
The Italian National Survey for Prader–Willi syndrome: An epidemiologic study
Upload
independentCategory
view
0download
0
Nosocomial Acquisition of Cadida parapsilosis: An Epidemiologic Study VERONICASANCHEZ, M.D., Detroit, Michigan, JOSEA. VAZQUEZ, M.D., DANIELBARTH-JONES, M.P.H., LOUISE DEMBRY, M.D., Detroit, Michigan, andRoya/Dak, Michigan, JACK D. SOBEL, M.D., Detroit, Michigan, MARCUS J. ZERVOS, M.D., Detroit, Michigan, and Royal Oak, Michigan
OJ!MKTMQ The purpose of this study was to determine aspects of the epidemiology of nosoco- mial infection due to Candida parapailosds. Can- &da specie43 are important nosocomial patho- genq however, little epidemiologic information is available.
PATIENTS AND =ODSz We prospectively cul- turtxlspecimensfrom98patientsadmittedtothe bonemarrowkanspbmtunitandamedkiuein- tensivecareunit(ICU)ofatertkycarehospital. &&mensfromhandsofpersonnelandenviron- msncal~W~also-~-tal
cxlhalmWere~befOrepe~~Were&dmitted
toastudieduniLRe+Wk&m~analysis (RZA)ofchromawwlalDNAwasusedasatyp~ qWt4!!mtodeWmhietherela~of~
RESULTS C. parap&o&was idenMed from five patif3ut8$sixhandl?ultWsfromfour~staff, andtwoen -tall3u&ce%Allfivepatients hadIMgatlvehlitkllc&lllWl#UdaCquhX!dCjW ap?3&J&aft%radmis&mtothestudyunitaThere wereno&ni&xmtdiffer0ncesbelxveenpatien~ and~tE-olsUbje@Jinage,~diclegse,im- m~therapy,andh&nunentation The duration of autibiotic therapy (mediam 328 velw311J3days#p=OS06)andthedurationinthe unit(me4~30.1ve~3us16.1days,p=0.048)was longer in patlenta than in controls. No common sourcewasiden~REAlwealedthreestrahl typee;-,Oll0f3tdltypewaSideolticalh
fourpatlentS#threestaffmemberi%andtwoenvi- ronmental-
CONCLUSION: Them redts suggest exogenous acquisition of C. pa.ra@osk Based upon isola- tion of identical patient straius of C. parap~&~& from inanimate surf&es before patients were ad- mitted to a study unit, there is evidence that the organism may have been acquired from the hos-
From the Departments of Internal Medicine (VS. JAV. LD. JDS. MJZ) and Biostatistics @B-J). Division of Infectious Disease (VS, JAV. LD, JDS, MJZ). Wayne State University School of Medicine, Detroit, Michigan, and William Beaumont Hospital (JAV, DB-J, LD, MJZ), Royal Oak, Michigan.
This study was supported in part by the William Beaumont Hospital Research Institute, Royal Oak, Michigan.
Requests for reprints should be addressed to Marcus Zervos. M.D., Division of Infectious Diseases, William Beaumont Hospital, 3601 West 13 Mile Road, Royal Oak, Michigan 48072.
Manuscript submitted February 28, 1992, and accepted in revised form November 6, 1992.
pital enviroument. The principal mechanism of . .
trammmon was probably indirect contact via the hands of hospital personnel.
P athogenic Candida species are ubiquitous or- ganisms usually confined to human and animal
reservoirs, but they can be recovered from soil, food, and the hospital environment. They are normal in- habitants of the female genital tract and the entire gastrointestinal tract, including the oropharynx, rec- tum, and perineum. Candida species are increasing- ly important nosocomial pathogens in immunocom- promised patients, including intensive care and postoperative patients [l-23]. C. parapsilosis has been particularly associated with infections in hospi- talized patients [12-231. Knowledge of the epidemi- ology of nosocomial Candida infection is incomplete because of the lack of a reliable typing system to evaluate strain relatedness. Previous typing systems have relied on serotyping and biotyping that do not reflect true strain differences.
Recent advances in the use of restriction fragment analysis has facilitated the development of a typing system at a molecular level. These techniques have been used to study diverse groups of organisms in- cluding bacteria, viruses, and fungi [24-351. Molecu- lar typing of Candida species (“DNA fingerprint- ing”) can differentiate closely related strains with phenotypic similarities [24-29,351. These tests have high discriminatory power. This typing system was used in this study to investigate aspects of the epide- miology of C. parapsilosis colonization and infec- tion. In this prospective study, we used molecular typing of C. parapsilosis to further clarify the pa- tient and hospital reservoirs of infection and modes of Candida transmission between high-risk patients.
PATIENTS AND METHODS Harper Hospital is a 900-bed tertiary care teach-
ing hospital in Detroit, Michigan. Patients in the medical intensive care unit (ICU) and bone marrow transplant (BMT) unit were studied. The medical ICU is an eight-bed private-room unit. Patients hos- pitalized in the ICU (ICUl) were transferred halfway through the study period to a separate IO-bed unit on a different floor with 4 open beds and 6 private beds. This new unit (ICU2) had previously been used as a
June 1993 The Amerlcen Journal of Medicine Volume 94 577
NOSOCOMIAL CAND/DA PARAPSILOSIS / SANCHEZ ET AL
surgical intensive care unit and underwent renovation prior to the transfer of patients. The same hospital personnel cared for patients in each ICU. The BMT unit is a 24-bed private room unit with a hospital staff different from that of the ICU. Patients were occa- sionally transferred between the BMT unit and the ICU, depending on the severity of their illness. Hou- sestaff and medical students rotate between Harper Hospital and five other Wayne State University hospitals.
We prospectively studied all patients who provided informed consent and who had been hospitalized in the BMT unit or ICU during a 7.5month period. Demographic and clinical data, including date of hos- pitalization, date of discharge, age, sex, ward, and medical service, were recorded by one of us (VS). The use of urinary catheterization and the dates and sites of vascular catheter placement were also noted. A careful record of bed assignments was kept. Move- ment within the hospital before discharge and expo- sure to antibiotic agents, cytotoxic agents, and immu- nosuppressive agents was also recorded. We defined colonization and infection according to established criteria: colonization was indicated when Candida species were isolated from a site without signs or symptoms of infection. Infection was diagnosed using criteria published for nosocomial infection: organism isolated from a body site concurrent with accompany- ing signs and symptoms of infection (e.g., fever great- er than or equal to 38OC, leukocytosis in nonneutro- penic patients, increased wound drainage, dysuria or pyuria, ophthahnitis). The severity of illness was de- termined using the criteria of McCabe and Jackson [36]. Death was considered related to Candida spe- cies if the patient died within 72 hours after a positive culture had been obtained on a sample from a normal- ly sterile site, and the clinical profile was consistent with septicemia including hypotension, hypothermia or hyperthermia, tachycardia, tachypnea, and inade- quate perfusion of at least one organ system.
Specimens for culture were obtained from all pa- tients and plated on Sabouraud dextrose agar. Clini- cal specimens were also plated on blood agar. Cultures were obtained when patients were admitted to the study unit, and then weekly for patients in the BMT unit and biweekly for patients in the ICU until dis- charge from the unit. Oropharyngeal, rectal, and urine cultures were obtained from all patients. Speci- mens from other sites such as wounds, vaginal areas, skin, and blood were also obtained when clinically indicated. The dates, sites, and colony counts of posi- tive cultures for yeast were recorded. Oropharyngeal and rectal specimens were obtained using a sterile cotton swab. Urine samples were obtained through clean-catch voiding or were taken from syringe-aspi- rated catheters. An environmental culture survey per- formed in every patient room included at least one
578 June 1993 The American Journal of Medicine Volume 94
culture of surfaces in contact with hands of personnel or patients, ventilator tubing, nebulizers, and humidi- fiers, one floor culture, and one sink faucet area culture.
Specimens from the hands of hospital personnel were obtained by producing an impression with the hands on a Petri dish that contained Sabouraud dex- trose agar. Cultures of selected environmental sur- faces from the study units were done using Rodac plates (Falcon Inc, Oxnard, CA). Cultures of surfaces and hands were performed at 60-day intervals during the study period. Cultures of the surfaces in the medi- cal ICU were obtained when the location of the unit was changed during the study period, including be- fore any patients were hospitalized in the new unit.
Patients from whom C. parapsilosis was isolated were matched by time of admission to the unit with three control patients without Candida species colo- nization. The statistical significance of data from pa- tients and control subjects was assessed using tests of homogeneity of proportions and Fisher’s exact test for bivariate analysis of dichotomous outcome data. The significance of continuous variables was deter- mined with the Mann-Whitney U test. A multivariate linear-regression model was used to analyze the inde- pendence of risk factors.
All C. parapsilosis isolates were identified by neg- ative germ tube formation, morphology, and Yeast API 20°C Systems (Sherwood Medical, Plainview, NY). Strains were initially isolated on Sabouraud dextrose agar (Difco, Detroit, MI), stored in a 1:l concentration of brain-heart infusion broth (Difco) and glycerol, and frozen at -7OOC until analysis. Con- trol strains of C. parapsilosis were obtained from five patients located in a geographically separate hospital and C. parapsilosis ATCC strain #22019.
Isolates were evaluated for molecular relatedness using restriction enzyme analysis (REA). REA was done by a blinded investigator (JV). For the isolation of DNA, yeast cells were grown on Sabouraud agar plates for 24 hours at 30°C. The method used to pre- pare the DNA is a modification of the method de- scribed by Petes et al [37]. The cells were suspended in 5.0 mL of 0.2M TRIS-HCl 5% mercaptoethanol and incubated in a water bath at 37OC for 30 minutes. After incubation, 10 mL of 1M sorbitol-0.004M potas- sium phosphate was added to the cells and pelleted. The cells were then resuspended in 2.5 mL of sorbitol- potassium phosphate-zymolyase 20T (ICN Biomedi- cal, Lisle, IL) to promote spheroplast formation as per Torres-Bauxa and Riigsby [38]. The spheroplasta were then lysed using a solution of 0.2M sodium chlo- ride-O.lM EDTA-5% sodium dodecyl sulfate-50mM TRIS (pH 8.5) -20 H pronase (Sigma, St. Louis, MO), and incubated at 60°C for 30 minutes in a water bath. Nucleic acids were extracted using a saturated solution of 1OmM TRIS-1mM EDTA (pH 8.3)-phe-
NOBOCOMIAL CAiVNDA PARMSUOSS J BANCNEZ ET AL
nol-chloroform in a ratio of 25~2524 and precipitated with two volumes of cold ethanol. The cell suspension
TABLE I
was frozen for 1 hour at -7OOC. Afterwards, the nu- Recovery of C. pampsisilosis by Body Site and as a Percentage d Total
cleic acids were dried and resuspended in 1 mL of TE study Candida SpKies koMes
buffer (1mM TRIS, -O.lmM EDTA, pH 8.0) and reprecipitated with potassium acetate 3M (20 rL/0.5 mL) and two volumes of cold ethanol, then frozen for either 1 hour at -7OOC or overnight at -20°C. The Orophatynx 3 119 2.5
nucleic acids were again dried in a vacuum oven for 30 Stool 3 138 2.2
minutes and resuspended in 106 rL of TE. The sam- ples were stored at 4OC until electrophoresis. The
Urine 0 77 0
concentration of DNA resulting from this procedure Vaginal 1 36 2.8
varies from 4 to 5 &pL. For the electrophoresis of Blood 0 4 0
samples, 5 & of DNA was digested with 50 U of the restriction endonucleasea EcoRI and MspI (BRL,
Wound 1 14 7.1
Gaithersburg, MD), according to the recommenda- Sputum 0 2 0
tions of the manufacturer. Agarose gel electrophoresis Total a 390 2.0
of the purified DNA was then performed using a 0.7% agarose horizontal gel apparatus at 30V for 16 hours. The gel was stained in a solution of 0.5 &mL of ethidium bromide for 20 minutes, then destained in TABLE II
water for 60 minutes before being photographed. Patient Location With Acquisition of C. pafapsibsis Grouping was done by visual inspection of the band- ing patterns. Total Patients WiiNew With Cobniis at
Unit at Unit Acquisitien Transfer to Unit
RESULTS ICU2 44 During the study period, we followed 98 patients BMT 54 ; :
with 106 admissions (49 males and 49 females) hospi- Total 98 5 0
talized in the BMT unit and the ICU. Six patients had U2 = intensive care unit 2; BMT = bane marrow transplant.
two admissions each, and one patient had a total of three admissions. Patients ranged in age from 5 to 66 years (mean: 46.8 years). Six patients were trans- ferred between the BMT unit and the ICU during their hospital stay. Patients in the ICU were hospital- ized a mean of 11.3 days (range: 2 to 43 days) and in the BMT unit for a mean of 27.4 days (range: 3 to 73 days).
cultures were done. The other two patients had repeat cultures from which C. parapsilosis wan not isolated. One patient received systemic amphotericin B for 6 days prior to the first culture of C. parapsilosis. None of the other patients received topical or systemic anti- fungal therapy prior to culturing of C. parapsilosis.
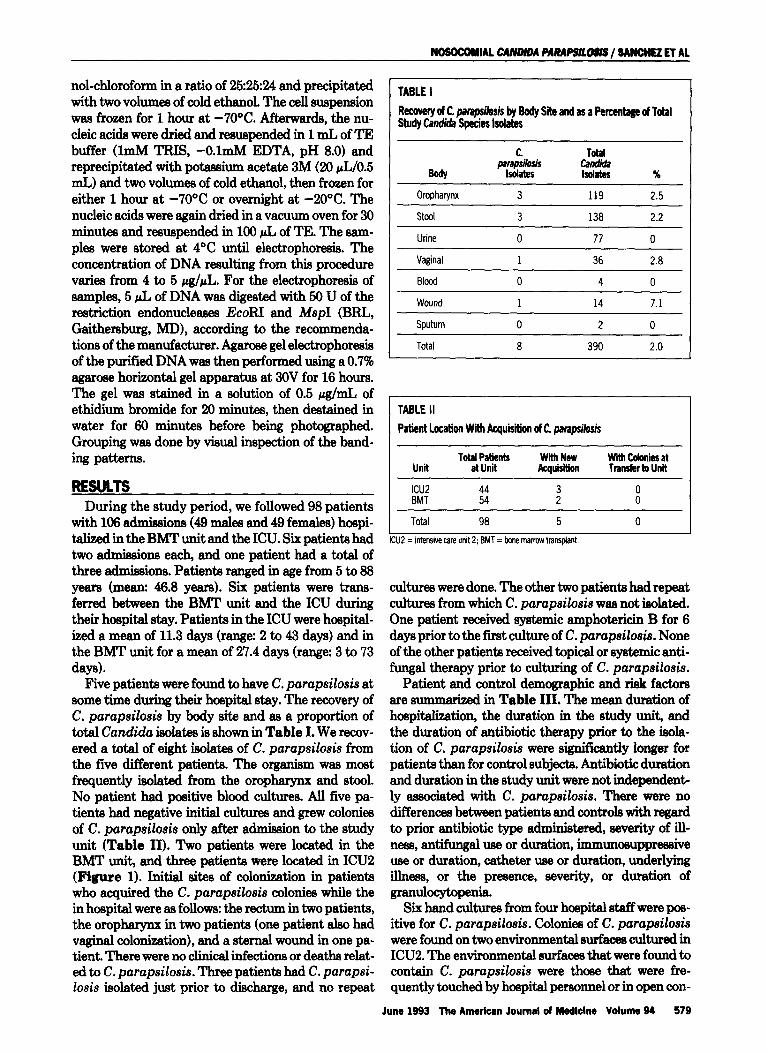
Five patients were found to have C. parapdosis at some time during their hospital stay. The recovery of C. parapsilosis by body site and as a proportion of total Candida isolates is shown in Table I. We recov- ered a total of eight isolates of C. parapsilosis from the five different patients. The organism was most frequently isolated from the oropharynx and stool. No patient had positive blood cultures. All five pa- tients had negative initial cultures and grew colonies of C. parapsilosis only after admiiion to the study unit (Table II). Two patients were located in the BMT unit, and three patients were located in ICU2 (Figure 1). Initial sites of colonization in patients who acquired the C. parapsiZosis colonies while the in hospital were as follows: the rectum in two patients, the oropharynx in two patients (one patient also had vaginal colonization), and a sternal wound in one pa- tient. There were no clinical infections or deaths relat- ed to C. parapsilosis. Three patients had C. parapsi- Zosis isolated just prior to discharge, and no repeat
Patient and control demographic and risk factors are summa&ed in Table III. The mean duration of hospit&ation, the duration in the study unit, and the duration of antibiotic therapy prior to the isola- tion of C. parapsilosis were significantly longer for patients than for control subjects. Antibiotic duration and duration in the study unit were not independent- ly associated with C. parapsilosis. There were no differences between patients and controls with regard to prior antibiotic type admmistered, severity of ill- ness, antifungal use or duration, immunosuppressive use or duration, catheter use or duration, underlying illness, or the presence, severity, or duration of granulocytopenia.
Six hand cultures from four hoepital staff were pos- itive for C. parapsilosis. Colonies of C. parapsilosis were found on two environmental surfaces cultured in ICUS. The environmental surfaces that were found to contain C. parapsilosis were those that were fre- quently touched by hospital personnel or in open con-
June 1993 The Americen Journal of Medlclne Volume 94 579
NOSOCOMIAL CANDIDA PARAPSILOSIS / SANCHEZ ET AL
BMTUJ
14
2
16
2l
22
23
24
Figure 1. Schematic floor plan of the medical intensive care unit (ICU2) and bone marrow transplant (EMT) unit. H = pa- tient with acquisition of C. parapsilosis in the unit; * = posi- tive environmental culture for C. parapsilosis; ** = hand cul- ture positive for C. parapsilosis. Numbers 1 to 24 and 25 to 34 denote patient room numbers.
tact with patients. Colonies of C. parapsilosis were cultured from a sink and from an air-conditioning vent in the ICU. These isolates were obtained before patients were moved into the new ICU. A patient hospitalized in the room where C. parapsilosis was cultured from the air-conditioning vent had negative initial cultures but later had an identical strain of C. parapsilosis first cultured from a sternal wound. There was no common source (vehicle) identified.
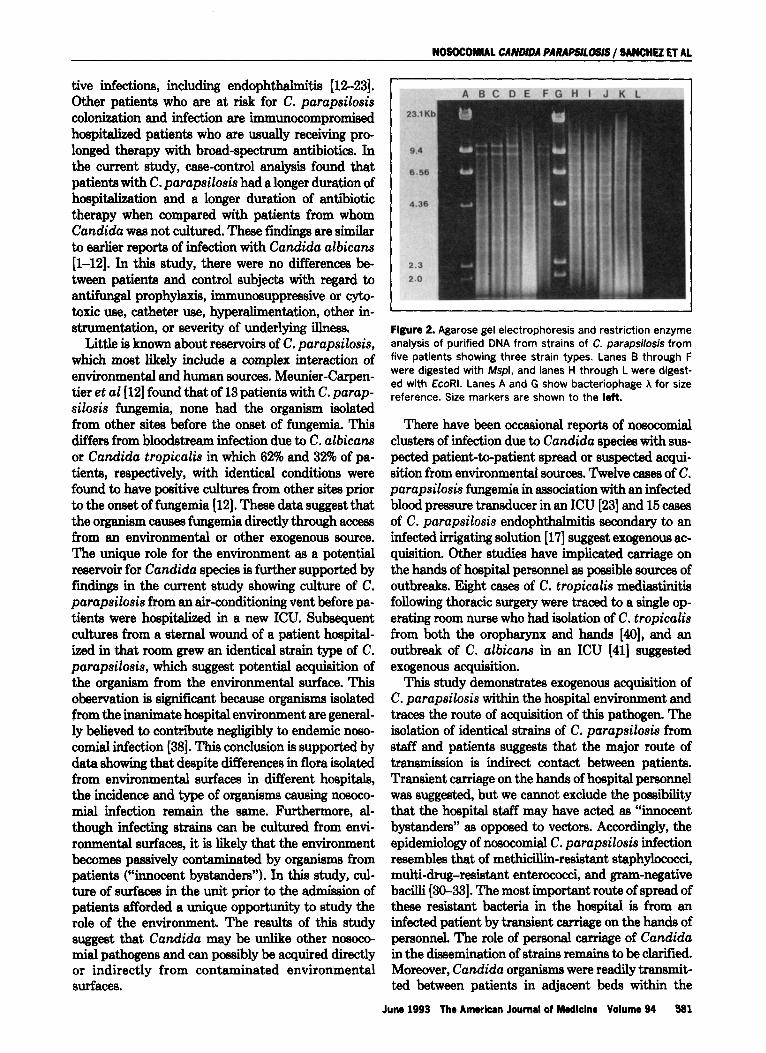
All C. parapsilosis isolates were evaluated by REA. There were eight isolates from five patients, six hand cultures from four hospital staff, two environ- mental isolates, six control strains, and one ATCC strain. REA revealed a total of 3 different restriction enzyme patterns (strain types) among the 23 strains examined. One strain type was identical in four pa- tients (three in ICU2), three staff (two nurses and one respiratory therapist), and two environmental sur- faces (sink and air vent in ICUB) (Figure 2). The isolates from the remaining patient, staff, and control
580 June 1993 The Amerfcan Journal of Medlclne Volume 94
TABLE III
Patient and Control Demographic and Risk Factor Characteristics
ZZ” Range
Sex (F/M)
Duration in unit(d) Mean Range
Prior antibiotics
Duration antibiotics (d) Median Range
Prior antiiungal therapy (topical or systemic)
Patients Controls (n = 5) (n = 15) V&e
38.4 47.2 1965 25-88
4/l 817
30.1 16.1 p = 0.048 11-51 3-41
5 13
32.8 11.8 p = 0.05 11-45 o-61
1 7
Immunosuppressive therapy 2 6
Granulocytopania 2 4
Underlying illness Cardiac disease Neurologic disease : 2” Hematologic Malignancy 2 7 Other - 2
strains, were separate strain types having unique re- striction fragment patterns. Evaluation of isolates colonizing different body sites within an individual patient showed that this patient was colonized with two strain types of C. parapsilosis in the oropharynx. One of the pharyngeal strain types was the same as that cultured from the vaginal specimen of the same patient.
COMMENTS C. parapsilosis is an infrequent opportunistic
pathogen but is of special interest because of its abili- ty to infect seriously ill hospitalized patients. C. par- apsilosis does not appear to be a commensal organ- ism. Isolates of C. parapsilosis have been recovered from urine, oropharynx, and stool of hospitalized pa- tients [l-21]. Dick et al [S] found C. parapsilosis to be an infrequent isolate representing 4% of yeast iso- lates recovered from oncology patients at the Johns Hopkins Hospital. Bloodstream infection due to C. parapsilosis is not uncommon and has been identi- fied in up to 28% of all fungemias [13]. C. parapsilosis appears to be tiquely related to intravascular cathe- ter infection. Extravascular infection and invasive candidiasis are uncommon.
Serious infections due to C. parapsilosis have been described among intravenous drug users, recipients of parental nutrition solutions, persons with intravascu- lar blood pressure monitoring transducer devices, and hemodialysis recipients, and are a cause of postopera-
NOSOCOMML CANDIDA PARAPSJLOSJS / SANCHEZ ET AL
tive infections, including endophthahnitis [12-231. Other patients who are at risk for C. parupsilosis colonization and infection are immunocompromised hospitalized patients who are usually receiving pro- longed therapy with broad-spectrum antibiotics. In the current study, case-control analysis found that patients with C. parupsilosis had a longer duration of hospital&ion and a longer duration of antibiotic therapy when compared with patients from whom Candidu was not cultured. These findings are similar to earlier reports of infection with Candida albicans [l-12]. In this study, there were no differences be- tween patients and control subjects with regard to antifungal prophylaxis, immunosuppressive or cyto- toxic use, catheter use, hyperalimentation, other in- strumentation, or severity of underlying ilhress.
Little is known about reservoirs of C. parapsilosis, which most likely include a complex interaction of environmental and human sources. Meunier-Carpen- tier et al [12] found that of 13 patients with C. parap- silosis fungeti, none had the organism isolated from other sit.ee before the onset of fungemia. This differs from bloodstream infection due to C. albicans or Candida tropicalis in which 62% and 3% of pa- tients, respectively, with identical conditions were found to have positive cultures from other sites prior to the onset of fungemia [12]. These data suggest that the organism causes fungemia directly through access from an environmental or other exogenous source. The unique role for the environment as a potential reservoir for Candida species is further supported by fmdings in the current study showing culture of C. parupsilosis from an air-conditioning vent before pa- tients were hospitalized in a new ICU. Subsequent cultures from a sternal wound of a patient hospital- ised in that room grew an identical strain type of C. parupsilosis, which suggest potential acquisition of the organism from the environmental surface. This observation is significant because organisms isolated from the inanimate hospital environment are general- ly believed to contribute negligibly to endemic noso- comial infection [38]. This conclusion is supported by data showing that despite differences in flora isolated from environmental surfaces in different hospitals, the incidence and type of organisms causing nosoco- mial infection remain the same. Furthermore, al- though infecting strains can be cultured from envi- ronmental surfaces, it is likely that the environment becomes passively contaminated by organisms from patients (%mocent bystanders”). In this study, cul- ture of surfaces in the unit prior to the admission of patients afforded a unique opportunity to study the role of the environment. The results of this study suggest that Candida may be unlike other nosoco- mial pathogens and can possibly be acquired directly or indirectly from contaminated environmental surfaces.
Flgure 2. Agarose gel electrophoresis and restriction enzyme analysis of purified DNA from strains of C. parapsilosis from five patients showing three strain types. Lanes B through F were digested with Mspl, and lanes l-l through L were digest- ed with EcoRI. Lanes A and G show bacteriophage X for size reference. Size markers are shown to the left.
There have been occasional reports of nosocomial clusters of infection due to Candida species with sus- petted patient-to-patient spread or suspected acqui- sition from environmental sources. Y&velve cases of C. parapsilosis fungemia in association with an infected blood pressure transducer in an ICU [23] and 15 cases of C. parapsilosis endophthalmitis secondary to an infected irrigating solution [17] suggest exogenous ac- quisition. Other studies have implicated carriage on the hands of hospital personnel as possible sources of outbreaks. Eight cases of C. tropicalis mediastinitis following thoracic surgery were traced to a single op- erating room nurse who had isolation of C. tropicalis from both the oropharynx and hands [40], and an outbreak of C. albicans in an ICU [41] suggested exogenous acquisition.
This study demonstrates exogenous acquisition of C. parapsilosis within the hospital environment and traces the route of acquisition of this pathogen. The isolation of identical strains of C. parapsilosis from staff and patients suggests that the major route of trensmission is indirect contact between patients. Transient carriage on the hands of hospital personnel was suggested, but we cannot exclude the possibility that the hospital staff may have acted ss “innocent bystanders” as opposed to vectors. Accordingly, the epidemiology of nosocomial C. parapsilosis infection resembles that of methicillin-resistant staphylococci, multi-drug-resistant enterococci, and gram-negative bacilli [30-331. The most important route of spread of these resistant bacteria in the hospital is from an infected patient by transient carriage on the hands of personnel. The role of personal carriage of Candida in the dissemination of strains remains to be clarified. Moreover, Candida organisms were readily transmit- ted between patients in adjacent beds within the
June 1993 The Amerlun Journal of Medlclne Volume 94 581

NOSOCOMIAL CANDIDA PARAPSllDSIS/ SANCHEZ ET AL
ICUs. Proximity to a patient with infection or coloni- zation increased the risk of acquisition of Candida. The source (reservoir) of C. parapsilosis is probably the respiratory tract, gastrointestinal tract, or genito- urinary tract of colonized patients. Although no de% nite symptomatic infections occurred in the patients who became colonized in this study, the ability of C. parapsilosis to cause serious infection in hospitalized patients has been amply demonstrated in other stud- ies [B-23].
The epidemiology of nosocomial C. parapsilosis infection is complex. Potential hospital reservoirs -in- clude colonized patients, hospital personnel, and the inanimate hospital environment. The mechanism of acquisition of C. parapsilosis in our patients remains uncertain; however, indirect contact transmission is most likely. A potential role for the environment as a source for Candida cannot be excluded. Our findings demonstrate that nosocomial C. parapsilosis coloni- zation is a result of the exogenous acquisition of strains. The potential for dissemination of C. parap- silosis in hospitalized patients is disturbing. Further prospective studies are needed to more accurately define patient and hospital reservoirs of infection, as well as the mode of transfer and measures for pre- venting spread.
REFERENCES 1. Bodey GP. Candkiiiis in cancer patients. Am J Med 1984: 77(Suppl4D): 13-9.
2. Horn R. Wong B. Kiehn TE, Armstrong D. Fungemia in a wnwr hospital: changing
frequency, earlier onset, and resuits of therapy. Rev Infect Dis 1985; 7: 646-55.
3. Gains JO. Remington JS. Disseminated candid&is in the surgical patient. Sur-
gery 1972; 72: 730-6.
4. Klein JJ, Watanakunakorn C. Hospital acquired fungemia. Its natural course and
clinical signiinw. Am J Med 1979; 67: 51-8.
5. Sobet JD. Vazquez J. Candidemia and systemic wndkfiasis. Semin Respir Infect
1990; 5: 123-37.
6. Dick JD. Merz WG, Sara1 R. Incidence of polyene-resistant yeasts recovered from
diniwl specimens. Antimicrob Agents Chemother 1980; 158-63.
7. Bross J, Talbot GM, Maislin G, Hurwitz S, Strom BL. Risk factors for nosocomial
wndiiemia: a case-control study in adults without leukemia. Am J Med 87: 614-20.
8. Burnie JP. Matthews R, Lee W, Philpott-Howard J, Brown R. Four outbreaks of
nosocomial systemic wndidiasis. Epiwmiol Infect 1987; 99: 201-11.
9. Vaudry WL, Tiemey Al. Wenman WM. Investigation of duster of systemic Candk
da ahiwns infections in a neonatal intensive care unit. J Infect Dis 1988; 158:
1375-9.
10. Wey SB, Motomi M, Pfaller MA, Woolson RF, Wenzel RP. Hospital-acquired
wndkfemia: the attributable mortality and excess length of stay. Arch Intern Med
1988; 148: 2642-7.
11. Wey SB. Motomi M, Pfaller MA. Woolson RF. Wenzel RP. Risk factors for
hospital-acquired wndkfemia: a matched wsecontrol study. Arch Intern Mad
1989; 149 2349-53.
12. Meunier-Carpantier F, Kiehn TE, Armstrong D. Fungemia in the compromised
host. Am J Med 1981; 71: 353-70.
13. Mayer AR, Brown A, Weintraub RA. Ragni M, Postic B. Successful medical
therapy for endowrditis due to Candida parapsiosis. Chest 1978: 73: 546-9.
14. D’Day DM, Head WS, Robinson RD. An outbreak of Candida parapsilosis en-
dophthalmitis; analysis of strains by enzyme profile and antifungal suswptibilii. Br
J Ophthalmol 1987; 71: 126-9.
15. DeClerck L. Dequeker J, Westhovens R, HaJustaine D. Candida parapsiosis
in a patient receiving chronic hemodialysis. J Rheumatol 1988; 15: 72-4.
16. McCray E. Rampell N. Solomon SL, Bond WN, Martone WJ, D’Day D. Outbreak
of Candida parapsihsis endophthalmitis after cataract extraction and intraocular
lens implantation. J Clin Microbial 1986; 24: 625-8.
17. Stern WH, Tamura E, Jacobs RA, eta/. Epidemic postsurgiwl Candidaparapsk
losis endophthalmitis. Clinical findings and management of 15 consecutive wses.
Ophthalmology 1985; 92: 1701-g.
18. Law EJ, Holder IA, MacMillian BG. Candida parapsilosis fungemia in burn
patients: report of three cases. Burns, Including Thermal Injury 1984; 10: X3-6.
19. Solomon SL. Khabbaz RF, Parker RH, Anderson RL, Geraghty MA. An outbreak
of Candida parapsiloss bloodstream infections in patients receiving parenteral
nutrition. J Infect Dis 1984; 149 98-102.
20. Younkin S, Evarts CM, SteigMgel RT. Candida parapsilosis infection of a total
hip-joint replacement: successful reimplantation after treatment with amphoteridn
B and 5fluorocytosine. A case report. J Bone Joint Surg [Am] 1984; 66: 142-3.
21. Faix FIG. Candida parapsilosis meningitis in a premature infant. Pediatr Infect
Dis 1983; 2: 462-4
22. Walter B. Nolte J, Kappe R, Muller J. Relapsing fur-gal septicemia caused by
Candidaparapsilosisfollowing staphylcwccal septicemia. Mycoses 1988; Suppl 1:
54-B.
23. Weems JJ, Chamberland ME, Ward J. Wtlly M, Padnye AA, Solomon SL. Candi
da parapsilosis fungemia associated with parenteral nutrition and contaminated
blood pressure transducers. J Clin Microbial 1987; 25: 1029-32.
24. Kaufmann CS, Merz WG. Electrophoretic karyotypes of Torulopsisglabrata. J
Clin Microbiil 1989; 27: 2165-8.
25. Matthews R, Bumie J. Assessment of DNA fingerprinting for rapid identiiwtion
of outbreaks of systemic wndidiasis. BMJ 1989; 298: 354-7.
26. Merz WG, Conneliy C, Hieter P. Variation of electrophoretic karyotypes among
clinical isolates of Candida albicans. J Clin Microbial 1988; 26: 842-5.
27. Stevens DA, Odds FC. Scherer S. Applications of DNA typing methods to
Candida albicans epidemiology and correlations With phenotype. Rev Infect Dis
1990: 12: 25866.
28. Su CS, Meyer SA. Restriction endonudease analysis of mitochondrial DNA from
Candida parapsilosis and other Candida species. Yeast 1989; 5: S355-60.
29. Schlitzer RL, Ahearn DG. Characterization of a typical Candida tropicais and
other uncommon clinical yeast isolates. J Clin Microbial 1982; 15: 51 l-6.
3O.Zervos MJ, Dembinski S, Mikesell T, Schaberg DR. High-level resistance to
gentamicin in Streptococcus faecak risk factors and evkienw for exogenous
acquisition of infection. J Infect Dis 1986; 153: 1075-82.
31. Farrar WE Jr. Molecular analysts of plasmids in epkiemiologiwl investigation. J
Infect Dis 1983: 148: l-6.
32. Schaberg DR. Tompkins LS, Falkow S. Use of agarose gel electrophoresis of
plasmid deoxyribonucleic acid to finger print gramnegative bacilli. J Clin Miaobiol
1981; 13: 1105-8.
33. McGowan JE Jr, Terry PM, Huang T Sr. Houk CL, Davies J. Nosocomial infec-
tions with gentamicin resistant Staphylococcus aureus: plasmid analysis as an
epidemiologic tool. J Infect Dis 1979: 140 86472.
34. Vazquez JA, Bed&y A, Sot& JD, Zervos MJ. Comparison of restriction enzyme
analysts versus pulsed-field gradient gel electrophoresis as a typing system for
Candida albicans. J Clin Microbial 1991; 291 962-7.
35. Fox BC, Mobley HLT, Wade JC. The use of a DNA probe for epidamiologiwl
studies of wndidiasis in immunocompromised hosts. J Infect Dis 1989; 159
488-94.
36. McCabe WR. Jackson GG. Gram-negative bacteremia. I. Etiology and ecology.
Arch Intern Med 1962: 110: 847-55.
37. Petes TD, Hereford LM, Skryabin K. Characterization of two types of yeast
ribosomal DNA genes. J Bacterial 1978; 134: 295-x)5.
38. Torres-Bauza U, Riggsby WS. Protoplasts from yeast and mycelial forms of
Candida albiwns. J Gen Microbial 1980; 119: 341-9.
39. Maki DG, Alvarado CJ, Hassemr CA, Zi!z MA. Relation of the inanimate hospital
environment to endemic nosocomial infection, N Engi J Med 1982: 307: 15626.
40. lsenberg HD, Tucoi V. Cintron F, Singer C, Weinstein GS, Tyras DH. Singie
source outbreak of Candida fropicaliscompliwting coronary bypass surgery. J Clin
Microbial 1989; 27: 2426-B.
41. Bumie JP, Odds FC. Lee W, Webster C, Williams JD. Outbreak of systemic
Candida albicans in an intensive care unit caused by cross infection. BMJ 1985;
290 746-8.
582 June 1993 The American Journal of Medicine Volume 94
Copyright © 2022 FDOKUMEN


![[Reducing the incidence of ventilator-associated pneumonia following heart surgery: 13-year experience of epidemiologic surveillance in a teaching hospital]](https://static.fdokumen.com/doc/165x107/633733ca9c13609c6c0ee513/reducing-the-incidence-of-ventilator-associated-pneumonia-following-heart-surgery.jpg)

















