Basilar bifurcation: a comparison of prenatal and postnatal cases


For Peer Review
PANCREATIC CANCER STEM CELLS –
NEW INSIGHTS & PERSPECTIVES
Jorge Dorado, Enza Lonardo, Irene Miranda-Lorenzo, Christopher Heeschen
Stem Cells & Cancer Group, Clinical Research Programme, Spanish National Cancer Research
Centre (CNIO), Madrid, Spain
Correspondence: Dr. Christopher Heeschen, MD, PhD
Clinical Research Programme, Stem Cells & Cancer Group
Spanish National Cancer Research Centre (CNIO)
Madrid, Spain, E-mail: [email protected]
Short title: Pancreatic cancer stem cells
Abbreviations: CSC: cancer stem cells; GEM: gemcitabine;
Keywords: cancer stem cells, tumor-initiating cells, pancreatic cancer
Total word count 5,781
Page 1 of 21
((The Japanese Society of Gastroenterology))
((Journal of Gastroenterology))
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
ABSTRACT
Since the identification of self-renewing cells in the hematopoietic system several decades ago,
stem cells have changed the way we study biology and medicine. Solid tumors contain a distinct
subpopulation of cells, which bear stem cell characteristics and are responsible for exclusively
driving tumorigenesis. This has led to the development of the stem cell concept for cancer, which
purports that a subpopulation of self-renewing tumor cells, also termed cancer stem cells is
responsible for tumorigenesis and metastasis. This contrasts with the stochastic model of tumor
development, which advances that all tumor cells are capable of tumor initiation. Different
subpopulations of cancer stem cells have also been identified in pancreatic ductal
adenocarcinoma based on the use of combinations of surface markers that allowed their isolation,
propagation, and further characterization. Importantly, cancer stem cells are not only capable of
self-renewal and differentiation, but also may confer virulence via immune evasion and multidrug
resistance, and potentially via vasculogenic mimicry and transition to migratory and
metastasizing derivatives. Therapeutic targeting of this subset of cells and the pathways defining
their virulence holds great promise for the development of more effective strategies for
amelioration and eradication of this most lethal form of cancer.
Page 2 of 21
((The Japanese Society of Gastroenterology))
((Journal of Gastroenterology))
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
INTRODUCTION
Pancreatic adenocarcinoma is the fourth most frequent cause of cancer-related deaths. Despite its
incidence is moderated when compared to the whole of the solid cancers, it accounts for one of
the highest mortality rates (1). Responsible for this are its late diagnosis due to lack of early
symptoms, common impossibility to resect the tumor, extensive metastasis and high resistance to
treatment. Despite intensive research activity in the field of pancreatic cancer and significant
advancements have been achieved in the understanding of the mechanisms underlying pancreatic
cancer, these advancements over the past decades have had modest clinical relevance. Little
progress has been done since the introduction in the late 90’s of the chemotherapeutic agent
gemcitabine, a nucleoside-analogue, which improved clinical response in terms of pain reduction
and loss of weight (2). Nowadays gemcitabine remains the first-line chemotherapeutic agent in
pancreatic cancer. However, the prognosis of patients diagnosed with pancreatic cancer remains
extremely poor: 5-year survival rate of 1-4% and median survival period of 4-6 months. The
incorporation of the only other approved agent, erlotinib, to the therapeutic cocktail has not
resulted in major improvement in survival (3). Very recent data suggest the existence of different
subtypes of pancreatic ductal adenocarcinoma with erlotinib being more effective in classical
subtype cell lines (4), although this still needs to be validated in clinical samples.
A new horizon has emerged in the therapeutic strategies against pancreatic cancer with the advent
of increasing evidence supporting the existence of cancer stem cells (CSCs) in both
hematopoietic and solid cancers, including pancreatic cancer. CSCs represent a subpopulation of
cells distinguishable from the bulk of the tumor based on their exclusive ability to drive
tumorigenesis and are blamed for their crucial role in relapse of the disease (5). Therefore, the
elucidation of the mechanisms underlying pancreatic tumorigenesis and specially pancreatic
CSCs is of crucial relevance for the development of clinically more efficient therapies.
Page 3 of 21
((The Japanese Society of Gastroenterology))
((Journal of Gastroenterology))
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
CANCER STEM CELL CONCEPT
Over the past years, different models were developed trying to explain the origin and progression
of carcinogenesis. Classical models of carcinogenesis imply that any mutant tumor cell of any
organ can be expanded during tumorigenesis (6) being the entire tumor a functionally
homogeneous cell mass. Emerging data suggest that the majority of tumors, including pancreatic
ductal adenocarcinomas, display significant functional heterogeneity in their respective cell
populations, where a small subpopulation of tumor cells that acquired the same somatic mutations
but are epigenetically distinct, are responsible for tumor initiation, growth and metastasis (5).
This model is based on a hierarchical organization of the tumor, where a stem cell can give rise to
the heterogeneous tumor cell mass, while maintaining the ability to self-renew (Figure 1).
Specifically, the latest consensus definition of a CSC represents a cell within a tumor that has
exclusively self-renewal capacities, can give rise the entire cancer cell lineages within a tumor,
and are exclusively tumorigenic in vivo (7, 8). First descriptive evidence for the cancer stem cell
hypothesis was generated in leukemia and myeloma (9, 10), but further proof has now been
provided in leukemia (11) as well as several solid cancers including breast cancer (7),
glioblastoma (12), colorectal (13), liver (14), and pancreatic cancer (8, 15).
Conceptually, CSCs are characterize by additional traits including the ability for
asymmetric/symmetric cell division, enabling CSCs to maintain and expand themselves (16), a
distinct surface markers expression profile, that is actually being linked with poor prognosis.
Chemo- or radiotherapy against pancreatic cancer are rather ineffective and are mostly following
by tumor relapse and spreading. Intriguingly, it has been shown that CSCs are highly resistant to
standard therapy (8, 17). Given these findings, many investigators have hypothesized that CSCs
Page 4 of 21
((The Japanese Society of Gastroenterology))
((Journal of Gastroenterology))
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
arise from somatic stem or progenitor cells with genetic, since normal stem cells survive longer in
tissues, they are more likely to accumulate mutations over the time.
Indeed, this has now been experimentally proven for several tumor entities (18). Accumulation of
sequential mutations has been defined as a main common mechanism giving rise to
tumorigenesis, especially in tissues such as the intestine (19). Alternatively, CSCs may arise via
dedifferentiation of lineage committed cells that (re-)acquire stem cell characteristics through
acquisition of genetic alterations (20). Tracking the “cell of origin” in tissues with a less clearly
defined hierarchy such as the pancreas is challenging and will also require a better understanding
of the processes involving tissue maintenance and regeneration. Indeed, the process of generating
CSC in different tissues may also vary on an individual basis considering the context of tumor
development including inflammation and exposure to carcinogens.
MARKERS FOR PROSPECTIVELY ITENTIFYING PANCREATIC CANCER STEM CELLS
First evidence for the existence of CSCs in pancreatic cancer was provided by Li et al, 2007 (15).
The authors identified a highly tumorigenic CD44+CD24
+EpCAM
+ subpopulation using a
xenograft model of immunocompromised mice for primary human pancreatic adenocarcinoma.
As few as 102 CD44
+CD24
+EpCAM
+ cells were able to generate a tumor in 50% of the animals
indicating strong enrichment for the tumorigenic fraction. In contrast, cells negative for all three
markers (CD44–CD24
–EpCAM
–) were not capable of initiating pancreatic cancer until 10
4 or
more cells were implanted. CD44+CD24
+EpCAM
+ cells displayed
typical stem cell features such
as self-renewal, activation of developmental
signaling pathways (e.g. Shh), generation of
progenies, and recapitulation of the phenotype of the parental tumor from which they were
derived. Unfortunately, the authors did not investigate the tumorigenicity of the remaining cell
Page 5 of 21
((The Japanese Society of Gastroenterology))
((Journal of Gastroenterology))
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
populations other than those that were negative for all three markers. Since EpCAM identifies
cells in the tumor that are committed to the epithelial lineage, their EpCAM negative counterparts
may be contaminated by non-epithelial inflammatory, stromal and vascular cells (15).
In a second study, Hermann et al. showed that expression of CD133 in freshly isolated primary
human pancreatic cancers discriminates for cells with the capacity for self-renewal, sphere
formation, and, most importantly, in vivo tumorigenicity (8). Importantly, CD133 positive cells
maintained their tumor-initiating capability during serial passaging in vivo. Interestingly, the
authors further showed partial, but not complete overlap of the CD133+
population with the
CD44+CD24
+EpCAM
+ subpopulation. Further studies will be required in order to determine
whether these markers (CD44+CD24
+EpCAM
+ and CD133
+) define two distinct pancreatic CSC
populations, or whether the use of a combination of these markers confers a higher enrichment in
pancreatic tumor initiating cells (Table 1).
More recently, additional markers have also been associated with pancreatic CSCs like ALdehyde
DeHydrogenase 1 (ALDH-1), that has been associated with the tumorigenic cells in pancreatic
cancer (21-23), although more recent data suggest an abundant expression of ALDH-1 in normal
pancreas tissue (24), which may limit the utility of ALDH-1 as a marker for CSCs. Indeed,
ALDH1 can be best used for tumors whose corresponding normal tissues express ALDH1 in
relatively restricted or limited levels such as breast, lung, ovarian, or colorectal. Moreover, side
populations (SP) cells, which are identified by their ability to exclude the dye Hoechst 33342
through the over expression of the ABCG2 transporters, proved to be enriched for cancer-
initiating cells in several cancers (25). Consistently, Kabashima and colleagues reported for
established pancreatic a CSCs that the contained SP cells are enriched for cells with cancer stem
cell features and bear strong potential of the epithelial to mesenchymal transition (EMT),
invasion, and metastasis (26). Since the homeobox gene MSX2 appears to represent an important
Page 6 of 21
((The Japanese Society of Gastroenterology))
((Journal of Gastroenterology))
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
inducer of EMT in pancreatic cancer and MSX2 turned out to correlate with chemoresistance,
subsequent analysis of the MSX2-target gene identified ABCG2, a defining feature of SP cells, as
the responsible gene (27). Together these findings do not only suggest that SP cells are strongly
enriched in CSC, but also validate an intriguing regulatory mechanism of the cancer stem cell-
related phenotype, which could represent novel therapeutic target.
Table 1: CSC markers in pancreatic cancer
Pancreatic ductal adenocarcinoma Markers Reference
EpCAM+ CD44
+ CD24
+ (15)
CD133+ (8)
Tumor-initiating population
ALDH-1+
Side population / ABCG2
(21-23)
(26, 27)
Migrating cancer stem cells CD133+ CXCR4
+ (8)
Taken together, none of the above listed markers appear to be capable of selectively identifying a
pure population of CSCs rather than enrich for a population containing CSC. Single cell
experiments have mostly failed to produce tumor formation and largely depend on the use of the
immunological competence of the secondary recipient (28, 29). Importantly, exposure of cancer
cells to therapeutic interventions prior to their isolation may lead to changes in the expression of
these makers, which could affect their utility to identify tumor-initiating cells. A broader
consensus on the use of the most appropriate markers is certainly desirable and would increase
the probabilities for producing consistent data in pancreatic cancer and other tumor entities.
Page 7 of 21
((The Japanese Society of Gastroenterology))
((Journal of Gastroenterology))
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
CANCER STEM CELLS ARE HETEROGENOUS POPULATIONS OF CELLS
CSCs are unlikely to represent a homogenous population rather than evolve over time into
different clones, some of them providing them with advantages features including proliferation,
anti-apoptosis, DNA damage response, resistance to hypoxia, invasion, and metastasis (Figure 2).
Based on the CSC concept, only CSC should be equipped with metastatic potential as the bear
exclusive tumorigenic capacity, Indeed, while many cancer cells appear to circulate in the
peripheral blood, only a subset of these cells are eventually directed through lymphatic or blood
vessels toward specific secondary sites to form metastases and establish secondary lesions.
Whether all CSC are equipped with this potential or whether this is restricted to a subpopulation
had not been investigated until recently.
Herman et al. identified two distinct subsets of CD133+ CSC based on the additional expression
of the chemokine receptor CXCR4 (8). CXCR4 is a chemokine receptor responding to
chemotactic gradients of its specific ligand stromal cell derived factor 1 (SDF-1) and was
originally identified in the context of homing of leukocyte and hematopoietic progenitors. Out of
the heterogeneous population of CD133+ cells, two different subpopulations were identified by
means of expression of CXCR4. While CD133+ CXCR4
– were responsible for the initiation and
growth promotion of the primary tumor, the other subset of cells characterize by co-expression of
CXCR4 resulting in CD133+CXCR4
+ cells had exclusive metastatic potential. Depletion of the
CSC population for CD133+CXCR4
+ cells did not affect the tumor initiating potential of the cells
but completely abrogated their metastatic capacity. Consistently, significantly higher numbers of
CD133+CXCR4
+ migrating CSCs were observed in patients with lymph node metastasis (pN1+),
demonstrating the clinical relevance and prognostic potential for the detection of migrating CSCs.
While these cells could also be detected in the portal vein of the mice orthotopically transplanted
with CD133+CXCR4
+ cells, it remains to be demonstrated whether these cells can also be
Page 8 of 21
((The Japanese Society of Gastroenterology))
((Journal of Gastroenterology))
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
detected in the circulation of patients with advanced pancreatic cancer. They may serve as
independent predictors for the clinical course of the patients and may be used as novel markers
for monitoring of CSC-targeted treatment.
Interestingly, CSC can acquire an invasive phenotype as a consequence of epigenetic changes
suggesting that the evaluation of metastatic CSC may not only require genetic alterations but may
also be achieved by epigenetic changes responding to microenvironmetal clues (Figure 2).
Indeed, Epithelial-Mesenchymal-Transition (EMT) as a reversible dedifferentiation process has
been demonstrated to equip cancer (stem) cells with strong migratory capacity, while maintaining
their stemness features, allowing the production of progenies during metastasis. This is associated
with loss of E-cadherin and de novo expression of vimentin. In this context, Wellner et al.
recently showed for pancreatic cancer that the EMT-activator ZEB1 represents an important
promoter of metastasis by suppressing E-cadherin. Most interestingly, the stem cell phenotype
was maintained in the context of EMT by suppression of miR-200 family members that usually
target stem cell factors such as Sox2 and Klf4 (30).
It remains to be determined, which cell populations in the heterogeneous populations of the tumor
are actually capable of undergoing EMT in vivo. In fact, if also the progenies of the CSC may be
able to undergo EMT and, in this context, obtain the capacity to self-renew, the CSC population
would represent a moving target making their elimination even more challenging. Future studies
will have to elucidate whether transit-amplifying progenitors as the immediate progenies of CSC
or even differentiated epithelial cells can undergo EMT.
Page 9 of 21
((The Japanese Society of Gastroenterology))
((Journal of Gastroenterology))
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
CANCER STEM CELL-TARGETED THERAPY
Despite huge efforts for the identification of more effective therapies, pancreatic cancer continues
to be one of the deadliest cancer-related diseases in the world (31). The development of advanced
therapeutic strategies still represents a prerequisite to eventually achieve better outcome as
sufficiently early detection of pancreatic cancer is unlikely to occur in the near future. Recent
studies base on mathematical modeling for the evaluation of metastatic pancreatic cancer suggest
that metastatic processes in pancreatic cancer take place many years prior to current diagnosis
(32). Thus, an improvement of the currently available imaging methods used for the diagnosis of
pancreatic cancer is of crucial need for improving the prognosis of these patients.
Nevertheless, treatment of pancreatic cancer with the standard chemotherapy agent gemcitabine is
still not capable of eliminating the CSC subpopulation rather than resulted in a remaining G0/1
population of CSC. These cells may represent the source for rapid disease relapse.
Comprehensive cell tracking experiments will be needed to determine whether this is a remaining
quiescent CSC population that does not respond to chemotherapy and/or whether chemotherapy
results in cell cycle arrest. Most importantly, (a subpopulation of) CSC did not undergo apoptosis
and, as soon as gemcitabine was withdrawn, these cells immediately started to expand again
resulting in tumor relapse (8). The mechanistic basis of resistance to chemotherapy might not
only be linked to a quiescent subpopulation but also to their enhanced anti-apoptotic mechanisms
(33), distinct DNA repair mechanism (34), or the presence of membrane transporters that rapidly
eliminated administered drugs from these cells (35).
There are mainly two non-exclusive scenarios for depleting CSC populations. First, developing
therapeutic agents that selectively kill CSCs by targeting their self-renewal machinery without
affecting normal stem cells. Secondly, identifying cues to force CSCs into differentiation, since
Page 10 of 21
((The Japanese Society of Gastroenterology))
((Journal of Gastroenterology))
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
this process may be reversible due to enhanced plasticity of cancer cells, these treatment
modalities most certainly need to be accompanied by cytotoxic or other targeted therapies.
Stem cells and CSC share features as they both strongly express ABC membrane transporters, in
particular ABCG2 and MDR1, that can exclude cytotoxic substances from the cell (35) and have
an extraordinarily high capacity to repair DNA damage. CSC also display a reduced
immunogenicity and are characterized by an increased expression of anti-apoptotic genes such as
Bcl-XL that can allow the incorporation of normal nucleosides, but not toxic analogues (36).
Most importantly, however, CSC seem to contain a quiescent subpopulation, that will evade the
effects of most cytotoxic drugs simply because they are not proliferating. As a consequence, it
seems that stem cells survive conventional cancer chemotherapy and radiation (37). Of note, CSC
resistance to radiation in glioblastoma and breast cancer could be counteracted by a preferential
activation of DNA damage response mechanisms, which seem to be restricted to CSC (38, 39).
Importantly, recent studies suggested that CSCs also express high levels of telomerase despite the
quiescence of at least a subpopulation of these cells (40-43). Therefore telomerase, which is
essential for tumor progression, appears to be a critical marker in many cancers and most likely
for all cancer cells despite the inherent cellular heterogeneity of solid tumors. Because of this,
telomerase inhibition has emerged as an almost universal tumor target. It has been reported that
the combination of standard chemotherapy with telomerase inhibitors is more effective for solid
tumors such as prostate cancer (44). Several therapeutic approaches for telomerase inhibition are
now being developed and tested in solid tumors including pancreatic cancer, although most of the
candidate molecules are still in preclinical development (42). Most importantly, whether this new
treatment modality will also be capable of eliminating CSCs still remains to be determined.
Successful targeted CSC elimination may require the inhibition of multiple stemness pathways as
Page 11 of 21
((The Japanese Society of Gastroenterology))
((Journal of Gastroenterology))
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
a consequence of their redundancy and/or non-exclusiveness. One of the most promising
approaches to target stem cells is certainly the inhibition of stem cell-associated pathways (e.g.
sonic hedgehog, mTOR, notch, BMI, BMP). The Sonic Hedgehog (Shh) pathway has been shown
to be critical for the embryonic development of the pancreas (45), but has also been deeply
implied in the maintenance and progression of pancreatic cancer (46, 47). More recently, this
pathway has been considered as a crucial element for the maintenance of CSCs. Inhibition of Shh
signaling improved survival in a mouse model of pancreatic cancer (48) and therapeutic blockade
of this pathway in a xenograft model induced tumor regression and decreased the CSC content
(22). Moreover, Feldmann and colleagues (23) also showed that Hedgehog signaling blockade
abrogates pancreatic cancer metastases, a process which has been linked to the evasion of
migrating CSCs from the primary tumor.
Although several genetically engineered mouse models have been established to investigate a
causative role of Shh signaling in pancreatic tumorigenesis, none of them distinguished paracrine
versus autocrine canonical versus ligand-independent Shh signaling in pancreatic cancer. Yauch
et al. recently demonstrated a paracrine requirement for the Shh pathway in xenograft models of
pancreatic cancer, where Shh ligand is produced by tumor cells and the pathway is activated by
the adjacent stroma (49). To address whether a paracrine Shh signal is present in autochthonous
mouse pancreatic tumors, and to test if epithelial cancer cells is competent to transduce the Shh
signal, Tian el al. used an oncogenic form of smoothened to activate the pathway cell
autonomously (50). These data indicated that Shh signaling is restricted to tumor stroma,
contradicting previous reports that suggest a key role for ligand-driven epithelial Shh signaling in
tumor cell growth. However, these studies are still consistent with the observation that a
subpopulation of CSCs, which do not express markers of epithelial differentiation, rely on Shh
signaling (15, 23). Therefore, more work is needed to comprehensively define the precise
mechanism by which Hh pathway activation in stromal cells may also generate a
Page 12 of 21
((The Japanese Society of Gastroenterology))
((Journal of Gastroenterology))
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
microenvironment providing a CSC niche in pancreatic cancer.
Interestingly, Mueller et al. have recently shown that neither Shh inhibition alone nor as a
supplement to chemotherapy were capable of effectively diminishing the CSC pool (51). They
were also able to show that CD133 positive cells in pancreatic cancers show particularly high
activity for mTOR signaling suggesting that this pathway may also play are dominant role in the
CSC population. The mammalian Target Of Rapamycin (mTOR) is a serine/threonine kinase,
which belongs to the phosphatidylinositol 3-kinase (PI3K) superfamily, and is the target of a
widely branched signaling pathway that activates mTOR among other downstream effectors (52).
For pancreatic CSCs, the authors were indeed able to demonstrate that single-agent therapy with
rapamycin alone resulted in a significant decrease in CD133 positive CSCs.
However, inhibition of the mTOR pathway by rapamycin, as also observed for Shh pathway
inhibition, was not sufficient to eliminate CSCs completely. Only the combined inhibition of Shh
and mTOR together with chemotherapy resulted in the desired complete targeting of the CSC.
This triple (CRG) therapy resulted in a virtually complete depletion of the pancreatic CSC pool.
Implantation of cells that were pre-treated ex vivo consistently demonstrated that the in vivo
tumorigenic activity as the most important endpoint was completely abrogated. In a clinically
most relevant setting, the authors then investigated the effects of the triple therapy on established
pancreatic cancers utilizing patient-derived pancreatic cancer tissues (51). For the first time, the
authors were thus able to show that a multimodal therapy, involving the inhibition of two relevant
stem cell pathways and additional chemotherapy, represents a very promising approach, resulting
in virtually complete elimination of CSCs, significantly reduced tumorigenic and metastatic
activity, and long-term event-free survival. Future studies will now have to demonstrate the
transferability of these findings to the clinical scenario.
Page 13 of 21
((The Japanese Society of Gastroenterology))
((Journal of Gastroenterology))
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
The results from a recent study in glioblastoma indicate that inhibition of Notch by use of an
inhibitor of γ-secretase (GSI-18) is also capable of significantly reducing the CD133+ Notch
+ cell
population and consistently led to the eradication of cmedulloblastoma SP cells (53). Since
medulloblastoma cells treated with GSI-18 did no longer expand in vivo, it was concluded that
CSCs were effectively eradicated. These findings might be also applicable to pancreatic CSCs as
Notch 2 has also been implicated in pancreatic cancer progression (54), but further studies are
certainly warranted to determine the role of Notch in pancreatic CSCs.
CONCLUSIONS
The increasing evidence demonstrating a hierarchical organization for many cancers and the
identification of CSC, their prospective isolation, and characterization in pancreatic cancer has
now paved the way for the development of novel therapies targeting CSC as the putative root.
Still much work needs to be done in order to completely understand their origin in pancreatic
cancer as well as mechanisms regulating their stemness features in the tumorigenic process and
their increased resistance to chemo- and radiotherapy. But the knowledge gained during the last
years now provides an increasingly solid starting-point for the development of new research lines.
Eventually, specifically eliminating this subpopulation of cells should improve the clinical
outcome of patients suffering from the deadly pancreatic cancer. For this purpose, new clinical
endpoints need to be defined as tumor regression per se is unlikely to serve as a good predictor of
successful CSC targeting. While tracking of circulating CSC is still hampered by technological
challenges, treatment of patients in a neo-adjuvant setting with tumor biopsies prior to initiation
of treatment and a second tissue collection after treatment during surgical resection of the primary
tumor could serve as a suitable platform to track changes in CSC content.
Page 14 of 21
((The Japanese Society of Gastroenterology))
((Journal of Gastroenterology))
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
REFERENCES
1. Jemal, A., Siegel, R., Xu, J., and Ward, E. 2010. Cancer statistics, 2010. CA Cancer J
Clin 60:277-300.
2. Burris, H.A., 3rd, Moore, M.J., Andersen, J., Green, M.R., Rothenberg, M.L., Modiano,
M.R., Cripps, M.C., Portenoy, R.K., Storniolo, A.M., Tarassoff, P., et al. 1997.
Improvements in survival and clinical benefit with gemcitabine as first-line therapy for
patients with advanced pancreas cancer: a randomized trial. J Clin Oncol 15:2403-2413.
3. Moore, M.J., Goldstein, D., Hamm, J., Figer, A., Hecht, J.R., Gallinger, S., Au, H.J.,
Murawa, P., Walde, D., Wolff, R.A., et al. 2007. Erlotinib plus gemcitabine compared
with gemcitabine alone in patients with advanced pancreatic cancer: a phase III trial of
the National Cancer Institute of Canada Clinical Trials Group. J Clin Oncol 25:1960-
1966.
4. Collisson, E.A., Sadanandam, A., Olson, P., Gibb, W.J., Truitt, M., Gu, S., Cooc, J.,
Weinkle, J., Kim, G.E., Jakkula, L., et al. 2011. Subtypes of pancreatic ductal
adenocarcinoma and their differing responses to therapy. Nat Med 17:500-503.
5. Reya, T., Morrison, S.J., Clarke, M.F., and Weissman, I.L. 2001. Stem cells, cancer, and
cancer stem cells. Nature 414:105-111.
6. Nowell, P.C. 1976. The clonal evolution of tumor cell populations. Science 194:23-28.
7. Al-Hajj, M., Wicha, M.S., Benito-Hernandez, A., Morrison, S., and Clarke, M.F. 2003.
Prospective identification of tumorigenic breast cancer cells. Proc Natl Acad Sci USA
100:3983-3988.
8. Hermann, P., Huber, S., Herrler, T., Aicher, A., Ellwart, J., Guba, M., Bruns, C., and
Heeschen, C. 2007. Distinct Populations of Cancer Stem Cells Determine Tumor Growth
and Metastatic Activity in Human Pancreatic Cancer. Cell Stem Cell 1:313-323.
9. Bruce, W.R., and Van Der Gaag, H. 1963. A Quantitative Assay for the Number of
Murine Lymphoma Cells Capable of Proliferation in Vivo. Nature 199:79-80.
10. Park, C.H., Bergsagel, D.E., and McCulloch, E.A. 1971. Mouse myeloma tumor stem
cells: a primary cell culture assay. J Natl Cancer Inst 46:411-422.
11. Bonnet, D., and Dick, J.E. 1997. Human acute myeloid leukemia is organized as a
hierarchy that originates from a primitive hematopoietic cell. Nat Med 3:730-737.
12. Singh, S.K., Hawkins, C., Clarke, I.D., Squire, J.A., Bayani, J., Hide, T., Henkelman,
R.M., Cusimano, M.D., and Dirks, P.B. 2004. Identification of human brain tumour
initiating cells. Nature 432:396-401.
13. Ricci-Vitiani, L., Lombardi, D., Pilozzi, E., Biffoni, M., Todaro, M., Peschle, C., and De
Maria, R. 2007. Identification and expansion of human colon-cancer-initiating cells.
Nature 445:111-115.
14. Ma, S., Chan, K., Hu, L., Lee, T., Wo, J., Ng, I., Zheng, B., and Guan, X. 2007.
Identification and Characterization of Tumorigenic Liver Cancer Stem/Progenitor Cells.
Gastroenterology 132:2542-2556.
15. Li, C., Heidt, D., Dalerba, P., Burant, C., Zhang, L., Adsay, V., Wicha, M., Clarke, M.,
and Simeone, D. 2007. Identification of Pancreatic Cancer Stem Cells. Cancer Research
67:1030-1037.
Page 15 of 21
((The Japanese Society of Gastroenterology))
((Journal of Gastroenterology))
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
16. Wicha, M.S. 2006. Cancer stem cells: an old idea--a paradigm shift. Cancer Research
66:1883-1890; discussion 1895-1886.
17. Bar, E.E., Chaudhry, A., Lin, A., Fan, X., Schreck, K., Matsui, W., Piccirillo, S.,
Vescovi, A.L., DiMeco, F., Olivi, A., et al. 2007. Cyclopamine-mediated hedgehog
pathway inhibition depletes stem-like cancer cells in glioblastoma. Stem Cells 25:2524-
2533.
18. Campbell, P.J., Yachida, S., Mudie, L.J., Stephens, P.J., Pleasance, E.D., Stebbings, L.A.,
Morsberger, L.A., Latimer, C., McLaren, S., Lin, M.L., et al. 2010. The patterns and
dynamics of genomic instability in metastatic pancreatic cancer. Nature 467:1109-1113.
19. Fearon, E.R., and Vogelstein, B. 1990. A genetic model for colorectal tumorigenesis. Cell
61:759-767.
20. Notta, F., Mullighan, C.G., Wang, J.C., Poeppl, A., Doulatov, S., Phillips, L.A., Ma, J.,
Minden, M.D., Downing, J.R., and Dick, J.E. Evolution of human BCR-ABL1
lymphoblastic leukaemia-initiating cells. Nature 469:362-367.
21. Rasheed, Z.A., Yang, J., Wang, Q., Kowalski, J., Freed, I., Murter, C., Hong, S.M.,
Koorstra, J.B., Rajeshkumar, N.V., He, X., et al. 2010. Prognostic Significance of
Tumorigenic Cells With Mesenchymal Features in Pancreatic Adenocarcinoma. J Natl
Cancer Inst.
22. Jimeno, A., Feldmann, G., Suarez-Gauthier, A., Rasheed, Z., Solomon, A., Zou, G.M.,
Rubio-Viqueira, B., Garcia-Garcia, E., Lopez-Rios, F., Matsui, W., et al. 2009. A direct
pancreatic cancer xenograft model as a platform for cancer stem cell therapeutic
development. Mol Cancer Ther 8:310-314.
23. Feldmann, G., Dhara, S., Fendrich, V., Bedja, D., Beaty, R., Mullendore, M., Karikari,
C., Alvarez, H., Iacobuzio-Donahue, C., Jimeno, A., et al. 2007. Blockade of hedgehog
signaling inhibits pancreatic cancer invasion and metastases: a new paradigm for
combination therapy in solid cancers. Cancer Res 67:2187-2196.
24. Rovira, M., Scott, S.G., Liss, A.S., Jensen, J., Thayer, S.P., and Leach, S.D. 2010.
Isolation and characterization of centroacinar/terminal ductal progenitor cells in adult
mouse pancreas. Proc Natl Acad Sci U S A 107:75-80.
25. Hirschmann-Jax, C., Foster, A.E., Wulf, G.G., Nuchtern, J.G., Jax, T.W., Gobel, U.,
Goodell, M.A., and Brenner, M.K. 2004. A distinct "side population" of cells with high
drug efflux capacity in human tumor cells. Proc Natl Acad Sci U S A 101:14228-14233.
26. Kabashima, A., Higuchi, H., Takaishi, H., Matsuzaki, Y., Suzuki, S., Izumiya, M., Iizuka,
H., Sakai, G., Hozawa, S., Azuma, T., et al. 2009. Side population of pancreatic cancer
cells predominates in TGF-beta-mediated epithelial to mesenchymal transition and
invasion. Int J Cancer 124:2771-2779.
27. Hamada, S., Satoh, K., Hirota, M., Kanno, A., Umino, J., Ito, H., Masamune, A., Kikuta,
K., Kume, K., and Shimosegawa, T. 2011. The homeobox gene MSX2 determines
chemosensitivity of pancreatic cancer cells via the regulation of transporter gene ABCG2.
J Cell Physiol.
28. Quintana, E., Shackleton, M., Sabel, M.S., Fullen, D.R., Johnson, T.M., and Morrison,
S.J. 2008. Efficient tumour formation by single human melanoma cells. Nature 456:593-
598.
Page 16 of 21
((The Japanese Society of Gastroenterology))
((Journal of Gastroenterology))
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
29. Ishizawa, K., Rasheed, Z.A., Karisch, R., Wang, Q., Kowalski, J., Susky, E., Pereira, K.,
Karamboulas, C., Moghal, N., Rajeshkumar, N.V., et al. Tumor-initiating cells are rare in
many human tumors. Cell Stem Cell 7:279-282.
30. Wellner, U., Schubert, J., Burk, U.C., Schmalhofer, O., Zhu, F., Sonntag, A., Waldvogel,
B., Vannier, C., Darling, D., zur Hausen, A., et al. 2009. The EMT-activator ZEB1
promotes tumorigenicity by repressing stemness-inhibiting microRNAs. Nat Cell Biol
11:1487-1495.
31. Philip, P.A., Mooney, M., Jaffe, D., Eckhardt, G., Moore, M., Meropol, N., Emens, L.,
O'Reilly, E., Korc, M., Ellis, L., et al. 2009. Consensus report of the national cancer
institute clinical trials planning meeting on pancreas cancer treatment. J Clin Oncol
27:5660-5669.
32. Yachida, S., Jones, S., Bozic, I., Antal, T., Leary, R., Fu, B., Kamiyama, M., Hruban,
R.H., Eshleman, J.R., Nowak, M.A., et al. 2010. Distant metastasis occurs late during the
genetic evolution of pancreatic cancer. Nature 467:1114-1117.
33. Visvader, J.E., and Lindeman, G.J. 2008. Cancer stem cells in solid tumours:
accumulating evidence and unresolved questions. Nat Rev Cancer 8:755-768.
34. Gallmeier, E., Hermann, P.C., Mueller, M.T., Machado, J.G., Ziesch, A., De Toni, E.N.,
Palagyi, A., Eisen, C., Ellwart, J.W., Rivera, J., et al. Inhibition of Ataxia Telangiectasia-
and Rad3 -Related Function Abrogates the In Vitro and In Vivo Tumorigenicity of
Human Colon Cancer Cells Through Depletion of the CD133(+) Tumor-Initiating Cell
Fraction. Stem Cells 29:418-429.
35. Goodell, M.A., Brose, K., Paradis, G., Conner, A.S., and Mulligan, R.C. 1996. Isolation
and functional properties of murine hematopoietic stem cells that are replicating in vivo.
J Exp Med 183:1797-1806.
36. Shi, X., Liu, S., Kleeff, J., Friess, H., and Buchler, M.W. 2002. Acquired resistance of
pancreatic cancer cells towards 5-Fluorouracil and gemcitabine is associated with altered
expression of apoptosis-regulating genes. Oncology 62:354-362.
37. Wilson, A., Laurenti, E., Oser, G., van der Wath, R.C., Blanco-Bose, W., Jaworski, M.,
Offner, S., Dunant, C.F., Eshkind, L., Bockamp, E., et al. 2008. Hematopoietic stem cells
reversibly switch from dormancy to self-renewal during homeostasis and repair. Cell
135:1118-1129.
38. Bao, S., Wu, Q., Mclendon, R., Hao, Y., Shi, Q., Hjelmeland, A., Dewhirst, M., Bigner,
D., and Rich, J. 2006. Glioma stem cells promote radioresistance by preferential
activation of the DNA damage response. Nature 444:756-760.
39. Phillips, T.M., McBride, W.H., and Pajonk, F. 2006. The response of CD24(-
/low)/CD44+ breast cancer-initiating cells to radiation. J Natl Cancer Inst 98:1777-1785.
40. Armanios, M., and Greider, C.W. 2005. Telomerase and cancer stem cells. Cold Spring
Harb Symp Quant Biol 70:205-208.
41. Bhagwandin, V.J., and Shay, J.W. 2009. Pancreatic cancer stem cells: fact or fiction?
Biochim Biophys Acta 1792:248-259.
42. Harley, C.B. 2008. Telomerase and cancer therapeutics. Nat Rev Cancer 8:167-179.
43. Phatak, P., Cookson, J.C., Dai, F., Smith, V., Gartenhaus, R.B., Stevens, M.F., and
Burger, A.M. 2007. Telomere uncapping by the G-quadruplex ligand RHPS4 inhibits
Page 17 of 21
((The Japanese Society of Gastroenterology))
((Journal of Gastroenterology))
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
clonogenic tumour cell growth in vitro and in vivo consistent with a cancer stem cell
targeting mechanism. Br J Cancer 96:1223-1233.
44. Marian, C.O., and Shay, J.W. 2009. Prostate tumor-initiating cells: a new target for
telomerase inhibition therapy? Biochim Biophys Acta 1792:289-296.
45. Ingham, P.W., and McMahon, A.P. 2001. Hedgehog signaling in animal development:
paradigms and principles. Genes Dev 15:3059-3087.
46. Bailey, J.M., Mohr, A.M., and Hollingsworth, M.A. 2009. Sonic hedgehog paracrine
signaling regulates metastasis and lymphangiogenesis in pancreatic cancer. Oncogene
28:3513-3525.
47. Morton, J.P., Mongeau, M.E., Klimstra, D.S., Morris, J.P., Lee, Y.C., Kawaguchi, Y.,
Wright, C.V., Hebrok, M., and Lewis, B.C. 2007. Sonic hedgehog acts at multiple stages
during pancreatic tumorigenesis. Proc Natl Acad Sci U S A 104:5103-5108.
48. Olive, K.P., Jacobetz, M.A., Davidson, C.J., Gopinathan, A., McIntyre, D., Honess, D.,
Madhu, B., Goldgraben, M.A., Caldwell, M.E., Allard, D., et al. 2009. Inhibition of
Hedgehog signaling enhances delivery of chemotherapy in a mouse model of pancreatic
cancer. Science 324:1457-1461.
49. Yauch, R.L., Gould, S.E., Scales, S.J., Tang, T., Tian, H., Ahn, C.P., Marshall, D., Fu, L.,
Januario, T., Kallop, D., et al. 2008. A paracrine requirement for hedgehog signalling in
cancer. Nature 455:406-410.
50. Tian, H., Callahan, C.A., DuPree, K.J., Darbonne, W.C., Ahn, C.P., Scales, S.J., and de
Sauvage, F.J. 2009. Hedgehog signaling is restricted to the stromal compartment during
pancreatic carcinogenesis. Proc Natl Acad Sci U S A 106:4254-4259.
51. Mueller, M.T., Hermann, P.C., Witthauer, J., Rubio-Viqueira, B., Leicht, S.F., Huber, S.,
Ellwart, J.W., Mustafa, M., Bartenstein, P., D'Haese, J.G., et al. 2009. Combined
Targeted Treatment to Eliminate Tumorigenic Cancer Stem Cells in Human Pancreatic
Cancer. Gastroenterology.
52. Inoki, K., Corradetti, M.N., and Guan, K.L. 2005. Dysregulation of the TSC-mTOR
pathway in human disease. Nat Genet 37:19-24.
53. Fan, X., Matsui, W., Khaki, L., Stearns, D., Chun, J., Li, Y.M., and Eberhart, C.G. 2006.
Notch pathway inhibition depletes stem-like cells and blocks engraftment in embryonal
brain tumors. Cancer Res 66:7445-7452.
54. Mazur, P.K., Gruner, B.M., Nakhai, H., Sipos, B., Zimber-Strobl, U., Strobl, L.J., Radtke,
F., Schmid, R.M., and Siveke, J.T. 2010. Identification of epidermal Pdx1 expression
discloses different roles of Notch1 and Notch2 in murine Kras(G12D)-induced skin
carcinogenesis in vivo. PLoS One 5:e13578.
Page 18 of 21
((The Japanese Society of Gastroenterology))
((Journal of Gastroenterology))
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
FIGURE LEGENDS
Figure 1. Cancer stem cell model. Like somatic stem cells, cancer stem cells are on top of a
hierarchical organization. They possess the ability to self-renew and therefore maintain the pool
of cancer stem cells within a tumor. Upon sequential differentiation they generate progenitor cells
representing the bulk of the tumor. Depending on the plasticity of the progenies, they may be
capable of contributing to the replenishment of the cancer stem cell pool. Epithelial-
Mesenchymal-Transition (EMT) may lead to the generation of a more mesenchymal stem cell
population bearing strong metastatic capacity.
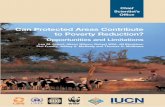
Figure 2. Cancer stem cell heterogeneity. CSCs can undergo both symmetric and asymmetric
divisions. Symmetric divisions result in two daughter CSCs, contributing to the expansion of the
CSC pool. In an asymmetric division, a CSC generates another CSC plus a differentiated cell.
Moreover, CSCs evolve within the tumor due to genetic and epigenetic changes and influences
from their microenvironment that can result in the acquisition of no features of the CSC. A more
invasive phenotype could lead to the evasion of the CSC from the primary tumor, circulation and
eventually generation of metastatic lesion.
Page 19 of 21
((The Japanese Society of Gastroenterology))
((Journal of Gastroenterology))
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review
Stem
cells
Progenitor
cells
Transit-
amplifying
cells
Differentiated
cells
Somatic
stem cells
Cancer
stem cells
Mesenchymal
phenotype
Increased
plasticity ?
Figure 1 – Dorado et al.
Page 20 of 21
((The Japanese Society of Gastroenterology))
((Journal of Gastroenterology))
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer ReviewCSC’
CSC
CSC
CSC
CSC
Cancer stem cells
CSC
Mos
tly
Sym
met
ric
divi
sion
CSC
High percentage of CSCs
Undifferentiated state
Poor clinical outcome
Symm
etric &
asymm
etric
division
Low percentage of CSCs
More differentiated state
Better clinical outcome
CSC evolution
Genetic & epigenetic changes
Microenvironment
CSC’
CSC
Tumor evasion
CSC’
CSC’
CSC’
Metastasis
Circulating
CSC
Figure 2 – Dorado et al.
Page 21 of 21
((The Japanese Society of Gastroenterology))
((Journal of Gastroenterology))
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Copyright © 2022 FDOKUMEN