
Quality of Vision after Bilateral Multifocal Intraocular Lens Implantation
Upload
independentCategory
view
0download
0
Optical quality of the eye after lens replacementwith a pseudoaccommodating intraocular lens
Robert Montes-Mico, PhD, Teresa Ferrer-Blasco, MSc, W. Neil Charman, PhD,Alejandro Cervino, PhD, Jose F. Alfonso, MD, PhD, Luis Fernandez-Vega, MD, PhD
PURPOSE: To examine the optical quality of healthy presbyopic eyes before and after implantationof the pseudoaccommodating AcrySof ReSTOR Natural intraocular lens (IOL) (Alcon Laboratories)by measuring visual acuity and wavefront aberrations.
SETTING: University of Valencia, Fernandez-Vega Ophthalmological Institute, Valencia, Spain.
METHODS: Monocular refraction and photopic distance (6 m) and near (0.33 m) visual acuitieswere determined before and after clear lens extraction with bilateral AcrySof ReSTOR NaturalIOL implantation in 30 hyperopic eyes (C0.50 to C4.00 diopters [D]) of presbyopic patientswith low astigmatism (%1.00 D). Postsurgical binocular visual acuity was measured over a rangeof effective distances. Wavefront aberrations were measured before and after surgery. Aberrationsfor 2 pupil diameters (3.0 mm and 5.0 mm) were decomposed using Zernike polynomials; total,defocus, astigmatism spherical, and coma aberration terms were studied separately. Postimplan-tation results were compared with preoperative values.
RESULTS: Safety and efficacy indices for distance vision were 1.01 and 0.96, respectively. At near,they improved to 1.07 and 1.06, respectively. Vision at intermediate distances was noticeably poor-er. Total, defocus, and spherical aberrations changed after IOL implantation with both pupil diam-eters (P<.01). Total and defocus aberrations were significantly reduced postoperatively. Sphericalaberration coefficients changed to negative and less positive values for a 3.0 mm and a 5.0 mmpupil, respectively.
CONCLUSIONS: Implantation of the pseudoaccommodating IOL in healthy eyes yielded uncorrectedlevels of high-contrast, distance, and near acuities comparable to preoperative best correctedvalues. Higher-order aberration levels appeared to be similar to the preoperative values.
J Cataract Refract Surg 2008; 34:763–768 Q 2008 ASCRS and ESCRS
ARTICLE
Pseudoaccommodating intraocular lenses (IOLs) aredesigned to reduce dependence on eyeglasses fordistance and near vision after cataract surgery or clearlens extraction (CLE). They are gaining acceptance asa potential refractive surgical option for selectedpatients. Although monofocal IOLs provide excellentvisual function, in many cases their limited depth-of-focus means that these IOLs cannot provide clearvision at both distance and near unless they are usedin a monovision arrangement. Patients with tradi-tional monofocal IOLs usually require glasses fornear tasks such as reading. With the introduction ofpseudoaccommodating IOLs, cataract and refractivesurgeons can offer patients the potential for a fullrange of uncorrected vision, from near to far.
Approaches to pseudoaccommodating IOLs can bebroadly categorized as refractive or diffractive. Dif-fractive IOLs, the first to be evaluated clinically,
Q 2008 ASCRS and ESCRS
Published by Elsevier Inc.
initially showed significant optical deficiencies.1–3
Refractive zonal-progressive IOLs were developed toavoid the problems of diffractive IOLs, giving, despitetheir bias toward distance vision, acceptable distanceand near visual performance when implanted.4,5
New diffractive IOL designs are reported to offer bet-ter visual quality than earlier models.6,7 The retinal im-age quality with refractive IOLs depends on pupildiameter because of the zonal nature of the power pro-file. Full-aperture diffractive IOLs are less pupildependent than refractive IOLs, with advantages innear vision,8 because the diffractive surface effectivelygenerates a superimposed distance and near correc-tion over its full aperture. However, the superpositionof (at distance) an in-focus distance retinal imageformed by the distance correction and an out-of-focusimage formed by the near correction leads to a loss inretinal image contrast.9 A similar effect occurs at near.
0886-3350/08/$dsee front matter 763doi:10.1016/j.jcrs.2008.01.017

764 OPTICAL QUALITY OF THE EYE WITH THE ACRYSOF RESTOR IOL
These losses in contrast lead to night-vision distur-bances and a reduction in contrast sensitivity.6,7,10
A new optical concept, refractive–diffractive optics,was recently applied to pseudoaccommodating IOLdesign. The AcrySof ReSTOR IOL (Alcon Laborato-ries) uses this hybrid concept in an attempt to reducethe disadvantages of conventional refractive anddiffractive IOLs.11 The central diffractive zone diame-ter is restricted to 3.6 mm, and the outer zones of thelens correspond to the distance correction. Within thediffractive region, diffractive efficiency is arranged todecrease as the zonal radius increases (apodization).Therefore, the fraction of the light contributing to thenear image progressively decreases as the pupil radiusincreases. The overall result is that under mesopic,large-pupil, night-driving conditions, the IOL actssimilar to an IOL giving distance monofocalcorrection, with little loss in contrast for the imagesof distant objects and minimal halos or other distur-bances. On the other hand, under photopic small-pupilconditions, near and distance corrections are simulta-neously available, with similar amounts of light(nominally about 40%) contributing to each of the 2corresponding retinal images.11 Although some stud-ies found this IOL provides a satisfactory full rangeof vision in terms of visual acuity and contrast sensitiv-ity under bright and dim conditions and has a lowincidence of visual disturbances after cataractsurgery12,13 and CLE,14 others found less satisfactoryresults with regard to visual disturbances, with evi-dence of marked increases in halos and glare afterIOL implantation in up to 30% of patients.15–18
If these IOLs are to be useful in CLE surgery, postim-plantation visual performance at distance and nearmust show significant improvement over that of the
Accepted for publication January 8, 2008.
From the Optometry Research Group (Montes-Mico, Ferrer-Blasco,Cervino), Optics Department, University of Valencia, and theFernandez-Vega Ophthalmological Institute (Alfonso, Fernandez-Vega), Valencia, and the Surgery Department (Alfonso, Fernandez-Vega), School of Medicine, University of Oviedo, Oviedo, Spain;Faculty of Life Sciences (Charman), University of Manchester, Man-chester, United Kingdom.
No author has a financial or proprietary interest in any material ormethod mentioned.
Supported in part by a Universitat de Valencia research grant (UV-AE-20070225) (Dr. Montes-Mico).
Corresponding author: Robert Montes-Mico, PhD, Optometry Re-search Group, Optics Department, Faculty of Physics, Universityof Valencia, C/Dr. Moliner, 50. 46100, Burjassot (Valencia), Spain.E-mail: [email protected].
J CATARACT REFRACT SU
natural presbyopic eye. Distance acuity should be atleast as good as that of the natural presbyopic eyeand performance at intermediate and near distances,markedly superior. As yet, the optical performanceof eyes with these IOLs has not been systematicallycompared with that of natural phakic eyes, althoughpostoperative wavefront analysis after cataractsurgery with AcrySof ReSTOR IOL implantationyielded total and higher-order ocular aberrations sim-ilar to those found in eyes with amonofocal IOL.16,17,19
Spherical aberration is reported to be significantly lessthan with monofocal IOLs.17,19
The best way to assess the in vivo performance ofthese IOLs is to compare the optical quality of thewhole eye before and after IOL implantation. Thus,the aim of this study was to evaluate the changes inoptical quality in terms of wavefront aberrations (totaland higher order) as well as changes in visual perfor-mance in 30 healthy, noncataractous eyes before andafter CLE combined with bilateral pseudoaccommo-dating IOL implantation in the capsular bag.
PATIENTS AND METHODS
This study included 15 hyperopic patients (30 eyes). Thestudy followed the tenets of the Declaration of Helsinki.Informed consent was obtained from all patients after thenature and possible consequences of the study wereexplained. All patients had bilateral implantation of theAcrySof ReSTOR Natural multifocal IOL (model SN60D3)to correct ametropia and presbyopia. Inclusion criteriawere age between 50 and 60 years and the desire to no longerwear spectacle or contact lens correction for distance andnear vision. Exclusion criteria included ocular disease (eg,cataract, glaucoma, macular degeneration, corneal or neuro-ophthalmic disease), best corrected distance visual acuityworse than 20/25 (logMAR 0.10) in either eye, a history ofocular surgery or inflammation, and astigmatism greaterthan 1.00 diopter (D).
Intraocular Lens Characteristics
The AcrySof ReSTORNatural multifocal IOL combines anapodized diffractive region and a refractive region.11 Theapodized diffractive optics is within the central 3.6 mm opti-cal zone of the IOL; because of the magnifying effect of thecornea, this zone appears to be approximately 4.1 mm inthe entrance pupil of the eye. This apodized area comprises12 concentric annuli of gradually decreasing (1.3 to 0.2 mm)step heights. The combined effect of the diffractive annuliis to produce superimposed diffracted wavefronts, 1 ofwhich contributes to the distance correction and the otherto the near addition. The refractive region of the optic sur-rounds the apodized diffractive region. This area directslight to a distance focal point with larger pupil diametersand is dedicated to distance vision. The overall diameter ofthe IOL is 13.0 mm and the optical diameter, 6.0 mm. TheIOL power varies from C10.0 to C30.0 D; the nominal dif-fractive near addition (add) is C4.0 D, equivalent to approx-imately 3.2 D in the spectacle plane.11 Because diffractivepower is directly proportional to wavelength, the actualadd power would be expected to vary by a factor of nearly
RG - VOL 34, MAY 2008

765OPTICAL QUALITY OF THE EYE WITH THE ACRYSOF RESTOR IOL
2 across the visible spectrum. If, as is likely, the add power of3.2 D is specified at a wavelength of about 550 nm, it willdecrease to approximately 2.3 D at 400 nm and increase to4.1 D at 700 nm; the exact powers vary with the distancepower of the IOL and the individual eye. However, thisvariation is counterbalanced by the natural longitudinalchromatic aberration (approximately 1.5 D across the visiblespectrum) of the eye’s cornea and media. Because this is ofopposite sign, it reduces the importance of the variationwith wavelength in the add power of the IOL; at near, theeye should be approximately corrected for longitudinal chro-matic aberration.20 Diffractive efficiency also varies withwavelength and probably decreases toward the extremesof the spectrum.
Patient Evaluations and Surgical Technique
Before the CLE procedure, patients had a completeophthalmologic examination, including manifest and cyclo-plegic refractions, keratometry, slitlamp biomicroscopy,Goldmann applanation tonometry, and binocular indirectophthalmoscopy through a dilated pupil. Axial length andanterior segment size were measured with the DGH-5100Ebiometer (DGH Technology, Inc.).
The Holladay 2 formula was used for IOL power calcula-tion. The targeted refraction was emmetropia.
All surgeries comprised phacoemulsification using topicalanesthesia and a 2.8 to 3.2 mm clear corneal incision. Phaco-emulsification was followed by irrigation and aspiration ofthe cortex and IOL implantation in the capsular bag. Clearlens extraction was performed in both eyes within 2 weeks.
Distance (6 m) measurements included monocular uncor-rected visual acuity (UCVA) and best corrected visual acuity(BCVA). At near (0.33m), uncorrected near visual acuity andbest distance corrected near visual acuity were determined;logMAR charts were used for all measurements. The meanchart luminance level was approximately 80 cd/m2 so thatthe measurements were photopic and the pupil diameterswere modest (approximately 4.0 mm). Measurements wererecorded preoperatively and postoperatively in all patients.Postoperative assessments were routinely performed at 1week and 1 and 3months. Through-focus binocular logMARacuity was also measured 3 months after surgery. Patientsobserved a distance logMAR chart through pairs of negativelenses that increased from 0.00 to �5.00 D in 0.50 D steps.
Wavefront aberration analysis was performed with theLADARWave aberrometer (Alcon Laboratories), which isbased on the Hartmann-Shack aberrometer.21 Wavefrontmeasurements with the LADARWave aberrometer arereported to have good reproducibility.22 The wavefrontmaps were analyzed with a 3.0 mm and 5.0 mm pupil diam-eter, corresponding approximately to the range of pupildiameters encountered under normal photopic conditionsin the patients’ age group. The diffractive add (diameter ap-proximately 4.1 mm in the entrance pupil) fills the 3.0 mmpupil but not the 5.0 mm pupil. The measurements wereperformed in a darkened room to avoid the need for pharma-cologic pupil dilation. Patients were instructed to blink 3 or 4times and fixate on a distant image created by the aberrom-eter while keeping their eyes wide open. One imagewas cap-tured with the aberrometer 3 seconds postblink in all eyes,avoiding temporal air–tear film changes.23,24 Each patienthad 2 separate aberrometer examinations before and afterIOL implantation. The mean Zernike coefficients were usedto calculate the total monochromatic wavefront aberration.
J CATARACT REFRACT SU
This study focused on the Zernike terms of defocus, astigma-tism, coma, and spherical aberration because these termshave the greatest potential visual impact.
Statistical Analysis
Data were analyzed using SPSS for Windows (version12.0, SPSS Inc.). Normality was assessed by the Shapiro-Wilk test, and the t test was used to compare preoperativeand postoperative outcomes. Differences were consideredto be statistically significant when the P value was lessthan 0.01 (ie, at the 1% level).
RESULTS
The study included 13 women and 2 men. Table 1shows the patients’ demographics. There were nointraoperative complications in any case.
Preoperatively, all patients had relatively low hy-peropiawith low levels of astigmatism (Table 1). Threemonths after IOL implantation, the residual meanspherical equivalent refractive error was 0.23 D G0.18 (SD). After surgery, no eye required secondaryintervention. No potentially sight-threatening compli-cations such as persistent corneal edema, pupillaryblock, retinal detachment, or endophthalmitis wereobserved during the postoperative period. In addition,no eye required neodymium:YAG capsulotomy up tothe last postoperative visit. Slitlamp assessmentshowed good IOL centration in relation to the visualaxis in all cases and no IOL tilt in any eye.
Table 2 shows the visual acuity values before andafter the IOL implantation for distance and near. Thepostoperative uncorrected distance acuity and uncor-rected near acuity were comparable to the preopera-tive best corrected values; in particular, good
Table 1. Patient demographics.
Characteristic Value
Mean age (y) G SD 55.2 G 2.7Mean IOL power (D) G SD C23.93 G 2.95Preoperative sphere (D)Mean G SD C2.18 G 1.17Range C0.50 to C4.00
Preoperative cylinder (D)Mean G SD �0.38 G 0.45Range 0.00 to �1.00
Preoperative keratometry (D)Mean K1 G SD 43.31 G 1.73Mean K2 G SD 43.73 G 1.92Range 40.75 to 45.00
Axial length (mm)Mean G SD 22.60 G 1.12Range 20.61 to 23.90
IOL Z intraocular lens
RG - VOL 34, MAY 2008
766 OPTICAL QUALITY OF THE EYE WITH THE ACRYSOF RESTOR IOL
uncorrected acuity was achieved at near. The safety in-dex (ratio of postoperative and preoperative BCVAs)for distance vision was 1.02. The efficacy index (ratioof postoperative UCVA and preoperative BCVA)was 0.91. Safety and efficacy indices for near visionwere 1.10 and 1.12, respectively, although the differ-ences in best corrected acuities were not significant.
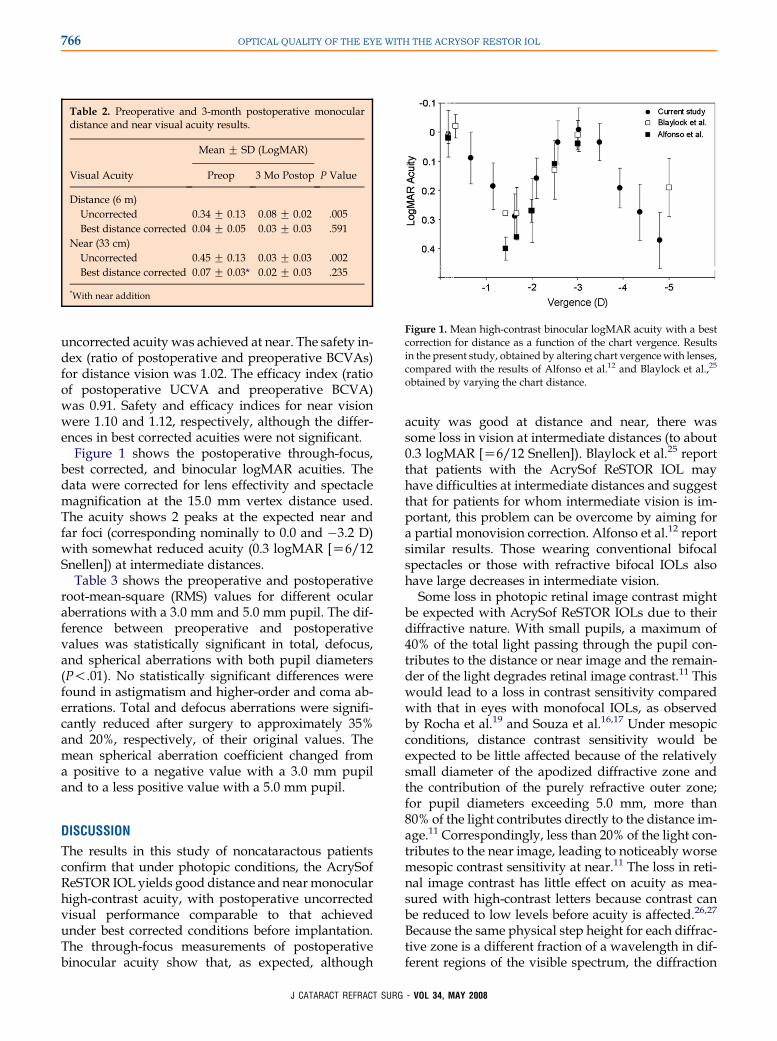
Figure 1 shows the postoperative through-focus,best corrected, and binocular logMAR acuities. Thedata were corrected for lens effectivity and spectaclemagnification at the 15.0 mm vertex distance used.The acuity shows 2 peaks at the expected near andfar foci (corresponding nominally to 0.0 and �3.2 D)with somewhat reduced acuity (0.3 logMAR [Z6/12Snellen]) at intermediate distances.
Table 3 shows the preoperative and postoperativeroot-mean-square (RMS) values for different ocularaberrations with a 3.0 mm and 5.0 mm pupil. The dif-ference between preoperative and postoperativevalues was statistically significant in total, defocus,and spherical aberrations with both pupil diameters(P!.01). No statistically significant differences werefound in astigmatism and higher-order and coma ab-errations. Total and defocus aberrations were signifi-cantly reduced after surgery to approximately 35%and 20%, respectively, of their original values. Themean spherical aberration coefficient changed froma positive to a negative value with a 3.0 mm pupiland to a less positive value with a 5.0 mm pupil.
DISCUSSION
The results in this study of noncataractous patientsconfirm that under photopic conditions, the AcrySofReSTOR IOL yields good distance and nearmonocularhigh-contrast acuity, with postoperative uncorrectedvisual performance comparable to that achievedunder best corrected conditions before implantation.The through-focus measurements of postoperativebinocular acuity show that, as expected, although
Table 2. Preoperative and 3-month postoperative monoculardistance and near visual acuity results.
Mean G SD (LogMAR)
Visual Acuity Preop 3 Mo Postop P Value
Distance (6 m)Uncorrected 0.34 G 0.13 0.08 G 0.02 .005Best distance corrected 0.04 G 0.05 0.03 G 0.03 .591
Near (33 cm)Uncorrected 0.45 G 0.13 0.03 G 0.03 .002Best distance corrected 0.07 G 0.03* 0.02 G 0.03 .235
*With near addition
J CATARACT REFRACT SU
acuity was good at distance and near, there wassome loss in vision at intermediate distances (to about0.3 logMAR [Z6/12 Snellen]). Blaylock et al.25 reportthat patients with the AcrySof ReSTOR IOL mayhave difficulties at intermediate distances and suggestthat for patients for whom intermediate vision is im-portant, this problem can be overcome by aiming fora partial monovision correction. Alfonso et al.12 reportsimilar results. Those wearing conventional bifocalspectacles or those with refractive bifocal IOLs alsohave large decreases in intermediate vision.
Some loss in photopic retinal image contrast mightbe expected with AcrySof ReSTOR IOLs due to theirdiffractive nature. With small pupils, a maximum of40% of the total light passing through the pupil con-tributes to the distance or near image and the remain-der of the light degrades retinal image contrast.11 Thiswould lead to a loss in contrast sensitivity comparedwith that in eyes with monofocal IOLs, as observedby Rocha et al.19 and Souza et al.16,17 Under mesopicconditions, distance contrast sensitivity would beexpected to be little affected because of the relativelysmall diameter of the apodized diffractive zone andthe contribution of the purely refractive outer zone;for pupil diameters exceeding 5.0 mm, more than80% of the light contributes directly to the distance im-age.11 Correspondingly, less than 20% of the light con-tributes to the near image, leading to noticeably worsemesopic contrast sensitivity at near.11 The loss in reti-nal image contrast has little effect on acuity as mea-sured with high-contrast letters because contrast canbe reduced to low levels before acuity is affected.26,27
Because the same physical step height for each diffrac-tive zone is a different fraction of a wavelength in dif-ferent regions of the visible spectrum, the diffraction
Figure 1. Mean high-contrast binocular logMAR acuity with a bestcorrection for distance as a function of the chart vergence. Resultsin the present study, obtained by altering chart vergencewith lenses,compared with the results of Alfonso et al.12 and Blaylock et al.,25
obtained by varying the chart distance.
RG - VOL 34, MAY 2008

767OPTICAL QUALITY OF THE EYE WITH THE ACRYSOF RESTOR IOL
Table 3. Preoperative and 3-month postoperative RMS of total and higher-order aberrations by pupil diameter.
Mean RMS (mm) G SD
3.0 mm Pupil 5.0 mm Pupil
Aberration Preop 3 Mo Postop Preop 3 Mo Postop
Total 0.755 G 0.126 0.275 G 0.111† 1.948 G 0.542 0.724 G 0.306†
Higher order 0.054 G 0.005 0.074 G 0.020 0.319 G 0.071 0.241 G 0.026Defocus 0.731 G 0.146 0.113 G 0.136† 1.727 G 0.703 0.432 G 0.299†
Astigmatism 0.081 G 0.092 0.141 G 0.070 0.481 G 0.330 0.372 G 0.221Coma 0.017 G 0.012 0.040 G 0.025 0.123 G 0.036 0.094 G 0.031Spherical* 0.016 G 0.005 �0.015 G 0.008† 0.212 G 0.065 0.082 G 0.029†
RMS Z root mean square*Zernike coefficient Z(4,0)†Statistically significant (P!.01)
efficiency and figures for the percentages of light in the2 images will be wavelength dependent.
The reductions in total and defocus wavefrontaberrations after IOL implantation in our study reflectthat the original spherical refractive errors werelargely corrected after IOL implantation. We canconvert from the 2nd-order Zernike RMS aberrationvalue C(2,0) (mm) to the corresponding dioptric defo-cus using
DefocusZ�4:
ffiffiffi3p �
C02=R
2 diopters
where R is the pupil radius (mm).28 With a 3.0 mmpupil, the preoperative and postoperative RMS defo-cus values convert to a mean spherical focus error of2.25 D and 0.35 D, respectively, and with a 5.0 mmpupil, to errors of 1.91 D and 0.48 D, respectively.These values are compatible with the mean refractiveerrors found clinically (2.18 D and 0.23 D, respec-tively). The mean postoperative total RMS aberrationwith a 5.0 mm pupil in our study is comparable tothat found by Rocha et al.19 (0.24 mm and 0.35 mm,respectively).
More interesting are the before and after compari-sons between the total higher-order (3rd and above)Zernike aberrations. With the 3.0 mm pupil, the levelsof total higher-order aberration before and afterimplantation were low (approximately a tenth ofa wavelength) and thus had a negligible effect on ret-inal image quality. With the 5.0 mm pupil, there wasa slight reduction in total higher-order RMS aberra-tion. If this is expressed in terms of the equivalentdefocus (the defocus that gives the same RMS aberra-tion), it corresponds to reducing equivalent dioptricblur from approximately 0.35 to 0.27 D, a rather smallamount. There were no significant changes in astigma-tism or coma-like or 3rd-order aberrations, suggestingthat the IOLs were centered and with little tilt. The
J CATARACT REFRACT SU
only individual change that reached significance wasspherical aberration, which changed in the negativedirection. This is presumably because the IOL, withits homogeneous and relatively high refractive index(1.55) and different surface curvatures, produces lesspositive spherical aberration than the natural, gradi-ent-index crystalline lens. The mean level of postim-plantation spherical aberration (0.08 G 0.03 mm) wascomparable to that found by Rocha et al.19 (0.09 G0.05 mm) in patients with the same IOL type and5.0 mm pupils. Although statistically significant, thesechanges were too small to have obvious visual impact.
Regarding the aberration measurements, somedoubts exist over what any aberrometer is trulymeasuringwhen apatient has a diffractive IOL.29,30 Be-cause the IOL has 2 powers, and hence produces2 wavefronts, there is ambiguity about whether thedistance or near wavefront is being measured. In thepresent study, the correspondence between the defo-cus aberration value and the clinical refractive errorand the fact that diffractive efficiency is probably lowat the infrared wavelength used for measurement(820 nm for the LADARWave Shack-Hartmann instru-ment) suggest that the ‘‘distance’’ aberrationwas likelyrecorded.A further limitation of aberrometermeasure-ments to assess optical image quality is that they fail togive a direct indication of the effects of light scatter inthe retinal image. The effects may be severe with theAcrySof ReSTOR Natural IOL because approximately20% of the light is likely to be scattered or diffractedinto unwanted higher-order images.11
Originally, the hyperopic presbyopic patients in ourstudy had poor acuity at distance and near and re-quired optical corrections for both distances to seeclearly. Patient satisfaction with the IOLs was there-fore high, largely because the significant improvementin uncorrected acuity at distance and near gave free-dom from the need to wear a correction for most
RG - VOL 34, MAY 2008

768 OPTICAL QUALITY OF THE EYE WITH THE ACRYSOF RESTOR IOL
purposes. Presumably, when younger, these patientswith relatively low hyperopia were able to dispensewith correction much of the time by using their still-active accommodation and wished to regain this free-dom. In contrast, patients with low myopia might beexpected to gain less benefit because their uncorrectedvision at near may be good and a correction may be re-quired for distance vision only. Excimer laser surgerycan be used to refine the correction in all patients withsignificant residual uncorrected refractive errors andthus a lower level of distance acuity.31
To summarize, the present study of patients whowere originally low hyperopes with low astigmatismconfirms findings in earlier studies that showed theapodized diffractive AcrySof ReSTOR Natural IOLcan yield good high-contrast, photopic, uncorrectedvisual acuity at distance and near. Intermediate visionis slightly impaired, as is vision of low-contrast objects.Aberration levels after implantation appear to be sim-ilar to those in the natural eye.
REFERENCES1. Percival SPB. Prospective study of the new diffractive bifocal in-
traocular lens. Eye 1989; 3:571–575
2. Jay JL, Chakrabarti HS, Morrison JD. Quality of vision through
diffractive bifocal intraocular lenses. Br J Ophthalmol 1991;
75:359–366
3. Akutsu H, Legge GE, Luebker A, et al. Multifocal intraocular
lenses and glare. Optom Vis Sci 1993; 70:487–495
4. Montes-Mico R, Alio JL. Distance and near contrast sensitivity
function after multifocal intraocular lens implantation. J Cataract
Refract Surg 2003; 29:703–711
5. Montes-Mico R, Espana E, Bueno I, et al. Visual performance with
multifocal intraocular lenses; mesopic contrast sensitivity under
distance and near conditions. Ophthalmology 2004; 111:85–96
6. Alfonso JF, Fernandez-Vega L, Senaris A, Montes-Mico R. Qual-
ity of vision with the Acri. Twin asymmetricdiffractive bifocal intra-
ocular lens system. J Cataract Refract Surg 2007; 33:197–202
7. Fernandez-Vega L, Alfonso JF, Baamonde MB, Montes-Mico R.
Symmetric bilateral implantation of a distance-dominance dif-
fractive bifocal intraocular lens. J Cataract Refract Surg 2007;
33:1913–1917
8. Walkow T, Liekfeld A, Anders N, et al. A prospective evaluation
of a diffractive versus a refractive designed multifocal intraocular
lens. Ophthalmology 1997; 104:1380–1386
9. Bradley A, Rahman HA, Soni PS, Zhang X. Effects of target dis-
tance and pupil size on letter contrast sensitivity with simultaneous
vision bifocal contact lenses. Optom Vis Sci 1993; 70:476–481
10. Allen ED, Burton RL, Webber SK, et al. Comparison of a diffrac-
tive bifocal and a monofocal intraocular lens. J Cataract Refract
Surg 1996; 22:446–451
11. Davison JA, Simpson MJ. History and development of the apo-
dized diffractive intraocular lens. J Cataract Refract Surg 2006;
32:849–858
12. Alfonso JF, Fernandez-Vega L, Baamonde MB, Montes-Mico R.
Prospective visual evaluation of apodized diffractive intraocular
lenses. J Cataract Refract Surg 2007; 33:1235–1243
13. Alfonso JF, Fernandez-Vega L, Baamonde MB, Montes-Mico R.
Correlation of pupil size with visual acuity and contrast sensitivity
after implantation of an apodized diffractive intraocular lens.
J Cataract Refract Surg 2007; 33:430–438
J CATARACT REFRACT SUR
14. Fernandez-Vega L, Alfonso JF, Rodrıguez PP, Montes-Mico R.
Clear lens extraction with multifocal apodized diffractive intraoc-
ular lens implantation. Ophthalmology 2007; 114:1491–1498
15. Kohnen T, Allen D, Boureau C, et al. European multicenter study
of the AcrySof ReSTOR apodized diffractive intraocular lens.
Ophthalmology 2006; 113:578–584
16. Souza CE, Gerente VM, Chalita MR, et al. Visual acuity, contrast
sensitivity, reading speed, and wavefront analysis; pseudophakic
eye with multifocal IOL (ReSTOR) versus fellow phakic eye in
non-presbyopic patients. J Refract Surg 2006; 22:303–305
17. Souza CE, Muccioli C, Soriano ES, et al. Visual performance of
AcrySof ReSTOR apodized diffractive IOL: a prospective com-
parative trial. Am J Ophthalmol 2006; 141:827–832
18. Chiam PJT, Chan JH, Aggarwal RK, Kasaby S. ReSTOR intra-
ocular lens implantation in cataract surgery: quality of vision.
J Cataract Refract Surg 2006; 32:1459–1463
19. Rocha KM, Chalita MR, B. Souza CE, et al. Postoperative wave-
front analysis and contrast sensitivity of a multifocal apodized
diffractive IOL (ReSTOR) and three monofocal IOLs. J Refract
Surg 2005; 21:S808–S812
20. Atchison DA, Ye M, Bradley A, et al. Chromatic aberration and
optical power of a diffractive bifocal contact lens. Optom Vis
Sci 1992; 69:797–804
21. Cervino A, Hosking SL, Montes-Mico R, Bates K. Clinical ocular
wavefront analyzers: a review. J Refract Surg 2007; 23:603–616
22. Lewis CD, Krueger RR. Reproducibility of wavefront measure-
ments using the LADARWave aberrometer. J Refract Surg
2006; 22:S971–S979
23. Montes-Mico R, Alio JL, Munoz G, et al. Postblink changes in total
andcornealocularaberrations.Ophthalmology2004;111:758–767
24. Montes-Mico R, Alio JL, Munoz G, Charman WN. Temporal
changes in optical quality of air-tear film interface at anterior
cornea after blink. Invest Ophthalmol Vis Sci 2004; 45:1752–
1757. Available at: http://www.iovs.org/cgi/reprint/45/6/1752.
Accessed February 4, 2008
25. Blaylock JF, Si Z, Vickers C. Visual and refractive status at differ-
ent focal distances after implantation of the ReSTOR multifocal
intraocular lens. J Cataract Refract Surg 2006; 32:1464–1473
26. Regan D, Neima D. Low-contrast letter charts as a test of visual
function. Ophthalmology 1983; 90:1192–1200
27. Post CT Jr. Comparison of depth of focus and low-contrast acu-
ities for monofocal versus multifocal intraocular lens patients at 1
year. Ophthalmology 1992; 99:1658–1663; discussion by DD
Koch, 1663–1664
28. Thibos LN. Wavefront data reporting and terminology. J Refract
Surg 2001; 17:S578–S583
29. Charman WN, Montes-Mico R, Radhakrishnan H. Can we mea-
sure wave aberration in patients with diffractive IOLs? J Cataract
Refract Surg 2007; 33:1997
30. Charman WN, Montes-Mico R, Radhakrishnan H. Problems in
the measurement of wavefront aberration for eyes implanted
with diffractive bifocal and multifocal intraocular lenses. In press,
J Refract Surg 2008
31. Fernandez-Vega L, Alfonso JF, Montes-Mico R, Amhaz H.
Visual acuity tolerance to residual refractive errors in patients
with an apodized diffractive intraocular lens. In press, J Cataract
Refract Surg 2008
First author:Robert Montes-Mico, PhD
Optometry Research Group, OpticsDepartment, Faculty of Physics,Universityof Valencia, Valencia, Spain
G - VOL 34, MAY 2008
Copyright © 2022 FDOKUMEN




















