
Optimum Recombinant Human Thyrotropin Dose in Patients with Differentiated Thyroid Carcinoma and...
12
Authors and Disclosures Fabián Pitoia, MD, 1 Veronica Ilera, MD, 2 Maria B. Zanchetta, MD, 1 Adriana Foffano, MD, 1 and Hugo Niepomniszcze, MD, PhD 1 1 Division of Endocrinology, Hospital de Clinicas, University of Buenos Aires, Buenos Aires, Argentina 2 Division of Endocrinology, Hospital Aleman, Buenos Aires, Argentina. Disclosure: Fabián Pitoia is an external medical advisor for Genzyme Corporation. From Endocrine Practice Optimum Recombinant Human Thyrotropin Dose in Patients With Differentiated Thyroid Carcinoma and End-stage Renal Disease Fabián Pitoia, MD; Veronica Ilera, MD; Maria B. Zanchetta, MD; Adriana Foffano, MD; Hugo Niepomniszcze, MD, PhD Posted: 02/10/2009; Endocrine Practice. 2008;14(8):961-966. © 2008 American Association of Clinical Endocrinologists Abstract and Introduction Abstract Objective: To evaluate serum thyrotropin (TSH) concentrations after conventional (0.9 mg) or half-dose (0.45 mg) administration of recombinant human TSH (rhTSH) injections intramuscularly in patients with end-stage renal disease and differentiated thyroid cancer. Methods: In this case series, we administered 2 doses of 0.9-mg rhTSH or 2 doses of 0.45-mg rhTSH to 3 patients with renal failure and differentiated thyroid cancer who were receiving hemodialysis. Basal serum TSH concentrations were assessed while the patients were taking thyroid hormone therapy. Serum TSH was measured on days 2, 3, 5, 8, 10, 14, and 17 of the study. Thyroglobulin and thyroglobulin antibodies were also measured on days 5 and 7. Patients were asked to report any adverse effects. Results: Patient 1, who received 2 injections of 0.9-mg rhTSH administered on days 1 and 3, had persistently elevated serum TSH levels for approximately 11 days. Peak serum TSH measured on day 5 was 644 mIU/L. Self-limited diarrhea was the only reported adverse effect. Patients 2 and 3 received 0.45 mg of rhTSH on 2 consecutive days (days 1 and 2), and both exhibited persistently elevated serum TSH levels for 12 days. The peak serum TSH values on day 3 were 402 mIU/L in Patient 2 and 386 mIU/L in Patient 3. No adverse events were observed in these 2 patients. Patient 2
Transcript of Optimum Recombinant Human Thyrotropin Dose in Patients with Differentiated Thyroid Carcinoma and...
Authors and Disclosures
Fabián Pitoia, MD,1 Veronica Ilera, MD,
2 Maria B. Zanchetta, MD,
1 Adriana
Foffano, MD,1 and Hugo Niepomniszcze, MD, PhD
1
1Division of Endocrinology, Hospital de Clinicas, University of Buenos Aires, Buenos
Aires, Argentina 2Division of Endocrinology, Hospital Aleman, Buenos Aires, Argentina.
Disclosure: Fabián Pitoia is an external medical advisor for Genzyme Corporation.
From Endocrine Practice
Optimum Recombinant Human
Thyrotropin Dose in Patients With
Differentiated Thyroid Carcinoma and
End-stage Renal Disease
Fabián Pitoia, MD; Veronica Ilera, MD; Maria B. Zanchetta, MD; Adriana Foffano,
MD; Hugo Niepomniszcze, MD, PhD
Posted: 02/10/2009; Endocrine Practice. 2008;14(8):961-966. © 2008 American
Association of Clinical Endocrinologists
Abstract and Introduction
Abstract
Objective: To evaluate serum thyrotropin (TSH) concentrations after conventional (0.9
mg) or half-dose (0.45 mg) administration of recombinant human TSH (rhTSH)
injections intramuscularly in patients with end-stage renal disease and differentiated
thyroid cancer.
Methods: In this case series, we administered 2 doses of 0.9-mg rhTSH or 2 doses of
0.45-mg rhTSH to 3 patients with renal failure and differentiated thyroid cancer who
were receiving hemodialysis. Basal serum TSH concentrations were assessed while the
patients were taking thyroid hormone therapy. Serum TSH was measured on days 2, 3,
5, 8, 10, 14, and 17 of the study. Thyroglobulin and thyroglobulin antibodies were also
measured on days 5 and 7. Patients were asked to report any adverse effects.
Results: Patient 1, who received 2 injections of 0.9-mg rhTSH administered on days 1
and 3, had persistently elevated serum TSH levels for approximately 11 days. Peak
serum TSH measured on day 5 was 644 mIU/L. Self-limited diarrhea was the only
reported adverse effect. Patients 2 and 3 received 0.45 mg of rhTSH on 2 consecutive
days (days 1 and 2), and both exhibited persistently elevated serum TSH levels for 12
days. The peak serum TSH values on day 3 were 402 mIU/L in Patient 2 and 386
mIU/L in Patient 3. No adverse events were observed in these 2 patients. Patient 2

received thyrotropin alfa for injection to confirm disease status. Patient 3 also received a
radioiodine dose because of presumed persistent disease.
Conclusion: High serum TSH levels achieved after conventional and half-dose
administration of rhTSH suggest that a dose adjustment might be considered in patients
with end-stage renal disease. (Endocr Pract. 2008;14:961-966)
Introduction
Differentiated thyroid cancer has an excellent prognosis in most patients after the initial
treatment. The usual treatment approach involves total thyroidectomy, often followed
by radioiodine ablation of the thyroid remnant.[1]
Adequate uptake of radioiodine by remnant or remaining malignant thyroid tissue is
dependent on an elevated level of thyrotropin (TSH) in the blood. In the past, it was
necessary to withdraw thyroid hormone-suppressive therapy for several weeks to cause
TSH elevation, and a somewhat arbitrary target level of greater than 25 mIU/L was
used.[2,3]
Children may have sufficiently elevated TSH concentrations after shorter
periods of withdrawal.[4]
Levothyroxine withdrawal is nearly always associated with signs and symptoms of
hypothyroidism, which are generally not well tolerated.[5,6]
The hypothyroid state
usually impairs the quality of life of patients with thyroid cancer, reduces productivity,
and can also promote thyroid tumor growth and worsen comorbid diseases.[7] Moreover,
patients asked to undergo repeated hypothyroid periods have documented lower
compliance with followup.[8]
The human gene that encodes the TSH β subunit was identified in 1988,[9] and methods
were established to synthesize the dimeric form of recombinant human TSH (rhTSH) in
vitro soon thereafter.[10] The rhTSH produced the same effects in in vitro assays as did
natural human TSH[11] and was soon shown to be active in healthy volunteers.
[12,13]
Extensive clinical studies followed. Between 1997 and 2007, more than 40 centers
around the world studied patients with differentiated thyroid cancer who received
rhTSH as a part of their evaluation or treatment.[14-16]
Despite the extensive experience using rhTSH, there are seldom reports of its use in
patients with renal failure.[17-19]
In such patients, the quality of life is, per se, affected by
several circumstances including the frequency of hemodialysis and higher frequencies
of infections, etc, and thyroid hormone withdrawal may aggravate this situation.
Recombinant human TSH would seem to be a good alternative in patients with renal
disease, but because of the extensive renal clearance of rhTSH, the proper dosage has
never been firmly established.
In this case series, we present the results observed in 3 patients with end-stage renal
disease and thyroid cancer who were receiving hemodialysis 3 times per week. In 1
patient, we used 2 injections of 0.9-mg rhTSH, and in the other 2 patients, we
administered 2 injections of 0.45-mg rhTSH.
Patients and Methods
Patient 1

A 46-year-old woman with a body mass index of 26 kg/m2 underwent partial
parathyroidectomy because of tertiary hyperparathyroidism 7 years earlier. During
surgery, a multinodular goiter was discovered. Total thyroidectomy was performed, and
pathologic examination revealed a 0.7-cm papillary thyroid carcinoma. A suspicious
jugular lymph node was also intrasurgically analyzed, and findings revealed the
presence of neoplastic thyroid cells. A modified neck dissection (levels II-III-IV and
VI) was then performed. The pathologic results showed the presence of metastases in 12
of 40 removed lymph nodes. Remnant ablation was performed with 100 mCi of iodine I
131 (131I) after thyroid hormone withdrawal. The hypothyroid state was poorly
tolerated, and the patient refused thyroxine withdrawal for several years thereafter, thus
impairing her follow-up evaluations.
A persistently detectable thyroglobulin concentration (between 1.2 and 1.9 ng/mL)
while the patient was taking thyroid hormone-suppressive therapy (with normal findings
from neck ultrasonography examinations) led us to offer injections of rhTSH followed
by therapeutic high activity 131I. A 0.9-mg dose of rhTSH was injected intramuscularly
on days 1 and 3.
Patient 2
A 59-year-old woman with a body mass index of 28 kg/m2 and a history of bilateral
nephrectomy underwent a partial parathyroidectomy. The discovery of a thyroid nodule
led to a surgical biopsy, the findings of which showed papillary thyroid cancer. Total
thyroidectomy was performed. Pathologic examination showed a multicentric and
bilateral papillary microcarcinoma. Thyroxine was withdrawn, and ablation of the
thyroid remnant was accomplished using 70 mCi 131I.
A follow-up evaluation of stimulated thyroglobulin/thyroglobulin antibody
measurement was proposed 1 year later. In view of the results of the first case, we
decided to use a lower rhTSH dose (2 consecutive 0.45-mg injections on days 1 and 2).
Patient 3
A 40-year-old man with chronic renal failure and a body mass index of 23 kg/m2 had a
partial parathyroidectomy 3 years earlier. A thyroid micronodule was discovered during
surgery, and the intrasurgical analysis showed the presence of papillary thyroid cancer.
Total thyroidectomy was performed, and a 0.7-cm papillary microcarcinoma with
capsule invasion was found in the right thyroid lobe. No affected lymph nodes were
found after the analysis of 16 operated nodes. Levothyroxine was withdrawn, and
remnant ablation using 100 mCi 131I was performed 1 month later, but the hypothyroid
symptoms were poorly tolerated.
A persistently detectable thyroglobulin concentration of 1.51 ng/mL while on thyroid
hormone-suppressive therapy (with normal findings from neck ultrasonography
examinations) led us to administer 60 mCi 131I after 0.45-mg rhTSH injections on 2
consecutive days.
Protocol

TSH concentrations were measured using an immunometric assay in solid phase with a
functional sensitivity of 0.03 µIU/mL. Thyroglobulin concentrations were measured by
immunochemiluminometric assay (IMMULITE, Diagnostics Products Corporation, Los
Angeles, California). Thyroglobulin antibodies were measured by radioimmunoassay
(RSR Limited, Pentwyn, Cardiff, United Kingdom) with a detection limit lower than 0.5
IU/mL.
The clinical protocol used in Patient 1 was as follows:
Measurement of basal serum TSH concentration while taking thyroid hormone therapy
Day 1: Hemodialysis followed by intramuscular injection of 0.9-mg rhTSH
(thyrotropin alfa for injection [Thyrogen], Genzyme Pharmaceuticals,
Cambridge, Massachusetts)
Day 2: Serum TSH measurement
Day 3: Hemodialysis followed by a second intramuscular injection of 0.9 mg of
rhTSH
Day 4: Administration of 100 mCi 131I
Day 5: Measurement of serum TSH, thyroglobulin, and thyroglobulin antibodies
followed by hemodialysis
Day 7: Serum thyroglobulin and thyroglobulin antibody measurement
Day 8
and 10:
Hemodialysis followed by serum TSH measurement
Day 11: Post-dose whole body scan
Day 12: Hemodialysis
Day 14: Serum TSH measurement
Day 15: Hemodialysis
Day 17: Hemodialysis followed by serum TSH measurement
The protocol for Patients 2 and 3 was identical to the protocol for Patient 1 except that
rhTSH was administered on 2 consecutive days (days 1 and 2), and the injected dose
was 0.45 mg (half ampoule) on each day. Patient 2 received thyrotropin alfa for
injection (Thyrogen) to confirm disease status. Patient 3 also received a radioiodine
dose because of presumed persistent disease. The timing of TSH measurements was
identical in the 3 patients and is shown in Table 1 .
[ CLOSE WINDOW ]
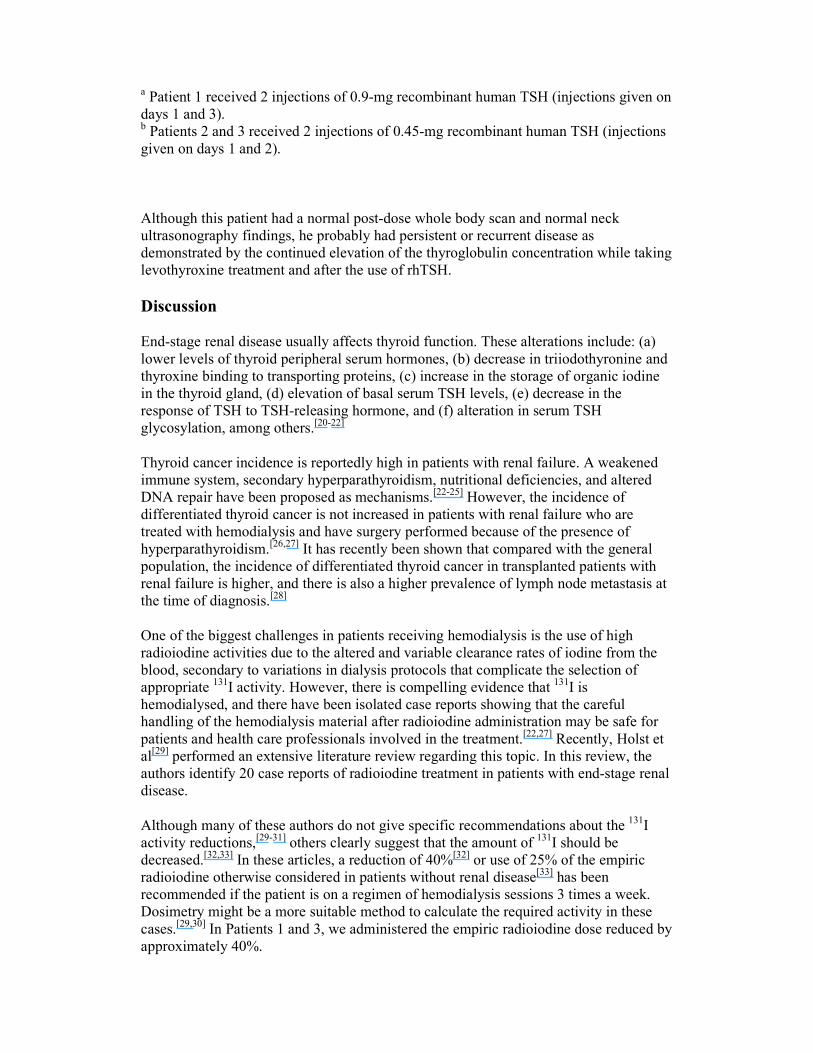
Table 1. Serum Thyrotropin (TSH) Concentrations in 3 Patients With
Differentiated Thyroid Cancer and End-stage Renal Disease After Administration
of Recombinant Human TSH
TSH, mIU/L
Patient Basal Day 2 Day 3 Day 5 Day 8 Day 10 Day 14 Day 17
1a 0.8 456 521 644 175 49 12 2.4

2b 0.23 261 402 210 47 22 12 4
3b 0.03 276 386 203 51 19 9 1.9
a Patient 1 received 2 injections of 0.9-mg recombinant human TSH (injections given on
days 1 and 3). b Patients 2 and 3 received 2 injections of 0.45-mg recombinant human TSH (injections
given on days 1 and 2).
All 3 patients gave written voluntary consent to receive rhTSH. Patients 1 and 3
received explanation about the offlabel use of a therapeutic radioiodine dose after 2
injections of 0.9-mg rhTSH, and Patients 2 and 3 were provided explanations about the
empiric choice of a lower rhTSH dose to achieve similar serum TSH levels as observed
in patients with normal renal function. Procedures were applied in agreement with the
ethical guidelines of our institution.
Results
Patient 1
TSH measurements are shown in Table 1 and in Figure 1. The serum TSH level on day
5 was 644 mIU/L, and it remained elevated for at least 11 days. The serum
thyroglobulin concentration measured 48 hours after the second rhTSH injection was
0.9 ng/mL. In the same sample, thyroglobulin antibodies were undetectable. On day 7,
the thyroglobulin concentration was 1.2 ng/mL, and thyroglobulin antibodies were
again undetectable. On day 11, a whole body scan showed only a faint thyroid bed
uptake (2%). Self-limited diarrhea was observed 48 hours after the first rhTSH
injection.
Table 1. Serum Thyrotropin (TSH) Concentrations in 3 Patients With
Differentiated Thyroid Cancer and End-stage Renal Disease After Administration
of Recombinant Human TSH
TSH, mIU/L
Patient Basal Day 2 Day 3 Day 5 Day 8 Day 10 Day 14 Day 17
1a 0.8 456 521 644 175 49 12 2.4
2b 0.23 261 402 210 47 22 12 4
3b 0.03 276 386 203 51 19 9 1.9
a Patient 1 received 2 injections of 0.9-mg recombinant human TSH (injections given on
days 1 and 3).

b Patients 2 and 3 received 2 injections of 0.45-mg recombinant human TSH (injections
given on days 1 and 2).
Figure 1. Serum thyrotropin (TSH) levels after the administration of recombinant
human TSH (rhTSH) in 3 patients with differentiated thyroid cancer and endstage renal
disease. Patient 1 received 2 injections of 0.9-mg rhTSH (given on days 1 and 3).
Patients 2 and 3 received 2 injections of 0.45-mg rhTSH (given on days 1 and 2).
The patient was considered free of disease, and after 3 years of follow-up, she continues
to have undetectable thyroglobulin levels with undetectable thyroglobulin antibodies
and normal neck ultrasonography findings while taking thyroid hormone-suppressive
therapy.
Patient 2
The serum thyroglobulin level assayed 72 hours after the second 0.45-mg rhTSH
injection was undetectable (<0.2 ng/mL), as were thyroglobulin antibodies. The serum
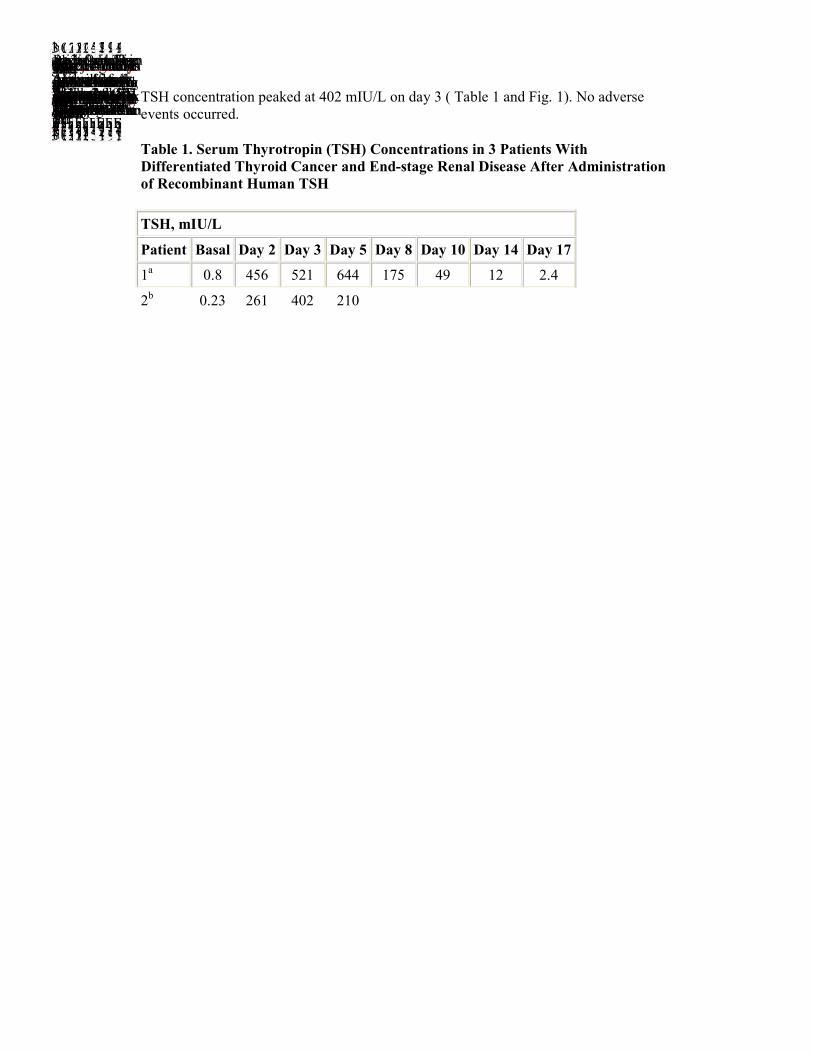
TSH concentration peaked at 402 mIU/L on day 3 ( Table 1 and Fig. 1). No adverse
events occurred.
Table 1. Serum Thyrotropin (TSH) Concentrations in 3 Patients With
Differentiated Thyroid Cancer and End-stage Renal Disease After Administration
of Recombinant Human TSH
TSH, mIU/L
Patient Basal Day 2 Day 3 Day 5 Day 8 Day 10 Day 14 Day 17
1a 0.8 456 521 644 175 49 12 2.4
2b 0.23 261 402 210
47 22 12 4 3b 0.03 276 386 203 51 19 9 1.9 a Patient 1 received 2 injections of 0.9-mg recombinant human TSH (injections given on days 1 and 3). b Patients 2 and 3 received 2 injections of 0.45-mg recombinant human TSH (injections given on days 1 and 2). As a low-risk patient, she was considered free of disease after an undetectable stimulated thyroglobulin level associated with normal neck ultrasonography findings. Patient 3 The serum thyroglobulin level measured 72 hours after the last 0.45-mg rhTSH injection was 4.1 ng/mL, while thyroglobulin antibodies were undetectable. The peak serum TSH concentration was 386 mIU/L on day 3 ( Table 1 and Fig. 1). No adverse events occurred. Table 1. Serum Thyrotropin (TSH) Concentrations in 3 Patients With Differentiated Thyroid Cancer and End-stage Renal Disease After Administration of Recombinant Human TSH TSH, mIU/L Patient Basal Day 2 Day 3 Day 5 Day 8 Day 10 Day 14 Day 17 1a 0.8 456 521 644 175 49 12 2.4 2b 0.23 261 402 210 47 22 12 4 3b 0.03 276 386 203 51 19 9 1.9
a Patient 1 received 2 injections of 0.9-mg recombinant human TSH (injections given on
days 1 and 3). b Patients 2 and 3 received 2 injections of 0.45-mg recombinant human TSH (injections
given on days 1 and 2).
Although this patient had a normal post-dose whole body scan and normal neck
ultrasonography findings, he probably had persistent or recurrent disease as
demonstrated by the continued elevation of the thyroglobulin concentration while taking
levothyroxine treatment and after the use of rhTSH.
Discussion
End-stage renal disease usually affects thyroid function. These alterations include: (a)
lower levels of thyroid peripheral serum hormones, (b) decrease in triiodothyronine and
thyroxine binding to transporting proteins, (c) increase in the storage of organic iodine
in the thyroid gland, (d) elevation of basal serum TSH levels, (e) decrease in the
response of TSH to TSH-releasing hormone, and (f) alteration in serum TSH
glycosylation, among others.[20-22]
Thyroid cancer incidence is reportedly high in patients with renal failure. A weakened
immune system, secondary hyperparathyroidism, nutritional deficiencies, and altered
DNA repair have been proposed as mechanisms.[22-25]
However, the incidence of
differentiated thyroid cancer is not increased in patients with renal failure who are
treated with hemodialysis and have surgery performed because of the presence of
hyperparathyroidism.[26,27]
It has recently been shown that compared with the general
population, the incidence of differentiated thyroid cancer in transplanted patients with
renal failure is higher, and there is also a higher prevalence of lymph node metastasis at
the time of diagnosis.[28]
One of the biggest challenges in patients receiving hemodialysis is the use of high
radioiodine activities due to the altered and variable clearance rates of iodine from the
blood, secondary to variations in dialysis protocols that complicate the selection of
appropriate 131I activity. However, there is compelling evidence that
131I is
hemodialysed, and there have been isolated case reports showing that the careful
handling of the hemodialysis material after radioiodine administration may be safe for
patients and health care professionals involved in the treatment.[22,27]
Recently, Holst et
al[29] performed an extensive literature review regarding this topic. In this review, the
authors identify 20 case reports of radioiodine treatment in patients with end-stage renal
disease.
Although many of these authors do not give specific recommendations about the 131I
activity reductions,[29-31]
others clearly suggest that the amount of 131I should be
decreased.[32,33]
In these articles, a reduction of 40%[32] or use of 25% of the empiric
radioiodine otherwise considered in patients without renal disease[33]
has been
recommended if the patient is on a regimen of hemodialysis sessions 3 times a week.
Dosimetry might be a more suitable method to calculate the required activity in these
cases.[29,30]
In Patients 1 and 3, we administered the empiric radioiodine dose reduced by
approximately 40%.
Patients with renal failure usually have a low quality of life that makes it hard to accept
withdrawal of thyroid hormone-suppressive therapy to perform the follow-up of
differentiated thyroid cancer. Recombinant human TSH is currently approved by the US
Food and Drug Administration and the European Medicines Agency to be used for
diagnostic purposes,[34] and it was recently also approved for thyroid remnant ablation
by both organizations.[35] The rhTSH-aided radioiodine treatment has been presented in
many isolated reports and has recently been reviewed.[14,16]
We have also shown the
usefulness of this procedure for the ablation of thyroid remnants and for the treatment of
patients with metastatic thyroid cancer.[15]
In our experience with patients with normal renal function, the mean serum TSH level
after administration of 2 consecutive 0.9-mg rhTSH injections—measured 24 hours
after the last injection—was 117 ± 34 mIU/L (range, 90-178 mIU/L),[15] which is
similar to serum levels seen by others.[34]
In Patient 1, we decided to administer 2 doses of 0.9-mg rhTSH. Because of technical
reasons, we had to administer the 2 rhTSH injections 48 hours apart. Although the
laboratory result showed a high serum TSH concentration after the first injection, this
TSH value was not available until 3 days later. The detectable thyroglobulin level while
Patient 1 was taking thyroid hormone-suppressive therapy was probably a laboratory
error. A detectable thyroglobulin level while a patient with differentiated thyroid cancer
is receiving suppressive thyroid hormone therapy usually indicates the presence of
persistent disease. This situation led us to administer a high radioiodine dose to evaluate
the situation after a post-dose whole body scan. Although we measured a thyroglobulin
concentration lower than 2 ng/mL after hyperstimulation with very high TSH levels, we
cannot be sure of the disease-free status of this patient because a very small percentage
of patients with persistent disease might have undetectable stimulated thyroglobulin
levels that become measurable after some years of followup.[36] Considering the faint
uptake observed in the thyroid bed only, it is probable that the thyroglobulin level was
produced by nonneoplastic thyroid cells that remained after the radioiodine ablation.
In Patients 2 and 3, we decided to use half of the rhTSH dose, yet quite high serum TSH
levels were still observed. The TSH levels remained elevated for at least 11 days in
Patient 1 and 12 days in Patients 2 and 3.
In the previously reported cases in which rhTSH was used in patients with renal failure,
serum TSH levels were often observed to be higher than 400 mIU/L, and 1 patient had
persistent nausea that lasted 10 days.[17,18]
We observed self-limited diarrhea in Patient 1
only. In the phase 1 study of rhTSH, headache and nausea were associated with very
high TSH levels.[37] These symptoms were not reported by any of the 3 patients in our
study. One possible reason is that nausea and headache are usually frequent symptoms
in patients with end-stage renal disease and perhaps they did not consider them to be
adverse effects.
Conclusion
The high serum TSH levels achieved after conventional and half-dose administration of
rhTSH indicate that dosage adjustments might be considered in patients with end-stage
renal disease to take into consideration that rhTSH seems to be cleared mainly by the
kidney. However, it is probable that rhTSH is a nonhemodialysed compound. The use
of a half dose (0.9 mg) divided into 2 injections seems to produce a more than
adequately high serum TSH level, but since no data are forthcoming about the
therapeutic response experienced by the patients given these 2 doses of rhTSH, it is
difficult to know if they are equivalently efficacious. In any event, we believe that it is
unlikely that a prospective study to define the correct rhTSH dose in patients with end-
stage renal disease will be performed because of the infrequent co-occurrence of
endstage renal disease and differentiated thyroid cancer. Thus, clinical decisions about
use of rhTSH and radioiodine will continue to be made on practical grounds, informed
by the accumulated published experience.
[ CLOSE WINDOW ]
References
1. Schlumberger MJ. Papillary and follicular thyroid carcinoma. N Engl J Med.
1998;338:297-306.
2. Liel Y. Preparation for radioactive iodine administration in differentiated thyroid cancer patients. Clin Endocrinol (Oxf). 2002;57:523-527.
3. Golger A, Fridman TR, Eski S, Witterick IJ, Freeman JL, Walfish PG. Three-
week thyroxine withdrawal thyroglobulin stimulation screening test to detect
low-risk residual/recurrent well-differentiated thyroid carcinoma. J Endocrinol
Invest. 2003;26:1023-1031.
4. Kuijt WJ, Huang SA. Children with differentiated thyroid cancer achieve
adequate hyperthyrotropinemia within 14 days of levothyroxine withdrawal. J
Clin Endocrinol Metab. 2005;90:6123-6125.
5. Dow KH, Ferrel BR, Anello C. Quality-of-life changes in patients with thyroid cancer after withdrawal of thyroid hormone therapy. Thyroid. 1997;7:613-619.
6. Schroeder PR, Haugen BR, Pacini F, et al. A comparison of short-term changes in health-related quality of life in thyroid carcinoma patients undergoing
diagnostic evaluation with recombinant human thyrotropin compared with
thyroid hormone withdrawal. J Clin Endocrinol Metab. 2006;91:878-884.
7. Luster M, Felbinger R, Dietlein M, Reiners C. Thyroid hormone withdrawal in
patients with differentiated thyroid carcinoma: a one hundred thirty-patient pilot
survey on consequences of hypothyroidism and a pharmacoeconomic
comparison to recombinant thyrotropin administration. Thyroid. 2005;15:1147-
1155.
8. Cohen O, Dabhi S, Karasik A, Zila Zwas S. Compliance with follow-up and the informative value of diagnostic whole-body scan in patients with differentiated
thyroid carcinoma given recombinant human TSH [erratum in Eur J Endocrinol.
2005;153:627]. Eur J Endocrinol. 2004;150:285-290.
9. Wondisford FE, Radovick S, Moates JM, Usala SJ, Weintraub BD. Isolation and
characterization of the human thyrotropin beta-subunit gene. Differences in gene
structure and promoter function from murine species. J Biol Chem.
1988;263:12538-12542.
10. Thotakura NR, Desai RK, Bates LG, Cole ES, Pratt BM, Weintraub BD.
Biological activity and metabolic clearance of a recombinant human thyrotropin
produced in Chinese hamster ovary cells. Endocrinology. 1991;128:341-348.
11. Huber GK, Fong P, Concepcion ES, Davies TF, et al. Recombinant human thyroid-stimulating hormone: initial bioactivity assessment using human fetal
thyroid cells. J Clin Endocrinol Metab. 1991;72:1328-1331.
12. Ramirez L, Braverman LE, White B, Emerson CH, et al. Recombinant human
thyrotropin is a potent stimulator of thyroid function in normal subjects. J Clin
Endocrinol Metab. 1997;82:2836-2839.
13. Torres MS, Ramirez L, Simkin PH, Braverman LE, Emerson CH. Effect of
various doses of recombinant human thyrotropin on the thyroid radioactive
iodine uptake and serum levels of thyroid hormones and thyroglobulin in normal
subjects. J Clin Endocrinol Metab. 2001;86:1660-1664.
14. Luster M, Lippi F, Jarzab B, et al. rhTSH-aided radioiodine ablation and
treatment of differentiated thyroid carcinoma: a comprehensive review. Endocr
Relat Cancer. 2005;12:49-64.
15. Pitoia F, Tamer EE, Schere DB, Passerieu M, Bruno OD, Niepomniszcze H.
Usefulness of recombinant human TSH aided radioiodine doses administered in
patients with differentiated thyroid carcinoma. Medicina (B Aires).
2006;66:125-130.
16. Robbins RJ, Driedger A, Magner J, U.S. and Canadian Thyrogen Compassionate
Use Program Investigator Group. Recombinant human thyrotropin-assisted
radioiodine therapy for patients with metastatic thyroid cancer who could not
elevate endogenous thyrotropin or be withdrawn from thyroxine. Thyroid.
2006;16:1121-1130.
17. Jawa A, Pendergrass M. A case of recombinant TSH for the treatment of
papillary thyroid cancer in a patient with end stage renal disease. Abstract
presented at: 75th Annual Meeting of the Thyroid Association; September 2003;
Palm Beach, Florida.
18. Pellegriti G, Scollo C, Giuffrida D, Vigneri R, Squatrito S, Pezzino V. Usefulness of recombinant human thyrotropin in the radiometabolic treatment of
selected patients with thyroid cancer. Thyroid. 2001;11:1025-1030.
19. Pitoia F, El Tamer E, Zanchetta MB, Danilowicz K, Lucas S, Niepomniszcze H.
Niveles séricos de TSH luego de la administración de TSH recombinante en un
paciente con carcinoma diferenciado de tiroides e insuficiencia renal terminal
[article in Spanish]. Rev Arg Endocrinol Metab. 2006;43:83-89.
20. Lim VS. Thyroid function in patients with chronic renal failure. Am J Kidney Dis. 2001;38:S80-84.
21. Kaptein EM, Quion-Verde H, Chooljian CJ, et al. The thyroid in end-stage renal
disease. Medicine (Baltimore). 1988;67:187-197.
22. Kaptein EM. Thyroid hormone metabolism and thyroid diseases in chronic renal
failure. Endocr Rev. 1996;17:45-63.
23. Vamvakas S, Bahner U, Heidland A. Cancer in end-stage renal disease: potential factors involved -editorial. Am J Nephrol. 1998;18:89-95.
24. Sinsakul M, Ali A. Radioactive 131I use in end-stage renal disease: nightmare
or nuisance? Semin Dial. 2004;17:53-56.
25. Wang TH, Lee CH, Tseng LM, Liu RH. The management of well-differentiated
thyroid cancer with end-stage renal disease. Endocrine. 2003;21:227-231.
26. Seehofer D, Rayes N, Klupp J, et al. Prevalence of thyroid nodules and carcinomas in patients operated on for renal hyperparathyroidism: experience
with 339 consecutive patients and review of the literature. World J Surg.
2005;29:1180-1184.
27. Demirer AN, Kemal Y, Gursoy A, Sahin M, Tutuncu NB. Clinicopathological
characteristics of thyroid cancer in patients on dialysis for end-stage renal
disease. Thyroid. 2008;18:45-50.
28. Pond F, Serpell JW, Webster A. Thyroid cancer in the renal transplant
population: epidemiological study. ANZ J Surg. 2005;75:106-109.
29. Holst JP, Burman KD, Atkins F, Umans JG, Jonklaas J. Radioiodine therapy for thyroid cancer and hyperthyroidism in patients with end-stage renal disease on
hemodialysis. Thyroid. 2005;15:1321-1331.
30. Morrish DW, Filipow LJ, McEwan AJ, et al. 131I treatment of thyroid papillary
carcinoma in a patient with renal failure. Cancer. 1990;66:2509-2513.
31. Magné N, Magné J, Bracco J, Bussière F. Disposition of radioiodine (131)I
therapy for thyroid carcinoma in a patient with severely impaired renal function
on chronic dialysis: a case report. Jpn J Clin Oncol. 2002;32:202-205.
32. Howard N, Glasser M. Iodine 131 ablation therapy for a patient on maintenance
haemodialysis. Br J Radiol. 1981;54:259.
33. Daumerie C, Vynckier S, Caussin J, et al. Radioiodine treatment of thyroid carcinoma in patients on maintenance hemodialysis. Thyroid. 1996;6:301-304.
34. Haugen BR, Pacini F, Reiners C, et al. A comparison of recombinant human thyrotropin and thyroid hormone withdrawal for the detection of thyroid
remnant or cancer. J Clin Endocrinol Metab. 1999;84:3877-3885.
35. Pacini F, Ladenson PW, Schlumberger M, et al. Radioiodine ablation of thyroid
remnants after preparation with recombinant human thyrotropin in differentiated
thyroid carcinoma: results of an international, randomized, controlled Study. J
Clin Endocrinol Metab. 2006;91:926-932.
36. Kloos RT, Mazzaferri EL. A single recombinant human thyrotropin-stimulated
serum thyroglobulin measurement predicts differentiated thyroid carcinoma
metastases three to five years later. J Clin Endocrinol Metab. 2005;90:5047-
5057.
37. Meier CA, Braverman LE, Ebner SA, et al. Diagnostic use of recombinant
human thyrotropin in patients with thyroid carcinoma (phase I/II study). J Clin
Endocrinol Metab. 1994;78:188-196.
Reprint Address
Dr. Fabián Pitoia, Esmeralda 961 PB "J," (1007) Buenos Aires, Argentina. E-mail:
Abbreviation Notes
rhTSH = recombinant human thyrotropin; TSH = thyrotropin
Endocrine Practice. 2008;14(8):961-966. © 2008 American Association of Clinical
Endocrinologists




















