanotherlarge study of lung cancer in nonsmokingwomen20 that identified an OR of approx-imately 1.3 due to exposure to greater than40 pack-years of spousal smoking.
In earlier studies, the most com-monly reported index of passive smokingexposure has been the presence or ab-sence ofa smoking spouse. In our data set,no elevated risk was noted for this vari-able. Since our study was limited towomen, part ofthe difference between ourfindings and those of earlier studies maybe due to differences in the effects of pas-sive smoke exposure by gender. The Na-tional Research Council's summary of 13studies21 found overall relative risks oflung cancer in nonsmokers due to spousalsmoking of 1.32 for women and 1.62 formen (although the estimate for men wasbased on few cases). It is possible thatmen are exposed to other factors (e.g.,
occupational exposures) that may interactwith passive smoke exposure to increaserisk above that observed in women. Pres-ence or absence of a smoking spouse is arelatively crude measure ofpassive smokeexposure, with a potential for wide vari-ability in actual exposure. It was noted inone survey, for example, that 47% ofwomen married to smokers reported zerohours of passive smoke exposure athome.37 It has also been shown that con-sidering spousal exposure alone may un-derestimate total household passivesmoke exposure.38 Another factor thatmay account for the differences in lungcancer risk due to spousal smoking be-tween our study and earlier studiesmaybetime trends in smoldng patterns. The de-clining prevalence of smoking amongmen39 has probably resulted in decreasingyears and perhaps levels of exposure topassive smoke in the home among non-smokingwomen whose husbands smoke.
Contrary to the findings oftwo earliercase-control studies,7.26 our data showedno evidence ofexcess lung cancer riskdueto passive smoke exposure in childhood.The risk of lung cancer due to childhoodpassive smoking may have some analogyto risk among ex-smokers. After 10 yearsof abstinence, the lung cancer risk for ex-smokers declines to 30% to50% ofthe riskfor continuing smokers.40 Similarly, lungcancer risk due to passive smoke expo-sure in childhood may decline by adult-hood, especially in the absence of adult-
American Journal of Public Health 1527November 1992, Vol. 82, No. 1 1

Bwnson et aLt
hood exposure. In addition, there may below reliability for quantitative measures(intensity and duration) of passive smokeexposure in childhood,41'42 which makes
assessment of lung cancer risk due to pas-sive smoke exposure in childhood partic-ularly difficult. Reliability and validity ofmeasures of childhood exposure may be
especially problematic when a large per-centage of surrogate interviews are con-ducted (as in our study). Partially becauseof these limitations, few studies of child-
1528 American Journal of Public Health November 1992, Vol. 82, No. 11

Passve SMOking and Lng Cane
hood passive smoking and lung cancerhave been conducted, and further re-search in this area is needed.
Our analyses by histologic typeshowed the largest increase in risk forother/mixed celi types and, although theestimatewasbasedonverysmall numbers,for small cell carcinoma. Previous studiesare inconsistent and often lacking in samplesize when evaluating risk by cell type.Garfinkel et al.1O found an elevated risk forsquamous cell carcinoma and for other/mixed cell types. Others5.18 have observedlarger elevations for squamous and smallcell carcinoma than for adenocarcinoma.In contrast, Wu et al."1 and Fontham etal.20 found larger increases for adenocarci-noma. An additional difficulty in evaluatingprevious studies of passive smoking andlung cancer by histologic ype is that fewstudies have conducted systematic pathol-ogy reviews to verify cell type.
Our study has several major strengths.These include the lage sample size-one ofthe largest series ofnonsmolinglungcancercases to date. In addition, we had relativelyhigh response rates from both case patientsand control subjects. Fnaly, we conducteda pathology review of cases.
The main limitation of our study isthe possibility of recall bias for passivesmoke exposure variables. The less quan-titative measures of passive exposure(i.e., light, moderate, or heavy exposure)resulted in larger risk estimates than morequantitative estimates such as pack-years.Because there is no way to confirm pre-vious passive smoke exposure, it is diffi-cult to determine the best index for esti-mating exposure. However,we found thatlung cancer risk due to adulthood passivesmoke exposure was elevated at the high-est quartile of exposure whether we useda more quantitative (e.g., pack-years) orless quantitative (e.g., heavy exposure)variable.
Another possible source ofbias in ourstudy is the large number of surrogate in-terviews for cases. Earlier studies,38.43however, have shown relatively closeagreement on most passive smoke expo-sure variables as reported by subjects andspouses.Wefound fairlyminor alterationsin risk estimates when analyses were re-stricted to directly interviewed cases. Inaddition, we compared sociodemographiccharacteristics of direct and surrogatecase-group interviews and found closeagreement for most variables. As onemight expect, the exceptionwas age; therewas a tendency toward moreyounger casepatients in direct interviews.
In summary, our study and othersconducted during the past decade suggesta small but consistent elevation in the riskof lung cancer in nonsmokers due to pas-sive smoldng. The proliferation offederal,state, and local regulations that restrictsmoking in public places and work sites44is well founded. [
AcknowledgmentsThis study was supported in part by NationalCancer Institute contracts N01-CP7-1096-01and N01-CP7-1096-02.
The authors gratefully acknowledge theassistance of numerous individuals and organi-zations who made this study possible: SandiEzrine, Patsy Henderson, Joan Huber, andother staffofSurvey Research Associates, Inc,for valuable help in all phases of the study; Dr.Jian Chang, Carlene Anderson, Debbie Pinney,and Jeanie Shanebarger ofthe Missouri CancerRegistry, Missouri Department of Health, forassistance in data collection and patient track-ing; Dr. Ellis Ingram of the University of Mis-souri School of Medicine and Dr. Jeffrey Mey-ers of the Mayo Clinic for their assistance inreviewing pathology slides; Drs. William Blotand Jay Lubin of the National Cancer Institutefor helpful comments on the manuscript; andthe Missouri Department of Revenue and theHealth Care Finance Administration for theirhelp in selecting population-based controls.
References1. Kabat GC, Wynder EL. Lung cancer in
nonsmokers. Cancer. 1984;53:1214-1221.2. Pathak DR, Samet JM, Humble CG, Skip-
per BJ. Determinants of lung cancer risk incigarette smokers in New Mexico. JNatlCancer Inst. 1986;76:597-604.
3. Higgins IT, Wynder EL. Reduction in riskoflung cancer among ex-smokers with par-ticular reference to histologic type. Cancer.1988;62:2397-2401.
4. Schoenberg JB, Wilcox HB, Mason TJ,Bill J, Stemhagen A. Variation in smoking-related lung cancer risk among New Jerseywomen. Am J EpidemioL 1989;130:688-695.
5. Dalager NA, Piclde LW, Mason TJ, et al.The relation of passive smoking to lungcancer. Cancer Res. 1986;46:4804-7.
6. Garfinkel L. Time trends in lung cancermortality among nonsmokers and a note onpassive smoking.JNatICancerInst. 1981;66:1061-1066.
7. Correa P, Pickle LW, Fontham E, Lin Y,Haenszel W. Passive smoking and lungcancer. Lancet. 1983;2:595-597.
8. Trichopoulos D, Kalandidi A, Sparros L.Lung cancer and passive smoking: conclu-sion of Greek study. Lancet. 1983;2:677-678.
9. HirayamaT. Cancermortalityinnonsmok-ing women with smoking husbands basedon a large-scale cohort study in Japan.PrevMeL 1984;13:680-690.
10. Garfinkel L, Auerbach 0, Joubert L. In-voluntary smoking and lung cancer: a case-control study. INatiCancerInst. 1985;75:463-469.
11. Wu AH, Henderson BE, Pike MC, Yu
MC. Smoking and other risk factors forlung cancer in women.JNad CancerInst.1985;74:747-751.
12. Akiba S, Kato H, Blot WJ. Passive smok-ing and lung cancer among Japanesewomen. CancerRes. 1986;46:4804-07.
13. Brownson RC, Reif JS, Keefe TJ, Fergu-son SW, Pritzl JA. Risk factors for adeno-carcinoma of the lung. Am J EpdemioL1987;125:25-34.
14. Gao YT, Blot WJ, Zheng W, et al. Lungcancer among Chinese women. IntJ Can-cer. 1987;40:604-609.
15. Hole DJ, Giflis CR, Chopra C, HawtreVM. Passive smoking and cardoespiratoryhealth in a general population in the west ofScoland. BrMed J. 1989-,299:.423-427.
16. Humble CG, Samet JM, Pathak DR. Mar-riage to a smoker and lung cancer risk.AAmJPublic Healt 1987;77:598-602.
17. Lam TH, Kung 1TM, Wong CM, et al.Smoking, passive smo and histoicaltypes in lung cancer in Hong Kong Chiesewomen. BrJ Cancer. 1987;56:673-678.
18. Pershagen G, Zdenek H, Svensson C. Pas-sive smoking and lung cancer in Swedishwomen. AmJ EpidemidoL 1987;125:17-24.
19. Kalandidi A, Katsouyanni K, VoropoulouN, et al. Passive smoking and diet in theetiology of lung cancer among non-smok-ers. Cancer Causes ControL 1990;1:15-21.
20. Fontham ETH, Correa P, Wu-Williams A,et al. Lung cancer in nonsmoking women:a multi-center case-control study. CancerEpidemiolBiomarkersPrev. 1991;1:35-43.
21. National Research Council, Board on En-vironmental Studies and Toxicology, Com-mittee on Passive Smoking. EnvironmentalTobacco Smoke: Measuring Exposuresand Assessing Health Effects. Washing-ton, DC: National Academy Press; 1986.
22. National Institute for Occupational Safetyand Health. Environental Tobacco Smnkein the Wolmace- Ig Cancer and OtherHealth Effects. Cincinnati, Ohio: NationalInstitute forOccupational Safetyand Health;1991. DHHS publication NIOSH 91-108.Current Intelligence Bulletin 54.
23. Chan WC, Fung SC. Lung cancer in non-smokers in Hong Kong. In: Grundmann E,Clemmesen J, Muir CS, eds. Cancer Cam-pair VoL 6: Geogniphical Pathology iCancer Epidemiology. New York, NY:Gustav Fischer Verlag; 1982:199-202.
24. BuffierPA, Pickle LW, Mason TJ, ContantC. The causes of lung cancer in Texas. In:Mizell M, Correa P, eds. Lung Cancer:Causes and Prevention. New York, NY:Verlag-Chemie International, Inc; 1984.
25. Lee PN, Chamberlain J, Alderson MR. Re-lationship ofpassive smoking to riskoflungcancer and other smoking-associated dis-eases. BrJ Cancer. 1986;54:97-105.
26. Janerich DT, Thompson WD, Varela LR,et al. Lung cancer and exposure to tobaccosmoke in the household. N EngI J Med.1990;323:632-636.
27. Wu-Williams AH, Dai XD, Blot WJ, et al.Lung cancer among women in northeastChina. BrJ Cancer. 1990;62:982-987.
28. Brownson RC, Davis JR, Chang JC,DiLorenzo TM, Keefe TJ, Bagby JR Jr. Astudy of the accuracy of cancer risk factorinformation reported to a central registrycompared with that obtained by interview.Am JEpidemioL 1989;129:616-624.
November 1992, Vol. 82, No. 11 American Joumal of Public Health 1529

Brwnsou et aL
29. World Health Organization. The WorldHealth Organization histologic typing oflung tumors, 2nd ed. Am J Cin PathoL1982;77:123-136.
30. Koss LG. Diagnoric Cytologyand its His-topathologi Bases. 3rd ed. Philadelphia,Pa: JB Lippincott Co; 1979.
31. Hatten J. Medicare's common denomina-tor: the covered population. Health CareFinance Rev. 1980;2:53-64.
32. Wynder EL, Goodman MT, Hoffmann K.Lung cancer etiology: challenges of the fu-ture. Carr&ngenesis. 1985;8:39-61.
33. Breslow NE, Day NE. StatisticalMethodsin CancerResearch Volume I-TheAnal-ysis of Case-Control Studies. Lyon,France: International Agency of Researchon Cancer; 1980. [ARC publication 32.
34. Mantel N. Chi-square testswithone degreeof freedom, extensions of the Mantel-Haenszel procedure. Am Stat Assoc J.1963;58:690-700.
35. Wynder El, Goodman MT. Smoking andlung cancer: some unresolved issues. Epi-demiol Rev. 1983;5:177-207.
36. Alavanja MCR, Brownson RC, Boice JD,Jr, Hock ET. Nonmalignant lung diwaseand lung cancer in nonsmoking women.AmJ EpidemioL In press.
37. Friedman GD, Petitti DB, Bawol RD.Prevalence and correlates ofpassive smok-ing.Am JPublic Healtk 1983;73:401-405.
38. Cummings KM, Markeilo SJ, MahoneyMC, Marshall JR. Measurement of lifetimeexposure to passive smoke. Am J Epide-mioL 1989;130:122-132.
39. Fiore MC, Novotny TE, Pierce JP, Hatzi-andreu EJ, PatelKM, Davis RM. Trends incigarette smoking in the United States: thechanging influence of gender and race.JAMA. 1989;261:49-55.
40. US Dept of Health and Human Services.The Health Benefis of Smokdng Cessa-
tion. Rockville, Md: Centers for DiseaseControl; 1990. DHHS publication CDC90-8416.
41. Pron GE, Burch JD, Howe GR, Miler AB.The reliability of passive smoking hisoriesreported in a case-control study of lung can-cer.AmJEpiderioL 1988;127:267-273.
42. Coultas DB, Peake GT, Samet JM. Ques-tionnaire assessment of lifetime and recentexposure to environmental tobacco smoke.AmJEpidemioL 1989;130:338-347.
43. Lerchen ML, Samet JM. An assessment ofthe validity ofquestionnaire responses pro-vided by a sulviving spouse. Am J Epide-mioL 1986;123:481-489.
44. Rigotti NA, Pashos CL. No-smoking lawsin the United States: an analysis of stateand city actions to limit smoking in publicplaces and workplaces. JAMA4. 1991;266:3162-3167.
1530 American Journal of Public Health November 1992, Vol. 82, No. 11






![Passive design[1]](https://static.fdokumen.com/doc/165x107/63215c9580403fa2920cb59b/passive-design1.jpg)