Panic attack symptom dimensions and their relationship to illness characteristics in panic disorder
8
Panic attack symptom dimensions and their relationship to illness characteristics in panic disorder Alicia E. Meuret a, * , Kamila S. White b , Thomas Ritz a , Walton T. Roth c , Stefan G. Hofmann d , Timothy A. Brown d a Department of Psychology, Southern Methodist University, 6424 Hilltop Lane, Dallas, TX 75205, USA b Department of Psychology, University of Missouri-Saint Louis, One University Boulevard, St. Louis, MO 63121, USA c Department of Psychiatry and Behavioral Sciences, Stanford School of Medicine Stanford, and the VAPA HCS, 3801 Miranda Avenue, Palo Alto, CA 94304, USA d Center for Anxiety and Related Disorders at Boston University, 648 Beacon Street, Boston, MA 02215, USA Received 3 June 2005; received in revised form 12 September 2005 Abstract Subtyping panic disorder by predominant symptom constellations, such as cognitive or respiratory, has been done for some time, but criteria have varied considerably between studies. We sought to identify statistically symptom dimensions from intensity ratings of 13 DSM-IV panic symptoms in 343 panic patients interviewed with the Anxiety Disorders Interview Schedule for DSM-IV Lifetime Version. We then explored the relation of symptom dimensions to selected illness characteristics. Ratings were submitted to explor- atory maximum likelihood factor analysis with a Promax rotation. A three-factor solution was found to account best for the variance. Symptoms loading highest on the first factor were palpitations, shortness of breath, choking, chest pain, and numbness, which define a cardio-respiratory type (with fear of dying). Symptoms loading highest on the second factor were sweating, trembling, nausea, chills/ hot flashes, and dizziness, which defines a mixed somatic subtype. Symptoms loading highest on the third factor were feeling of unre- ality, fear of going crazy, and fear of losing control, which defines a cognitive subtype. Subscales based on these factors showed mod- erate intercorrelations. In a series of hierarchical multiple regression analyses, the cardio-respiratory subscale was a strong predictor of panic severity, frequency of panic attacks, and agoraphobic avoidance, while the cognitive subscale mostly predicted worry due to panic. In addition, patients with comorbid asthma had higher scores on the cardio-respiratory subscale. We conclude that partly inde- pendent panic symptom dimensions can be identified that have different implications for severity and control of panic disorder. Ó 2005 Elsevier Ltd. All rights reserved. Keywords: Panic disorder; Panic attack; Symptom dimensions; Respiratory subtype; Agoraphobia 1. Introduction Considerable heterogeneity exists in the clinical pre- sentation of panic disorder. DSM-IV criteria require intense distress or fear and 4 out of 13 symptoms to be present for a diagnosis of panic. However, these symptoms seem to have several sources: the autonomic nervous system (e.g., pounding heart, sweating), the respiratory system (shortness of breath, chest tightness), and the central nervous system/cognitive processing (e.g., depersonalization, fear of losing control, fear of dying). A substantial number of symptoms are sugges- tive of hypocapnia, such as lightheadedness or dizziness, paresthesias, numbness, and tingling sensations. This has fueled discussions on the role of hyperventilation 0022-3956/$ - see front matter Ó 2005 Elsevier Ltd. All rights reserved. doi:10.1016/j.jpsychires.2005.09.006 * Corresponding author. Tel.: +1 214 768 3422; fax: +1 214 768 3910. E-mail address: [email protected] (A.E. Meuret). www.elsevier.com/locate/jpsychires Journal of Psychiatric Research 40 (2006) 520–527 J OURNAL OF P SYCHIATRIC RESEARCH
Transcript of Panic attack symptom dimensions and their relationship to illness characteristics in panic disorder

JOURNAL OF
www.elsevier.com/locate/jpsychires
Journal of Psychiatric Research 40 (2006) 520–527
PSYCHIATRIC
RESEARCH
Panic attack symptom dimensions and their relationship toillness characteristics in panic disorder
Alicia E. Meuret a,*, Kamila S. White b, Thomas Ritz a, Walton T. Roth c,Stefan G. Hofmann d, Timothy A. Brown d
a Department of Psychology, Southern Methodist University, 6424 Hilltop Lane, Dallas, TX 75205, USAb Department of Psychology, University of Missouri-Saint Louis, One University Boulevard, St. Louis, MO 63121, USA
c Department of Psychiatry and Behavioral Sciences, Stanford School of Medicine Stanford, and the VAPA HCS, 3801 Miranda Avenue,
Palo Alto, CA 94304, USAd Center for Anxiety and Related Disorders at Boston University, 648 Beacon Street, Boston, MA 02215, USA
Received 3 June 2005; received in revised form 12 September 2005
Abstract
Subtyping panic disorder by predominant symptom constellations, such as cognitive or respiratory, has been done for some time,but criteria have varied considerably between studies. We sought to identify statistically symptom dimensions from intensity ratings of13 DSM-IV panic symptoms in 343 panic patients interviewed with the Anxiety Disorders Interview Schedule for DSM-IV LifetimeVersion. We then explored the relation of symptom dimensions to selected illness characteristics. Ratings were submitted to explor-atory maximum likelihood factor analysis with a Promax rotation. A three-factor solution was found to account best for the variance.Symptoms loading highest on the first factor were palpitations, shortness of breath, choking, chest pain, and numbness, which define acardio-respiratory type (with fear of dying). Symptoms loading highest on the second factor were sweating, trembling, nausea, chills/hot flashes, and dizziness, which defines a mixed somatic subtype. Symptoms loading highest on the third factor were feeling of unre-ality, fear of going crazy, and fear of losing control, which defines a cognitive subtype. Subscales based on these factors showed mod-erate intercorrelations. In a series of hierarchical multiple regression analyses, the cardio-respiratory subscale was a strong predictor ofpanic severity, frequency of panic attacks, and agoraphobic avoidance, while the cognitive subscale mostly predicted worry due topanic. In addition, patients with comorbid asthma had higher scores on the cardio-respiratory subscale. We conclude that partly inde-pendent panic symptom dimensions can be identified that have different implications for severity and control of panic disorder.� 2005 Elsevier Ltd. All rights reserved.
Keywords: Panic disorder; Panic attack; Symptom dimensions; Respiratory subtype; Agoraphobia
1. Introduction
Considerable heterogeneity exists in the clinical pre-sentation of panic disorder. DSM-IV criteria requireintense distress or fear and 4 out of 13 symptoms to
0022-3956/$ - see front matter � 2005 Elsevier Ltd. All rights reserved.
doi:10.1016/j.jpsychires.2005.09.006
* Corresponding author. Tel.: +1 214 768 3422; fax: +1 214 7683910.
E-mail address: [email protected] (A.E. Meuret).
be present for a diagnosis of panic. However, thesesymptoms seem to have several sources: the autonomicnervous system (e.g., pounding heart, sweating), therespiratory system (shortness of breath, chest tightness),and the central nervous system/cognitive processing(e.g., depersonalization, fear of losing control, fear ofdying). A substantial number of symptoms are sugges-tive of hypocapnia, such as lightheadedness or dizziness,paresthesias, numbness, and tingling sensations. Thishas fueled discussions on the role of hyperventilation

A.E. Meuret et al. / Journal of Psychiatric Research 40 (2006) 520–527 521
in panic disorder and its relationship with chronichyperventilation syndrome (Bass, 1997; Bass and Gard-ner, 1985).
Distinct subtypes of panic attacks in patients withpanic disorder have been assumed to be identifiable onthe basis of predominant symptom constellations. Inparticular, two symptom clusters, respiratory and cogni-tive, have been postulated. The first cluster can berelated either to the hyperventilation theory of panic(Ley, 1985) or to the suffocation alarm theory of panic(Klein, 1993). Accordingly, Nardi et al. (2004) observedthat patients responding to a voluntary hyperventilationchallenge in the laboratory also reported more respira-tory symptoms during attacks in their daily life, andBiber and Alkin (1999) found that a respiratory sub-group of patients was more sensitive to CO2 challenge.Moreover, respiratory subgroups of patients have beenshown to have later panic onset (Nardi et al., 2004),longer illness duration, higher cigarette consumption,and increased agoraphobia (as evidenced on the PanicAgoraphobia Score; Biber and Alkin, 1999) have beenfound in respiratory subgroups. Lack of tolerance forrespiratory symptoms in agoraphobic panic patientswas observed by Telch et al. (2003). Because a higherprevalence of asthma occurs in panic patients (Carr,1998), the respiratory symptom constellation may belinked to comorbidity with this disease.
A cognitive symptom cluster would be characterizedby few symptoms of autonomic arousal or respiratorydysregulation but a strong feeling of distress or feartogether with cognitive symptoms (Clark, 1986; Ley,1992). However, empirical evidence for a cognitive sub-type is scanty. Schmidt et al. (2002) found that patientswho reacted with high subjective distress but little phys-iological activation to an inhaled CO2 challenge hadfewer cognitive symptoms than did patients who showedboth high subjective distress and strong physiologicalactivation. Similarly, Forsyth et al. (2000) found littlesupport for a cognitive subtype applying the same clas-sification to the reactions of healthy volunteers to a CO2
challenge.Two studies with larger patient samples that
attempted to diagnose subtypes of panic by symptomreport gave inconsistent results. Briggs et al. (1993) ana-lyzed retrospective symptom reports of patients� lastmajor panic attack using factor and cluster analysisand identified. However, in addition to shortness ofbreath, choking/smothering sensation, and chest pain/discomfort, the criteria for this subtype included fearof dying, a symptom with obvious relevance to the cog-nitive domain. Although some symptoms of hyperventi-lation, tingling and numbness, were included, faintnessand dizziness were not. A study by Shioiri et al. (1996)yielded three clusters by factor analysis with a mix ofautonomic, respiratory and cognitive symptoms, whichwas difficult to interpret: cluster 1 included dyspnea,
choking, sweating, nausea, flushes/chills, cluster 2, dizzi-ness, palpitations, trembling/shaking, depersonaliza-tion, agoraphobia, and anticipatory anxiety, andcluster 3, fear of dying, fear of going crazy, paresthesias,and chest pain/discomfort.
The low consistency and plausibility of these findingsmay result from a number of factors. First, dichotomousresponse formats for symptom report precluded the useof factor analysis as a common strategy to identifydimensions of self-report from an item pool. Second,items from prior versions of the DSM were used, and,as in the case of Shioiri et al. (1996), ratings of agora-phobia and anticipatory anxiety were also included inthe item pool. Even smaller variations in item pool suchas these can lead to changes in the factorial structure.Third, cultural differences can be expected in symptompatterns. While Shioiri et al. (1996) used a sample ofJapanese out patients, the study of Briggs et al. (1993)was based on data from a multinational sample ofpatients from Europe and in North and South America.
1.1. Aims of the study
The goal of our study was twofold: to explore dimen-sions of panic symptoms in patients with a principaldiagnosis of panic disorder with or without agoraphobiaand to explore the association of the identified symptomdimensions with specific illness characteristics. We pre-fer to view symptom constellations as dimensions ratherthan distinct categories, given the clinical and empiricalevidence on varying severity of individual symptoms andtheir partial intercorrelation. We expected to find evi-dence for a respiratory dimension of panic symptoms,and possibly also for a cognitive dimension. Based ontheory and previous empirical work, we hypothesizedthat respiratory symptoms would be associated withlater panic onset at a older age, longer illness duration,higher cigarette consumption, greater severity of agora-phobic avoidance, and comorbidity with asthma.Because a number of these variables previously associ-ated with respiratory panic symptoms seemed to indi-cate a greater overall severity of panic, we expectedstronger associations of these symptoms with other indi-cators of severity such as panic frequency, degree ofinterference with daily life, and amount of distresscaused by panic. Cognitive symptoms were expected tobe specifically associated with worrying about futureattacks.
2. Materials and methods
2.1. Patients
Our sample was 343 consecutive outpatients present-ing to an anxiety disorders specialty clinic for assessment

522 A.E. Meuret et al. / Journal of Psychiatric Research 40 (2006) 520–527
and treatment of anxiety and/or mood disorders.Patients met the criteria for a principal diagnosis of panicdisorder, with or without agoraphobia, as diagnosed bythe anxiety disorders interview (ADIS-IV-L, Di Nardoet al., 1994).
Patients were predominantly female, middle-aged,Caucasian, and unmarried. The majority had at leastCollege education and was working full-time at the timeof assessment (Table 1).
2.2. Procedure and instruments
Patients were prescreened over the phone for havinga current problem with anxiety or depression. Patientsreporting current or recent substance abuse, suicidalideation, or psychotic symptoms were referred else-where. Potential patients were then invited for a face-to-face structured diagnostic assessment using theAnxiety Disorders Interview Schedule for DSM-IV:Lifetime Version (ADIS-IV-L, Di Nardo et al., 1994).This highly reliable, semi-structured diagnostic inter-view (Brown et al., 2001) comprehensively evaluatesDSM-IV anxiety and mood disorders and screens forother major psychological disorders. In this study, itwas administered by instrument-trained clinical psy-chologists and advanced doctoral students in clinicalpsychology.
The ADIS-IV-L is designed to comprehensively eval-uate current and lifetime DSM-IV mood, anxiety, andsubstance use disorders as well as selected somatoformdisorders. For each diagnosis, interviewers assign a0–8 clinical severity rating (CSR) that indicates thedegree of distress and impairment associated with thedisorder (0 = ‘‘none’’ to 8 = ‘‘very severely disturbing/disabling’’). In patients with two or more current diagno-
Table 1Demographics and panic characteristics (N = 343)
Gender (women, %) 63.3Age (years, mean/SD) 34.0 (10.5)Race (non-Caucasians, %) 10.9Marital status (married, %) 37.8Household income (annual $ > 75K, %) 31.0Educational level (college or higher, %) 61.2Working status (full-time employed, %) 65.8Psychotropic medication (current, %) 64.3Treatment for medical condition (current, %) 30.3Smoking status (current smokers, %) 23.1Current asthma (%) 13.1Panic with agoraphobia (%) 94.5Illness duration (years, mean/SD) 5.0 (7.4)Panic attack frequency (last month, median/range) 2 (0–150)Panic attack severity (last month, mean/SD) 5.3 (0.9)Interference with daily life (mean/SD) 4.9 (1.2)Distress due to panic (mean/SD) 5.4 (1.0)Worry/apprehension due to panic (mean/SD) 5.3 (1.7)Severity of agoraphobic avoidance (mean/SD) 5.4 (0.9)
ses, the ‘‘principal’’ diagnosis is the one receiving thehighest CSR. For current and lifetime disorders thatmeet or surpass the threshold for a formal DSM-IV diag-nosis, CSRs of 4 (‘‘definitely disturbing/disabling’’) orhigher are assigned as ‘‘clinical’’ diagnoses. In additionto the diagnostic information, this instrument containsa 22-item agoraphobia scale in which clinicians assessand rate the patient�s avoidance of commonly avoidedsituations (e.g., public transportation, theaters) on a 0(no avoidance/apprehension) to 8 (very severe avoid-ance/apprehension) scale. The diagnostic reliability ofthe ADIS-IV-L for principal DSM-IV anxiety and mooddisorders is good to excellent in rater agreement(j = 0.77 for PDA principal diagnosis; Brown et al.,2001), and the agoraphobia rating score has shown tobe unidimensional and associated with excellent inter-rater reliability (0.86, Brown et al., 2001).
Each of the 13 DSM-IV symptoms items were ratedon intensity scales from 0 to 8 (‘‘none’’ to ‘‘very severe’’)for current full panic attacks. In addition, the followingvariables were extracted from the ADIS-IV-L: the num-ber of full panic attacks in the last month (frequency,transformed using natural logarithm), severity ratingof the panic, degree of interference with life, the amountof distress from attacks, the amount of worrying/appre-hension about an attack, and the degree of interferenceand distress of agoraphobic situations (each on a scaleof 0–8, ‘‘none’’ to ‘‘very severe’’). As additional criticalvariables suggested by the literature, we analyzed ageat panic onset, illness duration, smoking status, pack-years of smoking, and comorbidity with asthma.
2.3. Statistical analysis
Ratings on 13 items were submitted to exploratorymaximum likelihood factor analysis with Promax rota-tion. In a series of hierarchical multiple regression anal-yses that controlled for age and gender in a first step wethen explored the potential of scores on the identifiedfactors in predicting panic frequency, interference anddistress due to panic and agoraphobia, worry/apprehen-sion about panic, and agoraphobic avoidance.
3. Results
3.1. Panic symptom severity
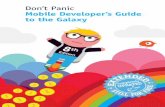
‘‘Heart palpitations’’ (M = 4.6, SD = 2.1), ‘‘dizzi-ness’’ (M = 4.3, SD = 2.2), and ‘‘shortness of breath’’(M = 3.9, SD = 2.5) were rated the most severe symp-toms while ‘‘choking’’ (M = 1.6, SD = 2.3), ‘‘chestpain’’ (M = 2.4, SD = 2.5), and ‘‘numbness’’ (M = 2.5,SD = 2.3) were rated lowest. Among the 13 symptomitems, a significant gender difference with higher scoresfor women was only found for ‘‘heart palpitations’’

A.E. Meuret et al. / Journal of Psychiatric Research 40 (2006) 520–527 523
(t(341) = 2.17; p = 0.031), a finding that may be due tochance given the large number of comparisons (Fig. 1).
3.2. Factor analysis
The eigenvalues of the first five factors of the unro-tated solution were 3.33, 1.58, 1.26, 0.99, and 0.97. Wedecided to extract the three factors (44.1% of the totalvariance) as they gave the most parsimonious solution,accounting for 28.9% of the variance after Promax rota-tion. Symptoms loading highest on the first factor(18.8% of the variance explained) were palpitations,shortness of breath, choking, and chest pain, sensationsof numbness, and fear of dying, which were suggestive ofa predominantly cardio-respiratory dimension (Table 2).Symptoms loading highest on the second factor (6.4%)were sweating, trembling, nausea, chills/hot flashes,and dizziness, which defines a mixed autonomic/somaticdimension. Symptoms loading highest on the third fac-tor (3.8%) were feelings of unreality and fear of going
Severity ratings of panic symptoms
0
1
2
3
4
5
6
7
8
Palpita
tions
Sweatin
g
Trem
bling
Shortn
ess o
f bre
ath
Chokin
g
Chestp
ain
Nause
aChil
ls
Dizzine
ss
Unrea
lity
Numbn
ess
Fear o
f dyin
g
Going
craz
y
Loos
ing co
ntro
l
Rat
ing
[0-8
]
Fig. 1. Means of panic symptom intensity ratings (N = 343).
Table 2Promax-rotated pattern matrix for 13 DSM-IV Axis I panic symptoms (N =
Factor 1
Cardio-re
Palpitations, pounding heart, or accelerated heart rate 0.48
Sweating �0.08Trembling or shaking 0.19Shortness of breath, or smothering sensations 0.65
Feeling of choking 0.36
Chest pain or discomfort 0.64
Nausea or stomach distress �0.09Chills or hot flushes �0.04Dizziness, unsteady feelings, lightheadedness, or faintness 0.24Feelings of unreality or being detached from oneself 0.06Numbness or tingling sensations 0.37
Fear of dying 0.59
Fear of going crazy �0.00Fear of doing something uncontrolled �0.13
crazy or doing something uncontrolled, which definesa cognitive dimension. A substantial secondary loading(a2 > 0.30) for choking is also present on this factor.Extracing two factors instead of three did not affect themake-up of the cardio-respiratory factor, but lumpedtogether somatic/autonomic and cognitive dimensionsand reduced communalities further. We thus decided tointerpret the three-factor solution because of its greaterheuristic value at this stage of research.
Subscales formed from the three factors showed onlylow to moderate intercorrelations, r(343) = 0.35, 0.24and 0.34, for correlations between cardio-respiratoryand autonomic/somatic, cardio-respiratory and cogni-tive, and autonomic/somatic and cognitive subscales,respectively. Partly due to the small number of items,subscale reliability estimates by internal consistencywere low, with Cronbach�s a = 0.69, 0.62 and 0.51, forthe cardio-respiratory, mixed autonomic/somatic, andcognitive subscale, respectively. After correcting forattenuation by low reliability, correlation coefficientswere r = 0.54, 0.40 and 0.60, for associations betweencardio-respiratory and autonomic/somatic, cardio-respi-ratory and cognitive, and autonomic/somatic and cogni-tive subscales, respectively.
Fig. 2 shows patients� location in the three-dimen-sional space defined by the three subscales. Visualinspection revealed little evidence for concentrations ofpatient in distinct clusters. As can be inferred from theintercorrelations, particular symptom combinationswere less likely, such as high cardio-respiratory or highcognitive symptoms combined with low autonomic/somatic symptoms.
3.3. Correlation between symptom dimension and illness
characteristics
In a series of hierarchical multiple regression analyses(Table 3), the cardio-respiratory dimension was strongly
343)
Factor 2 Factor 3 h2
spiratory Autonomic/somatic Cognitive
0.05 0.00 0.260.55 �0.03 0.260.48 �0.02 0.34�0.04 0.07 0.43�0.25 0.34 0.24
0.06 �0.23 0.400.45 0.08 0.200.47 0.11 0.260.37 0.02 0.280.14 0.38 0.240.20 0.09 0.29�0.11 0.01 0.30
0.14 0.42 0.240.04 0.58 0.31

88
Mix
ed
0
2
66
4
6
8
44
CognitiveRespiratory22
00
Fig. 2. Three-dimensional plot of scores of the three panic symptomsubscales.
524 A.E. Meuret et al. / Journal of Psychiatric Research 40 (2006) 520–527
associated with panic severity, panic attack frequency,and agoraphobic avoidance. The autonomic/somaticand cognitive subscales were associated with interfer-ence in everyday life, and the cognitive subscale, partic-ularly with worry about panic. Overall, 6.0–17.1% of the
Table 3Results of hierarchical multiple regression analyses with cardio-respiratory, acontrolling for age and gender
B SE
Panic severityCardio-respiratory 0.12 0.03Autonomic/somatic 0.14 0.03Cognitive 0.05 0.03
Panic attack frequencyCardio-respiratory 0.04 0.04Autonomic/somatic 0.08 0.04Cognitive �0.01 0.03
Agoraphobic scoreCardio-respiratory 1.74 0.50Autonomic/somatic 1.30 0.54Cognitive 0.78 0.40
Interference with lifeCardio-respiratory 0.09 0.05Autonomic/somatic 0.18 0.05Cognitive 0.08 0.04
Distress due to panicCardio-respiratory 0.11 0.04Autonomic/somatic 0.16 0.04Cognitive 0.06 0.03
Worry about future attacksCardio-respiratory 0.12 0.06Autonomic/somatic 0.30 0.07Cognitive 0.14 0.05
variance of these variables was explained by the threesubscales after controlling for age and gender.
Patients with a current diagnosis of asthma reportedsignificantly higher levels of the cardio-respiratory symp-tom group (t(340) = 2.42; p = 0.016), but no difference inother symptom groups. No differences in symptoms werefound regarding smoking status. Furthermore, there wasno significant correlation between pack-years of smok-ing, age of onset or duration of illness (after controllingfor age), and scores on symptom subscales.
4. Discussion
The goal of this study was to examine dimensions ofsymptoms in panic patients. In contrast to previousstudies we used continuous intensity ratings rather thandichotomous symptom items, which is a basic require-ment for proper factor analytic procedures. The threeidentified dimensions were interpreted as cardio-respira-tory, mixed somatic-autonomic, and cognitive symp-toms. The cardio-respiratory symptom group wassomewhat similar to the respiratory subtype identifiedby Briggs et al. (1993): In addition to the three itemsmore directly related to the mechanics of respiration,shortness of breath, choking, and chest tightness, twomore items, numbness and fear of dying, were also part
utonomic/somatic, and cognitive symptom subscales as predictors after
b p R2 df
0.171 33360.21 0.0010.23 0.0010.11 0.043
0.060 33340.19 0.0010.11 0.067�0.11 0.834
0.104 33250.19 0.0010.14 0.0180.11 0.055
0.103 33170.11 0.0590.21 0.0010.12 0.036
0.135 33200.16 0.0040.22 0.0010.12 0.033
0.158 33310.11 0.0500.26 0.0010.16 0.003

A.E. Meuret et al. / Journal of Psychiatric Research 40 (2006) 520–527 525
of their respiratory subtype. This symptom constellationis fairly consistent with the suffocation alarm theory ofpanic (Klein, 1993). Interestingly, palpitations alsoclearly loaded on this factor, which is not in agreementwith prior subtyping studies, but is reasonable consider-ing cardio-respiratory physiological coupling (Richterand Spyer, 1990). On the other hand, while numbnessand tingling also add to the interpretation of the car-dio-respiratory dimension as a hyperventilation cluster(together with shortness of breath), another symptomtypical of hypocapnia, ‘‘dizziness’’, loaded on the mixedsomatic-autonomic symptom dimension. Sweating andtrembling were more exclusively associated with the sec-ond factor, while in the study of Briggs et al. (1993), likethe palpitation item, they did not contribute to thedistinction between respiratory and nonrespiratorysymptom groups found by cluster analysis. Overall,the latter dimension could also be interpreted as anon-specific ‘‘illness/not feeling well’’ dimension, a con-text in which feelings of dizziness may be more reported.The third cognitive symptoms dimension reflected inpart that discussed in the literature, in which respiratory,somatic, or autonomic symptoms play a subordinaterole (Ley, 1985). Fear of dying did not even surface withsecondary loadings on this factor, which supports of thechanges in the panic symptom list introduced withDSM-III-R, in which fear of dying was separated fromfear of going crazy or losing control, although essen-tially it is also a cognitive item. While at least some con-vergence was noted between our findings and those inthe multinational sample of Briggs et al. (1993), ourfindings were quite different from those of the Japanesesample of Shioiri et al. (1996). In addition to culturalfactors, differences in item pools could have contributedto the divergent findings: their item pool consisted of 13DSM-III-R symptoms and ratings of agoraphobia andavoidance. Moreover, the composition of our sample,with an overwhelming majority of PD with agorapho-bia, was quite different from Shioiri et al�s sample, inwhich only 40.9% of the patients had agoraphobia.
We found that scores on the subscales constructed onthe basis of the identified panic symptom dimensionsshowed moderate intercorrelations, with up to 17.1%shared variance (or 36% for the estimated true scoreassociation) between subscales. It remains to be shownwhether such subscales lend themselves to the identifica-tion of subgroups of panic patients in which panicattacks are dominated by experience of these particularsubgroups of symptoms. Intercorrelations suggested thatpatients of certain subtypes, such as purely respiratory orcognitive symptoms, are very rare. Also, estimations ofthe reliability of these subscales by internal consistencywere only partly satisfactory. The modest communalitiesas well as the small number of items contributed to thisproblem. The cognitive subscale particularly shouldprofit from a larger item number: According to the
Spearman–Brown prophecy formula, if the number ofitems were doubled, an alpha of 0.67 would be achieved,approaching the internal consistency of the cardio-respi-ratory subscale. For an alpha of 0.80, 11 or more itemswould be needed. In addition, stability of patient differ-ences on these or similar subscales must be demonstratedby retesting before they would be suitable for diagnosisof individual patients. Eventually, a replication of thefactor structure using confirmatory factor analysis witha sufficiently large sample would be advisable. At thisconceptual stage it is probably too early to move beyondan exploration of dimensions. Also, our sample size wastoo limited to address both exploratory and confirma-tory issues in a meaningful way.
A limitation of our study was that the item pool wasrestricted to the 13 symptoms arising from the DSM-IV consensus, which do not cover the range of potentialsymptoms experienced in panic nor exemplify all vari-ants of symptoms possible in individual subgroup. Phe-nomenological studies of panic have turned upadditional symptoms, such as thought blocking, heartskipping beats, being fidgety, and difficulty swallowing(Aronson and Logue, 1988). Inclusion of these mightbolster the identified symptom groups or lead to the iden-tification of additional dimensions. Because sympathetic,fight-flight-like surges in activation are characteristic forpanic attacks (Barlow, 2002), additional symptomslinked to this autonomic state, such as dryness of themouth, muscle tension, or cold extremities (i.e., coldhands and feet), might also be candidates for inclusionin panic symptom lists. Using more detailed lists of dysp-nea items, Perna et al. (2004) showed that sensationsrelated to the work and effort of breathing, which arenot included in the DSM-IV list, are central to the expe-rience of CO2-induced panic attacks. These symptomscould help construct a more distinct respiratory symp-tom subscale. Additional cardiovascular symptomsmight help identification of a cardiovascular subtype.Symptoms related to chronotropic and inotropic activa-tion of the heart, heart racing and heart pounding, whichmay be experienced separately at times are lumpedtogether in one symptom item in DSM-IV. Additionalitems such as these might improve the dimensionaldescription of panic symptom constellations within apatient sample, with sufficient items of varying difficultycovering all relevant symptom facets across a continuumof mild to severe panic cases. In contrast with that, thecurrent DSM-IV list is a limited set of the most typicalsymptoms for binary diagnostic decisions. While increas-ing the number of items will improve the psychometricalproperties of the subscales, helping to locate individualsmore precisely on several of panic-related trait-likedimensions, it may have the disadvantage of inflatingthe prevalence of diagnosed panic disorder. As a partialsafeguard against this, adjustments would have to bemade on cut-off scores or critical numbers of items for

526 A.E. Meuret et al. / Journal of Psychiatric Research 40 (2006) 520–527
diagnosis, comparing them with previous panic criteriaand independent psychiatric evaluations.
In the light of these limitations, the presented evi-dence for differential relationships of symptom subscaleswith illness characteristics must be viewed with caution.After controlling for age and gender, cardio-respiratorysymptoms were particularly predictive of such majorcharacteristics as panic severity, agoraphobia, and panicattack frequency. For the latter, this symptom dimen-sion was the sole predictor. The higher occurrence ofcardio-respiratory symptoms in patients with comorbidasthma strengthened our confidence in the validity ofthis dimension. Whether this is simply due to a symptomoverlap between panic and asthma or whether it is indic-ative of a causal link between these illnesses as suggestedby the suffocation alarm theory (Klein, 1993) and recentprospective epidemiological research (Hasler et al.,2005) is an open question. Because asthma was onlyassessed by self-report, the association between thecardio-respiratory symptoms and asthma may reflect atendency to overreport symptoms. However, two obser-vations are at variance with this interpretation. First,while the 13.1% prevalence of asthma in our panicpatient sample was indeed higher than in typical adultpopulation surveys (National Heart, Lung, and BloodInstitute, 2003), a greater prevalence of asthma in panicpatients has been noted for some time (Carr, 1998), andother data on cross-sectional comorbidity with or with-out physician-based diagnosis of asthma confirm ourprevalence findings (e.g., Hasler et al., 2005; Goodwin,2003). Second, a simple tendency to overreport symp-toms should also have affected the somatic/autonomicand cognitive symptom dimensions, but these dimen-sions showed no association with the diagnosis ofasthma.
Autonomic/somatic symptoms surfaced as major pre-dictors for panic severity, interference with life, distress,and worry about future attacks, perhaps because theyare good indicators of the general quality of life of panicpatients. As expected, cognitive symptoms showed theirstrongest relationship with worry about future attacks.However, their contribution as predictors in the multipleregression analyses was only modest, and they were notsubstantially associated with agoraphobic avoidancecontrary to earlier suggestions (Craske and Barlow,1988). Although in contemporary treatment approachescognitive symptoms are central, they may largely be per-sonal attributions concerning causes or consequences ofthe attack, and thus be epiphenomenal to the experienceof panic (Barlow, 2002). The low reliability of the cogni-tive symptom subscale may have attenuated some of theassociations in our study, which might be more evidentwith better instruments.
A serious limitation of trying to define subtypes ofpanic disorder from retrospective reports of panic symp-toms as done in this and other studies (Briggs et al.,
1993; Shioiri et al., 1996) is that they do not necessarilyreflect patients� symptomatic response in actual panicattacks (Barlow et al., 1994). Biases in selective memoryencoding or retrieval, or interference from personal cog-nitive schemata can affect such retrospective reports.Assessment of perceived symptoms during actualattacks in daily life or in the laboratory using standardprovocation techniques is not subject to this limitation.Also, the contribution of halo effects to the symptomstructure cannot be ruled out. Although interviewerswere naı̈ve with respect to the aims of this study, it ispossible that expected stereotypes of the interviewerscould have produced intercorrelations between particu-lar types of symptoms. It should also be noted that theassociations explored are cross-sectional, and that theconstructed subscales define differences between patientsin terms of their predominant symptoms at a singlepoint of time. Different association between symptomsubgroups may appear over time in individual patients;theories have hypothesized temporal sequences involv-ing all three-symptom groups. Future research onsuch temporal associations would complement ourcross-sectional view.
Research up to now has focused on validations of arespiratory subtype. Briggs et al. (1993) demonstratedmore favorable treatment response of respiratory sub-type patients to imipramine compared with non-respira-tory patients. Using the respiratory symptom clusteridentified by Briggs et al. (1993), Beck et al. (2000) foundin respiratory compared with nonrespiratory subtypepatients lower basal levels of pCO2 and greater tidal vol-ume variability in response to low O2 challenge, but nodifference in panic symptoms to challenge. Similarly,Biber and Alkin (1999) found a higher percentage ofrespiratory subtype patients responded to 35% CO2
inhalation with anxiety. Lower basal pCO2 values werealso observed in respiratory subtype patients by Hegeland Ferguson (1997), who identified a respiratory sub-type by a 12-item questionnaire of hypocapnia symp-toms, and by Meuret et al. (submitted), who used fourof the five respiratory symptoms. Also, lower levels ofpCO2 during recovery from hyperventilation wereobserved by Meuret et al. (submitted) in patients whohad at least four of the following five symptoms: short-ness of breath, chocking, chest pain, dizziness, andnumbness. However, response to voluntary hyperventi-lation, a behavioral test often used to identify respira-tory subgroup patients, did not distinguish respiratoryfrom nonrespiratory subtypes in the latter study(Meuret et al., 2005). The current findings also suggestan important role for the (cardio-)respiratory symptomdomain, but at the same time document that a subtypewith isolated respiratory symptoms is probably veryrare.
In summary, our findings suggest that distinct dimen-sions of panic symptomatology can be identified, with

A.E. Meuret et al. / Journal of Psychiatric Research 40 (2006) 520–527 527
cardio-respiratory symptoms including fear of dyingconstituting the most prominent dimension. Thesedimensions show substantial and partly diverging rela-tionships with other illness characteristics, such as sever-ity, attack frequency, and agoraphobic avoidance. Morestudies on dimensions of panic and the validity of defi-nitions of patient subgroups are needed using a broaderrange of symptoms than currently included in DSM-IV.
References
Aronson TA, Logue CM. Phenomenology of panic attacks: adescriptive study of panic disorder patients� self-reports. Journalof Clinical Psychiatry 1988;49:8–13.
Barlow DH. Anxiety and its disorders. 2nd ed. New York: GuilfordPress; 2002.
Barlow DH, Brown TA, Craske MG. Definitions of panic attacks andpanic disorder in the DSM-IV: implications for research. Journal ofAbnormal Psychology 1994;24:553–64.
Bass C. Hyperventilation syndrome: a chimera? Journal of Psychoso-matic Research 1997;24:421–6.
Bass C, Gardner WN. Respiratory and psychiatric abnormalities inchronic symptomatic hyperventilation. British Medical Journal(Clinical Research Edition) 1985;290:1387–90.
Beck JG, Shipherd JC, Ohtake P. Do panic symptom profiles influenceresponse to a hypoxic challenge in patients with panic disorder? Apreliminary report. Psychosomatic Medicine 2000;62:678–83.
Biber B, Alkin T. Panic disorder subtypes: differential responses toCO2 challenge. American Journal of Psychiatry 1999;156:739–44.
Briggs AC, Strech DD, Brandon S. Subtyping of panic disorder bysymptom profile. British Journal of Psychiatry 1993;163:201–9.
Brown TA, Campbell LA, Lehman CL, Grisham JR, Mancill RB.Current and lifetime comorbidity of the DSM-IV anxiety andmood disorders in a large clinical sample. Abnormal Psychology2001;110:585–99.
Carr RE. Panic disorder and asthma: causes, effects and researchimplications. Journal of Psychosomatic Research 1998;44:43–52.
Clark DM. A cognitive approach to panic. Behaviour Research andTherapy 1986;24:461–70.
Craske MG, Barlow DH. A review of the relationship between panicand avoidance. Clinical Psychology Review 1988;8:667–85.
Di Nardo SC, Brown TA, Barlow DH. Anxiety Disorders InterviewSchedule for DSM-IV: lifetime version (ADIS-IV-L). San Anto-nio (TX): Psychological Corporation/Graywind PublicationsInc.; 1994.
Forsyth JP, Eifert GH, Canna MA. Evoking analogue subtypes ofpanic attacks in a nonclinical population using carbon dioxide-enriched air. Behaviour Research and Therapy 2000;38:559–72.
Goodwin RD. Asthma and anxiety disorders. In: Brown ES, editor.Asthma: social and psychological factors and psychosomaticsyndromes. Brown ES, editors. Advances in psychosomatic med-icine, vol. 24. Karger: Basel; 2003. p. 51–71.
Hasler G, Gergen PJ, Kleinbaum DG, Ajdacic V, Gamma A, Eich D,Rossler W, Angst J. Asthma and panic in young adults: A 20 yearprospective community study. American Journal of Respiratoryand Critical Care Medicine 2005;171:1224–30.
Hegel MT, Ferguson RJ. Psychophysiological assessment of respira-tory function in panic disorder: evidence for a hyperventilationsubtype. Psychosomatic Medicine 1997;59:224–30.
Klein DF. False suffocation alarms, spontaneous panics, and relatedconditions. Archives of General Psychiatry 1993;50:306–17.
Ley R. Agoraphobia, the panic attack and the hyperventilationsyndrome. Behaviour Research and Therapy 1985;23:79–81.
Ley R. The many faces of Pan: psychological and physiologicaldifferences among three types of panic attacks. Behaviour Researchand Therapy 1992;30:347–57.
Meuret AE, Ritz T, Wilhelm FH, Roth WT. Voluntary hyperventi-lation in the treatment of panic disorder-functions of hyperventi-lation, their implications for breathing training, andrecommendations for standardization. Clinical Psychology Review2005;25:285–306.
Meuret AE, Wilhelm FH, Ritz T, Roth WT, submitted. Effects ofcapnometry-assisted breathing therapy on symptoms and respira-tion in panic disorder.
Nardi AE, Lopes FL, Valenca AM, Nascimento I, Mezzasalma MA,Zin WA. Psychopathological description of hyperventilation-induced panic attacks: a comparison with spontaneous panicattacks. Psychopathology 2004;37:29–35.
National Heart, Lung, and Blood Institute. Expert panel report:guidelines for the diagnosis and management of asthma. Update onselected topics 2002. NIH publication #02-5074. Bethesda (MD):National Institutes of Health; 2003.
Perna G, Caldirola D, Namia C, Cucchi M, Vanni G, Bellodi L.Language of dyspnea in panic disorder. Depression and anxiety2004;20:32–8.
Richter RA, Spyer KM. Cardiorespiratory control. In: Loewy AD,Spyer KM, editors. Central regulation of autonomic func-tion. New York: Oxford University Press; 1990. p. 189–207.
Schmidt NB, Forsyth JP, Santiago HT, Trakowski JH. Classificationof panic attack subtypes in patients and normal controls inresponse to biological challenge: implications for assessment andtreatment. Journal of Anxiety Disorders 2002;16:625–38.
Shioiri T, Someya T, Murashita J, Takahashi S. The symptomstructure of panic disorder: a trial using factor and cluster analysis.Acta Psychiatrica Scandinavica 1996;93:80–6.
Telch MJ, Jacquin K, Smits JA, Powers MB. Emotional responding tohyperventilation as a predictor of agoraphobia status amongindividuals suffering from panic disorder. Journal of BehaviorTherapy and Experimental Psychiatry 2003;34:161–70.