P50 sensory gating in panic disorder
6
P50 sensory gating in panic disorder Eduardo S. Ghisolfi a,b, * , Elizeth Heldt c , Ana Paula Zanardo b , Ivo M. Strimitzer Jr. b , Alexandre S. Prokopiuk b , Jefferson Becker d , Aristides V. Cordioli c , Gisele G. Manfro c , Diogo R. Lara a a Departamento de Cie ˆncias Fisiolo ´ gicas, Faculdade de Biocie ˆncias da, Pontifı ´cia Universidade Cato ´ lica do Rio Grande do Sul (PUCRS), Av. Ipiranga, 6681 – Pre ´dio 12 A, 90619-900 Porto Alegre, RS, Brazil b Departamento de Bioquı ´mica do Instituto de Cie ˆncias Ba ´ sicas da Sau ´ de, Universidade Federal do Rio Grande do Sul (UFRGS), Brazil c Servic ¸o de Psiquiatria, Hospital de Clı ´nicas de Porto Alegre, Brazil d Servic ¸o de Neurologia, Hospital de Clı ´nicas de Porto Alegre e Unidade de Neurofisiologia, Universidade Luterana do Brasil (ULBRA), Brazil Received 4 October 2005; received in revised form 2 February 2006; accepted 20 February 2006 Abstract Previous studies with prepulse inhibition in panic disorder (PD) have suggested that the early stages of sensory information pro- cessing are abnormal in patients with PD. To further investigate sensory gating function in panic disorder we performed a case-con- trol study in a sample of 28 patients with PD, compared to 28 normal subjects and 28 schizophrenic subjects evaluating auditory mid-latency evoked potential P50 in a double-click paradigm as a measure of sensory gating. PD subjects showed weaker sensory gating as evidenced by higher P50 ratios as compared to normal subjects (62.5% vs. 45.4%, p = 0.03) and higher S2 (test) amplitude (3.5 lV vs. 2.1 lV, p = 0.01). Schizophrenic subjects when compared to healthy controls showed higher P50 ratios as compared to normal subjects (79.2% vs. 45.4%, p < 0.01) and higher S2 amplitude (3.3 lV vs. 2.1 lV, p = 0.01), but were not statistically different from PD subjects (p > 0.1). The present study corroborates recent findings of sensory gating dysfunction in PD. Further studies are still necessary to better understand the pathophysiology of this neurophysiological dysfunction and its nature as a trait or a state marker. Ó 2006 Elsevier Ltd. All rights reserved. Keywords: Panic disorder; Sensory gating; EEG; Anxiety 1. Introduction Auditory brain evoked potentials and other neuro- physiological examinations have been performed in panic disordered patients in order to understand its underlying pathophysiology. Panic disordered patients were found to exhibit significantly larger N1 amplitudes associated initially to abnormal temporal processing (Knott et al., 1991) and N3 latency abnormalities, corre- lated to pontine activation, probably through locus ceru- leus (Levy et al., 1996). These patients also showed enlarged prefrontal P300 in response to stimulus change, related to prefrontal-limbic pathways that could affect the processing of incoming information, supposedly dis- rupted in panic disorder (PD) (Clark et al., 1996; Turan et al., 2002) or even related to reticulothalamic struc- tures plus septohippocampal limbic system (Gordeev et al., 2003). A standard two-tone discrimination task study (oddball task) showed amplitudes that are also suggestive of alteration of early information processing in PD, specifically N1 and N2 amplitudes for target tones and the N1 amplitude for non-target tones were significantly larger in the PD patients (Iwanami et al., 1997). Another odd-ball study replicated findings of an 0022-3956/$ - see front matter Ó 2006 Elsevier Ltd. All rights reserved. doi:10.1016/j.jpsychires.2006.02.006 * Corresponding author. Tel.: +55 51 3320 3545; fax: +55 51 3320 3612. E-mail address: ghisolfi@pucrs.br (E.S. Ghisolfi). www.elsevier.com/locate/jpsychires Journal of Psychiatric Research xxx (2006) xxx–xxx J OURNAL OF P SYCHIATRIC RESEARCH ARTICLE IN PRESS
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of P50 sensory gating in panic disorder

JOURNAL OF
ARTICLE IN PRESS
www.elsevier.com/locate/jpsychires
Journal of Psychiatric Research xxx (2006) xxx–xxx
PSYCHIATRIC
RESEARCH
P50 sensory gating in panic disorder
Eduardo S. Ghisolfi a,b,*, Elizeth Heldt c, Ana Paula Zanardo b,Ivo M. Strimitzer Jr. b, Alexandre S. Prokopiuk b, Jefferson Becker d,
Aristides V. Cordioli c, Gisele G. Manfro c, Diogo R. Lara a
a Departamento de Ciencias Fisiologicas, Faculdade de Biociencias da, Pontifıcia Universidade Catolica do Rio Grande do Sul (PUCRS),
Av. Ipiranga, 6681 – Predio 12 A, 90619-900 Porto Alegre, RS, Brazilb Departamento de Bioquımica do Instituto de Ciencias Basicas da Saude, Universidade Federal do Rio Grande do Sul (UFRGS), Brazil
c Servico de Psiquiatria, Hospital de Clınicas de Porto Alegre, Brazild Servico de Neurologia, Hospital de Clınicas de Porto Alegre e Unidade de Neurofisiologia, Universidade Luterana do Brasil (ULBRA), Brazil
Received 4 October 2005; received in revised form 2 February 2006; accepted 20 February 2006
Abstract
Previous studies with prepulse inhibition in panic disorder (PD) have suggested that the early stages of sensory information pro-cessing are abnormal in patients with PD. To further investigate sensory gating function in panic disorder we performed a case-con-trol study in a sample of 28 patients with PD, compared to 28 normal subjects and 28 schizophrenic subjects evaluating auditorymid-latency evoked potential P50 in a double-click paradigm as a measure of sensory gating. PD subjects showed weaker sensorygating as evidenced by higher P50 ratios as compared to normal subjects (62.5% vs. 45.4%, p = 0.03) and higher S2 (test) amplitude(3.5 lV vs. 2.1 lV, p = 0.01). Schizophrenic subjects when compared to healthy controls showed higher P50 ratios as compared tonormal subjects (79.2% vs. 45.4%, p < 0.01) and higher S2 amplitude (3.3 lV vs. 2.1 lV, p = 0.01), but were not statistically differentfrom PD subjects (p > 0.1). The present study corroborates recent findings of sensory gating dysfunction in PD. Further studies arestill necessary to better understand the pathophysiology of this neurophysiological dysfunction and its nature as a trait or a statemarker.� 2006 Elsevier Ltd. All rights reserved.
Keywords: Panic disorder; Sensory gating; EEG; Anxiety
1. Introduction
Auditory brain evoked potentials and other neuro-physiological examinations have been performed inpanic disordered patients in order to understand itsunderlying pathophysiology. Panic disordered patientswere found to exhibit significantly larger N1 amplitudesassociated initially to abnormal temporal processing(Knott et al., 1991) and N3 latency abnormalities, corre-lated to pontine activation, probably through locus ceru-
0022-3956/$ - see front matter � 2006 Elsevier Ltd. All rights reserved.
doi:10.1016/j.jpsychires.2006.02.006
* Corresponding author. Tel.: +55 51 3320 3545; fax: +55 51 33203612.
E-mail address: [email protected] (E.S. Ghisolfi).
leus (Levy et al., 1996). These patients also showedenlarged prefrontal P300 in response to stimulus change,related to prefrontal-limbic pathways that could affectthe processing of incoming information, supposedly dis-rupted in panic disorder (PD) (Clark et al., 1996; Turanet al., 2002) or even related to reticulothalamic struc-tures plus septohippocampal limbic system (Gordeevet al., 2003). A standard two-tone discrimination taskstudy (oddball task) showed amplitudes that are alsosuggestive of alteration of early information processingin PD, specifically N1 and N2 amplitudes for targettones and the N1 amplitude for non-target tones weresignificantly larger in the PD patients (Iwanami et al.,1997). Another odd-ball study replicated findings of an

2 E.S. Ghisolfi et al. / Journal of Psychiatric Research xxx (2006) xxx–xxx
ARTICLE IN PRESS
abnormal N2 in PD (Wang et al., 2003). More recently,studies focusing sensory gating based in the pre-pulseinhibition (PPI) were carried out in PD. Panic disorderpatients in remission exhibited normal startle reactivity,reduced habituation and significantly reduced pre-pulseinhibition (PPI) and these alterations were more pro-nounced in patients with high trait and state anxiety(Ludewig et al., 2002). Increased startle response anddecreased habituation were found in PD patients thatwere not under treatment and correlated significantlywith higher cognitive dysfunction scores, but this wasnot the case for PPI (Ludewig et al., 2005).
The suppression of the P50 component of the audi-tory event-related potential has been used as an indexof sensory gating in neuropsychiatric research (Freed-man et al., 1983; Adler et al., 1998). The P50 wave isa small amplitude, positive wave occurring about50 ms after an auditory stimulus. In the P50 suppres-sion paradigm, when two stimuli are presented 500 msapart, the amplitude of the second peak (S2), comparedto the first (S1), is usually attenuated in healthy subjects(S2/S1 ratio <0.5), whereas in patients with schizophre-nia, acute mania or post-traumatic stress disorder thissuppression is impaired (S2/S1 ratio > 0.5) (Adleret al., 1998; Ghisolfi et al., 2004). The hippocampus,as well as structures of brainstem and temporal cortexhave been suggested as mediators of P50 suppressionand it is generally assumed that impaired suppressiondue to an inhibitory deficit, which leads to an overflowof information and diminished capacity to filter outirrelevant stimuli (Adler et al., 1998). The neurochemi-cal basis of P50 suppression is not yet completelyunderstood, but cholinergic, GABAergic and monoam-inergic systems have been proposed to modulate thisphenomenon (Adler et al., 1998; Hershman et al.,1995; Light et al., 1999) and more recently adenosinehas been implicated in P50 dysfunction (Ghisolfiet al., 2002).
Despite the cumulative evidence for the involvementof auditory sensory processing and for disturbed sensorygating in PD, studies on P50 auditory gating are lacking,as far as we know. This work was designed to compareP50 auditory gating between PD patients and controlhealthy volunteers as well as schizophrenic patients asan additional control group.
2. Materials and methods
2.1. Subjects
This study was approved by the Institutional ReviewBoard of Hospital de Clınicas de Porto Alegre. Partici-pants were recruited and signed an informed consentform after complete explanation about the protocol,the purpose and potential risks of this study.
Twenty-eight PD outpatients, previously diagnosedaccording to DSM-IV criteria assessed by clinical inter-view and the Mini International Neuropsychiatric Inter-view (MINI) (Sheehan et al., 1998), were included (10men and 18 women, mean age of 43.3 ± 10.1 years). Atthe time of P50 measurements, six PD subjects werenot on pharmacological treatment, 11 were on antide-pressants alone and 11 were on combined treatment withantidepressants and benzodiazepines. Characteristics ofPD subjects are shown on Table 1. Twenty-eight healthyvolunteers were recruited for this study among universitystudents and local hospital employees (10 men and 18women, mean age of 39.7 ± 7.8 years, all non-smokers).As an additional comparison group, 28 schizophreniaoutpatients, previously diagnosed according to DSM-IV were included (12 men and 16 women, mean age of37.5 ± 7.4 years). The three groups did not differ regard-ing age and gender. Healthy volunteers were screened bypsychiatrists using a structured clinical interview. Exclu-sion criteria for healthy volunteers were a DSM-IV axis Idiagnosis of any disorder, clinical illness and any currentpharmacotherapy, current use of alcohol and drugs ofabuse, except for nicotine and oral contraceptives. Nocontrol subjects were currently taking psychotropic med-ication, but some PD patients were on pharmacologicaltreatment. Subjects with family history of schizophreniaor other psychotic disorders, in first or second degree,were also excluded. Participants could not use tobaccoin the preceding 2 h, neither caffeine nor any beveragescontaining methylxanthines over the 4 h preceding therecordings. All schizophrenic patients were on treatmentwith typical antipsychotics, which do not correct P50sensory gating deficit (Adler et al., 1998).
2.2. Electrophysiological recordings
The method for electrophysiological recordings wasbased on previously described protocols, with slightmodifications (Nagamoto et al., 1996) as used by ourgroup in previous works that replicated the classicalfindings for schizophrenia (Ghisolfi et al., 2002) andpost-traumatic stress disorder (Ghisolfi et al., 2004). Inbrief, subjects were recorded seated, relaxed, and awakewith eyes open and fixed on a distant target to decreasedrowsiness during the recording. Electroencephalo-graphic activity was recorded from a disk electrode(positive reference) affixed to the vertex (Cz) and refer-enced to both ears. Electroencephalogram (EEG) wasprovided using a Nihon–Kohden MEM-4104K systemin 4 channels for recording of evoked responses inte-grated with auditory stimulator. The mean signal wasregistered in two channels (A1 and A2), one for eachmastoid and amplified 20,000 times with a bandpass fil-ter between 1 Hz and 10 kHz. EEG was collected for1000 ms for each paired stimulus presented. Additionalchannels were used to record the electro-oculogram

Table 1Clinical features and P50 ratio of panic disorder subjects (n = 28)
Age(years)
Gender Disorderduration(years)
HAM-A CGI Currenttreatment
Currentcomorbidity
Lifetimedepression
Smoking P50ratio(%)
54 F 24 13 1 None None N N 2142 M 8 52 6 AD + BZD Dp/Dyst/GAD/SP Y Y 2522 M 8 30 5 AD + BZD SP Y N 2937 F 9 12 2 AD + BZD Dp/Dyst N Y 3144 M 4 8 1 AD None N N 3544 F 8 41 5 AD + BZD GAD N Y 3736 F 0 32 5 AD + BZD SP Y N 3832 M 7 40 5 AD + BZD SP Y N 4155 F 4 41 5 AD + BZD GAD/SP Y N 4551 F 13 5 2 AD None Y N 4657 F 43 6 1 None None Y N 5041 M 2 19 4 AD GAD N N 5139 F 11 21 4 AD None Y N 5439 M 9 6 2 AD None N Y 5553 F 17 13 1 None None N Y 5648 F 9 30 2 AD + BZD Dp/Dyst/SP Y Y 5951 F 30 29 5 AD Dist N N 6640 F 26 43 6 AD + BZD GAD/SP N N 7448 M 5 13 1 None None N N 7546 M 7 20 4 None Dp/Dyst/SP Y N 8047 F 27 4 2 None SP N N 8241 F 3 51 4 AD + BZD Dp/Dyst/GAD/SP Y N 8338 F 9 6 1 AD None N N 8939 F 11 10 1 AD None Y N 9153 F 20 2 1 AD SP N N 9659 M 39 24 5 AD + BZD SP Y N 10833 F 7 25 6 AD SP N N 11224 M 11 8 1 AD None N N 120
M = male, F = female, Y = yes, N = no, AD = antidepressants, BZD = benzodiazepines, Dyst = Dysthymic disorder, GAD = Generalized anxietydisorder, SP = Social phobia, HAM-A = Hamilton scale for anxiety, CGI = Clinical global index.
E.S. Ghisolfi et al. / Journal of Psychiatric Research xxx (2006) xxx–xxx 3
ARTICLE IN PRESS
(EOG) between the superior orbita and lateral canthus.Trials were rejected if they contained artifacts indicatedby a response of ±50 lV over the area of P50 for evokedpotentials or the EOG recordings. Auditory stimuli werepresented in a conditioning testing paradigm with aninterpair interval of 500 ms and intertrial interval (ITI)of 10 s. A 0.1 ms square wave pulse was amplified inthe auditory frequencies (20–12.000 Hz) and deliveredthrough earphones that produce 1 ms sound with anintensity of 60 dB sound pressure level above the audi-tory threshold. In case of startle reaction, sound inten-sity was lowered 5 dB until startle reaction was absent.The auditory threshold of each subject was measured15 min before the recordings. Thirty non-rejected waveswere added together to give a grand average signal,which was used for analysis. Two grand average waveswere collected in sequence and the mean of both wasconsidered for analysis. The most positive peak between40 and 90 ms after the conditioning stimulus wasselected as the P50 final latency and the wave amplitude(S1) was measured relative to the previous negativity,determining the initial latency and the first P50 wave.The second wave (test) was determined using the corre-sponding peak between 500 ± 10 ms away from latency
of the first wave form (conditioning) and its amplitude(S2) also measured relative to the previous negativepeak. Tracings were analysed by a trained rater blindto the diagnosis, so that the test peaks that were awayfrom the predicted interval (approximately 5%) werenot overlooked. Averages with no discernible condition-ing P50 waves were excluded from analysis. S1 and S2
amplitudes were obtained for each grand average wavein the two derivations (Cz-A1 and Cz-A2) and test/conditioning ratios were calculated by dividing the testP50 amplitude (S2) by the conditioning P50 amplitude(S1). This ratio was multiplied by 100, thus representinga percentage. The mean value was obtained to composeboth derivations for the first grand average (trials: 1–30),further the same treatment was performed for thesecond grand average (trials: 31–60). Then other meanvalues representative of S1, S2 and P50 ratio wereobtained, generating two grand average forms, whichwere used for all the analysis.
2.3. Clinical features
Some clinical features were assessed in order to bettercharacterize the PD sample, such as the Hamilton Scale

P50 Ratio (S2/S1)
0
20
40
60
80
100
120
140
160
180
Healthy Panic Schizo%
*p=0.035
* p<0.001
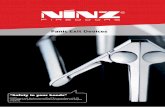
Fig. 1. Dot-plot of P50 ratio (%) in patients with panic disorder(n = 28) with (r) and without (e) treatment, healthy comparisonsubjects (n = 28) and schizophrenia comparison subjects (n = 28).ANOVA (F(2,81) = 9.279, p < 0.001) followed by Dunnett’s T3 aspost-hoc test. PD vs. healthy (p = 0.035). Schizophrenic vs. healthy(p < 0.001). PD vs. schizophrenic (p = 0.172).
4 E.S. Ghisolfi et al. / Journal of Psychiatric Research xxx (2006) xxx–xxx
ARTICLE IN PRESS
for Anxiety (HAM-A) (Hamilton, 1959) and ClinicalGlobal Index (CGI) in the occasion of P50 measure-ments, duration of panic disorder, age of onset of panicdisorder or concomitant common illness (as social pho-bia, dysthymia, depression, and generalized anxiety dis-order). Life-time history of depression was alsoconsidered. The PD subjects were also categoricallylabeled regarding smoking status and use of benzodiaze-pines and/or antidepressants.
2.4. Statistical analysis
P50 ratio (i.e. S2/S1), amplitudes (S1 and S2) andlatencies, considered apart as dependent variables, werecompared between groups (PD, schizophrenia orcontrols).
Data for the three evaluated groups were analyzedwith one-way ANOVA preceded by Levene’s test forhomogeneity of variances and followed by LSD post-hoc test when significant ANOVA was obtained. WhenLevene’s test was significant, Dunnett’s T3 was used aspost-hoc test.
Data considering P50 variables and clinical PD char-acteristics (gender, age, age of onset, smoking, history ofpast or present illness, use of benzodiazepines or antide-pressants, HAM-A and CGI scores) were analyzed by alinear regression model.
The level of significance was defined as p < 0.05 (two-tailed). All analyses were implemented with the SPSS10.0 for Windows (Chicago, IL). Data are shown asmean ± SD for all results.
Conditioning Amplitudes (S1)
0
2
4
6
8
10
12
14
Healthy Panic Schizo
mic
ro v
olt
s
Fig. 2. Dot-plot of P50 conditioning amplitudes (S1) in patients withpanic disorder (n = 28) with (r) and without (e) treatment, healthycomparison subjects (n = 28) and schizophrenia comparison subjects(n = 28). Non-significant ANOVA (F(2,81) = 1.538, p = 0.221).
3. Results
Table 1 presents relevant clinical features and P50ratios of PD subjects. Both grand average signals(blocks) yielded similar results, so the average of bothis expressed.
P50 ratio, S1 and S2 amplitudes and latencies are pre-sented on Table 2 (mean ± SD) for each group. Analysisof variance did not show significant differences forlatency (F(2,81) = 0.931, p = 0.398).
P50 ratios were compared between groups withANOVA (F(2,81) = 9.279, p < 0.001) followed by Dun-nett’s T3 as post-hoc test. Both patient groups showed
Table 2P50 ratio, amplitudes and latencies in patients with panic disorder (n = 28),
Group P50 ratio (%) (S2/S1) Conditioning (lV
Healthy controls 45.4 ± 20.9 5.6 ± 2.9Panic disorder 62.5 ± 27.7* 6.5 ± 3.3Schizophrenia 79.2 ± 37.3** 5.2 ± 3.1
Data presented as mean ± SD.*p < 0.05, **p < 0.01 significant difference compared to healthy controls. No si
higher P50 ratios compared to healthy controls: PDvs. healthy (p = 0.035), schizophrenic vs. healthy(p < 0.001). There was no significant difference betweenpanic and schizophrenic patients (p = 0.172) (Fig. 1).
Analysis of variance did not show significant differ-ences for S1 amplitude (F(2,81) = 1.538, p = 0.221)(Fig. 2).
A significant ANOVA was obtained for S2 ampli-tudes (F(2,81) = 6.299, p = 0.003) followed by Dun-nett’s T3 as post-hoc test. Both patient groups showedhigher S2 (test) amplitudes compared to healthy con-
healthy controls (n = 28) and schizophrenia subjects (n = 28)
) (S1) Test (lV) (S2) Latency (ms) (conditioning)
2.1 ± 1.1 56.3 ± 5.53.5 ± 1.7* 55.6 ± 7.63.3 ± 1.8** 57.8 ± 5.5
gnificant difference was found between panic and schizophrenic groups.

Test Amplitudes (S2)
0
1
2
3
4
5
6
7
8
9
Healthy Panic Schizo
mic
ro v
olt
s
* p=0.013
* p=0.003
Fig. 3. Dot-plot of P50 test amplitudes (S2) in patients with panicdisorder (n = 28) with (r) and without (e) treatment, healthycomparison subjects (n = 28) and schizophrenia comparison subjects(n = 28). ANOVA (F(2,81) = 6.999, p = 0.003) followed by Dunnett’sT3 as post-hoc test. PD vs. healthy (p = 0.013). Schizophrenic vs.healthy (p = 0.003). PD vs. schizophrenic (p = 0.976).
E.S. Ghisolfi et al. / Journal of Psychiatric Research xxx (2006) xxx–xxx 5
ARTICLE IN PRESS
trols: PD vs. healthy (p = 0.013), schizophrenic vs.healthy (p = 0.003). There was no significant differencebetween panic and schizophrenic patients (p = 0.976)(Fig. 3).
A linear regression model with the demographic,pharmacologic (including smoking status) and comor-bidity variables at entrance and a backward exclusioncut off significance criterion of 10% (R = 0.800,R2 = 0.640, adjusted R2 = 0.529) was obtained for P50ratio. The generated model showed as major predictorvariables social phobia (B = 30.3, p = 0.085) and gener-alized anxiety disorder (B = 23.8, p = 0.074) increasingP50 ratio and use of benzodiazepines (B = �43.1,p = 0.004) diminishing P50 ratio. The remaining vari-ables were excluded according to the criteria.
4. Discussion
In the present study PD patients showed diminishedsensory gating, expressed by a deficit in P50 suppression,compared to healthy subjects. This deficit was mainlydue to a failure to suppress S2 response. The magnitudeof this alteration was mostly indistinguishable from thefindings in our schizophrenic patients, which replicatedprevious results from the literature (Adler et al., 1998).Deficit of P50 suppression was positively associated withanxiety disorders and negatively associated with benzo-diazepine use.
The deficit to suppress the response to test stimulus isinterpreted as reflecting an impaired central inhibitoryactivity. The present results may also indicate a dysfunc-tion in brain regions responsible for P50 suppression,among which the hippocampus has been considered(Adler et al., 1998). This inhibitory deficit can affect sen-sory gating from external stimuli, but could also beinterpreted in the case of PD patients as an impairedability to filter out the perception of internal stimuli.
Among the putative candidate neurochemical sys-tems that mediate this inhibitory deficit are the choliner-gic system through a-7 receptors and GABAergic systemthrough GABA-B receptors (Adler et al., 1998), as wellas adenosine, an inhibitory neuromodulator releasedupon neuronal stimulation (Ghisolfi et al., 2002). Thepresent data also suggest that GABA-A receptors oranxiety status can also influence sensory gating giventhe association of benzodiazepine use with lower P50ratio. Also the noradrenergic system may be involved,as the a-2 antagonist yohimbine can both induce panicattacks (Charney et al., 1987) and disrupt P50 sensorygating in healthy subjects (Adler et al., 1994). However,the present protocol is not suitable to identify which ofthese factors are involved in P50 alterations in PDpatients.
GABA-B receptors may also be involved since theGABA-B agonist baclofen has been shown to reducepanic symptoms (Breslow et al., 1989) and GABA-Bantagonists decreased sensory gating suppression in ananimal model mostly due to effects on test response(Hershman et al., 1995). Although the benzodiazepinediazepam failed to alter P50 parameters in healthy vol-unteers (Van Luijtellar, 2003), this does not exclude thatsuch GABA-A co-agonists could affect sensory gating insubjects with anxiety disorders, as suggested by the pres-ent results.
The neuromodulator adenosine may also underliesuch alterations on P50 sensory gating in PD. Caffeineis a non-selective antagonist of adenosine A1 and A2receptors that has been shown to induce panic attacksand anxiety. PD patients showed hypersensitivity toanxiogenic and non-anxiogenic effects of caffeine andmay consume less caffeine (DeMet et al., 1989; Leeet al., 1988). Genetic studies have also reported an asso-ciation between A2A receptor polymorphism and riskfor panic disorder (Deckert et al., 1998; Yamada et al.,2001; Hamilton et al., 2004) and risk for caffeine-induced anxiety (Alsene et al., 2003). Regarding theP50 evoked potential, theophylline, which is a metabo-lite of caffeine and also an antagonist of adenosinereceptors, impaired P50 sensory gating in normal volun-teers (Ghisolfi et al., 2002). Also caffeine impaired P50sensory gating, and increase S2 wave amplitude wasfound in subject with low habitual intake of caffeine(Ghisolfi et al., 2006).
Limitations to our study include current use of med-ication in patient groups and the presence of comorbid-ities. In fact, the positive association with other anxietydisorders suggest that the findings in PD patients are notspecific for this disorder and may reflect a commondiathesis for anxiety disorders, e.g., harm avoidance.
In conclusion, this study extends previous neuro-physiological findings suggesting a sensory gating deficitin PD. Also, growing data support the notion that alter-ations in P50 sensory gating are not restricted to patients

6 E.S. Ghisolfi et al. / Journal of Psychiatric Research xxx (2006) xxx–xxx
ARTICLE IN PRESS
with schizophrenia. Nevertheless, the common altera-tions in P50 parameters observed in several neurologicaland psychiatric disorders does not imply that the under-lying substrate for changes in sensory gating are thesame. Further studies are necessary to better understandthe pathophysiology of this neurophysiological dysfunc-tion and its nature as a trait or state marker in anxietydisorders.
References
Adler LE, Hoffer L, Nagamoto HT, Waldo MC, Kisley MA, GiffithJM. Yohimbine impairs P50 auditory sensory gating in normalsubjects. Neuropsychopharmacology 1994;10:249–57.
Adler LE, Olincy A, Waldo M, Harris JG, Griffith J, Stevens K, et al..Schizophrenia, sensory gating, and nicotinic receptors. Schizophre-nia Bulletin 1998;24:189–202.
Alsene K, Deckert J, Sand P, de Wit H. Association between A2areceptor gene polymorphisms and caffeine-induced anxiety. Neu-ropsychopharmacology 2003;28:1694–702.
Breslow MF, Fankhauser MP, Potter RL, Meredith KE, Misiaszek J,Hope Jr DG. Role of gamma-aminobutyric acid in antipanic drugefficacy. American Journal of Psychiatry 1989;146:353–6.
Charney DS, Woods SW, Goodman WK, Heninger GR. Neurobio-logical mechanisms of panic anxiety: biochemical and behavioralcorrelates of yohimbine-induced panic attacks. American Journalof Psychiatry 1987;144:1030–6.
Clark CR, McFarlane AC, Weber DL, Battersby M. Enlarged frontalP300 to stimulus change in panic disorder. Biological Psychiatry1996;39:845–56.
Deckert J, Nothen MM, Franke P, Delmo C, Fritze J, Knapp M,et al.. Systematic mutation screening and association study of theA1 and A2a adenosine receptor genes in panic disorder suggest acontribution of the A2a gene to the development of disease.Molecular Psychiatry 1998;3:81–5.
DeMet E, Stein MK, Tran C, Chicz-DeMet A, Sangdahl C, Nelson J.Caffeine taste test for panic disorder: adenosine receptor supersen-sitivity. Psychiatry Research 1989;30:231–422.
Freedman R, Adler LE, Waldo MC, Pachtman E, Franks RD.Neurophysiological evidence for a defect in inhibitory pathways inschizophrenia: comparison of medicated and drug-free patients.Biological Psychiatry 1983;18:537–51.
Ghisolfi ES, Prokopiuk AS, Becker J, Ehlers JA, Belmonte-de-AbreuP, Souza DO, et al.. The adenosine antagonist theophyllineimpairs P50 auditory sensory gating in normal subjects. Neuro-psychopharmacology 2002;27:629–37.
Ghisolfi ES, Margis R, Becker J, Zanardo AP, Strimitzer IM, LaraDR. Impaired P50 sensory gating in post-traumatic stress disordersecondary to urban violence. International Journal of Psychophys-iology 2004;51:209–14.
Ghisolfi ES, Schuch A, Strimitzer Jr IM, Luersen G, Martins FF,Ramos FL, Becker J, Lara DR. Caffeine modulates P50 auditorysensory gating in healthy subjects. European Neuropsychophar-macology 2006;16:204–10.
Gordeev SA, Ryabokon IV, Fedotova AV, Tabeeva GR, Vein AM.Evaluation of nonspecific brain systems in patients with panicdisorders by the method of P300 cognitive evoked potentials.Bulletin of the Experimental and Biological Medicine2003;136:522–4.
Hamilton M. The assessment of anxiety states by rating. BritishJournal of Medical Psychology 1959:50–5.
Hamilton SP, Slager SL, De Leon AB, Heiman GA, Klein DF, HodgeSE, et al.. Evidence for genetic linkage between a polymorphism inthe adenosine 2A receptor and panic disorder. Neuropsychophar-macology 2004;29:558–65.
Hershman KM, Freedman R, Bickford PC. GABAB antagonistsdiminish the inhibitory gating of auditory response in the rathippocampus. Neuroscience Letters 1995;190:133–6.
Iwanami A, Isono H, Okajima Y, Kamijima K. Auditory event-relatedpotentials in panic disorder. European Archives of Psychiatry andClinical Neuroscience 1997;247:107–11.
Knott V, Lapierre YD, Fraser G, Johnson N. Auditory evokedpotentials in panic disorder. Journal of Psychiatry Neuroscience1991;16:215–20.
Lee MA, Flegel P, Greden JF, Cameron OG. Anxiogenic effects ofcaffeine on panic and depressed patients. American Journal ofPsychiatry 1988;145:632–5.
Levy D, Kimha R, Barak Y, Demmer M, Harel M, Elizur A.Brainstem auditory evoked potentials of panic disorder patients.Neuropsychobiology 1996;33:164–7.
Light GA, Malaspina D, Geyer MA, Luber BM, Coleman EA,Sackeim HA, Braff DL. Amphetamine disrupts P50 suppression innormal subjects. Biological Psychiatry 1999;46(7):990–6.
Ludewig S, Ludewig K, Geyer MA, Hell D, Vollenweider FX.Prepulse inhibition deficits in patients with panic disorder. DepressAnxiety 2002;15:55–60.
Ludewig S, Geyer MA, Ramseier M, Vollenweider FX, Rechsteiner E,Cattapan-Ludewig K. Information-processing deficits and cogni-tive dysfunction in panic disorder. Journal of Psychiatry andNeuroscience 2005;30:3037–43.
Nagamoto HT, Adler LE, Hea RA, Griffith JM, McRae KA,Freedman R. Gating of auditory P50 in schizophrenics: uniqueeffects of clozapine. Biological Psychiatry 1996;40:181–8.
Sheehan DV, Lecrubier Y, Harnett SK, Amorin P, Janavs J, Weiller E,et al.. The Mini International Neuropsychiatric Interview (MINI).The development and validation of a structured diagnosticpsychiatric interview. Journal of Clinical Psychiatry 1998;59:22–33.
Turan T, Esel E, Karaaslan F, Basturk M, Oguz A, Yabanoglu I.Auditory event-related potentials in panic and generalised anxietydisorders. Progress in Neuropsychopharmacology and BiologicalPsychiatry 2002;26:123–6.
Van Luijtellar G. The effect of diazepam on sensory gating in healthyvolunteers. Neuroscience Letters 2003;341:65–8.
Wang J, Miyazato H, Randall M, Hokama H, Hiramatsu K, Ogura C.The N200 abnormalities of auditory event-related potentials inpatients with panic disorder. Progress in Neuropsychopharmacol-ogy and Biological Psychiatry 2003;27:1013–21.
Yamada K, Hattori E, Shimizu M, Sugaya A, Shibuya H, YoshikawaT. Association studies of the cholecystokinin B receptor and A2aadenosine receptor genes in panic disorder. Journal of NeuralTransmission 2001;108:837–48.