
Novi Dewan Indian Life and Health Insurance Industry
182
Novi Dewan Indian Life and Health Insurance Industry
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Novi Dewan Indian Life and Health Insurance Industry

Novi Dewan
Indian Life and Health Insurance Industry

GABLER EDITION WISSENSCHAFTInternational Management ScienceEditorsMichael Frenkel, WHU – Otto Beisheim School of ManagementFrank Himpel (Managing Editor), University of MainzAnshuman Khare, Athabasca UniversityPete Nye, University of WashingtonKatharina J. Auer-Srnka, University of Vienna
Editorial Advisory BoardKlaus Bellmann, University of MainzMarc Förstemann, A.T. KearneyRené Haak, German Federal Ministry of Education and ResearchEvi Hartmann, European Business SchoolSabine T. Köszegi, University of ViennaMarkus Pütz, University of WuppertalJürgen Schröder, University of MannheimPaula M.C. Swatman, University of South AustraliaMichael Weller, Clifford ChanceJochen Wittmann, Dr Ing hc F Porsche AG
The aim of International Management Science is to promote interna-tional research and understanding of strategic issues in managementtopics. The series embraces a wide range of methodologies, approa-ches, traditions, and schools of thought. The mission of InternationalManagement Science is to meet the demands of the scholarly community sharing an interest in the management of strategic contextsin the regions of North America, Europe, Asia, and Australia.

Novi Dewan
Indian Life and Health Insurance IndustryA Marketing Approach
With forewords by Martin Fassnacht and Dirk Schmidt-Gallas
GABLER EDITION WISSENSCHAFT

Bibliographic information published by Die Deutsche NationalbibliothekDie Deutsche Nationalbibliothek lists this publication in the Deutsche Nationalbibliografie;detailed bibliographic data is available in the Internet at <http://dnb.d-nb.de>.
1st Edition 2008
All rights reserved© Betriebswirtschaftlicher Verlag Dr. Th. Gabler | GWV Fachverlage GmbH, Wiesbaden 2008
Editorial Office: Frauke Schindler / Anita Wilke
Gabler-Verlag is a company of Springer Science+Business Media.www.gabler.de
No part of this publication may be reproduced, stored in a retrieval systemor transmitted, mechanical, photocopying or otherwise without priorpermission of the copyright holder.
Registered and/or industrial names, trade names, trade descriptions etc. cited in this publica-tion are part of the law for trade-mark protection and may not be used free in any form or byany means even if this is not specifically marked.
Cover design: Regine Zimmer, Dipl.-Designerin, Frankfurt/MainPrinted on acid-free paperPrinted in Germany
ISBN 978-3-8349-0946-6

Foreword
The Indian market with its one billion plus population, presents lucrative and diverseopportunities for various industries. However, the intricacies that make up this mar-ket are not very well known to most people, particularly those living in developedcountries. India with its numerous and varied sub-cultures presents a microcosmicview of the world itself – it constitutes a small, representative system that has analo-gies to a larger world in configuration and/or development. This makes the study ofthe Indian insurance industry especially pertinent and appealing as it goes beyond theIndian market, facilitating an understanding of the dynamics of other countries/mar-kets with similar growth paths.
In her book, Novi Dewan provides an insight into the history, development, currentsituation and the emerging challenges and opportunities of the insurance industry inIndia. She methodically focuses on the marketing aspects of the life and health insur-ance industry with respect to the four Ps (product, price, place, promotion). In orderto substantiate her findings, Miss Dewan has conducted and presented the results ofan empirical study that comprises standardized interviews with decision makers ofIndian insurance companies.
The book is divided into four main sections. In the first section, the author presentsan understanding of the overall Indian Insurance Industry vis-à-vis other markets.Additionally, the rapid changes in the regulatory environment and the consequenteconomic impact on the industry are discussed. In the second and third sections,Miss Dewan systematically elaborates on the life and health insurance industry inlight of classical elements of marketing – the 4Ps and her empirical findings. Thebook ends with an outlook and prescriptive approach summarizing the best practicesfor the two industries.
It is indeed an excellent book for anyone interested in an in depth understanding ofinsurance in general, the Indian insurance industry in specific, the correspondingmarketing facets and best practices and a consequent comprehension of the insurancesector in countries with similar trajectories of growth.
Professor Martin FassnachtWHU – Otto Beisheim School of Management
Associate Dean and Holder of theOtto Beisheim Endowed Chair of Marketing and Commerce

Foreword
The heat is on. While many mature insurance markets are halting in stagnation, newand fast-growing economies are appearing on the international stage of the insurancebusiness and are offering opportunities that sometimes leave the bystanders breathless.
This has not gone unnoticed. Major players from across the globe have been joiningthe gold rush and entering promising markets such as India or China to conquer theAsia-Pacific region and reap the benefits from the enormous growth materialisingthere. Due to regulatory requirements, most of them enter partnerships to avoid settingup a distribution network from scratch or to benefit from a partner’s local experience.
India is, by all accounts, a prime target of this movement. Once a crown jewel ofthe British Empire, it is already on its way towards developing into a gem of the glob-al insurance industry.
However, the market today is still comparably small. Its gross written premiums ofabout 25 billion USD (world: 3,151 billion USD) only put it in fourth place in theAsia-Pacific, well behind Japan holding roughly 64% of the region’s market, SouthKorea (approx. 11%) and China (approx. 8%). India currently only accounts forslightly more than three percent of the region’s premium.
This market’s charm, however, stems from its enviable growth story. The potentialseems enormous. International comparisons show, for example, that only countrieslike Egypt or Mexico have a lower penetration of life insurance (India approx. 2.5%),looking meagre compared to Taiwan’s staggering 11%. More than 100 million house-holds are well aware of the life insurance concept without owning one. The potentialof those who are not yet educated about insurance seems to offer even bigger poten-tial in light of a population of over one billion.
But India is catching up at a fast pace. While the whole region has grown by lessthan four percent in 2005, India’s growth stands at 14%. New life policies havegrown by more than 35% in 2005, and privately held insurance companies (as op-posed to the public sector offering insurance) have realised an even more impressivegrowth rate of above 73%.
The outlook continues to be bold: The Indian insurance market is forecasted to havegrown by more than 60% in 2010, considerably outpacing the dynamic developmentof the Asia-Pacific region (which will have grown by 23% in the same time frame).
A brief look back into history – During its colonial aftermath, the Indian insurancemarket was private, then taken over by the government. Since 2000, more and morerights have been granted to private insurance providers.
While the public providers still hold a market share of about 80%, privately heldinsurance companies by far outpace them as mentioned above. Legal privatisation is

followed by an unstoppable factual privatisation, driven by the expertise that top-notch foreign partners inject into the partnerships with local experts to provide supe-rior products and services. While only 73% of all grievances are solved by publics,the ratio of privates stands at more than 93%.
Other markets have gone down this road already and they are vivid testimonials tothe dangers along the way. Price wars, loss-leading products without cross-sellingever materialising, a focus on growth that sacrifices profits, and returns that are hard-ly attractive to investors can be the disappointing results.
India is not immune. Since January 2007, the formerly regulated tariffs have beenopened to the free market game play. It is important, however, to understand that theIndian market is coming from much less than a balance. While fire and motor poli-cies, for example, have been very profitable, others such as health and marine insur-ance were cross-subsidised. It remains to be seen whether deregulation will lead tofire and motor prices falling and even more importantly, if the prices of health, ma-rine and others can be brought up to compensate. Increasing prices have always beenthe kingpin of all pricing measures, only mastered by few.
The current state of pricing in China warrants a word of caution, as India may fol-low a similar path. The underwriting discipline and capability of many Chinese play-ers is very low. Growth is put before profitability and the appetite for risk seems insa-tiable. Rogue pricing is used to buy market share.
Consequently in India, a well-defined appetite for risk must be underscored bysound underwriting practices that have yet to be established and costs should be con-tained by proven measures to fight fraud (such as in Indonesia, where the insurancecompany dictates the repair shop that has to be used when a motor claim is made).This is important since risk costs are the lower boundaries of price and therefore vitalfor proper tariff-setting in a market economy.
The price, however, is only the flip-side of the value provided to the customer.Hence, the challenges run deeper than can be tackled with proper underwriting andrisk-based pricing. As of April 2008, not only the prices but also the terms and condi-tions can be set freely by insurance companies in India.
Novi Dewan’s book impressively shows that today’s insurance products in Indiaare lacking differentiation and that the customer segmentation currently used is inap-propriate, as it is mainly based on demographics or life-cycle stages. As a conse-quence, delivering real customer value that would justify profitable prices will provea daunting task.
The author also demonstrates the idiosyncratic characteristics of the Indian insur-ance market that will make the simple transfer of existing models from other parts ofthe world impossible. Among them are:
VIII Foreword

• Geography: 75% of all households in Bangalore possess life insurance, whereasthe overall penetration is less than three percent.
• Society: Despite a strong middle class, the divide between rich and poor seems towiden, calling for a multi-tiered approach to develop the market.
• Demographics: Younger generations turning their backs on rural India to pursuetheir happiness in the big cities render traditional models of retirement fundingfragile.
• Culture: The Indian consumer considers himself indestructible and therefore not inneed of insurance – behaviour well-known from other markets such as Malaysia.
Miss Dewan goes well beyond a pure description of the status quo. She uses a com-prehensive and well-proven arsenal of scientific instruments to render managerially-relevant prescriptions. She concentrates her studies on life and health insurance.These two business lines are wisely chosen: Life insurance constitutes 80% of thepresent insurance business in India and health insurance used to be a loss-leadingproduct that may well serve as the acid test of whether the free market will only serveto drive prices down or whether insurers succeed in translating product value into ahealthy bottom-line.
The author systematically develops a marketing concept for the Indian insurancemarket. Much of what she derives for the life and health markets should be conceptu-ally transferable to the general insurance arena. She includes all aspects of the classi-cal marketing mix, the 4 Ps of product, price, placement and promotion.
The scientific work is never done as a l’art pour l’art, but always yields tangiblepractical implications. This is garnished with the results from an empirical studyamong stakeholders of the Indian insurance market such as senior executives as wellas the regulator and best practices from current players.
The reader can expect three types of lessons:
1. A comprehensive description of the status quo of the Indian insurance market.2. Hands-on advice for successful insurance marketing in this environment.3. Insights for other markets that may follow a similar trajectory.
What is this book about? At the very core, it is about market excellence which I de-fine as the ability of an insurance company to
• understand customer, competitor and sales dynamics• define innovative and powerful value propositions based on this understanding• deliver exceptional value to the customer• extract this value to the benefit of the insurer by charging high prices, not low
prices.
Foreword IX

Our projects show that this skill set is largely underdeveloped in the insurance world.Our comparative studies show that many other industries are well ahead of the insur-ance sector. Even the banking industry as a very traditional industry is three to fiveyears ahead of insurers.
The insurance industry in general is inward-looking, resistant to change, sees thecustomer as a cost-driver rather than a profit-driver, poor in designing customer-ori-ented value propositions and believes that pricing should be based on risk and othercosts.
However, cost-based pricing is something that other more advanced and customer-oriented industries have abandoned decades ago. It’s the value that counts. The typi-cal excuses that insurance products allegedly are commodities that are being soldrather than bought do not carry any weight.
What does that mean for successful marketing in India? There have to be differen-tiated offerings for a polarised society with a strong middle class. Customer segmen-tation has to be done based on benefits, not demographics. Price elasticities, the rela-tionship between price adjustments and their impact on volumes have to be re-searched to allow pricing that optimises the bottom-line.
The low financial literacy of the Indian consumer makes customer perceptionsmuch more important than objective measures. Typically, the insurance industryturns a blind eye on such psychological phenomena.
Finally, the trade-off between growth and profits must be addressed early. Manymarkets have been drawn into price wars in the past by insurance executives puttinggrowth before profits hoping that as soon as a high market share has been realised,profits will follow. In most cases, this has not materialised.
India and other comparable markets offer ample opportunity for breathtaking prof-itable growth. Will insurance executives reap the benefits of this growth without de-stroying their profits?
Dr. Dirk Schmidt-GallasPartner and Global Head of Insurance,
Simon-Kucher & Partnerswww.simon-kucher.com
X Foreword

Preface
India, with a population of over 1 billion, offers magnanimous potential for insuranceby virtue of two aspects foundational to the concept of insurance: [a] risk reductionthrough pooling and [b] probability theory and law of large numbers.
India’s rapid rate of economic growth over the past decade has been one of themore significant developments in the global economy. This growth has its roots in theintroduction of economic liberalization in the early 1990s, which has allowed Indiato exploit its economic potential and raise the population’s standard of living. Insur-ance has a very important role in this process. Health insurance and pension systemsare fundamental to protecting individuals against the hazards of life. Private insur-ance systems complement social security systems and add value by matching riskand price. Accurate risk pricing is one of the most powerful tools for setting the rightincentives for the allocation of resources, a feature which is key to a fast developingcountry like India. By nature of its business, insurance is closely related to saving andinvesting. Life insurance, funded pension systems and (to a lesser extent) non-life in-surance, will accumulate huge amounts of capital over time which can be investedproductively in the economy. In developed countries (re)insurers often own morethan 25% of the capital markets. The mutual dependence of insurance and capitalmarkets can play a powerful role in channeling funds and investment expertise tosupport the development of the Indian economy. (Sinha)
The massive population, sound economic fundamentals, huge consuming middleclass, an improvement in the insurance regulatory framework and increasing aware-ness amongst Indians about the relevance of health and life insurance in India as in-struments of risk mitigation, security, tax-savings and even investment (with ULIPs),call for an understanding of the insurance industry in India.
This study forms the master thesis which is part of the 16-month MBA program atthe WHU – Otto Beisheim School of Management, in collaboration with SimonKucher and Partners. The main purpose of this study is to understand the current sta-tus of the Indian Insurance Industry in general and life and health insurance industryin specific from a marketer’s point of view. This report intends to serve as a researchinput by projecting a picture of the Indian Insurance Market and thereby helpingreaders understand the insurance paradigm of other emerging markets – like LatinAmerica and certain markets in Asia, that closely mirror India’s development pattern.
Moreover, the aim of this report is to provide a strategic marketing perspective;hence I have sought to make the report comprehensive by adopting a scientific ap-proach through – the projection of best practices, marketing methodologies and tools,mapping empirical data from latest insurance journals, magazines and specialized

books onto these tools and finally summarizing primary data which includes inter-views/surveys of insurance executives/senior management.
The study begins with an analysis of evolution of insurance in India to understandits relevance in today’s context; it then moves on to understanding the dynamic mar-ket environment owing to the changes in the Indian insurance backdrop that have beenbrought about through deregulation and now de-tariffing of the general insurancearea. An understanding of the role of the regulator (Insurance Regulatory Develop-ment Authority of India) is crucial in order to comprehend the regulator’s contributionin shaping and promoting the Indian insurance business through laws that seek to pro-tect the policyholder’s interest, enhance the competitive environment, promote inno-vation and improve the sophistication of customer service. The study then analysesthe status quo of the Indian market vis-à-vis the Asian and Global insurance market.
The study develops to analyze the life and health insurance market in depth in lieuof the elements of marketing mix; projecting best practices and empirical evidencevia the survey “Emerging Opportunities and Challenges for the Insurance Industry inIndia.” The report concludes with an outlook for the Indian insurance industry and asummary of best practices.
The report intends to provide an overview of the health and life insurance industry;the data from this report should be furthered in order to enhance research in any par-ticular facet of marketing of the two areas – life and health. Moreover, the scope ofthis research may be augmented by considering other areas of insurance in India. Fi-nally, as mentioned previously, the insights from this report can be used to serve as amodel basis for other emerging markets, thus an analysis of insurance in similar mar-kets may be developed along the lines of this study.
Acknowledgment
This study has been plausible because of the impetus, contribution and relentless helpand support of several people. I would like to thank my parents, Mr. Bhushan Dewanand Dr. (Mrs) Ranjna Dewan for their constant support and ideas even while they aremiles away in India. I would like to thank Jan Richard and Matthew Armstrong foreverything. They also re-revised my thesis and supported me during my phases of dif-ficulty. My friends and mentors – Ravi Punjabi, Zeeshan Sultan and Kabir Wadiwalafor being my strongest pillars of encouragement since I have known them. I wouldlike to thank the perfect financial services team at Simon Kucher & Partners who of-fered diligent support and guidance even though I was working from home.
Alexander Dechent, my mentor at Simon Kucher, who, despite his ongoing projectdeliveries and responsibilities at SKP, offered exceptional suggestions, precisethought process, relentless guidance, continual follow-up and an immense amount of
XII Preface

time and efforts, that played a key role in the direction and formulation of my thesis.Moreover, Vanessa Behling for her presence, Daniel Loskamp for his philanthropiccontribution to my research via an article that he sent.
I would like to thank Heidi Hoffmann, the program manager of the MBA program,for a well-designed program and the endless and kind support she offered me andseveral others in helping us integrate into the lovely environment of the school andculture, my classmates, for their exotic complementarities and attributes; that servedas a steady source of entertainment and learning. Prof. Dr. Jurgen Weigand, the Deanof the program, an exceptional professor and a constant source of rock steady inspira-tion and help. He guided, spoke, discussed and suggested each and every time hecould despite his busy schedule and endless commitments. Prof. Dr. MichaelFrenkel, the Dean of the school, one of the best professors, the kindest and most hum-ble individual with his untiring spirit for the school, the program and its students; andhis conscientious effort towards improving the school and paying attention to everylittle feedback and/or complaint.
Dr. Dieter Lauszus, SKP, who interviewed me and was very kind and approachableeven on the interview day, Dr Dirk Schmidt-Gallas, also leading the financial servic-es team at SKP, who interviewed me on business and domain knowledge and skills;and merely by his style of interviewing taught me the critical ways of addressingbusiness problems and arriving at thought-process-driven and logic-driven appropri-ate solutions in an efficient and yet meticulous way. Dr. Schmidt-Gallas was the oneresponsible for giving me this prospect to work on the “Insurance Industry in India”and integrating me in his team at Franfurt. Dr. Lauszus’ and Dr. Schmidt-Gallas’ re-search papers on insurance and pricing served contributory to several sections of mythesis. Prof. Dr. Hermann Simon, the CEO of Simon Kucher and Partners, who wasso kind to personally meet with me on my interview day and bestow me with thelovely opportunity to work with his esteemed organization. I would like to thankDr. Frank Himpel, editor, Anita Wilke, editorial office at Gabler and Mr. Baier, whoformatted the manuscript, for their incessant support and follow-up while editing thisbook. They offered me their time and insightful ideas on how to go about publishingthis study into a book. Without them this book would not be a possibility.
Last, but not the least, I would like to thank Prof. Dr. Martin Fassnacht, the Associ-ate Dean of WHU, my supervising professor. An outstanding professor, he taught usmarketing in a way that was unique, enjoyable and engaging. A meticulous mentor,who always took pains to read, made contributory suggestions, and offered hisrevered views and opinion to everything that I presented to him for advice and an un-varying teacher, who appreciated and cared for his students in his own kind way.
Novi Dewan
Preface XIII

Contents
Foreword Prof. Fassnacht . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Foreword Dr. Schmidt-Gallas . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Preface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table of Illustrations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1 Insurance Industry in India . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1.1 Insurance – Introduction and History . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1.2 An Analysis of Evolution of Insurance in India . . . . . . . . . . . . . . . . . . . . .1.3 Dynamic Market Environment for Insurance in India . . . . . . . . . . . . . . . .1.4 Authorities and Regulatory Environment . . . . . . . . . . . . . . . . . . . . . . . . . .1.5 Status Quo – The Indian Market vis-à-vis other Markets . . . . . . . . . . . . . .
2 Life Insurance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2.1 Industry Outlook and Major Players . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2.2 Market Opportunities and Challenges: Empirical Results and Analysis . .2.3 Urgent Needs and Customer Segmentation . . . . . . . . . . . . . . . . . . . . . . . .2.4 Products . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2.5 Pricing Criteria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2.6 Distribution Channels . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2.7 Communication Strategy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3 Health Insurance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3.1 Industry Outlook and Major Players . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3.2 Market Opportunities and Challenges: Empirical Results and Analysis . .3.3 Urgent Needs and Customer Segmentation . . . . . . . . . . . . . . . . . . . . . . . .3.4 Products . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3.5 Pricing Criteria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3.6 Distribution Channels . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3.7 Communication Strategy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4 Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4.1 Outlook for the Life and Health Insurance Market in India . . . . . . . . . . . .4.1 Summary of the Best Practices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Appendix . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Bibliography . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
About the Author . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
V
VII
XI
126
142732
4546525662707690
101102108112118126130139
143144147
151
165
169
XVII

Table of Illustrations
Fig. 1: Financial Savings of the Household Sector (Graph) . . . . . . . . . . . . . . . 6Fig. 2: Financial Savings of the Household Sector (Table) . . . . . . . . . . . . . . . . 7Fig. 3: Milestones of Evolution of Insurance before Nationalization . . . . . . . . 8 Fig. 4: Rural Share of Life Insurance Business in India . . . . . . . . . . . . . . . . . . 9Fig. 5: Milestones of Evolution of Insurance after Nationalization in 1956 . . . 11Fig. 6: Relationship between national savings and life insurance
premium, 1950–1991 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Fig. 7: Convergence of Efficiency amongst the 4 public sector general
insurers (1997–2003) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Fig. 8: Factors influencing the Company Marketing Strategy . . . . . . . . . . . . . 15Fig. 9: PEST Analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Fig. 10: Facets while considering effects of de-tariffing . . . . . . . . . . . . . . . . . . . 19Fig. 11: Porter’s Five Force Analysis of the Insurance Industry . . . . . . . . . . . . . 20Fig. 12: Anita McGahan’s Model for Strategies in Dynamic Environments . . . 24Fig. 13: LUDI’s Internationalization Cube . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26Fig. 14: Status of Grievances – Non-Life Insurers (2005–2006) . . . . . . . . . . . . 28Fig. 15: Status of Grievances – Life Insurers (2005–2006) . . . . . . . . . . . . . . . . 28Fig. 16: Investment Regulations for the Life Insurance Business . . . . . . . . . . . . 30Fig. 17: Investment Regulations for the General Insurance Business . . . . . . . . . 31Fig. 18: Key Highlights of Indian Insurance vis-à-vis Asia Pacific & Global
Insurance Markets . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34Fig. 19: Market Value Comparison Chart . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35Fig. 20: Market Value (Growth Rate) Comparison Chart . . . . . . . . . . . . . . . . . . 36Fig. 21: Market Segmentation: Life and Non-Life . . . . . . . . . . . . . . . . . . . . . . . 36Fig. 22: Market Segmentation: By Geography . . . . . . . . . . . . . . . . . . . . . . . . . . 37Fig. 23: Market Value Forecast: 2010 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39Fig. 24: Market Value (% growth) forecast: 2010 . . . . . . . . . . . . . . . . . . . . . . . . 40Fig. 25: Insurance Penetration Comparison Chart in the Life Insurance Area . . 41Fig. 26: Insurance Penetration Comparison Chart in the Non-Life Area . . . . . . 41Fig. 27: Insurance Density Comparison Chart in the Life Insurance Area . . . . . 42Fig. 28: Insurance Density Comparison Chart in the Non-Life Insurance Area . 43Fig. 29: Market Share development for first year, renewal and total premium
for Life Insurers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47Fig. 30: New Policies Issued: Life Insurers Development and Market Share . . . 48Fig. 31: SEC for Urban India . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57Fig. 32: SEC for Rural India . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58

Fig. 33: Relation between SEC and HPI . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60Fig. 34: Pricing Levels based on Profit Potential and Professionalism . . . . . . . 72Fig. 35: New Business Underwritten through various Intermediaries in Life
Insurance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78Fig. 36: Representation of Relationships of Agents and Brokers with Insurers I 83Fig. 37: Representation of Relationships of Agents and Brokers with Insurers II 83Fig. 38: Key Differences between Brokers and Agents . . . . . . . . . . . . . . . . . . . 83Fig. 39: The Role of Service Communications in determining Marketing and
Firm Value . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 91Fig. 40: IMC Audience Contact Tools . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 93Fig. 41: TV Advertisement Volumes for the year 2006 by Category . . . . . . . . . 94Fig. 42: Seasonality Trend of Advertising for the Insurance sector on TV:
2005–2006 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 94Fig. 43: Top 3 Channels contributed 52% of ad volumes in the Insurance Sector
on TV: 2006 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 95Fig. 44: Top 5 Advertisers of the Insurance Sector on TV in 2006 . . . . . . . . . . . 95Fig. 45: Options of Service Communications for making Services Tangible . . . 96Fig. 46: Approach proposed for Financing of Health Expenditure . . . . . . . . . . . 104Fig. 47: Overall Healthcare Financing Situation in India . . . . . . . . . . . . . . . . . . 104Fig. 48: Health Insurance Development (in Rupees Billion) . . . . . . . . . . . . . . . 105Fig. 49: Development of Number of Policies issued year wise . . . . . . . . . . . . . 106Fig. 50: The Stimulus-Organism-Response Model . . . . . . . . . . . . . . . . . . . . . . 112 Fig. 51: Health Matters Survey and SOR Model . . . . . . . . . . . . . . . . . . . . . . . . 113Fig. 52: Asian Attitude Comparisons to risk and insurance . . . . . . . . . . . . . . . . 114Fig. 53: Customer Segments and Segmentation Variables for Bajaj Allianz . . . 116Fig. 54: Five Patterns of Target Market Selection . . . . . . . . . . . . . . . . . . . . . . . . 117Fig. 55: Shortcomings & Innovations in the Development of the Mediclaim
Policy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 121Fig. 56: Evolution of Medical Insurance Business . . . . . . . . . . . . . . . . . . . . . . . 122Fig. 57: A Health Insurer’s Cost Sheet . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 126Fig. 58: Types of “Risks” subject to “Downstream Delegation” or Outsourcing 132Fig. 59: Workflow for the Cashless Treatment . . . . . . . . . . . . . . . . . . . . . . . . . . 133Fig. 60: Top Growing Segments of Insurance Sector for TV Advertising in the
year 2006 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 140
XVIII Table of Illustrations

Chapter 1:Insurance Industry in India
This chapter starts with an analysis of evolution of insurance in India which isessential because insurance in India commenced with a de-regulated environ-ment (or private firms), moved to a regulated/government owned environ-ment and finally completed a full circle with de-regulation in the year 2000.The next sub-chapter discusses the dynamic market environment for insur-ance in India, in lieu of the changing regulations, de-tariffing of the generalinsurance industry and discussions about increase in foreign-equity cap. Thissub-chapter examines the environmental factors from the insurer’s point ofview, de-tariffing and its consequences, the porter’s 5 forces analysis, thekind of change and trajectory that the industry is expected to undergo, thetype of internationalization strategy that a foreign player must pursue. Thenext sub-chapter details the role of the authority/regulator in shaping and pro-moting the business environment and enlists the statutory functions of the IR-DA (the regulator). The final sub-chapter examines the Indian Market as-isvis-à-vis other markets; the Asian and Global Insurance markets illustratingmarket value, market value forecast, premium share of the total market acrossgeographies and categories, insurance penetration, insurance density andcompetitive landscape comparisons.

2 1 Insurance Industry in India
1.1 Insurance – Introduction and History
Introductory Terms to Insurance
An essential commodity in terms of social security, insurance simplistically definedhas two fundamental characteristics
– Transferring or shifting risk from one individual to a group– Sharing losses, on some equitable basis, by all members of the group
From an individual’s point of view, insurance is an economic device whereby the in-dividual substitutes a small certain cost (the premium) for a large uncertain financialloss (the contingency insured against) that would exist if it were not for the insurance.The primary function of insurance is to create a counterpart of risk, which is security.
From a social point of view, insurance is an economic device for reducing andeliminating risk through the process of combining a sufficient number of homoge-nous exposures into a group to make the losses predictable for the group as a whole(Vaughan and Vaughan).
Insurance Sector Revisited
Looking back in the Time Machine
Interesting accounts of ancient commerce have revealed the initial attempts of hu-mans at insurance. Around 6000 years ago, Babylonians, whose home in the Tigris-Euphrates Valley lay at the crossroads of early world traffic, had developed businesspractices to high degrees of sophistication. Babylon, a territory where all importantland trade routes converged, became the clearing house of trade. Though Babylonbuilt up a worthy commercial system, and its people were the first to enjoy the fruitsof political economy, the travelers were exposed to risks of robbery, pirates and un-canny winds at the seas. Human ingenuity was set to work and, in course of time, apractice developed that debt of the trader, both principal and interest, should be ab-solved if certain specified contingencies occur. By 2000 BC, the Babylonians and an-cient Hindus were familiar with the essentials of the insurance contract as indicatedby the provisions included in the codes of Hammurabi and Manu; the Babyloniancontract and the code of Hammurabi applying mostly to caravans, and Manu Dhar-mashastra referring to both seaborne and overland traffic.
Better and more sophisticated insurance came of age in the 11th century, on thebeach of Hastings, when King Harold (who carried a large Personal Disability Insur-ance) was shot dead by a Norman bowman firing through a narrow slit in the defensewall. His queen immediately got in touch with the insurance company enclosing a

plan, as required on the claim form showing the path of the arrow. The insurers exam-ined the policy for a few days and grew desperate at their inability to find a way of le-gitimately escaping the deal, when a bright “employee” noticed a gap in the defenses.Keeping the defenses without gap was a policy condition and was Harold’s responsi-bility, “Here”, he said, “if the gap wasn’t there, the arrow would never have gottenthrough, so there can be no claim” and that was how the “loophole” entered the histo-ry of insurance or more precisely said the ingenuity in drafting the policy documentwith clauses and “if-conditions” (Ayyar).
Understanding Insurance
Insurance is a service, which is sought to be commoditized for better conceptualiza-tion in keeping with the other unification trends running across the world. Insurerssell a promise to pay or defray on a future date for a predefined contingency. Thefunction of insurance is to protect a few against the heavy financial impact of the ex-pected loss by dispersing the losses among many who are exposed to homogenousrisks.
Initially insurance business structure was architected in three dimensions:
– The cross section of people, property or interest– Pre-determinable risks– Time ambit of coverage (Mishra and Mishra)
Insurance products were designed around such dimensions. Then started the era ofclassification of such products – choices of handling the assorted products createdtwo classes of insurers – life and non-life; life meant human life.
The discovery driven insurance industry encountered the problem of size. To prunethe vertical risk size another class of insurance business evolved, which is now fa-mous as reinsurance (Mishra and Mishra).
Augmentation of the Sector
Insurance products slowly incorporated other developments in the society and eco-nomics. Monetization of economy assorted the income of people into propensity toconsume and propensity to save. Such individual savings were pooled to classes ofinvestments depending on the economies of scope, scale and prioritization for thepurpose of common social good. There was need to internalize functional efficiencyin mobilizing the savings. Functional efficiency consists of allocative and operativeefficiency. Insurance sector got the share of these savings in the equilibrating processof allocative efficiency. Thus, the insurance sector found a new way to augment itsbusiness. Insurance products packaged savings features with risk management fea-
1.1 Insurance – Introduction and History 3

4 1 Insurance Industry in India
tures. The demand for operative efficiency forced insurers to define their core com-petencies; thus called for compartmentalization of insurance activities either by dic-tates of operative efficiency or by statutory and prudential regulations.
Originally meant to be a support service, the sector proved its excellence like a sol-id sphere and developed hydra-headed growth characteristics. The possibilities werepruned by regulations and that seemed to be the only constraining factor for the all-engulfing growth possibilities of the sector; which explains, as the global thrust onderegulation and liberalization compels nations to open up doors for the insurancesector growth, there is a stampede to enter into the sector.
The cardinal attraction of the insurance sector is harnessing long term funds forlong term investments in ever expanding sectors like infrastructure, technology andR & D. The earning potential of these sectors seem almost endemic (Mishra andMishra).

Tools and Methodology
Tools and methodologies have been used in order to contextually understand the In-dian life and health insurance market through a scientifically driven approach. Theyare as follows
– Porter’s 5 Forces for Industry Analysis– The PEST Framework for Macroeconomic Environmental Analysis– Anita McGahan’s Model for evaluating the Dynamic Market Environment– Ludi’s Internationalization Cube to understand the Internationalization strategy of
foreign players in India– Ansoff’s Matrix to understand the Marketing Strategy pursued by an insurer– The 4Ps of Marketing analyzed in depth to understand the Marketing Facets for
both Life and Health Insurance in India– Certain Service Marketing Tools used, since Insurance is a service
Moreover, certain information has been “boxed” in order to bring specific issues tothe foreground
– The “Management in Action” boxes intend to depict certain strategies that insurersin India have implemented; serving as best practices or role models for the rest ofthe industry.
– “The Regulator Says” boxes throw light on the regulatory developments of conse-quential importance to the Indian Insurance scenario.
– “Critical Support Functions” boxes detail the significance of certain functions likeClaims Management, Underwriting and Risk Management.
– “Customer Management and Retention” boxes seek to discuss aspects critical tocustomer centricity and orientation like Customer Relationship Management, Sim-plicity of Insurance Contracts etc.
– “Consumer Insight” boxes detail latest survey results or studies offering a deeperunderstanding of the Indian consumer thus a subsequent enhancement of latest lo-cal market knowledge.
1.1 Insurance – Introduction and History 5

1.2 An Analysis of Evolution of Insurance in India
An account of the Indian Economy and Insurance in Context
The Indian economy has been growing rapidly and the growth impulses continuedduring 2005–2006. There has been sustained manufacturing activity and impressiveperformance of the services sector along with a reasonable recovery in the agricultur-al sector. The agricultural and allied activities registered a growth of 3.9% due to im-provement in the agricultural production. The industrial sector improved by 7.6%and the services sector maintained a higher growth of 10.3%. Thus, the growth in realGDP was 8.4% during 2005–2006 as opposed to 7.5% in 2004–2005. Within theservices sector, there has been an improved performance in finance, insurance, realestate and business services. There has been a substantial increase in the GDP ema-nating from insurance. The deregulation of the sector in 2000 has contributed to in-surance growth. GDP from insurance sector which constituted 12% of the GDP in2000–2001, has increased to 19.3% in 2004–2005. The gross domestic savings, acomponent of which is the financial savings of the household sector, as a percentageof GDP increased to 29.1% in 2004–2005.
6 1 Insurance Industry in India
Figure 1: Financial Savings of the Household Sector – Gross (IRDA)

Financial Savings as a Percentage of GDP
The financial savings of the household sector as a percentage of the GDP has in-creased from 11.9% in 2000–2001, to 16.7% in 2005–2006. Moreover, of this finan-cial savings of the household sector, insurance funds equated to 13.6% in 2000–2001,which increased to 14.2% in 2005–2006, peaking at 16% in 2004–2005. All in all, in-surance funds as a component of the financial savings formed 1% of the GDP in1991, 1.5% in 2000, 1.6% in 2001 to a 2.4% in 2006 (IRDA). Please see the illustra-tions below which elucidate a development of financial savings of the household sec-tor.
1.2 An Analysis of Evolution of Insurance in India 7
Item 2000– 2001– 2002– 2003– 2004– 2005–2001 2002 2003 2004 2005 2006
Financial savings (FS) 11,90% 12,70% 13,10% 13,80% 14,00% 16,70%as a % of GDP
Currency (as a % of FS) 6,30% 9,70% 8,90% 11,20% 8,50% 8,80%
Currency (as a % of GDP) 0,70% 1,20% 1,20% 1,50% 1,20% 1,50%
Deposits (as a % of FS) 41,00% 39,40% 40,90% 38,30% 37,00% 47,40%
Deposits (as a % of GDP) 4,90% 5,00% 5,40% 5,30% 5,20% 7,90%
Shares and Debentures 4,10% 2,70% 1,70% 0,10% 1,10% 4,90%(as a % of FS)
Shares and Debentures 0,50% 0,30% 0,20% 0,00% 0,20% 0,80%(as a % of GDP)
Claims on Governement 15,70% 17,90% 17,40% 23,00% 24,40% 14,70%(as a % of FS)
Claims on Governement 1,90% 2,30% 2,30% 3,20% 3,40% 2,50%(as a % of GDP)
Insurance Funds (as a % of FS) 13,60% 14,20% 16,10% 13,70% 16,00% 14,20%
Insurance Funds (as a % of GDP) 1,60% 1,80% 2,10% 1,90% 2,20% 2,40%
Provident and Pension Funds 19,30% 16,10% 15,00% 13,60% 12,90% 10,00%(as a % of FS)
Provident and Pension Funds 2,30% 2,00% 2,00% 1,90% 1,80% 1,70%(as a % of GDP)
Figure 2: Financial Savings of the Household Sector – Gross (IRDA)
Insurance in India has completed a full circle; from being private with minimalgovernment intervention before 1956, to the nationalization of life insurance and for-mation of a monopoly (with Life Insurance Corporation of India) in 1956, and na-tionalization of general insurance in 1972 and finally back to deregulation in 2000.

First, I will present the milestones of the insurance industry before nationalization,essentially because the denationalized structure brought back to play (in 1999) im-portant legal rules from 1938.
Milestones of the Evolution of Insurance before nationalization in 1956
The Insurance Act, 1938 was the first comprehensive piece of legislation for Insur-ance in India. It covered both life and general insurance companies and clearly de-fined what would come under the life insurance business, the fire insurance businessand so on. It covered aspects ranging from deposits, supervision of insurance compa-nies, investments, commissions of agents, directors appointed by the policyholders,among others. This act lost its significance after nationalization in 1956 (of Life In-surance) and in 1972 (of General Insurance). With the privatization in the late 20th
century, it has returned as the backbone of the current legislation of insurance compa-nies (Sinha).
8 1 Insurance Industry in India
Figure 3: Milestones of Evolution of Insurance before Nationalization (Sinha)

Rationale for Nationalization of the Life Insurance Business in 1956
The genesis of nationalization of life insurance in India came from a document pro-duced by Mr. H.D. Malaviya (on behalf of the Indian National Congress) called “In-surance Business in India”. In his document, Mr. Malaviya made four importantclaims to justify nationalization. First, he argued that insurance is a “cooperative en-terprise”, under a socialist form of government; therefore it is more suited for thegovernment to be in the insurance business on behalf of the people. Second, heclaimed that Indian insurance companies were excessively expensive. Third, he ar-gued that private competition had not improved services to the “public” or to the pol-icyholders. Preventive activities like better public health, medical check-up, hazardprevention had not improved, according to him. Fourth, he commented that the lapseratios of life policies were very high and leading to “national waste” (Sinha). Severalof his arguments that were analyzed proved to stand on rather weak grounds. For ex-ample, his claim that Indian insurance companies were very expensive was justifiedby comparing the overall expenses of life insurers in India with those of the UK andthe USA. However, the base or denominator he used for India resulted in amplifica-tion of the figures beyond credible.
Anyway, the nationalization of the Life Insurance business in 1956 was justified bythe government on three distinct grounds. First, the government wanted to use the re-sources for its own purpose. This clearly meant that the government was unwilling to
1.2 An Analysis of Evolution of Insurance in India 9
Figure 4: Rural Share of Life Insurance Business in India (Annual Reports of LIC for differentyears)

pay the market return on assets (otherwise they could have raised the capital whetherinsurance companies were public or private). Second it sought to increase the marketpenetration through nationalization. There can be two reasons why nationalizationwould make more sense than privatization for market penetration (Sinha). [a] Thegovernment, by virtue of being a monopoly, could generate huge economies of scaleand thereby reduce costs of operation and thus reap higher volumes, by transferringthe lower costs into lower prices for the public. [b] Through nationalization, the gov-ernment may be able to take life insurance to rural areas where it may not be possiblefor private insurers to be profitable. This goal was definitely achieved by the newlyformed monopoly to a considerable extent. Please see the illustration below “Ruralshare of Life Insurance Business”. The last reason cited for nationalization was thatthe government found the number of failures of life insurance companies to be unac-ceptable.
Thus, with the Life Insurance Corporation Act of 1956, the 245 insurance compa-nies of both Indian and foreign origin in 1956 were nationalized by the governmentacquisition of the management of the companies; and the Life Insurance Corporationof India was created on 1st September, 1956, as a result; LIC has grown to be thelargest insurance company in India as of 2007.
Rationale for the non-nationalization of the General Insurance Business in 1956
However, general insurance was not nationalized in 1956. The then Finance Ministeraddressed it in his speech as follows, “I would like to explain briefly why we have de-cided not to bring in general insurance into the public sector. The considerationwhich influenced us the most is the basic fact that general insurance is a part and par-cel of the private sector of trade and industry and functions on a year to year basis.Errors of omission and commission in the conduct of the business do not directly af-fect the individual citizen. Life Insurance Business, by contrast, directly concerns theindividual citizen whose savings, so vitally needed for economic development, maybe affected by any acts of folly or misfeasance on the part of those in control or be re-tarded by their lack of imaginative policy.”
Milestones of the Evolution of Insurance after Nationalization in 1956
The diagram below illustrates the key milestones in the evolution of insurance in In-dia from the nationalization of life insurance in 1956, to the IRDA (Insurance Regu-latory and Development Authority) act in 1999 that led to the deregulation of the in-surance industry in India.
10 1 Insurance Industry in India

Nationalization of General Insurance in 1972
General Insurance was nationalized in 1972 (with effect from January 1st, 1973).There were 107 general insurers operating at that time. These were mainly large cityoriented companies catering to the organized sector (trade and industry). They wereof different sizes, operating at different levels of sophistication and were assigned tofour different subsidiaries (roughly of equal size) of the General Insurance Corpora-tion (GIC). The four subsidiaries were [1] the National Insurance Company, [2] theNew India Assurance Company, [3] the Oriental Insurance Company, [4] the UnitedIndia Insurance Company with head offices in Calcutta (now Kolkata), Bombay(now Mumbai), New Delhi, and Madras (now Chennai) respectively, collectivelyknown as NOUN for their initials. There were several goals for setting up such astructure [a] the subsidiaries were expected to “set up standards of conduct and soundpractices in the general insurance business and render efficient customer service”, [b]the GIC would assist controlling their expense, [c] the GIC would help in the chan-neling of funds, [d] this structure would help bring general insurance in rural areas,[e] GIC was also designated as the national reinsurer, [f] finally, all four subsidiarieswere expected to compete with one another. Most of these goals remained rather elu-sive and were not achieved to a massive degree (Sinha).
1.2 An Analysis of Evolution of Insurance in India 11
Figure 5: Milestones of Evolution of Insurance after Nationalization in 1956 (Sinha)

Development of the Life Insurance Industry during the Nationalized Era
By 2000, LIC had 100 divisional offices in 7 zones with 2,048 branches. There wereover 680,000 active agents across India with a total of 117,000 employees in the LIC.I will now present facets that explicate the development of the life insurance marketin India.
The largest product category of the life insurance market in India has been individ-ual life insurance. The types of the policies sold were mainly whole life, endowmentand “money back” policies. Money back policies return a fraction of the nominal val-ue of the premium paid by the policyholder at the termination of the contract. Untilrecently, term life policies were not available in the Indian market. Note that even in2001, individual life business accounted for 92% of all life insurance market. Thenumber of new policies sold each year went from about 0.95 million a year in 1957 toaround 22.49 million in 2001. The total number of policies in force increased from5.42 million in 1957 to 125.79 million in 2001. Thus, on both counts there has been a25-fold increase in the number of policies sold. Of course, during the same period,the population has grown from 413 million in 1957 to over 1,033 million in 2001. Ona per capita basis, there were 0.0023 new policies in 1957 compared with 0.0218 newpolicies in 2001. Total policies per capita went from 0.0131 in 1957 to 0.1218 in2001. Thus, whether we examine the new policies sold or the total number of policiesin force, there has been a tenfold increase during that period. Therefore, if we exam-ine the headcount of policies as an indication of penetration, there has been a substan-tial rise. A part of this rise is directly attributable to a deliberate policy of rural expan-sion of the Life Insurance Corporation. Between 1985 and 2001, total life businesshad grown from below 18 billion rupees to over 500 billion rupees. During that peri-od, the price index increased fourfold. Thus, if there were no change in life insurancebought in real terms, it would have accounted for 78 billion rupees worth of business(Sinha).
In recent years, life insurance saving has played a bigger role in national savings.Please see the figure below.
Note: The figure is plotted with Gross Domestic Savings as a percent of GDP onthe horizontal axis and Gross Life Premium as a percent of GDP on the vertical axis.Thus, there are fifty-two data points each pair representing data for a given year.
It clearly reveals a nonlinear relationship between these two variables. Specifical-ly, at relatively lower levels of saving rate (that correspond to a lower level of in-come), a rise in saving rate does not lead to a rise in life insurance premium expressedas a fraction of GDP. However, beyond a threshold; with the threshold value of sav-ing rate being 20% for India, the life premium as a percent of GDP starts to grow rap-idly. India seems to have reached that deflection point.
12 1 Insurance Industry in India

Moreover, we have already seen earlier in this chapter that insurance savings as apercentage of financial savings has increased over the years (till 2006).
1.2 An Analysis of Evolution of Insurance in India 13
Figure 6: Relationship between national savings and life insurance premium, 1950–1991(Calculated based on data from the Central Statistical Organization Database)
Deregulation of Insurance in India with the IRDAAct, 1999
With effect from 1st, January, 2000, with the passage of the IRDA Act, the Indian In-surance Industry was privatized or deregulated. The deregulation was brought aboutwith the following objectives: to increase coverage of population, propel a choice ofbetter products with informed decisions, promote competition, encourage the en-trance and joint partnership of foreign players with the Indian insurers, boost innova-tion, advance economy of operations, enhance customer centricity and service excel-lence and improve the efficiency of the public sector companies. The Insurance Reg-ulatory and Development Authority (IRDA) was formulated as an independent bodythat would monitor and shape the insurance business in India. The IRDA has separat-ed out life, non-life and reinsurance insurance businesses and therefore a companyhas to have separate licenses for each line of business. Each license has its own capi-tal requirements (around USD 24 million for life and non-life and USD 48 million forreinsurance business). The role and the statutory functions of the IRDA will be dis-cussed in chapter 1.3 that deals with Authorities and Regulatory environment.
To illustrate the positive direct or indirect effects of deregulation of insurance in In-dia, I have presented a graph below, which represents the convergence of efficiencyof the four public sector general insurers (now independent of the GIC): [1] the Na-

tional Insurance Company, [2] the New India Assurance Company, [3] the OrientalInsurance Company, [4] the United India Insurance Company, in 2003. The technicalefficiency of each of the above is used as a parameter of comparison, with the numberof employees (labor), the number of offices (physical capital) and commission paidas the inputs, and premiums and claims as two alternative measures of outputs. Therelative efficiency was calculated using the data envelopment analysis (DEA), amathematical programming framework (Sinha)
The graph depicts that New India Insurance has consistently stayed as the companywith the highest technical efficiency. Moreover, it shows that after some initialchange the relative efficiency level among the public sector general insurance com-panies converged, in 2003.
14 1 Insurance Industry in India
Figure 7: Convergence of Efficiency amongst the four public sector general insurers1997–2003 (Sinha)
1.3 Dynamic Market Environment for Insurance in India
An Era of Change
The insurance industry has experienced significant change over the past few decades.But never before have the changes been so pronounced, the pace so rapid and thescope so broad. Insurers are in the midst of a true paradigm shift. Their governingrules are changing. Their functional bodies are blurring. Buyers are becoming moresophisticated about services and value, and are ever more demanding. This height-ened form of consumerism is spurring a new demand pressure on insurance products.
At the same time, the industry is experiencing traditional financial pressures, aswell as new competition, new market entrants, new substitutes for traditional insur-

ance offerings. The industry is responding in many ways. For example, there is an en-hanced focus on market selection, new and varied distribution channels, bundlingand unbundling of products and services, all in an effort to customize and achievegreater value while re-engineering and consolidating for efficiency.
The Dynamic Environment and the Insurer’s point of View
In view of the ever-changing landscape of the Insurance Industry in India, insurersneed to revisit the core competencies and the cardinal features of their underlyingstrategy.
The schematic diagram below illustrates the key aspects influencing the insurer’sstrategy, conducive to the marketing point of view.
1.3 Dynamic Market Environment for Insurance in India 15
Figure 8: Factors Influencing Company Marketing Strategy (Kotler and Lane)
PEST Analysis
Of the facets illustrated above, it would make logical sense to take an outside-in viewand begin by analyzing the environment, a backdrop amidst which a new firm wouldlike to enter or an existing insurer would like to relook its strategy. Thus, I have illus-trated all factors contributory to the environment via the PEST (P-Political/Legal

Factors, E- Economical Factors, S – Social/Cultural Factors, T – Technological/Phys-ical Factors) framework.
Political Factors: The regulatory aspects of the political factors will be discussedin chapter 1.3. De-tariffing, the opening up of the market to free pricing and flexiblepolicy terms and conditions (which came into effect on the 1st January, 2007), is themost essential aspect that is set to revolutionalize the face of the insurance industryby directly affecting the insurers, concerned intermediaries, customers and stake-holders; thus, a separate subsection detailing its prime characteristics will be dedicat-ed to de-tariffing.
16 1 Insurance Industry in India
Figure 9: PEST Analysis (Research and Understanding gathered from several sources andAuthor)
Economical Factors:
– Increase in contribution of insurance to the GDP: GDP from insurance sector con-stituted 12% of GDP in 2000–01, increased to 19.3% in 2004–2005.
– Gross domestic savings as a per cent of GDP increased to 29.1% in 2004–2005.Savings in the form of life insurance funds accounted for 15.1% of the gross finan-cial savings.
– A decline in the savings in the form of insurance funds was witnessed, even thoughlife insurers increased their business during the year.
Economic Factors– Increase in contribution of insurance to the GDP– Increase in gross domestic savings as a
percentage of GDP– Decline in savings in the form of insurance funds– Buoyancy in the Indian stock market– Insurance business (first year premium) grew at
47.93% in 2005–2006
Political Factors– De-tariffing of general insurance with effect
from 1st Jan, 2007– Safety valve imposed by the IRDA, of not
changing the terms and conditions of thepolicies till 31st Mar, 2008
– Investment regulations– Social and rural sector obligations
Technological Factors– Building up data warehouses– Increase in CRM solutions– Increased use of online portals for policy
purchase, renewal, claims processing etc.– Impending importance of technology to lower
costs in a de-tariffed scenario– Grievance redressal cells– Online Complaints reporting mechanisms with
the regulatory body– Using bank databases to cross sell insurance
products through bancassurance
Social Factors– Insurance penetration stood at 2.53% for life
insurance, 0.62% for non-life insurance,thus huge scope
– Huge middle class– Increase in lifestyle diseases– Higher demand for old age provisions– Increasing awareness among the population– Growth of insurance catering to certain
groups – Islamic insurance, micro insuranceetc.
PEST
– Buoyancy in the Indian stock market due to strong macroeconomic fundamentals,robust corporate results, positive investment climate and sound business outlook.
– Insurance business (first year premium) grew at 47.93% in 2005–2006, surpassingthe growth of 32.49% in 2004–2005
Technological and Social Factors: These are self-explanatory in the illustration. The“Grievance Redressal Cell” of the technological factors will be elaborated upon insection 1.3.
De-tariffing and its consequences
A tariff market is one where the premium rates, policy terms and deductibles are con-trolled and to be applied uniformly by all the underwriters. The market portfolio mixfor general insurers on tariff/non-tariff covers during the tariff regime were as fol-lows: 73.09% of the overall premiums were tariffed, and 29.91% was non-tariffed.Health formed a part of the non-tariffed portfolio which implied that insurers couldset their own prices and adopt flexible policy terms and conditions.
The primary effects of the tariffed regime were
– Cross subsidization: Profitable businesses like fire and motor which were tariffedpaid for un-profitable businesses of a company like health and marine cargo insur-ance (which were non-tariffed), thus making these (health and marine cargo insur-ance) available to customers at throw away prices. The profitable businesses, thuscross-subsidized the unprofitable businesses. This is also the core reason for theabsence of any standalone health insurance company until 2006, because such aninsurer would not be able to compete with the general insurers, for whom healthinsurance was one of the businesses that could be easily subsidized despite exorbi-tant claim-to-premium ratios at 130%.
– “Good” customers paid for “bad” customers: In a tariffed regime, where priceswere uniform, all the “good” customers, who had a better risk management historywith lower risks and thus consequently fewer claims, ended up paying for “bad”customers with higher risks. In fact the tariffed regime, induced complacency inthe customer, who had no incentive to improve their risk profile or management ashe would get reimbursed anyway.
– Underwriting skills smothered: The biggest defect of the tariffed regime was thecomplete dearth of underwriting skills. For businesses that were tariffed, under-writing was rule based rather than risk based (as it should be for insurance); and forbusinesses that weren’t tariffed, underwriting did not matter on account of depend-ency on the profitable tariffed businesses. Thus although underwriting is the core
1.3 Dynamic Market Environment for Insurance in India 17

activity defining the profitability of an insurance company, the tariffed regime nul-lified its significance.
– Complete lack of quality data: Risk profiling, customer history, data warehouse,data mining, management information systems were deemed insignificant and justinvestments with a rather negative net present value because of their irrelevance tothe pricing of an insurance product; thus subsequently leading to complete lack ofquality data available to insurers and intermediaries, and reliance on outdated in-formation that was provided by the Tariff Advisory Committee.
The movement from a tariffed to a de-tariffed regime will occur in a phased manner
In order to prevent cut-throat competition with the lifting of tariffs, the IRDA has de-cided to move from the tariffed to a de-tariffed regime in a phased manner. Thisphased process would act as a safety valve for insurers and help preserve the sanctityof the industry.
– Phase 1: • What is it? Opening up of the free market pricing policy with effect from 1st of
January, 2007. However, insurers cannot change their policy terms and condi-tions during this phase (of the businesses that belonged to the tariffed part of theportfolio mix)
• Process of Preparation in this phase includes:• – Data compilation and stratification• – Data warehousing, analysis of data and sending data to the appointed actuary
– Phase 2:• What is it? With effect from 1st April, 2008, insurers can change their policy
terms, conditions, wordings, tariff rules and regulations. This phase would in-clude launching new or redefined products.
• Process of Preparation in this phase includes:• In order to launch new products with options to choose perils and add-on covers
and considerations on “what are the most urgent requirements of the customer?”,define product concepts like [a] policies purely on first loss covers, [b] policieson selective perils basis, [c] policies considering agreed value covers etc.
Effects and Consequences of Lifting of Tariffs
In order to understand the consequences of de-tariffing, I will present its impact onvarious facets of the Indian insurance archetype that would invariably alter the trailof progression of the industry as a whole. This account of effects would also serve inunderstanding the nature of change and trajectory of industry evolution on Anita McGahan’s Model for strategies in dynamic environments.
18 1 Insurance Industry in India

Please see the illustration below depicting the various facets while considering ef-fects of de-tariffing.
1.3 Dynamic Market Environment for Insurance in India 19
Figure 10: Facets while considering the effects of de-tariffing (Author)
Please find below Porter’s 5 Forces for industry analysis, as there are several ele-ments in the 5 forces analysis that overlap with the current rage that de-tariffingbrings. Thus they will have to be discussed in congruence.
Note with respect to the Porter’s 5 Forces Illustration: All aspects related to de-tar-iffing are marked with a “D” followed by a “+” sign indicating it has a positive effecton insurers, “–” sign indicating it has a negative effect on insurers, and “+/–” sign if ithas both positive and negative effect on insurers. The points in the illustration that arenot preceded with a “D” are unrelated to the de-tariffing aspect and would have pro-gressively occurred irrespective of the de-tariffed scenario.
TPA = Third Part AdministratorFacets explicated
Marketing Facets
– Pricing: • Industry experts predict that fire and motor premiums would go down by
30–35% (these were part of the tariffed, thus profitable businesses). This is at-tributed to the tendency of players to undercut one another, due to free market

pricing policy, thus resulting in some type of cut-throatism and a price war. [Ini-tial ill effects of a de-tariffed scenario – Industry Rivalry, Porter’s 5 forces.]
• Health and marine premiums will have to rise due to end of cross-subsidizationby their profitable counterparts (motor and fire).
• There will be a rise of sophisticated price segmentation methods: for example,having location based pricing in place, people in cities would pay higher premi-ums than those in suburbs.
– Products:• De-tariffing will propel competition because of a need to differentiate, thus pro-
mote heightened innovation in product design; for example, there may be healthinsurance products developed for people with specific hereditary diseases whichwere not in existence earlier.
– Distribution channels:• Need of an innovative combination of distribution channels to increase the num-
ber of touch points with the customers and maximize customer reach via channeleffectiveness.
20 1 Insurance Industry in India
Figure 11: Porter’s Five Force Analysis of the Insurance Industry (Author throughaccumulated readings and research)
Buyer/Customer Power✔ D+ Widening product range
✔ D– Increasing pricesensitivity of customers
✔ D± Increased competitionin a de-tariffed scenario
✔ D– Large corporate clients✔ D– Switching costs
✔ D+ Good risk customerwill not longer subsidize bad
risk customer✔ Low penetration, thus less
number of buyers✔ Yearly renewal for non-life
products✔ Multiple distribution
✔ Sale of Bancassurance
Suppliers’ Power✔ D– Reduced commission
offered by reinsurancecompanies with de-tariffing
✔ D- Increased efficiency ofBrokers necessitated
✔ Limited actuaries in themarked
✔ Reinsurance concentration✔ Lock in & high switching
costs for firms✔ Cession to the National
Insurer✔ Dependence on IT providers
✔ Dependence on TPAs✔ Orphaned customers due
to high attribution ofagents
Barriers to Entry✔ FDI Ceiling
✔ Capital requirements✔ Experience with respect to
understanding of the market✔ Elaborate distribution requirements
✔ “Lock-in” of buyers
Threat of Substitutes✔ D– Increased competition, thus
substitutes due to de-tariffing✔ Government pension schemes
✔ Tax savings instruments✔ Emerging substitutes
✔ Switching costs of customers✔ Dependence on Children in rural
India
Industry Rivalry✔ D– Initial effects ofDetarifed scenario
✔ Industry concentration in bothlife and non-life
✔ Foreign players entering✔ Restricted competition due
to regulations✔ Solvent Margin requirements
✔ Low penetration ofinsurance

• Achieving operational efficiencies in channels would be inevitable; as priceswould go down initially and costs will have to be kept at an all time low, if thestipulated solvency margins have to be maintained.
Customers
– “Good” customers will cease to subsidize “bad” customers, as each customerwould pay premiums based on his/her risk profile [Good customers will no longersubsidize bad customers – Buying Power, Porter’s 5 Forces]
– Due to de-tariffing, competition would heighten and consequently result in newand innovative products, thus resulting in increased consumer choice and height-ened customer centricity and service. [Increased competition in a de-tariffed sce-nario – Buying Power, Porter’s 5 forces]
– Price sensitivity of customers will increase in areas where competition results in aninitial price fight. [Increasing price sensitivity of customers – Buying Power,Porter’s 5 forces]
– The obvious consequence of the de-tariffed regime is increasing customer aware-ness and aggravated premium tension.
– The moral hazard will end with high risk customers coming in the spot light asthey can no longer find “cover” under the low risk customers.
– The information asymmetry would reduce as customers would be willing to dis-close more information to get a better risk rating in case they are good customers;thus complete and furnished information from customers would be rewarded withdiscounts.
– Policyholders would be incentivized to improve their risk portfolio, as doing sowould be compensated for.
– Large corporate clients’ bargaining power would be enhanced in the fire and motorportfolio where prices will be slashed; however, corporate clients would be lost in thehealth insurance area where prices will have to be increased to ensure the profitabilityof these businesses. [Large Corporate Clients – Buying Power, Porter’s 5 forces.]
Reserving
– The IRDA (regulatory authority) has stipulated regulations with respect to the sol-vency margin that companies must adhere to; solvency margin is the extent towhich assets need to be over the liabilities for the insurer. In lieu of the same, insur-ers cannot indulge in price wars to the extent that their solvency margins will behurt, thus serving as a necessary evil. Moreover, insurers are answerable to theshareholders for their bottom line, which is why they cannot afford to let it get af-fected too drastically.
1.3 Dynamic Market Environment for Insurance in India 21

Regulations
– The IRDA (regulatory authority) has disallowed cross subsidization of businessesin light of the solvency margin argument; however, if insurers do need to crosssubsidize, they can do so by presenting a proposal to the IRDA with a justificationfor the same.
– Actuaries have been appointed to insurers to help them in their underwriting activ-ities and rate making process.
– The phased process sequenced by the IRDA acts as a safety valve (as discussedearlier).
Reinsurance
– If competition based on price increases, it would imply reduced prices, howeversame liabilities or better put, increased liability for the same price suggests that theinsurers would pass on more liabilities to the reinsurer (who in turn gives commis-sion to the insurer for the percentage of premium received and obviously even car-ries partial risk of the insurer in return). More liabilities to the reinsurer withoutcorresponding increase in premium would reduce the commissions that insurerscan get out of reinsurers. [Reduced commission offered by reinsurers in case of de-tariffing – Supplier’s Power , Porter’s 5 forces.]
Investments
– Price reduction by insurers would call for more efficient management of their in-vestment portfolio and thus cautious and conscientious pooling of resources toreap maximum returns, in order to be able to augment their bottom line and sustaintheir solvency margins.
Risk Management and Underwriters
– The switch from a tariffed to a de-tariffed regime calls for a transition from rulebased underwriting to risk profile based underwriting.
– This would imply classification of risks into class rated risks and individual ratedrisks.• Class rates: where risks of a class have similar risk factors and individual varia-
tions are not financially significant; for example motor risks in India• Individual rates: where each risk has significant variation in risk factors and the
financial magnitude justifies individual rating – for example engineering risks(Bhattacharya).
– More time and money will need to be invested in risk profiling through and datacollection.
22 1 Insurance Industry in India

– Low pricing will not be the basis for creating the best company; it will be based up-on risk acceptance, service delivery standards and commensurate remunerativepricing.
– Efforts will have to be made to overcome the steep learning curve with respect tosophistication in risk management practices.
– Underwriters will have to team up with the marketing department and rate policiesbased on claims data collected at a micro level which would include [a]productlevel knowledge per se, [b]enhanced customer domain knowledge and correspon-ding merit rating of the same
– Use of IT and innovative techniques to improve decision making via data ware-housing, data mining and other business intelligence systems augmenting microlevel data analysis will have to be used to improve efficiency and quality of deci-sion making.
Brokers
– The de-tariffed regime would enhance the broker’s role and transform him into afinancial advisor; as Mr. Sunderasan, the Chair Professor of National InsuranceAcademy put it “The Broker will be the eyes of the insurer and the voice of thecustomer.” This means he will use his proximity to the customer and market intel-ligence to help design new products, develop new markets and improve pricingstrategies. The broker’s role as the voice of the customer would imply: a require-ment analysis of the prospective insured, matching the price within the desiredbudget, using customer (insured) response to provide feedback to the insurers, andenhancing his value addition by providing a bundle of services. [Increased effi-ciency of the brokers necessitated – Supplier’s Power, Porter’s 5 Forces]
– Brokers may face reduced margins from insurers (on account of price cuttingmechanisms the effects of which will have to be borne by all the intermediaries in-volved) and may even be compelled to switch from a commission based model to afee based one.
Transition to a de-tariffed regime will have deep, certain and temporary financial im-pact on the insurers before the industry cycles settle. In order to find a way to create alasting value in the customer’s mind, there is a need to ensure fair pricing, balancebetween the interests of insurer, insured and other stakeholders. Since a price war isin the offing, unmindful viability of the insurers will need to be kept in check and itwould be essential to moor pricing on sound technical base to prevent the marketfrom going out of control. Finally priorities with respect to growth versus profit needto be defined as both may elude for some time.
1.3 Dynamic Market Environment for Insurance in India 23

Anita Mc Gahan’s Model for Strategies in Dynamic Environments
Anita Mc Gahan’s model helps analyze the nature of change and interpret the trajec-tory of industry evolution. Based on the kind of change (architectural or foundation-al), the nature of the industry trajectory is determined. In architectural change, coreactivities and in foundational change, core assets are threatened.
24 1 Insurance Industry in India
Figure 12: Anita McGahan’s Model (McGahan & Mapping and Interpretation by Author)
Core activities are defined as recurring actions that create value both by making theindustry’s suppliers more willing to transact and by generating greater willingness topay among industry’s buyers. Core assets are durable resources that make the firmmore efficient or effective at performing core activities and can include intangiblessuch as brand and knowledge capital. Core assets are threatened with obsolescencewhen a new approach accelerates their real rate of depreciation (McGahan).
Thus in this case,
– The old “core” activities include [a] rule based underwriting, [b] reliance on oth-ers: intermediaries like Third Party Administrators for activities like claims man-agement and with minimal interference by insurers.
– Core assets would be [a] historical customer data [b] distribution network [c] rela-tionship with intermediaries [d] cushion of assets over liabilities (solvency mar-gin) [e] investment portfolio.

In context of [i] the account on consequences of de-tariffing and [ii] the increasing ofthe FDI cap (equity participation that foreign investors can have in their Indian coun-terparts from 26% to 49%) that is in the offing, the nature of change can be defined as“intermediating” wherein core activities are threatened but core assets are not. Thenew core activities would be [a] accurate risk assessment & management, [b] riskdriven underwriting, [c] efficient and responsive claims management and [d] effec-tive fraud management minimizing errors of omission and commission replacing old“core” activities which include [a] rule based underwriting, [b] detachment on insur-ers with respect to claims management, by ignorant dependence on Third Party Ad-ministrators. However, core assets remain intact and will only have to be strength-ened to improve their efficiency and effectiveness towards the newly established coreactivities.
LUDI’s Internationalization Cube (Kaufmann, Panhans and Poovan)
To conclude our discussions on the dynamic market environment and industry analy-sis, I would present the suggested internationalization strategy for foreign insurers inIndia by means of the Ludi’s Internationalization cube.
In the cube
– National Focus: when the concerned firm decides to expand base within its homecountry without venturing abroad.
– Export Orientation: when the firm would like to make use of the market opportuni-ties abroad and export products while not setting base in the foreign location.
– Business Transfer: would imply the firm setting base in the foreign location as areplica of the business done back home, however, this would be customized toserve the local market in the foreign base through local partners, investment andstrategy.
– Global Integration: would imply when this contribution from business transferwould be looped into the supply chain of providing the finalized product to theworld market or a subset of it.
The current best strategy for foreign players in India is Business Transfer, with for-eign value creation and independence with respect to integration across borders (as inthe business at the foreign location – India in this case, would not be dependent on thebusiness at the home location). Moreover, foreign firms must pursue entry by meansof a joint venture with Indian insurers or partners in order to get access to the marketknow how and existing customer base and consequently share their risk managementexpertise and responsiveness in claims management.
1.3 Dynamic Market Environment for Insurance in India 25

Please see the illustrations below.
26 1 Insurance Industry in India
Figure 13: LUDI’s Cube (Kaufmann, Panhans and Poovan & Mapping and Interpretation byAuthor)

1.4 Authorities and Regulatory Environment 27
1.4 Authorities and Regulatory Environment
The Insurance Regulatory and Development Authority (IRDA) is a nationalagency of the Government of India, based in Hyderabad. It was formed by an act ofIndian Parliament known as IRDAAct 1999, which was amended in 2002 to incorpo-rate some emerging requirements. Mission of IRDA as stated in the act is “to protectthe interests of the policyholders, to regulate, promote and ensure orderly growth ofthe insurance industry and for matters connected therewith or incidental thereto.”
The role of the IRDA as a developer
The role of the IRDA as a developer includes
• Shouldering the responsibility of developing a nascent insurance market• Striking a right balance between developing and regulating the industry• Protection of Policy holders’ Interests – Mission of IRDA• Interests of policy holders as the prime objective while framing regulations (Prab-
hakara)
The Statutory functions of the IRDA
The statutory functions of the IRDA include
1. Issue to the applicant a certificate of registration, renew, modify, withdraw, suspendor cancel such registration. The applicants may be the insurer, broker or the TPA.
The Regulator Says: License to Operate for an Insurer
An insurance company gets a license to operate from the regulator once it re-ceives approvals for the 3-staged application process (R1 through R3) from theIRDA. The IRDA by clearing an R1 (stage 1) application gives in-principle ap-proval to a proposed insurance venture. The R1 application contains the detailsof promoters of the proposed insurance company, capital structure, directors andkey persons, proposed external auditors, financial projections, regions in whichbusiness will be transacted, and the manner in which rural and social obligationswill be fulfilled. The R2 application contains details of geographical spread, dis-tribution, sales promotions, underwriting, investments, IT, customer services, re-tention limits and reinsurance training, internal controls, expenses of administra-tion, premium rates for products along with rebates. The R3 application containsthe classes of business which may be transacted and a confirmation from thestakeholders on the company’s capitalization (Syed).

2. Protection of the interests of the policyholders in matters concerning assignmentof policy, nomination by policyholders, insurable interest, settlement of insuranceclaim, surrender value of policy and other terms and conditions of contracts of in-surance.The mission statement of the authority attaches immense importance to the pro-tection of the policyholders’ interest. In order to achieve this, the IRDA has set upa cell that handles grievances against insurers. Grievances received by the authori-ty are taken up with insurers for examination/re-examination and speedy resolu-tion. A greater awareness amongst the policyholders was seen about the existenceof a Grievance Cell at the Authority. The Regulations for Protection of Policy-holders’ interests, 2002 requires every insurer to have an effective grievance re-dressal system. Policyholders who have complaints against insurers are requiredto first approach the grievance/customer cell of the concerned insurer. If they donot receive a response from the insurer within a reasonable period of time or are
28 1 Insurance Industry in India
Insurer Grievances Reported Total Resolved Pending Break up according as on during during as on to the nature31st March, the year the year 31st March, of grievance2005 2006 2006 2006
(i) (ii) (iii) (iv)
Public 707 1331 2038 1488 550 279 101 149 21Sector (73.01%)
Private 23 196 219 204 15 9 0 6 0Sector (93.15%)
Total 730 1527 2257 1692 565 288 101 155 21(74.97%) 50.9% 17.88% 27.43% 3.72%
Figure 14: Status of Grievances – Non-Life Insurers 2005–2006 (IRDA)
Insurer Grievances Reported Total Resolved Pending Break up according as on during during as on to the nature31st March, the year the year 31st March, of grievance2005 2006 2006 2006
(i) (ii) (iii) (iv)
Public 992 851 1843 467 1376 109 212 590 465Sector (25.33%)
Private 133 540 673 270 403 36 92 157 118Sector (40.11%)
Total 1125 1391 2516 737 1779 145 304 747 583(29.29%) 8.15% 17.08% 41.98% 32.77%
Figure 15: Status of Grievances – Life Insurers 2005–2006 (IRDA)

dissatisfied with the response of the company, they may approach the GrievanceCell of the IRDA. Please see the tables below, depicting the status of grievances ofnon-life insurers and life insurers in 2005–2006. The figures 1692 in the first table and 737 in the second table depict the number ofgrievances resolved by Insurance ombudsmen in non-life and life areas respec-tively over the year 2005–2006. In the table (i) through (iv) signify the following:
(i) signifies grievance due to non-settlement/delay in settlement of claim(ii) signifies grievance due to repudiation/partial settlement of claim(iii) signifies policy issues (non-renewal/cancellation/non-issuance/other issues
related to policy)(iv) signifies other reasons
3. Specifying requisite qualifications, code of conduct and practical training for in-termediaries or insurance intermediaries and agents.The IRDA has specified mandatory training and pre-recruitment exams for indi-vidual and corporate agents that they need to clear before licensing.
4. Specifying the code of conduct for surveyors and loss assessors.The code of conduct for surveyors and loss assessors is specified in the IRDARegulations for Surveyors and Loss Assessors, 2000.
5. Promoting efficiency in the conduct of insurance business.For example, the Authority raised the limit of losses required to be surveyed by alicensed surveyor and loss assessor for settlement of claims for the flash floods inSurat, Gujrat as a special case for a period of two months from the date of issue ofthe order.
6. Promoting and regulating professional organizations connected with insuranceand reinsurance business.IIRM (the Institute of Insurance and Risk Management), in order to achieve itsmission of spreading insurance education, continues to receive cooperation frominternational bodies, relevant institutions and insurance regulatory authorities.
7. Levying fees and other charges for carrying out the purposes of the Act.The Authority levies both registration and renewal fees from the insurers and vari-ous intermediaries associated with the insurance business. The registration fee foran insurer for example, is Rs. 50,000 and the renewal fees are 1/10th of 1 percentof gross direct premium written in India, subject to a minimum of Rs. 50,000 anda maximum of Rs. 50 million.
8. Calling for information from, undertaking inspection of, conducting enquiries andinvestigations including audit of the insurers, intermediaries, insurance intermedi-aries and other organizations connected with the insurance business.
1.4 Authorities and Regulatory Environment 29

9. The de-tariffing of the general insurance business and file and use guidelinesprescribed by the IRDA to best deal with de-tariffing; setting up an agenda for in-surers to permit a desired switch, in order to smoothly transit from a tariffedregime which called for no underwriting skills to a regime where prices need tobe set based on prudent risk assessment and underwriting.
10. Specifying the form and manner in which books of accounts shall be maintainedand statements of accounts shall be rendered by insurers and other insurance in-termediaries.
11. Regulating investment of funds by the insurance companies.Please see the illustrations below; they depict the investment regulations for lifeand non-life insurance businesses.
12. Regulating maintenance of margin of solvency.Every insurer is required to maintain a certain solvency margin. Solvency mar-gin is defined as the excess of assets over liabilities; the main purpose of which isto ensure that insurers have sufficient financial muscle especially in a servicelike insurance, where costs cannot be pre-accounted for, implying costs are real-ized after the price/premium has already been paid for, making the businesshighly susceptible to uncertainty.
13. Adjudication of disputes between insurers and intermediaries or amongst vari-ous insurance intermediaries (IRDA).
14. Specifying the percentage of life insurance business and general insurance busi-ness to be undertaken by the insurers in the rural and social sector.As part of the initiatives to increase the spread of insurance to rural and sociallybackward sectors, the Authority notified the Regulations on obligations of insur-
30 1 Insurance Industry in India
Type of Investment Percentage
1 Government Securities 25%
2 Government Securities or other approved securities Not less (Including 1 above) than 50%
3 Approved investments as specified in ScheduleInfrastructure and Social Sector: Not lessExplanation: Infrastructure and Social Sector shall have the meaning as than15%in given in regulation 2(h) of IRDA (Registration of Indian InsuranceCompanies) Regulations, 2000 and as defined in the IRDA (Obligationsto Rural and Social Sector) Regulations, 2000 respectively. Others to be governed by Exposure/Prudential norms specified Not exceedingin Regulation 5 20%
4 Other than in Approved Investments to be governed by Not exceedingExposure/Prudential norms specified in Regulation 5 15%
Figure 16: Investment Regulations for the Life Insurance Business (IRDA)

ers to the rural and social sectors in the year 2000 consequent upon the amend-ment of the Insurance Act, 1938. The obligations require
– Life Insurers to fulfill – 7, 9, 12, 14, 16 and 18% of total policies in first sixyears of operation as rural obligations.
– General Insurers to fulfill – 2, 3 and 5% of total gross premium in I, II andsubsequent years as rural obligations.
– 5000, 7000, 10000, 15000, 20000 and 25000 of lives as social sector obli-gations by all insurers in first six years of operation (Prabhakara)
15. Moreover, by virtue of the IRDA’s regulatory role in the area of consumer pro-tection, the Authority has been instrumental in implementing the following:
– Introduction of cashless transactions by third party administrators in health in-surance
– Maintenance of minimum solvency margins as mentioned earlier– Protection of policyholder’s interests regulations, 2002– Widening of distribution channels in order to increase insurance accessibility– Entry of banks in the “bancassurance” model– Monitoring of the underwriting policy through file and use– Formulation of the Grievance Redressal Cell as discussed– Formulation of a committee to study existing grievances’ mechanisms to for-
mulate uniform guidelines and prescribe improvement steps for the insurers
1.4 Authorities and Regulatory Environment 31
Type of Investment Percentage
1 Central Government Securities being not less than 20%
2 State Government Securities and other Guaranteed securitiesincluding (i) above being not less than 30%
3 Housing and loans to State Government for Housing and Fire Fightingequipment, being not less than 5%
4 Investments in Approved Investments as specified in Schedule 2a Infrastructure and Social Sector:
Explanation: Infrastructure and Social Sector shall have the meaning Not less thanas in given in regulation 2(h) of IRDA (Registration of Indian 10%Insurance Companies) Regulations, 2000 and as defined in theIRDA (Obligations to Rural and Social Sector) Regulations,2000 respectively.
b Others to be governed by Exposure/Prudential norms specified in Not exceedingRegulation 5 30%
5 Other than in Approved Investments to be governed by Not exceeding Exposure/Prudential norms specified in Regulation 5 25%
Figure 17: Investment Regulations for the General Insurance Business (IRDA)

– Promotion of micro-insurance to reach rural areas – Prescribing guidelines for insurers with respect to simplicity of contracts et al
to reduce the principal agent problem between the insurer and the insured andthereby diminish the occurrence of grievances on account of errors of omis-sion, or frauds on account of errors of commission.
The Regulator Says: FDI Cap
“Overseas companies are allowed to own a maximum insurance companies inIndia” unshackled the industry control seven years ago as part of a phased lib-eralization financial services business. However, a federal proposal owner-ship limit to 49% has run into political headwinds, communists and unionslobbying against higher Recently (18th, May 2007), Allianz, based in Munichpartnered with Bajaj Auto in ventures for general and has been granted the op-tion to raise its equity holdings companies from 26% to 50% (Bhattacharjee);thus [a] the state is considering the proposal (put forth raise the cap on over-seas ownership of insurance companies a full-fledged regulation is definitelyin the offing.
1.5 Status Quo – The Indian Market as-is vis-à-vis other Markets
This section will primarily deal with establishing the context of the Indian insurancemarket vis-à-vis the Asian and the Global Insurance market.
The primary results for this chapter include
– Market Value• India: The Indian insurance market grew by 14% in 2005 to reach a value of
$ 25.1 billion (Datamonitor).• Asia: The Asia-Pacific insurance market grew by 3.7% in 2005 to reach a value
of $ 763.5 billion (Datamonitor).• World: The global insurance market grew by 4.7% in 2005 to reach a value of
$ 3,151 billion (Datamonitor).
– Market Value Forecast• India: In 2010, the market is forecast to have a value of $ 40.5 billion, an in-
crease of 61.3% since 2005 (Datamonitor).
32 1 Insurance Industry in India

• Asia: In 2010 the market is forecast to have a value of $ 941.5 billion, an in-crease of 23.3% since 2005 (Datamonitor).
• World: In 2010, the market is forecast to have a value of $ 3,997 billion, an in-crease of 26.9% since 2005 (Datamonitor).
– Market Segmentation I
• India: Life insurance accounts for 80.6% of gross premiums written within themarket (Datamonitor).
• Asia Pacific: Life insurance accounts for 75.2% of gross premiums writtenwithin the market (Datamonitor).
• World: Life insurance accounts for 57.6% of gross premiums written within themarket (Datamonitor).
– Market Segmentation II
• India: India accounts for 3.3% of gross premiums written within the Asia-Pacif-ic insurance (Datamonitor).
• Asia: Japan accounts for 63.5% of gross premiums written within the market(Datamonitor).
• World: The Americas account for 39.9% of gross premiums written within themarket (Datamonitor).
Market Definition
The insurance market consists of the non-life insurance sector and the life insurancesector. The value of the market is shown in terms of gross premium incomes. The lifeinsurance sector covers all life insurance products including annuities, which can belinked to retirement savings plans. The non-life insurance sector consists of the acci-dent and health and the property and casualty insurance segments.
The insurance market depends on a variety of economic and non-economic factorsand future performance is difficult to predict. The forecast given below is not basedon a complex economic model, but is intended to propose a rough idea, thereby sug-gesting the direction in which the market is likely to move. This forecast is based on acorrelation between past market growth and growth of base drivers, such as houseprice growth, GDP growth and long-term interest rates. Any currency conversionsused in the following information have been calculated using constant 2005 annualaverage exchange rates.
For the purpose of the data, Asia-Pacific comprises of Australia, China, India,Japan, South Korea, Singapore, and Taiwan. Europe comprises Belgium, the CzechRepublic, Denmark, France, Germany, Hungary, Italy, the Netherlands, Norway,
1.5 Status Quo – The Indian Market as-is vis-à-vis other Markets 33

Poland, Russia, Spain, Sweden, and the United Kingdom. The Americas comprisesthe US, Canada, Brazil, and Mexico. The global market comprises Asia-Pacific, Eu-rope, and the Americas (Datamonitor).
Illustration 1: The illustration below gives key highlight and a comparison be-tween the Indian, Asia-Pacific, and Global Insurance Market.
34 1 Insurance Industry in India
Criteria Indian Asia Pacific GlobalInsurance Insurance InsuranceMarket Market Market
Total Gross Premiums in 2005 $ 25.1 Billion $ 763.5 Billion $ 3150.7 Billionand CAGR for the 5 year period and 15.3% and 2.5% and 5%(2001 to 2005)
Most lucrative segment in 2005, Life Insurance, Life Insurance, Life Insurance,Premium written, Equivalent to $ 20.2 Billion, $ 574.4 Billion, $ 1,815.6 billion,what % of market value 80.6% 75.2% 57.6%
Performance of the market, Performance Performance PerformanceAnticipated CAGR for the forecasted to forecasted to forecasted to5 year period, decelerate, 10%, accelerate, 4.3%, decelerate, 4.9%,Market Value by the end of 2010 Gross premium Gross premium Gross premium
of $ 40.5 billion of $ 941.5 billion of $ 3,997 billion
Figure 18: Illustration 1 – Key highlights of the Indian Insurance vis-à-vis the Asia Pacific andGlobal Insurance Markets (Datamonitor)
Illustration 2: The illustration below gives the insurance market value in USDBillion for the market in India vis-à-vis that of Asia Pacific and the World.
Note: The Market Value measured in $ Billion represents the amount of premiumcollected by the respective industry in $ Billion. If one gives a quick glance at thegraph, one might feel that the Indian Insurance Market forms a fair proportion of theAsia-Pacific Insurance Market, which in turn contributes to a fair amount of theGlobal Insurance premium. However, a closer look would reveal that the vertical axisscale is logarithmic, implying the units in which the scale proceeds are not constant,in fact represent a geometric progression. I had to make use of this scale, in order tobe able to view the market value of the Indian Insurance on the graph, which was al-most invisible in a constant distance scale. However, before one jumps to conclu-sions, one would have to note that for comparison sake, all premiums have been con-verted into USD. Thus there are two points to note from this graph [a] The Indian In-surance Industry is in a highly nascent stage in the global scenario, as is vivid by the
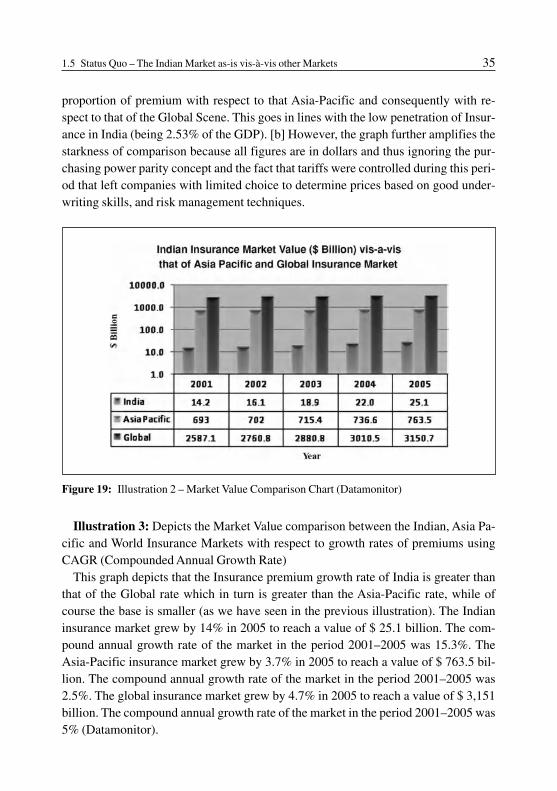
proportion of premium with respect to that Asia-Pacific and consequently with re-spect to that of the Global Scene. This goes in lines with the low penetration of Insur-ance in India (being 2.53% of the GDP). [b] However, the graph further amplifies thestarkness of comparison because all figures are in dollars and thus ignoring the pur-chasing power parity concept and the fact that tariffs were controlled during this peri-od that left companies with limited choice to determine prices based on good under-writing skills, and risk management techniques.
1.5 Status Quo – The Indian Market as-is vis-à-vis other Markets 35
Figure 19: Illustration 2 – Market Value Comparison Chart (Datamonitor)
Illustration 3: Depicts the Market Value comparison between the Indian, Asia Pa-cific and World Insurance Markets with respect to growth rates of premiums usingCAGR (Compounded Annual Growth Rate)
This graph depicts that the Insurance premium growth rate of India is greater thanthat of the Global rate which in turn is greater than the Asia-Pacific rate, while ofcourse the base is smaller (as we have seen in the previous illustration). The Indianinsurance market grew by 14% in 2005 to reach a value of $ 25.1 billion. The com-pound annual growth rate of the market in the period 2001–2005 was 15.3%. TheAsia-Pacific insurance market grew by 3.7% in 2005 to reach a value of $ 763.5 bil-lion. The compound annual growth rate of the market in the period 2001–2005 was2.5%. The global insurance market grew by 4.7% in 2005 to reach a value of $ 3,151billion. The compound annual growth rate of the market in the period 2001–2005 was5% (Datamonitor).
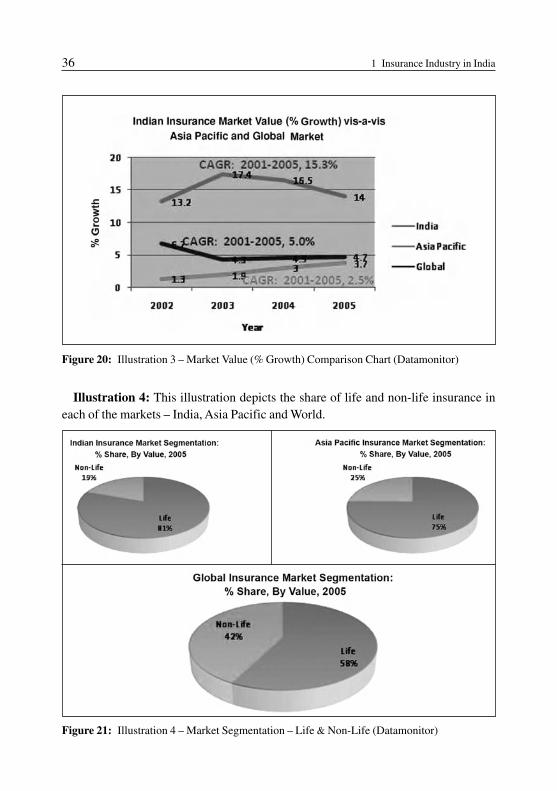
Illustration 4: This illustration depicts the share of life and non-life insurance ineach of the markets – India, Asia Pacific and World.
36 1 Insurance Industry in India
Figure 20: Illustration 3 – Market Value (% Growth) Comparison Chart (Datamonitor)
Figure 21: Illustration 4 – Market Segmentation – Life & Non-Life (Datamonitor)

Illustration 5: Depicts the Indian Insurance’s contribution to the Asia Pacific Mar-ket Value as a percentage of premium, and in turn Asia Pacific Insurance contributionto the Global Insurance Paradigm as a percentage of premium. It gives geography-based market segmentation.
Graph [a] indicates that India accounts for 3.3% of gross premiums written withinthe Asia-Pacific insurance market. In comparison, China generates a further 7.9% ofAsia-Pacific market value.
1.5 Status Quo – The Indian Market as-is vis-à-vis other Markets 37
Figure 22: Illustration 5 – Market Segmentation – By Geography (Datamonitor)
Graph [b] indicates that the Americas account for 39.9% of gross premiums writ-ten within the global insurance market. In comparison, Europe and Asia Pacific gen-erate a further 35.8% and 24.2% respectively of global gross premiums written.
Thus India accounted for 0.7986% of the global gross premiums written in 2005.

A Snapshot of the Competitive Landscape
[a] The competitive landscape of the Indian Insurance Market
India’s large rural population is migrating to urban areas, creating a large “new cus-tomer” demographic for India’s insurance companies. India’s booming economy isalso conducive to a positive performance from insurance companies. India’s leadinginsurance company is the Life Insurance Corporation of India (LIC). The companyhas more than 2,000 branch offices located all over India, with its corporate office inMumbai.
India’s second largest insurance company and its largest non-life insurance compa-ny, New India Assurance, is India’s first entirely Indian-owned general insurancecompany. The company’s revenue for the fiscal year 2005 increased 37.5% on theprevious year to reach a 2005 of $18.6 billion. India’s public sector general insurancecompanies are in the process of restructuring their operations to cope with the com-petitive pressures unleashed by the private players.
[b] The competitive landscape of the Asia-Pacific Insurance Market
Japan’s life insurance market continues to dominate Asia-Pacific’s insurance land-scape. However, the declining birth rate and aging population of Japan have created asubstantial alteration in the insurance needs of the Japanese. As the consumer demo-graphic diversifies, companies need to widen their insurance packages, particularlywith regard to life insurance. Nippon Life Insurance Company, the leading insurancecompany in Japan and Asia-Pacific, is responding to this by focusing more on theirmedical insurance plans as opposed to death protection.
Nippon’s revenue in the fiscal year ending March 2006 reached $ 62.9 billion; thisrepresents a 6.5% increase on the previous year, a recovery from the declining rev-enues Nippon Life Insurance Company faced in the previous fiscal year. Income frominsurance and reinsurance premiums constituted 70% of the company’s revenue.
Dai-Ichi Mutual Life Insurance Company, Asia-Pacific and Japan’s second largestinsurance company, had 11.5 million individual insurance policies in force in the fis-cal year ending March 2006. The company’s premium income was $ 30.9 billion, a4% fall on the previous year, although its total revenues rose by 6% to $ 45.9 billion.
[c] The competitive landscape of Global Insurance Market
Fiscal year 2005 was marked by the impact of hurricanes in the US and other naturaldisasters, which threatened earnings for insurers. This followed a year of below aver-age major damage costs in 2004.
Allianz Group is one of the leading companies in the global insurance market. Infiscal 2005, its gross premiums written in property and casualty increased by 0.6% to
38 1 Insurance Industry in India

$ 54.8 billion, while life and health statutory premiums rose by 6.5% to $ 59.8 bil-lion. Allianz considers Europe to be its core market, and France, Germany, and Italyshowed strong growth in premiums written.
Another major player in the global market is AIG. In fiscal 2005, it reported that inits general insurance division net premiums written had increased by 3% on 2004, toreach $ 41.9 billion. The group has an extensive international property and casualtyinsurance operation, and also a personal lines business focused on high net worthclients and car insurance. In its life insurance and retirement services business, pre-miums, deposits, and other income amounted to $ 66.4 billion, a marginal decreaseon the previous fiscal year.
Both Allianz and AIG have partnered with Indian counterparts and have venturedinto the Indian foray – Allianz with the Bajaj group (the biggest producer of twowheelers in India) and AIG with the Tata Group (one of the biggest conglomerates inthe country).
Illustration 6: Depicts market value forecast in $ billion for the Indian Insurancemarket vis-à-vis the Asia Pacific and Global Insurance market. It suggests; in 2010,the Indian insurance market is forecast to have a value of $ 40.5 billion, an increase of61.3% since 2005. In 2010 the Asia-Pacific insurance market is forecast to have a val-ue of $ 941.5 billion, an increase of 23.3% since 2005. In 2010, the global insurancemarket is forecast to have a value of $ 3,997 billion, an increase of 26.9% since 2005.
1.5 Status Quo – The Indian Market as-is vis-à-vis other Markets 39
Figure 23: Illustration 6 – Market Value Forecast – 2010 (Datamonitor)

Notice the use of the logarithmic scale here as well, in order to permit viewing ofthe Indian market vis-à-vis the Asian and World.
Illustration 7: Suggests the market value forecast up to 2010, in terms of the com-pounded annual growth rate (CAGR). The CAGR of the Indian Insurance market inthe period 2005–2010 is predicted to be the highest at 10%, followed by the GlobalInsurance CAGR at 4.9%, and the Asia Pacific CAGR at predicted to be 4.3%. Thesmaller base obviously for the CAGR in India justifies the higher growth rate; how-ever, the current CAGR from 2000–2005 for India stood at 15.3%. The decrease inthe relative CAGR from 15.3% to 10% for the Indian insurance market can be ex-plained because the base has obviously increased for India from 2001 to the newpoint of comparison in 2005; thus an apparent reduction in CAGR is justified.
40 1 Insurance Industry in India
Figure 24: Illustration 7 – Market Value (%Growth) Forecast – 2010 (Datamonitor)
Illustration 8: Projects the development of insurance penetration in the life areaacross continents and selected countries over the years 2003 through 2005. Insurancepenetration is measured as the ratio (in percent) of the premium to the GDP. Insur-ance penetration for a country is a measure depicting reach. Interesting facets to notefor the same are: the world life insurance penetration stood at 4.34%, the US at4.14%, Germany at 3.06%, Asia at 5.16%, Japan at 8.32%, Taiwan remarkably highat 11.17%, China at 1.78%, India at 2.53% and Mexico at 0.68%.

1.5 Status Quo – The Indian Market as-is vis-à-vis other Markets 41
Figure 25: Illustration 8 – Insurance Penetration Comparison Chart in the Life Insurance Area(IRDA)
Illustration 9: Projects the Insurance Density comparison chart for the life insur-ance area across continents and selected countries. Insurance density is defined as theinsurance premium per capita or the ratio of the insurance premium of the nation to
Figure 26: Illustration 9 – Insurance Penetration in the Non-Life Insurance Area for the years2003 through 2005 (IRDA)

the population of the nation. Two points to note are [a] the scale used in the illustra-tion below is logarithmic scale to permit visualization of the figures of countries likeIndia, China, Egypt and Latin America. [b] However, since the figures depict the in-surance density in dollars, it does not factor in the purchasing power parity concept.The Insurance density (in 2005) for the world life stood at 299.5, the US at 1753.2,Germany at 1042.1, Asia at 149.6, Japan at 2956.3, Taiwan remarkably high at1699.1, China at 30.5, India at 18.3 and Mexico at 49.9. It is interesting to note that a“small” country like Taiwan has such high insurance penetration and insurance den-sity rates. Although Mexico had a very low penetration rate in the Life Area 0.68%,its insurance density is almost 3 times of India.
Illustration 10: Projects the Insurance penetration rates comparison chart for thenon-life insurance area for the years 2003–2005. The world over, insurance penetra-tion in life is higher than that of non-life areas.
42 1 Insurance Industry in India
Figure 27: Illustration 10 – Insurance Density in the Life Insurance Area for the years 2003through 2005 (IRDA)
Illustration 11: Projects the insurance density development comparison chart fornon-life areas. In general, the insurance density for non-life is lower than that of life.In the case of India it was as low as 4.4 for non-life in 2005.

1.5 Status Quo – The Indian Market as-is vis-à-vis other Markets 43
Figure 28: Illustration 11 – Insurance Density in the Non-Life Insurance Area for the years2003 through 2005 (IRDA)

Chapter 2:Life Insurance
“Industry outlook and the Main Players” for life insurance in India discussesthe market share, the profits for life insurers and exemplifies the strategiesthat work for them by discussing the generic approaches of the Life InsuranceCorporation of India. The next sub-chapter discusses empirical data via re-sponses and views of insurance executives and knowledge leaders on the out-look of insurance over the next 5 years. The “Urgent Needs and CustomerSegmentation” reveals the socio-economic-classification (SEC) used to cate-gorize the population of India, which serves as an input to the customer seg-mentation exercise. It throws light on the HPI (Household Potential Index)which overcomes the drawbacks of SEC by categorizing individuals based ontheir consumption propensity rather than a rigid approach of the SEC whichmay not correspond to the lifestyle consumption patterns of a household. Fur-thermore, customer segmentation at a micro level has been explicatedthrough best practices. The chapter on “Product” discusses common life in-surance policies in force in India, riders that can be judiciously used to offercustomized solutions, best practices in product design and finally best prac-tices in the way product offerings are structured. “Pricing” discusses the im-portance of combining cost-plus pricing with a outside-in customer-orientedview on pricing. “Distribution Channels” throws light on various lateral dis-tribution channels with a focus on the potential of bancassurance and the roleof agents. Finally, “Communication Strategy” discusses television advertis-ing as a key communication element for insurance in India, concluding with aTV ad-analysis.

46 2 Life Insurance
2.1 Industry Outlook and Major Players
Introduction
When it was part of the British Empire, India with its splendor and natural riches, wasknown as the “jewel in the crown.” Today, foreign insurance companies, especiallythose in the life sector, tend to view India in a similar, if less lyrical light. With its rap-idly expanding economy, burgeoning middle class and overall population of morethan a billion, India is seen as a land of promise (O’Connor). Joint venture is recog-nized as the preferred route into the Indian insurance market, for reasons beyond theforeign direct investment cap. Joint ventures help in combining local knowledge, dis-tribution network and infrastructure with global experience. The year on year growthfor private insurers in the life insurance industry has exceeded 100%, with private in-surers now gaining 20% of the market share. Peter Alexander Smyth, the regionalgeneral manager of ING Asia Pacific said to this outstanding growth “Outside man-agers are likely to be unused to high growth rates like these; however, Indian man-agers are unfazed by this”; which is why although foreign players bring in a lot of ex-perience, managers feel this may not be everything. It is essential to think locally in adynamic environment and understand the rhythm and cycles of the local market be-fore exacting a business model from the foreign location onto a new market. This dis-cussion helps us to further the base established in the previous chapter with respect tothe kind of internationalization strategy that a foreign player must pursue, whereinwe concluded it should be “business transfer” with a “joint venture”.
The Life Insurance Industry in India recorded a premium income of Rs.1058.7 bil-lion (1Euro is approximately Rs. 55) during 2005–2006 as against Rs. 828.5 billionin the previous financial year recording a growth of 27.78%. The contribution of thefirst year premium, single premium and renewal premium to the total premium wasRs. 212.7 billion (20.09%), Rs. 175.09 billion (16.54%) and Rs. 670.90 billion(63.37%), respectively. The private sector with a total premium of Rs. 150.8 billionformed 14.25% of the total premium. The Life Insurance Corporation (LIC) which isthe only public sector company in the life insurance area, with a premium of Rs.907.9 billion formed the remaining 85.75% of the total premium underwritten in theindustry. Overall, the size of the life insurance market increased on the strength ofgrowth in the economy and concomitant increase in per capita income (IRDA).
Market Share
With these premiums underwritten, the private sector and the LIC experienced a95.19% and 20.85% growth respectively, over the previous year (2004–2005). The

2.1 Industry Outlook and Major Players 47
higher growth for the private insurers needs to be viewed in context of the lower base.However, the private insurers have improved their market share from 9.33% in2004–2005 to 14.25% in 2005–2006.
Please see the illustrations below that reflect the market share development overthe years 2004–2005 to 2005–2006 for the LIC and private insurers with respect tothe first year premium, renewal premium and total premium.
Figure 29: Market Share Development for first year, renewal and total premium for LifeInsurers (IRDA)
Increase in the renewal premium is a good measure of the quality of the businessesunderwritten by the insurers. It reflects increase in their persistency ratio and enablesinsurers to bring down their overall costs of doing business. The renewal premiumunderwritten by the life insurance industry recorded a growth of 18.46% during2005–2006 as against 20.85% in 2004–2005. The private insurers and LIC reportedgrowths of 122.56% and 14.32% respectively during the year.
The proportion of the linked and non-linked business has changed to 44.78% and55.22% respectively in 2005–2006 as against 32.54% and 67.46% for linked to non-

Management in Action: Customer Satisfaction Survey
Tata AIG Life Insurance Company aces the VOICE Customer SatisfactionSurvey
A survey conducted by the Voluntary Organization in Interest of Consumer Edu-cation (VOICE) revealed Tata AIG Life Insurance Company (Tata AIG Life) asthe clear winner in terms of customer satisfaction in the life insurance categoryin 2006. This was India’s first-ever customer satisfaction study for the insurancesector.Furthermore, the survey revealed that Tata AIG Life had a high recall as a reput-ed brand name. The ability to provide innovative and customer-focused servicesuch as allowing the maximum grace period for premium payment has not onlyfurther distinguished Tata AIG Life from other life insurance companies but alsoappealed to consumers.Commenting on the survey results, Trevor Bull, managing director, Tata AIGLife Insurance Company, said, “The quest of the company has always been to bethe best at what we do rather than adopting a simplistic market share at all costsapproach. Achieving this VOICE recognition required huge effort from Tata AIGLife team; however retaining the number one position will be tougher. Beingranked the best in the life insurance category by an independent consumer group
48 2 Life Insurance
linked in 2004–2005. This shift in preference towards linked products has coincidedwith the positive developments in the stock market.
New policies issued by life insurers showed an overall growth of 35.29% in2005–2006 as opposed to a decline of 8.44% in the previous year. Please see the illus-tration below depicting the new policies issued by life insurers in India. The firstbracket “y-o-y” indicates year on year growth over the previous year, and the secondbracket indicates the market share (with respect to the number of new policies issued)for that particular year.
Insurer 2004–2005 2005–2006
Private 2233075 (34.62% y-o-y) (9% of total) 3871410 (73.37% y-o-y)(11% of total)Sector
LIC 23978123(–11.09% y-o-y) (91% of total) 31590707 (31.75% y-o-y) (89% of total)
Total 26211198 (–8.44% y-o-y) 35462117 (35.29% y-o-y)
Figure 30: New Policies Issued – Life Insurers, Development and Market Share 2004–2005,2005–2006 (IRDA)

2.1 Industry Outlook and Major Players 49
is an encouraging and fitting manifestation of our successful completion of fiveyears of service in the insurance industry. We look forward to the challenges thatlie ahead and are confident of maintaining and improving further our currentstandards of service and efficiency.”The survey, which was conducted across eight cities and covered around 1,250life insurance customers, evaluated the different life insurance companies on theparameters of tangibility, problem solving ability, reliability, responsiveness, as-surance and empathy. The objective of the survey was to understand and meas-ure overall customer satisfaction within the insurance sector. The Voluntary Or-ganization in Interest of Consumer Education (VOICE) is a voluntary actiongroup, whose objective is to protect and further the interests of the consumer.Tata AIG Life Insurance Company (Tata AIG Life) is a joint venture company,formed by the Tata Group and American International Group, Inc (AIG). TataAIG Life combines the Tata Group’s pre-eminent leadership position in Indiaand AIG’s global presence as the world’s leading international insurance and fi-nancial services organization. The Tata Group holds 74 per cent stake in the in-surance venture with AIG holding the balance 26 per cent. Tata AIG Life pro-vides insurance solutions to individuals and corporate. Tata AIG Life InsuranceCompany was licensed to operate in India on February 12, 2001 and started op-erations on April 1, 2001 (Press).
Profits for the Life Insurers and the Strategy of LIC
The Life Insurance industry is capital intensive and insurers are required to injectcapital at frequent intervals to achieve growth in premium income. Given the highrates of commissions payable (22.52% of the premiums was the industry average in2005–2006), expenses towards setting up operations, training costs incurred towardsdeveloping the agency force, creating a niche for its products, achieving reasonablelevels of persistency, providing for policy liabilities, and maintaining the solvencymargin, make it difficult for insurers to earn profits in the initial 5–7 years of their op-erations. SBI Life Insurance Company was the first private insurer to turnaroundwith a net profit of Rs. 20.3 million in 2005–2006. SBI (State Bank of India) is one ofthe largest banks in the country; thus bancassurance continued to be SBI Life’s keydistribution channel contributing to 43% of the premium underwritten, consequentlymassively reducing costs of operations, leading to an earlier break even. All privateinsurers reported a deficit in their revenue accounts 2005–2006 and thus necessitat-ing further injection of capital by shareholders. LIC continued to report a surplus of

50 2 Life Insurance
Rs. 127 billion, of which Rs. 6.2 billion was transferred to the Government of India intune with the provisions of Section 28 of the LIC Act, 1956 (IRDA).
LIC, which has been in existence since 1956, is the largest life insurer of the coun-try and had a market share of 85.75% in 2005–2006. Despite liberalization and thusincreased competition on account of new entrants, LIC continues to maintain its posi-tion, profitability, government obligations and is also successfully achieving mam-moth growth rates despite its colossal base. A critical analysis of LIC’s strategy inlieu of the generic methods of competition proposed by Michael Porter would thus beof immense help as it serves amongst areas of learning for the rest of the industry.
Management in Action: Best or Worst Practices – LIC’s Strategies
On opening up of the insurance market, whichever offers the same product at thelowest premium would thrive and prosper. This is “cost leadership” in insurance.LIC has both advantages and disadvantages in this aspect with respect to new en-trants. Its first mover advantage, existing distribution network through estab-lished agency system and walk-in business potentials gives a degree of cost ad-vantage. Its rigidities in organizational structure, systems in place, state of tech-nology in conflict with the existing level of manpower may give it a cost disad-vantage. However, there are economies of scale in the huge number of policies ithas achieved, and economies of scope, especially in the case of renewal premi-um and new related products. (I will briefly discuss LIC’s product portfolio inchapter 2.3.) The investment income arising out of deployment of premium in-come will contribute to cost leadership, in other words lowering of premium. If,however, new entrants enter the market with state-of-the-art investment technol-ogy and successfully append their premium income to other investible resourcesto match the size of the LIC investments, then LIC’s cost leadership will be un-der pressure. This will typically be the case if banks and development bankscome into competition with LIC. The second generic strategy is one of “differen-tiation”. LIC has earned phenomenal brand equity as the life insurer of the na-tion. Any new entrant has to compete with this cardinal differentiation, whereLIC scores an advantage in the short and medium term. For price sensitive cus-tomers, LIC has policies which can be catered for a very low premium like LIC’sTerm Assurance policy, thus achieving a “cost focus”. Any new entrants servingsuch customers will be fraught with high transaction costs and will not be able tomatch premiums.“Jeevan Surabhi”, “Money Back Policy”, “Beema Sandesh”, “Jeevan Griha”,“Jeevan Shri” are examples of LIC marketed policies with various unbundling,

2.1 Industry Outlook and Major Players 51
rebundling of risks and addition of frills to make them more attractive to seg-ments of customers, thus achieving a “differentiation focus”. The fifth competi-tive strategy “speed” without sacrificing any of the aforesaid advantages can beachieved by pro-actively positioning itself into the top echelon, through strategicalliances and corresponding arrangements with – for example the Indian Postetc, and restructuring its business around the core competencies (Mishra andMishra).
The Players
The various players in the Indian life insurance industry include one public sectorplayer – The Life Insurance Corporation and 15 private insurers (since liberalizationin 2000), which include several joint ventures between foreign insurance playerswith Indian companies. They are as follows in descending order of premiums under-written (premiums underwritten in 2005–2006 are mentioned in brackets)
– ICICI Prudential (Rs. 42.6 billion)– Bajaj Allianz (Rs. 31.3 billion)– HDFC Standard Life Insurance (Rs. 15.69 billion)– Birla Sun Life Insurance (Rs. 12.59 billion)– SBI Life Insurance (Rs. 10.75 billion)– Tata AIG Life (Rs. 8.80 billion)– Max New York Life (Rs. 7.88 billion)– Mahindra Kotak Life (Rs. 6.21 billion)– Aviva Life (Rs. 6.00 billion)– ING Vysya (Rs. 4.25 billion)– Reliance Life (Rs. 2.24 billion)– Met Life (Rs. 2.05 billion)– Sahara Life (Rs. 0.27 billion)– Shriram Life (Rs. 0.103 billion)– Bharati AXA ( no premiums in 2005–2006, as 2006 was its first year of operation)
Conclusion
The economy and capital markets play a dominant role in the life insurance market;this is the supply side phenomenon. Improving operations, proper distribution, after-sales services and a full service product range can only improve the demand-sidephenomenon. The hallmark of life insurers operations historically has been conser-

52 2 Life Insurance
vatism. Life insurers tend to enjoy favorable gains in investments, mortality and of-fice productivity, which beget predominantly solid balance sheets. Given the rela-tively inelastic demand for life insurance products, companies seem largely immuneto external changes in markets or in the economy. However, although the market con-ditions affect firms to varying degrees, the overall economic environment’s impacton the life insurer’s performance is potentially significant, a critical issue as this per-formance is of direct consequence to various stakeholders – policyholders, benefici-aries, investors, capital markets and government. In the life insurance industry, thereare evident trends towards emphasis on returns on investment, tax efficiency, and onproduct performance. Projections for social security, national insurance systems andrising longevity are leading to an encouragement of retirement savings (Mishra andMishra). Moreover, the introduction of ULIPs (Unit Linked Insurance Plans) hasbeen the most significant innovation in the life insurance industry since the productdesign of ULIPs addresses several concerns like liquidity, flexibility and transparen-cy and at the same time providing increased autonomy (and corresponding risk) tothe insured. It may be interesting to note that in 2005, only a small portion of the lifeinsurers’ business was reinsured; however, this may be offset by the increased riskborne by policyholders, through the increase in ULIPs in the Life Insurance Busi-ness. All in all, consumer demands in the life insurance industry are tending to en-courage a focus on the marketing of individual investment vehicles with a more ho-listic view of overall financial management.
2.2 Market Opportunities and Challenges –Empirical Results and Analysis
Introduction
This section highlights the results from the survey questionnaire (please see appen-dix). The purpose of the survey was to understand the esteemed opinion of insuranceexecutives on the emerging opportunities and challenges and the outlook for the next5 years for the insurance industry in India. The survey was sent to the senior manage-ment of various insurers in India, faculty at the best insurance institute in India: Na-tional Insurance Academy, associates employed by the regulatory body and the deci-sion maker: IRDA and other opinion leaders and insurance knowledge experts. I de-veloped the questionnaire based on current relevant research and an understanding ofdebatable issues pertinent to the development and evolutionary path for the insurancemarket in India. In order to make the survey holistic and accommodate for various

2.2 Market Opportunities and Challenges – Empirical Results and Analysis 53
facets contributory to the emerging opportunities and challenges and outlook for theIndian insurance milieu, the survey was developed around six primary sections: [1]Tariffed vs. De-tariffed regime, [2] Foreign players’ participation, [3] Health Insur-ance, [4] Life Insurance, [5] IRDA: its role and developments and [6] Innovation andBest Practices. Respondents were asked to project their opinion as applicable (Forexample life insurers who do not have health insurance products, would obviouslyleave the “health insurance” section out). On account of the limited time availableand the exhaustiveness of the survey, the number of responses per industry was limit-ed. While this means that the data cannot be statistically projected (for per industrybasis); however, majority of the questions in the survey were expert opinion relatedor subjective, which help divulge the inclination of industry experts on the whole.Thus a subjective elucidation of the same is deemed essential; else one fears loss ofsubstance while attempting to convert the information from the subjective to the ob-jective.
Whilst sections 1, 2, 5 and 6 are applicable to the insurance industry in general andthus both health and life insurance, section 3 is explicitly structured around healthand section 4 around life insurance. In this chapter, I will depict the views as per theresponses to section 4. In chapter 3.2, I will present the opinions as per responses tosection 3. And finally, the responses to section 1, 2, 5 and 6 would be illustrated inchapter 4.1 (which is “Future Outlook for the Insurance Industry in India”). Heresome statistical methods have been used on account of a reasonable number of re-sponses, which includes responses of both health and life insurers, as these questions(1, 2, 5 and 6) were by and large pertinent to both industries.
For the results below, please refer to the corresponding questions of section 4 of thesurvey in the appendix.
Results
To 4[a], the CEO of one key life insurer responded that their customer segmentationincludes individuals between the age of 0 and 50, living in metros and tier-2 townsand earning incomes across the range. He added that their product and distributionsuite are “multi-crossing” across several segments, implying that a product being of-fered to one customer segment, may also be offered to another segment and that sev-eral such crossovers exist across their entire gamut of products. However, to cater tothe rural and social sector requirements, they have a specialist rural/social sector dis-tributions and products unit in place. Whilst, most products are offered to individualstill the age of 50, and after that age limit, only renewals are possible, some insurershave elevated the age limit to draw a policy from 50 years to 60 years.

54 2 Life Insurance
4[b]: the claims to premium ratio for the main life insurance product of life insur-ers averages at 50%.
4[c]: the retention rate for life insurance products in general ranges from 70% to85%. The purpose of understanding the retention rate in life insurance is to reveallapses in a business where terms of policies are obviously longer than those for motoror health insurance. Moreover, it is an industry wide known fact that a policyholder’sact of ceasing to pay the premium before the term ends or before maturity has a high-er direct negative financial impact on him compared to the insurer.
4[d]: While one industry expert unaffiliated to an insurance company stated that onan average, frauds detected by a life insurer in a year are about 50, the CEO of a lifeinsurer disclosed that his company detected in excess of 400 frauds across all productlines, annually.
4[e]: Since there were multiple views on this, I would present the views of insurersas opposed to those of faculty or members of the group of respondents not affiliateddirectly to the insurance companies, on grounds that senior management can opinion-ate on the course of the business environment as it happens. Thus, the most urgent re-quirements for the Indian life insurance industry were in the order as follows, 1 beingthe most urgent requirement: [1] Increasing professionalism amongst agents and bro-kers, [2] reaching out (selling policies) to the segment of society that is below thepoverty line, [3] moving from the perception of life insurance policies solely as taxsavings vehicles to investment vehicles, [4] right pricing strategies based on accuraterisk assessment (differences between good and bad risk) and underwriting skills, [5]not punishing the rightful claimant on account of the misconduct of fraudulentclaimants, [6] customer satisfaction with respect to efficient and quick claims settle-ment, [7] use of CRM tools and data warehousing for linking historical customer in-formation and thereby coming up with accurate assessments, [8] tracking fraudulentclaims, [9] simplicity of contracts and contract language, [10] developing life insur-ance products that also incorporate other functionalities, like ULIPs, credit insurance,children’s marriage savings plans etc. The above also reflect primarily the views ofthe CEO respondent in 4[d]. It is thus fascinating to note that despite 400 frauds de-tected across all product lines annually in his company, contrary to what one wouldintuitively believe to be on his radar for the industry, he ranks “tracking fraudulentclaims” as number 8. Thus implying, something as seemingly urgent as this, is essen-tial but not deemed as essential as the 7 other factors ranked above it.
4[f]: Most effective mediums of advertising/promotion for the core life insuranceproducts are ranked as follows, with 1 being the most effective channel driftingdownwards: [1] Newspaper, [2] Television, [3] Outdoors (billboards etc), [4] Maga-zines, [5] Radio, [6] Internet. However, some respondents did mention in the “others”

2.2 Market Opportunities and Challenges – Empirical Results and Analysis 55
column, that the most effective promotional activities are realized by distributionpartners and through word of mouth recommendations, adding customers from simi-lar reference groups, like family members or organization circle or friends.
4[g]: Life insurers are opting for several channels of distribution to maximize reachand optimize penetration. Respondents had the following views towards the effective-ness of 7 different distribution channels on a “likert scale” that runs from least effec-tive [1] to most effective [5]. The primary views included: more effective [4] or mosteffective [5] for bancassurance, neither effective nor ineffective [3] for telcassurance,less effective [2] to neither effective nor ineffective [3] for online distribution, neithereffective nor ineffective [3] for malls and supermarkets (this channel is still being test-ed for majority of the insurers). Certain extremes exist in opinions, with some respon-dents claiming that no life insurer has a tie up with postal services yet, while somedeeming it to be neither effective nor ineffective [3]. This may technically indicatesimilar things, as the survey has not provided for an option to check a NA (not applica-ble) box, thus a interfacial deficiency of the survey, unless it was penned down next toit. Automobile tie-ups on the other hand was another contradiction, where one insurerresponded that it was not applicable to life insurers, while some deemed it more effec-tive [4], which are obviously two very different aspects. Another area mirroring con-tradicting views is medical tie-ups, with some respondents rating it [1] least effectivewhile others rating it [4] more effective. However, this needs to be viewed in light ofthe necessity of existential infrastructure in place to appropriately use medical tie upsin an efficient manner for life insurance products, via cross selling life insurance poli-cies to primarily health insurance customers. Furthermore, question 4[g] requested re-spondents to answer in lieu of their individual companies’ competencies, thus clearlyjustifying outliers or a so-called extremism in opinion.
Having said that, the responses on the life insurance industry reveal the followingkey highlights:
1. New policies are issued to customers between ages 0 and 50, with some insurerselevating the age limit to 60.
2. Many crossovers exist between customer segments and the products and distribu-tion suite.
3. Social and rural obligations necessitate a separate specialist rural/social distribu-tions and products unit.
4. Claims to premiums ratio average at 50%, much more positive figures than healthinsurance figures will later reveal.
5. Retention rate for life insurance policies ranges between 70 and 85%.6. Frauds are company dependent, and are as high as 400 frauds across product lines
(annually) for some companies.
7. Increasing the professionalism amongst agents and brokers, increasing reach tothe segment of society that is below poverty line and moving from the perceptionof life insurance policies seen as tax savings vehicles to protection, savings andinvestment vehicles are the three most urgent requirements for the life insuranceindustry in India.
8. Promotion through distribution partners, word of mouth recommendations, news-papers and television are the most effective channels of communication.
9. Bancassurance is deemed as the most effective distribution channel over andabove the conventional agency model; malls and supermarkets are growing as al-ternative channels of distribution but are still in the testing stage for majority ofthe insurers.
2.3 Urgent Needs and Customer Segmentation
Socio Economic Classification of India – Urban and Rural India
“Life insurance business” which means the business of effecting contracts of insur-ance upon human life, is the most lucrative category of insurance globally with thehighest penetration and reach. Moreover, the IRDA recently framed regulations onthe obligations of insurers towards the rural and social sectors, binding all insurers tofulfil their requirements on an annual basis. 18% of the total policies in the first 6years of operation of a Life Insurer must be policies extended to lives in rural areas.The Life Insurance Corporation of India (the leading Life Insurance Company in In-dia) has been extending coverage to the economically weaker sections of the societythrough various social security group schemes targeting masses and non-convention-al groups in the unorganized sector.
Coming up next is an essential examination of the possible customer segments, byuncovering the foundational Socio-Economic Classification (SEC) of India; this is ofconsequential importance for the following reasons. First, empirical evidence showsthat the Indian Life Insurance penetration (percentage of the premium to GDP) is2.53% (which is below the global average of 4.34%), thus implying huge potential inthe middle and lower segment of society. Second, the rural and social obligations im-posed by the authority necessitate an un-biased examination of the overall market.Finally, the actuality that serving the rural/weaker sections is, if truth be told, givingimpetus to both market share and profitability of the life insurers in India, making thecustomer segments insurers would have earlier ignored, an indispensable current pri-ority.
56 2 Life Insurance

Education
Occupation
Unskilled Worker E2 E2 E1 D D D D
Skilled Worker E2 E1 D C C B2 B2
Petty Traders E2 D D C C B2 B2
Shop Owners D D C B2 B1 A2 A2
Business/Industrialistwith Number ofEmployees
[a] None D C B2 B1 A2 A2 A1
[b] 1 to 9 C B2 B2 B1 A2 A1 A1
[c] 10+ B1 B1 A2 A2 A1 A1 A1
Self-Employed/ D D D B2 B1 A2 A1Professional
Clerical Job/Salesman D D D C B2 B1 B1
Supervisory Level D D C C B2 A2 A2
Officer/Executives C C C B2 B1 A2 A2– Junior
Officers/Executives B1 B1 B1 B1 A2 A1 A1– Middle, Senior
Figure 31: SEC for Urban India (Exchange4Media)
Illit
erat
e
4 ye
ars
of S
choo
l
5–9
year
s of
Sch
ool
SSC
/HSC
(equ
iva-
lent
to 1
0than
d 12
th
Gra
de r
espe
ctiv
ely)
SSC
/HSC
but n
ot G
radu
ate
Gra
duat
e/P
ost-
Gra
duat
e G
ener
al
Gra
duat
e/P
ost-
G
radu
ate
Pro
fess
iona
l
2.3 Urgent Needs and Customer Segmentation 57
The SEC Classification
SEC, that is Socio-economic Classification is a classification made in the urban andthe rural sector, to identify the consumption pattern and the household purchase be-havior. Based on education levels, occupation, type of household, the population isdivided into separate bands, called the Socio-economic Classes.
The Urban Sector in India is divided into SEC A1, A2, B1, B2, C, D, E1, and E2.These classes are calculated as a function of Educational qualifications of the ChiefWage Earner1 and his occupation. The table below details the categorization based onthe various criteria.
1 Chief Wage Earner = CWE and is the person who contributes the most to the household expenses

58 2 Life Insurance
Similarly, the Rural Sector in India is divided into SEC R1, R2, R3 and R4. Theseclasses are calculated as a function of Educational Qualifications of the CWE (ChiefWage Earner) and the type of the household he stays in – Pucca (Solid), Semi Pucca(Semi Solid Houses) or Kaccha (Houses made of weak material like earth or hay).Please see the table below for the rural SEC categorization.
Education of the Type of HouseChief Wage Earner(CWE) Pucca Semi-Pucca Kutcha
Illiterate R4 R4 R4
Self-learning /No School R3 R4 R4
Up to Grade 4 R3 R3 R4
Up to Grade 9 R3 R3 R4
SSC/HSC R2 R3 R3
College R1 R2 R3
Graduate/Post-Graduate General R1 R2 R3
Graduate/Post-Graduate Professional R1 R2 R3
Figure 32: SEC for Rural India (Exchange4Media)
More generally speaking, urban Indian households have broadly been classified as
✓ ‘high’ socioeconomic class referring to SEC A & SEC B✓ ‘mid’ socioeconomic class referring to SEC C, and✓ ‘low’ socioeconomic class referring to SEC D & SEC E.
However, an analysis of the SEC classification indicates that consumption patternsmay not be completely reflected in an education vs. occupation chart and lifestylepatterns would thus reflect the consumption patterns more closely and effectivelythan the income levels.
The Drawbacks of SEC
“Socio Economic Classification (SEC) is often said to be lacking in discriminatingthe truly potential households and audience. Also, as we recognize, SEC is an indica-tor or a pointer towards the “likely to consume” set but often defies the reality of notpointing clearly towards the “consuming class”, which is the purpose of any targetingby a marketer. The drawback of using Monthly Household Income (MHI) lies in thedifficulty of capturing the correct data, as the respondent is hesitant to disclose thecorrect MHI” (Sodhani).

2.3 Urgent Needs and Customer Segmentation 59
The various assumed variables augmenting the SEC (like durable ownership, fre-quency of travel by air, intensity of consuming various products and services, recentpurchase date etc.) come with the negative aspect of “judgment” of the individualsconcerned. This is because the variables are defined around the specific ownership ofa particular product or service, which is rather subjective considering the vast spec-trum of Indian preferences and micro cultures, thus also highly skewed if some indi-viduals happen to posses those very goods or services. An alternative method whicheradicates this problem will thus be discussed below.
The Concept of HPI
The above argument has given rise to a more subjective (rather than objective) per-spective to the calculation of SEC and thus is a debatable classification. An alterna-tive to the traditional MHI is the concept of HPI, or Household Potential Index. Ex-perts believe that it is a more scientific method used to segregate and target the “con-suming” class. HPI enables a direct comparison of the urban and rural population onthe same scale.
It divides the population into 3 classes:
a) Upper most segment of the consuming class (the “lakhpathis” or “crorepathis”who also spend and consume)“Lakhpati” is a Hindi word used loosely to describe a person who is rich and ownlakhs of rupees, where 1 lakh Rupees = 100, 000 Rupees. Similarly “Crorepati” issomebody who owns crores of rupees, where 1 crore is equivalent to 10 million or100 lakhs.
b) Middle segment which is the core target for growth of several categories, consid-ering the rising middle class in India.
c) The lower most segment, which is the “volume generator” for many FMCG cate-gories and lower end durables and services (Sodhani).
Another advantage of the HPI method is that it permits factoring in of the premiumgoods. “Premium” goods are those that are “wanted by many” but “consumed byfew”. Simply put, “premuimness” is defined as the inverse of penetration. If the pen-etration level of a good is low, it commands a higher premium. For example 41 percent of all homes in India have Television. But only 2 per cent have a flat TV. Hencehomes with a flat TV are considered to be “premium” by the HPI measure (Sodhani).Thus ‘premiumness’ thus needs to be factored in while deciding the classification inorder to reflect a consumption pattern associated with lifestyle; which can be cateredby the HPI calculation, but not by SEC method. The concept of HPI allocates high
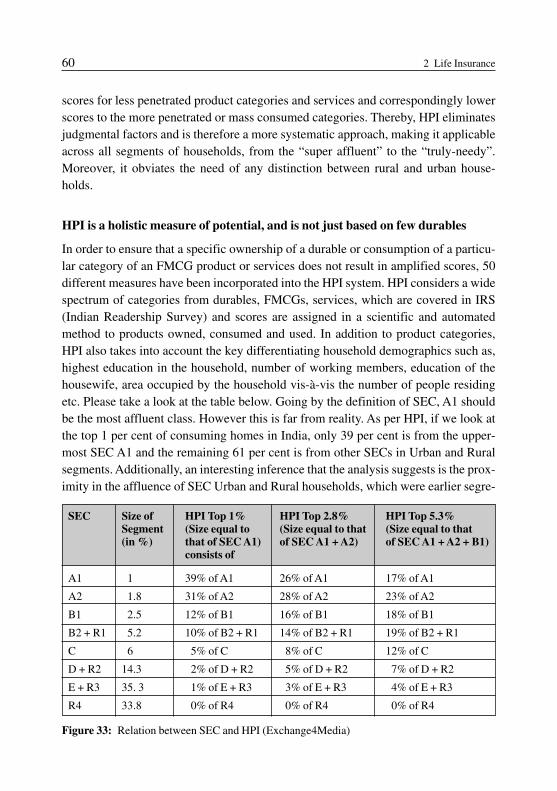
60 2 Life Insurance
scores for less penetrated product categories and services and correspondingly lowerscores to the more penetrated or mass consumed categories. Thereby, HPI eliminatesjudgmental factors and is therefore a more systematic approach, making it applicableacross all segments of households, from the “super affluent” to the “truly-needy”.Moreover, it obviates the need of any distinction between rural and urban house-holds.
HPI is a holistic measure of potential, and is not just based on few durables
In order to ensure that a specific ownership of a durable or consumption of a particu-lar category of an FMCG product or services does not result in amplified scores, 50different measures have been incorporated into the HPI system. HPI considers a widespectrum of categories from durables, FMCGs, services, which are covered in IRS(Indian Readership Survey) and scores are assigned in a scientific and automatedmethod to products owned, consumed and used. In addition to product categories,HPI also takes into account the key differentiating household demographics such as,highest education in the household, number of working members, education of thehousewife, area occupied by the household vis-à-vis the number of people residingetc. Please take a look at the table below. Going by the definition of SEC, A1 shouldbe the most affluent class. However this is far from reality. As per HPI, if we look atthe top 1 per cent of consuming homes in India, only 39 per cent is from the upper-most SEC A1 and the remaining 61 per cent is from other SECs in Urban and Ruralsegments. Additionally, an interesting inference that the analysis suggests is the prox-imity in the affluence of SEC Urban and Rural households, which were earlier segre-
SEC Size of HPI Top 1% HPI Top 2.8% HPI Top 5.3%Segment (Size equal to (Size equal to that (Size equal to that(in %) that of SEC A1) of SEC A1 + A2) of SEC A1 + A2 + B1)
consists of
A1 1 39% of A1 26% of A1 17% of A1
A2 1.8 31% of A2 28% of A2 23% of A2
B1 2.5 12% of B1 16% of B1 18% of B1
B2 + R1 5.2 10% of B2 + R1 14% of B2 + R1 19% of B2 + R1
C 6 5% of C 8% of C 12% of C
D + R2 14.3 2% of D + R2 5% of D + R2 7% of D + R2
E + R3 35. 3 1% of E + R3 3% of E + R3 4% of E + R3
R4 33.8 0% of R4 0% of R4 0% of R4
Figure 33: Relation between SEC and HPI (Exchange4Media)

2.3 Urgent Needs and Customer Segmentation 61
gated; SEC R1, SEC R2 are close to SEC B2, SEC D of urban respectively. Con-versely speaking, 61 per cent of SEC A1 does not feature in the Top 1 per cent of theconsuming households.
Concluding remarks on HPI and SEC Methodology
Finally, another advantage that works for HPI is that HPI scores can be modified andrecomputed with time. As penetration increases, products consequently lose their rel-ative level of premium over time and hence new variables need to be introduced asand when the need is felt. For example, motorcycle, which is a growing category to-day, need not be one of the parameters in HPI (say 5 years hence) if majority of theconsuming homes possess one in the year 2010 (Sodhani).
By an astute combination of HPI with the SEC system, marketers and plannercan now refine the market prioritization. From a Marketer’s perspective – whilstSEC entails understanding the “potential” of markets, HPI indicates the “consump-tion intensity” of markets, which can be understood from the mean HPI scores ofmarkets.
Micro Segmentation
While the SEC classification enhanced by the HPI methodology is useful for themacro segmentation of the life insurance market, these techniques cannot be deemedadequate to serve as inputs for product design formulation. These techniques mustthereby be augmented by a subsequent needs analysis method (to trace the most ur-gent needs), thus calling for micro-segmentation within these major classifications.
The primary segmentation variables for the Indian Life Insurance market are ageand stage of life. While age helps estimate the ballpark for the most urgent needs, thestage of life or circumstance helps design customized products to suit the event.
Says Shivaji Dam, Managing Director of OM Kotak Mahindra Life Insurance,“Any event that may change considerably the financial course of your life warrants areview of your insurance cover. These could be anything from landing with a job togetting married to having a child to taking a home loan to the retirement of one’s par-ents.” Debashish Sarkar, Senior Vice-President, Marketing, Max New York Life In-surance asserts: “Assessing your life insurance needs is not a one-time exercise. It isa dynamic process that must be revised as often as possible.” In fact, he argues, it is agood practice for your life insurance advisor to visit you every year, “not just to col-lect the premium for your policy, but to understand how your life circumstances havechanged over the year” (N. Krishnamurthy).

62 2 Life Insurance
Management in Action: Best Practices – Segmentation
HDFC Standard Life Insurance offers life plans based on the stage of the life orcircumstance that one belongs to. Please see the stages and the correspondingneeds that can be satiated by the products offered for the respective stages.
Stages Main Needs
[1] Young and Single [a] Save for a home and wedding[b] Tax Planning[c] Saving for Golden Years (retirement)
[2] Just Married [a] Planning for a home/securing your home loan liabili-ty
[b] Saving for a vacation[c] Saving for the first child
[3] Proud Parents [a] Providing for children’s education[b] Safeguarding family against loan liabilities[c] Savings for post-retirement
[4] Planning for [a] Provide for regular income post–retirementretirement [b] Immediate tax benefits
[c] Lead a secure, comfortable & independent lifestylewhen retired
(HDFC Standard Life Insurance)
Similarly Max New York Life (MNYL) has designed its products [1] By LifeStages and [2] By needs. By life stages includes stages [a] Single, [b] Married,[c] Married with children, [d] Planning for retirement. By needs includes [a]Savings [b] Investment [c] Education for children [d] Marriage for children [e]Protection. (Max New York Life) The products of MNYL will be discussed inthe following chapter.
2.4 Products
Common Life Insurance Policies in India
Insurance sector reforms have introduced structural reforms to bring competition andgreater efficiency to the insurance market. The underlying idea of the insurance sec-tor is to unleash the enormous financial assets held by households by expanding the

2.4 Products 63
range of investment options with a promise of increasing returns to the users. The un-leashed funds can be used to create matching term assets.
The basic customer needs met by life insurance policies are protection and savings.Policies that provide protection benefits are designed to protect the policyholders (orhis/her dependents) from the financial consequences of unwelcomed events such asdeath, disability or long term sickness. Policies that are designed as savings contractsallow the policyholders to build up funds to meet specific investment objectives suchas income in retirement or repayment of a loan. Most life insurance policies provide amixture of savings and protection benefits. The common types of life insurance poli-cies in force in India are as follows
1. The Endowment Assurance: with two basic variants [a] Non-participating (with-out profit) and [b] Participating (with profit) endowment assurance. Non-partici-pating policy offers a guaranteed amount of money at the maturity date, in ex-change of a single premium at the start of the policy or a series of premiumsthroughout the term of the policy. If the policyholder dies before maturity, a sum ispaid on his death. Policyholder can surrender the policy before maturity and re-ceive a lump sum (called the surrender or cash value) at the time. The policyhold-er can keep the policy in force without paying further premiums; in this case, a re-duced sum may be granted. There is usually a provision to take a loan up to 90%of the surrender value in the policy provision. In case of participating polices, thepolicyholder is entitled to receive profits in the form of bonus as regular cash pay-ments.
2. Money Back Plan is a popular savings plan providing for lump sum period at peri-od intervals (like 20% at the end of 5 years, then 10 years, 15 years and 40% at theend of 20 years). Here too the policy can be offered in a non-participating or par-ticipating format. In case of the death of the insured, the assured sum plus an addi-tional guarantee would be received. This kind of policy usually has no loan facili-ty; but does have a surrender value.
3. Whole Life Assurance provides a benefit on the death of the policyholder whenev-er that may occur during the currency of the policy. It is a pure protection instru-ment providing for long-term financial protection to the dependents. Paid up valueassured option may be granted in case of early death of the insured.
4. Term Assurance Policy is a measure of pure protection, however for a limited pe-riod or term. It is the cheapest policy available; generally no payment is made ifthe policyholder survives. These policies are structured with no “surrender value”and “paid up” policy options.
5. Immediate Annuity meets the policyholder’s need for a regular income (in ex-change of a single premium) after her retirement. The policy can also be struc-

64 2 Life Insurance
tured to provide an income for a limited period of time for nominal expenses. Thepolicy usually comes with no surrender value option.
6. Deferred Annuity; here the policyholder pays regular premiums for a period up tothe specified “vesting date”, when the sum assured may be offered in full or partof the pension, also meeting any cash obligation at that time, like a housing loanpayment (Bhattacharya).
Riders or Customized Solutions
The riders in the Life Insurance policy have been likened to toppings of a pizza whichcan be ordered as per one’s needs. Just as the cost of the pizza changes by the top-pings that one prefers, the cost of the policy (or the total premium) also changes withthe rider that a policyholder orders for herself. The convenience of having riders in apolicy eliminates the want to obtain a separate policy for each of the needs. By takingjust one policy, several needs can be fulfilled by going in for several riders; thus of-fering a great deal of flexibility by means of a customized solution to the policyhold-ers. The overriding factor, however, is that these riders have to be paid for and insome cases can be quite expensive.
The liberalization of the insurance industry in India and the foreign entrants hastriggered the importance of riders with several insurers offering riders with their basepolicies, thus serving as a value enhancement. A look at some of the riders would en-able a clearer understanding of their role.
1. Accident Death Rider is the oldest and the most popular among several riders. Un-der this rider, the beneficiary receives an additional amount (besides the sum as-sured under the policy), if the policyholder were to die in an accident. The term“accident” covers a wide range of events and the premium for this rider is afford-able, making it doubly attractive. Nevertheless, there is a maximum limit put onthe amount of coverage of the policy and an upper age limit as well (usually 70years).
2. Premium Waiver Benefit Rider is one where the payment of further premiums bythe policyholder is totally waived if the policyholder were to be afflicted with oneof the covered crippling eventualities and be disabled to live a normal life. Thepolicy continues as if the premiums are being remitted regularly and the policy isin full force.
3. Guaranteed Insurability Rider is one wherein the further renewal of the policywhen the present term ends is guaranteed without proving further insurability,which one would have to do normally (without the presence of this rider). Be-sides, in case the insured would like to surrender his policy (which is rather un-

2.4 Products 65
profitable if the term was long), the rider gives him the flexibility of choosingshorter terms with guaranteed insurability at the end.
4. Critical Illness Rider is one wherein a policyholder can combine the advantage ofa health insurance without going in for a separate health insurance policy, provid-ing coverage against a list of diseases restricted as per age, personal and familyprofile of the policyholder.
5. Family Income Benefit Rider is an accentuated value addition to the policy, as itensures a regular stream of income for the family if the sole breadwinner of thefamily dies during the active working period, hence taking care of both the cashand income needs of the family.
Insurers are leveraging on the utilities of these riders to come up with customized so-lutions rather than rigid bundled products, while offering only a few base products.While this sounds very customer friendly and dynamic, the public awareness of lifeinsurance in all its glory and benefits is not at an elevated level; and insurance is pri-marily seen as an investment tool by a large section of people. Thus the public is un-used to getting no return on investment for these riders at maturity or a surrender val-ue. Considering the exclusive risk coverage features of the riders, IRDA initially pre-scribed an upper limit (30% of the premium paid on the base policy) on the premiumpaid towards the coverage of riders in a life insurance policy. This has nonethelesscaused furore in the industry and would change with improved awareness and per-haps active lobbying (Jawaharlal).
Best Practices: Product Design Innovation – Unit Linked Insurance Plans
The introduction of unit-linked insurance plans (ULIPs) has been, possibly, thesingle-largest innovation in the field of life insurance in the past several decades.In a swoop, it has addressed and overcome several concerns that customers hadabout life insurance – liquidity, flexibility and transparency and their lack there-of. These benefits are possible because ULIPs are differently structured productsand leave many choices to the policyholder. Broadly speaking, ULIPs are bestsuited for those who have a conceptual understanding of financial markets andare genuinely looking for a flexible, long-term savings-cum-insurance solution.Simply put, ULIPs are structured such that the protection (insurance) elementand the savings element can be distinguished and hence managed according toone’s specific needs.Traditionally, the savings element of insurance has been opaque, giving policy-holders no control over asset allocation, no transparency, no flexibility to match

one’s lifestyle, inexplicable returns and an expensive, complicated exit. ULIPs,by separating the two parts within the same product and managing them inde-pendently, offer insurance buyers what no traditional policy had – continuous in-formation about how their policy is working for them. For those who want a con-venient, economical, one-stop solution, ULIPs are the best bet.The key to good financial planning is to understand one’s current and future fi-nancial goals, risk appetite and portfolio mix. This done, the next step is to allo-cate assets across different categories and systematically adhere to an investmentpattern, so that they work in tandem to meet one’s requirements over the nextmonth, year or decade. Because of their flexibility to adjust to different life stageneeds, ULIPs fit in very well with financial planning efforts. What is more, as asystematic investment plan, ULIPs greatly diminish the hazards of investing in avolatile market and using the concept of ‘Rupee Cost Averaging’ allows the poli-cyholder to earn real returns over the long term.When buying a ULIP, customers are advised to look for and understand the nu-ances as [A] Charges: First, understanding all the charges levied on the productover its tenure, not just the initial charges, which would include the fixed admin-istrative charges, the fund management charges, mortality charges and spreads,and that too, not only in the first year but also through the term of the policy.Some companies levy a spread between the buy and sell rates of the units, whichcan significantly reduce the value of the investment over the long-term. Closeexamination and questioning of such aspects will reveal the growing power ofone’s investment. [B] Fund Options and Management: Next, understandingthe various fund options available and the fund management philosophy and ob-jectives of each of them. This would entail examination of the track record of thefunds thus far and how they are performing in comparison to benchmarks. Ques-tions such as – who manages the funds and what experience do they have? Arethere adequate controls? Looking at how easily one can access information aboutthe fund’s performance when one needs it – are there daily NAVs? Is the portfo-lio disclosed regularly?[C] Features: Most ULIPs are rich in features such as allowing customers totop-up or switch between funds, increase or decrease their protection level, orpremium holidays. Carefully understanding the conditions and charges associat-ed with each of these is crucial. For instance, is there a minimum amount thatmust be switched? Is there a charge on the same? Must one go through medicalunderwriting if one needs to increase the sum assured? [D] Company: Cus-tomers must insure with a brand they can trust would honor its commitment and
66 2 Life Insurance

2.4 Products 67
service them according to their requirements. [E] Monitoring: Having bought aULIP, the customer must check at least once a quarter how his fund is perform-ing, and consider a switch if there is a change in the level of risk he is willing totake or in his personal market view (Nanda).
Management in Action: Max New York Life Products
As discussed in the previous chapter, Max New York Life (MNYL) has struc-tured its product offerings along [a] Various Stages of Life or [b] Needs as theprimary segmentation variables.I would now go on to elucidate the various products offered by MNYL in the re-spective stages and/or need areas.
The Products by Life Stage are1. Single
a. Whole Life (Participating) for Protection (the need being fulfilled is pro-tection)
b. Level Term Plan (Non-Participating) for Protectionc. Five Year Term Renewable & Convertible (Non-Participating) for Pro-
tectiond. Life Maker Unit Linked Plan which is Unit Linked, thus flexible invest-
ment2. Married includes the above 1[a] to [d] and
a. Life Pay Money Back Plan for Savingsb. Life Partner Plus (Money Back) for Protectionc. Life Invest which is Unit Linked
3. Married with children which includes products 1[a], 1[d], 2[a], 2[c] and a. Child Endowment for Children. It is a participating policy.b. Stepping Stones (Money Back) for Children. It is a participating policy. c. Life Gain Endowment Plan (Participating) for Savingsd. Life Gain Plus a Limited Pay Endowment Plan (Participating) for Savings
4. Planning for Retirement which includes 1[a], 1[d], 3[c], 3[d], 2[b], 2[c]anda. Easy Life Retirement Plan (Participating) for Retirementb. Life Maker Pension Plan which is Unit Linked
The Products by Needs are1. Savings which includes 1[a], 1[d], 2[a], 2[b], 3[a], 3[b], 3[c], 4[a] and 4[b] 2. Investments which includes 1[a], 1[d], 2[c], 3[c], 3[d] and 4[b]

68 2 Life Insurance
3. Education for children which includes 1[a], 1[d], 3[a], 3[b], 2[a] and 2[c] 4. Marriage for children which includes 1[a], 1[d], 3[a], 3[b], 2[a], 2[c], 3[c]
and 3[d]5. Protection which includes 1[a], 1[b] and 1[c]
A bird’s eye view of the product categorization depicts the sophistication withwhich needs and life stages are matched with the product offerings. Moreover, itis interesting to note how products 1[a] and 1[d] are marketed for every need orstage of life, thus serving as the base products across categories. Furthermore,each of these offerings can be augmented by opting for additional customizationsvia riders. These offerings are dealt with in detail highlighting the core needs’ ful-fillment of the same, in the company’s website and brochures, thus helping con-sumers choose the most apt and fitting products (Max New York Life).
Product Level Concepts
A product is a bundle of satisfaction. It is more than just a tangible offering; a productis anything that can be offered to a market to satisfy a need or want. In planning itsmarket offering, the marketer needs to address 5 product levels, with each leveladding more customer value and the 5 constituting a customer value hierarchy (Kotlerand Keller). The fundamental level is “core benefit”; in insurance the core benefitwould correspond to protection, savings or investment or all. The next level is the “ba-sic product”. The basic product would be one that satisfies any or all the core benefitsas deemed necessary. For example the plain Vanilla Whole Life policy serves the Pro-tection benefit. The next level “expected product” includes the set of attributes andconditions that buyers normally expect when they purchase the product. For example– besides the product itself, the buyer would expect effective claims managementwhen the insured event occurs. Several riders’ options now form a part of the expectedproduct level category, as all insurers provide for the same and thus the provision ofthe same no longer serving as a differentiator. The “augmented product” level, whichexceeds customer expectations and thereby acts as the core differentiator for the insur-er, would include features like speedy and proactive claims settlement, minimal errorsof commission especially in a highly emotional and sensitive scenario like death ofthe insured and genuine empathy on behalf of the insurer by providing exclusive serv-ice at home at a time as comfortable by the dependants or family of the deceased. Fi-nally the “potential product” would encompass all possible augmentations and trans-formations the product or offering might undergo in the future.

2.4 Products 69
Thus, claims management is a highly critical “support” function that fulfills the ex-pected product requirement, however, if enhanced to the augmented product level,efficient, timely and empathetic claims settlement could be a core differentiator forthe life insurer.
Critical Support Functions: Claims Settlement
Customer services become even more important when it is a one-time purchaseand majority of the customers are unaware of the product variations available inthe market. Life insurance is one such industry. A satisfied customer is the great-est brand ambassador and one negative experience by a customer can cost the in-surance company very dearly. This is especially valid in death claims on accountof the seriousness and grief of the occasion. The fact that the occasions of interac-tion are few, imply less cumulative effort on behalf of the insurer, however with ahigher “weight” allocated to the experience. Life insurers do not have to deal withyear on year renewals and thus lapses. Any lapse that occurs due to non-paymentof premiums costs the insured more. Even an early surrender of a policy has anegative net present value for the insured, which is why customer lifetime value(CLV) sustenance can be achieved by a life insurer with greater ease than it can beby general insurers. A good experience would translate into heightened customerloyalty thus enhanced CLV for the insured (in case of the maturity claim) or de-pendent (in case of a death claim) and their family members.Unlike tangibles, where it is possible to examine the product prior to purchase,the real test of insurance is after purchase – at the time of claims settlement. Thusclaims settlement in life insurance can be classified as the single, most crucial re-alization of product satisfaction. Claims settlement has become one of the cor-nerstones for continued customer loyalty for LIC. LIC has laid great emphasis onexpeditious settlement of maturity and death claims. LIC settles 1.43 claimsevery second with highly transparent and fair claims settlement operations. Onlyin case of suppression of material information, is a claim repudiated. However,the number of claims repudiated is very small since the extent of moral hazard isrelatively lower in life insurance as opposed to non-life insurance. Nonetheless,in such a case the claimants can make a representation for consideration by theClaims Review Committees (CRCs) at the zonal and central offices. The claimssettlement operations of LIC improved from 4.02 million “claims settled” and0.144 million “claims outstanding” in 1994–95 to 10.3 million “claims settled”and 0.016 million “claims outstanding” in 2003–04, thus making enhancedclaims management as the Key Success Factor of LI (Rajesh).

70 2 Life Insurance
2.5 Pricing Criteria
Insurance sector uniqueness and Indian Life Insurance in context
Insurance sector is unique in its core financial technology. The sector has high levelof behavioral inputs in recognition of income, expenses, liabilities and profits. Herethe system intuitively follows target costing or in case of a structural imbalance ofcosts the system goes for reverse engineering. The insurance sector determines theprice first and then looks askance at the cost of underwritten risk claims (Mishra andMishra, Insurance Sector Revisited).
In India, where the insurance sector is at a nascent stage, rate making or pricing ininsurance consists of arriving at plain vanilla or naked price of funding the futurepromises. The ideal price is arrived at by applying a principle propounded by oneS.S. Huebner known as the principle of “life displacement cost” of an individual orfamily. This life’s displacement cost or alternatively human life value is equal to thediscounted present value of income less the life’s own consumption over its remain-ing lifetime. The extent to which this benchmark optimal human life value will beconverted into life policy depends on the paying capacity of the customer, positionaladvantage of the customer to self insure the risk and relative opaqueness of the insur-ance products to the investment decision-maker in the family (Mishra and Mishra,Getting Closer to Life Insurance).
For majority of the general insurance businesses in India which until 31st Decem-ber 2006 were still operating in a tariffed regime, a transition from rule based pricingto risk based pricing is already a herculean task, essentially because of the dearth ofunderwriting skills in the tariffed regime. Actuarial science, accurate risk profilingand enhancement in underwriting quality in India have momentous scope for im-provement. In the life insurance area, underwriting is relatively easy on account ofthe certainty of the eventuality – death or maturity, thus definitely accounted forwhile “pricing”. However, even in the life insurance area pricing is still cost-plus andsubject to the quality of underwriting skills, which is why improvements in risk pro-filing and underwriting will augment the overall profit potential of the Indian Life In-surance Industry.
Actuary Method and Pricing Elements for a Whole Life Policy
For example let us consider the plain vanilla life insurance policy is a whole life poli-cy without profit. Annual premiums are payable until the death for sum assured. Themethod through which such a premium is determined is known as actuary evaluation.Actuary method relies on the theory of large numbers and uncertainty ingrained in

2.5 Pricing Criteria 71
the probable happening of a certain event like death during and after the durationconfined between now and the life expectancy at birth as prevailing on the date ofevaluation. A careful analysis of the sentence is essential to understand the elementsinvolved. The core pricing elements for a whole life policy are as follows
– Larger is the number of lives insured the better for the theory of large numbers towork.
– Life expectancy at birth keeps on changing due to changes in the health care andother welfare activities in the society. The greater the life expectancy, the less willbe the premium for the sum assured.
– As individuals may predecease or live beyond their life expectancy, the riskinessof the premium depends on the extent of such observed variation. The premiumshould be relatively more for larger variations.
– There are phases in life expectancy duration where the death shows unsteady pat-tern. That is why providers avoid contracting such covers during childhood and be-yond a cut-off old age limit. The covers are available during the phase of steadystate of distribution of death. (Although a higher premium should be charged forthe “outlier” phases instead of not offering a cover at all; this would benefit bothparties: the insurer and the insured.)
– Within the steady state, the earlier one opts for the policy, lesser is the amount ofthe premium.
– If the payment of premium is monthly or quarterly, the premium gets divided withresultant adjustments downwards for earlier payments but upwards for increasedtransaction costs.
– The policy provides the self-assessed and agreed displacement cost of human val-ue to the nominee of the life insured.
– If the same policy was with bonuses, which are calculated on a yearly basis perthousand of the sum assured, the premium would obviously accommodate forthese additional bonuses.
Management in Action: Best Practice in Risk Profiling
SBI Life Insurance launches “Agency Online” Portalto help insurance advisors understand customer risk profiles
SBI Life Insurance Company Limited launched the ‘Agency Online’, an exclu-sive portal designed to meet the needs of its growing insurance adviser base onthe 16th of May, 2007. The CEO Uday Sankar Roy said in a press release:“Agency Online is an initiative towards empowering our insurance advisers with

72 2 Life Insurance
tools that facilitate self-learning and delivering right advice.” A key feature is‘Profile Score’ that helps understand customer's risk profile and offer solutionsthat meet investment objectives. Moreover, “The portal offers advisors’ cus-tomer friendly tools that include premium calculators, understanding risk pro-file, customer portfolios, product flip charts and policy tracker” he added. SBILife Insurance is a joint venture between the State Bank of India(SBI) and CardifSA of France with the paid-up capital of Rs. 500 crore (US $ 123 Million) (PTI).
Professional Price Management Process
Although a preliminary business concept, most managers tend to forget that not onlyis price a profit driver (by virtue of the statement profit = pric e* quantity – costs), butit is also the strongest profit driver; implying no other variable change (of the profitequation) gives as much impetus to the profit as does price. Moreover, price is astrong marketing instrument, a change in which provokes customer and competitorresponse (Fassnacht).
Simply put, price is the strongest lever to increase profits (Schmidt-Gallas andLauszus). In an industry like insurance, where majority of the costs are incurred (viaclaims) after the pricing is already set, it becomes crucial to fully exploit the profitpotential of pricing: [a] to serve as reserves for the future, [b] to abide by the solvency
Figure 34: Pricing Levels based on the Profit Potential and Professionalism (Fassnacht)

2.5 Pricing Criteria 73
margins regulations and [c] finally, to make profits over and above the reserves thatmay be paid out in claims.
As illustrated above, as a firm moves from cost-plus pricing to competitive pricingto value-based pricing, the potential to make profits increases. In India, streamliningand honing the underwriting skills would be the pillar of cost-plus pricing. Althoughvalue-based pricing is essential, it is of utmost criticality to be able to cover the costs(due to solvency margin regulations), which is why speedy, efficient and accuraterisk profiling and underwriting is a foundational precursor to value-based pricing.Thus please see the “Critical Support Functions” box below on best practice sugges-tions for underwriting in life insurance.
Next, to fully reveal the profit potential of pricing the entire marketing value chain– from product to the price to distribution must be professionally managed. This in-volves mastering 5 tasks.
1. Value Pricing and Segmentation2. Knowledge about the price elasticity3. Cross selling4. Sales optimization5. Optimization of the pricing process (Schmidt-Gallas and Lauszus)
Let us look at each of these tasks in the Indian Life Insurance Context
1. Value pricing and segmentation: The price set must skim the customers’ willing-ness to pay. Thus it is essential to understand the following.
a. Which parameters offer the “must-have” value to customers? (Schmidt-Gallasand Lauszus) For example for a whole life policy the “must-have” value is pro-tection. In a money back policy, the most urgent need is savings and in a unitlinked policy, the most urgent requirement is transparent and flexible investment.
b. Are there any innovative new parameters? (Schmidt-Gallas and Lauszus) Theriders like accident death rider, premium waiver rider, family benefit rider,guaranteed insurability rider and critical illness riders are innovative new pa-rameters, a combination of which can provide customized solutions. These fea-tures can be better understood by a conjoint analysis which reveals the price-value proposition of the individual attributes thus suggesting an optimal pric-ing for the final product.
Critical Support Functions: Underwriting in Life Insurance
A risk which cannot be quantified cannot be underwritten is the golden rule ofinsurance. Underwriting is the process of selecting and classifying exposures

74 2 Life Insurance
and the lifeblood of insurance business. Knowledgeable underwriting is the keyto a gainful future for an insurance company. Underwriting profits are directlyproportional to the skill level of the underwriters. The old systems of underwrit-ing were quite slow and expensive. The exercise used to take an hour or more in-volving culling out medical information from the prospect and completing theapplication with over a 100 questions that needed answers. Traditional under-writing makes sales difficult and the issue of policy expensive. It is cost-effec-tive only for big size policies. The total time taken is sometimes of the order of 6weeks. There is a growing need to upgrade underwriting skills in tune with theimprovement in mortality.In Underwriting – faster, cheaper and better delivery is the mantra. The processof underwriting can be streamlined by mechanizing most of the decisions. Thereduction of human intervention in the underwriting process will reduce subjec-tivity and also enhance the risk management practices of the insurance company.This also aids to even out the processing load which shows high variations in thelife insurance business. A tool that can enhance the speed of the underwritingprocess and the issue of insurance policies, several times over is tele-underwrit-ing. Many insurance companies are gearing up to adopting tele-underwriting.The move would help them lower acquisition cost, speed up application process,maintain the mortality goals and of course help customer friendliness. It reducespaper work thereby helping the field staff to sell more without digressions; es-sentially totally transforming the underwriting functions.“Tele-underwriting” had its origin in the early nineties. The modus operandi is:the call center professionals conduct telephonic interviews with insurance appli-cants with the exclusive aim of ordering medical records. Thereby this leads toboth cost and time saving for the insurance companies. A great idea, it has thepotential for substantial savings. It is a step in the right direction and is a big ben-efit to the advisor. It reduces for the agent the burden of taking a personal historyor asking an applicant medical questions. As a consequence it would allow themmore time to concentrate on selling. It is a win-win situation as the client is bene-fited – because of tele-underwriting being a “once-and-done” method. Even theinsurance company reaps benefits as it is able to obtain quality underwriting in-formation. The reasons are not far to seek – the personnel asking the questionsare experienced underwriters. Reflexive (drill-down) medical questions are usedto get an accurate picture of applicants. This neutral third-party interview ismuch superior to an agent or an underwriter interview in terms of the quality ofinformation obtained.

2.5 Pricing Criteria 75
The essential precursor for success of tele-underwriting rests on the capability toelicit risk salient information with the least number of questions. The better thequality of questions, the superior is the protective information. All in all, the suc-cess potential of tele-underwriting is vivid and far-reaching – tele-underwritinghas lead to a significant drop in the cycle time; that is the intervening period be-tween the submission of an application and the time the policy is issued; the fig-ures are touted at 40% to 50% (T. S. Rao).
2. Knowledge about the price elasticity: Before making any changes in the price, itis essential to understand the corresponding price elasticity that is how the quanti-ty in sales would change if the prices are increased or decreased. This is essentialbecause a price increase is justified only to the extent that the impact of sales lostis not ousting the price, in a way that causes the profit to plummet. Nevertheless, acertain increase in premium would result in lesser sales lost with respect to thebottom line of the company.
3. Cross selling: This would include targeted bundling of insurance benefits andtheir conjoint offering in the market (Schmidt-Gallas and Lauszus). For exampleunder the “Married with Children” stage Max New York Life offers products tar-geted towards savings for education or marriage of children over and above thebasic policies (whole life and term policies). Each of these products encapsulate adifferent set of product features satisfying related but non-overlapping needs, thusmaking these products complementary and consequently achieving cross sellingof the products. This level of product design sophistication goes a long way inhelping command the right prices based on the value proposition of the bundle,and thus exhausting the profit potential of pricing via cross selling.
4. Sales Optimization: The Management needs optimize its sales force, keeping inmind the importance of the on-location sales representative; thus calling for an op-timal balance between effectiveness (proximity to the customer) and efficiency(costs reduction through online sales) (Schmidt-Gallas and Lauszus). Besides, thecurrent incentive system of the agency force in India is a commission model basedon revenue, thus misdirecting the sales personnel to focus on volumes rather thanthe profit or bottom line. This could serve as a key learning for a new entrant intothe Indian market, who could now use a margin-based commission model to in-centivize his sales force, thus giving impetus in the right direction.
5. Optimization of pricing process: In companies with a high “pricing IQ”, all price-related decisions are organized systematically and clearly. Three decisive ele-ments characterize a pricing process: the components, the input dimensions and

76 2 Life Insurance
the chronological structure. The components are the information, methods, mod-els, guidelines for decision making, qualifications, competencies, incentive sys-tems and timing. Aside from objective information such as data on revenue, cus-tomers and competition, the input dimensions are subjective dimensions like theassessments and experiences of the management. Finally, there is the chronologi-cal structure: Supported by the pricing strategy, an audit must objectively andhonestly check the current practices, success and improvement potential of pric-ing. Based on this review of the status quo, price decisions concerning the key as-pects discussed above have to be made and established in the market by means ofa systematic implementation plan (Schmidt-Gallas and Lauszus).
Finally it is important to combine the internal pricing view of the company with theexternal market oriented view, by essentially combining the underwriting skills, riskmanagement perspective and actuarial experience (of the internal pricing view of thefirm) with the marketer’s view, the one closest to the market, which begets an indepth understanding of the willingness to pay of potential policyholder, in order tomaximize the capacity of a right pricing technique.
2.6 Distribution Channels
The three ‘A’s for spreading the message of insurance, as an instrument of financialsecurity, are: (i) the affordability of the product to the consumer, (ii) its acceptability,as need based and necessary at the given cost and (iii) its easy accessibility if the oth-er two ‘A’s are found acceptable to the consumer (Rao). The distribution channel isthe third A: accessibility and plays the role of discovering and highlighting the riskexposure needs of the consumer and supplying him with the product that best serveshis needs. The speed with which the insurer reaches the market place, the quality ofinteraction, and the constituents of the distribution channels i.e. the intermediarieshave at the market place will decide the growth graph of the company. The marketshare of the entity will depend on the share of heart, mind and wallet of the customerand it is no wonder organizations globally are continuously engaging themselves inupgrading the capabilities of their intermediaries. Agents of insurers, brokers repre-senting the consumers as their agents and direct selling by insurers constitute the coreof the distribution chain of the marketing of insurance products. One very interestingdimension of the whole process of intermediation (in insurance industry) is thatworld over the tied agency channel has yielded place to multiple distribution chan-nels. This is primarily to ensure that through capacity building, economies of scale

2.6 Distribution Channels 77
are achieved, the reach is increased, and the customer base is enlarged, in order tohave an adequate channel mix for different segments of market and to ultimately en-sure growth in volumes. This transformation has happened not without any basis, for,today, markets are moving from being product driven to customer driven. Hence ithas become essential for companies to reinvent themselves, in their run to be aheadof the competitors (Viswanathan).
Since the entry of private players in 2000, there have been substantial shifts in thedistribution of insurance in India. While many of these changes echo internationaltrends and the expertise brought in by private players, the Indian life (or non-life forthat matter) insurance distribution is predominantly agency driven. The transforma-tion which has been brought in by the opening of the sector has changed the valueproposition for the distribution channels. Today the customer has multiplicity ofchoices of service providers; of products and services; distribution channels etc. As asequel to this, the distribution channels have to be customer focused as compared toproduct focused, keep in mind the long term results as against the low hanging fruits,migrate from a push orientation to a pull orientation and move to strategy-driven ac-tivities vis-à-vis transaction-driven activities. Building a distribution network is ex-pensive and time consuming. Nonetheless, if insurers want to keep up with their cur-rent mammoth growth rates, developing innovative and efficient distribution chan-nels that bridge the reach and give impulsion to the penetration is of utmost criticali-ty. Additionally, the measuring rod for the efficacy of each constituent of the distribu-tion channels will be the pace and ease with which the new paradigm shifts is adoptedby them.
Status quo
The charts below depict the contribution of various intermediaries in underwritingnew businesses in the life insurance sector of India. The information suggeststhe dominance of the agency driven model (primarily individual agents) for the LifeInsurance Corporation of India (Government owned). However, the private playersthat arrived post 2000 (liberalization of the insurance industry in India), have pursueda conscientious mix of several intermediaries to generate business. Although theprivate life insurers, like the LIC, do derive a majority of their business from theindividual agents, a substantial portion of their new life premium is written by inter-mediaries like corporate agents (banks and others), brokers, referral and direct busi-ness.
I will now evaluate the essential distribution channels against the backdrop of theIndian life insurance development.

78 2 Life Insurance
Bancassurance
Bancassurance is the provision of insurance and banking products and servicesthrough a common distribution channel or to a common client base. India has a sav-ings rate of 26% of which savings with banks constitute more than 50% of the do-mestic household savings. This presents an enviable opportunity for insurers to takeadvantage of banks in India, both domestic and foreign, have networks that span thewhole country, thus reaching the most remote locations and cutting across all socialclasses. Increasing customer sophistication is leading banks to devise holistic finan-cial solutions including insurance, long-term savings and retirement (Sahgal).
The relevance of bancassurance in the Indian sector works as a hand-in-glove situ-ation for both insurance companies and banks. Integration of the financial service in-dustry in terms of banking, securities business and insurance is a growing worldwidephenomenon (R. Krishnamurthy).
Figure 35: New Business Underwritten through various intermediaries in Life Insurance(Annual Report, IRDA, 2005–2006)

2.6 Distribution Channels 79
1. Banks are the key pillars of India’s financial system and the common Indian pub-lic has immense faith in banks as is elucidated from the fact above: wherein sav-ings with banks constitute more than 50% of the domestic household savings.
2. The agency network of insurance has not been successful in penetrating many ar-eas as is obvious by the insurance penetration and density in India.2 With about65,000 branches across India and an estimated average of 16,500 customers perbranch (Sahgal), banks, on the contrary enjoy immense reach to households andconsiderable goodwill in the rural regions as well. A majority of customers contin-ue to visit their bank’s branch to meet their savings and credit needs; bancassur-ance thus provides an availability of scale to insurers.
3. Banks have an enormous retail base, showing huge retail thrust with a growth of50% (Bhaskaran). Share of ‘individuals’ as a category in bank accounts is steadilyincreasing. Rural and semi-urban bank accounts constitute close to 60% in termsof number of accounts, indicating the number of potential lives that could be cov-ered by insurance with the frontal involvement of banks (R. Krishnamurthy).
4. The huge customer data available at banks provide for immense cross selling op-portunities. Banks can put their energies into the ‘small-commission customers’that insurance agents would tend to avoid. Banks’ entry in distribution helps to en-large the insurance customer base rapidly. This helps to popularize insurance as animportant financial protection product.
5. Bancassurance helps to lower the distribution costs of insurers. Acquisition cost ofinsurance customer through banks is low. Selling insurance to existing mass mar-ket banking customers is far less expensive than selling to a group of unknown cus-tomers. Experience in Europe has shown that bancassurance firms have a lower ex-pense ratio. This benefit could go to the insured public by way of lower premiums.
6. Banks have an important role to play in the pension sector. Low cost of collectingpension contributions is the key element in the success of developing the pensionsector. Money transfer costs in Indian banking are low by international standards.Portability of pension accounts is a vital requirement which banks can fulfill in acredible framework (R. Krishnamurthy).
Having understood the benefits of bancassurance for insurers, let us now analyzewhat bancassurance has to offer to banks.
1. Banks world over have realized that offering value-added services such as insur-ance, helps to meet client expectations. Competition in the Personal Financial Ser-
2 Insurance penetration which is measured as a ratio (in percent) of premium to the GDP is2.53% for the life insurance sector in India, while being 11.17% for a country like Taiwan. In-surance density, measured as the premium per capita, is USD 18.3.

80 2 Life Insurance
vices area is getting ‘hot’ in India. Banks seek to retain customer loyalty by offer-ing them a vastly expanded and more sophisticated range of financial productsfulfilling an assortment of needs.
2. Insurance distribution helps to increase the fee-based earnings of banks to a con-siderable extent. Insurance activities contribute significantly to banks’ total do-mestic retail revenues. Margins for Indian banks are being squeezed – in 1994,banks borrowed money at 10% and lent out at 14%; now banks borrow at 9% andhave to lend at 9.5%, giving them a very small window for profits. Thus a fee-based model would help banks improve their bottom-line.
3. There is an increasing emphasis on ROE (return on equity) and productivity and aglobal pressure on banks to become financial powerhouses; thus pure bankingdoes not seem to be a viable option any more.
4. Fee-based selling helps to enhance the levels of staff productivity in banks. This isvitally important to bring higher motivation levels in banks in India.
5. Retail thrust and a growing sense of customer segmentation implies that banks areoffering financial products to customers at a more micro level, consequently indi-cating a higher risk for customers and banks and the need for risk managementproducts (Bhaskaran).
The main types of bancassurance are [a] corporate agency, wherein banks can earnfees, [b] referral arrangements, where banks share customer database with insurancecompanies, [c] joint ventures, where banks and insurance companies develop newproducts together (Bhaskaran).
Despite the rapid growth of the life insurance industry in India (at 144% year onyear increase in the first 7 months of 2006), bancassurance in India is still in its nas-cent stages, with the business generated by bancassurance for life insurance in totalbeing less than 7%, (IRDA) whereas in markets like Italy and Spain, the same ac-counts for more than 50% of the total new business (Sahgal). In Asian markets suchas Singapore, Hong Kong and Taiwan, bancassurance has a share approaching 40%.In the year 2006 up to January 2007, bancassurance generated almost 22 to 25% ofthe business in the private sector, suggesting a significant shift from the purelyagency sales model prevalent prior to 2002 and a welcome endorsement of the ban-cassurance-led-strategy pioneered in India by Aviva. Aviva today is a leading bancas-surer with 30 agreements and 65% of its new business premium being generatedfrom this channel3 (Sahgal).
3 In India total sales from the Aviva and Dabur Group joint venture increased to $135 millionwith over 21,000 agents (FD Wire).

2.6 Distribution Channels 81
The primary models of bancassurance in India are [a] Natural partnerships for ex-ample SBI Life and SBI, (which include a parent and a subsidiary relationship) [b]Banks partnering with single insurance companies [c] Insurance companies partner-ing with different banks for example, Aviva has partnered with ABN Amro/AMEX toreach corporate and urban customers, with Canara Bank to reach national masses,with LVB to reach the local population of the state of Tamil Nadu. [d] Insurance com-panies may have separate partners for their life and non-life insurance business. [e] Abank may partner with several insurance companies, (more like a supermarket of in-surance products) (Bhaskaran).
Future growth and trends in the bancassurance area suggest that strategic align-ment and expeditious execution are increasingly being recognized as the key driversof success. Insurers need to select partners, through a judicious analysis of the banks’business, products, processes and customers. Banks are primarily doing “walk-in”business, however this mindset of “walk-in” business has to be adapted to suit the“selling” business that suits insurance products. One of the critical dilemmas ofbranch persons, deciding the priority between a bank product, insurance product andmutual fund, has to be dealt with through a common understanding and training ofsales staff. The primary purpose of bancassurance, as the name suggests, is to sellboth insurance and bank products; thus selling just one of the two products would de-feat the purpose of the channel and subsequently not bring any significant synergiesor substantial cost advantages, which can be derived through economies of scope (ofselling two products through the same channel). Increased sophistication in bundlingproducts and selling a whole gamut of financial instruments would benefit bothbanks and insurers. Unfortunately, the dual regulator environment (for banks and in-surance companies) does hinder operational freedom of such alliances. Moreover, ifa bank wishes to manufacture and sell insurance products, it needs to have a networth of Rs. 5 billion and establish a separate business unit or a subsidiary to do so.Until regulations are completely favorable, insurance companies must definitely usethe bancassurance channel, as is and aim to exhaust its potential to reach out to theuntapped customer network base, as are advanced markets like Europe.
Role of Agents
Despite the growing importance of bancassurance, the Indian life insurance sectoris still primarily agency driven; 86% of the new business premium (for public andprivate insurers in total) in 2005–2006 was underwritten through individual agents(IRDA). Tied agents have traditionally been the primary channels for insurance dis-tribution in the Indian market. The LIC has branches in almost all parts of the countryand has attracted local people to become their agents, apparent by the verity that the

82 2 Life Insurance
LIC still generated 98.37% (2005–2006) of its first year business through individualagents. Traditionally, a person who has lived in a locality for many years sells theproducts of the insurance company with a local branch nearby. While these agentsmay not have been sufficiently knowledgeable about the different products offeredand may not have sold the best possible product to customers, the customers trustedthe company and the agents as locals (Sinha). In lieu of status-quo, it would pay tounderstand the role and importance of the traditional agency system, and discuss es-sential steps to enhance its current standing.
The key features of an agent are as follows
– He acts as the face of the insurance company and allocates primacy to the insurer’sinterest. He collects premium on behalf of the insurance company.
– An agent has an exclusive single insurer relation, implying he cannot representmultiple insurers and hence is “tied” to a single insurer.
– The agent identifies prospective clients for the insurance company and carries outa “Sell” transaction with the customers.
– He does not require any kind of capital investment to start his services; however hedoes require undergoing some training and clearing agents’ examinations, spon-sored by a single insurer.
– Since he is more or less the face of the insurer, the insurer is responsible for theconduct of an insurer.
– Agents can only make straightjacket or un-negotiated offers.– Normally, switching of agents is discouraged (Ramachandaran) (ICICI Lombard).
While brokers act as intermediaries too, the relationship of brokers and agents withthe insurance companies differs substantially. (Please see the illustrations below tounderstand the differences between the two.) However, the skill sets requirements forthe two are similar to a large extent, the foremost requirements being
– understanding insurer’s business and risk management philosophy,– detailed knowledge of the available insurance market and capacities, – high customer orientation, – advising customer according to their needs, – ability to sell multiple products to the same customer at the same time (thus cross
selling) or over a period of time (thus enhancing the customer lifetime value (CLV)of the customer),
– providing market intelligence to the insurers by giving them latest consumer in-sights and feedback, contributing to new product development and/or existingproduct modifications,
– a good working knowledge of the IRDA regulations and a willingness to adhere tothem

2.6 Distribution Channels 83
Figure 36: Representation of the Relationships of Agents and Brokers with Insurers – I(Sawhney)
Figure 37: Representation of the Relationships of Agents and Brokers with Insurers – II(Sawhney)
Agent Broker
Procures premium for his insurer Offers advice for optimal cover
Exclusive single insurer relationship Works with multiple insurers
Identifies prospective clients Identifies prospective risk issues
No capital investment Minimum Rs. 5 Million + Capital
Straight jacket offer Negotiated covers
Figure 38: Key Differences between Brokers and Agents (Ramachandaran)

84 2 Life Insurance
Challenges and Complexities:In the distribution of Life Insurance Policies
In spite of the collapse of the traditional protection mechanisms such as jointfamily and community support, the need for life insurance is yet to be fully ap-preciated in the Indian society. This is possibly due to the fact that while theground realities have changed, the mindsets are still in transition. Selling lifeinsurance, therefore, is not merely about presenting the features and benefits ofthe products and helping the customer choose the right plan. On most occa-sions, it starts at the more basic level of dispelling wrong notions about life in-surance and convincing the prospect about the need for the same. This is whatmakes distribution the toughest of the chain of activities in the business of lifeinsurance. This is also why, of all the financial products, life insurance is ratedas the most difficult to sell.The resistance to life insurance in our society casts an additional burden on thedistribution network and induces a higher degree of fatigue. It also leads tolower conversion rates (number of sales to number of sales attempted) resultingin lower productivity levels of the agents. The costs of distribution, both directand indirect, are also on the higher side due to higher commissions and incen-tives, which cannot be avoided due to the above reasons. The training costs arealso quite high in view of the constant need to give inputs, motivate and en-thuse the sales persons to keep them in performing mode. The higher percent-age of commissions and other incentives notwithstanding, attrition rate amonglife insurance agents is extremely high (up to 50%), not only further adding tothe costs in terms of pre-licensing training expenses but also wasting the orga-nizational efforts in training and hand-holding these agents.Adverse fallout of this attrition is that policies sold by the terminated agentsend up as ‘orphans‘ (which means the customer is left stranded without anagent). A majority of such policies are lapsed, putting both the insurer and poli-cy holder to loss (Kumar).“Orphans” that is policyholders and insurers bereft of their agents, has been agrowing stigma for life insurers in India. I will thus present a case study to ex-plicate how Max New York Life dealt with the impending issue of high agentattrition and orphaned policyholders, and earned profitability and accoladesfrom industry experts by tackling the problem through early thought leader-ship.

2.6 Distribution Channels 85
Management in Action:Best Practice in Customer Retention and Management
Case Study: Max New York Life Insurance:Orphan Policy or Direct Customer – A Paradigm Shift
Max New York Life Insurance co. Ltd is a life insurance company, formedthrough a partnership between Max India Limited and New York Life, a Fortune100 company.As a life insurer, a few “firsts” that Max New York Life is proud of are
– First to offer “free look” period on all policies– First to be awarded the ISO 9001:2000 certification– First to have a customer toll free number– First to launch a formal Six Sigma program– First to have a whole life policy with coverage up to 100 years– First US GAAP profitable company in India– First to pay cash bonuses to its policyholders– First to have a Direct Customer Service Program
An orphan policy holder is one who is now bereft of his agent. However, the pol-icy holders are not the only ones that are orphaned; the insurers who lose theiragents are orphaned as well.

86 2 Life Insurance
The voice of an “Orphan Policyholder”
– I do not have an agent, what happens to me now?– The agent I know is gone. How will you help me?– Whom do I call now, for any help?– How will the company keep in touch with me?– Shouldn’t I get out of the relationship while I can?
What do these customers want?
Concerns for the life insurer
– Growing customer attrition in the segment where the agent is no longer there– High customer complaints in this segment– Adverse impact on goodwill and image– Poor proof of customer centricity– Direct and indirect opportunity loss
Looking at the big picture

2.6 Distribution Channels 87
Early thought leadership matters; In 2002 Max New York Life saw this asan opportunity to
– Provide services “directly” to such customers– Provide services in a manner the best agents would have done for the cus-
tomers– Retain and delight this segment of customers– Ensure that customer expectations are met– Arrest policy lapses
Instead of asking these customers to send letters, redirecting them to customerhelp lines, asking them to visit the branch office or buying time by waiting forthe customer to call or write in, MNYL decided to take a “Feet on street” ap-proach through the launch of their “Direct Customer Services Program”. Thisentailed an employee of the company to act as an agent; he would visit the cus-tomer at his doorstep; this employee was the Customer Relationship Manager(CRO) with a sales background and trained with high customer centricity.
The Direct Customer Services Program
Their initial engagement model was based on premium size:
• First MNYL focused on category A• In 2003, they focused on category A and B• Now (2007), they focus on all four categories – A, B, C, D

88 2 Life Insurance
The Activities that MNYL does to complementthe Direct Customer Services Program include
– Customer relationship officer (CRO) recruitment and training– Introduce CROs to customers– Pro-actively engage with customers– Act like Agents– Meet with customers often– Focus on customer complaints– Provide Point of Sales services– Remind customers about renewals– Trace non-contactable customers– Keep customers updated– Reinstate lapsed policies– uild relationship with customers– Help with Claim process– Generate leads– Renewals follow up

Results of implementing the Program and the Engagement
Model: Indicate the success
MNYL has moved from retention to service to delight, to now up selling andcross selling.
2.6 Distribution Channels 89
(Thomas M. Daniel, Max New York Life)
Role of Brokers
In India, brokers are now emerging as powerful outsourced vendors for insurancemarketing. While brokers have done well and captured a good share in the non-lifebusiness, their contribution on the life side has been relatively insignificant. Further-more, de-tariffing of the general insurance lines of business, and its corresponding ef-fect on health insurance, will give further momentum to the role of brokers in healthinsurance. I will thus build upon the information provided in this chapter (with re-spect to agents and brokers) in chapter 3.6 (distribution channels in health insurance)and throw some light on the role of brokers in the Indian context.
Other Relevant Emerging Channels
Automobile Tie ups
Automobile tie-ups involve distributing life insurance through automobile compa-nies like Maruti, Hyundai, Honda, and Toyota depending upon the target customer

90 2 Life Insurance
segment. The auto industry is booming currently thanks to the ease of access to carloans and the rapid consumer spending of the middle class (Sawhney). As the insur-ance density and penetration in India is abysmally low compared to other emergingmarkets, such an agreement would take the insurer to a place where target customersfrequently visit in sizeable numbers. Innovative and emotional advertising shouldpromote the cause as people could be made to realize that – while the purchase of carinsurance is natural and mandatory, their lives are more precious than the car itselfand hence the life insurance policy too would be advisable.
Indian Post
Earlier, in this chapter, I mentioned the importance of capacity building andeconomies of scale to enhance the reach and volumes achieved by insurers in India.The Indian Post has 150,000 outlets, thus creating a reach far more valuable than anybancassurance tie-up. Moreover, this would give the Post to earn up to 15% in agencycommission (Hindu Business Line).
Malls and Supermarkets
Selling insurance policies through malls and supermarkets is gaining momentum es-pecially with the youth in India. However, retailing of life insurance products requirewell educated interfaces on account of the complexities that the products carry. More-over, it is crucial for the insurance advisor to provide the right advice keeping in mindthe long-term interests of the policy holder. They say a satisfied customer of an advi-sor is like a never ending referral database. The atmosphere in a mall or supermarketmay not be necessarily conducive to such an objective – as it converts the “financialadvisory” role to appear more or less like a “sales” person role. Thus the use of mallsand supermarkets as distribution channels, needs to be revisited and streamlined.
2.7 Communication Strategy
Value Contribution of Branding and Communications
Service communications affect the value of a service firm in various ways. Servicecommunications are
– A driver of customers’ perceived service quality– A driver of customers’ brand image– A driver of customers’ behavior directly, for example by presenting special offers
and enticing the customers to trigger the purchase.
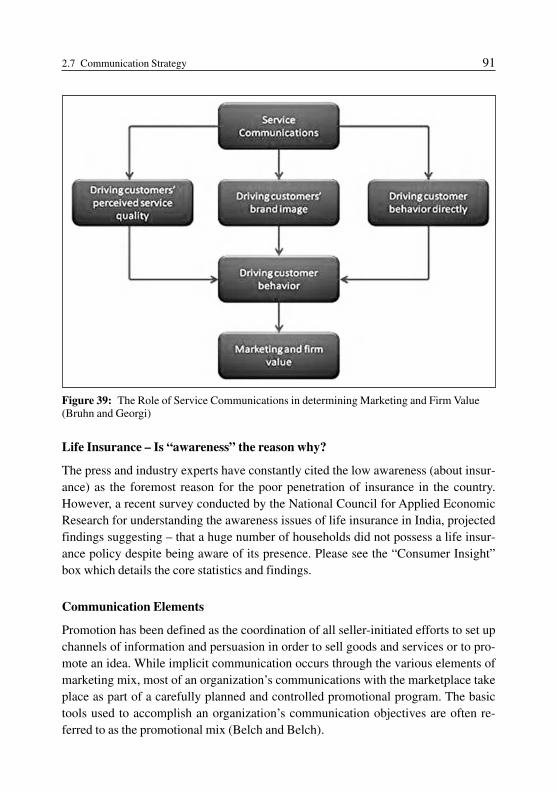
2.7 Communication Strategy 91
Life Insurance – Is “awareness” the reason why?
The press and industry experts have constantly cited the low awareness (about insur-ance) as the foremost reason for the poor penetration of insurance in the country.However, a recent survey conducted by the National Council for Applied EconomicResearch for understanding the awareness issues of life insurance in India, projectedfindings suggesting – that a huge number of households did not possess a life insur-ance policy despite being aware of its presence. Please see the “Consumer Insight”box which details the core statistics and findings.
Communication Elements
Promotion has been defined as the coordination of all seller-initiated efforts to set upchannels of information and persuasion in order to sell goods and services or to pro-mote an idea. While implicit communication occurs through the various elements ofmarketing mix, most of an organization’s communications with the marketplace takeplace as part of a carefully planned and controlled promotional program. The basictools used to accomplish an organization’s communication objectives are often re-ferred to as the promotional mix (Belch and Belch).
Figure 39: The Role of Service Communications in determining Marketing and Firm Value(Bruhn and Georgi)

92 2 Life Insurance
Consumer Insight: Life Insurance Survey Results
78 million households in rural India and 31 million in urban Indiawere aware of Life Insurance but did not possess any policy
Notwithstanding increased savings in bank deposits and post office schemes, In-dians are still averse to saving money in life insurance policies, a survey con-ducted by National Council for Applied Economic Research has found.Main Statistics: Seventy-eight million households in rural India and thirty-onemillion in urban India were aware of life insurance but did not possess any poli-cy, the report said on 12 April.The main reason for not possessing a policy: “A misplaced optimism and the‘nothing will happen to me’ syndrome was a major reason behind several Indianhouseholds being reluctant to go in for insurance cover,” said Rajesh Sud, Execu-tive Director Distribution, Max Newyork Life, which commissioned the survey.Survey details and statistics: The survey, which covered a sample of 63,016households in 1976 villages and 2,255 urban wards, and was conducted duringOctober 2006 and September 2006 found that
• 88% households in urban areas saved their money through various instru-ments while the proportion in rural areas was 79%.
• Bank deposits continued to be the most preferred form of savings with 50.9%of people opting for it. About 36% preferred to keep their money at home andjust 5% deposited in post office. Only 0.1% purchased bonds.
• Among the reasons for savings, education and emergency provisioning toppedthe list with nearly 80% and 82% saving for those purposes.
• A total of 62.7% saved for social ceremonies while 22.4% saved for consumergoods, the report said.
• Nearly 20.7% people borrowed money in rural areas while only 7.4% tookloans in urban wards.
• 51% people took loans for the purchase of consumer durables while 19% bor-rowed money to meet education expenses. Around 14% households headed tobanks to meet their health expenses.
• Both Karnataka and the capital city of Karnataka, Bangalore were above thenational average in terms of ownership of life insurance. While 92% house-holds in Karnataka were aware of it, 53% owned it and 75% of Bangalorehouseholds owned a policy.
• Only 14% female life insurance owners existed as compared to 86% beingmen (PTI)

2.7 Communication Strategy 93
Integrated marketing communications (IMC) involves co-ordination of variouspromotional elements and other marketing activities that communicate with a firm’scustomers. In developing an IMC strategy, a company combines the various promo-tional mix elements, balancing the strengths and weaknesses of each to produce aneffective communications program (Belch and Belch).
Despite the growing importance of IMC and enhancing the customer experience atall plausible touch points through innovative methods, most senior management (re-spondents of my survey on “Emerging Opportunities and Challenges for the IndianInsurance Industry”) consistently cited television and newspaper as the first and sec-ond most effective media of communication.
Figure 40: IMC Audience Contact Tools (Belch and Belch)
Television Advertising and the Insurance Industry – Status Quo
Since television was cited as the most effective medium of advertising and it doeshave the widest reach, I would like to present trends with respect to television adver-tising in the Insurance sector.
First, in a country like India, where a huge population lives below poverty line, itmight be interesting to note that Indians love their television – number of householdsowning television sets was 66.1% in 2004–2005; (Agencies) thus implying a mag-nanimous reach in a country where the literacy rate is at barely 60% (CIA – TheWorld Factbook).
The key findings of a survey conducted by Adex India with respect to “InsuranceSector Advertising on Television” were as follows
– The Insurance sector accounts for 27 per cent share of ad volumes in Banking/Finance/Investment Industry on TV in the year 2006.

94 2 Life Insurance
– The Insurance sector saw a growth of 47% in advertisement volumes on TV in theyear 2006 over 2005.
– Insurance advertising on television was lead by ‘Life Insurance’ with 89 per centshare of volumes in the year 2006.
– Life Insurance saw a rise of 47% in ad volumes on television in 2006 compared tothe previous year.
Figure 41: (AdEx Analysis)
Figure 42: (AdEx Analysis)
TV Ad Volumes for the year 2006 by category
Seasonality trend of advertising for Insurance sectoron TV across the years 2005–2006

2.7 Communication Strategy 95
– Q1 (January to March) saw the highest number of advertisements of insurancecompanies on television across both years 2005 and 2006.
– Highest advertisement volumes of Insurance sector were contributed by HindiNews channels.
Figure 43: (AdEx Analysis)
Figure 44: (AdEx Analysis)
Top 3 channels contributed 52% share of ad volumesin Insurance sector on TV in year 2006
Top 5 advertisers of the Insurance sector on TV in 2006

96 2 Life Insurance
– Private players dominated advertising with 81 per cent share on television in year2006.
– ‘HDFC Standard Life Insurance’ topped the advertisers list on television with a24% advertisement volumes share (AdEx Analysis).
Advertisement Analysis – HDFC Standard Life Insurance
The last graph shows that HDFC Standard Life Insurance topped the advertisers liston television with a 24% advertisement volumes share. In order to understand thekind of advertising that is deemed effective in India, I will present a storyboard of anHDFC Life ad and map the same to a matrix that deals with “options of service com-munications for making services tangibles”.
An important task of mass communications is to make the intangible tangible. Dueto their process character, services are intangible and therefore cannot be examinedphysically or be touched. Therefore, mass communications use certain means tomake services tangibles which refer to one of the two functions: materialization andpersonification. The materialization strategy aims at presenting physical elements ofthe service resources, process or outcome. The personification function establishesan association between the recipient and other persons in order to make the servicetangible (Bruhn and Georgi).
Tangibilization Means Materialization Personification
Service Factors
External Factors – Before–after comparisons – Seeing reference customers– Packaging of service objects – Testimonials– Visualizing need satisfaction – Celebrities
Internal Factors – Material internal factors – Top management– Object samples – Employees– Utilization of symbols – Visualization of service process
Figure 45: Options of service communications for making services tangible

2.7 Communication Strategy 97
Storyboard of an HDFC Standard Life Insurance TV Ad, with translation
As his daughter comes homedejected, her father asks, “Kyahua Neha?” (English: “Whathappened Neha? Anythingwrong?”)
She replies sadly, “U.S. kischolarship mili, par aadhi.”(“I received the scholarshipfor the US, but just half theamount”)
Her aunt assures her, “Baakiapne U.S. wale Uncle bhardenge.” (“Your Uncle fromthe US will pay the remaininghalf, child.”)
But her father is against takinga favor from someone

98 2 Life Insurance
… as he adds, “Koi hai toaapke liye paison ka intezaamkar raha hai … jab aap itni sithi.” (“Somebody has beensaving for you, since you werethis tiny.”)
As the girl realizes that herfather has been saving up forher, she is overjoyed.
Voiceover: “HDFC StandardLife Insurance ke Children’sPlans … Double InsuranceBenefit ke saath.” (HDFCStandard Life Insurance’sChildren Plans with DoubleInsurance benefits)
As her father remarks how shehas grown up, the girl says,“Nahi Papa, main to itni sihun!” (“No, Papa, I am justthis tiny!”)

2.7 Communication Strategy 99
Ad analysis
– The tag line and the musical for the Ad is – “Sar uthaa ke Jiyo” which meanslive your life with your head held high (implying respectfully).
– The ad touches on emotional elements that bind a family in India, and touchesemotions like self-respect, self-sufficiency, and self-esteem etc the qualitiesparents would like their children to develop.
– It vividly connects to middle class families because for most of the youth inIndia, the preferable foreign destination for higher studies is the US; however,the cost for the education is definitely above ones means, connecting the ad toreality.
– Thus, the ad achieves “personification” through “reference customer”, theambitious young girl who dreams of building a wonderful career by opting foreducation in the US.
– The ad achieves “materialization” of service communications through a“visualization of needs satisfaction”
Chapter 3:Health Insurance
“Industry outlook and the Main Players” for health insurance in India dis-cusses key consumer insights, the health insurance industry in contextualbackground with the health expenditure in the country, number of uninsured,health insurance premium and policies development over a time line; also ex-emplifying the main issues and challenges for health insurance in India. Thenext sub-chapter discusses empirical data via responses and views of insur-ance executives and knowledge leaders on the outlook of insurance over thenext 5 years. The “Urgent Needs and Customer Segmentation” reveals the re-sults of a survey with respect to key consumer insights, and projects thesefindings onto the S-O-R model. The chapter highlights regional differences inperspectives, needs and attitudes across selected nations in Asia with respectto health insurance. Furthermore, through best practices, it explicates cus-tomer segmentation at a micro level. The chapter on “Product” discusseshealth insurance product design facets, product development history of the“mediclaim” policy and the concept of managed health care which is gainingmomentum in the global health insurance development. The chapter suggestsa product range to suit various customer segments and the best practices inproduct offerings are elaborated upon. “Pricing” discusses the key pricingcriteria and the increased importance of accurate pricing in health insurance,supplemented by accounts of policy discussions reflecting the pricing crite-ria, the premiums charged and the sums insured. “Distribution Channels” pri-marily discusses the role & contribution of and effectiveness-enhancingmeasures for TPAs and role of brokers. Finally, “Communication Strategy”concludes with a TV ad-analysis.

3.1 Industry Outlook and Major Players
The Mind of the Indian Consumer
While researching for his book, “Best Guide to Buy Health Insurance”, Mr. SureshSethi, CEO of RIA Insurance Brokers Private Limited, discovered myths abouthealth insurance that are core to the average, naive Indian consumer. They were
– “I will not have to go in for hospitalization, it won’t happen to me.” (undying unre-alistic optimism with a “sound” backing of faith in the Gods and Goddesses)
– “I will buy health insurance when I need it.” (unrealistic expectations from healthinsurance, rooting from low awareness about the purpose that a health insurancepolicy fulfills and the way it truly works)
– When told that a health insurance policy cannot be simply purchased on the occur-rence of the disease, as that defies the very purpose of insurance which is meant tocover events that cannot be predicted (illness in this case) and therefore this newfound disease would have to be excluded from the coverage, he says “I am smartenough to manage Health Insurance at a short notice, I have contacts and will man-age it.” (self-confidence beyond realism)
The main inferences that one can draw from the statements above and the current In-dian health insurance context are
– The average Indian consumer is living in denial as far health insurance is con-cerned.
– He is aware of the existence of health insurance, but is not sure why he would needit “before time”.
– He has probably heard of the poor claims settlement ratio in the Indian health in-surance scenario and fears that the insurance companies are “out to scam him.”
– He fears procedural delays that are so often heard of in claim settlements in the In-dian health insurance context.
– This consumer probably does possess a life insurance policy but will refrain frompurchasing a health insurance policy because death is inevitable and out of his con-trol; however, health is within his control, and he is confident that “nothing canhappen to him.”
– Moreover, constant paralleling with life insurance policies compels him to aban-don the idea of possessing a health insurance policy on grounds that a health insur-ance policy gives him no returns (at the end of the term), as do several life insur-ance money-back and endowment policies.
102 3 Health Insurance

A knowledge and understanding of these consumer inferences are critical to compre-hending the landscape in which the Indian health insurance industry is emerging.Furthermore, the above validate some drastic figures that were revealed by a recentWorld Bank Study. (Please see consumer insight box below.)
Consumer Insights: World Bank Study Statistics
– 85% of the working population in India do not have Rs. 500,000 as instantcash
– 14% do have Rs. 500,000 instant cash but will face a financial crunch sub-sequently
– Only 1% can afford to spend Rs. 500,000 instantly and easily– 99% of the Indians will face a financial crunch in case of any illness (Sethi)
To help place the above figures in perspective, the hospitalization costs of sometreatments are as follows- Rs. 200,000 to 250,000 for angioplasty, Rs. 250,000 to350,000 for open heart surgery, Rs. 30,000 to 50,000 for a hernia surgery (Sethi).
Indian Health Insurance in Context – Status quo
Health insurance constitutes a paltry 10% of the total industry revenue and has notkept in pace with the expansion of the healthcare industry on the whole. India standsat a humble 127th position in the Human Development Report, 2005. Other health in-dicators also appear to be equally somber. The total health expenditure in India is6.1% of the Gross Domestic Product (GDP), out of which public expenditure is just1.3% of the GDP. The per capita spending on health is USD 96. Compared to this,other developing countries like Brazil and Jordan in the moderate development slotspend 7.9% and 9.8% of the GDP on health respectively. Their per capita spending onhealth is also higher at USD 611 and USD 418 respectively (Oza).
The World Health Organization has defined a possible approach of financing ofhealth expenditure. Please see the illustration below.
In context with the illustration above, public spending in health care is squat at17% of the health care financing. Additionally, the market is underdeveloped andlargely financed out of pocket: over 85% of the health care expenses are substantiatedby out of pocket expenses (unplanned for, non-contributory spending) (Parera).
Population profile of the Indian Population indicates that 55% of the Indian popu-lation (605 million) is below 35 years of age, 25% (275 million) is between 36–50years of age and 20% (220 million) is above 50 years of age. In India, an issue that re-
3.1 Industry Outlook and Major Players 103

cently raised concerns and invited negative publicity of health insurers has been theirceasing to insure individuals above 50 years of age. However, the IRDA has recentlyset up a committee (focusing on senior citizens) with an aim to address this issue.
With a population of 1.1 billion and a health insurance premium of Rs. 17.19 bil-lion in 2004–2005, the per capital health insurance premium in India stood at a negli-gible amount of Rs. 15.63. On the other hand, the Pharmaceutical Industry, anotherindustry part of the healthcare sector of India had revenues of over Rs. 350 billion,clearly reflecting the incongruence of pace within the health sector itself (Sethi).
104 3 Health Insurance
1.1 Billion Total Population
–17 million Private Medical Insurance (Mediclaim)
–38 million Employees State Insurance Scheme
–40 million Central Government Health Scheme (CGHS)
– 7 million Indian Railways
–55 million Public Sector Enterprises
–50 million Community Insurance
893 million Uninsured
Figure 47: Overall Healthcare Financing Situation in India (Mendiratta)
Figure 46: Approach for Financing of Health Expenditure (Parera)

Adding another dimension to the profile above; of the total population of 1.1 bil-lion, 356 million belong to the middle income group, of which only 17 million arecovered by a private health insurance scheme. The situation of overall healthcare fi-nancing in India is as elucidated below.
The overall health insurance premium development over the last couple years hasbeen illustrated in the graph below
3.1 Industry Outlook and Major Players 105
Figure 48: Health Insurance Premium Development – In Rupees Billion (Sethi)* The figures in 2006–2007 represent a projected value.
Although the base is small, the health insurance sector is growing at an encourag-ing pace of 35% year-on-year, thus making it one of the fastest growing segments inthe non-life area. Furthemore, the health insurance penetration has increased from0.1% of the population in 1991–1992 to 1.5% in 2005–2006, another indicator ofprogress in the right direction. The illustration below depicts the number of policiesissued year wise (2001–02 to 2005–06) for 3 of the 4 public sector companies.
Data for the private insurers was unavailable. Moreover, the private insurers en-tered the market only in 2001. The 4 public sector insurers developed their corehealth insurance product “Mediclaim” in 1986. The graph above illustrates that NewIndia Assurance is the best performing company in terms of the number of policies is-sued. Whilst United India was not performing as well initially, the liberalization trig-gered competition; and in 2005–2006 United India seems to have caught up with Na-tional.

Main Issues and Challenges for Health Insurance in India
An understanding of the key issues and challenges for health insurance in India is vi-tal to the development of a new strategy or amendment of an existing one.
1. Tariffed Regime: With claims-to-premium ratio at 130% (on an average), thehealth insurance sector in India has been a loss making portfolio. However, thiswas triggered on account of complacency in underwriting skills, and competingon price for health products, while seeking cross subsidization of this loss makingsegment by profitable businesses (motor).
2. Dearth of Underwriting Skills: Insurers lacked rational pricing. A shift to the de-tariffed regime, will now cause cross subsidization to end and will give impetus tohealth insurance as a profit making business. However, this poses a new problemfor non-life insurers: honing appropriate underwriting skills that were dormantenough to disappear in the tariffed regime will be a staggering task.#
3. Price Hikes and Attrition: Appropriate pricing strategies (that reap initial profitsnow, and sustained profitable growth in the future) would imply that insurers haveto be on their toes in order to address customer reaction to the price hikes. This re-action may include attrition (on account of price sensitivity), which is further ag-gravated by the yearly renewal of policies and thus a corridor for customers tostep down, in turn making it herculean for insurers to acquire new customers.
106 3 Health Insurance
Figure 49: Development of Number of Policies issued year wise (Sethi)

Thus a price hike has to be complemented/ justified by customized product solu-tions, creative bundling and unbundling of risks, increased awareness of products,and innovation in various facets of the marketing value chain from product designto pricing to distribution channels.
4. Moral Hazard Dilemma: On one hand, insurers have to seek to reduce moral haz-ard and adverse selection; whilst on the other hand, by virtue of judicious acumen,they have to seek to increase number of policies sold, for “insurance” as a conceptto make sense: via pooling of risk on account of law of large numbers.
5. Information Asymmetry and Fraudulent Claims: Reducing information asymme-try and installing effective systems preventing fraudulent claims are the need ofthe hour. These would also help reduce errors of omission wherein a validclaimant is denied claim amount or has to face unnecessary delays.
6. Provider unpreparedness: There is no standardization with respect to treatmentprotocols and quality, either through registration or accreditation. There is no wayof controlling claims as prices vary from one hospital to another and over time.
7. Intermediary unpreparedness: Third Party Administrators (TPAs) were rammedin the scene in lieu of the procedural handling of cashless transactions, unfortu-nately, without provision of adequate information systems and streamlinedprocesses. Thus training TPAs and extending support to them via responsive andeffective claims settlement tools is an impending need. This would help insurersreduce the incongruence between themselves and the TPAs; who by most cus-tomers are regarded as the face of the insurer, thus a cardinal touch point.
8. Regulatory barrier: The 26% foreign equity cap is definitely a challenge and it isdifficult to find a “local” partner in a risky, less understood business which wasde-regulated only 6 years ago. Additionally, there exists a high capital require-ment of USD 22 million suggesting that in the first few years of operations, insur-ers will have to charge premiums that are sufficient to compensate for the invest-ment, however, sacrificing volumes on account of price sensitivity and once againposing a hindrance in achieving the law of large numbers.
9. Payer unpreparedness: The insurer is unable to design schemes that are profitabledue to lack of comprehensive data on health requirements and usage patterns ofdifferent socio economic segments.
The Key Players
The players in the health insurance sector in India include all the general insurers (ornon-life insurance companies). The LIC, although primarily into life insurance prod-
3.1 Industry Outlook and Major Players 107

ucts, does offer products that cater to the needs of the health insurance market. Thelist of players as of 2005–2006 includes
– New India Assurance Co. Ltd– National Insurance Co. Ltd– The Oriental Insurance Co. Ltd– United India Insurance Co. Ltd– Bajaj Allianz General Insurance Co. Ltd– Cholamandalam MS General Insurance Co. Ltd– HDFC Chubb General Insurance Co. Ltd– ICICI Lombard General Insurance Co. Ltd– IFFCO-Tokio General Insurance Co. Ltd– Reliance General Insurance Co. Ltd– Royal Sundaram Alliance Insurance Co. Ltd– Tata AIG General Insurance Co. Ltd– Star Health and Allied Insurance Co. Ltd
3.2 Market Opportunities and Challenges –Empirical Results and Analysis
Having already established the context for empirical results and analysis in chapter2.2, without further ado, I will present to you the results and analysis of Section 3 ofthe questionnaire. Please refer to the same in the appendix for any clarifications.
Results
3[a]: the responses of the CEO of Bajaj Allianz will be discussed in the followingchapter amongst best practices. Due to the subjectivity of the question, not all respon-dents listed the customer segments precisely. Nevertheless, most respondents didenumerate the segmentation variables, offering significant cues to the key attributesused for deriving primary customer categories and groups in the health insurance are-na. For some respondents, their primary customer segment included individuals liv-ing in metropolitan cities (Mumbai, Delhi, Kolkata, Chennai, Hyderabad and Banga-lore) in age group 35 to 55. Their firms also had employee group schemes with rele-vant corporate clients. Another respondent belonging to the senior management of areputed insurer specified that the primary customer segment at his organization in-cluded middle class individuals in the age group 35–45 living in metros. “Health in-
108 3 Health Insurance

surance, I believe, is a long term contract despite it having to be renewed on a yearlybasis; thus it has been our target to develop a long term relationship with the popula-tion which would grow in income levels”, he added. This is justified because of theever burgeoning income levels of the Indian middle class. He further clarified, “Un-fortunately, we have currently narrowed our focus to the Metros, because medicalpractices across the country are not uniformly well developed or sophisticated andthus do not provide grounds for managed care solutions where we would like to buildour expertise and forte in.” Another respondent (who’s company provides products inboth life and health areas) claimed that his firm offered products across all segments(age, sex and income), except the rural segment where minimum premiums would in-hibit purchase for a large cross section of the population. Additionally, the insurerprovides for traditional life and ULIP policies to which medical riders can be at-tached. Some respondents precisely defined that their main customer segmentswould include city dwelling, middle class families with children where age of the pri-mary insured is less than 45 years; certain classes of rural customers; and employees(and their families) belonging to huge corporations, thereby implying group schemesand consequently benefiting from cost economies of scope and scale.
3[b]: responses were varied and ranging from less than 50% to almost peaking at130%. The ranges above 110% would normally entail, claims to premium ratios forgroup schemes. Despite the range, responses were skewed within a limited band-width in the lower end. While there were varied figures above 100%, which included105%, 110%, 120%, 124%, 130%, anything below 100% was also below 60%. Thissignifies that firms were either pricing their products backed by sound underwritingand pricing mechanisms thus providing for a cushion for additional administrative,sales and employee costs and decent margins, or they were breeding obvious lossmaking portfolios with certain categories, where the claims to premium ratio wasabove 100%; and this doesn’t even include costs besides the claims.
3[c]: responses averaged at about 80%. One respondent revealed individual figuresfor both individual and group policies, with the retention rates being more than 95%and more than 80% respectively. This is counterintuitive and rather alarming, consid-ering that one would believe that group policies, by virtue of being tied up with theemployer would be easily renewed. However, this can mean one of two things. One,there is a reduction in the number of overall groups attached to an insurer’s groupscheme. This would necessitate, the retention rate to be defined as (total number ofgroups renewed in n+1)/(total number of groups enrolled in year n.) Two, there is anelevated employee attrition in corporate Indian firms, thus projecting a lower overallretention rate for the group schemes. Contextually, here, the retention rate will haveto be defined as (total number of individuals who renewed their policies that belongs
3.2 Market Opportunities and Challenges – Empirical Results and Analysis 109

to a group scheme in year n+1)/(total number of individuals who were enrolled bymeans of the group scheme policy in year n).
3[d]: the number of frauds detected ranged between 60 and 150, although most re-spondents admitted that they “suspect” a higher figure. The fact that insurers suspecthigher frauds reveals an obvious flaw of the system: one that breeds on a principalagent problem, leaving both parties insecure and constantly anxious and wondering ifeach is being “scammed”, thus resulting in unfriendly measures or exaggeration onboth sides.
3[e]: obviously, not all respondents replied similarly. In order to better comprehendthe responses, I would present the “mode” and “mean” rank corresponding to everyone of the 10 criteria. For “Right pricing strategies based on accurate risk assessmentand underwriting skills”, the mode ranks were 1 and 3 with equal number of occur-rences and the mean was 2. For “Tracking fraudulent claims”, the mode and meanranks were both 8. For “Customer satisfaction with respect to efficient and quickclaims settlements”, the mode was 2 and mean was 2.25. For “Enhanced and im-proved service provided by TPAs”, a mode did not exist due to varied answers, butthe mean was 5.25. This was an outlier, with some respondents claiming that this wasa very urgent requirement while some others giving it the least importance with arank of 10. For “Increasing professionalism amongst agents and brokers”, the modeand mean ranks were both 3. For “Reaching out to the segment of society that is be-low the poverty line”, the mode was 9 and the mean 6.75. The mean was pushed upbecause of some responses that suggested this aspect was an urgent requirement. For,“Developing health insurance products that cover different diseases”, the mode was 7and the mean 8. For, “Developing health insurance products that cover day-to-daydoctor visits”, the mode was 6 and mean 7.25. For, “Use of CRM tools and Datawarehousing for linking historical customer information and thereby coming up withaccurate assessments”, the mode did not exist due to varied answers, and the meanwas 6. For, “Simplicity of contracts and contract language”, the mode is undefined asit was varied, and mean was 6.5.
3[f]: a similar approach (as 3[e]) has been adopted to understand the effectivenessof promotional media. The effectiveness was rated as follows is as follows: News-papers with a mode and mean of 2 and 2, Television with a mode and mean of 1 and1.25, Radio with a mode and mean of 5 and 4, Magazines with a mode and mean of 6and 4.75, Internet and Outdoor each with no definite mode but a mean of 4.5.
3[g]: Health insurers are opting for several channels of distribution to maximizereach and optimize penetration. Respondents had the following views towards theeffectiveness of 7 different distribution channels on a “likert scale” that runs fromleast effective [1] to most effective [5]. The primary views included [5] most effec-
110 3 Health Insurance

tive for bancassurance, [1] least effective for medical tie-ups, with one outlier claim-ing it to be [5] most effective for the rural population, [4] more effective to [5] mosteffective for automobile tie-ups, with one outlier claiming it to be neither effectivenor ineffective, [2] less effective to [3] neither effective nor ineffective for malls andsupermarkets, with a few companies testing this channel, while others finding it lesseffective. There exists one outlier, with this channel being rated [4] more effective.Postal service was rated [5] most effective primarily for the rural segment anddeemed [2] less effective otherwise. Life insurers who have ventured into health in-surance products claimed that they do not have any postal tie-ups yet. Telcassurancewas rated [5] most effective or [4] more effective by a few respondents who felt thatthis channel had proven effective for families in middle and upper middle class orfor first time customers. Other respondents had company specific varied answers tothis channel. To, online distribution, the responses varied across the gradient of thelikert scale.
Having said that, the responses on the health insurance industry reveal the follow-ing key highlights:
1. The main customer segments include middle class families with children with thekey insured between ages 35 to 55 and employee group schemes with huge corpo-rations, thus permitting cost economies.
2. The claims to premium ratio ranges between 50% and 130%, with anything below100%, being skewed at less than 60% and anything above 100% being uniformlydistributed till 130%. Moreover, the group schemes seem to be the loss makingportfolios
3. The retention rate averages at 80% with some insurers projecting a retention rateof 95% for individual schemes and 80% for group schemes; counterintuitive butjustifiable figures.
4. The frauds range between 60 and 150, with some insurers suspecting a highernumber.
5. The most urgent requirements for the Indian health insurance industry are [1]Right pricing strategies based on accurate risk assessment (differences betweengood and bad risk) and underwriting skills, [2] Customer satisfaction with respectto efficient and quick claims settlement, [3] Increasing professionalism amongstagents and brokers and [4] Enhanced and improved service provided by ThirdParty Administrators.
6. The most effective channels of communication are [1] Television and [2] News-paper.
7. The most effective distribution channels are [1] Bancassurance across urban andrural segments and [2] Postal services specifically for the rural sector.
3.2 Market Opportunities and Challenges – Empirical Results and Analysis 111

3.3 Urgent Needs and Customer Segmentation
The Socio Economic Classification and the Household Potential Index that was cov-ered earlier in the Life Insurance Segment is of acute importance in the Indian HealthInsurance Scenario as well, as health insurance in India is a highly under-penetratedarea (with a lower relative penetration to life insurance in India4), thus implying high-er level of “premiumness” (a concept which implies that a product or service is“wanted by many” but “consumed by few”), consequently suggesting that health in-surance consumption in India would correspond to higher HPI score and would ini-tially be a profitable business by aiming for the higher socio-economic classes. In or-der to precisely and holistically uncover the most urgent customer needs and corre-sponding profitable customer segments for the Health Insurance Market in India, Ihave relied on my analysis of empirical data that was disclosed in a recent uniqueHealth Survey “Health Matters” Index 2006 conducted by one of the leading LifeInsurance Companies: Tata AIG Life that seeks to enter into the health insurance areain the de-tariffed era (which would imply profitability after an initial predicted pricewar hopefully settles). “Health Matters” is a comprehensive, first-of-its-kind surveyto assess the awareness and the need for accident and health insurance as well as crit-ical illness covers in India. The survey was conducted with a sample size of 1200 re-spondents across Mumbai, Delhi, Hyderabad, Kolkata, Chandigarh and Bangalore.
4 Indian non-life penetration is lower than the life penetration where penetration is measured asa ratio of the percentage of premium to GDP. Although the life insurance penetration in India islower than the global average for the same, the non-life penetration in India is relatively muchlower compared to the global average of the non-life insurance penetration. Thus I used theterm “relatively” to compare the penetration of life and non-life insurance in India. To be pre-cise, in 2005, the life insurance penetration in India was 2.53% vs. the global 4.34%, whilst thenon-life insurance penetration in India was a meager 0.61% vs. a global 3.81% (Novi).
112 3 Health Insurance
Figure 50: The Stimulus-Organism-Response Model (Philip Kotler)
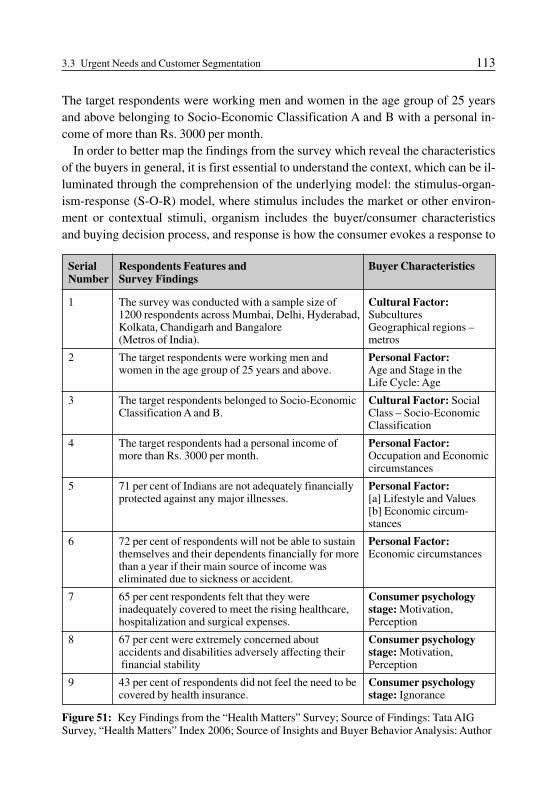
The target respondents were working men and women in the age group of 25 yearsand above belonging to Socio-Economic Classification A and B with a personal in-come of more than Rs. 3000 per month.
In order to better map the findings from the survey which reveal the characteristicsof the buyers in general, it is first essential to understand the context, which can be il-luminated through the comprehension of the underlying model: the stimulus-organ-ism-response (S-O-R) model, where stimulus includes the market or other environ-ment or contextual stimuli, organism includes the buyer/consumer characteristicsand buying decision process, and response is how the consumer evokes a response to
3.3 Urgent Needs and Customer Segmentation 113
Serial Respondents Features and Buyer CharacteristicsNumber Survey Findings
1 The survey was conducted with a sample size of Cultural Factor:1200 respondents across Mumbai, Delhi, Hyderabad, Subcultures Kolkata, Chandigarh and Bangalore Geographical regions – (Metros of India). metros
2 The target respondents were working men and Personal Factor:women in the age group of 25 years and above. Age and Stage in the
Life Cycle: Age
3 The target respondents belonged to Socio-Economic Cultural Factor: SocialClassification A and B. Class – Socio-Economic
Classification
4 The target respondents had a personal income of Personal Factor:more than Rs. 3000 per month. Occupation and Economic
circumstances
5 71 per cent of Indians are not adequately financially Personal Factor:protected against any major illnesses. [a] Lifestyle and Values
[b] Economic circum-stances
6 72 per cent of respondents will not be able to sustain Personal Factor:themselves and their dependents financially for more Economic circumstancesthan a year if their main source of income waseliminated due to sickness or accident.
7 65 per cent respondents felt that they were Consumer psychologyinadequately covered to meet the rising healthcare, stage: Motivation,hospitalization and surgical expenses. Perception
8 67 per cent were extremely concerned about Consumer psychologyaccidents and disabilities adversely affecting their stage: Motivation,financial stability Perception
9 43 per cent of respondents did not feel the need to be Consumer psychologycovered by health insurance. stage: Ignorance
Figure 51: Key Findings from the “Health Matters” Survey; Source of Findings: Tata AIGSurvey, “Health Matters” Index 2006; Source of Insights and Buyer Behavior Analysis: Author

make the purchase. Once in context, the findings of the survey can be appreciatedbetter. Please see the illustration below, depicting the S-O-R model and projecting thefacets encompassing each of these: stimulus, organism and response.
The “Health Matters” survey suggests vital findings which offer cues to imminentneed of health insurance amidst the Indian market milieu. In the table (Fig. 51) be-low I have proposed corresponding buyer characteristics and consumer psychology(in reference to the S-O-R model) for the respective respondents’ features and surveyfindings.
The 9th finding in the table above is “43% of the respondents did not feel the needto be covered by health insurance”: This is significantly alarming and indicates a lackof awareness towards the relevance and need for health insurance, in the backdrop ofrising healthcare costs and an increasingly stressful life that leads to a higher suscep-
114 3 Health Insurance
Country India Hongkong Singapore Malaysia Thailand
Customer NeedsDerived from
% of individuals 72% 50% 55% 71% 38%who will run outof funds in case ofcritical illnesswithin a year
Amount of savings Rs. 200,000 Rs. 545,842 Rs. 538,849 Rs. 229,455 Rs. 432,000required to cover (4927 USD) (HK$ (Sng$ (RM $ (Baht$medical expenses 95,174) 18,731) 43,855) 351,429)for a critical (13448 (13204 (5642 (10631illness USD) USD) USD) USD)
Multiple of annual 2.6 times 6.2 times 6.8 times 3.3 times 5.8 timesincome requiredfor insurancecoverage
% of individuals 68% 66% 49% 78% 74%who do not havepost retirementmedical coverage
% of people who 69% 50% 34% 45% NAstarted investingin their twenties
Types of insurance Hospital/ Critical Critical NA NAthat consumers are surgical illness illnessmost interested in expenses and and hospital/
and life income surgicalinsurance protection expenses
Figure 52: Asian Attitudes Comparisons to risk and insurance (Tata AIG)

tibility to major illnesses. Thus, although the low penetration of health insurance inIndia suggests optimism with respect to the achievable potential of the market, thisparticular finding poses a considerable challenge to health insurers since the con-sumer psychology stage suggested by this finding is that of ignorance.
A comparison with a similar survey commissioned by the AIG to assess the Asianregion’s attitudes to insurance and risk revealed the following insightful differencesbetween the attitudes and primary needs of Indians and individuals belonging to oth-er Asian economies.
The survey also evaluated the perceptions of consumers towards various benefitsoffered by accident and medical insurance products and revealed that about 65 percent respondents rate cashless hospitalization admission and care as an extremely im-portant attribute in selecting a medical insurance product. Interestingly, the survey re-vealed a high preference among respondents, of about 79 per cent, who expressedtheir desire to purchase a health insurance product for their children. It further re-vealed that the average age of owning an insurance policy in India is 28 years whichis a positive sign and indicates a growing awareness amongst the youth towards theneed and importance of insurance. While 41 per cent of respondents expressed a pref-erence for private medical care post retirement, only 27 per cent expressed a desirefor public medical care post retirement.
The “Health Matters” Index survey is an initiative by Tata AIG Life aimed at as-sessing and understanding the needs and expectations of consumers for insuranceproducts. This survey will be an annual exercise of Tata AIG Life with the objectiveof evaluating and understanding the changing market needs for products like acci-dent/health insurance. Whilst the survey provides interesting insights about the per-ception and orientation of consumers towards life and health insurance, it will alsohelp create an annual index that would track the progress of the growth of this sectorand benchmark India against other Asian countries. The findings of this survey canaid in customizing suite and offering innovative insurance solutions to the Indianconsumer (Mr. Bimal Balasingham).
Segmentation Process for the Health Insurance Market in India
Markets are not homogenous. A company cannot connect with all customers in large,broad and diverse markets. Consumers vary on many dimensions and often can begrouped according to one or more characteristics. A company needs to identify whichmarket segments it can serve effectively. Such decisions require a keen understand-ing of consumer behavior and careful strategic thinking (Kotler and Lane, MarketSegmentation).
3.3 Urgent Needs and Customer Segmentation 115

I will use the results of my survey “Emerging Opportunities and Challenges in theHealth Insurance Industry in India” (Please see appendix) in order to illuminate thesegmentation process for the health insurance market in India. I will consider the bestpractices as adopted by Bajaj-Allianz (a joint venture between Bajaj Auto Limited ofIndia and Allianz AG of Germany). The respondent is a senior management personwho represented his views based on the current and next 3 years outlook for Bajaj Al-lianz in India.
The major segmentation variables are geographic, demographic and behavioral.Please see the table below depicting the main customer segments and the correspon-ding variables used for segmentation for Bajaj-Allianz’s health insurance products.
116 3 Health Insurance
Serial Customer Segment Segmentation VariablesNumber
1 Age group 25–55 years, Middle Class Demographic: Age, Socio-economic & Upper Middle Class, living in ClassMetros and Major cities Geographic: region
2 Self employed, Upper Middle Class, Demographic: Socio-economic Class,in Metros and Major cities Occupation
Geographic: region
3 Salaried and Self employed, Demographic: Socio-economic Class,Middle Class and Upper Middle Class, Occupationin Smaller cities Geographic: region
4 Employees of small and medium sized Demographic: Occupationbusiness organization Behavioral: Usage rate is heavy as it
includes buyers who are part ofmembership groups (social factors); furthermore renewal premium is boundto be high.
5 Large corporate in manufacturing and Demographic: Occupationservice industry Behavioral: Usage rate is heavy as it
includes buyers who are part ofmembership groups (social factors);moreover renewal premium is bound tobe high due to the group scheme, thusgiving impetus to loyalty status.
Figure 53: Customer Segments and Segmentation Variables for Bajaj Allianz (Emerging Op-portunities and Challenges for the Indian Insurance Industry, Author)
In the segmentation process, it is essential to analyze the segment profitability. Al-though, it was difficult to get micro data revealing profitability at the segment level,the degree of product profitability does signal soundness of the underlying segmenta-

tion policy. Implying, since an accurate segmentation policy represents the necessary(but insufficient condition) for the success of the corresponding products, an analysisof the claims-to-premium ratio for an insurance product can conversely depict the de-gree of attractiveness of the underlying segmentation policy. Responses to my surveyon “Emerging Opportunities and Challenges for the Indian Insurance Industry” revealthat: the main health insurance product for Bajaj-Allianz is “Health Guard” with aclaims-to-premium ratio of 67% in 2006–2007. This means that for every Rs. 100 ofpremium collected, Rs. 67 is the claims paid out. This is an exceptional ratio, consid-ering non-life insurance market was still tariffed until 1st of Jan, 2007 and companieswere unable to decide their prices. Moreover, several non-life companies have hadhealth claims-to-premium ratio as lofty as 130%, thus calling for the potential crosssubsidization of the unprofitable health insurance business by the other more prof-itable businesses, in order to maintain the stipulated solvency margin. This can also becited as the single main reason for the dearth of standalone health insurance compa-nies in the Indian insurance environment until recently. However, the claims-to-pre-mium ratio for group health schemes at Bajaj-Allianz has been over 120%. This obvi-ous unprofitability suggests that Bajaj Allianz needs to either redefine or drop thegroup scheme related segments, before going in for the next target market selection.
3.3 Urgent Needs and Customer Segmentation 117
Figure 54: Five Patterns of Target Market Selection (Philip Kotler)

The retention ratio for Bajaj-Allianz stands at 85% for their health insurance productsin general; this again suggesting an overall segmentation policy success.
Finally, the pattern of target market selection for Bajaj Allianz (as most other non-life insurance companies) is selective specialization implying the selection of multi-ple segments, each of course objectively attractive and appropriate, promising to be amoneymaker (Abell). Please see the illustrations of the “Patterns of Target MarketSelection” below.
3.4 Products
Health Insurance Product Design Facets
Every upside has its downside. The Indian healthcare sector has made impressivestrides and is surging ahead with an annual growth rate of 13% per annum. Increasedliteracy rate, higher levels of income and an increased awareness have been contribu-tory factors. The downside includes cost escalation; declining budget provisions forpublic health; emergence of new killer diseases like aids and innovation in the wronghands thus further soaring costs.
For the health insurance industry, even the upside has added complexity. TheHealth Insurance Industry in India has not been able to keep pace with burgeoning ofthe economy and rise of the middle class; moreover, the downside of the healthcaresector has further pulled down its momentum. While regulations like the 26% cap onforeign equity and high capital investment requirements hinder the plausible growth,these are unavoidable circumstances and the issue lies primarily in the way the healthinsurance products are designed. If designed meticulously and in sync with all thefacets going into its development, this very product could augment partnerships withintermediaries, providers (hospitals etc), enhance customer satisfaction, promotecustomer life time value and subsequently extract its deserved value through premi-ums that are profitable.
The facets that determine the health insurance “product” delivery are those thathave to be essentially considered during the design and development of the product.Thus the product design aspects are
– Hazards in claims settlement: Delays and errors of omission in claims settlementwas considered as a hindrance (for their selection of the product) for 70% of a pop-ulation in a survey by Srabanti Chakravati (Chakravati).
– Information Lag: 60% of the population sampled claimed information lag was ahindrance in their selection of the product (Chakravati). This arises from unclearand in-transparent policy contract; complex and hidden clauses in contracts.
118 3 Health Insurance

– Adverse selection: In the tariffed regime, a “good-risk” customer paid as muchpremium as a “bad-risk” customer. Insurance companies adversely selected badrisk customers as well; which meant that good customers were suffering at the ex-penses of the bad ones. The problem of adverse selection can now be sorted by dif-ferent products for different segments, and differential pricing methodologies cou-pled with a database with claims data record.
– Introduction of cashless hospitalization without infrastructure in place: Althougha customer oriented advancement, cashless hospitalization products need to besupported by the right infrastructure and systems in place. This would require clos-er tie ups with hospitals, assuring standardization of pricing strategies, less fre-quent changes in price and training and support of TPAs.
– Fraud Management: Transparency of contracts, full disclosure of clauses wouldminimize frauds in health insurance; because information asymmetry triggersmoral hazard or revengeful attitude in consumers to scam the insurer as they mighthave felt when the policy was thrust before them. Moreover, data warehouses withdetailed information that can assist in data mining and drawing correlations wouldassist in tracking fraudulent behavior.
– Tenure of renewal: Products with increased term of renewal is the call of thehour; these would help reduce decisions triggered by price sensitivity, provide awindow to build customer loyalty, improve CLV, reward good-risk customers withclaims bonuses, increase the number of customers through network effects by lur-ing other customers belonging to the same reference group (for example familymembers).
– Focused Products satiating Focused Needs: India with its huge population, hasscores of people infected by several diseases. Health Insurance products could in-clude coverage of a certain group of diseases like diabetes (ICICI Prulife intro-duced a product called “Diabetes Care” for those who might be afflicted by it andare within 25–60 years of age).
– Age no bar: Instead of barring individuals above the age of 50 from health insur-ance coverage, insurers must devise customized products for this age group withcorrespondingly higher premiums on account of higher probability of occurrenceof diseases or insured events.
– Location Wise: Insurers must devise different product or lines extensions for dif-ferent locations, depending on whether it is a rural or urban location, depending onthe propensity of the kinds of diseases probable, depending on the slightly tweakeddemographics; all of these would call for different pricing mechanisms; which isjustified because health care costs in rural areas are negligible compared to the spi-raling costs in the metros.
3.4 Products 119

– Group Policies Impetus: Insurers need to seek out group contracts not just big cor-porates, but groups that include: student bodies, colleges, schools, doctors, profes-sional organizations members etc. Group policies imply discount to the group andbenefits to the insurer via economies of scale and scope thus reduced acquisition,retention and administrative costs.
– Group Policies Portability: Portability of insurance from group to individual poli-cy must be permitted when an individual leaves the group or gets retired; addition-ally, this does not affect the insurer, who continues to enjoy the law of large num-bers. Furthermore, customers must be allowed transfer to a new one (or retain hisexisting policy), as he desires, when he changes employers and thus the correspon-ding insurers that the employer has tied up with.
Regular Checkups Coverage: In India, although hospitalization costs have sky-rock-eted, the regular checkups (or more commonly referred to as Out Patient Departmentcharges) have not risen beyond affordability. However, most individuals visit doctorsfor curing daily infections which does not call for hospitalization. Most insurers inIndia do not cover these expenses (perhaps on account of the expected fraud, due tonon-mechanization of private hospitals’ billing system). But, the survey by Srabanti,revealed that lack of out-patient coverage was quoted as the biggest hindrance fornon-consideration of a health insurance policy by 80% of the sampled population(Chakravati).
The Regulator Says: The Finance Minister raised the tax exemption limit for health insurance
The finance minister of India, P. Chidambaram, in his reply to the debate of the fi-nance bill said “Honorable Members may also note that we have raised the exemp-tion limit for health insurance premium from Rs. 10,000 to Rs. 15,000 for individu-als and in the case of senior citizens to Rs. 20,000. A senior citizen will get a mini-mum relief of Rs. 2,000 per year.” (P. Chidambaram) The primary motive for insur-ance policies is supposed to be risk mitigation. However, until recently, the Indianconsumer saw the insurance policy, primarily as a tax saving instrument. In fact, in-surers even advertised the insurance policies in a similar light: with the extent oftax saved being projected as the key incentive to take up the policy. Although, withthe increasing awareness of the Indian consumer, risk coverage has become theessence; however, the traditional mindset remains and tax savings can still be usedto lure consumers. Thus, the piece of information above (the FM’s reply to the fi-nance bill debate), brings good news for both the insurers and the insured.
120 3 Health Insurance

Product Development History of the “Mediclaim” Policy
Health insurance in India was initiated by the launch of the “Mediclaim” policy bythe four general insurance companies (the current public sector general insurers) in1986. Thus understanding the developments of the Mediclaim policy would unveilthe development of health insurance products over time. The Mediclaim provides re-imbursement of hospitalization and domiciliary hospitalization expenses (expensesfor treatment of such illness which would normally require hospitalization but whichis treated at home under compelling circumstances as per doctor’s advice only.) Thetreatment taken in India qualifies for reimbursement. Under Third-Party-Administra-tion (TPA) system, there has been an initiation of cashless service in case of hospital-ization, up to a limited extent.
The table below traces the innovations in medical insurance due to inadequacies ofMediclaim scheme in India.
3.4 Products 121
Limitations in Mediclaim Solutions Introduced
New Born not covered Cradle Care
As age increases, income drops Bhavishya Arogya granted with higher in old age premiums
Premium only, thus becomes an Asha Deep, Jeevan Asha, Nav Prabhat outgo if no claims lodged (coveringlimited diseases and life cover)
Does not offer cash benefits for change of Dreaded Disease Coverlifestyle, specialized treatments and equipments
Attendants’ costs, donor’s expenses, ambulance Tertiary Carecharges not covered
Dental Treatment Excluded Smile Care
Spend first claim later reimbursement policy Hospital tie up and introduction of TPA sas intermediaries for cashlesshospitalization
Health Cover not suitable for economically Jana Arogyabackward class
Renewal hassles & possibility of policy Long term hospitalizationdiscontinuity
Costs not covered- private nursing care, Health Quarter Planhealth check up; admission to hospital notassured; provider vigilance not offered;health tips and guidance not gives
For negotiations possible in group policies Group Tailored covers
Figure 55: Shortcomings and Innovations in the Development of the Mediclaim Policy(Mishra and Mishra)

Managed Health Care
Until recently, we identified health as merely the absence of disease. Doctors concen-trated on fighting acute illnesses such as tuberculosis, polio and small pox that threat-ened entire communities. Biomedical researchers focused their efforts on identifyingviruses and bacteria that cause disease and then developing “silver bullets” such asantibiotics and vaccines to fight them. Our definition of health now would include amarriage of body, mind and environment. General insurers can be leaders in this newhealthcare paradigm. Such companies can build partnerships among doctors and oth-er health professionals who provide patients with a full spectrum of coordinated careservices from preventive efforts and primary care to specialty treatment and follow-up. These seamless systems can help patients control their symptoms everyday athome, work or school, rather than waiting to visit the doctor when they are seriouslyill. Instead of managing the cost of healthcare, member establishments or planprocuring companies can focus on managing the care itself. At each point along thecontinuum of care, such companies can use information-driven programs to improvetheir care-receiver’s health and quality of life. The major components of the caremanagement approach include: disease prevention and wellness; early detection; themanagement of chronic illness; and partnerships to improve healthcare quality.
122 3 Health Insurance
Figure 56: Evolution of Medical Insurance Business (Chatagny)
3.4 Products 123
This transformation from a fragmented, fee-for-service, biomedical model to a pre-paid system based on coordination, health management and wellness would requireinvestments in information systems, re-engineering programs and mergers designedto achieve economies of scale. It would necessitate insurers expanding their geo-graphic markets, forming strategic alliances with healthcare providers, pharmaceuti-cal companies, information management vendors and even competitors; resulting ina cost reduction, access to new markets and achievement of their business and statu-tory objectives (Mishra and Mishra).
Product Range to Suit Various Segments
The following products have been suggested to suit various segments
1. Long Term Hospitalization/Domiciliary Hospitalization (DH) Insurance Policy;with term periods choice of 1, 5, 10 years.
2. Tertiary Care Insurance; which could cover major ailments like strokes, open andclose heart surgeries, malignancy, neurosurgery, joint replacement, grievous in-jury including multiple fractures, encephalitis and nephritis.
3. Long Term Retirement Benefit Plan, with reimbursement options for the completelifetime of an individual without age restrictions; however, by use of differentialpricing for increasing amounts insured.
Consumer Insight: De-tariffing and Group Health Insurance Schemes
There will be a reduction in the Group Insurance Schemes in the IndianHealth Insurance Industry. Following the lifting of price controls, experts pre-dict that this year there will be an increase in cases of cancellation of grouphealth policies. This is the initial side-effect of 'de-tariffing' with effect from Jan-uary this year. Earlier, the Indian non-life insurance industry followed tariffs setby the Tariff Advisory Committee. There were tariffs for fire, engineering andmotor lines of businesses ensuring profitability for the insurance companies. Onthe other hand, health, marine and personal accident were non-tariff lines ofbusinesses. Here, corporates especially, the IT, ITES and engineering companieshad to pay negligible premium on their group health policies, if they had a largeproperty or engineering policy. Under the new system, because of the end ofcross-subsidization, insurers are hesitant to offer large discounts on group healthcovers. Already, companies such as Oriental Insurance, ICICI Lombard, BajajAllianz and others have hiked the premiums for group health insurance and theyare underwriting the portfolio on a stand-alone basis.

124 3 Health Insurance
Says Sandeep Dadia, director, Enam Insurance Brokers, “There could be a situa-tion where insurance companies get aggressive on market share or volumes andunderwrite group health insurance at a low premium.” According to him, some-times the insurance company expects to control losses over time. But when theyare unable to do so and the claim-to-premium ratio rises, the insurer renegotiatesthe pricing with the corporate. Then, it is left to the corporate to either accept thenew rate or look for a cheaper option. For an option. For an employee, thingscould change quite dramatically. Sandeep added “Earlier, you had the luxury offree health insurance for yourself and your family, as well. Now you may have toeither take family floaters or take separate health insurance products for familymembers. That means that you have to shell out the money from your own pock-et.” Moreover, said Anoop Mathur, vice-president, corporate accounts at How-den Insurance Brokers, “Individuals should avail of an individual health insur-ance policy, especially in high attrition sectors such as IT, ITES and financialservices, depending on their age profile. The premium paid against such healthinsurance policies also gets benefits under income tax laws, up to Rs. 15,000.This effectively brings down the overall cost of health insurance.” (Syed, FreeHealth Insurance from Office? No More!)The two reasons cited above [a] increase in cancellation of group health insur-ance policies by corporates [b] and increased attrition rate at these corporates im-ply: that individuals will now be more conscientious and aware of the availableindividual health insurance schemes, by virtue of selective perception.
4. Seafarer’s Health policy, which is justified because there are over 40,000 seafar-ers in Mumbai itself. These individuals are covered by the government only whileat sea, which may be 6 months a year. The policy could include [a]hospitalizationand DH, could cover the seafarers, while they are back on port and their families,the year around, [b]personal accident continuous cover for both the seafarer andhis family, [c] long term retirement benefit plan for the seafarer and his spouse.
5. Destination India, designed for NRI (non-resident Indians) who visit India and/ortheir families for only a short duration, about once in 2 years. This would be ashort period policy offered for a maximum of 180 days, with covers on personalaccident, medical & repatriation, personal baggage, delayed baggage, loss of pass-port, personal liability and hijack benefit.
6. Health Quarter’s Plan, designed for the parents and family of the NRIs in India,providing for health insurance package with accident insurance; with an emotion-al appeal to children settled abroad, reminding them to take care of their parents.

3.4 Products 125
(ICICI Bank has already launched one such policy called “Rishtey” which in Hin-di is a word for close relations with an emotional connotation.)
Gram Arogya Yojna (Hindi phrase for Village Disease-Free Policy); which would re-ly on economies of scale, for covering the entire village in a standardized fashion.Any number of members above the average family size would pay additional premi-um. “Floaters” would be used to permit usage of the insured sum by one or all mem-bers of the family within the policy period (Mishra and Mishra).
Best Practices: Bajaj Allianz General Insurance Co Ltd’s“Health Guard” Policy
To my survey “Emerging Opportunities and Challenges for the Insurance Indus-try in India”, Kamlesh Goyal, the CEO of Bajaj Allianz responded that his mainhealth product for individuals is “Health Guard” with a claims ratio at 67% (agood ratio when the industry average is almost at 110%) and a retention rate of85%. Thus the policy deserves to be elucidated.
How will the Health Guard Policy benefit the insured? Core features
– Covers medical expenses for the insured and his family during hospitalization– Covers pre and post hospitalization expenses– Covers emergency ambulance charges (upto Rs. 1000)– Provides cashless facility– Provides cumulative bonus of 5% to the sum assured for every claims free year
Exclusions: [1] All diseases/injuries existing at the time of proposing this insur-ance. [2] Any disease contracted during the first 30 days of commencement of thepolicy. [3] Certain diseases such as hernia, piles and cataract (liability restricted to10% of SI, max up to Rs. 25,000), and sinusitis shall be covered after waiting peri-od of 2 years. [4] Non allopathic medicine. [5] Congenital diseases. [6] All ex-penses arising from AIDS and related diseases. [7] Cosmetic, aesthetic or relatedtreatment. [8] Use of intoxicating drugs, alcohol. [9] Joint replacement surgery(other than due to accidents shall have a waiting period of four years).
Eligible Age– 5 to 55 years– Age at entry should not be over 55 years– Children below 5 eligible if their parents are concurrently insured by Bajaj-
Allianz
Restrictions on the Value of the Sum Insured– Sum insured value of Rs. 750,000–Rs. 1,000,000 is available only up to 40
years of age (subject to clean proposal form and medical tests)– Sum insured value of above Rs. 300,000 is not available for citizens above 50
years of age

3.5 Pricing Criteria
126 3 Health Insurance
Details of Coverage that the policy covers: The member has access to cashlessfacility at various empanelled hospitals in India (subject to exclusions and condi-tions). In case the member opts for hospitals besides the empanelled ones, the ex-penses incurred by him shall be reimbursed within 14 days from submission of alldocuments. Pre and post hospitalization expenses covers relevant medical expens-es incurred 60 days prior to and 90 days after hospitalization. 10% copayment is tobe paid by the member if treatment is carried out in hospitals other than networkhospitals. Family discounts of 10% as applicable; health check-up in BA diagnos-tic centers or reimbursement upto Rs. 1000 at the end of 4 claims free years.
Premium Rs. 100
Less commission paid Rs. 17.5
TPA Rs. 10
Net Rs. 72.5
Claim Rs. 140 to Rs. 180
Loss Rs. 107.5
Figure 57: A Health Insurer’s Cost Sheet (Sethi)
The above table depicts the cost situation for health insurance in the tariffed regime –for every Rs. 100 collected in premium, the insurer incurred a loss of Rs. 107.5. Thistable offers a very crucial insight – the criticality of rate making (pricing) in the de-tariffed scenario, and how this would determine the financial muscle of an insurer,the adherence to the stipulated solvency margin and finally the existence of the insur-er in a few years from now.
It is normally believed that any insurance pricing exercise is expected to give aprice that will cover the cost of all likely claims, popularly known as “pure premi-um”. However, this unfortunately does not include the claim settlement/adjustmentexpenses and insurer’s administrative expenses. Even if the price does project for thesame, there are several disadvantages to be found in this cost plus pricing method.The biggest catch lies here–we are talking about estimating future claims cost on aportfolio of risks that are yet to be written. One would thereby suggest relying on [a]past claims data, [b] picking up a homogeneous portfolio of risks, [c] fit a suitabledistribution to claims frequency and claims severity, and [d] estimate the likelyclaims frequency and claims severity for future. However, extrapolating for the fu-ture on the basis of what happened in the past hinges on a very basic assumption that

is the past will repeat itself in the future, which may not mirror the way we wouldwant it to. The following factors could materially alter the future claims experience
1. Expected inflation in the future different from reality – suggesting the claimscould be much higher with an increased rate of inflation.
2. There may be an underlying trend or pattern of an upswing or downturn of theclaims frequency and severity; this trend and the underlying causal factors (whichmay be seasonal issues, macro economical factors, and changes in related serviceproviders like hospitals) needs to be identified and factored in.
3. Business mix might have changed over the period. This may materially affect thefrequency and severity projections. Even though the claims analysis might havebeen carried out for each homogeneous group of risks separately, the data quantityand credibility issue would force some heterogeneity in the data. For example, agroup covered for critical illness may seem like they have fairly homogenousrisks, however, a closer look would reveal that individual differences in familyhistory, profiles, genetic diseases would result in a highly differential claim filingpattern.
4. A change in the claims administration will alter the expenses: for example the in-troduction of TPAs to manage the cashless facility.
5. Regulatory and legislative changes may also alter the claims severity and/or fre-quency of certain classes of insurance.
6. A slight change in the policy terms and conditions can impact the claims frequen-cy and severity substantially. For example an introduction or withdrawal of de-ductibles would not only have an immediate corresponding financial impact, butalso an indirect one by altering perception. For instance, an introduction of a de-ductible implies that the insured would have to pay for a share of the initial claims,thus reducing the tendency of moral hazards or frauds.
All of the above facts illustrate that a sole reliance on the cost-plus approach of pric-ing would be unwise and would have to be substantiated by a judicious use of pricemanagement techniques hinging on the willingness to pay of the customer, thusadopting an outside in approach.
Premiums Charged and Corresponding Sum Insured
I will now elaborate on the pricing dimensions of two health insurance policies forICICI Lombard (which has been ranked as the number 1 insurer amongst privateplayers and has earned reputation and success in its few years of operation). Theproduct highlights, policy coverage information, key benefits, eligibility and the coreneed of critical care have been further illustrated to justify the pricing dimensions.
3.5 Pricing Criteria 127

Currently the primary pricing dimensions [a] Age of the Insured and [b] Sum Insured.[c] The Number of Adults and kids in the family seeking the policy.
Product 1: Critical Care (ICICI Lombard)
[a] Product Information: Critical Care protects the insured and spouse against loss ofincome on diagnosis of any of the 9 major medical illnesses and procedures. The firstof its kind, it offers a lump sum benefit on diagnosis of Cancer, Bypass Surgery,Heart Attack, Kidney Failure, Major Organ Transplant, Stroke, Paralysis, HeartValve Replacement Surgery or Multiple Sclerosis. Critical Care Insurance also pro-vides cover against accidental death and permanent total disablement.
[b] Policy Coverage: Critical Care offers a choice of coverage on both the sum in-sured and the tenure of the policy. One can choose the sum insured of Rs. 600,000 orRs. 1,200,000 over a period of 3 or 5 years. The premium would be calculated ac-cordingly.
[c] Key Benefits: The key benefits include (i) Comprehensive Cover – Lump sumbenefit on diagnosis of any of 9 Critical Illnesses, Personal Accident and PermanentTotal Disablement (PTD) Cover, (ii) Policy Coverage (see [b]), (iii) No health checkup required (iv)No 30 day waiting period (cooling off period), benefit paid immedi-ately on diagnosis.
[d] Eligibility: The eligibility criteria include (i) The insured can be one or one’sspouse, (ii) The insured needs to be between 20 and 45 years of age, (iii) Age is calcu-lated as on the date the policy is issued (age completed as on last birthday).
[e] Need for Critical Care: The need for critical arises on account of – (i) India ishome to 60 million Coronary Heart patients, (ii) India’s economic loss due to heartrelated disease could be $236 billion till 2015, (iii) At any given time there will be 3million cancer patients in India (World Health Organization)
[f] Premium Table:
128 3 Health Insurance
Policy Tenure/ Sum Insured = Rs. 600,000 Sum Insured = Rs. 1,200,000Age Groups (Years)
3 Years (Rs.) 5 Years (Rs.) 3 Years (Rs.) 5 Years (Rs.)
20–25 5,800 9,700 11,600 19,400
26–30 6,600 11,280 13,200 22,600
31–35 8,300 14,000 16,600 28,000
36–40 10,300 18,400 20,600 36,800
41–45 20,500 38,200 41,000 76,440

Product 2: Family Floater Health Plan (ICICI Lombard)
[a] Product Information: A single policy taking care of the hospitalization expensesof the entire family. Family Floater Health Plan takes care of all the medical ex-penses during sudden illness, surgeries and accidents.
[b] Policy Coverage: The policy covers medical expenses: (i) Incurred as an inpa-tient during hospitalization for more than 24 hours, including room charges, doctor/surgeon’s fee, medicines, etc. (ii) 30 days prior to hospitalization (iii) 60 days posthospitalization (iv) Day care expenses incurred on advance technological surgerieslike dialysis, radiotherapy, chemotherapy, requiring less than 24 hours of hospital-ization (v) Pre-existing diseases can be covered after the 4th year provided the poli-cy is renewed for 4 consecutive years.
[c] Key Benefits: Key benefits of the policy include (i) one policy for the entirefamily, (ii) income tax benefit under section 80 D, (iii) 5% discount on premium forevery claim free year, (iv) digitally signed policy available online, (v)no healthcheckup required till the age of 45 years, (vi) hassle free claims, (vii) cashless facil-ity available at over 3500 hospital networks in more than 175 cities in India, (viii)multiple payment options; and up to 2 year policies without increased premium inthe second year or renewal hassles.
[d] Eligibility: The eligibility criteria include (i) The enrolment age (of the seniormost family member) should be between 19 years to 60 years, (ii) Other membersin the plan can be less than 19 years of age (i.e. up to 91 days), (iii) The policy coveris renewable till the age of 70 years, (iv) The customer can buy the policy for anyfamily member(s), (v) For the purpose of income tax exemption u/s Sec. 80D, thepolicy should be bought only for self, spouse, dependent children and dependentparents.
[e] Need for Floater: The need for the Floater is justified on the followinggrounds (i) Healthcare costs have been rising at more than 20 percent on an annual-ized basis and out of pocket spending on healthcare still continues to be around 75percent (Times of India), (ii) Tax Savings up to Rs. 3366 u/s 80 D of the Income TaxAct Supplements employer-based health plans with higher sum insured and med-ical benefits, (iii) Individuals require to have an insurance that caters solely to theirhealth needs, apart from life insurance and investments, that provides cover againstexpenses incurred during hospitalization, as well as before and after, (iv) Availcashless hospitalization through ICICI Lombard’s network of 3500 hospitals acrossIndia.
3.5 Pricing Criteria 129

[f] Premium Table:
130 3 Health Insurance
Plan Details Plan A Plan B Plan C
Individual 2 Adults 2 Adults & 1 Kid
Age of senior 1 L 2 L 3 L 2 L 3 L 2 L 3 Lmost familymember
5–18 yrs. 1790 1990 2290 – – – –
19–35 yrs. 2490 2690 3100 4035 4650 5229 6024
36–45 yrs. 3120 3370 3744 5055 5616 6249 6990
46–55 yrs. 5700 6000 6667 9600 10667 10794 12041
56–60 yrs. 8167 11760 13067 12954 14441
Plan Details Plan D Plan E Plan F
2 Adults & 2 Kids 1 Adult & 1 Kid 1 Adult & 2 Kids
Age of senior 2 L 3L 2 L 3 L 2 L 3 Lmost familymember
5–18 yrs. – – – – – –
19–35 yrs. 6423 7398 3533 4069 4406 5073
36–45 yrs. 7443 8364 4094 4600 4916 5556
46–55 yrs. 11988 13415 6593 7378 7188 8082
56–60 yrs. 14148 15815 7782 8698 8268 9282
Note: “L” means lakhs where 1 lakh =100,0002nd row which includes 1 L etc indicates the amount of sum insured (ICICI Lombard).
3.6 Distribution Channels
An Introduction to Marketing Channels
Marketing channels are sets of independent organizations involved in the process ofmaking the product or service available for use or consumption. Decisions about themarketing channel system are amongst the most critical facing the management. Infact the channels chosen, affect all other marketing decisions – pricing for one wouldbe highly dependent on the kind of channel selected (Kotler and Lane, Designing andManaging Value Networks and Channels.) While channels play an essential role indelivery of products, their importance in services is actually contributory to the real-ization of the service itself. In insurance for example, the “product” is realized [a]

while selling the insurance policy and [b] during the claim settlement process. Thusany party concomitant to accomplishment of the processes responsible for the finaldelivery of service, form the essence of distribution channels. What is more, theseparties on account of their proximity to the customer can best alter their purchase de-cision and additionally provide insights to the insurers or the service producers.
In managing its intermediaries a firm must decide how much effort to devote topush versus pull marketing. A push strategy involves the producer using its salesforce and trade promotion money to induce intermediaries to carry, promote, and sellthe products/services to its end users. Push strategy is appropriate where there is lowbrand loyalty in a category, brand choice is made in the store, the product is an im-pulse item, and product benefits are well understood. A pull strategy involves themanufacturer using advertising and promotion to persuade consumers to ask interme-diaries for the product, thus inducing the intermediaries to order it. Pull strategy is ap-propriate when there is high brand loyalty and high involvement in the category,when people perceive differences between brands, and when people choose the brandbefore they go to the store (Kotler and Lane, Designing and Managing Value Net-works and Channels). A mixture of pull and push strategies may be employed byhealth insurer – pull because an insurance policy is a high involvement product; pushhowever, because the new introduction of policies, “free-look” period and shorterterm periods, induce customers to adopt policies on a trial and error basis.
Introduction of TPAs in the Indian Health Insurance Milieu
Claims management in Health Insurance in India is a no-win situation with the insur-er feeling that claims are always exaggerated, and hence is looking for opportunitiesof cutting corners; the client, on the other hand, is aware of the insurer’s propensity orthe tendency to cut corners and feels compelled to make exaggerated claims. Anotheraspect of health insurance claims settlement is the extent of preconditions that aremade mandatory in the policy. For example, the insurance is covered for cases whichnecessitate hospitalization for at least 24 hours. In such a scenario, the policyholderhas the tendency to enforce upon himself the hospitalization for the minimum periodso that his or her claim can be settled. It would, on the contrary, make more sense tohave in place the actual cause of hospitalization as a factor for passing the claimrather than insisting on a condition like minimum time of hospitalization, which in-duces moral hazard and cost hikes. In such a scenario, it would be better if there ismechanism which could work as a go-between and the role of the TPA would thus fillthe gap here in normal circumstances. Thus the TPA concept was introduced post-opening up of the industry, to introduce cashless hospitalization and propel health-care and promote health insurance amongst Indians (Jawaharlal and Kumar).
3.6 Distribution Channels 131
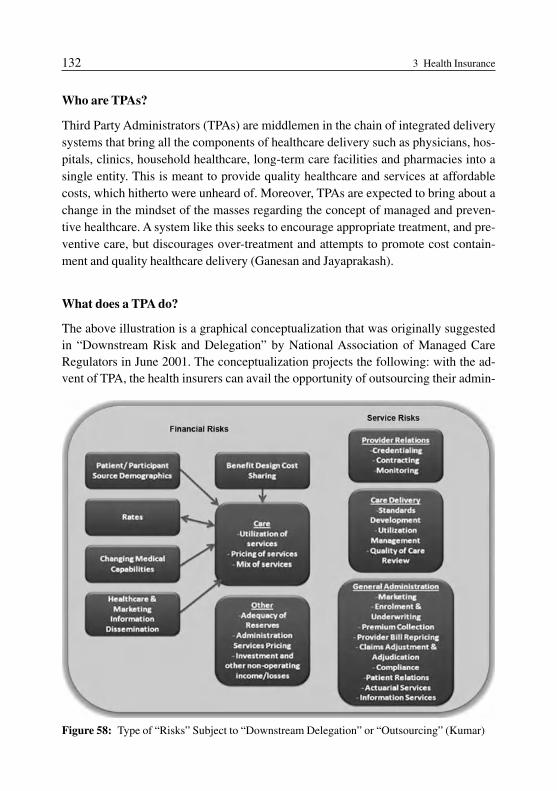
Who are TPAs?
Third Party Administrators (TPAs) are middlemen in the chain of integrated deliverysystems that bring all the components of healthcare delivery such as physicians, hos-pitals, clinics, household healthcare, long-term care facilities and pharmacies into asingle entity. This is meant to provide quality healthcare and services at affordablecosts, which hitherto were unheard of. Moreover, TPAs are expected to bring about achange in the mindset of the masses regarding the concept of managed and preven-tive healthcare. A system like this seeks to encourage appropriate treatment, and pre-ventive care, but discourages over-treatment and attempts to promote cost contain-ment and quality healthcare delivery (Ganesan and Jayaprakash).
What does a TPA do?
The above illustration is a graphical conceptualization that was originally suggestedin “Downstream Risk and Delegation” by National Association of Managed CareRegulators in June 2001. The conceptualization projects the following: with the ad-vent of TPA, the health insurers can avail the opportunity of outsourcing their admin-
132 3 Health Insurance
Figure 58: Type of “Risks” Subject to “Downstream Delegation” or “Outsourcing” (Kumar)

istrative services including claims settlement to them. A TPA will attend to all the ad-ministrative duties and will charge a single clubbed fee for all. It will have to assumeall the risks associated with those functions. The risk portfolio of the insurers can bebroadly classified into two types: financial risks and service risks. Financial risks in-volves activities like pricing products (insurance plans), setting reserves, determiningand implementing investment policy, and other measures. Service risks include theduties of insurers like provider relations activities, care management, delivery-relat-ed functions as well as marketing, underwriting, premium collection and benefit pay-ment. TPAs assume significant portion of both the afore-mentioned types of risksthus availing the insurers a cost cutting medium (Kumar).
Role of the TPA
Currently the role and services of the TPA entail bearing primarily the service risks,whilst the insurer will be the sole bearer of the financial risks. The TPAs in Indiapresently cater only to the corporate clients. Furthermore, the entry of TPAs implies
3.6 Distribution Channels 133
Figure 59: Workflow for the Cashless Treatment (Ganesan and Jayaprakash)

the arrival of the cashless system of payment for healthcare services. The policy-holders would receive every healthcare facility required, depending on their needsand high medical costs would not be a deterrent. Cashless hospitalization means thatthe policyholder will be able to avail medical services at designated hospitals and hisbills will be settled through TPAs (instead of tracking insurers for claims later), whowill additionally offer a 24-hour toll free helpline, access to physicians, specialists,diagnostic centers and ambulance services. By January 2005, 10 out of 14 TPAs hadbeen shortlisted by state insurers with fees for the same set at 5.5% (of the total busi-ness volume) for the north and south zones, 5.4% for the east and west zones. In caseof private insurers, the fee set was around 10 to 11% (Ganesan and Jayaprakash).
The illustration below depicts the workflow of the processes carried out in case of acashless facility, highlighting the role of the TPA within.
Stumbling Blocks in Operational Issues (of the functioning of TPAs)
The core reason for the failure of TPA s in India has been the lack of coordination be-tween TPAs and insurers. These hindrances have risen on account of agonies and is-sues faced by all of the involved parties participating in the service provision – hospi-tals, insurers and TPAs.
Hospitals
– First unhappy with the initial fee they had to pay for TPAs to empanel them asmembers. Hospitals do not feel the need to pay to belong to a network, as they aregetting volumes of business anyway.
– There is dissatisfaction by the hospitals due to the delayed payment and huge out-standing bills of the patients. Hospitals have reported that some bills have beenpending for 6 months to a year and that TPAs/insurers need to speed up theirclaims settlement processes.
– TPAs do not have an exhaustive network of member hospitals, implying limitedcoverage: one of the main reasons cited for the lackluster take off of the TPAs.
– Some doctors do not appreciate the fact that some third party needs to validatetheir style of treatment to verify the authenticity of the claim.
– Finally, in some cases it is felt that doctors use insured individuals as an opportuni-ty to earn more money, thus slapping exaggerated expenses onto insurers.
Insurers
– Initially when the services were introduced, there was agitation on behalf of the in-surance employees who feared a loss of their jobs. Thus the initial startup suffereda setback.
134 3 Health Insurance

– The service fee provided by the insurers is still quite low.– Many insurers believe that TPAs are interfering in the companies’ state of affairs;
as is apparent by the option for the policyholder to choose between the TPA or not,and pay a lower premium if they do not use TPA services, a highly de-motivatingmove against the TPAs (Ganesan and Jayaprakash).
– Finally, insurers are displeased with the regulatory restriction on the selection ofTPAs – which states that public sector general insurers can appoint 5 TPAs but notmore than 2 in one region, making the functioning straight jacketed for the insur-ance companies and the TPAs (Jawaharlal and Kumar).
TPAs
– A disparity in fees and in-transparency in charges of various hospitals has addeddifficulty to the claims data forecast thus making the smooth functioning of theTPA a distant reality. Despite attempts to change the system and suggest standardi-zation by way of grading of hospitals and treatments as super-major, major, inter-mediate and minor categories and fixing the ceiling accordingly, little has pro-gressed on this front.
– The regulatory restriction against marketing of healthcare products by the TPA hassqueezed the scope of TPAs in providing service to the healthcare industry.
– Moreover, they are required to pay a 1% of their income as fee to the regulator overand above the Rs. 20,000 as license fee. The minimum working capital of Rs. 10million and a minimum asset worth of Rs. 2.5 million at any point of time, coupledwith a 26% cap on the foreign equity make functioning rather stringent (Jawaharlaland Kumar).
– The lack of coordination between the insurer and TPA creates drastic dilemmas like
• Inability to estimate the number of policyholders in the spectrum.• Delay in payments for service charges.• The “free-look” period of 15 days wherein the customer can cancel his policy
poses a problem for the TPA who is not promptly informed; this delay leading toadded confusion and waste of time and opportunity cost in examining data that isof no relevance any more.
– TPAs are allocated to specif0ic regions; however since their only clients are corpo-rate clients, they need to open offices in zones where the client is: implying in-creased unprecedented costs.
– Weak profit margins for the TPAs leave them with less employees handling cus-tomer queries and educating customers on health insurance conditions and exclu-sions.
3.6 Distribution Channels 135

– The issuance of identity cards to customers is not streamlined and automated(Ganesan and Jayaprakash).
Corrective Measures to Improve the TPA Situation
Fine tuning the relationship between the TPAs and Insurers can solve several prob-lems and thereby improve the quality of the marketing channel, and consequently thebrand image of the insurer itself.
– A centralized regional office can be established to control the issue of all health in-surance policies and its administration. A representative officer from the TPA canbe positioned here who would function as a coordinator between the TPA and in-surer.
– The servicing issues of the TPA for regions other than authorized regions can bedelegated to nodal TPAs of the respective regions – similar to the cellular phonenetworks in India.
– An effective software system should be developed for deployment across TPAsand insurers, to monitor fund performance, its needs; whenever the flow reaches acritical level, the system would alert the insurer and TPAs with rules engines de-ployed for the same.
– Mandatory periodic meetings between the TPAs and insurers to improve commu-nication and discuss impending issues.
– A common database should be created wherein important fields like disease, sex,age, region etc which needs to be shared with TPAs and insurers; such a databasewould help in identifying patterns of diseases, regional variations, cost controlmeasures, identification of fraudulent cases, bringing down claims ratio, increas-ing professionalism among insurers, hospitals and TPAs and knowledge manage-ment and training of TPAs (Ganesan and Jayaprakash).
Brokers and their role in the Health Insurance Segment
Having already discussed brokers in the life insurance chapter 2.6, I would now ad-vance the discussion by highlighting the role of the broker, key broker traits, what thebrokers bring to the client and what they bring to the insurer. The concept of insur-ance broking was introduced in India in 2002 and is still at a nascent stage. Presentlythere are about 250 brokers and around 15 per cent of general insurance kitty isthrough direct brokers (Press Trust of India).
136 3 Health Insurance

Role of the Broker
– Understanding the clients business and risk management philosophy.– Detailed knowledge and comprehension of the available insurance market and ca-
pacities.– The broker sells and markets the products (thus reducing the marketing costs) and
the insurer underwrites it.– The broker renders assistance during the claims settlement process.– The broker assists in understanding the risk retention policy of the insurer.– He provides periodic market updates.
The Broker Traits essential in a de-tariffed regime are
– Inspiring confidence and trust,– Furnishing complete information,– Explanation of the insurance contract terms to the client,– And quicker response time with respect to market information, settlement of claims.
Brokers will bring the following to the client
– Peace of mind and tranquility.– Take care of the entire documentation, especially as far as the claims portfolio is
concerned.– Quality of service is regularly upgraded.– Contract certainty; thus clearly defining and explaining all clauses and conditions,
helping interpret all aspects of the contract, making what-if scenarios for the clientand thereby minimizing the tendency of grievance occurrence.
– Value added services like asset valuation, human resource management, calculat-ing the life displacement cost (which is the discounted cash flow of future earningsin a life investment plan).
Brokers will bring the following to the insurer
– Fair competition amongst insurers by representing the customer rather than the in-surer,
– Sound rating of risks,– Reduction in marketing time and costs; improving response time and market
knowledge of the insurer by virtue of their proximity to the customers and fair rep-resentation of the customers,
– Develop or co-produce the products suited for the market,– Selling the right product to the right person based on the apt understanding of risk
appetite of the clients and knowledge and experience in risk rating.
3.6 Distribution Channels 137

The Regulator Says: Regional Rural Banks (RRBs) can now jointhe insurance play
RBI has permitted RRBs to take up corporate agency for insurancecompanies
Reserve Bank of India (RBI), the regulator for banks in India has come out withnorms for regional rural banks (RRBs), enabling them to take up corporateagency of insurance companies. Until now RRBs have been acting as insuranceintermediaries by referring their customer base to insurers but were not permit-ted to sell directly or take up corporate agency. In terms of the new guidelines,RRBs can become corporate agents for insurance companies after qualifying un-der the Insurance Regulatory and Development Authority’s norms for corporateagency.This will open a new revenue stream for RRBs as first year commissions on saleof insurance policies are very high: up to 20% for a bank on an average. In its cir-cular to all RRBs, RBI has said as a measure of providing further business op-portunities, RRBs would be allowed to take up corporate agency business, with-out risk participation, for distribution of all insurance products, including healthinsurance and animal insurance.“RRBs need not obtain prior approval of RBI for taking up corporate agencybusiness for distribution of insurance products without risk participation. How-ever, a report may be sent to the concerned Regional Office of Reserve Bankwithin 15 days of commencing the insurance agency business,” the central banksaid in its circular. According to insurance companies, the entry of RRBs will im-prove penetration of health insurance in rural areas since they have the distribu-tion network. Besides, since they are part of the payment system, insurers can of-fer premium collection service locally without having a local branch. The entryof RRBs will also enable insurance companies in pushing forward with their mi-cro-insurance plans.RBI has said besides complying with IRDA regulations for a composite corpo-rate client, RRBs cannot adopt any restrictive practice of forcing its customers togo in only for a particular insurance company in respect of assets financed by thebank. As the participation by a bank’s customer in insurance products is purelyon a voluntary basis, it should be stated in all publicity material distributed bythem in a prominent way. There should be no ‘linkage’ either direct or indirectbetween the provisions of banking services offered by the bank to its customersand use of the insurance products. (Times News Network (TNN)) The last state-
138 3 Health Insurance

3.7 Communication Strategy 139
ment, although in consumer interest, seems to suggest a potential hindrance tothe RRBs with respect to bundling insurance products with their bank products.This, unfortunately obviates the banks and insurance companies from exploitingthe profit potential of product bundling, subsequently preventing the two fromfully realizing the benefits of bancassurance. This may also be cited as a negativeside effect of the “dual regulator” scene: Reserve Bank of India (RBI) for banksand the Insurance Regulatory Authority of India (IRDA) for insurers.
3.7 Communication Strategy
Consumer Insight: Health Insurance in India; is awareness the key?
In an interview with the Times of India, Dr. Prasad, CEO of the Apollo HospitalChains in India explained, “Certain state-of-the-art treatments can be expensivefor the common man. That’s the reason why we need to make health insurancemandatory. People need to be informed about it. There’s an urgent need forawareness about health insurance. When you buy a bike you have to pay up theinsurance. Why not be more particular about human life. It’s precious.”Vijay Reddy an associate with the Insurance Institute of India added, “70 percent of middle class families’ savings are spent on healthcare. Sometimes peopleeven end up selling their property to pay up their expenses. But investing inhealth insurance will make a difference. Insurance is something that you neednot when you have an emergency but way in advance (Sanam).Shantanu Dutta, a journalist for a news portal commented “Health insurance,which is what most of the developed world lives by has not “really” taken off inthe country as with large population living just in survival mode, coping withtroubles and issues today is their concern and not the difficulties that may cropup tomorrow” (Dutta).
Service communications is a tool for value delivery in the marketing value chainwhich alters customers’ brand image, customers’ perceived service quality and cus-tomer’s behavior directly; thereby altering the marketing and firm value (Bruhn andGeorgi).
The above illustration projects health and accident insurance as the second largestgrowing segment for Television advertising in the year 2006, with a growth rate of82%. The CEO of Bajaj Allianz General Insurance Co. Ltd believes that televisionadvertising is by far the most effective channel of communication in India with re-

140 3 Health Insurance
Figure 60: Information Source: Adex Analysis
Having made her purchases anold woman steps out of a shop
spect to reach and coverage, specially because the number of households possessinga television set (as a % of the population) is greater than the literacy percentage of thepopulation. Insurance is a long term business and carefully planned value propositioncreation that is consistently and perennially projected in the advertising, promotionand integrated marketing communication activities of an insurer, is the essence ofbrand identification, recollection, and customer loyalty initiation. Let us thus take alook at the storyboard of one of the television ads and draw an analysis from thesame.
Storyboard of New India Assurance Television AD (Agency FAQs)

3.7 Communication Strategy 141
Three goons spot her andfollow her with plans to robher
Just as they close in, a call“Mom” makes them stop andturn around
A guy standing at the shopcalls out to the lady, “Mom,wait”
As the son walks in, therogues quickly turn awaylooking strangely busy tyingtheir laces and praying

Analysis of the AD
– Emotional orientation and connection, efficiently achieving “personifica-tion” and “materialization”
– A very well improvised situation, where the “goons” are implicitly comparedto an unlikely event or uncertainty and the “son” who is watching what is go-ing on is implicitly compared to the health insurance policy.
– The core need satisfied by the product is communicated very distinctly – withan uncertain situation in the offing but a “protection” or “security” in place tocombat its occurrence or impact.
– Moreover, the emotional angle of the ad is enhanced because it is left for theviewer to imagine whether the “son” who called out was really the lady’s sonor a passerby who happened to observe the situation and intelligently savedthe lady on time, without creating a traditional “fight scene”. If this “son” isimagined to be a stranger doing a good deed – once again the product has beenimprovised into someone who is dormant but comes to rescue you when youare in dire straits.
– A humor aspect enhances the message effectiveness by the way the “goons”react pretending to pray, tie their shoe lace etc when the “son” approachesagain paralleling it to instant risk evasion when the security is around.
– Finally the MVO (male voice over) subtly but succinctly conveys the message“Where you go, often depends on what you have with you. New India Assur-ance, Assurance of the Leader” (New India Assurance is truly the leader in thegeneral insurance area)
142 3 Health Insurance
MVO: “Where you go oftendepends on what you havewith you. New India Assur-ance, Assurance of the leader”
Chapter 4:Conclusion
This is the concluding chapter which discusses the outlook for the health andlife insurance industry based on primary data from the “emerging opportuni-ties and challenges for the insurance market in India” survey. The thesis clos-es with a summary of the best strategies and practices in the Industry.

4.1 Outlook for the Life and Health Insurance Marketin India
The new wave of regulations, increased foreign players’ entry, rising consumerismand awareness, insurmountable insurance business growth rates, innovativedistribution channels, profit determining product designs and pricing techniques,emotional advertising and the looming necessity of making speedy businessdecisions, all embellish the current insurance business environment in India.Having discussed these varied aspects in the report, the reality that precedes and de-termines the future can now be best exemplified through a candid evaluation of thesurvey (Emerging Opportunities and Challenges for the Insurance Market in India)results.
Every response to the survey has been evoked by an opinion leader and/or chief ex-ecutive or key senior management of the corresponding insurance company. As eachof these individuals is also the prime decision maker of his/her company and shapesthe business evolution of the firm in concern and in turn the industry, each of these re-sults will highlight a projected pattern from time t (where t is May 2007) and trajecto-ry of development from then on for the firm in specific and consequently the industryin general.
Thus, I will now summarize the findings of the survey (sections 1, 2, 5 and 6)which serves as a directional outlook to the industry. Please refer to the questionnairein the appendix for the corresponding detailed questions.
Section 1 “Tariffed vs. De-tariffed Regime” Results:
1. The results for the “biggest defects of a tariffed regime” were averaged, with themost prominent defects being (in this order) ii) Lack of underwriting skills, asprices were determined by the Tariff Advisory Committee and iv) Companieslacked quality data to understand whether the pricing policies made sense orwhether the companies are running smoothly.
2. The “biggest challenges that come with a de-tariffed regime” are as follows (inthis order) ii) Initial price cuts, iii) Collection of risks and its link to claims’ dataand i) Developing responsible underwriting skills.
3. The responses for “positive developments in a de-tariffed regime” include theability to deliver the “appropriate price” to the individual customer through differ-ential pricing, ability to use customer insight and underwriting expertise to deliverprofitable growth, a better understanding of “risk”, differentiation through riskmanagement and risk profiling and the ability to hone customer centric innova-tion.
144 4 Conclusion
Section 2 “Foreign Players’Participation” Results:
1. To the foreign player cap hike question, most responses stated that it should be in-creased to 49% (option iii). However, one respondent believed otherwise suggest-ing that the foreign cap is alright at 26% (option i) under the following justifiablegrounds: “I personally believe that there is no real value add in increasing theshareholding except in reducing the exposure of the Indian entity. Unless the for-eign entities can demonstrate their ability to adapt to the nuances of the Indian In-surance market, increase in shareholding does not automatically imply an increasein penetration, customization or even introduction of products benefiting the Indi-an consumer”
2. Question 2[b] is concerned with understanding the expertise that foreign playersbring on a likert scale ranging from 1 which implies least contribution to 5 which isthe most contribution of foreign players for each of the factors. The results to thisanswer have been portrayed statistically by the usage of mode to understand themost frequent response, and mean to understand the average of all responses. Theresults are as follows: Foreign players bring in: “good underwriting skills and there-by help formulate better pricing techniques for insurance products” with 4 and 5both as modes and a mean of 4.2, “product innovation expertise and thereby helpformulate more customized solutions” with 3 and 5 both as modes and a mean of 4,“an operational edge through technological efficiency” with 5 as mode and 3.8 asmean, “good risk perception and risk management skills” with mode of 4 and mean4.4, “increased brand awareness amongst end customers” with mode 3 and mean3.2, “expertise through more innovative distribution channels” with 4 and 5 asmodes and 4 as mean, “sufficient amount of capital that Indian players may nothave” with mode of 4 and mean of 4.4, “best practices in recruiting and trainingstaff” with mode of 5 and mean of 3.8, “expertise with respect to efficient andspeedy claims management” with modes of 5 and 4 and mean of 4, “bring in expert-ise with respect to fraud management” with mode of 4 and mean of 4.4. Thus, basedon the highest averages, the maximum contribution of foreign players is felt in goodrisk perception and risk management skills, sufficient amount of capital that Indianplayers may not have and expertise with respect to fraud management.
3. There were mixed responses to question 2[c] on whether the respondents felt thata foreign player with an Indian partner is better off than a standalone foreign sub-sidiary, however a slight majority responded with a “yes”, less than half indicateda “no” and few others a “neither disagree nor agree”.
4. To understand the reasons why foreign players with Indian partners were betteroff than standalone foreign partners, scores had to be allocated to 5 statementssuch that they add up to 50 for the 5. This question was to be answered only by
4.1 Outlook for the Life and Health Insurance Market in India 145

those who responded with a “yes” in the previous question. However, despite asmaller subset responding, the following are the core results: brand awareness ofthe Indian partner and its existing customer base are seen as biggest advantages tothe foreign counterpart.
Section 5 “IRDA – Its role and Developments” Results:
1. For question 5[a], a similar data analysis method is used as above (Section 2 Re-sults, Point 2). Here too a likert scale has been used with 1 being least effectiveand 5 the most effective in the concerned task. Thus a projection of the mode andmean is used to analyze the effectiveness of the role of the IRDA in developmentand regulation of the insurance market in India. The results for the contribution ofthe IRDA in the various areas are as follows: “promoting product innovation”with mode of 4 and mean of 3.2, “addressing customer grievances” with mode of3 and mean of 3.6, “addressing insurance companies’ concerns” with mode 3 andmean 3.4, “laying guidelines for agents and intermediaries” with mode 4 andmean 4, “quick and speedy changes with respect to optimum business environ-ment” with modes of 3 and 4 and mean of 3.2, “reach with respect to various cus-tomer segments with modes of 3 and 4 and mean of 3.2, “providing support to for-eign players in the Indian insurance market” with mode 3 and mean 3.2. Thus, rel-atively, the most effective areas of contribution of the IRDA towards the develop-ment and regulation of the insurance market in India are “laying guidelines foragents/intermediaries” and “addressing customer grievances”.
2. For the detailed questions in 5[b], please refer to the questionnaire in the appen-dix. To [1] Solvency margins, an equal majority said that it was “tough to adhereto, but necessary” and “achievable and necessary”, thus the underlying facet beingthat individual firms with different capital structures find it difficult or achievable(as the case may be) to adhere to these regulations, but all of respondents agreethat these regulations are necessary for the smooth functioning of a cost-first anduncertain business like insurance. To [2] Social and Rural Obligations, a majorityresponded with “Achievable and necessary”. To [3] De-tariffing safety valve, amajority responded with a “Yes”. To [4] Permission from IRDA with respect tocross-subsidization, there was a mixed response with an equal number of respon-dents indicating a “yes” and a “no”. To each [5] Investment Regulations, [6]Agents’ qualifications requirements, [7] Board of Members’ approval for under-writing, the majority replied with a “yes”.
3. The responses for the most essential change or development that the IRDA mustimplement for the overall development of the Indian insurance market were as fol-lows: establish regulations for the improvement in claims service, enhance the ac-
146 4 Conclusion

counting regulations which has a mismatch in the recognition of revenues andcosts, allow for more innovative product approvals and begin to improve penaltiesfor non-compliance/misconduct versus regulations. A reasonable number of re-spondents felt that the IRDA must grant more freedom to the insurer in transactingits core business, and that the primary role of a regulator should be to ensure thesolvency of the underwriter and must be limited to the fiscal and financial sound-ness of the firm; thus implying that the IRDA must refrain itself from getting intothe micro management of every aspect of business for which they lack expertise.
Section 6 “Innovation and Best Practices” Results:
1. Most questions in this section are company specific; thus I will present the generalinformation that helps elucidate an industry trend, and mention the company spe-cific information of one company “Tata-AIG”.
2. To 6[a], all respondents felt the importance of a data warehouse for the company,thus responding with option [i].
3. To 6[b], whilst 40% said that “it already existed”, the remaining 60% stated that adata warehouse was “in progress of development” in his/her respective firm.
4. TATA – AIG’s Responses: (All responses include only publically available infor-mation, in lieu of the confidentiality of the insurer). Tata-AIG’s CEO Trevor Bullfeels that “Invest Assure Gold” is their star product on account of its uniqueness,though he suspects that it would continue to remain their star product for morethan 2 years, suggesting the dynamicity of the industry’s products. The number ofpolicies and premium collected for this product is unavailable since it is a recentlylaunched product. Some of the innovations that Tata-AIG is proud of are as fol-lows: Tata-AIG: is the first life insurance company to launch a standalone medicalproduct, the first life insurer to launch micro insurance products following the reg-ulations last year (2006), was voted as number 1 in customer satisfaction by theVOICE survey, is one of the only two private insurers to have a balance of tradi-tional life and ULIP products with a 50–50 split on a portfolio basis; others are de-pendent on ULIP with more than 80% now. Finally Tata-AIG prides itself in itsunique agency model that minimizes agent attrition and reaps economies.
4.2 Summary of the Best Practices
In conclusion, I would like to reinstate the best marketing strategies employed byvarious life and health insurers. These strategies serve as industry wide best practicesand stand out primarily because of efficiency, uniqueness and/or local market prox-
4.2 Summary of the Best Practices 147

imity of the implementation or formulation of the strategy. The account of the bestpractices in the Indian insurance industry includes:
Life Insurance:
1. TATA-AIG for its 50–50 portfolio balance in ULIP and traditional life insuranceproducts. Most life insurers currently pride themselves in the huge profits thatULIPs bring to them and are thus constantly adjusting their portfolio of businessesin favor of ULIPs; all except two life insurers (one of the two being Tata-AIG)have now a portfolio mix of 85:15 for ULIPS versus traditional products. Whilst,this may seem like a profitable strategy now, since ULIPs are primarily invest-ment vehicles linked to the stock market and additionally transfer the burden ofinvestment to the policyholder, it is however short-lived to imagine that infinitegrowth based on this product alone, is possible. In their book on Corporate Fi-nance, Brealey and Meyers proved that according to the market efficiency theory,it was impossible for investors to make abnormal returns on the stock market con-tinually and if so this would only be in lieu of additional information that wasn’tpublicly available to the market as a whole. In light of this theory, it is only wisefor Tata-AIG to maintain a reasonably balanced portfolio of ULIP versus tradi-tional life products. Moreover, in the two day national conference on “Emergingopportunities and challenges for insurance market” at Jaipur, India Feb 2007, ex-perts like Prof Sunderasan of the National Insurance Academy at Pune stated that,life insurers must focus in developing products that first cater to the true and basicneeds of insurance: security and savings.
2. For customer segmentation in life insurance, marketers and planners must use anastute combination of the HPI with the SEC system, and thereby refine their mar-ket prioritization. From a Marketer’s perspective: whilst SEC entails understand-ing the “potential” of markets, HPI elaborates on the “consumption intensity” ofmarkets.
3. HDFC Standard Life Insurance establishes the best practice in needs satisfactionby offering products based on the stage of life or the circumstance that one be-longs to. For every stage, HDFC has products satisfying different needs. The mainstages around which the product offerings are structured are: Young and Single,Just Married, Proud Parents and Planning for Retirement.
4. Riders provide the flexibility of choosing amongst several options without havingto sign a separate policy for every need. Hence, they offer customized solutions,without having to opt for rigidly bundled product offerings. The key riders thatcan be “added on” to a life insurance policy include accident death rider, premiumwaiver benefit rider, guaranteed insurability rider, critical illness rider and familyincome benefit rider.
148 4 Conclusion

5. Although overreliance on Unit Linked Insurance Plans may prove detrimental tothe fiscal soundness of a firm in the long run, there is no denying that ULIPs areamongst the best practices with respect to product design innovations providingfor liquidity, flexibility, transparency and control over asset allocation to the pol-icyholder. Besides offering the above benefits to the policyholder, ULIPs alsotransfer the investment burden from the insurer to the policyholder.
6. Max New York Life offers a whole gamut of products serving various life stages(like HDFC Standard Life Insurance) and needs. The main life stages includeSingle, Married, Married and with Children and Planning for Retirement, and themain needs around which products are structured include Savings, Investments,Education for Children, Marriage for Children and Protection.
7. The best practices in life pricing includes SBI Life Insurance’s “Agency Online”portal developed to help insurance advisors understand customer risk profiles.Moreover, best strategies entail combining the cost-plus: efficient underwritingand rate making approach with the professional price management approachthrough the mastering of 5 main tasks: value pricing and segmentation, knowl-edge about price elasticity, sales optimization and optimization of the pricingprocess. Additional best practices includes tele-underwriting, a procedure thatserves to streamline processes and enhance efficiency by mechanizing most ofthe decisions and thereby reducing subjectivity.
8. In distribution channels, bancassurance provides for a hand-in-glove or comple-mentary situation for both insurers and banks, benefiting the insurers with a thehuge retail base of the bank, the existing customer network and lowered distribu-tion costs, and the banks with increased fee-based earnings, retail thrust and agrowing sense of customer segmentation by provision of a whole range of finan-cial products.
9. Max New York Life’s “Direct Customer Services Program”, the feet-on-streetmodel to address the orphan policyholders is a best practice solution giving im-petus to distribution via increased customer proximity and consequently in-creased CLV.
10. Television advertising is the most effective medium of communication for lifeinsurers in India and HDFC Standard Life’s advertisement on children endow-ment plans elicits best practice in aptly communicating through emotional adver-tising and achieving both “materialization” via “visualization of needs satisfac-tion” and “personification” via “reference customers”.
Health Insurance:
1. The segmentation methodology used by Bajaj Allianz, aptly defining segmentsbased on an astute mix of demographic, geographic and behavioral variables, cou-
4.2 Summary of the Best Practices 149

pled with the pattern of target market selection which includes “selective special-ization” based on competencies are amongst best practices underlying urgentneeds identification and the corresponding customer categories.
2. Managed health care, the major components of which include seamless systemsmanaging disease prevention and wellness, early disease detection, the manage-ment of chronic illness and valuable partnerships to improve healthcare quality,are amongst the forward looking product related best practices for the health in-surance industry in India. Certain insurers, like ICICI Lombard are already mov-ing in the right direction by providing insurance covers for hereditary diseases likeDiabetes.
3. Bajaj Allianz’s “Health Guard” policy with a retention rate of 85% and a claims-to-premium ratio of 67%, with cashless facilities and wide eligibility spanning in-dividuals between 5 and 55 years of age, is one of the better designed and prof-itable policies in the health insurance arena today.
4. ICICI Lombard’s “Critical Care” policy and “Family Floater Health Plan” areamongst the more sophisticated products designs adopting differential pricingtechniques based on various criteria: age of the insured, sum insured, number ofadults and number of children in the family.
5. Brokers and TPAs are the key intermediaries in the value chain for health insurers;however, the current situation demands improvements in managing the qualityand contribution of the two mediators: by enhancing interaction between the in-surer and them, providing for continual and flawless support through automatedenvironments and finally, grooming and enhancing their role to permit truly valueadditive activities towards both policyholders and insurers.
6. New India Assurance stands out in its emotionally oriented and subtle communi-cation strategy with impactful materialization and personification.
150 4 Conclusion
Appendix
Emerging Opportunities and Challengesfor the Indian Insurance Market
A Survey for Insurance Executives
Dear Sir/ Ma’am,
The purpose of this survey is to understand your esteemed opinion on the emergingopportunities and challenges for the insurance industry in India. The survey has beendivided into 6 sections – 1] Tariffed vs. De-tariffed regime, 2] Foreign players’ partic-ipation, 3] Health Insurance, 4] Life Insurance, 5] IRDA – its role and developments6] Innovation and Best Practices.
Please answer the questions based on how it may relate to you or your company or toyour overall understanding of the industry as a whole.
This information is being used for research purposes by Novi Dewan, under the men-torship of Prof. Martin Fassnacht, Head of the Marketing Chair at WHU – OttoBeisheim School of Management.
Thank you very much for your time and efforts.
Warmest Regards,Novi DewanMarketing Speaker,WHU – Otto Beisheim School of ManagementBurgplatz 2, Vallendar 56179Germany
[email protected]@gmail.com
Tel.: 0049 173 6719 826

Points to Note
1. Section 1] “Tariffed vs. De-tariffed regime” has three main questions a), b)and c)
2. Section 2] “Foreign players’ participation” has four main questions a), b), c)and d)
3. Section 3] “Health Insurance” has seven main questions a), b), c), d), e), f), g)4. Section 4] “Life Insurance” has seven main questions a), b), c), d), e), f), g)5. Section 5] “IRDA – its role and developments” has three main questions a),
b), c)6. Section 6] “Innovation and Best practices” has nine main questions a), b), c),
d), e), f), g), h), i)7. Please try and answer all sections 1 through 6 and fill in whichever may be appli-
cable to you.8. Respondents from insurance companies –
a. Please fill in sections 1), 2), 3), 4), 5), 6)b. Based on whether you are a non-life or life insurance company, you can choose
between 3) and 4) respectively.9. Respondents who are not from insurance companies, but from bodies affiliated
with the insurance industry like News agencies, Institutes, Regulatory Body orother Independent Bodies – a. Please fill in sections 1), 2), 5) and b. Also please try and fill as much as applicable from sections 3), 4) and 6).
1) Tariffed vs. de-tariffed regime
a) What were the biggest defects of a tariffed regime?
Give each of the following statements a score (or weight) so that the sum of indi-vidual scores is 50. For example … (i) 10, (ii) 5, (iii) 15, (iv) 9, (v) 11; Thereforesum of (i) + (ii) + (iii) + (iv) + (v) = 50. A higher score indicates a higher weightallocated to the particular statement.
i) Cross subsidization of loss making businesses by the profit incurring businessii) Lack of Underwriting skills, as prices were determined by the Tariff Adviso-
ry Committeeiii) Good customer paid for the bad customer, due to a single non-historical pric-
ing policy iv) Companies lacked quality data; thus lacked an understanding of whether the
pricing policies made sense or whether companies ran smoothlyv) No incentive on the part of the insured to improve his/her risk portfolio
152 Appendix

b) What are the biggest challenges that come with a de-tariffed regime?
Give each of the following statements a score (or weight) so that the sum of indi-vidual scores is 50. For example… (i) 10, (ii) 5, (iii) 15, (iv) 9, (v) 11; Thereforesum of (i) + (ii) + (iii) + (iv) + (v) = 50. A higher score indicates a higher weightallocated to the particular statement.
i) Developing responsible underwriting skills
ii) Initial price cuts
iii) Collections of risks and its link to claims’ data
iv) Differentiation through customer relationship management
v) Developing innovative products and distribution channels
c) What, according to you, will be the positive developments in a de-tariffedregime? Please name at least two.
2) Foreign players’ participation
a) Most private insurance companies in India are joint ventures between Indi-an banks or insurance companies and foreign players. However, the currentcap for foreign player participation in an insurance company in India is26%.
Please select the option that you think will be most beneficial to the Indianinsurance industry in general. Please select one option only.
i) Foreign player cap is alright at 26% �ii) Foreign player cap should be increased to 35% �iii) Foreign player cap should be increased to 49% �
b) 2000 saw the de-regulation of the Indian Insurance Industry, thereby wit-nessing the entrance of several foreign players into the Industry. What arethe primary benefits for an Indian company to team up with foreign playersin the Indian Insurance market? What expertise do the foreign playersbring?
Please score the following statements on a scale of 1 to 5, 1 indicating the leastlevel of importance with respect to the contribution by the foreign player and 5indicating the maximum level of importance for the corresponding statement.
Please mark against one number only reflecting the level of contribution for everystatement.
Appendix 153

Foreign players bring in 1 2 3 4 5Least Less Neither less More Mostcontri- contri- nor more contri- contri-bution bution contribution bution bution
A] Good underwriting skills, and thereby � � � � �help formulate better pricingtechniques for insurance products
B] Product innovation expertise and � � � � �thereby help formulate morecustomized solutions
C] An operational edge through � � � � �technological efficiency
D] Good risk perception and risk � � � � �management skills
E] Increased brand awareness amongst � � � � �the end customers
F] Expertise through more innovative � � � � �distribution channels
G] Sufficient amount of capital that � � � � �Indian players may not have
H] Best practices in recruiting and � � � � �training staff
I] Expertise with respect to efficient � � � � �and speedy claims management
J] Bring in expertise with respect to � � � � �fraud management
K] Others (if so, please name at least � � � � �one such)
c) Do you think that foreign players with Indian partners are better off than astandalone foreign subsidiary? Please select one option only.
i) Yes �ii) No �iii) Neither agree nor disagree �
d) If yes, then why do you think foreign players in a joint venture with Indianpartner are better off than a standalone foreign subsidiary in India?
Give each of the following statements a score (or weight) so that the sum of indi-vidual scores is 50. For example … (1) 10, (2) 5, (3) 15, (4) 9, (5)11; Therefore
154 Appendix

sum of (1) + (2) + (3) + (4) + (5) = 50. A higher score indicates a higher weight al-located to the particular statement.
(1) Brand awareness of the Indian partner brand
(2) An existing customer base
(3) An existing distribution network
(4) Knowhow of the Indian market and customer segments
(5) Awareness of customer related frauds
3) Health Insurance, Please answer the following questions if your companydeals with health insurance products.
a) Please name at least 3 main customer segment categories for your health in-surance products. For example Customer Segment 1 – Age Group 25 to 50,Upper Middle Class, Living in Metros. Please define the customer segmentsbased on as many characteristics as you like.
b) What is the “claims to premium ratio” for your main health insurance prod-uct?
c) What is the retention rate for your health insurance products in general?
d) How many frauds (frauds/claims) has your company detected in the lastyear?
e) What according to you are the most urgent requirements for the Indianhealth insurance industry?
Please rank the following criteria based on the level of urgency, 1 being the mosturgent and 10 being the least urgent. Please make sure that no two items have thesame rank.
(1) Right pricing strategies based on accurate risk assessment (differences be-tween good and bad risk) and underwriting skills
(2) Tracking fraudulent claims
(3) Customer satisfaction with respect to efficient and quick claims settlement
(4) Enhanced and improved service provided by Third Party Administrators(TPAs)
(5) Increasing professionalism amongst agents and brokers
Rank
Appendix 155

(6) Reaching out (selling policies) to the segment of society that is belowpoverty line
(7) Developing health insurance products that cover different diseases
(8) Developing a health insurance product that covers day-to-day doctor visits
(9) Use of CRM tools and Data Warehousing for linking historical customerinformation and thereby coming up with accurate assessments
(10) Simplicity of contracts and contract language
f) What are the most effective (maximum reach and thereby maximum salesachieved) mediums of advertising/promotion for core health insurance prod-ucts of your company?
Please rank the following channels/media for promotion based on the level of ur-gency, 1 being the most effective and 7 being the least effective. Please make surethat no two items have the same rank.
(1) Newspaper
(2) Television
(3) Radio
(4) Magazines
(5) Internet
(6) Outdoor (Billboards etc)
(7) Others (please mention in case there are more) Please add the “others”here
g) Health Insurance companies these days are opting for several channels ofdistribution for maximizing reach and optimizing penetration.
On a scale of 1 (1 being least effective) to 5 (5 being most effective), please indi-cate the overall effectiveness of the distribution channel with respect to its salesto a desired customer segment from the perspective of your company or as peryour knowledge for health insurance in general.
Please mark against one number for each distribution channel that reflects thelevel of effectiveness according to you. Please mention the customer segmentmost suitable to the distribution channel, for example “Bank customers”,“Teenagers”, “Middle aged , lower middle class” etc.
156 Appendix
Rank

4) Life Insurance. Please answer the following questions if your company dealswith life insurance products.
a) Please name at least 3 main customer segment categories for your life insur-ance products. For example Customer Segment 1 – Age Group 25 to 50, Up-per Middle Class, Living in Metros. Please define the customer segmentsbased on as many characteristics as you like.
b) What is your “claims to premium ratio” for your main life insurance prod-uct?
Appendix 157
Distribution Channel 1 2 3 4 5 Name theLeast Less Neither More Most Customer effective effective effective effective effective Segment
nor most suit-ineffective able to the
channel
1) Bancassurance (using � � � � �banks for distributionof insurances)
2) Medical tie-ups � � � � �(tie-ups with hugeprivate and publichospital chains)
3) Automobile tie-ups � � � � �(distribution ofinsurance policiesthrough automobilecompanies)
4) Telcassurance � � � � �(distribution throughtelephone marketing)
5) Online distribution � � � � �(through your companywebsite or any otherinternet portal medium)
6) Malls and Supermarkets � � � � �(distribution ofinsurance policies)
7) Postal services � � � � �(the Indian Post)
8) Others (kindly � � � � �mention at least one)

c) What is the retention rate for your life insurance products in general? (Thisquestion is being asked to understand whether some people stop paying theirlife insurance premiums)
d) How many frauds (frauds/claims) has your company detected in the last year?
e) What according to you are the most urgent requirements for the Indian lifeinsurance industry?
Please rank the following criteria based on the level of urgency, 1 being the mosturgent and 10 being the least urgent. No two items must have the same rank.
(1) Right pricing strategies based on accurate risk assessment (differences be-tween good and bad risk) and underwriting skills.
(2) Tracking fraudulent claims
(3) Customer satisfaction with respect to efficient and quick claims settlement
(4) Not punishing the rightful claimant on account of the misconduct of fraudu-lent claimant
(5) Increasing professionalism amongst agents and brokers
(6) Reaching out (selling policies) to the segment of society that is belowpoverty line
(7) Developing life insurance products that also incorporate other functionali-ties, for examples ULIPs, Credit Insurance, Children’s Marriage SavingsPlan etc.
(8) Moving from the perception of a life insurance policy solely as a tax sav-ings instrument to a savings, protection and investment vehicle
(9) Use of CRM tools and Data Warehousing for linking historical customer in-formation and thereby coming up with accurate assessments
(10) Simplicity of contracts and contract language
f) What are the most effective (maximum reach and thereby maximum salesachieved) mediums of advertising/promotion for core life insurance prod-ucts of your company?
Please rank the following channels/media for promotion based on the level of ur-gency, 1 being the most effective and 7 being the least effective. No two itemsmust have the same rank.
158 Appendix
Rank

1. Newspaper
2. Television
3. Radio
4. Magazines
5. Internet
6. Outdoor (Billboards etc)
7. Others (please mention in case there are more)Please add the “others” here
g) Life Insurance companies these days are opting for several channels of dis-tribution for maximizing reach and optimizing penetration.
On a scale of 1 (1 being least effective) to 5 (5 being most effective), please indi-cate the overall effectiveness of the distribution channel with respect to its salesto a desired customer segment from the perspective of your company or as peryour knowledge for life insurance companies in general.
Please select one number that reflects the level of effectiveness according to you.
Please mention the customer segment most suitable to the distribution channel, forexample “Bank customers”, “Teenagers”, “Middle aged , lower middle class” etc.
Appendix 159
Distribution Channel 1 2 3 4 5 Name theLeast Less Neither More Most Customer effective effective effective effective effective Segment
nor most suit-ineffective able to the
channel
1) Bancassurance (using � � � � �banks for distributionof insurances)
2) Medical tie-ups � � � � �(tie-ups with hugeprivate and publichospital chains)
3) Automobile tie-ups � � � � �(distribution ofinsurance policiesthrough automobilecompanies)
Rank

5) IRDA – its role and developments
a. IRDA is playing an essential role in the development and regulation of the in-surance market in India.
Please select one number that reflects the level of effectiveness according to you.
160 Appendix
Distribution Channel 1 2 3 4 5 Name theLeast Less Neither More Most Customer effective effective effective effective effective Segment
nor most suit-ineffective able to the
channel
4) Telcassurance � � � � �(distribution throughtelephone marketing)
5) Online distribution � � � � �(through your companywebsite or any otherinternet portal medium)
6) Malls and Supermarkets � � � � �(distribution ofinsurance policies)
7) Postal services � � � � �(the Indian Post)
8) Others (kindly � � � � �mention at least one)
Contribution of IRDA 1 2 3 4 5in the following areas Least Less Neither More Most
effective effective effective effective effectivenorineffective
A] Promoting Product Innovation � � � � �
B] Addressing customer grievances � � � � �
C] Addressing insurance � � � � �companies’ concerns
D] Laying Guidelines for Agents/ � � � � �Intermediaries

b. IRDA has several laws in place keeping in mind the overall well being of theindustry.
Some laws/regulations and the reasons for their existence have been explainedbelow. Please select your opinion for each of the regulations.
1. Solvency Margin: The IRDA expects every insurance company to have acertain solvency margin (assets > liabilities by a certain amount) which ismeant to act as a safety buffer.
Do you feel the solvency margin for you is (please select just one option)
a. Too tough to adhere to, and unnecessary �b. Tough to adhere to, but necessary �c. Neither tough nor easy �d. Achievable and necessary �e. Easy to adhere, must be made more stringent �
2. Social and Rural Obligations: The IRDA has prescribed certain social andrural obligations.
Do you think these obligations are (please select just one option)
a. Too tough to adhere to, and unnecessary �b. Tough to adhere to, but necessary �c. Neither tough nor easy �d. Achievable and necessary �e. Easy to adhere, must be made more stringent �
3. De-tariffing safety valve: The de-tariffing of general insurance took effecton the 1st of Jan, 2007. However, IRDA stated that the policies and terms
Appendix 161
Contribution of IRDA 1 2 3 4 5in the following areas Least Less Neither More Most
effective effective effective effective effectivenorineffective
E] Quick and speedy changes with � � � � �respect to optimum businessenvironment
F] Reach with respect to various � � � � �customer segments
G] Support to foreign players in the � � � � �Indian insurance market

and conditions with respect to the policies cannot be changed until the 1stof April, 2008. The purpose of this was to serve as a safety valve, so thatinsurance companies do not engage in a “bloody war”.
Do you think this is justified? (Please select just one option)
a. Yes �b. No �c. Neither Agree nor Disagree �
4. Permission from IRDA with respect to cross-subsidization: One of the ma-jor goals of de-tariffing has been to discontinue the cross subsidization ofloss making areas like health insurance by the more profitable areas likemotor insurance. However the IRDA has a regulation that permits com-panies to cross subsidize certain lines, wherein the Board of Directors canpresent their case with a valid reason for cross-subsidization.
Do you think this is a good option to have? (Please select just one option)
a. Yes �b. No �c. Neither Agree nor Disagree �
5. Investment requirements: The IRDA has prescribed investment regula-tions for both Life and General Insurance Business with respect to invest-ments in Central Government Securities, State Government Securities,Infrastructure and Social Sector, Housing Loans etc.
Do you think these are in general fair? (Please select just one option)
a. Yes �b. No �c. Neither Agree nor Disagree �
6. Agents’ qualifications requirement: IRDA has prescribed lower limits ofqualifications and training requirements for agents to improve the overallquality of this staff.
Do you think these requirements are sufficient? (Please select just one option)
a. Yes �b. No �c. Neither Agree nor Disagree �
7. Board of Members Approval for Underwriting: IRDA has formulated aregulation, wherein the Board of Directors needs to approve the under-
162 Appendix

writing strategy of the management. Besides ensuring that the Board isinformed, this makes the Board directly accountable for the underwritingstrategy. Moreover, insurers now have to spend time on their underwrit-ing skills, as this new law will reduce information asymmetry between theBoard and the Insurer. Of course, however this involves the Board in theoperations of the company.
Do you think this regulation/strategy makes sense? (Please select just one op-tion)a. Yes �b. No �c. Neither Agree nor Disagree �
c. Mention one most essential change or development that the IRDA must im-plement, for the overall development of the Indian Insurance Market
i.
5) Innovation and Best Practices
a. Do you feel the importance of a data warehouse for your company? (Pleaseselect just one option)
i. Yes �ii. No �iii. Neither agree nor disagree �
b. If so, what is the state of development for the same in your company? Pleaseselect the statement applicable. (Please select just one option)i. Already there �ii. In Progress of development �iii. Will begin development in the next 1 year �iv. Planning to develop it �
c. Please name one product that you think is your star product
i.
d. Why do you think this is your star product?
i.
Appendix 163

e. What is the number of policies sold in your star product? (information on amonthly or annual basis, please mention the month or year)
i.
f. What is the premium collected for this product? (information on a monthlyor annual basis, please mention the month or year whichever you may use)
i.
g. Do you think this will continue to be your star product in the next 2 years?
i.
h. If not, which product do you think will be your new star product?
i.
i. What are the one or more innovations that your company is particularlyproud of?
i.
164 Appendix
Bibliography
Abell, Derek. “Five Patterns of Target Market Selection.” Kotler, Philip and Kevin Lane. Mar-keting Management 12e. New Jersey: Pearson, Prentice Hall, 2006. 262.
AdEx Analysis. Insurance Sector Advertising on TV in the year 2006. 27 March 2007. 21 May2007 <http://us.indiantelevision.com/tamadex/y2k7/mar/tam13.php>.
Agencies. Even rural India shining: Survey. 02 May 2007. 21 May 2007 <http://www.ex-pressindia.com/fullstory.php?newsid=85866>.
Agency FAQs. Agency Faqs>Advertising>Television>Storyboard>New India Assurance. 18November 2004. 2 June 2007 <http://www.agencyfaqs.com/perl/advertising/storyboard/in-dex.html?id=1881>.
Ayyar, V Sesha. “Insurance: Origin and Developments.” Kumar, K B S. Non-Life Insurance.Hyderabad: ICFAI University Press, 2006. 132–133.
Belch, George and Michael Belch. “An introduction to Integrated Marketing Communication.”Advertising and Promotions – An Integrated Marketing Communications Perspective. SanDiego: McGraw Hill, 2006. 1–36.
Bhaskaran, R. “Bancassurance – Developments in India.” Two Day National Conference on“Emerging opportunities and challenges in the Indian Insurance Indsutry”. Jaipur: InsuranceTimes and Government of Rajasthan State Insurance, 8, 9 February 2007.
Bhattacharya, Anabil. “General Insurance Market Leading to a Tariff Free Regime.” The Insur-ance Times. Jaipur: The Insurance Times, 2007. 30–41.
Bhattacharya, Anabil. “Life Insurance Products & Strategies for successful marketing in Urbanand Rural India.” Life Insurance Today (2006): 5–7.
Bruhn, Manfred and Dominik Georgi. “Communicating Service Value.” Bruhn, Manfred andDominik Georgi. Services Marketing – Managing the Service Value Chain. England: PrenticeHall, 2006. 268–297.
Chakravati, Srabanti. “Reasons Behind Low Penetration of Health Insurance Schemes in In-dia.” Kumar, K B S. Non Life Insurance. Hyderabad: ICFAI Press, 2006. 35–44.
Chatagny, Jean Michael. “Why has Health Insurance not taken off?” Insurance Summit CII.Mumbai: Swiss Re, 10 October 2006.
CIA – The World Factbook. CIA World Factbook. 21 May 2007 <https://www.cia.gov/library/publications/the-world-factbook/geos/in.html>.
Datamonitor. Global Insurance. Market Analysis. New York: Datamonitor, 2006.–. Insurance in Asia Pacific. Market Analysis. New York: Datamonitor, 2006.–. Insurance in India. Market Analysis. New York: Datamonitor, 2006.–. “Multiple reports on the Indian Insurance, Asia Pacific Insurance and Global Insurance Mar-
ket.” New York: Datamonitor, 2006.Dutta, Shantanu. The paradox of silent cradles and obese generals. 4 May 2007. 20 May 2007
<http://www.merinews.com/catFull.jsp?articleID=124960>.Exchange4Media. Socio Economic Classification (SEC) of India. 13 July 2005. 13 May 2007
<http://www.exchange4media.com/e4m/media_matter/matter_130705.asp>.Fassnacht, Prof. Martin. “Importance of Price.” Brand and Price - Price Management . Koblenz:
Marketing Chair at WHU, MBA Class of 2007.Ganesan, S and S Jayaprakash. “TPAs in India: Can they be Turning Point Administrators?” Ku-
mar, KBS. Non-Life Insurance. Hyderabad: ICFAI Press, 2006. 69–78.HDFC Standard Life Insurance. Knowledge Centre - Know more about insurance. 27 May 2007
<http://www.hdfcinsurance.com/knowledgecenter/lifestages.asp#young>.

Hindu Business Line. Oriental Insurance Products through post offices – Pilot project kicked offin 7 states. 5 February 2004. 21 May 2007 <http://www.thehindubusinessline.com/2004/02/05/stories/2004020502241000.htm>.
ICICI Lombard. “Financial Intermediaries in Non-Life Insurance.” FICCI, 16 October 2001.ICICI Lombard. Health Insurance Policy India. 01 June 2007 <http://www.icicilombard.com/
app/PersonalProducts/Health/criticalcare.asp>.IRDA. Annual Report 2005–2006. Annual Report. Hyderabad: IRDA Journal, 2005–2006.IRDA. Annual Report IRDA 2005–2006. Annual Report. Hyderabad: IRDA, 2006.–. Annual Report, IRDA, 2005–2006. Annual Report. Hyderabad: IRDA, 2005–2006.Jawaharlal, U and K B S Kumar. “The Teething Troubles of TPAs.” Kumar, KBS. Non Life In-
surance. Hyderabad: ICFAI Press, 2006. 79–87.Jawaharlal, U. “Riders or Customized Solutions?” Kumar, K B S. Insurance – Customer Ser-
vice. Hyderabad: ICFAI Press, 2006. 104–107.Kaufmann, Lutz, et al. China Champions. Koblenz: EMP, 2005.Kedia, Sanjay. “Strategies and Experiences in Managing Risk Transfers – A Broker’s Perspec-
tive.” New Delhi: IFC, 22 August 2006.Kotler, Philip and Kevin Lane Keller. “Setting Product Strategy.” Kotler, Philip and Kevin Lane
Keller. Marketing Management 12e. New Jersey: Pearson and Prentice Hall, 2006. 371–399.Kotler, Philip and Kevin Lane. “Defining Marketing for the 21st Century.” Kotler, Philip and
Kevin Lane. Marketing Management 12e. New Jersey: Prentice Hall, 2006. 3–31.Kotler, Philip and Kevin Lane. “Designing and Managing Value Networks and Channels.”
Kotler, Philip and Kevin Lane. Marketing Management 12 e. New Jersey: Prentice Hall andPearson, 2006. 466–501.
Kotler, Philip and Kevin Lane. Market Segmentation. New Jersey: Pearson, Prentice Hall,2006.
Krishnamurthy, Narayan. “At Every Step of Life...” Kumar, K B S. Insurance – Customer Ser-vice. Hyderabad: ICFAI Press, 2006. 32–37.
Krishnamurthy, R. Bancassurance in Insurance Distribution: Key Issues in the Indian Context .New Delhi, 15 October 2001.
Kumar, K B S. “TPAs: A Cure for the Indian Health Sector.” Kumar, K B S. Non-Life Insurance.Hyderabad: ICFAI Press, 2006. 63–68.
Kumar, V. Sai. “Life Insurance Products in India – Issues in Distribution.” IRDA (December2006): 22–23.
Max New York Life. Max New York Life India: Easy Plan Finder. 27 May 2007<http://www.maxnewyorklife.com/Home/Tools%20and%20Planners/Easy%20Plan%20Finder.aspx>.
–. Max New York Life India: Easy Plan Finder, Planning Retirement, Savings, Investment, In-surance. 27 May 2007 <http://www.maxnewyorklife.com/Home/Tools%20and%20Planners/Easy%20Plan%20Finder.aspx>.
McGahan, Anita M. How Industries Evolve. Boston: HBS Press, 2004.Mendiratta, Deepak. “Rise of Health Insurance in India.” Health Insurance Conference 2007,
IFC. Washington DC: International Finance Corporation, 20 April 2007.Mishra, K C and Simita Mishra. “Getting Closer to Life Insurance.” Mishra, K C and Simita
Mishra. The Game is Changing – Insurance Reloaded. Hyderabad: ICFAI Press, 2005. 7–16.Mishra, K C and Simita Mishra. “Health Insurance to Managed Care.” Mishra, K C and Simita
Mishra. The Game is Changing – Insurance Reloaded. Hyderabad: ICFAI Press, 2005.145–167.
Mishra, K C and Simita Mishra. “Insurance Sector Revisited.” Mishra, K C and Simita Mishra.The Game is Changing – Insurance Reloaded. Hyderabad: ICFAI Press, 2005. 1–6.
166 Bibliography

Mishra, K C and Smita Mishra. “Insurance Sector Revisited .” Mishra, K C and Smita Mishra.The Game is Changing – Insurance Reloaded. Hyderabad: ICFAI University Press, 2005. 1–6.
Mishra, K C and Smita Mishra. The Game is Changing – Insurance Reloaded. Hyderabad: IC-FAI Press, 2005.
Mr. Bimal Balasingham, Director, Tata AIG Life Insurance Company Ltd. Media Releases; TataAIG. 21 December 2006. 17 May 2007 <http://www.tata.com/tata_aig_life>.
Nanda, Puneet. Investing in ULIPs - Read This First. 20 May 2005. 27 May 2007 <http://in.red-iff.com/money/2005/may/20perfin.htm>.
O’Connor, Robert. “For Life Writers, India Looms as Another “Jewel”.” BestWeek. AM BestCompany Inc, April 2007.
Oza, Arman. “Health Insurance: Awaiting Congruence.” Kumar, K B S. Non-Life Insurance.Hyderabad: ICFAI Press, 2006. 19–27.
P. Chidambaram. Full Text of Finance Minister’s reply to the debate on Finance Bill. 4 May2007. 20 May 2007 <http://economictimes.indiatimes.com/News/Economy/Policy/Full_text_of_FMs_reply_to_debate_on_Finance_Bill_/articleshow/1999172.cms>.
Parera, Russell. “Health Insurance in India - Devising an Appropriate Model.” New Delhi:KPMG, 18 October 2004.
Prabhakara, G. Importance of Sound Awareness and Education on Risks and Insurance issues.Istanbul, 13 April 2007.
Press Trust of India. Enam Insurance Broker gets IRDA license. 17 May 2007. 18 May 2007<http://economictimes.indiatimes.com/News/News_By_Industry/Finance__Insurance/In-surance/Enam_Insurance_Broker_gets_IRDA_licence/articleshow/2057688.cms>.
Press. Tata Group: Tata AIG LIfe Insurance: Media Releases. 10 May 2006. 18 May 2007<http://tata.com/tata_aig_life/releases/20060510.htm>.
PTI. Indians need awareness on life insurance – a survey. 12 April 2007. 20 May 2007<http://www.livemint.com/2007/04/12211610/Indians-need-awareness-on-life.html>.
–. SBI Life Launches a Technology Initiative for Advisors – Business Live News – The Eco-nomic Times. 18 May 2007. May 18 2007 <http://economictimes.indiatimes.com>.
Rajesh, J. “Claims Settlement: The Key Success Factor of LIC.” Kumar, K B S. Insurance –Customer Service. Hyderabad: ICFAI Press, 2006. 88–94.
Ramachandaran, K. “Role of Brokers: Redefining Products and Service Excellence.” NewDelhi: International Finance Corporation, 22 August 2006.
Rao, GV. “Brokers in India and Other Markets.” IRDA Journal (December 2006): 11–14.Rao, T S Ramakrishna. “Tele-Underwriting in Life Insurance.” IRDA Journal October (2006):
18–20.Sahgal, Anil. “Bancassurance helps tap household savings.” Two Day National Conference on
“Emerging Opportunities and Challenges in the Insurance Industry” February 2007: 73–74.Sanam, Chitra. Don’t fall ill, unless you’re rich. 5 May 2007. 20 May 2007 <http://timesofind-
ia.indiatimes.com/Cities/City_Supplements/Hyderabad_Times/Dont_fall_ill_unless_youre_rich/articleshow/2005097.cms>.
Sawhney, Banit Singh. Distribution Challenges – How will the insurance industry respond? Pa-per. Pune, 2006.
Schmidt-Gallas, Dr Dirk and Dieter Lauszus. “Profitable Growth: Manage your Pricing or LoseMoney.” Simon Kucher and Partners (2006): 1–9.
Sethi, Suresh. “Developments in Health Insurance in India.” National Conference on “Emerg-ing Challenges and Opportunities in the Insurance Industry”. Jaipur: The Insurance Times,2007. Slide 3.
Sinha, Tapen. An Analysis of Evolution of Insurance in India. An Analysis. Mexico, 2004.–. The Indian Insurance Industry – Challenges and Prospects. Analysis. UK: University of Not-
tingham, 2004–2005.
Bibliography 167

Sinha, Tapen. The Indian Insurance Industry – Challenges and Prospects. Analysis. UK: Univer-sity of Nottingham, 2004–2005.
Sinha, Tapen. The Indian Insurance Industry: Challenges and Prospects. A report. UK, 2003.Sodhani, Vineet. Target your truly consuming homes better, HPI from IRS. 13 July 2005. 17
May 2007 <http://www.exchange4media.com/e4m/media_matter/matter_130705.asp>.Syed, Falaknaaz. Free Health Insurance from Office? No More! 7 May 2007. 21 May 2007
<http://inhome.rediff.com/money/2007/may/07perfin3.htm>.–. Three more insurers on the horizon. 18 May 2007. 18 May 2007 <http://www.business-stan-
dard.com/banking/storypage.php?tab=r&autono=284795&subLeft=1&leftnm=2>.Thomas M. Daniel, Max New York Life. “Orphan Policy or Direct Customer – A Paradigm
Shift.” Two Day National Conference on Emerging Opportunities and Challenges in IndianInsurance Industry. Jaipur: The Insurance Times, 2007.
Times News Network (TNN). RRBs can join Insurance Play, but can’t take any risk. 4 May2007. 20 May 2007 <http://economictimes.indiatimes.com/News/News_By_Industry/Fi-nance_Insurance/Banking/RRBs_can_now_join_insurance_play_but_cant_take_any_risk/articleshow/1999694.cms>.
Vaughan, Emmet and Therese Vaughan. Essentials of Insurance – A Risk Management Perspec-tive. Iowa: John Wiley and Sons, Inc, 1995.
Viswanathan, S. “Role of Distribution Channels.” IRDA (December 2006): 20–21.Wikipedia. Insurance in India. 22 May 2007 <http://en.wikipedia.org/wiki/Insurance_in_In-
dia#Life_Insurance_Corporation_Act.2C_1956>.
168 Bibliography
About the Author
Novi Dewan, an Engineer by profession recently
completed her MBA as Valedictorian of the MBA
Class of 2007 at the WHU – Otto Beisheim School
of Management, Germany with international mod-
ules at Kellogg School of Management, North-
western University, US; Indian Institute of Manage-
ment (IIM), Bangalore, India; and CEIBS, Shang-
hai, China. She is currently a research scholar at the
Chair of Microeconomics and Industrial Organization at WHU. She was selected
amongst a pool of high caliber candidates for the Harvard Program for Asian and
International Relations (HPAIR) which was held in Hong Kong, in August, 2007.
Her paper on shakeout theories titled “When entrepreneurial spirit is not enough”
was published and selected for the Max Planck Annual Conference at Indian Institute
of Management, Bangalore in October, 2007. Her main areas of interest include
Neuroeconomics and Social Entrepreneurship. In her free time, Novi enjoy traveling,
exploring new cultures and sub-cultures, hiking, writing, solving Sudoku puzzles,
bowling and learning new adventure sports.




















