Örebro Studies in Medicine 110 MATHIAS VON BECKERATH
82
Photodynamic therapy in the Head and Neck
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Örebro Studies in Medicine 110 MATHIAS VON BECKERATH

Photodynamic therapy in the Head and Neck

To my family, the light of my life that cures all my ailments
Mathias

Örebro Studies in Medicine 110
MATHIAS VON BECKERATH
Photodynamic Terapy in the Head and Neck

© Mathias von Beckerath, 2014
Title: Photodynamic therapy in the Head and Neck
Publisher: Örebro University 2014 www.oru.se/publikationer-avhandlingar
Print: Örebro University, Repro 08/2014
ISSN 1652-4063 ISBN 978-91-7529-039-3

Abstract Mathias von Beckerath (2014): Photodynamic therapy in the Head and Neck. Örebro Studies in Medicine Photodynamic therapy, PDT, is a method to diagnose and treat cancer. In PDT a sensitizer is administered to the patient and this sensitizer is accumulated in tumors. If the sensitizer-containing tumor is subjected to a laser of a specific wavelength the tumor is fluorescing allowing diag-nostics. If other wavelengths are used a process involving reactive oxy-gen species and singlet oxygen is started and the tumor cells are killed. This process thus requires oxygen as well.
This thesis investigates how UV-induced damage of the skin and dif-ferent physiological factors of the skin influences the uptake of 5-aminolevulinic acid, ALA, and its conversion to the active sensitizer protoporphyrin IX, PpIX. It shows that UV-induced damage affects both the uptake and production of PpIX. UV-induced damage lowers the PpIX produced after ALA application both if the damage is acute and in chronically UV-affected skin.
The PpIX production differs inter and intra individually. When look-ing how different physiological factors affect the PpIX production after topically applied ALA the thesis shows that an increase of temperature increases the production. No correlation between the formation of PpIX and the density of hair follicles was found and a weak correlation was seen comparing the epidermal and total dermal thickness and PpIX production
The thesis also shows how PDT is used in treating laryngeal malig-nancies. It shows that it is possible to cure laryngeal tumors (both squa-mous cell carcinomas and sarcomas) using PDT primarily, and that the cure rate as well as outcome of voice and patient safety is comparable to the conventional treatment modalities.
PDT can also be used as a function and organ sparing treatment for re-curring laryngeal cancers, both squamous cell carcinomas and sarcomas. Keywords: Photo Dynamic Therapy, Cancer, Skin, Larynx, 5-ALA, UV-radiation, sarcoma, squamous cell carcinoma, porfimer sodium, temo-porfin, voice
Mathias von Beckerath, School of Medicine Orebro University, SE-701 82, Örebro, Sweden [email protected]


Table of Contents/Innehållsförteckning
ABBREVIATIONS ............................................................................................. 9
THE THESIS IS BASED ON THE FOLLOWING STUDIES .................. 10
INTRODUCTION: ............................................................................................ 11 A short history of PDT: ....................................................................................... 11 Photodynamic action ........................................................................................... 13 Sensitizers .............................................................................................................. 15 Oxygen: ................................................................................................................. 18 Lasers and other light sources: ........................................................................... 19 Light delivery: ....................................................................................................... 21
ORGANS AND TISSUE STUDIED .............................................................. 21 Skin ......................................................................................................................... 21
Skin tumors ...................................................................................................... 22 PDT in dermatology ....................................................................................... 22
Larynx ................................................................................................................... 23 Laryngeal tumors ............................................................................................. 25 PDT in the Head and Neck ........................................................................... 26
AIMS .................................................................................................................... 27
MATERIALS ...................................................................................................... 28 Animals: ................................................................................................................ 28 Healthy volunteers: .............................................................................................. 28 Patients ................................................................................................................. 28
METHODS ......................................................................................................... 32 Sensitizers ............................................................................................................. 32 UV-exposure: ........................................................................................................ 33 Topical application: ............................................................................................. 34 Fluorescence measurements: .............................................................................. 34 Physiological parameters: .................................................................................... 34 Spots measured: ................................................................................................... 34 Treatment of patients with laryngeal malignancies ........................................... 35 Sensitizer in patients ........................................................................................... 36 Illumination of patients treated ......................................................................... 38 Follow up ............................................................................................................. 40

Results of treatment of patients with laryngeal malignancies (Study three and four) ........................................................................................................... 46
DISCUSSION ..................................................................................................... 51 UV-exposure ......................................................................................................... 51 Factors influencing PpIX production ............................................................... 52 Topical sensitizers in the head and neck area ................................................... 54 PDT in laryngeal malignancies ............................................................................ 55 Laryngeal recurrences .......................................................................................... 57 Illumination of the larynx ................................................................................... 59 Systemic sensitizers ............................................................................................. 59 Sarcomas ............................................................................................................... 59 Voice .................................................................................................................... 60 Costs .................................................................................................................... 60 Safety .................................................................................................................... 60 Future .................................................................................................................... 61
CONCLUSION .................................................................................................. 62
ACKNOWLEDGEMENTS ............................................................................. 63
REFERENCES .................................................................................................... 65
PAPERS ............................................................................................................... 76 The influence of UV exposure on 5-aminolevulinic acid-induced protoporphyrin IX production in skin .............................................................. 76 Influence of Physiological Parameters on the Production of Protoporphyrin IX in Human Skin by Topical Application of 5-Aminolevulinic Acid and its Hexylester. ............................................................................................................ 81 Outcome of primary treatment of early laryngeal malignancies using photodynamic therapy ....................................................................................... 90 Outcome of treatment of recurring laryngeal malignancies using photodynamic therapy ........................................................................................ 98
RESULTS ............................................................................................................ 40

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 9
Abbreviations ALA 5-aminolevulinic acid BC Before Christ CoA Coenzyme A CR Complete Response ENT Ear, Nose and Throat EU European Union Hex-ALA Hexyl-aminolevulinic acid HpD Hematoporphyrine Derivate HPV Human Papilloma Virus IR Infrared LE Laryngectomy LED Light Emitting Diode m-THPC meta-tetra-hydroxy-phenylchloride (temo-
porfin) TLE Total Laryngectomy MED Minimal Erythema Dose Met-ALA Methyl-aminolevulinic acid Mo Months nm Nano Meter PBDG Porphobilinogen Deaminase PDD Photodynamic diagnostics PDT Photodynamic therapy PLE Partial Laryngectomy PpIX Protoporphyrin IX PR Partial Response PS Photo Sensitizer RT Radio Therapy SCC Squamous Cell Carcinoma Tis Tumor in situ TLS Trans oral Laser Surgery UV Ultraviolet USÖ Örebro University Hospital w/w Weight to weight

10 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
The Thesis is based on the following studies 1. von Beckerath M, Juzenas P, Ma LW, Iani V, Löfgren L, Moan J. The influence of UV exposure on 5-aminolevulinic acid-induced protoporphyrin IX production in skin. Photochem Photobiol. 2001 Dec;74(6):825-8. PubMed PMID: 11783939. 2. Beckerath Mv, Juzenas P, Löfgren L, Ma L-W, Iani V, Malik Z, et al. Influence of Physiological Parameters on the Production of Proto-porphyrin IX in Human Skin by Topical Application of 5-Aminolevulinic Acid and its Hexylester. Journal of Medical Sciences. 2006;6(4):546-53. 3. von Beckerath MP, Reizenstein JA, Berner AL, Nordqvist KW, Landstrom FJ, Lofgren AL, et al. Outcome of primary treatment of early laryngeal malignancies using photodynamic therapy. Acta Otolaryngol. 2014 Aug;134(8):852-8. PubMed PMID: 24856450. 4. Mathias P. von Beckerath, MD;Johan A. Reizenstein, MD; Fredrik J. Landström, MD; Gun-Britt Adamsson, RN ; Claes G Möller MD, PhD. Outcome of treatment of recurring laryngeal malignancies using pho-todynamic therapy, In Manuscript

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 11
Introduction: Photo Dynamic Therapy, PDT, is a technique whereby cancer can be treat-ed and diagnosed. It has a long history and is in some medical specialties a common and accepted treatment of cancer. One example is the treatment of non-melanoma skin cancer (1). In this thesis the use of PDT in both skin and other tissues in the head and neck area will be studied.
In the head and neck area PDT has been used for decades in a research setting but it wasn’t until the 1990’s that sensitizers were commercially available.
A sensitizer can be administered systemically (intravenously or orally) or topically (a cream or a patch).
This thesis consists of four studies. The first two parts are studies in a la-boratory setting concerning factors that influence a topically applied sensi-tizer. The other two studies evaluate the clinical effect of PDT in primary laryngeal cancer and as a treatment of recurrences of laryngeal cancer.
Lennart Löfgren was the pioneer who introduced PDT at the ENT-clinic in Örebro. He introduced it in the late 1980’s and worked with PDT active-ly until his retirement.
Since the introduction over 200 treatments on over 130 patients have been performed at the clinic. The great majority of patients have been treated for malignant tumors. Other indications have been laryngeal papil-loma and basalioma (one patient with Gorlins syndrome was treated more than 40 times).
The first two studies in this thesis were in collaboration with prof Moans group at Radiumhospitalet in Oslo, Norway. This group has a long experi-ence in PDT, especially topically applied ALA and its esters.
The two later studies are based on treatments at the University Hospital in Örebro.
The author, Mathias von Beckerath, is a head and neck surgeon, trained and working at the ENT-clinic at the University Hospital in Örebro, Swe-den since 1995. He has actively worked with PDT since 1997.
A short history of PDT: Light as therapy has been used for several thousand years starting in India, Egypt and China. The first description of the combination of a sensitizer and light is from 1400 BC. In one of India’s sacred books Atha-rava-veda there is a description on how the seeds of the plant Psoralea Cory-

12 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
lifolia can be used for the treatment of vitiligo (2). Psoralens are a group of sensitizers.
Fig 1: Psoralea Corylifolia, picture from Wikimedia
The concept of PDT is over one hundred years old. It was first described by Raab(3). He studied the toxic effect of the malaria drug chinin on parame-cium. During incubation experiments there was one instance when the paramecium only survived 1,5 hours instead of 15 hours. The observant Raab noted that the only difference between the experiments had been a thun-derstorm and thus he stumbled on the combined effect of sensitizer and light. It was however his supervisor von Tappeiner who coined the name Photodynamic (4).
A number of experiments were carried out during the years 1908-13 using hematoporphyrine in different cultures and animals. The German doctor Friedrich Meyer Betz tried to inject himself with 200 mg hematoporpyrine and became very photosensitive for two months (5). Dyes were also used in treatment of tumors and short term results were seen but there was no long time follow up. During this time the antitumor effect of ionizing radiation

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 13
was discovered and this attracted a much larger interest and PDT attracted less interest and was more or less forgotten (2).
Fig 2: Friedrich Meyer Betz during and after the photodynamic effect.(5)
The modern PDT started with the work of Dougherty and coworkers who in 1978 at Roswell Park (re)discovered the anti-tumor effects of PDT. Their work resulted in the first commercial PDT sensitizer Photofrin (6).
Photodynamic action Three prerequisites are necessary for PDT to work:
• A sensitizer • Light of a specific wavelength • Oxygen.
Another fundament of PDT is that each part required for PDT is harmless by itself (in clinical doses) or if one of the prerequisites is absent. But to-gether they are lethal for the cells that take part in the action.
Photosensitizer + Light gives a singlet state photosensitizer. This singlet state photosensitizer can either give away fluorescence or convert to a more stable triplet state by intersystem crossing. This triplet state photosensitizer is sufficiently long lived to partake in a photodynamic action (7).

14 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
Fig 3: Photochemical reactions of the excited photosensitizers (Jablonski diagram). A schematic illustration of photodynamic therapy: The Photosensitizer, PS initially absorbs a photon that excites it to the first excited singlet state and this can relax to the more long-lived triplet state. This triplet PS can interact with molecular oxygen in two pathways, type I and type II, leading to the formation of reactive oxygen species (ROS) and singlet oxygen respectively.(8)
The photodynamic action can be of two kinds. It can either partake in an electron or hydrogen transfer reaction producing reactive intermediates that are harmful to cells, such as superoxides, hydroperoxyl (Type I). Or, it can react with oxygen creating singlet oxygen, which is highly reactive (Type II). It is generally considered that Type II photodynamic action is the main source of photodynamic cell toxicity. After the triplet state sensitizer has partaken in the photodynamic reaction it is returned to its original state and can thereby re-enter the process again if there is an activating light and oxy-gen.
Singlet oxygen can in sufficient doses cause necrosis of the cell. In lower concentrations it will cause apoptosis (9).
Singlet oxygen has a short lifetime and range (10) and this is the reason why the PDT-effect is contained in the target cell. The effect stays in the cell where the sensitizer was located and the light was directed at.

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 15
PDT also affects the stroma of the tumor. The vasculature is damaged by the PDT effect. Some sensitizers have less effect on the vasculature (like 5-aminolevulinic acid, ALA) and other sensitizers have more (like porfimer sodium) (11). :
Fig 4: Type II PDT effects can be summarized by a figure by Oleinick and Kessel (12).
Sensitizers A perfect sensitizer would be one that is specifically taken up in tumor cells, which doesn’t accumulate in skin (in head and neck PDT) or normal cells, reaches the target cells quickly, is non toxic, is cheap, is able to be adminis-tered by different ways (e.g. orally, topically) and is activated by light of adequate wavelengths.
Today there are several different sensitizers with different properties. The sensitizers on the market today can be divided into three different groups (13):

16 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
• Porphyrines examples are HpD, porfimer sodium (Photofrin), 5-Aminolevulinic Acid (ALA, Levulan)
• Chlorophylls example is temoporfin (Foscan®) • Dye example is Phthalocyanine (Photosens)
In this thesis HpD, porfimer sodium, 5-Aminolevulinic Acid and temo-porfin have been used.
Hematoporphyrine Derivate, HpD, was the earliest sensitizer used in modern PDT. Its properties as a sensitizer were studied already in the 1960’s. One problem with HpD is that it is a mixture of many molecules with different properties. Therefore when porfimer sodium was extracted from HpD by Thomas J. Dougherty, (6) it was a big step for PDT.
Porfimer sodium is more efficient than HpD and can therefore be used in smaller doses. It is most often used with the dose 2 mg/kg and activation with a laser of 630 nm is done 48 hours later. The time of activation is de-cided by when there is a sufficient level of sensitizer in the tumor cells and when the ratio between normal and tumor cells is most favorable. It is not clearly understood or known why HpD and porfimer sodium is accumulated in a higher degree in tumor cells. HpD and porfimer sodium are today commercial products. Porfimer sodium is sold under the name of Photo-frin®. HpD and porfimer sodium are both given systemically in most treatments but have also been administered topically as injections.
5-Aminolevulinic acid or ALA is a precursor in the synthesis of Hem. It occurs naturally in the cells, in the mitochondria. It is in several steps con-verted into hem and one of those steps is protoporphyrin IX (PpIX). There is a negative feedback so the process is halted when the levels of hem are high enough but this feedback works on the step before ALA (Succinyl CoA + Glycine). Therefore the production of PpIX is not halted when we admin-ister ALA (7). The activity of porphobilinogendeaminase seems also to be high in some tumors (14). The step between PpIX and Hem, the enzyme Ferrochelatase, has a limited capacity (15).

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 17
Fig 5: Hem biosynthesis pathway showing how increased intracellular amounts of 5-ALA can increase the amount of Protoporphyrine IX, PpIX (14)
This means that if ALA is administered a high dose it will give a high con-centration of PpIX, the active PDT molecule, and ALA is therefore a pre-cursor. ALA can be administered as a topical application in a cream, thermo gel or bio adhesive patch, or be taken orally, inhaled as an aerosol or injected in-travenously. It is among other indications used in neurosurgery for diagnos-tic purposes and in dermatology in treatment of non-melanoma skin cancers and for treatment of precancerous lesions. Many different esters of ALA such as Met-ALA and Hex-ALA are used as well. They have different properties compared to ALA. Another reason for research of esters is that they can be patented and can thereby yield a higher economic gain than ALA, which is an orphan drug.
Temoporfin or meta-tetra-hydroxy-phenylchloride (m-THPC) is sold un-der the name Foscan® and was the first PDT-sensitizer that was registered in Europe. It was first registered for use in the head and neck area. It is more potent than HpD or porfimer sodium and the dose used is normally
and for treatment of precancerous lesions.

18 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
0,15 mg/kg. The time between the injection of temoporfin and activation is 4 days. This means that less sensitizer is needed but the side effects are similar as with other systemically used sensitizers. The activation of temo-porfin is with a laser of the wavelength 650 nm and that is an advantage compared to the previously mentioned porphyrines because that wavelength penetrates deeper into tissue than 630 nm does (16).
Fig 6: Molecular structure of temoporfin
Temoporfin is also subject to many studies where it is used in liposomal formulation, as nanoparticles. The idea is that it would give the sensitizer new properties such as a higher ratio between tumors and normal tissue as well as faster uptake in tumors. So far it seems as if both Foslip® and Fospeg® (temoporfin in liposomes) are promising as intravenous and topical sensitizers. There are also studies on modification of the m-THPC molecule to change its properties (compare with ALA and met-ALA or hex-ALA) (17)
A possibility to use temoporfin topically would very much facilitate the clinical use. The patient light sensitivity and the time between injection and activation are two issues that pose problems for the patient and makes the PDT more expensive since the treatment often is not done in an outpatient setting. The injection can also for some patients be painful.
Oxygen: One of the important parts of PDT is the presence of oxygen. This is more difficult to control than sensitizer or light activation. It is important during the treatment to allow as much oxygen into the tissue as possible. Therefore

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 19
one should avoid local anesthetics containing adrenaline for example. It is probably important that the patient refrains from smoking at the time of treatment. This is however not proven in studies. Another way of increasing the possibilities of a high oxygen level is to fractionate the treatment whereby the concentration of oxygen is allowed to rise during the dark peri-ods (18).
Lasers and other light sources: When PDT is used as a diagnostic (PDD, Photo Dynamic Diagnostics) either the auto fluorescence in the tumor or the fluorescence from a low dose sensitizer such as ALA is used. The auto fluorescence is much lower or absent in malignant or premalignant tissue so it is possible to see a differ-ence compared to normal tissue. If the patient is given ALA, as an inhala-tion, cream or orally it will result in a fluorescence that is higher in tumors than in normal tissue and thereby the tumor is visualized (19)
Fig 7: Picture from Kraft et al(19). Invasive carcinoma. White light endoscopy (A) demonstrates a bulging tumor of the right vocal fold. Auto fluorescence endoscopy (B) shows a marked loss of auto fluorescence, whereas induced fluorescence endos-copy (C) displays a strong protoporphyrin IX fluorescence.
The light that is used for diagnostics is of a shorter wavelength than that used for treatment. The wavelength is around 4-500 nm and therefore it doesn’t penetrate as deep into the tissue, it can only penetrate to 3-500 μm. This should be taken into consideration during diagnosis. The energy need-ed to visualize fluorescence is sufficiently achieved by using a normal light source.
When PDT is used as a treatment however other wavelengths of light and stronger light sources are needed. In order to activate the sensitizer a light of a certain wavelength and of a sufficient energy is required. A laser is

20 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
very useful for PDT since it gives light of a very specific wavelength and it can produce high energy.
The wavelength is the most important factor of penetration. An increase in wavelength increases the penetration depth up to a wavelength of about 1100 nm. The increase of depth is quite significant with light between 500 and 900 nm (20).
Fig 8: The optical penetration depth of human skin (above) and mucosa (below). The optical penetration depth is the depth where the light intensity has dropped to 1/e (close to 37 %)(20) Note that the penetration in mucosa is much higher.
Different lasers and light sources can be used for PDT. In ALA-PDT a laser is not required so red light diodes (LED) giving a wavelength of 630 nm are sufficient. For HpD and porfimer sodium a gold-vapor laser that gives a red

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 21
light of 628 nm can be used. This wavelength is ideal for porphyrines. For temoporfin a special diode-laser from Biolitec® that emits a light of the wavelength 652 nm is often used.
Light delivery: The light can be delivered to the tumor or the area subject to diagnostics in different ways.
Diagnostics need a lower light intensity and therefore it is sufficient to use a conventional light source equipped with filters. One example is Storz D-light®. It is also possible to use computer-enhanced pictures and soft-ware to further facilitate the PDD (Photo Dynamic Diagnostics). The light therefore can be delivered by the means we normally use, such as through endoscopes.
In the treatment setting the light that has to be delivered needs to be much more intense. Therefore a laser is often needed. The light from the laser is guided through a fiber and delivered to the intended site. At the site the light can be delivered by a variety of means. Most commonly a micro lens is used for surface application.
To reach deeper into tissue, for example to treat tumors that are thicker than one centimeter, the light has to be administered interstitially. This can clinically be done by either a cylindrical diffusor that is put in an arterial catheter or a preformed applicator that can be inserted into the tissue. In treatment of laryngeal cancer a vocal cord applicator can be used, which is an example of the latter.
It is also possible to control the positions of the interstitial fibers with ul-trasound or computer tomography. Organs and tissue studied Skin The skin’s purpose is to protect. It keeps the body’s internal environment and protects against mechanical trauma, heat, cold, light, chemical sub-stances and microorganisms from the outside.
The skin consists of three layers: the epidermis, the dermis and the sub-cutaneous layer. In the epidermis there is a keratin layer that is an im-portant part of the skin’s protection (21). In PDT this layer is hard to pene-trate for topically applied sensitizers. Since skin tumors have a damaged keratin layer this accounts for some of the selectivity of PDT. If you how-

22 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
ever prepare the skin over the tumor further with curettage it does not in-crease the PDT effect (22).
The skin also has adnexa such as hair follicles and sebaceous glands. It has been shown that these sebaceous glands take up sensitizers to a higher de-gree than normal skin (23).
Skin tumors UV-exposure because of sunlight is the most common etiology of skin can-cer. The tumors in the skin range from slow growing non-metastatic tumors such as most basal cell cancers to malignant melanoma that can be life threatening. Skin cancers are normally easy to reach with both topical sensi-tizers and lasers. It is in this group that PDT has the most common use.
PDT in dermatology Today treatment with the sensitizers 5-ALA and Met-ALA are used clinical-ly in a large scale. The sensitizers are used topically and normally applied under an occlusive dressing. One of the mechanisms of PDT selectivity is that tumors often have a damaged stratum corneum and this facilitates the penetration of the sensitizer.
The light sources are both non-coherent and lasers. Non-coherent light sources have many advantages; they are cheaper, can cover larger areas and require less maintenance. They however have a lower irradiance and there-fore require longer treatment time (24)
In dermatology PDT is used for a variety of pathologies. Examples are Squamous Cell Carcinoma, Actinic Keratosis, Acne Vulgaris, Basal Cell Carcinoma, Actinic Chelitis, Viral infections, cutaneous T-cell lymphoma and various cosmetic applications (25).
When it comes to non melanoma skin tumors the advantages are a prov-en good effect (except SCC where there is insufficient data), good cosmetic outcome and it is preferred by patients compared to other therapies (1). Especially patients who have recurring dermatologic tumors such as patients with Gorlins syndrome and patients who have received organ transplants have a benefit of PDT (26).
In the present study the variability of PpIX production is studied. It is frequently observed that there clinically is a large variability among
patients with respect to the sensitivity of normal skin to PDT. Further-more, the sensitivity of skin on different body localizations appears to be different, there is an inter and intra individual difference. Different parts of

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 23
the body also react differently to exposure from solar radiation, mostly be-cause of the history of sun exposure
The chronic changes in solar exposed skin are mostly induced by the UV-radiation. The skin protects itself against prolonged UV-radiation by tan-ning and thickening of the epidermis (27, 28). UV-radiation also causes non-tumorous acute changes such as erythema, pigment regeneration and skin thickening (29). These reactions are thought to be in response to the UV-radiations carcinogenic effects (30).
It has been shown that ALA-PDT delays the development of UV-induced skin tumors in hairless mice (31).
In short there is one acute reaction to UV-radiation and one chronic. Since UV-light is one of the most important etiologies for tumors of the skin and ALA-PDT is able to both delay and treat skin tumors it would be interesting to see whether the skins UV-induced changes influences ALA-PDT.
The large differences between individuals and in an individual also make ALA-PDT efficiency unpredictable (32, 33). It is known that factors such as high activity in the rate limiting enzyme porphobilinogen deaminase (PBDG) (34), temperature (35), permeability and integrity of the overlying skin (36) and vehicle composition (37) play a role. In our study we looked at factors that vary between individuals and are easily measurable. We looked at how these factors influenced PpIX production in skin after application of topical ALA and its esters.
Larynx The larynx has two main purposes. One is to generate sound that can be converted into speech in the oral cavity and the other is to protect the air-way from aspiration of food and drink destined for the esophagus.
The larynx extends superiorly to the dorsal side of the epiglottis and infe-riorly to the caudal edge of the cricoid. Peripherally it includes the laryngeal framework that consists of the cartilage of the thyroid and cricoid.
The subdivisions of the larynx are subglottic (below the vocal cords), glot-tis and supraglottic (above the vocal folds).
24 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
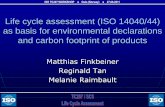
Fig 9: Cross section of the larynx. From a from a public domain edition of Gray's Anatomy.
The muscles of the larynx are divided into intrinsic, that move the vocal cords to phonate or to facilitate breathing, and the extrinsic that support and position the larynx. Innervation is by the superior and recurrent laryn-geal nerves that both originate from the vagal nerve (38).
The vocal folds, or vocal cords, are stretched between the arytenoid carti-lage and the anterior commissure at the thyroid cartilage. Above the vocal folds are the false cords or folds.

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 25
The vocal folds have a delicate lining below the mucosa and exteriorly of the vocal ligament called Reinke’s space. This space is important to voice quality and is easily disturbed by treatments of the larynx or chronic irrita-tion i.e. smoking.
Laryngeal tumors Tumors in the larynx are one of the most common tumors in the Head and Neck Area (39, 40). The most common tumors are squamous cell carcino-mas. The most common etiology is smoking (41) but alcohol is also associat-ed with increased risk (42).
The larynx is in some patients the site for troublesome papilloma virus in-fections and it has now been established that HPV also is a risk factor for laryngeal cancer (43).
There are also carcinoid tumors and sarcomas of the larynx but these are much more unusual.
Laryngeal cancer has a worldwide incidence of 1.6 per 100,000 in males and 0.4 per 100,000 in females (age-standardized rate); in Sweden, the inci-dences are 3.1 and 0.6 per 100,000, respectively . Laryngeal cancer is the third most common head and neck cancer in Sweden (39).
Currently, laryngeal cancers are generally treated with surgery or radia-tion therapy. The more common surgical treatment for early laryngeal can-cer is presently trans-oral laser surgery (TLS); open laryngeal surgery for early laryngeal cancer is less common (44).
Radiation therapy and TLS provide comparable cure rates and voice out-comes (45). However, TLS has some disadvantages. TLS can be technically complicated and results are closely linked to the experience of the individual surgeon (46). The vocal cords also must be readily visualized to allow laser surgery.
Radiotherapy is a more lengthy therapy and also requires experience. Fur-thermore, if the area has been irradiated previously, radiotherapy may be hazardous and thus is usually avoided. This treatment can also induce future cancers in the long term (47).
The results of early laryngeal cancer treatment are very good. However, sometimes neither of the two dominant treatment modalities is suitable.
Primary treatment of laryngeal T1 and T2 cancer has similar curates for RT, 66--‐95%, and TLS, 76--‐96% (48). But if recurrences occur there is some controversy over the best treatment. Total laryngectomy is the most successful relapse treatment but organ-sparing treatments such as TLS and partial laryngectomy are options. The results of those treatments are well

26 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
described when TLS is used as a relapse treatment after radiotherapy and about 1/3 of the recurrences after RT are considered to be suitable for TLS (49). Fewer studies have been conducted on treatment of a relapse after TLS and it seems that retreatment with TLS after recurrence after TLS is associ-ated with decreased survival and larynx preservation (50).
PDT in the Head and Neck Tumors in the head and neck area are in many ways suitable for PDT. They are often visible and therefore available to illumination. In the US and EU Barrett's esophagus, obstructing esophageal carcinoma and early and obstructing tracheobronchial carcinoma is approved using the photosensitizer porfimer sodium (Photofrin®). In Europe temoporfin (Fos-can®) is approved in early head and neck cancer as well as a palliative treat-ment for head and neck cancer (European Medicines Agency EMEA/H/C/000318).
Tumors of the oral cavity, both malignant and pre-malignant have been successfully treated as well as naso- oro and hypopharyngeal cancers. Benign lesions such as hygroma and vascular lesions are also possible to treat with PDT (51).
At our clinic we have experience in treating head and neck cancers with PDT since 1988. We have used HpD, porfimer sodium and temoporfin. The treated tumors have included nasopharynx, tongue, floor of mouth, bucca, oropharynx, hypopharynx, skin and larynx.
We have treated laryngeal cancer with PDT in over 20 cases when the conventional therapies were less suitable.

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 27
Aims The aim of this thesis were to:
• Investigate whether UV-induced erythema has any influence on the ability of mouse skin to produce PpIX from ALA.
• Compare PpIX-fluorescence in human skin frequently exposed to solar radiation with skin exposed rarely to solar radiation.
• Investigate and compare the production of PpIX from ALA and its hexylester derivative with respect to various physiological parame-ters of human skin.
• Evaluate results of primary PDT in laryngeal cancer, (squamous cell carcinomas (SCC) and sarcomas).
• Describe the results of photodynamic treatment of recurring laryn-geal cancer after primary treatment with radiation or surgery.

28 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
Materials Animals: 26 Female nude BALB/c mice 8-24 weeks of age were used for the animal experiments in study one. BALB/c mice have been frequently used in PDT-studies. The choice of nude mice was done to facilitate cream application and occluding dressing. Animals were used in study one.
Healthy volunteers: Seven healthy male volunteers age 25-55 (mean 36.9 years) were included in the studies on locally applied ALA in humans. None of the volunteers had a history of skin disease or excessive burning of the sun. One had a signifi-cantly less history of sun exposure of cultural reasons. Healthy volunteers were used in study one and two.
Patients Örebro University Hospital, USÖ, is a tertiary referral hospital. Between 1993 and 2012 we had 310 cases of malignant laryngeal tumors. The treat-ment and local outcome of the T1 and T2 tumors is shown here:

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 29
Tab 1: Early malignant laryngeal tumors and their treatment according to T-stage. RT-Radio Therapy, Rec – recurrence, PDT – Photodynamic therapy, Surgery de-notes surgery with or without laser.
PAPER IV
9
7. Biel M. Advances in photodynamic therapy for the treatment of head and neck cancers. Lasers Surg Med. 2006 Jun;38(5):349-‐55. PubMed PMID: 16788923.
8. von Beckerath MP, Reizenstein JA, Berner AL, Nordqvist KW, Landstrom FJ, Lofgren AL, et al. Outcome of primary treatment of early laryngeal malignancies using photodynamic therapy. Acta Otolaryngol. 2014 Aug;134(8):852-‐8. PubMed PMID: 24856450.
9. Hartl DM. Evidence-‐based practice: management of glottic cancer. Otolaryngol Clin North Am. 2012 Oct;45(5):1143-‐61. PubMed PMID: 22980690.
10. Abdurehim Y, Hua Z, Yasin Y, Xukurhan A, Imam I, Yuqin F. Transoral laser surgery versus radiotherapy: systematic review and meta-‐analysis for treatment options of T1a glottic cancer. Head Neck. 2012 Jan;34(1):23-‐33. PubMed PMID: 21374753.
11. Biel MA. Photodynamic therapy treatment of early oral and laryngeal cancers. Photochem Photobiol. 2007 Sep-‐Oct;83(5):1063-‐8. PubMed PMID: 17880501.
12. Matoscevic K, Graf N, Pezier TF, Huber GF. Success of Salvage Treatment: A Critical Appraisal of Salvage Rates for Different Subsites of HNSCC. Otolaryngol Head Neck Surg. 2014 Jun 3. PubMed PMID: 24894422.
13. Zbaren P, Weidner S, Thoeny HC. Laryngeal and hypopharyngeal carcinomas after (chemo)radiotherapy: a diagnostic dilemma. Curr Opin Otolaryngol Head Neck Surg. 2008 Apr;16(2):147-‐53. PubMed PMID: 18327034.
14. Zbaren P, Nuyens M, Curschmann J, Stauffer E. Histologic characteristics and tumor spread of recurrent glottic carcinoma: analysis on whole-‐organ sections and comparison with tumor spread of primary glottic carcinomas. Head Neck. 2007 Jan;29(1):26-‐32. PubMed PMID: 17103406.
15. Schweitzer VG. PHOTOFRIN-‐mediated photodynamic therapy for treatment of early stage oral cavity and laryngeal malignancies. Lasers Surg Med. 2001;29(4):305-‐13. PubMed PMID: 11746107. Epub 2001/12/18. eng.
16. Freche C, De Corbiere S. Use of photodynamic therapy in the treatment of vocal cord carcinoma. J Photochem Photobiol B. 1990 Jul;6(3):291-‐6. PubMed PMID: 2120406. Epub 1990/07/01. eng.
17. Rigual NR, Thankappan K, Cooper M, Sullivan MA, Dougherty T, Popat SR, et al. Photodynamic therapy for head and neck dysplasia and cancer. Arch Otolaryngol Head Neck Surg. 2009 Aug;135(8):784-‐8. PubMed PMID: 19687399. Pubmed Central PMCID: 2810853.
18. Yoshida T, Kato H, Okunaka T, Saeki T, Ohashi S, Okudaira T, et al. Photodynamic therapy for head and neck cancer. Diagn Ther Endosc. 1996;3(1):41-‐51. PubMed PMID: 18493416. Epub 1996/01/01. eng.
19. Kraft M, Betz CS, Leunig A, Arens C. Value of fluorescence endoscopy for the early diagnosis of laryngeal cancer and its precursor lesions. Head Neck. 2011 Jul;33(7):941-‐8. PubMed PMID: 21674669.
134 T1
97 RT
9 Rec
4 Surgery
3 Cured
5 PDT
2 Cured after
additional
surgery
3 Cured after
PDT
25 Surgery
2 Rec
1 PDT 1 Cured
1 No treatment
11 PDT
3 Rec
2RT 2 Cured
1 New PDT
1 Cured
1 No treatment
74 T2
68 RT
8 Rec
5 Surgery
3 Cured
3 PDT
2 Cured after
additional
surgery
1 Cured after
PDT alone
6 Surgery
2 Rec
1 Laryngectomy
Cured
1 PDT and then
Laryngectomy
Cured

30 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
All patients that are diagnosed with a head and neck malignancy or are re-ferred to Örebro University Hospital go through a three-day program as inpatients in our clinic. At that time diagnostics such as CT and pathology evaluation are looked at and completed, if needed. A head and neck sur-geon, if needed under general anesthesia, examines all patients. If needed additional examinations and tests are performed. Many patients and all laryngeal cancer patients are also examined by a phoniatrician. At the end of the three days a multi disciplinary tumor board (MDT) is held where all patients are presented, most often in person. There the decision is made what therapy is best suited for the patient. In study three and four the re-sults of patients treated with PDT for laryngeal cancer are shown.
As demonstrated in the graphics above most patients were considered best treated by RT. The number of patients treated with surgery has in-creased in later years with an increase of TLS but the numbers of patients treated by RT are still much higher. This trend is in concurrence with inter-national trends (44).
At times neither RT nor TLS is suitable as a treatment. TLS is less suita-ble for example if the visualization during direct laryngoscopy is impaired, the surgeon is inexperienced, and the anterior commissure is involved. RT can be a bad choice for example if the area has been radiated before, the tumor is less suitable for radiation treatment or the patient has claustro-phobia.
When used to treat recurrences TLS is only suitable in 1/3 of the cases (49) and RT can normally not be repeated. Therefore PDT was used to a higher degree in recurrences than in primary tumors.
In our material PDT was chosen most often when there were contraindi-cations like the ones described but three patients also chose PDT on their own accord. When PDT was chosen as a recurrence therapy the reason was most often to avoid laryngectomy.
MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 31
Pat nr Age Sex Smo-
ker Location T AI Histol-ogy
1 73 Female No Supraglottis 1 No SCC 2 80 Male Yes Glottis 1 No SCC 3 86 Male Yes Glottis 1 Yes SCC 4 70 Male Yes Glottis 1 No SCC
5 60 Male Previ-ous Glottis 1 Yes SCC
6 58 Male Previ-ous Glottis 1 No
Chon-drosar-coma
7 78 Male Yes Glottis 1 Yes SCC
8 48 Male No Subglottis 1 No Liposar-coma
9 56 Male No Subglottis 1 No Chon-drosar-coma
10 35 Female Yes Subglottis 1 No
Pleo-morphic Undif-ferenti-
ated sarcoma
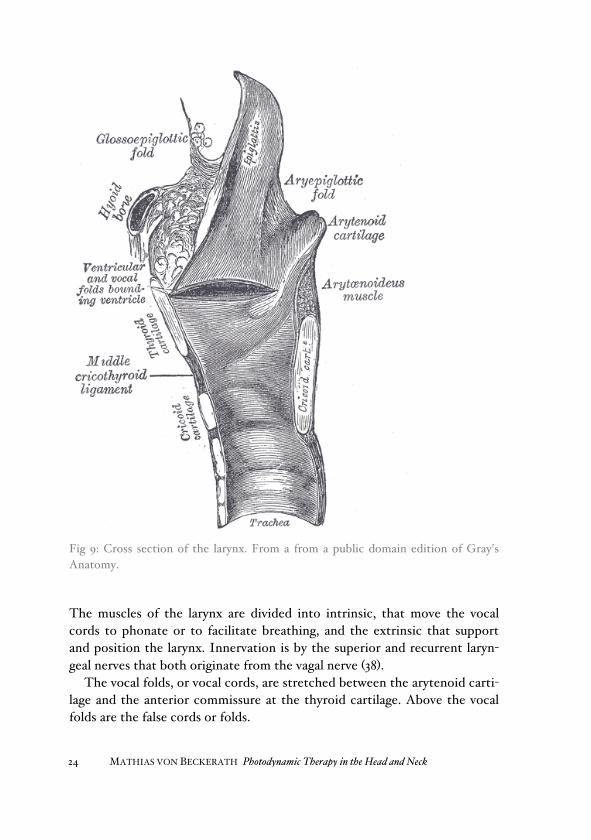
Tab 2: Above: Details of the10 patients that were treated with PDT as primary treatment. T – Tumor stage, SCC – Squamous cell carcinoma AI- Aneterior Comis-sure involvement

32 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
Nr Age T Histology Previous Treatment
1 58 T2 SCC PLE/TLS
2 40 T3 SCC RT
3 81 T2 SCC RT
4 74 T1a SCC RT
5 65 T2 SCC RT/PLE/TLS
6 70 T1a Fibrosarcoma TLS
7 54 T1a SCC RT
8 74 T1a SCC RT
9 46 T2 SCC RT
10 62 T1 SCC RT, TLS
11 35 T1 Pleomorphic Undifferenti-‐ated sarcoma
PDT
Tab 3: Above: Details of the 11 patients treated with PDT for recurrence. PLE- Partial Laryngectomy, SCC-Squamous cell carcinoma, T- Tumor stage, RT-Radiotherapy, TLS-Trans Oral Laser Surgery. N.B. Patient 11 is identical with pa-tient 10 in the group treated primarily with PDT.
Methods Sensitizers We used ALA in study one and two and its hexylester derivate (ALA-Hex) in study two, both obtained from Photocure ASA, Oslo, Norway, Both were used as topical application. We used porfimer sodium (Photofrin®, Pinna-cle Biologics, Bannockburn, IL, USA) or temoporfin (Foscan®, Biolitec Pharma Ltd, Dublin, Ireland) in patients with laryngeal malignancies.

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 33
UV-exposure: The acute UV-exposure of the mice in study one was achieved with a com-mercial sunlamp (Philips, The Netherlands), where the IR sources were blocked with two aluminum sheets. To prevent overheating the mouse was also protected with aluminum except for a hole that was 2 cm in diameter. Only one side of the mouse was subjected to UV-light allowing the mouse to be its own control. The total radiation fluence rate was approximately 70mW/cm2 and the fluence rate of UVA radiation (310-400 nm) was 1,8mW/cm2 at the position of mouse exposure.
The minimal erythema dose (MED) was calculated by exposing mice to the UV-source. Different parts of the skin were subjected to UV-light for 1, 2, 4, 7, 14 and 21 minutes and the skin reactions were evaluated after 24 hours. An obvious edema and redness was noted after 7 min of exposure and increased exposure did not increase the effect.
Fig 10: Emission spectrum of the Philips TLD 18W/08 lamp tube that was used for erythema induction in mice. The graph shows the intensity at the position of the exposed mouse skin. During UV-exposure and at the beginning of the cream application the mice were anesthetized with an intraperitoneal injection of fenta-nyl/fluanisone (Hypnorm®) and midazolam (Dormicum®). Only during the ALA-application they were kept in the dark.

34 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
For the humans in study one spots on the body were chosen that resem-bled each other in pairs but differed in chronic sun exposure, the skin of the arm below and above the T-shirt sleeve.
Topical application: The ALA compounds used in study one and two were dissolved in an oint-ment (Unguentum Merck, Merck, Darmstadt, Germany) on a weight-to-weight basis (w/w). Approximately 0,1 g of freshly prepared cream was ap-plied on selected spots and covered with a transparent dressing (OpSite Flexigrid, Smith and Nephew Medical Ltd, Hull, UK).
Fluorescence measurements: The amount of PpIX induced by ALA in study one and two was measured by measuring PpIX fluorescence according to a method described by Moan et al (52). In short a luminescence spectrometer (Perkin Elmer LS50B, Nor-walk, CT, USA) equipped with a photomultiplier (R928, Hamamatsu, Japan) and an non-invasive fiber optic probe. The excitation wavelength was 407 nm and the fluorescence measured was at 637 nm. This corresponds to the maxima of PpIX excitation and emission in skin and is a good way of meas-uring the PpIX concentrations in skin (53).
Physiological parameters: In study two the influence of physiological parameters on PpIX production was studied. The number of hair follicles was counted with a magnifying glass in an area of 0,8 cm2. The temperature was measured with a thermal couple (KM45 Kane-May Ltd, Welwyn Garden City, UK) immediately before the application of the cream. An ultrasound machine with a 30 MHz transducer (DermaScan C ver 3, Cortex Technology, Hadsuns, Denmark) was used to measure the epidermal and skin thickness.
Spots measured: In the study of UV-exposure (study one) mice were their own control so the mice were measured on both sides of the body while only one side had been subjected to UV-light. They were measured every hour through the ALA cream except in the short-term analysis where the cream was removed after ten minutes.
On humans spots were chosen above and below the T-shirt sleeve (upper and lower arm) for the UV-study (study one). In the study of physiological

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 35
parameters (study two) the following spots were chosen: upper and lower arm, the neck above and below the collar, on the back and side of thorax and in four subjects on the top of the ear and behind it. In humans PpIX production was measured every hour for five or six hours.
Treatment of patients with laryngeal malignancies In study three and four treatment of laryngeal malignancies with PDT was studied. If the MDT deemed PDT to be the most suitable treatment the patient was planned for the treatment within one month. The patient was admitted to the ENT-ward as an inpatient and was given an injection of the sensitizer the first day.
Tab 4: Below: Details of the PDT when used as primary treatment
Pat nr Sensitizer Dose Illumination Wavelangth
of laser Energy
given
1 Porfimer Sodium
5 mg/kg Surface 628 nm 40 J/cm2
2 Temoporfin 0,15 mg/kg Surface 652 nm 20 J/cm2
3 Porfimer Sodium
2 mg/kg
Surface & Interstitial 628 nm
80 J/cm fibre, 100
J/cm2
4 Temoporfin 0,15 mg/kg Interstitial 652 nm 30 J/cm
fibre
5 Temoporfin 0,15 mg/kg Interstitial 652 nm 30 J/cm
fibre
6 Temoporfin 0,15 mg/kg Surface 652 nm 20 J/cm2
7 Temoporfin 0,15 mg/kg Interstitial 652 nm 30 J/cm
fibre
8 Temoporfin 0,15 mg/kg Interstitial 652 nm 30 J/cm
fibre
9 Temoporfin 0,15 mg/kg Interstitial 652 nm 30 J/cm
fibre
10 Porfimer Sodium
2 mg/kg Surface 630 nm 100
J/cm2

36 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
Sensitizer in patients The sensitizer was more often HpD or porfimer sodium in the first patients and temoporfin more often in the later patients. The reason for this was availability of HpD and porfimer sodium early in the series. Later temo-porfin was approved for head and neck cancer and this explained the change. HpD was given in the dose 2 mg/kg except in one case (patient 1 in the group primarily treated with PDT) where the dose was 5 mg/kg. The dose temoporfin was 0,15 mg/kg except in one patient where it was about ¼ of the dose, 0,0375 mg/kg (patient 5 in the group treated with PDT for a recur-rence). If HpD or porfimer sodium was used, the injection was given two days be-fore the treatment and if temoporfin was used, the injection was given four days before the treatment. In one case the illumination of the patient was delayed because of a laser malfunction. A patient that had received HpD was illuminated after five days. The patients were kept under light restriction and were allowed 100 lux day one and after that 100 lux times the number of days after injection. The light exposure was assessed using a lux-meter that was monitored by the patient.

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 37
Pat nr Sensitizer Dose Illumination Wavelangth
of laser Energy
given
1 Porfimer Sodium x 2
2 mg/kg Surface 628 nm 43-208
J/cm2
2 Temoporfin 0,15 mg/kg Surface 652 nm 39 J/cm2
3 Temoporfin 0,15 mg/kg
Surface & Interstitial 652 nm
25 J/cm fibre, 20
J/cm2
4 Temoporfin x 2
0,15 mg/kg
Surface later Interstitial 652 nm
20J/cm2 & 30 J/cm fibre
5 Temoporfin x 2
0,0375 mg/kg
Surface w cylindrical
fibre 652 nm
35 &45 J/cm fibre
6 Temoporfin 0,15 mg/kg
Surface w cylindrical
fibre 652 nm 30 J/cm
fibre
7 Porfimer Sodium
2 mg/kg
Surface & Interstitial 628 nm
100J/cm2 &240 J/cm fibre
8 Temoporfin x 2
0,15 mg/kg
Surface & Interstitial 652 nm
20 J/cm2 & 25 J/cm
fibre
9 Temoporfin 0,15 mg/kg Interstitial 652 nm 30 J/cm
fibre
10 Temoporfin 0,15 mg/kg Interstitial 652 nm 30 J/cm
fibre
11 Temoporfin 0,15 mg/kg Surface 652 nm 20 J/cm2
Tab 5: Above: Details of PDT when used as treatment for recurrence. X2 stands for two separate treatments. NB Patient 11 is identical as patient 10 in the table before.

38 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
Illumination of patients treated All of the treatments were conducted under general anesthesia. Ventilation was achieved using a microlaryngoscopy tube. A rigid laryngoscope was used, and the light used during laryngoscope placement was kept at the lowest possible level.
To get the light into the treatment area different methods were used. Surface illumination was performed with either a laser fiber equipped with a microlens (QLT, Vancouver, Canada) or a cylindrical fiber. The cylindrical fiber could be shielded on one side. If a microlens was used it was held above the vocal cord in a contraption that held it still.
Fig 11: A vocal cord diffusor
On some patients an interstitial technique was used. One way was to use a custom-built laser fiber; a vocal-cord diffuser (CeramOptec, Bonn, Germa-ny; fig 11). The tip was sharp and rigid and provided cylindrical diffusion of light at a length of 10 or 15 mm. It was introduced into the vocal cords using a special instrument constructed at Örebro University Hospital. The fiber was introduced into the vocal cords at several places so that the tumor and a

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 39
region of approximately 1 cm around the tumor were illuminated. Normally, this was accomplished by introducing the fiber at two or three sites. Anoth-er way to achieve interstitial illumination is to use an intra-arterial catheter and putting a cylindrical fiber inside it (fig 12).
Fig 12: Interstitial illumination schematics
The advantage of the method with the arterial catheter is that the length of the cylindrical fiber can be longer, between 1 and 9 cm long. The same fiber can be used in different locations in the same patient.
The treatment illumination was performed using two different lasers, ei-ther a Biolitec Laser (Biolitec, Jena, Germany) delivering 652 nm light or a gold vapor laser delivering 628 nm light. A physicist calculated the energy to be delivered, and each fiber was calibrated immediately before the treat-ment. The interstitial fiber was also calibrated after each treatment to check for changes. No changes affecting the light emission were noted.

40 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
Follow up After the anesthesia the patient was kept in the ward for another period of four to seven days under continued light restriction. The reason for the prolonged inpatient period was to monitor for adverse events. When the patient went home the light restriction continued according to the same plan and the patient was given a lux meter. The light restriction was continued for six weeks except for the injection site that was recom-mended to keep out of direct sunlight for four months. The reason for this is that there is a suspicion that there may be sensitizer left there for a longer time.
All patients were followed up every two months the first year, every three months the second and third year and biannually for another two years. The indication for direct laryngoscopy and biopsy was very liberal.
To compare costs of the different treatments the hospital’s economic de-partment was asked what a referral hospital would have paid for a typical RT, TLS and PDT patient had it been November 2011.
Results In study one and two the typical PpIX fluorescence spectra with emission peaks at 636 and 705 nm were observed in all spots where ALA was topically applied in both human and mouse skin.
Study one shows how acute UV-damage influenced the uptake and trans-portation of ALA and the PpIX production after a short application time of ALA was looked at. There was a difference between mouse skin with an erythema and the control with a lower transportation and uptake in UV-damaged skin.

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 41
Fig 13: Build-up of PpIX fluorescence in control and UV-exposed mouse skin after 10 min. of topical application of 10% ALA-cream. ALA was applied 24 h after UV-exposure. Error bars show one standard deviation
When the PpIX production in acutely UV-damaged skin was studied it was shown that the production was lower in the damaged skin. This difference was more obvious and could be shown when we applied the cream 24 and 48 hours after the UV-exposure. This is shown in the graphs below.

42 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
4 h
24 h
48 h.
Fig 14: Build-up of PpIX fluorescence in control and UV-exposed mouse skin during continuous topical application of 10% ALA-cream. ALA-cream was applied 4, 24 and 48 h after UV-exposure. Error bars show one standard deviation

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 43
A chronicall UV-damage in human skin did also give a lower PpIX produc-tion. The number of hair follicles, skin thickness and temperature did not differ between the sites and the tanning of skin at the time of the experi-ment was negligible since it was done in early spring.
Fig 15:Build-up of PpIX fluorescence in human skin on upper and lower arm after continuous topical application of 10% ALA-cream. Data represent averages from 6 persons. Error bars show one standard deviation.
In the study of physiological parameters (study two) it was shown that there was a difference between the PpIX productions at different body locations. It could vary as much as a factor two. The spots with a history of sun expo-sure had a lower PpIX production.
44 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
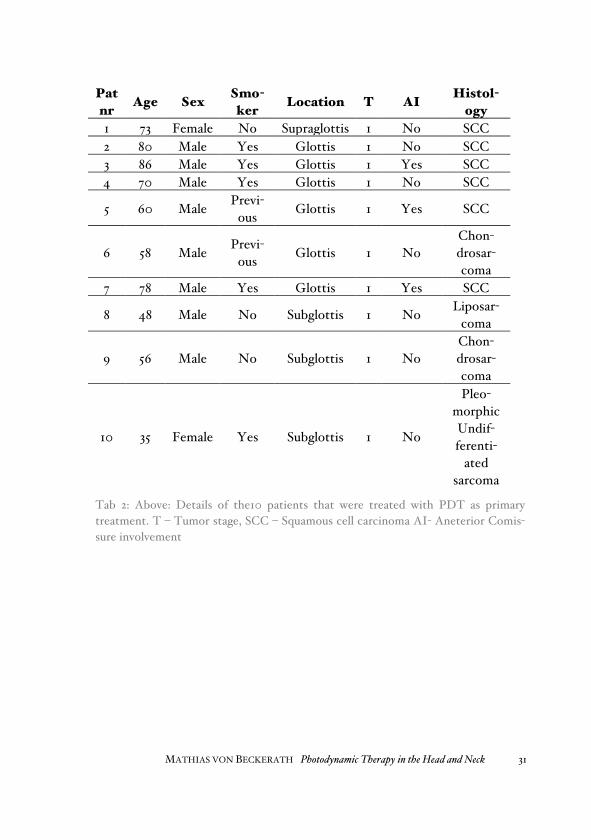
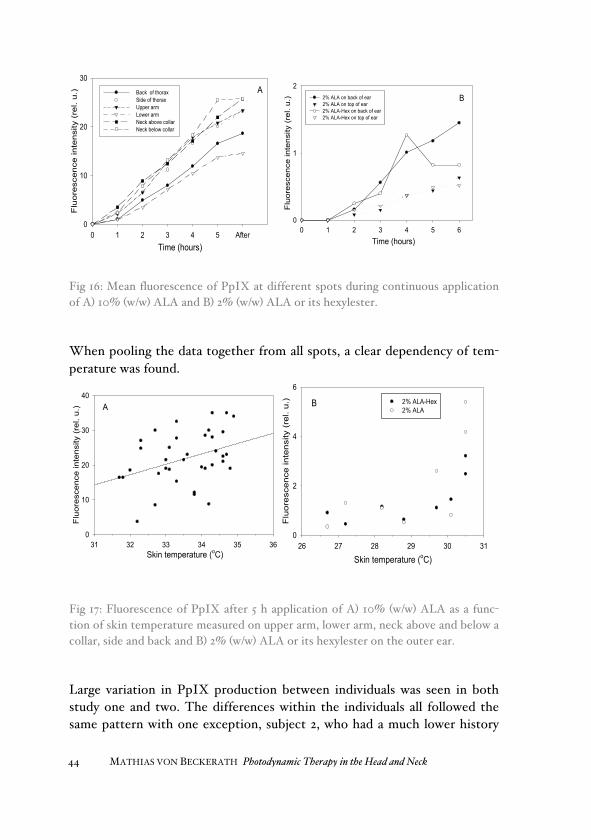
Fig 16: Mean fluorescence of PpIX at different spots during continuous application of A) 10% (w/w) ALA and B) 2% (w/w) ALA or its hexylester.
When pooling the data together from all spots, a clear dependency of tem-perature was found.
Fig 17: Fluorescence of PpIX after 5 h application of A) 10% (w/w) ALA as a func-tion of skin temperature measured on upper arm, lower arm, neck above and below a collar, side and back and B) 2% (w/w) ALA or its hexylester on the outer ear.
Large variation in PpIX production between individuals was seen in both study one and two. The differences within the individuals all followed the same pattern with one exception, subject 2, who had a much lower history
A
Time (hours)0 1 2 3 4 5 After
Flu
ores
cenc
e in
tens
ity (
rel.
u.)
0
10
20
30
Back of thoraxSide of thoraxUpper arm Lower arm Neck above collar Neck below collar
0 1 2 3 4 5 60
1
22% ALA on back of ear2% ALA on top of ear2% ALA-Hex on back of ear2% ALA-Hex on top of ear
Time (hours)
Flu
ores
cenc
e in
tens
ity (
rel.
u.) B
31 32 33 34 35 36
Flu
ores
cenc
e in
tens
ity (
rel.
u.)
0
10
20
30
40
Skin temperature (oC)
A B
Skin temperature (oC)26 27 28 29 30 31
Flu
ores
cenc
e in
tens
ity (
rel.
u.)
0
2
4
6
2% ALA-Hex2% ALA

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 45
of sun exposure for cultural reasons and also a noticeable lower pigmenta-tion in sun exposed areas compared with the other subjects.
Fig 18: Fluorescence of PpIX for different individuals after 5 h application of ALA. The data represent Left: 10% ALA (w/w), Right: 10% ALA (w/w) corrected for the temperature Upper arm (empty bars) Lower arm filled bars.
Fig 19: Fluorescence of PpIX for different individuals after 5 h application of ALA. The data represent Left: 2% ALA (w/w), Right: 10% ALA (w/w) corrected for the temperature Back of ear (empty bars) Top of ear filled bars.
No correlation between the formation of PpIX and the density of hair folli-cles was found and a weak correlation was seen comparing the epidermal and total dermal thickness and PpIX production in study two.
1 2 3 4 5 60
10
20
30Upper arm Lower arm
Fluo
resc
ence
Inte
nsity
(rel
. u.)
Subject #
A
Subject #1 2 3 4 5 6
0
10
20
30Upper arm Lower arm
B
Flu
ores
cenc
e In
tens
ity (
rel.
u.)
1 2 3 40
1
2
3Back of ear Top of ear
C
Fluo
resc
ence
Inte
nsity
(rel
. u.)
Subject # 1 2 3 40
1
2
3Back of ear Top of ear
Flu
ores
cenc
e In
tens
ity (
rel.
u.) D
Subject #

46 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
Fig 20: PpIX production correlated to number of hairs, epidermal thickness and total skin thickness
Results of treatment of patients with laryngeal malignancies (Study three and four)
The follow-up of the patients was between 2 and 170 months. None of the patients died from a local disease. Three patients in the group treated with PDT for recurrence died of regional and distant metastasis despite a laryn-gectomy. No other patients died of their laryngeal cancer
Number of hairs0 10 20 30
Flu
ores
cens
e in
tens
ity (
rel.
u.)
0
10
20
30
40
Epidermal thickness (mm)0.15 0.20 0.25 0.30
Flu
orsc
ence
inte
nsity
(re
l. u.
)
0
10
20
30
40
Skin thickness (mm)1 2 3 4 5 6
Flu
ores
cenc
e in
tens
ity (
rel.
u.)
0
10
20
30
40

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 47
Pat nr Follow up Time until
relapse,
Voice after PDT- treat-ment
Results
1 2 months
Died 2 months after PDT of intercurrent disease
Impossible to assess
Residual laryngeal tu-mor
2 4,7 years 10 months Improved Tumor free after radia-tion treatment of re-lapse
3 32 months 10 months Unchanged Tumor free after radia-tion treatment of re-lapse
4 5,6 years No relapse Improved Tumor free PDT sole modality
5 5,0 years No relapse Unchanged Tumor free PDT sole modality
6 5,9 years No relapse Unchanged Tumor free PDT sole modality
7 4,8 years No relapse Improved Tumor free PDT sole modality
8 24 months No relapse Improved Tumor free PDT sole modality
9 18 months No relapse Improved Tumor free PDT sole modality
10 9,0 years 7 months Unchanged Tumor free after se-cond PDT with temo-porfin
Tab 6: Above: Results of PDT in patients treated primarily
MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 47
Pat nr Follow up Time until
relapse,
Voice after PDT- treat-ment
Results
1 2 months
Died 2 months after PDT of intercurrent disease
Impossible to assess
Residual laryngeal tu-mor
2 4,7 years 10 months Improved Tumor free after radia-tion treatment of re-lapse
3 32 months 10 months Unchanged Tumor free after radia-tion treatment of re-lapse
4 5,6 years No relapse Improved Tumor free PDT sole modality
5 5,0 years No relapse Unchanged Tumor free PDT sole modality
6 5,9 years No relapse Unchanged Tumor free PDT sole modality
7 4,8 years No relapse Improved Tumor free PDT sole modality
8 24 months No relapse Improved Tumor free PDT sole modality
9 18 months No relapse Improved Tumor free PDT sole modality
10 9,0 years 7 months Unchanged Tumor free after se-cond PDT with temo-porfin
Tab 6: Above: Results of PDT in patients treated primarily
Voice after PDT-treatment
48 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
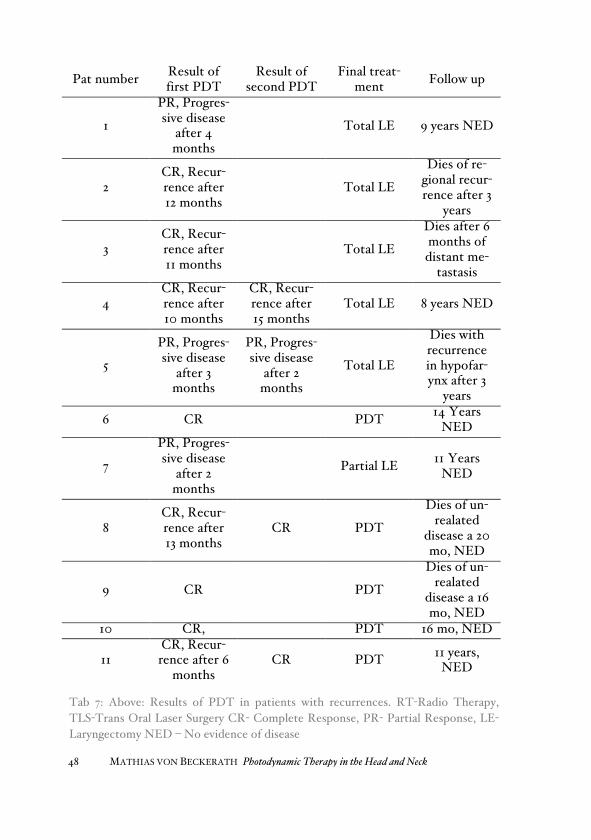
Pat number Result of first PDT
Result of second PDT
Final treat-ment Follow up
1
PR, Progres-sive disease
after 4 months
Total LE 9 years NED
2 CR, Recur-rence after 12 months
Total LE
Dies of re-gional recur-rence after 3
years
3 CR, Recur-rence after 11 months
Total LE
Dies after 6 months of distant me-
tastasis
4 CR, Recur-rence after 10 months
CR, Recur-rence after 15 months
Total LE 8 years NED
5
PR, Progres-sive disease
after 3 months
PR, Progres-sive disease
after 2 months
Total LE
Dies with recurrence in hypofar-ynx after 3
years
6 CR PDT 14 Years NED
7
PR, Progres-sive disease
after 2 months
Partial LE 11 Years NED
8 CR, Recur-rence after 13 months
CR PDT
Dies of un-realated
disease a 20 mo, NED
9 CR PDT
Dies of un-realated
disease a 16 mo, NED
10 CR, PDT 16 mo, NED
11 CR, Recur-rence after 6
months CR PDT 11 years,
NED
Tab 7: Above: Results of PDT in patients with recurrences. RT-Radio Therapy, TLS-Trans Oral Laser Surgery CR- Complete Response, PR- Partial Response, LE- Laryngectomy NED – No evidence of disease

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 49
One serious adverse event was noted. Patient 10 in the recurrence group required a tracheostomy two months after treatment. It was removed after another two months but was replaced again after another 6 months. None of the times he required the tracheostomy it was not done acutely but after about one week of consideration. Ten of the 20 patients did not experience hoarseness after the treatment. One of the 20 patients (Patient 1, primary treatment) had a tracheotomy before the treatment; therefore, hoarseness could not be assessed. Other side effects were one swollen lip and one swol-len tongue (1/20 patients). This was most likely caused by light from the operation microscope that was not fully shielded. In the group treated for recurrences three had pain that required pharmaceutical treatment and four required antibiotics for infections. None in the primarily treated group required pharmaceutical treatment.
In the primarily treated patients, three patients had a tumor relapse. Two relapses occurred 10 months after treatment. Those patients were then successfully treated with radiotherapy. One patient suffered relapse seven months after the PDT and was treated with PDT again, but this time was sensitized with temoporfin instead of HpD. This treatment was successful, with no relapse occurring during nine years of follow-up.
PDT alone cured 7/10 patients in the patients treated with PDT primari-ly. These patients were the last patients treated in this study, and all were sensitized with temoporfin. They have been followed for between one and a half and 9 years. One patient presented with a new laryngeal cancer after five years; however, this was considered a new tumor rather than a relapse because the patient had had a SCC and had been tumor-free for five years. The new tumor was on the same site as the first and the patient was now treated with a laryngectomy.
Five of the 20 patients had sarcomas. If PDT had not been used, they would have been treated surgically with a partial or total laryngectomy. Of the seven sarcomas treated at our clinic since 1988 four were treated suc-cessfully with PDT primarily, one was cured with PDT after repeated at-tempts with TLS and two were treated with open surgery (one partial and one total laryngectomy). The patient treated with a partial laryngectomy died with but not of a recurrence. In all of the patients treated with PDT, the larynx was spared.
All three patients treated primarily with PDT who had a tumor affecting the anterior commissure were treated with interstitial illumination using the vocal cord diffuser, and one of these patients required radiation after the

50 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
PDT. All of the patients were recurrence-free after their treatment with a follow up of 2,6 to 5 years.
The voice assessment was only done in the group treated primarily with PDT. It was difficult to evaluate in 2/10 patients. Patient 1 had an advanced tumor in the oral cavity and had a weak voice. Patient 3 also had a weak voice that was difficult to assess but was considered unchanged.
Of the remaining eight patients, two had good voices both pre- and post-PDT; one had an unchanged, well-functioning voice after PDT; and five had an improved voice after PDT.
The costs of the different treatments in our hospital are shown in the ta-ble below.
Costs nov 2011 TLS PDT RT
Surgery 1 310 € (60 min)
1 310 € (60 min)
Anaesthesia 390 € (90 min)
390 € (90 min)
Postop care 254 € (240 min)
254 € (240 min)
Sensitizer (Temoporfin) 7 998 €
RT 62,5 Gy 7 880 €
In patient care 2 087 € (3 days)
6 260 € (9 days)
Hotel 1 778 € Total 4 041 € 16 212 € 9 658 €
Tab 8: Above: What the referring hospital is charged for treatment costs as of No-vember 2011

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 51
Discussion UV-exposure We have investigated the influence of UV-exposure and other physiological parameters on topical ALA induced PpIX fluorescence in mouse and hu-man skin. Fluorescence and/or production of PpIX at various times after UV-exposure seem to be influenced by UV-induced processes in the skin. The PpIX production also shows an inter and intra individual variation. Some variations can be explained by physiological parameters such as tem-perature and skin thickness.
ALA-diffusion (penetration) can be distinguished from PpIX-production by applying ALA for relatively short and long times, respectively. We have earlier found that the penetration of ALA through the stratum corneum can be measured by applying the drugs for a short time and then, after removal of the drugs, determining the fluorescence intensity of PpIX as a function of time (54). During a short application time (around 10 min.) practically no PpIX is produced, so that the later production is directly related to the amount of ALA that has penetrated into the tissue during short application time. Thus, after a short application time the fluorescence of PpIX is pro-portional to the number of ALA molecules that has diffused through the epidermis. Lower PpIX fluorescence is observed in UV-exposed skin possi-bly indicating decreased ALA penetration in skin (Fig. 13). When ALA is applied continuously on skin, the amount of drug penetrating to the living cells will be larger than after short application time and the amount of PpIX produced will be related to the rate of PpIX-production in the cells (35). Continuous application of ALA after UV-exposure reveals a lasting skin damage. Significant difference in PpIX fluorescence was seen at late times after UV-exposure (Fig. 14).
Disrupted stratum corneum has a marked response to ALA and light (55). Moreover, when ALA and light is applied on sun-exposed areas of human skin such as face and arms, a mild edema is observed, while a combination of ALA and light produces no effect on sun-unexposed areas (56). It is sup-posed that permeability of the stratum corneum may have been altered by UV-exposure and enhanced penetration of ALA occurs through the stratum corneum (31). Prolonged UV-exposure of skin induces stronger skin damage and leads to a higher PpIX production rate after application of ALA-methyl ester in UV-exposed skin than in normal skin (57). Oppositely, we observed lower PpIX fluorescence in skin for short time UV-exposures. This contra-

52 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
diction may lead to a conclusion, that early UV-induced damage lowers PpIX fluorescence, while prolonged UV-induced damage results in in-creased PpIX fluorescence in skin. Furthermore, we cannot exclude two possible differences of normal and UV-damaged skin: 1) altered penetration of ALA and 2) altered metabolism in skin, which contribute to the observed differences in PpIX fluorescence after ALA application.
The model of UV-exposed mouse skin was compared with that of human skin. The lower part of an arm shows a decreased PpIX fluorescence as compared to the upper part of an arm (Fig. 18). All the volunteers included in this study frequently wore T-shirts during summer time, resulting in a prolonged exposure of the lower arm to solar radiation, while the upper arm stays covered for most of the time. This correlates with the present animal experiments, showing reduced PpIX production in skin exposed to single UV doses. For the case of solar pigmentation of human skin, PpIX fluores-cence could be partially influenced by absorption of blue excitation light by melanin, that is present in pigmented skin. However, in our case the tanning of volunteers’ skin was minimal or absent at the time of experiment.
In conclusion, UV-radiation induces alterations in the skin that has a prolonged influence on its ability to produce PpIX from ALA. Thus, it seems possible to assess the degree of skin damage by a topical application of ALA followed by fluorescence spectroscopy: for early UV-induced dam-age lower PpIX fluorescence is observed while prolonged UV-induced dam-age results in increased PpIX fluorescence in skin. The alteration persists for at least 48 h after single UV-exposure in mouse skin. Daily solar radia-tion on human skin results in a reduced ALA-induced PpIX fluorescence. Observed differences in PpIX fluorescence after ALA application may be due to altered penetration of ALA through stratum corneum and/or altered metabolizing ability of normal and UV-damaged skin. Further investigations of such UV-induced inhibition of PpIX synthesis are of great interest.
Factors influencing PpIX production There is a large variation of PpIX production in skin from person to person and from skin site to skin site. This is true for both ALA and its hexylester derivative. Skin temperature certainly varies from person to person and from one skin site to another (58) Temperature is an important determinant for PpIX formation. Even a small temperature increase may give rise to a significantly elevated production of PpIX (59). Our data indicate that skin temperature is a major determinant for PpIX production in human skin. This is in agreement with our, as well as others’, earlier work where the

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 53
temperature of the skin of mice and humans was manipulated artificially (35, 60). In the present study the temperature dependency of PpIX formation is confirmed by natural variations of the skin temperature. An artificial cool-ing of mouse skin from around 36 to 30oC reduced the PpIX fluorescence by a factor of 2-3 (61). This is in a good agreement with the present data obtained from human skin. An increase of 2oC on an ear roughly doubles the fluorescence both for ALA and ALA-Hex (Fig. 17 B). On other body sites the average dependency is less expressed, giving a rise of around 20% for 1oC (Fig. 17 A).
Furthermore, skin thickness varies from person to person and from one body site to another. The impact of this variation is hard to foresee. On one hand, thick skin would retard the downward penetration of drug, but on the other hand, thick skin contains more cells, also living ones, that may con-tribute to PpIX synthesis. Production of PpIX was found to be only slightly dependent on the skin thickness (Fig. 20). There seemed to be no propor-tionality between the amount of PpIX formed and skin thickness, since regression lines do not pass through the origo. The statement is not strong because of the large scatter of the points, but, if true, it indicates a limited penetration downwards in the skin, even in the skin epidermis. It should be kept in mind that the excitation wavelength used for the fluorescence meas-urements was 407 nm and probes mainly superficial skin layers down to around 1 mm (62). This may partly explain why PpIX fluorescence is inde-pendent on the thickness of the whole skin (epidermis and dermis). The density of hair follicles also shows large individual variations. It has been shown that hair follicles in the skin of mice are preferentially damaged by ALA-PDT (23). This may be due to the fact that after application of ALA, fluorescence of PpIX is mainly located in tumors, epidermis, hair folli-cles(63) and sebaceous glands ( 64). Surprisingly, PpIX formation was found to be independent on the density of hair follicles (Fig. 20). It may indicate that, even though individual follicles exhibit a strong PpIX fluorescence after ALA application (23), the density of them is rather low so they do not contribute significantly to overall skin fluorescence. The discrepancy be-tween our studies and microscopic studies is probably related to the meth-odology. Fluorescence microscopy enables distinguishing of fluorescence pattern as a function of a fine skin structure. In our case the fiber-optic probe ensures an integrated record of fluorescence signal over a relatively large skin area (around 0.3 cm2). This may be an advantage whenever fast and reliable pharmacological in situ comparisons are needed, but the fine structure of the fluorescence pattern will be lost.

54 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
Sun exposure seems to play a role, since in most cases more PpIX was produced at skin sites shielded from the sun (upper arm) than on similar skin sites (of similar thickness and temperature) more regularly exposed to the sun (lower arm). Skin on the back of the ear produced twice as much PpIX as skin on the top of the ear (Fig. 19). This may be related to differ-ences in both temperature and history of sun exposure (65). However, the results are surprising in view of animal experiments, which showed larger PpIX formation in UV-exposed mouse skin than in unexposed skin (66, 67). The reason for this discrepancy may be that in the animal experiments we studied skin with acute UV-damage while in the present work we consider body localizations with different long-time exposure to sunlight.
The present results show large individual variations in PpIX production in skin. Increased PpIX production in skin with elevated temperature is indicated. Thus, heating may be a clinically relevant method of increasing the efficacy of ALA-PDT. This is probably also true in other tissue than skin. There was only a weak dependence of PpIX production on skin thick-ness and no dependence on the density of hair follicles. However, the histo-ry of sun exposure, which is an important factor in dermatology, seemed to play a role in that less PpIX formation was found in sun exposed than in unexposed skin.
Topical sensitizers in the head and neck area In the head and neck area most tumors appear in the mucosa. We have done pilot studies on topical application on the mucosa and have seen that the PpIX levels after ALA application rise much faster than on skin. This is probably due to the lack of stratum corneum and therefore a much faster penetration of ALA. A faster penetration means shorter application times. A shorter application time could increase the importance of temperature, since the temperature dependence can be attributed to a greater enzyme activity and therefore increased ALA to PpIX conversion.
Other ways of increasing the PpIX formation have also been tried, such as the use of ultrasound (68).
There have been several attempts to use topical PDT in the head and neck area (69, 70). Especially precancerous lesions have been the targets of this treatment. A topical application would have many benefits: no systemic light sensitivity, higher specificity, shorter hospital stay and lower costs. Ways of administering the ALA are already designed, such as patches that stick to mucosa and deliver ALA (71). Other ways that seem promising are thermosetting gels (72). Since light penetration is deeper in the mucosa, the

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 55
head and neck area is perhaps even more suitable for PDT than the skin (20).
PDT in laryngeal malignancies PDT can be used to treat laryngeal cancer. We present the results of PDT of primary laryngeal cancer (73) and when used for recurrence of laryngeal cancer.
The current treatments of choice for early laryngeal cancer are radiother-apy or TLS. Both treatments yield excellent results. The use of open surgery has declined in the past decade (74). There is a discussion about what treat-ment is the best and so far it seems as if the results after radiotherapy and TLS are similar concerning local control, overall survival, disease-specific survival, and post treatment voice quality (75). The preservation of the lar-ynx seems to be higher in the TLS group (76). Local control is high in both treatment groups.
However, some patients with laryngeal tumors are not suited to either treatment. Radiation can be less appropriate if the patient has previously received radiation to the laryngeal area, is claustrophobic or has a tumor that is less radio sensitive. In the case of young patients, one must consider the risk of a future radiation-induced tumor. Additionally, a six-week radia-tion treatment can pose problems for many patients. Successful TLS re-quires experience, particularly if the anterior commissure is involved (77). TLS also requires a good laryngoscopic view. In experienced hands, TLS is an excellent therapy, but there is a learning curve (46).
The use of PDT in the treatment of early laryngeal cancer has been de-scribed by several authors (78-88). The results varied, but Feyh and Biel ob-served a complete response rate of up to 90%. Generally PDT has mostly been used to treat squamous cell carcinomas, the most common type of laryngeal cancer. While different photosensitizers have been used, HpD was utilized for 93% of the patients in the scientific reports.

56 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
Study # Pri-mary T
Sen-sitiz-er
CR
PR
NR
His-tolo-gy
Airway prob-lems
Feyh 12
Not dis-closed
Tis - T2 (3 CIS) HpD 11 1 SCC
1 de-layed extuba-tion
Wenig 1 Yes T1 HpD 1 SCC No
Freche 32
24 prim, 8 recur
17 T1, 15 Tis HpD 25 7 SCC No
Schweitzer 10 Mixed Tis-T2 HpD 8 2
9 SCC, 1 Sar-coma No
Gluckman 5 No T1-T3 HpD 2 1 2 SCC
3 prophy-lactic trach
Biel 115 Mixed Tis T1 T2 HpD 105
10 SCC No
Rigual 3 1 rec T1 HpD 2 1 SCC No
Lorenz 1 No T3 Tem-porfin 1 SCC
Yo-shida 15
2 re-curr after RT T1-T3
Tala-porfin 12 3 SCC? 1 trach
Sum 194 166 18 10
Tab 9: Earlier publications of PDT of laryngeal cancer. # - Number of subjects, T – Tumor stage according to TNM, HpD – Porfimer Sodium, SCC – Squamous cell carcinoma CR- Complete Response, PR- Partial Response, NR- No response
We have conducted a retrospective, descriptive study, where we evaluated our use of PDT as a primary treatment for patients with laryngeal malignan-

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 57
cies referred to Örebro University Hospital, that were less suitable for radia-tion therapy or TLS. Over the past 22 years, the center has treated 381 cases of laryngeal cancer. During the past 10 years, nine patients were considered best treated with PDT primarily by our multidisciplinary tumor boards (MDTs). Previously, we had treated only one laryngeal cancer patient with PDT, in 1988, and this patient was included in this study.
The number of patients treated with PDT is small, which we believe is because the other modalities provide good results. The reason for the in-crease of use of PDT is probably because of our increased experience with PDT in other areas of the head and neck.
Seven of the 10 patients first treated with PDT had a complete response after PDT treatment alone and did not require any other therapy. These patients were all treated with temoporfin, and five of the seven had intersti-tial illumination.
Two patients had a complete response, but recurred after 10 months and were then treated with radiation and cured. The one patient who was not cured was our first laryngeal PDT patient; she died from a simultaneous cancer only a few months post-treatment.
Laryngeal recurrences Early laryngeal cancer has a good prognosis but there are of course instances of recurrence. The recurrences can also be treated by several different mo-dalities. The safest and most effective treatment is total laryngectomy. Treatment or retreatment with TLS after radiation treatment also shows promising results, if used in correct patients. Studies have shown that about one third of the recurrences are best treated by conservation surgery, such as TLS or partial laryngectomy (49). The reason for this is possibly the fact that recurrence of early laryngeal cancer presents itself more advanced. Studies have shown that recurrences are difficult to diagnose, even if the patients are subjected to laryngoscopies under general anesthesia with biop-sies (89). It has also been shown that recurrences often have more than one foci after failed radiotherapy (90) and this could lead to false radical mar-gins.
The present study shows that PDT is an option in treating recurrences of laryngeal cancer. Five out of eleven patients were cured with this organ spar-ing technique and the other six were able to get conventional treatment resulting in local control. On the other hand three patients died of regional or distant failures and these failures may have been avoided with an earlier laryngectomy. These were patients with recurrences of larger primary tu-

58 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
mors, 1/1 T3 and 2/4 T2. The study is too small to be compared to results from other modalities. It does however concur with earlier studies with PDT (80, 81, 85, 87, 88).
Study # T Histology Sensitizer CR Followup Schweitzer 6 Tis-
T2 5 SCC, 1 Sarcoma
HpD 4 of 6 21-52 mo
Freche 8 Tis-T1
SCC HpD 6 of 8 1 - 4 years
Rigual 1 T1 SCC HpD 0 of 1 Biel 33 T1-
T2 SCC HpD At least
23 of 33 mean 84 months
Yoshida 2 T1-T2
SCC Talaporfin 2 of 2 Recurrence after 5 & 13 mo
Beckerath 11 T1-T3
9 SCC, 2 Sarcomas
HpD and Temoporfin
8 of 11 12 - 170 mo, 3 CR recurred
Tab 10: Studies including PDT for recurrences of laryngeal cancer # - Number of subjects, T – Tumor stage according to TNM, CR – Complete Respeonse HpD – Porfimer Sodium, SCC – Squamous cell carcinoma
This study supports further studies of PDT as an organ and function sparing treatment for recurring laryngeal cancer. The advantage of PDT could be, that since it is a selective treatment, it has a possibility to treat areas with foci that are not clinically obvious.
Since PDT also can be used as a diagnostic tool it could be used as a combination. A patient that is sensitized could first be subjected to blue light to determine where the tumor, its boundaries and possible subclinical further tumors are (19).
A study where PDT is used for selected patients with recurrence of early laryngeal cancer after radiotherapy or TLS would be most interesting. The recurrent tumor should be rT1 and selected rT2 with no suspicion of growth in cartilage since this could hinder light penetration. Sensitization should be with temoporfin or porfimer sodium and illumination with an interstitial laser fiber emitting light at the correct wavelength. The area covered by light should be the primary tumor and the present tumor with an addition

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 59
of 5-10 mm. PDT in the larynx seems to be easier than TLS technically and it requires less visualization.
Illumination of the larynx An interstitial mode to deliver light to the tumor was used in 12/20 of the cases. The vocal cord diffuser with the introduction instrument was prefer-able to a surface illumination with a micro lens. It was easy to apply the illumination to the correct site, and the diffuser remained in place during the entire lighting cycle. A surgeon with some experience of performing surgery in the larynx will have no problem with the technique. It also re-quires less visualization than when performing TLS. The PDT effect reach-es further than the area that is directly viewed. This gives PDT a longer reach than working with a CO2-laser.
The results of the patients that have received interstitial illumination in these studies seem to be better, but this can coincide with other factors since they are more common later in the studies.
Systemic sensitizers In most other studies of PDT for laryngeal cancer, the sensitizer used was HpD. In these studies temoporfin was mostly used (18/24 treatments), and it appears that this sensitizer has at least comparable results.
The patient treated with a fourth of the normal dose of temoporfin got a quick recurrence suggesting this dose to be inadequate.
Sarcomas The use of sensitizers in treatment of sarcomas was already described by Cohen and Schwartz in 1966 (91). In these studies we successfully treated five laryngeal sarcomas. To the best of our knowledge, PDT of only one sarcoma in the larynx, an angiosarcoma, has been described before in the literature (81).
Sarcomas are often less sensitive to radiation therapy; in many cases, par-tial or total laryngectomy is used as the treatment (92). In the case of low malignant sarcomas, PDT appears to be a good option, particularly because it is an organ- and function-preserving therapy. PDT cured all five sarcomas, although two had a relatively short follow-up period (one and a half and two years).

60 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
The studies also demonstrate that PDT can be used for laryngeal sarco-mas that have been treated by surgery but recurred or as a repeated treat-ment.
Voice The voice outcome of PDT was studied in the primarily treated group and appears to be comparable to those of the other treatment modalities (93), with at least half of the patients experiencing an improved voice and none having a worse voice. This is in concordance with other studies of voice outcome after PDT for laryngeal Tis and T1 tumors (94). This shows that PDT is both organ and function sparing.
Costs The cost of PDT as a primary treatment in this study exceeded that of TLS or radiation. There is hope that the difference in cost can be reduced in the near future: For safety reasons, the patients in this study were kept in the hospital under close surveillance for many days until it was deemed entirely certain that the swelling caused by the treatment had subsided so to ensure that the airway was not compromised. The in-patient cost accounted for approximately 40% of the total cost. However, none of the patients had any problems with airway patency or swallowing difficulties, nor was the protec-tion from intense light a problem. Therefore a shorter hospital stay is feasi-ble in the future. The injection may well be given in an outpatient setting, thereby further limiting patient costs. Nonetheless, even with a shorter hospital stay, PDT would remain more expensive than radiation and TLS because of the high cost of the sensitizer. New or less expensive sensitizers would increase the usefulness of PDT.
Safety PDT is a safe primary treatment for early laryngeal cancer. We did not ex-perience any unexpected side effects or airway problems. The side effects were minor, with hoarseness as the most common symptom (4/10). This finding is consistent with those of earlier studies. Of the 194 reported cases only one patient required a tracheotomy after the treatment. In one study, however, three out of five patients were given a prophylactic tracheotomy. The lack of airway complications when PDT is used in the larynx is in con-trast to reports of airway problems when PDT is used in base of tongue (95).

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 61
One patient got a second tumor in the treated area five years after the PDT. The question whether this tumor could be induced by PDT arises, but we have not found any indications in the literature that temoporfin has any carcinogenic properties.
Patients who received PDT as a treatment for a recurring cancer did have more side effects that required pharmacological treatment for pain and infections. This was more common in the group previously treated with RT. It is known that RT affects tissue for a long time and this could be the cause (96). One serious adverse event was noted in this group, one patient re-quired a tracheostomy, although it wasn’t acute. The patient got the trache-otomy after a week of consideration. One reason could be that he continued smoking and did not follow given instructions to use antibiotics and saline inhalations.
Future The clinical studies conducted by us are some of few but it suggests an in-creased study of and use of PDT. The number of patients and the selection of patients need to be improved in future studies. The biggest obstacles for PDT in treatment of laryngeal cancers are the excellent outcome of today’s treatments, costs and lack of randomized studies. Randomized controlled studies need to be done to see if PDT is an alternative to the conventional treatments. It would be of special interest to investigate if low-malignant sarcomas are best treated by PDT. In the meantime PDT should mostly be used when conventional treatments are unavailable or less suitable.
Topical application is a good option for future treatments in the head and neck area. It would minimize adverse reactions like skin sensitivity. Topical application is also much faster with hours between administration of sensitizer and treatment instead of days. A possibility of one day treat-ments in the head and neck are, much like in dermatology, very promising.
PDT for precancerous lesions would also be more feasible with a topical application.

62 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
Conclusion This thesis confirms that there is an inter and intra individual difference in levels of PpIX produced after ALA application. The thesis has demonstrat-ed that one of the major reasons seems to be temperature dependence where more PpIX is produced at higher temperatures. This indicates that a topically applied ALA could be a good way to administer sensitizers in the mucosa.
The thesis shows that both very short term and long term UV-damage of the skin affects the PpIX production after topical ALA by lowering it.
Study three shows that PDT could be an option for the primary treat-ment of laryngeal cancers. The same study also demonstrated that it is pos-sible to cure laryngeal tumors (both SCCs and sarcomas) using PDT primari-ly, including temoporfin-mediated PDT.
The findings in study four suggest that PDT also can be used for treat-ment of recurrences of laryngeal cancers, both SCC and sarcomas.
The voice outcome of PDT appears to be comparable to those of the conventional treatment modalities (93), with at least half of the patients experiencing an improved voice and none having a worse voice.
For patients who are less suitable for conventional treatments, PDT is a viable and safe option with cure rates comparable to those of other treat-ments. It is technically easier to perform PDT than TLS. For many larynge-al sarcomas, PDT appears to be an option that could spare organs and func-tions. Further studies of PDT treatment for primary and recurring laryngeal cancer and sarcomas are warranted.
MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 63
Acknowledgements I would like to express my gratitude to all that have made this thesis possi-ble and would like to mention the following
• Claes Möller, my main supervisor, for all the invaluable help and ex-cellent advice. You saved the thesis!
• Johan Moan, Petras Juzenas, Vladimir Iani and Li-Wei Ma for the help introducing me to PDT research and the work behind papers one and two at Radium Hospitalet in Oslo.
• Lennart Löfgren for starting the PDT tradition at our hospital, in-troducing me to PDT and for conducting many of the procedures in article three and four.
• My colleagues at the Örebro ENT-clinic who have taken the clini-cal load when the thesis was written. A special thanks to the head and neck surgeons in the “blue-team” for all the help, cooperation and support.
• My colleagues at the oncology department. Special thanks to Johan Reizenstein for all the sound judgement concerning our patients and for the work with article three and four and to Bengt Johansson for good ideas and cooperation.
• Fredrik Landström for research cooperation and honest opinions over a beer or two.
• Hans Gustafsson for all the constructive criticism. • All former and present, nurses, secretaries and staff members at the
ENT-clinic in Örebro for all the help with the patients treated with PDT
• Gun-Britt Adamsson for amoung other things aiding me with in-formation from our cancer registry.
• Örebro University Hospital and Örebro County Council for finan-cial support making this thesis possible.
• My parents, Mare and Jan-Paul for always being there for me. • Maja, Lova and Embla, my wonderful daughters who always care
about me and support me. The best moments in life is are with you • Ann-Sofie for your care and support of the family and me even
when the hours are long.


MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 65
References 1. Braathen L, Szeimies R, Bassetseguin N, Bissonnette R, Foley P, Pariser
D, et al. Guidelines on the use of photodynamic therapy for nonmela-noma skin cancer: An international consensus. J Am Acad Dermatol. 2007;56(1):125-43.
2. Moan J, Peng Q. An outline of the hundred-year history of PDT. Anti-cancer Res. 2003 Sep-Oct;23(5A):3591-600. PubMed PMID: 14666654.
3. Raab O. Ueber die Wirkung fluoreszierender Stoffe auf Infusorien. Z Biol Munich). 1900;39:524-46.
4. Von Tappeiner H, Jodlbauer A. Die Sensibilisierende Wirkung fluorieszierender Substanzer Gesammte Untersuchungen uber die pho-todynamische Erscheinung. Leipzig: F. C. W. Vogel; 1907.
5. Meyer-Betz F. Untersuchungen uber die biologische (photodynamische) wirkung des hamatoporphyrins und anderer derivative des blut-und Gallenfarbstoffs. Deutches Archiven Klin Med. 1913;112:476-503.
6. Dougherty TJ. Photodynamic therapy (PDT) of malignant tumors. Crit Rev Oncol Hematol. 1984;2(2):83-116. PubMed PMID: 6397270. Epub 1984/01/01. eng.
7. Calzavara-Pinton PG, Venturini M, Sala R. Photodynamic therapy: up-date 2006. Part 1: Photochemistry and photobiology. J Eur Acad Derma-tol Venereol. 2007 Mar;21(3):293-302. PubMed PMID: 17309449.
8. Dai T, Fuchs BB, Coleman JJ, Prates RA, Astrakas C, St Denis TG, et al. Concepts and principles of photodynamic therapy as an alternative anti-fungal discovery platform. Front Microbiol. 2012;3:120. PubMed PMID: 22514547. Pubmed Central PMCID: 3322354.
9. Agarwal ML, Clay ME, Harvey EJ, Evans HH, Antunez AR, Oleinick NL. Photodynamic therapy induces rapid cell death by apoptosis in L5178Y mouse lymphoma cells. Cancer Res. 1991 Nov 1;51(21):5993-6. PubMed PMID: 1933862.
10. Moan J, Berg K. The photodegradation of porphyrins in cells can be used to estimate the lifetime of singlet oxygen. Photochem Photobiol. 1991 Apr;53(4):549-53. PubMed PMID: 1830395. Epub 1991/04/01. eng.

66 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
11. Peng Q, Nesland JM. Effects of photodynamic therapy on tumor stroma. Ultrastruct Pathol. 2004 Sep-Dec;28(5-6):333-40. PubMed PMID: 15764581.
12. Biel M, Betz C, Dougherty T, Edell E, Goldenberg D, Hopper C, et al. Photodynamic Therapy of Diseases of the Head and Neck. Biel M, edi-tor: Plural Publishing; 2008.
13. Allison RR, Downie GH, Cuenca R, Hu XH, Childs CJH, Sibata CH. Photosensitizers in clinical PDT. Photodiagnosis Photodyn Ther. 2004 May;1(1):27-42. PubMed PMID: WOS:000208590400008. English.
14. Peng Q, Berg K, Moan J, Kongshaug M, Nesland JM. 5-Aminolevulinic acid-based photodynamic therapy: principles and experimental research. Photochem Photobiol. 1997 Feb;65(2):235-51. PubMed PMID: 9066303.
15. Castano AP, Demidova TN, Hamblin MR. Mechanisms in photodynam-ic therapy: part one—photosensitizers, photochemistry and cellular lo-calization. Photodiagnosis Photodyn Ther. 2004;1(4):279-93.
16. Senge MO, Brandt JC. Temoporfin (Foscan(R), 5,10,15,20-tetra(m-hydroxyphenyl)chlorin)--a second-generation photosensitizer. Photo-chem Photobiol. 2011 Nov-Dec;87(6):1240-96. PubMed PMID: 21848905.
17. Senge MO. mTHPC--a drug on its way from second to third generation photosensitizer? Photodiagnosis Photodyn Ther. 2012 Jun;9(2):170-9. PubMed PMID: 22594988.
18. Sotiriou E, Apalla Z, Chovarda E, Goussi C, Trigoni A, Ioannides D. Single vs. fractionated photodynamic therapy for face and scalp actinic keratoses: a randomized, intraindividual comparison trial with 12-month follow-up. J Eur Acad Dermatol Venereol. 2012 Jan;26(1):36-40. PubMed PMID: 21366709.
19. Kraft M, Betz CS, Leunig A, Arens C. Value of fluorescence endoscopy for the early diagnosis of laryngeal cancer and its precursor lesions. Head Neck. 2011 Jul;33(7):941-8. PubMed PMID: 21674669.
20. Bashkatov AN, Genina EA, Kochubey VI, Tuchin VV. Optical proper-ties of human skin, subcutaneous and mucous tissues in the wavelength range from 400 to 2000 nm. Journal of Physics D-Applied Physics. 2005 Aug 7;38(15):2543-55. PubMed PMID: WOS:000231406800005. English.

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 67
21. Rorsman H, Björnberg A. Dermatologi Venerologi. 5 ed: Studentlittera-tur; 1993.
22. Moseley H, Brancaleon L, Lesar AE, Ferguson J, Ibbotson SH. Does surface preparation alter ALA uptake in superficial non-melanoma skin cancer in vivo? Photodermatol Photoimmunol Photomed. 2008 Apr;24(2):72-5. PubMed PMID: 18353086. Epub 2008/03/21. eng.
23. Divaris DX, Kennedy JC, Pottier RH. Phototoxic damage to sebaceous glands and hair follicles of mice after systemic administration of 5-aminolevulinic acid correlates with localized protoporphyrin IX fluores-cence. Am J Pathol. 1990 Apr;136(4):891-7. PubMed PMID: 2327473.
24. Choudhary S, Nouri K, Elsaie ML. Photodynamic therapy in dermatolo-gy: a review. Lasers Med Sci. 2009 Nov;24(6):971-80. PubMed PMID: 19653060.
25. Babilas P, Karrer S, Sidoroff A, Landthaler M, Szeimies RM. Photody-namic therapy in dermatology--an update. Photodermatol Photoim-munol Photomed. 2005 Jun;21(3):142-9. PubMed PMID: 15888131.
26. Loncaster J, Swindell R, Slevin F, Sheridan L, Allan D, Allan E. Efficacy of Photodynamic Therapy as a Treatment for Gorlin Syndrome-related Basal Cell Carcinomas. Clin Oncol. 2009;21(6):502-8.
27. Bataille V, Bykov VJ, Sasieni P, Harulow S, Cuzick J, Hemminki K. Photoadaptation to ultraviolet (UV) radiation in vivo: photoproducts in epidermal cells following UVB therapy for psoriasis. Br J Dermatol. 2000 Sep;143(3):477-83. PubMed PMID: 10971317.
28. Bech-Thomsen N, Wulf HC. Photoprotection due to pigmentation and epidermal thickness after repeated exposure to ultraviolet light and pso-ralen plus ultraviolet A therapy. Photodermatol Photoimmunol Pho-tomed. 1996 Oct-Dec;11(5-6):213-8. PubMed PMID: 8738717.
29. de Gruijl FR. Photocarcinogenesis: UVA vs UVB. Methods Enzymol. 2000;319:359-66. PubMed PMID: 10907526.
30. Moan J, Dahlback A, Setlow RB. Epidemiological support for an hy-pothesis for melanoma induction indicating a role for UVA radiation. Photochem Photobiol. 1999 Aug;70(2):243-7. PubMed PMID: 10461463.
31. Stender IM, Bech-Thomsen N, Poulsen T, Wulf HC. Photodynamic therapy with topical delta-aminolevulinic acid delays UV photocarcino-

68 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
genesis in hairless mice. Photochem Photobiol. 1997 Oct;66(4):493-6. PubMed PMID: 9337620.
32. Dougherty TJ, Gomer CJ, Henderson BW, Jori G, Kessel D, Korbelik M, et al. Photodynamic therapy. J Natl Cancer Inst. 1998 Jun 17;90(12):889-905. PubMed PMID: 9637138.
33. Stefanidou M, Tosca A, Themelis G, Vazgiouraki E, Balas C. In vivo fluorescence kinetics and photodynamic therapy efficacy of delta-aminolevulinic acid-induced porphyrins in basal cell carcinomas and ac-tinic keratoses; implications for optimization of photodynamic therapy. Eur J Dermatol. 2000 Jul-Aug;10(5):351-6. PubMed PMID: 10882942.
34. Krieg RC, Messmann H, Rauch J, Seeger S, Knuechel R. Metabolic characterization of tumor cell-specific protoporphyrin IX accumulation after exposure to 5-aminolevulinic acid in human colonic cells. Photo-chem Photobiol. 2002 Nov;76(5):518-25. PubMed PMID: 12462647.
35. Moan J, Berg K, Gadmar OB, Iani V, Ma L, Juzenas P. The temperature dependence of protoporphyrin IX production in cells and tissues. Pho-tochem Photobiol. 1999 Oct;70(4):669-73. PubMed PMID: 10546563.
36. van den Akker JT, Holroyd JA, Vernon DI, Sterenborg HJ, Brown SB. Comparative in vitro percutaneous penetration of 5-aminolevulinic acid and two of its esters through excised hairless mouse skin. Lasers Surg Med. 2003;33(3):173-81. PubMed PMID: 12949947.
37. McCarron PA, Donnelly RF, Andrews GP, Woolfson AD. Stability of 5-aminolevulinic acid in novel non-aqueous gel and patch-type systems in-tended for topical application. J Pharm Sci. 2005;94(8):1756-71.
38. Bailey B, Johnson J, Newlands SD. Head and neck surgery–otolaryngology: Lippincott Williams & Wilkins; 2006.
39. Sweden OSo. Cancer Incidence in Sweden 2011. 2012.
40. Siegel R, Ward E, Brawley O, Jemal A. Cancer statistics, 2011: the im-pact of eliminating socioeconomic and racial disparities on premature cancer deaths. CA Cancer J Clin. 2011 Jul-Aug;61(4):212-36. PubMed PMID: 21685461.
41. Kjaerheim K, Gaard M, Andersen A. The role of alcohol, tobacco, and dietary factors in upper aerogastric tract cancers: a prospective study of

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 69
10,900 Norwegian men. Cancer Causes Control. 1998 Jan;9(1):99-108. PubMed PMID: 9486469.
42. Ahmad Kiadaliri A, Jarl J, Gavriilidis G, Gerdtham UG. Alcohol drink-ing cessation and the risk of laryngeal and pharyngeal cancers: a system-atic review and meta-analysis. PLoS One. 2013;8(3):e58158. PubMed PMID: 23469267. Pubmed Central PMCID: 3585880.
43. Li X, Gao L, Li H, Gao J, Yang Y, Zhou F, et al. Human papillomavirus infection and laryngeal cancer risk: a systematic review and meta-analysis. J Infect Dis. 2013 Feb 1;207(3):479-88. PubMed PMID: 23175764.
44. Ambrosch P, Fazel A. Functional organ preservation in laryngeal and hypopharyngeal cancer. GMS Curr Top Otorhinolaryngol Head Neck Surg. 2011;10:Doc02. PubMed PMID: 22558052. Pubmed Central PMCID: 3341579. Epub 2011/01/01. eng.
45. Hartl DM, Ferlito A, Brasnu DF, Langendijk JA, Rinaldo A, Silver CE, et al. Evidence-based review of treatment options for patients with glot-tic cancer. Head Neck. 2011;33(11):1638-48.
46. Bernal-Sprekelsen M, Blanch JL, Caballero-Borrego M, Vilaseca I. The learning curve in transoral laser microsurgery for malignant tumors of the larynx and hypopharynx: parameters for a levelled surgical approach. Eur Arch Otorhinolaryngol. 2013 Feb;270(2):623-8. PubMed PMID: 22996081.
47. Barrett B, Stiles M, Patterson J. Radiation risks: critical analysis and commentary. Prev Med. 2012 Mar-Apr;54(3-4):280-2. PubMed PMID: 22227282.
48. Feng Y, Wang B, Wen S. Laser surgery versus radiotherapy for T1-T2N0 glottic cancer: a meta-analysis. ORL J Otorhinolaryngol Relat Spec. 2011;73(6):336-42. PubMed PMID: 22005723. Epub 2011/10/19. eng.
49. Agra IM, Ferlito A, Takes RP, Silver CE, Olsen KD, Stoeckli SJ, et al. Diagnosis and treatment of recurrent laryngeal cancer following initial nonsurgical therapy. Head Neck. 2012 May;34(5):727-35. PubMed PMID: 21484925.
50. Huang J, Yu Z, Fang J, Chen X, Chen X, Huang Z. Salvage transoral laser microsurgery for early recurrent glottic carcinoma after primary la-

70 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
ser treatment. Acta Otolaryngol. 2013 May;133(5):531-7. PubMed PMID: 23350599.
51. Green B, Cobb AR, Hopper C. Photodynamic therapy in the manage-ment of lesions of the head and neck. Br J Oral Maxillofac Surg. 2013 Jun;51(4):283-7. PubMed PMID: 23245464.
52. Moan J, Peng Q, Sorensen R, Iani V, Nesland JM. The biophysical foundations of photodynamic therapy. Endoscopy. 1998 May;30(4):387-91. PubMed PMID: 9689514.
53. Pottier RH, Chow YF, LaPlante JP, Truscott TG, Kennedy JC, Beiner LA. Non-invasive technique for obtaining fluorescence excitation and emission spectra in vivo. Photochem Photobiol. 1986 Nov;44(5):679-87. PubMed PMID: 3809258.
54. Juzenas P, Sorensen R, Iani V, Moan J. Uptake of topically applied 5-aminolevulinic acid and production of protoporphyrin IX in normal mouse skin: dependence on skin temperature. Photochem Photobiol. 1999 Apr;69(4):478-81. PubMed PMID: 10212580.
55. Goff BA, Bachor R, Kollias N, Hasan T. Effects of photodynamic thera-py with topical application of 5-aminolevulinic acid on normal skin of hairless guinea pigs. J Photochem Photobiol B. 1992 Aug 31;15(3):239-51. PubMed PMID: 1453276.
56. Kennedy JC, Pottier RH, Pross DC. Photodynamic therapy with endog-enous protoporphyrin IX: basic principles and present clinical experi-ence. J Photochem Photobiol B. 1990 Jun;6(1-2):143-8. PubMed PMID: 2121931.
57. Juzenas P, Sharfaei S, Moan J, Bissonnette R. Protoporphyrin IX fluo-rescence kinetics in UV-induced tumours and normal skin of hairless mice after topical application of 5-aminolevulinic acid methyl ester. J Photochem Photobiol B. 2002 May;67(1):11-7. PubMed PMID: 12007462.
58. Liang MT, Norris S. Effects of skin blood flow and temperature on bioe-lectric impedance after exercise. Med Sci Sports Exerc. 1993 Nov;25(11):1231-9. PubMed PMID: 8289609.
59. Moan J, van den Akker JT, Juzenas P, Ma L, Angell-Petersen E, Gadmar ÖB, et al. On the basis for tumor selectivity in the 5-aminolevulinic acid

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 71
induced synthesis of protoporhyrin IX. Journal of Porphyrins and Phtatalocyanines. 2001;5:170-6.
60. van den Akker JT, Boot K, Vernon DI, Brown SB, Groenendijk L, van Rhoon GC, et al. Effect of elevating the skin temperature during topical ALA application on in vitro ALA penetration through mouse skin and in vivo PpIX production in human skin. Photochem Photobiol Sci. 2004 Mar;3(3):263-7. PubMed PMID: 14993942.
61. Juzeniene A, Juzenas P, Iani V, Moan J. Topical application of 5-aminolevulinic acid and its methylester, hexylester and octylester deriva-tives: considerations for dosimetry in mouse skin model. Photochem Photobiol. 2002 Sep;76(3):329-34. PubMed PMID: 12403455.
62. Juzenas P, Juzeniene A, Kaalhus O, Iani V, Moan J. Noninvasive fluores-cence excitation spectroscopy during application of 5-aminolevulinic acid in vivo. Photochem Photobiol Sci. 2002 Oct;1(10):745-8. PubMed PMID: 12656473.
63. van der Veen N, de Bruijn HS, Berg RJ, Star WM. Kinetics and localisa-tion of PpIX fluorescence after topical and systemic ALA application, observed in skin and skin tumours of UVB-treated mice. Br J Cancer. 1996 Apr;73(7):925-30. PubMed PMID: 8611408.
64. Bissonnette R, Shapiro J, Zeng H, McLean DI, Lui H. Topical photody-namic therapy with 5-aminolaevulinic acid does not induce hair regrowth in patients with extensive alopecia areata. Br J Dermatol. 2000 Nov;143(5):1032-5. PubMed PMID: 11069515.
65. von Beckerath M, Juzenas P, Ma LW, Iani V, Lofgren L, Moan J. The influence of UV exposure on 5-aminolevulinic acid-induced protopor-phyrin IX production in skin. Photochem Photobiol. 2001 Dec;74(6):825-8. PubMed PMID: 11783939.
66. van den Akker JT, de Bruijn HS, Beijersbergen van Henegouwen GM, Star WM, Sterenborg HJ. Protoporphyrin IX fluorescence kinetics and localization after topical application of ALA pentyl ester and ALA on hairless mouse skin with UVB-induced early skin cancer. Photochem Photobiol. 2000 Sep;72(3):399-406. PubMed PMID: 10989612.
67. Sharfaei S, Juzenas P, Moan J, Bissonnette R. Weekly topical application of methyl aminolevulinate followed by light exposure delays the appear-

72 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
ance of UV-induced skin tumours in mice. Arch Dermatol Res. 2002 Jul;294(5):237-42. PubMed PMID: 12115027.
68. Charoenbanpachon S, Krasieva T, Ebihara A, Osann K, Wilder-Smith P. Acceleration of ALA-induced PpIX fluorescence development in the oral mucosa. Lasers Surg Med. 2003;32(3):185-8. PubMed PMID: 12605424.
69. Lin HP, Chen HM, Yu CH, Yang H, Wang YP, Chiang CP. Topical photodynamic therapy is very effective for oral verrucous hyperplasia and oral erythroleukoplakia. J Oral Pathol Med. 2010 Sep;39(8):624-30. PubMed PMID: 21054548. Epub 2010/11/09. eng.
70. Kvaal SI, Angell-Petersen E, Warloe T. Photodynamic treatment of oral lichen planus. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013 Jan;115(1):62-70. PubMed PMID: 23217536. Epub 2012/12/12. eng.
71. McCarron PA, Donnelly RF, Zawislak A, Woolfson AD. Design and evaluation of a water-soluble bioadhesive patch formulation for cutane-ous delivery of 5-aminolevulinic acid to superficial neoplastic lesions. Eur J Pharm Sci. 2006;27(2-3):268-79.
72. Bourre L, Thibaut S, Briffaud A, Lajat Y, Patrice T. Potential efficacy of a delta 5-aminolevulinic acid thermosetting gel formulation for use in photodynamic therapy of lesions of the gastrointestinal tract. Pharmacol Res. 2002 Feb;45(2):159-65. PubMed PMID: 11846630.
73. von Beckerath MP, Reizenstein JA, Berner AL, Nordqvist KWO, Land-ström FJ, Löfgren AL, et al. Outcome of primary treatment of early lar-yngeal malignancies using photodynamic therapy. Acta Otolaryngol. 2014:1-7.
74. Silver CE, Beitler JJ, Shaha AR, Rinaldo A, Ferlito A. Current trends in initial management of laryngeal cancer: the declining use of open surgery. Eur Arch Otorhinolaryngol. 2009;266(9):1333-52.
75. Hartl DM. Evidence-based practice: management of glottic cancer. Oto-laryngol Clin North Am. 2012 Oct;45(5):1143-61. PubMed PMID: 22980690.
76. Abdurehim Y, Hua Z, Yasin Y, Xukurhan A, Imam I, Yuqin F. Tran-soral laser surgery versus radiotherapy: systematic review and meta-analysis for treatment options of T1a glottic cancer. Head Neck. 2012 Jan;34(1):23-33. PubMed PMID: 21374753.

MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck 73
77. Sachse F, Stoll W, Rudack C. Evaluation of treatment results with re-gard to initial anterior commissure involvement in early glottic carcino-ma treated by external partial surgery or transoral laser microresection. Head Neck. 2009;31(4):531-7.
78. Feyh J. Photodynamic treatment for cancers of the head and neck. J Photochem Photobiol B. 1996 Nov;36(2):175-7. PubMed PMID: 9002255.
79. Wenig BL, Kurtzman DM, Grossweiner LI, Mafee MF, Harris DM, Lobraico RV, et al. Photodynamic therapy in the treatment of squamous cell carcinoma of the head and neck. Arch Otolaryngol Head Neck Surg. 1990 Nov;116(11):1267-70. PubMed PMID: 2146969.
80. Freche C, De Corbiere S. Use of photodynamic therapy in the treatment of vocal cord carcinoma. J Photochem Photobiol B. 1990 Jul;6(3):291-6. PubMed PMID: 2120406. Epub 1990/07/01. eng.
81. Schweitzer VG. PHOTOFRIN-mediated photodynamic therapy for treatment of early stage oral cavity and laryngeal malignancies. Lasers Surg Med. 2001;29(4):305-13. PubMed PMID: 11746107. Epub 2001/12/18. eng.
82. Gluckman JL. Hematoporphyrin photodynamic therapy: is there truly a future in head and neck oncology? Reflections on a 5-year experience. Laryngoscope. 1991 Jan;101(1 Pt 1):36-42. PubMed PMID: 1701843.
83. Biel MA. Photodynamic therapy and the treatment of neoplastic diseas-es of the larynx. Laryngoscope. 1994 Apr;104(4):399-403. PubMed PMID: 8164476. Epub 1994/04/01. eng.
84. Biel MA. Photodynamic therapy and the treatment of head and neck neoplasia. Laryngoscope. 1998 Sep;108(9):1259-68. PubMed PMID: 9738739.
85. Rigual NR, Thankappan K, Cooper M, Sullivan MA, Dougherty T, Popat SR, et al. Photodynamic therapy for head and neck dysplasia and cancer. Arch Otolaryngol Head Neck Surg. 2009 Aug;135(8):784-8. Pub-Med PMID: 19687399. Pubmed Central PMCID: 2810853.
86. Lorenz KJ, Maier H. Photodynamic therapy with meta-tetrahydroxyphenylchlorin (Foscan) in the management of squamous cell carcinoma of the head and neck: experience with 35 patients. Eur Arch Otorhinolaryngol. 2009 Dec;266(12):1937-44. PubMed PMID: 19290535.

74 MATHIAS VON BECKERATH Photodynamic Therapy in the Head and Neck
87. Yoshida T, Kato H, Okunaka T, Saeki T, Ohashi S, Okudaira T, et al. Photodynamic therapy for head and neck cancer. Diagn Ther Endosc. 1996;3(1):41-51. PubMed PMID: 18493416. Epub 1996/01/01. eng.
88. Biel MA. Photodynamic therapy treatment of early oral and laryngeal cancers. Photochem Photobiol. 2007 Sep-Oct;83(5):1063-8. PubMed PMID: 17880501.
89. Zbaren P, Weidner S, Thoeny HC. Laryngeal and hypopharyngeal carci-nomas after (chemo)radiotherapy: a diagnostic dilemma. Curr Opin Oto-laryngol Head Neck Surg. 2008 Apr;16(2):147-53. PubMed PMID: 18327034.
90. Zbaren P, Nuyens M, Curschmann J, Stauffer E. Histologic characteris-tics and tumor spread of recurrent glottic carcinoma: analysis on whole-organ sections and comparison with tumor spread of primary glottic car-cinomas. Head Neck. 2007 Jan;29(1):26-32. PubMed PMID: 17103406.
91. Cohen L, Schwartz S. Modification of radiosensitivity by porphyrins. II. Transplanted rhabdomyosarcoma in mice. Cancer Res. 1966 Aug;26(8):1769-73. PubMed PMID: 5923175.
92. Bathala S, Berry S, Evans RA, Brodie S, Altaan O. Chondrosarcoma of larynx: review of literature and clinical experience. J Laryngol Otol. 2008 Oct;122(10):1127-9. PubMed PMID: 17908358.
93. Goor KM, Peeters AJGE, Mahieu HF, Langendijk JA, Leemans CR, Verdonck-de Leeuw IM, et al. Cordectomy by CO2 laser or radiotherapy for small T1a glottic carcinomas: Costs, local control, survival, quality of life, and voice quality. Head Neck. 2007;29(2):128-36.
94. Silbergleit AK, Somers ML, Schweitzer VG, Gardner GM, Peterson E. Vocal fold vibration after photofrin-mediated photodynamic therapy for treatment of early-stage laryngeal malignancies. J Voice. 2013 Nov;27(6):762-4. PubMed PMID: 24119638.
95. Story W, Sultan AA, Bottini G, Vaz F, Lee G, Hopper C. Strategies of airway management for head and neck photo-dynamic therapy. Lasers Surg Med. 2013 Aug;45(6):370-6. PubMed PMID: 23775429.
96. Dörr W. Late effects of chemotherapy and radiation. In: Davis MP, Feyer PC, Ortner P, Zimmermann C, editors. Supportive Oncology2011. p. 429-37.

Publications in the series
Örebro Studies in Medicine
1. Bergemalm, Per-Olof (2004). Audiologic and cognitive long-term sequelae from closed head injury.
2. Jansson, Kjell (2004). Intraperitoneal Microdialysis. Technique and Results.
3. Windahl, Torgny (2004). Clinical aspects of laser treatment of lichen sclerosus and squamous cell carcinoma of the penis.
4. Carlsson, Per-Inge (2004). Hearing impairment and deafness. Genetic and environmental factors – interactions – consequences. A clinical audiological approach.
5. Wågsäter, Dick (2005). CXCL16 and CD137 in Atherosclerosis.
6. Jatta, Ken (2006). Inflammation in Atherosclerosis.
7. Dreifaldt, Ann Charlotte (2006). Epidemiological Aspects on Malignant Diseases in Childhood.
8. Jurstrand, Margaretha (2006). Detection of Chlamydia trachomatis and Mycoplasma genitalium by genetic and serological methods.
9. Norén, Torbjörn (2006). Clostridium difficile, epidemiology and antibiotic resistance.
10. Anderzén Carlsson, Agneta (2007). Children with Cancer – Focusing on their Fear and on how their Fear is Handled.
11. Ocaya, Pauline (2007). Retinoid metabolism and signalling in vascular smooth muscle cells.
12. Nilsson, Andreas (2008). Physical activity assessed by accelerometry in children.
13. Eliasson, Henrik (2008). Tularemia – epidemiological, clinical and diagnostic aspects.
14. Walldén, Jakob (2008). The influence of opioids on gastric function: experimental and clinical studies.
15. Andrén, Ove (2008). Natural history and prognostic factors in localized prostate cancer.
16. Svantesson, Mia (2008). Postpone death? Nurse-physician perspectives and ethics rounds.

17. Björk, Tabita (2008). Measuring Eating Disorder Outcome – Definitions, dropouts and patients’ perspectives.
18. Ahlsson, Anders (2008). Atrial Fibrillation in Cardiac Surgery.
19. Parihar, Vishal Singh (2008). Human Listeriosis – Sources and Routes.
20. Berglund, Carolina (2008). Molecular Epidemiology of Methicillin-Resistant Staphylococcus aureus. Epidemiological aspects of MRSA and the dissemination in the community and in hospitals.
21. Nilsagård, Ylva (2008). Walking ability, balance and accidental falls in persons with Multiple Sclerosis.
22. Johansson, Ann-Christin (2008). Psychosocial factors in patients with lumbar disc herniation: Enhancing postoperative outcome by the identification of predictive factors and optimised physiotherapy.
23. Larsson, Matz (2008). Secondary exposure to inhaled tobacco products.
24. Hahn-Strömberg, Victoria (2008). Cell adhesion proteins in different invasive patterns of colon carcinoma: A morphometric and molecular genetic study.
25. Böttiger, Anna (2008). Genetic Variation in the Folate Receptor-α and Methylenetetrahydrofolate Reductase Genes as Determinants of Plasma Homocysteine Concentrations.
26. Andersson, Gunnel (2009). Urinary incontinence. Prevalence, treatment seeking behaviour, experiences and perceptions among persons with and without urinary leakage.
27. Elfström, Peter (2009). Associated disorders in celiac disease.
28. Skårberg, Kurt (2009). Anabolic-androgenic steroid users in treatment: Social background, drug use patterns and criminality.
29. de Man Lapidoth, Joakim (2009). Binge Eating and Obesity Treatment – Prevalence, Measurement and Long-term Outcome.
30. Vumma, Ravi (2009). Functional Characterization of Tyrosine and Tryptophan Transport in Fibroblasts from Healthy Controls, Patients with Schizophrenia and Bipolar Disorder.
31. Jacobsson, Susanne (2009). Characterisation of Neisseria meningitidis from a virulence and immunogenic perspective that includes variations in novel vaccine antigens.

32. Allvin, Renée (2009). Postoperative Recovery. Development of a Multi-Dimensional Questionnaire for Assessment of Recovery.
33. Hagnelius, Nils-Olof (2009). Vascular Mechanisms in Dementia with Special Reference to Folate and Fibrinolysis.
34. Duberg, Ann-Sofi (2009). Hepatitis C virus infection. A nationwide study of assiciated morbidity and mortality.
35. Söderqvist, Fredrik (2009). Health symptoms and potential effects on the blood-brain and blood-cerebrospinal fluid barriers associated with use of wireless telephones.
36. Neander, Kerstin (2009). Indispensable Interaction. Parents’ perspectives on parent–child interaction interventions and beneficial meetings.
37. Ekwall, Eva (2009). Women’s Experiences of Gynecological Cancer and Interaction with the Health Care System through Different Phases of the Disease.
38. Thulin Hedberg, Sara (2009). Antibiotic susceptibility and resistance in Neisseria meningitidis – phenotypic and genotypic characteristics.
39. Hammer, Ann (2010). Forced use on arm function after stroke. Clinically rated and self-reported outcome and measurement during the sub-acute phase.
40. Westman, Anders (2010). Musculoskeletal pain in primary health care: A biopsychosocial perspective for assessment and treatment.
41. Gustafsson, Sanna Aila (2010). The importance of being thin – Perceived expectations from self and others and the effect on self-evaluation in girls with disordered eating.
42. Johansson, Bengt (2010). Long-term outcome research on PDR brachytherapy with focus on breast, base of tongue and lip cancer.
43. Tina, Elisabet (2010). Biological markers in breast cancer and acute leukaemia with focus on drug resistance.
44. Overmeer, Thomas (2010). Implementing psychosocial factors in physical therapy treatment for patients with musculoskeletal pain in primary care.
45. Prenkert, Malin (2010). On mechanisms of drug resistance in acute myloid leukemia.

46. de Leon, Alex (2010). Effects of Anesthesia on Esophageal Sphincters in Obese Patients.
47. Josefson, Anna (2010). Nickel allergy and hand eczema – epidemiological aspects.
48. Almon, Ricardo (2010). Lactase Persistence and Lactase Non- Persistence. Prevalence, influence on body fat, body height, and relation to the metabolic syndrome.
49. Ohlin, Andreas (2010). Aspects on early diagnosis of neonatal sepsis.
50. Oliynyk, Igor (2010). Advances in Pharmacological Treatment of Cystic Fibrosis.
51. Franzén, Karin (2011). Interventions for Urinary Incontinence in Women. Survey and effects on population and patient level.
52. Loiske, Karin (2011). Echocardiographic measurements of the heart. With focus on the right ventricle.
53. Hellmark, Bengt (2011). Genotypic and phenotypic characterisation of Staphylococcus epidermidis isolated from prosthetic joint infections.
54. Eriksson Crommert, Martin (2011). On the role of transversus abdominis in trunk motor control.
55. Ahlstrand, Rebecca (2011). Effects of Anesthesia on Esophageal Sphincters.
56. Holländare, Fredrik (2011). Managing Depression via the Internet – self-report measures, treatment & relapse prevention.
57. Johansson, Jessica (2011). Amino Acid Transport and Receptor Binding Properties in Neuropsychiatric Disorders using the Fibroblast Cell Model.
58. Vidlund, Mårten (2011). Glutamate for Metabolic Intervention in Coronary Surgery with special reference to the GLUTAMICS-trial.
59. Zakrisson, Ann-Britt (2011). Management of patients with Chronic Obstructive Pulmonary Disease in Primary Health Care. A study of a nurse-led multidisciplinary programme of pulmonary rehabilitation.
60. Lindgren, Rickard (2011). Aspects of anastomotic leakage, anorectal function and defunctioning stoma in Low Anterior Resection of the rectum for cancer.

61. Karlsson, Christina (2011). Biomarkers in non-small cell lung carcinoma. Methodological aspects and influence of gender, histology and smoking habits on estrogen receptor and epidermal growth factor family receptor signalling.
62. Varelogianni, Georgia (2011). Chloride Transport and Inflammation in Cystic Fibrosis Airways.
63. Makdoumi, Karim (2011). Ultraviolet Light A (UVA) Photoactivation of Riboflavin as a Potential Therapy for Infectious Keratitis.
64. Nordin Olsson, Inger (2012). Rational drug treatment in the elderly: ”To treat or not to treat”.
65. Fadl, Helena (2012). Gestational diabetes mellitus in Sweden: screening, outcomes, and consequences.
66. Essving, Per (2012). Local Infiltration Analgesia in Knee Arthroplasty.
67. Thuresson, Marie (2012). The Initial Phase of an Acute Coronary Syndrome. Symptoms, patients’ response to symptoms and opportunity to reduce time to seek care and to increase ambulance use.
68. Mårild, Karl (2012). Risk Factors and Associated Disorders of Celiac Disease.
69. Fant, Federica (2012). Optimization of the Perioperative Anaesthetic Care for Prostate Cancer Surgery. Clinical studies on Pain, Stress Response and Immunomodulation.
70. Almroth, Henrik (2012). Atrial Fibrillation: Inflammatory and pharmacological studies.
71. Elmabsout, Ali Ateia (2012). CYP26B1 as regulator of retinoic acid in vascular cells and atherosclerotic lesions.
72. Stenberg, Reidun (2012). Dietary antibodies and gluten related seromarkers in children and young adults with cerebral palsy.
73. Skeppner, Elisabeth (2012). Penile Carcinoma: From First Symptom to Sexual Function and Life Satisfaction. Following Organ-Sparing Laser Treatment.
74. Carlsson, Jessica (2012). Identification of miRNA expression profiles for diagnosis and prognosis of prostate cancer.
75. Gustavsson, Anders (2012): Therapy in Inflammatory Bowel Disease.

76. Paulson Karlsson, Gunilla (2012): Anorexia nervosa – treatment expectations, outcome and satisfaction.
77. Larzon, Thomas (2012): Aspects of endovascular treatment of abdominal aortic aneurysms.
78. Magnusson, Niklas (2012): Postoperative aspects of inguinal hernia surgery – pain and recurrences.
79. Khalili, Payam (2012): Risk factors for cardiovascular events and incident hospital-treated diabetes in the population.
80. Gabrielson, Marike (2013): The mitochondrial protein SLC25A43 and its possible role in HER2-positive breast cancer.
81. Falck, Eva (2013): Genomic and genetic alterations in endometrial adenocarcinoma.
82. Svensson, Maria A (2013): Assessing the ERG rearrangement for clinical use in patients with prostate cancer.
83. Lönn, Johanna (2013): The role of periodontitis and hepatocyte growth factor in systemic inflammation.
84. Kumawat, Ashok Kumar (2013): Adaptive Immune Responses in the Intestinal Mucosa of Microscopic Colitis Patients.
85. Nordenskjöld, Axel (2013): Electroconvulsive therapy for depression.
86. Davidsson, Sabina (2013): Infection induced chronic inflammation and its association with prostate cancer initiation and progression.
87. Johansson, Benny (2013): No touch vein harvesting technique in coronary by-pass surgery. Impact on patency rate, development of atherosclerosis, left ventricular function and clinical outcome during 16 years follow-up.
88. Sahdo, Berolla (2013): Inflammasomes: defense guardians in host-microbe interactions.
89. Hörer, Tal (2013): Early detection of major surgical postoperative complications evaluated by microdialysis.
90. Malakkaran Lindqvist, Breezy (2013): Biological signature of HER2-positive breast cancer.

91. Lidén, Mats (2013): The stack mode review of volumetric datasets – applications for urinary stone disease.
92. Emilsson, Louise (2013): Cardiac Complications in Celiac Disease.
93. Dreifaldt, Mats (2013): Conduits in coronary artery bypass grafting surgery: Saphenous vein, radial and internal thoracic arteries.
94. Perniola, Andrea (2013): A new technique for postoperative pain management with local anaesthetic after abdominal hysterectomy.
95. Ahlstrand, Erik (2013): Coagulase-negative Staphylococci in Hematological Malignancy.
96. Sundh, Josefin (2013): Quality of life, mortality and exacerbations in COPD.
97. Skoog, Per (2013): On the metabolic consequences of abdominal compartment syndrome.
98. Palmetun Ekbäck, Maria (2013): Hirsutism and Quality of Life with Aspects on Social Support, Anxiety and Depression.
99. Hussain, Rashida (2013): Cell Responses in Infected and Cystic Fibrosis Respiratory Epithelium.
100. Farkas, Sanja (2014): DNA methylation in the placenta and in cancer with special reference to folate transporting genes.
101. Jildenstål, Pether (2014): Influence of depth of anaesthesia on post-operative cognitive dysfunction (POCD) and inflammatory marker.
102. Söderström, Ulf (2014): Type 1 diabetes in children with non-Swedish background – epidemiology and clinical outcome
103. Wilhelmsson Göstas, Mona (2014): Psychotherapy patients in mental health care: Attachment styles, interpersonal problems and therapy experiences
104. Jarl, Gustav (2014): The Orthotics and Prosthetics Users´ Survey: Translation and validity evidence for the Swedish version
105. Demirel, Isak (2014): Uropathogenic Escherichia coli, multidrug-resistance and induction of host defense mechanisms
106. Mohseni, Shahin (2014): The role of ß-blockade and anticoagula-tion therapy in traumatic brain injury

107. Bašić, Vladimir T. (2014): Molecular mechanisms mediating development of pulmonary cachexia in COPD
108. Kirrander, Peter (2014): Penile Cancer: Studies on Prognostic Factors
109. Törös, Bianca (2014): Genome-based characterization of Neisseria meningitidis with focus on the emergent serogroup Y disease
110. von Beckerath, Mathias (2014): Photodynamic therapy in the Head and Neck