Acute paroxysmal Subsequently there were 28 additional
7
ment of the endometrium or Johnson's lymphoid struct- ure; yet ample evidence is obtainable that endometrial diseases frequently occur in the history of splenic dis- ease. The symptoms of splenic hypertrophy are divided into two classes, first constant and second occasional. Of the first we have progressively enlarging abdomen, pain, weight and dragging sensation, anorexia, nau- sea and frequently most obstinate vomiting, vertigo, insomnia, dyspnea, emaciation and enemia. The occasional symptoms are hematuria, epistaxis and hematemesis. I wish in this connection to remark upon the constancy of insomnia as a symptom. In almost every detailed report it is mentioned and may be explained, I think, by the existing anemia. I do not think it necessary to discuss here the phys- ical diagnosis of splenic tumors and hypertrophy. Our acquaintance with intra-abdominal disorders is so much more intimate than formerly that in the future errors in diagnosis will be quite the exception. There are two complications which occur in the life history of enlarged spleen deserving special mention, torsion of the pedicle and ascites. I am able to gather altogether eight cases of torsion of the pedicles. To these if it were proper I would add a ease reported by me in the Medical News, April 1890, of splenic hypertrophy with torsion of the pedi- cle, diagnosticated as uterine fibroma with torsion of the pedicle. The woman died while preparations were being made for operation, the autopsy revealed the true nature of the case. Of the eight cases I reported all were women, six were multípara?, two may have been though were not so stated. In four cases symptoms of torsion became quite manifest after labor or abor- tion. The symptoms of rotation of the spleen briefly stated are the following: Acute paroxysmal pain of the twisting character, more or less sharp; nausea, vomiting, frequently obstinate constipa- tion so much so as to suggest intestinal obstruction; sausage tympany; tumor enlarges rapidly, becomes hard, tense and very tender. These symptoms remarkably simulate hemorrhagic pancreatitis. The second complication to which I would call your attention is that of accumulation of ascitic fluid. It was present in eleven cases; nine of these patients died. Death was due to hemorrhage no doubt, though it is not so stated. The splenic hypertrophy in these cases was associated with, if not due to, hepatic cirrho- sis, and after removal of the spleen by reason of the obstruction offered to the portal circulation there were double causes for increased vascular tension. There- fore a patient presenting this complication is predis- posed to hemorrhage, a fact that should have due weight in determining the propriety of an operation. The first operation done in America was performed by Alston. Subsequently there were 28 additional operations performed, resulting in 11 deaths and 17 recoveries. Our honored fellow, Prof. E. S. Lewis of New Orleans, appears as the most successful American operator, he having removed the spleen in two cases of malarial hypertrophy. In one case the physical signs warranted the diagnosis of uterine fibroma. When the abdomen was opened he quickly discovered his error, but drew up the spleen, ligated its long pedicle and removed it. The second case was correctly diagnosed, as an enlarged and displaced spleen. Both patients recovered. Our honorable president Dr. Louis McLean Tiffany kindly gives me the following notes of his case: Mrs.-, age 45, came into my care December, 1893, suffer- ing from a tumor in the left side of the abdomen. It was freely movable from side to side as well as up and down, but always extended six inches below the left ribs. When stand- ing the tumor presented below the navel in the middle line ; toward the linea alba the finger could be pressed underneath the tumor recognizing a more or less sharp border, broken in two places by depressions which suggested that the tumor was an enlarged spleen. The history of the patient showed that she had suffered for years from irregular attacks of malarial fever and that the tumor had grown for seven or eight years slowly. It was thought at first that the attacks of malarial fever were accompanied by pain in the tumor. At present not only is discomfort complained of, but inability to eat and digest food also. Examination of the blood showed slight rel- ative increase in white blood cells. The spleen was removed Dec. 29, 1893. An incision sufficiently long was made from the umbilicus downward to the left of the linea alba, and from the - umbilicus upward and outward as far as necessary. The spleen at once came into view with a long pedicle. The omen- tum was adherent to the under surface and was tied off in segments. The vessels entering the spleen at the hilum were separately uncovered and tied. Two small spleens not larger than walnuts were left. All went well, the patient recovered without trouble. Examination of the tumor showed that it was 25 c. long, 14^ c. wide, 7 c. thick and weighed 11,000 gr. It was hard and inelastic ; the capsule tense and much thick- ened. In places it was very opaque, apparently by fibrous deposit. On section it was of a dark red color, nearly black ; the pulp could easily be pressed out leaving large and prominent trabeculae which crossed in all directions. Microscopic sections were stained with eosin and hematoxylon. They showed enlarged blood vessels, the spaces between the trabeculas con- tained large numbers of red corpuscles and a good many white ones. The sections looked like hemorrhagic infarctions, the walls of the blood vessels were thickened and infiltrated with small round cells. The capsule was thickened and infiltrated similarly, the glomeruli were seen with difficulty. Trabecuke were increased in size and number and infiltrated with round cells. There was much 'coloring matter present and there appeared to be a general increase in connective tissue through- out the whole organ. The appearance justified the diagnosis of subacute indurate splenitis. The blood was normal when the patient left the hospital. AMERICAN OPERATORS. Goodell, leukemia, death ; Markoe, simple hypertrophy, recovery ; Miner, simple hypertrophy, death ; Powell, wound and hernia, recovery ; Alston, wound and hernia, recovery ; Myers, malarial hypertrophy, recovery ; Markham, wound and hernia, recovery ; Markoe, malarial hypertrophy, recovery ; Strong, leukemia, death ; Willien, wound, death ; McGraw, malarial hypertrophy, recovery ; McGraw, simple hypertrophy, death ; Nilsen, simple hypertrophy, recovery ; Deaver, trau- matism, death : Simmons, malarial hypertrophy, death ; Rod- dick, traumatism, death ; McCann, simple hypertrophy, recov- ery ; Conklin, simple hypertrophy with torsion, recovery ; Bond, simple hypertrophy with torsion, death ; Pane, malarial hyper- trophy, recovery ; Bark, leukemia, death ; Saurason, malarial hypertrophy, recovery ; Penrose, simple hypertrophy, death ; Yourkin, simple hypertrophy, recovery ; Stephen, simple hypertrophy, recovery ; Lewis, malarial hypertrophy, recovery ; Lewis, malarial hypertrophy, recovery ; Tiffany, malarial hypertrophy, recovery ; Douglas, malarial hypertrophy, recov- ery ; total number 29, deaths 11, recoveries 18. THE EXTENSION CORSET AND ITS INDICA- TIONS. BY ALEX. C. WIENER, M.D. CHICAGO. Lewis A. Sayre revolutionized the treatment of tubercular processes of the spinal column by the prop- aganada of absolute immobilization and freedom from pressure of the diseased portion. That the results obtained by his method were unprecedented is amply evidenced by the fact that his principles have made a triumphal tour around the civilized world and that the use of the plaster of paris corset has come to be considered indispensable in the treatment of Pott's disease. The symptoms of tubercular infection of the spinal DownloadedFrom:http://jama.jamanetwork.com/byaUniversityofArizonaHealthSciencesLibraryUseron06/08/2015
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Acute paroxysmal Subsequently there were 28 additional

ment of the endometrium or Johnson's lymphoid struct-ure; yet ample evidence is obtainable that endometrialdiseases frequently occur in the history of splenic dis-ease.
The symptoms of splenic hypertrophy are dividedinto two classes, first constant and second occasional.Of the first we have progressively enlarging abdomen,pain, weight and dragging sensation, anorexia, nau-sea and frequently most obstinate vomiting, vertigo,insomnia, dyspnea, emaciation and enemia. Theoccasional symptoms are hematuria, epistaxis andhematemesis. I wish in this connection to remarkupon the constancy of insomnia as a symptom. Inalmost every detailed report it is mentioned and maybe explained, I think, by the existing anemia.
I do not think it necessary to discuss here the phys-ical diagnosis of splenic tumors and hypertrophy.Our acquaintance with intra-abdominal disorders isso much more intimate than formerly that in the futureerrors in diagnosis will be quite the exception. Thereare two complications which occur in the life historyof enlarged spleen deserving special mention, torsionof the pedicle and ascites. I am able to gatheraltogether eight cases of torsion of the pedicles.To these if it were proper I would add aease reported by me in the Medical News, April1890, of splenic hypertrophy with torsion of the pedi-cle, diagnosticated as uterine fibroma with torsion ofthe pedicle. The woman died while preparationswere being made for operation, the autopsy revealed thetrue nature of the case. Of the eight cases I reported allwere women, six were multípara?, two may have beenthough were not so stated. In four cases symptomsof torsion became quite manifest after labor or abor-tion. The symptoms of rotation of the spleenbriefly stated are the following: Acute paroxysmalpain of the twisting character, more or less sharp;nausea, vomiting, frequently obstinate constipa-tion so much so as to suggest intestinal obstruction;sausage tympany; tumor enlarges rapidly, becomeshard, tense and very tender. These symptomsremarkably simulate hemorrhagic pancreatitis.
The second complication to which I would call yourattention is that of accumulation of ascitic fluid. It waspresent in eleven cases; nine of these patients died.Death was due to hemorrhage no doubt, though it isnot so stated. The splenic hypertrophy in thesecases was associated with, if not due to, hepatic cirrho-sis, and after removal of the spleen by reason of theobstruction offered to the portal circulation there weredouble causes for increased vascular tension. There-fore a patient presenting this complication is predis-posed to hemorrhage, a fact that should have dueweight in determining the propriety of an operation.The first operation done in America was performedby Alston. Subsequently there were 28 additionaloperations performed, resulting in 11 deaths and 17recoveries. Our honored fellow, Prof. E. S. Lewis ofNew Orleans, appears as the most successful Americanoperator, he having removed the spleen in two cases ofmalarial hypertrophy. In one case the physical signswarranted the diagnosis of uterine fibroma. When theabdomen was opened he quickly discovered his error,but drew up the spleen, ligated its long pedicle andremoved it. The second case was correctly diagnosed,as an enlarged and displaced spleen. Both patientsrecovered.
Our honorable president Dr. Louis McLean Tiffanykindly gives me the following notes of his case:
Mrs.-, age 45, came into my care December, 1893, suffer-ing from a tumor in the left side of the abdomen. It wasfreely movable from side to side as well as up and down, butalways extended six inches below the left ribs. When stand-ing the tumor presented below the navel in the middle line ;toward the linea alba the finger could be pressed underneaththe tumor recognizing a more or less sharp border, broken intwo places by depressions which suggested that the tumor wasan enlarged spleen. The history of the patient showed thatshe had suffered for years from irregular attacks of malarialfever and that the tumor had grown for seven or eight yearsslowly. It was thought at first that the attacks of malarialfever were accompanied by pain in the tumor. At present notonly is discomfort complained of, but inability to eat anddigest food also. Examination of the blood showed slight rel-ative increase in white blood cells. The spleen was removedDec. 29, 1893. An incision sufficiently long was made from theumbilicus downward to the left of the linea alba, and from the
-umbilicus upward and outward as far as necessary. Thespleen at once came into view with a long pedicle. The omen-tum was adherent to the under surface and was tied off insegments. The vessels entering the spleen at the hilum wereseparately uncovered and tied. Two small spleens not largerthan walnuts were left. All went well, the patient recoveredwithout trouble. Examination of the tumor showed that itwas 25 c. long, 14^ c. wide, 7 c. thick and weighed 11,000 gr.It was hard and inelastic ; the capsule tense and much thick-ened. In places it was very opaque, apparently by fibrousdeposit. On section it was of a dark red color, nearly black ; thepulp could easily be pressed out leaving large and prominenttrabeculae which crossed in all directions. Microscopic sectionswere stained with eosin and hematoxylon. They showedenlarged blood vessels, the spaces between the trabeculas con-tained large numbers of red corpuscles and a good many whiteones. The sections looked like hemorrhagic infarctions, thewalls of the blood vessels were thickened and infiltrated withsmall round cells. The capsule was thickened and infiltratedsimilarly, the glomeruli were seen with difficulty. Trabecukewere increased in size and number and infiltrated with roundcells. There was much 'coloring matter present and thereappeared to be a general increase in connective tissue through-out the whole organ. The appearance justified the diagnosisof subacute indurate splenitis. The blood was normal whenthe patient left the hospital.
AMERICAN OPERATORS.Goodell, leukemia, death ; Markoe, simple hypertrophy,
recovery ; Miner, simple hypertrophy, death ; Powell, woundand hernia, recovery ; Alston, wound and hernia, recovery ;Myers, malarial hypertrophy, recovery ; Markham, wound andhernia, recovery ; Markoe, malarial hypertrophy, recovery ;Strong, leukemia, death ; Willien, wound, death ; McGraw,malarial hypertrophy, recovery ; McGraw, simple hypertrophy,death ; Nilsen, simple hypertrophy, recovery ; Deaver, trau-matism, death : Simmons, malarial hypertrophy, death ; Rod-dick, traumatism, death ; McCann, simple hypertrophy, recov-ery ; Conklin, simple hypertrophy with torsion, recovery ; Bond,simple hypertrophy with torsion, death ; Pane, malarial hyper-trophy, recovery ; Bark, leukemia, death ; Saurason, malarialhypertrophy, recovery ; Penrose, simple hypertrophy, death ;Yourkin, simple hypertrophy, recovery ; Stephen, simplehypertrophy, recovery ; Lewis, malarial hypertrophy, recovery ;Lewis, malarial hypertrophy, recovery ; Tiffany, malarialhypertrophy, recovery ; Douglas, malarial hypertrophy, recov-ery ; total number 29, deaths 11, recoveries 18.
THE EXTENSION CORSET AND ITS INDICA-TIONS.
BYALEX.C.WIENER,M.D.CHICAGO.
Lewis A. Sayre revolutionized the treatment oftubercular processes of the spinal column by the prop-aganada of absolute immobilization and freedom frompressure of the diseased portion. That the resultsobtained by his method were unprecedented is amplyevidenced by the fact that his principles have made a
triumphal tour around the civilized world and thatthe use of the plaster of paris corset has come to beconsidered indispensable in the treatment of Pott'sdisease.
The symptoms of tubercular infection of the spinal
Downloaded From: http://jama.jamanetwork.com/ by a University of Arizona Health Sciences Library User on 06/08/2015

column, first described by Perceval Pott in 1783, havebeen dilated upon by Sayre in so clear and scholarlya manner that every physician ought to memorize hiswords, so as to always have them at command; forhow many beginners in practice fail to diagnose prop-erly the early stages of Pott's disease and owing totheir lack of skill expose themselves to the seriouscharge of perpetuating for life in a fellow creature a
deformity which is the constant source of physicaland mental agony ? We are still further indebted toLewis A. Sayre when we observe that his principlesare now being applied to the treatment of tuberculardiseases of the hip and knee joint, thus constantlylessening the indications for operative interference,so that the young patient may be spared an extensiveoperation, painful treatment and a tedious sickbed.
Although Sayre, Phelps and others have clearlydemonstrated the utter uselessness of the Taylorbrace, these bandages are nevertheless sold in largequantities to the public by truss makers, who appar-ently have faith in the suggestive value of such a sup-port, as it is impossible for them to demonstrate thata real extension and support is exercised by an appa-ratus which slips down upon the pelvis or excoriatesthe skin when charged with the weight of the headand trunk. But unfortunately, unlike hysteria, Pott'sdisease is caused by infection with the tuberclebacillus and precious time is wasted in using worth-less instruments, the serious consequences of whichare not slow to make themselves felt.
A. M. Phelps in his valuable paper on Spinal Sup-ports, makes the following remarks on this importantsubject. "Previous to Sayre's investigations the Tay-lor brace has been exclusively used for the extensionand fixation of the vertebrae, but many disadvantagesresulted from its use, in that a mother or nurse beingable to remove it at any time often handled the childin such a manner as to produce traumatism and injuryto the diseased vertebra?. Further, the steel barshad to be frequently removed or excoriations wouldaccur. When they do give support, they are uncom-fortable, which is one of the strongest argumentsagainst their use in Pott's disease of the spine. Inplace of this troublesome instrument, which is devisedin a hundred different forms, Lewis Sayre introducedthe plaster of paris corset to be applied while thepatient is hanging in Sayre's suspension apparatus.
"We all agreed," continues Phelps, "that the bestorthopedic instrument ever devised is the humanhand. Guided by intelligence it applies forces forthe correction of deformity more delicately and per-fectly than any inanimate object ever invented.Plaster of paris is applied to the deformity. While itis yet in a plastic state the hand molds it to the cor-rect position and holds it there until it becomes hard-dened or set. Can you not see that now the plasterof paris is effective as a brace or support only in pro-portion to the amount of cerebral matter concernedin its use? In the absence of the latter it is worth-less."
Phelps' specific statement of the requirements of abrace brings us to the leading principle of the exten-sion corset, which was first made by Hessing. Everyinch of the bars used in the construction of the corsetmust be fitted to the figure, so that when the variousparts are put together no pressure will be felt any-where on the underlying soft, parts. The work of fit-ting and correcting must be prosecuted with untiringexactness, until eveTy part fits the body snugly, rest-
ing upon it without pressure. Herein lies the chiefobjection. The vast amount of labor which every cor-set involves is the principal reason why these corsetswill never supplant the plaster of paris corsets in theclinical practice. A mechanic can prepare the steelbars according to given measurements, but the realwork, that of fitting inch by inch, must be done bythe orthopedic surgeon himself with hammer and rulein hand and the anvil at his side. These instrumentsare of equal importance in the operating room of theorthopedic surgeon as are those which are used inoperations. In this method in adjusting steel barsthe requirements made by Phelps are complied with.Just as the plaster of paris is molded by the hand ofthe surgeon in applying the Sayre corset, so the sur-
geon guided by a thorough anatomic knowledge fitsthe steel bars to the configuration of the body, makingample use of his "cerebral matter,"' Phelps' paraphraseof common sense, for which a substitute never wasand never will be found.
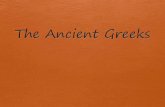
Extension Corset for lateral curvature of the spine.A plaster of paris cast is taken of the patient while
hanging in Sayre's apparatus. This cast filled withplaster represents the figure of the patient. A corsetis cut according to measurements from French coutil,which should fit accurately but somewhat loosely, toleave room for the braces. The hip part consists of asteel bar which, starting backward from the os coccygis,runs upward to the spina posterior superior, andcrossing the crest of the iliac bone laps over the an-terior abdominal wall, terminating one inch above thePoupart ligament, thus riding, as it were, and restingon the crest of the iliac bone, with both shanks clasp-ing the whole iliac region. A steel ring is then fittedin the arm-pit, xipon which the shoulder rests firmly,as upon a crutch. After both these parts have beenconnected by steel bars, which must also closely fol-low the outlines of the body, so that their combinedlength will be greater than that of the spinal column,it is evident that, since the whole weight of the
Downloaded From: http://jama.jamanetwork.com/ by a University of Arizona Health Sciences Library User on 06/08/2015

shoulder and head rests upon the lower part of thecorset, the deformed spinal column will first berelieved and then extended. After the spinal columnhas been raised so far that the given length of theside bars has been reached and no further extensioncan take place, the screws in the longitudinal slit ofthe bars must then be loosened, the space betweenthe pelvis and the arm rest enlarged and fastened in thisposition. Thus, the correction conforms with thegrowth of the body as well as the improved conditionof the diseased spine. The corset should always bedrawn tight, fitting the body closely and if possible,should be worn at night. Elastic bands properlyplaced enhance the efficiency of the steel bars in thecorrection of the deformity.
At the end of his article Phelps gives the followingindications for the different devices: 1, plaster ofparis corsets for acute Pott's disease; 2, wooden cor-set for lateral curvature and cured or convalescentcases of Pott's disease; 3, the Beely corset for mildforms of lateral curvature, especially in girls; 4, thealuminum (Phelps) corset far permanent bracing; 5,the celluloid corset (Lorenz) in a way takes the placeof aluminum.
Extension Corset, side view.
While fully recognizing the value of these variousapparatus, more especially on account of the sim-plicity of their construction, still the superiority ofthe extension corset for permanent extension must beacknowledged, because the effected spine is equallyrelieved from pressure and immobilized. This is evi-dent from the instantaneous cessation of the reflexmuscular spasms and pain. The length of the sidebars can be readily adjusted. The corset may betaken off for constitutional treatment with ease (baths,etc. ). Above all, it does not in any way interfere withextensive open air exercise which is essential in thetreatment of these affections. Hoffa and Heusner arethe most enthusiastic advocates of the extension corsetin Germany, while Lorenz, too, uses the Hessing devicein the construction of his corset, excepting only that thepelvis bar is replaced by a capsule of celluloid. TheLorenz corset, however, is too heavy and inflexibleand the celluloid casting does not conform to the sub-sequent changes in the trunk during the course oftreatment, as does the elastic French coutil. If theseat of disease be at the thoracic or cervical vertebra?,a collar should be added which is wider at the back ofthe head and finds its support on the mastoid process
and forward under the lower jaw. Exactly in thecenter of the mastoid process a steel bar projects fromeach side which conforms accurately to the depres-sions between the muscles of the neck and the pro-truding collar-bone and reaches downward to the mid-dle of the trunk. Here the bar is attached to theshoulder brace by means of an elastic band. Thehead may be immobilized or kept movable, accordingas the screws are drawn.
Admission to a hospital is desirable in having thecorset prepared, so that the patient may be always onhand. Even after the corset is finished it is betterfor the patient to remain a few weeks longer, so thatany defect may be noted and remedied and instructionmay be given the mother or nurse as to the exactmanner of fitting the corset.
It is easy to understand that at first patients, especi-ally if children, feel uncomfortable in the corset. Inthe beginning, therefore, it is advisable to leave thecorset on for only a few hours and to draw the stringgradually until the maximum is reached. Care mustbe taken to distinguish between the feeling of discom-fort wdiich is common to almost every new garmentand the actual pressure of a steel bar, which is indi-
Extension Corset, back view.
cated by a redening and soreness of the skin and mustbe relieved at once.
Constitutional treatment should go hand in handwith local treatment. The majority of children suffer-ing from tuberculosis of the bones are afflicted withanemia, lack of appetite, a tendency to nervousnessand weakness of the heart. They have a pronounceddislike of nitrogenous foods, i.e., meat and eggs andfrequently milk also. Obedient to this hint of natureI have for a number of years prescribed a vegetariandiet with strict exclusion of beverages and of medi-cines, containing alcohol and have had the satisfac-tion of observing an increase in appetite and subse-quent gain in weight. Beginning with milk, rice andapple sauce we change to heavier foods as the childrenare allowed freedom of movement, such as buckwheat,oatmeal, barley, sago, spinach, peas, beans, potatoes,the fruits of the season raw and cooked, etc. Smallquantities of rich unskimmed and freshly cooked milkmay be given and raised by degrees until a quart a
day is reached. Often Horlick's malted milk provesuseful for a change. Cod liver oil combined withphosphorus, lactophosphate of lime (Merck's) andextract of malt or iodids should only be given after
Downloaded From: http://jama.jamanetwork.com/ by a University of Arizona Health Sciences Library User on 06/08/2015

the children have gained in strength and their useshould be discontinued if nausea or loss of appetiteresult. An effective means of improving the appetiteand general health is warm sea-salt baths. It is ad-visable to begin with washing the whole body withsea-salt solution in a well warmed room, the waterbeing lukewarm in the morning and warm in theevening. The whole procedure should not last morethan three minutes and the skin should be dried, notby rubbing with a towel, but by gentle touching, soas not to wipe off the salt crystals which are precip-itated in the pores of the skin. When the bathsare found to agree with the patients, full bathsshould be taken three times a week, the duration notto exceed five minutes and the temperature of thewater being about 98 degrees. In proportion as thepatient grows stronger the temperature of the watermay be gradually lowered. In the beginning thebaths should be warmer, about 98 degrees, and shouldnot last longer than five minutes, especially if thereis any complication of the heart, By degrees thetemperature may be lowered to 90 degrees and theduration may be increased to thirty minutes. It isdifficult to give any special rules in this connection.The frequency, duration and temperature of the bathsare regulated by the condition of the patient and thegood judgment of the physician. In general, bathsshould not be given more than four times a week andthe temperature should not be under 90 degrees. Theloss of calorics from the system is not excessive. Thestimulation of the peripheral nerves is so much greaterin cooler water, which is of importance, first, onaccount of the strong irritation of the sensible nerveends on the surface of the skin, as wTell as an irritationof the cerebral centers of sensibility, and, second, onaccount of hardening the system. By hardening wemean the accustoming of the nerves of the skin andof the mucous membrane of the upper air passages toexposure to cold, which leads to an increased genera-tion of warmth with increase of appetite and stimu-lated metabolism in the organism and also stimulationof breathing. The salt contained in the water exer-cises a merely mechanical action, since after drying,the crystals of salt remain in the pores of the skin,where they act as an irritant on the nerve ends andWood vessels of the skin. For feverish patients thereis no more reliable and gentle means of lowering thetemperature and relieving the tormenting thirst aswell as the debilitating night sweats. After the baththe patient should remain in bed for one hour and becareful to prevent perspiration, so that the pressure ofthe blood is not lowered to too great an extent and theheart's action weakened. Special care should be takenin the case of patients with complications of theheart and lungs. When possible visits should bemade to the seashore during the season, wdiere bath-ing in the surf, and the sea breezes exercise very salu-tary effects. The excellent results I have observed fromthe sea-salt baths makes me im enthusiastic advocateof this treatment in every case where there are evi-dences of constitutional disturbances cither of tuber-cular or rachitic origin. But many mothers anxiousthat their children be restored to health as quickly as
possible overdo the bathing to such an extent as tocounteract the good effects. The physician, therefore,should insist on seeing the patient at least twice amonth and should not allow the baths to be givenlonger than two months in succession.
In the natural course of tubercular infection of the
spine a cold abscess will be formed surrounded byspongy granulations which penetrating into the spinalchannel press on the spinal cord. It is very rarely thecase, however, that pressure symptoms alone attend de-generated and sunken vertebra?. In these serious cases,in which paraplegia and total paralysis of the lowerextremities have developed, the immediate applicationof an extension corset is necessary, which must beworn day and night, or for which a weight extensionon the head may be substituted at night. Laminect-omy is justified only when the pressure of the tuber-culous pus and granulated tissue has become so greatas to paralyze the bladder and rectum, and the patient'slife is threatened by septicemia due to bed sores.
Although a discussion of the operative treatment ofPott's disease is beyond the scope of the presentpaper, still it may not be irrelevant to state that froma critical review of'the literature in this connection theultimate results of this operation are not such as to ^
warrant the procedure without positive indications.Beside septic infection, hemorrhage and the difficultyof access to the diseased part, a miliary infection hasbeen observed in some and a return of the paralysis inothers, although all pathologic symptoms may havedisappeared with surprising rapidity immediately afterthe operation. Another fact which has not receivedproper attention is, that an edematous swelling hasbeen observed at that portion of the spinal cordwhich corresponds in the diseased portion of the ver-
tebra?, and this continued after the removal of thepressure and eventually resulted in a return of theparalysis of the extremities. This edema lasts abouttwo years. As yet its anatomic cause is not demon-strated. It is not improbable that iodid of potassiummay reduce this edema and in this way the mysteri-ous specific effect of this remedy on paralysis inPott's disease may be explained.
In so far as the spinal cord is relieved from pres-sure, there is certainly a promising future in storefor the operative treatment of Pott's disease. Judg-ing from the effects of operative procedure on themore accessible joints, however, one is inclined todoubt that such procedure will ever bring the processto a standstill, and, for the present, conservativeorthopedic treatment will have the better results toshow as its methods are perfected. The universalintroduction of the extension corset together withSayre's plaster of paris corset will mark a most impor-tant advance.
I will restrict myself to a fewT typical instances.The following case was referred to me by Dr. E. W.Lee in the accompanying letter:
Dear Doctor:—I herewith send you a boy ten years of age,whom I saw for the first time only a few days ago. I foundhim with a temperature of 102.5 degrees, pulse 140 weak andirregular, vomiting and constant nausea, so that he could notkeep anything on his stomach. A tenderness was found in theupper cervical region. The head was turned to the right likea torticollis, almost resting on the right shoulder ; loud bruiton the mitral valve. 1 suspected a local meningitis startingfrom a tuberculosis of the upper cervical vertebra?.
Yours etc. E. W. Lee.Passive and active motion of the head was impos-
sible. No swelling was to be found. Digital percus-sion of the occiput and the subsequent rapid improve-ment fortunately failed to substantiate Dr. Lee's wellfounded suspicions. From the symptoms, I concludedthat the process was seated in the atlo-axoid articula-
Downloaded From: http://jama.jamanetwork.com/ by a University of Arizona Health Sciences Library User on 06/08/2015

tion, and this was confirmed by the great tendernessin the region extending from the first to the thirdvertebra on the right side.
The boy was admitted to St, Josephs Hospital andan extension with weights applied. The weights were
gradually increased from one to seven pounds. Seasalt baths were prescribed and gave immediate com-fort and relief. As soon as the vomiting had sub-sided vegetarian diet with plenty of milk was insti-tuted. The corset was at once prepared. The boywas discharged at the end of four weeks, lookingbright and well, with a gain in weight of eight poundsand wearing a tight but comfortably fitting corsetwith a leather collar attached, which held hishead corrected to the left side, Without supportthe head had an inclination to turn to the right, butcould be moved without pain, the tenderness ofthe upper cervical vertebra? on palpation havingentirely disappeared. The apparatus he wears isalmost entirely concealed under his clothes.
Karl B., Gase 2.
How serious would have been the consequences hadthis boy been compelled to stay in bed or even weara jury mast! WTith this strange-looking instrumenthe would have confined himself to the house fright-ened away through the taunts of his comrades, thuswanting the stimulus of outdoor exercise and cheerful-ness, whose importance can not be overestimated inrestoring metabolism and augmenting the vital forcesin chronic diseases.
Through the kindness of Dr. Fischer I had an
opportunity in Buda Pesth last September to examinea remarkable case of tubercular caries of the thoracicportion of the spinal column involving the second tothe seventh vertebra?. Carl B., 28 years of age, hasthe following history: Both parents died of tuber-culosis of the lungs. He had a kyphosis since hisseventh year, which gradually and imperceptibly in-creased in size without causing him any pain. In thebeginning of January 1891 suddenly without anyapparent cause pain set in in the middle of thekyphotic part, which was soon followed by paralysis
of the lower extremities, the legs ceasing to actalmost instantly. The reflex action in the legs in-creased, the sensibitity decreased. When seated thepatient held his shoulders so high that they were on a
level with the tops of his ears. The kyphotic part formedan angle of 90 degrees. A lateral deviation was notnoticeable. About one centimeter below the mostprominent part of the kyphosis there was a painfulspot, and from this point emanated the paralytic feel-ing above mentioned. The action of the bladder andof the bowels was not disturbed. Diagnosis: Tuber-cular kyxiliosis of the thoracic vertebra?, complicatedwith compression of the spinal cord. Every othermeans of treatment having failed he was admitted to
Karl B., with corset and collar.Fischer's orthopedic hospital in Buda Pesth to betreated with an extension corset. Suspension of buta few minutes' duration relieved him very much andenabled him to lift his feet with ease, the kyphoticpart becoming stretched about one centimeter and thespinal cord being relieved from pressure. At first thepatient could hardly wear the corset, but he graduallybecame accustomed to it. After ten days the constantreflex contractions of the legs ceased and he made hisfirst step in a frame support. To make the extensionof the spine as effective as possible the patient was
provided with a leather collar embracing the posteriorpart of the head and chin, by means of which thehead was supported and the vertebra? stretched stillmore. When the writer saw the patient two yearslater, he walked about without a corset, only usingtwo canes on the street. The pain in the back hadleft him and the reflex action and sensibility in thelower extremities were normal. His general healthwas very good.
In cases of lateral curvature of the spine in the sec-
Downloaded From: http://jama.jamanetwork.com/ by a University of Arizona Health Sciences Library User on 06/08/2015

oiid and third stage, the extension corset has provenindispensable. In these cases the spinal column isonly supported in order to prevent the muscles, whichhave been greatly strengthened by daily gymnasticexercises and massage, from again losing their tonethrough over-exertion. Special care must be takento construct the corset so as to conform to the rapidchanges in configuration. From the foregoing it isapparent that all patients suffering from injury to thespine and in need of temporary relief are enabled towalk about by the wearing of these corsets, whereaswithout this support they would have been compelledto remain in the extension bed. In this connection Iwould refer to my paper, " Ambulatory Treatmentof Fractures of the Lower Extremities," published inthe Railway Surgeon in February, 1896, in which thesame principles were discussed.
So far we have been considering only diseases of thespinal column, whereas the universal character of theextension corset is still more in evidence in the suc-cessful treatment of an affection of the spinal cord,in the therapy of which even neurologists haveachieved but indifferent success, that much investi-gated disease, locomotor ataxia.
Recent research has shed but little light on thenature of this malady of the posterior column, whichin its first stages is characterized by symptoms so
vague and baffling that only a neurologist is in a posi-tion to make an accurate diagnosis, binder these cir-cumstances Leyden acknowledged that no plausibletheory has yet been advanced for the progressivedegeneration of the nervous system and that we mustfor the present be content to consider themas peculiar processes. Even the strenuous effortsof Charcot and his pupils to classify locomotorataxia among the systemic diseases were futile.In the therapy of the disease, too, but littlelittle progress has been made within the last decade,although it would have seemed, that the fact, that inabout 80 per cent, of the cases the disease was pre-ceded by syphilitic infection would have given rise tobetter results by the institution of an antisyphilistictreatment, The suspension method is the only origi-nal innovation, which has been made in the treatmentof locomotor ataxia. Added to the electric treatment,which is imperative, it is a mechanical means ofgreat value, although it is by no means all that can bedesired. This mechanical treatment of locomotorataxia was first employed by Dr. Motschukowsky, ofOdessa, with great success, and his results were pub-lished in the Wratsch in 1883. Dr. Motschukowskyreached the following conclusions:
1. For two or three hours after suspension walkingbecomes easier and steadier. After eight or ten sit-tings it becomes permanently firm and steady.
2. The shooting pains cease entirely and do notrecur even during thunder storms and changes in theatmospheric pressure. Some patients who had pre-viously experienced much pain during north andnorthwest winds became entirely indifferent to thechanges of wind.
3. The retarded pain current is considerably hast-ened, while the paresthetic feelings, such as chills,formication and girdle sensation subsided.
4. After twenty to thirty sittings there is a gradualsubsiding of the ataxic symptoms. The Rombergsymptom disappears, the tactile sense improves andthe atrophied muscles increase in size.
5. Urination and defecation are once more under
the control of the patient. The quantity of indicanin the urine decreases, the sexual functions are re-
stored, the gastric pains become milder and lessfrequent.
6. In some cases the eyesight is improved; thepupils become more movable and dilated; there is a
gain in weight. In no case has a return of the kneephenomena been observed, and no improvement hasbeen noticed in the dilatory skin and musclereflexions.
Motschukowsky has ascertained by exact measure-
ments, that the length of the spinal column increasesfrom one to three centimeters while suspended inSayre's apxiaratus, in consequence of which the rela-tion of the spinal cord to the spinal channel is un-
doubtedly altered, so that the nerve roots assume amore vertical position, though without being percep-tibly stretched. Suspension also increases the pres-sure of the blood, the breathing becomes costal andthe vital capacity of the lungs grows larger. Mot-schukowsky is of the opinion that the white substancenot yet infected may preserve its physiologic func-tions for some time by favoring the establishment ofcollateral circulation. What Motschukowsky espe-cially commends in his method is its mildness as
compared with operative and mechanical stretchingof the nervi ischii, which succeed in reaching butone part at a time and the first of which is frequentlyfollowed by trophic disorders, the second being annoy-ing and painful to the patients.
As contra-indications to his method Motschukow-sky enumerates the following:
1. Disease of the heart and compensative derange-ments.
2. Sclerosis of the arteries and aneurysms, anemiain a high degree and a tendency to faint.
3. Pulmonary cavities and emphysema.4. Previous apoplectic, epileptic or epileptoid at-
tacks.The success of the treatment is less apparent in the
first stages than in the secondary.Charcot, in the Progrès Méd., 1889, fully confirmed
the statements made by Motschukowsky. Out offourteen cases he had observed eight that were con-siderably improved by suspension. Win. J. Mortonconcurs with him in the following words: "My ex-
perience leads me to confirm in every particular theresults observed in the eight cases at Salpetrière, Weshall have to admit that the aggregate of improve-ments and cures, whether temporary or permanent, isfar beyond that which has been attained by any othermeans, and for that reason this method must be re-garded as the most signal advance yet made in thetreatment of this hitherto intractable disease."
Weir Mitchell has modified Sayre's apparatus forthis special case so ingeniously that even those seri-ously ill may be safely treated with it. Yet notwith-standing these indisputable facts the suspension treat-ment has of late years been entirely discarded, chiefly,in my opinion, because the majority of patients grow-ing tired of frequent suspension even in the mostcomfortable apparatus, would not allow the physicianto carry the treatment to a satisfactory end. Onlyrecently, however, Dr. Brower, in an elaborate articlepublished in The Corpuscle in 1895, refers to theabandoned treatment in the following words: "Myexperience has taught me that suspension is of valuein the stage of incoordination. I would recommendsuspension treatment three times a week, lasting from
Downloaded From: http://jama.jamanetwork.com/ by a University of Arizona Health Sciences Library User on 06/08/2015

Uve to fifteen minutes, according to the effect on thepatient. I think it should be continued as long as
possible,"Bechterew is convinced that even where no ana-
tomic changes are found in the eye the power of visionis materially increased by suspension. (Neurolog.Centralblatt, 1893; On the Influences of Suspensionon Visual Derangements in Affections of the SpinalCord.)
It is impossible to assert that the statements of men
like Charcot, Brower and Morton are erroneous. Whyis it, then, that the treatment of locomotor ataxia bysuspension has been abandoned? When we considerthat, although suspension should last but half a min-ute at first, and should only gradually be increased tothirty minutes, and further that the patient should be,treated only every other day, the salutary effects ofthis method are nevertheless apparent in the extensionof the vertebra? as well as in the probable stretchingof the nerve roots, the question involuntarily arises:Why are not the vertebra? kept permanently stretchedund the good effects perpetuated? No instrument isbetter adapted to this purpose than the extension cor-
set, the application of which removes the contra-indi- cations mentioned by Motschukowsky and does awaywith the disadvantages of the suspension apparatus.The corset should, therefore, be regarded as a perma-dent suspension apparatus, the object of which is tocheck the degenerative process in the spinal cord with-out interfering with the electric, medical and hydro-pathic treatment of the patient. In other words, thepiatient should continue under the specialist's care
while wearing the corset, just as the treatment remainsin the hands of the physician while the bloody nerve
extension is made by the surgeon. In both cases thesurgeon's skill is at the command of the neurologist,
The following case of locomotor ataxia is reportedby Prof. Dr. von Jürgensen, Tübingen, Germany, whopersonally observed its progress with great care.
History: While taking the waters at Kissingen in1884 the patient was suddenly afflicted with constipa-tion and want of appetite. Later on a heaviness inthe legs set in, the power of locomotion decreased andthe carriage became stooping. In March, 1885, afterhaving attended a dancing party he suddenly experi-enced a feeling of contraction and numbness in differ-ent parts of the skin, especially about the breast andarms, and at times the sexual functions were weak-ened. Evacuation was effected only by artificialmeans. Nervous pains were frequent. Treatmentwith massage and electricity and the use of the watersof Wiesbaden resulted in an improvement in the gen-eral health, but the above mentioned symptoms didnot entirely disappear. In March, 1888, there was a
severe relapse. He experienced a sensation of con-
traction at the throat, which made speaking and swal-lowing of food very difficult. He suffered from fre-quent and violent nervous spells. There was a rapidloss in weight. Professor Mendel, of Berlin, findinghis treatment of little avail, recommended the wearingof an extension corset, which Hessing himself con-structed. The neuralgic pains, the girdle sensationand the numbness of the skin rapidly disappeared.The appetite increased and digestion became normal.His gait became firmer. Although he had resumedliis business vocations, it did not in any way retardimprovement, and the patient could walk five mileswithout being fatigued. With the exception of a
slight uneasiness when walking in the dark, he felt
perfectly well. His finger nails, which had previ-ously been distorted, resumed their normal shape.
Equal success is not likely to be experienced inevery case of locomotor ataxia, as 25 per cent, of thecases are not in any way, even temporarily, influ-enced by artificial stretching. In the remaining 75per cent, of the cases which react more or less aftera suspension of so short duration, permanent exten-sion may be expected to effect a definite improvementin coordination.
The remaining diseases of the spinal cord—sclero-sis of the lateral cords, diffuse chronic myelitis andchronic meningo-myelitis—wTill not be influenced bysuspension at all, and permanent extension will alsoprove ineffectual. On the other hand, suspension willcause a material improvement in defective functionsof the nervi erigentes which originate in the first tothird sacral nerves and the center of erection, whichis located in the lumbar part, In cases of paralysisafter poliomyelitis acuta, it is necessary to use thecorset in combination with supporting apparatus forthe lower extremities, a description of which, how-ever, would take up too much space for insertion inthis article.
CONCLUSIONS.
1. The essential requirements for the successfultreatment of Pott's disease, viz., extension and immo-bilization of the spinal column, are met in an idealmanner by Sayre's plaster of paris corset.
2. The Taylor brace does not meet either of thesetwTo requirements: It is therefore of no value intreating Pott's disease and for this reason should bediscarded.
3. The extension corset acts like the plaster corsetwhich is constructed according to Sayre's method,except that steel bars and French coutil are used in-stead of plaster. It fits as snug to the body as a
plaster corset, and both form an outer skeleton, to theinner side of which the muscles of the trunk adhereclosely, a. The plaster corset is preferable to the ex-tension corset in the first stages of Pott's disease forchildren under 6 years of age, and its cheapness adaptsit to clinical practice, o. The extension corset, on theother hand, can be readily adapted to the changes inconfiguration by readjusting the steel bars. It canbe taken off with ease for constitutional treatmentand at night, and it does not interfere with extensiveoutdoor exercise.
4. To insure the ultimate success of the treatmentit is of the utmost importance that the surgeon him-self adjusts the steel bars and exercises a generalsupervision, occasionally making such alterations inthe fit as are deemed advisable.
5. The value of the discovery of Motschukowskyin the treatment of locomotor ataxia will not beappreciated to its full extent by the profession at largeuntil permanent suspension by means of the exten-sion corset has replaced temporary suspension.
Venetian Building.
From the Washington Star:—"You feel verysluggish, do you not?" said the physician. "Doc,"said the patient confidentially, " bein' ez yer mephysician, I'll tell ye somethin'. I've been a profes-sional pugilist in me time, an' between me an' you,that sluggish feelin' ye hear 'em talkin' so muchabout is gin'rally a complete bluff."
Downloaded From: http://jama.jamanetwork.com/ by a University of Arizona Health Sciences Library User on 06/08/2015