
Is Mode Switching Beneficial? A Randomized Study in Patients With Paroxysmal Atrial Tachyarrhythmias
Upload
independentCategory
view
0download
0
The Journal of Emergency Medicine, Vol 14, No 1, 39-5 1, 1996 pp Copyright 0 1996 Elsevier Science Inc. Printed in the USA. All rights reserved
0736-4679/96 $15.00 + .OO
ELSEVIER SSDI 0736-4679(95)02061-6
Selected Topics: Cardiology Commentary
PAROXYSMAL SUPRAVENTRICULAR TACHYCARDIAS
Steven R. Lowenstein, MD, MPH,** Blair D. Halperin, MD,t and Michael J. Reiter, MD, PHDt
Divisions of *Emergency Medicine and tCardiology and SColorado Emergency Medicine Research Center, University of Colorado Health Sciences Center, Denver, Colorado
Reprint Address: Steven R. Lowenstein, MD, MPH, University of Colorado Health Sciences Center, Division of Emergency Medicine, Box B-21 1, 4200 East Ninth Avenue, Denver, CO 80262
q Abstract-Paroxysmal supraventricular tachycardia (PSVT) is a distinct clinical syndrome. Most patients present with the abrupt onset of palpitations, dizziness, dyspnea, or chest pain. The electrocardiogram (ECG) demonstrates a fast heart rate (150-250 beats per min), a regular rhythm, and most often, a narrow QRS com- plex. The P wave is usually hidden within the QRS com- plex. PSVT is caused by reentry, and the tachycardias are classified, electropbysiologically, according to the an- atomic location of the reentry circuit. Atrioventricular nodal reentry is the most common form of PSVT. In A- V nodal reentry, there are two conducting pathways (alph and beta) that have different conduction times and refractory periods; both pathways are confined to the A- V nodal and perinodal atria1 tissue. The other common form of PSVT, termed atrloventricular reciprocating tachycardia, depends on an anatomically distinct, or “ac- cessory,” pathway that may conduct impulses between the atria and the ventricles, while bypassing the AV node. The two forms of PSVT may be distinguised in many cases by examining the 12-lead electrocardiogram. In the majority of cases of A-V nodal reentry, the atria and ventricles are depolarized simultaneously, and the P waves are hidden in the QRS complex. If the reentry circuit includes an accessory pathway, the P wave always follows the QRS, and usually the R-P interval exceeds 70 msec.
Several principles should guide the management of PSVT: (a) Unstable patients require emergent electrical cardioversion; (b) A 1Zlead ECG should be obtained immediately to confirm that the tachycardia has a nar-
row complex (ventricular tachycardia may masquerade as PSVT if only a single lead is examined); (c) Vagal maneuvers may be attempted (the Valsalva maneuver is safer and more efficacious, especially in the elderly); and (4) In most patients, adenosine is the first-line agent to treat PSVT. Contraindications to adenosine and drug interactions are noted in this article. In addition, the use of adenosine in wide complex tachycardias and the indications for admission and referral for electrophysio- logic evaluation are discussed.
0 Keywords-supraventricular tachycardia; reentry; Wolff-Parkinson-White syndrome; adenosine
INTRODUCTION
Eight years ago, an article in this journal reviewed the management of tachycardias (1). The differential diagnosis of wide-complex tachycardias was empha- sized. In the present article, we discuss recent develop- ments in the diagnosis and treatment of paroxysmal supraventricular tachycardia (PSVT), a common nar- row-complex tachycardia. We emphasize the manage- ment of PSVT. Atria1 fibrillation, atria1 flutter, and multifocal atria1 tachycardia are mentioned only briefly.
Although this article was written to highlight new discoveries in pharmacotherapy and electrophysiology,
Cardiology Commentary is coordinated by Steven R. Lowenstein, MD, MPH, of the University of Colorado Health Sciences Center, Denver, Colorado
RECEIVED: 3 August 1994; FINAL SUBMISSION RECEIVED: 9 August 1995; ACCEPTED: 21 August 1995
39
40 S. R. Lowenstein et al.
readers are reminded of the importance of promptly evaluating each patient’s hemodynamic status. Patients who present with a faint or unobtainable pulse, hypo- tension, altered mentation, angina, or pulmonary edema require emergent electrical cardioversion. No diagnostic maneuvers should defer initiation of electri- cal therapy.
BASIC MECHANISMS OF SUPRAVENTRICULAR TACHYCAIWIAS
Automaticity
The two principal mechanisms of the genesis of cardiac dysrhythmias are enhanced automaticity and reentry (2,3). Automaticity is a normal property of some specialized cardiac cells; it is responsible for sinus node function and for the appearance of subsidiary (“escape”) pacemaker activity seen in atrial, A-V nodal, and His-Purkinje cells. Common automatic dysrhythmias include sinus tachycardia and multifocal atria1 tachycardia (2,4). Acute infe- rior wall myocardial infarction and digitalis toxic- ity often increase A-V nodal automaticity; the result is nonparoxysmal junctional tachycardia, another common automatic tachycardia.
Reentry
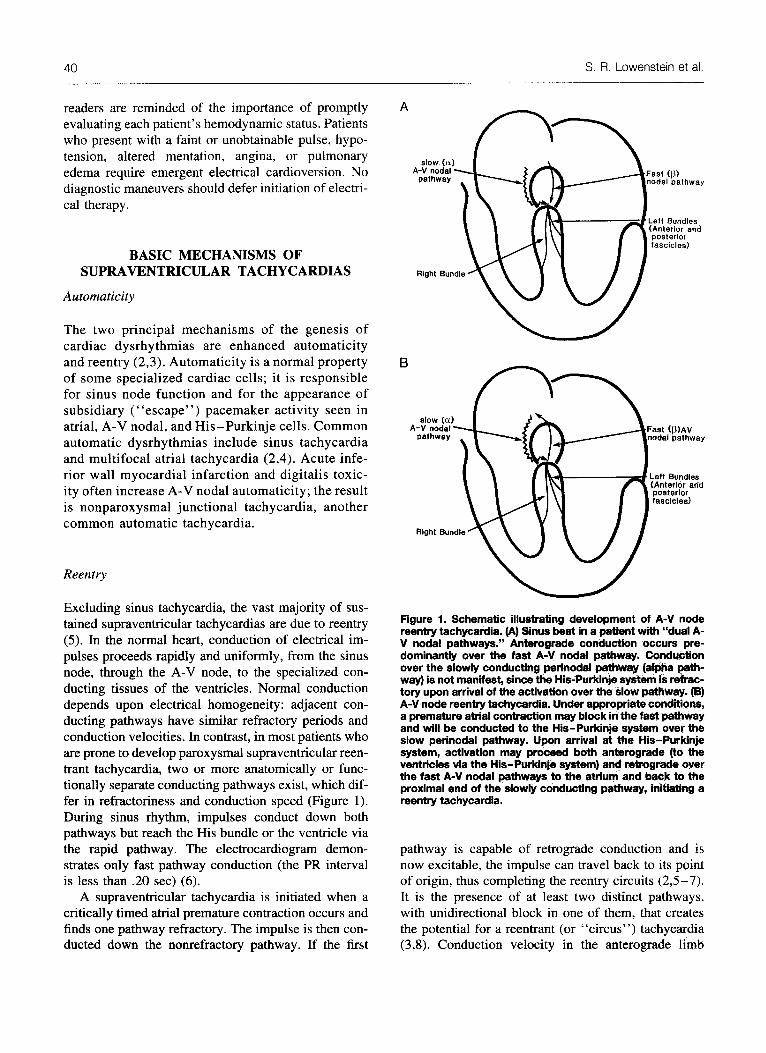
Excluding sinus tachycardia, the vast majority of sus- tained supraventricular tachycardias are due to reentry (5). In the normal heart, conduction of electrical im- pulses proceeds rapidly and uniformly, from the sinus node, through the A-V node, to the specialized con- ducting tissues of the ventricles. Normal conduction depends upon electrical homogeneity: adjacent con- ducting pathways have similar refractory periods and conduction velocities. In contrast, in most patients who are prone to develop paroxysmal supraventricular reen- trant tachycardia, two or more anatomically or func- tionally separate conducting pathways exist, which dif- fer in refractoriness and conduction speed (Figure 1). During sinus rhythm, impulses conduct down both pathways but reach the His bundle or the ventricle via the rapid pathway. The electrocardiogram demon- strates only fast pathway conduction (the PR interval is less than .20 set) (6).
A supraventricular tachycardia is initiated when a critically timed atrial premature contraction occurs and finds one pathway refractory. The impulse is then con- ducted down the nonrefractory pathway. If the first
Figure 1. Schematic illustrating development of A-V node reentry tachyoerdia. (A) Sinus beat in a patient with “dual A- V nodal pathways.” Anterograde conduction occurs pre- dominantly over the fast A-V nodal pathway. Conduction over the slowly conducting p&nodal pathway (afpha path- way) is not manifest, since the His-Purkinje system is refrac- tory upon arrival of the activation over the slow pathway. (B) A-V node reentry tachycardia. Under appropriate conditions, a premature atrial contractfon may block in the fast pathway and will be conducted to the His-Purkinje system ovar the slow perinodal pathway. Upon arrival at the His-Purkinje system, activation may proceed both anterograde (to the ventricles via the His-Purkinje system) and retrograde over the fast A-V nodal pathways to the atrium and back to the proximal end of the slowly conducting pathway, initiating a reentry tachycardia.
pathway is capable of retrograde conduction and is now excitable, the impulse can travel back to its point of origin, thus completing the reentry circuits (2,5-7). It is the presence of at least two distinct pathways, with unidirectional block in one of them, that creates the potential for a reentrant (or “circus”) tachycardia (3,8). Conduction velocity in the anterograde limb
Supraventricular Tachycardia 41
must be slower than the refractory period of the return limb; the leading edge of the wavefront must always meet excitable tissue, or the tachycardia cannot be sus- tained (7,9). The two pathways that participate in a reentrant tachycardia may be anatomically distinct. One example is the accessory Kent bundle of the Wolff-Parkinson-White syndrome (10). Commonly, the two pathways cannot be distinguished anatomi- cally, and in most patients with paroxysmal supraven- tricular tachycardia, the two pathways both lie within or near the AV node.
The differentiation between automatic and reentrant tachycardias is important therapeutically. Supraven- tricular tachycardias due to reentry can be terminated with electrical cardioversion or pacing, whereas auto- matic tachycardias cannot. Reentry tachycardias in- volving the A-V node as part of the reentry circuit can also be terminated by vagal maneuvers. Vagal maneu- vers usually induce A-V block in automatic tachycar- dias or reentry tachycardias confined to the atrium.
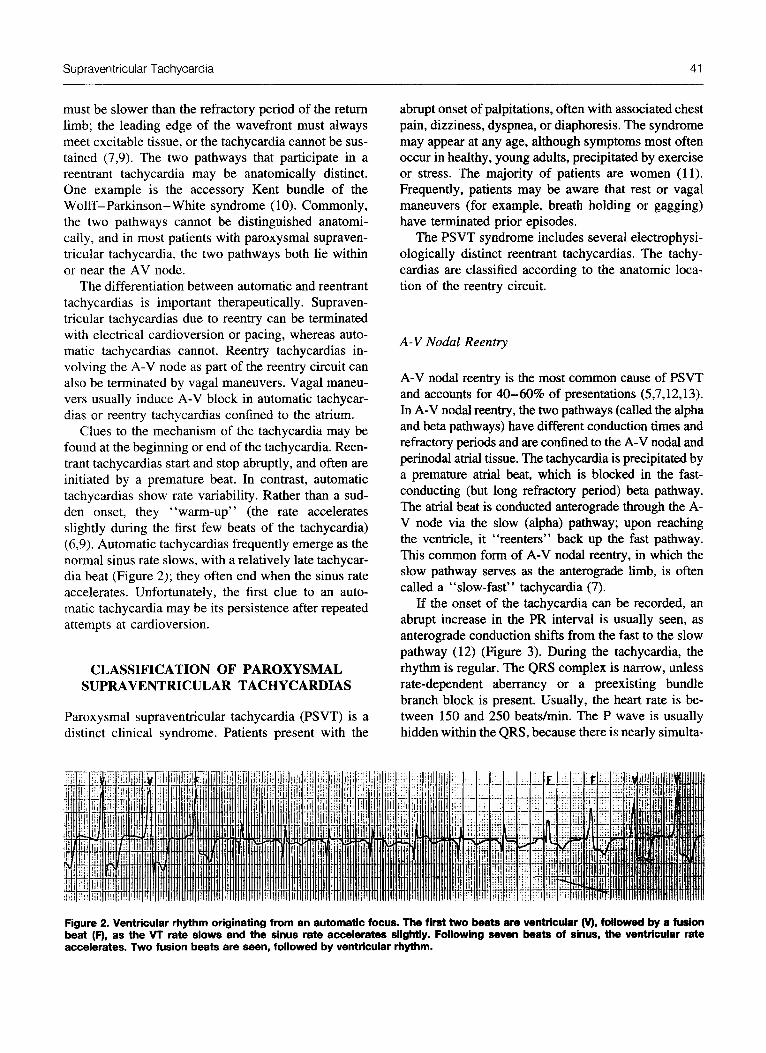
Clues to the mechanism of the tachycardia may be found at the beginning or end of the tachycardia. Reen- trant tachycardias start and stop abruptly, and often are initiated by a premature beat. In contrast, automatic tachycardias show rate variability. Rather than a sud- den onset, they “warm-up” (the rate accelerates slightly during the first few beats of the tachycardia) (6,9). Automatic tachycardias frequently emerge as the normal sinus rate slows, with a relatively late tachycar- dia beat (Figure 2); they often end when the sinus rate accelerates. Unfortunately, the first clue to an auto- matic tachycardia may be its persistence after repeated attempts at cardioversion.
CLASSIFICATION OF PAROXYSMAL SUPRAVENTRICULAR TACHYCARDIAS
Paroxysmal supraventricular tachycardia (PSVT) is a distinct clinical syndrome. Patients present with the
abrupt onset of palpitations, often with associated chest pain, dizziness, dyspnea, or diaphoresis. The syndrome may appear at any age, although symptoms most often occur in healthy, young adults, precipitated by exercise or stress. The majority of patients are women (11). Frequently, patients may be aware that rest or vagal maneuvers (for example, breath holding or gagging) have terminated prior episodes.
The PSVT syndrome includes several electrophysi- ologically distinct reentrant tachycardias. The tachy- cardias are classified according to the anatomic loca- tion of the reentry circuit.
A-V Nodal Reentry
A-V nodal reentry is the most common cause of PSVT and accounts for 40-60% of presentations (5,7,12,13). In A-V nodal reentry, the two pathways (called the alpha and beta pathways) have different conduction times and refractory periods and are confined to the A-V nodal and perinodal atrial tissue. The tachycardia is precipitated by a premature atrial beat, which is blocked in the fast- conducting (but long refractory period) beta pathway. The atrial beat is conducted anterograde through the A- V node via the slow (alpha) pathway; upon reaching the ventricle, it “reenters” back up the fast pathway. This common form of A-V nodal reentry, in which the slow pathway serves as the anterograde limb, is often called a “slow-fast” tachycardia (7).
If the onset of the tachycardia can be recorded, an abrupt increase in the PR interval is usually seen, as anterograde conduction shifts from the fast to the slow pathway (12) (Figure 3). During the tachycardia, the rhythm is regular. The QRS complex is narrow, unless rate-dependent aberrancy or a preexisting bundle branch block is present. Usually, the heart rate is be- tween 150 and 250 beats/min. The P wave is usually hidden within the QRS, because there is nearly simulta-
Figure 2. Ventricular rhythm originating from an automatic focus. The first two beats are ventricular (V), followed by a fusion beat (F), as the VT rate slows and the sinus rate accelerates slightly. Following seven beats of sinus, the ventricular rate accelerates. Two fusion beats are seen, followed by ventricular rhythm.

42 S. R. Lowenstein et al.
neous activation of the atria and the ventricles. At times, a P wave can be seen on the terminal portion of the QRS complex, but the R-to-P interval is always very short (less than 70 millisec) (7,12) (Figure 4A). If P waves are seen, they are upright in lead V1 (“Pseudo R-waves”) and negative in leads 2, 3, and AVF (‘ ‘Pseudo S-waves”), indicating a low-to-high, superiorly directed, atria1 activation sequence (5,6,13).
Vagal maneuvers result in slight slowing (with per- sistence of the tachycardia) or abrupt termination. Va- gal maneuvers cannot cause A-V block with persis- tence of the tachycardia, because the A-V nodal con- ducting tissue is an integral part of the electrical circuit (6). A-V nodal reentry tachycardia is effectively termi- nated by intravenous adenosine, verapamil, or electri- cal cardioversion. Chronic therapy to prevent tachycar- dia is indicated in individuals with frequent symptom- atic recurrences and is often initiated with diltiazem or verapamil, calcium channel blocking drugs that have significant antidromic effects on the A-V node (14).
Atrio-Ventricular Reciprocating Tachycardia
The second most common cause of PSVT, termed atrio-ventricular reciprocating tachycardia, depends on an anatomically distinct, or “accessory,” pathway. Pa- tients with the Wolff-Parkinson-White syndrome are the most widely recognized. They have one or more accessory connections capable of conducting from the atrium to the ventricle. During sinus rhythm, antero- grade conduction bypasses the usual physiological de- lay of the A-V node and eccentrically and prematurely activates a part of the ventricle that is normally acti- vated late. This accounts for the characteristic electro- cardiographic features during sinus rhythm: (a) a PR
Figure 3. Paroxysmal supraventricular tachycardia second- ary to A-V node reentry tachycardia. A premature atrial con- traction (Arrow) after a sinus beat (SR) initiates tachycardia. An increase in the PR interval is seen in the last pretachycar- dia beat, as anterograde conduction shiis abruptly to the slow pathway.
interval less than 120 millisec; (b) a slurred QRS onset (delta wave); and (c) a QRS duration greater than 120 millisec (10).
A reciprocating tachycardia is usually initiated by a premature atria1 beat. In most cases, the accessory pathway has the longer refractory period and is blocked. The PAC is conducted anterograde through the normal A-V node, and the accessory pathway is utilized in a retrograde direction, giving rise to a reen- trant tachycardia with a normal QRS complex (Figures 4B, 4C, & 5).
In approximately 40-50% of individuals with PSVT, there exists an accessory pathway that is only capable of retrograde conduction. In sinus rhythm, there is no electrocardiographic evidence of the pathway (it is ‘ ‘con- cealed”); however, it may participate in a tachycardia identical to that described above. In fact, patients with atrio-ventricular reentrant tachycardias caused by con- cealed accessory pathways are more numerous than are patients with the Wolff-Parkinson-White syndrome (WV
In atrio-ventricular reciprocating tachycardias, as in A-V nodal reentry, the QRS is regular and normal in morphology, unless a preexisting bundle branch block or rate-dependent aberrant conduction is present. In recipro- cating tachycardias, P-waves typically follow the QRS complex by 70 millisec or more (Figures 4B & 4C). The P waves are upright in V, , and they are negative in leads 2, 3, and AVF, where they often notch or indent the T wave after each QRS. The reason for this R-P relationship is easily understood. In A-V reciprocating tachycardia, unlike A-V nodal reentrant tachycardia, the electrical cir- cuit includes a portion of the ventricle. After the wave- front has passed anterograde through the A-V node, it must traverse a portion of the ventricle; only then can it access the accessory pathway that forms the retrograde limb of the tachycardia circuit (9).
Vagal maneuvers result in slight slowing or abrupt termination of the atrio-ventricular reciprocating tachy- card&. Verapamil, adenosine, and cardioversion are ap- propriate for termination. Because of the involvement of an accessory pathway in the tachycardia circuit, class IA antidysrhythmic agents are also effective for termination or prevention.
Atria1 Flutter
Atria1 flutter and atrial fibrillation are also reentrant supraventricular tachycardias (6). In both, the reentry circuits reside completely within the atria. In atrial flutter, the atria1 rate is typically 250 to 350 beats/min, but it may be slower in patients receiving antidysrhyth-

Supraventricular Tachycardia 43
mic therapy. Typical flutter waves are seen in leads 2, 3, AVF, and Vi, and the ventricular rate is usually half the atria1 rate, due to 2: 1 block in the A-V node. Higher degrees of block, variable A-V block or, rarely, 1:l A-V conduction may be encountered. Vagal maneu- vers or administration of adenosine or verapamil may increase the A-V block (but not terminate the tachycar- dia), causing a sudden drop in the ventricular rate and the appearance of flutter waves.
Atria1 Fibrillation
Atria1 fibrillation is the most common reentrant tachy- cardia. In atria1 fibrillation, polymorphous reentrant circuits occur within the atrium and result in atria1 rates exceeding 350 beats/min (15), The ventricular rhythm is irregular. No atria1 activity is apparent on a surface ECG, although an esophageal lead may record rapid, irregular, sharp atria1 depolarizations.
MORE ON THE TACHYCARDIAS OF THE WOLFF-PARKINSON-WHITE SYNDROME
The Wolff-Parkinson-White (WPW) syndrome is characterized by the presence of an accessory atrio- ventricular connection that is capable of anterograde conduction. As noted above, the most common tachy- cardia in patients with WPW is atrio-ventricular re- ciprocating tachycardia (7,lO). The QRS complex is usually narrow, because anterograde conduction pro- ceeds through the normal A-V node. This tachycardia is commonly termed orthodromic reciprocating tachy- cardia.
Antidromic reciprocating tachycardia occurs rarely in patients with WPW (7). Here, the circuit is re- versed: the anterograde limb is the accessory path- way, and retrograde conduction occurs through the A-V node. This results in a wide-complex, regular tachycardia. Only patients with the WPW syn- drome-not those with concealed accessory path- ways-can develop antidromic reciprocating tachy- cardia. The morphology of the QRS complex in each of the 12 standard leads is identical to the delta wave morphology in the same lead during sinus rhythm (Figure 6). P waves may be seen before or after each QRS complex.
Vagal maneuvers often will terminate an antidromic reciprocating tachycardia, since the A-V node is an obligatory part of the tachycardia circuit. In cases where anterograde conduction is occurring over the accessory pathway, intravenous verapamil and digoxin
should be avoided. It is often difficult to distinguish antidromic tachycardia from atria1 fibrillation or atria1 flutter with 2:l conduction. Both verapamil and di- goxin may accelerate conduction over the accessory pathway (16- 19).
Approximately 15% of tachycardias in patients with the Wolff-Parkinson-White syndrome are atria1 fibrillation. This tachycardia may be life-threatening. Because the accessory pathway can have a short re- fractory period and may be capable of rapid antero- grade conduction, accelerated ventricular rates may result, with the potential to deteriorate into ventricular fibrillation (20). A rapid, irregular rhythm, with heter- ogeneity of QRS complexes (occasionally narrow. but frequently preexcited and wide) should alert the clini- cian to the possibility of atria1 fibrillation with preex- citation (6,7).
COMMON QUESTIONS ABOUT DIAGNOSIS AND TREATMENT
1. When a patient presents in stable condition and has a rhythm strip demonstrating a narrow-complex supraventricular tachycardia, what is thejrst step that should be taken?
A 12-lead ECG should be obtained immediately to confirm that the tachycardia does, in fact, have narrow QRS complexes. Ventricular tachycardia may mas- querade as a narrow-complex tachycardia if only a single lead is examined (21).
2. Should vagal maneuvers be attempted in the initial management of stable patients with PSVT.?
Yes, probably. Vagotonic maneuvers, such as ca- rotid sinus massage, the Valsalva maneuver, the head- down position, deep inspiration, and application of ice to the face can terminate episodes of PSVT (22,23). Success rates above 85% are often quoted (22-24). However, in most published studies, vagal maneuvers have been applied to highly selected patients-usually those with catheter-induced PSVT undergoing electro- physiologic testing in the laboratory (24). In these cases, vagotonic procedures are initiated almost imme- diately after induction of the tachycardia. In this artifi- cial setting, even spontaneous reversion to sinus rhythm is very common. Indeed, when PSVT is in- duced artifically at the time of electrophysiologic study, the cumulative response rate to boluses of pla- cebo is 16% (25).
Patients with PSVT who present for care in emer- gency departments may have a more refractory dys- rhythmia. Their tachycardia is usually of longer dura- tion, is less likely to revert spontaneously, and may be

S. R. Lowenstein et al.
“pseudo R-prime”
AV Node Reentry Tachycardia. CL-490 msec. RP Interval-65 msec
retrograde P waves
Orthodromic Reciprocating Tachycardia, CL-390 meet. RP interval-115 msec
Figure 4(A and 6). Electrocardiograms of 2 types of paroxysmal supraventricular tachycardia illustrating utilii of the “R-P” relationship in distinguishing underlying mechanism. (A) A-V node reentry tachycardia. The activation of the vet’tttWea and atrla are near& simultaneous (R-P interval = 65 msec) and the P wave merges with the QRS complex. The cyds length of the tachycardia is 490 msec, corresponding to a rate of 122 beats/min. (B) Orthodromic reciproceting tacbycardia @iii&g a conce#ed atrioventricular accessory pathway. Note that activation of the atria follows ventricular a&vat&n by 115 meet. The cycle Ien@ is CW msec, equal to 154 beats/min.

Supraventricular Tachycardia
40 Hz 25.0 mm/s 10.0 mm/mV 4 by 2.56 + 1 rhythm Id MACVU 002C 12SLtm v260
Figure 4(C). This electrocardiogram was obtained in a 33-year-old man who presented with chest tightness and pa@itations. The ECG demonstrates atrio-ventricular reciprocating tachycardia. The P waves are negative in leads 2,3, and AVF, and are upright in lead V,, indiing a low-to-high, superiorly directed atrial activation sequence. The R-P interval is long (>70 msec), because the rebograde limb of the reentry circuit includes a portion of the ventricle. He converted spontaneously to a normal sinus rhythm. The 1Blead ECG in sinus rhythm was normal, suggesting a concealed accessory pathway. El-ologic studies were not performed.
more difficult to treat because of heightened sympa- thetic tone. In one recent emergency department study, 17 patients with PSVT were treated with carotid sinus massage, Valsalva maneuver, or a head-down tilt, sin- gly and in combination; only 3 patients converted to sinus rhythm (24).
Side effects of Valsalva maneuvers are seldom en- countered. Occasionally, however, carotid sinus mas- sage may provoke bradycardia or asystole in elderly patients who have sinoatrial conduction system dis- ease. In addition, cerebrovascular accidents may fol- low carotid sinus massage in patients with carotid ar- tery disease (26).
In addition to its attendant risks, carotid sinus mas- sage is less effective than other vagal maneuvers. A recent study demonstrated that the Valsalva maneuver was effective in terminating PSVT 3 times more often than right carotid sinus massage and 10 times more often than left carotid massage (27). These data (and a recent clinical decision model published by Grnato et al.) (24) suggest that in young, healthy patients, vago- tonic maneuvers should be tried, and that the Valsalva maneuver should be attempted first. In the elderly and
in others with cardiovascular disease, carotid sinus mas- sage is contraindicated. The Valsalva maneuver may be attempted, followed by pharmacological treatment. 3. When a patient presents with PSVT, what are the
best clues to the mechanism of the tachycardia? Spe- ci&ally, how does one tell if an accessory pathway is present?
An accessory pathway is a part of the tachycardia circuit in about 30% of cases of PSVT. The patient’s history is helpful if aware of an accessory pathway or the Wolff-Parkinson-White syndrome. If an electro- cardiogram in sinus rhythm is available, it may demon- strate a short PR interval and a delta wave, confirming the diagnosis of WPW.
A 12-lead ECG should be performed if time permits. The most important electrocardiographic clues pertain to the timing of the retrograde activation of the atria (7). In the majority of cases of A-V nodal reentrant tachycardia, the atria and ventricles are depolarized simultaneously, and the P waves are hidden in the QRS complex. Occasionally, a P wave is seen after the QRS, but the QRS-P interval is almost always less than 70 millisec. If the reentry circuit includes an accessory

46 S. R. Lowenstein et al.
HRA -f-
Figure 5. A schematic diagram and corresponding ECG of the most common tachycardia in pat&tts with the Wolff-Parkinson- Whii syndrome: orthodromic reciprocating tachycardia. To illustrate the mechanism, we have Wized data from a whom pacing from the high right atrium (HRA) followed by an early atrial stimulus (3rd beat) inMates Who&on& tachycardia. The A-V node is represented by a circle, and the sinus node is labeled (SA). During slnus rhythm or atrial pacing (A, fiit two illustrated beats), the ventricular depolarization is a fusion of anterograde conduction over the atrioventricu+ar accessory pathway and the A-V node His-Purkinje system. Under appropriate conditions (e.g., a spontaneous or paoed premature atrial contraction) (PAC, third beat), anterograde block may occur in the accessory pathway, nonnafMng the Gf?S and setting up a reentry tachycardia (subsequent beats) that travels anterograde from the atrium through the A-V node and His-Purkinje system, to the ventricles. Retrograde conduction takes place over the accessory pathway (last 4 illustrated beats).
pathway (atrio-ventricular reciprocating tachycardia), the P wave always follows the QRS. Usually, the R- P interval exceeds 70 millisec. Sustained aberration (more than 10 set) is uncommon in AV nodal reentrant tachycardia; its presence suggests a bypass tract. The presence of QRS alternans also favors the diagnosis of atrio-ventricular reciprocating tachycardia incorpo- rating a bypass track (12).
4. If a patient with PSVT is suspected of having WPW or another preexcitation syndrome, is it still safe to use intravenous verapamil?
If preexcitation is suspected, adenosine is a safer agent. Verapamil is contraindicated if the QRS is wide.
5. In stable patients with PSVT, should adenosine or verapamil be used first?
Verapamil and adenosine are equally effective in converting PSVT to sinus rhythm (25). Both agents have success rates greater than 90%. Yet, adenosine
is now the treatment of choice (11,28). Intravenous verapamil has three important disadvantages. First, it often causes hypotension, especially in patients with poor left ventricular function (29). Second, the half-life of intravenous verapamil is protracted; after a single intravenous dose of five milligrams, the physiological effects last 15-30 min. Third, verapamil can cause accelerated conduction in accessory pathways. Often, these accessory pathways are not recognized before treatment begins.
Adenosine is an endogenous nucleotide that is pres- ent in all body cells. Adenosine is rapidly degraded enzymatically or cleared from the circulation by vascu- lar endothelial cells (28). After a bolus of adenosine, the half-life is approximately 6-10 set (25). Flushing, chest pain, and dyspnea often occur after adenosine ad- ministration, but these discomforts are brief (28). Simi- larly, if hypotension occurs, it lasts only a few seconds.

Supraventricular Tachycardia
Figure 6. Antidromic reciprocating tachycardia in a patient with the WPW syndrome. (A) 1Blead ECG during sinus rhythm. Delta wave morphology is positive in leads I, II, aVL, V,-V,; the delta wave is negative in leads Ill, aVR, V,, and isoelectric in lead aVF. (B) ECG during antidromic tachycardia. Note similarity of QRS complex to delta wave morphology seen in sinus rhythm in each of the 12 leads.

48 S. R. Lowenstein et al.
In contrast to verapamil, adenosine appears to be safe in patients who present with hypotension, in pa- tients with heart failure, in those receiving concurrent beta-blocker therapy, and in those with accessory pathways (30,31). While acceleration of anterograde conduction in accessory pathways has been docu- mented in electrophysiologic studies, this effect is extremely short-lived. Adverse effects of adenosine in patients with WPW have been reported on rare occasions (32); yet, adenosine is less likely to be dele- terious than verapamil. Adenosine is not likely to be effective, nor is it recommended, in patients with pre- excitation and atria1 fibrillation (32). The preferred emergency agent in such patients is procainamide.
Intravenous beta-blockers are seldom indicated to manage PSVT; they may cause bronchoconstriction, hypotension, or cardiac dysfunction, and they are less effective than verapamil or adenosine. Intravenous digoxin has a delayed onset and is dangerous in the presence of accessory pathwaves.
6. How should adenosine be used for greatest efi- cacy and safety? What are the important contraindica- tions and drug interactions?
The initial dose of adenosine should be 6 mg intra- venously. If the tachycardia persists, a second dose of 6 mg or 12 mg may be administered 1 to 2 min later (28,33). Adenosine must be administered as a rapid bolus through a large intravenous catheter placed in an antecubital or other proximal vein.
Two drug interactions are noteworthy. First, the- ophylline is a potent adenosine receptor antagonist, and patients receiving theophylline may be refractory to adenosine. An opposite interaction has been ob- served with carbomazepine and dipyridamole; these agents prolong the half-life and physiological effect of adenosine.
There are few medical contraindications to adeno- sine. However, adenosine may provoke bronchospasm and therefore should not be used in patients who are wheezing. Since adenosine administration frequently results in brief periods of bradycardia or asystole, this drug should be used cautiously in patients with sinus node dysfunction.
One limitation of adenosine is its cost. One 6 mg dose costs $22 (wholesale price), compared to $3 for verapamil (5 mg). Another limitation of adenosine is its short half-life. In some patients (between 8 and 35% in one reported series), PSVT recurs within minutes of administration of adenosine. Verapamil may be needed to achieve long-lasting control (25,30,34,35).
7. How can adenosine be utilized in the diagnosis of narrow complex tachycardias?
Adenosine has an obvious therapeutic role in PSVT.
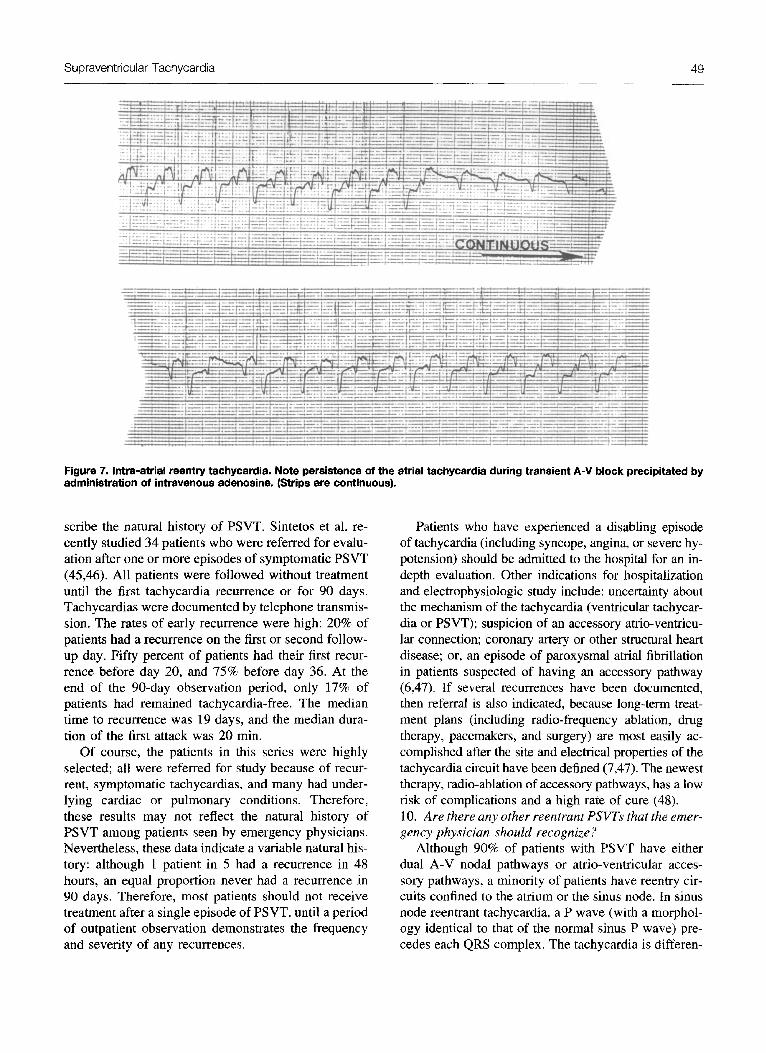
In addition, adenosine may be useful in the differential diagnosis of narrow complex tachycardias. The effect of adenosine is highly specific for reentrant tachycar- dias that include the A-V node (36). Thus, as noted earlier, in A-V nodal reentry, the usual response to adenosine is abrupt termination of the tachycardia. Atrio-ventricular reciprocating tachycardias also cease after adenosine; however, since adenosine blocks the A-V node but not the bypass pathway, the first few sinus beats in the postconversion period often demon- strate marked preexcitation (delta waves). Indeed, some have advocated the administration of adenosine during sinus rhythm to uncover latent preexcitation (37). When adenosine is administered to patients with atria1 reentrant tachycardias, A-V block may be in- duced with continuation of the tachycardia (Figure 7). A similar response occurs if the presenting tachycardia is atria1 tachycardia, atria1 flutter, or atria1 fibrillation.
8. Can adenosine be used safely if the QRS complex is wide? Should it be used for diagnostic purposes?
The vast majority of wide complex tachycardias are ventricular tachycardias (VT). In most series, 85% of patients with a wide complex tachycardia have VT; among patients with known coronary artery disease or congestive heart failure, this proportion rises to 95%. In most cases, the history and electrocardiogram provide robust clues to the diagnosis of ventricular tachycardia (l), and there is no reason to use adenosine where VT is highly likely. It is also well-established that adminis- tration of intravenous verapamil for patients with VT may cause catastrophic hemodynamic collapse (38-41).
While the safety of adenosine in wide complex tachycardias has not been defined in large clinical tri- als, the brevity of its actions suggests an important theoretical advantage over verapamil. In several small studies, administration of adenosine in patients with VT did not cause adverse consequences (31,33- 35,42,43). The response to adenosine in ventricular tachycardia is variable. Many patients with VT have 1: 1 retrograde ventriculo-atria1 conduction. After aden- osine, V-A conduction may be abolished, allowing A- V dissociation, capture beats, or fusion beats to emerge. If seen, these responses confirm a ventricular origin of the wide complex tachycardia. Alternatively, there may be no response to adenosine, suggesting (but not proving) that the diagnosis is VT (42-44).
9. After treatment for PSVT, what is the likelihood of a recurrence of PSVT? What are the indications for long-term treatment, hospital admission, and referral?
The reentrant tachycardias have been studied exten- sively in electrophysiology laboratories, but they have received little attention in ambulatory and emergency settings. Thus, there are few data available that de-
Supraventricular Tachycardia
Figure 7. Intra-atrial reentry tachycardia. Note persistence of the atrial tachycardia during transient A-V block precipitated by administration of intravenous adenosine. (Strips are continuous).
scribe the natural history of PSVT. Sintetos et al. re- cently studied 34 patients who were referred for evalu- ation after one or more episodes of symptomatic PSVT (45,46). All patients were followed without treatment until the first tachycardia recurrence or for 90 days. Tachycardias were documented by telephone transmis- sion. The rates of early recurrence were high: 20% of patients had a recurrence on the first or second follow- up day. Fifty percent of patients had their first recur- rence before day 20, and 75% before day 36. At the end of the 90-day observation period, only 17% of patients had remained tachycardia-free. The median time to recurrence was 19 days, and the median dura- tion of the first attack was 20 min.
Of course, the patients in this series were highly selected; all were referred for study because of recur- rent, symptomatic tachycardias, and many had under- lying cardiac or pulmonary conditions. Therefore, these results may not reflect the natural history of PSVT among patients seen by emergency physicians. Nevertheless, these data indicate a variable natural his- tory: although 1 patient in 5 had a recurrence in 48 hours, an equal proportion never had a recurrence in 90 days. Therefore, most patients should not receive treatment after a single episode of PSVT, until a period of outpatient observation demonstrates the frequency and severity of any recurrences.
Patients who have experienced a disabling episode of tachycardia (including syncope, angina, or severe hy- potension) should be admitted to the hospital for an in- depth evaluation. Other indications for hospitalization and electrophysiologic study include: uncertainty about the mechanism of the tachycardia (ventricular tachycar- dia or PSVT); suspicion of an accessory atrio-venticu- lar connection; coronary artery or other structural heart disease; or, an episode of paroxysmal atria1 fibrillation in patients suspected of having an accessory pathway (6,47). If several recurrences have been documented, then referral is also indicated, because long-term treat- ment plans (including radio-frequency ablation, drug therapy, pacemakers, and surgery) are most easily ac- complished after the site and electrical properties of the tachycardia circuit have been defined (7,47). The newest therapy, radio-ablation of accessory pathways, has a low risk of complications and a high rate of cure (48). 10. Are there any other reentrant PSVTs that the emer- gency physician should recognize?
Although 90% of patients with PSVT have either dual A-V nodal pathways or atrio-ventricular acces- sory pathways, a minority of patients have reentry cir- cuits confined to the atrium or the sinus node. In sinus node reentrant tachycardia, a P wave (with a morphol- ogy identical to that of the normal sinus P wave) pre- cedes each QRS complex. The tachycardia is differen-

50
tiated from sinus tachycardia by its abrupt onset and termination (6). In addition, the clinical setting may raise the possibility of sinus node reentrant tachycar- dia: whereas sinus tachycardia occurs in response to acute volume depletion, pain, fever, hypoxia, or an- other physiological stress, sinus node reentrant tachy- cardia may be observed at rest.
Intra-atria1 reentrant tachycardia is also character- ized by a sudden onset and termination; here, the P wave is different from the P wave of sinus rhythm. Another electrocardiographic clue is observation of an unchanged tachycardia during episodes of A-V block. Pharmacologic A-V nodal blockade will not terminate
5.
IO.
11.
12.
13.
S. R. Lowenstein et al.
intra-atria1 reentry tachycardia, in sharp contrast to A- V node reentry and reciprocating tachycardias. Both sinus node and atria1 reentrant tachycardias are un- common, and both usually terminate spontaneously. Both tachycardias will respond to electrical cardiover- sion in emergent situations. When pharmacological treatment is required, sinus node reentrant tachycardia will usually respond to adenosine, calcium channel blockers, or beta blockers, the same agents that are effective in A-V node reentry. Intra-atria1 reentrant tachycardia will respond to agents that are used to treat atria1 flutter or fibrillation, including type IA anti- dysrhythmic agents.
REFERENCES
Lowenstein SR, Harken AH. A wide, complex look at cardiac dysrhythmias. J Emerg Med. 1987;5(6):519-31. Wit AL. Cellular electrophysiologic mechanisms of cardiac ar- rhythmias. Cardio Clin. 1990;8(3):393-409. Hoffman BF, Rosen MR. Cellular mechanisms for cardiac ar- rhythmias. Circ Res. 1981;49(1):1-1.5. Schwartz M, Lowenstein SR, Rodman D. Recognition and treat- ment of multifocal atria1 tachycardia: a critical review. J Emerg Med. 1994; 12(3):353-60. Wu D, Denes P, Amat-Y -Leon F, et al. Clinical, electrocardio- graphic and electrophysiologic observations in patients with par- oxysmal supraventricular tachycardia. Am J Cardiol. 1978; 41:1045-51. Sager PT, Bhandari AK. Narrow complex tachycardias. Differen- tial diagnosis and management. Cardiol Clin. 1991;9(4):619-40. Wu D. Supraventricular tachycardias. JAMA. 1983;249(24): 3357-60. Rosen MR. The links between basic and clinical cardiac electro- physiology. Circulation. 1988;77(2):251-63. Benditt DG, Goldstein MA, Reyes WJ, Milstein S. Supraventric- ular tachycardias: mechanisms and therapies. Hosp Pratt. 1988;23(8):161-73,176-80,183-5. Wellens HJ, Brugada P, Penn OC. The management of preexci- tation syndromes. JAMA. 1987;257(17):2325-33. Ganz LI, Friedman PL. Supraventricular tachycardia. N Engl J Med. 1995;332:162-173. Josephson ME, Wellens HJ. Differential diagnosis of supraven- tricular tachycardia. Cardiol Clin. 1990; 8(3):41 l-42. Bar FW, Brugada P, Dassen WR, Wellens HJ. Differential diag- nosis of tachycardia with narrow QRS complex (shorter than 0.12 second). Am J Cardiol. 1984;54(6):555-60.
14. Mauritson DR, Winniford MD, Walker WS, Rude RE, Cary JR, Hillis LD. Oral verapamil for paroxysmal supraventricular tachycardia: a long-term, double-blind randomized trial. Ann Intern Med. 1982;96(4):409-12.
15. Flagel KM. From delirium cordis to atria1 fibrillation: historical development of a disease concept. Ann Intern Med. 1995; 122:867-73.
28. Camm AJ, Garratt CJ. Adenosine and supraventricular tachycar- dia. N Engl 3 Med. 1991:325(23):1621-9.
29. Kuhn M, gchriger DL. Verapa&l’administration to patients with contraindications: is it associated with adverse outcomes? Ann Emerg Med. 1991;20(10):1094-9.
30. Rankin AC, McGovern BA. Adenosine or verapamil for the acute treatment of supraventricular tachycardia? Ann Intern Med. 1991; 114(6):513-5.
16. Wellens HJ, Durrer D. Effect of digitalis on atrioventricular conduction and circus-movement tachycardias in patients with Wolff-Parkinson-White syndrome. Circulation. 1973;47(6): 1229-33.
17. Gulamhusein S, Ko P, Carruthers SG, Klein GJ. Acceleration of the ventricular response during atrial fibrillation in the Wolff- Parkinson-White syndrome after verapamil. Circulation. 1982:65(2):348-54.
31. McCabe JL, Adhar GC, Menegazzi JJ, Paris PM. Intravenous adenosine in the prehospital treatment of paroxysmal supraven- tricular tachycardia. Ann Emerg Med. 1992; 21(4):358-6 I
32. Exner DV, Muzyka T, Gillis AM. Proarrhythmia in patients with the Wolff-Parkinson-White syndrome after standard doses of intravenous adenosine. Ann Intern Med. 1995; 122:351-2.
33. Adenosine and the diagnosis of tachycardias. Lancet. 1992;339(8791):464-5.
18. Jacob AS, Nielsen DH, Gianelly RE. Fatal ventricular fibrillation 34. Cairns CB, Niemann JT. Intravenous adenosine in the emer-
following verapamil in Wolff-Parkinson-White syndrome with atria1 fibrillation. Ann Emerg Med. 1985; 14(2):159-60.
19. McGovern B, Garan H, Ruskin JN. Precipitation of cardiac arrest by verapamil in patients with Wolff-Parkinson-White syndrome. Ann Intern Med. 1986; 104(6):791-4.
20. Klein GJ, Bashore TM, Sellers TD. Pritchett EL, Smith WM, Gallagher JJ. Ventricular fibrillation in the Wolff-Parkinson- White syndrome. N Engl J Med. 1979;301(20):1080-5.
21. Marriott HJL. Practical electrocardiography (8th edn). Balti- more: Williams and Wilkins; 1988.
22. Waxman MB, Wald RW, Sharma AD, Huerta F, Cameron DA. Vagal techniques for termination of paroxysmal supraventricular tachycardia. Am J Cardiol. 1980;46(4):655-64.
23. Waxman B, Bonet JF, Finley JP, Wald RW. Effects of respira- tion and posture on paroxysmal supraventricular tachycardia. Circulation. 1980;62(5): 101 l-20.
24. Omato JP, Hallagan LF, Reese WA, et al. Treatment of paroxys- mal supraventricular tachycardia in the emergency department by clinical decision analysis. Am J Emerg Med. 1988;6(6):555- 60.
25. DiMarco JP, Miles W, Akhtar M, et al. Adenosine for paroxys- mal supraventricular tachycardia: dose ranging and comparison with verapamil. Assessment in placebo-controlled, multicenter trials. The Adenosine for PSVT Study Group. Ann Intern Med. 1990;113(2):104-10.
26. Bastulli JA. Stroke as a complication of carotid sinus massage. Crit Care Med. 1985;869.
27. Mehta D, Wafa S, Ward DE, Camm AJ. Relative efficacy of various physical manoeuvres in the termination of junctional tachycardia. Lancet. 1988; 1(8596): 1181-5.

Supraventricular Tachycardia 51
gency department management of paroxysmal supraventricular tachycardia. Ann Emerg Med. 1991;20(7):717-21.
35. Rankin AC, Oldroyd KG, Chong E, Rae AP, Cobbe SM. Value and limitations of adenosine in the diagnosis and treatment of narrow and broad complex tachycardias. Br Heart J. 1989;62(3):195-203. - -
36. DiMarco JP. Sellers TD. Lerman BB. Greenberg ML, Beme
42.
43.
AA RM, Belardinelli L. Diagnostic and therapeutic u&of adenosine in patients with supraventricular tachyarrhythmias. J Am Co11 Cardiol. 1985;6(2):417-25.
--’
37. Garratt CJ, Antoniou A, Griffith MI, Ward DE, Camm AJ. Use ,,< of intravenous adenosine in sinus rhythm as a diagnostic test -” for latent oreexcitation. Am J Cardiol. 1990:65(13):868-73. ,_
38. Stewart RB, Bardy GH, Greene HL. Wide complex tachycardia: misdiagnosis and outcome after emergent therapy. Ann Intern Med. 1986; 104(6):766-71.
39. Dancy M, Camm Al, Ward D. Misdiagnosis of chronic recurrent ventricular tachycardia. Lancet. 1985;2(8450):320-3.
40. Buxton AE, Marchlinski FE, Doherty JU, Flores B, Josephson ME. Hazards of intravenous verapamil for sustained ventricular tachycardia. Am J Cardiol. 1987;59(12):1107-10.
41. Rankin AC, Rae AP, Cobbe SM. Misuse of intravenous vera- pamil in patients with ventricular tachycardia. Lancet. 1987; 2(8557):472-4.
40.
47.
48.
Griffith MJ, Linker NJ, Ward DE, Camm AJ. Adenosine in the diagnosis of broad complex tachycardia. Lancet. 1988; 1 (8587):672-5. Sharma AD, Klein GJ, Yee R. Intravenous adenosine triphos- phate during wide QRS complex tachycardia: safety, therapeutic efficacy, and diagnostic utility. Am J Med. 1990;88(4):337-43. Lerman BB. Belardinelli L, West GA, Beme RM, DiMarco JP. Adenosine-sensitive ventricular tachycardia: evidence sug- gesting cyclic AMP-mediated triggered activity. Circulation. 1986;74(2):270-80. Pritchett EL, McCarthy EA, Lee KL. Clinical behavior of parox- ysmal atria1 tachycardia. Am J Cardiol. 1988;62(6):3D-9D. Sintetos AL, Roark SF, Smith MS, McCarthy EA. Lee KL, Pritchett EL. Incidence of symptomatic tachycardia in un- treated patients with paroxysmal supraventricular tachycar- dia. Arch Intern Med. 1986; 146(11):2205-9. Prystowsky EN. Indications for intracardiac electrophysio- logic studies in patients with supraventricular tachycardia. Circulation. 1987;75(4 Pt 2):IIII 19-24. Jackman WM, Beckman KJ, McClelland JH, et al. Treatment of supraventricular tachycardia due to atrioventricular nodal reentry, by radiofrequency catheter ablation of slow-pathway conduction. N Engl J Med. 1992;327(5):313-8.
Copyright © 2022 FDOKUMEN














