Outcome of post-liver transplant ischemic and nonischemic biliary stenoses treated with percutaneous...
11
ORIGINAL ARTICLE Outcome of Post–Liver Transplant Ischemic and Nonischemic Biliary Stenoses Treated With Percutaneous Interventions: The Bologna Experience Emanuela Giampalma, 1 Matteo Renzulli, 1 Cristina Mosconi, 1 Giorgio Ercolani, 2 Antonio Daniele Pinna, 2 and Rita Golfieri 1 1 Radiology Unit, Department of Digestive Diseases and Internal Medicine, and 2 Liver and Multiorgan Transplant Unit, Department of General Surgery, Sant’Orsola-Malpighi Hospital, University of Bologna, Bologna, Italy In liver transplantation (LT), biliary strictures (BSs) are among the most common complications. The aim of this study was to evaluate the efficacy of percutaneous treatments in the management of post-LT BSs. Between 1999 and 2007, 48 patients underwent percutaneous treatments for posttransplant BSs. We divided the population into 2 groups according to the cause [ischemic (n ¼ 14) or nonischemic (n ¼ 34)] and into further subgroups according to the site [anastomotic (n ¼ 34) or nonanastomotic (n ¼ 14)]. All patients were treated with bilioplasty; in 9 patients who were refractory to bilioplasty, metallic stents were implanted. A technical success rate of 90% was achieved without differences between the ischemic and nonischemic groups or between the anastomotic and nonanastomotic subgroups (P ¼ 0.10). The major complication rate was 4%. The overall 1- and 3-year primary patency rates were 94% and 45%, respectively, and better results were found for patients with nonischemic stenoses versus patients with ischemic stenoses (P ¼ 0.032). The overall secondary patency rates were 94% and 83% at 1 and 3 years, respectively, and there were no statistical differences between the is- chemic and nonischemic groups or between the anastomotic and nonanastomotic groups. In the stent subgroup, the overall primary 1- and 2-year patency rates were 100% and 71%, respectively, and the secondary patency rates were 100% and 100%, respectively. In conclusion, a percutaneous approach is highly effective for the treatment of post-LT BSs, and the best results are obtained for patients with simple, nonischemic BSs (technical success rate ¼ 94%, 3-year primary patency rate ¼ 81%, 3-year secondary patency rate ¼ 75%). For patients with ischemic BSs, closer follow-up and retreatment are more frequently needed to achieve secondary patency rates comparable to (or even better than) those for patients with non- ischemic stenoses. Liver Transpl 18:177-187, 2012. V C 2011 AASLD. Received June 6, 2011; accepted October 3, 2011. In liver transplantation (LT), biliary complications are the second most common cause of graft dys- function after rejection, 1 and they have been called the Achilles’ heel of LT, despite advances in surgical techniques, immunosuppression, and postoperative management. In the past, they were seen in one- third of transplants and accounted for approximately 50% of post-LT deaths, 2 but now they are reported in 10% to 40% of transplants from cadaveric donors 3-12 and rarely lead to death; some may not require interventions. Conversely, in living donor LT and pediatric transplantation, they are the most fre- quent cause of postoperative morbidity with rates of 30% to 60% 13-15 ; these high rates are related to the Abbreviations: BS, biliary stricture; C-C, choledochocholedochostomy; C-J, choledochojejunostomy; H-J, hepaticojejunostomy; LT, liver transplantation; NS, not significant; PIT, percutaneous interventional technique. Address reprint requests to Emanuela Giampalma, M.D., Radiology Unit, Department of Digestive Diseases and Internal Medicine, Sant’Orsola-Malpighi Hospital, University of Bologna, Via Albertoni 15, Bologna, Italy 40138. Telephone: þ390516362311 or þ390516362307; FAX: þ390516362699; E-mail: [email protected] DOI 10.1002/lt.22450 View this article online at wileyonlinelibrary.com. LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases LIVER TRANSPLANTATION 18:177-187, 2012 V C 2011 American Association for the Study of Liver Diseases.
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Outcome of post-liver transplant ischemic and nonischemic biliary stenoses treated with percutaneous...
ORIGINAL ARTICLE
Outcome of Post–Liver Transplant Ischemicand Nonischemic Biliary Stenoses TreatedWith Percutaneous Interventions:The Bologna ExperienceEmanuela Giampalma,1 Matteo Renzulli,1 Cristina Mosconi,1 Giorgio Ercolani,2
Antonio Daniele Pinna,2 and Rita Golfieri11Radiology Unit, Department of Digestive Diseases and Internal Medicine, and 2Liver and MultiorganTransplant Unit, Department of General Surgery, Sant’Orsola-Malpighi Hospital, University of Bologna,Bologna, Italy
In liver transplantation (LT), biliary strictures (BSs) are among the most common complications. The aim of this study wasto evaluate the efficacy of percutaneous treatments in the management of post-LT BSs. Between 1999 and 2007, 48patients underwent percutaneous treatments for posttransplant BSs. We divided the population into 2 groups according tothe cause [ischemic (n ¼ 14) or nonischemic (n ¼ 34)] and into further subgroups according to the site [anastomotic (n ¼34) or nonanastomotic (n ¼ 14)]. All patients were treated with bilioplasty; in 9 patients who were refractory to bilioplasty,metallic stents were implanted. A technical success rate of 90% was achieved without differences between the ischemicand nonischemic groups or between the anastomotic and nonanastomotic subgroups (P ¼ 0.10). The major complicationrate was 4%. The overall 1- and 3-year primary patency rates were 94% and 45%, respectively, and better results werefound for patients with nonischemic stenoses versus patients with ischemic stenoses (P ¼ 0.032). The overall secondarypatency rates were 94% and 83% at 1 and 3 years, respectively, and there were no statistical differences between the is-chemic and nonischemic groups or between the anastomotic and nonanastomotic groups. In the stent subgroup, the overallprimary 1- and 2-year patency rates were 100% and 71%, respectively, and the secondary patency rates were 100% and100%, respectively. In conclusion, a percutaneous approach is highly effective for the treatment of post-LT BSs, and thebest results are obtained for patients with simple, nonischemic BSs (technical success rate ¼ 94%, 3-year primary patencyrate ¼ 81%, 3-year secondary patency rate ¼ 75%). For patients with ischemic BSs, closer follow-up and retreatment aremore frequently needed to achieve secondary patency rates comparable to (or even better than) those for patients with non-ischemic stenoses. Liver Transpl 18:177-187, 2012. VC 2011 AASLD.
Received June 6, 2011; accepted October 3, 2011.
In liver transplantation (LT), biliary complicationsare the second most common cause of graft dys-function after rejection,1 and they have been calledthe Achilles’ heel of LT, despite advances in surgicaltechniques, immunosuppression, and postoperativemanagement. In the past, they were seen in one-third of transplants and accounted for approximately
50% of post-LT deaths,2 but now they are reportedin 10% to 40% of transplants from cadavericdonors3-12 and rarely lead to death; some may notrequire interventions. Conversely, in living donor LTand pediatric transplantation, they are the most fre-quent cause of postoperative morbidity with rates of30% to 60%13-15; these high rates are related to the
Abbreviations: BS, biliary stricture; C-C, choledochocholedochostomy; C-J, choledochojejunostomy; H-J, hepaticojejunostomy; LT,liver transplantation; NS, not significant; PIT, percutaneous interventional technique.
Address reprint requests to Emanuela Giampalma, M.D., Radiology Unit, Department of Digestive Diseases and Internal Medicine,Sant’Orsola-Malpighi Hospital, University of Bologna, Via Albertoni 15, Bologna, Italy 40138. Telephone: þ390516362311 or þ390516362307;FAX: þ390516362699; E-mail: [email protected]
DOI 10.1002/lt.22450View this article online at wileyonlinelibrary.com.LIVER TRANSPLANTATION.DOI 10.1002/lt. Published on behalf of the American Association for the Study of Liver Diseases
LIVER TRANSPLANTATION 18:177-187, 2012
VC 2011 American Association for the Study of Liver Diseases.
greater technical difficulties in biliary tractreconstruction.
Biliary complications after LT are mainly due to bili-ary leaks, biliary strictures (BSs), biliary stones/sludge, bile cast syndrome, and bile duct necro-sis.7,16-21 The most common complications are biliaryleaks and BSs.22 Biliary leaks are reported in 1% to25% of all LT cases,23,24 and anastomotic stricturesare reported in 4% to 9% of adult LT patients. BSsmay also occur at locations other than the biliaryanastomosis, and these are called nonanastomoticstrictures and have an incidence ranging from 5% to15%.12
The critical anatomical element in the biliary treegraft is represented by vascularity and is strictly de-pendent on the hepatic artery alone. This conditionexplains the high incidence of biliary complications inpatients with hepatic arterial thrombosis (up to 80%)or hepatic artery stenosis (up to 67%).25-32
For the most part, BSs at the site of the bile ductanastomosis are thought to result from the surgicaltechnique and/or local ischemia33; the primary treat-ment for anastomotic BSs is surgical repair, but thefailure rate increases after each subsequent repair.34
The exact mechanisms resulting in nonanastomoticBSs are not well understood; the initial reports ofnonanastomotic BSs after LT described an associationwith hepatic artery thrombosis resulting in bile ductischemia,35 but later reports described intrahepaticBSs in patients without hepatic artery thrombosis.36
This suggests that several mechanisms may cause in-trahepatic BSs. Nonanastomotic BSs can present achallenging problem because they are more difficult totreat, and surgical repair is usually not an option.22 Auniform algorithm for the management of these biliarycomplications has not yet been adopted by transplantcenters worldwide.22 Percutaneous interventionaltechniques (PITs) are being increasingly used for thetreatment of biliary complications33; in the past fewyears, there has been significant progress in the use
of PITs for the management of benign biliary compli-cations such as BSs,37 and they have also become al-ternative therapies for the post-LT population.
In the literature, great variability in the results ofPITs for the treatment of post-LT BSs has beenreported, and this has been related to broad differen-ces in the technical procedures.
In this article, we report our experience with astandardized percutaneous treatment protocol forpost-LT anastomotic and nonanastomotic BSs, andwe evaluate its efficacy in terms of the success rateand the primary and secondary patency rates accord-ing to the underlying ischemic or nonischemic cause.
PATIENTS AND METHODS
Patients
This study complied with the principles of the Decla-ration of Helsinki and subsequent amendments andwas performed at a tertiary liver care center. Theinstitutional review boards approved the study, andwritten informed consent was obtained from allpatients.
From January 1999 to December 2007, 48 patients[30 men (62%); mean age ¼ 51 6 11 years (range ¼13-68 years)] were referred to our interventional radi-ology unit for the elective percutaneous treatment ofpost-LT BSs. The characteristics of these patients andthe wider cohort of transplant patients during thestudy period are summarized in Table 1.
The clinical and laboratory signs of BSs includedrecurrent cholangitis, pyrexia, leukocytosis, andincreases in blood chemistry indices of biliary stasis(serum bilirubin, alkaline phosphatase, c-glutamyl-transferase, and guanosine triphosphate/glutamicoxaloacetic transaminase). Abdominal ultrasound, colorDoppler ultrasound, and magnetic resonance cholan-giography were performed in all cases before the PITs;
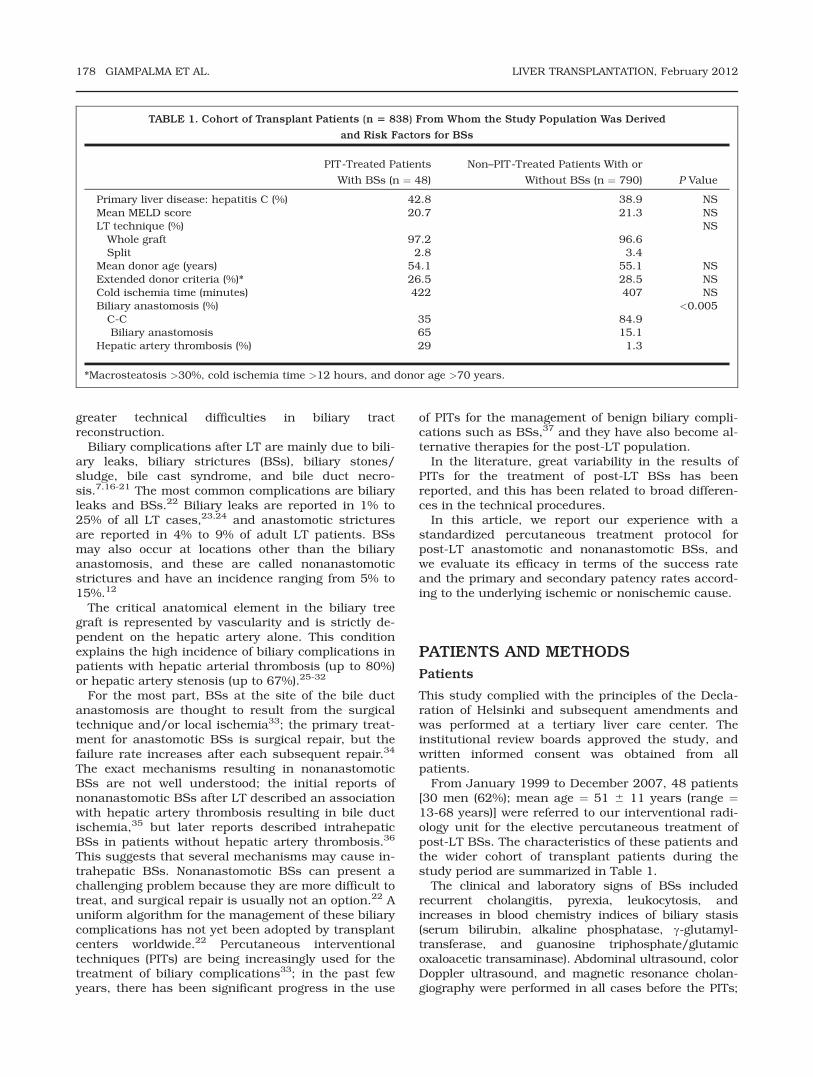
TABLE 1. Cohort of Transplant Patients (n 5 838) From Whom the Study Population Was Derived
and Risk Factors for BSs
PIT-Treated Patients
With BSs (n ¼ 48)
Non–PIT-Treated Patients With or
Without BSs (n ¼ 790) P Value
Primary liver disease: hepatitis C (%) 42.8 38.9 NSMean MELD score 20.7 21.3 NSLT technique (%) NSWhole graft 97.2 96.6Split 2.8 3.4
Mean donor age (years) 54.1 55.1 NSExtended donor criteria (%)* 26.5 28.5 NSCold ischemia time (minutes) 422 407 NSBiliary anastomosis (%) <0.005C-C 35 84.9Biliary anastomosis 65 15.1
Hepatic artery thrombosis (%) 29 1.3
*Macrosteatosis >30%, cold ischemia time >12 hours, and donor age >70 years.
178 GIAMPALMA ET AL. LIVER TRANSPLANTATION, February 2012
computed tomography/magnetic resonance angiogra-phy, conventional angiography, or both were performedin all cases with suspected hepatic artery thrombosisor hepatic artery stenosis on Doppler ultrasound.
Seventeen of the 48 patients (35%) underwent chol-edochocholedochostomy (C-C). Seven of these 17patients with anastomotic BSs refused endoscopic ret-rograde cholangiopancreatography as the primarytreatment; the other 10 patients had nonanastomoticintrahepatic BSs, so a PIT was used. Thirty-onepatients (65%) underwent biliary jejunostomy with aRoux-en-Y loop; 21 of these patients (68%) underwenthepaticojejunostomy (H-J), and 10 patients (32%)underwent choledochojejunostomy (C-J).
We defined as ischemic BSs those strictures associ-ated with a vascular problem (as demonstrated bycomputed tomography/magnetic resonance angiogra-phy or conventional angiography), such as hepatic ar-tery thrombosis, significant hepatic artery stenosis(>50% narrowing of the diameter of the artery), portalvein thrombosis, or ABO-incompatible LT. Nonische-mic BSs were defined as those not associated with theaforementioned vascular injuries.
The patients were divided into groups according tothe cause of the BSs (groups 1 and 2) and to the siteof the stenosis (groups A and B; Table 2).
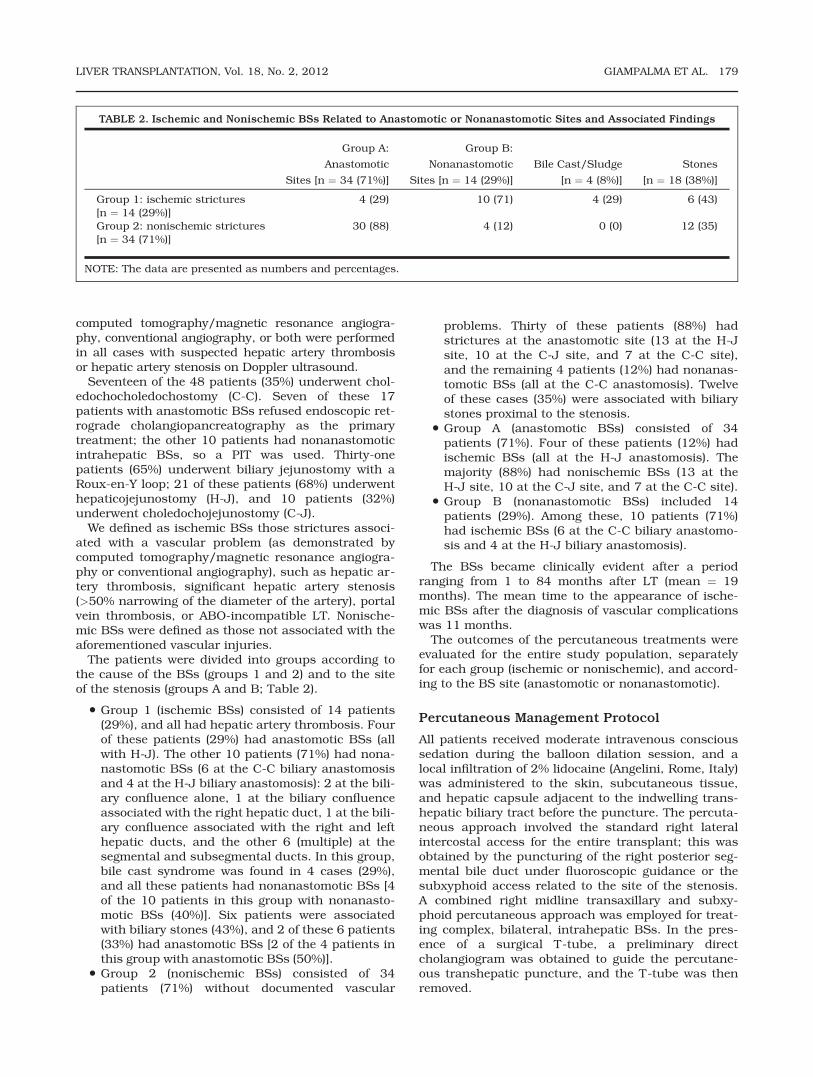
• Group 1 (ischemic BSs) consisted of 14 patients(29%), and all had hepatic artery thrombosis. Fourof these patients (29%) had anastomotic BSs (allwith H-J). The other 10 patients (71%) had nona-nastomotic BSs (6 at the C-C biliary anastomosisand 4 at the H-J biliary anastomosis): 2 at the bili-ary confluence alone, 1 at the biliary confluenceassociated with the right hepatic duct, 1 at the bili-ary confluence associated with the right and lefthepatic ducts, and the other 6 (multiple) at thesegmental and subsegmental ducts. In this group,bile cast syndrome was found in 4 cases (29%),and all these patients had nonanastomotic BSs [4of the 10 patients in this group with nonanasto-motic BSs (40%)]. Six patients were associatedwith biliary stones (43%), and 2 of these 6 patients(33%) had anastomotic BSs [2 of the 4 patients inthis group with anastomotic BSs (50%)].
• Group 2 (nonischemic BSs) consisted of 34patients (71%) without documented vascular
problems. Thirty of these patients (88%) hadstrictures at the anastomotic site (13 at the H-Jsite, 10 at the C-J site, and 7 at the C-C site),and the remaining 4 patients (12%) had nonanas-tomotic BSs (all at the C-C anastomosis). Twelveof these cases (35%) were associated with biliarystones proximal to the stenosis.
• Group A (anastomotic BSs) consisted of 34patients (71%). Four of these patients (12%) hadischemic BSs (all at the H-J anastomosis). Themajority (88%) had nonischemic BSs (13 at theH-J site, 10 at the C-J site, and 7 at the C-C site).
• Group B (nonanastomotic BSs) included 14patients (29%). Among these, 10 patients (71%)had ischemic BSs (6 at the C-C biliary anastomo-sis and 4 at the H-J biliary anastomosis).
The BSs became clinically evident after a periodranging from 1 to 84 months after LT (mean ¼ 19months). The mean time to the appearance of ische-mic BSs after the diagnosis of vascular complicationswas 11 months.
The outcomes of the percutaneous treatments wereevaluated for the entire study population, separatelyfor each group (ischemic or nonischemic), and accord-ing to the BS site (anastomotic or nonanastomotic).
Percutaneous Management Protocol
All patients received moderate intravenous conscioussedation during the balloon dilation session, and alocal infiltration of 2% lidocaine (Angelini, Rome, Italy)was administered to the skin, subcutaneous tissue,and hepatic capsule adjacent to the indwelling trans-hepatic biliary tract before the puncture. The percuta-neous approach involved the standard right lateralintercostal access for the entire transplant; this wasobtained by the puncturing of the right posterior seg-mental bile duct under fluoroscopic guidance or thesubxyphoid access related to the site of the stenosis.A combined right midline transaxillary and subxy-phoid percutaneous approach was employed for treat-ing complex, bilateral, intrahepatic BSs. In the pres-ence of a surgical T-tube, a preliminary directcholangiogram was obtained to guide the percutane-ous transhepatic puncture, and the T-tube was thenremoved.
TABLE 2. Ischemic and Nonischemic BSs Related to Anastomotic or Nonanastomotic Sites and Associated Findings
Group A:
Anastomotic
Sites [n ¼ 34 (71%)]
Group B:
Nonanastomotic
Sites [n ¼ 14 (29%)]
Bile Cast/Sludge
[n ¼ 4 (8%)]
Stones
[n ¼ 18 (38%)]
Group 1: ischemic strictures[n ¼ 14 (29%)]
4 (29) 10 (71) 4 (29) 6 (43)
Group 2: nonischemic strictures[n ¼ 34 (71%)]
30 (88) 4 (12) 0 (0) 12 (35)
NOTE: The data are presented as numbers and percentages.
LIVER TRANSPLANTATION, Vol. 18, No. 2, 2012 GIAMPALMA ET AL. 179

After preliminary percutaneous transhepatic chol-angiography, the stenosis was usually crossed withhydrophilic guide wires (Radifocus Guide Wire M, Ter-umo, Tokyo, Japan) and dilated with angioplasty-typeballoon catheters (BlueMax or Wanda, Boston Scien-tific, Medi-Tech, Watertown, MA), which were chosenaccording to the location of the stricture and the di-ameter of the normal bile duct adjacent to the stric-ture (range ¼ 4-14 mm). The balloon was inflated 2 to3 times consecutively for 1 to 5 minutes to reach thepressure required to eliminate a balloon waist. Thesuccess of each dilation was defined as the disappear-ance of the balloon waist during inflation.25,38
The dilation procedure (bilioplasty) was repeated inadditional sessions whenever a preliminary cholangio-graphic check showed residual/recurrent stenosisgreater than 30% (despite improvements in BSsaccording to images obtained at the end of the previ-ous session) with balloon size increments of 1 to 2mm. The stricture dilation was repeated every 15 to20 days; 4- to 8-mm balloons were used for the dila-tion of BSs extending into the secondary bile ducts,and 8- to 14-mm balloons were used for the dilationof extrahepatic strictures. After each dilation session,a transhepatic internal-external biliary catheter ofadequate caliber (8- to 14-Fr) for percutaneous trans-hepatic biliary drainage (Flexima, Boston Scientific,Medi-Tech) was left in place across the stenosis topreserve the lumen during the healing process and toallow external drainage for 1 to 2 days after each dila-tion in order to check for transient hemobilia; it wasthen capped for internal drainage until the re-evalua-tion. Transhepatic catheters were externally openedonly in cases of fever and/or cholangitis.
In those cases complicated by lithiasis, sludge/bili-ary casts, or both after bilioplasty, mechanical litho-tripsy was performed during the same session with a10-mm occlusion balloon catheter (Boston Scientific)and/or a Dormia basket (Olympus Medical SystemsCorp., Tokyo, Japan) to fragment and remove thestones. This was followed by multiple injections of acontrast medium or a saline solution to clean the bili-ary tree.
After each PIT, prophylaxis with short-term sys-temic antibiotics was used as recommended to pre-vent septic complications.33,39
The sequential treatment was considered completedand successfully concluded whenever no residualstricture could be seen or the residual stenosis wasless than 30%; therefore, the required number of dila-tion sessions was not limited to 3 sessions as previ-ously described by Zajko et al.25 The biliary drainagecatheter was subsequently removed after the assess-ment of the bile duct patency when the patient wasasymptomatic and did not have altered liver functiontests for 2 weeks after the drainage was capped.
Whenever the patency of the bile ducts was notrestored through dilation alone (ie, no cholangio-graphic response to balloon dilation with a balloonsize 20% to 25% larger than the estimated true size ofthe main biliary duct), stenosis recoil during subse-
quent cholangiography was observed, or the balloonwaist was absent during bilioplasty, metallic stentswere implanted (Wallstent, Boston Scientific, Medi-Tech) with diameters ranging from 7 to 12 mm. Stentpositioning was used only in patients refusing surgeryand in patients who had undergone H-J but whoseclinical/anatomical condition was not favorable forsurgical revision of the biliary anastomosis.
The follow-up consisted of clinical assessments andlaboratory examinations every 3 months; ultrasoundand magnetic resonance cholangiography were usedonly if the recurrence was suspicious.
PIT-related complications, which included majorcomplications [sepsis, hemobilia requiring a bloodtransfusion, bile leaks, pneumothorax, and death]and minor complications (transfusion and postdila-tion cholangitis),40-42 were recorded.
Statistical Analysis
For statistical analysis, PIT technical failure wasdefined as the inability to cross a BS with a percuta-neous route. Primary patency was defined as the timefrom the first balloon dilation to the diagnosis of therecurrent obstruction or the end of follow-up. Second-ary patency was defined as the total time from thefirst balloon dilation (including all subsequent PITinterventions) to the end of follow-up with a function-ing graft, retransplantation, or death.43
Fisher’s exact test was used to analyze the differen-ces in terms of the technical success rate betweenpatients with ischemic and nonischemic BSs andbetween patients with anastomotic and nonanasto-motic BSs. The primary and secondary patency rateswere estimated with the Kaplan-Meier method. AP value <0.05 was considered statistically significant.The log-rank test was used to analyze the differencesin terms of the primary and secondary patency ratesbetween patients with ischemic and nonischemic BSsand between patients with anastomotic and nonanas-tomotic BSs.
RESULTS
During the study period, the overall incidence of BSswas 7% (58 of 838 patients). Ten of the 58 patients(17%) with BSs after a C-C anastomosis were treatedwith endoscopic retrograde cholangiopancreatogra-phy. The remaining 48 patients (83%) with BSs weretreated percutaneously, and they constituted thestudy population: in 65% of these patients, the biliaryreconstruction was made with an H-J.
Vascular problems due to hepatic artery thrombosis(almost one-third of the study population) were themain reasons that a percutaneous approach wasrequired for BSs, and most showed intrahepatic BSs.
The technical success rate of PITs was 90%: a PITwas successful in 43 of the 48 patients. There were 5technical failures (10%). Four of these patients under-went C-C; 3 patients belonged to group 1 [3 of 14patients (21%)] with diffuse nonanastomotic BSs and
180 GIAMPALMA ET AL. LIVER TRANSPLANTATION, February 2012
underwent retransplantation; and 2 patients belongedto group 2 [2 of 34 patients (6%)] with anastomoticBSs after C-C and, after unsuccessful endoscopic ret-rograde cholangiopancreatography, ultimately under-went the surgical conversion of their C-C into an H-Jwith successful biliary reconstruction. There were nostatistical differences in terms of the technical suc-cess rates between the ischemic and nonischemicgroups (P ¼ 0.10) or between the anastomotic andnonanastomotic groups (P ¼ 0.10).
In the patients who were treated successfully (43patients), 2 different interventional radiologicalapproaches were used:
1. Bilioplasty alone and subsequent percutaneoustranshepatic biliary drainage were used in 34patients (79%): 26 with nonischemic BSs (76%)and 8 with ischemic BSs (24%). In cases compli-cated by lithiasis and/or sludge/biliary casts (22patients), mechanical lithotripsy was performedafter bilioplasty during the same session.
2. Bilioplasty was followed by metallic stent inser-tion in 9 of the 43 patients (21%; 2 after C-C and7 after H-J): 3 with ischemic BSs (33%) and 6with nonischemic stenoses (67%). Among thepatients with ischemic stenoses, 1 patient whohad multiple BSs received 3 metallic stents, 1received 2 stents, and the last received only 1stent. Among the patients with nonischemic BSs,1 patient received 3 stents, and the othersreceived only 1 stent. Seven of the 9 patients(78%) had undergone H-J; the remaining 2patients, who had nonischemic anastomoticstrictures on the C-C anastomosis (22%),received 1 stent each.
In group 1 (n ¼ 14), there were 3 technical failures;in 11 patients, bilioplasty was repeated 3 times on av-erage (range ¼ 1-7; Fig. 1). Bilioplasty alone was effec-tive in 8 patients; in the remaining 3, the insertion ofa metallic stent was necessary. Nine patients (82%)were recurrence-free. In the remaining 2 patients(18%) who were previously treated with metallicstents, the recurrence of BSs 36 and 12 months afterthe treatment (which was due to mucosal hyperplasiaassociated with stones) was percutaneously retreatedwith good results (secondary patency times of 96 and31 months, respectively, at the time of this writing).
In group 2 (n ¼ 34), there were 2 technical failures;32 patients underwent repeated bilioplasty for an av-erage of 2.4 times (range ¼ 1-11). Bilioplasty alonewas effective in 26 patients; 23 of these patients(88%) were recurrence-free, whereas 3 patients (12%)experienced BS recurrence and were then percutane-ously retreated.
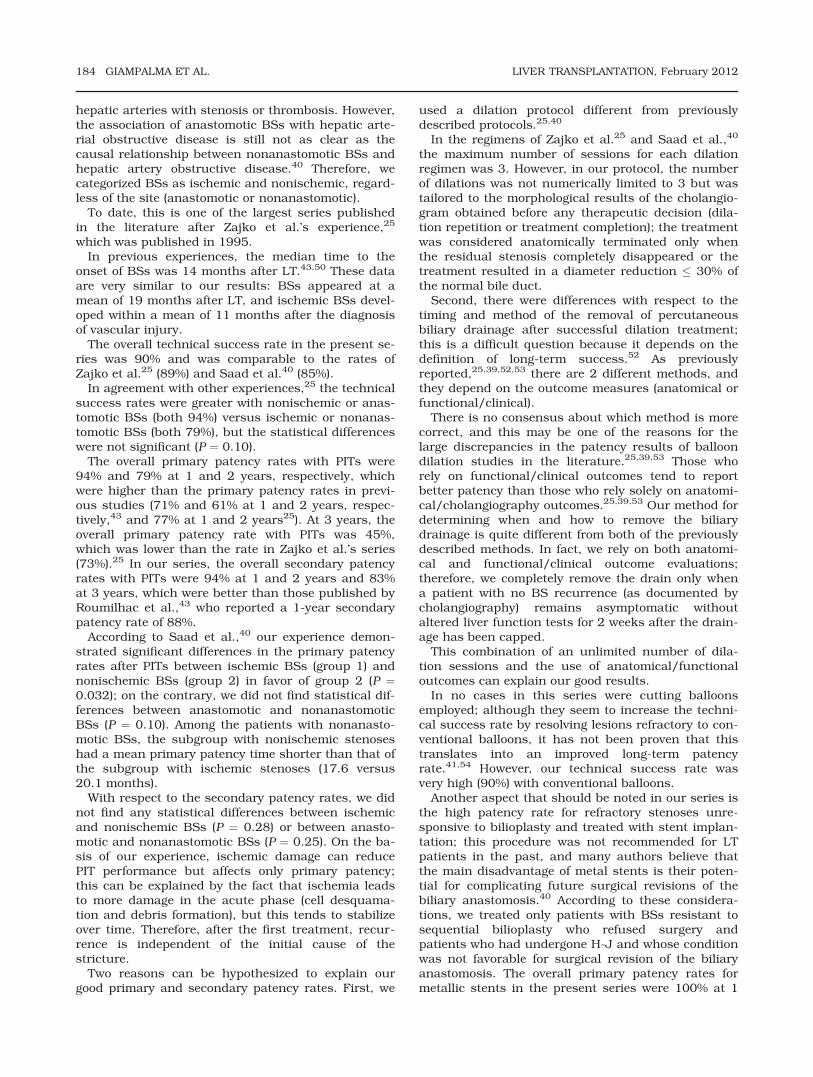
Bilioplasty alone was ineffective in 6 patients, sometallic stents were implanted. In 1 patient (17%),there was a recurrence of intrastent stenosis 13months after positioning because of mucosal hyper-plasia without stones. This was percutaneouslyretreated with good results (a secondary patency timeof 26 months; Fig. 2).
Forty-three of the 48 patients were treated success-fully, and 6 patients died from causes unrelated tobiliary complications.
Patency Rates According to Ischemic (Group 1)
and Nonischemic Etiologies (Group 2)
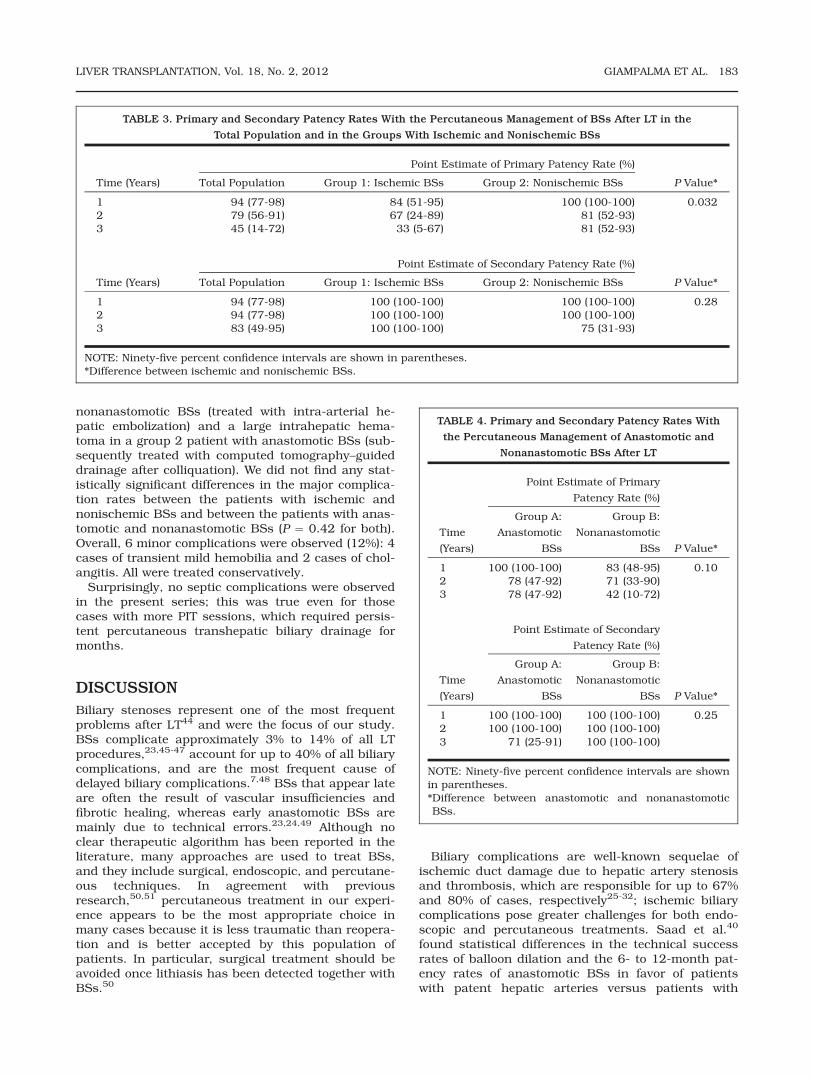
The primary and secondary patency rates with PITs inthe entire study population and in groups 1 and 2 aresummarized in Table 3. The primary patency rateswith PITs in the entire study population were 94%,79%, and 45% at 1, 2, and 3 years, respectively, andthe secondary patency rates were 94%, 94%, and83%. The differences in the primary patency ratesbetween groups 1 and 2 were statistically significantin favor of nonischemic BSs (P ¼ 0.032); in contrast,the differences in the secondary patency rates werenot statistically significant (P ¼ 0.28; Table 3).
Patency Rates According to Anastomotic
(Group A) and Nonanastomotic Sites (Group B)
for Biliary Stenoses
The 1-, 2-, and 3-year primary patency rates wereslightly better in group A versus group B, but they didnot differ statistically (P ¼ 0.10), and the secondarypatency rates were very similar (100%, 100%, and71% in group A and 100%, 100%, and 100% in groupB; Table 4). Among the patients with nonanastomoticBSs, those with nonischemic stenoses (n ¼ 4) hadslightly worse outcomes than those with ischemicstenoses with mean primary patency times of 17.6and 20.1 months, respectively.
Patency Rates of the Stent Subgroup
This group included 9 patients: 3 (33%) in group 1 [allwith nonanastomotic (H-J) BSs] and 6 (67%) in group2 [4 with nonanastomotic (H-J) BSs and 2 with anas-tomotic BSs on the C-C anastomosis]. As a result, 2patients (22%) were in group A (anastomotic BSs),and 7 patients (78%) were in group B (nonanasto-motic BSs).
The primary 1- and 2-year patency rates of thewhole group were 100% and 71%, respectively, andthe secondary patency rates were 100% and 100%,respectively.
Among the 6 patients with nonanastomotic intrahe-patic BSs treated with stents, 4 had primary patencytimes of 13, 17, 18, and 23 months, respectively; theremaining 2 patients had recurrent strictures due tostones associated with intrastent mucosal hyperpla-sia, and they were retreated percutaneously with sec-ondary patency times of 96 and 31 months,respectively.
Complications
Two major complications (4%) related to PITs wereobserved: severe hemobilia due to a distal arteriobili-ary fistula in a group 1 patient with multiple
LIVER TRANSPLANTATION, Vol. 18, No. 2, 2012 GIAMPALMA ET AL. 181
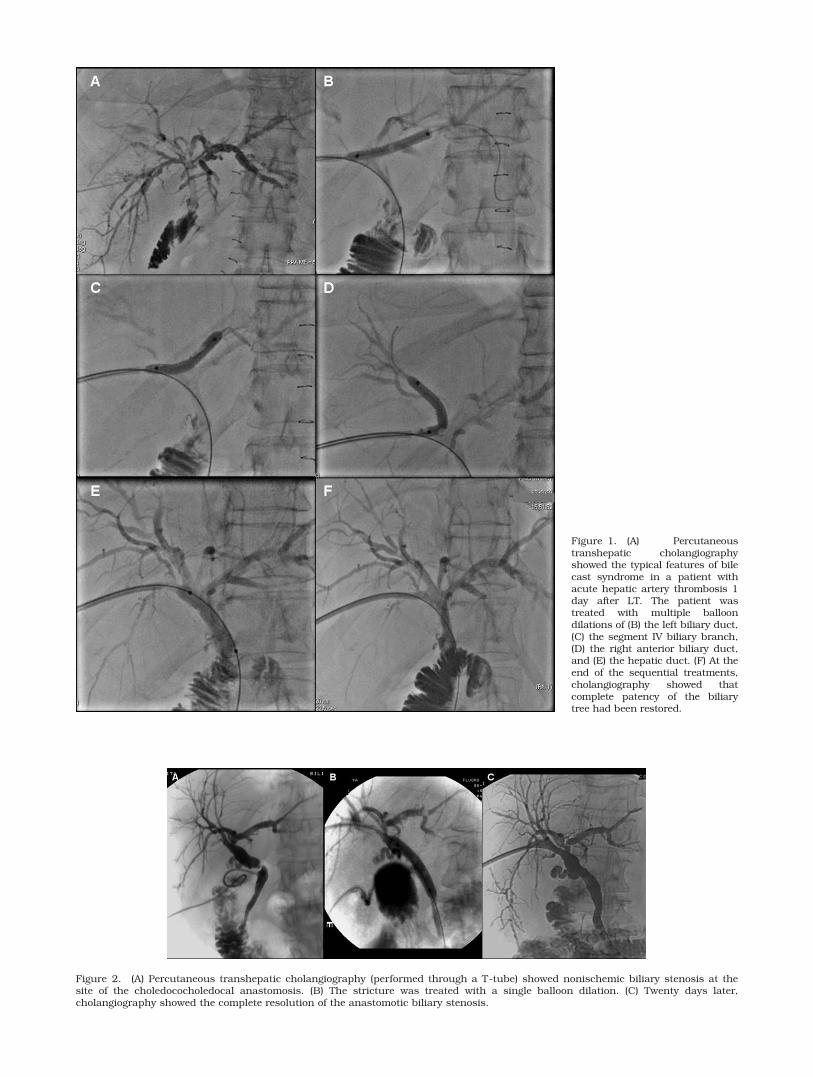
Figure 2. (A) Percutaneous transhepatic cholangiography (performed through a T-tube) showed nonischemic biliary stenosis at thesite of the choledococholedocal anastomosis. (B) The stricture was treated with a single balloon dilation. (C) Twenty days later,cholangiography showed the complete resolution of the anastomotic biliary stenosis.
Figure 1. (A) Percutaneoustranshepatic cholangiographyshowed the typical features of bilecast syndrome in a patient withacute hepatic artery thrombosis 1day after LT. The patient wastreated with multiple balloondilations of (B) the left biliary duct,(C) the segment IV biliary branch,(D) the right anterior biliary duct,and (E) the hepatic duct. (F) At theend of the sequential treatments,cholangiography showed thatcomplete patency of the biliarytree had been restored.
nonanastomotic BSs (treated with intra-arterial he-patic embolization) and a large intrahepatic hema-toma in a group 2 patient with anastomotic BSs (sub-sequently treated with computed tomography–guideddrainage after colliquation). We did not find any stat-istically significant differences in the major complica-tion rates between the patients with ischemic andnonischemic BSs and between the patients with anas-tomotic and nonanastomotic BSs (P ¼ 0.42 for both).Overall, 6 minor complications were observed (12%): 4cases of transient mild hemobilia and 2 cases of chol-angitis. All were treated conservatively.
Surprisingly, no septic complications were observedin the present series; this was true even for thosecases with more PIT sessions, which required persis-tent percutaneous transhepatic biliary drainage formonths.
DISCUSSION
Biliary stenoses represent one of the most frequentproblems after LT44 and were the focus of our study.BSs complicate approximately 3% to 14% of all LTprocedures,23,45-47 account for up to 40% of all biliarycomplications, and are the most frequent cause ofdelayed biliary complications.7,48 BSs that appear lateare often the result of vascular insufficiencies andfibrotic healing, whereas early anastomotic BSs aremainly due to technical errors.23,24,49 Although noclear therapeutic algorithm has been reported in theliterature, many approaches are used to treat BSs,and they include surgical, endoscopic, and percutane-ous techniques. In agreement with previousresearch,50,51 percutaneous treatment in our experi-ence appears to be the most appropriate choice inmany cases because it is less traumatic than reopera-tion and is better accepted by this population ofpatients. In particular, surgical treatment should beavoided once lithiasis has been detected together withBSs.50
Biliary complications are well-known sequelae ofischemic duct damage due to hepatic artery stenosisand thrombosis, which are responsible for up to 67%and 80% of cases, respectively25-32; ischemic biliarycomplications pose greater challenges for both endo-scopic and percutaneous treatments. Saad et al.40
found statistical differences in the technical successrates of balloon dilation and the 6- to 12-month pat-ency rates of anastomotic BSs in favor of patientswith patent hepatic arteries versus patients with
TABLE 3. Primary and Secondary Patency Rates With the Percutaneous Management of BSs After LT in the
Total Population and in the Groups With Ischemic and Nonischemic BSs
Time (Years)
Point Estimate of Primary Patency Rate (%)
P Value*Total Population Group 1: Ischemic BSs Group 2: Nonischemic BSs
1 94 (77-98) 84 (51-95) 100 (100-100) 0.0322 79 (56-91) 67 (24-89) 81 (52-93)3 45 (14-72) 33 (5-67) 81 (52-93)
Time (Years)
Point Estimate of Secondary Patency Rate (%)
P Value*Total Population Group 1: Ischemic BSs Group 2: Nonischemic BSs
1 94 (77-98) 100 (100-100) 100 (100-100) 0.282 94 (77-98) 100 (100-100) 100 (100-100)3 83 (49-95) 100 (100-100) 75 (31-93)
NOTE: Ninety-five percent confidence intervals are shown in parentheses.*Difference between ischemic and nonischemic BSs.
TABLE 4. Primary and Secondary Patency Rates With
the Percutaneous Management of Anastomotic and
Nonanastomotic BSs After LT
Time
(Years)
Point Estimate of Primary
Patency Rate (%)
P Value*
Group A:
Anastomotic
BSs
Group B:
Nonanastomotic
BSs
1 100 (100-100) 83 (48-95) 0.102 78 (47-92) 71 (33-90)3 78 (47-92) 42 (10-72)
Time
(Years)
Point Estimate of Secondary
Patency Rate (%)
P Value*
Group A:
Anastomotic
BSs
Group B:
Nonanastomotic
BSs
1 100 (100-100) 100 (100-100) 0.252 100 (100-100) 100 (100-100)3 71 (25-91) 100 (100-100)
NOTE: Ninety-five percent confidence intervals are shownin parentheses.*Difference between anastomotic and nonanastomoticBSs.
LIVER TRANSPLANTATION, Vol. 18, No. 2, 2012 GIAMPALMA ET AL. 183
hepatic arteries with stenosis or thrombosis. However,the association of anastomotic BSs with hepatic arte-rial obstructive disease is still not as clear as thecausal relationship between nonanastomotic BSs andhepatic artery obstructive disease.40 Therefore, wecategorized BSs as ischemic and nonischemic, regard-less of the site (anastomotic or nonanastomotic).
To date, this is one of the largest series publishedin the literature after Zajko et al.’s experience,25
which was published in 1995.In previous experiences, the median time to the
onset of BSs was 14 months after LT.43,50 These dataare very similar to our results: BSs appeared at amean of 19 months after LT, and ischemic BSs devel-oped within a mean of 11 months after the diagnosisof vascular injury.
The overall technical success rate in the present se-ries was 90% and was comparable to the rates ofZajko et al.25 (89%) and Saad et al.40 (85%).
In agreement with other experiences,25 the technicalsuccess rates were greater with nonischemic or anas-tomotic BSs (both 94%) versus ischemic or nonanas-tomotic BSs (both 79%), but the statistical differenceswere not significant (P ¼ 0.10).
The overall primary patency rates with PITs were94% and 79% at 1 and 2 years, respectively, whichwere higher than the primary patency rates in previ-ous studies (71% and 61% at 1 and 2 years, respec-tively,43 and 77% at 1 and 2 years25). At 3 years, theoverall primary patency rate with PITs was 45%,which was lower than the rate in Zajko et al.’s series(73%).25 In our series, the overall secondary patencyrates with PITs were 94% at 1 and 2 years and 83%at 3 years, which were better than those published byRoumilhac et al.,43 who reported a 1-year secondarypatency rate of 88%.
According to Saad et al.,40 our experience demon-strated significant differences in the primary patencyrates after PITs between ischemic BSs (group 1) andnonischemic BSs (group 2) in favor of group 2 (P ¼0.032); on the contrary, we did not find statistical dif-ferences between anastomotic and nonanastomoticBSs (P ¼ 0.10). Among the patients with nonanasto-motic BSs, the subgroup with nonischemic stenoseshad a mean primary patency time shorter than that ofthe subgroup with ischemic stenoses (17.6 versus20.1 months).
With respect to the secondary patency rates, we didnot find any statistical differences between ischemicand nonischemic BSs (P ¼ 0.28) or between anasto-motic and nonanastomotic BSs (P ¼ 0.25). On the ba-sis of our experience, ischemic damage can reducePIT performance but affects only primary patency;this can be explained by the fact that ischemia leadsto more damage in the acute phase (cell desquama-tion and debris formation), but this tends to stabilizeover time. Therefore, after the first treatment, recur-rence is independent of the initial cause of thestricture.
Two reasons can be hypothesized to explain ourgood primary and secondary patency rates. First, we
used a dilation protocol different from previouslydescribed protocols.25,40
In the regimens of Zajko et al.25 and Saad et al.,40
the maximum number of sessions for each dilationregimen was 3. However, in our protocol, the numberof dilations was not numerically limited to 3 but wastailored to the morphological results of the cholangio-gram obtained before any therapeutic decision (dila-tion repetition or treatment completion); the treatmentwas considered anatomically terminated only whenthe residual stenosis completely disappeared or thetreatment resulted in a diameter reduction � 30% ofthe normal bile duct.
Second, there were differences with respect to thetiming and method of the removal of percutaneousbiliary drainage after successful dilation treatment;this is a difficult question because it depends on thedefinition of long-term success.52 As previouslyreported,25,39,52,53 there are 2 different methods, andthey depend on the outcome measures (anatomical orfunctional/clinical).
There is no consensus about which method is morecorrect, and this may be one of the reasons for thelarge discrepancies in the patency results of balloondilation studies in the literature.25,39,53 Those whorely on functional/clinical outcomes tend to reportbetter patency than those who rely solely on anatomi-cal/cholangiography outcomes.25,39,53 Our method fordetermining when and how to remove the biliarydrainage is quite different from both of the previouslydescribed methods. In fact, we rely on both anatomi-cal and functional/clinical outcome evaluations;therefore, we completely remove the drain only whena patient with no BS recurrence (as documented bycholangiography) remains asymptomatic withoutaltered liver function tests for 2 weeks after the drain-age has been capped.
This combination of an unlimited number of dila-tion sessions and the use of anatomical/functionaloutcomes can explain our good results.
In no cases in this series were cutting balloonsemployed; although they seem to increase the techni-cal success rate by resolving lesions refractory to con-ventional balloons, it has not been proven that thistranslates into an improved long-term patencyrate.41,54 However, our technical success rate wasvery high (90%) with conventional balloons.
Another aspect that should be noted in our series isthe high patency rate for refractory stenoses unre-sponsive to bilioplasty and treated with stent implan-tation; this procedure was not recommended for LTpatients in the past, and many authors believe thatthe main disadvantage of metal stents is their poten-tial for complicating future surgical revisions of thebiliary anastomosis.40 According to these considera-tions, we treated only patients with BSs resistant tosequential bilioplasty who refused surgery andpatients who had undergone H-J and whose conditionwas not favorable for surgical revision of the biliaryanastomosis. The overall primary patency rates formetallic stents in the present series were 100% at 1
184 GIAMPALMA ET AL. LIVER TRANSPLANTATION, February 2012

year and 71% at 2 years; these results are morepromising than those of larger series,33 which havereported unsatisfactory primary patency rates for ex-pandable stents of 68% and approximately 51% at 1and 2 years, respectively. The secondary patencyrates in the stent subgroup were 100% at 1 and 2years and 75% at 3 years; the rate at 3 years wasslightly lower than the rate observed by Culp et al.33
(94%, approximately 93%, and 88% at 1, 2, and 3years, respectively), probably because of our unfavor-able bias selection.
In our series, only uncovered, self-expandablestents were used; covered stents did not prove suc-cessful because the first results obtained with coveredstents did not confirm the expectations of higher pat-ency rates.50
The last aspect that should be noted is the accept-ably low rate of complications in our series; the majorcomplication rate was 4%, and there were no statisti-cal differences between the ischemic and nonischemicgroups or between the anastomotic and nonanasto-motic groups. In our series, we observed 1 case ofsevere hemobilia and 1 wide intrahepatic hematoma,but we did not experience any other serious complica-tions such as sepsis. One reason might be that theuse of short-term systemic antibiotics prevented thesecomplications effectively; this has been reported byother authors.33,39 Another more important reasonmight be the absence of donors after circulatory deathin our LT series. This is one of the strategies used toincrease the donor pool; it has been applied in a fewcountries, but at the moment is not allowed in Italy. Itis well known that BSs are among the most frequentcomplications after LT involving donors after circula-tory death; retransplantation is often required.55,56
Because we did not use donors after circulatory deathin the present series, this may in part explain the ab-sence of severe septic complications in our patientswith BSs. The minor complication rate was 12%.These data cannot be compared to those of other pub-lished studies because they were evaluated withrespect to the number of patients and not to theprocedures.
In conclusion, an excellent technical success ratewith long-term primary and secondary patency andvery low rates of septic complications (or none) can beachieved with PITs for post-LT BSs in experiencedcenters using a standardized protocol. The results areindependent of the BS location (anastomotic or nona-nastomotic). The best results can be obtained forpatients with simple, nonischemic BSs (technical suc-cess rate ¼ 94%, 3-year primary patency rate ¼ 81%,3-year secondary patency rate ¼ 75%). For ischemicand complex BSs, which pose greater challenges forany treatment other than retransplantation, even afterdiscouraging 2- and 3-year primary patency rates of67% and 33% were obtained, more promising 2- and3-year secondary patency rates of 100% and 100%were observed, which were similar to or even betterthan those for nonischemic stenoses (100% and 75%,respectively). Ischemic stenoses should, therefore, be
more strictly monitored and more frequently treatedthan nonischemic stenoses in order to obtain satisfac-tory long-term results. In our series, in the last 10years, retransplantation has never been required forBSs.
More recently, retrievable covered stents werereported to be more suitable for treating BSs afterLT57-59; however, these preliminary experiences dealtwith small groups of LT recipients (<8) during shortfollow-up periods57,58 or with only anastomotic BSs.59
Therefore, while we are awaiting more consistentresults for these new and promising devices, bilio-plasty should always be considered the first-lineapproach for the management of BSs and especiallymultiple nonanastomotic intrahepatic BSs. Metallic,self-expandable stents can be proposed as a second-line treatment for refractory stenoses in selectpatients, such as those who have undergone unsuc-cessful H-J and are not candidates for surgical revi-sion because of unfavorable clinical/anatomical con-ditions. In these patients, stent placement as the lasttherapeutic choice allows stricture resolution withgood long-term patency and thus prevents immediateretransplantation in the present era of long transplantwaiting lists.
REFERENCES
1. Quiroga S, Sebastia MC, Margarit C, Castells L, Boye R,Alvarez-Castells A. Complications of orthotopic livertransplantation: spectrum of findings with helical CT.Radiographics 2001;21:1085-1102.
2. Shaw AS, Ryan SM, Beese RC, Sidhu PS. Ultrasound ofnon-vascular complications in the post liver transplantpatient. Clin Radiol 2003;58:672-680.
3. Holbert BL, Campbell WL, Skolnick ML. Evaluation ofthe transplanted liver and postoperative complications.Radiol Clin North Am 1995;33:521-540.
4. Nghiem HV, Tran K, Winter TC III, Schmiedl UP, AlthausSJ, Patel NH, Freeny PC. Imaging of complications inliver transplantation. Radiographics 1996;16:825-840.
5. D’Alessandro AM, Kalayoglu M, Pirsch JD, Sollinger HW,Reed A, Knechtle SJ, et al. Biliary tract complications af-ter orthotopic liver transplantation. Transplant Proc1991;23:1956.
6. Colonna JO II, Shaked A, Gomes AS, Colquhoun SD,Jurim O, McDiarmid SV, et al. Biliary strictures compli-cating liver transplantation. Incidence, pathogenesis,management, and outcome. Ann Surg 1992;216:344-350.
7. Greif F, Bronsther OL, Van Thiel DH, Casavilla A, Iwat-suki S, Tzakis A, et al. The incidence, timing and man-agement of biliary tract complications after orthotopicliver transplantation. Ann Surg 1994;219:40-45.
8. Rossi G, Lucianetti A, Gridelli B, Colledan M, CaccamoL, Albani AP, et al. Biliary tract complications in 224orthotopic liver transplantations. Transplant Proc 1994;26:3626-3628.
9. Neuhaus P, Blumhardt G, Bechstein WO, Steffen R, PlatzKP, Keck H. Technique and results of biliary reconstruc-tion using side-to-side choledochocholedochostomy in300 orthotopic liver transplants. Ann Surg 1994;219:426-434.
10. Verran DJ, Asfar SK, Ghent CN, Grant DR, Wall WJ. Bili-ary reconstruction without T tubes or stents in livertransplantation: report of 502 consecutive cases. LiverTranspl Surg 1997;3:365-373.
LIVER TRANSPLANTATION, Vol. 18, No. 2, 2012 GIAMPALMA ET AL. 185
11. Moser MA, Wall WJ. Management of biliary problems af-ter liver transplantation. Liver Transpl 2001;7(suppl 1):S46-S52.
12. Thethy S, Thomson BNJ, Pleass H, Wigmore SJ, Madha-van K, Akyol M, et al. Management of biliary tract com-plications after orthotopic liver transplantation. ClinTransplant 2004;18:647-653.
13. Icoz G, Kilic M, Zeytunlu M, Celebi A, Ersoz G, Killi R,et al. Biliary reconstructions and complications encoun-tered in 50 consecutive right-lobe living donor livertransplantations. Liver Transpl 2003;9:575-580.
14. Gondolesi GE, Varotti G, Florman SS, Munoz L, FishbeinTM, Emre SH, et al. Biliary complications in 96 consecu-tive right lobe living donor transplant recipients. Trans-plantation 2004;77:1842-1848.
15. Kawachi S, Shimazu M, Wakabayashi G, Hoshino K,Tanabe M, Yoshida M, et al. Biliary complications inadult living donor liver transplantation with duct-to-ducthepaticocholedochostomy or Roux-en-Y hepaticojejunos-tomy biliary reconstruction. Surgery 2002;132:48-56.
16. Stratta RJ, Wood RP, Langnas AN, Hollins RR, BruderKJ, Donovan JP, et al. Diagnosis and treatment of biliarytract complications after orthotopic liver transplantation.Surgery 1989;106:675-683.
17. Letourneau JG, Hunter DW, Payne WD, Day DL. Picto-rial essay. Imaging of and intervention for biliary compli-cations after hepatic transplantation. AJR Am JRoentgenol 1990;154:729-733.
18. Barton P, Steininger R, Maier A, Muhlbacher F, LechnerG. Biliary sludge after liver transplantation: 2. Treatmentwith interventional techniques versus surgery and/or oralchemolysis. AJR Am J Roentgenol 1995;164:865-869.
19. Kuo PC, Lewis WD, Stokes K, Pleskow D, Simpson MA,Jenkins RL. A comparison of operation, endoscopic ret-rograde cholangiopancreatography, and percutaneoustranshepatic cholangiography in biliary complications af-ter hepatic transplantation. J Am Coll Surg 1994;179:177-181.
20. Srinivasaiah N, Reddy MS, Balupuri S, Talbot D, JaquesB, Manas D. Biliary cast syndrome: literature review anda single centre experience in liver transplant recipients.Hepatobiliary Pancreat Dis Int 2008;7:300-303.
21. Shah JN, Haigh WG, Lee SP, Lucey MR, Brensinger CM,Kochman ML, et al. Biliary casts after orthotopic livertransplantation: clinical factors, treatment, biochemicalanalysis. Am J Gastroenterol 2003;98:1861-1867.
22. Buck DG, Zajko AB. Biliary complications after ortho-topic liver transplantation. Tech Vasc Interv Radiol 2008;11:51-59.
23. Tung BY, Kimmey MB. Biliary complications of ortho-topic liver transplantation. Dig Dis 1999;17:133-144.
24. Jagannath S, Kalloo AN. Biliary complications after livertransplantation. Curr Treat Options Gastroenterol 2002;5:101-112.
25. Zajko AB, Sheng R, Zetti GM, Madariaga JR, Bron KM.Transhepatic balloon dilation of biliary strictures in livertransplant patients: a 10-year experience. J Vasc IntervRadiol 1995;6:79-83.
26. Zajko AB, Campbell WL, Bron KM, Schade RR, KoneruB, Van Thiel DH. Diagnostic and interventional radiologyin liver transplantation. Gastroenterol Clin North Am1988;17:105-143.
27. Orons PD, Sheng R, Zajko AB. Hepatic artery stenosis inliver transplant recipients: prevalence and cholangio-graphic appearance of associated biliary complications.AJR Am J Roentgenol 1995;165:1145-1149.
28. Lerut JP, Gordon RD, Iwatsuki S, Starzl TE. Humanorthotopic liver transplantation: surgical aspects in 393consecutive grafts. Transplant Proc 1988;20(suppl 1):603-606.
29. Tzakis AG. The dearterialized liver graft. Semin Liver Dis1985;5:375-376.
30. Sanchez-Urdazpal L, Gores GJ, Ward EM, Maus TP,Wahlstrom HE, Moore SB, et al. Ischemic-type biliarycomplications after orthotopic liver transplantation. He-patology 1992;16:49-53.
31. Egawa H, Inomata Y, Uemoto S, Asonuma K, Kiuchi T,Fujita S, et al. Biliary anastomotic complications in 400living related liver transplantations. World J Surg 2001;25:1300-1307.
32. Margarit C, Hidalgo E, Lazaro JL, Murio E, Charco R,Balsells J. Biliary complications secondary to late he-patic artery thrombosis in adult liver transplant patients.Transpl Int 1998;11(suppl 1):S251-S254.
33. Culp WC, McCowan TC, Lieberman RP, Goertzen TC,LeVeen RF, Heffron TG. Biliary strictures in liver trans-plant recipients: treatment with metal stents. Radiology1996;199:339-346.
34. Pitt HA, Miyamoto T, Parapatis SK, Tompkins RK, Long-mire WP Jr. Factors influencing outcome in patients withpostoperative biliary strictures. Am J Surg 1982;144:14-21.
35. Zajko AB, Campbell WL, Logsdon GA, Bron KM, TzakisA, Esquivel CO, Starzl TE. Cholangiographic findings inhepatic artery occlusion after liver transplantation. AJRAm J Roentgenol 1987;149:485-489.
36. Sanchez-Urdazpal L, Sterioff S, Janes C, Schwerman L,Rosen C, Krom RA. Increased bile duct complications inABO incompatible liver transplant recipients. TransplantProc 1991;23(pt 2):1440-1441.
37. Rieber A, Brambs HJ, Lauchart W. The radiological man-agement of biliary complications following liver transplan-tation. Cardiovasc Intervent Radiol 1996;19:242-247.
38. Z’graggen K, Wehrli H, Metzger A, Buehler M, Frei E,Klaiber C. Complications of laparoscopic cholecystectomyin Switzerland. A prospective 3-year study of 10,174patients. Swiss Association of Laparoscopic and Thoraco-scopic Surgery. Surg Endosc 1998;12:1303-1310.
39. Ward EM, Kiely MJ, Maus TP, Wiesner RH, Krom RA.Hilar biliary strictures after liver transplantation: cholan-giography and percutaneous treatment. Radiology 1990;177:259-263.
40. Saad WE, Saad NE, Davies MG, Lee DE, Patel NC, SahlerLG, et al. Transhepatic balloon dilation of anastomoticbiliary strictures in liver transplant recipients: the signif-icance of a patent hepatic artery. J Vasc Interv Radiol2005;16:1221-1228.
41. Saad WE, Davies MG, Saad NE, Waldman DL, SahlerLG, Lee DE, et al. Transhepatic dilation of anastomoticbiliary strictures in liver transplant recipients with useof a combined cutting and conventional balloon protocol:technical safety and efficacy. J Vasc Interv Radiol 2006;17:837-843.
42. Winick AB, Waybill PN, Venbrux AC. Complications ofpercutaneous transhepatic biliary interventions. TechVasc Interv Radiol 2001;4:200-206.
43. Roumilhac D, Poyet G, Sergent G, Declerck N, Karoui M,Mathurin P, et al. Long-term results of percutaneousmanagement for anastomotic biliary stricture after ortho-topic liver transplantation. Liver Transpl 2003;9:394-400.
44. Cameron AM, Busuttil RW. Ischemic cholangiopathy af-ter liver transplantation. Hepatobiliary Pancreat Dis Int2005;4:495-501.
45. Thuluvath PJ, Pfau PR, Kimmey MB, Ginsberg GG. Bili-ary complications after liver transplantation: the role ofendoscopy. Endoscopy 2005;37:857-863.
46. Graziadei IW. Recurrence of primary sclerosing cholangi-tis after liver transplantation. Liver Transpl 2002;8:575-581.
186 GIAMPALMA ET AL. LIVER TRANSPLANTATION, February 2012
47. Goss JA, Shackleton CR, Farmer DG, Arnaout WS, SeuP, Markowitz JS, et al. Orthotopic liver transplantationfor primary sclerosing cholangitis. A 12-year single cen-ter experience. Ann Surg 1997;225:472-481.
48. Porayko MK, Kondo M, Steers JL. Liver transplantation:late complications of the biliary tract and their manage-ment. Semin Liver Dis 1995;15:139-155.
49. Testa G, Malago M, Broelseh CE. Complications of biliarytract in liver transplantation. World J Surg 2001;25:1296-1299.
50. Righi D, Cesarani F, Muraro E, Gazzera C, Salizzoni M,Gandini G. Role of interventional radiology in the treat-ment of biliary strictures following orthotopic liver trans-plantation. Cardiovasc Intervent Radiol 2002;25:30-35.
51. Bouttier E, Arrive L, Rotenberg L, Balladur P, Chazouil-leres O, Mostefa-Kara N, et al. Non-surgical treatment ofbiliary stenoses after hepatic transplantation [in French].J Radiol 1997;78:485-489.
52. Saad WE. Percutaneous management of postoperativeanastomotic biliary strictures. Tech Vasc Interv Radiol2008;11:143-153.
53. McDonald V, Matalon TA, Patel SK, Brunner MC, Sank-ary H, Foster P, Williams J. Biliary strictures in hepatictransplantation. J Vasc Interv Radiol 1991;2:533-538.
54. Atar E, Bachar GN, Bartal G, Mor E, Neyman H, GraifF, Belenky A. Use of peripheral cutting balloon in
the management of resistant benign ureteral andbiliary strictures. J Vasc Interv Radiol 2005;16(pt 1):241-245.
55. Foley DP, Fernandez LA, Leverson G, Anderson M, Mez-rich J, Sollinger HW, D’Alessandro A. Biliary complica-tions after liver transplantation from donation aftercardiac death donors: an analysis of risk factors andlong-term outcomes from a single center. Ann Surg2011;253:817-825.
56. Wigmore SJ. Current challenges in liver transplantationfollowing donation after cardiac death. Transplantation2010;90:1048-1049.
57. Petersen BD, Timmermans HA, Uchida BT, Rabkin JM,Keller FS. Treatment of refractory benign biliary stenosesin liver transplant patients by placement and retrieval ofa temporary stent-graft: work in progress. J Vasc IntervRadiol 2000;11:919-929.
58. Kuo MD, Lopresti DC, Gover DD, Hall LD, Ferrara SL.Intentional retrieval of Viabil stent-grafts from the bili-ary system. J Vasc Interv Radiol 2006;17(pt 1):389-397.
59. Kim J, Ko GY, Sung KB, Gwon DI, Lee SG, Kim KM,et al. Percutaneously placed covered retrievable stentsfor the treatment of biliary anastomotic strictures follow-ing living donor liver transplantation. Liver Transpl2010;16:1410-1420.
LIVER TRANSPLANTATION, Vol. 18, No. 2, 2012 GIAMPALMA ET AL. 187