
Pulmonary Hypertension in Sickle-Cell Disease: Comorbidities and Echocardiographic Findings
Upload
independentCategory
view
4download
0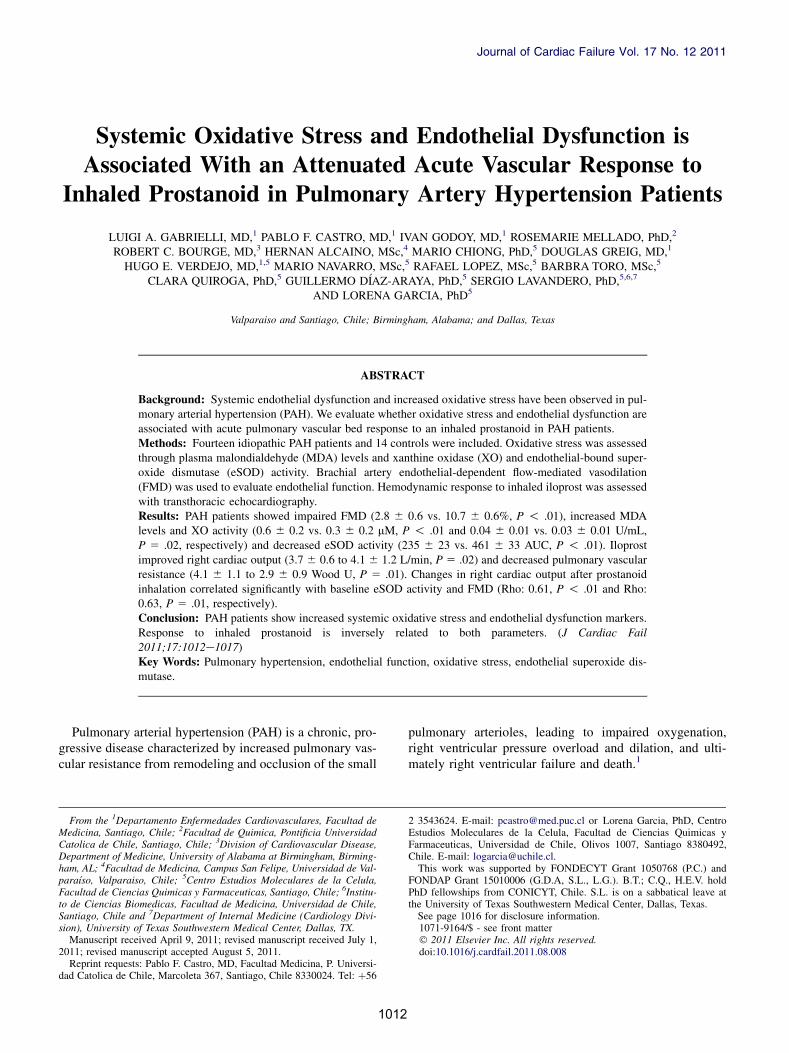
Journal of Cardiac Failure Vol. 17 No. 12 2011
Systemic Oxidative Stress and Endothelial Dysfunction isAssociated With an Attenuated Acute Vascular Response to
Inhaled Prostanoid in Pulmonary Artery Hypertension Patients
LUIGI A. GABRIELLI, MD,1 PABLO F. CASTRO, MD,1 IVAN GODOY, MD,1 ROSEMARIE MELLADO, PhD,2
ROBERT C. BOURGE, MD,3 HERNAN ALCAINO, MSc,4 MARIO CHIONG, PhD,5 DOUGLAS GREIG, MD,1
HUGO E. VERDEJO, MD,1,5 MARIO NAVARRO, MSc,5 RAFAEL LOPEZ, MSc,5 BARBRA TORO, MSc,5
CLARA QUIROGA, PhD,5 GUILLERMO D�IAZ-ARAYA, PhD,5 SERGIO LAVANDERO, PhD,5,6,7
AND LORENA GARCIA, PhD5
Valparaiso and Santiago, Chile; Birmingham, Alabama; and Dallas, Texas
From the 1DepaMedicina, SantiagCatolica de ChileDepartment of Meham, AL; 4Facultapara�ıso, ValparaiFacultad de Ciencto de Ciencias BioSantiago, Chile asion), University o
Manuscript rece2011; revised man
Reprint requestdad Catolica de C
ABSTRACT
Background: Systemic endothelial dysfunction and increased oxidative stress have been observed in pul-monary arterial hypertension (PAH). We evaluate whether oxidative stress and endothelial dysfunction areassociated with acute pulmonary vascular bed response to an inhaled prostanoid in PAH patients.Methods: Fourteen idiopathic PAH patients and 14 controls were included. Oxidative stress was assessedthrough plasma malondialdehyde (MDA) levels and xanthine oxidase (XO) and endothelial-bound super-oxide dismutase (eSOD) activity. Brachial artery endothelial-dependent flow-mediated vasodilation(FMD) was used to evaluate endothelial function. Hemodynamic response to inhaled iloprost was assessedwith transthoracic echocardiography.Results: PAH patients showed impaired FMD (2.8 6 0.6 vs. 10.7 6 0.6%, P ! .01), increased MDAlevels and XO activity (0.6 6 0.2 vs. 0.3 6 0.2 mM, P ! .01 and 0.04 6 0.01 vs. 0.03 6 0.01 U/mL,P 5 .02, respectively) and decreased eSOD activity (235 6 23 vs. 461 6 33 AUC, P ! .01). Iloprostimproved right cardiac output (3.7 6 0.6 to 4.1 6 1.2 L/min, P 5 .02) and decreased pulmonary vascularresistance (4.1 6 1.1 to 2.9 6 0.9 Wood U, P 5 .01). Changes in right cardiac output after prostanoidinhalation correlated significantly with baseline eSOD activity and FMD (Rho: 0.61, P ! .01 and Rho:0.63, P 5 .01, respectively).Conclusion: PAH patients show increased systemic oxidative stress and endothelial dysfunction markers.Response to inhaled prostanoid is inversely related to both parameters. (J Cardiac Fail2011;17:1012e1017)Key Words: Pulmonary hypertension, endothelial function, oxidative stress, endothelial superoxide dis-mutase.
Pulmonary arterial hypertension (PAH) is a chronic, pro-gressive disease characterized by increased pulmonary vas-cular resistance from remodeling and occlusion of the small
rtamento Enfermedades Cardiovasculares, Facultad deo, Chile; 2Facultad de Quimica, Pontificia Universidad, Santiago, Chile; 3Division of Cardiovascular Disease,dicine, University of Alabama at Birmingham, Birming-d de Medicina, Campus San Felipe, Universidad de Val-so, Chile; 5Centro Estudios Moleculares de la Celula,ias Quimicas y Farmaceuticas, Santiago, Chile; 6Institu-medicas, Facultad de Medicina, Universidad de Chile,nd 7Department of Internal Medicine (Cardiology Divi-f Texas Southwestern Medical Center, Dallas, TX.ived April 9, 2011; revised manuscript received July 1,uscript accepted August 5, 2011.s: Pablo F. Castro, MD, Facultad Medicina, P. Universi-hile, Marcoleta 367, Santiago, Chile 8330024. Tel: þ56
1012
pulmonary arterioles, leading to impaired oxygenation,right ventricular pressure overload and dilation, and ulti-mately right ventricular failure and death.1
2 3543624. E-mail: [email protected] or Lorena Garcia, PhD, CentroEstudios Moleculares de la Celula, Facultad de Ciencias Quimicas yFarmaceuticas, Universidad de Chile, Olivos 1007, Santiago 8380492,Chile. E-mail: [email protected] work was supported by FONDECYT Grant 1050768 (P.C.) and
FONDAP Grant 15010006 (G.D.A, S.L., L.G.). B.T.; C.Q., H.E.V. holdPhD fellowships from CONICYT, Chile. S.L. is on a sabbatical leave atthe University of Texas Southwestern Medical Center, Dallas, Texas.See page 1016 for disclosure information.1071-9164/$ - see front matter� 2011 Elsevier Inc. All rights reserved.doi:10.1016/j.cardfail.2011.08.008

Peripheral Markers in Pulmonary Hypertension � Gabrielli et al 1013
Impaired endothelial function and increased oxidativestress in the pulmonary vascular bed are key elements inPAH pathogenesis.2 Endothelial cell damage modifies thevascular milieu promoting increased vascular tone and vas-cular structural remodeling characteristic of PAH.2 Interest-ingly, when compared to controls, PAH patients exhibitimpaired endothelium-dependent vasoreactivity in conduitvessels, which appears to correlate with pulmonaryvascular response to vasodilators.3 Together with increasedoxidative stress,4e8 another paramount finding in PAH,these linked processes lead to vascular remodeling and dis-ease progression.9,10
We hypothesize that systemic oxidative stress markersand peripheral endothelial function tests may serve as bio-markers for identifying PAH patients responsive to inhaledprostanoids.
Methods
Patients
Cross-sectional study (Registration Trial Number FONDECYT1050768, CONICYT, Chile). Fourteen PAH patients (group I fromthe Dana Point classification11) evaluated in a university hospitalbetween December 2007 and May 2009 and 14 healthy volunteerswere included. All participants signed an informed consent ap-proved by our local Ethics Review Board. Patients were includedif they fulfill the following eligibility criteria: 1) age 18 or older;2) diagnosis of idiopathic PAH according to the Dana Point Clas-sification; 3) mean pulmonary artery pressure (mPAP) $25 mmHg12 at rest with a pulmonary capillary wedge pressure (PCWP)!15 mm Hg at the time of right heart catheterization (RHC); 4)stable treatment and stable clinical condition with no new medica-tion started within the past 3 months; and 5) no evidence of throm-boembolic disease in a computed tomographic pulmonaryangiogram performed within 6 months. All patients had RHCand a normal spirometric study at the time of diagnosis. Patientswere considered non-responders to adenosine if they failed to de-crease mPAP by at least 10 mm Hg to an absolute level of 40 mmHg or less without a decrease in cardiac output after adenosine ad-ministration.11 Exclusion criteria were: 1) pregnancy; 2) chroniciloprost use; 3) concurrent medical conditions that might affect de-termination of oxidative stress status, such as renal failure (plasmacreatinine O 2 mg/dL), autoimmune disease (defined as the ab-sence of anamnestic data suggestive autoimmune disease, negativerheumatoid factor, and negative antinuclear antibodies), neoplasticor advanced liver or pulmonary disease, acute or chronic inflam-mation; 4) systemic hypertension; 5) use of any anti-inflammatory drug, corticosteroids, aspirin or statins; and 6) activesmoker. For baseline comparisons, the study included a controlgroup of healthy nonsmoker volunteers matched by age andgender.Within 2 weeks after RHC, patients underwent acute pulmonary
vasoreactivity test using aerosolized iloprost (20 mg/4.5 mL in sa-line solution, Ventavis�, Bayer-Schering Pharma, Germany) ap-plied by a jet nebulizer over 10 minutes. This dose has beenreported as safe and effective and had been used in previous stud-ies of acute pulmonary vasoreactivity.13 Echocardiographic re-sponders were defined as those patients who did exhibit a rightcardiac output improvement of any magnitude accompanied by
a decrease in pulmonary vascular resistance 45 minutes afteriloprost inhalation.14,16
Assessment of Peripheral Endothelial Function
All endothelial function studies were performed before 9 AM.Patients fasted overnight and rested 30 minutes in supine positionin a quiet room before the examination. A 7.5-MHz linear arrayultrasound probe was employed to perform longitudinal sectionscans of the brachial artery 3 to 5 cm above the elbow pleat.Flow-mediated vasodilation (FMD) was assessed by placinga blood pressure cuff around the forearm and inflating it up to300 mm Hg. After 5 minutes of arterial occlusion, the cuff wasdeflated. An increase in vessel diameter of less than 8% was con-sidered evidence of endothelial dysfunction.15 Endothelial-independent vasodilation was evaluated 10 minutes after cuffdeflation, by measuring brachial artery diameter at baseline and3 minutes after administration of isosorbide dinitrate 1.25 mg sub-lingual spray (Schwarz Pharma AG, Swiss).
Assessment of Pulmonary Vascular Response
Transthoracic Doppler echocardiography was performed in allsubjects at baseline, and then 15 and 45 minutes after iloprost in-halation by a single blinded trained operator with a Phillips IE 33(S5-1 1-5 MHz transducer) within 2 weeks of RHC. MPAP, pul-monary vascular resistance (PVR), tricuspid annular plane systolicexcursion (TAPSE), systolic wave velocity of lateral tricuspid an-nulus with tissue Doppler (s0 wave), right outflow tract time-volume integral (RTVI), and right cardiac output (RCO) wereevaluated.16
Evaluation of Oxidative Stress
Malondialdehyde (MDA) levels and endothelium-bound en-zyme xanthine oxidase (eXO) activity were determined as markersfor reactive oxygen species (ROS) generation while endothelialsuperoxide dismutase (eSOD) activity as index of antioxidant en-zyme status.4e8 A venous blood sample from the antecubital veinof the nondominant arm was obtained at baseline. Then, a heparinbolus (5000 IU) was injected into the brachial artery of the samearm, and blood samples are taken at fixed intervals from the ante-cubital vein (1, 3, 5, 7, and 10 minutes after heparin injection).eSOD activity was calculated as the area under the curve (AUC)of the plasmatic SOD activity expressed as unit per milliliter ofplasma as previously described.17
eXO activity was calculated as the difference between plasmaXO at baseline and after 5 minutes of intra-arterial heparin injec-tion18,19 and was expressed as absorbance units (AU) per milliliterof plasma per minute.Plasma MDA levels, a marker for lipid peroxidation, were de-
termined by examining the content of thiobarbituric acid-reactive substances as previously described.9
Statistical Analysis
Baseline differences between PAH patients and control groupwere performed using chi-square or Mann-Whitney U test as ap-propriate. Hemodynamic parameter changes after iloprost inhala-tion were evaluated using Wilcoxon’s rank sum test. Correlationbetween hemodynamic response to inhaled iloprost and FMD oroxidative stress markers was evaluated with Spearman’s method.Categorical variables are expressed as percent and continue
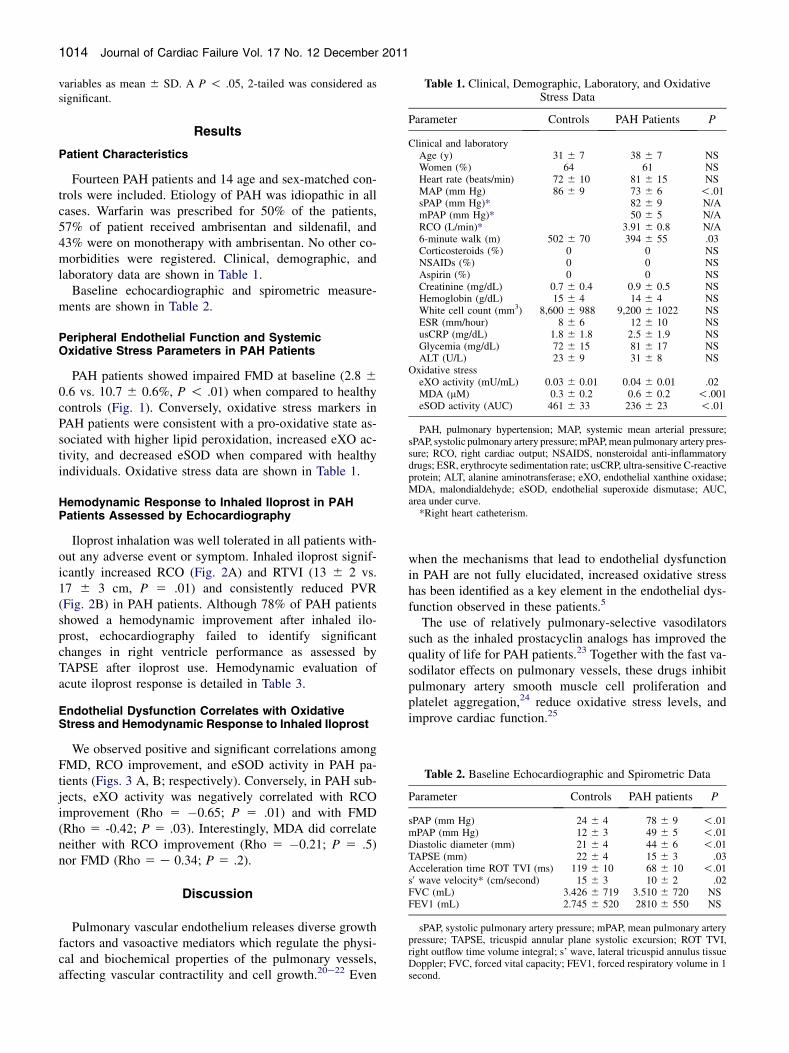
Table 1. Clinical, Demographic, Laboratory, and OxidativeStress Data
Parameter Controls PAH Patients P
Clinical and laboratoryAge (y) 31 6 7 38 6 7 NSWomen (%) 64 61 NSHeart rate (beats/min) 72 6 10 81 6 15 NSMAP (mm Hg) 86 6 9 73 6 6 !.01sPAP (mm Hg)* 82 6 9 N/AmPAP (mm Hg)* 50 6 5 N/ARCO (L/min)* 3.91 6 0.8 N/A6-minute walk (m) 502 6 70 394 6 55 .03Corticosteroids (%) 0 0 NSNSAIDs (%) 0 0 NSAspirin (%) 0 0 NSCreatinine (mg/dL) 0.7 6 0.4 0.9 6 0.5 NSHemoglobin (g/dL) 15 6 4 14 6 4 NSWhite cell count (mm3) 8,600 6 988 9,200 6 1022 NSESR (mm/hour) 8 6 6 12 6 10 NSusCRP (mg/dL) 1.8 6 1.8 2.5 6 1.9 NSGlycemia (mg/dL) 72 6 15 81 6 17 NSALT (U/L) 23 6 9 31 6 8 NS
Oxidative stresseXO activity (mU/mL) 0.03 6 0.01 0.04 6 0.01 .02MDA (mM) 0.3 6 0.2 0.6 6 0.2 !.001eSOD activity (AUC) 461 6 33 236 6 23 !.01
PAH, pulmonary hypertension; MAP, systemic mean arterial pressure;sPAP, systolic pulmonary artery pressure;mPAP,mean pulmonary artery pres-sure; RCO, right cardiac output; NSAIDS, nonsteroidal anti-inflammatorydrugs; ESR, erythrocyte sedimentation rate; usCRP, ultra-sensitive C-reactiveprotein; ALT, alanine aminotransferase; eXO, endothelial xanthine oxidase;MDA, malondialdehyde; eSOD, endothelial superoxide dismutase; AUC,area under curve.
*Right heart catheterism.
Table 2. Baseline Echocardiographic and Spirometric Data
Parameter Controls PAH patients P
sPAP (mm Hg) 24 6 4 78 6 9 !.01mPAP (mm Hg) 12 6 3 49 6 5 !.01Diastolic diameter (mm) 21 6 4 44 6 6 !.01TAPSE (mm) 22 6 4 15 6 3 .03Acceleration time ROT TVI (ms) 119 6 10 68 6 10 !.01s0 wave velocity* (cm/second) 15 6 3 10 6 2 .02FVC (mL) 3.426 6 719 3.510 6 720 NSFEV1 (mL) 2.745 6 520 2810 6 550 NS
sPAP, systolic pulmonary artery pressure; mPAP, mean pulmonary arterypressure; TAPSE, tricuspid annular plane systolic excursion; ROT TVI,right outflow time volume integral; s’ wave, lateral tricuspid annulus tissueDoppler; FVC, forced vital capacity; FEV1, forced respiratory volume in 1second.
1014 Journal of Cardiac Failure Vol. 17 No. 12 December 2011
variables as mean 6 SD. A P ! .05, 2-tailed was considered assignificant.
Results
Patient Characteristics
Fourteen PAH patients and 14 age and sex-matched con-trols were included. Etiology of PAH was idiopathic in allcases. Warfarin was prescribed for 50% of the patients,57% of patient received ambrisentan and sildenafil, and43% were on monotherapy with ambrisentan. No other co-morbidities were registered. Clinical, demographic, andlaboratory data are shown in Table 1.
Baseline echocardiographic and spirometric measure-ments are shown in Table 2.
Peripheral Endothelial Function and SystemicOxidative Stress Parameters in PAH Patients
PAH patients showed impaired FMD at baseline (2.8 60.6 vs. 10.7 6 0.6%, P ! .01) when compared to healthycontrols (Fig. 1). Conversely, oxidative stress markers inPAH patients were consistent with a pro-oxidative state as-sociated with higher lipid peroxidation, increased eXO ac-tivity, and decreased eSOD when compared with healthyindividuals. Oxidative stress data are shown in Table 1.
Hemodynamic Response to Inhaled Iloprost in PAHPatients Assessed by Echocardiography
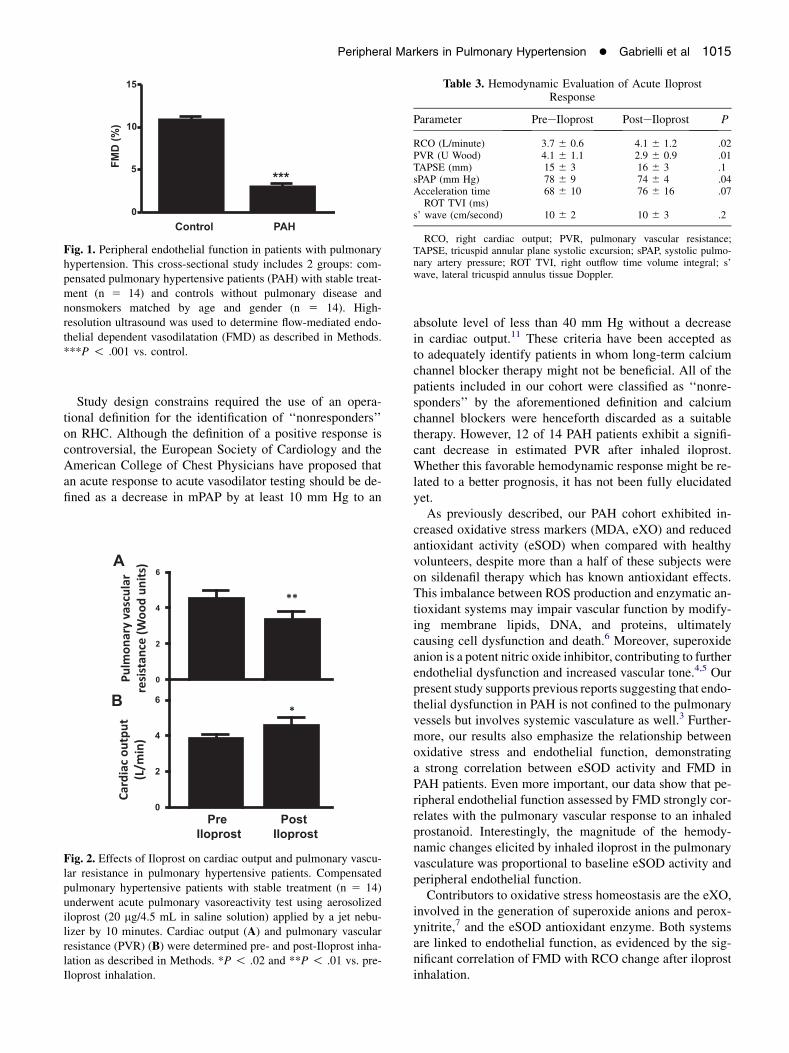
Iloprost inhalation was well tolerated in all patients with-out any adverse event or symptom. Inhaled iloprost signif-icantly increased RCO (Fig. 2A) and RTVI (13 6 2 vs.17 6 3 cm, P 5 .01) and consistently reduced PVR(Fig. 2B) in PAH patients. Although 78% of PAH patientsshowed a hemodynamic improvement after inhaled ilo-prost, echocardiography failed to identify significantchanges in right ventricle performance as assessed byTAPSE after iloprost use. Hemodynamic evaluation ofacute iloprost response is detailed in Table 3.
Endothelial Dysfunction Correlates with OxidativeStress and Hemodynamic Response to Inhaled Iloprost
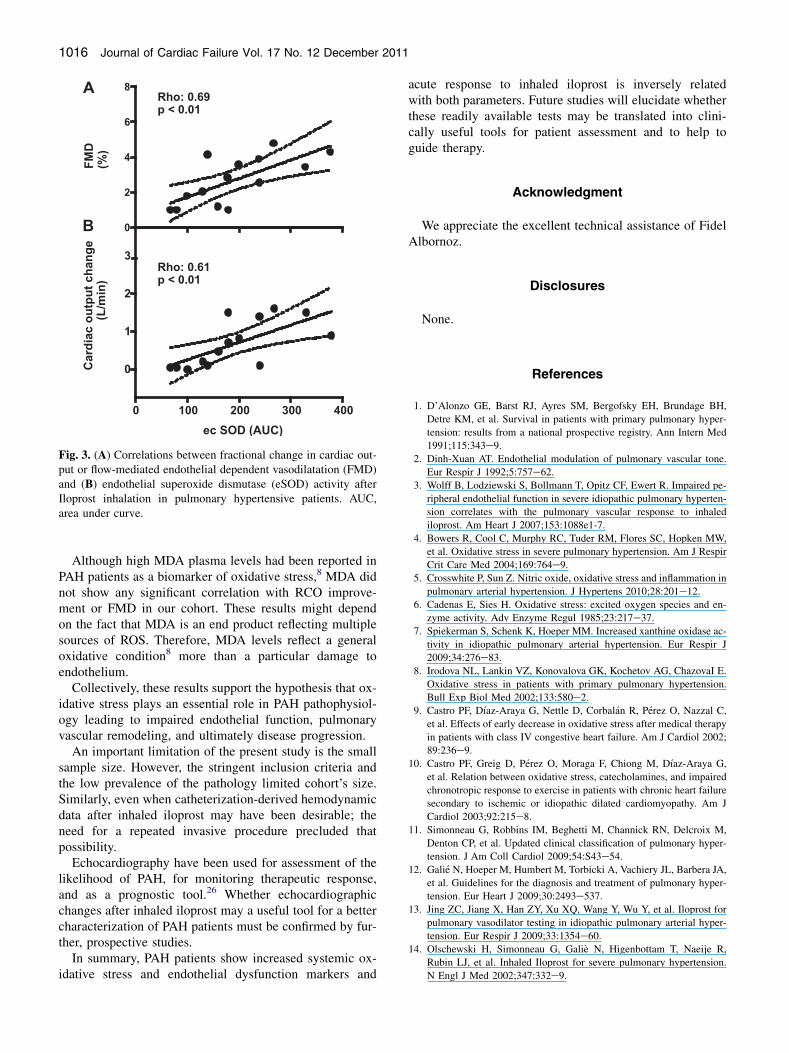
We observed positive and significant correlations amongFMD, RCO improvement, and eSOD activity in PAH pa-tients (Figs. 3 A, B; respectively). Conversely, in PAH sub-jects, eXO activity was negatively correlated with RCOimprovement (Rho 5 �0.65; P 5 .01) and with FMD(Rho 5 -0.42; P 5 .03). Interestingly, MDA did correlateneither with RCO improvement (Rho 5 �0.21; P 5 .5)nor FMD (Rho 5 e 0.34; P 5 .2).
Discussion
Pulmonary vascular endothelium releases diverse growthfactors and vasoactive mediators which regulate the physi-cal and biochemical properties of the pulmonary vessels,affecting vascular contractility and cell growth.20e22 Even
when the mechanisms that lead to endothelial dysfunctionin PAH are not fully elucidated, increased oxidative stresshas been identified as a key element in the endothelial dys-function observed in these patients.5
The use of relatively pulmonary-selective vasodilatorssuch as the inhaled prostacyclin analogs has improved thequality of life for PAH patients.23 Together with the fast va-sodilator effects on pulmonary vessels, these drugs inhibitpulmonary artery smooth muscle cell proliferation andplatelet aggregation,24 reduce oxidative stress levels, andimprove cardiac function.25
15
10
5
0
Control PAH
FM
D (%
)
***
Fig. 1. Peripheral endothelial function in patients with pulmonaryhypertension. This cross-sectional study includes 2 groups: com-pensated pulmonary hypertensive patients (PAH) with stable treat-ment (n 5 14) and controls without pulmonary disease andnonsmokers matched by age and gender (n 5 14). High-resolution ultrasound was used to determine flow-mediated endo-thelial dependent vasodilatation (FMD) as described in Methods.***P ! .001 vs. control.
Table 3. Hemodynamic Evaluation of Acute IloprostResponse
Parameter PreeIloprost PosteIloprost P
RCO (L/minute) 3.7 6 0.6 4.1 6 1.2 .02PVR (U Wood) 4.1 6 1.1 2.9 6 0.9 .01TAPSE (mm) 15 6 3 16 6 3 .1sPAP (mm Hg) 78 6 9 74 6 4 .04Acceleration timeROT TVI (ms)
68 6 10 76 6 16 .07
s’ wave (cm/second) 10 6 2 10 6 3 .2
RCO, right cardiac output; PVR, pulmonary vascular resistance;TAPSE, tricuspid annular plane systolic excursion; sPAP, systolic pulmo-nary artery pressure; ROT TVI, right outflow time volume integral; s’wave, lateral tricuspid annulus tissue Doppler.
Peripheral Markers in Pulmonary Hypertension � Gabrielli et al 1015
Study design constrains required the use of an opera-tional definition for the identification of ‘‘nonresponders’’on RHC. Although the definition of a positive response iscontroversial, the European Society of Cardiology and theAmerican College of Chest Physicians have proposed thatan acute response to acute vasodilator testing should be de-fined as a decrease in mPAP by at least 10 mm Hg to an
A
B
Fig. 2. Effects of Iloprost on cardiac output and pulmonary vascu-lar resistance in pulmonary hypertensive patients. Compensatedpulmonary hypertensive patients with stable treatment (n 5 14)underwent acute pulmonary vasoreactivity test using aerosolizediloprost (20 mg/4.5 mL in saline solution) applied by a jet nebu-lizer by 10 minutes. Cardiac output (A) and pulmonary vascularresistance (PVR) (B) were determined pre- and post-Iloprost inha-lation as described in Methods. *P ! .02 and **P ! .01 vs. pre-Iloprost inhalation.
absolute level of less than 40 mm Hg without a decreasein cardiac output.11 These criteria have been accepted asto adequately identify patients in whom long-term calciumchannel blocker therapy might not be beneficial. All of thepatients included in our cohort were classified as ‘‘nonre-sponders’’ by the aforementioned definition and calciumchannel blockers were henceforth discarded as a suitabletherapy. However, 12 of 14 PAH patients exhibit a signifi-cant decrease in estimated PVR after inhaled iloprost.Whether this favorable hemodynamic response might be re-lated to a better prognosis, it has not been fully elucidatedyet.
As previously described, our PAH cohort exhibited in-creased oxidative stress markers (MDA, eXO) and reducedantioxidant activity (eSOD) when compared with healthyvolunteers, despite more than a half of these subjects wereon sildenafil therapy which has known antioxidant effects.This imbalance between ROS production and enzymatic an-tioxidant systems may impair vascular function by modify-ing membrane lipids, DNA, and proteins, ultimatelycausing cell dysfunction and death.6 Moreover, superoxideanion is a potent nitric oxide inhibitor, contributing to furtherendothelial dysfunction and increased vascular tone.4,5 Ourpresent study supports previous reports suggesting that endo-thelial dysfunction in PAH is not confined to the pulmonaryvessels but involves systemic vasculature as well.3 Further-more, our results also emphasize the relationship betweenoxidative stress and endothelial function, demonstratinga strong correlation between eSOD activity and FMD inPAH patients. Even more important, our data show that pe-ripheral endothelial function assessed by FMD strongly cor-relates with the pulmonary vascular response to an inhaledprostanoid. Interestingly, the magnitude of the hemody-namic changes elicited by inhaled iloprost in the pulmonaryvasculature was proportional to baseline eSOD activity andperipheral endothelial function.
Contributors to oxidative stress homeostasis are the eXO,involved in the generation of superoxide anions and perox-ynitrite,7 and the eSOD antioxidant enzyme. Both systemsare linked to endothelial function, as evidenced by the sig-nificant correlation of FMD with RCO change after iloprostinhalation.
Rho: 0.69
p < 0.01
0
2
4
6
8F
MD
(%
)
100 200 300 400
0
1
2
3
ec SOD (AUC)
C
ard
ia
c o
utp
ut c
ha
ng
e
(L
/m
in
)
Rho: 0.61
p < 0.01
0
A
B
Fig. 3. (A) Correlations between fractional change in cardiac out-put or flow-mediated endothelial dependent vasodilatation (FMD)and (B) endothelial superoxide dismutase (eSOD) activity afterIloprost inhalation in pulmonary hypertensive patients. AUC,area under curve.
1016 Journal of Cardiac Failure Vol. 17 No. 12 December 2011
Although high MDA plasma levels had been reported inPAH patients as a biomarker of oxidative stress,8 MDA didnot show any significant correlation with RCO improve-ment or FMD in our cohort. These results might dependon the fact that MDA is an end product reflecting multiplesources of ROS. Therefore, MDA levels reflect a generaloxidative condition8 more than a particular damage toendothelium.
Collectively, these results support the hypothesis that ox-idative stress plays an essential role in PAH pathophysiol-ogy leading to impaired endothelial function, pulmonaryvascular remodeling, and ultimately disease progression.
An important limitation of the present study is the smallsample size. However, the stringent inclusion criteria andthe low prevalence of the pathology limited cohort’s size.Similarly, even when catheterization-derived hemodynamicdata after inhaled iloprost may have been desirable; theneed for a repeated invasive procedure precluded thatpossibility.
Echocardiography have been used for assessment of thelikelihood of PAH, for monitoring therapeutic response,and as a prognostic tool.26 Whether echocardiographicchanges after inhaled iloprost may a useful tool for a bettercharacterization of PAH patients must be confirmed by fur-ther, prospective studies.
In summary, PAH patients show increased systemic ox-idative stress and endothelial dysfunction markers and
acute response to inhaled iloprost is inversely relatedwith both parameters. Future studies will elucidate whetherthese readily available tests may be translated into clini-cally useful tools for patient assessment and to help toguide therapy.
Acknowledgment
We appreciate the excellent technical assistance of FidelAlbornoz.
Disclosures
None.
References
1. D’Alonzo GE, Barst RJ, Ayres SM, Bergofsky EH, Brundage BH,
Detre KM, et al. Survival in patients with primary pulmonary hyper-
tension: results from a national prospective registry. Ann Intern Med
1991;115:343e9.2. Dinh-Xuan AT. Endothelial modulation of pulmonary vascular tone.
Eur Respir J 1992;5:757e62.
3. Wolff B, Lodziewski S, Bollmann T, Opitz CF, Ewert R. Impaired pe-
ripheral endothelial function in severe idiopathic pulmonary hyperten-
sion correlates with the pulmonary vascular response to inhaled
iloprost. Am Heart J 2007;153:1088e1-7.
4. Bowers R, Cool C, Murphy RC, Tuder RM, Flores SC, Hopken MW,
et al. Oxidative stress in severe pulmonary hypertension. Am J Respir
Crit Care Med 2004;169:764e9.
5. Crosswhite P, Sun Z. Nitric oxide, oxidative stress and inflammation in
pulmonary arterial hypertension. J Hypertens 2010;28:201e12.6. Cadenas E, Sies H. Oxidative stress: excited oxygen species and en-
zyme activity. Adv Enzyme Regul 1985;23:217e37.
7. Spiekerman S, Schenk K, Hoeper MM. Increased xanthine oxidase ac-
tivity in idiopathic pulmonary arterial hypertension. Eur Respir J
2009;34:276e83.
8. Irodova NL, Lankin VZ, Konovalova GK, Kochetov AG, ChazovaI E.
Oxidative stress in patients with primary pulmonary hypertension.
Bull Exp Biol Med 2002;133:580e2.9. Castro PF, D�ıaz-Araya G, Nettle D, Corbal�an R, P�erez O, Nazzal C,
et al. Effects of early decrease in oxidative stress after medical therapy
in patients with class IV congestive heart failure. Am J Cardiol 2002;
89:236e9.
10. Castro PF, Greig D, P�erez O, Moraga F, Chiong M, D�ıaz-Araya G,
et al. Relation between oxidative stress, catecholamines, and impaired
chronotropic response to exercise in patients with chronic heart failure
secondary to ischemic or idiopathic dilated cardiomyopathy. Am J
Cardiol 2003;92:215e8.
11. Simonneau G, Robbins IM, Beghetti M, Channick RN, Delcroix M,
Denton CP, et al. Updated clinical classification of pulmonary hyper-
tension. J Am Coll Cardiol 2009;54:S43e54.
12. Gali�e N, Hoeper M, Humbert M, Torbicki A, Vachiery JL, Barbera JA,
et al. Guidelines for the diagnosis and treatment of pulmonary hyper-
tension. Eur Heart J 2009;30:2493e537.
13. Jing ZC, Jiang X, Han ZY, Xu XQ, Wang Y, Wu Y, et al. Iloprost for
pulmonary vasodilator testing in idiopathic pulmonary arterial hyper-
tension. Eur Respir J 2009;33:1354e60.14. Olschewski H, Simonneau G, Gali�e N, Higenbottam T, Naeije R,
Rubin LJ, et al. Inhaled Iloprost for severe pulmonary hypertension.
N Engl J Med 2002;347:332e9.

Peripheral Markers in Pulmonary Hypertension � Gabrielli et al 1017
15. Celermajer DS. Testing endothelial function using ultrasound. J Cardi-
ovasc Pharmacol 1998;32:S29e32.
16. Selimovic N, Rundqvist B, Bergh CH, Andersson B, Petersson S,
Johansson L, et al. Assessment of pulmonary vascular resistance by
Doppler echocardiography in patients with pulmonary arterial hyper-
tension. J Heart Lung Transplant 2007;26:927e34.
17. Castro PF, Miranda R, Verdejo HE, Greig D, Gabrielli LA, Alcaino H,
et al. Pleiotropic effects of atorvastatin in heart failure: role in oxida-
tive stress, inflammation, endothelial function, and exercise capacity.
J Heart Lung Transplant 2008;27:435e41.
18. Prajda N, Weber G. Malignant transformation-linked imbalance: de-
creased xanthine oxidase activity in hepatomas. FEBS Lett 1975;59:
245e9.
19. Landmesser U, Spiekermann S, Dikalov S, Tatge H, Wilke R,
Kohler C, et al. Vascular oxidative stress and endothelial dysfunc-
tion in patients with chronic heart failure: role of xanthine-
oxidase and extracellular superoxide dismutase. Circulation 2002;
106:3073e8.
20. Madden JA, Vadula MS, Kurup VP. Effects of hypoxia and other va-
soactive agents on pulmonary and cerebral artery smooth muscle cells.
Am J Physiol 1992;263:L384e93.
21. Morrell NW, Adnot S, Archer SL, Dupuis J, Jones PL, MacLean MR,
et al. Cellular and molecular basis of pulmonary arterial hypertension.
J Am Coll Cardiol 2009;54:S20e31.
22. Farber HW, Loscalzo J. Pulmonary arterial hypertension. N Engl J
Med 2004;351:1655e65.23. Yildiz P. Molecular mechanisms of pulmonary hypertension. Clin
Chim Acta 2009;403:9e16.
24. Jacobs W, Vonk-Noordegraf A. Epoprostenol in pulmonary arterial hy-
pertension. Expert Opin Drug Metab Toxicol 2009;5:83e90.
25. Shinmura K, Tamaki K, Sato T, Ishida H, Bolli R. Prostacyclin attenuates
oxidative damage of myocytes by opening mitochondrial ATP-sensitive
Kþ channels via the EP3 receptor. Am J Physiol 2005;288:H2093e210.26. Habib G, Torbicki A. The role of echocardiography in the diagnosis
and management of patients with pulmonary hypertension. Eur Respir
Rev 2010;19:288e99.
Copyright © 2022 FDOKUMEN




















