
Oncoplastic surgery of the breast: Rationale and experience of 30 cases
9
The Breast (2007) 16, 411–419 THE BREAST ORIGINAL ARTICLE Oncoplastic surgery of the breast: Rationale and experience of 30 cases Andre´Vallejo da Silva a, , Claudinei Destro a , Wilhermo Torres b a Breast Service, Anto ˆnio Pedro Universitary Hospital, Federal Fluminense University, Nitero ´i, Rio de Janeiro, Brazil b Pathology Service, Anto ˆnio Pedro Universitary Hospital, Federal Fluminense University, Nitero ´i, Rio de Janeiro, Brazil Received 21 November 2006; accepted 31 January 2007 KEYWORDS Breast cancer; Reconstructive surgi- cal procedures; Oncoplastic surgery; Oncological safety Summary A definition of oncoplastic surgery of the breast is presented, and its objectives and advantages over the usual conservative procedures are discussed. The oncological safety of these procedures are demonstrated, especially in surgery of larger tumors. Technical possibilities are discussed and a classification of the procedures presented. Data from 30 cases operated in our institution are depicted. The need for better training of the breast surgeon is discussed and the advantages of the same surgeon to perform the whole procedure presented. & 2007 Elsevier Ltd. All rights reserved. Introduction Oncoplastic surgery of the breast defines the set of techniques used along with oncological techniques for the prevention or correction of breast defor- mities caused by surgical cancer treatment. The goals of modern breast cancer surgery include the cure of the patient, preserving the breast as much as possible and satisfying the woman by giving her physical and psychological welfare. Mostly, the response of breast surgeons to this challenge has been the use of traditional ablative techniques based on margin-free resection and primary synthesis of the tissues This approach, though appropriate from the pure oncological point of view, usually do not satisfy the patient’s esthetic hopes, creating dissatisfaction with her body image, which may lead to several problems, including treatment non-compliance and even worse oncological outcome. Conservative surgery has an esthetic goal. The reason behind its existence is to preserve the normal aspect of the breast as much as possible, contributing to the women’s body image and self- esteem. Otherwise, we would still be performing mastectomies for all cases, considering this is the ARTICLE IN PRESS www.elsevier.com/locate/breast 0960-9776/$ - see front matter & 2007 Elsevier Ltd. All rights reserved. doi:10.1016/j.breast.2007.01.014 Corresponding author. Tel.: +5521 26227279; fax: +55 21 26227279. E-mail address: [email protected] (A. Vallejo da Silva).
Transcript of Oncoplastic surgery of the breast: Rationale and experience of 30 cases
ARTICLE IN PRESS
The Breast (2007) 16, 411–419
THE BREAST
0960-9776/$ - sdoi:10.1016/j.b
�Correspondifax: +55 21 262
E-mail addr(A. Vallejo da S
www.elsevier.com/locate/breast
ORIGINAL ARTICLE
Oncoplastic surgery of the breast: Rationale andexperience of 30 cases
Andre Vallejo da Silvaa,�, Claudinei Destroa, Wilhermo Torresb
aBreast Service, Antonio Pedro Universitary Hospital, Federal Fluminense University, Niteroi,Rio de Janeiro, BrazilbPathology Service, Antonio Pedro Universitary Hospital, Federal Fluminense University, Niteroi,Rio de Janeiro, Brazil
Received 21 November 2006; accepted 31 January 2007
KEYWORDSBreast cancer;Reconstructive surgi-cal procedures;Oncoplastic surgery;Oncological safety
ee front matter & 2007reast.2007.01.014
ng author. Tel.: +55 2127279.ess: andre@saudedamailva).
Summary A definition of oncoplastic surgery of the breast is presented, and itsobjectives and advantages over the usual conservative procedures are discussed.The oncological safety of these procedures are demonstrated, especially in surgeryof larger tumors. Technical possibilities are discussed and a classification of theprocedures presented. Data from 30 cases operated in our institution are depicted.The need for better training of the breast surgeon is discussed and the advantages ofthe same surgeon to perform the whole procedure presented.& 2007 Elsevier Ltd. All rights reserved.
Introduction
Oncoplastic surgery of the breast defines the set oftechniques used along with oncological techniquesfor the prevention or correction of breast defor-mities caused by surgical cancer treatment.
The goals of modern breast cancer surgeryinclude the cure of the patient, preserving thebreast as much as possible and satisfying thewoman by giving her physical and psychologicalwelfare.
Elsevier Ltd. All rights reserv
26227279;
ma.org
Mostly, the response of breast surgeons to thischallenge has been the use of traditional ablativetechniques based on margin-free resection andprimary synthesis of the tissues
This approach, though appropriate from the pureoncological point of view, usually do not satisfy thepatient’s esthetic hopes, creating dissatisfactionwith her body image, which may lead to severalproblems, including treatment non-compliance andeven worse oncological outcome.
Conservative surgery has an esthetic goal. Thereason behind its existence is to preserve thenormal aspect of the breast as much as possible,contributing to the women’s body image and self-esteem. Otherwise, we would still be performingmastectomies for all cases, considering this is the
ed.

ARTICLE IN PRESS
Figure 1
A. Vallejo da Silva et al.412
gold standard for the surgical treatment of breastcancer.
So said, results like that in Fig. 1 may beperfectly acceptable from the oncological point ofview, but are a disaster to the patient’s cosmeticaspirations.
The use of oncoplastic procedures brings the bestof both worlds: While it allows optimal oncologicaltreatment, it satisfies the woman’s desire for anormal body look, as it has been demonstrated bymany authors.1–6
Advantages
Advantages of oncoplastic surgery include:
(1)
The possibility of treating larger tumors with aconservative approach, preserving the breast ofa greater number of women. This preservationmay include (and usually do) procedures on thecontra lateral breast to ensure a symmetricalappearance.(2)
Larger margins free of tumors are achieved,since it’s possible to resect larger amounts ofbreast tissue, what shall result in less localrelapses.7–9(3)
Resecting more then 400 g of breast tissue,especially when the contra lateral breast is alsoreduced, brings a risk reduction of 40% ormore.10(4)
Better quality radiotherapy can be delivered tolarge and fatty breast, because of better dosehomogeneity.11,12The association of the above factors leads to abetter oncological outcome. It is to be noted that a
better psychological profile is believed to help inthis outcome.
Oncological safety
Although the cosmetic result is important totreatment, it cannot impair the oncologicalresult. We know that conservative surgery isfeasible whenever it does not impair theoverall survival of the patient. When severalmodalities of conservative treatment are to becompared, low local recurrence rates are theultimate goal.
The main causes of local relapses are insufficientresection (positive margins) and multifocallity.Holland, in his classic paper,13 demonstrated thatthe possibility of obtaining free marginsrelated to the extensiveness of the excision, andthat multimodality was not different in tumorsbelow or above 2 cm. Macmillan, studying thecavities of 300 lumpectomies, found 39.3% ofresidual disease, not related to the tumor size.14
A very interesting paper from Vaidya et al.15
analyzes 30 mastectomies specimens, relatingmultifocality to tumor size, but showing that thesize of the ablative margin to obtain free specimensis the same, regardless of tumor size. Asgerisson etal.16 revised the main prospective and retrospec-tive papers which analyzed tumor size as aprognostic factor for local relapse, and found thatthere is no reason to exclude the possibility ofconservative surgery on tumor size grounds exclu-sively. Not to be forgotten is the paper from Kannaet al.17 that have operated conservatively tumorsup to 12 cm with no local relapses when freemargins were obtained. Also, it is widely acceptednow that all patients treated with less then a totalmastectomy should receive radiotherapy as part ofthe treatment, to avoid unacceptable rates of localrecurrences.18,19
The conclusion that can be drawn from literatureis that although we do not know what is the idealintraoperative free margin to obtain the bestresults, it is unacceptable to live viable tumor cellsat the margins of resection20 and that the like-lihood of local relapses are related to the possibi-lity of obtaining free margins, not the tumor size byitself.
In face of all this evidence, we must say thatconservative surgery is possible every time that:
(1)
Free margins can be obtained. (2) There are no contraindications to radiotherapy. (3) The breast/tumor volume ratio allows a resec-tion with good cosmesis.

ARTICLE IN PRESS
Oncoplastic surgery of the breast: Rationale and experience of 30 cases 413
Technical possibilities
We divide the technical approaches to oncoplasticsurgery into three categories:
(1)
T
ATHP
Classical mamaplasty techniques (Pitanguy,Liacyr Ribeiro, wise pattern, etc.).
(2)
Usage of distant flaps for partial reconstruction(i.e. latissimus dorsi flaps).(3)
Atypical local flaps from breast tissue.We cannot stress enough the importance ofpreoperatory planning, that has to be doneconsidering in advance the kind of reconstructionintended. That shall be done by the breast surgeonhimself, if he is to perform the whole procedure, orby him and the reconstructive surgeon in a two-team approach. Though the former has consider-able advantages21 it is still less common to havesurgeons with experience in both areas. Intra-operatory margin control performed by the pathol-ogist is also mandatory.
Large breasts (‘‘donator breasts’’) are moresuitable to 1 and 3 procedure type, while smallones (‘‘receptor breasts’’) are more likely to need atype 2 procedure.
Techniques best suited for particular tumorlocations are discussed below in this paper.
Material and methods
We reviewed the charts of all patients submitted tooncoplastic surgery for breast cancer in ourinstitution between 2003 and 2006, including thosewho had neoadjuvant chemotherapy for tumorreduction, which we use whenever seems indi-cated. All patients were operated by the two seniorbreast surgeons of our breast service (AVS and CD)who are trained in both oncological and recon-structive procedures. All patients had sentinellymph node examination after blue dye localization(tumors up to 3 cm without previous chemotherapy)or axillary dissection (all others and positivesentinel patients). Patients were studied for age,tumor size, histological type, location, margin
able 1
Mean Range
ge 48.6 34–67umor size 2.58 0.7–8 cmistological typereop. chemoterapy
status on frozen and permanent sections, surgicaltechnique used for reconstruction, preoperatorychemotherapy, surgical complications and localrelapse occurrence. Resected specimens wereassessed by the pathologist just after resections.Specimens are inked, margins measured and anysuspect limit examined by cytology and frozensections, according to our institution protocol.Paraffin sections are then obtained for histolo-pathological and immunohistochemical studies.Margins considered to be positive or close areimmediately enlarged by the surgeon. Oncologicalsafety being of ultimate importance, any suspecttissue is resected, regardless of the impact it mayhave in the process of reconstruction. All surgicalinstruments are then exchanged, and local recon-struction is carried out with the most suitabletechnique by the same breast surgeon that re-sected the tumor. Immediate contralateral syme-trization is accomplished in all cases where theclinical status allows for longer procedures, beingthe standard approach. After discharge from thehospital, all patients are seen by the clinicaloncologists, which prescribe the appropriate ad-juvant treatment and radiotherapy protocol thathas been given to every patient (5500 cGy dividedin 4 weeks plus a local boost when advised by theradiotherapist). Patients are then followed forlifetime every 6 months, with mammograms beingthe standard radiological method, complementedby ultrasound whenever needed. Breast MRI is notcurrently available in our institution.
Results
Patient, procedures and tumor characteristics ofthe 30 patients are summarized in Tables 1–6. Witha median follow-up of 15.5 months, ranging from4 to 27.8 months, only one patient relapsed10 months after radiotherapy in the form ofinvasive carcinoma in the same site of the primarytumor, indicating insufficient resection. She hadbeen operated for a 3 cm invasive carcinoma atthe superior half of the breast, with a 5mmfree margin. On intraoperative frozen sections,
Infiltrating ductal—28 In situ ductal-2Yes-2 No-18

ARTICLE IN PRESS
Table 2
Technique Liacyr I Liacyr III Liacyr V Pitanguy Latissimus dorsi L-shape Round block Atypical
No. of cases 15 3 2 5 2 1 1 1
Table 3
Location SUP RA INF JEXT JINT
No. of cases 14 4 5 4 3
SUP: superior quadrants; RA: retroareolar; INF: inferior quadrants; JEXT: external quadrants intersection; JINT: internalquadrants intersection.
Table 4
Margin status Free Close Positive
No. of cases 28 1 1Average margin (cm) 1.4 0.1 —
Range (cm) 0.3–6.0 — —
Table 5
pT No. of cases
pTis 2pT1 16pT2 10pT3 2
Table 6
Surgical complications
Wound infection 2Areolar necrosis 1Areolar depigmentation 1
A. Vallejo da Silva et al.414
high-grade intraductal carcinoma was found on themedial, lateral and deep surfaces that wereenlarged by the surgeon, then obtaining free limits,which were confirmed in permanent sections. Totalmastectomy has been her secondary procedure.
As for the complications, two patients had smallwound infections at the junction of the ‘‘T’’ scarthat were managed conservatively and healed well.
One patient had depigmentation of both areolas,but the patient declared to be satisfied with thefinal result and declined dermopigmentation. Onepatient had suspicious tissue under the areola closeto the areolar pedicle region at the time of surgeryand that tissue was removed. We decided to livethe areola in place as we were not certain of itsviability. It evolved with dry necrosis, that wasmanaged conservatively, and that occurrence didnot postpone her adjuvant radiotherapy. She isplanned to have nipple-areolar reconstruction 6months after the conclusion of adjuvance.
One patient had negative margins on frozensections but became positive on permanent sec-tions. As it was considered a focal involvement, shedecided to have chemo and radiotherapy only,without further surgery. This patient is now with 24months of follow-up with no sign of relapse.
Discussion
Tumor size varied from 7mm to 8 cm. This broadrange, that includes very small tumors that couldcertainly be resected by standard techniques withgood cosmesis, shows that our approach aims thebest overall outcome. This way, even small tumorsin large breasts are handled by oncoplastic techni-ques with contralateral symetrization, so that thepatient can have the oncological benefits of largemargins and better radiotherapy, plus achieving abetter esthetic appearance, usually much betterthen before the operation. Most of these patientsalready wished for reductive breast surgery thatthey could not have for economical reasons, so theoncoplastic approach acts like a plus, diminishingher stress with the overall situation. Figure 2 shows

ARTICLE IN PRESS
Figure 2
Figure 3
Oncoplastic surgery of the breast: Rationale and experience of 30 cases 415
an example where symetrization was done in asecond procedure, and allows for observation ofthe difference in the quality of life that can beachieved with such approach. Even in cases likeFig. 3a and b, where the breast are more ptoticthen large, the final result brings great joy for thepatient, thus allowing for much better acceptanceof the treatment and of the whole situation.
As it has been shown, if clear margins can beachieved and intraoperative monitoring is of greathelp in this pursue, though even then no one canguarantee that all neoplastic cells have beenresected,22,23,24 tumor size is of no concern,because its importance is about overall survivaland not about local relapses.
The ideal situation is that where the surgeon istrained in both oncological and reconstructivesurgery, so that he can plan the most suitableapproach from the very first time the patients areseen. One obvious advantage of this approach isthat though multidisciplinary teams are desired, inthe real world, especially in developing countries,it’s not always feasible to have different teamsworking closely on all stages of the process, fromthe initial visits to the operating room and after.Even when this is possible, is our opinion thathaving one professional handling both problemsultimately leads to better results, for the flow ofthinking is continuous. Not to be forgotten is theeconomical advantage. This idea has beenshared by many breast surgeons around theworld,25,21,2,26–28 and represents a natural evolu-tion of our specialty.
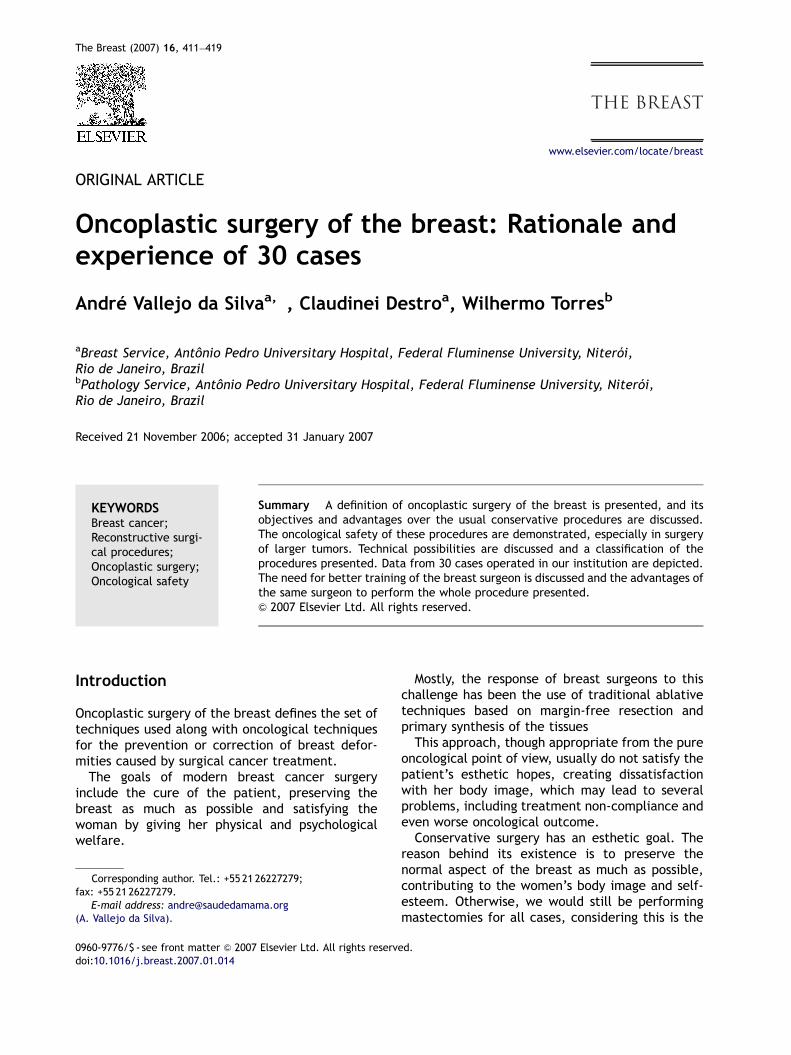
Concerning the technique used for reconstruc-tion, we found that in the tumors of the upperquadrants, the inferior gland flaps developed by
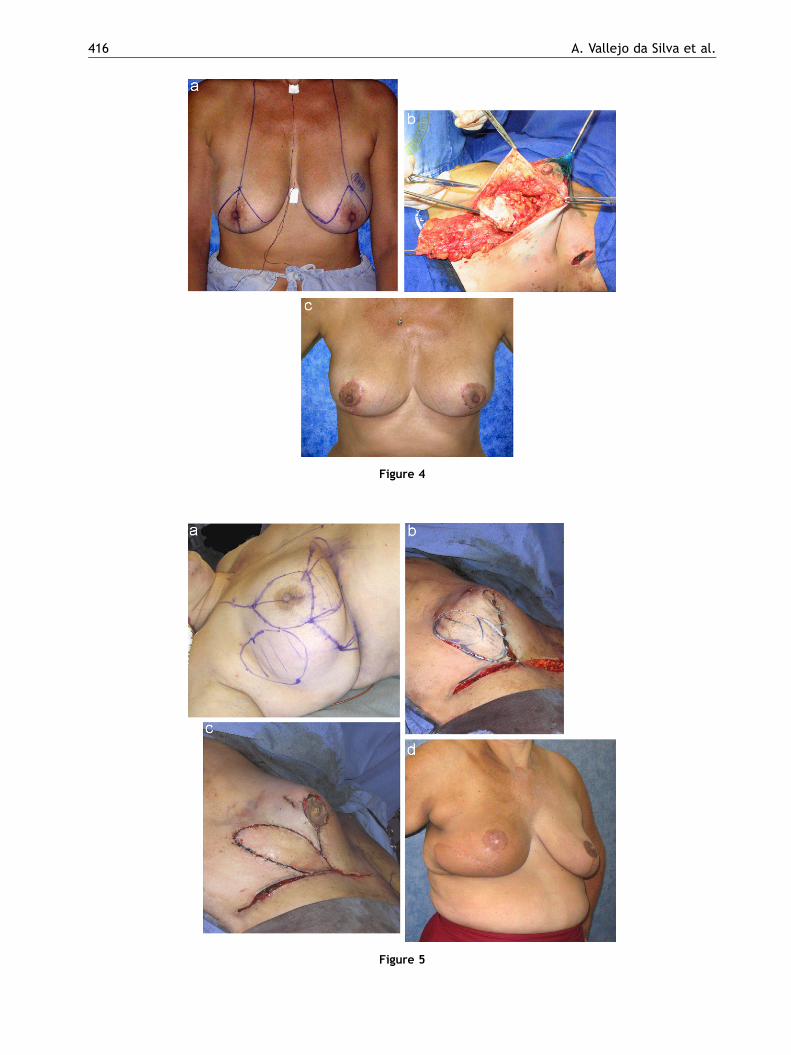
Dr. Liacyr Ribeiro (types I, III and V)29,30 are themost useful for replacing the glandular defects atthe same time that reshape the breast in a easy andpredictable way. When skin is not invaded, resec-tions can be done from below after underminingthe necessary inferior periareolar skin, removingthe inferior-lateral portions of the gland (the wholeinferior breast tissue will be used in the type IIIflap) and shaping the inferior flap, as shown inFigs. 4a–c. This greatly facilitates the treatment oftumors in the internal quadrants, which are usuallymore difficult to handle in a cosmetic way. Evenwhen skin above the tumor is to be removed, theuse of such flaps with its original skin can provideall the necessary tissue for the repair of the area(Figs. 5a–d).
Tumors in the inferior quadrants are usu-ally easily handed by most of the available
ARTICLE IN PRESS
Figure 4
Figure 5
A. Vallejo da Silva et al.416

ARTICLE IN PRESS
Figure 6
Oncoplastic surgery of the breast: Rationale and experience of 30 cases 417
mammaplasty techniques, because most of theminclude the resection of the inferior, medial andlateral pole of the breast. The gold standard forthese procedures is the ancient Pitanguy techni-que, mother of all others.31,32
The so called receptor breast, small glands that donot have spare tissue to donate, are better handledwith use of distant flaps, being latissimus dorsi themore useful among them. Along with the simplicityof its execution, it can be used with or without skin,depending on the patients needs, and when used forvolume replacement of lateral gland defects, themuscle only can be retrieved by the same incisionused for the oncological resection (Figs. 6a–c) aspreviously demonstrated,33,34 thus sparing anotherscar, along with it’s own complications.
Small tumors in moderate-sized breast withelastic skin and little ptosis can be well managedwith the periareolar round-block technique, whichgives excellent approach to the tumor and thesmallest scars possible (Figs. 7a and b).
There are plenty of other techniques that can beused creatively to solve particular problems ofparticular patients. The greater the knowledge andskill of the surgeon in the use of such procedures, thebetter will be the chances that every patient willreceive the best-tailored treatment for her problem.
Free margins are much easier to achieve with thisapproach then with conventional techniques, since
the amount of tissue that can be resected yet givingexcellent cosmetic results is much greater. Thisalone would be enough reason for its use. Alongwith the fact that it allows us to treat conserva-tively patients that otherwise would be doomed tomastectomy and eventually whole breast recon-struction (which is a much more complicatedprocedure with results that not always stand upfor patients expectations) oncoplastic surgery is tobe considered an excellent tool that should be inevery breast surgeon arsenal.
Another possibility that must be evaluated in thefuture, considering the current protocols underinvestigation on intraoperative radiotherapy (IOR),which seems to demonstrate that whole breastirradiation may not be necessary in all cases, is thatoncoplastic techniques that often allow for all thetissue around the tumor that would be irradiated inIOR to be removed (specially in the lower poletumors), may avoid the need of radiotherapy at all.
Conclusion
The use of oncoplastic techniques in conservativesurgery of the breast offers a wide range ofpossibilities to the breast cancer patients. We cannow offer breast conservation in larger tumors, yetproviding better margins and therefore a better

ARTICLE IN PRESS
Figure 7
A. Vallejo da Silva et al.418
local prognosis. Reductions in breast volume, oftenbilaterally, also enhance the patient’s chances ofa better oncological outcome, by reducing thepossibilities of methacronic tumors to appear, andby allowing radiotherapy to be more effective.
Preserving the women self image by preservingher breast normal look and many times evenenhancing its appearance, greatly improves thepatient’s adherence to the treatment, and may alsoresult in higher cure rates, for the psychologicalrepercussion on the immune system.
Our experience with oncoplastic proceduresshowed that creative use of reconstructive techni-ques can yield excellent results, fulfilling all theseexpectations with a minimum rate of morbidity. Sowe conclude that oncoplastic surgery should be thestandard approach to breast cancer treatmentwhenever feasible.
For all of that can be a reality in the near future,training of breast surgeons must be planned to beas complete as possible, so that they can achieveproper expertise in all areas of breast surgery.
References
1. Clough KB, Kroll SS, Audretsch W. An approach to the repairof partial mastectomy defects. Plast Reconstr Surg1999;104(2):409–20.
2. Clough KB, Lewis JS, Couturaud B, Fitoussi A, Nos C, FalcouMC. Oncoplastic techniques allow extensive resections forbreast-conserving therapy of breast carcinomas. Ann Surg2003;237(1):26–34.
3. Stolier A, Allen R, Linares L. Breast conservation therapywith concomitant breast reduction in large-breastedwomen. Breast J 2003;9(4):269–71.
4. Woerdeman LAEM, Hage JJM, Thio EAM, Zoetmulder FANM,Rutgers L, Emiel J. Breast-conserving therapy in patientswith a relatively large (T2 or T3) breast cancer: long-termlocal control and cosmetic outcome of a feasibility study.Plastic Reconstruct Surg 2004;113(6):1607–16.
5. Baildam AD. Oncoplastic surgery of the breast. Br J Surg2002;89(5):532–3.
6. Giacalone PL, Roger P, Dubon O, El Gareh N, Daures JP,Laffargue F. Lumpectomy vs oncoplastic surgery for breast-conserving therapy of cancer. A prospective study about 99patients. Ann Chir 2006.
7. Katz A, Strom EA, Buchholz TA, Theriault R, Singletary SE,McNeese MD. The influence of pathologic tumor character-istics on locoregional recurrence rates following mastect-omy. Int J Radiat Oncol Biol Phys 2001;50(3):735–42.
8. Park CC, Mitsumori M, Nixon A, Recht A, Connolly J, GelmanR, et al. Outcome at 8 years after breast-conserving surgeryand radiation therapy for invasive breast cancer: influenceof margin status and systemic therapy on local recurrence.J Clin Oncol 2000; 18(8):1668–75.
9. Bland KI. Surgical margins in breast cancer: how wide? Howaccurate? How big? Does it make a difference? Curr Surg2001;58(3):248–53.
10. Brinton LA, Persson I, Boice Jr. JD, McLaughlin JK, FraumeniJFJ. Breast cancer risk in relation to amount of tissueremoved during breast reduction operations in Sweden.Cancer 2001;91(3):478–83.

ARTICLE IN PRESS
Oncoplastic surgery of the breast: Rationale and experience of 30 cases 419
11. Moody AM, Mayles WP, Bliss JM, A’Hern RP, Owen JR, Regan J,et al. The influence of breast size on late radiation effectsand association with radiotherapy dose inhomogeneity.Radiother Oncol 1994;33(2):106–12.
12. Neal AJ, Torr M, Helyer S, Yarnold JR. Correlation of breastdose heterogeneity with breast size using 3D CT planningand dose-volume histograms. Radiother Oncol 1995;34(3):210–8.
13. Holland R, Veling SH, Mravunac M, Hendriks JH. Histologicmultifocality of Tis, T1-2 breast carcinomas. Implications forclinical trials of breast-conserving surgery. Cancer1985;56(5):979–90.
14. Macmillan RD, Purushotham AD, Mallon E, Love JG, GeorgeWD. Tumour bed positivity predicts outcome after breast-conserving surgery. Br J Surg 1997;84(11):1559–62.
15. Vaidya JS, Vyas JJ, Chinoy RF, Merchant N, Sharma OP, MittraI. Multicentricity of breast cancer: whole-organ analysis andclinical implications. Br J Cancer 1996;74(5):820–4.
16. Asgeirsson KS, McCulley SJ, Pinder SE, Macmillan RD. Size ofinvasive breast cancer and risk of local recurrence afterbreast-conservation therapy. Eur J Cancer 2003;39(17):2462–9.
17. Khanna MM, Mark RJ, Silverstein MJ, Juillard G, Lewinsky B,Giuliano AE. Breast conservation management of breasttumors 4 cm or larger. Arch Surg 1992;127(9):1038–41discussion 1041.
18. Gennaro M, Ferraris C, Guida V, Tomasic G, Carcangiu ML,Greco M. Conservative surgery in breast cancer. Signifanceof resection margins. Breast 2001;10(5):432–7.
19. Fisher B, Anderson S, Redmond CK, Wolmark N, WickerhamDL, Cronin WM. Reanalysis and results after 12 years offollow-up in a randomized clinical trial comparing totalmastectomy with lumpectomy with or without irradiation inthe treatment of breast cancer. N Engl J Med 1995;333(22):1456–61.
20. Singletary SE. Surgical margins in patients with early-stagebreast cancer treated with breast conservation therapy. AmJ Surg 2002;184(5):383–93.
21. Rainsbury RM. Training and skills for breast surgeons in thenew millennium. ANZ J Surg 2003;73(7):511–6.
22. Haga S, Makita M, Shimizu T, Watanabe O, Imamura H,Kajiwara T, et al. Histopathological study of local residualcarcinoma after simulated lumpectomy. Surg Today1995;25(4):329–33.
23. Akazawa K, Tamaki Y, Taguchi T, Tanji Y, Miyoshi Y, Kim SJ, etal. Preoperative evaluation of residual tumor extent bythree-dimensional magnetic resonance imaging in breastcancer patients treated with neoadjuvant chemotherapy.Breast J 2006;12(2):130–7.
24. Wazer DE, Schmidt-Ullrich RK, Schmid CH, Ruthazer R,Kramer B, Safaii H, et al. The value of breast lumpectomymargin assessment as a predictor of residual tumor burden.Int J Radiat Oncol Biol Phys 1997;38(2):291–9.
25. Rew DA. Towards a scientific basis for oncoplastic breastsurgery. Eur J Surg Oncol 2003;29(2):105–6.
26. Acea-Nebril B, Lopez S, Cereijo C, Bazarra A, Pais P, UriarteI, et al. Impact of conservative oncoplastic techniques in asurgery program for women with breast cancer. Cir Esp2005;78(3):175–82.
27. Baum M. Is it time for a paradigm shift in the training ofbreast surgeons as a sub-speciality? Breast 2003;12(3):159–60.
28. Hoffmann J. Is it time for a paradigm shift in the training ofbreast surgeons as a sub-speciality? Breast 2004;13(1):83.
29. Ribeiro L. Pedıculos em mamoplastia. Rio de Janeiro:Guanabara Koogan; 2005.
30. Ribeiro L, Accorsi Jr. A, Buss A, Marcal-Pessoa M. Creationand evolution of 30 years of the inferior pedicle in reductionmammaplasties. Plast Reconstr Surg 2002;110(3):960–70.
31. Pitanguy I. Mammaplasty. Study of 245 consecutive casesand presentation of a personal technic. Rev Bras Cir1961;42:201–20.
32. Pitanguy I. A new technic of plastic surgery of the breast.Study of 245 consecutive cases and presentation of apersonal technic. Ann Chir Plast 1962;7:199–208.
33. Rainsbury RM. Breast-sparing reconstruction with latissimusdorsi miniflaps. Eur J Surg Oncol 2002;28(8):891–5.
34. Dixon JM, Venizelos B, Chan P. Latissimus dorsi mini-flap:a technique for extending breast conservation. Breast 2002;11(1):58–65.






![CIVIL CASES] [FRESH (FOR ADMISSION) - CRIMINAL CASES]](https://static.fdokumen.com/doc/165x107/633739bdd63e7c790105b19d/civil-cases-fresh-for-admission-criminal-cases-1682892728.jpg)













