Oncothermia Journal 22 v5.pdf
228
ONCOTHERMIA JOURNAL A publication of Oncotherm ® ISSN 2191-6438 Volume 22 - February 2018 WWW.ONCOTHERMIA-JOURNAL.COM 8 20 22 32 46 57 67 85 103 116 151 178 206 208 Effects of moderate whole-body hyperthermia and complementary medicine in the treatment of rheumatoid arthritis: a preliminary study Combining hyperthermia with the new biologic and immunotherapy drugs Non-oncological & oncological whole-body hyperthermia and a new immunological road to attack cancer? - some treatment procedures Retrospective observational Clinical Study on Relapsed Malignant Gliomas Treated with Electro- hyperthermia Lower and less toxic doses of chemotherapy by combining it with hyperthermia and complementary treatments Modulated Electro-Hyperthermia: Role in Developing Countries Local oncothermia treatment fights against systemic malignancy Oncothermia development in Hungary Effects of moderate whole-body hyperthermia and complementary medicine in the treatment of rheumatoid arthritis: a preliminary study Redefining Hyperthermia: A Not Temperature-Dependent Solution of The Temperature Problem Oncothermia in brain tumours Basic principle and new results of Oncothermia Cooperation of Academic and Industrial Partners to Fight Tumorous Diseases Electrokinetics of Temperature for Development and Treatment of Effusions
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Oncothermia Journal 22 v5.pdf
ONCOTHERMIA JOURNAL
ONCOTHERMIA JOURNAL A publication of Oncotherm®
A publication of Oncotherm®
ISSN 2191-6438
Volume 22 - February 2018
Volume 21 - November 2017
Volume 21 - November 2017
Volume 21 - November 2017
Volume 22 - January 2018
Volume 21 - November 2017
Volume 21 - November 2017
Volume 21 - November 2017
WWW.ONCOTHERMIA-JOURNAL.COM
8
20
22
32
46
57
67
85
103
116
151
178
206
208
Effects of moderate whole-body hyperthermia and complementary medicine in the treatment of rheumatoid arthritis: a preliminary study Combining hyperthermia with the new biologic and immunotherapy drugs Non-oncological & oncological whole-body hyperthermia and a new immunological road to attack cancer? - some treatment procedures Retrospective observational Clinical Study on Relapsed Malignant Gliomas Treated with Electro-hyperthermia Lower and less toxic doses of chemotherapy by combining it with hyperthermia and complementary treatments Modulated Electro-Hyperthermia: Role in Developing Countries Local oncothermia treatment fights against systemic malignancy Oncothermia development in Hungary Effects of moderate whole-body hyperthermia and complementary medicine in the treatment of rheumatoid arthritis: a preliminary study Redefining Hyperthermia: A Not Temperature-Dependent Solution of The Temperature Problem Oncothermia in brain tumours Basic principle and new results of Oncothermia Cooperation of Academic and Industrial Partners to Fight Tumorous Diseases Electrokinetics of Temperature for Development and Treatment of Effusions Redefining Hyperthermia: A Not Temperature-Dependent Solution of The Temperature Problem Oncothermia in brain tumours Cooperation of Academic and Industrial Partners to Fight Tumorous Diseases Electrokinetics of Temperature for Development and Treatment of Effusions

Oncothermia Journal, Volume 22 February 2018
2
Editorial
Liebe Oncotherm-Anwender, Liebe Leser, Ich freue mich, Ihnen den 22. Band unseres Oncothermia Journals (OJ) vorstellen zu können. Unser öffentlich zugängliches Journal ist zu einem wichtigen Forum für den Austausch von Ideen und Informationen über die moderne onkologische Hyperthermie und den damit verbundenen medizinischen Bereichen geworden. Ich hoffe, dass unsere Veröffentlichungen dazu beitragen, die 2000 Jahre alte medizinische Methode auf den neusten Stand der modernen Medizin zu bringen. Der aktuelle OJ-Band bietet wieder ein breites Spektrum an Erkenntnissen an, darunter einige Publikationen zur Ganzkörper-Hyperthermie, welche sich hervorragend mit allen lokalen Anwendungen kombinieren lassen. Ein neuer Ansatz der Onkologie, die Betrachtung der Immun-Aktivitäten, wird ebenfalls präsentiert und zeigt die enorme Flexibilität der onkologischen Hyperthermie. Weitere relevante Themen wie beispielsweise die Glioblastom Therapie und die allgemeinen komplementären Therapien werden ebenfalls besprochen. Die Rolle der Oncothermie in Entwicklungsländern wird diskutiert, ebenso die Entwicklungen in Ungarn. Eine erfreuliche Nachricht ist in diesem Zusammenhang zum Beispiel die bemerkenswerte Unterstützung der ungarischen Behörden bei der Entwicklung eines internationalen Bildungs- und Therapiezentrums für Oncothermie-Anwendungen an der Semmelweis Universität in Budapest. Zusätzlich finden Sie im Journal Ausschnitte von Vorträgen, die auf der Jahreskonferenz der International Clinical Hyperthermia Society (ICHS), welche in Guangzhou, China, im November 2017 stattfand, gehalten wurden. Die Konferenz wurde in einem neuen medizinischen Zentrum, ausgestattet mit 2000 Betten, im Bezirk Panyu, Clifford Estates veranstaltet. Die sehr sorgfältig organisierte Konferenz war sehr luxuriös und lockte mehr als 1000 Teilnehmer an. Prof. Dr. Clifford Pang war der Gastgeber, Vorsitzender und Präsident der Konferenz. Die Präsentationen von Oncotherm haben Verbindungen zwischen den östlichen und westlichen medizinischen Ansätzen hervorgehoben. Die Debatte über die Rolle der Temperatur in der Hyperthermie wird in einem der wissenschaftlichen Artikel angeregt und besprochen. Dieser Artikel wird voraussichtlich zu einer ausführlicheren Diskussion zu diesem ungeklärten Thema führen. Die Diskussion ist umso wichtiger geworden, da die FDA die Therapie TTF-Methode für Gliombehandlungen genehmigt hat. Ich wünsche Ihnen viel Spaß beim Lesen, dass Sie viele neue Informationen erhalten und dass das Journal für alle Leser aus verschiedenen Arbeitsbereichen hilfreich ist. Mit freundlichen Grüßen, Prof. Dr. Andras Szasz
Dear Oncothermia User, Dear Reader, I am pleased to introduce the 22nd volume of our Oncothermia Journal (OJ). It seems to me that our open-access journal became an important forum of exchanging ideas and information in modern oncological hyperthermia and the connected medical fields. I hope our communication helps to renew the 2000 years old medical method fit the state-of-art medicine. The present volume of OJ gives a wide range of knowledge again including some whole-body hyperthermia publications which are in excellent combination with any local applications. The new line of oncology, the immune-activities are also presented showing the massive flexibility of oncological hyperthermia adopting all actual modern therapies. Such relevant topics as the glioblastoma therapy and the general complementary therapies are also included. The role of oncothermia in developing countries is also discussed together with the specialties of the Hungarian developments. I am more than happy to see the remarkable support of the Hungarian authorities to develop an International Education and Therapy Center for oncothermia applications at Semmelweis University, Budapest. It is an excellent opportunity for OJ to publish one small part of the presentations of the International Clinical Hyperthermia Society (ICHS) held in Guangzhou China in November 2017. This large conference was opened in a new, 2000 bed medical center in Panyu District, Clifford Estates. The very carefully organized conference with high luxury conditions attracted more than 1000 participants. The Host and Chairman of the conference was the President of ICHS in 2017, Prof.Dr. Clifford Pang. Oncotherm presentations formed a clear connection between the Eastern and Western medical approaches showing the necessity of the complex unification of the deductive and inductive approaches to the medicine. A real debate on the role of the temperature in hyperthermia is initialized and discussed in one of the papers, which probably will initialize a more extensive discussion on this “enigmatic” topic. This debate is even more important as the FDA approved the therapy TTF-method for glioma treatments. I wish learning and enjoyment by reading the articles in this volume, hoping it benefits for all the readers from laboratories to the paient’s bed side. Sincerely yours, Prof. Dr. Andras Szasz

Oncothermia Journal, Volume 22, February 2018 3
Editor-in-Chief Prof. Dr. András Szász Head of the Department of Biotechnics, St. Istvan University, Godollo, Hungary Chief Scientific Officer (CSO), Oncotherm GmbH, Belgische Allee 9, 53842 Troisdorf, Germany Tel: +49 2241 31992-0; + 36 23 555 510; E-mail: [email protected]
Managing Editors Dr. Janina Leckler Oncotherm GmbH, Belgische Allee 9, 53842 Troisdorf, Germany Tel: +49 2241 31992-0; E-mail: [email protected] and
Ms. Zsófia Hahn Oncotherm Kft., Gyár u. 2. 2040, Budaörs, Hungary Tel: + 36 23 555 510, E-mail: [email protected]
Editorial Board Prof. Dr. Alexander Herzog Chief-physician, Fachklinik Dr. Herzog, Germany
Prof. Dr. Clifford L. K. Pang Managing Director of Clifford Group, P.R. China
Dr. Friedrich Douwes Director Klinik St. Georg, Bad Aibling, Germany,
President of the German Oncological Society DGO
Prof. Dr. Gabriella Hegyi Department of Complementary Medicine, Medical School, University of Pecs, Hungary
Dr. Olivér Szász CEO of Oncotherm Group, Germany and Hungary
Dr. Marcell A. Szász Cancer Center, Semmelweis University, Budapest, Hungary
Prof. Dr. Giammaria Fiorentini Oncology Unit, San Giuseppe General Hospital, Italy
Dr. Gurdev Parmar Director of Integrated Health Clinic, Canada
Dr. Chi Kwan-Hwa President, Taiwan Society Hyperthermic Oncology
Mr. Samuel Yu- Shan Wang Molecular Medicine and Biochemical Engineering
National Chiao Tung University, Hsinchu, Taiwan
Mr. Balázs Tóth Managing Partner, RWU Consulting
Imprint

Oncothermia Journal, Volume 22 February 2018
4
As the editorial team we are committed to a firm and coherent editorial line and the highest possible printing standards. But it is mainly you, the author, who makes sure that the Oncothermia Journal is an interesting and diversified magazine. We want to thank every one of you who supports us in exchanging professional views and experiences. To help you and to make it easier for both of us, we prepared the following rules and guidelines for abstract submission. Als redaktionelles Team vertreten wir eine stringente Linie und versuchen, unserer Publikation den höchst möglichen Standard zu verleihen. Es sind aber hauptsächlich Sie als Autor, der dafür Sorge trägt, dass das Oncothermia Journal zu einem interessanten und abwechslungsreichen Magazin wird. Wir möchten allen danken, die uns im Austausch professioneller Betrachtungen und Erfahrungen unterstützen. Um beiden Seiten die Arbeit zu erleichten, haben wir die folgenden Richtlinien für die Texterstellung entworfen. 1. Aims and Scope The Oncothermia Journal is an official journal of the Oncotherm Group, devoted to supporting those, who would like to publish their results for general use. Additionally, it provides a collection of different publications and results. The Oncothermia Journal has an open-minded character, but it should particularly contain complete study-papers, case-reports, reviews, hypotheses, opinions, and all the informative materials which could be helpful for the international Oncotherm community. Advertisement connected to the topic is also welcome.
• Clinical Studies: Regional or local or multilocal oncothermia or electro cancer therapy (ECT) treatments, case-reports, practical considerations in complex therapies, clinical trials, physiological effects, Oncothermia in combination with other modalities, and treatment optimization.
• Biological Studies: Mechanisms of oncothermia, thermal-or non-temperature dependent effects, response to electric fields, bioelectromagnetic applications for tumors, Oncothermia treatment combination with other modalities, effects on normal and malignant cells and tissues, immunological effects, physiological effects, etc.
• Techniques of oncothermia: Technical development, new technical solutions, proposals. • Hypotheses, suggestions, opinions to improve oncothermia and electro-cancer-therapy methods, intending the
development of the treatments. Further information about the Journal, including links to the online sample copies and content pages can be found on the website of the journal: www.Oncothermia-Journal.com. 1. Selbstverständnis und Ziele Das Oncothermia Journal ist das offizielle Magazin der Oncotherm Gruppe und soll diejenigen unterstützen, die ihre Ergebnisse der Allgemeinheit zur Verfügung stellen möchten. Das Oncothermia Journal ist neuen Inhalten gegenüber offen, sollte aber vor allem Studienarbeiten, Fallstudien, Hypothesen, Meinungen und alle weiteren informativen Materialien, die für die internationale Oncotherm-Gemeinschaft hilfreich sein könnten, enthalten. Werbung mit Bezug zum Thema ist ebenfalls willkommen.
• Klinische Studien, regionale, lokale oder multilokale Oncothermie oder Electro Cancer Therapy (ECT) Behandlungen, Fallstudien, praktische Erfahrungen in komplexen Behandlungen, klinische Versuche, physiologische Effekte, Oncothermie in Kombination mit anderen Modalitäten und Behandlungsoptimierungen.
• Biologische Studien. Mechanismen der Oncothermie, thermale oder temperaturunabhängige Effekte, Ansprechen auf elektrisches Feld, bioelektromagnetische Anwendungen bei Tumoren, Kombination von Oncothermie und anderen Modalitäten, Effekte auf normale und maligne Zellen und Gewebe, immunologische Effekte, physiologische Effekte etc.
• Oncothermie-Techniken. Technische Entwicklungen, neue technische Lösungen. • Hypothesen, Meinungen, wie die Oncothermie- und ECT-Methoden verbessert werden können, um die Behandlung zu
unterstützen. 2. Submission of Manuscripts All submissions should be made online via email: [email protected]. 2. Manuskripte einreichen Manuskripte können online eingereicht werden: [email protected] 3. Preparation of Manuscripts Manuscripts must be written in English, but other languages can be accepted for special reasons, if an English abstract is provided. Texts should be submittedin a format compatible with Microsoft Word for Windows (PC). Charts and tables are considered textual and should also besubmitted in a format compatible with Word. All figures (illustrations, diagrams, photographs) should be provided in JPG format.
Rules for submission
Oncothermia Journal, Volume 22, February 2018 5
Manuscripts may be any length, but must include:
• Title Page. Title of the paper, authors and their affiliations, 1-5 keywords. At least one corresponding author should belisted, whose email address and full contact information has to be provided.
• Abstracts. Abstracts should include the: purpose, materials, methods, results and conclusions. • Test. Unlimited volume. • Tables and Figures. Tables and figures should be referred to in the text (numbered figures and tables). Each table and/or
figure must have a legend that explains its purpose without a reference to the text. Figure files will ideally be submitted as jpg-file (300dpi for photos).
• References. Oncothermia Journal uses the Vancouver (Author-Number) system to indicate references in the text, tables and legends, e.g. [1], [1-3], [1-3]. The full references should be listed numerically in order of appearance, and presented following the text of the manuscript.
3. Manuskripte vorbereiten Manuskripte müssen in englischer Sprache vorliegen. Andere Sprachen können in Ausnahmefällen akzeptiert werden, wenn ein englisches Abstract vorliegt. Texte sollten in einem mit Microsoft Word für Windows (PC) kompatiblen Format eingereicht werden. Tabellen sollten in einem Word-kompatiblen Format eingefügt werden. Alle Graphiken (Illustrationen, Diagramme, Photographien) sollten im jpg Format vorliegen. Manuskripte können jede Längen haben, müssen aber die folgenden Punkte enthalten:
• Titelseite. Titel der Arbeit, Autor, Klinikzugehörigkeit, 1-5 Schlüsselworte. Es muss mindestens ein Autor ausgewiesen sein, dessen Email-Adresse und Kontaktdetails angegeben werden.
• Abstracts. Abstracts müssen enthalten: Zielsetzung, Material und Methoden, Ergebnisse, Fazit. • Text. Beliebige Länge. • Abbildungen und Tabellen. Abbildungen und Tabellen sollten im Text erläutert werden (nummeriert). Jede Abbildung /
Tabelle muss eine erklärende Bildunterschrift haben. Bilder sollten als jpg verwendet werden (300 dpi). • Zitate. Das Oncothermia Journal verwendet die Vancouver Methode (Autornummer), um Zitate auszuweisen, z.B. [1], [1-
3], [1-3]. Die Bibliographie erfolgt numerisch in Reihenfolge der Erwähnung im Text. 4. Copyright It is a condition of publication that authors assign copyright or license the publication rights in their articles, including abstracts to the journal. The transmitted rights are not exclusive, the author(s) can use the submitted material without limitations, but Oncothermia Journal also has the right to use it. 4. Copyright Es ist eine Publikationsvoraussetzung, dass die Autoren die Erlaubnis zur Publikation ihres eingereichten Artikels und des dazugehörigen Abstracts unterschreiben. Die überschriebenen Rechte sind nicht exklusiv, der Autor kann das eingereichte Material ohne Limitation nutzen. 5. Electronic Proofs When the proofs are ready, the corresponding authors will receive an e-mail notification. Hard copies of proofs will not be mailed. To avoid delays in the publication, corrections to proofs must be returned within 48 hours, by electronic transmittal or fax. 5. Elektronische Korrekturfahne Wenn die Korrekturfahnen fertig gestellt sind, werden die Autoren per Email informiert. Gedruckte Kopien werden nicht per Post versandt. Um Verzögerungen in der Produktion zu verhindern, müssen die korrigierten Texte innerhalb von 48 Stunden per Email oder Fax zurückgesandt werden. 6. Offprints and Reprints Author(s) will have the opportunity to download the materials in electronic form and use it for theirown purposes. Offprints or reprints ofthe Oncothermia Journal are not available. 6. Sonderdrucke und Nachdrucke Die Autoren haben die Möglichkeit, das Material in elektronischer Form herunterzuladen, Sonderdrucke und Nachdrucke des Oncothermia Journals sind nicht erhältlich. 7. Advertising The Oncothermia Journal accepts advertising in any language but prefers advertisements in English or at least partially in English. The advertising must have a connection tothe topics in the Oncothermia Journal and must be legally correct, having checked that all information is true.

Oncothermia Journal, Volume 22 February 2018
6
7. Werbung Das Oncothermia Journal akzeptiert Werbeanzeigen in allen Sprachen, wünscht aber die zumindest teilweise Gestaltung in englischer Sprache. Die Werbung muss eine Beziehung zu den Themen des Oncothermia Journals haben und der Wahrheit entsprechende Inhalte aufweisen. 8. Legal responsibility Authors of any publications in the Oncothermia Journal are fully responsible for the material which is published. The Oncothermia Journal has no responsibility for legal conflicts due to any publications. The editorial board has the right to reject any publication if its validity has not been verified enough or the board is not convinced by the authors. 8. Haftung Die Autoren aller im Oncothermia Journal veröffentlichten Artikel sind in vollem Umfang für ihre Texte verantwortlich. Das Oncothermia Journal übernimmt keinerlei Haftung für die Artikel der Autoren. Der redaktionelle Beirat hat das Recht, Artikel abzulehnen. 9. Reviewing The Oncothermia Journal has a special peer-reviewing process, represented by the editorial board members and specialists, to whom they are connected. To avoid personal conflicts the opinion of the reviewer will not be released, and her/his name will be handled confidentially. Papers which are not connected to the topicsof the journal could be rejected without reviewing. 9. Bewertung Die Texte für das Oncothermia Journal werden vom redaktionellen Beirat kontrolliert. Um Konflikte zu vermeiden, werden die Namen des jeweiligen Korrektors nicht öffentlich genannt. Artikel, die nicht zu den Themen des Journals passen, können abgelehnt werden.

Oncothermia Journal, Volume 22, February 2018 7
Contents
Contents
Effects of moderate whole-body hyperthermia and complementary medicine in the treatment of rheumatoid arthritis: a preliminary study................................................................................................................... 8
Combining hyperthermia with the new biologic and immunotherapy drugs ............................................ 20
Non-oncological & oncological whole-body hyperthermia and a new immunological road to attack cancer? - some treatment procedures ........................................................................................................................ 22
Retrospective observational Clinical Study on Relapsed Malignant Gliomas Treated with Electro-hyperthermia ........................................................................................................................................................................ 32
Lower and less toxic doses of chemotherapy by combining it with hyperthermia and complementary treatments ........................................................................................................................................... 46
Modulated Electro-Hyperthermia: Role in Developing Countries .................................................................... 57
Local oncothermia treatment fights against systemic malignancy ............................................................... 67
Oncothermia development in Hungary ..................................................................................................................... 85
Effects of moderate whole-body hyperthermia and complementary medicine in the treatment of rheumatoid arthritis: a preliminary study............................................................................................................... 103
Redefining Hyperthermia: A Not Temperature-Dependent Solution of The Temperature Problem 116
Oncothermia in brain tumors ........................................................................................................................................ 151
Basic principle and new results of Oncothermia .................................................................................................. 178
Cooperation of Academic and Industrial Partners to Fight Tumorous Diseases .................................... 206
Electrokinetics of Temperature for Development and Treatment of Effusions ....................................... 208
Advertisement ................................................................................................................................................................... 225

Oncothermia Journal, Volume 22 February 2018
8
Effects of moderate whole-body hyperthermia and complementary medicine in the treatment of rheumatoid arthritis: a preliminary
study
Siddarth Agrawal Integrative Medical Center Sp. z o. o.
Poland
Presented at 35th ICHS, Guangzhou, 2017
Cite this article as: Agrawal S. (2018): Effects of moderate whole-body hyperthermia and complementary medicine in the treatment of rheumatoid arthritis: a
preliminary study; Oncothermia Journal 22:8-19 www.oncothermia-journal.com/journal/2018/Effects_of_moderate -
whole_body.pdf

Oncothermia Journal, Volume 22, February 2018 9
Effects of moderate whole-body hyperthermia and complementary medicine in the
treatment of rheumatoid arthritis: a preliminary study
Abstract
It is estimated that more than two-thirds of patients with rheumatoid arthritis (RA) use
complementary and alternative medicine (CAM). The rationale for the use of some CAM
therapies is supported by reasonable evidence. 8 patients with RA were included in the
preliminary study. Patients received treatment that included whole-body hyperthermia,
ozone major autohemotherapy, intravenous vitamin C and individual nutrition counselling
for 4 weeks. The patient’s perceptions of pain, stiffness, and fatigue were measured on a
100-mm visual analogue scale and were considered as primary outcomes. In all patients,
a significant improvement was seen at the end of the treatment and post-treatment. Pain
and stiffness reduced over 40%, while fatigue nearly 60% for patients with RA. More
importantly, the treatment was found to be safe and did not relate with any adverse
events. The results of this study are encouraging and may become a platform for future
planning of long-term studies with the complementary treatments in combination with
existing standard therapies in RA.
Introduction
Rheumatoid arthritis (RA) is a symmetric, inflammatory, peripheral polyarthritis of
unknown aetiology, which affects multiple small joints of the hands and feet. The evolution
of hyperplastic synovial tissue, leads to deformity through the stretching of tendons and
ligaments and destruction of joints through the erosion of cartilage and bone.
It is estimated that 60% to 90% of persons with arthritis, particularly those with
rheumatoid arthritis, have used complementary and alternative medicine (CAM) [1]. The
rationale for the use of some therapies is supported by a reasonable and fairly consistent
body of evidence.
Oncothermia Journal, Volume 22 February 2018
10
Heat treatment in patients with rheumatic disorders has been used through the ages.
Initially,
the application of hyperthermia treatment was mainly empirical. In the last few decades
evidence from clinical studies documented its beneficial effects in RA [2,3]. Pain and
stiffness decrease, and grip strength and range of motion improve after application of local
hyperthermia [4]. Some studies reported beneficial effects of whole-body hyperthermia
(WBH) [5,6].
In this preliminary study, the effectiveness of whole-body hyperthermia and
complementary therapies in the treatment of rheumatoid arthritis was evaluated.
Material and methods
8 patients with RA were included in the study. Patients received treatment for 4 weeks.
After oral and written information about the treatment and the possible clinical effects of
applied therapies, patients were invited to the study. Informed consent was obtained from
all patients. Clinical measurements were performed before the start of the treatment, at
the end of the 4-week period of therapy and one month after the end of the treatment
series. The patient’s perceptions of pain [7], stiffness [8], and fatigue [9–11] were measured
on a 100-mm visual analogue scale and were considered as primary outcomes.
Statistical analysis
The conformity assessment was carried out by the Shapiro-Wilk test. The homogeneity of
variance was tested with Bartlett's test. The significance of differences in mean values (M)
in more than two populations for parameters of normal distribution and of homogeneous
variances was assessed with analysis of variance (ANOVA). In case of rejection of the null
hypothesis of homogeneity of variance, to verify the differences between the mean values
in pairs, post-hoc tests were performed (Scheffe test). The level p = 0.05 was assumed as
the critical significance level. Data was expressed as M±SD and analysed with the statistical
program STATISTICA v.12 (StatSoft, Inc. Tulsa, USA).

Oncothermia Journal, Volume 22, February 2018 11
Treatment protocol
The treatment protocol consisted of: 4 moderate whole-body hyperthermia sessions (once
every week), 8 sessions (twice every week) of ozone major autohemotherapy (MAHT) and
intravenous vitamin C (IVC), as well as two individual nutrition counselling.
Results
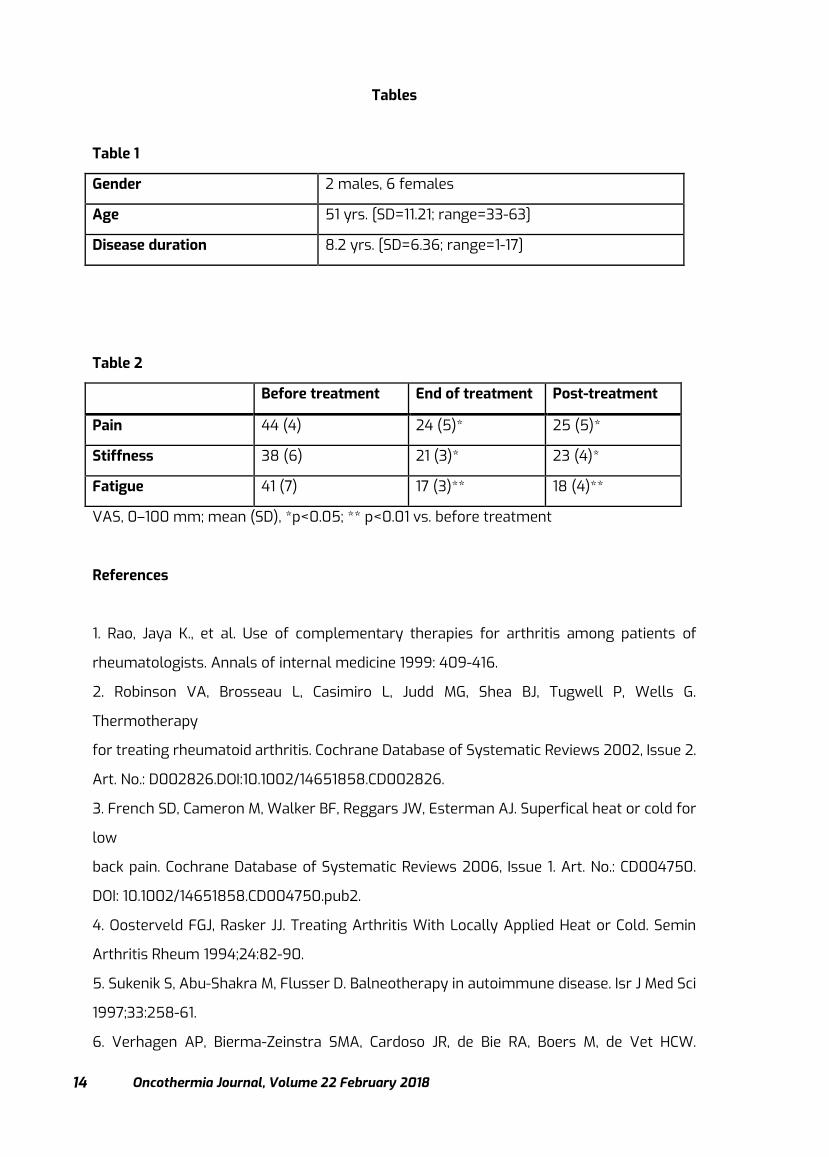
Patient characteristics. A total of 8 patients (6 female, 2 male) with RA were included in
the study with mean age of 51 (Table 1). One patient dropped out in the treatment period
due to nonmedical reasons and could not be measured for follow-up. Hence, the mean
group results of 7 patients are presented in Table 2. Pain and stiffness (p<0.05) as well as
fatigue (p<0.001) significantly decreased at the end of the treatment and post-treatment
periods.
Discussion
In all patients, a clinically significant improvement was seen at the end of the treatment
and post-treatment. Pain and stiffness reduced over 40%, while fatigue nearly 60% for
patients with RA (Table 2). The effect of whole-body hyperthermia upon local joint
inflammation or disease activity is not clear. The findings of earlier studies were
ambiguous [12-18], and many studies have no optimal quality as summarized in the
COCHRANE study [2]. It is known that whole-body hyperthermia can enhance immune
surveillance, including increased mobility and activity of white blood cells [19,20]. It is
hypothesized that increased temperature can modulate the immune response by targeting
the intracellular signalling pathways, cytokines, and other mediators of the phases of RA.
Ozone major autohemotherapy was first described in 1954 [21] and since then, after Wolff's
modification [22], it has been carried out worldwide millions of times without side-effects
and with therapeutic results [23]. The rationale for the use of ozone is based on its
immunosoppressive action if it is used at high concentration (45-65 μg/ml) [24]. Several
studies described its anti-inflammatory and analgesic effects [25,26], the functional
recovery of muscle and joint groups [27,28], as well as perfusion improvement of

Oncothermia Journal, Volume 22 February 2018
12
microcirculation [29]. A study by Chang et al. demonstrated that ozone applied externally
ameliorated the inflammatory reaction of RA without toxicity or serious side effects [30].
The authors found that the decrease in cytokine synthesis and secretion was due to the
pouring of ozone into the inflamed and infiltrated area via oxidation and eliminating the
hyperplastic synovial fibroblasts. Our study showed that ozone in the form of MAHT was
well-tolerated and contributed to the beneficial outcome of the therapy.
Oxidative stress and severe systemic inflammation have been considered as important
pathophysiologic mechanisms involved in the development of RA [31, 32]. Oxidative stress
occurs in response to the oxidative damage resulting from imbalance between antioxidant
and scavenging ability and the active oxidants produced by a harmful stimulant [32, 33].
Previous reports showed that significantly elevated production of reactive oxygen species
(ROS) in the serum of RA patients can be observed comparing with healthy donors [34].
ROS are indirectly involved in joint damage as the secondary messengers in inflammatory
and immunological cellular response in RA, which also can degrade directly the joint
cartilage, influencing its proteoglycan and inhibiting its synthesis [35, 36].
In this study, the rationale for the use of IVC and diet modification has been based on their
anti-inflammatory action. Vitamin C has direct antioxidant capacity and contributes to the
protection of cells from the damaging effects of endogenously produced or exogenous
reactive oxygen radicals and reactive nitrogen species, e.g. during immune activation.
Vitamin C prevents oxidative damage to lipids, proteins, and DNA, which has been
implicated as a major contributing factor in the development of chronic diseases such as
cardiovascular disease, cancer, and cataract, respectively [37,38]. Evidence further
suggests that vitamin C provides indirect antioxidant protection by regenerating other
biologically important antioxidants such as glutathione and vitamin E to their active state
[39]. The nutritional and physiological aspects of this essential nutrient have been widely
reviewed in a large number of comprehensive publications on vitamin C [37,40]. To our
knowledge, this is the first study that evaluated the demonstrated that IVC is safe and does
not correlate with any adverse events.
Among a number of small clinical trials of dietary manipulation in RA, modest benefit has
been noted for high-dose omega-3 fatty acids, fasting, vegetarian diet, and Mediterranean-
type diet [41-43]. In a recent study by Tedeschi et al. [44] 24.0% of subjects in a prospective,
Oncothermia Journal, Volume 22, February 2018 13
longitudinal RA registry reported that foods affect their RA symptoms, and 24.3% avoid
foods due to worsening of their RA. Among a list of 20 specific foods, blueberries and
spinach were most often noted to improve RA, while soda with sugar and desserts were
most commonly reported to worsen RA. Past work has shown that greater consumption
of sugar-sweetened beverages is associated with increased risk for developing RA [45].
In this study, a certified nutritionist provided face-to-face counselling that was individually
tailored to each patient. Each counselling session lasted 30 to 60 minutes, during which
nutritionists educated and strongly recommended patients to follow an anti-inflammatory
diet. The Western-type diet, which is high in red meat, high-fat dairy products, refined
grains, and simple carbohydrates, has been associated with higher levels of CRP and IL-6
[46]. On the other hand, the anti-inflammatory Mediterranean diet, which is high in whole
grains, fish, fruit and green vegetables, and associated with moderate alcohol and olive oil
intake and low intake of red meat and butter has been associated with lower levels of
inflammation [47–51]. Diets high in fruit and vegetable intake have been associated with
lower levels of CRP [52–54]. Specific nutrients such as (n-3) fatty acids [55–56], fiber [57–
58], moderate alcohol intake [59-60], vitamin C [61-62], β-carotene [63-64], and
magnesium [65-66] have also consistently been shown to be associated with lower levels
of inflammation. In our study, we observed that individual counselling can greatly affect
engagement and compliance to the prescribed diet. Post-treatment all patients reported
that they follow the dietary guidelines.
In conclusion, WBH and complementary therapies were safe and well-tolerated when given
up to 4 weeks. Although our present data are limited in terms of small sample size and
lack of control group they are encouraging and may become a platform for future planning
of long-term studies with the complementary treatments in combination with existing
standard therapies in RA. The multifaceted approach presented in this research consisted
of immunomodulating heat therapy in the form of WBH, immunosuppressive and
regenerative therapy in the form of MAHT and anti-inflammatory IVC and nutritional
counselling. While we cannot draw strong conclusions based on this study, the suggested
multimodal approach may be beneficial in the management of refractory RA.
Oncothermia Journal, Volume 22 February 2018
14
Tables
Table 1
Gender 2 males, 6 females
Age 51 yrs. [SD=11.21; range=33-63]
Disease duration 8.2 yrs. [SD=6.36; range=1-17]
Table 2
Before treatment End of treatment Post-treatment
Pain 44 (4) 24 (5)* 25 (5)*
Stiffness 38 (6) 21 (3)* 23 (4)*
Fatigue 41 (7) 17 (3)** 18 (4)**
VAS, 0–100 mm; mean (SD), *p<0.05; ** p<0.01 vs. before treatment
References
1. Rao, Jaya K., et al. Use of complementary therapies for arthritis among patients of
rheumatologists. Annals of internal medicine 1999: 409-416.
2. Robinson VA, Brosseau L, Casimiro L, Judd MG, Shea BJ, Tugwell P, Wells G.
Thermotherapy
for treating rheumatoid arthritis. Cochrane Database of Systematic Reviews 2002, Issue 2.
Art. No.: D002826.DOI:10.1002/14651858.CD002826.
3. French SD, Cameron M, Walker BF, Reggars JW, Esterman AJ. Superfical heat or cold for
low
back pain. Cochrane Database of Systematic Reviews 2006, Issue 1. Art. No.: CD004750.
DOI: 10.1002/14651858.CD004750.pub2.
4. Oosterveld FGJ, Rasker JJ. Treating Arthritis With Locally Applied Heat or Cold. Semin
Arthritis Rheum 1994;24:82-90.
5. Sukenik S, Abu-Shakra M, Flusser D. Balneotherapy in autoimmune disease. Isr J Med Sci
1997;33:258-61.
6. Verhagen AP, Bierma-Zeinstra SMA, Cardoso JR, de Bie RA, Boers M, de Vet HCW.
Oncothermia Journal, Volume 22, February 2018 15
Balneotherapy for rheumatoid arthritis Cochrane Database of Systematic Reviews 2004
Issue 1. Art. No:CD000518.DOI:10.1002/14651858.CD000518.
7. Melzack R, Katz J (1994) Pain measurement in persons in pain. In: Wall PD, Melzack R
(eds) Textbook of pain. 3rd edn. Churchill Livingstone, Edinburgh, pp 337–351
8. Oosterhof J (1992) The reliability of Visual Analogue Scale measurements for stiffness
in patients with rheumatoid arthritis. NPI, Amersfoort
9. Riemsma RP, Rasker JJ, Taal E, Griep EN, Wouters JMGW, Wiegman O (1998) Fatigue in
rheumatoid arthritis: the role of self-efficacy and problematic social support. Br J
Rheumatol 37:1042–1046
10. van Tubergen A, Coenen J, Landewe R, Spoorenberg A, Chorus A, Boonen A, van der
Linden S, van der Heijde D (2002) Assessment of fatigue in patients with ankylosing
spondylitis: a psychometric analysis. Arthritis Rheum 47(1):8–16 Feb
11. Jones SD, Koh WH, Steiner A, Garrett SL, Calin A (1996) Fatigue in ankylosing spondylitis:
its prevalence and relationship to disease activity, sleep, and other factors. J Rheumatol
23:487–490
12. Licht S (1982) Physical therapy in arthritis. In: Lehman JF (ed) Therapeutic heat and cold.
3rd edn. Williams & Wilkins, Baltimore, pp 263–269
13. Kirk JA, Kersley GD (1968) Heat and cold in the physical treatment of rheumatoid
arthritis of the knee. Ann Phys Med 9:270–274
14. Mainardi CL, Walter JM, Spiegel PK, Goldkamp OG, Harris ED (1979) Rheumatoid arthritis:
failure of daily heat therapy to affect its progression. Arch Phys Med Rehabil 60:390–393
15. Schmidt KL, Mäurer R, Rusch D (1980) Zum Verhalten der Hauttemperatur über
entzündeten Kniegelenken unter täglicher Kryotherapie. Z Phys Med 9:58–59
16. Zivkovic M, Cvetkovic S, Jovic D (1986) Effects of thermotherapy on acute phase
reactants in rheumatoid arthritis and ankylosing spondylitis. Arthritis Rheum 29:57 (suppl)
17. Schmidt KL, Ott VR, Rocher G, Schaller H (1979) Heat, cold and inflammation (a review).
Z Rheumatol 38:391–404
18. Oosterveld FGJ, Rasker JJ (1994) Treating arthritis with locally applied heat or cold.
Semin Arthritis Rheum 24:82–90
19. Nahas GG, Tannieres ML, Lennon JF. Direct measurement of leukocyte motility: effects
of pH and temperature. Proc Soc Exp Biol Med. 1971; 138: 350±52.
20. Moore TC, Nur K, Storm FK. Localized deep hyperthermia increases the traffic of
lymphocytes through peripheral lymph nodes of sheep in vivo. J Surg Oncol 1987;
35:75±81.
Oncothermia Journal, Volume 22 February 2018
16
21. Wehrli F, Steinbart H. Erfahrungen mit der hamatogen oxidation therapie (hot) Ars
Medici. 1954;10:44–51.
22. Wolff HH. Die Behandlung peripherer Durchblutungsstorungen mit Ozon. Erfahr Hk.
1971;23:181–184.
23. Bocci, V. (2013). Oxygen-ozone therapy: a critical evaluation. Springer Science &
Business Media.
24. Plopper CG, Duan X, Buckpitt AR, Pinkerton KE. Dose-dependent tolerance to ozone. IV.
Site-specific elevation in antioxidant enzymes in the lungs of rats exposed for 90 days or
20 months. Toxicol Appl Pharmacol 1994;127(1):124-31.
25. Christian DL, Chen LL, Scannell CH, Ferrando RE, Welch BS, Balmes JR. Ozone-induced
inflammation is attenuated with multiday exposure. Am J Respir Crit Care Med
1998;158:532–
537
26. Clavo B, Perez JL, Lopez L, Suarez G, Lloret M, Rodriguez V, et al. Effect of ozone therapy
on muscle oxygenation. J Altern Complement Med 2003;9:251–6
27. Sroczyński J, Antoszewski Z, Rudzki H, Matyszczyk B, Kuźniewicz R. Various parameters
of lipid metabolism after intra-arterial injections of ozone in patients with ischemia of the
lower extremities and diabetes mellitus. Pol Tyg Lek1990; 45(47-48):953-5.
28. Rovira G, Ralindo N. La ozonoterapia en el tratamiento de las ulceras cronicas de las
extremidades inferiors. Angiologia 1991;2:47-50
29. Peralta C, Leon OS, Xaus C, Prats N, Jalil EC, Planell ES, et al. Protective effect of ozone
treatment on the injury associated with hepatic ischemia-reperfusion: antioxidant-
prooxidant
balance. Free Radic Res 1999; 31:191–6
30. Chang, J.D.S., Lu, HS., Chang, YF. et al. Rheumatol Int (2005) 26: 142.
31. Meng J, Yu P, Jiang H, Yuan T, Liu N, Tong J, Chen H, Bao N and Zhao J. Molecular hydrogen
decelerates rheumatoid arthritis progression through inhibition of oxidative stress. Am J
Transl Res 2016; 8: 4472-4477.
32. Matyska-Piekarska E, Luszczewski A, Lacki J and Wawer I. The role of oxidative stress
in the etiopathogenesis of rheumatoid arthritis]. Postepy Hig Med Dosw (Online) 2006; 60:
617- 623.
33. Filippin LI, Vercelino R, Marroni NP and Xavier RM. Redox signalling and the
inflammatory response in rheumatoid arthritis. Clin Exp Immunol 2008; 152: 415-422.
Oncothermia Journal, Volume 22, February 2018 17
34. Mateen S, Moin S, Khan AQ, Zafar A and Fatima N. Increased reactive oxygen species
formation and oxidative stress in rheumatoid arthritis. PLoS One 2016; 11: e0152925.
35. Mirshafiey A and Mohsenzadegan M. The role of reactive oxygen species in
immunopathogenesis of rheumatoid arthritis. Iran J Allergy Asthma Immunol 2008; 7: 195-
202.
36. Hadjigogos K. The role of free radicals in the pathogenesis of rheumatoid arthritis.
Panminerva
Med 2003; 45: 7-13.
37. Dietary Reference Intakes for vitamin C, vitamin E, selenium, and carotenoids. A report
of
the Panel on Antioxidants and Related compounds, Standing Committee on the Scientific
Evaluation of Dietary Reference Intakes; Food and Nutrition Board, Institute of Medicine.
Washington, National Academy Press, 2000, chapter 5: Vitamin C, pp 95–185.
38. Carr AC, Frei B: Toward a new recommended dietary allowance for vitamin C based on
antioxidant and health effects in humans. Am J Clin Nutr 1999; 69: 1086–1107.
39. Ames BN, Shigenaga MK, Hagen TM: Oxidants, antioxidants, and the degenerative
diseases of aging. Proc Natl Acad Sci USA 1993; 90: 7915–7922.
40. Jacob RA: The integrated antioxidant system. Nutr Res 1995; 15: 755–766.
41. Panush RS, Carter RL, Katz P, Kowsari B, Longley S, Finnie S. Diet therapy for rheumatoid
arthritis. Arthritis and Rheumatism 1983;26:462-71.
42. Kremer JM, Lawrence DA, Petrillo GF, et al. Effects of high-dose fish oil on rheumatoid
arthritis after stopping nonsteroidal anti-inflammatory drugs. Clinical and immune
correlates. Arthritis and Rheumatism 1995;38:1107-14.
43. Tedeschi SK, Costenbader KH. Is there a role for diet in the therapy of rheumatoid
arthritis? Current Rheumatology Reports 2016;18:23.
44. Tedeschi, S. K., Frits, M., Cui, J., Zhang, Z. Z., Mahmoud, T., Iannaccone, C., Lin, T.-C., Yoshida,
K., Weinblatt, M. E., Shadick, N. A. and Solomon, D. H. (2017), Diet and Rheumatoid Arthritis
Symptoms: Survey Results From a Rheumatoid Arthritis Registry. Arthritis Care &
Research. Accepted Author Manuscript. doi:10.1002/acr.23225
45. Hu Y, Costenbader KH, Gao X, et al. Sugar-sweetened soda consumption and risk of
developing rheumatoid arthritis in women. The American Journal of Clinical Nutrition
2014;100:959-67.
46. Esmaillzadeh A, Kimiagar M, Mehrabi Y, Azadbakht L, Hu FB, Willett WC. Dietary patterns
and markers of systemic inflammation among Iranian women. J Nutr. 2007;137:992–8
Oncothermia Journal, Volume 22 February 2018
18
47. Dalziel K, Segal L, de Lorgeril M. A mediterranean diet is cost-effective in patients with
previous myocardial infarction. J Nutr. 2006;136:1879–85.
48. Chrysohoou C, Panagiotakos DB, Pitsavos C, Das UN, Stefanadis C. Adherence to the
Mediterranean diet attenuates inflammation and coagulation process in healthy adults:
The ATTICA Study. J Am Coll Cardiol. 2004;44:152–8.
49. Esposito K, Marfella R, Ciotola M, Di Palo C, Giugliano F, Giugliano G, D'Armiento M,
D'Andrea F, Giugliano D. Effect of a Mediterranean-style diet on endothelial dysfunction
and markers of vascular inflammation in the metabolic syndrome: a randomized trial.
JAMA. 2004;292:1440–6.
50. Estruch R, Martinez-Gonzalez MA, Corella D, Salas-Salvado J, Ruiz-Gutierrez V, Covas
MI, Fiol M, Gomez-Gracia E, Lopez-Sabater MC, et al. Effects of a Mediterranean-style diet
on cardiovascular risk factors: a randomized trial. Ann Intern Med. 2006;145:1–11.
51. Serrano-Martinez M, Palacios M, Martinez-Losa E, Lezaun R, Maravi C, Prado M, Martinez
JA, Martinez-Gonzalez MA. A Mediterranean dietary style influences TNF-alpha and VCAM-
1 coronary blood levels in unstable angina patients. Eur J Nutr. 2005;44:348–54.
52. Gao X, Bermudez OI, Tucker KL. Plasma C-reactive protein and homocysteine
concentrations are related to frequent fruit and vegetable intake in Hispanic and non-
Hispanic white elders. J Nutr. 2004;134:913–8.
53. Watzl B, Kulling SE, Moseneder J, Barth SW, Bub A. A 4-wk intervention with high intake
of carotenoid-rich vegetables and fruit reduces plasma C-reactive protein in healthy,
nonsmoking men. Am J Clin Nutr. 2005;82:1052–8.
54. Esmaillzadeh A, Kimiagar M, Mehrabi Y, Azadbakht L, Hu FB, Willett WC. Fruit and
vegetable intakes, C-reactive protein, and the metabolic syndrome. Am J Clin Nutr.
2006;84:1489–97.
55. Ferrucci L, Cherubini A, Bandinelli S, Bartali B, Corsi A, Lauretani F, Martin A, Andres-
Lacueva C, Senin U, et al. Relationship of plasma polyunsaturated fatty acids to circulating
inflammatory markers. J Clin Endocrinol Metab. 2006;91:439–46.
56. Lopez-Garcia E, Schulze MB, Manson JE, Meigs JB, Albert CM, Rifai N, Willett WC, Hu FB.
Consumption of (n-3) fatty acids is related to plasma biomarkers of inflammation and
endothelial activation in women. J Nutr. 2004;134:1806–11.
57. Bo S, Durazzo M, Guidi S, Carello M, Sacerdote C, Silli B, Rosato R, Cassader M, Gentile L,
et al. Dietary magnesium and fiber intakes and inflammatory and metabolic indicators in
middle-aged subjects from a population-based cohort. Am J Clin Nutr. 2006;84:1062–9.
Oncothermia Journal, Volume 22, February 2018 19
58. King DE, Egan BM, Geesey ME. Relation of dietary fat and fiber to elevation of C-reactive
protein. Am J Cardiol. 2003;92:1335–9. Erratum in: Am J Cardiol 2004;93:812.
59. Avellone G, Di Garbo V, Campisi D, De Simone R, Raneli G, Scaglione R, Licata G. Effects
of moderate Sicilian red wine consumption on inflammatory biomarkers of
atherosclerosis. Eur J Clin Nutr. 2006;60:41–7.
60. Sierksma A, van der Gaag MS, Kluft C, Hendriks HFJ. Moderate alcohol consumption
reduces plasma C-reactive protein and fibrinogen levels; a randomized, diet-controlled
intervention study. Eur J Clin Nutr. 2002;56:1130–6.
61. van Herpen-Broekmans WM, Klopping-Ketelaars IA, Bots ML, Kluft C, Princen H, Hendriks
HF, Tijburg LB, van Poppel G, Kardinaal AF. Serum carotenoids and vitamins in relation to
markers of endothelial function and inflammation. Eur J Epidemiol. 2004;19:915–21.
62. Chien CT, Chang WT, Chen HW, Wang TD, Liou SY, Chen TJ, Chang YL, Lee YT, Hsu SM.
Ascorbate supplement reduces oxidative stress in dyslipidemic patients undergoing
apheresis. Arterioscler Thromb Vasc Biol. 2004;24:1111–7.
63. Gunter MJ, Stolzenberg-Solomon R, Cross AJ, Leitzmann MF, Weinstein S, Wood RJ,
Virtamo J, Taylor PR, Albanes D, et al. A prospective study of serum C-reactive protein and
colorectal cancer risk in men. Cancer Res. 2006;66:2483–7.
64. Erlinger TP, Guallar E, Miller ER III, Stolzenberg-Solomon R, Appel LJ. Relationship
between systemic markers of inflammation and serum beta-carotene levels. Arch Intern
Med. 2001;161:1903–8.
65. King DE, Mainous AG III, Geesey ME, Woolson RF. Dietary magnesium and C-reactive
protein levels. J Am Coll Nutr. 2005;24:166–71.
66. Song Y, Li TY, van Dam RM, Manson JE, Hu FB. Magnesium intake and plasma
concentrations of markers of systemic inflammation and endothelial dysfunction in
women. Am J Clin Nutr. 2007;85:1068–74.

Oncothermia Journal, Volume 22 February 2018
20
Combining hyperthermia with the new biologic and immunotherapy drugs
Dr. Joseph Brenner
"New-Hope" center for integrative cancer treatments Tel-Aviv/Israel
Presented at 35th ICHS, Guangzhou, 2017
Cite this article as: Brennner J. (2018): Combining hyperthermia with the new biologic and
immunotherapy drugs; Oncothermia Journal 22:20-21 www.oncothermia-
journal.com/journal/2018/Combining_hyperthermia.pdf

Oncothermia Journal, Volume 22, February 2018 21
Combining hyperthermia with the new biologic and immunotherapy drugs
The combined synergistic effect of hyperthermia with radiation, chemotherapy, supplements, photodynamic therapy and more, is well known. In the recent years, many new anti-cancer agents appeared and become an important part of any cancer treatments. These are the biologic agents affecting intracellular processes and related to genetic changes in the tumor cells. In addition, there are in use several new immunotherapy agents affecting the possibility of cancer cells to hide from the body own immune system. Laboratory and clinical studies as well as case reports, published in the medical literature, are indicating that these new biologic and immunologic agents work synergistically with hyperthermia. Antiangiogenic agents such as bevacizumab (Avastin) are more effective when combined with hyperthermia which is an antiangiogenic by itself, in lung, ovarian and other cancer types. In an Indian study, all 6 patients with advanced H&N cancer treated with cetuximab, radiation and hyperthermia achieved a complete response. In a Dutch study only one out of 7 advanced cervical cancer progressed after treatment with cisplatin, lapatinib and hyperthermia. Similar impressive effects were observed combining sutent, sorafenib, gefitinib, bortezumab, mapatuzumab and several immunotherapy agents with hyperthermia. The scientific basis of these combined effects and studies details will be presented.

Oncothermia Journal, Volume 22 February 2018
22
Non-oncological & oncological whole-body hyperthermia and a new immunological road to attack cancer?
- some treatment procedures
Alexander von Ardenne Dr. rer. nat. Von Ardenne Institute of Applied Medical Research, Germany
Presented at 35th ICHS, Guangzhou, 2017
Cite this article as: Von Ardenne A. (2018): Non-oncological & oncological whole-body
hyperthermia and a new immunological road to attack cancer? - some treatment procedures; Oncothermia Journal 22:22-31
www.oncothermia-journal.com/journal/2018/Non_oncological.pdf
Oncothermia Journal, Volume 22, February 2018 23
Non-oncological & oncological whole-body hyperthermia and a new immunological road to attack cancer? -some treatment procedures
There is an increasing number of publication-based non-oncological indications in which the application of modern whole-body hyperthermia (WBH) can bring about an alleviation for the patients. Some of these indications are arterial hypertension, chronic back pain, fibromyalgia syndrome, psoriatic arthritis, ankylosing spondylitis, systemic scleroderma and major depressive disorder. This presentation wants to inform about the procedure in the mentioned indications. In a first Table 1 “Publication-Based Treatment Procedures for WBH for some Non-Oncological Indications” are the main parameters for the WBH procedure given with some remarks and together with the publications behind the procedure.
Furthermore, the application of WBH adjuvant to the conventional methods for the treatment of cancer patients - surgery, radiotherapy and chemotherapy - could be helpful. By WBH before operation, which increases the microcirculation and activates the immune system, the risk of wound infection after surgery is reduced. WBH increases with its intensified perfusion the oxygen partial pressure in tumors for higher x-ray sensitivity. WBH combined with chemotherapy for the treatment of cancer patients in a therapy resistant, metastatic or advanced stage of solid malignancies can improve the response rate and increases the quality of life.
Last but not least a view onto the immune system. It is still not proved by (published) clinical trials with cancer patients but there is a good probability that WBH with temperatures until fever-range supports the efficacy of checkpoint inhibitors. Also, not proved by clinical trials is the proposal of Hatfield & Sitkovsky to activate the cytotoxic T-cells to kill cancer cells by increasing the Oxygen partial pressure in the tumor, followed by a reduced adenosine concentration in the tumor microenvironment, and in connection with an adoptive immunotherapy. Fever-range WBH could support this process by increasing the killing efficiency of the cytotoxic T-cells. In a second Table 2 “For Discussion: Treatment Procedures regarding Adjuvant Treatment of Cancer Patients with WBH” is given a proposal of the main parameters for the WBH procedure with the rationale of the procedure and remarks together with the associated publications.
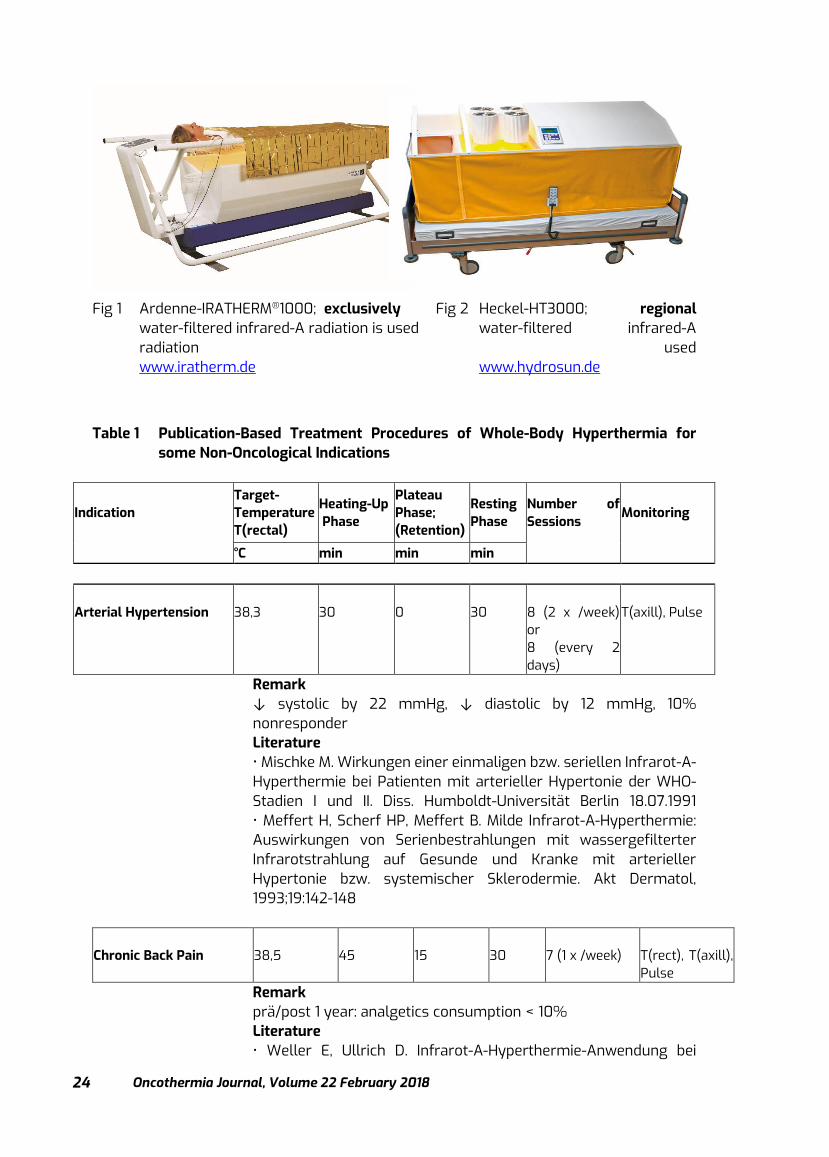
For all the mentioned indications and procedures are currently two leading devices used, realizing body-core temperatures from mild until extreme WBH (s. Fig 1 and Fig 2):
Oncothermia Journal, Volume 22 February 2018
24
Fig 1 Ardenne-IRATHERM®1000; exclusively Fig 2 Heckel-HT3000; regional
water-filtered infrared-A radiation is used water-filtered infrared-A radiation used www.iratherm.de www.hydrosun.de
Table 1 Publication-Based Treatment Procedures of Whole-Body Hyperthermia for
some Non-Oncological Indications
Indication Target-Temperature T(rectal)
Heating-Up Phase
Plateau Phase; (Retention)
Resting Phase
Number of Sessions
Monitoring
°C min min min
Arterial Hypertension
38,3
30
0
30
8 (2 x /week) or 8 (every 2 days)
T(axill), Pulse
Remark ↓ systolic by 22 mmHg, ↓ diastolic by 12 mmHg, 10% nonresponder Literature • Mischke M. Wirkungen einer einmaligen bzw. seriellen Infrarot-A-Hyperthermie bei Patienten mit arterieller Hypertonie der WHO-Stadien I und II. Diss. Humboldt-Universität Berlin 18.07.1991 • Meffert H, Scherf HP, Meffert B. Milde Infrarot-A-Hyperthermie: Auswirkungen von Serienbestrahlungen mit wassergefilterter Infrarotstrahlung auf Gesunde und Kranke mit arterieller Hypertonie bzw. systemischer Sklerodermie. Akt Dermatol, 1993;19:142-148
Chronic Back Pain
38,5
45
15
30
7 (1 x /week)
T(rect), T(axill), Pulse
Remark prä/post 1 year: analgetics consumption < 10% Literature • Weller E, Ullrich D. Infrarot-A-Hyperthermie-Anwendung bei

Oncothermia Journal, Volume 22, February 2018 25
Patienten mit Analgetica-Abusus wegen chronischer Rückenschmerzen. Vortrag auf dem 95. Kongreß der Gesellschaft für Phys Med und Rehab 5.10.1990
Fibromyalgia Syndrome
38,1
40
15
30
6 (2 x /week), or 6 (every 2 days) or 6 consecutive days
T(axill), Pulse
Remark prä/post 6 month 20% below basic painacc. to "Fibromyalgia Impact Questionaire"/FIQ Literature • Brockow T, Wagner A, Franke A, Offenbächer M, Resch KL. A Randomized Controlled Trial on the Effectiveness of Mild Water-filtered Near Infrared Whole-body Hyperthermia as an Adjunct to a Standard Multimodal Rehabilitation in the treatment of Fibromyalgia. Clin J Pain 2007;1:67-75 • Walz J, Hinzmann J, Haase I, Witte T. Ganzkörperhyperthermie in der Schmerztherapie – eine kontrollierte Studie an Patient. mit Fibromyalgiesyndrom. Schmerz 2013;1:38-45 • Romeyke T, Stummer H. Multi-modal pain therapy of fibromyalgia syndrome with integration of systemic whole-body hyperthermia – effects on pain intensity and mental state: A non-randomised controlled study. J Musculoskel Pain 2014;4:341-55 • Schleenbecker HG, Schmidt KL. Zur Wirkung einer iterativen milden Ganzkörper-hyperthermie auf den Fibromyalgieschmerz. Phys. Rehab. Kur Med, 1998;8:113-117
Psoriatic Arthritis
38,5
45
15
30
6 (in 8 days) or 6 consecutive days
T(rect), T(axill), Pulse
Remark prä/post 6 month alleviation of pain, ↓ Disease-Activity Score (DAS 28) 3 month (DAS28 = activity and function parameter) Literature • Lange U, Schwab F, Müller-Ladner U, Dischereit G. Wirkung iterativer Ganzkörperhyperthermie mit wassergefilterter Infrarot-A-Strahlung bei Arthritis psoriatica – eine kontrollierte, randomisierte, prospektive Studie. Akt Rheumatol 2014;05:310-16

Oncothermia Journal, Volume 22 February 2018
26
Axial Spondyloarthritis
38
30
15
120 in bed
6 (2 x /week)
T(axill), Pulse
Remark prä/post 3 months pain reduction Literature • Stegemann I, Hinzmann J, Haase I, Witte T. Ganzkörperhyperthermie mit wassergefilterter Infrarot-A-Strahlung bei Patienten mit axialer Spondyloarthritis. Orthopäd. & Unfallchirurg. Praxis 2013;10:458-463
Ankylosing Spondylitis
38,5
45
15
30
6 (in 8 days) or 6 consecutive days
T(rect), T(axill), Pulse
Remark ↓ disease activity index (BASDAI) 3 month, ↓ blood sedimentation rate 3 month, ↑ TLR-4, IL-10 (BASDAI = Bath AS Disease Activity Index Literature • Lange U, Müller-Ladner U, Dischereit G. Effectiveness of whole-body hyperthermia by mild water-filtered infrared-A radiation in ankylosing spondylitis – a controlled, randomized, prospective study. Akt Rheumatol 2017; 2:122-128 • Zauner D, Quehenberger F, Hermann J, Dejaco C, Stadner MH, et al. Whole-body hyperthermia treatment increases interleukin 10 and toll-like receptor 4 expression in patients with ankylosing spondylitis: a pilot study. Int J Hyperthermia 2014; 6:393-401
Systemic Scleroderma
38,3
30
0
30
15 (2 x /week) or 15 (every 2 days)
T(axill), Pulse
Remark in the follow-up period of two years for about 50% of the female patients the frequency and severity of Raynaud attacks were sustained reduced Literature • Meffert H, Scherf HP, Meffert B. Milde Infrarot-A-Hyperthermie: Auswirkungen von Serienbestrah-lungen mit wassergefilterter Infrarotstrahlung auf Gesunde und Kranke mit arterieller Hypertonie bzw. systemischer Sklerodermie. Akt Dermatol, 1993;19:142-148 • Förster J, Fleischanderl S, Wittstock S, Storch A, Meffert H. Letter to the Editor: Infrared-Mediated Hyperthermia is Effective in the Treatment of Scleroderma-Associated Raynaud’s Phenomenon. J Investig Dermatol, 2005;6:1313-16

Oncothermia Journal, Volume 22, February 2018 27
Major Depressive Disorder
38,5
110
60
0
1
T(rect), T(axill), Pulse
Remark a single session of whole-body hyperthermia produced a significant antidepressant effect apparent within a week of treatment that persisted for 6 weeks after treatment. Literature • Janssen CW, Lowry CA, Mehl MR, Allen JJB, Kelly KL, Gartner DE, Medrano A, Begay TK, Rentscher K, White JJ, Fridman A, Roberts LJ, Robbins ML, Hanusch KU, Cole SP, Raison CL. Whole-Body Hyperthermia for the Treatment of Major Depressive Disorder – A Randomized Clinical Trial. JAMA Psychiatry 2016; 8:789-95 • Meesters Y, Beersma DGM, Bouhuys AL, vdHoofdakker RH. Prophylactic Treatmet of Seasonal Affective Disorder (SAD) by Using Light Visors: Bright White or Infrared Light. Soc Biol Psychiatry 1999; 46:239-246
Table 2 For Discussion: Treatment Procedures regarding Adjuvant Treatment of
Cancer Patients with Whole-Body Hyperthermia
Procedure Rationale
Target-Temperature T(rectal)
Heating-Up Phase
Plateau Phase; (Retention)
Resting Phase
Number of Sessions
Monitoring
°C min min min Surgery + Whole-Body Hyperthermia
whole-body hyperthermia before surgery activates the immune system and reduces the risk of a postoperative infection. Hypothesis: better wound care on the side of the body-own immune defense
+ 0,35
30
0
0
1 x right before surgery
T(axill)
Remark 421 patients with clean breast, varicose vein, or hernia surgery randomized in control- and treatment group. Whole-body hyperthermia device was left in situ until just before surgery. Follow-up: 2 and 6 weeks postoperatively: wound infections were reduced from 14% (control group) to 5% (hyperthermia group). post OP: hyper gr. TNF-𝝰, HSP ‘s 60+90 increased Literature • Melling AC, Ali B, Scott EM, Leaper DJ. Effects of preoperative warming on the incidence of wound infection after clean surgery: a randomised controlled trial. Lancet 2001;358:876-80
Oncothermia Journal, Volume 22 February 2018
28
• Sulyok L, Fleischmann E, Stift A, Roth G, Eichinger DL, Kasper D, Spittler A, Kimberger O. Effect of preoperative fever-range whole-body hyperthermia on immunological markers in patients undergoing colorectal cancer surgery. Br J Anaesth 2012; 5:754-61 • Wong PF, Kumar S, Bohra A, Whetter D, Leaper DJ. Randomized clinical trial of perioperative systemic warming in major elective abdominal surgery. Br J Surg 2007; 4:421-26
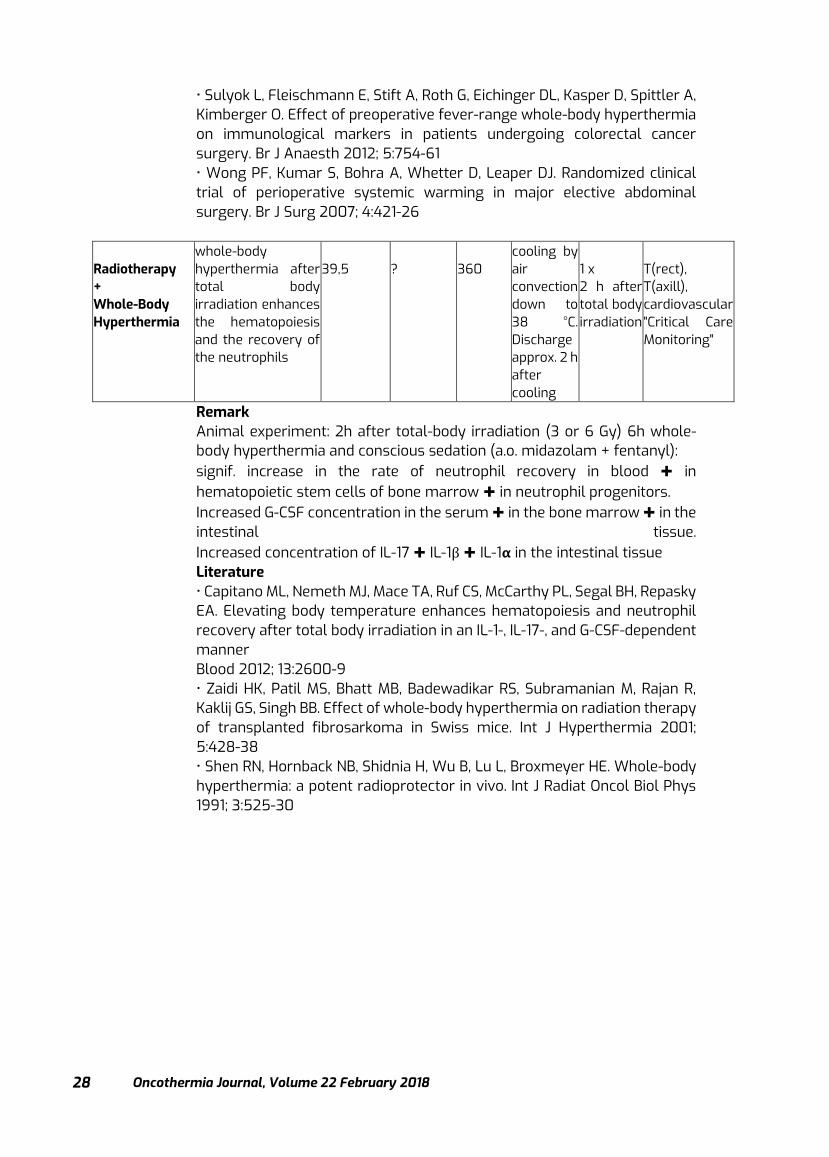
Radiotherapy + Whole-Body Hyperthermia
whole-body hyperthermia after total body irradiation enhances the hematopoiesis and the recovery of the neutrophils
39,5
?
360
cooling by air convection down to 38 °C. Discharge approx. 2 h after cooling
1 x 2 h after total body irradiation
T(rect), T(axill), cardiovascular "Critical Care Monitoring"
Remark Animal experiment: 2h after total-body irradiation (3 or 6 Gy) 6h whole-body hyperthermia and conscious sedation (a.o. midazolam + fentanyl): signif. increase in the rate of neutrophil recovery in blood ✚ in hematopoietic stem cells of bone marrow ✚ in neutrophil progenitors. Increased G-CSF concentration in the serum ✚ in the bone marrow ✚ in the intestinal tissue. Increased concentration of IL-17 ✚ IL-1β ✚ IL-1𝝰 in the intestinal tissue Literature • Capitano ML, Nemeth MJ, Mace TA, Ruf CS, McCarthy PL, Segal BH, Repasky EA. Elevating body temperature enhances hematopoiesis and neutrophil recovery after total body irradiation in an IL-1-, IL-17-, and G-CSF-dependent manner Blood 2012; 13:2600-9 • Zaidi HK, Patil MS, Bhatt MB, Badewadikar RS, Subramanian M, Rajan R, Kaklij GS, Singh BB. Effect of whole-body hyperthermia on radiation therapy of transplanted fibrosarkoma in Swiss mice. Int J Hyperthermia 2001; 5:428-38 • Shen RN, Hornback NB, Shidnia H, Wu B, Lu L, Broxmeyer HE. Whole-body hyperthermia: a potent radioprotector in vivo. Int J Radiat Oncol Biol Phys 1991; 3:525-30

Oncothermia Journal, Volume 22, February 2018 29
Chemotherapy + Whole-Body Hyperthermia
whole-body hyperthermia raises the chemotherapy-induced tumor-response by combination with special chemotherapy protocol (here: Cisplatin, Gemcitabine and Interferon-𝝰: proof in preclinical model followed by phase I/II study)
40,0
60
360
cooling by air convection down to 38 °C. Discharge approx. 2 h after cooling
up to 7 sessions
T(rect), T(axill), T(skin), cardiovascular "Critical Care Monitoring"
Remark 37 patients with therapy-resistant, metastatic or advanced solid malignancies. Conscious sedation (a.o. midazolam + fentanyl): 43% response rate (best: pancreas ca. with 5/7) ✚ LQ-improvement w.r.t. pain, weight, fatigue. Extreme whole-body hyperthermia (Trect > 42°C) in the scope of the systemic Cancer Multistep Therapy is not considered here Literature • Bull JMC, Scott GL, Strebel FR, Nagle VL, Oliver D, Redwine M, Rowe RW, Ahn CW, Koch SM. Fever-range whole-body thermal therapy combined with cisplatin, gemcitabine and daily interferon-α: A description of a phase I-II protocol. Int J Hyperthermia 2008; 8: 649-662 • Kraybill WG, Olenki T, Evans SS, Ostberg JR, O’Leary KA, Gibbs JF, Repasky EA. A phase I study of fever-range whole-body hyperthermia in patients with advanced solid tumors: correlation with mouse models. Int J Hyperthermia 2002; 3:253-66 • Hildebrandt B, Dräger J, Kerner T, Deja M, Löffel J, Strosczczynski C, Ahlers O, Felix R, Riess H, Wust P. Whole-body hyperthermia in the scope of von Ardenne’s systemic cancer multistep therapy (sCMT) combined with chemotherapy in patients with metastatic colorectal cancer: a phase I/II study. Int. J. Hyperthermia 2004; 3:317-33

Oncothermia Journal, Volume 22 February 2018
30
Next Steps? Checkpoint Immunotherapy (Immunoncolog. Therapy) + Whole-Body Hyperthermia
checkpoint-inhibitors reduce the suppression of cytotoxic T-cells and activate these to damage cancer cells. Preclinically: killing efficiency of T cells against cancer cells reaches its maximum at 39.5 °C ( 3 times higher than at 37 °C)
39,5
45
60
60 preferably in bed (thermally well insulated) to increase the thermal dose
e.g. 6 sessions (in 2 weeks Mo, We, Fr)
T(rect), T(axill), cardiovascular "Critical Care Monitoring"
Remark Currently focused on melanoma patients. Simultaneously during application of checkpoint-inhibitors a number of whole-body hyperthermia sessions should run in phases of high efficacy of checkpoint-inhibitors under consideration of the pharmacodynamics of the checkpoint-inhibitors (time constant betw. application & inhibition?). Attention SE: activation of cytotoxic T-cells by checkpoint-inhibitors attracts systemically and it attracts therefore also against normal cells in inflammation regions! Literature Still no clinical publication available! → However, hint to meaningfulness: • Schadendorf D. Entscheidungsfindung für die klinische Praxis: Aktuelle Konzepte und Behandlungsalgorithmen mit Immun-Checkpoint-Inhibitoren beim Melanom. Oncol Res Treat 2016;39/4:8-12 • Larkin J, Sileni VC, Gonzalez R, et al. Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. N Engl J Med 2015; 373:23-34 • Weigelin B, activating serial killers of cancer cells with artificial fever: Hyperthermia as supporting strategy for immunotherapy of cancer. Symposium - Modern Hyperthermia, Krakow, 14.11.2015 • Kobayashi Y, Ito Y, Ostapenko VV, Sakai M, Matsushita N, Imai K, Shimizu K, Aruga A, Tanigawa K. Fever-range whole-body heat treatment stimulates antigen-specific T-cell responses in humans. Immunology Letters 2014; 162:256-61
Adoptive Immunotherapy + Respiratory Hyperoxia + Whole-Body Hyperthermia
hypoxia in tumors leads to high adenosine concentration in the tumor microenviron-ment and activates in zytotoxic T cells immunosuppressive factors such as PD-1 and CTLA-4. Respiratory
39,5
45
60
60 preferably in bed (thermally well insulated) to increase the
e.g. 6 sessions (in 2 weeks Mo, We, Fr)
T(rect), T(axill), cardiovascular "Critical Care Monitoring"
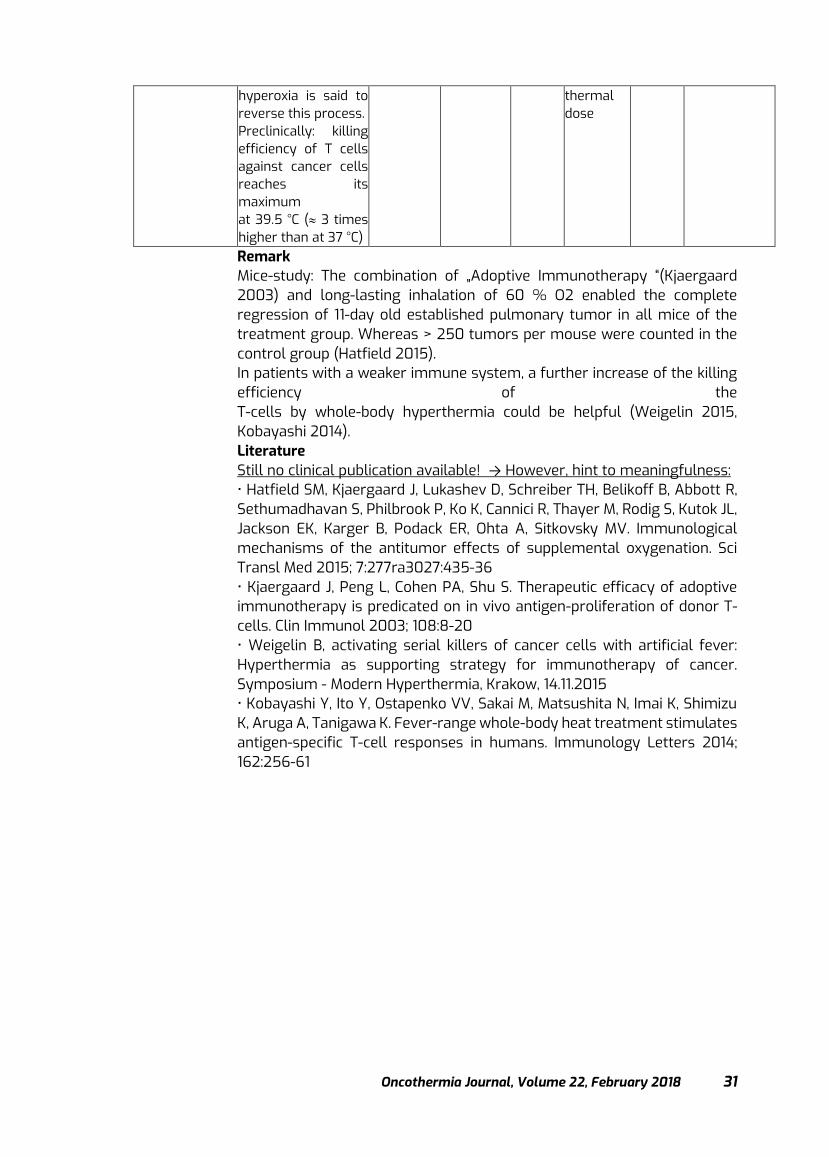
Oncothermia Journal, Volume 22, February 2018 31
hyperoxia is said to reverse this process. Preclinically: killing efficiency of T cells against cancer cells reaches its maximum at 39.5 °C ( 3 times higher than at 37 °C)
thermal dose
Remark Mice-study: The combination of „Adoptive Immunotherapy “(Kjaergaard 2003) and long-lasting inhalation of 60 % O2 enabled the complete regression of 11-day old established pulmonary tumor in all mice of the treatment group. Whereas > 250 tumors per mouse were counted in the control group (Hatfield 2015). In patients with a weaker immune system, a further increase of the killing efficiency of the T-cells by whole-body hyperthermia could be helpful (Weigelin 2015, Kobayashi 2014). Literature Still no clinical publication available! → However, hint to meaningfulness: • Hatfield SM, Kjaergaard J, Lukashev D, Schreiber TH, Belikoff B, Abbott R, Sethumadhavan S, Philbrook P, Ko K, Cannici R, Thayer M, Rodig S, Kutok JL, Jackson EK, Karger B, Podack ER, Ohta A, Sitkovsky MV. Immunological mechanisms of the antitumor effects of supplemental oxygenation. Sci Transl Med 2015; 7:277ra3027:435-36 • Kjaergaard J, Peng L, Cohen PA, Shu S. Therapeutic efficacy of adoptive immunotherapy is predicated on in vivo antigen-proliferation of donor T-cells. Clin Immunol 2003; 108:8-20 • Weigelin B, activating serial killers of cancer cells with artificial fever: Hyperthermia as supporting strategy for immunotherapy of cancer. Symposium - Modern Hyperthermia, Krakow, 14.11.2015 • Kobayashi Y, Ito Y, Ostapenko VV, Sakai M, Matsushita N, Imai K, Shimizu K, Aruga A, Tanigawa K. Fever-range whole-body heat treatment stimulates antigen-specific T-cell responses in humans. Immunology Letters 2014; 162:256-61

Oncothermia Journal, Volume 22 February 2018
32
Retrospective observational Clinical Study on Relapsed Malignant Gliomas Treated with Electro-hyperthermia
Giammaria Fiorentini1, Donatella Sarti1, Carlo Milandri4, Patrizia Dentico4, Andrea
Mambrini2, Stefano Guadagni3 1 Onco-Ematology Department, Azienda Ospedaliera “Ospedali Riuniti Marche Nord”, 61122
Pesaro, Italy 2 Oncology Department, Carrara General Hospital, 54033 Carrara, Italy
3 Department of Applied Clinical Sciences and Biotechnology, Section of General Surgery, University of L’Aquila, 67100 L’Aquila, Italy
4 Oncology Department, NuovoOspedale San Giuseppe, 50053, Empoli (Florence), Italy
Presented at 35th ICHS, Guangzhou, 2017
Cite this article as: Fiorentini G., Sarti D., Milandri C., Dentico P., Mambrini A., Guadagni S.
(2018): Retrospective observational Clinical Study on Relapsed Malignant Gliomas Treated with Electro-hyperthermia Oncothermia Journal 22:32-
45 www.oncothermia-
journal.com/journal/2018/Retrospective_observational.pdf

Oncothermia Journal, Volume 22, February 2018 33
Correspondence to: Dr. Giammaria Fiorentini, Onco-Ematology Department, Azienda Ospedaliera “Ospedali Riuniti Marche Nord”, Via Lombroso 1, 61122 Pesaro, Italy. [email protected] Telephone: +39-0721-364005 Fax: +39-0721-364094 Abstract AIM: to evaluate the efficacy and tolerability of electro-hyperthermia (ET) for the treatment of relapsed malignant glioma. Methods: this was a retrospective observational clinical study. Patients were included in the study if they had >18 years, informed consent signed, histological diagnosis of malignant glioma, failure of previous temozolamide-based chemotherapy and radiotherapy, indication for treatment with ET. Hyperthermia was performed with short radiofrequency waves of 13.56 MHz using a capacitive coupling technique keeping the skin surface at 26 C°. The applied power ranged between 40-150 Watts and the calculated average equivalent temperature in the tumors was above 40 C° for more than 90% of the treatment duration (20-60 minutes gradually). Results: 24 consecutive patients were enrolled in the study, 19 (79%) had glioblastoma multiforme (GBM) 13 were of grade 1-3 and 6 of rade 4, 5 (21%) ASTROCYTOMA. Tumor response analysis two months after ET showed 2 (8%) complete remission (astrocytomas) and 5 (21%) partial remission ( 2 ASTROCYTOMA, and 3 glioblastomas), with a response rate of 29%. The median duration of response was 16 months (range 6-120). The median survival of whole study population was 19.5 months (range 2-156), 55% survival rate at 1 year, and 15 % at two years. We observed 3 long survivors at 156, 60, 62 months in atrocitomas. Conclusions: ET appears to have promising efficacy in adults with relapsed malignant glioma. Keywords: relapsed malignant glioma, electro-hyperthermia, survival, tumor response
Oncothermia Journal, Volume 22 February 2018
34
Introduction
The use of Hyperthermia has been known for long time, since it was found out that heat had the ability to kill cells. In the last decade, hyperthermia has been increasingly used as treatment choice for several types of cancer, because tumor cells are more sensible to heat than normal cells (1). Several methods of hypertermia for cancer treatment are currently available, such as magnetic nanoparticles (mNPs) inducing intracellular hyperthermia, external Radio-Frequency (RF), hyperthermic perfusion; frequency enhancers associated to magnetic field; catheter mediated hypertermia (2-4).
Hyperthermia can be used alone or in association with chemotherapy or radiotherapy in order to improve and prolong their benefit (5-7). The synergic effect of traditional hyperthermia (41–43°C) with chemo and radio-therapy is due to apoptosis induction, angiogenesis inhibition, chemo- and radio-sensitivity activation and high drug concentration induction inside the lesion. The heat, moreover, can induce the externalization of new antigens, thus increasing the tumor sensitivity to immunotherapy (8, 9). Gliomas represent the majority (80%) of malignant brain cancers (10). According to the glioma grading system of the World Health Organization (WHO), the astrocytomas are classified by four grades (I, II, III, and IV); and oligodendrogliomas and oligoastrocytomas, by two grades (II and III). The most aggressive and common glioma is glioblastoma (a grade IV astrocytoma) (10). Glioblastoma multiforme (grade IV) (GBM) represent 65% of all gliomas (11). The prognosis is poor, especially for GBM patients, because of infiltration in surrounding brain tissues, and resistance to chemo- and radio-therapy (10). Anaplastic glioma (grade III) includes anaplastic astrocytoma, oligodendroglioma and oligoastrocytoma. It is less frequent and has a better prognosis than GBM (12). There are only few target therapy or biological drugs available for gliomas (13). The gold standard treatment consists of surgery followed by RT for high grade gliomas (HGG) (14). When surgey is not indicated radiation and chemotherapy in association with temozolomide (TMZ) is the most used choice for GBM (12-17). The effectiveness of chemotherapy is not clear, but most indicated adjuvant therapy is the association of temozolomide to radiation, resulting in longer overall survival (16, 17). However, most of HGG have disease recurrence. Median overall survival of recurrent HGG is 30-33 weeks, for this reason HGG therapy is very challenging. Treatment choices for recurrent HGG are surgical resection, re-irradiation (re-RT), chemotherapy, anti-angiogenic agents, and combination therapies of hypertermia with chemo- or radio-therapy (14). However, there is currently no standard treatment option, and surgery is indicated only for a limited group of patients with high performance status, small lesion, and young age (18). Radiofrequency (RF) and electro-hyperthermia can be applied intra- and extra-cranially and have efficacy of this treatment for brain-tumors (19, 20). As shown in randomized, controlled studies. (21). For this reason, the United States Food and Drug Administration approved brain-hyperthermia for HGG. Reports on electro-hyperthermia for MG are few (22-26). One retrospective study shows only palliative results (22). Hager et al. (23) treated 35 patients with 13.56 MHz capacitive coupled device hyperthermia, reporting good tolerability for HGG with 11% of adverse events. He also reported improvement of survival and quality of life. In our previous study, we treated with ET 12 patients with relapsed malignant gliomas and reported a response rate of 29% with a median duration of response of 10 months (range 4-32) (12, 9). The purpose of this study was to extend our previous experiences to better evaluate the activity and toxicity of ET on relapsed malignant glioma patients. This article reports our
Oncothermia Journal, Volume 22, February 2018 35
experiences to the recent advancements in ET treatment of patients with gliomas, in recurrent setting. Materials and Methods Patients selection Patients were included in this study if had: >18 years old, informed consent signed, diagnosis of HGG relapsed, Eastern Cooperative Oncology Group (ECOG) performance status ≥2, normal hematological values and vital signs, previous temozolamide-based chemotherapy and radiotherapy. From April 2003 to January 2016, twenty-four patients with relapsed HGG were enrolled in the study. Description of the device EHT was administered with Oncotherm EHY-2000 device. This machine delivered a non-ionizing therapy that elevates the temperature of the tumour macro and micro-environments, in a controlled manner, to a therapeutic range of 40 –43°C (37-40). The device employs modulated electro-hyperthermia (mEHT) to achieve the controlled heating of a target anatomy (41,42) The device is a capacitive coupled impedance matching solid state electrical system that incorporates two electric capacitive plates (electrodes). One electrode is situated under the patient and is built into the treatment table, running the full length and width of the table platform. The second is a mobile electrode positioned over the patient’s target anatomical area, as directed by the prescribing physician. The electrodes are coupled to the patient with electrically conductive temperature controlled water bolus to conduct and distribute electric current into tissue, as well as help cool the skin’s surface. The capacitive system generates a 40-150-Watt radiofrequency (RF) carrier signal at 13.56 MHz, which is further modulated (amplitude modulation) for absorption by the tumour (41-44). Electro-hyperthermia protocol All patients received pre-procedural medications with a suspension of glycerol 18% and dexamethasone 12 mg before each ET session. ET with short RF waves of 13.56 MHz was applied with capacitive coupling technique maintaining 26 C° at skin contact. ET was performed with an EHY 2000 device (CE0123, Oncotherm, Traisdorf, Germany). We used a power from 40 up to 150 Watt, resulting in an average equivalent temperature of >40 C° in the tumors, for more than 90% of the treatment duration (from 20 up to 60 minutes). The targeted area was selectively treated using an electrode system cover, excluding the eye-area from the field. ET was performed in three sessions per week, increasing the power and time each session. First treatment was always at 40 Watt for 20 minutes. Time was gradually raised from 20 to 60 minutes and power from 40 up to 150 Watt in two weeks. Hyperthermia was given with short radiofrequency waves of 13.56 MHz using a capacitive coupling technique keeping the skin surface at 22°C. The applied power ranged between 40-150 Watts and the calculated average equivalent temperature in the tumors was above 40.5°C for more than 90% of the treatment duration. Duration treatment increases from 20 to 60 min. One treatment is: 3 session/wk for 4 weeks and recycle if evidence of clinical benefit or stable desease. Each patient received 24 sessions (range 12 – 64).
Oncothermia Journal, Volume 22 February 2018
36
Outcome measures The tumor responses were evaluated by MR or CT scan every two months. A complete remission (CR) was considered the complete disappearance of the tumor. A partial remission (PR) was considered the reduction of at least 20% in the two greatest diameters. A stable disease (SD) was considered when no tumor reduction or reduction <20% was observed. Progression was established when tumor size increased. The ECOG performance status scale was used to evaluate the functional recovery. Statistical Analysis Descriptive statistical analysis was performed. Continuous date was reported as median and ranges. Proportions were reported as percentages. Results Sample characteristics Twenty-four patients were enrolled in the study. Nineteen (79%) patients had glioblastoma multiforme (13 were of grade 1-3 and 6 of grade 4), 5 (21%) astrocytoma (table 1). Most patients 22 (92%) were pre-treated with surgery, and all patients were pre-treated with temozolomide associated to radiotherapy. Thirteen (54%) were females and 11 (46%) were males, median age was 60 (22-81). All patients were pre-treated with surgery (22/24), temozolomide and radiotherapy. Tumor response and survival Tumor response analysis two months after ET showed 2 (8%) complete remission (astrocytomas) and 5 (21%) partial remission (2 ASTROCYTOMA, and 3 glioblastomas), with a response rate of 29%. The median duration of response was 6 months 6 months (4-24) for gliomas, and 44 months for atrocitomas (14-156+). Stable disease was observed in 8 (33%) of patients and progression in 9 (38%) patiens. The median survival of whole study population was 19.5 months (range 2-156), 55% survival rate at 1 year, and 15 % at two years. We observed 3 long survivors at 156, 60, 62 months in atrocitomas. Ten patients had an objective clinical benefit as resulting from an increase of their ECOG from 3 to 1 in 4 (16%) patients and to 0 in 2 (8%) patients. Five-year survival trends Median overall survival was 14 months for gliomas and 61 months for astrocitomas (71% survival rate at 1 year, 50% at 2 and 29% at 3 years). Astrocytoma patients had longer survival: 60,60+,156+,62,60,63 months (fig. 1-4). The 5-year survival data for the patients with the seven most commonly treated cancer types and stages was plotted on a Kaplan-Meier curve. This data was then compared to survival data for standard of care using the Surveillance, Epidemiology and End Results (SEER) database as a control for the evaluation of an integrative approach where LRHT was the primary variable being explored (fig.5). The graphs consist of survival probability on the vertical axis and Time from Diagnosis (in years) on the horizontal axis. Tolerability ET toxicity was mostly mild (G1). We observed one (4%) head pain, one (4%) scalp burn, five (21%) epilepsy that was resolved with a medication including diazepam 10 mg in 100 ml of saline and levetiracetam in tablets without any further attack.
Oncothermia Journal, Volume 22, February 2018 37
Discussion The first-line therapy for newly diagnosed HGG are several, including surgery, radiotherapy, chemotherapy with nitrosourea, temozolomide, bevacizumab, and irinotecan, alone or guided in combination and radiation alone or combined to temozolomide (27). There is currently no standard treatment for relapsed HGG, and several potentially active systemic drugs are not effective because of blood brain barrier blockade (28). Maintenance therapy and treatments for recurrent HGG widely vary according to physician, hospital and country and include surgery, re-radiation, second/third-line chemotherapies, biodegradable carmustine wafers, gene therapy and hyperthermia (28-32, 19-21). The use of Electric Capacitive Transference hypertermia increases heat of brain tumor and is harmless for surrounding brain tissue that in no case reaches a temperature > 39.2°C (20). Most common side effects of hyperthermia are pain, burns or discomfort, but they are temporary and most of normal tissues are not damaged during the therapy. Tumor cell are more sensible than normal cells to heat, and hypertermia inhibits the DNA repair system of tumor cells. For this reason, classic hyperthermia (42-43 °C) is often associated to chemotherapy or radiotherapy. This association is safe and well tolerated and increases the efficacy on overall survival and progression free survival (16, 18). We previously reported the results of ET treatment of 12 recurrent HGG patients (14). We showed 1 CR and 2 PR with a response rate of 25% and a median duration of response of 10 months (12), without severe toxicity. The patient with CR is still alive with a progression free survival of 156 months. In this paper we report our experiences in ET treatment of a larger number of 24 recurrent HGG patients. Tumor response analysis showed a similar response to that of our past paper with a response rate of 29 % two months after ET 2 (8%) complete remission (astrocytomas) and 5 (21%) partial remission ( 2 ASTROCYTOMA, and 3 glioblastomas). The median duration of response was longer 16 months (range 6-120) than our previous study 10 months (13). Tumor response was coupled to an improvement of performance status in 6 (24%) patients. Moran and colleagues reported a higher response rate 66%, however they observed only SD or PR and none CR (20). Tanaka et al. Had higher responses when treated 16 patients with brain cancers adopting hyperthermia with 13.56- MHz RF capacitive heating machine and showed a 50% of PR (19). However, the combination of hyperthermia with other methods did not allow to draw any conclusion about the efficacy of hyperthermia alone. The median OS of whole study population was 19.5 months, 55% survival rate at 1 year, and 15 % at two years. Of particular interest we underline the presence of 3 long survivors at 156, 60, 62 months. OS was higher than that of magnetic hypertermia that resulted in survival ranging from 2.1 to 7.9 months (33). OS was comparable to that reported by Sneed et al. 31% at the 2 years follow up (22) Limitation of our study are the absence of an active comparator, non-randomization, and low number of patients. Further multicenter randomized studies with a larger number of patients are required to confirm our data. Conclusions ET hyperthermia therapy for recurrent HGG is feasible and may increase tumor response and survival. ET is a non-invasive method to treat HGG without severe toxicity

Oncothermia Journal, Volume 22 February 2018
38
References 1. Soares PI, Ferreira IM, Igreja RA, Novo CM and Borges JP: Application of
hyperthermia for cancer treatment: recent patents review. Recent Pat Anticancer Drug Discov 7: 64-73, 2012.
2. Datta NR, Krishnan S, Speiser DE, Neufeld E, Kuster N, Bodis S, Hofmann H. Magnetic nanoparticle-induced hyperthermia with appropriate payloads: Paul Ehrlich's "magic (nano)bullet" for cancer theranostics? Cancer Treat Rev. 2016 Nov;50:217-227. doi: 10.1016/j.ctrv.2016.09.016. PMID: 27756009
3. Kim KS, Hernandez D, Lee SY. Time-multiplexed two-channel capacitive radiofrequency hyperthermia with nanoparticle mediation. Biomed Eng Online. 2015 Oct 24;14:95. doi: 10.1186/s12938-015-0090-9. PMID: 26499058
4. Solari N, Sucameli F, Gipponi M, De Cian F, Cafiero F. Laparoscopic hyperthermic isolated limb perfusion a new minimally invasive approach for HILP. Int J Hyperthermia. 2017 Apr 24:1-5. doi: 10.1080/02656736.2017.1315179. PMID: 28540806
5. Lee SY, Lee NR, Cho DH, Kim JS. Treatment outcome analysis of chemotherapy combined with modulated electro-hyperthermia compared with chemotherapy alone for recurrent cervical cancer, following irradiation. Oncol Lett. 2017 Jul;14(1):73-78. doi: 10.3892/ol.2017.6117. PMID: 28693137
6. Ranieri G, Ferrari C, Palo AD, Marech I, Porcelli M, Falagario G, Ritrovato F, Ramunni L, Fanelli M, Rubini G, Gadaleta CD. Bevacizumab-Based Chemotherapy Combined with Regional Deep Capacitive Hyperthermia in Metastatic Cancer Patients: A Pilot Study. Int J Mol Sci. 2017 Jul 6;18(7). pii: E1458. doi: 10.3390/ijms18071458. PMID: 28684680
7. Brüningk SC, Ijaz J, Rivens I, Nill S, Ter Haar G, Oelfke U. A comprehensive model for heat-induced radio-sensitisation. Int J Hyperthermia. 2017 Jul 5:1-11. doi: 10.1080/02656736.2017.1341059. PMID: 28641499
8. Moy AJ, Tunnell JW. Combinatorial immunotherapy and nanoparticle mediated hyperthermia. Adv Drug Deliv Rev. 2017 Jun 15. pii: S0169-409X(17)30092-3. doi: 10.1016/j.addr.2017.06.008. PMID: 28625829
9. Baronzio G, Gramaglia A, Fiorentini G. Hyperthermia and immunity. A brief overview. In Vivo. 2006;20:689–695. [PubMed]
10. . Louis, D. N., Perry, A., Reifenberger, G., von Deimling, A., Figarella-Branger, D., Cavenee, W. K., et al. (2016). The 2016 world health organization classification of tumors of the central nervous system: a summary. Acta Neuropathol. 131, 803–820. doi: 10.1007/s00401-016-1545-110.1007/s00401-016-1545-1
11. Ostrom, Q.T., H. Gittleman, J. Fulop, M. Liu, R. Blanda, www.impactjournals.com/oncotarget 80099 Oncotarget C. Kromer, Y. Wolinsky, C. Kruchko, and J.S. BarnholtzSloan. CBTRUS Statistical Report: Primary Brain and Central Nervous System Tumors Diagnosed in the United States in 2008-2012. Neuro Oncol. 2015; 17 Suppl 4: iv1- iv62
12. Rees JH: Diagnosis and treatment in neuro-oncology: an oncological perspective. Br J Radiol 84: S82-S89, 2011

Oncothermia Journal, Volume 22, February 2018 39
13. Uhm JH, Porter AB. Treatment of Glioma in the 21st Century: An Exciting Decade of Postsurgical Treatment Advances in the Molecular Era. Mayo Clin Proc. 2017 Jun;92(6):995-1004. doi: 10.1016/j.mayocp.2017.01.010. PMID: 28578786
14. Fiorentini G, Giovanis P, Rossi S, Dentico P, Paola R, Turrisi G and Bernardeschi P: A phase II clinical study on relapsed malignant gliomas treated with electro-hyperthermia. In Vivo 20: 721-724, 2006.
15. Heo J, Kim SH, Oh YT, Chun M, Noh OK. Concurrent hyperthermia and re-irradiation for recurrent high-grade gliomas. Neoplasma. 2017 Jun 8. doi: 10.4149/neo_2017_520. PMID: 28592133
16. Stupp R, Hegi ME, Mason WP, et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised Phase III study: 5-year analysis of the EORTC-NCtrial IC. Lancet Oncol. 2009;10(5):459–466. [PubMed]
17. Clarke JL, Iwamoto FM, Sul J, et al. Randomized Phase II trial of chemoradiotherapy followed by either dose-dense or metronomic temozolomide for newly diagnosed glioblastoma. J. Clin. Oncol. 2009;27(23):3861–3867. [PMC free article] [PubMed]
18. Wust P, Hildebrandt B, Sreenivasa G, Rau B, Gellermann J, Riess H, Felix R and Schlag PM: Hyperthermia in combined treatment of cancer. Lancet Oncology 3: 487-497, 2002.
19. Tanaka R, Kim CH, Yamada N and Saito Y: Radiofrequency hyperthermia for malignant brain tumors: preliminary results of clinical trials. Neurosurgery 21(4): 478-483, 1987.
20. Moran CJ, Marchosky JA, Wippold FJ 2nd, DeFord JA and Fearnot NE: Conductive interstitial hyperthermia in the treatment of intracranial metastatic disease. J Neurooncol 26(l): 53-63, 1995.
21. Ley-Valle A: Non invasive intracranial hyperthermia with capacitive transference –ECT- intratumoral and cerebral thermometry results. Neurocirurgia 14 (1): 41-45, 2003
22. Sneed PK, Stauffer PR, McDermott MW, Diederich CJ, Lamborn KR, Prados MD, Chang S, Weaver KA, Spry L,Malec MK, Lamb SA, Voss B, Davis RL, Wara WM, Larson DA, Phillips TL and Gutin PH: Survival benefit of hyperthermia in a prospective randomized trial of brachytherapy boost +/–hyperthermia for glioblastoma multiforme, Int J Radiat Oncol Biol Phys 40(2): 287-295, 1998.
23. Hager D, Dziambor H, App EM, Popa C, Popa O and Hertlein M: The treatment of patients with high-grade malignant gliomas with RF-hyperthermia. Abs No. 470, 39th Proceedings ASCO, 2003.
24. Wismeth C, Dudel C, Pascher C, Ramm P, Pietsch T, Hirschmann B, Reinert C, Proescholdt M, Rümmele P, Schuierer G, Bogdahn U, Hau P. Transcranial electro-hyperthermia combined with alkylating chemotherapy in patients with relapsed high-grade gliomas: phase I clinical results. J Neurooncol. 2010;98(3):395-405. doi: 10.1007/s11060-009-0093-0. PMID: 20033471

Oncothermia Journal, Volume 22 February 2018
40
25. Cha J, Jeon TW, Lee CG, Oh ST, Yang HB, Choi KJ, Seo D, Yun I, Baik IH, Park KR, Park YN, Lee YH. Electro-hyperthermia inhibits glioma tumorigenicity through the induction of E2F1-mediated apoptosis. Int J Hyperthermia. 2015;31(7):784-92. doi: 10.3109/02656736.2015.1069411. PMID: 26367194
26. Sun J, Guo M, Pang H, Qi J, Zhang J, Ge Y. Treatment of malignant glioma using hyperthermia. Neural Regen Res. 2013;8(29):2775-82. doi: 10.3969/j.issn.1673-5374.2013.29.009. PMID: 25206588
27. Yamaguchi F. Therapy Decisions for Patients with High-Grade Glioma and Their Families. World Neurosurg. 2017 Jun;102:671-672. doi: 10.1016/j.wneu.2017.03.094. PMID: 28359926
28. Stöckelmaier L, Renovanz M, König J, Nickel K, Hickmann AK, Mayer-Steinacker R, Nadji-Ohl M, Ganslandt O, Bullinger L, Wirtz CR, Coburger J. Therapy for Recurrent High-Grade Gliomas: Results of a Prospective Multicenter Study on Health-Related Quality of Life. World Neurosurg. 2017 Jun;102:383-399. doi: 10.1016/j.wneu.2017.02.061. PMID: 28288921
29. Buonerba C, Di Lorenzo G , Marinelli A, Federico P, Palmieri G, Imbimbo M, Conti P, Peluso G, De Placido S, Sampson JH. A comprehensive outlook on intracerebral therapy of malignant gliomas. Crit Rev Oncol Hematol. 2011 Oct;80(1):54-68. doi: 10.1016/j.critrevonc.2010.09.001. PMID: 20888252
30. Burger MC, Mildenberger IC, Wagner M, Mittelbronn M, Steinbach JP, Bähr O. Bevacizumab for Patients with Recurrent Gliomas Presenting with a Gliomatosis Cerebri Growth Pattern. Int J Mol Sci. 2017 Mar 29;18(4). pii: E726. doi: 10.3390/ijms18040726. PMID: 28353668
31. Sai K, Zhong MG, Wang J, Chen YS, Mou YG, Ke C, Zhang XH, Yang QY, Lin FH, Guo CC, Chen ZH, Zeng J, Lv YC, Li X, Gao WC, Chen ZP. Safety evaluation of high-dose BCNU-loaded biodegradable implants in Chinese patients with recurrent malignant gliomas. J Neurol Sci. 2014 Aug 15;343(1-2):60-5. doi: 10.1016/j.jns.2014.05.022. PMID: 24874252
32. Glaser T, Han I, Wu L, Zeng X. Targeted Nanotechnology in Glioblastoma Multiforme. Front Pharmacol. 2017;8:166. doi: 10.3389/fphar.2017.00166. eCollection 2017. PMID: 28408882
33. Silva AC, Oliveira TR, Mamani JB, Malheiros SM, Malavolta L, Pavon LF, Sibov TT, Amaro E Jr, Tannús A, Vidoto EL, Martins MJ, Santos RS, Gamarra LF. Application of hyperthermia induced by superparamagnetic iron oxide nanoparticles in glioma treatment. Int J Nanomedicine. 2011;6:591-603. doi: 10.2147/IJN.S14737. PMID: 21674016
34. Lee Titsworth W1, Murad GJ, Hoh BL, Rahman M. Fighting fire with fire: the revival of thermotherapy for gliomas. Anticancer Res. 2014;34(2):565-74. PMID: 24510985
35. Hegyi G, Szigeti GP, Szász A. Hyperthermia versus Oncothermia: Cellular Effects in Complementary Cancer Therapy. Evid Based Complement Alternat Med. 2013;2013:672873. doi: 10.1155/2013/672873. PMID: 23662149
Oncothermia Journal, Volume 22, February 2018 41
36. Heo J, Kim SH, Oh YT, Chun M, Noh OK. Concurrent hyperthermia and re-irradiation for recurrent high-grade gliomas. Neoplasma. 2017;64(5):803-808. doi: 10.4149/neo_2017_520.
37. Szentgyorgi A. Electronic biology and cancer. New York, NY, USA: Marcel Dekker; 1998.
38. Singh BB. Hyperthermia--a new dimension in cancer treatment. Indian J Biochem Biophys. 1990;27(4):195-201.
39. Warburg O. Oxygen,the creator of differentiation, biochemical energetics. New York, NY, USA: Academic Press; 1966.
40. Warburg O. The prime cause and prevention of cancer, revised lecture at the meeting of the nobel-laureates . . June 30, 1966.
41. Szasz A, Szasz O, Szasz N. Electrohyperthermia: A new paradigm in cancer therapy. In: 33rd ed., 2001:91-99.
42. Szasz O, Szasz A. Oncothermia – nano-heating paradigm. J Cancer Sci Ther. 2014;1(6):117-121.
43. Szasz A, Szasz O, Szasz N. Physical background and technical realization of hyperthermia, in: Locoregional radiofrequency-perfusional- and wholebody- hyperthermia in cancer treatment: New clinical aspects. ; 2006.
44. Szasz A, Vincze G, Szasz O, Szasz N. An energy analysis of extracellular hyperthermia. Electromagnetic Biology and Medicine. 2003;1(22):103-115)

Oncothermia Journal, Volume 22 February 2018
42
Table 1) Chracteristics of the sample ID Sex Age Type of glioma MGMT
metilated
IDH1 Response
OS (months)
01 F 41 ASTROCYTOMA YES YES PR 60 02 M 26 ASTROCYTOMA NO YES RC 60 03 M 22 ASTROCYTOMA YES YES RC 156 04 F 56 ASTROCYTOMA III NO NO SD 62 05 M 63 ASTROCYTOMA/GBM YES NO SD 60 06 M 58 GBM IV NO NO SD 2 07 M 45 GBM IV NO NO SD 14 08 F 67 GBM IV NO NO PD 10 09 M 66 GBM IV NO NO PD 9 10 M 54 GBM ND ND PD 14 11 F 46 GBM YES YES PR 24 12 M 65 GBM ND ND PD 5 13 F 75 GBM ND ND SD 8 14 F 76 GBM ND ND PD 6 15 M 62 GBM IV NO NO PD 14 16 M 74 GBM NO NO SD 15 17 F 81 GBM ND ND PD 8 18 M 53 GBM ND ND SD 36 19 M 66 GBM ND ND PR 25 20 F 66 GBM ND NF SD 15 21 F 33 GBM ND ND PD 32 22 F 49 GBM ND ND PD 32 23 M 52 GBM IV YES ND PR 24 24 F 66 ASTROCYTOMA III ND ND PR 63 25 F 34 NOT DEFINED ND ND PR 5

Oncothermia Journal, Volume 22, February 2018 43
Figure 1) ASTROCYTOMA G III (G.E. 32 yrs) 1-Response
2013/12/0
4
2016/23/0
8
Figure 2) Astrocytoma GIII (g.e. 32 yrs) 2-response
2013/12/04 2016/23/08
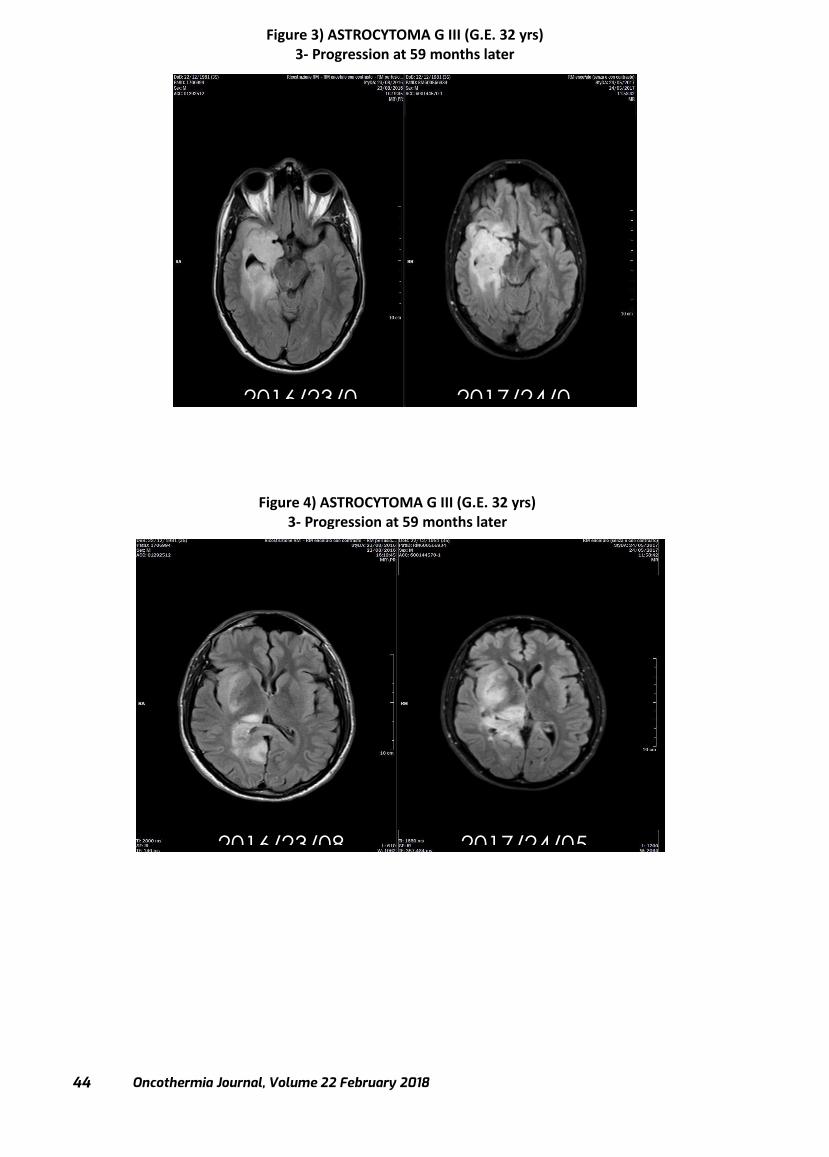
Oncothermia Journal, Volume 22 February 2018
44
Figure 3) ASTROCYTOMA G III (G.E. 32 yrs) 3- Progression at 59 months later
2016/23/0 2017/24/0
2016/23/08 2017/24/05
Figure 4) ASTROCYTOMA G III (G.E. 32 yrs) 3- Progression at 59 months later
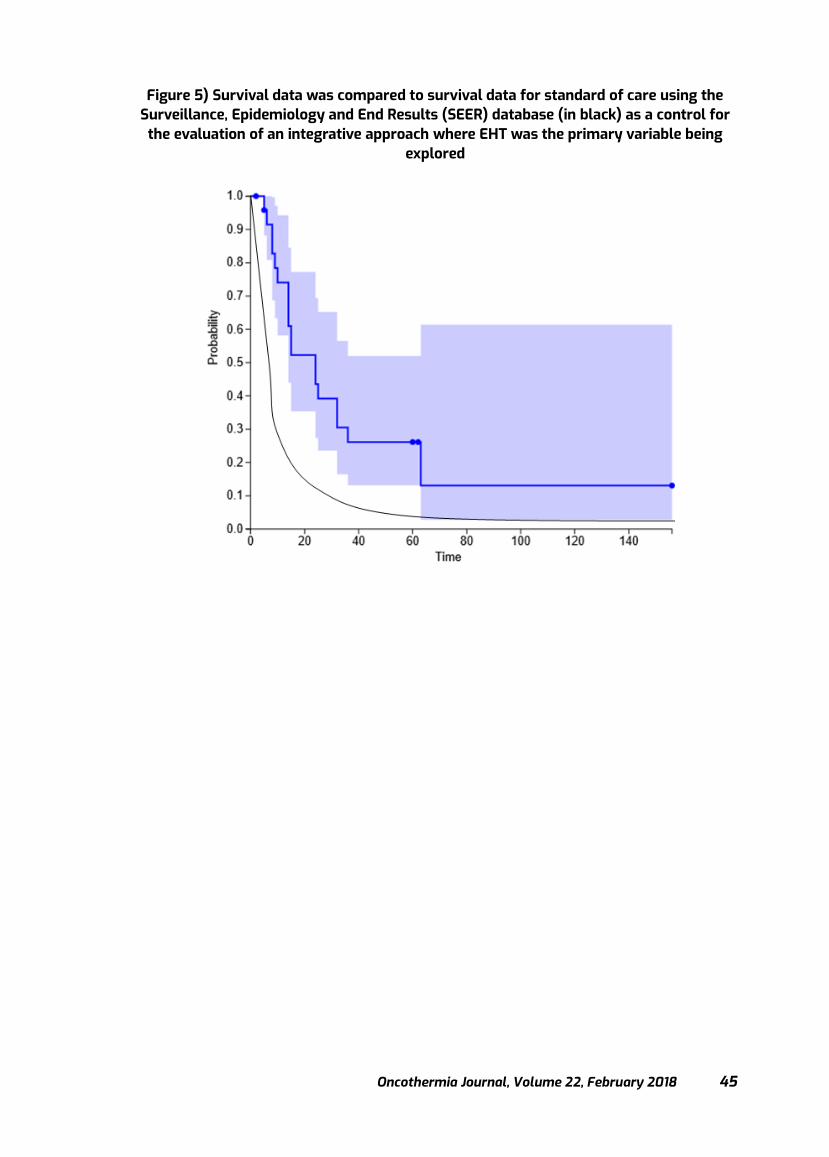
Oncothermia Journal, Volume 22, February 2018 45
Figure 5) Survival data was compared to survival data for standard of care using the Surveillance, Epidemiology and End Results (SEER) database (in black) as a control for the evaluation of an integrative approach where EHT was the primary variable being
explored

Oncothermia Journal, Volume 22 February 2018
46
Lower and less toxic doses of chemotherapy by combining it with hyperthermia and complementary treatments
Prof. Dr. med. Alexander Herzog
Chief-physician, Fachklinik Dr. Herzog, Germany
Presented at 35th ICHS, Guangzhou, 2017
Cite this article as: Herzog A. (2018): Lower and less toxic doses of chemotherapy by combining it with hyperthermia and complementary treatments;
Oncothermia Journal 22:46-56 www.oncothermia-journal.com/journal/2018/Lower_and_less_toxic.pdf

Oncothermia Journal, Volume 22, February 2018 47
Lower and less toxic doses of chemotherapy by combining it with hyperthermia and complementary treatments.
Introduction: Hyperthermia is an important tool to improve the efficacy of chemotherapy and radiation in cancer. Numerous studies have been published about hyperthermia treatment in cell cultures, in animal experiments but also in patients. These studies include randomized studies, phase 2 studies but also many successful case reports providing evidence for the benefit of hyperthermia. In neoadjuvant treatment the goal would be a higher remission rate and faster and more complete shrinkage of the tumors so that surgery would be easier. In curative treatment the goal would be to achieve a higher rate of cure. In palliative treatment, however, the focus would be not so much on high remission rates as a remission itself is not as important as the overall survival time. Achieving a higher remission rate with very toxic chemotherapy even may result in shorter survival time (and reduced quality of life in the remaining time). As hyperthermia increases the efficacy of chemotherapy and radiation we have to consider in the palliative setting a dose reduction of chemotherapy when given together with hyperthermia. By controlling a malignant disease with less toxic treatments not only quality of life would be preserved, also survival time may be prolonged as patients would suffer from less toxicity. Methods: Hyperthermia means heating up cancer tissue up to 42°C (107.6°F). In several experiments it has been shown that chemotherapy works more efficient if the temperature of cancer tissue is increased. There can be a linear or even an exponential increase of the activity of cytostatic drugs. Hyperthermia for healthy tissues is not dangerous but in cancer cells hyperthermia already alone may have a damaging effect. This includes disturbances of the regulation of cell membranes, denaturation of p-glycoproteins (which are responsible for resistancies of tumor cells against chemotherapy or radiation), increased blood flow into tumor tissues and also possibly getting cells out of a dormant status. There are different types of hyperthermia: Local hyperthermia includes superficial hyperthermia with infrared radiation or microwaves and deep regional hyperthermia using short wave irradiation. Depending on the devices and technical features energies up to 600 W and more may be used. (We use the Oncotherm device with 13.56 MHz and energies up to 150 Watts). Local hyperthermia treatment takes 1 hour for each session. The treatment can be repeated frequently (the gap between 2 treatments should be at least 48 hours to avoid thermal tolerance). Chemotherapy is given simultaneously to a local hyperthermia session. The efficacy of hyperthermia even can be increased if a tumor is treated with chemo- embolization. By this procedure tumors are less perfused which allows higher accumulation of heat tumor as the cooling effect of the bloodstream is reduced.

Oncothermia Journal, Volume 22 February 2018
48
In whole body hyperthermia the body core temperature is heated up 41.5°C (106.7° F). This is only possible in analgo-sedation and intensive care monitoring. The temperature of the body is increased by whole body water filtered infrared-irradiation using energies up to 2000 Watts. This radiation heats up the small blood vessels under the skin and in this way the blood gradually heats up the body core until the desired level is reached. Chemotherapy is given at the peak temperature of whole body hyperthermia (Image 1). The chemotherapy protocols for hyperthermia depend on the different diseases. But the chemotherapy can be modified in a way that lower and less toxic doses may be given if combined with hyperthermia. Results for a selection of different cancers: ENT-Cancers: Advanced ENT -cancers are difficult to treat by surgery as often tumors are surrounded by vulnerable structures in face, throat, skull base and neck. Standard chemotherapy in this condition would be a rather toxic program of 5 days Cisplatin together with 5-FU as continuous infusion. Together with hyperthermia a 4 day program would be sufficient. (Image 2) Together with local hyperthermia this treatment is efficient even in large tumors. (Image 3). Lung cancer: In patients with non-small cell lung cancer whole body hyperthermia and local hyperthermia together with chemotherapy can be highly efficient. The dose regime would follow a platin based chemotherapy, but the doses of Carboplatin and Gemcitabine or Vinorelbine could be reduced about 20%. Not only the primary tumors in the lung often respond quite well, also in metastatic disease fast changes can be noticed resulting in reduction of symptoms. (Image 4). Colorectal cancer: The chemotherapy protocols in colorectal cancer are mainly the FOLFOX and the Folfiri protocol, which can be combined with the antibodies Bevacizumab or Cetuximab. Together with hyperthermia the oxaliplatin dose would be kept at the standard level. Irinotecan could be reduced and also 5-FU significantly could be reduced it given as chronomodulated treatment overnight with 50% of the total dose between 2 a.m. and 6 a.m. Also, Capecitabine may be used together with hyperthermia in a reduced dose (Image 5). Even patients with a high tumor load and predicted short survival time in which a standard chemotherapy is not possible any more may benefit from this treatment. In a patient with subtotal liver involvement using local hyperthermia and chemotherapy with sequential use of FOLFOX, later FOLFIRI and later Capecitabine a nearly three-year survival could be achieved (Image 6). In a patient with very advanced rectal cancer protruding out of the anus but no distant metastases using local hyperthermia and neoadjuvant FOLFOX first a very good partial remission could be achieved. Continuing local hyperthermia with neoadjuvant radiation plus Capecitabine finally a nearly complete remission was achieved. The patient could be operated in a way that normal bowel passage was achieved. Seven years later the patient is still free of disease (Image 7).

Oncothermia Journal, Volume 22, February 2018 49
Ovarian and cervical cancers: In ovarian and cervical cancer standard chemotherapy is Carboplatin and the neurotoxic drug Paclitaxel. Together with hyperthermia Carboplatin could be combined with the less toxic Cyclophosphamide which is a drug with enhancement of its activity under hyperthermic conditions (Image 8). In a 28-year-old patient with very advanced inoperable ovarian cancer a complete remission could be achieved with whole body hyperthermia and Carboplatin in moderate doses (AUC 4-4,5) plus Cyclophosphamide resulting in survival until today, 9 years later (Image 9). In patients with recurrent cervical cancer a combination of local hyperthermia and chemo-embolisation can be successful. By chemo-embolisation the perfusion of the tumor is reduced so that hyperthermia heats the tumor up more selected. In a patient with a very large cervical recurrence filling nearly the complete small pelvis, causing subtotal compression of the bladder requiring nephrostomas on both sides and heavy vaginal bleeding and pain as symptom a fast remission could be achieved with the patient free of symptoms. The nephrostomas could be exchanged to ureteral splints when the bladder got back its capacity (Image 10). Breast cancer: In breast cancer patients often are pretreated by neoadjuvant or adjuvant chemotherapy. Therefore, in patients with local recurrence or with metastases chemotherapy options are limited. Using a chemotherapy with moderate doses of Vinorelbine and Mitomycin a high rate of responses can be achieved. But whole-body hyperthermia also can be applied in the neoadjuvant situation (Image 11) but also in wide spread disease around the chest wall and around breast implants (Image 12). In a small study we could show that between 70% and 80% of consecutive patients with breast cancer respond to a treatment program with whole body and local hyperthermia together with moderate doses of chemotherapy (image13). Hyperthermia is a treatment which does not have dangerous side effects. Most patients tolerate it very well. After local hyperthermia sometimes “hot spots” occur in fatty tissues. In whole body hyperthermia the risk of local superficial burns is about 4% (depending on the experience of the therapist). Discussion: Together with hyperthermia it is possible to use chemo-therapy in more moderate doses. This reduces toxicity and helps patients in particular in the palliative situation to preserve quality of life. It also allows to perform treatments more regular and over a longer period of time which possibly is very important to achieve longer survival times. This report presents a number of patients with very advanced diseases difficult to treat. In all of these patients using standard treatment protocols similar responses would not have been expected. International studies exist up to now for patients with cancer of the cervix uteri, for patients with sarcoma, for patients with recurrent breast cancer but also colorectal and ovarian cancer. However, the number of these studies is limited and often they are not performed in a randomized form. Randomized studies on the other hand are difficult to perform nowadays as chemotherapy treatment guidelines change very fast, sometimes every year. So, performing a randomized study with hyperthermia using a certain chemotherapy protocol after 2 years would not be up-to-date anymore as other chemotherapies would be standard. Also
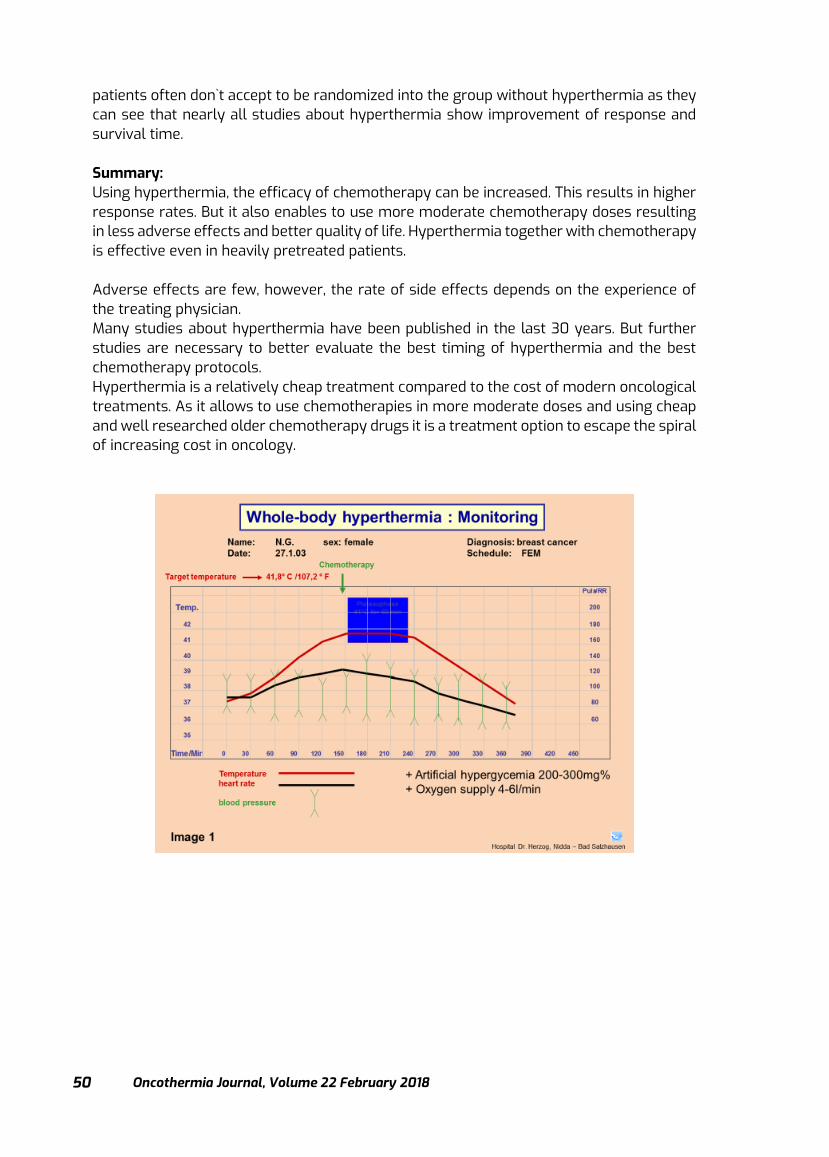
Oncothermia Journal, Volume 22 February 2018
50
patients often don`t accept to be randomized into the group without hyperthermia as they can see that nearly all studies about hyperthermia show improvement of response and survival time. Summary: Using hyperthermia, the efficacy of chemotherapy can be increased. This results in higher response rates. But it also enables to use more moderate chemotherapy doses resulting in less adverse effects and better quality of life. Hyperthermia together with chemotherapy is effective even in heavily pretreated patients. Adverse effects are few, however, the rate of side effects depends on the experience of the treating physician. Many studies about hyperthermia have been published in the last 30 years. But further studies are necessary to better evaluate the best timing of hyperthermia and the best chemotherapy protocols. Hyperthermia is a relatively cheap treatment compared to the cost of modern oncological treatments. As it allows to use chemotherapies in more moderate doses and using cheap and well researched older chemotherapy drugs it is a treatment option to escape the spiral of increasing cost in oncology.

Oncothermia Journal, Volume 22, February 2018 51
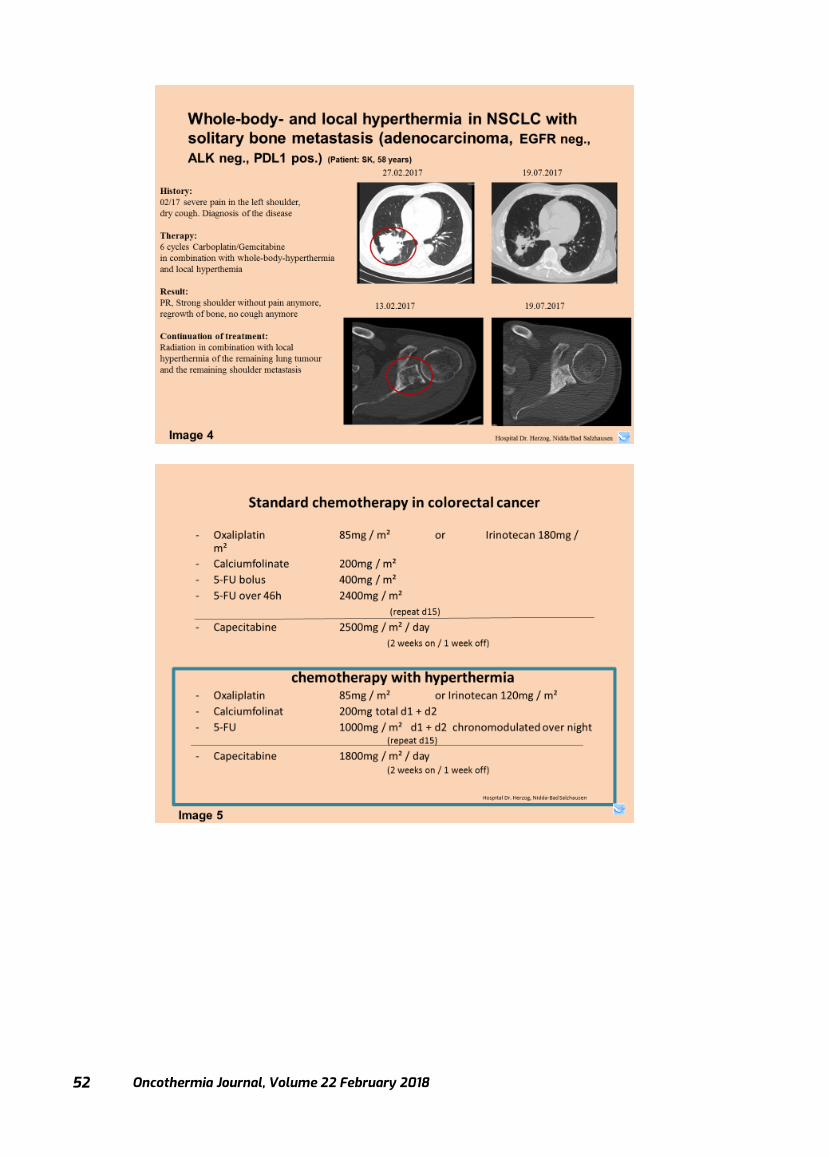
Oncothermia Journal, Volume 22 February 2018
52

Oncothermia Journal, Volume 22, February 2018 53
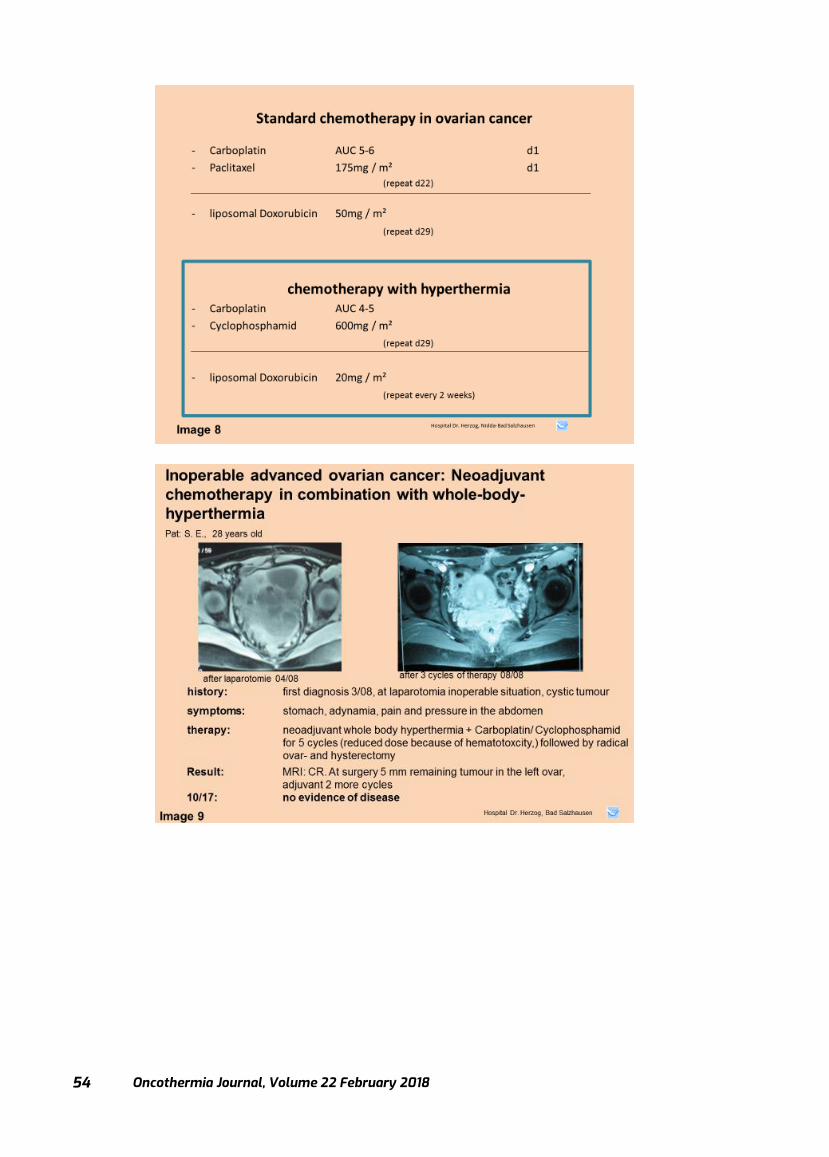
Oncothermia Journal, Volume 22 February 2018
54
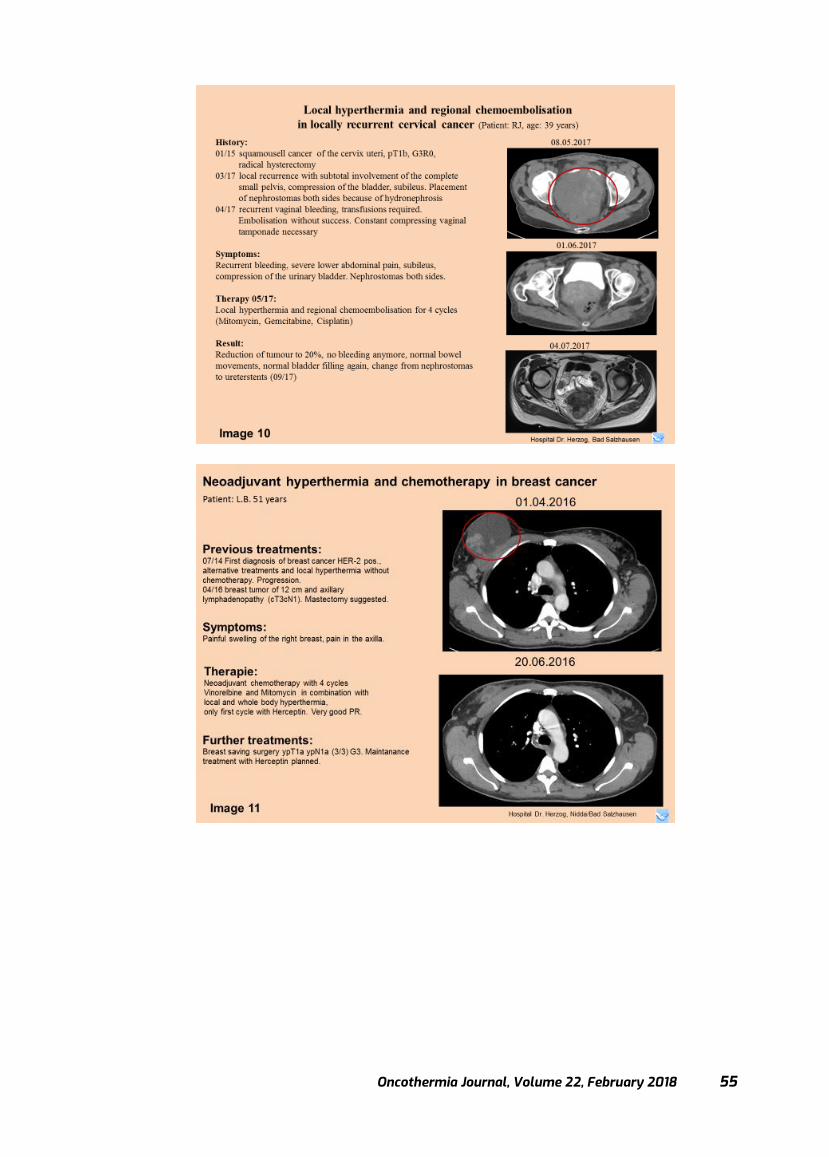
Oncothermia Journal, Volume 22, February 2018 55
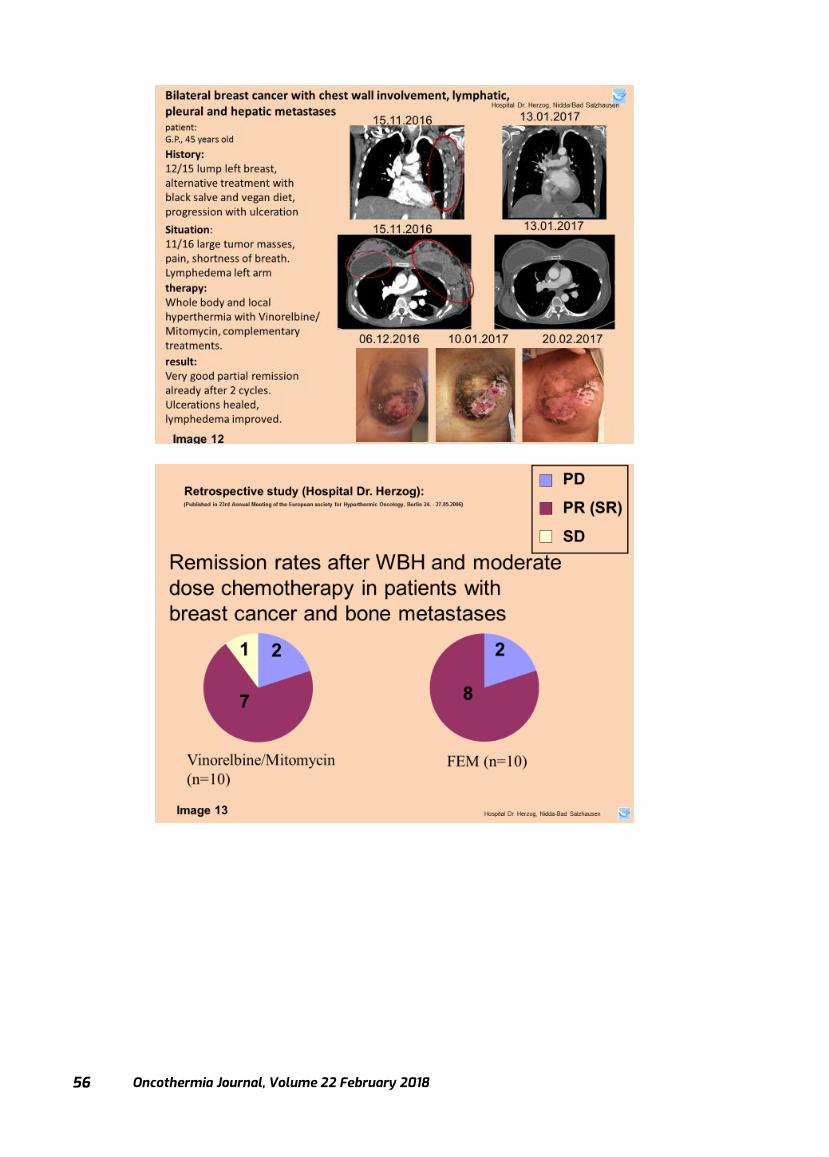
Oncothermia Journal, Volume 22 February 2018
56

Oncothermia Journal, Volume 22, February 2018 57
Modulated Electro-Hyperthermia: Role in Developing Countries
C.A. Minnaar; 1 J.A. Kotzen 1; A. Baeyens 1 2 1Radiobiology, Radiation Sciences, University of the Witwatersrand, Johannesburg, South
Africa 2Radiobiology, Basic Medical Sciences, Ghent University, Ghent, Belgium
Presented at 35th ICHS, Guangzhou, 2017
Cite this article as:
Minnaar C.A., Kotzen J.A., Baeyens A. (2018): Modulated Electro-Hyperthermia: Role in Developing Countries; Oncothermia Journal 22: 57-
66 www.oncothermia-
journal.com/journal/2018/Modulated_Electro_Hyperthermia.pdf
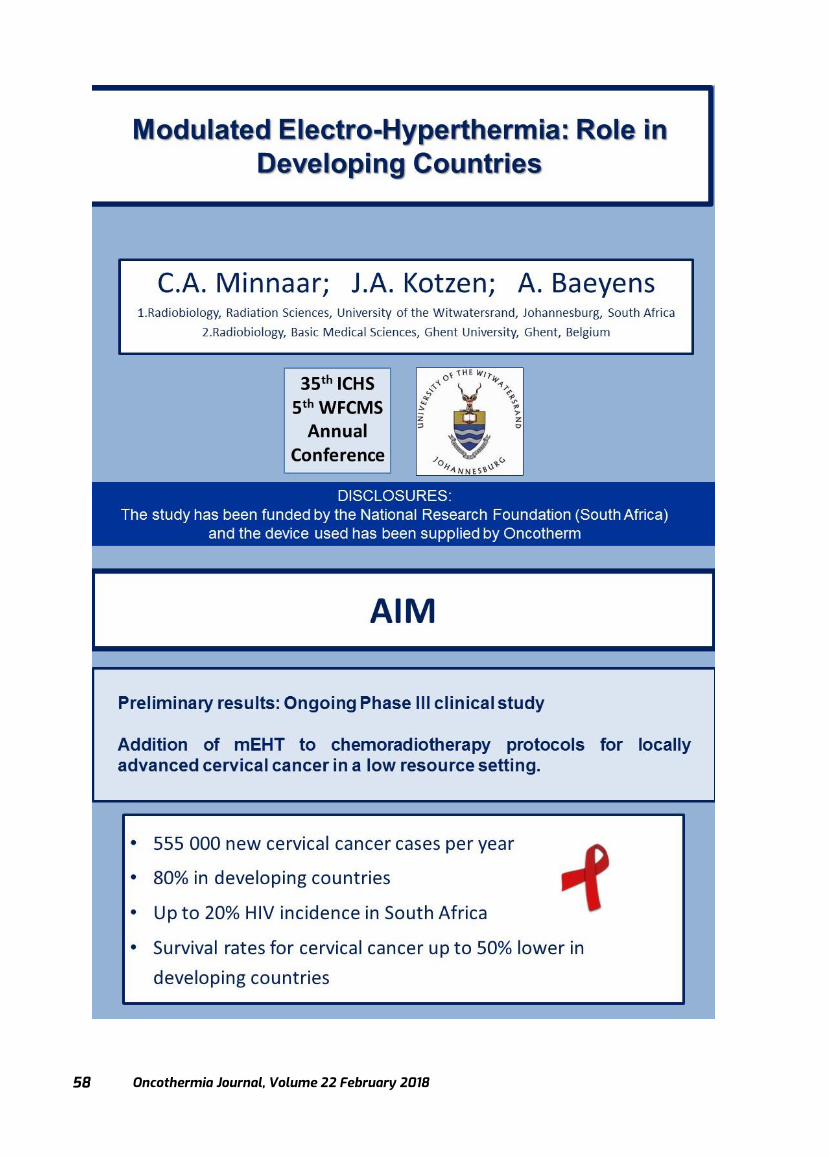
Oncothermia Journal, Volume 22 February 2018
58
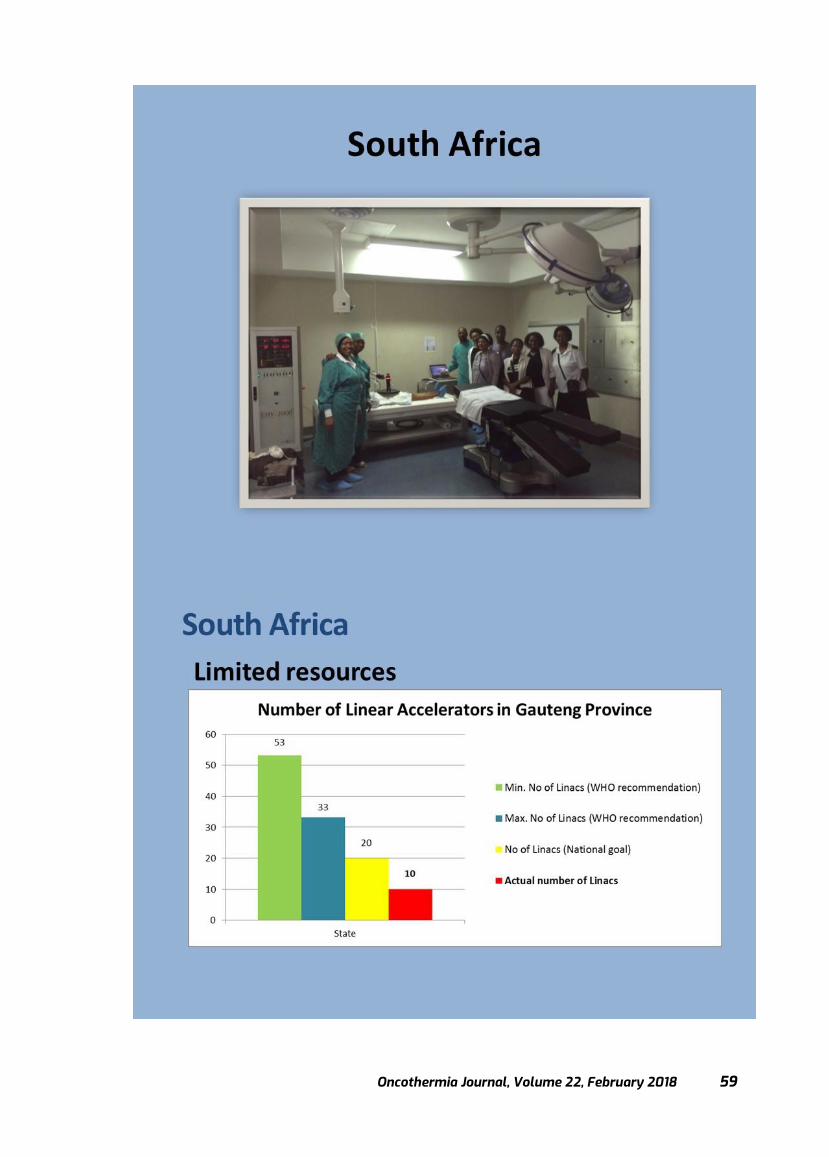
Oncothermia Journal, Volume 22, February 2018 59
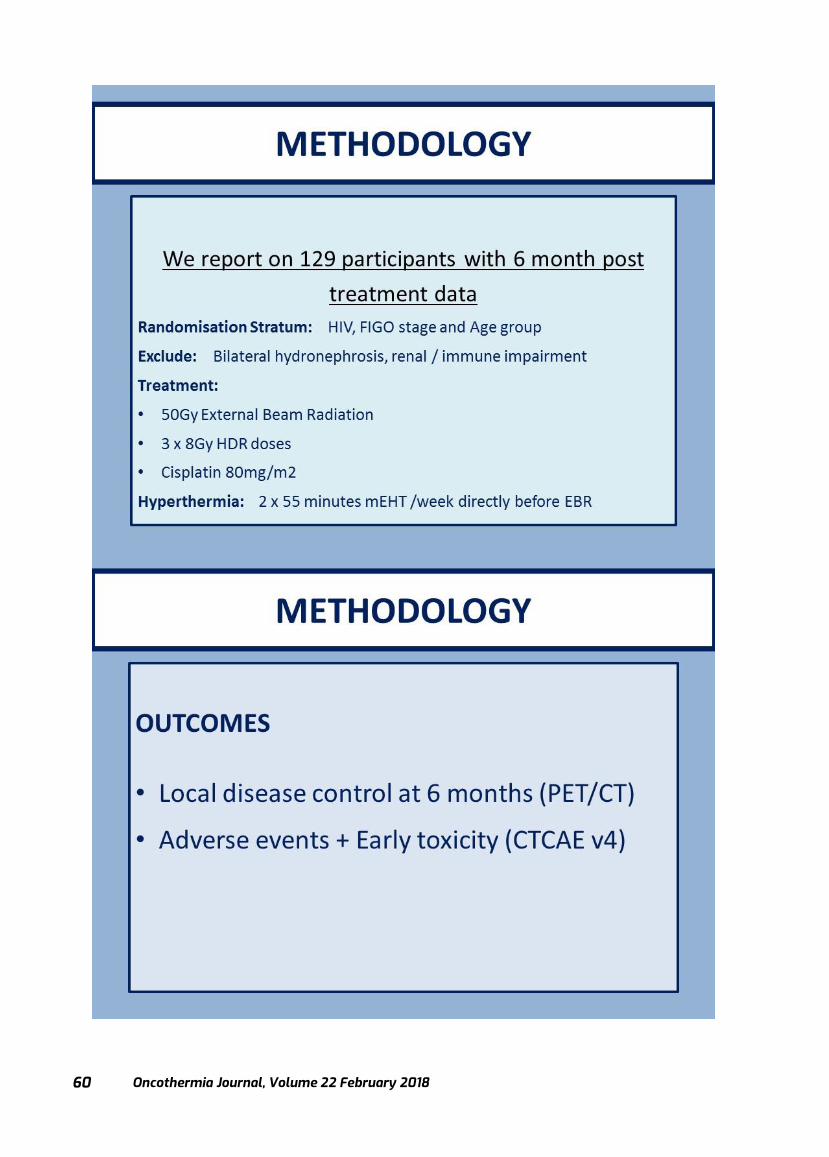
Oncothermia Journal, Volume 22 February 2018
60
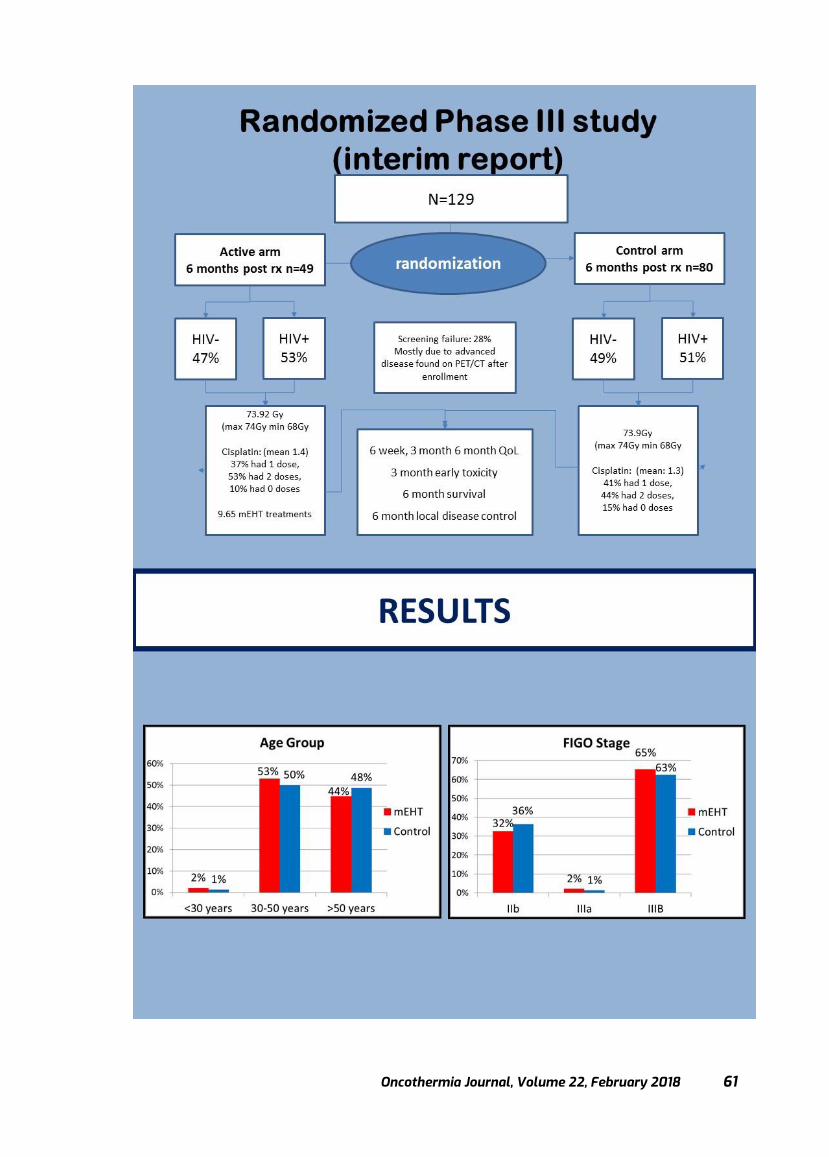
Oncothermia Journal, Volume 22, February 2018 61
Oncothermia Journal, Volume 22 February 2018
62
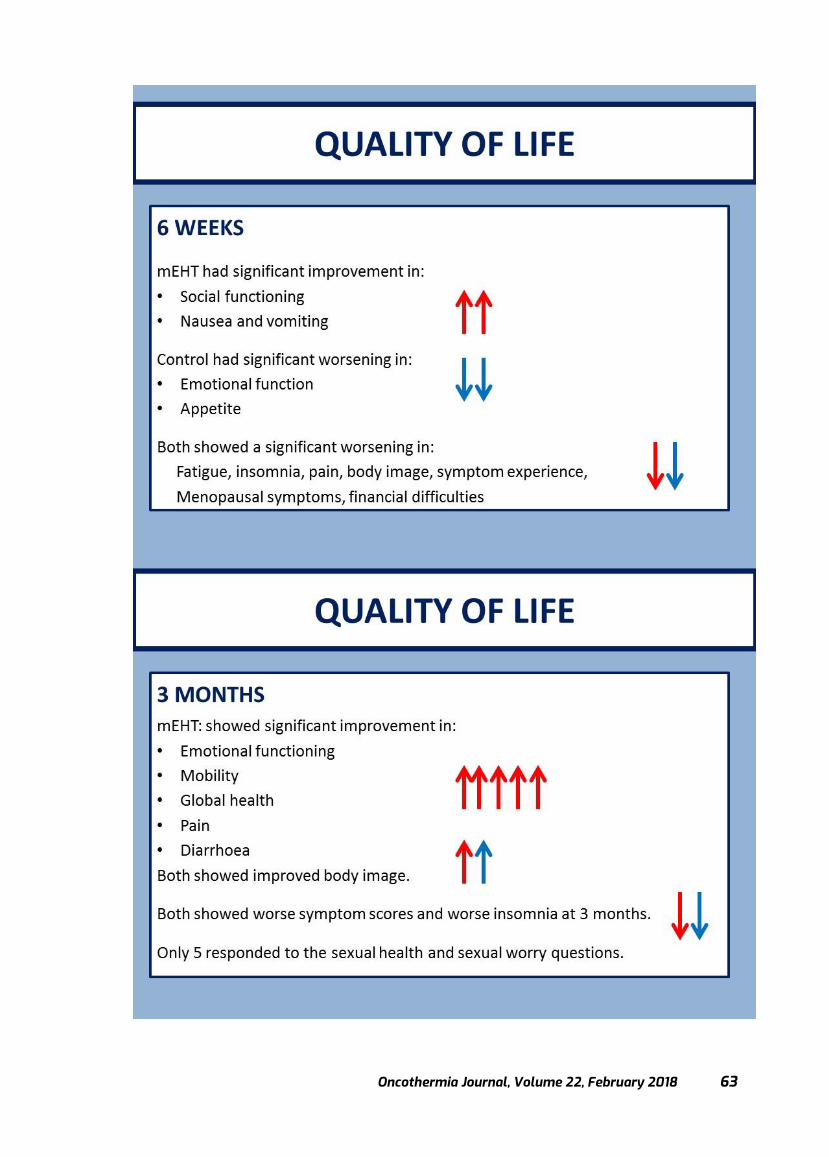
Oncothermia Journal, Volume 22, February 2018 63

Oncothermia Journal, Volume 22 February 2018
64
Oncothermia Journal, Volume 22, February 2018 65

Oncothermia Journal, Volume 22 February 2018
66

Oncothermia Journal, Volume 22, February 2018 67
Local oncothermia treatment fights against systemic malignancy
Prof. Dr. Andras Szasz Professor of physics & biophysics
Chair, Department of Biotechnics, St. Istvan University, Hungary & Visiting professor (bioelectromagnetics) in Pazmany P. Catholic University, Hungary &
Visiting professor (fractal physiology) in Chiba University, Japan & Chief Scientific Officer (CSO), Oncotherm GmbH, Troisdorf, Germany
Presented at 35th ICHS, Guangzhou, 2017
Cite this article as:
Szasz A. (2018) Local oncothermia treatment fights against systemic malignancy; Oncothermia Journal 22:67-84
www.oncothermia-journal.com/journal/2018/Local_oncothermia_treatment.pdf
Oncothermia Journal, Volume 22 February 2018
68
Oncothermia Journal, Volume 22, February 2018 69
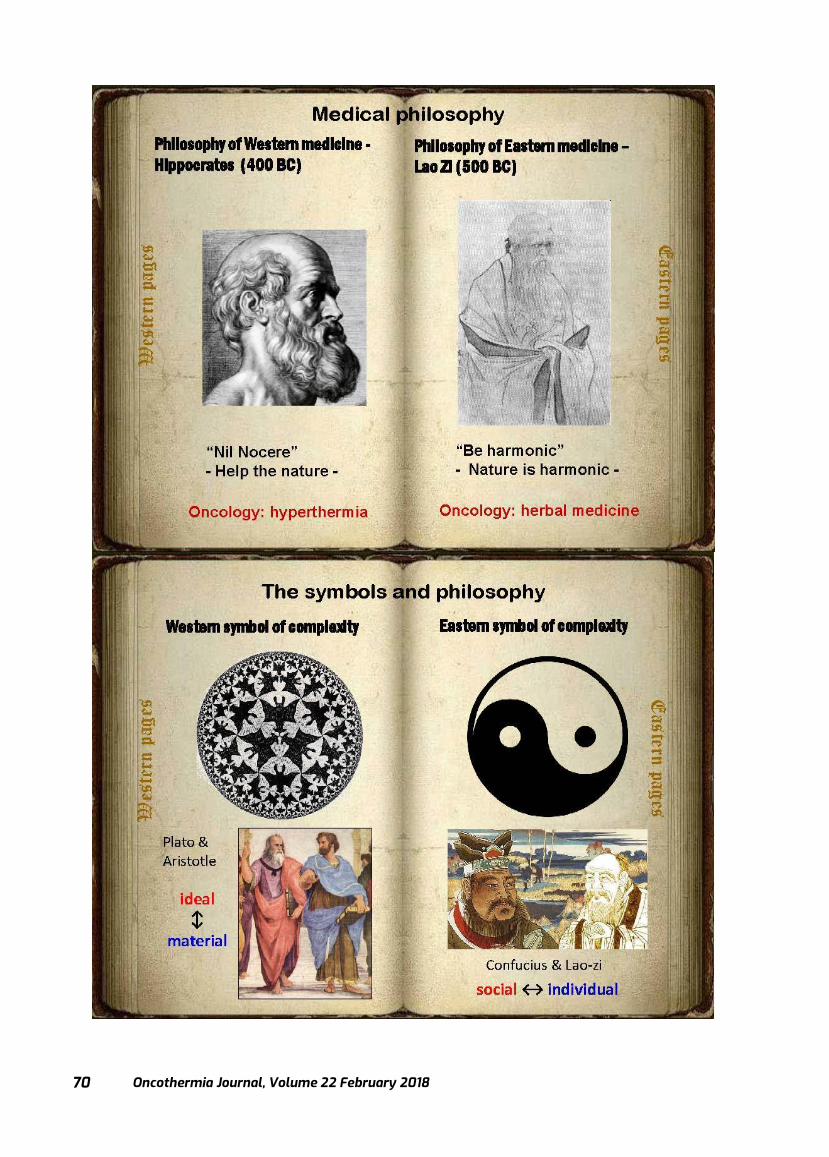
Oncothermia Journal, Volume 22 February 2018
70

Oncothermia Journal, Volume 22, February 2018 71

Oncothermia Journal, Volume 22 February 2018
72
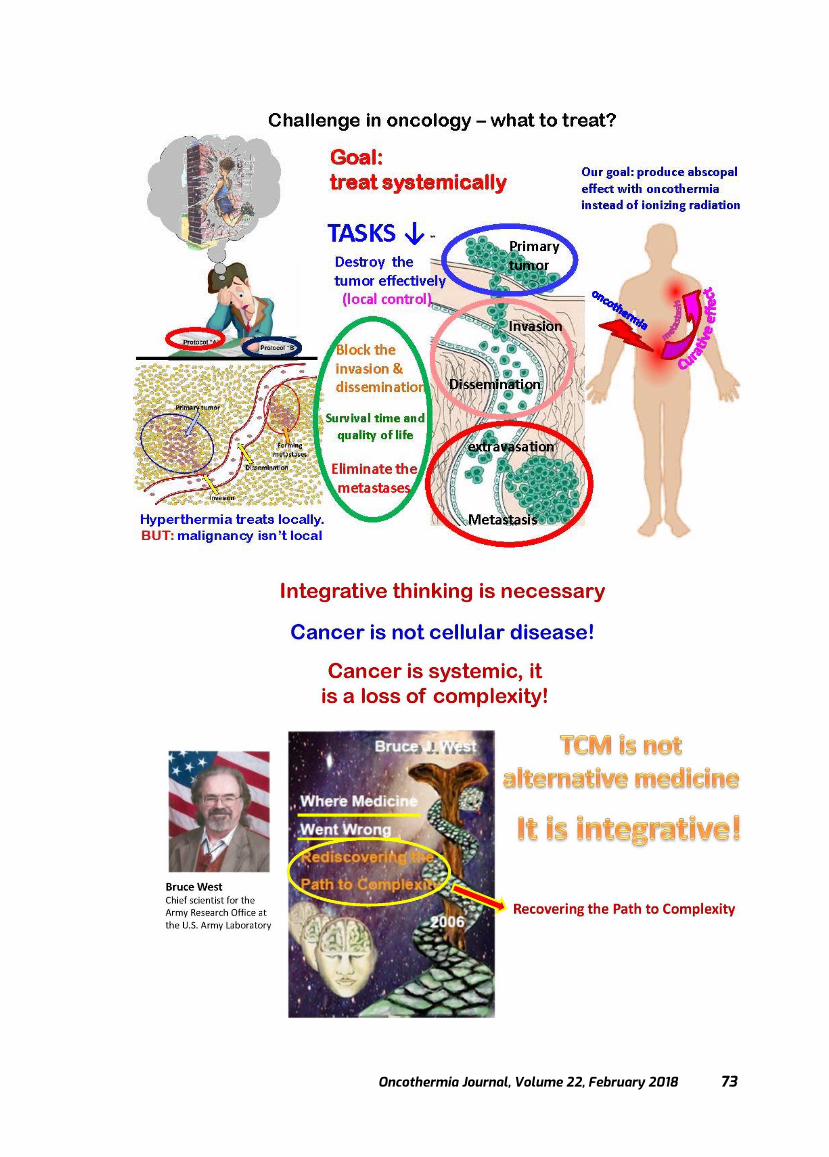
Oncothermia Journal, Volume 22, February 2018 73
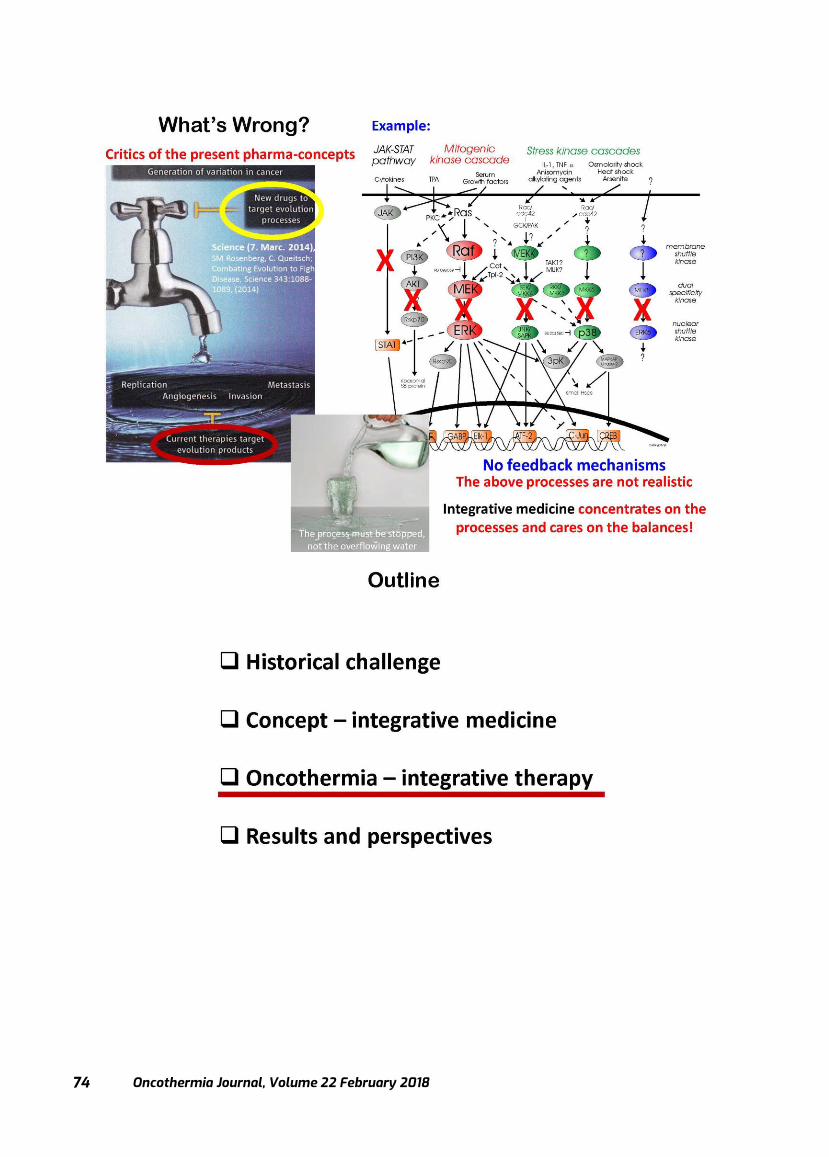
Oncothermia Journal, Volume 22 February 2018
74

Oncothermia Journal, Volume 22, February 2018 75
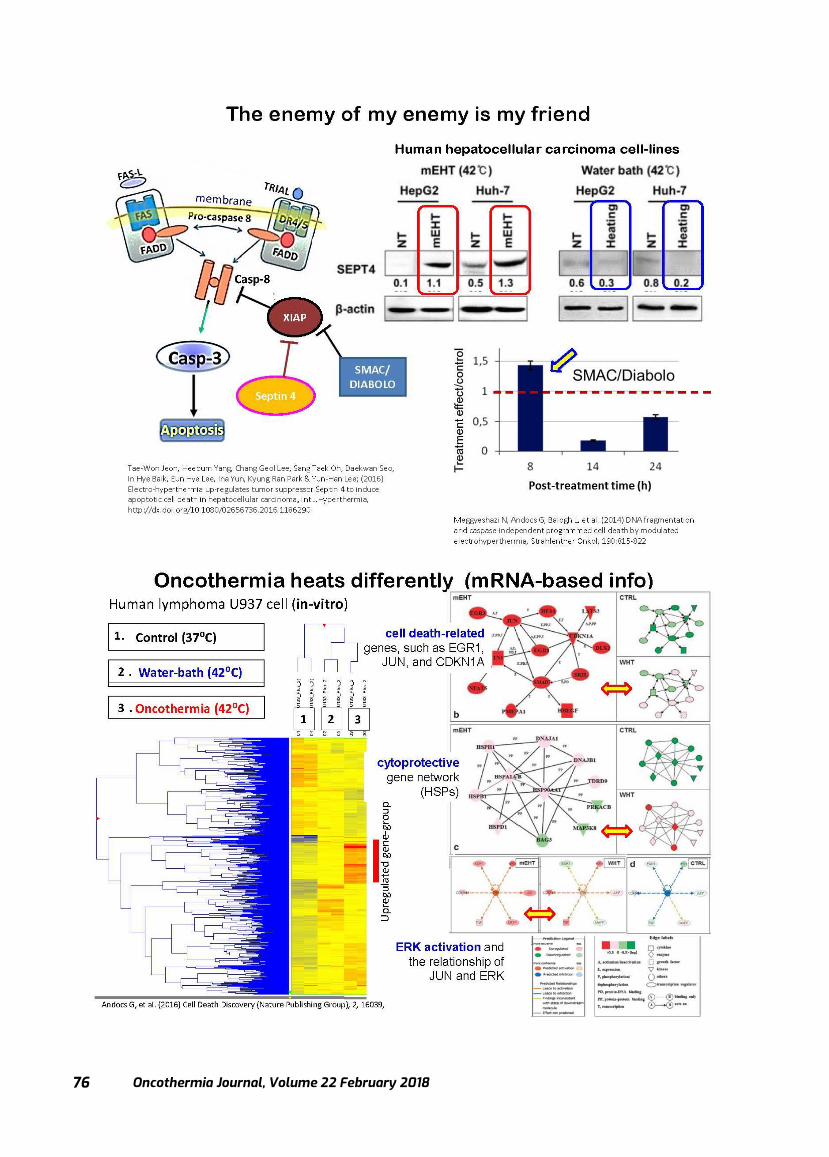
Oncothermia Journal, Volume 22 February 2018
76
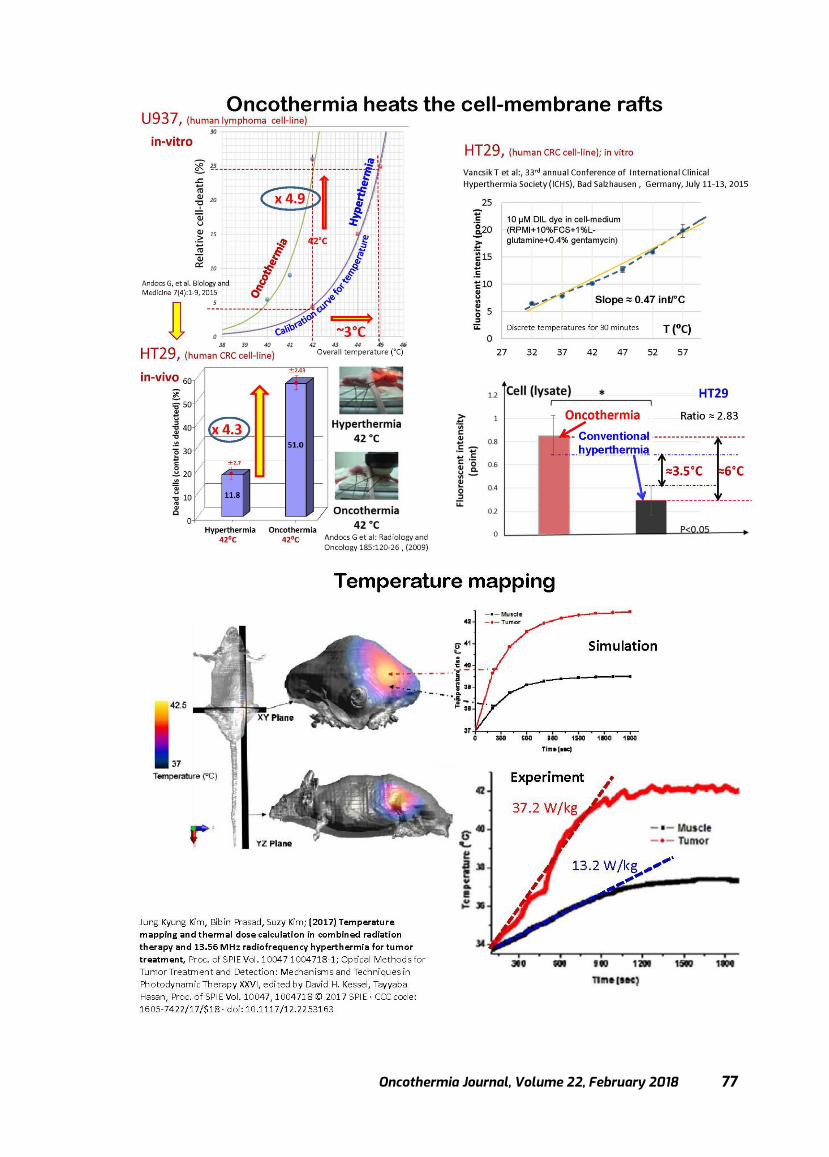
Oncothermia Journal, Volume 22, February 2018 77
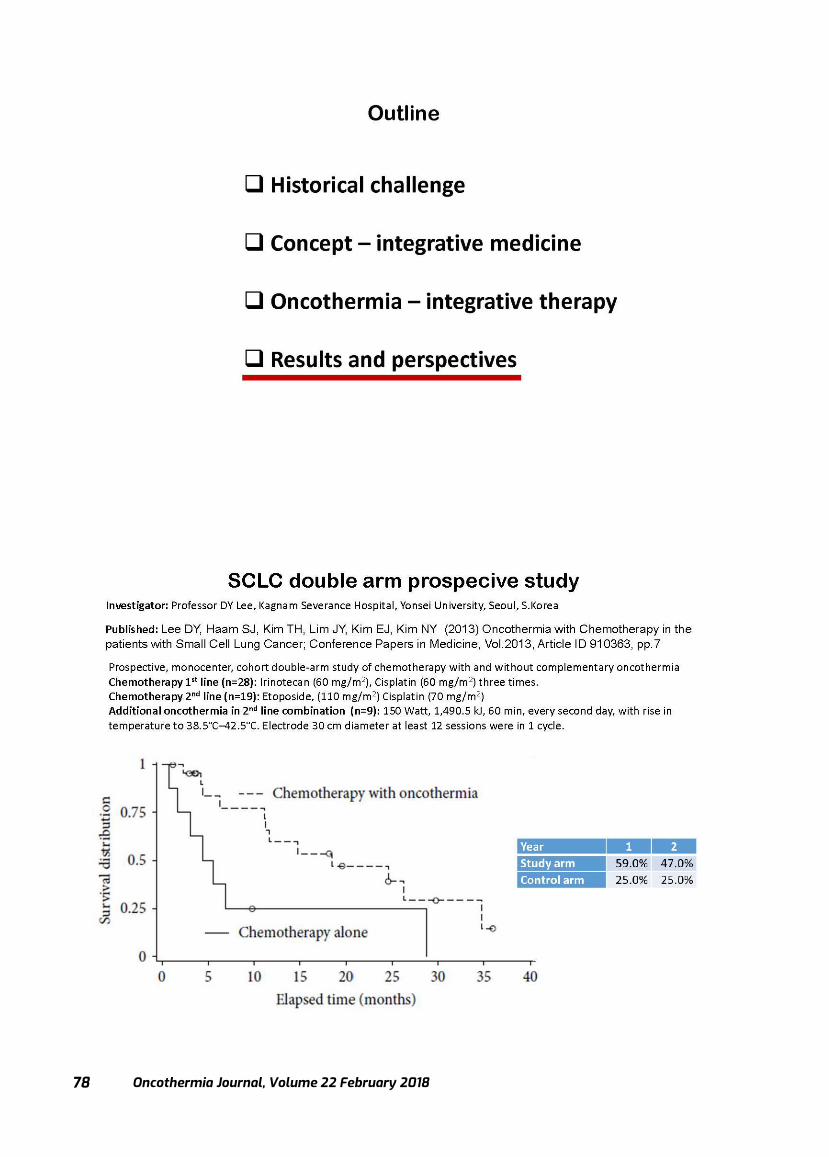
Oncothermia Journal, Volume 22 February 2018
78
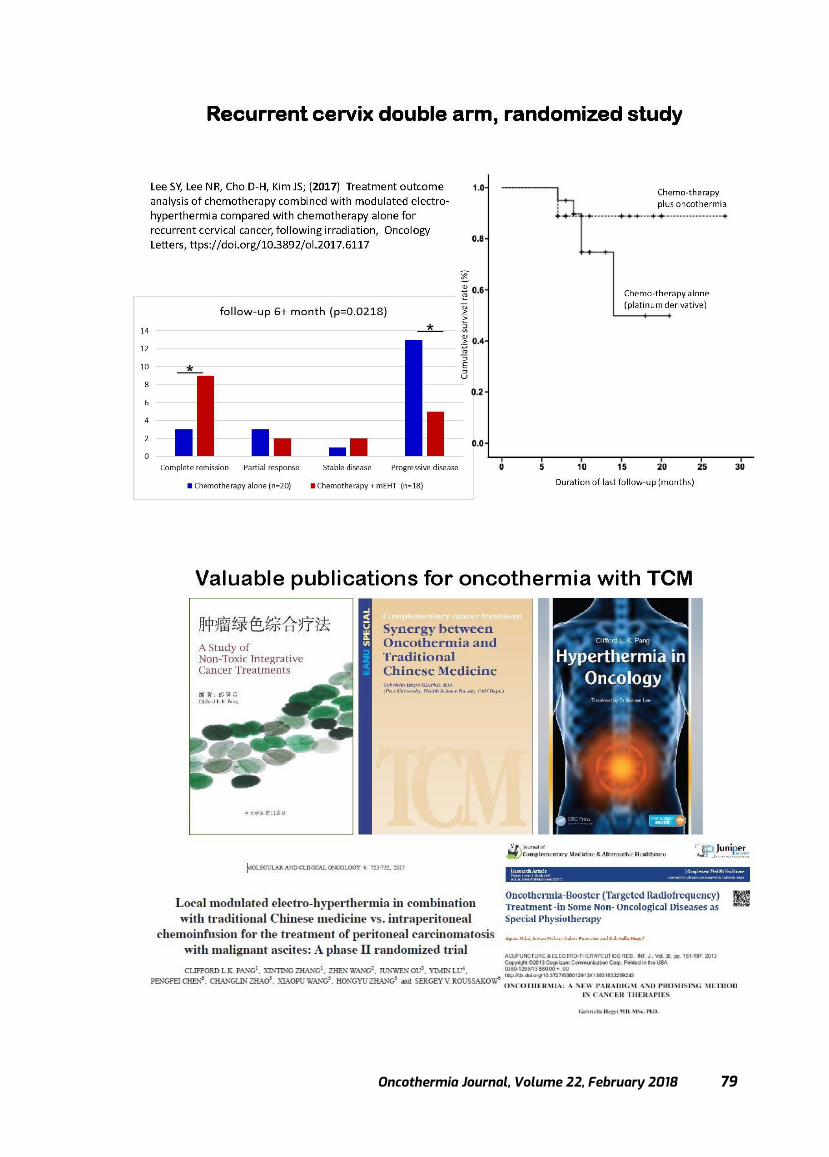
Oncothermia Journal, Volume 22, February 2018 79
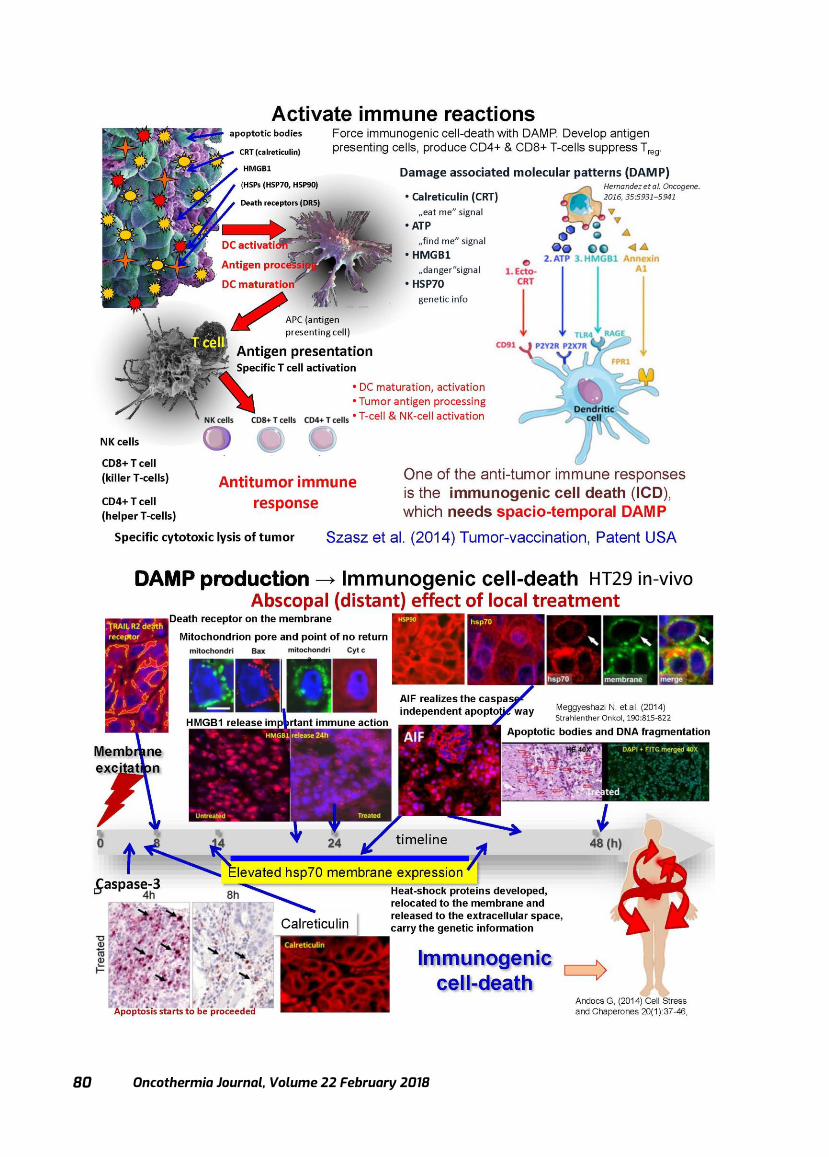
Oncothermia Journal, Volume 22 February 2018
80

Oncothermia Journal, Volume 22, February 2018 81

Oncothermia Journal, Volume 22 February 2018
82

Oncothermia Journal, Volume 22, February 2018 83
Oncothermia Journal, Volume 22 February 2018
84

Oncothermia Journal, Volume 22, February 2018 85
Oncothermia development in Hungary
Dr. Oliver Szasz Assoc. Professor
Department of Biotechnics, St. Istvan University, Hungary, CEO, Oncotherm GmbH, Troisdorf, Germany,
CEO, Oncotherm Kft., Budaörs, Hungary
Presented at 35th ICHS, Guangzhou, 2017
Cite this article as:
Szasz O. (2018): Oncothermia development in Hungary; Oncothermia Journal 22: 85-102 www.oncothermia-
journal.com/journal/2018/Oncothermia_development_in_Hungary-pdf

Oncothermia Journal, Volume 22 February 2018
86
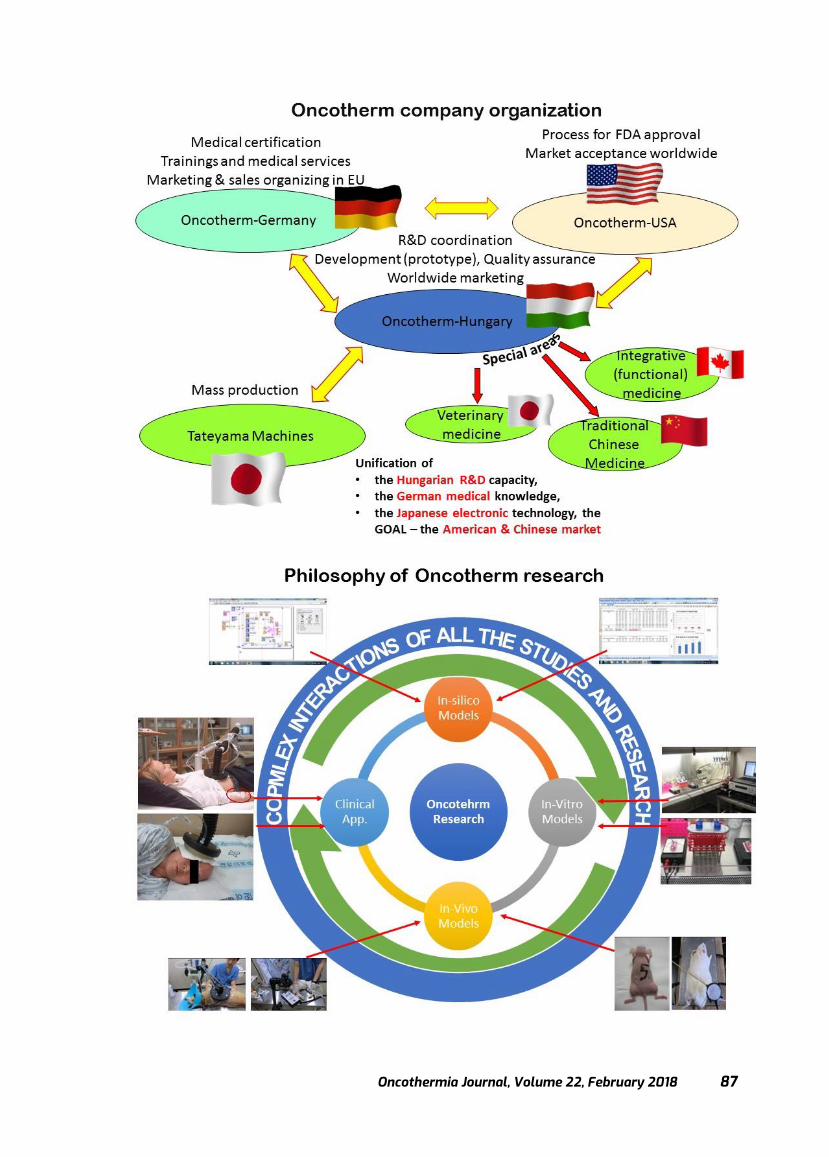
Oncothermia Journal, Volume 22, February 2018 87
Oncothermia Journal, Volume 22 February 2018
88
Oncothermia Journal, Volume 22, February 2018 89
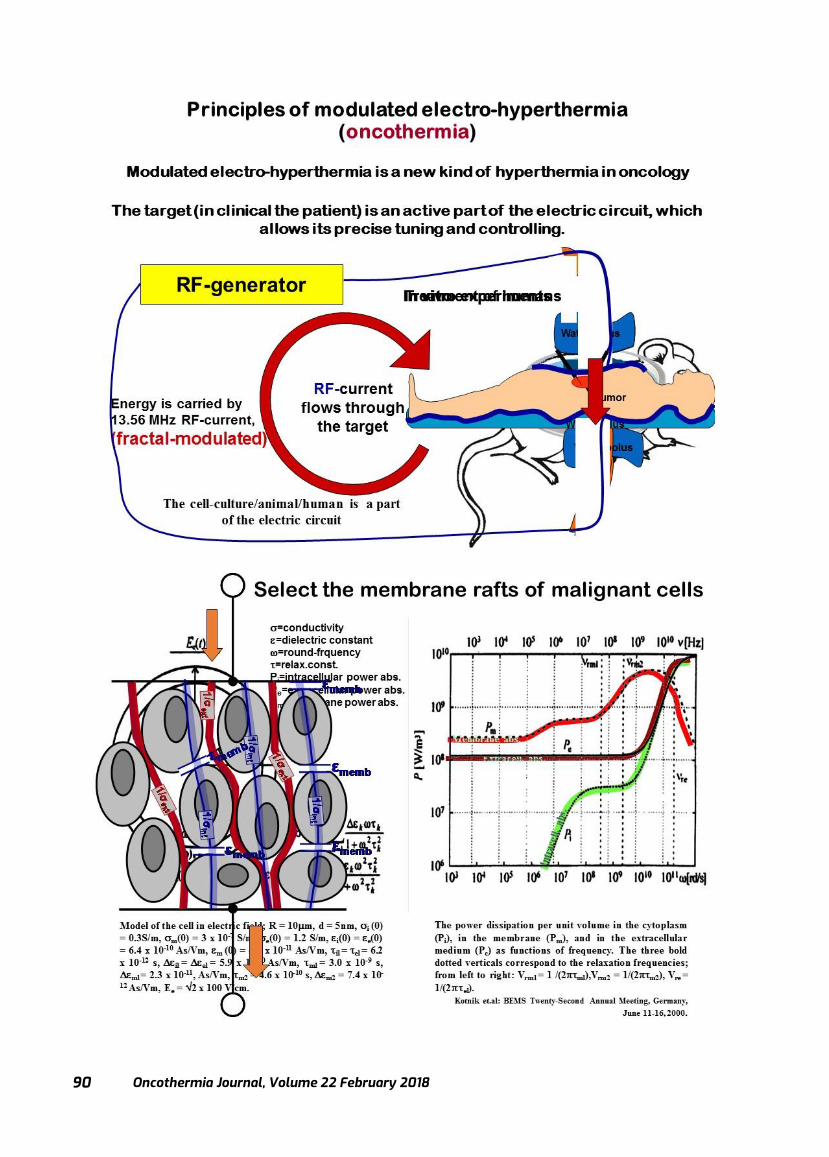
Oncothermia Journal, Volume 22 February 2018
90

Oncothermia Journal, Volume 22, February 2018 91
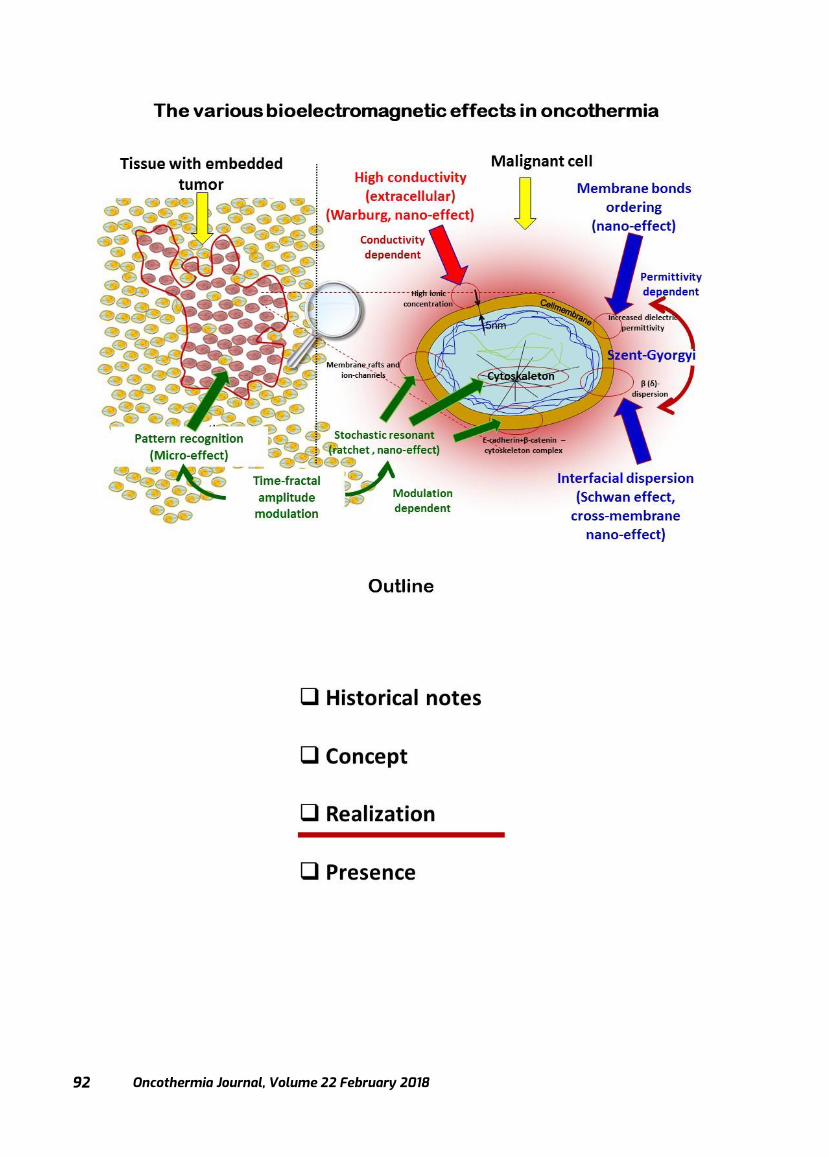
Oncothermia Journal, Volume 22 February 2018
92
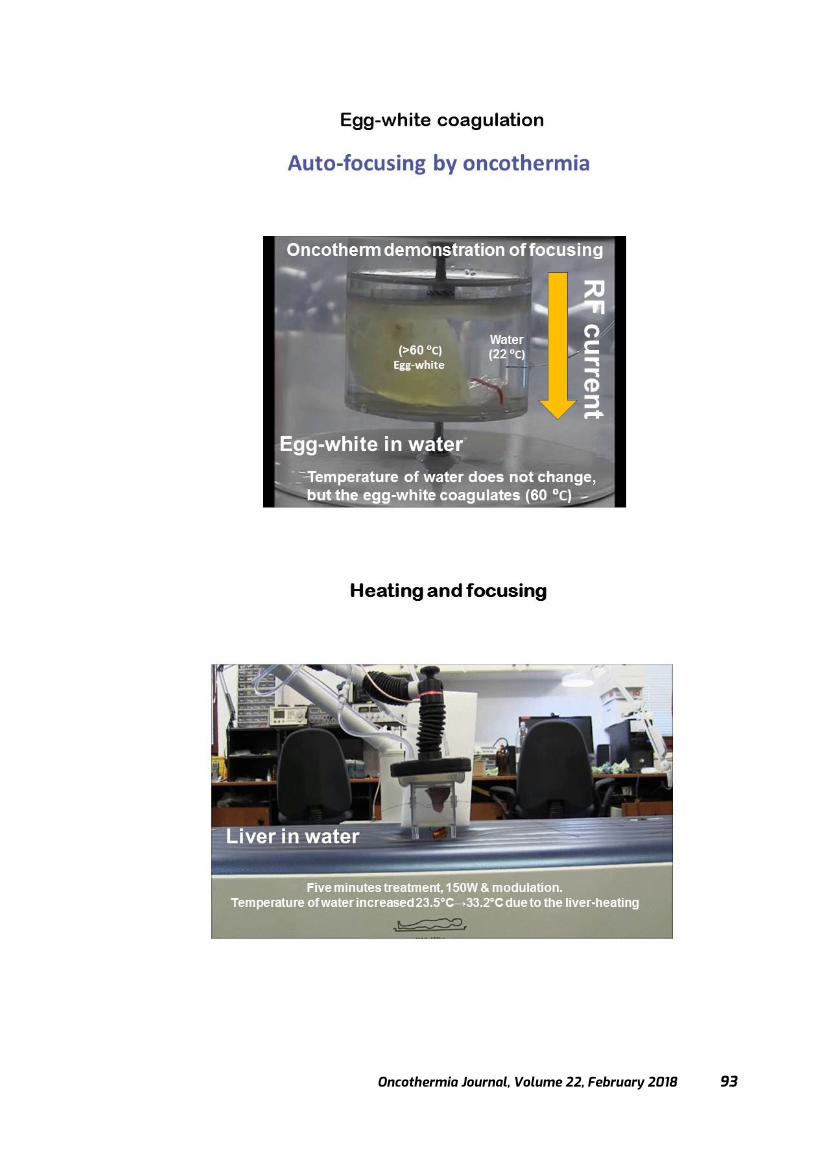
Oncothermia Journal, Volume 22, February 2018 93
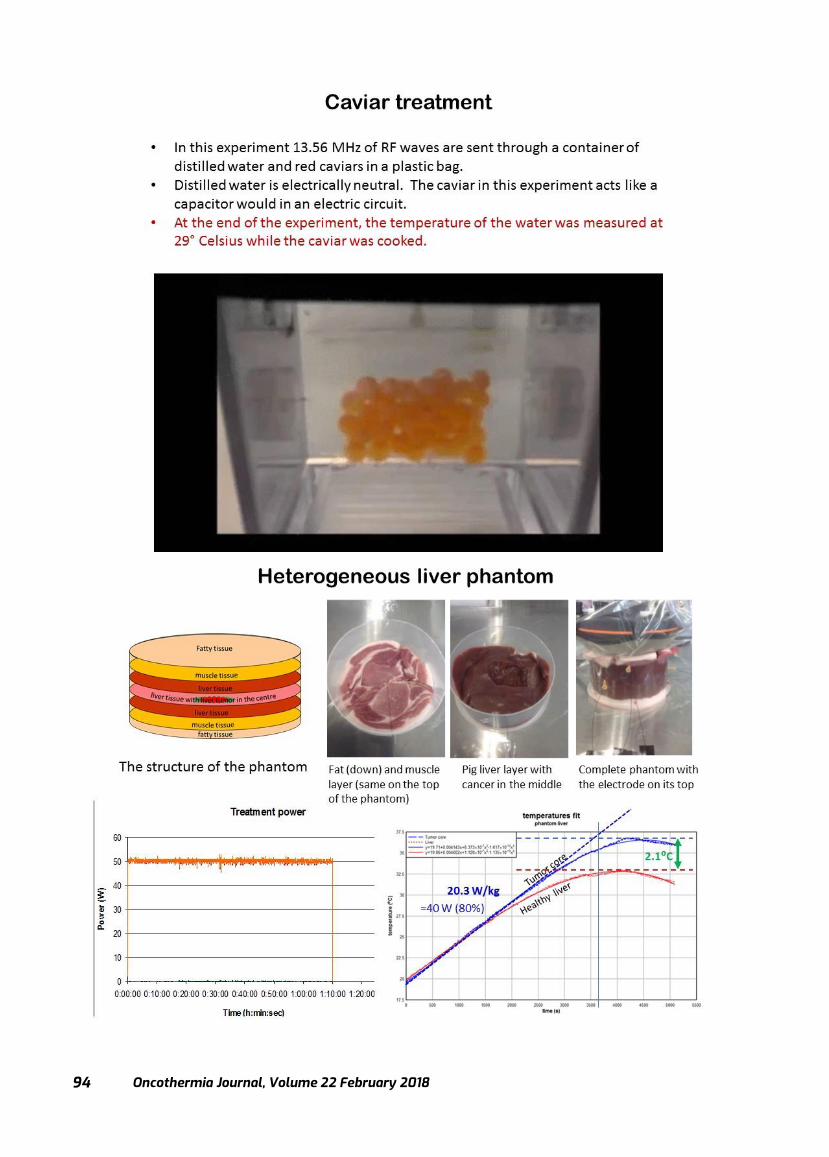
Oncothermia Journal, Volume 22 February 2018
94
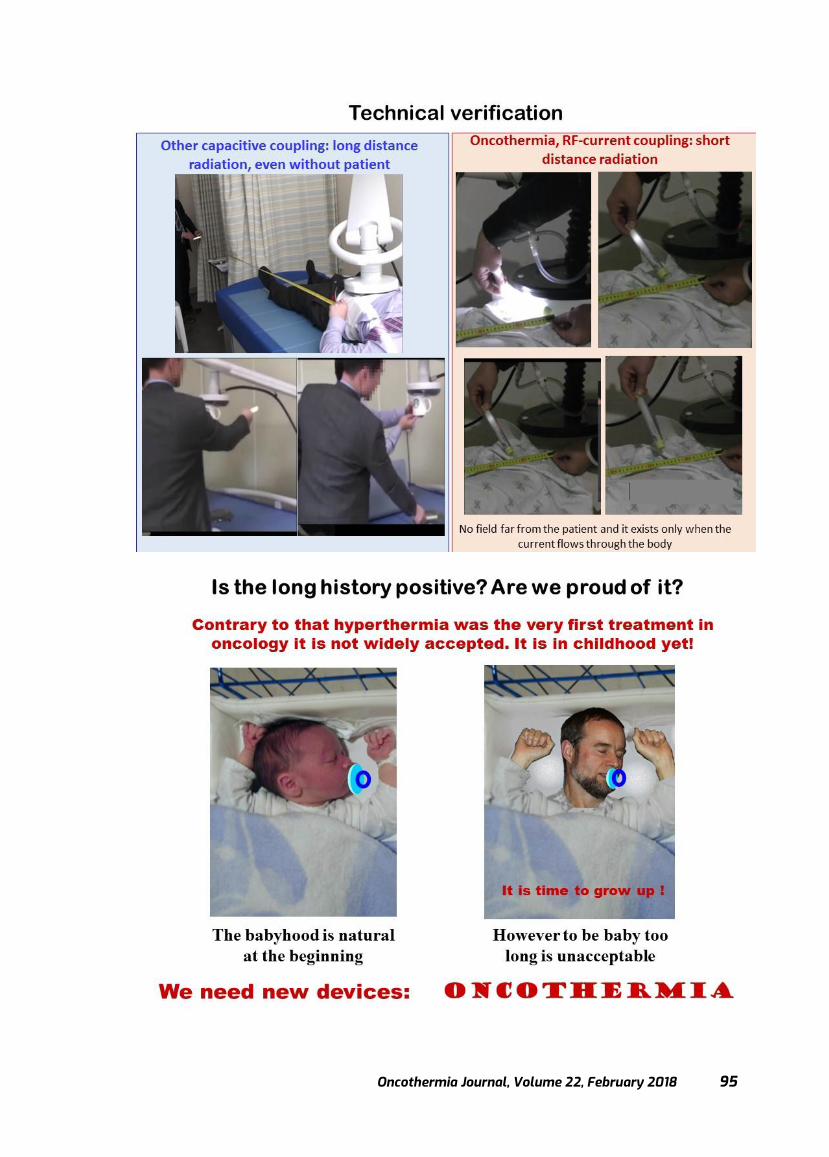
Oncothermia Journal, Volume 22, February 2018 95

Oncothermia Journal, Volume 22 February 2018
96
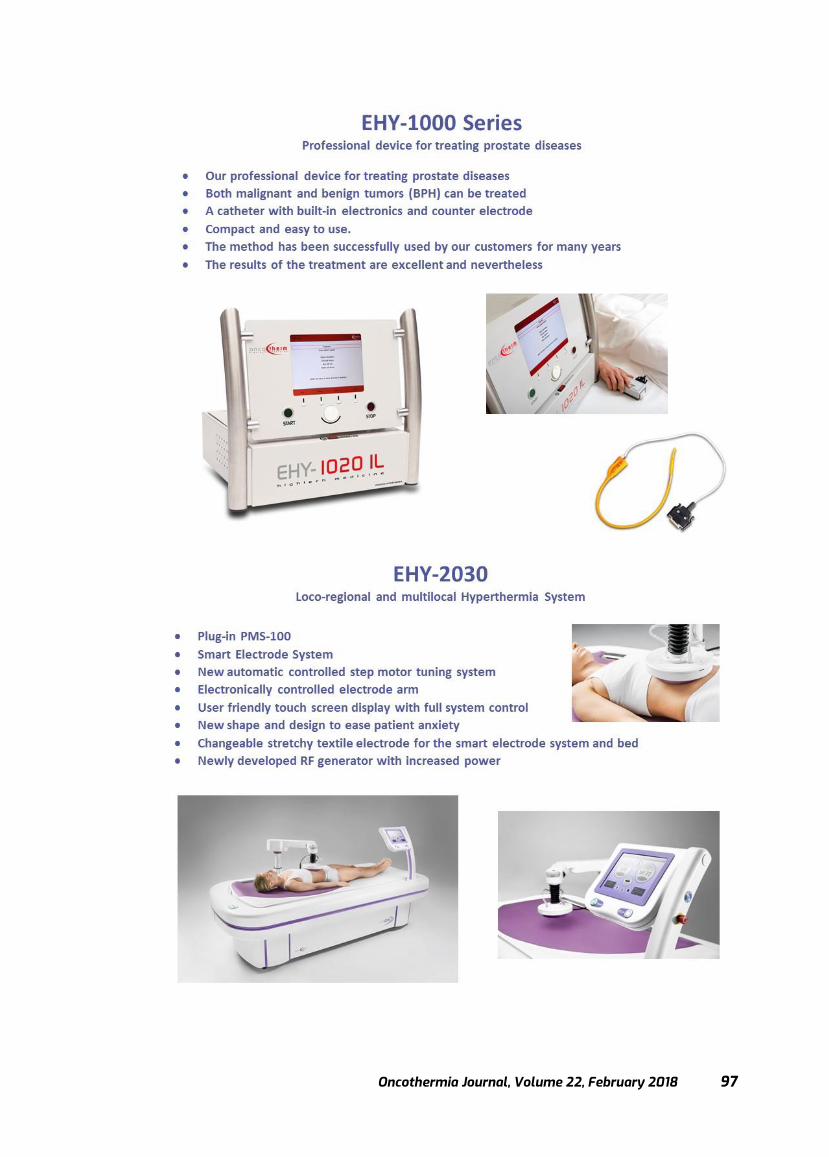
Oncothermia Journal, Volume 22, February 2018 97

Oncothermia Journal, Volume 22 February 2018
98

Oncothermia Journal, Volume 22, February 2018 99
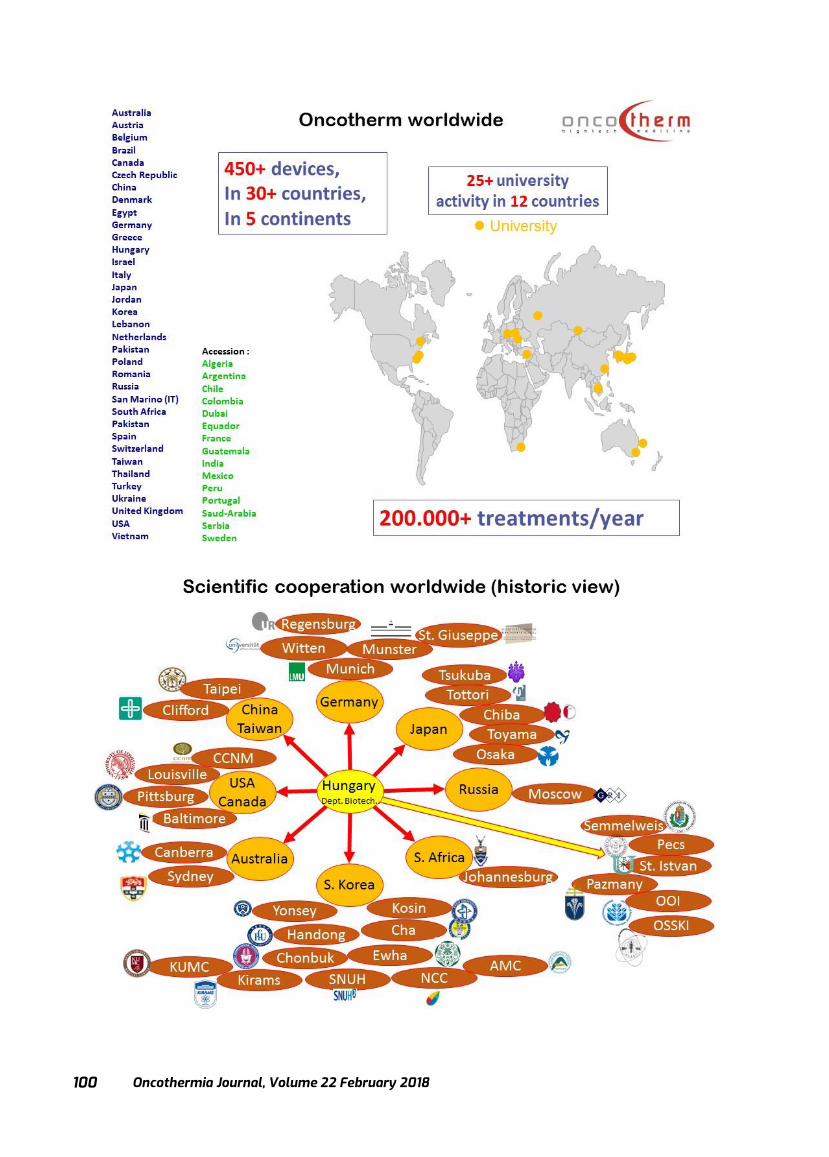
Oncothermia Journal, Volume 22 February 2018
100
Oncothermia Journal, Volume 22, February 2018 101
Oncothermia Journal, Volume 22 February 2018
102

Oncothermia Journal, Volume 22, February 2018 103
Effects of moderate whole-body hyperthermia and complementary medicine in the treatment of rheumatoid arthritis: a preliminary study
Preeti Agrawal MD, PhD Fellow in Integrative Medicine (University of Arizona, USA)
Presented at 35th ICHS, Guangzhou, 2017
Cite this article as:
Agrawal P. (2018): Effects of moderate whole-body hyperthermia and complementary medicine in the treatment of rheumatoid arthritis: a
preliminary study; Oncothermia Journal 22: 103-115 www.oncothermia-journal.com/journal/2018/Effects_of_moderate.pdf

Oncothermia Journal, Volume 22 February 2018
104
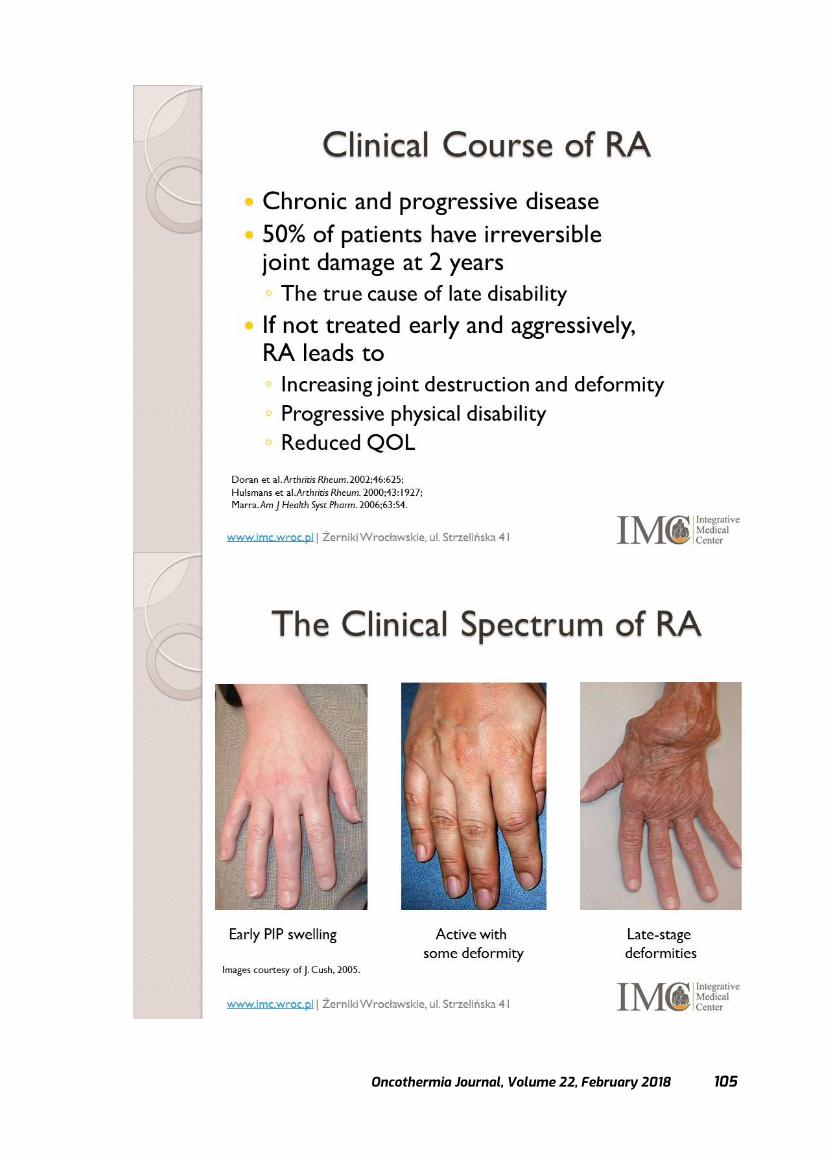
Oncothermia Journal, Volume 22, February 2018 105
Oncothermia Journal, Volume 22 February 2018
106
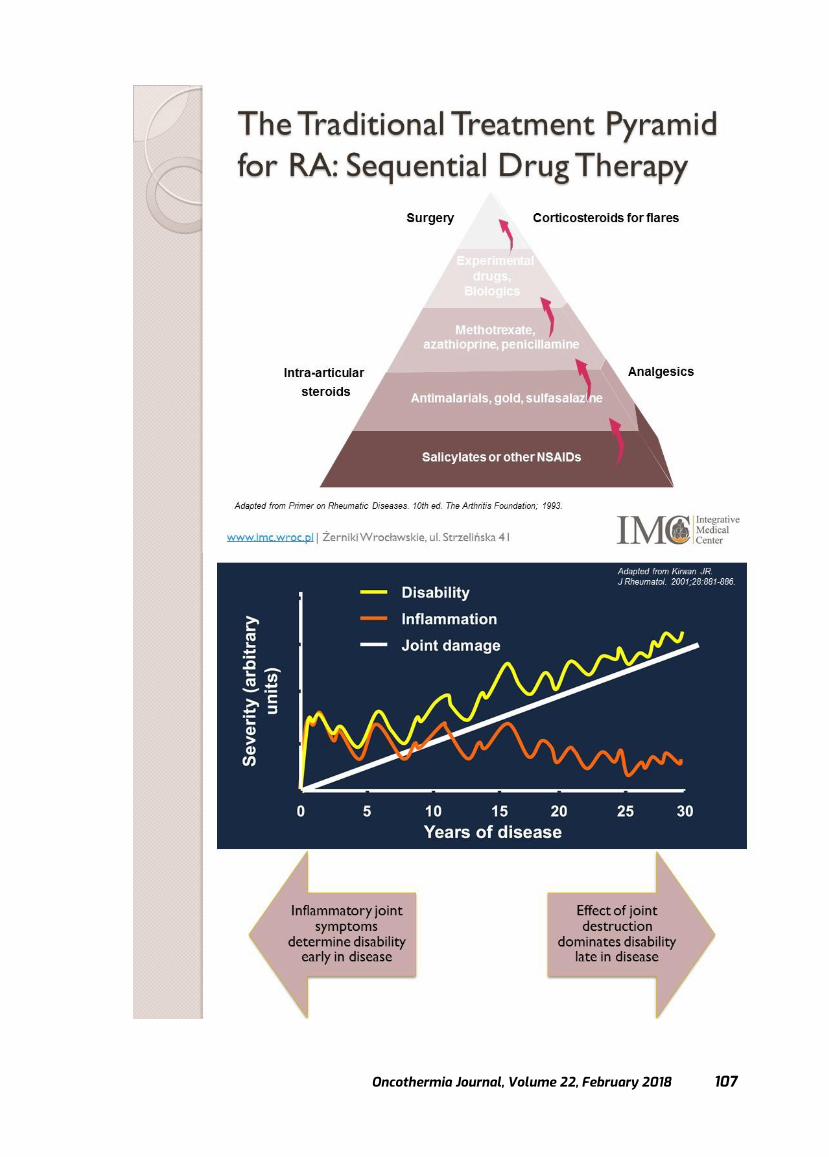
Oncothermia Journal, Volume 22, February 2018 107
Oncothermia Journal, Volume 22 February 2018
108
Oncothermia Journal, Volume 22, February 2018 109
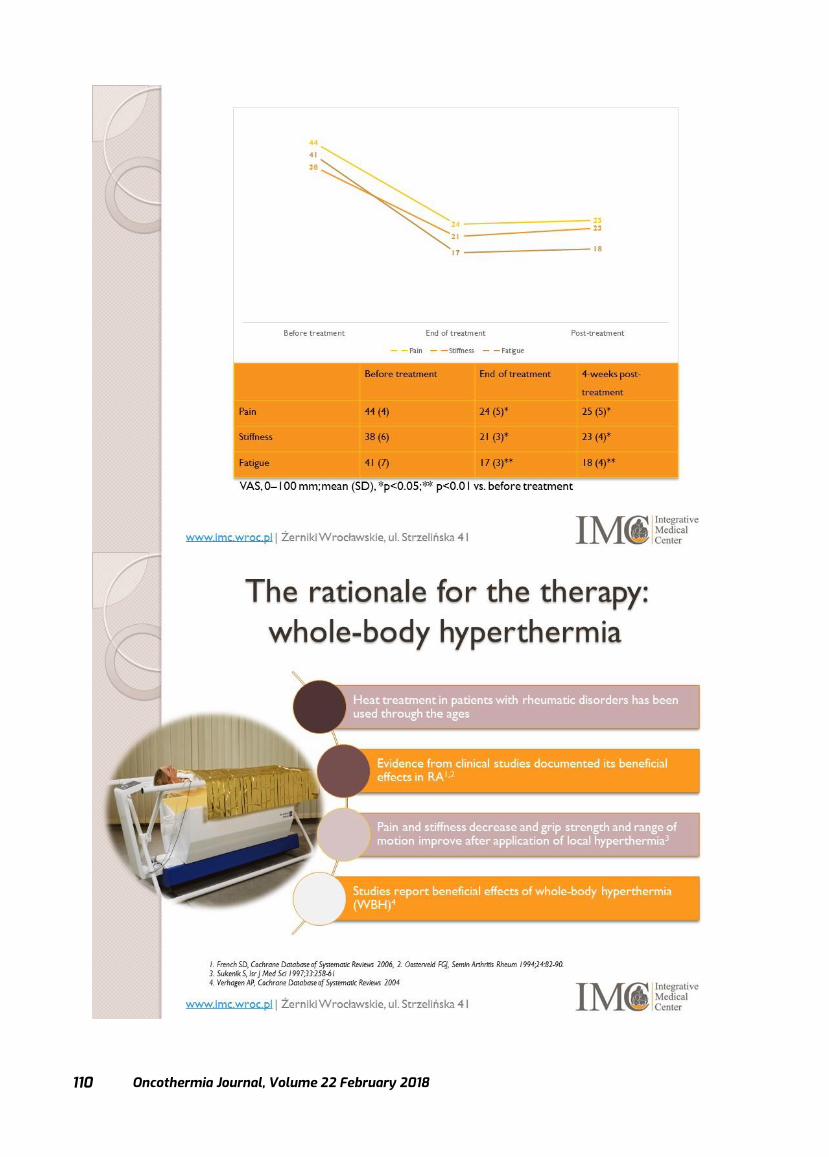
Oncothermia Journal, Volume 22 February 2018
110
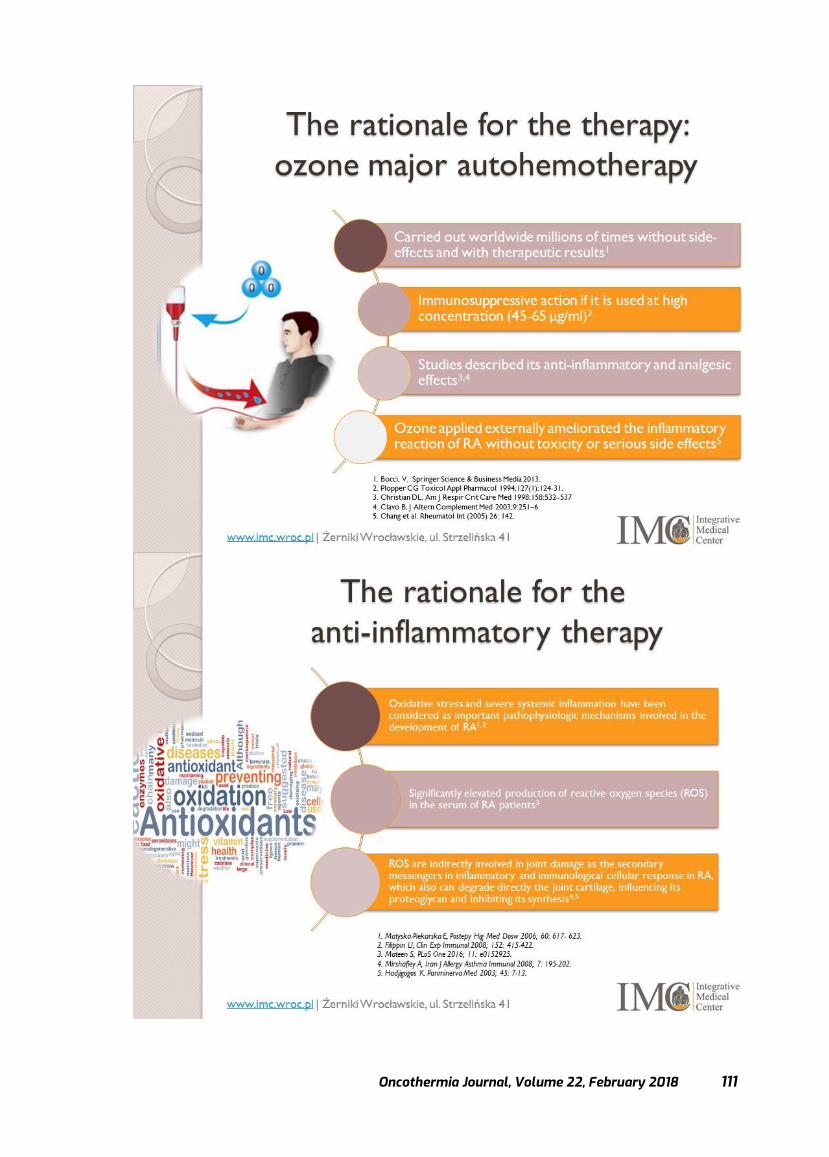
Oncothermia Journal, Volume 22, February 2018 111

Oncothermia Journal, Volume 22 February 2018
112
Oncothermia Journal, Volume 22, February 2018 113

Oncothermia Journal, Volume 22 February 2018
114

Oncothermia Journal, Volume 22, February 2018 115

Oncothermia Journal, Volume 22 February 2018
116
Redefining Hyperthermia: A Not Temperature-Dependent Solution of The Temperature Problem
Sergey Roussakow, MD, PhD Galenic Research Institute
Presented at 35th ICHS, Guangzhou, 2017
Cite this article as: Roussakow S. (2018): Redefining Hyperthermia: A Not Temperature-
Dependent Solution of The Temperature Problem; Oncothermia Journal 22: 116-150
www.oncothermia-journal.com/journal/2018/Redefining_Hyperthermia.pdf
Oncothermia Journal, Volume 22, February 2018 117

Oncothermia Journal, Volume 22 February 2018
118
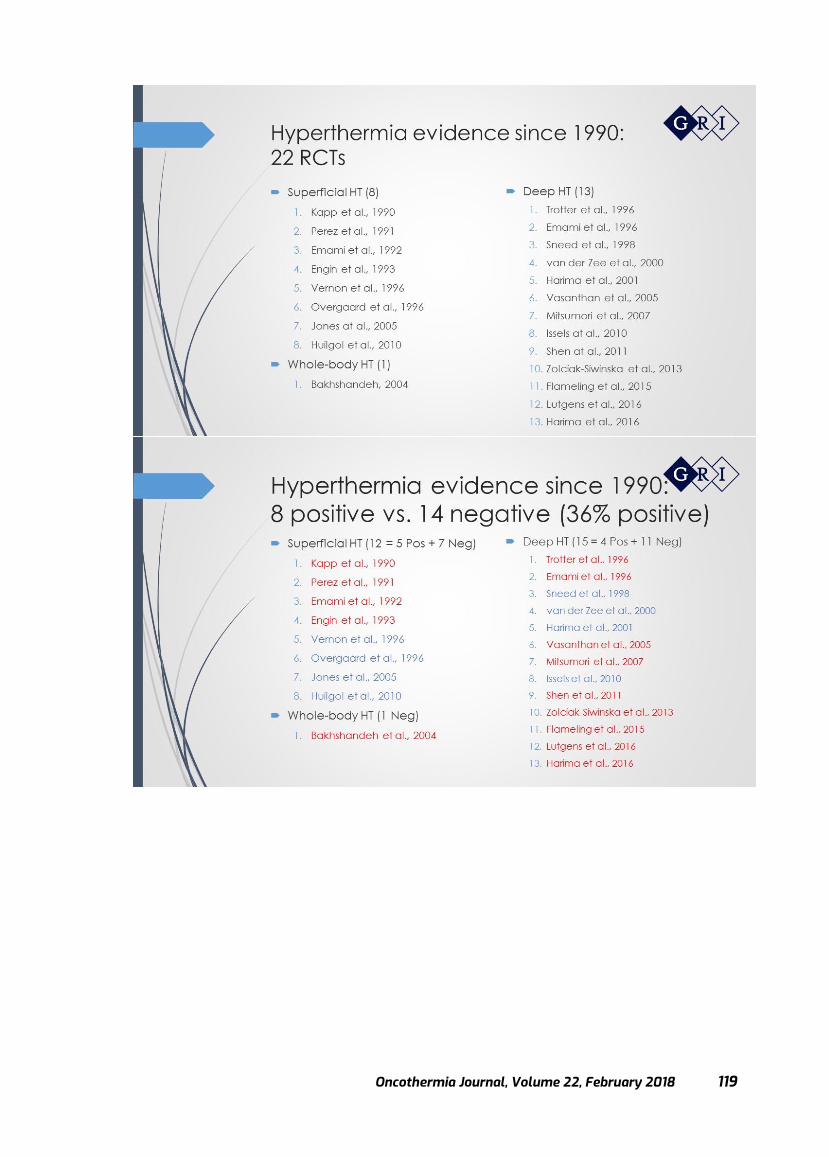
Oncothermia Journal, Volume 22, February 2018 119
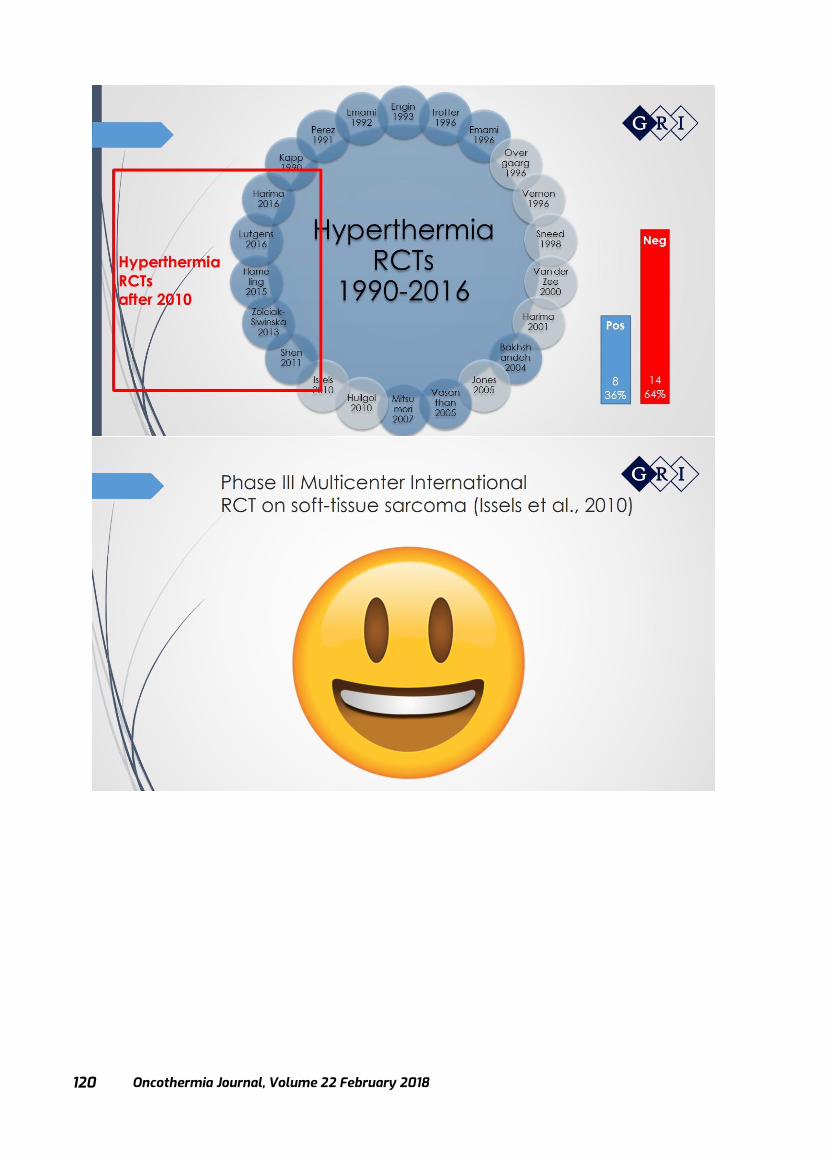
Oncothermia Journal, Volume 22 February 2018
120

Oncothermia Journal, Volume 22, February 2018 121
Oncothermia Journal, Volume 22 February 2018
122

Oncothermia Journal, Volume 22, February 2018 123
Oncothermia Journal, Volume 22 February 2018
124
Oncothermia Journal, Volume 22, February 2018 125

Oncothermia Journal, Volume 22 February 2018
126
Oncothermia Journal, Volume 22, February 2018 127

Oncothermia Journal, Volume 22 February 2018
128

Oncothermia Journal, Volume 22, February 2018 129
Oncothermia Journal, Volume 22 February 2018
130
Oncothermia Journal, Volume 22, February 2018 131
Oncothermia Journal, Volume 22 February 2018
132
Oncothermia Journal, Volume 22, February 2018 133
Oncothermia Journal, Volume 22 February 2018
134
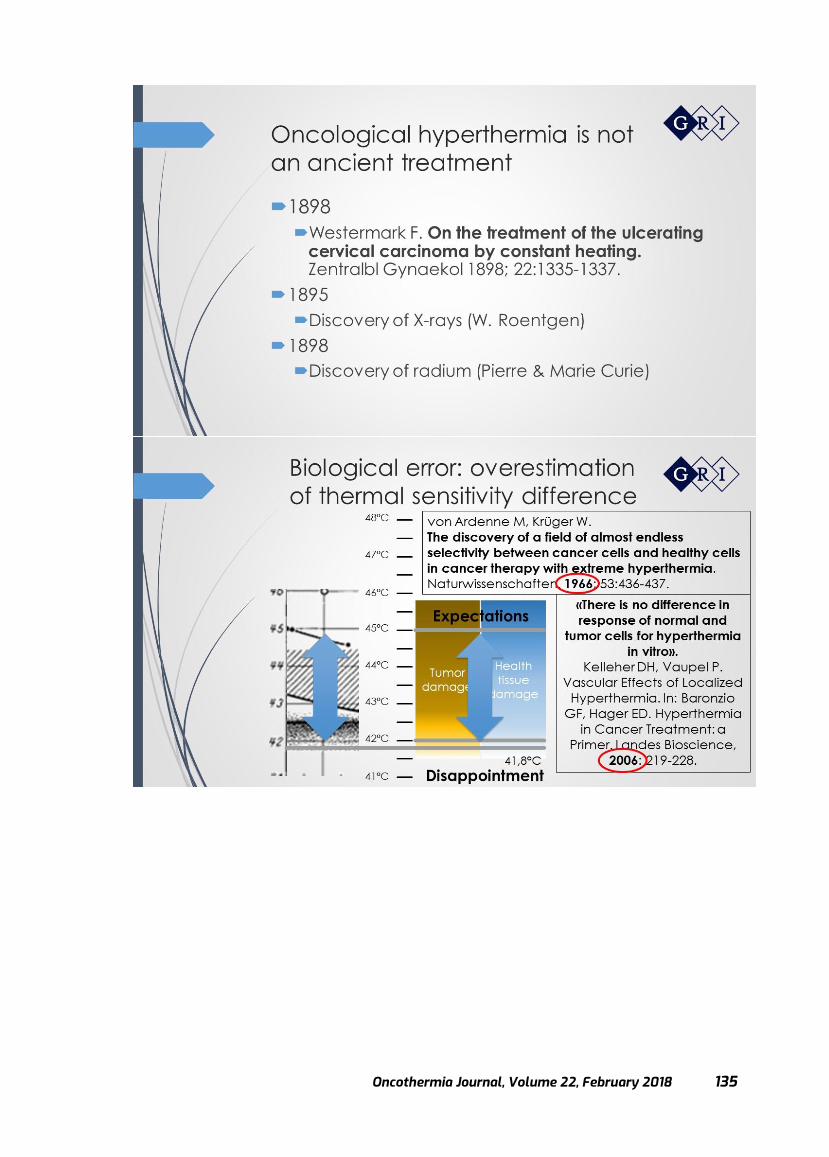
Oncothermia Journal, Volume 22, February 2018 135

Oncothermia Journal, Volume 22 February 2018
136
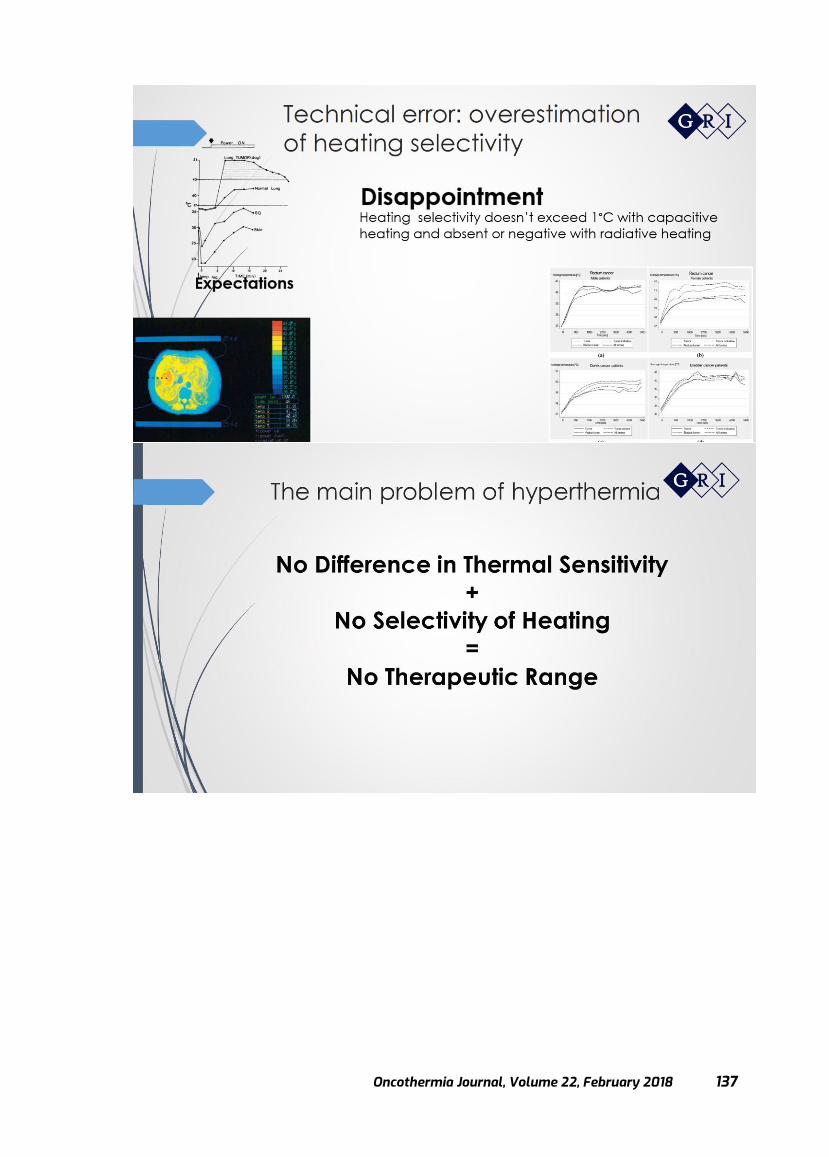
Oncothermia Journal, Volume 22, February 2018 137

Oncothermia Journal, Volume 22 February 2018
138

Oncothermia Journal, Volume 22, February 2018 139

Oncothermia Journal, Volume 22 February 2018
140
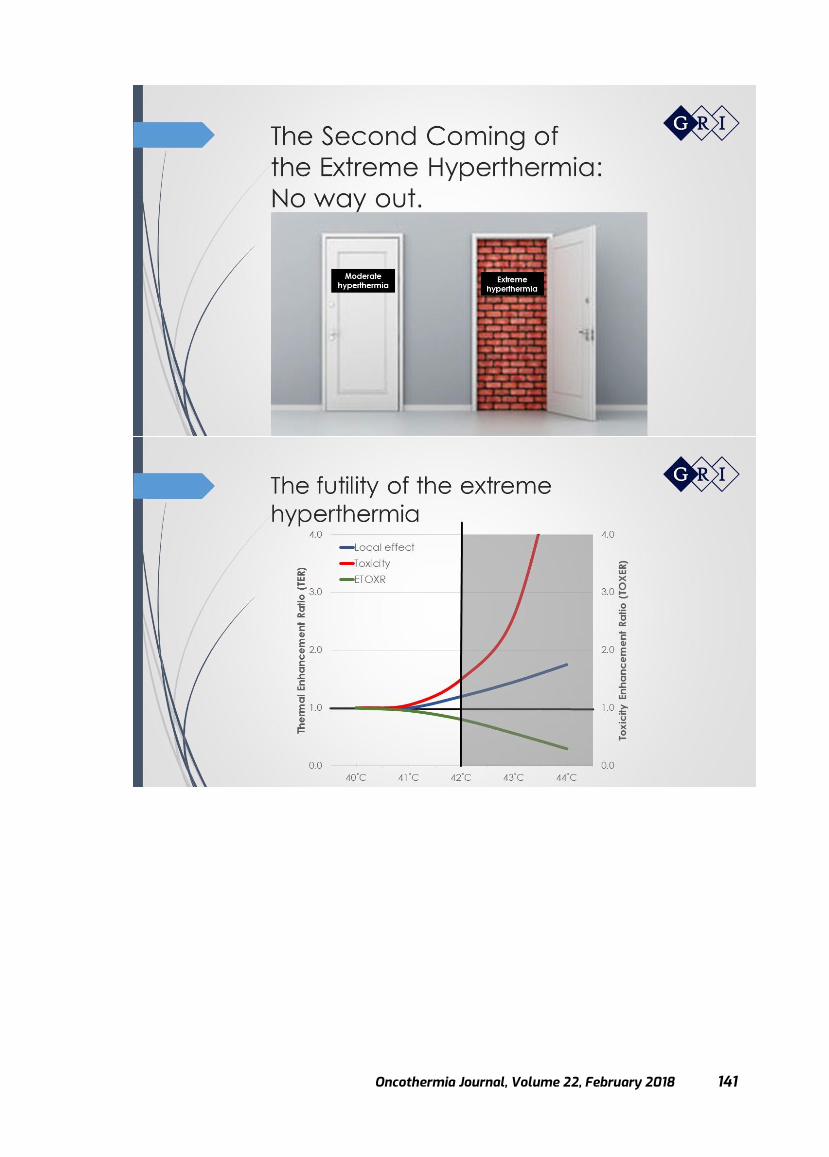
Oncothermia Journal, Volume 22, February 2018 141
Oncothermia Journal, Volume 22 February 2018
142

Oncothermia Journal, Volume 22, February 2018 143

Oncothermia Journal, Volume 22 February 2018
144
Oncothermia Journal, Volume 22, February 2018 145
Oncothermia Journal, Volume 22 February 2018
146
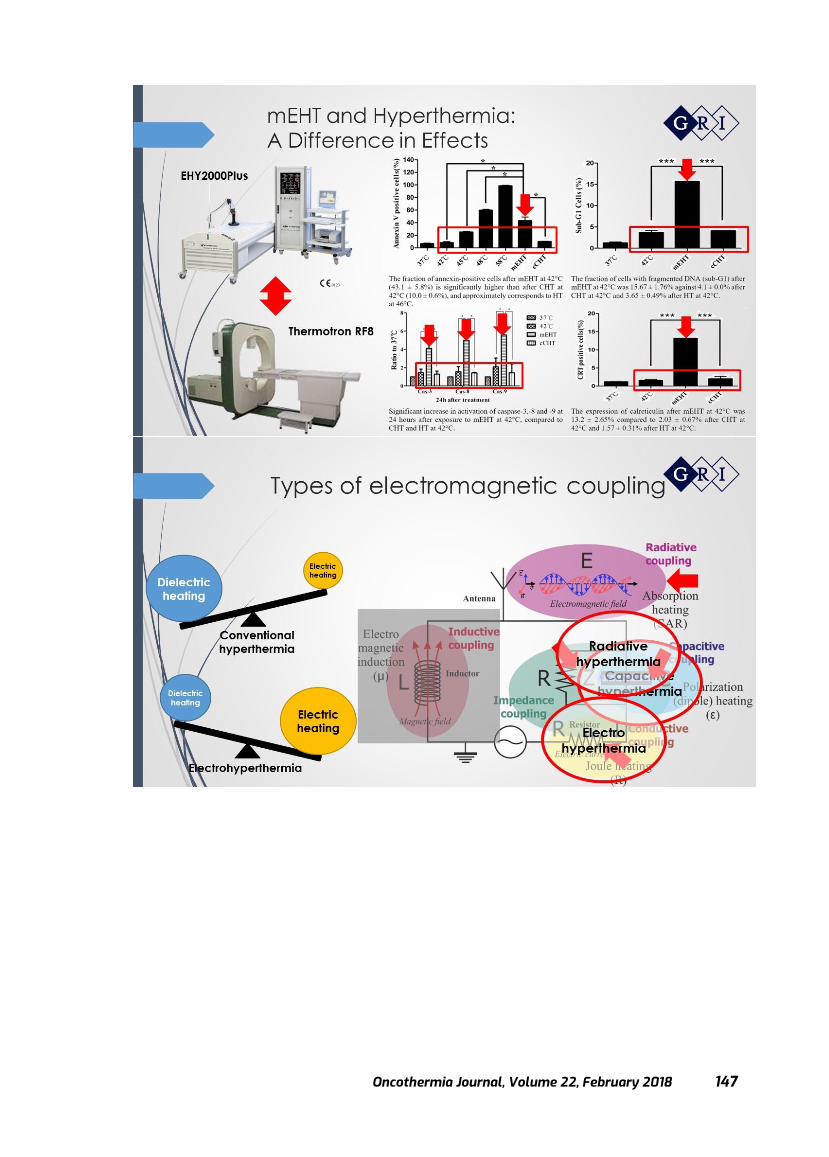
Oncothermia Journal, Volume 22, February 2018 147

Oncothermia Journal, Volume 22 February 2018
148
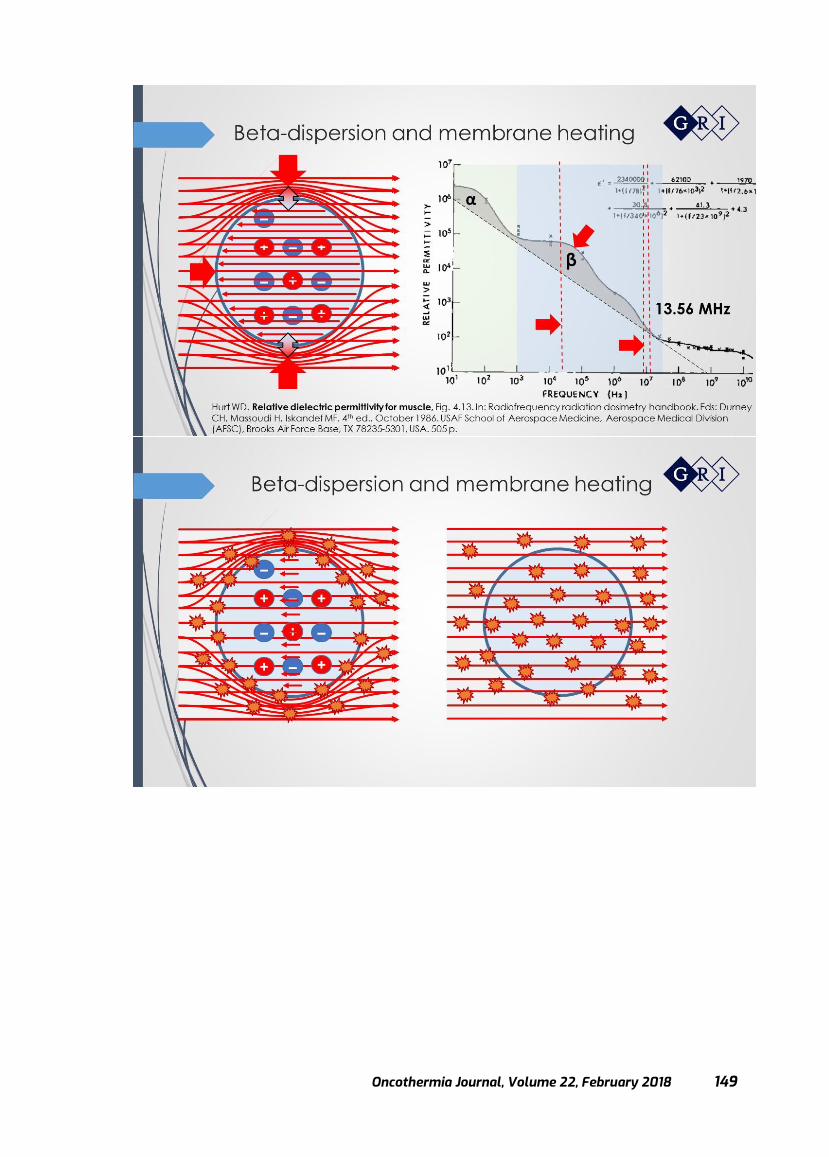
Oncothermia Journal, Volume 22, February 2018 149

Oncothermia Journal, Volume 22 February 2018
150

Oncothermia Journal, Volume 22, February 2018 151
Oncothermia in brain tumors
Prof. Giammaria Fiorentini Department of Onco- Hematology, Azienda Ospedaliera Marche Nord,
Pesaro, Italy
Presented at 35th ICHS, Guangzhou, 2017
Cite this article as:
Fiorentini G. (2018): Oncothermia in brain tumours; Oncothermia Journal 22: 151-177
www.oncothermia-journal.com/journal/2018/Oncothermia_in_brain_tumours.pdf

Oncothermia Journal, Volume 22 February 2018
152

Oncothermia Journal, Volume 22, February 2018 153
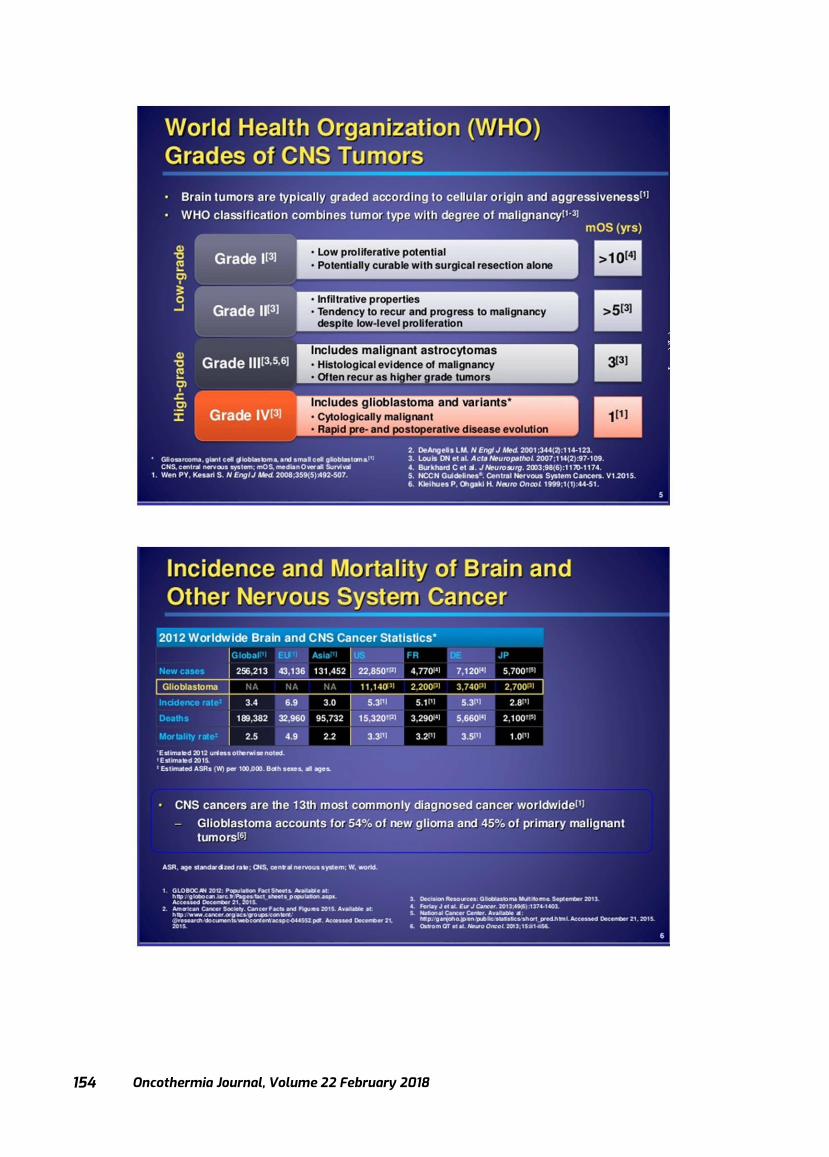
Oncothermia Journal, Volume 22 February 2018
154

Oncothermia Journal, Volume 22, February 2018 155

Oncothermia Journal, Volume 22 February 2018
156
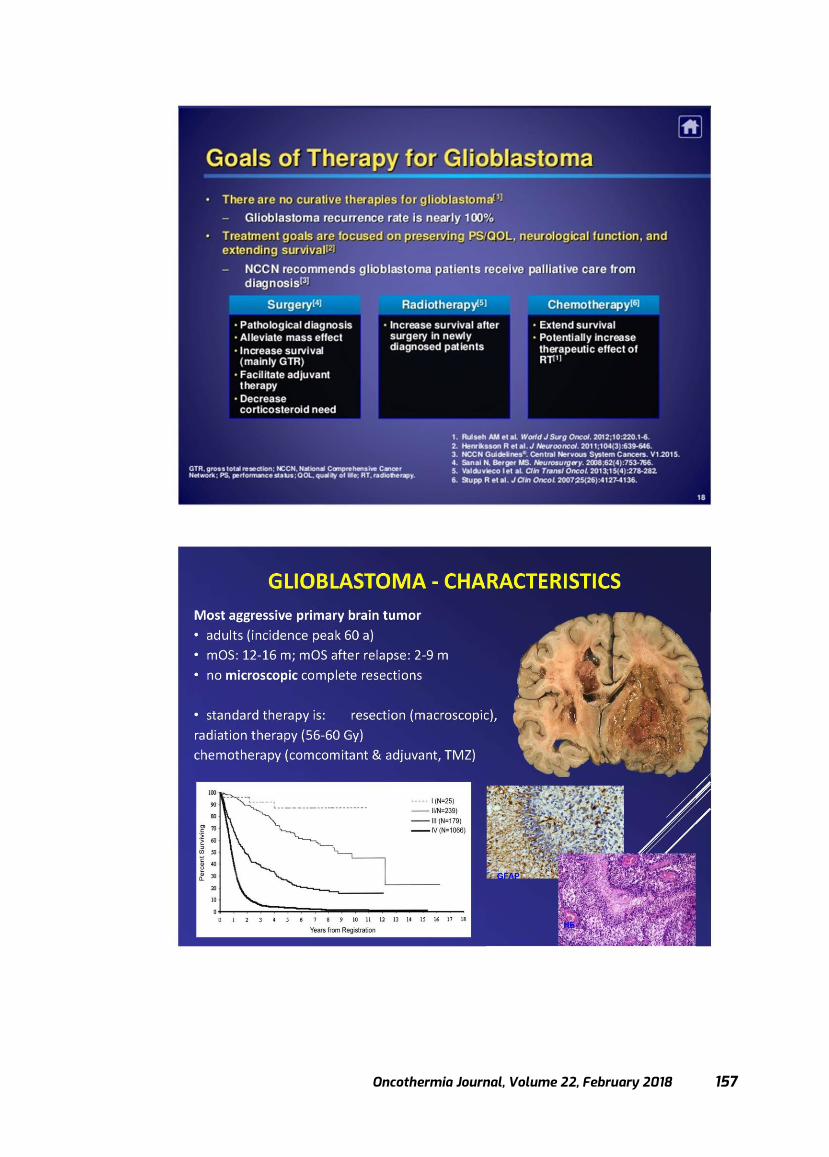
Oncothermia Journal, Volume 22, February 2018 157

Oncothermia Journal, Volume 22 February 2018
158
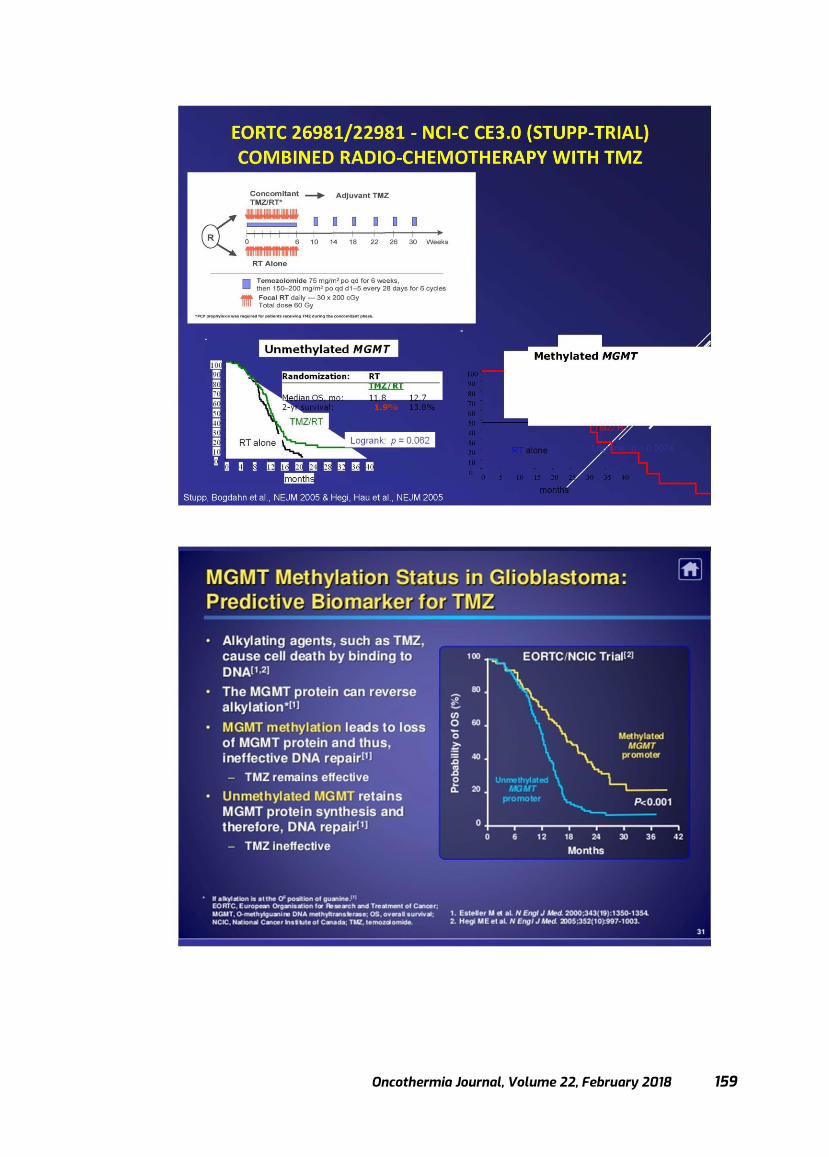
Oncothermia Journal, Volume 22, February 2018 159
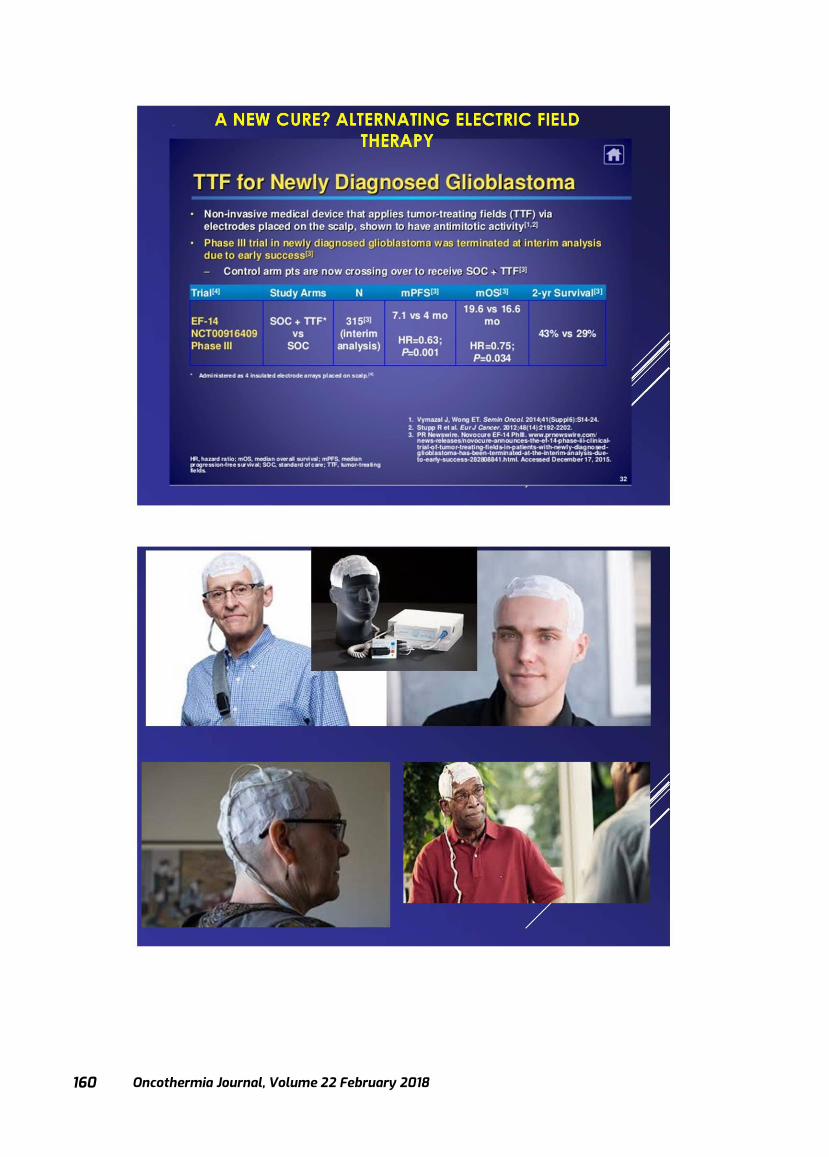
Oncothermia Journal, Volume 22 February 2018
160

Oncothermia Journal, Volume 22, February 2018 161

Oncothermia Journal, Volume 22 February 2018
162

Oncothermia Journal, Volume 22, February 2018 163

Oncothermia Journal, Volume 22 February 2018
164

Oncothermia Journal, Volume 22, February 2018 165

Oncothermia Journal, Volume 22 February 2018
166
Oncothermia Journal, Volume 22, February 2018 167

Oncothermia Journal, Volume 22 February 2018
168
Oncothermia Journal, Volume 22, February 2018 169

Oncothermia Journal, Volume 22 February 2018
170
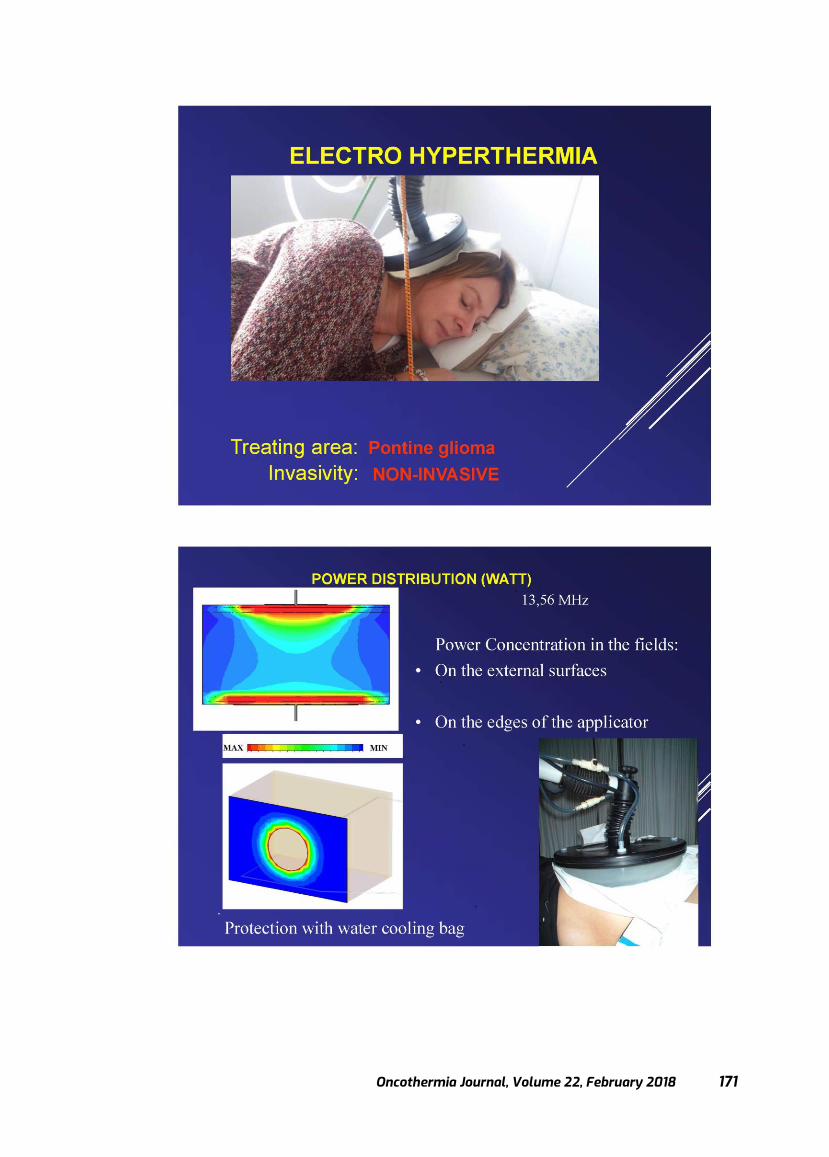
Oncothermia Journal, Volume 22, February 2018 171

Oncothermia Journal, Volume 22 February 2018
172
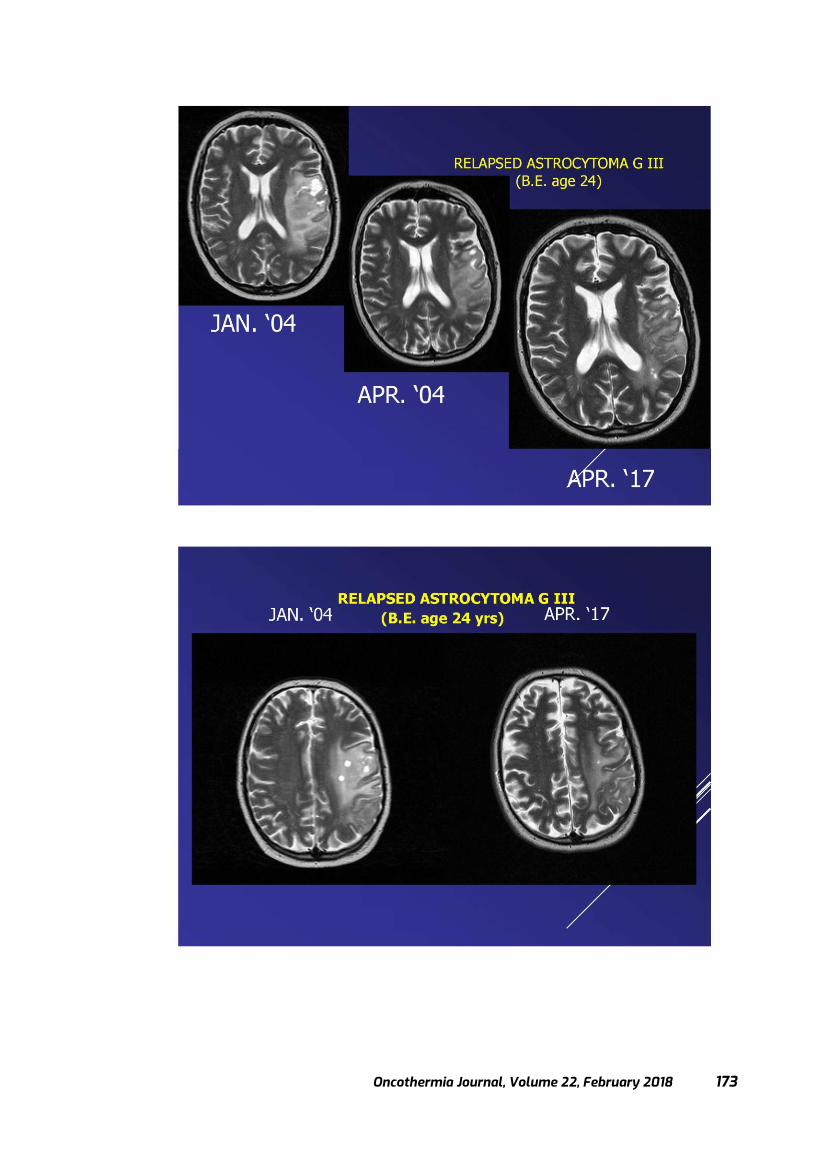
Oncothermia Journal, Volume 22, February 2018 173
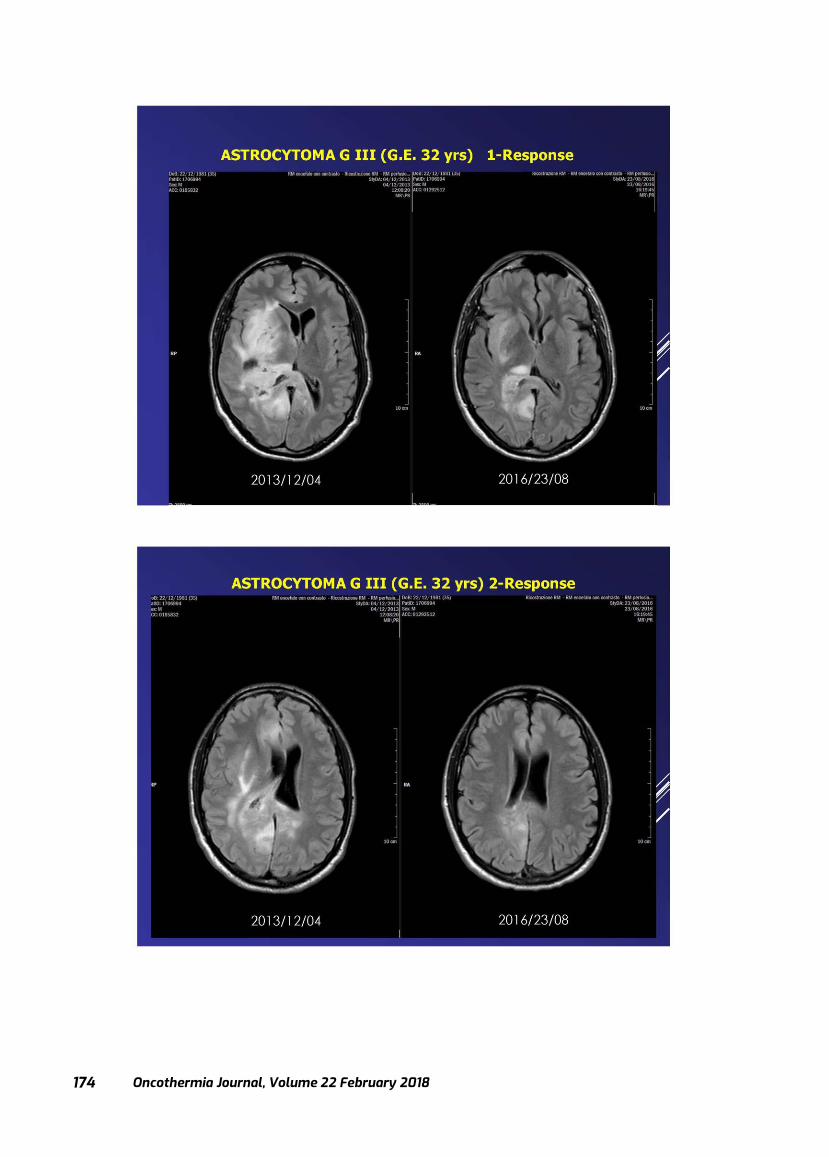
Oncothermia Journal, Volume 22 February 2018
174
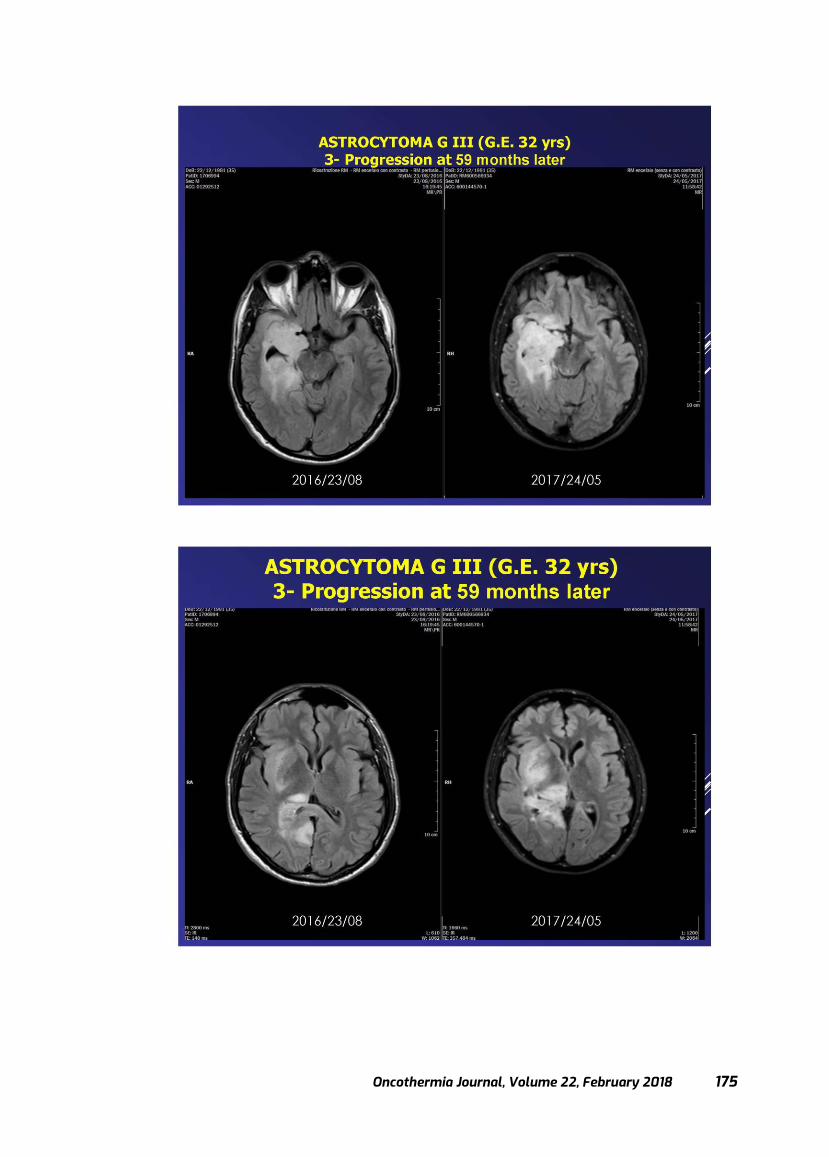
Oncothermia Journal, Volume 22, February 2018 175
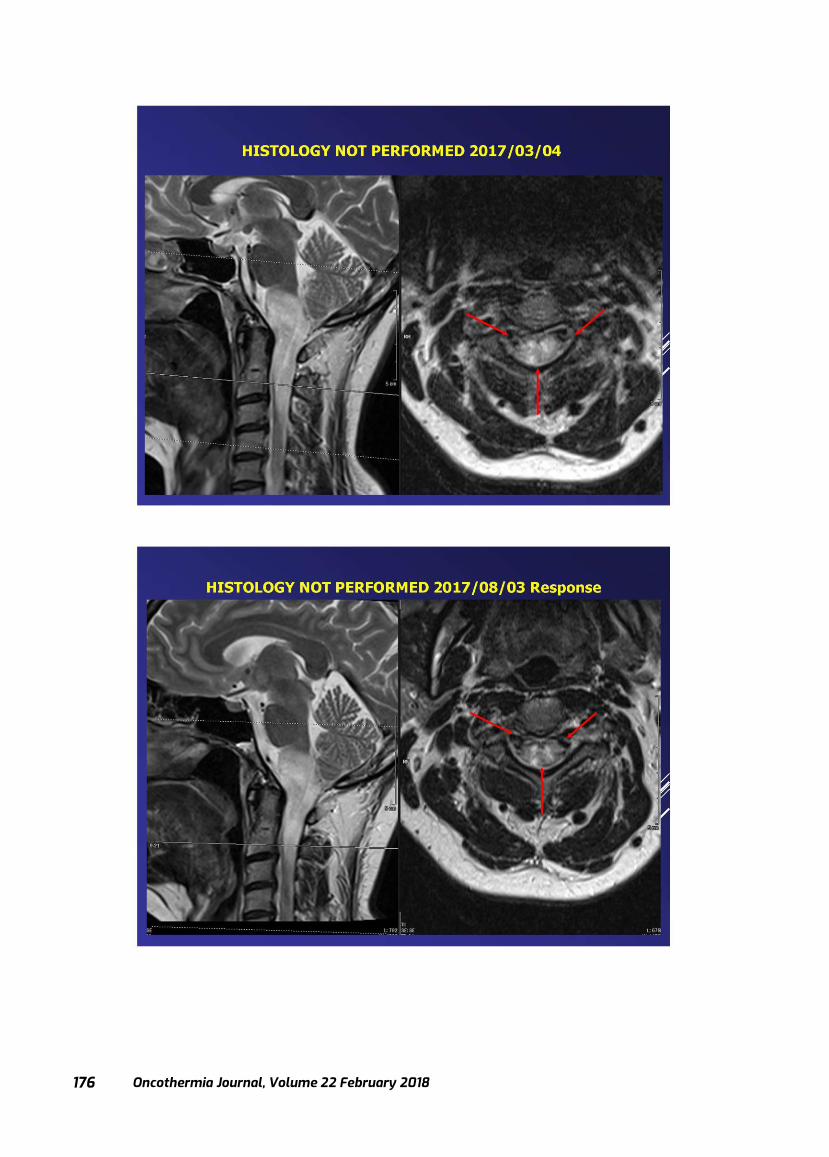
Oncothermia Journal, Volume 22 February 2018
176
Oncothermia Journal, Volume 22, February 2018 177

Oncothermia Journal, Volume 22 February 2018
178
Basic principle and new results of Oncothermia
Prof. Dr. Andras Szasz
Professor of physics & biophysics Chair, Department of Biotechnics, St. Istvan University, Hungary &
Visiting professor (bioelectromagnetics) in Pazmany P. Catholic University, Hungary & Visiting professor (fractal physiology) in Chiba University, Japan &
Chief Scientific Officer (CSO), Oncotherm GmbH, Troisdorf, Germany
Presented at KOSG Daejeon, 2017
Cite this article as:
Szasz A. (2018): Basic principle and new results of Oncothermia; Oncothermia Journal 22: 178-205
www.oncothermia-journal.com/journal/2018/Basic_principle_and_new _results_of _Oncothermi.pdf
Cite this article as:
Szasz O., Szigeti GyP., Szasz AM,. (2017): Electrokinetics of Temperature for Development and Treatment of Effusions
http://www.scirp.org/Journal/PaperInformation.aspx?PaperID=80707
Oncothermia Journal, Volume 22, February 2018 179
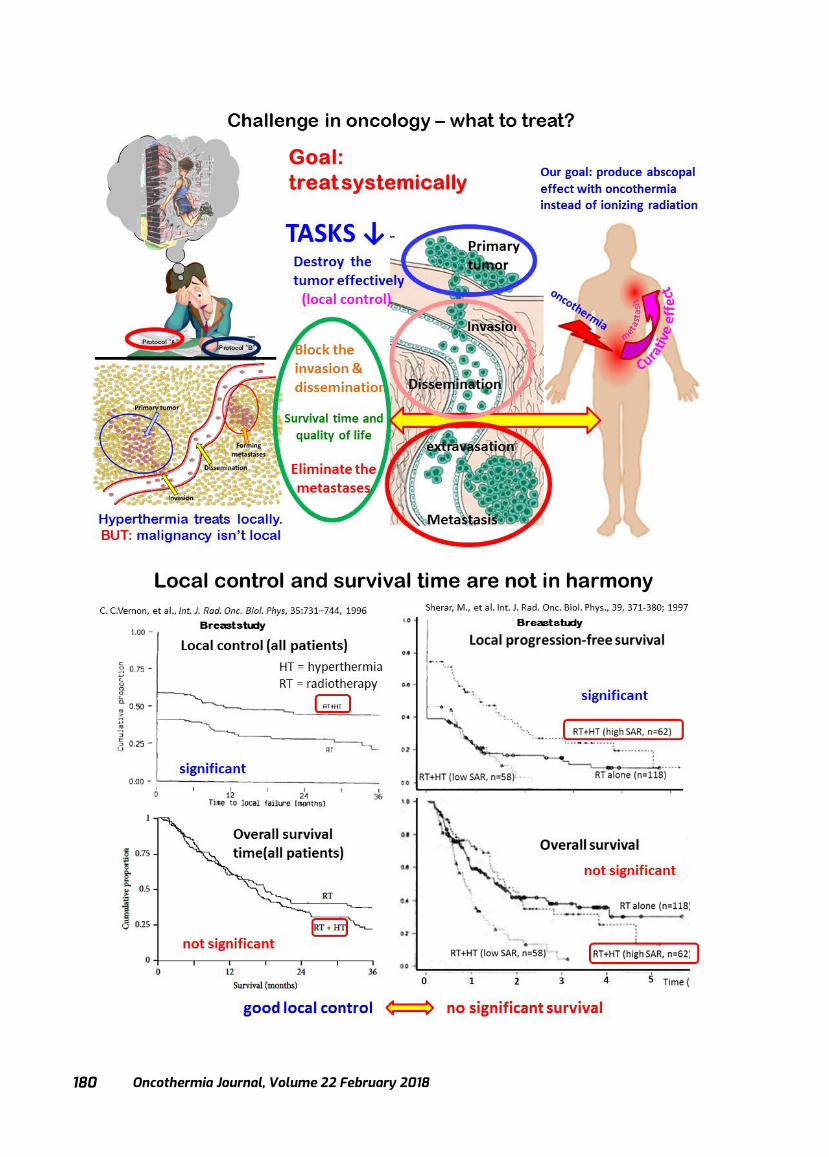
Oncothermia Journal, Volume 22 February 2018
180
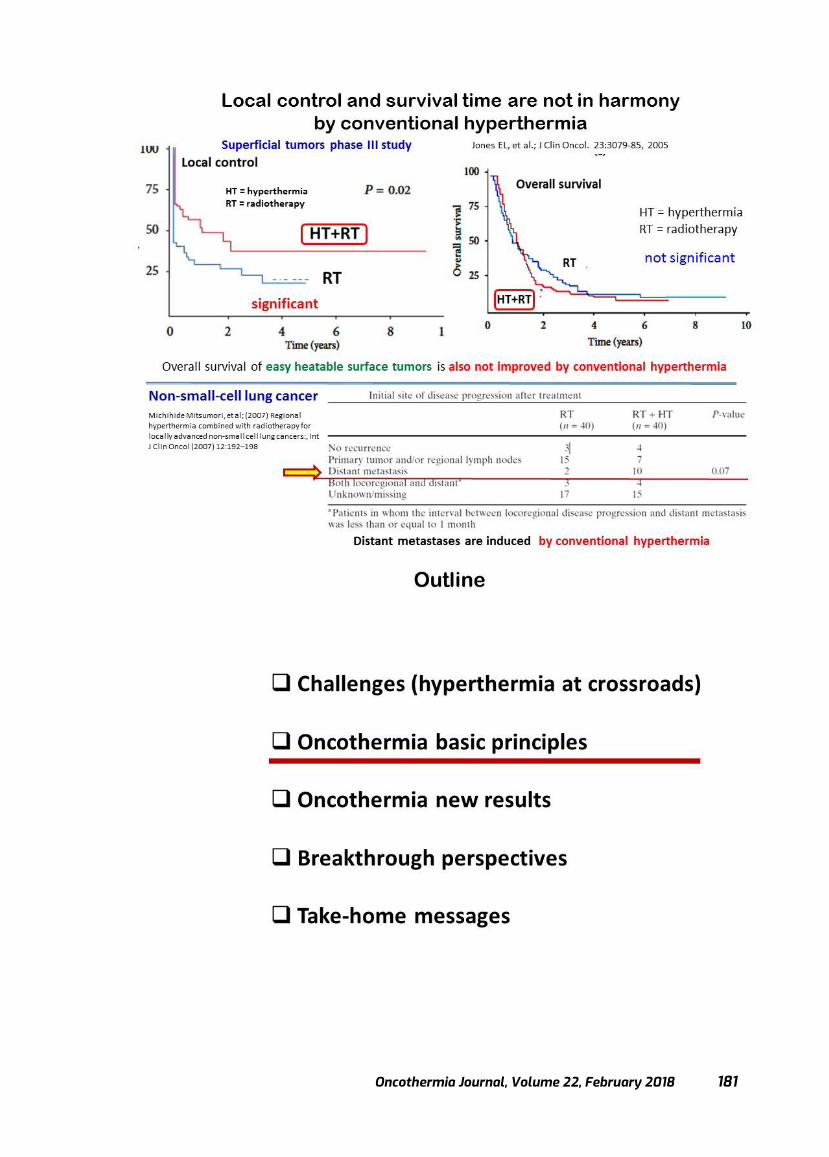
Oncothermia Journal, Volume 22, February 2018 181
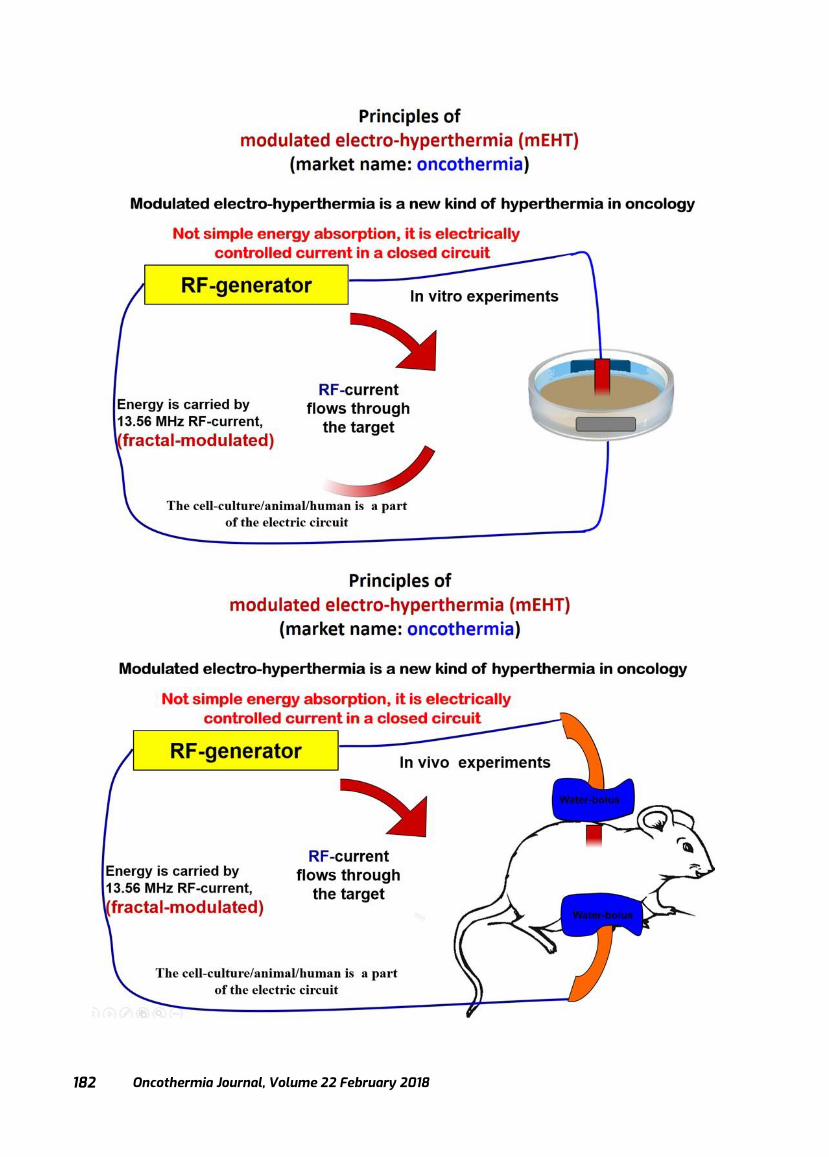
Oncothermia Journal, Volume 22 February 2018
182
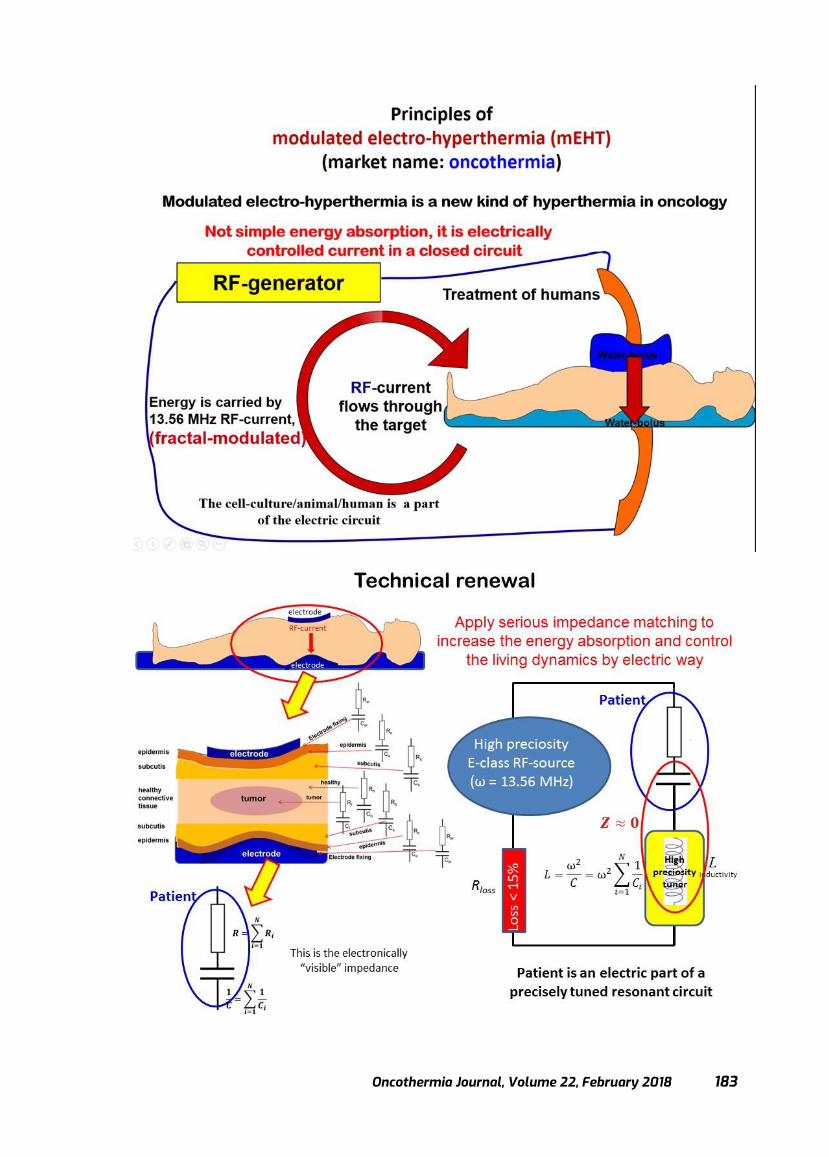
Oncothermia Journal, Volume 22, February 2018 183
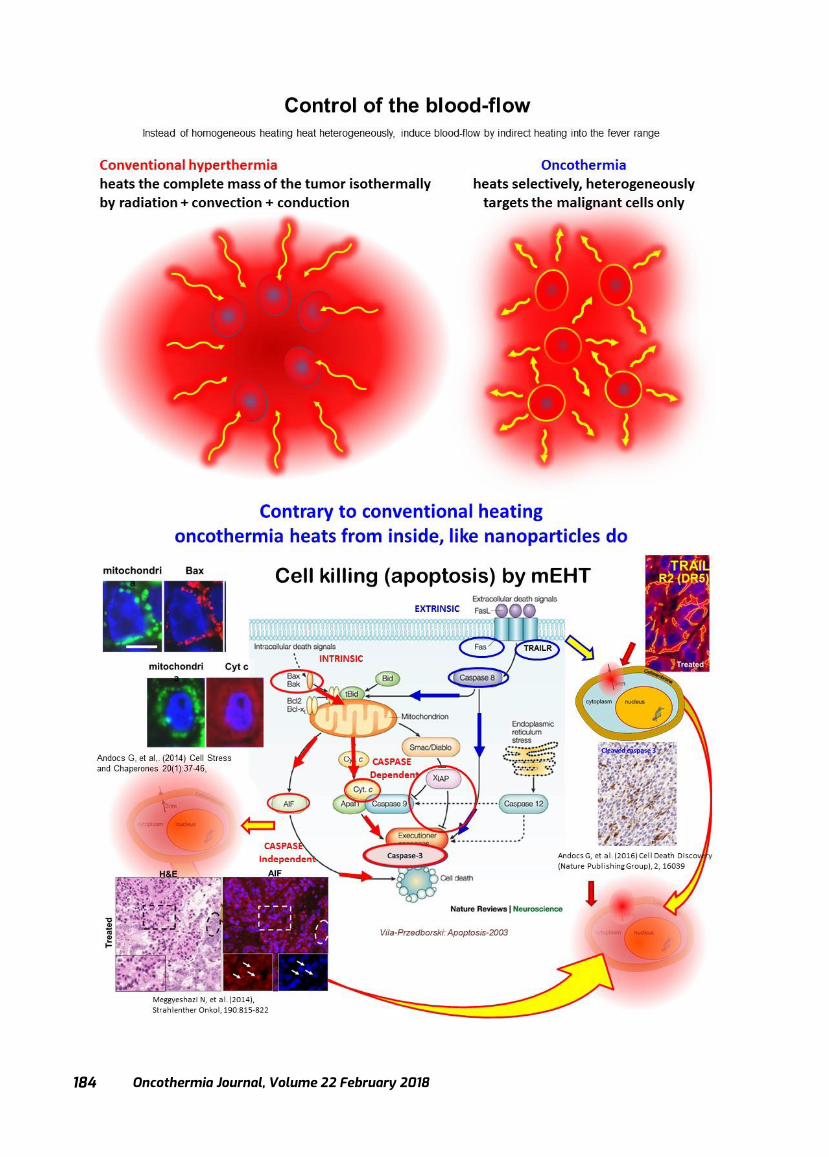
Oncothermia Journal, Volume 22 February 2018
184
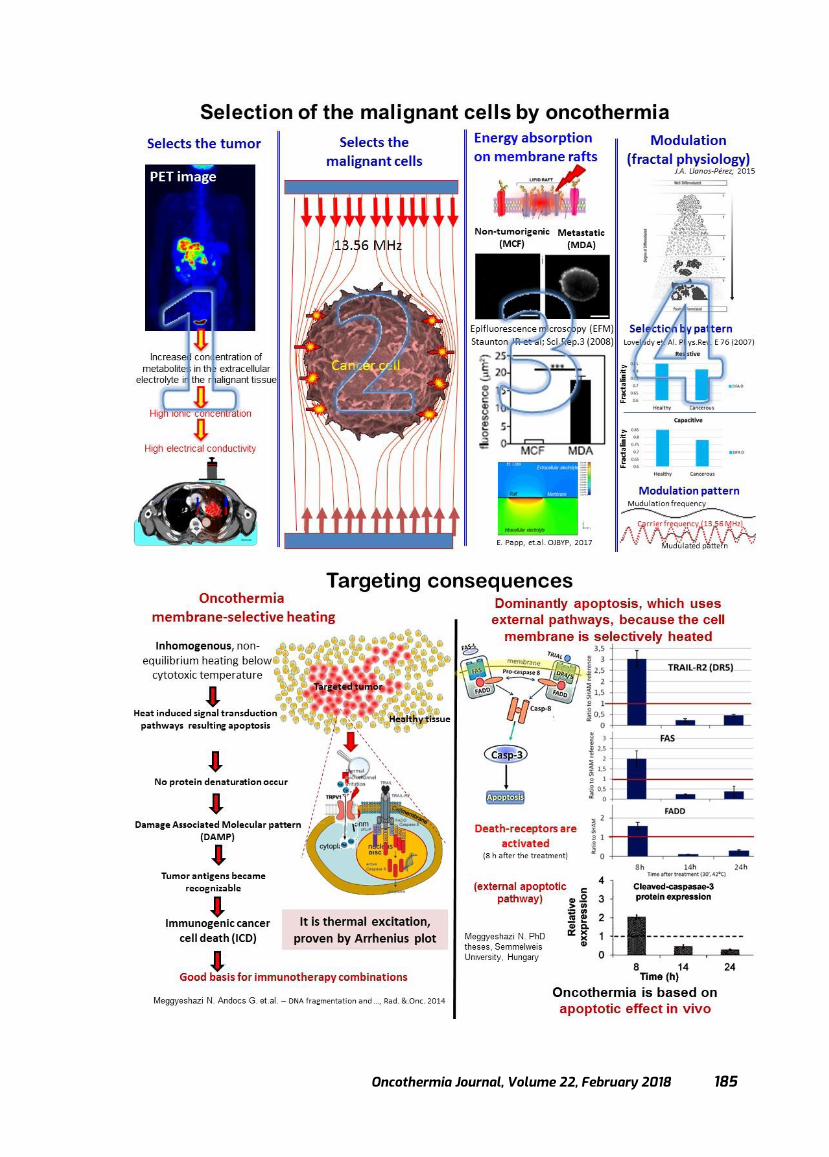
Oncothermia Journal, Volume 22, February 2018 185

Oncothermia Journal, Volume 22 February 2018
186
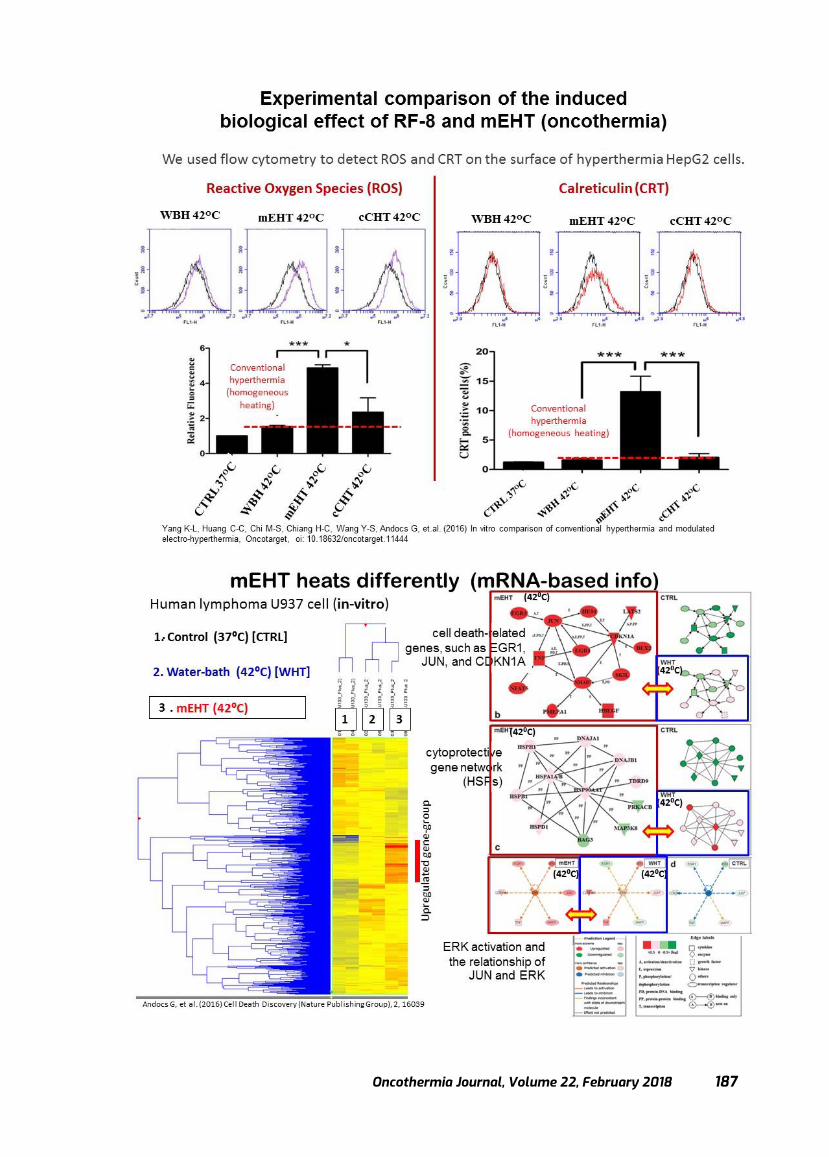
Oncothermia Journal, Volume 22, February 2018 187
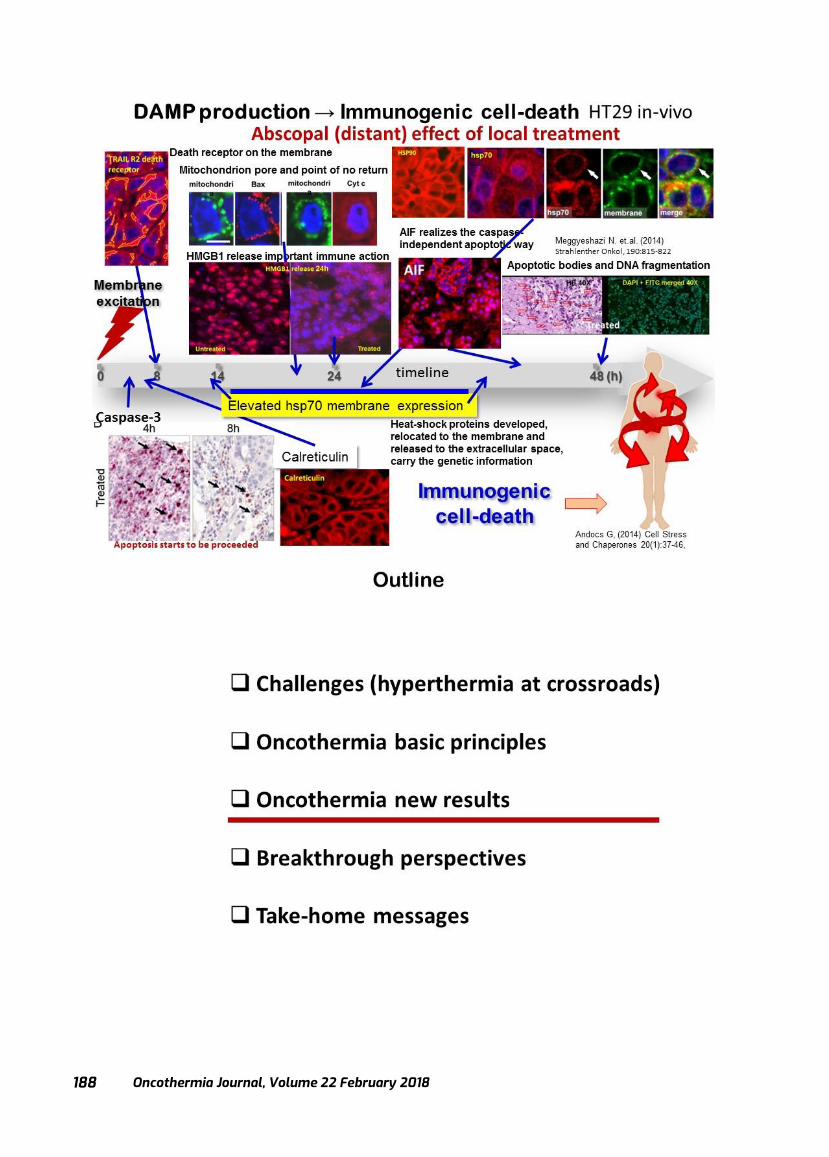
Oncothermia Journal, Volume 22 February 2018
188

Oncothermia Journal, Volume 22, February 2018 189
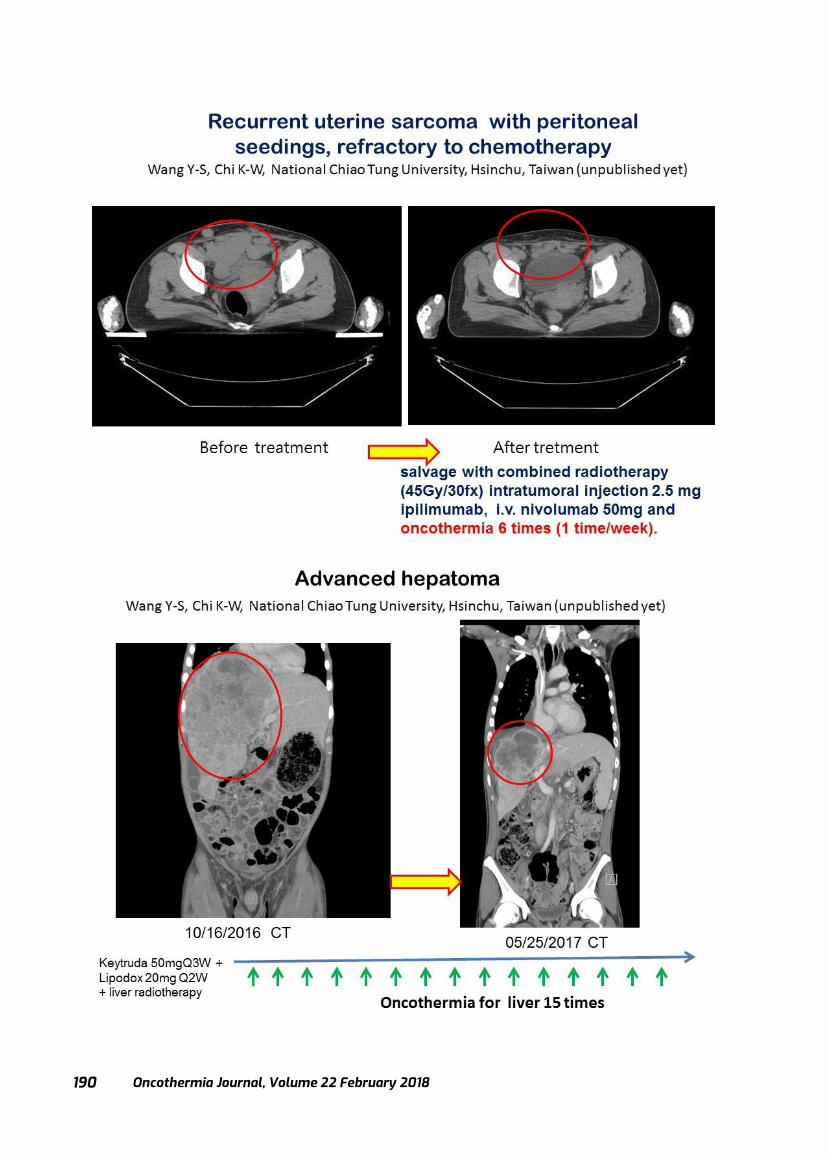
Oncothermia Journal, Volume 22 February 2018
190
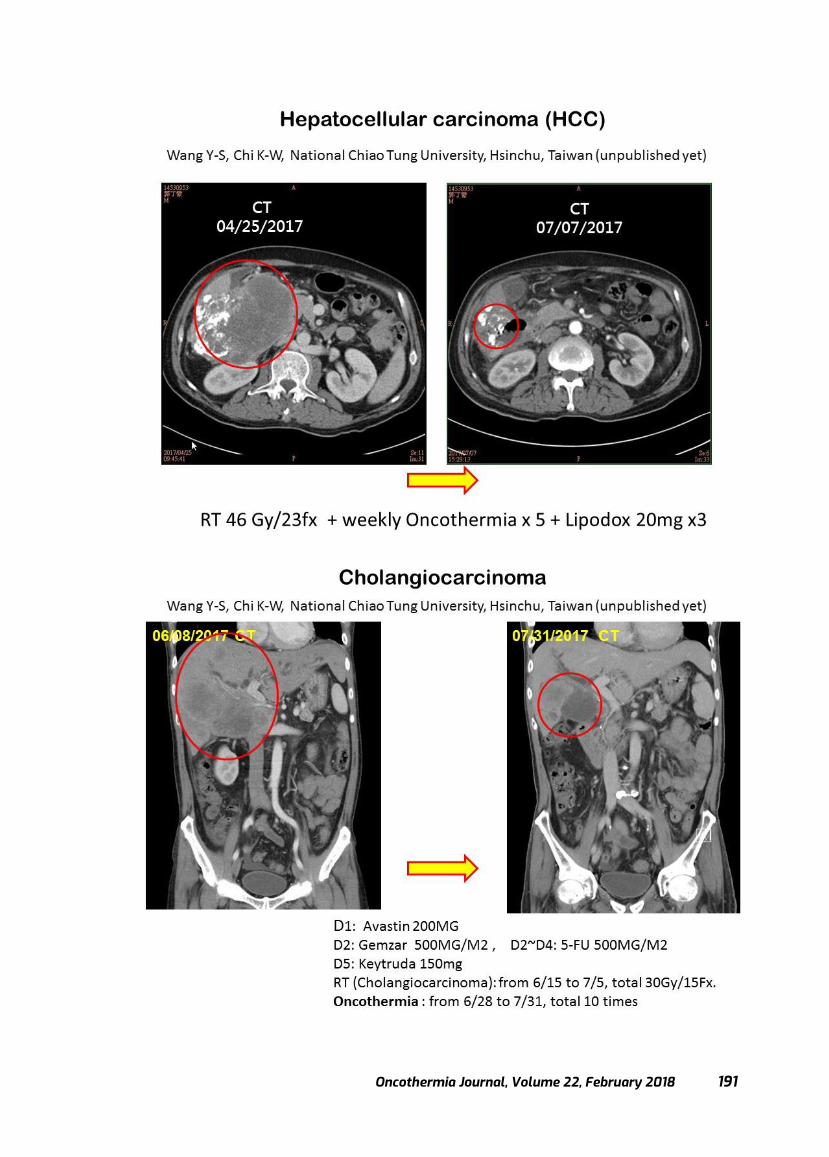
Oncothermia Journal, Volume 22, February 2018 191

Oncothermia Journal, Volume 22 February 2018
192
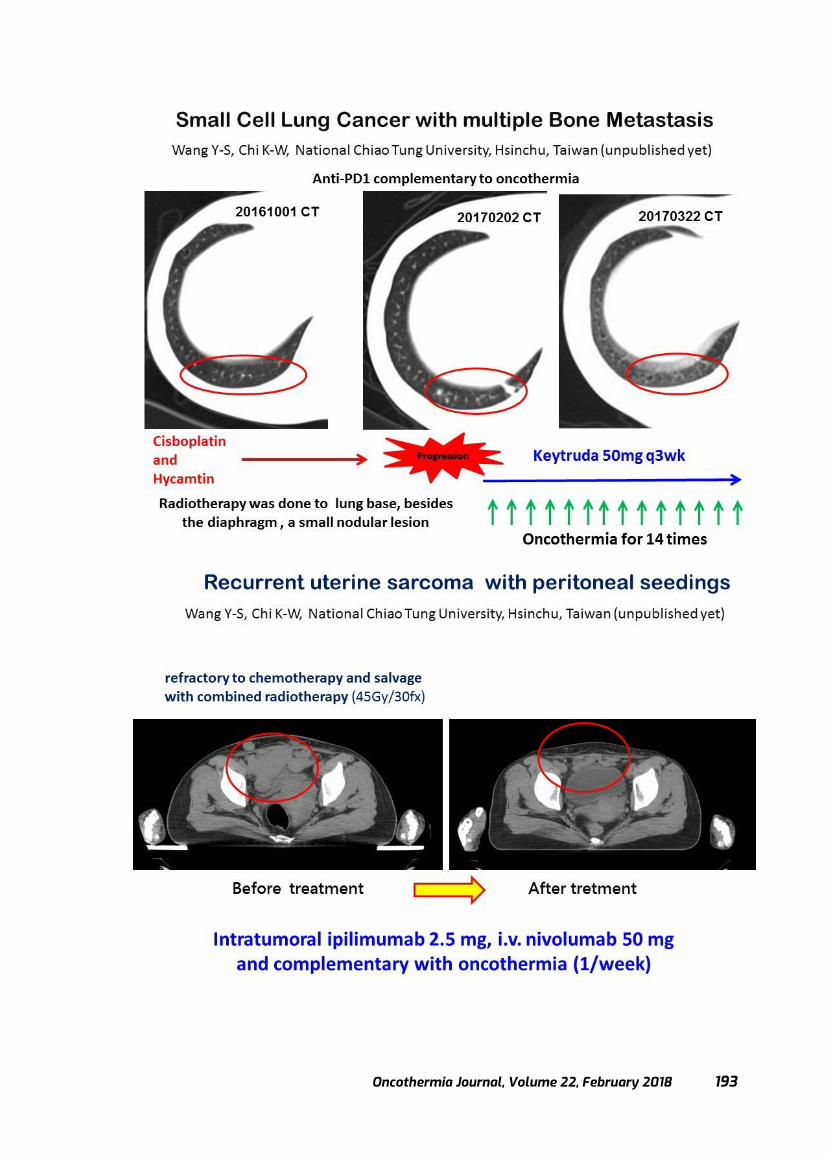
Oncothermia Journal, Volume 22, February 2018 193
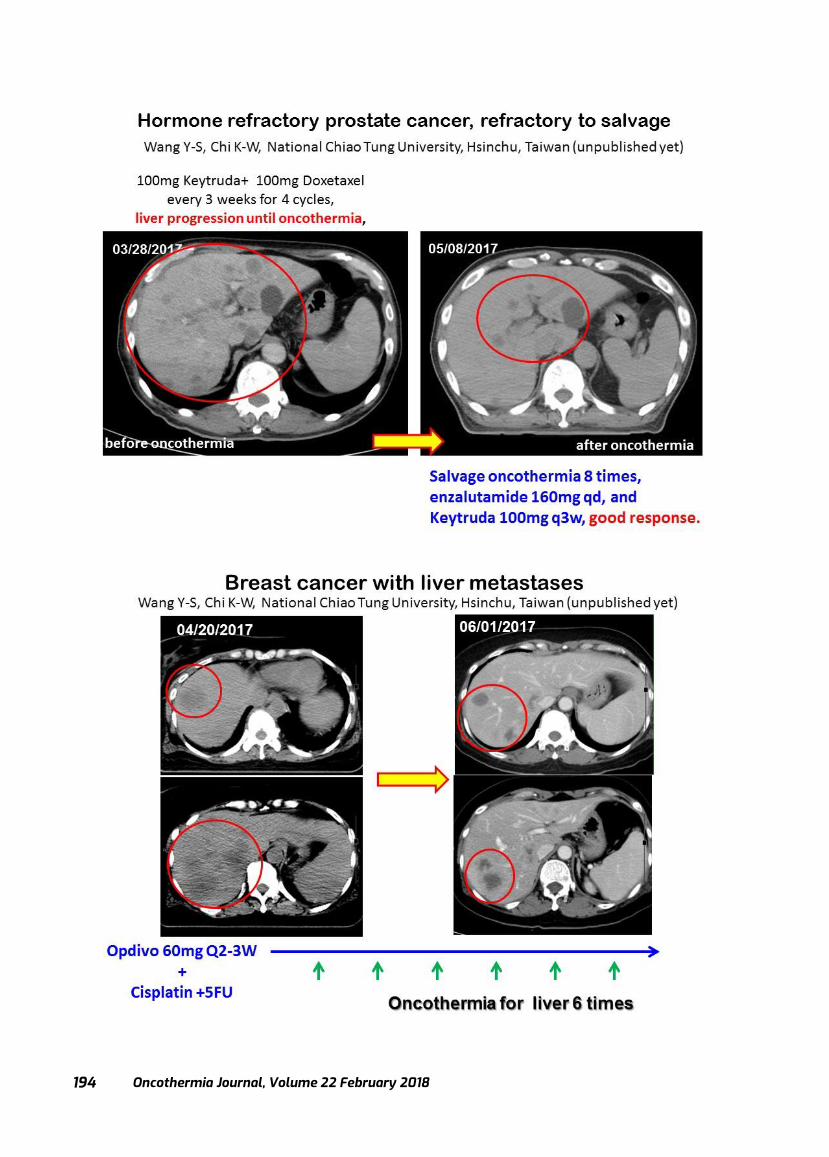
Oncothermia Journal, Volume 22 February 2018
194

Oncothermia Journal, Volume 22, February 2018 195
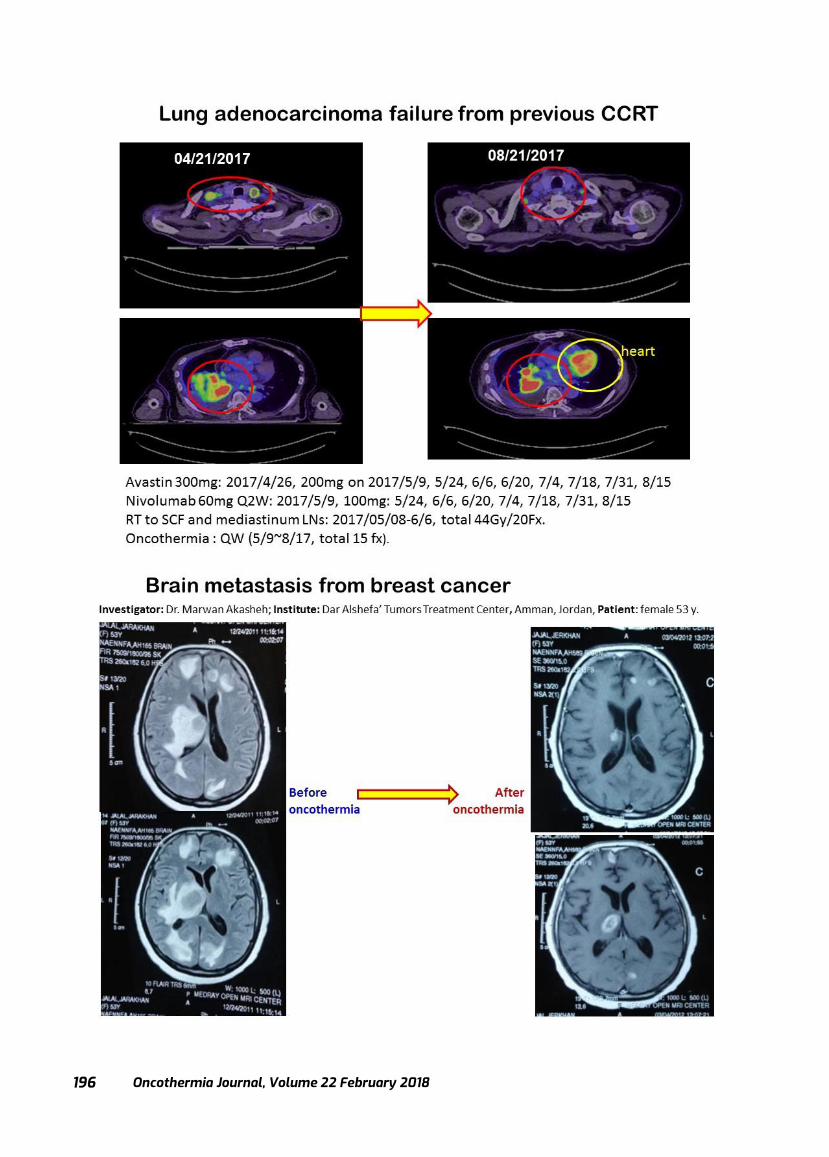
Oncothermia Journal, Volume 22 February 2018
196

Oncothermia Journal, Volume 22, February 2018 197
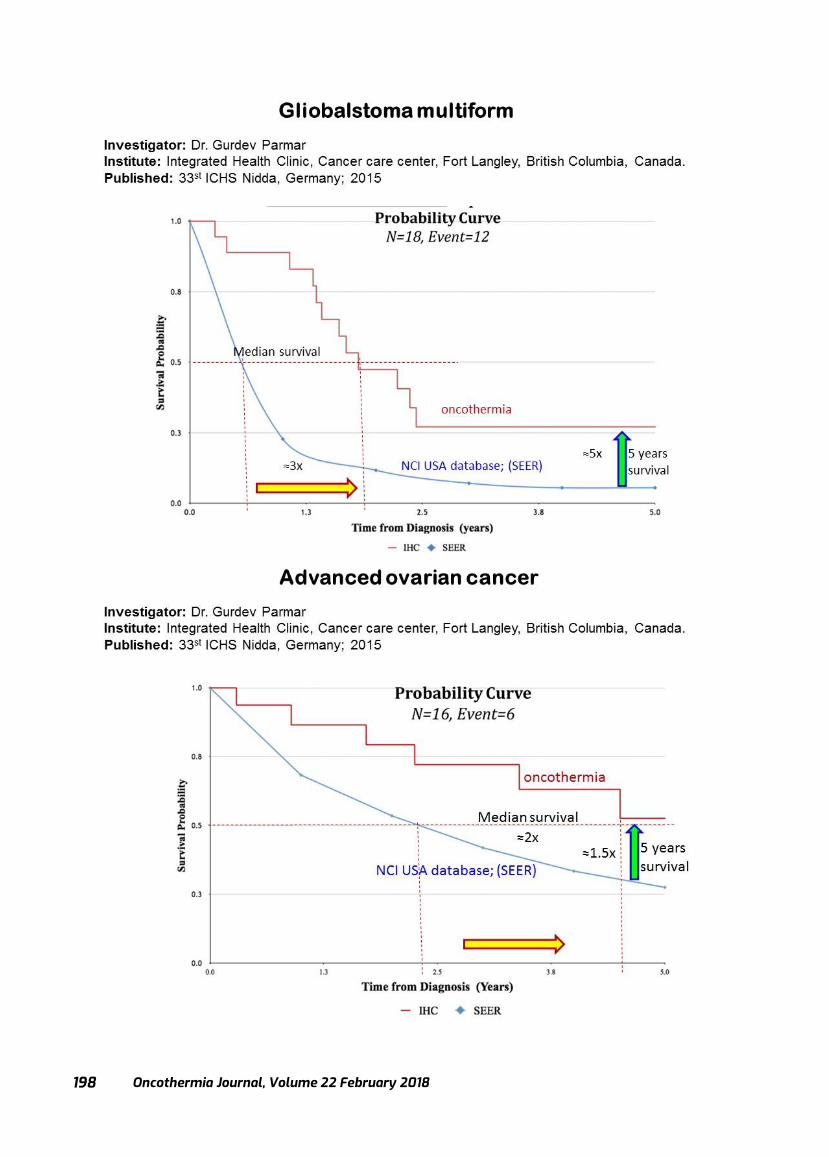
Oncothermia Journal, Volume 22 February 2018
198
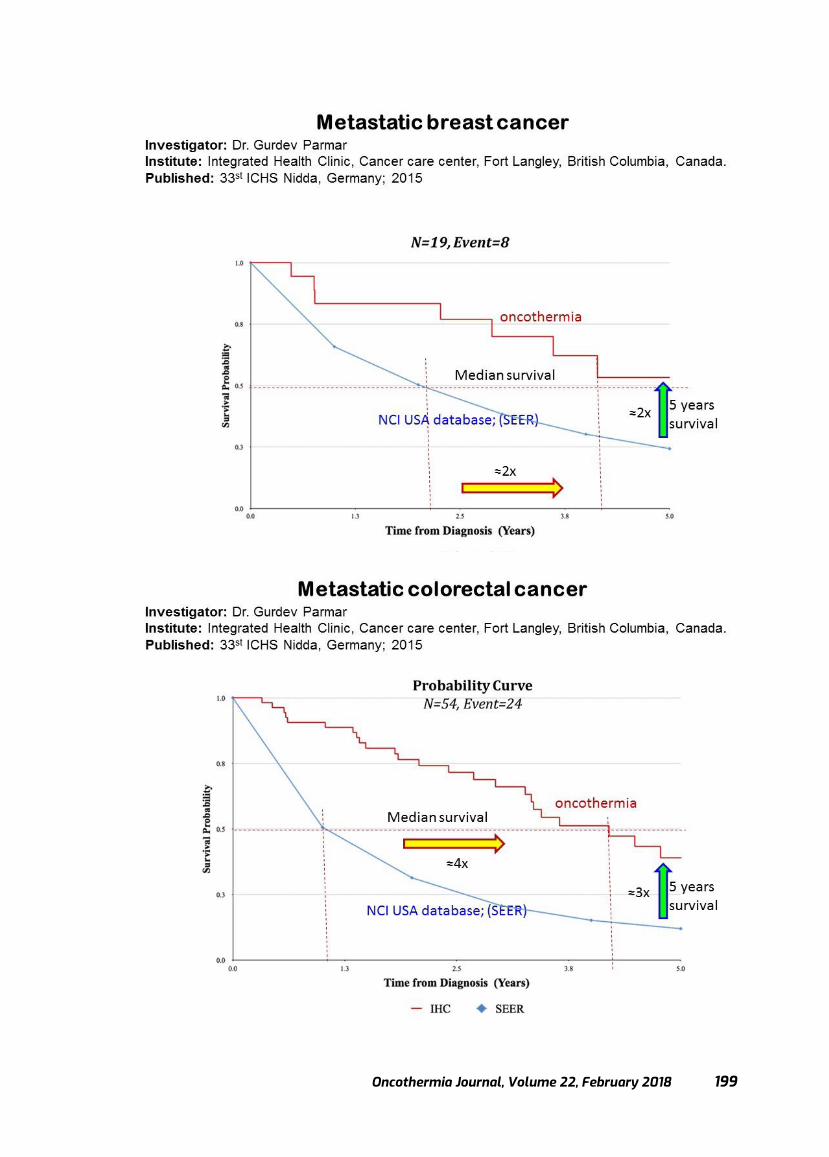
Oncothermia Journal, Volume 22, February 2018 199
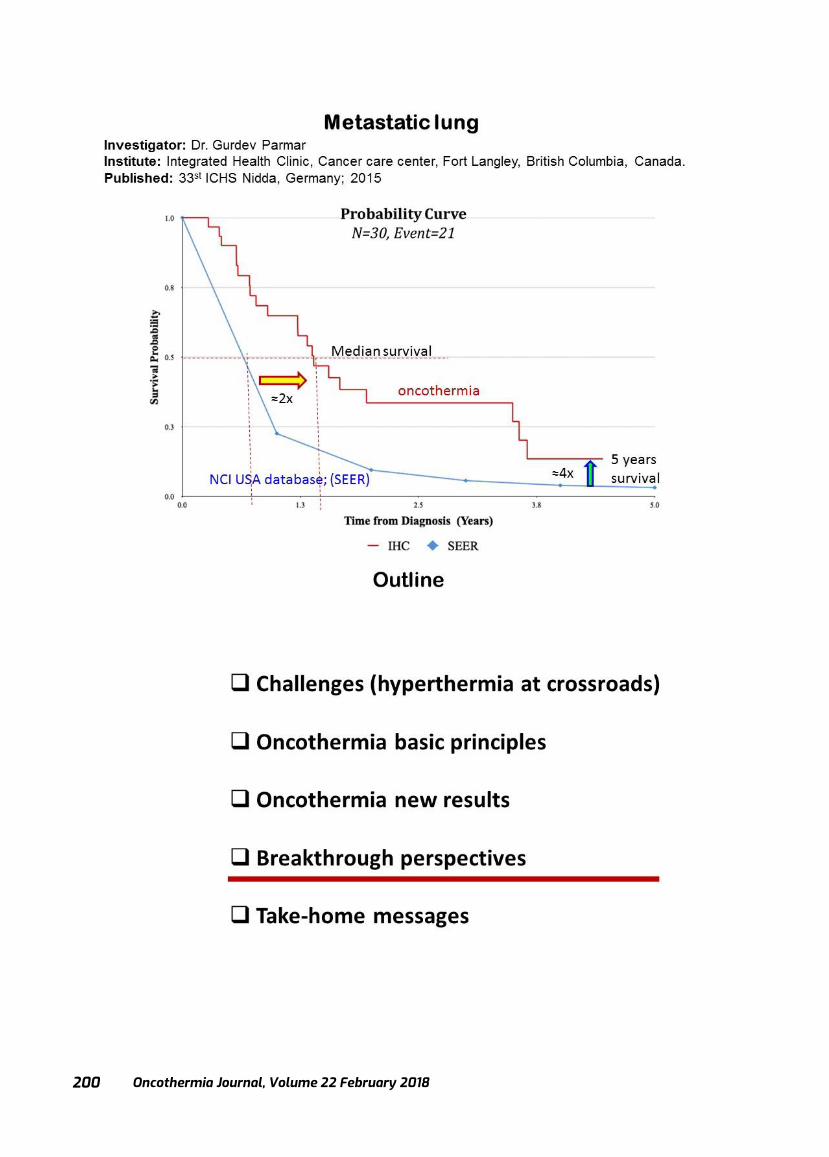
Oncothermia Journal, Volume 22 February 2018
200
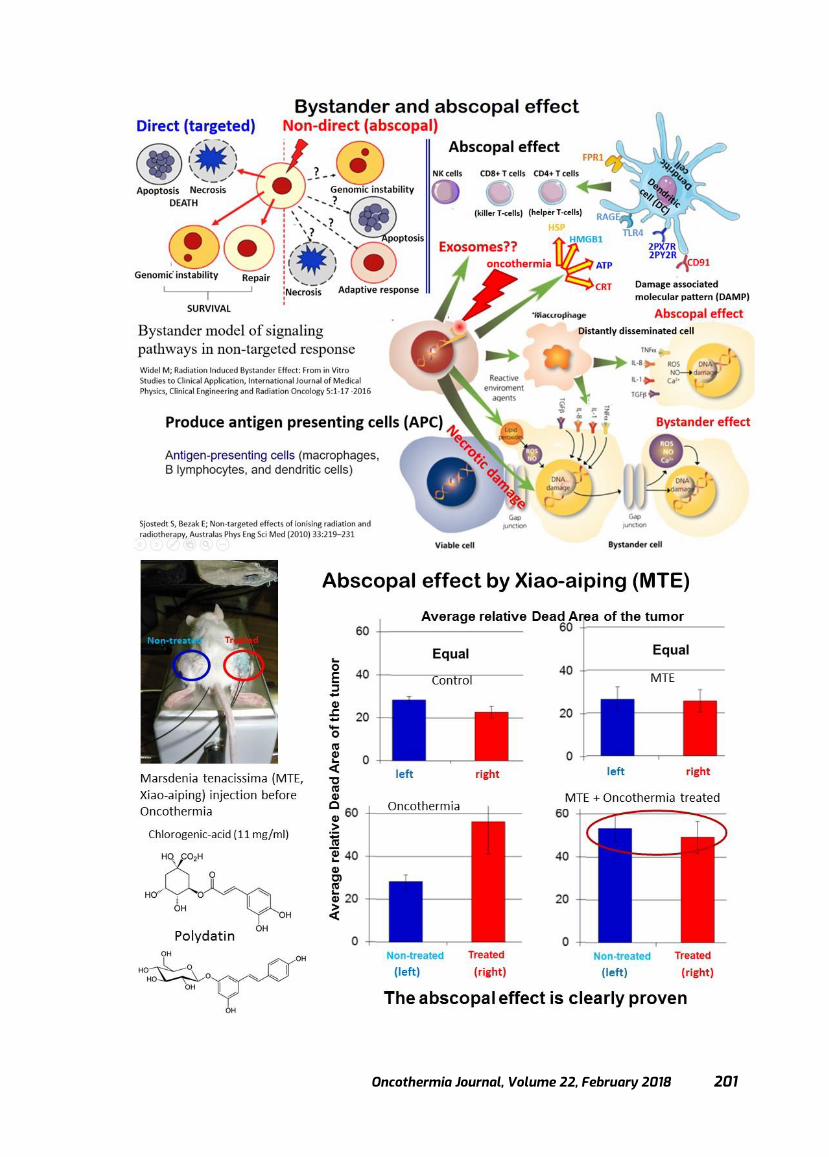
Oncothermia Journal, Volume 22, February 2018 201

Oncothermia Journal, Volume 22 February 2018
202
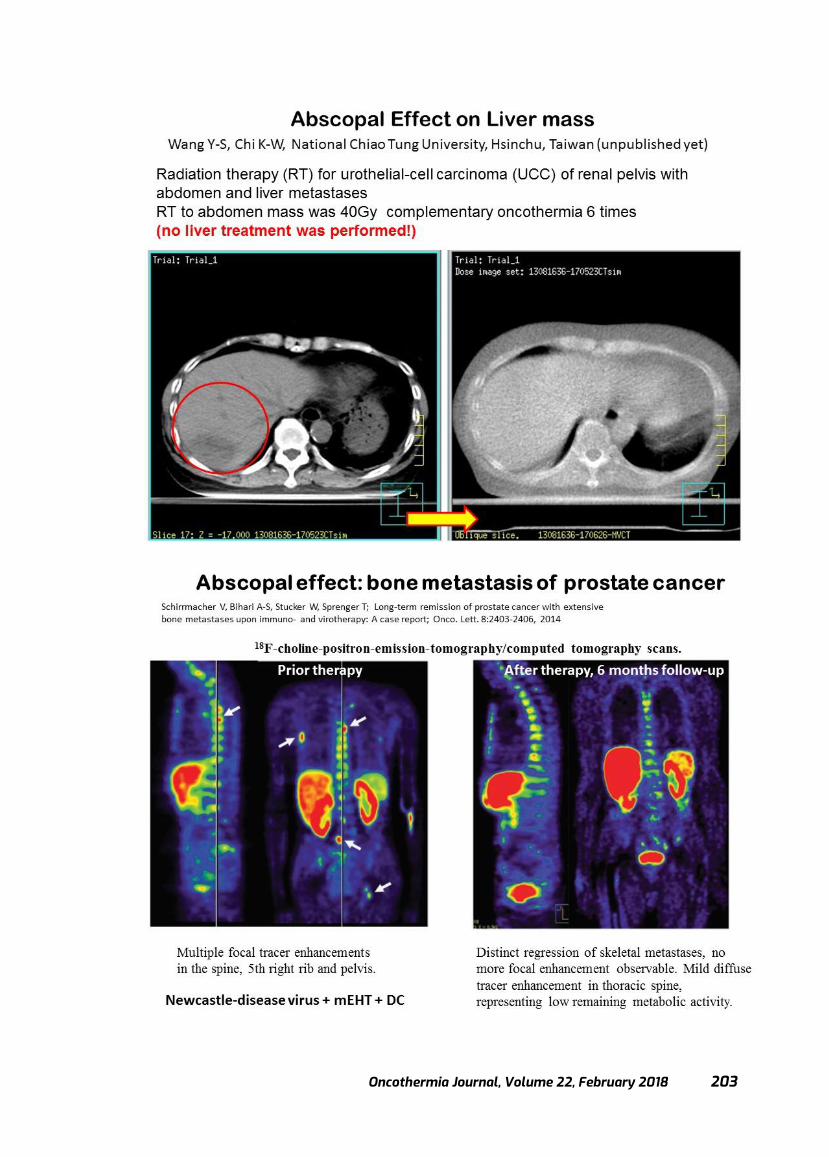
Oncothermia Journal, Volume 22, February 2018 203
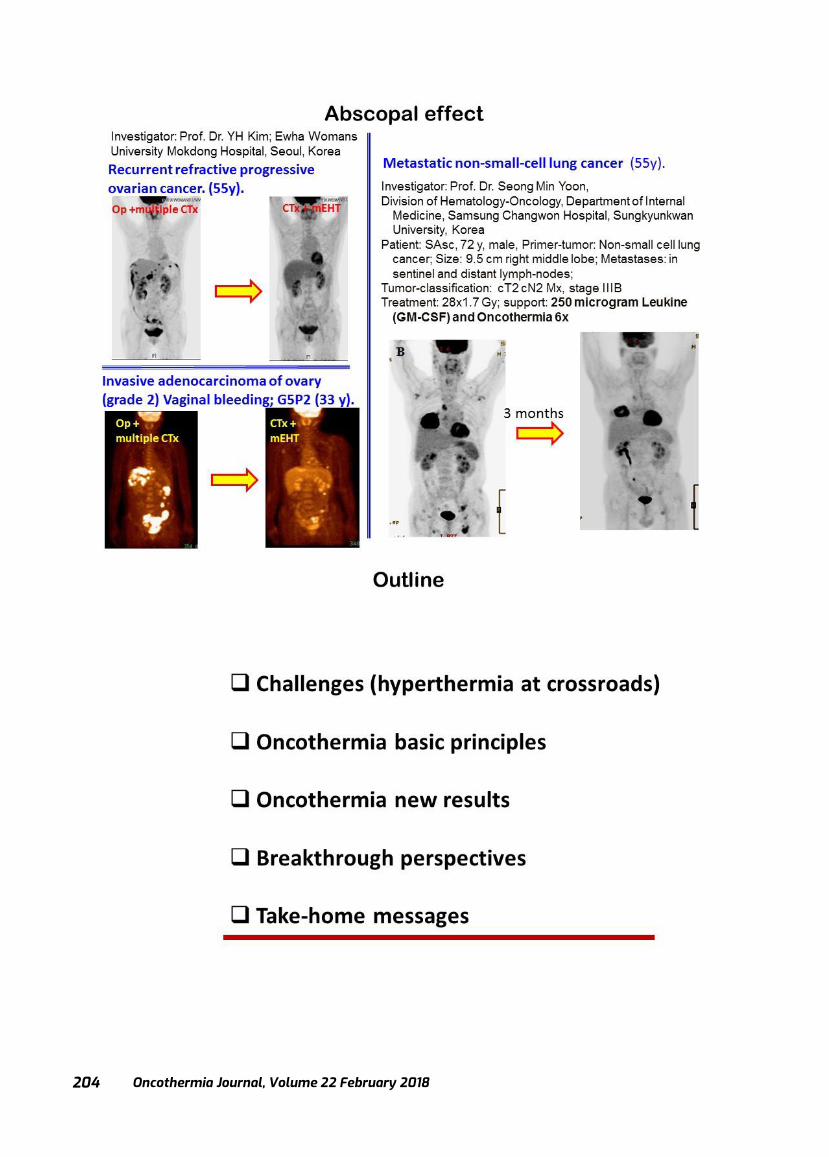
Oncothermia Journal, Volume 22 February 2018
204
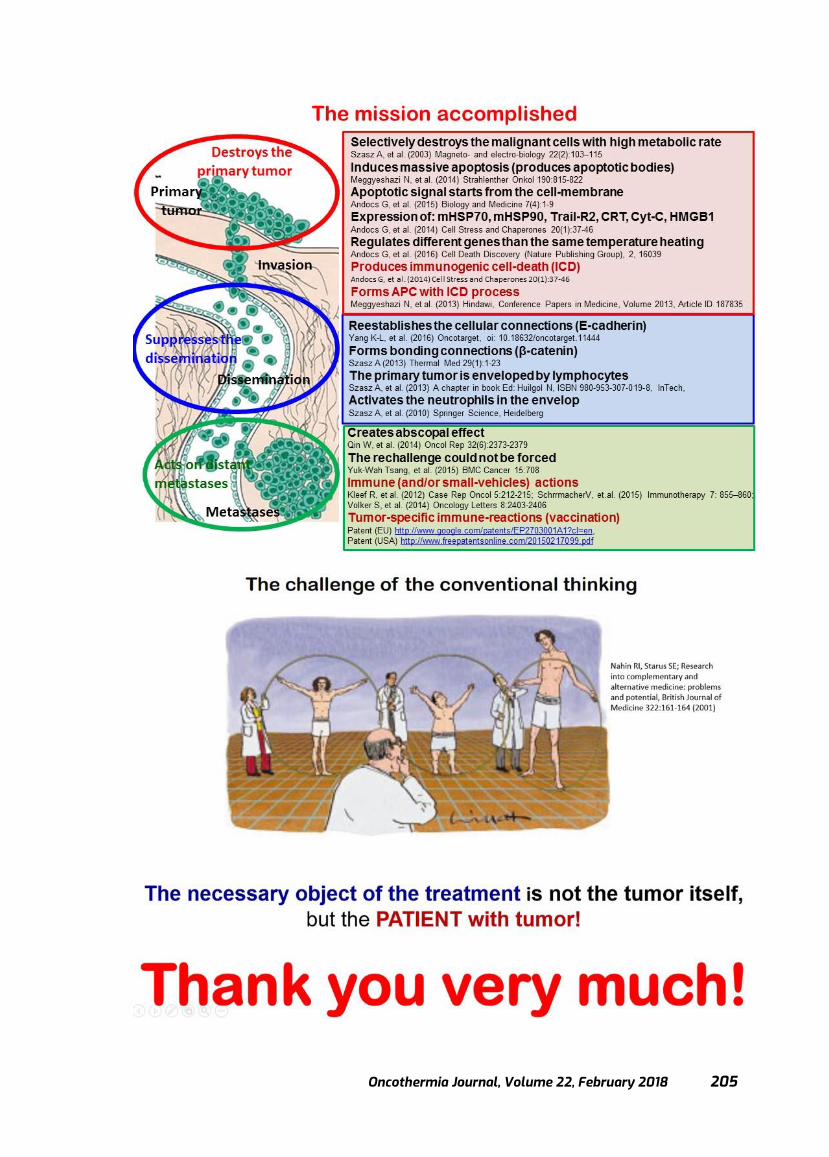
Oncothermia Journal, Volume 22, February 2018 205
Oncothermia Journal, Volume 22 February 2018
206
Press release
Cooperation of Academic and Industrial Partners to Fight Tumorous Diseases
http://oncotherm.com/en/news-events/cooperation-academic-and-industrial-partners-fight-tumorous-diseases
The objective of the National Competitiveness and Excellence Program (NVKP-16) was to provide funding for projects that aim at increasing the efficiency of the therapy of diseases of public health significance via Research, Development and Innovation (RDI). Our grant proposal entitled “Efficiency improvement, market introduction and preparations for integration into oncological therapeutic practice of an electromagnetic tumour therapeutic device” received a total of 1,472 billion Hungarian forints for a period of three years. The project is being realized within the framework of a consortium comprising the Semmelweis University and its partner, Oncotherm Kft, a company that played a leading role in the development of oncothermia, a novel therapeutic procedure. The gist of the method is in situ radio-frequency stimulation of tumour cells; the method elicits, via physico-chemical effects, responses such as local inhibition of tumour growth and a tumour-specific immunoreaction through immunogenic cell death of tumour cells. As a consequence of the latter response, the treatment of the primary tumour can be turned into a systemic anti-tumour process that allows prevention of metastasis formation and therapeutic control of existing metastases. The method is already used in clinical practice as an adjuvant therapy. According to Director Dr Zoltán Benyó, Principal Investigator of the project, the objective of the research is to improve the efficiency of the method. The program is based on three pillars, namely preclinical and clinical studies and instrument development. The preclinical module is coordinated by the Institute of Clinical Experimental Research, where the local and systemic effects of oncothermia treatment and the underlying cell-, organ- and organism-level processes are studied on experimental animal models. The aim is to identify and understand, at the molecular level, those tumour immunological and tumour angiogenetic processes, which can be effectively influenced by oncothermia treatment, creating the possibility for clinical application of the method to treat several high-prevalence tumorous diseases with poor prognosis (e.g. breast carcinoma, melanoma, glioblastoma). Funding covers significant instrument development. The first half-year of the project term is spent with provision of equipment and setting up methodologies and experimental models. Rapid success in these efforts is guaranteed, on the one hand, by the employment of new staff members with considerable experience in tumour biological research and, on the other hand, by the establishment of collaborations between the Institute and other University Departments performing international level, cutting-edge oncological research, such as the 1st Department of Pathology and Experimental Cancer Research, the Department of Biophysics and Radiation Biology and the Department of Laboratory Medicine. Research in the clinical module is performed in the Cancer Centre and is led by Prof. Dr. Magdolna Dank. A new oncothermia apparatus has been installed within the framework of the project; it is being used mainly for the therapy of patients suffering in malignancies whose treatment has been reported in the special literature to have produced positive results, such as pancreas carcinoma. The clinical research team has enrolled a significant number of pancreas carcinoma patients in these studies aiming at the development of novel therapeutic recommendations for the selection of the appropriate target group and
Oncothermia Journal, Volume 22, February 2018 207
the formulation of a therapeutic protocol that will ensure optimal performance of oncothermia therapy. The objective of the industrial partner of the consortium is targeted development of the apparatus based on the results of preclinical studies and on clinical experience, in order to create a device that can meet strong market demand. A significant result of the cooperation is that Oncotherm Kft has undertaken the establishment of an international demonstration and training centre at the Semmelweis University. Nearly 30 researchers support staff participate in this project funded by the National Research, Development and Innovation Office. The cooperation of the partners is a good example for the simultaneous realization of academic research objectives and a practical, marketable product.

Oncothermia Journal, Volume 22 February 2018
208
Electrokinetics of Temperature for Development and Treatment of Effusions
Oliver Szasz1, Gyula Peter Szigeti2, Attila Marcell Szasz3
1Department of Biotechnics, Istvan University, Budaors, Hungary 2Institute of Human Physiology and Clinical Experimental Research, Semmelweis
University, Budapest, Hungary 3Cancer Center, Semmelweis University, Budapest, Hungary
Cite this article as:
Szasz O., Szigeti GyP., Szasz AM. (2018): Electrokinetics of Temperature for Development and Treatment of Effusions; Oncothermia Journal
22:208-224 Reprinted from:
http://www.scirp.org/Journal/PaperInformation.aspx?PaperID=80707

Oncothermia Journal, Volume 22, February 2018 209

Oncothermia Journal, Volume 22 February 2018
210

Oncothermia Journal, Volume 22, February 2018 211

Oncothermia Journal, Volume 22 February 2018
212

Oncothermia Journal, Volume 22, February 2018 213
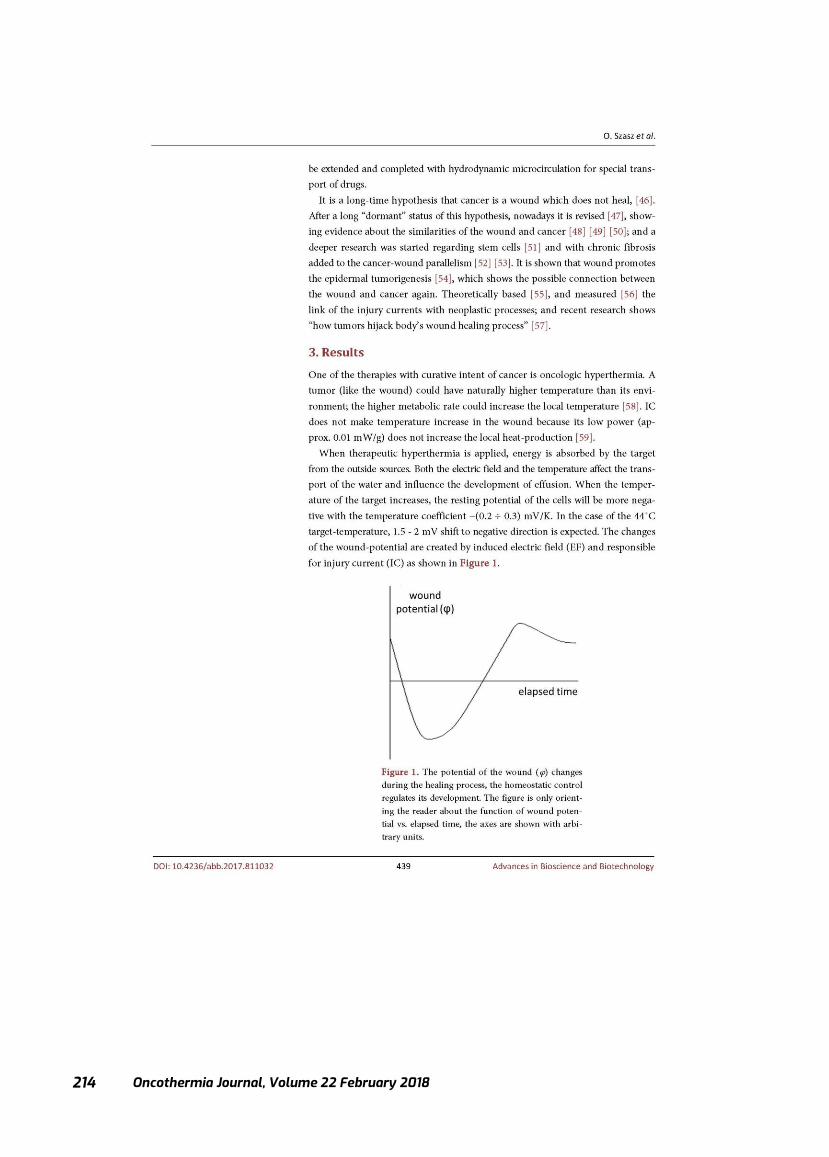
Oncothermia Journal, Volume 22 February 2018
214

Oncothermia Journal, Volume 22, February 2018 215

Oncothermia Journal, Volume 22 February 2018
216

Oncothermia Journal, Volume 22, February 2018 217

Oncothermia Journal, Volume 22 February 2018
218

Oncothermia Journal, Volume 22, February 2018 219
Oncothermia Journal, Volume 22 February 2018
220
Oncothermia Journal, Volume 22, February 2018 221

Oncothermia Journal, Volume 22 February 2018
222
Oncothermia Journal, Volume 22, February 2018 223

Oncothermia Journal, Volume 22 February 2018
224
Oncothermia Journal, Volume 22, February 2018 225
Advertisement

Oncothermia Journal, Volume 22 February 2018
226

Oncothermia Journal, Volume 22, February 2018 227
32nd Annual Meeting of the European Society for Hyperthermic Oncology
16–19 May 2018 • Berlin/Germany www.esho2018.eu
Registration deadline: 28th February
Venue: Langenbeck- Virchow- Haus
Luisenstraße 58/59 10117 Berlin (DE)
Oncothermia Journal, Volume 22 February 2018
228
THE ONCOTHERMIA METHOD & DEVICES
THE ONCOTHERMIA METHOD & DEVICES
EHY-2030
EHY-2030
EHY-2000plus
EHY-2000plus
EHY-3010
EHY-3010
EHY-1020
EHY-1020
The EHY-2030 is our latest development in the treatment of loco-regional
(including deep and surface) tumors. The newly designed device includes the
Smart Electrode Seystem (SES), the plug-in Patient Management System
(PMS-100) and a user-friendly touch screen display with full system control.
The new RF generator with increased power has been developed with a new
intelligently controlled step motor tuning system for rapid impedance
matching to achieve faster tuning times.
The EHY-2030 is our latest development in the treatment of loco-regional
(including deep and surface) tumors. The newly designed device includes the
Smart Electrode Seystem (SES), the plug-in Patient Management System
(PMS-100) and a user-friendly touch screen display with full system control.
The new RF generator with increased power has been developed with a new
intelligently controlled step motor tuning system for rapid impedance
matching to achieve faster tuning times.
The EHY-2000plus is a widely accepted system for loco-regional deep mEHT
applications. This model has been used for treatment worldwide for more than
20 years. Popular, versatile device, applicable for a range of solid tumors and
improved over the years through feedback from our doctors and experts and the
requirements of patients and the people treating them. The EHY-2000plus is an
easy to use and highly reliable device.
The EHY-2000plus is a widely accepted system for loco-regional deep mEHT
applications. This model has been used for treatment worldwide for more than
20 years. Popular, versatile device, applicable for a range of solid tumors and
improved over the years through feedback from our doctors and experts and the
requirements of patients and the people treating them. The EHY-2000plus is an
easy to use and highly reliable device.
The EHY-3010 is designed for the simultaneous multi-local treatment of
advanced, metastatically disseminated, malignant, solid tumors. Within the
range of Oncothermia systems, it is the pioneering breakthrough in the field of
multi-local tumor therapy. Instead of a bolus electrode, this system uses textile
electrodes, which are even more flexible to better adjust to the treatment area.
The EHY-3010 is designed for the simultaneous multi-local treatment of
advanced, metastatically disseminated, malignant, solid tumors. Within the
range of Oncothermia systems, it is the pioneering breakthrough in the field of
multi-local tumor therapy. Instead of a bolus electrode, this system uses textile
electrodes, which are even more flexible to better adjust to the treatment area.
The EHY-1020 is specifically designed to treat prostate diseases. Both malignant and benign
tumors (BPH) can be treated using this system. It uses a catheter with built-in electronics and
counter electrode. The EHY-1020 system is compact and easy to use. The method has been
successfully used by our customers since 2010 with high success rates and minimal side effect.
The EHY-1020 is specifically designed to treat prostate diseases. Both malignant and benign
tumors (BPH) can be treated using this system. It uses a catheter with built-in electronics and
counter electrode. The EHY-1020 system is compact and easy to use. The method has been
successfully used by our customers since 2010 with high success rates and minimal side effect.
HUNGARY
Oncotherm Kft.
Gyár utca 2.
2040 Budaörs, Hungary
Phone (+36) 23-555-510
Fax (+36) 23-555-515
www.oncotherm.hu
HUNGARY
Oncotherm Kft.
Gyár utca 2.
2040 Budaörs, Hungary
Phone (+36) 23-555-510
GERMANY
Oncotherm GmbH
Belgische Allee 9
53842 Troisdorf, Germany
Phone (+49) 2241-319920
Fax (+49) 2241-3199211
www.oncotherm.de
GERMANY
Oncotherm GmbH
Belgische Allee 9
53842 Troisdorf, Germany
Phone (+49) 2241-319920
USA
Oncotherm Ltd.
LLC, 1942 Broadway Street
Suite 314C
Boulder CO 80302
United States
Phone: (406) 225-7009
www.oncotherm.com
USA
Oncotherm Ltd.
LLC, 1942 Broadway Street
Suite 314C
Boulder CO 80302
Oncothermia is based on the classical method of Hyperthermia, one of the oldest cancer treatment methods. Unlike conventional
Hyperthermia, Oncothermia does more than simply warm up deep layers of tissue. It combines such warming with a modulated
electric field, with a carrier frequency of 13.56 MHz, which is generated by two active electrodes.
Oncothermia is based on the classical method of Hyperthermia, one of the oldest cancer treatment methods. Unlike conventional
Hyperthermia, Oncothermia does more than simply warm up deep layers of tissue. It combines such warming with a modulated
electric field, with a carrier frequency of 13.56 MHz, which is generated by two active electrodes.