After Affects. Zealous Zombies, Panic Prevention, Crowd Simulation

Available online at www.sciencedirect.com
General Hospital Psychiatry 34 (2012) 671–680
Emergency Psychiatry in the General HospitalThe emergency room is the interface between community and health care institution. Whether through outreach or in-hospital service, the psychiatrist in the general
hospital must have specialized skill and knowledge to attend the increased numbers of mentally ill, substance abusers, homeless individuals, and those with greater
acuity and comorbidity than previously known. This Special Sectionwill address those overlapping aspects of psychiatric,medicine, neurology, psychopharmacology,
and psychology of essential interest to the psychiatrist who provides emergency consultation and treatment to the general hospital population.
Treatment of panic in chest pain patients from emergency departments:efficacy of different interventions focusing on panic management☆
André Marchand, Ph.D.a,b,⁎, Geneviève Belleville, Ph.D.c, Richard Fleet, M.D., Ph.D.d,Gilles Dupuis, Ph.D.a,e, Simon L. Bacon, Ph.D.e, f,g, Julien Poitras, M.D.h,
Jean-Marc Chauny, M.D. i, Alain Vadeboncoeur, M.D.j, Kim L. Lavoie, Ph.D.a,e,gaPsychology Department, Université du Québec à Montréal, Montreal, Canada
bFernand-Séguin Research Center, Montreal, CanadacSchool of Psychology, Laval University, Quebec, Canada
dResearch Chair in Emergency Medicine Laval University, CHAULévis Hospital, Quebec, CanadaeResearch Centre, Montreal Heart Institute, Montreal, Canada
fDepartment of Exercise Science, Concordia University, Montreal, CanadagResearch Center, Hôpital du Sacré-Coeur de Montréal, Montreal, Canada
hEmergency Medicine Research Axis, Hôtel-Dieu de Lévis Hospital, Quebec, CanadaiEmergency Department, Hôpital du Sacré-Coeur de Montréal, Montreal, Canada
jEmergency Department, Montreal Heart Institute, Montreal, Canada
Received 7 February 2012; accepted 12 June 2012
Abstract
Objective: The aim was to assess the efficacy of two brief cognitive–behavioral therapy (CBT)-based interventions (7×1-h sessions and1×2-h session) and a pharmacological treatment (paroxetine), compared to supportive usual care, initiated in the emergency department (ED)for individuals suffering from panic disorder (PD) with a chief complain of noncardiac chest pain (NCCP). We hypothesized that theinterventions would be more efficacious than supportive usual care on all outcomes.Method: A 12-month follow-up study of patients who received a diagnosis of NCCP in the ED and who met diagnostic criteria for PD(n=71) was performed. Assessments included several psychological questionnaires and a structured interview. A series of repeated-measuresanalyses of variances, using a split-plot design, were conducted, as well as planned comparisons to examine the differences.Results: The seven-session CBT (n=19), one-session panic management (n=24) and pharmacotherapy (n=13) led to greater improvementsin PD severity (primary outcome) compared to supportive usual care (n=15) at posttest, and no significant difference was noted between thethree active interventions. On the other measures, patients improved in all conditions, and the therapeutic gains were maintained up to 1 yearfollowing the visit to the ED.Conclusions: These results suggests that early intervention, in particular seven sessions of CBT, one session of PM or pharmacotherapy(generic paroxetine), should be considered for the treatment of PD patients consulting the ED with a discharge diagnosis of NCCP.© 2012 Elsevier Inc. All rights reserved.
Keywords: Panic disorder; Noncardiac chest pain; Emergency department; Cognitive–behavioral therapy; CBT; Pharmacotherapy
☆ Sources of support: This research was funded by a grant to the first author from the Canadian Institutes of Health Research (153245), as well aspostdoctoral scholarships to the second author from theResearch Group on agoraphobia and panic.
⁎ Corresponding author. Psychology Department, UQAM, P.O. Box 8888, Downtown Station, Montreal, Quebec, Canada H3C 3P8.E-mail address: [email protected] (A. Marchand).
0163-8343/$ – see front matter © 2012 Elsevier Inc. All rights reserved.http://dx.doi.org/10.1016/j.genhosppsych.2012.06.011

672 A. Marchand et al. / General Hospital Psychiatry 34 (2012) 671–680
Chest pain is found to be the second most frequent reasonfor consultations in hospitals, especially in emergencydepartments (EDs) [1,2]. In the United States, approximatelysix million individuals per year consult the ED with achief complain of chest pain [2–4]. Between 50% and 90%of those individuals are diagnosed with noncardiac chestpain (NCCP) or chest pain with minimal risk of heart disease[5–11]. Interestingly, it has been estimated that up to 88% ofpatients diagnosedwith NCCP also have a psychiatric disorder[12–15]. Panic disorder (PD) has been found to be the mostfrequent, followed by major depressive disorder [16–19].
The probable association between PD and NCCP in medicalsettings (e.g., cardiac outpatients, EDs) has been previouslyinvestigated. It has been found that 24%–70%ofNCCPpatientshave concurrent PD [11,14,20–26], which are considerablyhigher than rates observed in the general population (e.g. 4.7%[27]). The high prevalence of PD among NCCP patients in theED is thought to be linked to similarities between many of thecardiovascular symptoms (e.g., heart palpitations, breathless-ness, chest tightness or discomfort) experienced by PD patientsand their tendency to interpret them as dangerous and indicativeof an imminent heart attack. PD patients’ tendency to focus onthese physical symptomsmakes themmore inclined to seek helpin medical settings [28–30].
Despite the high prevalence of PD in individuals withNCCP, more than 90% of cases are not detected or diagnosed[10,14,23,31]. Even when PD is detected, standard mentalhealth treatments are not commonly offered [32–37].Physician reassurance regarding absence of cardiovasculardisease appears to be the norm. Unfortunately, withouttreatment addressing PD, these symptoms, including chestpain, tend to persist [27,38–40], resulting in repetitive medicalconsultations, particularly in the ED [41]. This vicious cycleemphasizes the importance of offering both timely andefficacious intervention adapted to PD patients with NCCP.
Although PD is a common cause for NCCP in ED patients,few treatments studies have been conducted for patients seen inthis clinical setting. To date, only nine studies have assessedthe efficacy of psychological interventions [primarily based oncognitive–behavioral therapy (CBT) approaches] in medicalsettings for individuals consulting for NCCP [42–50]. Overall,the results have demonstrated that these interventions outper-form usual care evaluation only or wait-list control in terms ofreducing symptoms of anxiety and depression, as well as chestpain and health service/medication use. They have also beenshown to improve functional limitations and quality of life. Inspite of these promising results, no studies have yet evaluatedthe efficacy of psychological treatments for PD patientspresenting at the ED with NCCP.
With regards to pharmacological treatments in PD patientsconsulting medical services for chest pain, the results have beenencouraging. Three studies have demonstrated the efficacy ofbenzodiazepines in reducing frequency of panic attacks andchest pain episodes [51–53]. However, benzodiazepines areassociated with risk of drug dependence and are notrecommended for long-term use [54]. Instead, the recom-
mended first-line pharmacological treatment for PD is selectiveserotonin reuptake inhibitors (SSRIs). However, only one studywith a short-term follow-up (8 weeks) has assessed theirefficacy in PD patients consulting the ED with NCCP [36].Results showed a reduction in PD symptoms after 4 weeks oftreatment, but given the fact that SSRIs tend to demonstrate theirmaximum therapeutic effects only after 8–16 weeks oftreatment, the results should be cautiously interpreted pendinglonger treatment and follow-up studies [55].
This study assessed the efficacy of two brief CBT-basedinterventions and a pharmacological treatment (SSRI) initiatedin the ED for individuals suffering from PDwith chief complainof chest pain. Specifically, we assessed the efficacy of (a) a one-session panic management intervention (PM), (b) a seven-session weekly CBT intervention and (c) paroxetine treatmenton 1-year PD severity (primary outcome) and several secondaryoutcome measures (e.g., the number of panic attacks,agoraphobia and daily interference attributed to panic) in asample of PD patients presenting to the ED with NCCP. Wehypothesized that both brief psychological interventions andSSRI treatmentwould bemore efficacious than supportive usualcare on all outcomes. We also expected that the seven-sessionCBT intervention would be more efficacious than the one-session PM and pharmacological treatment.
1. Method
1.1. Participants
A total of 71 patients were recruited between November2005 and December 2009 from one of three EDs in theprovince of Quebec: Montreal's Sacre-Coeur Hospital, theMontreal Heart Institute and the Hôtel-Dieu de LévisUniversity Affiliated Hospital. They presented to the EDwith a chief complaint of chest pain and were diagnosed withPDby onsite graduate students in clinical psychology using theAnxiety Disorder Interview Schedule for the Diagnostic andStatisticalManual ofMentalDisorders, FourthEdition (DSM-IV) (ADIS-IV). Inclusion criteria included being 18 years andolder, having a primary diagnosis of PD and having a diagnosisof NCCP or chest pain highly unlikely to be of cardiac origin(e.g., patient had negative serial electrocardiogram and cardiacenzyme tests). Exclusion criteria were current or recentpsychotherapy (past 6 months), and any medical or psycho-logical condition that could invalidate the procedure (e.g.,apparent medical causes for NCCP, intoxication, bipolardisorder, schizophrenia, dementia, cognitive impairment).
1.2. Measures
Sociodemographic and medical history characteristicswere obtained via structured interview.
1.2.1. PD diagnosis and severity: primary outcome measureThe ADIS-IV [56] is a structured diagnostic interview
that allows for the diagnosis and severity classification ofanxiety, mood, somatoform and substance-related disorders

673A. Marchand et al. / General Hospital Psychiatry 34 (2012) 671–680
according to DSM-IV criteria [54]. The ADIS-IV allows foran assessment of PD severity on a scale from 0 to 8, withhigher scores indicating greater severity. PD of clinicalseverity is assumed to be associated with a score of 4 orhigher; this criterion was used to include participants in thestudy and was also used as the primary outcome measure. PDdiagnoses were assessed by eight research assistants whowere supervised by licensed clinical psychologists. Allinterviews were audio recorded, and a random sample of30% was rated independently to determine the reliability ofPD diagnoses, which was 92%.
1.2.2. Self-report questionnaires: secondaryoutcome measures
Participants completed the following standard psycho-logical tests each assessing different important characteris-tics of panic anxiety: Panic and Agoraphobia Scale (PAS)[57,58], Agoraphobic Cognitions Questionnaire (ACQ) [59],Anxiety Sensitivity Index (ASI) [60,61], Body SensationsQuestionnaire (BSQ) [59], Spielberger State–Trait AnxietyInventory (STAI) [62], Beck Depression Inventory-Revised(BDI-II) [63], McGill Pain Questionnaire (MPQ) [64] andthe Medical Outcomes Study 36-Item Short-Form HealthSurvey (SF-36) [65]. They all display good to excellentpsychometric properties and are frequently used in assess-ment and treatment studies for PD.
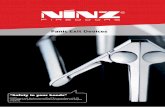
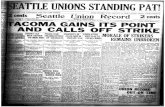
Fig. 1. Flowchart o
1.3. Procedure
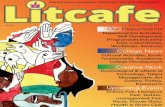
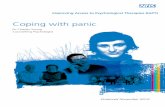
After being diagnosed with NCCP by the emergencyphysician, 246 potentially eligible participants wereapproached by a trained clinical research assistant to undergoa psychological assessment (Fig. 1). Of those, 99 eligiblepatients meeting DSM-IV criteria for PD were informed ofthe nature of the study and invited to participate. Seventy-one agreed and completed the pretreatment assessment andwere sequentially assigned to one of four interventionconditions according to the ‘study period’ in which they wererecruited. Intervention condition (cohort) was randomizedrather than individual according to a predetermined sequence(Fig. 2), allowing one cohort to be recruited during a 3-month period for every year of recruitment. Separate consentforms were used for each treatment condition and supportiveusual care to minimize negative expectancy biases. Treat-ment was initiated by a study psychologist (one-session PMand seven-session CBT groups) or a study emergencyphysician (pharmacotherapy group) as soon as possible afterthe baseline evaluation, usually within 2 weeks. Posttreat-ment assessments were performed by a trained clinicalresearch assistant in hospital 14 weeks after the beginning oftreatment. Participants were reassessed by the same clinicalresearch assistant in hospital 3, 6 and 12 months after theposttreatment assessment. Reasons for refusal to participatein the study included general lack of interest, lack of interest
f recruitment.

Fig. 2. Randomization on sequence of cohorts.
674 A. Marchand et al. / General Hospital Psychiatry 34 (2012) 671–680
for the specific treatment option offered, transportationissues for the scheduled meetings and lack of time.
1.4. Treatments
Four treatment modalities were used in the present study.The first consisted of seven 1-h sessions of CBTwith a licensedclinical psychologist. The main components were psychoedu-cation (about chest pain and the nature and development of PD),demystification of panic symptoms, in vivo exposure to panicsymptoms and cognitive restructuring. The intervention wasmanual-based and adapted for use with PD patients with chestpain from the protocol developed by Marchand and colleagues[66], and all patients received an adapted version of the manual.The second modality was a 2-h session of CBT limited tomanagement of panic symptoms (PM). With the exception ofexposure to physical sensations and in vivo exposure, the samestrategies as those in the seven-session intervention were used,but were delivered in a single session. Patients also received thesamemanual as those in the seven-sessionCBTgroup at the endof their single session. All CBT sessions were audio recorded,and 30% were randomly selected for independent evaluation ofthe presence of planned treatment strategies according to thestudy's protocol by two graduate students in psychology.Treatment integrity was determined to be 99%. The thirdtreatment was a pharmacotherapy, consisting of genericparoxetine, and was initiated and managed by an emergencyphysician (one per study site). The initial dose was 10 mg andwas gradually increased to 40mg. That dosewasmaintained for4 months and then gradually tapered down over a 4-weekperiod, which means that the patients were taking themedication over a 6-month period. Treatment adherence wasevaluated with pill counts, and 91% of the participants werejudged to be adherent (i.e., took all prescribed doses accordingto study protocol). The last modality was supportive usual care.
Although participants received no active intervention (asidefrom what may have been ordered by the emergency physicianas part of routine care, which usually included a thoroughmedical evaluation and information that the patient's chest painwas noncardiac in origin), they did undergo a series of follow-upassessments that totalled approximately 6 h. The time andattention received by the participants resulted in this being amore supportive than purely usual care condition.
1.5. Data analyses
To assess the differential effect of the four interventionson the main outcomes (PD severity, panic attacks,agoraphobia and daily interference caused by panic), a seriesof 2×4 repeated-measures analyses of variance (ANOVAs),using a split-plot design, were conducted. The two-levelwithin-group factor was Time (baseline and posttreatment),and the four-level between-groups factor was Condition(CBT, PM, pharmacotherapy and supportive usual care).Significant interactions were followed by ANOVAs com-paring the four conditions conducted for baseline andposttreatment scores separately; in the case of significanteffects, planned comparisons were used to specify the natureof the differences. According to the hypothesis, threeplanned comparisons were conducted: the first one comparedall treatment arms (CBT, PM and pharmacotherapy) tosupportive usual care, the second compared CBT andpharmacotherapy to PM, and the third compared CBT topharmacotherapy. To assess maintenance of therapeuticgains on the four main outcomes, a series of 4×4 repeated-measures ANOVAs, using a split-plot design, wereperformed. The four-level within-group factor was Time(posttreatment and 3-, 6- and 12-month follow-ups), and thefour-level between-group factor was Condition (CBT, PM,pharmacotherapy, supportive usual care).

675A. Marchand et al. / General Hospital Psychiatry 34 (2012) 671–680
To assess the differential impact of the four interventionson ancillary measures, a series of 5×4 repeated-measuresANOVAs, using a split-plot design, were performed. Thefive-level within group factor was Time (pretreatment,posttreatment and 3-, 6- and 12-month follow-ups), and thefour-level between-group factor was Condition (CBT, PM,pharmacotherapy, supportive usual care).
1.6. Missing data
All participants who completed the baseline evaluation andwere assigned to an intervention were kept in the analyses(intend to treat analysis). Missing data were replaced with thelast observation carried forward.
2. Results
2.1. Description of sample
The final sample was composed of 71 individuals whoconsulted an ED for chest pain who were determined to haveNCCP by the treating physician and later diagnosed ashaving PD by the research team. The majority of the sample(54%) was male, which is uncommon in treatment studies forPD but may be attributed to the fact that participants wererecruited in the ED [24]. Several participants (40%) reportedhaving consulted a psychiatrist or a psychologist in the past.The characteristics of participants according to the conditionto which they were assigned are presented in Table 1. Therewere no significant differences between groups regardingage, sex, civil and employment status, annual income andreport of past psychological or psychiatric consultation.
2.2. Main outcomes
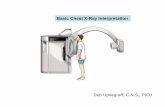
Findings for the four main outcome measures — PDseverity according to the ADIS, panic attacks, agoraphobiaand daily interference attributed to panic measured by thePAS— are illustrated in Fig. 3. For PD severity according tothe ADIS, a significant Time main effect [F(1,67)=93.05,Pb.001] indicated that, across all four conditions, partici-pants improved after treatment. The Condition main effect
Table 1Characteristics of participants
Pharmacotherapy(n=13)
CBT (n=
Age (mean, SD) 40.31 (11.74) 46.26 (1Female (n) 6 10Married or in a common-law relationship 5 12Annual income0–29,999 6 530,000–59,999 2 660,000+ 3 8EducationUncompleted or completed secondary 5 6Completed postsecondary 6 13Employed 9 12Past psychological/psychiatric consultation 5 9
did not reach statistical significance [F(3,67)=2.21, P=.095],suggesting no systematic differences between the conditions.However, the Condition×Time interaction was statisticallysignificant [F(3,67)=3.62, P=.017]. Only the first compar-ison was significant [t (67)=−2.98, P=.004], which meansthat the treatments are more effective than supportive usualcare on the PD severity.
A similar pattern of results was obtained for the panicattacks subscale of the PAS (Fig. 3). There were a significantTime effect [F(1,57)=82.83, Pb.001] showing improve-ments across all four conditions, no Condition effect[F(3,57)=1.43, P=.244] and a significant Condition×Timeinteraction [F(3,67)=2.82, P=.047]. Further examination ofthe results indicated that groups were not equivalent atbaseline on this measure [F(3,63)=4.15, P=.010], with thesupportive usual care condition having significantly lowerscores than the pharmacotherapy condition, but there was nosignificant difference between conditions after treatment[F(3,61)=.472, P=.703]. The results on the agoraphobiasubscale of the PAS (Fig. 3) showed a significant Time effect[F(1,57)=40.91, Pb.001], indicating that participants in allfour conditions improved after the intervention. Neither theCondition effect [F(3,57)=1.10, P=.359] nor the Condi-tion×Time interaction [F(3,57)=0.94, P=.426] was statisti-cally significant.
The results on the daily interference subscale of thePAS (Fig. 3) showed a significant Time effect [F(1,57)=28.23, Pb.001], indicating that participants across allfour conditions improved after the intervention. Neitherthe Condition effect [F(3,57)=0.67, P=.576] nor theCondition×Time interaction [F(3,57)=2.22, P=.096] wasstatistically significant.
2.3. Maintenance of therapeutic gains
Maintenance of therapeutic gains was assessed bycomparing posttreatment and follow-up evaluations betweenthe four conditions. There were no significant Time effectson the four main outcomes, indicating maintenance ofgains up to 1 year after the visit to the ED. There wereno Condition effects or Time×Condition interactions;
19) One-session panicmanagement (n=24)
Supportive usualcare (n=15)
Total sample(N=71)
3.61) 40.79 (13.73) 38.93 (11.97) 41.77 (13.03)11 6 3316 7 40
5 4 209 5 228 6 25
12 7 3012 8 3917 11 4910 5 29

Fig. 3. Evolution of PD, severity panic attacks, agoraphobia and daily interference caused by panic according to treatment groups.
676 A. Marchand et al. / General Hospital Psychiatry 34 (2012) 671–680
maintenance of gains did not differ according to theintervention that was offered.
2.4. Ancillary measures
The effect of the four conditions was also evaluated onother aspects of panic and anxiety, as well as pain,depression and quality of life. For all ancillary measures
Table 2Means and standard deviations of ancillary measures of panic and anxiety, depres
Pretreatment Posttreatment 3-mont
PAS — anticipatory anxiety 2.84 (2.15) 1.30 (1.87) 1.49 (PAS — concerns about health 3.90 (1.92) 1.80 (1.86) 2.06 (ACQ 1.46 (0.21) 1.36 (0.22) 1.34 (ASI 28.65 (10.30) 21.51 (12.36) 21.17 (BSQ 2.86 (0.86) 2.42 (0.89) 2.36 (STAI — state 44.32 (11.29) 38.21 (11.04) 37.47 (STAI — trait 47.28 (8.94) 41.30 (10.13) 40.71 (BDI-II 4.02 (1.18) 3.08 (1.54) 3.07 (MPQ — sensory pain 3.16 (1.34) 2.47 (1.36) 2.36 (MPQ — affective pain 1.96 (1.01) 1.46 (0.98) 1.34 (SF-36 — physical functioning 77.64 (21.90) 81.81 (22.70) 81.88 (SF-36 — physical role 41.29 (41.25) 58.96 (44.10) 64.55 (SF-36 — bodily pain 47.86 (22.39) 57.74 (26.64) 61.00 (SF-36 — general health 53.50 (20.30) 57.62 (21.13) 60.46 (SF-36 — vitality 41.99 (12.88) 49.28 (16.25) 49.71 (SF-36 — social functioning 57.17 (26.48) 69.57 (26.30) 73.62 (SF-36 — emotional role 40.86 (43.70) 58.97 (44.79) 60.42 (SF-36 — mental health 48.53 (12.80) 54.35 (15.47) 57.62 (
(with the exception of the SF-36's Physical Functioningsubscale), a significant Time effect was observed, indicatingimprovements across all four conditions, but no Conditioneffect or Condition×Time interaction was obtained. Since nodifferences were detected between the intervention condi-tions, only means and standard deviations of the wholesample as well as statistics associated with Time effects arereported (Table 2).
sion, pain and quality of life
h FU 6-month FU 12-month FU Time effect P
1.75) 1.52 (1.76) 1.41 (1.68) F(4,220)=15.15 .0002.00) 1.95 (1.83) 1.92 (1.76) F(4,220)=28.51 .0000.22) 1.31 (0.23) 1.31 (0.23) F(4,260)=22.66 .00011.36) 20.96 (11.02) 20.32 (11.00) F(4,268)=22.40 .0000.94) 2.32 (0.88) 2.31 (0.88) F(4,256)=20.08 .00010.81) 37.17 (11.24) 37.20 (11.07) F(4,264)=17.26 .0009.86) 39.96 (10.39) 39.74 (10.30) F(4,264)=26.05 .0001.47) 2.91 (1.54) 2.77 (1.58) F(4,268)=29.77 .0001.44) 2.31 (1.54) 2.31 (1.54) F(4,240)=11.94 .0001.07) 1.35 (1.05) 1.41 (1.02) F(4,240)=9.52 .00023.63) 82.03 (23.95) 83.26 (22.21) F(4,256)=2.22 .06840.16) 63.06 (40.91) 60.82 (43.13) F(4,248)=9.56 .00027.39) 60.39 (26.55) 60.59 (26.49) F(2.244)=8.80 .00022.04) 62.06 (21.73) 61.23 (21.67) F(4,256)=10.05 .00017.08) 51.59 (15.89) 52.83 (17.29) F(4,256)=12.99 .00024.52) 73.44 (24.18) 74.17 (24.41) F(4,256)=13.89 .00044.00) 60.42 (44.39) 63.02 (44.49) F(4,232)=7.34 .00016.58) 58.03 (16.26) 59.48 (16.52) F(4,256)=14.95 .000

Table 3Sample distribution according to levels of end-state functioning
Pretreatment Posttreatment
AllPoor 43 (67%) 21 (33%)Moderate 18 (28%) 23 (37%)Good 3 (5%) 19 (30%)1-session PMPoor 14 (67%) 11 (48%)Moderate 5 (24%) 6 (26%)Good 2 (9%) 6 (26%)PharmacotherapyPoor 6 (50%) 1 (9%)Moderate 6 (50%) 6 (55%)Good 0 (0%) 4 (36%)CBTPoor 13 (76%) 5 (31%)Moderate 3 (18%) 6 (38%)Good 1 (6%) 5 (31%)Usual carePoor 10 (71%) 4 (31%)Moderate 4 (29%) 5 (38%)Good 0 (0%) 4 (31%)
677A. Marchand et al. / General Hospital Psychiatry 34 (2012) 671–680
2.5. End-state functioning clinical significance
Pre- and postintervention levels of functioning arepresented in Table 3. Before the intervention, 67% of thesample had a poor level of functioning. After theintervention, 37% had a moderate level of functioning, and30% had a good level of functioning. The proportion ofposttreatment good level of functioning was similar acrossall four conditions. The proportion of individuals with a poorlevel of functioning appeared somewhat lower in thepharmacological treatment condition (9%) and higher inthe one-session PM condition (48%).
3. Discussion
The present study aimed to evaluate the efficacy of twobrief CBT-based interventions and pharmacotherapy for thetreatment of PD among patients presenting to the ED with achief complaint of chest pain who were discharged with adiagnosis of NCCP. To our knowledge, this study is the firstto assess the efficacy of these treatments compared tosupportive usual care in this population. PD severity, panicattacks, agoraphobia and daily interference were improvedirrespective of treatment condition, including supportiveusual care. The seven-session CBT, the one-session PMintervention and the pharmacotherapy interventions led togreater improvements in PD severity compared and usualcare at posttest. There are no significant differences betweenthe three interventions. On the other measures, patientsimproved in all conditions, and the therapeutic gains weremaintained up to 1 year following the visit to the ED.
The efficacy of the seven-session CBT intervention isconsistent with previous studies on PD patient [67,68].However, our results do not support the superiority of seven-
session CBT, one-session PM and pharmacotherapy oversupportive usual care for the treatment of panic attacks,agoraphobia and daily interference. These latter findingswere unexpected, though several possible explanations canbe posited. First, results suggesting a time effect may reflectthe fact that patients had received reassurance from the EDphysician of the absence of organic or cardiac disease priorto discharge. This may have had a therapeutic effect on allthe main measures of this study, except for PD severity. Arecent review highlights the role of medical reassurance forchest pain [15] and demonstrates that it may be effective onreducing chest pain and medication use only if providedbefore exercise stress testing. However, we are unaware ofany studies that have directly assessed this in a PDpopulation with NCCP. Second, participants receivedapproximately 6 h of individual attention from a PhD-levelpsychology student throughout the course of the studyassessments. Therefore, these assessments could have beenexperienced as very supportive by the participants and couldhave contributed to many of the improvements observedacross all treatment conditions. This is in part why we electedto label our control condition ‘supportive usual care’ ratherthan ‘usual care’ alone.
3.1. Study limitations and strengths
The results of this study should be interpreted in light ofsome methodological limitations. First, many of our negativefindings may have been due to our small sample size, whichlikely reduced statistical power to detect between groupeffects. Second, our study may be limited by the fact that itwas not a traditional randomized controlled trial in thatindividual participants were not randomly assigned to theconditions. Rather, the order of the four interventioncondition cohorts was predetermined, a design chosen forlogistical reasons. Third, our sample was one of conve-nience, which may reduce the generalizability of the results.Fourth, because assessors were not blinded to treatmentallocation of participants, this may have introduced infor-mation bias, which may have influenced internal validity[68]. Finally, we currently do not have data on health serviceuse across the four intervention groups, which would haveallowed us to conduct a cost–benefit analysis of theseinterventions. However, we are currently in the process ofcollecting these data, which requires accessing provincialelectronic database records and unfortunately incurs signif-icant delays.
Despite the above limitations, this study also has severalimportant strengths. First, patients were assessed at multipletime points by highly qualified personnel in order to ensurethe reliability and validity of the assessments. Second, highlyvalidated and reliable instruments were used for allassessments. Third, all study psychologists received stan-dardized training and supervision, and both psychotherapyinterventions were manualized, ensuring treatment integrityacross patients. Independent assessments of treatment

678 A. Marchand et al. / General Hospital Psychiatry 34 (2012) 671–680
integrity were conducted and revealed an excellent integrity.Fourth, the use of multiple recruitment centers also ensured amore representative sample and enhances generalizability ofthe results. Fifth, we used separate consent forms for all threeintervention conditions and the control condition in order toreduce negative expectancy bias in patients who were notrandomized to their preferred treatment condition. We alsoattempted to control for possible seasonal effects by usingnonsynchronized recruitment periods between the recruit-ment centers, which also adds to the quality of the study. Theinclusion of several follow-up assessments through 1 yearpost index ED visit may also be viewed as a significantstrength of the study. Finally, the use of ‘intention to treat’analyses increased the external validity of results [68].
4. Conclusion
These results highlight that early intervention with eitherseven sessions of CBT, one session of PM or pharmaco-therapy (generic paroxetine) should be considered for thetreatment of PD patients consulting the ED with a dischargediagnosis of NCCP. Our study shows that these threetreatments may significantly improve PD severity relative tosupportive usual care. A recent study [69] underlines theeconomic burden of PD in ED. These three interventionscould decrease health service utilization and reduce itseconomic burden, including ED overcrowding [70]. Theycould also decrease the risk of chronicity of panic attacks andhelp these patients to improve their overall well-being. Thefinding that the vast majority of the outcome measuresassessed were significantly improved posttest and gains weremaintained at 6- and 12-month follow-ups suggests that allfour interventions may be offered in clinical practiceand may similarly improve psychological and functionaloutcomes among PD patients with NCCP. Given the range oftechniques used in the interventions, future researchshould investigate the ‘active’ therapeutic ingredients forPD patients with NCCP presenting to the ED. Futureresearch could also consider testing the efficacy ofpharmacological or psychological treatments according tothe different subtypes of PD patients in order to personalizetreatment plans and optimize outcomes [71,72]. Meanwhile,efforts should be made to continue to improve recognitionrates of PD in the ED, as early intervention appearsefficacious in improving several important clinical andfunctional outcomes.
References
[1] Eslick GD. Noncardiac chest pain: epidemiology, natural history,health care seeking, and quality of life. Gastroenterol Clin North Am2004;33:1–23.
[2] Ly N, McCaig LF. National Hospital Ambulatory Medical Care Survey:2000 outpatient department summary. Adv Data 2002;327:1–27.
[3] Eslick GD, Coulshed DS, Talley NJ. Review article: the burden ofillness of non-cardiac chest pain. Aliment Pharmacol Ther 2002;16:1217–23.
[4] Kahn S. The challenge of evaluating the patient with chest pain. ArchPathol Lab Med 2000;124:1418–9.
[5] Bahr R. Chest pain centers: moving toward proactive acute coronarycare. Int J Psychiatry 2000;72:101–10.
[6] Goldman L, Weinberg M, Weisberg M, Olshen R, Cook EF, SargentRK, et al. A computer-derived protocol to aid in the diagnosis ofemergency room patients with acute chest pain. N Eng J Med 1982;307:588–96.
[7] Karlson BW, Herlitz J, Pettersson P, Ekvall HE, Hjalmarson A.Patients admitted to the emergency room with symptoms indicative ofacute myocardial infarction. J Intern Med 1991;230:251–8.
[8] Kroenke K, Mangelsdorff AD. Common symptoms in ambulatorycare: incidence, valuation, therapy, and outcome. Am J Med 1989;86:262–6.
[9] Lee TH, Cook EF, Weisberg M, Sargent RK, Wilson C, Goldman L.Acute chest pain in the emergency room. Identification andexamination of low-risk patients. Arch Intern Med 1985;145:65–9.
[10] Wulsin LR, Arnold LM, Hillard JR. Axis I disorders in ER patientswith atypical chest pain. Int J Psychiatry Med 1991;21:37–46.
[11] Wulsin LR, Yingling K. Psychiatric aspects of chest pain in theemergency department. Med Clin North Am 1991;75:1175–88.
[12] Alexander PJ, Prabhu SG, Krishnamoorthy ES, Halkatti PC. Mentaldisorder in patients with noncardiac chest pain. Acta Psychiatr Scand1994;89:291–3.
[13] Bass C, Wade C, Hand D, Jackson G. Patients with angina with normaland near normal coronary arteries: clinical and psychosocial state 12months after angiography. Br Med J (Clin Residency Ed) 1983;287:1505–8.
[14] Foldes-Busque G, Marchand A, Chauny JM, Poitras J, Diodati J, DenisI, et al. Unexplained chest pain in the ED: could it be panic? Am JEmerg Med 2011;29:743–51.
[15] White KS. Assessment and treatment of psychological causes of chestpain. Med Clin North Am 2010;94:291–318.
[16] Beitman BD, Basha IM, DeRosear L, Flaker G, et al. Comparing panicdisorder uncomplicated and panic disorder with agoraphobia incardiology patients with atypical or nonanginal chest pain. J AnxietyDisord 1987;1:301–12.
[17] Hocaoglu C, Gulec MY, Durmus I. Psychiatric comorbidity in patientswith chest pain without a cardiac etiology. Isr J Psychiatry Relat Sci2008;45:49–54.
[18] Katon W, Hall ML, Russo J, Cormier L, Hollifield M, Vitaliano PP,et al. Chest pain: relationship of psychiatric illness to coronaryarteriographic results. Am J Med 1988;84:1–9.
[19] White KS, Raffa SD, Jakle KR, Stoddard JA, Barlow DH, Brown TA,et al. Morbidity of DSM-IV Axis I disorders in patients withnoncardiac chest pain: psychiatric morbidity linked with increasedpain and health care utilization. J Consult Clin Psychol 2008;76:422–30.
[20] Beitman BD, Mukerji V, Russell JL, Grafting M. Panic disorder incardiology patients: a review of the Missouri Panic/Cardiology Project.J Psychiatr Res 1993;27:35–46.
[21] Carter C, Maddock R, Amsterdam E, McCormick S, Waters C, BillettJ. Panic disorder and chest pain in the coronary care unit.Psychosomatics 1992;33:302–9.
[22] Dammen T, Ekeberg O, Arnesen H, Friis S. The detection of panicdisorder in chest pain patients. Gen Hosp Psychiatry 1999;21:323–32.
[23] Fleet RP, Dupuis G, Marchand A, Burelle D, Arsenault A, BeitmanBD. Panic disorder in emergency department chest pain patients:prevalence, comorbidity, suicidal ideation, and physician recognition.Am J Med 1996;101:371–80.
[24] Fleet RP, Marchand A, Dupuis G, Kaczorowski J, Beitman BD.Comparing emergency department and psychiatric setting patients withpanic disorder. Psychosomatics 1998;39:512–8.

679A. Marchand et al. / General Hospital Psychiatry 34 (2012) 671–680
[25] Fleet RP, Lavoie KL, Beitman BD. Is panic disorder associated withcoronary artery disease? A critical review of the literature.J Psychosom Res 2000;48:347–56.
[26] Yingling KW, Wulsin LR, Arnold LM, Rouan GW. Estimatedprevalences of panic disorder and depression among consecutivepatients seen in an emergency department with acute chest pain. J GenIntern Med 1993;8:231–5.
[27] Kessler RC, Chiu WT, Jin R, Ruscio AM, Shear K, Walters EE. Theepidemiology of panic attacks, panic disorder, and agoraphobia in theNational Comorbidity Survey Replication. Arch Gen Psychiatry 2006;63:415–24.
[28] Clark DM. A cognitive approach to panic. Behav Res Ther 1986;24:61–470.
[29] Pauli P, Marquardt C, Hartl L, Nutzinger DO, Holzl R, Strian F.Anxiety induced by cardiac perceptions in patients with panic attacks:a field study. Behav Res Ther 1991;29:137–45.
[30] White KS, Barlow DH. Panic disorder and agoraphobia. In: &Barlow DH, editor. Anxiety and its disorders: the nature andtreatment of anxiety and panic. New York: The Guilford Press;2004, pp. 328–79.
[31] Weissman MM. The hidden patient: unrecognized panic disorder.J Clin Psychiatry 1990;51:5–8.
[32] Dammen T, Bringager CB, Arnesen H, Ekeberg O, Friis S. A 1-yearfollow-up study of chest-pain patients with and without panic disorder.Gen Hosp Psychiatry 2006;28:516–24.
[33] Fifer SK, Mathias SD, Patrick DL, Mazonson PD, Lubeck DP,Buesching DP. Untreated anxiety among adult primary care patients ina health maintenance organization. Arch Gen Psychiatry 1994;51:740–50.
[34] Mathias SD, Fifer SK, Mazonson PD, Lubeck DP, Buesching DP,Patrick DL. Necessary but not sufficient: the effect of screening andfeedback on outcomes of primary care patients with untreated anxiety.J Gen Intern Med 1994;9:606–15.
[35] Montgomery S, Bullock T, Fineberg N. Serotonin selectivity forobsessive compulsive and panic disorders. J Psychiatry Neurosci 1991;16:30–5.
[36] Wulsin LR, Liu T, Storrow A, Evans S, Dewan N, Hamilton C. Arandomized, controlled trial of panic disorder treatment initiation in anemergency department chest pain center. Ann Emerg Med 2002;39:139–43.
[37] Yelin E, Mathias SD, Buesching DP, Rowland C, Calucin RQ, Fifer S.The impact on unemployment of an intervention to increaserecognition of previously untreated anxiety among primary carephysicians. Soc Sci Med 1996;42:1069–75.
[38] Fleet RP, Lavoie KL, Martel JP, Dupuis G, Marchand A, Beitman BD.Two-year follow-up status of emergency department patients withchest pain: was it panic disorder? CJEM 2003;5:247–54.
[39] Kessler RC, Chiu WT, Demler O, Merikangas KR, Walters EE.Prevalence, severity, and comorbidity of 12-month DSM-IV disordersin the National Comorbidity Survey Replication. Arch Gen Psychiatry2005;62:617–27.
[40] Roy-Byrne PP, Stein MB, Russo J, Mercier E, Thomas R, McQuaidJR, et al. Panic disorder in the primary care setting: comorbidity,disability, service utilization, and treatment. J Clin Psychiatry 1999;60:492–9.
[41] Zane RD, McAfee AT, Sherburne S, Billeter G, Barsky A. Panicdisorder and emergency services utilization. Acad Emerg Med 2003;10:1065–9.
[42] Dyckman JM, Rosenbaum RL, Hartmeyer RJ, Walter LJ. Effects ofpsychological intervention on panic attack patients in the emergencydepartment. Psychosomatics 1999;40:422–7.
[43] Swinson RP, Soulios C, Cox BJ, Kuch K. Brief treatment ofemergency room patients with panic attacks. Am J Psychiatry 1992;149:944–6.
[44] Cott A, McCully J, Goldberg WM, Tanser PH, Parkinson W.Interdisciplinary treatment of morbidity in benign chest pain.Angiology 1992;43:195–202.
[45] Esler JL, Barlow DH, Woolard RH, Nicholson RA, Nash JM, ErogulMH. A brief-cognitive behavioral intervention for patients withnoncardiac chest pain. Behav Ther 2003;34:129–48.
[46] Klimes I, Mayou RA, Pearce MJ, Coles L, Fagg JR. Psychologicaltreatment for atypical non-cardiac chest pain: a controlled evaluation.Psychol Med 1990;20:605–11.
[47] Mayou RA, Bryant BM, Sanders D, Bass C, Klimes I, Forfar C. Acontrolled trial of cognitive behavioural therapy for non-cardiac chestpain. Psychol Med 1997;27:1021–31.
[48] Van Peski-Oosterbaan AS, Spinhoven P, van Rood Y, van Does JW,Bruschke AV, Rooijmans HG. Cognitive–behavioral therapy fornoncardiac chest pain: a randomized trial. Am J Med 1999;106:424–9.
[49] Potts SG, Lewin R, Fox KA, Johnstone EC. Group psychologicaltreatment for chest pain with normal coronary arteries. QJM 1999;92:81–6.
[50] Sanders D, Bass C, Mayou RA, Goodwin S, Bryant BM, Tyndel S.Non-cardiac chest pain: why was a brief intervention apparentlyineffective? Psychol Med 1997;27:1033–40.
[51] Beitman BD, Mukerji V, Flaker G, Basha IM. Panic disorder,cardiology patients, and atypical chest pain. Psychiatr Clin NorthAm 1988;11:387–97.
[52] Beitman BD, Mukerji V, Lamberti JW, Schmid L, DeRosear L,Kushner M, et al. Panic disorder in patients with chest pain andangiographically normal coronary arteries. Am J Cardiol 1989;63:1399–403.
[53] Wulsin LR, Maddock R, Beitman B, Dawaher R, Wells VE.Clonazepam treatment of panic disorder in patients with recurrentchest pain and normal coronary arteries. Int J Psychiatry Med 1999;29:97–105.
[54] APA. Diagnostic and statistical manual of mental disorders, fourthedition, text revised. Washington, D.C: American Psychiatric Asso-ciation; 2000.
[55] Mavissakalian MR, Ryan MT. The role of medication. In: Roth WT, &Yalom ID, editors. Treating anxiety disorders. San Francisco: Josey-Bass; 1997.
[56] DiNardo PA, Brown TA, Barlow DH. Anxiety Disorders InterviewSchedule for DSM-IV (ADIS-IV): Lifetime Version (ADIS-IV-L). SanAntonio, 1994.
[57] Bandelow B. Panic and agoraphobia scale (PAS). Seattle, WA:Hogrefe & Huber Publishers; 1999.
[58] Bandelow B. Assessing the efficacy of treatments for panic disorderand agoraphobia II. The panic and agoraphobia scale. InternationalClin Psychopharmacol 1995;10:73–81.
[59] Chambless DL, et al. Assessment of fear of fear in agoraphobics: thebody sensations questionnaire andthe agoraphobic cognitions ques-tionnaire. J Consult Clin Psychol 1984;52:1090–7.
[60] Reiss S, et al. Anxiety sensitivity, anxiety frequency, and the predictionof fearfulness. Behav Res Ther 1986;24:1–8.
[61] Peterson RA, Reiss S. Anxiety sensitivity index revised test manual.Worthington, OH: IDS Publishing Corporation; 1993.
[62] Spielberg CD, et al. Manual for the state-trait anxiety inventory (STAIform Y). Palo Alto, CA: Mind Garden; 1983.
[63] Beck AT, Steer RA, Brown GK. Manual for the BDI-II. San Antonio,TX: The Psychological Corporation; 1996.
[64] Melzack R. The short-form McGill Pain Questionnaire. Pain 1987;30:191–7.
[65] Ware JE. SF-36 health survey: manual and interpretation guide.Boston: The Health Institute, New England Medical Center; 1993.
[66] Marchand A, Letarte A. La peur d'avoir peur (3rd ed.). Montréal:Stanké; 2004.
[67] Côté G, Gauthier JG, Laberge B, Cormier HJ, Plamondon J. Reducedtherapist contact in the cognitive behavioral treatment of panicdisorder. Behav Ther 1994;25:123–45.
[68] Kazdin AE. Methodological and interpretive problems of single-case experimental designs. J Consult Clin Psychol 1978;46:629–42.

680 A. Marchand et al. / General Hospital Psychiatry 34 (2012) 671–680
[69] Coley KC, Saul MI, Seybert AL. Economic burden of not recognizingpanic disorder in the emergency department. J Emerg Med 2009;36:3–7.
[70] Rucci P, Miniati M, Oppo A, Mula M, Calugi S, Frank E, et al. Thestructure of lifetime panic–agoraphobic spectrum. J Psychiatr Res2009;43:366–79.
[71] Poirier-Bisson J, Marchand A, Roberge P, Pelland M-E, Lessard M-J, Dupuis G, Fleet R. Incremental cost-effectiveness of pharmaco-
therapy and two brief cognitive-behavioral therapies compared tousual care for panic disorder and non cardiac chest pain. J NervMent Dis; [In Press].
[72] Marchand A, Coutu M-F, Dupuis G, Fleet R, Borgeat F, Todorov C,Mainguy N. Treatment of panic disorder with agoraphobia: random-ized placebo-controlled trial of efficacy of combined pharmacologicaland cognitive-behavioural interventions. Cogn Behav Ther 2008;37:146–59.
Copyright © 2022 FDOKUMEN