Orthopedic Surgery in the United States Army - Oxford Academic
7
MILITARY MEDICINE, Vol. 176, June 2011 689 MILITARY MEDICINE, 176, 6:689, 2011 INTRODUCTION Although only recognized as an independent discipline at the end of the 19th century, orthopedic surgery had developed over the course of millennia with many significant develop- ments engendered during times of war. Although this associa- tion between military surgery and what we presently accept as orthopedics reaches back to the ancient period, the contribu- tions of American military practitioners to the development of orthopedic surgery cannot be overlooked. Arguably, the experiences of American military surgeons in conflicts from the Civil War to the present have continued to reinvigorate the orthopedic discipline, resulting in important developments within the field, as well as scientific discoveries that have gone on to benefit the civilian and military communities. Before the technological advancements that potentiated the modern sur- gical specialties, it is even possible to maintain that the major- ity of what constituted American military combat surgery, from the Revolution to the First World War, was orthopedic in nature: removal of bullets and shrapnel, soft tissue care, set- ting of fractures, and extremity amputation. The goal of this review is to survey the U.S. Army’s ortho- pedic experience from the period of the American Revolution to the current conflicts in Iraq and Afghanistan. It is hoped that, through this report, the reader may gain a better apprecia- tion for the significant contributions American combat ortho- pedics has made to the development of the field as a whole. EARLY BEGINNINGS: THE AMERICAN REVOLUTION (1775) TO 1860 The United States Army Medical Department and the Medical Corps trace their origins to the founding of the United States Army Hospital department on July 27, 1775, only 10 days after the Battle of Bunker Hill. 1 The department, under the direction of Surgeon General Benjamin Church, was charged with supplying the fledgling units of the Continental Army with military surgeons who could provide battlefield care and administer to the wounded. Each Army regiment was autho- rized 1 surgeon. At the time, medical education within the United States was not standardized and the vast majority of physicians obtained their education through an apprentice system. Almost none of the American military surgeons had prior combat experience, including the Surgeon General. The surgeons of the Continental Army had limited resources, as well as a truncated understanding of the patho- physiological mechanisms of trauma, infection, and wound healing. These individuals were most effective at removing bullet fragments or shrapnel from superficial wounds, debrid- ing devitalized tissue, and setting fractured limbs. 1–4 The fear of sepsis led to a substantial reliance on extremity amputa- tions, particularly in the event of soft-tissue compromise or comminuted fractures. In most instances, wounds were not cleansed at all or they were irrigated with what standing water was available. During the Battle of Harlem Heights (1776), however, Continental Army Surgeon Charles Gillman used alcohol to treat combat wounds and later reported on the ben- efits of this process. His practices, however, were not adopted by other practitioners in the Continental Army. 3 In an effort to standardize some of the practices used to treat American war wounded, Continental Army Surgeon John Jones (Fig. 1) authored the first American surgical text “[O]n the Treatment of Wounds and Fractures: Designed for the Use of Young Military Surgeons in North America.” 5 The text, devoted almost entirely to what would now be consid- ered the purview of an orthopedic surgeon, cautioned army surgeons to respect the soft tissue envelope, remove bone fragments and foreign bodies as atraumatically as possible, and use bark emollients as a means of cautery. Amputations, unless needed to save a soldier’s life, were to be delayed until the individual was determined to be stable from a medical standpoint. Open fractures were to be treated with debride- ment and an attempt at reduction. 5 Although other surgeons expounded principles from the standpoint of medical theory, Jones was one of the few military Orthopedic Surgery in the United States Army: A Historical Review MAJ Andrew J. Schoenfeld, MC USA ABSTRACT The contribution of American military surgeons to the development of orthopedic surgery has not previously been explored. The experiences of American military surgeons in conflicts from the Civil War to Iraq and Afghanistan have advanced the orthopedic discipline, resulting in important developments within the field, as well as sci- entific discoveries that have benefited both the civilian and military communities. From advances in wound care, to spinal surgery, intramedullary nailing of long bone fractures, and external fixation, American military surgeons have been pio- neers of orthopedic surgery. The goal of this review was to survey the American military orthopedic experience from the American Revolution to the wars in Iraq and Afghanistan. Department of Orthopaedic Surgery, William Beaumont Army Medical Center, Texas Tech University Health Sciences Center, 5005 North Piedras Street, El Paso, TX 79920. Downloaded from https://academic.oup.com/milmed/article/176/6/689/4345447 by guest on 20 July 2022
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Orthopedic Surgery in the United States Army - Oxford Academic

MILITARY MEDICINE, Vol. 176, June 2011 689
MILITARY MEDICINE, 176, 6:689, 2011
INTRODUCTION Although only recognized as an independent discipline at the end of the 19th century, orthopedic surgery had developed over the course of millennia with many signifi cant develop-ments engendered during times of war. Although this associa-tion between military surgery and what we presently accept as orthopedics reaches back to the ancient period, the contribu-tions of American military practitioners to the development of orthopedic surgery cannot be overlooked. Arguably, the experiences of American military surgeons in confl icts from the Civil War to the present have continued to reinvigorate the orthopedic discipline, resulting in important developments within the fi eld, as well as scientifi c discoveries that have gone on to benefi t the civilian and military communities. Before the technological advancements that potentiated the modern sur-gical specialties, it is even possible to maintain that the major-ity of what constituted American military combat surgery, from the Revolution to the First World War, was orthopedic in nature: removal of bullets and shrapnel, soft tissue care, set-ting of fractures, and extremity amputation.
The goal of this review is to survey the U.S. Army’s ortho-pedic experience from the period of the American Revolution to the current confl icts in Iraq and Afghanistan. It is hoped that, through this report, the reader may gain a better apprecia-tion for the signifi cant contributions American combat ortho-pedics has made to the development of the fi eld as a whole.
EARLY BEGINNINGS: THE AMERICAN REVOLUTION (1775) TO 1860 The United States Army Medical Department and the Medical Corps trace their origins to the founding of the United States Army Hospital department on July 27, 1775, only 10 days after the Battle of Bunker Hill. 1 The department, under the direction of Surgeon General Benjamin Church, was charged
with supplying the fl edgling units of the Continental Army with military surgeons who could provide battlefi eld care and administer to the wounded. Each Army regiment was autho-rized 1 surgeon. At the time, medical education within the United States was not standardized and the vast majority of physicians obtained their education through an apprentice system. Almost none of the American military surgeons had prior combat experience, including the Surgeon General.
The surgeons of the Continental Army had limited resources, as well as a truncated understanding of the patho-physiological mechanisms of trauma, infection, and wound healing. These individuals were most effective at removing bullet fragments or shrapnel from superfi cial wounds, debrid-ing devitalized tissue, and setting fractured limbs. 1–4 The fear of sepsis led to a substantial reliance on extremity amputa-tions, particularly in the event of soft-tissue compromise or comminuted fractures. In most instances, wounds were not cleansed at all or they were irrigated with what standing water was available. During the Battle of Harlem Heights (1776), however, Continental Army Surgeon Charles Gillman used alcohol to treat combat wounds and later reported on the ben-efi ts of this process. His practices, however, were not adopted by other practitioners in the Continental Army. 3
In an effort to standardize some of the practices used to treat American war wounded, Continental Army Surgeon John Jones ( Fig. 1 ) authored the fi rst American surgical text “[O]n the Treatment of Wounds and Fractures: Designed for the Use of Young Military Surgeons in North America.” 5 The text, devoted almost entirely to what would now be consid-ered the purview of an orthopedic surgeon, cautioned army surgeons to respect the soft tissue envelope, remove bone fragments and foreign bodies as atraumatically as possible, and use bark emollients as a means of cautery. Amputations, unless needed to save a soldier’s life, were to be delayed until the individual was determined to be stable from a medical standpoint. Open fractures were to be treated with debride-ment and an attempt at reduction. 5
Although other surgeons expounded principles from the standpoint of medical theory, Jones was one of the few military
Orthopedic Surgery in the United States Army: A Historical Review
MAJ Andrew J. Schoenfeld , MC USA
ABSTRACT The contribution of American military surgeons to the development of orthopedic surgery has not previously been explored. The experiences of American military surgeons in confl icts from the Civil War to Iraq and Afghanistan have advanced the orthopedic discipline, resulting in important developments within the fi eld, as well as sci-entifi c discoveries that have benefi ted both the civilian and military communities. From advances in wound care, to spinal surgery, intramedullary nailing of long bone fractures, and external fi xation, American military surgeons have been pio-neers of orthopedic surgery. The goal of this review was to survey the American military orthopedic experience from the American Revolution to the wars in Iraq and Afghanistan.
Department of Orthopaedic Surgery, William Beaumont Army Medical Center, Texas Tech University Health Sciences Center, 5005 North Piedras Street, El Paso, TX 79920.
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/176/6/689/4345447 by guest on 20 July 2022

Orthopedic Surgery in the U.S. Army
690 MILITARY MEDICINE, Vol. 176, June 2011
surgeons who could speak from prior experience. Formally trained in medicine in Europe, Jones had apprenticed under famed surgeons such as Percival Pott and John Hunter. He had also served as a British Army surgeon during the French and Indian War (1755–1763). Interestingly, the revolutionary con-fl ict now pitted Jones against his former mentor, John Hunter, who was serving as Surgeon General of the British Armed Forces. 4
At the end of the revolution, the Army Medical Corps was dissolved and would only be reconstituted during times of war until 1818, when it was offi cially mandated as a standing por-tion of the peacetime Armed Forces. 1 The lack of a profes-sional military medical service retarded the development of combat casualty care in the nascent U.S. Army. Nonetheless, advancements continued to be made by enterprising physi-cians serving within the ranks. For example, during the War of 1812, American surgeons advocated the performance of emer-gent extremity fasciotomies to treat elevated compartment pressures in the setting of fractures, burns, or severe combat-related soft-tissue damage. 4
THE CIVIL WAR (1861–1865) The medical departments of both the Federal American forces, as well as the Confederacy, at the start of the Civil War were grossly understaffed and unprepared for the shear number of casualties that were to arise from the confl ict. 6–8 At
the start of the Civil War, less than 100 physicians staffed the U.S. Army and some of these resigned their commissions to serve in the Confederate Medical Corps. 7,8 Most medical per-sonnel on both sides were recruited from the civilian ranks of what was still a rudimentary, nonstandardized, medical edu-cation system. Even medical students were considered worthy of appointments as full-fl edged combat surgeons. 6 Assistant Surgeon William W. Keen ( Fig. 2 ), of the 5th Massachusetts Infantry, had less than 1 month of formal medical school train-ing before he was pressed into service. 6 His experiences at the Battle of Bull Run (1861), the fi rst major Civil War battle, are extremely telling of the orthopedic nature of combat sur-gery at the time. Within the fi rst hours of the battle, Keen was asked to perform a shoulder amputation and set a fracture of the upper extremity. 6
Over the course of the 4-year confl ict, the ranks of the Medical Corps of the U.S. Army, as well as the Confederacy, burgeoned to over 15,000 surgeons. 7–10 Both sides produced
FIGURE 1. John Jones, MD. Arguably America’s fi rst military surgeon. Jones trained under Percival Pott and John Hunter and composed On the Treatment of Wounds and Fractures: Designed for the Use of Young Military Surgeons in North America during the American Revolution. Courtesy of the National Library of Medicine.
FIGURE 2. Assistant Surgeon William W. Keen of the 5th Massachusetts Infantry. Keen served in the Federal Army Medical Corps during all 4 years of the Civil War and performed an emergent surgical decompression on a wounded soldier at Gettysburg (1863). Courtesy of the National Library of Medicine.
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/176/6/689/4345447 by guest on 20 July 2022

Orthopedic Surgery in the U.S. Army
MILITARY MEDICINE, Vol. 176, June 2011 691
medical texts attempting to inform the treatment of war wounded, and “A Manual of Military Surgery for the Use of Surgeons in the Confederate Army” even provided an algo-rithm for performing amputations. 8 With approximately 70% of survivable Civil War injuries involving the extremities, the combat medical experience of this confl ict provided ample exposure to fracture care. 9,10
Although popular conception associates the Civil War sur-geon with the rapid performance of extremity amputations (indeed more than 60,000 amputations were performed by Federal surgeons alone 3 ), some practitioners pioneered novel approaches to fracture care and wound management. The aforementioned Dr. Keen performed an emergent decompres-sion of the cervical spine in the setting of a gunshot wound at the Battle of Gettysburg (1863) successfully reversing an incomplete spinal cord injury. 11 Benjamin Howard, of the New York militia, performed open reduction and internal fi xation of femur fractures using metal wire, 7,9,10 and some Confederate surgeons attempted to fi x fractures with brass pins, 6 whereas others experimented with external fi xation. 12 George Otis, a staff surgeon with Surgeon General Joseph Barnes, avoided extremity amputations by performing resection arthroplasty on damaged shoulder and hip joints. 10
The American medical experience during the Civil War galvanized the recognition of orthopedics as an indepen-dent fi eld from general surgery. Within 20 years of the con-fl ict, independent orthopedic societies, such as the American Orthopedic Association (AOA), were being founded across the country. Indeed, a substantial portion of the AOA’s mem-bership, as well as 2 of its fi rst 6 presidents, were medical vet-erans of the Civil War. 6
A GROWING SERVICE: THE INDIAN WARS TO WORLD WAR I (1866–1918) Although after the Civil War orthopedics was recognized as an independent medical specialty, no dedicated orthopedic surgeons existed within the Army Medical Corps. The medi-cal service in the American West consisted of surgeons who administered all facets of medical care to the soldiers they served. However, orthopedic-related injuries comprised a siz-able portion of combat wounds, particularly during the Indian Wars (1866–1890). Throughout the Indian confl icts in the American West, 2 assistant surgeons were typically assigned to each military formation and service could be hazardous. In addition to performing battlefi eld amputations, care of gun-shot wounds, and managing a soldier with a spinal cord injury from gunshot associated fracture, 2 of the 3 surgeons assigned to the 7th Cavalry lost their lives at the Battle of the Little Bighorn (1876). 13
During this period, the use of Listerian antiseptic tech-niques were adopted by the Medical Corps and applied to all military surgeries. 4 Hospital barges were utilized for the rapid evacuation and treatment of wounded personnel dur-ing the Spanish–American War (1898). 3 These hospital ships also contained X-ray machines that allowed surgeons to pre-
cisely localize bullet fragments, as well as fractures, and treat such injuries more expeditiously, as well as precisely. These advances contributed to a remarkable decrease in the mortality and amputation rates during this confl ict. 2,3 Among the 1,990 American servicemen injured during the Spanish–American War, only 29 extremity amputations were performed and the mortality rate was 7.4%. 3
During World War I, 3 years of observation as a neutral country allowed the Army Medical Corps the time to antic-ipate the orthopedic needs of combat-injured soldiers. As a result, once American involvement in the confl ict appeared imminent, the Army War Department petitioned the AOA to assist in the development of an Orthopedic Section within the American Expeditionary Force (AEF). 4,14 The Department of Military Orthopedic Surgery was formed within the Offi ce of the Surgeon General in 1916 under MAJ Brackett EG. 15
The responsibility for orthopedic services in the combat zone, however, fell to the Division of Orthopedic Surgery of the AEF, under the command of COL Joel Goldthwait and COL Nathaniel Allison ( Fig. 3 ). 14,15 Both Goldthwait and Allison were Harvard-trained surgeons, as were many members of the initial orthopedic cadre of the AEF. The division comprised 42 orthopedic surgeons, almost entirely from Harvard or Johns Hopkins, and 12 nurse assistants. 14,15 The unit did not oper-ate as a specifi c entity but rather was spread across the entire Western Front, where physicians applied splints in the front line trenches and performed surgical interventions at hospi-tals in the rear. Military experiences in World War I resulted in the transformation of orthopedic surgery from a discipline focused on splinting and amputation as surgical mainstays to a service that actively sought to surgically intervene in frac-ture care. Open injuries were irrigated with Dakin’s solution, debrided, and left open for a minimum of 24 to 48 hours. 16 The mortality rate for open femur fractures in the American forces remained below 20%, whereas it approached 80% for simi-larly injured servicemen in the armies of other combatants. 14 Following the experiences of World War I, the American Academy of Orthopaedic Surgeons (AAOS) was formed and residency training for the orthopedic specialty was standard-ized. Similar to the situation after the Civil War, many of the leaders of orthopedic surgery in the interwar period were veterans of the AEF, including 4 of the fi rst 9 presidents of the AAOS. 14
WORLD WAR II AND KOREA (1941–1953) A number of factors culminated to engender signifi cant advances in the fi eld of orthopedic surgery during, and imme-diately following, World War II (1941–1945). 2,3,15,17,18 Chief among these were technical developments, such as the discov-ery of antibiotics and blood replacement that enabled orthope-dic surgeons to more aggressively intervene in their manner of fracture care and internal fi xation. 18 Second, the Army Sur-geon General during World War II, MG Norman Kirk ( Fig. 4 ), was himself an orthopedic surgeon and strongly promoted the benefi ts of his specialty to American combat-injured. 3,17
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/176/6/689/4345447 by guest on 20 July 2022

Orthopedic Surgery in the U.S. Army
692 MILITARY MEDICINE, Vol. 176, June 2011
MG Kirk was instrumental in the development of special Army orthopedic hospitals and amputee centers and galvan ized the development of hand surgery when he charged Dr. Sterling Bunnell with the task of training young military surgeons in hand microsurgical and reconstructive techniques. 17,18
During World War II, American military surgeons experi-mented with the use of bone grafting, limb salvage, and sur-gical debridement for the treatment of osteomyelitis. 17–20 External fi xation, a technique initially described by American surgeons during the Civil War 12 , was refi ned and its applica-tion was established in the aftermath of Pearl Harbor. 18 The Army was very interested in facilitating the widespread use
of external fi xators but the devices fell out of favor with prac-titioners because of a high infection rate and a propensity to cause pseudarthrosis. 18 Particularly poor outcomes in the European theater resulted in the complete removal of external fi xators from fi eld hospitals. 18 Internal fi xation was used spar-ingly, but with some remarkable success. 17,18 In 71 instances of open reduction and internal fi xation performed at the 46th General Hospital, no cases of signifi cant postoperative infec-tion were reported. 18 At the end of the war, the experience of American POWs who had been treated in Germany with Gerhard Kuntscher’s intramedullary devices, led to the accep-tance of this technology as an approach to the treatment of combat-related long bone fractures. 2,17
The orthopedic experience during World War II also resulted in a revolution in the manner in which amputations were per-formed. At the start of the confl ict, both guillotine and open circular amputations were advocated as equivalent techniques. However, based on the experience of large hospital sections, such as that of the 3rd Army, the decision was made to aban-don the guillotine in favor of the circular technique, 18 a variant of which is still in use today. This was because the guillotine technique resulted in diffi culties with soft-tissue coverage and often necessitated revision surgery. 18
During the Korean War (1950–1953), the use of the heli-copter enabled rapid evacuation of wounded soldiers to med-ical treatment facilities. For the fi rst time in the history of military medicine, fi xed military hospitals allowed soldiers to receive rapid medical and surgical intervention similar to that which they could receive in a civilian setting. 2,3 This facili-tated relatively rapid surgical intervention for the treatment of fractures, traumatic amputations, and spinal cord injury. Orthopedic surgeons were a core component of cadre at Mobile Army Surgical Hospitals (MASHs). 3 All soldiers with penetrating cervical wounds received decompressive lamine-ctomies during the Korean confl ict 11 and the use of intramed-ullary fi xation became standard among soldiers with lower extremity long-bone injuries. 2,15
FIGURE 3. Colonel Nathaniel Allison of the American Expeditionary Force. Colonel Allison was the Assistant Director of the Division of Orthopaedic Surgery during World War I (1917–1918). Courtesy of the National Library of Medicine.
FIGURE 4. Major General Norman T. Kirk, MD (seated, second from right) and his staff during World War Two (1941–1945). Major General Kirk was responsible for several initiatives which advanced the fi eld of orthope-dic surgery during, and after, the war. Courtesy of the National Library of Medicine.
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/176/6/689/4345447 by guest on 20 July 2022

Orthopedic Surgery in the U.S. Army
MILITARY MEDICINE, Vol. 176, June 2011 693
THE VIETNAM CONFLICT (1965–1973) The capabilities of fi xed army hospitals and MASHs were fur-ther expanded during the Vietnam era and the treatment of war wounded was doctrinally refi ned, approaching the mod-ern echelons of care system used in the military today. 2,21 Wounded soldiers were treated emergently and stabilized in smaller medical units close to the combat zone, then succes-sively evacuated to larger military medical facilities that con-tained more robust resources and were capable of defi nitive intervention. 22,23 Orthopedic surgeons were integral to the treatment of servicemembers at the large military centers, but many could also be found among the medical teams serving near the front lines. 22 Combat injuries to the extremities were treated with wound exploration, debridement, and open pack-ing. Pulsatile lavage was used to treat contaminated war inju-ries, and primary closure was avoided in country. 22
Although previously injuries to major and collateral ves-sels were considered absolute indications for amputations, surgeons of the Vietnam era attempted to salvage limbs by performing vascular repair or reconstruction. Primary amputa-tions were avoided and, if deemed necessary, were performed at the most distal site possible. 22 Approximately 55% of all combat-related injuries in Vietnam involved the extremities 23 and relatively modern approaches to internal fi xation and limb reconstruction were utilized in their treatment. 22 Surgical exploration of the spine was also performed in instances of wounds caused by gunshot or explosive mechanisms. 11
THE MODERN ERA: GRENADA TO 9/11 (1983–2001) In the 10-year period from the end of Vietnam to the invasion of Grenada, the American military underwent a transforma-tion to a more mobile, rapidly deployable fi ghting force. 2,3,21 Unfortunately, the doctrinal approach of the Medical Corps was not revised to refl ect this fact. As a result, the fi rst MASH was not operational in Grenada until 4 days following the start of hostilities. 24 This led to a reconsideration of the way the Army deployed its medical assets and a revolution in the administra-tion of combat-related healthcare that continues to this day. 21 Following Grenada, the Army began to train highly mobile airborne surgical squads, which could be parachuted behind assault teams to provide close medical support. 24,25 One ortho-pedic surgeon was assigned to each of these 20-man surgi-cal squads, which would eventually develop into the Forward Surgical Teams (FSTs) employed in combat today. 21,24,25
The fi rst forward surgical squads made combat jumps during the Panama invasion (1989), which represented the fi rst major American confl ict to transpire during the period of modern orthopedic instrumentation and the largest night-time airborne assault since World War II. In total, U.S. forces sustained 252 casualties during this operation with more than 80% of injuries considered orthopedic in nature. 26 Many inju-ries occurred during the initial jump and a high proportion of these included spinal fractures. 11,26
The concomitant use of Kevlar helmets and individual body armor on a large scale at the start of the Persian Gulf War
(1990–1991) signifi cantly increased the proportion of orthope-dic injuries encountered on the fi eld of battle. 3,27 Additionally, advances in medical capabilities combined with military tech-nology to create situations where soldiers were able to sur-vive previously lethal combat-related injuries, but still endure devastating extremity wounds that posed substantial chal-lenges to orthopedic specialists. 27,28 The fast-paced, and rap-idly mobile, realities of desert warfare also led to the effective elimination of MASH units from the Army’s medical doc-trine. 3,21,24,25 Following the Gulf War, these hospitals, whose history extended back to the Korean War, were replaced by the more versatile FSTs and Combat Support Hospitals (CSHs) developed during the 1980s. 3,21
THE UNITED STATES’ CURRENT CONFLICTS: IRAQ AND AFGHANISTAN (2001–PRESENT) At the start of the Afghanistan invasion, the 274th and 250th FSTs were the fi rst medical units to deploy in direct support of American forces in Operation Enduring Freedom (OEF). 24,25 Eventually, these units were followed by larger CSHs, who established fi xed facilities in country. Doctrinally, 1 orthope-dic surgeon is assigned to an FST, whereas up to 3 orthopedic practitioners may support a CSH. 21 Orthopedic interventions at an FST are limited to those necessary to save life and/or limb, such as emergent amputation, irrigation and debri-dement, and/or application of external fi xation. 21,24,25 More robust medical capabilities are present at a CSH, but ortho-pedic interventions remain similar to those performed at an FST. 21 For American military personnel, defi nitive orthopedic intervention is reserved until wounded soldiers arrive at facili-ties in Germany or within the continental United States. 21,28
Reports from the 274th and 250th FSTs in the initial phases of OEF revealed a high proportion of cases fell to the orthopedic surgeon on the team, including external fi x-ation of fractures, amputations, and fasciotomies. 24,25 At the 250th FST, extremity procedures represented 65% of all cases performed from October 2001–April 2002. 25 In 2003, the 250th FST redeployed to Operation Iraqi Freedom (OIF) and actively supported the 173rd Airborne Brigade in its inva-sion of Northern Iraq. 24 Here, 51% of all combat injuries were found to involve the extremities. 24 During the initial invasion of Iraq, the 555th and 745th FSTs traveled in the wake of the 3rd Infantry Division, which was responsible for spearhead-ing the assault. 29
Of all the military confl icts in which the United States has previously been engaged, we possess the greatest knowledge regarding the orthopedic experience in both OIF and OEF because of the publication of recent prospective reports and the Joint Theater Trauma Registry. 30–32 Publications regard-ing the spectrum of orthopedic injuries in OIF/OEF reveal a prevalence of 54% among all those injured. 30,31 Owens et al 30,31 found that explosions were the cause of 75% of all orthopedic injuries, whereas gunshot wounds were responsible for only 16%. Similar fi ndings were endorsed in the work of Belmont et al. 32 Here, approximately 50% of all injuries involved the
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/176/6/689/4345447 by guest on 20 July 2022
Orthopedic Surgery in the U.S. Army
694 MILITARY MEDICINE, Vol. 176, June 2011
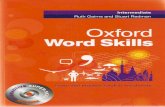
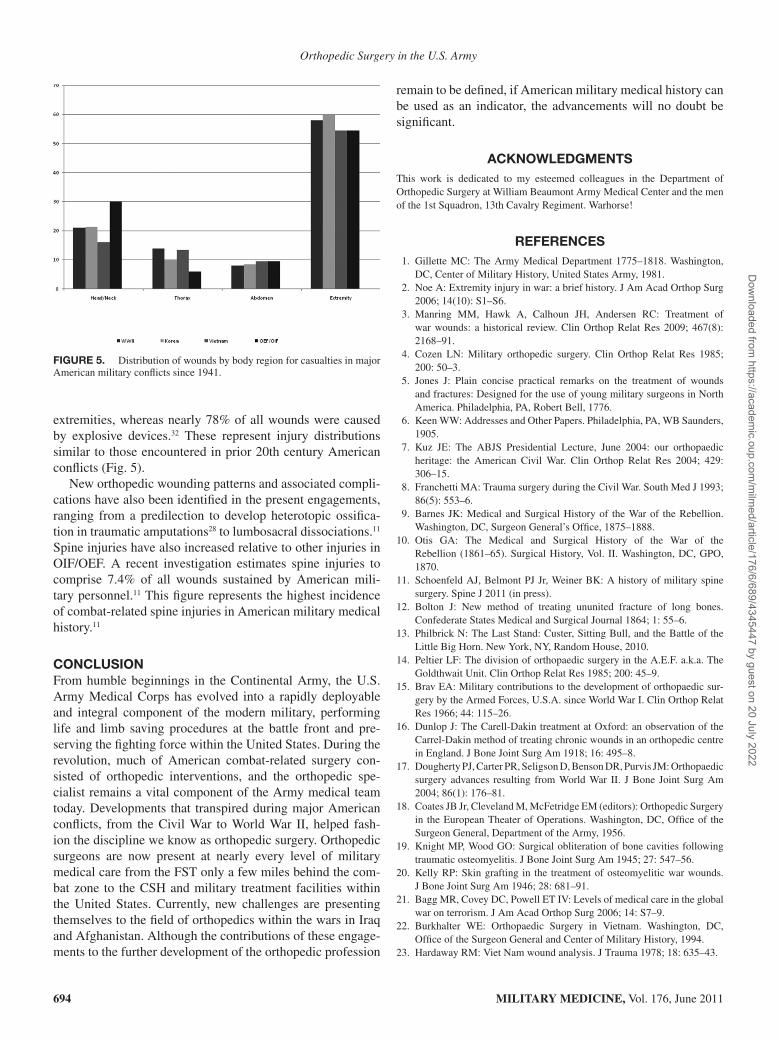
extremities, whereas nearly 78% of all wounds were caused by explosive devices. 32 These represent injury distributions similar to those encountered in prior 20th century American confl icts ( Fig. 5 ).
New orthopedic wounding patterns and associated compli-cations have also been identifi ed in the present engagements, ranging from a predilection to develop heterotopic ossifi ca-tion in traumatic amputations 28 to lumbosacral dissociations. 11 Spine injuries have also increased relative to other injuries in OIF/OEF. A recent investigation estimates spine injuries to comprise 7.4% of all wounds sustained by American mili-tary personnel. 11 This fi gure represents the highest incidence of combat-related spine injuries in American military medical history. 11
CONCLUSION From humble beginnings in the Continental Army, the U.S. Army Medical Corps has evolved into a rapidly deployable and integral component of the modern military, performing life and limb saving procedures at the battle front and pre-serving the fi ghting force within the United States. During the revolution, much of American combat-related surgery con-sisted of orthopedic interventions, and the orthopedic spe-cialist remains a vital component of the Army medical team today. Developments that transpired during major American confl icts, from the Civil War to World War II, helped fash-ion the discipline we know as orthopedic surgery. Orthopedic surgeons are now present at nearly every level of military medical care from the FST only a few miles behind the com-bat zone to the CSH and military treatment facilities within the United States. Currently, new challenges are presenting themselves to the fi eld of orthopedics within the wars in Iraq and Afghanistan. Although the contributions of these engage-ments to the further development of the orthopedic profession
remain to be defi ned, if American military medical history can be used as an indicator, the advancements will no doubt be signifi cant.
ACKNOWLEDGMENTS This work is dedicated to my esteemed colleagues in the Department of Orthopedic Surgery at William Beaumont Army Medical Center and the men of the 1st Squadron, 13th Cavalry Regiment. Warhorse!
REFERENCES 1. Gillette MC : The Army Medical Department 1775–1818 . Washington,
DC , Center of Military History, United States Army , 1981 . 2. Noe A : Extremity injury in war: a brief history . J Am Acad Orthop Surg
2006 ; 14 (10) : S1 – S6 . 3. Manring MM , Hawk A , Calhoun JH , Andersen RC : Treatment of
war wounds: a historical review . Clin Orthop Relat Res 2009 ; 467 (8) : 2168 – 91 .
4. Cozen LN : Military orthopedic surgery . Clin Orthop Relat Res 1985 ; 200: 50 – 3 .
5. Jones J : Plain concise practical remarks on the treatment of wounds and fractures: Designed for the use of young military surgeons in North America . Philadelphia, PA , Robert Bell , 1776 .
6. Keen WW : Addresses and Other Papers . Philadelphia, PA , WB Saunders , 1905 .
7. Kuz JE : The ABJS Presidential Lecture, June 2004: our orthopaedic heritage: the American Civil War . Clin Orthop Relat Res 2004 ; 429: 306 – 15 .
8. Franchetti MA : Trauma surgery during the Civil War . South Med J 1993 ; 86 (5) : 553 – 6 .
9. Barnes JK : Medical and Surgical History of the War of the Rebellion . Washington, DC , Surgeon General’s Offi ce , 1875–1888 .
10. Otis GA : The Medical and Surgical History of the War of the Rebellion (1861–65) . Surgical History, Vol. II . Washington, DC , GPO , 1870 .
11. Schoenfeld AJ , Belmont PJ Jr , Weiner BK : A history of military spine surgery . Spine J 2011 (in press ).
12. Bolton J : New method of treating ununited fracture of long bones . Confederate States Medical and Surgical Journal 1864 ; 1: 55 – 6 .
13. Philbrick N : The Last Stand: Custer, Sitting Bull, and the Battle of the Little Big Horn . New York, NY , Random House , 2010 .
14. Peltier LF : The division of orthopaedic surgery in the A.E.F. a.k.a. The Goldthwait Unit . Clin Orthop Relat Res 1985 ; 200: 45 – 9 .
15. Brav EA : Military contributions to the development of orthopaedic sur-gery by the Armed Forces, U.S.A. since World War I . Clin Orthop Relat Res 1966 ; 44: 115 – 26 .
16. Dunlop J : The Carell-Dakin treatment at Oxford: an observation of the Carrel-Dakin method of treating chronic wounds in an orthopedic centre in England . J Bone Joint Surg Am 1918 ; 16: 495 – 8 .
17. Dougherty PJ , Carter PR , Seligson D , Benson DR , Purvis JM : Orthopaedic surgery advances resulting from World War II . J Bone Joint Surg Am 2004 ; 86 (1) : 176 – 81 .
18. Coates JB Jr , Cleveland M , McFetridge EM (editors): Orthopedic Surgery in the European Theater of Operations . Washington, DC , Offi ce of the Surgeon General, Department of the Army , 1956 .
19. Knight MP , Wood GO : Surgical obliteration of bone cavities following traumatic osteomyelitis . J Bone Joint Surg Am 1945 ; 27: 547 – 56 .
20. Kelly RP : Skin grafting in the treatment of osteomyelitic war wounds . J Bone Joint Surg Am 1946 ; 28: 681 – 91 .
21. Bagg MR , Covey DC , Powell ET IV : Levels of medical care in the global war on terrorism . J Am Acad Orthop Surg 2006 ; 14: S7 – 9 .
22. Burkhalter WE : Orthopaedic Surgery in Vietnam . Washington, DC , Offi ce of the Surgeon General and Center of Military History , 1994 .
23. Hardaway RM : Viet Nam wound analysis . J Trauma 1978 ; 18: 635 – 43 .
FIGURE 5. Distribution of wounds by body region for casualties in major American military confl icts since 1941.
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/176/6/689/4345447 by guest on 20 July 2022

Orthopedic Surgery in the U.S. Army
MILITARY MEDICINE, Vol. 176, June 2011 695
24. Rush RM Jr , Stockmaster NR , Stinger HK , et al : Supporting the Global War on Terror: a tale of two campaigns featuring the 250th Forward Surgical Team (Airborne) . Am J Surg 2005 ; 189: 564 – 70 .
25. Place RJ , Rush RM Jr , Arrington ED : Forward surgical team (FST) work-load in a Special Operations environment: the 250th FST in Operation Enduring Freedom . Curr Surg 2003 ; 60: 418 – 22 .
26. Parsons TW III , Lauerman WC , Ethier DB , et al : Spine injuries in com-bat troops—Panama, 1989 . Mil Med 1993 ; 158: 501 – 2 .
27. Uhorchak JM , Rodkey WG , Hunt MM , Hoxie SW . Institute report no. 469: Casualty data assessment team Operation Desert Storm . San Francisco, CA , Letterman Army Institute of Research , 1992 .
28. Belmont PJ Jr , Schoenfeld AJ , Goodman GP . Epidemiology of combat wounds in Operation Iraqi Freedom and Operation Enduring Freedom: orthopaedic burden of disease . J Orthop Surg Adv 2010 ; 19: 2 – 7 .
29. Patel TH , Wenner KA , Price SA , Weber MA , Leveridge A , McAtee SJ : A U.S. Army Forward Surgical Team’s experience in Operation Iraqi Freedom . J Trauma 2004 ; 57: 201 – 7 .
30. Owens BD , Kragh JF Jr , Macaitis J , Svoboda SJ , Wenke JC : Characterization of extremity wounds in Operation Iraqi Freedom and Operation Enduring Freedom . J Orthop Trauma 2007 ; 21: 254 – 7 .
31. Owens BD , Kragh JF , Wenke JC , Macaitis J , Wade CE , Holcomb JB : Combat wounds in Operation Iraqi Freedom and Operation Enduring Freedom . J Trauma 2008 ; 64: 295 – 9 .
32. Belmont PJ Jr , Goodman GP , Zacchilli M , Posner M , Evans C , Owens BD : Incidence and epidemiology of combat injuries sustained during “the surge” portion of Operation Iraqi Freedom by a U.S. Army brigade combat team . J Trauma 2010 ; 68: 204 – 10 .
Dow
nloaded from https://academ
ic.oup.com/m
ilmed/article/176/6/689/4345447 by guest on 20 July 2022