
Noninvasive Remote Sensing Techniques for Infrastructures Diagnostics
Catheterization and Cardiovascular Diagnosis 9:55-62 (1983)
Noninvasive Evaluation of a Left Ventricular Pseudoaneurysm: Complementary Role of Echocardiographic and Nuclear Techniques
Michael J. Ptacin, MD, Virinderjit S. Bamrah, MD,
Lee S. Wann, MD, Gordon N. Olinger, MD, and Rajinder Singh, MD
This 45-year-old white male was evaluated for congestive heart failure initially ascribed to a rapidly progressive cardiomyopathy. Both radionuciide ventricuiography and echocardiography correctly identified a left ventricular pseudoaneurysm as the cause for heart failure. Thallium-201 scintigraphy, by demonstrating a large perfusion defect, suggested a large ostium of the pseudoaneurysm. Following resection of the false aneurysm, a Dacron prosthesis was required to close a large posterior wail defect. We conclude that both radionuciide ventricuiography and echocardiography can in- dependently demonstrate a ieR ventricular pseudoaneurysm. The combined nonin- vasive approach is able to delineate various anatomical aspects of the pseudoaneu- rysm and help in planning adequate surgical intervention.
Key words: radionuclide ventricuiography, pseudoaneurysm, two-dimensional echocardiog- raPhY
INTRODUCTION
Cardiac rupture continues to be a frequent complication of acute myocardial infarction and can be seen in as many as 10% of fatal infarctions [ 11. Although rupture of the free wall of the left ventricle is universally fatal, certain forms of heart rupture are amenable to surgical correction. Surgical repair of ruptured or dysfunctioning papillary muscle, acquired ventricular septa1 defect, and ventricular pseudoaneurysm have been reported [2,31.
Although several etiologies for pseudoaneurysm of the left ventricle have been reported, acute myocardial infarction and cardiac surgical procedures continue to be the most
From the Veterans Administration Medical Center, Wood (Milwaukee), The Medical College of Wisconsin, Milwaukee, and Veterans Administration Medical Center, North Chicago, Illinois.
Address reprint requests to Dr. Michael J . Ptacin. Cardiovascular Sectionil I IM. Veterans Administration Medical Center. Wood. WI 53193.
Received June 10, 1982; revision accepted September 4, 1982.
0098-6569/83/0901-0055$02.50 0 1983 Alan R. Liss, Inc.
56 Ptacin et al
common causes. Until recently, only contrast left ventriculography could accurately demonstrate pseudoaneurysm formation. Recent reports, however, have shown two-di- mensional echocardiography and radionuclide ventriculography to be useful tools in eval- uating pseudoaneurysms.
Described below is a patient evaluated at our institution for congestive heart failure initially thought to be the basis of a rapidly progressive cardiomyopathy . Subsequently, noninvasive studies demonstrated a left ventricular pseudoaneurysm as the cause of heart failure. The false aneurysm was successfully resected, and the resultant large defect in the left ventricular wall was closed with a Dacron prosthesis.
CASE REPORT
A 45-year-old white male (R.P.V.) was seen at the Wood Veterans Administration Medical Center (VAMC) in April, 1980, for evaluation of dyspnea and cardiomegaly. Prior to this admission the patient was evaluated in May 1979, for chest discomfort at North Chicago VAMC. Multiple examiners at that institution did not feel that the chest pain was of an ischemic origin. Electrocardiogram (EKG) on that admission was not suggestive of ischemia. Chest X ray showed severe cardiomegaly and pulmonary vascular redistribution. Review of past chest X rays showed this to be a new finding since 1977. Two-dimensional echocardiography demonstrated a large diffusely hypokinetic left ven- tricle with a posterior pericardial effusion. A perfusion lung scan was suggestive of a pulmonary embolus, and heparin was administered for seven days without angiographic documentation of pulmonary embolism. The poor left ventricular function was ascribed to cardiomyopathy of unknown etiology.
In the 6 months prior to admission to the Wood VAMC, the patient developed worsening exertional dyspnea. He showed only mild improvement after the initiation of digoxin (0.25 mg) and furosemide (40 mg) daily. He did not complain of further chest discomfort. He was again reevaluated at the North Chicago VAMC where a two-dimensional echo- cardiogram was suggestive of a posterior pseudoaneurysm. The patient was transferred to Wood VAMC for further evaluation and management.
Physical examination on admission revealed a well-developed, well-nourished white male in no apparent distress. The blood pressure was 120/80. The pulse was 80 and regular. The carotid upstrokes were brisk and of normal volume. The apex had a heaving quality and was palpable in the sixth intercostal space in the anterior axillary line. The first heart sound was soft, the second split normally. There was no third heart sound. A grade 3/6 holosystolic murmur was heard at the apex and radiated to the axilla. No thrill was noted. The lung fields were tympanic to percussion and clear to auscultation. No hepatosplenomegaly was noted. No peripheral edema was present.
An EKG revealed a normal sinus rhythm, normal axis, left atrial enlargement, and inverted T waves in the inferolateral leads.
A chest X ray showed severe cardiomegaly suggestive of biventrical enlargement, prominent posterior bulging of the cardiac silhouette, and pulmonary vascular redistri- bution.
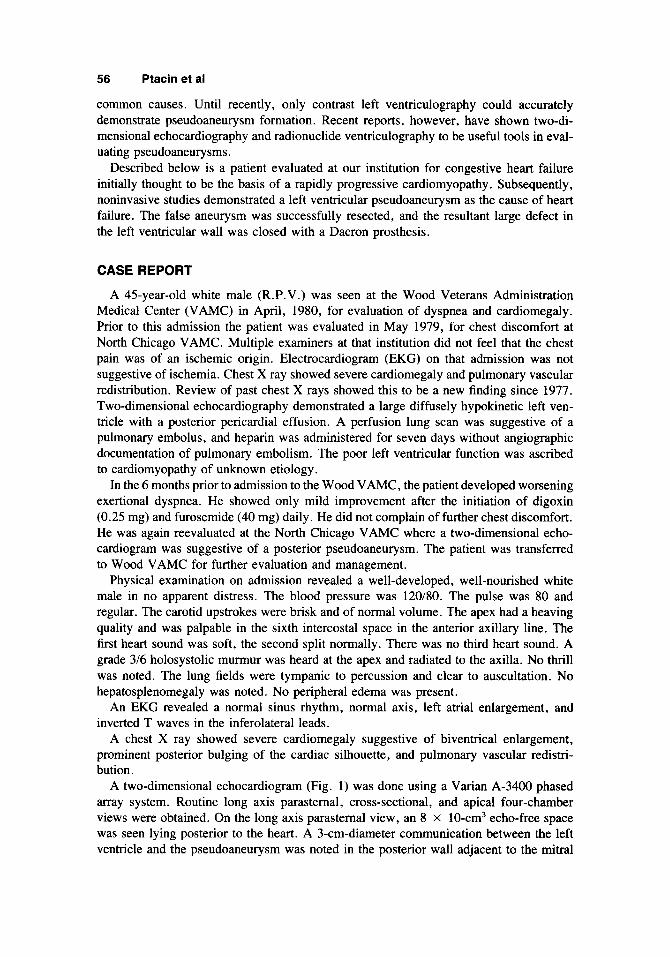
A two-dimensional echocardiogram (Fig. 1) was done using a Varian A-3400 phased array system. Routine long axis parastemal, cross-sectional, and apical four-chamber views were obtained. On the long axis parastemal view, an 8 x 10-cm3 echo-free space was seen lying posterior to the heart. A 3-cm-diameter communication between the left ventricle and the pseudoaneurysm was noted in the posterior wall adjacent to the mitral

Left Ventricular Pseudoaneurysm 57
Fig. 1. Two-dimensional sector scan in the long axis parasternal view showing a retrocardiac PSA chamber filled with clot and connected to the LV cavity through a relatively narrow ostium. (LV = left ventricle; LA = left atrium; PSA = pseudoaneurysm; Ao = aorta).
valve. Echo-dense material consistent with thrombus lined the pseudoaneurysm and in places protruded into the cavity. The remainder of the left ventricle appeared normal.
Radionuclide ventriculography , using 25 mCi of technetium-99m pertechnitate with in vivo red cell labeling, was canied out in the standard anterior and 45" left anterior oblique views. Imaging was performed with a Searle L.E.M. gamma camera and processed with Medical Data Systems computer. In the 45" left anterior oblique projection, a large noncontracting chamber was seen posterior to the left ventricle. Communication between the left ventricle and pseudoaneurysm appeared to involve much of the posterior wall of the left ventricle. The true left ventricular cavity appeared to have normal dimensions and wall motion (Fig. 2).
A resting thallium-20 1 perfusion scintigram demonstrated a large posterior defect that was in the area of communication between the left ventricle and the pseudoaneurysm (Fig. 3). This suggested that the defect in the posterior wall was extensive and probably larger than that seen on two-dimensional echocardiogram.
The patient underwent cardiac catheterization on April 15, 1980. Hemodynamics (Table I) showed mild elevation of the right atrial pressure. There was moderate pulmonary arterial and venous hypertension. There was no significant "V" wave noted in the pul- monary artery wedge tracing. The left ventricular end diastolic pressure was markedly elevated. Forward flow was normal by the cardiogreen dilution method.
Biplane left ventriculography demonstrated a large pseudoaneurysm posteriorly. The ostium of the aneurysm was located in the posterolateral segment and was large in diameter. The other segments of the left ventricle displayed normal wall motion (Fig. 4).
Coronary angiography revealed a dominant right system, which was normal. The left main and left anterior descending vessels were normal. The circumflex was occluded in its distal portion after the origin of a small third marginal vessel.
Since the patient's heart failure was considered to be on the basis of the pseudoaneu- rysm, surgical intervention was recommended. At surgery, gross inspection showed dense adhesions between the pseudoaneurysm and the left lung. After placing the patient on cardiopulmonary bypass, the cavity of the pseudoaneurysm was entered. Necrotic tissue and clot were found lining the attenuated wall of the pseudoaneurysm. Following de-

58 Ptacin et al
Flg. 2. End dlastollc (ED) and end systollc (ES) frames of radlonucllde ventrlculogram In 45" left anterlor obllque view. A large posterolateral pseudoaneurysm (PSA) communlcatlng with left ventricle (LV) through a large ostlum Is seen. Left ventricular wall motlon other than the posterolateral segment Is normal.
Fig. 3. Thallium-201 (Tl-201) myocardial perfusion scintigraphy in 45" left anterior oblique view showing a large and dense perfusion defect in the posterolateral segment of left ventricle (LV). Note the complete absence of T1-201 activity in an area corresponding to the pseudoaneurysm.

Left Ventricular Pseudoaneurysm 59
TABLE 1. Pre- and Postoperatlve Hemodynamlc Results
CI A-V 0 2 (liters
RA PA PAW LV A 0 difference /mid SI ( m H g ) ( m H g ) ( m H g ) ( m H g ) ( m H g ) (ml%) m2) (ml) LVEFRN
95 95 3.4 3.1 34 0.43 - - - 56 - - Preoperative 8 28 38 28 32 64 78
51 - - 91 - 85 5.0 3.1 34 0.36 - - Postoperative 11 20 Tl 18 21 52 67
RA, right atrium; PA, pulmonary artery; PAW, pulmonary artery wedge; LV, left ventricle; Ao, aorta; A-V 0 2 difference, arteriovenous oxygen difference; CI, cardiac index; SI, stroke index; LVEFw, radionuclide left ventricular ejection fraction (pseudoaneurysm not included in the calculation of ejection fraction).
Flg. 4. Contrast left ventrlculogram In 60" left anterlor obllque vlew showlng a large retrocardlac pseudoaneurysm connected through a large ostlum (A0 = aorta; LV = left ventricle; PSA = pseudoaneurysm).
bridement, the communication between the left ventricle and pseudoaneurysm was found to be 8 x 10 cm2 in size. Primary closure of the defect could not be undertaken, as it would have excessively diminished left ventricular cavity size. Instead, an oval Dacron prosthesis was preclotted and incorporated into the posterior wall.
Microscopic examination showed the aneurysmal sac to be composed of dense fibrous tissue. No myocardial cells were noted in the numerous sections of the aneurysm wall.
Cardiac catheterization was repeated postoperatively. The left ventricular end diastolic pressure was moderately elevated (Table I). Left ventricular angiography showed slight

60 Ptacin et al
dilatation in the area of the patch. The remaining segments of the left ventricle showed slightly decreased systolic contraction as compared to the preoperative study (Fig. 5).
Postoperative radionuclide ventriculograph demonstrated the posterolateral segment to be akinetic and aneurysmal, although much less than in the previous study (Fig. 5). Repeat two-dimensional echocardiography showed a sizeable area of akinesis and dy- skinesis in the posterior wall. The patient was placed on digoxin and furosemide. He was discharged and continues to do well one year postoperatively with minimal functional impairment.
DISCUSSION
Pseudoaneurysm of the left ventricle is a form of cardiac rupture that is contained by the pericardium or extracardiac tissue and freely communicates with the left ventricle. Pseudoaneurysms of the left ventricle have several etiologies, the most common being acute myocardial infarction and past open heart surgery [4]. Unlike true aneurysms of the left ventricle, pseudoaneurysms tend to enlarge progressively and are associated with a high incidence of rupture within the first year of their discovery [5,6]. The propensity for rupture has made early evaluation and surgical correction a necessity in this entity
In the past, contrast left ventriculography was the only definitive means of identifying pseudoaneurysm. Angiographic evidence of a chamber filling from the left ventricle through a narrow ostium has been considered a classic criterion for left ventricular pseudoaneurysms. A chamber adjacent to the lateral or posterior wall of the heart is felt to be more compatible with a pseudoaneurysm than a true aneurysm. Coronary angiog- raphy has also proved helpful. The wall of a pseudoaneurysm is not composed of myo- cardial elements. The pseudoaneurysm then is not traversed by the coronary arteries. On the other hand, the coronary arteries in true aneurysm can be seen to follow a nondisplaced path over the effected segment of the left ventricle.
~ 3 1 .
Fig. 5. (Left panel) Postoperatlve end systolic (ES) frame of radlonucllde ventrlculogram In 45" left anterlor oblique vlew showing a posterlorly bulglng left ventrlcle (LV) segment corm spondlng to the Dacron patch. (Right panel) Postoperatlve ES frame of contrast left ventrlcu- logram showing a Dacron patch (RV = rlght Ventricle; Ao = aorta).

Left Ventricular Pseudoaneurysm 61
As demonstrated by the present case, radionuclide ventriculography and echocardiog- raphy represent a significant advance for detecting left ventricular pseudoaneurysm. The typical features shown by these techniques consist of a left ventricle and pseudoaneurysm chamber lying adjacent to each other and communicating through a narrow ostium [8,9]. On occasion, dyskinetic motion of the pseudoaneurysm may be visualized by these techniques [ 10,111. The first pass radionuclide angiocardiography is of considerable diagnostic importance in this entity. Since the narrow ostium between the left ventricle and the pseudoaneurysm may impede a rapid mixing of their contents, late filling of the pseudoaneurysm on first pass study is highly suggestive of a pseudoaneurysm [ 121.
Assessment of the relative size of the pseudoaneurysm is more easily undertaken with radionuclide ventriculography . This is frequently difficult on contrast ventriculography , as well as on two-dimensional echocardiography, because it is difficult to include the left ventricle and the pseudoaneurysm in the same frame simultanewsly. In the present case, radionuclide ventriculography suggested a relatively large ostium of the pseudoaneurysm. Resting thallium-201 scintigraphy was employed to assess the orifice size in the posterior lateral wall. A striking cutoff in myocardial activity was seen posteriorly and was far more pronounced than usually seen in an uncomplicated posterior infarct. We attributed this to a large orifice between the left ventricle and pseudoaneurysm. Further, the lack of usual lung background posterior to the heart suggests an avascular area, which at the time of surgery corresponded to a large clot [ 131.
The use of echocardiography has been previously reported for detecting left ventricular pseudoaneurysms [ 14-20]. Suggestive echocardiographic features include: (1) sharp dis- continuity of the endocardia1 image at the site of communication between the pseudo- aneurysm and the left ventricle; (2) saccular or globular contour of the false aneurysm; and (3) presence of a relatively narrow orifice compared to the diameter of the pseudo- aneurysm [20]. Quantitative methods of looking at maximal aneurysm diameter to its orifice diameter have been developed. If the ratio of the orifice opening to the maximal diameter of the aneurysm is less than 0.5, a pseudoaneurysm is suspected. Although in our case this relationship was found, the two-dimensional echocardiography study under- estimated the size of the pseudoaneurysm orifice. The problem of adequately evaluating the orifice size has been commented on by previous authors [19,20]. Numerous views of the orifice are required to evaluate its dimension adequately.
The adequate preoperative delineation of orifice size can be helpful in determining the surgical approach. If the orifice size is thought to be small (as is usually the case), surgical resection of the pseudoaneurysm and primary closure of the orifice are the procedures of choice. In the present case, the communication was unusually large, requiring aneurys- mectomy and patch repair of the posterior wall. This large orifice may have reflected a molding process of the infarcted posterior wall with time. Preoperative evaluation of a pseudoaneurysm may benefit from all three previously described noninvasive procedures, which permit adequate assessment of the total extent of the aneurysm, orifice size, presence, and extent of clot. These three noninvasive techniques were clearly comple- mentary in this case.
The clinical presentation in this case was unusual. The clinical diagnosis of acute myocardial infarction was overlooked due to the absence of typical chest pain and EKG findings. Rather, the patient was diagnosed as having a pulmonary embolism on the basis of pleuorpericardial chest pain and suggestive lung scan. .Another interesting aspect of this case was the limited nature of his coronary artery disease. He showed distal left circumflex occlusion. Most cases of left ventricular pseudoaneurysm reported in the literature had more proximal and multivessel coronary artery disease.

62 Ptacin et al
SUMMARY
An unusual case of pseudoaneurysm of the left ventricle is presented with atypical clinical findings and single vessel coronary artery disease. A diagnosis of pseudoaneurysm was made in the absence of clinical features pointing to this. Although a diagnosis of pseudoaneurysm was made independently by nuclear and echocardiographic means, these noninvasive tests proved complementary to one another in devising the surgical approach.
REFERENCES
1. Bates RJ, Beutler S , Resnekov L, Anagnostopoulos CE: Cardiac rupture-challenge in diagnosis and
2. Harper RW, Sloman G, Westlake G: Successful surgical resection of a chronic false aneurysm of the left
3. Gueron M, Wanderman KL, Hirsch M, Borman J: Pseudoaneurysm of the left ventricle after myocardial
4. Higgins CB, Lipton M, Johnson A, et al: False aneurysms of the left ventricle. Radiology 127:21, 1978. 5 . Vlodaver F, Coe J, Edwards JE: True and false aneurysms of the left ventricle propensity for the latter to
6. VanTAssel RA, Edwards J: Rupture of heart complicating myocardial infarction. Analysis of 40 cases
7. Spindola-Franc0 H, Kronacher N: Psuedoaneurysm of the left ventricle. Radiology 127:29, 1978. 8. Onik G, Recht L, Edwards JE, et al: False left ventricular aneurysm: diagnosis by noninvasive means. J
9. Sweet S, Sterline R, McCormick J, et al: Left ventricular false aneurysm after coronary artery bypass
management. Am J Cardiol 40:429, 1977.
ventricle. Chest 67:359, 1975.
infarction. A curable form of myocardial rupture. J Thorac Cardiovasc Surg 69(5):736, 1975.
rupture. Circulation 51567, 1975.
including nine examples of left ventricular false aneurysm. Chest 61(2):104, 1972.
Nucl Med 21:177, 1980.
surgery: radionuclide diagnosis and surgical resection. Am J Cardiol 43: 154, 1979. 10. Perkins P: Radioisotopic diagnosis of false left ventricular aneurysm. Am J Radiol 132:l 17. 1979. 11. Botvinick E, Shames D, Hutchinson J, et al: Noninvasive diagnosis of a false left ventricular aneurysm
with radioisotope gated blood pool imaging: differentiation from true aneurysm. Am J Cardiol 37:1089, 1976.
12. Dymond D, Elliott AT, Banim S: Detection of a false left ventricular aneurysm by first pass radionuclide ventriculography. J Nucl Med 202351, 1979.
13. Winzelberg G. Miller SW, Okada RD. et al: Scintigraphic assessment of false left ventricular aneurysms. Am J Radiol 135:569. 1980.
14. Grube E, Redel D, Janson R: Noninvasive diagnosis of a false left ventricular aneurysm by echocardiography and pulsed Doppler echocardiography. Br Heart J 43:232, 1980.
15. Davidson KH, Parisi AF, Harrington J, et al: Pseudoaneurysm of the left ventricle: an unusual echocar- diographic presentation. AM Intern Med 86:430, 1977.
16. Van Mechelen R, Van Henel N, Vanrigh PP: Noninvasive diagnosis of pseudoaneurysms of the left ventricle. Br Heart J 40:812, 1978.
17. Roelandt J, Van den Branc M, Vlelter W, et al: Echocardiographic diagnosis of pseudoaneurysm of the left ventricle. Circulation 52:466, 1975.
18. Sears TD, Ong YS, Starke H, Forker AD: Left ventricular pseudoaneurysm identified by cross-sectional echocardiography. AM Intern Med 90:935, 1979.
19. Gatewood RP, Nanda NC: Differentiation of left ventricular pseudoaneurysm from true aneurysm with two-dimensional echocardiography. Am J Cardiol 46:869, 1980.
20. Cathenvood E, Mintz GS, Kotler MN, et al: Two-dimensional echocardiographic recognition of left ventricular pseudoaneurysm. Circulation 62:294, 1980.
Copyright © 2022 FDOKUMEN




















